SPATIAL AND EPIDEMIOLOGICAL ASPECTS OF PLAGUE IN INDIA: A CASE STUDY OF MAMLA VILLAGE AND SURAT...
11
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of SPATIAL AND EPIDEMIOLOGICAL ASPECTS OF PLAGUE IN INDIA: A CASE STUDY OF MAMLA VILLAGE AND SURAT...
21
SPATIAL AND EPIDEMIOLOGICAL ASPECTS OF PLAGUE IN INDIA: A CASE STUDY OF MAMLA VILLAGE AND SURAT CITY
HARSHIT SINHA
Public System Group, Indian Institute of Management, Ahmedabad - 380015
ABSTRACT
The outbreak of Plague in India in 1994 was of global concern. The imbalance between ecology and environment has not only reinvited the unforgotten scourge of mankind after a gap of twenty-six years but has puzzled the entire world. Different theories and related issues have led to a series of doubts in the minds of people as to whether the outbreak was really "plague". Tracing etiological and epidemiological aspects, the present article explores the reality to elucidate factors responsible for the current outbreaks of Plague and discuss the critical issues pertaining to its spread.
Keywords: Mamla, Surat, plague, environment, rodent surveillance.
INTRODUCTION
Plague is a disease of great antiquity, recorded in the ancient writings of India as well as in the Bible. Three pandemics have swept across the world claiming many millions of lives and causing untold misery. Even today "Plague continues to smoulder in population of wild rodents in natural foci throughout the world, and occasional outbreaks of human plague bring a reminder of the devastation it has caused in the past. Changed ecological circumstances in a plague focus may release an epizootic wave that could lead to a serious epidemic of this fearful disease in humans unless constant vigilance is maintained in the danger areas of the world" I.
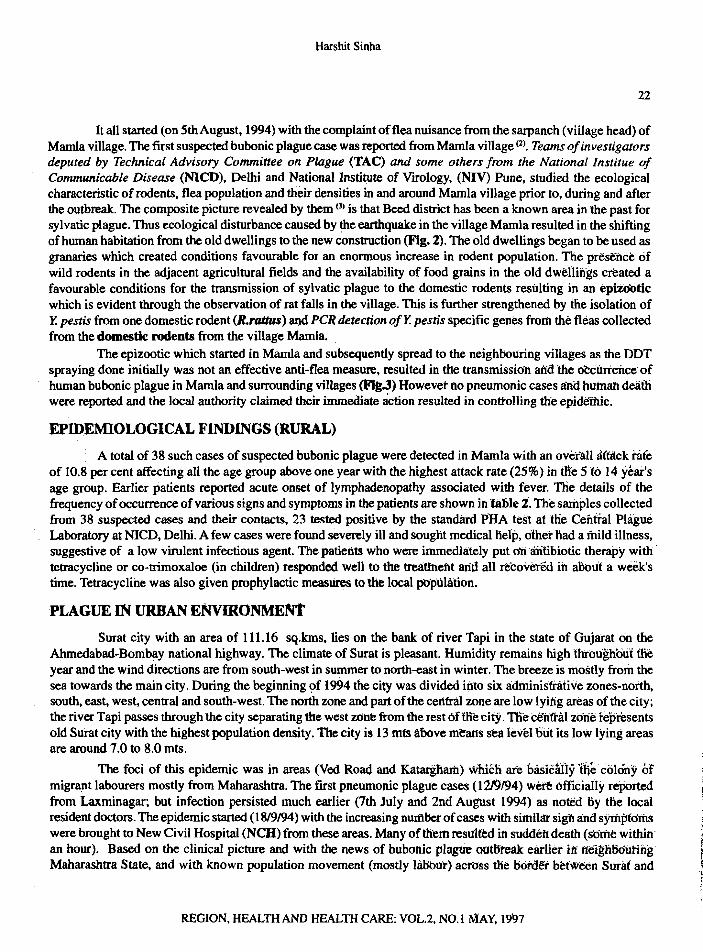
