
Carbon Monoxide Inhalation Protects Rat Intestinal Grafts from Ischemia/Reperfusion Injury
Short and Long Term Effects of (-)-Epicatechin on Myocardial Ischemia Reperfusion Injury
Katrina Go Yamazaki*, Diego Romero-Perez*, Maraliz Barraza-Hidalgo*, Michelle Cruz*, Maria Rivas*, Brenda Cortez-Gomez*, Guillermo Ceballos#, Francisco Villarreal*
*University of California, San Diego, Department of Medicine, San Diego, CA, #Escuela Superior de Medicina del Instituto Politécnico Nacional, Departamento de Farmacologia, Mexico
City, Mexico
Running head: Cardioprotection by epicatechin
Francisco Villarreal M.D. Ph.D. Professor of Medicine UCSD Cardiology 9500 Gilman Dr. 0613J BSB 4028 La Jolla, CA 92093 tel (858) 534-3630 lab (858) 534-1314 fax (858) 534-0522 email: [email protected]
Articles in PresS. Am J Physiol Heart Circ Physiol (June 20, 2008). doi:10.1152/ajpheart.00413.2008
Copyright © 2008 by the American Physiological Society.
H-00413-2008-R1
2
Abstract
Epidemiological studies have shown a correlation between flavonoid-rich diets and improved
cardiovascular prognosis. Cocoa contains large amounts of flavonoids, in particular flavanols
(mostly catechins and epicatechins). Flavonoids possess pleiotropic properties that may confer
protective effects to tissues during injury. We examined the ability of epicatechin to reduce short
and long-term ischemia reperfusion (IR) myocardial injury. Epicatechin (1mg/kg/day) pre-
treatment (Tx) was administered daily via oral gavage to male rats for 2 or 10 days. Controls
received water. Ischemia was induced via a 45 min coronary occlusion. Reperfusion was
allowed until 48 h or 3 weeks while Tx continued. We measured infarct (MI) size (%),
hemodynamics, myeloperoxidase (MPO) activity, tissue oxidative stress, and matrix
metalloproteinase-9 (MMP-9) activity in 48 h groups. Cardiac morphometry was also evaluated
in 3 week groups. With 2 days of Tx, no reductions in MI size occurred. After 10 days, a
significant ~50% reduction in MI size occurred. Epicatechin rats demonstrated no significant
changes in hemodynamics. Tissue oxidative stress was significantly reduced in the epicatechin
group vs. controls. MMP-9 activity demonstrated limited increases in the infarct region with
epicatechin. By 3 weeks, a significant 32% reduction in infarct size was observed with Tx,
accompanied with sustained hemodynamics and preserved chamber morphometry. In
conclusion, epicatechin Tx confers cardioprotection in the setting of IR injury. The effects are
independent of changes in hemodynamics, are sustained over time, and are accompanied by
reduced levels of indicators of tissue injury. Results warrant the evaluation of cocoa flavanols as
possible therapeutic agents to limit ischemic injury.
Keywords: myocardial infarction, catechin, epigallocatechin, cocoa, chocolate
H-00413-2008-R1
3
Introduction
Known risk factors for the development of cardiovascular disease (CVD) include hypertension, a
poor diet, obesity, lack of physical activity, smoking and diabetes. Diet has been established as
one of the most important lifestyle factors that can strongly influence the incidence of CVD.
Polyphenols are widely distributed in plants and are known as flavonoids (30). Flavonoids can
be divided into 4 classes, flavones, flavanols, flavonols and anthocyanins (34). All 4 classes
have in common phenolic rings with variations in the number and arrangement of the hydroxyl
groups as well as the nature and extent of alkylation and/or glycosylation of these groups (34).
Flavonoids have been long recognized for their free radical scavenging activity (34).
Epidemiological evidence indicates a negative correlation between consumption of flavonoid
rich foods or beverages and incidence of cardiovascular disease (CVD) (20, 23, 25, 26). Wine
has garnered attention because its polyphenol concentration is relatively high and may be partly
responsible for the prolonged longevity associated with the “French Paradox” (2, 13). However,
cocoa powder contains by far the largest amount of flavonoids, in particular the subtype known
as flavanols (up to 10% flavanols by weight) (11). Main flavanols in cocoa are catechins and
epicatechins present in mono- or multimeric forms (11, 26). Interest in the beneficial effects of
cocoa derived flavonols emerged from observations of Kuna Indians living off Panama. Kuna
islanders have a very low incidence of CVD in particular, hypertension. The low incidence of
CVD is related to environmental factors and not genetic since protection is lost when Kuna
Indians migrate to mainland (21, 29). Kuna islanders drink large amounts of cocoa rich in
flavanols vs. mainland migrants. Studies relate the low indices of CVD to the consumption of
cocoa beverages and not other factors such as fruit or protein, physical activity or alcohol
intake. In addition to their free radical scavenging activity, there are other clues as to the
mechanisms that may explain cocoa effects. Consumption of flavanol rich cocoa leads to
vasodilation which can be reversed by the use of the NO synthesis inhibitors (12, 18). Other
H-00413-2008-R1
4
effects of flavanoids/flavanols include the inhibition of platelet adhesion, low-density lipoprotein
(LDL) oxidation, inflammation, reactive oxygen species generation, eicosanoid synthesis and
insulin resistance (for reviews see, (10, 33). Recent reports link the effects of cocoa to
epicatechin. The ingestion of epicatechin in humans can reproduce the hypotensive, antioxidant
and insulin sensitizing effects of cocoa (35).
In spite of the identification of many candidate compounds, which have the potential to
reduce infarct size, none have demonstrated the capacity to retain the effect over the long-term
(3, 24, 45). Most pharmacological agents studied to date have only managed to postpone cell
death. On the basis of the reported pleiotropic actions of flavanols, it is reasonable to propose
that on the short-term, these agents may ameliorate tissue injury secondary to ischemia
reperfusion (IR) and that in the long-term their continued actions may lead to improved
outcomes. We hypothesize that the administration of epicatechin to rats leads to a sustained
reduction in infarct size and that this phenomena is secondary to a suppression of mediators of
reperfusion injury.

H-00413-2008-R1
5
Materials and Methods
Animal Groups and Epicatechin treatment
Adult male Sprague-Dawley rats (Harlan, Indianapolis, IN) weighing 250-300 g (~8 weeks of
age) were used. All procedures were approved by the Institutional Animal Care and Use
Committee and conform to published NIH guidelines for animal research. Epicatechin (1
mg/kg/day; Sigma-Aldrich, St. Louis, MO) or vehicle (water) was administered by oral gavage
once/day beginning either 2 or 10 days before thoracotomy and continuing until the time of the
terminal study (48 h or 3 weeks). This dose was noted in humans to reproduce the vascular (i.e.
hypotensive) effects of dark chocolate (35). Groups of normal (i.e. no surgery was performed in
these groups) animals were treated with water (n=6) or epicatechin (n=6) for 10 d and were
used solely to evaluate the effects of epicatechin on baseline hemodynamics. For 48 h studies,
groups included IR (n=21), IR + 2 d epicatechin (n=7) and IR + 10 d epicatechin (n=15) and
were used to measure infarct size. Subgroups of 10 d treatment (n=8 per each) were used to
measure hemodynamics. For 48 h biochemical determinations subgroups included IR (n=8) and
IR + 10 d epicatechin (n=7). The 48 h timepoint was selected to be able to clearly distinguish
regions of necrotic tissue from viable myocardium. For 3 week studies, groups included sham
(n=5), sham + 10 d epicatechin (n=4), IR (n=7) and IR + 10 d epicatechin (n=8). Sham animals
underwent a thoracotomy but were not subjected to IR.
