
Spinal cord perfusion after extensive segmental artery sacrifice: can paraplegia be prevented?
6
Spinal cord perfusion after extensive segmental artery sacrifice: can paraplegia be prevented? § Christian D. Etz a, * , Tobias M. Homann a , Konstadinos A. Plestis a , Ning Zhang a , Maximilian Luehr a , Donald J. Weisz b , George Kleinman c , Randall B. Griepp a a Department of Cardiothoracic Surgery, Mount Sinai School of Medicine, New York, New York, USA b Department of Neurophysiology, Mount Sinai School of Medicine, New York, New York, USA c Department of Pathology, Mount Sinai School of Medicine, New York, New York, USA Received 10 September 2006; received in revised form 28 December 2006; accepted 5 January 2007; Available online 12 February 2007 Abstract Objective: Understanding the ability of the paraspinal anastomotic network to provide adequate spinal cord perfusion pressure (SCPP) critical for both surgical and endovascular repair of thoracoabdominal aortic aneurysms (TAAA). Methods: To monitor pressure in the collateral circulation, a catheter was inserted into the distal end of the divided first lumbar segmental artery (SA) of 10 juvenile Yorkshire pigs (28.9 3.8 kg). SA pairs from T3 through L5 were serially sacrificed at 32 8C; SCPP and function — using motor-evoked potentials (MEPs) — were continuously monitored until 1 h after clamping the last SA. Intermittent aortic and SCPP monitoring was continued for 5 days postoperatively, along with evaluation of motor function. Results: A mean of 14.4 0.7 SAs were sacrificed without loss of MEP. SCPP (mmHg) dropped from 68 7 before SA clamping (77% of aortic pressure) to 22 6 at end clamping, and 21 4 after 1 h, reaching its lowest point — 19 4 — after 5 h. Postoperatively, SCPP recovered to 33 6 at 24 h; 42 10 at 48 h; 56 14 at 72 h; 62 15 at 96 h, returning to baseline (63 20) at 120 h. Despite comparable SCPP patterns, four pigs did not fully regain the ability to stand. Six animals recovered: two could stand and four could walk. Conclusions: Interruption of all SAs at 32 8C in this pig model results in a spectrum of cord injury, with normal function in a majority of pigs postoperatively. The short duration of low SCPP suggests that hemodynamic manipulation lasting only 24—48 h may allow routine complete preservation of normal cord function despite sacrifice of all SAs. # 2007 European Association for Cardio-Thoracic Surgery. Published by Elsevier B.V. All rights reserved. Keywords: Spinal cord perfusion/protection; Paraplegia; Segmental artery sacrifice; Thoracoabdominal aortic aneurysm repair (TAA/A) 1. Introduction The mortality and morbidity of even extensive thora- coabdominal replacement has improved markedly in recent years [1]. However, postoperative paraplegia remains a devastating complication and its occurrence is still somewhat unpredictable [2—6]. Most often, neurologic injury becomes apparent immedi- ately postoperatively, and is attributed to ischemic injury during intraoperative aortic cross-clamping and/or inade- quate postoperative spinal cord perfusion. However, a small fraction of patients awaken from anesthesia neurologically normal, but develop delayed onset paraplegia hours to weeks later. The pathogenesis of both types of paraplegia, but particularly of delayed onset deficit, is still poorly under- stood [7]. Consequently, the effectiveness of different strategies for minimizing intraoperative spinal cord ische- mia, and for managing intercostal and lumbar arteries during repair of thoracic and thoracoabdominal aortic aneurysms (TAA/A) in order to prevent paraplegia remains controversial [3,8—14]. The studies described in this report were undertaken to try to gain a better understanding in an animal model of the impact of extensive sacrifice of segmental arteries (SAs) on spinal cord perfusion intraoperatively and in the immediate postoperative period, under experimental conditions which approximate the circumstances prevailing during clinical thoracoabdominal aortic surgery. Previous studies with this model established the feasibility of routine extensive SA sacrifice without loss of function because of the existence of a dense and complex collateral arterial network feeding the spinal cord [15,16]. It is hoped that further investigation of the usual physiological and functional response of the collateral spinal cord perfusion network to the sacrifice of important contributors to its blood supply — and especially of www.elsevier.com/locate/ejcts European Journal of Cardio-thoracic Surgery 31 (2007) 643—648 § Presented at the joint 20th Annual Meeting of the European Association for Cardio-thoracic Surgery and the 14th Annual Meeting of the European Society of Thoracic Surgeons, Stockholm, Sweden, September 10—13, 2006. * Corresponding author. Address: Mount Sinai School of Medicine, Depart- ment of Cardiothoracic Surgery, One Gustave L. Levy Place, PO-Box: 1028, New York, NY 10029, USA. Tel.: +1 212 659 6800; fax: +1 212 659 6818. E-mail address: [email protected] (C.D. Etz). 1010-7940/$ — see front matter # 2007 European Association for Cardio-Thoracic Surgery. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.ejcts.2007.01.023
-
Upload
uni-leipzig -
Category
Documents
-
view
5 -
download
0
Transcript of Spinal cord perfusion after extensive segmental artery sacrifice: can paraplegia be prevented?

