Southern Sudan: an opportunity for NTD control and elimination?
14
Southern Sudan: An opportunity for NTD control and elimination? John Rumunu 1 , Simon Brooker 2,3 , Adrian Hopkins 4 , Paul Emerson 5 , Fasil Chane 6,7 , and Jan Kolaczinski 2,8,* 1 Ministry of Health, Government of Southern Sudan 2 Department of Infectious & Tropical Diseases, London School of Hygiene & Tropical Medicine, London, United Kingdom. 3 Malaria Public Health and Epidemiology Group, KEMRI/Wellcome Trust Collaborative Programme, Nairobi, Kenya 4 Mectizan Donation Program, Decatur, Georgia, USA 5 The Carter Center, Atlanta, Georgia, USA 6 Christoffel Blindenmission (CBM), Southern Sudan 7 Southern Sudan Onchocerciasis Task Force, Rumbek, Southern Sudan 8 Malaria Consortium Africa, Kampala, Uganda Abstract Southern Sudan has been ravaged by decades of conflict and is thought to have one of the highest burdens of neglected tropical diseases (NTDs) in the world. Health care delivery, including efforts to control or eliminate NTDs, is severely hampered by a lack of infrastructure and health systems. However, the post-conflict environment and Southern Sudan's emerging health sector provide the unprecedented opportunity to build new, innovative programmes targeting NTDs. This article describes the current status of NTDs and their control in Southern Sudan and outlines the opportunities for the development of evidence-based, innovative implementation of NTD control. Keywords neglected tropical diseases; control; elimination; post-conflict; Southern Sudan An opportunity for coordinated control Neglected tropical diseases (NTDs) are a range of diseases that occur in conditions of poverty and frequently overlap in endemic countries [http://www.who.int/ neglected_diseases/en]. Funding for their control and elimination has recently seen a dramatic expansion, with an emphasis on co-administration of preventive chemotherapy (PCT) [1]. However, operational experience in delivering PCT packages has, to date, been from countries with relatively well-established health systems [e.g. 2-5]. Little is known about implementation in post-emergency settings, where delivery structures are less developed or absent. One such setting is Southern Sudan which, until recently, was plagued by a series of conflicts since independence in 1956 [6]. The cessation of conflict coupled with the commitment of the Ministry of Health (MoH) of the Government of Southern Sudan (GoSS) has yielded new opportunities and funding for NTD control, notably support from the US Agency for International Development to develop an integrated NTD control programme. There exists therefore a unique opportunity to develop an integrated programme from scratch, and to generate crucial evidence on cost and cost-effectiveness in the process. * Corresponding author: Malaria Consortium Africa, Plot 2A, Sturrock Road, Kololo, Kampala, Uganda, PO Box 8045; [email protected], Phone: (256-0312) 300430, Fax: (256-0312) 300425. Europe PMC Funders Group Author Manuscript Trends Parasitol. Author manuscript; available in PMC 2009 August 19. Published in final edited form as: Trends Parasitol. 2009 July ; 25(7): 301–307. doi:10.1016/j.pt.2009.03.011. Europe PMC Funders Author Manuscripts Europe PMC Funders Author Manuscripts
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Southern Sudan: an opportunity for NTD control and elimination?

Southern Sudan: An opportunity for NTD control andelimination?
John Rumunu1, Simon Brooker2,3, Adrian Hopkins4, Paul Emerson5, Fasil Chane6,7, andJan Kolaczinski2,8,*
1 Ministry of Health, Government of Southern Sudan 2 Department of Infectious & TropicalDiseases, London School of Hygiene & Tropical Medicine, London, United Kingdom. 3 MalariaPublic Health and Epidemiology Group, KEMRI/Wellcome Trust Collaborative Programme,Nairobi, Kenya 4 Mectizan Donation Program, Decatur, Georgia, USA 5 The Carter Center,Atlanta, Georgia, USA 6 Christoffel Blindenmission (CBM), Southern Sudan 7 Southern SudanOnchocerciasis Task Force, Rumbek, Southern Sudan 8 Malaria Consortium Africa, Kampala,Uganda
AbstractSouthern Sudan has been ravaged by decades of conflict and is thought to have one of the highestburdens of neglected tropical diseases (NTDs) in the world. Health care delivery, including effortsto control or eliminate NTDs, is severely hampered by a lack of infrastructure and health systems.However, the post-conflict environment and Southern Sudan's emerging health sector provide theunprecedented opportunity to build new, innovative programmes targeting NTDs. This articledescribes the current status of NTDs and their control in Southern Sudan and outlines theopportunities for the development of evidence-based, innovative implementation of NTD control.
Keywordsneglected tropical diseases; control; elimination; post-conflict; Southern Sudan
An opportunity for coordinated controlNeglected tropical diseases (NTDs) are a range of diseases that occur in conditions ofpoverty and frequently overlap in endemic countries [http://www.who.int/neglected_diseases/en]. Funding for their control and elimination has recently seen adramatic expansion, with an emphasis on co-administration of preventive chemotherapy(PCT) [1]. However, operational experience in delivering PCT packages has, to date, beenfrom countries with relatively well-established health systems [e.g. 2-5]. Little is knownabout implementation in post-emergency settings, where delivery structures are lessdeveloped or absent. One such setting is Southern Sudan which, until recently, was plaguedby a series of conflicts since independence in 1956 [6]. The cessation of conflict coupledwith the commitment of the Ministry of Health (MoH) of the Government of SouthernSudan (GoSS) has yielded new opportunities and funding for NTD control, notably supportfrom the US Agency for International Development to develop an integrated NTD controlprogramme. There exists therefore a unique opportunity to develop an integrated programmefrom scratch, and to generate crucial evidence on cost and cost-effectiveness in the process.
* Corresponding author: Malaria Consortium Africa, Plot 2A, Sturrock Road, Kololo, Kampala, Uganda, PO Box 8045;[email protected], Phone: (256-0312) 300430, Fax: (256-0312) 300425.
