
Safety & Efficacy of Boceprevir/Peginterferon/Ribavirin for HCV G1 Compensated Cirrhotics:...
10
Safety and efficacy of boceprevir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta-analysis of 5 trials John M. Vierling 1,⇑, , Stefan Zeuzem 2 , Fred Poordad 3 , Jean-Pierre Bronowicki 4 , Michael P. Manns 5 , Bruce R. Bacon 6 , Rafael Esteban 7 , Steven L. Flamm 8 , Paul Y. Kwo 9 , Lisa D. Pedicone 10,à , Weiping Deng 10 , Frank J. Dutko 10 , Mark J. DiNubile 10 , Kenneth J. Koury 10 , Frans A. Helmond 10 , Janice Wahl 10 , Savino Bruno 11, 1 Baylor College of Medicine, Houston, TX, USA; 2 JW Goethe University Hospital, Frankfurt, Germany; 3 University of Texas Health Science Center, San Antonio, TX, USA; 4 INSERMU954, CHU de Nancy, Université de Lorraine, Vandoeuvre-lès-Nancy, France; 5 Medical School of Hannover, Hannover, Germany; 6 Saint Louis University School of Medicine, St. Louis, MO, USA; 7 Vall d’Hebron University Hospital, Barcelona, Spain; 8 Northwestern Feinberg School of Medicine, Chicago, IL, USA; 9 Indiana University School of Medicine, Indianapolis, IN, USA; 10 Merck Sharp & Dohme Corp., Whitehouse Station, NJ, USA; 11 A.O. Fatebenefratelli e Oftalmico, Milan, Italy Background & Aims: HCV-infected cirrhotics may urgently need therapy but are often under-represented in clinical trials result- ing in limited data to guide their management. We performed a meta-analysis of well-compensated cirrhotic patients from five Phase 3 trials. Methods: Patients received P/R (peginterferon/ribavirin; 4 weeks) followed by BOC (boceprevir)/P/R or P/R for 24, 32, or 44 weeks. Sustained virologic response (SVR) rates were calcu- lated by Metavir score. Multivariate logistic regression (MLR) models identified baseline and on-treatment predictors of SVR. Safety was evaluated by adverse-event (AE) reporting and labora- tory monitoring. Results: Pooled meta-estimates for SVR rates (95% confidence interval) in 212 F4 (cirrhotic) patients were 55% (43, 66) with BOC/P/R vs.17% (0, 41) with P/R. MLR identified 4 predictors of SVR in F3/F4 patients: undetectable HCV-RNA at treatment week (TW) 8; P1 log 10 decline in HCV-RNA from baseline at TW4; male; and baseline HCV-RNA 6800,000 IU/ml. SVR rate was 89% (65/73) in F4 patients who were HCV-RNA undetectable at TW8. No F3 (0/5) or F4 (0/17) patients with <3 log 10 decline and detectable HCV-RNA at TW8 achieved SVR. Anemia and diar- rhea occurred more frequently in cirrhotic than non-cirrhotic patients. Serious AEs, discontinuations due to an AE, interven- tions to manage anemia, infections, and thrombocytopenia occurred more frequently in cirrhotics with BOC/P/R than P/R. Potential hepatic decompensation and/or sepsis were identified in 2 P/R and 3 BOC/P/R recipients. Conclusions: BOC/P/R appears to have a generally favorable ben- efit-risk profile in compensated cirrhotic patients. SVR rates were particularly high in cirrhotic patients with undetectable HCV-RNA at TW8. Ó 2014 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved. Introduction Cirrhotic patients with chronic hepatitis C continue to present a therapeutic challenge in the era of directly acting antiviral agents because of lower SVR rates and poorer tolerability of therapy compared with non-cirrhotics [1]. Yet there is a clear benefit in treating cirrhotics and in many cirrhotics, an urgency to treat before patients advance to decompensated cirrhosis at which point interferon-based antiviral therapies are contraindicated. Initial experience with BOC/P/R was obtained in the two pivotal Phase 3 trials; the SVR rates in 79 cirrhotics ranged from 31% to 77% and safety was similar compared to patients with mild to moderate fibrosis [2]. An additional perspective was provided by the CUPIC study, which evaluated triple combination regimens with either telaprevir or BOC in a wider range of treatment-expe- rienced cirrhotic patients (many of whom would not have quali- fied for pivotal trials) [3]. The SVR rate in CUPIC at 12 weeks after end of therapy with BOC/P/R was 41% (79/190) [4]. However, the safety profile in CUPIC differed from the pivotal trial experience and both regimens with boceprevir or telaprevir were poorly tolerated, especially in those subjects with low platelet counts and albumin levels at baseline. The ultimate goal of this analysis was to understand the over- all risk to benefit ratio of BOC/P/R treatment in well-compensated cirrhotic patients using expanded data from 5 Phase 3 clinical Journal of Hepatology 2014 vol. xxx j xxx–xxx Keywords: Hepatitis C; Cirrhosis; Chronic HCV. Received 2 December 2013; received in revised form 12 March 2014; accepted 19 March 2014 ⇑ Corresponding author. Address: Baylor College of Medicine, One Baylor Plaza, Houston, TX 77030, USA. Tel.: +1 832 355 1400; fax: +1 713 610 2482. E-mail address: [email protected] (J.M. Vierling). These authors contributed equally to this work. à Former employee of Merck Sharp & Dohme Corp., Whitehouse Station, NJ, USA. Abbreviations: HCV, hepatitis C virus; BOC, boceprevir; P/R, peginterferon/ribavi- rin; SVR, sustained virologic response; MLR, multivariate logistic regression; AE, adverse event; TW, treatment week; SAE, serious adverse event; CI, confidence interval. Research Article Please cite this article in press as: Vierling JM et al. Safety and efficacy of boceprevir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta- analysis of 5 trials. J Hepatol (2014), http://dx.doi.org/10.1016/j.jhep.2014.03.022
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Safety & Efficacy of Boceprevir/Peginterferon/Ribavirin for HCV G1 Compensated Cirrhotics:...

Research Article
Safety and efficacy of boceprevir/peginterferon/ribavirin for HCVG1 compensated cirrhotics: Meta-analysis of 5 trials
John M. Vierling1,⇑,�, Stefan Zeuzem2, Fred Poordad3, Jean-Pierre Bronowicki4, Michael P. Manns5,Bruce R. Bacon6, Rafael Esteban7, Steven L. Flamm8, Paul Y. Kwo9, Lisa D. Pedicone10,�,
Weiping Deng10, Frank J. Dutko10, Mark J. DiNubile10, Kenneth J. Koury10, Frans A. Helmond10,Janice Wahl10, Savino Bruno11,�
1Baylor College of Medicine, Houston, TX, USA; 2JW Goethe University Hospital, Frankfurt, Germany; 3University of Texas Health Science Center,San Antonio, TX, USA; 4INSERMU954, CHU de Nancy, Université de Lorraine, Vandoeuvre-lès-Nancy, France; 5Medical School of Hannover,Hannover, Germany; 6Saint Louis University School of Medicine, St. Louis, MO, USA; 7Vall d’Hebron University Hospital, Barcelona, Spain;
8Northwestern Feinberg School of Medicine, Chicago, IL, USA; 9Indiana University School of Medicine, Indianapolis, IN, USA; 10Merck Sharp &Dohme Corp., Whitehouse Station, NJ, USA; 11A.O. Fatebenefratelli e Oftalmico, Milan, Italy
Background & Aims: HCV-infected cirrhotics may urgently needtherapy but are often under-represented in clinical trials result-ing in limited data to guide their management. We performed ameta-analysis of well-compensated cirrhotic patients from fivePhase 3 trials.Methods: Patients received P/R (peginterferon/ribavirin;4 weeks) followed by BOC (boceprevir)/P/R or P/R for 24, 32, or44 weeks. Sustained virologic response (SVR) rates were calcu-lated by Metavir score. Multivariate logistic regression (MLR)models identified baseline and on-treatment predictors of SVR.Safety was evaluated by adverse-event (AE) reporting and labora-tory monitoring.Results: Pooled meta-estimates for SVR rates (95% confidenceinterval) in 212 F4 (cirrhotic) patients were 55% (43, 66) withBOC/P/R vs.17% (0, 41) with P/R. MLR identified 4 predictors ofSVR in F3/F4 patients: undetectable HCV-RNA at treatment week(TW) 8; P1 log10 decline in HCV-RNA from baseline at TW4;male; and baseline HCV-RNA 6800,000 IU/ml. SVR rate was 89%(65/73) in F4 patients who were HCV-RNA undetectable atTW8. No F3 (0/5) or F4 (0/17) patients with <3 log10 declineand detectable HCV-RNA at TW8 achieved SVR. Anemia and diar-rhea occurred more frequently in cirrhotic than non-cirrhoticpatients. Serious AEs, discontinuations due to an AE, interven-tions to manage anemia, infections, and thrombocytopenia
Journal of Hepatology 20
Keywords: Hepatitis C; Cirrhosis; Chronic HCV.Received 2 December 2013; received in revised form 12 March 2014; accepted 19March 2014⇑ Corresponding author. Address: Baylor College of Medicine, One Baylor Plaza,Houston, TX 77030, USA. Tel.: +1 832 355 1400; fax: +1 713 610 2482.E-mail address: [email protected] (J.M. Vierling).
