
Sciences Journal - CiteSeerX
106
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1 211 VCare For Life Sciences Journal Online ISSN: 2231-9522 Vol.4, Issue 1 April 2014 http://vcareforlife.org/vcfl-science-journal ISSN: 2231-9522
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Sciences Journal - CiteSeerX

VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
211
VCare For Life
Sciences Journal Online
ISSN: 2231-9522
Vol.4, Issue 1
April 2014
http://vcareforlife.org/vcfl-science-journal
ISSN: 2231-9522
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
212
Patron V Care for Life Medical and Healthcare services private limited
Editor in Chief Dr. P. G Bagali Executive Editor Dr. C. R. V. Murthy Associate Editor Dr. H S Naik Editorial Board Members Dr. Vijay Kumar (Env.Health/UK) Dr. Sampath Kumar (Family Medicine/ USA) Dr. Ngin Cin Khai ( Immunology / Japan) Dr. Shivaprasad (Physiology/USA) Dr. Sreenivasa Jayachandra (Physiology/Malaysia) Dr. Mallikarjuna MS (ENT/India) Dr. Harshavardhana (Microbiology/India) Dr. Than Win (Medicine/ Myanmar) Dr. Abdul Hameed (Pathology/Libya) Dr. Ramana Gouda (Veterinary Science/USA) Dr Manjunath S (Biochemistry/India) Indexing & Archiving Index Copernicus getCITED Jour Informatics Google Scholar Research Bible ourGlocal Journal Database DRJI MYJurnal DOAJ Web Designer & Publication Coordinator For Your Web Pvt. Ltd
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
213
V Care For Life
Sciences Journal ISSN: 2311-9522
We are proud to announce that V Care For Life Sciences Journal has embarked on to a new journey in the community of scientific journals.
V Care For Life Sciences Journal has been indexed with the following
Index Copernicus
getCITED
Jour Informatics
Google Scholar Research Bible ourGlocal Journal Database DRJI MYJurnal DOAJ
It is also a Member of
The Committee on Publication Ethics (COPE)
Asia pacific association of Medical Editors (APAME)
World Association of Medical Editors (WAME)
Global Impact Factor
0.466
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
214
Contents
STUDY OF CERTAIN BIOCHEMICAL INDICES TO ASSESS LIVER FUNCTIONAL STATUS IN SICKLE CELL DISEASE PATIENTS WITH ANAEMIC CRISES ................................................. 215
A STUDY OF DIGIT RATIO (2D:4D) COMPARISON IN MALE AND FEMALE HUMAN BEINGS. .................................................................................................................................... 224
INDIAN PERSPECTIVE OF INFLAMMATORY GRANULOMA IN A TERTIARY CARE HOSPITAL .................................................................................................................................... 232
BOMB BLAST INJURIES – NEW FACE OF TERROR: RADIOLOGISTS' PERSPECTIVES BASED ON THE EXPERIENCE IN INDIA ............................................................................................. 248
STRANGULATED INTERNAL HERNIA .............................................................................. 266
A RARE CASE PRESENTING WITH ACUTE SMALL BOWEL OBSTRUCTION. ........................ 266
DIAGNOSTIC EFFICACY OF ENDOSCOPY IN EVALUATION OF DYSPHAGIA ....................... 271
STUDY OF SELLAR BRIDGES IN DRY HUMAN SKULLS OF NORTH INTERIOR KARNATAKA . 275
STUDY OF VARIATION IN HIP JOINT ANGLES AND MEASUREMENTS AMONG REGIONAL URBAN POPULATION OF SOUTH INDIA- A CONTRIBUTION TO TRIBOLOGY .................... 286
USEFULNESS OF FINE NEEDLE ASPIRATION CYTOLOGY IN THE EVALUATION OF THE NODULAR GOITER WITH HISTOPATHOLOGICAL CORRELATION ...................................... 298
IMPACT OF STANDARDIZED FEEDING REGIME ON INCIDENCE OF NECROTIZING ENTEROCOLITIS IN LOW BIRTH WEIGHT BABIES ............................................................ 305

VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
215
Study of certain biochemical indices to assess liver functional
status in sickle cell disease patients with anaemic crises
Prashant Nigam1, Purnima Dey Sarkar2
1Dept. of Biochemistry, Chhattisgarh Institute of Medical Sciences, Bilaspur (C.G.),
2Dept. of Biochemistry, MGMC, Indore (M.P.).
Corresponding Author
Prashant Nigam E mail: [email protected]
Abstract
Sickle cell disease is characterized by
presence of HbS in RBC. It is a genetic
disorder in which substitution of glutamate
by valine produces abnormal hemoglobin.
Multi-organ failure is often occurred in SCD
if it is not managed well. Liver is one of the
most important organ affected in sickle cell
disease. Due to multi-factorial causes,
pathophysiology of liver is not easy to
understand. The manifestation of
biochemical parameters related to liver are
very useful to understand to severity of
liver damage as well as its pathophysiology.
Hemolysis, transfusion management,
vasoocclusion, and other defects which are
not associated with sickle cell disease can
cause hepatic complications in Sickle cell
disease. In this study we were investigated
biochemical findings of patients with sickle
cell disease in order to determine the
extent of liver damage.
Key Words
Liver Function, Sickle Cell Disease, Crises,
Steady State.
Introduction
Initially sickle cell was believed to be
familial until it was later found that sickle
cell anaemia was an autosomal recessive
inheritable disease associated with the
sickling of the red blood cell as a result of
oxygen depletion (Davis et al 1997). The
incidence of liver disease in sickle cell
disorders is difficult to ascertain despite
being a component of the multi-organ
failure that occurs in sickle cell disease. The
clinical manifestations of different causes of
liver failure is also similar and inter related
thus making the pathophysiology complex.
The liver function abnormalities may be due
to hemolytic anaemia of sickle cell disease,
complications to the liver due to the part of
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
216
treatment in sickle cell disease such as
transfusion management, hepatobiliary
abnormalities due to the consequences of
sickling and vaso occlusion and
abnormalities of the liver not related to the
sickle cell disease mainly viral hepatitis.
Abnormalities of liver function tests have
been reported to be common and relatively
mild in sickle cell patients in steady state.
Hepatomegaly as a common symptom
observed both in disease and trait groups.
The clinical manifestation of sickle cell in
India seems to be milder than in Africa and
Jamaica (Mohanty et al 2002). The clinical
spectrum of SCD ranges from mild to severe
liver function and clinical crises with
marked hyperbilirubinemia and liver failure.
Multiple factors may contribute to the
aetiology of the liver disease, including
ischemia, transfusion related viral hepatitis,
iron overload, and gallstones (Banerjee S. Et
al 2001).
Materials & Methods
This study included 50 patients with an
established diagnosis of SCD. All are
homozygous sickle cell disease patients. All
the patients were in crisis state of the
disease. The diagnosis of disease was
confirmed by Hb electrophoresis in alkaline
pH using fully automatic electrophoresis
instrument, Genio, Italy. A general
examination was done on all the patients
before blood sampling were taken for
biochemical studies.
Statistical Analysis
Data were analyzed by using SPSS version
16.0 software. Association between clinical
data was assessed by cross tabulation and
two tailed T – test was used for laboratory
parameters. Analysis of Variance (ANOVA)
was then used to compare the parameters
of each group. Level of significance for all
tests was set at 95% confidence interval.
Result
In this study we included patients under age
of 16 years. The mean age was 12 year
(Range 4 – 16 year), 62% were male & 38%
were female. All patients were presented
with crisis. The level of SGPT as well as
SGOT was increased. ALP level was also
present beyond its normal reference
interval. The level of GGT also observed
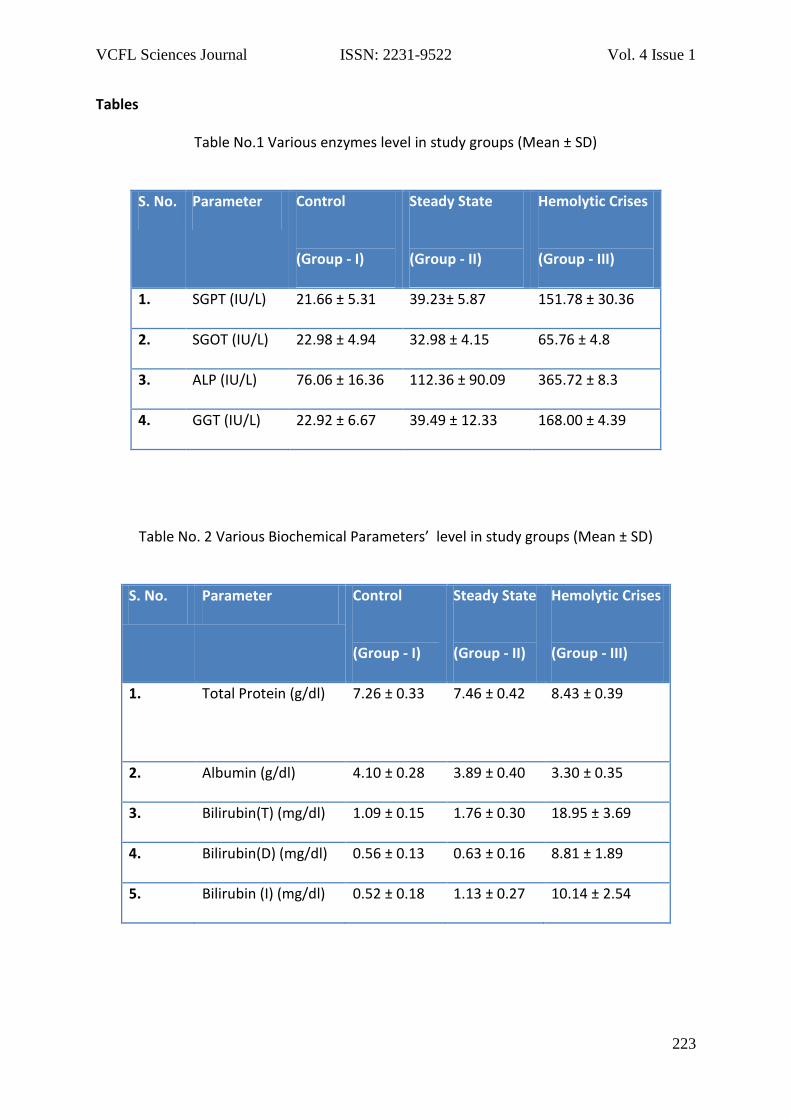
elevated (Table No. 1). There was no
significant correlation found between these
enzymes, age and sex. Total protein and
albumin level was observed within normal
limit or higher side of normal reference
interval. The level of total bilirubin was
higher in all patients without any
correlation with age and sex (Table No. 2).
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
217
Discussion
Liver abnormality release SGPT and SGOT,
which makes useful test for detecting liver
damage. Hemolysis also raises SGOT and
SGPT levels in SCD. Nsiah K et al (2011)
reported higher activity of SGOT and SGPT
in sickle hepatopathy with various crises
associated with sickle cell disease. In the
present study levels of SGPT and SGOT were
found higher in haemolytic crisis when
compared to other two groups (I & II
p<0.001). Level of ALP also found highly
significant in group – III when compared to
other groups (p<0.001). Oparinde DP et al
(2006) conducted biochemical assessment
regarding severity of sickle cell anemia with
reference to role of hepatic enzyme and
found that a significant increase in serum
ALT, ALP and GGT levels in SCA with
persistent hepatomegaly over those
without hepatomegaly (p < 0.05, p < 0.05
and p < 0.01 respectively). All the index
scores and the final aggregate severity
scores were also significantly higher in SCA
subjects with persistent hepatomegaly.
Only GGT demonstrated a fairly positive
and significant correlation (r = 0.46, P <
0.05) with increased clinical severity among
the hepatic enzymes. Yahaya et al (2012)
conducted a study in which activities of
alkaline phosphatase, alanine
aminotransferase and aspartate
aminotransferase were significantly higher
(P<0.05) in the HbSS patients than the
control subjects. This study made a
conclusion that level of total protein and
albumin is not very much altered in sickle
cell crises. Our study was also in agreement
with above study although we were found
statistically significant difference between
group I and Group III as the level of total
protein and albumin fall higher side of the
normal reference interval. However in
present study group III shows highly
significant mean difference when compared
to group I, it may be due to the
inflammatory response against viral
infection, induced over production of
antibody. Statistically insignificant
difference of albumin in above group
supports this study. Same findings were
also reported by U. P. ISICHEF (1979). The
protein patterns seen in his study are
interesting in many respects. A comparison
of the serum protein values shows definite
evidence of relative hyperproteinaemia as
well as hyperglobulinaemia in sickle cell
disease. Whereas the albumin levels were
almost the same in all groups, the globulin
values in sicklers were significantly greater
than in normal children of the same age,
showing that the globulin fraction is largely
accountable for the high total protein.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
218
Marked hyperbilirubinemia of up to 57
mg/dL, in most cases predominantly
conjugated with only a mild elevation in ALT
levels, has been described by Buchanan et
al. (1977) in 6 children with minimal or no
symptoms. In the present study we found
highly significant Bilirubin mean differences
among all the groups (p<0.001). Similar
pattern was also observed by Ebert EC et al
(2010), reported the most common
laboratory abnormality is an elevation of
unconjugated bilirubin level. Bilirubin and
lactate dehydrogenase levels correlate with
one another, suggesting that chronic
hemolysis and ineffective erythropoiesis,
rather than liver disease, are the sources of
hyperbilirubinemia. Highly significant
bilirubin level may be due to combination of
ongoing hemolysis, intra hepatic cholestasis
and renal impairment encountered in sickle
cell hepatopathy in comparison with
remaining disease groups. Abdominal pain
is very common in SCD and is usually due to
sickling, even in the steady state Bilirubin is
significantly high with the asymptomatic
jaundice. In the present study the total
serum bilirubin concentration was also
significantly increased in haemolytic crisis
(mean 18.95, p<0.001) above the steady
state level. Bilirubin concentration in
haemolytic crisis was much more higher
when compared to other groups(Group I &
II), is due to access hemolysis of RBC in the
crisis which is not present up to that extent
steady state SCD. Ojuwa et al (1994) studied
thirty children with SCA and assayed serum
alanine aminotransferase, alkaline
phosphatase, total protein, albumin and
bilirubin, during vaso-occlusive crisis and at
recovery. Alanine aminotransferase,
alkaline phosphatase and bilirubin levels
were significantly higher during crisis than
at recovery, (p < 0.005) especially in the
young patient. However, the total protein
and albumin levels were not significantly
different in crisis and at recovery. A
transient hepatic functional derangement
during vaso-occlusive crisis is a probable
explanation for the reported changes.
Bone changes are common in SCD but the
pathogenesis is not fully understood
(Nouraie M et al 2011). The level of alkaline
phosphatase indicates severity of bone
damage and is a useful guide of progress in
the management of bone pains in sickle
cell(Afonja OA et a 1986). Bone disease with
osteoporosis and osteomalacia are common
in SCD. Some patients have vitamin D
deficiency and low bone mineral density.
Delayed growth and bone destruction may
contribute to the elevated levels of alkaline
phosphatase. Higher levels of alkaline
phosphatase may be due to associated
vasoocclussive crises involving the bones

VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
219
rather than pathology of the liver (Kotila T
et al 2005, Mohammed SM et al 1991). The
level of the heat-labile alkaline phosphatase
indicates severity of bone damage and is a
useful guide of progress in the management
of bone pains in sickle cell. In the present
study we found highly significant level of
alkaline phosphatase in group II & III when
compare with normal (p <0.001), which is
similar to a study conducted by Isichei UP
(1980). Brody JI et al (1975) studied
behaviour of ALP in sickle cell anemia
patients and found Physical and
biochemical criteria identified bone alkaline
phosphatase as the principal, although not
necessarily the sole, enzyme fraction that
increases during
symptomatic sickle cell crises. Moreover,
there appeared to be concordance between
crisis severity, serum levels of alkaline
phosphatase, and isoenzyme patterns;
electrophoretic and biochemical
abnormalities could be detected even when
the patients were asymptomatic. GGT is
another useful enzyme to assess hepatic
function in SCD. In our study we found
statistically highly significant raised level of
GGT among all the group when compared
to normal (p <0.001). Similar findings were
obtained by Oparinde DP et al (2006)
concluded, Only GGT demonstrated a fairly
positive and significant correlation (r = 0.46,
P < 0.05) with increased clinical severity
among the hepatic enzymes. It shows,
serum alkaline phosphatase level may be an
additional marker of the degree, frequency,
and persistence of tissue injuries that occur
in sickle cell anemia.
Conclusion
The present data suggest that abnormalities
in liver functions have been assumed to be
common and mild in steady state and to
become more severe in crisis. Liver function
tests are normal in majority of the sickle cell
disease patients, who progressed to
hepatobiliary complications they shown
significant elevated levels of hepatobiliary
enzymes.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
220
Reference
1. Afonja OA, Boyd AE (1986). Plasma
alkaline phosphatase and osteoblastic
activity in sickle cell . J Trop Pediatr.
32(3): 115–6.
2. Banerjee S, Owen C, Chopra S. (2001)
Sickle cell hepatopathy. Hepatology.;
33(5):1021–8.
3. Brody JI, Ryan WN, Haidar MA (1975).
Serum alkaline phosphatase isoenzymes
in sickle cell anemia.JAMA. 19;
232(7):738-41.
4. Buchanan GR, Glader BE (1977). Benign
course of extreme hyperbilirubinemia in
sickle cell anemia: analysis of six cases. J
Pediatr, 91:21-24.
5. Davies SC, Oni L. The management of
patients with sickle cell disease. Br.
(1997). Med. J. 315: 656-660.
6. Ebert EC, Nagar M, Hagspiel KD (2010).
Gastrointestinal and hepatic
complications of sickle cell disease.Clin
Gastroenterol Hepatol. Jun; 8(6):483-9;
quiz e70. doi:
10.1016/j.cgh.2010.02.016.
7. Isichei UP (1980). Liver function and the
diagnostic significance of biochemical
changes in the blood of African children
with sickle cell disease. J Clin Pathol.
Jul;33(7):626-30.
8. Kotila T, Adedapo K, Adedapo
A, Oluwasola O, Fakunle E, Brown B.
(2005) Liver dysfunction in steady
state sickle cell disease. Ann Hepatol.
Oct-Dec; 4(4):261-3.
9. Mohammed SM, Suleiman SA, Addae SK,
Annobil SH, Adzaku FK, Kadoummi OF,
Richards JT (1991). Urinary
hydroxyproline and serum alkaline
phosphatase in sickle cell disease. Clin
Chim Acta. 203(2–3):285–94.
10. Mohanty D, Mukheriee M (2002): Sickle
Cell Disease in India; Haematology. 9(2):
117-122.
11. Nouraie M, Cheng K, Niu X, Moore-King
E, Fadojutimi-Akinsi MF, Minniti CP, et al
(2011). Predictors of osteoclast activity
in sickle cell disease patients.
Haematologica. 96.
doi:10.3324/haematol.2011.042499.
12. Nsiah K, Dzogbefia VP, Ansong D, Osei
Akoto A, Boateng H, Ocloo D (2011).
Pattern of AST and ALT changes in
relation to hemolysis in sickle cell
disease. Clin Med Insight Blood
Disord.;4:1–9.
13. Ojuawo A, Adedoyin MA, Fagbule D
(1994). Hepatic function tests in
children with sickle cell during vaso
occlusive crisis. Cent Afr J Med.
Dec;40(12):342-5.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
221
14. Oparinde DP, Oghagbon EK, Okesina
AB, Olatunji PO, Ojuawo AO (2006). Role
of hepatic enzymes in the biochemical
assessment of the severity
of sickle cell anemia. Trop
Gastroenterol. Jul-Sep;27(3):118-21.
15. U. P. Isichef (1979). Serum protein
profile in sickle cell disease. Journal of
Clinical Pathology, 32, 117-121
16. Yahaya IA (2012). Biochemical features
of hepatic dysfunction in Nigerians
with sickle cell . Niger Postgrad Med J.
Dec;19(4):204-7.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
223
Tables
Table No.1 Various enzymes level in study groups (Mean ± SD)
S. No. Parameter Control
(Group - I)
Steady State
(Group - II)
Hemolytic Crises
(Group - III)
1. SGPT (IU/L) 21.66 ± 5.31 39.23± 5.87 151.78 ± 30.36
2. SGOT (IU/L) 22.98 ± 4.94 32.98 ± 4.15 65.76 ± 4.8
3. ALP (IU/L) 76.06 ± 16.36 112.36 ± 90.09 365.72 ± 8.3
4. GGT (IU/L) 22.92 ± 6.67 39.49 ± 12.33 168.00 ± 4.39
Table No. 2 Various Biochemical Parameters’ level in study groups (Mean ± SD)
S. No. Parameter Control
(Group - I)
Steady State
(Group - II)
Hemolytic Crises
(Group - III)
1. Total Protein (g/dl)
7.26 ± 0.33 7.46 ± 0.42 8.43 ± 0.39
2. Albumin (g/dl) 4.10 ± 0.28 3.89 ± 0.40 3.30 ± 0.35
3. Bilirubin(T) (mg/dl) 1.09 ± 0.15 1.76 ± 0.30 18.95 ± 3.69
4. Bilirubin(D) (mg/dl) 0.56 ± 0.13 0.63 ± 0.16 8.81 ± 1.89
5. Bilirubin (I) (mg/dl) 0.52 ± 0.18 1.13 ± 0.27 10.14 ± 2.54
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
224
A Study of Digit Ratio (2d:4d) Comparison in Male and Female
Human Beings.
Ravi P Bangalore1, Vinod A2, Prashanth S3, Praveenkumar I. Inamadar4
1Assistant Professor, Department of Psychiatry, SSIMS&RC, Davangere, Karnataka.
2Senior Resident, Department of Psychiatry, S Nijalingappa Medical College, HSK (Hanagal
Shree Kumareshwar) Hospital and Research Centre Bagalkot. Karnataka
3Associate Professor, Department of Neurology, SSIMS&RC, Davangere, Karnataka
4Professor and Head - Dept. of Forensic Medicine & Toxicology, HIMS & RC, Hassan,
Karnataka
Corresponding Author
Dr Ravi P Bangalore
Email: [email protected]
Abstract
The digit ratio is the ratio of the lengths of
different digits, fingers or toes, typically as
measured from the bottom crease where
the finger joins the hand to the tip of the
finger. It has been suggested that the ratio
of two digits in particular, the 2nd (index
finger) and 4th (ring finger) is affected by
exposure to androgens such as testosterone
while in the uterus. This study was
conducted with objective of comparing the
digit ratio (2D:4D) in males & female human
beings. The subjects included 30 males and
30 females who met the inclusion and
exclusion criteria and were assessed with
measurement of digit ratio in both the
hands by transperancy method. The results
were analysed by applying chi square test
for categorical variables and independent T
test for continuous variables. We found that
men have longer ring finger (4D) than index
finger (2D), where as in females both are of
nearly equal length. The digit ratio was
higher in females compared to males in
both the hands but the difference was not
statistically significant.
Keywords
Digit ratio; 2D:4D.
Introduction
The digit ratio is the ratio of the lengths of
different digits, fingers or toes, typically as
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
225
measured from the bottom crease where
the finger joins the hand to the tip of the
finger. It has been suggested by some
scientists that the ratio of two digits in
particular, the 2nd (index finger) and 4th
(ring finger) is affected by exposure to
androgens such as testosterone while in the
uterus and that this 2D:4D ratio can be used
as a crude measure for prenatal gonadal
exposure.
2D:4D is sexually dimorphic: in men, the
second digit tends to be shorter than the
fourth, and in females the second tends to
be the same size or slightly longer than the
fourth.1 Several studies have shown that
the length of the second digit in adults is
directly proportional to the average plasma
estrogen concentration in the individual. In
the same fashion, the length of the fourth
finger is directly proportional to the average
plasma concentration of androgens.2, 3, 4
The fact that the proportion between the
length of the above two digits (second:
fourth) is already fixed around the
thirteenth week of intrauterine life5 has led
to the conclusion that the length of the two
digits is also representative of the foetal
concentrations of oestrogens and
androgens. Their measurements therefore
represent a “smoking gun” of what were
the concentrations of an individual’s sexual
hormones in utero.2, 3, and 4
Smaller ratio reflects higher foetal
testosterone and lower estrogen,6 the
relationship between the gonad
differentiation and formation of fingers and
toes led to suggestion that patterns of digit
and toe morphology may correlate with
gonad function in the fetus and adult.3
According to hypothesis of manning and
Bundred (2000), the2D: 4D may be used as
an indicator and predictive factor in a
variety of disorders associated with a
disturbed testosterone/estrogen hormone
balance like gender identity disorder7,4
dyslexia, migraine, stammering, immune
dysfunction. There are some studies which
have thrown light on testosterone/estrogen
hormonal imbalance in schizophrenia.
According to Mihaly arato et al, 2004 low
fetal androgen/estrogen ratio may have a
predisposing role in development of
schizophrenia.8 More feminized digit ratio
have been demonstrated in schizophrenia
compared to same sex controls.9
Materials and Methods
The study was based on the hypothesis that
digit ratio is sexually dimorphic trait with
females having higher digit ratio than the
males.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
226
Aim of the study
To compare the second to fourth digit
length ratio between male and female
participants
Methodology:
The study group comprised male (n= 30)
and female (n=30) who were selected from
NIMHANS staff, their families and the
neighbourhood of local guardian of the
main investigator provided -
1. They did not have any medical and
surgical conditions that would lead to
errors in measuring 2D:4D ratio like
syndactaly, polydactaly, trauma,
amputation, contracture etc.
2. They were ready to give informed
consent.
After obtaining informed consent, subjects
who met the above said criteria were
assessed. Digit ratio (second finger to fourth
finger lengths) measurement was taken
using a vernier calliper by transparency
method, in which the hand in straight
continuation position of forearms was
placed over the table with dorsum of hand
facing table. A transparent sheet was placed
over the palm. The proximal crease and tip
of the second and fourth finger was
marked. Digit lengths (2Dand 4D) was
obtained by measuring the distance
between proximal crease and tip of the
finger using simple scale by three different
raters blind to the gender of subject. The 2D
and 4D lengths were measured for both
hands. This 2D: 4D ratio was compared
between males and female participants.
Statistical analysis was done using the
Statistical package for social sciences (SPSS)
version-13. Continuous variables were
assessed using the t-test and categorical
variables were assessed using the chi-
square test
Results
In this study 60 participants (males=30,
females=30) were participated. There was
statistically significant difference between
two groups in terms of marital status,
education, occupation, socio economic
status and place. These were of lesser
significance as the digit ratio not affected by
these parameters.
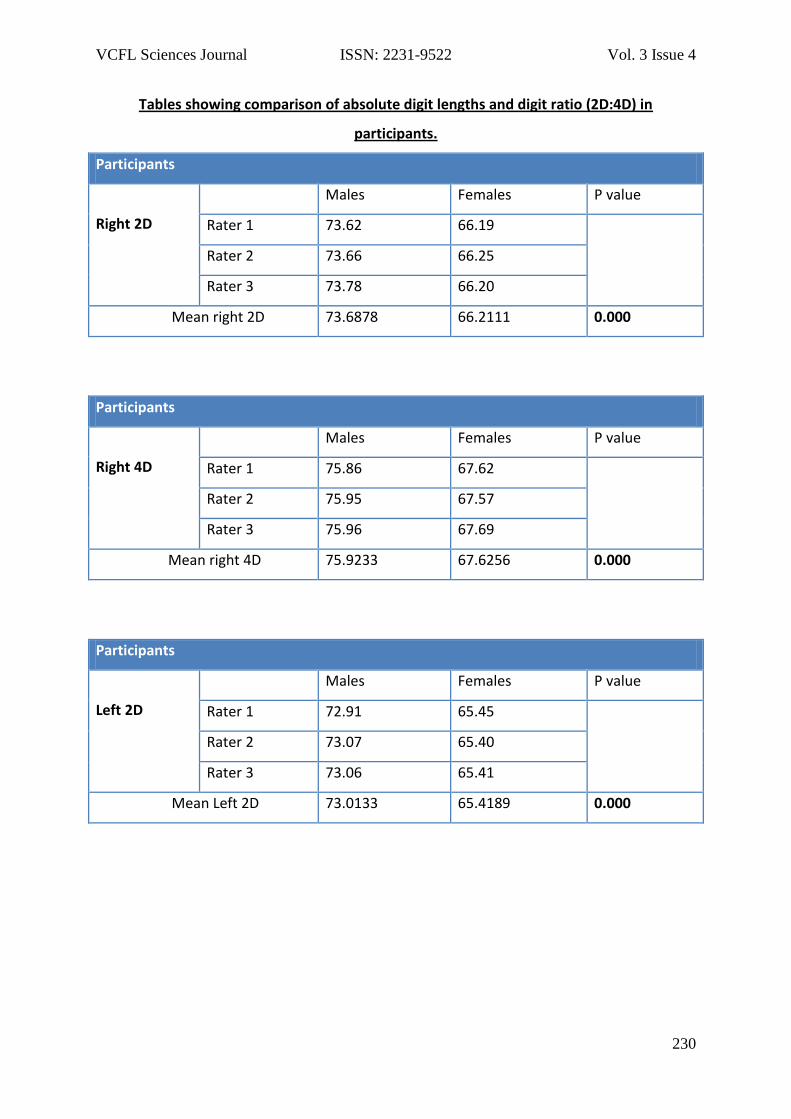
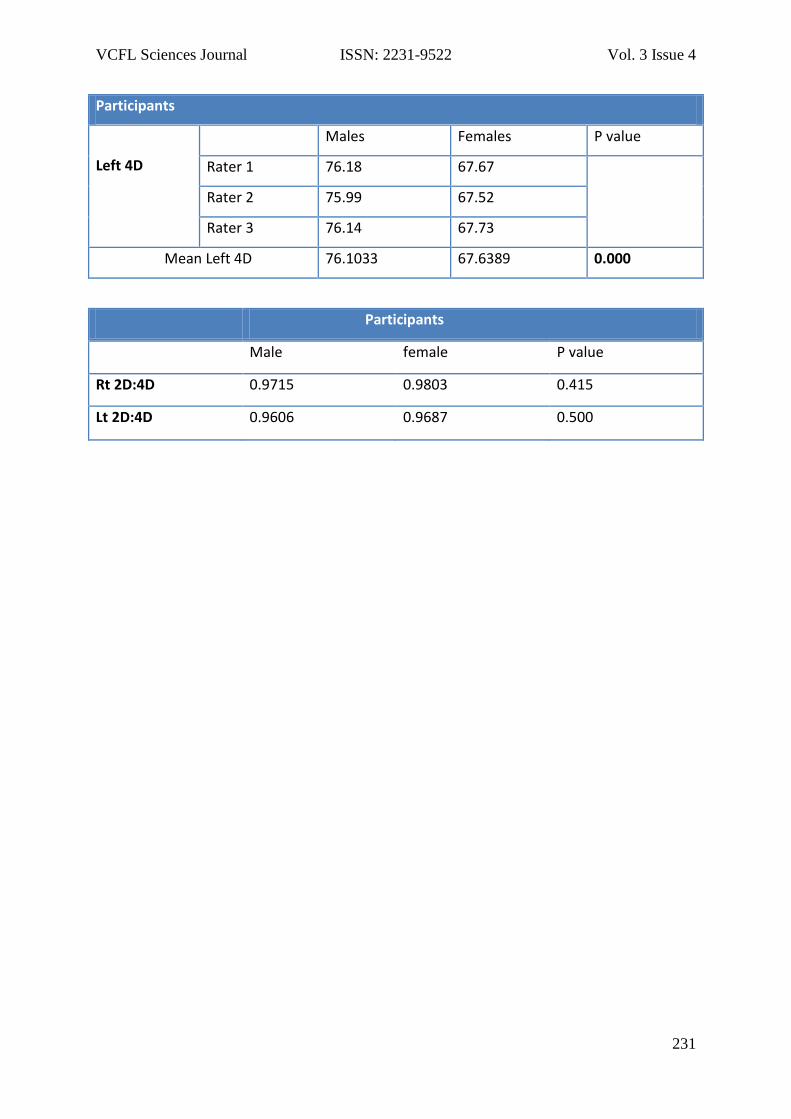
Comparison of digit lengths showed that
length of 2D and 4D was more in males
than females and the difference was
statistically significant(p=0.00). The
comparison of digit ratio (2D:4D) showed
that the ratio is higher in females than
males but the difference was not
statistically significant (p=0.415 for right
side and p=0.500 for left side).
