Diabetes and Its Management
32
Diabetes & Its Management
-
Upload
dibakardas -
Category
Documents
-
view
3 -
download
0
Transcript of Diabetes and Its Management
Diabetes & Its Management

DiabetesDiabetes- Greek word which means Syphon.A disease characterized by polyuria i.e. excessive urination.
Classificatio
n:Diabetes
Diabetes Mellitus Diabetes Incipidus
Type 1It happens when pancreas can’t produce insulin
at all.
Type 2It happens when
pancreas can produce insulin but not sufficiently.

Common symptoms of Diabetes
If left untreated, the level of glucose in the blood can become very high, inducing coma and possibly death.
Frequent Urination
Weight Loss
Excess Thirst
Lack of Energy
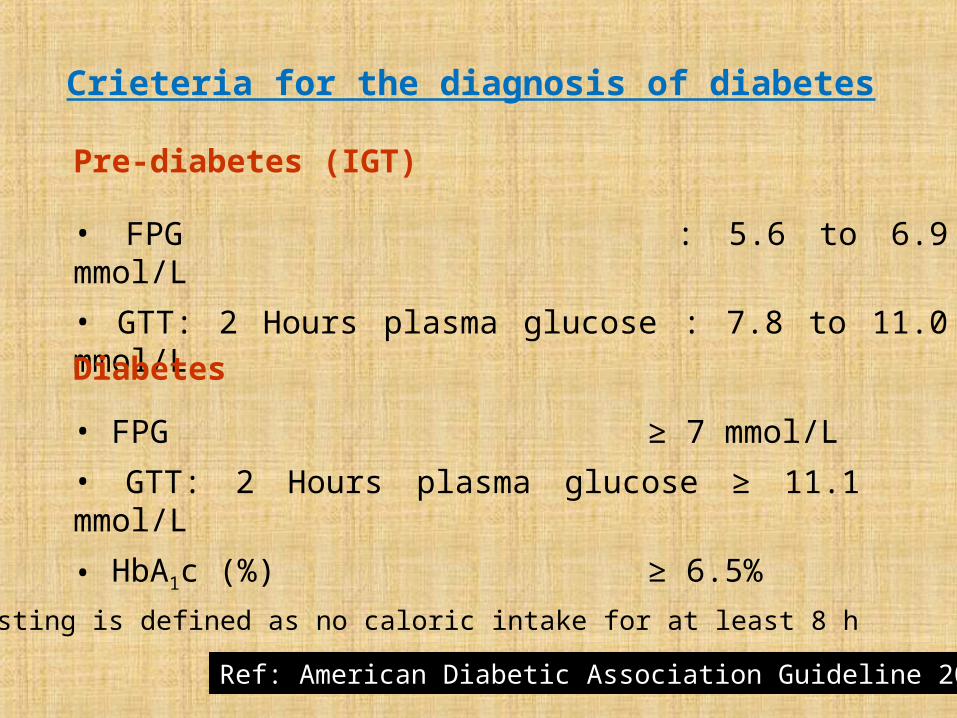
Crieteria for the diagnosis of diabetes
Pre-diabetes (IGT)
• FPG : 5.6 to 6.9 mmol/L• GTT: 2 Hours plasma glucose : 7.8 to 11.0 mmol/LDiabetes • FPG ≥ 7 mmol/L• GTT: 2 Hours plasma glucose ≥ 11.1 mmol/L• HbA1c (%) ≥ 6.5%
* Fasting is defined as no caloric intake for at least 8 h
Ref: American Diabetic Association Guideline 2011
Diabetes is ManagableBut is not Curable
GOAL:To maintain target
blood glucose
• Diet• Diet + Discipline • Diet + Discipline + Drug (3D Theory)
Management of diabetes
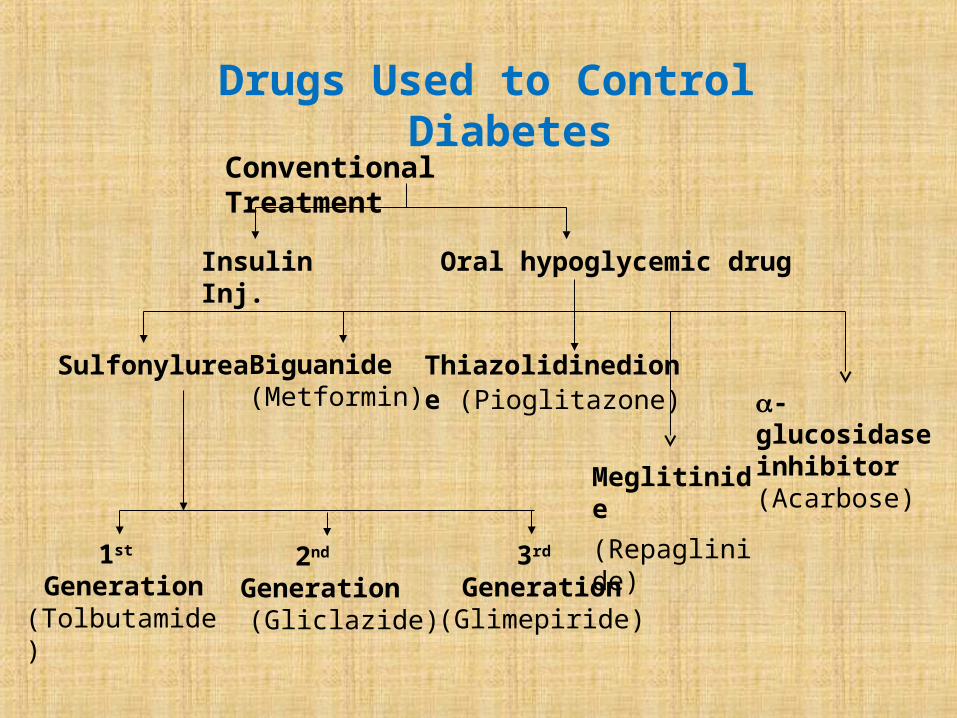
Drugs Used to Control Diabetes
Conventional Treatment
Insulin Inj.
Oral hypoglycemic drug
SulfonylureaBiguanide(Metformin)
Thiazolidinedione (Pioglitazone)
Meglitinide (Repaglinide)
1st Generation
(Tolbutamide)
2nd Generation
(Gliclazide)
3rd Generation
