
Development of a process to manufacture PEGylated orally bioavailable insulin

L
PhD
FAPMAM
a
ARAA
KRTS
1
l
A
Gf
h1
Digestive and Liver Disease 46 (2014) 826–832
Contents lists available at ScienceDirect
Digestive and Liver Disease
journa l h om epage: www.elsev ier .com/ locate /d ld
iver, Pancreas and Biliary Tract
egylated interferon � plus ribavirin for the treatment of chronicepatitis C: A multicentre independent study supported by the Italianrug Agency�
loriano Rosinaa,∗, Maria Elena Tostib, Elisabetta Borghesioc, Maria Masoccob,lfonso Meleb, Carmine Coppolad, Michele Milellae, Guglielmo Borgia f,ietro Andreoneg, Maurizio Kochh, Anna Linda Zignegoi, Mario Romanoj,aurizio Carrarak, Piero Luigi Almasio l, Emilio Azzolam, Gerardo Nardonen,
ntonio Benedettio, Giampiero Carosip, Francesco Mazzottaq, Evangelista Sagnelli r,ario Rizzettoc, for the AIFA Study Group1
r t i c l e i n f o
rticle history:eceived 7 January 2014ccepted 18 May 2014vailable online 28 June 2014
eywords:ibavirinreatmentustained virological response (SVR)
a b s t r a c t
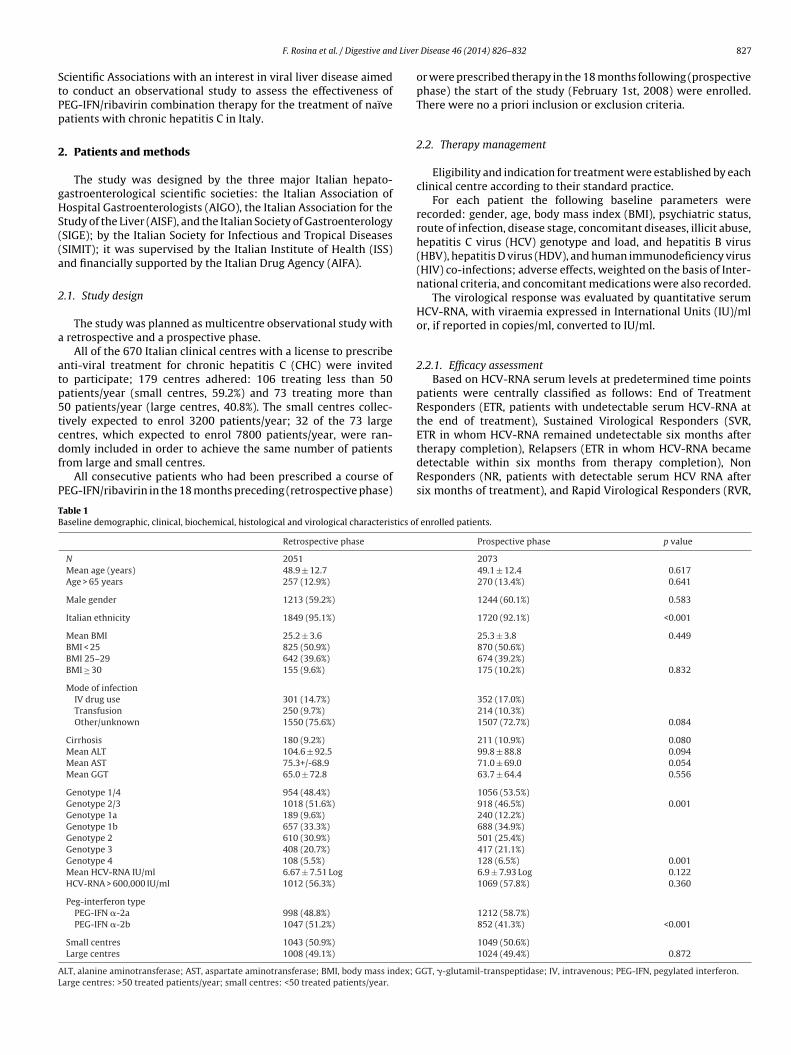
Background: Data on the efficacy of Peg-interferon/ribavirin therapy for chronic hepatitis C are mostlyderived from treatment of selected patients enrolled in clinical trials. This study aimed to assess theeffectiveness of Peg-interferon/ribavirin therapy in “real world” chronic hepatitis C patients in Italy.Methods: Independent observational multicentre study including consecutive patients receiving Peg-interferon/ribavirin in the 18 months before (retrospective phase) and after (prospective phase) the startof the study.Results: 4176 patients were eligible. The final study population consisted of 2051 patients in the retro-spective and 2073 in the prospective phase.
Sustained virological response was achieved by 1036 patients (50.5%) during the retrospective phase:325 were genotypes 1/4 (34.1%) and 684 were genotypes 2/3 (67.2%) and by 800 patients (38.6%) duringthe prospective phase: 300 were genotypes 1/4 (28.4%) and 473 were genotypes 2/3 (51.5%).
During multivariate analysis genotypes 2/3 were significantly associated with higher sustained viro-
logical response rates; cirrhosis and �-glutamil-transpeptidase >2 times the normal limit were associatedwith poorer response.Conclusions: The response to Peg-interferon/ribavirin therapy in “real world” clinical practice is distinctlylower than in registration trials. The difference in response rates was more pronounced among easy-to-treat than among difficult-to-treat hepatitis C virus genotypes.© 2014 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All rights reserved.
. Introduction
The addition of ribavirin to standard interferon � in theate 1990s, followed by the introduction of pegylated interferon
� Source of support: The study was funded by the Governmental Italian Druggency (Associazione Italiana per il FArmaco (AIFA)).a Gastroenterology & Hepatology Unit, Gradenigo Hospital, Torino, Italyb−r See Appendix A.1 See Appendix B for AIFA Study Group Collaborators.∗ Corresponding author at: S.C. Gastroenterologia & Epatologia, Presidio Sanitarioradenigo, C.so Regina Margherita 10, 10133 Torino, Italy. Tel.: +39 011 8151375;
ax: +39 011 8151375; mobile: +39 347 0128577.E-mail address: [email protected] (F. Rosina).
ttp://dx.doi.org/10.1016/j.dld.2014.05.014590-8658/© 2014 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All
(PEG-IFN), has significantly improved the cure rates of chronic hep-atitis C [1].
Much of the information available on the use of PEG-IFNs isderived from clinical trials. As a rule, however, results of such trialsmay be biased by several factors including the use of restrictive cri-teria to avoid confounding the results, and strict patient supervisionto improve compliance.
Therefore, the setting of a clinical trial may not reflect real-worldexperiences, where patients often present complex co-morbidities,and support facilities are variable.
Since only fragmentary information was available on the use ofPEG-IFN in Italy, data on the effectiveness of PEG-IFNs in routinepractice were needed. By including virtually all of the 670 medicalcentres qualified nationwide to prescribe PEG-IFN, the major Italian
rights reserved.