� These authors contributed equally to this work.� Former employee of Merck Sharp & Dohme Corp., Whitehouse Station, NJ,
USA.Abbreviations: HCV, hepatitis C virus; BOC, boceprevir; P/R, peginterferon/ribavi-rin; SVR, sustained virologic response; MLR, multivariate logistic regression; AE,adverse event; TW, treatment week; SAE, serious adverse event; CI, confidenceinterval.
Please cite this article in press as: Vierling JM et al. Safety and efficacy of bocepanalysis of 5 trials. J Hepatol (2014), http://dx.doi.org/10.1016/j.jhep.2014.03.
occurred more frequently in cirrhotics with BOC/P/R than P/R.Potential hepatic decompensation and/or sepsis were identifiedin 2 P/R and 3 BOC/P/R recipients.Conclusions: BOC/P/R appears to have a generally favorable ben-efit-risk profile in compensated cirrhotic patients. SVR rates wereparticularly high in cirrhotic patients with undetectableHCV-RNA at TW8.� 2014 European Association for the Study of the Liver. Publishedby Elsevier B.V. All rights reserved.
Introduction
Cirrhotic patients with chronic hepatitis C continue to present atherapeutic challenge in the era of directly acting antiviral agentsbecause of lower SVR rates and poorer tolerability of therapycompared with non-cirrhotics [1]. Yet there is a clear benefit intreating cirrhotics and in many cirrhotics, an urgency to treatbefore patients advance to decompensated cirrhosis at whichpoint interferon-based antiviral therapies are contraindicated.Initial experience with BOC/P/R was obtained in the two pivotalPhase 3 trials; the SVR rates in 79 cirrhotics ranged from 31%to 77% and safety was similar compared to patients with mildto moderate fibrosis [2]. An additional perspective was providedby the CUPIC study, which evaluated triple combination regimenswith either telaprevir or BOC in a wider range of treatment-expe-rienced cirrhotic patients (many of whom would not have quali-fied for pivotal trials) [3]. The SVR rate in CUPIC at 12 weeks afterend of therapy with BOC/P/R was 41% (79/190) [4]. However, thesafety profile in CUPIC differed from the pivotal trial experienceand both regimens with boceprevir or telaprevir were poorlytolerated, especially in those subjects with low platelet countsand albumin levels at baseline.
The ultimate goal of this analysis was to understand the over-all risk to benefit ratio of BOC/P/R treatment in well-compensatedcirrhotic patients using expanded data from 5 Phase 3 clinical
14 vol. xxx j xxx–xxx
revir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta-022

Research Article
trials. Specifically, we sought to identify baseline and on-treat-ment variables that could help to predict response and to guideclinical decisions about BOC/P/R therapy for cirrhotic patients,including decisions about discontinuation for futility (low likeli-hood of achieving SVR) and decisions regarding the duration oftreatment. We examined efficacy and safety in the cirrhoticpopulation. We also evaluated potential early stopping rules (atweeks 4 and 8) as well as the utility of response-guidedparadigms to potentially shorten duration of therapy to<48 weeks in carefully selected patients.Materials and methods
Objectives
The primary objectives of this retrospective study were to estimate the SVR rateand adverse-event profile for BOC (VICTRELIS� (boceprevir), Merck & Co., Inc.,Whitehouse Station, NJ, USA) plus P/R in compensated cirrhotic (Metavir fibrosisscore F4) patients with chronic hepatitis C genotype 1 infection based on pooleddata from 5 Phase 3 clinical studies (P05101 [RESPOND-2 [5]], P05216 [SPRINT-2[6]], P05514 [PROVIDE; [7]], P05685 [Peginterferon alfa-2a Study [8]], andP06086 [Anemia Management Study; [9]] (Supplementary Table 1).
ClinicalTrials.gov Identifiers: NCT00708500, NCT00705432, NCT01023035,NCT00845065, NCT00910624.
Assessment of cirrhosis
Cirrhosis was determined by liver biopsies performed on all patients and cen-trally read by a single pathologist. Cirrhosis was defined as Metavir score F4;advanced fibrosis without cirrhosis as Metavir score F3.
Statistical analysis plan
The pooled analysis was conducted using individual participant data from 5 clin-ical studies (P05101, P05216, P05514, P05685, and P06086) with a total numberof 2522 patients. No formal hypothesis-testing or multiplicity adjustments wereplanned.
Efficacy analyses
The primary efficacy analysis was conducted on the pooled patients from theBOC/P/R arms who received P1 dose of any study medication and who werefibrosis score F4 (cirrhotics), F3 or F0–F2. An SVR was defined as having undetect-able HCV-RNA (‘‘Target Not Detected’’ or ‘‘HCV-RNA Not Detected’’) in the plasma24 weeks after completion or discontinuation of therapy. HCV-RNA was mea-sured using a Roche COBAS� TaqMan� assay with a lower limit of detection of9.3 IU/ml. Meta-analysis methods were used to estimate the SVR rate for the pri-mary analysis in the pooled cirrhotic patients as well as for pooled F0–F2 and F3patients treated with BOC/P/R.
The relationship between baseline factors and SVR for patients receiving BOC/P/R with different fibrosis scores (F0–F2, F3/F4) was explored using multivariatelogistic regression analysis. The multivariate logistic regression analysis was per-formed on pooled F3 and F4 patients in order increase the power to identify addi-tional predictors of SVR.
Safety analyses
For all safety analyses, the results from all patients who received P1 dose of anystudy medication were analyzed by treatment (BOC/P/R vs. P/R) and fibrosis score(F0/F1/F2, F3, and F4). The numbers of patients reporting any AEs and serious AEs(SAEs; including deaths and hospitalizations), and AEs leading to study drug dis-continuations were tabulated. Laboratory assessments during treatment focusedon anemia, neutropenia, and thrombocytopenia. The following parameters wereconsidered to potentially represent hepatic decompensation: new onset of asci-tes, encephalopathy, bleeding esophageal varices, jaundice, sepsis (in the contextof declining liver function); increase in bilirubin (total >4.0 with at least 50%direct), or prothrombin time >10% above laboratory reference range [10,11].
Please cite this article in press as: Vierling JM et al. Safety and efficacy of bocepanalysis of 5 trials. J Hepatol (2014), http://dx.doi.org/10.1016/j.jhep.2014.03.
2 Journal of Hepatology 201
Patients with the above findings, regardless of the Metavir classification, wereadjudicated by John Vierling and Savino Bruno who were blinded to the treat-ment regimen and Metavir score.
Results
Patient accounting and baseline characteristics
The distributions of patients according to treatment (BOC/P/R vs.P/R) and fibrosis scores in the pooled data are presented inSupplementary Table 1. Eighty percent (1925/2415) of patientscame from the BOC/P/R arms of the 5 studies, and 20% (490/2415) of patients came from the P/R arms of 3 studies (P05101,P05216, and P05685; no P/R arms were included in P05514 andP06086). Fibrosis scores were distributed as: F0/F1/F2, 86%(2074/2415); F3, 5% (129/2415); and F4, 9% (212/2415). Of the212 F4 patients, 32 (15%) patients received P/R and 180 (85%)received BOC/P/R. The number of patients, prior treatment his-tory (treatment naïve or previous treatment failure), and treat-ment assignments (P/R, BOC/P/R for 48 weeks, and ResponseGuided Therapy [RGT] for BOC/P/R if applicable) from each study,as well as fibrosis scores by treatment assignment, are providedin Supplementary Table 2.
Baseline characteristics are shown in Table 1. F4 patients trea-ted with BOC/P/R were approximately 53 yr (compared to 50 yrfor F0–F2 patients), 62% male, 83% White, 10% Black, with a meanbody mass index of 29.8 (compared to 28 for F0–F2). Approxi-mately 51% of F4 patients treated with BOC/P/R were infectedwith HCV subtype 1a. In F4 patients, mean platelet count was166 � 109/L (compared to approximately 250 � 109/L for F0–F2patients), 44% had mean platelet counts <150 � 109/L (comparedto 6% of F0–F2 patients), and 12% had serum albumin levels<35 g/dl (compared to 2% of F0–F2 patients).
