
Role of free radical in atherosclerosis, diabetes and dyslipidemia: larger-than-life
17
Role of free radical in atherosclerosis, diabetes and dyslipidaemia: larger-than-life Randhir Singh 1 * Sushma Devi 1 Rakesh Gollen 2 1 MM College of Pharmacy, Maharishi Markandeshwar University, Mullana, Ambala, India 2 Department of Pharmaceutical Sciences, Long Island University, Brooklyn, New York, NY 11201, USA *Correspondence to: Randhir Singh, Associate Professor, Maharishi Markandeshwar College of Pharmacy, Maharishi Markandeshwar University, Mullana, Ambala, India. E-mail: randhirsingh.dahiya@gmail. com Abstract During the past few decades, there have been numerous studies related to the Q1 field of free radical chemistry. Free radicals including reactive oxygen species (ROS) and reactive nitrogen species are generated by the human body by various endogenous systems, exposure to different physiochemical conditions, or pathological states, and thus, they participate in the pathogenesis of increasing numbers of diseases. These free radicals are also the common by-products of many oxidative biochemical reactions in cells. In the past few years, there have been more attention and focus towards the field of free radical chemistry. If free radicals overwhelm the body’s ability to regulate them, a condition known as oxidative stress ensues. Thus, they adversely alter lipids, proteins, and DNA, which triggers a number of human diseases. In a number of pathophysiological conditions, the delicate equilibrium between free radical production and antioxidant capability is distorted leading to oxidative stress and increased tissue injury. ROS which are mainly produced by vascular cells are implicated as possible underlying pathogenic mechanisms in a progression of cardiovascular diseases including ischemic heart disease, atherosclerosis, cardiac arrhythmia, hypertension, and diabetes. This review summarizes the key roles played by free radicals in the pathogenesis of atherosclerosis, diabetes, and dyslipidaemia. Although not comprehensive, this review will also provide a brief perspective on some of the current research being conducted in this area for a better under- standing of the role free radicals play in the pathogenesis of atherosclerosis, diabetes, and dyslipidaemia. Copyright © 2014 John Wiley & Sons, Ltd. Keywords free radicals; ROS; atherosclerosis; diabetes; dyslipidaemia Introduction The recent growth in the knowledge of free radicals including reactive oxygen species (ROS) and reactive nitrogen species (RNS) in biology is producing a medical revolution that promises a new age of health and disease management and pathogenesis of various disorders and diseases. A free radical can be de- fined as any molecular species capable of independent existence that contains an unpaired electron in an atomic orbital. Many radicals are unstable and highly reactive in their present state, which can either accept one electron or donate from other molecules; therefore, they behave as oxidants or reductants, respectively [1]. The life span of free radicals ranges from the high reactivity of hydroxyl (*OH), which has a half-life of 1 ns, to the low reactivity of melanin REVIEW ARTICLE Received: 25 September 2013 Revised: 17 April 2014 Accepted: 29 April 2014 Copyright © 2014 John Wiley & Sons, Ltd. DIABETES/METABOLISM RESEARCH AND REVIEWS Diabetes Metab Res Rev 2014 Published online in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/dmrr.2558 Journal Code Article ID Dispatch: 21.05.14 CE: Mary Charlane Payuan D M R R 2 5 5 8 No. of Pages: 14 ME: 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105 106 107 108 109 110 111 112 113 114 115 116 117 118 119 120 121 122 123 124 125 126 127
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Role of free radical in atherosclerosis, diabetes and dyslipidemia: larger-than-life

Role of free radical in atherosclerosis, diabetes anddyslipidaemia: larger-than-life
Randhir Singh1*Sushma Devi1
Rakesh Gollen2
1MM College of Pharmacy, MaharishiMarkandeshwar University, Mullana,Ambala, India2Department of PharmaceuticalSciences, Long Island University,Brooklyn, New York, NY 11201, USA
*Correspondence to: Randhir Singh,Associate Professor, MaharishiMarkandeshwar College ofPharmacy, MaharishiMarkandeshwar University,Mullana, Ambala, India.E-mail: [email protected]
Abstract
During the past few decades, there have been numerous studies related to the Q1
field of free radical chemistry. Free radicals including reactive oxygen species(ROS) and reactive nitrogen species are generated by the human body by variousendogenous systems, exposure to different physiochemical conditions, orpathological states, and thus, they participate in the pathogenesis of increasingnumbers of diseases. These free radicals are also the common by-products ofmany oxidative biochemical reactions in cells. In the past few years, there havebeen more attention and focus towards the field of free radical chemistry. If freeradicals overwhelm the body’s ability to regulate them, a condition known asoxidative stress ensues. Thus, they adversely alter lipids, proteins, and DNA,which triggers a number of human diseases. In a number of pathophysiologicalconditions, the delicate equilibrium between free radical production andantioxidant capability is distorted leading to oxidative stress and increased tissueinjury. ROS which are mainly produced by vascular cells are implicated aspossible underlying pathogenic mechanisms in a progression of cardiovasculardiseases including ischemic heart disease, atherosclerosis, cardiac arrhythmia,hypertension, and diabetes. This review summarizes the key roles played by freeradicals in the pathogenesis of atherosclerosis, diabetes, and dyslipidaemia.Although not comprehensive, this review will also provide a brief perspectiveon some of the current research being conducted in this area for a better under-standing of the role free radicals play in the pathogenesis of atherosclerosis,diabetes, and dyslipidaemia. Copyright © 2014 John Wiley & Sons, Ltd.
Keywords free radicals; ROS; atherosclerosis; diabetes; dyslipidaemia
Introduction
The recent growth in the knowledge of free radicals including reactive oxygenspecies (ROS) and reactive nitrogen species (RNS) in biology is producing amedical revolution that promises a new age of health and disease managementand pathogenesis of various disorders and diseases. A free radical can be de-fined as any molecular species capable of independent existence that containsan unpaired electron in an atomic orbital. Many radicals are unstable andhighly reactive in their present state, which can either accept one electron ordonate from other molecules; therefore, they behave as oxidants or reductants,respectively [1]. The life span of free radicals ranges from the high reactivity ofhydroxyl (*OH), which has a half-life of 1 ns, to the low reactivity of melanin
REVIEW ARTICLE
Received: 25 September 2013Revised: 17 April 2014Accepted: 29 April 2014
Copyright © 2014 John Wiley & Sons, Ltd.
DIABETES/METABOLISM RESEARCH AND REVIEWSDiabetes Metab Res Rev 2014Published online in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/dmrr.2558
Journal Code Article ID Dispatch: 21.05.14 CE: Mary Charlane PayuanD M R R 2 5 5 8 No. of Pages: 14 ME:
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127

with the half-life of a few day, whereas nitric oxide (NO*)and ubisemiquinone have half-life of ~10 s and 10 ms,respectively, and show intermediate reactivity [2]. Theformation of free radicals as by-products of metabolismand cellular respiration is also known to be synthesizedby enzyme systems (nicotinamide adenine dinucleotidephosphate (NADPH) oxidase, myeloperoxidases), andby exposure to ionizing radiation, smoking, herbicides,pesticides, fried foods, etc. [3–6]. The most importantoxygen-containing free radicals formed in human body,which are also responsible for different disease statesinclude hydroxyl radical (*OH), superoxide anion radical(O2*), hydrogen peroxide (H2O2), oxygen singlet (O2*),hypochlorite (ClO*), nitric oxide radical (NO*), andperoxynitrite radical (ONOO*). Collectively, they arecalled ROS and RNS. ROS also forms different radicals,e.g. R*, ROO*, RO*, RS*, RSO2*, RSO*, etc. [7]. Thesefree radicals are highly reactive species, capable ofdamaging biologically relevant molecules such as DNA,proteins, carbohydrates, and lipids in the nucleus, and inother cell membranes. They are formed by several knownpathways, which may be either a result of homolyticcleavage of covalent bond of molecule or as the result ofloss and/or addition of single electron to a stable mole-cule [8,9]. These free radicals and the resultant oxidativestress were explored after the discovery of enzyme super-oxide dismutase (SOD) [8], which catalyses thedismutation of highly reactive O2* into H2O2 [10] and,thus, acts as an intracellular generator of H2O2. Ascharged O2* is unable to diffuse through intracellularmembranes, cells express distinct SOD isoforms in thecytosol (Cu, Zn-SOD) and mitochondria (Mn-SOD),where they locally scavenge O2* leading to productionof H2O2. This H2O2 is most efficiently scavenged by theenzyme glutathione peroxidase (GPx), which requiresglutathione (GSH) as the electron donor. Oxidized gluta-thione (GSSG or glutathione disulphide) is reduced backto GSH by the enzyme glutathione reductase which usesNADPH as the electron donor in the organism [11,12].This oxidized glutathione (GSSG) is accumulated insidethe cells, and the ratio of GSH/GSSH is a measure of oxida-tive stress in humans. Some transition metals (e.g. Fe2+,Cu+ among others) can break H2O2 to the reactive hydroxylradical (*OH) which can cause alteration of DNA bases,break DNA strands, inactivate proteins, and result in lipidperoxidation. [13–15]. This lipid peroxidation is anotherpathway for the formation of ROS, where, lipid hydro-peroxide reacts quickly with Fe2+ to form a lipid oxyl radical(LO*) or much more slowly with Fe3+ to form a lipidperoxyl radical (LOO*). The hydroxyl radical can alsoremove an electron from polyunsaturated fatty acid and inthe presence of molecular oxygen, results in a LOO* [16],and if lipid peroxyl radical is further not reduced by antiox-idants, this results in the process of lipid peroxidation [17].
LOO* can be reduced within the membrane by the reducedform of vitamin E and can form a lipid hydro-peroxide and aradical of vitamin E [18]. The regeneration of vitamin Eoccurs with vitamin C (ascorbic acid) where the vitamin Eradical is reduced back to vitamin E by ascorbic acid andleaves behind the ascorbyl radical (Asc*) [19]. The GSSGand the ascorbyl radical (Asc*) are reduced back to GSHand ascorbatemonoanion (AscH*), respectively, cooperatingwith NADPH and the dihydrolipoic acid (DHLA). ThisDHLA itself is converted to α-lipoic acid [20–22] and alsoregenerates back from α-lipoic acid using NADPH reaction.Coenzyme Q10 (CoQ10) (ubiquinone), in its reduced form,inhibits lipid peroxidation and can protect mitochondrialinner-membrane proteins and DNA from oxidative damage.It is the most widely used co-factor supplement in the treat-ment of mitochondrial disorders [23].
Free radicals attack important macromolecules leadingto cell damage and homeostatic disruption. There issignificant evidence, showing that most of the degenerativediseases that afflict humanity have their origin from delete-rious free radical reactions. Cancer, atherosclerosis, inflam-matory joint disease, asthma, diabetes, senile dementia,and degenerative eye diseases and ageing are salient ‘freeradical’ diseases [24]. According to a World Health Organi-zation report, cardiovascular disease (CVD) remains themajor cause of mortality throughout the world, typicallycausing one third of all deaths [25,26]. The oxidativeevents may affect CVD; therefore, they have the potentialto provide enormous benefits to human well-being. Thereare different known causes for cardiovascular disordersincluding atherosclerosis, diabetes, dyslipidaemia, obesity,and hypertension. The primary cause of CVD is atheroscle-rosis, which refers to the hardening of arteries [27]. Studieson atherosclerosis reveal the probability that the diseasemay be due to free radical reactions involving diet-derivedlipids in the arterial wall and serum to yield peroxides andother substances. Poly unsaturated fatty acids occur as amajor part of low density lipoproteins (LDL) in the blood,and oxidation of these lipid components in LDL plays a vitalrole in atherosclerosis, which progresses slowly during aperson’s lifetime and typically begins before adulthood.This slow progression and its complex etiology havechallenged attempts to identify the initial atherogenic eventso that it remains elusive [28]. The other important knowncause of CVD is diabetes, which confers a fourfold risk foratherosclerosis, manifested in the vessel wall as intimalthickening, smooth muscle hypertrophy, lipid accumula-tion, extracellular matrix expansion, and inflammatory cellinfiltration [29]. There is much known evidence regardingthemechanisms responsible for accelerated atherosclerosis,which occurs in patients with diabetes, and it is believedthat proteins in blood containing amadori glucose adductsmay play a substantive role and are strongly linked to thepathogenesis of vascular complications of diabetes [30].
2 R. Singh et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127