www.elsevier.com/locate/ejctsEuropean Journal of Cardio-thoracic Surgery 31 (2007) 643—648
Spinal cord perfusion after extensive segmental artery sacrifice:can paraplegia be prevented?§
Christian D. Etz a,*, Tobias M. Homann a, Konstadinos A. Plestis a, Ning Zhang a,Maximilian Luehr a, Donald J. Weisz b, George Kleinman c, Randall B. Griepp a
aDepartment of Cardiothoracic Surgery, Mount Sinai School of Medicine, New York, New York, USAbDepartment of Neurophysiology, Mount Sinai School of Medicine, New York, New York, USA
cDepartment of Pathology, Mount Sinai School of Medicine, New York, New York, USA
Received 10 September 2006; received in revised form 28 December 2006; accepted 5 January 2007; Available online 12 February 2007
Abstract
Objective: Understanding the ability of the paraspinal anastomotic network to provide adequate spinal cord perfusion pressure (SCPP) criticalfor both surgical and endovascular repair of thoracoabdominal aortic aneurysms (TAAA). Methods: To monitor pressure in the collateralcirculation, a catheter was inserted into the distal end of the divided first lumbar segmental artery (SA) of 10 juvenile Yorkshire pigs(28.9 � 3.8 kg). SA pairs from T3 through L5 were serially sacrificed at 32 8C; SCPP and function — using motor-evoked potentials (MEPs) —were continuously monitored until 1 h after clamping the last SA. Intermittent aortic and SCPP monitoring was continued for 5 dayspostoperatively, along with evaluation of motor function. Results: A mean of 14.4 � 0.7 SAs were sacrificed without loss of MEP. SCPP (mmHg)dropped from 68 � 7 before SA clamping (77% of aortic pressure) to 22 � 6 at end clamping, and 21 � 4 after 1 h, reaching its lowest point —19 � 4 — after 5 h. Postoperatively, SCPP recovered to 33 � 6 at 24 h; 42 � 10 at 48 h; 56 � 14 at 72 h; 62 � 15 at 96 h, returning to baseline(63 � 20) at 120 h. Despite comparable SCPP patterns, four pigs did not fully regain the ability to stand. Six animals recovered: two could standand four could walk. Conclusions: Interruption of all SAs at 32 8C in this pig model results in a spectrum of cord injury, with normal function in amajority of pigs postoperatively. The short duration of low SCPP suggests that hemodynamic manipulation lasting only 24—48 h may allow routinecomplete preservation of normal cord function despite sacrifice of all SAs.# 2007 European Association for Cardio-Thoracic Surgery. Published by Elsevier B.V. All rights reserved.
Keywords: Spinal cord perfusion/protection; Paraplegia; Segmental artery sacrifice; Thoracoabdominal aortic aneurysm repair (TAA/A)
1. Introduction
The mortality and morbidity of even extensive thora-coabdominal replacement has improved markedly in recentyears [1]. However, postoperative paraplegia remains adevastating complication and its occurrence is still somewhatunpredictable [2—6].
Most often, neurologic injury becomes apparent immedi-ately postoperatively, and is attributed to ischemic injuryduring intraoperative aortic cross-clamping and/or inade-quate postoperative spinal cord perfusion. However, a smallfraction of patients awaken from anesthesia neurologicallynormal, but develop delayed onset paraplegia hours to weekslater. The pathogenesis of both types of paraplegia, but
§ Presented at the joint 20th Annual Meeting of the European Association forCardio-thoracic Surgery and the 14th Annual Meeting of the European Societyof Thoracic Surgeons, Stockholm, Sweden, September 10—13, 2006.* Corresponding author. Address: Mount Sinai School of Medicine, Depart-
ment of Cardiothoracic Surgery, One Gustave L. Levy Place, PO-Box: 1028, NewYork, NY 10029, USA. Tel.: +1 212 659 6800; fax: +1 212 659 6818.
E-mail address: [email protected] (C.D. Etz).
1010-7940/$ — see front matter # 2007 European Association for Cardio-Thoracicdoi:10.1016/j.ejcts.2007.01.023
particularly of delayed onset deficit, is still poorly under-stood [7]. Consequently, the effectiveness of differentstrategies for minimizing intraoperative spinal cord ische-mia, and for managing intercostal and lumbar arteries duringrepair of thoracic and thoracoabdominal aortic aneurysms(TAA/A) in order to prevent paraplegia remains controversial[3,8—14].
The studies described in this report were undertaken totry to gain a better understanding in an animal model of theimpact of extensive sacrifice of segmental arteries (SAs) onspinal cord perfusion intraoperatively and in the immediatepostoperative period, under experimental conditions whichapproximate the circumstances prevailing during clinicalthoracoabdominal aortic surgery. Previous studies with thismodel established the feasibility of routine extensive SAsacrifice without loss of function because of the existence ofa dense and complex collateral arterial network feeding thespinal cord [15,16]. It is hoped that further investigation ofthe usual physiological and functional response of thecollateral spinal cord perfusion network to the sacrifice ofimportant contributors to its blood supply — and especially of
Surgery. Published by Elsevier B.V. All rights reserved.