(Glimepiride)
-glucosidase inhibitor (Acarbose)

Modern Treatment
DPP-4 inhibitors (Vildagliptin SitagliptinSaxagliptinLinagliptin)
GLP-1 Analogues
(LiraglutideExenatide)
Insulin The word “Insulin” comes from the Latin “Insula”, which means Islet or Island.
Insulin is a polypeptide hormone produced from the beta cells of the Islets of Langerhans in pancreas.
Advantages & Disadvantages of Insulin
Advantages: •Quicker action than oral
hypoglycemic drugs•The only therapy for type 1 diabetic patients•Comparatively safer•Early initiation may reduce beta cell damage
Disadvantages: • May cause hypoglycemia
• Expensive
Increased glucose in blood
Secretion of Insulin
Glucose enters into beta cells
Ca2+ channel opens due to increased glucose conc.
Contraction of beta cells
Insulin is released
Role of Insulin on DiabetesInsulin- Increases glucose transport from blood to tissue
Increases glucose uptake by liver Stimulates glycogenesis (Synthesis of glycogen from glucose)
Inhibits glycogenolysis (Breakdown of glycogen to glucose)
Inhibits gluconeogenesis (Synthesis of glucose from protein & fat)
Basal & Bolus Insulin Basal insulin is the insulin which is produced in our body to control blood glucose between meals & overnight. As Insulin N, Glargine, Detemir etc. also give similar action they are called basal insulin.
Bolus insulin is the insulin which is produced in our body to control blood glucose when food is eaten. As Insulin R, Aspart, Lispro, Glulisine etc. also give similar action they are called bolus insulin.
