Study of prevalence and sonographic diagnosis of benign prostate hypertrophy and malignant tumours...
11
Global Research Journal of Public Health and Epidemiology: ISSN-2360-7920 2(4): pp xxx-xxx, April, 2014. Copyright © 2014 Spring Journals Full Length Research Paper Study of prevalence and sonographic diagnosis of benign prostate hypertrophy and malignant tumours among Ghanaian men Raphael Obu Sonography Unit, Agbeve Herbal Hospital, Msc Prostate Cancer, Ghana Faculty of Health and Well-being, Post graduate Office,T/DR. Abdul Wahab Agbeve, OPD Agbeve Herbal Hospital, Ghana Sheffield Hallam University, UK. E-mail: [email protected] Accepted19th Marc, 2014 Study of prevalence of Benign Prostate Hypertrophy and likely malignant tumors among Ghanaian men. The study was carried in Agbeve Herbal Hospital in Sowutuom, Accra-Ghana to assess the age- standardized prevalence of BPH and/or LUTS among Ghanaian men in a probability sample of 875 men aged 20-70 in the ultrasound unit at the Hospital, Sowutuom, Accra-Ghana, with no evidence of biopsy-confirmed prostate cancer. No PSA test and digital rectal examination (DRE). Information on LUTS was based on the Herbal doctor’s assessment of the patient’s symptom and the International Prostate Symptom Score (IPSS) was not used. BPH was estimated using the Ultrasound Scan of the prostate to assess the patient’s prostate volume and echotexture. The prevalence of BPH using ultrasound detected enlarged prostate was 95.4%, (an estimate of prostate volume ≥ 40 cm3) was 40.0%. BPH and/or LUTS appear to be quite common among older Ghanaian men. It was found that after age standardization, the prevalence of ultrasound detected enlarged prostate in Ghanaian men is higher with high prevalence of LUTS and erectile dysfunction. Keywords: benign prostatic hypertrophy, malignant tumour, Ghanaian men, sonographic patterns, prevalence, herbal hospital INTRODUCTION Benign prostatic hyperplasia (BPH) is the most common prostate problem in men and is a significant cause of urinary symptoms in the aging Ghanaian male. Although much is unknown about the pathophysiology of BPH, the condition results in a diminished quality of life for many patients. The symptoms of BPH can be broadly divided into obstructive and irritative components. The former symptoms include a weakened urinary stream, hesitancy, and the need to push or strain to initiate micturition. Irritative symptoms can be much more bothersome for many men and include frequency, nocturia, and urgency. When assessing the importance and magnitude of BPH, one must consider several factors. First, the typical symptoms of BPH are nonspecific. There are many other potential causes of urinary symptoms in aging men, including diabetes mellitus, Parkinson’ s disease, and stroke, which can lead to the same urinary problems seen in men with prostatic enlargement. Second, unlike most other common, chronic medical disorders such as diabetes, hypertension, or hypercholesterolemia, there is no standardized medical test or measurement that can be used to quantify the problem or assess the response to treatment for men with BPH. Rather than lowering blood pressure or maintaining blood glucose levels in the desired range, the primary goal in the management of BPH for most patients is a subjective improvement in urinary symptoms and quality of life. Although objective measurements such as urinary flow rate and postvoid residual urine volume can be used to evaluate BPH, the reproducibility and correlation of these measures with urinary symptoms is often limited. Finally, much is unknown about the natural history of BPH, and this may dramatically impact our understanding of the magnitude and prevalence of the
Transcript of Study of prevalence and sonographic diagnosis of benign prostate hypertrophy and malignant tumours...

Global Research Journal of Public Health and Epidemiology: ISSN-2360-7920 2(4): pp xxx-xxx, April, 2014. Copyright © 2014 Spring Journals
Full Length Research Paper
Study of prevalence and sonographic diagnosis of benign prostate hypertrophy and malignant tumours
among Ghanaian men
Raphael Obu
Sonography Unit, Agbeve Herbal Hospital, Msc Prostate Cancer, Ghana Faculty of Health and Well-being, Post graduate Office,T/DR. Abdul Wahab Agbeve, OPD Agbeve Herbal Hospital, Ghana
Sheffield Hallam University, UK.
E-mail: [email protected]
Accepted19th Marc, 2014
Study of prevalence of Benign Prostate Hypertrophy and likely malignant tumors among Ghanaian men. The study was carried in Agbeve Herbal Hospital in Sowutuom, Accra-Ghana to assess the age-standardized prevalence of BPH and/or LUTS among Ghanaian men in a probability sample of 875 men aged 20-70 in the ultrasound unit at the Hospital, Sowutuom, Accra-Ghana, with no evidence of biopsy-confirmed prostate cancer. No PSA test and digital rectal examination (DRE). Information on LUTS was based on the Herbal doctor’s assessment of the patient’s symptom and the International Prostate Symptom Score (IPSS) was not used. BPH was estimated using the Ultrasound Scan of the prostate to assess the patient’s prostate volume and echotexture. The prevalence of BPH using ultrasound detected enlarged prostate was 95.4%, (an estimate of prostate volume ≥ 40 cm3) was 40.0%. BPH and/or LUTS appear to be quite common among older Ghanaian men. It was found that after age standardization, the prevalence of ultrasound detected enlarged prostate in Ghanaian men is higher with high prevalence of LUTS and erectile dysfunction. Keywords: benign prostatic hypertrophy, malignant tumour, Ghanaian men, sonographic patterns, prevalence, herbal hospital
INTRODUCTION Benign prostatic hyperplasia (BPH) is the most common prostate problem in men and is a significant cause of urinary symptoms in the aging Ghanaian male. Although much is unknown about the pathophysiology of BPH, the condition results in a diminished quality of life for many patients.
