
Students' perceptions of a multimedia computer-aided instruction resource in histology
13
behaviour, the cross-sectional study design precludes the attribution of causal explanations to the relationships documented. This is also exemplified by the behaviours mentioned in the previous paragraph, viz. having had sexual intercourse and going out at night beyond the neighbourhood and walking home alone; each of these behaviours serves as a predictor of the other. To the extent that these variables may be causally related, it is impossible to detennine the 'direction' in which this causality operates. Longitudinal studies are required to elucidate questions of this nature. The authors would like to thank the foHowing people for their contribution to the series of articles of which this article comprises the 10th part: Derek Yach, of the Medical Research Council, for providing an enormous amount of encouragement and advice at all stages of the project and for facilitating the acquisition of funding; Debbie Bradshaw, A1ex Butchart, Blanche de Wet, Theunis Kotze, Cathy Mathews, Mehrunisha Mohamed, Char1es Parry, Malcolm Steinberg and Hester van der Wait, for comments on the protocol or one or more of the manuscripts; the many people who assisted in the piloting, data gathering, coding, punching, and cleaning (especially Margie Joyi. Abe Koch, and Merieth P1aatjies of the Department of Psychiatry of the University of Cape Town); Donald Berry, Shar1ene Heath and John Seager, of the Medical Research Council, for contributing in the initial stages of the analysis; and the educationalists and students involved with the project, for co-operating with the researchers. Financial support was provided by the Medical Research Council and the Department of Psychiatry, University of Cape Town. We would also like to thank Dabble Bradshaw, Carol Metcalf. Charles Parry and Derek Yach for providing comments on an earlier version of this article. REFERENCES 1. FlisheI" AJ, Ziervogel CF, Cttalton DO. Leget PH, Roben:son BA. Risk-taking behaviour of cape Peninsula hlgh-school students: Evidence for a syndrome of aOolesc6nt risll behaviour. S AfrMedJ 1996; 86: 1088-1091 (this issue). 2. Jessor R, Jessot" SL Problem and PsychoslxiaJ Development: A LOilgitudinaJ Study of YotIttr. New Yor1c Academic Press, 1977. 3. FIi$her Al. ZiervogeI CF, Chalton 00. Aobertson BA. Risk-laking behaviour of Cape Peninsula high-school students: Part I. Intnxluction and methods. S AIr Med J 1993; 4. Gillmore MR, Butlel" SS, Lotv" MJ, Gi'cMst L Substance use and other factOl!J associated with risky sexual behaviour amotlQ pn!gI'W'It aOoIescents. FaIn Plant! Perspet;r 1992; 24: 255-268. 5. Kandel O. Drug and einking behavior emong youth. Annu Rev Sociology 1980; 6: 2:i5- 285. 6. Kandel D. Stages .... adolescoot involvement in drug use. Science 1975; 190: 912-914. 7. Single E, Kandel D, Faust R. Patterns of multiple drug use in high schoOl. J Health Sac Behav 1974; 15; 344-357. 8. Bailey GW. Cutrem perspectives on substance use in YQUth. JAm Acad Child AdoJesc P$yf;hiarry 1989; 28: 151-162. 9. Berman AL., Scl'lwanz RH. Suicide attempts among adoIescenl drug US@f$. Am J Dis Child 1990; 144: 310-314. 10. cams AB, G, Neckem'l<ill HJ. Suicidal btihaviour in aggressive adolescents. J CJin Child PsychoI1988; 17: 296-309. 11. CnunIey FE Substance abuse and adolescent suil::idaI behavicr. .lAMA 1990; 2S3: 3051-3056. 12. Garrison cz. McKeown RE. 1/ak)is RF, Vncent ML Aggression. substanCe use. and suicidal behavicn in higt1 sr::hooI $tueemS. Am J Pl.lbIic HN/lJIl993; 83; 179-184. 13. Sha1fer D. SuiOOe i'l childhood and earty adolesa!nce. J ChtJd Psychd Psychi;my 1974: 15: 275-291. 14. Wailer I-LJ. vaughan AD, Arrnstroog B. er al. Sexual, assaultive, and sUcidaJ behaviot'S among urban minority junior high school students. J Am Acad Child AdoIesc Psychiarry 1995: 34: 73-80. 15. Shaffer D. Garland A. Gould M. FIsher P, Trautmafl P. Preventing teenage suIcide: a critical rl!View. JAm Acad Child AdoJesc P$ychiatry 1988; 27: 675-687. 16. Shatler D. Garland A, Vieland V, Unde.-wood M, Busner C. The impact of curriculum- based suicide prt!VenOOn programs for teenagE.'l1i. J Am At;ad Child AdoIesc P$ychiarry 1991; 30: 588-596. 17. Pearee CM, Martin G. Prec:ictinq suicide attempts among adole$cena Acts Psydriatr Scanct 1994; 9Q; 324-32£1- 18. Choquel: M, Mantred R. Sexual inten::olne. OJillia::eptiO". and risk-t:ilki'lg behaviour among lnSeIect'ed Ft&nCh aged 11-20 years. J Adolesc HNIrh 1992; 12: 623-<'lO. 19. Goode E. Drug use and sexual actMtyOl'l a college campus. Am J PsyCNarry 19n; 128: 92·96. 20. lrwin CE. MllIstein $G. Biopsychosocial correlates of riSk-taJUng behaviots during adolescence. Can the physician itTterv8tle7 J AdoJesc HeaJr!I Care 1986; 7: 82$-96S. 21. Oryfoos J. FulI-!SNIIice SchooJs. A RevohJDon in Health and SodaJ ServIces frJl' Children, Youth, and Families. San Francisco: Jossey-Bass. 1994. Accepted 16 Oct 1995. Students' perceptions of a multimedia computer-aided instruction resource in histology Maurice Mars, Michelle McLean Objective. To develop an interactive muttimedia-based computer-aided instruction (CAI) programme, to detennine its educational worth and efficacy in a multicuttural academic environment and to evaluate its usage by students with differing levels of computer literacy. Design. A prospective descriptive study evaluating pre- and post-module testing, student usage tracking and a questionnaire survey. Setting. University of Natal Medical School. Participants. Thirty-four volunteers from the class of 125 second-year M.B. Ch.B. students who participated in the CAI study; 13 of these were not computer-literate. Intervention. The stUdy group used the CAI module for 2 weeks as part of the course. Main outcome measures, Post·test scoring and evaluation of questionnaire responses. Results. Results of pre- and post-tests show that CAI users' scores were slightly lower on pre-testing (22.1 % v. 23.2%), while their post-test scores were higher (65.6% v. 60.7%). Lack of computer literacy did not restrict or hinder students in their use of the programme. Responses to a questionnaire completed by all CAI users indicate consensus that the programme helped the students to learn (94%), that it provided important basic knowledge (88%) and that it was a helpful learning experience (88%). All but 1 student wished to have more programmes like this available in histology. Conclusions. The CAI programme reduced the time spent by students in the histology microscopy laboratory and did not negatively affect their marks in post-course evaluation. The concept of muttimedia-based CAI in medical education was posmvely received by the students who participated. S Afr Med J 1996; 86: 1098-1102. Recognising the worldwide reappraisal of medical teaching and curricula, the University of Natal Medical School is investigating an integrated, problem-based (or problem- solving) curriculum. Fundamental to these methods is the Department of Physiology, University of Natal, Ourban Maurice Mars. M.B. CH.B. Michelle McLean. Pl-LO. 1098 Volumt 86 No. 9 Stprtmber 1996 SAMJ
Transcript of Students' perceptions of a multimedia computer-aided instruction resource in histology

behaviour, the cross-sectional study design precludes theattribution of causal explanations to the relationshipsdocumented. This is also exemplified by the behavioursmentioned in the previous paragraph, viz. having had sexualintercourse and going out at night beyond the neighbourhoodand walking home alone; each of these behaviours serves asa predictor of the other. To the extent that these variablesmay be causally related, it is impossible to detennine the'direction' in which this causality operates. Longitudinalstudies are required to elucidate questions of this nature.
The authors would like to thank the foHowing people for theircontribution to the series of articles of which this articlecomprises the 10th part: Derek Yach, of the Medical ResearchCouncil, for providing an enormous amount of encouragementand advice at all stages of the project and for facilitating theacquisition of funding; Debbie Bradshaw, A1ex Butchart, Blanchede Wet, Theunis Kotze, Cathy Mathews, Mehrunisha Mohamed,Char1es Parry, Malcolm Steinberg and Hester van der Wait, forcomments on the protocol or one or more of the manuscripts; themany people who assisted in the piloting, data gathering, coding,punching, and cleaning (especially Margie Joyi. Abe Koch, andMerieth P1aatjies of the Department of Psychiatry of the Universityof Cape Town); Donald Berry, Shar1ene Heath and John Seager,of the Medical Research Council, for contributing in the initialstages of the analysis; and the educationalists and studentsinvolved with the project, for co-operating with the researchers.Financial support was provided by the Medical Research Counciland the Department of Psychiatry, University of Cape Town.