Liver
StPp
2
gHS((a
2
a
atp5tcdf
P
TB
AL
F. Rosina et al. / Digestive and
cientific Associations with an interest in viral liver disease aimedo conduct an observational study to assess the effectiveness ofEG-IFN/ribavirin combination therapy for the treatment of naïveatients with chronic hepatitis C in Italy.
. Patients and methods
The study was designed by the three major Italian hepato-astroenterological scientific societies: the Italian Association ofospital Gastroenterologists (AIGO), the Italian Association for thetudy of the Liver (AISF), and the Italian Society of GastroenterologySIGE); by the Italian Society for Infectious and Tropical DiseasesSIMIT); it was supervised by the Italian Institute of Health (ISS)nd financially supported by the Italian Drug Agency (AIFA).
.1. Study design
The study was planned as multicentre observational study with retrospective and a prospective phase.
All of the 670 Italian clinical centres with a license to prescribenti-viral treatment for chronic hepatitis C (CHC) were invitedo participate; 179 centres adhered: 106 treating less than 50atients/year (small centres, 59.2%) and 73 treating more than0 patients/year (large centres, 40.8%). The small centres collec-ively expected to enrol 3200 patients/year; 32 of the 73 largeentres, which expected to enrol 7800 patients/year, were ran-
omly included in order to achieve the same number of patientsrom large and small centres.All consecutive patients who had been prescribed a course ofEG-IFN/ribavirin in the 18 months preceding (retrospective phase)
able 1aseline demographic, clinical, biochemical, histological and virological characteristics of
Retrospective phase
N 2051
Mean age (years) 48.9 ± 12.7
Age > 65 years 257 (12.9%)
Male gender 1213 (59.2%)
Italian ethnicity 1849 (95.1%)
Mean BMI 25.2 ± 3.6
BMI < 25 825 (50.9%)
BMI 25–29 642 (39.6%)
BMI ≥ 30 155 (9.6%)
Mode of infectionIV drug use 301 (14.7%)
Transfusion 250 (9.7%)
Other/unknown 1550 (75.6%)
Cirrhosis 180 (9.2%)
Mean ALT 104.6 ± 92.5
Mean AST 75.3+/-68.9
Mean GGT 65.0 ± 72.8
Genotype 1/4 954 (48.4%)
Genotype 2/3 1018 (51.6%)
Genotype 1a 189 (9.6%)
Genotype 1b 657 (33.3%)
Genotype 2 610 (30.9%)
Genotype 3 408 (20.7%)
Genotype 4 108 (5.5%)
Mean HCV-RNA IU/ml 6.67 ± 7.51 Log
HCV-RNA > 600,000 IU/ml 1012 (56.3%)
Peg-interferon typePEG-IFN �-2a 998 (48.8%)
PEG-IFN �-2b 1047 (51.2%)
Small centres 1043 (50.9%)
Large centres 1008 (49.1%)
LT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; Garge centres: >50 treated patients/year; small centres: <50 treated patients/year.
Disease 46 (2014) 826–832 827
or were prescribed therapy in the 18 months following (prospectivephase) the start of the study (February 1st, 2008) were enrolled.There were no a priori inclusion or exclusion criteria.
2.2. Therapy management
Eligibility and indication for treatment were established by eachclinical centre according to their standard practice.
For each patient the following baseline parameters wererecorded: gender, age, body mass index (BMI), psychiatric status,route of infection, disease stage, concomitant diseases, illicit abuse,hepatitis C virus (HCV) genotype and load, and hepatitis B virus(HBV), hepatitis D virus (HDV), and human immunodeficiency virus(HIV) co-infections; adverse effects, weighted on the basis of Inter-national criteria, and concomitant medications were also recorded.
The virological response was evaluated by quantitative serumHCV-RNA, with viraemia expressed in International Units (IU)/mlor, if reported in copies/ml, converted to IU/ml.
2.2.1. Efficacy assessmentBased on HCV-RNA serum levels at predetermined time points
patients were centrally classified as follows: End of TreatmentResponders (ETR, patients with undetectable serum HCV-RNA atthe end of treatment), Sustained Virological Responders (SVR,ETR in whom HCV-RNA remained undetectable six months after
therapy completion), Relapsers (ETR in whom HCV-RNA becamedetectable within six months from therapy completion), NonResponders (NR, patients with detectable serum HCV RNA aftersix months of treatment), and Rapid Virological Responders (RVR,enrolled patients.
Prospective phase p value
207349.1 ± 12.4 0.617270 (13.4%) 0.641
1244 (60.1%) 0.583
1720 (92.1%) <0.001
25.3 ± 3.8 0.449870 (50.6%)674 (39.2%)175 (10.2%) 0.832
352 (17.0%)214 (10.3%)1507 (72.7%) 0.084
211 (10.9%) 0.08099.8 ± 88.8 0.09471.0 ± 69.0 0.05463.7 ± 64.4 0.556
1056 (53.5%)918 (46.5%) 0.001240 (12.2%)688 (34.9%)501 (25.4%)417 (21.1%)128 (6.5%) 0.0016.9 ± 7.93 Log 0.1221069 (57.8%) 0.360
1212 (58.7%)852 (41.3%) <0.001
1049 (50.6%)1024 (49.4%) 0.872
GT, �-glutamil-transpeptidase; IV, intravenous; PEG-IFN, pegylated interferon.
8 d Liver
ps
p
2
rrCo
2
Ma
l
2
i
TD
SPL
28 F. Rosina et al. / Digestive an
atients with an undetectable serum HCV-RNA one month aftertarting treatment).
Patients lacking the HCV-RNA assessment six months after stop-ing therapy were classified as NR.
.2.2. Adherence assessmentAdherence was centrally evaluated according to the 80/80/80
ule (>80% of the expected PEG-IFN dose, >80% of the expectedibavirin dose, >80% of the expected length of treatment) [2].omparison was based on the doses and length of treatment rec-mmended by AISF [3].
.3. Data quality assurance and management procedures
The data were conveyed to the Contract Research OrganizationAF Servizi – Torino, Italy – for centralised elaboration and quality
ssurance.Data entry was administered by a dedicated website, and col-
ection was performed via an online e-Case Report Form.
