
HLA-B52 allele in giant cell arteritis may indicate diffuse large ...
Upload
independentCategory
view
4download
0
1 23
Pediatric Cardiology ISSN 0172-0643 Pediatr CardiolDOI 10.1007/s00246-011-0025-6
Takayasu’s Arteritis Mimicking UnilateralPulmonary Artery Agenesis in a ChildWith Severe Pulmonary Hypertensionand Right Heart Failure: A DiagnosticDilemmaSudeep Kumar, Nagaraja Moorthy, AdityaKapoor & Sunil Kumar
1 23
Your article is protected by copyright and
all rights are held exclusively by Springer
Science+Business Media, LLC. This e-offprint
is for personal use only and shall not be self-
archived in electronic repositories. If you
wish to self-archive your work, please use the
accepted author’s version for posting to your
own website or your institution’s repository.
You may further deposit the accepted author’s
version on a funder’s repository at a funder’s
request, provided it is not made publicly
available until 12 months after publication.

CASE REPORT
Takayasu’s Arteritis Mimicking Unilateral Pulmonary ArteryAgenesis in a Child With Severe Pulmonary Hypertensionand Right Heart Failure: A Diagnostic Dilemma
Sudeep Kumar • Nagaraja Moorthy •
Aditya Kapoor • Sunil Kumar
Received: 18 March 2011 / Accepted: 19 May 2011
� Springer Science+Business Media, LLC 2011
Abstract Affliction of the pulmonary arteries in Taka-
yasu’s arteritis is uncommon. Moreover the incidence of
pulmonary artery involvement in this condition is often
underestimated because of asymptomatic nature in most
patients. Severe involvement may however present with
pulmonary artery hypertension and hemoptysis, which
may prove to be fatal. This case report describes a 9-year-
old girl with severe pulmonary hypertension and right
heart failure secondary to total occlusion of the right
pulmonary artery. Detailed clinical examination and
computed tomography (CT) angiography confirmed this
diagnosis.
Keywords Pulmonary artery agenesis �Pulmonary hypertension � Takayasu’s arteritis
Pulmonary artery (PA) involvement in Takayasu’s arteritis
is not only uncommon but often remains asymptomatic,
leading to significant underestimation of its overall fre-
quency [7]. Presentation with PA hypertension, hemopty-
sis, and right heart failure as a manifestation of PA
involvement in Takayasu’s arteritis is very rare. We report
a young girl with Takayasu’s arteritis who had total ostial
occlusion of the right PA.
A high index of suspicion is needed to make the correct
diagnosis. The disease is associated with a high incidence
of morbidity and a significant risk of premature death.
Takayasu’s arteritis most often affects the aorta and its
branches, and the involvement of pulmonary arteries is
underestimated [7].
Case Report
A 9-year-old girl presented with recent onset progressive
distension of the abdomen, pedal edema, and recurrent
hemoptysis during the preceding 6 months. Before the
onset of symptoms, she had experienced an episode of
febrile illness accompanied by arthralgia and mild short-
ness of breath, which had subsided within a week. An
echocardiography showed a dilated left ventricle (LV) with
severely reduced LV function (LV ejection fraction, 25%).
The girl’s disorder had been labeled as postmyocarditis
dilated cardiomyopathy with severe LV dysfunction, and
she subsequently was referred to our Institute.
The girl also reported gradually worsening claudication
in both lower limbs for the preceding 3 months. Clinical
examination showed sinus tachycardia (heart rate,
100 bpm), mild pallor, bilateral pitting pedal edema, and
elevated jugular venous pressures, with prominent a and v
waves. The left upper limb, the left carotid, both lower
limbs, and abdominal aortic pulsations were absent. The
blood pressure in her right upper limb was 100/70 mmHg,
whereas it was unrecordable in both lower limbs and the
left upper limb.
Auscultation exhibited a loud pulmonary component of
the second heart sound, a prominent pan systolic murmur at
Electronic supplementary material The online version of thisarticle (doi:10.1007/s00246-011-0025-6) contains supplementarymaterial, which is available to authorized users.