SVR rates
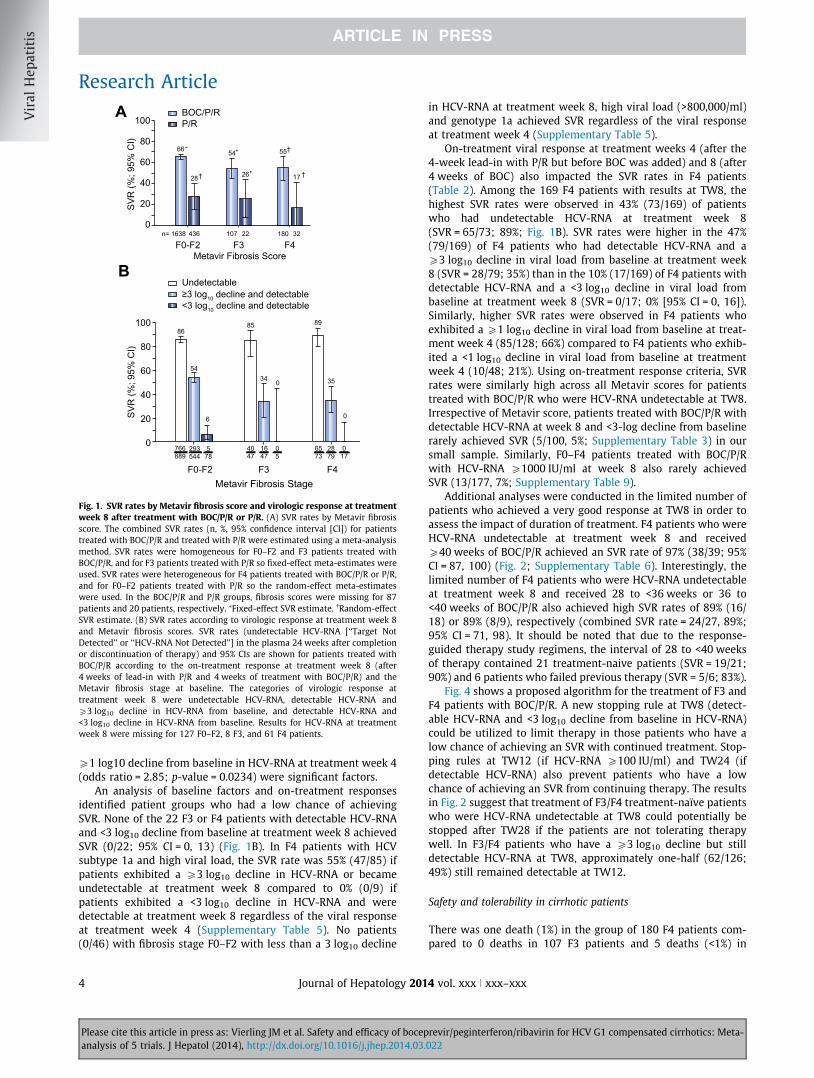
A meta-analysis was performed in order to estimate the SVR ratesaccording to pooled data by fibrosis score (Fig. 1A; Supplemen-tary Figs. S1 and S2). The meta-estimates of the SVR rates were55% (95% confidence interval [CI]: 43, 66) vs. 17% (95% CI: 0,41) for F4 patients treated with BOC/P/R or P/R, respectively (pre-liminary results were presented at EASL [12]). Among patientstreated with BOC/P/R, the meta-estimates for the SVR rates werecomparable in F4 (55%) and F3 patients (54%; 95% CI: 45, 64) andwere numerically lower than the SVR rates in F0–F2 (66%; 95% CI:63, 68) patients.
Several factors that predicted achievement of an SVR in F3/F4patients were identified with multivariate logistic regressionmodels. Undetectable HCV-RNA at treatment week 8, aP1 log10 decline from baseline in HCV-RNA at treatment week4, low baseline viral load (6800,000 IU/ml), and male genderwere significant factors that predicted SVR in F3/F4 patients(Fig. 3; Supplementary Table 3). The most significant factor forachieving an SVR was undetectable HCV-RNA at treatment week8 in F3 and F4 patients. In F0–F2 patients, undetectable HCV-RNAat treatment week 8, a P1 log10 decline from baseline in HCV-RNA at treatment week 4, non-black and HCV subtype 1b weresignificant predictors of SVR (Supplementary Table 4). If achieve-ment of an SVR was analyzed by multivariate logistic regressionin only F4 patients, then only low undetectable HCV-RNA attreatment week 8 (odds ratio = 10.90; p value <0.0001) and a
revir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta-022
4 vol. xxx j xxx–xxx
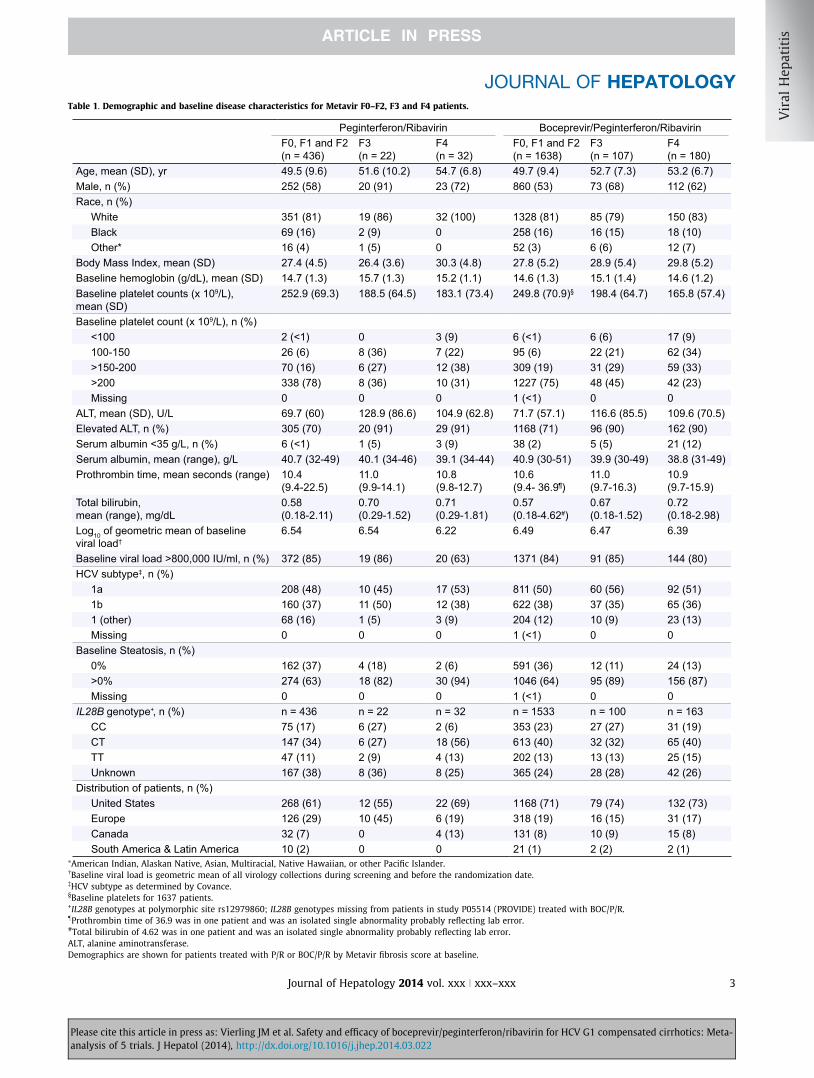
Table 1. Demographic and baseline disease characteristics for Metavir F0–F2, F3 and F4 patients.