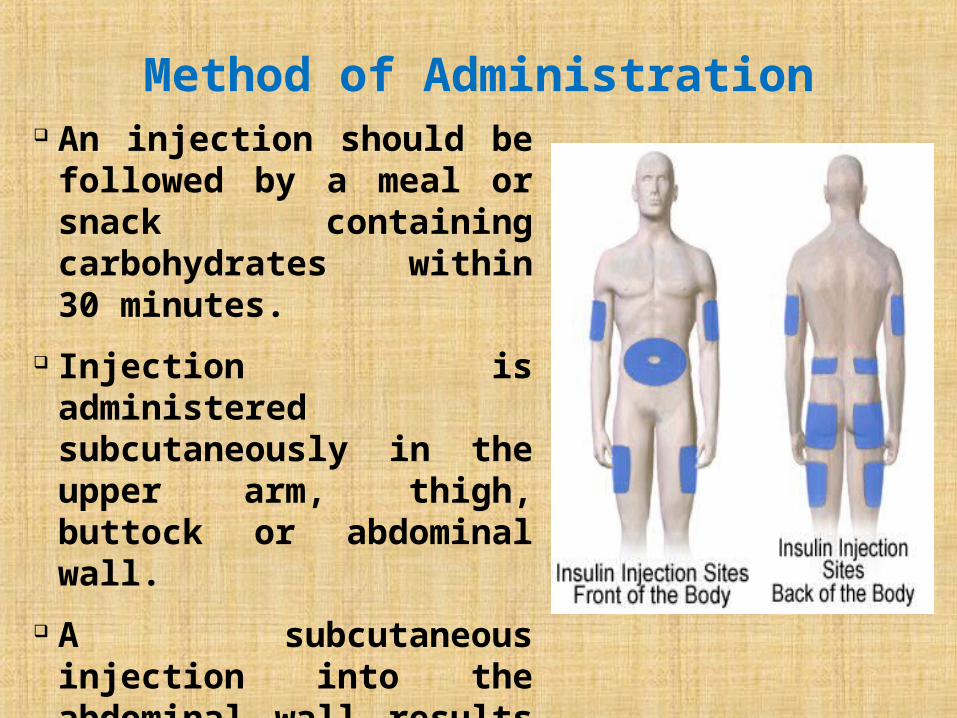
Method of Administration An injection should be followed by a meal or snack containing carbohydrates within 30 minutes.
Injection is administered subcutaneously in the upper arm, thigh, buttock or abdominal wall.
A subcutaneous injection into the abdominal wall results in a faster absorption than from other injection sites.
Preparation Before Use Clean your hands. Shake or rotate the vial gently to mix the solution uniformly and check if the insulin has the normal appearance.
In case of using a new vial, flip off the plastic protective cap and wipe the rubber plug with an alcohol swab.
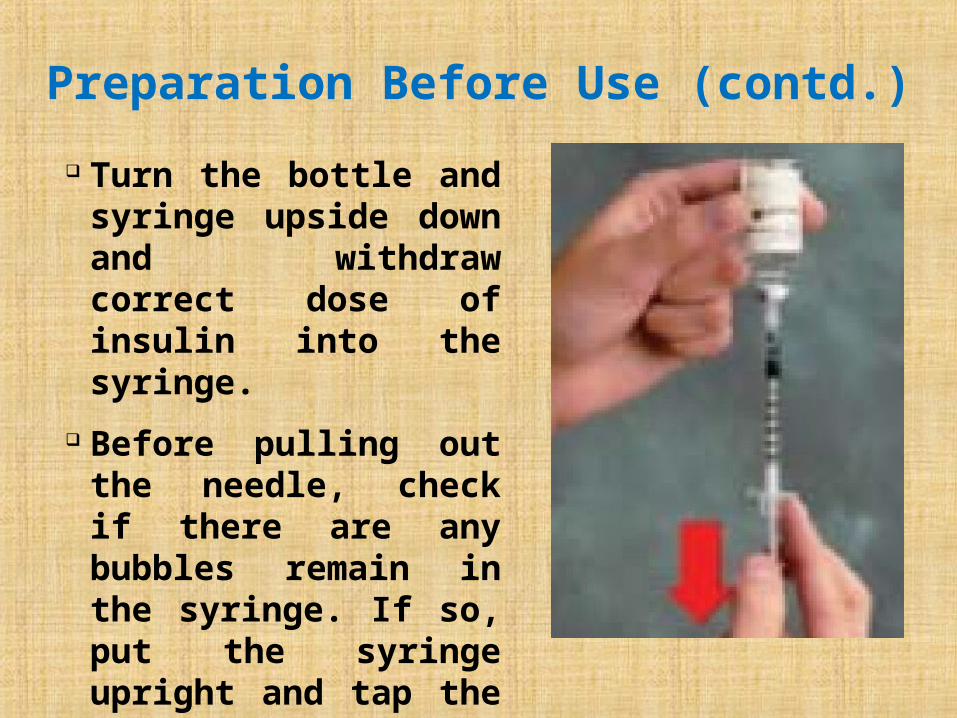
Preparation Before Use (contd.) Turn the bottle and syringe upside down and withdraw correct dose of insulin into the syringe.