Europe PMC Funders GroupAuthor ManuscriptTrends Parasitol. Author manuscript; available in PMC 2009 August 19.
Published in final edited form as:Trends Parasitol. 2009 July ; 25(7): 301–307. doi:10.1016/j.pt.2009.03.011.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

Post-conflict progress and challengesSouthern Sudan and the Khartoum Government signed on 9 January 2005 theComprehensive Peace Agreement, ending decades of civil war. Health systems are nowbeing rebuilt, providing opportunities and funding to integrate the control of multiple NTDs.However, the country's recent history, as well as its sheer size, also pose several challenges[7]. Southern Sudan covers an area of 231,177 square miles (Figure 1) but has an estimatedpopulation of 11 million at the most, which equates to 47 people per square mile. Migrantpopulations and the return of refugees and internally displaced persons result in constantlyfluctuating population figures. In 2004, 98% of the population lived in rural areas [Factsabout South Sudan (http://www.codecan.org/media/PLS-%20Facts%20about%20South%20Sudan%202008.pdf)]. Physical, health and education infrastructure is largely absent andmany areas are only accessible by plane, boat, four-wheel drive, or foot, especially duringthe rainy season. The proportion of the population with access to a health facility has beenestimated below 25% [7,8], while in 2002 just over 20% of school-age children wereenrolled in schools [Towards a baseline: Best estimates of social indicators for SouthernSudan (http://www.unicef.org/media/media_21825.html)].
Notwithstanding such challenges, the ongoing transition towards development and itsassociated lack of entrenched government structures and processes provide greatopportunities to improve public health, including NTD control. For such improvements totake place, it is essential to build up a credible evidence-base to understand theepidemiology of infection and disease, and develop, as well as appropriately implement,intervention strategies.
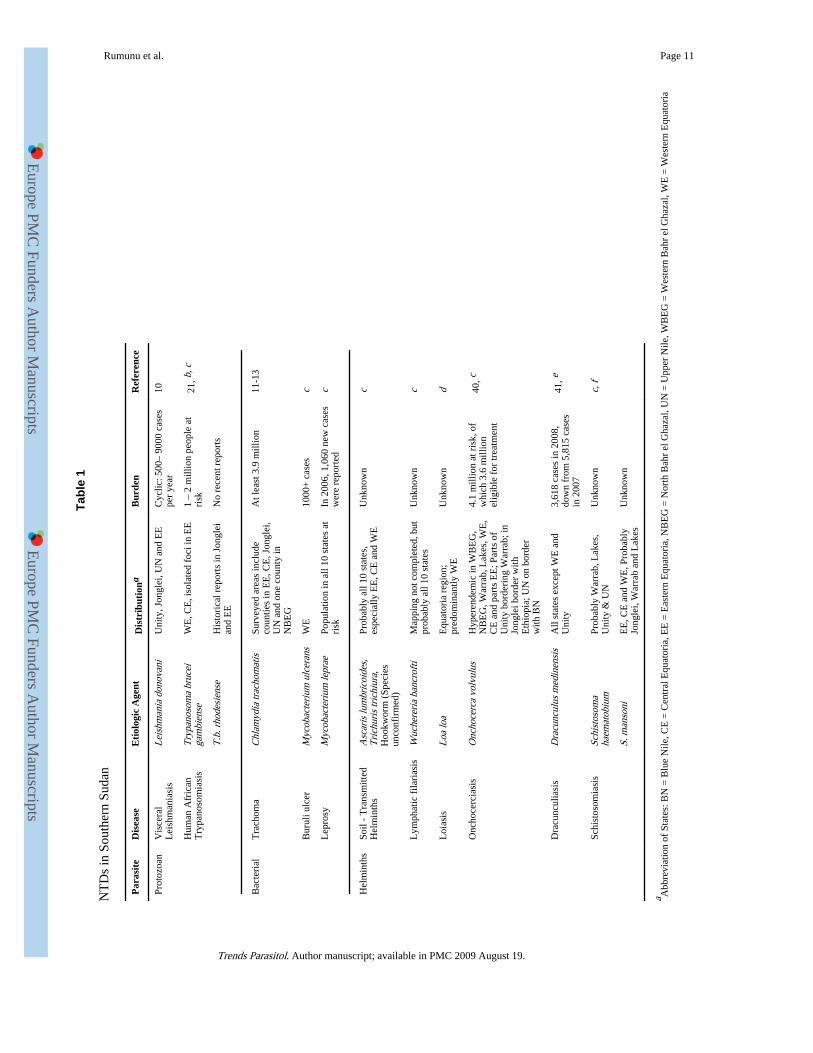
Neglected tropical diseases in Southern SudanTwelve NTDs are endemic to Southern Sudan (Table 1) [Neglected Tropical Disease inSouthern Sudan (http://www.malariaconsortium.org/data/files/pages/ntds_southern_sudan.pdf)]. However, as in all post-conflict settings, reliable diseasesurveillance data are sparse. Estimates of incidence or prevalence are based either on passivecase-detection [9,10] or localized surveys undertaken in areas where specific NTDs areknown or suspected to occur [11-14]. Although comprehensive empirical data are few, thosethat do exist indicate that lymphatic filariasis (LF), schistosomiasis, soil-transmittedhelminth (STH) and trachoma are endemic over large areas, whereas visceral leishmaniasis(VL), human African trypanosomiasis (HAT), Buruli ulcer and leprosy occur more focally.To date, comprehensive epidemiological mapping has been undertaken for onlyonchocerciasis, loiasis and Guinea worm. Determining the prevalence and distribution of theother NTDs remains an important operational necessity, because NTD transmission isheterogeneous and scarce resources for control need to be geographically targeted [15].
