
ro0122i.pdf - Review of Optometry
86
Answering the “Myopia or Glaucoma?” Question, P. 60 • Clinical Quandaries: Herpes Zoster, P. 20 January 15, 2022 • reviewofoptometry.com Leadership in clinical care Recognizing them as an individual shaped by their life experiences will help you assess their health risks better and communicate more effectively. The Role of Race and Ethnicity in Optometry, p. 22 Connecting Across Cultures: How to Reach Out to Hispanics, p. 28 Breaking Down Barriers: The Black Experience in Optometry, p. 36 Evaluating Patients with Neurodevelopmental Conditions, p. 42 How to Offer Inclusive Care for LGBTQ+ Patients, p. 48 How to Defuse a Difficult Patient, p. 52 Making Your Practice Kid-Friendly, p. 56 Who is Your Patient? EARN 2 CE CREDITS 10 Questions on Digital Devices and Eye Health —Answered! Page 66 Soon all will be revealed. A new addition from the makers of the lens that Feels Like Nothing ™ is on its way. You will be able to fit more patients, more of the time, which is great for your patients and your practice. See product instructions for complete wear, care and safety information. © 2021 Alcon Inc. US-DTA-2100012 SURFACING SOON. Look for an ultimate in comfort and stability. Scan QR code to see what’s surfacing soon.
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of ro0122i.pdf - Review of Optometry
Answering the “Myopia or Glaucoma?” Question, P. 60 • Clinical Quandaries: Herpes Zoster, P. 20
January 15, 2022 • reviewofoptometry.com Leadership in clinical care
Recognizing them as an individual shaped by their life experiences
will help you assess their health risks better
and communicate more effectively.
The Role of Race and Ethnicity in Optometry, p. 22
Connecting Across Cultures: How to Reach Out to Hispanics, p. 28
Breaking Down Barriers: The Black Experience in Optometry, p. 36
Evaluating Patients with Neurodevelopmental Conditions, p. 42
How to Offer Inclusive Care for LGBTQ+ Patients, p. 48
How to Defuse a Diffi cult Patient, p. 52
Making Your Practice Kid-Friendly, p. 56
Who is Your Patient?
EARN 2 CE CREDITS
10 Questions on Digital Devices
and Eye Health—Answered!
Page 66
Soon all will be revealed. A new addition from the makers of the lens that Feels Like Nothing™ is on its way. You will be able to � t more patients, more of the time, which is great for your patients and your practice.
See product instructions for complete wear, care and safety information.© 2021 Alcon Inc. US-DTA-2100012
SURFACING SOON. Look for an ultimate in comfort and stability.
Scan QR code to see what’s surfacing soon.

Answering the “Myopia or Glaucoma?” Question, P. 60 • Clinical Quandaries: Herpes Zoster, P. 20
January 15, 2022 • reviewofoptometry.com Leadership in clinical care
Recognizing themas an individual shapedby their life experiences
will help you assesstheir health risks better
and communicatemore effectively.
The Role of Race and Ethnicityin Optometry, p. 22
Connecting Across Cultures:How to Reach Out to Hispanics, p. 28
Breaking Down Barriers: The BlackExperience in Optometry, p. 36
Evaluating Patients withNeurodevelopmental Conditions, p. 42
How to Offer Inclusive Carefor LGBTQ+ Patients, p. 48
How to Defuse a Diffi cult Patient, p. 52
Making Your Practice Kid-Friendly, p. 56
Who is YourPatient?Patient?Patient?
EARN 2 CE CREDITS
10 Questionson Digital Devices
and Eye Health—Answered!
Page 66

NOW APPROVEDScan to be among the first
to learn about VUITY.™
VuityPro.com
©2021 AbbVie Inc. North Chicago, IL 60064 US-VUI-210131 11/21

JANUARY 15, 2022 | REVIEW OF OPTOMETRY 3
Emmetropization duringearly child development isthought to be affected byage and initial refractive error
(RE), with greater initial RE leadingto faster rates. Currently, the AmericanAcademy of Ophthalmology (AAO)bases its recommendations for glasseson specific RE ranges at specific ages;however, researchers pointed out in anew study that these recommendationsare based mainly on expert consensusand that application varies amongprescribing doctors.
To help doctors make more in-formed decisions, researchers con-ducted a retrospective cohort study tobetter understand the proportion ofchildren with high RE during infancythat emmetropize to a point where itwould alter their clinical management.
The researchers studied 362 eyesof 194 infants (mean age at first exam:seven months), 168 hyperopic eyesof 92 children, 40 myopic eyes of 27children and 201 astigmatic eyes of 114children. A total of 26 children receivedglasses at their first exam. All childrenunderwent cycloplegic refraction at six,eight, 12 and 24 months. The childrenalso had, during earlier periods, a REin one or both eyes of hyperopia +3.5Dor greater, myopia -2.0D or greater or
astigmatism +1.5D or greater. The re-searchers didn’t include children withocular disease that could affect RE orocular growth.
Here are their key findings:
“We found that eyes with hypero-pia or astigmatism emmetropized to agreater degree than eyes with myopia,and the greatest degree of emme-tropization occurred among eyes with
high astigmatism, followed by thosewith moderate astigmatism, moder-ate hyperopia and high hyperopia, inthat order,” they explained in theirpaper. “Our observations stand incontrast with prior studies that showedno significant improvement in REin hyperopic eyes of older children.Our results suggest a different patternearlier in childhood.”
They say their results support “somebut not all” of the AAO’s recommenda-tions for prescribing glasses to infantsunder age one. “Prescribing glassesearly for children with high myopiamay be clinically appropriate as theyare unlikely to emmetropize sufficient-ly by two years,” they wrote. “Thedecision to prescribe glasses early isless clear in infants with high hypero-pia, as one quarter of children will nolonger meet AAO guidelines whenthey are one year of age. Finally, almosttwo thirds of infants with astigmatismhigh enough to meet AAO guidelinesemmetropize sufficiently to no longermeet guidelines for age one to lessthan two years. It appears appropriateto delay giving glasses and recheck RElater in these children.”
Schein Y, Yu Y, Ying G, et al. Emmetropization during earlychildhood. Ophthalmology. November 29, 2021. [Epubahead of print].
Rethink Glasses in Infants with Astigmatism, Hyperopia
news reviewClinical, legislative and practice development updates for ODs.
Red-light Therapy for Myopia CONTROL, p. 4 >> Wet AMD Patients skipping Treatment Lost VA, p. 6 >> Evidence FOR Vascular Hypothesis For GlaucomA , p. 8
Get the latest atwww.reviewofoptometry.com/news
Stories post every weekday
Most of these eyes emmetropized to a greater degree than eyes with myopia.
Photo: Getty Images
Delaying giving glasses prescriptionsto infants may result in better visualoutcomes, this study found.
IN BRIEFPostmarketing reports of adverseevents such as retinal vasculitis(RV) and retinal occlusive vasculitis(RO) with brolucizumab (Beovu) usetriggered an investigation by Novar-tis and an external safety commit-tee, which concluded that patients
receiving brolucizumab injectionsmay be at increased risk for RVand/or RO, usually accompanied byintraocular inflammation (IOI).
More recently, a research teamlooking at two large databasesof patients with wet AMD (21,815eyes total) who received at leastone brolucizumab injection found
the incidence rate of IOI and/orRO to be about 2.4%, as was theincidence of RV and/or RO (0.6%). The researchers identified the fol-lowing two risk factors: a history ofIOI and/or RO occurring within theprevious year and female gender(although the latter was much lesssignificant).
Due to study limitations, brolu-cizumab cannot be tied directly tothese inflammatory events, the au-thors note. More controlled studies will help better determine causality.Khanani AM, Zarbin MA, Barakat MR, et al. Safetyoutcomes of brolucizumab in neovascular age-relatedmacular degeneration: results from the IRIS registryand Komodo Healthcare Map. JAMA Ophthalmol.November 24, 2021. [Epub ahead of print].
Improvement (% patients)
Large Moderate Small
High astigmatism 48% 29% 23%
Moderate astigmatism 30% 23% 47%
High hyperopia 19% 24% 57%
Moderate hyperopia 27% 25% 48%
Moderate/high myopia 5% 27% 68%

