Sharad Pawar Dental College and Hospital - Datta Meghe ...
159
Sharad Pawar Dental College and Hospital, Sawangi (Meghe), Wardha Department of prosthodontics, Crown and Bridge “Evaluation of the effect of functional contouring of the palatal vault of maxillary complete denture on clarity of speech sounds in edentulous patients.” An In-Vivo Study By Dr. Surekha Godbole Dubey Research Supervisor Dr. Ashok J. Pakhan Professor and Dean Department of Prosthodontics, Crown and Bridge Sharad Pawar Dental College and Hospital,
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Sharad Pawar Dental College and Hospital - Datta Meghe ...

Sharad Pawar Dental College and Hospital,
Sawangi (Meghe), Wardha
Department of prosthodontics, Crown and Bridge
“Evaluation of the effect of functional contouring of the palatal
vault of maxillary complete denture on clarity of speech sounds in
edentulous patients.”
An In-Vivo Study
By
Dr. Surekha Godbole Dubey
Research Supervisor
Dr. Ashok J. Pakhan
Professor and Dean
Department of Prosthodontics, Crown and Bridge
Sharad Pawar Dental College and Hospital,
Sawangi (Meghe), Wardha
2017
Introduction
3 | P a g e
Declaration by the Candidate
I hereby declare that the thesis entitled “Evaluation of the effect of functional
contouring of the palatal vault of maxillary complete denture on clarity of
speech sounds in edentulous patients.”- An In-Vivo Study is a bonafide and a
genuine research work carried out by me, under the guidance of Dr. Ashok J.
Pakhan, Professor and Dean, Department Of Prosthodontics, Crown and
Bridge, S.P.D.C.
I hereby solemnly affirm that the contents of this thesis have not been
submitted earlier in candidature for any degree elsewhere. The university is
permitted to have legal rights for subsequent uses.
Date:
Place: Sawangi (Meghe), Wardha
Dr. Surekha Godbole Dubey
Ph.D. Scholar
Department Of Prosthodontics, Crown and
Bridge.
Sharad Pawar Dental College and Hospital,
Sawangi (Meghe), Wardha

Introduction
4 | P a g e
Department of Prosthodontics, Crown and Bridge
Sharad Pawar Dental College and Hospital, Sawangi (Meghe), Wardha
Datta Meghe Institute of Medical Sciences (Deemed University)
Certificate
This is to certify that the work embodied in this thesis for the degree of
Doctor of Philosophy (Prosthodontics, crown and bridge) of Datta Meghe
Institute of Medical Sciences (Deemed University), Nagpur, entitled
“Evaluation of the effect of functional contouring of the palatal vault of
maxillary complete denture on clarity of speech sounds in edentulous
patients.” An In-Vivo Study, was undertaken by Dr. Surekha Godbole Dubey
and was carried out in the Department of Prosthodontics, Sharad Pawar Dental
College, Sawangi (Meghe), Wardha, under my guidance and direct supervision
to my satisfaction.
This thesis fulfills the basic ordinance governing the submission of
thesis laid down by Datta Meghe Institute of Medical Sciences University,
Nagpur.
Date:
Place: Sawangi (Meghe), Wardha.
Dr. Ashok J Pakhan
Ph.D. Supervisor
Professor and Dean
Department of Prosthodontics.
Sharad Pawar Dental College and Hospital,
Sawangi (Meghe), Wardha
Department of Prosthodontics, Crown and Bridge

Introduction
5 | P a g e
Sharad Pawar Dental College and Hospital, Sawangi (Meghe), Wardha
Datta Meghe Institute of Medical Sciences Deemed University
Certificate
This is to certify that the work “Evaluation of the effect of functional
contouring of the palatal vault of maxillary complete denture on clarity of
speech sounds in edentulous patients.” An In-Vivo Study for the degree of
Doctor of Philosophy (Prosthodontics, crown and bridge) of Datta Meghe
Institute of Medical Sciences (Deemed University), Nagpur 2013-2016 is
undertaken by Dr. Surekha Godbole Dubey, Professor and Head, Department
of Prosthodontics, crown and bridge, Sharad Pawar Dental College and
Hospital, Sawangi (Meghe), Wardha.
I have great pleasure in forwarding this thesis to Datta Meghe Institute
of Medical Sciences (Deemed University), Nagpur.
Date:
Place: Sawangi (Meghe), Wardha.
Dr. Ashok J Pakhan
Dean
Sharad Pawar Dental College and Hospital,
Sawangi (Meghe), Wardha

Introduction
6 | P a g e
Sharad Pawar Dental College and Hospital,
Sawangi (Meghe), Wardh
Datta Meghe Institute of Medical Sciences (DU), Nagpur.
This is to certify that the work “Evaluation of the effect of functional
contouring of the palatal vault of maxillary complete denture on clarity of
speech sounds in edentulous patients.” An In-Vivo Study for the degree of
Doctor of Philosophy (Prosthodontics, crown and bridge) of Datta Meghe
Institute of Medical Sciences (Deemed University), Nagpur 2013-2016 is
undertaken by Dr. Surekha Godbole Dubey, Professor and Head, Department
of Prosthodontics, crown and bridge, Sharad Pawar Dental College and
Hospital, Sawangi (Meghe), Wardha.
I have great pleasure in forwarding this thesis to Datta Meghe Institute
of Medical Sciences (Deemed University), Nagpur.
Date :
Place :
Dr Sunita Shrivastava
Dean Academics
Sharad Pawar Dental College
Sawangi (M)
Introduction
7 | P a g e
All creatures great and small, even the tiny amoeba are connected in an
endless ebb and flow of messages. The process that makes this connection possible is
the process of communication. Communication is the essence of life. The act of
communication is a process, not an entity. In its simplest form it consists of the
transfer of a message (M) from a sender (S) to a receiver (R) However, the fastest
mode of communication for human being is through speech. In this mode of
communication, there is a speaker and one or more listeners. To produce speech the
participation of various systems is required. Speaking is a complex and highly
coordinated process involving many systems of the human body. Any problem in the
structure and function or the coordination between the systems may lead to
impairment in speech.1
“Say now shiboleth; and he said siboleth, for he could not frame to
pronounce it right……….”- Judges xii;6
According to the Bible, failure to pronounce this single word correctly not
only cost the Ephraimite who mispronounced it his life, but forty and two thousand of
his fellow tribes’ men were slain in the ensuring battle with the Giledites. It is likely
that the consequence of a single oral inaccuracy is unparalleled in history, but this
classic report is indicative of the significant role speech has played in shaping man’s
destiny.2
As speech is the basic fundamental means of communication become the
cornerstone for the establishment and organization of society. In the highly complex
international society of today with the sophisticated systems for transmitting the
voice, the spoken word becomes increasingly important in establishing and
maintaining a niche in the social structure. Today man is judged not only by what he
says, but equally by the way he says it. Proper speech is a reflection of education,
careless speech is an imputation of slovenliness and faulty speech is a handicap
directly proportionate to the speech incapability.
The dental profession, as the guardian of oral health is engaged to a great
extent in altering structures within the oral cavity to alleviate the ravages of disease
and developmental abnormalities. A major portion of speech articulation takes place

Introduction
8 | P a g e
within the oral cavity and any alteration of structures therein will adversely affect
speech proportionate to the location and magnitude of the alteration.2
Phonetics was studied as early as 2500 years ago in ancient India, with
Panini’s account of the place and manner of articulation of consonants in his 5th
century BC treatise on Sanskrit. The major Indian alphabets today order their
consonants according to Panini's classification.
The ability to produce, manipulate and articulate with sounds is called speech.
Speech is such an accepted part of man’s makeup that we seldom pause to consider
that this is a learned function.
Phonetics is the science of sounds used in speech. It is derived from the Greek
word ‘phone’ meaning ‘sound/voice’ and is branch of linguistics that comprises the
study of the sounds of human speech. It is concerned with the physical properties of
speech sounds (phonemes) and the processes of their physiological production,
auditory reception and neurophysiological perception.3
Thus, speech consists of a discrete series of sounds that corresponds to the
letters and words of a written language. Producing and recognizing the sounds of a
language is a highly complex motor and perceptual skill that involve considerable
mental processing. The development of vocal sounds into a meaningful speech was
one of the major accomplishments that has enabled man to reach the pinnacle of the
animal kingdom. Thus, speech is essential to human life but is often taken for
granted.2
The production of various speech sounds is done by the articulatory system,
which consists of several structures of the oral cavity – tongue, lips, teeth, hard palate
and soft palate8. Any alteration or loss of these structures therein will adversely affect
speech sounds produced. This is especially true in case of an edentulous patient who
has lost the teeth and adjacent structures resulting in poor quality of speech sounds,
which the clinician should take note of during fabrication of complete denture.
Though complete dentures are less than perfect replacements for the natural teeth,
they have proven to be effective for countless individuals and are comfortable to
wear, if a person has reasonable expectations and recognizes that there will be an
adaptation phase.

Introduction
9 | P a g e
A successful denture is one in which the three cardinal factors of mechanics ,
esthetics and phonetics are so completely and perfectly harmonized that the patient
not only chews his food but also experiences satisfaction from the contribution of his
denture to the facial expression and speech. Problems in speech is a very common ,
unpleasant and embarrassing experience faced by the patient using new complete
dentures, despite all the efforts made by the dentist in clinical and laboratory
procedures of denture fabrication. Ability to speak clearly while adapting to new
dentures, significantly reinstates the patient’s confidence, a factor that is usually given
secondary importance by the general dental practitioner.4
Of the above mentioned three major factors, considerable progress has been
made in improving the first two factors, mechanics and esthetics but phonetics has not
been given its due attention. This can be reasoned by the fact that most patients get
used to the dentures over a period of time and improve their speech. 4
A scientific approach to the phonetic factor in denture construction often
places the burden on the tongue to adapt, so as to compensate speech changes. If
dentures are to contribute effectively to the functions of speech dentist should utilize
the studies in speech science field to implement their clinical knowledge of the
phonetic factor in denture construction.3
A missing bicuspid will permit a lateral emission, which is intolerable to the
precise speaker or singer. A missing anterior tooth will permit an anterior emission
which impairs speaking until an accommodating articulation pattern is learned. Gross
removal of gingival tissue denies the tongue its usual soft tissue contact and leaves
potential escape of the air stream between the interspaces of the exposed root portions
of the teeth. Mechanical movement of the tooth or teeth in the maxillary arch, as well
as the expansion or constriction of the arch, will increase or decrease the area for
speech articulation. Therefore, it behooves the dental practitioner to be familiar with
speech articulations, particularly those which take place within the oral cavity, in
order to prognosticate the effect of intraoral remedial procedure on speech. Speech
rehabilitation following dental treatment is an obligation of the profession, and failure
to include phonetics in the dental curriculum is not coincident with the high standards
established by dental educators to provide maximum health service.
The poorly contoured replacement for a single tooth can cause speech
impediment, and larger prosthetic restorations fabricated without regard for speech

Introduction
10 | P a g e
articulation will impair speech until an accommodating articulation pattern is learned.
A very high percentage of the English speaking sound are produced by contact of the
tongue with some portion of the palate and teeth. Since these contact areas are
replaced or covered by the complete denture, speech rehabilitation for the edentulous
patient becomes the onerous task of the Prosthodontist. Failure to contour the palate to
accommodate normal tongue contact usually results in poor speech for a period of
several days or several weeks, depending upon the aptitude of the patient and the
discrepancy in palatal contour. This inarticulate period, generally accepted as getting
used to dentures, could be markedly reduced or completely eliminated if proper
attention were given to palatal contour at the time of the waxed trial denture try-in.
Faulty speech is never desirable, even for short periods of time. It is unpleasant for the
listener, embarrassing to the patient, and adds to the burden of adaptation to dentures.
The fact that most denture patients recover from improper articulation after a post-
insertion practice period does not justify neglect of this phase in complete denture
construction nor minimize the Prosthodontist’s responsibility for speech rehabilitation
following delivery of dentures. Contour of palate for proper tongue contact is not
difficult, time consuming, or expensive; however it does require some knowledge of
the fundamentals of phonetics and a precise knowledge of the normal tongue contact
areas for speech articulation. 2
The complete denture may modify speech due to the following reasons –
• Changes in surface will affect resonance and articulation.
• Thickness of the denture in the palatal area reduces the tongue space, again
affecting the resonance and articulation.
• It will also affect the sensory feedback mechanism.
• Emotional behavior of the patients.
Thus, though initial experiences in speech disturbance are transient, the
treatment objective should be to make the dentures conform to the individual patient’s
existing neuromuscular pattern. The dentist should therefore recognize the role of
prosthetic treatment on speech activity4
Speech has been used in the prosthodontic practice to achieve proper anterior
tooth positioning, vertical dimension and in general to simplify the designing of
dentures. Allen (1958)6, Pound E.(1951)
7, Silvermann M.M.(1953)
8, H. Tanaka

Introduction
11 | P a g e
(1973)9, B. Goyal and P. Greenstein (1982)
10 have done pioneering work through
several studies on phonetics in relation to complete denture, in an attempt to
improvise the clarity and intelligibility speech of the edentulous patients who are
acclimatizing to new dentures. However, there have been very few studies in the
literature that use sound spectrographic analysis in combination with individual
perceptions to analyze changes that use of dentures would produce. Hence, the
following study is conducted to assess the changes in the speech sound production in
edentulous patients after rehabilitation with complete dentures after functionally
contouring the palatal vault of the maxillary complete denture.
Complete maxillary and mandibular dentures are required to serve the three
basic functions in the oral cavity: mastication, esthetics and speech. Because
mastication and esthetics assume higher priority from the patient’s point of view and
during the edentulous period speech is not impaired to the same extent as esthetics
and mastication, these two categories have been given more consideration than the
function of speech when dentures have been made. Another factor that reduces the
incentive to improve speech is that most patients learn to speak fairly well once the
tongue “gets used to” and “adapts to” the presence of dentures in the oral cavity. Thus
maxillary complete denture continue to be made with arbitrarily contoured polished
palatal surfaces and depend on the adaptability of the patient to provide “normal
speech” which might takes a few weeks to a few months. So this study was designed
to contour the palatal vault of the maxillary complete denture according to the
individual tongue-to-palate contact and incorporation of newly developed contour in
the same denture10
.Therefore the objective of the present investigation is to develop a
procedure in denture construction which would enable the patient to speak clearly at
the time of insertion of denture thus reducing the getting used period.

Research Question
12 | P a g e
Research Gap Analysis
The speech is the basic fundamental means of communication. The production
of various speech sounds is done by the articulatory system, which consists of several
structures of the oral cavity- tongue, lips, teeth, hard palate and soft palate. Any
alteration or loss of these structures will adversely affect speech sound produced. This
is especially true in case of edentulous patients who lost the teeth and adjacent
structures resulting in poor quality of speech sounds. Complete dentures are proven to
effective for countless individuals as substitute for replacement of natural teeth. A
successful complete denture is one in which three cardinal factors of mechanics,
esthetics and phonetics are so completely and perfectly harmonized that the patient
should be able to perform not only mastication but also experiences satisfaction from
contribution of his denture to facial expression and speech.
Considerable progress has been made in improving the first two factors,
mechanics and esthetics but phonetics has not given its due attention, this can be
reasoned by the fact that most patients get used to the dentures over a period of time
and improve their speech. A very high percentage of sounds are produced by contact
of tongue with different areas of palate and teeth, since these contacts are replaced by
complete denture and failure to contour the palatal morphology results in poor speech.
So this study was designed to contour the palatal vault of the maxillary complete
denture according to the individual's tongue- to-palate contact and incorporation of
newly developed contour for that particular denture, therefore the purpose of the
present investigation was to develop a procedure in denture construction which would
enable the patient to speak clearly at the time of denture insertion and there on. Faulty
speech is never desirable even for the short periods of time. It is unpleasant for the
listener, embarrassing to the patient and adds to the burden of adaptation to the
dentures. The fact that most denture patients recover from improper articulation after
a post insertion practice period does not justify neglect of this phase in complete
denture construction nor minimize the prosthodontist's responsibility for speech
rehabilitation following delivery of dentures. This gap of 8 to 10 days adaptation
period after denture delivery or insertion needs to be minimized. This study is an
attempt to overcome this vital issue in prosthetic dentistry.

Research Question
13 | P a g e
• Various experiments done in past to contour the palate with different materials
like waxes, hydrocolloids, auto polymerizing resin ,rubber base materials, relining
materials which has their own drawbacks.
• So this study was designed to functionally contour the palatal vault of maxillary
complete denture according to the individual’s tongue-to-palate contact by
application of visible light cure resin material which can be molded by tongue
pressure. Results in the improvement in quality of speech
Research Question
Does the functional contouring of palatal vault using visible light cure resin in
maxillary complete denture of edentulous patient improves the quality of speech
sounds?
Generated Hypothesis
Functional contouring of palatal vault using visible light cure acrylic resin in
the maxillary complete denture may improve the quality of speech in edentulous
patients.
Null hypothesis
• There is no improvement in the quality of speech after functional contouring of
palatal vault using visible light cure resin in maxillary denture of edentulous
patients.

Aim and Objectives
14 | P a g e
AIM:-
To evaluate and compare the quality of speech sounds in edentulous patients
before and after functional contouring of palatal vault using visible light cure resin in
Maxillary complete denture.
OBJECTIVES: -
• To evaluate the quality of speech sounds in edentulous subjects wearing
conventional complete dentures without modification of palatal vault using
spectrograph.-(G1)
• To evaluate the quality of speech sounds in edentulous subjects wearing
functionally contoured palatal vault of maxillary complete dentures by visible
light cure acrylic resin using spectrograph .(G2)
• To compare the changes in the quality of speech sounds produced by dentures
made for both the groups –( G1 and G2)
• To establish the association between quality of speech improvement and
functional contouring of palate.

Mechanism of Speech
15 | P a g e
The sound of the voice is unique. It is sufficiently universal to be understood
by millions of people throughout the world who speak the same language, and at the
same time it is sufficiently particular to identify the individual. It is so simple that the
child learns it as speech, and so complicated that a room full of electronic equipment
manipulated by experts cannot simulate it. The cacophony of modern environment
should make it easy to recall that any vibrating body will produce sound and that the
prerequisites for sound are a source of energy and a vibrator. The sound of energy for
the voice is air in the lungs which breathing automatically maintain sufficient quantity
to accomplish the vital exchange of impure gases of metabolism. Lung capacity
varies with the physiology of the individual but with training can be increased to
accommodate the most vicious physical exercise or to permit the opera singer to attain
and sustain a high note on the musical scale.2
Speech, language and communication
Human communication has several modalities, such as speaking, reading,
writing, use of gestures, signing. However, we talk, we listen, and we “think” using
language and speech.
Humans communicate with others about the present, as do other living
creatures but the complexity of language usage and intellectual capacity allows
communication attention to matters of the past and future as well. Human
communication is not bound by time. It is not limited to “here and now”.
Communication is the process of exchanging and / or sharing information – thoughts,
ideas and opinions via the use of language. Language as defined by Lahey, suggest it
to be “a code whereby ideas about the world are represented through a conventional
system of arbitrary signals for communication.”
Communication is a two way process which involves receiving information and
sending information. In verbal communication we receive the message by ear or by
listening and we send the message by speaking i.e., by mouth or orally. During non-
verbal communication receiving the message is mainly based on the visual sense. Here
information by writing the message, through gestures, signs and signing system.
Speech may be called as the communication through vocal and oral symbols.
According to Van Riper, “speech is an audible manifestation of language”. Speech is
very rapid, complex activity and requires very finely tuned muscle movements.

Mechanism of Speech
16 | P a g e
According to Simon (1957) speech can be viewed as learned behavior, social
phenomenon, novel responses, and oral gestures and as means of establishing
interpersonal relation, maintaining emotional homeostasis and manipulating human
behavior.1
Mechanism of speech production
Now imagine the phone rings, you pick it up and say “Hello”. To say this there
is a complex chain of events between the thought and the spoken message. While
saying “hello” you see a whole series of nerves, muscles and body organs. We will try
to understand the processes by which air in the lungs is transformed into the
meaningful sequence of sounds i.e. speech. Speech is a highly coordinated fine motor
act. It involves a high integration and co-ordination between various structures. The
structures involved in speech production are the organs and structures that are a part
of the systems in the human body that participate in the speech production. These
structures include:
FIG 1
• Structures in the respiratory system: lungs, trachea, bronchi, the rib cage,
diaphragms and other muscles of respiration.
• Structures in the phonatory system: larynx, the vocal folds in the larynx and the
muscles of the larynx.
• Structures in the articulatory system: Lips, tongue, teeth, jaw, teeth, and palate.
Mechanism of Speech
17 | P a g e
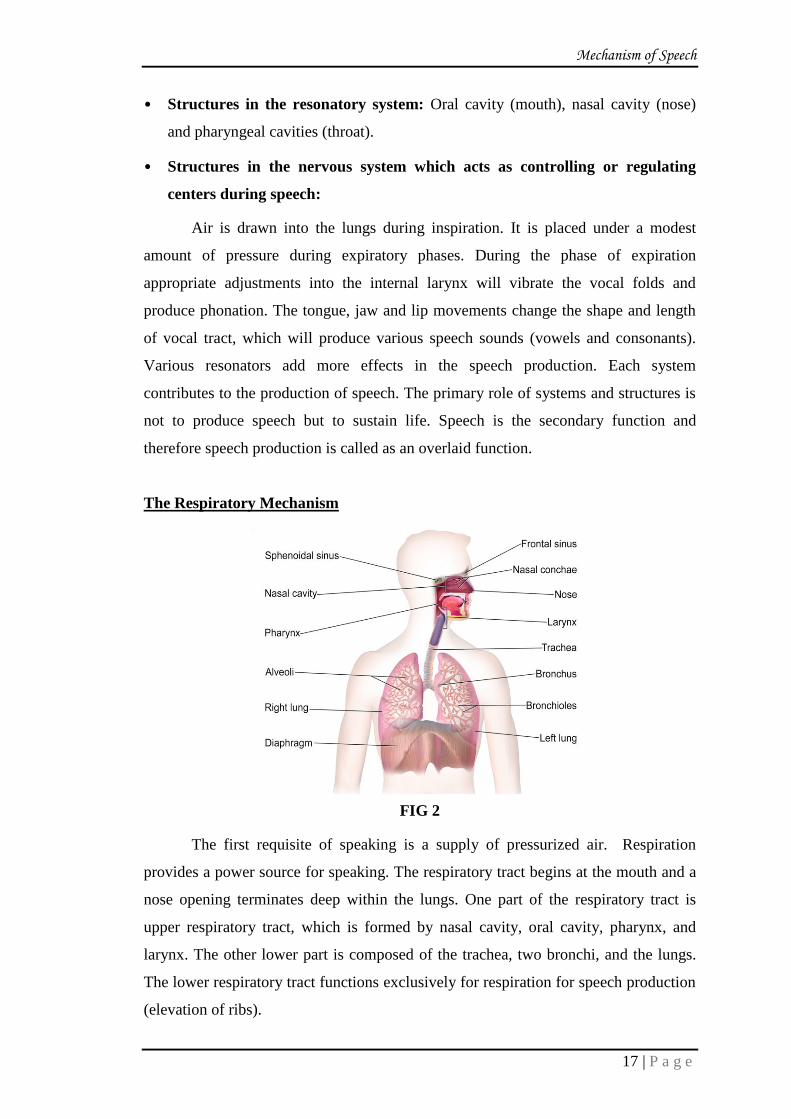
• Structures in the resonatory system: Oral cavity (mouth), nasal cavity (nose)
and pharyngeal cavities (throat).
• Structures in the nervous system which acts as controlling or regulating
centers during speech:
Air is drawn into the lungs during inspiration. It is placed under a modest
amount of pressure during expiratory phases. During the phase of expiration
appropriate adjustments into the internal larynx will vibrate the vocal folds and
produce phonation. The tongue, jaw and lip movements change the shape and length
of vocal tract, which will produce various speech sounds (vowels and consonants).
Various resonators add more effects in the speech production. Each system
contributes to the production of speech. The primary role of systems and structures is
not to produce speech but to sustain life. Speech is the secondary function and
therefore speech production is called as an overlaid function.
The Respiratory Mechanism
FIG 2
The first requisite of speaking is a supply of pressurized air. Respiration
provides a power source for speaking. The respiratory tract begins at the mouth and a
nose opening terminates deep within the lungs. One part of the respiratory tract is
upper respiratory tract, which is formed by nasal cavity, oral cavity, pharynx, and
larynx. The other lower part is composed of the trachea, two bronchi, and the lungs.
The lower respiratory tract functions exclusively for respiration for speech production
(elevation of ribs).