Peginterferon/Ribavirin Boceprevir/Peginterferon/RibavirinF0, F1 and F2(n = 436)
F3(n = 22)
F4(n = 32)
F0, F1 and F2(n = 1638)
F3(n = 107)
F4(n = 180)
Age, mean (SD), yr 49.5 (9.6) 51.6 (10.2) 54.7 (6.8) 49.7 (9.4) 52.7 (7.3) 53.2 (6.7)Male, n (%) 252 (58) 20 (91) 23 (72) 860 (53) 73 (68) 112 (62)Race, n (%)
White 351 (81) 19 (86) 32 (100) 1328 (81) 85 (79) 150 (83)Black 69 (16) 2 (9) 0 258 (16) 16 (15) 18 (10)Other* 16 (4) 1 (5) 0 52 (3) 6 (6) 12 (7)
Body Mass Index, mean (SD) 27.4 (4.5) 26.4 (3.6) 30.3 (4.8) 27.8 (5.2) 28.9 (5.4) 29.8 (5.2)Baseline hemoglobin (g/dL), mean (SD) 14.7 (1.3) 15.7 (1.3) 15.2 (1.1) 14.6 (1.3) 15.1 (1.4) 14.6 (1.2)Baseline platelet counts (x 109/L), mean (SD)
252.9 (69.3) 188.5 (64.5) 183.1 (73.4) 249.8 (70.9)§ 198.4 (64.7) 165.8 (57.4)
Baseline platelet count (x 109/L), n (%)<100 2 (<1) 0 3 (9) 6 (<1) 6 (6) 17 (9)100-150 26 (6) 8 (36) 7 (22) 95 (6) 22 (21) 62 (34)>150-200 70 (16) 6 (27) 12 (38) 309 (19) 31 (29) 59 (33)>200 338 (78) 8 (36) 10 (31) 1227 (75) 48 (45) 42 (23)Missing 0 0 0 1 (<1) 0 0
ALT, mean (SD), U/L 69.7 (60) 128.9 (86.6) 104.9 (62.8) 71.7 (57.1) 116.6 (85.5) 109.6 (70.5)Elevated ALT, n (%) 305 (70) 20 (91) 29 (91) 1168 (71) 96 (90) 162 (90)Serum albumin <35 g/L, n (%) 6 (<1) 1 (5) 3 (9) 38 (2) 5 (5) 21 (12)Serum albumin, mean (range), g/L 40.7 (32-49) 40.1 (34-46) 39.1 (34-44) 40.9 (30-51) 39.9 (30-49) 38.8 (31-49)Prothrombin time, mean seconds (range) 10.4
(9.4-22.5)11.0 (9.9-14.1)
10.8 (9.8-12.7)
10.6 (9.4- 36.9¶)
11.0 (9.7-16.3)
10.9 (9.7-15.9)
Total bilirubin, mean (range), mg/dL
0.58 (0.18-2.11)
0.70 (0.29-1.52)
0.71 (0.29-1.81)
0.57 (0.18-4.62#)
0.67 (0.18-1.52)
0.72 (0.18-2.98)
Log10 of geometric mean of baseline viral load†
6.54 6.54 6.22 6.49 6.47 6.39
Baseline viral load >800,000 IU/ml, n (%) 372 (85) 19 (86) 20 (63) 1371 (84) 91 (85) 144 (80)HCV subtype‡, n (%)
1a 208 (48) 10 (45) 17 (53) 811 (50) 60 (56) 92 (51)1b 160 (37) 11 (50) 12 (38) 622 (38) 37 (35) 65 (36)1 (other) 68 (16) 1 (5) 3 (9) 204 (12) 10 (9) 23 (13)Missing 0 0 0 1 (<1) 0 0
Baseline Steatosis, n (%)0% 162 (37) 4 (18) 2 (6) 591 (36) 12 (11) 24 (13)>0% 274 (63) 18 (82) 30 (94) 1046 (64) 95 (89) 156 (87)Missing 0 0 0 1 (<1) 0 0
IL28B genotype+, n (%) n = 436 n = 22 n = 32 n = 1533 n = 100 n = 163CC 75 (17) 6 (27) 2 (6) 353 (23) 27 (27) 31 (19)CT 147 (34) 6 (27) 18 (56) 613 (40) 32 (32) 65 (40)TT 47 (11) 2 (9) 4 (13) 202 (13) 13 (13) 25 (15)Unknown 167 (38) 8 (36) 8 (25) 365 (24) 28 (28) 42 (26)
Distribution of patients, n (%)United States 268 (61) 12 (55) 22 (69) 1168 (71) 79 (74) 132 (73)Europe 126 (29) 10 (45) 6 (19) 318 (19) 16 (15) 31 (17)Canada 32 (7) 0 4 (13) 131 (8) 10 (9) 15 (8)South America & Latin America 10 (2) 0 0 21 (1) 2 (2) 2 (1)
⁄American Indian, Alaskan Native, Asian, Multiracial, Native Hawaiian, or other Pacific Islander.�Baseline viral load is geometric mean of all virology collections during screening and before the randomization date.�HCV subtype as determined by Covance.§Baseline platelets for 1637 patients.+IL28B genotypes at polymorphic site rs12979860; IL28B genotypes missing from patients in study P05514 (PROVIDE) treated with BOC/P/R.–Prothrombin time of 36.9 was in one patient and was an isolated single abnormality probably reflecting lab error.#Total bilirubin of 4.62 was in one patient and was an isolated single abnormality probably reflecting lab error.ALT, alanine aminotransferase.Demographics are shown for patients treated with P/R or BOC/P/R by Metavir fibrosis score at baseline.
JOURNAL OF HEPATOLOGY
Please cite this article in press as: Vierling JM et al. Safety and efficacy of boceprevir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta-analysis of 5 trials. J Hepatol (2014), http://dx.doi.org/10.1016/j.jhep.2014.03.022
Journal of Hepatology 2014 vol. xxx j xxx–xxx 3
66 54 55
28 26 17
20
0
40
60
80
100A
SVR
(%; 9
5% C
I)
F0-F2 F3 F4Metavir Fibrosis Score
BOC/P/RP/R
32436 22n= 1638 180107
†
†
†
*
*
*
86
54
6
293544
578
05
766889
4047
6573
2879
017
1647
85
34 0
89
35
0
0
20
40
60
80
100
F0-F2 F3 F4
SVR
(%; 9
5% C
I)
Metavir Fibrosis Stage
≥3 log10 decline and detectable<3 log10 decline and detectable
UndetectableB
Fig. 1. SVR rates by Metavir fibrosis score and virologic response at treatmentweek 8 after treatment with BOC/P/R or P/R. (A) SVR rates by Metavir fibrosisscore. The combined SVR rates (n, %, 95% confidence interval [CI]) for patientstreated with BOC/P/R and treated with P/R were estimated using a meta-analysismethod. SVR rates were homogeneous for F0–F2 and F3 patients treated withBOC/P/R, and for F3 patients treated with P/R so fixed-effect meta-estimates wereused. SVR rates were heterogeneous for F4 patients treated with BOC/P/R or P/R,and for F0–F2 patients treated with P/R so the random-effect meta-estimateswere used. In the BOC/P/R and P/R groups, fibrosis scores were missing for 87patients and 20 patients, respectively. ⁄Fixed-effect SVR estimate. �Random-effectSVR estimate. (B) SVR rates according to virologic response at treatment week 8and Metavir fibrosis scores. SVR rates (undetectable HCV-RNA [‘‘Target NotDetected’’ or ‘‘HCV-RNA Not Detected’’] in the plasma 24 weeks after completionor discontinuation of therapy) and 95% CIs are shown for patients treated withBOC/P/R according to the on-treatment response at treatment week 8 (after4 weeks of lead-in with P/R and 4 weeks of treatment with BOC/P/R) and theMetavir fibrosis stage at baseline. The categories of virologic response attreatment week 8 were undetectable HCV-RNA, detectable HCV-RNA andP3 log10 decline in HCV-RNA from baseline, and detectable HCV-RNA and<3 log10 decline in HCV-RNA from baseline. Results for HCV-RNA at treatmentweek 8 were missing for 127 F0–F2, 8 F3, and 61 F4 patients.
Research Article
P1 log10 decline from baseline in HCV-RNA at treatment week 4(odds ratio = 2.85; p-value = 0.0234) were significant factors.
An analysis of baseline factors and on-treatment responsesidentified patient groups who had a low chance of achievingSVR. None of the 22 F3 or F4 patients with detectable HCV-RNAand <3 log10 decline from baseline at treatment week 8 achievedSVR (0/22; 95% CI = 0, 13) (Fig. 1B). In F4 patients with HCVsubtype 1a and high viral load, the SVR rate was 55% (47/85) ifpatients exhibited a P3 log10 decline in HCV-RNA or becameundetectable at treatment week 8 compared to 0% (0/9) ifpatients exhibited a <3 log10 decline in HCV-RNA and weredetectable at treatment week 8 regardless of the viral responseat treatment week 4 (Supplementary Table 5). No patients(0/46) with fibrosis stage F0–F2 with less than a 3 log10 decline
Please cite this article in press as: Vierling JM et al. Safety and efficacy of bocepanalysis of 5 trials. J Hepatol (2014), http://dx.doi.org/10.1016/j.jhep.2014.03.
4 Journal of Hepatology 201
in HCV-RNA at treatment week 8, high viral load (>800,000/ml)and genotype 1a achieved SVR regardless of the viral responseat treatment week 4 (Supplementary Table 5).
On-treatment viral response at treatment weeks 4 (after the4-week lead-in with P/R but before BOC was added) and 8 (after4 weeks of BOC) also impacted the SVR rates in F4 patients(Table 2). Among the 169 F4 patients with results at TW8, thehighest SVR rates were observed in 43% (73/169) of patientswho had undetectable HCV-RNA at treatment week 8(SVR = 65/73; 89%; Fig. 1B). SVR rates were higher in the 47%(79/169) of F4 patients who had detectable HCV-RNA and aP3 log10 decline in viral load from baseline at treatment week8 (SVR = 28/79; 35%) than in the 10% (17/169) of F4 patients withdetectable HCV-RNA and a <3 log10 decline in viral load frombaseline at treatment week 8 (SVR = 0/17; 0% [95% CI = 0, 16]).Similarly, higher SVR rates were observed in F4 patients whoexhibited a P1 log10 decline in viral load from baseline at treat-ment week 4 (85/128; 66%) compared to F4 patients who exhib-ited a <1 log10 decline in viral load from baseline at treatmentweek 4 (10/48; 21%). Using on-treatment response criteria, SVRrates were similarly high across all Metavir scores for patientstreated with BOC/P/R who were HCV-RNA undetectable at TW8.Irrespective of Metavir score, patients treated with BOC/P/R withdetectable HCV-RNA at week 8 and <3-log decline from baselinerarely achieved SVR (5/100, 5%; Supplementary Table 3) in oursmall sample. Similarly, F0–F4 patients treated with BOC/P/Rwith HCV-RNA P1000 IU/ml at week 8 also rarely achievedSVR (13/177, 7%; Supplementary Table 9).
Additional analyses were conducted in the limited number ofpatients who achieved a very good response at TW8 in order toassess the impact of duration of treatment. F4 patients who wereHCV-RNA undetectable at treatment week 8 and receivedP40 weeks of BOC/P/R achieved an SVR rate of 97% (38/39; 95%CI = 87, 100) (Fig. 2; Supplementary Table 6). Interestingly, thelimited number of F4 patients who were HCV-RNA undetectableat treatment week 8 and received 28 to <36 weeks or 36 to<40 weeks of BOC/P/R also achieved high SVR rates of 89% (16/18) or 89% (8/9), respectively (combined SVR rate = 24/27, 89%;95% CI = 71, 98). It should be noted that due to the response-guided therapy study regimens, the interval of 28 to <40 weeksof therapy contained 21 treatment-naive patients (SVR = 19/21;90%) and 6 patients who failed previous therapy (SVR = 5/6; 83%).