REVIEW OF OPTOMETRY | JANUARY 15, 20224
NEWS REVIEW | Get the latest at www.reviewofoptometry.com/news
Researchers recently testeda new strategy for myopiacontrol in children calledlow-level red-light therapy,
abbreviated as RLRL, with encourag-ing results. The approach involvesdelivering light to the retina directly,repeatedly, for a short duration. Brightlight exposure outdoors has beendemonstrated to be protective againstmyopia, but the study authors pointout that certain approaches, such asrenovating classrooms with glass wallsand ceilings, are expensive and notnecessarily practical.
Instead, they used a device thatemits red light at a wavelength of650nm to try to simulate this effect.“It has already been approved andwidely used for amblyopia treat-ment in China,” the authors wrote.Unpublished anecdotal findings haveobserved choroidal thickness, bloodflow and axial elongation stabilizationin children who used the device foramblyopia treatment.
The multicenter, randomized clini-cal trial enrolled 264 children betweenthe ages of eight and 13, 246 of whichwere included in the analysis. All sub-jects had myopia with a cycloplegicspherical equivalent refraction (SER)of -1.0D to -5.0D, astigmatism ≤2.5D,anisometropia ≤1.5D and BCVA≥0.0logMAR (Snellen 1.0 or 20/20).
The researchers assigned childrenrandomly to the intervention group(n=117) to receive RLRL plus single-vision spectacle (SVS) or to the controlgroup (n=129) to receive SVS only.RLR treatment was done with a desk-top light therapy device that emittedred light at a wavelength of 650nm,1,600lux and 0.29mW for a 4mmpupil. The test sessions lasted threeminutes and were done twice daily ata minimum interval of four hours, fivedays per week.
Here are some of the study’sfindings:
• The adjusted 12-month axialelongation and SER progression were0.13mm and -0.20D for the RLRLgroup and 0.38mm and -0.79D for theSVS group, respectively.
• The difference between groups inaxial elongation and SER progressionwas 0.26mm and -0.59D, respectively.
• The researchers reported nosevere adverse events, functionalvisual loss (by BCVA) or structuraldamage (observed on OCT).
“Orthokeratology, speciallydesigned spectacles and atropine eyedrops are the most common opticaland pharmacological interventionsfor myopia control,” the researcherswrote. Though studies show thesemethods achieve between 30% and59% efficacy in myopia control,ortho-K has a “small but significantrisk of developing sight-threateningcorneal infection, and compliancewith wearing a tight contact lensevery night can be challenging.”Additionally, they noted that atropine,used at 0.01% to 0.05% concentration,has a 50% efficacy in myopia control.
“In addition to orthokeratology andatropine eye drops, two recent innova-tively designed lenses which imposemyopic defocus on the retina, the De-focus Incorporated Multiple Segment(DIMS) lens and Highly AsphericalLenslet Target (HALT) lens, haveshown strong myopia-controllingeffects of 52% and reduced axial elon-gation by 62% when compared overtwo years with SVS. A further reporthas shown that this myopia controleffect is sustained in the third year.While study design differences makedirect comparison difficult, the RLRLefficacy results reported here appearat least competitive with these othertreatment modalities,” the team said.
“In our study, we demonstrate thatRLRL treatment was able to achievegreater than 0.05mm axial length short-ening in 70.1% of participants at one
month and 31.6% at 12 months,” theycontinued. They also found choroidalthickness changes at two of their studysites and increasing thickness by anaverage of 16.1µm at the one-monthfollow-up visit.
“Axial shortening was measured as-0.04mm at this visit; axial shorteningtherefore cannot be fully explainedby choroidal thickening either,” theywrote. “As recent evidence confirmsscleral hypoxia as a promoter for scleralremodeling and myopia development,we hypothesized that the RLRLtreatment increases blood flow andmetabolism of the fundus, thus ame-liorating scleral hypoxia and restorationof scleral collagen levels.”
They noted that treatment efficacyincreased with improved treatmentcompliance. “This strong dose-response effect may imply that anextension of the treatment durationfrom three minutes to a longer treat-ment time per session may result inimproved treatment efficacy.” Theauthors concluded that RLRL is apromising new alternative treatmentfor myopia control, but advocated forfurther research using with double-masked, placebo-controlled designs.
Jiang Y, Zhu Z, Tan X, et al. Effect of repeated low-levelred-light therapy in myopia control in children: a multicenterrandomized controlled trial. Ophthalmology. December 1,2021. [Epub ahead of print].
Red-light Therapy Promising for Myopia ControlThe treatment was well-accepted and kids demonstrated no functional or structural damage.
Photo: Getty Images
Over two-thirds of the myopic childrenachieved a 0.05mm axial length shorteningthrough red-light therapy.

Lenstar MyopiaTrack myopia. Educate. Monitor your treatment plan.
For myopia management,Lenstar Myopia is head of the class.
lenstarmyopia.com© 2022 Haag-Streit USA. All Rights Reserved.
When myopia is undiagnosed or untreated it can lead to more serious issues. With the Lenstar Myopia from Haag-Streit, featuring EyeSuite™ Myopia software, you can accurately measure axial length, and track the progression of myopia in young patients. The measurements you take now can make a big impact later.
• Developed in conjunction with leading myopia experts.
• Track precise axial length measurements for early detection of myopia onset,using growth curves from myopia experts.
• State-of-the-art graphical visualizations and printable report for easyeducation.