Mechanism of Speech
18 | P a g e
The lungs are housed in the bony rib cage, which formed by 12 pairs of ribs.
The first pair of ribs is joined directly to the sternum by cartilage and it is immovable.
The second to seventh pairs of ribs are attached in thoracic vertebrae by synovial
stern-costal joints with the sternum and are therefore mobile. The eighth to tenth pairs
are inter-costal joints to costal cartilage above and is called as “false ribs”. The last
two pairs are called as “floating ribs” because they are indirectly attached to the
sternum. All the ribs are joined to each other by muscles which are called as
intercostal muscles.
The lungs are composed of elastic, non-muscular tissue surrounding the
alveoli or air. They are supplied profusely with blood vessels. The lungs are capable
of expansion and contraction only by intervention of the respiratory movements
activated by the muscles of respiration. It enters the lungs through the passage of
nose, pharynx, larynx, trachea and bronchi. The trachea is made up of about 16-20
rings which are made up of cartilage. There is bifurcation of last cartilage into 2
bronchi. Bronchi are divide into bronchioles. These bronchioles open into alveoli.
Larynx and Bronchial Tree
FIG 3
The actual gaseous exchange between the blood and oxygen rich air takes
place in the lungs. The oxygen is absorbed from the air by blood circulating through
capillaries of air-sacs. While at the same time carbon dioxide passes from the blood
into the air sacs to be exhaled during exhalation. There is dome shaped muscle the
Mechanism of Speech
19 | P a g e
diaphragms, which lies on each side below the lungs. It separated the thoracic cavity
and abdominal cavity.
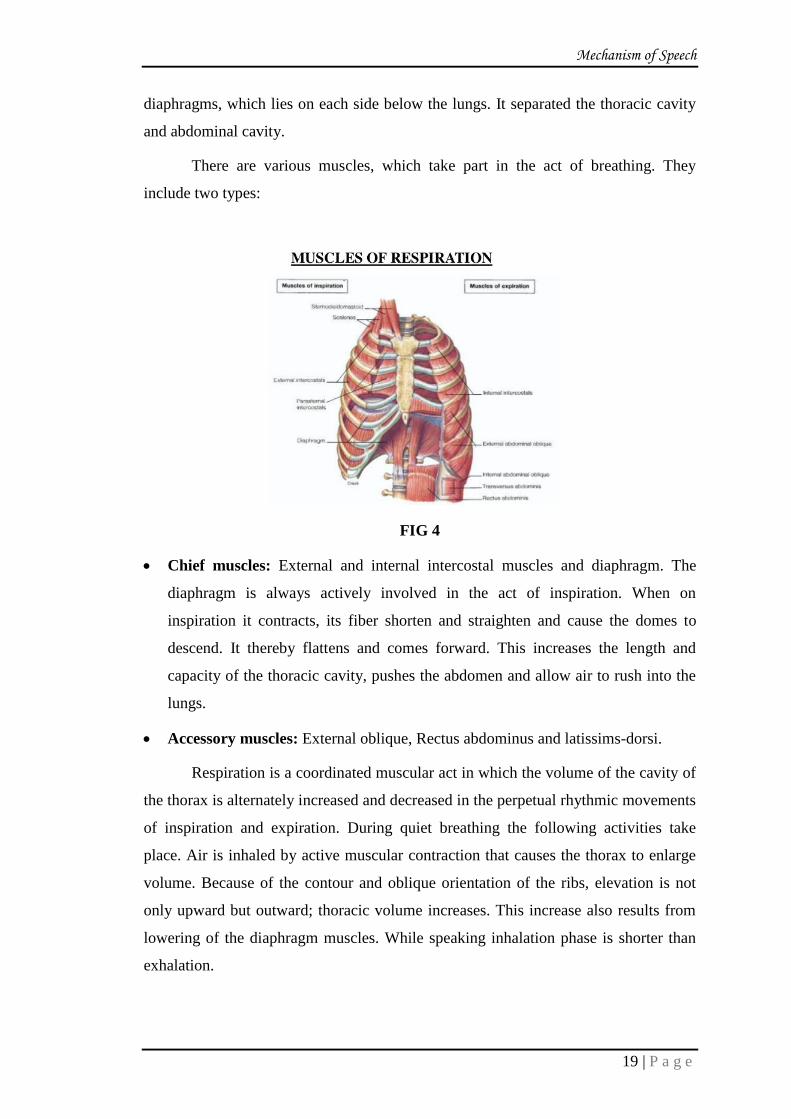
There are various muscles, which take part in the act of breathing. They
include two types:
FIG 4
Chief muscles: External and internal intercostal muscles and diaphragm. The
diaphragm is always actively involved in the act of inspiration. When on
inspiration it contracts, its fiber shorten and straighten and cause the domes to
descend. It thereby flattens and comes forward. This increases the length and
capacity of the thoracic cavity, pushes the abdomen and allow air to rush into the
lungs.
Accessory muscles: External oblique, Rectus abdominus and latissims-dorsi.
Respiration is a coordinated muscular act in which the volume of the cavity of
the thorax is alternately increased and decreased in the perpetual rhythmic movements
of inspiration and expiration. During quiet breathing the following activities take
place. Air is inhaled by active muscular contraction that causes the thorax to enlarge
volume. Because of the contour and oblique orientation of the ribs, elevation is not
only upward but outward; thoracic volume increases. This increase also results from
lowering of the diaphragm muscles. While speaking inhalation phase is shorter than
exhalation.
Mechanism of Speech
20 | P a g e
Quiet breathing is usually under subconscious reflex control, predominantly
driven by elastic forces and the level of CO2.Quiet breathing requires little physical
energy, as it is relaxing. The average quiet respiration airflow is about 500 ml, 12-18
times per minute. The ratio of inhalation and exhalation is equal. Quiet respiration
primarily involves nasal breathing, respiration provides the power source for the act
of speaking. We speak during expiration. During the act of speaking there is quick
inhalation and prolonged exhalation.
Phonatory Mechanism
After the air has been inhaled during inspiration the larynx acts on the exhaled
air stream to create voice. This act is called as “phonation”. Voice is produced by the
vibration of the two vocal folds (also called vocal cords) in the larynx.
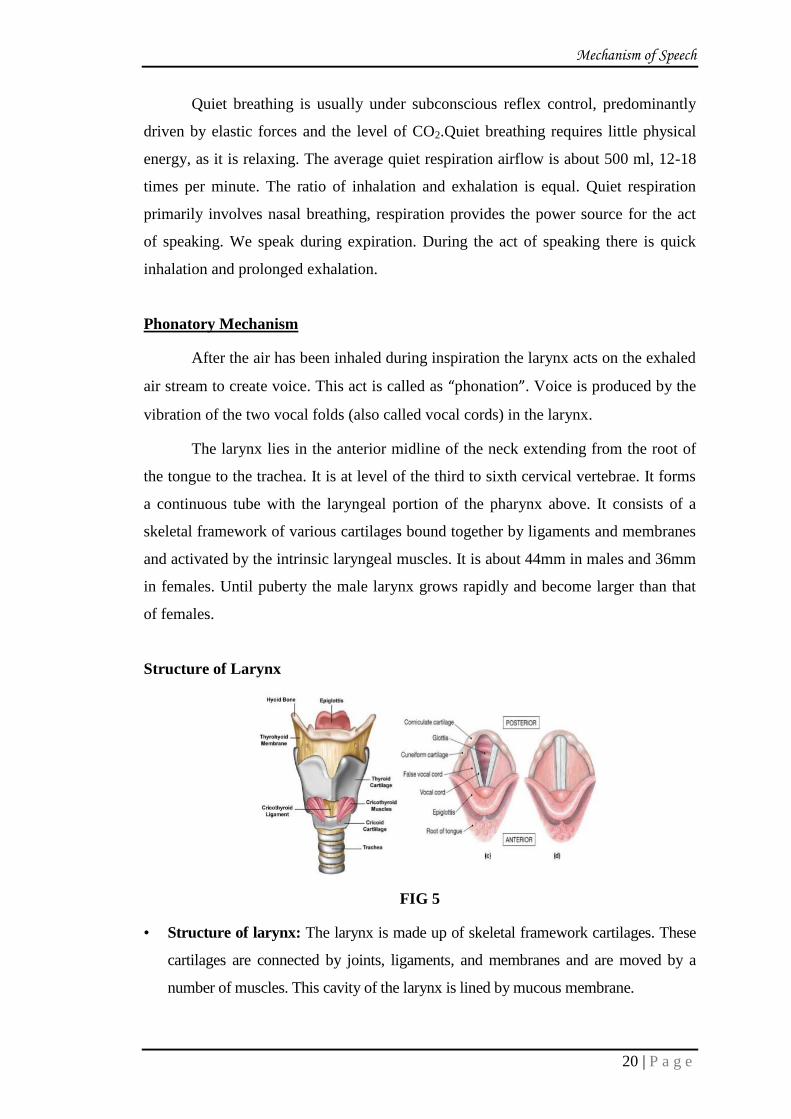
The larynx lies in the anterior midline of the neck extending from the root of
the tongue to the trachea. It is at level of the third to sixth cervical vertebrae. It forms
a continuous tube with the laryngeal portion of the pharynx above. It consists of a
skeletal framework of various cartilages bound together by ligaments and membranes
and activated by the intrinsic laryngeal muscles. It is about 44mm in males and 36mm
in females. Until puberty the male larynx grows rapidly and become larger than that
of females.
Structure of Larynx
FIG 5
• Structure of larynx: The larynx is made up of skeletal framework cartilages. These
cartilages are connected by joints, ligaments, and membranes and are moved by a
number of muscles. This cavity of the larynx is lined by mucous membrane.
Mechanism of Speech
21 | P a g e
The skeleton of larynx is made up of 9 cartilage, 3 paired and 3 unpaired .The
unpaired cartilages are thyroid cartilage, cricoid cartilage and epiglottis.
• Thyroid cartilage: This is the largest cartilage of the larynx. It is shaped like a
shield and can be thought as shielding the structures inside. The most anterior
angle of this cartilage is commonly referred to as the Adam’s apple, which can be
seen on the neck in some men. Thyroid cartilage is composed of two plates of
cartilage, joined at midline to form an angle. Posteriorly thyroid cartilage has two
horns or cornea. The superior horn connects hyoid bone and the inferior connects
the cricoid cartilage. The vocal folds extend from the interior thyroid angle to the
arytenoids across the laryngeal cavity.
• Cricoid cartilage: It’s a ring shaped cartilage, narrow in front and broad behind.
It is attached to the thyroid cartilage on its upper end and to the first tracheal ring.
• Epiglottis: It is a leaf shaped larger cartilage. It is not considered important for
phonation. It is attached to the posterior cricoid elevation and the root of tongue. It
funnels the food to the esophagus and away from the laryngeal inlet.
The paired cartilages are arytenoids cartilages, corniculate cartilages and
cuneiform cartilages. The corniculates are small coned shaped cartilages that form
the apex of the arytenoids. The cuneiform cartilages are small rod shaped
cartilages found within the ary-epiglottic-fold, a fold of tissue and muscle
coursing from the arytenoids to the epiglottis.
• Arytenoids cartilages: These two cartilages each positioned on either side of the
midline on the supra-posterior surface of the cricoid cartilage. They are roughly
pyramidal in shape. The most anterior angle of the base of the arytenoids is called
vocal process. On this the vocal folds are attached. The body of vocal folds are
made of thyroartenoid muscle. There are various muscles attached to these
cartilages. Some, muscles are extrinsic muscles, which alter the position of the
larynx. Other muscles are called intrinsic muscles, which help in phonation.
The vocal folds are two muscle bands that serve to open and close the trachea
by vibrating to and fro. When the vocal folds are open, free flow of air from the
trachea to the oral and nasal cavities is possible. The opening between the two vocal
folds is called the glottis. During the normal breathing, the vocal folds are separated
from each other (glottis is open), allowing air to flow easily. When the vocal folds
Mechanism of Speech
22 | P a g e
vibrate to and fro, the air stream coming from the lungs is released into the cavities
above the larynx in small air puffs. This results in the production of a complex sound
called the laryngeal tone. (Phonation) The laryngeal muscles play an important part in
opening and closing the glottis. The glottis can be completely open when the vocal
folds are away from each other and it can be completely closed when the vocal folds
are tightly closed against each other. The laryngeal muscles can also close the glottis
only lightly so that the vocal folds can be parted by air pressure from the lungs,
causing rhythmic opening and closing of the glottis for phonation. During phonation,
the vocal folds follow a rhythmic cycle:
• Vocal folds come together.
• Air pressure below the glottis is increased.
• Due to the pressure the vocal folds open up.
• Emission of puff of air.
• Vocal folds close again due to the decrease in air pressure and constant muscle
tension.
When the vocal folds close, air pressure below the glottis again increase and
the pattern is repeated. The resulting periodic puffs of breath give the sound of voice.
The frequency at which the vocal folds vibrate (number of vibrations per
second) determines the fundamental frequency of the voice. The fundamental
frequency of the voice depends on an interaction between the height of the larynx in
the neck and the length, thickness and tension of the vocal folds. The vocal folds of
males vibrate at a lower frequency while that of females vibrate at a higher
fundamental frequency, the frequency of vibration is highest in the children. The
fundamental frequency of vibration decides the individual’s vocal pitch. When the
increase in air pressure below the glottis is considerable, the vocal folds are forced
farther apart during the close - open - close cycle. The pitch and loudness of the voice
can be voluntarily changes by an individual to some extent.
Mechanism of Speech
23 | P a g e
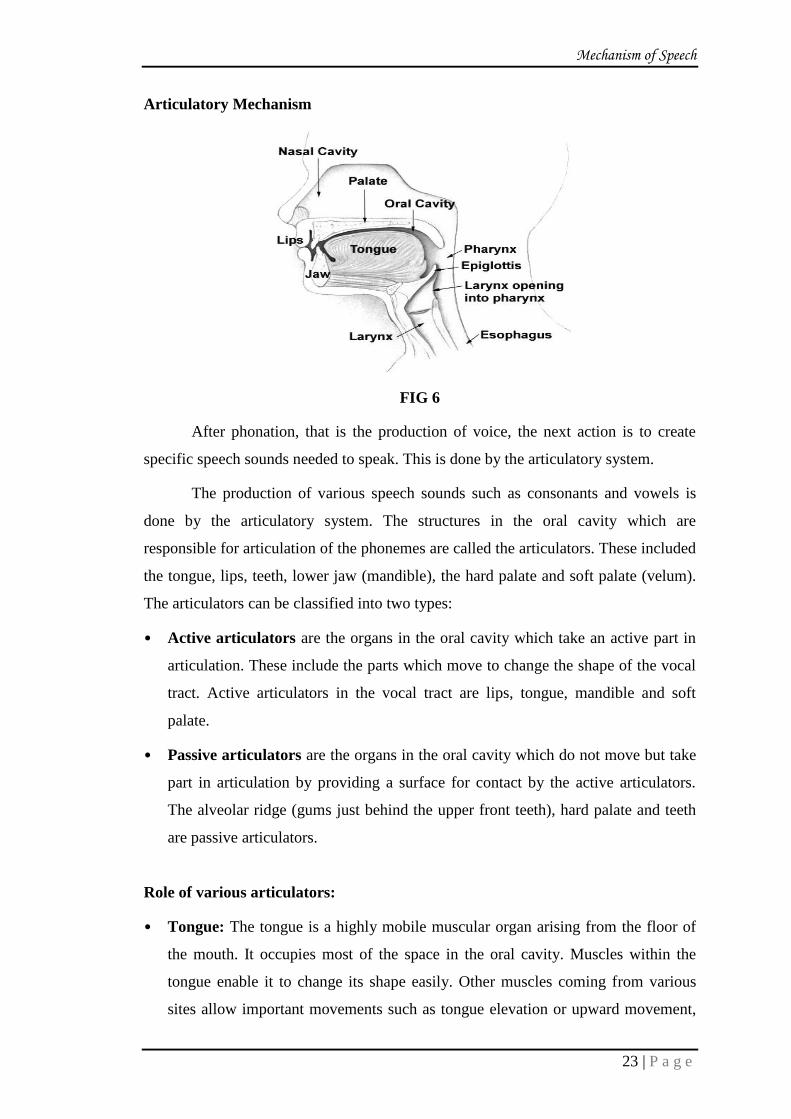
Articulatory Mechanism
FIG 6
After phonation, that is the production of voice, the next action is to create
specific speech sounds needed to speak. This is done by the articulatory system.
The production of various speech sounds such as consonants and vowels is
done by the articulatory system. The structures in the oral cavity which are
responsible for articulation of the phonemes are called the articulators. These included
the tongue, lips, teeth, lower jaw (mandible), the hard palate and soft palate (velum).
The articulators can be classified into two types:
• Active articulators are the organs in the oral cavity which take an active part in
articulation. These include the parts which move to change the shape of the vocal
tract. Active articulators in the vocal tract are lips, tongue, mandible and soft
palate.
• Passive articulators are the organs in the oral cavity which do not move but take
part in articulation by providing a surface for contact by the active articulators.
The alveolar ridge (gums just behind the upper front teeth), hard palate and teeth
are passive articulators.
Role of various articulators:
• Tongue: The tongue is a highly mobile muscular organ arising from the floor of
the mouth. It occupies most of the space in the oral cavity. Muscles within the
tongue enable it to change its shape easily. Other muscles coming from various
sites allow important movements such as tongue elevation or upward movement,
Mechanism of Speech
24 | P a g e
protrusion or outward movement, retraction or backward movement and
lateralization or side to side movement. The tongue can be divided into its tip,
middle portion and back. The tongue can narrow and point as it does for the sound
l as in letter, or it can present a broad front surface as it does in the production of
the sound sh as in shirt. The back of the tongue can be elevated independently of
the front portion as in the production of the sound k as in kite. The vowels and
diphthongs of our speech are produced primarily by the movement of the tongue.
The tongue is the most important structure for articulate speech. In some children
there may be tongue tie, the tongue tip may not be free and hence may cause
difficulty in raising the tongue. This will cause the child to have difficulty in
producing sounds which require tongue elevations, such as l, t and r.
• Lips: The lips are made up mainly of facial muscles which make it possible for
them to spread, round, come together or pucker. They are most visible structures
of the mouth and are also used in various facial expressions. The lips can close to
stop the air stream as in the production of sounds such as p in parrot, b in bag and
m in mummy. The lower lip can touch the upper front teeth for production of
sounds such as f in father and v in van. Rounding the lips and changing the degree
of lip opening contributes to the production of vowel sounds such as u in pull and
o in four. If there is structural defect such as cleft lip it may cause speech problem.
• Teeth: The teeth that are most important for production of speech sounds are the
four front teeth in each jaw lower and upper. They are used in the production of
speech sounds are such an f in father, v in van, s in six and z in zebra. If teeth are
mal-aligned they will affect the speech.
• Alveolar ridge: This is the gum ridge just behind the upper front teeth. This is an
important point of contact for sounds such as t in ten, d in dog, n in nose, l in
letter, s in six and z in zebra.
• Mandible: The lower jaw or the mandible helps in opening or closing of the
mouth (oral cavity). It also changes the size and shape of the oral cavity required
for different vowels. Mandibular movements are also important in maintaining
optimal vocal resonance.
• Palate: This is the structure separating the oral and the nasal cavities. It extends
from the alveolar ridge to the back of the mouth. The part of the palate just behind
Mechanism of Speech
25 | P a g e
the alveolar ridge is bony and hard. This is called hard palate. The part toward the
back of the oral cavity is soft, muscular and mobile. This is known as the soft
palate or the velum. His hard palate helps to direct the air stream towards the front
of the mouth during consonants articulation. It also contributes to vowel
resonance. It provides various points of contact by the tongue for articulation of
different speech sounds. The soft palate is a mobile structure and can be raised or
lowered. When elevated, it is in contact with the wall of the throat (posterior
pharyngeal cavities to the nasal cavity. When it is not elevated, air can flow from
the oral and pharyngeal cavities to the nasal cavities. This is required in the
production of nasal sounds like m in mat and n in nose. The velum also serves as a
point of contact for the back of the tongue during production of sounds such as k
in kite and g in go. Any structural defect such as cleft palate will have its effect on
speech.
Resonatory Mechanism
The physical (acoustic) changes made in the original vocal tone are called as
resonance phenomenon. The excitation of the air in the spaces above the larynx, in the
pharynx and oral cavity is created by the laryngeal tone. The sound waves created by
vibrations in the larynx travel up through the other structures of the airway, primarily
the hypopharynx, the oropharynx, oral cavity, nasopharynx and nasal cavity.
The place where the velum meets pharynx is the beginning of nasopharynx,
which leads to the nasal cavity. The site is known as the “velopharyngeal port”. When
the velum hangs down during breathing, it connects nasal cavity with oral cavity. This
nasal-oral coupling is required for nasal resonance for nasal consonants m, n. When
the velum is lifted by the muscular action the velopharyngeal port is closed. This
closed position is required for the oral resonance of all vowels and consonants except
nasal sounds. Failure to move the velum rapidly enough, when required can result in
excessively nasal utterance which is called “hypernasality”. Sometimes the
nasopharynx, the pharynx above the velar closure site may become blocked with the
swollen tissues (perhaps because of the allergies and colds) that will block the passage
of the sound waves and airflow through the nasal cavities. Excessive tonsil and
adenoid tissue in nasopharynx and nasal cavities will sometimes create enough
obstruction to give the voice a denasal vocal quality.

Mechanism of Speech
26 | P a g e
Nervous System (Regulatory System)
FIG 7
The role of nervous system is to control the ongoing speech activity. The
ability to communicate effectively is primarily related to the complex nervous system.
This system permits and facilitates communication between a person and his
environment, other creatures and people. It is our brain that allows us to understand
and use the complex structure language. It is the ultimate mediator of most of our
voluntary behavior as well as immediate environment. The system investigates and
transmits neural impulses that stimulate our muscle to contract. At the same time
muscle contraction and movements about the joints initiate neural impulses, and they
turn travel back to the coordinating centers of the brain to “tell it” what is happening
and if things are happening as planned.
The nervous system is divided into a central nervous system and peripheral
nervous system. The central nervous system consists of the brain and spinal cord. The
brain consists of cerebral hemispheres which have different lobes such as frontal lobe,
temporal lobe, parietal lobe, occipital lobe, cerebellum and brainstem. The brain stem
finally leads to the spinal cord. The peripheral nervous system is divide into voluntary
part (cranial nerves and spinal nerves) and involuntary part (autonomous nervous
system).
There are specialized centers in the brain respectively for the various speech
and language functions. The functions of these centers are discussed below:

Mechanism of Speech
27 | P a g e
• The Broca’s Area: It is located on frontal lobe of the left hemisphere. The
Broca’s area is responsible for motor speech. This area is responsible for
originating, planning and carrying out the transmission of messages. Damage to
the area leads to a problem in production of speech and comprehension of spoken
language may also affected but to a lesser degree.
• The Wernike’s Area: Wernike’s area is located in the temporal lobe of the left
hemisphere in most of the individuals. This area is responsible for comprehension
(understanding).
• Cerebellum: The role of cerebellum is coordination of movements required for
production of speech.
• Cranial nerves: The command centers in the cerebral hemispheres relay orders to
the specific muscle groups of speech production and receive information from the
sense organ of hearing through the peripheral nervous system. This is done
through the cranial nerves. There are 12 pairs of cranial nerves. They emerge from
the base of the brain and are named primarily according to the function they serve.
For the control of speech mechanism the fifth (trigeminal), seventh (facial), ninth
(glossopharyngeal), tenth (vagus) and twelfth (hypoglossal) nerves play important
roles. The eighth cranial nerve is the auditory nerve, which is responsible for
hearing and balance.
Parameters of Speech
Speech is produced by a complex interaction between the processes of
respiration, phonation, articulation and resonation. Speech has a number of
parameters that are considered to be a result of various processes involved in the
production of speech. The main parameters of speech are voice, articulation, fluency
and prosody.
Voice: Voice is the sound (tone) generated by the vocal folds in the larynx (voice
box). It is the result of the processes respiration, phonation and resonance. The
various parameters of the vibration of the vocal folds determine the parameters of
voice. Different aspects of the respiratory and resonatory processes also affect the
parameters of voice. Voice can be described in terms of its pitch – which depends
on the fundamental frequency of vibration of the vocal folds, loudness-which

Mechanism of Speech
28 | P a g e
depends on the amplitude of the vibration of the vocal folds and quality – which
depends mainly on the resonatory effects. Very often, the parameters of speech
discussed above are referred to in a different way that categorizes them into the
segmental, non-segmental and the supra- segmental aspects of speech. In that
view voice may be considered as non-segmental feature.
Ling (1976) provides an extensive discussion about these aspects for the purpose
of teaching of speech to the hearing impaired. According to Ling, non-segmental
features of speech are:
Pitch and its control
Loudness and its control
Duration and its control
Quality.
• Articulation: the process of sound production is called articulation. It consists of
a series of finely coordinated overlapping movements to the articulators, placing
varying degrees of obstruction to the outgoing air stream and simultaneously
modifying the size, shape and coupling of the resonating cavities. Correct
articulation of speech sounds require accuracy in the placement of articulators,
timing, direction of movement, strength of movement, speed of movement and the
coordination of all events. Speech sounds are classified mainly as vowels and
consonants. Consonants are further classified depending on the place of
articulation, manner of articulation and presence of voicing during articulation.
• Fluency: Fluency is the smoothness with which sounds, syllables, words and
phrases are joined together during speaking. Speech that flows uninterrupted, at an
optimal rate and easily without unusual hesitations, pauses or breaks is considered
as fluent. In other words, appropriate and timely sequencing of these units of
speech is necessary to maintain the fluency of speech. Fluent speech , then , is that
which is :
Relatively effortless
Relatively free of abnormal pauses or discontinuities
Moves forward quite rhythmically and easily
Spoken at an optimal rate, which is neither too fast nor too slow.
Mechanism of Speech
29 | P a g e
• Rhythm or prosody or supra segmental: prosodic features of speech are those,
which give speech its melody and rhythm. Speech rhythm carries meaning aids
under-standing, conveys emotional state and expresses esthetic qualities. Rhythm
features are produced by changes in voice and articulation, and usually by a
combination of the two.
Features such as intonation, emphasis, phrasing and rate of speech contributes to
the prosody of speech. Because prosodic features such as stress, intonation and
emphasis are often spread over more than a single consonants or vowels, they are
often referred to as the “suprasegemental” aspects of speech.
Rhythm features that are relevant to speech include:
• Emphasis: Increased stress to a word in a phrase. Emphasis is produced primarily
by an increase in intensity and duration of syllables within the stressed word. An
accompanying change in frequency also occurs. The stress on a word or a syllable
will give more meaning.
• Intonation: Change in pitch from syllable to syllable, rather than from word to
word. Important linguistic information can be conveyed through intonation
without using additional words. There are different intonation patterns we use to
convey meaning. For example, while asking a question we use a rising intonation,
while for statement we use falling intonation.
• Phrasing: Organization of words into groups related to units of meaning. It has
two components- the words linked in speech and the pauses between phrases.
Pause help the speaker to inhale air, to mark grammatical boundaries and to
provide time for planning of new material while speaking. If there are no pauses
then speech will be difficult to follow. Also if the pauses then speech will be
difficult to follow. Also if pauses are given at inappropriate places then it will
change the meaning. For example “go slow work in progress”. In this sentence if
the pause is taken before the word slow then meaning of sentence will be “go,
slow work in progress”. And if we take a pause after the word slow then the
sentence will become “go slow, work in progress”.
• Rate: Number of syllables uttered in per unit of time. Individuals vary in the rate
at which they talk. Rate is usually measured as the number of words per minute or
Mechanism of Speech
30 | P a g e
the number of syllables per second. Most adults read only from 160 to 180 words
per minute. In connected conversational speech, we average 5 to 5.5 syllables per
second or about 270 words per minute. If the speech is very fast it will be difficult
to flow. If it is too slow then it will be too boring to listen.
Speech Intelligibility
Intelligibility refers to the degree to which a message can be understood. It is
the clarity with which an average listener can understand one’s utterances. In other
words, it is that aspect of oral speech language output that allows a listener to
understand what a speaker is saying. We therefore describe a person’s speech in terms
of its intelligibility. For example, when we understand everything that Mr. X say that
“Mr. X’s speech intelligibility is good”.
Intelligibility of speech depends on various factors such as:
• Appropriate use of the speech parameters discussed above,
• Listener’s ability to predict parts of the message,
• Location of pauses,
• Speed with which the utterances are produced, and
• Grammatical complexity of the sentences.
Functions of Speech
Speech is one of the fastest and most efficient mode of communication. It is
most fundamental to human beings. Speech can serve a number of functions. Some of
these are:
• Gaining attention: The most primary function of speech can be that of helping an
individual in gaining attention of another person. In a crowded place calling out
someone’s name or using some predetermined words to signal someone rather
than whistling are examples of this.
• Exchange of information: Individuals can give and get information about a lot of
things by speaking. As it is very commonly seen, information spreads very fast
by” word of mouth”. Exchange of information can occur not only between two
individuals, but also between members of two groups, two cities, two countries

Mechanism of Speech
31 | P a g e
and two generations. Important about legacies, traditions, religious rituals, etc. is
passed from one generation to another through speech.
• Sharing of emotions: Speech is an important medium through which an
individual expresses his or her emotions and feelings. It helps individuals to elate
better with each other, build interpersonal relations with each other and promote
intimacy. Speech also serves as a medium for ventilating one’s pent –up emotions.
• Speech as a controlling medium: Through speech an individual can influence
and control the behavior of another individual. Speech can be used for intents such
as requesting, asking, reprimanding, convincing, warning and many more, which
help in changing, monitoring or effectively for gaining cooperation of other
persons in a cooperative Endeavour. It is through speech that great leaders could
gate the respect and cooperation of their countrymen.
• Speech reflects individuality: Every individual has his ways to communicate. An
individual can express his or her individuality by speaking his or her mind or by
expressing his or her opinion in his own style. It is through speech that an
individual can achieve his or her identity and entity. Actors and other public
figures are often remembered by their unique styles of speaking.
• Speech as recreation: Through silent movies, mime acts and other forms of non-
speech entertainment are available, they are not as popular. Some of the best
forms of recreation and entertainment use speech as the medium. Theatre, cinema,
drama, mimicry and singing all make use of the oral mode of communication. The
functions of speech thus can be summarized as follows:
• To gain attention
• To give information
• To get information.
• To bind one generation to another.
• To express emotions.
• To promote intimacy.
• To influence other’s behavior.
• To facilitate cooperative activities
• To express individuality

Mechanism of Speech
32 | P a g e
Characteristics of Normal Speech
For the speech to be effective and contribute to appropriate social interactions,
it must have certain characteristics. We will now discuss these:
• Purposiveness: For speech to be effective, it should be purposeful. It should serve
the purpose with which the speech was initiated to begin with. If speech is meant
to seek information about something, it should do so. If it intends to express an
emotion, it should do so correctly. Speech that does not serve its purpose is not
effective.
• Communicativeness: Speech should be purposive and should carry a sense of
personal contact and rapport with the listeners. Communicativeness is possible
only when there is a full realization of the meaning s that are being conveyed.
Also, for speech to be communicative, it should be direct and logical.
• Agreeable voice quality: To be most effective as an instrument of
communication, the speaker’s voice should be of good quality. It should not be
breathy, harsh, shrill, excessively nasal or unpleasant. It should be age and gender-
appropriate, of optimum pitch and adequately loud.
• Flexibility: Flexibility of speech refers to flexibility if features such as pitch,
loudness, rate, quality and stress, without flexibility, speech will become
monotonous and boring. Flexibility refers to variations that a speaker creates
while speaking. This can be achieved by varying the quality of speech i.e., varying
the length of the sentences, varying the rate of speech and varying the number and
length of pauses.
• Adequate projection: Projection refers to speech and voice that is sufficiently
strong. Good projection arises from a good voice mechanism, proper use of the
voice mechanism, interest, enthusiasm and animation on the part of the speaker.
Failure to open the mouth adequately, failure to provide adequate breath stream
and indistinctly articulation lead to inadequate projection.
• Adequate articulation: Distinctness of speech requires flexibility and agility of
speech organs. For correct and adequate articulation, the sounds in the language
should be formed at the right place of articulation and in correct manner of
articulation.

Mechanism of Speech
33 | P a g e
• Correct pronunciation: The pronunciation of a good speaker should be
acceptable by the listeners. This is especially relevant to the variations in the
pronunciation of a particular word in different dialects and religion.
• Ease of bearing: The posture and the body language of the speaker convey a lot
about the speaker. Awkwardness, stiffness and an immovable and inflexible
posture may not convey ease and comfort on the part of the speaker. An erect
posture, but not an arrogant or rigidly tense one, may be more effective.
• Absence of excessive fear and timidity: A wholesome attitude towards speaking,
one that is free of fear, anxiety and timidity will definitely be more effective to the
listener. If the speaker reflects these feelings, it may give an expression that the
speaker is not well versed with the topic of discussion.
• Semantic/linguistic soundness: A good and effective speaker is one who makes
good and apt choice of the right words in the right context. A powerful vocabulary
with good knowledge of linguistic rules contributes immensely to effective
speech.
Speech as an Overlaid Function
Overlaid means secondary function. The overlaid function has a great
importance along with the primary function. It is often paradox that our body does not
have any special organ for speech production. All the systems, which are involved in
speech production, have many biological functions on which our body is entirely
dependent on for survival. Without speech an individual can live but without lungs he
cannot survive. As far as speech is concerned it is secondary function of each organ,
which is directly or indirectly helpful for production of speech. However, it has been
found that the various organs of our body, which have other primary functions, like
eating, chewing, respiration (breathing) etc., help in production of speech. Thus speech
is an imposed function on them and it is therefore said to be overlaid. According to
Negus (1923). Speech is overlaid upon non-vegetative functions”. Thus speech
production is a secondary process for various organs whose main function is to perform
various primary biological functions to keep the human being alive. The respiratory,
phonatory, resonatory and articulatory systems along with nervous coordination
combine to form a whole body functional unit during the production of speech.

Mechanism of Speech
34 | P a g e
All the above structures and the muscles involved in speech production are
used for other bodily activities that are important for sustaining life. Breathing which
provides the airstream for speaking is very necessary for life. The lungs transfer
oxygen to the blood and then to the muscles and remove impurities. The larynx or the
voice box has the basic function of preventing the foreign objects and food from
entering the lungs. The vocal folds also help to cough up anything, such as food and
phlegm, which the lungs reject. The larynx also help in fixation of the chest cavity
during activities such as pushing, pulling, lifting heavy objects and childbirth. The
structures in the articulators are basically used for chewing and swallowing which are
also functions necessary for life. The tongue directs food to the back of the cavity, the
lips help in keeping the food from escaping out of the mouth, the teeth cut, grind and
chew the food, the palate provides a hard upper surface for swallowing and the velum
or soft palate keeps food from entering the nasal cavity. The resonating structures are
the cavities through which necessary food or air passes. But these same organs are
also used to produce very delicately and very accurately modulated chains of sound
through which we communicate. Because the speech process utilizes the same
structures that are used in important biological (bodily) functions, speech is called an
overlaid function. This means that speech is a secondary function of the organs which
basically works towards sustaining life.1
COMPONENTS OF SPEECH
Kantner and West divided speech into 5 components:-
Respiration, phonation, resonations, articulations and neurologic integrations,
Chierici and Lawson added audition, or the ability to hear sounds, to this list. The
successful performance of these functions is necessary for the production of
acceptable speech.
• RESPIRATION:-
During respiration, inhalations and expirations are approx., equal in duration
and the airflow and regular and repetitive. During speech, however, the inhalation
phase is shortened and the exhalation phase in prolonged and not repetitive. In
normal discourse, the volume and pressure of the expelled air is comparable to the
vegetative breathing. Upward movement of the diaphragm with contraction of the

Mechanism of Speech
35 | P a g e
costal cartilage and contiguous musculature creates an intrapulmonary pressure which
is greater than atmospheric pressure, the permitting air to be expelled from the lungs.
Prolongation of exhalation is achieved by the valve mechanism along the laryngeal,
pharyngeal, oral and nasal components of the respiratory tract these valves impede the
expired air and help to create speech signals. Subglottic pressure is maintained by the
balanced elasticity between the inspiratory intercostal musculature and the expiratory
abdominal musculature. If the vital capacity of lungs is compromised, as in
emphysema, speech will be perceived as “breathy”. The poor projections of the voice,
in such cases are due to the reduced volume and pressure of the expired air.
• PHONATION:-
The larynx provided the first level of constrictions for controlling the
respiration air stream. The primary function of vocal cords is to protect the lungs and
the lower respiratory tract from inhalation of particulate matter. This mechanism
requires a simple, forceful approximation of the vocal folds. Speech, conversely,
requires a multitude of positions, varying tensions and vibratory cycles, and an
intricate co-ordination of the vocal folds with other structures. If the vocal folds are
partially or completely adducted or closed, they impede the expired air. With the
proper degree of tension and sufficient sub-glottal pressure, the vocal cords may set in
vibration and thus impart phonation to air stream. Whereas phonation is essential for
certain speech sounds, other speech signals do not require phonation, hence, the vocal
folds are abducted or open. The tension and position of vocal folds will, in part,
determine the pitch of the phonated sound. In the production of low pitched sounds,
the vocal folds are relatively thick and flaccid. In high-pitched sounds, the margins of
the approximated folds are thin and tense.
• RESONATION:-
The sounds produced at the level of vocal folds, is not the final acoustic signal
with is perceived as speech. This sound is augmented and modified by the chambers
and structures above the level of glottis. The pharynx, the oral cavity and the nasal
cavity act as resonating chambers and the structures above the level of glottis. The
pharynx being a muscular tube, services as an excellent resonating chamber. This
tube is formed by 3 closely associated muscles namely: - inferior, middle and superior
Mechanism of Speech
36 | P a g e
constrictor. These muscles are unique in that they share common insertions, the
medial pharyngeal raphe, but have a different anterior origin. Also, it appears that
each muscle constrictor, as well as portions of each muscle can contact selectively.
The dimensional changes imparted by this muscular action influence the resonant
characteristics of the pulsating air stream as it emerges from the larynx. The
velopharngeal mechanism proportions the sound and / or air stream between the oral
and nasal cavities and influences voice quality (or the basic sound) that is perceived
by the listener. If velopharangeal closure is compromised, or if the structural integrity
or relative size of the oral, pharyngeal or nasal cavities has been altered, voice quality
can be compromised.
• ARTICULATION:-
Amplified, resonated sound is formulated into meaningful speech by the
articulators, namely, the lips, tongue, cheek, teeth and palate, by changing the relative
spatial relationship of these structures. The tongue is considered to be the single most
important articulator of speech because of its ability to affect rapid changes in
movement and shape. The tongue may impede, selectively restrict, and channel the air
stream with precise contact against the teeth and palatal areas, thus articulating the
basic laryngeal sound, or the non-phonated air stream, into recognizable speech. If
oral structures such as the tongue, adjacent soft tissues, jaws or lips, are altered
surgically and / or neurologically, articulation may be compromised.
• NEURAL INTEGRATION: -
Speech is integrated by the central nervous system both at the peripheral and
central level. The sequential and simultaneous movements required throughout the
speech this complex demand precise co-ordination.
Neurologic impairments may compromise, a specific component of the speech
mechanism. Such as the vocal folds, soft palate or tongue, or it may indirectly affect
the entire speech system. A cerebro-vascular accident may compromise the ability of
the patient to comprehend and / or formulate meaningful speech, even though all
structures used to produce speech are anatomically within normal limits. In addition, a
neurologic impairment may produce a specific type of speech deformity. Example:
The loss of motor innervations to the soft palate may compromise elevation and
velopharyngeal closure.

Mechanism of Speech
37 | P a g e
• AUDITION:-
Audition, or the ability to receive acoustic signals, is vital for normal speech.
Hearing permits receptions and interpretation of acoustic signals and allows the
speaker to monitor and control speech output. Compromised hearing can preclude
accurate feedback and hence, affect speech. Speech development and subsequent
speech therapy is hampered in-patient with hearing impairments.
NEUROPHYSIOLOGICAL BACKGROUND
A very complex neuro-physiological mechanism governs the production of
speech. A large number of oral mechano-sensitive receptors (tactile and kinesthetic)
are involved in its molar control. Therefore, all prosthodontic treatment will, more or
less, have an influence on speech performance because a great number of these
structures will be involved.
Speech production includes large number and sequences of innate and learned
motor acts produced in sequences of 12-16 sounds/sec in a rhythmic behavior. It has
been hypothesized that less cortex area is required for processing of skills as they
become automatic. Once automatized, speech control becomes localized in certain
areas such as the pre-motor and motor cortex. For the precise movements executed in
speech production the pyramidal motor system has the primary role.
Feedback plays a dynamic and flexible role in the control of most motor
events, including sequencing and timing of speech movements, there seems to be a
subconscious but learned type of pattern recognitions, or feedback, of afferent
information’s used to guide central pattern generator (CPG’s) and a central program.
The CGPs are thus important in the basic rhythm generation and timing of motor
activity. Other neural networks are also very active in the rapid transformations of the
shape of the oral cavity from one fixed configurations to another. Proprioceptive
mechano-sensitive afferents will establish the timing of certain aspects of the very fast
motor pattern and will, in synergy with cortical information, generate the final motor
output and rhythm. A precise co-ordination between different articulators is essential
for the final sound production.
A prerequisite for the satisfactory speech sounds and adaptation is an intact
general feedback system, that is orosensory and audio feed back with auditory
Mechanism of Speech
38 | P a g e
feedback regarded as an every important mechanism. When impaired hearing is
present, speech production will deteriorate. Adaptation after an oral rehabilitation also
may create problems in the formation of new neuromuscular pathways.
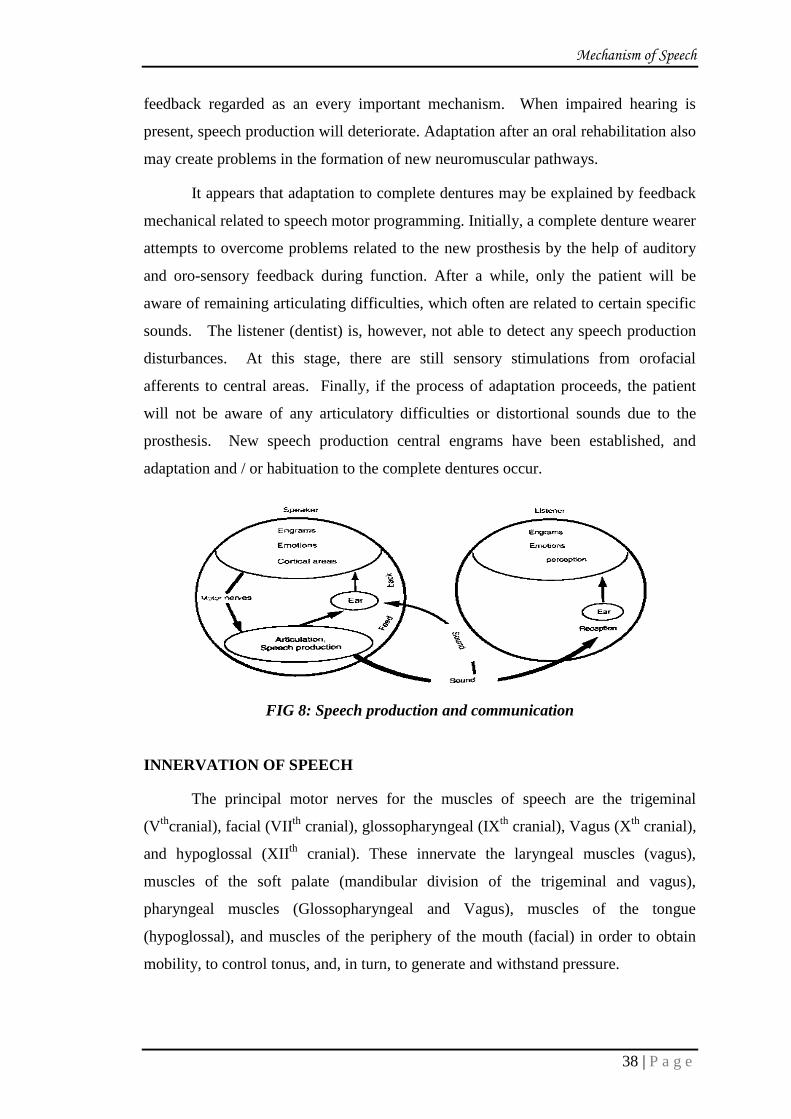
It appears that adaptation to complete dentures may be explained by feedback
mechanical related to speech motor programming. Initially, a complete denture wearer
attempts to overcome problems related to the new prosthesis by the help of auditory
and oro-sensory feedback during function. After a while, only the patient will be
aware of remaining articulating difficulties, which often are related to certain specific
sounds. The listener (dentist) is, however, not able to detect any speech production
disturbances. At this stage, there are still sensory stimulations from orofacial
afferents to central areas. Finally, if the process of adaptation proceeds, the patient
will not be aware of any articulatory difficulties or distortional sounds due to the
prosthesis. New speech production central engrams have been established, and
adaptation and / or habituation to the complete dentures occur.
FIG 8: Speech production and communication
INNERVATION OF SPEECH
The principal motor nerves for the muscles of speech are the trigeminal
(Vth
cranial), facial (VIIth
cranial), glossopharyngeal (IXth
cranial), Vagus (Xth
cranial),
and hypoglossal (XIIth
cranial). These innervate the laryngeal muscles (vagus),
muscles of the soft palate (mandibular division of the trigeminal and vagus),
pharyngeal muscles (Glossopharyngeal and Vagus), muscles of the tongue
(hypoglossal), and muscles of the periphery of the mouth (facial) in order to obtain
mobility, to control tonus, and, in turn, to generate and withstand pressure.