C.D. Etz et al. / European Journal of Cardio-thoracic Surgery 31 (2007) 643—648644
the time course of the response — will help to elucidate howbest to prevent even the rare occurrence of paraplegia afterextensive SA sacrifice. Avoiding spinal cord injury despiteocclusion of most SAs is critical not only for surgical repair butalso for the eventual successful endovascular treatment oflarge thoracoabdominal aneurysms.
2. Materials and methods
2.1. Study design
Ten female juvenile Yorkshire pigs (Animal BiotechIndustries, Allentown, NJ, USA), 4—5months of age, weighing28—32 kg, were used for this experiment. In all animals, thedescending thoracic and abdominal aortas were exposed, andall segmental arteries were carefully dissected. Thereafter,the segmental artery feeding L1 was identified and clampedproximally, and an arterial catheter was placed for monitor-ing spinal cord perfusion pressure (SCPP), generated by flowin the collateral pathway. With the L1 catheter in place, allthoracic and abdominal segmental arteries were sequentiallyclamped in a craniocaudal direction during mild hypothermia(32 8C), allowing a 3-min interval between clamping ofsuccessive arteries. In addition to hemodynamic variables —arterial pressure and SCCP — myogenic motor-evokedpotentials (MEPs) were monitored. Functional recoverywas evaluated for 5 days using a modification of the Tarlovscore, and histopathological examination was carried outafter sacrifice.
This experimental model closely simulates the procedureused for resection of descending thoracic and thoracoab-dominal aneurysms clinically at our institution. However, itshould be noted that the anatomy of the pig differs from thatof humans in having 13 thoracic (and five lumbar) segmentalarteries, which arise together from the descending aorta andsubsequently divide. The subclavian arteries and the mediansacral arteries are both important parts of the collateralperfusion of a continuous spinal cord vascular network in bothspecies; in humans, however, the iliac arteries provide amuch greater proportion of the flow into the collateralnetwork. In the clinical situation, cross-clamping of the aortais occasionally required for an open distal anastomosis, anddistal perfusion and spinal fluid drainage are routinelyutilized to minimize intraoperative spinal cord ischemia. Thisexperimental model is simplified to allow an uncomplicatedfocus on the input to the collateral network in the wake ofsegmental artery sacrifice. Previous experiments with thismodel have demonstrated that the spinal cord collateral flowin the pig behaves in ways very similar to what is observedunder comparable circumstances clinically in humans[15,16].
2.2. Perioperative management and anesthesia
All animals received humane care in compliance with theguidelines of ‘Principles of Laboratory Animal Care’ for-mulated by the National Society for Medical Research and the‘Guide for the Care and Use of Laboratory Animals’ publishedby the National Institute of Health (NIH Publication No. 88-23, revised 1996). The Mount Sinai Institutional Animal Care
and Use Committee approved the protocols for all experi-ments.
After pretreatmentwith intramuscular ketamine (15 mg/kg) and atropine (0.03 mg/kg), animals were anesthetizedwith intravenous sodium thiopenthal (20 mg/kg). Followingendotracheal intubation, the pigs were ventilated mechani-cally with an FiO2 of 0.5 and anesthesia was maintainedwith an infusion of ketamine 15 mg/kg/h and sufentanil5 mg/kg/h. This anesthetic regimen has no major effect onMEP responses, and has been described previously [12].Paralysis for intubation was achieved with intravenouspancuronium (0.1 mg/kg), but no further doses wereadministered subsequently to avoid interfering with mea-surement of MEPs.
The ventilator rate and the tidal volume were adjusted tomaintain the arterial carbon dioxide tension at 35—40 mmHg.End-expiratory carbon dioxide (PPG Biomedical Systems,Model 2010-200 R, Lenexa, KS, USA) was monitoredcontinuously. Arterial oxygen tension was maintained>90 mmHg. A bladder catheter (Foley 8—10 F) was insertedfor online measurement of urine output, and temperatureprobes were placed in the esophagus and the rectum.Electrocardiographic measurements were recorded continu-ously. An arterial line was placed in the right brachial arteryfor pressure monitoring and blood sampling (pH, oxygentension, carbon dioxide tension, oxygen saturation, baseexcess, hematocrit, hemoglobin and glucose, lactate, BloodGas Analyzer, Ciba Corning 865, Chiron Diagnostics, Norwood,MA, USA).
2.3. Body temperature management
After inducing anesthesia (see protocol above), the pigswere cooled to 32 8C rectal temperature by covering themwith packs of artificial refrigerants for a period of 30 min. Inaddition, a cooling blanket was used even after the targettemperature was reached to maintain hypothermia andprevent an upward temperature drift during the procedure.The operating room temperature was reduced to 14 8C. Nolocal cooling of the vertebral column was undertaken. Theanimals were subsequently warmed using a heating blanketand a heating lamp, usually for 90—100 min, and by raisingthe operating room temperature to 24 8C. To prevent anyintraoperative temperature drift, the small left thoracotomyin the fourth intercostal space was temporarily closed afterclamping the thoracic spinal arteries.
2.4. Monitoring of postoperative systemic and spinalcord perfusion pressure (SCPP)
Two arterial lines were placed: one in the descendingaorta and another in the distal arm of the segmental arteryfeeding the first lumbar segment. These lines enabledsystemic and lumbar perfusion pressure monitoring andblood sampling (pH, oxygen tension, carbon dioxide tension,oxygen saturation, base excess, hematocrit, hemoglobin andglucose, lactate; Blood Gas Analyzer, Ciba Corning 865,Chiron Diagnostics, Norwood, MA, USA) prior to, during, andafter radical sacrifice of all thoracic and abdominalsegmental arteries.