We would also like to thank Dabble Bradshaw, Carol Metcalf.Charles Parry and Derek Yach for providing comments on anearlier version of this article.
REFERENCES
1. FlisheI" AJ, Ziervogel CF, Cttalton DO. Leget PH, Roben:son BA. Risk-taking behaviourof cape Peninsula hlgh-school students: Evidence for a syndrome of aOolesc6nt risllbehaviour. S AfrMedJ 1996; 86: 1088-1091 (this issue).
2. Jessor R, Jessot" SL Problem 8ehav~and PsychoslxiaJ Development: A LOilgitudinaJStudy of YotIttr. New Yor1c Academic Press, 1977.
3. FIi$her Al. ZiervogeI CF, Chalton 00. Aobertson BA. Risk-laking behaviour of CapePeninsula high-school students: Part I. Intnxluction and methods. S AIr Med J 1993;83:46~73.
4. Gillmore MR, Butlel" SS, Lotv" MJ, Gi'cMst L Substance use and other factOl!Jassociated with risky sexual behaviour amotlQ pn!gI'W'It aOoIescents. FaIn Plant!Perspet;r 1992; 24: 255-268.
5. Kandel O. Drug and einking behavior emong youth. Annu Rev Sociology 1980; 6: 2:i5285.
6. Kandel D. Stages .... adolescoot involvement in drug use. Science 1975; 190: 912-914.7. Single E, Kandel D, Faust R. Patterns of multiple drug use in high schoOl. J Health Sac
Behav 1974; 15; 344-357.8. Bailey GW. Cutrem perspectives on substance use in YQUth. JAm Acad Child AdoJesc
P$yf;hiarry 1989; 28: 151-162.9. Berman AL., Scl'lwanz RH. Suicide attempts among adoIescenl drug US@f$. Am J Dis
Child 1990; 144: 310-314.10. cams AB, Pet~ G, Neckem'l<ill HJ. Suicidal btihaviour in aggressive adolescents.
J CJin Child PsychoI1988; 17: 296-309.11. CnunIey FE Substance abuse and adolescent suil::idaI behavicr. .lAMA 1990; 2S3:
3051-3056.12. Garrison cz. McKeown RE. 1/ak)is RF, Vncent ML Aggression. substanCe use. and
suicidal behavicn in higt1 sr::hooI $tueemS. Am J Pl.lbIic HN/lJIl993; 83; 179-184.13. Sha1fer D. SuiOOe i'l childhood and earty adolesa!nce. J ChtJd Psychd Psychi;my
1974: 15: 275-291.14. Wailer I-LJ. vaughan AD, Arrnstroog B. er al. Sexual, assaultive, and sUcidaJ behaviot'S
among urban minority junior high school students. J Am Acad Child AdoIesc Psychiarry1995: 34: 73-80.
15. Shaffer D. Garland A. Gould M. FIsher P, Trautmafl P. Preventing teenage suIcide: acritical rl!View. JAm Acad Child AdoJesc P$ychiatry 1988; 27: 675-687.
16. Shatler D. Garland A, Vieland V, Unde.-wood M, Busner C. The impact of curriculumbased suicide prt!VenOOn programs for teenagE.'l1i. J Am At;ad Child AdoIesc P$ychiarry1991; 30: 588-596.
17. Pearee CM, Martin G. Prec:ictinq suicide attempts among adole$cena Acts PsydriatrScanct 1994; 9Q; 324-32£1-
18. Choquel: M, Mantred R. Sexual inten::olne. OJillia::eptiO". and risk-t:ilki'lg behaviouramong lnSeIect'ed Ft&nCh~ aged 11-20 years. J Adolesc HNIrh 1992; 12:623-<'lO.
19. Goode E. Drug use and sexual actMtyOl'l a college campus. Am J PsyCNarry 19n;128: 92·96.
20. lrwin CE. MllIstein $G. Biopsychosocial correlates of riSk-taJUng behaviots duringadolescence. Can the physician itTterv8tle7 J AdoJesc HeaJr!I Care 1986; 7: 82$-96S.
21. Oryfoos J. FulI-!SNIIice SchooJs. A RevohJDon in Health and SodaJ ServIces frJl'Children, Youth, and Families. San Francisco: Jossey-Bass. 1994.
Accepted 16 Oct 1995.
Students' perceptions of amultimedia computer-aidedinstruction resource inhistologyMaurice Mars, Michelle McLean
Objective. To develop an interactive muttimedia-basedcomputer-aided instruction (CAI) programme, to detennine
its educational worth and efficacy in a multicutturalacademic environment and to evaluate its usage by
students with differing levels of computer literacy.
Design. A prospective descriptive study evaluating preand post-module testing, student usage tracking and a
questionnaire survey.
Setting. University of Natal Medical School.Participants. Thirty-four volunteers from the class of 125
second-year M.B. Ch.B. students who participated in theCAI study; 13 of these were not computer-literate.
Intervention. The stUdy group used the CAI module for 2weeks as part of the course.
Main outcome measures, Post·test scoring and
evaluation of questionnaire responses.Results. Results of pre- and post-tests show that CAI
users' scores were slightly lower on pre-testing (22.1 % v.23.2%), while their post-test scores were higher (65.6% v.
60.7%). Lack of computer literacy did not restrict or hinder
students in their use of the programme. Responses to aquestionnaire completed by all CAI users indicate
consensus that the programme helped the students tolearn (94%), that it provided important basic knowledge
(88%) and that it was a helpful learning experience (88%).
All but 1 student wished to have more programmes like
this available in histology.Conclusions. The CAI programme reduced the time
spent by students in the histology microscopy laboratory
and did not negatively affect their marks in post-course
evaluation. The concept of muttimedia-based CAI in
medical education was posmvely received by the studentswho participated.
S Afr Med J 1996; 86: 1098-1102.
Recognising the worldwide reappraisal of medical teachingand curricula, the University of Natal Medical School isinvestigating an integrated, problem-based (or problemsolving) curriculum. Fundamental to these methods is the
Department of Physiology, University of Natal, Ourban
Maurice Mars. M.B. CH.B.
Michelle McLean. Pl-LO.
1098 Volumt 86 No. 9 Stprtmber 1996 SAMJ

concept of small-group discussions as opposed to didacticclass lectures. With the aid of facilitators, and with theprovision of suitable resource material, students will beexpected to drive their own learning experience. They will beexpected to discover information and acquire knowledgethemselves. It is envisaged that the changes will take placein the 3 preclinical years of study.
The second year currently consists of courses in anatomyand physiology, the latter including biochemistry andhistology. Both courses entail a large laboratory component.Given the possibility that students will progress at differentrates and in different directions, logistical problems areexpected in terms of provision of staffing and laboratoryresources for these small groups. Computer-aidedinstruction (CAI) is seen as a possible solution. Throughnetworked software, CAI resources can be made availableto students, laboratory experiences can be simulated andstudents can gauge their progress through self-assessmentand drill-type exercises. In addition, studenVstaff contacttime can be directed to activities more productive thanlaboratory supervision.
While it is often argued that CAI is potentially useful as aneducational tool, tertiary education in South Africa has notintegrated such technology widely into curricula. Reluctanceto do so may in part be due to the lack of vividness orrealism of presentations, but may also be ascribed toeconomic, practical and administrative constraints. Withrapid advances in sound, video and image management onpersonal computers, interactive multimedia is now availableat relatively low cost, and may act as a catalyst to realisethe full potential of CAI. Mayers' suggested that ifmultimedia components were included in CAI, the learnerwould be enticed into and experience an enriched learningenvironment.
While multimedia-based CAI appears an attractivesolution, several questions must be asked beforewidespread implementation is attempted. Has it been shownto be any better than existing forms of CAI? Does it work inour multicultural educational environment? Is it a resourcethat will help close the gap for educationally disadvantagedstudents, or will it disadvantage them further? As fewstudents at our medical school have had exposure tocomputers and computing, what is the effect of a lack ofcomputing skills and computer literacy on successful use ofinteractive GAl?
While much research is under way to evaluate multimediabased CAI, the response to all four questions is the same the technology is too new to provide a valid answer.
As a pilot study, one section of the second-year course inhistology, viz. the eye, was chosen in which to introduce theuse of CAI as an additional resource, and to evaluate itsworth, before a decision about more widespreadimplementation was made. The present histology courseconsists of one didactic lecture per week, and 3 - 4 hoursper week of supervised laboratory microscopy. Thelaboratory is open at all times for self-study. The coursehandbook provides objectives, key references and slideinformation. The students take regUlar self-assessment testsand, at the end of each of the 6 units, take a mark-earningcompetency test. This test consists of tissue and cellidentification from histological slides and photographs andtrue/false questions, and requires brief written answers.
