The posterior segmental maxillary osteotomy: Recent applications
Upload
charite-deCategory
view
3download
0
Ultrasound in Med. & Biol., Vol. 37, No. 3, pp. 474–483, 2011Copyright � 2011 World Federation for Ultrasound in Medicine & Biology
Printed in the USA. All rights reserved0301-5629/$ - see front matter
asmedbio.2010.12.007
doi:10.1016/j.ultrd Original Contribution
SPATIAL-TEMPORAL MAPPING OF BONE STRUCTURAL AND ELASTICPROPERTIES IN A SHEEP MODEL FOLLOWING OSTEOTOMY
BERND PREININGER,* SARA CHECA,* FERENC L. MOLNAR,*x PETER FRATZL,y
GEORG N. DUDA,*zx and KAY RAUM*xk
*Julius Wolff Institute and Center for Musculoskeletal Surgery, Charit�e–Universit€atsmedizin Berlin, Berlin, Germany; yMaxPlanck Institute of Colloids and Interfaces, Department of Biomaterials, Research Campus Golm, Potsdam Golm, Germany;zBerlin-Brandenburg Center for Regenerative Therapies, Berlin, Germany; xBerlin-Brandenburg School for Regenerative
Therapies, Berlin, Germany; and kDepartment of Orthopedics, Martin Luther University of Halle-Wittenberg, Halle, Germany
(Received 19 July 2010; revised 6 December 2010; in final form 8 December 2010)
AInstitutCharit�eBerlin,
Abstract—The course of bone healing in animal models is conventionally monitored by morphologic approaches,which donot allow the determination of thematerial properties of the tissues involved.Mechanical characterizationtechniques are either dedicated to themacroscopic evaluation of the entire organ or to themicroscopic evaluation ofthe tissue matrix. The latter provides insight to regionally specific alterations at the tissue level in the course ofhealing. In this study, quantitative scanning acousticmicroscopywas used at 50MHz to investigatemicrostructuraland elastic alterations of mineralized callus and cortical tissue after transverse osteotomy in sheep tibiae. Analyseswere performed after 2, 3, 6 and 9weeks of consolidation with stabilization by either a rigid or a semi-rigid externalfixator. Increased stiffness and decreased porosity were observed in the callus tissue over the course of the healingprocess,whichwas dependent on the fixator type. In the adjacent cortical tissue, stiffness decreasedduring the first 3weeks. Cortical porosity increased over time but the time-dependence was different between the two fixator types.The changes of stiffness of cortical and callus tissues were measured with respect to the distance to the periostealcortex-callus boundary. Stiffness of cortex and callus tissue smoothly decreased as a function of the distancefrom the inner cortical region.The data obtained in this study canhelp to understand the processes involved in tissuematuration during endogenous bone healing. (E-mail: [email protected]) � 2011 World Federation forUltrasound in Medicine & Biology.
Key Words:Acoustic microscopy, Acoustic impedance, Bone, Callus, Elasticity, Healing, Microscopy, Callus, Frac-ture healing, Mechanical properties, Stiffness, Ultrasound.
INTRODUCTION
Bone regeneration is usually an efficient process but de-layed healing and non-unions are still severe clinicalcomplications that may occur following certain fracturesor osteotomies. Numerous small and large animal modelshave been developed for the study of bone regeneration.These models are useful to characterize and better under-stand the various stages of bone healing. Histologic andhistomorphometric analyses are commonly used to inves-tigate the effect of mechanical stimulation, e.g., inducedby varying the fixator stability, on the bone healing
ddress correspondence to: Prof. Dr. Kay Raum, Julius Wolffe and Berlin Brandenburg School for Regenerative Therapies,–Universit€atsmedizin Berlin, Augustenburger Platz 1, D-13353Germany. E-mail: [email protected]
474
process (Lienau et al. 2005; Schell et al. 2006).However, little is known about the material propertiesof the tissues involved.
An ideal diagnostic method should yield morpho-logic and functional information during the entire healingcourse without considerable impact on the healingprocess. However, the experimental assessment anddescription of the biomechanical competence of thecomplex callus/bone compound is still a challengingissue, mainly due to the fact that currently no method isable to capture all structural and compositional featuresthat determine the biomechanical function. In vivoimaging techniques based on X-rays (conventional X-ray projections, CT and mCT scans) are limited to theevaluation of mineralized tissues (MTs). Although mCTprovides detailed three-dimensional (3-D) morphologicinformation about MTs, it is time consuming and poten-tially dangerous to the animal due to the anaesthesia and

Elastic mapping of bone healing by SAM d B. PREININGER et al. 475
radiation exposure levels needed for the examination.Moreover, the bone mineral density (BMD) or tissuedegree of mineralization (DMB) accessible with quantita-tive X-ray devices is only an indirect predictor of bonemechanical stability and the correlation between BMDand biomechanical tests found in previous studies weremoderate (Reichel et al. 1998). High resolution magneticresonance imaging MRI can also be used for the assess-ment of the 3-D morphology of mineralized tissue (Liuet al. 2010b). In combination with contrast agents, MRIhas the potential to assess bone blood flow in variousdisease and injury states, which is essential in estimatingthe risk of avascular necrosis and subsequent rates ofhealing (Dyke and Aaron 2010).
Nanoindentation studies have shown that themechanical properties of the newly formed tissues areconsiderably different at different locations within thecallus region and that the changes in tissue stiffnessover the healing period are also site-specific (Leong andMorgan 2008; Manjubala et al. 2009). However, due totechnical limitations, these studies have been limited tothe evaluation of small regions-of-interest (ROI) or fewspecific locations within the regenerating region. More-over, no information about the spatial and temporal vari-ations of local mechanical properties of the cortical tissuedirectly adjacent to the repair zone is currently available.