6 REVIEW OF OPTOMETRY | JANUARY 15, 2022
As COVID-19 continues tohave rippling effects acrossthe globe, researchers look for
clues on how eye care was impactedduring the lockdown and ways toapply lessons learned two years intothe pandemic. Two recent studiespublished in Retina considered howCOVID has impacted the continuityof care for wet AMD patients, withone international study citing notablevision loss based on fewer anti-VEGFtreatments and the other suggestingthe effectiveness of an “injection-only”approach.
The first investigation consideredthe lockdown’s impact on about 5,800eyes of 4,700 individuals who hadeither wet AMD, DME or RVO andresided in either Australia, France,Ireland, Italy, the Netherlands, NewZealand, Spain or Switzerland.1 Allparticipants received anti-VEGFinjections prior, during and after the na-tional lockdown. The baseline visit wasdefined as the last visit within threemonths prior to lockdown, and pre- andpost-lockdown periods were six monthsbefore and after lockdown.
The researchers found eyes withwet AMD (n=4,649) lost vision in allcountries in proportion to the reducednumber of injections. VA changepost-lockdown ranged from -0.4 to -3.8logMAR letters, while the number ofinjections/visits decreased from 4-5/4-7to 2-4/2-4 post-lockdown. Vision lossoccurred even after the condition hadbeen prioritized in all the national andinternational clinical guidelines, theauthors noted.
Clinical outcomes in DME and RVOeyes were slightly different, as intravit-real injections for both were deferredin favor of wet AMD patients in all theparticipating countries. Specifically,the VA change in DME (n=654) andRVO (n=479) eyes ranged from -2.8
to +1.7 letters and -1.6 to +0.1 letters,respectively. Additionally, the numberof injections/visits decreased from 2.5-5/4-6 to 1-3/2-4 in DME eyes and from3-5.5/4-5 to 1-3.5/2-3.5 in RVO eyes.
In general, countries that only missedone injection (Australia, France and theNetherlands) had better outcomes (VAloss of less than one letter) comparedwith those that reduced their treatmentrate by two injections (Ireland, Italy,Spain), with the exception of NewZealand, which had one or fewer letterslost and two fewer injections.
Six months into lockdown, RVOpatients had the highest treatmentdropout rate at 28%, followed by 27%for individuals with DME and 20%for wet AMD patients. These findingsmay help clinicians prepare strate-gies to mitigate vision loss in futurepandemics, the investigators suggested.“It appears appropriate to prioritizeintravitreal therapy for eyes with wetAMD in this scenario,” they wrote.
The second investigation foundpatients who temporarily stoppedintravitreal injections during thelockdown showed increased exudativeactivity with worsened visual andanatomical parameters compared withpatients who pursued an “injection-only” treatment approach, where
exams and OCT were omittedbut therapy was given.2 Whileanatomical parameters recoveredto pre-lockdown values, visualfunction did not recover entirely inpatients who delayed treatment.
This study was a retrospectivereview of 314 patients (394 eyes)who were scheduled to receiveinjections during the Swiss lock-down between March 17 and April27 of 2020. Researchers comparedoutcomes of 215 individuals whocontinued to receive scheduledanti-VEGF treatment without clini-
cal consultation and 179 patients whocompletely deferred treatment.
Not surprisingly, the baseline andpost-lockdown VA were about the samein those who continued treatment.On the other hand, participants whodeferred treatment had a significantdeterioration in their vision comparedwith baseline. Although these patients’VA improved slightly after injectionsresumed, it didn’t reach baseline levels.
The findings suggest that visual ben-efits of therapy may be lost if regulardosing is not maintained, showing nodifference in relation to the type ofanti-VEGF agent in use, the research-ers suggested. Furthermore, treatmentduring a lockdown was a never-before-seen unique scenario that could reoccurin the future, they added.
“Our experience denotes the fea-sibility of an ‘injection-only’ manage-ment plan for implementation in futurepandemics, especially in a cohort ofpatients following an observe-and-planregimen,” the researchers concluded.
1. Zarranz-Ventura J, Nguyen V, Creuzot-Garcher C, et al.International impact of the COVID-19 pandemic lockdownon intravitreal therapy outcomes: Fight Retinal Blindnessregistry. Retina. December 1, 2021. [Epub ahead of print].2. Montesel A, Gigon A, Giacuzzo C, et al. Treatmentdeferral during COVID-19 lockdown: functional andanatomical impact on neovascular age-related maculardegeneration patients. Retina. December 2, 2021. [Epubahead of print].
NEWS REVIEW | Get the latest at www.reviewofoptometry.com/news
Wet AMD Patients Who Skipped Treatment Lost VAThose who deferred injections during lockdowns lost up to 3.8 letters in one study, whilea second found those who delayed therapy showed increased exudative activity.
Photo: Leonid Skorin Jr., DO, OD, MS
Lockdowns have caused many wet AMD patientsto miss or skip anti-VEGF injections, which hasresulted in negative visual outcomes.
6
The Vantage BIO is great for ROP screening! It’s lightweight, has settings for different pupil sizes, a cool, white LED light and the longest battery ever!!”
I’m a big fan of the All Pupil BIO. I had issues with other models so when I started [my practice], I knew the All Pupil would be my go-to BIO...I greatly appreciate the new custom fit Keeler BIO shields as an added safety layer.”
I chose my [Vantage Plus] for the optics and value...with other brands, I had difficulty focusing up close during my dilated fundus exams. [The oculars] made my eyes feel more relaxed, and I felt like my view was better.”
[I’ve] been seeing emergent and urgent cases every day during the COVID19 pandemic. I really like [the Vantage BIO] because [it’s a] very good quality and provides a super clear view.”
Dra. Paulina Ramirez Neria
Dr. Annie BaconDr. Michelle Hammond Dr. Reza Moradi
Helping Heroes See Clear And Stay Safe
A world without vision loss
www.keelerusa.com • 3222 Phoenixville Pike - Bldg. #50 • Malvern, PA 19355Tel No: 1-610-353-4350 • Toll Free: 1-800-523-5620 • Fax: 1-610-353-7814
Choose option #1 or #2 below when you purchase (or lease) a BIO*(Expires March 31, 2022)
Contact us at 800-523-5620 or [email protected] to learn more or place your order. This promo cannot be combined with any other Keeler offers.
RECEIVE A 24-MONTH RECEIVE
lease as low as $128/month*bottles of phenylephrine
2.5%, 15mLcredit towards any PPE
$850 0% 10 FREE
*Valid for wireless indirects: Vantage Plus and/or All Pupil II
*All Pupil II: $127.92/month; Vantage Plus: $155/month (shipping and taxes not included).
*If you lease the BIO, you may also choose the PPE credit OR the phenylephrine option.
NEWS REVIEW | Get the latest at www.reviewofoptometry.com/news
While intraocular pressure(IOP) is the driving forcebehind glaucomatous optic
neuropathy (GON), those with low-tension glaucoma (LTG) don’t presentwith elevated pressures. Researcherssay there are other variables at playthat can cause cellular injury in theinitiation and/or progression of GONbesides IOP.
“Genetic predisposition, inflamma-tory and immune responses, structuraland mechanical stress, mitochondrialdysfunction, oxidative stress and vas-cular dysfunction may modulate thepressure-associated perceived stress ofthe retinal ganglion cell or may evenact in an IOP-independent mecha-nism,” the researchers explained intheir paper.
Their study reported that multiplesystemic, vascular-associated condi-tions are associated with LTG, includ-ing systemic hypertension and hypo-tension, diabetes, migraine headache,peripheral vascular disease, Raynaud’ssyndrome and anemia. “This studystrengthens evidence for the vascularhypothesis of LTG,” they noted.
They conducted a retrospectivecase-control study to identify patientsseen at the Mayo Clinic Departmentof Ophthalmology for LTG between2005 and 2015 (n=277). An age- andsex-matched control group was alsoincluded (n=277). Researchers select-ed patients with LTG because “GONis likely a multifactorial disease witha number of systemic risk factorsincluding those that may affect a pa-tient’s hemodynamics and ultimatelytheir ocular perfusion pressure.”
They reported that the LTG grouphad more myopic refractive errors(-1.6D vs. -1D), lower IOP (14.2mmHg vs. 15.2mm Hg) and a highercup-to-disc ratio (0.7 vs. 0.3) than thecontrol group. They also noted thatthe LTG group was less likely to beobese (BMI >30).
Additionally, the low tensionglaucoma group had a higher preva-lence of certain systemic conditions,including hypertension, diabetes,peripheral vascular disease, migraineheadache, anemia, systemic hypoten-sion, Raynaud’s syndrome, angioten-sin-converting enzyme inhibitor andcalcium channel blocker use. Theresearchers reported no significantdifferences regarding hyperlipidemia,obstructive sleep apnea (OSA), coro-nary artery disease, carotid stenosis,stroke, statin, ACE inhibitor, angio-tensin receptor blocker, beta blockeror metformin use.
The researchers say that accordingto the vascular hypothesis, sys-temic vascular dysregulation “mayplay a more prominent role in LTGcompared with other types of open-angle GON.” Patients with high orlow blood pressure, anemia, cardiacdisease or stroke are more likely toexperience lower-end organ perfusionand systemic vascular dysregulation,they said.
“From a blood pressure standpoint,our study supports the parabolicnature of risk with both systemichypertension and hypotension beingrisk factors for LTG,” they wrote.“Coronary artery disease and strokehave been reported to have an as-sociation with glaucoma; however, our
study did not find an association witheither condition.”
The significant associations be-tween LTG and Raynaud’s syndromeand between LTG and migraine inthe study also support the idea ofreduced perfusion as a factor in GON,the researchers explained. Raynaud’ssyndrome is caused by peripheralvasospasm, leading to dysregulationof peripheral perfusion. “It’s beensuggested to be an independent riskfactor for LTG.”
They wrote that systemic inflam-mation and metabolic stress (e.g.,diabetes, obesity and OSA) maydisrupt axonal transport and lead toretinal ganglion cell death. Whilethey noted that diabetes and othercauses of metabolic stress may havemultiple mechanisms contributing toretinal damage, overall, they said thatdiabetic patients have demonstratedhigher rates of LTG prevalence andglaucoma progression. “Our datashow that LTG patients were morelikely to have diabetes, supportingthe hypothesis for diabetes being arisk factor for LTG.”
Overall, the researchers say theirstudy supports the vascular hypoth-esis for glaucomatous neuropathy.
Funk RO, Hodge DO, Kohli D, et al. Multiple systemic vascu-lar risk factors are associated with low tension glaucoma. JGlaucoma. November 3, 2021. [Epub ahead of print].
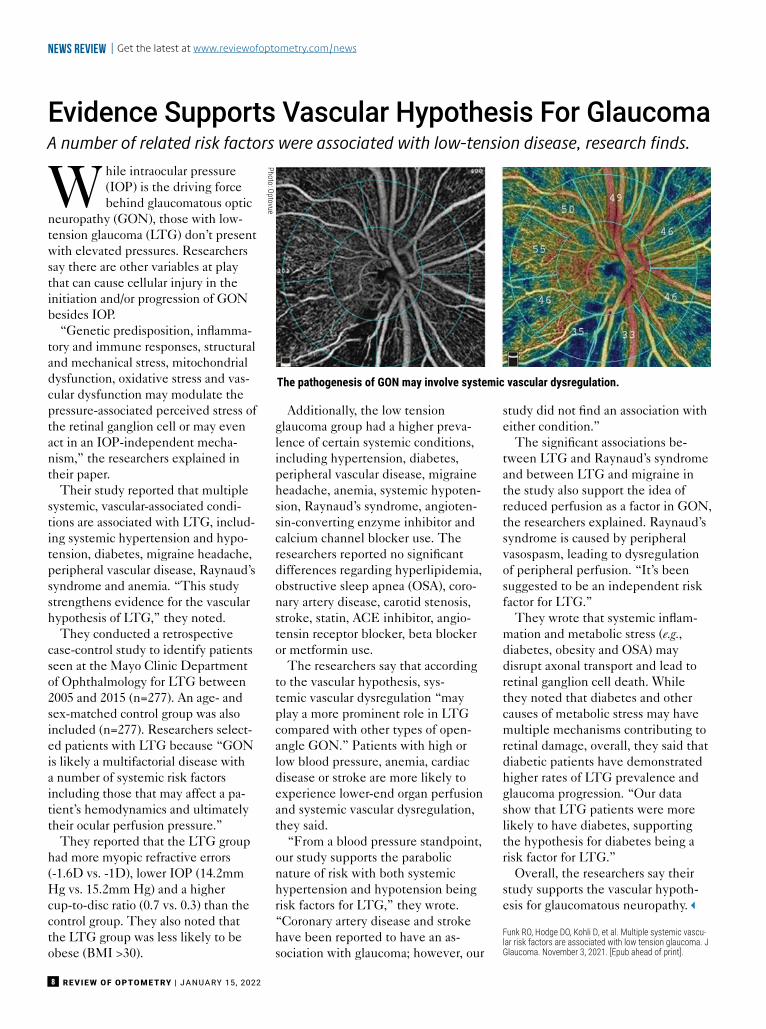
Evidence Supports Vascular Hypothesis For GlaucomaA number of related risk factors were associated with low-tension disease, research finds.
Photo: Optovue
The pathogenesis of GON may involve systemic vascular dysregulation.
REVIEW OF OPTOMETRY | JANUARY 15, 20228
Need Ocular Surface Repair?*
©2021 Akorn Pharmaceuticals JA022 Rev. 11/2021 1925 West Field Court, Suite 300, Lake Forest, IL 60045
*AcellFX is an HCT/P (human cells, tissues, and cellular and tissue-based product) that is intended for homologous use, providing protection or covering in ocular surface repair.
Learn more at AcellFX.com
ACELLFXAcellular Amniotic MembraneACELLFXAcellular Amniotic Membrane
Amniotic membrane enlarged and darkened
to show detail
Amnioticenlarged
to
• Air-dried, not chemically dried
• Ready for immediate use without thawing or rinsing
• Flexible membrane with no ring required
• Convenient storage at room temperature
We’ve Got You Covered!

