
Stereotactic planning software for human neurotransplantation: suitability in 22 surgical cases of...
10
AUTHOR COPY Restorative Neurology and Neuroscience 32 (2014) 259–268 DOI 10.3233/RNN-130340 IOS Press 259 Stereotactic planning software for human neurotransplantation: Suitability in 22 surgical cases of Huntington’s disease William Omar Contreras Lopez a,b , Guido Nikkhah c , Elisabeth Sch ¨ ultke a,b , Luciano Furlanetti a,b and Michael Trippel a,∗ a Department of Stereotactic and Functional Neurosurgery, University Medical Center, Freiburg, Germany b Laboratory of Stereotaxy and Interventional Neurosciences, University Medical Center, Freiburg, Germany c Department of Neurosurgery, University of Erlangen, Schwabachanlage, Erlangen, Germany Abstract. Purpose: Intrastriatal neural transplantation using multiple grafts is an experimental approach to the treatment of Huntington’s disease (HD). Brain atrophy makes stereotactic plans in these patients a tedious procedure with a risk of suboptimal spatial distribution of the grafts in transplantation procedures. Here we present a self-developed software to optimize the surgical stereotactic planning for bilateral neurotransplantation procedures. It allows close to symmetrical distribution of the stereotactic coordinates in relation to the mid-commissural point (MCP), proposing automatically the planning coordinates for the first transplanted hemisphere and mirrored coordinates to be used in the contra-lateral hemisphere. Methods: Twenty-two consecutive HD patients underwent bilateral stereotactic striatal transplantation. Two caudate nucleus and four putaminal tracks were planned bilaterally. For the second, contra-lateral transplantation, the coordinates were mirrored in order to determine contralateral targets and trajectories. Intra-individual comparison between software given coordinates and finally used coordinates was performed. Results: No statistical significance was found comparing a) the differences between coordinates proposed by the software and the final coordinates and b) the distribution of the transplantation sites in relation to the midline for the right vs. left hemisphere. No intra- or postoperative transplantation-related adverse events occurred. Conclusions: The use of model-based and mirrored coordinates allowed optimal spatial distribution of the grafts. Minor changes were required comparing right to left coordinates giving proof-of principle. The initial use of the software suggests that it may be useful in experimental transplantation trials where neural cell grafts are to be implanted into predefined target sites in the human brain, whether unilateral or bilateral. Keywords: Huntington’s disease, human fetal striatal transplantation, anterior commissure-posterior commissure line (AC-PC), mid-commissural point (MCP), whole ganglionic eminence (WGE), caudate nucleus, putamen ∗ Corresponding author: Dr. Michael Trippel, Department of Stereotactic and Functional Neurosurgery, University Medical Cen- ter, Breisacher Str. 64, 79106 Freiburg, Germany. Tel.: +49 761 270 50620; Fax: +49 761 270 93150; E-mail: michael.trippel@ uniklinik-freiburg.de. 0922-6028/14/$27.50 © 2014 – IOS Press and the authors. All rights reserved
-
Upload
sysbiomed-erlangen -
Category
Documents
-
view
0 -
download
0
Transcript of Stereotactic planning software for human neurotransplantation: suitability in 22 surgical cases of...
AU
THO
R C
OP
Y
Restorative Neurology and Neuroscience 32 (2014) 259–268DOI 10.3233/RNN-130340IOS Press
259
Stereotactic planning software for humanneurotransplantation: Suitability in 22surgical cases of Huntington’s disease
William Omar Contreras Lopeza,b, Guido Nikkhahc, Elisabeth Schultkea,b, Luciano Furlanettia,b
and Michael Trippela,∗aDepartment of Stereotactic and Functional Neurosurgery, University Medical Center, Freiburg, GermanybLaboratory of Stereotaxy and Interventional Neurosciences, University Medical Center, Freiburg, GermanycDepartment of Neurosurgery, University of Erlangen, Schwabachanlage, Erlangen, Germany
Abstract.Purpose: Intrastriatal neural transplantation using multiple grafts is an experimental approach to the treatment of Huntington’sdisease (HD). Brain atrophy makes stereotactic plans in these patients a tedious procedure with a risk of suboptimal spatialdistribution of the grafts in transplantation procedures. Here we present a self-developed software to optimize the surgicalstereotactic planning for bilateral neurotransplantation procedures. It allows close to symmetrical distribution of the stereotacticcoordinates in relation to the mid-commissural point (MCP), proposing automatically the planning coordinates for the firsttransplanted hemisphere and mirrored coordinates to be used in the contra-lateral hemisphere.Methods: Twenty-two consecutive HD patients underwent bilateral stereotactic striatal transplantation. Two caudate nucleusand four putaminal tracks were planned bilaterally. For the second, contra-lateral transplantation, the coordinates were mirroredin order to determine contralateral targets and trajectories. Intra-individual comparison between software given coordinates andfinally used coordinates was performed.Results: No statistical significance was found comparing a) the differences between coordinates proposed by the software andthe final coordinates and b) the distribution of the transplantation sites in relation to the midline for the right vs. left hemisphere.No intra- or postoperative transplantation-related adverse events occurred.Conclusions: The use of model-based and mirrored coordinates allowed optimal spatial distribution of the grafts. Minor changeswere required comparing right to left coordinates giving proof-of principle. The initial use of the software suggests that it maybe useful in experimental transplantation trials where neural cell grafts are to be implanted into predefined target sites in thehuman brain, whether unilateral or bilateral.
Keywords: Huntington’s disease, human fetal striatal transplantation, anterior commissure-posterior commissure line (AC-PC),mid-commissural point (MCP), whole ganglionic eminence (WGE), caudate nucleus, putamen
∗Corresponding author: Dr. Michael Trippel, Department ofStereotactic and Functional Neurosurgery, University Medical Cen-ter, Breisacher Str. 64, 79106 Freiburg, Germany. Tel.: +49 761270 50620; Fax: +49 761 270 93150; E-mail: [email protected].
0922-6028/14/$27.50 © 2014 – IOS Press and the authors. All rights reserved

AU
THO
R C
OP
Y
260 W.O.C. Lopez et al. / Stereotactic planning software for human neurotransplantation
1. Introduction
Huntington’s disease (HD) is a fatal inheritedgenetic disorder caused by mutation of the gene (IT15)on the chromosome 4p16.3, causing an abnormal num-ber of CAG repeats (>36) within its 5′-end codingsequence. The huntingtin gene was identified in 1993by the Huntington’s Disease Collaborative Researchgroup, but until today the molecular pathways that endcausing cell death remain poorly elucidated.
HD is a neurodegenerative disorder present world-wide. The highest prevalence of the disease is infamilies of Caucasian descent, calculated to be 5–7.5in 100.000 people (Warby et al., 2011). Importantconcentrations of HD patients are also found in Juande Acosta near Barranquilla in Colombia and in thestate of Zulia, on the east coast of Lake Maracaiboin Venezuela, with 700 cases per 100.000 being thehighest concentrated population reported. The diseaseis generally of low occurrence in Asian and Africanpopulations (Kaplan, 2012).