Numerical methods, such as finite element models,have received increasing attention as they allow, (1) inves-tigation of arbitrary elastic and plastic deformationscenarios of the tissue (Grimal et al. 2008), (2) stochasticstudies ofmultiple parameter interactions and their effectson macroscopic mechanical function (Parnell and Grimal2009) and (3) identification of mechanical or biologicregulation rules of the healing process (Andreykiv et al.2008; Isaksson et al. 2006, 2008, 2010). For thesemodels, the mesh generation and assignment of elasticproperties to the elements is usually based on CTimages using simplified relations between bone densityand elastic modulus (Shefelbine et al. 2005). However,to date, there is overwhelming evidence that no generalrelation between these material properties exists(Austman et al. 2008) and reliable conversions can onlybe achieved with additional site-specific and customizedanatomical information (Austman et al. 2009).
Quantitative ultrasound (QUS) is a class of nonde-structive techniques that is sensitive to elastic and struc-tural variations of the interrogated material (Raum et al.2005). Low-intensity in vivo QUS in the kHz to MHz-range has been established as a first class diagnostic toolfor the prediction of fracture risk (Gluer 2008). With thedevelopment of sophisticated sound propagation simula-tion tools, QUS has also proved its suitability for the eval-uation of fracture healing (Dodd et al. 2007; Kaufmanet al. 2008; Protopappas et al. 2007). Because of easy
accessibility, previous numerical and experimentalstudies have focused sound propagation properties inaxial transmission configurations (Protopappas et al.2008). However, a common limitation of previous numer-ical studies was the use of simplified callus geometries,neglected microstructure and assumed (not experimen-tally confirmed) isotropic and homogenous materialproperties.
In vitro scanning acoustic microscopy (SAM) iscurrently the only microelastic imaging technique thatprovides large scale (cm range) structural and elasticproperties at the tissue level with spatial resolutiondown to the mm-range (Raum 2008). Such large scaledistributions of structural and elastic properties withmicroscopic resolution were previously assessed by 50-MHz SAM in rat fracture (Harten Jr. et al. 1997) andsheep callus distraction osteotomy models (Hube et al.2006). Hube et al. (2006) have shown that the combina-tion of structural and anisotropic elastic properties ofcallus and cortical tissues determine the macroscopicresistance to failure (R2 5 0.86).
Site-matched analyses of the acoustic impedanceobtained by SAM and tissue degree of mineralizationDMB obtained by synchrotron radiation microcomputedtomography (SRmCT) (Raum et al. 2006a, 2006b, 2007a)have shown that the elastic stiffness of bone is morestrongly correlated with the acoustic impedance (R2 50.996) than with mineral or mass density (R2 5 0.310).Therefore, we anticipate that SAM measurements of theentire repair zone will provide comprehensive andcomplementary information of temporal and spatialvariations of structural and elastic material variationsthat is not accessible with the aforementioned techniques.
In the present study, the mechanical and structuralproperties (stiffness, porosity and area) of cortical andcallus bone tissues have been evaluated in vitro withrespect to consolidation time and fixator stability (rigidand semi-rigid) in a sheep osteotomy model. It washypothesized that (1) callus formation and stiffeningcoincide initially with a softening and at later time pointswith remodeling of the adjacent cortical bone tissue; (2)medial (external fixator side) callus stiffening is lesspronounced than that of the lateral side; (3) stiffness ofthe periosteal callus decreases with respect to the distanceto the cortical boundary; and (4) the time course of callusstiffening depends on the fixator stability.
MATERIALS AND METHODS
Sample preparationEmbedded longitudinal sections from previous
bone healing studies were used in this investigation(Lienau et al. 2005; Manjubala et al. 2009). All animalexperiments were carried out according to the policies

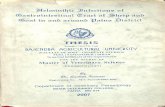
Fig. 1. Exemplary grey-scale stiffness map (9 weeks consolida-tion time, semi-rigid fixator) obtained by SAM measurements.The overlaid colors indicate segmented evaluation regions(red 5 excluded non-mineralized tissue and embedding mate-rial; green 5 cortical tissue; yellow 5 callus tissue). The colorbar indicates the values for the derived elastic coefficient c11.
476 Ultrasound in Medicine and Biology Volume 37, Number 3, 2011
and principles established by the AnimalWelfare Act, theNIH Guide for Care and Use of Laboratory Animals andthe national animal welfare guidelines. The animal studywas approved by the local legal representative.
The samples were obtained from healthy femaleMerino sheep (N 5 32; age: 2 years; mean weight: 63 67 kg) that received a 3-mm osteotomy at the right tibia.The osteotomies were stabilized with either a rigid ora semi-rigid monolateral external fixator attached to themedial aspect of the tibia (Lienau et al. 2005). Briefly,a monolateral external fixator, consisting of six 5-mmSchanz screws (Synthes, Umkirch, Germany) and two10-mm steel rods (Synthes, Germany), acted as a rigid fix-ator. The distance between the skin and the inner bar was15 mm. For the semi-rigid fixator, the inner bar of the fix-ator was modified with a custom-made sliding joint. Thedistance between the skin and the inner bar was reducedto 10 mm to prevent excessive interfragmentary move-ments. In the semi-rigid fixator, the bending stiffness inthe mediolateral plane was approximately 50% reducedcompared with that of the rigid one, whilst both fixatorsystems showed similar resistance to axial compression.
After predefined time points (2, 3, 6 and 9 weekspostoperative), the animals were sacrificed (eight andfour animals per time point and fixation type, respec-tively). In the 6- and 9-week groups, left and right tibiaewere biomechanically tested until failure. For all animals,3-mm slices sectioned in the frontal plane were dehy-drated and embedded in methylmethacrylate for histo-logic analysis (Lienau et al. 2005). Quantitative backscattered electron imaging and nanoindentation were per-formed on the remaining section blocks in the rigid fixa-tor group in small regions of the newly formed periostealcallus near the cortex (Manjubala et al. 2009). After-wards, all sample blocks were forwarded to SAMmeasurements. Flat surfaces of the longitudinal sectionblocks were prepared by a grinding and polishingprotocol described elsewhere (Raum 2008).