Ischemia/ Reperfusion Surgery
Animals were anesthetized by intraperitoneal injection of ketamine (100 mg/kg) and xylazine (10
mg/kg), intubated, and positive-pressure ventilated. A left thoracotomy was then performed. In
IR animals, the left anterior descending coronary artery was ligated for 45 min, released and the
suture left in place as a point of reference. The chest was closed in layers and animals allowed
H-00413-2008-R1
6
to recover. Successful occlusion and reperfusion was verified by visual inspection of left
ventricle (LV) color.
Hemodynamics
For hemodynamic measurements, animals were anesthetized with 5% isoflurane and
maintained with 1-2% isoflurane. The right carotid artery was exposed via a neck dissection.
Carotid and LV pressures were acquired using a micromanometer (2 French, 140 cm; Millar
instruments Inc. Houston, TX) introduced via the carotid artery. Hemodynamics were digitally
recorded for subsequent analysis using WINDAQ software (version 2.15, DATAQ Instruments
Inc).
Terminal Studies
Hearts were excised and weighed. In 48 h hearts, the area at risk (AAR) was determined by the
reocclusion of the snare and infusion of trypan blue into the cannulated aorta. Hearts was
sectioned into five 2 mm rings and stained using triphenyltetrazolium chloride. Computer
assisted image analysis was used using blinded operators. Results are expressed as infarct
area (IA) as a function of the area at risk (AAR). For 3 week studies, hearts were processed as
above and sectioned to identify the infarct (i.e. scar) area. The images of unfixed, stained rings
were also used to measure internal and external chamber diameters, and anterior and septal
wall thicknesses.
Tissue collection
The 48 h excised hearts were perfused with cold saline to remove blood. LV free wall was
separated, and divided into two parts, the infarct region and the border zone. The right ventricle
was also taken to be used as the remote or non-ischemic region.
Gelatin zymography
H-00413-2008-R1
7
Heart samples ( 50 mg) were homogenized in 10 mM HEPES, pH 7.5, 150 mM NaCl, 0.2 mM
EDTA, 25% glycerol, 100 µg/ml phenylmethylsulfonyl fluoride, and 0.2 kallikrein inhibitory
units/ml aprotinin. Samples (10 µg of protein) were analyzed by SDS-PAGE as described (14).
An internal control (human MMP-2/MMP-9, Chemicon, Temecula, CA) was loaded to normalize
between gels. Bands of gelatinolytic activity were digitally quantified (Kodak 1D, Eastman
Kodak, Rochester, NY).
Myeloperoxidase (MPO) Assay
The MPO assay was performed as previously described with modification (14). Tissue samples
were homogenized in MPO lysis buffer (50 mmol/L KH2PO4 pH 6.0, 0.5%
hexadecyltrimethylammonium bromide) and incubated on ice for 30 min. Following
centrifugation, the supernatants were reacted with 0.4 mmol/L tetramethylbenzidine (Sigma)
and 0.006% H2O2 in 50 mmol/L phosphate at pH 6.0. Absorbance was monitored and MPO
activity expressed as relative units/min.
Glutathione (GSH/GSSG) Assay
Tissue samples were homogenized in ice cold homogenization buffer (154mM KCl, 5mM
diethylenetriaminepentaacetic acid (DPTA), and 0.1 M potassium phosphate, pH 6.8). After
centrifugation, an aliquot was removed for protein determination using the bicinchoninic acid
method (Pierce Chemical Co., Rockford, IL). Immediately after an aliquot was taken, one
volume of cold acid buffer (40mM HCl, 10mM DPTA, 20mM ascorbic acid, and 10%
trichloroacetic acid (TCA) was added to one volume of homogenate. The suspension was
centrifuged and the resulting supernatant solution was centrifuged through a 0.45-µm
microcentrifuge filter (Millipore Corp., Bedford, MA). Reduced and oxidized glutathione, GSH
and GSSG respectively, levels were determined as previously described by Senft et al., using
the fluorophore o-phthalaldehyde (OPA) (37).
H-00413-2008-R1
8
Statistical Analysis
Results are expressed as mean ± S.E.M. Comparisons between means were analyzed, as
appropriate, by student’s t-tests or one-way ANOVA followed by Bonferroni t-test. A value of
p<0.05 was considered statistically significant.
H-00413-2008-R1
9
Results
Hemodynamics
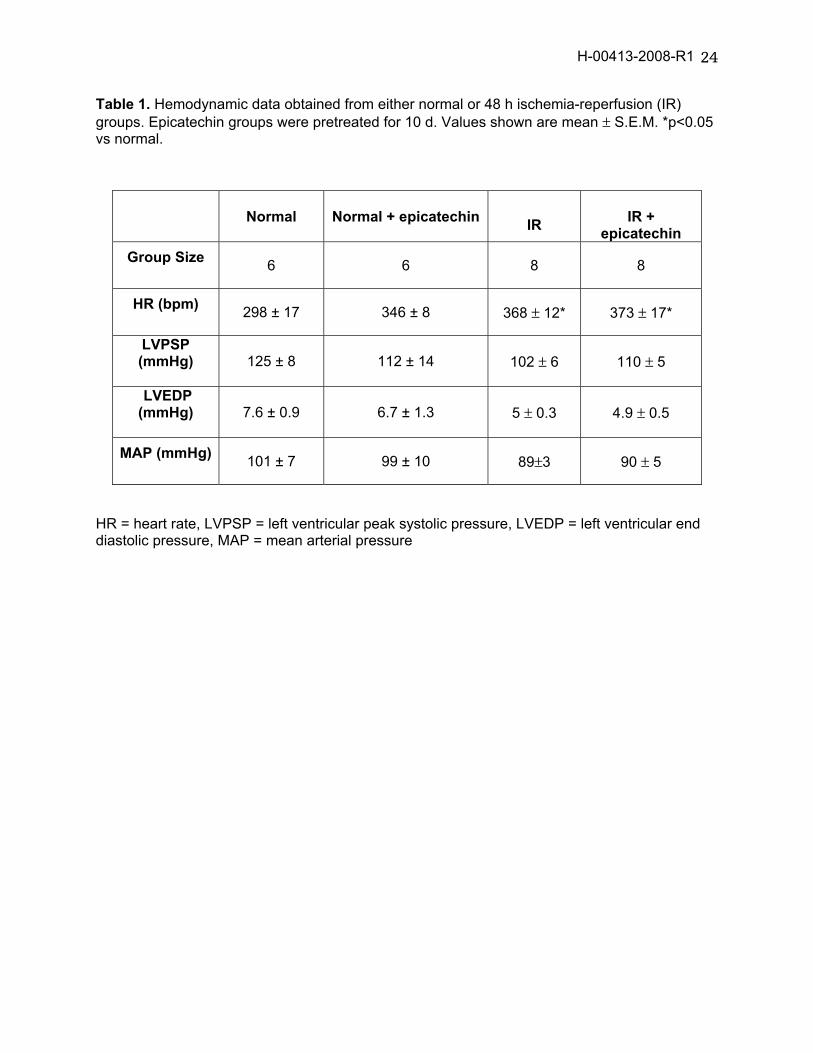
Hemodynamic parameters were measured in normal, and normal + 10 d epicatechin rats.