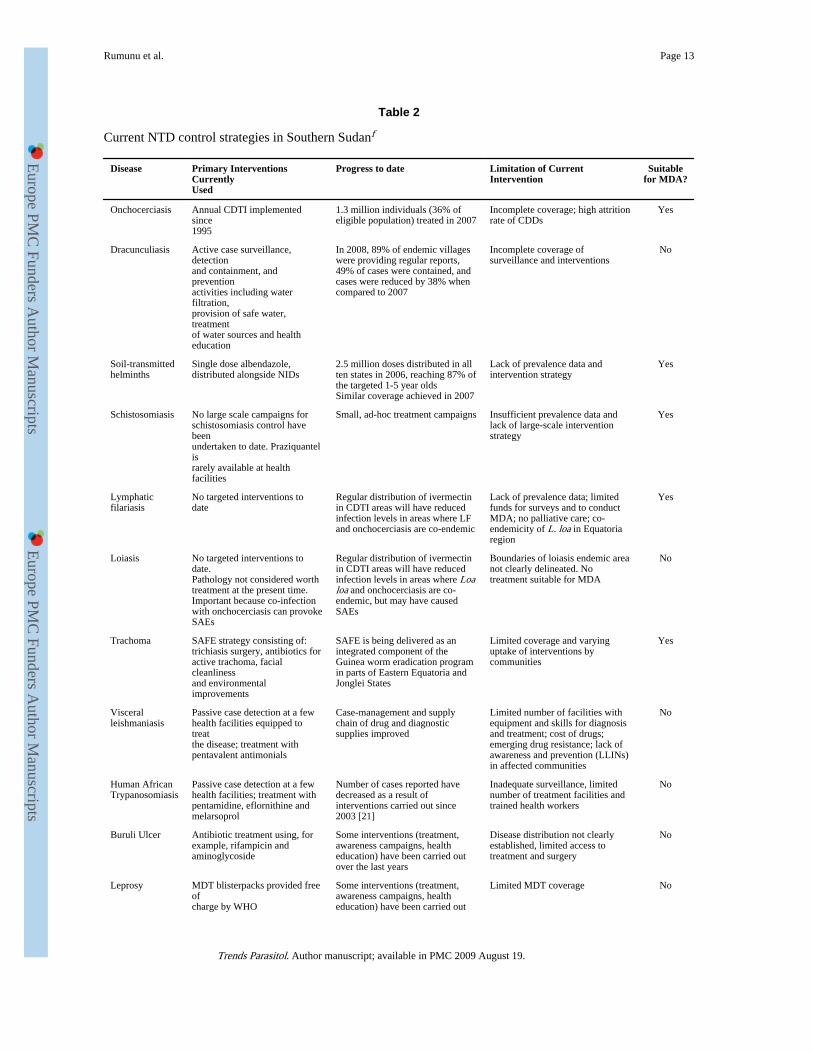
Current NTD control strategiesDespite decades of civil unrest, progress has been made with the control of some NTDs(Table 2). These efforts can be broadly categorised as: (i) large-scale programmes targetingat least 10% of the population (onchocerciasis and Guinea worm; see Figure 1); (ii) smaller,ad-hoc public health campaigns (STH and trachoma); and (iii) treatment provided, tovarying degrees, by health facilities on an in-patient basis (VL, HAT) and through outreach(Buruli ulcer, leprosy). Since the populations at risk are not precisely known, it is generallynot possible to reliably estimate coverage rates or their change over recent years.
Implementation of both onchocerciasis and Guinea worm control is through community-based structures, utilizing volunteers for community-directed treatment with ivermectin(CDTI) and for distribution of water filters and surveillance, respectively. Trachoma control
Rumunu et al. Page 2
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
is currently integrated with the Guinea worm eradication program in Eastern Equatoria andJonglei States, and consists of the SAFE strategy with its four components of eyelid surgery(S), antibiotics to treat the community pool of infection (A), facial cleanliness (F), andenvironmental changes (E). To date, deworming against STH has been carried out duringnational immunization days and schistosomiasis treatment is being provided by some healthfacilities.
Treatments for VL, HAT, leprosy and Buruli ulcer are considered too toxic, lengthy ordifficult to be delivered through community-based mechanisms, and are only available athealth facilities or through outreach, if at all. Historically, treatment services for VL andHAT were provided by non-governmental organizations during epidemics (see, for example,Ref [16]), allowing temporary expansion of service coverage [17,18]. Activities werescaled-back shortly after the disease was considered to be under control, leaving opportunityfor disease resurgence [19-21]. Current access to and quality of treatment to VL and HAT,as well as leprosy and Buruli ulcer, remains inadequate [10].
Building on existing MDA structuresOngoing post-conflict reconstruction provides a number of key opportunities to improve oncurrent NTD control, which are outlined below and in Box 1. An immediate opportunity forexpanding NTD control is through integration of PCT delivery into the CDTI onchocerciasisnetwork. Delivery of albendazole can readily be added to annual ivermectin distribution inareas where onchocerciasis and LF are co-endemic, with the collateral benefit of controllingSTH, scabies and lice [22]. Southern Sudan will start co-administration of ivermectin andalbendazole through CDTI structures in 2009.
In some Guinea worm endemic areas, health education and distribution of antibiotics fortrachoma control have been integrated into the community-based Guinea worm activities.Anecdotal reports suggest that this has been popular with the communities. Once thetransmission of Guinea worm has been interrupted and the network needs to be maintainedfor surveillance, Southern Sudan will have the opportunity to expand the existingintegration, both geographically and in scope.
Together the CDTI and Guinea worm network provide about 80% geographic coverage(Figure 1). This means that other mechanisms are required to deliver PCT to parts of thecountry where neither onchocerciasis nor Guinea worm are endemic, as well as withinadministrative units where distribution of these two diseases is focal and where the existingnetworks do not reach all individuals eligible for other treatments. This is particularlyrelevant for elimination of LF, a disease that tends to be endemic over large areas [23]. Co-administration through the expanded programme on immunization provides one alternativedelivery structure, as it was successfully used in 2006 and 2007 for mass de-worming withalbendazole. Another option may be de-worming for schistosomiasis and STH throughschools; an approach that is already well established elsewhere in the region [24-26].However, distribution through schools, as well as modification of the curriculum to improveknowledge, attitudes and practices related to NTD control, will only become viable oncerebuilding of infrastructure has progressed and school attendance has substantiallyincreased. Meanwhile, ongoing campaigns for distribution of long-lasting insecticidal nets(LLINs) present an interim opportunity for PCT distribution until LLIN coverage has beenscaled-up [3].