In the majority of patients, symptoms appearbetween the third and fourth decade of life. Clini-cal features are the consequence of severe cell loss(up to 60% of type II Golgi-neurons) and atrophy inthe striatum, with consequent loss of thalamic inhi-bition, and hyperactivation of the direct basal gangliacircuit (Lobo, 2009). Such neurodegeneration causesprogressive motor, cognitive, and behavioral deterio-ration with progressive dementia (Foroud et al., 1999;Rosser, 2012). Mortality appears unequivocally in aperiod of 7 to 10 years after onset of symptoms and fre-quently from complications such pneumonia and heartdisease (Sorensen and Fenger, 1992; Zuccato et al.,2010).
At present there are no curative treatments forHD and there is a lack of effective symptomatictherapies. Bilateral stereotactic human fetal striataltransplantation (HFST) is a promising experimentaltherapy for patients with HD. The feasibility, safetyand proof-of-principle of neuronal transplantation hadbeen demonstrated in open clinical trials (Peschanski,1995; Kopyov, 1998; Freeman, 2000, 2011; Rosser,NEST-UK 2002; Hauser, 2002; Bachoud-Levi, 2006;Reuter, 2008; Gallina, 2008; Ruwani, 2011).
Studies in humans are still experimental and HFSTis not yet a standard treatment since clinical out-come has not yet been established conclusively. Safetyof the procedure is an essential requirement for anyclinical study. However as with any other surgi-
cal procedure, complications can occur. Intracranialhemorrhages, symptomatic subdural hygromas, andinfections related to donor origin and graft-rejectionhave been previously reported (Hauser, 2002; Krys-tkowiak, 2007). Transplanted tissue has little migratorycapacity and mostly remains at the surgical implanta-tion site (Bachoud-Levi, 2000; Gallina, 2008), makingadequate caudate-putaminal graft distribution crucialto increase the chances of a successful transplantation(appropriate donor-host cells connectivity).
The transplantation technique involves the surgi-cal implantation of the donor tissue by means ofa stereotactic procedure. Coordinates of the targetsare currently calculated on workstations using directtarget visualization on MRI images onto stereotac-tic equipment (Gallina, 2008) or MRI plus contrastmedium computed tomography (CCT) image fusion.Such strategy requires time consuming planning ses-sions, defining the individual targets and trajectories,optimizing spatial distribution and safety.
Hoping to fulfill the need of an easier, faster, andmore precise way to achieve a safe and homogeneousintrastriatal graft distribution, we report and proposethe use of an original software that allows fast distri-bution of the stereotactic coordinates in relation to theMCP, proposing to the user automatically the planningcoordinates for transplantation with two entry pointsand six trajectories. Planning can be modified man-ually, according to anatomy or presence of vesselson direct image visualization and mirrored coordi-nates to be used on the contra-lateral side. Trajectoriesproposed by the software can be moved as a wholeor as individual trajectories. An evaluation of clini-cal benefit of the transplantation procedure is out ofthe scope of this manuscript. This will be part of thefinal analysis of the ongoing multicenter MIG-HDTrial.
2. Methods
Twenty two consecutive patients of genetically con-firmed HD underwent bilateral stereotactic HFSTusing six striatal trajectories: Two in the head of thecaudate nucleus and four in the putamen, employingtwo 6 mm width burr holes on each hemisphere as entrypoints.
All patients had a clinically symptomatic and geneti-cally confirmed Huntington’s disease (number of CAGrepeats ≥ 36), were 25 to 65 years old, with an early
AU
THO
R C
OP
Y
W.O.C. Lopez et al. / Stereotactic planning software for human neurotransplantation 261
Table 1
Data of stereotactic procedures in 22 HD patients undergoing HFST with a two entry points approach. CAG: Genetic CAG repeat expansion;M: Mean, SD∗: Standard deviation; KPS: Karnofsky index performance scale; Tx group: Transplantation group, early (A) vs. late (B); R: right,
L: left
Patient Age Sex CAG Symptoms KPS% Time between Tx #Tracts #Embryos(Years) duration (Years) procedures (Weeks)
Group R L R L
1 43 M 44 8 70 9 B 6 6 2 22 45 M 46 9 60 10 B 6 6 2 23 42 M 44 8 90 4 A 5 5 2 24 50 F 46 5 80 1 B 6 6 4 25 32 F 51 3 80 14 A 6 6 2 26 45 F 47 12 70 2 A 6 6 4 47 36 F 45 4 90 10 A 6 6 2 48 38 M 43 5 70 3 B 5 6 2 29 31 F 41 7 60 4 B 6 5 2 210 46 F 50 3 70 5 A 6 6 2 311 35 F 50 3 90 3 A 6 6 2 212 39 M 42 5 90 7 B 6 6 2 113 54 M 46 4 90 7 A 6 6 2 214 50 M 44 8 80 9 A 6 6 1 215 41 F 43 7 80 3 A 6 6 2 216 49 F 43 5 80 7 A 6 4 2 217 40 M 45 9 70 3 B 6 6 2 218 50 M 42 7 60 3 A 6 6 2 219 41 M 44 4 70 3 A 6 6 2 220 38 M 51 6 80 3 A 6 6 2 221 46 F 46 4 80 4 A 6 6 2 222 30 F 46 3 80 7 A 6 6 2 2M 41.8 45.4 5.8 76.8 5.5 5.9 5.8 2.1 2.1SD 6.64 2.87 2.43 9.94 3.3 0.2 0.5 0.6 0.6
to moderate stage of the disease. All had a motor score>=5 on the Unified Huntington’s Disease Rating Scale(UHDRS) and a largely preserved autonomy in every-day life. The procedure was approved by the localEthics committee at the Freiburg University MedicalCenter as part of a European multicenter study (MIG-HD). Only patients who were aware of the full extent oftheir illness and who had appropriate decisional capac-ity and legal empowerment were included and asked togive their informed consent to medical care. Patientswho had advanced disease, severe comorbidity, acutepsychiatric disturbances, or severe cortical atrophy onthe CT and MRI images and/or positive HIV serol-ogy, active hepatitis (B and C) or HTLV 1 and 2 wereexcluded (Table 1).
Patients treated were assessed preoperatively for atleast six months and postoperatively by clinical, neu-ropsychological, psychiatric, neurophysiological andneuroimaging (MRI and PET) tests.
Transplantation surgery was performed in two sepa-rate surgical sessions, with a minimum interval of twoweeks. The first transplantation was performed alwaysin the right hemisphere, followed by a second surgeryinto the left hemisphere.
