
Lung Cancer in Nonsmoking Women: A Multicenter Case-Control Studyl

UUCMU
ea
Safety and outcomes of cryoablation for ventriculartachyarrhythmias: Results from a multicenter experienceLuigi Di Biase, MD, PhD, FHRS,�,†,‡ Amin Al-Ahamad, MD,§ Pasquale Santangeli, MD,�
Henry H. Hsia, MD,§ Javier Sanchez, MD,* Rong Bai, MD, FHRS,* Shane Bailey, MD,*Rodney Horton, MD,* G. Joseph Gallinghouse, MD,* David J. Burkhardt, MD, FHRS,*Dhanunjay Lakkireddy, MD,¶ Yanfei Yang, MD,# Nitish Badhwar, MD,# Melvin Scheinman, MD,#
Roderick Tung, MD,‡‡ Antonio Dello Russo, MD,** Gemma Pelargonio, MD,** Michela Casella, MD,**Gery Tomassoni, MD,†† Kalyanam Shivkumar, MD,‡‡ Andrea Natale, MD, FACC, FESC, FHRS*
From *Texas Cardiac Arrhythmia Institute at St. David’s Medical Center, Austin, Texas, †Department of Cardiology,niversity of Foggia, Foggia, Italy, ‡Department of Biomedical Engineering, University of Texas, Austin, Texas, §Stanfordniversity, Palo Alto, California, �Catholic University, Rome, Italy, ¶University of Kansas, Kansas City, Kansas, #UCSF/ardiac Electrophysiology, San Francisco, California, **Arrhythmia Department, Institute of Cardiology, University ofilan, IRCCS–Centro Cardiologico Monzino, Milan, Italy, ††Central Baptist Hospital, Lexington, Kentucky, and ‡‡UCLAniversity, Los Angeles, California.
ftfw
Csrcdvpr
KV
A
BACKGROUND Catheter ablation of ventricular arrhythmias (VAs)with cryoenergy has not been widely reported.
OBJECTIVE The purpose of this study was to assess the feasibilityand safety of cryoablation for VA.
METHODS Cases where cryoablation of VA was attempted as theinitial strategy or was considered to prevent potential damage toother structures such as the coronary arteries, phrenic nerve, andHis bundle were collected. Thirty-three patients with either normalheart or structural heart disease undergoing VA ablation usingcryoenergy at six different institutions were enrolled in the study.Epicardial access was obtained when appropriate.
RESULTS Fifteen patients (7 men) underwent endocardial ab-lation, 13 (9 men) epicardial ablation (from the coronary sinusin 7), and 5 (2 men) aortic cusp ablation. Mean age was 54 �8 years, and ejection fraction was 45% � 5%. In 15 (45%)patients, VAs were successfully ablated, whereas cryoablationwas unsuccessful in the remaining 18 (55%) patients. Cryoab-lation was successful in all parahisian cases (100%). In three
pa
ienvw
com. (Received August 9, 2010; accepted February 24, 2011.)
1547-5271/$ -see front matter © 2011 Heart Rhythm Society. All rights reserved
ailed attempts with open irrigated catheter. An aortic dissec-ion occurred during catheter placement in the aortic cusp. Atollow-up of 24 � 5 months, all patients with acute successere free from clinical VA.
ONCLUSION Use of cryoenergy for ablation of VA has excellentuccess for arrhythmias near the His bundle; however, successates at other sites appear less favorable. Cryoablation may beonsidered as an alternative approach for reducing complicationsuring ablation of VAs originating from sites close to other rele-ant cardiac structures (conduction system, coronary arteries,hrenic nerve) and, in rare cases, could be used epicardially whenadiofrequency energy applications have failed.
EYWORDS Cardiomyopathy; Cryocatheter ablation; Normal heart;entricular tachycardia
BBREVIATIONS RF � radiofrequency; VA � ventricular arrhyth-mia; VT � ventricular tachycardia
(Heart Rhythm 2011;8:968–974) © 2011 Heart Rhythm Society. All
patients, epicardial cryoablation was successful after several rights reserved.IntroductionSignificant advances in radiofrequency (RF) catheter abla-tion of ventricular arrhythmias (VAs) both endocardiallyand epicardially have been made in recent years as a resultof improved technologic tools and a better understanding ofthe physiopathology.1–3 The role of alternative source ofnergy, such as cryoenergy, for treatment of endocardialnd epicardial VA has not been established or widely re-
Address reprint requests and correspondence: Dr. Andrea Natale,Texas Cardiac Arrhythmia Institute at St. David’s Medical Center, 3000 N.I-35, Suite 720, Austin, Texas 78705. E-mail address: dr.natale@gmail.
orted. The aim of this study was to assess the feasibilitynd safety of cryoablation for VA.
Consecutive cases in which cryoablation was used werencluded in this study. Cryoablation was used as the primarynergy source if the optimal ablation site was believed to beear a critical structure (His bundle, coronary arteries oreins, phrenic nerve) or in cases where irrigated RF ablationas unsuccessful.