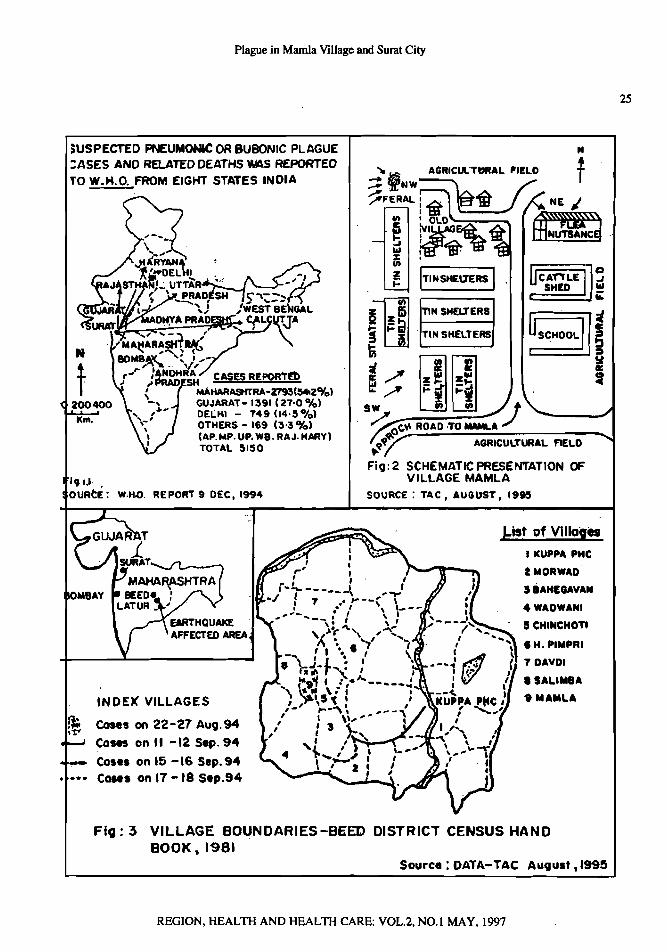
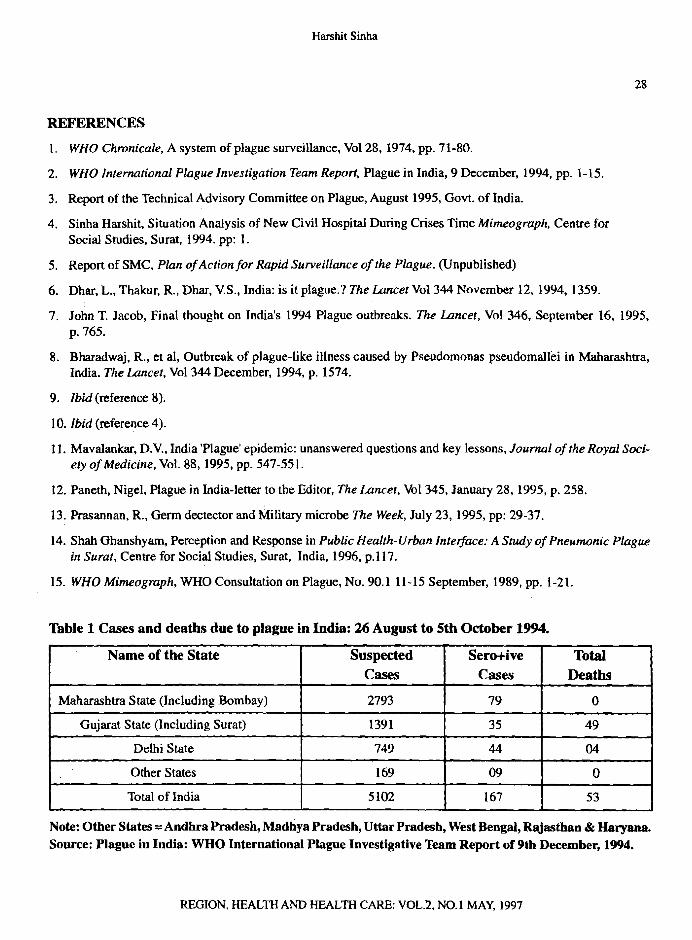
However with improved hygiene and living standards, the availability of effective drugs for treatment and prophylaxis and the large-scale application of insecticides, a remarkable decline in the number of cases and deaths due to plague was observed in the entire world during 20th century. After the last reported cases in 1967, there have been no laboratory confirmed case of human plague in India, until its reappearance in September 1994 (Fit- 1). About four persons tested positive for bubonic plague in Beed (Maharashtra), followed by an outbreak of pneumonic plague in Surat (Gujarat). During August 26 to October 5, 1994 a total of 5150 suspected pneumonic or bubonic plague cases and 53 (crude case-fatality ratio=l.O%) related deaths was reported to the WHO from eight states in India (Table 1). Inspite of many controversies about the nature of the epidemic, effective measures taken by the authorities in India brought the Surat outbreak rapidly under control and the chain of infection could not spread to other countries.
OBJECTIVES & METHODOLOGY
Based on personal experience, incorporating experts' view and referring to technical reports, the present article explores the reality to elucidate factors responsible for the current outbreaks of plague and discusses the critical issues pertaining to its spread.
PLAGUE IN RURAL ENVIRONMENT
The plague hit Mamla village is located about 35 KIn from the district headquarter town of Beed in the Beed district of Maharashtra state. This village has a population of 325 with relatively low rainfall. The climate of the district is pleasant for the major part of the year. However seeing the undulating topography, climatic variation are found within the district.
