Strength at the extracellular matrix–muscle interface
11
Strength at the extracellular matrix–muscle interface M. D. Grounds 1 , L. Sorokin 1,2, *, J. White 1 1 School of Anatomy and Human Biology, The University of Western Australia, Perth, WA, Australia, 2 Experimental Pathology, Lund University, Lund, Sweden Corresponding author: Miranda D. Grounds, School of Anatomy and Human Biology, The University of Western Australia, Crawley, Perth, WA 6009, Australia. Tel: 161 8 6488 3480, Fax: 161 8 6488 1051, E-mail: [email protected] http://school.anhb.uwa.edu.au/PersonalPages/Grounds Accepted for publication 15 March 2005 Mechanical force is generated within skeletal muscle cells by contraction of specialized myofibrillar proteins. This paper explores how the contractile force generated at the sarcomeres within an individual muscle fiber is transferred through the connective tissue to move the bones. The initial key point for transfer of the contractile force is the muscle cell membrane (sarcolemma) where force is transferred laterally to the basement membrane (specialized extracel- lular matrix rich in laminins) to be integrated within the connective tissue (rich in collagens) before transmission to the tendons. Connections between (1) key molecules outside the myofiber in the basement membrane to (2) molecules within the sarcolemma of the myofiber and (3) the internal cytoplasmic structures of the cytoskeleton and sarcomeres are evaluated. Disturbances to many components of this complex interactive system adversely affect skeletal muscle strength and integrity, and can result in severe muscle diseases. The mechanical aspects of these crucial linkages are discussed, with particular reference to defects in lami- nin-a2 and integrin-a7. Novel interventions to potentially increase muscle strength and reduce myofiber damage are mentioned, and these are also highly relevant to muscle diseases and aging muscle. Force is generated within skeletal muscle cells by contraction of specialized myofibrillar proteins. These are highly organized into sarcomeres (Lloyd et al., 2004), and complex movement between the actins, myosins and many other proteins results in shortening of the muscle fiber. The central question addressed in this paper is ‘‘how is this force, gener- ated at the sarcomeres within an individual muscle fiber, transferred through the tissue to move the bones?’’ In simple terms, this requires connection of the sarcomeres through the cytoplasm to the inner face of the cell membrane of the muscle cell, and then connection through the cell membrane (sarcolemma) to the connective tissue that is attached to bones. The interstitial connective tissue that surrounds and lies between individual myofibers is referred to as the endomysium, which is a dynamic complex of many extracellular matrix (ECM) components. A great deal of attention has focused on the mechanical properties of this collagen-rich endomysium, which is organized at the ends of the myofibers into tendons. There have been many excellent publica- tions on force transmission through the interstitial connective tissue (see review by Kjaer, 2004), but these will not be covered in this review. Instead, we will focus on force transmission through the sarco- lemma and examine the intimate association of the interstitial connective tissue with the surface of the myofiber where specialized ECM components are organized into the basement membrane (also widely referred to as basal lamina or external lamina). The basement membrane is anchored to the interstitial ECM through a microfilament network rich in col- lagen VI (Wiberg et al., 2002). The basement mem- brane is linked through the myofiber cell membrane to the interior of the muscle cells and the sarcomeres through a complex series of molecules that form an integrated mechanism for the transfer of the con- tractile force (generated by the sarcomeres) to out- side the muscle cell. Force transmission through the sarcolemma Linkage through the muscle membrane is the key point for transfer of the contractile force. It is important to note that this force transfer occurs at the surface over the entire perimeter of each myofi- ber, as well as at the ends where tendons are attached (discussed in detail by Huijing, 1999; Purslow, 2002; Trotter, 2002). It seems that most of the force *Visiting Professor at the University of Western Australia. Scand J Med Sci Sports 2005: COPYRIGHT & BLACKWELL MUNKSGAARD 2005 Printed in Denmark . All rights reserved DOI: 10.1111/j.1600-0838.2005.00467.x 1
-
Upload
uni-muenster -
Category
Documents
-
view
1 -
download
0
Transcript of Strength at the extracellular matrix–muscle interface

Strength at the extracellular matrix–muscle interface
M. D. Grounds1, L. Sorokin
1,2,*, J. White1
1School of Anatomy and Human Biology, The University of Western Australia, Perth, WA, Australia, 2Experimental Pathology,Lund University, Lund, SwedenCorresponding author: Miranda D. Grounds, School of Anatomy and Human Biology, The University of Western Australia,Crawley, Perth, WA 6009, Australia. Tel: 161 8 6488 3480, Fax: 161 8 6488 1051, E-mail: [email protected]://school.anhb.uwa.edu.au/PersonalPages/Grounds
Accepted for publication 15 March 2005
Mechanical force is generated within skeletal muscle cellsby contraction of specialized myofibrillar proteins. Thispaper explores how the contractile force generated at thesarcomeres within an individual muscle fiber is transferredthrough the connective tissue to move the bones. The initialkey point for transfer of the contractile force is the musclecell membrane (sarcolemma) where force is transferredlaterally to the basement membrane (specialized extracel-lular matrix rich in laminins) to be integrated within theconnective tissue (rich in collagens) before transmission tothe tendons. Connections between (1) key molecules outsidethe myofiber in the basement membrane to (2) molecules
within the sarcolemma of the myofiber and (3) the internalcytoplasmic structures of the cytoskeleton and sarcomeresare evaluated. Disturbances to many components of thiscomplex interactive system adversely affect skeletal musclestrength and integrity, and can result in severe musclediseases. The mechanical aspects of these crucial linkagesare discussed, with particular reference to defects in lami-nin-a2 and integrin-a7. Novel interventions to potentiallyincrease muscle strength and reduce myofiber damage arementioned, and these are also highly relevant to musclediseases and aging muscle.
Force is generated within skeletal muscle cells bycontraction of specialized myofibrillar proteins.These are highly organized into sarcomeres (Lloydet al., 2004), and complex movement between theactins, myosins and many other proteins results inshortening of the muscle fiber. The central questionaddressed in this paper is ‘‘how is this force, gener-ated at the sarcomeres within an individual musclefiber, transferred through the tissue to move thebones?’’In simple terms, this requires connection of the
sarcomeres through the cytoplasm to the inner faceof the cell membrane of the muscle cell, and thenconnection through the cell membrane (sarcolemma)to the connective tissue that is attached to bones. Theinterstitial connective tissue that surrounds and liesbetween individual myofibers is referred to as theendomysium, which is a dynamic complex of manyextracellular matrix (ECM) components. A greatdeal of attention has focused on the mechanicalproperties of this collagen-rich endomysium, whichis organized at the ends of the myofibers intotendons. There have been many excellent publica-tions on force transmission through the interstitialconnective tissue (see review by Kjaer, 2004), but
these will not be covered in this review. Instead, wewill focus on force transmission through the sarco-lemma and examine the intimate association of theinterstitial connective tissue with the surface of themyofiber where specialized ECM components areorganized into the basement membrane (also widelyreferred to as basal lamina or external lamina). Thebasement membrane is anchored to the interstitialECM through a microfilament network rich in col-lagen VI (Wiberg et al., 2002). The basement mem-brane is linked through the myofiber cell membraneto the interior of the muscle cells and the sarcomeresthrough a complex series of molecules that form anintegrated mechanism for the transfer of the con-tractile force (generated by the sarcomeres) to out-side the muscle cell.
