Target Level for Hemoglobin Correction in Patients With Diabetes and CKD: Primary Results of the...
14
Target Level for Hemoglobin Correction in Patients With Diabetes and CKD: Primary Results of the Anemia Correction in Diabetes (ACORD) Study Eberhard Ritz, MD, PhD, Maurice Laville, MD, PhD, Rudy W. Bilous, MD, PhD, Donal O’Donoghue, MD, PhD, Armin Scherhag, MD, Ulrich Burger, PhD, and Fernando de Alvaro, MD, PhD, on behalf of the ACORD Investigators and Coordinators Background: Patients with diabetes and anemia are at high risk of cardiovascular disease. The Anemia CORrection in Diabetes (ACORD) Study aimed to investigate the effect of anemia correction on cardiac structure, function, and outcomes in patients with diabetes with anemia and early diabetic nephropathy. Methods: One hundred seventy-two patients with type 1 or 2 diabetes mellitus, mild to moderate anemia, and stage 1 to 3 chronic kidney disease were randomly assigned to attain a target hemoglobin (Hb) level of either 13 to 15 g/dL (130 to 150 g/L; group 1) or 10.5 to 11.5 g/dL (105 to 115 g/L; group 2). The primary end point was change in left ventricular mass index (LVMI). Secondary end points included echocardiographic variables, renal function, quality of life, and safety. Results: Median Hb level and LVMI were similar in groups 1 and 2 (Hb, 11.9 and 11.7 g/dL [119 and 117 g/L]; LVMI, 113.5 and 112.3 g/m 2 , respectively). At study end, Hb levels were 13.5 g/dL (135 g/L) in group 1 and 12.1 g/dL (121 g/L) in group 2 (P 0.001). No significant differences were observed in median LVMI at month 15 between study groups (group 1, 112.3 g/m 2 ; group 2, 116.5 g/m 2 ). Multivariate analysis showed a nonsignificant decrease in LVMI (P 0.15) in group 1 versus group 2. Anemia correction had no effect on the rate of decrease in creatinine clearance, but resulted in significantly improved quality of life in group 1 (P 0.04). There were no clinically relevant differences in adverse events between study groups. Conclusion: In patients with diabetes with mild to moderate anemia and moderate left ventricular hypertrophy, correction to an Hb target level of 13 to 15 g/dL (130 to 150 g/L) does not decrease LVMI. However, normalization of Hb level prevented an additional increase in left ventricular hypertrophy, was safe, and improved quality of life. Am J Kidney Dis 49:194-207. © 2007 by the National Kidney Foundation, Inc. INDEX WORDS: Diabetes; chronic kidney disease (CKD); left ventricular mass index; quality of life; renal function. D iabetes has become the most common co- morbid condition of end-stage renal dis- ease in Europe and the United States. 1,2 In addi- tion, diabetes is recognized as a major risk factor for cardiovascular disease, 3,4 and the risk is am- plified further by the presence of diabetic ne- phropathy. Accordingly, patients with both end- stage renal disease and diabetes have a worse prognosis than those without diabetes. 5 Left ventricular hypertrophy (LVH) is ob- served in approximately 75% of patients entering dialysis therapy, and in addition, other cardiovas- cular complications, such as chronic heart failure, coronary artery disease, and peripheral arterial dis- ease, are common. 6,7 The burden of cardiovascular disease therefore is greater; consequently, survival rates are worse in patients with diabetes entering dialysis than in those without this condition. 5,8,9 From the Department of Internal Medicine, University of Heidelberg; Medical Clinic I, University Hospital Mann- heim, Germany; Department of Nephrology, Edouard Her- riot Hospital, Lyon, France; Education Centre, James Cook University Hospital, Middlesbrough; Department of Renal Medicine, Hope Hospital, Salford, UK; F. Hoffmann-La Roche Ltd, Basel, Switzerland; and Servicio Nefrología, Hospital Universitario La Paz, Madrid, Spain. Received July 14, 2006; accepted in revised form Novem- ber 2, 2006. Originally published online as doi:10.1053/j.ajkd.2006.11.032 on January 3, 2007. Support: The study was sponsored by F. Hoffmann-La Roche Ltd. Potential conflicts of interest: E.R. and D.O. received honoraria as speakers from Hoffmann-La Roche. A.S. and U.B. are employees of F. Hoffmann-La Roche Ltd. Trial registration: www.clinicaltrials.gov; study number: NCT00354341. Address reprint requests to Eberhard Ritz, MD, PhD, Department of Internal Medicine, Bergheimerstrasse 58, Heidelberg 69115 Germany. E-mail: [email protected] © 2007 by the National Kidney Foundation, Inc. 0272-6386/07/4902-0005$32.00/0 doi:10.1053/j.ajkd.2006.11.032 American Journal of Kidney Diseases, Vol 49, No 2 (February), 2007: pp 194-207 194
Transcript of Target Level for Hemoglobin Correction in Patients With Diabetes and CKD: Primary Results of the...

Detfppsp
HhrUMRH
b
o
1
Target Level for Hemoglobin Correction in Patients WithDiabetes and CKD: Primary Results of the Anemia Correction
in Diabetes (ACORD) Study
Eberhard Ritz, MD, PhD, Maurice Laville, MD, PhD, Rudy W. Bilous, MD, PhD,Donal O’Donoghue, MD, PhD, Armin Scherhag, MD, Ulrich Burger, PhD,
and Fernando de Alvaro, MD, PhD, on behalf of the ACORD Investigators and Coordinators
Background: Patients with diabetes and anemia are at high risk of cardiovascular disease. The AnemiaCORrection in Diabetes (ACORD) Study aimed to investigate the effect of anemia correction on cardiac structure,function, and outcomes in patients with diabetes with anemia and early diabetic nephropathy.
Methods: One hundred seventy-two patients with type 1 or 2 diabetes mellitus, mild to moderateanemia, and stage 1 to 3 chronic kidney disease were randomly assigned to attain a target hemoglobin(Hb) level of either 13 to 15 g/dL (130 to 150 g/L; group 1) or 10.5 to 11.5 g/dL (105 to 115 g/L; group 2).The primary end point was change in left ventricular mass index (LVMI). Secondary end points includedechocardiographic variables, renal function, quality of life, and safety.
Results: Median Hb level and LVMI were similar in groups 1 and 2 (Hb, 11.9 and 11.7 g/dL [119 and117 g/L]; LVMI, 113.5 and 112.3 g/m2, respectively). At study end, Hb levels were 13.5 g/dL (135 g/L) ingroup 1 and 12.1 g/dL (121 g/L) in group 2 (P � 0.001). No significant differences were observed inmedian LVMI at month 15 between study groups (group 1, 112.3 g/m2; group 2, 116.5 g/m2).Multivariate analysis showed a nonsignificant decrease in LVMI (P � 0.15) in group 1 versus group 2.Anemia correction had no effect on the rate of decrease in creatinine clearance, but resulted insignificantly improved quality of life in group 1 (P � 0.04). There were no clinically relevant differences inadverse events between study groups.
Conclusion: In patients with diabetes with mild to moderate anemia and moderate left ventricularhypertrophy, correction to an Hb target level of 13 to 15 g/dL (130 to 150 g/L) does not decrease LVMI.However, normalization of Hb level prevented an additional increase in left ventricular hypertrophy, wassafe, and improved quality of life.Am J Kidney Dis 49:194-207. © 2007 by the National Kidney Foundation, Inc.
INDEX WORDS: Diabetes; chronic kidney disease (CKD); left ventricular mass index; quality of life;renal function.
sdccedrd
iabetes has become the most common co-morbid condition of end-stage renal dis-
ase in Europe and the United States.1,2 In addi-ion, diabetes is recognized as a major risk factoror cardiovascular disease,3,4 and the risk is am-lified further by the presence of diabetic ne-hropathy. Accordingly, patients with both end-tage renal disease and diabetes have a worserognosis than those without diabetes.5
From the Department of Internal Medicine, University ofeidelberg; Medical Clinic I, University Hospital Mann-eim, Germany; Department of Nephrology, Edouard Her-iot Hospital, Lyon, France; Education Centre, James Cookniversity Hospital, Middlesbrough; Department of Renaledicine, Hope Hospital, Salford, UK; F. Hoffmann-Laoche Ltd, Basel, Switzerland; and Servicio Nefrología,ospital Universitario La Paz, Madrid, Spain.Received July 14, 2006; accepted in revised form Novem-
er 2, 2006.Originally published online as doi:10.1053/j.ajkd.2006.11.032
n January 3, 2007.
American Journal of Kid94
Left ventricular hypertrophy (LVH) is ob-erved in approximately 75% of patients enteringialysis therapy, and in addition, other cardiovas-ular complications, such as chronic heart failure,oronary artery disease, and peripheral arterial dis-ase, are common.6,7 The burden of cardiovascularisease therefore is greater; consequently, survivalates are worse in patients with diabetes enteringialysis than in those without this condition.5,8,9
Support: The study was sponsored by F. Hoffmann-Laoche Ltd. Potential conflicts of interest: E.R. and D.O.
eceived honoraria as speakers from Hoffmann-La Roche..S. and U.B. are employees of F. Hoffmann-La Roche Ltd.Trial registration: www.clinicaltrials.gov; study number:
CT00354341.Address reprint requests to Eberhard Ritz, MD, PhD,
epartment of Internal Medicine, Bergheimerstrasse 58,eidelberg 69115 Germany. E-mail: [email protected]© 2007 by the National Kidney Foundation, Inc.0272-6386/07/4902-0005$32.00/0
RrA
N
DH
doi:10.1053/j.ajkd.2006.11.032
ney Diseases, Vol 49, No 2 (February), 2007: pp 194-207

apphacloAet
mplspmtisltwioe
tleqd
Samloyetomttfcp
S
ocDps
tesTi
S
pcc(ag
gfiigb(gogwgnwm
mtmfdeso
Ra
Stfitcwcs
Target Level for Hemoglobin Correction in Diabetes 195
Anemia is a common feature of renal diseasend is associated with increased mortality inatients with chronic kidney disease (CKD),articularly those with diabetes.5 Anemia alsoas an effect on left ventricular mass. For ex-mple, in a large prospective Canadian multi-enter study, each decrease in hemoglobin (Hb)evel of 0.5 g/dL (5 g/L) resulted in an increaseddds ratio for left ventricular mass by 32%.10
nemia also is an independent predictor of non-lective hospitalization before and after initia-ion of renal replacement therapy.11,12
In patients with end-stage renal disease, treat-ent of anemia with recombinant human erythro-
oietin (epoetin) improves overall and cardiovascu-ar event–free survival.11,13,14 Observational studiesuggested that early treatment of anemia in theredialysis stage of CKD has a beneficial effect onortality after the patients are on dialysis
herapy.15-17 Two uncontrolled observational stud-es18,19 and 1 small randomized controlled trial20
howed that anemia correction with epoetin led toess rapid deterioration in renal function and preven-ion, or even regression, of LVH21-23 in patientsith advanced CKD. Furthermore, small-scale stud-
es showed that epoetin treatment improved qualityf life in patients with diabetes with anemia andarly renal disease.24,25
In view of these observations, it was proposedhat early and complete, as opposed to partialate, anemia correction would have beneficialffects on left ventricular mass index (LVMI),uality of life, and renal function in patients withiabetes with mild to moderate anemia and CKD.