Quantitative ultrasound measurementsThe samples were scanned with a custom-made
scanning acoustic microscope (SAM200Ex; Q-BAM,Halle, Germany). A spherically focused 50-MHz trans-ducer (Valpey Fisher, Hopkinton, MA, USA) provideda spatial resolution of 23 mm in water (Hube et al. 2006;Raum et al. 2005; Raum 2008). The measurements wereperformed in distilled and degassed water at 25�C asdescribed by Hube et al. (2006). Calibrated maps of theacoustic impedance Z were converted into maps of theelastic coefficient c11 (Fig. 1) using a calibration methodand empirical relations between impedance and elasticcoefficients, as described in previous studies (Hube et al.2006; Lakshmanan et al. 2007; Raum et al. 2004, 2005,2007b; Raum 2008; Saied et al. 2008). For clarity, we
summarize here the major steps for deriving thesecalibrated elastic maps.
Relation between acoustic impedanceand elastic stiffness
The acoustic impedance is defined as the product ofmass density (r) and compressional wave velocity (nP)and is usually expressed in Mrayl (1 rayl5 1 kgm22s21).In anisotropic materials such as bone, the acoustic imped-ance is a tensor quantity (Lakshmanan et al. 2007).
The amplitude of plane waves reflected at normalincidence at the boundary between the coupling fluidand the anisotropic bone matrix is described by theacoustic impedances Z of the two media. The matrixelements of the acoustic impedance tensor Zn of theanisotropic bone matrix are linked to the scalar massdensity and to the coefficients of the elastic stiffnesstensor C. For example, for a compressional wave propa-gation in the x-direction (hereinafter defined as the direc-tion normal to the longitudinal section surface), thecorresponding impedance is:
ðZnxÞxx5ffiffiffiffiffiffiffiffiffiffiffic11$r
p: (1)
c11 is one component of the elastic stiffness tensor C. Itshould be noted that the index 1 assumes the elastic

Elastic mapping of bone healing by SAM d B. PREININGER et al. 477
symmetry to be parallel to the x-axis. Similarly, theimpedance for a compressional wave propagating in thez-direction (hereinafter defined as the direction parallelto bone long axis) is:
ðZnzÞzz5ffiffiffiffiffiffiffiffiffiffiffic33$r
p: (2)
The impedance for the propagation not parallel to anelastic symmetry direction can easily be obtained by rota-tion of the elastic stiffness tensor C (Lakshmanan et al.2007; Raum 2008). For the transverse isotropic caserotation in the xz plane yields:
cðqÞ5c33cos4q12ðc1312c44Þsin2qcos2q1c11sin
4q; (3)
where q is the rotation angle. c(q) is equivalent to theelastic coefficient c33 of the rotated tensor. It can beseen that cð0�Þ5c33 and cð90�Þ5c11. Combining (1)with (3) gives:
ðZnqÞq5ffiffiffiffiffiffiffiffiffiffiffiffifficðqÞ$r
p; (4)
hereinafter simply referred to as apparent impedance Z(q)and stiffness c(q).
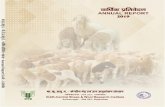
The acoustic impedance Z(q) and the density r havebeen determined independently in various bone tissues,anatomical sites and directions at the microscale, i.e.,with acoustic frequencies between 50 and 200 MHz, bysite-matched analyses (Raum et al. 2006a, 2006b,2007a). Figure 2a shows the relation between c(q) calcu-lated using (4) and the density r derived from the tissuedegree of mineralization (DMB) assessed by synchrotronmicrocomputed tomography (SRmCT) for mature humanradius and mice femur samples. There are clearly rela-tions between these quantities in each of the tissues but
Fig. 2. Relationships mass density and elastic stiffness (a) andbone from different species, anatomical sites, measurement difrom Raum et al. (2006a, 2006b, 2007a). The lines indicate exf*(Z) 5 mrb, whereas a 5 b(2-b)21 and l 5 ma11 that werehuman radius; dotted 5 embedded longitudinal sections of m
was used for the pre
the relations differ between the tissues. This can be dueto different fibril orientations, embedding or other differ-ences in the collagenous organic matrix. Similar differ-ences in the relation between stiffness and density werepreviously observed between mineralized cartilage andbone in humans (Gupta et al. 2005). Very remarkably,this notable difference is much less apparent when oneplots Z(q) as a function of c(q) (Fig. 2b). Since we didnot determine the density in the various compartmentsof the callus, we therefore approximate the relationbetween Z(q) and c(q) by a single regression function:
cðqÞ50:608$ZðqÞ1:923; (5)
that is also plotted in Figure 2b. Despite the fact that theopen and closed symbols follow different graphs (corre-sponding to the different relations between c(q) andr in Fig. 2a), the data points are sufficiently close(RMSE 5 1.35 GPa) to use this approximation at leastfor bone from different origin. Moreover, since theacoustic measurements have been conducted in onedirection only, the symmetry direction could not be deter-mined and we call c11 simply the elastic coefficient in thedirection perpendicular to the surface.
We note that to obtain the Young’s modulus, it isnecessary to know additional parameters. However,with the commonly used assumption of isotropic proper-ties and a Poisson ratio of n 5 0.3 (Rho et al. 2002; Xuet al. 2003), the relation between elastic stiffness Ciso
and Young’s modulus Eiso is:
Eiso5ð11nÞð122nÞ
ð12nÞ $Ciso50:7429$Ciso: (6)
acoustic impedance and elastic stiffness (b) for corticalrections and sample preparation. The data were collatedponential functions of the form c 5 f(r) 5 lra, and c 5fitted to the data (dashed 5 native transverse sections ofice femora). The fit of the combined data (solid lines)diction of c11.