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
227
Discussion
Our study replicated the finding that men
have longer ring finger (4D) than index
finger (2D), where as in females both are of
nearly equal length which is consistent with
findings from the previous studies.3
In our study the digit ratio was higher in
females than males in both the hands but
the difference was not statistically
significant. The earlier studies have found
that the digit ratio was higher in females
than males3, 8, and 9 which was partly
supported by this study. This could be
because of the racial differences in digit
ratio which need to be explored.
Sexual differences in 2D:4D are mainly
caused by the shift along the
common allometric line with non-zero
intercept, which means 2D:4D necessarily
decreases with increasing finger length, and
the fact that men have longer fingers than
women, 10 which may be the basis for the
sex difference in digit ratios and/or any
putative hormonal influence on the ratios.
The 2D:4D ratio in mice is controlled by the
balance of androgen to estrogen signaling
during a narrow window of digit
development.11 The formation of the digits
in humans, in utero, is thought to occur by
13 weeks, and the bone-to-bone ratio is
consistent from this point into an
individual’s adulthood.5 During this period if
the fetus is exposed to androgens, the exact
level of which is thought to be sexually
dimorphic, the growth rate of the 4th digit
is increased, as can be seen by analyzing the
2D:4D ratio of opposite sex dizygotic twins,
where the female twin is exposed to excess
androgens from her brother in utero, and
thus has a significantly lower 2D:4D ratio.12
Hox genes responsible for digit
development13 have been implicated in
affecting these multiple traits such as
otoacoustic emissions and arm-to-trunk
length ratio (pleiotropy). Direct effects of
sex hormones on bone growth might be
responsible, either by regulation of Hox
genes in digit development or
independently of such genes. Further
studies with large number of subjects are
required to throw some more lights in this
aspect.
The strengths of study being the method
used for the measurement of digits was
direct (transparency method) than the
photocopies of the hands, measurement
was done using vernier callipers which is
more sensitive than ruler and
measurements were done by 3 raters blind
to the gender of participants which
increases the inter rater reliability.
Limitation of the study may be lesser
number of subjects.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
228
References
1. George R. Human finger types.
Anatomical Record. 1930; 46:199–
204.
2. Manning JT, Bundred PE. The ratio
of 2nd to 4th digit length: a new
predictor of disease predisposition?.
Med Hypotheses. 2000; 54:855-7.
3. Manning JT, Scutt D, Wilson J. The
ratio of 2nd to 4th digit length: a
predictor of sperm numbers and
concentrations of testosterone,
luteinizing hormone and oestrogen.
Hum Reprod. 1998; 13:3000-4.
4. Williams T, Pepitone ME,
Christiansen SE, Cooke BM,
Huberman AD, Breedlove TJ, Jordan
CL, Breedlove SM. Finger-length
ratios and sexual orientation.
Nature. 2000; 404:455–6.
5. Garn S, Burdi AR, Babler WJ, Stinson
S. Early prenatal attainment of adult
metacarpal-phalangeal rankings and
proportions. Am J Phys Anthropol.
1975; 43:327–332.
6. Manning JT, Barley L, Walton J et al.
The 2nd:4th digit ratio, sexual
dimorphism, population differences,
and reproductive success. Evidence
for sexually antagonistic genes
Evolution and Human
Behavior. 21(3); 2000163–183.
7. Green ED, Yan WL, Guan XY.
Childhood-onset
schizophrenia/autistic disorder and t
(1; 7) reciprocal translocation:
identification of a BAC contig
spanning the translocation
breakpoint at 7q21. Am J Med
Genet. 2000;96:749-53
8. Arato M, Frecska E, Beck C, An M,
Kiss H. Digit length pattern in
schizophrenia suggests disturbed
prenatal hemispheric lareralization.
Prog Neuropsychopharmacol Biol
Psychiatry. 2004; 28(1):191-4.
9. Walder DJ, Seidman LJ, Cullen N,
SuJ, Tsuang MT, Goldstein JM. Sex
differences in language dysfunction
in schizophrenia. Am J Psychiatry.
2006; 163(3):470-7.
10. Kratochvíl L, Flegr J. Differences in
the 2nd to 4th digit length ratio in
humans reflect shifts along the
common allometric line. Biology
Letters. 2009; 5(5): 643–6.
11. Zhengui Z., Cohn MJ. Developmental
basis of sexually dimorphic digit
ratios. Proceedings of the National
Academy of Sciences of the United
States of America. 2011;
108(39):16289–16294.
12. Van Anders SM, Vernon PA, Wilbur
CJ. Finger-length ratios show

VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
229
evidence of prenatal hormone-
transfer between opposite-sex
twins. Hormones and Behavior.
2006; 49(3): 315–9.
13. Dickman S. HOX gene links limb,
genital defects. Science. 1997;
275 (5306):1568–9.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 3 Issue 4
230
Tables showing comparison of absolute digit lengths and digit ratio (2D:4D) in
participants.
Participants
Right 2D
Males Females P value
Rater 1 73.62 66.19
Rater 2 73.66 66.25
Rater 3 73.78 66.20
Mean right 2D 73.6878 66.2111 0.000
Participants
Right 4D
Males Females P value
Rater 1 75.86 67.62
Rater 2 75.95 67.57
Rater 3 75.96 67.69
Mean right 4D 75.9233 67.6256 0.000
Participants
Left 2D
Males Females P value
Rater 1 72.91 65.45
Rater 2 73.07 65.40
Rater 3 73.06 65.41
Mean Left 2D 73.0133 65.4189 0.000
VCFL Sciences Journal ISSN: 2231-9522 Vol. 3 Issue 4
231
Participants
Left 4D
Males Females P value
Rater 1 76.18 67.67
Rater 2 75.99 67.52
Rater 3 76.14 67.73
Mean Left 4D 76.1033 67.6389 0.000
Participants
Male female P value
Rt 2D:4D 0.9715 0.9803 0.415
Lt 2D:4D 0.9606 0.9687 0.500
VCFL Sciences Journal ISSN: 2231-9522 Vol. 3 Issue 4
232
Indian perspective of inflammatory granuloma in a Tertiary Care
Hospital
Dr. Rajkumar S Y1, Dr. Pavitra2, Dr. Dipu Bhuyan3, Dr. Gautam Goswami4
1Assistant professor, Department of Radiology, S.S.I.M.S & R.C., Davangere, Karnataka,
India; 2Postgraduate resident, Department of Pharmacology, JJM medical college,
Davangere, Karnataka, India; 3Associate professor, Department of Radiology, Gauhati
Medical College and Hospital, Guwahati-32, Assam, India; 4Professor and Head, Department
of Radiology, Gauhati Medical College and Hospital, Guwahati-32, Assam, India.
Corresponding Author
Dr. Rajkumar S. Y.
Email: [email protected]
Abstract
Central nervous infections presenting as
episode of seizure is frequently
encountered in clinical scenario.
Neurocysticerosis and Tuberculoma
constitutes majority of inflammatory
granuloma is a public-health problem,
especially in developing countries including
India. Systematic population-based studies
are lacking in most parts of the country;
hence it is difficult to estimate the disease
burden in India. It becomes difficult in some
cases where infective conditions with
similar clinical and radiological conditions
with low sensitivity and specificity in
serological and immunological screening.
With recent advances in computed
tomography (CT) and magnetic resonance
imaging (MRI) technology, our study was
aimed to study incidence, various stages of
neurocysticercosis, location, enhancement
pattern, to differentiate neurocysticercosis (
NCC) and tuberculomas based on imaging
findings and in difficult cases magnetic
resonance spectroscopy and clinical
response to medical therapy with interval
follow up helped us to come to conclusion.
This study helps in the early medical
intervention, decrease morbidity and
improves quality of life in the endemic and
high prevalence disease population in
developing countries especially in India.
Key Words
Central nervous infections (CNS),
Neurocysticerosis (NCC), Computed
tomography (CT), Magnetic resonance
Imaging (MRI), Magnetic resonance
spectroscopy (MRS), Fluid attenuated
VCFL Sciences Journal ISSN: 2231-9522 Vol. 3 Issue 4
233
inversion recovery sequence (FLAIR),
Diffusion weighted images (DWI).
Introduction
Epilepsy is a largely unrecognized but
increasing burden on the welfare and
economies of developing countries like
India. Poor hygiene, living conditions,
immune status, poor nutrition are some of
risk factors. Neurocysticerosis and
tuberculomas are the major cause of
inflammatory granuloma frequently
presenting as partial or generalized tonic
clonic seizures. Neurocysticercosis is caused
by the encysted larval stage, 'cysticercus
cellulosae' of the pork tapeworm Taenia
solium. The parenchymal cysts may remain
dormant for many years, and symptoms
(e.g. seizures) usually coincide with larval
death and subsequent intense
inflammatory reaction induced by larval
antigens. Subsequently, the cyst then
shrinks and granuloma eventually calcify or
more frequently disappear completely1.
Imaging and clinical features of
tuberculoma are exceedingly similar to that
of neurocysticercosis and it is difficult to
differentiate between these two conditions
1. This distinction is an important issue
because cysticercus granuloma is a benign,
self-limiting condition which is preventable
and potentially eradicable, whereas
tuberculoma is an active infection that
requires prolonged therapy with potentially
toxic drugs 2. Due to the scarcity of relevant
literature about the incidence, various
stages and differentiating features on CT
and MRI, wherein the case load is
enormous which inspired us to take up this
prospective study in northeastern part of
India.
Materials and Methods
This prospective study was carried out in
the department of Radiology, Gauhati
Medical College and Hospital, Guwahati
from July 2007 to November 2009.
Inclusion criteria:
Our study was carried out in 90 consecutive
patients presenting with seizure and
clinically high suspicion of CNS infection,
particularly common types of inflammatory
granulomas- neurocysticercosis and
tuberculoma from neurology referral and
out patients. Out of which 80 cases were
studied, 10 cases were excluded due to
exclusion criteria.
Exclusion Criteria:
Hypoxic ischemic encephalopathy, trauma,
congenital CNS abnormalities, metabolic
disorders, stroke, drug abuse and brain
tumors.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 3 Issue 4
234
Data Analysis: Were done using rate,
ratios and statistical percentage of different
diagnoses and outcome is computed.
CT evaluation was carried out using a
SIEMENS SPIRIT DUAL SLICE SPIRAL
SCANNER. Axial 4 mm slices, plain followed
by contrast with intravenous 50-60 ml of
non-ionic contrast media.
MRI evaluation was carried out using
SIEMENS TIM AVANTO 1.5T SCANNER.
Multiplanar T1W, T2W, Fluid attenuated
inversion recovery (FLAIR), Diffusion
weighted (DWI), Apparent diffusion
coefficient (ADC) and Post Gadolinium T1W,
SWI and Magnetic resonance spectroscopy
(MRS) in selected cases.
Results and Discussion:
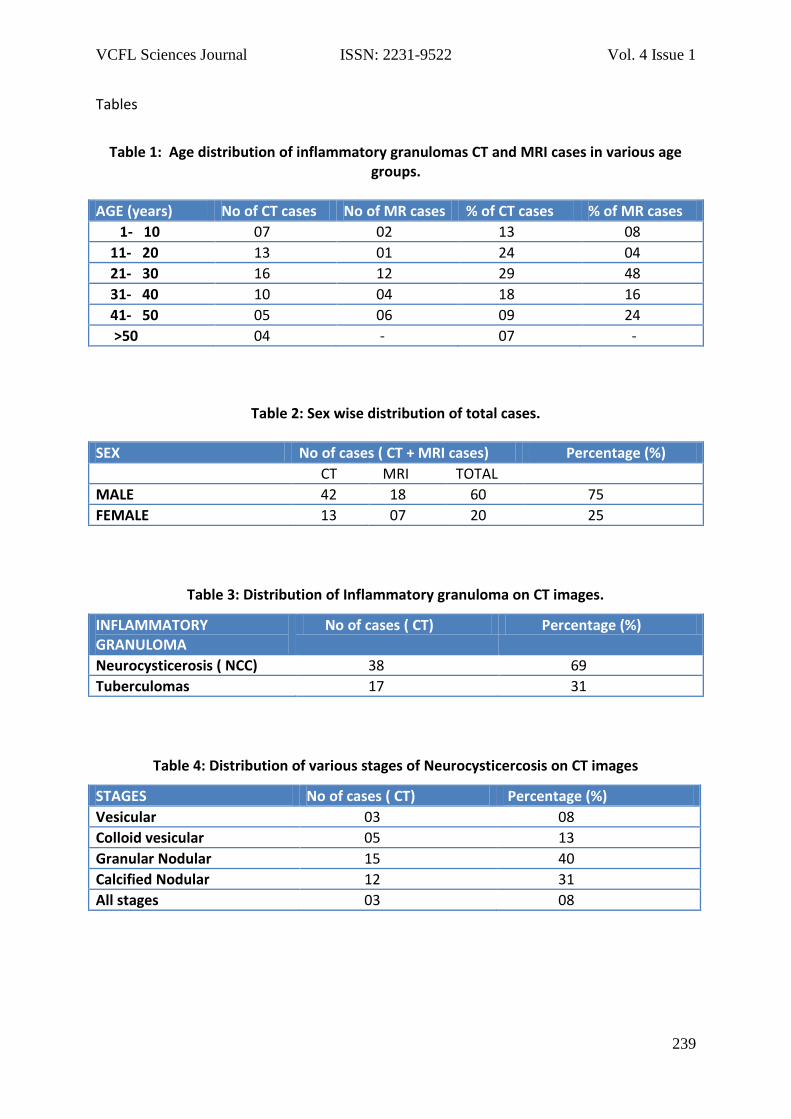
Out of 80 patients, 55 cases on CT and 25
cases on MRI was studied. 16 cases (29 %)
were 21-30 age group followed by 13 cases
(24%) in 11-20 age groups on CT. 12 cases
(48 %) were 21-30 age group and 6 (24 %) in
41-50 age groups on MRI. Single enhancing
CT lesions, seen in India, are common in
children and younger patients. Chopra et al
3 observed that 78 % of 122 patients of their
series were between 11 and 20 years of
age. Sethi et al 4 noted that approximately
46 % of 186 patients were below 15 years
of age and only one patient was over 60
years of age. Male were three times more
common than female (75: 25).
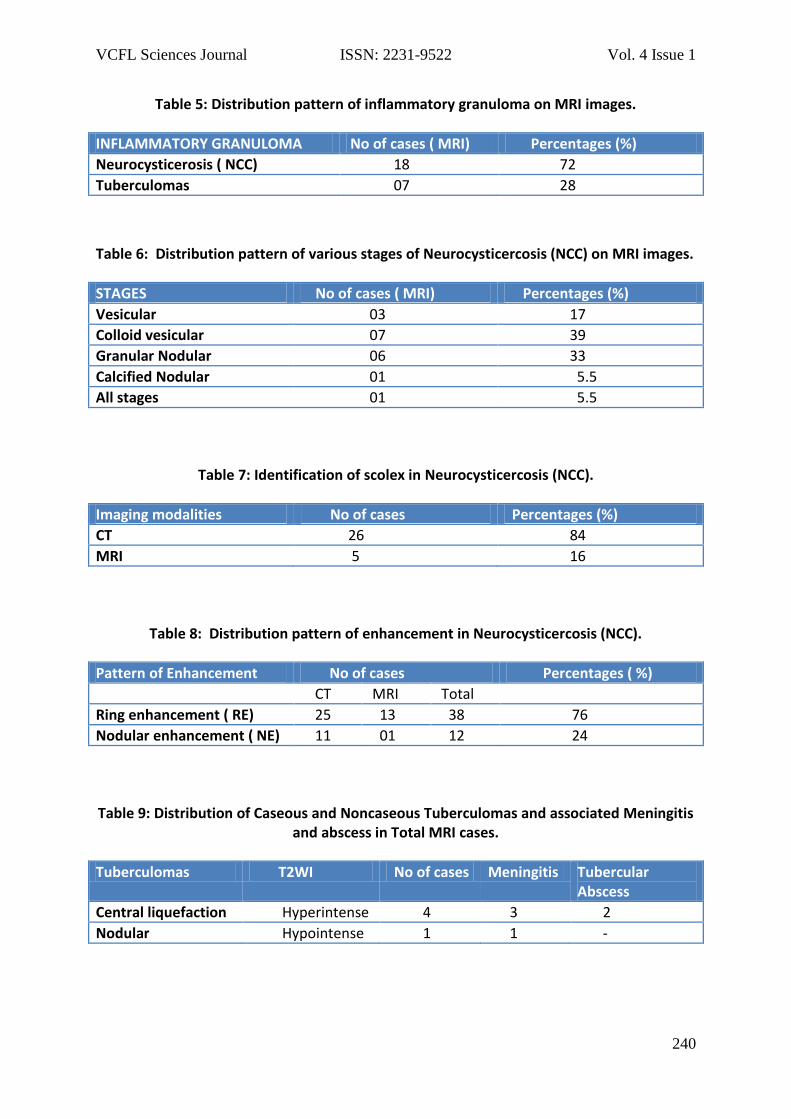
Neurocysticerosis (NCC) comprises of 69 %
on CT and 72 % on MRI and Tuberculomas
comprises of 31 % on CT and 28 % on MRI.
Our study showed 66 % and 60 % solitary
NCC on CT and MRI respectively of total
cases. Vedantam Rajashekhar et al5 stated
that solitary cerebral cysticercus granuloma
(SCCG) is one of the commonest causes of
seizures in Indian patients.
Rajshekhar et al, in a prospective study of
210 patients, observed that single
enhancing lesions completely resolved at
different time intervals. At 3 months 19%
had completely resolved; at 1 year
approximately 63% had disappeared.
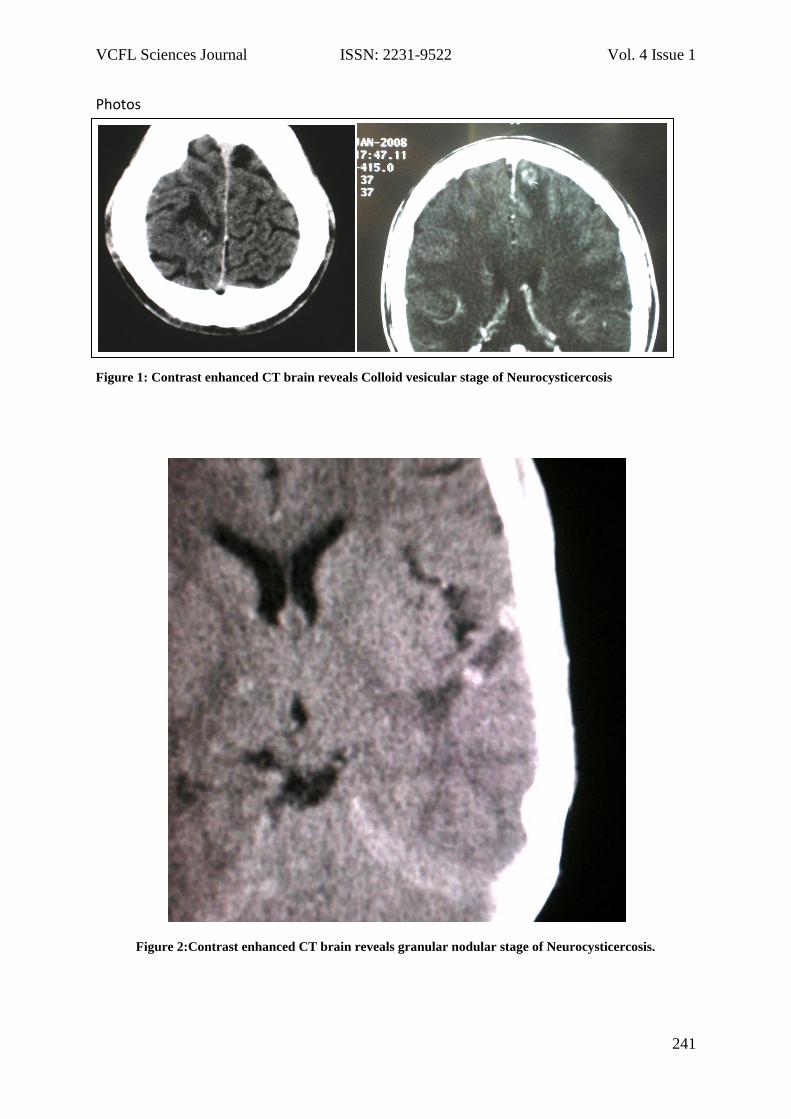
Our study showed 40 % granular nodular
stage, followed by 31 % calcified nodular
and 8 % disseminated neurocysticercosis on
CT images and 39 % colloidal vesicular, 33
% granular nodular and 6 % disseminated
stages of neurocysticercosis on MRI images.
The presence of cystic lesions
demonstrating the scolex can be considered
pathognomonic from a diagnostic
standpoint in a NCC. The scolex is visualized
as a bright nodule within the cyst,
producing the so-called "hole-with-dot"
imaging that is seen in some vesicular cysts
VCFL Sciences Journal ISSN: 2231-9522 Vol. 3 Issue 4
235
located in the brain parenchyma, the
subarachnoid space, or the ventricular
system 6. Our study showed 26 cases on CT
(84%) and 5 cases (16 %) on MRI. The scolex
was frequently observed in vesicular stage
of neurocysticercosis with high percentage
detected on CT. On MRI FLAIR and proton
density (PD) sequences were useful in
detecting the scolex.
According to D Kishore et al7 in a study of
100 patients with NCC, majority of the cases
had a ring like enhancement 88 out of 100
(88%) patients. Only 12% had disc- like
enhancement. An eccentric dot inside the
ring representing the cysticercus larva was
seen in only 19 out of 88 (21.6%) patients.
In our study 76 % cases had ring enhancing
lesion, 24 % had nodular enhancement and
39 % had scolex.
According to D Kishore et al7, the most
favored site was the parietal lobe (52%)
followed by fronto-parietal (19%), later
either at parieto-occipital region or
temporo-parietal region. These regions
form the watershed areas of cerebral
circulation and hematogenous spread of
infective agents are more likely to lodge in
these regions, because of the end arteries 7.
In this study, the maximum number of
lesions was seen in the parietal lobe (40%)
followed by the frontal lobe. Moreover
85% of the granulomas were at the grey
matter or the grey-white matter junction.
Diagnosis of NCC was greatly improved by
the introduction of CT and MR imaging.
These imaging techniques depict the
location and number of lesions and their
stages and the degree of inflammatory
response to the parasite (perilesional
edema and blood-brain barrier breakdown).
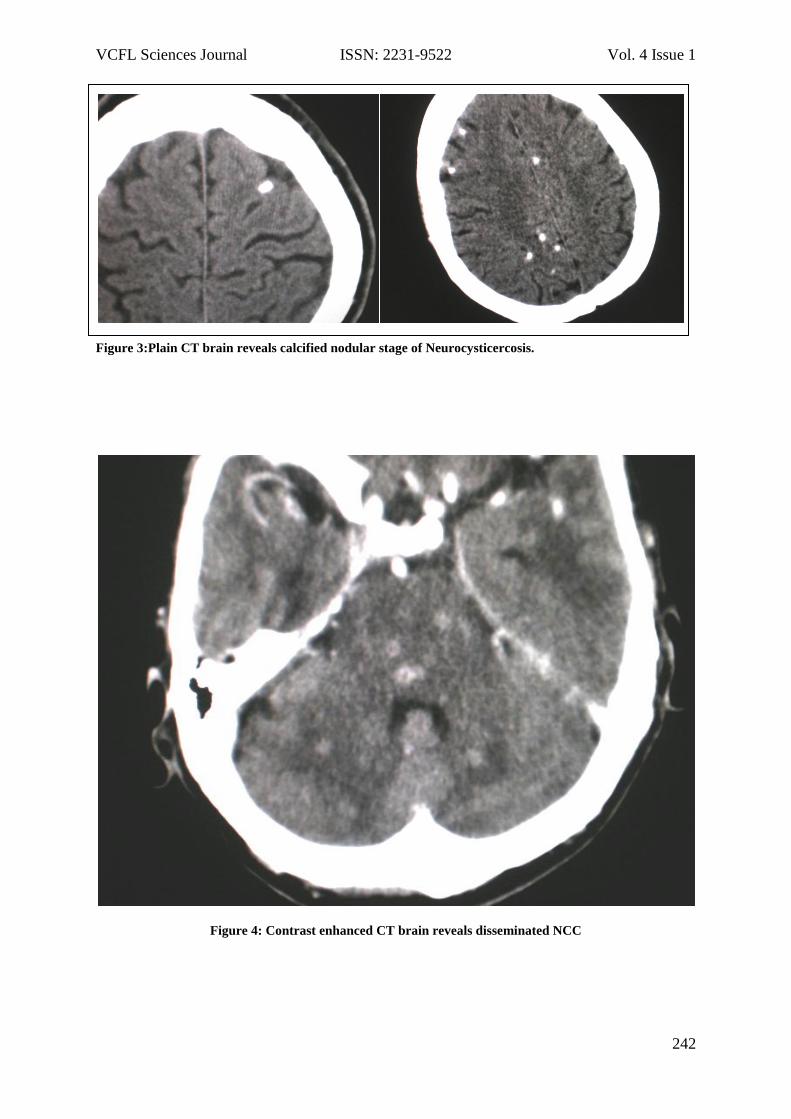
In a study by HR Martinez et al 8, inactive
forms were observed better with CT (23%
vs 14%). Our study showed, the inactive
form, i.e. calcified nodular stage was seen
better on CT than MRI (31 % vs 6 %).
MRI is considered the best neuro-imaging
tool for the detection of degenerating and
innocuous (viable) cysticerci, while CT is the
best for calcified lesions 11. The added
advantage of MRI is that it can differentiate
the stages of the parasite, which CT fails to
do. Moreover, MRI with gradient echo
sequence phase imaging has been reported
as good as CT for the detection of the scolex
in cystic lesions and also the calcified stage
of the parasite10. Although MRI allows
better detection of the active parasites but
some calcified parasites may be missed,
especially in absence of gradient echo
sequence.
The incidence of tuberculoma varies from
3.3% to 40.5% in different studies by Dastur

VCFL Sciences Journal ISSN: 2231-9522 Vol. 3 Issue 4
236
and Desai et al 9. Our study showed the
incidence of tuberculomas was 31% on CT
and 28 % on MRI. 57 % cases with liquefied
center and 14 % with nodular
enhancement. Few of the cases are
associated with meningitis and tubercular
abscess.
The distinction between cysticercal
granuloma & tuberculoma is controversial,
often associated with single enhancing CT-
documented lesions. This is because the
clinical and imaging features are quite
similar; both diseases are common in
endemic areas and may coexist in the same
patient. Rajshekhar et al, have attempted to
differentiate between the two entities on
the basis of clinical and imaging features.
Based on these findings and their
experience, Rajshekhar V, Prakash and
Chandy 5, suggested that cysticerci are
usually round in shape, 20mm or smaller in
size, with ring enhancement or a visible
scolex; cerebral edema severe enough to
produce midline shift or focal neurological
deficit is not seen. Tuberculomas by
contrast are usually irregularly shaped, solid
and greater than 20mm in size. They are
often associated with severe perifocal
edema and focal neurological deficit.
Various metabolites were studied using
magnetic resonance spectroscopy (MRS) in
neurocysticercosis and tuberculoma. On
MR spectroscopy, neurocysticercosis (NCC)
shows Lactate 1.33, Alanine 1.47, Acetate
1.92, Succinate 2.4 ppm(parts per million) 10
and tuberculoma shows high lipid lactate
peaks, doublet lactate peak at 0.9 and 1.3
ppm10.
Whenever, in a difficult case on
conventional magnetic resonance imaging,
we sort the help of MR spectroscopy
findings and follow up cases with good
clinical response after medical treatment of
albendazole or antitubercular therapy.
Conclusion
In this part of India, NCC and tuberculomas
are alarming high in communities with low
socioecomic status, lack of basic education,
decreased environmental awareness and
high HIV prevalence. Since cysticercosis is a
preventable and eradicable disease,
appropriate measures like health education,
mass awareness, better medical facilities,
mass treatment of T. solium carriers, and
restriction on sale of measly pork may help
to reduce the disease burden in the
endemic areas. Tuberculoma is an active
infection that requires prolonged therapy
with potentially toxic drugs in a high HIV
prevalence population. With recent
advances in CT and MRI technology, NCC
and tuberculoma are better localized,
characterized and differentiated.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 3 Issue 4
237
Background knowledge helps in the early
medical intervention, decrease morbidity
and improves quality of life in the endemic
and high prevalence disease population in
developing countries especially in India.
Acknowledgement
To my parents for constant support and
care.
To technical staff and patients.
Fund Support: None
Conflict of Interest: None
VCFL Sciences Journal ISSN: 2231-9522 Vol. 3 Issue 4
238
REFERENCES:
1. Shah GV. Central nervous system
tuberculosis. Neuroimaging Clin North
Am 2000; 10:355-74.
2. Garg RK. Diagnostic criteria for
neurocysticercosis: Some modifications
are needed for Indian patients. Neurol
India 2004; 52:171-7.
3. Chopra JS, Sawhney IMS, Suresh N, et al.
Vanishing CT lesions in epilepsy. J
Neurol Sci 1992; 107:40-9.
4. Sethi PP, Wadia RS, Kiyawat DP et al.
Ring or disc enhancing lesions in
epilepsy in India. J Trop Med Hyg 1994;
97:347-53.
5. Rajshekhar V, Haran RP, Prakash GS et
al. Differentiating solitary small
cysticercus granuloma and tuberculoma
in patients with epilepsy. Clinical and
computerized tomographic criteria. J
Neurosurg 1993; 78:402-7.