The symptoms of BPH can be broadly divided into obstructive and irritative components. The former symptoms include a weakened urinary stream, hesitancy, and the need to push or strain to initiate micturition. Irritative symptoms can be much more bothersome for many men and include frequency, nocturia, and urgency. When assessing the importance and magnitude of BPH, one must consider several factors. First, the typical symptoms of BPH are nonspecific. There are many other potential causes of urinary symptoms in aging men, including diabetes mellitus, Parkinson’s disease, and stroke, which can lead to the same urinary problems seen in men with
prostatic enlargement. Second, unlike most other common, chronic medical disorders such as diabetes, hypertension, or hypercholesterolemia, there is no standardized medical test or measurement that can be used to quantify the problem or assess the response to treatment for men with BPH. Rather than lowering blood pressure or maintaining blood glucose levels in the desired range, the primary goal in the management of BPH for most patients is a subjective improvement in urinary symptoms and quality of life. Although objective measurements such as urinary flow rate and postvoid residual urine volume can be used to evaluate BPH, the reproducibility and correlation of these measures with urinary symptoms is often limited.
Finally, much is unknown about the natural history of BPH, and this may dramatically impact our understanding of the magnitude and prevalence of the

Figure 1. Image courtesy www.: trialx.com
problem. An enlarged prostate is common in men after the age of about 50. What is benign prostatic hypertrophy? You may hear an enlarged prostate called benign prostatic enlargement (BPE) or benign prostatic hyperplasia (BPH). Having an enlarged prostate does not mean you have cancer. In some cases, an enlarged prostate can cause the urethra to narrow which can slow down or stop the flow of urine. About 4 out of every 10 men over the age of 50 (40 per cent) and 3 out of 4 men in their 70s (75 per cent) have urinary symptoms that are caused by an enlarged prostate.
BPH is one of the most common diseases found in aging men. It is associated with lower urinary tract symptoms that affect the quality of life by interfering with daily activities and normal sleep patterns
BPH commonly presents with obstructive (or 'voiding') and irritative (or 'storage') lower urinary tract symptoms. Lower urinary tract symptoms, as defined by the International Continence Society, reflect changes in voiding patterns that lead a patient to seek medical attention(figure 1) Epidemiology
The prevalence of BPH increases with age. Histologic BPH is present in approximately 8% of men aged 31 to 40, 50% of men aged 51 to 60, 70% of men aged 61 to 70, and 90% of men aged 81 to 90. Correspondingly, symptomatic (clinical) BPH is present in approximately 26% of men in the fifth decade of life, 33% of men in the sixth decade, 41%
of men in the seventh decade, and 46% of men in the eighth decade of life and beyond
The prevalence of lower urinary tract symptoms secondary to BPH in the U.S. population is 41% in black men and 34% in white men
The incidence of BPH is 34.4 per 1,000 persons per year in the U.S. in men over age 55
In developed countries, the prevalence of serious BPH complications, including urosepsis, renal failure, acute urinary retention, recurrent urinary tract infection (UTI), and large bladder diverticula, is less than 10% Causes/risk factors
Testosterone is produced by the Leydig cells of the testes and is converted by 5α-reductase to dihydrotestosterone (DHT). Testosterone and DHT promote prostatic epithelial and stromal cell proliferation, apoptosis inhibition, and prostatic angiogenesis. Balance between cellular proliferation and apoptosis exists in patients with normal intraprostatic levels of androgen and estrogen, but DHT imbalance occurs with advancing age, favoring prostatic epithelial and stromal cell proliferation
Obstructive lower urinary tract symptoms are produced via two mechanisms: o o The enlarged prostate can obstruct the prostatic urethra and impede continuous urinary flow o The prostatic stromal smooth muscle cells, which are controlled by α-adrenergic stimulation, can become hyperactive and constrict the prostatic urethra. Hyperactivity may be secondary to certain medications, including tricyclic antidepressants (imipramine, amitriptyline, nortriptyline, doxepin), anticholinergic agents (propantheline, tolterodine, oxybutynin), diuretics (furosemide, thiazides), narcotics (morphine, codeine), first-generation
o antihistamines (fexofenadine, diphenhydramine, chlorpheniramine), and decongestants (phenylpropanolamine)
Irritative (storage) urinary symptoms result from bladder instability. The obstructing prostate increases the intravesicular pressure, and the bladder's smooth muscles adapt by increasing in size. When the bladder muscles become hypertrophic, the bladder becomes hypersensitive and unstable, causing irritative (storage) urinary symptoms. Risk factors Demographic factors
The prevalence of BPH increases with age
The risk of acquiring BPH is 47% higher among black men Genetic factors
There is a three-fold increase in the risk of BPH in monozygotic twins with an affected sibling, suggesting that family history may be a risk factor; however, the exact role of familial transmission remains ambiguous
Other genetic factors that may be related to BPH development include: o Vitamin D3—vitamin D receptor regulates both epithelial and cell growth proliferation o Cytochrome P45017 mediates sex steroid hormone synthesis, which may influence BPH risk o Steroid-5α-reductase enzyme converts testosterone to DHT, which promotes prostate cell proliferation Behavioral and comorbid factors Obesity
The risk of BPH increases by 10% for each 0.05-increase in the waist-to-hip ratio