Hyperlipidaemia or multiple-type hyper-lipoproteinemia isthe responsible factor for CVD and increases platelet activity.Oxidized LDL is antherogenic and cytotoxic and plays asignificant role in the formation of atherosclerosis plaques[31]. Atherosclerosis, diabetes, and dyslipidaemia areknown as the major causes of CVD, and are linked to havesome kind of interconnection with free radicals. Thus, thereview emphasizes the relationships between free radicals,atherosclerosis, diabetes, and dyslipidaemia.
Relationship between free radicals andatherosclerosis
In the past, the role of free radicals in the development ofatherosclerosis is widely understood [32]. The develop-ment of atherosclerosis is a multifactorial process in whichboth elevated plasma cholesterol levels and proliferationof smooth muscle cells (SMC) play central roles [33].Considerable in vivo studies support the role of free radi-cal reactions in atherogenesis and atherosclerotic-relatedcoronary heart disease. Free radicals are involvedthroughout the atherogenic process beginning from endo-thelial dysfunction up to the rupture of a lipid-rich athero-sclerotic plaque, which further leads to acute myocardialinfarction or sudden death [34]. An increased concentra-tion of plasma LDL cholesterol plays a major role in thedevelopment of atherosclerosis. Epidemiological, clinical,and genetic studies convincingly demonstrate that LDLpromotes atherosclerosis. However, the precise mecha-nism(s) by which LDL promotes the development of theearly fatty-streak lesion still remain to be elucidated[35]. LDL is composed of a hydrophilic surface layer ofphospholipid, free cholesterol, and hepatically derivedapoB100 to package the particle and to add stability.The core of the particle includes esterified cholesteroland triglyceride together with the fatty acid tails of thephospholipid. LDL may be oxidative modified by all majorcell types of the arterial wall including endothelial cells,SMC, and macrophages via their extracellular release ofROS [35]. Additionally, the initiation of peroxidationcatalysed by a hydroxyl radical within the LDL moleculegives rise to conjugated dienes, and lipid hydroperoxyradicals (LOO*) [36]. Hydrogen peroxide also has beenreported to increase vascular permeability, prostacyclinrelease, and translocation of P-selectin to the endothelialcell surface [37,38]. The free radical chain reaction isself-propagating, so that LOO* can attack adjacent fattyacids until complete fatty acid chain fragmentation occurs[34]. During free peroxidation, reactive products then ac-cumulate in the LDL particle, including malondialdehyde(MDA) and lysophosphatides (FigureF1 1) [4]. These prod-ucts interact with the amino side chain of the apoB100and modify it to form new epitopes which are not
recognized by the LDL receptor [34]. Antioxidants likeB-carotene or vitamin E play a vital role in the preventionof various CVD. Whereas apoprotein E (apoE) is reportedto impede sub-endothelial LDL retention, it is an earlyproatherogenic event and protects against oxidative stressand apoptosis. ApoE has an anti-oxidant activity andinhibits LDL oxidation; it also prevents LDL retention inthe artery wall and delivers lipid antigens to CD1 indendritic cells for presentation to T-cells. This alsoincludes apoE-mediated inhibition of platelet aggregationand smooth-muscle-cell migration and proliferation [39].Oxidized and glycated LDL are taken up by the macro-phage scavenger receptors such as SRB1, CD36, and TR4[40]. Oxidized LDL may also form oxidized LDL–antibodycomplexes which can be taken up by the macrophagefoam cell receptor. Scavenger receptor uptake is not regu-lated and leads to macrophage cholesterol accumulationand foam cell formation in the arterial intima [35]. Thefoam cell recruits more monocyte/macrophages to convertto foam cells. Accumulating LDL-laden foam cells beneatharterial endothelium lay the foundation for the fattystreak, the earliest histopathological evidence of thedevelopment of atherosclerotic plaque [41]. Endothelial
Figure 1. Pathways of ROS formation and lipid peroxidationprocess O2•
� is dismutated by SOD into H2O2 and further, H2O2 effi-ciently scavenged by GPx. Transition metal (Fe2+) can breakdownH2O2 into •OH which removes an electron from polyunsaturatedfatty acid to give rise to a lipid radical (L•) and finally leads to theformation of lipid peroxyl radical (LOO•). Abbreviations: GSH—glutathione, GSSG—oxidized glutathione, H2O2—hydrogenperoxide, L•—lipid radical, LO•—lipid alkoxyl radical, LOO•—lipidperoxyl radical, MA—deoxyadenosine adduct, MC—deoxycytidineadduct, MG—deoxyguanosine adduct, MDA—malondialdehyde,NADPH—nicotinamide adenine dinucleotide phosphate,O2•
�—superoxide radical, •OH—hydroxyl radical
Role of Free Radicals in Atherosclerosis, Diabetes and Dyslipidaemia 3
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127

dysfunction is a known biomarker of cardiovascular riskfactors, and it precedes the development of atherosclerosis.Endothelial dysfunction is also involved in lesion formationby the promotion of both the early and late mechanisms ofatherosclerosis including up-regulation of adhesion mole-cules, increased chemokine secretion, leukocyte adherence,increased cell permeability, enhanced low-density lipopro-tein oxidation, platelet activation, cytokine elaboration,and vascular SMC proliferation and migration. A dysfunc-tional endothelium promotes many processes involved inatherogenesis. These include decreased bioavailability ofnitric oxide (NO*), migration of SMC, and/or an increasein endothelium-derived contracting factors and prolifera-tion which contribute to the neointimal formation betweenthe endothelium and the inner elastic lamina [42,43].Oxidized LDL also stimulates the release of monocyte-derived tumour necrosis factor-α (TNF-α) and IL-1β, leadingto SMC proliferation [44]. SMC elaborate collagen andelastin and provide the foundation for plaque formationand fibrosis [45]. Oxidized lipids, derived from oxidativemodified LDLs, which accumulate in the intima, stronglymodulate inflammation-related gene expression, throughinvolvement of various signalling pathways [46]. Theoxidative stress factors and oxidative modification ofbiomolecules are also involved in a number of other knownphysiological and pathophysiological processes such asaging, inflammation, carcinogenesis, and drug toxicity.Lipid peroxidation is another process which involves asource of secondary free radical; thus, it acts as a secondmessenger or can directly react with other biomolecules,further enhancing the biochemical lesions. This processmainly occurs in polysaturated fatty acid located on the cellmembranes, which further leads to radical chain reaction.Hydroxyl radical is thought to initiate ROS, by removinghydrogen atoms, thus producing lipid radicals, whichfurther converted into conjugate dienes. After the additionof oxygen, this conjugate diene forms a peroxyl radical,which is a highly reactive radical. It then attacks anotherfatty acid resulting in the formation of lipid hydro-peroxide(LOOH*) and additional free radical. Lipid peroxides alsoinhibit the synthesis of prostacyclin, which is used to inhibitplatelet aggregation resulting in platelet adherence [47].The aggregation of platelets further lays the foundationfor formation of thrombus [42]. Platelet release growthfactor subsequently leads to SMC proliferation andmigration to intima. Measurement of this intima-mediathickness using high resolution B-mode ultrasonographyhas emerged as one of the methods of choice for determin-ing the anatomic extent of preclinical atherosclerosis andfor assessing cardiovascular risk related to it [48]. Increasednumber of ROS formation in mitochondria results in mito-chondrial DNA damage, and progressive respiratory chaindysfunction, which are associated with atherosclerosis orcardiomyopathy in human and animal studies of oxidative
stress [49]. It has also been reported that, especially inindividuals with aging and various types of cancer, DNA isconsidered to be a major target [50]. Free radical-inducedalterations in the endothelial cells of arterial the wall havebeen implicated in the pathogenesis and progression ofatherosclerosis. Endothelial cell injury is measured bydecrease count in protein, glyceride, and phospholipidsynthesis. The concurrent increases in lipid peroxidationand cholesterol synthesis may explain the relationshipbetween free radical injury and the pathogenesis of athero-sclerosis [51]. HDL is inherently capable of exerting anti-atherogenic effects by metabolizing and transporting lipidoxidation products as well as cholesterol from the cells tothe liver by virtue of paraoxonase-1 (PON-1), lecithin-cholesterol acyltransferase, phospholipase A-2, and platelet-activating factor acetyl hydrolase [52]. The oxidativemodification of HDL impairs the ‘reverse cholesterol trans-port’ ability of apoA-I and also the anti-inflammatoryfunction of HDL [53]. It is assumed that HDL is oxidizedessentially by the same oxidants, and also by the samemechanisms as LDL. It has been found that HDL is a majorcarrier of lipid hydro-peroxides.
Relationship between free radicals anddiabetes
Diabetes is a group of chronic diseases characterized byhyperglycaemia. Indeed, coronary heart disease andperipheral vascular disease are the leading causes ofmorbidity and mortality due to diabetes mellitus [54].Diabetes is associated with the formation of the ROS bydifferent pathogenic pathways [55]. Free radical activityhas been previously implicated in the development ofdiabetic vascular complications in type- I diabetes mellitus.It plays an important role in both micro-vascular andmacro-vascular complications during diabetes mellitus,which is a known metabolic disorder, characterized byhyperglycaemia resulting from a deficiency in insulin actionor secretion and associated with several vascular complica-tions. Long-term complications of diabetes mellitus areassociated with various oxidative reactions, increased freeradical generation, and subsequent increase in oxidativestress [56], particularly those which are catalysed by de-compartmentalized transition metals playing a significantrole in diabetic tissue damage [57,58]. In hyperglycaemia,ROS is produced by various processes: glucose oxidation,glucose toxicity [59], and oxidative phosphorylation [60].Chronic exposure to hyperglycaemia can lead to cellulardysfunction which may become irreversible over time by aprocess called glucose toxicity [61]. Multiple biochemicalpathways and mechanisms of action for glucose toxicityinclude glucose autoxidation, protein kinase C activation,methyl-glyoxal formation and glycation, hexosamine
4 R. Singh et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127