MethodsThirty-three patients who underwent VA ablation usingcryoenergy at seven different institutions were enrolled in
this study. All patients provided written informed consent,. doi:10.1016/j.hrthm.2011.02.038
969Di Biase et al Cryoablation for Ventricular Arrhythmias
and the study was approved by the local institutional reviewboards.
Inclusion criteriaAny patient who received cryoablation therapy for ventric-ular arrhythmias was included in this study.
ProcedureVascular access was obtained in the femoral vein and fem-oral artery via standard techniques. Intracardiac echocardi-ography was used in all patients to locate cardiac structures,monitor for potential complications, and assist in transseptalpuncture when necessary. A quadripolar catheter was placedinto the right ventricular apex.
Programmed ventricular stimulation was performed us-ing up to three extrastimuli from two different sites atbaseline and after isoproterenol administration.
Conventional mapping techniques included pace map-ping, activation mapping, and entrainment mapping, whichhelped determining the mechanism of the arrhythmias andidentify the potential critical isthmus.
In all patients, mapping was performed with a conven-tional 4-mm-tip ablation catheter or a 3.5-mm-tip open-irrigation catheter (Biosense Webster, Diamond Bar, CA,USA). A three-dimensional electroanatomic mapping sys-tem was used in all patients. In patients with no structuralheart disease, standard activation mapping was performedusing a surface QRS complex during the arrhythmia as thereference. Optimal ablation sites were determined by locat-ing the earliest intracardiac signal compared to the refer-ence, preferably at least 20 ms prior to the earliest QRSsignal on the surface ECG. In addition, pace mapping tech-niques and entirely negative unipolar catheter signals atthese sites were used to confirm suitable ablation locations.
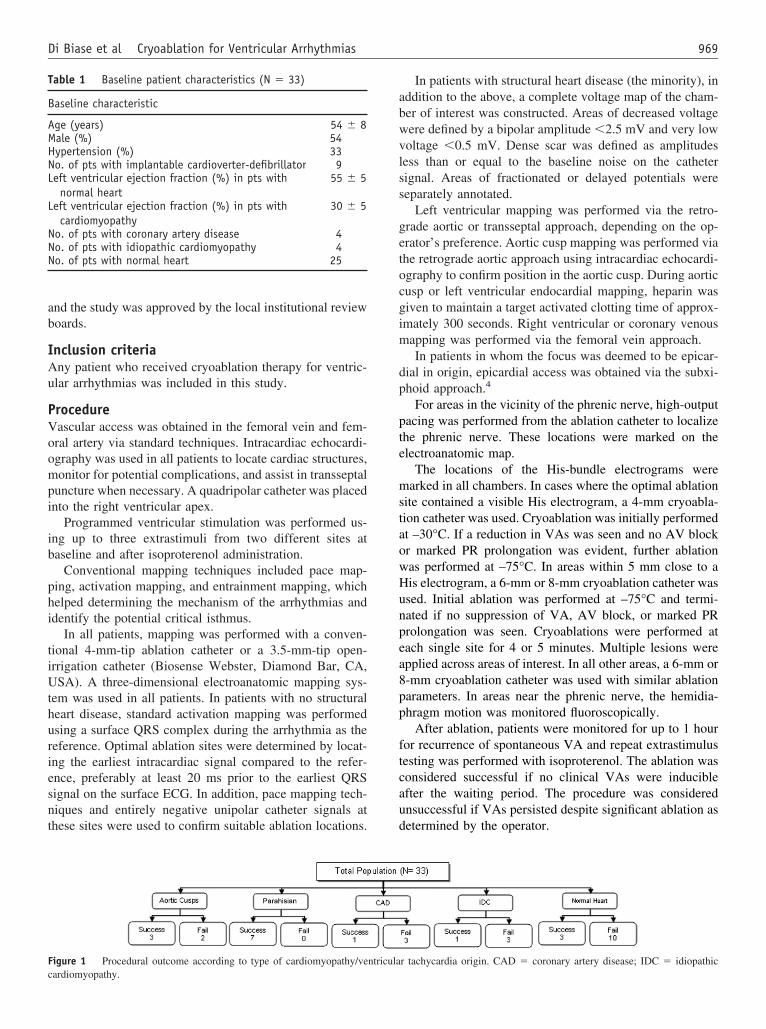
Figure 1 Procedural outcome according to type of cardiomyopathy/ve
Table 1 Baseline patient characteristics (N � 33)
Baseline characteristic
Age (years) 54 � 8Male (%) 54Hypertension (%) 33No. of pts with implantable cardioverter-defibrillator 9Left ventricular ejection fraction (%) in pts with
normal heart55 � 5
Left ventricular ejection fraction (%) in pts withcardiomyopathy
30 � 5
No. of pts with coronary artery disease 4No. of pts with idiopathic cardiomyopathy 4No. of pts with normal heart 25
cardiomyopathy.