The increase in adipose aromatization of testosterone to estrogen and the altered levels of testosterone and sex hormone–binding globulin in patients with increased adipose stores promote prostatic epithelial and stromal proliferation
Obesity is also associated with an increase in sympathetic tone, which promotes prostatic cellular proliferation through a mechanism that is not well understood. Although still inconclusive, various mechanisms have been proposed to explain the relationship between obesity and increased sympathetic tone, including: . Insulin levels increasing in proportion to the
amount of adipose stores increase sympathetic neural activity Leptin, a protein hormone secreted by adipocytes, increases sympathetic neural activity Activation of the renin-aldosterone-angiotensin system enhances sympathetic tone
Moderate to vigorous exercise reduces the risk of BPH by 25% Dietary factors
High intake of polyunsaturated fats increases the risk of BPH (relative risk [RR], 1.17)
A diet high in beef products increases the risk of BPH by 25%
A fatty acid–rich diet increases the substrate for the synthesis of cholesterol, which increases the substrate for androgen synthesis
Alcohol consumption appears to have a protective effect on BPH development. The risk decreases by 50% in men who consume three drinks of alcohol per day. The association is thought to be related to alcohol's cardiovascular effects and modulation of steroid hormone metabolism Other factors
Systemic hypertension increases the risk of severe lower urinary tract symptoms by 76%
Elevated fasting plasma glucose increases the risk of BPH. Glucose regulation is hypothesized to influence prostate growth. Elevated insulin levels are associated with increased prostate volume
Cirrhosis of the liver is protective against BPH development, potentially because of the high level of estrogen relative to androgen present
There is no clear association between smoking and BPH. For most men, these nightly bathroom runs may be the first sign of an enlarged prostate. Other symptoms may include trouble starting a stream of urine, leaking, or dribbling. And, like gray hair, an enlarged prostate is a natural by-product of getting older, doctors say. Trouble is, the nightly bathroom runs become more frequent -- eventually edging their way into the daytime routine."They can't sit through a meeting or a plane flight without getting up," says Kevin Slawin, MD, a professor of urology at Baylor School of Medicine in Houston. "It's very annoying … and when they have to go, they really have to go." It's a problem that has several names -- enlarged prostate, benign prostate hyperplasia, or simply BPH. According to the National Kidney and Urological Disease Information Clearinghouse, the most common prostate problem for men over 50 is prostate enlargement. By age 60, over one-half of men have

BPH; by age 85, the number climbs to 90%, according to the American Urological Association (AUA). Enlarged prostate symptoms and causes In men, urine flows from the bladder through the urethra. BPH is a benign (noncancerous) enlargement of the prostate that blocks the flow of urine through the urethra. The prostate cells gradually multiply, creating an enlargement that puts pressure on the urethra -- the "chute" through which urine and semen exit the body. As the urethra narrows, the bladder has to contract more forcefully to push urine through the body. Over time, the bladder muscle may gradually become stronger, thicker, and overly sensitive; it begins to contract even when it contains small amounts of urine, causing a need to urinate frequently. Eventually, the bladder muscle cannot overcome the effect of the narrowed urethra so urine remains in the bladder and it is not completely emptied. Symptoms of enlarged prostate can include:
A weak or slow urinary stream
A feeling of incomplete bladder emptying
Difficulty starting urination
Frequent urination
Urgency to urinate
Getting up frequently at night to urinate
A urinary stream that starts and stops
Straining to urinate
Continued dribbling of urine
Returning to urinate again minutes after finishing When the bladder does not empty completely, you
become at risk for developing urinary tract infections. Other serious problems can also develop over time, including bladder stones, blood in the urine, incontinence, and acute urinary retention (an inability to urinate). A sudden and complete inability to urinate is a medical emergency; you should see your doctor immediately. In rare cases, bladder and/or kidney damage can develop from BPH. Ghanaian men must understand that having an
enlarged prostate does not put them at greater risk of getting prostate cancer. The two conditions begin in different areas of the prostate gland. However, it is possible to have both an enlarged prostate and prostate cancer at the same time. In most cases, early prostate cancer does not cause any urinary symptoms. Medications for an enlarged prostate Several drugs are FDA-approved to relieve common symptoms of an enlarged prostate. Each works differently, says Westney. They either shrink the
enlarged prostate or stop the prostate cell growth, she explains. "For many men, medications are very effective," Westney tells WebMD. "They have a significant change in symptoms, and side effects are very uncommon … so medications are an attractive treatment." Doctors use the BPH Index to gauge how the patient responds to medication, Westney adds. "We see how symptoms are progressing … if they've stabilized or not." Alpha blockers These drugs don't reduce the size of the prostate, but they are very effective at relieving symptoms. They work by relaxing the muscles around the prostate and bladder neck, so urine can flow more easily. These drugs work quickly, so symptoms improve within a day or two. They are most effective for men with normal to moderately enlarged prostate glands.