In the medium-term, Southern Sudan will have the opportunity to develop an innovativeplatform for community directed delivery of PCT and other interventions (e.g. LLINs andvitamin A supplementation). Building on a recent TDR study [Community DirectedInterventions for major health problems in Africa (http://www.who.int/tdr/svc/publications/
Rumunu et al. Page 3
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

tdr-research-publications/community-directed-interventions-health-problems)], astandardized delivery platform could be developed. A common set of interventions could beidentified that address Southern Sudan's needs and are suitable for integration, and donorswould then be asked to invest into the platform, instead of supporting specific diseases. Thedelivery platform could be part of a health facility – community linkage, and pre-servicetraining of the country's new nurses and doctors could emphasize supervision andmanagement of the platform as a central part of their job. To inform the development ofsuch platform, more in-country experience with integration will be needed.
For VL, HAT, leprosy and Buruli ulcer, where confirmative diagnosis is required beforeinfected individuals receive treatment [27-30], the existence of community-based MDAstructures cannot be harnessed to provide mass treatment, but presents an opportunity toimprove treatment outcomes and to reduce transmission through prevention. CDDs can betrained to provide health education, case identification, early referral and community follow-up.
Integration into multi-functional health care deliveryFor those NTDs not suitable for MDA, both diagnosis and treatment are only available at afew facilities, often many hours if not days away from endemic communities. As a result,infected individuals generally present late or not at all, resulting in high morbidity andmortality [e.g. 31]. With Southern Sudan having the highest caseload of VL in Africa [32]and being among the top three endemic countries for HAT [21] there is an obvious andurgent need for improvement. As mentioned above, such improvement should involve theaffected communities where feasible, but also requires better and more accessible case-management. Ongoing upgrading of facility-based health care undertaken by the MoH-GoSS and partners provides an important opportunity to ensure that the skills and supplies toprovide routine NTD diagnosis and treatment are put in place, and that a link between thefacilities and the communities is being established. Initial steps to do so have been taken bythe MoH-GoSS with considerable support from WHO and other agencies. The requireddrugs and other supplies have been included in the essential drug kit list and training ofnational staff, including those operating at the periphery, on diagnostic and treatmentprocedures is ongoing.
New policies and strategiesUntil 2005, communicable diseases in Southern Sudan were either managed using strategiesdeveloped by the Khartoum Government or according to the protocols of individual aidagencies. Since then, the MoH-GoSS has put in place a number of new or revised strategieswith the aims of: i) standardizing diagnosis, treatment and prevention among implementingpartners operating in the South, and ii) providing a framework for the MoH-GoSS and otherdevelopment partners to allocate funding. The most recently addition specifically addressesintegrated NTD control [Integrated Control of Neglected Tropical Diseases (http://www.malariaconsortium.org/data/files/ntd_ss_strategic_plan_june_2008_final.doc).
Revision or development of new strategies continues to provide opportunities to include newevidence and to identify specific areas requiring further in-country research (see below).Due to the absence of large government bureaucracies such strategic planning processes canbe undertaken relatively quickly and with extensive consultation. This dynamic environmentalso allows for specific implementation needs, such as a strong government commitment tocommunity-based delivery, to be readily incorporated into emerging health policies.
More generally, improvements in environmental hygiene are the ultimate answer to thecontrol and elimination of many NTDs, but for Southern Sudan as for many low-income
Rumunu et al. Page 4
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

countries these are expensive and represent long-term objectives. Multiple agencies areworking with the GoSS to strengthen water, hygiene and sanitation infrastructure, andefforts should be made to ensure integration between NTD control and governmentdepartments coordinating the provision of water and sanitation. Here there is opportunity forcross-sectoral collaboration and influencing strategies and policies, for example to formulatestandardised, rather than disease-specific, education on water and sanitation and to target theconstruction of new boreholes and latrines to areas with high population densities and a highrisk of specific NTDs.
Strengthening the evidence-baseIntegrated NTD control has now been initiated in at least ten African countries, although todate, there are few empirical data on the health benefits and cost savings of an integratedapproach over and above single-disease control programmes [4,33,34]. There thus remainsan urgent need to strengthen the evidence-base for integrated control. Southern Sudanprovides particular opportunities to do so, because all of the targeted NTDs are endemic andmost of them have not been mapped. This means that extensive epidemiological surveys areneeded. With the aim of saving time and money, the feasibility of an integrated survey toolcovering a range of NTDs is being investigated. Integrated surveys will need to overcome anumber of important difference in epidemiologies and survey methodologies of NTDs[15,35], and thus generate useful information to guide similar undertakings elsewhere.
It is also apparent that the commonly quoted annual MDA cost of US$ 0.4 – 0.5 per person[36,37] are not applicable in Southern Sudan. Actual cost data is thus being collected andwill be used to generate evidence on cost and cost-effectiveness of this approach. Themethodology and costing templates used will be available for similar data collectionelsewhere, providing an opportunity to generate figures that can be readily comparedbetween countries.
Lastly, the planned expansion of co-administration of PCT through community-basedstructures and campaigns will require exploration of new and innovative deliveryapproaches, to ensure that full coverage (both geographically and of the eligible population)is achieved and can be retained. Amongst others, this will provide opportunities tocontribute to the evidence-base on recruitment, training, supervision and retention ofcommunity drug distributors (CDDs), and on factors associated with coverage. At present,the Southern Sudan Onchocerciasis Task Force already faces the challenge that about 30%of CDDs discontinue their involvement in CDTI every year, resulting in considerable costsfor recruitment and training of new volunteers. Useful insight on improving CDD retentionhas been gained from other countries with well-established onchocerciasis controlprogrammes [e.g. 42], as has been on factors associated with coverage [e.g. 43]. However,there is as yet limited evidence on how best to address these issues once a package of drugsor other interventions is delivered through community-based mechanisms, though TDR andothers have recently started to fill this knowledge gap [44, Community DirectedInterventions for major health problems in Africa (http://www.who.int/tdr/svc/publications/tdr-research-publications/community-directed-interventions-health-problems)].