The Anemia CORrection in Diabetes (ACORD)tudy is designed to investigate the effects ofnemia correction with epoetin beta (NeoRecor-on; F. Hoffmann-La Roche Ltd, Basel, Switzer-
and) on cardiac structure, function, and clinicalutcomes in patients with diabetes and CKD notet on renal replacement therapy. The primarynd point was the effect of early versus latereatment strategy for correction of renal anemian LVH assessed by echocardiographic measure-ent of LVMI. Secondary objectives included
he effect of early and complete anemia correc-ion on left ventricular volumes, left ventricularunction, renal function, and various other clini-al parameters, including quality of life and,
articularly, safety. cMETHODS
tudy Population
ACORD was an international, multicenter, randomized,pen-label, parallel-group study involving 64 centers in 16ountries. The study was performed in accordance with theeclaration of Helsinki and guidelines for good clinicalractice.26 The study protocol was approved by the respon-ible ethical review boards at all participating centers.
The ACORD Study enrolled adult patients with type 1 orype 2 diabetes mellitus, mild to moderate anemia, andarly-stage (stages 1 to 3) CKD. Major inclusion and exclu-ion criteria used to ascertain study eligibility are listed inable 1. All patients gave written informed consent before
nclusion in the study.
tudy Design
The ACORD Study design is shown in Fig 1. Eligibleatients who fulfilled the stipulated inclusion and exclusionriteria were randomly assigned to receive either early andomplete anemia correction to attain normal Hb levelstarget Hb, 13 to 15 g/dL [130 to 150 g/L]; group 1) or partialnemia correction (target Hb, 10.5 to 11.5 g/dL [105 to 115/L]; group 2).Randomization was performed centrally into 2 treatment
roups by using a block-size randomization procedure strati-ed by country and use of angiotensin-converting enzyme
nhibitors and/or angiotensin receptor blockers. Patients inroup 1 were started immediately on subcutaneous epoetineta treatment to reach a target Hb level of 13 to 15 g/dL130 to 150 g/L) within approximately 3 months. Patients inroup 2 were started on subcutaneous epoetin beta treatmentnly when their Hb level had decreased to less than 10.5/dL (�105 g/L) on 2 consecutive visits at an interval of 2eeks or if their Hb level decreased to less than 10 g/dL (100/L) at a single determination. The starting dose of subcuta-eous epoetin beta in both groups was 2,000 IU onceeekly, self-administered using the Reco-Pen (F. Hoff-ann-La Roche Ltd) delivery device.All patients had a clinical assessment at 6 weeks and 3onths after starting treatment and at 3-monthly intervals
hereafter. In addition, during the correction phase of treat-ent, patients must have returned to the clinic every 2 weeks
or assessment of Hb and any adjustment to epoetin betaose necessary to achieve a rate of increase in Hb notxceeding 1 g/dL (10 g/L) every 4 weeks. The study wascheduled to end after each patient had completed 15 monthsf follow-up.
ole of the Funding Sourcend Study Committees
The trial was designed, implemented, and overseen by atudy Steering Committee, together with representatives of
he sponsor, F. Hoffmann-La Roche Ltd. The sponsor identi-ed participating centers together with the Steering Commit-
ee and was responsible for monitoring the centers, dataollection, and data cleaning. The statistical analysis planas agreed with the Steering Committee before database
losure. The Steering Committee was granted access to alltudy data. Interpretation of all study data was done in close
ollaboration between the Steering Committee and the sponsor.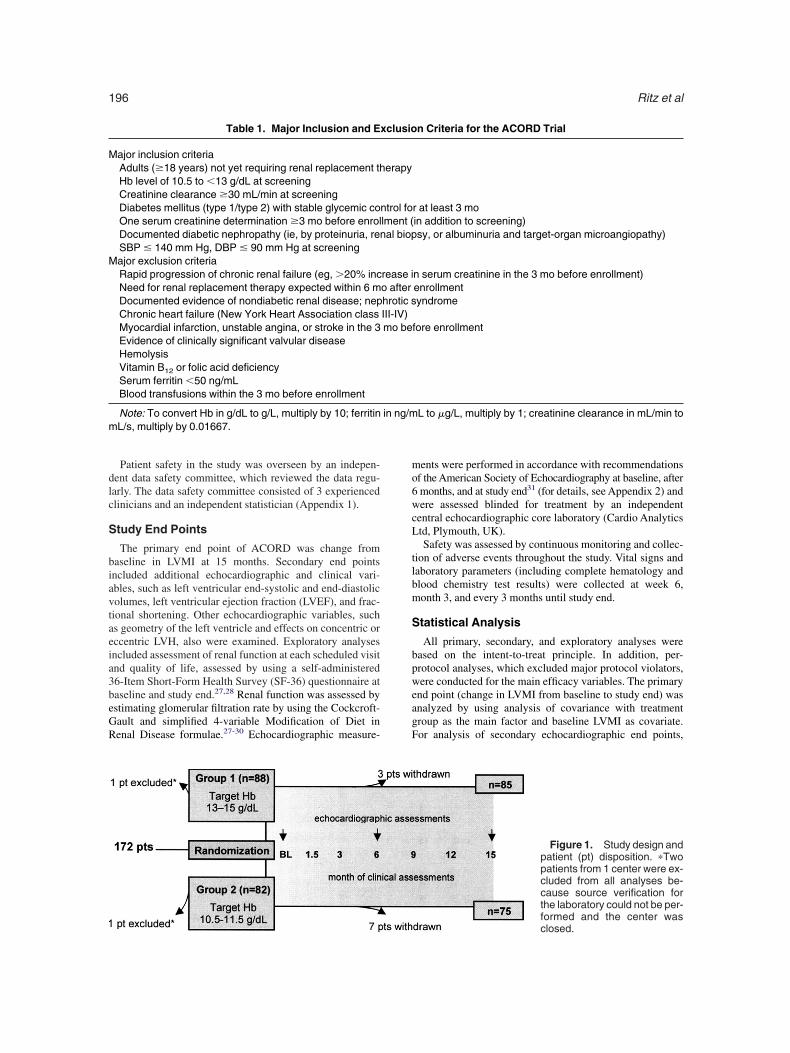
dlc
S
biavtaeia3beGR
mo6wcL
tlbm
S
bpweagF
M
M
m
Ritz et al196
Patient safety in the study was overseen by an indepen-ent data safety committee, which reviewed the data regu-arly. The data safety committee consisted of 3 experiencedlinicians and an independent statistician (Appendix 1).
tudy End Points
The primary end point of ACORD was change fromaseline in LVMI at 15 months. Secondary end pointsncluded additional echocardiographic and clinical vari-bles, such as left ventricular end-systolic and end-diastolicolumes, left ventricular ejection fraction (LVEF), and frac-ional shortening. Other echocardiographic variables, suchs geometry of the left ventricle and effects on concentric orccentric LVH, also were examined. Exploratory analysesncluded assessment of renal function at each scheduled visitnd quality of life, assessed by using a self-administered6-Item Short-Form Health Survey (SF-36) questionnaire ataseline and study end.27,28 Renal function was assessed bystimating glomerular filtration rate by using the Cockcroft-ault and simplified 4-variable Modification of Diet inenal Disease formulae.27-30 Echocardiographic measure-
Table 1. Major Inclusion and E
ajor inclusion criteriaAdults (�18 years) not yet requiring renal replacement thHb level of 10.5 to �13 g/dL at screeningCreatinine clearance �30 mL/min at screeningDiabetes mellitus (type 1/type 2) with stable glycemic coOne serum creatinine determination �3 mo before enrolDocumented diabetic nephropathy (ie, by proteinuria, renSBP � 140 mm Hg, DBP � 90 mm Hg at screeningajor exclusion criteriaRapid progression of chronic renal failure (eg, �20% incNeed for renal replacement therapy expected within 6 mDocumented evidence of nondiabetic renal disease; nepChronic heart failure (New York Heart Association classMyocardial infarction, unstable angina, or stroke in the 3Evidence of clinically significant valvular diseaseHemolysisVitamin B12 or folic acid deficiencySerum ferritin �50 ng/mLBlood transfusions within the 3 mo before enrollment
Note: To convert Hb in g/dL to g/L, multiply by 10; ferritinL/s, multiply by 0.01667.
ents were performed in accordance with recommendationsf the American Society of Echocardiography at baseline, aftermonths, and at study end31 (for details, see Appendix 2) andere assessed blinded for treatment by an independent
entral echocardiographic core laboratory (Cardio Analyticstd, Plymouth, UK).Safety was assessed by continuous monitoring and collec-
ion of adverse events throughout the study. Vital signs andaboratory parameters (including complete hematology andlood chemistry test results) were collected at week 6,onth 3, and every 3 months until study end.
tatistical Analysis
All primary, secondary, and exploratory analyses wereased on the intent-to-treat principle. In addition, per-rotocol analyses, which excluded major protocol violators,ere conducted for the main efficacy variables. The primary
nd point (change in LVMI from baseline to study end) wasnalyzed by using analysis of covariance with treatmentroup as the main factor and baseline LVMI as covariate.or analysis of secondary echocardiographic end points,
n Criteria for the ACORD Trial
r at least 3 moin addition to screening)sy, or albuminuria and target-organ microangiopathy)
n serum creatinine in the 3 mo before enrollment)enrollmentyndrome
fore enrollment
L to �g/L, multiply by 1; creatinine clearance in mL/min to
Figure 1. Study design andpatient (pt) disposition. �Twopatients from 1 center were ex-cluded from all analyses be-cause source verification forthe laboratory could not be per-
xclusio
erapy
ntrol folment (al biop
rease io afterhrotic sIII-IV)mo be
in ng/m
formed and the center wasclosed.