Force transmission through the sarcolemma
Linkage through the muscle membrane is the keypoint for transfer of the contractile force. It isimportant to note that this force transfer occurs atthe surface over the entire perimeter of each myofi-ber, as well as at the ends where tendons are attached(discussed in detail by Huijing, 1999; Purslow, 2002;Trotter, 2002). It seems that most of the force*Visiting Professor at the University of Western Australia.
Scand J Med Sci Sports 2005: COPYRIGHT & BLACKWELL MUNKSGAARD 2005
Printed in Denmark .All rights reservedDOI: 10.1111/j.1600-0838.2005.00467.x
1

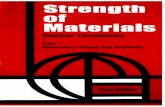
generated by sarcomere contraction may be trans-mitted laterally, across the sarcolemma rather thanlongitudinally, through the sarcoplasm (Bloch &Gonzalez-Serratos, 2003). Because of many complex-ities of muscle architecture, it is difficult to calculatethe extent, in vivo, to which this force transmission atthe sarcolemma (over the myofiber perimeter) isinitially transferred laterally through the endomy-sium to adjacent myofibers, to affect the wholemuscle, compared with the extent of direct forcetransmission longitudinally at the myotendinous(Huijing, 1999; Purslow, 2002) or myomyonal junc-tions (Paul et al., 2002). It has been proposed that atleast 50% of the force generated may be transmittedlaterally through the endomysium (see Fig. 1).A large role for integrated tension delivery across
all myofibers within a muscle fascicle is stronglysupported by studies in muscles where myofibers donot run from tendon to tendon but are joined endto end at myomyonal junctions (Paul et al., 2002;Purslow, 2002; Sheard et al., 2002). It was concludedthat the forces produced by individual motor unitsare integrated within the muscle’s connective tissueand distributed across all fibers before being trans-mitted evenly to the tendon across the entire muscle–tendon interface. Such an arrangement of myofibreswith intrafasicular terminations is common in largemammals, where muscles with fascicles longer than35mm are composed of multiple sets of overlappingarrays of short muscle fibres each with their ownneuromuscular junction (NMJ). It is noted that thisarrangement of in-series multiply innervated myofi-
bers is not common in humans and other primates(macaque monkey): despite their large size, usuallyonly simple muscles with a single myofibre stretchingfrom tendon to tendon occurs, even in muscle fas-cicles as long as 140mm (Paul, 2001).Connection of (1) key molecules in the basement
membrane outside the myofiber to (2) molecules on thesurface of and within the sarcolemma of the myofiber,through to (3) the internal cytoplasmic structures ofthe cytoskeleton and sarcomeres will be discussed withreference to generation of mechanical force.
Costameres
Before proceeding to discuss such complex molecularconnections, it is pertinent to mention costameres.Costameres are specialized sites of transmembranecomplexes, occurring over the entire sarcolemma,where the transmission of force is concentrated(Bloch & Gonzalez-Serratos, 2003). Costamereswere first recognized as rib-like structures over theZ lines of the underlying myofibrils (Fig. 1). The termhas since been used to include similar sarcolemmalstructures over M lines or parallel to the long axis ofmuscles (Bloch et al., 2002; Bloch & Gonzalez-Serratos, 2003). Costameres overlying the Z lineswere first identified as concentrations of severalstructural and peripheral membrane proteins: themost widely studied of these protein complexescontain dystrophin and dystroglycans and othersinclude vinculin (focal adhesion complex) and spec-
1a Interstitial connective tissueCollagen types I, III , VIFibronectinVitronectinTenascins (4 forms) Proteoglycans: decorin, biglycan
1b. Basement membraneLaminins −2/4, 8/9,10/11Entactin/nidogen-1Collagen type IV Proteoglycans: perlecan, agrin
1a. Interstitial connective tissue
3. Sarcomeres and cytoskeleton
1b. Basement membrane
2. Cell membrane
1.ECM
MTJ MTJ
Main ECM Types
costamers
NMJ
Fig. 1. Overview of the extracellular matrix (ECM)/muscle interface. The diagram of a skeletal muscle fiber indicates the linesof lateral force transmission across the sarcolemma at the costamers (long arrows) and myotendinous junctions (MTJ) (shortarrows). Much (50%) of this force may be transmitted laterally to adjacent myofibers so that tension is integrated and thendelivered to the tendon. The neuromuscular junction (NMJ) is also indicated. The inset shows a portion of the muscle interfaceviewed by electron microscopy, illustrating (1) the ECM with (1b) the basement membrane in intimate association with themyofiber surface, (2) the cell membrane (sarcolemma) and (3) the cytoplasm (sarcoplasm) where the cytoskeleton andsarcomeres (specialized contractile proteins) are located. The major molecules in the interstitial compartment of the ECM andthe specialized basement membrane appear in the box.
Grounds et al.
2

trin. Laminin is also concentrated at the costameresbut, unlike dystroglycan and dystrophin, is hard todetect at intercostameric regions (Bloch et al., 2002).As a result of the firm connection between thecontractile apparatus and the sarcolemmna at costa-meres, the intercostal region may bulge out or‘‘festoon’’ slightly during contraction and muscleshortening (Bloch & Gonzalez-Serratos, 2003).In general, the same molecules that are co-located
at the sarcolemma and sub-sarcolemmal regionaround the whole myofiber are upregulated at thecostamers and also where the myofiber connects tothe tendon at the myotendinous junction (MTJ),although exceptions exist. One potential majorexception to this trend, the laminin b1 chain, isdiscussed below under basement membrane. Manystudies have described the enrichment of suchmolecules at MTJ and the consequences of mechan-ical loading in both normal and dystrophicmuscles (Tidball, 1991a, b; Law et al., 1995). Preciseinformation on the relative distribution of such mole-cules is important to critically evaluate the mechanicsof molecular interactions around the myofiber.This trend for a greater concentration at MTJ is
supported by pronounced immunostaining for thebasement membrane protein, laminin b2 (as a2b2g1:laminin-4) at the specialized MTJ and NMJ and alsodistinct localization around the extrasynaptic sarco-lemma (Wewer et al., 1997). Laminin b2 was initiallyreported to be restricted to the MTJ and NMJ(Noakes et al., 1986; Hunter et al., 1989), but thisbroader distribution (Wewer et al., 1997) has subse-quently been confirmed in independent studies(Sasaki et al., 2002). Other studies show that lamininimmunofluorescent staining is concentrated at thecostameres but is hard to detect at intercostamericregions, although the chain specificity of the lamininantibody used was not mentioned (Bloch et al.,2002). A pattern of low concentration over thesarcolemma with marked concentration at regionsspecialized for submitting tension (costamers, MTJand interfasicular junctions) is also seen for integrina7B that co-localized with dystrophin in rat andguinea-pig muscles (Paul et al., 2002). It is interestingthat a similar localization pattern for integrin a7Ahas been described in the rat but not other species,indicating that inter-species differences exist, withbroad sarcolemmal distribution being seen in theguinea-pig (Paul et al., 2002).The main link between the sarcolemma and the
myofibrils is by intermediate filaments at the Z linesand also the M lines. At the Z lines, the main proteinis desmin with its associate proteins, synemin andparanemin. A second distinct set of intermediatefilaments composed of cytokeratins also helps alignthe costameres with the underling contractile appa-ratus, and only the cytokeratins are found at the M
line (Bloch & Gonzalez-Serratos, 2003). This recti-linear array forms a lattice organization on the sur-face of mature myofibers.
