
Subcutaneous Methylnaltrexone for the Treatment of Opioid-Induced Constipation in Patients with...
9
Subcutaneous Methylnaltrexone for Treatment of Opioid-Induced Constipation in Patients With Chronic, Nonmalignant Pain: A Randomized Controlled Study Edward Michna,* E. Richard Blonsky, y,x Seth Schulman, z Evan Tzanis, z Amy Manley, z Haiying Zhang, z Shrividya Iyer, z and Bruce Randazzo z *Brigham and Women’s Hospital, Boston, Massachusetts. y Pain & Rehabilitation Clinic of Chicago, Chicago, Illinois. z Pfizer Inc, Collegeville, Pennsylvania. x Deceased. Abstract: Methylnaltrexone is effective for opioid-induced constipation (OIC) in advanced illness pa- tients. This 4-week, double-blind, randomized, placebo-controlled study investigated the effect of subcutaneous methylnaltrexone on OIC in patients receiving opioids for chronic, nonmalignant pain. Patients (N = 460) received subcutaneous methylnaltrexone 12 mg once daily (QD) or every other day (alternating with placebo) compared with placebo. Assessments included bowel movement count, time of bowel movement, straining, sense of complete evacuation, Bristol Stool Form Scales, and quality of life. Within 4 hours of first dose, 34.2% of patients in both methylnaltrexone groups had rescue-free bowel movements (RFBMs) versus 9.9% on placebo (P< .001). The estimated number needed to treat was about 4. On average, 28.9% of methylnaltrexone QD and 30.2% of methylnaltrex- one alternate-day dosing resulted in RFBMs within 4 hours versus 9.4% QD and 9.3% alternate-day placebo injections (both P< .001). Both methylnaltrexone groups had significantly shorter time to first RFBM (P < .001) and greater increase in number of weekly RFBMs (P< .05) versus placebo. Adverse events included abdominal pain, diarrhea, nausea, and hyperhidrosis. Bristol Stool Form Scale scores (P= .002) and sensation of complete evacuation (P < .04) were significantly superior with methylnal- trexone QD; both methylnaltrexone groups reported no or mild straining during RFBMs in the first 2 weeks (P< .02). At 4 weeks, a significantly greater improvement in patient-reported, constipation- specific quality of life was seen in the alternate-day dosing (P < .05) and QD (P < .001) groups. Perspective: We present data demonstrating that subcutaneous methylnaltrexone 12 mg given once daily (QD) or every other day provides significant relief of OIC and was generally well tolerated in patients with chronic, nonmalignant pain. These results expand on prior effectiveness observed for the treatment of OIC in advanced illness patients to a broader population. ª 2011 by the American Pain Society Key words: Methylnaltrexone, palliative care, constipation, abdominal pain, opioids, mu-opioid receptor antagonist, opioid-related disorders, chronic disease. O pioid analgesics are increasingly used to treat chronic, nonmalignant pain in patients with a wide variety of conditions. 8 While the long- term utility of opioids for pain management in these patients has been questioned, Noble et al 15 recently ex- amined 17 studies of long-term (6- to 48-week) opioid use in patients with chronic, noncancer-related pain and found that pain scores improved in patients remain- ing on treatment for at least 6 months. However, a sub- stantial number of patients withdrew prior to 6 months because of adverse events. Analysis of these adverse events revealed that 32.5% of patients taking oral opioids and 17.5% of those using transdermal opioids Received May 11, 2010; Revised September 2, 2010; Accepted November 8, 2010. This research was funded by Wyeth Research, which was acquired by Pfizer Inc in October 2009. Pfizer Inc provided funding for writing support, provided by On Assignment Clinical Research, a paid consultant to Pfizer in connection with the development of this manuscript, and for editorial support, provided by Peloton Advantage, LLC. Drs. Schulman, Zhang, Randazzo, and Iyer, Mr. Tzanis, and Ms. Manley are employees of Pfizer Inc. At the time of this study, they were employees of and stockholders in Wyeth. No author received an honorarium or other form of financial support related to the development of this manuscript. Address reprint requests to Edward Michna, MD, Brigham and Women’s Hospital, 75 Francis Street, Department of Anesthesia, Boston, MA 02115. E-mail: [email protected] 1526-5900/$36.00 ª 2011 by the American Pain Society doi:10.1016/j.jpain.2010.11.008 554 The Journal of Pain, Vol 12, No 5 (May), 2011: pp 554-562 Available online at www.sciencedirect.com
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Subcutaneous Methylnaltrexone for the Treatment of Opioid-Induced Constipation in Patients with...
The Journal of Pain, Vol 12, No 5 (May), 2011: pp 554-562Available online at www.sciencedirect.com
Subcutaneous Methylnaltrexone for Treatment of Opioid-Induced
Constipation in Patients With Chronic, Nonmalignant Pain: A
Randomized Controlled Study
Edward Michna,* E. Richard Blonsky,y,x Seth Schulman,z Evan Tzanis,z Amy Manley,z
Haiying Zhang,z Shrividya Iyer,z and Bruce Randazzoz
*Brigham and Women’s Hospital, Boston, Massachusetts.yPain & Rehabilitation Clinic of Chicago, Chicago, Illinois.zPfizer Inc, Collegeville, Pennsylvania.xDeceased.
Received8, 2010.This resePfizer Insupport,to PfizereditorialZhang, Rof PfizerstockholNo authorelated tAddressHospital,E-mail: e
1526-590
ª 2011 b
doi:10.10
554
Abstract: Methylnaltrexone is effective for opioid-induced constipation (OIC) in advanced illness pa-
tients. This 4-week, double-blind, randomized, placebo-controlled study investigated the effect of
subcutaneous methylnaltrexone on OIC in patients receiving opioids for chronic, nonmalignant
pain. Patients (N = 460) received subcutaneous methylnaltrexone 12 mg once daily (QD) or every other
day (alternating with placebo) compared with placebo. Assessments included bowel movement
count, time of bowel movement, straining, sense of complete evacuation, Bristol Stool Form Scales,
and quality of life. Within 4 hours of first dose, 34.2% of patients in both methylnaltrexone groups
had rescue-free bowel movements (RFBMs) versus 9.9% on placebo (P < .001). The estimated number
needed to treat was about 4. On average, 28.9% of methylnaltrexone QD and 30.2% of methylnaltrex-
one alternate-day dosing resulted in RFBMs within 4 hours versus 9.4% QD and 9.3% alternate-day
placebo injections (both P < .001). Both methylnaltrexone groups had significantly shorter time to first
RFBM (P < .001) and greater increase in number of weekly RFBMs (P < .05) versus placebo. Adverse
events included abdominal pain, diarrhea, nausea, and hyperhidrosis. Bristol Stool Form Scale scores
(P = .002) and sensation of complete evacuation (P < .04) were significantly superior with methylnal-
trexone QD; both methylnaltrexone groups reported no or mild straining during RFBMs in the first 2
weeks (P < .02). At 4 weeks, a significantly greater improvement in patient-reported, constipation-
specific quality of life was seen in the alternate-day dosing (P < .05) and QD (P < .001) groups.