Our full-service, dedicated team is here to assist you and your staff with all your REFRESH® needs.
©2021 AbbVie. All rights reserved. All trademarks are the property of their respective owners. REF138377 07/20
DISCOVER EXCLUSIVE ACCESS TO ALL THINGS REFRESH®.
Call us and see how REFRESH® Concierge can help you bring relief to your patients.
833-REF-SMPL 7:30 a.m.–7 p.m. CT, M–F
REFRESH®
SAMPLESPATIENT
COUPONSPRODUCT
EDUCATIONREFRESH® DIRECT
ECOMMERCE
OPEN YOUR EYES TO
creo

JANUARY 15, 2022 | REVIEW OF OPTOMETRY 11
REVIEW OF OPTOMETRY • Vol. 159, No. 1 • JANUARY 15, 2022
48How to Offer Inclusive Care for LGBTQ+ Patients
Recognize inherent biases in practices and implement more supportive behavior to interact with members of this communityrespectfully. By Matthew J. Roberts, OD, and Paula McDowell, OD
22The Role of Race and Ethnicity in Optometry
Biologic factors combined with social customs create distinct patterns in how eye diseases manifest. Though not foolproof,these give us at least a sense of a patient’s elevated risk for certain conditions. By Brian Chou, OD
42Evaluating Patients with Neurodevelopmental Conditions
Learn how to modify your practice and clinical approach to best manage this population. By Catherine Heyman, OD
60Tackling the “Myopiaor Glaucoma?”Question
As the prevalence of both increase, ODs will be on the frontlines, relying on a growing set of tools to aid proper diagnosisand management. By Andrew Rouse, Tej Ramdass, LaurenSabol, Anupam Laul, OD, and Richard Madonna, OD
REVIEW OF OPTOMETRY • Vol. 159, No. 1 • JANUARY 15, 2022
36Breaking Down Barriers: The Black Experience in Optometry
How to establish trust and provide effective communication to create a stronger connectionbetween optometrists and the Black community. By Essence Johnson, OD
28Connecting Across Cultures: How to Reach Out to HispanicsThis burgeoning group offers an ideal example of the need to develop “cultural competence” in the clinic.
Other distinct communities are profi led here as well. By Hector C. Santiago, OD
56Making Your Practice Kid-Friendly
How to simplify exams and make them fun while minimizing stress for you, the pediatric patients and their parents. By Sarah Galt, OD
features
6610 Questions on DigitalDevices and Eye Health—Answered!
With screen time rising in children and adults, ODs mustunderstand the potential ocular impact. By Lisa Ostrin, OD, PhD
EARN 2 CE CREDITS
REVIEW OF OPTOMETRY | JANUARY 15, 202212
departments3NEWS REVIEWClinical, legislative and practice development updates.
16THROUGH MY EYESNew BeginningsStart preparing for the therapeutics potentiallycoming this year.
Paul M. Karpecki, OD
REVIEW OF OPTOMETRY • JANUARY 15, 2022
18CHAIRSIDETime to Go DeepReady to uncover what’s lurking beneath thesurface?Montgomery Vickers, OD
74CORNEA AND CONTACT LENS Q+AKCN Again?Keratoconus development post-cornealtransplantation may be harder to explain, buttimely detection and treatment is the best courseof action for successful visual outcomes.
Joseph P. Shovlin, OD
We Welcome Your CommentsFeedback from the community provides important insights about clinical practice. If you
would like to share your thoughts on the topics discussed in this issue—or the wider field of optometry at large—please write to: [email protected]
14OUTLOOKThis Time, It’s PersonalA look at the many ways your patient’s lifeexperiences matter inside the clinic, too.
Jack Persico, Editor-in-Chief
20CLINICAL QUANDARIESShingle RepairChronic, debilitating pain following herpes zostermust be managed promptly.
Paul C. Ajamian, OD
76URGENT CARENot the Usual SuspectUnilateral proptosis, pain and decreased vision led toan uncommon diagnosis.Alison Bozung, OD
82DIAGNOSTIC QUIZKnow When to Fold ’emDo the findings here provide a definitive diagnosis,or merely a clue to the full story?
Andrew S. Gurwood, OD, Michael Rebar, OD
78THE ESSENTIALSIn The NOFind out how nitric oxide plays a role in thetreatment of POAG by boosting the efficacy ofprostaglandin analogs.
Bisant A. Labib, OD
Facebook: www.facebook.com/revoptomTwitter: twitter.com/revoptom
Instagram: www.instagram.com/revoptomVISIT US ON SOCIAL MEDIA
BRING BETTER BALANCE.Refract safely from across the room or across the Internet with the most advanced Phoroptor®, Phoroptor® VRx, and the
pixel-perfect ClearChart® 4 Digital Acuity System. Multitasker Lisa Genovese, OD, has brought balance to her practice andpersonal life all while managing Insight Eye Care’s multiple locations. She e� ciently juggles being a full-time optometrist,
a full-time entrepreneur, and a full-time parent with the help of Reichert’s complete line of digital refraction devices.
· © 2021 AMETEK, Inc. & Reichert, Inc. (08-2021) · Phoroptor and ClearChart are registered trademarks of Reichert, Inc. · Phoroptor and ClearChart are designed & assembled in USA.
LEARN
MORE
REICHERT.COM/VRXWATCH THE VIDEOS AT
BRING BETTER BALANCE.Refract safely safely from from across across the the room room or or across across across the the Internet Internet with with the the most most advanced advanced Phoroptor®, Phoroptor®, Phoroptor® Phoroptor® VRx, VRx, and and the the
pixel-perfect ClearChart® ClearChart® 4 4 Digital Digital Acuity Acuity System. System. Multitasker Multitasker Lisa Lisa Lisa Genovese, Genovese, OD, OD, has has brought brought balance balance to to her her practice practice practice and andpersonal life life all all while while managing managing Insight Insight Eye Eye Care’s Care’s multiple multiple locations. locations. She She e� e� ciently ciently ciently e� ciently e� juggles juggles being being a a full-time full-time optometrist, optometrist,
a full-time full-time entrepreneur, entrepreneur, and and a a full-time full-time parent parent with with the the help help of of Reichert’s Reichert’s complete complete line line of of digital digital refraction refraction devices. devices.
· · © © 2021 2021 AMETEK, AMETEK, Inc. Inc. & & Reichert, Reichert, Inc. Inc. (08-2021) (08-2021) · · Phoroptor Phoroptor and and ClearChart ClearChart are are registered registered trademarks trademarks of of Reichert, Reichert, Inc. Inc. · · Phoroptor Phoroptor and and ClearChart ClearChart are are designed designed & & assembled assembled in in USA. USA.
LEARN
MORE
REICHERT.COM/VRXWATCH THE THE VIDEOS VIDEOS AT AT
creo