Outside the myofiber: the basement membrane andinterstitial ECM
The main ECM components of the interstitial con-nective tissue and of the basement membrane aresummarized in Fig. 1. These different molecules formmany linkages between components of the basementmembrane and the interstitial matrix to form acomplex interrelated mesh of molecules, some ofwhich are sticky and adhesive, whereas others aremore structural. The multiplicity of linkages is illu-strated for collagen VI that links the basementmembrane to the interstitial ECM: this importantrole is illustrated by binding to integrins, basementmembrane components like collagen IV and perle-can, proteoglycans like biglycan and decorin and thefibrillar collagens type I and II (Wiberg et al., 2002),and defects in collagen VI cause muscle weaknessand human myopathies (Bonnemann & Laing, 2004).Similarly, myogenic laminins (laminins 2/4, 8/9, 10/11) not only self-assemble to form a network con-stituting an integral part of the muscle fiber basementmembrane but also interact with the collagen type IVnetwork both directly and via binding to nidogens,and bind to the heparan sulfate proteoglycan, perle-can. Loss of laminin 2/4 or mutations in the laminina2 chain result in congenital muscular dystrophies inboth humans and mice (Xu et al., 1994; Arahataet al., 1995; Miyagoe-Suzuki et al., 2000).The ECM plays many roles during muscle devel-
opment, homeostasis and regeneration but these willnot be addressed here. We will focus on the basementmembrane (Sanes, 2003) and, in particular, thelaminins (Sasaki et al., 2004) that are found only inthis specialized ECM in mature muscle. All lamininsare composed of three chains, a, b and g, that eachoccur in multiple forms and combine to form up to15 different heterotrimers (Table 1) (Colognato &Yurchenco, 2000). In mature skeletal muscle, lami-nins containing the a2 chain are the main componentof the basement membrane (Fig. 2). The only otherlaminins that occur on skeletal muscle, characterizedby the presence of laminin a4 and a5 chains, have amore restricted localization at NMJ in maturemuscle(Sorokin et al., 1997; Ringelmann et al., 1999;Patton, 2000). The situation is different in developingskeletal muscle where, although laminin a2 is thedominant laminin chain, laminin a4 and a5 chainsare more broadly distributed. The reader is referredto an elegant review by Gullberg et al. (1999), whichclearly outlines expression of the laminins at differentstages of muscle development (Gullberg et al., 1999).
Strength at the extracellular matrix–muscle interface
3

Laminin a2 chain
It is significant that in mature muscle, the predomi-nant laminin a2 chain is combined with both lamininb1 and b2 chains around most of the sarcolemna aslaminin-2 (a2b1g1) and laminin-4 (a2b2g1) (Sasakiet al., 2002), while only laminin-4 (a2b2g1) occurs atthe NMJ where the synapse connects the nerve to themuscle. Laminin-4 (a2b2g1) also appears to be theonly laminin isoform concentrated at the MTJ wherethe ends of the myofiber are connected to thetendons; laminin a1, a3, a4, b1, b3, g2 or g3 chains
are absent at this site, while laminin a5 may bepresent at very low levels depending on the species(Patton, 2000). The pattern of immunostaining forlaminin-2 (a2b1g1), which is conspicuous aroundthe sarcolemma but not at the MTJ, appears to bea striking exception to the trend for higher concen-trations of sarcolemmal-associated molecules at theMTJ. If true, this has major functional (mechanicaland signalling) implications for different propertiesof the laminin b1 and b2 chains at these specializedregions of cell contact on the myofiber surface. Yet,on the basis of the similarity of their molecularstructure, such a striking functional difference ap-pears unlikely.To clarify this anomaly, the accuracy of the
immunostaining data supporting elevated b1 aroundthe sarcolemma, but not at the MTJ, should bere-evaluated with different laminin b1 and b2 chainantibodies. Much of the past confusion concerninglocalization of laminin b chains is because of theuse of monoclonal antibodies to laminin b2, whichexhibit weaker staining (Hunter et al., 1989) than themore recently developed polyclonal antibodies (Sa-saki et al., 2002). Although the staining patternsobtained with the laminin b2 monoclonal and poly-clonal antibodies are essentially the same, the mono-clonal antibodies highlight the NMJ and MTJ andstain the rest of the sarcolemma basement membraneweakly, while polyclonal laminin b2 antibodies stainthe entire sarcolemma basement membrane equally.
Table 1. Laminin isoforms and their chain composition
Laminin isoform Chain composition
Laminin-1 a1 b1 g1Laminin-2 a2 b1 g1Laminin-3 a1 b2 g1Laminin-4 a2 b2 g1Laminin-5 a3 b3 g2Laminin-6 a3 b1 g1Laminin-7 a3 b2 g1Laminin-8 a4 b1 g1Laminin-9 a4 b2 g1Laminin-10 a5 b1 g1Laminin-11 a5 b2 g1Laminin-12 a2 b1 g3Laminin-13* a3 b2 g3Laminin-14 a4 b2 g3Laminin-15 a5 b2 g3
*It is debated whether laminin-13 exists in vivo, as there is only
circumstantial evidence for its existence (Libby et al., 2000).
α2
β1 γ1
Myotendinous Junction (MTJ)Laminin-4 α2β2y1Integrins α7Aβ1D
SarcolemnaLaminin-2 α2β1y1Integrin α7Cβ1D
MTJLaminin-4 α2β2y1Integrins α7Aβ1D
Neuromuscular Junction (NMJ)Laminin-4 α2β2y1Integrins α7Aβ1D
α7Bβ1Dα7Cβ1D
α7Bβ1D α7Bβ1D
Laminin-2 Laminin-8 Laminin-10
Integrin α7β1
Integrins
+ α-dystroglycan
+ Lutheran blood group antigen
MYOBLAST AND MYOTUBE SURFACE
Integrins αvβ3
Integrins α6β1
α7β1 + Lutheran blood group antigen
(a)
(b) (c)α2
β1 γ1
α4β γ
α5
β γ
MUSCLE FIBRE SURFACE
Laminin-2 (and -4)
Integrin α7β1+ α-dystroglycan
Fig. 2. Laminins and integ-rins on muscle cells. Dia-gram (a) indicates the mainlaminin a2 and integrin a7isoforms associated with thesurface of a mature musclefiber (adapted from Burkin& Kaufman, 1999). Note:we query the apparent lackof laminin a2b1 at themyotendinous junctions(see text). (b) During myo-genesis (associated with de-velopment or regeneration),different combinations of la-minins and integrins are ex-pressed by myoblasts andmyotubes (the boxed mole-cules are not detected onmyoblasts) and (c) on thesarcolemma of mature myo-fibers only, laminin a2 ispresent (mainly as laminin-2 but also as laminin-4)bound to integrin a7b1 anda-dystroglycan.