Perspective: We present data demonstrating that subcutaneous methylnaltrexone 12 mg given
once daily (QD) or every other day provides significant relief of OIC and was generally well tolerated
in patients with chronic, nonmalignant pain. These results expand on prior effectiveness observed for
the treatment of OIC in advanced illness patients to a broader population.
ª 2011 by the American Pain Society
Key words: Methylnaltrexone, palliative care, constipation, abdominal pain, opioids, mu-opioid
receptor antagonist, opioid-related disorders, chronic disease.
May 11, 2010; Revised September 2, 2010; Accepted November
arch was funded by Wyeth Research, which was acquired byc in October 2009. Pfizer Inc provided funding for writingprovided by On Assignment Clinical Research, a paid consultantin connection with the development of this manuscript, and forsupport, provided by Peloton Advantage, LLC. Drs. Schulman,andazzo, and Iyer, Mr. Tzanis, and Ms. Manley are employeesInc. At the time of this study, they were employees of and
ders in Wyeth.r received an honorarium or other form of financial support
o the development of this manuscript.reprint requests to Edward Michna, MD, Brigham and Women’s75 Francis Street, Department of Anesthesia, Boston,MA [email protected]
0/$36.00
y the American Pain Society
16/j.jpain.2010.11.008
Opioid analgesics are increasingly used to treatchronic, nonmalignant pain in patients witha wide variety of conditions.8 While the long-
term utility of opioids for pain management in thesepatients has been questioned, Noble et al15 recently ex-amined 17 studies of long-term (6- to 48-week) opioiduse in patients with chronic, noncancer-related painand found that pain scores improved in patients remain-ing on treatment for at least 6 months. However, a sub-stantial number of patients withdrew prior to 6 monthsbecause of adverse events. Analysis of these adverseevents revealed that 32.5% of patients taking oralopioids and 17.5% of those using transdermal opioids

Michna et al The Journal of Pain 555
withdrew from the study, with opioid-induced constipa-tion (OIC) among the most common side effects leadingto discontinuation.15
Constipation commonly occurs with the use of opi-oids.21 Unlike other opioid-induced gastrointestinal (GI)side effects (eg, nausea or vomiting), wherein tolerancemay develop and symptoms abate with continued use,constipation typically persists throughout treatment.13
Information from the 2004 National Health andWellnessSurvey performed in the United States, United Kingdom,France, and Germany demonstrated that during long-term opioid use, patients with OIC experience signifi-cantly more missed time from work, greater work andnonwork-related activity impairment, and greaterhealth care resource utilization compared with patientswithout OIC (P < .05 for all comparisons).1 Additionally,patients with OIC were noted to have significantly lowerhealth-related quality of life (HRQOL) scores, indicatinggreater impairment, as measured by both the physicaland mental component of the Short Form-8 HealthSurvey24 questionnaire, compared with those withoutOIC (P < .05 for both comparisons).1
When opioids are prescribed over the long term,prophylactic measures used in an attempt to preventOIC may include increasing fluid intake, increasing phys-ical activity, and establishing a daily toileting schedule.17
Unfortunately, these interventions only provide limitedbenefit in OIC,17 especially in patients who requireincreasing opioid doses. Despite their frequent use, laxa-tive treatments for OIC are unpredictable and are associ-ated with side effects, such as bloating, increased gasproduction, and abdominal cramping.16 A survey of pa-tients receiving opioid therapy for noncancer-relatedpain found that only 46% of those requiring laxativesfor constipation achieved the desired results more than50% of the time compared with 84% of those withchronic noncancer-related pain not treated with opi-oids.16 This finding is not unexpected given that laxativesdo not address the underlying mechanism of OIC.Opioid receptors have a wide distribution throughout
the GI tract and the central nervous system (CNS).11
While a centrally mediated effect of opioids has beenpostulated for the development of OIC, its predominantmechanism is thought to be peripherally mediated.27
Opioid receptor agonists in the GI tract cause slowedbowel motility by decreasing effective peristaltic con-tractions and increasing sphincter tone. Additionally,opioids may also delay GI transit by reducing gut secre-tions and increasing the absorption of fluids from thegut,10 thus providing a mechanism by which constipa-tion could manifest.Methylnaltrexone (Relistor; Pfizer Inc, Philadelphia,
PA, and Progenics Pharmaceuticals, Tarrytown, NY), a se-lective, peripherally acting mu-opioid receptor antago-nist available as a subcutaneous injection, is approvedfor the treatment of OIC in patients with advanced ill-ness receiving palliative care whose response to laxativetherapy has not been sufficient.18,25 Owing to its highpolarity and low lipid solubility, methylnaltrexone hasrestricted ability to cross the blood-brain barrier28;thus methylnaltrexone decreases the constipating
effects of opioids without affecting centrally mediatedanalgesia.26
Studies have shown that methylnaltrexone decreasesthe adverse effects of opioids on the GI tract, includingdelayed gastric emptying14 and delayed oral-cecal transittime.30,32,33 Methylnaltrexone has demonstrated theability to induce laxation in methadone maintenancepatients with OIC.29,31 Additionally, methylnaltrexonehas demonstrated efficacy and safety in the treatment ofOIC in advanced-illness patients, the majority of whomhad cancer-relatedpain forwhich theywere receivingopi-oids.19,22 This study is the first to assess the effectivenessand safety of subcutaneous methylnaltrexone for thetreatment of OIC in patients with chronic, nonmalignantpain.Results from this study were presented in poster for-
mat at the 28th and 29th Annual Scientific Meetings ofthe American Pain Society, May 7-9, 2009 in San Diego,CA, and May 6-8, 2010, in Baltimore, MD, respectively,and at the International Society of Pharmacoeconomicsand Outcomes Research 12th Annual European Con-gress, October 24-27, 2010, in Paris, France.2,5,7
Methods
PatientsAdults (aged 18 years and older) with OIC and chronic
pain caused by a nonmalignant condition were screenedto participate in this study. After providing informed con-sent, patients entered a 14-day screening period. Eligiblepatients had fewer than 3 rescue-free bowel movements(RFBMs; bowelmovement[s] occurringwithout theuseofany laxative in the prior 24 hours) per week that wereassociated with 1 or more of the following signs andsymptoms: hard or lumpy stools, straining during bowelmovements, or a sensation of incomplete evacuationafter a bowel movement. All patients had a history ofchronic pain lasting at least 2 months prior to study en-rollment and were taking opioid medications for at least1 month, with an average daily dose greater than 50-mgoral morphine equivalents for at least 2 weeks. Patientswere excluded from the study if they had a history ofinflammatory bowel disease within the prior 6 months,evidence of bowel obstruction or impaction, history ofrectal bleeding not due to hemorrhoids or fissures,history of malignancy within the previous 5 years, or ahistory of chronic constipation before starting opioidtherapy. Patients were also excluded if they had a historyof alcohol or drug abuse within the year prior to enroll-ing, if they were pregnant or breastfeeding, or if theyhadpreviously received subcutaneousmethylnaltrexone.The study was approved by independent ethics
committees at each participating institution and wasconducted in accordance with the International Confer-ence on Harmonisation Guideline for Good ClinicalPractice and the Declaration of Helsinki.