2.1. Transformation of stereotactic coordinates tomid commissural point (MCP) coordinatesthe MCP coordinates system
For every procedure, the stereotactic coordinatesor the mid commissural point
−−−→MCP were calculated
as middle of the two vectors−→AC and
−→PC
−−−→MCP =
(−→AC + −→
PC)/2. The unit vectors defining the MCPcoordinate system for each patient were determined
as follows: the stereotactic coordinates→u ,
→v ,
→w of the
anterior commissure (AC), the posterior commissure(PC), the upper (MU) and lower midline (ML) points
were determined forming the vectors→A = −→
AC − −→PC
and→M = −−→
MU − −→ML. The cross vector product
→R
of→A and
→M was calculated ((�R = �A × �M)) indicat-
ing to the right direction. The cross product→V of
the vectors→R and
→A gave the third upwards-directed
coordinate (( �V = �R × �A)). These vectors→R,
→A,
→V
were normalized to the unit vectors→X,
→Y ,
→Z show-
ing right, anterior and upwards (( �X = �R /∣∣�R∣
∣ ; �Y =�A /
∣∣∣ �A
∣∣∣ ; �Z = �V/
∣∣ �V ∣
∣)). These three orthogonal unit
AU
THO
R C
OP
Y
262 W.O.C. Lopez et al. / Stereotactic planning software for human neurotransplantation
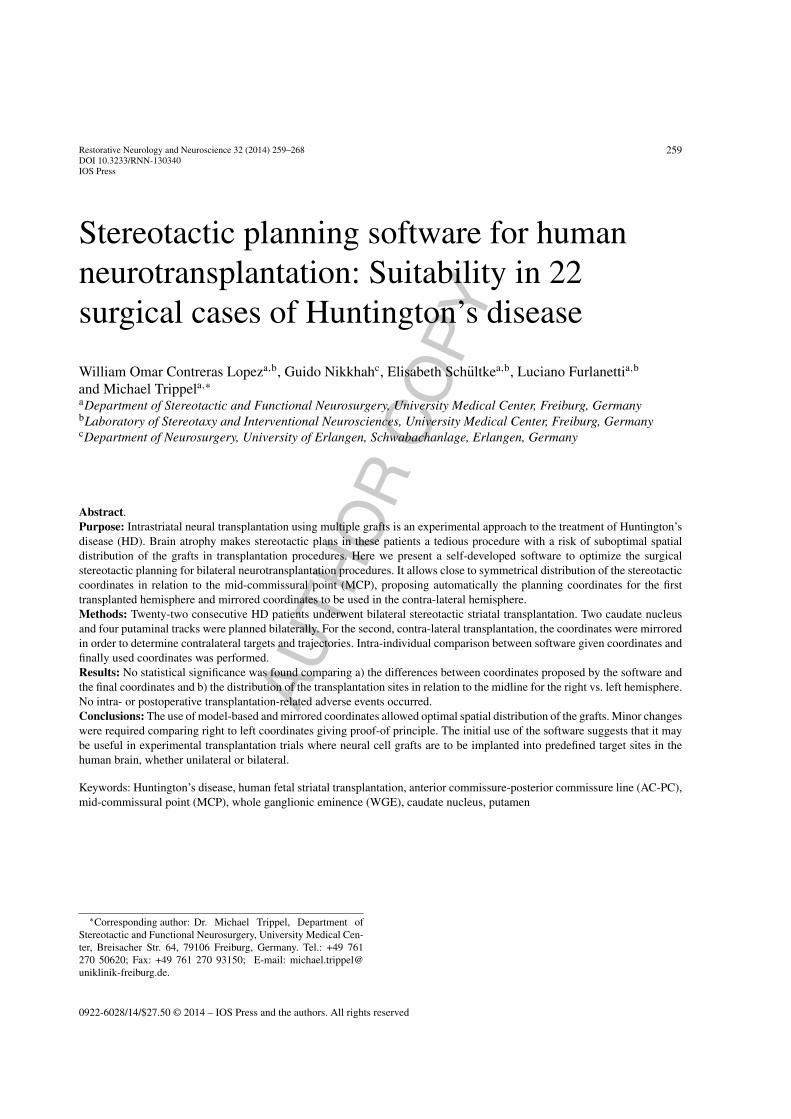
Fig. 1. MRI T1w, showing typical views obtained from the STP3 –planning workstation. Three coronal projections with tracts going to thecaudate nucleus and to the putamen on the left side.
vectors built up the lines of the matrix TM, based onwhich the inverse matrix T = TM−1. To transform anystereotactic coordinate point S into the MCP coordinatesystem the vector difference �D = �S − −−−→
MCP was cal-culated and multiplied with the inverse transformationmatrix T to obtain MCP coordinates (( �M = [T ] ∗ �D).
Thus, the stereotactic coordinates of target and entrypoints were transformed into MCP - coordinates forall patients. The points on the left side of the headwith negative X – MCP - coordinates were mirroredto the right side by inverting the sign of the X coordi-nate. From these transformed target points, the spatialcenter of each cluster, its distribution and standarddeviation was calculated. Points belonging to a clusterwith a distance of more than 2.25 standard devia-tions from the center were eliminated to improve dataquality.
These coordinates allow for the identification of thetargets, where the eight tissue deposits along the tra-jectory are given, and can be used in the planning ofthe transplantation, aiming for a safer and faster tar-get planning (Fig. 1). The coordinates in the putamenand caudate nucleus were identified in Three-TeslaMagnetic Resonance imaging and transformed intomid-commissural point (MCP) coordinates. From thisdata a model-based atlas was created. For the second,contra-lateral transplantation, the MCP coordinateswere mirrored to the opposite side in order to determinecontralateral targets and trajectories.
The decision of performing five or six trajectories isbased on the individual atrophy of the striatal nuclei,which may reduce the number of possible trajectories,avoiding the last post commissural putaminal trajec-tory (Gallina, 2008). The number of grafts therefore, is
Table 2
Mean length of each tract from cortex to target and AC-PC line in mil-limetres PCP2 (Putamen posterior), PCP1 (Putamen posterior), CP(Putamen anterior), PP (Putamen anterior), CC (Caudate anterior),PC (Caudate posterior), AC-PC line (anterior commissure-posterior
commissure) connecting anterior and posterior commissure
Name Mean length of the tract
PCP2 63.95 mmPCP1 63.63 mmCP 63.22 mmPP 62.71 mmCC 58.92 mmPC 58.17 mmAC-PC 25.15 mm
customized for each patient based on the degree of atro-phy and accessibility, with a distance of 1 mm betweenindividual grafts (Bachoud-Levi, 2000).
2.2. Transplantation technique
The grafts consisted of striatal tissue obtained fromthe striatal primordia. Fetal striatal primordia arelocated bilaterally in the whole ganglionic eminences(WGE) of 7 to 12 weeks-old human fetuses. The tissuewas the product of a voluntary interruption of preg-nancy and was obtained in accordance with the localethical committee guidelines and legal regulations ofthe Federal Republic of Germany and the EuropeanUnion (EU) with informed consent of the donors.