REGION, HEALTH AND HEALTH CARE: YOL.2, NO.1 MAY, 1997 (21-30)
Harshit Sinha
22
It all started (on 5thAugust, 1994) with the complaint offlea nuisance from the sarpanch (viiIage head) of Mamla village. The first suspected bubonic plague case was reported from Mamla village (2). Teamsofinvestigators deputed by Technical Advisory Committee on Plague (TAC) and some others from the National Institue of Communicable Disease (NICD), Delhi and National Institute of VIrology, (NIV) Pune, studied the ecological characteristic of rodents, flea population and their densities in and around Mamla village prior to, during and after the outbreak. The composite picture revealed by them (3) is that Beed district has been a known area in the past for sylvatic plague. Thus ecological disturbance caused by the earthquake in the village Mamla resulted in the shifting of human habitation from the old dwellings to the new construction (Fig. 2). The old dwellings began to be used as granaries which created conditions favourable for an enormous increase in rodent population. The presence of wild rodents in the adjacent agricultural fields and the availability of food grains in the old dwellings created a favourable conditions for the transmission of sylvatic plague to the domestic rodents resulting in an epizootic which is evident through the observation of rat falls in the village. This is further strengthened by the isolation of Y. pestis from one domestic rodent (R.rattus) and PCR detection ofY. pestis specific genes from the fleas collected from the domestic rodents from the village Mamla.
The epizootic which started in Mamla and subsequently spread to the neighbouring villages as the DDT spraying done initially was not an effective anti-flea measure, resulted in the transmission and the OCcurrence of human bubonic plague in Mamla and surrounding villages (FIt.J) Howevet nopneumonic cases andhumandeath were reported and the local authority claimed their immediate action resulted in conttolling the epidemic.
EPIDEMIOLOGICAL FINDINGS (RURAL)
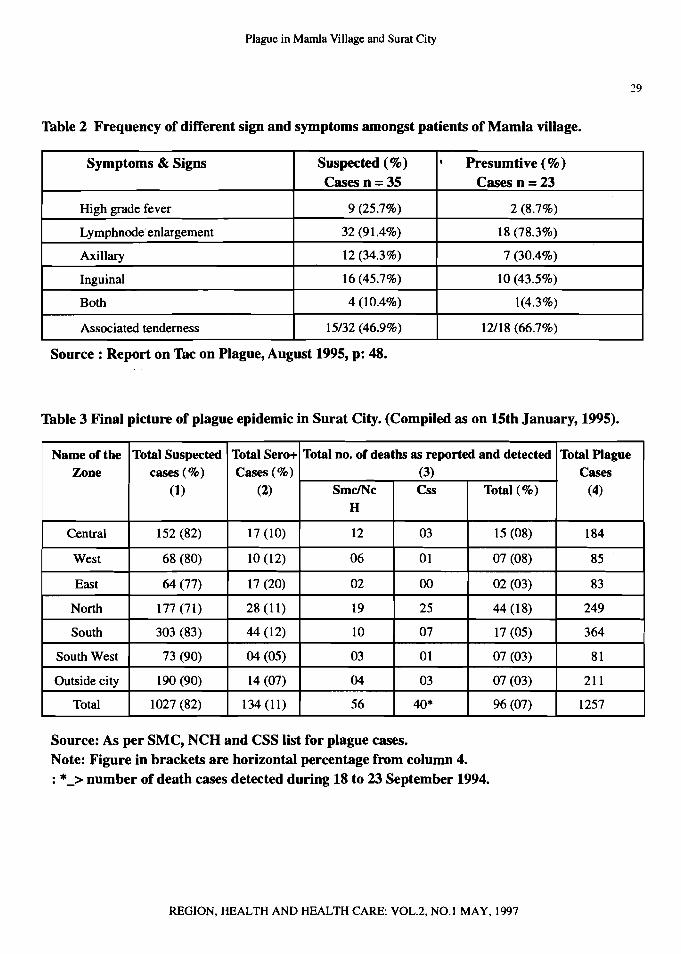
A total of 38 such cases of suspected bubonic plague were detected in Mamla with an overall Mtack ra(e of 10.8 per cent affecting all the age group above one year with the highest attack rate (25%) in tile 5 to 14 year's age group. Earlier patients reported acute onset of lymphadenopathy associated with fever. The details of the frequency ofoccurrence of various signs and symptoms in the patients are shown in 'UlJ)le z, The samples collected from 38 suspected cases and their contacts, 23 tested positive by the standard PlIA test at the Central Plague Laboratory at NICD, Delhi. A few cases were found severely ill and sought medical help, other "ad a mild illness, suggestive of a low virulent infectious agent. The patients who were immediately put onlfutibiotic therapy with . tetracycline or co-trimoxaloe (in children) responded well to the treatment arid all recovered in about a week's time. Tetracycline was also given prophylactic measures to the local population.
PLAGUE IN URBAN ENVIRONMENT
Surat city with an area of 111.16 sq.kms, lies on the bank of river Tapi in the state of Gujarat on the Ahmedabad-Bombay national highway. The climate of Surat is pleasant. Humidity remains high throughout the year and the wind directions are from south-west in summer to north-east in winter. The breeze is mostly from the sea towards the main city. During the beginning of 1994 the city was divided into six administrative zones-north, south, east, west, central and south-west. The north zone and part ofthe central zone are low lying areas of the city; the river Tapi passes through the city separating the west zOn~ from the rest oHIle city. The d:'nfhlI ZOne represents old Surat city with the highest population density. The city is 13 mts lloove means sea level out its low lying areas are around7.0 to 8.0 mts.