Study DesignThis multicenter, double-blind, randomized, placebo-
controlled phase 3 study was conducted from August

556 The Journal of Pain Methylnaltrexone for Opioid-Induced Constipation
2007 to November 2008. Eligible patients were randomlyassigned via a computer-generated randomizationschedule in a 1:1:1 ratio to receive subcutaneous methyl-naltrexone 12mg once daily (QD dosing group), subcuta-neous methylnaltrexone 12 mg once every other day(alternate-day dosing group), or subcutaneous placebofor 4 weeks. Allocation assignments were provided on-line to investigators. Each site’s randomization assign-ments were distributed in blocks of 6 to mitigate therisk that investigatorswould be able to predict a patient’sdosing regimen. Methylnaltrexone and placebo wereprovided in identically appearing vials. All patients, localtrial personnel, and the sponsor’s Study Team wereblinded to treatment allocation. Since all patients re-ceived 1 injection daily, patients in the methylnaltrexonealternate-day dosing group received placebo on dayswhen active treatment was not administered. Patientsreceived study treatment for 4 weeks, after which theywere eligible to enter an 8-week open-label as-neededdosing phase, with a subsequent 14-day follow-up pe-riod after active treatment was completed. Patients dis-continued all laxatives taken prior to study enrollment.Rescue laxatives were permitted during the study if thepatient had no bowel movement for 3 consecutivedays, atwhich point bisacodyl tablets (1 dose, up to 4 tab-lets orally) were provided by the study sponsors. Nomorethan 1 dose of a rescue laxative was permitted withina 24-hour period and, when used, was administered atleast 4 hours after any dose of study drug.
EvaluationsThe coprimary efficacy end points were the proportion
of patients having a RFBM within 4 hours of the firstdose, and the percentage of active injections per patientresulting in a RFBM within 4 hours. Secondary efficacyend points included time to first RFBM after injection,change in weekly number of RFBMs, and improvementsin Bristol Stool Form Scale scores, straining, and com-pleteness of evacuation. Efficacy was measured usingdaily patient diary information, including number andtime of bowel movements, the Bristol Stool Form Scale,9
Straining Scale (assessed as 0 [none] to 4 [very severe]),Sense of Complete Evacuation Scale (assessed as either0 [no] or 1 [yes]), and use of rescue laxatives. Pain inten-sity scores and either subjective or objective evidenceof opioid withdrawal (Subjective Opiate WithdrawalScale [SOWS] and Objective Opiate Withdrawal Scale[OOWS]) were also assessed. Patient-reported constipa-tion-specific quality of life was assessed at baseline, day14, and day 28 using the Patient Assessment of Constipa-tion–Qualify of Life (PAC-QOL) questionnaire.12
Statistical AnalysisThe efficacy analysis included all patients who received
at least 1 dose of study drug (modified intent-to-treat[mITT] population). The overall familywise Type I errorratewas controlledat level .05usingafixed-sequence test-ing approach. Three comparisons for the 2 coprimary endpointswereperformedsequentially. Thecombinedmethyl-naltrexone QD and alternate-day dosing groups were
compared with placebo using a 2-sided chi-square testfor the first coprimary end point. If the P value was lessthan5%, thenmethylnaltrexoneQDgroupwas tobecom-pared with placebo using a 2-sided t test for the secondcoprimary end point. If that P value was less than 5%, themethylnaltrexone alternate-day dosing group was com-pared with placebo for the second coprimary end point.For the secondary efficacy end point of time to first
RFBM after injection, the combined methylnaltrexoneQD/alternate-day dosing groups were compared withplacebo using a 2-sided log-rank test. Change in weeklynumber of RFBMs from baseline between themethylnal-trexone QD and placebo groups and between the meth-ylnaltrexone alternate-day dosing group and placebogroups was compared using an analysis of covariance(ANCOVA)model with treatment as a factor and baselineweekly number of RFBMs as a covariate. Pain intensity,SOWS, OOWS, and constipation-specific quality of lifescores were compared between treatment and placebogroups using ANCOVA, with treatment as a factor andbaseline value of the measurements as a covariate.A sample size of 157 patients for each treatment group
was calculated basedon the coprimary endpoints. A sam-ple size of 314 patients in the combined methylnaltrex-one treatment groups and 157 patients in the placebogroup was estimated to have a statistical power of 95%todetect a treatmentdifferenceof15%in theproportionof patients having a RFBM within 4 hours after the firstdose, based on a 2-sided chi-square testwith a .05 2-sidedsignificance level. This sample size would also have 95%power to detect amean difference of 15%of active injec-tions resulting in any RFBMwithin 4 hours of dose admin-istration, based on a 2-sided t test at the a level of .05,assuming a 33% common standard deviation.
Results
PatientsOf1,037 patientswhowere screened, 469met the inclu-
sion criteria and were randomized to double-blind treat-ment groups. Of these, 460 patients received at least 1dose of study drug (Fig 1). These patients were includedin the mITT and safety populations, with 150 receivingmethylnaltrexoneQD, 148 receivingmethylnaltrexoneev-ery other day, and 162 receiving placebo QD. Of the 568patients screened but not randomized to the study,38.2%were ineligiblebecause they failed tomeet the con-stipation criteria of 2 or fewer RFBMs perweek,while 15.7and 10.4% of this group failed to comply with diary com-pletionor rescue laxativeusage, respectively.Nomajordif-ferences existed between the treatment and placebogroups in baseline demographics or clinical characteristics(Table 1). Back pain was the most common condition forwhich opioid therapy was prescribed, occurring in 278(60.4%) patients in the study population. Three hundredeighty-eight patients completed the double-blind phase.
EfficacyIn the combined group who received methylnaltrex-
one, 34.2% of patients achieved a RFBM within 4 hours

Figure 1. Disposition of patients in the modified intent-to-treat population. mITT, modified intent-to-treat.