The drugs: Flomax (tamsulosin), Uroxatral (alfuzosin), Hytrin (terazosin), Cardura (doxazosin), and Rapaflo (silodosin).
Alpha blockers were originally created to treat high blood pressure; dizziness is the most common side effect; other side effects are generally mild and controllable. Possible side effects include headache, stomach irritation, and stuffy nose. These drugs are not for men with significant urine retention and frequent urinary tract infections. Alpha reductase inhibitors These drugs can partially shrink the prostate by reducing levels of a male hormone -- dihydrotestosterone (DHT) -- which is involved in prostate growth. These drugs take longer to work than alpha blockers, but there is urine flow improvement after three months. These drugs can reduce risk of acute retention (inability to urinate) -- and also reduce the need for prostate surgery. You may need to take them for 6 to 12 months to see if they work. The drugs: Proscar (finasteride) and Avodart
(dutasteride). Possible side effects include erection problems,
decreased sexual desire, and reduced amount of semen. These side effects are generally mild and may go away when you stop taking the drugs -- or after the first year of taking the drugs. There is also drug combination therapy, which may
be effective against symptoms associated with BPH. Some examples of combined drugs include an alpha-blocker and a 5-alpha-reductase inhibitor; or an alpha-blocker and an anticholinergic.

Minimally invasive treatments for an enlarged prostate When medications don't help your enlarged prostate, several procedures can relieve symptoms -- without surgery. They are performed in a doctor's office. "These procedures use various types of heat energy to shrink a portion of the prostate," explains Westney. "They are very effective." TUMT (transurethral microwave thermotherapy) This therapy for mild to moderate blockage reduces urinary frequency, urgency, straining, and intermittent flow -- but does not correct any bladder-emptying problems. In this procedure, computer-regulated microwaves are used to heat portions within the prostate to destroy select tissue. A cooling system protects the wall of the urethra during the procedure. TUMT is performed in a doctor's office and requires only topical anesthesia and pain medications. Possible side effects include painful urination for several weeks. Temporary urgency and frequency of urination is also possible. There may be less semen ejaculated. Many men must have this procedure repeated, either because symptoms return or do not improve. TUNA (transurethral radio frequency needle ablation) This procedure also destroys prostate tissue to improve urine flow and relieve symptoms. It involves heating the tissue with high-frequency radiowaves transmitted by needles inserted directly into the prostate (some anesthesia is used). The procedure does not require a hospital stay. Possible side effects include painful, urgent, or frequent urination for a few weeks. Prostatic stents In some cases, a tiny metal coil called a stent can be inserted in the urethra to widen it and keep it open. Stenting is done on an outpatient basis under local or spinal anesthesia. Usually, stents are only for men who are unwilling or unable to take medications -- or who are reluctant or unable to have surgery. The majority of doctors don't consider stents a good option for most men.
There could be serious side effects, and some men find that stents don't improve their symptoms. Sometimes a stent shifts position, which can worsen the symptoms. In some cases, men experience painful urination or have frequent urinary tract
infections. Stents are expensive, and there can be difficulty in removing them. Surgery for an enlarged prostate For most men with very enlarged prostates, surgery can relieve symptoms, but there are both risks and benefits with each type of operation. Discuss them with your doctor. After a careful evaluation of your situation and your general medical condition, your doctor will recommend which is best for you. TURP (transurethral resection of the prostate) This is the most common surgery for an enlarged prostate, and considered to bring the greatest reduction in symptoms. Only the tissue growth that is pressing against the urethra is removed to allow urine to flow easily. The procedure involves an electrical loop that cuts tissue and seals blood vessels. Most doctors suggest using TURP whenever surgery is required, as it is less traumatic than open surgery and requires shorter recovery time.
With the TURP procedure, patients can expect to have retrograde ejaculation afterwards, says Westney. This is a condition in which a man ejaculates backward into the bladder instead of through the urethra. "Retrograde ejaculation generally isn't painful," she tells WebMD. "It shouldn't be an issue unless fertility is a concern." Other possible side effects include blood loss requiring transfusion (rare), painful urination, recurring urinary tract infections, bladder neck narrowing, and blood in the urine.