metabolism, sorbitol formation, and oxidative phosphor-ylation. There are many potential mechanisms wherebyexcess glucose metabolites travelling along thesepathways might cause beta cell damage. However, allof these pathways have in common the formation ofROS that, in excess and over time, cause chronic oxida-tive stress, which in turn can result in defective insulingene expression and insulin secretion as well asincreased apoptosis [62]. The destruction of β cells byautoimmune cells occurs not only in type-I diabetes,but also in type-II diabetes. Insulin resistance in type-IIdiabetes mellitus may be the consequence of abnormalproduction of anti-insulin receptor antibodies, but isgenerally due to post-receptor defects [63–65].
Also, a recent study has shown that thyroid ROS areelevated in experimental diabetic rats, which is a conse-quence of low-serum thyroid-stimulating hormone andinsulin, but is also related to hyperglycaemia [66]. Toxicamounts of reactive oxygen intermediates are releasedby endothelial cells and infiltrating macrophages duringislet inflammation [63]. It is known that islet cells haveinsufficient defence systems against free radical attacks,which makes them susceptible to reactive oxygen inter-mediates, leading to the destruction of these cells [8].Macrophages are innate immune cells derived frommonocytes, which have many important roles in theinnate and adaptive immune response, as well as in tissuehomeostasis. These macrophages are known to be centralplayers in diabetes, which act in two different ways. Thefirst one triggers inflammatory responses which initiateinsulitis and pancreatic β cell death during type-I diabe-tes, whereas the other regulates type-I diabetes nega-tively, by decreasing the glucose level hyperglycaemia,insulitis, and inflammation in the pancreas, therebynegatively regulating type-I diabetes [67]. These oxygenradicals not only play a significant role in the pathogenesisof diabetes, but are also involved in some of the complica-tions seen in long-term diabetes [56,68]. In autoimmunediabetes, the interactions between CD4-T cells and macro-phages are critical to the development and progression ofinflammatory events in the pancreatic islet lesion. Cyto-kines and chemokine produced by auto reactive CD4-Tcells lead to recruitment and activation of macrophages,which, upon activation, produce additional inflammatorymediators and become effector cells during pathogenesis[69]. In patients with diabetes mellitus, LDL oxidationby macrophages is also increased due to the activation ofseveral pro-oxidant systems, as well as due to the deple-tion of antioxidants such as the paraoxonases (PONs),which protect against atherogenesis by exerting a protec-tive role against diabetes mellitus development by stimu-lating insulin secretion from β cells, and also by theirunique antioxidant properties [70]. ROS also regulatesmacrophage scavenger receptor in type-I diabetes, but
not in type-II, in the human monocyte cell line. Oxidativestress also contributes to increased activity in macrophagescavenger receptor (MSR) by stabilizing MSR-I mRNA[71]. Further, hyperglycaemia also increases the expres-sion of growth factors and cytokines such as transforminggrowth factor-β, vascular endothelial growth factor, plate-let-derived growth factor, insulin-like growth factor, andTNF-α. ROS are found to be important arbitrator factorsinvolved in all these events, and they activate intracellularsignal transduction and transcription cascades in whichmitogen activated protein kinases (MAPKs) and nuclearfactor kappa B play the most significant roles [17,72–74].Proteins, lipids, and nucleic acids are damaged by oxida-tion (Figure F22). Osmotic stress from sorbitol accumulationhas also been postulated as an underlying mechanism inthe development of diabetic microvascular complications,including diabetic retinopathy and nephropathy [75].During hyperglycaemia, the polyol pathway has increasedactivity, and these pathways are responsible for the reduc-tion of glucose to sorbitol via the aldose reductaseenzyme, utilizing the cofactor NADPH [72]. This reduc-tion reaction leads to increased sorbitol accumulation inthe cells and results in cellular and organ damage [76].Additionally, excessive accumulations of sorbitol result inthe decrease of myo-inositol in the peripheral nerves.
Figure 2. ROS-induced DNA damage activates PARP and modifiesGAPDH and mechanism of hyperglycaemia induced cellulardamage. In case of diabetes and hyperlipidaemia, the level ofglucose increases which further increases the level of free radicals.The increased level of ROS is responsible for activation of PARPwhich is involved in modification of GAPDH. Modified GAPDH isinvolved in different pathological mechanisms like activation ofprotein kinase C and increased production of advanced glycationend-products and hexamine pathways, etc.; these pathways alongwith free radicals play a significant role in the pathogenesis of dia-betic complications. Abbreviations: AGEs—advanced glycation endproducts, GAPDH—glyceraldehyde phosphate dehydrogenase,NAD+-nicotinamide adenine dinucleotide, PARP—poly (ADP-ribose) polymerase, PKC—protein kinase C, ROS—reactive oxygenspecies, ADPR—ADP ribose, NA—nicotinamide, PW—pathway
Role of Free Radicals in Atherosclerosis, Diabetes and Dyslipidaemia 5
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127

When myo-inositol is decreased, there is a resultingdecrease in Na+, or K+-ATPase activity, which is essentialfor nerve conduction [77]. It is known that increase in theproduction of ROS leads to more oxidative stress, whichfurther simulates the dysfunction and destruction of βcell, and leads to the impairment of insulin function[78]. Auto-oxidative glycosylation is important inexplaining free radical formation and protein damage indiabetes [79]. High glucose concentration facilitates theeicosanoid pathway and, consequently, production of thesuperoxide. In the endothelial cells, NO is synthesizedfrom arginine by NO synthase and is quenched by super-oxide, resulting in peroxynitrite anion formation. Inhibi-tion of the nitric oxide action reduces vasodilatation andenhances endothelial dysfunction in diabetes [80].Hyperglycaemia also elicits oxidative stress by directlyimpairing the cellular mechanisms, which, in turn, elicitsendothelial dysfunction [81]. Moreover, hyperglycaemiais also responsible for the generation of NO* and O* inexcess through activation of nitric oxide synthases (NOSs)and NADPH oxidase, respectively. O2* reacts with NO* toproduce OONO*, another oxidant which increases oxida-tive stress and elicits endothelial dysfunction by promot-ing tissue injury [82]. O2* is converted to H2O2 bySODs, which not only increases oxidative stress, but alsogenerates endothelial dysfunction by modulating intracel-lular signalling and transcription factors [82,83]. In addi-tion to O2*, hyperglycaemia also stimulates the synthesisof NO via increased enzymatic activity of endothelialand inducible isoforms of NOS [81–84]. According toDesco et al. (2002), ketone, especially acetoacetate, isinvolved in free radical formation in type-I diabetes [79].The production of ketone bodies is especially important inbrain metabolism, which, under normal circumstances,depends mainly on glucose [85,86]. Glucose is not toxic atphysiological conditions; however, at higher concentra-tions, it undergoes auto-oxidation, and noncyclic proteinsare non-enzymatically glycated by high levels of noncyclicglucose. Glucose is also able to modify proteins by theattachment of its oxidation derived aldehydes, thus leadingto the development of novel protein fluorophores andfragment protein via free radical mechanisms [67]. How-ever, the metal chelators and free radical scavengers caninhibit the fragmentation of these proteins [87]. Transitionelements (for example iron) are involved in free radicalproduction (Fe2+« Fe3+), and iron (II) ions are also knownto induce oxidation of ascorbic acid and glucose [88]. Thesimultaneous episodes of glycation and oxidation furthersupport the hypothesis that tissue damage is associatedwith diabetes [87,89,90]. Xanthine oxidase, a superoxide-generating enzyme, is also involved in free radical produc-tion in patients with type-I diabetes, which can be protectedby allopurinol [77]. Generation of high levels of ONOO* ionsinitiates the onset of different processes like mitochondrial
dysfunction, which is a part of premature aging of the endo-thelium [91]. Hyperglycaemia-induced overproduction ofsuperoxide by the mitochondrial electron transport chainactivates the four major pathways of hyperglycaemicdamage by inhibiting glyceraldehyde phosphate dehydroge-nase (GAPDH) activity [72], which includes (1) hexosaminebiosynthetic pathway [92], (2) sorbitol-aldose reductasepathway [93], (3) MAPK [94], and (4) protein kinase C[95]. GADPH is a classic glycolytic enzyme that alsomediatescell death by its nuclear translocation under oxidative stress[96]. Hyperglycaemia-induced mitochondrial superoxideproduction further inhibits GAPDH by activating PARP[72]. Abnormally high levels of free radicals and the simulta-neous decline of antioxidant defencemechanisms can lead todamage of cellular development of insulin resistance. Theconsequences of this oxidative stress also promote the devel-opment of diabetes mellitus and its complications [97].
Relationship between free radicals anddyslipidaemia
It is well known that free radicals play a crucial role in thepathogenesis of fatty liver disease and increase metabolicalterations [98]. As discussed earlier, high lipid or choles-terol (LDL) levels are important factors responsible forvarious cardiac diseases since they lead to developmentof hyperlipidaemia, atherosclerosis, and ischemic heartdisease. ROS are known to be associated with the forma-tion of oxidized LDL that, in turn, stimulates the releaseof ROS and enhanced adhesion molecule expression aswell as platelet activity with pro-atherogenic effects inthe vasculature [99]. Hyperlipidaemia is characterizedby increased LDL and triglyceride concentrations, whichis often accompanied by decreased HDL [100]. Type-IIhyper-cholesterolemia causes changes in the structure andfluidity of erythrocyte plasma membranes since the excesscholesterol affects the normal rheology of blood throughits interaction with erythrocytes. Hyper-cholesterolemiamay also decrease the deformability of red blood cells,which impairs their haemorheological behaviour and thuspromotes atherosclerosis. It also impairs the function andstructure of plasma membrane proteins [101]. Evolutionof hyper-cholesterolemia is also associated with endothelialcell dysfunction, a near complete abrogation in vascular NObioavailability, elevated oxidative stress, and creation ofpro-inflammatory condition; these are symptoms whichcan culminate in profound impairments/alterations tovascular reactivity [9]. Dyslipidaemia, with or withoutatherosclerosis, is one of the major metabolic/CVD statesin which the enhanced formation of ROS is of pivotalpathogenic importance [102]. Hyperlipidaemia withelevated levels of triglycerides, chylomicron remnants, andfree fatty acids results in oxidative stress and inflammation
6 R. Singh et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127

and may independently potentiate the adverse effects ofhyperglycaemia [103]. It is well known that NO rapidlyreacts with O2* to form the cytotoxic species (ONOO*),and hyperlipidaemia has been shown to increase productionof ROS including ONOO* in the vasculature, which results ina deterioration of cardiac function. Hyperlipidaemia alsoincreases the plasma nitro-tyrosine level, which is a markerfor systemic ONOO* generation [104]. Some known cyto-toxic effects of ONOO* include lipid peroxidation, nitrationof tyrosine residues, oxidation of sulfhydryl groups, tissueinjury, and DNA-strand breakage [105]. The detrimentaleffects of increased oxidative stress result in dysfunction ofendogenous NO*, production and inactivation of NO* byoxygen-derived radicals (eliciting the formation of thecytotoxic and genotoxic ONOO*), or altered function ofNOS [106]. Excessive formation ofONOO* is associatedwitha significant decrease in cellular glutathione content and,subsequently, of NOS as well as of soluble guanylate cyclaseactivity (e.g. through oxidation of thiol groups {�SH} [107].Enhanced lipid peroxidation and decreased antioxidant en-zyme activity also represent early events in the developmentof hyperlipidaemia in humans [108]. In high lipid conditions,decreased activities of SOD and GPx are observed. Thus,there is insufficient detoxification of these ROS by antioxi-dant enzymes thatmay lead to an imbalance between antiox-idant and oxidant systems [109]. This oxidant–antioxidantstatus has a major impact, not only on the rate of LDL oxida-tion, but also on the development of atherosclerosis [110]. Itis possible that a potential risk of atherosclerosis in the hyper-lipidaemia population is associated with LDL oxidation anddecreased antioxidant enzyme activity. Further hypertriglyc-eridemia and hypercholesterolemia are associated with LDLperoxidation, protein glycation, glucose auto-oxidation, andthus lead to excess production of free radicals, which mayfurther elevate the oxidative stress in hyperlipidaemiapopulation [111].
Relationship of nitric oxide withatherosclerosis, diabetes, anddyslipidaemia
NO is an endogenous anti-atherogenic molecule. The dualrole of NO as a protective and toxic molecule depends onseveral factors. Primarily, it depends on the isoform ofNOS involved, and there are three main isoforms of theenzyme: neuronal NOS (nNOS), inducible NOS (iNOS),and endothelial NOS (eNOS). They differ in their depen-dence on Ca2+, as well as in their expression and activities[112]. The important factor includes eNOS, which are theonly NOS isoform expressed in normal coronary arteries,and it offers protection against atherosclerosis [113].iNOS is proatherogenic, so it decreases atheroscleroticplaque areas [114]. Additionally, nNOS might modulate
atherosclerosis by directing the flow of NO* towardparticular targets [115]. The important isoform in theregulation of insulin resistance is iNOS. Understandingthe molecular mechanisms regulating the iNOS pathwayin normal and hyperglycaemic conditions would help toexplain some of the vascular abnormalities observed intype-II diabetes mellitus [116]. The other factors include,but are not limited to, the concentration of NO* type cellsin which NO* is synthesized, the availability of thesubstrate L-arginine, generation of guanosine 3,5′-cyclicmonophosphate (cGMP) from guanosine triphosphate ca-talyse by soluble guanylate cyclise (sGC), and the overallextra and intracellular environment in which NO* isproduced. NOS activation as a result of trauma (calciuminflux) or infection leads to NO* production, whichactivates its downstream receptor sGC to synthesise cGMPand/or leads to protein nitrosylation. This may lead to oneor more systemic effects including altered neurotransmis-sion, which can be protective or toxic vaso/broncho dila-tation in the cardiovascular and respiratory systems, andenhanced immune activity against invading pathogens[117]. NO* also regulates critical lipid membranes andlipoprotein oxidation events either by contributing to theformation of more potent free radicals from superoxide(i.e. ONOO*) or by its antioxidant properties throughtermination reactions with lipid radicals to potentially lessreactive secondary nitrogen-containing products [118,119].In addition to being a potent vasodilator, it may inhibit anumber of key processes in atherogenesis, including vascu-lar SMC proliferation [120], platelet adherence or aggrega-tion [121], generation of oxygen-derived free radicals [122],and monocyte adherence and infiltration (possibly byinhibiting the expression or activity of endothelial adhesionmolecules or chemotactic proteins) [123–126]. Protein-bound nitrotyrosine (NO2Tyrosine), a post-translationalmodification specific for protein oxidation by NO-derivedoxidants, is markedly enriched within human atheroma.Further, recent clinical studies demonstrate that systemiclevels of protein-bound NO2Tyrosine serve as an indepen-dent predictor of atherosclerotic risk [127].
The impairment of NO* activity by hypercholesterol-emia, diabetes mellitus, or hypertension plays a significantrole in the initiation of atherosclerosis [124]. For example,in a traumatic arterial injury, the loss of endothelialinfluence facilitates platelet plug formation and vasoconstric-tion, thereby promoting homeostasis [126]. This becomes apathophysiologic mechanism when the endothelium isdysfunctional due to a systemic disorder (hyperlipidaemia).Further, platelet adherence to the dysfunctional endothe-lium promotes thrombosis and the growth of vascularlesions [127]. Deficiency of nitric oxide is responsible forreduced nerve blood flow and response in the developmentof endoneurial ischemia in diabetic rats [128]. There is anincreased production of NO* observed immediately after
Role of Free Radicals in Atherosclerosis, Diabetes and Dyslipidaemia 7
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127