Michna et al The Journal of Pain 557
of the first dose of study medication compared with9.9% of the placebo group (P < .001; number neededto treat [NNT] z 4). When the 2 methylnaltrexonegroups were assessed separately, the differences com-pared with placebo remained significant. In the methyl-naltrexone QD group, 33.3% of patients had a RFBMwithin 4 hours of the first dose administered (P < .001versus placebo), while those in the methylnaltrexonealternate-day dosing group had a similar response(35.1%; P < .001 versus placebo).The second coprimary end point evaluated the per-
centage of active injections per patient resulting ina RFBM within 4 hours of dose. An average of 28.9% ofmethylnaltrexone QD injections resulted in a RFBMwithin 4 hours compared with 9.4% with placebo(P < .001). In the methylnaltrexone alternate-day group,30.2% of active study drug injections resulted in a RFBM(P < .001 versus placebo), while 9.3% of injections wereeffective on alternating days when placebo wasadministered.The time to first bowel movement was significantly
shorter among patients receiving methylnaltrexone QDor every other day compared with those receiving pla-cebo (P < .001) (Fig 2). Among patients in the combinedmethylnaltrexone treatment groups, 46% had a RFBMwithin 24 hours, whereas 25.3% of those receivingplacebo had a response within 24 hours.Patients in the methylnaltrexone treatment groups
experienced a significantly increased number ofweekly RFBMs compared with the placebo group. Theadjusted mean change from baseline in the numberof weekly RFBMs was 3.1 in the methylnaltrexone QDgroup (P < .001 versus placebo) and 2.1 in the methyl-naltrexone alternate-day dosing group (P = .01 versusplacebo) compared with 1.5 in the placebo group
(Fig 3). The increase in weekly RFBMs with active treat-ment was significant with methylnaltrexone QD versusplacebo in each of the 4 weeks of the double-blindperiod (P < .001 for all) and at weeks 1 and 3 (P < .01for each week) in those receiving methylnaltrexone ev-ery other day. Significantly more patients receivingdaily methylnaltrexone had at least 3 RFBMs perweek over the entire double-blind phase and duringeach respective week compared with placebo (P < .01for all comparisons) and at weeks 1 through 3 in thosetaking methylnaltrexone every other day (P < .05).Overall, 58.7% of patients in the methylnaltrexoneQD group, 45.3% in the alternate-day dosing group,and 38.3% in the placebo group had at least 3 RFBMsper week during the double-blind period (NNT z 5for methylnaltrexone QD; NNT z 14 for methylnaltrex-one alternate-day dosing).Additional secondary efficacy end points included
assessments of straining, completeness of evacuation,and Bristol Stool Form Scale scores with RFBMs. Com-pared with patients receiving placebo, either regimenof methylnaltrexone treatment provided a changefrom baseline in the percentage of RFBMs with strainingrated as ‘‘none’’ or ‘‘mild’’ that was significantly differentduring the first 2 weeks of treatment (Week 1: 28.1%,28.5% versus 14.0%; Week 2: 26.9%, 26.8%, versus15.2% for methylnaltrexone QD, alternate-day dosing,and placebo groups, respectively; P < .02) and at week3 in those receiving methylnaltrexone QD (29.0% versus14.4%; P = .002). Additionally, the change from baselinein the percentage of RFBMswith a sensation of completeevacuation was significant in patients receiving methyl-naltrexone QD (27.4% versus 19.9%; P < .04), as were im-provements from baseline in average Bristol Stool FormScale scores of RFBMs (1.4 versus .9; P = .002) over the
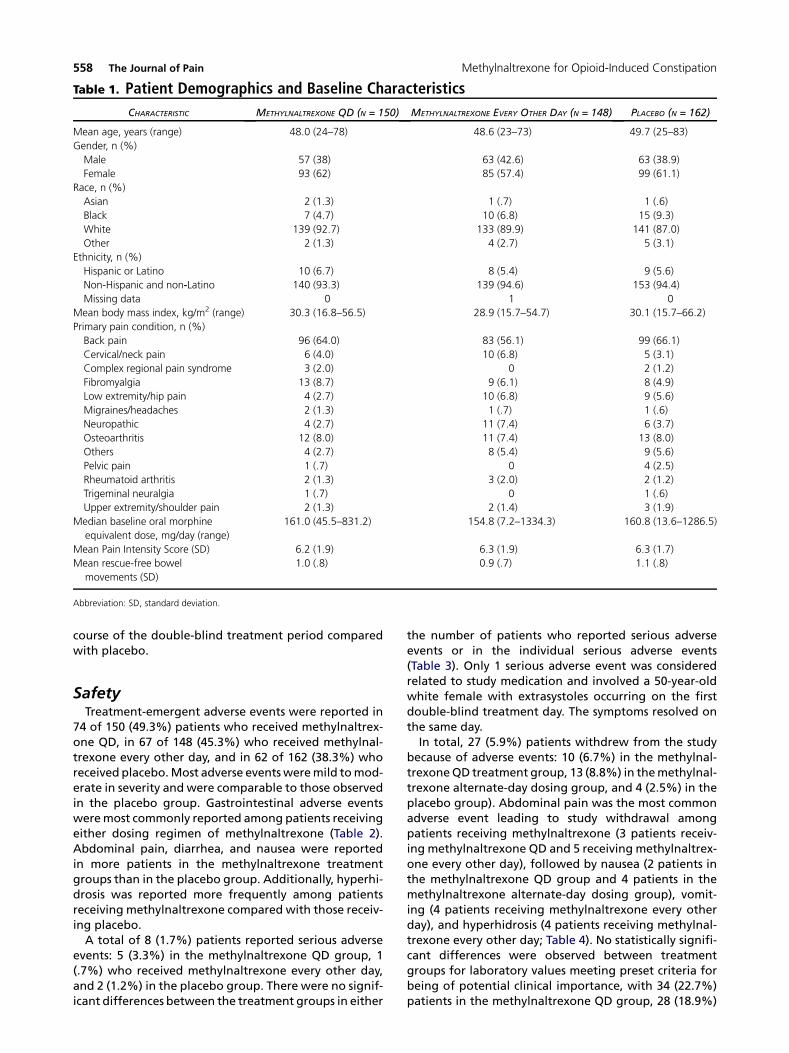
Table 1. Patient Demographics and Baseline Characteristics
CHARACTERISTIC METHYLNALTREXONE QD (N = 150) METHYLNALTREXONE EVERY OTHER DAY (N = 148) PLACEBO (N = 162)
Mean age, years (range) 48.0 (24–78) 48.6 (23–73) 49.7 (25–83)
Gender, n (%)
Male 57 (38) 63 (42.6) 63 (38.9)
Female 93 (62) 85 (57.4) 99 (61.1)
Race, n (%)
Asian 2 (1.3) 1 (.7) 1 (.6)
Black 7 (4.7) 10 (6.8) 15 (9.3)
White 139 (92.7) 133 (89.9) 141 (87.0)
Other 2 (1.3) 4 (2.7) 5 (3.1)
Ethnicity, n (%)
Hispanic or Latino 10 (6.7) 8 (5.4) 9 (5.6)
Non-Hispanic and non‑Latino 140 (93.3) 139 (94.6) 153 (94.4)
Missing data 0 1 0
Mean body mass index, kg/m2 (range) 30.3 (16.8–56.5) 28.9 (15.7–54.7) 30.1 (15.7–66.2)
Primary pain condition, n (%)
Back pain 96 (64.0) 83 (56.1) 99 (66.1)
Cervical/neck pain 6 (4.0) 10 (6.8) 5 (3.1)
Complex regional pain syndrome 3 (2.0) 0 2 (1.2)
Fibromyalgia 13 (8.7) 9 (6.1) 8 (4.9)
Low extremity/hip pain 4 (2.7) 10 (6.8) 9 (5.6)
Migraines/headaches 2 (1.3) 1 (.7) 1 (.6)
Neuropathic 4 (2.7) 11 (7.4) 6 (3.7)
Osteoarthritis 12 (8.0) 11 (7.4) 13 (8.0)
Others 4 (2.7) 8 (5.4) 9 (5.6)
Pelvic pain 1 (.7) 0 4 (2.5)
Rheumatoid arthritis 2 (1.3) 3 (2.0) 2 (1.2)
Trigeminal neuralgia 1 (.7) 0 1 (.6)
Upper extremity/shoulder pain 2 (1.3) 2 (1.4) 3 (1.9)
Median baseline oral morphine
equivalent dose, mg/day (range)
161.0 (45.5–831.2) 154.8 (7.2–1334.3) 160.8 (13.6–1286.5)
Mean Pain Intensity Score (SD) 6.2 (1.9) 6.3 (1.9) 6.3 (1.7)
Mean rescue-free bowel
movements (SD)
1.0 (.8) 0.9 (.7) 1.1 (.8)
Abbreviation: SD, standard deviation.