SAMJARTICLES
The aims of this pilot study were to write an interactivemultimedia CAI programme on the histology of the eye, toevaluate the software and its effect on student performance, .to evaluate the students' response to both the software andthe concept of CAI, and to assess the effect of lack ofcomputer literacy and experience on the use of multimediabased CAI.
Method
Programme content and developmentProgramme content was structured around the courseobjectives. A list was compiled of questions frequentlyasked by students when looking at microscopy sections ofthe eye, and of questions asked by teaching staff of thestudents. A preliminary questionnaire on problem areas inhistology had shown that 65% of the students had difficultyin identifying specific structures and cells in histologicalpreparations. These questions, their answers and theidentified areas of difficulty, including adequate labelling ofcells and/or structures, were subsequently addressed withinthe programme. A script was written for each screen of theprogramme, detailing the image to be displayed, theaccompanying text, the effect of interactions accessed bythe clicking on of words or images on the screen, and thetext of the voice/sound file to be played with the screen orits interactions.
Software was then written by the authors withinWindows™, using a commercial software authoringprogramme, Authorware Professional™. Images weredigitised from 35 mm photographic colour slides ofhistological sections of the eye with a video camera, a video'grabber' card and software. Care was taken to ensure thatthe colour reproduction of the computer images was faithfulto the normal colours seen with light microscopy. Imageswere filtered and enhanced with commercial software whennecessary, and resized to occupy a quarter of the screenwhen presented from within the programme. Severaldiagrams were drawn on a digitised pad for use in theprogramme.
Liberal use was made of voice/sound files to introducenew concepts, to give advice on the use of the interactionsin the programme, to ask questions and to supply answersto incorrectly answered questions. The voice used was thatof the staff member responsible for teaching the section onthe eye. An attempt was made to use a conversational stylein the sound recordings, so as to give the student theimpression of having an individual tutorial with their lecturer.Sound files were recorded with a microphone linked to thesound card in the computer.
Several standard interactions were used. Within the textwindow, interactivity was indicated by a word or phrase inred. Clicking of the mouse cursor on a red word resulted invarious actions, such as the highlighting of an area of thehistological image, labelling or animation of the image,presentation of additional text or sound information, or aself-assessment question relating to the topic. Otherinteractions related to alternative methods of asking andanswering questions.
A modular approach was adopted. The introdUctorymodule contained instructions on the use of a mouse, use of
SAMJ Volumr86 No.9 Srprembrr 1996 _

the programme, features of the programme such as anorientation option and interactive words, instruction on howto exit the programme, and the course objectives withregard to the histology of the eye. A dictionary of new wordsencountered in the course, including their derivations, andthe key references in the prescribed textbooks were alsoprovided.
The menu offered access to any of the 5 remainingmodules - the corneoscleraJ layer, the middle vascularlayer, the retina, the accessory structures and a slide test.Three of the 4 modules on the components of the eyeincluded self-assessment questions, which were asked inthe course of the module. Questions were either multiplechoice, true/false, text response-based or they required a'drag and drop' labelling, a method in which a label isdragged by the mouse cursor to the appropriate site on theimage. The text responses were programmed to allow forcommon spelling errors. In the event of a spelling error, the'voice' informed the student that although they hadanswered correctly, they should check the correct spellingthat appeared on the screen. Incorrect answers produced averbal explanation as to why the answer was wrong.
The fifth module, the 'slide quiz', consisted only ofquestions or structures to be identified. A total of 93questions were included in the programme, 50 in modules 1,2 and 4, and 43 questions in the slide quiz. On exiting anymodule, the student was informed of the number ofquestions attempted and the percentage of correct answers,based on the number of questions answered correctly at thefirst attempt.
Programme deliveryThe completed software comprised the 6 modules, eachcompiled as a separate programme. These were loaded onthe faculty local area network (lAN) and accessed via the 13computers in the student computing facility in the facuttylibrary. The computers were 486SX IBM™ clones, with 4megabytes of RAM, a 512k VGA card, a 0.28 colour monitor,a SoundblastefM card with attached headphones,connected via ethernet cards to the LAN file-server runningNovel! Netware 3.1. When switched on, the computers wereset to run to WindowsnA
• The icon to initiate the eyeprogramme was the only icon shown on the start-up screen,and the only instruction given the students was to press theenter key to start the programme. Further instruction on theuse of the programme and the mouse was given from withinthe programme. The programme was available to thestudents for 2 weeks. It was later made available on the LANfor a week for revision purposes.
StUdent trackingOnce within the introductory/menu module, students wereobliged to log on and enter a password in order to proceed.This information was used to generate unique files of eachstudent's progress through the programme, with the filesbeing updated and saved on the LAN file-server on exit froma module. New data were appended to each file every timea module was accessed. Information stored included thestudent's name, password, log-on time, the module chosen,time spent on the module, the number of questionsattempted and the number of questions answered correctly
at the first attempt. These files were reviewed at the end ofthe course.
Programme evaluationGiven that there were only 13 computers, we initiallyplanned to caH for 20 volunteers from the second-year classof 125 students. Thirty-four students volunteered and allwere included in the study. The students were asked to usethe programme as an alternative method of completing thesection on the eye. They did, however, also have access tothe microscopy lab if they desired.
All 125 students in the class completed a 20-question pretest on the eye before teaching commenced. At the end ofthe semester, after the final tests had been written, the sametest was re-administered. At the post-test, the stUdy groupcompleted a 38-point questionnaire covering the student'scomputing experience, programme evaluation and CAJevaluation, and five questions requiring a written response.
ResultsThe 6 modules comprising the whole programme totalled18.5 megabytes, and required apprOXimately 70 hours ofprogramming, and apprOXimately 50 hours of script writing,image acquisition and audio recording. No difficulties wereencountered with either multi-user access, or graphic andsound transmission on the LAN.
A total of 374 modules were accessed by the 34 studentsduring the 2 weeks that the programme was available on thelAN, an average of 11 ± 6.9 modules per student (range4 - 30). Five students did not complete all the modules. Theslide quiz, module 5, was the most frequently accessedmodule (Fig. 1). Students averaged 2 ± 1.2 sessions at thecomputer (range 1 - 5). Total time spent on the computer,excluding the introductory module, averaged 90 ± 71 minutes(range 31 - 328 minutes). Students in the study group spentsignificantly less time (an average of 92 minutes) in themicroscopy laboratory than the remainder of the class (170minutes) (P < 0.0001, Hest). Seven students used only theprogramme and did not use the microscopy laboratory.
96100
"0 80'"U>U>
'" 60""'" 40U>
'"E 20i=
0mod 1 mod 2 mod 3 mod 4 mod 5
Fig. 1. The number of times each module was accessed by the 34students during the 2-week study period.
All students improved their self-assessment scores withrepeated use of a module (Fig. 2). Approximately half thestudents attempted a module only once, and their selfassessment scores were on average 7 - 9% higher than thefirst-try scores of those who repeated modules.
1100 Volume 86 No. 9 September 1996 SAb,tJ
MVSJ\MJ\SJ\
September 1996
• • • A • • •• A ~.:-...... CARE ,~, ~_v__-__\.._-_~_.._J '-v
QUALITY ~~2V-':'2WFacts, trends and knowledge for doctors in today's changing health care environment
SHe negotiations successfully concluded!
Algorithm
The revised
Individual
Provider
Agreement of
Southern
HealthCare JV
meets with
the essential
principles
required by
MASA.
In this•IssueContracts page 1
Ne\'\'sand trends page 2Capitation page3&4
Letters &questions pageS
Med-DirectBank page 6ProstaticHyperplasia page 7
Prescription-of-the-month page 7
page 8
'We are therel/ \vas the general commentfrom a satisfied MASA negotiation teamafter concluding the final discussions on theSouthern HealthCare IV (SHC) contract on28 August.
The revised SHe provider contract, or'Individual Provider Agreement', as it iscalled, was initiated by MASA four monthsago, as certain aspects of the contract causedsome concern.
The revised SHC document incorporates theessential principles of the pro forma contractthat was drawn up by MASA's legaldepartment in conjunction with a legalexpert on managed care in the USA, NoahRosenberg. The pro forma contract has beenaccepted by the relevant specialist andspecial interest groups as a basis for futurenegotiations with health care £unders.
The negotiation team consisting of OrRichard Tuft, chairman of the PrivatePractice Committee, and Drs Paul Cooke,Alistair Lamont, Jos van Niekerk andChristo Botha, confirmed in a statementthat
• The revised Individual ProviderAgreement of Southern HealthCare JVincorporates the essential principles ofMASA's pro forma contract, which hasbeen accepted by the relevant MASAgroups as a basis for future negotiationswith health care funders.