Epicatechin treatment only raised heart rate vs. normal. Values recorded 48 h after IR (table 1)
demonstrate no significant changes in either heart rate, LV end-diastolic/peak systolic pressure,
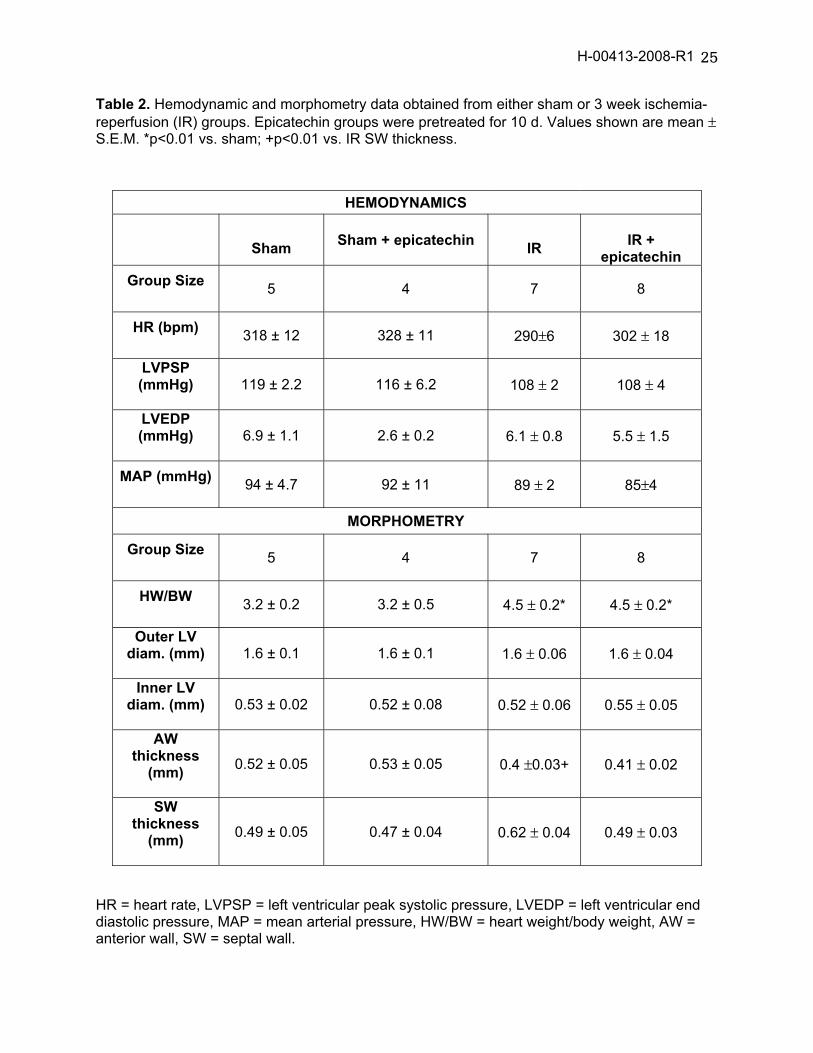
or mean aortic pressure between IR groups. In 3 week studies (table 2), hemodynamic
parameters were recorded in sham and IR animals and results were comparable between
untreated vs. treated groups.
Infarct size and morphometry
For the 2 day pre-treatment study, the AAR was 50±4% and 56±2% and were statistically not
different between the IR and IR + 2 d epicatechin groups respectively. The IR group and the IR
+ 2 d epicatechin group also had comparable (p>0.05) infarct areas (infarct area/area at risk) of
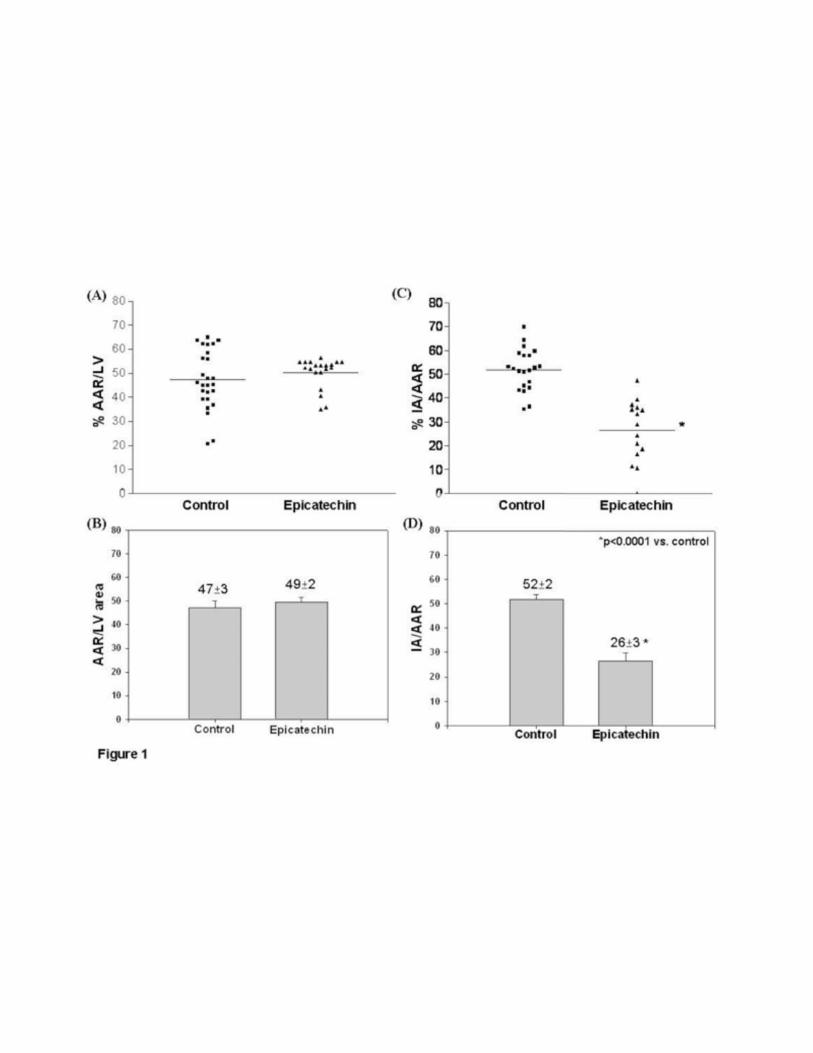
41±8% and 34±4% respectively. In the 10 day pre-treatment study (figure 1), infarct area was
52 ± 2% vs. 26 ±3% (p<0.0001). There was no difference in the area at risk, 47±3% and 49±2%,
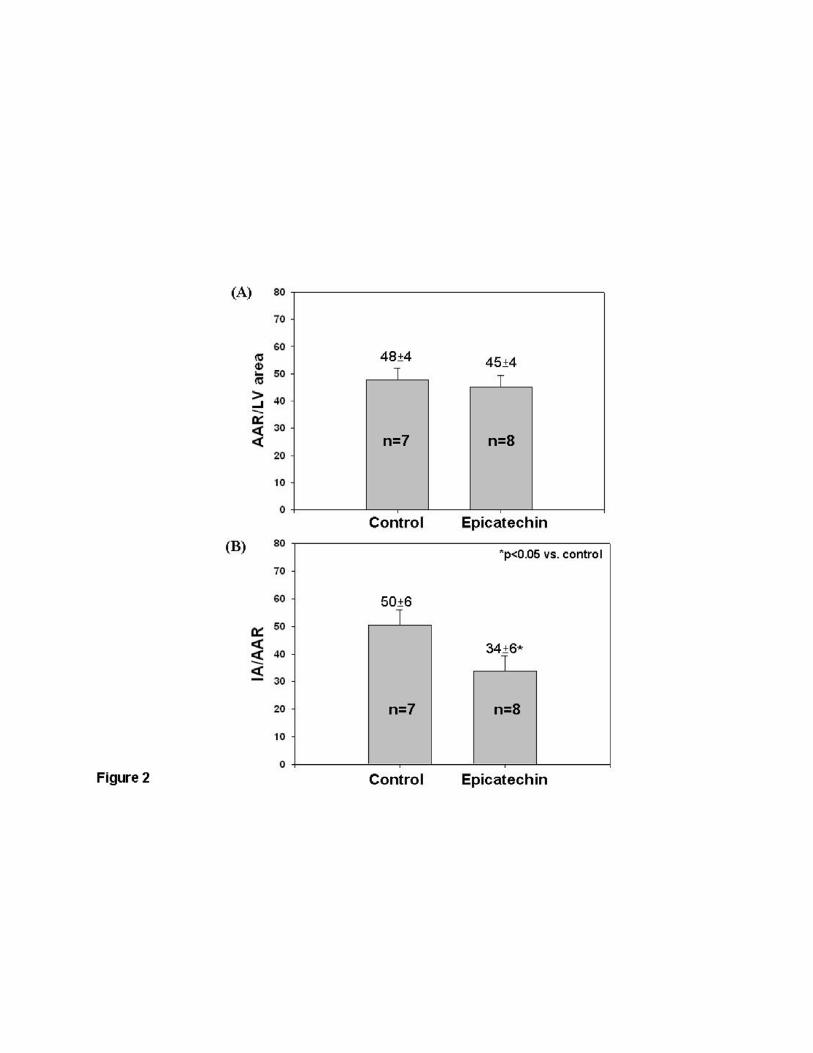
between the two groups. Figure 2 summarizes the 3 week results. The IR animals infarct area
was 50±6% vs. 34±6% (p<0.05). The two groups had similar area at risks (48±4% and 45±4%).