Before pulling out the needle, check if there are any bubbles remain in the syringe. If so, put the syringe upright and tap the syringe to discharge the air bubbles.
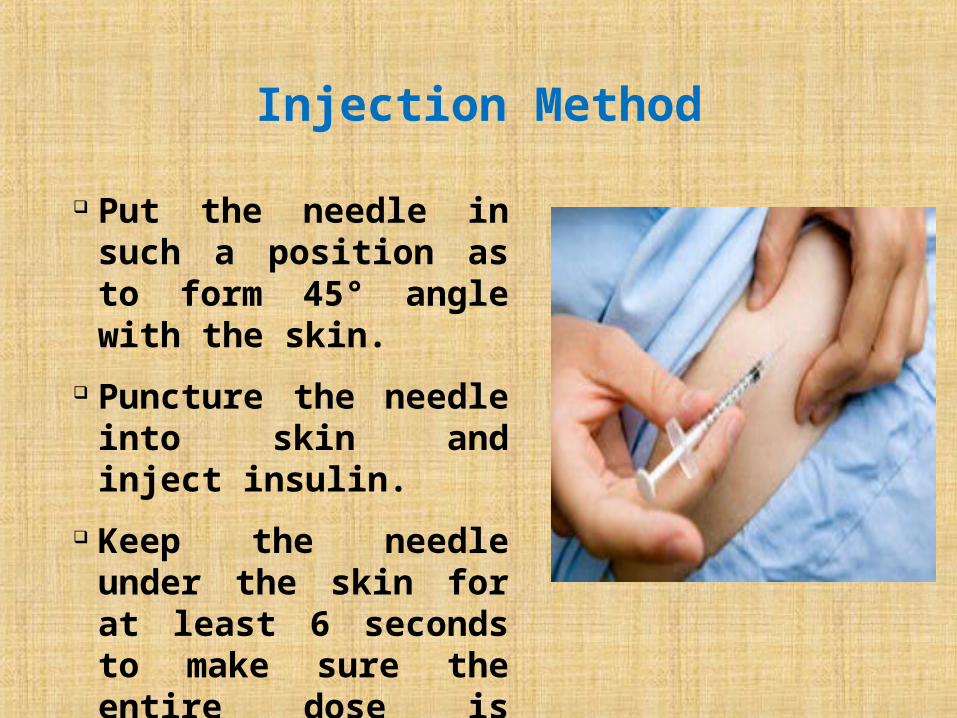
Injection Method Put the needle in such a position as to form 45° angle with the skin.
Puncture the needle into skin and inject insulin.
Keep the needle under the skin for at least 6 seconds to make sure the entire dose is injected.