• MASA does not comment on the tariffoffered by SHC JV. Acceptance of the tariffis a business decision of the individualdoctor, following advice from MASA'sspecialist and special interest groupsand/or specific IPAs.
The most important revisions concernthe following:
• SHC accepting financial responsibility forincorrectly confirming a member's
eligibility for benefits;
• confidentiality of medical records meetsacceptable norms set by MASA;
• prior authorisation for treatment andhospital admissions;
• SHC will make use of MASA's clinicalguidelines;
• regular review of the fee schedules;
• payment for after-hours services.
To facilitate communication behveen theprofession and SHC, MASA has beeninvited to nominate representatives on theSHC Management Advisory Committee.This committee will consider issues such asguideline development, admissionrequirements, fee schedule development,confidentiality and contract amendments.
MASA will also have the right to nominatea 'participating provider' on SHe's QualityAssurance and Credentialling Committees.Doctors will receive the revised agreementsshortly.
News on Sanlam HealthThe prediction that Sanlam Health's finalprovider contract will be released to theprofession in August onwards, as reportedMC&QR of August 1996, has not beenrealised, but a few draft versions of thecontract have since seen the light.
MASA has requested a meeting withSanlam Health to discuss the final contractbefore its release to the profession. Thismeeting is scheduled to take place onAugust 30.
The Private Practice Committee askedmembers not to sign Sanlam Health'scontract until so advised by their grouprepresentatives, as certain clauses in thecontract were regarded as unacceptable.
This publication has been made possible by Sanlam in the interest ofquality managed health care for South Africa. mSanlam
Don't buy newsoftw'are packages ormake drastic changesto your hardware atthis stage in order toaccommodate thenew CTP-4 (CurrentProceduralTerminology) codingsystem, warns DrGeorge Veliotes,Head, PrivatePractice of MASAand member ofPHISC, the taskgroup exploring themost cost-effectiveway to implementCPT.
Page 2
Top pharmaceutical andmedical companiesThere are six pharmaceutical and medicalcompanies listed among the JSE's top 300industrial companies, measured by total assets.They are:
• SA Druggists (ranked 52) with total assetsworth RI 584 million, a net profit ofR 12~ million and a turnover ofR ~68 million (August '94 to '95).
• Clinics (ranked 68) with total marketassets worth R 1 079,5 million, a netprofit of R 42,1 million and a turnover ofR 840,8 million (September '94 to '95).
• Adcock Ingram (ranked 93) with totalassets worth R 713,7 million, a net profitof R 131,1 million and a turnover ofR 1 165,8 million (September '94 to '95).
• Presmed (ranked 173) with total assets ofR 162,1 million, a net profit ofR 14,0 million and a turnover ofR 171,5 million (February '94 to '95).
• Medex (ranked 175) with total assets ofR 157,7 million, a net profit ofR 10,6 million, and a turnover ofR 51,1 million (April '94 to '95).
• Aukland (ranked 259) with total assets ofR 28,5 million, a net profit of R 2,6million and a turnover of R 41,5 million(June '94 to '95).
Source: Filwllcial Mail SpecialSlIroey of Top Companies inSOllth Africa, 28 June 1996.
New clinic group competeon the PHC marketPharma Clinic, a new division of themedical supply company Medhold Lld,announced its entrance into the managedcare market on the primary care level with aplan to convert more than 400 retailpharmacies into private care centres overthe next three years.
Each of these pharmacies will offer a lowcost private health care package toemployed people without medical cover,according to general manager, MarkHyrnan.
He said at a media launch at Summer Placein Johannesburg, property of the Krokfamily, that health care principles will beapplied in these centres. Clinics would bestaffed by a primary health care nurse,supported by a general practitioner.
Fee-for-service patients would payR30 for a PHC nurse consultation,diagnosis and treatment, dispensed by thepharmacist. Further treatment would be fortheir own account.
Capitation patients would be recruitedthrough employer groups and pay monthlyfees of behveen RI04 and R120 permember per month for nurse and GPconsultations and treahnent, as ,vell asaccess to further treatment on referral.
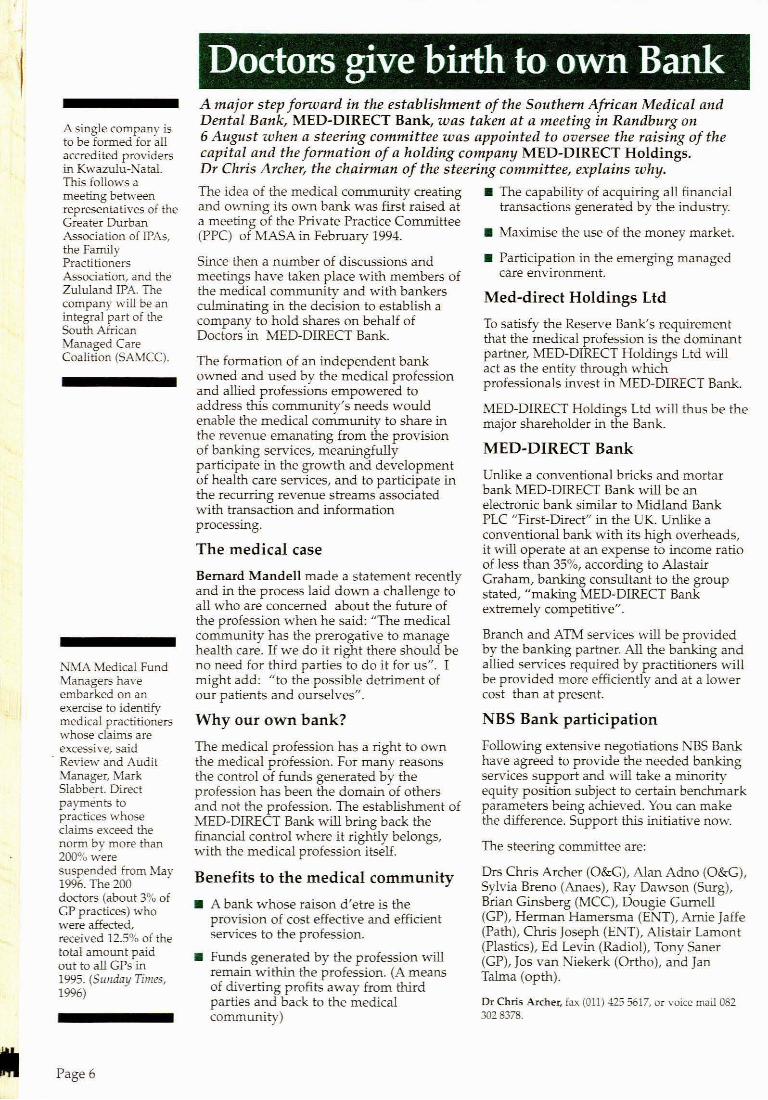
Ranking of medicalschemes administratorsMedscheme (Pty) was ranked first amongmedical schemes administrators in thelatest Financial Mail Special Suroey of TopCompanies in South Africa, (28 June 1996) inthe category for average members,contributions received and administrationfees and AMA second. D&E was rankedfirst in the categories for administrationsfees as a percentage of contributions, aswell as for administration costs per month.
MEDICAL SCHEMESADMINISTRATORS 199~
Contri-Average butions Admin
memOOs received fee;Name 1994 (Rm) Rank (Rm)
Medscheme (Ply) 543922 3155,0 1 195$AMA 193 270 1172,7 2 67.4D&E 117 631 6535 3 323Sanmed 93559 fJ:6,9 4 34.8Northern mm 492,0 5 371Old Mutual 66865 BP 6 27.1
Adminfees Admin
as%of costscontri· I""
Name butions Rank month Rank
Medscheme (Ply) 611 4 30,00 3AMA i75 3 79JJ3 2D&E 4.9-l 1 = 15anrned i74 2 30,'J7 4Northern 756 5 40,20 6Old Mutual 7.74 6 13;9 5
Soun:e' Gm Thieny
The 1996 DiRdwJ of SoaIILAfJkaDCliDkaI guideIiaes tIut4f • JUdy{lit pages PLUS tIm!e-, S npdares~,earl, is _ a.ailabJe at Il198 formembemand1l298__emhrs Itcanbe onte.ed m- Roget Maaf4mald,MASA P....... at" Cape 1'owD;.llI!l(021) Sl:h1lItlI,. _ lax (82l) 531-4126.

1Jelieve me, it will not go away' (part 3)
In this third article in a series based on workshops held in SOllth Africa, Dr RichardF. Corlin, a gastroenterologist in private practice in Santa Monica, California, andspeaker of the American Medical Association (AMA) HOllse of Delegates, expandsfllrther on the topic of risk-sharing.
At some point
you will need
to negotiate a
capitation rate
with the funder.
You cannot do
that without
data or
information.