Mechanism of Speech
39 | P a g e
The speech mechanism is characterized by motility, by the capacity to exert
pressure, by the capacity to resist pressure, and by the ability of the talker to identify
through habitual pressures against familiar structures of the conditions for a particular
sound. The motor innervations involved derives from three pathways; the cortico-
bulbar pathway, extra pyramidal paths, and cerebellar paths. The first of these, the
corticobulbar-corticospinal, or pyramidal tract permits the conscious control of
precise movements required, e.g., in the articulation of speech sounds. This tract
becomes important in the relearning of speech habits to accommodate new intra oral
structures. The extra pyramidal tract also conveys some voluntary impulses as well as
the control of muscle tonus, the regulation and inhibition of opposing sets of muscles,
and the coordination of depth of breathing, tension of vocal folds, the lips, the cheeks,
the tongue, and the pharyngeal walls. The third pathway, from the cortex to the
speech muscles, is the cerebellar one, the route of the automatic coordination. This
one takes over much of speech after childhood until violent changes in the speech
mechanism or the functioning of the mechanism are introduced.
PHYSIOLOGIC VALVES IN SPEECH PRODUCTION
The primary functions of the respiratory and digestive tract in relation to their
secondary function of producing and modifying sounds may be understood by
recognizing that the speech mechanism includes three principal physiologic valves.
• Valve I , the glottis
• Valve II, the palato-pharyngeal region
• Valve III, the orifice of the mouth.
FIG. 9
Mechanism of Speech
40 | P a g e
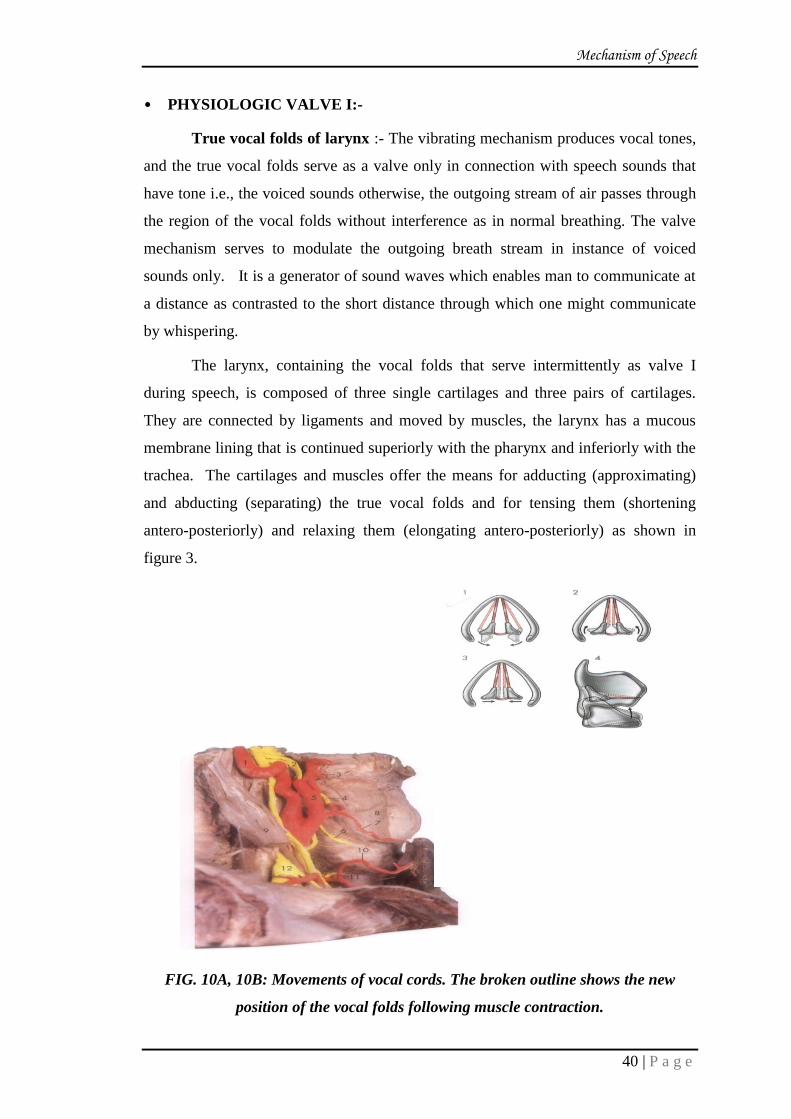
• PHYSIOLOGIC VALVE I:-
True vocal folds of larynx :- The vibrating mechanism produces vocal tones,
and the true vocal folds serve as a valve only in connection with speech sounds that
have tone i.e., the voiced sounds otherwise, the outgoing stream of air passes through
the region of the vocal folds without interference as in normal breathing. The valve
mechanism serves to modulate the outgoing breath stream in instance of voiced
sounds only. It is a generator of sound waves which enables man to communicate at
a distance as contrasted to the short distance through which one might communicate
by whispering.
The larynx, containing the vocal folds that serve intermittently as valve I
during speech, is composed of three single cartilages and three pairs of cartilages.
They are connected by ligaments and moved by muscles, the larynx has a mucous
membrane lining that is continued superiorly with the pharynx and inferiorly with the
trachea. The cartilages and muscles offer the means for adducting (approximating)
and abducting (separating) the true vocal folds and for tensing them (shortening
antero-posteriorly) and relaxing them (elongating antero-posteriorly) as shown in
figure 3.
FIG. 10A, 10B: Movements of vocal cords. The broken outline shows the new
position of the vocal folds following muscle contraction.

Mechanism of Speech
41 | P a g e
The true vocal folds are casually related to voice as opposed to whisper. The
folds are attached anteriorly to the thyroid cartilage and posteriorly to the arytenoid
muscles. When in a position of rest, as in quiet breathing, the free edges of the folds
form a triangular opening which has its apex located anteriorly and its base
posteriorly the opening or aperture between them when they are not approximated is
called rima glottidis. When voice is desired, the folds are approximated, and air is
pushed against them from below with sufficient force to blow the edges of these
elastic folds apart. The overload of air pressure is momentarily spent. Tension
restores the folds to a closed position. This cycle is repeated and becomes
quasivibratory. The acoustic output is called voice.
The muscles that control the vocal folds are divided into two classes:-
• Those within the organ itself (intrinsic) and
• Those that act upon it from out (extrinsic).
The intrinsic muscles have two main functions:-
• To adduct and abduct the folds
• To regulate the degree of their tension and length.
Intrinsic Muscles of Larynx
FIG11A, 11B
Mechanism of Speech
42 | P a g e
The muscle that open the rimaglottidis are posterior Crico-arytenoids. They
are attached to the posterior surfaces of the arytenoid and cricoid cartilages. Thus,
they may rotate the arytenoid cartilages laterally and separate the true vocal cords.
Closure of rima glottides is effected by the arytenoid and lateral crico-
arytenoid muscle. They rotate the arytenoid cartilages medially and cause the true
vocal folds to be approximated. The arytenoids muscle extends from the posterior and
lateral surfaces of one arytenoid cartilage to the corresponding surface of the other.
These bring the arytenoids cartilage together, consequently narrowing the
rimaglottidis. The most important muscle used in lengthening and tensing the true
vocal folds is the cricothyroid.
The vocal folds are relaxed and shortened by the thyroaryteniod muscle.
The extrinsic (accessory) muscles act upon the larynx as a whole, connecting
the larynx with the hyoid bone, the sternum, the tongue and the pharynx. By means
of these muscles, the larynx may be elevated, depressed and tilted.
• PHYSIOLOGIC VALVE II:-
Palatopharyngeal region:-The pharynx is made up primarily of a constrictor band of
broad, flat muscles inserting into a median raphe along its posterior wall. The
pharynx may be divided arbitrarily into three parts (as shown in Fig. 5):-
• The nasal pharynx is a continuation of nasal cavity posteriorly; it is bounded
inferiorlyby the soft palate and terminates along the posterior pharyngeal wall
near the atlas (1st cervical vertebra). It’s only function is respiratory.
• The oral pharynx is a continuation, inferiorly, of the nasal pharynx to the
laryngeal pharynx, i.e. above the level of hyoid bone. Its function are respiratory
and digestive.
• The laryngeal pharynx is the inferior portions of the pharynx. It extends
inferiorly from the oral pharynx and terminates in the esophagus at about the level
of the VIth
cervical vertebra. Its function is strictly digestive. The palato-
pharyngeal valve is located in the region in which the respiratory and digestive
tracts cross each other (pharyngeal Isthmus). Both in the act of swallowing and in
speech, this valve divide the pharynx into naso-pharyngeal and oro-pharyngeal
cavities. The principal closure is affected by movement of the soft palate into
contact with the posterior wall of the pharynx...

Mechanism of Speech
43 | P a g e
Schematic picture of the different valves and articulators
FIG. 12
• PHYSIOLOGIC VALVE III:-
The Mouth:-The mouth is a complicated valve, capable of making many changes,
both in capacity and in size of the orifices. It is modified by many articulators, the
chief one being the tongue.
The three physiologic valves serve to form a number of more specific articulatory
valves, such as:-
• Mandibular lip against the maxillary lip.
• Mandibular lip against the maxillary teeth.
• Tip of the tongue against the alveolar ridge etc.
These valves are formed by momentary intrusions of some segment of the
physiologic valves into the path of the outgoing stream.5
Description of Speech Sounds
In verbal communication we combine words to form sentences. The words are
formed by combining various syllabus / speech sounds. The speech sound production
is a complex process. In the process the speech organs move together in a coordinated
manner. During these movements various speech sounds such as vowels, consonants
and diphthongs are produced. The branch of linguistics that deals with the
characteristics of speech sounds is called phonetics. There are further subdivisions
Mechanism of Speech
44 | P a g e
such as Articulatory phonetics, Acoustic Phonetics and auditory Phonetics. It is
Articulatory Phonetics which deals with the production of sounds by organs of
speech. Articulation is usually to be a joining of parts, however, speech articulation
takes place when any approximation or movement of the articulators constricts,
impedes, and diverts the air stream to produce a single sound. The single sound that
the physiologic airstream mechanism are capable of producing are varied and
innumerable. Many occur as noise and are unclassified, but those that are learned as
speech are called phones. Many of the phones are so similar in character that they
cannot be recognized as separate sounds by other than an expert or when pronounced
very slowly and carefully. These closely related phones have been combined to form
recognizable sounds and are classified as phonemes. The phoneme, then, is the unit of
speech by which we distinguish one utterance from another and which, collectively
(about 40) make up the phonemics of the language. Speech is further classified
according sonority into surds, sonants and consonants. The surd is any voiceless
sound and is produced by separation of vocal folds with no marginal vibration.
Consonants are articulated speech sounds and all require articulation to impede,
constrict, divert or stop the airstream at the proper place and time to produce the
desired sound.
Consonants
Consonants of speech sounds which are produced by closure or narrowing of the air
passage so that the air stream is blocked completely or partially in the mouth or come
out with an audible noise. In the production of consonants airflow out of the mouth is
completely blocked, greatly restricted or diverted through the nose. This gives
consonants a noisy, less melodic quality than vowels. Vowels are produced with an
unobstructed vocal tract .They are produced in a relatively open vocal tract, that is,
without any closure, or narrowing that will produce audible friction. The vowels
require laryngeal tone (voicing), and they provide the carrying power of voice. The
quality of a vowel depends on the shapes of the cavities of the pharynx, the mouth and
nose, which in turn depend on the positions of the soft palate, the tongue and the
lips. A diphthong is a vowel whose quality or timbre changes considerably during its
articulation. For example, the vowel of the word “my “is produced by starting with the
tongue in a low back position and then moving with the tongue up to high front
Mechanism of Speech
45 | P a g e
position ai. The combination of two sounds is known as clusters or blends, tr in train,
br in brown are few examples of blends.
Classification of consonants
Consonants can be classified by: (i) Place of articulation, (ii) Manner of articulation
(iii) Voicing.
(i) Place of articulation: the exact point in the vocal tract at which the air stream is
modified – that is the lips, teeth, alveolar ridge, etc.
(ii) Manner of articulation: the way the air stream from the mouth is modified
(blocked, restricted, diverted, etc.)
(iii) Voicing: whether vocal cords are vibrating or not vibrating. A segment is
described as voiced or voiceless.
Place of articulation
The place of articulation dimension uses the names of the various parts of the
vocal tract. The names are given according to the parts of the vocal tracts. The names
are given according to the articulators that take part in production of that consonant.
• Bilabial
• Labio-dental
• Linguo-dental
• Linguo-alveolar
• Linguo-palatal
• Linguo-velar
• Bilabial Sounds: - The sounds b, p and m are made by contact of the lips.
Insufficient support of lips by teeth and / or denture base can cause these sounds to
be defective. Therefore, the anterior-posterior position of the anterior teeth and the
thickness of the labial flange can affect the production of these sounds like wise an
incorrect vertical dimension of occlusion (VDO) or teeth positioning hindering
proper lip closure, might influence these sounds.
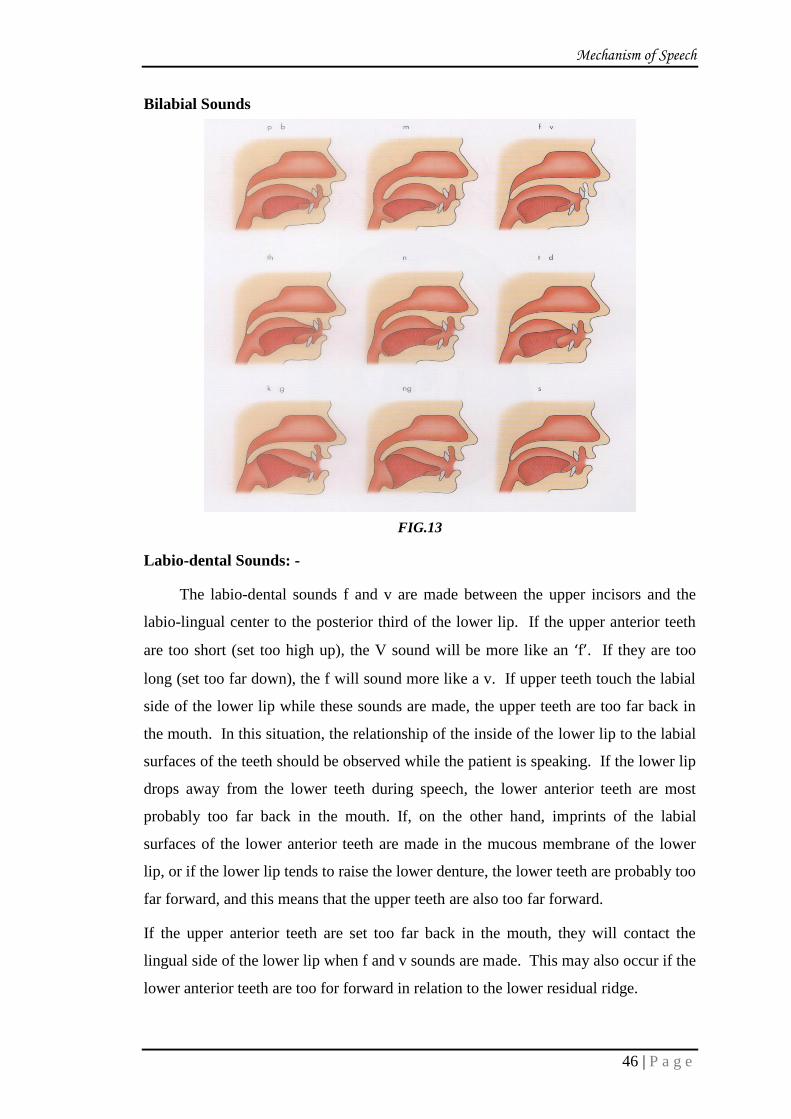
Mechanism of Speech
46 | P a g e
Bilabial Sounds
FIG.13
Labio-dental Sounds: -
The labio-dental sounds f and v are made between the upper incisors and the
labio-lingual center to the posterior third of the lower lip. If the upper anterior teeth
are too short (set too high up), the V sound will be more like an ‘f’. If they are too
long (set too far down), the f will sound more like a v. If upper teeth touch the labial
side of the lower lip while these sounds are made, the upper teeth are too far back in
the mouth. In this situation, the relationship of the inside of the lower lip to the labial
surfaces of the teeth should be observed while the patient is speaking. If the lower lip
drops away from the lower teeth during speech, the lower anterior teeth are most
probably too far back in the mouth. If, on the other hand, imprints of the labial
surfaces of the lower anterior teeth are made in the mucous membrane of the lower
lip, or if the lower lip tends to raise the lower denture, the lower teeth are probably too
far forward, and this means that the upper teeth are also too far forward.
If the upper anterior teeth are set too far back in the mouth, they will contact the
lingual side of the lower lip when f and v sounds are made. This may also occur if the
lower anterior teeth are too for forward in relation to the lower residual ridge.

Mechanism of Speech
47 | P a g e
FIG. 14
• Linguodental Sounds:-
Dental sounds are made with the tip of the tongue extending slightly between
the upper and lower anterior teeth. This sound is actually made closer to the alveolus
(the ridge) than to the tip of the teeth. Careful observation of the amount of tongue
that can be seen with the words – this, that, these and those will provide information
as to the labio-lingual position of the anterior teeth. If about 3mm of the tip of the
tongue is not visible, the anterior teeth are probably too far forward, or there may be
an excessive vertical overlap that does not allow sufficient space for the tongue to
protrude between the anterior teeth. If more than6mm of the tongue extends out
between the teeth when such sounds are made, the teeth are probably too lingual.

Mechanism of Speech
48 | P a g e
FIG.15
• Linguoalveolar Sounds:-
Alveolar sounds (ex. t, d, s, z, v & l) are made with the valve formed by
contact of the tip of the tongue with the most anterior part of the palate (the alveolus)
or the lingual sides of the anterior teeth. The sibilants (sharp sounds) s, z, sh, ch& j
(with ch& j being affricatives) are alveolar sounds, because the tongue and alveolus
forms the controlling valve. The important observations when these sounds are
produced are the relationship of the anterior teeth to each other. The upper and lower
incisors should approach end to end but not touch. A phrase such as “I went to church
to see the judge” will cause the patient to use these critical sounds, and the relative
position of the incisal edges will provide a check on the total length of the upper and
lower teeth (including their vertical overlap).
A failure of the incisal edge to approach exactly end to end indicates a possible
error in the anterior of horizontal overlap of the anterior teeth.

Mechanism of Speech
49 | P a g e
FIG. 16
THE ‘S’ SOUND
From a dental point of view, the S sound is the most interesting one. This is
the case because its articulation is mainly influenced by the teeth and palatal part of
the maxillary prosthesis Clinical experience suggests that s and t can cause most
problems suggests that s and t can cause most problems in a prosthodontic context. In
nearly all languages of the world, S is a common speech sound. The inter individual
variation in articulatory details may be great due to individual variation in teeth,
palate, lower jaw and tongue shape and size. However, the following phonetic
properties are common to all s sounds.

Mechanism of Speech
50 | P a g e
FIG. 17
Linguopalatal and Articulatory characteristics:-
• The tip of the tongue is placed far forward, coming but never touching the upper
front incisors.
• The sagittal groove is made in the upper front part of the tongue, with a small cross
sectional area.
• The tongue dorsum is flat.
• Normally, the mandible will move forward and upward, with the teeth almost in
contact.
Auditory Characteristics
• The sound is fairly loud, with a light, sibilant (sharp) quality.
The S sound can be considered dental and alveolar speech sounds because
they are produced equally well with too different tongue positions, but there can be
some variations even behind the alveolus. Most people make the S sound with the tip
of the tongue against the alveolus in the area of the rugae, but with a small space for
air to escape between the tongue and alveolus. The tongue’s anterior dorsum forms a
narrow groove near the midline, with a cross section of about 10mm2. The size and
shape of this small space will determine the quality of the sound. Part of the sibilant
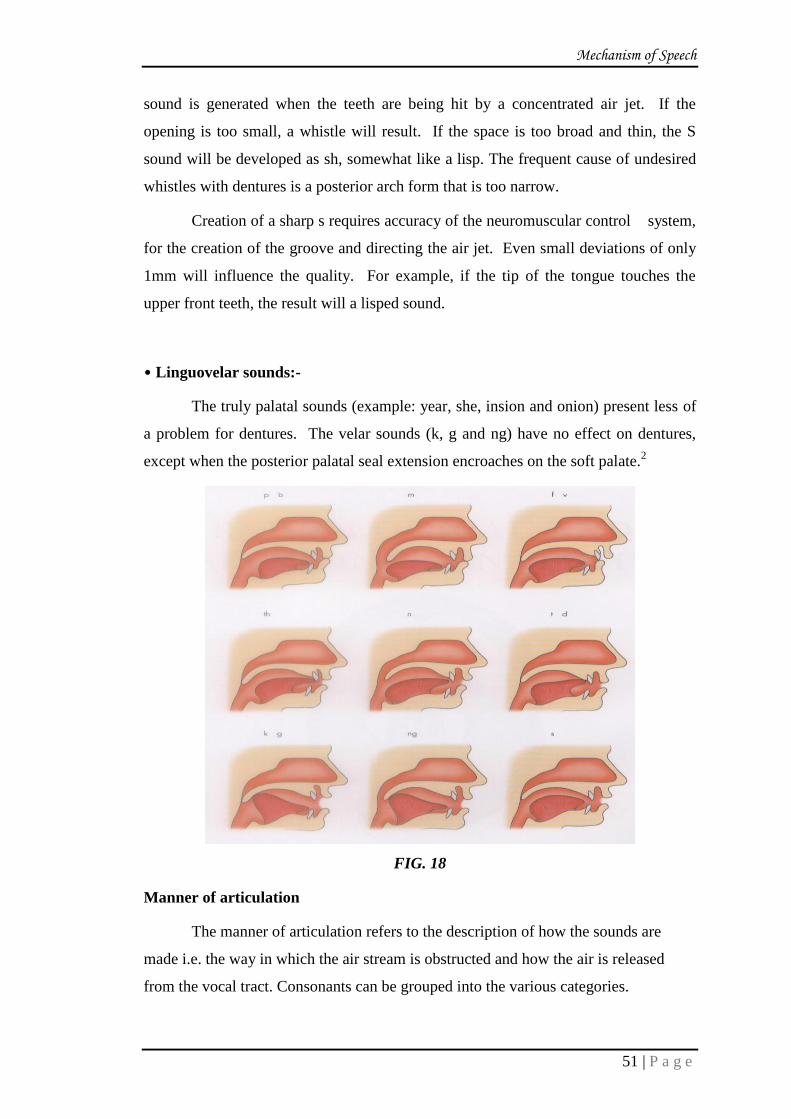
Mechanism of Speech
51 | P a g e
sound is generated when the teeth are being hit by a concentrated air jet. If the
opening is too small, a whistle will result. If the space is too broad and thin, the S
sound will be developed as sh, somewhat like a lisp. The frequent cause of undesired
whistles with dentures is a posterior arch form that is too narrow.
Creation of a sharp s requires accuracy of the neuromuscular control system,
for the creation of the groove and directing the air jet. Even small deviations of only
1mm will influence the quality. For example, if the tip of the tongue touches the
upper front teeth, the result will a lisped sound.
• Linguovelar sounds:-
The truly palatal sounds (example: year, she, insion and onion) present less of
a problem for dentures. The velar sounds (k, g and ng) have no effect on dentures,
except when the posterior palatal seal extension encroaches on the soft palate.2
FIG. 18
Manner of articulation
The manner of articulation refers to the description of how the sounds are
made i.e. the way in which the air stream is obstructed and how the air is released
from the vocal tract. Consonants can be grouped into the various categories.

Mechanism of Speech
52 | P a g e
• Stops :- Are characterized by stoppage and sudden release of the air stream and
require complete occlusion of the articulators involved ; the plosives P and B are
produced by closure of the lips to permit momentary buildup of the air stream,
followed by a sudden explosive release, and t & d are produced by tongue
contacting the hard palate to stop the air stream before suddenly releasing it; and
the K sounds are produced by tongue and soft palate closing the oral cavity at the
same time the soft palate and pharynx close the nasal cavity to stop the air stream
prior to plosive release.
• Fricatives:-Are produced by the air stream being forced through loosely closed
articulators or a narrow passageway. For the labiodentals f and v, the lower lip
articulates with the maxillary anterior teeth to constrict the air stream. The linguo-
dental ‘th’ is produced by incomplete articulation of tongue lip maxillary incisors
to construct the air stream. The sibilants s, z, zh, sh are produced by tongue blade
articulating with the lateral aspects of the hard palate, permitting the air stream to
be forced through the groove created in the tongue apex.
• The Affricatives: - “j” and “ch” are produced by a combination of stop and
friction, accomplished by articulation of the tongue and anterior hard palate.
• Diversions: -Of the air stream is characterized by stoppage at one point to permit
escape at another. The nasal m is produced by the lips occluding to seal the oral
cavity and permit emission through the nose. The nasal n is produced by
articulation of the tongue and hard palate closing the oral cavity while the sound
escapes through the nasal cavity. The nasal ng is produced by the tongue and soft
palate closing off the oral cavity to permit nasal emission. For the lateral “l”, the
tongue apex occludes the anterior portion of the oral cavity while sound escapes
through the lateral portions.
Voicing
This is the third dimension commonly used for classifying consonant sounds.
This is a binary dimension and refers to whether or not a consonant is accompanied
by laryngeal tone. Consonants that are produced with vocal fold activity are termed
voiced. Voiceless is the term applied to consonants that are not produced with vocal
fold vibration.

Review of Literature
53 | P a g e
In order to produce articulate speech in complete denture patients, an effective
tongue to palate contact is an important factor. Unfortunately, very few attempts are
made to modify the palatal contours of maxillary dentures to produce the desired
normal speech. There are sporadic references in the literature identifying specific area
of tongue contact on the palate during pronunciation of various consonants in
dentulous, edentulous and denture wearing individuals. However, this information is
rarely used to modify the palatal contour of artificial maxillary denture. In 1958
Allen6 carried out a comparative analysis of the palatograms made by dentulous
subjects He developed the palatogram on thin methyl methacrylate artificial palate
dusted with unscented talcum powder .The tracings made by different subjects were
compared and analyzed. The study concluded that though there is a pattern of tongue
to palate contact in pronunciation of given consonant, no two patients contacted
exactly the same area of the palate in pronouncing it. He further concluded that the
thickness of the palatal vault is critical to speech only in the anterior region from
canine to canine also advised that thickening the area of the incisive papilla facilitates
proper enunciation and eliminates much of the post insertion practice period.
Palmer44
a speech pathologist, indicated that some patients develop problems
after the insertion of complete dentures because they experience a loss of tactile
location skills. He recommended that a non-anatomic papilla be placed on the oral
surface of the denture just posterior to the location of the incisive papilla to foster
normal speech also suggested to incorporate a transversely elongated rugae like
papilla to be identified by patient’s tongue.
History states the untiring efforts that numerous pioneers have taken for the
improvement of speech in the edentulous patient using complete denture. From the
olden times till this contemporary era, the literature reviews the significant studies and
research work that has been done.
The review of literature has been described separately under the following heads:
• Physiology and analysis of speech.
• Speech as used for designing of dentures.
• Studies to evaluate the denture in relation to speech.
• Incorporation of rugae

Review of Literature
54 | P a g e
• PHYSIOLOGY AND ANALYSIS OFSPEECH
E. McDowell(1936)11
stated that overtones in speech are dampened by the
walls of the mouth but minimized the effect with fallowing statement ‘the size and
shape of the hard palate which acts as a sounding board, probably have much to do
with the quality of voice. Nevertheless, so many other factors more potential in
selecting frequencies are operating simultaneously that the degree of influence of the
textures of the lining of the cavities is probably very small.
C. Van Riper (1954)12
stated that there are various ways to make all speech
sounds, the compensatory activity of the tongue can substitute for anatomic
abnormalities of the lips and jaws. The outcome can also occur after the dentist has
interfered with habitual movements. There is however, an additional factor of
personal discomfort of the patient as he is called upon to make new movements and
difficult adjustment and to run the risk of uttering odd speech.
Barnett Kessler (1955)13
analyzed the tongue factor and its functioning areas
in dental prosthesis. He suggested that comprehension of the tongue function and its
operating area in both the buccal cavity and the vestibular space is a prerequisite in
achieving or approaching the ideal dental prosthesis. The tongue is a necessary part of
the instrument of articulate speech; and also moistens the lips to facilitate speech. It
acts like a reed in a wood-wind instrument to effect variations of sound qualities. It
has the transient and permanent power to change form in order to effect better speech
patterns or in general function of maturation. Tooth alignment should be effective
without encroachment upon the tongue functioning space. The base of the tongue is
frequently “hooked” by the lower second molars resulting in unstable lower dentures.
In cases of tongue enlargement the author has suggested to lessen the mechanical
irritation. The tongue use the upper and lower teeth as a spring board in capitulating
words. The tip of the tongue possess an extremely noticeable tactile sense. Thus the
authors has outlined the tongue factor in speech.
Alexander L. Martone (1962)14
wrote a series of eight articles on “An
approach to prosthodontics through speech science” titled as –„The phenomenon of
function in complete denture prosthodontics‟ described the physiology of speech to
provide a basis for a scientific approach to the phonetic factor in denture construction.
In Part I of the series he has described the „Anatomy of the mouth and related
structures‟. According to him, all the facial features act as diagnostic aids to the
Review of Literature
55 | P a g e
dentist as he first sees his patient. But as the patient begins to relax and speak, the
dentist has an opportunity to observe the fleeting facial movements and mannerisms
characteristic of that individual. This has been termed the fourth dimension, the
vitality factor, or anatomy in action.
PartII15
of the series, Alexander Martone describes how the complex
interplay of bone and musculature is apparent in any facial expression. These complex
structures are responsible for the functions of speech, respiration, mastication, and
deglutition. Analysis of the facial expression and speech and the study of dissection of
the muscles of facial expression had indicated that these muscles, act as combined
units and are attached to fixed and movable bone, and play a role in mandibular
movements associated with the functions of speech and facial expression.
Part III16
of the series the author describes how the various parts of the oral
cavity that lie within the poly-functional pyramid carry out several functional
activities like speech, respiration, deglutition and mastication with miraculous
smoothness. The role of tongue, hard and soft palate has been explained that together
they act as a resonating sound board, and also serve as deflectors of airstream, thus
giving vocal colour to the speech sounds.
Part IV17
the author has discussed in detail the physiology of speech to
provide a background for the practical application of principles of speech science to
prosthodontic practice. The primary physiologic functions of respiratory and digestive
tracts in relation to their secondary function of producing and modifying sounds has
been explained by describing the role of three valves – glottis, Palatopharyngeal
valve, and the oral cavity in the speech mechanism.
Part V18
Alexander Martone highlights on how speech entails the use of
structures and muscles that shape and reshape the oral cavity from second to second.
The innervation of these muscles is such that habitual and rapid formation of sounds
is provided. The dentist who is constructing dentures for a patient has choices which
permit greater or less interference with the habits of speech. Construction of a denture
will preclude his forming new habits of articulation of speech sounds. Since the
quality of voice and speech is inherent and serves as a major area of identification of
an individual, the prosthodontic implication of maintaining this identity has to be
understood.