In patients with structural heart disease (the minority), inaddition to the above, a complete voltage map of the cham-ber of interest was constructed. Areas of decreased voltagewere defined by a bipolar amplitude �2.5 mV and very lowvoltage �0.5 mV. Dense scar was defined as amplitudesless than or equal to the baseline noise on the cathetersignal. Areas of fractionated or delayed potentials wereseparately annotated.
Left ventricular mapping was performed via the retro-grade aortic or transseptal approach, depending on the op-erator’s preference. Aortic cusp mapping was performed viathe retrograde aortic approach using intracardiac echocardi-ography to confirm position in the aortic cusp. During aorticcusp or left ventricular endocardial mapping, heparin wasgiven to maintain a target activated clotting time of approx-imately 300 seconds. Right ventricular or coronary venousmapping was performed via the femoral vein approach.
In patients in whom the focus was deemed to be epicar-dial in origin, epicardial access was obtained via the subxi-phoid approach.4
For areas in the vicinity of the phrenic nerve, high-outputpacing was performed from the ablation catheter to localizethe phrenic nerve. These locations were marked on theelectroanatomic map.
The locations of the His-bundle electrograms weremarked in all chambers. In cases where the optimal ablationsite contained a visible His electrogram, a 4-mm cryoabla-tion catheter was used. Cryoablation was initially performedat –30°C. If a reduction in VAs was seen and no AV blockor marked PR prolongation was evident, further ablationwas performed at –75°C. In areas within 5 mm close to aHis electrogram, a 6-mm or 8-mm cryoablation catheter wasused. Initial ablation was performed at –75°C and termi-nated if no suppression of VA, AV block, or marked PRprolongation was seen. Cryoablations were performed ateach single site for 4 or 5 minutes. Multiple lesions wereapplied across areas of interest. In all other areas, a 6-mm or8-mm cryoablation catheter was used with similar ablationparameters. In areas near the phrenic nerve, the hemidia-phragm motion was monitored fluoroscopically.
After ablation, patients were monitored for up to 1 hourfor recurrence of spontaneous VA and repeat extrastimulustesting was performed with isoproterenol. The ablation wasconsidered successful if no clinical VAs were inducibleafter the waiting period. The procedure was consideredunsuccessful if VAs persisted despite significant ablation asdetermined by the operator.
r tachycardia origin. CAD � coronary artery disease; IDC � idiopathic
ntricula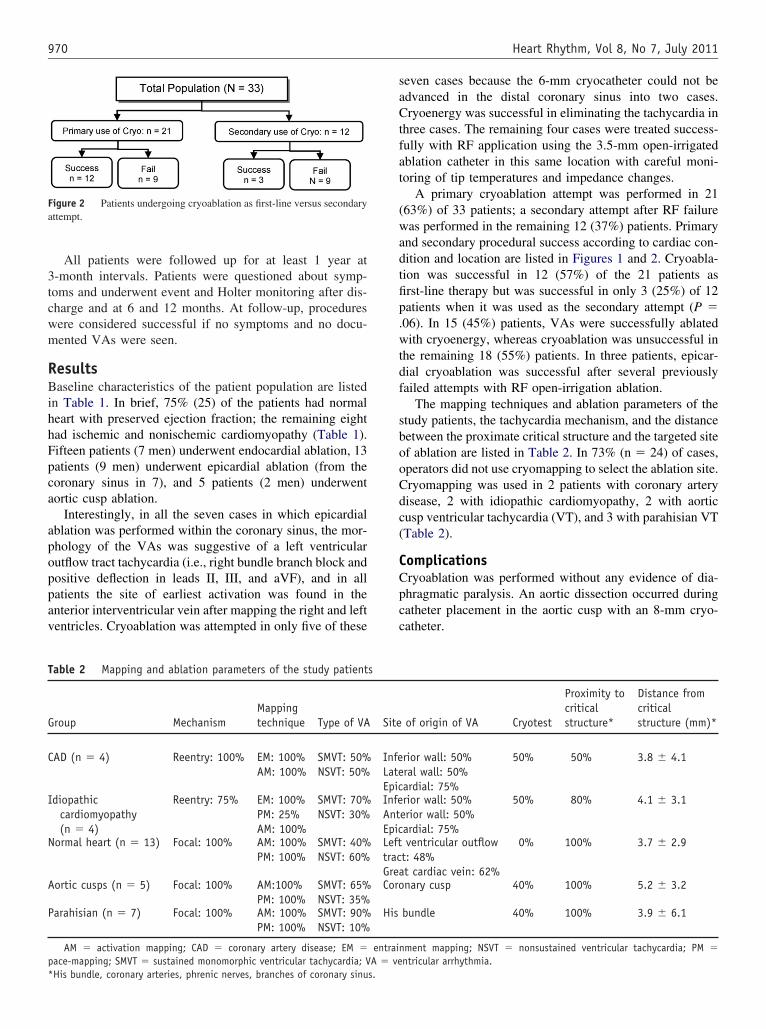
a
C
I
N
A
970 Heart Rhythm, Vol 8, No 7, July 2011
All patients were followed up for at least 1 year at3-month intervals. Patients were questioned about symp-toms and underwent event and Holter monitoring after dis-charge and at 6 and 12 months. At follow-up, procedureswere considered successful if no symptoms and no docu-mented VAs were seen.