sumt
sccactw
pigahgtp
P
d8cptsbv
Ttmi1
SAWBSDT
T
DHH
R
L
SF
ftm
Target Level for Hemoglobin Correction in Diabetes 197
uch as left ventricular end-systolic and end-diastolic vol-mes, LVEF, and fractional shortening, a similar covarianceodel was used with treatment group as the main factor and
he respective baseline value as covariate.For quality of life, mean total score on the SF-36 sub-
cales at the end of the study were calculated, and analysis ofovariance was performed using baseline as an independentofactor. Other variables were analyzed qualitatively. Percent-ges of patients with stable Hb levels, as well as otheromparisons between groups, were done by using chi-squareest. All values are reported as mean � SD or median valueith the respective range or interquartile range (IQR).Sample-size calculation for ACORD was based on the
rimary outcome variable, LVMI. The expected mean changen LVMI from baseline to follow-up between the 2 studyroups was 20 g/m2. With a sample size of at least 64ssessable patients per treatment arm, ACORD would havead 80% power to show this difference between studyroups. Assuming a 20% dropout rate during the course ofhe study, it was calculated that recruitment of at least 160atients (80 per treatment arm) was needed.
Table 2. Patient Ch
Group 1 Target Hb(n � 88
ex (% men) 51ge (y) 58 (49-69eight (kg)* 75.6 (50.0-1ody mass index (kg/m2) 28.5 (24.9-3BP (mm Hg) 134 (126-1BP (mm Hg) 78 (70-80ype 1 diabetes (%) 27Time since diagnosis (y) 20 (17-30
ype 2 diabetes (%) 73Time since diagnosis (y) 16 (11-21iabetic retinopathy (%) 84bA1c (%) 8.2 (7.2-9.ematology/iron variablesHb (g/dL) 11.9 (11.3-1Ferritin (ng/mL) 99 (69-16Transferrin saturation (%) 22 (17-31enal functionUrine protein excretion (g/24 h) 1.3 (0.5-3.Creatinine clearance (mL/min) 51 (39-67Serum creatinine (mg/dL) 1.58 (1.21-1
ipid variablesLow-density lipoprotein
cholesterol (mg/dL)116 (89-14
High-density lipoproteincholesterol (mg/dL)
50 (39-66
Total cholesterol (mg/dL) 197 (166-2Triglycerides (mg/dL) 151 (97-20
tatin treatment (%) 46ibrate treatment (%) 7
Note: Values expressed as percent or median (IQR) unleerritin in ng/mL to �g/L, multiply by 1; creatinine clearanceo �mol/L, multiply by 88.4; low-density lipoprotein cholestg/dL to mmol/L, multiply by 0.02586; triglycerides in mg/d
*Median (range).RESULTS
atients and Baseline Characteristics
One hundred seventy-two patients were ran-omly assigned to the 2 treatment arms (group 1,9 patients; group 2, 83 patients), of which 160ompleted the study as planned (group 1, 85atients; group 2, 75 patients; Fig 1). Two pa-ients from a single center were randomly as-igned, but were excluded from all analysesecause the center was closed due to majoriolation of Good Clinical Practice guidelines.Patient baseline characteristics are listed in
ables 2 and 3. In general, baseline characteris-ics were similar in the 2 groups. However,edian body weight, body mass index, and creat-
nine clearance were significantly greater in groupcompared with group 2. Furthermore, a greater
ristics at Baseline
g/dL Group 2 Target Hb, 10.5-11.5 g/dL(n � 82) P
50 0.94157 (47-66) 0.366
70.0 (41.5-110.0) 0.00925.6 (23.1-29.5) 0.005133 (126-139) 0.88680 (71-80) 0.188
35 0.29124 (21-31) 0.174
65 0.29114 (9-19) 0.256
83 0.9177.9 (6.8-8.7) 0.078
11.7 (11.3-12.0) 0.151125 (62-212) 0.68722 (18-29) 0.435
0.8 (0.4-2.9) 0.32246 (35-55) 0.020
1.63 (1.26-2.17) 0.334
124 (104-159) 0.110
50 (43-62) 0.828
201 (174-232) 0.377133 (97-213) 0.502
35 0.2089 0.779
ed otherwise. To convert Hb in g/dL to g/L, multiply by 10;in to mL/s, multiply by 0.01667; serum creatinine in mg/dL
gh-density lipoprotein cholesterol, and total cholesterol inol/L, multiply by 0.01129.
aracte
, 13-15)
)06.1)0.7)40))
)
)
2)
2.2)3))
1)).93)
3)
)
36)4)
ss notin mL/merol, hiL to mm
pgPvsc
azbruwt3mmta
A
(gaitptl(2dwgaggt2gglsim(17Sp(D
CI
CLPVEO
Ritz et al198
roportion of patients had type 2 diabetes inroup 1 (73%) compared with group 2 (65%).revious myocardial infarction and peripheralascular disease were the most commonly ob-erved concomitant cardiovascular diseases (ex-luding hypertension; Table 3).
In total, 89% and 84% of patients in group 1nd group 2 received angiotensin-converting en-yme inhibitors and/or angiotensin receptorlockers with or without other antihypertensives,espectively. Calcium channel blockers, loop di-retics, and �-blockers were prescribed, with orithout angiotensin-converting enzyme inhibi-
ors and/or angiotensin receptor blockers, in 52%,8%, and 23% of patients, respectively. Use ofultiple antihypertensive medications was com-on, with only 19.8% of patients receiving mono-
herapy. Half the patients received 3 or morentihypertensive agents.
Table 3. Cardiovascular Diseases at Baseline
Group 1(n � 88)
Group 2(n � 82)
hronic heart failure (%) 5 2schemic heart disease (%) 25 14
Previous myocardial infarction 17 7Coronary artery disease 5 7erebrovascular disease, stroke (%) 6 5VH (%) 5 4eripheral vascular disease (%) 11 6alvulopathies (%) 1 4lectrocardiogram abnormalities (%) 5 1ther cardiovascular diseases (%) 13 12
Note: LVH as reported by treating physician.
nemia Correction
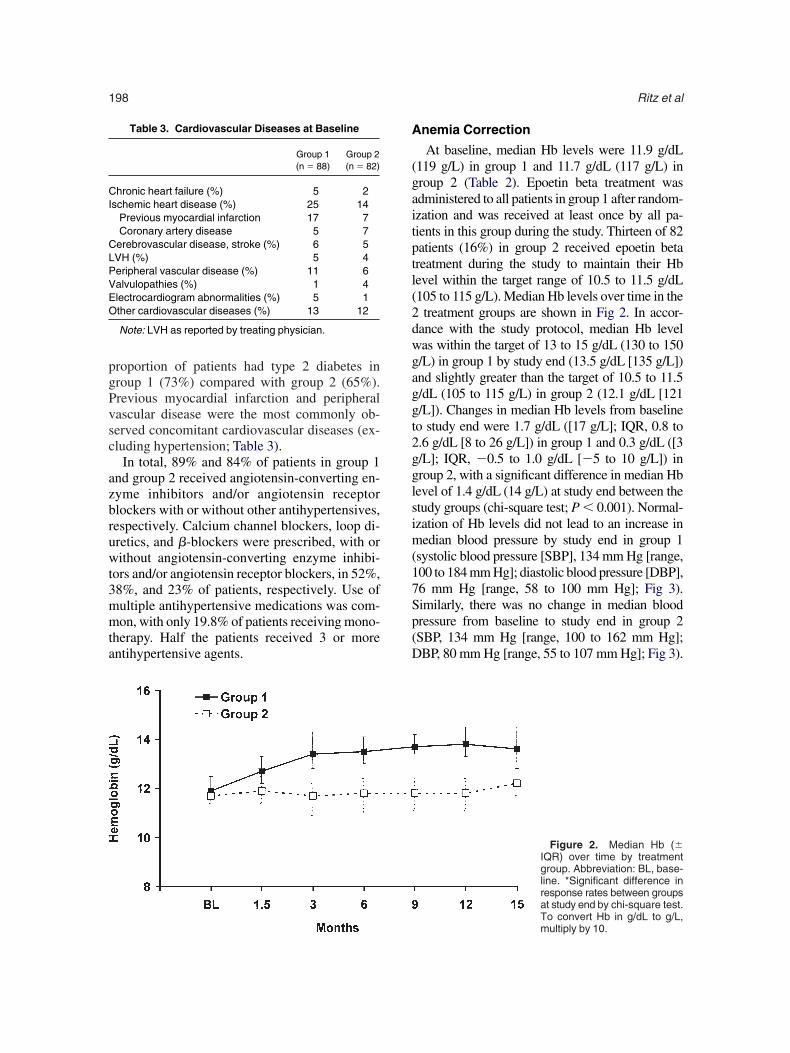
At baseline, median Hb levels were 11.9 g/dL119 g/L) in group 1 and 11.7 g/dL (117 g/L) inroup 2 (Table 2). Epoetin beta treatment wasdministered to all patients in group 1 after random-zation and was received at least once by all pa-ients in this group during the study. Thirteen of 82atients (16%) in group 2 received epoetin betareatment during the study to maintain their Hbevel within the target range of 10.5 to 11.5 g/dL105 to 115 g/L). Median Hb levels over time in the
treatment groups are shown in Fig 2. In accor-ance with the study protocol, median Hb levelas within the target of 13 to 15 g/dL (130 to 150/L) in group 1 by study end (13.5 g/dL [135 g/L])nd slightly greater than the target of 10.5 to 11.5/dL (105 to 115 g/L) in group 2 (12.1 g/dL [121/L]). Changes in median Hb levels from baselineo study end were 1.7 g/dL ([17 g/L]; IQR, 0.8 to.6 g/dL [8 to 26 g/L]) in group 1 and 0.3 g/dL ([3/L]; IQR, �0.5 to 1.0 g/dL [�5 to 10 g/L]) inroup 2, with a significant difference in median Hbevel of 1.4 g/dL (14 g/L) at study end between thetudy groups (chi-square test; P � 0.001). Normal-zation of Hb levels did not lead to an increase inedian blood pressure by study end in group 1
systolic blood pressure [SBP], 134 mm Hg [range,00 to 184 mm Hg]; diastolic blood pressure [DBP],6 mm Hg [range, 58 to 100 mm Hg]; Fig 3).imilarly, there was no change in median bloodressure from baseline to study end in group 2SBP, 134 mm Hg [range, 100 to 162 mm Hg];BP, 80 mm Hg [range, 55 to 107 mm Hg]; Fig 3).