6. RA Suss, KR Maravilla and J Thompson
MR imaging of intracranial cysticercosis:
comparison with CT and
anatomopathologic features. , American
Journal of Neuroradiology, Vol 7, Issue 2
235-242.
7. Short course of Oral Prednisolone on
disappearance of lesion and seizure
recurrence in patients of Solitary
Cysticercal Granuloma with Single small
enhancing CT lesion: An Open Label
Randomized Prospective Study, D
Kishore, S Misra; JAPI • VOL. 55 • JUNE
2007.
8. HR Martinez, R Rangel-Guerra, G
Elizondo, J Gonzalez, LE Todd, J Ancer
and SS Prakash MR imaging in
neurocysticercosis: a study of 56 cases.
(American Journal of Neuroradiology,
Vol 10, Issue 5 1011-1019).
9. Dastur H.M., and Desai A.D:1965; Brain,
88: 375-396.
10. Rakesh K. Gupta and Robert B. Lufkin et.
al, MR Imaging and Spectroscopy of
Central Nervous System Infection, book:
Kluwer Academic Publishers, 2001.
11. García HH, Del Brutto OH, Imaging
findings in neurocysticercosis. Acta
Trop. 2003 Jun; 87(1):71-8.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
239
Tables
Table 1: Age distribution of inflammatory granulomas CT and MRI cases in various age groups.
AGE (years) No of CT cases No of MR cases % of CT cases % of MR cases
1- 10 07 02 13 08
11- 20 13 01 24 04
21- 30 16 12 29 48
31- 40 10 04 18 16
41- 50 05 06 09 24
>50 04 - 07 -
Table 2: Sex wise distribution of total cases.
SEX No of cases ( CT + MRI cases) Percentage (%)
CT MRI TOTAL
MALE 42 18 60 75
FEMALE 13 07 20 25
Table 3: Distribution of Inflammatory granuloma on CT images.
INFLAMMATORY GRANULOMA
No of cases ( CT) Percentage (%)
Neurocysticerosis ( NCC) 38 69
Tuberculomas 17 31
Table 4: Distribution of various stages of Neurocysticercosis on CT images
STAGES No of cases ( CT) Percentage (%)
Vesicular 03 08
Colloid vesicular 05 13
Granular Nodular 15 40
Calcified Nodular 12 31
All stages 03 08
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
240
Table 5: Distribution pattern of inflammatory granuloma on MRI images.
INFLAMMATORY GRANULOMA No of cases ( MRI) Percentages (%)
Neurocysticerosis ( NCC) 18 72
Tuberculomas 07 28
Table 6: Distribution pattern of various stages of Neurocysticercosis (NCC) on MRI images.
STAGES No of cases ( MRI) Percentages (%)
Vesicular 03 17
Colloid vesicular 07 39
Granular Nodular 06 33
Calcified Nodular 01 5.5
All stages 01 5.5
Table 7: Identification of scolex in Neurocysticercosis (NCC).
Imaging modalities No of cases Percentages (%)
CT 26 84
MRI 5 16
Table 8: Distribution pattern of enhancement in Neurocysticercosis (NCC).
Pattern of Enhancement No of cases Percentages ( %)
CT MRI Total
Ring enhancement ( RE) 25 13 38 76
Nodular enhancement ( NE) 11 01 12 24
Table 9: Distribution of Caseous and Noncaseous Tuberculomas and associated Meningitis and abscess in Total MRI cases.
Tuberculomas T2WI No of cases Meningitis Tubercular Abscess
Central liquefaction Hyperintense 4 3 2
Nodular Hypointense 1 1 -
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
241
Photos
Figure 1: Contrast enhanced CT brain reveals Colloid vesicular stage of Neurocysticercosis
Figure 2:Contrast enhanced CT brain reveals granular nodular stage of Neurocysticercosis.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
242
Figure 3:Plain CT brain reveals calcified nodular stage of Neurocysticercosis.
Figure 4: Contrast enhanced CT brain reveals disseminated NCC
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
243
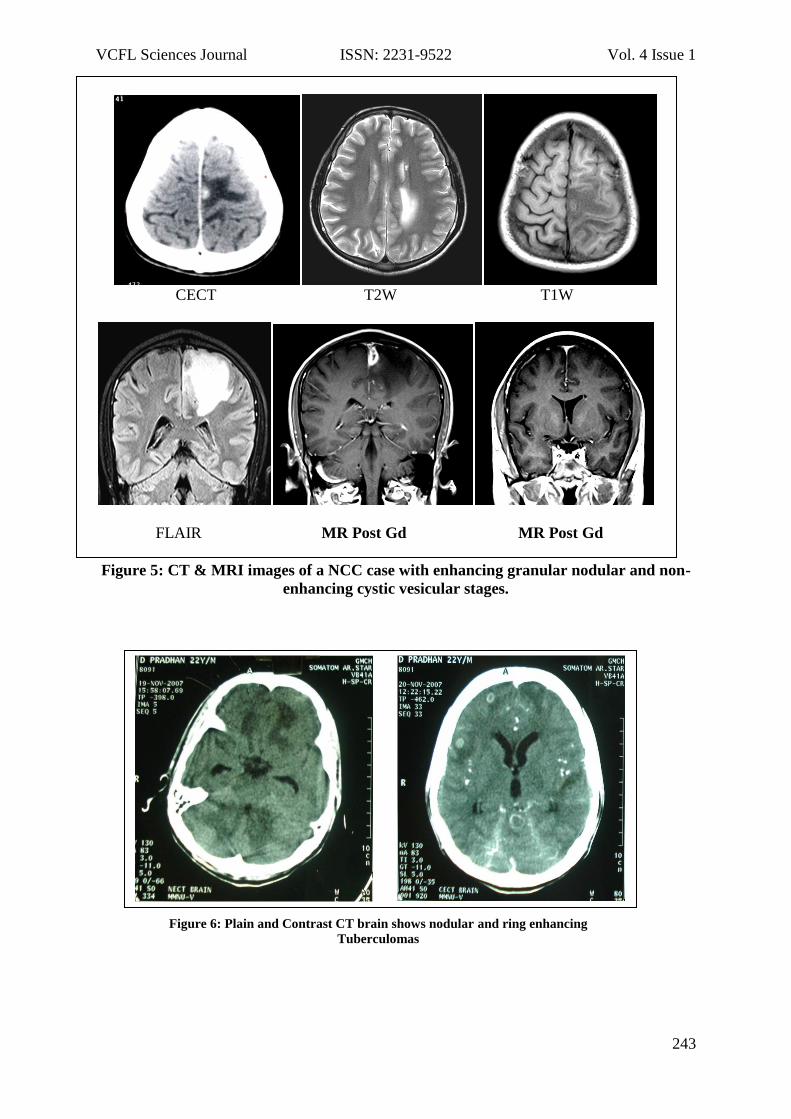
CECT T2W T1W
FLAIR MR Post Gd MR Post Gd
Figure 5: CT & MRI images of a NCC case with enhancing granular nodular and non-
enhancing cystic vesicular stages.
Figure 6: Plain and Contrast CT brain shows nodular and ring enhancing
Tuberculomas
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
244
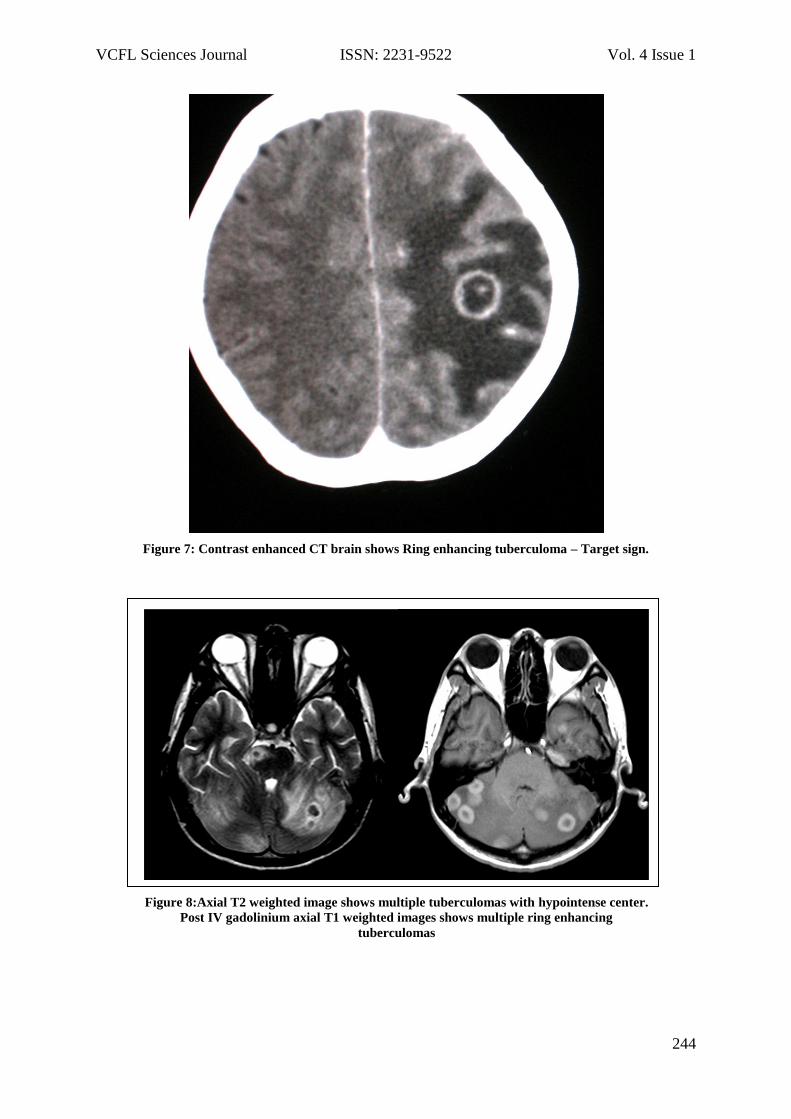
Figure 7: Contrast enhanced CT brain shows Ring enhancing tuberculoma – Target sign.
Figure 8:Axial T2 weighted image shows multiple tuberculomas with hypointense center.
Post IV gadolinium axial T1 weighted images shows multiple ring enhancing
tuberculomas
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
245
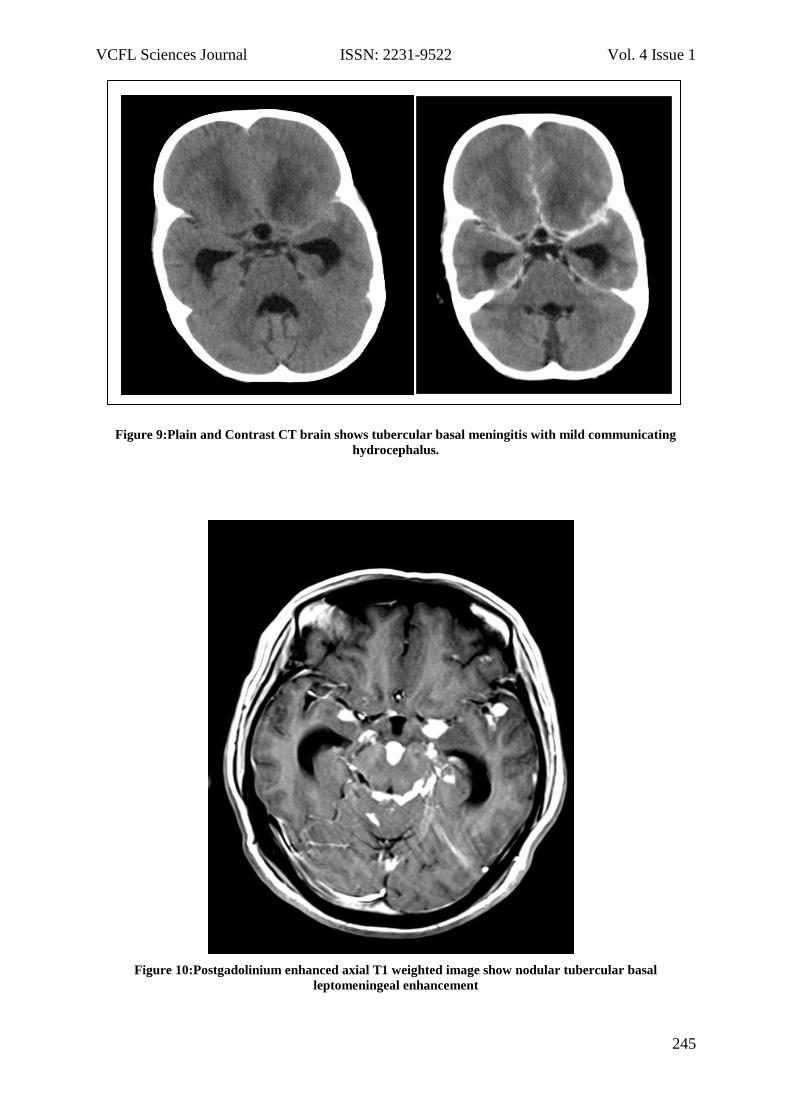
Figure 9:Plain and Contrast CT brain shows tubercular basal meningitis with mild communicating
hydrocephalus.
Figure 10:Postgadolinium enhanced axial T1 weighted image show nodular tubercular basal
leptomeningeal enhancement
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
246
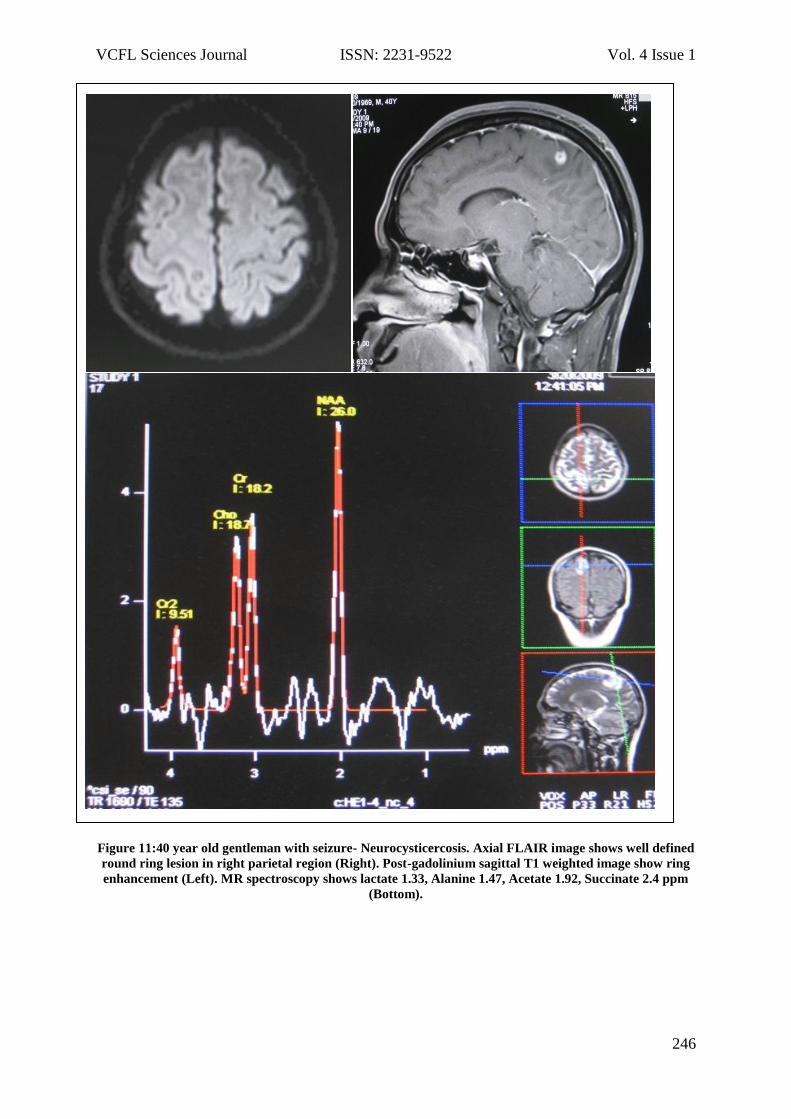
Figure 11:40 year old gentleman with seizure- Neurocysticercosis. Axial FLAIR image shows well defined
round ring lesion in right parietal region (Right). Post-gadolinium sagittal T1 weighted image show ring
enhancement (Left). MR spectroscopy shows lactate 1.33, Alanine 1.47, Acetate 1.92, Succinate 2.4 ppm
(Bottom).
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
247
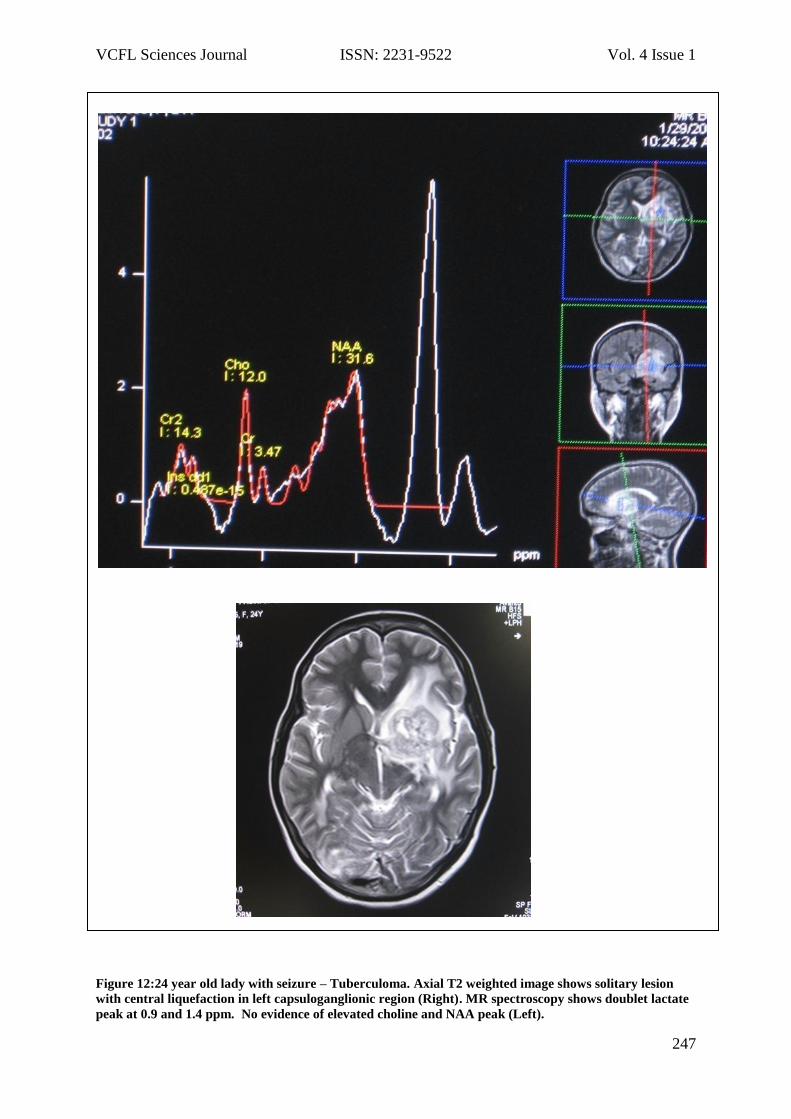
Figure 12:24 year old lady with seizure – Tuberculoma. Axial T2 weighted image shows solitary lesion
with central liquefaction in left capsuloganglionic region (Right). MR spectroscopy shows doublet lactate
peak at 0.9 and 1.4 ppm. No evidence of elevated choline and NAA peak (Left).
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
248
Bomb blast injuries – New face of terror: radiologists' perspectives
based on the experience in India Rajkumar S Yalawar1, Pavitra2, Ramesh Desai3, Dipu Bhuyan4
1Department of Radiology, S.S.I.M.S & R.C., Davangere, Karnataka, India.
2Department of Pharmacology, JJM medical college, Davangere, Karnataka, India.
3Department of Radiology, Gauhati Medical College and Hospital, Guwahati-32, Assam,
India.
Corresponding Author
Dr. Rajkumar S Yalawar
Email: [email protected].
Abstract
Objectives: To understand the nature and
patterns of bomb blast injuries, to
familiarize with the imaging the radiologist
might expect to see in a mass casualty
terrorist, the role of radiology in the
management and planning for a mass
casualty terrorist incident.
Materials and Methods: A prospective
study of 126 bomb blast victims, 100
patients were included due to imaging and
26 patients were excluded due to critical
conditions and brought dead. Study
conducted in the department of Radiology,
Gauhati Medical College and Hospital at
Guwahati from July 2007 to January 2010.
Results: Males were more common to
female (70 / 30), 53% in young productive
15-29 years, followed by 21 % in 30-44
years. Multiple complex injuries of head
and neck, chest and abdomen, skeletal and
vascular injuries are noted. 23 % patients
shifted to ICU care for ventilation and
priority nursing care, 62 % victims
underwent surgical procedures and 19 were
reported dead.
Conclusion: Imaging should be fast, in order
to help identify major injuries that need
immediate management and to help in the
triage of injured individuals. With the
limited hospital resources, tailored
protocol for patient evaluation, triage,
training to doctors and supporting staff,
better management and optimal outcome
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
249
in victims during terrorist attack in any
region of the world.
Keywords
Mass Casualty Incidents (MCI), Intensive
care unit (ICU), Focused assessment with
sonography for trauma (FAST), Extended
FAST (eFAST), Computed tomography (CT)
Introduction
After the horrific mass-casualty terror
attack on the United States on September
11, 2001, Israel bomb blast injuries of 2000-
2003 and London Underground tube blasts
of 7 July 2005, the world has changed.
Bomb blast injuries was a part of
emergency department in the hospital
when I was training my residency in the
northeastern part of India. I share my
experience, owing to the complexity of
injuries and mass casualty incidents
encountered in terror attack victims. New
challenges, skills, clinically inapparent cases
where fast and accurate imaging plays an
essential role in triage and identification of
abnormalities associated with injuries. The
radiologist becomes a crucial part of the
first-line team of doctors treating these
patients. A need to understand the nature
and patterns of bomb blast injury,
particularly in confined spaces. We highlight
the value of using a standardized imaging
protocol to find clinically undetected
multisystem and complex injuries
encountered in the bomb blast victims.
Knowledge and skills in managing the
victims by using optimal imaging facilities
can enhance the strength and endurance of
society against terror.
Materials and Methods
This prospective study was carried out in
the department of Radiology, Gauhati
Medical College and Hospital at Guwahati
from July 2007 to January 2010.
Inclusion criteria: Total of 126 patients of
bomb blast victims referred to our hospital
for tertiary care and management, 100
patients were sent for imaging. 26 patients
were excluded due to critical conditions and
brought dead.
Exclusion Criteria: Critical and unstable
patients, brought dead, severe burns.
Data Analysis: Were done using rate,
statistical percentage and outcome is
computed.
Imaging Protocols:
1. Fluoroscopy: To screen out any metallic
objects.
2. Spine, chest, abdomen and extremity
radiographs: To screen out metallic
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
250
objects, fractures, pneumothorax,
pneumomediastinum,
pneumoperitoneum – life threatening
conditions.
3. Ultrasonography of abdomen: FAST to
exclude solid organ injuries and
hemoperitoneum.
4. CT evaluation using SIEMENS spirit dual
slice spiral scanner and 16 slice Toshiba
CT scanner. Plain CT scan for brain or
whole body single venous phase CT scan
including head, neck, chest and
abdomen using 100-150 ml of non-ionic
contrast media.
Results
Out of 126 bomb blast victims, 100 were
included due to imaging workup. Males
were more common to female (70 / 30),
53% in young productive 15-29 years,
followed by 21 % in 30-44 years. Multiple
complex body injuries: Traumatic brain
injuries (79%) - Countercoup injury,
Subdural hematoma, extradural hematoma,
Faciomaxillary complex fractures, nasal and
temporal bone fractures, Spine and cord
injuries (19%)- Multilevel compression and
burst fractures, shrapnel’s in bony canal,
Chest injuries (39%) – Multilevel rib
fractures, tension pneumothorax,
pneumomediastinum, lung contusions,
surgical emphysema , vascular injury,
Abdominal and pelvic injuries ( 43%)- liver,
splenic and pancreatic lacerations, blunt
and penetrating injury to kidneys, hemo-
pneumoperitoneum, mesenteric /bowel
injuries, extremities (62%) – comminuted
fractures and open wounds. Depending
upon severity, internal and external body
injuries patients were triaged and
categorized to mild, moderate and severe.
Urgent attention and care to severe
category shifting to ICU care, surgical
theatre, minor procedures, hospitalization.
23 % patients shifted to ICU care for
ventilation and priority nursing care. Most
of the patients 60% were discharged within
7 days, 19% within 2 week and 21 % longer
duration. 62 % victims underwent surgical
procedures esp. liver and splenic
lacerations, bowel / mesenteric injury,
pelvic and femoral bone fractures, aortic
injury in 2 cases and minor procedures in
causality like suturing, repair. 23 cases had
severe burns were isolated and treated, 1
patient after a week died. Out of
hospitalized victims, 19 deaths was
reported, 72 % died within a week, 11%
within 2 week.
Discussion
Terror-related injuries have become a
threat for populations all over the world [1].
As long as gunpowder and explosives are
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
251
used to solve disagreements between
nations, ethnic groups and individuals,
victims of blast injury continue to arrive at
trauma centers around the world [5]. Bomb
blast injuries are often more complex but
easiest and least costly methods of
achieving the terrorist goals of large-scale
casualties. This explains why
multidisciplinary team including Radiologist,
Surgeons, Paediatrians, Orthopedics
surgeons and supporting staffs must be
integrally involved in the field of disaster
management, local hospitals and tertiary
care centers. We must develop the
necessary expertise that we now tend to
lack in the biology of explosive injury, its
known patterns of severity and the unique
principles of mass casualty management
that are so different from our routine
approaches to trauma [3].
Only lifesaving procedures should be
performed during the initial phase. Later,
medical care is directed at patients moved
to ICUs. Prompt evacuation after necessary
lifesaving procedures in the field, proper
triage and distribution, prudent hospital
triage and surgical care and last but not
least, expert critical care provide the best
possible outcome in such circumstances.
The mortality among critically injured
survivors of terrorist bombing disasters is
directly related to the magnitude of
overtriage [4]. Therefore rapid and accurate
triage is essential to minimize mortality
among survivors.
During a detonation, the explosive
substance transforms from a solid state to a
gaseous one, creating the blast wave. When
the explosion occurs in a closed space, the
blast damage is amplified owing to
reflection of the blast wave ranging from
wind velocity of 125 mph (201 km/h) to the
velocity of a hurricane, because of the low
density of air, high-velocity winds can be
produced even by small changes in
pressure. The objects that can be found at
a local hardware store such as nails, screws,
bolts, and ball bearings; the included
metallic objects may add up to 10 kg to a
single bomb[1]. The large number of
metallic objects, along with the complex
internal injuries they may inflict requires a
multimodality imaging approach. Places
like crowded markets, shops, bus stops and
railway station are targeted. These places
are difficult to access for hospitals, first-aids
and fire stations.
The clinical presentation depends on
whether the blast occurs in open or
confined quarters, open air or water, the
pattern of injury inflicted on the body is
relatively consistent [5]. Injury from
explosion may be due to the direct cussive
effect of the blast wave (primary), being
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
252
struck by material propelled by the blast
(secondary), to whole-body displacement
and impact (tertiary) or to miscellaneous
effects from burns, toxic acids and so on6.
Three systems are prone to injury. The first
is the auditory system, with damage to the
eardrum in milder cases and inner-ear
injury in more severe cases. Second is
alimentary tract with contusions,
hematoma and less frequently perforation
of a hollow viscus. Solid organs injuries are
noticed in survivors of blast injury but the
hallmark of blast injury is the involvement
of the respiratory system. Pulmonary injury
is characterized by pneumothorax,
parenchymal hemorrhage, and alveolar
rupture where later is responsible for the
arterial air embolism that is the principle
cause of early mortality [6]. Close proximity
to the blast can impose traumatic
amputation of limbs (i.e., arms and legs)
and ear lobes [5]. The most common fatal
injury is brain damage [7].
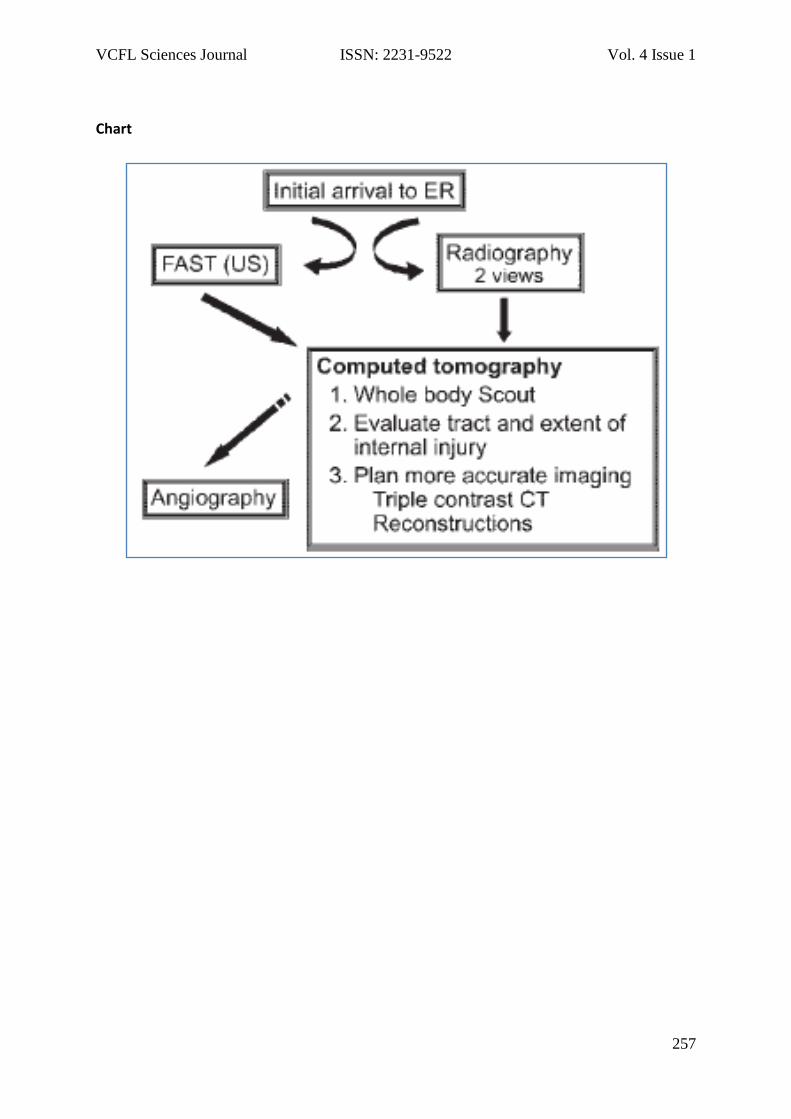
The heart of every hospital is the
emergency department - core of decision
makers whose choices determine how the
emergency response will evolve. The
radiologist becomes a crucial part of the
first-line team of doctors in mass casualty
incidents and in disaster management. The
workflow pattern is described in the given
chart [⁴].