ResultsBaseline characteristics of the patient population are listedin Table 1. In brief, 75% (25) of the patients had normalheart with preserved ejection fraction; the remaining eighthad ischemic and nonischemic cardiomyopathy (Table 1).Fifteen patients (7 men) underwent endocardial ablation, 13patients (9 men) underwent epicardial ablation (from thecoronary sinus in 7), and 5 patients (2 men) underwentaortic cusp ablation.
Interestingly, in all the seven cases in which epicardialablation was performed within the coronary sinus, the mor-phology of the VAs was suggestive of a left ventricularoutflow tract tachycardia (i.e., right bundle branch block andpositive deflection in leads II, III, and aVF), and in allpatients the site of earliest activation was found in theanterior interventricular vein after mapping the right and leftventricles. Cryoablation was attempted in only five of these
Figure 2 Patients undergoing cryoablation as first-line versus secondaryttempt.
Table 2 Mapping and ablation parameters of the study patient
Group MechanismMappingtechnique Type of VA
AD (n � 4) Reentry: 100% EM: 100%AM: 100%
SMVT: 50%NSVT: 50%
diopathiccardiomyopathy(n � 4)
Reentry: 75% EM: 100%PM: 25%AM: 100%
SMVT: 70%NSVT: 30%
ormal heart (n � 13) Focal: 100% AM: 100%PM: 100%
SMVT: 40%NSVT: 60%
ortic cusps (n � 5) Focal: 100% AM:100%PM: 100%
SMVT: 65%NSVT: 35%
Parahisian (n � 7) Focal: 100% AM: 100%PM: 100%
SMVT: 90%NSVT: 10%
AM � activation mapping; CAD � coronary artery disease; EM �pace-mapping; SMVT � sustained monomorphic ventricular tachycardia; V
*His bundle, coronary arteries, phrenic nerves, branches of coronary sinus.seven cases because the 6-mm cryocatheter could not beadvanced in the distal coronary sinus into two cases.Cryoenergy was successful in eliminating the tachycardia inthree cases. The remaining four cases were treated success-fully with RF application using the 3.5-mm open-irrigatedablation catheter in this same location with careful moni-toring of tip temperatures and impedance changes.
A primary cryoablation attempt was performed in 21(63%) of 33 patients; a secondary attempt after RF failurewas performed in the remaining 12 (37%) patients. Primaryand secondary procedural success according to cardiac con-dition and location are listed in Figures 1 and 2. Cryoabla-tion was successful in 12 (57%) of the 21 patients asfirst-line therapy but was successful in only 3 (25%) of 12patients when it was used as the secondary attempt (P �.06). In 15 (45%) patients, VAs were successfully ablatedwith cryoenergy, whereas cryoablation was unsuccessful inthe remaining 18 (55%) patients. In three patients, epicar-dial cryoablation was successful after several previouslyfailed attempts with RF open-irrigation ablation.
The mapping techniques and ablation parameters of thestudy patients, the tachycardia mechanism, and the distancebetween the proximate critical structure and the targeted siteof ablation are listed in Table 2. In 73% (n � 24) of cases,operators did not use cryomapping to select the ablation site.Cryomapping was used in 2 patients with coronary arterydisease, 2 with idiopathic cardiomyopathy, 2 with aorticcusp ventricular tachycardia (VT), and 3 with parahisian VT(Table 2).
ComplicationsCryoablation was performed without any evidence of dia-phragmatic paralysis. An aortic dissection occurred duringcatheter placement in the aortic cusp with an 8-mm cryo-catheter.
of origin of VA Cryotest
Proximity tocriticalstructure*
Distance fromcriticalstructure (mm)*
rior wall: 50%ral wall: 50%ardial: 75%
50% 50% 3.8 � 4.1
rior wall: 50%erior wall: 50%ardial: 75%
50% 80% 4.1 � 3.1
ventricular outflowt: 48%t cardiac vein: 62%
0% 100% 3.7 � 2.9
nary cusp 40% 100% 5.2 � 3.2
bundle 40% 100% 3.9 � 6.1
ment mapping; NSVT � nonsustained ventricular tachycardia; PM �ntricular arrhythmia.
s
Site
InfeLateEpicInfeAntEpicLefttracGreaCoro
His
entrainA � ve
emanocolta
971Di Biase et al Cryoablation for Ventricular Arrhythmias
Follow-upAt 24 � 5 months of follow-up, all 15 patients with acuteprocedural success were free from clinical VA. Of the 9patients who failed cryoablation as the primary energysource, 8 underwent a second procedure with RF. At 7 � 3months of follow-up, 7 of the 8 patients were free fromVAs. In patients who failed cryo-VT ablation after a previ-ous RF attempt, no additional ablation was performed.