As shown in table 2, IR animals treated with epicatechin demonstrate comparable post IR
morphometric changes to those of 3 week untreated IR animals. Anterior wall vs. septal wall
thicknesses yielded a statistical difference only in the vehicle treated IR group. Changes in
infarct size and morphometry appear independent from altered hemodynamics since
epicatechin did not modify these in a manner that would explain the observed results. No
differences in survival rates were noted between any groups.

H-00413-2008-R1
10
MPO Activity
We assessed the capacity of epicatechin to alter inflammatory cell infiltration in the myocardium
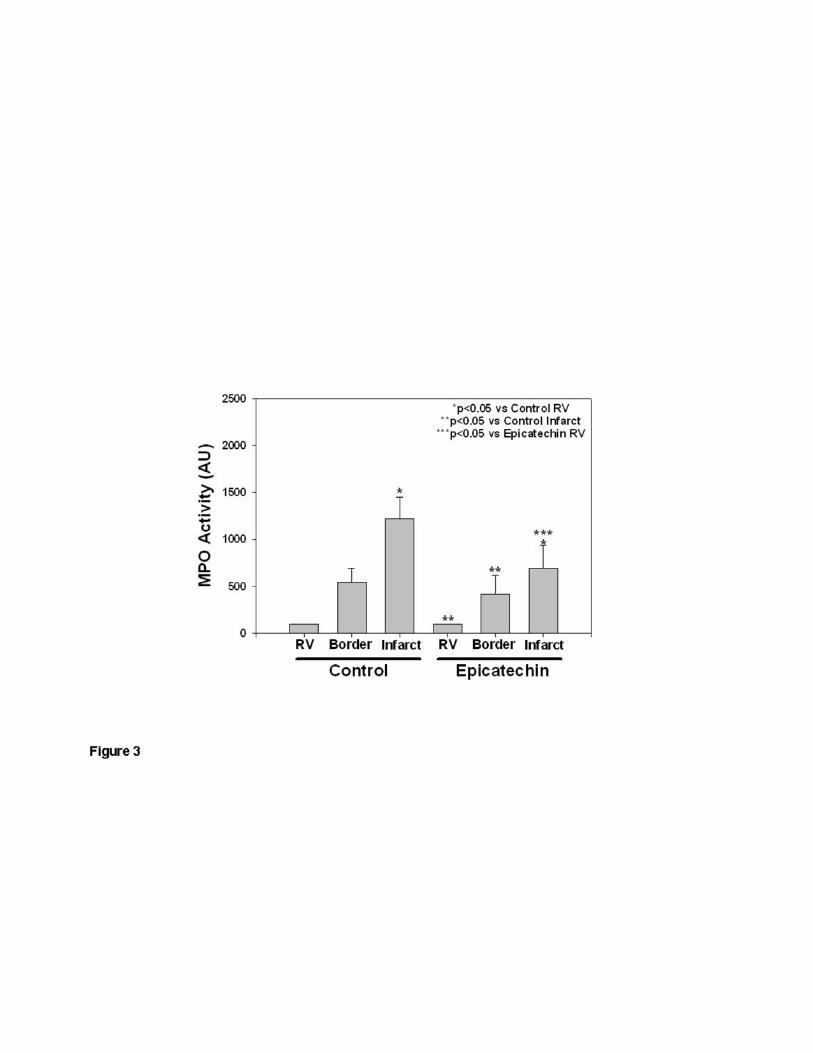
by measuring MPO activity using a colorimetric assay (14). As shown in figure 3, in both the 48
h IR and IR + 10 d epicatechin groups, MPO in the infarct region was higher when compared to
the RV (p<0.05), indicating infiltration of inflammatory cells into the border zone and ischemic
regions. No differences in MPO levels were noted between IR and IR + 10 d epicatechin at any
of the analyzed regions.