Fig. 4 shows a proposed algorithm for the treatment of F3 andF4 patients with BOC/P/R. A new stopping rule at TW8 (detect-able HCV-RNA and <3 log10 decline from baseline in HCV-RNA)could be utilized to limit therapy in those patients who have alow chance of achieving an SVR with continued treatment. Stop-ping rules at TW12 (if HCV-RNA P100 IU/ml) and TW24 (ifdetectable HCV-RNA) also prevent patients who have a lowchance of achieving an SVR from continuing therapy. The resultsin Fig. 2 suggest that treatment of F3/F4 treatment-naïve patientswho were HCV-RNA undetectable at TW8 could potentially bestopped after TW28 if the patients are not tolerating therapywell. In F3/F4 patients who have a P3 log10 decline but stilldetectable HCV-RNA at TW8, approximately one-half (62/126;49%) still remained detectable at TW12.
Safety and tolerability in cirrhotic patients
There was one death (1%) in the group of 180 F4 patients com-pared to 0 deaths in 107 F3 patients and 5 deaths (<1%) in
revir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta-022
4 vol. xxx j xxx–xxx

Table 2. Adverse events by Metavir fibrosis stage.
n (%)Peginterferon/Ribavirin Boceprevir/Peginterferon/Ribavirin
F0-2 F3 F4 F0-2 F3 F4Adverse events (AE) n = 436 n = 22 n = 32 n = 1638 n = 107 n =180
Treatment-emergent AE 427 (98) 22 (100) 32 (100) 1621 (99) 106 (99) 179 (99)Treatment-related treatment-emergent AE 424 (97) 22 (100) 32 (100) 1618 (99) 106 (99) 178 (99)Serious AE 36 (8) 3 (14) 2 (6) 189 (12) 13 (12) 33 (18)Death 4 (1) 0 0 5 (<1) 0 1 (1)Life-threatening treatment-emergent AEDose modification due to an AE
Dose modification due to anemia
4 (1) 0 0 25 (2) 3 (3) 7 (4)95 (22) 5 (23) 13 (41) 642 (39) 43 (40) 78 (43)55 (13) 1 (5) 5 (16) 414 (25) 29 (27) 58 (32)
Study drug discontinuation due to AE 59 (14) 1 (5) 1 (3) 226 (14) 16 (15) 28 (16)
Specific clinical AE
Specific laboratory AE
4 (1) 0 0 25 (2) 4 (4) 2 (1)
Transfusions 2 (<1) 0 0 38 (2) 8 (7) 13 (7)Treatment-emergent infections 154 (35) 3 (14) 9 (28) 548 (33) 37 (35) 74 (41)
Hemoglobin n = 432 n = 22 n = 32 n = 1629 n = 107 n = 178<10 g/dL 127 (29) 7 (32) 7 (22) 870 (53) 60 (56) 113 (63)8.5-<10 g/dL 110 (25) 7 (32) 5 (16) 741 (45) 43 (40) 85 (48)<8.5 g/dL 17 (4) 0 2 (6) 129 (8) 17 (16) 27 (15)EPO use, n (%) 104 (24) 6 (27) 7 (22) 690 (42) 49 (46) 95 (53)
Platelets (x 109/L) n = 430 n = 21 n = 32 n = 1638 n = 107 n = 178>100 (grade 0) 374 (87) 13 (62) 16 (50) 1206 (74) 45 (42) 46 (26)70-100 (grade 1) 48 (11) 6 (29) 10 (31) 285 (17) 40 (37) 50 (28)50-<70 (grade 2) 3 (1) 2 (10) 2 (6) 99 (6) 14 (13) 45 (25)25-<50 (grade 3) 5 (1) 0 4 (13) 37 (2) 6 (6) 35 (20)<25 (grade 4) 0 0 0 2 (<1) 2 (2) 2 (1)Thrombopoietin use, n 0 0 0 0 0 0Change from baseline in minimum platelets, mean (SD)
-94.8 (54.3) -68.3 (42.4) -73.1 (39.6) -114.3 (56.8) -92.7 (46.7) -84.3 (43.0)
Neutrophils (x109/L) n = 432 n = 22 n = 32 n = 1629 n = 107 n = 178>1.5 (grade 0) 96 (22) 7 (32) 8 (25) 235 (14) 7 (7) 19 (11)1.0-1.5 (grade 1) 156 (36) 9 (41) 8 (25) 437 (27) 36 (34) 47 (26)0.75-<1.0 (grade 2) 103 (24) 3 (14) 7 (22) 419 (26) 29 (27) 46 (26)0.5-<0.75 (grade 3) 59 (14) 3 (14) 6 (19) 389 (24) 25 (23) 41 (23)<0.5 (grade 4) 18 (4) 0 3 (9) 149 (9) 10 (9) 25 (14)G-CSF use, n (%) 28 (6) 1 (5) 4 (13) 176 (11) 11 (10) 19 (11)
Lymphocytes (x109/L) N = 432 N = 22 N = 32 N = 1629 N = 107 N = 178>0.5 (grade 0) 367 (85) 19 (86) 23 (72) 1236 (76) 85 (79) 125 (70)>0.2-0.5 (grade 1) 63 (15) 3 (14) 8 (25) 376 (23) 21 (20) 50 (28)>0.1-0.2 (grade 2) 2 (<1) 0 1 (3) 13 (1) 1 (1) 3 (2)≤0.1 (grade 3) 0 0 0 4 (<1) 0 0
Common adverse event (≥25%*) n = 436 n = 22 n = 32 n = 1638 n = 107 n = 180Any adverse event 427 (98) 22 (100) 32 (100) 1621 (99) 106 (99) 179 (99)
Anemia 124 (28) 6 (27) 7 (22) 786 (48) 49 (46) 100 (56)Fatigue 253 (58) 10 (45) 17 (53) 965 (59) 60 (56) 102 (57)Dysgeusia 72 (17) 5 (23) 4 (13) 627 (38) 39 (36) 75 (42)Nausea 171 (39) 10 (45) 12 (38) 783 (48) 47 (44) 70 (39)Headache 188 (43) 9 (41) 8 (25) 725 (44) 46 (43) 65 (36)Diarrhea 85 (19) 2 (9) 6 (19) 425 (26) 27 (25) 64 (36)Chills 114 (26) 3 (14) 9 (28) 482 (29) 35 (33) 54 (30)Neutropenia 85 (19) 3 (14) 7 (22) 404 (25) 22 (21) 47 (26)Pyrexia 129 (30) 6 (27) 7 (22) 437 (27) 34 (32) 46 (26)
JOURNAL OF HEPATOLOGY
Please cite this article in press as: Vierling JM et al. Safety and efficacy of boceprevir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta-analysis of 5 trials. J Hepatol (2014), http://dx.doi.org/10.1016/j.jhep.2014.03.022
Journal of Hepatology 2014 vol. xxx j xxx–xxx 5

93%83% 100% 94%89%
0
25
50
75
100
<28 wk 28-36 wk 36-40 wk >40 wk
SV
R, %
(95%
CI)
1518
7884
66
89
1718
91%
279306
1618
96% 97%
351367
3839
89%43%40%
37
44%
58132
25
F3F4
F0-F2
Fig. 2. SVR according to treatment duration in patients receiving BOC/P/Rwith undetectable HCV-RNA at treatment week 8. SVR rates (undetectableHCV-RNA [‘‘Target Not Detected’’ or ‘‘HCV-RNA Not Detected’’] in the plasma24 weeks after completion or discontinuation of therapy) and 95% CIs are shownfor patients treated with BOC/P/R and undetectable HCV-RNA at treatment week8 (after 4 weeks of lead-in with P/R and 4 weeks of treatment with BOC/P/R)according to the duration of treatment received and the Metavir fibrosis score atbaseline. Treatment-naive patients and those with previous treatment failurewere combined.
TW8: undetectable vs.detectable HCV-RNA
TW4: ≥1 log10 decline vs.<1 log10 decline
Male vs. female
Baseline viral load≤800,000 IU/ml
vs. >800,000 IU/mlG1b vs. G1a
Non-black vs. black
42 31Odds Ratio (95% CI)
5 6 7 8 9 10
10.57 (5.23-21.36); p <0.0001
2.64 (1.33-5.21); p = 0.0053
2.23 (1.18-4.24) p = 0.0141
2.55 (1.05-6.20) p = 0.0383
1.76 (0.90-3.44); p = 0.0971
1.08 (0.43-2.72); p = 0.8636
Fig. 3. Predictors of SVR by multivariate logistic regression analysis in F3/F4patients receiving BOC/P/R. The relationship between baseline factors and SVRfor patients receiving BOC/P/R with baseline fibrosis scores of F3 or F4 wasexplored using multivariate logistic regression analysis, with SVR as thedependent variable and using demographic and baseline disease characteristics(e.g., race, baseline viral load, gender, genotype, previous treatment history) andon-treatment responses at TW4 and TW8 as independent variables in order toidentify predictors of SVR for patients with different fibrosis scores. Once the on-treatment response at TW8 was in the model, IL28B genotype [17] was no longerpredictive of SVR. The figure shows the multivariate logistic regression analysisfor F3 and F4 patients (odds ratio; 95% CI; p value) which were pooled in orderincrease the power to identify predictors of SVR. Factors with p values <0.05:filled ovals; factors with p values >0.05: open ovals.