S. Kumar (&) � N. Moorthy � A. Kapoor
Department of Cardiology, Sanjay Gandhi Postgraduate Institute
of Medical Sciences, Lucknow 226014, India
e-mail: [email protected]
S. Kumar
Department of Radiology, Sanjay Gandhi Postgraduate Institute
of Medical Sciences, Lucknow 226014, India
123
Pediatr Cardiol
DOI 10.1007/s00246-011-0025-6
Author's personal copy
the left lower sternal border suggestive of tricuspid regur-
gitation (TR), and a continuous bruit over the D10-L1
vertebrae. Abdominal examination showed ascites with
gross hepatomegaly.
An electrocardiogram showed sinus tachycardia, right
axis deviation, and evidence of right ventricular (RV)
hypertrophy. The chest radiograph showed absence of right
PA shadow with relative hyperlucency on the right side,
with no significant volume loss noted (Fig. 1a).
Routine blood investigations exhibited a hemoglobin
level of 9 g/dl, an erythrocyte sedimentation rate of 20 mm
at 1 h, and elevated serum C-reactive protein levels (4 mg/
dl). The serology results for connective tissue disorders
were negative.
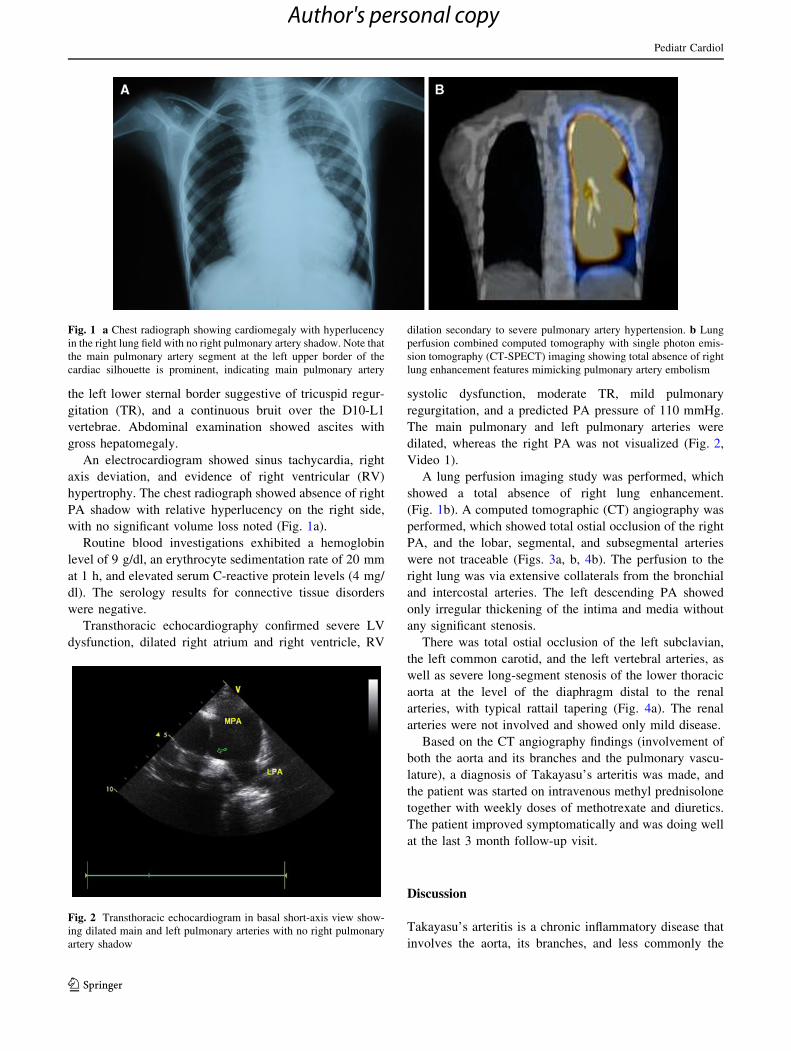
Transthoracic echocardiography confirmed severe LV
dysfunction, dilated right atrium and right ventricle, RV
systolic dysfunction, moderate TR, mild pulmonary
regurgitation, and a predicted PA pressure of 110 mmHg.