558 The Journal of Pain Methylnaltrexone for Opioid-Induced Constipation
course of the double-blind treatment period comparedwith placebo.
SafetyTreatment-emergent adverse events were reported in
74 of 150 (49.3%) patients who received methylnaltrex-one QD, in 67 of 148 (45.3%) who received methylnal-trexone every other day, and in 62 of 162 (38.3%) whoreceived placebo.Most adverse eventsweremild tomod-erate in severity and were comparable to those observedin the placebo group. Gastrointestinal adverse eventsweremost commonly reported among patients receivingeither dosing regimen of methylnaltrexone (Table 2).Abdominal pain, diarrhea, and nausea were reportedin more patients in the methylnaltrexone treatmentgroups than in the placebo group. Additionally, hyperhi-drosis was reported more frequently among patientsreceiving methylnaltrexone compared with those receiv-ing placebo.A total of 8 (1.7%) patients reported serious adverse
events: 5 (3.3%) in the methylnaltrexone QD group, 1(.7%) who received methylnaltrexone every other day,and 2 (1.2%) in the placebo group. There were no signif-icant differences between the treatment groups in either
the number of patients who reported serious adverseevents or in the individual serious adverse events(Table 3). Only 1 serious adverse event was consideredrelated to study medication and involved a 50-year-oldwhite female with extrasystoles occurring on the firstdouble-blind treatment day. The symptoms resolved onthe same day.In total, 27 (5.9%) patients withdrew from the study
because of adverse events: 10 (6.7%) in the methylnal-trexoneQD treatment group, 13 (8.8%) in themethylnal-trexone alternate-day dosing group, and 4 (2.5%) in theplacebo group). Abdominal pain was the most commonadverse event leading to study withdrawal amongpatients receiving methylnaltrexone (3 patients receiv-ing methylnaltrexone QD and 5 receiving methylnaltrex-one every other day), followed by nausea (2 patients inthe methylnaltrexone QD group and 4 patients in themethylnaltrexone alternate-day dosing group), vomit-ing (4 patients receiving methylnaltrexone every otherday), and hyperhidrosis (4 patients receiving methylnal-trexone every other day; Table 4). No statistically signifi-cant differences were observed between treatmentgroups for laboratory values meeting preset criteria forbeing of potential clinical importance, with 34 (22.7%)patients in the methylnaltrexone QD group, 28 (18.9%)
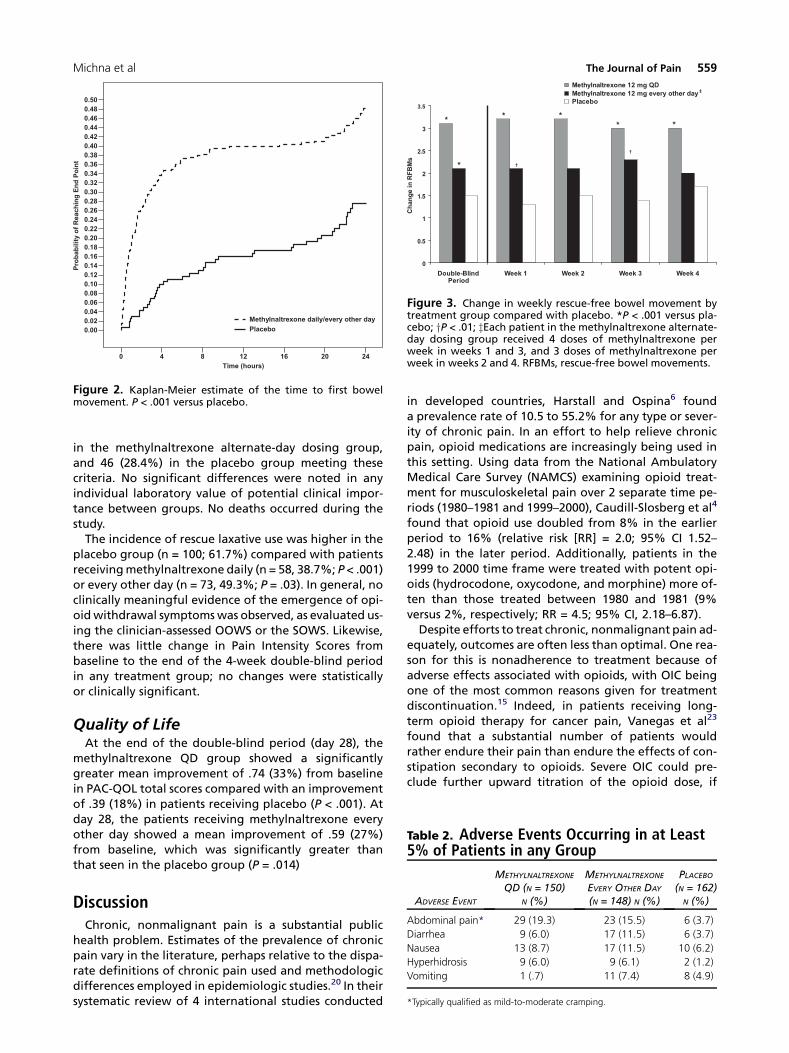
Figure 2. Kaplan-Meier estimate of the time to first bowelmovement. P < .001 versus placebo.
Figure 3. Change in weekly rescue-free bowel movement bytreatment group compared with placebo. *P < .001 versus pla-cebo; yP < .01; zEach patient in the methylnaltrexone alternate-day dosing group received 4 doses of methylnaltrexone perweek in weeks 1 and 3, and 3 doses of methylnaltrexone perweek in weeks 2 and 4. RFBMs, rescue-free bowel movements.
Table 2. Adverse Events Occurring in at Least5% of Patients in any Group
Michna et al The Journal of Pain 559
in the methylnaltrexone alternate-day dosing group,and 46 (28.4%) in the placebo group meeting thesecriteria. No significant differences were noted in anyindividual laboratory value of potential clinical impor-tance between groups. No deaths occurred during thestudy.The incidence of rescue laxative use was higher in the
placebo group (n = 100; 61.7%) compared with patientsreceivingmethylnaltrexone daily (n = 58, 38.7%; P < .001)or every other day (n = 73, 49.3%; P = .03). In general, noclinically meaningful evidence of the emergence of opi-oidwithdrawal symptomswas observed, as evaluated us-ing the clinician-assessed OOWS or the SOWS. Likewise,there was little change in Pain Intensity Scores frombaseline to the end of the 4-week double-blind periodin any treatment group; no changes were statisticallyor clinically significant.