DiscussionMain findingsThis is the first large ablation series to report cryoenergy as theenergy source for treatment of VA originating either endocar-dially or epicardially. Our results demonstrate that cryoenergymay be used as an alternative energy source during selectedcases of VA ablation originating from sites in close proximityto the coronary arteries, conduction system, phrenic nerve, andother cardiac structures or after RF ablation has failed.
RF lesions compared to cryolesionsAblations were performed with a 4-mm, 6-mm, or 8-mm-tipcryocatheter at all institutions. RF ablation with open-irri-
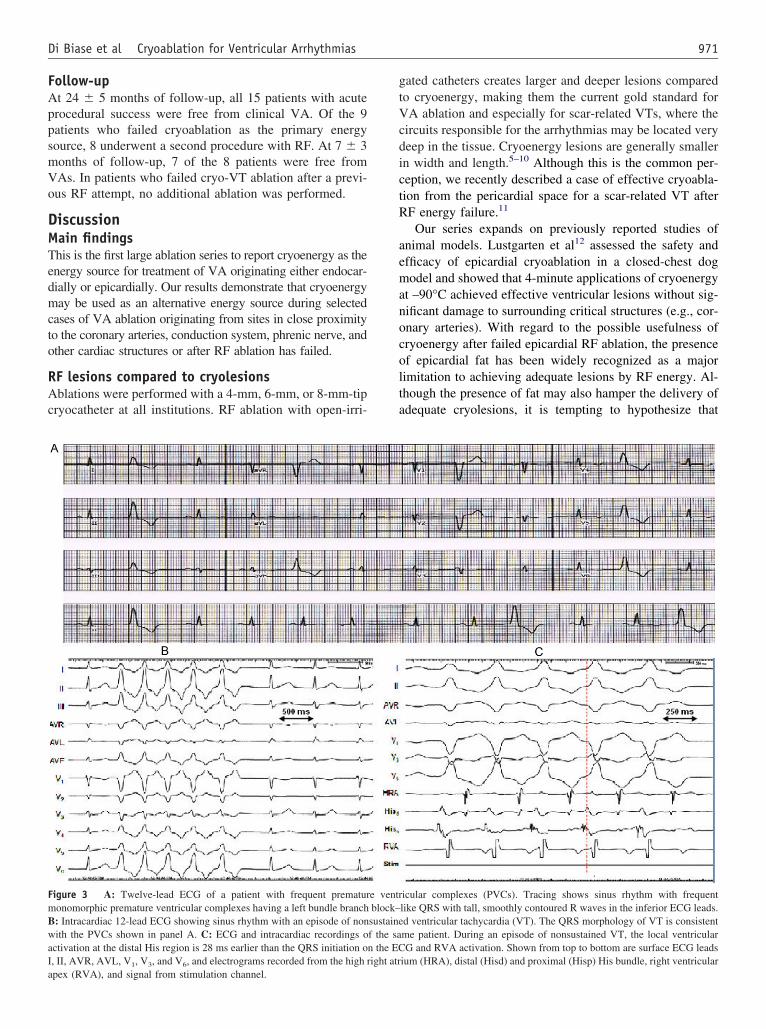
Figure 3 A: Twelve-lead ECG of a patient with frequent prematurmonomorphic premature ventricular complexes having a left bundle branchB: Intracardiac 12-lead ECG showing sinus rhythm with an episode of nonwith the PVCs shown in panel A. C: ECG and intracardiac recordings oactivation at the distal His region is 28 ms earlier than the QRS initiation oI, II, AVR, AVL, V , V , and V , and electrograms recorded from the high r
1 3 6apex (RVA), and signal from stimulation channel.
gated catheters creates larger and deeper lesions comparedto cryoenergy, making them the current gold standard forVA ablation and especially for scar-related VTs, where thecircuits responsible for the arrhythmias may be located verydeep in the tissue. Cryoenergy lesions are generally smallerin width and length.5–10 Although this is the common per-ception, we recently described a case of effective cryoabla-tion from the pericardial space for a scar-related VT afterRF energy failure.11
Our series expands on previously reported studies ofanimal models. Lustgarten et al12 assessed the safety andfficacy of epicardial cryoablation in a closed-chest dogodel and showed that 4-minute applications of cryoenergy
t –90°C achieved effective ventricular lesions without sig-ificant damage to surrounding critical structures (e.g., cor-nary arteries). With regard to the possible usefulness ofryoenergy after failed epicardial RF ablation, the presencef epicardial fat has been widely recognized as a majorimitation to achieving adequate lesions by RF energy. Al-hough the presence of fat may also hamper the delivery ofdequate cryolesions, it is tempting to hypothesize that
icular complexes (PVCs). Tracing shows sinus rhythm with frequentlike QRS with tall, smoothly contoured R waves in the inferior ECG leads.d ventricular tachycardia (VT). The QRS morphology of VT is consistentme patient. During an episode of nonsustained VT, the local ventricularG and RVA activation. Shown from top to bottom are surface ECG leads
ium (HRA), distal (Hisd) and proximal (Hisp) His bundle, right ventricular
e ventrblock–sustainef the san the ECight atr
V
rcaic
sratthsl
stphnda
mdatipnfa
972 Heart Rhythm, Vol 8, No 7, July 2011
cryoenergy would result in a deeper lesion than RF due tothe different conductivity behavior of human fat tissue toheat or cold thermal energy.13,14 This series of patientsshowed that in 55% of cases, cryoablation failed to achieveprocedural success.