Myocardial Oxidative Stress
We determined if epicatechin ameliorates the generation of oxidative stress within the
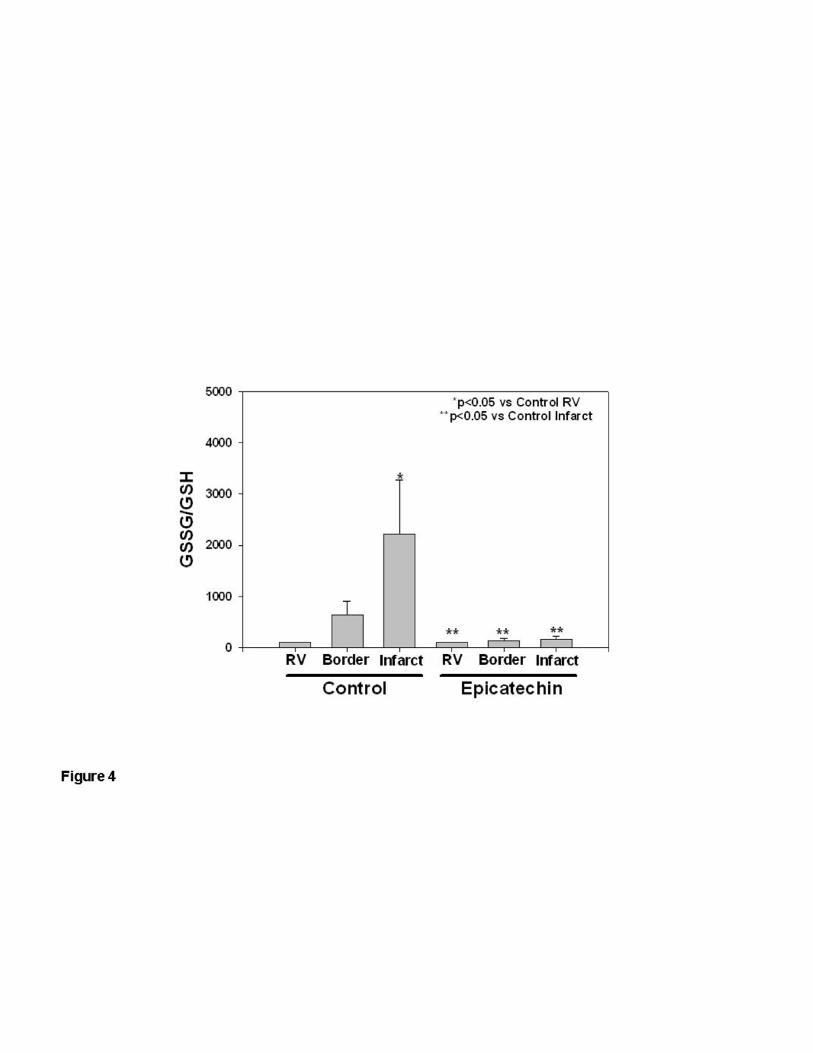
myocardium of rats subjected to IR. Results are shown as a ratio of oxidized glutathione to
reduced glutathione (GSSG/GSH), which is a measure of total tissue oxidative stress. Oxidative
stress was significantly increased (p<0.05) in the infarct region compared to the RV in the IR
group, and this increase was significantly attenuated (p<0.05) in the border zone and ischemic
regions of the IR + 10 d epicatechin group (figure 4).
Zymography Results
We determined if epicatechin decreases levels of MMP-2 and/or MMP-9 activity. Gelatin
zymography of tissue homogenates from the RV, border, and infarct region only revealed bands
corresponding to 92 kDa MMP-9 and 75 kDa MMP-2 (Figure 5a). The 86 kDa MMP-9 and 72
kDa MMP-2 were not visible. Densitometric analysis revealed that 92 kDa MMP-9 levels were
significantly increased (p<0.01) in the infarct region compared to the RV in the IR group, but not
in the IR + 10 d epicatechin group (Fig. 5B). As observed in the gel image and by densitometric
analysis, no notable differences were identified in 75 kDa MMP-2 levels.
H-00413-2008-R1
11
Discussion
Our results indicate that 10 d pre- and continuous epicatechin Tx significantly reduced
infarct size in rats 48 h after IR injury. The smaller infarct size observed in treated animals is
accompanied by significant reductions in tissue oxidative stress at the infarct region. These
results were accompanied by a preservation of local inflammation and lesser degrees of MMP-9
activity in treated, injured myocardium. More importantly, a sustained reduction in infarct size
was observed three weeks after IR injury.
Since the length of exposure to cocoa flavanols appears to determine bioactivity, we first
examined if short term pre-treatment with epicatechin could confer cardioprotective effects. Two
days of epicatechin pre-treatment did not significantly reduce MI size. These results contrast to
those of others where cardioprotection with flavanols can be generated immediately upon
treatment. Wang et al demonstrated the capacity of a synthetic flavanol, administered at 5
mg/kg just prior to reperfusion to reduce MI size in sheep while also decreasing ROS
generation, improving coronary blood flow and NO metabolite levels (42). Aneja et al reported
similar effects with epigallocatechin-3-gallate (EGCG) at 10 mg/kg given just prior to reperfusion
to rats (1). An important difference arises when comparing our 2 day results with these studies.
Flavanol doses used by these investigators were significantly higher than those of our study
(~5-10 fold). It is well known that higher doses of flavanols attain greater antioxidant effects
thus, effectively mitigating (with increased efficacy) the damaging effects of ROS during IR. This
observation is supported by data that indicates that serum concentrations of the order of ~0.01
mM allow flavonoids to act as effective in vivo ROS scavengers (17). The serum concentration
reported in animals treated with 1 mg/kg/day would only approximate 1/10th of this. The fact that
short term treatment with 1 mg/kg/day epicatechin does not confer cardioprotection suggests
that changes in myocardial gene expression and/or protein levels may need to develop with

H-00413-2008-R1
12
longer Tx times (11, 40). Alternatively, changes in epicatechin metabolism may be required to
generate IR protection (11).
In studies performed in patients suffering from hypertension, sustained reductions in
blood pressure were observed when Tx was given with high flavanol cocoa for at least 7 days
(15). Our results demonstrate that in animals with 10 days of pre- and continuous epicatechin
Tx, a significant, ~50%, reduction in infarct size was observed. A potential mechanism by which
epicatechin may decrease MI size is a reduction in afterload. Ten days of epicatechin treatment
in normal and IR animals did not reduce blood pressure and thus, changes in afterload fail to
explain the observed effects.
In the setting of myocardial ischemia, the lack of oxygen and associated ATP production
can lead to cell death (necrosis). Upon reperfusion, the reintroduction of blood flow to the
previously ischemic area leads to the activation of an injury pathway associated with
reoxygenation (4, 45). Reperfusion injury activates an inflammatory response, which can lead to
loss of contractile function, arrythmias, and may promote cell death in ischemic myocytes (4).
Major mediators of IR injury are neutrophils, oxygen radicals, proteases, and calcium overload
(4, 45). Compounds that target “single” mediators of IR related injury, such as antioxidants,
have shown to improve indicators of tissue injury in animal models. However, the translation of
these improvements into the clinical setting has not been successful (3, 24, 45). Similar failures
have been observed with strategies that target tissue inflammation (i.e. neutrophil infiltration) or
protease activity where again, promising results in animal models did not translate into the
clinical setting (3, 24, 45). This leads to the question of: Are small molecules that possess
pleiotropic actions potentially a better strategy to limit IR injury? Studies have demonstrated that
flavonoids including flavanols are pleiotrophic. Flavonoids possess antioxidant (17, 43, 44), anti-
inflammatory (1, 9, 36, 39), and antithrombotic properties (19, 31). Flavonoids can also induce
NO-mediated vasodilation (12, 22, 35). Interestingly, several flavonoid properties mirror those of
H-00413-2008-R1
13
adenosine, the only agent that has shown some promise as a cardioprotectant (3, 24). It is
interesting to note that for adenosine to act as a prophylactic cardioprotector, the doses required
would likely yield hypotension and thus, be impractical for daily use. However, studies using
flavonoids have yet to identify any toxic or significant side effects, including notable hypotension
in normotensive individuals (6, 12).
It is well established that during the acute phase of IR injury, inflammatory cells are
recruited to the site of injury either infiltrating the tissue and/or causing microvascular plugging
(i.e. no-reflow phenomenom). Inflammatory cells release proteases, such as MMPs, and
generate an oxidative burst (4, 45). Previous studies have investigated the effects of catechins
on tissue inflammation. Dona et al., examined the effects of epigallocatechin gallate (EGCG) to
modulate in vitro and in vivo lung inflammatory responses (9). EGCG reduced ROS activity,
inhibited apoptosis, and reduced chemokine-induced neutrophil chemotaxis in vitro. EGCG
significantly reduced pulmonary inflammatory responses and fibrosis. Aneja et al, also
investigated the effects of EGCG on neutrophil activation in rats subjected to IR (1).