Radiologic examinations including plain
radiography, fluoroscopy, Computed
tomography (CT), sonography, and
angiography are used to assess the site,
extent of injuries and can help determine
which patients will be triaged to immediate
surgery and which will be followed up
conservatively. Large numbers of casualties
whose complicated injuries are due to blast
and shrapnel’s require the most
sophisticated imaging but are often
admitted with no or minimal early warning
to the radiology department during a brief
period.
As in any trauma / blast victims, chest,
cervical spine, and pelvic radiographs are
routinely obtained as part of the initial
work-up. The role of conventional
radiography in localizing foreign objects is
limited when shrapnel’s are multiple,
scattered in body parts and therefore
helping detect which parts of the body need
further imaging usually with Computed
tomography (CT). The radiographs are
requested to exclude any metallic density
shrapnel’s, fractures, live threatening
pneumothorax, pneumomediastinum,
pneumoperitoneum, hollow viscus injuries.
Chest radiological findings from pulmonary
contusions, chest wall injury including bony
fractures and soft tissue injury to
pneumothorax, hemothorax,
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
253
hemopericardium and vascular injury.
Abdominal radiographs to look for free air
under diaphragm. However with best
possible, internal injuries cannot be
excluded from radiographs. It warrants
computed tomography for detailed and
precise information and guides further
surgical management.
The primary function of the radiologist is to
perform focused abdominal sonography in
trauma or FAST, in order to evaluate for
free peritoneal fluid and to exclude
hemodynamically significant abdominal
injuries. This quick study takes 1–2 minutes
per patient. To provide rapid reports that
could be used instantly, we have developed
colored stickers that are attached the
patient’s chart: red when positive for free
peritoneal fluid, green when negative, and
yellow when indeterminate, which will alert
the staff as to whether the patient needs
prompt further evaluation1.
The extended FAST (eFAST) [10] allows for
the examination of both lungs by adding
bilateral anterior thoracic sonography to
the FAST exam. This allows for the
detection of a pneumothorax with the
absence of normal ‘lung-sliding’ and
‘comet-tail’ artifact. Compared with supine
chest radiography with CT or clinical course
as the gold standard, bedside sonography
has superior sensitivity (49–99 versus 27–
75%), similar specificity (95–100%) and can
be performed in under a minute [10].
Immediate bedside detection of a
pneumothorax confirms, often ambiguous
physical findings in unstable patients and
guides immediate chest decompression. In
addition, in the patient undergoing positive-
pressure ventilation, the detection of an
otherwise ‘occult’ pneumothorax prior to
CT scanning may hasten treatment and
subsequently prevent development of a
tension pneumothorax, a deadly
complication if not treated immediately and
deterioration in the radiology suite (in the
CT scanner) [11].
FAST is most useful in trauma patients who
are hemodynamically unstable. A positive
result suggests hemoperitoneum; often CT
scan will be performed if the patient is
stable [12] or a laparotomy if unstable. In
those with a negative FAST result, a search
for extra-abdominal sources of bleeding
may still need to be performed [12]
Computed tomography (CT) is a superior
modality for demonstrating the course a
penetrating object has traveled and the
resulting injuries. Radiologist should be
stationed at every CT console to aid in
planning the best protocol and to give real-
time interpretations of the scans. On arrival
at the CT suite, a whole body scout image
should be obtained initially. This may depict
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
254
additional unsuspected sites of shrapnel
that were not detected on the emergency
department. Shrapnel in the pelvis may
warrant rectal administration of contrast
material prior to CT to aid in evaluating
injuries to the colon. Then dedicated region
of interest was planned with single venous
contrast and later multiplanar and
reformatted images was performed.
Angiography is a minimally invasive
examination that should be reserved for
patients in whom there is a clinical
suspicion of vascular injury. Angiography
has the added benefit of allowing for
therapy in certain cases, such as the
treatment of active bleeding by means of
embolization.
Males were more common to female (70 /
30), 53% in young productive 15-29 years,
followed by 21 % in 30-44 years. Multiple
complex body injuries- brain, chest and
abdominal, skeletal and vascular injuries.
Depending upon severity, internal and
external body injuries patients were triaged
and categorized to mild, moderate and
severe. Urgent attention and care to severe
category shifting to ICU care, surgical
theatre, minor procedures and
hospitalization. In damage control for
abdominal trauma, bail-out laparotomy for
achieving hemostasis and preventing
uncontrolled spillage of intestinal contents
or urine [8]. 23 % patients shifted to ICU
care for ventilation and priority nursing
care. 62 % victims underwent surgical
procedures esp. liver and splenic
lacerations, bowel / mesenteric injury,
pelvic and femoral bone fractures, aortic
injury in 2 cases and minor procedures in
causality like suturing, repair and wound
debridement. 23 cases had burns were
isolated and treated, 1 patient after a week
died. Out of hospitalized victims, 19 deaths
was reported, 72 % died within a week, 11%
within 2 week. Deaths were due to third
space volume loss, septicemia and in some
victims without obvious external injuries,
cardiac dysrhythmia or air emboli caused
cardiac arrest and eventual death [9].
Conclusion
Take home message, there are four
components of knowledge are required as
critical to master by medical teams
intending to treat victims admitted
following explosions. a) detonation- the
physics of the explosion, b) wound ballistics
- understanding the resultant injury
patterns, c) triage - the art of sorting
patients according to the severity of injury
and d) medical concerns - treating multiple
patients with multidimensional injuries and
special injury patterns [9].
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
255
In Mass Casualty Incidents (MCI), imaging
should be fast, in order to help identify
major injuries that need immediate
management and to help in the triage of
injured individuals.
The observations in this article have
implications for treatment, preparedness of
hospital resources, tailored protocol for
patient evaluation and training to treat
patients after a terrorist attack in any
region of the world. Disaster management
plans should include the possibility of
terrorist bombing, and medical
preparedness should anticipate that a large
proportion of the injuries will be nonfatal.
Fund Support: None
Conflict of Interest: None
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
256
References
1. Kobi Peleg, Limor Aharonson-Daniel,
Michael Stein. Gunshot and Explosion
Injuries: Characteristics, Outcomes and
Implications for Care of Terror-Related
Injuries in Israel. Ann Surg. 2004 March;
239(3): 311–18.
2. Jacob Sosna, Tamar Sella, Dorith
Shaham. The role of radiology in terror
attacks. Radiology 2005; 237:28–36.
3. Eric R. Frykberg. Principles of Mass
Casualty Management Following
Terrorist Disasters. Ann Surg. 2004
March; 239(3): 319–21.
4. Frykberg ER. Medical management of
disasters and mass casualties from
terrorist bombings. How can we cope? J
Trauma. 2002; 53:201–12.
5. Stein M, Hirshberg A. Medical
consequences of terrorism: the
conventional weapon threat. Surg Clin
North Am. 1999; 79:1537–52.
6. Philips YY. Primary blast injuries. Ann
Emerg Med. 1986; 15:1446–50.
7. Cooper GJ, Maynard RL, Cross NL.
Casualties from terrorist bombings. J
Trauma. 1983; 23:955–67.
8. Hirshberg A, Walden R. Damage control
for abdominal trauma. Surg Clin North
Am. 1997; 77:813–20
9. Kluger Y. Bomb explosions in acts of
terrorism-detonation, wound ballistics,
triage and medical concerns. Isr Med
Assoc J. 2003; 5:235–40.
10. Kirkpatrick AW, Sirois M, Laupland KB. J
Trauma, 2004; 57(2):288–95.
11. Davis JA. Critical Diagnosis in Bedside
Ultrasonography. Diagnostics & Imaging
2007.
12. Scalea T, Rodriguez A, Chiu W,
Brenneman F (1999). "Focused
Assessment with Sonography for
Trauma (FAST): results from an
international consensus conference".
Journal of Trauma 46 (3): 466–72.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
257
Chart
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
258
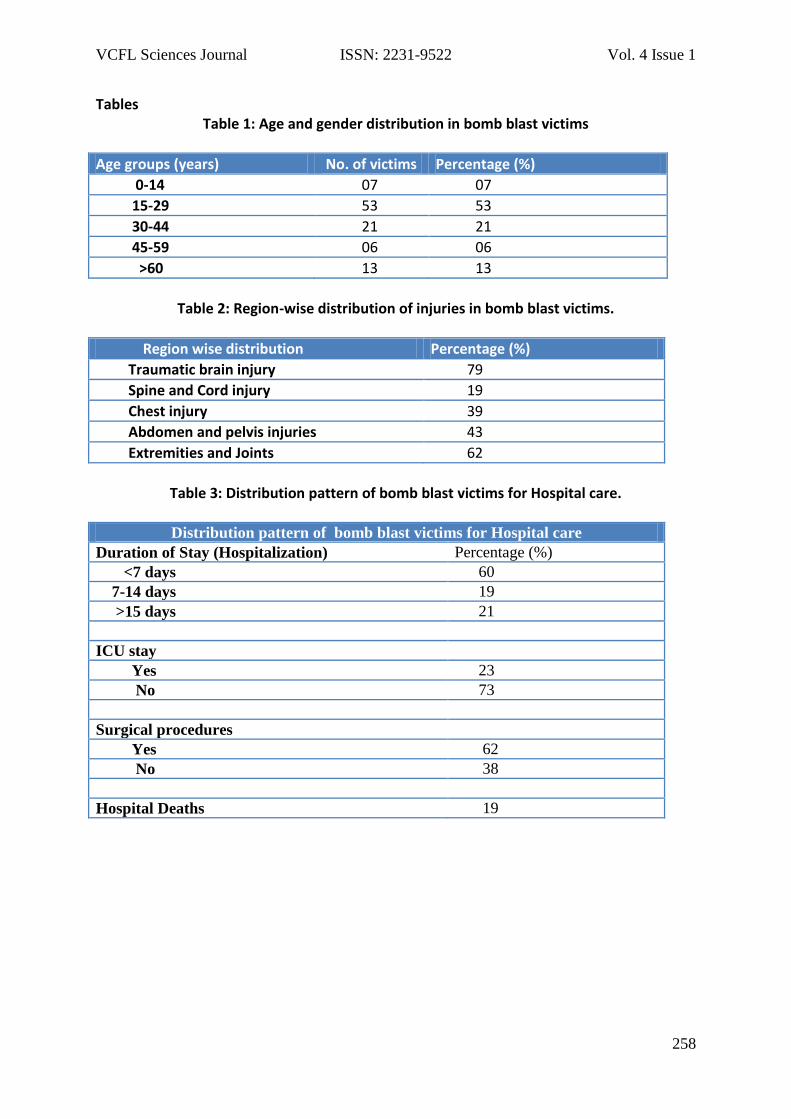
Tables Table 1: Age and gender distribution in bomb blast victims
Age groups (years) No. of victims Percentage (%)
0-14 07 07
15-29 53 53
30-44 21 21
45-59 06 06
>60 13 13
Table 2: Region-wise distribution of injuries in bomb blast victims.
Region wise distribution Percentage (%)
Traumatic brain injury 79
Spine and Cord injury 19
Chest injury 39
Abdomen and pelvis injuries 43
Extremities and Joints 62
Table 3: Distribution pattern of bomb blast victims for Hospital care.
Distribution pattern of bomb blast victims for Hospital care
Duration of Stay (Hospitalization) Percentage (%)
<7 days 60
7-14 days 19
>15 days 21
ICU stay
Yes 23
No 73
Surgical procedures
Yes 62
No 38
Hospital Deaths 19
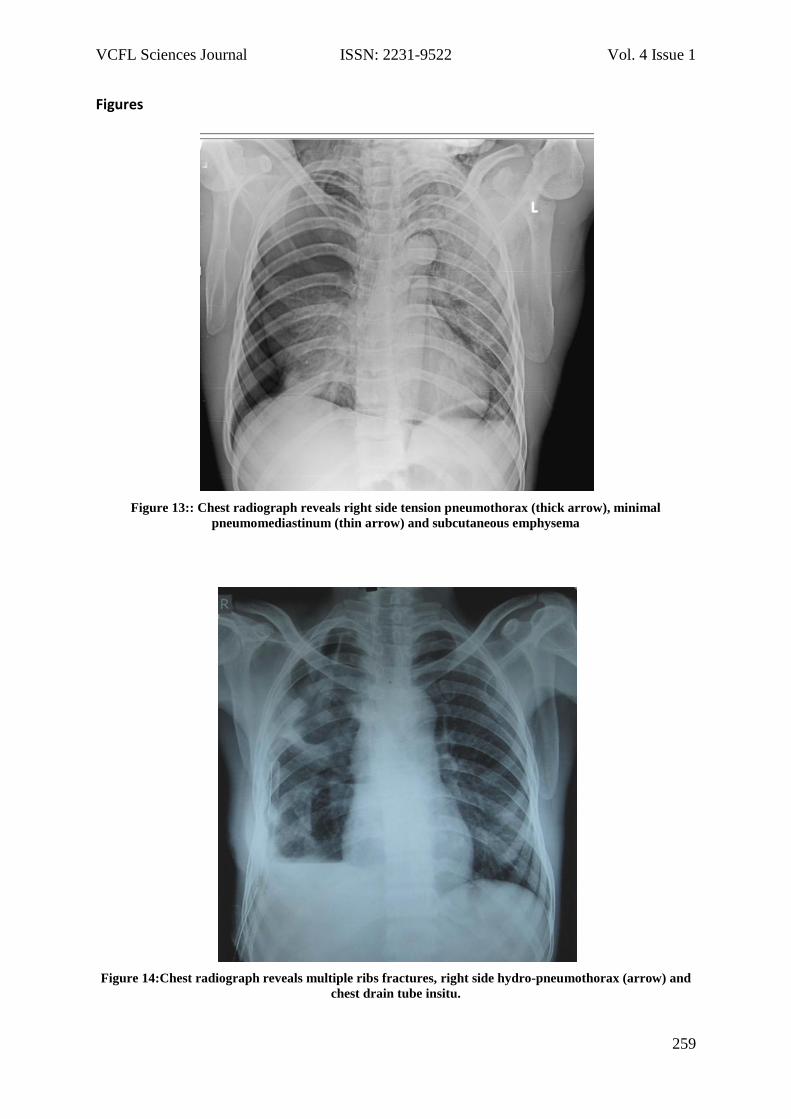
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
259
Figures
Figure 13:: Chest radiograph reveals right side tension pneumothorax (thick arrow), minimal
pneumomediastinum (thin arrow) and subcutaneous emphysema
Figure 14:Chest radiograph reveals multiple ribs fractures, right side hydro-pneumothorax (arrow) and
chest drain tube insitu.
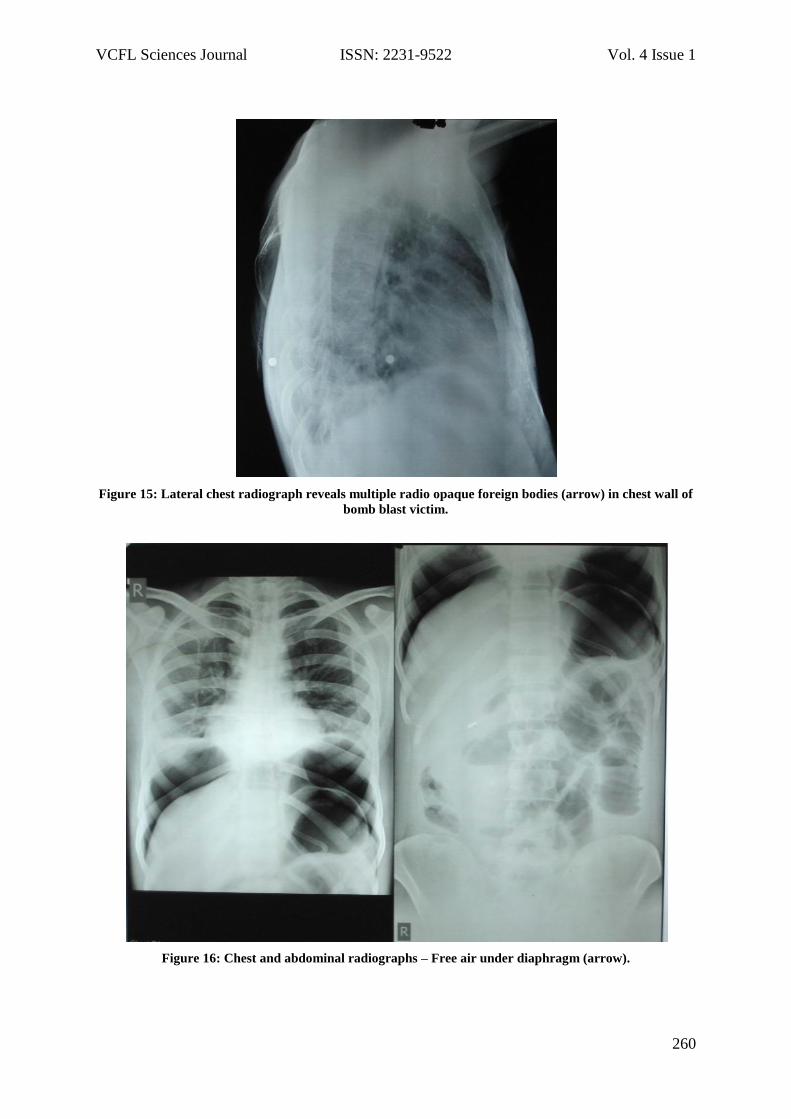
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
260
Figure 15: Lateral chest radiograph reveals multiple radio opaque foreign bodies (arrow) in chest wall of
bomb blast victim.
Figure 16: Chest and abdominal radiographs – Free air under diaphragm (arrow).

VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
261
Figure 17: Pelvic radiograph reveals comminuted intertrochanteric fracture of right femur
Figure 18: Radiograph of right leg reveals comminuted fractures of tibia and fibula.
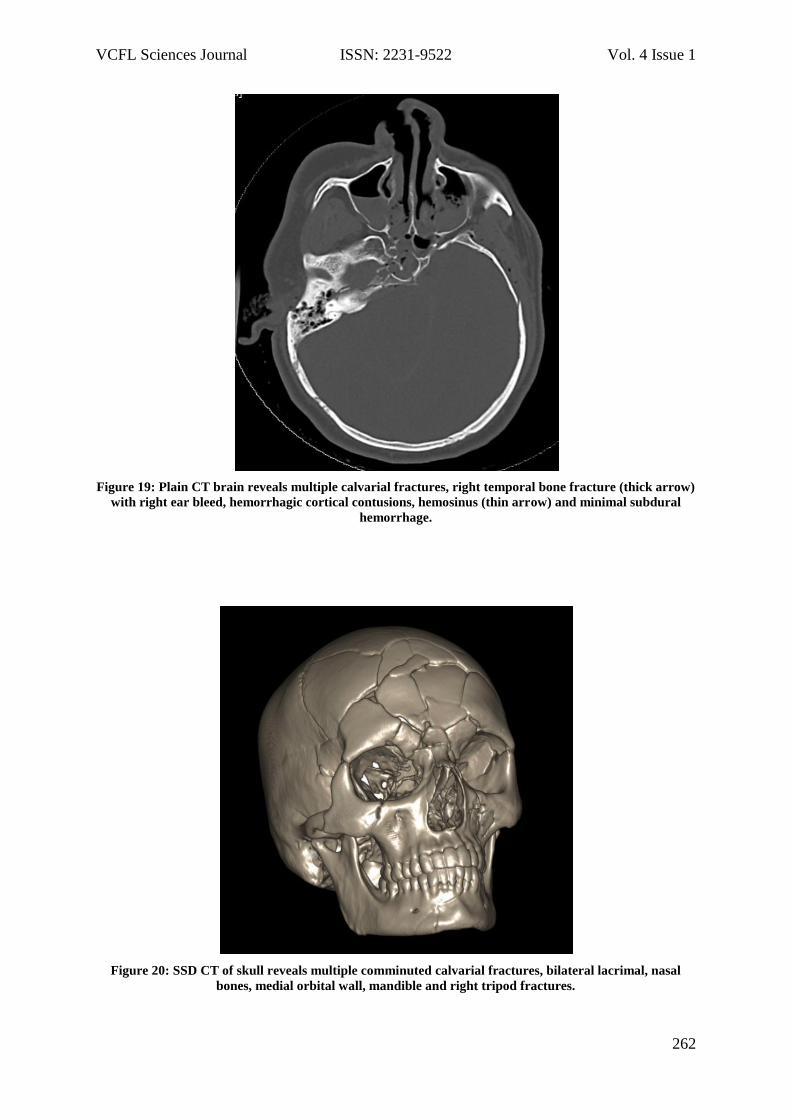
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
262
Figure 19: Plain CT brain reveals multiple calvarial fractures, right temporal bone fracture (thick arrow)
with right ear bleed, hemorrhagic cortical contusions, hemosinus (thin arrow) and minimal subdural
hemorrhage.
Figure 20: SSD CT of skull reveals multiple comminuted calvarial fractures, bilateral lacrimal, nasal
bones, medial orbital wall, mandible and right tripod fractures.
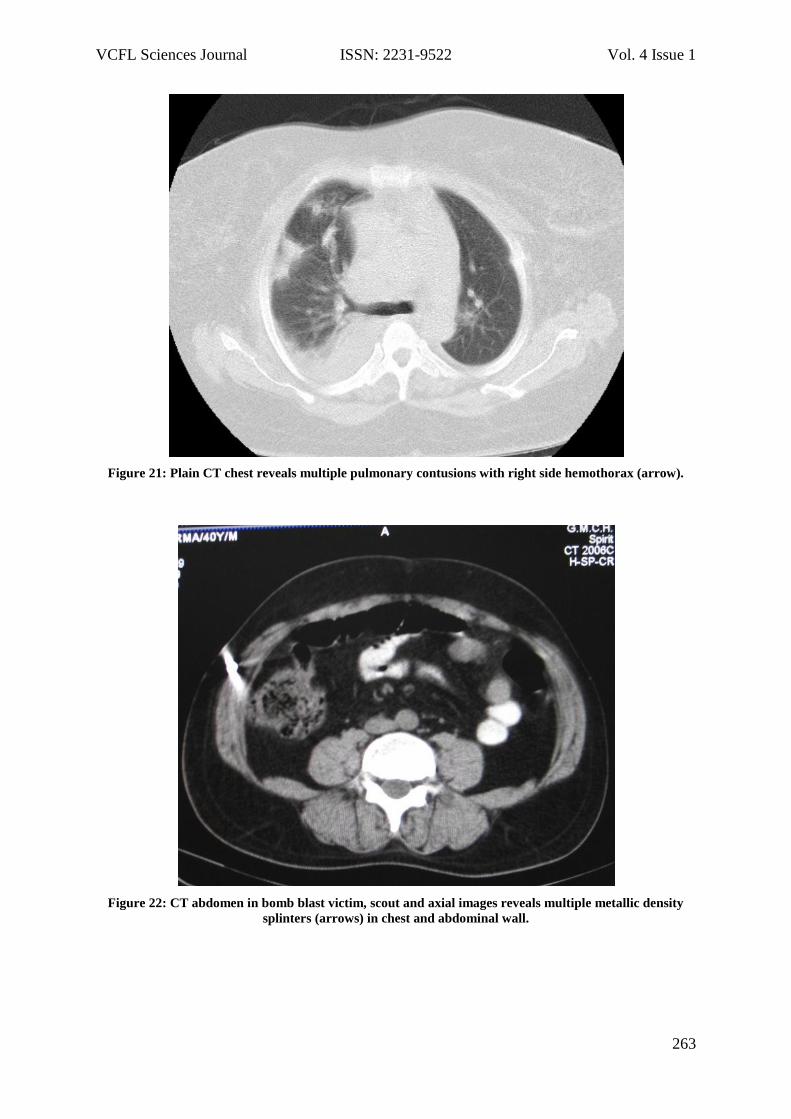
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
263
Figure 21: Plain CT chest reveals multiple pulmonary contusions with right side hemothorax (arrow).
Figure 22: CT abdomen in bomb blast victim, scout and axial images reveals multiple metallic density
splinters (arrows) in chest and abdominal wall.
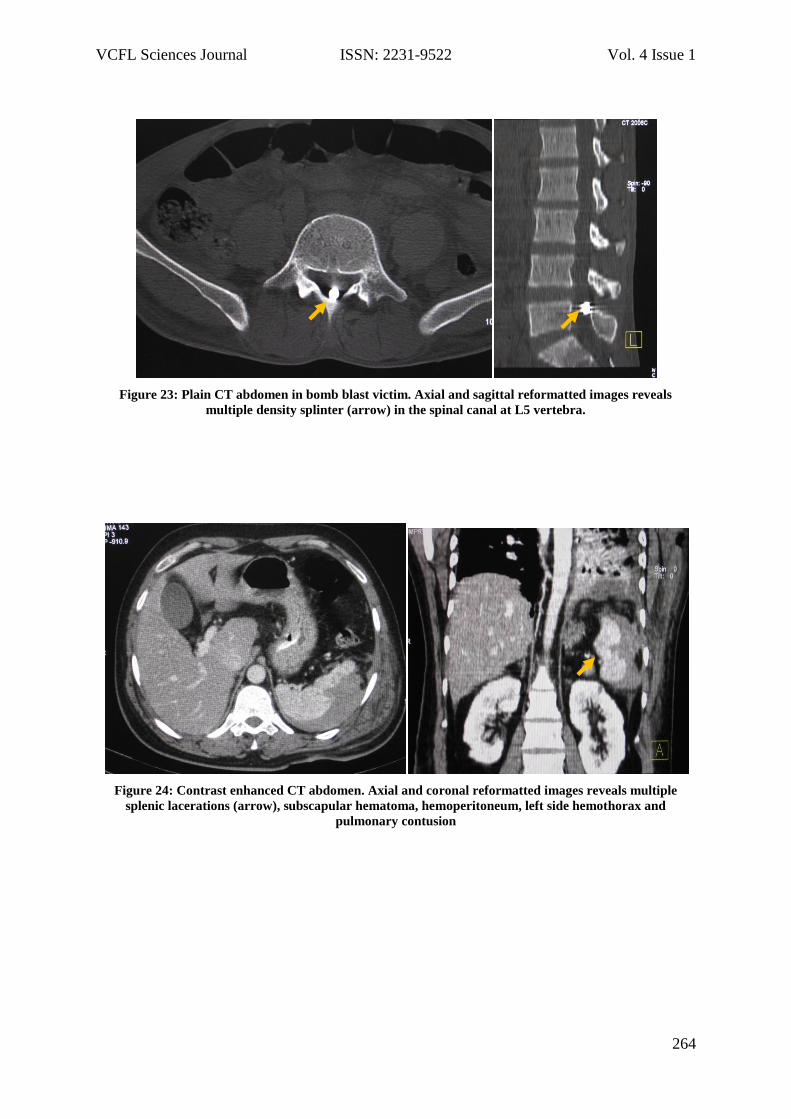
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
264
Figure 23: Plain CT abdomen in bomb blast victim. Axial and sagittal reformatted images reveals
multiple density splinter (arrow) in the spinal canal at L5 vertebra.
Figure 24: Contrast enhanced CT abdomen. Axial and coronal reformatted images reveals multiple
splenic lacerations (arrow), subscapular hematoma, hemoperitoneum, left side hemothorax and
pulmonary contusion
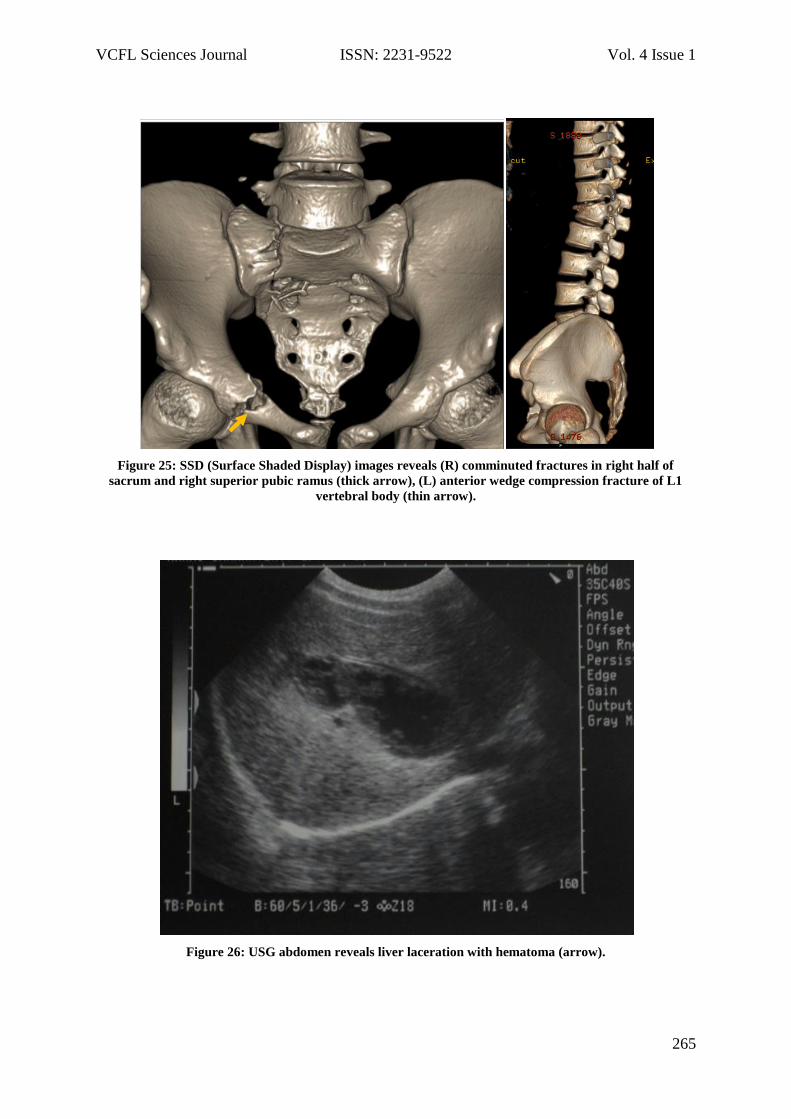
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
265
Figure 25: SSD (Surface Shaded Display) images reveals (R) comminuted fractures in right half of
sacrum and right superior pubic ramus (thick arrow), (L) anterior wedge compression fracture of L1
vertebral body (thin arrow).
Figure 26: USG abdomen reveals liver laceration with hematoma (arrow).