Concluding remarksInformation on the distribution and burden of NTDs in Southern Sudan is limited, butexisting data consistently indicate that this is a country with a high burden and great need. Initself, this is not unlike many other developing countries. What sets Southern Sudan apart isthat most NTDs are endemic, that most of them have benefited from little control and thatinfrastructure and systems are practically absent. Though this presents great challenges, italso offers great potential to increase treatment coverage for co-endemic NTDs, integrate
Rumunu et al. Page 5
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

more complex case-management into facility-based health care delivery and strengthen thelink between communities and health facilities. This unprecedented opportunity to buildevidence-based systems for NTD control or elimination needs to be maximised now whilerebuilding of the health sector is ongoing.
Box 1
Key opportunities and outstanding key questions for Southern Sudan
Opportunities1. To build on existing solid structures for MDA delivery developed during the
war, and expand their scope and geographical coverage at a unique time ofhealth sector rebuilding. In the medium term, a common delivery platform forPCT and other interventions (e.g. LLINs, vitamin A supplementation) couldbe developed as part of a health facility – community linkage.
2. To address the control of NTDs not suitable for MDA through appropriateintegration into multi-functional health care delivery at facility level, andthrough strengthening of the link between communities and health facilities.
3. To ensure that new policies and strategies incorporate MDA of PCT andother NTDs treatment and prevention as part of Primary Health Care.
4. To generate essential evidence that may allow better coordination/integrationof mapping and MDA activities, thus reducing time and costs associated withoperating in very difficult terrain, as well as contributing to the internationalunderstanding of the cost and cost-effectiveness of NTD control/elimination.
Questions1. Which NTDs are endemic where? Both MDA and health facility based NTD
interventions need to be targeted based on disease prevalence. For the majorityof NTDs this information is not available in sufficient detail.
2. How best to integrate the various criteria for NTD mapping? Trachoma, inparticular, requires costly and detailed epidemiological surveys beforeazithromycin donation can be requested. There is an urgent need to developsimplified mapping procedures for trachoma and to establish how best tointegrate survey procedures for LF, schistosomiasis, and STH, as well astrachoma.
3. What is the actual cost of conducting MDA of PCT? Few cost data fordelivery of integrated MDA are currently available. A cost analysis, followingguidelines for economic evaluation of health care programmes, will be requiredto allow appropriate budgeting and to be used in the cost-effectivenessevaluation of integrated MDA.
4. What is/are the vector(s) of lymphatic filariasis and what is the vectorialcapacity? It is assumed that Anopheles gambiae and A. funestus mosquitoes areresponsible for LF transmission in Southern Sudan, based on data fromneighboring Uganda [38]. Whether this is the case and what the competence ofthe vector(s) is should be determined, as it is an important determinant of thenumber of MDAs required and hence of the overall cost of LF elimination [39].
5. How to monitor and evaluate the integrated NTD programme? Standardizedtool for monitoring and evaluation are need that address issues such as: i) Howbest to collect data, particularly once prevalence decreases, ii) Which datacollection methods can be integrated, and iii) How frequently data need to be
Rumunu et al. Page 6
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

collected, particularly in areas where communications are poorly developed andwhere population access is intermittent and expensive.
AcknowledgmentsWe wish to thank all the individuals and organizations that have contributed to the control of NTDs in SouthernSudan over the last decades. Without their dedication, many lives would have been lost and many people would nothave been cured from disabilities.
The information presented in this publication was collated for a comprehensive situation analysis on NTDs recentlypublished by the Ministry of Health, Government of Southern Sudan (http://www.malariaconsortium.org/data/files/pages/ntds_southern_sudan.pdf). Major contributions to the analysis were made by Jose Ruiz, Michaleen Richer,Samson Baba, Lasu Hickson, Karinya Lewis, Steven Becknell and Samuel Makoy. Development of the situationanalysis was led by Malaria Consortium [http://www.malariaconsortium.org] and funded by COMDIS, a ResearchProgramme Consortium coordinated by the Nuffield Centre for International Health and Development, Universityof Leeds, with funds from the Department for International Development, UK. COMDIS also funded MalariaConsortium to lead writing of this publication. Simon Brooker is supported by a Wellcome Trust CareerDevelopment Fellowship (081673). Current scale-up of integrated NTD control in Southern Sudan is funded by theUS Agency for International Development, through RTI International.
References1. Lawrence D. Bush's plan for tackling parasitic diseases set out. Lancet Infect. Dis. 2008; 8:743.
2. Hopkins DR, et al. Lymphatic filariasis elimination and schistosomiasis control in combination withonchocerciasis control in Nigeria. Am. J. Trop. Med. Hyg. 2002; 67:266–272. [PubMed: 12408665]
3. Blackburn BG, et al. Successful integration of insecticide-treated bed net distribution with massdrug administration in central Nigeria. Am. J. Trop. Med. Hyg. 2006; 75:650–655. [PubMed:17038688]
4. Kolaczinski JH, et al. Neglected tropical diseases in Uganda: the prospect and challenge ofintegrated control. Trends Parasitol. 2007; 23:485–493. [PubMed: 17826335]
5. Mohammed KA, et al. Triple co-administration of ivermectin, albendazole and praziquantel inZanzibar: A safety study. PLoS Negl. Trop. Dis. 2008; 2:e171. [PubMed: 18235853]
6. Stephen, MJ.; de Waal, A. Can Sudan Escape its Intractability?. In: Crocker; Chester, A.; Hampson,Fen Osler; Aall, Pamel, editors. Grasping the Nettle: Analyzing Cases of Intractable Conflict.United States Institute of Peace; Washington, D.C.: 2005. p. 161-182.