The foci of this epidemic was in areas (Ved ROaQ and Katargham) wmen are blisic~t)y 'file colony Of migrant labourers mostly from Maharashtra. The first pneumonic plague cases (1219194) were officially reported from Laxminagar; but infection persisted much earlier (7th July and 2nd August 1994) as noted By the local resident doctors. The epidemic started (1819194) with the increasing number ofcases with similar sign and symptoms were brought to New Civil Hospital (NCR) from these areas. Many of them resulted in suddeh death (some within an hour). Based on the clinical picture and with the news of bubonic plague outBteak earlier iff neighBOuting Maharashtra State, and with known population movement (mostly hlBolit) aertsss ilie l)6roei' bet"woon Sural and
t t t I
~ t
f ,I f
t t r
REGION,HEALTH AND HEALTH CARE: VOL.2,NO.1 MAY, 1997
23 l2
of rs of :al ler
for ng as of h ;tic lof ted
Dr
ni(e ~ar's I the eted igue ~ess,
with Eek's
II the jUlie fit the Ioith, I city; :gents areas
~tiy of torted local ~ofu:s
within ,oong at and
Plague in Mamla Village and Surat City
different parts of Maharashtra a clinical diagnosis was made by local expert ofNCH. A "safety pin" -like organism as demonstrated on Wayson strain in sputum smears and after intensive discussions, finally declared the epidemic as "Plague" 4. Thus seeing the magnitude of the problem and designating the new Civil Hospital as the isolation and treatment centre, "do and die" efforts were made for early detection, referral services, providing prophylactic treatment, spraying of insecticide, health education and preventive measures against the disease 5. The case fatality rates came down rapidly after the initial high levels in the first few days.
DISEASE DISTRIBUTION
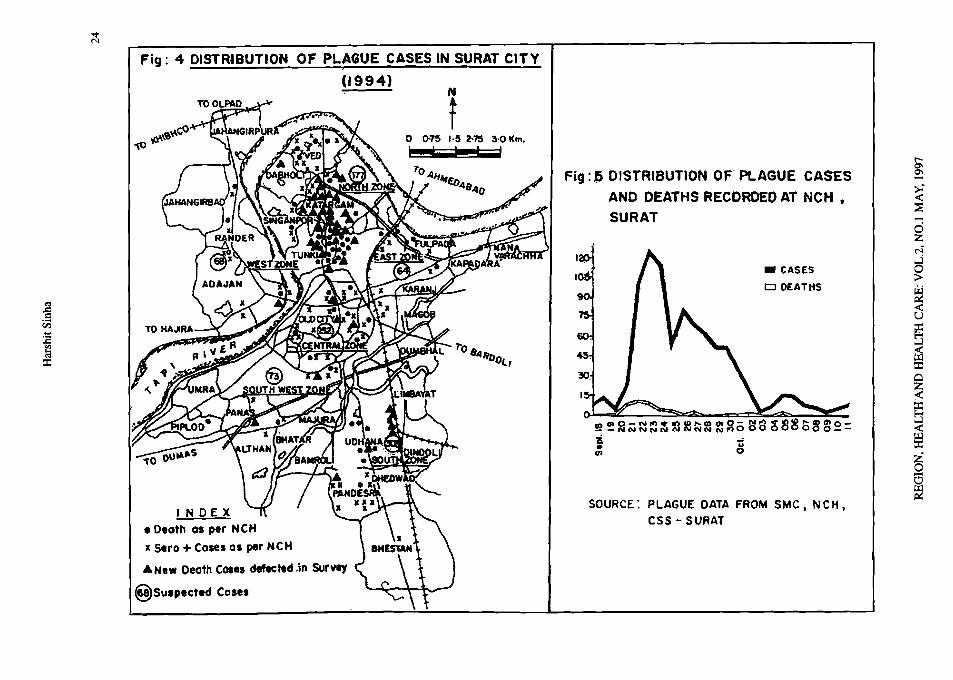
As per the survey conducted by Centre for Social Studies (CSS), Surat, the NCD admitted plaguesuspected patients from almost all parts of the city (Fig.4). The largest number of deaths and sero positive cases were found in low lying (Ved Road, Tunki, Singanpore and Katargham) areas of the northern part. These areas were flooded before the outbreak of the epidemic. A clustering of cases and deaths was noted in the north and central Zones, (Fig.4) where most of the deaths occurred within a radius of 1.5 km. Besides, clustering of deaths was also observed in many areas within a 100 meter range. In the southern part of the city, Udhana and Pandesara had the largest number (303) of suspected cases. Udhana had more incidence of deaths, whereas Pandesara had more cases of sero positive. This is followed by eight deaths and 14 sero positive cases in central Zone, which is the most congested part having highest population density. The death and sero positive cases in the central zone were not located in one particular neighbourhood as it was found in Ved Road. They were found scattered in various locality
It is astonishing to note that plague death was also reported even in the posh localities like the Athawa lines in the south west zone. Incidence of deaths was also reported from the middle class locality of Rander in the western part. However what is striking is that (Slums like Dindoli, Limbayat, Dumbhal and Karanj) in the southeastern part escaped from the calamity. Varachha road in the eastern part which has many similar characteristics to Ved Road had very few plague patients. The final status of plague is described in the table 3, that indicates more number of pneumonic plague cases with deaths occurred within and beyond city limit during early days of the epidemic. Since there was no direct evidence of mortality with this epidemic, such cases were not registered neither at SMC nor at NCH. Thus one can see very different nature of virulence and uneven distribution of the disease in the city from the very first day. The number of patients steeply rose to 110 and on the 23rd. There were as many as 411 patients on the 24th. The inflow of new patients continued thereafter but the rate declined from the 26th day onwards (Fig.5).