Figure 2. Median Hb (�IQR) over time by treatmentgroup. Abbreviation: BL, base-line. *Significant difference inresponse rates between groupsat study end by chi-square test.
To convert Hb in g/dL to g/L,multiply by 10.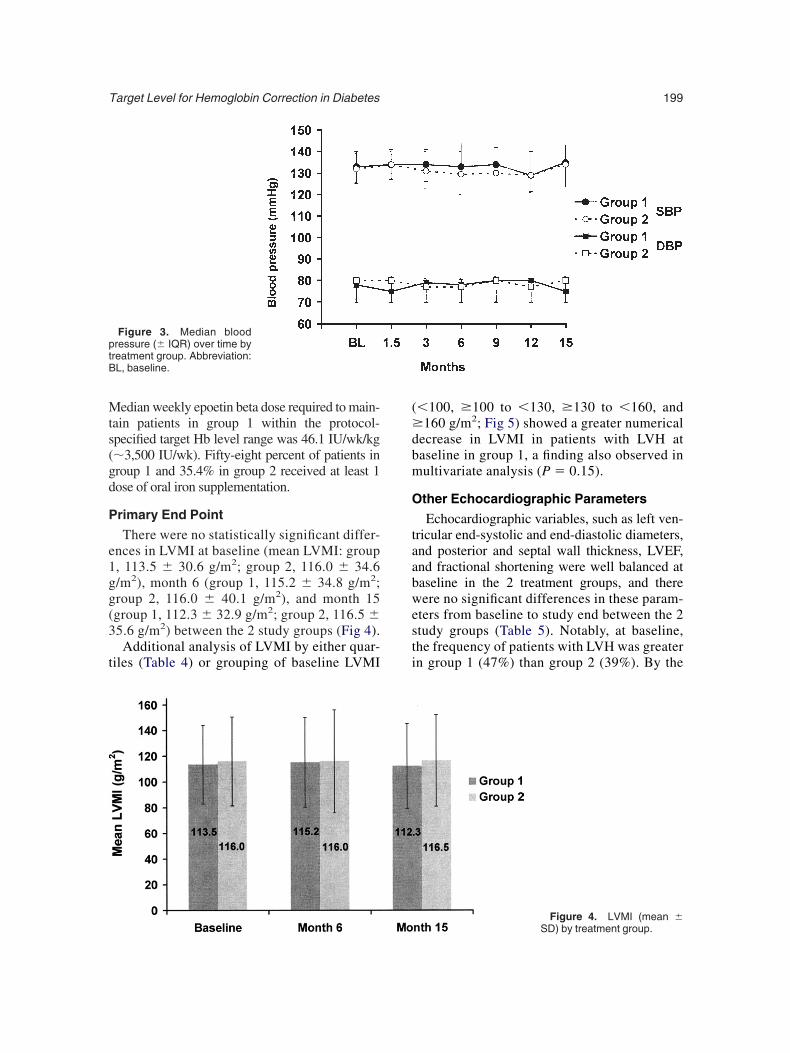
Mts(gd
P
e1gg(3
t
(�dbm
O
taabwesti
ptB
Target Level for Hemoglobin Correction in Diabetes 199
edian weekly epoetin beta dose required to main-ain patients in group 1 within the protocol-pecified target Hb level range was 46.1 IU/wk/kg�3,500 IU/wk). Fifty-eight percent of patients inroup 1 and 35.4% in group 2 received at least 1ose of oral iron supplementation.
rimary End Point
There were no statistically significant differ-nces in LVMI at baseline (mean LVMI: group, 113.5 � 30.6 g/m2; group 2, 116.0 � 34.6/m2), month 6 (group 1, 115.2 � 34.8 g/m2;roup 2, 116.0 � 40.1 g/m2), and month 15group 1, 112.3 � 32.9 g/m2; group 2, 116.5 �5.6 g/m2) between the 2 study groups (Fig 4).Additional analysis of LVMI by either quar-
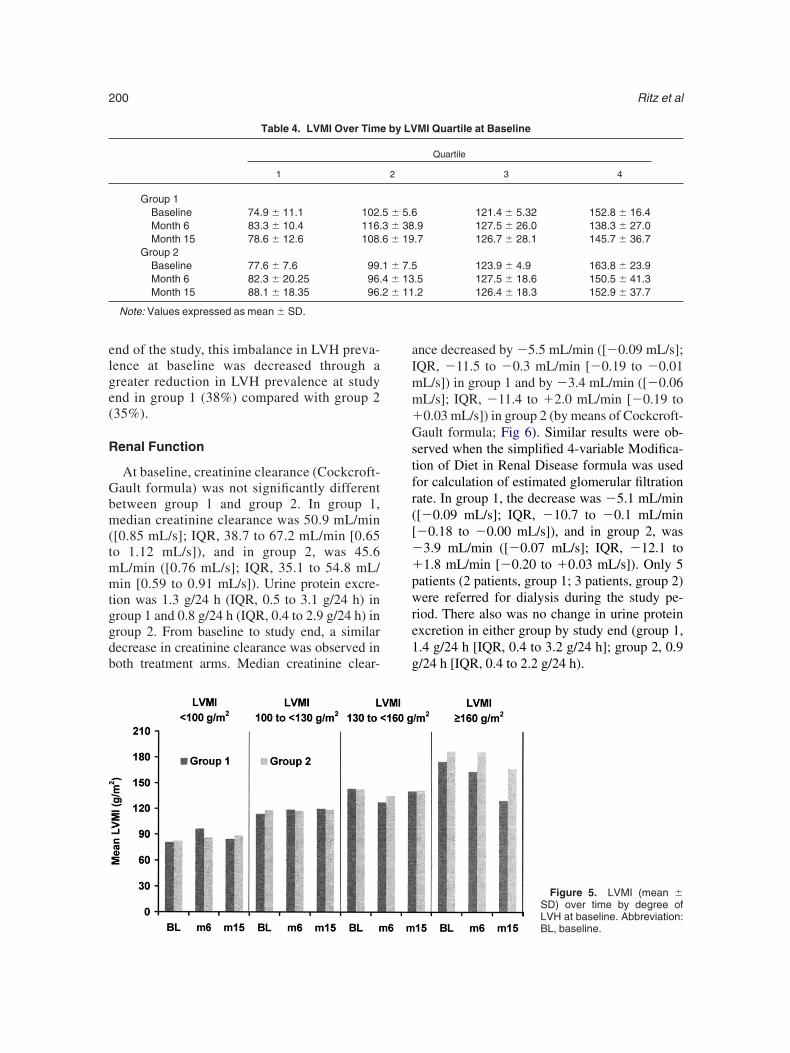
iles (Table 4) or grouping of baseline LVMI
Figure 3. Median bloodressure (� IQR) over time byreatment group. Abbreviation:L, baseline.
�100, �100 to �130, �130 to �160, and160 g/m2; Fig 5) showed a greater numerical
ecrease in LVMI in patients with LVH ataseline in group 1, a finding also observed inultivariate analysis (P � 0.15).
ther Echocardiographic Parameters
Echocardiographic variables, such as left ven-ricular end-systolic and end-diastolic diameters,nd posterior and septal wall thickness, LVEF,nd fractional shortening were well balanced ataseline in the 2 treatment groups, and thereere no significant differences in these param-
ters from baseline to study end between the 2tudy groups (Table 5). Notably, at baseline,he frequency of patients with LVH was greatern group 1 (47%) than group 2 (39%). By the
Figure 4. LVMI (mean �SD) by treatment group.
elge(
R
Gbm(tmmtggdb
aImm�Gstfr([��pwre1g
Ritz et al200
nd of the study, this imbalance in LVH preva-ence at baseline was decreased through areater reduction in LVH prevalence at studynd in group 1 (38%) compared with group 235%).
enal Function
At baseline, creatinine clearance (Cockcroft-ault formula) was not significantly differentetween group 1 and group 2. In group 1,edian creatinine clearance was 50.9 mL/min
[0.85 mL/s]; IQR, 38.7 to 67.2 mL/min [0.65o 1.12 mL/s]), and in group 2, was 45.6L/min ([0.76 mL/s]; IQR, 35.1 to 54.8 mL/in [0.59 to 0.91 mL/s]). Urine protein excre-
ion was 1.3 g/24 h (IQR, 0.5 to 3.1 g/24 h) inroup 1 and 0.8 g/24 h (IQR, 0.4 to 2.9 g/24 h) inroup 2. From baseline to study end, a similarecrease in creatinine clearance was observed inoth treatment arms. Median creatinine clear-
Table 4. LVMI Over Time
1
Group 1Baseline 74.9 � 11.1 102.Month 6 83.3 � 10.4 116.Month 15 78.6 � 12.6 108.
Group 2Baseline 77.6 � 7.6 99.Month 6 82.3 � 20.25 96.Month 15 88.1 � 18.35 96.
Note: Values expressed as mean � SD.