the onset of diabetes. NO* may be responsible for theglomerular hyper filtration observed in diabetic kidneys byinducing vasodilation of the afferent arteriole [129,130].In addition, hypercholesterolemia is associated with theloss of nitric oxide-induced vasodilation and the subsequentincrease in blood pressure [131].
Relationship of free radicals withatherosclerosis, diabetes, anddyslipidaemia
The relationship between oxidant generation, oxidativestress, oxidative damage, and various disorders like athero-sclerosis, diabetes, dyslipidaemia, ischemic pain, etc. is nowwell known (FigureF3 3). In many scientific publications,oxidative stress is solely used to describe impaired ROS orRNS systems which may develop secondary hypertension,atherosclerosis, or hyperglycaemia [132]. There is greaterrisk of developing atherosclerosis and its complications:stroke, myocardial infarction, and peripheral vasculardisease in diabetic populations as compared to non-diabeticones [68,133]. Artherogenesis has been associated with
lipid disorders characterized by hypertriglyceridemia, andincreased levels of VLDL and LDL without diabetes.However, diabetic populations with relatively normal plasmalipid and lipoprotein concentrations still have an increasedlevel of atherosclerosis [134]. Therefore, increased incidenceof vascular diseases in diabetic patients may involvedyslipidaemia or other factors unique to diabetes. Severalrisk factors have been proposed to explain the increased riskof CVD with diabetes, e.g. hyperglycaemia, dyslipidaemia[132], accelerated formation of advanced glycation end(AGEs) products, increased oxidative stress, and othergenetic factors [135]. Advanced oxidative stress is generatedby hyperglycaemia and, in many diabetic patients, also bydyslipidaemia which accelerates endothelial dysfunction asthe first step in the development of angiopathy [80]. Inthe diabetic state, the accelerated formation of amadori-modified glycated serum proteins and lipoproteins fostersthe pathogenesis of atherosclerosis [15]. MDA formation,which is a marker of oxidative stress, is altered in differentstages of development of hyperlipidaemia and is also animportant risk factor of atherosclerosis [136,137]. Accordingto Renard et al., (2004) diabetes increases lesion initiation,and diabetes-induced dyslipidaemia leads to a progression
Figure 3. Relationship between free radicals, atherosclerosis, diabetes, and dyslipidaemia. Diabetes and hyperlipidaemia triggerprejudicial pathways like PKC, AGE, and polyol, leading to excessive generation of ROS. As a consequence of redox imbalance, oxidativestress is enhanced leading to increased prevalence of atherosclerosis and other diabetic complications. Abbreviations: FFA—free fattyacid, SMC—smooth muscle cell, PKC—protein kinase C, AGE—advanced glycation end-products, ROS—reactive oxygen species
Colouronlin
e,B&W
inprint
8 R. Singh et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127

of atherosclerotic lesions, and their transformation intomoresevere condition of lesions which are prone to rupture andthrombosis [138]. Many epidemiological studies have alsoestablished that risk factors for diabetes and atherosclerosiscoexist [139]. Further, endothelial dysfunction supportsatherosclerosis [34]. Glucose and free fatty acids overwhelmthe Krebs cycle, stimulate excess production of NAD+whichoutpaces the capacity for oxidative phosphorylation andcreates free radicals [140]. Postprandial in diabetes is complexand involves a variety of factors including hyperinsulinemia,insulin resistance, hyperglycaemia, and disturbed fatty acidmetabolism. Postprandial oxidative stress triggers a numberof atherogenic changes including increases in inflammation,sympathetic tone, vasoconstriction, thrombogenicity, andoxidation of LDL in diabetic and non-diabetic populations[141]. Numerous clinical studies have shown that postpran-dial dyslipidaemia is associated with endothelial dysfunctionin type-II diabetes and with alterations in other surrogatemarkers in the cascade of atherosclerosis [142].
Type-I diabetes is associated with early impairment ofcommon carotid artery structure and function, and thisdiabetic state may be the main risk factor for commoncarotid artery wall stiffening and thickening, which areof considerable concern as possible early events in thegenesis of atheroma [143]. Substantial clinical and exper-imental evidence suggest that both diabetes and insulinresistance cause a combination of endothelial dysfunc-tions, which may diminish the anti-atherogenic role ofthe vascular endothelium. Oxidative stress due to highglucose can also lead to a number of proatherogenicevents [56]. The elucidation of themechanisms of oxidativestress in diabetes and their relationship with atherosclerosiscould potentially identify molecular targets of therapy forthis condition and its cardiovascular consequences [135].Blood flow restriction is achieved by vasoconstrictiondespite increased production of NO*, and the vasodilationeffects of which are overridden by catecholamine (and alsoby angiotensin-II and endothelia). Decreased blood flowreduces the availability of oxygen, provoking massiveglycolysis (hyperglycaemic conditions), which results inthe production of lactate which is exported to the liver forfurther processing [144]. However, this produces localacidosis, which elicits the rapid dissociation ofoxyhaemoglobin, freeing bursts of oxygen in localizedzones of the tissue. The excess oxygen (and nitric oxide)induces the production of ROS, which deeply affects theendothelial, blood, and adipose cells, inducing oxidativeand nitrosative damage, and eliciting an increased immuneresponse, which translates into inflammation, and thenleads to atherosclerosis [145]. Cholesterol-enriched diet-induced hyperlipidaemia results in an increase in cardiacONOO* formation and decrease in the bioavailability ofNO*, both of which contribute to the deterioration ofcardiac performance and may lead to further cardiac
pathologies [104]. Control of hyperglycaemia thus remainsthe best way to improve endothelial function and to preventatherosclerosis and other cardiovascular complications ofdiabetes [81]. Dehydro-ascorbic acid (oxidized form ofvitamin C) is transported into mammalian cells via facilita-tive glucose transporters. Hyperglycaemia inhibits thisprocess by competitive inhibition. This inhibited transportmay promote oxidative stress and contribute to the increasein atherosclerotic CVD observed in patients with diabetesmellitus [146].
Micro-albuminuria is now considered to be an atheroscle-rotic risk factor and predicts future CVD risk in diabeticpatients [144]. A wide range of micro-albuminuria cut-offvalues are currently used for diagnosing the early stagesof nephropathy in patients with type-II diabetes. However,in the same early stage of diabetic nephropathy, there is asignificant correlation between different levels of micro-albuminuria and markers of oxidative stress. Serumconjugated dienes have emerged as the main marker forevaluating kidney damage in diabetic nephropathy [147].Numerous experimental studies suggest that diabetes/hyperglycaemia accelerates atherosclerotic lesion initiation,but not progression of pre-existing lesions. This effect maybe mediated by increased glycosaminoglycan depositionand monocyte recruitment [139]. Maternal hypercholester-olemia during pregnancy is known to be responsible forcascade of pathogenic events. It is also associated withgreatly increased fatty streak formation in human foetalarteries and accelerated progression of atherosclerosisduring the early stages of life [148]. Impaired lipid andglucose metabolism is a typical feature in diabetes. Diabetesis associated with formation of ROS by different pathogenicpathways. Advanced generation of ROS may further accel-erate glycation, sorbitol, protein kinase C, or hexosaminepathways which are activated by high glucose and lipids.These pathogenic mechanisms are closely linked to oxida-tive stress, which has been recognized as the main causefor development of the endothelial dysfunction [149].Further endothelial dysfunction increases permeability ofendothelial cell monolayers, pro-coagulant activity, expres-sion of adhesionmolecules and intracellular oxidative stress[132,150]. Additionally, they serve as the nidus for athero-sclerotic lesion formation. Increased levels of oxidants alsofunction as a link between diabetes, dyslipidaemia, and freeradicals, which respond to atherosclerosis [151]. A majormechanism appears to be the hyperglycaemia/hyperlipid-aemia induced intracellular ROS, produced by the protonelectromechanical gradient generated by the mitochondrialelectron transport chain and resulting in increased produc-tion of superoxide [152]. Two other mechanisms have beenproposed to elucidate the role of hyperglycaemia in ROSformation. One mechanism involves the transition metal-catalysed autoxidation of free glucose; glucose itself initiatesan auto-oxidative reaction and free radical production,
Role of Free Radicals in Atherosclerosis, Diabetes and Dyslipidaemia 9
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127
yielding superoxide anion and hydrogen peroxide [153]. Theother mechanism involves the transitional metal-catalysedautoxidation of protein-bound amadori products, whichyield superoxide and hydroxyl radicals and highly reactivedi-carbonyl compounds [132,154].
Discussions and future prospective
The development of procedures to ameliorate undesirableROS production may be one of the central issues in thefield of research studying aging and other oxidativestress-related diseases [18,155]. Now, it has becomepossible to accurately quantify in vivo and ex vivo ROSconcentrations under different pathophysiological andexperimental conditions by electron paramagnetic reso-nance or electron spin resonance spectroscopy [156].There are some encouraging reports regarding the use ofSOD/CAT mimetic in certain experimental systems.Dietary antioxidants are widely used to ameliorate exces-sive oxidative stress, but scientific proof of their efficacy isscarce. There is, nevertheless, a strong possibility that theprocess of senescence and disease-related wasting results,at least to some extent, from a progressive shift inbiochemical conditions that may not be irreversible inprinciple [18]. Hyperlipidaemia stimulates the generationof ONOO* in the heart, which further leads to myocardialdysfunction. Targeting ONOO* with pharmacologicalactive agents may be an exciting new strategy to protectthe heart and the vasculature in the event of hyperlipi-daemia [104]. Hyperglycaemia induces endothelial celldysfunction, which further activates multiple pathwaysincluding enhanced glycolysis (ROS), the build-up ofglycolytic intermediates (polyol pathway, hexosaminepathway, PKC activation, and AGE formation), and AGEmodification of proteins (ROS, PKC). Given the inter-dependent nature of these pathways, it is not surprisingthat inhibitors targeting one of them can profoundly affecthyperglycaemia-induced alterations in endothelial cellfunction [157]. Apo E is a well-known blood circulatingprotein with pleiotropic atheroprotective properties thathave emerged as a strong candidate for treating hyper-cholesterolemia and other cardiovascular disorders [40].
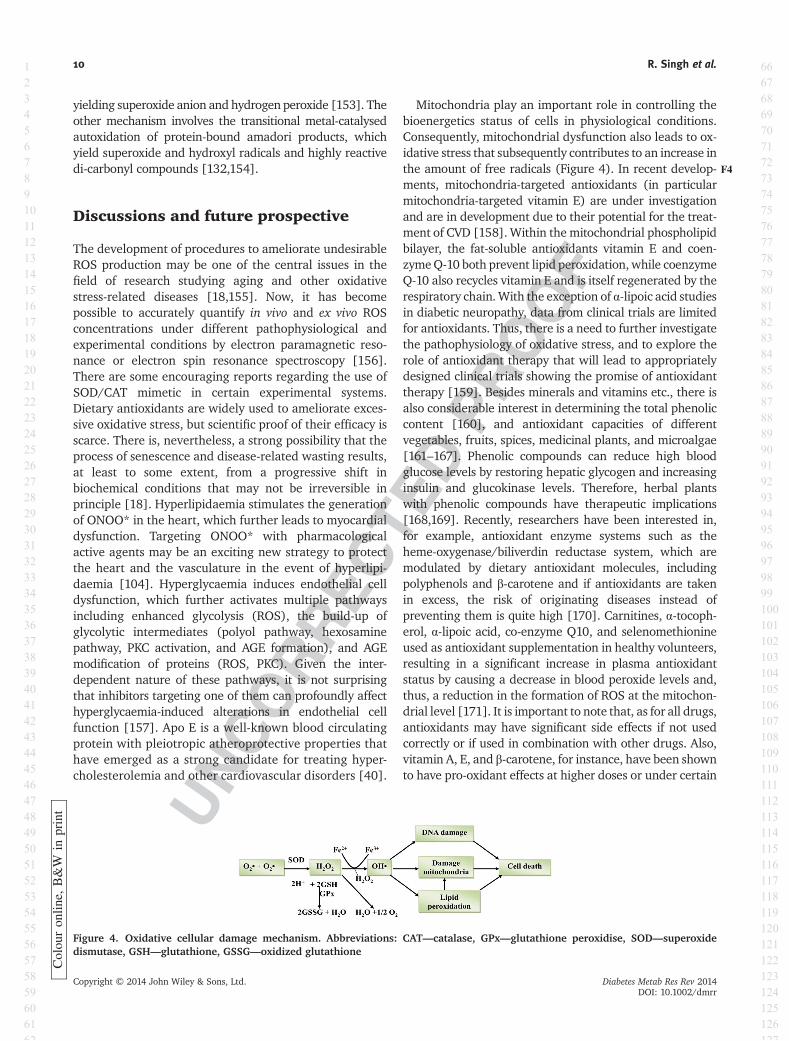
Mitochondria play an important role in controlling thebioenergetics status of cells in physiological conditions.Consequently, mitochondrial dysfunction also leads to ox-idative stress that subsequently contributes to an increase inthe amount of free radicals (Figure F44). In recent develop-ments, mitochondria-targeted antioxidants (in particularmitochondria-targeted vitamin E) are under investigationand are in development due to their potential for the treat-ment of CVD [158]. Within the mitochondrial phospholipidbilayer, the fat-soluble antioxidants vitamin E and coen-zymeQ-10 both prevent lipid peroxidation, while coenzymeQ-10 also recycles vitamin E and is itself regenerated by therespiratory chain.With the exception of α-lipoic acid studiesin diabetic neuropathy, data from clinical trials are limitedfor antioxidants. Thus, there is a need to further investigatethe pathophysiology of oxidative stress, and to explore therole of antioxidant therapy that will lead to appropriatelydesigned clinical trials showing the promise of antioxidanttherapy [159]. Besides minerals and vitamins etc., there isalso considerable interest in determining the total phenoliccontent [160], and antioxidant capacities of differentvegetables, fruits, spices, medicinal plants, and microalgae[161–167]. Phenolic compounds can reduce high bloodglucose levels by restoring hepatic glycogen and increasinginsulin and glucokinase levels. Therefore, herbal plantswith phenolic compounds have therapeutic implications[168,169]. Recently, researchers have been interested in,for example, antioxidant enzyme systems such as theheme-oxygenase/biliverdin reductase system, which aremodulated by dietary antioxidant molecules, includingpolyphenols and β-carotene and if antioxidants are takenin excess, the risk of originating diseases instead ofpreventing them is quite high [170]. Carnitines, α-tocoph-erol, α-lipoic acid, co-enzyme Q10, and selenomethionineused as antioxidant supplementation in healthy volunteers,resulting in a significant increase in plasma antioxidantstatus by causing a decrease in blood peroxide levels and,thus, a reduction in the formation of ROS at the mitochon-drial level [171]. It is important to note that, as for all drugs,antioxidants may have significant side effects if not usedcorrectly or if used in combination with other drugs. Also,vitamin A, E, and β-carotene, for instance, have been shownto have pro-oxidant effects at higher doses or under certain
Figure 4. Oxidative cellular damage mechanism. Abbreviations: CAT—catalase, GPx—glutathione peroxidise, SOD—superoxidedismutase, GSH—glutathione, GSSG—oxidized glutathione
Colou
ron
line,
B&W
inprint
10 R. Singh et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127