Grounds et al.
4

Laminin a1 is not detected normally in muscletissue (Schuler & Sorokin, 1995; Tiger & Gullberg,1997). Yet, when it is experimentally overexpressedin muscles that lack laminin a2, the laminin a1 chainappears to effectively replace the missing endogenouslaminin isoform (Gawlik et al., 2004). Such substitu-tion for the native laminin a2 chain does not occurnaturally (Tiger & Gullberg, 1997; Ringelmann et al.,1999) and is also not seen on mature myofiberswith either the endogenous laminin a4 or a5 chains(Sorokin et al., 2000).
Laminin a4 and a5 chains
Laminins with the a4 or a5 chain are also associatedwith mature muscle at the NMJ. The NMJ hasthree different laminin a chains present as laminin-4(a2b2g1), laminin-9 (a4b2g1) and laminin-11(a5b2g1), with laminin-4 and -11 present in thesynaptic folds and laminin-9 also present in the clefts(Patton, 2000; Sanes, 2003). Defects in laminin a2, a4and b2 chains all result in synaptic defects of differenttypes: dy/dy mice lacking laminin-4 in the synapticbasement membrane have fold dysgenesis and nerveterminal detachment, while laminin b2-null mice,which lack laminin-4, -9 and -11 but gain laminin-8(because of Schwann cell intrusion into the synapse),have fold dysgenesis, nerve terminal detachment pluspoor presynaptic differentiation (Noakes et al., 1995;Patton, 2000). In mice lacking laminin a4, activezones and junctional folds form in normal numbers,but are not precisely apposed to each other. Thus, theformation and localization of synaptic specializa-tions are regulated separately, and laminin-9 iscritical in the latter process (Patton et al., 2001). Itis noted that while laminin a2 and a5 are made bymuscle cells in culture and in vivo, a4 appears to bemade predominantly by fibroblasts (L Sorokin, un-published data and Frieser et al., 1997). However, theorigin of laminin a2, a4 and a5 chains at the NMJ isnot clear.Apart from the NMJ, laminin a4 and a5 chains
also occur in the basement membranes of bloodvessels in mature muscle, being present as laminins-8 (a4b1g1) and 10 (a1b1g1).During embryogenesis, the a4 or a5 chains are also
present in the basement membrane surroundingdeveloping myotubes in mice (Sorokin et al., 1997;Ringelmann et al., 1999; Sorokin et al., 2000) andhumans (Petajaniemi et al., 2002) (Fig. 2(b)). Com-pensatory upregulation of laminin a4 and a5 chainsis seen in dy/dymice that lack laminin a2, with the a5chain being observed on young myotubes at day 1after birth for dy/dy muscles (but not controls) butnot at 1 week of age, and laminin a4 persisting longeraround developing myotubes (Ringelmann et al.,1999; Sorokin et al., 2000). The a4 and a5 laminin
chains are also detectable in small amounts in base-ment membrane surrounding myotubes in maturemuscle regenerating after damage (Sorokin et al.,2000) and are transiently elevated in basement mem-branes of myotubes of regenerating dy/dy muscle(Sorokin et al., 2000). However, the fact that there isno long-term compensation for the laminin a2 defectin mature muscle emphasizes that the functionalproperties of the laminin a2, a4 and a5 chains aredistinct (Gullberg et al., 1999; Ringelmann et al.,1999; Sorokin et al., 2000).The laminins are key molecules that connect the
basal lamina to the myofiber and without them, thecontractile force of the myofiber cannot be trans-ferred effectively to the interstitial connective tissue.Laminin is concentrated at the costameres and ishard to detect at intercostameric regions (Blochet al., 2002). While laminin a2 does not appear tobe necessary for assembly of the costameric frame-work, it is required for maintaining the stability andorganization of the structure in mature muscle and isof central importance since it binds to both thedystroglycan/sarcoglycan complex and to integrina7 (Yurchenco et al., 2003).The critical importance of laminin is clearly de-
monstrated by genetic defects in the laminin a2 chainthat result in severe congenital muscular dystrophy inhumans, and there are mouse models of such defectswhere the a2 chain is reduced (dy/dy), truncated(dy2J) or completely absent (dyw & dy3k) (Guoet al., 2003). Absence of the laminin a2 chain leadsto severe muscle weakness. The associated defects ofnerve and synaptic function probably play a majorrole in this pathology. It is noted that the pro-nounced wasting of the laminin-deficient musclesmay be a result, in large part, of denervation atrophy(and the wasting may be further confounded bynutritional problems of feeding, swallowing anddigestion), since membrane fragility as measured bypenetration of Evans Blue Dye into myofibers (as amarker of myofiber leakiness) is not pronounced inthe laminin a2-deficient mice (Straub et al., 1997). It isnot clear whether the low level of sarcolemmal da-mage in the absence of laminin a2 is largely because of(a) the impaired neural function that may result inrelatively little electrical stimulation and contractionof the myofibers and thus little opportunity forsarcolemmal damage, or (b) no marked direct effecton sarcolemmal strength in the absence of this lamininlinkage to the proteins in the sarcolemma.
The myofiber surface: molecules in the sarcolemma
Two main classes of membrane-associated moleculesare responsible for force transmission: the dystrogly-can/sarcoglycan complex and integrins (see Fig. 3).
Strength at the extracellular matrix–muscle interface
5

The crucial importance of transmembrane linkage innormal muscle function and strength is demonstratedby the wide range of clinical muscle disorders thatresult from defects of one of the many molecules inthis complex network of structural components(Campbell & Stull, 2003; Lapidos et al., 2004) (seeFig. 3). A weak link in the transmembrane complexresults in myofiber fragility where exercise and thecontractile force of sarcomeres damage the myofiberand can lead to sarcolemmal lesions and myofibernecrosis. While necrosis normally results in muscleregeneration, this is impaired or ultimately fails to beeffective in severe myopathies like Duchenne musculardystrophy (DMD), where there are repeated cycles ofmuscle necrosis (because of membrane fragility) andmuscles are replaced by fat and fibrous connectivetissue. It is noted that this pattern of pathologycontrasts with the consequences of defects in (1)ECM proteins such as laminin and (3) the cytoskeletalcomponents where weakness is not generally accom-panied by myofiber necrosis. These consequences needto be considered in light of the roles that different
groups of proteins play in the generation and subse-quent transfer of the contractile force.Because of their medical importance, much atten-
tion has been focused on molecules associated withthe dystroglycan/sarcoglycan complex (Michele &Campbell, 2003), and these will not be consideredin detail here. The discussion will be confined to theintegrins. Both the dystroglycan/sarcoglycan com-plex and integrin a7 (the main integrin in maturemuscle) bind to laminin-2. Integrins are composed ofone a and one b subunit (Belkin & Stepp, 2000) andintegrate the inside of the cell with the ECM: theintracellular integrin domain interacts with morethan 20 molecules (Brakebusch & Fassler,2003) and the extracellular domain binds to ECMmolecules such as laminins, fibronectin andtenascin.