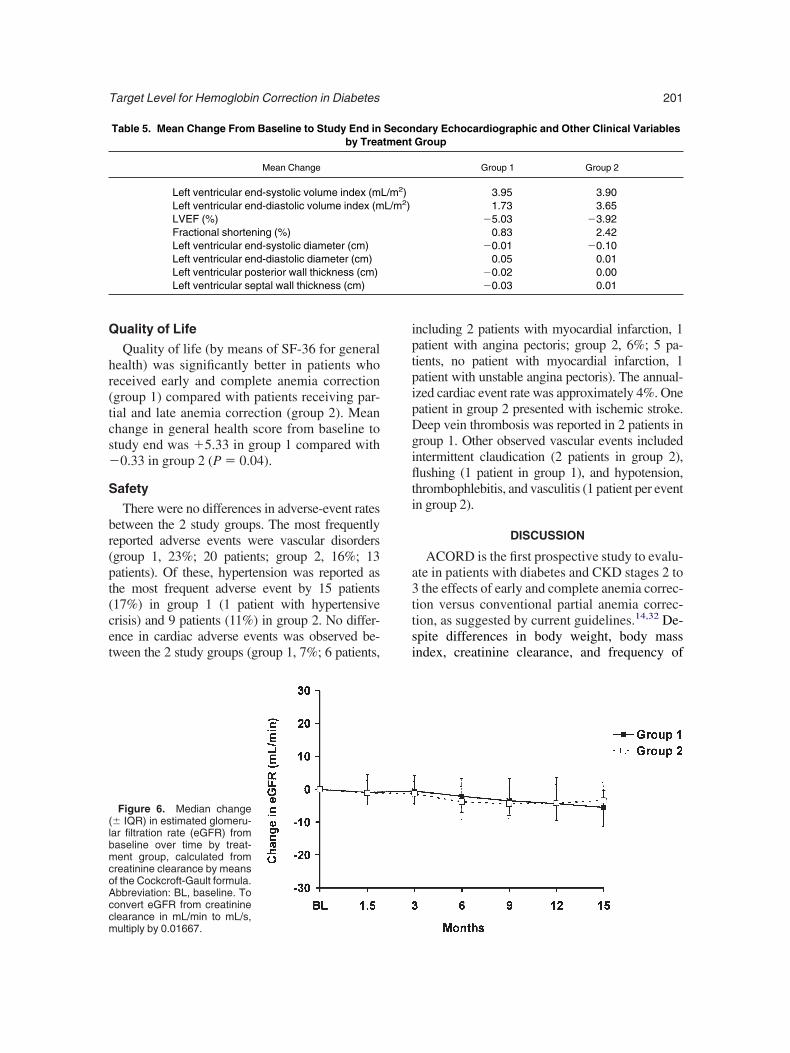
nce decreased by �5.5 mL/min ([�0.09 mL/s];QR, �11.5 to �0.3 mL/min [�0.19 to �0.01L/s]) in group 1 and by �3.4 mL/min ([�0.06L/s]; IQR, �11.4 to �2.0 mL/min [�0.19 to0.03 mL/s]) in group 2 (by means of Cockcroft-ault formula; Fig 6). Similar results were ob-
erved when the simplified 4-variable Modifica-ion of Diet in Renal Disease formula was usedor calculation of estimated glomerular filtrationate. In group 1, the decrease was �5.1 mL/min[�0.09 mL/s]; IQR, �10.7 to �0.1 mL/min�0.18 to �0.00 mL/s]), and in group 2, was3.9 mL/min ([�0.07 mL/s]; IQR, �12.1 to1.8 mL/min [�0.20 to �0.03 mL/s]). Only 5
atients (2 patients, group 1; 3 patients, group 2)ere referred for dialysis during the study pe-
iod. There also was no change in urine proteinxcretion in either group by study end (group 1,.4 g/24 h [IQR, 0.4 to 3.2 g/24 h]; group 2, 0.9/24 h [IQR, 0.4 to 2.2 g/24 h).
Figure 5. LVMI (mean �SD) over time by degree of
MI Quartile at Baseline
Quartile
3 4
121.4 � 5.32 152.8 � 16.4.9 127.5 � 26.0 138.3 � 27.0.7 126.7 � 28.1 145.7 � 36.7
123.9 � 4.9 163.8 � 23.9.5 127.5 � 18.6 150.5 � 41.3.2 126.4 � 18.3 152.9 � 37.7
by LV
2
5 � 5.63 � 386 � 19
1 � 7.54 � 132 � 11
LVH at baseline. Abbreviation:BL, baseline.
Q
hr(tcs�
S
br(pt(cet
iptpipDgiflti
a3ttsi
(lbmcoAccm
Target Level for Hemoglobin Correction in Diabetes 201
uality of Life
Quality of life (by means of SF-36 for generalealth) was significantly better in patients whoeceived early and complete anemia correctiongroup 1) compared with patients receiving par-ial and late anemia correction (group 2). Meanhange in general health score from baseline totudy end was �5.33 in group 1 compared with0.33 in group 2 (P � 0.04).
afety
There were no differences in adverse-event ratesetween the 2 study groups. The most frequentlyeported adverse events were vascular disordersgroup 1, 23%; 20 patients; group 2, 16%; 13atients). Of these, hypertension was reported ashe most frequent adverse event by 15 patients17%) in group 1 (1 patient with hypertensiverisis) and 9 patients (11%) in group 2. No differ-nce in cardiac adverse events was observed be-ween the 2 study groups (group 1, 7%; 6 patients,
Table 5. Mean Change From Baseline to Study End inby Trea
Mean Change
Left ventricular end-systolic volume index (mLeft ventricular end-diastolic volume index (mLVEF (%)Fractional shortening (%)Left ventricular end-systolic diameter (cm)Left ventricular end-diastolic diameter (cm)Left ventricular posterior wall thickness (cm)Left ventricular septal wall thickness (cm)
Figure 6. Median change� IQR) in estimated glomeru-ar filtration rate (eGFR) fromaseline over time by treat-ent group, calculated from
reatinine clearance by meansf the Cockcroft-Gault formula.bbreviation: BL, baseline. Toonvert eGFR from creatinine
learance in mL/min to mL/s,ultiply by 0.01667.ncluding 2 patients with myocardial infarction, 1atient with angina pectoris; group 2, 6%; 5 pa-ients, no patient with myocardial infarction, 1atient with unstable angina pectoris). The annual-zed cardiac event rate was approximately 4%. Oneatient in group 2 presented with ischemic stroke.eep vein thrombosis was reported in 2 patients inroup 1. Other observed vascular events includedntermittent claudication (2 patients in group 2),ushing (1 patient in group 1), and hypotension,
hrombophlebitis, and vasculitis (1 patient per eventn group 2).
DISCUSSION
ACORD is the first prospective study to evalu-te in patients with diabetes and CKD stages 2 tothe effects of early and complete anemia correc-
ion versus conventional partial anemia correc-ion, as suggested by current guidelines.14,32 De-pite differences in body weight, body massndex, creatinine clearance, and frequency of
dary Echocardiographic and Other Clinical VariablesGroup
Group 1 Group 2
3.95 3.901.73 3.65
�5.03 �3.920.83 2.42
�0.01 �0.100.05 0.01
�0.02 0.00�0.03 0.01
Secontment
L/m2)L/m2)

tigr0ialwmatssr(det
sptiactc1Ccd1sosdecais0mi
trLsd
bcsooia
LLicwtwtelt(Hgbt
pepaffigac
ttmvdcptLi
gebt
Ritz et al202
ype 2 diabetes at baseline, there were no majormbalances at baseline between study groups. Inroup 1, anemia correction with epoetin betaesulted in a significant increase in Hb level (P �.001) compared with group 2. However, thenitial hypothesis of this study, namely, that earlynd complete anemia correction to an Hb targetevel of 13 to 15 g/dL (130 to 150 g/L; group 1)ould result in a significant decrease in LVMI atonth 15 compared with maintaining patients atlower Hb target level of 10.5 to 11.5 g/dL (105
o 115 g/L; group 2), was not confirmed. Ashown in Fig 4, mean LVMI was stable in bothtudy groups across the entire observation pe-iod. In line with the primary efficacy parameterLVMI), there were no statistically significantifferences in any of the secondary or otherxploratory echocardiographic parameters be-ween the 2 study groups.
The finding for the primary end point of thistudy contrasts with previous reports in whichartial reversal of LVH was seen with epoetinreatment.33,34 Importantly, in these previous stud-es, Hb values at baseline were markedly lowernd mean LVMI values were markedly higherompared with the present study enrolling pa-ients with mild to moderate anemia (inclusionriterion, Hb level of 10.5 to 12.5 g/dL [105 to25 g/L]) and well-controlled blood pressure.omparison of mean LVMI in this study with thelassification of the American Society of Echocar-iography (“moderately abnormal”: in women,01 to 112 g/m2; in men, 117 to 130 g/m2)35
hows that in the present study, mean LVMI wasnly moderately abnormal, possibly pointing tolowly improving management of patients withiabetes with renal failure, although we cannotxclude a selection artifact. At any rate, thehance of seeing reversal thus was lessened. Onelso might argue that despite a clinically mean-ngful (�1.4 g/dL [14 g/L]) and statisticallyignificant difference in median Hb levels (P �.001) between the 2 study groups, the differenceight have been insufficient to have a significant
mpact on LVMI.The primary result of this study adds addi-
ional evidence to results of 3 recent studieseported by Roger et al,36 Parfrey et al,37 andevin et al.38 In all 3 studies conducted in highlyelected and well-controlled predialysis36,38 or
ialysis patients37 who had no severe LVH at vaseline, no significant effects of Hb level in-rease by epoetin treatment on LVMI was ob-erved. Our finding of no significant regressionf LVH in patients without increased LVMI andnly moderate degrees of anemia at baseline alsos in line with previous observations of Foley etl39 and McMahon et al.40
When we assessed patients with increasedVMI at baseline in a subanalysis, a decrease inVMI was observed that was more pronouncedn group 1 with early and complete anemiaorrection (Table 4; Fig 5). Regression of LVMIas seen in the recent open-label intervention
rial of Ayus et al41 investigating patients with orithout diabetes and comprising a high propor-
ion of patients with LVH (68.3%). In this study,poetin was administered only if Hb level wasess than 10 g/dL (�100 g/L), with the objectiveo increase Hb to values greater than 12 g/dL�120 g/L). In patients receiving epoetin, meanb level increased from 9.1 g/dL (91 g/L) to 11.3/dL (113 g/L; P � 0.001), and mean LVMI ataseline significantly decreased from 157 � 55.7o 142 � 55.7 g/m2 (P � 0.007) within 6 months.