Under general anesthesia with additional local anes-thesia, the stereotactic frame was fixed to the head ofthe patients. Stereotactic contrast-enhanced CT (2 mmslices-Siemens Somatom plus) was performed andthe images transferred to a workstation for fusion
AU
THO
R C
OP
Y
W.O.C. Lopez et al. / Stereotactic planning software for human neurotransplantation 263
A B C
D E F
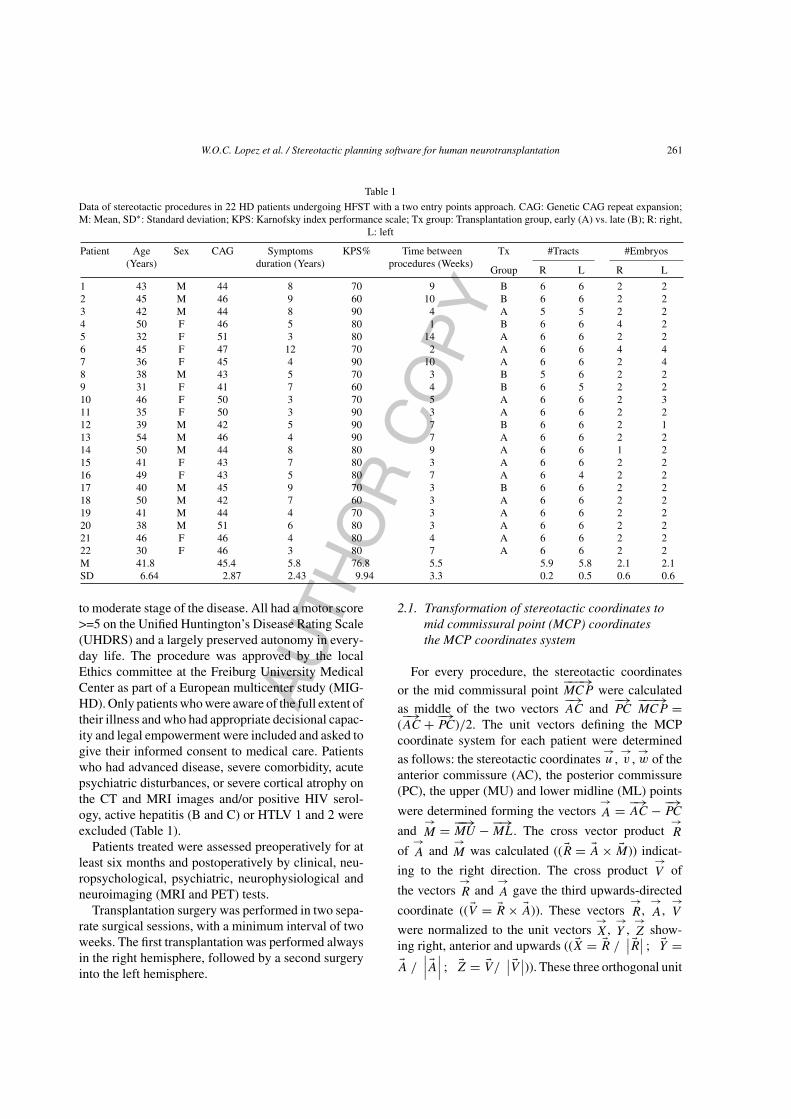
Fig. 2. The figure shows an overview of the stepwise planning approach to transplantation as well as a post-operative image control in thesame patient. A: MRI T1w contrast-enhancement sagittal image, planning begins by identification and registration of AC-PC line (thick yellowarrow) and midline (purple line, five-tipped star) starting from the posterior part of the brainstem (corresponding colored starts help to identifythe lines in the picture). B: Axial view of a contrast MRI T1w sequence image, showing stereotactic planning of the six targets (two in the headof the caudate nucleus (CN) (yellow arrow) and four into the Putamen (short red arrow) with two independent entry points for CN and putamentargets. C: Sagittal MRI T1w sequence image showing planned trajectories and clear necessity of two entry points. D: Picture shows the setupat the time of transplantation. It shows the stereotactic Riechert-Mundinger frame with its aiming bow, the patient is under general anesthesiaand the transplantation is performed with a Hamilton syringe attached to the aiming bow (Inomed, Medizintechnik GmbH Emmendingen,Germany); Transplantation is performed delivering 5 µl of tissue suspension in 8 deposits per each trajectory. E: Postoperative MRI (T1w,Siemens TRIO), axial view, of the same patient three days after left striatal transplantation. The longer yellow arrow shows the deposits intothe head of the left CN and the short red arrow indicates the deposits into the putamen. This patient was previously transplanted on the rightside where it is possible to identify the grafted area. F: MRI (T1w, TRIO, Siemens) of the same patient in a sagittal view 3 days after left-sidedtransplantation; the yellow arrow shows a characteristic local hyperintensity indicative of the deposits sites.
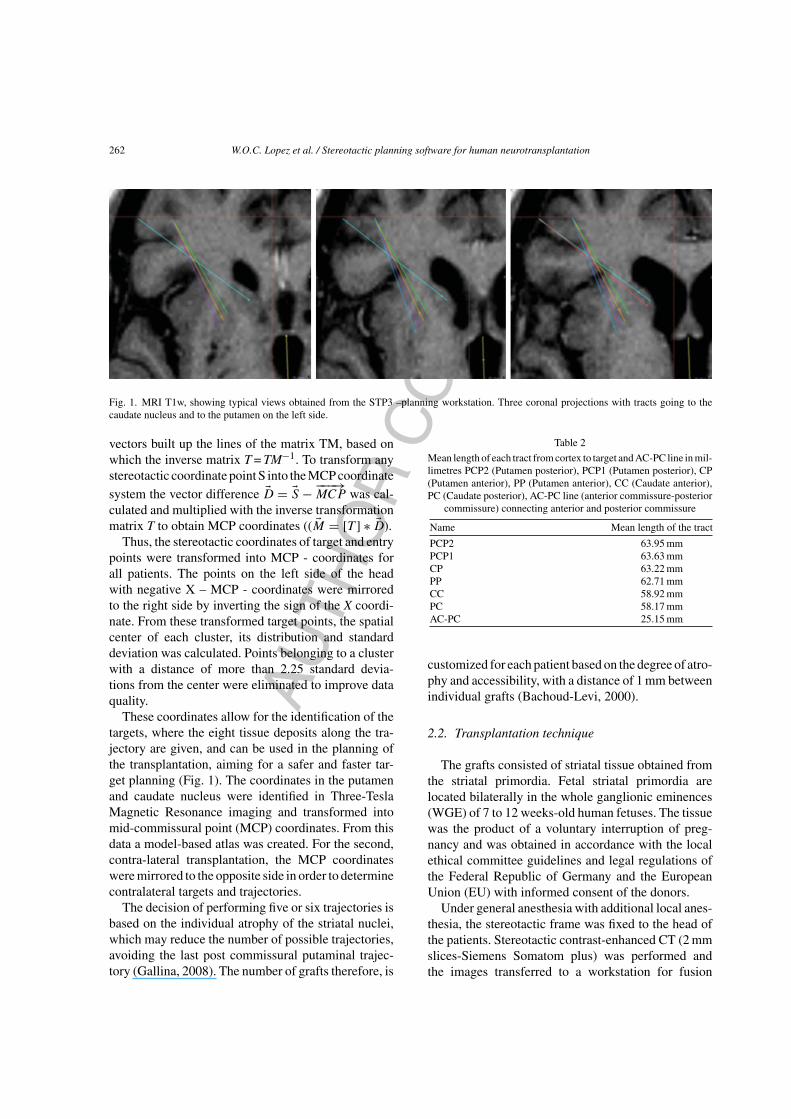
Table 3
Stereotactic coordinates. On the left: MCP-Coordinates (tx, ty, tz) of the target (t), in millimetres. Four targets in the putamen, two posterior: PCP2and PCP1, two anterior: CP and PP and two targets in the caudate nucleus: CC and PC. SD (standard deviation). On the right: MCP-Coordinates(ex, ey, ez) of the entry points (e) in millimetres, posterior putamen: PCP2 and PCP1, Anterior: CP and PP and caudate nucleus: CC and PC.
