
Salmonella enterica Serovar Typhi-Specific Immunoglobulin A Antibody Responses in Plasma and...
8
CLINICAL AND VACCINE IMMUNOLOGY, Nov. 2009, p. 1587–1594 Vol. 16, No. 11 1556-6811/09/$12.00 doi:10.1128/CVI.00311-09 Copyright © 2009, American Society for Microbiology. All Rights Reserved. Salmonella enterica Serovar Typhi-Specific Immunoglobulin A Antibody Responses in Plasma and Antibody in Lymphocyte Supernatant Specimens in Bangladeshi Patients with Suspected Typhoid Fever Alaullah Sheikh, 1 † M. Saruar Bhuiyan, 1 † Farhana Khanam, 1 Fahima Chowdhury, 2 Amit Saha, 1 Dilruba Ahmed, 1 K. M. A. Jamil, 1 Regina C. LaRocque, 2 Jason B. Harris, 2 Mian Mashhud Ahmad, 3 Richelle Charles, 2 W. Abdullah Brooks, 1 Stephen B. Calderwood, 2,4,5 Alejandro Cravioto, 1 Edward T. Ryan, 2,4,6 and Firdausi Qadri 1 * International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B), Dhaka, Bangladesh 1 ; Division of Infectious Diseases, Massachusetts General Hospital, Boston, Massachusetts 2 ; Dhaka Medical College Hospital, Dhaka, Bangladesh 3 ; Department of Medicine, Harvard Medical School, Boston, Massachusetts 4 ; Department of Microbiology and Molecular Center, Harvard Medical School, Boston, Massachusetts 5 ; and Department of Immunology and Infectious Diseases, Harvard School of Public Health, Boston, Massachusetts 6 Received 29 July 2009/Returned for modification 28 August 2009/Accepted 31 August 2009 Many currently available diagnostic tests for typhoid fever lack sensitivity and/or specificity, especially in areas of the world where the disease is endemic. In order to identify a diagnostic test that better correlates with typhoid fever, we evaluated immune responses to Salmonella enterica serovar Typhi (serovar Typhi) in indi- viduals with suspected typhoid fever in Dhaka, Bangladesh. We enrolled 112 individuals with suspected typhoid fever, cultured day 0 blood for serovar Typhi organisms, and performed Widal assays on days 0, 5, and 20. We harvested peripheral blood lymphocytes and analyzed antibody levels in supernatants collected on days 0, 5, and 20 (using an antibody-in-lymphocyte-supernatant [ALS] assay), as well as in plasma on these days. We measured ALS reactivity to a serovar Typhi membrane preparation (MP), a formalin-inactivated whole-cell preparation, and serovar Typhi lipopolysaccharide. We measured responses in healthy Bangladeshi, as well as in Bangladeshi febrile patients with confirmed dengue fever or leptospirosis. We categorized suspected typhoid fever individuals into different groups (groups I to V) based on blood culture results, Widal titer, and clinical features. Responses to MP antigen in the immunoglobulin A isotype were detectable at the time of presentation in the plasma of 81% of patients. The ALS assay, however, tested positive in all patients with documented or highly suspicious typhoid, suggesting that such a response could be the basis of improved diagnostic point- of-care-assay for serovar Typhi infection. It can be important for use in epidemiological studies, as well as in difficult cases involving fevers of unknown origin. Salmonella enterica serovar Typhi (serovar Typhi) is the cause of typhoid fever, an illness that affects over 20,000,000 individuals worldwide each year, killing over 200,000 (5, 8, 16). The largest burden of typhoid fever is borne by impoverished individuals in resource-poor areas of the world. Serovar Typhi is a human-restricted invasive enteric pathogen which, after ingestion, crosses the intestinal mucosa, is taken up by gut- associated lymphoreticular tissues, and enters the systemic cir- culation. Both mucosal and systemic host immune responses are stimulated after infection. Serovar Typhi is an intracellular pathogen, and antibody and cell-mediated immune responses occur after infection or immunization with live oral attenuated typhoid vaccines (10, 25, 34). Diagnostic tests for typhoid fever often lack sensitivity and/or specificity, especially in areas of the world that are endemic for typhoid fever, where clinically distinguishing ty- phoid fever from other febrile illnesses is difficult (5, 17, 39). Microbiologic culturing of blood is approximately 30 to 70% sensitive, with the highest sensitivity being associated with an absence of prior use of antibiotics and the culturing of larger volumes of blood, features that complicate this mode of diag- nosis in young children (5, 6, 8, 36). Microbiologic culturing of bone marrow aspirates is more sensitive than blood but often clinically impractical (1, 11, 12). Serum Widal assay titers are often nonspecific in endemic settings and are of limited value unless titers are markedly elevated or are analyzed for changes from acute to convalescent phases of illness (18, 33, 38). Mo- lecular diagnostic assays including PCR are promising, but issues of practicality, contamination, and quality control have limited their use in many resource-poor areas of the world (14). Since serovar Typhi interacts with both the mucosal and the systemic immune systems, we were interested to determine whether analyses of mucosal immune responses would give improved insight into this human-restricted infection. Acti- vated mucosal lymphocytes migrate from intestinal tissue and * Corresponding author. Mailing address: Immunology Unit, Labo- ratory Sciences Division, International Centre for Diarrhoeal Disease Research, Bangladesh, Dhaka, Bangladesh. Phone: 88-02-8860523-32, ext. 2431. Fax: 88-02-8823116. E-mail: [email protected]. † A.S. and M.S.B. contributed equally to this study. Published ahead of print on 9 September 2009. 1587 by on October 30, 2009 cvi.asm.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Salmonella enterica Serovar Typhi-Specific Immunoglobulin A Antibody Responses in Plasma and...

CLINICAL AND VACCINE IMMUNOLOGY, Nov. 2009, p. 1587–1594 Vol. 16, No. 111556-6811/09/$12.00 doi:10.1128/CVI.00311-09Copyright © 2009, American Society for Microbiology. All Rights Reserved.