REVIEW OF OPTOMETRY | JANUARY 15, 202214
Founded 1891Founding Editor, Frederick Boger
EDITOR-IN-CHIEFJACK PERSICO
(610) 492-1006 • [email protected]
SENIOR EDITORJULIE SHANNON
(610) 492-1005 • [email protected]
SENIOR ASSOCIATE EDITORCATHERINE MANTHORP
(610) 492-1043 • [email protected]
SENIOR ASSOCIATE EDITORMARK DE LEON
(610) 492-1021 • [email protected]
ASSOCIATE EDITORLEANNE SPIEGLE
(610) 492-1026 • [email protected]
SPECIAL PROJECTS MANAGERJILL GALLAGHER
(610) 492-1037 • [email protected]
SENIOR ART DIRECTORJARED ARAUJO
(610) 492-1032 • [email protected]
DIRECTOR OF CE ADMINISTRATIONREGINA COMBS
(212) 274-7160 • [email protected]
Clinical Editors
Chief Clinical Editor • Paul M. Karpecki, OD
Associate Clinical EditorsJoseph P. Shovlin, OD, Christine W. Sindt, OD
Clinical & Education Conference AdvisorPaul M. Karpecki, OD
Case Reports Coordinator • Andrew S. Gurwood, OD
Clinical Coding Editor • John Rumpakis, OD, MBA
Columnists
Chairside – Montgomery Vickers, OD
Clinical Quandaries – Paul C. Ajamian, OD
Cornea and Contact Lens Q+A – Joseph P. Shovlin, OD
Diagnostic Quiz – Andrew S. Gurwood, OD
The Essentials – Bisant A. Labib, OD
Focus on Refraction – Marc Taub, OD, Paul Harris, OD
Glaucoma Grand Rounds – James L. Fanelli, OD
Ocular Surface Review – Paul M. Karpecki, OD
Retina Quiz – Mark T. Dunbar, OD
Surgical Minute – Derek Cunningham, OD, Walter Whitley, OD
Therapeutic Review – Joseph W. Sowka, OD
Through My Eyes – Paul M. Karpecki, OD
Urgent Care – Alison Bozung, OD
Editorial Offices
19 Campus Blvd., Suite 101• Newtown Square, PA 19073
Jobson Medical Information/WebMD395 Hudson Street, 3rd Floor, New York, NY 10014
Subscription inquiries: (877) 529-1746Continuing Education inquiries: (800) 825-4696
Printed in USA
By Jack PersicoEditor-in-Chief
OUTLOOK
We always aim to ensure that thescientific merit of the clinicalguidance we publish shinesthrough. Articles often give
diagnostic or treatment advice in a waythat’s so evidence-based it almost, in away, makes the patient irrelevant. Howthey feel, speak or act doesn’t factorinto your clinical assessment, right?
Wrong. Patients are more than just asa set of eyes to be examined, of course;they’re complex, unique people withpersonalities and values shaped bytheir lives, families and peers.
This month, we’re bringing the indi-vidual into the equation with a series ofarticles that explores how race, ethnic-ity, culture, sexual orientation and othermarkers of identity can manifest in theexam room. Why, you may ask? To fillin an important part of the puzzle that’soften ignored, to the detriment of thedoctor-patient relationship and possiblythe outcomes of the care provided.
At last fall’s Academy of Optometryannual meeting, guest speaker BeverlyDaniel Tatum, PhD, a psychologistwho studies cross-racial dynamics, dis-cussed an exercise she uses to uncoverdeep-seated feelings of marginalization.If you ask a group of people to describethemselves as many ways as possiblein 15 seconds, you’ll get a lot of resultsabout jobs, hobbies, family responsi-bilities and so on—what they do. Butpeople whose race, ethnicity, religion,gender or orientation differs from thebroader society will write down thosecharacteristics, too—what they are.
“If you are seen as outside the norm,people remind you of that and youhave it as part of your social under-standing of the world and so it becomessalient for you,” Dr. Tatum explained.
Recognizing these experiences and thefeelings of discrimination or alienationthat often accompany them is the firststep toward building a stronger rapportwith people of different backgrounds.
However, it’s important to avoidconceiving of a person from a differ-ent walk of life as some exotic “other”to be studied like a rare plant or bird.Striking the right balance can be tricky:we should aim to recognize individualdistinctions and understand their im-plications, but then pivot to findingcommon ground. Hopefully, a con-certed effort might eventually reducedisparities in health care among variousgroups (along with lowering tensions).
In our corner of the world, a recentstudy in the Ophthalmology journalfound that the normative databases ofOCT devices are largely comprisedof data from Caucasian individuals,leading to false readings of possibleglaucomatous damage in some Asianpatients, who can have thinner-than-average RNFLs. That’s one small wayeye care is engineered for the past—when US demographics were more ho-mogenous—instead of the present andfuture. Deeming one group “normal”skews the delivery of care toward theirneeds (and away from that of others).
Unfortunately, some of these topicshave become politicized, creating fric-tion over pronoun use, racial repre-sentation and other hot-button issues.Consider: aside from the social benefitsof striving for greater inclusivity, there’svaluable data to be gleaned from seeingall facets of your patient. You wouldn’tdo an eye exam and fail to look at theretina. Bring that same inquisitivenessand attention to the rest of the personto get the complete picture. g
A look at the many ways your patient’s life experiencesmatter inside the clinic, too.
This Time, It’s Personal

®2021 Menicon Co. Ltd. See instructions for use in the Package Insert. US-MI053
A new generation of silicone hydrogel material balanced for health and comfort incorporating a unique combination of high oxygen and ultra low modulus.
Miru 1day UpSide contact lenses are always the right way up and ready to wear, thanks to Smart Touch™ technology.
Miru 1day UpSideIntroducing,
silicone hydrogel contact lenses with Smart Touch™ technology.
www.meniconamerica.com
Find us on:
7 th1951- 2021anniversary7
creo

16 REVIEW OF OPTOMETRY | JANUARY 15, 2022
There is something special aboutbeginnings. It’s an opportunityto start again, learn from the pastand anticipate and even accelerate
the future. If you position your practicenow for what is likely to come, you canthrive in the new year. Fortunately,there are numerous exciting innova-tions we can anticipate in 2022 that willallow us to do exactly that.
Prepare for PresbyopiaWith Vuity (Allergan) recently hittingthe market—the first FDA-approvedeye drop to treat presbyopia—andanother low-dose pilocarpine that ispreservative-free potentially com-ing in 2022, we have to anticipate thepresbyopia opportunity, especially sincethere are about 32 million patients whohave never seen an optometrist and usereading glasses.1
The first visit requires a comprehen-sive eye exam, binocular vision testing,a dilated fundus evaluation, assessmentof chronic inflammation and advancedpupil testing.
The opportunity is more than just anew therapeutic for reading via pupilconstriction, it’s also about educat-ing patients about PALs, presbyopiccontact lenses and, in some cases, light-adjusting or multifocal IOLs.
Dilating Drops ReplacementA new microdose (8µL) dispenserknown as MydCombi (Eyenovia) maybecome available this year. Comparedwith three drops at 30µL to 50µL each(topical anesthetic, phenylephrine andtropicamide), the option of deliveringa dilating agent through an easy-to-use
dispenser seems appealing for doctors(cost-saving and quicker administra-tion) and patients (minimal burning,reduced tearing, less makeup smearingand only one application). It may alsoincrease efficiency and possibly reducethe duration of dilation after the exam.
MGD/DED Lipid Solubilizing AgentThere is also a good chance we will seea new therapeutic from Bausch + Lombthat can solubilize thickened meibum.It’s the first dry eye drug in the UnitedStates that achieved a statistically sig-nificant improvement in pre-specifiedsigns and symptoms in only two phaseIII clinical trials. If you consider thefact that 86% of all DED involvesMGD, having a drop that could liquifyhardened meibum would be a valuableaddition.
With the recent approval of Tyrvaya(Oyster Point) and availability of Para-sym Plus Eyes (TJ Nutrition), we cantackle the neurological component ofDED. Likewise, the use of these neu-rological agents results in stimulation ofmeibum, mucin and aqueous.
Taming DemodexThe first drug for Demodex blephari-tis, TP-03 (Tarsus Pharmaceuticals),
achieved positive results in trials andmay be approved this year. Cur-rently, mechanical blepharoexfolia-tion (Blephex, Alcon) and a Manukahoney extract/coconut oil cleanser(MyboClean) coupled with a uniquesilicone brush is showing success inmanaging Demodex.
It has been shown that 58% of allpatients observed in an optometricoffice show the presence of collarettes(clear sleeves at the base of the lashesthat are pathognomonic for Demodex).It’s time to begin the new year byhaving patients look down while atthe slit lamp and scanning across thebase of the lashes.
Dry Macular DegenerationAn exciting potential injection totreat dry AMD, which constitutes90% of all cases in the United States,may see approval. The drug, fromApellis, works on the complementsystem and was shown to reduce thesize of geographic atrophy in patientswith dry AMD. But even patientswith wet AMD may see a significantadvancement with Susvimo (Genen-tech), which was FDA-approved afew months ago. It’s a port system fordelivering anti-VEGF into the vitre-ous to alleviate the need for frequentinjections and office visits. I suggeststarting to educate your dry AMDpatients now about a potential treat-ment that may be available soon.
The inevitable future can some-times be slowed but, as it’s beensaid, what you resist, persists. So, inthe best interest of patients and yourpractice, the most prudent thing youcan do is prepare and accelerate toensure you thrive as each key devel-opment comes to fruition. ■
1. Heath DA, Spangler JS, Wingert TA, et al. 2017 nationaloptometry workforce survey. Accessed December 20,2021.
Start preparing for the therapeutics potentially coming this year.New Beginnings
Dr. Karpecki is the director of Cornea and External Disease for Kentucky Eye Institute, associate professor at KYCO and medical director for Keplr Vision and theDry Eye Institutes of Kentucky and Indiana. He is also chair of the New Technologies & Treatments conferences. He consults for a wide array of ophthalmic clients,including ones discussed in this article. Dr. Karpecki’s full disclosure list can be found in the online version of this article at www.reviewofoptometry.com.
AboutDr. Karpecki
By Paul M. Karpecki, ODChief Clinical Editor
Through my eyes
In the interest of patients andyour practice, the most prudentthing you can do is prepare andaccelerate to ensure you thriveas each key development comesto fruition.
2021. MacuLogix, Inc. All rights reserved. MM-658
By combining structural and functional assessments, optometry has conquered glaucoma. It’s time to do the same for AMD!
Your optometric peers are implementing the AdaptDx Pro® guided by Theia™, as the functional complement to structural imaging to better detect and monitor AMD. Discover how our AMD Excellence Program® empowers you to change the future of AMD care for your patients and your practice.
THE FUTUREOF AMD CARESTARTS NOW
GET THE LATEST MUST-HAVE AMD RESOURCE:
19 of your peers share their experiences in making
dark adaptation testing a reality in their offices. maculogix.com/ebook