The main pulmonary and left pulmonary arteries were
dilated, whereas the right PA was not visualized (Fig. 2,
Video 1).
A lung perfusion imaging study was performed, which
showed a total absence of right lung enhancement.
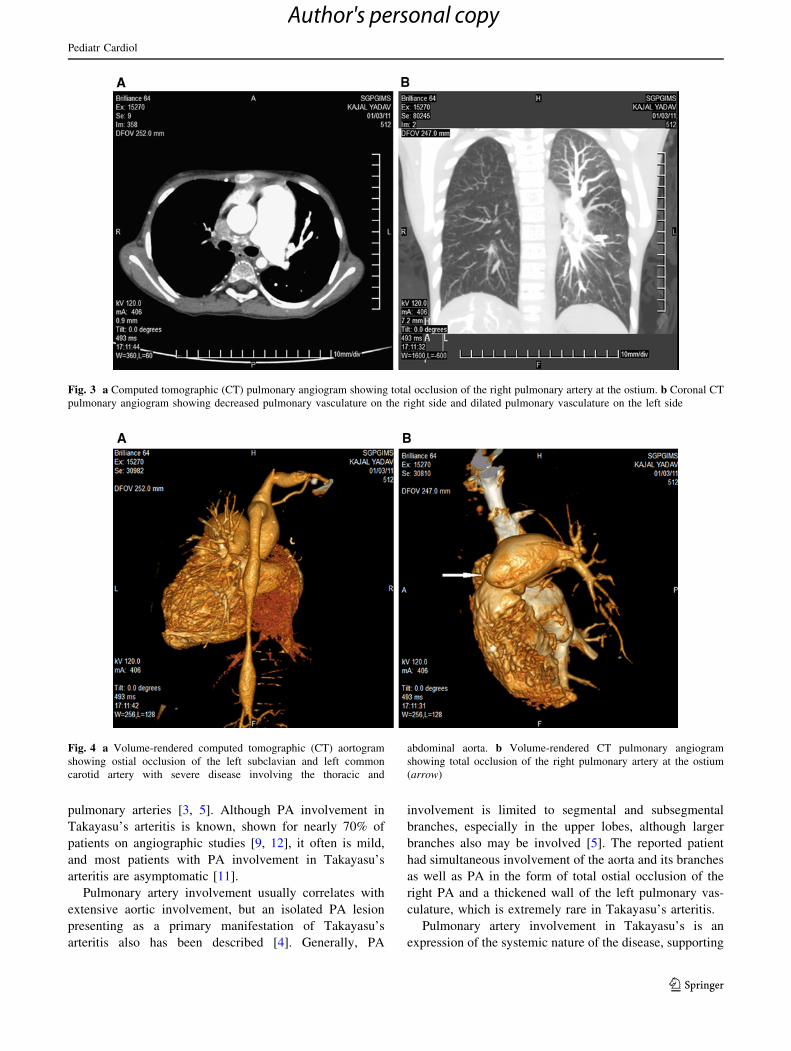
(Fig. 1b). A computed tomographic (CT) angiography was
performed, which showed total ostial occlusion of the right
PA, and the lobar, segmental, and subsegmental arteries
were not traceable (Figs. 3a, b, 4b). The perfusion to the
right lung was via extensive collaterals from the bronchial
and intercostal arteries. The left descending PA showed
only irregular thickening of the intima and media without
any significant stenosis.
There was total ostial occlusion of the left subclavian,
the left common carotid, and the left vertebral arteries, as
well as severe long-segment stenosis of the lower thoracic
aorta at the level of the diaphragm distal to the renal
arteries, with typical rattail tapering (Fig. 4a). The renal
arteries were not involved and showed only mild disease.
Based on the CT angiography findings (involvement of
both the aorta and its branches and the pulmonary vascu-
lature), a diagnosis of Takayasu’s arteritis was made, and
the patient was started on intravenous methyl prednisolone
together with weekly doses of methotrexate and diuretics.