sdx, sdy, sdz, sdt (standard deviation for the target and entry points in the x, y, z direction and total)
Target tx ty tz sdx sdy sdz sdt ex ey ez sdx sdy sdz sdt
PCP2 21.34 13.78 −0.66 1.81 2.39 1.73 3.47 33.84 42.67 54.94 3.74 5.36 7.83 10.20PCP1 20.92 16.12 −1.41 1.97 2.00 1.66 3.26 34.03 41.56 55.27 3.65 6.35 7.90 10.77CP 20.22 19.00 −2.22 1.55 1.59 1.30 2.57 34.02 41.52 55.05 3.69 6.24 7.80 10.65PP 19.57 21.84 −2.73 1.56 1.52 1.38 2.57 34.07 41.40 54.95 3.72 6.21 7.56 10.46CC 12.44 21.84 2.10 1.79 1.56 1.27 2.69 47.83 37.28 46.41 6.82 7.39 8.01 12.86PC 13.16 24.63 0.88 1.84 1.48 1.18 2.63 47.61 37.51 46.01 6.25 7.31 7.82 12.40
AU
THO
R C
OP
Y
264 W.O.C. Lopez et al. / Stereotactic planning software for human neurotransplantation
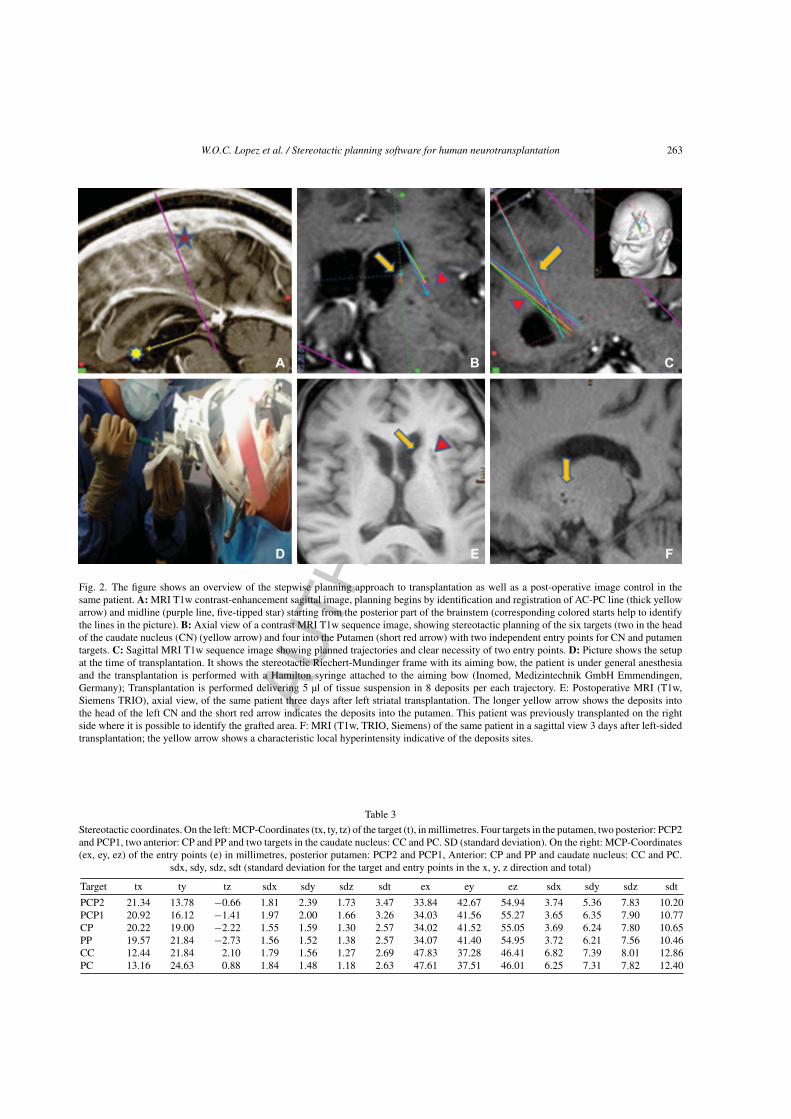
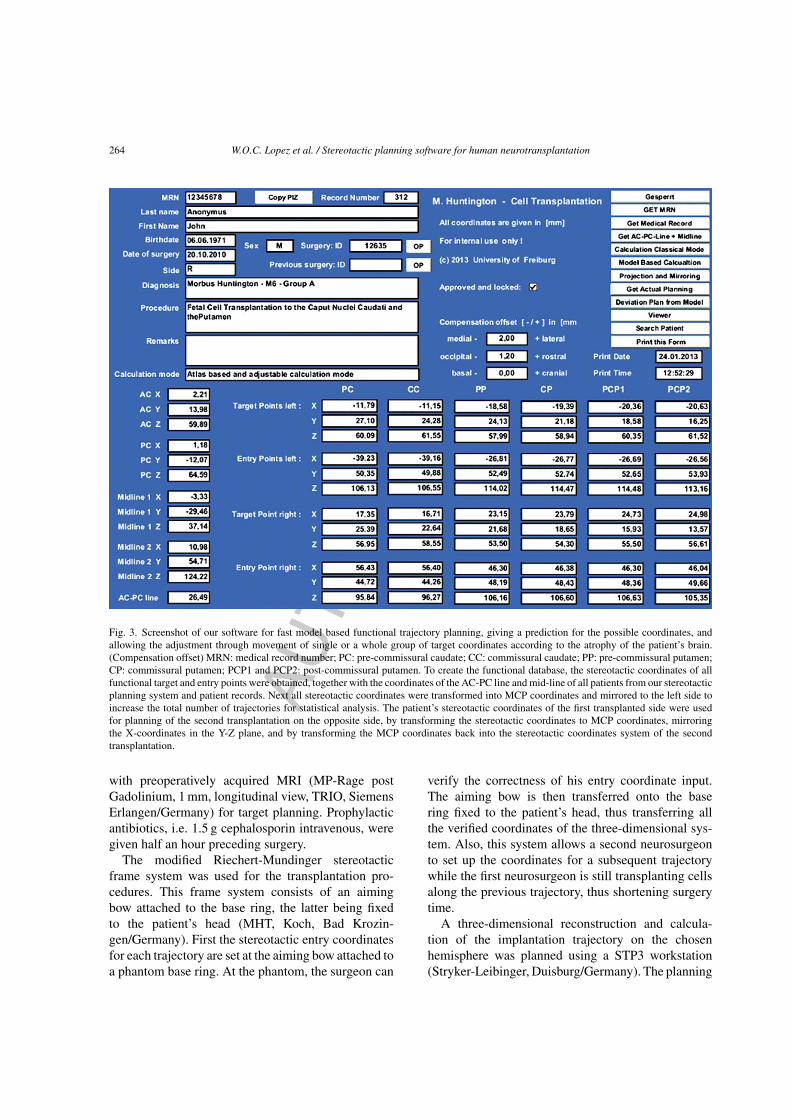
Fig. 3. Screenshot of our software for fast model based functional trajectory planning, giving a prediction for the possible coordinates, andallowing the adjustment through movement of single or a whole group of target coordinates according to the atrophy of the patient’s brain.(Compensation offset) MRN: medical record number; PC: pre-commissural caudate; CC: commissural caudate; PP: pre-commissural putamen;CP: commissural putamen; PCP1 and PCP2: post-commissural putamen. To create the functional database, the stereotactic coordinates of allfunctional target and entry points were obtained, together with the coordinates of the AC-PC line and mid-line of all patients from our stereotacticplanning system and patient records. Next all stereotactic coordinates were transformed into MCP coordinates and mirrored to the left side toincrease the total number of trajectories for statistical analysis. The patient’s stereotactic coordinates of the first transplanted side were usedfor planning of the second transplantation on the opposite side, by transforming the stereotactic coordinates to MCP coordinates, mirroringthe X-coordinates in the Y-Z plane, and by transforming the MCP coordinates back into the stereotactic coordinates system of the secondtransplantation.