Cardioprotection was associated with decreased IL-6 production and neutrophil infiltration as
measured by MPO activity. In our study, epicatechin treatment did not reduce in a significant
manner MPO activity in the infarct region, indicating that at 48 h post-IR there is a preservation
of acute inflammation. There is continuing controversy as to the wisdom of the potential benefit
to be derived from therapies intended to suppress acute inflammation in the setting of
myocardial infarction. While the reduction of neutrophil infiltration can reduce IR injury in
animals, the use of anti-inflammatory agents in patients has led to adverse outcomes, including
ventricular rupture (38). In a study performed in our laboratory, the continuous use of steroids
after coronary occlusion led post-MI adverse remodeling (14).
In the setting of IR injury, oxidative stress has a number of deleterious biochemical
effects on the heart. ROS produced in IR injury can contribute to mitochondrial damage, which
H-00413-2008-R1
14
can lead to cell death by necrosis and apoptosis (4, 45). ROS can also activate pro-enzymes,
such as pro-MMPs, and promote calcium overload (4, 45). There are several endogenous
antioxidants found in tissues, including reduced glutathione (GSH). It is known that GSH plays a
central role in intracellular endogenous antioxidant defenses as it is involved in all lines of
protection against ROS (28). In the course of IR, GSH is converted into its oxidized form,
GSSG, and the level of ROS exceeds the antioxidant capacity of the cell, leading to oxidative
stress (28). A study by Chen et al. investigated the effect of tea catechin on the Pb2+-induced
change of intracellular thiol levels (5). They demonstrated that Pb2+ significantly increased tissue
oxidative stress in a concentration-dependent manner. Supplementation of the cells with (-)-
epicatechin or (-)-epicatechin gallate resulted in reduced oxidative stress. These results match
ours in that we showed a significant increase in the GSSG/GSH ratio in the infarct regions
compared to the non-infarct regions in control hearts, with epicatechin significantly attenuating
this increase. In our study, we utilized doses of epicatechin that are low and would appear on
the basis of expected blood concentrations (~0.002 mM) to yield limited antioxidant activity (17).
Thus, the manner in which low doses of epicatechin significantly reduce tissue oxidative stress
needs further investigation as it raises a wide spectrum of possibilities. One such possibility is
that epicatechin over the course of several days is concentrated intracellularly several fold vs.
blood levels and allows it to act as an effective antioxidant.
The activation of MMPs with IR injury has also been described. We and others have
documented the upregulation of MMP-2 and MMP-9 activity in infarcted myocardium (16, 27).
MMPs contribute to the loss of contractile function and damage the integrity of the extracellular
matrix. Our results showed significant increases in MMP-9 activity in the infarct region
compared to the non-infarct region in the vehicle group, and a lack of a significant increase in
the necrotic region with epicatechin Tx. This correlates with the findings of Dell’agli et al, who
studied the effects of EGCG on MMP-9. Results indicate that EGCG directly inhibited MMP-9
H-00413-2008-R1
15
activity (8). Interestingly, the reduction in tissue oxidative stress observed in our study may
have also led to decrease levels of MMP-9 activity via inhibition of the cysteine switch activation
mechanism, which is known to be ROS dependent (32).
The purpose behind the study of 3 weeks post-IR animals was to determine the extent to
which there was a sustained reduction in tissue injury with treatment. Results yield a reduction
in scar (infarct) size of ~32%. Our 3 week results are encouraging in that most studies have
failed to demonstrate the capacity of candidate cardioprotective agents to yield sustained (long-
term) effects (3, 24, 45). The observed preservation of post-MI chamber morphometry is also
important since little is known about what impact the pleiotropic effects of flavonoids may have
on post-MI wound healing/remodeling. To our knowledge as noted above, only the use of the
pleiotrophic agent adenosine has shown promise as a possible cardioprotector and promoter of
either preserved or reduced post-MI remodeling (7, 41).
Since the sustained beneficial effects of cocoa flavanols depend on their continued
intake it implies that their possible use as cardioprotective agents at the time of reperfusion or
soon afterwards would appear unlikely. However, cocoa induced vasodilation can be
reproduced by a select group of metabolites (35) thus, there is the possibility that future studies
using flavanol derivatives may allow for their examination as “immediate” cardioprotectors.
Alternatively, there is the possibility that higher does of flavanols may yield immediate
cardioprotection. This possibility will need to be explored. The concept of feasible prophylactic
cardioprotection has been proposed. Bolli et al., have noted that the most practical strategy for
limiting infarct size and improving clinical outcome may be to induce a chronically protected
cardiac phenotype where this property would be operative at the onset of ischemia (3). The
observation that Kuna Indians have low incidences of cardiovascular disease is supportive of
this idea. However, this population is not representative of the poorer health status observed in
developed countries general population. The concept of suggesting that humans consume

H-00413-2008-R1
16
traditional cocoa based products high in flavanol content is not a practical one given their high
caloric content. Alternatively, it is more likely to conceive of the production of cocoa based
“supplements” devoid of calories to be used for daily prophylactic use. This is a concept that has
been proposed as viable on the basis of observations derived from the use of the flavonoid
resveratrol on animals exposed to unhealthy diets (2).
On the basis of the results presented, more work needs to be performed to validate
these results and identify key underlying mechanisms of action of epicatechin. The
reproducibility of these observations by independent groups is warranted. In addition, further
preclinical studies need to be performed using small and large animal models of human disease
such as those with hypertension, diabetes, stroke prone, aging and importantly, to verify the
variability of the effects on the basis of gender. Nonetheless, the results presented provide
support towards the consideration of cocoa flavanols as possible therapeutic agents intended to
prevent and/or limit the development of ischemic heart disease.
H-00413-2008-R1
17
Acknowledgements
We wish to acknowledge the support of NIH HL-43617 and HL-67922 to Dr. F. Villarreal, a
CONACYT-UC MEXUS doctoral fellowship to D. Romero-Perez, an undergraduate diversity
supplement to B. Cortez-Gomez (HL-80049) and a pre-doctoral NIH fellowship (HL-07444) to K.
Yamazaki.
H-00413-2008-R1
18
References
1. Aneja R, Hake PW, Burroughs TJ, Denenberg AG, Wong HR, and Zingarelli B.
Epigallocatechin, a green tea polyphenol, attenuates myocardial ischemia reperfusion injury in
rats. Mol Med 10: 55-62, 2004.
2. Baur JA, Pearson KJ, Price NL, Jamieson HA, Lerin C, Kalra A, Prabhu VV, Allard JS,
Lopez-Lluch G, Lewis K, Pistell PJ, Poosala S, Becker KG, Boss O, Gwinn D, Wang M,
Ramaswamy S, Fishbein KW, Spencer RG, Lakatta EG, Le Couteur D, Shaw RJ, Navas P,
Puigserver P, Ingram DK, de Cabo R, and Sinclair DA. Resveratrol improves health and survival
of mice on a high-calorie diet. Nature 444: 337-342, 2006.
3. Bolli R, Becker L, Gross G, Mentzer R, Jr., Balshaw D, and Lathrop DA. Myocardial
protection at a crossroads: the need for translation into clinical therapy. Circ Res 95: 125-134,
2004.
4. Buja LM and Entman ML. Modes of myocardial cell injury and cell death in ischemic
heart disease. Circulation 98: 1355-1357, 1998.
5. Chen L, Yang X, Jiao H, and Zhao B. Effect of tea catechins on the change of
glutathione levels caused by Pb(++) in PC12 cells. Chem Res Toxicol 17: 922-928, 2004.