Integrin b1 subunit
In muscle, b1 is the only b integrin subunit identified,and b1D is the only isoform expressed in adult
Fig. 3. Sarcolemnal-associated molecular complexes. The laminin a2/integrin complex and laminin a2/dystroglycan complex,in particular, are illustrated with connections to cytoskeletal and sarcomeric proteins (adaption of diagram by Straub,unpublished). Defects in many of these molecules (indicated by bold typeface) result in human muscle diseases (based onBonnemann & Laing, 2004).
Grounds et al.
6

muscle. The b1 subunit is present at the costamers,NMJ and MTJ (Burkin & Kaufman, 1999), andappears to be essential for myoblast fusion to formmyotubes (Schwander et al., 2003). There is only asingle report of the b3 integrin subunit being ex-pressed by cultured human myoblasts, althoughimmunocytochemical staining is required to confirmthat the b3 integrin was actually present on myo-blasts since other cell types are present in suchprimary cultures (Blaschuk et al., 1997).
Integrin a subunits (a7, a3, av)
Of the 12 a integrin subunits associated with the b1integrin, mainly a7, a3 and av are present in matureskeletal muscle. Minor skeletal muscle integrins in-clude a6, and possibly also a10 and a11 (Mayer,2003). The integrins a7, a6, a3 and av bind to severallaminin isoforms, while integrin av also binds otherECM molecules, such as vitronectin and fibronectin.The main integrin a subunit in mature skeletal
muscle is a7 (Burkin & Kaufman, 1999), whichoccurs as three splice variants, A, B and C (Fig. 2).In general, the integrin a7C form is located over theperipheral sarcolemna where it is concentrated in thecostamers, and also at the NMJ. The reverse patternis seen for integrins a7A and a7B that are concen-trated at the MTJ, NMJ (Burkin & Kaufman, 1999)and intrafascicular myofiber terminations (Paulet al., 2002; Mayer, 2003), although this patternmay vary between different species as indicated above.Integrin a7b1 binds to laminin a2 and these pro-
teins co-localize on mature muscle fibers (Fig. 2).Interactions also occur between integrin a7b1 andother molecules, such as ADAM12, which play im-portant roles in skeletal muscle formation and func-tion (Moghadaszadeh et al., 2003; Zhao et al., 2004),and it is suggested that laminin and the DC domain ofADAM12 represent two functional ligands for integ-rin a7b1 that trigger different cellular responses.Elimination of integrin a7 in mice results in a mild
but progressive muscular dystrophy that developssoon after birth (Mayer et al., 1997), and patientshave been identified with a primary integrin a7deficiency (Hayashi et al., 1998). Histologically, thedystrophy appears mild with little necrosis or varia-tion in muscle fiber size. However, the defect is mostprominent at the MTJ, where the digit-like exten-sions at this site are lost and the sarcomere isretracted from the muscle membrane, suggestingimpaired MTJ function. This may explain the muscleweakness in human patients despite the rather mildmyofiber damage. The ligand for integrin a7b1 at theMTJ is not clear; however, the predominance oflaminin-4 at this site suggests potential interaction.Overexpression of integrin a7 appears to be able to
compensate partially for defects in the dystrophin/
dystroglycan (Burkin et al., 2001) and sarcoglycancomplex (Allikian et al., 2004), further confirmingthat integrin a7 and the dystrophin/glycoproteincomplex (Fig. 3) are parallel pathways (that bind tolaminin-2) for the maintenance of mature musclemembrane integrity.Integrins of the av series (predominantly avb1 and
avb3) bind to the laminin a5 chain of laminin-10(a5b1g1) (Sasaki & Timpl, 2001). Interestingly,both avb1 and laminin a5 have been reported tooccur at the NMJ; however, whether an associat-ion occurs is not clear. Although laminin a5- andintegrin av-null mice exist, neither has been investi-gated for a NMJ defect.A minor skeletal muscle integrin, which warrants
mention here as it binds both laminin a4- and a5-containing isoforms, is a6b1. Like laminin a4 and a5chains, it is transiently present on young myotubes(Fig. 2) but not mature myofibers (von der Market al., 1991; Sorokin et al., 2000), it is upregulated onsome young myotubes of the dy/dy mouse (Sorokinet al., 2000) and in mature tissues it is normally foundon blood vessels and nerves. Integrin a6 is notpresent on mature myofibers (even in mice lackingintegrin a7), indicating that it cannot compensate forintegrin a7 function. This is analogous to the inabil-ity of other laminin a chains to compensate for theabsence of laminin a2 chain on mature skeletalmuscle fibers and again emphasizes the precise func-tional role of such specific isoforms.
Inside the myofiber: the cytoskeleton and sarcomeres
Linkage between the membrane complexes at themyofiber surface and sarcomeric proteins within themuscle cell involves many cytoskeletal proteinsincluding actin, a-actinin, desmin and spectrin (asindicated in Fig. 3). For other diagrams, see Bonne-mann & Laing (2004); Paulin et al. (2004). Desminforms a 3D scaffold around the Z-disks of sarco-meres and interconnects the entire contractile appa-ratus with the sarcolemmal skeleton, the nuclei andother organelles (Paulin et al., 2004). Desmin isparticularly abundant at MTJ and NMJ; it alsoappears to be concentrated at costameres as dovinculin and spectrin. Desmin is closely associatedwith a-B-crystallin, synemin and plectin and ankyrinmay be involved in linkage to the sarcolemma(Paulin et al., 2004). Desmin is not required formuscle formation during embryogenesis but lack ofdesmin makes muscle more susceptible to exercise-induced damage and myofibrillogenesis is disorga-nized in regenerating muscle (Paulin et al., 2004).The cytoskeletal structure of the myoblasts affects
the formation of sarcomeres in newly formed myo-fibers (Berendse et al., 2003) and it appears that
Strength at the extracellular matrix–muscle interface
7

sarcomere assembly in skeletal muscle starts at pointswhere non-muscle g-actin is attached to the cellmembrane (Lloyd et al., 2004). The sarcomerestretches from one Z-disk to the next and is thefundamental unit of striated muscle contraction,although the precise mechanism of contraction re-mains controversial (Pollack, 1996). Many novelproteins associated with the sarcomere are beingidentified and these include not only structural com-ponents but also enzymes and signalling molecules(for an excellent description and review, see Bonne-mann & Laing, 2004). Many more connectionsbetween sarcomeric proteins and the nucleus are nowbecoming apparent (Bonnemann & Laing, 2004)beyond the binding of desmin to nuclear lamins(Paulin et al., 2004).Defects in a great many of these proteins are
associated with different human myopathies as dis-cussed in recent reviews (Bonnemann & Laing, 2004;Paulin et al., 2004). As a generalization, many ofthese defects result in weakness, sometimes of distalmuscles, but without membrane damage. This isbecause the internal contractile protein architectureis weak and thus does not generate the optimal forceand accordingly, there is no overload of the sarco-lemma to result in membrane damage. This outcomeis in striking contrast to situations where the fullforce is generated by the normal sarcomeric archi-tecture, but defects at the level of force transferacross the sarcolemma to the ECM cause majorsarcolemmal damage.