After TURP, the odds of erection problems range from 5% to 35%. However, this is often temporary -- and the ability to have an erection and an orgasm returns after a few months. TUIP (transurethral incision of the prostate) This procedure involves making cuts in the prostate instead of removing prostate tissue. These cuts reduce pressure on the urethra, making urination easier. Patients go home the same day, and wear a catheter for a day or two. Symptom relief is slower with TUIP, compared with TURP. However, most men are satisfied with their ultimate symptom relief from this. Also, retrograde ejaculation is less common and less severe than after TURP. Risk of erection problems is similar to TURP. Laser Surgery This procedure uses a high energy vaporizing laser to destroy prostate tissue. It is done under general

anesthesia and may require an overnight stay at the hospital. It provides immediate relief of symptoms, yet men may suffer from painful urination for a few weeks. In general this procedure causes less blood loss, and side effects can include retrograde ejaculation. These procedures include:
Transurethral holmium laser ablation of the prostate (HoLAP)
Transurethral holmium laser enucleation of the prostate (HoLEP)
Holmium laser resection of the prostate (HoLRP)
Photoselective vaporization of the prostate (PVP) Open Prostate Surgery (Prostatectomy) When a transurethral procedure cannot be used, open surgery (which requires an incision in the abdomen) may be used. This allows the surgeon to remove tissue in the prostate. Open prostatectomy is typically done when the prostate gland is greatly enlarged, when there is bladder damage, if there are bladder stones, or if the urethra is narrowed. The inner part of the prostate is removed. This surgery is done under general or spinal anesthesia, and recovery can take a few weeks to several months. Side effects are similar to TURP, including blood loss requiring a transfusion, urinary incontinence, erection problems, and retrograde ejaculation. Herbal therapies for an enlarged prostate Several herbal supplements are marketed for enlarged prostates. Saw palmetto, beta-sitosterol, and pygeum are all are widely used in Europe. They are available in the U.S. and now in Ghana and don't require a prescription. Saw palmetto Saw palmetto is one of the most popular herbal supplements taken for BPH. The extract comes from ripened berries of the saw palmetto shrub. Extracts are thought to prevent testosterone from breaking down and triggering prostate tissue growth, similar to the 5-alpha reductase inhibitor medications. Studies of this supplement have had varied results.
"Saw palmetto does not work," Slawin tells WebMD. He points to a recent "very nicely done" randomized study that found palmetto was no more effective than a placebo in relieving BPH symptoms. However, other studies have found it to be as effective as Proscar, a BPH medication. Varying quality of herbal products (dosages, ingredients, or purity) may account for the
conflicting results, researchers say. Also, many studies of herbals have not been well-controlled. Beta-sitosterol This compound is extracted from pollen of rye grass. There has been some evidence that it provides relief from urinary symptoms. However, in four studies the supplement did not increase urinary flow rates, shrink the prostate, or improve bladder emptying. Pygeum This extract comes from the bark of the African plum tree. Numerous studies have found positive results for pygeum. In 18 studies, this extract relieved BPH symptoms twice as often as the placebo; it also increased urinary flow by nearly 25%. Pumpkin Reduces inflammation of the prostate and the urinary bladder, and expels intestinal parasites. There are many cultivated varieties of pumpkins, which render fruit weighing from half a kilogram to more than fifty. Croton Membranaceus The root extract of croton membranaceus is used in formulations for the treatment and management of prostate and related cancers and measles in Ghana (Mshana et al 2000) Enlarged prostate treatments in the pipeline Researchers continue to investigate new therapies for enlarged prostates. "Another category of drugs is under development," says Slawin. "We've come a long way in treating BPH. It's no longer the life-threatening disease it once was. Now, in treatment, we're working on quality of life issues… reducing side effects of treatment."