Quality of LifeAt the end of the double-blind period (day 28), the
methylnaltrexone QD group showed a significantlygreater mean improvement of .74 (33%) from baselinein PAC-QOL total scores compared with an improvementof .39 (18%) in patients receiving placebo (P < .001). Atday 28, the patients receiving methylnaltrexone everyother day showed a mean improvement of .59 (27%)from baseline, which was significantly greater thanthat seen in the placebo group (P = .014)
ADVERSE EVENT
METHYLNALTREXONE
QD (N = 150)N (%)
METHYLNALTREXONE
EVERY OTHER DAY
(N = 148) N (%)
PLACEBO(N = 162)
N (%)
Abdominal pain* 29 (19.3) 23 (15.5) 6 (3.7)
Diarrhea 9 (6.0) 17 (11.5) 6 (3.7)
Nausea 13 (8.7) 17 (11.5) 10 (6.2)
Hyperhidrosis 9 (6.0) 9 (6.1) 2 (1.2)
Vomiting 1 (.7) 11 (7.4) 8 (4.9)
*Typically qualified as mild-to-moderate cramping.
DiscussionChronic, nonmalignant pain is a substantial public
health problem. Estimates of the prevalence of chronicpain vary in the literature, perhaps relative to the dispa-rate definitions of chronic pain used and methodologicdifferences employed in epidemiologic studies.20 In theirsystematic review of 4 international studies conducted
in developed countries, Harstall and Ospina6 founda prevalence rate of 10.5 to 55.2% for any type or sever-ity of chronic pain. In an effort to help relieve chronicpain, opioid medications are increasingly being used inthis setting. Using data from the National AmbulatoryMedical Care Survey (NAMCS) examining opioid treat-ment for musculoskeletal pain over 2 separate time pe-riods (1980–1981 and 1999–2000), Caudill-Slosberg et al4
found that opioid use doubled from 8% in the earlierperiod to 16% (relative risk [RR] = 2.0; 95% CI 1.52–2.48) in the later period. Additionally, patients in the1999 to 2000 time frame were treated with potent opi-oids (hydrocodone, oxycodone, and morphine) more of-ten than those treated between 1980 and 1981 (9%versus 2%, respectively; RR = 4.5; 95% CI, 2.18–6.87).Despite efforts to treat chronic, nonmalignant pain ad-
equately, outcomes are often less than optimal. One rea-son for this is nonadherence to treatment because ofadverse effects associated with opioids, with OIC beingone of the most common reasons given for treatmentdiscontinuation.15 Indeed, in patients receiving long-term opioid therapy for cancer pain, Vanegas et al23
found that a substantial number of patients wouldrather endure their pain than endure the effects of con-stipation secondary to opioids. Severe OIC could pre-clude further upward titration of the opioid dose, if
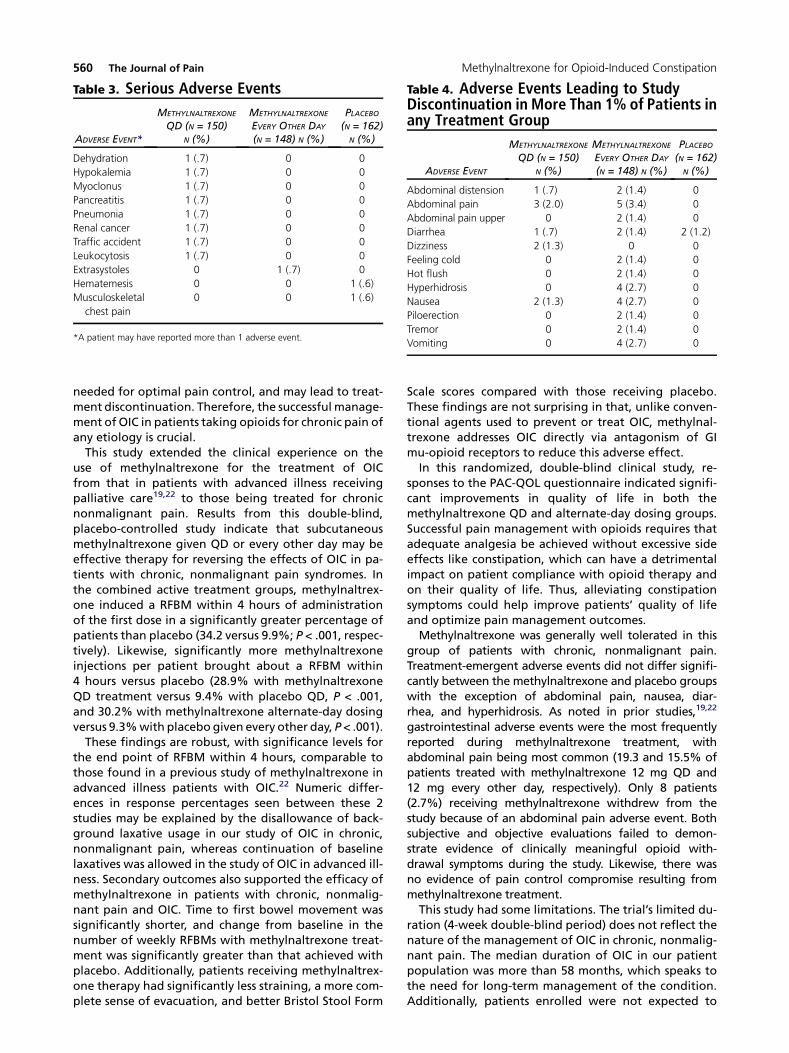
Table 4. Adverse Events Leading to StudyDiscontinuation in More Than 1% of Patients inany Treatment Group
ADVERSE EVENT
METHYLNALTREXONE
QD (N = 150)N (%)
METHYLNALTREXONE
EVERY OTHER DAY
(N = 148) N (%)
PLACEBO(N = 162)
N (%)
Abdominal distension 1 (.7) 2 (1.4) 0
Abdominal pain 3 (2.0) 5 (3.4) 0
Abdominal pain upper 0 2 (1.4) 0
Diarrhea 1 (.7) 2 (1.4) 2 (1.2)
Dizziness 2 (1.3) 0 0
Feeling cold 0 2 (1.4) 0
Hot flush 0 2 (1.4) 0
Hyperhidrosis 0 4 (2.7) 0
Nausea 2 (1.3) 4 (2.7) 0
Piloerection 0 2 (1.4) 0
Tremor 0 2 (1.4) 0
Vomiting 0 4 (2.7) 0
Table 3. Serious Adverse Events
ADVERSE EVENT*
METHYLNALTREXONE
QD (N = 150)N (%)
METHYLNALTREXONE
EVERY OTHER DAY
(N = 148) N (%)
PLACEBO(N = 162)
N (%)
Dehydration 1 (.7) 0 0
Hypokalemia 1 (.7) 0 0
Myoclonus 1 (.7) 0 0
Pancreatitis 1 (.7) 0 0
Pneumonia 1 (.7) 0 0
Renal cancer 1 (.7) 0 0
Traffic accident 1 (.7) 0 0
Leukocytosis 1 (.7) 0 0
Extrasystoles 0 1 (.7) 0
Hematemesis 0 0 1 (.6)
Musculoskeletal
chest pain
0 0 1 (.6)
*A patient may have reported more than 1 adverse event.