The information
you need
includes all the
things you do
in significant
quantities, and
how many you
do for each
funder.
THE payment strategies of managed careorganisations often go through differentphases. Initially it will be some version ofwhatever they pay you now. Then themanaged care organisations will try tointroduce a reduced fee for service rate inreturn for more patients as everybody won'tbe on the contract, and in return for earlierpayment.
The next step will be a capitated system - towhich I am not fundamentally opposed - butyou will have to knOVl hov..r to work with it.
One of the minimal advantages under acapitated system is that billing costs areremarkably reduced because you only haveto keep track of how many people areenrolled in the plan. You also get a fixedamount of money per member per month.
You also need to know that at some pointyou will be asked to negotiate a capitationrate with the funder. You cannot negotiatethat rate blindly and without data orinformation.
So what data or information do you need?Firstly a computer system and a soft-warepackage that allm·\' you to obtain certaininformation from your system.
You will need information on all the thingsyou do in significant quantities, and on howmany you do for each funder. For examplehow many consultations, office visits,gastroscopes, endoscopes. And you'd betterbe able to get the information off youcomputer, because if you have to ask thefunder for the information he will think thatyou are an idiot.
Without that information you cannotnegotiate a capitated rate. Now why \·\,ouldthey want to negotiate a capitated rate'Because they want to transfer the risk ofaccess utilisation of patients from them toyou. If you are on a capitated rate, the MHCcompany can predict its costs accurately,and you take the risk.
Before you can negotiate, you need to knowhow many people they have covered undera certain plan. And you need to ask themho'" many people they had covered duringeach of those months.
With that information you will be able to
tell if the capitated rate they offer, is fair. Forexample, if I did an average of 12colonoscopies per month for people in aplan for the last two years, and they paidme S 400 per colonoscopy, I would get$ 4 800 per colonoscopy per month. If therewere 1 000 people in the plan, I would do12 colonoscopies for a I 000 patients permonth, and if 10 000, 1.2 colonoscopiesper 1 000 patients per month for the sameamount. In gastroenterology the typicalcapitated rate offered by MHC companiesstarts at SOc per member per month. Thequestion is: \''lhat does that 30c mean? Is itenough? Is it more than enough, or is itless?
How do I work that out? If there are 10 000people in the plan at SOc per member permonth, it will mean S 5 000 a month for acolonoscopy. 1 were previously paid S 4 800.Under the capitated system it would meanthat I \vill receive more or less the sameamount. Tcan live with that.
If, however, they only have 1 000 membersin their plan and they offer me SOc permember per month, I will only get S 500 permember per month where I used to get S 4800, and I cannot begin to live with that.And if they have 20 000 members in theirplan I would receive $10 000 a monthinstead of $ -+ 800, which is a huge bonus.
The point is that if you don't have thedata, you won't know if a negotiated rateof SOc per member per month is areasonable, or a great rate, or whether itwill it drive you into bankruptcy.
Let's recap some of what was said in thefirst two articles: What will be the outcomeof a properly run managed care system?
• A significant drop in hospital patient daysof at least 50%.
• More work will be done in your roomsand you will notice tha t for every $1000dollars you generate in your office, it costsyou a lot more to generate the same amountin hospitals.
• Because more work will be done at yourpractice instead of at the hospital, youroverheads will tend to rise. You \·\,ill have tocut on overheads as far as possible.
Page 3

Risk-sharing: Capitation fees
Things to doand records tokeep:
Patient files
Capitationservice contractfile
Register ofpatientconsultations
Patienteducationprogrammes
Records oroutcome andtreatment
An average of 45%of all primary caremedical senrices inthe USA covered byHMOs are capitated,according to a recentsurvey by lnterStudyPublication, aresearchorganisation. ~10spaid 27.30
0 ofprimary health careservices under fee-for-servicearrangements, 7.2%through relativevalue scale systems,and 8.5% to salariedhealth care workers.(American HealtJzline,9 July 1996).
Page -!
CAPITATION is when a fixed amount ispaid to a provider by a health plan to coverthe cost of health care delivered for aperson. The term usually refers to anegotiated rate per member per month paidto the health care provider, regardless of theuse of services. The provider is responsiblefor delivering or arranging for the deliveryof all health services required by thecovered person under the conditions of theprovider contract.
This differs from fee-far-service contracts inthat the funder carries the volume risk andthe medical practitioner submits a feeaccount far every patient who attends.Under capitation the funder has cappedtheir liability by the amount of thecapitation fee and the medical practitionercarries the risk relative to the number ofpatients who attend.
Practice management must change so thatthe medical practitioner is fully aware of theimplications of capitation contracts.
The first implication for your practice willbe in the area of record-keeping. Thepractitioner needs to maintain the followingrecords and statistics:
• Patient file: This would continue as in thepast to contain clinical history of the patientin the prescribed manner.
• Capitation Service contract file: This filewill include the details of the definedservices which are to be provided in termsof the contract. The file will need to beupdated with further definition of servicesthat result from enquiry and funderupdates. It is important to understand whenthe patient mayor may not be referred to aspecialist and the terms of referral asprescribed by the fund er. If a patient isincorrectly referred, the funder may refusepayment and seek payment from thepractitioner or the patient. Similarly, therules for admitting a patient to a day clinicor hospital need to be understood andfollowed to protect both practitioner andpatient from embarrassment. Conversely,the practitioner will not want to carry out aprocedure which can be referred to aspecialist against payment by the fund.
• Register of patients: This is an extremelyimportant function. The patient may onlyreceive attention under the contract if they
are still paid up members of the fund. Themonthly returns from the funder will adviseof changes in membership and if thepractitioner is not kept advised of a changethe patient could receive attention when nolonger a member of the fund. This willlead to drawn-out fee collection proceduresar even bad debts. The practitioner willintroduce a process whereby the fund'smembership list is checked against theregister of members before the start of eachmonth. When a patient presents for aconsultation the practitioner will check theeligibility of the patient against the registerbeforehand.
• Register of patient consultations: Feeaccounts are no longer prepared by thepractitioner. The introduction of a registerwhich records each patient visit and theprocedures carried out for each visit hasbecome important for two reasons:
1. the funder may require statistics. Thefunder used to collate statistics fromfee-for-service accounts and now seeksanother method of information collection;
2. the practitioner will need to have basicprocedure volumes to manage the practiceand as a base far future fee negotia tions.
• Patient education programme: Theobjective is to improve the health status ofthe patient without adding to the averagenumber of visits per patient per annum. Toachieve this end the funder and thepractitioner must work together to educatethe patient on matters such as preventivemedicine, early consultation, self-diagnosis,self-medication and healthy living habits.The practitioner will develop and introducean ongoing patient education programmeusing material supplied by the Funder andother organizations.
• Outcome and cost of treatmentawareness: Practitioners have in the pastenjoyed practice habits which carried littleor no risk to their income and lifestyle. Theintroduction of capitation means that therisk has been transferred. It will now benecessary to maintain records of theoutcomes of particular treatment regimes sothat the most cost effective protocol can beadopted for treating patients in the future.
Malcolm Bro\l\o"ll CA (SA), Health Care Consultant, tel
and fax (012) 47-f>l68.

Speak your mind! Letters and questions
Strategic HealthCare Systems(Stratmed), inwhich ThebeHealth Care holds acontrolling interest,secured a tender ofRlOO million torenovate theNorthernProvince'5 heal thservices. 1t willinclude the trainingof hospitalpersonnel in thehandling,distribution andstoring of medicalsupplies, thehandling ofmedication andestablishing of amedical database(Beeld, 5 July, 1996).
The principles of set-off
D.L Peannain, Legal Advisor, ANLA (Pty)LTD, writes: The subject of set-off is poorlyunderstood within the health care industry.In an article on the Sou them HealthCare JV(SHC) provider contract (MC&QR, May1996) the writer observes that SHC hasagreed to review a clause which gives SHethe right to reverse payment for thetreatment of a patient not eligible forbenefits.
This is called set-off, but set-off within ahealth care context is not usually illegal.The clause proposed by SHC is legal.Indeed, set-off will automatically applywhere there is a contract. Set-off applies toall commercial affairs, includingtransactions within the health care industry.
Set-off is a method by which debts may becancelled. Debts arise from contracts butthey can also arise where no contract exists,e.g. where one person has been unjustifiablyenriched at another's expense.
Set-off occurs when parties are reciprocallyindebted to each other. Set-off can occurbehveen the scheme and its men1bers \".iherethere is no contract to the contrary behveenthe scheme and the provider. Whereoverpayment is made to a provider inrespect of a patient A and patient Asubsequently incurs further medicalexpenses with the same provider and thenclaims these from the scheme, the laterclaim may be offset against the earlieroverpayrnent.
Set-off can also occur \vhere there is acontract behveen the provider and thescheme, regardless of whether the claimsconcerned are for different patients.Contracts do not have to be \'\'ritten to bevalid.