478 Ultrasound in Medicine and Biology Volume 37, Number 3, 2011
It should be noted, however, that bone is notisotropic and the anisotropic Poisson ratios may varybetween 0.15 and 0.45 (Lakshmanan et al. 2007; Rupinet al. 2010). Therefore, eqn (6) should be used withcaution and is used herein only for comparison of ourdata with previously reported elastic data obtained bynanoindentation (Manjubala et al. 2009).
Calibrated maps of the elastic coefficient c11 (Fig. 1)were further analyzed. Subsequent image and statisticalanalyses were performed with custom-made softwarefunctions using Matlab (The Mathworks Inc., Natick,MA, USA).
Fig. 3. Histograms of the elastic coefficient of callus andcortical tissue obtained within the ROIs indicated in Figure 1.The red lines show Gauss functions fitted to the histograms.
Image segmentation and definition of regions of interestA primary segmentation between mineralized tissue
and embedding material was achieved using a threshold(Zthreshold 5 3.50 Mrayl) well above the impedance valueof the embeddingmaterial (ZPMMA5 3.206 0.05Mrayl).According to eqns (4) and (5), the threshold value corre-sponds to an elastic coefficient and indentation modulusof c11 5 5.8 GPa and Er 5 4.3 GPa, respectively, whichis below the value of indentation modulus of 6 GPa re-ported by (Manjubala et al. 2009) for the onset of miner-alization in the soft callus (after fixation and embeddingin PMMA). The definition of ROI was based on previ-ously established ROIs in histologic investigations(Lienau et al. 2005). The selection of these ROIs wasdone semiautomatically by drawing polygon linesdefining the osteotomy gap edges manually. These lineswere translated 1.5 times the gap width in the distal andproximal directions, to define 4.5 mm regions adjacentto the gap. Afterwards, the contour of the cortical tissuewas selected manually. Cortical and newly formed callustissue could be easily distinguished in the acoustic imagesbecause of apparent structural and elastic differences.The remaining areas within the region demarcated bythese lines were automatically defined as endosteal, peri-osteal and intracortical callus regions. Moreover, corticaltissue fragments and new fracture gap areas induced byprevious biomechanical tests were excluded manually.
Within each ROI an adaptive threshold method wasapplied to separate the voids from the mineralized tissuematrix (Lakshmanan et al. 2007). Within each ROI, thetissue area, porosity and the distribution histograms ofthe elastic coefficient c11 were evaluated (Fig. 3). Forthe estimation of the tissue porosity, the total mineralizedtissue area within a ROI was first detected by applyinga morphologic closing operation to the segmented binaryimage. Porosity (%) was defined as the ratio of the voidarea to the total mineralized tissue area. In addition tothe distribution parameters of a normal distribution func-tion fitted to histograms (Fig. 3), the means, medians andstandard deviations of the distributions were extracted. Inmany cases, the distribution did not follow a normal
distribution. Therefore, for further statistical analysesthe medians were used.
Statistical analysisThe relative effect of tissue and fixator types, consol-
idation time and anatomical region within the osteotomysite on the elastic coefficient c11, porosity and callus areawere investigated using the nonparametric Kruskal-Wallis tests followed by post hoc Tukey-Kramer multiplecomparison tests. The confidence level was set to p 50.05. The strength of significant effects is provided bymeans of c2 values. All statistical computations were per-formed with the Matlab Statistics Toolbox (The Math-works Inc.)
Moreover, the spatial variation of the elastic coeffi-cient c11 was investigated in both tissue types with respectto the distance from the cortical-callus boundaries. Thiswas done by averaging the measured c11 values of thematrix stepwise with a 40-mm increment relative to thecallus-cortical tissue boundary over the entire ROI. Forquantification, exponential growth and decay functionswere fitted to the resulting graphs.
RESULTS
Mineralized callus formationMineralized callus tissue, i.e., tissue with c11 . 5.8
GPa, was found adjacent to the site of the osteotomy gapat all time points. Callus porosity, callus area and matrixstiffness could not be assessed reliably at the 2-week timepoint because of the small mineralized callus area. At thelater time points, the mineralized callus area was signifi-cantly affected by the consolidation time (rigid group:c2 5 37.3; semi-rigid group: c2 5 61.5) as well as by

Fig. 5. Course of cortical softening and callus stiffening at theevaluated consolidation time points. A decrease of the stiffnessof the cortical bone was observed between weeks 2 and 3 forboth fixator groups. The onset of callus stiffening occurs ata later time point in the semi-rigid group compared with therigid (after 6 and 3 weeks, respectively). Significant differencesare marked by connecting bars. The solid and dashed lines indi-
Elastic mapping of bone healing by SAM d B. PREININGER et al. 479
the fixator type (c2 5 3.9). While a continuous increaseup to the last evaluated time point (9 weeks) was observedin the semi-rigid group, the maximum callus area in therigid group was found after 6 weeks of consolidation.Callus porosity significantly decreased in both fixatorgroups from the 6- to the 9-week time point (rigid group:c2 5 46.6; semi-rigid group: c2 5 72.1) (Fig. 4). Thestiffness (as estimated by eqn (5) from the acousticimpedance) of the newly formed mineralized callus tissuesignificantly increased over time in both groups (rigidgroup: c2 5 88.6; semi-rigid group: c2 5 70.4). Theonset of this increase of stiffness occurred after week 3and week 6 in the rigid and semi-rigid groups, respec-tively (Fig. 5). Moreover, the increase of callus tissuestiffening was similar on the medial and lateral sides.