REVIEW OF OPTOMETRY | JANUARY 15, 202218
Doctors, it’s time to take a mo-ment for introspection. No, thisis not a column about colonos-copies (again). Google “intro-
spection.” It’s way different. Now,let’s all take a deep cleansing breathand be honest with ourselves andeach other. It’s calming, I promise!
1. What’s the first thing that popsinto your head when I say the word“optometry”? Your profession?Your income? Helping people seestuff? Vision plans? Online refrac-tions? (For me? Lunch. I wouldhave turned into a raving loon manyyears ago if it weren’t for my lunchbreaks.)
2. What’s the first thing that popsinto your head when I say the words“contact lenses”? Sclerals? CRT?Overwear? Ulcers? (For me? Lunch,again. That’s when, every day, I tryanother multifocal to see if it worksbetter.)
3. What’s the first thing that popsinto your head when I say the word“family”? Your kids? Your grandkids?Your mom and dad? Too much hub-bub? (For me? Yet again, lunch—youguessed right! It’s the only time afamily member isn’t jabbering in myear.)
4. What’s the first thing that popsinto your head when I say the word“lunch”? Vickers, quit talking aboutlunch? (For me? Uh, I can’t reallythink of anything. Come back to meagain later.)
Okay, you get it. We are a part of ahuge machine involving life in gen-eral. It’s easy to get sucked into theblack hole of activities, products and,
well, lunch. Stuff is constantly pop-ping into our puny minds. Maybe weall need to stop for a second and letourselves breathe. But if we do that,the vast majority of us optometristswill feel, unfortunately, awkward.
You heard me right. Why awk-ward? It’s because we have allowedthe outside world to dominate theinside world. This creates stress andanxiety, and the only way to curestress and anxiety is to look within,but we have all forgotten how to dothat, right?
In the mid-80s (not my mid-80s,the mid-80s!), I had a three-yearbout with anxiety and agoraphobia.Married with two young children, Ionly felt “normal” at the office andat home. In many instances,I could barely leave homeunless I was going towork. The low point waswhen I almost didn’t gowith my wife to seeBarry Manilow inconcert. Now thatI think aboutit, all thingsconsidered, thatmay have been anadvantage, but Barrysurprised me and turnedout to be pretty good afterall.
I finally visited a psy-chiatrist. It reminded me ofthe Soupy Sales show, achildren’s TV show frommy era way back when. Inone scene, this guy comesto Soupy’s front door and
says, “Hey! You gotta help me! Mywife thinks she’s a couch!” Soupyanswers, “Why don’t you take her toa psychiatrist?” The guy responds,“We need the extra furniture whencompany comes over!”
So, I saw the doctor three times.I told him that I was too anxiousto even go to optometry meetingsbecause I was afraid I might passout. He calmly responded, “You’re ina room full of doctors. I think they’llknow what to do.” I thought aboutmy colleagues giving me mouth-to-mouth. This mental image onlymade things worse for me, muchworse.
He gave me a prescription forValium (diazepam, Roche). Therewere no real anxiety meds at thattime. I never took it, but, for somereason, carrying the bottle around inmy pocket seemed to help enoughto make a difference.
We did one session of biofeed-back. I was cured. This taught me
instantly that I had the powerto basically meditate my anxi-ety away. It also made me feel
like a dork for paying thatguy for three vis-its when I hadthe cure insideme the wholetime.
So, what’s thefirst thing thatpops into yourhead when I
say “peace”?Folks, you’ve had the
cure inside you fromthe start. Look within,
breathe and calm yourselfdown. What’s the worst that could
happen? After all, you may needthe extra furniture when companycomes over. g
Ready to uncover what’s lurking beneath the surface?
Time to Go Deep
Dr. Vickers received his optometry degree from the Pennsylvania College of Optometry in 1979 and was clinical director at Vision Associates in St. Albans, WV, for36 years. He is now in private practice in Dallas, where he continues to practice full-scope optometry. He has no financial interests to disclose.
AboutDr. Vickers
By Montgomery Vickers, OD
ChairSide
– Dr. Paul Karpecki, OD, FAAO
F r o m t h e e x p e r t s
Answered by Dr. Paul Karpecki, OD, FAAO
Why encourage patients to follow an eye hygiene regimen?
Increased digital device use caused a dramatic rise in ocular surface disease symptoms in our clinic, making hygiene more important than ever. This comprehensive kit makes it easy to satisfy patient needs at a time they are more motivated to follow a recommended regimen.
to remove build up, oil, dirt, pollen, and debris that may cause eye irritation and infectionpure 0.02% HOCl solution to help reduce bacteria and inflammationto naturally unclog meibomian glands and relieve dry eye symptoms
Wipe
Spray
Warm
Have a question or want to learn more? Give us a call at 888-827-8337 or email [email protected]
©2021 Bruder Healthcare Company Alpharetta, GA 30004
Ready to bring relief to your patients? Visit order.bruder.com.
Whatever treatment strategy you plan for a patient, it should include the Bruder Moist Heat Eye Compress — recommended by more doctors than any other moist heat eye compress — and Bruder Hygienic Eyelid Cleansing products.
and inflammationto naturally unclog meibomian glands and relieve dry eye symptoms
Whatever treatment strategy you plan for a patient, it should Bruder Moist Heat Eye Compress — recommended
by more doctors than any other moist heat eye compress — and