.4. Statistical analysis
The sample size calculation was based on the planned compar-son between PEG-IFN �-2a and �-2b in terms of effectiveness. A
able 2emographic, clinical, biochemical, histological and virological characteristics of patients
Retrospective phase
SVR No SVR
N 1036 (50.5%) 1015 (49.5%)
Mean age (years) 48.6 ± 12.9 49.2 ± 12.4
Age < 65 years 879 (50.6%)
Age ≥ 65 years 133 (51.8%)
Male gender 583 (48.1%)
Female gender 452 (54.1%)
Italian ethnicity 938 (50.7%)
Other ethnicity 45 (46.9%)
Mean BMI 25.1 ± 3.6 25.3 ± 3.6
BMI < 25 432 (52.4%)
BMI 25–29 312 (48.6%)
BMI ≥ 30 81 (52.3%)
Mode of infectionIV drug use 144 (47.8%)
Transfusion 106 (53.0%)
Other 786 (50.7%)
Cirrhosis 54 (30.0%)
No cirrhosis 946 (53.4%)
Mean ALT 103.1 ± 94.5 106.2 ± 90.5
Mean AST 71.8 ± 71.7 79.0 ± 65.6
Mean GGT 52.3 ± 57.2 78.8 ± 84.4
Genotype 1/4 325 (34.1%)
Genotype 2/3 684 (67.2%)
Genotype 1a 72 (38.1%)
Genotype 1b 211 (32.1%)
Genotype 2 452 (74.1%)
Genotype 3 232 (56.9%)
Genotype 4 42 (38.9%)
Mean HCV RNA IU/ml 6.79 ± 7.61 Log 6.49 ± 7.3 Log
<600,000 IU/ml 453 (57.6%)
≥600,000 IU/ml 475 (46.9%)
PEG-IFN�-2a 526 (52.7%)
PEG-IFN �-2b 509 (48.6%)
Small centres 494 (47.4%)
Large centres 542 (53.8%)
VR, sustained virological response; ALT, alanine aminotransferase; AST, aspartate aminotEG-IFN, pegylated interferon.arge centres: >50 treated patients/year; small centres: <50 treated patients/year.
Disease 46 (2014) 826–832
minimum of 5% difference in effectiveness was considered clin-ically relevant. With a probability of type I error ̨ = 0.05 and apower ̌ = 0.80, enrolment of 1600 patients per group was plannedto identify the expected difference.
In the comparison between PEG-IFN �-2a and �-2b in termsof effectiveness, the effect of possible confounders was taken intoaccount during data analysis by means of a multivariate logisticmodel. Factors to be included in the models were chosen by step-wise selection. A factor selected for one model (retrospective orprospective phase) was included in both models. Statistical analysiswas conducted by STATA software (version 11.2).
3. Results
Four thousand one hundred and seventy-six naïve patients wereeligible for the study: 2091 during the retrospective phase and 2085during the prospective phase. A limited subset of patients receiv-ing PEG-IFN alone (40/2091 during the retrospective, and 12/2085during the prospective phase) was excluded from the analysis.
The final study population consisted of 2051 patients (males59.2%, mean age 48.9 ± 12.7 years) enrolled during the retrospec-tive phase, and 2073 patients (males 60.1%, mean age 49.1 ± 12.4years) enrolled during the prospective phase.
according to response.
Prospective phase
p SVR No SVR p
800 (38.6%) 1273 (61.4%) <0.001
0.275 48.3 ± 12.7 49.5 ± 12.2 0.034690 (39.5%)
0.725 95 (35.2%) 0.179
446 (35.8%)0.007 354 (42.8%) 0.001
673 (39.1%)0.461 64 (43.2%) 0.326
0.307 25.0 ± 3.9 25.4 ± 3.7 0.035365 (42.0%)273 (40.5%)
0.336 61 (34.9%) 0.217
127 (36.1%)92 (43.0%)
0.502 581(38.6%) 0.261
53 (25.1%)<0.001 703 (40.8%) <0.001
0.453 98.4 ± 91.6 100.7 ± 86.9 0.5770.022 67.9 ± 63.9 73.1 ± 72.1 0.094
<0.001 51.5 ± 52.5 71.8 ± 70.1 <0.001
300 (28.4%)<0.001 473 (51.5%) <0.001
74 (30.8%)183 (26.6%)279 (55.7%)194 (46.5%)
<0.001 43 (33.6%) <0.001
0.042 6.42 ± 7.19 Log 7.06 ± 8.03 0.007342 (43.7%)
<0.001 401 (37.5%) 0.007
444 (36.6%)0.064 355 (41.7%) 0.021
429 (40.9%)0.004 371 (36.2%) 0.029
ransferase; BMI, body mass index; GGT, �-glutamil-transpeptidase; IV, intravenous;
F. Rosina et al. / Digestive and Liver Disease 46 (2014) 826–832 829
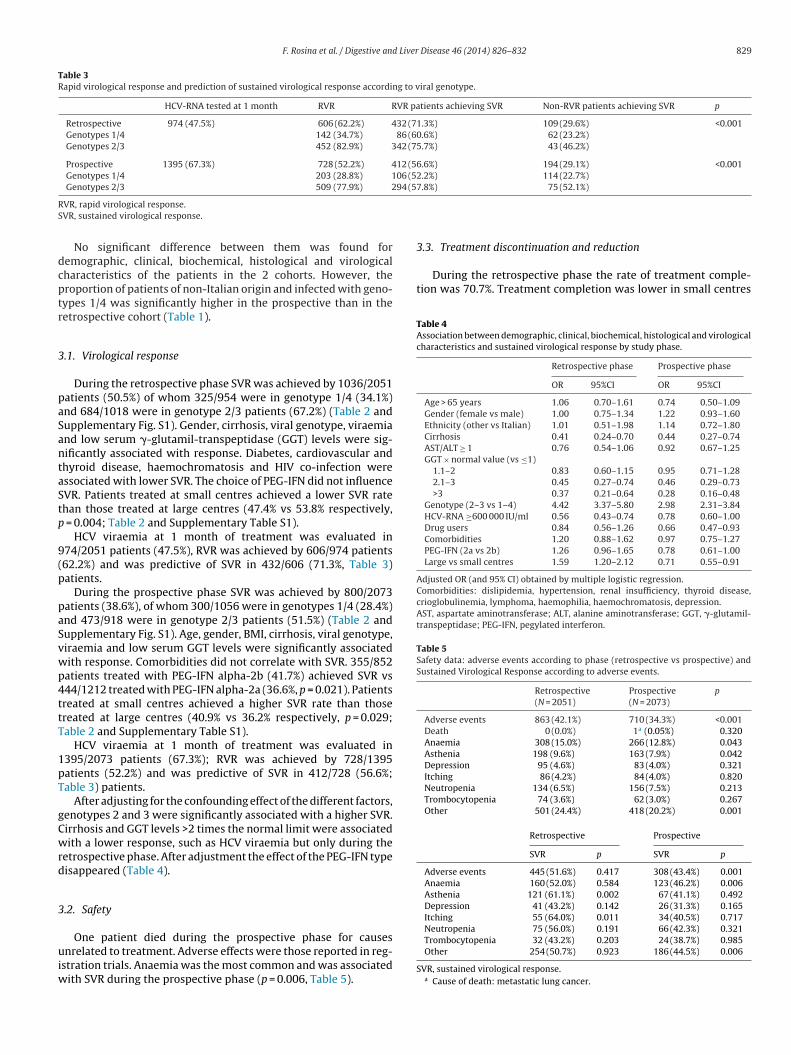
Table 3Rapid virological response and prediction of sustained virological response according to viral genotype.