7. Wakabi W. Peace has come to southern Sudan, but challenges remain. Lancet. 2006; 368:829–830.[PubMed: 16958158]
8. Moszynski P. Lack of trained personnel thwarts Sudan's plans to rebuild health services. BMJ. 2008;337:a2954. [PubMed: 19074225]
9. Collin SM, et al. Conflict and kala-azar: Determinants of adverse outcomes of kala-azar amongpatients in Southern Sudan. Clin. Infect. Dis. 2004; 38:612–619. [PubMed: 14986243]
10. Kolaczinski JH, et al. Kala-azar epidemiology and control, Southern Sudan. Emerg. Infect. Dis.2008; 14:664–666. [PubMed: 18394290]
11. Ngondi J, et al. The epidemiology of trachoma in Eastern Equatoria and Upper Nile States,Southern Sudan. Bull. WHO. 2005; 83:904–912. [PubMed: 16462982]
12. Ngondi J, et al. Prevalence and cause of blindness and low vision in Southern Sudan. PLoS Med.2006; 3:e477. [PubMed: 17177596]
13. King JD, et al. The burden of trachoma in Ayod county of Southern Sudan. PLoS Negl. Trop. Dis.2008; 2:e299. [PubMed: 18820746]
14. Deganello R, et al. Schistosoma haematobium and S. mansoni among children, Southern Sudan.Emerg. Infect. Dis. 2007; 13:1504–1506. [PubMed: 18257996]
15. Brooker S, et al. Rapid mapping of schistosomiasis and other neglected tropical diseases in thecontext of integrated control programmes in Africa. Parasitology. 2009 in press.
16. Seaman J, et al. The epidemic of visceral leishmaniasis in Western Upper Nile, Southern Sudan:course and impact from 1984-1994. Int. J. Epidemiol. 1996; 25:862–871. [PubMed: 8921468]
Rumunu et al. Page 7
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

17. Ritmeijer K, Davidson R. Royal Society of Tropical Medicine and Hygiene Joint Meeting withMédecins Sans Frontières at Manson House, London, 20 March 2003. Field research inhumanitarian medical programmes. Médecins Sans Frontières interventions against kala-azar inthe Sudan, 1989-2003. Trans. R. Soc. Trop. Med. Hyg. 2003; 97:609–613. [PubMed: 16134257]
18. Balasegaram M, et al. Examples of tropical disease control in the humanitarian medicalprogrammes of MSF and Merlin. Trans. R. Soc. Trop. Med. Hyg. 2006; 100:327–334. [PubMed:16289631]
19. Moore A, et al. Resurgence of sleeping sickness in Tambura county, Sudan. Am. J. Trop. Med.Hyg. 1999; 61:315–318. [PubMed: 10463686]
20. Moore A, Richer M. Re-emergence of epidemic sleeping sickness in Southern Sudan. Trop. Med.Int. Health. 2001; 6:342–347. [PubMed: 11348529]
21. Simarro PP, et al. Eliminating human African trypanosomiasis: where do we stand and what comesnext? PLoS Negl. Trop. Dis. 2008; 5:e55.
22. Ottesen EA, et al. The Global Programme to Eliminate Lymphatic Filariasis: Health impact after 8years. PLoS Negl. Trop. Dis. 2008; 2:e317. [PubMed: 18841205]
23. Gyapong JO, Remme JH. The use of grid sampling methodology for rapid assessment of thedistribution of bancroftian filariasis. Trans. R. Soc. Trop. Med. Hyg. 2001; 95:681–686. [PubMed:11816445]
24. Guyatt HL, et al. Evaluation of efficacy of school-based anthelmintic treatments against anaemia inchildren in the United Republic of Tanzania. Bull. WHO. 2001; 79:695–703. [PubMed: 11545325]
25. Kabatereine NB, et al. Impact of a national helminth control programme on infection andmorbidity in Ugandan schoolchildren. Bull. WHO. 2007; 85:91–99. [PubMed: 17308729]
26. Brooker S, et al. Cost and cost-effectiveness of nationwide school-based helminth control inUganda: intra-country variation and effects of scaling-up. Health Policy Plan. 2008; 23:24–35.[PubMed: 18024966]
27. Walker SL, Lockwood DNJ. Leprosy. Clin. Dermatol. 2007; 25:165–172. [PubMed: 17350495]
28. Chappuis F, et al. Visceral leishmaniasis: what are the needs for diagnosis, treatment and control?Nat. Rev. Microbiol. 2007; 5:873–882. [PubMed: 17938629]
29. Fèvre EM, et al. Human African trypanosomiasis: Epidemiology and control. Adv. Parasitol. 2006;61:167–221. [PubMed: 16735165]
30. Wansbrough-Jones M, Phillips R. Buruli ulcer: emerging from obscurity. Lancet. 2006; 367:1849–1858. [PubMed: 16753488]
31. Collin SM, et al. Unseen Kala-Azar Deaths in Southern Sudan (1999-2002). Trop. Med. Int.Health. 2006; 2:509–512. [PubMed: 16553934]
32. Reithinger R, et al. Visceral leishmaniasis in eastern Africa - current status. Trans. R. Soc. Trop.Med. Hyg. 2007; 101:1169–1170. [PubMed: 17632193]
33. Brady P, et al. Projected benefits from integrating NTD programs in sub-Saharan Africa. TrendsParasitol. 2006; 22:285–291. [PubMed: 16730230]
34. Lammie PJ. A blueprint for success: integration of neglected tropical disease control programmes.Trends Parasitol. 2006; 22:313–321. [PubMed: 16713738]
35. Brooker S, Utzinger J. Integrated disease mapping in a polyparasitic world. Geospatial Health.2007; 2:141–146. [PubMed: 18686239]