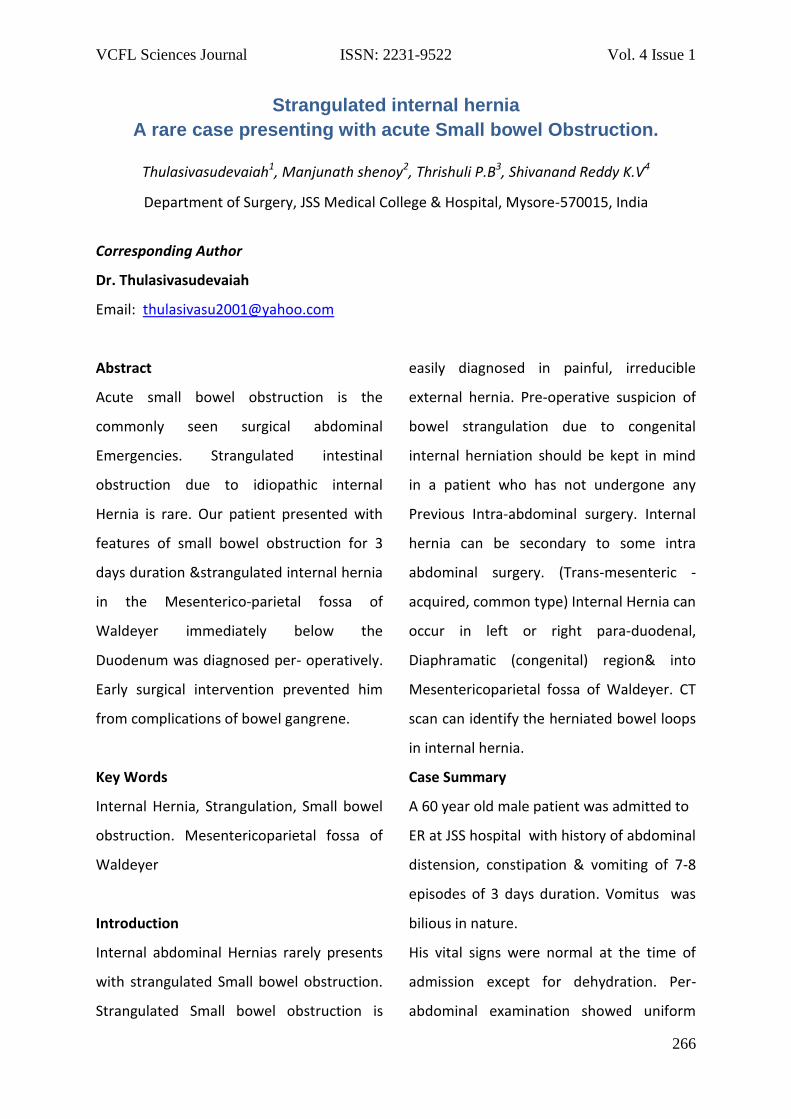
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
266
Strangulated internal hernia
A rare case presenting with acute Small bowel Obstruction.
Thulasivasudevaiah1, Manjunath shenoy2, Thrishuli P.B3, Shivanand Reddy K.V4
Department of Surgery, JSS Medical College & Hospital, Mysore-570015, India
Corresponding Author
Dr. Thulasivasudevaiah
Email: [email protected]
Abstract
Acute small bowel obstruction is the
commonly seen surgical abdominal
Emergencies. Strangulated intestinal
obstruction due to idiopathic internal
Hernia is rare. Our patient presented with
features of small bowel obstruction for 3
days duration &strangulated internal hernia
in the Mesenterico-parietal fossa of
Waldeyer immediately below the
Duodenum was diagnosed per- operatively.
Early surgical intervention prevented him
from complications of bowel gangrene.
Key Words
Internal Hernia, Strangulation, Small bowel
obstruction. Mesentericoparietal fossa of
Waldeyer
Introduction
Internal abdominal Hernias rarely presents
with strangulated Small bowel obstruction.
Strangulated Small bowel obstruction is
easily diagnosed in painful, irreducible
external hernia. Pre-operative suspicion of
bowel strangulation due to congenital
internal herniation should be kept in mind
in a patient who has not undergone any
Previous Intra-abdominal surgery. Internal
hernia can be secondary to some intra
abdominal surgery. (Trans-mesenteric -
acquired, common type) Internal Hernia can
occur in left or right para-duodenal,
Diaphramatic (congenital) region& into
Mesentericoparietal fossa of Waldeyer. CT
scan can identify the herniated bowel loops
in internal hernia.
Case Summary
A 60 year old male patient was admitted to
ER at JSS hospital with history of abdominal
distension, constipation & vomiting of 7-8
episodes of 3 days duration. Vomitus was
bilious in nature.
His vital signs were normal at the time of
admission except for dehydration. Per-
abdominal examination showed uniform
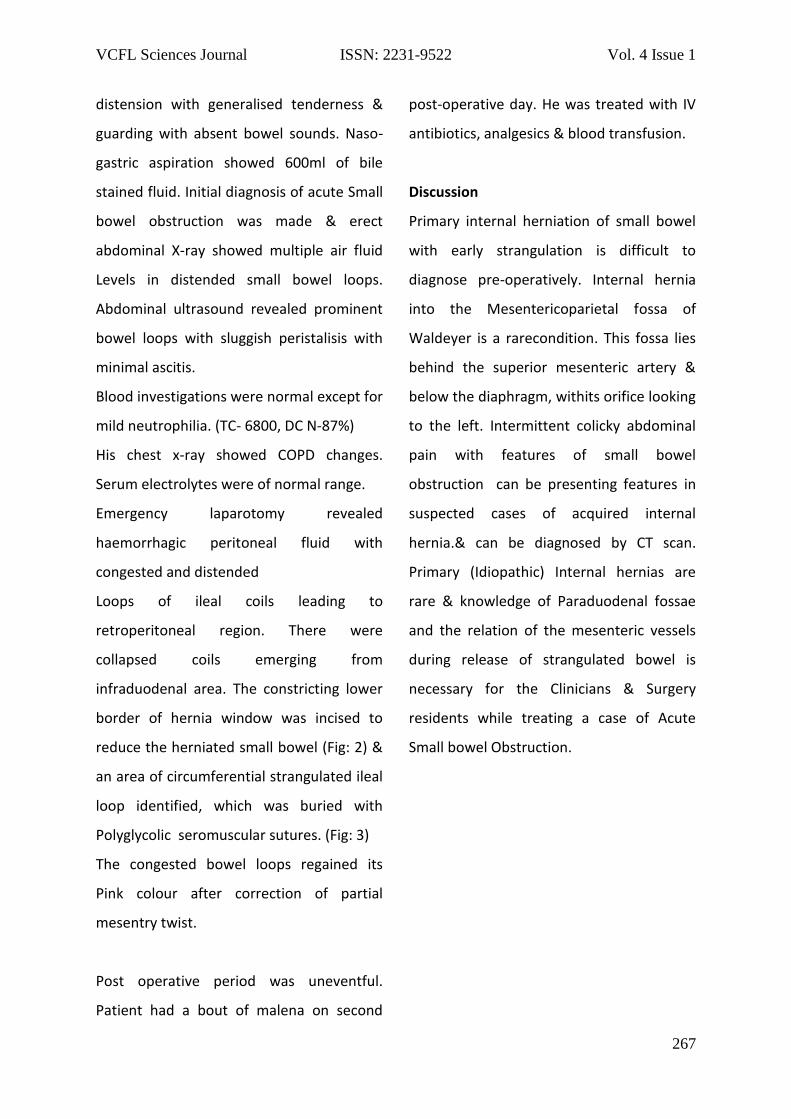
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
267
distension with generalised tenderness &
guarding with absent bowel sounds. Naso-
gastric aspiration showed 600ml of bile
stained fluid. Initial diagnosis of acute Small
bowel obstruction was made & erect
abdominal X-ray showed multiple air fluid
Levels in distended small bowel loops.
Abdominal ultrasound revealed prominent
bowel loops with sluggish peristalisis with
minimal ascitis.
Blood investigations were normal except for
mild neutrophilia. (TC- 6800, DC N-87%)
His chest x-ray showed COPD changes.
Serum electrolytes were of normal range.
Emergency laparotomy revealed
haemorrhagic peritoneal fluid with
congested and distended
Loops of ileal coils leading to
retroperitoneal region. There were
collapsed coils emerging from
infraduodenal area. The constricting lower
border of hernia window was incised to
reduce the herniated small bowel (Fig: 2) &
an area of circumferential strangulated ileal
loop identified, which was buried with
Polyglycolic seromuscular sutures. (Fig: 3)
The congested bowel loops regained its
Pink colour after correction of partial
mesentry twist.
Post operative period was uneventful.
Patient had a bout of malena on second
post-operative day. He was treated with IV
antibiotics, analgesics & blood transfusion.
Discussion
Primary internal herniation of small bowel
with early strangulation is difficult to
diagnose pre-operatively. Internal hernia
into the Mesentericoparietal fossa of
Waldeyer is a rarecondition. This fossa lies
behind the superior mesenteric artery &
below the diaphragm, withits orifice looking
to the left. Intermittent colicky abdominal
pain with features of small bowel
obstruction can be presenting features in
suspected cases of acquired internal
hernia.& can be diagnosed by CT scan.
Primary (Idiopathic) Internal hernias are
rare & knowledge of Paraduodenal fossae
and the relation of the mesenteric vessels
during release of strangulated bowel is
necessary for the Clinicians & Surgery
residents while treating a case of Acute
Small bowel Obstruction.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
268
References
1. Internal hernia- An increasingly
common cause of SBO. –Blachar.A
FederleMP,Division of abdominal
imaging, Dept of radiology, University
of Pittsburgh medical center
2. Lee McGregor`s synopsis of surgical
Anatomy.-Duodenal fossae-page 33-35.
3. Congenital & acquired internal hernia-
Unusual causes of small bowel
obstruction- NewsomBD,Kukora JS Dept
of Surgery ,University of Mississipi chool
of medicine,Jackson MS USA
4. Internal hernia –a brief review, Hernia
Vol17,issue 3June 201
5. Right paradudenal hernia in an adult
patient ,diagnostic approach & surgical
management.Case reports in
Gastroenterology 2011 may-Aug 5(2)
www.karger.com
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
269
Figures
Figure 27: Reduction of herniated coils of ileum from retroperitoneum after transecting the constricting
band
Figure 28: Reduction of herniated bowel loops
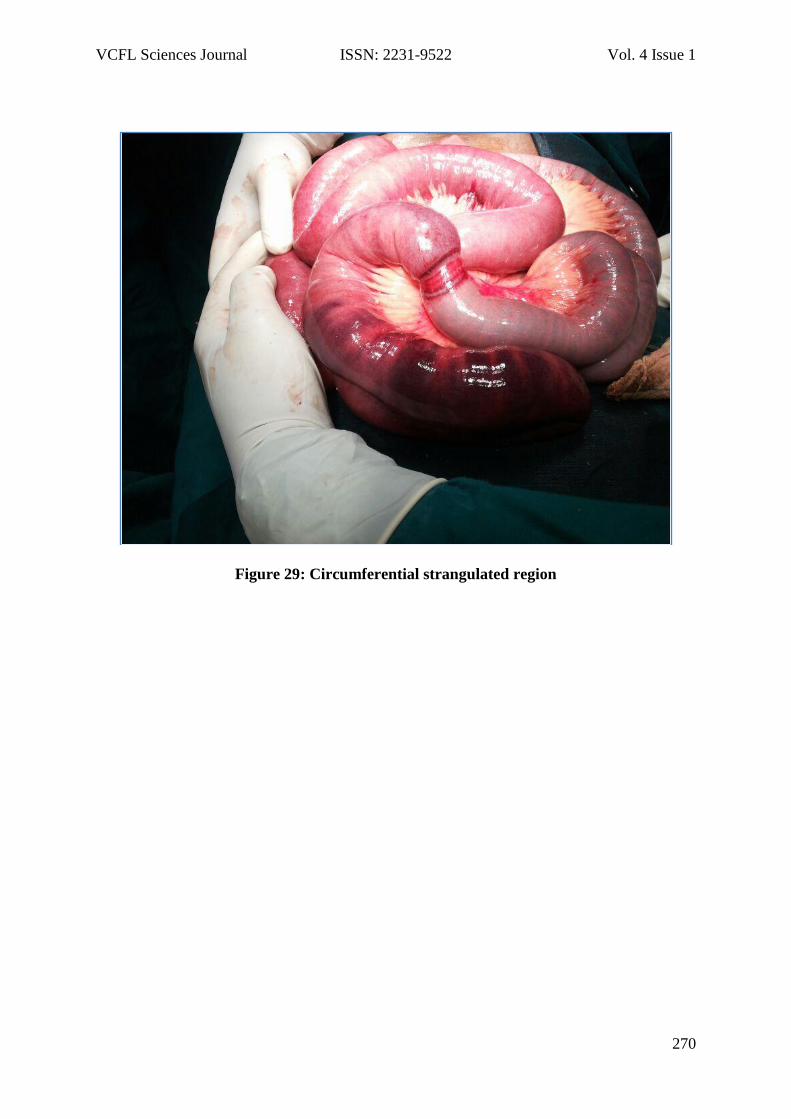
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
270
Figure 29: Circumferential strangulated region

VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
271
Diagnostic Efficacy of Endoscopy in Evaluation Of Dysphagia
Zameerulla T1, Praveen Devarbhavi2
1Associate professor, Department of general surgery, SSIMSRC, Davanagere 2Associate professor, Department of Medicine, SSIMSRC, Davanagere
Corresponding Author
Dr. Zameerulla T
Email: [email protected]
Abstract
Background: Dysphagia is a common
complaint in the patients attending the
surgical OPD. It is common especially in the
elderly population and more so in females.
Many investigative modalities have been in
use in the evaluation of this complaint
including barium swallow and more
recently with the invention of flexible
endoscopy it has become the gold standard
of investigations in dysphagia owing to its
advantages over others.
In the present retrospective study, data was
collected and evaluated from the registry of
endoscopy department of SSIMSRC,
regarding the cases of upper GI endoscopy
done by the author for the evaluation of
dysphagia from January 2008 to December
2013. Patients with known diagnosis or who
have come for repeat endoscopy were
excluded from the study.
Conclusion: Dysphagia being a common
complaint, yet could be a symptom of
malignancy, has to be evaluated properly.
Upper gastro intestinal endoscopy is of
immense value in the initial evaluation of
the same.
Key words
Efficacy, Dysphagia, Endoscopy.
Introduction
Dysphagia is defined as Difficulty in
swallowing or inability to swallow1.
Dysphagia is a common complaint
especially in ageing persons. Approximately
7 to 10 percent of adults above 50 years
have dysphagia, although this number may
be lower in comparison to the reality
because many patients may never seek
medical care2, 3. About 25 percent of
patients in hospitals and 30 to 40 percent of
patients in nursing homes experience
swallowing problems.4, 5. Before the advent
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
272
of endoscopy physicians had rely upon
barium studies for the evaluation of
dysphagia. In 1988, the first published
description of the use of flexible
laryngoscopy to evaluate oropharyngeal
dysphagia was published by Langmore,
Schatz, and Olsen6. Now fibreoptic
endoscopy is in common use and in
combination with barium swallow the
diagnostic accuracy of this is reported to be
85%7.
Materials and Methods
The data was collected from the registry
maintained in the department of endoscopy
at SSIMSRC Davangere regarding the cases
of upper gastro intestinal endoscopy done
by the author in the patients with
predominant complaint of difficulty in
swallowing from January 2008 to December
2013. Both outpatient and admitted
patients were included in the study.
Patients with known diagnosis and
previously done endoscopy cases were
excluded.
The data collected was evaluated regarding
the pre procedure clinical diagnosis, the
endoscopy findings, weather biopsy was
taken and the pathological diagnosis.
Statistical analysis was done using SPSS
statistical tool. The results were compared
with the other international studies.
Results
In the present study, total of 187 patients
were included, out of which 106 were males
and 81 were females. Endoscopy was able
to find some pathology in 122 patients
(65%) and was normal in 65. The most
common diagnosis was malignancy of the
esophagus , 46% of the total number of
patients, out of this malignancy of upper,
middle and lower third of esophagus
constituted 14(), 15() and 57() patients
respectively. Among 14 patients of upper
third malignancy, 6 patients were found to
have carcinoma of post cricoid region and
among 57 patients of lower third
malignancies, 6 patients were found to
have carcinoma of Gastro Esophageal
junction. Other lesions discovered were
carcinoma of posterior pharyngeal wall in 6
patients, stricture of the esophagus in 6,
carcinoma of pyriform fossa in 4, reflux
esophagitis in 3, hiatus hernia in 3,
esophageal candidiasis and erosive gastritis
in 2 patients each, carcinoma of
paraepiglottic region, pyloric stenosis and
esophageal web was found in one patient
each.
Discussion
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
273
Dysphagia is a common symptom in the
patients attending the surgical and ENT
outpatient departments. Cause for such a
symptom can be minor disorders such as
pharyngitis or laryngitis in some. But the
cause can also be dreaded diseases such as
malignancy of the upper gastrointestinal
tract such as esophagus and gastro
esophageal junction and can also be a
symptom of malignancy of upper aero
digestive tract.
The most common cancer of the gastro
intestinal tract in southern India is that of
esophagus8. Esophageal cancer is one of the
least treatment responsive cancers all over
the world9. In India, Squamous cell
carcinoma of the esophagus is the third
leading cancer in men and fourth in
women10, 11, and 12. Males are more
commonly affected13, 14. In the present
study also there is male preponderance
noted.
In our study, about 65% of the patients
evaluated for dysphagia were found to have
some or the other pathological lesion as a
cause for their complaint, majority of them
were found to have malignancy, mainly of
the esophagus and the gastro esophageal
junction. This finding may not reflect with
the general population and this alarming
percentage of patients with malignancy can
be because of the fact that a significant
percentage of the patients were referred to
the author from the department of
oncosurgery.
Our study demonstrated that although
majority of the patients with dysphagia will
either be have some clinically diagnosed
disease or will be normal, there are some
‘diagnostic surprises’ possible such as we
found esophageal candidiasis, GERD, pyloric
stenosis, esophageal web and erosive
gastritis as a cause for the patients’
complaints.
Conclusion
Upper gastro intestinal endoscopy is an
important tool in the initial evaluation of
patients with dysphagia. Being an
outpatient procedure and done without any
form of sedation or anesthesia in most of
the patients and being safer even in elderly
patients, it can be considered even with
slightest suspicion of malignancy. Multiple
biopsies can be taken from any suspected
areas and subjected for histopathology. If
found to be normal patient can be safely
evaluated further with other investigative
tools.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
274
Reference
1. The American Heritage® Medical
Dictionary Copyright © 2007, 2004 by
Houghton Mifflin Company.
2. Lindgren S, Janzon L. Prevalence of
swallowing complaints and clinical findings
among 50–79-year-old men and women in
an urban population. Dysphagia. 1991;
6:187–92.
3. Tibbling L, Gustafsson B. Dysphagia and
its consequences in the elderly. Dysphagia.
1991; 6:200–2.
4. Brin MF, Younger D. Neurologic disorders
and aspiration. Otolaryngol Clin North Am.
1988; 21:691–9.
5. Layne KA, Losinski DS, Zenner PM, Ament
JA. Using the Fleming index of dysphagia to
establish prevalence. Dysphagia. 1989;
4:39–42.
6. Langmore SE, Schatz K, Olsen N.
Fiberoptic endoscopic examination of
swallowing safety: a new procedure.
Dysphagia 1988; 2:216–219.
7. Wilkins WE, WalkerJ, McNulty MR,
Britton DC, Gough K.
The organisation and evaluation of an open
access dysphagia
clinic. Ann R Coll Surg Engl 1984; 66:115-6.
8.Chitra S, Ashok L, Anand L, Srinivasan V,
Jaynath V. Risk factors for esophageal
cancer in Coimbatore;SouthernIndia;A
hospital based care control study. Indian J
Gastroenterology 2004; 23:19-21.
9. Kamangar F, Malekzadeh R, Dawsey SM,
Saidi F.et al Esophageal cancer in North
Eastern Iran: A review. Arch Iran Med 2007;
10:70-82.
10. Malkan G, Mohandas KM.
Epidemiology of digestive tract cancers in
India. Gut 1997; 16:98-101.
11. Malhotra SL. Geographical
distribution of gastrointestinal cancers in
India with special reference to causation.
Gut 1967; 8:376-72.
12. Ansari MM, Haleem S, Beg MH.
Clinicopathological profile of carcinoma
esophagus at Aligarh. J Indian Med Assoc
1991; 89:217-19.
13. Farin K, Graca MD, William FA. Patterns
of cancer incidence, mortality and
prevalence across five continents: Defining
priorities to reduce cancer disparities in
different geographic regions of the world. J
Clin Oncol 2006; 24:2137-50
14. Sankaranarayanan R, Duffy SV, Padma
Kumaray G, Nair SM, Day NE, Pandanabhan
TK. Risk factors for cancer of the esophagus
in Kerala, India. Ind J cancer 1991; 49:485-
89

VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
275
Study of Sellar Bridges in Dry Human Skulls of North Interior
Karnataka
P.S.Bhusaraddi1, S. D. Desai2, sunkeswari sreepadma3
1Associate Professor, Department of Anatomy, KIMS, Hubli, India
2Principal, Sridevi Institute of Medical Sciences & RH, Tumkur, India
3Department of Anatomy, S D M Medical College, Dharawad, India
Corresponding Author Dr P.S.Bhusaraddi Introduction
The ossified interclinoid ligament forms a
bony bridge between the anterior, middle
and posterior clinoid processes of the
sphenoid bone. These bony bridges are
known as sellar bridge.
The microsurgical and radiological anatomy
of the clinoid processes and their bridging
structures give neurosurgeons more details
about the anterior, middle and the
posterior clinoid processes and their
relations to the vascular and nervous
relations during intradural and extradural
clinoidectomy, thus making the operatives
procedures successful and safer.
Excision of the anterior clinoid process may
be required for many skull based surgical
procedures and the presence of the
carotico clinoid foramen may pose
problems. The study of these structures
around the sella is immensely beneficial and
especially related to neurosurgeons and
radiologists
Objectives
To know the prevalence of Sellar bridges
among the skull samples studied.
To study the Different types of Sellar
bridges in relation to unilateral or bilateral
Methodology
Source of data:
For the present study, dry unknown human
skulls were obtained from North interior
Karnataka region collected in the
department of Anatomy of Shri B. M. Patil
Medical College Hospital and Research
Centre, BLDE University Bijapur.
Method of Data Collection
Sample size- 223 dry unknown human
skull were taken for the study.
Sampling procedure- Skulls were
observed for different types of sellar
bridges.
Type 1
Type 2
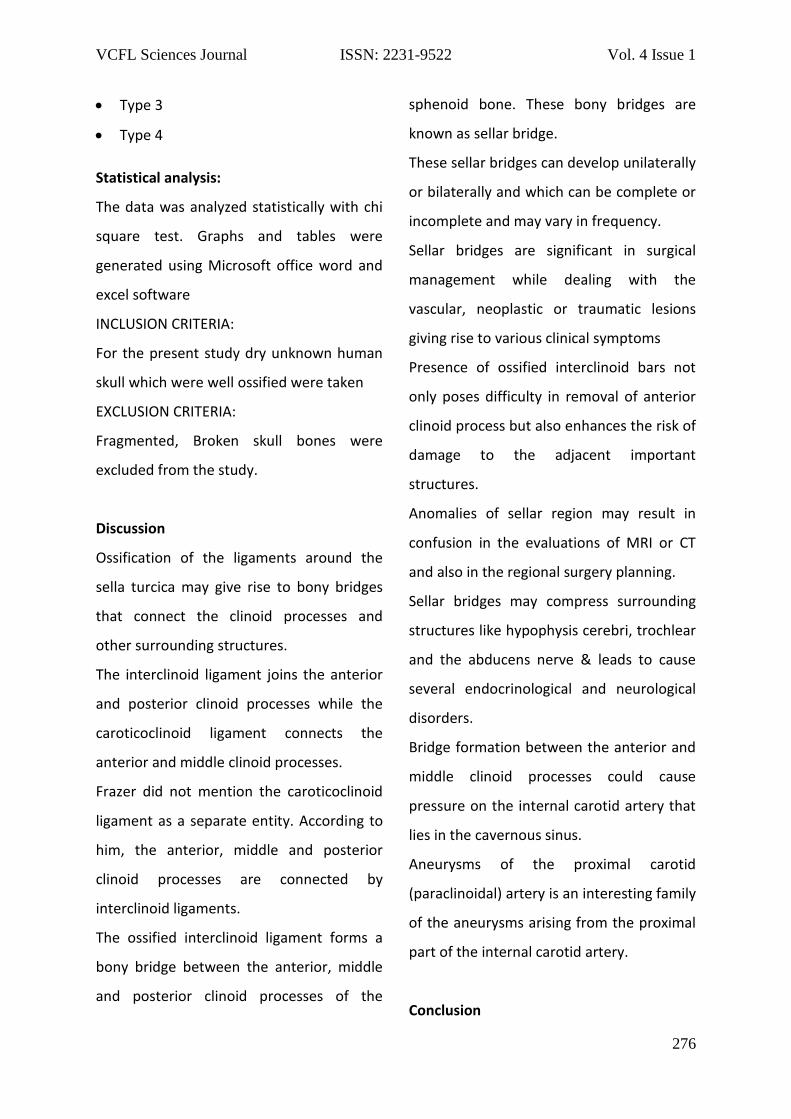
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
276
Type 3
Type 4
Statistical analysis:
The data was analyzed statistically with chi
square test. Graphs and tables were
generated using Microsoft office word and
excel software
INCLUSION CRITERIA:
For the present study dry unknown human
skull which were well ossified were taken
EXCLUSION CRITERIA:
Fragmented, Broken skull bones were
excluded from the study.
Discussion
Ossification of the ligaments around the
sella turcica may give rise to bony bridges
that connect the clinoid processes and
other surrounding structures.
The interclinoid ligament joins the anterior
and posterior clinoid processes while the
caroticoclinoid ligament connects the
anterior and middle clinoid processes.
Frazer did not mention the caroticoclinoid
ligament as a separate entity. According to
him, the anterior, middle and posterior
clinoid processes are connected by
interclinoid ligaments.
The ossified interclinoid ligament forms a
bony bridge between the anterior, middle
and posterior clinoid processes of the
sphenoid bone. These bony bridges are
known as sellar bridge.
These sellar bridges can develop unilaterally
or bilaterally and which can be complete or
incomplete and may vary in frequency.
Sellar bridges are significant in surgical
management while dealing with the
vascular, neoplastic or traumatic lesions
giving rise to various clinical symptoms
Presence of ossified interclinoid bars not
only poses difficulty in removal of anterior
clinoid process but also enhances the risk of
damage to the adjacent important
structures.
Anomalies of sellar region may result in
confusion in the evaluations of MRI or CT
and also in the regional surgery planning.
Sellar bridges may compress surrounding
structures like hypophysis cerebri, trochlear
and the abducens nerve & leads to cause
several endocrinological and neurological
disorders.
Bridge formation between the anterior and
middle clinoid processes could cause
pressure on the internal carotid artery that
lies in the cavernous sinus.
Aneurysms of the proximal carotid
(paraclinoidal) artery is an interesting family
of the aneurysms arising from the proximal
part of the internal carotid artery.
Conclusion
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
277
The variations in clinoid processes of the
sphenoid bone should be carefully studied
by all neurosurgeons.
Complete or partial removal of the anterior
clinoid process is an important step in the
superior approach to the cavernous sinus.
Knowledge of the prevalence sellar bridges
will help the neurosurgeons for pre-
operative scanning and precautions to be
taken implications in surgical procedures to
assess the pituitary gland, cavernous sinus
and internal carotid artery to prevent fatal
complications during surgery.
The osseous carotico clinoid foramen is an
underestimated structure which has
important neuronal and vascular relations
and is both clinically and surgically
important.
Knowledge of the detailed anatomy of the
carotico clinoid foramen and its content can
increase the success of diagnostic
evaluation and surgical approaches to the
region.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
278
References
1. Avci E, Bademci G, Ozturk A.
Microsurgical Landmarks for Safe
Removal anterior clinoid
process.Minim Invas Neurosurg
2005; 48: 268-72.
2. Seoane E, Rhoton AL, Oliveira E
.Microsurgical anatomy of the dural
collar (carotid collar) and rings
around the clinoid segment of the
internal carotid artery.
Neurosurgery 1998;42:869–86.
3. Archana R, Anita R, Jyoti C, Punita
M, Rakesh D. Incidence of osseous
interclinoid bars in Indian
population.Surg Radiol Anat
2010;32:383–7.
4. Ozdogmus O, Saka E, Tulay C, Gurdal
E, Uzun I, Cavdar S. Ossification of
interclinoid ligament and its clinical
significance. Neuroanatomy 2003;
2:25–7.
5. Peker T, Anıl A , Gülekon N, Turgut
HB, Pelin C , Karaköse M.The
incidence and types of sella and
sphenopetrous bridges. Neurosurg
Rev 2006;29: 219–23.
6. Bilodi AKS. Study of sella turcica and
associated anomalies in human
skulls, Journal of Institute of
Medicine 2005;27: 3-6.
7. Erturk M, Kayalioglu G, Govsa F
.Anatomy of the clinoidal region
with special emphasis on the
caroticoclinoid foramen and
interclinoid osseous bridge in a
recent Turkish population.
Neurosurg Rev 2004; 27:22–6.
8. Dyke CG, DavidoV LM
Demonstration of normal cerebral
structures by means of
encephalography: choroid plexus.
Bull Neurol Inst NY 1932;2:331–46
9. Rengachari SS, Ellenbogen RE
.Intracranial aneurysm. In: Principles
of Neurosurgery. 2nd ed. USA:
Elsevier Mosby; 2005.p 222-5.