HCV-RNA tested at 1 month RVR RVR patients achieving SVR Non-RVR patients achieving SVR p
Retrospective 974 (47.5%) 606 (62.2%) 432 (71.3%) 109 (29.6%) <0.001Genotypes 1/4 142 (34.7%) 86 (60.6%) 62 (23.2%)Genotypes 2/3 452 (82.9%) 342 (75.7%) 43 (46.2%)
Prospective 1395 (67.3%) 728 (52.2%) 412 (56.6%) 194 (29.1%) <0.001Genotypes 1/4 203 (28.8%) 106 (52.2%) 114 (22.7%)Genotypes 2/3 509 (77.9%) 294 (57.8%) 75 (52.1%)
RS
dcptr
3
paSantaStp
9(p
paSvwp4ttT
1pT
gCwrd
3
uiw
3.3. Treatment discontinuation and reduction
During the retrospective phase the rate of treatment comple-tion was 70.7%. Treatment completion was lower in small centres
Table 4Association between demographic, clinical, biochemical, histological and virologicalcharacteristics and sustained virological response by study phase.
Retrospective phase Prospective phase
OR 95%CI OR 95%CI
Age > 65 years 1.06 0.70–1.61 0.74 0.50–1.09Gender (female vs male) 1.00 0.75–1.34 1.22 0.93–1.60Ethnicity (other vs Italian) 1.01 0.51–1.98 1.14 0.72–1.80Cirrhosis 0.41 0.24–0.70 0.44 0.27–0.74AST/ALT ≥ 1 0.76 0.54–1.06 0.92 0.67–1.25GGT × normal value (vs ≤1)
1.1–2 0.83 0.60–1.15 0.95 0.71–1.282.1–3 0.45 0.27–0.74 0.46 0.29–0.73>3 0.37 0.21–0.64 0.28 0.16–0.48
Genotype (2–3 vs 1–4) 4.42 3.37–5.80 2.98 2.31–3.84HCV-RNA ≥600 000 IU/ml 0.56 0.43–0.74 0.78 0.60–1.00Drug users 0.84 0.56–1.26 0.66 0.47–0.93Comorbidities 1.20 0.88–1.62 0.97 0.75–1.27PEG-IFN (2a vs 2b) 1.26 0.96–1.65 0.78 0.61–1.00Large vs small centres 1.59 1.20–2.12 0.71 0.55–0.91
Adjusted OR (and 95% CI) obtained by multiple logistic regression.Comorbidities: dislipidemia, hypertension, renal insufficiency, thyroid disease,crioglobulinemia, lymphoma, haemophilia, haemochromatosis, depression.AST, aspartate aminotransferase; ALT, alanine aminotransferase; GGT, �-glutamil-transpeptidase; PEG-IFN, pegylated interferon.
Table 5Safety data: adverse events according to phase (retrospective vs prospective) andSustained Virological Response according to adverse events.
Retrospective Prospective p(N = 2051) (N = 2073)
Adverse events 863 (42.1%) 710 (34.3%) <0.001Death 0 (0.0%) 1a (0.05%) 0.320Anaemia 308 (15.0%) 266 (12.8%) 0.043Asthenia 198 (9.6%) 163 (7.9%) 0.042Depression 95 (4.6%) 83 (4.0%) 0.321Itching 86 (4.2%) 84 (4.0%) 0.820Neutropenia 134 (6.5%) 156 (7.5%) 0.213Trombocytopenia 74 (3.6%) 62 (3.0%) 0.267Other 501 (24.4%) 418 (20.2%) 0.001
Retrospective Prospective
SVR p SVR p
Adverse events 445 (51.6%) 0.417 308 (43.4%) 0.001Anaemia 160 (52.0%) 0.584 123 (46.2%) 0.006Asthenia 121 (61.1%) 0.002 67 (41.1%) 0.492Depression 41 (43.2%) 0.142 26 (31.3%) 0.165Itching 55 (64.0%) 0.011 34 (40.5%) 0.717Neutropenia 75 (56.0%) 0.191 66 (42.3%) 0.321
VR, rapid virological response.VR, sustained virological response.
No significant difference between them was found foremographic, clinical, biochemical, histological and virologicalharacteristics of the patients in the 2 cohorts. However, theroportion of patients of non-Italian origin and infected with geno-ypes 1/4 was significantly higher in the prospective than in theetrospective cohort (Table 1).
.1. Virological response
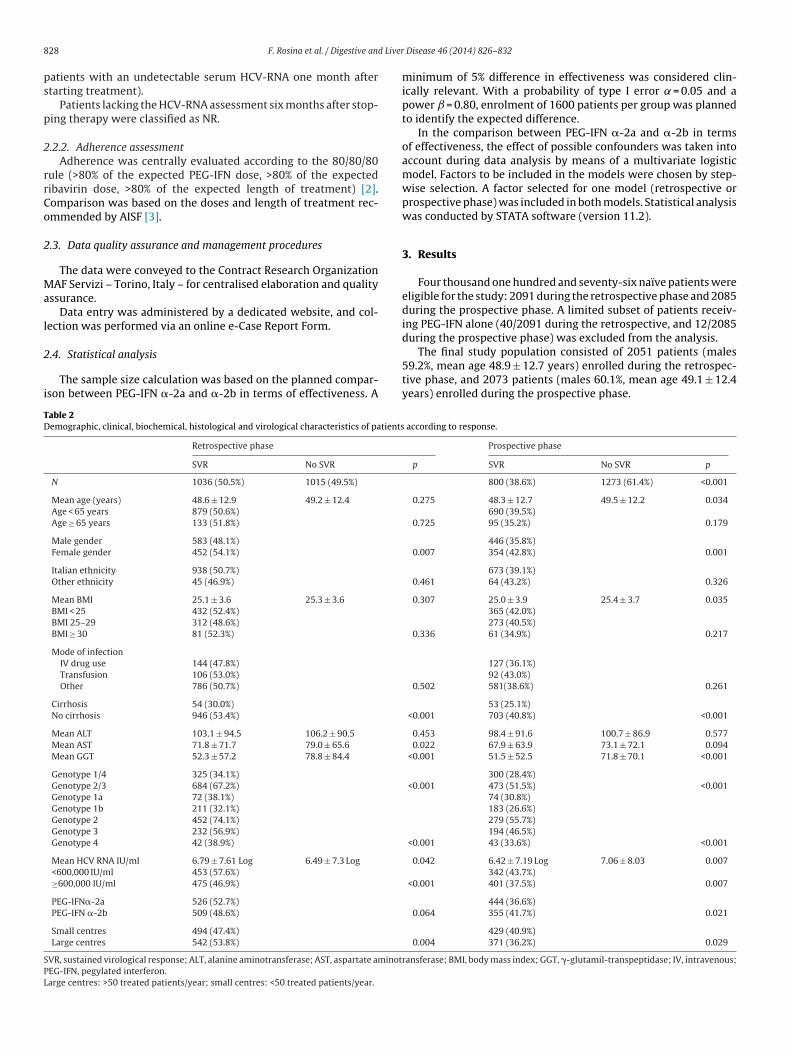
During the retrospective phase SVR was achieved by 1036/2051atients (50.5%) of whom 325/954 were in genotype 1/4 (34.1%)nd 684/1018 were in genotype 2/3 patients (67.2%) (Table 2 andupplementary Fig. S1). Gender, cirrhosis, viral genotype, viraemiand low serum �-glutamil-transpeptidase (GGT) levels were sig-ificantly associated with response. Diabetes, cardiovascular andhyroid disease, haemochromatosis and HIV co-infection weressociated with lower SVR. The choice of PEG-IFN did not influenceVR. Patients treated at small centres achieved a lower SVR ratehan those treated at large centres (47.4% vs 53.8% respectively,
= 0.004; Table 2 and Supplementary Table S1).HCV viraemia at 1 month of treatment was evaluated in
74/2051 patients (47.5%), RVR was achieved by 606/974 patients62.2%) and was predictive of SVR in 432/606 (71.3%, Table 3)atients.