Also being studied is a procedure called water-induced thermotherapy (WIT), an experimental procedure that involves destroying excess prostate tissue utilizing heated water and an air-filled balloon, which protects normal prostate tissue. The procedure is performed with only local anesthesia. Results may not be fully apparent for three to four months. However, preliminary studies examining WIT have shown positive results, with a near doubling in urine flow. However, the American Urological Association has not thus far endorsed WIT as a viable treatment
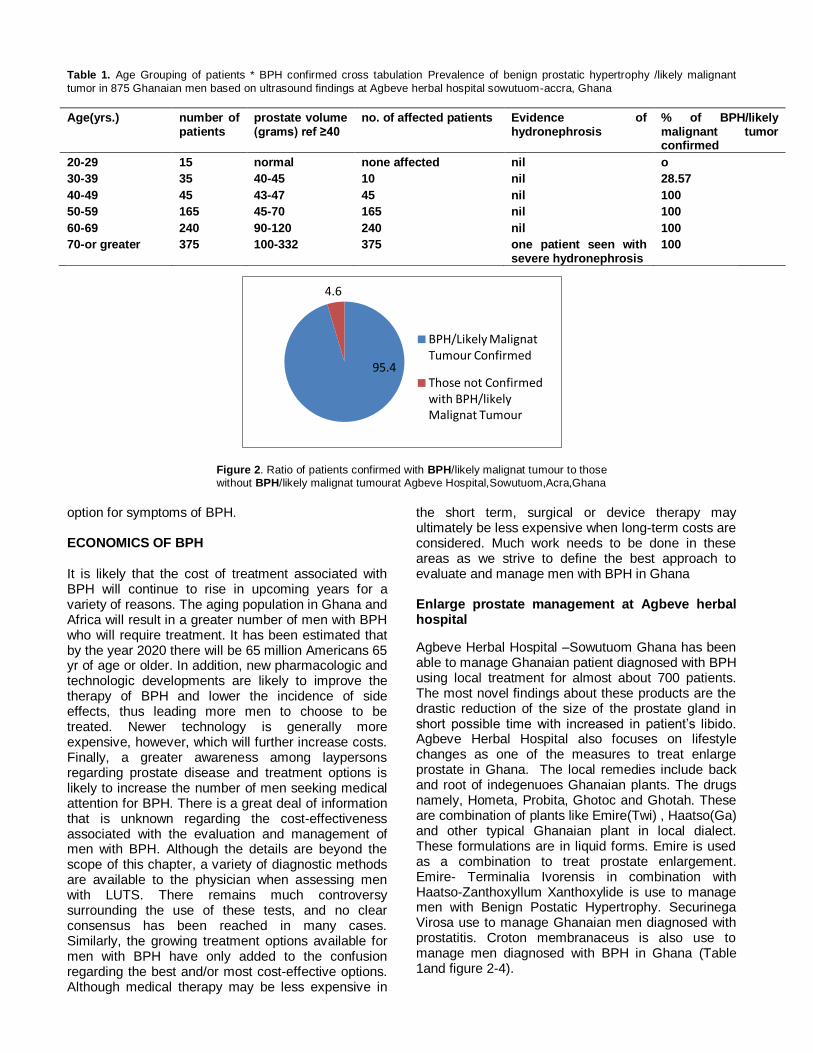
Table 1. Age Grouping of patients * BPH confirmed cross tabulation Prevalence of benign prostatic hypertrophy /likely malignant
tumor in 875 Ghanaian men based on ultrasound findings at Agbeve herbal hospital sowutuom-accra, Ghana
Age(yrs.) number of patients
prostate volume (grams) ref ≥40
no. of affected patients Evidence of hydronephrosis
% of BPH/likely malignant tumor confirmed
20-29 15 normal none affected nil o
30-39 35 40-45 10 nil 28.57
40-49 45 43-47 45 nil 100
50-59 165 45-70 165 nil 100
60-69 240 90-120 240 nil 100
70-or greater 375 100-332 375 one patient seen with severe hydronephrosis
100
Figure 2. Ratio of patients confirmed with BPH/likely malignat tumour to those without BPH/likely malignat tumourat Agbeve Hospital,Sowutuom,Acra,Ghana
option for symptoms of BPH. ECONOMICS OF BPH It is likely that the cost of treatment associated with BPH will continue to rise in upcoming years for a variety of reasons. The aging population in Ghana and Africa will result in a greater number of men with BPH who will require treatment. It has been estimated that by the year 2020 there will be 65 million Americans 65 yr of age or older. In addition, new pharmacologic and technologic developments are likely to improve the therapy of BPH and lower the incidence of side effects, thus leading more men to choose to be treated. Newer technology is generally more expensive, however, which will further increase costs. Finally, a greater awareness among laypersons regarding prostate disease and treatment options is likely to increase the number of men seeking medical attention for BPH. There is a great deal of information that is unknown regarding the cost-effectiveness associated with the evaluation and management of men with BPH. Although the details are beyond the scope of this chapter, a variety of diagnostic methods are available to the physician when assessing men with LUTS. There remains much controversy surrounding the use of these tests, and no clear consensus has been reached in many cases. Similarly, the growing treatment options available for men with BPH have only added to the confusion regarding the best and/or most cost-effective options. Although medical therapy may be less expensive in
the short term, surgical or device therapy may ultimately be less expensive when long-term costs are considered. Much work needs to be done in these areas as we strive to define the best approach to evaluate and manage men with BPH in Ghana Enlarge prostate management at Agbeve herbal hospital
Agbeve Herbal Hospital –Sowutuom Ghana has been able to manage Ghanaian patient diagnosed with BPH using local treatment for almost about 700 patients. The most novel findings about these products are the drastic reduction of the size of the prostate gland in short possible time with increased in patient’s libido. Agbeve Herbal Hospital also focuses on lifestyle changes as one of the measures to treat enlarge prostate in Ghana. The local remedies include back and root of indegenuoes Ghanaian plants. The drugs namely, Hometa, Probita, Ghotoc and Ghotah. These are combination of plants like Emire(Twi) , Haatso(Ga) and other typical Ghanaian plant in local dialect. These formulations are in liquid forms. Emire is used as a combination to treat prostate enlargement. Emire- Terminalia Ivorensis in combination with Haatso-Zanthoxyllum Xanthoxylide is use to manage men with Benign Postatic Hypertrophy. Securinega Virosa use to manage Ghanaian men diagnosed with prostatitis. Croton membranaceus is also use to manage men diagnosed with BPH in Ghana (Table 1and figure 2-4).