In contrast to the overall neutral finding for therimary and secondary echocardiographic param-ters, quality of life improved significantly inatients for whom anemia was corrected earlynd completely (P � 0.04). With respect to renalunction, no difference in estimated glomerularltration rate was observed between the 2 studyroups. Importantly, there was no difference indverse events between groups and the annualardiac event rate was remarkably low, ie, 4%.
Baseline data from the ACORD Study showhat a substantial proportion of the enrolled pa-ients failed to meet treatment targets recom-ended by current practice guidelines for pre-
enting cardiovascular disease in patients withiabetes.42 The recommended targets were ex-eeded for median SBP (�130 mm Hg) in ap-roximately 67% to 72%, for low-density lipopro-ein cholesterol level (�96.7 mg/dL [�2.5 mmol/]) in 53% to 66%, and for HbA1c level (6.1%)
n 84% to 88% of patients.Although in principle, all patients were eli-
ible for treatment with angiotensin-convertingnzyme inhibitors and/or angiotensin receptorlockers, only 84% to 89% were administeredhese agents. �-blockers, proved to reduce cardio-
ascular mortality and morbidity,43-45 were
lt
mtl3tlE
ipstpcbgtspi
AsiHclrernqprogpo
goahe
rdc
rCmcmscpcahv
gadsLTseepsnr
r3iZfSHVaos
DHLCBsOH
Target Level for Hemoglobin Correction in Diabetes 203
argely underprescribed, with only 23% of pa-ients receiving these agents.
Despite the reported benefits of statin treat-ent for reducing low-density lipoprotein choles-
erol levels and reducing the risk of cardiovascu-ar events in patients with diabetes,42,46,47 only5% to 46% were administered statins and 53%o 66% had low-density lipoprotein cholesterolevels greater than those recommended by theuropean guidelines (96.7 mg/dL [2.5 mmol/L]).42
Assessment of quality-of-life parameters us-ng the SF-36 scale showed that early and com-lete anemia correction was associated with aignificantly greater improvement from baselineo study end in general health compared withartial anemia correction. Although not signifi-ant, there also was greater improvement fromaseline in vitality in group 1 compared withroup 2. These improvements were similar tohose observed by Rossert et al.48 Both studieshowed the beneficial impact that early and com-lete anemia correction can have on patient qual-ty of life.
In the Cardiovascular Risk Reduction in Earlynaemia Trial with Epoetin beta (CREATE)
tudy, earlier start of dialysis treatment was notedn some patients randomly assigned to a higherb level target.49 In the present study, serum
reatinine concentration was monitored regu-arly. Creatinine clearance and doubling of se-um creatinine level were not significantly differ-nt in the 2 treatment groups, suggesting a similarate of progression of CKD. Similarly, there waso difference between treatment groups in fre-uency of patients requiring dialysis (group 1, 2atients; group 2, 3 patients). Findings withespect to renal function confirm the observationf Rossert et al,48 who found no significantlyreater decrease in glomerular filtration rate inatients randomly assigned to an Hb target levelf 13 to 15 g/dL (130 to 150 g/L).Importantly, safety profiles of the 2 study
roups were very similar in terms of frequencyf adverse events. In contrast to previous reports,lthough the most frequent adverse event wasypertension, there were no significant differ-nces in blood pressure until study end.
A remarkably low annual cardiovascular eventate of approximately 4% was observed, with noifferences between study groups. This cardiovas-
ular event rate is much less than cardiac event Sates reported in previous studies, eg, 15% in aanadian cohort study examining patients withild to moderate renal insufficiency.10 The low
ardiovascular event rate observed in our studyay be explained by excluding patients with
evere anemia. Furthermore, an Hb level de-rease to less than 10.5 g/dL (�105 g/L) wasrevented by protocol. In addition, use of suchardioprotective agents as �-blockers, statins,spirin, and angiotensin-converting enzyme in-ibitors may have contributed to the low cardio-ascular event rate.In conclusion, this study is designed to investi-
ate the effect of early and complete versus latend partial anemia correction in patients withiabetes with mild to moderate anemia and CKDtages 2 to 3. Overall, no significant decrease inVMI was seen in the overall study population.his finding is explained most plausibly by thetrict inclusion criteria of the study, resulting innrollment of a study population with only mod-rately increased LVMI. Of note, early and com-lete anemia correction was associated with aignificant improvement in quality of life and didot result in increased cardiac risk or acceleratedenal progression.
ACKNOWLEDGMENTThe authors thank all investigators who contributed to the
ecruitment and successful conduct of the study (Appendix); Caesar Escrig, MD, and Chris Dougherty, MD, who werenvolved closely in the early phase of the study; Michelaug, PharmD, for reviewing patient data from case report
orms and assistance in drafting the manuscript; Reginechrumpf, for the operational leadership of the study; Rachelosie, for leading data collection and data management;iktor Nendel, for his support with the statistical analyses;nd all clinical monitors of the study, without whose continu-us commitment to the collection of high-quality data thistudy would not have been possible.
APPENDIX 1: STUDY ORGANIZATION
Study Steering Committee: Professor E. Ritz,epartment of Internal Medicine, University ofeidelberg, Heidelberg, Germany; Professor M.aville, Department of Nephrology, Universitélaude Bernard, Lyon, France; Professor R.ilous, Education Centre, James Cook Univer-
ity Hospital, Middlesbrough, UK; Dr D.’Donoghue, Department of Renal Medicine,ope Hospital, Salford, UK; Dr F. de Alvaro,
ervicio de Nefrología, Hospital Universitario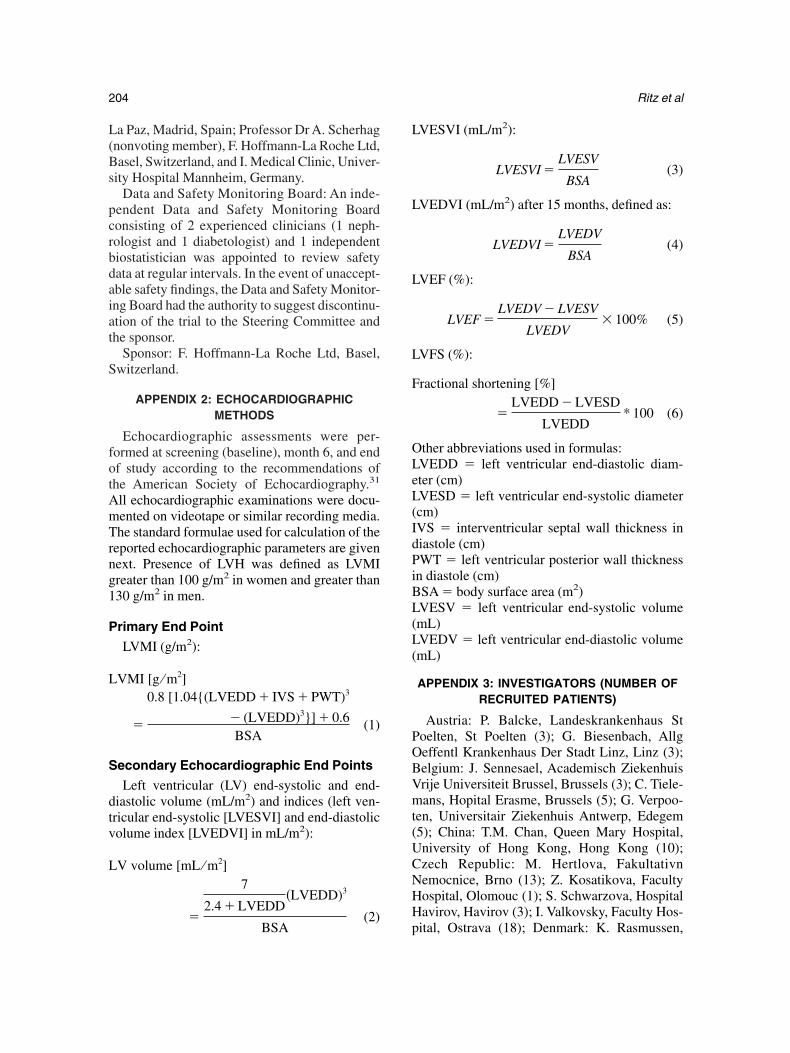
L(Bs
pcrbdaiat
S
fotAmTrng1
P
L
S
dtv
L
L
L
L
L
F
OLeL(IdPiBL(L(
POBVmt(UCNHH
Ritz et al204
a Paz, Madrid, Spain; Professor Dr A. Scherhagnonvoting member), F. Hoffmann-La Roche Ltd,asel, Switzerland, and I. Medical Clinic, Univer-
ity Hospital Mannheim, Germany.Data and Safety Monitoring Board: An inde-
endent Data and Safety Monitoring Boardonsisting of 2 experienced clinicians (1 neph-ologist and 1 diabetologist) and 1 independentiostatistician was appointed to review safetyata at regular intervals. In the event of unaccept-ble safety findings, the Data and Safety Monitor-ng Board had the authority to suggest discontinu-tion of the trial to the Steering Committee andhe sponsor.
Sponsor: F. Hoffmann-La Roche Ltd, Basel,witzerland.