conditions [170]. The use of natural antioxidants toaugment physiological antioxidant mechanisms is particu-larly attractive, but potential difficulties exist, for examplein situations where most of the diseases where oxidativedamage has been demonstrated, free radical generation isnot the primary cause of the disease; rather, it plays a rolein further complicating/worsening the disease condition.The possibility of antioxidant therapy may also be harmful
which can be a potential possibility is for any syntheticagent, but it may also be true for natural antioxidant agentstaken in excess which is needed to be investigated further.
Conflict of interest
None declared.
References
1. Winter. Organic radical’s battery.Electrochem Soc Interface 2005: 32–36.Q3Q4
2. Valdez LB, Arnaiz SL, Bustamante J,Alvarez S, Costa LE, Boveris A. Freeradical chemistry in biological systems.Biol Res 2000: 33.Q5
3. Blake DR, Allen RE, Lunec J. Freeradicals in biological systems-a revieworientated to inflammatory processes.Br Med J 1987; 43: 371–385.
4. De Zwart LL, John H, Meerman N, et al.Biomarkers of free radical damageapplications in experimental animalsand in humans. Free Radic Biol Med1999; 26: 202–226.
5. Inoue M, Sato EF, Nishikawa M. Mito-chondrial generation of reactive oxygenspecies and its role in aerobic life. CurrMed Chem 2003; 10: 2495–2505.
6. Kumar S. Free radicals and antioxidants:Human and food system. Adv Appl SciRes 2011; 2: 129–135.
7. Funda SP. K›ymet T. Free radicals: Ourenemies or friends? Adv Appl Mol Biol2007; 1: 63–69.
8. McCord JM, Fridovich I. Superoxidedismutase: an enzyme functions forerythromycin (haemocuprein). J BiolChem 1969; 244: 6049–6055.
9. Karlsson J. Introduction to nutraologyand radical formation. In Antioxidantsand Exercise. Human Kinetics Press:Illinois, 1997; 1–143.
10. Landis GN, Tower J. Superoxidedismutase evolution and life span regu-lation. Mech Ageing Dev 2005; 126:365–379.
11. Pastore A, Federici G, Bertini E, PiemonteF. Analysis of glutathione: Implication inredox and detoxification. Clin Chim Acta2003; 333: 19–39.
12. Vasdev S, Gill VD, Singal PK.Modulationof oxidative stress induced changes inhypertension and atherosclerosis byantioxidants. Exp Clin Cardiol 2006; 11:206–216.
13. Leonard SS, Harris GK, Shi XL. Metal-induced oxidative stress and signaltransduction. Free Radic Biol Med2004; 37: 1921–1942.
14. Valko M, Morris H, Cronin MT. Metals,toxicity and oxidative stress. Curr MedChem 2005; 12: 1161–1208.
15. Chobot V, Hadacek F. Iron and itscomplexation by phenolic cellular
metabolites from oxidative stress tochemical weapons. Plant Signal Behav2010; 5: 1–5.
16. Valko M, Leibfritz D, Moncol J, CroninMT, Mazur M, Telser J. Free radicalsand antioxidants in normal physiologi-cal functions and human disease. Int JBiochem Cell Biol 2007; 39: 44–84.
17. Marnett LJ. Lipid peroxidation- DNAdamage by malondialdehyde. Mut.Res-Fund. Mol Mech Muta 1999; b:83–95.
18. Meagher EA, Barry OP, Lawson JA,Rokach J, FitzGerald GA. Effects ofvitamin E on lipid peroxidation inhealthy persons. JAMA 2001; 285:1178–1182.
19. Huang HY, Appel LJ, Croft KD, MillerER, Mori TA, Puddey IB. Effects ofvitamin C and vitamin E on in vivo lipidperoxidation: results of a randomizedcontrolled trial. Am J Clin Nutr 2002;76: 549–555.
20. Brzezińska-Ślebodzińska E,ŚlebodzińskiAB, Pietras B, Wieczorek G. Antioxidanteffect of vitamin E and glutathione onlipid peroxidation in boar semen plasma.Biol Trace Elem Res 1995; 47: 69–74.
21. Biewenga GP, Guido RM, Haenen M,Bast A. The pharmacology of the anti-oxidant lipoic acid. Gen Pharmacol1997; 29: 315–331.
22. Song K, Lee WJ, Koh J. α-Lipoic acidprevents diabetes mellitus in diabetes-prone obese rats. Biochem Biophys ResCommun 2004; 326: 197–202.
23. Turunen M, Olsson J, Dallner G.Metabolism and function of coenzymeQ. Biochim Biophys Acta 2004; 1660:171–199.
24. Tomás-Zapico C, Coto-Montes A. Mela-tonin as antioxidant under pathologicalprocesses. Recent Pat Endocr MetabImmune Drug Discov 2007; 1: 63–82.
25. http://www.who.int/mediacentre/factsheets/fs317/en/.
26. Yusuf S, Ôunpuu S, Anand S. The globalepidemic of atherosclerotic cardiovas-cular disease. Med Princ Prac 2002; 11:3–8.
27. Frostegård J. Immunity, atherosclerosisand cardiovascular disease. BMC Med2013; 11: 117–117.
28. Maria EL, Dennis JM, Stocker R.Actions of“antioxidants”in the protection
against atherosclerosis. Free Radic BiolMed 2012; 53: 863–884.
29. Hansson GK. Inflammation, atheroscle-rosis and coronary artery disease. NewEng J Med 2005; 352: 1685–1695.
30. Cohen MP, Ziyadeh FN, Chen S.Amadori-modified glycated serumproteins and accelerated atherosclero-sis in diabetes: Pathogenic and thera-peutic implications. J Lab Clin Med2006; 147: 211–219.
31. Stapleton PA, Goodwill AG, James ME,Brock RW, Frisbee JC. Hypercholester-olemia and microvascular dysfunction:Interventional strategies. J Inflamm2010; 7: 54–54.
32. Vogiatzi G, Tousoulis D, Stefanadis C.The role of oxidative stress in athero-sclerosis. Hellenic J Cardiol 2009; 50:402–409.
33. Davignon J, Ganz P. Role of endothelialdysfunction in atherosclerosis. Circula-tion 2004; 109: III27–III32.
34. Fruchart JC, Duriez P. Free radicalsand atherosclerosis. In Free RadicalDamage and its Control, Rice-EvansCA, Burdon RH (eds). Elsevier Science1994; 257–281. Q6
35. Gerald HT. Daphne. LDL as a cause ofatherosclerosis. Open Atheroscl ThrombJ 2012; 5: 13–21.
36. Mimić-Oka J, Simić DV, Simić TP. Freeradicals in cardiovascular diseases. SciJ FACTA UNIVERSITATIS Series: MedBiol 1999; 6: 11–22.
37. Prasad CVB, Kodliwadmath MV,Kodliwadmath GB. Erythrocyte super-oxide dismutase, catalase activitiesand hydrogen peroxide induced lipidperoxidation in leprosy. Leprosy Rev2007; 78: 391–397.
38. Maia MDS, Bicudo SD, Sicherle CC,Rodello L, Gallego ICS. Lipid peroxida-tion and generation of hydrogen perox-ide in frozen-thawed ram semencryopreserved in extenders with anti-oxidants. Ani Reprod Sci 2010; 122:118–123.
39. Harris JD, Evans V, Owen JS. ApoEgene therapy to treat hyperlipidemiaand atherosclerosis. Curr Opin MolTher 2006; 8: 1–13.
40. Chung M, Lichtenstein AH, Ip S, Lau J,Balk EM. Comparability of methods forLDL subfraction determination: a
Role of Free Radicals in Atherosclerosis, Diabetes and Dyslipidaemia 11
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127
DAHIYA
Cross-Out
DAHIYA
Cross-Out
DAHIYA
Sticky Note
Hiroyaki Nishidae, Takio Suga
DAHIYA
Sticky Note
Winter
DAHIYA
Cross-Out
DAHIYA
Inserted Text
(2): 65-70.
DAHIYA
Inserted Text
London, United Kingdom.