95.4
4.6
BPH/Likely Malignat Tumour Confirmed
Those not Confirmed with BPH/likely Malignat Tumour

Figure 3. Age against number of Patients affected by BPH/Likely Malignant Tumour
Figure 4. Number of patients attended/ number of patients affected by BPH/Likely Malignant Tumor/ evidence of
hydronephrosis
DISCUSSION A. Demography and BPH A total of 875 trans-abdominal pelvic ultrasound scanned images of Men were analyzed out of which 835 representing 95.4% were confirmed to have BPH. The finding is consistent with available data which suggest that BPH and LUTS are the most common men problems causing symptoms in old Ghanaian men with the overall with the overall prevalence of BPH increasing to over 85%. The mean, standard deviation and range of the age of the sampled population (confirmed BPH cases; n = 875) were patient’s who attended the Hospital for their prostate solution. The study indicated that the highest prevalence (95.4%) of the BPH cases was found
among men aged 40-70 years and the lowest (4.6%) recorded among men aged less
than 39years. The current study showed that men aged between 30-39 years also recorded significant percentage of 28.57% of BPH. The above results agree with similar findings conducted elsewhere which suggest that BPH by sonography(figure 5) is very common among men in their early 40’s and late 50 .The study also recorded 95.4% of Ghanaian men who visited the hospital told the herbal doctors that they had erectile problems.
The recorded situation in Ghana is worrying in view of health and other risk implications. BPH has social, economic and medical implications in the men populace. Ghanaian men constitute about 40% of the Ghanaian population(2010 Ghana population Census) and are strong component of the country’s workforce
0
20
40
60
80
100
120
% of BPH/Likely Malignat …
0
50
100
150
200
250
300
350
400
20-29 30-39 40-49 50-59 60-69 70 or greater
number of patients affected by BPH/likely Malignat Tumour
Number of patients
Evidence of hydronephrosis

Figure 5. Songoraphic diagnosis of Benign Prostatic Hypertrophy
and thus contribute immensely to the economy. Their role in the development of the economy therefore cannot be over emphasized. The Ghanaian man is engaged in government and non-governmental businesses and has seen a tremendous growth which is an indication that men are the breadwinners in Ghana.
Therefore managing the health of the Ghanaian man is essential for the socio-economic growth of the country. The study also agreed with studies which put age as a key risk factor for BPH and Prostate Cancer. The study also clearly tells us about the life cycle of the prostate gland corresponding to age. The entire prostate is surrounded by a dense, fibrous capsule. As we age, our prostate naturally grows. This is due to the muscular tissue, since all muscles grow with age and use. Prior to puberty, men prostate is quiet small, about the size of a marble. After puberty, it goes through a rather rapid growth spurt. During young and middle adulthood, the prostate is roughly, the size of a golf ball. Under healthy conditions, it should rather remain about this size for many, many years. Then, after about age 50, it begins to grow again. How much it grows, and is inflamed, depends upon a variety of factors. There are several problems, which might occur relative to the prostate gland as the aging process takes place. It is therefore essential that Ghanaian men understand and be able to identify these problems in their early stages. For, it is at this time when prevention methods have their greatest effect.
Statically it can also be deduced from the research at Agbeve Herbal Hospital that 4 in 5 Ghanaian men that visit the Hospital will be diagnosed with BPH /likely malignant Tumor in his lifetime. It also appears that Ghanaian men present LUTS to the Hospital when their symptoms appears getting worse, Some also already knows they have the problem before visit
the Hospital for solution. It was also seen that 30% of the prostate gland assessed show areas loss of glandular architecture and results in the hypoechoic mass likely to be prostate cancer which means about 3 out of 10 Ghanaian men will be diagnosed with prostate cancer in their lifetime.
Prostate cancer is typically described as a hypoechoic lesion on sonography. However, approximately 40% of malignant lesions are isoechoic and an additional 1% may appear hyperechoic. Furthermore, prostate cancer differs from other visceral neoplasms in that it is frequently multifocal in origin. The attitude of I don’t care must change and Ghanaian men must be proactive about their health. Ghanaian women appear to be more proactive about their health and they must also support their husbands in this fight and stand by them. MATERIALS AND METHODS A. Characteristics of the ultrasound machine used in the study The ultrasound scanning machine used in the study has the following characteristics;
Mobile Ultrasound machine
Model: Sonoscape A6 diagnostic ultrasound system.
Probe type: Convex transducer of frequency 3.5 MHz B. Exam type i. Tran abdominal approach of the Prostate ii. Full Bladder for easy visualization of the prostate

CONCLUSION BPH is an important cause of diminished quality of life among aging Ghanaian men, and the prevalence of this condition in the Ghana is likely to grow as the population ages. A variety of definitions of BPH is available based on the presence of urinary symptoms, prostatic enlargement, and/or the histologic finding of hyperplastic glands. In addition,
urodynamic results demonstrating decreased urinary flow rates or bladder outlet obstruction may also be used to help define the presence of BPH. Although nonspecific, the presence of LUTS such as frequency, hesitancy, or nocturia are most commonly used to define the prevalence
of BPH. Overall, the introduction and validation of symptom questionnaires such as the I-PSS has added greatly to our understanding of the extent and magnitude of BPH in a variety of populations.
A number of epidemiologic factors have been investigated among men with BPH. Although aging clearly has the most important effect on the development of prostatic enlargement and urinary symptoms, a variety of other factors may also play a role in the occurrence of BPH.