An important advantage of cryoenergy is the reduced risk ofdamage to surrounding structures, such as during application inclose proximity to the conduction system, phrenic nerve, andcoronary arteries. In addition, cryoenergy has the advantage ofcreating reversible and smaller lesions.
Histologic evaluation shows that cryolesions have lessendothelial disruption and a homogeneous border zone withpreservation of extracellular collagen compared to RF.5–10
The latter is of particular interest when ablating near criticalstructures, including the His bundle and vessels, which areencased by a thin layer of connective tissue.15 Finally is the“cryoadherence” effect of the cooling energy. Ablationcatheters are more stable during the cardiac cycle, thusfavoring “effective” transmural lesions.
The results obtained in this series suggest that cryoabla-tion could be considered an “effective” alternative energysource, especially for ablation of specific type of Vas. It isimportant to note that parahisian VA cases can simulate aright ventricular outflow tract tachycardia on the ECG. Thisoccurred in 5 of our 7 cases. The possibility of a parahisianorigin should be suspected, and in these cases cryoablationshould be considered an optional first-line approach (Fig-ures 3–7). We achieved success in all 7 cases of parahisianVT. The success rate in these cases is important because indifferent VT ablations series, RF ablations at sites close tothe AV node have not been attempted or have resulted incomplete AV block.16–19 In 3 of the 5 cases of aortic cusp
T, cryoablation was successful. Considering the potential
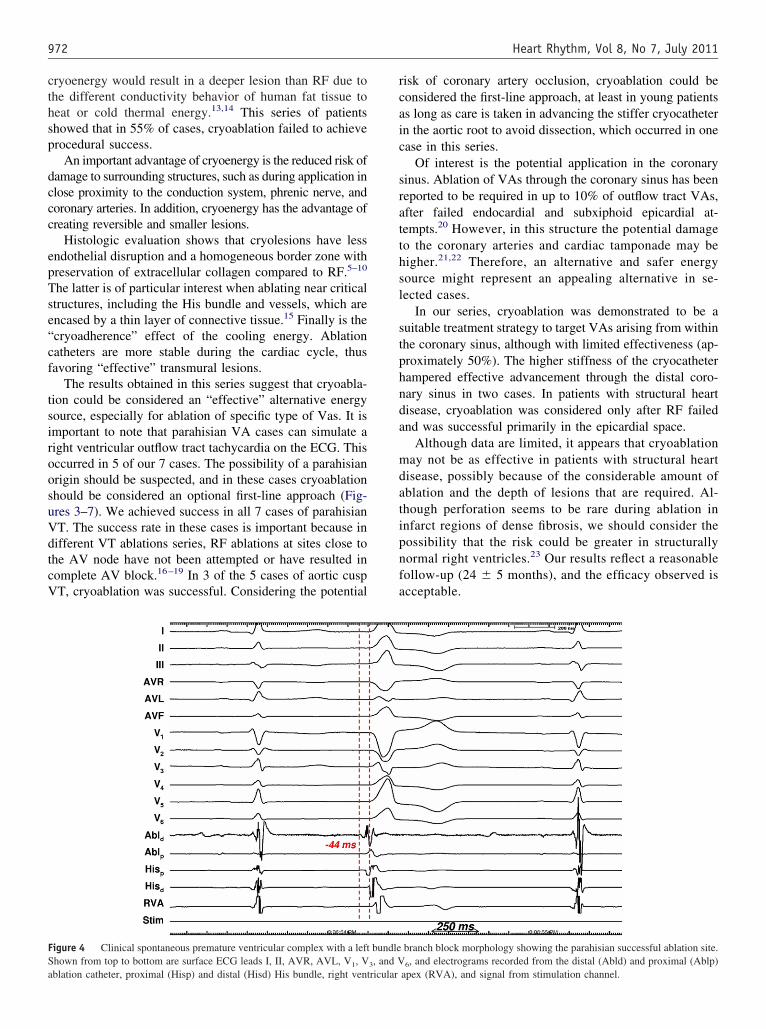
Figure 4 Clinical spontaneous premature ventricular complex with a leftShown from top to bottom are surface ECG leads I, II, AVR, AVL, V , V
1 3ablation catheter, proximal (Hisp) and distal (Hisd) His bundle, right ventricular
isk of coronary artery occlusion, cryoablation could beonsidered the first-line approach, at least in young patientss long as care is taken in advancing the stiffer cryocathetern the aortic root to avoid dissection, which occurred in onease in this series.