with preoperatively acquired MRI (MP-Rage postGadolinium, 1 mm, longitudinal view, TRIO, SiemensErlangen/Germany) for target planning. Prophylacticantibiotics, i.e. 1.5 g cephalosporin intravenous, weregiven half an hour preceding surgery.
The modified Riechert-Mundinger stereotacticframe system was used for the transplantation pro-cedures. This frame system consists of an aimingbow attached to the base ring, the latter being fixedto the patient’s head (MHT, Koch, Bad Krozin-gen/Germany). First the stereotactic entry coordinatesfor each trajectory are set at the aiming bow attached toa phantom base ring. At the phantom, the surgeon can
verify the correctness of his entry coordinate input.The aiming bow is then transferred onto the basering fixed to the patient’s head, thus transferring allthe verified coordinates of the three-dimensional sys-tem. Also, this system allows a second neurosurgeonto set up the coordinates for a subsequent trajectorywhile the first neurosurgeon is still transplanting cellsalong the previous trajectory, thus shortening surgerytime.
A three-dimensional reconstruction and calcula-tion of the implantation trajectory on the chosenhemisphere was planned using a STP3 workstation(Stryker-Leibinger, Duisburg/Germany). The planning

AU
THO
R C
OP
Y
W.O.C. Lopez et al. / Stereotactic planning software for human neurotransplantation 265
began with the identification of the anterior and pos-terior commissural points to set up the denominatedAC-PC line, allowing more precision and the possi-bility to use either model based planning or mirroredcoordinates obtained from the first surgery, speedingup planning of the second surgery (Fig. 2).
The software was developed for a fast model-basedplanning, giving a prediction for the possible coordi-nates, allowing where required individual or multipleadjustments by moving a whole group of target coordi-nates according to the atrophy of the patient’s brain. Amodel-based functional database of stereotactic coor-dinates of target and entry points was created, togetherwith the coordinates of the AC-PC line and mid-lineof the patients, which were obtained from the stereo-tactic planning system and patient records (Table 2).Next, all stereotactic coordinates were transformedinto MCP coordinates and mirrored to one side toincrease the total number of trajectories for statisticalanalysis. The typical MCP - coordinates of all targetand entry points were calculated using cluster analysis,excluding patients with a spatial distance of more than2.25 standard deviations from the center of the corre-sponding cluster. After registration of a new patient,the patient’s coordinates were included in the databaseimproving statistics for all succeeding patients. Thusa self-learning functional database of coordinates wascreated. The patient’s stereotactic coordinates of thefirst transplanted hemisphere were used for planningof the second transplantation procedure on the con-tralateral hemisphere, by first transforming stereotacticstandard coordinates to MCP coordinates, then mir-roring the X - Coordinates in the Y-Z plane, and byfinally transforming the MCP coordinates back intothe actual stereotactic coordinates system of the sec-ond transplantation (Fig. 3). In this way the target andentry points must only be adjusted to avoid blood ves-sels on the surface of the brain and in the path of thetrajectories (Table 3). In some of the patients, with a faradvanced state of striatal degeneration, it was impos-sible to make a plan for all four-target points in theputamen. In these cases the most posterior trajectorywas omitted.
A frontal pre-coronal entry point was chosen with a6 mm burr hole for the two caudate nucleus trajectories,and a second entry point more medial to accommo-date the four trajectories to the putamen (Table 4). Theaim was to perform: two separate trajectories in thehead of the caudate nucleus; two trajectories in the pre-commissural and commissural region of the putamen
and two trajectories in the post-commissural region ofthe putamen bilaterally.
50 �l of tissue suspension were aspirated into aHamilton syringe through a 0.6 mm diameter needle(Hamilton™ Company- Bonaduz, Switzerland). Thetip of the needle was inserted in the target along theplanned trajectory, and then 5 �l of tissue suspensionwere deposited. After a waiting period of 2 minutes,the needle was retracted 1 mm, repeating the depositeach time over a distance of 7 mm. Thus eight graftswere deposited along each trajectory (Fig. 2).
All patients received bilateral HFST in two separateprocedures under general anesthesia. Transplantationwas always performed first in the right hemisphere, andafter a minimum of two weeks (mean: 5.5, SD: 3.3)transplantation in the left hemisphere was performed.For the second surgery, the software automaticallyprovided the coordinates based on the previous con-tralateral surgery, proposing mirrored coordinates forintra-individual planning. In total a number of 94 WGEfrom 47 embryos were obtained and transplanted.The number of embryos transplanted per side rangedbetween one and four, with a mean of 2.15 embryos,for each procedure (SD: 0.6).
3. Results
The intended number of targets was six (two tar-gets into the head of the caudate nucleus and fourinto the putamen). All patients were planned usingthe software for that purpose, however, it was notalways possible to achieve this objective. Four patientsreceived transplantation along five trajectories, and onepatient four trajectories only in one hemisphere. In twocases this was due to a reduced quantity of suspension,and in three cases due to increased cerebral atrophyrequired reduction in the number of trajectories. Thoseresults agree with the report of Gallina (2008). In thisstudy, the extend of brain atrophy was assessed in 8consecutive HD patients before human fetal striataltransplantation, giving an atrophy score based on thevisual rating of the shape of the lateral wall of thefrontal ventricular horn and of the size of the caputnuclei caudate. The score slightly differed between thetwo hemispheres only in two patients, being equal inthe other six.