Salmonella enterica Serovar Typhi-Specific Immunoglobulin AAntibody Responses in Plasma and Antibody in Lymphocyte
Supernatant Specimens in Bangladeshi Patients withSuspected Typhoid Fever�
Alaullah Sheikh,1† M. Saruar Bhuiyan,1† Farhana Khanam,1 Fahima Chowdhury,2 Amit Saha,1Dilruba Ahmed,1 K. M. A. Jamil,1 Regina C. LaRocque,2 Jason B. Harris,2
Mian Mashhud Ahmad,3 Richelle Charles,2 W. Abdullah Brooks,1Stephen B. Calderwood,2,4,5 Alejandro Cravioto,1
Edward T. Ryan,2,4,6 and Firdausi Qadri1*International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B), Dhaka, Bangladesh1; Division of Infectious Diseases,
Massachusetts General Hospital, Boston, Massachusetts2; Dhaka Medical College Hospital, Dhaka, Bangladesh3; Department ofMedicine, Harvard Medical School, Boston, Massachusetts4; Department of Microbiology and Molecular Center,
Harvard Medical School, Boston, Massachusetts5; and Department of Immunology and Infectious Diseases,Harvard School of Public Health, Boston, Massachusetts6
Received 29 July 2009/Returned for modification 28 August 2009/Accepted 31 August 2009
Many currently available diagnostic tests for typhoid fever lack sensitivity and/or specificity, especially inareas of the world where the disease is endemic. In order to identify a diagnostic test that better correlates withtyphoid fever, we evaluated immune responses to Salmonella enterica serovar Typhi (serovar Typhi) in indi-viduals with suspected typhoid fever in Dhaka, Bangladesh. We enrolled 112 individuals with suspected typhoidfever, cultured day 0 blood for serovar Typhi organisms, and performed Widal assays on days 0, 5, and 20. Weharvested peripheral blood lymphocytes and analyzed antibody levels in supernatants collected on days 0, 5,and 20 (using an antibody-in-lymphocyte-supernatant [ALS] assay), as well as in plasma on these days. Wemeasured ALS reactivity to a serovar Typhi membrane preparation (MP), a formalin-inactivated whole-cellpreparation, and serovar Typhi lipopolysaccharide. We measured responses in healthy Bangladeshi, as well asin Bangladeshi febrile patients with confirmed dengue fever or leptospirosis. We categorized suspected typhoidfever individuals into different groups (groups I to V) based on blood culture results, Widal titer, and clinicalfeatures. Responses to MP antigen in the immunoglobulin A isotype were detectable at the time of presentationin the plasma of 81% of patients. The ALS assay, however, tested positive in all patients with documented orhighly suspicious typhoid, suggesting that such a response could be the basis of improved diagnostic point-of-care-assay for serovar Typhi infection. It can be important for use in epidemiological studies, as well as indifficult cases involving fevers of unknown origin.
Salmonella enterica serovar Typhi (serovar Typhi) is thecause of typhoid fever, an illness that affects over 20,000,000individuals worldwide each year, killing over 200,000 (5, 8, 16).The largest burden of typhoid fever is borne by impoverishedindividuals in resource-poor areas of the world. Serovar Typhiis a human-restricted invasive enteric pathogen which, afteringestion, crosses the intestinal mucosa, is taken up by gut-associated lymphoreticular tissues, and enters the systemic cir-culation. Both mucosal and systemic host immune responsesare stimulated after infection. Serovar Typhi is an intracellularpathogen, and antibody and cell-mediated immune responsesoccur after infection or immunization with live oral attenuatedtyphoid vaccines (10, 25, 34).
Diagnostic tests for typhoid fever often lack sensitivityand/or specificity, especially in areas of the world that are
endemic for typhoid fever, where clinically distinguishing ty-phoid fever from other febrile illnesses is difficult (5, 17, 39).Microbiologic culturing of blood is approximately 30 to 70%sensitive, with the highest sensitivity being associated with anabsence of prior use of antibiotics and the culturing of largervolumes of blood, features that complicate this mode of diag-nosis in young children (5, 6, 8, 36). Microbiologic culturing ofbone marrow aspirates is more sensitive than blood but oftenclinically impractical (1, 11, 12). Serum Widal assay titers areoften nonspecific in endemic settings and are of limited valueunless titers are markedly elevated or are analyzed for changesfrom acute to convalescent phases of illness (18, 33, 38). Mo-lecular diagnostic assays including PCR are promising, butissues of practicality, contamination, and quality control havelimited their use in many resource-poor areas of the world(14).
Since serovar Typhi interacts with both the mucosal and thesystemic immune systems, we were interested to determinewhether analyses of mucosal immune responses would giveimproved insight into this human-restricted infection. Acti-vated mucosal lymphocytes migrate from intestinal tissue and
* Corresponding author. Mailing address: Immunology Unit, Labo-ratory Sciences Division, International Centre for Diarrhoeal DiseaseResearch, Bangladesh, Dhaka, Bangladesh. Phone: 88-02-8860523-32,ext. 2431. Fax: 88-02-8823116. E-mail: [email protected].
† A.S. and M.S.B. contributed equally to this study.� Published ahead of print on 9 September 2009.
1587
by on October 30, 2009
cvi.asm.org
Dow
nloaded from

circulate within peripheral blood before rehoming to mucosaltissues (20, 31). This migration peaks 1 to 2 weeks after intes-tinal infection and may be measured by using peripheral bloodmononuclear cells (PBMC) in an antibody-secreting cell(ASC) assay (19, 26) or in supernatants recovered from har-vested PBMC (the “antibody in lymphocyte supernatant”[ALS] assay) (7, 31). Although ALS and ASC responses havepreviously been measured after immunization with oral liveattenuated typhoid vaccines, detailed analyses of ALS or ASCresponses in individuals with wild-type typhoid fever are lack-ing (21, 24). In order to gain further insight into mucosalimmune responses during wild-type serovar Typhi infection,we undertook a study to characterize the serum and ALSresponses to serovar Typhi among individuals with suspectedtyphoid fever in Bangladesh.
MATERIALS AND METHODS
Study participants and specimens. Individuals 3 to 59 years of age whopresented to the International Centre for Diarrhoeal Disease Research, Bang-ladesh (ICDDR,B)-Dhaka Hospital or Dhaka Medical College Hospital withfever of 3 to 7 days duration (�39°C), without an obvious focus of infection andlacking an alternate diagnosis, were eligible for enrollment. Because of thewidespread availability of antibiotics in Bangladesh, prior use of antibiotics wasnot an exclusion criterion for the present study. Individuals were queried regard-ing headache, abdominal discomfort or pain, constipation, diarrhea, vomiting,myalgia, and loss of appetite and were assessed for lymphadenopathy, organo-megaly, rash, rose spots on the lower chest and upper abdomen, coated tongue,and relative bradycardia. We collected venous blood (5 ml from children �5years old, and 10 ml from all others) at enrollment (day 0) and 5 and 20 dayslater. For children �5 years of age, 3 ml of day 0 blood was microbiologicallycultured; for older individuals, 5 ml of day 0 blood was microbiologically cul-tured. All patients suspected of having typhoid fever were initially treated withoral ciprofloxacin (10 mg/kg of body weight twice a day, up to 500 mg twice daily)or cefixime (4 mg/kg of body weight twice a day, up to 200 mg twice daily) orinjectable ceftriaxone (100 mg/kg of body weight, up to 1 g/day), and this wascontinued for up to 14 days at the discretion of the attending physician.