EPIDEMIOLOGICAL FINDINGS (URBAN)
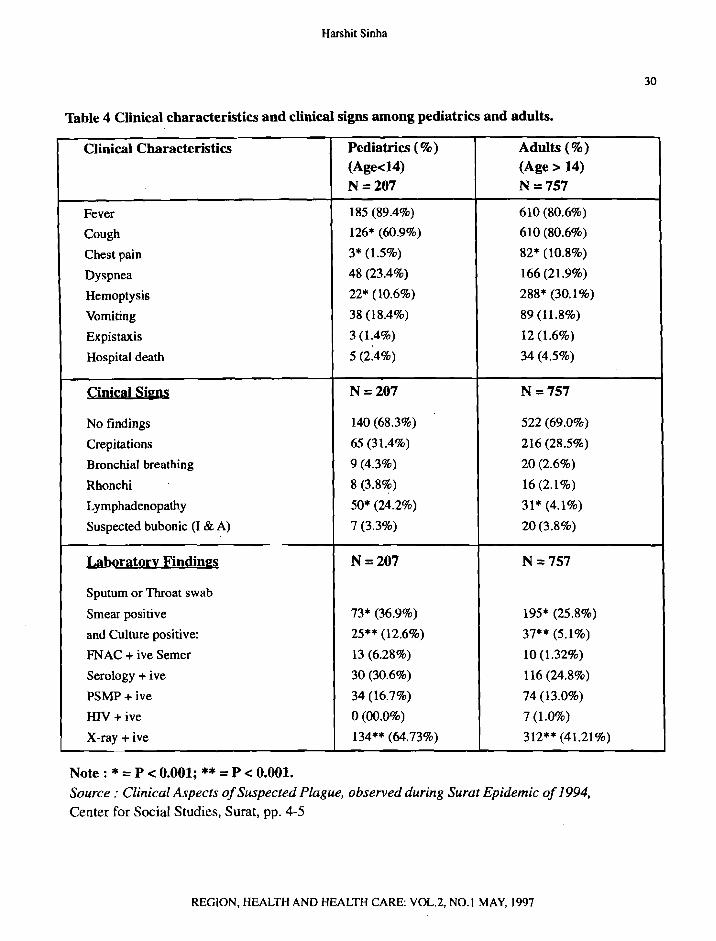
According to the information provided by NCD, the clinical analysis done at CSS reveals that some 1013 patients were admitted from 21st September to 3rd November. However reliable clinical records were only available for 964 patients. Of these, 260 (27%) were females and 704 (73%) were males from all age groups, The means age of patients was 25.36 (+ 14.59 with the range of I month to 85 years). Of the total cases, 207 (21.5%) patients were below 14 years of age (treated by paediatric department) and 757 (78.5%) were adults. Table 4 indicates different clinical and laboratory parameters in paediatrics and adult's groups. Fever was most common in adults than in paediatric patients. Similarly Haemoptysis and chest pain were far more common in adults than in paediatric patients (P<O.OOl). All respiratory signs were present in both the group with more or less equal frequency except rhonchi which were common in paediatric patients. Lymphnode enlargement was significantly more in paediatric age group (p,O.OOOl). All positive cultures were sensitive to Tetracycline's, Aminoglycosides, Chloramphenicol, Streptomycin, Ceftriaxone, Ceftazidime and Ofloxacin.
REGION, HEALTH AND HEALTH CARE: VOL.2. NO.1 MAY, 1997
,r",.t, ' _, ffjr' ;7;i~\'Jl1 .~ ~
• CASES
CJ OEATtiS
u o ~•~
SOURCE: PLAGUE DATA FROM SMC. N CH • C55 - SURAl
Fig ~ ~ DISTRIBUTION OF' PLAGUE CASES
AND DEATHS RECORDED AT NCH ,
SURAT
1 o 1>15 '·5 2-1'5 3·0 Km. I ; . !
Fig: 4 DISTRIBUTION OF PL.~GUE CASES IN SURAT CITY
(t994l
INDEX • Oeoth os per NCH
x Sero + Cases as per NCH
• New Death Cose, defected .in Survey
8Su.pected Cosel
~
~
:E ~ :r::
.§ v.i
o
IIIb.'.'.....