C.D. Etz et al. / European Journal of Cardio-thoracic Surgery 31 (2007) 643—648 645
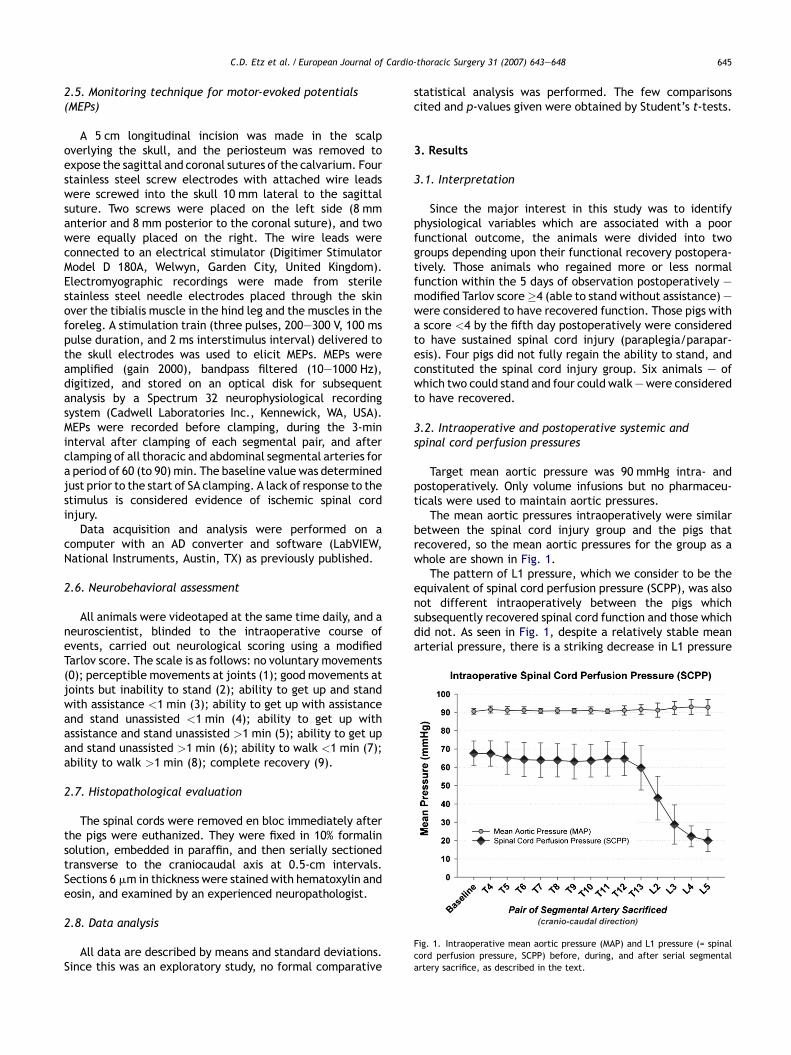
Fig. 1. Intraoperative mean aortic pressure (MAP) and L1 pressure (= spinalcord perfusion pressure, SCPP) before, during, and after serial segmentalartery sacrifice, as described in the text.
2.5. Monitoring technique for motor-evoked potentials(MEPs)
A 5 cm longitudinal incision was made in the scalpoverlying the skull, and the periosteum was removed toexpose the sagittal and coronal sutures of the calvarium. Fourstainless steel screw electrodes with attached wire leadswere screwed into the skull 10 mm lateral to the sagittalsuture. Two screws were placed on the left side (8 mmanterior and 8 mm posterior to the coronal suture), and twowere equally placed on the right. The wire leads wereconnected to an electrical stimulator (Digitimer StimulatorModel D 180A, Welwyn, Garden City, United Kingdom).Electromyographic recordings were made from sterilestainless steel needle electrodes placed through the skinover the tibialis muscle in the hind leg and the muscles in theforeleg. A stimulation train (three pulses, 200—300 V, 100 mspulse duration, and 2 ms interstimulus interval) delivered tothe skull electrodes was used to elicit MEPs. MEPs wereamplified (gain 2000), bandpass filtered (10—1000 Hz),digitized, and stored on an optical disk for subsequentanalysis by a Spectrum 32 neurophysiological recordingsystem (Cadwell Laboratories Inc., Kennewick, WA, USA).MEPs were recorded before clamping, during the 3-mininterval after clamping of each segmental pair, and afterclamping of all thoracic and abdominal segmental arteries fora period of 60 (to 90) min. The baseline value was determinedjust prior to the start of SA clamping. A lack of response to thestimulus is considered evidence of ischemic spinal cordinjury.
Data acquisition and analysis were performed on acomputer with an AD converter and software (LabVIEW,National Instruments, Austin, TX) as previously published.