systematic review. Atherosclerosis2009; 20: 342–348.
41. Howard SK, Huang W, Ishii I, ZhangWY. Macrophage foam cell formationwith native low density lipoprotein. JBiol Chem 2002; 277: 34573–34580.
42. Louis SF, Zahradka P. Vascular smoothmuscle cell motility: From migrationto invasion. Exp Clin Cardiol 2010; 15:e75–e85.
43. Steven OM, Jain HT, Marks AR. Vascu-lar smooth muscle cell proliferation inrestenosis. Circulation: CardiovascInterv 2011; 4: 104–111.
44. Kaul N, Devaraj S, Jialal I. α-Tocopheroland Atherosclerosis. Exp Biol Med 2001;226: 5–12.
45. Lim AK, Barry NP, Miyazaki-Anzai S,et al. ultimodal CARS microscopydetermination of the impact of diet onmacrophage infiltration and lipidaccumulation on plaque formation inApoE-deficient mice. J Lipid Res 2010;51: 1729–1737.
46. Leonarduzzi G, Gamba P, Gargiulo S,Biasi F, Poli G. Inflammation-relatedgene expression by lipid oxidation-derived products in the progression ofatherosclerosis. Free Radic Biol Med2012; 52: 19–34.
47. Gonza´ lez-correa JA, Arrebola MM,Guerrero J, et al. Influence of vitaminE on the antiplatelet effect ofacetylsalicylic acid in human blood.Platelets 2005; 16: 171–179.Q7
48. Poredos P. Markers of preclinical ath-erosclerosis and their clinical rele-vance. Open Atheroscl Thromb J 2011;4: 1–10.
49. Madamanchi NR, Runge MS. Mitochon-drial Dysfunction in Atherosclerosis. CircRes 2007; 100: 460–473.
50. Woo RA, McLure KG, Lees-Miller SP,Rancourt E. DNA-dependent proteinkinase acts upstream of p53 in responseto DNA damage. Nature 1998 Aug 13;394(6694): 700–4.
51. Kozar RA, McKeone BJ, Pownall HJ.Free radical-induced alterations inendothelial cell function. J Surg Res1994; 56: 32–36.
52. Van Lenten BJ, Navab M, Shih D,Fogelman AM, Lusis AJ. The role ofhigh-density lipoproteins in oxidationand inflammation. Trends CardiovascMed 2001; 11: 155–161.
53. Navab M, Reddy ST, Van Lenten BJ,Anantharamaiah GM, Fogelman AM.The role of dysfunctional HDL in ath-erosclerosis. J Lipid Res 2009; 50:S145–S149.
54. Berry C, Tardif JC, Bourassa MG. Coro-nary Heart disease in patients with diabe-tes part I: recent advances in preventionand noninvasive management free. J AmCol Cardiol 2007; 49: 631–642.
55. Alfadda AA, Sallam RM. Reactiveoxygen species in health and disease.J Biomed Biotech 2012; 2012: 1–14.
56. Giacco F, Brownlee M. Oxidative stressand diabetic complications. Circ Res2010; 107: 1058–1070.
57. Wolff SP. Diabetes mellitus and freeradicals. Free radicals, transition metalsand oxidative stress in the aetiology ofdiabetes mellitus and complications.Br Med Bull 1993; 49: 642–652.
58. Shaath JS. Islet amyloid and selectedtrace elements among type 2 diabetesmellitus patients in Gaza city, IslamicUniversity-Gaza 2012; 5: 33. Q8
59. Kaneto H, Nakatani Y, Kawamori D,Miyatsuka T, Matsuoka T. Involvementof oxidative stress and the JNKpathway in glucose toxicity. Rev Dia-betic Stud 2004; 1: 165–174.
60. Green K, Brand MD, Murphy MP.Prevention of mitochondrial oxidativedamage as a therapeutic strategy indiabetes. Diabetes 2004; 53: S110–S118.
61. Robertson RP, Harmon J, Tran PO,Tanaka Y, Takahashi H. Glucose toxicityin beta-cells: type 2 diabetes, goodradicals gone bad, and the glutathioneconnection. Diabetes 2003; 52: 581–587.
62. Robertson RP. Chronic Oxidative Stressas a Central Mechanism for GlucoseToxicity in Pancreatic Islet Beta Cellsin Diabetes. J Biol Chem 2004; 279:42351–42354.
63. Yoon JW, Jun HS. Autoimmune destruc-tion of pancreatic beta Cells. Am Jf Ther2005; 12: 580–591.
64. Arioglu E, Andewelt A, Diabo C, Bell M,Taylor SI, Gorden P. Clinical course ofthe syndrome of autoantibodies to theinsulin receptor (type B insulin resis-tance): a 28-year perspective. Medicine(Baltimore) 2002; 81: 87–100.
65. Elbein SC. Perspective: the search forgenes for type 2 diabetes in the post-genome era. Endocrinology 2002; 143:2012–2018.
66. Santos MCS, Louzada RAN, Souza ECL,et al. Diabetes mellitus increases reac-tive oxygen species production in thethyroid of male rats. Endocrinol 2013;13: 1930–1930.
67. Espinoza-Jiménez A, Peón AN, TerrazasLI. Alternatively activated macrophagesin Types 1 and 2 Diabetes.Med Inflamm2012; 2012: 1–10.
68. Fowler MJ. Microvascular and macro-vascular complications of diabetes.Clin Diabetes 2008; 26: 77–82.
69. Cantor J, Haskins K. Interactions ofmacrophages and T cells in autoim-mune diabetes. Drug Discov Today DisMech 2006; 3: 381–385.
70. KaplanM, AviramM,Hayek T. Oxidativestress and macrophage foam cell forma-tion during diabetes mellitus-inducedatherogenesis: Role of insulin therapy.Pharmacol Therape 2012; 136: 175–185.
71. De Kimpe SJ, Anggârd EE, Carrier MJ.Reactive oxygen species regulatemacrophage scavenger receptor type I,but not type II, in the human monocyticcell line THP-1. Mol Pharmacol 1998;53: 1076–1082.
72. Brownlee M. The pathobiology ofdiabetic complications a unifying mech-anism. Banting Lecture 2004. Diabetes2005; 54: 1615–1625.
73. Wolf G. Role of reactive oxygen speciesin angiotensin II-mediated renal growth,differentiation, and apoptosis. AntioxidRedox Signal 2005; 7: 1337–1345.
74. Lee KY, D’Acquisto F, Hayden MS, ShimJH, Ghosh S. PDK1 nucleates T cellreceptor-induced signaling complexfor NF-κB activation. Science 2005;308: 114–118.
75. Fong DS, Aiello LP, Ferris FL, Klein R.Diabetic retinopathy. Diabetes Care2004; 27: 2540–2553.
76. Oyama T, Miyasita Y, Watanabe H,et al. The role of polyol pathway in highglucose-induced endothelial celldamages. Diabetes Res Clin Pract 2006;73: 227–234.
77. Oka M, Kato N. Aldose reductase inhibi-tors. J Enzyme Inhib 2001; 16: 465–473.
78. David James FAA. The free radical thattriggers insulin resistance and Type 2diabetes. Proc Natl Acad Sci U S A 2009. Q9 Q10
79. Desco MC, Asensi M, Ma´rquez R, et al.Xanthine oxidase is involved in freeradical production in type 1 diabetesprotection by allopurinol. Diabetes2002; 51: 1118–1124.
80. Sˇkrha J. Diabetes and vascular disease:From pathogenesis to treatment Arevascular effects of hypoglycemic andhypolipidemic drugs independent oftheir metabolic effects? Diabetes &Metabolic Syndrome. Clin Res Rev2007; 1: 61–69. Q11
81. Hadi HAR, Suwaidi JAI. Endothelialdysfunction in diabetes mellitus. VascHealth Risk Manage 2007; 3: 853–876.
82. Shi Y, Vanhoutte PM. Reactive oxygen-derived free radicals are key to theendothelial dysfunction of diabetes. JDiabetes 2009; 1: 151–162.
83. Graier WF, Pusch K, Wascher T.Increased superoxide formation in endo-thelial cells during hyperglycemia. Dia-betes Res Clin Pract 1999; 45: 153–160.
84. Cosentino F, Hishikawa K, Katusic ZS,Luscher TF. High glucose increasesNOS expression and superoxide aniongeneration in human aortic endothelialcells. Circulation 1997; 96: 25–28.
85. Pierre K, Pellerin L. Monocarboxylatetransporters in the central nervous sys-tem: distribution, regulation and func-tion. J Neurochem 2005; 94: 1–14.
86. Thaler S, Choragiewicz TJ, Rejdak R,et al. Neuroprotection by acetoacetateand β-hydroxybutyrate against NMDA-induced RGC damage in rat-possibleinvolvement of kynurenic acid. Graefe’sArch Clin Exp Ophthalmol 2010; 248:1729–1735.
87. Umamaheswari M, Chatterjee TK. In-vitro antioxidant activities of the frac-tions of Coccinia grandis L. leaf extract.Afr J Tradit Complement Alternate Med2008; 5: 61–73.
88. Mlakar A, Batna A, Dudda A, SpitellerG. Iron (II) ions induced oxidation ofascorbic acid and glucose. Free RadRes 1996; 25: 525–539.
89. Ali Ebrahimzadeh M, Nabavia SM,Nabavia SF, Bahramianc F, Bekhradnia
12 R. Singh et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127
DAHIYA
Cross-Out
González-Correa JA, Arrebola MM, Guerrero A,
DAHIYA
Cross-Out
DAHIYA
Sticky Note
Science is the name of the journal.
DAHIYA
Cross-Out
Hoehn KL, Salmon AB, Hohnen-Behrens C et al. Insulin resistance is a cellular antioxidant defense mechanism. Proc Natl Acad Sci USA. 2009 Oct 20;106 (42):17787-92
DAHIYA
Cross-Out
DAHIYA
Cross-Out
DAHIYA
Cross-Out
Jan Škrha