APPENDIX 2: ECHOCARDIOGRAPHICMETHODS
Echocardiographic assessments were per-ormed at screening (baseline), month 6, and endf study according to the recommendations ofhe American Society of Echocardiography.31
ll echocardiographic examinations were docu-ented on videotape or similar recording media.he standard formulae used for calculation of the
eported echocardiographic parameters are givenext. Presence of LVH was defined as LVMIreater than 100 g/m2 in women and greater than30 g/m2 in men.
rimary End Point
LVMI (g/m2):
VMI [g ⁄ m2]
�
0.8 [1.04{(LVEDD � IVS � PWT)3
� (LVEDD)3}] � 0.6BSA
(1)
econdary Echocardiographic End Points
Left ventricular (LV) end-systolic and end-iastolic volume (mL/m2) and indices (left ven-ricular end-systolic [LVESVI] and end-diastolicolume index [LVEDVI] in mL/m2):
V volume [mL ⁄ m2]7
2.4 � LVEDD�LVEDD)3
�BSA
(2)p
VESVI (mL/m2):
LVESVI �LVESV
BSA(3)
VEDVI (mL/m2) after 15 months, defined as:
LVEDVI �LVEDV
BSA(4)
VEF (%):
LVEF �LVEDV � LVESV
LVEDV� 100% (5)
VFS (%):
ractional shortening [%]
�LVEDD � LVESD
LVEDD* 100 (6)
ther abbreviations used in formulas:VEDD � left ventricular end-diastolic diam-ter (cm)VESD � left ventricular end-systolic diametercm)VS � interventricular septal wall thickness iniastole (cm)WT � left ventricular posterior wall thickness
n diastole (cm)SA � body surface area (m2)VESV � left ventricular end-systolic volumemL)VEDV � left ventricular end-diastolic volumemL)
APPENDIX 3: INVESTIGATORS (NUMBER OFRECRUITED PATIENTS)
Austria: P. Balcke, Landeskrankenhaus Stoelten, St Poelten (3); G. Biesenbach, Allgeffentl Krankenhaus Der Stadt Linz, Linz (3);elgium: J. Sennesael, Academisch Ziekenhuisrije Universiteit Brussel, Brussels (3); C. Tiele-ans, Hopital Erasme, Brussels (5); G. Verpoo-
en, Universitair Ziekenhuis Antwerp, Edegem5); China: T.M. Chan, Queen Mary Hospital,niversity of Hong Kong, Hong Kong (10);zech Republic: M. Hertlova, Fakultativnemocnice, Brno (13); Z. Kosatikova, Facultyospital, Olomouc (1); S. Schwarzova, Hospitalavirov, Havirov (3); I. Valkovsky, Faculty Hos-
ital, Ostrava (18); Denmark: K. Rasmussen,
RlSSFspBMLGGF(Ed(SSBAc(MgGstVHPCBA(S“SCAOOOSePVJrIN
OSd(GUtMPHFeK#SbpZeCVLGdCCdFNsdTb(UeW(TNKvkFCNcFd(
Target Level for Hemoglobin Correction in Diabetes 205
oskilde Amtssygehuset, Roskilde (9); K. Soel-ing, Holbaek Centralsygehus, Holbaek (1); G.teffensen, Fredericia Sygehus, Fredericia (8);. Strandgaard, Herlev Amtssygehus, Herlev (10);inland: A. Koistinen, Keski-Suomen Keskus-airaala, Jyvaeskylae (16); J. Mustonen, Tam-ere University Hospital, Tampere (4); France: P.ataille, Centre Hospitalier de Boulogne Surer, Boulogne (10); B. Canaud, Chu Hopital
apeyronie, Montpellier (7); G. Choukroun,roupe Hospitalier Sud, Amiens (8); C. Combe,roupe Hospitalier Pellegrin, Bordeaux (5); B.aller, Centre Hospitalier Louis Pasteur, Colmar6); J.P. Grunfeld, Group Hopitalier Necker-nfants Malades, Paris (5); M. Kessler, Hopital’Adultes de Brabois, Vandoeuvre-Lès-Nancy4); M. Laville, Hopital H. Herriot, Lyon (5); F.chillinger, Centre Hospitalier, Troyes (2); P.imon, Centre Hospitalier la Beauchee, Saintrieuc (13); L. Yver, Centre Hospitalier,ngouleme (8); Germany: U Frei, Charite, Vir-
how Klinikum, Humboldt Universtitaet, Berlin6); L. Schramm, Facharztpraxis Fuer Innere
edizin, Wuerzburg (2); G. Schultze, Nephrolo-isches Zentrum, Villingen-Schwenningen (5);reece: D. Memmos, Hippokratio Hospital, Thes-
aloniki (4); C. Stathakis, Laiko General Hospi-al, Athens (6); D. Tsakiris, General Hospital oferia, Veria (5); Ireland: P.J. Conlon, Beaumontospital, Dublin (1); Italy: S. David, Ospedale diarma, Parma (6); P. Altieri, Ospedale G. Brotzu,agliari (2); G. Buccianti, Ospedale Civileassini, Cinisello Balsamo (3); S. Cantaro,zienda Ospedale Universita di Padova, Padova
4); V. de Cristofaro, Ospedale Civile di Sondrio,ondrio (3); C. de Pascale, Azienda OspedalieraD. Cotugno”, Napoli (4); S. di Guilio, Ospedale. Camillo, Roma (1); A. Giangrande, Ospedal diircolo, Busto Arsizio (2); F. Locatelli, Ospedalelessandro Manzoni, Lecco (20); C. Meloni,spedale S. Eugenio, Roma (7); G. Panzetta,spedale di Cattinara, Trieste (3); A. Sessa,spedale Civile di Vimercate, Vimercate (1); C.tallone, Ospedale Casa Sollievo della Soffer-nza, San Giovanni Rotondo (3); S. Stefoni,oliclinico S. Orsola-Malpighi, Bologna (6); G.illa, Fondazione S. Maugeri, Pavia (8); Mexico:
.A. Barbosa, Centro de Investigacion del No-oeste, Tijuana (9); T.M. Bochicchio, Unidad denvestigacion Clinica Cuernavaca, Mexico (12);
orway: H. Gudmundsdottir, Ullevael Sykehus, (slo (7); Poland: K. Bidas, Wojewodzki Szpitalpecjalistyczny, Kielce (9); M. Klinger, Aka-emia Medyczna im. Piastow Slaskich, Wroclaw17); B. Rutkowski, SPSK Nr 1 ACK AM,dansk (13); W. Sulowicz, Collegium Medicumniwersytetu Jagielonskiego, Krakow (25); Por-
ugal: A.C. Nogueira, Hospital Sams, Lisboa (1);.J. Pais, Hospital Sta. Cruz, Carnaxide (4); M.
estana, Hospital Sao Jao, Porto (3); P. Ponces,ospital Garcia de Horta, Almada (3); Russianederation: V. Ermolenko, Russian MedicalAcad-my of Postgraduate Education, Moscow (4); N.hasabov, Central Republican Clinical Hospital2, Moscow (4); M. Komandenko, St Petersburgtate Medical Academy Mechnikov, St Peters-urg (1); N. Tomilina, Research Institute of Trans-lantology and Artificial Organs, Moscow (4); A.emtchenkov, St. Petersburg State Medical Acad-my Mechnikov, St Petersburg (5); Spain: J.-M.ruz, Fundacion Hospital Universitario La Fe,alencia (4); J.L. de Miguel Alonso , Hospital dea Paz, Madrid (12); J.L. Fernandez , Hospitaleneral Universitario Gregorio Maranon, Ma-rid (9); L. Palop, Hospital General de Grananaria Doctor Negrin, Las Palmas de Grananaria (2); L. Piera, Hospital General Vall’Hebron, Barcelona (8); Sweden: C. Frisenette-ich, Laenssjukhuset Ryhov, Jonkoping (5); F.D.ielsen, Sas Boras Hospital, Boras (3), E. Olaus-
on, Sundsvall Hospital, Sundsvall (4); M. Soe-erhaell, Karolinska Hospital, Stockholm (7); M.idman, Oerebro Medical Center Hospital, Öre-ro (6); L.G. Weiss, Central Hospital, Karlstad5); Taiwan: J.-J. Huang, National Cheng Kungniversity Hospital, Tainan (20); K.-S. Shu, Vet-
rans General Hospital, Taichung (11); K.-D.u, National Taiwan University Hospital, Taipei
13); C.-C. Yu, Chang Gung Memorial Hospital,aoyuan (6); Thailand: D. Lumlertgul, Maharajakorn Chiang Mai Hospital, Chiang Mai (4);. Vareesangthip, Siriraj Hospital, Mahidol Uni-ersity Faculty of Medicine, Bangkok (8); Tur-ey: M. Arici, Hacettepe University of Medicineaculty, Ankara (2); E. Erek, Istanbul Universityerrahpasa Medical Faculty, Istanbul (1); G.ergisoglu, Ankara University Faculty of Medi-
ine, Ankara (10); M. Ozkahya, Ege Universityaculty of Medicine, Izmir (10); United King-om: P. Andrews, St. Helier Hospital, Carshalton4); E. Brown, Charing Cross Hospital, London
1); I. Macdougall, King’s College Hospital,
LttFW
RoM
id1
c
af1
aN
PP4
iH
d4
yI
ld
haep
ah
tc2
pmT
pm
Mera
Aa1
Kee1
Aer1
KdK
eeA
JhD
osh1
Wt
Gp4
Gw2
MM
S(
RfitA
Ritz et al206
ondon (15); A.P. Maxwell, Belfast City Hospi-al, Belfast (12); M. Rogerson, Royal Southamp-on Hospital, Southampton (9); R. Wilkinson,reeman Hospital, Newcastle Upon Tyne (3), G.ood, Hope Hospital, Salford (1).