2.6. Neurobehavioral assessment
All animals were videotaped at the same time daily, and aneuroscientist, blinded to the intraoperative course ofevents, carried out neurological scoring using a modifiedTarlov score. The scale is as follows: no voluntary movements(0); perceptible movements at joints (1); good movements atjoints but inability to stand (2); ability to get up and standwith assistance <1 min (3); ability to get up with assistanceand stand unassisted <1 min (4); ability to get up withassistance and stand unassisted >1 min (5); ability to get upand stand unassisted >1 min (6); ability to walk <1 min (7);ability to walk >1 min (8); complete recovery (9).
2.7. Histopathological evaluation
The spinal cords were removed en bloc immediately afterthe pigs were euthanized. They were fixed in 10% formalinsolution, embedded in paraffin, and then serially sectionedtransverse to the craniocaudal axis at 0.5-cm intervals.Sections 6 mm in thickness were stained with hematoxylin andeosin, and examined by an experienced neuropathologist.
2.8. Data analysis
All data are described by means and standard deviations.Since this was an exploratory study, no formal comparative
statistical analysis was performed. The few comparisonscited and p-values given were obtained by Student’s t-tests.
3. Results
3.1. Interpretation
Since the major interest in this study was to identifyphysiological variables which are associated with a poorfunctional outcome, the animals were divided into twogroups depending upon their functional recovery postopera-tively. Those animals who regained more or less normalfunction within the 5 days of observation postoperatively —modified Tarlov score�4 (able to stand without assistance) —were considered to have recovered function. Those pigs witha score <4 by the fifth day postoperatively were consideredto have sustained spinal cord injury (paraplegia/parapar-esis). Four pigs did not fully regain the ability to stand, andconstituted the spinal cord injury group. Six animals — ofwhich two could stand and four could walk —were consideredto have recovered.
3.2. Intraoperative and postoperative systemic andspinal cord perfusion pressures
Target mean aortic pressure was 90 mmHg intra- andpostoperatively. Only volume infusions but no pharmaceu-ticals were used to maintain aortic pressures.
The mean aortic pressures intraoperatively were similarbetween the spinal cord injury group and the pigs thatrecovered, so the mean aortic pressures for the group as awhole are shown in Fig. 1.
The pattern of L1 pressure, which we consider to be theequivalent of spinal cord perfusion pressure (SCPP), was alsonot different intraoperatively between the pigs whichsubsequently recovered spinal cord function and those whichdid not. As seen in Fig. 1, despite a relatively stable meanarterial pressure, there is a striking decrease in L1 pressure

C.D. Etz et al. / European Journal of Cardio-thoracic Surgery 31 (2007) 643—648646
Fig. 2. Postoperative L1 (= spinal cord perfusion pressure, SCPP) after gradualsacrifice of all thoracic and lumbar segmental artery pairs. No differences werefound between pigs having functional recovery according to a modified Tarlovscore, and those with spinal cord injury, as detailed in the text. Note that thetime scale, in hours, is not linear.
Fig. 3. Postoperative mean aortic pressure (MAP), in mmHg � standard devia-tion, corresponding to the measurements of L1 pressure shown in Fig. 2.Pressures did not differ significantly over time, or between recovery andparaplegia/paraparesis groups except at 5 h, when MAP was significantlyhigher in the group with functional recovery (according the modified Tarlovscore) compared with MAP in those pigs which did not recover function,p = 0.04.
Fig. 4. Postoperative neurobehavioral recovery using a modified Tarlov score,as detailed in the text. Recovery was defined as a score�4, which requires thepig to be able to stand unassisted.
with the sacrifice of the last of the SAs intraoperatively. Amean of 14.4 � 0.7 SAs were sacrificed, all without loss ofMEP. Intraoperatively, SCPP dropped from 68 � 7 mmHgbefore SA clamping (77% of mean aortic pressure) to22 � 6 mmHg at end clamping.
Postoperatively (Fig. 2), SCPP continued to drop further:to 21 � 4 mmHg at 1 h, and to its lowest point — 19 � 4 mmHg— 5 h after sacrifice of the last segmental artery. Thereafter,there was recovery, reaching (in mmHg) 33 � 6 at 24 h;42 � 10 at 48 h; 56 � 14 at 72 h; 62 � 15 at 96 h, andreturning to baseline (63 � 20) at 120 h. There was nodifference in the SCCP between the groups which recoveredand which did not recover function postoperatively at any ofthe postoperative time points.
Postoperative mean aortic pressures are shown in Fig. 3.Despite the intent to maintain aortic pressures constant,there is a suggestion that the mean pressure was higher in thegroup which recovered function than in those that did not atthe 5-h postoperative measurement ( p = 0.04), when theSCPP was seen to reach its lowest point. Except for the 5-hpoint, there was no apparent difference in the mean aorticpressures over time throughout the postoperative period, orbetween the pigs which recovered function and those whichdid not.
3.3. MEP monitoring
MEP monitoring was carried out to assess the impact onfunction as the SAs were being serially sacrificed, asdescribed in detail previously, and until 1 h after the lastof them had been sacrificed: later monitoring is not possiblewithout prolonging the duration of anesthesia. It is a littledisturbing that MEPs after extensive SA sacrifice were intacteven in those pigs that subsequently suffered a loss of spinalcord function. Our hypothesis is that critical ischemiaoccurred in these pigs after the last measurement of MEPshad been carried out (1 h after the last of the SAs had been
occluded), at a time when SCPP remained very low but MEPscould no longer be obtained.