In the intra-cortical region, for the rigid group, theformation of mineralized tissue was observed fromweek 3 to 6 (c2 5 9.1) while tissue stiffness increasedsignificantly from week 6 to 9 (c2 5 6.1). A similar trendwas observed in the semi-rigid group. However, thechanges of mechanical and structural properties werenot significant.
cate mean 6 standard deviation of c11 in intact cortical tissue.
Cortical tissue alterationsTo estimate the decrease of cortical tissue stiffness in
the repair region relative to intact cortical tissue, corticalcentral ROIs distant from both, the osteotomy gap and thepin locations have been evaluated in the 2-week groups.The average values for cortical porosity and elastic
Fig. 4. Course of cortical and callus porosities at the evaluatedconsolidation time points. A decrease of callus porosity wasfound in both groups from 3 to 9 weeks while the porosityincreased in the cortical tissue. Significant differences aremarked by connecting bars. The solid and dashed lines indicatemean 6 standard deviation of porosity in intact cortical tissue.Porosity was not assessed in the callus tissue of the 2-week
group.
coefficient in these ROIs were 1.4 6 0.6% and 33.8 61.8 GPa, respectively.
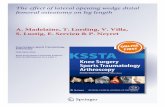
Remarkable changes of structural properties, i.e., theoccurrence of resorption lacunae and the subsequentsynthesis of new tissue within these lacunae wereobserved from 6 weeks onwards (Fig. 6). This was re-flected by a significant increase in tissue porosity in the6- and 9-week groups compared with the earlier timepoints (rigid group: c2 5 26.9; semi-rigid group: c2 527.0) (Fig. 4). Moreover, a significant decrease of thecortical tissue stiffness was observed even at the earliesttime points (between weeks 2 and 3) in both fixatorgroups (rigid group: c2 5 11.5; semi-rigid group: c2 510.2) (Fig. 5). At the later time points, the average stiff-ness remained at a lower level compared with the valuesobtained in the intact tissue. The course of these structuralalterations was not influenced by the fixator type.
Local variations of stiffness gradientsThe local variations within cortical and callus tissue
were evaluated by averaging the elastic coefficients c11 inthe direction parallel to the cortex-callus boundary in theperiosteal side (Fig. 7). It should be noted that negativeand positive x values define cortical and callus tissueregions, respectively, and x 5 0 mm defines the cortex-callus boundary. The resulting profile plots revealeda well pronounced step function at the cortex-callusboundary with a sharp transition from high to low valuesat week 2 (data not shown). At the later time points,

Fig. 6. Comparison of elastic stiffness maps obtained after 3 (a) and 9 (b) weeks of consolidation at the medial side(cortical and periosteal callus ROIs). Per 5 periosteal region; End 5 endosteal region.
480 Ultrasound in Medicine and Biology Volume 37, Number 3, 2011
a gradual decrease of the cortical stiffness toward thecallus boundary was observed. The cortical tissue areaaffected by this gradual stiffness alteration increasedwith time. The stiffness values were fitted to an exponen-tial growth function:
cCt11ðxÞ5�cCt:dist11 2cCt:bound11
�eðCt:B=xÞ1cCt:bound11
x˛ð23; 0Þmm ; (7)
whereas the superscript Ct indicates cortical tissue, cCt:dist11
and cCt:bound11 are the stiffness values in the cortical tissue ata large distance from the callus-cortex boundary (i.e., inthe central part of the cortex) and at the boundary,respectively. Ct.B defines the gradual change from thecallus-cortex boundary toward the central cortex region.Similarly, the stiffness values in the callus tissues werefitted to an exponential decay function:
cCa11 ðxÞ5�cCa:bound11 2cCa:dist11
�eð2x=Ca:BÞ1cCa:dist11
x˛ð0; 3Þmm ; (8)
whereas the superscript Ca indicates callus tissue, cCa:dist11
and cCa:bound11 are the stiffness values in the callus tissue ata large distance from the callus-cortex boundary and atthe boundary, respectively. Ca.B defines the gradualchange from the callus-cortex boundary toward the outerboundary of the periosteal callus. A strong gradient of thestiffness was observed at week 3. At week 6, the gradientwas less pronounced and the stiffness in the distant callusregions reached approximately the same value as theregions at the boundary. It should be noted that cCa:bound11
was almost equivalent at weeks 3 and 6. At week 9,increased values in the entire callus region togetherwith a more pronounced gradient were observed. The fitparameters for the representative graphs of Figure 7 aresummarized in Table 1.
The difference of cCt:bound11 and cCa:bound11 decreasedfrom 8.4 GPa at week 3 to 2.2 GPa at week 9.
DISCUSSION
The current work is the first one to provide compre-hensive analysis of variations of tissue porosity and oneelastic coefficient in cortical and mineralized callustissues in the course of healing in a sheep osteotomymodel. Quantitative 50-MHz scanning ultrasoundmicroscopy was used to map the elastic stiffness coeffi-cient c11 (derived from the acoustic impedance) witha spatial resolution of 23 mm. It is well known that tissueformation during the course of bone healing is influencedby the mechanical boundary conditions in the repair zone.Toward a better understanding of the interrelationsbetween mechanics and biology, it is essential not onlyto characterize the material behavior of the external stabi-lization but also the dynamic alterations of the tissuesinvolved in the healing process. It was hypothesizedthat elastic tissue alterations over the course of healingdo not only occur in the callus tissue as a result of miner-alization but also in the cortical tissue adjacent to therepair zone. Moreover, we anticipated a dependency ofstructural and elastic tissue alterations in the course ofhealing with respect to the external mechanical boundaryconditions (fixator stiffness).