All patients:lead-in
with P/R for 4 weeks
Add BOC at TW4
Recommend stopping*
≥3 log10decline in HCV-RNA at
TW8
Continue to wk 12
STOP
HCV-RNA ≥100 IU/ml at TW12 or detectable
HCV-RNA at TW24
Undetectable HCV-RNA at
TW12 and TW24
Continue to wk 48†
<3 log10 declineand detectable
HCV-RNAat TW8
Fig. 4. Proposed treatment algorithm for cirrhotic (F4) and F3 patientstreated with BOC/P/R. A potential algorithm for the treatment of F4 and F3patients was derived from the on-treatment viral responses at weeks 8, 12, and24. Because no F3 or F4 patients (0/22; 95% CI = 0, 13) with a detectable HCV-RNAand <3 log10 decline in viral load from baseline at Week 8 achieved SVR, stoppingtherapy in these patients should be considered. Because treatment-naïve F3 andF4 patients with undetectable viral load at treatment week 8 and thereafterachieved similar SVR rates with durations of treatment between 28 and 40 weekscompared to P40 weeks, therapy of treatment-naive cirrhotic patients might bestopped after week 28 if the regimen is poorly tolerated. HCV-RNA levels shouldbe monitored at Treatment Weeks 4, 8, 12, and 24, at the end of treatment, andduring treatment follow-up. Use of a sensitive real-time reverse-transcriptionpolymerase chain reaction (RT-PCR) assay for monitoring HCV-RNA levels duringtreatment is recommended. The assay should have a lower limit of HCV-RNAquantification of equal to or less than 25 IU/ml, and a limit of HCV-RNA detectionof approximately 10–15 IU/ml. Discontinuation of therapy is recommended in allpatients with (1) Detectable HCV-RNA and <3 log10 decline from baseline in HCV-RNA at TW8, (2) HCV-RNA levels of greater than or equal to 1000 IU per ml atTW8; (3) HCV-RNA levels of P100 IU/ml at TW12, or (4) confirmed detectableHCV-RNA levels at TW24. ⁄Recommend stopping therapy based on low chance ofSVR in F3 and F4 patients with detectable HCV-RNA and <3 log10 decline in HCV-RNA from baseline (SVR = 0/22; 0%; 95% CI [0, 13]). �Recommend stoppingtreatment of treatment-naïve patients after TW28 if undetectable HCV RNA fromTW8 through TW24.
Research Article
1638 F0–F2 patients in this meta-analysis who were treated withBOC/P/R (Table 3). The frequency of serious adverse events washigher in F4 patients treated with BOC/P/R (33/180; 18%) thanF0–F2 patients (13/107; 12%) or F3 (189/1638; 12%). The discon-tinuation rates due to an AE were similar in F4 (16%), F3 (15%)and F0–F2 (14%) patients. The percentage of patients withhemoglobin <10 g/dl was higher in F4 patients treated withBOC/P/R (113/180; 63%) than F0–F2 patients (870/1638; 53%)
⁄Adverse events of P25% in F4 patients treated with BOC/P/R; listed in decreasing frequAdverse events, specific clinical adverse events, specific laboratory adverse events, andMetavir fibrosis stage. Results for hemoglobin, platelets, neutrophils or lymphocytes we
Please cite this article in press as: Vierling JM et al. Safety and efficacy of bocepanalysis of 5 trials. J Hepatol (2014), http://dx.doi.org/10.1016/j.jhep.2014.03.
6 Journal of Hepatology 201
(Supplementary Table 7). Baseline hemoglobin was the strongestpredictor of on-study anemia among the covariates considered inF4 patients treated with BOC/P/R with an estimated odds ratio of0.59 (Supplementary Table 10). Similarly, the percentage ofpatients with hemoglobin <8.5 g/dl was higher in F4 patientstreated with BOC/P/R (27/180; 15%) than F0–F2 patients (129/1638; 8%). The kinetics of the decrease in hemoglobin levels weresimilar in F4, F3, and F0–F2 patients treated with BOC+PR(Supplementary Fig. 4). Interventions to manage anemia wereused more frequently in the cirrhotics. The rates of dose modifi-cation due to anemia were 32% in F4, 27% in F3, and 25% in F0–F2patients treated with BOC/P/R. The rates of transfusions werehigher in F4 (13/180; 7%) and F3 (8/107; 7%) treated withBOC/P/R than F0–F2 (38/1638; 2%). The rates of EPO use werehigher in F4 (53%) than in F0–F2 patients treated with BOC/P/R(42%) and the rate of EPO use in F3 patients was 46%. On-treatment decrease in platelets (grade 4) was higher in F4 onBOC/P/R (25/178; 14%) than F0–F2 (149/1629; 9%) or F3(10/107; 9%), potentially reflecting lower baseline platelet levels.
The frequency of common adverse events (frequency of P25%in F4 patients treated with BOC/P/R) by Metavir fibrosis stage isshown in Table 2. The frequency of anemia was higher in F4patients treated with BOC/P/R (100/180; 56%) than F3 (49/107;
ency in F4 patients treated with BOC/P/R.common adverse events are shown for patients treated with P/R or BOC/P/R byre missing for some patients.
revir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta-022
4 vol. xxx j xxx–xxx

Table 3. Five patients with potential hepatic decompensation or sepsis.
Patient ID(study)
Baseline data Event Treatment regimen (weeks of treatment)
Outcome
Cirrhotic patients
016301(PROVIDE)
Male, 64 yr; F4.history of ascites;Platelets 108 x109/LAlbumin 3.7 g/dL
Decompensated cirrhosis with ascites and encephalopathy (confusion)
BOC/P/R(TW6)
Discontinued treatment; events resolved
012072(RESPOND-2)
Female, 51 yr; F4Platelets 170 x109/LAlbumin 3.5 g/dL
Bleeding esophageal varices and portal hypertension
P/R(TW2)
Discontinued treatment;events resolved
000603(PEG2a study)
Male, 48 yr; F4Diabetic, IVDUPlatelets 135 x109/LAlbumin 3.8 g/dL
Multi-organ failure with total bilirubin peak 17.4 mg/dL(Staphylococcus pneumonia, resulting in multi-organ failure)
BOC/P/R(TW12)
Died of multi-organ failure
Non-cirrhotic patients
000005(PEG2a study)
Male, 52 yr; F2Platelets 280 x109/LAlbumin 4.2 g/dL
Possible urosepsis(Negative blood and urine cultures)
P/R(TW3)
Discontinued treatment; event resolved
001868(SPRINT-2)
Male, 58 yr; F2Platelets 192 x109/LAlbumin 3.5 g/dL
Ascites(Hospitalized with severe epiglottis and neutropenia; developed acute renal failure. Treatment discontinued. Ascites and edema noted 12 days later)
12 days after discontinuing BOC/P/R (TW12)
Discontinued treatment for other AEs; ascites resolved
JOURNAL OF HEPATOLOGY
46%) and F0–F2 (786/1638; 48%) patients treated with BOC/P/R.The frequency of diarrhea was higher in F4 patients treated withBOC/P/R (64/180; 36%) than F3 (27/107; 25%) and F0–F2 (425/1638; 26%) patients treated with BOC/P/R.
Five patients with potential hepatic decompensation or sepsiswere adjudicated by J. Vierling and S. Bruno who were blinded tothe treatment regimens and Metavir scores (Table 3). Threepatients were F4 and two were F2 at baseline. The three F4patients had events of decompensated cirrhosis with ascitesand encephalopathy (confusion) at TW6 (BOC/P/R), bleedingesophageal varices and portal hypertension at TW2 (P/R), ormulti-organ failure with total bilirubin peak of 17.4 mg/dl atTW12 (BOC/P/R). The two F2 patients had events of possible uro-sepsis at TW3 (P/R), or ascites at 12 days after discontinuing BOC/P/R (TW12). All of the events of decompensated cirrhosis resolvedexcept for the patient with multi-organ failure who died. In addi-tion, there were two F4 patients with hepatocellular carcinoma(one patient on P/R and one patient on BOC/P/R; ‘‘More Informa-tion on the Two F4 Patients with Hepatocellular Carcinoma’’ inthe Supplemental Material for more information about these 2patients). When a safety composite endpoint of death, hepaticdecompensation, and severe infection (grade 3 or 4 or requiringhospitalization) was analyzed in the cirrhotic cohort using logis-tic regression (13 subjects with event, 167 subjects withoutevent), no association was found between the composite end-point and baseline albumin and baseline platelets levels. How-ever, this result should be viewed with caution due to of thesmall number of events (13) in this cirrhotic cohort.
Discussion
In the 2 registration trials, the SVR rates in 79 cirrhotic (F4) HCVG1 patients on BOC/P/R ranged from 31% to 77% compared to64–67% in non-cirrhotics [2]. Achieving an SVR reduces the risk
Please cite this article in press as: Vierling JM et al. Safety and efficacy of bocepanalysis of 5 trials. J Hepatol (2014), http://dx.doi.org/10.1016/j.jhep.2014.03.