560 The Journal of Pain Methylnaltrexone for Opioid-Induced Constipation
needed for optimal pain control, and may lead to treat-ment discontinuation. Therefore, the successful manage-ment of OIC in patients taking opioids for chronic pain ofany etiology is crucial.This study extended the clinical experience on the
use of methylnaltrexone for the treatment of OICfrom that in patients with advanced illness receivingpalliative care19,22 to those being treated for chronicnonmalignant pain. Results from this double-blind,placebo-controlled study indicate that subcutaneousmethylnaltrexone given QD or every other day may beeffective therapy for reversing the effects of OIC in pa-tients with chronic, nonmalignant pain syndromes. Inthe combined active treatment groups, methylnaltrex-one induced a RFBM within 4 hours of administrationof the first dose in a significantly greater percentage ofpatients than placebo (34.2 versus 9.9%; P < .001, respec-tively). Likewise, significantly more methylnaltrexoneinjections per patient brought about a RFBM within4 hours versus placebo (28.9% with methylnaltrexoneQD treatment versus 9.4% with placebo QD, P < .001,and 30.2% with methylnaltrexone alternate-day dosingversus 9.3%with placebo given every other day, P< .001).These findings are robust, with significance levels for
the end point of RFBM within 4 hours, comparable tothose found in a previous study of methylnaltrexone inadvanced illness patients with OIC.22 Numeric differ-ences in response percentages seen between these 2studies may be explained by the disallowance of back-ground laxative usage in our study of OIC in chronic,nonmalignant pain, whereas continuation of baselinelaxatives was allowed in the study of OIC in advanced ill-ness. Secondary outcomes also supported the efficacy ofmethylnaltrexone in patients with chronic, nonmalig-nant pain and OIC. Time to first bowel movement wassignificantly shorter, and change from baseline in thenumber of weekly RFBMs with methylnaltrexone treat-ment was significantly greater than that achieved withplacebo. Additionally, patients receiving methylnaltrex-one therapy had significantly less straining, a more com-plete sense of evacuation, and better Bristol Stool Form
Scale scores compared with those receiving placebo.These findings are not surprising in that, unlike conven-tional agents used to prevent or treat OIC, methylnal-trexone addresses OIC directly via antagonism of GImu-opioid receptors to reduce this adverse effect.In this randomized, double-blind clinical study, re-
sponses to the PAC-QOL questionnaire indicated signifi-cant improvements in quality of life in both themethylnaltrexone QD and alternate-day dosing groups.Successful pain management with opioids requires thatadequate analgesia be achieved without excessive sideeffects like constipation, which can have a detrimentalimpact on patient compliance with opioid therapy andon their quality of life. Thus, alleviating constipationsymptoms could help improve patients’ quality of lifeand optimize pain management outcomes.Methylnaltrexone was generally well tolerated in this
group of patients with chronic, nonmalignant pain.Treatment-emergent adverse events did not differ signifi-cantly between the methylnaltrexone and placebo groupswith the exception of abdominal pain, nausea, diar-rhea, and hyperhidrosis. As noted in prior studies,19,22
gastrointestinal adverse events were the most frequentlyreported during methylnaltrexone treatment, withabdominal pain being most common (19.3 and 15.5% ofpatients treated with methylnaltrexone 12 mg QD and12 mg every other day, respectively). Only 8 patients(2.7%) receiving methylnaltrexone withdrew from thestudy because of an abdominal pain adverse event. Bothsubjective and objective evaluations failed to demon-strate evidence of clinically meaningful opioid with-drawal symptoms during the study. Likewise, there wasno evidence of pain control compromise resulting frommethylnaltrexone treatment.This study had some limitations. The trial’s limited du-
ration (4-week double-blind period) does not reflect thenature of the management of OIC in chronic, nonmalig-nant pain. The median duration of OIC in our patientpopulation was more than 58 months, which speaks tothe need for long-term management of the condition.Additionally, patients enrolled were not expected to

Michna et al The Journal of Pain 561
require further titration of their opioid dosage; however,in clinical practice, exacerbations of painmay necessitateupward opioid titration. An 8-week open-label phase ofthe trial was designed to further assess durability ofresponse found in the acute double-blind study. Theseresults have been reported separately, with similar effi-cacy findings for treatment of OIC as were found in theacute-phase trial.3 The use of face-value measures ofsubjective effects, such as constipation outcomes, painintensity scores, and opioid withdrawal, is another limi-tation. In addition, the population studied was limitedto North American participants. This trial also showedthe use of subcutaneous methylnaltrexone in the man-agement of OIC, specifically in the setting of chronic,nonmalignant pain patients. Additional research to in-vestigate the use of methylnaltrexone in other settingsin which OIC is a significant clinical problem, such asacute or subacute use of high-dose opioids, would beuseful.Clinicians continually strive to provide adequate pain
relief for their patients with chronic, nonmalignantpain, and many patients will be prescribed opioidanalgesia. As constipation appears to be an almostunavoidable side effect of this therapy, and given the
negative impact that constipation can have on patientoutcomes, clinicians should have a tool in their arma-mentarium that can reduce the morbidity related toOIC. In that regard, methylnaltrexone may represent aneffective therapeutic option for patients with chronic,nonmalignant pain and OIC. An oral formulation ofmethylnaltrexone is currently under investigation for thetreatment of OIC. If evidence dictates that oral methyl-naltrexone is safe and effective for OIC managementand regulatory approval is obtained, the oral formula-tionmay provide potential advantages over the subcuta-neous formulation, including a less invasive route ofadministration leading to increasedpatient acceptability.
AcknowledgmentsThe authors thank Cheryl Jones of On Assignment
Clinical Research, a paid consultant to Pfizer in connec-tion with the development of this manuscript, for writ-ing support, and John H. Simmons, MD, of PelotonAdvantage for editorial support, which was funded byPfizer Inc. This manuscript is presented in memory ofDr. Richard Blonsky.