3.4. Behavioral score
The pattern of behavioral scores is shown in Fig. 4. Thesescores, as previously noted, were assessed on the basis ofvideotapes of postoperative behavior taken at the same timeeach day, and interpreted in a blinded format by aneurophysiologist. After the final assessment on the fifthpostoperative day, the animals were sacrificed and their spinalcords were harvested for histopathological examination.
3.5. Histopathological findings
In paraparetic/paraplegic animals, there was no evidenceof necrosis in the cervical and higher thoracic segments.

C.D. Etz et al. / European Journal of Cardio-thoracic Surgery 31 (2007) 643—648 647
Fig. 5. Examples of low power (2�) transverse sections of the spinal cord,stained with hematoxylin and eosin, from two pigs 5 days after extensivesacrifice of segmental arteries. The levels along the craniocaudal axis fromwhich the sections are taken are indicated: C = cervical, T = thoracic, L = lum-bar. Recovery sections are from a pig that recovered function, and show anormal population of neurons in the gray matter of the spinal cord at all levels.There is no evidence of comprehensive necrosis. Paraplegia sections are from apig that was paraparetic, and show necrosis of the gray matter and surroundingwhite matter (so called ‘pencil necrosis’), sparing a thin peripheral rim ofwhite matter below the pia mater. The affected sections extend from T9 to L4,corresponding to the vascular territory of the anterior spinal artery.
From the lower thoracic to the upper sacral segments,however, paraparetic/paraplegic animals showed distinctivenecrosis of the gray matter involving the posterior andanterior horns and surrounding white matter (so called‘pencil necrosis’), sparing a thin peripheral rim of whitematter below the pia (Fig. 5). The areas in which necrosis wasfound in the animals with functional evidence of spinal cordinjury correspond to the vascular territory of the anteriorspinal artery.
In pigs which regained function, all segments showed anormal population of neurons and intact gray matter at alllevels at the magnification shown in Fig. 5. There was noevidence of comprehensive segmental necrosis, althoughhigher power evaluation showed rare minute areas withnecrotic cells in sections from the lower thoracic and lumbarlevels.
4. Discussion
Although most aortic surgeons try to minimize intraopera-tive ischemic spinal cord injury by utilizing mild hypothermiaand other adjuncts such as left heart bypass, they also liberallyreimplant segmental arteries, especially in the lumbar region,with the idea that paraplegia results principally frominadequate postoperative spinal cord perfusion. But, on thebasis of previous experimental studies in the pig model, andclinical studies showing very low paraplegia rates, it can beargued that postoperative spinal cord perfusion adequate toprevent immediate paraplegia is achievable without reim-plantation of any segmental arteries [17,18]. The freedom toocclude segmental arteries without fear of spinal cord injury isa prerequisite for the success of endovascular treatment ofextensive thoracoabdominal aneurysms.
The severity of the acute intraoperative ischemic insult —the duration of aortic cross-clamping, for example, and thetemperature at which it is carried out — certainly plays acritical role in whether acute spinal cord injury occurs [16].
However, the ways in which the spinal cord collateralcirculation responds to intraoperative injury — how itcompensates for the sacrifice of large numbers of SAs, andthe time required for full recovery — remain largely unknown[19,20]. The observations in this study document that therecoveryof spinal cordperfusionpressure in thepresenceof anadequate mean arterial pressure takes longer than 24 h. Verylow SCPPs are present, beginning 1 h after sacrifice of the lastSA: these pressures remain very low for at least 5 h, and arestill well below baseline values at 24 h. Since not all of the pigsrecovered function in the presence of these very lowpressures, it seems reasonable to suppose that these pressuresare very close to the threshold for intolerable ischemia duringthe recovery phase postoperatively. The discovery, uponhistopathological examination, of evidence of minute areas ofischemia even in pigs with apparent complete functionalrecoveryconfirms theprecariousness of theblood supplyundercurrent operative conditions. Determination of the minimalamplitude of blood pressure/flow which will assure recoveryof spinal cord function and of the duration for which thisminimum perfusion requirement needs to be sustained, willrequire further investigation.
Within the first few hours postoperatively, any fall inarterial pressure could make a critical difference, as issuggested by the graph in Fig. 3, which shows slightly butsignificantly higher arterial pressures at the critical 5-h nadirof SCPP in the group which eventually recovered. Theobservations suggest that it is very likely that meticulousattention to preserving good perfusion pressures — includingpharmacological manipulations — not only intraoperativelybut for at least the first 24 h postoperatively may be effectivein further reducing the incidence of spinal cord injury. Thevery low measured pressures in the collateral circulation tothe spinal cord make it quite conceivable that the smallcontribution in lowering outflow resistance provided bycerebrospinal fluid (CSF) drainage could have a considerableimpact in improving functional outcome by helping toimprove SCPP, as has been documented in both clinical andexperimental studies [21—23].
The most important and not previously noted observationarising from this study is that the interval of low perfusionpressure following SA sacrifice is limited in duration:perfusion pressures nearly at baseline levels are once againpresent 48—72 h postoperatively in the absence of any patentSAs. This new observation underlines the clinical importanceof maintaining high normal systemic pressures during the firstfew days postoperatively, and continuing to carefully andfrequently monitor spinal cord function during this vulner-able interval. The data suggest that after 48 h, whenpressures return to within the preoperative range, loss ofspinal cord integrity is much less likely to occur.