For all patients and target points: Two caudatenucleus tracks were performed in all the 22 patientsbilaterally; two pre-commissural putamen tracks were
AU
THO
R C
OP
Y
266 W.O.C. Lopez et al. / Stereotactic planning software for human neurotransplantation
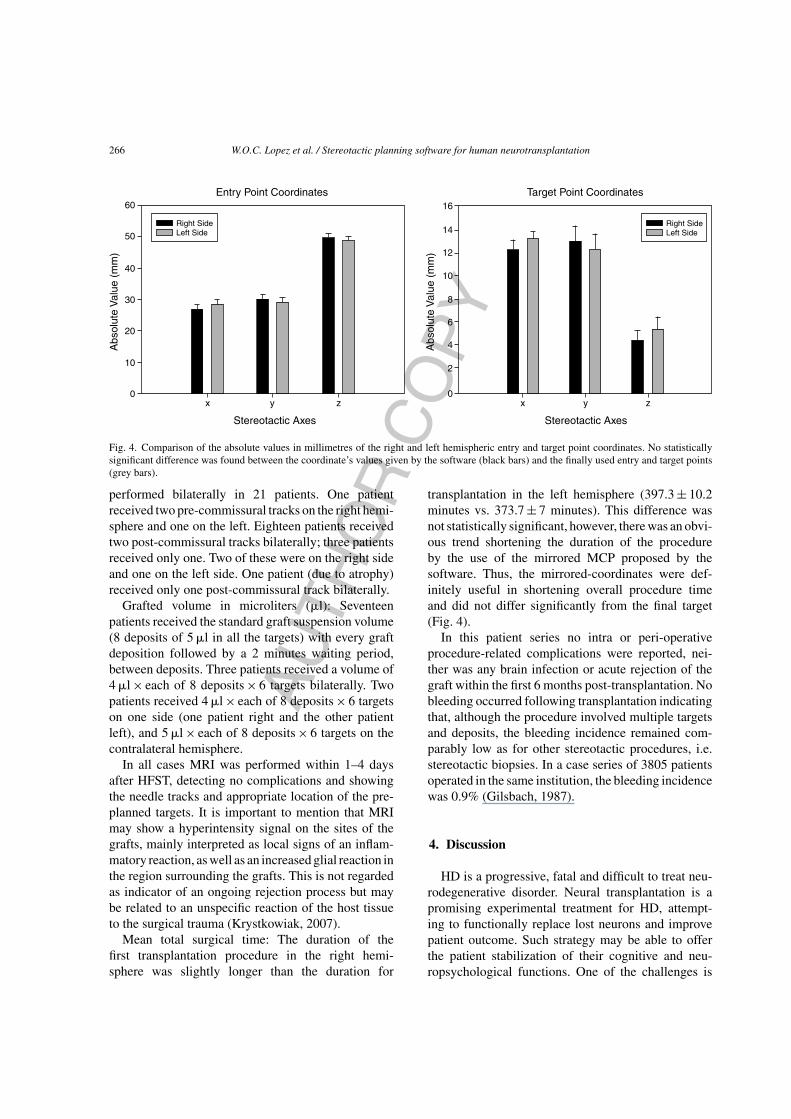
Fig. 4. Comparison of the absolute values in millimetres of the right and left hemispheric entry and target point coordinates. No statisticallysignificant difference was found between the coordinate’s values given by the software (black bars) and the finally used entry and target points(grey bars).
performed bilaterally in 21 patients. One patientreceived two pre-commissural tracks on the right hemi-sphere and one on the left. Eighteen patients receivedtwo post-commissural tracks bilaterally; three patientsreceived only one. Two of these were on the right sideand one on the left side. One patient (due to atrophy)received only one post-commissural track bilaterally.
Grafted volume in microliters (�l): Seventeenpatients received the standard graft suspension volume(8 deposits of 5 �l in all the targets) with every graftdeposition followed by a 2 minutes waiting period,between deposits. Three patients received a volume of4 �l × each of 8 deposits × 6 targets bilaterally. Twopatients received 4 �l × each of 8 deposits × 6 targetson one side (one patient right and the other patientleft), and 5 �l × each of 8 deposits × 6 targets on thecontralateral hemisphere.
In all cases MRI was performed within 1–4 daysafter HFST, detecting no complications and showingthe needle tracks and appropriate location of the pre-planned targets. It is important to mention that MRImay show a hyperintensity signal on the sites of thegrafts, mainly interpreted as local signs of an inflam-matory reaction, as well as an increased glial reaction inthe region surrounding the grafts. This is not regardedas indicator of an ongoing rejection process but maybe related to an unspecific reaction of the host tissueto the surgical trauma (Krystkowiak, 2007).
Mean total surgical time: The duration of thefirst transplantation procedure in the right hemi-sphere was slightly longer than the duration for
transplantation in the left hemisphere (397.3 ± 10.2minutes vs. 373.7 ± 7 minutes). This difference wasnot statistically significant, however, there was an obvi-ous trend shortening the duration of the procedureby the use of the mirrored MCP proposed by thesoftware. Thus, the mirrored-coordinates were def-initely useful in shortening overall procedure timeand did not differ significantly from the final target(Fig. 4).
In this patient series no intra or peri-operativeprocedure-related complications were reported, nei-ther was any brain infection or acute rejection of thegraft within the first 6 months post-transplantation. Nobleeding occurred following transplantation indicatingthat, although the procedure involved multiple targetsand deposits, the bleeding incidence remained com-parably low as for other stereotactic procedures, i.e.stereotactic biopsies. In a case series of 3805 patientsoperated in the same institution, the bleeding incidencewas 0.9% (Gilsbach, 1987).
4. Discussion
HD is a progressive, fatal and difficult to treat neu-rodegenerative disorder. Neural transplantation is apromising experimental treatment for HD, attempt-ing to functionally replace lost neurons and improvepatient outcome. Such strategy may be able to offerthe patient stabilization of their cognitive and neu-ropsychological functions. One of the challenges is

AU
THO
R C
OP
Y
W.O.C. Lopez et al. / Stereotactic planning software for human neurotransplantation 267
to deposit multiple grafts in such an atrophic brain.This requires fine-tuning of the stereotactic proce-dure, beginning with the planning process to assurethe safety of the procedure.
The selected targets allow the distribution of graftsin the caudate nucleus, anterior putamen (areas primar-ily associated with cognitive and neuropsychologicalfunction) (Farrer, 1986; Freeman, 1995; Olanow, 1996)and post-commissural putamen (primary involved inmotor circuits) (Hauser, 2002; Wijeyekoon, 2011).
To date, several studies have reported that neuralcell replacement therapy is not associated with serioussurgical complications (Kopyov, 1998; Rosser, 2002).Subdural hematoma seems to be the most frequent oneand has been directly related to the degree of cerebralatrophy. This may suggest that surgery performed in anearlier stage of the disease could minimize this problem(Hauser, 2002). Common post-operative complica-tions such as subdural hygromas (SDHs), generally theconsequence of chronic subdural hematomas, are com-monly seen in elderly patients. Large hygromas maycause secondary localized mass effect on the adjacentbrain parenchyma. SDHs are reported in the literatureas a notable adverse event in HD transplantations stud-ies. Intraoperative CSF loss causes brain “shrinkage”and shift in HD patients who had cerebral atrophy,expanding the subdural space, predisposing to post-operative SDHs (Freeman, 2011). Therefore, the riskof developing SDHs after neurotransplantation may bedirectly related to the degree of cerebral atrophy, andcould be reduced by covering the burr hole with bonecement or fibrin glue (Hauser, 2002; Freeman, 2000).For the same reason we decided to apply two separatesmall burr holes for each hemisphere instead of onelarger craniotomy. In our experience this significantlydecreases the likelihood of SDH.