During the prospective phase SVR was achieved by 800/2073atients (38.6%), of whom 300/1056 were in genotypes 1/4 (28.4%)nd 473/918 were in genotype 2/3 patients (51.5%) (Table 2 andupplementary Fig. S1). Age, gender, BMI, cirrhosis, viral genotype,iraemia and low serum GGT levels were significantly associatedith response. Comorbidities did not correlate with SVR. 355/852atients treated with PEG-IFN alpha-2b (41.7%) achieved SVR vs44/1212 treated with PEG-IFN alpha-2a (36.6%, p = 0.021). Patientsreated at small centres achieved a higher SVR rate than thosereated at large centres (40.9% vs 36.2% respectively, p = 0.029;able 2 and Supplementary Table S1).
HCV viraemia at 1 month of treatment was evaluated in395/2073 patients (67.3%); RVR was achieved by 728/1395atients (52.2%) and was predictive of SVR in 412/728 (56.6%;able 3) patients.
After adjusting for the confounding effect of the different factors,enotypes 2 and 3 were significantly associated with a higher SVR.irrhosis and GGT levels >2 times the normal limit were associatedith a lower response, such as HCV viraemia but only during the
etrospective phase. After adjustment the effect of the PEG-IFN typeisappeared (Table 4).
.2. Safety
One patient died during the prospective phase for causesnrelated to treatment. Adverse effects were those reported in reg-
stration trials. Anaemia was the most common and was associatedith SVR during the prospective phase (p = 0.006, Table 5).
Trombocytopenia 32 (43.2%) 0.203 24 (38.7%) 0.985Other 254 (50.7%) 0.923 186 (44.5%) 0.006
SVR, sustained virological response.a Cause of death: metastatic lung cancer.

830 F. Rosina et al. / Digestive and Liver
Table 6Incidence of discontinuation and dose modification by study phase.
Retrospective phase Prospective phase
Treatment discontinuationOverall 562 (29.3%) 613 (32.9%)For death 0 (0.0%) 1 (0.05%)For adverse events 215 (11.2%) 188 (10.1%)For non compliance 56 (2.9%) 99 (5.3%)For treatment inefficacy 238 (12.4%) 229 (12.3%)For loss to follow-up 53 (2.8%) 96 (5.2%)
Dose reductionPEG-IFN 165 (8.0%) 131 (6.3%)Ribavirin 250 (12.2%) 179 (8.6%)
P
tdp8f
ttd(8f
4
dmt
tcrn
wwwgofpo(imssSi[
oa
ppi
c
expected. Though the percentage of cirrhosis was only around 10%,
EG-IFN, pegylated interferon.
han in large centres (68.9% vs 72.6% respectively, p = 0.077). Theoses of PEG-IFN and ribavirin were reduced in 165 (8.0%) and 250atients (12.2%) respectively. Adherence, assessed according to the0/80/80 rule, was confirmed in 1406/2051 patients (68.5%): 58.3%or genotypes 1/4 and 77.5% for genotypes 2/3 (Table 6).
During the prospective phase the rate of treatment comple-ion was 67.1%. Treatment completion was higher in small centreshan in large centres (69.0% vs 65.1% respectively, p = 0.078). Theoses of PEG-IFN and ribavirin were reduced in 131 (6.3%) and 1798.6%) patients respectively. Adherence, assessed according to the0/80/80 rule, was confirmed in 1477/2073 patients (71.2%): 63.7%or genotypes 1/4 and 80.0% for genotypes 2/3 (Table 6).
. Discussion
This observational independent nationwide study aimed atetermining the performance of antiviral therapy for CHC in Italianedical practice in comparison with results derived from clinical
rials.The study design comprised two different cohorts (retrospec-
ive and prospective) in order to minimise the selection bias thatould occur in an exclusively retrospective study. Nonetheless, theetrospective phase was designed to ensure the enrolment of a highumber of patients in a short period of time.
The overall SVR rates in the retrospective phase of the studyere similar to those reported in registration trials [4–6]. However,hen the response rate was analysed according to genotype, SVRas 13% lower than in trials for genotypes 1/4 and 14% lower for
enotypes 2/3 (Supplementary Fig. S1). The discrepancy betweenverall and per genotype comparison is accounted for by a dif-erent genotype distribution: in registration trials 62–68% of theatients had genotype 1 infection while in the retrospective phasef this study difficult and easy to treat genotypes were balanced48% genotypes 1/4 vs 52% genotypes 2/3). The genotype balances likely to reflect an attitude to treat patients with easy genotype
ore often than with difficult genotypes. The findings of the retro-pective phase are in keeping with those from other retrospectivetudies of CHC patients treated in clinical practice where overallVR rates of 49–66% have been reported, with rates of 37–61%n genotype 1 and around 70% in genotypes 2/3 infected patients7–14].
In the prospective phase SVR rates were distinctly lower, withnly 28.4% of genotype 1/4 and 51.5% of genotype 2/3 patientschieving a response (Supplementary Fig. S1).
The different results between the retrospective and prospectivehases could not be accounted for by differences in age, gender,resence of cirrhosis, viral genotype or viral load, which were sim-
lar.After adjustment by multiple logistic regression, virological and
linical factors associated with SVR were genotype, cirrhosis, GGT
Disease 46 (2014) 826–832
and HCV viral load (only during the retrospective phase); otherfactors as age, sex and BMI showed no association.