We also collected single blood and stool samples from healthy Bangladeshiadults (n � 32) who denied any illness, fever, or diarrhea in the preceding 3months and were of the same socioeconomic status as the patients (30). We alsoanalyzed immune responses using previously collected acute and convalescent-phase serum specimens from patients with culture-confirmed cholera (n � 5) (2)and febrile illnesses due to serologically confirmed dengue (n � 5) and lepto-spirosis (n � 5) (23). The study and all sample collections and analyses wereapproved by the ethical and research review committees of the ICDDR,B.
Diagnosis of typhoid fever by blood culture and Widal test. Microbiologicalculturing of day 0 blood was performed by using a BacT/Alert automated system,and positive bottles were subcultured on MacConkey agar. Colonies were iden-tified by standard biochemical tests and by reaction with Salmonella-specificantisera (35). Antimicrobial sensitivity was assessed by the disc diffusion methodon a Mueller-Hinton agar plate with Oxoid disks (Oxoid, Hampshire, UnitedKingdom) containing ampicillin, ceftriaxone, ciprofloxacin, nalidixic acid, nitro-furantoin, trimethoprim, cefixime, and gentamicin (3). Widal assays were per-formed using twofold dilutions of plasma by a slide agglutination test withtyphoid-specific antigens (Omega Diagnostics, Scotland, United Kingdom). Atiter of �320 for serovar Typhi H and/or O antigen was considered a positiveresponse (27, 28).
Isolation of PBMC and collection of plasma and ALS specimens. We dilutedheparinized blood in phosphate-buffered saline (PBS; 10 mM [pH 7.2]) andisolated PBMC by density gradient centrifugation on Ficoll-Isopaque (Pharma-cia, Uppsala, Sweden). We resuspended isolated PBMC to a concentration of107cells/ml in RPMI complete medium RPMI 1640 (Gibco, Gaithersburg, MD)with 10% heat-inactivated fetal bovine serum (HyClone, Ogden, UT), 100 U ofpenicillin/ml, 100 �g of streptomycin/ml, 100 mM pyruvate, and 200 mM L-glutamine (Gibco) (31). We incubated cells for 48 h at 37°C with 5% CO2,collected supernatants, and added a protease inhibitor solution as previouslydescribed (21, 31). Plasma and ALS specimens were tested for typhoid-specificantibodies by enzyme-linked immunosorbent assay (ELISA).
Serovar Typhi antigens used in the study. In the present study, we used aserovar Typhi lipopolysaccharide (LPS) preparation, a formalin inactivated
whole-cell (WC) preparation, and a membrane preparation (MP). LPS wasprepared from a wild-type clinical isolate of serovar Typhi (strain ST004) isolatedin Bangladesh, using a previously reported phenol-water extraction procedure,followed by enzyme treatment with proteinase K, DNase, and RNase and ultra-centrifugation (9, 13). For preparation of WC extract, we cultured the wild-typeclinical isolate on nutrient agar plates and harvested into PBS. After addition offormalin (0.5%) and vortexing, we placed the cell suspension in a petri dish andincubated overnight at 37°C and confirmed the absence of viability by streakingan aliquot on a MacConkey agar plate, followed by additional overnight incu-bation at 37°C. We adjusted the suspension to 10 ml with PBS, centrifuged for 8min at 6,000 � g, washed once with PBS, and adjusted the optical density to 0.40at 600 nm with PBS (�1010 CFU/ml). We prepared MP antigen by using apreviously described procedure (4). Briefly, we cultured the strain on sheepblood agar plates (n � 20) and harvested in Tris buffer (10 mM Tris [pH 8.0], 5mM MgCl2). We sonicated the mixture, centrifuged at 1,400 � g for 10 min,transferred the supernatant to fresh tubes, centrifuged at 14,900 � g for 30 min,suspended the pellet in 10 ml of Tris buffer, and determined the protein contentby the Bio-Rad protein assay (37).
Detection of typhoid-specific antibodies in specimens by ELISA. We assayedimmunoglobulin A (IgA), IgG, and IgM isotype-specific antibody responses toLPS, WC, and MP by using ELISA. We coated microtiter plates (Nunc F; Nunc,Denmark) with 100 �l of LPS (2.5 �g/ml), WC (108 CFU/ml), and MP (2 �g/mlfor plasma and 10 �g/ml for ALS) and blocked them with 1% bovine serumalbumin in PBS (29, 31). To detect antigen-specific responses, we added 100 �lof dilutions of plasma in PBS-Tween 0.1% bovine serum albumin (1:25 for IgAand IgM and 1:50 for IgG isotypes) or 100 �l (1:2 dilution for IgA) of ALSspecimens to coated plates, which were then incubated for 90 min at 37°C. Aftera washing step with 0.05% PBS-Tween, we detected responses using horseradishperoxidase-conjugated antibodies to either human IgA, IgG (Jackson Laborato-ries, Bar Harbor, ME) or IgM (Southern Biotech, Birmingham, AL) (1:100 inPBS-Tween for IgA and IgM isotypes and 1:500 for IgG isotypes), developedplates with ortho-phenylene diamine (Sigma Chemical Co., St. Louis, MO) in 0.1M sodium citrate buffer and 0.1% hydrogen peroxide, and read the plateskinetically at 450 nm for 5 min at 19-s intervals as previously described (13). Themaximal rate of optical density change was expressed as milli-optical densityabsorbance units per minute. To control among plates, readings of unknownswere divided by readings of an in-house pooled convalescent-phase standard seraof blood culture-confirmed typhoid patients, multiplied by 100, and expressed asELISA units. A positive response was defined as being a value greater than twostandard deviations (SD) above the geometric mean of healthy controls (32).
Statistical analysis. We used SigmaStat (version3.1), Prism4, and SPSS (ver-sion 12.0 for Windows) for data management, analysis, and graphical presenta-tion. Statistical evaluation of differences between groups was performed by usingthe Mann-Whitney U test, and evaluation of differences between study days in agroup were performed by using the Wilcoxon signed-rank test.