~~2N~~~~~~~~~oSS3~8b~~~=
s 01->'« ::;-c z C'i'
5 > ~ -c u ~ :.J
s:r:: o z ~
B s:r:: ~ @ ~
t
l ...~._~ _SsT t1 i
Plague in Mamla Village and Surat City
25 4
!>USPECTEO PNEUMONIC OR BUBONIC PLAGUE
100400 Km.
N
:ASES AND RELATED DEATHS WAS REPORTED -:: bi AGRICUl'TURAL 'IELO T TO W.H.O. FROM EIGHT STATES INOlA
- ':Jf:NW~.A.A r".~FERAL !1i' I~ ;. ME ,
en : OLD ~" ~ r~AG~ tt t!1~UTSANCg II'%: •
~iitlit en r----- ~ ImlSHEII'ERS I
fiz:1 n"~E.' ~ i=i! TINSHELTERS
~
~~./' z~&! ~z::/ i=!, t=, SW '" en I t
, ~O(,~ ROAD ,TO.......A ./
'l-q-': AGRICULTURAL FIELD to
FiCJ: 2 SCHEMATICPRESEN'rAT10N a: VIL.LAGE MAML.AI'I.J,
OURtE: W.H.Q, REPORT 9 DEC, 1994 SOURCE: TAC I AUGUST I 1915
bisl of VlIIo,es I ICUPPA PHC
2 MORWAD
SiAH!GAYAN
4WADWANI
5 CHINCHOTI
IH.PIMPRI
7 DAVDI
• SALUI8A
9MAMUINDEX' VILLAGES
~ cases on 22-21 Aug.94 CaMS on II -12 Sep. 94
_ Co.e. on 15 -16 Sep.94 ••** Cases on 17 - 18 S,p.94
FiCJ: 3 VILLAGE BOUNDARIES-SEED DISTRICT CENSUS HAND BOOK ~ 1981
Source: DATA-TAC August ,'995
REGION, HEALTH AND HEALTH CARE: VOL.2, NO.1 MAY, 1997
Harshit Sinha
26
EVIDENCE OF PLAGUE
Following the suspected outbreak of bubonic plague without any mortality in Mamla village and absence of secondary (bubonic) plague cases with low mortality (52) in the Surat, there was much controversy about the causative agents. Possibility for Hanltl VII'IU (6), Melodises (7), Plasmodmonas Pseudomalleri (8) etc, were predicted while some experts raised objections about the procedure adopted in collection and pathological testing of the victims.
No human specimens could be obtained from the disease outbreak in Beed district and thus have to rely on the serum of rodent. While in Surat serum of human, rodents and dogs were processed. As per TAC, the work was initiated at Defence Research and Development Establishment (DRDE) Gwalior on the specimens that were processed earlier (by Worlds Health Org8nization & Intemational Plague Investigative Team) or were kept stored in different institutions. It strongly supports the occurrence of bubonic plague in human and of enzootic plague involving recent infection among rodent and dogs with Yersinia pestis.
After establishing growth characteristic, morphology, straining and biochemical reactions, fluorescent antibody testing and specific phage lysis of the isolates were undertaken by experts working in different institutions in India. Further, with the efforts of Government of India (GOI) and three WHO Collaborating Centres for Plague, successes were made in detecting Yersinia pestis as unique and never recorded in the world. Confirming the uniqueness of the protein profile, the Russian Institute, on the basis of additional test, reported that Surat strain was a weak Pathogen. The new strain has been classified under group 'S'(9).
UNANSWERED QUESTIONS ABOUT PLAGUE
As discussed earlier that Beed district has been a known area in the past of sylvatic plague which resulted in an epizootic. However situation in Surat city (Urban) was different from the (rural) Mamla village. Inspite of isolating Y.Pestis from the stored cultures of specimens obtained from Surat, many conditions conducive for epizootic plague still remain unanswered.
The reasons for the origin of the epidemic in the city could not be established as no rat falls were witnessed and the possibility of transmission of the disease was ruled out, as the agricultural land on either side of the Tapi river was found to harbour the field rodent B.bengalensis. However a small circumscribed pocket of feral habitat with scanty population of Tatera indica was found near the bank of Tapi, about 2.5 kID away from the Lakshmi Nagar colony, believed to be indexed case locality during the 1994 September outbreak of plague. From an ecological standpoint, the support system is not believed to be conducive to the initiation of an epizootic of plague in T.indica for a spillover through a 2.5 kms distance into the domestic biotype at the index case locality (Lakshmi Nagar). The absence of proper ecological linkages between diverse habitats conducive for the dynamics of plague transmission is therefore not supportive of bubonic plague in Surat city with its origin inferal habitat (10).
Mode or transmission: An important factor for the prevention and control of the spread of the disease, still remains a riddle because in India, last plague cases occurred in 1967. However a small number ofplague cases were reported in 1983 in a small village of Himachal Pradesh when 17 of the 22 affected persons died. Thereafter bubonic cases were first identified in Beed district of Maharashtra which is in the neighbouring state 300 kIDaway from Surat. Inspite of hundreds of bubonic cases being reported from Beed there has been no pneumonic case or death in that district. As the disease is known to be air borne, the annual Ganapati festival with close intermingling of huge crowds of people beside river Tapi and migration from Maharashtra state could have facilitated the spread. There is no evidence of any secondary bubonic plague cases conducive for the diffusion of this disease were ever detected in Surat (l1).