Decreased cortical tissue stiffness values wereobserved in all evaluated tissue regions adjacent to the os-teotomy gap in comparison with values in cortical tissuein the 2-week group in regions far away from both, the os-teotomy gap and the pin locations. At this time point, onlymarginal mineralization of the callus tissue and nogradual decrease of the cortical stiffness toward the peri-osteal cortex-callus boundary were observed. It should be

Fig. 7. Gradients of elastic coefficients relative to the cortex-callus boundary developed with consolidation time. After 3and 6 weeks (a) and (b), distinct steps can still be recognized.After 9 weeks (c) of consolidation a smooth elastic transitionbetween the cortical tissue and the periosteal callus tissue hasdeveloped. The solid and dashed lines indicate mean6 standard
deviation of c11 in intact cortical tissue.
Elastic mapping of bone healing by SAM d B. PREININGER et al. 481
noted, however, that the selected control regions may alsohave been altered compared with intact contralateralcortical tissue. However, this finding is well in line withthe reduction of mineral particle size in the cortex nearthe fracture gap prior to resorption, as previouslyobserved with small-angle x-ray scattering in similarsamples (Liu et al. 2010a). At later time points, thisreduction was complemented by an increase of porosity,predominantly induced by resorption lacunae. At thelatest evaluated time points, some of these resorptionlacunae have been refilled by new mineralized, but yetsofter tissue (data not shown). This cascade has severalimportant impacts on the course of the healing process.In the initial phase (up to week 3), no or only a few osteo-clasts have been observed (Schell et al. 2006). We specu-late that during this time, calcium and phosphate neededfor the mineralization of the newly formed callus tissuecould be provided by the directly adjacent environment,e.g., the intact bonematrix. The observed decrease of stiff-ness may be related to a partial demineralization of thecortical bonematrixwhile providing the required hydroxy-apatite, which needs to be confirmed by additional site-matched investigations of the mineral and organic phases.The combination of these structural and elastic changesleads to a softening of the cortical tissue directly adjacentto the newly formed callus tissue. This assumption isfurther supported by the observed gradients of stiffnessfrom the central cortical regions toward the periostealcallus tissue, which showed a change from a step-like toa smooth transition at the interface between week 2 and 9.
In contrast to the gradual decrease of stiffness incortical tissue, the stiffness in callus tissue increasedfrom week 3 to week 9, which is in agreement with nano-indentation data measured in the periosteal region of therigid-fixator group by Manjubala et al. (2009). Their re-ported indentation modulus values are in good agreementwith the elastic coefficients estimated from our acousticmeasurements. For example, with the aforementionedassumption of a Poisson ratio of 0.3, the Young’s modulusderived from the acoustic measurement in intact corticaltissue is Ea5 25.26 1.3 GPa. The values measured in thecortical ROIs at the osteotomy site, Ea5 22.66 1.1 GPa,compare well with the indentation modulus Er5 20.6 64.5 GPa reported previously. The slightly smaller inden-tation based values may well be explained by the differentevaluated ROIs, i.e., only the region directly adjacent tocallus has been analyzed by Manjubala et al. (2009).Our data suggest that these regions exhibit consolidationtime-dependent decreased stiffness values compared withthe central cortical regions. Also, the range of indentationmodulus values in callus tissue (between 6 and 15 GPa)was equivalent to the values derived from the acousticmeasurement. However, it should be noted that with

Table 1. Fit parameter for cortical and callus gradients from eqns (7) and (8) and Figure 7
Cortical tissue Callus tissue
cCt:dist11 [GPa] cCt:bound11 [GPa] Ct.B [mm21] R2 cCa:dist11 [GPa] cCa:bound11 [GPa] Ca.B [mm21] R2
3 weeks 31.2 25.3 0.2 0.72 6.8 16.9 1.9 0.876 weeks 33.8 25.6 0.7 0.86 12.8 15.7 5.2 0.249 weeks 30.4 21.7 0.3 0.91 16.1 19.5 0.9 0.59
R2 is the goodness of the fit.
482 Ultrasound in Medicine and Biology Volume 37, Number 3, 2011
both techniques, the anisotropic Poisson ratios would beneeded for the derivation of the Young’s modulus.Rupin et al. (2009) have recently observed by site-matched evaluation of acoustic impedance Z, indentationmodulus En and tissue degree of mineralization DMB inhuman cortical bone samples that (1) Z and En are highlycorrelated (R2 5 0.67, RMSE 5 1.9 GPa); (2) bothparameters were correlated with DMB, but the correla-tion was higher with Z (R2 5 0.53) than with En (R
2 50.38); and (3) potential variations in the Poisson’s ratiowould strongly affect the Young’s modulus derivedfrom the acoustic measurement, but to a much lesserextent En. Therefore, the correlation of Z(q) and c(q)found in cortical tissues of human and mice implies thatreliable estimates of the elastic coefficients, but notnecessarily of the Young’s modulus can be made fromthe acoustic measurements. Moreover, the empirical rela-tion of eqn (5) depends on the elastic properties of organicmatrix (and embedding medium) and it may be differentin the various tissues within the callus (Gupta et al. 2005;Raum et al. 2006a). Thus, the elastic values presentedhere have to be taken with some caution. Animprovement in the quantification of elastic constantsfrom ultrasound reflection by a combination with localdensity and collagen fibril orientation determination,e.g., by back-scattered electron imaging (Roschgeret al. 2008) and polarized Raman spectroscopic imaging(Kazanci et al. 2007), respectively, may be a subject forfurther development of the technique.
We anticipate that the combination of the observedstructural and elastic changes in cortical and callus tissueduring healing results in a rather homogeneous straindistribution. With such concept, potentially harmfulstrain peaks at the cortical-callus boundary would beminimized during the healing process.