RESULTS
Clinical and microbiological features in study subjects. Atotal of 112 febrile subjects met the inclusion criteria andcompleted the follow-up appointments. The median age was24 years, with a range of 3 to 59 years (see Table 1 for theclinical characteristics). Of these, 26 participants (23%) werepositive by blood culture for serovar Typhi. Of the isolatedserovar Typhi organisms, 16 (62%) were resistant to ampicillin,16 (62%) were resistant to trimethoprim-sulfamethoxazole, 24(92%) were resistant to nalidixic acid, and 7 (27%) were re-sistant to ciprofloxacin, but all (100%) remained susceptible togentamicin, cefixime, and ceftriaxone. Of the 112 study partic-ipants, 51(46%) reported antibiotic use prior to enrollment. Ofthe 26 blood culture-confirmed patients, 7 (27%) reported useof ciprofloxacin prior to presenting for medical care, and all 7grew a serovar Typhi strain that was resistant to ciprofloxacin.Another 13 individuals (12%) had a negative blood culture, buta fourfold increase of Widal titer comparing either day 5 or day20 blood samples to day 0 samples. Of these, 5 (38%) reportedciprofloxacin use before presenting for medical care. A total of41 participants (37%) had a negative blood culture and did not
1588 SHEIKH ET AL. CLIN. VACCINE IMMUNOL.
by on October 30, 2009
cvi.asm.org
Dow
nloaded from

have a fourfold change in Widal titer but did have at least oneWidal titer of �320; of these, 18 (44%) reported use of cip-rofloxacin before presenting for medical care. For the remain-ing 32 patients, 21 (66%) reported the use of any antibioticbefore presenting for medical care. After enrollment, all pa-tients were treated with antimicrobial agents, and 42 (38%)were hospitalized at the discretion of the attending physician.By day 5, 80 (71%) were afebrile, and by day 20 all wereafebrile and well. There was no clinically evident intestinalhemorrhage or perforation, and no patient died.
Subgrouping of study subjects for analyses. Patients werecategorized as follows. For comparison purposes, we groupedpatients into a number of groups: group I, illness characterizedwith at least 3 days of high-grade fever and positive bloodculture (n � 26); group II, compatible illness and a fourfoldincrease in Widal assay from day 0 baseline sample to conva-lescent period (n � 13); group III, compatible illness and aWidal titer of �320 (n � 41); group IV, an illness suspiciousfor clinical typhoid fever, but with a negative blood culture andWidal titer but with an anti-serovar Typhi IgA response in theALS assay that was �2 SD above the geometric mean mea-sured in healthy Bangladeshi controls (�10 ELISA units) (n �14); and group V, patients with an illness compatible withenteric fever but negative by all tests (n � 18). There were nopatients in more than one group. Healthy controls ranged inage from 24 to 35 years (median, 27 years).
Plasma antibody responses. LPS-specific IgA and IgG re-sponses were increased in patient groups I to III at all time
FIG. 1. LPS-specific IgA and IgG antibody responses in plasma specimens of different study groups on different study days. Groups: group I(Gr-I), blood culture positive; GrII, fourfold change in Widal; GrIII, Widal titer of �320; GrIV, negative culture and Widal but an anti-serovarTyphi IgA titer of �10 ELISA units in an ALS assay; GrV, all assays negative; HC, healthy controls. Geometric means with standard errors of themean (SEM) are shown for day 0 (D0), day 5 (D5), and day 20 (D20). The responder rate was calculated with a cutoff of �GM plus two SD ofhealthy controls (55 and 119 ELISA units for IgA and IgG, respectively). Statistical difference compared to healthy controls: ***, P � 0.0001; **,P � 0.005; *, P � 0.05. Statistical difference compared to GrV: �, P � 0.05.
TABLE 1. Clinical features in study participants
Feature Value
Baseline dataSample size............................................................. 112Median age in yr (25th, 75th percentile) ........... 24 (15, 30)No. of patients with serovar Typhi in
blood (%) ....................................................... 26 (23.2)Median maximum temp in °C
(25th, 75th percentile) .................................. 39 (39, 40)
GenderNo. of males (%) .................................................. 52 (44)No. of females (%) ............................................... 60 (54)
Clinical featuresDuration of fever in days at presentation
(25th, 75th percentile) .................................. 5 (4, 6)No. of patients (%) with:
Headache............................................................ 92 (82)Abdominal pain................................................. 62 (55)Constipation....................................................... 38 (34)Coated tongue ................................................... 63 (56)Diarrhea ............................................................. 17 (15)Vomiting............................................................. 10 (9)Rose spot............................................................ 10 (9)Rash .................................................................... 7 (6)
Median pulse/min (25th, 75th percentile).......... 83 (74, 88)
VOL. 16, 2009 ANTIBODY RESPONSES IN PATIENTS WITH TYPHOID FEVER 1589
by on October 30, 2009
cvi.asm.org
Dow
nloaded from

points compared to healthy controls and compared to group Vpatients (P � 0.05 to �0.0001). In group IV patients, the LPSIgA response was increased at the acute stage only (Fig. 1).Compared to healthy controls, elevated LPS-IgM responseswere seen at all time points and in all group I to IV patients(P � 0.001; data not shown). Patients in group V did not haveincreased serovar Typhi LPS-specific responses at any timepoint in any antibody isotype.
Anti-WC (killed WC bacterial preparation) IgA and IgGresponses were seen in group I to III patients compared tohealthy controls (Fig. 2). Group IV and V patients were notstatistically different from healthy controls in either IgA or IgGanti-WC responses. Using a cutoff value of healthy controlgeometric mean plus 2 SD, 17/26 (65%) blood culture-positivepatients had positive WC-specific IgA responses on day 0blood, 23 (88%) on day 5 blood, and 14 (53%) on day 20 blood.Similarly, using a cutoff value of healthy control geometricmean plus 2 SD, 19/26 (73%) blood culture positive patientshad positive anti-WC IgG responses on day 0 blood, 23 (88%)on day 5 blood, and 21 (81%) on day 20 blood. Significantanti-WC IgM responses compared to healthy controls wereonly seen in group I patients and were low in magnitude (datanot shown).
MP-specific IgA responses were seen at presentation ingroup I to IV patients and at presentation and at later timepoints in group I to III patients compared to healthy controls(Fig. 3). Using a cutoff value of healthy control geometricmean plus two SD, 21/26 (81%) blood culture-positive patients
had positive anti-MP IgA responses at the time of presentation(day 0). Of the 13 patients in group II, 8 (58%) were alsopositive for MP-IgA responses at presentation. Of those ingroup III, 18/41 (43%) patients were positive for MP-IgA re-sponses on study day 0; 22/41 (54%) were positive on day 5,and 14/41 (44%) were positive on day 20. The MP IgG re-sponses were only different from healthy controls in bloodculture-confirmed (group I) patients at later time points andnot in the day 0 plasma samples. The MP IgG responses werealso not different from healthy controls in any other group atany other time point. Anti-MP IgM responses were not signif-icantly different in any group at any time point compared tothose measured in healthy controls (data not shown).