The patient improved symptomatically and was doing well
at the last 3 month follow-up visit.
Discussion
Takayasu’s arteritis is a chronic inflammatory disease that
involves the aorta, its branches, and less commonly the
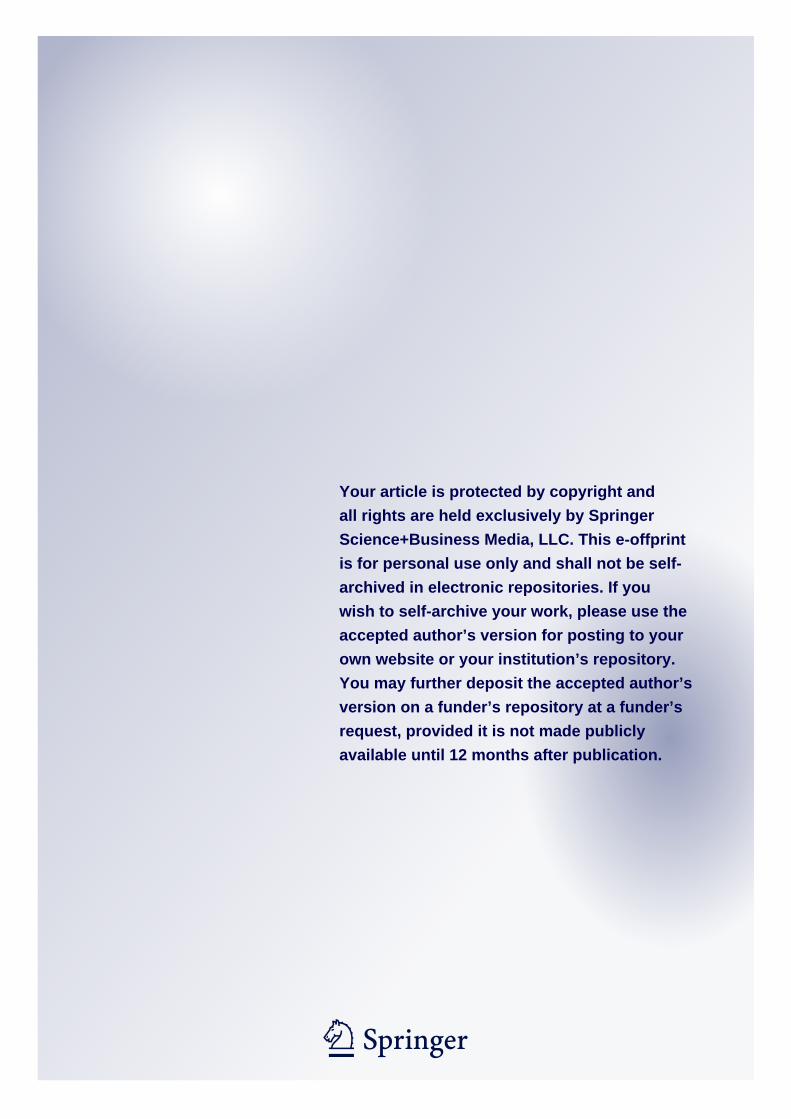
Fig. 1 a Chest radiograph showing cardiomegaly with hyperlucency
in the right lung field with no right pulmonary artery shadow. Note that
the main pulmonary artery segment at the left upper border of the
cardiac silhouette is prominent, indicating main pulmonary artery
dilation secondary to severe pulmonary artery hypertension. b Lung
perfusion combined computed tomography with single photon emis-
sion tomography (CT-SPECT) imaging showing total absence of right
lung enhancement features mimicking pulmonary artery embolism
Fig. 2 Transthoracic echocardiogram in basal short-axis view show-
ing dilated main and left pulmonary arteries with no right pulmonary
artery shadow
Pediatr Cardiol
123
Author's personal copy
pulmonary arteries [3, 5]. Although PA involvement in
Takayasu’s arteritis is known, shown for nearly 70% of
patients on angiographic studies [9, 12], it often is mild,
and most patients with PA involvement in Takayasu’s
arteritis are asymptomatic [11].