In the present patient series, no operative or post-operative complications occurred, and the procedurewas well tolerated by all patients. There were noadverse events attributable to either anesthesia or tothe neurosurgical procedure. The grafted areas couldbe identified on MRI scans as appropriately placedinto the caput nuclei caudate and putamen. The model-based coordinates predicted by the software optimizedthe surgical planning, which is considered as a keypart of the procedure. The presented technique canalso be applied in neurotransplantation for other neu-rodegenerative diseases, for instance in patients withParkinson’s disease. To the best of our knowledge, thisis the largest reported patient series and therefore it
was especially suited to create a database for targetcoordinates.
5. Conclusions
The software presented here allowed us to achievea fast determination of the stereotactic coordinates inrelation to the MCP for the first surgery providingmirrored coordinates for the contralateral transplanta-tion, facilitating an optimized spatial distribution of thegrafts. The stereotactic trajectories have to be adaptedfor anatomical variations, according to the disease-related brain atrophy and to the presence of bloodvessels. The proposed use of such a data base for coor-dinates can shorten stereotactic planning time and thusincrease the safety of the overall procedure.
Acknowledgments
We thank the centers involved in the multicenterstudy Euro-HD phase II trial, the Department of Neu-roradiology in Freiburg and the French collaborationgroup lead by Prof. Dr. A. Bachoud-Levi as well asthe NECTAR group for their close collaboration. Thesoftware presented here was developed by MichaelTrippel, MD. We thank Thomas Gunter from our localworkshop and InomedTM (Emmendingen/Germany)for their constant support in the development and opti-mization of the surgical instrumentation.
References
The Huntington’s disease Collaborative Research, Group, (1993). Anovel gene containing a trinucleotide repeats that is expandedand unstable on Huntington’s disease chromosomes. Cell,72(6), 971-983.
Kaplan, A. & Stockwell, B. (2012). Therapeutic approaches topreventing cell death in Huntington disease. Progress in Neu-robiology PRONEU, 1241, 1-19.
Warby, S.C. & Hayden, M. (2011). HTT haplotypes contribute todifferences in Huntington disease prevalence between Europeand East Asia. Eur J Hum Genet, 19(5), 561-566.
Lobo, M. (2009). Molecular Profiling of Striatonigral and Stri-atopallidal Medium Spiny Neurons: Past, Present, and Future.International Review of Neurobiology, 89, 1-35.
Foroud, T. & Conneally, M. (1999). Differences in duration of Hunt-ington’s disease based on age at onset. J Neurol NeurosurgPsychiatry, 66, 52-56.
Rosser, A.E. & Barker, R.A., NEST-UK consortium (2002). Uni-lateral transplantation of human primary fetal tissue in fourpatients with Huntington’s disease: NEST-UK safety report

AU
THO
R C
OP
Y
268 W.O.C. Lopez et al. / Stereotactic planning software for human neurotransplantation
ISRCTN no 36485475. J Neurol Neurosurg Psychiatry, 73,678-685.
Sorensen, S.A. & und Fenger, K. (1992). Causes of death in patientswith Huntington’s disease and in unaffected first degree rela-tives. J Med Genet, (29)S, 911-914.
Zuccato, C., Valenza, M. & Cattaneo, E. (2010). Molecular mech-anisms and potential therapeutical targets in Huntington’sdisease. Physiol Rev, (90)S, 905-981.
Peschanski, M., Cesaro, P. & Hantraye, P. (1995). Rationale forintrastriatal grafting of striatal neuroblasts in patients withHuntington’s disease. Neuroscience, 68, 273-285.
Kopyov, O.V., Jacques, S., Lieberman, A., Duma, C.M. & Eagle,K.S. (1998). Safety of intrastriatal neu-rotransplantation forHuntington’s disease patients. Exp Neurol, 149, 97-108.
Freeman, T.B., Hauser, R.A., Sanberg, P.R. & Saporta, S. (2000).Neural transplantation for the treatment of Huntington’s dis-ease. Prog Brain Res, 127, 405-411.
Hauser, R.A., Furtado, S., Cimino, C.R. & Freeman, T.B. (2002).Bilateral human fetal striatal transplantation in Huntington’sdisease. Neurology, 58, 687-695.
Bachoud-Levi, A.C. & Peschanski, M. (2006). Effect of fetal neuraltransplants in patients with Huntington’s disease 6 years aftersurgery: a long-term follow-up study. Lancet Neurol, (5), 303-309.
Reuter, I. & Piccini, P. (2008). Long-term clinical and positronemission tomography outcome of fetal striatal transplantationin Huntington’s disease. J Neurol Neurosurg Psychiatry, (79),948-951.
Gilsbach J. & Mundinger F. (1987). A new safety device to preventbleeding complications during stereotactic: The stereotacticDoppler sonography. Act Neurochir, (89), 77-79.
Gallina P., & Di Lorenzo N. (2008). Human fetal Striatal Transplan-tation in Huntington’s Disease. A Refinement of the StereotacticProcedure. Stereotactic and Functional Neurosurgery, 86, 308-313.
Bachoud-Levi, A., Bourdet, C. & Brugieres, P. et al. (2000). Safetyand tolerability assessment of intrastriatal neural allografts infive patients with Huntington’s disease. Exp Neurol, (161), 194-202.
Wijeyekoon R. & Barker R.A. (2011). The Current Status of NeuralGrafting in the Treatment of Huntington’s Disease, a Review.Front Integr Neurosci, (5), 78.
Krystkowiak P. & Bachoud-Levi, A. (2007). Alloimunisation toDonor Antigens and Immune Rejection Following Fetal Neuralgrafts to the Brain in Patients with Huntington’s disease. PloSOne, 24(1), 166.
Farrer, L.A. (1986). Suicide and attempted suicide in Huntingtondisease: Implications for preclinical testing of persons at risk.Am J Med Genet, (24), 305-311.
Freeman, T.B., Olanow, C.W. & Hauser, R.A. et al. (1995). Bilateralfetal nigral transplantation into the postcommissural putamenin Parkinson’s disease. Ann Neurol, (38), 379-388.
Olanow, C.W., Kordower, J.H. & Freeman, T.B. (1996). Fetal nigraltransplantation as a therapy for Parkinson’s disease. TrendsNeurosci, (19), 102-109.
Freeman, T.B., Cicchetti, F., Bachoud-Levi, A.C. & Dunnett, S.B.(2011). Technical factors that influence neural transplant safetyin Huntington’s disease. Exp Neurol, 227(1), 1-9.




