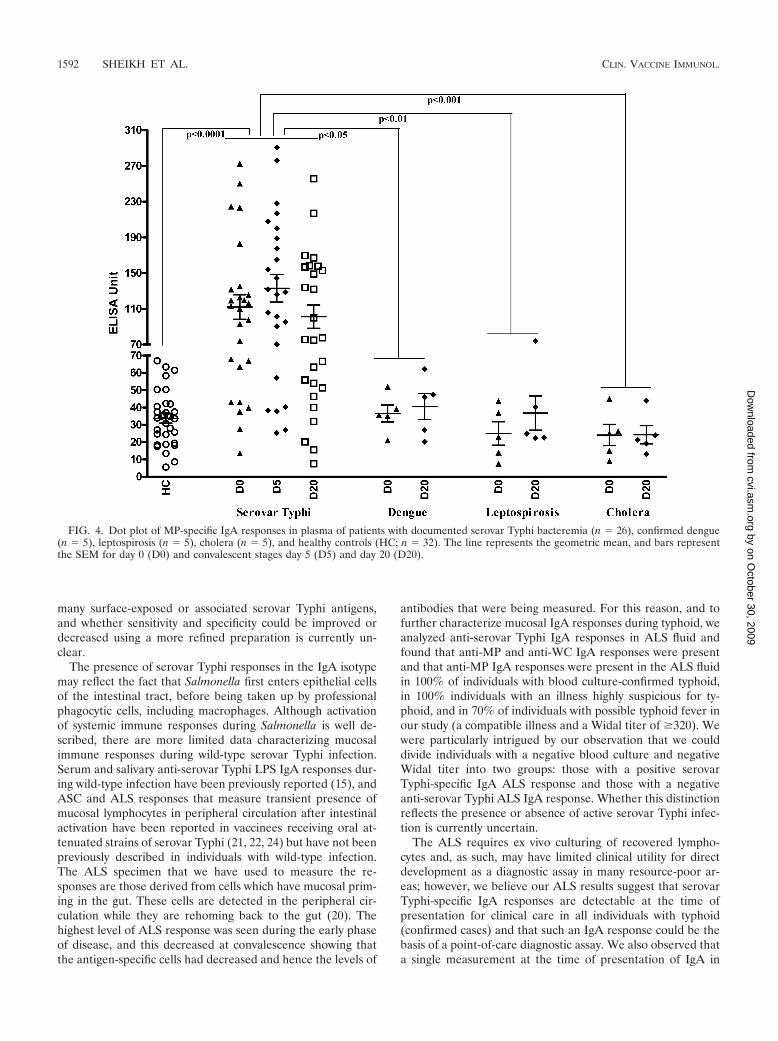
Comparison to reactivity in other illnesses using plasma.We compared the MP IgA responses in serovar Typhi bloodculture-positive individuals for MP IgA responses in plasmaobtained from patients with other confirmed causes of febrileillness or enteric disease caused by V. cholerae O1 (Fig. 4). TheMP IgA responses were elevated at all time points in serovarTyphi blood culture-confirmed patients compared to individu-als with confirmed dengue, leptospirosis, and cholera andhealthy controls (P � 0.05 to 0.001). Focusing on blood drawnat the time of presentation (day 0 sample) and using a cutoffvalue of geometric mean of healthy controls plus two SD (61ELISA units), a positive plasma anti-MP IgA on day 0 was ca.76% sensitive and 87% specific for blood culture-confirmedserovar Typhi infection versus all comparison groups and 76%sensitive and 100% specific when blood culture-confirmed
FIG. 2. Formalin-inactivated Salmonella Typhi WC-specific IgA and IgG antibody responses in plasma specimen of different groups ondifferent study days (see Fig. 1 legend for details). Geometric means with the SEM are shown for day 0 (D0), day 5 (D5), and day 20 (D20).The responder rate was calculated with a cutoff of �GM plus two SD of healthy controls (59 and 114 ELISA units for IgA and IgG,respectively). Statistical difference compared to healthy controls: ***, P � 0.0001; **, P � 0.005; *, P � 0.05. Statistical difference comparedto GrV: �, P � 0.05.
1590 SHEIKH ET AL. CLIN. VACCINE IMMUNOL.
by on October 30, 2009
cvi.asm.org
Dow
nloaded from

cases were compared to febrile cases caused by other illnesses(leptospirosis and dengue). When considering only those indi-viduals with blood culture-confirmed serovar Typhi bacteremia(as a confirmed positive; n � 26), and all febrile and healthycontrols (as confirmed negatives; n � 42), having a day 0plasma MP-IgA level greater than 61 had a positive predictivevalue of 88%, and having a value of �60 was associated with anegative predictive value of 89%.
Serovar Typhi-specific response in ALS specimens. In orderto more directly evaluate mucosal IgA responses, we also mea-sured anti-serovar Typhi responses in ALS fluid of individualswith suspected typhoid. Compared to healthy controls, theanti-WC- and anti-MP-specific IgA responses in ALS fluid ingroup I to IV patients was significantly elevated at all timepoints, including in the sample collected at the time of presen-tation, with the MP-specific responses being of higher magni-tude than the WC-specific responses (Fig. 5).
Comparison of IgA responses in plasma and ALS specimensto MP at the acute stage of disease (day 0). We comparedanti-MP IgA responses in ALS and plasma in our differentgroups of patients in acute-phase samples collected at the timeof presentation (Table 2). Defining a positive response as beinggreater than two SD above the geometric mean of healthycontrols (�61 ELISA units, plasma; �10 ELISA units, ALS),21/26 (81%) of group I and 8/13 (58%) of group II patients hadpositive plasma responses on day 0, and 100% of both groupshad positive ALS responses. Moreover, 18/41 (43%) group IIIpatients with a Widal titer of �320 were positive in plasma,and 70% were positive in ALS. Of the remaining 32 patients,
14 (44%) had a positive ALS response, and of these 9 (28%)were also positive in plasma.