Pulmonary artery involvement usually correlates with
extensive aortic involvement, but an isolated PA lesion
presenting as a primary manifestation of Takayasu’s
arteritis also has been described [4]. Generally, PA
involvement is limited to segmental and subsegmental
branches, especially in the upper lobes, although larger
branches also may be involved [5]. The reported patient
had simultaneous involvement of the aorta and its branches
as well as PA in the form of total ostial occlusion of the
right PA and a thickened wall of the left pulmonary vas-
culature, which is extremely rare in Takayasu’s arteritis.
Pulmonary artery involvement in Takayasu’s is an
expression of the systemic nature of the disease, supporting
Fig. 3 a Computed tomographic (CT) pulmonary angiogram showing total occlusion of the right pulmonary artery at the ostium. b Coronal CT
pulmonary angiogram showing decreased pulmonary vasculature on the right side and dilated pulmonary vasculature on the left side
Fig. 4 a Volume-rendered computed tomographic (CT) aortogram
showing ostial occlusion of the left subclavian and left common
carotid artery with severe disease involving the thoracic and
abdominal aorta. b Volume-rendered CT pulmonary angiogram
showing total occlusion of the right pulmonary artery at the ostium
(arrow)
Pediatr Cardiol
123
Author's personal copy

the hypothesis of an immunologic etiology [5]. The lesions
in the pulmonary arteries are inflammatory or granuloma-
tous, involving the elastic, medial, and adventitial layers,
often culminating in thickness, stenosis, and even short-
ening of the artery in some cases [5, 8]. Although occlusion
of unilateral pulmonary arteries can occur in advanced
cases [6, 12], it is extremely rare.
Because most patients remain asymptomatic despite
extensive involvement of the PA vasculature, the incidence
of PA involvement in Takayasu’s arteritis often is under-
estimated. Hence, it is important to evaluate the pulmonary
arteries in all cases of Takayasu’s arteritis, even in the
absence of any significant respiratory symptoms. In fact, it
is important to consider and rule out late-phase Takayasu’s
arteritis in cases of chronic PA obstruction of unknown
cause, especially in endemic areas, where Takayasu’s
arteritis is common [2].
Pulmonary hypertension generally is moderate and
found to be severe in only a few cases. Although pul-
monary hypertension increases the probability of pulmon-
ary vascular involvement, normal pressures do not exclude
lesions in the pulmonary vasculature.
Diffuse wall thickening and stenosis or dilations are the
most frequent PA changes detected by CT in patients with
Takayasu’s arteritis. These signs are suggestive of PA
involvement and often are associated with ascending aorta
involvement, as seen in the reported patient. Visualization
of a systemic PA shunt on a thoracic aortogram or a
selective bronchial arteriogram in Takayasu’s arteritis has
already been described [12]. In the reported patient, these
shunts led to an anterograde opacification of the distal
pulmonary vasculature through extensive bronchial and
intercostal collaterals. Such systemic PA shunts appear to
be indicative of extensive PA involvement in Takayasu’s
arteritis [12].
Heart failure from Takayasu’s arteritis is common in
children and an important cause of mortality. Hypertension
is the most common reason for heart failure, but it may
occur in the absence of severe hypertension [10]. Myo-
carditis, coronary arterial involvement, organic valvular
involvement, or PA involvement may cause or contribute
to the heart failure. Frequently, children with Takayasu’s
arteritis who experience heart failure are misdiagnosed as
having dilated cardiomyopathy because the echocardio-
gram shows systolic ventricular dysfunction, and hyper-
tension may be missed. Heart failure in the absence of
hypertension suggests myocarditis as a cause for ventric-
ular dysfunction.
Radiologically, PA involvement in Takayasu’s arteritis
with a total cutoff of the PAs, as happened in the reported
case, may mimic congenital unilateral PA agenesis [1].