REFERENCES1. US Renal Data System: USRDS 2004 Annual Data
eport. The National Institutes of Health, National Institutef Diabetes and Digestive and Kidney Diseases, Bethesda,D, 20042. Stengel B, Billon S, Van Dijk PC, et al: Trends in the
ncidence of renal replacement therapy for end-stage renalisease in Europe, 1990-1999. Nephrol Dial Transplant8:1824-1833, 20033. American Diabetes Association: Standards of medical
are in diabetes. Diabetes Care 27:15-35, 20044. Grundy SM, Benjamin IJ, Burke GL, et al: Diabetes
nd cardiovascular disease: A statement for healthcare pro-essionals from the American Heart Association. Circulation00:1134-1146, 19995. Ma JZ, Ebben J, Xia H, Collins AJ: Hematocrit level
nd associated mortality in hemodialysis patients. J Am Socephrol 10:610-619, 19996. Harnett JD, Foley RN, Kent GM, Barre PE, Murray D,
arfrey PS: Congestive heart failure in dialysis patients:revalence, incidence, prognosis and risk factors. Kidney Int7:884-890, 19957. Parfrey PS, Harnett JD, Foley RN: Heart failure and
schemic heart disease in chronic uremia. Curr Opin Nephrolypertens 4:105-110, 19958. Foley RN, Culleton BF, Parfrey PS, et al: Cardiac
isease in diabetic end-stage renal disease. Diabetologia0:1307-1312, 19979. Arkouche W, Traeger J, Delawari E, et al: Twenty-five
ears of experience with out-center hemodialysis. Kidneynt 56:2269-2275, 1999
10. Levin A, Thompson CR, Ethier J, et al: Left ventricu-ar mass index increase in early renal disease: Impact ofecline in hemoglobin. Am J Kidney Dis 34:125-134, 199911. Locatelli F, Conte F, Marcelli D: The impact of
aematocrit levels and erythropoietin treatment on overallnd cardiovascular mortality and morbidity—The experi-nce of the Lombardy Dialysis Registry. Nephrol Dial Trans-lant 13:1642-1644, 199812. Holland DC, Lam M: Predictors of hospitalization
nd death among pre-dialysis patients: A retrospective co-ort study. Nephrol Dial Transplant 15:650-658, 200013. National Kidney Foundation: K/DOQI Clinical Prac-
ice Guidelines for Chronic Kidney Disease: Evaluation,lassification, and stratification. Am J Kidney Dis 39:S1-49, 2002 (suppl 2)14. Locatelli F, Aljama P, Barany P, et al: Revised Euro-
ean best practice guidelines for the management of anae-ia in patients with chronic renal failure. Nephrol Dialransplant 19:Sii1-Sii47, 2004 (suppl 2)15. Fink J, Blahut S, Reddy M, Light P: Use of erythro-
oietin before the initiation of dialysis and its impact on
ortality. Am J Kidney Dis 37:348-355, 2001 c16. Lu WX, Jones-Burton C, Zhan M, Salzberg DJ,oore J Jr, Fink JC: Survival benefit of recombinant human
rythropoietin administration prior to onset of end-stageenal disease: Variations across surrogates for quality of carend time. Nephron Clin Pract 101:c79-c86, 2005
17. Xue JL, St Peter WL, Ebben JP, Everson SE, CollinsJ: Anemia treatment in the pre-ESRD period and associ-
ted mortality in elderly patients. Am J Kidney Dis 40:1153-161, 2002
18. Kuriyama S, Tomonari H, Yoshida H, Hashimoto T,awaguchi Y, Sakai O: Reversal of anemia by erythropoi-
tin therapy retards the progression of chronic renal failure,specially in nondiabetic patients. Nephron 77:176-185,99719. Jungers P, Choukroun G, Oualim Z, Robino C, Nguyen
T, Man NK: Beneficial influence of recombinant humanrythropoietin therapy on the rate of progression of chronicenal failure in predialysis patients. Nephrol Dial Transplant6:307-312, 200120. Gouva C, Nikolopoulos P, Ioannidis JP, Siamopoulos
C: Treating anemia early in renal failure patients slows theecline of renal function: A randomized controlled trial.idney Int 66:753-760, 200421. Hayashi T, Suzuki A, Shoji T, et al: Cardiovascular
ffect of normalizing the hematocrit level during erythropoi-tin therapy in predialysis patients with chronic renal failure.m J Kidney Dis 35:250-256, 200022. Portoles J, Torralbo A, Martin P, Rodrigo J, Herrero
A, Barrientos A: Cardiovascular effects of recombinantuman erythropoietin in predialysis patients. Am J Kidneyis 29:541-548, 199723. Valderrabano F, for the Spanish Group for the Study
f the Anaemia and Left Ventricular Hypertrophy in Predialy-is Patients: Improvement and prevention of left ventricularypertrophy in predialysis patients. J Am Soc Nephrol1:0424A, 2000 (abstr)
24. Winkler AS, Marsden J, Chaudhuri KR, Hambley H,atkins PJ: Erythropoietin depletion and anaemia in diabe-
es mellitus. Diabet Med 16:813-819, 199925. Rarick MU, Espina BM, Colley DT, Chrusoskie A,
andara S, Feinstein DI: Treatment of a unique anemia inatients with IDDM with epoetin alfa. Diabetes Care 21:423-26, 199826. ICH: Harmonised Tripartite Guideline: Guideline for
ood Clinical Practice, adopted 1997. Available at: http://ww.ich.org/UrlGrpServer.jser?@_ID�276&_TEMPLATE�54. Accessed April 200527. Ware J, Kosinski M, Keller S: SF-36 Physical andental Health Summary Scales: A User’s Manual. Boston,A, The Health Institute, 199428. Ware JE Jr, Gandek B: Overview of the SF-36 Health
urvey and the International Quality of Life AssessmentIQOLA) Project. J Clin Epidemiol 51:903-912, 1998
29. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N,oth D: A more accurate method to estimate glomerularltration rate from serum creatinine: A new prediction equa-
ion. Modification of Diet in Renal Disease Study Group.nn Intern Med 130:461-470, 199930. Cockcroft DW, Gault MH: Prediction of creatinine
learance from serum creatinine. Nephron 16:31-41, 1976

dr
tAD
bc
Rth
mASWpE1
eu3N
Zpw2
rdA
ha
G
te1
esK
ap1
Ziss
bc
scSH2
Mwp
PtDc
cK
o
Target Level for Hemoglobin Correction in Diabetes 207
31. American Society of Echocardiography: Recommen-ations for continuous quality improvement in echocardiog-aphy. J Am Soc Echocardiogr 8:S1-S28, 1995 (suppl P2)
32. National Kidney Foundation: KDOQI Clinical Prac-ice Guidelines and Clinical Practice Recommendations fornemia in Chronic Kidney Disease in Adults. Am J Kidneyis 47:S16-S85, 2006 (suppl 3)33. Radermacher J, Koch KM: Treatment of renal anemia
y erythropoietin substitution. The effects on the cardiovas-ular system. Clin Nephrol 44:S56-S60, 1995 (suppl 1)
34. Silberberg J, Racine N, Barre P, Sniderman AD:egression of left ventricular hypertrophy in dialysis pa-
ients following correction of anemia with recombinantuman erythropoietin. Can J Cardiol 6:1-4, 199035. Lang RM, Bierig M, Devereux RB, et al: Recom-endations for chamber quantification: A report from themerican Society of Echocardiography’s Guidelines andtandards Committee and the Chamber Quantificationriting Group, developed in conjunction with the Euro-
ean Association of Echocardiography, a branch of theuropean Society of Cardiology. J Am Soc Echocardiogr8:1440-1463, 200536. Roger SD, McMahon LP, Clarkson A, et al: Effects of
arly and late intervention with epoetin alpha on left ventric-lar mass among patients with chronic kidney disease (stageor 4): Results of a randomized clinical trial. J Am Socephrol 15:148-156, 200437. Parfrey PS, Foley RN, Wittreich BH, Sullivan DJ,
agari MJ, Frei D: Double-blind comparison of full andartial anemia correction in incident hemodialysis patientsithout symptomatic heart disease. J Am Soc Nephrol 16:180-2189, 200538. Levin A, Djurdjev O, Thompson C, et al: Canadian
andomized trial of hemoglobin maintenance to prevent orelay left ventricular mass growth in patients with CKD.m J Kidney Dis 46:799-811, 200539. Foley RN, Parfrey PS, Morgan J, et al: Effect of
emoglobin levels in hemodialysis patients with asymptom-tic cardiomyopathy. Kidney Int 58:1325-1335, 2000
40. McMahon LP, Mason K, Skinner SL, Burge CM,
rigg LE, Becker GJ: Effects of haemoglobin normaliza- aion on quality of life and cardiovascular parameters innd-stage renal failure. Nephrol Dial Transplant 15:1425-430, 200041. Ayus JC, Go AS, Valderrabano F, et al: Effects of
rythropoietin on left ventricular hypertrophy in adults withevere chronic renal failure and hemoglobin �10 g/dL.idney Int 68:788-795, 200542. De Backer G, Ambrosioni E, Borch-Johnsen K, et
l: European guidelines on cardiovascular disease andrevention in clinical practice. Atherosclerosis 171:145-55, 200343. Cruickshank JM, Pennert K, Sorman AE, Thorp JM,
acharias FM, Zacharias FJ: Low mortality from all causes,ncluding myocardial infarction, in well-controlled hyperten-ives treated with a beta-blocker plus other antihyperten-ives. J Hypertens 5:489-498, 1987
44. Furberg CD, Cutler JA: Diuretic agents versus beta-lockers. Comparison of effects on mortality, stroke, andoronary events. Hypertension 13:157-161, 1989
45. Lindholm LH, Hansson L, Ekbom T, et al: Compari-on of antihypertensive treatments in preventing cardiovas-ular events in elderly diabetic patients: Results from thewedish Trial in Old Patients with Hypertension-2. STOPypertension-2 Study Group. J Hypertens 18:1671-1675,00046. Collins R, Armitage J, Parish S, Sleigh P, Peto R:RC/BHF Heart Protection Study of cholesterol-loweringith simvastatin in 5963 people with diabetes: A randomisedlacebo-controlled trial. Lancet 361:2005-2016, 200347. Colhoun HM, Betteridge DJ, Durrington PN, et al:
rimary prevention of cardiovascular disease with atorvasta-in in type 2 diabetes in the Collaborative Atorvastatiniabetes Study (CARDS): Multicentre randomised placebo-
ontrolled trial. Lancet 364:685-696, 200448. Rossert J, Levin A, Roger SD, et al: Effect of early
orrection of anemia on the progression of CKD. Am Jidney Dis 47:738-750, 200649. Drüeke TB, Locatelli F, Clyne N, et al: Normalization
f hemoglobin level in patients with chronic kidney disease
nd anemia. N Engl J Med 16:2071-2084, 2006