Can molecular interventions increase musclestrength?
Interventions to maintain or increase muscle strengthare of considerable interest for aging skeletal muscleand are under intense investigation for clinical ap-plications (Shavlakadze & Grounds, 2003; Lynchet al., 2004): many of these involve increasing theprotein content of myofibers and thus contractilestrength, and potentially have direct application tosports medicine. A related research field is the devel-opment of treatments for myopathies such as thelethal human X-linked disease DMD, where upregu-lation of many compensatory molecules or ‘‘boostergenes’’ to increase skeletal muscle strength andreduce myofiber necrosis have been explored forpotential therapeutic interventions. Such researchhas wider theoretical applications for increasing thestrength of normal muscles in sports medicine; there-fore, it is of interest to be aware of recent develop-ments in this area.In human DMD, as well as the mdx mouse model
of DMD, defects in the membrane-associated proteindystrophin predispose the cell membrane of skeletal
muscle fibers to breakdown, leading to necrosis.Overexpression of insulin-like growth factor-1(IGF-1) within dystrophic skeletal muscles of mdxmice helps to protect the myofibers from necrosis(Shavlakadze et al., 2004b) and this is of interest tosports medicine since IGF-1 is normally producedlocally by skeletal muscles in response to stretch andexercise. Modulating the expression of other genescan help salvage the integrity of dystrophic myofibers(Engvall & Wewer, 2003). For example, reduceddystropathology in mdx mice is seen when thegrowth factor myostatin is absent (Wagner et al.,2002) or blocked by specific antibodies (Bogdanovichet al., 2002), and by overexpression of membrane-associated proteins such as utrophin (Khurana &Davies, 2003), integrin a7 (Burkin et al., 2001) andADAM12 (Moghadaszadeh et al., 2003). While ge-netically engineered mice (transgenics and knock-outs) are very powerful tools to dissect theimportance of specific molecules, it can be difficultto translate these promising observations into theclinical situation (e.g. Shavlakadze et al., 2004a).Another approach that markedly reduces myofiber
necrosis of dystrophic mdx muscle is suppression ofthe inflammatory response. Such protection of myo-fibers has been demonstrated using pharmacologicalagents (already in wide clinical use to treat inflamma-tory diseases) that block activity of the pro-inflam-matory cytokine tumor necrosis factor-a (TNF-a) byeither specific antibodies (Grounds & Torrisi, 2004)or soluble receptors to TNF-a (Hodgetts, 2005,manuscript submitted). A similar protective effect isseen after depletion of host neutrophils (Hodgetts,2005, manuscript submitted) strongly implicatingthese cells in myofiber damage (McLoughlin et al.,2003; Nguyen & Tidball, 2003). These studies em-phasize the delicate balance between re-sealing ofmyofibers (Doherty & McNally, 2003) after exercise-induced minor sarcolemnal damage or the alternativefate of myofiber necrosis (Shavlakadze et al., 2004b).It is important to recognise that, while an excessiveinflammatory response (especially involving neutro-phils) may exacerbate myofiber damage, some in-flammatory cell activity seems to be required for theadaptive response to exercise-induced muscle da-mage. Thus, a careful balance involving an appro-priate (but not excessive) inflammatory cell responseis probably necessary for maintenance of skeletalmuscle integrity, repair and function.
Perspectives
There is much interest in making muscles stronger.This usually involves increasing the size of individualmuscle fibers by hypertrophy. The greater contractileforce must then be transferred from the muscle fiber
Grounds et al.
8

to the tendons to move the bones. An early criticalstep is lateral transmission of the force from thecontractile proteins, across the muscle surface mem-brane, through to the basal lamina and interstitialconnective tissue (the ECM) and adjacent myofibers.The molecules associated with this muscle/matrixinterface form a key link for effective transfer ofthe force. A thorough understanding of the complexinteractions and structural and signalling propertiesof these many molecules is fundamental to increasingthe strength of skeletal muscles. The importance ofthis functional linkage is clearly demonstrated clini-cally by a vast array of inherited muscle diseasesassociated with gene defects for many of thesemolecules. Therapeutic interventions to strengthenthese linkages (or replace defective components inmyopathies) have potential applications in sports
medicine. The extent to which molecules associatedwith the muscle surface might be upregulated toincrease overall strength for transfer of sarcomere-generated force, and to protect individual myofibersfrom sarcolemmal damage that can lead to myofibernecrosis, has hardly been explored.
Key words: basement membrane, sarcolemma, lami-nins, integrins, myofiber strength, skeletal muscle,exercise, muscle damage.
Acknowledgements
We thank Ulla Wewer (Copenhagen, Denmark) for her help-ful comments, and Volker Straub (Newcastle, UK) for gener-ous permission to use his original diagram.
References
Allikian MJ, Hack AA, Mewborn S,Mayer U, McNally EM. Geneticcompensation for sarcoglycan loss byintegrin alpha7beta1 in muscle. J CellSci 2004: 117: 3821–3830.
Arahata K, Ishii H, Hayashi YK.Congenital muscular dystrophies. CurrOpin Neurol 1995: 8: 385–390.
Belkin AM, Stepp MA. Integrins asreceptors for laminins. Microsc ResTech 2000: 51: 280–301.
Berendse M, Grounds MD, Lloyd CM.Myoblast structure affects subsequentskeletal myotube morphology andsarcomere assembly. Exp Cell Res2003: 291: 435–450.
Blaschuk KL, Guerin C, Holland PC.Myoblast alpha v beta3 integrin levelsare controlled by transcriptionalregulation of expression of the beta3subunit and down-regulation of beta3subunit expression is required forskeletal muscle cell differentiation. DevBiol 1997: 184: 266–277.
Bloch RJ, Capetanaki Y, O’Neill A, ReedP, Williams MW, Resneck WG, PorterNC, Ursitti JA. Costameres: repeatingstructures at the sarcolemma of skeletalmuscle. Clin Orthop 2002: S203–S210.
Bloch RJ, Gonzalez-Serratos H. Lateralforce transmission across costameres inskeletal muscle. Exerc Sport Sci Rev2003: 31: 73–78.
Bogdanovich S, Krag TO, Barton ER,Morris LD, Whittemore LA, AhimaRS, Khurana TS. Functionalimprovement of dystrophic muscle bymyostatin blockade. Nature 2002: 420:418–421.