DISCUSSION
In this study, we characterized antibody responses in indi-viduals with suspected enteric fever in Dhaka, Bangladesh.Definitive diagnosis of typhoid fever is problematic, complicat-ing the application of any gold standard to our study. Wetherefore considered responses based on the key assays avail-able in resource-poor areas of the world, blood culture posi-tivity, and Widal serology, and grouped patients into those withdefinitive typhoid, an illness highly suspicious for typhoid andwith a fourfold increase in Widal titer, and an illness that wecharacterized as possible typhoid (with a Widal titer of �320).We found serovar Typhi MP-specific IgA responses in themajority of individuals with confirmed and highly suspicioustyphoid fever, suggesting that IgA responses could be used toevaluate individuals with a febrile illness compatible with ty-phoid.
We analyzed serovar Typhi-specific responses using threeantigen preparations—LPS, WC, and a MP—and found thatboth IgG and IgA against LPS and WC were present across ourcharacterized groups but that MP-specific responses were re-stricted to the IgA isotype (with the exception that blood cul-tured confirmed patients also had a positive IgG anti-MP re-sponses). These results suggest that measurement of the MPIgA responses warrants further development as a diagnostictest for individuals with suspected typhoid. The MP includes
FIG. 3. IgA and IgG antibody responses to Salmonella Typhi MP in plasma specimen of different study groups on different study days (see Fig.1 legend for details). Geometric means with the SEM are shown for day 0 (D0), day 5 (D5), and day 20 (D20). Responder rates were calculatedwith a cutoff of �GM plus two SD of healthy controls (61 and 143 milliabsorbance units/min for IgA and IgG, respectively). Statistical differencecompared to healthy controls: ***, P � 0.0001; **, P � 0.005; *, P � 0.05. Statistical difference compared to GrV: �, P � 0.05.
VOL. 16, 2009 ANTIBODY RESPONSES IN PATIENTS WITH TYPHOID FEVER 1591
by on October 30, 2009
cvi.asm.org
Dow
nloaded from
many surface-exposed or associated serovar Typhi antigens,and whether sensitivity and specificity could be improved ordecreased using a more refined preparation is currently un-clear.
The presence of serovar Typhi responses in the IgA isotypemay reflect the fact that Salmonella first enters epithelial cellsof the intestinal tract, before being taken up by professionalphagocytic cells, including macrophages. Although activationof systemic immune responses during Salmonella is well de-scribed, there are more limited data characterizing mucosalimmune responses during wild-type serovar Typhi infection.Serum and salivary anti-serovar Typhi LPS IgA responses dur-ing wild-type infection have been previously reported (15), andASC and ALS responses that measure transient presence ofmucosal lymphocytes in peripheral circulation after intestinalactivation have been reported in vaccinees receiving oral at-tenuated strains of serovar Typhi (21, 22, 24) but have not beenpreviously described in individuals with wild-type infection.The ALS specimen that we have used to measure the re-sponses are those derived from cells which have mucosal prim-ing in the gut. These cells are detected in the peripheral cir-culation while they are rehoming back to the gut (20). Thehighest level of ALS response was seen during the early phaseof disease, and this decreased at convalescence showing thatthe antigen-specific cells had decreased and hence the levels of
antibodies that were being measured. For this reason, and tofurther characterize mucosal IgA responses during typhoid, weanalyzed anti-serovar Typhi IgA responses in ALS fluid andfound that anti-MP and anti-WC IgA responses were presentand that anti-MP IgA responses were present in the ALS fluidin 100% of individuals with blood culture-confirmed typhoid,in 100% individuals with an illness highly suspicious for ty-phoid, and in 70% of individuals with possible typhoid fever inour study (a compatible illness and a Widal titer of �320). Wewere particularly intrigued by our observation that we coulddivide individuals with a negative blood culture and negativeWidal titer into two groups: those with a positive serovarTyphi-specific IgA ALS response and those with a negativeanti-serovar Typhi ALS IgA response. Whether this distinctionreflects the presence or absence of active serovar Typhi infec-tion is currently uncertain.
The ALS requires ex vivo culturing of recovered lympho-cytes and, as such, may have limited clinical utility for directdevelopment as a diagnostic assay in many resource-poor ar-eas; however, we believe our ALS results suggest that serovarTyphi-specific IgA responses are detectable at the time ofpresentation for clinical care in all individuals with typhoid(confirmed cases) and that such an IgA response could be thebasis of a point-of-care diagnostic assay. We also observed thata single measurement at the time of presentation of IgA in
FIG. 4. Dot plot of MP-specific IgA responses in plasma of patients with documented serovar Typhi bacteremia (n � 26), confirmed dengue(n � 5), leptospirosis (n � 5), cholera (n � 5), and healthy controls (HC; n � 32). The line represents the geometric mean, and bars representthe SEM for day 0 (D0) and convalescent stages day 5 (D5) and day 20 (D20).
1592 SHEIKH ET AL. CLIN. VACCINE IMMUNOL.
by on October 30, 2009
cvi.asm.org
Dow
nloaded from

plasma reacting with the serovar Typhi MP had high positiveand negative predictive values in this endemic setting, includ-ing when comparing responses in individuals with other febrileillnesses difficult to clinically distinguish from typhoid fever inendemic settings (leptospirosis and dengue). Whether theseresults could be improved upon by use of a purified antigen oramplification of reactivity is currently unknown.
Our study has a number of shortcomings. The absence of agold standard for diagnosing typhoid means that we can onlyapproximate response rates across our clinical groups. The factthat many of our patients received antibiotics prior to present-
ing for medical care likely affected their likelihood of bloodculture positivity, as well as the host-pathogen interactions thatcould have occurred during infection, including antibody re-sponses. We feel, however, that our study represents an accu-rate clinical representation of how individuals with entericfever present in areas of endemicity, and our blood culturepositivity rate of almost 30% supports our observation thatmany of these individuals did indeed have serovar Typhi in-fection. Although serovar Typhi infection can cause a range ofillness, all individuals in the present study were ill enough toseek medical care, and all had a minimum of 3 days of highlevel fever (with a median of 5 days). Despite these shortcom-ings, our results suggest that an IgA response to serovar Typhi-specific antigens is present in the peripheral circulation ofmany individuals with serovar Typhi infection (documented orhighly suspected) at the time of presenting for clinical care andthat such a response of especially the ALS specimen could bethe basis of improved diagnostic point-of-care-assay for ty-phoid and warrants further evaluation.