Till date, seeing the low (Table 4) virulent behaviour, the nature of this epidemic was very much in debate. As discussed earlier, no deaths were reported from Beed district and uneven distribution of the disease
REGION, HEALTH AND HEALTH CARE: YOL.2, NO.1 MAY, 1997
27 ~6
:e Ie
eof
ly rk re :pt tic
:nt tu
ror ng lin
ted .of :pi
vitthe ~al
the :om ~ of !ity aics ,(\0)
ase, sses lfter way e or ling earl. ever
:h in ease
Plaguein Mamla Village and SuratCity
(Fig. 4) virulent behaviour, the nature of this epidemic was very much in debate. As discussed earlier, no deaths were reported from Beed district and uneven distribution of the disease (Fig.4) in the Surat city under similar condition raised many question about the authenticity of this epidemic as "Plague"(12).
The detection of extra band in the 25 KD region during protein profile analysis (done to understand the molecular epidemiology of Y.pestis) gave much speculation in the media that Surat isolates were "genetically engineered". In the USA, (13) the invention of biological integrated detection system (BIDS) for detecting germ in the air and sudden rise in the expenditure for germ defence programme in 1994 (Which was 54% more that the previous year), raised many possibilities, as it is no longer difficult to transport the germ, Since majority of plague cases had only occurred in communal riots (after the demolition of Babri Masjid in 1992) affected areas, the local people feel a revengeful act done by some anti social element (14). However nothing can be said so conclusively without concrete proof.
CRITICAL ISSUES
The Beed district (as discussed earlier) has been a known area in the past for sylvatic plague; But vigilance on communicable diseases is so lax that is allowed plague surveillance unit in Maharashtra to shut down in 1989. An adequate surveillance system depends on many critical factors (15). However in India surveillance system is still in a rudimentary state although several attempts had been made in the past to establish such a system on a national scale. As surveillance and response constitute the foundation of infectious disease control, total eradication of rodent population is impossible. However surveillance of rodent population control remains a more practical option.
CONCLUSION
It is a well-established fact that pneumonic outbreak in Surat city was due to Y.pestis and short term
investigation at Mamla village reveals favourable eco - entomological and serological condition conducive for plague transmission. But several gaps exist on the ecology of plague and natural history of Y. pestis in the region. Seeing the unique pattern as observed by WHO, long term systematic studies on plague ecology are needed. This can help to identify where natural form of plague in sylvatic settings exists, maintaining continuously the dynamic interaction of wild and domestic rodents and fleas. Thus efforts should be made for effective surveillance system to forecast disease outbreak when conditions were conducive for epizootic plague. Besides, in order to prevent the outbreak of plague, it is important to minimise the scope of rodents of different ecological habitat coming in close proximity to one another. Thus rodent population management essentially remains a national problem. It cans for a basic change in the attitude of both the urban and rural people as well as the government which should set up properly manned units to monitor rodent population periodically, specially in the plague prone belts of Andhra Pradesh, Tamil Nadu, Karnataka, Gujarat and Maharashtra.
Acknowledgment: The author is very thankful to Prof. Ghanshyam Shah (Director, Centre for Social Studies [CSS], Surat) for providing an opportunity to assist him in the project titled: Urban Society Interface: A study of Pneumonic Plague in Surat city (sponsored by CASA, The Netherlands). Dr. n.v. Mavlankar (Assist. Prof. Public system Group, India Institute of Management, [11M] Ahmedabad & member of State expert's committee
on Plague) and Dr. R.P. Sinha (Dy. Commissioner of Health, Surat Municipal Corporation, [SMC] for providing necessary information and their valuable suggestions).
REGION, HEALTH AND HEALTH CARE: VOL.2, NO.1 MAY, 1997
Harshit Sinha
28
REFERENCES
I. WHO Chronicale, A system of plague surveillance, Vol 28, 1974, pp. 71-80.
2. WHO International Plague Investigation Team Report, Plague in India, 9 December, 1994, pp. 1-15.
3. Report of the Technical Advisory Committee on Plague, August 1995, Govt. of India.
4. Sinha Harshit, Situation Analysis of New Civil Hospital During Crises Time Mimeograph. Centre for Social Studies, Surat, 1994. pp: I.
5. Report of SMC, Plan ofAction for Rapid Surveillance ofthe Plague. (Unpublished)
6. Dhar, L., Thakur, R., Dhar, V.S., India: is it plague.? The Lancet Vol 344 November 12, 1994, 1359.
7. John T. Jacob, Final thought on India's 1994 Plague outbreaks. The Lancet. Vol 346, September 16, 1995, p.765.
8. Bharadwaj, R., et al, Outbreak of plague-like illness caused by Pseudomonas pseudornallei in Maharashtra, India. The Lancet, Vol 344 December, 1994, p. 1574.
9. Ibid (reference 8).
10. Ibid (reference 4).
11. Mavalankar, D.V., India 'Plague' epidemic: unanswered questions and key lessons, Journal of the Royal Society ofMedicine, Vol. 88, 1995, pp. 547-551.