Bonnemann CG, Laing NG. Myopathiesresulting from mutations in sarcomericproteins. Curr Opin Neurol 2004: 17:529–537.
Brakebusch C, Fassler R. The integrin-actin connection, an eternal love affair.EMBO J 2003: 22: 2324–2333.
Burkin DJ, Kaufman SJ. The alpha 7 beta1 integrin in muscle development anddisease. Cell Tissue Res 1999: 296:183–190.
Burkin DJ, Wallace GQ, Nicol KJ,Kaufman DJ, Kaufman SJ. Enhancedexpression of the a7B1 integrin reducesmuscular dystrophy and restoresviability in dystrophic mice. J Cell Biol2001: 152: 1207–1218.
Campbell KP, Stull JT. Skeletal musclebasement membrane-sarcolemma-cyto-skeleton interaction minireview series.J Biol Chem 2003: 278: 12599–12600.
Colognato H, Yurchenco PD. Form andfunction: the laminin family ofheterotrimers. Dev Dyn 2000: 218:213–234.
Doherty KR, McNally EM. Repairingthe tears: dysferlin in muscle membranerepair. Trends Mol Med 2003: 9: 327–330.
Engvall E, Wewer UM. The new frontierin muscular dystrophy research:booster genes. FASEB J 2003: 17:1579–1584.
Frieser M, Nockel H, Pausch F, Roder C,Hahn A, Deutzmann R, Sorokin LM.Cloning of the mouse laminin alpha 4cDNA. Expression in a subset ofendothelium. Eur J Biochem 1997: 246:727–735.
Gawlik K, Miyagoe-Suzuki Y, Ekblom P,Takeda S, Durbeej M. Laminin alpha1chain reduces muscular dystrophy inlaminin alpha2 chain deficient mice.Hum Mol Genet 2004: 13: 1775–1784.
Grounds MD, Torrisi J. Anti-TNFa(Remicade) therapy protects
dystrophic skeletal muscle fromnecrosis. FASEB J 2004: 18: 676–682.
Gullberg D, Tiger C-F, Velling T.Laminins during muscle developmentand in muscular dystrophies. Cell MolLife Sci 1999: 56: 442–460.
Guo LT, Zhang XU, Kuang W, Xu H,Liu LA, Vilquin J-T, Miyagoe-SuzukiY, Takeda S, Ruegg MA, Wewer UM,Engvall E. Laminin [alpha]2 deficiencyand muscular dystrophy; genotype–phenotype correlation in mutant mice.Neuromusc Disord 2003: 13: 207–215.
Hayashi YK, Chou F-L, Engvall E,Ogawa M, Matsuda C, Hirabayashi S,Yokochi K, Ziober BL, Kramer RH,Kaufman SJ, Ozawa E, Goto Y-i,Nonaka I, Tsukahara T, Wang J-Z,Hoffman EP, Arahata K. Mutations inthe integrin a7 gene cause congenitalmyopathy. Nat Genet 1998: 19: 94–97.
Huijing PA. Muscle as a collagen fiberreinforced composite: a review of forcetransmission in muscle and whole limb.J Biomech 1999: 32: 329–345.
Hunter DD, Shah V, Merlie JP, Sanes JR.A laminin-like adhesive proteinconcentrated in the synaptic cleft of theneuromuscular junction. Nature 1989:338: 229–234.
Khurana TS, Davies KE.Pharmacological strategies formuscular dystrophy. Nat Rev DrugDiscovery 2003: 2: 379–390.
Kjaer M. Role of extracellular matrix inadaptation of tendon and skeletalmuscle to mechanical loading. PhysiolRev 2004: 84: 649–698.
Lapidos KA, Kakkar R, McNally EM.The dystrophin glycoprotein complex:signalling strength and integrity forthe sarcolemma. Circ Res 2004: 94:1023–1031.
Strength at the extracellular matrix–muscle interface
9

Law DJ, Caputo A, Tidball JG. Site andmechanics of failure in normal anddystrophin-deficient skeletal muscle.Muscle Nerve 1995: 18: 216–223.
Libby RT, Champliaud MF,Claudepierre T, Xu Y, Gibbons EP,Koch M, Burgeson RE, Hunter DD,Brunken WJ. Laminin expression inadult and developing retinae: evidenceof two novel CNS laminins. J Neurosci2000: 20: 6517–6528.
Lloyd CM, Berendse M, Lloyd DG,Schevzov G, Grounds MD. A novelrole for non-muscle gamma-actin inskeletal muscle sarcomere assembly.Exp Cell Res 2004: 297: 82–96.
Lynch G, Shavlakadze T, Grounds MD.Evaluation of strategies to reduce age-related skeletal muscle wasting. In:Rattan SIS, ed. Ageing interventionsand therapies. Singapore: WorldScientific Publishers, 2004, Chapter 4:63–84.
Mayer U. Integrin: redundant orimportant players in skeletal muscle? JBiol Chem 2003: 278: 14587–14590.
Mayer U, Saher G, Fassler R,Bornemann A, Echtermeyer F, vonder Mark H, Miosge N, Poschl E,von der Mark K. Absence of integrinalpha 7 causes a novel form ofmuscular dystrophy. Nat Genet 1997:17: 318–323.
McLoughlin TJ, Tsivitse SK, EdwardsJA, Aiken BA, Pizza FX.Deferoxamine reduces and nitric oxidesynthase inhibition increasesneutrophil-mediated myotube injury.Cell Tissue Res 2003: 313: 313–319.
Michele DE, Campbell KP. Dystrophin-glycoprotein complex: post-translational processing anddystroglycan function. J Biol Chem2003: 278: 15457–15460.
Miyagoe-Suzuki Y, Nakagawa M,Takeda S. Merosin and congenitalmuscular dystrophy. Microsc Res Tech2000: 48: 181–191.
Moghadaszadeh B, Albrechtsen R, GuoL, Zaik M, Kawaguchi N, Borup RH,FKronquist P, Schroder HD, DaviesKE, Voit T, Neielson FC, Engvall E,Wewer UM. Compensation fordystrophin-deficiency: ADAM 12overexpression in skeletal muscleresults in increased alpha 7 integrin,utrophin, and associated glyco-proteins. Hum Mol Genet 2003: 12:2467–2493.
Nguyen HX, Tidball JG. Interactionsbetween neutrophils and macrophagespromote macrophage killing of ratmuscle cells in vitro. J Physiol 2003:547: 125–132.
Noakes PG, Everett AW, Bennett MR.The growth of muscle nerves in relationto the formation of primary myotubesin the developing chick forelimb.
J Comp Neurol 1986: 248:245–256.
Noakes PG, Gautam M, Mudd J, SanesJR, Merlie JP. Aberrant differentiationof neuromuscular junctions in micelacking s-laminin/laminin beta 2.Nature 1995: 374: 258–262.
Patton BL. Laminins of theneuromuscular system. Microsc ResTech 2000: 51: 247–261.