Rates of SVR were lower also among the 56.3% of the patientswho achieved a RVR (80.2% in genotypes 2/3 and 30.9% in geno-types 1/4); the global SVR rate in these patients was 63.3% (66.1%for genotypes 2/3 and 55.7% for genotypes 1/4) versus a higherthan 80% rate reported in registration trials both for genotype 1and genotypes 2/3 [15–17]. Though the RVR rate of 31% achievedin genotype 1 patient was higher than the RVR rates in registra-tion trials, it does not differ greatly from the relatively high RVRrates observed in other studies in Europe [17–20]. Nevertheless itis likely that in some centres RVR rates were artificially increasedby the low sensitivity of the methods used for detecting HCV-RNA,and possibly by a prolonged time span for the RVR assay; both fac-tors would have accounted for a higher RVR and a lower positivepredictive value of this result [21,22].
Considering that the prospective phase provides the best rep-resentation of treatment performance, the overall effectiveness oftherapy for difficult-to-treat genotypes 1/4 and easy-to-treat geno-types 2/3 was 19% and 30% lower than achieved in registrationtrials; more surprisingly, the drop in SVR was higher for the easygenotypes than for the difficult genotypes.
The lower efficacy cannot be ascribed to inappropriate patientmanagement. Dosages of PEG-IFN and ribavirin were within therange established by the guidelines in 70% of the cases (69% in theretrospective, 71% in the prospective phase). Adherence was onlyslightly lower than the 77% reported in registration trials [2].
In contrast to other studies, the type of PEG-IFN used didnot influence results. During the retrospective phase there wasno difference in efficacy between the two PEG-IFNs; during theprospective study PEG-IFN alpha-2b was superior at univari-ate analysis but the difference was lost at multivariate analysis[17,19,23].
In order to provide a realistic analysis, this study monitoredas many Italian centres treating CHC as possible and warrantedthat patients enrolled from large volume centres (>50 treatedpatients/year) matched those from small volume centres (the latterbeing perhaps less familiar with treatment or equipped with fewersupport facilities). Treatment at a small volume centre resultedin a significantly lower likelihood of SVR during the retrospec-tive phase (47.4% vs 53.8%), but the trend was reversed in theprospective phase where patients treated at small centres wereshown to achieve a significantly higher overall SVR (40.9% vs 36.2%).Difference in SVR by centre volume could be partly explained bytreatment completion rate, which was higher in the large centres(p = 0.077) during the retrospective phase and in the small centres(p = 0.078) during the prospective phase, even though these differ-ences were not statistically significant. Treatment at a small centre,therefore, does not imply risk of a lower response. Our data agreewith the conclusion from the German Observational RetrospectivePractice study which has identified 20 treated cases per year as athreshold to acquire expertise in treating CHC [13].
Given the valid therapeutic expertise nationwide, the limitedantiviral efficacy which was achieved in this real-world practice islikely to depend on the type of patients scheduled for therapy. Inroutine practice a significant proportion of patients present factorswhich would lead to exclusion from clinical trials. Comorbiditieswere reported in up to 46% of our patients; though it is impossibleto estimate their negative impact on therapy, it is likely that theconfidence gained in treating CHC led many centres to “attempt”therapy in patients with substantial adverse predictors, in partic-ular in those with genotypes 2/3 for whom a higher response was
it is also likely that a substantial proportion of our patients, partic-ularly those in the prospective phase, had a more advanced diseasethan those in registration trials.

Liver
ota
Ctobsbamcwbrer2
C
a
R
A
L
A
b
mc
Id
Ge
f
Ng
Ph
Ri
vj
Ik
sl
sm
pn
Uo
Ap
B
F. Rosina et al. / Digestive and
Compliance to treatment is also a major submerged issue. Inur study the rate of treatment discontinuation was 1–10% higherhan in registration trials, with 50% of the discontinuations due todverse events and 50% due to treatment inefficacy.
The data in this study may be relevant to the management ofHC with the incoming new therapies [24–27]. PEG-IFN/ribavirinherapy is no longer standard of care, as guidelines now rec-mmend triple therapy with PEG-IFN plus ribavirin and eitheroceprevir or telaprevir as first line [28,29]. Though triple therapyignificantly increases the rate of SVR in genotype 1 patients, bothoceprevir and telaprevir cause significant adverse effects andlmost triple the cost of therapy. The routine use of triple therapyay thus increase the discrepancy between a high efficacy in
linical trials and a dramatically reduced effectiveness in real life,ith a paradoxical loss of therapeutic advantage. This scenario has
een anticipated in the extended access CUPIC Study, in which cir-hotic patients treated with triple therapy experienced severe sideffects in almost half of the cases (37% higher than that reported inegistration trials), leading to premature discontinuation in up to6% of the patients and to an unacceptable death rate of 2% [30].
onflict of interest
MR is a member of the International Advisory Board for MSDnd Janssen.
PA is a member of Advisory Board for Roche and MSD.M Romano is a member of the Macroregional Advisory Board for
oche.All other authors declare that they have no conflicts of interest.
cknowledgements
We thank Mrs. Sara Ghignone, Dr. Rosa Maria Pilato and Mr.orenzo Speranza for the administrative and secretarial support.