10. Narolewski R. Significance of
anatomic variants of bony
surroundings of the internal carotid
artery and their significance for
lateral surgical approaches to the
cavernous sinus. Ann Acad Med
Stetin 2003; 49:205-29.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
279
Figures
Figure 30: Normal Anatomy of Sellar Region
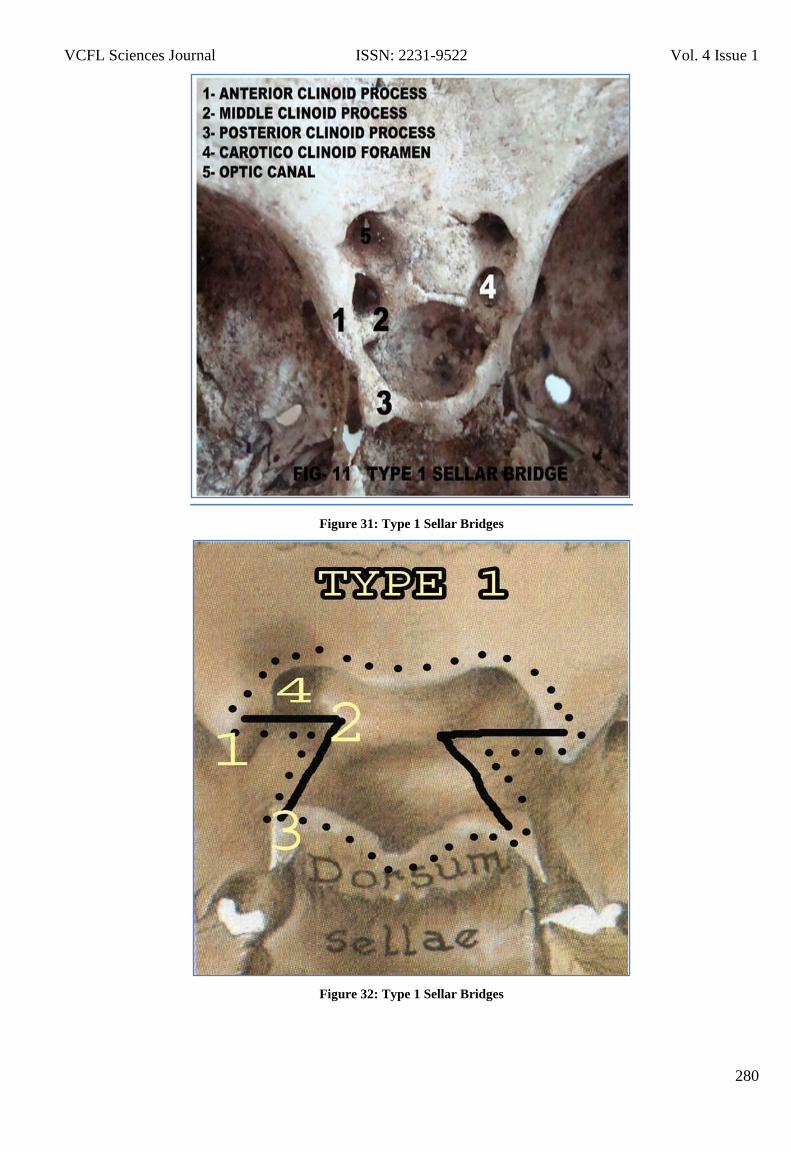
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
280
Figure 31: Type 1 Sellar Bridges
Figure 32: Type 1 Sellar Bridges
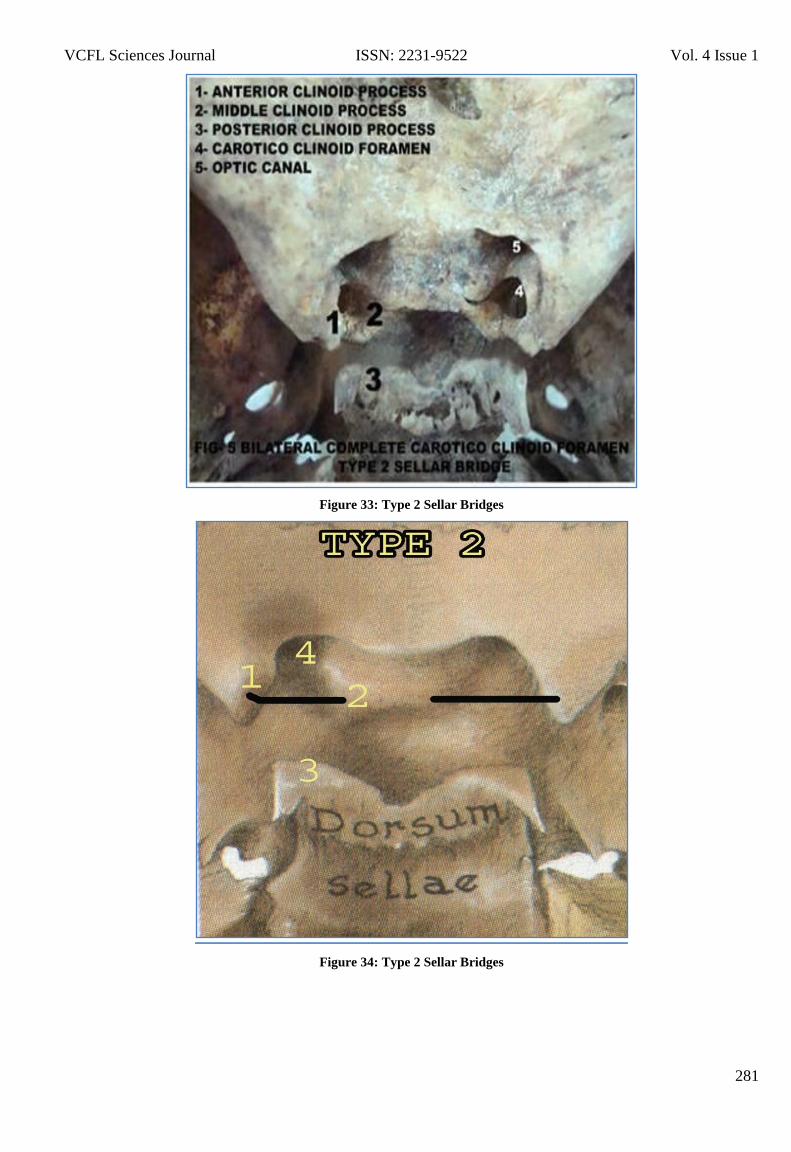
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
281
Figure 33: Type 2 Sellar Bridges
Figure 34: Type 2 Sellar Bridges
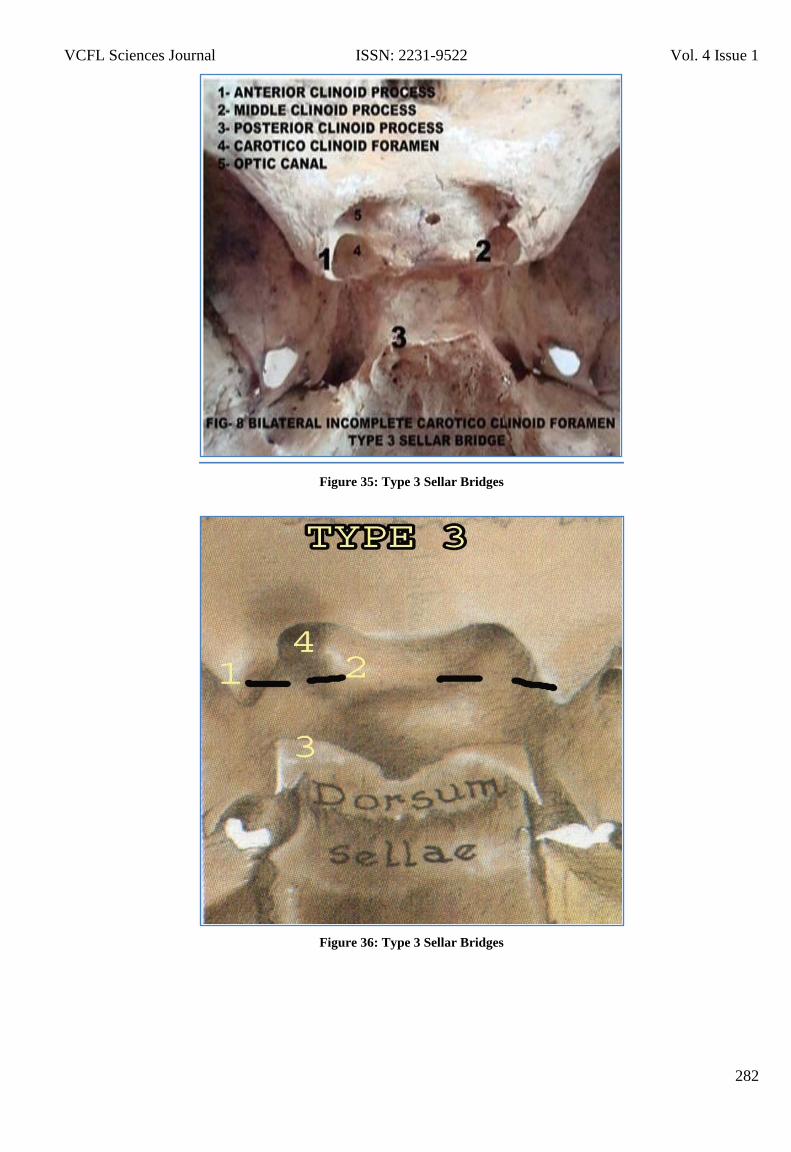
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
282
Figure 35: Type 3 Sellar Bridges
Figure 36: Type 3 Sellar Bridges
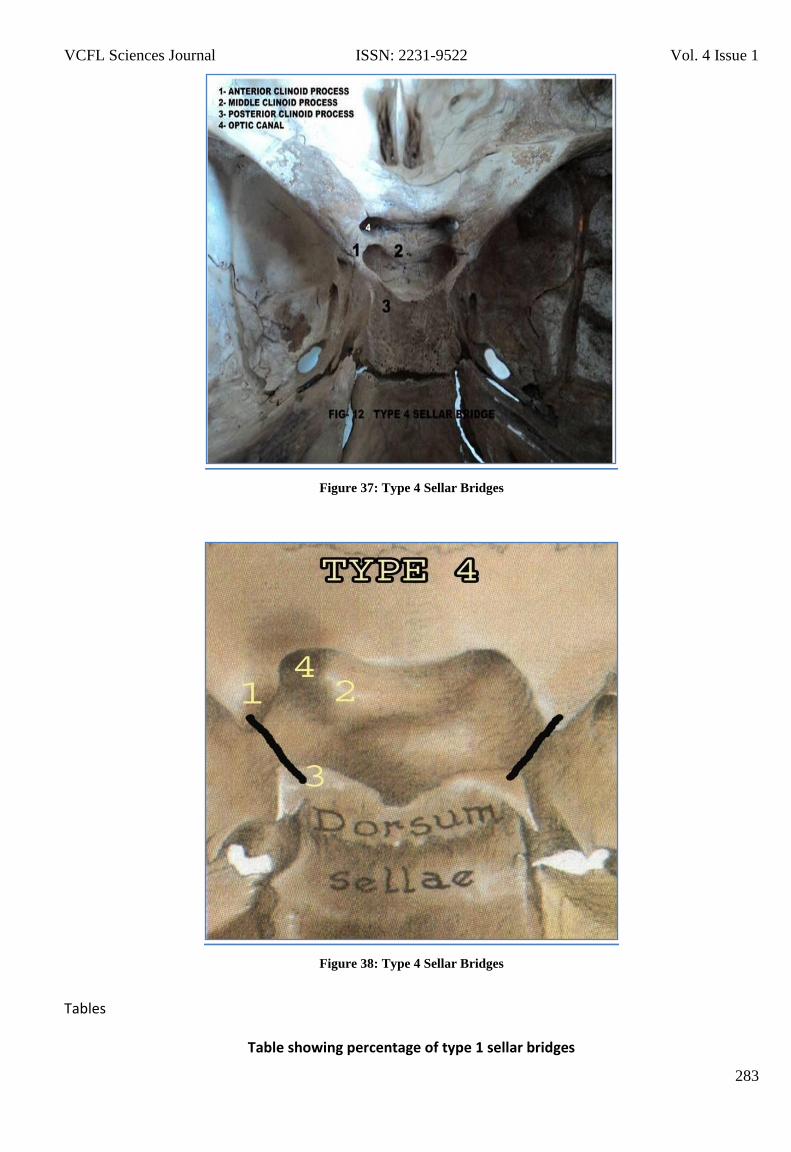
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
283
Figure 37: Type 4 Sellar Bridges
Figure 38: Type 4 Sellar Bridges Tables
Table showing percentage of type 1 sellar bridges
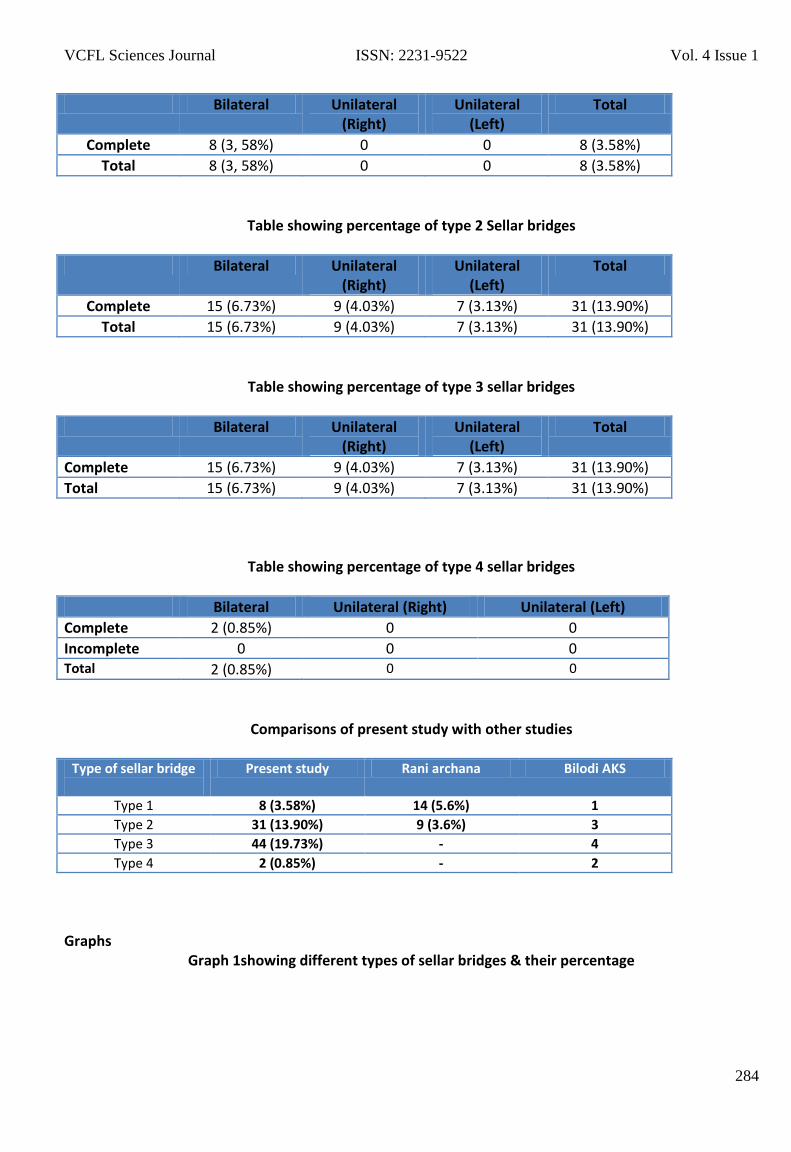
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
284
Bilateral Unilateral (Right)
Unilateral (Left)
Total
Complete 8 (3, 58%) 0 0 8 (3.58%)
Total 8 (3, 58%) 0 0 8 (3.58%)
Table showing percentage of type 2 Sellar bridges
Bilateral Unilateral (Right)
Unilateral (Left)
Total
Complete 15 (6.73%) 9 (4.03%) 7 (3.13%) 31 (13.90%)
Total 15 (6.73%) 9 (4.03%) 7 (3.13%) 31 (13.90%)
Table showing percentage of type 3 sellar bridges
Bilateral Unilateral (Right)
Unilateral (Left)
Total
Complete 15 (6.73%) 9 (4.03%) 7 (3.13%) 31 (13.90%)
Total 15 (6.73%) 9 (4.03%) 7 (3.13%) 31 (13.90%)
Table showing percentage of type 4 sellar bridges
Bilateral Unilateral (Right) Unilateral (Left)
Complete 2 (0.85%) 0 0
Incomplete 0 0 0 Total 2 (0.85%) 0 0
Comparisons of present study with other studies
Type of sellar bridge
Present study Rani archana Bilodi AKS
Type 1 8 (3.58%) 14 (5.6%) 1
Type 2 31 (13.90%) 9 (3.6%) 3
Type 3 44 (19.73%) - 4
Type 4 2 (0.85%) - 2
Graphs
Graph 1showing different types of sellar bridges & their percentage
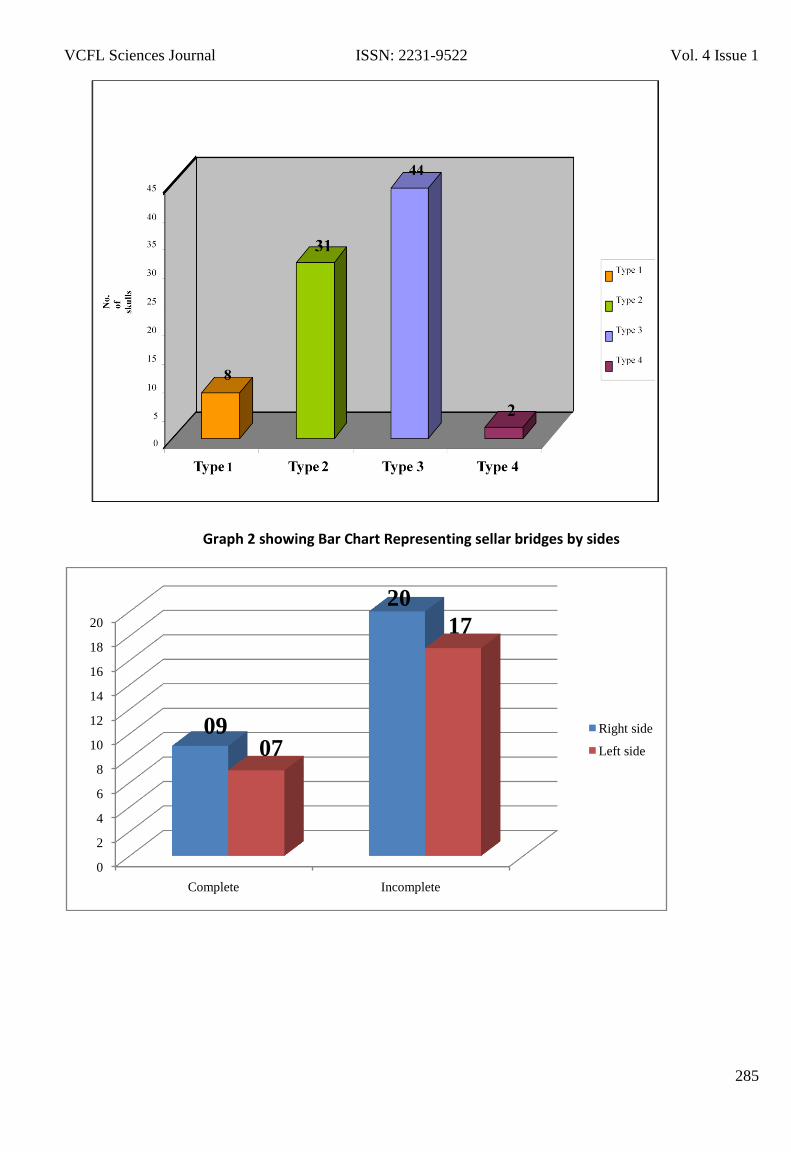
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
285
Graph 2 showing Bar Chart Representing sellar bridges by sides
0
2
4
6
8
10
12
14
16
18
20
Complete Incomplete
Right side
Left side
0907
20
17
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
286
Study of variation in hip joint angles and measurements among regional
urban population of south India- A Contribution to Tribology
Prashanth Nagaraj1, Gautham T Kiron2, Dinesh Golla3, Raghavendra Rao Dharmavaram4
1Assistant Professor, Department of Orthopaedics, M S Ramaiah Medical College, Bangalore
2Resident, Apollo Hospitals, Chennai
3Post graduate, Department of Orthopaedics, M S Ramaiah Medical College, Bangalore 4Assistant
Professor, Department of Orthopaedics, M S Ramaiah Medical College, Bangalore
Corresponding Author
Dr. Prashanth Nagaraj
Email: [email protected]
Abstract:
Background: Anatomical parameters of bony
components of the hip joint are essential for
better understanding of diseases and their
etiopathogenesis like primary osteoarthritis of
the hip joint.
Aims/Objectives: This study is planned to analyze
the outcome of various measurements and
geometrical angles around the normal hip joints
of representative sample size. It will help us to
know the same in our native population in terms
of averages creating a new insight into whether
any change in these parameters will help us to
better understand tribology and its application.
Design: prospective analytical observer non
population based study
Main outcome measures: acetabular
inclination ,Acetabular depth ,center edge
angle, neck length ,neck width, Neck shaft
angle, Distance from tip of greater
trochanter to center of head ,Tear drop to
femoral head distance and their averages.
Materials and methods: 80 Pelvic
radiographs of adult patients were
taken,32(64hips) were analyzed in 18 men
and 14 women, we measured the acetabular
inclination , Acetabular depth ,center edge
angle, neck length ,neck width, Neck shaft
angle, Distance from tip of greater
trochanter to center of head ,Tear drop to
femoral head distance using goniometer and
scale. The radiographs were taken from
patients with no underlying bone disease
between June 2011 and June 2012.
Conclusion: Sex and Age influences the
measurements of parameters around a
normal hip joint. Males had significantly
longer neck length in comparison to females
(p=0.001) .For neck diameter towards right
side .Males had significantly longer neck
diameter in comparison to females (p=0.004)
(report mean and SD as appropriate. Towards
left side Males had significantly longer neck
diameter in comparison to females
(p=0.011).Regarding Acetabular inclination,
Acetabular depth, Center edge angle ,Neck
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
287
shaft angle and Tear drop to head distance
there were no observable differences but for
Distance GT to center of femoral head
towards left hip Males had significantly
longer distance GT center head measurement
in comparison to females (p=0.041)This
information will assist clinicians in the region
to interpret analyze and design appropriate
implants to native Indian patients.
Key words
Hip joint, acetabulum, femur, measurements,
radiographs
Introduction
There has been an ongoing interest in degree
and patterns of variation of the medial
inclination of the femoral head and neck,
relative to its diaphysis at least since Charpy
(1885) and Humphry (1889), And with the
extreme vertical and horizontal positions
normally characterized as coxa valga and
coxa vara according to John. Y Anderson
1997. The hip joint is functionally a three-
dimensional ball and socket joint, known
commonly as a cotyloid joint because of its
anatomical feature, enabling movements in
three planes as rotation(Jeremid D,2011 ).
The acetabulum is a cup-shaped socket of the
hipbone that derives its name from its
resemblance to a shallow Roman vinegar cup
(Williams and Wilkins, 1992). In clinical
medicine, measurements of the acetabulum
and proximal femur are crucial in diagnosis,
monitoring of patient recovery,
determination of stability of the hip joint and
in assessment of acetabular dysplasia
(McCarthy, 1996).The decision for type of
operative treatment and the prostheses used
is often based on different radiographic
measurements and scores for which normal
values have been defined (Nelitz, 1999).
Therefore orthopaedic surgeons often use
combinations of measurements when
assessing hip joint parameter.
knowledge about various bony components
of the hip joint will not only help the
radiologists, but will be also of immense
importance to the orthopaedic surgeons and
tribologists to design suitable prosthesis. The
awareness about average dimensions of hip
bones joints in both sexes will also help in
early detection of disputed sex by forensic
experts (Jeremid D,2011).
Materials and Methods A total of 80
anteroposterior bilateral pelvic radiographs
were collected from June 2011 to June 2012
from our Hospital in Bangalore. Of these 48
were excluded: 34 had fractures of hip, 9 had
no clear boundaries, and 5 were out of focus.
32 bilateral pelvic radiographs 18 male and
14 female subjects were studied by
measuring acetabular inclination ,Acetabular
depth ,center edge angle, neck length ,neck
diameter, Neck shaft angle, Distance from tip
of greater trochanter to center of head ,Tear
drop to femoral head distance using a scale
and goniometer. The criteria for choosing
pelvic radiographs taken in neutral position
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
288
(Tonnis,1976) included: intact pelvis and hip
joint, intact Shenton's line, intact cortices at
the femoral heads, no history of fractures at
femoral necks and no hip or pelvic bone
disease(5). All films were taken at the object-
film distance of 5 cm (5) and focal-film
distance of 100 cm in the antero-posterior
view (Jeremid D, 2011)
Acetabular inclination: The acetabular
inclination is formed between the
intersection of a line joining the superior and
inferior margins of the acetabulum. A line
joining the ischeal tuberosity.
• Acetabular Depth (AD): The acetabular
depth is the length measured along a
perpendicular line after joining the superior
and inferior lips of the acetabulum, from the
midpoint of the lips to the deepest point of
the acetabulum.
• Centre Edge Angle (CEA): The centre edge
angle is formed by the intersection between
a perpendicular line passing through the
centre of the femoral head and the line
joining the centre of the femoral head to the
superior lateral part of the acetabulum
• Neck length: Distance on a line from the
center of the head intersecting the femoral
axis.
• Neck diameter: A perpendicular line to the
line drawn to measure the neck length. At the
most narrowest point of femur neck.
• Tear drop distance/medial joint space: A
vertical line drawn from the most medial
margin of the femoral head to that of the
outer cortex of pelvic tear drop.
Neck shaft angle: Angle formed by a line
drawn through the mid-axis of femoral shaft
and that of the femoral head and neck
Distance from tip of greater trochanter to
center of head. Two independent observers
calculated these measurements. The
measurements were recorded separately for
each sex and side of the hip
Results Analysis tool: SPSS Version 16.0
software Type of analysis: Descriptive &
Bivariate (student t-test; Chi-square test)
only. Multivariate analysis was irrelevant to
this study. Test of normality was done. This
study required parametric tests. Descriptive
statistics for demographics was conducted.
(Number/Percentage was reported). In cases
of continuous variable (age), mean and
standard deviation was reported. Bivariate
analysis using demographic (sex-
male/female) was compared to each of the
parameters being studied. Age was irrelevant
to be compared in this study.
Lau et al., (1995) defined hip dysplasia as
centre edge angle of less than 25° or
acetabular depth of less than 9 mm. Msamati
et al., (2003) explored prevalence of hip
dysplasia using center edge angle and further
investigation on association with gender.
Similar investigation using center edge angle
would be reported in this study. This study
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
289
could not classify hip dysplasia according to
acetabular depth; no such measurement
cases obtained. To assess association
between categorical variables in dysplasia, in
relation to gender; chi-square test was used
due to two categorical variables involvement.
Discussion
This study has demonstrated variation in
acetabular angles and depth between men
and women, but not the centre-edge angle.
The significant differences observed in
acetabular depth and angles could be due to
the wider pelvis of women that would appear
to reduce the acetabular angle and depth. In
a study of 23 radiographs of normal infants
aged 1-7 days, and 20 radiographs of normal
hips in children aged 11-24 months, Kleinberg
and Lieberman (6) found no sex differences
between them. It is possible that the changes
we have observed in women most likely set
in at puberty when hormonal changes occur
as an adaptation to child bearing in
adulthood. For neck length for right side
Males had significantly longer neck length in
comparison to females (p=0.004) (report
mean and SD as appropriate) Males had
significantly longer neck length in comparison
to females (p=0.001) .For neck diameter
towards right right side .Males had
significantly longer neck diameter in
comparison to females (p=0.004) (report
mean and SD as appropriate. Towards left
side Males had significantly longer neck
diameter in comparison to females
(p=0.011).Regarding Acetabular inclination,
Acetabular depth, Center edge angle ,Neck
shaft angle and Tear drop to head distance
there were no observable differences but for
Distance GT to center of femoral head
towards left hip Males had significantly
longer distance GT center head measurement
in comparison to females (p=0.041) .To
assess association between categorical
variables in dysplasia, in relation to gender;
chi-square test was used due to two
categorical variables involvement. We found
that it was not statistically Significant for both
hip and Findings conformed to the study by
Msamati et al., (2003)
Conclusions
Our study was primarily aimed at analyzing
the statistically significant differences in
various geometric angles around hip joints.
There have been certain demerits in our
study, the sample size is small, and
standardization could be more optimal if CT
scans are done for required sample size,
inter-observational and intra-observational
differences are minimized by choosing only
two observers with less chance of play and
kappa coefficient was not analyzed.
Regression to mean could not be established
due to smaller sample size. However our
study has established new insights to
understand various geometric changes in our
population. We hope this study will assist
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
290
clinicians in the region to interpret X-ray films
of the hip and to manage orthopaedic
problems of the hip. Further studies are
required, however, to generate more data on
age specific pelvic anthropometry and more
specifically cadaveric anthropometry of the
hip.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
291
References
1. Moore, L. The lower limb. In:
Clinically Oriented Anatomy 3rd Ed.
Baltimore: Williams and Wilkins, 1992;
373
2. McCarthy, J.J., Fox, J.S. and Gurd, A.R.
Innominate osteotomy in adolescents
and adults who have acetabular
dysplasia. J. Bone and Joint Surgery.
1996; 78:1455-1461.
3. Nelitz, M., Guenther, K.P., Gunkel, S.
and Puhl. Reliability of radiological
measurements in the assessment of hip
dysplasia in adults. Brit. J. Radiology.
1999; 72:331-334.
4. Tonnis, D. Normal values of the hip
joint for the evaluation of x-rays in
children and
adults. Clinical Orthopaedics and
Related Res. 1976; 119:39-47.
5. Geometric Measurements Of The
Acetabulum In Adult Malawians:
Radiographic Study. East African
Medical Journal Vol. 80 No. 10 October
2003 546 -549
6. Kleinberg, S. and Liberman, H.S. The
acetabular index in infants in relation to
congenital dislocation of the hip. Arch
Surgery. 1932; 32:1049-1054.
7. Sex differences in anatomical
parameters of acetabulum among
asymptomatic Serbian population.