ACKNOWLEDGMENTS
This study was supported by the ICDDR,B and grants from theNational Institutes of Health, including the National Institute of Al-lergy and Infectious Diseases (AI072599 [E.T.R.] and AI058935[R.C.C. and S.B.C.]), a Training Grant in Vaccine Development fromthe Fogarty International Center (TW05572 [A.S., M.S.B., and F.Q.]),and Career Development Awards (K01) from the Fogarty Interna-tional Center (TW007409 [J.B.H.] and TW07144 [R.C.L.]), and aPhysician-Scientist Early Career Award from the Howard HughesMedical Institute (R.C.L.).
FIG. 5. MP- and WC-specific IgA responses in ALS specimens of different study groups on different study days (see Fig. 1 legend for details).Geometric means with the SEM are shown for day 0 (D0), day 5 (D5), and day 20 (D20). Statistical difference compared to healthy controls: ***,P � 0.0001; **, P � 0.005; *, P � 0.05. Statistical difference compared to GrV: �, P � 0.05.
TABLE 2. MP specific IgA responses in plasma and ALSspecimens at the acute stage of diseasea
Group Characteristics Samplesize
IgA response (%)
Plasma ALS
I Blood culture positive 26 21 (81) 26 (100)II Fourfold Widal titer change 13 8 (58) 13 (100)III �320 Widal titer 41 18 (43) 29 (70)IV Culture negative, Widal negative
but a �10 ELISA unit ALSresponse
14 4 (29) 14 (100)
V Culture negative, Widal negativeand a �10 ELISA unit ALSresponse
18 5 (28) 0 (0)
a Analyses of specimens on study day 1 from patients subgrouped according todifferent clinical and immunological characteristics. Positive responses were cal-culated as �GM plus two standard deviations of healthy control results; plasmaMP-IgA response cutoff, �61 ELISA units; ALS MP-IgA response cutoff, �10ELISA units.
VOL. 16, 2009 ANTIBODY RESPONSES IN PATIENTS WITH TYPHOID FEVER 1593
by on October 30, 2009
cvi.asm.org
Dow
nloaded from

REFERENCES
1. Akoh, J. A. 1991. Relative sensitivity of blood and bone marrow cultures intyphoid fever. Trop. Doctor 21:174–176.
2. Asaduzzaman, M., E. T. Ryan, M. John, L. Hang, A. I. Khan, A. S. Faruque,R. K. Taylor, S. B. Calderwood, and F. Qadri. 2004. The major subunit of thetoxin-coregulated pilus TcpA induces mucosal and systemic immunoglobulinA immune responses in patients with cholera caused by Vibrio cholerae O1and O139. Infect. Immun. 72:4448–4454.
3. Begum, Y. A., K. A. Talukder, G. B. Nair, S. I. Khan, A. M. Svennerholm,R. B. Sack, and F. Qadri. 2007. Comparison of enterotoxigenic Escherichiacoli isolated from surface water and diarrhoeal stool samples in Bangladesh.Can. J. Microbiol. 53:19–26.
4. Bhuiyan, T. R., F. Qadri, A. Saha, and A. M. Svennerholm. 2009. Infectionby Helicobacter pylori in Bangladeshi children from birth to two years: rela-tion to blood group, nutritional status, and seasonality. Pediatr. Infect. Dis.J. 28:79–85.
5. Brooks, W. A., A. Hossain, D. Goswami, K. Nahar, K. Alam, N. Ahmed, A.Naheed, G. B. Nair, S. Luby, and R. F. Breiman. 2005. Bacteremic typhoidfever in children in an urban slum, Bangladesh. Emerg. Infect. Dis. 11:326–329.
6. Butler, T., A. Islam, I. Kabir, and P. K. Jones. 1991. Patterns of morbidityand mortality in typhoid fever dependent on age and gender: review of 552hospitalized patients with diarrhea. Rev. Infect. Dis. 13:85–90.
7. Chang, H. S., and D. A. Sack. 2001. Development of a novel in vitro assay(ALS assay) for evaluation of vaccine-induced antibody secretion from cir-culating mucosal lymphocytes. Clin. Diagn. Lab. Immunol. 8:482–488.
8. Crump, J. A., S. P. Luby, and E. D. Mintz. 2004. The global burden oftyphoid fever. Bull. W. H. O. 82:346–353.
9. Falklind-Jerkerus, S., F. Felici, C. Cavalieri, C. Lo Passo, G. Garufi, I.Pernice, M. M. Islam, F. Qadri, and A. Weintraub. 2005. Peptides mimickingVibrio cholerae O139 capsular polysaccharide elicit protective antibody re-sponse. Microbes Infect. 7:1453–1460.
10. Forrest, B. D. 1992. Indirect measurement of intestinal immune responses toan orally administered attenuated bacterial vaccine. Infect. Immun. 60:2023–2029.
11. Gasem, M. H., W. M. Dolmans, B. B. Isbandrio, H. Wahyono, M. Keuter,and R. Djokomoeljanto. 1995. Culture of Salmonella typhi and Salmonellaparatyphi from blood and bone marrow in suspected typhoid fever. Trop.Geogr. Med. 47:164–167.
12. Gilman, R. H., M. Terminel, M. M. Levine, P. Hernandez-Mendoza, andR. B. Hornick. 1975. Relative efficacy of blood, urine, rectal swab, bone-marrow, and rose-spot cultures for recovery of Salmonella typhi in typhoidfever. Lancet i:1211–1213.
13. Harris, J. B., R. C. Larocque, F. Chowdhury, A. I. Khan, T. Logvinenko, A. S.Faruque, E. T. Ryan, F. Qadri, and S. B. Calderwood. 2008. Susceptibility toVibrio cholerae infection in a cohort of household contacts of patients withcholera in Bangladesh. PLoS Negl. Trop. Dis. 2:e221.
14. Hatta, M., and H. L. Smits. 2007. Detection of Salmonella typhi by nestedpolymerase chain reaction in blood, urine, and stool samples. Am. J. Trop.Med. Hyg. 76:139–143.
15. Herath, H. M. 2003. Early diagnosis of typhoid fever by the detection ofsalivary IgA. J. Clin. Pathol. 56:694–698.
16. Iperepolu, O. H., P. E. Entonu, and S. M. Agwale. 2008. A review of thedisease burden, impact and prevention of typhoid fever in Nigeria. West Afr.J. Med. 27:127–133.
17. John, T. J., R. Samuel, V. Balraj, and R. John. 1998. Disease surveillance atdistrict level: a model for developing countries. Lancet 352:58–61.
18. Kalhan, R., I. Kaur, R. P. Singh, and H. C. Gupta. 1998. Rapid diagnosis oftyphoid fever. Indian J. Pediatr. 65:561–564.