Review of Literature
56 | P a g e
Part VI19
In The diagnostic phase of denture construction describes how
detailed patient evaluation, clinical examination, and vitality factor of the patient and
his speech, functional patterns are significant while fabricating dentures. The benefits
of incorporating a fluid or progressive diagnostic approach in Prosthodontic treatment
need to be recognized, to study the functional performances of various structures
during speech and to apply the additional knowledge gained to the procedural steps in
denture construction in relation to phonetics.
Part VII20
described as The recording phases of denture construction in which
the development of impressions and the registrations of Maxillo-mandibular relations
have been discussed and the significance of each step in re-establishing the patient’s
speech habits.
Part VIII21“The final phases of denture construction” in which speech plays
an important role in this verification, in esthetic determinations, and in the critical
evaluation of the completed dentures. The muscles responsible for facial expressions
in the regions of the lips and checks must be properly supported by the dentures so
that natural movements of facial expressions should not get disturbed. He described
the unique complexity of the oral cavity and adjacent structures and their role in
performing various functions like respiration, deglutition, mastication, facial
expression and speech. This presents a continuous challenge to the prosthodontist.
This article focuses on how several factors such as respiration, phonation, resonance,
speech articulation, audition, neurologic function and emotional behavior are
responsible for the overall speech mechanism in its totality. All these parameters need
to be considered by the clinician while constructing dentures.
Hamlet SL, Geoffrey VC, Barlett DM. (1976)22
in the article effect of a
dental prosthesis on speaker specific characteristics of voice. Proposed that every
individual produce sound is different and person specific no similar pattern of
articulation has been observed in the patients wearing removable dental prosthesis
John M. Palmer(1974)23
in his article Analysis of speech in prosthodontic
practice has discussed in detail three baseline features of speech sound production that
include acoustic events, aerodynamic characteristics and anatomy and physiology of
the speech apparatus; thereby providing a basic rationale for speech evaluation by the
clinician. He has also illustrated various speech problems like omission, substitution,

Review of Literature
57 | P a g e
and distortion that may occur in patients with dentures and has suggested general
approaches to alleviate these problems.
C. Andrew Burnett (1999)24
conducted a study to describe the mandibular
incisor positions for 24 consonant sounds of the English language. Incisal
relationships have been described in speech function at the S position and M position
while counting or recitation of any passage that simulate conversational speech. He
concluded from his study that the incisor position for each individual consonant was
unaffected by initial or final word placement of that sound. A sibilant sound always
produces the most anterior and superior position of the mandible.
The Rehabilitation Council of India1has provided a manual for patients with
speech and hearing difficulties titled “Fundamental of Speech and Speech Teaching.”
The structured literature consists of detailed description of mechanisms of speech
production, description of various speech sounds, their classification, development of
speech , habitual patterns, evaluation of speech , and defects or changes in speech
apparatus with age. Appendix for speech intelligibility rating scale that was
constructed by the National Teaching Institute for the Deaf, USA and followed by the
National Institute for the Hearing Handicapped in India have also been included.
Nitinkumar Agarwal and Ruchir Tripathi25
in their book “Complete
Denture Prosthodontics” have included an entire chapter on Speech Considerations
with Complete Denture Patients. According to them, speech production is an
autonomous unconscious activity. Hence, description of the various factors
responsible for its production has enlisted such as neural factor, muscular factor,
mechanical factor, aerodynamic factor, and auditory factor.
Fenn, Liddelow, and Gimsons26
in their book “Clinical Dental Prosthesis”
included an entire chapter on phonetics in which the mechanism of speech and factors
in denture designing affecting speech have been discussed in detail.
A. Ylppo (1954)27
in his article “The effect of dentures on speech” surveyed
the work of other authors and divided it into:
• Ordinary normal cases,
• Congenital and acquired cleft palate cases for the effect of dentures on speech. He
concluded that the best results were obtained by placing the upper incisors so that
edges hardly show below the lower border of the upper lip.

Review of Literature
58 | P a g e
He also stated that during the articulation of the dentals i.e. t, d, l, s, z the tip of
the tongue either touches the hard palate or the back portion of the front teeth.
Any variations thus made in the palatal aspect of the upper anterior teeth leads
to different articulation from the original.
Anthony K. Kaires Part 1 (1956)28
in his article “Palatal pressures of the
tongue in phonetics and deglutition” quantitatively measured the variations in the
palatal pressures of the tongue at definite vertical dimensions:
• During pronunciation of palatolingual sounds
• During swallowing.
In addition to this, an attempt was also made to find out the change in the
phonetic values with a change in the vertical dimension. It was concluded that the
tongue was capable of adapting itself to the different predetermined vertical
dimensions of occlusion. However, it was noted that during the pronunciation of
certain sounds containing words – /t/, /d/, /m/, all the strain gauges were affected. It
was also stated that highlighting the effect of altering vertical dimension on the
various speech sounds was a difficult procedure. This was due to the adaptability of
the patient to the predetermined vertical dimensions. The patient, however, faced
certain amount of difficulty in the pronunciation of sibilants. He stated that co-
coordinated movements and an unrestricted tongue are dependents for the act of
speaking and swallowing.
II. SPEECH AS USED FOR DESIGNING OF DENTURES
Landa J.S. in (1935)29
suggested the use of the s sound to determine the
adequacy of freeway space and the m sound as a relaxing subject so as to establish a
desirable rest position while treating complete denture patients. He also used the f and
v labiodental sounds as an adjunct to the arrangement of maxillary teeth.
Sears V.H. in (1949)30
reported that clearer s pronunciation will result by
fashioning the area of the anterior median ridge according to the type of the tongue.
He recommended making a groove in this area of the maxillary complete denture for a
broad tongue with a slight median sulcus and building a ridge in this area for the
tongue with a deep median sulcus.

Review of Literature
59 | P a g e
Pound E.in (1951)7 made his patient pronounce s and he observed the
clearance of the anterior teeth. He stated that reproduction of a reverse curve in the
maxillary complete denture facilitated proper production of s and sh sounds.
Silvermann M.M (1953)8in his article "The speaking method in measuring
vertical dimension‟, had arranged the vertical height of complete dentures such that
they provided the “closest speaking space” of 1 to 2mm depending on the facial
appearance and comfort of the patient, thereby using speech as a physiologic phonetic
method for re-establishing the lost vertical dimension in the edentulous patient.
Kessler H.E. (1957)31
stated that dentistry and all its specialties play a leading
role both in maintaining normal speech and in helping to correct certain speech
defects that occur in complete denture patients. Some dentures are made phonetically
correct and in certain others, the patients compensate with their tongues or lips for the
phonetic shortcomings of their dentures. The author emphasized that a tape recorder
should be an important part of the prosthodontists equipment. A comparison should
be made between the recordings made before extraction, at wax try-in, practice
sessions and final recording. This procedure gives the patient a little needed ear
training and some understanding of where his tongue touches while he still has his
natural oral sensation. After experimentation, the author concluded that artificial
rugae are a hindrance to speech as they make the region thick. The largest share of
responsibility for the denture wearer’s speaking voice rests on the dentist. It can be
fulfilled by correct construction of dentures and giving each patient as much
education in phonetics as is needed.
For the purpose of speech therapy by the dentist. The author used anterior
teeth of many different brands of material for complete denture prosthesis treatment,
one after another, in the mouth of different patients and recorded the patients’ voices
each time on tape. He concluded that the dentist and the speech therapist both bear a
responsibility towards the phonetic considerations of the patients. This should be
overcome by a proper analysis of speech and education of the patient for a more
phonetically correct prosthesis.
Allen L.R (1958)6 carried out a comparative analysis of the palatograms made
by dentulous subjects. He developed the palatogram on a thin methyl methacrylate
artificial palate dusted with unscented powder. The tracings made by different

Review of Literature
60 | P a g e
subjects were compared and analyzed. The study concluded that although there is a
pattern in tongue-to-palate contact in pronunciation of a given consonant, no two
patients contacted exactly the same area of palate in pronouncing it. He further
concluded that the thickness of the palatal vault is critical to speech only in the
anterior section from canine to canine. He also advised that thickening the area of the
incisive papilla facilitates proper enunciation and eliminates much of the post-
insertion practice period.
Morrison (1959)2suggested the use of the words „sixty-six‟ and ‘Mississippi’
and several short poems containing many sibilants to determine the closest speaking
space and to establish an acceptable vertical dimension of occlusion in the denture.
Rothman R (1961)32
described the action of the lips, tongue, teeth and soft
palate in the production of speech as is related to denture construction. In his article
‘Phonetic Considerations in Denture Prosthesis’ described how for normal speech
production - The primary concern in phonetics is the change in the stream of air as it
passes through the oral cavity. The tongue plays a major role by changing its shape
and position for pronunciation of vowels and contacting a specific part of the teeth,
ridge or palate for each consonant. If these structures are replaced by dentures the
dentist must know where the tongue contacts them. Correct vertical dimension,
occlusal plane, contour of palate, and position of anterior teeth are the primary
requirements for speech sounds.
Mehringer E.J. (1963)33
adjusted the occlusal rims to provide an incisal
separation of 1- 1.5mm for sibilants, 2- 4 mm for nasal sibilants, and 5-10mm for
diphthongs. The author has quoted the recording of speech as the first and the most
logical step in recording functional positions. The neuromuscular pattern that controls
speech is not affected by the loss of teeth. This article discusses how the speech
patterns develop physiologically, illustrates graphically the basic phonetic formats
established by neuromuscular patterns in articulate speech and shows how such
patterns can be utilized under functional conditions for maling records.
Paul Gibbson (1963)34
in response to “The use of speech patterns as an aid in
prosthodontic reconstruction- by Edward J. Mehringer”, has appreciated how several
authors have become aware of the role of speech and have come to the consensus that
speech can be used as an aid in selecting and checking the vertical dimension of

Review of Literature
61 | P a g e
occlusion, height of occlusal plane, and position of teeth in relation to the lips, tongue
and cheek.
Silverman M.M.(1967)35
in his article titled “The Whistle and Swish Sound
in Denture Patients” explained how common abnormal sounds, such as whistling and
swishing, occur in speech of patients wearing fixed and removable restorations.
Etiology and treatment of these undesirable conditions were discussed in this article.
According to him, for proper enunciations of the “s” sound - the sides of the tongue
are pressed against the sides of the palate up to, but not including the central incisors
and air passes through a narrow groove; while for “sh” sound – the entire tongue is
drawn back and slightly broadened; for “s” & ”z” sounds - maxilla and mandible are
in their closest speaking relation; teeth are edge to edge in a horizontal relation and
sufficient vertical overlap is present. The whistle and swish sounds can be corrected
by maintaining a vertical overlap equal to the closest speaking space and by
incorporation of reverse curves in the processed denture. All abnormal sounds can be
avoided by using pre-extraction records in patients with normal speech and placement
of teeth in exact locations they previously occupied
Donald P. Erb (1967)36
attempted to provide information on various aspects
of speech effects of the maxillary retainer. According to his observations the thickness
of the maxillary retainer has to be as thin as possible in the anterior alveolar area (1-
1.5mm). Most patients adapted to speech with their denture within two weeks.
Adjusting the retainer, grooving it, and roughening it in the anterior alveolar area
appeared to improve speech. Roughening the region in the anterior alveolar area
seems to allow the patient to find the correct tongue placement for speech. The
grooving allows for a sharper quality to the sibilants. It helps correct a substitution of
“sh” or “th” for “s” sound. Patterns in articulate speech and shows how such patterns
can be utilized under functional conditions for making records.
W. Alan Lawson and E.K. Bond (1969)37
in their review article under
“Speech and its relation to dentistry and the effect of speech on variations in the
design of dentures” discussed the changes in the speech due to various denture shapes.
They pointed out the following changes:

Review of Literature
62 | P a g e
• If upper anteriors placed back palatally (centrals alone or centrals, laterals and
canines) it produces a total blockage of the air channel and affects /t/, /d/, /tsh/,
/dz/, /th/, /s/ and /z/ sounds.
• If there is thick gum present behind the upper anteriors, the air channel is blocked
again resulting in changes in the /t/, /d/, /th/ sounds.
They concluded that the elimination of speech defects of dental origin can be
possible by understanding general mechanism of speech and by knowledge of the role
played by oral structures in speech articulation.
Pound E (1970)38
attempted to utilize speech to simplify a personalized
denture service. Maxillary anterior teeth should be positioned so the incisal edges
make a definite seal against the lower lip, when the patient is pronouncing the "F" or
"V" sounds. This position sets the stage for the positions of all the remaining teeth.
The mandibular anterior teeth are set using the "S" sound, slightly lingual to the labial
edges of the upper incisors with a space of 1-1.5 mm between them. The "S" position
is also utilized for recording of the patient’s original class of occlusion, vertical
dimension, centric relation, and incisal guidance. A technique of progressive
refinement is outlined utilizing diagnostic treatment dentures, tissue treatment
material, and resin blocks on the posterior of the mandibular denture. After occlusion
is developed and tissues are in good tone, patient is comfortable, and esthetics are
satisfied these dentures are used as a mockup for the making of "continuance"
dentures.
George A. Murrell (1970)39
in his article occlusal considerations in esthetic
tooth positioning has put forth an opinion that to achieve protrusive balance, dentists
have minimized the horizontal and vertical overlap when positioning anterior teeth for
dentures. This factor increases denture stability but at the expense of natural tooth
position, esthetics and phonetics. The dentist should be concerned with developing the
following three functions in the dentures. First, the phonetic function is developed so
that the incisal edges of maxillary anteriors form a seal with the vermilion border of
lower lip when the patient says “f”. A soft block of wax is contoured as the patient
says “s” to determine the position of the lower anteriors. Second, a balanced occlusion
is developed on the articulator and a masticator function is incorporated by
eliminating the occlusal interferences during chewing and swallowing.

Review of Literature
63 | P a g e
Francis W. Shaffer, Robert A. Kutz (1972)40
in their article on Phonetics
and swallowing to determine palatal contours of dentures, suggested a method for
using soft wax to physiologically develop the palatal-rugae surface of a denture prior
to fabrication in acrylic resin. This technique is based on the movements and
pressures made by the tongue during swallowing and speech.
George A. Murrell (1974)41
has reviewed the positioning of anterior teeth for
esthetics and phonetics. The production of the “f” sound is used to determine the
positions of the upper anteriors. The procedure of using speaking wax placed on
stabilized lower base as used for the diagnosis of anterior occlusion is explained.
Using the established anterior stop, a procedure is described to record the occlusal
vertical relation and centric relation. The article also provides a brief review of the
atypical “s” sounds produced under classes I, II and III of occlusion and methods to
overcome these obstacles in recording the occlusal vertical and centric relations.
Pound E. (1977)42
stated that it is necessary to develop clarity of speech in
patients who wear dentures. The author reviewed the use of the sound /s / for
designing of dentures. The principles of using speech for designing of dentures
encompass two factors. The most forward, most closed position of the mandible is
assumed when the /s/ sounds are enunciated at conversational speed and another that
no teeth or denture parts should ever make contact during speech. Even after the teeth
are lost, the mandible is carried to the precise established relation during the
pronunciation of the /s/ sound. This position is as definitive and recordable as the
terminal hinge position of the condyles. The /s/ sound can be used to determine the
correct position of the maxillary and mandibular incisors along with the vertical
dimension of the patient. It is important, however, that the patient produces the sound
at conversational speed as slow speech creates larger incisal space during /s/ sound.
The posterior speaking space may vary with the skeletal jaw relation of the patient
being about 1 to 3mm for classes I and III occlusion and may be as much as 10 mm in
class II patients. The author has described a method of obtaining protrusive
registration after the anterior teeth have been set to the correct vertical and horizontal
overlap.
George Chierici and Lucie Lawson (1973)43
studied the clinical speech
considerations in prosthodontics, from the perspective of a prosthodontist and speech

Review of Literature
64 | P a g e
pathologist. They considered the various dimensions of speech production separately.
For this seven related functions and their importance were assessed.
• Respiration: The phenomenon of respiration is generated by the intercostal
muscles and the diaphragm. During speech the rate of air exchange per minute is
accelerated, the number of breaths per minute is decreased, breathing is deeper,
the rate of inspiration is slightly increased and rate of expiration is decreased.
A prosthetic treatment which interferes with the normal physiologic
process of respiration during speech should be avoided.
• Phonation: During speech the breath stream through the trachea initiates the
vibration of the vocal cords.
• Resonance: The sound produced at the site of the vocal cords is modified when it
passes through various chambers, example: pharynx, the oral cavity, the nasal
cavity. The excessive bulk of dentures alters the size of the oral cavity by reducing
it and may affect the resonance pattern.
• Speech articulation: The air column, thus produced is radiated outwards. It is
formed into meaningful elements of speech by the movements of the palate,
mandible, teeth, tongue and lips. This is referred to as “articulation”.
Precise articulation requires the tongue contact with the teeth, the alveolar
area, the hard or soft palate. Missing anterior teeth require the compensation for
linguodental or the labiodental sounds. Though intelligible speech can develop,
however, the precise articulation is rarely accomplished.
• Audition: It is important to recognize any form of hearing impairment in the
patients. This is to say that distortions in the speech articulations may be
associated with hearing disorders.
• Neurologic function: It is of utmost significance to distinguish speech defects
associated with neurologic disorders, from those related to prosthodontic
treatment.
• Emotional behavior: The emotional attitude of the patients towards the
prosthodontic treatment influences the patients. Such a situation requires
psychotherapeutic counseling.

Review of Literature
65 | P a g e
He concluded that each patient’s condition should be thoroughly evaluated so
that the prosthesis is able to provide an optimal environment for its accommodation
and acceptance towards a more natural speech.
John M. Palmer(1979)44
stated that in the absence of any clearly identifiable
pathologic condition, the prosthodontic patient demonstrating speech problems after
insertion of complete dentures must be having problems with loss of turbulence,
because of diminution of tactile location skills in speaking, or both. Potential aids to
improve speech are a non-anatomic papilla placed on the oral surface of the denture
just posterior to the location of the incisive papilla, a transversely elongated rugae-like
papilla at the same location, a roughened region at that spot, or an indentation
sufficient for the patient’s tongue to identify. The location and effectiveness of such
structural changes can be planned and judged with the cooperation of a qualified
speech pathologist.
G.M. Ritchie and Yusnidar T.Ariffin (1981)45
conducted a study on
sonographic analysis of speech sounds with varying positions of the upper anterior
teeth. This study was done to investigate the effect of the varying position of the
anterior teeth on the speech of denture wearers and the adaptability of the tongue to
altered intraoral dimensions. Complete dentures were constructed for each subject.
Six replica of upper dentures were constructed using a duplication technique and
fabricated to articulate with complete lower dentures. The position of the upper
anterior teeth was altered and these alterations were termed as conditions. The
different conditions were of seven types:
Condition I– subject without wearing dentures.
Condition II– upper central incisors 12mm from incisive papilla.
Condition III– same teeth positioning but thinning of rugae area.
Condition IV– upper central incisors 2mm anterior to the standard position as in
condition II.
Condition V– upper central incisors 4mm anterior to the standard position as in
condition II.
Condition VI– upper central incisors 2mm posterior to the standard position as in
condition II.
Condition VII– upper central incisors 4mm posterior to the standard position as in
condition II.

Review of Literature
66 | P a g e
Test sounds chosen were tee, chee, see and recordings were made in a sound
proof room with the mike at a distance of 40cm from the subject. Spectrographic
analysis was done subsequently. They mentioned that the tee sounds are formed with
the tip of tongue touching the lingual surfaces of the upper anterior teeth and leaving
with an explosive sound or “Burst”. A change in tee sound was noted in different
conditions during spectrographic analysis. The authors concluded that spectrographs
can be employed to analyze and interpret speech difficulties related to prosthetic
treatment.
J F McCord, H J Firestone, A A Grant (1985)46
in their article „Phonetic
determinants of tooth placement in complete dentures‟ - The provision of satisfactory
complete dentures requires that dentist, technician, and patient adequately fulfill their
respective roles in the provision of, and adaptation to, these dentures. The clinician
should combine clinical skills and appropriate patient management, in addition to an
appreciation of post-extraction resorptive changes in the alveolar ridges, if clinically
acceptable dentures are to be prescribed. An increasing number of replacement
dentures are being prescribed for older patients; thus, the need to utilize functional
factors to determine tooth placement has been reviewed.
Emily A. Tobey and Israel M. Finger (1983)69
put forth a view that since
anterior teeth play a major role in the production of certain sounds any prosthesis
placed near or replacing teeth alters speech production. According to the authors since
the volume of the oral cavity is changed on insertion of the prosthesis a variation in
the speech articulation is observed. For this purpose the authors carried out an
acoustic study of sounds produced with and without dentures and active versus
passive adaptation. A number of 10 subjects were selected and special target stimulus
words were recorded at two different intervals 1) without dentures and 2) Immediately
after wearing dentures. They concluded that passive acoustic affects are noted for
sounds produced with high-tongue to palate relationships; however active articulatory
changes were observed when there was a low tongue to palate relationship.
J.E Riski, E. DeLong (1984)47
conducted a study on articulation development
of children with cleft lip/palate and suggested that as the severity of clefting increases
the severity of the articulation deficit does also. Age and type of cleft were
statistically significant factors in the development of normal articulation skills.
Children with cleft lip appeared to be a homogeneous speaking group characterized

Review of Literature
67 | P a g e
by normal articulation development. However, children with palatal clefts remained at
a heterogeneous group with regard to their articulation test performance.
Samuel G. Fletcher (1988)48
investigated changes in the dimensions and
patterns of aticulation to compensate for different amounts of tongue tissue excised
during partial glossectomy and observed that place of articulation was shifted to parts
of the vocal tract congruent with the speakers' surgically altered lingual morphology.
Certain metrical properties of the articulatory gestures, such as width of the sibilant
groove, were maintained.
K.C. White, M.E. Connelly (1989)49
described a simple method of
duplicating natural palatal rugae to a complete denture has been described. For those
patients who have difficulty with their speech patterns accommodating to the
introduction prove helpful. This article describes methods of incorporating palatal
rugae in a newly fabricated and existing complete denture.
G.E.Turner, W.N.Williams. (1991)50
stated that optimal prosthetic
management of the palato pharyngeal part requires close interaction between the
prosthodontist and speech pathologist in the use of video fluoroscopy and video naso-
endoscopy for design, placement, and modification of the prosthesis. Function of the
palato-pharyngeal port during production of controlled samples of connected speech
can be observed from multi-view fluoroscopy, including lateral and frontal
projections. Like fluoroscopy, naso-endoscopy can be used to observe and record
function of the palato-pharyngeal port during speech.
C.A. Burnett and T.J. Clifford (1993)51
studied the closest speaking space
during the production of sibilant sounds and its value in establishing the vertical
dimension of occlusion. The purpose of their investigation was to determine whether
the production of sibilant sounds involved adapting a jaw position that corresponded
to the closest vertical speaking space. 30 young adult subjects had their closest
speaking space determined during three separate phonetic tests by using a
Kinesiograph and a Bio-pak jaw tracking software programme. It was concluded that
the subjects varied with the respect to the group of sibilant sounds produced and that a
single sibilant word sound does not give a reliable indication of the smallest speaking
vertical dimension.
Patrick A. Mattie and Rodney D. Phoenix (1996)52
have described a precise
method for fabricating metal denture base with appropriate placement and contouring

Review of Literature
68 | P a g e
of metal-resin finish lines, such that the resultant prosthesis should exhibit surfaces
that re-establish proper anatomic, physiologic and phonetic contours .
Vijay Prataph Singh, Girish Bharadwaj and K.Chandrashekaran Nair
(1997)53
conducted a clinical study to observe the tongue position in speech and
tongue position for four selected consonants, /s/, /k/, /l/, and /t/, through an opening in
the cheek of a patient and found that the variations in tongue position were negligible.
Although the patient had a large facial defect, speech clarity was also not affected.
D.W Farley, J.D Jones, R.J Cronin (1998)54
presented a review of the
mechanics of speech as well as common speech problems encountered with a
removable maxillary prosthesis. The use of a palatogram to aid the clinician in the
assessment and resolution of speech problems associated with a maxillary denture
were demonstrated.
T. Tachimura, K. Nohara, H. Hara, T. Wada (1999)55
conducted a clinical
study to evaluate the change in levator palatine muscle activity of normal speakers in
association with elevation of velum using experimental palatal lift prosthesis and they
concluded that the severity of velopharyngeal incompetence might be related in part
to change in levator activity in association with oral air pressure. The effect of a
speech appliance to correct velopharyngeal incompetence might consist not only of
mechanical obturation of the velopharynx but also of alteration of velopharyngeal
function to become similar to normal speakers. Moreover, it is likely that the
velopharyngeal system could be well regulated so as to exhibit a consistent outcome
of velopharyngeal function.
C. Andrew Burnett and Thomas J. Clifford (1999)56
in their study on the
mandibular speech envelope in subjects with and without incisal tooth wear described
a mandibular envelope of motion during speech for 2 subject groups. One subject
group with no tooth wear and the other with incisal tooth wear. The author concluded
that the envelope of mandibular movements during speech differed in dimension and
position for the two groups investigated.
Christina A. Gitto, Salvatore J. Esposito and Julius M. Draper
(1999)57
described how restoring patient’s speech is an important goal in complete
denture fabrication. For those patients who have difficulty with their speech patterns
accommodating to the introduction of a prosthesis, texture in the palatal region may

Review of Literature
69 | P a g e
prove helpful. This article describes methods of incorporating palatal rugae in a newly
fabricated and existing complete denture.
Eberhard Seifert, ChristophRunte, Michael Riebandt, Antoinette
Lamprecht-Dinnesen, and Friedhelm Bollmann (1999)58
stated that alterations to
the oral cavity caused by dental prostheses can affect speech articulation, whereas the
influence of dental prostheses on the voice is unknown. In their study they observed
that for 1 patient, the fundamental frequency rose by up to 5 semitones during speech
and his voice range was enlarged by up to 4 semitones when a thin denture was used
instead of his normal denture. This study evaluated the effects of changes in
phonation by varying the dentures of 20 subjects in line with those of the first patient.
They concluded that the variations of thickness and or volume of dentures and of the
vertical and horizontal dimension of occlusion may result in unpredictable audible
changes to the voice. Patients should be informed about possible effects of modified
or new dentures on their voice.
Stig.L.Karlsson (2004)4, in his chapter “Speech Consideration with Complete
Denture” as a contribution to the book “Prosthodontic treatment for the edentulous
patient: complete dentures and implant- supported prostheses” has described how the
various orodental morphological features influence and individual’s speech and the
role of prosthetic treatment on speech activity. He has also given an in depth
description of the neurophysiologic mechanism that governs the speech production
and how the various speech sounds are influenced by the variations in articulatory,
acoustic and auditory features/ characteristics of a person . The chapter also covers
methods for speech analysis and suggests simple and prudent ways to overcome /
minimize the speech problems that patients may encounter after prosthetic treatment.
G Schierano, M. Mozzati, F Bassi, G. Preti. (2001)59
conducted a clinical
study to evaluate the influence of the resin palatal vault on the closest speaking with
complete dentures and they concluded that thickening the resin palatal vault could be
a useful procedure to increase the VDO, in cases in which it is too low from the
aesthetic stand point.
Jana Rieger, John Wolfaard, Hadi Seikaly and Naresh Jha (2002)60
revealed that speech without an obturator is significantly different from the
preoperative stage, while speech with an obturator does not differ significantly from

Review of Literature
70 | P a g e
preoperative state, while speech with an obturator does not differ significantly poorer
nasalance values than individuals with involvement of the hard palate only and
concluded that rehabilitation with a maxillary obturator is successful in restoring
preoperative speech function. Rehabilitation of individuals with involvement of the
soft palate maybe more challenging.
Seiko Hongama, Masatoshi Ishikawa, Fumiaki Kawano and Tetsuo
Ichikawa (2002)61
described the fabrication of a complete denture with removable
palatal lift prosthesis and a clinical evaluation of the concluded that the dentures were
24.4% less stable when the palatal lift prosthesis was in place and were generally easier
to dislodge than were conventional dentures. This denture with removable palatal lift
prosthesis is useful for patients with dysfunction of the soft palate involving hypernasal
speech who have difficulty in retaining the prosthesis while eating.
B. Meier, O. Luck, W. Harzer (2003)62
concluded that the manual
registration method can be used only in connection with mm. consonants. Speaking
the word “Ohio” yielded excessively high values in all methods, so that this word has
to be rejected as a speech sample. Cephalometric registration produced values with
slight inter individual variations. In practice, however, this method is unsuitable for
use with orthodontic patients because of the additional radiation exposure involved in
producing an additional lateral cephalogram. For good reproducibility, practicing or
frequent repeating of the measuring method prior to definitive measuring is essential.
Mark A. Pigno, Jeff J. Funk (2003)63
described the prosthetic treatment of an
edentulous total glossectomy patient with an unconventional custom impression
procedure to develop and record proper lower lip and cheek support. They also discussed
some issues involved in the prosthetic management of the total glossectomy patient.
David M. Bohnenkamp, Lily T. Garcia, (2007)64
evaluated that the
fabrication, use, and wear instructions for complete dentures are often the factors
determining success. The dentist must help guide the mental attitude of the skeptical
patient to foster acceptance and success of complete dentures. A “feeling of looseness”
may be a condition experienced while patients learn to wear a new mandibular
complete denture. This type of patient requires more explanation, more advice, and
more instruction. A phonetic training technique, to demonstrate to the patient how to
retain and stabilize the mandibular denture, may be needed for some denture patients.

Review of Literature
71 | P a g e
This article reports the clinical use of phonetics and its effect on tongue position to
improve the retention and stability of a mandibular complete denture.
III. STUDIES TO EVALUATE THE DENTURE IN RELATION TO SPEECH -
Kaires AK. (1957)65
- in his article “Palatal pressures of the tongue in
phonetics and deglutition” ; conducted a study to measure quantitatively, by electronic
means, under predetermined vertical dimensions of occlusion, the palatal pressures of
the tongue in the pronunciation of selected palatolingual speech sounds and that
during the act of swallowing. Spectrographs were used to detect changes in phonetic
values in which the vertical dimension of occlusion was altered. A palatogram was
constructed for an old maxillary single denture wearer to determine the regions of
strain guage placement. Test maxillary dentures were made one with increased
vertical dimension and one with decreased vertical dimension. The results obtained
from the experimental dentures were compared with that obtained from the denture
that the patient had worn successfully for one year. The study concluded that in
speech and in swallowing, the compensatory tongue changes resulted not only in
changes of the magnitude of palatal pressures, but also in the time interval in which
those pressures were applied.
Agnello JG and Wictorin L (1972)66
conducted a study of phonetic changes
in edentulous patients to alter speech function following complete denture treatment.
The patients who have been completely edentulous for a minimum of six months prior
to making of dentures speech samples are taken
• In the edentulous state
• Immediately following denture insertion
• Two weeks following insertion of dentures
• Twelve weeks following the insertion of dentures.
They concluded that the voiced /th/ was least resistant to improvement after
the insertion of complete dentures and might need the attention of speech therapy.
Harley W.T. in (1972)67
in his article “Dynamic palatography - A study of
linguopalatal contacts during the production of selected consonant sounds. “Identified
areas of the palate contacted by the tongue during speech to assess the evidence of

Review of Literature
72 | P a g e
lingual laterality and to observe if a characteristic pattern linguopalatal temporal
sequencing exists. The speech material selected included the consonants /t /, /d /, /l /,
/n /, /s / and /k/ as control. The apparatus used for the study consisted of artificial resin
palates of uniform thickness (1.9 mm), which had twelve electrodes, embedded into
the lingual surface. It recorded the areas contacted by the tongue during speech. The
results of the study showed that the lateral aspects of the palate plus the incisive
papilla are the areas most commonly frequented by the tongue. The tongue appears to
function in a bilaterally symmetrical manner during speech and the dynamic manner
in which the tongue contacts and releases from the palate depends on whether an
“initial” or “ final” consonant is being articulated.
Hisatoshi Tanaka (1973)9studied the speech patterns of edentulous patients
and morphology of the palate in relation to phonetics. He made the following
conclusions-
• Most of the patients showed speech improvement when the dentures were first
inserted.
• With increased length of time of wearing new dentures, the speech intelligibility
was improved.
• Speech of patients can be improved by experience with their new dentures.
• Individuals showed difference in length of speech intelligibility and the level of
improvement with different lengths of denture usage.
• Acoustic distortions occurred more frequently in “s’, “sh”, “ch”, “zh”, “j” sounds
than in the “z”, “t”, “n”, “d”, and “l” sounds.
• “S” sound is a poor prognostic sound for speech intelligibility of speech.
• The palatal ridge formation of complete denture will affect the acoustic distortion
of affricative and fricative sound “s”.
Sandra Hamlet, Maureen Stone and Thomas McCartey (1978)68
studied the
feasibility of using conditioning prosthesis for speech adaptation. Seven subjects with
normal speech, hearing and no orthodontic treatment or experience in speaking with a
dental prosthesis formed the sample of the study. Each subject was given an artificial
palatal plate similar to an orthodontic appliance, with 1 mm base thickness and 4 mm
thickness at the alveolar region. A similar second prosthesis was constructed with 16

Review of Literature
73 | P a g e
electrode contacts to be used during speech sample recording. Speech sample
consisted of a set of short phrases. Recordings were made at three intervals:
• Immediately with unfamiliar prosthesis
• After two weeks of adaptation
• Approximately 1 month after the second recording.
During this interval, the subject did not wear the prosthesis. The study
concluded that speech improved with adaptation and this adaptation pattern is stored
as memory. The third recording was a progress from the initial recording towards the
adapted speech.
Bal.K.Goyal and P.Greenstein(1982)10
conducted a study that was designed
to develop a method by which the palatal contour of the maxillary complete denture
could be modified according to the individual’s tongue-to-palate contact for
enunciation of normal speech immediately on insertion of the dentures. The dentures
were modified using auto polymerising resin. The speech was recorded in three
modes without the dentures, with conventional maxillary complete dentures and with
modified maxillary complete dentures, while the patient was asked to say aloud ten
stimulus sentences for contouring the palatal vault of the dentures. The immediate
speech achieved by modification showed on improvement since the modified palatal
surface of the denture offers a more physiologic and “natural” tactile sensation to the
tongue during speech production as compared to the smooth surface of a conventional
complete denture.
Tobey E.A. and Finger I.M. (1983)69
explored active verses passive
adaptation to orofacial reconstruction in relation to the speech changes that
accompany volume changes in the oral cavity during edentulous verses a denture-
speaking condition and to what extent the passive acoustic and active articulatory
effects contribute to these changes. The study was conducted on ten subjects, with
previous history of denture wearing prior to current treatment. New dentures were
made, all subjects reported satisfactory with esthetics and masticatory function of
dentures. Target words were given in a carrier sentence in which the initial consonants
consisted of /t/, /s/, and /sh/, medial vowels were /e/ as in "seat" and /a/ as in "sat".
Subjects were tested in a quiet room and recorded without dentures and immediately
following insertion of the new denture. Analysis was done of the recordings with a