The SHC contract, in requiring the providernot to bill the patient, substitutes thescheme as the debtor. This is not illegal. Thelaw requires that a statement be sent to thepatient. The provider is not required todemand payment from the patient.
Set-off operates by operation of law. Set-offis not implemented by anyone. Unless it isspecifically excluded, set-off will occur assoon as the parties incur reciprocal debts.For set-off to occur, the claim must beliquidated. It must be evident that the debtis due and the amount thereof.
Many providers have tacit agreements withmedical schemes. The standard terms are asfollows:
• The provider agrees that if the schemeconsistently pays directlv all accmmtssubmitted in respect of members of thescheme, he/ she will consistently charge theRAMS recommended tariff (RRT).• Direct payments will be made only to thelimit of the RRT. Charges in excess of thiswill be reduced to the amount of the tariff.If the provider persists in charging in excessof the tariff, direct payment status will bewithdrawn.• The scheme is obliged to give reasonablenotice of termination of this arrangement.• The arrangement may be terminated if theprovider acts fraudulently or abuses theagreement.
The reason for the existence of suchcontracts is the mutual benefit of providersand schemes alike.
Esme PrillS, Manager: Legal Affairs ofMASA, llllSWers: The reversal of paymentpractised by medical schemes to recoverincorrect payment from doctors should onlybe allowed in exceptional circumstances. Inthe past year we obtained legal advice fromcouncil on two occasions to determinewhether schemes had the right to recovertheir losses in this manner.
MASA was advised that medical schemescould indeed reverse payment under certainconditions, but that each case should bedealt with individually. Tt would appearthat the system used by the schemes todetermine whether a patient qualifies forbenefits or not, is inefficient, and thatincorrect information is sometimesprovided. At its recent meeting the PrivatePractice Negotiating Committeerecommended tha t schemes should beencouraged to improve patient informationsystems to prevent under- and overpayment for services. This aspect would benegotiated with managed health careorganisations in future to eliminate thispractice.
If you have any questions, comments,or special issues you would like to seeaddressed in MQ&QR, we undertaketo get experts to answer it! Pleaseaddress your letters to: Ilia van derLinde, PO Box 27232, Lynnwood 0005.or fax: (012) 47-6101, e-mail:[email protected]
Page 5
Doctors give birth to own BankA major step forward in the establishment of the Southern African Medical andDental Bank, MED-DIRECT Bank, was taken at a meeting in Randburg on6 August when a steering committee was appointed to oversee the raising of thecapital and the formation of a holding company MED-DIRECT Holdings.Dr Chris Archer, the chairman of the steering committee, explains why,
The idea of the medical community creating • The capability of acquiring all financialand owning its own bank was first raised at transactions generated by the industry.a meeting of the Private Practice Committee(PPC) of MASA in February 1994. • Maximise the use of the money market.
A single company isto be formed for allaccredited providersin Kwazulu-NataLThis follows ameeting behV'eenrepresentatives of theGreater DurbanAssociation of IPAs,the FamilyPractitionersAssociation, and theZululand IPA. Thecompany \'\"ill be anintegral part of theSouth AfricanManaged CareCoalition (SAMCC).
NMA Medical FundManagers haveembarked on anexercise to identifymedical practitionerswhose claims areexcessive, said
. Review and AuditManager, MarkSlabber!. Directpayments topractices whoseclaims exceed thenorm by more than200% weresuspended from May1996. The 200doctors (about 3% ofGP practices) whowere affected,received 12.5% of thetotal amount paidout to all GPs in1995. (Sunday Times,1996)
Page 6
Since then a number of discussions andmeetings have taken place with members ofthe medical community and with bankersculminating in the decision to establish acompany to hold shares on behalf ofDoctors in MED-DIRECT Bank.
The formation of an independent bankowned and used by the medical profeSSionand allied professions empowered toaddress this community's needs wouldenable the medical community to share inthe revenue emanating from the provisionof banking services, meaningfullyparticipate in the growth and developmentof health care services, and to participate inthe recurring revenue streams associatedwith transaction and informationprocessing.
The medical case
Bemard Mandell made a statement recentlyand in the process laid down a challenge toall who are concerned about the future ofthe profession when he said: "The medicalcommunity has the prerogative to managehealth care. If we do it right there should beno need for third parties to do it for us". Imight add: "to the possible detriment ofour patients and ourselves".
Why our own bank?
The medical profession has a right to ownthe medical profession. For many reasonsthe control of funds generated by theprofession has been the domain of othersand not the profession. The establishment ofMED-DIRECT Bank will bring back thefinancial control where it rightly belongs,with the medical profession itself.
Benefits to the medical community
• A bank whose raison d'etre is theprovision of cost effective and efficientservices to the profession.
• Funds generated by the profession willremain within the profession. (A meansof diverting profits away from thirdparties and back to the medicalcommunity)
• Participation in the emerging managedcare environment.
Med-direct Holdings Ltd
To satisfy the Reserve Bank's requirementthat the medical profession is the dominantpartner, MED-DIRECT Holdings Lld willact as the entity through whichprofessionals invest in MED-DIRECT Bank.
MED-DIRECT Holdings Lld will thus be themajor shareholder in the Bank.
MED-DIRECT Bank
Unlike a conventional bricks and mortarbank MED-DIRECT Bank will be anelectronic bank similar to Midland BankPLC "First-Direct" in the UK. Unlike aconventional bank with its high overheads,it will operate at an expense to income ratioof less than 35%, according to AlastairGraham, banking consultant to the groupstated, "making MED-DIRECT Bankextremely competitive".
Branch and ATM services will be providedby the banking partner. All the banking andallied services required by practitioners willbe provided more efficiently and at a lowercost than at present.
NBS Bank participation
Following extensive negotiations NBS Bankhave agreed to provide the needed bankingservices support and will take a minorityequity position subject to certain benchmarkparameters being achieved. You can makethe difference. Support this initiative now.
The steering committee are:
Drs Chris Archer (O&G), Alan Adno (O&G),Sylvia Breno (Anaes), Ray Dawson (Surg),Brian Ginsberg (MCC), Dougie Gumell(GP), Hennan Hamersma (ENT), Amie Jaffe(Path), Chris Joseph (ENT), Alistair Lamont(Plastics), Ed Levin (Radiol), Tony Saner(GP), Jos van Niekerk (Ortho), and JanTalma (opth).
Or Chris Archer, fax (011) 425 5617, or voice mail 0823028378.

Benign prostatic hyperplasia (BPH)BPH is a consequence of aging affecting more than 70% of older men.It is associated with recurrent urinary infections, bleeding andbladder stones. Men with similar symptoms vary considerably in thedegree to which their condition bothers them.
Treatment
Many patients are willing to tolerate symptoms when fully informedabout the variable natural history of the condition, the risks andbenefits of possible treatments and the large placebo effect.
• Watchful waiting seems to be the safest and most cost-effectiveoption for men with mild and moderate symptoms. Clinicallydiagnosed, untreated BPH shows a variable pattern of exacerbationand remission. In a 7-year study 10% developed acute retention and48% had no symptoms at final follow-up. Acute retention at thebeginning was not associated with worse symptoms later. Prostatesize did not correlate with symptom severity" degee of obstruction ortreatment outcome.
• Alpha-blockers relax muscles in the bladder neck and prostate. Allseem to produce small improvements in a short time. Adverse effectsare usually minor though dizziness and tiredness may be severe.
• Finasteride \'\'ruch reduces the level of dihvdrotestosterone causesthe prostate to shrink. Reduction in sympto~s takes months. In 123patients sexual dysfunction affected 19%.
• Audits showed 1/4 failed to improve symptomatically aftertransurethral resection [TURF]. Men with severe symptoms weremost likely to benefit; those with mild or moderate symptoms ended
up worse. Impotence, incontinence andstrictures were long-term adverse effects.More than 70% experienced dry or retrogradeejaculation.
• Open prostatectomy leads to slightly higherrates of improvement. Re-operation rates arelower. Complications are more common.
• Incision of the prostate [TUIP] is onlysuitable for glands;::: 30g. In these men it is aseffective as TURP. It is quicker, uses fewerresources and causes less tissue damage thanother forms of surgery,
• Laser prostatectomy seems slightly lesseffective than TURF but is safer and causesless complications. Disadvantages includelengthy catheterisation, persistent irritation,dysuria and a delay in benefits,
• The effectiveness of thermotherapy,transurethral needle ablation [TUNA], highintensity ultrasound and balloon dilatation isdoubtful or unknown.
Adapted with permission for Effectiveness Matters Val.2(2) 1995. Univ. of York, l\THS Centre for Reviev.'s &Dissemination, Heslington, York, Y01 SDD,
Prescription-of-the-month
Bernard van de Wal, fax: (021) 932-2189, and VictoriaPinkney-Atkinson, fax: (012) 481-2100.