12. Paneth, Nigel, Plague in India-letter to the Editor, The Lancet, Vol 345, January 28,1995, p. 258.
13. Prasannan, R., Germ dectector and Military microbe The Week, July 23, 1995, pp: 29-37.
14. Shah Ghanshyam, Perception and Response in Public Health-Urban Interface: A Study ofPneumonic Plague in Surat, Centre for Social Studies, Surat, India, 1996, p.1l7.
15. WHO Mimeograph, WHO Consultation on Plague, No. 90.1 11-15 September, 1989, pp. 1-21.
Table 1 Cases and deaths due to plague in India: 26 August to 5th October 1994.
Name of the State Suspected Cases
Sero+ive Cases
Total Deaths
Maharashtra State (Including Bombay) 2793 79 0
Gujarat State (Including Surat) 1391 35 49
Delhi State 749 44 04
Other States 169 09 0
Total of India 5102 167 53
Note: Other States =Andhra Pradesh, Madhya Pradesh, Uttar Pradesh, West Bengal, Rajasthan & Haryana. Source: Plague in India: WHO International Plague Investigative Team Report of 9tb December, 1994.
REGION,HEALTH AND HEALTH CARE:VOL.2, NO.1 MAY, 1997
8 29
5,
ra,
ci-
rue
ma. I.
Plague in Mamla Village and Surat City
Table 2 Frequency of different sign and symptoms amongst patients of Mamla village.
Symptoms & Signs Suspected (%)
Cases n = 35
Highgradefever 9 (25.7%)
Lymphnode enlargement 32 (91.4%)
Axillary 12 (34.3%)
Inguinal 16 (45.7%)
Both 4 (10.4%)
Associated tenderness 15/32 (46.9%)
Source: Report on Tac on Plague, August 1995, p: 48.
, Presumtive (% )
Cases n =23
2 (8.7%)
18 (78.3%)
7 (30.4%)
10 (43.5%)
1(4.3%)
12/18 (66.7%)
Table 3 Final picture of plague epidemic in Surat City. (Compiled as on 15th January, 1995).
Name of the Total Suspected Total Sero+ Total no. of deaths as reported and detected Total Plague Zone cases (%) Cases (%) (3) Cases
(1) (2) SmclNc Css Total (%) (4) H
Central 152 (82) 17 (10) 12 03 15 (08) 184
West 68 (80) 10 (12) 06 01 07 (08) 85
East 64 (77) 17 (20) 02 00 02 (03) 83
North 177 (71) 28 (11) 19 25 44 (18) 249
South 303 (83) 44 (12) 10 07 17 (05) 364
SouthWest 73 (90) 04 (05) 03 01 07 (03) 81
Outside city 190 (90) 14 (07) 04 03 07 (03) 211
Total 1027 (82) 134 (11) 56 40* 96 (07) 1257
Source: As per SMC, NCD and CSS list for plague cases. Note: Figure in brackets are horizontal percentage from column 4. : *_> number of death cases detected during 18 to 23 September 1994.
REGION. HEALTH AND HEALTH CARE: VOL.2. NO.1 MAY, 1997
Harshit Sinha
30
Table 4 Clinical characteristics and clinical signs among pediatrics and adults.
Clinical Characteristics Pediatrics (%) (Age<14) N=207
Adults (%)
(Age> 14) N=757
Fever 185 (89.4%) 610 (80.6%)
Cough 126* (60.9%) 610 (80.6%)
Chest pain 3* (1.5%) 82* (10.8%)
Dyspnea 48 (23.4%) 166 (21.9%)
Hemoptysis 22* (10.6%) 288* (30.1%)
Vomiting 38 (18.4%) 89 (11.8%)
Expistaxis 3 (1.4%) 12 (1.6%)
Hospital death 5 (2.4%) 34 (4.5%)
Cinical Sips N=207 N=757
No findings 140 (68.3%) 522 (69.0%)
Crepitations 65 (31.4%) 216 (28.5%)
Bronchial breathing 9 (4.3%) 20 (2.6%)
Rhonchi 8 (3.8%) 16 (2.1%)
Lymphadenopathy 50* (24.2%) 31* (4.1%)
Suspected bubonic (I & A) 7 (3.3%) 20(3.8%)
Laboratory Findines
Sputum or Throat swab
N=207 N=757
Smear positive 73* (36.9%) 195* (25.8%)
and Culture positive: 25** (12.6%) 37** (5.1%)
FNAC + ive Semer 13 (6.28%) 10 (1.32%)
Serology + ive 30 (30.6%) 116 (24.8%)
PSMP+ ive 34 (16.7%) 74 (13.0%)
HIV + ive 0(00.0%) 7(1.0%)
X-ray + ive 134** (64.73%) 312** (41.21%)
Note: * = P < 0.001; **= P < 0.001. Source: Clinical Aspects ofSuspected Plague, observed during Surat Epidemic of1994, Center for Social Studies, Surat, pp. 4-5
REGION, HEALTH AND HEALTH CARE: VOL.2, NO.1 MAY, 1997