Of interest is the potential application in the coronaryinus. Ablation of VAs through the coronary sinus has beeneported to be required in up to 10% of outflow tract VAs,fter failed endocardial and subxiphoid epicardial at-empts.20 However, in this structure the potential damageo the coronary arteries and cardiac tamponade may beigher.21,22 Therefore, an alternative and safer energyource might represent an appealing alternative in se-ected cases.
In our series, cryoablation was demonstrated to be auitable treatment strategy to target VAs arising from withinhe coronary sinus, although with limited effectiveness (ap-roximately 50%). The higher stiffness of the cryocatheterampered effective advancement through the distal coro-ary sinus in two cases. In patients with structural heartisease, cryoablation was considered only after RF failednd was successful primarily in the epicardial space.
Although data are limited, it appears that cryoablationay not be as effective in patients with structural heart
isease, possibly because of the considerable amount ofblation and the depth of lesions that are required. Al-hough perforation seems to be rare during ablation innfarct regions of dense fibrosis, we should consider theossibility that the risk could be greater in structurallyormal right ventricles.23 Our results reflect a reasonableollow-up (24 � 5 months), and the efficacy observed iscceptable.
branch block morphology showing the parahisian successful ablation site., and electrograms recorded from the distal (Abld) and proximal (Ablp)
bundle, and V
6apex (RVA), and signal from stimulation channel.

timulati
R
973Di Biase et al Cryoablation for Ventricular Arrhythmias
Overall, the moderate success rate reported with cryoen-ergy in this series of patients for treatment of the VA issimilar to that reported with cryoenergy for treatment ofsupraventricular tachycardia.24
Study limitationsThe study has several limitations. First, the study was not acontrolled randomized trial. Second, the patients included in
Figure 5 Pacing-induced parahisian ventricular tachycardia showing –24catheter at this site perfectly matches clinical premature ventricular complexECG leads I, II, AVR, AVL, V1, V3, and V6, and electrograms recorded fdistal (Hisd) His bundle, right ventricular apex (RVA), and signal from s
Figure 6 Fluoroscopy during the procedure showing catheter positionsRight: left anterior oblique (LAO) view. The distance between the ablatioHis-bundle catheters (parahisian). Abl � ablation catheter; CS � coronar
VA � right ventricular apex catheter.
the study do not represent the real population of patientsundergoing VT ablations, who are sicker. Although weacknowledge such limitations, we believe this study can beconsidered a pilot guide for further investigations.
ConclusionThe use of cryoenergy for ablation of VA has shown onlymoderate success. However, cryoenergy can be considered
systolic recordings at the site of ablation. Pace-mapping from the ablationntricular tachycardia QRS morphology. Shown from top to bottom surfacedistal (Abld) and proximal (Ablp) ablation catheter, proximal (Hisp) and
on channel.
ame patient shown in Figure 3. Left: right anterior oblique (RAO) view.ter and the His region was 3.5 mm. Note close proximity of ablation andcatheter; His � His-bundle catheter; HRA � high right atrium catheter;
ms preand ve
rom the
in the sn cathey sinus

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
974 Heart Rhythm, Vol 8, No 7, July 2011
an alternative source of energy to reduce complicationsduring ablation of VTs originating from sites close to otherrelevant cardiac structures (e.g., conduction system, coro-nary arteries, phrenic nerve). Indeed, cryoablation was suc-cessful in all parahisian VT cases. In addition, in rare cases,cryoablation could be considered epicardially when RF en-ergy applications have failed.
AppendixPatients in this study were enrolled from the followinginstitutions: (1) Texas Cardiac Arrhythmia Institute at St.David’s Medical Center, Austin, Texas, USA; (2) StanfordUniversity, Palo Alto, California, USA; (3) University ofKansas, Kansas City, Kansas, USA; (4) UCSF/CardiacElectrophysiology, San Francisco, California, USA; (5)Catholic University, Rome, Italy; (6) Central Baptist Hos-pital, Lexington, Kentucky, USA; and (7) UCLA Univer-sity, Los Angeles, California, USA.
References1. Soejima K, Suzuki M, Maisel WH, et al. Catheter ablation in patients with
multiple and unstable ventricular tachycardias after myocardial infarction: shortablation lines guided by reentry circuit isthmuses and sinus rhythm mapping.Circulation 2001:104, 664–669.
2. Marchlinski FE, Callans DJ, Gottlieb CD, Zado E. Linear ablation lesions for
Figure 7 Electroanatomic (CARTO) map of the right ventricular out-flow tract. Left: right anterior oblique (RAO) view. Right: left anterioroblique (LAO) view. The ablation catheter is slightly superior to theHis-bundle region (parahisian). Red arrow indicates successful cryoabla-tion site. Blue arrows indicate unsuccessful ablation sites. The distancebetween the successful ablation site (red arrow) and the His-bundle regionwas 2.1 mm. His � His bundle; TV � tricuspid valve.
control of unmappable ventricular tachycardia in patients with ischemic andnonischemic cardiomyopathy. Circulation 2000;101:1288–1296.