Why the lowest SCPP in this experiment occurs quiteconsistently 5 h after sacrifice of the last SA is not readilyapparent from this study. We speculate that it may reflectvasodilatation of the collateral circulation in response toincreased metabolic requirements upon rewarming andrecovery from anesthesia.
The physiological observations of this study thus hold outhope that some further relatively simple hemodynamicadjustments, sustained until the spinal cord perfusionpressure spontaneously regains baseline values at about

C.D. Etz et al. / European Journal of Cardio-thoracic Surgery 31 (2007) 643—648648
48 h, may enable routine sacrifice of large numbers of SAs —during conventional thoracoabdominal surgery and perhapswith endovascular repairs — without provoking paraplegia.
References
[1] Svensson LG. Paralysis after aortic surgery: in search of lost cord function.Surgeon 2005;3(6):396—405.
[2] Coselli JS, LeMaire SA, Miller 3rd CC, Schmittling ZC, Koksoy C, Paqan J,Curling PE. Mortality and paraplegia after thoracoabdominal aorticaneurysm repair: a risk factor analysis. Ann Thorac Surg 2000;69(2):409—14.
[3] Bachet J, Guilmet D, Rosier J, Cron C, Dreyfus G, Goudot B, Piquois A,Brodaty D, Dubois C, de Lentdecker P. Protection of the spinal cord duringsurgery of thoraco-abdominal aortic aneurysms. Eur J Cardiothorac Surg1996;10(10):817—25.
[4] Kouchoukos NT, Rokkas CK. Hypothermic cardiopulmonary bypass forspinal cord protection: rationale and clinical results. Ann Thorac Surg1999;67(6):1940—2 [discussion 1953—8].
[5] Svensson LG, Patel V, Robinson MF, Ueda T, Roehm Jr JO, Crawford ES.Influence of preservation or perfusion of intraoperatively identified spinalcord blood supply on spinal motor evoked potentials and paraplegia afteraortic surgery. J Vasc Surg 1991;13(3):355—65.
[6] Yamauchi T, Takano H, Nishimura M, Matsumiya G, Sawa Y. Paraplegia andparaparesis after descending thoracic aortic aneurysm repair: a riskfactor analysis. Ann Thorac Cardiovasc Surg 2006;12(3):179—83.
[7] Huynh TT, Miller 3rd CC, Safi HJ. Delayed onset of neurologic deficit:significance and management. Semin Vasc Surg 2000;13(4):340—4.
[8] Minatoya K, Karck M, Hagl C, Meyer A, Brassel F, Harringer W, Haverich A.The impact of spinal angiography on the neurological outcome aftersurgery on the descending thoracic and thoracoabdominal aorta. AnnThorac Surg 2002;74(5):S1870—2 [discussion S1892—8].
[9] Lang-Lazdunski L, Bachet J, Rogers C. Repair of the descending thoracicaorta: impact of open distal anastomosis technique on spinal cordperfusion, neurological outcome and spinal cord histopathology. Eur JCardiothorac Surg 2004;26(2):351—8.
[10] Lang-Lazdunski L, Bachet J. Pharmacological spinal cord protection withmagnesium during replacement of the thoracic and thoracoabdominalaorta. Ann Thorac Surg 2001;72(6):2180—1.
[11] Griepp RB, Ergin MA, Galla JD, Klein JJ, Spielvogel D, Griepp EB. Mini-mizing spinal cord injury during repair of descending thoracic and thor-acoabdominal aneurysms: the Mount Sinai approach. Semin ThoracCardiovasc Surg 1998;10(1):25—8.
[12] Galla JD, Ergin MA, Lansman SL, McCullough JN, Nguyen KH, Spielvogel D,Klein JJ, Griepp RB. Use of somatosensory evoked potentials for thoracicand thoracoabdominal aortic resections. Ann Thorac Surg1999;67(6):1947—52 [discussion 1953—8].
[13] Ogino H, Sasaki H, Minatoya K, Matsuda H, Yamada N, Kitamura S.Combined use of adamkiewicz artery demonstration and motor-evokedpotentials in descending and thoracoabdominal repair. Ann Thorac Surg2006;82(2):592—6.
[14] Weigang E, Hartert M, von Samson P, Sircar R, Pitzer K, Gensdorfer J,Zentner J, Beyersdorf F. Thoracoabdominal aortic aneurysm repair:interplay of spinal cord protecting modalities. Eur J Vasc Endovasc Surg2005;30(6):624—31.
[15] Strauch JT, Spielvogel D, Lauten A, Zhang N, Shiang H,Weisz D, Bodian CA,Griepp RB. Importance of extrasegmental vessels for spinal cord bloodsupply in a chronic porcine model. Eur J Cardiothorac Surg 2003;24(5):817—24.
[16] Strauch JT, Lauten A, Spielvogel D, Rinke S, Zhang N, Weisz D, Bodian CA,Griepp RB. Mild hypothermia protects the spinal cord from ischemicinjury in a chronic porcine model. Eur J Cardiothorac Surg2004;25(5):708—15.