REVIEW OF OPTOMETRY | JANUARY 15, 202220
I have a patient that presentedwith shingles on his left arm and
trunk three months ago. The skin lesionsare resolving, but he is still in severepain. What is his prognosis, and whatcan he do to alleviate the suffering?
With nearly every adult in theUnited States exposed to the
varicella zoster virus (VZV), the samevirus that causes chickenpox, an indi-vidual has about a 30% lifetime risk ofthe virus reactivatingand causing herpeszoster (HZ). Posther-petic neuralgia (PHN)is the most commoncomplication, affecting20% of patients.1-6
PHN, or pain thatpersists at least 90 daysafter the initial rash,can be described assevere burning, electricshock-like sensationsor itching at the site ofthe original rash.1-3
“Many patients willsuffer from a modestamount of pain during the acute phaseonly to be blindsided with excruciatingpain weeks later when physically theyappear to be healing,” says Taia DeL-ano, OD, of Columbia, MO. “Watchyour older patients who have severepain in the acute phase, ophthalmicinvolvement, a more severe eruptionand underlying systemic conditions.”1
Acute TherapiesChronic pain therapy should start withappropriate management of the acute
phase of HZ. If possible, oral antiviralssuch as acyclovir (800mg five timesa day for seven days) or valacyclovir(1g TID for seven days) should beinitiated within the first 72 hours.3,4
While this doesn’t reduce PHN risk,it decreases the time that new lesionsform while speeding up the time to le-sions’ full crusting. It also reduces painduring the initial episode and reducesthe pain’s duration by about 50%.1,3,5
Glucocorticoids,oral analgesics andnonsteroidal anti-inflammatory drugsare often used inconjunction with oralantivirals for patientsin the acute phasewith mild-to-moderatepain.1,3
Dr. DeLano also sug-gests a cool compressto the affected area, asimple yet effectivetherapy that can beimplemented in-officeor at home.
Chronic TherapiesMany times, severe pain will needto be managed with systemic treat-ments by pain management specialists.First-line therapies include antidepres-sants such as amitriptyline (initial doseof 10mg to 25mg orally at bedtime,increased by 10mg to 25mg per weekto a target of 75mg to 150mg daily),and anticonvulsants such as gabapentin(300mg to 600mg three times a day).The latter can reduce pain by almost
half, but the time needed to achievethis makes it less desirable.1,3,4,7
Topically, two options have beenapproved for PHN treatment, althoughevidence to support either is lacking.A 5% lidocaine patch can help withshort-term pain control, and capsaicin0.075% cream has been used but doesnot offer substantial relief for most.1,4,7
Opioids offer good pain relief inPHN; however, due to their commonmisuse, addiction and high side-effectprofile, they are a third-line option.1,4,7
Newer treatments that warrantfurther investigation are more invasive.Botulinum toxin has been shown to of-fer relief for neuropathic pain. Neuro-modulation allows for a more targetedapproach and has shown promise inPHN prevention.2,7
“Prevention is key with HZ andPHN,” Dr. DeLano says. The recom-binant adjuvant Shingrix (GlaxoSmith-Kline) is the two-shot vaccine that ismuch more effective and lasts longerthan the Zostavax shot that is now offthe market. Dr. DeLano says this vac-cine is approved for adults 50 years andolder, even if they have had Zostavax.Its two doses are more than 90% effec-tive at preventing shingles and PHN.Protection stays above 85% for at leastthe first four years after vaccination. g
1. Saguil A, Kane S, Mercado M, Lauters R.Herpes zoster andpostherpetic neuralgia: prevention and management. Am FamPhysician. 2017;96(10):656-63.2. Han R, Guo G, Ni Y, et al. Clinical efficacy of short-term peripheral nerve stimulation in management of facial painassociated with herpes zoster ophthalmicus. Front Neurosci.202;14:574713.3. Tuft S. How to manage herpes zoster ophthalmicus. Com-munity Eye Health. 2020;33(108):71-2.4. Tyring SK.Management of herpes zoster and postherpeticneuralgia. J Am Acad Dermatol. 2007;57(6 suppl):S136-42.5. Singh, Grisuna, et al. Recombinant zoster vaccine (Shingrix):a new option for the prevention of herpes zoster and posther-petic neuralgia. Korean J Pain. 2020;33(3):201-7.6. Ernst E, Fialka V. Ice freezes pain? a review of the clinicaleffectiveness of analgesic cold therapy. J Pain Symptom Man-age. 1994;9(1):56-9.7. Shrestha M, Chen A. Modalities in managing postherpeticneuralgia. Korean J Pain. 2018;31(4):235-243.
Chronic, debilitating pain following herpes zoster must bemanaged promptly.
Shingle Repair
Dr. Ajamian is the center director of Omni Eye Services of Atlanta. He currently serves as general chairman of the education committee for SECO International.He has no financial interests to disclose.
AboutDr. Ajamian
Q
A
Edited by Paul C. Ajamian, OD
CLINICAL QUANDARIES
Even mild zoster lesions, as seenon the forehead, can cause severePHN.
© 2021 Visioneering Technologies, Inc. MKT-NVEM-PA1
Reference: 1. Chang W-H, Liu P-Y, Lin M-h, et al. Applications of hyaluronic acid in ophthalmology and contact lenses. Molecules. 2021;26:2485
Introducing New NaturalVue® (etafilcon A) Enhanced
Multifocal 1 Day™ contact lensesAcuity and comfort—together like never before
See what’s possible at vtivision.com For information about the management of myopia in your practice and how NaturalVue®
Multifocal can help, call 1-844-884-5367, ext.136, or email [email protected]
TripleTear® lubrication system, including hyaluronic acid, hydrates, lubricates, locks-in moisture and maintains a clean surface1
Ultra-Tapered Edge designed for optimal fit and comfort
Redefinethe patient experience
ENHANCEDCOMFORTNO REFIT REQUIRED
ENHANCEDENHANCEDCOMFORT
NEW
creo

22 REVIEW OF OPTOMETRY | JANUARY 15, 2022
The Role of Race and Ethnicityin Optometry
Biologic factors combined with social patterns create distinct patterns in how eye diseases manifest.Though not foolproof, these give us at least a sense of a patient’s elevated risk for certain conditions.
While race and ethnicity are oftenused interchangeably, racehas to do with biological andphysical features which gener-
ally cannot be hidden. Ethnicity refersmore to cultural identification, languageand customs adopted by people from ageographic region. Discussing race andethnicity is fraught these days. Blamesocial media for stoking tribalismwhile amplifying hate and polarization.Profitability for the social media giantslies in optimizing user engagement byappealing to our paleolithic emotions.Users stay glued to these platformswhen triggered into outrage, whichamplifies culture wars. By first recog-nizing that social media latches ontothe attention economy and succeedswhen we are emotionally triggered, wecan purposely begin a reflective, calmand meaningful discussion on the roleof race and ethnicity in eye care.
Knowing a patient’s race and ethnic-ity can help optometrists with diagnosisand treatment when it comes froma place of compassion and empathy.
What follows is a look intohow race and ethnicity factorinto diagnosing and treat-ing select ocular conditions,including glaucoma, macu-lar degeneration, diabeticeye disease, keratoconusand myopic degeneration.Finally, learn what to expectas healthcare moves fromassessing patient race towardindividual genetic make-up.
The Healthcare SystemIn law enforcement, racial andethnic profiling is frownedupon, as it can discriminateagainst a minority population based onnegative stereotypes. By comparison, inhealthcare, physicians use race and eth-nicity to predict disease risk and treat-ment efficacy. Classic medical exam-ples include how cystic fibrosis is morecommon in white patients, specificallythose of Northern European ancestry,and how sickle cell anemia affects pre-dominantly Black people. In eye care,a retinal hemorrhage in a Black patientmay signal sickle cell retinopathy. AnAsian patient who complains of eyeredness after drinking may be experi-
encing conjunctival hyperemia relatedto alcohol flush syndrome, as 60% to80% of East Asians have a reduced abil-ity to metabolize alcohol.1 Despite howrace and ethnicity can help a clinician,doing so comes with certain dangers.
The shortcoming of using race andethnicity to assess health risk is thatit involves stereotyping and applyingpopulational data to an individual. Asclinicians, we must ask ourselves if thisis always valid. Understandably, peopleof color may question race-basedhealthcare, particularly if it could leadto discriminatory care.
PEER REVIEWED
By brian chou, odsan diego
Dr. Chou practices at ReVision Optometry, a referral-based scleral contact lens and keratoconus clinic in San Diego. He authored Practical Spanish in Eyecare and hasserved on the Transitions Optical Diversity Advisory Board for over a decade. He has no financial interests to disclose.
Aboutthe author
Glaucomatous optic nerve with inferior notching.
R A C E, E T H N I C I T Y A N D E Y E D I S E A S EFeature