However, the absence of other signs suggestive of congenital
agenesis (ipsilateral contracted lung with a mediastinal
shift and hyperinflation of the contralateral lung) and sub-
sequent CT findings confirmed the reported case to be severe
ostial stenosis of the right pulmonary artery secondary to
Takayasu’s arteritis. Although similar x-ray findings may
occur in cases of pulmonary embolism, the latter more often
involves larger pulmonary branches such as the main pul-
monary, lobar, and segmental branches, especially the lower
lobe branches. Moreover, the presence of associated abnor-
malities in the aorta and its branches further support the
diagnosis of Takayasu’s arteritis.
The reported case is unique in several aspects. The
initial presentation simulated dilated cardiomyopathy,
probably secondary to myocarditis. However, at this stage,
Takayasu’s arteritis was either not suspected or missed
clinically due to the absence or clinically undetectable
involvement of the aorta and its branches. During the fol-
low-up period, the LV dysfunction responded to medica-
tions, but there was ongoing progression of the disease,
resulting in severe involvement of the aorta and its bran-
ches as well as the pulmonary vasculature, resulting in
severe pulmonary hypertension with congestive heart
failure.
Conclusion
Pulmonary artery involvement in Takayasu’s arteritis is not
so rare and may range from mild asymptomatic thickening
of the intima to total occlusion of the main or branch
pulmonary arteries. Pulmonary circulation should be rou-
tinely studied for all patients with suspected Takayasu’s
arteritis. The PA involvement may be responsible for
unexplained pulmonary hypertension with heart failure in
children and may be a diagnostic challenge.
Acknowledgment The authors thank Dr. Amithab Arya from
Department of Nuclear Medicine, SGPGIMS, for providing SPECT
CT lung perfusion images.
References
1. Grum CM, Yarnal JR, Cook SA, Cardasco EM, Tomashefski JF
(1981) Unilateral hyperlucent lung: noninvasive diagnosis of the
pulmonary artery agenesis. Angiology 32:194–207
2. Hayashi K, Nagasaki M, Matsunaga N et al (1986) Initial pul-
monary artery involvement in Takayasu arteritis. Radiology
159:401–403
3. Ishikawa K (1978) Natural history and classification of occlusive
thromboartopathy (Takayasu’s disease). Circulation 57:27–35
4. Lie JT (1996) Isolated pulmonary Takayasu arteritis: clinico-
pathological characteristics. Mod Pathol 9:469–474
5. Lupi-Herrera E, Sanchez-Torres G, Marcushamer J, Mispireta J,
Horwitz S, Vela JE (1977) Takayasu’s arteritis: clinical study of
107 cases. Am Heart J 93:94–103
Pediatr Cardiol
123
Author's personal copy

6. Matsunaga N, Hayashi K, Sakamoto I et al (1993) Coronary-to-
pulmonary artery shunts via the bronchial artery: analysis of
cineangiographic studies. Radiology 186:877–882
7. Paul J, Hernigou A, Lefe B et al (1999) Electron beam CT fea-
tures of the pulmonary artery in Takayasu’s arteritis. AJR Am J
Roentgenol 173:89–93
8. Saito Y, Hirota K, Ito I et al (1972) Clinical and pathological
studies of five autopsied cases of aortitis syndrome: Part 1.
Findings of the aorta and its branches, peripheral arteries and
pulmonary arteries. Jap Heart J 13:20
9. Sharma S, Kamalakar T, Rajani M, Talwar KK, Shrivastava S
(1990) The incidence and patterns of pulmonary artery involve-
ment in Takayasu’s arteritis. Clin Radiol 42:182–187
10. Shrivastava S, Srivastava RN, Tandon R (1986) Idiopathic
obstructive aortoarteritis in children. Indian Paediatr 23:403–410
11. Suzuki Y, Konishi K, Hisada K (1973) Radioisotope lung scan-
ning in Takayasu’s arteritis. Radiology 109:133–136
12. Yamada I, Shibuya H, Matsubara O, Umehard I, Makino T,
Numano F, Suzuki S (1992) Pulmonary artery disease in Takayasu’s
arteritis: angiographic findings. AJR Am J Roent 159:263–269
Pediatr Cardiol
123
Author's personal copy
Copyright © 2022 FDOKUMEN




