[17] Acher CW, Wynn MM. Thoracoabdominal aortic aneurysm. How we do it.Cardiovasc Surg 1999;7(6):593—6.
[18] Etz CD, Halstead JC, Spielvogel D, Lazala R, Shahani R, Weisz D, GrieppRB. Thoracic and thoracoabdominal aneurysm repair: is reimplantation ofspinal cord arteries a waste of time? Ann Thorac Surg 2006;82(5):1670—7.
[19] de Haan P, Kalkman CJ, Meylaerts SA, Lips J, Jacobs MJ. Development ofspinal cord ischemia after clamping of noncritical segmental arteries inthe pig. Ann Thorac Surg 1999;68(4):1278—84.
[20] Christiansson L, Ulus AT, Hellberg A, Bergqvist D, Wiklund L, Karacagil S.Aspects of the spinal cord circulation as assessed by intrathecal oxygen
tension monitoring during various arterial interruptions in the pig. JThorac Cardiovasc Surg 2001;121(4):762—72.
[21] Schepens M, Dossche K, Morshuis W, Heijmen R, van Dongen E, Ter Beek H,Kelder H, Boezeman E. Introduction of adjuncts and their influence onchanging results in 402 consecutive thoracoabdominal aortic aneurysmrepairs. Eur J Cardiothorac Surg 2004;25(5):701—7.
[22] Huynh TT, Miller 3rd CC, Estrera AL, Mohamed SG, Hassoun HT, SheinbaumR, Porat EE, Safi HJ. Correlations of cerebrospinal fluid pressure withhemodynamic parameters during thoracoabdominal aortic aneurysmrepair. Ann Vasc Surg 2005;19(5):619—24.
[23] Coselli JS, Lemaire SA, Koksoy C, Schmittling ZC, Curling PE. Cerebrosp-inal fluid drainage reduces paraplegia after thoracoabdominal aorticaneurysm repair: results of a randomized clinical trial. J Vasc Surg2002;35(4):631—9.
Appendix A. Conference discussion
Dr C. Olsson (Uppsala, Sweden): I have two questions for you.
First of all, are there any important differences in the anatomy of spinalcord supply between pig and man?
And secondly, do you see any way of clinically applying this monitoring inhuman beings?
Dr Etz: This slide shows a photograph of a vascular cast — which wasprepared in our laboratory prior to this study — of the collateral network in thepig. Yorkshire pigs have 15 segmental arteries arising from the thoracoab-dominal aorta (TAASA), whereas the first three branches arise from thesubclavian artery. Since the Yorkshire pig has one more thoracic segment thanman does, one can see the TAASA for the segments T4 to T13 and L1 to L5 here.The next slide displays the collateral network in humans: the gross anatomy —as you can see — is very similar.
With regard to your second question, we can learn from this study thatSCPP reaches a nadir 5 h after complete TAASA sacrifice, and that functionalrecovery is associated with themean aortic pressure during this period: this is avery important finding. Clinically translated, it means that stable post-operative hemodynamics are particularly crucial during the first 24 (to 48) h,because the collateral network has not yet recovered.
We believe that the drop in segmental artery pressure at 5 h seen in thisexperiment is potentially preventable using hemodynamic manipulation, andwe are currently conducting pilot pharmacological studies with the objectiveof accelerating the collateral network’s local response to segmental arterysacrifice.
Dr C. Rokkas (Athens, Greece): You’re defining spinal cord perfusionpressure as the intra-arterial pressure that supplies the spinal cord. That’s notthe definition we have so far in the literature. Spinal cord perfusion pressure isdefined as the intra-arterial pressure minus the intrathecal pressure of thecerebrospinal fluid.
My question here is whether you measure intrathecal pressures in thoseanimals and whether these changes in the pressures that you measure actuallyreflect changes within the intrathecal space.
Dr Etz: We agree that the contemporary definition of SCPP is mean aorticpressure (MAP) minus intrathecal pressure, although we think the latter islikely to be reflected not only by cerebrospinal fluid pressure, but also maydepend upon central venous pressure.We are not convinced that this definition— a rather theoretical calculation— is applicableafter extensiveTAASA sacrifice,when direct spinal cord perfusion from the aorta is disrupted and local perfusionpressure may therefore be more divorced from MAP than usual. We, therefore,prefer to put our trust in direct measurement, using a distally inserted TAASAcatheter: we believe this comes as close as one can get to reality.
The drop in SCPP occurred acutely after clamping the lower thoracic andabdominal segmental arteries — as was witnessed in the video presentation,and — even more importantly — could be reversed immediately by clipremoval. Rising intrathecal pressure — presumably related to spinal cordischemia and subsequent edema — does not occur in seconds, and would not belikely to be reversed acutely unless by CSF drainage.
CSF drainage in juvenile Yorkshire pigs is difficult in a survival experiment,since the anatomy of the spine requires a laminectomy to reliably place acatheter intrathecally, which potentially adds major risks to the postoperativecourse (and has thus far not been successfully accomplished in a comparablestudy). So we did not use CSF drainage in these 10 pigs, as we would have inhumans. But we speculate that further reduction of the paraplegia/paraparesis rate below 40% in our animals could be achieved if CSF drainagewere possible.




