Journal of Hepatology 201
of hepatocellular carcinoma, liver decomposition, and all-causemortality in patients with cirrhosis [13,14]. In these combinedregistration trials, serious AEs occurred in 16% of patients in theBOC-containing arms with cirrhosis compared to 11% of thosewithout cirrhosis. Based on the results from the 2 registration tri-als, 48 weeks of therapy (4 week lead-in with P/R and 44 weeksof BOC/P/R) was recommended for all patients with cirrhosis(F4) irrespective of baseline variables or early on-treatmentresponses. To better elucidate the risks and benefits of therapywith BOC/P/R in F4 patients with compensated cirrhosis, we ana-lyzed results from all arms of the 5 clinical trials of BOC/P/R inHCV G1 patients.
Previously, it was known that SVR was more likely in patientswith advanced fibrosis/cirrhosis who had P1.0 log10 decline inHCV-RNA at week 4 (the end of the lead-in with P/R), and in thosewith undetectable HCV-RNA at week 8 [2]. Here we show thatover one-half of all F4 patients treated with BOC/P/R can achievean SVR (SVR rate by meta-analysis = 55%). In addition, the SVRrates were particularly high (89%) in F4 patients who wereHCV-RNA undetectable at treatment week 8; these patientsaccounted for 43% of the total treated cirrhotic population. Fur-thermore, F3 and F4 patients with undetectable viral load attreatment week 8 achieved similar SVR rates with durations oftreatment between 28 and 40 weeks (33/38; 87%; 95% CI = 72,96) compared to P40 weeks (23/25; 92%; 95% CI = 74, 99). Theresults with shorter durations of treatment in F4 patients mainlyderived from treatment-naïve patients where the response-guided therapy regimen allowed a duration of 28 weeks of ther-apy in responsive patients. Thus, shorter durations of treatment(28–40 weeks) might be considered for treatment-naïve F4patients with undetectable HCV RNA from weeks 8 through 24if the patients are poorly tolerating therapy.
Predictors of SVR in F3 and F4 patients included male gender,low baseline viral load, and on-treatment viral responses atweeks 4 and 8. These factors can help clinicians identify patient
revir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta-022
4 vol. xxx j xxx–xxx 7

Research Article
profiles and early virologic responses associated with higher SVRrates. On the other hand, the frequency of SAEs, transfusions, ane-mia, and thrombocytopenia (grade 4) were higher in F4 patientstreated with BOC/P/R compared to F0–F2 patients. Therefore, ourresults demonstrate both the potential benefits and risks of treat-ing F4 patients.A potential algorithm for the treatment of F4 and F3 patientscan be derived from the on-treatment viral responses at weeks 8,12, and 24 (Fig. 4). Because no F3 or F4 patients (0/22; 95% CI = 0,13) with a detectable HCV-RNA and <3 log10 decline in viral loadfrom baseline at week 8 achieved SVR, stopping therapy in thesepatients is recommended. A similar stopping rule if HCV-RNA isP1000 IU/ml at week 8 is also recommended because the SVRrate was 0% (0/31) in these F3 or F4 patients. The U.S. FDA hasapproved a revision to the Prescribing Information for VICTRELIS�
(boceprevir) to add a futility rule for stopping therapy with BOC/P/R in all patients if HCV-RNA levels are greater than or equal to1000 IU per ml at TW8. The same futility rule has been acceptedby the CHMP for inclusion in the European Summary of ProductsCharacteristics, and is pending approval by the EuropeanCommission. Based on the upper bound of the 95% confidenceinterval, it is possible that up to 13% of F3 or F4 patients with a<3 log10 decline in viral load from baseline might yet achievean SVR. Because treatment-naïve F3 and F4 patients withundetectable viral load at treatment week 8 achieved similarSVR rates with durations of treatment between 28 and 40 weekscompared to P40 weeks, therapy of treatment-naive cirrhoticpatients might be stopped after week 28 if the regimen is poorlytolerated. Stopping rules will also be important with interferon-based triple therapy with simeprevir, faldaprevir, and sofosbuvirfor HCV genotype 1 infection, in particular in patients withcirrhosis [15].
There were several differences between the patient popula-tion from the 5 clinical trials with BOC/P/R and those in theFrench Early Access Programme (ANRS CO20-CUPIC) [3]. Mostimportantly, 40% of the 190 patients treated with BOC/P/R inCUPIC would have been excluded from the pivotal clinical trialswith BOC due to the exclusion criteria in the study protocols.Approximately 44% of the F4 patients treated with BOC/P/R inthe 5 clinical trials had failed previous treatment compared to97% of the patients in CUPIC (Supplementary Table 8). The F4patients treated with BOC/P/R in the 5 clinical trials were younger(53 years vs. 57 years), less often male (62% of the F4 patientstreated with BOC/P/R in the 5 clinical trials compared to 68% inCUPIC), and had a higher frequency of infection with HCV geno-type 1a (51% vs. 35%) and higher BMI (29.8 vs. 26.0) than thepatients in CUPIC. In addition, the mean baseline platelet countswere approximately 166,000/mm3 range = 49,000–393,000/mm3) in the F4 patients treated with BOC/P/R in the 5 clinical tri-als compared to approximately 144,000/mm3 (range = 34,000–346,000/mm3) in the F4 patients treated with BOC/P/R in CUPIC.The mean serum albumin levels were 38.8 g/dl in the F4 patientstreated with BOC/P/R in the 5 clinical trials compared to approx-imately 40 g/dl in the patients in CUPIC. Therefore, this meta-analysis and CUPIC are complementary and extend our knowl-edge about cirrhotics.
One limitation of the meta-analysis is that the 5 clinical trialswith BOC/P/R enrolled stable, well-compensated cirrhotics (dueto the requirement for platelets to be >100,000/mm3) who maydiffer from cirrhotic patients in clinical practice who need to betreated. Another limitation of our meta-analysis is that it was a
Please cite this article in press as: Vierling JM et al. Safety and efficacy of bocepanalysis of 5 trials. J Hepatol (2014), http://dx.doi.org/10.1016/j.jhep.2014.03.
8 Journal of Hepatology 201
retrospective analysis so the subgroups are not truly randomizedcomparisons; unidentified variables might explain some of theapparent differences in safety and efficacy between cirrhoticsand non-cirrhotics.
In conclusion, there is a generally favorable benefit:risk ratiofor BOC/P/R in well-compensated cirrhotics. Baseline and on-treatment parameters can be used to estimate the likelihood ofachieving SVR. The on-treatment response at TW8 is especiallyinformative in identifying patients with a high likelihood ofresponse and, on the other hand, could be the earliest point intime when patients could be discontinued because of a verylow likelihood of responding. The tolerability of BOC/P/R in cir-rhotics is manageable but cirrhotics need closer attention tomanagement of anemia. Data from CUPIC are important as theyextend the experience of BOC/P/R in cirrhotics and in particular,identify those who are likely to poorly tolerate therapy and mightbest be treated with interferon-free regimens [16].
Financial support
The study was sponsored and funded by Merck & Co., Inc., White-house Station, NJ, USA.
Conflict of interest
The authors report the following disclosures:J. Vierling had received research grants, consulting fees or
honorarium, and support for travel to meetings for the study orother purposes from Merck; consultancy fees from Bristol-MyersSquibb, Gilead, Vertex and Roche; expert testimony for the FDAand CDC; grants/grants pending from Excalenz, Hyperion, Ocera,Ikaria, Intercept, Mochida, Sundise, Abbott, Conatus, Gilead,GlobeImmune, Hyperion, Indenix-Novartis, Novartis, Pharmasset,Pfizer, Roche, Vertex, Zymogenetics, Bristol-Myers Squibb, andJohnson and Johnson; payment for CME lectures including serviceon speakers bureaus from Chronic Liver Diseases Foundation;patents (planned, pending, or issued) for HCV riboprobes andS.C.I.D mouse model; royalties from Liver Immunology 2ndEdition, Gershwin, Vierling and Manns, eds; travel/accommoda-tions/meeting expenses from NIH, NIDDK; is the DigestiveDiseases Week Secretary-Treasurer, and is a member of ClinicalResearch Centers of America.
Dr. Zeuzem reports consulting fees from Merck during theconduct of the study; consulting fees from Abbvie, Achillion,Bristol-Myers Squibb, Boehringer Ingelheim, Gilead, Idenix,Janssen, Novartis, Presidio, Roche, Santaris, and Vertex outsidethe submitted work.
F. Poordad has received consultancy fees from Abbvie,Achillion Pharmaceuticals, Anadys Pharmaceuticals, BiolexTherapeutics, Boehringer Ingelheim, Bristol-Myers Squibb, GileadSciences, GlaxoSmithKline, GlobeImmune, Merck, SantarisPharmaceuticals, Tibotec/Janssen, Theravance and Vertex; hasgrants/grants pending from Abbvie, Achillion Pharmaceuticals,Anadys Pharmaceuticals, Biolex Therapeutics, BoehringerIngelheim, Bristol-Myers Squibb, Genentech, Gilead Sciences,GlaxoSmithKline, GlobeImmune, Idenix Pharmaceuticals, IderaPharmaceuticals, Intercept Pharmaceuticals, Janssen, Medarex,Medtronic, Merck, Novartis, Santaris Pharmaceuticals, ScynexisPharmaceuticals, Vertex Pharmaceuticals, ZymoGenetics; and
revir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta-022
4 vol. xxx j xxx–xxx

JOURNAL OF HEPATOLOGY
has received educational and speaker honoraria from Gilead,Kadmon, Merck, Onyx/Bayer, Salix and Vertex.J.-P. Bronowicki has received board membership fees fromMerck, Roche, Gilead, Bristol-Myers Squibb, Janssen, and Bayer;consultancy fees from Merck, Boehringer Ingelheim, andNovartis; payment for lectures including service on speakersbureaus for Merck, Roche, Bayer and Bristol-Myers Squibb andtravel/accommodations/meeting expenses unrelated to activitieslisted from Roche.