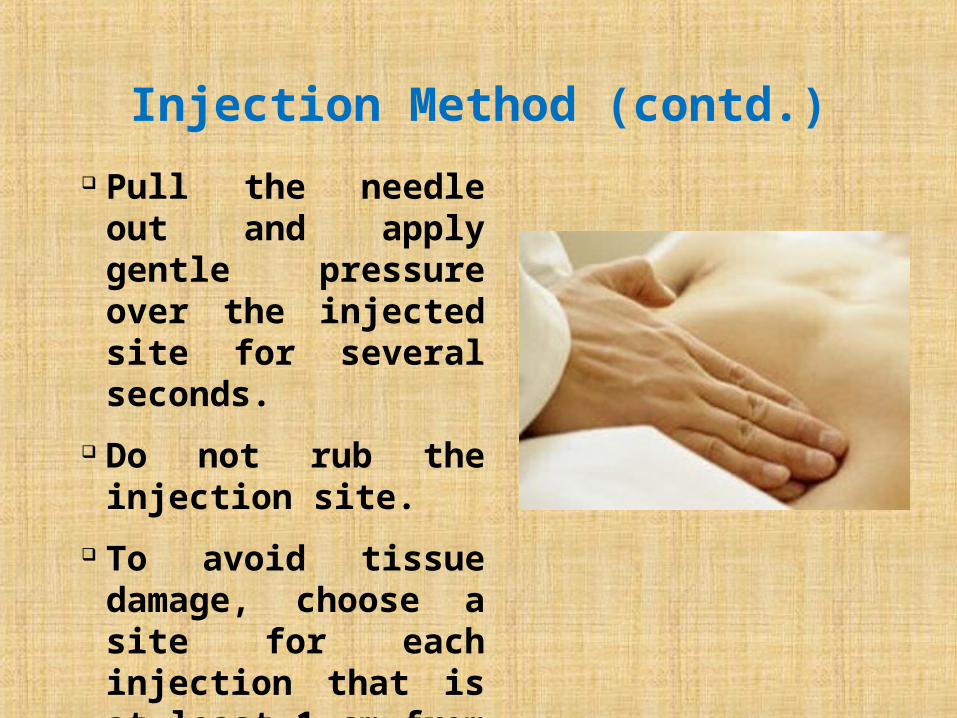
Injection Method (contd.) Pull the needle out and apply gentle pressure over the injected site for several seconds.
Do not rub the injection site.
To avoid tissue damage, choose a site for each injection that is at least 1 cm from the previous injection site.
Dosage Guideline Dosage depends on body weight, food intake, physical exercise and is determined by the physician. General dose for type 1 diabetes is 0.5-1.0 IU/kg/day. General dose for type 2 diabetes is 0.3-0.6 IU/kg/day.
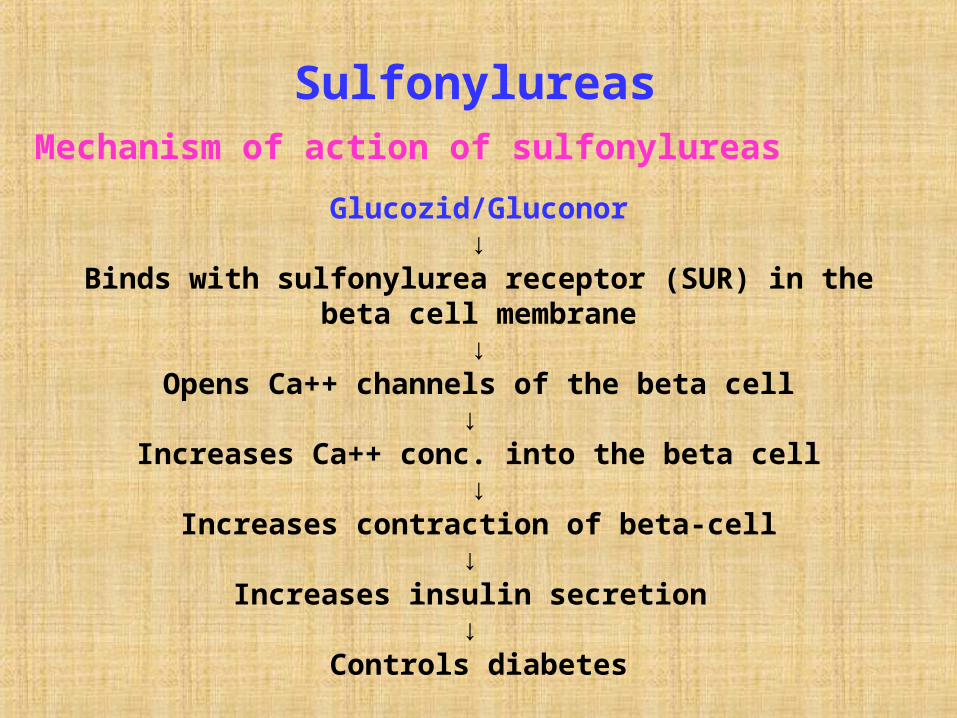
Glucozid/Gluconor↓
Binds with sulfonylurea receptor (SUR) in the beta cell membrane
↓Opens Ca++ channels of the beta cell
↓ Increases Ca++ conc. into the beta cell
↓Increases contraction of beta-cell
↓ Increases insulin secretion
↓ Controls diabetes