It appears that racial or ethnic background may play a minor role in the incidence of BPH. However, African-American men do not appear to be at increased risk compared with whites and other groups. Although a family history of BPH appears to increase the overall likelihood that
urinary symptoms and prostatic enlargement will occur, the ambiguity associated with the definition of BPH among relatives is a limiting factor. Among lifestyle factors, cigarette smoking seems to lower the risk of BPH, whereas obesity and a high-fat diet may increase the incidence
of prostatic enlargement. Conflicting results have been reported, however, in different studies, and the precise role of many factors in the development of BPH remains largely unknown. As the importance of BPH grows, it is likely that further information will become available
regarding the role of epidemiologic factors in BPH. There should be a collaboration between medical practitioners and Herbal Practitioners in Ghana as the Herbal sector in Ghana has excellent talented professional that can bring change in the development of the country and find antidote using local remedy for management of Benign Prostatic Hypertrophy in Ghana as it appears western medicine has fail to find solution for Ghanaian men leaving with BPH coupled with side effects of these treatment. Herbal Practitioners must also make it clear to patients in Ghana the difference between BPH and Prostate Cancer and refer those who with serious problems to see specialist as Practice in Agbeve Herbal Hospital, Ghana. There must also be a training workshop for
Herbal Practitioners on prostate gland and its management option by the Ghana Federation of Traditional Medicine (GHAFTRAM) members. There must also be awareness on the disease in Ghana as it appears most of the patents that come to the hospital already present with the problem to reduce the incidence rates among Ghanaian men. This study call for stakeholders approach towards prostate cancer in Ghana and the need for introduction of a specific policy on prostate cancer screening in Ghana as practiced in the UK and in the Caribbean’s –Jamaica to save the lives of so many Ghanaian men as some Herbal Practitioners ends up confusing some patients with the management of BPH and Prostate Cancer. The management of Prostate disorders is not the same as the management of prostate cancer depends upon the stage of the cancer and it’s also about time for collaboration in the Health Sector between herbal practitioners and expert to save lives in Ghana. ACKNOWLEDGMENTS The authors acknowledge the support and cooperation received from the staff of theAgbeve Herbal Hospital Sowutuom in Ghana for this study. Clifford Owusu Ansah of the sonography department , Mr. Addo Quaye of the security department and Ibrahim Kwesi of the laboratory department. Dr. Tanoh at the outpatient departments and the managing director of the Hospital Alhaji/T.Dr. Agbeve REFERENCES Chokkalingam AP, Yeboah ED, Demarzo A, Netto G, Yu
K, Biritwum RB, Tettey Y, Adjei A, Jadallah S, Li Y, Chu LW, Chia D, Niwa S, Partin A, Thompson IM, Roehrborn C, Hoover RN, Hsing AW(2012). Prevalence of BPH and lower urinary tract symptoms in West Africans.Prostate Cancer Prostatic Dis. (2):170-6. doi: 10.1038/pcan.2011.43. Epub 2011 Sep 13
Matter D, Spinelli G, Warter F, Bollack C, Warter P (1982). Suprapubic prostatic ultrasonography Sem Hop. 1982 May 6;58(18):1089-94.
Iko BO1, Monu JU, Mangete ED, Nduka NR (1987). Ultrasonography of the prostate: a preliminary report from Nigeria. Int Urol Nephrol. 1987;19(3):279-85.
Grond A1, Ostermann-Myrau M (1994). Benign and malignant diseases of the prostate. Versicherungsmedizin. 1;46(6):199-205.
Greenberg M, Neiman HL, Brandt TD, Falkowski W, Carter M (1981). Ultrasound of the prostate. Analysis of tissue texture and abnormalities.Radiology. 1981 December;141(3):757-62.
Abu-Yousef MM.(1985) Benign prostatic hyperplasia: tissue characterization using suprapubic ultrasound. Radiology. Jul;156(1):169-73.
Neil F, Wasserman MD(2006) Benign Prostatic Hyperplasia: A Review and Ultrasound Classification Radiologic Clinics of North America - Volume 44, Issue 5 (September 2006)

DOI: 10.1016/j.rcl.2006.07.005 Enlarged prostate | Prostate Cancer
www.http//UKprostatecanceruk.org/information/enlarged-prostate Reviewed on August 29, 2011 Enlarged Prostate Causes, Symptoms, and Treatments - WebMD www.webmd.com/men/...bph/.../enlarged-prostate-bph-complex-proble..
Benign Prostatic Hyperplasia Causes, Diagnosis and Treatments ...https://www.clinicalkey.com/topics/.../benign-prostatic-hyperplasia.html
Glenn S. Gerber, MD (nd) The Definition of Benign Prostatic Hyperplasia. Epidemiology and Prevalence pdf
George D. Paniplona-Roger,MD, (2006).Encyclopedia of Medicinal Plant, Ninth edition.vol2.P605 and 6 and 10 and 11 Eric KO, William KA, Ekow AA, Edmund KB, Benjamin Dabo
Sarkodie D-T, Klenam HO, Patrick KA, Jerry C (2004). J. Med. Appl. Biosci. Prevalence and sonographic patterns of uterine fibroid among Ghanaian women (Uterine Fibroid- The Ghanaian situation) (4): PDF