Despite significant differences in the amount ofcallus tissue formed on the medial (external fixator)and on the lateral side, as revealed by histomorphome-try (Lienau et al. 2005), no other differences betweenthese two regions could be identified in the distributionof the elastic coefficient c11. Fixator stiffness didneither influence the stiffening of mineralized callusformed through endochondral ossification (intracorticalgap region), nor the properties of the mineralized callus
formed through intramembranous ossification (perios-teal callus).
CONCLUSION
High resolution maps of tissue stiffness and porositywithin the callus and surrounding cortical bone providenew insights into themechano-regulation of bone healing.Until now, computer models of bone healing usuallyassume a simplified distribution of the material propertieswithin the callus region and, frequently, a homogeneous orconstant value for cortical bone stiffness (Andreykiv et al.2008; Isaksson et al. 2006; Lacroix and Prendergast2002). In this study, we have shown that cortical bone isby no means constant in stiffness during healing and,thus, represents an integral part of the remodelling ofthe callus. This presumably contributes to the dynamicsof the mechanical stimulation of the callus tissues.
For the first time, structural andmicroelasticmaterialproperties of the entire bone regeneration zone have beenevaluated with respect to consolidation time and fixatorstability over thewhole area of bone regeneration. In addi-tion to an increase of the elastic coefficient in the callustissue, a progressive decrease of cortical matrix stiffnessand at a later time, an increase of cortical porosity, wereobserved. This remodeling process suggests that thechanges of the material properties of the tissues in thehealing zone lead to a homogenization, maybe to reducemaximum strains at the boundaries between the tissuesto a minimum.
The principle findings and the data gained from thisstudy can be used to refine numerical modeling in a verysophisticated way. For example, the elastic maps inconjunction with information of the local tissue mineral-ization from recent qBEI studies of the same samples canbe used directly as input for more realistic sound propa-gation simulations. Moreover, the high spatial resolutionof SAM images allows stress-strain simulations withmicroscopic resolution. Thereby, further insights in thetransformation of external mechanical stimulation condi-tions to cellular responses can be gained.
Acknowledgments—This work has been conducted within the EuropeanAssociated Laboratory ‘‘Ultrasound Based Assessment of Bone’’(ULAB) and has been supported by the Deutsche Forschungsgemein-schaft DFG grants Ra1380/7 and SFB 760 (B-2, G-2.2).

Elastic mapping of bone healing by SAM d B. PREININGER et al. 483
REFERENCES
Andreykiv A, van KF, Prendergast PJ. Simulation of fracture healingincorporating mechanoregulation of tissue differentiation anddispersal/proliferation of cells. Biomech Model Mechanobiol2008;7:443–461.
Austman RL,Milner JS, Holdsworth DW, Dunning CE. The effect of thedensity-modulus relationship selected to applymaterial properties ina finite element model of long bone. J Biomech 2008;41:3171–3176.
Austman RL,Milner JS, Holdsworth DW, Dunning CE. Development ofa customized density-modulus relationship for use in subject-specific finite element models of the ulna. Proc Inst Mech Eng H2009;223:787–794.
Dodd SP, Miles AW, Gheduzzi S, Humphrey VF, Cunningham JL.Modelling the effects of different fracture geometries and healingstages on ultrasound signal loss across a long bone fracture. ComputMethods Biomech Biomed Eng 2007;10:371–335.
Dyke JP, Aaron RK. Noninvasive methods of measuring bone bloodperfusion. Ann N YAcad Sci 2010;1192:95–102.
Gluer CC. A new quality of bone ultrasound research. IEEE TransUltrason Ferroelectr Freq Control 2008;55:1524–1528.
Grimal Q, Raum K, Gerisch A, Laugier P. Derivation of the mesoscopicelasticity tensor of cortical bone from quantitative impedanceimages at the micron scale. Comput Methods Biomech BiomedEngin 2008;11:147–157.
Gupta HS, Schratter S, Tesch W, Roschger P, Berzlanovich A,Schoeberl T, Klaushofer K, Fratzl P. Two different correlationsbetween nanoindentation modulus and mineral content in thebone-cartilage interface. J Struct Biol 2005;149:138–148.
Harten RD Jr, Lee FY, Zimmerman MC, Hurowitz E, Arakal R,Behrens FF. Regional and temporal changes in the acoustic proper-ties of fracture callus in secondary bone healing. J Orthop Research1997;15:570–576.
Hube R, Mayr H, Hein W, Raum K. Prediction of biomechanicalstability after callus distraction by high resolution scanning acousticmicroscopy. Ultrasound Med Biol 2006;32:1913–1921.
Isaksson H, Harjula T, Koistinen A, Iivarinen J, Seppanen K,Arokoski JP, Brama PA, Jurvelin JS, Helminen HJ. Collagen andmineral deposition in rabbit cortical bone during maturation andgrowth: Effects on tissue properties. J Orthop Res 2010;28:1626–1633.
Isaksson H, van Donkelaar CC, Huiskes R, Ito K. Amechano-regulatorybone-healing model incorporating cell-phenotype specific activity.J Theor Biol 2008;252:230–246.
Isaksson H, Wilson W, van Donkelaar CC, Huiskes R, Ito K. Compar-ison of biophysical stimuli for mechano-regulation of tissue differ-entiation during fracture healing. J Biomech 2006;39:1507–1516.
Kaufman JJ, Luo G, Siffert RS. Ultrasound simulation in bone. IEEETrans Ultrason Ferroelectr Freq Control 2008;55:1205–1218.
Kazanci M, Wagner HD, Manjubala NI, Gupta HS, Paschalis E,Roschger P, Fratzl P. Raman imaging of two orthogonal planeswithin cortical bone. Bone 2007;41:456–461.
Lacroix D, Prendergast PJ. Three-dimensional simulation of fracturerepair in the human tibia. Comput Methods Biomech Biomed Eng2002;5:369–376.