Review of Literature
74 | P a g e
Kay Sonagraph machine and broad spectrograms were generated for each of the target
sound. They observed that –
• In the edentulous situation /a/ segments were longer than /e/ and increased in
duration with wearing of the dentures.
• The /sh/ sound was associated with the greatest % of change (3%), followed by /s/
(0.9%) and /t/ (0.7%).
• Speakers produce longer vowel segments when speaking with dentures than
without.
• Overall frequency relationships between vowels are achieved by variations in
tongue, position, and jaw opening.
• Lower frequencies during edentulous conditions may reflect subtle lengthening of
the oral cavity - a passive acoustic rather than active articulatory effect.
• Lower frequencies for /a/ may occur because speakers overcompensate for
dentures by using wider mouth opening or active articulation adjustment.
• Speakers actively change jaw position to accommodate the prosthesis if it may
potentially interfere with speech sounds like vowel production.
Thus, they concluded that examination of vowels, as well as consonants,
assists in delineating active articulatory versus passive acoustic changes to orofacial
reconstruction. Adjusting prostheses by listening to the changes in consonant sounds
may change only the passive acoustic characteristics of prostheses and may not
necessarily influence active articulatory accommodation by the patient.
Jeffrey M. Kestenberg (1983)70
studiedthe various types of speech tests such as
spontaneous samples, imitative samples, samples by reading, and deep samples have
been discussed. The clinical application of speech tests in relation to dentistry has also
been also outlined. A proposed speech articulation screening test for use in the dental
surgery has been suggested. The criteria to which the test was formulated are listed and
an analysis of the test is provided. It has been recommended that for difficult cases, that
a speech pathologist treats the patient in co-operation with the dentist.
A.Petrovic (1985)71
Evaluated the effects on speech sounds caused by
alterations of the oral cavity dimensions with complete dentures of different
morphology were analyzed. Different positions of upper incisors and different
Review of Literature
75 | P a g e
thickness of the denture palatal plate were used as changeable factors in the
longitudinal and transverse dimensions of the oral cavity. The method was based on
sounds spectrograms as carriers of information about individual voice characteristics.
The effects of these changes on the relative duration of separate sounds in a word and
the patient adaptation period were also analyzed. From the results some conclusions
of pragmatic value were obtained useful in the clinical procedures of denture
construction.
Howell (1986)72
conducted an investigation in which the dimensions of
movement of the mandible during the reading of a standard passage of text were
measured using a bar magnet (affixed to the mandibular incisors), magnetometers,
and computer software. This enabled a speech envelope to be described. They derived
from this study that the relationship between closest speaking space and the vertical
overlap of the incisor teeth shows that there is a trend in this direction, but it is not as
definitive a correlation as has been previously assumed. The relationship between the
anterior speaking space and the horizontal overlap of the incisor teeth shows a similar
trend but with a much reduced correlation. There was often a small space of
approximately 0.2 mm between the mandibular incisor teeth and the palatal aspects of
the maxillary incisor teeth that, although a common finding in this study, was by no
means a constant feature for all subjects.
Alexander J. Hassel and Thomas Holste (2006)73
conducted a study to
compare the improvement in speech function of maxillary complete dentures with and
without sand blasting of the palatal surface of the denture. They observed a significant
improvement in the speech after sand blasting the palatal surface of the maxillary
denture, especially for stops and fricatives.
Hyung-Jun Kong and Carl A. Hansen(2008)74
described a technique for
customizing palatal contours of a maxillary complete denture. This technique uses a
palatogram as a diagnostic tool, dynamic impression of the tongue and auto-
polymerizing resin to reproduce the functional contours of the palatal vault of the
maxillary denture. After inserting a trial / processed denture, the patient is asked to
pronounce a series of sibilant sounds while recording the dynamic impression of the
tongue. Though this method does not cause any significant impact on mastication,
retention and comfort, it does help the patient to easily adapt to the denture and
shorten the adjustment period for achievement of enunciation

Review of Literature
76 | P a g e
Bortum Cristina,Leretter Marius, Sandu Liiana (2004)75
proposed the
phonetic evaluation of the edentulous patient co-related with the various settings of
the artificial teeth assessed the phonetic alterations in complete denture wearers
caused by position, size and material of the frontal artificial teeth. This was performed
using the static palatographies and spectograms.
Earl Pound (2006)76
in the article utilizing the speech to simplify a
personalized denture service, stated that the extent of downward and forward
mandibular movements made during speech automatically restores the patients
original horizontal and vertical overlaps which can be used to control seven factors of
occlusion. The values derived by progressive function refinement of this information
through the controlled use of diagnostic treatment dentures incorporating tissue
treatment material, and a free running occlusal scheme have been reviewed .
Manashvini S. Patil, Sanjaygouda B. Patil et al (2008)77
in the critical
review of palatine rugae and their significance in clinical dentistry reviewed that the
patients whose speech is sensitive to a changed relationship of the tongue to a palatal
prosthesis may require surface texture to orient the tongue. Because surface portion of
a complete denture can impede proper articulation, one solution is to add palatine
rugae. Unfortunately the addition of rugae to a prosthesis is not a foolproof method of
eliminating speech problems.
F.STelzie, B.Urginovic C. Knipfer et al (2010)78
assessed automatic,
computer –based speech assessment on edentulous patients with and without complete
dentures- preliminary results. Speech accessibility assessment was done by expert
listeners and the automatic rating of the word accuracy by computer based speech
recognition system (ASR). Speech production is significantly reduced after complete
loss of teeth. Reconstitution of speech production quality is important part of dental
rehabilitation and can be improved for edentulous patients by means of complete
dentures. The (ASR) has proven to be a useful and easily applicable tool for automatic
speech assessment in a standardized way.
Jean –LueSchwarfz,Louis-Jean Boe Pierre Badin et al (2011)79
evaluated
grounding stop place systems in the perceptuo-motor substance of speech on the
universality of the labial–coronal-velar stop series. Authors have used an articulatory
acoustic model of the vocal tract to examine stop consonant place in terms of both
articulation and formant values. This allows them to locate each place of articulation
Review of Literature
77 | P a g e
in the F1-F2-F3 space and to demonstrate in “articulatory nomograms” how formants
evolve while closure is displaced from the front to the back of the vocal tract. Then
near universal labial-coronal-velar stop series i.e. (/b d g/or/p t k/) is a perceptually
optimal structure for stops just as /I a u/is for vowels, provided that it is embedded in
a suitable perceptuo-motor framework.
Victoria Artjomenko, Aldis Vidzis, Kristine Broka (2012)80
inthe problem
solving article. The assessment of speech quality and intelligibility after replacement
of lost teeth with removable dentures: review of literature .After analysis of data in
current literature conclude that alterations in oral cavity caused by tooth loss and
resorption of alveolar ridges can produce changes in speech quality and intelligibility.
Abdul-Aziz Abdullah Al Kherif and Ravikumar Ramakrishnaiah (2012)81
in the article ‘phonetics related to prosthodontics’ stated the correlation between
occlusion and speech, since there two factors are mostly not considered related to
each other , but during phonation the lower teeth function independently and there
should not be any constant with upper teeth. This article also highlights the utilization
of phonation as a tool for placement of upper anteriors in complete and partial denture
rehabilitation if pre extraction records have been lost. We us phonetics as a guideline
for proper placement of artificial teeth.
Vasmi Krishna, V. Vasmi Krishna Reddy et al (2012)82
performed the study
on dentures with phonetically contoured palate. A simple technique of adding
customized rugae and palate contours to the maxillary denture…..introduced this
technique for achieving normal speech after denture fabrication.
Rajya Laxmi Ravuri, Suchita Tella, Kiran Thota (2013)83
in their article
phonetics in complete denture- A prime concern stated that loss of teeth is through a
physiological process, many times it leads to psychological trauma to individuals due
to lack of confidence, esthetics and clarity of speech by fabrication of complete
dentures is always done but they consider it to be technique sensitive. They stated the
role of orodental structures in speech production so also denture thickness oral
peripheral outline , post dam area, vertical dimension, width of dental arches,
anterioposterior position of incisors relationship of upper anteriors to lower anteriors
and freeways play important role in speech production.

Review of Literature
78 | P a g e
Mariko Hattori, Yukal Smita, Hisaashi Taniguchi et al (2013)84
experimented the automatic evaluation of speech impairment caused by wearing a
dental appliance. The automatic test system detected a significant difference in speech
intelligibility, using the speech recognition score, in normal subjects with and without
placement of palatal plates. The results of the automatic test system and the
conventional evaluation system by human listeners were positively co-related their
findings suggest that the system can be used to evaluate speech intelligibility of
denture wearers.
Kristine Broka, Aldis Vidzis, Juris Grigorjevs et al (2013)85
reviewed the
influence of the design of removable dentures on patient’s voice quality. When
designing removable dental prosthesis it is important to evaluate the disposition of
artificial teeth (taking into account phonetic pronunciation) and to make a
phonetically beneficial construction of the base of dental prosthesis. It is necessary to
make the base of the prosthesis as thin as possible to improve good sound
pronunciation, however it is important not to change the resistance ability of dentures.
Spectrograms and palatograms are suitable methods of investigation to evaluate
phonetic quality of removable partial dentures.
Raghvendra Adki, Suresh Meshram, Shridevi Adaki (2013)86
performed a
study on Acoustic analysis and speech intelligibility in patients wearing conventional
dentures and rugae incorporated dentures. Reports of the acoustic analysis revealed
that pronunciation of S, SH, T, D. was clearer with rugae incorporated dentures than
conventional dentures. Amongst rugae incorporated dentures, customized rugae were
better than arbitrary rugae dentures. Intelligibility reports showed many substitutional
errors with conventional dentures. Special attention should be given to anterior palatal
region while fabricating the denture.
Hala M Abdel hameed and Mohamed E. El-Sayed (2014)87
studied the
effect of different techniques for palatal denture base configuration on speech quality
in complete denture wearer. The purpose of this study was carried out to evaluate the
effect of different techniques for palatal denture base configuration on pronunciation
of different speech sounds. Based on the results of this study, it could be concluded
that, with proper denture construction, the palatine rugae plays an important role in
speech pronunciation, as there should be some anatomical landmarks where tongue
can recognize and produce best particular sound.
Review of Literature
79 | P a g e
Ashish R Jain, M. K. Venkat Prasad and Padma ariga (2014)88
in the
article palatograms revisited describes a technique of obtaining palatogram and
customizing palatal contours of a maxillary complete denture with autopolymerising
acrylic resinto improve the clarity of speech.
Hamada Zaki Mahross and Kusai Baroudi (2015)89
did the spectrogram
analysis of complete dentures with different thickness and palatal rugae materials on
speech production. It is recommended to reproduce the rugae area in complete denture
because the phonetic quality of complete denture with rugae was superior to the
conventional denture. If the denture was too thick in the anterior region the result
would be a faculty /s h/d/z/ t /l/ sound .The dentures with metallic base can enhance
s/s h / t /d and z sound. The use of resilient acrylic to reproduce the rugae in complete
denture can enhance z/l/s/sh/t/ and d sounds.
Sleve Kelly, Alison Main, Graham Manley et al (2015)90
describes the
technique of electropalatography and the development of linguograph which is a user
friendly clinical instrument for measurement of tongue/palate contact, during speech.
Linguograph allows objective assessment of tongue function, appropriate targeting of
therapy is therefore possible. Visual feedback is also provided for therapy and an
objective measurement of occlusion is easily obtained. Technical aspect of linguograph
and of the trial results are presented here. These suggest that the investment will prove
useful in the assessment and management of many speech disorders.
Priya Vaswani, Pronob Sanyal, Ankur Prajapati (2015)91
demonstrated
comparison of speech articulation and intelligibility in palatally contoured dentures
using a novel rugae duplication technique stated that phonetics is better served by
keeping the posterior ridge area in the denture as thin as possible and confining the
palatal contour in anterior region. Irrespective of the depth of palatal vault, mucostatic
impression material is more appropriate as a material of choice for rugae duplication
and wax pattern fabrication.
Herman J.M. Steeneken92
wrote the chapter on the “Measurement of speech
intelligibility” suggesting that the present signal processing technologies, integrated in
personal computers, allows us to perform advance measurement on public address
system and telecommunication channels used for alert and warning messages,
professional use and entertainment

Review of Literature
80 | P a g e
Saurabh Chaturvedi, Narendrakumar Gupta, Ashok kumar Verma et al
(2015)93
in the article speech comprehension (prosthetic contemplation) is all the
steps of denture fabrication with its effect on speech which helps in construction of
perfect complete denture.
Christopher Jeannin et al (2016)94
did experiment on tongue pressure
recording during speech using complete denture. This describes an original
experimental procedure to measure mechanical interactions between tongue and teeth
during speech production .Using edentulous subjects, pressure transfuses are inserted
in their complete denture duplicate, physiology is respected during sound and pressure
recording as with standard complete denture original calibrations device is also
describe in order to know what kind of information can be extracted from the data.
The device permits the measurement of contact pressure without introducing any
additional perturbation other than the prosthesis itself. The preliminary results show a
well synchronization between the two signals.
Dr. Renu Gupta, Dr. R.P Luthra, Dr. Deepak Gautama (2016)95
in the
article Phonetics in complete denture- A review stated that replacement of missing
dentition with complete dentures is a major event in patient‘s life .This brings drastic
change to his /her activities. In complete denture the impressions accurate periphery
vertical dominions arch form posited of the anterior teeth etc. should be such that they
allow natural articulators such as tongue lips to work efficiently with the
morphological changes in the oral cavity thus results in each word to its fullest
perfection.
Martina Giovannetti, Alessio Casucci, Daniel Casucci et al. (2016)96
did
phonetic analysis and maxillary anterior tooth position signifies that clinicians take
care in determining the correct central incisor position in complete dentures in order
to avoid any undesirable phonetic distortions to patients complete dentures with
anterior teeth set too far palatally prevent many problems including aesthetic and
phonetic alternation ions sometimes result in whistle.
Anupama Neelakantan, Sunil Dhaded (2016)101
In the article rugae
duplication- different techniques of customizing palatal rugae in maxillary complete
denture to enhance phonetics discussed various techniques of customizing palatal
rugae in maxillary complete dentures to improve phonetics.

Material and Methodology
81 | P a g e
The present study was undertaken in the department of prosthodontics, Sharad
Pawar Dental College to evaluate the effect of functionally contouring the palatal
vault of maxillary complete denture on the quality of speech sounds produced in two
group of patients.
G1- this group used conventional dentures without modification of palatal
vault of maxillary complete denture.
In G2-group of patients palatal vault of maxillary complete denture had been
functionally contoured with visible light cure resin. In both the groups same set of
sounds has been recorded by microphone and analyzed spectrographically in terms of
amplitude and frequency. Following equipment and materials were used to perform
this study.
MATERIALS USED –
1. Materials used for complete denture fabrication (Ph.1)

Material and Methodology
82 | P a g e
2. Material used for functional contouring of palatal vault of maxillary complete
denture – Vocco’s visible light cure denture base resin. (Pink sheet) (Ph.2)
• Instrument used for fabrication of complete dentures (Ph. 3)
• Maxillary edentulous non perforated metal stock trays
• B.P. blade with handle
• Rubber bowl
• Plaster spatula
• Wax knife
• Lecron’s carver
• Camel hair brush
Material and Methodology
83 | P a g e
• Enamel bowl
• Varsity flask and clamp
• Acrylic finishing burs
• Glass Slab
• Cement Spatula
EQUIPMENT USED -
1. Sony entertainment copyrighted Sound Forge Pro System software Version 11
for recording the speech samples. (Ph.4)
2. Portable Microphone (VHF) (Ph.5)

Material and Methodology
84 | P a g e
3. Light Cure Unit (Delta India Ltd.) (Ph.6)

Material and Methodology
85 | P a g e
METHODOLOGY -
A) Selection of patients -
• 60 edentulous subjects of both gender aged between 40 to 70 years, were selected.
• The patients were selected randomly from the out-patient department of
Prosthodontics at Sharad Pawar Dental College, Sawangi (Meghe), Wardha.
• The subjects chosen were Co-operative in nature.
• They had no hearing disabilities.
• The subjects had basic education and could speak and read the local language
(Hindi or Marathi) fluently.
• All the subjects were informed about the procedure of the study and a written
consent was obtained. (Annexure 1)
B) Fabrication of complete denture by conventional method (Ph.7)
The selected patients were clinically thoroughly evaluated and relevant medical and
dental history was obtained. Complete dentures were then fabricated for the selected
subjects by conventional method .The preliminary impressions were made using
impression compound and this was poured into a plaster model. A special tray with
spacer was fabricated using autopolymerising resin. Border molding procedure was
performed using low fusing compound. Secondary impressions were made using Zinc
Oxide Eugenol impression paste. An accurate master cast was obtained in dental
stone. The occlusal rims were placed in the mouth and the jaw relations were
recorded. A face-bow transfer was done using waterpik spring bow face bow and
maxillary cast was mounted on to the articulator. Mandibular cast was mounted
against the maxillary cast using a centric relation record.

Material and Methodology
86 | P a g e
The anterior teeth were arranged based on guidelines marked on the maxillary rim and
the angulations of the adjustable incisal table. An anterior try in verification was done
with esthetics and phonetics principles. Then, protrusive records were made and the
articulator was programmed. The lateral condylar inclination was calculated using
Hanau’s formula.
L= H/8 + 12 where, H = Horizontal condylar inclination
L = Lateral condylar inclination.
The posterior teeth were arranged and the protrusive and lateral balance was obtained.
In the waxing stage the thickness of maxillary denture was kept 1 mm so as to
facilitate easy adaptation of light cure resin without altering the thickness of the
denture. Try-in verification was done and denture was fabricated with a heat
polymerized acrylic resin
C) Stimulus speech sounds used in the study (Ph.8)
Linguopalatal sounds were used for functionally contouring the palatal vault of the
maxillary complete denture. For this, the speech sounds used in local language (Hindi
/ Marathi) are as follows – T, TH, D, L, CH.. (ट, ठ, ड, ल, छ)
The classification for consonants in both Hindi and English languages is given in
Annexure II.
D) Recording of Speech Samples –(Ph.9)
The recording of speech for all the subjects is done in a sound proof room using a
portable microphone (VHF) and MP3 recording system (Sony entertainment’s
copyrighted Sound Forge Pro System software Version 11). The subjects were

Material and Methodology
87 | P a g e
askedto wear portable microphone where the distance of the microphone from the
mouth was kept constant. Training was provided to each patient with the help of
pictorial representation of the sounds (ph.8) and speech sound samples of various
linguopalatal sounds were recorded. Each speech sound was recorded thrice to ensure
proper recording of each sound.
E) Recording Speech Sounds without Modification of Palatal Vault of Maxillary
Complete Denture(Ph.10)
The first speech sound sample (group G1) was recorded by instructing the subject to
speak the 05 stimulus speech sounds with the maxillary complete denture without any
modifications on the palate. The sound spectrograph obtained is as follows

Material and Methodology
88 | P a g e
F) Recording Speech Sounds after functionally contouring the Palatal Vault of
Maxillary Complete Denture using visible light cure material (group G2)(Ph.11)
Visible light cure acrylic resin was adapted on the complete palatal surface of
maxillary complete denture.
The subject was then instructed to speak the 05 stimulus speech sounds to
functionally contour the palatal vault of the maxillary complete denture
(Ph.12)

Material and Methodology
89 | P a g e
After recording the various tongue–palate contact positions, the resin was
cured using light source. The sound spectrograph obtained is as follows (Ph.13)
spectrograph after functional molding
(G) Assessment of the sound samples -
The recorded sound samples of each subject post-denture insertion were analyzed by
using –
Quantitative analysis - Spectrogram – The software (Sony entertainment’s
copyrighted Sound Forge pro System software Version 11) used for recording the
sound samples displays each sample in the form of a spectrograph (sound waves)
(Fig. 14a, 14b,). The spectrograph provides the details of the mean frequencies (pitch
of sound) and mean decibel (intensity / loudness of sound) of each of the recordings.
A spectrograph is defined as a graphic representation of the sound in terms of their
component frequencies, in which time is shown on the horizontal axis, frequencies on
the vertical axis and intensity of each frequency at each moment in time by the
darkness of the mark.
Fig 14 a Fig 14 b
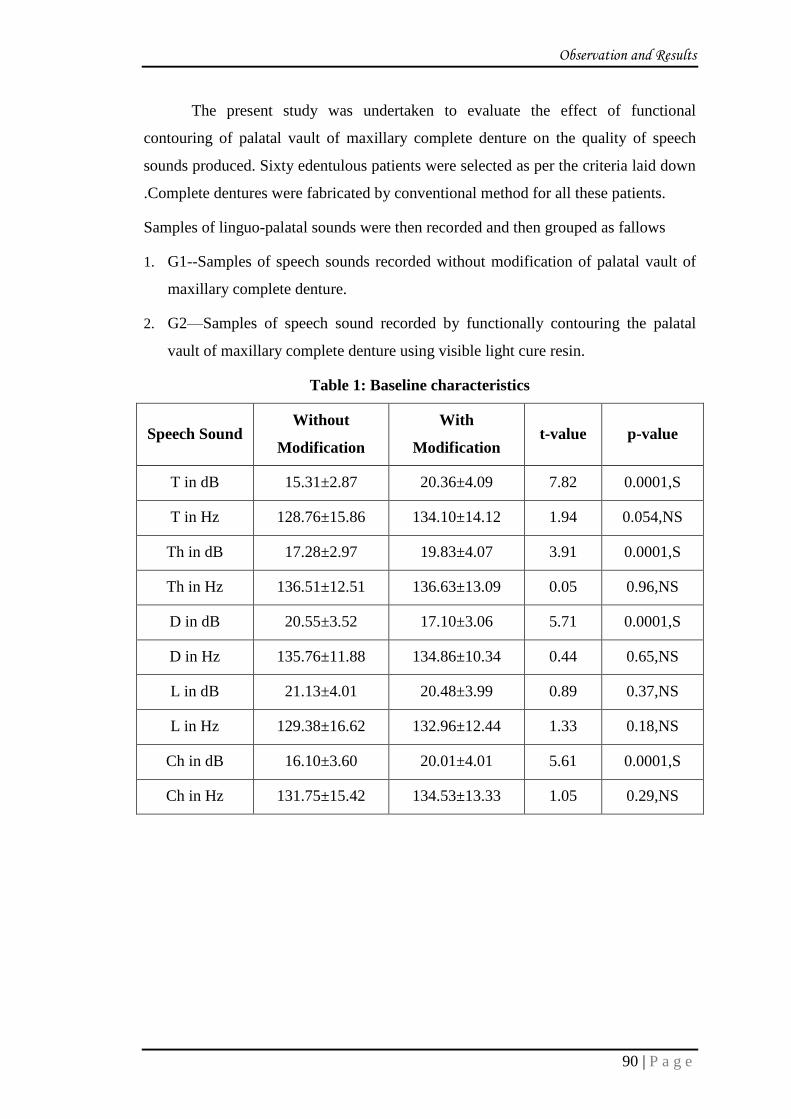
Observation and Results
90 | P a g e
The present study was undertaken to evaluate the effect of functional
contouring of palatal vault of maxillary complete denture on the quality of speech
sounds produced. Sixty edentulous patients were selected as per the criteria laid down
.Complete dentures were fabricated by conventional method for all these patients.
Samples of linguo-palatal sounds were then recorded and then grouped as fallows
1. G1--Samples of speech sounds recorded without modification of palatal vault of
maxillary complete denture.
2. G2—Samples of speech sound recorded by functionally contouring the palatal
vault of maxillary complete denture using visible light cure resin.
Table 1: Baseline characteristics
Speech Sound Without
Modification
With
Modification t-value p-value
T in dB 15.31±2.87 20.36±4.09 7.82 0.0001,S
T in Hz 128.76±15.86 134.10±14.12 1.94 0.054,NS
Th in dB 17.28±2.97 19.83±4.07 3.91 0.0001,S
Th in Hz 136.51±12.51 136.63±13.09 0.05 0.96,NS
D in dB 20.55±3.52 17.10±3.06 5.71 0.0001,S
D in Hz 135.76±11.88 134.86±10.34 0.44 0.65,NS
L in dB 21.13±4.01 20.48±3.99 0.89 0.37,NS
L in Hz 129.38±16.62 132.96±12.44 1.33 0.18,NS
Ch in dB 16.10±3.60 20.01±4.01 5.61 0.0001,S
Ch in Hz 131.75±15.42 134.53±13.33 1.05 0.29,NS
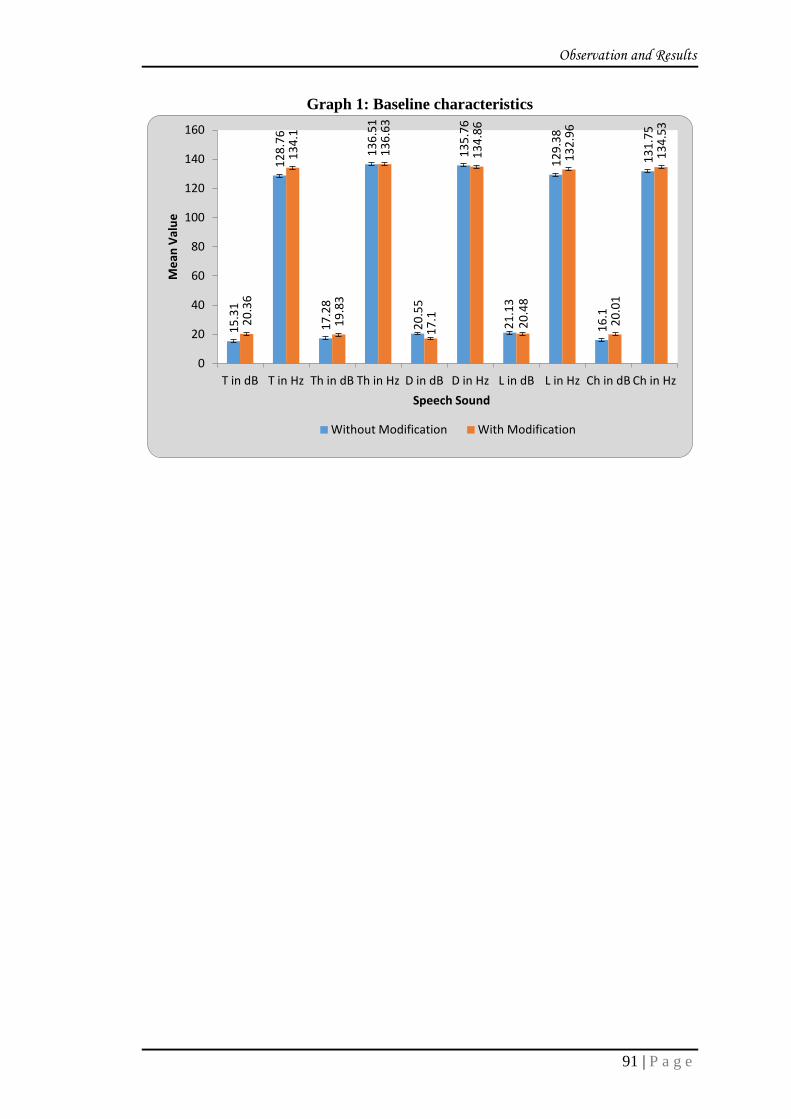
Observation and Results
91 | P a g e
Graph 1: Baseline characteristics
15
.31
12
8.7
6
17
.28
13
6.5
1
20
.55
13
5.7
6
21
.13
12
9.3
8
16
.1
13
1.7
5
20
.36
13
4.1
19
.83
13
6.6
3
17
.1
13
4.8
6
20
.48
13
2.9
6
20
.01
13
4.5
3
0
20
40
60
80
100
120
140
160
T in dB T in Hz Th in dB Th in Hz D in dB D in Hz L in dB L in Hz Ch in dB Ch in Hz
Me
an V
alu
e
Speech Sound
Without Modification With Modification
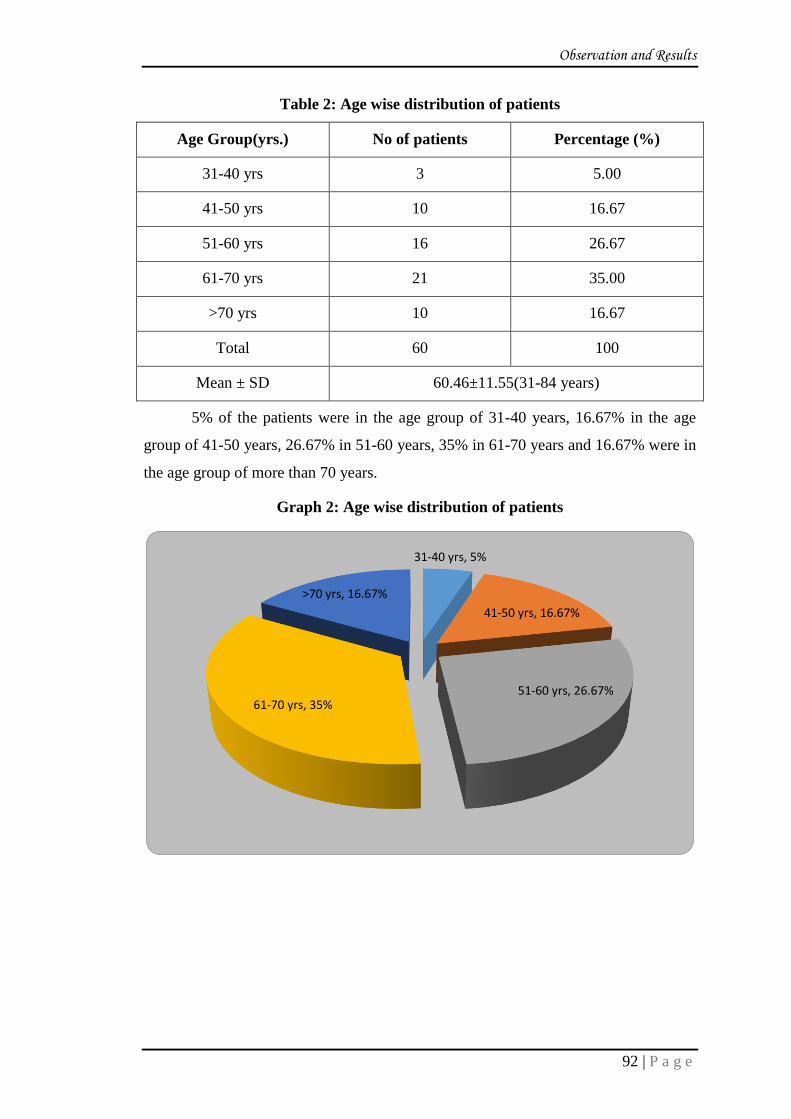
Observation and Results
92 | P a g e
Table 2: Age wise distribution of patients
Age Group(yrs.) No of patients Percentage (%)
31-40 yrs 3 5.00
41-50 yrs 10 16.67
51-60 yrs 16 26.67
61-70 yrs 21 35.00
>70 yrs 10 16.67
Total 60 100
Mean ± SD 60.46±11.55(31-84 years)
5% of the patients were in the age group of 31-40 years, 16.67% in the age
group of 41-50 years, 26.67% in 51-60 years, 35% in 61-70 years and 16.67% were in
the age group of more than 70 years.
Graph 2: Age wise distribution of patients
31-40 yrs, 5%
41-50 yrs, 16.67%
51-60 yrs, 26.67% 61-70 yrs, 35%
>70 yrs, 16.67%

Observation and Results
93 | P a g e
Table 3: Gender wise distribution of patients
Gender No of patients Percentage (%)
Male 35 58.33
Female 25 41.67
Total 60 100
58.33% of patients were males and 41.67% were females.
Graph 3: Gender wise distribution of patients
Male, 58.33%
Female, 41.67%

Observation and Results
94 | P a g e
Table 4: Comparison of speech sound T in dB in two groups
Group N Mean Std.
Deviation
Std. Error
Mean
t-
value p-value
Without Modification 60 15.31 2.87 0.37
7.82 0.0001,S
With Modification 60 20.36 4.09 0.52
Mean speech sound T in dB in without modification was 15.31±2.87 and in
with modification it was 20.36±4.09. By using Student’s unpaired t test statistically
significant difference was found in speech sound T in dB in two groups (7.82, p-
value=0.0001)
Graph 4: Comparison of speech sound T in dB in two groups
15.31
20.36
0
5
10
15
20
25
Without Modification With Modification
Me
an s
pe
ech
so
un
d T
in d
B

Observation and Results
95 | P a g e
Table 5: Comparison of speech sound T in Hz in two groups
Group N Mean Std.
Deviation
Std. Error
Mean t-value p-value
Without Modification 60 128.76 15.86 2.04
1.94 0.054,NS
With Modification 60 134.10 14.12 1.82
Mean speech sound T in Hz in without modification was 128.76±15.86 and in
with modification it was 134.10±14.12. By using Student’s unpaired t test statistically
no significant difference was found in speech sound T in Hz in two groups (1.94, p-
value=0.054)
Graph 5: Comparison of speech sound T in Hz in two groups
128.76
134.1
124
126
128
130
132
134
136
Without Modification With Modification
Me
an s
pe
ech
so
un
d T
in H
z &
SD

Observation and Results
96 | P a g e
Table 6: Comparison of speech sound Th in dB in two groups
Group N Mean Std.
Deviation
Std. Error
Mean t-value p-value
Without Modification 60 17.28 2.97 0.38
3.91 0.0001,S
With Modification 60 19.83 4.07 0.52
Mean speech sound Th in dB in without modification was 17.28±2.97 and in
with modification it was 19.83±4.07. By using Student’s unpaired t test statistically
significant difference was found in speech sound Th in dB in two groups (3.91, p-
value=0.0001).
Graph 6: Comparison of speech sound Th in dB in two groups
17.28
19.83
0
5
10
15
20
25
Without Modification With Modification
Me
an s
pe
ech
so
un
d T
h in
dB
an
d S
D

Observation and Results
97 | P a g e
Table 7: Comparison of speech sound Th in Hz in two groups
Group N Mean Std.
Deviation
Std.
Error
Mean
t-value p-value
Without Modification 60 136.51 12.51 1.61
0.05 0.96,NS
With Modification 60 136.63 13.09 1.69
Mean speech sound Th in Hz in without modification was 136.51±12.51 and
in with modification it was 136.63±13.09. By using Student’s unpaired t test
statistically no significant difference was found in speech sound Th in Hz in two
groups (0.05, p-value=0.96).
Graph 7: Comparison of speech sound Th in Hz in two groups
136.51 136.63
134
134.5
135
135.5
136
136.5
137
137.5
138
Without Modification With Modification
Me
an s
pe
ech
so
un
d T
h in
Hz
and
SD

Observation and Results
98 | P a g e
Table 8: Comparison of speech sound D in dB in two groups
Group N Mean Std.
Deviation
Std. Error
Mean t-value p-value
Without Modification 60 20.55 3.52 0.45
5.71 0.0001,S
With Modification 60 17.10 3.06 0.39
Mean speech sound D in dB in without modification was 20.55±3.52 and in
with modification it was 17.10±3.06. By using Student’s unpaired t test statistically
significant difference was found in speech sound D in dB in two groups (5.71, p-
value=0.0001).
Graph 8: Comparison of speech sound D in dB in two groups
20.55
17.1
0
5
10
15
20
25
Without Modification With Modification
Me
an s
pe
ech
so
un
d D
in d
B &
SD