Jeremid D, et al. Vojnosanit Pregl 2011;
volume 68; 935 - 939
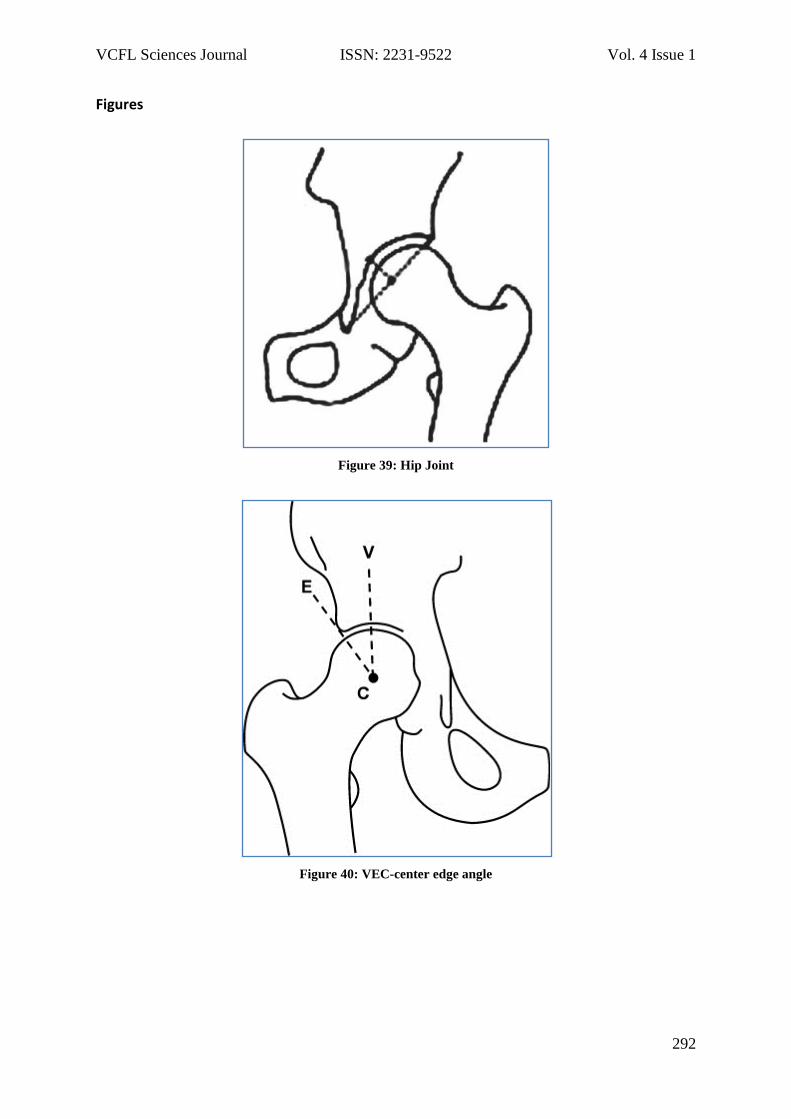
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
292
Figures
Figure 39: Hip Joint
Figure 40: VEC-center edge angle
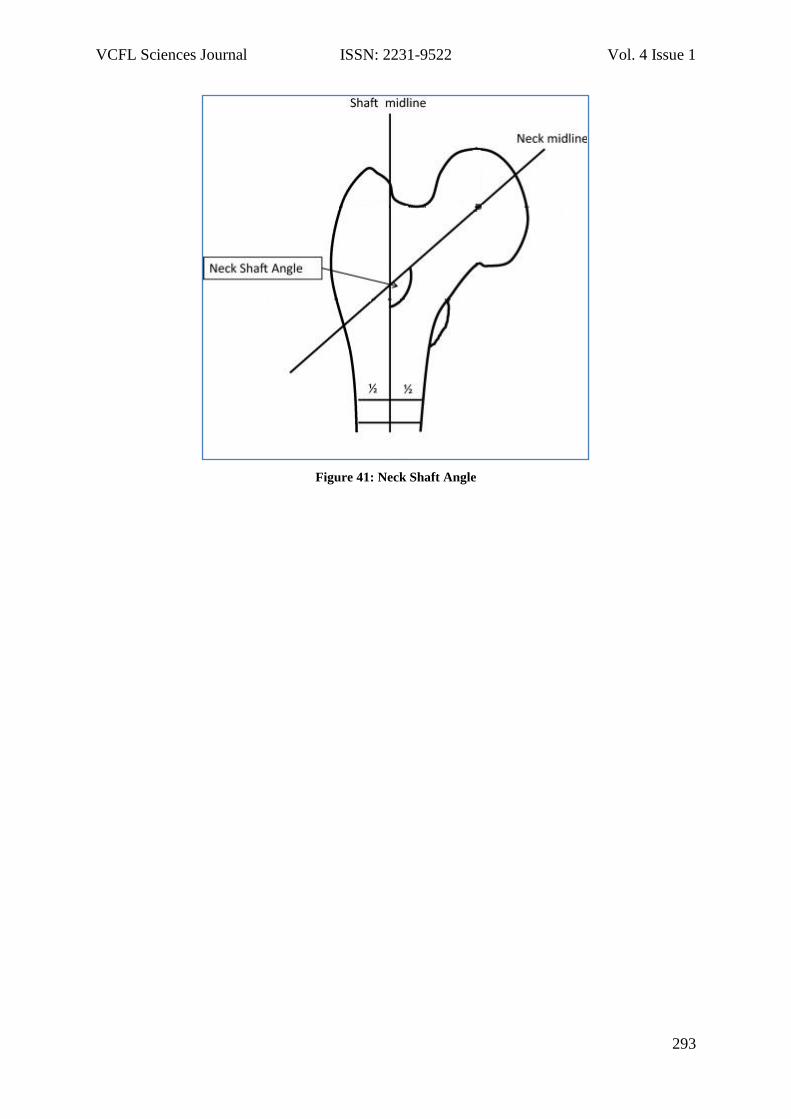
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
293
Figure 41: Neck Shaft Angle
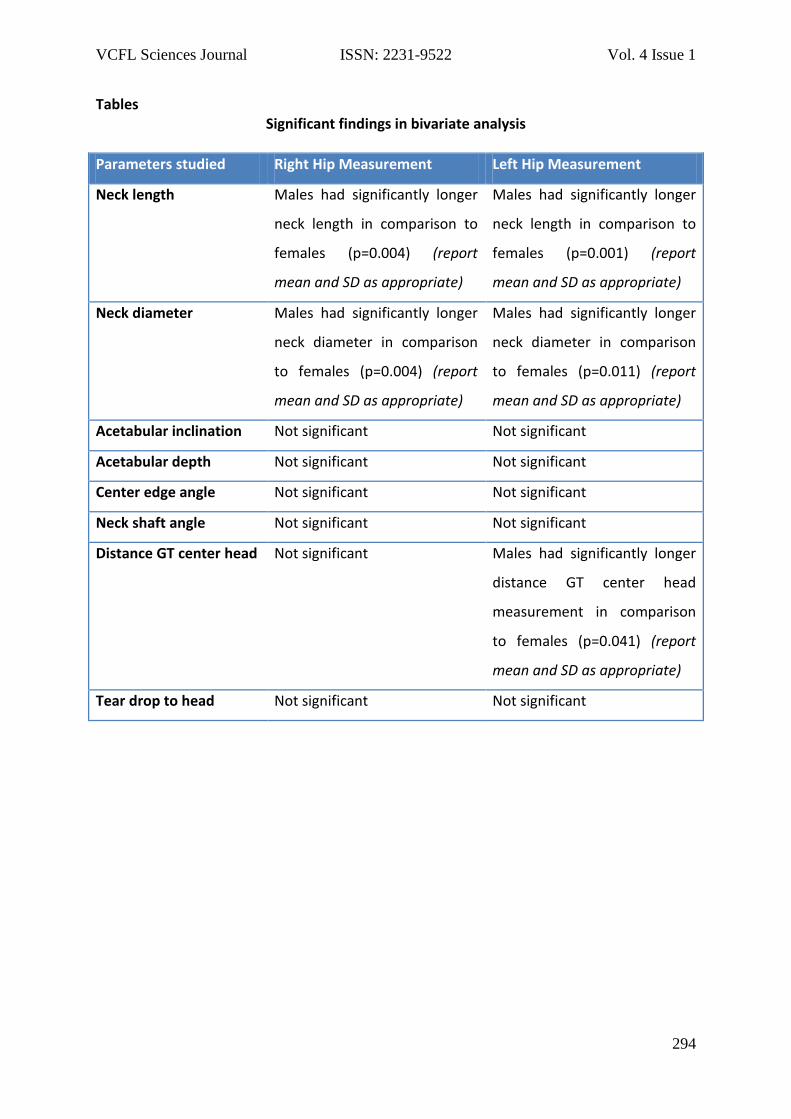
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
294
Tables Significant findings in bivariate analysis
Parameters studied Right Hip Measurement Left Hip Measurement
Neck length Males had significantly longer
neck length in comparison to
females (p=0.004) (report
mean and SD as appropriate)
Males had significantly longer
neck length in comparison to
females (p=0.001) (report
mean and SD as appropriate)
Neck diameter Males had significantly longer
neck diameter in comparison
to females (p=0.004) (report
mean and SD as appropriate)
Males had significantly longer
neck diameter in comparison
to females (p=0.011) (report
mean and SD as appropriate)
Acetabular inclination Not significant Not significant
Acetabular depth Not significant Not significant
Center edge angle Not significant Not significant
Neck shaft angle Not significant Not significant
Distance GT center head Not significant Males had significantly longer
distance GT center head
measurement in comparison
to females (p=0.041) (report
mean and SD as appropriate)
Tear drop to head Not significant Not significant
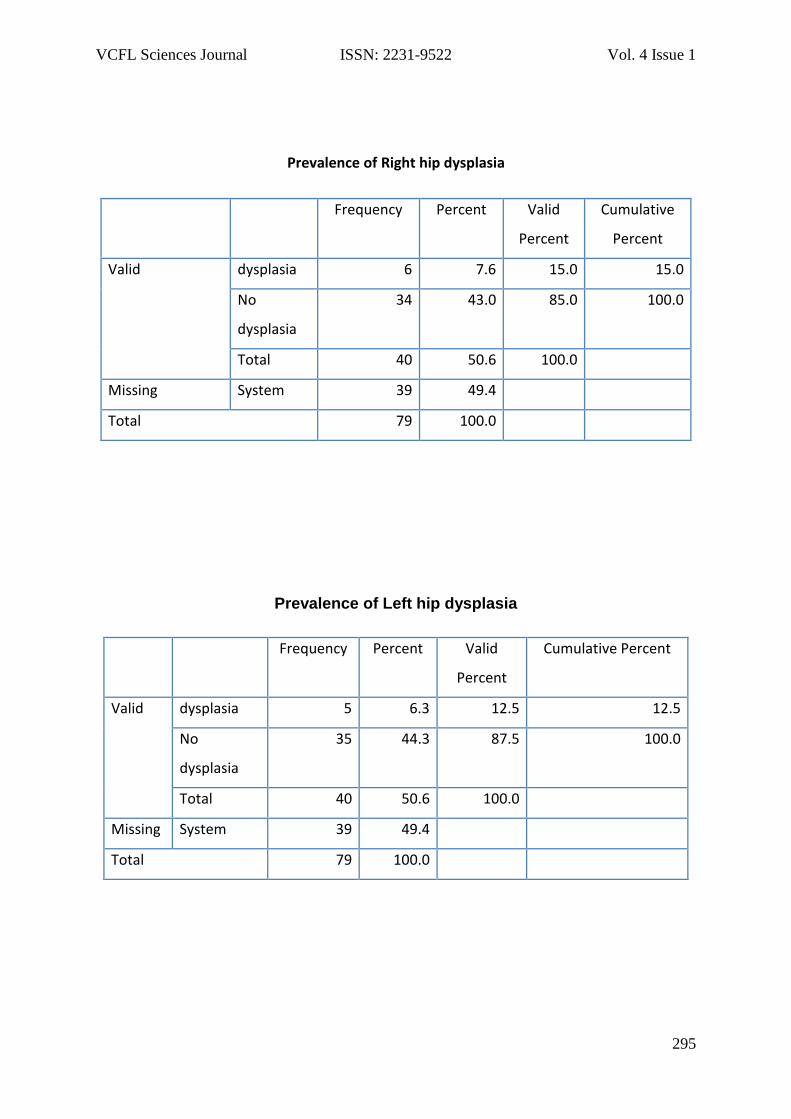
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
295
Prevalence of Right hip dysplasia
Frequency Percent Valid
Percent
Cumulative
Percent
Valid dysplasia 6 7.6 15.0 15.0
No
dysplasia
34 43.0 85.0 100.0
Total 40 50.6 100.0
Missing System 39 49.4
Total 79 100.0
Prevalence of Left hip dysplasia
Frequency Percent Valid
Percent
Cumulative Percent
Valid dysplasia 5 6.3 12.5 12.5
No
dysplasia
35 44.3 87.5 100.0
Total 40 50.6 100.0
Missing System 39 49.4
Total 79 100.0
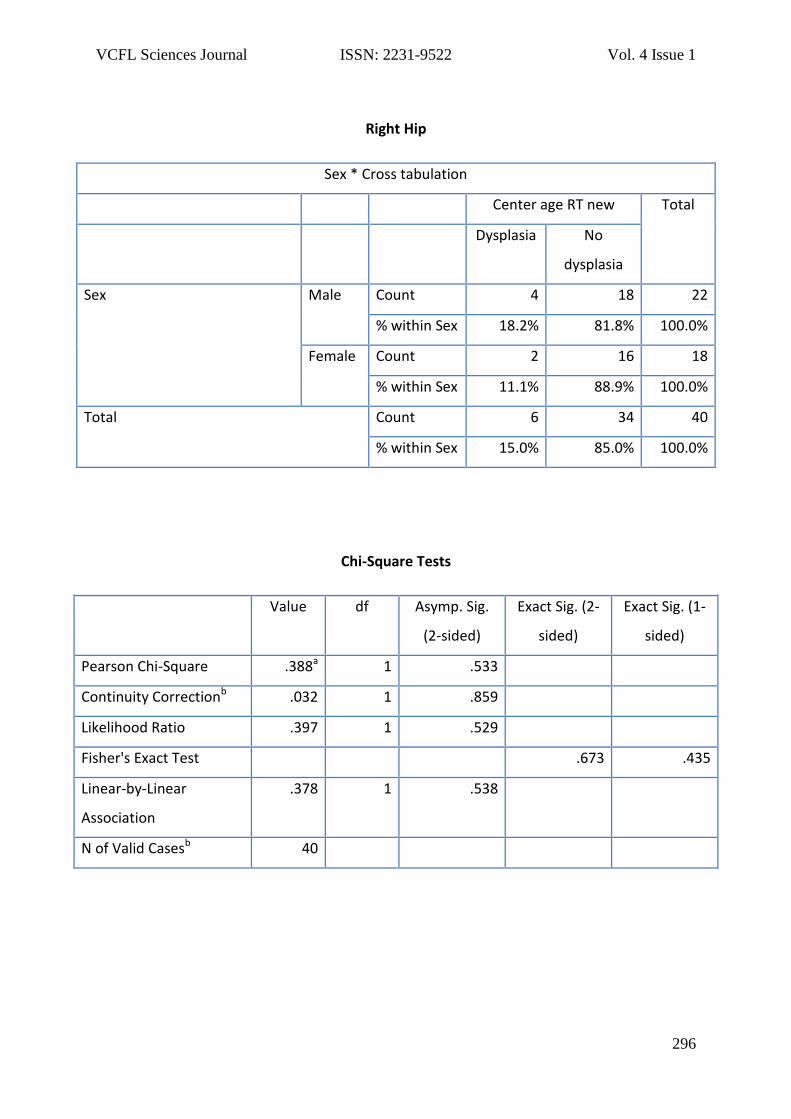
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
296
Right Hip
Sex * Cross tabulation
Center age RT new Total
Dysplasia No
dysplasia
Sex Male Count 4 18 22
% within Sex 18.2% 81.8% 100.0%
Female Count 2 16 18
% within Sex 11.1% 88.9% 100.0%
Total Count 6 34 40
% within Sex 15.0% 85.0% 100.0%
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig. (2-
sided)
Exact Sig. (1-
sided)
Pearson Chi-Square .388a 1 .533
Continuity Correctionb .032 1 .859
Likelihood Ratio .397 1 .529
Fisher's Exact Test .673 .435
Linear-by-Linear
Association
.378 1 .538
N of Valid Casesb 40
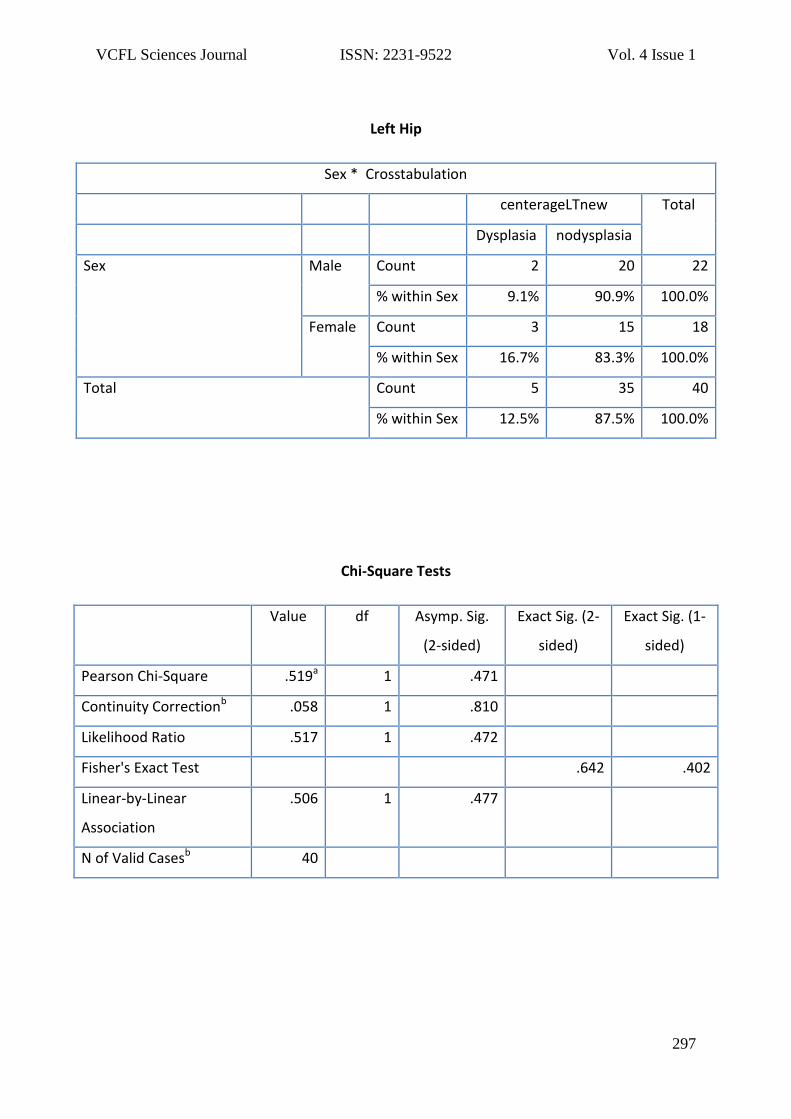
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
297
Left Hip
Sex * Crosstabulation
centerageLTnew Total
Dysplasia nodysplasia
Sex Male Count 2 20 22
% within Sex 9.1% 90.9% 100.0%
Female Count 3 15 18
% within Sex 16.7% 83.3% 100.0%
Total Count 5 35 40
% within Sex 12.5% 87.5% 100.0%
Chi-Square Tests
Value df Asymp. Sig.
(2-sided)
Exact Sig. (2-
sided)
Exact Sig. (1-
sided)
Pearson Chi-Square .519a 1 .471
Continuity Correctionb .058 1 .810
Likelihood Ratio .517 1 .472
Fisher's Exact Test .642 .402
Linear-by-Linear
Association
.506 1 .477
N of Valid Casesb 40

VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
298
Usefulness of Fine needle aspiration cytology in the evaluation of
the Nodular Goiter with histopathological correlation Purushotham Krishnappa1, Sowmya Ramakrishnappa2
1Consultant Pathologist & Faculty of Pathology, International Medical University, Kuala
Lumpur.
2Department of Community medicine, University Putra Malaysia, Kuala Lumpur.
Corresponding Author
Dr Purushotham Krishnappa E mail: [email protected] Abstract
Aim: To assess the usefulness of fine needle
aspiration (FNA) in making a diagnosis of
multinodular goiter by correlating with the
histopathology wherever possible.
Materials & methods: All the patients
presented with multinodular thyroid
swellings at the Karnataka Institute of
Medical Sciences, Hubliunderwent FNAC
procedure. After careful analysis of the
slides, a cytological diagnosis was made.
This diagnosis was compared with
histological diagnosis wherever possible.
Analyses were evaluated using descriptive
statistics.
Results: A total of 41 patients were included
in the study. The mean age was 39 years.
The majority of the patients were females
(85.4%). The results of thyroid FNA revealed
that 7.3% (3) of the samples were
inadequate and did not yield a diagnosis.
Overall, the results of the tests were good,
revealing the diagnostic accuracy of 89%.
Conclusion: Thyroid FNA is a useful test in
the evaluation of multinodular goiter.
Keywords
Fine-needle aspiration, malignancy,
multinodular goiter
Introduction
Thyroid nodules are common clinical
encounters1. Nodular goiter forms an
important group of thyroid lesions which is
a major problem across the globe. The main
challenge in the clinical practice is to
differentiate accurately the malignant
nodules from the more common and
benign nodules so that an accurate pre-
operative tissue diagnosis is made and
allows theappropriatemanagement of the
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
299
patient2.The incidence of malignancy in
multinodular goiter (MNG) ranges from 1%
to 10%3.
Fine-needle aspiration (FNA) cytology is a
well-established procedure in the primary
diagnosis of thyroid disorders4.However,
the usefulness of FNA in multinodular goiter
is controversial. The study done by Antonio
Rνos et al reported that FNA is not useful
for differentiating MNG with malignant
thyroid lesions, as more than 80% of
carcinomas go unnoticed5, whereas other
study reported the ability to discriminate
11.7% of patients with a 34% probability of
malignancy (suspicious/malignant cytology)
from 81.2% of patients (benign cytology)
with a probability of only 3% of
malignancy6.
The aim of this study was to assess the
ability of thyroid FNA in accurately
diagnosing the multinodular goiter.
Materials and methods
A total of 41 cases presented with nodular
swelling of thyroid to the pathology
department at Karnataka institute of
Medical sciences were included in the
study. After a detailed explanation of the
FNAC procedure, aninformed verbal
consent was obtained from all the patients.
The demographic details and a detailed
history were obtained from the patients.
With the aseptic precautions all the
patients underwent fine needle aspiration
cytology.11 out of 41 cases underwent
surgery with subsequent histopathological
studies. The diagnosis of which was
compared with cytological diagnosis.
Results
The study had majority of the patients as
females 35 (85.4%) and 6(14.6%) cases
were males. Patient’s age ranged from 10
to 80 years. With maximum number of
patients in the age group of 20 – 29 years.
(Table1)
Out of 41 cases, 36 were in euthyroid state
remaining 5 had clinical signs and
symptoms of hyperthyroidism. All of them
presented with thyroid enlargement which
was diffuse, smooth and firm in 8, diffuse
nodular in 7 and remaining 26 had solitary
nodule. Size of the enlarged thyroid varied
from 1to 8 cm with surface smooth to
multinodular. Duration of enlargement
ranged from 4days to 20 years.
Aspirate was hemorrhagic in 7 patients. In
the remaining 34 patients aspirate
consisted of 0.25 - 10 ml of brown /
chocolate brown fluid.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
300
Out of 41 samples, 3 samples yielded
inadequate follicular cells to conclude a
diagnosis and were reported as inadequate
samples. The remaining 38 cases were
diagnosed as nodular goiter. Aspirates were
cellular with honeycomb pattern of
follicular cells in 6 (14.6%) cases. Follicular
cells were arranged in small clusters and
singles in 35(73.1%) with few bare nuclei.
Pseudopapillary arrangement was seen in
2(4.8%) cases. Follicular cells showed mild
anisonucleosis in 38(92.6%). Fire flare was
observed in 11(26.8%). Askanazy cells were
present in 10 cases. Majority of these
showed abundant colloid (38 aspirates), in
the remaining 3 scant colloid was seen.
Foamy macrophages, sparse lymphocytes,
hemosiderin laden macrophages were seen
in most of the aspirates (Table 2).
Comparison of diagnosis of nodular goiter
by FNA and histopathology
Histopathological study was available in 11
cases. Cytological diagnosis of nodular
goiter was confirmed in 9 cases. The other
two cases were diagnosed as neoplastic
lesions with follicular adenoma and
follicular carcinoma respectively as shown
in the table 3.
Discussion:
In the current study we compared the
usefulness of FNA to histology results in
evaluating the thyroid nodules. There has
been series of clinical studies made on the
usage of fine needle aspiration cytology in
evaluating the thyroid nodules. However,
the utilization of this technique on the
multinodular goiter is not very much
established.
The study by Antonio Rios et al reports no
significant sensitivity and specificity of FNA
towards the diagnosis of nodular goiter6.
Furthermore this was supported by
Mandreker et al7 and Franklyn et al8. Our
study finds the diagnosis made by cytology
was 82% accurate when correlated with the
tissue diagnosis.
Review of literature has pointed out many
important issues in the varying results of
FNAC accuracy of diagnosing nodular
goiters9. One of the keyissues with MNG is
which nodule is to be aspirated10. A few
researchers claim that it is not
correct/ethical to aspirate all palpable
nodules when the clinical suspicion of
malignancy is minimal and they propose
that the aspiration should be done only
from the one or two of the prominent
thyroid nodules of each thyroid lobe and
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
301
from the nodules which are suspected to be
malignancy clicnially6.
FNA being a blind technique has limitations
like inadequateyield and false negative
results4. Inadequate samples results when
the lesions are cystic or vascular, yielding a
dilute specimen and few follicular cells.
False negative results occur majorly
because of wrong nodule being sampled11.
Literature also points out with addition of
ultrasound the efficacy of the FNA
technique increases greatly and reduces the
above mentioned limitations12.
Conclusion
FNAC is animportant baseline investigation
of thyroid disease with high specificity and
accuracy. We conclude that FNAC diagnosis
of nodular goiter is significant. However, we
caution about the false negative results
which can miss the possibility of a
neoplastic lesions. Thus, the final should be
based upon histopathology.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
302
References
1. TamasSolymosi, GyulaLukacsToth and
MiklosBodo: Diagnostic accuracy of fine
needle aspiration cytology of the
thyroid. Acta cytological 45: 669-674,
2001.
2. Sachmechi I, Miller E, Varatharajah R,
Chernys A, Carroll Z, Kissin E, et al.
Thyroid carcinoma in single cold nodules
and in cold nodules of multinodular
goiters. EndocrPract. 2000;6:5–
3. Vander JB, Gaston EA, Dawber TR. The
significance of nontoxic thyroid nodules.
Final report of a 15-year study of the
incidence of thyroid malignancy. Ann
Intern Med. 1968; 69:537–40. 7
4. P. Krishnappa, S. Ramakrishnappa, M.H.
Kulkarni. “Comparison of Free Hand
versus Ultrasound guided Fine Needle
Aspiration of Thyroid with
Histopathological correlation”. Journal
of Environmental pathology, Toxicology
& Oncology. 2013 Vol.32 Issue 2: 149-
155.
5. Ríos A, Rodríguez JM, Galindo PJ,
Montoya M, Tebar FJ, Sola J, et al. Utility
of fine-needle aspiration for diagnosis of
carcinoma associated with multinodular
goiter. ClinEndocrinol (Oxf) 2004;
61:732–7.
6. Cap J, Ryska A, Rehorkova P, Hovorkova
E, Kerekes Z, Pohnetalova I. Sensitivity
and specificity of the fine needle
aspiration biopsy of the thyroid: Clinical
point of view. ClinEndocrinol
(Oxf)1999;51:509–15
7. Mandreker SR, Nadkarni NS, Pinto RG,
Menezes S. Role of fine needle
aspiration cytology as the initial
modality in the investigation of thyroid
lesions. ActaCytol. 1995; 39:898–904.
8. Franklyn JA, Daykin J, Young J, Oates
GD, Sheppard MC. Fine needle
aspiration cytology in diffuse or
multinodular goiter compared with
solitary thyroid nodules. BMJ. 1993;
307:240.
9. Lopez LH, Canto JA, Herrera MF,
Gamboa-Dominguez A, Rivera R,
Gonzalez O, et al. Efficacy of fine-needle
aspiration biopsy of thyroid nodules:
Experience of a Mexican
institution. World J Surg.1997; 21:408–
11.
10. Gharib H. Fine needle aspiration biopsy
of thyroid nodules: Advantages,
limitations and effect. Mayo Clin
Proc. 1994; 69:44–9.
11. Md. Shafiqul I, Belayat H S, Nasima A,
Kazi S S, Mohammad A. Comparative
study of FNAC and histopathology in the
diagnosis of thyroid swelling.
Bangladesh J Otorhinolaryngol. 16 (1);
April 2010.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
303
12. E. Papini, R. Guglielmi, A. Bianchini et
al., “Risk of malignancy in non-palpable
thyroid nodules: predictive value of
ultrasound and color-doppler
features,” Journal of Clinical
Endocrinology and Metabolism 2002,
vol. 87(5), 1941–1946,
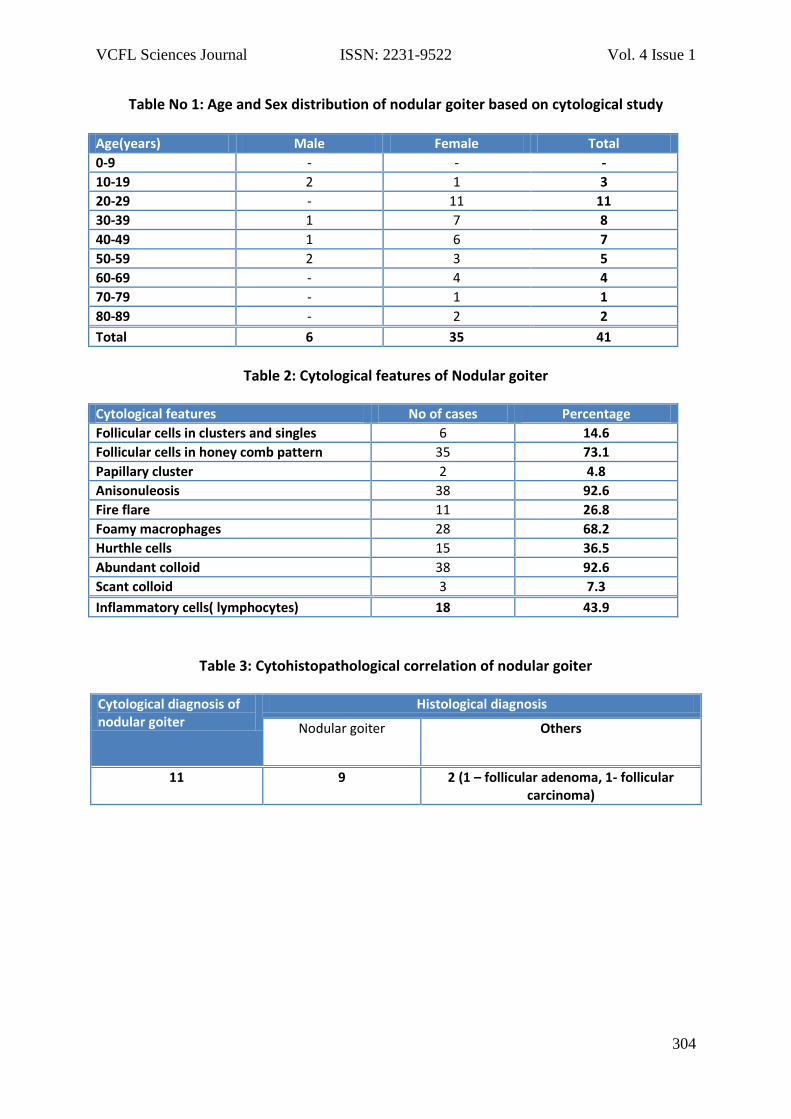
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
304
Table No 1: Age and Sex distribution of nodular goiter based on cytological study Age(years) Male Female Total
0-9 - - -
10-19 2 1 3
20-29 - 11 11
30-39 1 7 8
40-49 1 6 7
50-59 2 3 5
60-69 - 4 4
70-79 - 1 1
80-89 - 2 2
Total 6 35 41
Table 2: Cytological features of Nodular goiter
Cytological features No of cases Percentage
Follicular cells in clusters and singles 6 14.6
Follicular cells in honey comb pattern 35 73.1
Papillary cluster 2 4.8
Anisonuleosis 38 92.6
Fire flare 11 26.8
Foamy macrophages 28 68.2
Hurthle cells 15 36.5
Abundant colloid 38 92.6
Scant colloid 3 7.3
Inflammatory cells( lymphocytes) 18 43.9
Table 3: Cytohistopathological correlation of nodular goiter
Cytological diagnosis of nodular goiter
Histological diagnosis
Nodular goiter Others
11 9 2 (1 – follicular adenoma, 1- follicular carcinoma)

VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
305
Impact of Standardized Feeding Regime on Incidence of
Necrotizing Enterocolitis in Low Birth Weight Babies
Manjunatha Sarthi1, Mohamed HaseenBasha2, Chandini K3, Ashoka4, Prasad B S5
Associate professor1, Assistant professor2, Resident3, Associate professor4, Professor5
Department of pediatrics, S.S. Institute of Medical Sciences & Research Center
Davangere 577005, Karnataka, India
Corresponding Author
Dr.B.S.PRASAD
Email: [email protected]
Abstract
Objective: The objective of this study was
to evaluate the role of standardized feeding
regime in reducing the incidence of
Necrotising Enterocolitis (NEC) in Low Birth
Weight (LBW) babies.