Lakshmanan S, Bodi A, Raum K. Assessment of anisotropic tissue elas-ticity of cortical bone fromhigh-resolution, angular acousticmeasure-ments. IEEE Trans Ultrason Ferroelectr Freq Control 2007;54:1560–1570.
Leong PL, Morgan EF. Measurement of fracture callus material proper-ties via nanoindentation. Acta Biomater 2008;4:1569–1575.
Lienau J, Schell H, Duda GN, Seebeck P, Muchow S, Bail HJ. Initialvascularization and tissue differentiation are influenced by fixationstability. J Orthop Res 2005;23:639–645.
Liu Y, Manjubala I, Schell H, Epari DR, Roschger P, Duda GN, Fratzl P.Size and habit of mineral particles in bone and mineralized callusduring bone healing in sheep. J Bone Miner Res 2010a;25:2029–2038.
Liu XS, Zhang XH, Rajapakse CS, Wald MJ, Magland J, Sekhon KK,Adam MF, Sajda P, Wehrli FW, Guo XE. Accuracy of high-resolution in vivo micro magnetic resonance imaging for
measurements of microstructural and mechanical properties ofhuman distal tibial bone. J Bone Miner Res 2010b;25:2039–2050.
Manjubala I, Liu Y, Epari DR, Roschger P, Schell H, Fratzl P, Duda GN.Spatial and temporal variations of mechanical properties andmineral content of the external callus during bone healing. Bone2009;45:185–192.
Parnell WJ, Grimal Q. The influence of mesoscale porosity on corticalbone anisotropy. Investigations via asymptotic homogenization.J R Soc Interface 2009;6:97–109.
Protopappas VC, Kourtis IC, Kourtis LC, Malizos KN, Massalas CV,Fotiadis DI. Three-dimensional finite element modeling of guidedultrasound wave propagation in intact and healing long bones.J Acoust Soc Am 2007;121:3907–3921.
Protopappas VC, VavvaMG, Fotiadis DI,Malizos KN. Ultrasonic moni-toring of bone fracture healing. IEEE Trans Ultrason FerroelectrFreq Control 2008;55:1243–1255.
Raum K. Microelastic imaging of bone. IEEE Trans Ultrason Ferroe-lectr Freq Control 2008;55:1417–1431.
Raum K, Cleveland RO, Peyrin F, Laugier P. Derivation of elastic stiff-ness from site-matched mineral density and acoustic impedancemaps. Phys Med Biol 2006a;51:747–758.
RaumK, Hofmann T, Leguerney I, Saied A, Peyrin F, Vico L, Laugier P.Variations of microstructure, mineral density and tissue elasticity inB6/C3H mice. Bone 2007a;41:1017–1024.
Raum K, Kempf K, Hein HJ, Schubert J, Maurer P. Preservation of mi-croelastic properties of dentin and tooth enamel in vitro–A scanningacoustic microscopy study. Dent Mater 2007b;23:1221–1228.
Raum K, Leguerney I, Chandelier F, Bossy E, Talmant M, Saied A,Peyrin F, Laugier P. Bonemicrostructure and elastic tissue propertiesare reflected in QUS axial transmission measurements. UltrasoundMed Biol 2005;31:1225–1235.
Raum K, Leguerney I, Chandelier F, Talmant M, Saied A, Peyrin F,Laugier P. Site-matched assessment of structural and tissue proper-ties of cortical bone using scanning acoustic microscopy andsynchrotron radiation mCT. Phys Med Biol 2006b;51:733–746.
Raum K, Reisshauer J, Brandt J. Frequency and resolution dependenceof the anisotropic impedance estimation in cortical bone using time-resolved scanning acoustic microscopy. J BiomedMat Research PartA 2004;71A:430–438.
Reichel H, Lebek S, Alter C, Hein W. Biomechanical and densitometricbone properties after callus distraction in sheep. Clin Orthop RelatRes 1998;357:237–246.
Rho JY, Zioupos P, Currey JD, Pharr GM. Microstructural elasticity andregional heterogeneity in human femoral bone of various ages exam-ined by nanoindentation. J Biomech 2002;35:189–198.
Roschger P, Paschalis EP, Fratzl P, Klaushofer K. Bone mineraliza-tion density distribution in health and disease. Bone 2008;42:456–466.
Rupin F, Bossis D, Vico L, Peyrin F, RaumK, Laugier P, Saied A. Adap-tive remodeling of trabecular bone core cultured in 3D bioreactorproviding cyclic loading: An acoustic microscopy study. UltrasoundMed Biol 2010;36:999–1007.
Rupin F, Saied A, Dalmas D, Peyrin F, Haupert S, Raum K, Barthel E,Boivin G, Laugier P. Assessment of microelastic properties of boneusing scanning scoustic microscopy: A face-to-face comparisonwith nanoindentation. Jpn J Appl Phys 2009;48:1–6.
Saied A, Raum K, Leguerney I, Laugier P. Spatial distribution of aniso-tropic acoustic impedance assessed by time-resolved 50-MHz scan-ning acoustic microscopy and its relation to porosity in humancortical bone. Bone 2008;43:187–194.
Schell H, Lienau J, Epari DR, Seebeck P, Exner C, Muchow S,Bragulla H, Haas NP, Duda GN. Osteoclastic activity begins earlyand increases over the course of bone healing. Bone 2006;38:547–554.
Shefelbine SJ, Simon U, Claes L, Gold A, Gabet Y, Bab I, Muller R,Augat P. Prediction of fracture callus mechanical properties usingmicro-CT images and voxel-based finite element analysis. Bone2005;36:480–488.
Xu J, Rho JY, Mishra SR, Fan Z. Atomic force microscopy andnanoindentation characterization of human lamellar bone preparedby microtome sectioning and mechanical polishing technique.J Biomed Mat Research 2003;67A:719–726.
Copyright © 2022 FDOKUMEN