The patient should be admitted for a completephysical and psychological assessment andweaning off the present medication. Themanagement plan may include medicationlike non-narcotic analgesics, anticonvulsantsand antidepressants. Psychotherapy andpossibly hormonal treatment may beconsidered.
The management of chronic pain can be extremely difficult and oftenneeds teamwork by several clinical disciplines to assess all the
This prescription was sent to us by a group perfonning dn~g utilisation review. TIle main comment related to theabuse of the medical aid system by doctors. The prescription is undeniably un affordable. But we sense that thereis an underlying problem relating to the comprehensive management of a person living with chronic pain. Gurversion follows. We have not considered dn'g interactions - that is another story.
A patient with arachnoiditis is treated with the medication marked!. physical and psychological aspects of theZofran® is prescribed for the nausea caused by fentanyU Other condition and of the management.medications are given as indicated: Barlow's syndrome3
; idiopathic A fr th h'b' . f hioedema' ; hypermotility syndrome'; Zyrtec® for pruritus due to part. om eh pro J thhVelmincost 0 t s. .f t I prescnphon, t e ovenv e g impressIOn IS
en any , of a very desperate prescriber who has beenDilemmas forced to add on drugs to counteract the
fetanyl's side effects e.g, ondansetron,domperidone, scopolamine, cyclizine,lactulose, senna, cetrizine and even propanol,the diuretics and the lofepramine.
The prescription also presents a compellingargument against the use of opioid analgesics(like fentanyl) in the management of chronicnon-eancer pain. In this patient the opioidside effect could even explain themanifestations ascribed to the other diagnosedconditions.
Medication Dosage CostR1month
Durogesic TfS® (fentanyl) 100mcg/h' 72 hours 2089,12Durogesic TTS® (fentanyl) 50mcg/h l 72 hours 1 120,64
Emdalen® (lofepramine) 70mg' at night 155,03Zofran® ondansetron) 8mgt..: 12 hourly 4850,24Motilium® (domperidone) 10mg' 8 hourly 187,38ScopodermTIS® (scopolamine) 1,5mg 1 72 hourly 238,12Purbloka® (propranolol) 4Omg' 12 hourly 36,44Burinex-K® (bumetanide + KCl)' 2 daily 85,24Aldazide® (spironolactone + HCTZ)' 2 daily 146,89Zyrtec® (cetirizine Hcl) 4OOmg'·' daily 111,26Brufen® (ibuprofen) 6OOmg' 8 hourly 122,70Covamet® (cyclizine HO) 4 x day 127,20Duphalac Dry® (lactulose) pm 161,80Senokot® (sennosides) pm 32,69
TOTAL R9464,75
Page 7

Adult \,"ith low back painof <3 months durationand with no assessed
serious spinalconditions.
Pro\"ide assurance - educateabout back problems
Doesthe patient
need help to relieve YESsymptoms?
NO
Recommend acti\"ity alterations toa\-oid back irritation,
Review activity limitations (if any)due to back problem: encourage tocontinue or return to normalactivities (including \....ork, with orwithout restrictions) as soon aspossible.Encourage low stress aerobicexercise.
ACUTE LOW BACK PAINALGORITHM: TREATMENT
Recommend/prescribe comfort options based on risk/benefits and patient preferencefrom the list belo,,·:.
RECOMMENDED
Nonprescription analgesics
• Acetaminophen (safest) • NS}\.IDS (aspirin!, ibuprofen·).
Prescribed Pri'3Cri~d
pharmaceutical pl'ysical methodsmethods
Nonspecific low back Nonspecific low Sciaticasymptoms and/or back symptomssciatica
Other .:'-1SAIDs I Manipulation (inplace of medicationor a shorter trial ifcombined with:"5;\105)
OPTIONS
Nonspecific low back Nonspecific low Sciaticasymptoms and/or back symptomssciatica
• Muscle relaxants:J' . PhYSical agents · Manipulation (in• Opiods :'-'-1 & modalities~ place of medication
(only heat or cold or shorter trial iffor home combined ,..!ithprogrammes) NS."JDs). Shoe insoles~ · Physical agents
modalities
· Few days' rest
• Shoe insotes~
N 1. Aspirin and other I\SAIDs are not recommended or use in
0 combination with one another due to the risk of Cl complications.
T 2. Equivocal efficacy3. Significant potential for producing drowsiness and debilitation:
E potential for dependency.
S -I. Short courses of a few days only for 5e,"ere symptoms.
Symptoms improving?
YES
( Return to normal activity )
~-~
NO
Follow-up and e\'a!uation of the 510\\' torecover patient.
See October issue of Mnllaged Care andQuality Rrf/ieu;
Algorithm adapted by Victoria Pinkney-Atkinson, MASA Quality Care. From the US Agency for Health Care Policy and Research Clinical PracticeGuideline 1994 Acute Low Back Problems in Adults.
Managed Care & Quality Review is a publication of the Medical Association of South Africa, PO Box 20272, Alkantrant, 0005. Editor: loa van derUnde. Inquiries can be directed to the ~.ASA Quality Care Department, teI, (012) 481-2034, fax (012) 481-2100. e-mail: masah·[email protected]. The\'iews expressed in this publication are not necessarily !:hose of ~1A5A, the As..-.ociation's special interest groups, or our sponsors.
SAMJARTICLES
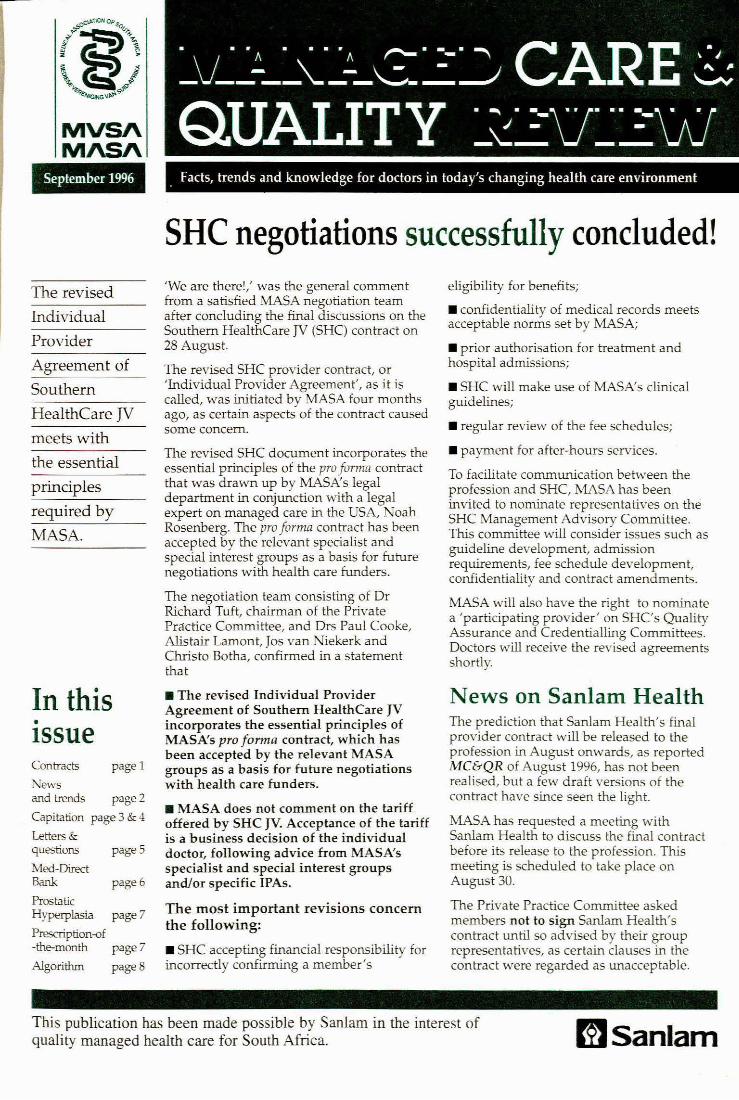
Fig. 2. The scores achieved on first and last attempt at each ofthe modules. The increases are significant for each module(P < 0.002, p~ired t-test).
I • First attempt D Last attempt I
Thirteen of the 34 students (38%) indicated that they hadhad no computer experience prior to taking part in thisstudy. These students spent less time in the laboratory andmore time using the computer (119 minutes) than theexperienced users (73 minutes). In addition they accessed,on average, 2 modules more per person than theexperienced computer users. There was no significantdifference between experienced users and new users in theirpattern of use of the programme, in the marks obtained inself-assessment scores within the modules, in their pre-and post-test scores (Table I) or in their end of block testmarks.