Mechanism of action of sulfonylureasSulfonylureas
Advantages: • Quick action• Once daily dose• Antioxidant properties
Disadvantages: • Causes damage of beta cell• May cause insulin resistance in long term use• May cause hypoglycemia (for short acting 1st generation drugs
Gliclazide
Advantages & disadvantages of sulfonylureas (Glucozid)
(Due to presence of azabicyclo-octyl ring)
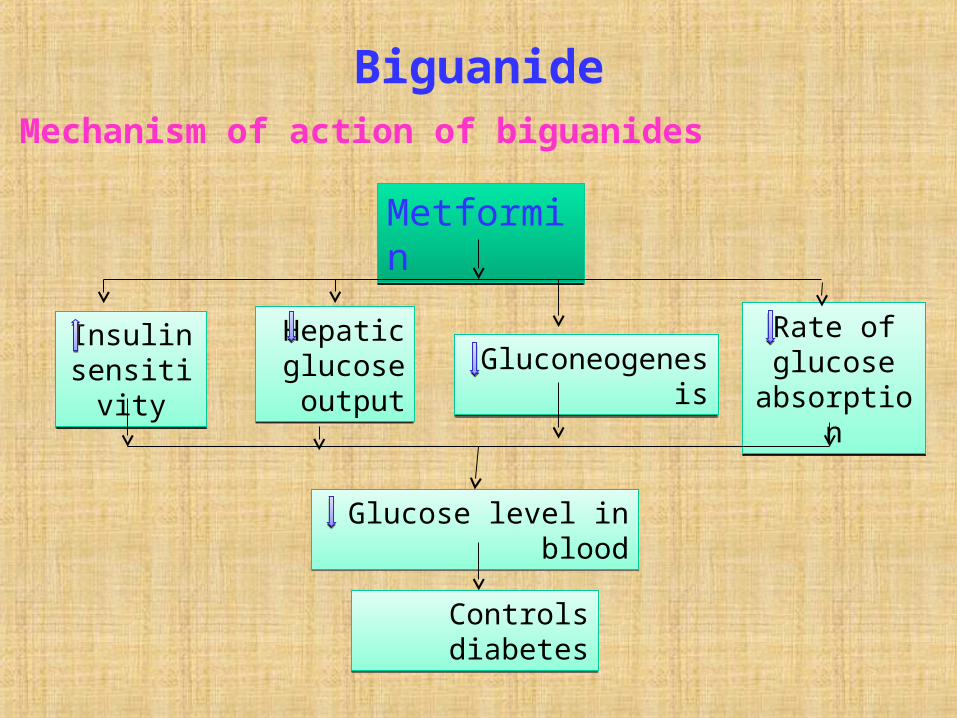
Biguanide
Metformin
Hepatic glucose output
Gluconeogenesis
Rate of glucose absorptio
n
Insulin sensitivity
Glucose level in blood
Controls diabetes
Mechanism of action of biguanides
Advantages:• No damage of beta cell• No insulin resistance• Doesn’t cause hypoglycemia• Helpful for infertile women• Helpful for obese patients
- both diabetic & non-diabetic
• Can be given in pregnancy safely