AR. Antioxidant and free radicalscavenging activity of H. officinalis L.Var. Angustifolius, V. odorata, B.hyrcana and C. speciosum. Pak JPharma Sci 2010; 23: 29–34.
90. Hunt JV, Wolff SP. Oxidative glycationand free radical production: a causalmechanism of diabetic complications.Free Rad Res Communication 1991;12–13: 115–123.
91. Stadler K, Jenei V, B¨olcsh´azy V,Somogyi A, Jakus J. Increased nitricoxide levels as an early sign of prema-ture aging in diabetes. Free Radic BiolMed 2003; 35: 1240–1251.
92. Schleicher ED, Weigert C. Role of thehexosamine biosynthetic pathway indiabetic nephropathy. Kidney Int Suppl2000; 77: S13–S8.
93. Dunlop M. Aldose reductase and therole of the polyol pathway in diabeticnephropathy. Kidney Int Suppl 2000;58: S3–S12.
94. Koshikawa M, Mukoyama M, Mori K,et al. Role of p38 mitogen-activatedprotein kinase activation in podocyteinjury and proteinuria in experimentalnephrotic syndrome. J Am Soc Nephrol2005; 16: 2690–2701.
95. Meier M, Menne J, Park JK, Haller H.Nailing down PKC isoform specificityin diabetic nephropathy-two’s company,three’s a crowd. Nephrol Dial Transplant2007; 22: 2421–2425.
96. Nakajima H, Amano W, Kubo T, et al.Glyceraldehyde-3-phosphate dehydro-genase aggregate formation partici-pates in oxidative stress-induced celldeath-An external file that holds apicture, illustration, etc. J Biol Chem2009; 284: 34331–34341.
97. Maritim AC, Sanders RA, Watkins JB.Diabetes, oxidative stress, and antioxi-dants: a review. J Biochem Mol Toxicol2003; 17: 24–38.
98. Blázovics A, Fehér E, Fehér J. Role ofFree Radical Reactions in ExperimentalHyperlipidemia in the Pathomechanismof Fatty Liver. Free Radicals and theLiver.
99. Peterson TE. Poppa V, Ueba H, Wu A,Yan C, Berk BC. Opposing effects ofreactive oxygen species and cholesterolon endothelial nitric oxide synthaseand endothelial cell caveolae. Cir-culation Res 1999; 85: 29–37. 1992;96–123.
100. Roberts WC. Preventing and arrestingcoronary atherosclerosis. Am Heart J1995; 130: 580–600.
101. Koter M, Franiak I, Strychalska K,Broncel M, Chojnowska-Jezierska J.Damage to the structure of erythro-cyte plasma membranes in patientswith type-2 hypercholesterolemia.Int J Biochem Cell Biol 2004; 36:205–215.
102. Schaffer SW, Jong CJ, Mozaffari M.Role of oxidative stress in diabetes-mediated vascular dysfunction: Unify-ing hypothesis of diabetes revisited.Vas Pharmacol 2012; 57: 139–149.
103. O’Keefe JH, Bell DSH. Postprandialhyperglycemia/hyperlipidemia (Post-prandial Dysmetabolism): Is a Cardio-vascular Risk Factor. Am J Cardiol2007; 100: 899–904.
104. Ónody A, Csonka C, Giricz Z,Ferdinandy P. Hyperlipidemia inducedby a cholesterol-rich diet leads toenhanced peroxynitrite formation inrat hearts. Cardiovas Res 2003; 58:663–670.
105. Vira´g L, Szabo´ E, Gergely P, Szabo C.Peroxynitrite-induced cytotoxicity:mechanism and opportunities forintervention. Toxicol Lett 2003; 140:113–124.
106. Hrabarova E, Juranek I, Soltes L. Pro-oxidative effect of peroxynitrite regard-ing biological systems: a special focuson high-molar-mass hyaluronan degra-dation. Gen Physiol Biophy 2011; 30:223–238.
107. Miller MR, Megson IL. Recent develop-ments in nitric oxide donor drugs. Br JPharmacol 2007; 151: 305–321.
108. Yang R. Effect of antioxidant capacityon blood lipid metabolism and lipopro-tein lipase activity of rats fed a high-fatdiet. Nutrition 2006; 22: 1185–1191.
109. Condell RA. Evidence for suitability ofglutathione peroxidase as a protectiveenzyme: studies of oxidative damage,restoration and proteolysis. ArchBiochem Biophys 1983; 223: 407–416.
110. Thomas MJ. Physiological aspects oflow-density lipoprotein oxidation. CurrOpin Lipidol 2000; 11: 297–301.
111. Keevil JG. Implications of cardiac riskand low-density lipoprotein cholesteroldistributions in the United States forthe diagnosis and treatment ofdyslipidemia: data from NationalHealth and Nutrition Examination Sur-vey 1999 to 2002. Circulation 2007;115: 1363–1370.
112. Andrew PJ, Mayer B. Enzymatic func-tion of nitric oxide synthases. CardiovasRes 1999; 43: 521–531.
113. Knowles JW, Reddick RL, Jennette JC,Shesely EG, Smithies O, Maeda N.Enhanced atherosclerosis and kidneydysfunction in eNOS(�/�)Apoe(�/�)mice are ameliorated by enalapril treat-ment. J Clin Invest 2000; 105: 451–458.
114. Kuhlencordt PJ, Chen J, Han F, AsternJ, Huang PL. Genetic deficiency ofinducible nitric oxide synthase reducesatherosclerosis and lowers plasma lipidperoxides in apolipoprotein E-knockoutmice. Circulation 2001;103: 3099–3104.
115. Lowenstein CJ. Beneficial Effects ofNeuronal Nitric Oxide Synthase in Ath-erosclerosis. Arterioscler Thromb VascBiol 2006; 26: 1417–1418.
116. Soski S, Dobutovi BD, Sudar EM, et al.Regulation of inducible nitric oxidesynthase (inos) and its potential rolein insulin resistance, diabetes and heartfailure. Open Cardiovas Med J 2011; 5:153–163.
117. Thippeswamy T, McKay JS, Quinn JP,Morris R. Nitric oxide, a biological
double-faced janus--is this good or bad?Histol Histopath 2006; 21: 445–458.
118. Beckman JS, Koppenol WH. Nitricoxide, superoxide, and peroxynitrite:the good, the bad, and ugly. Am JPhysiol 1996; 271: C1424–C1437.
119. Rubbo H, Batthyany C, Radi R. Nitricoxide-oxygen radical interactions inatherosclerosis. Biol Res 2000; 33:167–175.
120. Jeremy JY, Rowe D, Emsley AM, NewbyAC. Nitric oxide and the proliferation ofvascular smooth muscle cells. CardiovasRes 1999; 43: 580–594.
121. Chiang TM, Woo-Rasberry V. Effect ofnitric oxide on platelet progeneitorgrowth, posttranslational modificationof protein, and function. Open NitricOxide J 2008; 1: 1–4.
122. Sethi S, Sharma P, Dikshit M. Nitricoxide and oxygen derived free radicalgeneration from control andlipopolysaccharide-treated rat poly-morphonuclear leukocyte. Nitric Oxide2001; 5: 482–493.
123. Cooke JP. Role of nitric oxide in pro-gression and regression of atheroscle-rosis. West J Med 1996; 164: 419–424.
124. Barter PJ, Nicholls S, Rye KA,Anantharamaiah GM, Navab M,Fogelman AM. Antiinflammatoryproperties of HDL. Circulation Res2004; 95: 764–772.
125. Zheng L, Nukuna B, Brennan ML, et al.Apolipoprotein A-I is a selective targetfor myeloperoxidase-catalyzed oxida-tion and functional impairment insubjects with cardiovascular disease. JClin Invest 2004; 114: 529–541.
126. Rivera J, Lozano ML, Navarro-Núñez L,Vicente V. Platelet receptors and sig-naling in the dynamics of thrombusformation. Haematologica 2009; 94:700–711.
127. Etsuo N. Do free radicals play causalrole in atherosclerosis? Low densitylipoprotein oxidation and vitamin Erevisited. J Clin BioNut 2011; 48: 3–7.
128. Omawari N, Dewhurst M, Vo P,Mahmood S, Stevens E, TomlinsonDR. Deficient nitric oxide responsiblefor reduced nerve blood flow indiabetic rats: effects of L-NAME, L-arginine, sodium nitroprusside andevening primrose oil. Br J Pharmacol1996; 118: 186–190.
129. Cosenzi A, Bernobich E, Bonavita M,Trevisan R, Bellini G, Campanacci L.Early effects of diabetes on induciblenitric oxide synthase in the kidney.Acta Diabetol 2002; 39: 91–96.
130. Sokolovska J, Isajevs S, Baumanea L,et al. P5: Enhanced expression ofxanthine oxidase and NO synthasescausing the overproduction of NO inkidneys of diabetic animals can bereduced by 1,4-dihydropyridines. NitricOxide 2013; 31: S1–S15.
131. Kincer JF, Uittenbogaard A, Dressman J,et al. Hypercholesterolemia promotesa CD36-dependent and endothelialnitric-oxide synthase-mediated vascular
Role of Free Radicals in Atherosclerosis, Diabetes and Dyslipidaemia 13
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127