ppendix A. Co-author affiliations
National Centre for Epidemiology, Surveillance and Health Pro-otion, Italian National Institute of Health (ISS), Rome, Italy
Gastroenterology & Hepatology Unit, Torino University, Torino,talyHepatology & Interventional Ultrasound Unit, Gragnano Hospital,ragnano (NA), ItalyInstitute of Infectious Diseases, Bari University, Bari, ItalyInfectious and Parasitic Diseases Unit, Federico II University,apoli, ItalyDepartment of Medical and Surgical Sciences, Bologna University,oliclinico Sant’Orsola-Malpighi, Bologna, ItalyGastroenterology & Hepatology Unit, San Filippo Neri Hospital,ome, ItalyDepartment of Experimental and Clinical Medicine, Florence Uni-ersity, Florence, ItalyInternal Medicine I & Hepatology Unit, S. Pertini Hospital, Rome,talyHepatology Unit – Gastroenterology Unit, Orlandi Hospital, Bus-olengo (VR), ItalyGastroenterology & Hepatology Unit, Di.Bi.M.I.S., Palermo Univer-ity, Palermo, ItalyGastroenterology & Digestive Endoscopy Unit, Santa Corona Hos-
ital, Pietra Ligure (SV), ItalyDepartment of Clinical Medicine & Surgery, Gastroenterologynit, Federico II University, Napoli, Italy
Department of Gastroenterology, Marche Polytechnic University,ncona, ItalyInstitute of Infectious and Tropical Diseases, Brescia University,rescia, ItalyDisease 46 (2014) 826–832 831
q Infectious Diseases Unit, Azienda Sanitaria Firenze, Firenze, Italyr Infectious and Tropical Diseases Unit, S. Anna and S. SebastianoHospital, Naples Second University, Caserta, Italy
Appendix B. AIFA Study group collaborators
1. Italian Association for the Study of the Liver (AISF)
M.C. Mascolo (Gragnano, NA, Italy), C. Cursaro (Bologna, Italy), A.Scuteri (Bologna, Italy), J. Ranieri (Firenze, Italy), M. Monti (Firenze,Italy), S. Bellentani (Carpi, MO, Italy), A. Gasbarrini (Rome, Italy),M. Pompili (Rome, Italy), C. Puoti (Marino, Rome, Italy), L. Bellis(Marino, Rome, Italy), A. Regazzetti (San’Angelo Lodigiano, LO,Italy), E. Maffezzini (San’Angelo Lodigiano, LO, Italy), A. Pietrangelo(Modena, Italy), G. Abbati (Modena, Italy), G. Raimondo (Messina,Italy), L. Scribano (Padova, Italy), D. Martines (Padova, Italy), G.Svegliati Baroni (Ancona, Italy), G. Faraci (Ancona, Italy), S. Schi-anchi (Reggio Emilia, Italy), G. Fornaciari (Reggio Emilia, Italy), P.Fabris (Vicenza, Italy), S. Madonia (Palermo, Italy), G. Civitavecchia(Palermo, Italy), M. Pirisi (Novara, Italy), C. Smirne (Novara, Italy),A. Borghi (Modena, Italy), C. Sardini (Modena, Italy), M. Andreoletti(Lecco, Italy), F. Morisco (Napoli, Italy), N. Caporaso (Napoli, Italy),S. Fargion (Milano, Italy), E. Fatta (Milano, Italy), F. Masutti (Trieste,Italy), M.E. Bonaventura (Rieti, Italy), A. Autolitano (Mortara, PV,Italy), M. Russello (Catania, Italy), A. Bellia (Catania, Italy), P.Toniutto (Udine, Italy), D. Bitetto (Udine, Italy), F. Mecenate (Rome,Italy), L. Pasulo (Bergamo, Italy), M.G. Lucà (Bergamo, Italy), A.Picardi (Rome, Italy), U. Vespasiani (Rome, Italy), I. Grattagliano(Bari, Italy), G. Palasciano (Bari, Italy), D. Romagno (Bari, Italy), C.Crespi (Bologna, Italy), A. Gianstefani (Bologna, Italy), G. Gobbo(San Donato Milanese, MI, Italy), V. Monti (San Donato Milanese,MI, Italy), G. Giannelli (Bari, Italy), N. Napoli (Bari, Italy), Nosotti(Rome, Italy), A. Raspanti (Monza, Italy), Cuccorese (Barletta, Italy),A.E. Colombo (Como, Italy), Floridia (Baggiovara, MO, Italy)
2. Italian Society for Infectious and Tropical Diseases (SIMIT)
M.S. Plattella (Bari, Italy), P. Cassano (Bari, Italy), I. Gentile (Napoli,Italy), P.L. Blanc (Firenze, Italy), V. Messina (Caserta, Italy), S.Bonfante (Caltagirone, CT, Italy), P. Bellissima (Caltagirone, CT,Italy), M. Toti (Grosseto, Italy), J. Vecchiet (Chieti, Italy), K. Falasca(Chieti, Italy), V. Portelli (Trapani, Italy), G. De Stefano (Matera,Italy), G. Pietromatera (Matera, Italy), P. Viganò (Cuggiono, MI,Italy), T. Re (Cuggiono, MI, Italy), M. Andreoni (Biella, Italy), G.Raineri (Cuneo, Italy), M. Massari (Reggio Emilia, Italy), P.A. Grossi(Varese, Italy), S. Caputo (Varese, Italy), G. Cassola (Genova, Italy),M. Feasi (Genova, Italy), G. Foti (Reggio Calabria, Italy), A. Kunkar(Reggio Calabria, Italy), G. Corti (Firenze, Italy), F. Baragli (Firenze,Italy), L. Caterini (Viterbo, Italy), D. Migliorini (Viterbo, Italy),A. Chiodera (Macerata, Italy), G. Calleri (Torino, Italy), C. Spezia(Torino, Italy), C. Baiguera (Brescia, Italy), M. Puoti (Brescia, Italy),G. Brancaccio (Napoli, Italy), G.B. Gaeta (Napoli, Italy), S. Vento(Cosenza, Italy), A. Di Biagio (Genova, Italy), L. Nicolini (Genova,Italy), A. Liberti (Napoli, Italy), M.D. Iannece (Napoli, Italy), C.Contini (Ferrara, Italy), D. Tacconi (Arezzo, Italy), M. Caremani(Arezzo, Italy), P. Almi (Massa Carrara, Italy), M. Chimenti (MassaCarrara, Italy), Cosco (Catanzaro, Italy), D. Messeri (Pistoia, Italy),F.C. Esperti (Pistoia, Italy), A. Paffetti (Rome, Italy), C. Mastropietro(Rome, Italy)
3. Italian Association of Hospital Gastroenterologists (AIGO)
A. Moretti (Rome, Italy), A.L. Spagnolo (Rome, Italy), L. Lomonaco(Bussolengo, VR, Italy), A. Calì (Palermo, Italy), G. Mandelli (Como,

8 d Liver
IBrC(IC
4
A(IE(
A
So
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
tics 2012;35:647–62.
32 F. Rosina et al. / Digestive an
taly), G.C. Spinzi (Como, Italy), L. Framarin (Torino, Italy), M.errutti (Torino, Italy), S. Boccia (Ferrara, Italy), L. Simone (Fer-ara, Italy), P. Pazzi (Cesena, Italy), F. Fornari (Piacenza, Italy), G.omparato (Piacenza, Italy), T. Casetti (Ravenna, Italy), F.G. FoschiRavenna, Italy), T. Bertin (Vicenza, Italy), M. Salvagnini (Vicenza,taly), A. Samori (Senigallia, AN, Italy), E. Ferretti (Italy), M.A.asiraghi (Ferrara, Italy), R. Marin (Dolo, VE, Italy)
. Italian Society of Gastroenterology (SIGE)
. Ciancio (Torino, Italy), N. Campo (Pietra Ligure, SV, Italy), R. TestaPietra Ligure, SV, Italy), A. Rocco (Napoli, Italy), A. Federico (Napoli,taly), C. Loguercio (Napoli, Italy), S. Rizzo (Martina Franca, TA, Italy),.G. Giannini (Genova, Italy), M. Corbo (Genova, Italy), G. RieglerNapoli, Italy), P. Esposito (Napoli, Italy), G.L. Ricci (Rome, Italy),
ppendix C. Supplementary data
upplementary material related to this article can be found, in thenline version, at http://dx.doi.org/10.1016/j.dld.2014.05.014.
eferences
[1] Poynard T, Yuean M-F, Ratziu V, et al. Viral hepatitis C. Lancet2003;362:2095–100.
[2] Reddy KR, Mitchell L, Shiffman TR, et al. Impact of ribavirin dose reduc-tions in hepatitis C virus genotype 1 patients completing Peginterferonalpha 2a/ribavirin treatment. Clinical Gastroenterology and Hepatology2007;5:124–9.