Disadvantages: • Comparatively slow work• 2-3 times daily
Advantages & disadvantages of Biguanide (Metformin)
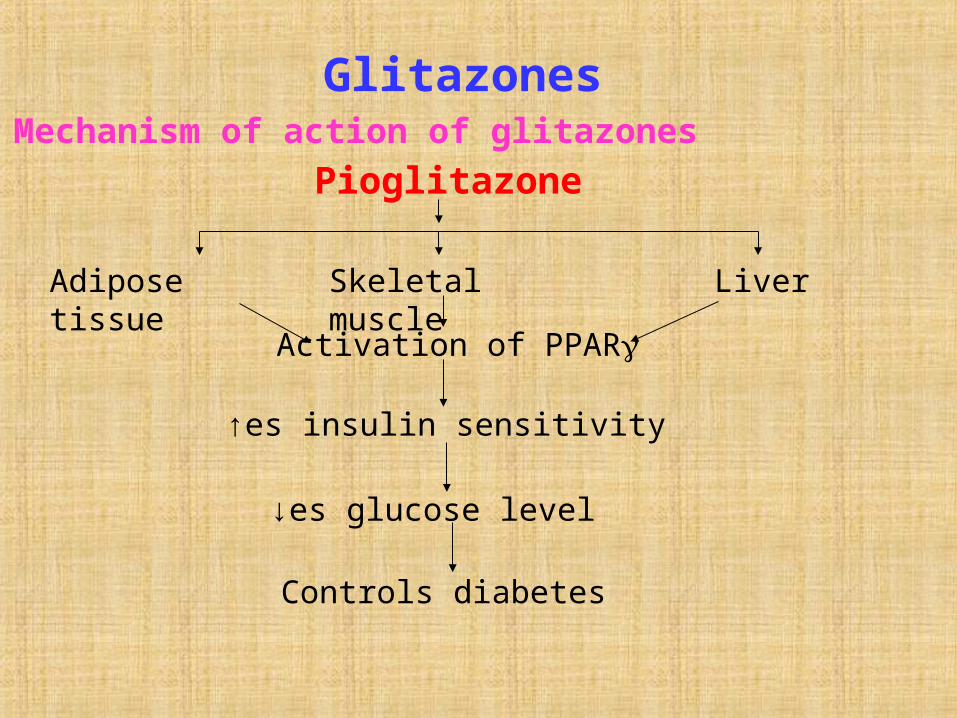
Glitazones
Pioglitazone
Adipose tissue
Skeletal muscle
LiverActivation of PPAR
↑es insulin sensitivity
↓es glucose level
Controls diabetes
Mechanism of action of glitazones
Advantages:• No damage of beta cell• No insulin resistance• Once daily
Disadvantages: • Comparatively slow work• Liver function should be monitored
Advantages & disadvantages of Glitazone (Pioglitazone)
So, Sulfonylureas increase insulin secretion &
Biguanides/Glitazones increase insulin sensitivity
As they work in two different ways, they can be given together to get
synergistic effect
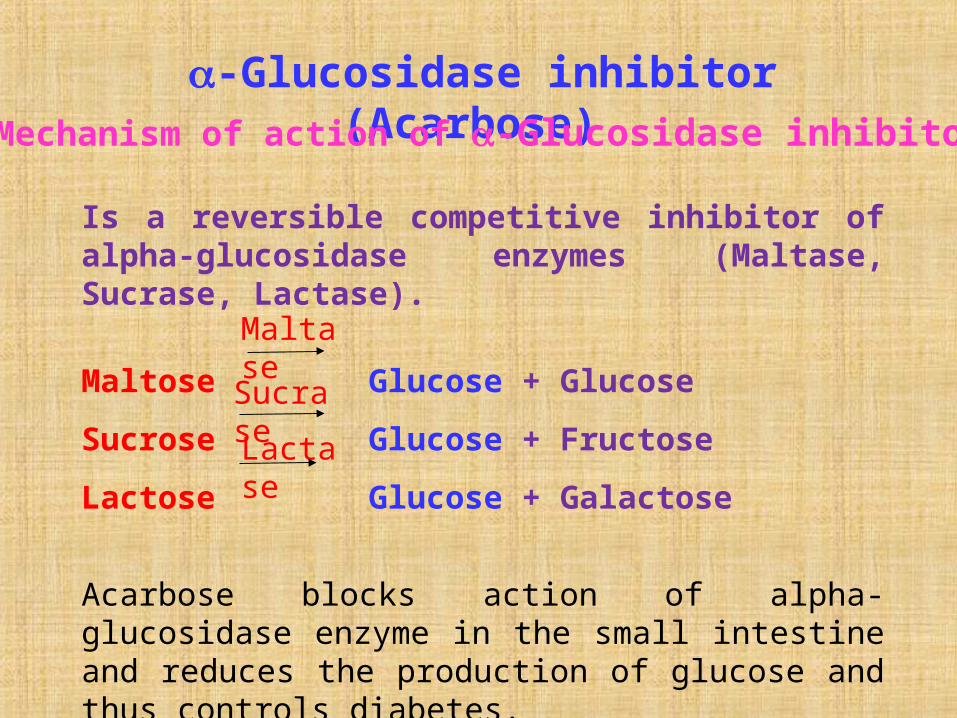
Is a reversible competitive inhibitor of alpha-glucosidase enzymes (Maltase, Sucrase, Lactase).