Patton BL, Cunningham JM, Thyboll J,Kortesmaa J, Westerblad H, EdstromL, Tryggvason K, Sanes JR. Properlyformed but improperly localizedsynaptic specializations in the absenceof laminin alpha4. Nat Neurosci 2001:4: 597–604.
Paul AC. Muscle length affects thearchitecture and pattern of innervationdifferently in leg muscles of mouse,guinea pig, and rabbit compared tothose of human and monkey muscles.Anat Rec 2001: 262: 301–309.
Paul AC, Sheard PW, Kaufman SJ,Duxson MJ. Localization of alpha 7integrins and dystrophin suggestspotential for both lateral andlongitudinal transmission of tension inlarge mammalian muscles. Cell TissueRes 2002: 308: 255–265.
Paulin D, Huet A, Khanamyrian L, XueZ. Desminopathies in muscle disease.J Pathol 2004: 204: 418–427.
Petajaniemi N, Korhonen M, KortesmaaJ, Tryggvason K, Sekiguchi K,Fujiwara H, Sorokin L, Thornell L-E,Wondimu Z, Assefa D, Patarroyo M,Virtanen I. Localization of lamininalpha4-chain in developing and adulthuman tissues. J. Histochem.Cytochem. 2002: 50: 1113–1130.
Pollack GH. Phase transitions and themolecular mechanism of contraction.Biophys Chem 1996: 59: 315–328.
Purslow PP. The structure and functionalsignificance of variations in theconnective tissue within muscle. CompBiochem Physiol A 2002: 133: 947–966.
Ringelmann B, Roder C, Hallmann R,Maley M, Davies M, Grounds M,Sorokin L. Expression of laminin a1,a2, a4 and a5 chains, fibronectin andtenascin-C in skeletal muscle ofdystrophic 129ReJ dy/dy mice. ExpCell Res 1999: 246: 165–182.
Sanes JR. The basement membrane/basallamina of skeletal muscle. J Biol Chem2003: 278: 12601–12604.
Sasaki T, Fassler R, Hohenester E.Laminin: the crux of basementmembrane assembly. J Cell Biol 2004:164: 959–963.
Sasaki T, Mann K, Miner JH, Miosge N,Timpl R. Domain IV of mouse lamininbeta1 and beta2 chains. Eur J Biochem2002: 269: 431–442.
Sasaki T, Timpl R. Domain IVa oflaminin alpha5 chain is cell-adhesive
and binds beta1 and alphaVbeta3integrins through Arg-Gly-Asp. FEBSLett 2001: 509: 181–185.
Schuler F, Sorokin LM. Expression oflaminin isoforms in mouse myogeniccells in vitro and in vivo. J Cell Sci1995: 108: 3795–3805.
Schwander M, Leu M, Stumm M,Dorchies OM, Ruegg UT, Schittny J,Muller U. beta1 integrins regulatemyoblast fusion and sarcomereassembly. Dev Cell 2003: 4:673–685.
Shavlakadze T, Grounds MD. Theraputicinterventions for age-related musclewasting: importance of innervation andexercise for preventing sarcopenia. In:Rattan S, ed. Modulating aging andlongevity, Vol. 5. the Netherlands:Kluwer Academic publisher, 2003,Chapter 9, 139–166.
Shavlakadze T, Rosenthal NA, Wynn N,Grounds MG. Reconciling data fromtransgenic mice that over-express IGF-1 specifically in skeletal muscle.Growth Hormone and IGF Research2004a: 15: 4–18.
Shavlakadze T, White J, Rosenthal N,Grounds MD. Targeted expression ofinsulin-like growth factor-1 reduces thenecrosis of dystrophic mdx muscle. MTherapy 2004b: 10: 829–843.
Sheard PW, Paul AC, Duxson MJ.Intramuscular force transmission. AdvExp Med Biol 2002: 508: 495–499.
Sorokin LM, Frieser M, Pausch F,Kroger S, Ohage E, Deutzmann R.Developmental regulation of thelaminin a5 chain suggests a role inepithelial and endothelial cellmaturation. Dev Biol 1997: 189:285–300.
Sorokin LM, Maley MAL, Moch H, vonder Mark H, von der Mark K,Cadalbert L, Karosi S, Davies MJ,McGeachie JK, Grounds MD.Laminin a4 and integrin a6 areupregulated in regenerating dy/dyskeletal muscle: comparativeexpression of laminin and integrinisoforms in muscles regenerating aftercrush injury. Exp Cell Res 2000: 256:500–514.
Straub V, Rafael JA, Chamberlain JS,Campbell KP. Animal modelsfor muscular dystrophy showdifferent patterns of sarcolemmaldisruption. J Cell Biol 1997: 139:375–385.
Tidball JG. Force transmission acrossmuscle cell membranes. J Biomech1991a: 24: 43–52.
Tidball JG. Myotendinous junction injuryin relation to junction structure andmolecular composition. Exerc Sport SciRev 1991b: 19: 419–445.
Tiger CF, Gullberg D. Absence oflaminin a1 chain in the skeletal muscle
Grounds et al.
10

of dystrophic dy/dy mice. MuscleNerve 1997: 20: 1515–1524.
Trotter JA. Structure-functionconsiderations of muscle-tendonjunctions. Comp Biochem Physiol A2002: 133: 1127–1133.
von der Mark H, Durr J, Sonnenberg A,von der Mark K, Deutzmann R,Goodman SL. Skeletal myoblastsutilize a novel beta 1-series integrin andnot alpha 6 beta 1 for binding to the E8and T8 fragments of laminin. J BiolChem 1991: 266: 23593–23601.
Wagner KR,McPherron AC,Winik N, LeeSJ. Loss of myostatin attenuates severityof muscular dystrophy in mdx mice. AnnNeurol 2002: 52: 832–836.
Wewer UM, Thornell LE, Loechel F,Zhang X, Durkin ME, Amano S,Burgeson RE, Engvall E, AlbrechtsenR, Virtanen I. Extrasynaptic locationof laminin beta 2 chain in developingand adult human skeletal muscle. Am JPathol 1997: 151: 621–631.
Wiberg C, Heinegard D, Wenglen C,Timpl R, Morgelin M. Biglycansorganizes collagen VI into hexagonal-like networks resembling tissuestructures. J Biol Chem 2002: 277:49120–49126.
Xu H, Christmas P, Wu X-R, WewerUM, Engvall E. Defective musclebasement membrane and lack of M-laminin in the dystrophic dy/dy mouse.
Proc Natl. Acad Sci USA 1994: 91:5572–5576.
Yurchenco PD, Cheng Y-S, campbell K,Li S. Loss of basement membrane,receptor and cytoskeletal latticesin a laminin-deficient musculardystrophy. J Cell Sci 2003: 117:735–742.
Zhao Z, gruszczynska-Biegala J,Cheuvront T, von der Mark H,von der Mark K, Kaufman SJ,Zolkiewska A. Interaction of thedisintegrin and cysteine-rich domainsof ADAM12 with integrin alpha 7 beta1. Exp Cell Res 2004: 298:28–37.
Strength at the extracellular matrix–muscle interface
11