19. Kantele, A. 1996. Peripheral blood antibody-secreting cells in the evaluationof the immune response to an oral vaccine. J. Biotechnol. 44:217–224.
20. Kantele, J. M., H. Arvilommi, S. Kontiainen, M. Salmi, S. Jalkanen, E.Savilahti, M. Westerholm, and A. Kantele. 1996. Mucosally activated circu-lating human B cells in diarrhea express homing receptors directing themback to the gut. Gastroenterology 110:1061–1067.
21. Kirkpatrick, B. D., M. D. Bentley, A. M. Thern, C. J. Larsson, C. Ventrone,M. V. Sreenivasan, and L. Bourgeois. 2005. Comparison of the antibodies in
lymphocyte supernatant and antibody-secreting cell assays for measuringintestinal mucosal immune response to a novel oral typhoid vaccine(M01ZH09). Clin. Diagn. Lab. Immunol. 12:1127–1129.
22. Kirkpatrick, B. D., R. McKenzie, J. P. O’Neill, C. J. Larsson, A. L. Bour-geois, J. Shimko, M. Bentley, J. Makin, S. Chatfield, Z. Hindle, C. Fidler,B. E. Robinson, C. H. Ventrone, N. Bansal, C. M. Carpenter, D. Kutzko, S.Hamlet, C. LaPointe, and D. N. Taylor. 2006. Evaluation of Salmonellaenterica serovar Typhi (Ty2 aroC-ssaV-) M01ZH09, with a defined mutationin the Salmonella pathogenicity island 2, as a live, oral typhoid vaccine inhuman volunteers. Vaccine 24:116–123.
23. LaRocque, R. C., R. F. Breiman, M. D. Ari, R. E. Morey, F. A. Janan, J. M.Hayes, M. A. Hossain, W. A. Brooks, and P. N. Levett. 2005. Leptospirosisduring dengue outbreak, Bangladesh. Emerg. Infect. Dis. 11:766–769.
24. Lundgren, A., J. Kaim, and M. Jertborn. 2009. Parallel analysis of mucosallyderived B- and T-cell responses to an oral typhoid vaccine using simplifiedmethods. Vaccine 27:4529–4536.
25. McGhee, J. R., and H. Kiyono. 1993. New perspectives in vaccine develop-ment: mucosal immunity to infections. Infect. Agents Dis. 2:55–73.
26. Nieminen, T., H. Kayhty, and A. Kantele. 1996. Circulating antibody secret-ing cells and humoral antibody response after parenteral immunization witha meningococcal polysaccharide vaccine. Scand. J. Infect. Dis. 28:53–58.
27. Pang, T., and S. D. Puthucheary. 1983. Significance and value of the Widaltest in the diagnosis of typhoid fever in an endemic area. J. Clin. Pathol.36:471–475.
28. Pohan, H. T. 2004. Clinical and laboratory manifestations of typhoid fever atPersahabatan Hospital, Jakarta. Acta Med. Indones. 36:78–83.
29. Qadri, F., T. Ahmed, F. Ahmed, M. S. Bhuiyan, M. G. Mostofa, F. J. Cassels,A. Helander, and A. M. Svennerholm. 2007. Mucosal and systemic immuneresponses in patients with diarrhea due to CS6-expressing enterotoxigenicEscherichia coli. Infect. Immun. 75:2269–2274.
30. Qadri, F., R. Raqib, F. Ahmed, T. Rahman, C. Wenneras, S. K. Das, N. H.Alam, M. M. Mathan, and A. M. Svennerholm. 2002. Increased levels ofinflammatory mediators in children and adults infected with Vibrio choleraeO1 and O139. Clin. Diagn. Lab. Immunol. 9:221–229.
31. Qadri, F., E. T. Ryan, A. S. Faruque, F. Ahmed, A. I. Khan, M. M. Islam,S. M. Akramuzzaman, D. A. Sack, and S. B. Calderwood. 2003. Antigen-specific immunoglobulin A antibodies secreted from circulating B cells arean effective marker for recent local immune responses in patients withcholera: comparison to antibody-secreting cell responses and other immu-nological markers. Infect. Immun. 71:4808–4814.
32. Rollman, E., T. Ramqvist, B. Zuber, K. Tegerstedt, A. Kjerrstrom Zuber, J.Klingstrom, L. Eriksson, K. Ljungberg, J. Hinkula, B. Wahren, and T.Dalianis. 2003. Genetic immunization is augmented by murine polyomavirusVP1 pseudocapsids. Vaccine 21:2263–2267.
33. Saha, S. K., M. Ruhulamin, M. Hanif, M. Islam, and W. A. Khan. 1996.Interpretation of the Widal test in the diagnosis of typhoid fever in Bang-ladeshi children. Ann. Trop. Paediatr. 16:75–78.
34. Sarma, V. N., A. N. Malaviya, R. Kumar, O. P. Ghai, and M. M. Bakhtary.1977. Development of immune response during typhoid fever in man. Clin.Exp. Immunol. 28:35–39.
35. Talawadekar, N., P. Vadher, D. Antani, V. Kale, and S. Kamat, and 1989.Chloramphenicol resistant Salmonella species isolated between 1978 and1987. J. Postgrad. Med. 35:79–82.
36. Wain, J., V. B. Pham, V. Ha, N. M. Nguyen, S. D. To, A. L. Walsh, C. M.Parry, R. P. Hasserjian, V. A. HoHo, T. H. Tran, J. Farrar, N. J. White, andN. P. Day. 2001. Quantitation of bacteria in bone marrow from patients withtyphoid fever: relationship between counts and clinical features. J. Clin.Microbiol. 39:1571–1576.
37. Wenneras, C., F. Qadri, P. K. Bardhan, R. B. Sack, and A. M. Svennerholm.1999. Intestinal immune responses in patients infected with enterotoxigenicEscherichia coli and in vaccinees. Infect. Immun. 67:6234–6241.
38. Willke, A., O. Ergonul, and B. Bayar. 2002. Widal test in diagnosis of typhoidfever in Turkey. Clin. Diagn. Lab. Immunol. 9:938–941.
39. Yew, F. S., S. K. Chew, K. T. Goh, E. H. Monteiro, and Y. S. Lim. 1991.Typhoid fever in Singapore: a review of 370 cases. J. Trop. Med. Hyg.94:352–357.
1594 SHEIKH ET AL. CLIN. VACCINE IMMUNOL.
by on October 30, 2009
cvi.asm.org
Dow
nloaded from




