9%
3%
15%3%
21%
12%
82%
85%
70%
94% 0% 6%
88% 3% 9%
88% 6% 6%
0% 6% 94%
15% 15% 70%
73% 15% 12%
The questions and answersprovided in the programmehelped me learn.
The programme provided mewith important basic knowledge.
Using the programme was ahelpful learning experience.
This programme disruptedmy studies.
I would like the programmeto tell me facts rather thanask me questions.
I would like the programmeto tell me how often my firstanswers were correct.
The interactive labelling mademore sense than beingpresented with an alreadylabelled image on the screen.
The information in theprogramme was presented ina logical, ordered fashion.
I would have liked thereto be more questionsin the programme.
Table 11. Questionnaire - sample of Questions and responses
Positive Neutral Negative92
mod 5
95.7
mod 3mod 2
97.5100
80
?fi 60
40
20
0mod 1
Table I. Mean scores obtained in the pre-test and post-test. Theimprovement in scores between groups was not statisticallysignificant
Study group Non-users P-value
Pre-test 22.1% 23.2% 0
Post-test 65.6% 60.7% 0
Improvement 43.5% 37.5% 0.12
QuestionnaireIn addition to the 13 students who had had no previouscomputer experience, 1 other had not used a mouse before.Of these 14, only 1 student claimed to have had difficulty inusing the mouse. No students found that their lack ofcomputer experience hindered their use of the programme.All felt that the instructions within the programme wereadequate and found it easy to work through the modules.All but one found it interesting to use the programme.Four students had difficulty in starting up the programmeand 6 did not know how to exit the programme, despite a'quit' button's being permanently displayed on the screen.
The questions and responses of the students to the worthof the programme and its content are summarised inTable 11. All but 1 student favour another programme like thisin histology. Sixty-seven per cent were in favour of CAlsbeing introduced into physiology and biochemistry, whileonly 1 (3%) was against this. Ail but 1 student felt that CAIhas a future in the teaching of medicine. (The dissenter wasthe same student in each case.)
Forty per cent of the students had had no previousexperience with a mouse, but this did not appear to be aproblem, as all the students found the instructions adequateand over 90% found it easy to use and work through theprogramme. There was consensus that the programmehelped students to learn (94%), provided important basicknowledge (88%) and was a helpful learning experience(88%).
In response to what students liked best about theprogramme, 'the graphics' and 'the interactive labelling'were the most common replies, with 'easy to learn from'being the next most common. Other responses included'ease of use', 'not having to use a microscope', 'the selfassessment questions', 'the sound' and the 'orientationfeature'.
Aspects of the programme they liked the least were thepoor sound quality, the lack of a 'zoom' facility to changemagnification at will and the inability to return to completedscreens. Several wanted more information given by voice.In response to what they would like to change within themodules, the response 'nothing' was the most frequent after'improve the sound'. Asked what they would like to seeadded to future programmes in histology, 'more questions','a zoom facility', and 'a return option' were most commonlyrequested. Several students wanted more slides, and 1asked for a slide gallery from which he could choose theslide that he wished to view.
During the week that the programme was available forrevision, an additional 30 students who were not in the studygroup accessed 122 modules of the programme. The slidequiZ was the one most frequently used.
SAMJ Volul1It' 86 No.9 St'ptt'mbt'f 1996 1101

DiscussionWhile the generally positive response of the students to thispilot study suggests that there may be a place for morewidespread implementation of multimedia-based CAI withina subject such as histology, the various questions asked ofmultimedia-based CAI and issues raised in the objectives ofthe pilot study need to be examined more closely.
The first objective was to produce an interactiveprogramme on the eye. Why write 'in-house' software? It isa common phenomenon in educational softwaredevelopment that educationists prefer to use a home-grownproduct: This preference is understandable in clinicalmedicine, where investigation and treatment algorithms mayvary in different countries and from centre to centre. Withinthe basic sciences, the need is less apparent, save topresent information in a specific form and at a specific level.Another advantage is that it is easier and cheaper to updateand modify the software as and when required. Multimediabased CAI is still so novel that Irttle commercial software isavailable, thereby necessitating self-development at present.
Much of the time spent on this project - 120 staff hours was taken up with finding solutions to programming problemsand improving the end product. Once over the learning curve,the final module of 3.7 megabytes was produced in under 3hours. The software was written without the services of acomputer programmer, which confirms that it is possible forthe 'average' computer-literate academic to producemultimedia CAI. While a programmer would reducedevelopment time, academic staff input is still required towrite the script and to edit the software.
Software evaluation can take place at different levels,ranging from student participation in software design anddevelopment, to academic peer review and end-userreview. J This programme has undergone peer and end-userreview. The students fanned two groups, the computerliterate. familiar with the standards of commercial softwareand games, and those with no standards against which tojudge the end product. The instructions within theprogramme were found to be adequate. Both groupsexpressed satisfaction with the content, the quality of thegraphics and the interactions, including the labelling. Thisapproval probably reflects the time taken to identify studentproblem areas before writing the script. The quality andquantity of the self-assessment questions, while generallyacceptable, did not meet the expectations of all thestudents, some of whom found them too easy while othersconsidered them too difficult. Academic peer review withinthe faculty was favourable_
The use of sound was considered a positive feature. Thepoor quality of the sound was, however, the major problemidentified in the programme_ This was partfy a consequenceof the quality of equipment used for making the recordings,the low recording sampling rate used to minimise file size,the standard of the sound card through which it was playedand the quality of the headphones used by the students.These are all issues that warrant attention if voice files are tobe used by students who have become used to the highquality of digital sound.
The lack of computer literacy and experience in the use ofa mouse was identified as a possible problem that mightrestrict the use and efficacy of multimedia CAI. The group ofstudents lacking computer literacy were nonetheless able to
use the programme and accessed, on average, 2 modulesmore than their more experienced peers. While this wasencouraging, the problem has not been fully resolved, asonly 13 of the 75 (17%) students with no computerexperience volunteered for the study. It is of interest that 4of these 13 students used only the computer programmeand did not make use of the microscopy laboratory.
The improvement in the post-test scores of the CAI usersis in keeping with other studies, which show that studentsexposed to CAI score better in unannounced testing. 4 Ofgreater importance is the finding that, despite a significantreduction in time spent in the microscopy laboratory, the CAIusers fared no worse than the rest of the class.Notwithstanding the bias of the sample in favour ofcomputer-literate students, only 1 student, an experiencedcomputer user, was not in favour of general implementationof multimedia CAI in histology.
While the students' response to multimedia CAI appearsfavourable, it is the response of administrators faced withfinancing the implementation of CAI that will dictate the futureof the medium in many institutions. The provision of initialinfrastructure is costty. A student computing facility isrequired. This should preferably be a lAN linked to a facultyor university network. An adequate number of computers isneeded to meet the demand of the student population. Thereis the additional cost of ownership of computer hardware,which conservatively requires replacement and/or upgradingevery 5 years. The students should have access to thecomputers after-hours, so that they may work at their ownpace and in their own time. Depending on the siting of thestudent LAN, this may have security and staffing implications.There is, in addition, the cost of software and softwaredevelopment in terms of both finance and staff time. Againstthis burden must be weighed the annual costs of laboratoryequipment purchase and maintenance, laboratory technicalstaff salaries, the provision of expendables. and academicstaff time given to laboratory supervision.
This pilot study was undertaken to assess the potentialuse of multimedia-based CAI as a resource in problembased teaching in a group of students with disparatecomputing skills, and as a means of reducing the need tostaff laboratories for small groups of students proceeding atdifferent speeds through their course. Use of CAI reducedstudent laboratory time and did not affect their marks. Lackof computing skills was not disadvantageous to studentsusing CAI. The lack of computing skills on the part ofsecond-year students has been identified, and computerliteracy is to be introduced into the first-year curriculum.Given the favourable response of the students, further CAIresource programmes will be designed.
This paper was presented in part at the InternationalConference on Computer Assisted Education and Training inDeveloping Countries, Pretoria, 1994. This work was funded bya grant from the University of Natal Research Office.
AEFERENCES
1. Mayen JTM. The 'M-Word·: Multimedia interfaces and their role in IMeractivelearning systems. In: Edwards AND, Holland S, ecs. Multim~la Inrl!rfaee DesignIn Education. Berlin: Springer-Verlag, 1992.
2. Mills KA. McGlade K. Computer based learning in general practIce - opuonsand Implementation. Med Tl!ach 1992; 14: 89-92.
3. Aeeves T. Evaluating interaclJVe multimedia. Educ Tech 1992; 32: 47-53.4. Garrud p. Chapman lA. Gordon SA. Herben N. Non verbal communication;
evaJuallon of a computer assisted learning package. Med Educ 1993: 27: 474-478.
Accepted 19 Mar 1996.
I 1102 \-'olumf' 86 No. 9 Sf'pumber 1996 SAM J




