6. Chengelis CP, Kirkpatrick JB, Regan KS, Radovsky AE, Beck MJ, Morita O, Tamaki Y,
and Suzuki H. 28-Day oral (gavage) toxicity studies of green tea catechins prepared for
beverages in rats. Food Chem Toxicol 46: 978-989, 2008.
7. Claeys MJ, Bosmans J, De Ceuninck M, Beunis A, Vergauwen W, Vorlat A, and Vrints
CJ. Effect of intracoronary adenosine infusion during coronary intervention on myocardial
reperfusion injury in patients with acute myocardial infarction. Am J Cardiol 94: 9-13, 2004.
8. Dell'agli M, Bellosta S, Rizzi L, Galli GV, Canavesi M, Rota F, Parente R, Bosisio E, and
Romeo S. A structure-activity study for the inhibition of metalloproteinase-9 activity and gene
expression by analogues of gallocatechin-3-gallate. Cell Mol Life Sci 62: 2896-2903, 2005.
H-00413-2008-R1
19
9. Dona M, Dell'Aica I, Calabrese F, Benelli R, Morini M, Albini A, and Garbisa S.
Neutrophil restraint by green tea: inhibition of inflammation, associated angiogenesis, and
pulmonary fibrosis. J Immunol 170: 4335-4341, 2003.
10. Engler MB and Engler MM. The emerging role of flavonoid-rich cocoa and chocolate in
cardiovascular health and disease. Nutr Rev 64: 109-118, 2006.
11. Fisher ND and Hollenberg NK. Flavanols for cardiovascular health: the science behind
the sweetness. J Hypertens 23: 1453-1459, 2005.
12. Fisher ND, Hughes M, Gerhard-Herman M, and Hollenberg NK. Flavanol-rich cocoa
induces nitric-oxide-dependent vasodilation in healthy humans. J Hypertens 21: 2281-2286,
2003.
13. Formica JV and Regelson W. Review of the biology of Quercetin and related
bioflavonoids. Food Chem Toxicol 33: 1061-1080, 1995.
14. Garcia RA, Go KV, and Villarreal FJ. Effects of timed administration of doxycycline or
methylprednisolone on post-myocardial infarction inflammation and left ventricular remodeling in
the rat heart. Mol Cell Biochem 300: 159-169, 2007.
15. Grassi D, Necozione S, Lippi C, Croce G, Valeri L, Pasqualetti P, Desideri G, Blumberg
JB, and Ferri C. Cocoa reduces blood pressure and insulin resistance and improves
endothelium-dependent vasodilation in hypertensives. Hypertension 46: 398-405, 2005.
16. Griffin MO, Jinno M, Miles LA, and Villarreal FJ. Reduction of myocardial infarct size by
doxycycline: a role for plasmin inhibition. Mol Cell Biochem 270: 1-11, 2005.
17. Hanasaki Y, Ogawa S, and Fukui S. The correlation between active oxygens scavenging
and antioxidative effects of flavonoids. Free Radic Biol Med 16: 845-850, 1994.
18. Heiss C, Dejam A, Kleinbongard P, Schewe T, Sies H, and Kelm M. Vascular effects of
cocoa rich in flavan-3-ols. Jama 290: 1030-1031, 2003.
H-00413-2008-R1
20
19. Heptinstall S, May J, Fox S, Kwik-Uribe C, and Zhao L. Cocoa flavanols and platelet and
leukocyte function: recent in vitro and ex vivo studies in healthy adults. J Cardiovasc Pharmacol
47 Suppl 2: S197-205; discussion S206-199, 2006.
20. Hertog MG, Kromhout D, Aravanis C, Blackburn H, Buzina R, Fidanza F, Giampaoli S,
Jansen A, Menotti A, Nedeljkovic S, and et al. Flavonoid intake and long-term risk of coronary
heart disease and cancer in the seven countries study. Arch Intern Med 155: 381-386, 1995.
21. Hollenberg NK, Martinez G, McCullough M, Meinking T, Passan D, Preston M, Rivera A,
Taplin D, and Vicaria-Clement M. Aging, acculturation, salt intake, and hypertension in the Kuna
of Panama. Hypertension 29: 171-176, 1997.
22. Karim M, McCormick K, and Kappagoda CT. Effects of cocoa extracts on endothelium-
dependent relaxation. J Nutr 130: 2105S-2108S, 2000.
23. Keen CL, Holt RR, Oteiza PI, Fraga CG, and Schmitz HH. Cocoa antioxidants and
cardiovascular health. Am J Clin Nutr 81: 298S-303S, 2005.
24. Kloner RA and Rezkalla SH. Cardiac protection during acute myocardial infarction:
where do we stand in 2004? J Am Coll Cardiol 44: 276-286, 2004.
25. Knekt P, Jarvinen R, Reunanen A, and Maatela J. Flavonoid intake and coronary
mortality in Finland: a cohort study. Bmj 312: 478-481, 1996.
26. Kris-Etherton PM and Keen CL. Evidence that the antioxidant flavonoids in tea and
cocoa are beneficial for cardiovascular health. Curr Opin Lipidol 13: 41-49, 2002.
27. Lindsey M, Wedin K, Brown MD, Keller C, Evans AJ, Smolen J, Burns AR, Rossen RD,
Michael L, and Entman M. Matrix-dependent mechanism of neutrophil-mediated release and
activation of matrix metalloproteinase 9 in myocardial ischemia/reperfusion. Circulation 103:
2181-2187, 2001.
28. Masella R, Di Benedetto R, Vari R, Filesi C, and Giovannini C. Novel mechanisms of
natural antioxidant compounds in biological systems: involvement of glutathione and
glutathione-related enzymes. J Nutr Biochem 16: 577-586, 2005.

H-00413-2008-R1
21
29. McCullough ML, Chevaux K, Jackson L, Preston M, Martinez G, Schmitz HH, Coletti C,
Campos H, and Hollenberg NK. Hypertension, the Kuna, and the epidemiology of flavanols. J
Cardiovasc Pharmacol 47 Suppl 2: S103-109; discussion 119-121, 2006.
30. Middleton E, Jr. Effect of plant flavonoids on immune and inflammatory cell function. Adv
Exp Med Biol 439: 175-182, 1998.
31. Murphy KJ, Chronopoulos AK, Singh I, Francis MA, Moriarty H, Pike MJ, Turner AH,
Mann NJ, and Sinclair AJ. Dietary flavanols and procyanidin oligomers from cocoa (Theobroma
cacao) inhibit platelet function. Am J Clin Nutr 77: 1466-1473, 2003.
32. Nelson KK and Melendez JA. Mitochondrial redox control of matrix metalloproteinases.
Free Radic Biol Med 37: 768-784, 2004.
33. Nijveldt RJ, van Nood E, van Hoorn DE, Boelens PG, van Norren K, and van Leeuwen
PA. Flavonoids: a review of probable mechanisms of action and potential applications. Am J
Clin Nutr 74: 418-425, 2001.
34. Rice-Evans CA, Miller NJ, and Paganga G. Structure-antioxidant activity relationships of
flavonoids and phenolic acids. Free Radic Biol Med 20: 933-956, 1996.
35. Schroeter H, Heiss C, Balzer J, Kleinbongard P, Keen CL, Hollenberg NK, Sies H, Kwik-
Uribe C, Schmitz HH, and Kelm M. (-)-Epicatechin mediates beneficial effects of flavanol-rich
cocoa on vascular function in humans. Proc Natl Acad Sci U S A 103: 1024-1029, 2006.