Observation and Results
99 | P a g e
Table 9: Comparison of speech sound D in Hz in two groups
Group N Mean Std.
Deviation
Std. Error
Mean t-value p-value
Without Modification 60 135.76 11.88 1.53
0.44 0.65,NS
With Modification 60 134.86 10.34 1.33
Mean speech sound D in Hz in without modification was 135.76±11.88 and in
with modification it was 134.86±10.34. By using Student’s unpaired t test statistically
no significant difference was found in speech sound D in Hz in two groups (0.44, p-
value=0.65).
Graph 9: Comparison of speech sound D in Hz in two groups
135.76 134.86
0
20
40
60
80
100
120
140
160
Without Modification With Modification
Me
an s
pe
ech
so
un
d D
in H
z &
SD

Observation and Results
100 | P a g e
Table 10: Comparison of speech sound L in dB in two groups
Group N Mean Std.
Deviation
Std. Error
Mean t-value p-value
Without Modification 60 21.13 4.01 0.51
0.89 0.37,NS
With Modification 60 20.48 3.99 0.51
Mean speech sound L in dB in without modification was 21.13±4.01 and in
with modification it was 20.48±3.99. By using Student’s unpaired t test statistically
no significant difference was found in speech sound L in dB in two groups (0.89, p-
value=0.37).
Graph 10: Comparison of speech sound L in dB in two groups
21.13 20.48
0
5
10
15
20
25
Without Modification With Modification
Me
an s
pe
ech
so
un
d L
in d
B &
SD

Observation and Results
101 | P a g e
Table 11: Comparison of speech sound L in Hz in two groups
Group N Mean Std.
Deviation
Std. Error
Mean t-value p-value
Without Modification 60 129.38 16.62 2.14
1.33 0.18,NS
With Modification 60 132.96 12.44 1.60
Mean speech sound L in Hz in without modification was 129.38±16.62 and in
with modification it was 132.96±12.44. By using Student’s unpaired t test statistically
no significant difference was found in speech sound L in Hz in two groups (1.33, p-
value=0.18).
Graph 11: Comparison of speech sound L in Hz in two groups
129.38
132.96
125
126
127
128
129
130
131
132
133
134
135
Without Modification With Modification
Me
an s
pe
ech
so
un
d L
in H
z &
SD

Observation and Results
102 | P a g e
Table 12: Comparison of speech sound Ch in dB in two groups
Group N Mean Std.
Deviation
Std. Error
Mean t-value p-value
Without Modification 60 16.10 3.60 0.45
5.61 0.0001,S
With Modification 60 20.01 4.01 0.51
Mean speech sound Ch in dB in without modification was 16.10±3.60 and in
with modification it was 20.01±4.01. By using Student’s unpaired t test statistically
significant difference was found in speech sound Ch in dBin two groups (5.61, p-
value=0.0001.
Graph 12: Comparison of speech sound Ch in dB in two groups
16.1
20.01
0
5
10
15
20
25
Without Modification With Modification
Me
an s
pe
ech
so
un
d C
h in
dB
& S
D

Observation and Results
103 | P a g e
Table 13: Comparison of speech sound Ch in Hz in two groups
Group N Mean Std. Deviation Std. Error Mean t-value p-value
Without Modification 60 131.75 15.42 1.99
1.05 0.29,NS
With Modification 60 134.53 13.33 1.72
Mean speech sound Ch in Hz in without modification was 131.75±15.42 and
in with modification it was 134.53±13.33. By using Student’s unpaired t test
statistically no significant difference was found in speech sound Ch in Hz in two
groups (1.05, p-value=0.29).
Graph 13: Comparison of speech sound Ch in Hz in two group
Statistical Analysis: Statistical analysis was done by using descriptive and
inferential statistics using Student’s unpaired t test and software used in the analysis
was SPSS 22.0 and p<0.05 is considered as level of significance.
131.75
134.53
128
129
130
131
132
133
134
135
136
Without Modification With Modification
Me
an s
pe
ech
so
un
d C
h in
Hz
& S
D

Observation and Results
104 | P a g e
STATISTICAL FORMULAS
Statistical analysis of assessment “Evaluation of the effect of functional
contouring of the palatal vault of maxillary complete denture on clarity of speech
sounds in edentulous patients “Analysis of the data was done by using descriptive and
inferential statistics both.
Descriptive statistics are used to describe the basic features of the data in a
study. They provide simple summaries about the sample and the measures. Together
with simple graphics analysis, they form the basis of virtually every quantitative
analysis of data.
Descriptive statistics are typically distinguished from inferential statistics.
With descriptive statistics you are simply describing what is or what the data shows.
With inferential statistics, you are trying to reach conclusions that extend beyond the
immediate data alone. For instance, we use inferential statistics to try to infer from the
sample data what the population might think. Or, we use inferential statistics to make
judgments of the probability that an observed difference between groups is a
dependable one or one that might have happened by chance in this study. Thus, we
use inferential statistics to make inferences from our data to more general conditions;
we use descriptive statistics simply to describe what's going on in our data.
The software used in the analysis were SPSS 17.0, EPI-INFO 6.0and Graph
Pad Prism 5.0 version and p<0.05 is considered as level of significance.
The statistical tests used for the analysis of the result were:
1. Student’s unpaired t test
Descriptive Statistics:
1. Arithmetic Mean: The arithmetic mean, or average, is the sum of the
values divided by the number of values.
Formula:

Observation and Results
105 | P a g e
Where:
2. Standard Déviation(SD) =
Inferential Statistics:
3. Student’s unpaired t-test:
Assumption:
1. The samples (n1 and n2) from two normal populations are independent.
2. One or both sample sizes are less than 30
3. The appropriate sampling distribution of the test statistic is the t distribution
4. The unknown variances of the two populations are not equal
To compute the two-sample t-test two major computations are needed before
computing the t-test. First, you need to estimate the pooled standard deviation of the
two samples. The pooled standard deviation gives a weighted average of the standard
deviations of the two samples. The pooled standard deviation is going to be between
the two standard deviations, with greater weight given to the standard deviation from
a larger sample. The equation for the pooled standard deviation is:

Observation and Results
106 | P a g e
In all work with two-sample t-test the degrees of freedom or DF is:
The formula for the two sample t-test is:

Discussion
107 | P a g e
Speech is an integral part of human communication, which makes the human
species superior to other life forms. Although every prosthodontist aims at providing
excellent complete denture prosthesis in terms of esthetics, functional efficiency and
comfort, a thorough evaluation of phonetics is too neglected with greater emphasis
placed on other three components. Loss of teeth is usually accompanied by eventual
loss of oral morphology responsible for the articulation of certain speech sounds.
Some patients do not experience any speech problems because it appears that tongue
makes compensatory adjustments for the absence of teeth. Allen had stated that
patient fitted with complete dentures generally adjust his speech pattern to the new
appliance and thus improves6.Mortone reported that older patients with complete
dentures show a resistance to speech improvement.18,19,20,21
Speech consists of
Respiration, Phonation, Resonation, Articulation, Neural integration and
Audition43
.Of these components articulation is mostly affected by construction of
complete dentures.
Articulation by definition is resonated sound formed into meaningful speech
by the movements of the mandible, lips, tongue, soft palate, hard palate and teeth. The
tongue, lips and soft palate are dynamic structures that control and direct the air
movement. Rapid and precise movements of tongue and lips occur across the static
structures. Their approximation to the teeth, hard palate and the alveolar processes
create valves for the production of specific sounds of speech like lingual-dental,
lingual-alveolar and palatal consonants. Tanaka H. (1973) reported that a reverse
curve exist in the sagittal and frontal sections of dentate patients9. This convexity is
important for the pronunciation of the sibilant sounds such as S and SH. If the anterior
palatal area is over contoured such that the air stream is excessively impeded, an S
sound may be heard as central or frontal lisp. However if this area is under-contoured,
resulting in an insufficient impeding of the air stream, “S” sound may be perceived as
whistle.91
Complete loss of teeth can cause a persistent speech disorder by altering dental
articulation areas. This severely reduces the quality of speech particularly the alteration
of frontal maxillary morphology leads to impairment of speech production. Removable
complete dentures can partly solve this problem. However, they disturb speech
production themselves as they restrict the flexibility of tongue, narrow the oral cavity
and alter the articulation areas of the palate and teeth. Speech production plays a

Discussion
108 | P a g e
significant role in patient’s general satisfaction with dentures. The patient’s contentment
co-relates with the acceptance of the denture therefore, speech production quality is an
essential feature for success or failure of dental rehabilitation.9
A phonetically correct articulation after a prosthodontic treatment in the form of
complete denture prosthesis is an important desideratum for a socially comfortable,
meaningful, and high quality of life. Moreover, the ability of correctly articulating the
phonemes and words, with no impediment in realizing the proper prosody is an
essential requirement in numerous professions, such as public relations- related
professions, law, teaching media, speakers. In all these fields of activity, normal natural,
fully modulated pronunciation is a crucial requirement. Researchers in dentistry and
psychology are aware of these facts. Dental treatment and prosthetics contribute to the
preservation of the normal speech ability, beyond contributing to the preservation and
re-establishing of the masticatory and esthetic functions. While the last two roles of the
dental treatment and prosthetics are well instituted and understood, the phonetic
recovering is still poorly comprehended and rather unvalued 103
Correction of faulty speech is the primary task of the speech specialist but the
complexity of the voice producing mechanism implores the services of the allied
health sciences .Successful treatment of the defective speech usually requires close
co-operation between the speech therapist and the practitioner in some branch of the
medical or dental profession.
This co-operation would be greatly enhanced if the medical and dental
practitioner were more aware of the fundamentals of the phonetics. Early and proper
diagnosis of speech abnormality is important for successful treatment and favorable
prognosis.
Articulation is usually considered to be a joining of parts however speech
articulation takes place when any approximation or movement of the articulators
constrict, impedes or diverts the airstream to produce a single sound.
The single sound that the physiologic airstream mechanism are capable of
producing are varied and innumerable. Many occur as noise and are un-classified, but
those that are learned as speech are called phones. Many of the phones are so similar
in character that they cannot be recognized as separate sounds by other than an expert
Discussion
109 | P a g e
or when pronounced very slowly and carefully. Those closely related phones have
been combined to form recognizable sounds and are classified as phonemes.
The Phoneme then is the unit of speech by which we distinguish one utterance
from another and which collectively (about 40) make up phonemics of the language.
Each phoneme has been given a phonetic symbol which represents its specific
sound in any language. The symbols of all phonemes together with their variance are
published by the International phonetic Association (IPA) as the Phonetic ‘Alphabet’.
Knowledge of this alphabet is an invaluable aid in learning different languages and it
is likely that phonetics will be better understood when it is mastered, because to learn
the alphabet it is necessary to learn the sounds which are universal and basic to any
language2.
Speech may be defined as formalized oral communication. It consist of four
components which are: 1-linguistic (conversational). The underlying thought and
grammatical form used in expression, 2-phonatory, the breath support as well as
laryngeal vibration in articulate speech, 3-articulatory, the neuromuscular controls
used to alter the oral and pharyngeal architecture to make definitive phonetic sounds,
and 4-auditory,the aural monitoring of one’s own speech.34
Speech is a very complex, sophisticated and autonomous activity.4 It is a
complex and highly coordinated process involving several systems of the body like
the respiratory system, phonatory system, articulatory system and resonatory system.1
Of these the articulatory system is of particular interest or significance to the dentist,
owing to the fact that the various components of the articulatory system consist of
structures of the oral cavity. The unique complexity of the oral cavity and adjacent
area presents a continual challenge to prosthodontic point. Functional movements
include those associate with respiration, deglutition, mastication, facial expression and
speech
Hence, knowledge of the phenomenon and mechanism of speech production is
an essential feature of comprehensive dental treatment.
Speech in matured man is a learned habitual neuromuscular pattern. The loss
of teeth and supporting structures alters the main articulator cavity and produce a
marked effect on the speech pattern.
Discussion
110 | P a g e
An empiric approach to the phonetic factor in denture construction frequently
place the burden for compensating for speech changes on the adaptability of the
tongue. While it is true that the tongue is very adaptable, it must be recognized that
this quality is far more significant in patients of orthodontic age than those who are
within a prosthodontic age range. In the latter group, functional patterns have been
established, and ability to adapt has decreased. Additionally significant is the fact that
the speech mechanism is highly susceptible to degenerative diseases. If dentures are
to contribute effectively to the function of speech, dentist should utilize studies in the
speech science field to augment their clinical knowledge of the phonetic factor in
denture construction.18
As Bloomer said, “surgeons and dentists who have labored carefully and
skillfully to fashion or restore anatomical form are frequently disappointed to find that
anatomical form is no guarantee of function” more important , of course , is the fact
that patient is sometimes equally or more disappointed when function does not equal
structure. Here, the function we will consider is speech –specifically, articulation or
phonetics.
For some time, prosthodontics main attention has been placed upon the patient’s
skill in talking after dentures have been made and fitted. Schlosser and Gehl said that”
correction of speech defects due to the partial or complete loss of natural teeth in
compliance with phonetic requirements was the third major objective for the fabrication
of a denture prosthesis. These authors were suggesting that a speech problem existed
before the patient had his dental treatment. It is perhaps equally important to identify
any speech problems which might develop after the denture has been fitted .The patient
will probably suspect that the denture itself is the cause of the speech problem.23
Patients usually maintain acceptable speech if the dentures satisfy the
requirements of function and esthetics however, some patients encounter difficulties,
and their speech becomes major concern. Accurate diagnosis of the speech problem is
essential in order to determine the appropriate clinical response. Of paramount
importance is the differentiation between 1) those speech defects which are associated
with changes in oral form and structure and2) those produced by other co existent
conditions in denture wearing patients. Since dentures constitute an obvious “reality”,
the patient with the speech defect may readily assume that all components of the
problem are ascribable to the dentures. However other concomitant conditions may be

Discussion
111 | P a g e
contributory to the speech defect or may be of major etiological significance. Older
patients, in particular, frequently have physical problems which are temporarily
overshadowed by their concern regarding the dentures.
Though the totality of the speech process should be emphasized for purposes
of differentiation, the various dimensions basic to speech production will be
considered separately. To clarify areas of mutual concern for prosthodontists and
speech pathologists, the following seven functions will be assessed: 1) respiration 2)
phonation 3) resonance 4) speech articulation 5) audition 6) neurologic function 7)
emotional behavior.22
The primary concern in phonetics is with the changes in the stream of air as it
passes through the oral cavity. Therefore, the enunciators or articulators are of
greatest interest to us. Of these, the tongue plays a major role. The tongue is the
principal articulator of the consonants and changes position and shape for the
pronunciation of each of the vowels. In pronouncing each consonant, the tongue
contacts a specific part of the teeth, alveolar ridge or hard palate. These structures are
covered or replaced by the denture, and the dentist must know where the tongue
contacts them so that they may be appropriately restored in the prosthesis.32
In as much as the neuromuscular patterns for speech are least affected by the
loss of the teeth, it follows that the recording of the speech, positions would be the
first and most logical step in recording functional positions. The study of phonetics
provides much useful information in formulating a treatment plan for the prosthetic
patient. In addition, knowledge of how the speech patterns develop, how they operate,
and what they are, is a most enlightening factor in understanding the performance of
all the oral functions.
The phonetic formats to be described are normal and average formats which
will physically produce the proper and intended speech sounds, and do not hold true
for retrognathic, prognathic, or any other. Although speech patterns are universal,
there are minor and individual variations, just as there are in the human gait for
walking. For this reason, functional positions assumed during speech can be recorded
only on an individual basis.33
This is true, especially, in case of the complete or partially edentulous patient,
wherein the loss of teeth and supporting structures alters the main articulatory cavity

Discussion
112 | P a g e
and produces a marked effect on the speech pattern. Wad M.A. and associates have
described the importance of speech for patient satisfaction with new dentures.97
They
showed that incorporation of dentures affects speech and familiarization may be a
protracted process. Quite often patient Complains about their inability to pronounce
certain sounds following insertion of complete dentures.
Such a complaint is more significant, especially for those engaged in a
profession where oration is an important entity like teachers, orators, singers, famous
personalities, politicians etc.
Superior speech performance was found to be related to a denture with better
fit.99
More emphasis has always been placed, by the clinician, on other key elements of
denture success like esthetics, function and comfort as compared to phonetics. Several
authors100,44,72
suggested that missing proprioceptors , change in sensory stimulus,
altered tooth positions , change in oral cavity dimension, gradual loss of hearing
(ageing process) might be responsible for problems in speech sound production
immediately post denture insertion.
The role of lips, teeth, tongue, hard palate, alveolar ridges and soft palate, in
production of speech sounds has been described eloquently by several
authors.14,15,16,17,18,19,22
Rothman32
termed these structures as "enunciators" and described
the mechanism of speech and how these structures added distinctness and clarity to
speech sounds. These structures act in unison to produce consonant sounds. Thus
consonants are articulatory speech sounds that require the articulatory structures of the
oral cavity to impede, construct, divert or stop air stream at the proper place and time
either actively or passively1 The production of consonant sounds have multiple
dimensions based on place of articulation (bilabial, dental, linguopalatal, velar,
labiodental), manner of articulation (plosives, fricatives, affricatives, flap, retroflex) and
voice (voiced / voiceless). Of these the tongue has been universally accepted as the
principal articulator for the consonants speech sounds which contacts the anterior,
middle and posterior portions of the hard palate in pronouncing many of them (t,d,n,s,l)2
A few have recognized the importance of palatal contour of the denture for
better phonation. Snow, as early in (1899) recommended restoring the anterior lingual
alveolar area to improve phonetics, particularly the pronunciation of S and SH.
Prendergast 1935 pointed out that proper thickening of the lingual alveolar area was
important for proper speech. Sears in (1949) recommended making a palatogram on

Discussion
113 | P a g e
cases where the median sulcus of the tongue does not coincide with the midline of the
palate. He recommended grooving of the palate just above the median sulcus for
patients who had little or no tongue sulcus and thickening this area for the patient who
had a deep tongue sulcus. Pound in (1951) was successful in improving phonetics by
contouring the entire lingual aspect of the maxillary denture to stimulate the normal
palate. In 1958 a method for restoring the lingual alveolar area by use of palatography
was published, and, in essence, that method together with several refinements found
to be advantageous.2
The precision of tongue palate contact relationship for a given sound has long
been a subject of interest, the use of palatograms has been well documented for this.54,
67Tanaka
9 studied the relationships between palatal contours and speech intelligibility
in both dentulous and edentulous subjects. He noted that in a sagittal section, the
natural anterior portion of the palate exhibits a reverse curve. This curve is crucial for
production of linguopalatal consonant sounds like t, d, n, l, s, sh, ch, jh. When
compared between dentate subjects and complete denture patients, Tanaka found that
this curvature was missing in most of the prostheses.
The role of palatal rugae as a land mark which the tongue recognizes in speech
has long been a point of contention. The palatal rugae contribute to a sensory input
which also serves as a bio feedback unit along with the tongue and the auditory
system, in production of various sounds. As this is surface is covered by an artificial
material, the feedback mechanism is weekend. The speech sound distortion might be
the result of substitution of plastic material against natural tissues in the palatal
region. Hence, the controversy as to whether or not to replace or reproduce the rugae
has been long standing.
Slaughter7 believes that the smoothness of the denture is disturbing, and
without the rugae, the tongue loses its capacity for local orientation. However,
Landa29, 33
states that the rugae are useless or even detrimental to most patients
because of the unnecessary additional thickness of the denture. When plataolingual
sounds t, d, s, n, l54
are produced, the excessive thickness causes phonetic difficulty
due to the premature contact of the tongue with the denture base. As there is no loss of
tissues on the palatal surface, the denture should be thin so tongue space will not be
reduced,6believed that entire lingual aspect of the maxillary denture should be

Discussion
114 | P a g e
contoured to simulate the palate, if phonetics is to be attained. Hence, many authors
recommended the reproduction of rugae as an adjunct to proper phonetics.
The simplest procedure involves hand carving the palatal surface of the
denture.49
However, this method is difficult to correct if improperly done and is
difficult to polish. Another more precise procedure uses electroplating to form a metal
plate that duplicates the form of the patient’s palate.49,52
K.C.White, M.E. Connelly
advocated the use of prefabricated palatal veneers and also described a technique for
making an individualized palatal pattern made of acrylic resin to duplicate the
rugae49
Alexander Hassel73
conducted a study and observed that there was a
significant improvement in the speech after sandblasting the palatal surface of the
maxillary denture, especially for stops and fricatives. Christina et al57
described a
method for incorporating rugae by the use of tinfoil trimmed and adapted to a cast
with prominent rugae. Shaffer and Kutz40
suggested a method of using soft wax to
physiologically develop the palatal rugae surface of a denture, based on the
movements and pressure made by the tongue during swallowing and speech.
Raghvendra Adaki, Suresh Meshram86
conducted study to evaluate the impact of
rugae on phonetics. Evaluation of speech was done by acoustic analysis and
intelligibility analysis. Reports revealed that pronunciation of s, sh, t, d, was clearer
with rugae incorporated denture than conventional denture. Amongst rugae
incorporated dentures customized rugae dentures were better than arbitrary rugae
dentures. Bit of modification in the anterior part of palate gives the better results
regarding pronunciations, thus enhancing patient’s confidence. We can do better
justice by inculcating this into our routine practice. In the past some investigators
stated that metal denture base can improve the quality of speech as it can be used in
thin sections. So tongue can adapt the oral environment easily as compared to acrylic
but fabrication of metal denture base is time consuming and costly. It cannot be
relined and cannot be contoured with any functional method. Sandblasting of the
palatal vault of denture was also performed to create the irregularities on the surface
to mimic the natural tissue morphology. These irregularities will entrap the food
particles which would be difficult to keep clean.
This aroused the need for the concept of customized palatal surface or
functional molding of the palatal vault with various materials like auto-polymerizing
resins, tissue conditioners, and physiologic wax74
. However, none of the methods is a

Discussion
115 | P a g e
direct method and can be put to use in routine clinical practice. Thus, though initial
experiences in speech disturbances are transient, the treatment objective should be to
make the dentures confirm to the individual patient's existing neuromuscular pattern.
The dentist should therefore recognize the role of prosthetic treatment on speech
activity. However there has been very few studies in the literature that use sound
spectrographic analysis to analyses the changes that use of dentures would produce.
Hence the present study is conducted to assess the changes in the speech sound
production in edentulous patients after rehabilitation with complete dentures where
functional contouring of the palatal vault of maxillary complete denture was done by
visible light cure resin.
In the present study, an attempt was made to improve the quality of speech
sounds produced immediately post denture insertion by customizing / functionally
contouring the palatal vault of maxillary complete denture using visible light cure
material and assessed if it can be put to use in routine clinical practice.
Immediately after insertion of dentures, the tongue is in a new environment
usually has to function against a highly polished palatal surface of the denture,
resulting in an altered speech pattern.10
It is possible the tongue might be able to adapt
to the new environment, and might even produce normal speech with the practice in
time. However, the approach in this study is to functionally contour the palatal surface
of the maxillary complete denture so that at the time of insertion and afterwards the
tongue does not have to adapt itself to the changed environment to produce normal
speech.
So in this study, sixty edentulous patients were selected who satisfied the
criteria laid down. Complete dentures were fabricated by standardizing the clinical
and laboratory steps for all these patients to avoid influence of variations. At the
denture insertion appointment, speech sounds were recorded with and without
modification of palatal vault of maxillary complete denture. The complete palatal
portion was functionally contoured by carefully adapting visible light cure resin
material. In the various studies conducted in past other materials had been used to
contour the palate functionally like waxes, reversible hydrocolloid, tissue
conditioners, auto polymerizing resins. Each has its own drawbacks, so the material
selected in this study is visible light cure resin, Light -activated resins are supplied as
premixed sheets or rope in light proof pouches which has fallowing advantages

Discussion
116 | P a g e
1-available in thin sheet forms
2-good working time
3-can be easily adapted manually by finger pressure
4-chemical bonding with the existing denture
5-no extra equipment required
6- biocompatible with pleasant colour
7- Easily moldable by tongue pressure
8- easy to polish. Repeatable procedure
9- cost effective, readily available
10-can be done chair side no lab procedure required
11- Changes are identifiable and visible
12- Light weight, less porosity, nontoxic
13- Reduced polymerization shrinkage
This palatal area was chosen because the tongue makes direct, firm contact
with the denture in this region and the normal anatomy of this area shows unevenness
due to presence of rugae.74
After adaptation of the material on the complete palatal
vault patient was asked to pronounce certain linguopalatal and linguoalveolar sounds
thrice so that proper molding should takes place. Denture was removed from the
patient’s oral cavity and cured. Again the sound recording been done which was
recorded in the form of spectrographs of that particular sound and analyzed in the
terms of frequency (pitch) and loudness. During the adaptation procedure there were
chances to increase the thickness of denture area in palatal region which would
adversely affect the quality of speech. So care has been taken while fabrication of
denture during wax-up stage. Thickness of the wax in the palatal region has been kept
1 mm, so that after addition of visible light cure resin thickness of denture should not
increase
In the previous studies the anterior area of the palate had given much more
importance than the posterior region in the production of speech sounds. As presence
of rugae in the anterior region became the major factor when compared to posterior
area, Duplication and incorporation of rugae has been done by many investigators but

Discussion
117 | P a g e
the results are controversial. Majority of them stated that rugae improved the quality
of speech by orosensory mechanism when compared with smooth glossy surface of
denture. Some investigators found the presence of rugae disturbing the quality of
speech.
As the hand carving and duplication of rugae from the other patient model
and transferring it to the denture require extra laboratory time and it is not matching
with the natural morphology of the palatal vault of that particular patient. So the
results achieved are not promising. This emphasized the need to contour the palate
functionally both in anterior and posterior region. Tongue makes contact in posterior
region in lateral sounds like labeling the principle articulator of the speech tongue
makes contact in both the anterior as well as posterior regions, so in this study
material has been adapted on the complete palatal vault.
Actual molding of palatal surface by patient by pronouncing certain
palatolingual sounds used in the study molded the palate uniquely and true for that
particular patient and improved the quality of sound in terms of frequency and
loudness measured in Hertz and Decibels respectively on the spectrograph. Even the
patient can be involved in the procedure and the change in the quality of speech can
be witnessed by the patient which improves the psyche of the patient dramatically and
gives confidence to patient. The palatal area was chosen because the tongue makes
direct, firm contact with the denture in this region and the normal anatomy of this area
shows unevenness due to presence of rugae.74
Hence, the speech sounds analyzed in this study were restricted to
linguopalatal sounds like t, d, ch, l, th in which the tongue made active contact with
the palate thereby functionally molding it. Other linguopalatal sounds s, dh, sh, jh,
were not included as they are formed by passive contact of tongue with the palate and
are also influenced by the position of the teeth. The subjects were trained prior to
recording and the records were made in local language Hindi. The polymerization was
done in the light curing unit
The sound recording and spectrographic analysis was done with the help of
Sony Entertainment Ltd. copyrighted Sound Forge Version 11.0 Sound Forge is a
two-track digital audio editor that includes a set of audio processes, tools, and is
compatible with any Windows sound card to create, record, and analyze audio files.
The speech sound samples of each subject were recorded immediately post denture

Discussion
118 | P a g e
insertion without any modification of the palatal surface of the denture. The recording
was repeated again after functional molding of the palatal vault of the maxillary
complete denture with visible light cure material. Spectrographic analysis of the
sound samples was done using the same software, for both frequency and decibel
comparison. This spectrum analysis allows user to perform FFT analysis and displays
the resulting data in a spectrum graph or sonogram display. The spectrum graph
allows real time monitoring of input and make it easy to navigate data and read audio
frequency and position. In the spectrum graph the horizontal axis represents frequency
and vertical axis represents amplitude in decibel (dB.)
The descriptive analysis of comparison of decibels between group G1 and,
group G2 showed that the mean value and standard deviation of the decibels of the
sound samples of "t" in group G1 was 15.31±2.87dB, and in G2 was 20.36±4.09 dB.
In "th” sound group G1 shows 17.28±2.97dB and G2 shows 19-83±4.07dB.Sound"d"
in G1 shows20.55±3-52 dB and G2 shows17.10±3.06dB.In sound "d' group shows
20.55±3.52 dB and G2 shows17.10±3.06 dB. In sound 'l" G1 shows21.31±4.01dB and
G2 shows20.48±3.99 dB. Sound "ch" in G1 shows16.10±3.60 dB and G2 shows
20.01±4-01 dB.
The descriptive analysis of comparison between decibels of group G1 and
group G2 showed that the mean value and standard deviation of sound samples in
group G1and G2 by using Student’s unpaired t test statistically significant difference
was found. All the sounds recorded after modification of palatal vault with visible
light cure material showed increase in dB. The scale for measuring intensity/loudness
of sound is the decibel scale. It was observed that group G2 had a higher decibel as
compared to group G1 indicating that the tongue had active contact with the
contoured palate to produce clear sounds as compared to group G1.
The frequency of a sound wave is measured as the number of complete back-
and-forth vibrations of a particle of the medium per unit of time. The sensation of a
frequency is commonly referred to as the pitch of a sound. A high pitch sound
corresponds to a high frequency sound wave and a low pitch sound corresponds to a
low frequency sound wave. The descriptive analysis of comparison of frequencies
between group G1 and group G2 showed that the mean value and standard deviation
of sound samples in GI for sound "t” was 128.76±15.86 Hz and in G2 it was
134.10±14.12 Hz. The sound "th" in group G1 it was136.51±12.51Hz and in G2 it

Discussion
119 | P a g e
was136.63±13.09Hz.Sound "d' in group G1 it was 135.76±11.88Hz and in G2
134.86±10.34 Hz. The sound "l" in G1 was 129.38±16.62 and in G2 it was
132.96±12.44 Hz. Sound 'ch" was 131.75±15.42 and in G2 it was 134.53±13.33 Hz.
The results showed that samples of group G2 had a higher frequency than group G1
indicating that functional contouring of the palatal vault resulted in an improvement in
the pitch of the speech.
Observing the combined results of frequency and decibels, it can be seen that
there was improvement in the pitch of speech and intensity/loudness of sound after
functional molding of palatal vault of maxillary complete denture.
When the tongue, a soft muscular structure, makes firm contact with relatively
smooth, glossy surface of the acrylic there is dampening of the sound as compared to
the relatively hard, rough / uneven surface of the set resin which simulates the
unyielding nature of tissues in that region. Thus, it can be concluded that the
orosensory feedback as well as the type of material, both, are responsible for
improvement in the pitch (frequency) and intensity (decibels), hence quality of the
speech sounds.
The improvement noticed may be due to the orosensory feedback by the
tongue-functional palate contact relation, leading to better adaptation and hence,
improvement in the quality of speech. Thus, the quantitative results affirmed that
functional contouring of the palatal vault of maxillary complete dentures significantly
improves the speech intelligibility.
There is a need for further studies with a larger sample size to investigate the
effect of alterations in dentures on other parameters. There is a necessity to evaluate
the effects of a longer duration of adaptation on all parameters. The study has proved
that functional contouring of the anterior portion of the palate is one of the major
factors that contributes to the clarity of speech but other factors like vertical
dimension, tooth position, arch form etc. have not been considered. Hence, there is
need for further investigation in this area.
PALATAL CONTOUR OF THE DENTURE
A few have recognized the importance of palatal contour of the denture for
better phonation. Snow (1899), recommended restoring the anterior lingual alveolar

Discussion
120 | P a g e
area to improve phonetics, particularly the pronunciation of s & sh. Prendergast
(1935) pointed out that proper thickening of the lingual alveolar area was important
for proper speech.
Sears (1949) recommended making a palatogram on cases where the median
sulcus of the tongue does not coincide with the midline of the palate. He
recommended grooving the palate just above the median sulcus for the patient who
had little or no tongue sulcus and thickening this area for the patient who had a deep
tongue sulcus. Pound (1951) was successful in improving phonetics by contouring
the entire lingual aspect of the maxillary denture to simulate the normal palate
PROSTHODONTIC CONSIDERATIONS OF SPEECH
The impact of denture on speech has been studied since 1950s in the papers of
pound42
and by Allen6and continued sporadically in 1960 by Rothman32
Martone
and Black17,18,19,20,21
and silverman35
during the last two decades, several groups
started investigating methodically the relationships between speech on one side and
dental treatment and prosthetic denture, on the other. These researchers were helped
by the new technologies of speech processing that flourished between 1990 and
2000.103
• Speech problems are usually identified immediately following phonetic treatment.
• After denture insertion, it is sometimes difficult to receive speech habits
immediately, but gradual process of retaining tongue positions good compensation
can be achieved in later periods.
• Speech adaptation to new complete dentures normally takes place within 2-4
weeks after insertion.
• During fabrication of denture, certain guidelines have to be followed in order to
achieve clarity of speech.
1) Effect of denture thickness and peripheral outlines
If the thickness of the denture base covering the palatal area is more, then lisping of
the sounds will occur.
Allen (1958) found that an additional thickness of 1mm in the anterior palatal area
made speech awkward and indistinct.

Discussion
121 | P a g e
The denture base thickness in the post dam area will irritate the dorsum of the tongue
which will impede the speech and there is a possibility in producing feeling of nausea
and denture may be unseated during sounds, which requires sudden repositioning of
the tongue to control and stabilize it.
The upper denture base in posterior region must be kept thin and the posterior border
should be merge with soft tissues.
If the lingual flange of the lower denture is too thick in the anterior region, will
encroach the space needed by the tongue and this results in faulty production of ‘s’
sound.
It can be corrected by arranging the artificial teeth, in same position as the natural
teeth will occupy and shaping the lingual flange so that there will be enough tongue
space to establish.
2) Effect of tooth position on speech
If the lower anterior teeth are arranged too lingually, the tongue is forced to arch itself
up to a higher position and the airway is to be too small and there will be faulty
pronunciation in ‘s’ and ‘z’ sounds.
If upper anteriors are too short of occlusal plane the word ‘v’ will more likely
pronounce as ‘f’. If upper anteriors are arranged below the occlusal plane the word ‘f’
will be pronounced like ‘v’.
The labiodental sounds like ‘f’, ‘v’ are helpful in determining the anteroposterior
positioning of the upper incisors and the occlusal plane.
3) Effect of dental arch form on speech:
If the arch is narrow, which will crumple the tongue which affects the size and shape
of the air channel results in faulty articulation of the consonants like ‘t, d, l, n, s, t’
where lateral margins of the tongue makes contact with palatal surfaces of the upper
posterior teeth.
The correction can be done by the slight thickening of the denture base in the center of the
palate, so that tongue does not have to extend up as far as into narrow palatal vault.