36. Fenwick A, et al. Achieving the millennium development goals. Lancet. 2005; 365:1029–1030.[PubMed: 15781095]
37. Champagna A, et al. Neglected Tropical Diseases: Challenges, progress, and hope. Minn. Med.2008; 91:42–44.
38. Onapa A, et al. Lymphatic filariasis in Uganda: Baseline investigation in Lira, Soroti and Katakwidistricts. Trans. R. Soc. Trop. Med. Hyg. 2001; 95:161–167. [PubMed: 11355548]
39. Kyelem D, et al. Determinants of success in national programs to eliminate lymphatic filariasis: Aperspective identifying essential elements and research needs. Am. J. Trop. Med. Hyg. 2008;79:480–484. [PubMed: 18840733]
40. Mukhtar MM, et al. The burden of Onchocerca volvulus in Sudan. Ann. Trop. Med. Parasitol.1998; 92(Suppl. 1):S129–S131. [PubMed: 9861278]
Rumunu et al. Page 8
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

41. Hopkins DR, et al. Dracunculiasis eradication: neglected no longer. Am. J. Trop. Med. Hyg. 2008;79:474–479. [PubMed: 18840732]
42. Katabarwa, et al. In rural Ugandan communities the traditional kinship/clan system is vital to thesuccess and sustainment of the African Programme for Onchocerciasis Control. Ann. Trop. Med.Parasitol. 2000; 94:485–495. [PubMed: 10983561]
43. Brieger, et al. Factors associated with coverage in community-directed treatment with ivermectinfor onchocerciasis control in Oyo State, Nigeria. Trop. Med. Int. Health. 2002; 7:11–18. [PubMed:11851950]
44. Ndyomugyenyi R, Kabatereine N. Integrated community-directed treatment for the control ofonchocerciasis, schistosomiasis and intestinal helminths infections in Uganda: advantages anddisadvantages. Trop. Med. Int. Health. 2003; 8:997–1004. [PubMed: 14629766]
Rumunu et al. Page 9
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts

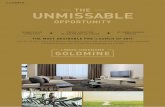
Figure 1.Maps showing (a) the location of Southern Sudan in Africa, its ten states and major towns,highlighting its large size and low population density, (b) areas of Southern Sudan withstructures for onchocerciasis control, either in the form of community-drug distributors (red,hatched) or supervision centres for community-directed treatment with ivermectin (red, nothatched), (c) areas covered by the community-based network for Guinea worm eradication,and (d) trachoma-endemic areas already targeted with the SAFE strategy through the Guineaworm network. Both community-based structures shown in (b) and (c) are suitable foradditional mass drug administration (MDA) of preventive chemotherapy (PCT).
Rumunu et al. Page 10
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
Rumunu et al. Page 11
Tabl
e 1
NT
Ds
in S
outh
ern
Suda
n
Par
asit
eD
isea
seE
tiol
ogic
Age
ntD
istr
ibut
iona
Bur
den
Ref
eren
ce
Prot
ozoa
nV
isce
ral
Lei
shm
ania
sis
Lei
shm
ania
don
ovan
iU
nity
, Jon
glei
, UN
and
EE
Cyc
lic: 5
00–
9000
cas
espe
r ye
ar10
Hum
an A
fric
anT
rypa
noso
mia
sis
Try
pano
som
a br
ucei
gam
bien
seW
E, C
E, i
sola
ted
foci
in E
E1
– 2
mill
ion
peop
le a
tri
sk21
, b, c
T.b
. rho
desi
ense
His
tori
cal r
epor
ts in
Jon
glei
and
EE
No
rece
nt r
epor
ts
Bac
teri
alT
rach
oma
Chl
amyd
ia tr
acho
mat
isSu
rvey
ed a
reas
incl
ude
coun
ties
in E
E, C
E, J
ongl
ei,
UN
and
one
cou
nty
inN
BE
G
At l
east
3.9
mill
ion
11-1
3
Bur
uli u
lcer
Myc
obac
teri
um u
lcer
ans
WE
1000
+ c
ases
c
Lep
rosy
Myc
obac
teri
um le
prae
Popu
latio
n in
all
10 s
tate
s at
risk
In 2
006,
1,0
60 n
ew c
ases
wer
e re
port
edc
Hel
min
ths
Soil
- T
rans
mitt
edH
elm
inth
sA
scar
is lu
mbr
icoi
des,
Tri
chur
is tr
ichi
ura,
Hoo
kwor
m (
Spec
ies
unco
nfir
med
)
Prob
ably
all
10 s
tate
s,es
peci
ally
EE
, CE
and
WE
Unk
now
nc
Lym
phat
ic f
ilari
asis
Wuc
here
ria
banc
roft
iM
appi
ng n
ot c
ompl
eted
, but
prob
ably
all
10 s
tate
sU
nkno
wn
c
Loi
asis
Loa
loa
Equ
ator
ia r
egio
n;pr
edom
inan
tly W
EU
nkno
wn
d
Onc
hoce
rcia
sis
Onc
hoce
rca
volv
ulus
Hyp
eren
dem
ic in
WB
EG
,N
BE
G, W
arra
b, L
akes
, WE
,C
E a
nd p
arts
EE
; Par
ts o
fU
nity
bor
deri
ng W
arra
b; in
Jong
lei b
orde
r w
ithE
thio
pia;
UN
on
bord
erw
ith B
N
4.1
mill
ion
at r
isk,
of
whi
ch 3
.6 m
illio
nel
igib
le f
or tr
eatm
ent
40, c
Dra
cunc
ulia
sis
Dra
cunc
ulus
med
inen
sis
All
stat
es e
xcep
t WE
and
Uni
ty3,
618
case
s in
200
8,do
wn
from
5,8
15 c
ases
in 2
007
41, e
Schi
stos
omia
sis
Schi
stos
oma
haem
atob
ium
Prob
ably
War
rab,
Lak
es,
Uni
ty &
UN
Unk
now
nc,
f
S. m
anso
niE
E, C
E a
nd W
E, P
roba
bly
Jong
lei,
War
rab
and
Lak
esU
nkno
wn
a Abb
revi
atio
n of
Sta
tes:
BN
= B
lue
Nile
, CE
= C
entr
al E
quat
oria
, EE
= E
aste
rn E
quat
oria
, NB
EG
= N
orth
Bah
r el
Gha
zal,
UN
= U
pper
Nile
, WB
EG
= W
este
rn B
ahr
el G
haza
l, W
E =
Wes
tern
Equ
ator
ia
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.

Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
Rumunu et al. Page 12b H
uman
Afr
ican
Try
pano
som
iasi
s (s
leep
ing
sick
ness
): E
pide
mio
logi
cal u
pdat
e. h
ttp://
ww
w.w
ho.in
t/wer
/200
6/w
er81
08.p
df
c Neg
lect
ed T
ropi
cal D
isea
se in
Sou
ther
n Su
dan:
Situ
atio
n A
naly
sis,
Gap
Ana
lysi
s an
d In
terv
entio
n O
ptio
ns A
ppra
isal
. http
://w
ww
.mal
aria
cons
ortiu
m.o
rg/d
ata/
file
s/pa
ges/
ntds
_sou
ther
n_su
dan.
d APO
C (
2005
) R
apid
ass
essm
ent o
f lo
iasi
s an
d on
choc
erci
asis
in E
quat
oria
reg
ion
of S
outh
ern
Suda
n. M
issi
on R
epor
t, A
fric
an P
rogr
amm
e fo
r O
ncho
cerc
iasi
s C
ontr
ol, 4
– 2
4 A
pril
2005
.
e Sout
hern
Sud
an G
uine
a W
orm
Era
dica
tion
Prog
ram
, Min
istr
y of
Hea
lth, G
over
nmen
t of
Sout
hern
Sud
an, F
inal
Rep
ort,
2008
f Atla
s of
the
Glo
bal D
istr
ibut
ion
of S
chis
toso
mia
sis.
http
://w
ww
.who
.int/w
orm
cont
rol/d
ocum
ents
/map
s/en
/
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.
Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
Rumunu et al. Page 13
Table 2
Current NTD control strategies in Southern Sudanf
Disease Primary InterventionsCurrentlyUsed
Progress to date Limitation of CurrentIntervention
Suitablefor MDA?
Onchocerciasis Annual CDTI implementedsince1995
1.3 million individuals (36% ofeligible population) treated in 2007
Incomplete coverage; high attritionrate of CDDs
Yes
Dracunculiasis Active case surveillance,detectionand containment, andpreventionactivities including waterfiltration,provision of safe water,treatmentof water sources and healtheducation
In 2008, 89% of endemic villageswere providing regular reports,49% of cases were contained, andcases were reduced by 38% whencompared to 2007
Incomplete coverage ofsurveillance and interventions
No
Soil-transmittedhelminths
Single dose albendazole,distributed alongside NIDs
2.5 million doses distributed in allten states in 2006, reaching 87% ofthe targeted 1-5 year oldsSimilar coverage achieved in 2007
Lack of prevalence data andintervention strategy
Yes
Schistosomiasis No large scale campaigns forschistosomiasis control havebeenundertaken to date. Praziquantelisrarely available at healthfacilities
Small, ad-hoc treatment campaigns Insufficient prevalence data andlack of large-scale interventionstrategy
Yes
Lymphaticfilariasis
No targeted interventions todate
Regular distribution of ivermectinin CDTI areas will have reducedinfection levels in areas where LFand onchocerciasis are co-endemic
Lack of prevalence data; limitedfunds for surveys and to conductMDA; no palliative care; co-endemicity of L. loa in Equatoriaregion
Yes
Loiasis No targeted interventions todate.Pathology not considered worthtreatment at the present time.Important because co-infectionwith onchocerciasis can provokeSAEs
Regular distribution of ivermectinin CDTI areas will have reducedinfection levels in areas where Loaloa and onchocerciasis are co-endemic, but may have causedSAEs
Boundaries of loiasis endemic areanot clearly delineated. Notreatment suitable for MDA
No
Trachoma SAFE strategy consisting of:trichiasis surgery, antibiotics foractive trachoma, facialcleanlinessand environmentalimprovements
SAFE is being delivered as anintegrated component of theGuinea worm eradication programin parts of Eastern Equatoria andJonglei States
Limited coverage and varyinguptake of interventions bycommunities
Yes
Visceralleishmaniasis
Passive case detection at a fewhealth facilities equipped totreatthe disease; treatment withpentavalent antimonials
Case-management and supplychain of drug and diagnosticsupplies improved
Limited number of facilities withequipment and skills for diagnosisand treatment; cost of drugs;emerging drug resistance; lack ofawareness and prevention (LLINs)in affected communities
No
Human AfricanTrypanosomiasis
Passive case detection at a fewhealth facilities; treatment withpentamidine, eflornithine andmelarsoprol
Number of cases reported havedecreased as a result ofinterventions carried out since2003 [21]
Inadequate surveillance, limitednumber of treatment facilities andtrained health workers
No
Buruli Ulcer Antibiotic treatment using, forexample, rifampicin andaminoglycoside
Some interventions (treatment,awareness campaigns, healtheducation) have been carried outover the last years
Disease distribution not clearlyestablished, limited access totreatment and surgery
No
Leprosy MDT blisterpacks provided freeofcharge by WHO
Some interventions (treatment,awareness campaigns, healtheducation) have been carried out
Limited MDT coverage No
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.

Europe PM
C Funders A
uthor Manuscripts
Europe PM
C Funders A
uthor Manuscripts
Rumunu et al. Page 14
Disease Primary InterventionsCurrentlyUsed
Progress to date Limitation of CurrentIntervention
Suitablefor MDA?
over the last years
fAbbreviations: CDD, community drug distributor; CDTI, community-directed treatment with ivermectin; LF, lymphatic filariasis; LLIN, long-
lasting insecticidal net; MDA, mass drug administration; MDT, multi-drug therapy; NID, national immunization day; SAE, severe adverse event;SAFE, strategy for trachoma control consisting of eyelid surgery (S), antibiotics to treat the community pool of infection (A), facial cleanliness (F),and environmental changes (E).
Trends Parasitol. Author manuscript; available in PMC 2009 August 19.