36. Selmi C, Mao TK, Keen CL, Schmitz HH, and Eric Gershwin M. The anti-inflammatory
properties of cocoa flavanols. J Cardiovasc Pharmacol 47 Suppl 2: S163-171; discussion S172-
166, 2006.
37. Senft AP, Dalton TP, and Shertzer HG. Determining glutathione and glutathione disulfide
using the fluorescence probe o-phthalaldehyde. Anal Biochem 280: 80-86, 2000.
38. Silverman HS and Pfeifer MP. Relation between use of anti-inflammatory agents and left
ventricular free wall rupture during acute myocardial infarction. Am J Cardiol 59: 363-364, 1987.
H-00413-2008-R1
22
39. Steffen Y, Schewe T, and Sies H. Myeloperoxidase-mediated LDL oxidation and
endothelial cell toxicity of oxidized LDL: attenuation by (-)-epicatechin. Free Radic Res 40:
1076-1085, 2006.
40. van Praag H, Lucero MJ, Yeo GW, Stecker K, Heivand N, Zhao C, Yip E, Afanador M,
Schroeter H, Hammerstone J, and Gage FH. Plant-derived flavanol (-)epicatechin enhances
angiogenesis and retention of spatial memory in mice. J Neurosci 27: 5869-5878, 2007.
41. Wakeno M, Minamino T, Seguchi O, Okazaki H, Tsukamoto O, Okada K, Hirata A, Fujita
M, Asanuma H, Kim J, Komamura K, Takashima S, Mochizuki N, and Kitakaze M. Long-term
stimulation of adenosine A2b receptors begun after myocardial infarction prevents cardiac
remodeling in rats. Circulation 114: 1923-1932, 2006.
42. Wang S, Dusting GJ, May CN, and Woodman OL. 3',4'-Dihydroxyflavonol reduces
infarct size and injury associated with myocardial ischaemia and reperfusion in sheep. Br J
Pharmacol 142: 443-452, 2004.
43. Waterhouse AL, Shirley JR, and Donovan JL. Antioxidants in chocolate. Lancet 348:
834, 1996.
44. Wippel R, Rehn M, Gorren AC, Schmidt K, and Mayer B. Interference of the polyphenol
epicatechin with the biological chemistry of nitric oxide- and peroxynitrite-mediated reactions.
Biochem Pharmacol 67: 1285-1295, 2004.
45. Yellon DM and Hausenloy DJ. Myocardial reperfusion injury. N Engl J Med 357: 1121-
1135, 2007.
H-00413-2008-R1
23
Figure Legends.
Figure 1. Infarct area as a function of area at risk (IA/AAR) in IR rats subjected to 10d vehicle or
epicatechin treatment and 48h reperfusion. Infarct size was determined by staining hearts with
trypan blue and triphenyltetrazolium chloride. (A) Dispersion plot of the area at risk in IR (n=21)
and IR +10 d epicatechin (n=15) in rats subjected to 48 h reperfusion. (B) Bar graphs of the
area at risks. (C) Dispersion plot of the infarct area in IR (n=21), and IR + 2d epicatechin (n=15)
subjected to 48 h reperfusion. (D)Bar graphs of the infarct areas. Values are mean ± S.E.M.
Figure 2. Infarct area as a function of area at risk (IA/AAR) in IR rats subjected to 10d vehicle or
epicatechin treatment and 3 weeks reperfusion. Infarct size was determined by staining hearts
with trypan blue and triphenyltetrazolium chloride. (A) Area at risk in IR (n=7) and IR +10 d
epicatechin (n=8) in rats subjected to 3 weeks reperfusion. (B) Infarct area in IR (n=7), and IR +
10 d epicatechin (n=8) subjected to 3 week of reperfusion. Values are mean ± S.E.M.
Figure 3. Myocardial myeloperoxidase (MPO) activity in IR (n=8) and IR + 10 d epicatechin
(n=7) hearts was determined by a recently described colorimetric assay. Values are mean ±
S.E.M.
Figure 4. Myocardial levels of oxidative stress (GSSG/GSH) in IR (n=8) and IR + 10 d
epicatechin (n=7) infarcted hearts were detected in IR hearts using the fluorophore o-
pthalaldehyde. Values are mean ± S.E.M.
Figure 5. Myocardial MMP-2 and MMP-9 levels in IR (n=8) and IR + 10 d epicatechin hearts
(n=7) as determined by gelatin zymography. (A) Representative gelatin zymograms of
myocardial MMP-2 and MMP-9 levels in IR and IR + 10 d epicatechin. (B) Densitometric
analysis of 92 kDa MMP-9 zymographic activity. Values are mean ± S.E.M. ‘Std’ = human MMP-
2/-9 standard.
H-00413-2008-R1
24
Table 1. Hemodynamic data obtained from either normal or 48 h ischemia-reperfusion (IR) groups. Epicatechin groups were pretreated for 10 d. Values shown are mean ± S.E.M. *p<0.05 vs normal.
Normal
Normal + epicatechin
IR
IR + epicatechin
Group Size 6 6 8 8
HR (bpm) 298 ± 17 346 ± 8 368 ± 12* 373 ± 17*
LVPSP (mmHg)
125 ± 8 112 ± 14 102 ± 6 110 ± 5
LVEDP (mmHg)
7.6 ± 0.9 6.7 ± 1.3 5 ± 0.3 4.9 ± 0.5
MAP (mmHg) 101 ± 7 99 ± 10 89±3 90 ± 5
HR = heart rate, LVPSP = left ventricular peak systolic pressure, LVEDP = left ventricular end diastolic pressure, MAP = mean arterial pressure
H-00413-2008-R1
25
Table 2. Hemodynamic and morphometry data obtained from either sham or 3 week ischemia-reperfusion (IR) groups. Epicatechin groups were pretreated for 10 d. Values shown are mean ± S.E.M. *p<0.01 vs. sham; +p<0.01 vs. IR SW thickness.
HEMODYNAMICS
Sham
Sham + epicatechin
IR
IR + epicatechin
Group Size 5 4 7 8
HR (bpm) 318 ± 12 328 ± 11 290±6 302 ± 18
LVPSP (mmHg)
119 ± 2.2 116 ± 6.2 108 ± 2 108 ± 4
LVEDP (mmHg)
6.9 ± 1.1 2.6 ± 0.2 6.1 ± 0.8 5.5 ± 1.5
MAP (mmHg) 94 ± 4.7 92 ± 11 89 ± 2 85±4
MORPHOMETRY
Group Size 5 4 7 8
HW/BW 3.2 ± 0.2 3.2 ± 0.5 4.5 ± 0.2* 4.5 ± 0.2*
Outer LV diam. (mm)
1.6 ± 0.1 1.6 ± 0.1 1.6 ± 0.06 1.6 ± 0.04
Inner LV diam. (mm)
0.53 ± 0.02 0.52 ± 0.08 0.52 ± 0.06 0.55 ± 0.05
AW thickness
(mm)
0.52 ± 0.05 0.53 ± 0.05 0.4 ±0.03+ 0.41 ± 0.02
SW thickness
(mm)
0.49 ± 0.05 0.47 ± 0.04 0.62 ± 0.04 0.49 ± 0.03
HR = heart rate, LVPSP = left ventricular peak systolic pressure, LVEDP = left ventricular end diastolic pressure, MAP = mean arterial pressure, HW/BW = heart weight/body weight, AW = anterior wall, SW = septal wall.

Copyright © 2022 FDOKUMEN




