Discussion
122 | P a g e
With the Every effort should be made, consistent with the general mechanical
principles, to place the lingual and palatal surfaces of the artificial teeth in the position
previously occupied by the natural dentition03
4) Effect of vertical dimension on speech:
Fymbo (1936) pointed out that defective speech is most frequently associated with
increased vertical dimension which may result in difficulty in pronouncing sounds
like ‘b, m, p, f, and v’.
Landa (1947) recommended various phonetic tests to determine proper vertical
dimension using sounds such as ‘s, c, z’.
Silverman (1956) stated that sibilient sound‘s’ as a mean for determining the correct
vertical dimension. He established the “closest speaking space” and used this as
clearance area between the dentures.
The bilabial sounds like ‘m’ is helpful in determining the vertical dimension, when
this sound is pronounced there will be passive contact between the upper and the
lower lip, which aid in obtaining the correct vertical dimension.
Seifert e, Runt C et al (2000) concluded that variations of thickness and or volume of
the dentures and of the vertical and horizontal dimension of occlusion may result in
unpredictable audible changes to the voive93
5) Whistle and Swish sounds:
Silverman (1967) stated that the Whistle and Swish sounds are produced during
speech due to air abnormally passing over the tongue and through the interincisal
space. These sounds may be caused due to decreased over jet.
6) Effect of denture esthetics on speech:
Speech is sometimes related to patient’s emotional attitudes towards the denture
esthetics.
Lawson (1973) stated that when there is any change in patient mouth, then there will
be anxiety reaction will occur some patients dissatisfied with their teeth appearance in
denture and to overcome this problem they shows abnormal movement of lip, jaws,
and tongue during speech.

Discussion
123 | P a g e
The Tongue Factor
The tongue, which is the most versatile of the articulators, is involved in the
production of all vowels and the vast majority of consonants. The versatility of the
tongue allows different sounds to be produced; these require different tongue
configurations .By altering tongue position and shape' the size of the oral cavity, and
therefore the resonating characteristics, are changed the tongue can also acts as a
place of closure, in the production sounds, where a buildup of intra oral air pressure is
required. Furthermore, by using the tongue to create a narrowing against the hard
palate or teeth, fricative sounds are produced90
The tongue is the principle articulator for speech, and learning its position for
a given sound is the key to speech learning. To divide its role in speech the dorsum of
the tongue is divided into a back portion, which approximates the soft palate, and a
front portion, which approximates the hard palate, and the sides are referred it’s as the
tongue blade and the apex is called the tongue tip, or apex.
To pronounce ‘a’ the dorsum of the tongue is arched and the blade contacting
the alveolar ridge and the tip resting behind the lower incisors. The position for ‘e’ is
essentially the same, except the dorsum is arched a little higher, with the blade in
heavier contact with the alveolar ridge and the tip raised slightly. To pronounce ‘i’,
the tongue is pulled back with the dorsum flattened at the beginning of the sound, but
raises to the ‘e’ position for the completion. To pronounce ‘U’ the tongue first
assumes the ‘e’ position then fills back with the dorsum flattened for the second part
of the sound. For the ‘o’ tongue is in its flattest and lowest position with no palatal
contact.
Functional Tongue Classification
The working range of the mobile tongue varies with the individual. Therefore,
classification and knowledge of the conditions that cause variations are indicated.
The degree of activity and the variation in functional type suggest the
following classification:-
• The occupational tongue.
• The still tongue
• The normal tongue

Discussion
124 | P a g e
• The habitual tongue.
The term “occupational tongue” was selected to apply to those people whose
activities require increased tongue action. This includes jurists, teachers, lecturers and
preachers.
The developed increased muscular positioning force will herein after be
designated “tongue power movements”.
The “still tongue” is at the opposite end of the classification. In these patients,
as a result of limited activity, due to injury, deformity, or undue timidity, a passive
tongue exists. An example is ankyloglossia.
The “normal tongue” exists between these two extreme ranges and refers to
the type of tongue function in people exhibiting a normal or average development.
These cases are welcomed by the prosthodontist, as they give a range within limits in
effecting desirable rehabilitation.
PALATOGRAMS
A palatogram is a graphic representation of the area of the palate contacted by
tongue during a specified activity, usually speech-GPT 8
Palatograms are the area of tongue contact for a given sound displayed on an
artificial palate through a medium of non-scented talcum powder.
Pre-Requisites of Making a Palatogram
1. The artificial palate must be accurately adapted and refined so that it can be worn
comfortably without an adhesive until speech is normal and natural. The subject who
does not accommodate or who gags after a 15 minutes practice speaking period
should not be used, because palatograms of faulty speech would be of dubious value
and gagging makes palatography impossible.
2. The subject should be trained to pronounce the sound distinctly, and then to open
his mouth with the tongue flat (out of contact with the palate) and not to attempt to
swallow until after the palate is removed. Several trials should precede the making of
the palatogram to ensure that the patient can pronounce the sound distinctly and
immediately open his mouth without a gain contacting the palate with the tongue.

Discussion
125 | P a g e
3. The tracing medium should not be distasteful in flavors or appearance and should
be of a consistency that will permit ease of application and removes from the artificial
palate. The colour of the medium should contrast with the palate sufficiently to
display readily the area of tongue contact.
4. The palate must be dried thoroughly before dusting with talc, and care must be
taken in inserting and removing the dusted palate to avoid finger contact, which
would smudge the tracing. In pronouncing the phoneme, the moist tongue removes
the talc from the contact area, leaving a clear tracing.
A palatographic study of all the vowels revealed tongue palatal contact for all
except ‘O’. The similarity of the tongue contact area on the palatograms is because
phenomes are usually composed of more than one phone and that each phone requires
separate articulation. The phone with, occurs singly in pronouncing the vowel ‘e’ and
is prevalent in a, i and u. It occurs as the initial sound in u (ee – o) and as the second
sound of a and i (i-ee)
Consonants cannot be used in making palatograms, because the vowels included
in the pronunciations involve tongue palatal contact, which would obscure the tracing
of the articulation for the stop or affricative. Example: in pronouncing t and d, the
occlusive articulations is made first followed by ‘e’, ‘a’ follows the affricative
articulations for J and the affricative articulation for K. In pronouncing S, n or l, the
mid-vowel ‘e’ precedes the articulations for the sibilant s, the nasal n, or the lateral l.
To make the palatographic study of consonantal articulation, the ‘O’ was used in
conjunction with the consonant to be studied, even though the combination did not
result in a standard English work as in pronouncing ‘O’, the tongue naturally drops
back out of contact with the palate and flattens, making it easy for the subject to
open his mouth without raising the tongue.
Speech Tests
The phonetic aspect of denture construction at least deserves equal
consideration with esthetics and mechanics and should be checked at the time of the
waxed try in when it is possible to alter palatal contour to accommodate speech
articulation. The trial denture evaluation should not be considered complete until a
phonetic test has been made and enunciation proved satisfactory to both the patient
and the operator.

Discussion
126 | P a g e
Waxing of the palatal portions of the trial denture should be confined to the
area adjacent to the teeth, with just enough wax added to ensure a smooth surface
between the base tray and collars of the teeth. It is presumed that the base trays are
comfortable, well adapted and approximate the tissues with nearly the same fidelity as
anticipated for the completed denture bases. Before the speech tests are started, the
mandibular trial denture should be secured with denture adhesive.
• The first test is of random speech and is best accomplished by engaging the
patient in conversation and obtaining a subjective speech analysis by asking the
patient how the dentures feel, how his speech sounds to him, and which words
seem most difficult to pronounce.
• The second test is to specific speech sounds. This is best accomplished by having
the patient pronounce six or eight words containing the sound and then combining
these words into a sentence. The following is a list of the sounds to be tested;
opposite the sounds are the words to be pronounced and a sentence composed of
these words :-
s and sh Six, sixty, ships, sailed,
Mississippi, sure, sign, sun,
shine.
Sixty-six ships sailed the
Mississippi. Sure sign of sunshine
t, d, n, and
l
Locator, located, tornado, near,
Toledo
The locator located the tornado near
Toledo.
Ch and j Joe, Joyce, Joined, George,
Charles, church
Joe and Joyce joined George and
Charles at the church.
K Committee, convened, political,
convention, Connecticut
The committee convened at the
political convention in Connecticut.
f and v Vivacious, Vivian, lived, five,
fifty-five, fifth, avenue
Vivacious Vivian lived at five fifty-
five Fifth Avenue.
In the third test, the patient is asked to read a short paragraph containing an
abundance of s, sh, and ch sounds.

Discussion
127 | P a g e
If the patient can complete the speech test distinctly, with no difficulty, and if
his random speech satisfies him and the operator, it would be unwise to contour the
palate to solve a speech problem that does not exist. If, however, problems are
encountered in one or more of the areas tested, then palatal contour is indicated and
can effectively be accomplished by palatography.
If the palate is to be altered, the entire palate should be contoured to
accommodate tongue contact for all palatal consonants. This is best accomplished by
systematically displaying each contact area with a palatogram and establishing normal
tongue contact.
Palatography for Proper Palatal Contour
The only additional equipment necessary for palatography is some non-
scented talc, in inexpensive soft bristle brush for dusting the talc on the palate, and a
glass marking pencil to outline the contact area. Palatograms can be easily and
quickly made on the trial denture if the following steps are recalled:-
• Use o with the consonant to be studied, even though the combination is not a
word; i.e., to study k, use KO; to study ch; use cho.
• Train the patient to pronounce the sound and open the mouth without again
contacting the palate.
• Dry the palate thoroughly before dusting on non-scented talc (do not use regular
or surgical talc) and shake off the excess powder.
• Avoid touching dusted palate with the fingers during insertion, but ensure that the
denture is well seated before the sound is pronounced.
• Be sure the patient makes definite palatal contact in pronouncing the sound, but
avoids palatal contact after opening the mouth.
• Avoid contacting the palate with the fingers when removing the denture.
• Outline the contact area with a wax carver where wax is present, and with a glass-
marking pencil where the base tray is exposed.
To avoid overlapping the tracing and recontouring one contact area to
accommodate another, a sequence of palatograms should be followed, and waxing of
the palate should be accomplished in steps. First, s and sh palatograms are made and

Discussion
128 | P a g e
outlines on the base trays. Where wax is present, the palatogram is outlined with the
carving end of the wax spatula; where the base tray is exposed, the outline is made
with a glass marking pencil. Before waxing is commenced, the patterns for s and sh
should be reviewed. The tongue contact for s is always higher and more anterior on
the palate, so that the outline for the s palatogram is the high line and includes some
of the anterior teeth, and the sh line is always lower and includes fewer anterior teeth.
The sh line (low line) is used as a guide in waxing the posterior alveolar area, and the
s line (high line) is used as guide in waxing the anterior alveolar area. The anterior
portion of the “sh” tracing is not waxed until last.
Waxing is started around the first molar by adding enough wax to provide a 1-
mm margin at the collar. Next, the low tracing line on the palate is sighted directly
below this tooth, and enough wax is added to the palate to permit an even contour
between this line and the margin of the molar. Then wax is added around the anterior
teeth delineated by the s tracing to provide a ½ mm margin at the collars. Enough
wax is then added between the tracing line and teeth to present an even contour.
Waxing in the bicuspid area is accomplished by using the anterior and molar regions
as a guide for adding wax around these teeth to complete for smooth, even contour
between these waxed areas and the palatal tracing line.
Waxing around the second molar consists of adding enough wax around this
tooth to complete the contour between palatal tracing line and the waxed first molar
area. After waxing on the other side of the palate is completed, a palatogram should
be taken to cheek to contour. If the area is properly contoured, the tongue tracing line
should be even and about 2mm above the original. If the tracing line rises abruptly in
a specific area, that area is too thick and should be reduced until the tracing line is
even. If the tracing line drops abruptly in a specific area, that area is not thick enough
and additional wax will be needed to provide an even tracing. If the entire tracing
rises markedly, the area has been over contoured and should be reduced.
The photographs of the waxing procedure of a case with considerable alveolar
ridge resorption, and using the palatogram to outline the area and waxing in steps as
described should aid the beginner in establishing normal tongue contact for these
cases. After some experience, the entire outlined areas can be waxed in one step.
Discussion
129 | P a g e
The palatogram can be used effectively for any case, including the immediate
denture, if the pattern for normal tongue contact is kept in mind and if sensible
observation is employed.
The line on the palate outlining the palatogram represents the lowest point of
tongue contact in pronouncing s, and the area between this line and the artificial tooth
should be of even contour and gradual slope without excessive convexity or concavity.
The amount of wax needed to complete this contour is dependent upon the extent and
degree of alveolar resorption, and wax should be added only where necessary to
compensate for alveolar deficiency. Many times it is not necessary to add wax as far
down as the tracing line to complete the contour, and sometimes, as in the case of slight
resorption or the immediate denture, it is not necessary to add wax at all, because
enough of the alveolar ridge remains to provide proper contour to the base tray.
After lateral tongue contact for s has been established on the trial denture, the
speech tests should be repeated, and if speech is satisfactory, further contouring is
unnecessary. However, it is usually necessary to contour the anterior aspect of the
palate to facilitate proper s pronunciation.
By using the palatogram to establish normal tongue blade contact in
pronouncing s, appropriate portions of the lateral aspects of the anterior alveolar area
are included in the contour, leaving only the region between the lateral contact areas
to be considered. The area of this region, which is the most critical to proper s
pronunciation, is the area midway between the lateral contacts and directly above the
median sulcus of the tongue. In pronouncing s, the tongue contacts the alveolar area
to occlude the lateral portion of the oral cavity and form a channel for the air stream
between the median sulcus and the palate. This channel narrows to a groove at the
tongue apex to constrict the air stream, so that is escapes as a hiss. Normally, this jet
of air exits at the incisal edges of the teeth to be heard as the typical s, but on the
denture, where tooth arrangement has been altered to accommodate mechanics and
esthetics, it is usually necessary to provide a path of exit on the palate in the area
directly above the groove in the tongue apex. This is best accomplished by inserting
the trial denture and instructing the patient to pronounce ess (not so) and hold it so
that the groove in the tongue apex can be observed. The chair should be tilted back
and slightly raised so that the operator can look up and into the oral cavity to
determine the character of the groove and its proximity to the palate. It is the area

Discussion
130 | P a g e
directly above the groove that must be altered according to the fault in pronunciation.
If the patient whistles and hisses when pronouncing s, the area between the groove
and denture base is excessive and will need to be thickened. For the patient with a
deep groove ,a slight elevation is usually required. If the patient lisps substitutes th
for s or has a muffled, indistinct s, there is not enough space between the groove and
the denture base, and the area will need to be thinned. If the groove in the tongue is
broad and shallow, a depression in the denture base may be required, and if there is no
groove in the tongue, a groove on the denture base directly above the median sulcus,
as recommended by Sears, will be necessary. If the patient substitutes sh for s, the jet
of air is probably escaping toward the vault and the area above the groove will need to
be extended toward the tongue. This extension must be made with care, because
overextension will occlude the air stream and it will occlude the air stream and sh will
be substituted for s.
There is no simple way of correcting faulty s pronunciation. The fault must be
analyzed the area contoured, and the sound tested, then reanalyzed, re-contoured, and
retested until satisfactory pronunciation is attained. The words best suited for testing
are short words containing the ess sound, such as “hess,” “guess,” “less,” “mess”.
The time required to correct an error in s pronunciation is time well spent, because it
is the commonest and most persistent oral inaccuracy of the denture patient and the
one that may remain as a characteristic denture whistle.
Proper palatal contour is the key to proper s pronunciation, or all other
pronunciation for that matter, and that the palate can be contoured to accommodate
phonetics for any sensible tooth arrangement, including the bizarre class II and severe
class III jaw relation cases. There is little doubt that the character of the air stream
directed between the upper and lower incisors in pronouncing s will be affected by the
relationship of these teeth at the time of exit therefore, it is possible to soften or
sharpen the s by increasing or decreasing the amount of over jet. However, the
direction of exit can be controlled by palatal contour to permit considerable leeway in
anterior tooth arrangement and still provide good quality to this sound.
Contour of the anterior palate is completed by adding the minimum amount of
wax between the low tracing line for sh and the lateral and mid-palatal contoured
areas to make a smooth junction. Care should be taken not to thicken the lateral
contact areas or alter the median contour. To ensure that enough wax was added to
Discussion
131 | P a g e
provide tongue contact for the occlusive t, d, and n, a palatogram of t, to should be
made. After completing the anterior palatal contour, usually no further contouring is
necessary, but the speech tests should be repeated with particular attention given to
the pronunciation of ch and j, because occasionally, in contouring the mid anterior
alveolar region, wax builds up on the palate below and will interfere with the
pronunciation of these sounds. If this happens, a palatogram should be made for ch,
cho to outline the area of tongue contact so that alteration can be confined to that area.
The use of palatograms for contouring the entire alveolar area will be useful to
those who adhere to the philosophy of placing the artificial teeth in the same relative
position as the dentition. If the posterior teeth are arranged near the center of the
alveolar ridge and the anterior teeth arranged to occupy approximately the same
position as the originals, then a palatogram on the trial denture is an aid in contouring
the palate for normal contact. If, however, the philosophy of arranging teeth
according to mechanical advantage is adhered to, then the palatogram would be of
limited value in contouring the posterior alveolar area, because the posterior teeth will
occupy a position lingual to the center of the ridge on this denture. A palatogram of
the s on the trial denture in this case would reveal limited tongue contact in the molar
alveolar area, progressively increasing to normal contact in the anterior region, and
adding wax to simulate a natural alveolar contour in the molar area would be a grosser
insult to phonetics then not adding wax to complete alveolar contour in this area on
the denture with center of the ridge tooth arrangement. Phonetics is better served in
these cases by keeping the posterior alveolar area as thin as possible and confining
palatal contour to the anterior region. Thickening the vault to narrow the channel for
the air stream, facilitate s pronunciation in this type of denture, but before wax is
added to the vault, a palatogram of k, KO should be made to delineate the area of
posterior palatal tongue contact so that this area can be excluded from the waxing.
Satisfactory phonetics can be accomplished with a constricted posterior tooth
arrangement so long as the anterior teeth are arranged to permit normal palatal
contact. However, if the anterior teeth are arranged lingual to the natural tooth
position, they will interfere with the tongue in making palatal contact and impede or
occlude the air stream after contact has been made in pronouncing s. For this reason,
in cases with severe resorption, where the anterior ridge affords no clue to natural
tooth position, a palatogram can advantageously be used in arranging the teeth to

Discussion
132 | P a g e
ensure that tongue palatal contact is not jeopardized. Considerably more leeway is
permitted in arranging teeth toward the labial, because tongue contact is unhampered
and the palate can be contoured to accommodate the arrangement.
Complete loss of teeth can cause a persistent speech disorder by altering dental
articulation areas. This severely reduces the quality of speech
1-Particularly’ the alteration of frontal maxillary morphology leads to impairment of
speech production
2-removable complete dentures can partly solve this problem.
3- However, they disturb speech production themselves as they restrict the flexibility
of tongue, narrow the oral cavity and alter the articulation areas of palate and teeth.
Speech production has a significant effect on patient’s general satisfaction with
dentures. The patient’s contentment correlates with acceptance of denture. Therefore
speech production quality is an essential feature for success or failure of dental
rehabilitation.78
The influence of design of removable dentures on patient’s voice quality
The voice of each person is unique and is generally determined by size of the
resonatory system (oral cavity. Larynx, pharynx, vocal folds and nasal sinuses) which
vibrates at different frequencies, producing different sounds .The voice quality is
characterized by speech intelligibility (relationship between the voice pitch, volume,
timbre and speech speed).One of the most frequent phonetic distortions is lisping,
omission, substitution, distortion, addition and nasality are also possible when
improper and functionally low quality dentures have been made. Restrictions or
alterations of the normal mandibular may impede the transmission of acoustic energy
through the oral cavity, thereby affecting both oral resonatory characteristics and oral
/nasal balance. The phonetic adaptation of the patients with complete dentures
depends on selection and placing of artificial teeth, the thickness, size and placement
of maxillary denture base, the optimal space of the tongue, Individual adaptation
capacity and patient’s sound recognizing capacity.85

Discussion
133 | P a g e
The changes of resonance and the methods of research
Resonance is one of the most important characteristics of human speech, the
resonance depends on the age, gender spoken language, and phonetic environment of the
phonetic sound, models and speech conventions. Dental prostheses can alter resonance,
resulting in increase or decrease of nasalance. It is not known if or to what extent
complete maxillary dentures alter the resonating characteristics of the oral cavity. There
exits two hypotheses. The first claims that the base of prosthesis which covers the entire
hard palate and extends on to the soft palate, could impede the passive transmission of
sound waves into the nasal cavity, thus reducing the overall nasal energy, resulting in
decreased nesalance. The second hypothesis claims that the presence of dental prosthesis
would decrease the volume of oral cavity and increase impedance thereby reducing the
oral energy component, what results in increased nasalance. Thus dental prosthesis can
alter resonance but the passive acoustic effect on the oral/nasal resonance balance, related
to the presence of dentures, is not fully understood.
Spectrograms and palatograms are non-invasive research and evaluation methods
to estimate voice quality. For the best analysis of the phonetic spectral characteristics in
the spectrogram. However, the palatography is a rather conditioned method to evaluate
speech quality. There are no definite norms to evaluate the results that are obtained with
palatography. Palatograms of the announcers and speech artists were used to determine
the parameters of palatography. These norms of palatography were compared with the
parameters of palatography of patients of the patients with dental prosthesis inserted.
Speech production has a significant effect on the patient’s general satisfaction with the
dentures. Different studies revealed that the quality of speech production increases after
some period of habituation, the functional quality (retention, stability support) of
prosthesis is the main pre condition for good sound pronunciation85
Effect of different techniques for palatal denture base configuration
Metals and metal alloys used in denture bases display excellent strength- to-
volume ratios may be cast in thin sheets maintaining rigidity and fracture resistance.
Thinner metallic denture bases decrease interference with phonation and ensure proper
palatal contours. Failure to achieve unobtrusive palatal contours may produce noticeable
changes in phonation. Metal bases also display desirable dimensional characteristics and
may be cast accurately. Little concern has been given to the perfection and optimization

Discussion
134 | P a g e
of the phonetic quality of denture users. However, insertion of prosthetic restorations may
lead to speech defects. Most of such defects are mild but, nevertheless, can be a source of
concern to the patient. For the dental practitioner, there are few guidelines for designing a
prosthetic restoration with maximum phonetic success one of these guidelines involves
the palatal configuration of the maxillary denture bases.87
The artificial palatal vaults of
maxillary denture often have a concave shape .In contrast, natural palatal vaults are of
convex shape in the alveolar region. So the palatal vaults of the maxillary complete
denture should be shaped like natural ones to facilitate correct pronunciation and the
quality of speech.89
The most important instruments for the investigation of speech and
sound production are the trained hearing of speech and language professional, spectral
analysis and palatography89
. Studies on speech sound production may have a clinical
impact because many patients attach great importance to undisturbed speech sound
production after dental treatment and Heylink et al found 21% of denture wearing
individual had speech problems.89
Dentures should be made to enable the patient to
produce voice and speech without deficiencies. About 25% of patients in clinical
dentistry are considered to suffer from temporary or permanent changes in articulation
due to the application of removable dentures. Articulatory errors may be due to denture
factors like altered vertical dimension, size, and position of the teeth thickness and the
contour of the denture base. Accurate approximation of the palatal contours of a maxillary
complete denture to a patients tongue can improve speech if other factors are
satisfactory.89
Pound in 1950 stated that anterior palatal portion plays an important role in
pronunciation of consonants. He termed it as "playground" of tongue because 90% of
tongue’s rapid manipulation while talking was restricted to this area and are lingual to
lower anterior teeth.89
Speech problems are frequently reported after complete denture placement
mainly expressed as problems with consonants, especially linguopalatal sounds. So
the linguopalatal sounds were selected and analyzed in the present study. Some
patients have remarkable adaptive capacity after repeating 5-6 key words. Analyzed
spectrograms are different by frequency of emitted sounds related to denture changes
and oral resonance cavity. Specific letters were selected because not all the letters can
be verified. According to Sinescue some sounds such as t, d, ch, z l, sh are more
sensible and more often compromised due to the changes of the oral structures and
demand for more precise articulation movements. Therefore, these sounds were
studied in this work89
Allen stated that the most widely used procedure to improve

Discussion
135 | P a g e
denture phonetics is the random thinning of the entire maxillary palatal surface to
create more space for the tongue. Such arbitrary removal of acrylic resin from the
palatal surface ignores the critical importance of correct palatal contours in the proper
formation of the sounds. The results of this study coincide with the results reported by
Ravishankar and Singh as they reported that the linguopalatal sounds like t, d, n, l, z,
th are formed by contact of the tip of the tongue with the most anterior part of the
palate called palato alveolar or palato lingual sounds.89
If the denture base in rugae
area is too thick the ‘t’ sounds like ‘d’ and ‘d’ sounds like ‘t’.
Speech Analysis:
Assessment of speech defects is initially subjective, relying on the clinical
judgment of the Speech and Language Therapist. This will involve both assessment of
the intelligibility and quality of the patient’s speech, and observation of the visible
aspects of articulation. However majority of the articulators are not visible during
speech. Additionally there is a growing need for evidence based intervention. The best
approach is to use perpetual assessment, to highlight potential areas of difficulty, then
objective, instrumental assessment of these areas, to confirm the nature and severity
of their involvement.90
Spectrographic analysis of speech is one of the most widely used techniques
for studying the acoustic- phonetic characteristics of different phonems in language. It
is an extension of the short term spectral analysis ,and primarily involves
representation of the 3- D spectral information obtained by computing the magnitude
spectrum over the short overlapped window segments, that is 2-D spectral content
varying with respect to time. The 3-D spectral information is represented on a 2-D
plane with the X- axis representing time, Y-axis representing frequency, and the third
dimension denoting the long- magnitude of the sinusoidal frequency components is
converted to a proportional intensity or grey value. The resulting representation is
referred to as a spectrogram.107
A spectrogram is a visual representation of the spectrum of frequencies in a
sound or other variable. Spectrograms are sometimes called spectral waterfalls, voice
prints or voice grams. Spectrograms can be used to identify spoken words
phonetically and to analyze the various calls of animals. They are used extensively in
the development of fields of music, sonar, radar, and speech processing, seismology

Discussion
136 | P a g e
Speech Instrumentation:
Studies on speech sound production may have a clinical impact because many
patients attach great importance to undisturbed speech sound production after dental
treatment and Heyink et al found that 28 (21%) of 131 denture wearing individuals
had speech problem.89
Important investigations of speech sounds are based on the Fourier spectrum
and on the short time Fourier spectrum (spectrogram) the most accurate
measurements methods were, as this study suggested, by Jindra et al, Kobayashi et al
and Outmen- Toller who choose speech sounds analysis by using standard signal
processing methods. The method with the best result was the Fourier method. Its
evaluation of the studied phenomena is both qualitatively and quantitatively valuable
making the reproducibility of the analysis applicable. The Fourier method for the
phonetic evaluation has been used because its graphic correspondence is simple and
facile to translate. The phonetic alterations are considered classic for the human voice
and could also be represented even for the higher spectrum. In the present study, the
spectrogram was used.89
Two popular spectrographic representations used for analysis
are wide band spectrogram and narrowband spectrogram, depending on the spectral
and temporal resolution preserved in the final representation in the frequency domain.
The measurement of tongue movement during speech is not easy, for the
simple reason that, for the majority of sounds, the tongue is obscured by lips or teeth.
Several methods of accurately determining the movement have been used. Tongue
strength can be measured by tongue force transducers. A flexible rubber bulb,
connected to a pressure transducer. The amount of pressure put on the bulb gives
measure of strength of movement .This gives no indication of mobility and movement
patterns, however both computerized tomography and Magnetic resonance imaging
MRI scans allow tongue placement for speech sounds to be accurately visualized. But
these cannot measure dynamic tongue movement.90
X-ray micro beams use a narrow beam of radiation to track the movement of
small gold pellets attached to various articulator, including the midline of the tongue.
Also Videofluroscopy gives a two dimensional moving image of the articulators.
Electromagnetic Articulography (EMI) gives similar as X-ray microbeams but without
radiation. The pellets are transducers and the subject is placed within the magnetic field. It
is invasive as transducers are to be glued to the articulators under investigation. The

Discussion
137 | P a g e
equipment is also extremely expensive and the images recorded are again two
dimensional. It has been used therapeutically, in the treatment of dyspraxia.90
Electromyography (EMG) is a system that detects the electrical activity in
muscle fibers. The more active a muscle is, the greater the signals which will be
recorded. Therefore the degree of involvement of different muscles during different
articulatory gestures can be measured and compared. EMG is invasive, since it
involves either surface electrodes or the insertion of needle electrodes into the
muscles
Ultrasound uses the reflection of ultrasonic energy from tissue in its path. It
therefore enables the calculation of distance and speed of movement. Images from the
transducer, mounted below the chin, and does not use ionizing radiation. However,
the image provided is not detailed, and skilled transducer placement and image
interpretation are required.90
ELECTROPALATOGRAPHY:
Electopalatography is an instrumental technique for determining tongue/
palate contact during speech. The subject is provided with an artificial palate, in
which electrodes have been embedded. Generally, these palates are custom made,
from dental impressions. They are made of thin but rigid acrylic, which clips to secure
them to the subjects teeth. The plate extends from the front incisors to the junction of
the hard palate and velum. Individual wires from each electrode emerge from the
palate in two bundles, which leave the subject s mouth, one on each side. While
electropalatography measures dynamic movement of the tongue during speech,
precise tongue placement, and the part of the tongue which makes contact with
electrodes, can only be inferred. IT is generally accepted that, to maximize the
usefulness of electropalatography, it should be used in conjunction with other
instruments. A number of different electropalatography systems have been
developed.90
RION DP-01 ELECTROPALATOGRAPH SYSTEM
An electropalatography system was developed in Japan in the 1960s mainly
for phonetic research. From this early research, the Rion system has been developed.
The original system was not PC based, but instead relied on direct activation of Light

Discussion
138 | P a g e
Emitting Diodes (LEDs).Each corresponding to a palate electrode, on a single, one-
palate display.
KEY PALATOMETER SYSTEM
This is the American system, developed by Fetcher. It is PC based, with a
sampling rate of 100 frames per second, Data can be recorded, replayed and analyzed
For the KEY palatometer, several palate configurations have been described, and each
utilizes a thin, flexible acrylic palate, custom made for each individual, THE
PALATE FITS over the teeth. The palatometer can be linked to Kay’s computerized
speech lab, allowing comparison of tongue/palate contact with other speech outcome
data, like spectrum analysis.
READING SYSTEM
This system was developed by the speech Research Laboratory at reading
University, initially as a phonetic research tool, which came to be used in Speech and
Language Therapy Clinics.....EPG2,EPG3 can be used for the analysis of recorded
data. Tongue palate contact patterns, and spectral information can be obtained by
moving a cursor along the displayed acoustic wave form.
LINGUOGRAPH
Linguograph was developed to meet the need for a clinical, user and patient
friendly, portable low cost electropalatography system .It was developed by a multi-
disciplinary team, comprising Engineers, SPEECH AND LANGUAGE THERAPIST,
and PLASTIC SURGEON AND DENTAL SURGEON. The system comprises an
artificial palate, a small electronics unit, and interfaces to a standard PC. Custom
software, running under MS-DOS, PROVIDES VISUAL DISPLAYS AND
ANALYSIS.
PALATE
To provide compatibility with the other system in use in Europe, the Palate
developed at the University of READING has been adopted for use with Linguograph
Discussion
139 | P a g e
LINGUOGRAPH UNIT
The palate connector plugs into the Linguograph unit, which hangs around the
neck of the patient's by means of the adjustable strap.
INTERFACE CARD AND SOFTWARE
The linguograph electronics unit connects to an Amplicon PC14AT
DIGITALI/O card housed within the PC, Data from the Linguograph unit is displayed
and analyzed by custom software running under DOS.

Conclusion
140 | P a g e
Speech difficulties as sequelae of oral rehabilitation with complete dentures
are generally a transient problem when encountered the difficulties may not be easily
solved. Therefore efforts should be made to avoid them by pretreatment records or
assessment of speech and provision of information to patients about likely initial
deviation from normal speech, immediately following oral rehabilitation. Hence a
prosthodontist play a pivotal in understanding the basic mechanism involved in the
various speech pathology and provide prudent treatment for the same to enhance an
individual's personality. More research needs to be carried out in this field to make
our rehabilitative treatment complete. With ideal esthetics and optimum function.88
AS defined several objectives and specific study methods and means for a new field
that called phonetic dentistry. Several plausible mechanisms that affect the phonetic
quality of prosthetic result have been derived based on articulatory mechanisms and
on morphologic factors resulting. The relationships between the articulatory facts and
the acoustic features have been emphasized and discussed in order to derive acoustic
methods and acoustic quantitative indices for assessment of speech.
Within the scope and limitations of this experimental study, the following conclusions
were established-
1) The speech quality immediately after denture insertion was found to be fair i.e. the
consonants can be appreciated but the acoustic quality of sounds was unclear.
2) Significant improvement in phonetics and acoustics was observed with complete
dentures made by functionally contouring the palatal vault using visible light cure
denture base resin.
3) Compared to the samples of group 1, there was significant improvement in the
clarity of the speech sounds after functional contouring of the palatal vault of
maxillary complete dentures using visible light cure material.
4) Since visible light cure denture base resin can be cured immediately after
functional molding, it has proved to be a direct method and can be used in routine
clinical practice for providing improved phonetics to edentulous patients in need
of complete dentures.

Conclusion
141 | P a g e
Implications of study
This study has attracted the attention of professionals towards the neglected
aspect of phonetics in complete denture. Which can be taken care off by incorporation
of this simple step in routine clinical practice. Use of spectrographic analysis for
quality of speech is proposed and recommended
This study anticipates the improvement in the quality of speech after
functional contouring of palatal vault of maxillary complete denture by visible light
cure resin which may reproduce the original oral morphology. This reduces the
training and waiting post insertion period which may improve the quality of life.
.