dysfunction. J Biol Chem 2002; 277:23525–23533.
132. Aronson D, Rayfield EJ. How hypergly-cemia promotes atherosclerosis: molec-ular mechanisms. Cardiovas Diabetol2002; 1: 1–10.
133. Cade WT. Diabetes-related microvascu-lar and macrovascular diseases in thephysical therapy setting. Phy Ther2008; 88: 1322–1335.
134. Bierman EL. Atherogenesis in diabetes.Arteriosclero Thromb 1992; 12: 647–656.
135. Jay D, Hitomi H, Griendling KK. Oxida-tive stress and diabetic cardiovascularcomplications. Free Radic Biol Med2006; 40: 183–192.
136. Roche LD, AcostaMedina E, Pe´rez AF,et al. Lipofundin-Induced hyperlipidemiapromotes oxidative stress and atheroscle-rotic lesions in new zealandwhite rabbits.Int J Vas Med 2012; 2012: 1–7.
137. Yang RL, Shi YH, Hao G, Li W, Le GW.Increasing oxidative stress withprogressive hyperlipidemia in human:Relation between malondialdehydeand atherogenic. J Clin Biochem Nut2008; 43: 154–158.
138. Renard CB, Kramer F, Johansson F.Diabetes and diabetes-associated lipidabnormalities have distinct effects oninitiation and progression of athero-sclerotic lesions. J Clin Invest 2004;114: 659–668.
139. Renard C, Van Obberghen E. Role ofdiabetes in atherosclerotic pathogene-sis. What have we learned from animalmodels? Diabetes Metabol 2006; 32:15–29.
140. Lee SC. Uncoupling protein-2 modula-tion of reactive oxygen species and cellviability in the pancreatic beta cell,2008; 1–17.
141. Ceriello A, Motz E. Is oxidative stressthe pathogenic mechanism underlyinginsulin resistance, diabetes, and cardio-vascular disease? Arteriosclerosis ThrombVasc Biol 2004; 24: 816–823.
142. Pastromas S, Terzi AB, Tousoulis D,Koulouris S. Postprandial lipemia: Anunder-recognized atherogenic factor inpatients with diabetes mellitus. Int JCardiol 2008; 126: 3–12.
143. Atabek EM, Selim K, Ozgur P, Murat B.Arterial wall thickening and stiffeningin children and adolescents with type1 diabetes. Diabetes Res Clin Prac2006; 74: 33–40.
144. Mario B, Assunta P, Di PN, et al. Adher-ence of uremic erythrocytes to vascularendothelium decreases endothelial nitricoxide synthase expression. Kidney Int2005; 67: 1899–1906.
145. AlemanyM. Regulation of adipose tissueenergy availability through blood flowcontrol in the metabolic syndrome. FreeRadic Biol Med 2012; 52: 2108–2119.
146. Price KD, Catherine SC, Price B,Reynolds RD. Hyperglycemia-induced
ascorbic acid deficiency promotesendothelial dysfunction and the devel-opment of atherosclerosis. Atheroscle-rosis 2001; 158: 1–12.
147. Shao N, Kuang HY, Wang N, et al. Rela-tionship between oxidant/antioxidantmarkers and severity of microalbu-minuria in the early stage of nephropa-thy in type 2 diabetic patients. JDiabetes Res 2013; 2013: 1–6.
148. Palinski W, Napoli C. The fetal originsof atherosclerosis: Maternal hypercho-lesterolemia, and cholesterol-loweringor antioxidant treatment during preg-nancy influence in utero programmingand postnatal susceptibility to athero-genesis. FAS Exper Biol J 2002; 16:1348–1360.
149. Giardino I, Edelstein D, Brownlee M.BCL-2 expression or antioxidantsprevent hyperglycemia-induced forma-tion of intracellular advanced glycationend products in bovine endothelial cells.J Clin Invest 1996; 97: 1422–1428.
150. Takei A, Huang Y, Lopes-Virella F.Intercellular adhesion molecule-1(ICAM-1) expression induced by oxLDLon human umbilical vein endothelialcells (HUVEC) depends on the stageof LDL oxidation. Diabetes 1998; 47:A115–A115.
151. Leopold JA, Loscalzo J. Oxidative riskfor atherothrombotic cardiovasculardisease. Free Radic Biol Med 2009; 47:1673–1706.
152. Nishikawa T, Edelstein D, Du XL, et al.Normalizing mitochondrial superoxideproduction blocks three pathways ofhyperglycemic damage. Nature 2000;404: 787–790.
153. Wolff SP. Diabetes mellitus and free rad-icals. Free radicals, transitionmetals andoxidative stress in the aetiology of diabe-tes mellitus and complications. Br MedBull 1993; 49: 642–652.
154. Baynes JW, Thorpe SR. Role of oxida-tive stress in diabetic complications: anew perspective on an old paradigm.Diabetes 1999; 48: 1–9.
155. Kangralkar VA, Patil SD, BandivadekarRM. Oxidative stress and diabetes: a re-view. Int J Pharma App 2010; 1: 38–45.
156. Mrakic-Sposta S, Gussoni M, MontorsiM, Porcelli S, Vezzoli A. Assessment ofa standardized ROS production profilein humans by electron paramagneticresonance. Oxid Med Cell Longevity2012; 2012: 1–10.
157. Funk SD, Jr AY, Orr AW. Hyperglycemiaand endothelial dysfunction in athero-sclerosis: Lessons from Type 1 Diabetes.Int J Vasc Med 2012; 2012: 1–19.
158. Rocha MR, García-Bou R, Enguix N,Hernández-Mijares A, Esplugues JV,Víctor VM. Mitochondria-targetedVitamin E antioxidant: An agent forcardiovascular protection. Vasc Dis Prev2009; 6: 36–46.
159. Johansen JS, Harris AK, Rychly DJ,Ergul A. Oxidative stress and the useof antioxidants in diabetes: Linkingbasic science to clinical practice.Cardiovas Diabetol 2005; 4: 1–11.
160. Fu L, Xu BT, Xu XR, et al. Antioxidantcapacities and total phenolic contentsof 62 fruits. Food Chem 2011; 129:345–350.
161. Cai YZ, Luo Q, Sun M, Corke H. Antiox-idant activity and phenolic compoundsof 112 traditional Chinese medicinalplants associated with anticancer. LifeSci 2004; 74: 2157–2184.
162. Gan RY, Kuang L, Xu XR, Zhang Y, XiaEQ, Song FL. Screening of naturalantioxidants from traditional Chinesemedicinal plants associated with treat-ment of rheumatic disease. Molecules2010; 15: 5988–5997.
163. Ghasemzadeh A, Jaafar HZE, RahmatA. Antioxidant activities, total pheno-lics and flavonoids content in twovarieties of Malaysia young ginger(Zingiber officinale Roscoe). Molecules2010; 15: 4324–4333.
164. Li HB, Cheng KW, Wong CC, Fan KW,Chen F, Jiang Y. Evaluation of antioxi-dant capacity and total phenolic con-tent of different fractions of selectedmicroalgae. Food Chem 2007; 102:771–776.
165. Li HB, Wong CC, Cheng KW, Chen F.Antioxidant properties in vitro andtotal phenolic contents in methanolextracts from medicinal plants. FoodSci Tech 2008; 41: 385–390.
166. Stangeland T, Remberg SF, Lye KA.Total antioxidant activity in 35 Ugan-dan fruits and vegetables. Food Chem2009; 113: 85–91.
167. Wong CC, Li HB, Cheng KW, Chen F. Asystematic survey of antioxidant acti-vity of 30 Chinese medicinal plantsusing the ferric reducing antioxidantpower assay. Food Chem 2006; 97:705–711.
168. Pattaneeya P, Reuthaithip S, Rin C,et al. Amelioration of hyperglycemia,hyperlipidemia, oxidative stress andinflammation in steptozotocin-induceddiabetic rats fed a high fat diet byriceberry supplement. J FunctionalFoods 2013; 5: 195–203.
169. Jung EH, Kim SR, Hwang IK, Youl HT.Hypoglycemic effects of a phenolic acidfraction of rice bran and ferulic acid inC57BL/KsJ-db/db mice. J Agri FoodChem 2007; 55: 9800–9804.
170. Brambilla D, Mancuso C, Scuderi MR,et al. The role of antioxidant supple-ments in immune system, neoplastic,and neurodegenerative disorders: apoint of view for an assessment of therisk/benefit profile. Nut J 2008; 7: 1–9.
171. Mosca L, Marcellini S, Perluigi M,et al. Biochem Pharmacol 2002; 63:1305–1314.
14 R. Singh et al.
Copyright © 2014 John Wiley & Sons, Ltd. Diabetes Metab Res Rev 2014DOI: 10.1002/dmrr
1234567891011121314151617181920212223242526272829303132333435363738394041424344454647484950515253545556575859606162
66676869707172737475767778798081828384858687888990919293949596979899100101102103104105106107108109110111112113114115116117118119120121122123124125126127

Author Query Form
Journal: Diabetes/Metabolism Research and Reviews
Article: dmrr_2558
Dear Author,
During the copyediting of your paper, the following queries arose. Please respond to these by annotating your proofs withthe necessary changes/additions.• If you intend to annotate your proof electronically, please refer to the E-annotation guidelines.• If you intend to annotate your proof by means of hard-copy mark-up, please refer to the proof mark-up symbols guide-lines. If manually writing corrections on your proof and returning it by fax, do not write too close to the edge of thepaper. Please remember that illegible mark-ups may delay publication.
Whether you opt for hard-copy or electronic annotation of your proofs, we recommend that you provide additional clar-ification of answers to queries by entering your answers on the query sheet, in addition to the text mark-up.
Query No. Query Remark
Q1 AUTHOR: Please check correction done.
Q2 AUTHOR: You must provide a statement regarding any possible conflicts ofinterest connected to this paper. Your paper will not be published until theProduction Editor has received a signed form from you.
Q3 AUTHOR: Winter capture as group name, please check.
Q4 AUTHOR: Please provide volume.
Q5 AUTHOR: Please provide volume.
Q6 AUTHOR: Please provide city location.
Q7 AUTHOR: Please check author names if capture correctly.
Q8 AUTHOR: Book or journal? Please confirm.
Q9 AUTHOR: Please provide volume and page no.
Q10 AUTHOR: Please check journal title if capture correctly.
Q11 AUTHOR: Please check this author name if capture correct.
DAHIYA
Text Box
YES
DAHIYA
Text Box
Authors declares no conflicts of interest connected to paper.
DAHIYA
Text Box
Name of authors have been changed.
DAHIYA
Text Box
Volume 2, 65-70
DAHIYA
Text Box
No Volume number.
DAHIYA
Text Box
London, United Kingdom.
DAHIYA
Text Box
González-Correa JA, Arrebola MM, Guerrero A,
DAHIYA
Text Box
Journal
DAHIYA
Text Box
106 (42):17787-92.
DAHIYA
Text Box
Correct
DAHIYA
Text Box
correct name is Jan Škrha
DAHIYA
Approved

USING e-ANNOTATION TOOLS FOR ELECTRONIC PROOF CORRECTION
Required software to e-Annotate PDFs: Adobe Acrobat Professional or Adobe Reader (version 7.0 or above). (Note that this document uses screenshots from Adobe Reader X) The latest version of Acrobat Reader can be downloaded for free at: http://get.adobe.com/uk/reader/
Once you have Acrobat Reader open on your computer, click on the Comment tab at the right of the toolbar:
1. Replace (Ins) Tool – for replacing text.
Strikes a line through text and opens up a text box where replacement text can be entered.
How to use it
Highlight a word or sentence.
Click on the Replace (Ins) icon in the Annotations section.
Type the replacement text into the blue box that appears.
This will open up a panel down the right side of the document. The majority of tools you will use for annotating your proof will be in the Annotations section, pictured opposite. We’ve picked out some of these tools below:
2. Strikethrough (Del) Tool – for deleting text.
Strikes a red line through text that is to be deleted.
How to use it
Highlight a word or sentence.
Click on the Strikethrough (Del) icon in the Annotations section.
3. Add note to text Tool – for highlighting a section to be changed to bold or italic.
Highlights text in yellow and opens up a text box where comments can be entered.
How to use it
Highlight the relevant section of text.
Click on the Add note to text icon in the Annotations section.
Type instruction on what should be changed regarding the text into the yellow box that appears.
4. Add sticky note Tool – for making notes at specific points in the text.
Marks a point in the proof where a comment needs to be highlighted.
How to use it
Click on the Add sticky note icon in the Annotations section.
Click at the point in the proof where the comment should be inserted.
Type the comment into the yellow box that appears.

USING e-ANNOTATION TOOLS FOR ELECTRONIC PROOF CORRECTION
For further information on how to annotate proofs, click on the Help menu to reveal a list of further options:
5. Attach File Tool – for inserting large amounts of text or replacement figures.
Inserts an icon linking to the attached file in the appropriate pace in the text.
How to use it
Click on the Attach File icon in the Annotations section.
Click on the proof to where you’d like the attached file to be linked.
Select the file to be attached from your computer or network.
Select the colour and type of icon that will appear in the proof. Click OK.
6. Add stamp Tool – for approving a proof if no corrections are required.
Inserts a selected stamp onto an appropriate place in the proof.
How to use it
Click on the Add stamp icon in the Annotations section.
Select the stamp you want to use. (The Approved stamp is usually available directly in the menu that appears).
Click on the proof where you’d like the stamp to appear. (Where a proof is to be approved as it is, this would normally be on the first page).
7. Drawing Markups Tools – for drawing shapes, lines and freeform annotations on proofs and commenting on these marks.
Allows shapes, lines and freeform annotations to be drawn on proofs and for comment to be made on these marks..
How to use it
Click on one of the shapes in the Drawing Markups section.
Click on the proof at the relevant point and draw the selected shape with the cursor.
To add a comment to the drawn shape, move the cursor over the shape until an arrowhead appears.
Double click on the shape and type any text in the red box that appears.




