Maltose Glucose + GlucoseSucrose Glucose + FructoseLactose Glucose + Galactose
Acarbose blocks action of alpha-glucosidase enzyme in the small intestine and reduces the production of glucose and thus controls diabetes.
-Glucosidase inhibitor (Acarbose)
Sucrase
Maltase
Lactase
Mechanism of action of -Glucosidase inhibitor

Advantages:• No hypoglycemia• No insulin resistance• No damage of beta cell
Disadvantages: • Flatulence• Diarrhea
Advantages & disadvantages of-Glucosidase inhibitor (Acarbose)
Repaglinide selectively stimulates insulin secretion in response to high glucose level in the prandial phase, which in turn controls blood glucose peaks – called prandial glucose regulation.
Meglitinide (Repaglinide)Mechanism of action of Repaglinide
Advantages:• No hypoglycemia• One meal, one dose
Disadvantages: • May cause insulin resistance• Frequent dosing
Advantages & disadvantages ofMeglitinide (Repaglinide)
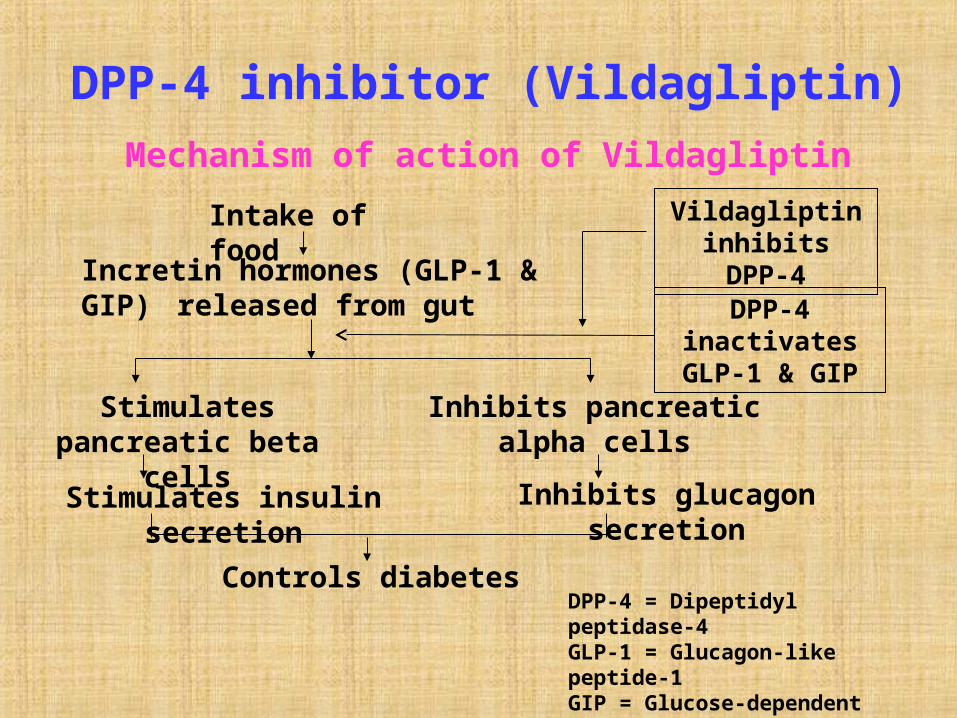
Mechanism of action of VildagliptinDPP-4 inhibitor (Vildagliptin)
Intake of foodIncretin hormones (GLP-1 &
GIP) released from gut
Stimulates pancreatic beta
cells
Inhibits pancreatic alpha cells
Stimulates insulin secretion
Inhibits glucagon secretion
Controls diabetes
DPP-4 inactivates GLP-1 & GIP
Vildagliptin inhibits DPP-4
DPP-4 = Dipeptidyl peptidase-4GLP-1 = Glucagon-like peptide-1GIP = Glucose-dependent insulinotropic peptide
Advantages:•No hypoglycemia•No weight gain•Improves beta cell function & insulin resistance
Advantages & disadvantages ofDPP-4 inhibitor (Vildagliptin)
Disadvantages:•Expensive•Should not be used in hepatic impaired patients





