3. Stevenson WG, Wilber DJ, Natale A, et al. Irrigated radiofrequency catheterablation guided by electroanatomic mapping for recurrent ventricular tachycar-dia after myocardial infarction: the Multicenter Thermocool Ventricular Tachy-cardia Ablation trial. Circulation 2008;118:2773–2782.
4. Sosa E, Scanavacca M, d’Avila A, Pilleggi F. A new technique to performepicardial mapping in the electrophysiology laboratory. J Cardiovasc Electro-physiol 1996;7:531–536.
5. Gage AA, Baust J. Mechanisms of tissue injury in cryosurgery. Cryobiology1998;37:171–186.
6. Garamy G. Engineering aspects of cryosurgery. In Rand R, Rinfret A, von LedenH, editors. Cryosurgery. Springfield, IL: Thomas, 1968, pp. 92–132.
7. Reek S, Geller JC, Schildhaus HU, et al. Feasibility of catheter cryoablation innormal ventricular myocardium and healed myocardial infarction. Pacing ClinElectrophysiol 2004;27:1530–1539.
8. Kovoor P, Daly MP, Pouliopoulos J, et al. Comparison of radiofrequencyablation in normal versus scarred myocardium. J Cardiovasc Electrophysiol2006;17:80–86.
9. Skanes AC, Klein G, Krahn A, et al. Cryoablation: potentials and pitfalls.J Cardiovasc Electrophysiol 2004;15:S28–S34.
0. Khairy P, Chauvet P, Lehmann J, et al. Lower incidence of thrombus formationwith cryoenergy versus radiofrequency catheter ablation. Circulation 2003;107:2045–2050.
1. Di Biase L, Saliba WI, Natale A. Successful ablation of epicardial arrhythmiaswith cryoenergy after failed attempts with radiofrequency energy. Heart Rhythm2009;6:109–112.
2. Lustgarten DL, Bell S, Hardin N, Calame J, Spector PS. Safety and efficacy ofepicardial cryoablation in a canine model. Heart Rhythm 2005;2:82–90.
3. Hatfield HS, Puch LG. Thermal conductivity of human fat and muscle. Nature1951;168:918–919.
4. Tarlochan F, Ramesh S. Heat transfer model for predicting survival time in coldwater immersion. J Biomed Eng 2005;17:159–166.
5. Sánchez-Quintana D, Yen Ho S. Anatomy of cardiac nodes and atrioventricularspecialized conduction system. Rev Esp Cardiol 2003;56:1085–1092.
6. Bogun F, Kim HM, Han J, Tamirissa K, et al. Comparison of mapping criteriafor hemodynamically tolerated, postinfarction ventricular tachycardia. HeartRhythm 2006;3:20–26.
7. Van der Burg AE, de Groot NM, van Erven L, Bootsma M, van der Wall EE,Schalij MJ. Long-term follow-up after radiofrequency catheter ablation of ven-tricular tachycardia: a successful approach? J Cardiovasc Electrophysiol 2002;13:417–423.
8. Calkins H, Epstein A, Packer D, et al. Catheter ablation of ventricular tachy-cardia in patients with structural heart disease using cooled radiofrequencyenergy: results of a prospective multicenter study. Cooled RF Multi CenterInvestigators Group. J Am Coll Cardiol 2000;35:1905–1914.
9. Soejima K, Stevenson WG, Sapp JL, Selwyn AP, Couper G, Epstein LM.Endocardial and epicardial radiofrequency ablation of ventricular tachycardiaassociated with dilated cardiomyopathy: the importance of low-voltage scars.J Am Coll Cardiol 2004;43:1834–1842.
0. Tanner H, Hindricks G, Schirdewahn P, Kobza R, et al. Outflow tract tachycar-dia with R/S transition in lead V3: six different anatomic approaches forsuccessful ablation. J Am Coll Cardiol 2005;45:418–423.
1. Aoyama H, Nakagawa H, Pitha JV, et al. Comparison of cryothermia andradiofrequency current in safety and efficacy of catheter ablation within thecanine coronary sinus close to the left circumflex coronary artery. J CardiovascElectrophysiol 2005;16:1218–1226.
2. Roberts-Thomson KC, Steven D, Seiler J, et al. Coronary artery injury due tocatheter ablation in adults: presentations and outcomes. Circulation 2009;120:1465–1473.
3. Coggins DL, Lee RJ, Sweeney J. et al. Radiofrequency catheter ablation as acure for idiopathic tachycardia of both left and right ventricular origin. J AmColl Cardiol 1994;23:1333–1341.
4. Friedman PL, Dubuc M, Green MS, et al. Catheter cryoablation of supraven-
tricular tachycardia: results of the multicenter prospective “frosty” trial. HeartRhythm 2004;1:129–138.Copyright © 2022 FDOKUMEN












![[Distribution of blaOXA genes in Acinetobacter baumannii strains: a multicenter study]](https://static.fdokumen.com/doc/165x107/6337b5c66f78ac31240eb601/distribution-of-blaoxa-genes-in-acinetobacter-baumannii-strains-a-multicenter.jpg)