Conclusion
142 | P a g e
Limitations of the present study
1. In this study only the palatal aspect or surface of the maxillary complete denture
has been taken into consideration.
2. Only palato lingual speech sounds were studied.
3. “Z” sound was excluded in the study.
Scope
Some of the correlations between the acoustic features and the dentition
deficiencies are already documented in literature, but much remains to be done for
establishing corpus of knowledge and tools that could constitute the solid foundation
of the emerging domain we call phonetic dentistry.
The use of indices such as SQI, SII and of the distances and indices suggested
in this study provides the practitioner with the grounds of an automated method for
assessing the quality of the performed prosthetic act. From the speech rehabilitation
perspective, this is a major step ahead in the current technology and solves a
fundamental problem in dentistry. At the same time. This assessment method lays
solid ground to the new field of phonetic dentistry.
1. There is need for further studies to investigate effect of alterations in other
parameters on quality of speech produced by such dentures
2. Evaluation of the effect of adaptation period on the quality of speech
3. Relating acoustic analysis to the characteristics of the prostheses and to their
design.
4. Study on linguo-palatal passive sounds.
Summary
143 | P a g e
Speech is critical and essential human activity that affects personal
communication and self-representation. Together with mechanics and esthetics,
speech is cardinal factor contributing to the ultimate success of a dental prosthesis.
The loss of teeth and supporting structures alters the main articulatory cavity and
produces a marked effect on speech pattern87
. An empiric approach to the phonetic
factor in denture construction frequently places the burden for compensating speech
depends on the adaptability of the tongue. While it is true that the tongue is very
adaptable, functional patterns have become firmly established, However , by
customizing palatal contours of a maxillary denture to the tongue, the patient may
easily adapt to the definitive denture contour, which in turn shortens or eliminates the
adjustment period for the achievement of proper pronunciation.87
There are persons
whose speech is sensitive to the changed relationships between lips, tongue, soft
palate, hard palate, alveolar ridge and teeth and have difficulty accommodating. These
patients often require a tactile sense to orient the tongue. The palatal rugae can often
serve as a cue because the lack of texture on the palatal portion of a complete denture
can impede proper articulation. There are some methods to duplicate palatal rugae,
one of the simplest method is to capture the patient's palatal rugae is by tin foil.
Beyond the unaesthetic acoustical appearance of the speech deficiencies
induced by imperfect dentition and by imperfect prosthetic denture, the decrease of
the linguistic expressive capacity is a significant social hurdle, even impairment. The
decrease in speech intelligibility may hinder the communication and may increase the
probability of confusion between words to levels that may require the abandon of a
profession and may even impose social quasi-isolation.
While progresses have been made in the analysis of the speech quality and in
understanding some of the involved mechanisms, the domain is still in its infancy.
The main needs are for relating acoustic analysis to the characteristics of the
prosthesis and to their design
The development of appropriate concepts, measuring method, and relevant
quantitative characteristics for assessing the changes in the vocal signals (speech) due
to imperfect prosthetic act remains a desideratum.
Summary
144 | P a g e
Correlation of the vocal signal changes with the characteristics of the
prosthesis and the specific types of errors in the prosthetic act would be an essential
achievement in the way of improving the outcome of the prosthetic action.1
The present study was conducted to evaluate the effect of functional
contouring of the palatal vault of maxillary complete denture on speech quality
without functional molding of palatal vault and with functional molding of palatal
vault of maxillary complete denture with visible light cure resin material. The
advantage of visible light cure denture base resin is that functional molding of the
palatal vault of the maxillary complete denture can be achieved at the stage of
insertion and can be cured immediately. The speech achieved immediately after
modification is much more clear and sharp, thereby eliminating the waiting and
training period after denture insertion.
Since the modification of the palatal vault is achieved by the functional
contact of the tongue during articulation, the tongue does not have to adapt to the
presence of the denture in order to achieve „normal speech‟. The advantage of this
method is the ease with which it can be performed in a clinical set up, so no special
skills are needed to achieve successful results in improving the quality of speech
sounds. It is the responsibility of the prosthodontist to construct dentures as accurately
as possible, so as to improve speech sound production with dentures, minimize the
period of adaptation and thereby, increase the self-confidence of the patient.
Therefore the objective of the present investigation is to develop a procedure
in denture construction which would unable the patient to speak clearly at the time of
insertion of denture.87
Speech difficulties as sequelae of oral rehabilitation with complete dentures
are generally a transient problem. When encountered the difficulties may not be easily
solved. Therefore efforts should be made to avoid them by pretreatment records or
assessment of speech and provision of information to patients about likely initial
deviation from normal speech, immediately following oral rehabilitation. If persistent
difficulties to pronounce certain sounds or other speech disorders persist for more
than 2 to 4 weeks, the following protocol is recommended –

Summary
145 | P a g e
1. If the patient has the previous complete denture experience, compare the new set
with the old one to diagnose possible design differences of significance for speech
production.
2. Make the necessary modifications; soft wax might be helpful.
3. Have the patient’s hearing checked. An auditory deficit will prolong the
adaptation period and render it more difficult.
4. If the reported/ perceived problem cannot be resolved by dental methods, the
patient should be referred to speech pathologist.
Not only the face but speech also reflects an individual’s inner being. Any
abnormality or defect in the same can affect his/ her psychology and social behavior.
Hence a prosthodontist play a pivotal role in understanding the basic mechanisms
involved in the various speech pathology and provide prudent treatment for the same
to enhance an individual’s personality

References
146 | P a g e
1. SadhanaRelekar, UshaDalvi, Anjali Kant. Manual on „Fundamental Of
Speech AndSpeech Teaching‟; Rehabilitation Council Of India, Kanishka
Publisher.
2. John J. Sharry. Complete denture Prosthodontics, 3rd edition, McGraw Hill
Book Company , 1962, pg130-148.
3. SaryuArora, Manpreetwalia, Shushantgarg-“phonetics its role in
Prosthodontics Indian Journal of Dental Sciences June 2011 Issue 2 Vol.3 Page
No. 36-40
4. Zarb and Bolender. „Prosthodontic treatment for the edentulous patient:
Complete dentures and Implant- supported prostheses‟, 12th edition , Elsevier
publication, 2004,pg 370-388.
5. Phonetics in complete Denture
6. Allen L.R. „Improved phonetics in denture construction.‟ J Prosthet Dent 1958;
8(5): 753-763.
7. Pound E. „Aesthetics and phonetics in complete denture construction.‟ Dent J
Australia 1951;23:126-134.
8. Silverman M.M. „The speaking method in measuring vertical dimension.‟ J
Prosthet Dent. March 1953; 3(2): 193-199.
9. Hisatoshi Tanaka. „Speech patterns of edentulous patients and morphology of
the palate in relation to phonetics.‟ J Prosthet Dent 1973;29(1):16-28.
10. BalK.Goyal, P.Greenstein. „Functional contouring of the palatal vault for
improving speech with complete dentures.‟ J. Prosthet Dent 1982; 48:6:640-646.
11. McDowell E: The role of speech training in a program of orthodontic
treatment,Int. J. Orthodontia 22:105-113, 1936.
12. Van Riper, C: Speech correction: Principles and Methods, ed. 3, New York,
1954, Prentice Hall, Inc.
13. Kessler B. “An analysis of the tongue factor and its functioning areas in dental
prosthesis”.J. Prosthet. Dent. 1955; 5(5): 628-635.

References
147 | P a g e
14. Martone, A. L. „Clinical Applications of Concepts of Functional Anatomy and
Speech‟: Part I – “Anatomy of mouth and related structures.” J Prosthet Dent
1962;11:1009-1018.
15. Martone A. L. „Clinical Applications of Concepts of Functional Anatomy and
Speech.‟ Part II – “Musculature of expression." J Prosthet Dent 1962;12:4-27.
16. Alexander L. Martone, Linden F. Edwards. „Anatomy of the mouth and related
structures.‟ Part III –“Functional anatomic considerations.” J Prosthet Dent 1962;
12(2):206-212.
17. Alexander L. Martone, John W. Black. „An approach to prosthodontics through
speech science.‟ Part IV – “Physiology of speech.” J Prosthet Dent 1962; 12(3):
409-419.
18. Martone A.L. and Black J.W. “The phenomenon of function in complete
denture prosthodontics.” Part V – „An approach to prosthodontics through speech
science. Speech Science Research of Prosthodontic significance‟. J Prosthet Dent
1962; 12(4): 628-636.
19. Alexander L. Martone. „Clinical applications of concepts of functional anatomy
and speech science to complete denture prosthodontics.‟ Part VI – “The
diagnostic phase.” J Prosthet Dent 1962; 12(5):817-834.
20. Alexander L. Martone. „Clinical applications of concepts of functional anatomy
and speech science to complete denture prosthodontics: Part VII- “ Recording
phases.” J Prosthet Dent 1963; 13(1):4-33.
21. Alexander L. Martone. „Clinical applications of concepts of functional anatomy
and speech science to complete denture prosthodontics‟: Part VIII – “The final
phases of denture construction.” J Prosthet Dent 1963; 13(2):204-228.
22.Hamlet SL, GeofferyVC,Barlett DM. -Effect of a dental prosthesis on speaker
specific characteristics of voice Jr Speech Hear Res 1976;19; 639-50
23. John M. Palmer. „Analysis of speech in prosthodontic practice.‟ J Prosthet
Dent1974; 31(6):605-614.
24. C. Andrew Burnett. “The Mandibular Speech Envelope in Subjects with and
without Incisal Tooth Wear.” International Journal of Prosthodontics, December
1999 ; 12(6):263-271.
References
148 | P a g e
25. Nitinkumar Agarwal, RuchirTripathi. „Complete Denture Prosthodontics‟, 1st
edition, Arora Medical Book Distributor.
26. Fenn, LiddelowAndGimson. „Clinical Dental Prosthetics‟-A. Roy McGregor,
3rd edition, Varghese Publishing House.
27. Yippo A, Dr. Odont “The effect of dentures on speech”. 1954; 5(2): 224-241.
28. Kaires A.K. “Palatal pressures of the tongue Kessler H.E. “Phonetics in denture
construction”. J. Am Dent. Assoc. 1957; 54: 347-351.
29. Landa J.F. „The Importance of phonetics in full denture prosthesis.‟ Dent Digest
1935;41 :154-160.
30. Sears V H. 1949. “Principles And Techniques For Complete Denture
Construction”, The C.V.Mosby Co., St.Louis, pg 312-319, 324-325.
31. H.E. Kessler. „Phonetics in Denture Construction.‟ J Am Dent Assoc 1957;54:
347–351.
32. Rothman R. “Phonetic considerations in denture prosthesis”. J Prosthet Dent.
1961; 11(2): 214-223.
33. Mehringer E.J. “The use of speech patterns as an aid in prosthodontic
reconstruction.” J Prosthet Dent 1963; 13(5): 825-836.
34. Paul Gibbson. Discussion of “The use of speech patterns as an aid in
prosthodontic reconstruction” by Edward J. Mehringer. J Prosthet Dent 1963;
13(5):837-838.
35. Silverman M.M. „The Whistle and Swish Sound in Denture Patients‟. J Prosthet
Dent 1967;17(2):144-148.
36.Donald P. Erb. „Speech effects of the maxillary retainer.‟ J Am Dent Assoc,
October1967; 37(9):298-303.
37. Lawson W.A. “Speech and its relation to dentistry”. Dent. Prosthet. 1969; 19(5):
150-157.
38. Earl Pound. “Utilizing speech to simplify a personalized denture service.” J
Prosthet Dent 1970;24(6):586-600.
39. George A. Murrell. „Occlusal considerations in esthetic tooth positioning‟. J
Prosthet Dent 1970; vol23, no5, 499-502.

References
149 | P a g e
40. Francis W. Shaffer, Robert A. Kutz. “Phonetics and swallowing to determine
palatal contours of dentures.” J Prosthet Dent October 1972; 28(4): 360-362.
41. George A. Murrell. “Phonetics, function, and anterior occlusion .”J Prosthet Dent
July 1974 ;32(1): 23-31.
42. Pound E. „Let /S/ be your Guide.‟ J Prosthet Dent 1977;38:482-489.
43. Chierici G. and Lawson L. “Clinical speech considerations in prosthodontics:
Perspectives of the prosthodontist and speech pathologist”. J. Prosthet. Dent.
1973; 29(1): 28-39.
44. John M. Palmer. “Structural changes for speech improvement in complete upper
denture fabrication.‟ J Prosthet Dent 1979, vol.41,5,507-510.
45. Ritchie G.M., Ariffin Y.T.45 “Sonographic analysis of speech sounds with
varying positions of the upper anterior teeth”. J. Dent. 1981; 10: 17-27.
46. J F McCord, H J Firestone, AA Grant. “Phonetic determinants of tooth
placement in complete dentures.” J Quintessence international 1985; 25(5):341-5.
47. Riski JE. Delong E.: Articulation development in children with cleft lip/palate.
Cleft Palate J. 1984 April. 21(2):57-64.
48 Fletcher S.G. “Speech production following partial glossectomy”. J Speech and
Hearing Disorders, 1988; 57: 232-238.
49. K.C. White D.D.S., M.E. Connelly. “Duplicating natural palatal contours in
acrylic resin complete dentures.” J Prosthet Dent April 1989;61(4): 508-510.
50. Turner G.E., Williams W.N. “Fluoroscopy and nasoendoscopy in designing
palatal lift prostheses”. J Prosthet Dent 1991; 66: 63-71.
51. Burnett C.A. and Clifford T.J. “Closest speaking space during the production
of sibilant sounds and its value in establishing the vertical dimension of
occlusion”. J Dent Res 1993; 72(6): 964-967.
52. Patrick A Mattie, Rodney D Phoenix . “A precise design and fabrication
method for metal base maxillary complete dentures.” J Prosthet Dent 1996;
76(5): 496-499.
53. Singh V.P., Bharadwaj G., Nair K.C. “Direct observation of tongue positions
in speech – A patient study”. Int J. Prosthodont 1997; 10: 231-234.

References
150 | P a g e
54. Farley DW, Jones JD, and Cronin RJ:Palatogram assessment of maxillary
complete dentures: J. Prosthodont. 1998 Jun; 7(2):84-90.
55. Tachimura T, Nohara K, Hara H, Wada T.: Effect of placement of a speech
appliance on levatorvelipalatini muscle activity during blowing. Cleft palate
Craniofac. . 1999 May: 36(3):224-32
56. Burnett C.A. and Clifford T.J. “The mandibular speech envelope in subjects
with and without incisal tooth wear”. Int J Prosthodont 1999; 12: 514-518.
57. Christina A. Gitto, Salvatore J. Esposito, Julius M. Draper .“A simple method
of adding palatal rugae to a complete denture.” J Prosthet Dent 1999;81(2):237-9.
58. Eberhard Seifert, ChristophRunte, Michael Riebandt, Antoinette
Lamprecht-Dinnesen, and FriedhelmBollmann. “Can dental prosthesis
influence?” J Prosthet Dent 1999; 81(5):579-585.
59. Schierano G, Mozzati M, Bassi F, Preti G. Influence of the thickness of the
resin palatal vault on the closest speaking space with complete dentures. J. Oral
Rehabil. 2001 Oct.28 (10)903-8.
60 Rieger J., Wolfaardt J., Seikaly H., Jha N. “Speech outcomes in patients
rehabilitated with maxillary obturator prostheses after maxillectomy: A
prospective study”. Int J Prosthodont 2002; 15: 139-144.
61. Hongama S., Ishikawa M., Kawano F. and Ichikawa T. “Complete denture
with a removable palatal lift prosthesis: A case report and clinical evaluation”.
Quintessence Int 2002; 33: 675-678
62 Meier B, Luck O, Harzer W: Interocclusal clearance during speech and in
Mandibular Rest Position A comparison between different measuring methods. J.
OrofacOrthop. 2003 Feb; 64(2):121-34
63 Pigno M.A., and Funk J.J. “Prosthetic management of a total glossectomy
defect after free flap reconstruction in an edentulous patient: A clinical report”. J
Prosthet Dent 2003; 89: 119-22.
64. David M. Bohnenkamp, Lily T. Garcia. “Phonetics and tongue position to
improve mandibular denture retention: A clinical report.” J Prosthet Dent 2007;
98(5): 344-347.

References
151 | P a g e
65. Kaires AK. Palatal pressures of the tongue in phonetics and deglutition. J Prosthet
Dent 1957; 7:305-317
66. Joseph G Agnello, LennatWictorin. “A Study of Phonetic changes in edentulous
patients following complete denture treatment.” J Prosthet Dent 1972; 27:133-139.
67. William Harley “Dynamic Palatogrpahy - A study of linguopalatal contacts during
production of selected consonant sounds” J ProsthetDent 1972;27:364-376.
68. Sandra Hamlet, Maureen Stone and Thomas McCartey. “Conditioning
Prostheses viewed from the standpoint of speech adaptation.” J ProsthetDent
1978;40:60-66.
69. Tobey E.A. and Finger I.M. “Active vs. Passive Adaptation: An Acoustic Study
of Vowels Produced with and without Dentures.” J Prosthet Dent 1983; 49:314-
320.
70. Jeffrey M. Kestenberg. “Speech Assessment In Dentistry.” Dent
JAustralia1983; 28(2):98-101.
71.. A. Petrović. „Speech sound distortions caused by changes in complete denture
morphology.‟ J Oral Rehabil 1985;12:69-79.
72. Howell PG.T. „Incisal Relationships During Speech.‟ J Prosthet Dent 1986;
56:93-99.
73. Alexander J. Hassel and Thomas Holste. “Improving the Speech Function of
Maxillary Complete Dentures: A Pilot Study.” Int J Prosthodontics
2006;19(5):499-503.
74. Hyung-Jun Kong and Carl A. Hansen. “Customizing palatal contours of a
denture to improve speech intelligibility.” J Prosthet Dent 2008 ; 199:243-248.
75. Bortun Cristina, LeretterMarius,Sandu Liliana et al-- phonetic evaluation of
the edentulous patient correlated with the various settings of the artificial teeth
Serbian Dental Journal 2004, 51
76.Earl Pound Utilizing speech to simplicity a personalized denture service JPD
2006 ; (1) Vol. 95:1-10
77. Manaswini Patil, Sanjaya gouda B Patil-- Palatine regae and their significance
in clinical dentistry- A review of literature JADA Nov. 2008 ;Vol.139: 1471-
1478.
References
152 | P a g e
78. F.Stelzie ,B Ugrinovic,CKnipffr et al -- Automatic , Computer based speech
assessment on edentulous patients with and without complete dentures-
Preliminary results. Journal of Oral Rehabilitation (2010);37:209-216
79 Jean-Lue schwartz Louis Jean Boe Pierre Badin et al Grounding stop place
systems in the perceptible-motor substance of speech :on the universality of the
labial-coronal velar stop series. Journal of phonetics2012:40:20-16
80. Kyo Nomura Akemi Utsumi,Kaori Tomita et alInfuence of command on
tongue elevation during swallowing examination of tongue pressure and
ultrasound imaging. Journal of Disability and oral Health 2011: 149-158
81. Abdule-Aziz Abdullah al kherit and RavikumarRamakshnaih Phonetics
Realated to Prosthodontics Middle –East Journal of Scientific Research
2012:1,31-35
82.Vasmikrisna,V, VasmkrishnaReddy,N Praveen Kumar et al“Denture with
phonetically contoured Palate: A Simple technique of Adding Customized Rugae
and Palatal Contours to the Maxillary Denture The Journal Comtempoaray
Dental practical 2012-March-April ;13(2):216-218
83. RajyaLaxmiRavari ,SuchitaTelaKiranThotaPhonetics in Complete Denture –
A Prime Concern Indian Journal of Dent Adv. 2013:5(3) Suppl 1:1341-1343
84. Mariko Hattori,YukaISmitaHisaashi Taniguchi Automatic evaluation of
speech impairment caused by wearing a dental appliance open Journal of
stomatology 20133) :365-369
85. KristineBrokaAldisVidzis Juris Grigorjevs el- The influence of the Design of
Removable Dentures on Patients Voice Quality Stomatologija, Baltic Dental and
Maxillofacial Journal 2013;(15) No.-120-25
86. RaghvendraAdaki, Suresh Meshram,ShrideviAdaki-Acoustic Analysis and
Speech Intelligibility in Patients Wearing Coventional Dentures and Rugae
IncarporatedDenruresJr Indian Prosthodont Soc. 2013 Dec 13 (4); 413-420
87. Hala M abdelhameed and MohnamedE,El –syed‘Effect of Different
Tecniques for palatal Denture Base configuration on Speech Quality in compelte
denture wearer Med.J.Cairo unvi,2014(1)Vol-82 :657-664
References
153 | P a g e
88. Ashish R. Jain M.K. Venkat Prasad and Padma Ariga Palatogram
RevistedContcmporary clinical Dentistry 2014Jan-March,5(1):138-141
89.HamadaZaki‘Spectogram analysis of complete Denture with different thickness
and palatal Rugae Materials on speech production .International Journal of
Dentistry volume 2015,Artide 606834
90. SleveKelly ,allsionMain,Graham Manley et al ‘Electopalatogfraphy and the
Logograph system 2015
91 PriyaVaswani, PronobSanyl, AnkurPrajapati-- Coparison of speech
articulation and Intelligibility in Pallatalt Contoured dentures using a novel rugae
duplication technique:A clinical study International jr of dental research, 3 (2)
(2015) 15-20
92 Hemen J.M steenkenTno Human factors, Soe‘The measurement of speech
Intelligibility
93. SaurabhChaturvedi, Narendra Kumar Gupta ,Ashok Kumar Verma et al
“Speech Comprehension (Prosthetic contemplation) IOSR-JDMS
July2015(7)Vol.14:34-36
94. Christophe Jeannin,Pascalperrier,YohanPayan et al Tongue Pressure
recodings during speech using complete denture 2016
95. Dr. Renu Gupta Dr. R.P. Luthra, Dr. Deepak Gautam‘Phonetic in complete
denture –A Rewire ‘International Journal of Heath care sciences Apri2016 (1)
Vol4:373-377
96. Martina GiovawnettiAlessiocasucci, Daniele Casucci et al ‘Phonetic Analysis
and maxillary anterior tooth position :a pilot study on preliminary outcomes
International Dentistry SA 2016,Vol11No5 32-39
97. Awad MA, Feine JS. “Measuring Patient Satisfaction with mandibular
prostheses.” Community Dent Oral Epidemiol 1998;26:400-405. Cited from:
98 Alexander J. Hassel and Thomas Holste.“Improving the Speech Function of
Maxillary Complete Dentures:A Pilot Study.” Int J
Prosthodontics2006;19(5):499-503.

References
154 | P a g e
99. Garrett NR, Kapoor KK, Perez P. “Effects of improvements of poorly fitting
dentures and new dentures on patient satisfaction” J ProsthoDent 1996;76:403-
413.
100. Pound E. „Controlling Anomalies of Vertical Dimension and Speech.‟ J
Prosthet Dent1976; 36:124-135.
101, AnupamaNeelkantan, Sunil dhaded Rugae Duplication -Different techniques
of custamizing palatal rugae in Maxillary complete denture to enhance
phonetics-Karnataka prosthodontics jr 2016 vol (1) 1-7
102. Christopher Runte, DjfarTawana, Dieter Dirksen, BettiniRunte, Antoinette
Lamprecht-Dinnesen, FriedhelmBollmann, Eberhard Seifert and
GholamrezaDanesh. “The influence of maxillary central incisor position in
complete dentures on /s/ sound production.”J Prosthet Dent 2001;85(5):485-495.
103.Sherman H. „Phonetic capability as a function of vertical dimension in complete
denture wearers- a preliminary report.‟ J Prosthet Dent 1970;23:621-632 .
104. Glossary of Prosthodontic terms.
105..R C. Goyal Research Methodology FOR health ProfessionalsMethods in .
Jaypee Publication,2013.
106. Kanji Gopal. Hundred Statistical Test, 1995, SAGE Publications Ltd., London.
107.Sterberg the Netherlands 2015
108AnupamaNeelakantan Sunil Dhaded Rugae Duplication-Different techniques of
customizing palatal Rugar in Maxillary complete denture to Enhance Phonetic
Karnataka Prosthodontics Journal 2016.Vol.(1) 1-7
109.S K, Lwanga,S. Lemeshow--Sample Size Determination In Health Studies--
W.H.O.Geneva 1991
110. Spectrogram From Wikipedia
111. H. N. L Teodorescu Voice analysis in dentistry; Journal of Romanian Medical
Dentistry, vol 14, issue 3, July/Sep 2010- Pg 171-186

Annexure
155 | P a g e
ANNEXURE – I

Annexure
156 | P a g e
ANNEXURE – II
Sharad Pawar Dental College & Hospital, Sawangi (Meghe), Wardha
Department of Prosthodontics
Consent Form
I, ____________________age ________resident of _________ hereby give my
willingness to be a subject (patient) for the study entitled:
“Evaluation of the effect of functional contouring of the palatal vault ofed
palatal maxillary complete denture on clarity of speech sounds in edentulous
patients- An in Vivo- study conducted by Dr Surekha .Godbole.
I have been given detail information about my involvement as a subject in the
study. I am personally satisfied with the protective measures taken. For this I
am ready to give my consent to participate in the recording my speech sample
as required.
I assure best of my co-operation during the period of study. I offer myself as a
subject voluntarily.
Sign of Researcher Sign of subject with Name
-------------------------- -------------------------------
Sign of Guide Sign of witness with Name
-------------------------- -------- ----------------------
Date:
Place:

Annexure
157 | P a g e
ANNEXURE – III
Classification of Consonants in English Language

Annexure
158 | P a g e
ANNEXURE – IV
Sr.
No. Name of the patient Age Sex OPD No.
Recording of speech sounds
Without modification With Modification
T Th D L Ch T Th D L Ch
dB Hz dB Hz dB Hz dB Hz dB Hz dB Hz dB Hz dB Hz dB Hz dB Hz
1 SangramLambe 42 M 1511170042 12 108 14 129 21 129 22 108 15 129 20 151 15 129 10 129 22 129 18 129
2 SuhilabaiMasathe 50 F 1512220131 11 110 13 132 22 131 18 112 18 129 19 129 14 132 12 131 19 130 21 129
3 RekhaJipkate 52 F 1601040096 15 108 17 136 24 135 26 118 19 131 22 132 18 136 14 135 28 129 22 131
4 Vinod Tiwari 40 F 1511270086 13 129 15 129 26 129 18 139 17 139 21 136 16 129 13 129 20 139 20 139
5 GautamKumbhare 60 M 1509080058 12 108 13 132 18 132 17 129 14 129 20 129 14 132 18 132 19 129 18 129
6 Priti Shukla 31 F 1511130011 16 151 18 180 17 129 14 151 15 132 24 132 19 180 14 129 16 151 17 132
7 Ramesh Sirsikar 65 M 1601040035 10 108 12 129 14 129 19 159 13 134 22 180 13 129 10 129 16 159 15 134
8 Ram Projen 45 M 1601040002 13 129 15 132 19 132 21 129 12 129 20 129 16 132 18 132 21 129 13 129
9 Nilkantporbat 67 M 1512040099 12 111 15 131 21 131 22 129 21 151 21 132 16 131 19 131 22 129 22 151
10 Ashok Panchbhai 64 M 1511020084 19 101 21 121 22 121 18 130 27 159 22 131 22 121 20 121 24 130 29 159
11 TulsiGosavi 55 F 1601040041 21 105 20 132 16 132 22 121 24 141 24 121 21 132 17 132 24 121 26 141
12 ShaziyaTabassum 68 F 1512110169 16 109 18 129 19 129 21 111 23 139 21 132 19 129 21 129 23 111 25 139
13 MadhuriPiprande 78 F 1411030030 13 129 15 149 21 149 31 151 21 129 28 149 16 149 16 149 33 151 22 129
14 KanhaiyaPrasapati 67 M 1506110074 11 127 16 147 14 147 21 156 18 129 29 131 17 147 18 147 24 156 21 129
15 SushilaBhalkar 52 F 1512110190 16 108 18 128 15 128 22 131 19 142 31 169 19 128 20 128 22 131 22 142
16 BhagwantThombare 58 M 1508070105 12 129 13 139 16 139 25 139 14 159 20 129 14 139 17 139 18 139 16 159
17 Baburao More 61 M 1512290066 15 129 12 149 18 149 18 149 18 151 23 131 13 149 19 149 21 149 20 151
18 Vijay Jaiswal 51 M 1512040155 18 108 20 129 19 129 19 120 19 129 26 132 21 129 21 129 22 120 21 129
19 Kalavati Hole 62 F 1601070029 15 151 18 132 21 132 12 101 21 142 15 129 19 132 22 132 15 101 23 142
20 DharmajiBabhulkar 55 M 1601010191 12 141 19 131 22 131 18 108 22 149 20 129 20 131 21 131 22 108 24 149
21 AmbadasNishan 62 M 1511050120 14 129 15 129 20 151 22 129 12 108 20 129 21 129 18 129 22 121 19 131
22 DevidasPatharkar 45 M 1510060133 13 132 14 132 19 129 19 130 11 110 18 132 22 131 15 149 21 132 15 129
23 VithbaiPethe 80 F 1601040053 17 136 18 136 22 132 28 129 15 108 19 131 24 135 16 147 19 129 14 132
24 MadhuriPiprande 55 M 1510050131 15 129 16 129 21 136 20 139 13 129 15 129 26 129 18 128 16 149 18 136
25 Kisan Chauhan 65 M 1601090024 13 132 14 132 20 129 19 129 12 108 14 132 18 132 13 139 17 147 16 129
26 BaliramRathod 66 M 1801200102 18 180 19 180 24 132 16 151 16 151 18 136 17 129 12 149 19 128 14 132
27 VitthalGawande 84 M 1601110065 12 129 13 129 22 180 16 159 10 108 16 129 14 129 20 129 14 139 19 180
28 SindutaiBhoge 70 F 1601130124 15 132 16 132 20 129 21 129 13 129 14 132 19 132 18 132 13 149 13 129

Annexure
159 | P a g e
29 SeetabaiBendre 75 F 1601090074 15 131 16 131 21 132 22 129 12 111 19 180 21 131 19 131 21 129 16 132
30 NasayahPohane 52 M 1601130967 18 121 22 121 22 131 24 130 19 101 13 129 22 121 15 129 19 132 16 131
31 BimraoShende 72 M 1512140056 19 132 21 132 24 121 24 121 21 105 16 132 16 132 14 132 20 131 22 121
32 JangaluChavhan 70 M 1601200105 18 129 19 129 21 132 23 111 16 109 16 131 19 129 18 136 21 129 21 132
34 Asha Chaudhari 60 M 1601200517 15 149 16 149 28 149 33 151 13 129 22 121 21 149 16 129 22 131 19 129
35 Fakri Chauhan 65 F 1601200106 16 147 17 147 29 131 24 156 11 127 21 132 14 147 14 132 24 135 16 149
36 SomeshwarPunewar 56 M 1601280097 18 128 19 128 31 169 22 131 16 108 19 129 15 128 19 180 26 129 17 147
37 Suleman Khan 58 M 1601210086 13 139 14 139 20 129 18 139 12 129 16 149 16 139 13 129 18 132 19 128
38 AshubaiBhagat 45 F 1509070033 12 149 13 149 23 131 21 149 15 129 17 147 18 149 16 132 17 129 14 139
39 Asha Chaudhari 50 F 1801200157 20 129 21 129 26 132 22 120 18 108 19 128 19 129 16 131 14 129 13 149
40 Suresh Ghodkhande 40 F 1306030091 18 132 19 132 15 129 15 101 15 151 14 139 21 132 22 121 19 132 21 129
41 Vilas Shrikhande 55 F 1601250058 19 131 20 131 20 129 22 108 12 141 13 149 22 131 21 132 21 131 19 132
42 Asha Hingave 45 F 1512170191 18 109 21 149 23 129 21 129 14 129 21 129 20 151 19 129 22 121 20 131
43 ShrikantWalake 62 F 1601270073 16 129 19 147 21 149 22 129 13 132 19 132 19 129 16 149 16 132 22 129
44 SindhuWani 55 F 1601270072 15 127 18 128 20 147 24 130 17 136 20 131 22 132 17 147 19 129 24 130
45 ApurvaKhadse 58 M 1602100001 12 108 15 139 18 128 24 121 15 129 22 129 21 136 19 128 21 149 24 121
46 Subhandrasidam 60 F 1601290034 13 129 17 149 19 139 23 111 13 132 24 130 20 129 14 139 14 147 23 111
47 NilkanthVyenrghe 78 M 1602030088 16 129 19 129 21 149 33 151 18 180 24 121 24 132 13 149 15 128 33 151
48 wasudevDarne 81 M 1601190123 18 108 21 132 22 129 24 156 12 129 23 111 22 180 21 129 16 139 24 156
49 vinodChaudhari 48 M 1601300071 21 151 20 131 21 132 22 131 15 132 33 151 20 129 19 132 18 149 22 131
50 Haribhav Bhil 65 M 1620100042 20 141 24 129 23 131 18 139 15 131 24 156 21 132 20 131 19 129 18 139
51 LalitaChaubey 65 M 1602010062 12 129 15 132 16 151 21 149 18 121 22 131 22 131 21 149 21 132 21 149
52 BebitaiBwane 50 F 1601120050 13 132 18 136 19 129 22 120 19 132 18 139 24 121 19 147 24 130 22 120
53 YadavBehanre 65 M 1602040112 14 136 16 129 17 132 15 101 18 129 21 149 21 132 18 128 24 121 15 101
54 kamlesh Mishra 69 M 1602040095 16 129 18 132 18 136 22 108 15 149 22 120 28 149 15 139 23 111 22 108
55 Prakash Padade 49 M 1602040109 11 132 12 180 13 129 22 131 16 147 15 101 29 131 17 149 33 151 22 131
56 LilabaiDarange 74 F 1602050083 20 180 22 129 24 132 18 139 18 128 22 108 31 169 19 129 24 156 18 139
57 NazmaKureshi 65 F 1602090141 15 129 17 132 20 180 21 149 13 139 22 131 20 129 21 132 22 131 21 149
58 FakiraKuputkar 80 M 1602100103 16 132 20 149 21 129 22 120 12 149 18 139 28 171 20 131 18 139 22 120
59 BabanDurbude 72 M 1602040091 18 131 21 147 22 132 15 101 20 129 21 149 21 158 18 129 21 149 24 129
60 Manjulabaizade 70 F 1602100124 19 121 22 128 24 131 22 108 18 132 22 120 22 129 12 108 22 120 26 131