Dr. Manns received financial compensation for consultancyand/or lecture activities from Roche, Bristol-Myers Squibb,Gilead, Boehringer Ingelheim, Novartis, Merck, Janssen, Idenixand GlaxoSmithKline, and research grants from Roche, Gilead,Novartis, Boehringer Ingelheim, Bristol-Myers Squibb, Merckand Janssen.
B. Bacon has received consultancy fees from Gilead, KadmonPharmaceuticals, Valeant, Vertex, and Human Genome Sciences;has grants and grants pending from Roche, Gilead, Bristol-MyersSquibb, Kadmon Pharmaceuticals, Valeant, Vertex, HumanGenome Sciences, Wyeth, and Romark Laboratories; paymentfor lectures including service on speakers bureaus for KadmonPharmaceuticals, Gilead, and Merck; and served on Data andSafety Monitoring Boards for Novartis, ISIS, Vertex, and Gilead.
Dr. Esteban received financial compensation from Merck,Janssen, Bristol-Myers Squibb, Abbvie, and Novartis, outside thesubmitted work.
S. Flamm has received grants from Merck, Vertex, Gilead, Nov-artis, Anadys, Achillion, Tibotec, and Bristol-Myers Squibb; con-sultancy fees from Vertex, Gilead, Boehringer Ingelheim, andNovartis; and payment for lectures including service on speaker’sbureaus from Merck and Vertex.
P. Kwo has received research grants, consulting fees or hono-rarium, and support for travel to meetings for the study or otherpurposes from Merck; consultancy fees from Abbott, Bristol-Myers Squibb, Gilead, Vertex, and Novartis; and payment for lec-tures including service on speakers bureaus from Merck, Vertex,and Genetech.
Dr. Bruno reports receiving fees for advisory board and speak-er’s bureau from Merck during the conduct of the study; andreceiving fees for speaker’s bureau from Roche, and Bristol-MyersSquibb outside the submitted work.
L. Pedicone, W. Deng, F. Dutko, M. DiNubile, K. Koury, F. Hel-mond, and J. Wahl are current or former employees of Merck &Co., Inc., Whitehouse Station, NJ and hold stock and/or stockoptions.
Potential competing interests
The opinions expressed in this report represent the consensus ofthe authors and do not necessarily reflect the formal position ofMerck or other institutions listed as authors’ affiliations. The cor-responding authors had full access to all of the data and take fullresponsibility for the veracity of the data and statistical analysis.
Authors’ contributions
All co-authors had full access to all pertinent data upon request.A penultimate version of the paper was reviewed by the sponsor.Each co-author has approved the final version of the manuscript.
Please cite this article in press as: Vierling JM et al. Safety and efficacy of bocepanalysis of 5 trials. J Hepatol (2014), http://dx.doi.org/10.1016/j.jhep.2014.03.
Journal of Hepatology 201
The corresponding authors had full access to all of the data andtake full responsibility for the veracity of the data and statisticalanalysis. The opinions expressed in this report represent the con-sensus of the authors and do not necessarily reflect the formalposition of Merck or the authors’ affiliated universities.
Acknowledgements
We are indebted to all the patients, healthcare providers, andinvestigators involved with the parent studies. We are particu-larly grateful to Dr. Scott Vuocolo of Merck for his advice and sup-port. The expert assistance of Victoria Enwemadu and KarynDavis from Merck in the preparation of this manuscript is verymuch appreciated.
Supplementary data
Supplementary data associated with this article can be found, inthe online version, at http://dx.doi.org/10.1016/j.jhep.2014.03.022.
References
[1] Bourliere M, Wendt A, Fontaine H, Hezode C, Pol S, Bronowicki JP. How tooptimize HCV therapy in genotype 1 patients with cirrhosis. Liver Int2013;33:46–55.
[2] Bruno S, Vierling JM, Esteban R, Nyberg LM, Tanno H, Goodman Z, et al.Efficacy and safety of boceprevir plus peginterferon-ribavirin in patientswith HCV G1 infection and advanced fibrosis/cirrhosis. J Hepatol2013;58:479–487.
[3] Hezode C, Fontaine H, Dorival C, Larrey D, Zoulim F, Canva V, et al. Tripletherapy in treatment-experienced patients with HCV-cirrhosis in a multi-centre cohort of the French Early Access Programme (ANRS CO20-CUPIC) –NCT01514890. J Hepatol 2013;59:434–441.
[4] Fontaine H, Hezode C, Dorival C, Larrey D, Zoulim F, de Ledinghen V, et al.SVR12 rates and safety of triple therapy including teleprevir or boceprevir in221 cirrhotic non responders treated in the French Early Access Program(ANRS CO20-CUPIC). J Hepatol 2013;58:S27.
[5] Bacon B, Gordon S, Lawitz E, Marcellin P, Vierling J, Zeuzem S, et al.Boceprevir for previously treated chronic HCV genotype 1 infection. N Engl JMed 2011;364:1207–1217.
[6] Poordad F, Bacon B, Bruno S, Mann M, Sulkowski M, Jacobson I, et al.Boceprevir for untreated chronic HCV genotype 1 infection. N Engl J Med2011;364:1195–1206.
[7] Vierling J, Davis M, Flamm S, Gordon S, Lawitz E, Yoshida E, et al. Sustainedvirologic response (SVR) in prior peginterferon/ribavirin (PR) treatmentfailures after retreatment with Boceprevir (BOC) + PR: the Provide studyinterim results. Gastroenterology 2012;142, [Supplement 1-S-931].
[8] Flamm SL, Lawitz E, Jacobson I, Bourliere M, Hezode C, Vierling JM, et al.Boceprevir with peginterferon alfa-2a-ribavirin is effective for previouslytreated chronic hepatitis C genotype 1 infection. Clin Gastroenterol Hepatol2013;11:81–87.
[9] Lawitz E, Zeuzem S, Nyberg L, Nelson D, Rossaro L, Balart L, et al. Boceprevir(BOC) combined with peginterferon alfa-2b/ribavirin (P/RBV) in treatment-naïve chronic HCV genotype 1 patients with compensated cirrhosis:sustained virologic response (SVR) and safety subanalyses from the anemiamanagement study. Hepatology 2012;56:216A.
[10] Garcia-Tsao G, Friedman S, Iredale J, Pinzani M. Now there are many (stages)where before there was one: in search of a pathophysiological classificationof cirrhosis. Hepatology 2010;51:1445–1449.
[11] Qamar AA, Grace ND, Groszmann RJ, Garcia-Tsao G, Bosch J, Burroughs AK,et al. Platelet count is not a predictor of the presence or development ofgastroesophageal varices in cirrhosis. Hepatology 2008;47:153–159.
[12] Vierling J, Zeuzem S, Poordad F, Bronowicki J, Manns M, Bacon B, et al. Safetyand efficacy of boceprevir/peginterferon/ribavirin (BOC/P/R) combinationtherapy for chronic HCV G1 patients with compensated cirrhosis: a meta-analysis of five phase 3 clinical trials. J Hepatol 2013;58:S576–S577.
revir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta-022
4 vol. xxx j xxx–xxx 9
Research Article
[13] Aleman S, Rahbin N, Weiland O, Davidsdottir L, Hedenstierna M, Rose N,et al. A risk for hepatocellular carcinoma persists long-term after sustainedvirologic response in patients with hepatitis C-associated liver cirrhosis. ClinInfect Dis 2013;57:230–236.
[14] van der Meer AJ, Veldt BJ, Feld JJ, Wedemeyer H, Dufour JF, Lammert F, et al.Association between sustained virological response and all-cause mortalityamong patients with chronic hepatitis C and advanced hepatic fibrosis.JAMA 2012;308:2584–2593.
Please cite this article in press as: Vierling JM et al. Safety and efficacy of bocepanalysis of 5 trials. J Hepatol (2014), http://dx.doi.org/10.1016/j.jhep.2014.03.
10 Journal of Hepatology 201
[15] Asselah T, Marcellin P. Second-wave IFN-based triple therapy for HCVgenotype 1 infection: simeprevir, faldaprevir and sofosbuvir. Liver Int2014;34:60–68.
[16] Liang TJ, Ghany MG. Current and future therapies for hepatitis C virusinfection. N Engl J Med 2013;368:1907–1917.
[17] Estrabaud E, Vidaud M, Marcellin P, Asselah T. Genomics and HCV infection:progression of fibrosis and treatment response. J Hepatol2012;57:1110–1125.
revir/peginterferon/ribavirin for HCV G1 compensated cirrhotics: Meta-022
4 vol. xxx j xxx–xxx



