References
1. Bell T, Annunziata K, Leslie JB: Opioid-induced constipa-tion negatively impacts pain management, productivity,and health-related quality of life: Findings from theNational Health and Wellness Survey. J Opioid Manag 5:137-144, 2009
2. Blonsky ER, Michna E, Schulman S, Tzanis E, Manley A,Zhang H, Randazzo B: Subcutaneous methylnaltrexone forthe treatment of opioid-induced constipation in patientswith chronic non-malignant pain [abstract]. Presented atthe 28th Annual Scientific Meeting of the American PainSociety, San Diego, CA, May 7-9, 2009
3. Blonsky ER, Watier A, Schulman S, Tzanis E, Manley A,Zhang H, Randazzo B: Subcutaneous methylnaltrexone forthe treatment of opioid-induced constipation in patientswith chronic non-malignant pain: Open-label results[abstract]. Presented at the 28th Annual ESRA Congress,Salzburg, Austria, September 9-12, 2009
4. Caudill-Slosberg MA, Schwartz LM, Woloshin S: Officevisits and analgesic prescriptions for musculoskeletal painin US: 1980 vs. 2000. Pain 109:514-519, 2004
5. Duerden M, Weil A, Yu D, Schulman S, Tzanis E, Zhang H,Manley A, Randazzo B: Subcutaneous methylnaltrexone forthe treatment of opioid-induced constipation in patientswith chronic, nonmalignant pain: Safety results in patientstreated for 12 weeks [abstract]. Presented at the 29thAnnual Scientific Meeting of the American Pain Society,Baltimore, MD, May 6-8, 2010
6. Harstall C, Ospina M: How prevalent is chronic pain? PainClin Update 11:1-4, 2003
7. Iyer S, Randazzo B, Tzanis E, Schulman S, Zhang H,Wang W, Manley A: Effect of subcutaneous (SC) methylnal-trexone on patient reported constipation specific quality of
life in a randomized double blind clinical trial [abstract].Value in Health 12:A349, 2009
8. Kalso E, Edwards JE, Moore RA, McQuay HJ: Opioids inchronic non-cancer pain: Systematic review of efficacy andsafety. Pain 112:372-380, 2004
9. Lewis SJ, Heaton KW: Stool form scale as a useful guideto intestinal transit time. Scand J Gastroenterol 32:920-924,1997
10. Loeser JD, Butler SH, Chapman CR, Turk DC (eds): Boni-ca’s Management of Pain, 3rd ed. Philadelphia, PA, Lippin-cott Williams & Wilkins, 2001
11. Manara L, Bianchetti A: The central and peripheral influ-ences of opioids on gastrointestinal propulsion. Annu RevPharmacol Toxicol 25:249-273, 1985
12. Marquis P, De La LC, Dubois D, McDermott A,Chassany O: Development and validation of the Patient As-sessment of Constipation Quality of Life questionnaire.Scand J Gastroenterol 40:540-551, 2005
13. McNicol E, Horowicz-Mehler N, Fisk RA, Bennett K,Gialeli-Goudas M, Chew PW, Lau J, Carr D: Manage-ment of opioid side effects in cancer-related andchronic noncancer pain: A systematic review. J Pain 4:231-256, 2003
14. Murphy DB, Sutton JA, Prescott LF, Murphy MB: Opioid-induced delay in gastric emptying: A peripheral mechanismin humans. Anesthesiology 87:765-770, 1997
15. Noble M, Tregear SJ, Treadwell JR, Schoelles K: Long-term opioid therapy for chronic noncancer pain: A system-atic review and meta-analysis of efficacy and safety. J PainSymptom Manage 35:214-228, 2008
16. Pappagallo M: Incidence, prevalence, and managementof opioid bowel dysfunction. Am J Surg 182(suppl 5A):11S-18S, 2001
562 The Journal of Pain Methylnaltrexone for Opioid-Induced Constipation
17. Plaisance L, Ellis JA: Opioid-induced constipation. Man-agement is necessary but prevention is better. Am J Nurs102:72-73, 2002
18. Relistor [package insert],Wyeth Pharmaceuticals Inc andProgenics Pharmaceuticals, Philadelphia, PA, and Tarrytown,NY, 2009
19. Slatkin N, Thomas J, Lipman AG, Wilson G,Boatwright ML, Wellman C, Zhukovsky DS, Stephenson R,Portenoy R, Stambler N, Israel R: Methylnaltrexone for treat-ment of opioid-induced constipation in advanced illnesspatients. J Support Oncol 7:39-46, 2009
20. Smith BH, Chambers WA, Smith WC: Chronic pain: Timefor epidemiology. J R Soc Med 89:181-183, 1996
21. Swegle JM, Logemann C: Management of commonopioid-induced adverse effects. Am Fam Physician 74:1347-1354, 2006
22. Thomas J, Karver S, Cooney GA, Chamberlain BH,Watt CK, Slatkin NE, Stambler N, Kremer AB, Israel RJ: Meth-ylnaltrexone for opioid-induced constipation in advancedillness. N Engl J Med 328:2332-2343, 2008
23. Vanegas G, Ripamonti C, Sbanotto A, De CF: Side effectsof morphine administration in cancer patients. Cancer Nurs21:289-297, 1998
24. Ware JE, Kosinski M, Dewey JE, Gandek B: How to Scoreand Interpret Single-Item Health Status Measures: AManualfor Users of the SF-8 Health Survey. Lincoln, RI, QualityMetricIncorporated, 2001
25. Yuan CS: Methylnaltrexone mechanisms of action andeffects on opioid bowel dysfunction and other opioid ad-verse effects. Ann Pharmacother 41:984-993, 2007
26. Yuan CS, Doshan H, Charney MR, O’Connor M,Karrison T, Maleckar SA, Israel RJ, Moss J: Tolerability, gut ef-fects, and pharmacokinetics of methylnaltrexone followingrepeated intravenous administration in humans. J Clin Phar-macol 45:538-546, 2005
27. Yuan CS, Foss JF: Antagonism of gastrointestinal opioideffects. Reg Anesth Pain Med 25:639-642, 2000
28. Yuan CS, Foss JF: Methylnaltrexone: Investigation ofclinical applications. Drug Dev Res 50:133-141, 2000
29. Yuan CS, Foss JF: Oral methylnaltrexone for opioid-induced constipation. JAMA 284:1383-1384, 2000
30. Yuan CS, Foss JF, O’Connor M, Karrison T, Osinski J,Roizen MF, Moss J: Effects of enteric-coated methylnal-trexone in preventing opioid-induced delay in oral-cecal transit time. Clin Pharmacol Ther 67:398-404,2000
31. Yuan CS, Foss JF, O’Connor M, Osinski J, Karrison T,Moss J, Roizen MF: Methylnaltrexone for reversal of consti-pation due to chronic methadone use: A randomized con-trolled trial. JAMA 283:367-372, 2000
32. Yuan CS, Foss JF, O’Connor M, Osinski J, Roizen MF,Moss J: Effects of intravenous methylnaltrexone on opioid-induced gut motility and transit time changes in subjects re-ceiving chronic methadone therapy: A pilot study. Pain 83:631-635, 1999
33. Yuan CS, Foss JF, O’Connor M, Toledano A,Roizen MF, Moss J: Methylnaltrexone preventsmorphine-induced delay in oral-cecal transit time with-out affecting analgesia: A double-blind randomizedplacebo-controlled trial. Clin Pharmacol Ther 59:469-475, 1996




