Methods: Prospective study conducted on
all LBW babies admitted to level III NICU
from July 2009 to June 2011.
Results: There were 250 LBW babies
admitted to NICU, out of these 20 were
excluded from the study. The remaining 230
were categorized in to 5 groups based on
the birth weight. In group I, two babies out
of 35 developed NEC (7.1%). In group II, one
baby out of 40 developed NEC (3.1%). In
group III, group IV and group V, none had
NEC.
Conclusion: Implementation of
standardized feeding regime in LBW babies
results in significant reduction in incidence
of NEC.
Keywords: Necrotising Enterocolitis (NEC),
Low Birth Weight (LBW), Feeding
guidelines.
Introduction
Premature birth is defined as birth of baby
before 37 completed weeks of gestation
from 1st day of last menstrual
period1.Premature infants are at greater risk
of short term complications like difficulty in
feeding, feed intolerance, vomiting,
necrotizing enterocolities1 and risk of
infection due to prolong intravenous
catheterization for parentral nutrition. The
long term complications include cognitive
dysfunction2, learning disability3, protein
energy malnutrition and gastro-esophagus
reflux disease and so on.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
306
Proper nutrition in postnatal age is essential
for normal growth, immunity, long term
health and optimal neurologic and cognitive
development. Providing adequate nutrition
to preterm infants is challenging because of
immaturity of bowel function, inability to
suck and swallow, high risk of necrotizing
enterocolitis (NEC) 1, illnesses that may
interfere with adequate enteral feeding
(e.g., RDS, PDA), sepsis causing feed
intolerance.NEC may result from initial
mucosal injury secondary to multiple
factors leading to a loss of mucosal integrity
in an immature gut 4, 5, 6. The combination
of bacterial colonization, mucosal injury and
enteral feedings predispose the baby to
develop NEC7.
Currently no single specific preventive
strategy exists for NEC.Many consider NEC
as almost unpreventable given its poorly
understood patho-physiology,and the
difficulties in preventing prematurity, the
single most important risk factor for
development of NEC8. Besides prematurity,
only enteral feeding has a firm association
with NEC, considering that only 10% of the
cases occur in neonates who have never
been fed9. Epidemilogical data strongly
suggest that NEC has an iatrogenic
component related to variations in clinical
practices including feeding strategies10.A
significant and prolonged decline in the
incidence of NEC, nearing virtual
elimination in some countries, has been
reported consistently since implementation
of a standardized feeding regimen (SFR) 11,
12.
Methods
This study was prospective study on LBW
babies from level III NICU of S. S. Institute of
Medical Science and research centre after
implementation of standardized feeding
regime. A standardized feeding regime was
developed through clinical consensus of the
faculty in the department on the basis of
review of literature and other center
feeding protocol. Study was conducted
from July 2009 to June 2011 for a period of
2 years.
All preterm (< 37 completed weeks of
gestation) babies admitted to NICU within
24hrs of life were enrolled in study.
The Exclusion criteria were
1. Congenital anomalies that interfere
with feeding like cleft palate,
esophageal atresia, trachioesophageal
fistula and so on.
2. Those babies admitted to hospital after
24hrs of birth.
3. Babies with respiratory distress due to
any cause.
4. Babies requiring ventilator care.
5. Hemodynamically unstable babies.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
307
6. Babies with hypoxic ischaemic
encephalopathy (>/= stage II of sarnat
classification of HIE)13
7. Babies who develops septicemia14
These babies were categorized based on
their birth weight as group I to V after
excluding those babies who met exclusion
criteria.
Assessment of gestation is done by using
modified Ballard`s chart 15. Babies were
weighed at admission and then daily on an
electronic weighing scale of ESSAE model
which has accuracy of ±10gm.
Written informed consent was taken from
parents before inclusion of babies in to
studies.Ethical clearance was taken from
Institute Ethical Committee. After inclusion,
a detailed history was taken for each
neonate to determine the risk factors for
LBW. Babies were categorized to five
groups on the basis of birth weight and
feeding was started according to birth
weight with a standardized feeding regime
through nasogastric tube as shown in table
1. All babies were started with mother`s
milk and in case if mother milk is not
available, Low birth weight formula feed
has been given. The outcome were
measured in the form of necrotizing
enterocolitis, feed intolerance, abdominal
distension and weight gain pattern during
hospital stay.
Babies with <32 weeks postmenstrual age
were given nasogastric tube feeding
intermittently as their sucking and
swallowing mechanism is immature. Direct
Breast feeding was started in such babies
after reaching corrected gestational age of
32 weeks, and is clinically stable and has
sucking and swallowing coordination. The
transition from tube to breast was gradual
and was managed by the nursing staffs.
Mothers will be encouraged to follow a
breast-feeding regimen i.e. an increase in
length and frequency of breast feeds and a
reduction in volume and frequency of tube
top ups. Feeds were stopped immediately,
if there is any clinical evidence of NEC
(modified Bell’s stage >/=1)17or features of
bowel obstruction like Increasing abdominal
distension, heavily bile-stained vomitus or
aspirates, having significant gastrointestinal
bleeding. Feed tolerance monitored by
abdominal girth and abdominal distention
and growth by daily Weighing.
Results
There were 250 LBW babies admitted to
NICU, out of these 20 were excluded from
the study as 11 babies required ventilator
support for Respiratory Distress Syndrome
and 9 babies had sepsis.Among 230
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
308
babies,119 were males and 111 were
females. Table 2 showing demographic
details and basal data of patients including
the weeks of gestation, hours of life at the
time of admission and birth weight.
In group I, there were 35 babies of which 28
were enrolled. Weeks of gestation was
ranging from 28 to 30 weeks, hours of life at
the time of admission was ranging from 1 to
5 Hrs and Birth weight was ranging from
860 to 980 grams. In group II, there were 40
babies of which 32 were enrolled. Weeks of
gestation was ranging from 28 to 32 weeks,
hours of life at the time of admission was
ranging from 2 to 7 Hrs and Birth weight
was ranging from 1100 to1240 grams. In
group III, there were 60 babies of which 58
were enrolled. Weeks of gestation was
ranging from 30 to 35 weeks, hours of life at
the time of admission was ranging from 2 to
10 Hrs and Birth weight was ranging from
1260 to 1480 grams. In group IV, there were
60 babies of which 58 were enrolled. Weeks
of gestation was ranging from 34 to 36
weeks, hours of life at the time of admission
was ranging from 2 to 18 Hrs and Birth
weight was ranging from 1560 to 1800
grams. In group V, there were 55 babies of
which 54 were enrolled. Weeks of gestation
was ranging from 34 to 36 weeks, hours of
life at the time of admission was ranging
from 2 to 10 Hrs and Birth weight was
ranging from 1820 to 1880 grams.
Table 3 showing the Mean and SD of full
feeding reached, weight gain started days,
discharge weight and hospital stay in days
in each group and incidence and % of
incidence of NEC. In group I, full feed was
reached by 15-19days, weight gain started
from 21-26 days, discharge weight was
ranging from 1200 to 1320grams, and total
duration of hospital stay was ranging from
34-48 days. Two patients out of 35
developed NEC (7.1%) in this group. In
group II, full feed reached by 8-14 days,
weight gain started from 11-19 days,
discharge weight was ranging from 1200 to
1400grams, and total duration of hospital
stay was ranging from 18-40 days. One
patient out of 40 developed NEC (3.1%).In
group III, full feed reached by 6-10 days,
weight gain started from 9-16 days,
discharge weight was ranging from 1260 to
1500 grams, and total duration of hospital
stay was ranging from 11-27 days. None
had NEC in this group. In group IV, full feed
reached by 5-9 days, weight gain started
from 7-14 days, discharge weight was
ranging from1480 to 1800grams, and total
duration of hospital stay was ranging from
9-18 days. None had NEC in this group. In
group V, full feed reached by 4-5 days,
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
309
weight gain started from 7-9 days,
discharge weight was ranging from 1700 to
1820 grams, and total duration of hospital
stay was ranging from 8-14 days. None had
NEC in this group.
Discussion
Currently no single specific strategy exists
for preventing NEC.Prematurity is one of
the most important risk factor for NEC18,
which is most difficult to control. With
improvement in care of preterm babies, the
survival of preterm babies has improved
further. Besides prematurity, only enteral
feeding has a firm association with
NEC.There are limited number of studies to
compare the incidence of NEC and
implementation of the standardized feeding
regime.
Our study showed a prevalence of NEC is
about1.3% which is comparable with 5% of
prevalence of NEC of total NICU admissions,
i.e., implementation of standardized
feeding regime has reduced the incidence
of NEC in high risk group. The benefit of
feeding regimen could be related to
decreasing variations in enteral feeding
practices as well as increased awareness
leading to early detection and management
of feed intolerance. Variations in enteral
feeding strategies in clinical practice has
been proposed to be iatrogenic component
of NEC.19, 20
Variations in enteral feeding strategies for
preterm neonates have also been reported
by parole et al.21Given such evidence and
the consistent reports of significant and
prolonged decline in the incidence of NEC
after implementation of SFR,it is almost
certain that variations in clinical practice
contribute to the incidence of
NEC.Kamitsuka et al,22 developed a SFR to
reduce variability in feeding practice for
neonates weighing >1250 gm. The risk of
NEC was reduced by 84% after the
introduction of feeding schedules. Before
the feeding schedules, those who
developed NEC were more likely (73.3% v
52.1%) to have been started on formula and
receive it as the first feed(83% v 20%) than
those who developed NEC after
implementation of the feeding
schedules.Brown et al,23reported that NEC
was virtually eliminated from their nursery
after they implemented a cautious and
conservative feeding schedule.Spritzer et
al,24 introduced a cautious a SFR based on
the recommendations of Brown et al,and
reported their experience as dramatic
decrease in the incidence of NEC.
The process per se developing and
implementing aSFR is associated with an
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
310
increased awareness of the existing
evidence and with early detection and
management of NEC.The benefits of SFR
may be related to the process of developing
and implementing the SFR as well as to the
constituents of the SFR itself. The
differences in the population
characteristics, clinical practices and
constituents of SFR in the various studies,
however indicate that the benefits are most
probably related to the process of
developing and implementing the SFR
rather than its specific constituents.
Our study was a hospital based study the
prevalence of the NEC and outcome may be
different from a community setting. In our
study the feeding was started and
categorization was on the basis of birth
weight and gestational age was not
considered which has direct correlation
with gut prematurity and high incidence of
NEC. We didnot make different feeding
regime for IUGR babies and AGA babies
which might also have some influence on
outcome.
CONCLUSION:
Our study showed that
implementation of SFR can reduce the
incidence of NEC in high risk group.The
benefit of feeding regimen could be related
to decreasing variations in enteral feeding
practices as well as increased awareness
leading to early detection and management
of ‘’feeding intolerance” and early NEC.
ACKNOWLEDGEMENTS:
The authors would like to thank all the
babies and their parents, their
colleagues for their participation and
cooperation in this study.
CONFLICT OF INTEREST: None
ETHICAL CLEARENCE: Institutional ethical
clearance obtained
SOURCE OF FUNDING: Self
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
311
REFERENCES:
1)Klingman,Stanton,St.Geme,Schor, Behrman, Prematurity and intrauterine growth restriction, Nelson text book of pediatric,19th edition, 555 2)Aizenman E, White WF, Loring RH, Rosenberg PA (August 1990). "A 3,4-dihydroxyphenylalanine oxidation product is a non-N-methyl-D-aspartate glutamatergic agonist in rat cortical neurons". Neuroscience Letters116 (1-2): 168–71. PMID1979663. 3) Frye RE, Landry SH, Swank PR, Smith KE (2009). "Executive dysfunction in poor readers born prematurely at high risk".Developmental Neuropsychology34 (3): 254-71.doi10.1080/87565640902805727. PMC2692028.PMID 19437202.: 4)Koloske AM. Pathogenesis and prevention of necrotizing enterocolities. Pediatrics 2010; 125; 777-785. 5)Reber KM. Neonatal intestinal circulation: physiology and pathophysiology. ClinPerinatol 2002; 29:23-39. 6) Wynn JL,Wong H R. pathophysiology and treatment of septic shock in neonate: clinPerinatol 2010; 30:50-54. 7)Kosloske AM. Pathogenesis and prevention of necrotizingenterocolities.Pediatric 1984; 74:1086-1092. 8) Singh, singh,&shikha,2007.a prospective analysis of etiology and outcome of preterm labour. The journal of obstrics and Gyneclogy OG india.57 (1), 48-52. 9) Samantha S. et al. Feeding the low birth weight infants. Indian J PractPediatr 2005;7 (4):304.
10) NNF. Neonatal morbidity and mortality - Report of National Neonatal, Perinatal data base.Indian Pediatr 1997; 34. 11)Kliegman, Behrman,Jenson, Stanton, The high risk infant, Nelson edition18, pg no 702 12)GuilletR,StollBJ,CottonCM,et al. Association of h2 blocker therapy and higher incidence of necrotizing enterocolities in very low birth weight infants. Pediatrics 2006;117: e 137-142. 13) Korszun P, Dubiel M, Breborowicz G, et al. Fetal superior mesenteric arteryblood flow velocimetry in normal and high-risk pregnancy. J Perinat Med 2002; 30:235. 14) Blott M, Greenough A, Gamsu HR, et al. Antenatal factors associated with obstruction of the gastrointestinal tract by meconium. BMJ 1988; 296:250. 15)Robel-TilligE,Vogtmann C, Bennek J. Prenatal hemodynamic disturbance pathophysiological background of intesnal motility disturbances in small for gestational age infants. Eur J PediatrSurg 2002; 12:175–9. 16)Mihatsch, WA, von Schenaich P, Fahnenstich H et al. The significance of gastric residual in the early enteral feeding advancement of extremely low birth weight infants.Pediatrics 2002; 109:457-459. 17) Srinivas PS, Brandler MD. Necrotizing enterocolities: Clin in perinatal 2008; 35; 251-272. 18)Bell EF,Acarregui MJ. Restricted versus liberal water intake for preventing mortality in preterm infants, Cochrane. Database Syst Rev 3 (2001): CD000503.
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
312
19) Agwu JC, Narchi H. In a preterm infant, dose blood transfusion increases the risk of necrotizing enterocolities. Arch Dis Child 2005; 90(1):102-03. 20) RG Bury, Tudehope D. Enteral antibiotics for preventing necrotizing enterocolities in low birth weight or preterm infants. Cochrane Database Syst Rev 1(2001):CD000405. 21) DB McElhinney, et al. “Necrotizing enterocolities in neonates with congenital heart disease: risk factors and outcomes.” Pediatrics 2005; 106(5):1080-7. 22) Berseth CL, Bisquera JA Paje VU, Prolonging small feeding volumes early in the life decreasing the incidence of necrotizing enterocolities in very low birth weight infants. Pediatrc 2003; 111(3):529-34. 23) Soto TT, Oldham K.T. Abdominal drain placement versus laproscopy for NEC with perforation: Clin in perinatol2004; 24:577-589. 24) McGuire W. Slow advancement of feedvolume to prevent necrotizing enterocolities in very low birth weight infants. Cochrane Database syst Rev-01 JAN 2008 (2):CD001241.
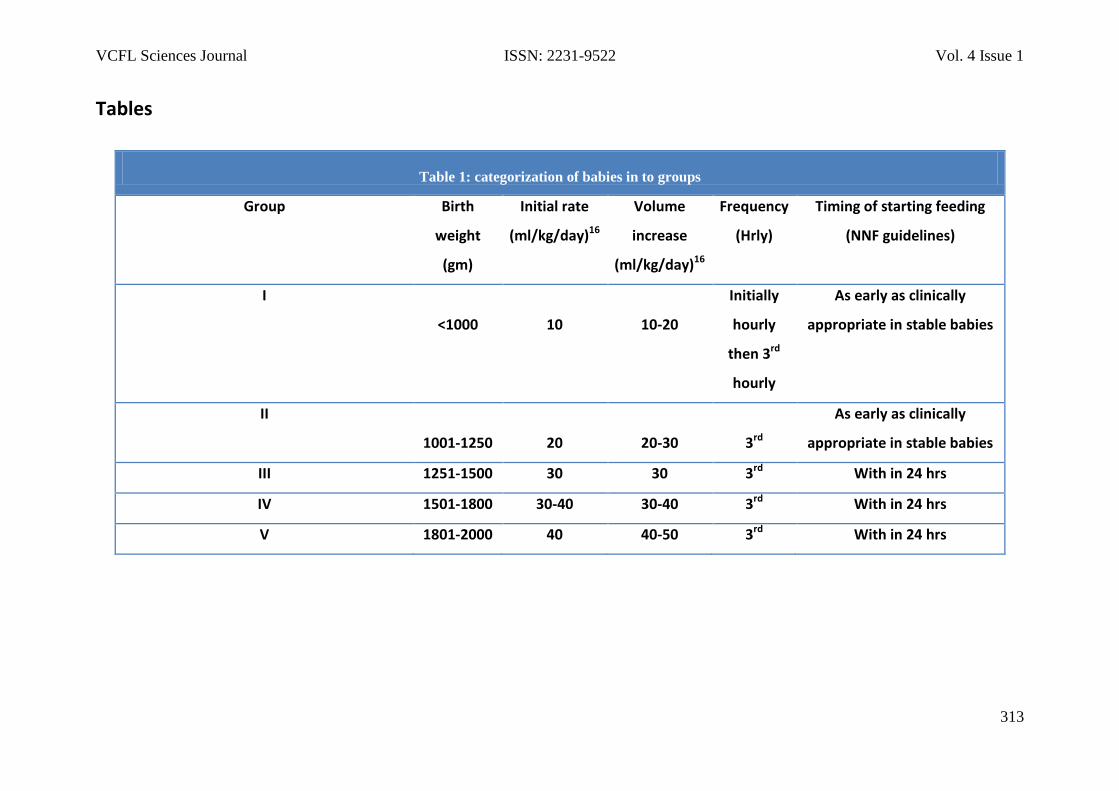
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
313
Tables
Table 1: categorization of babies in to groups
Group Birth
weight
(gm)
Initial rate
(ml/kg/day)16
Volume
increase
(ml/kg/day)16
Frequency
(Hrly)
Timing of starting feeding
(NNF guidelines)
I
<1000
10
10-20
Initially
hourly
then 3rd
hourly
As early as clinically
appropriate in stable babies
II
1001-1250
20
20-30
3rd
As early as clinically
appropriate in stable babies
III 1251-1500 30 30 3rd With in 24 hrs
IV 1501-1800 30-40 30-40 3rd With in 24 hrs
V 1801-2000 40 40-50 3rd With in 24 hrs
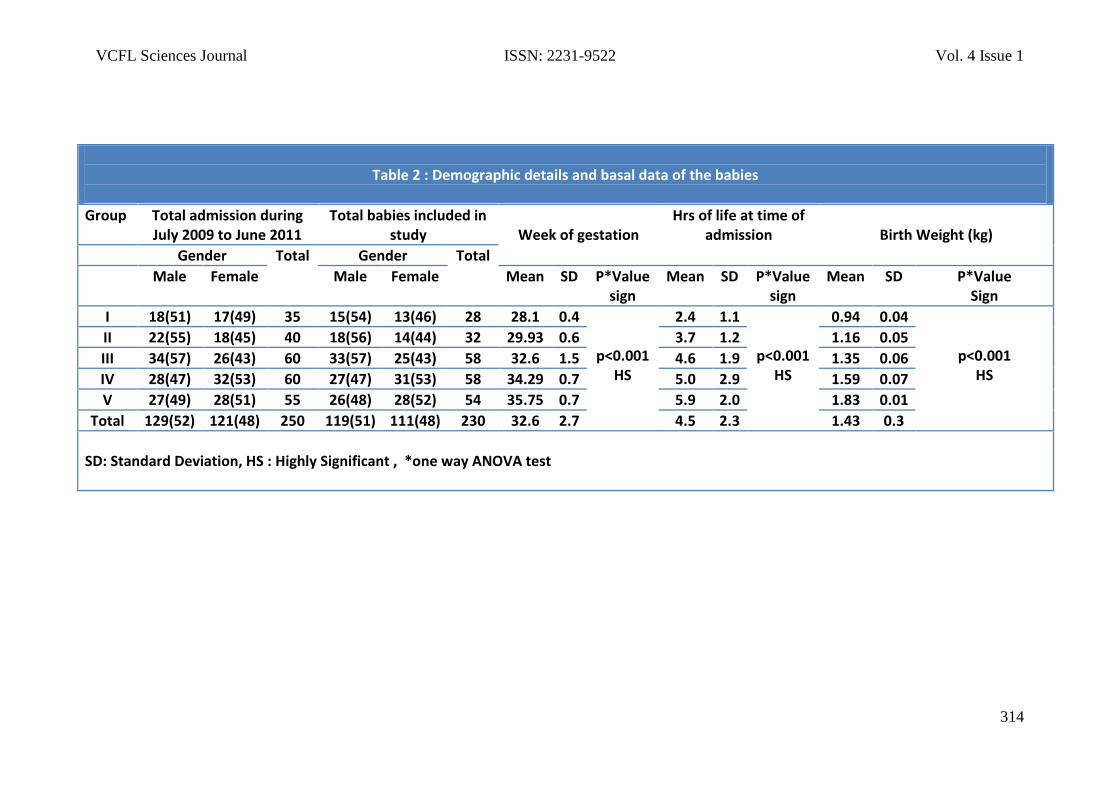
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
314
Table 2 : Demographic details and basal data of the babies
Group Total admission during July 2009 to June 2011
Total babies included in study
Week of gestation
Hrs of life at time of admission
Birth Weight (kg)
Gender Total Gender Total
Male Female Male Female Mean SD P*Value sign
Mean SD P*Value sign
Mean SD P*Value Sign
I 18(51) 17(49) 35 15(54) 13(46) 28 28.1 0.4
p<0.001 HS
2.4 1.1
p<0.001 HS
0.94 0.04
p<0.001 HS
II 22(55) 18(45) 40 18(56) 14(44) 32 29.93 0.6 3.7 1.2 1.16 0.05
III 34(57) 26(43) 60 33(57) 25(43) 58 32.6 1.5 4.6 1.9 1.35 0.06
IV 28(47) 32(53) 60 27(47) 31(53) 58 34.29 0.7 5.0 2.9 1.59 0.07
V 27(49) 28(51) 55 26(48) 28(52) 54 35.75 0.7 5.9 2.0 1.83 0.01
Total 129(52) 121(48) 250 119(51) 111(48) 230 32.6 2.7 4.5 2.3 1.43 0.3
SD: Standard Deviation, HS : Highly Significant , *one way ANOVA test
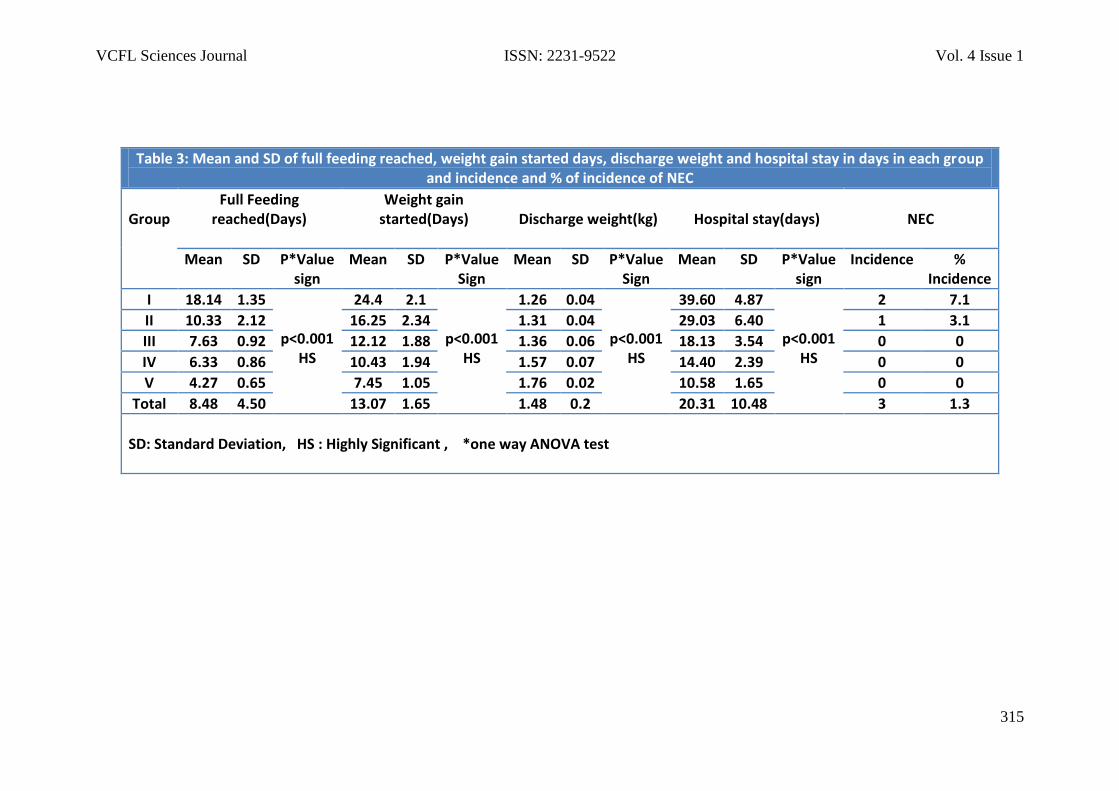
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
315
Table 3: Mean and SD of full feeding reached, weight gain started days, discharge weight and hospital stay in days in each group and incidence and % of incidence of NEC
Group
Full Feeding reached(Days)
Weight gain started(Days)
Discharge weight(kg)
Hospital stay(days)
NEC
Mean SD P*Value sign
Mean SD P*Value Sign
Mean SD P*Value Sign
Mean SD P*Value sign
Incidence % Incidence
I 18.14 1.35
p<0.001 HS
24.4 2.1
p<0.001 HS
1.26 0.04
p<0.001 HS
39.60 4.87
p<0.001 HS
2 7.1
II 10.33 2.12 16.25 2.34 1.31 0.04 29.03 6.40 1 3.1
III 7.63 0.92 12.12 1.88 1.36 0.06 18.13 3.54 0 0
IV 6.33 0.86 10.43 1.94 1.57 0.07 14.40 2.39 0 0
V 4.27 0.65 7.45 1.05 1.76 0.02 10.58 1.65 0 0
Total 8.48 4.50 13.07 1.65 1.48 0.2 20.31 10.48 3 1.3
SD: Standard Deviation, HS : Highly Significant , *one way ANOVA test
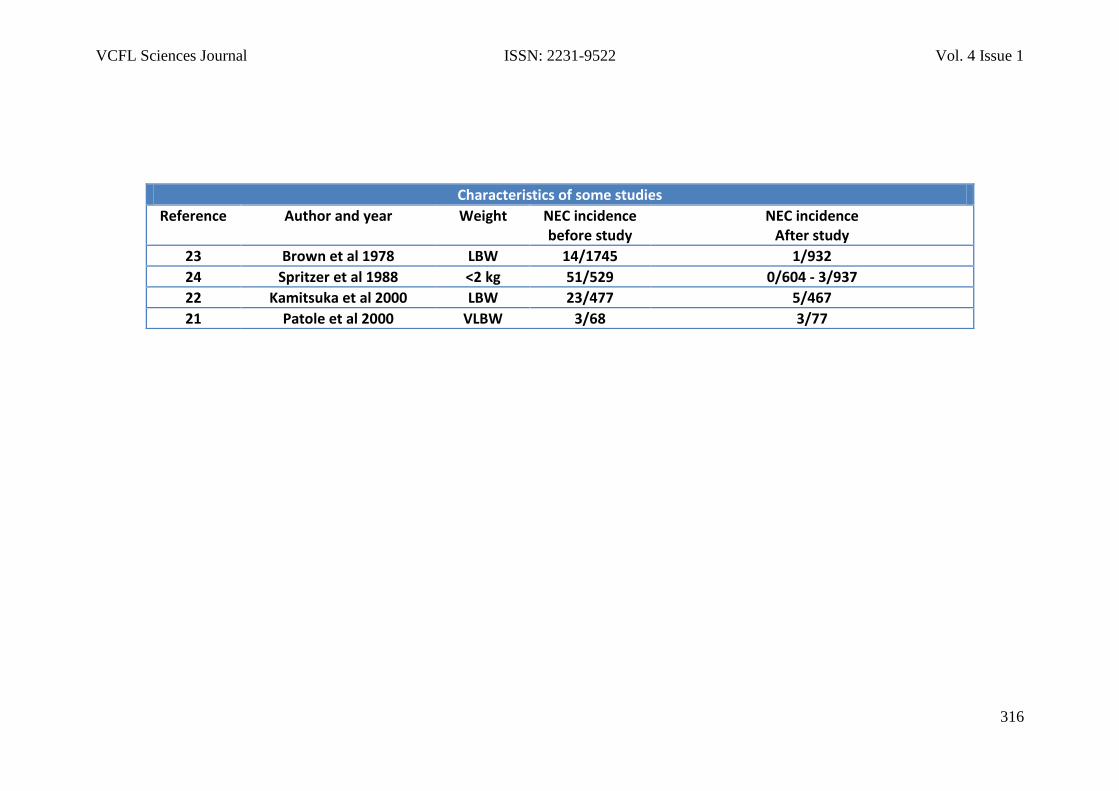
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
316
Characteristics of some studies
Reference Author and year Weight NEC incidence before study
NEC incidence After study
23 Brown et al 1978 LBW 14/1745 1/932
24 Spritzer et al 1988 <2 kg 51/529 0/604 - 3/937
22 Kamitsuka et al 2000 LBW 23/477 5/467
21 Patole et al 2000 VLBW 3/68 3/77
VCFL Sciences Journal ISSN: 2231-9522 Vol. 4 Issue 1
317
VCare For Life
Sciences Journal Online
ISSN: 2231-9522
Global Impact
Factor
0.466
Vol. 4, Issue 1
April 2014




