[3] Prati D, Gasbarrini A, Mazzotta F, et al. Practice guidelines for the treatmentof hepatitis C: recommendations from an AISF/SIMIT/SIMAST Expert OpinionMeeting. Digestive and Liver Disease 2010;42:81–91.
[4] Fried MW, Shiffman ML, Reddy KR, et al. Peginterferon alpha-2a plus rib-avirin for chronic hepatitis C virus infection. New England Journal of Medicine2002;347:975–82.
[5] Hadziyannis SJ, Sette Jr H, Morgan TR, et al. Peginterferon alpha-2a and ribavirincombination therapy in chronic hepatitis C: a randomized study of treatmentduration and ribavirin dose. Annals of Internal Medicine 2004;140:346–55.
[6] Manns MP, McHutchison JG, Gordon SC, et al. Peginterferon alpha-2b plus rib-avirin compared with interferon alpha-2b plus ribavirin for initial treatment ofchronic hepatitis C: a randomized trial. Lancet 2001;358:958–65.
[7] Witthoft T, Moller B, Wiedmann KH, et al. Safety tolerability and efficacy ofpeginterferon alpha-2a and ribavirn in chronic hepatitis C in clinical practice:the German Open Safety Trial. Journal of Viral Hepatitis 2007;14:788–96.
[8] Gheorghe L, Iacob B, Sporea I, et al. Efficacy, tolerability and predictive fac-tors for early and sustained virological response in patients treated withweight-based dosing regimen of PegIFN alpha-2b and Ribavirin in real lifehealthcare setting. Journal of Gastrointestinal and Liver Diseases 2007;16:23–9.
[9] Sagir A, Heintges T, Akyazi E, et al. Therapy outcome in patients with chronichepatitis C: role of therapy supervision by expert hepatologists. Journal of Viral
Hepatitis 2007;14:633–8.10] Thomson BJ, Kwong G, Ratib S, et al. Response therapy to combination ther-apy for chronic HCV infection in a clinical setting and derivation of probabilitytables for individual patient management. Journal of Viral Hepatitis 2008;15:271–8.
[
Disease 46 (2014) 826–832
11] De Kaita K, Wong S, Renner E, et al. Treatment outcomes in a centralized spe-cialty clinic for hepatitis C virus are comparable with those from clinical trials.Canadian Journal of Gastroenterology 2006;20:87–90.
12] Borroni G, Andreoletti M, Casiraghi MA, et al. Effectiveness of pegylatedinterferon/ribavirin combination in real world patients with chronic hepati-tis C virus infection. Alimentary Pharmacology and Therapeutics 2008;27:790–7.
13] Witthoeft T, Hueppe D, John C, et al. Efficacy and tolerability of peginterferonalpha-2a or alpha-2b plus ribavirin in the daily routine treatment of patientswith chronic hepatitis C in Germany: the PRACTICE study. Journal of ViralHepatitis 2010;17:459–68.
14] Hansen N, Obel N, Christensen PB, et al. Effectiveness of treatment with pegy-lated interferon and ribavirin in an unselected population of patients withchronic hepatitis C: a Danish nationwide cohort study. BMC Infectious Diseases2011;11:177.
15] Ferenci P, Fried MW, Shiffman ML, et al. Predicting sustained virologicalresponses in chronic hepatitis C patients treated with peginterferon alpha-2a(40 KD)/ribavirin. Journal of Hepatology 2005;43:425–33.
16] Poordad FF. Review article. The role of rapid virological response in determin-ing treatment duration for chronic hepatitis C. Alimentary Pharmacology andTherapeutics 2010;31:1251–67.
17] Marcellin P, Cheinquer H, Curescu M, et al. High sustained virologic responserates in rapid virologic response patients in the large real-world PROPH-ESYS cohort confirm results from randomized clinical trials. Hepatology2012;56:2039–50.
18] Hwang EW, Thomas IC, Cheung R, et al. Implications of rapid virologicalresponse in hepatitis C therapy in the US veteran population. Alimentary Phar-macology and Therapeutics 2012;35:105–15.
19] Rumi MG, Aghemo A, Prati GM, et al. Randomized study ofpeginterferon-alpha2a plus ribavirin vs peginterferon-alpha2b plus ribavirinin chronic hepatitis C. Gastroenterology 2010;138:108–15.
20] Bonardi R, Tabone M, Manca A, et al. Short duration treatment in genotype 1chronic hepatitis C patients with rapid virologic response to pegylated inter-feron plus ribavirin. Biomedicine and Pharmacotherapy 2011;65:303–6.
21] Carlsonn T, Quist A, Weiland O. Rapid viral response and treatment outcomein genotype 2 and 3 chronic hepatitis C: comparison between two HCV-RNAquantitation methods. Journal of Medical Virology 2008;80:803–7.
22] Kanda T, Imazeki F, Yonemitsu Y, et al. Quantification of hepatitis C virus inpatients treated with peginterferon-alpha 2a plus ribavirin treatment by COBASTaqMan HCV test. Journal of Viral Hepatitis 2011;18:e292–7.
23] Ascione A, De Luca M, Tartaglione MT, et al. Peginterferon-alpha 2a plus rib-avirin is more effective than peginterferon-alpha 2b plus ribavirin for treatingchronic hepatitis C virus infection. Gastroenterology 2010;138:116–22.
24] Bacon BR, Gordon SC, Lawitz E, et al. Boceprevir for previously treatedchronic HCV genotype 1 infection. New England Journal of Medicine2011;364:1207–17.
25] Jacobson IM, McHutchison JG, Dusheiko G, et al. Telaprevir for previouslyuntreated chronic hepatitis C virus infection. New England Journal of Medicine2011;364:2405–16.
26] Poordad F, McCone Jr J, Bacon BR, et al. Boceprevir for untreated chronic HCVgenotype 1 infection. New England Journal of Medicine 2011;364:1195–206.
27] Zeuzem S, Andreone P, Pol S, et al. Telaprevir for retreatment of HCV infection.New England Journal of Medicine 2011;364:2417–28.
28] Myers RP, Ramji A, Bilodeau M, et al. An update on the management of hepatitisC: consensus guidelines from the Canadian Association for the Study of theLiver. Canadian Journal of Gastroenterology 2012;26:359–75.
29] Ramachandran P, Fraser A, Agarwal K, et al. UK consensus guidelines forthe use of the protease inhibitors boceprevir and telaprevir in genotype 1chronic hepatitis C infected patients. Alimentary Pharmacology and Therapeu-
30] Hezode C, Fontaine H, Dorival C, et al. Triple therapy in treatment-experiencedpatients with HCV-cirrhosis in a multicentre cohort of the French EarlyAccess Programme (ANRS CO20-CUPIC) – NCT01514890. Journal of Hepatology2013;59:434–41.
Copyright © 2022 FDOKUMEN




