23JANUARY 15, 2022 | REVIEW OF OPTOMETRY
Indeed, there is evidence that racialand ethnic bias and stereotyping canlead to inequities in quality of care. Forexample, a 2016 study in Proceedings ofthe National Academy of Science investi-gated why Black Americans are system-ically undertreated for pain comparedwith white Americans.2 The researchersfound that half of medical students andresidents surveyed believed that Blackand white people are biologically dif-ferent and that Black people are moretolerant of pain. This assumption wasborn from the slavery era when it wasthought that Black people have thickerskin than white people, according tothe researchers.
Black patients are almost four timesmore likely to suffer from kidney fail-ure than non-Hispanic white patients.3
There is ongoing debate in nephrologyon whether it is appropriate for doctorsto routinely apply a “race correction” totheir formula for the estimated glomer-ular filtration rate (GFR). This “correc-tion” results in Black patients endingup with higher GFR values, suggestingbetter kidney function. In turn, thiscan contribute to worse kidney carefor Black patients. For this reason, agrowing number of medical institutionsare abandoning race adjustment forestimated GFR. Critics say that lowerhealth indicators among Black patientsreflect the experience of being Black.
Finally, the COVID-19 pandemichas exposed differences in access tohealthcare and preventive measures.People of color disproportionately bearthe brunt of COVID-19 illness andmortality. However, Black and Hispanicpeople are not genetically more suscep-tible to coronavirus; rather, it appearsthat external factors hold greater influ-ence.4 People of color commonly livein more crowded situations with lesshealthcare access, and a larger numbertend to work in the food service andtransportation industries where thereis an increased contagion risk, a higherburden of cardiovascular and otherchronic diseases and elevated exposureto stress related to violence and racism,all of which contribute to higher ratesof COVID-19 illness and mortality.5
In 2020, the House Waysand Means Committeerequested input from profes-sional societies in healthcareto re-examine how race ismisused within clinical care.6
In part, this was prompted byan article in the New EnglandJournal of Medicine, whichhighlighted examples of racecorrection used in cardiology,nephrology, obstetrics andurology and considered howthese clinical algorithms canperpetuate or even amplifyrace-based health inequities.7
Let’s now turn towardselect eye conditions and the role raceand ethnicity play in each.
GlaucomaThe world’s leading cause of irrevers-ible vision loss, glaucoma is a group ofeye conditions that cause optic nervedamage, leading to blindness andvisual impairment. Primary open-angleglaucoma shows increased prevalenceand greater clinical severity in popula-tions of African ancestry compared withthose of European or Asian origin. It issix to eight times more likely to causeblindness and 15 times more likelyto cause visual impairment in AfricanAmericans than Caucasians.8,9 Theage-adjusted prevalence of open-angleglaucoma among African American resi-dents of Baltimore receiving Medicareis 7.84% compared with 1.96% amongtheir Caucasian counterparts.10
There is also a high prevalence ofopen-angle glaucoma among self-identified Latinos of primarily Mexicanancestry 40 years and older. Accordingto the Los Angeles Latino Eye Study,in which 6,142 participants underwenta complete ophthalmologic examina-tion at a clinical center, the prevalenceof open-angle glaucoma was 4.74%.11
Despite the high prevalence of open-angle glaucoma among African Ameri-cans and Hispanics, the largest affectedgroup in the United States is oldernon-Hispanic white women. However,this is expected to shift to Hispanicmen over the next few decades.12
In terms of glaucoma detection,researchers recently suggested thatnormative databases for commercialOCTs must shift from predominantlyCaucasian-based to include more eth-nic-specific data. This would decreasethe chances of glaucoma misclassifica-tion in different patient demographicswhose OCT findings may vary.13
Importantly, a recent study publishedin Ophthalmology found that in a repre-sentative sample of Medicare benefi-ciaries with glaucoma, significant racialdisparities exist in eye care utilization.14
After stratification by socioeconomicstatus, Black beneficiaries were lesslikely than whites to have outpatientfollow-up and glaucoma testing butmore likely to undergo proceduralintervention for glaucoma. The authorsconcluded that this suggests systemicracism may independently drive thesedifferences in Blacks, whereas dis-parities between Hispanic and Asianvs. white beneficiaries were largelyexplained by socioeconomic status.
Another recent paper, also in Oph-thalmology, found that Black adults withglaucoma are significantly less likely tosee an ophthalmologist or optometristfor glaucoma care, which may contrib-ute to worse visual outcomes.15
Certain types of glaucoma are morecommon in specific groups. Vietnamesepatients have a much higher prevalenceof narrow angles and a greater risk ofangle-closure glaucoma than whitepatients.16 Japanese American patients
Pigmentary changes in dry AMD.

24 REVIEW OF OPTOMETRY | JANUARY 15, 2022
are at a much greater risk of normaltension glaucoma than white patients.17
Scandinavian patients are more likelyto develop pseudo-exfoliative glau-coma.18
Glaucoma treatment can have dif-ferent effects depending on a patient’srace. Prostaglandin analogs are thefirst-line pharmaceutical treatmentdue to their efficacy in reducing IOP,once-daily dosing and excellent safetyprofile.19 Curiously, the drug travoprosthas greater efficacy among AfricanAmericans. In a large Phase III trial,travoprost 0.004% lowered IOP in Afri-can American patients by almost 2mmHg more than non-African Americans.20
Furthermore, a higher percentage ofAfrican American patients respondedto travoprost 0.004% and reached lowertarget IOPs than with either latanoprost0.005% or timolol 0.5%.
On the other hand, certain glaucomasurgeries such as trabeculectomy maybe less successful for Black patientsdue to an exaggerated healing re-sponse, suggested by a tendency forthe conjunctivae of Black patients tocontain more fibroblasts and conjuncti-val macrophages.21
Macular DegenerationAMD, a degenerative retinal diseaseimpacting the elderly, arises from acomplex relationship between genet-ics, age and external factors includingsmoking and diet. AMD is the lead-ing cause of vision loss and blindness
in Americans aged 65 andolder.22
Older white patients are atthe greatest risk of developingAMD. In 2010, 2.5% of whiteadults aged 50 and older hadAMD, whereas 0.9% each ofBlacks, Hispanics and peopleof other races had AMD.23
Multiple studies havereported a higher rate ofAMD in white vs. Blackpatients. Pooled data from theBaltimore Eye Survey, BlueMountains Eye Study, BeaverDam Eye Study, RotterdamStudy, Melbourne Vision
Impairment Project and SalisburyEye Evaluation Project showed thatin whites aged 80 and older, 16.4% ofwomen and 11.9% of men had AMD.24
The same meta-review of pooled datafor Black people from the BarbadosEye Study, Baltimore Eye Surveyand Salisbury Eye Evaluation Projectshowed that female and male Blacksaged 80 and older had an AMD preva-lence of 2.4% and 1.6%, respectively.
Caucasians with light irises may bemore prone to AMD, according to onestudy.25 However, a meta-study foundthat it is not clear if this is always thecase.26
A leading hypothesis is that thegreater amount of melanin in RPEcells in Black populations may protectthe RPE cells and Bruch’s mem-brane, either by acting as a free radicalscavenger or absorbing high-energywavelength light, and reduce drusenformation and pigmentary changes.27
Optometrists should anticipate olderCaucasian patients’ concerns aboutAMD and take a proactive stance todiscuss lifestyle modifications to mini-mize risk. In the same breath, this doesnot mean that optometrists should dis-regard the potential of AMD in otherpatient populations. It is possible thatpractitioners have bias in under-detect-ing and under-treating AMD in otherracial groups. Studies have found thatBlack patients with AMD are 23% lesslikely to receive intravitreal anti-VEGFtreatment and 18% less likely to have
regular eye examinations comparedwith their white counterparts, althoughit is not known if this reflects clinicianbias or other factors.28
Diabetic Eye DiseaseAmong the US population, numbersfrom 2018 estimated that 34.2 mil-lion people of all ages, or 10.5%, haddiabetes.29 Diabetes is well-known todisproportionately impact racial andethnic minorities.30 There are multiplefactors that underlie these disparities,including biological, clinical, health sys-tem-related and social factors. Diabetescan increase the risk for cataract andglaucoma and lead to sight-threateningoutcomes such as diabetic retinopathy.
The prevalence of diagnosed dia-betes in US adults aged 18 and olderis greatest among American Indiansand Alaska natives (14.7%), followedby Hispanics (12.5%), non-HispanicBlacks (11.7%), non-Hispanic Asians(9.2%) and non-Hispanic whites(7.5%).29
A retrospective study of 53,900American Indians and Alaska nativeswith diabetes served by the IndianHealth Services’ teleophthalmologyprogram using ultra-widefield imagingfound that 28.6% had diabetic retinopa-thy, 3% had diabetic macular edemaand 3% had sight-threatening disease.31
The Veterans Affairs Diabetes Trial,involving 1,283 patients (~20% His-panics and ~20% African Americans),found that severe diabetic retinopathywas more frequent in Hispanics and Af-rican Americans than in non-Hispanicwhites.32 The authors indicated thatthese differences did not seem to beexplained by age, duration of diabetesdiagnosis, A1c or other standard riskfactors. Although it might appear thatBlacks are biologically at a greater riskfor developing type 2 diabetes, a studypublished in 2017 in the Journal of theAmerican Medical Association suggeststhat this may not be the case and thatobesity is the primary culprit for thedifference.33
Furthermore, among adult patientswith diabetic macular edema whoreceived intravitreal injections of beva-
Diabetic retinal and vitreal hemorrhages.
R A C E, E T H N I C I T Y A N D E Y E D I S E A S EFeature
cizumab, Black patients had a signifi-cantly lower likelihood of visual acuity improvement compared with white and Hispanic patients.34
As every optometrist knows, an eye exam may be the first indicator of systemic disease, including diabetes. Due to lower rates of racial and ethnic minorities seeking general healthcare, optometrists can play an important role in reinforcing why and when our patients need to see a physician to maintain their general health.
There are several online resources serving minority groups with elevated prevalence of diabetes. For example, the CDC has the Native Diabetes Wellness Program.35 The National Eye Institute and the National Eye Health Education Program have tip sheets encouraging clinicians to help African Americans and Hispanics/Latinos to reduce their risk of diabetic eye disease with the acronym TRACK: taking their medications, reaching and maintaining a healthy weight, adding physical activ-ity to their daily routine, controlling their blood sugar, blood pressure and cholesterol, and kicking the smoking habit.36,37 To help communicate with native Spanish speakers, the National Eye Institute has Spanish language brochures on diabetic retinopathy avail-able for download.38
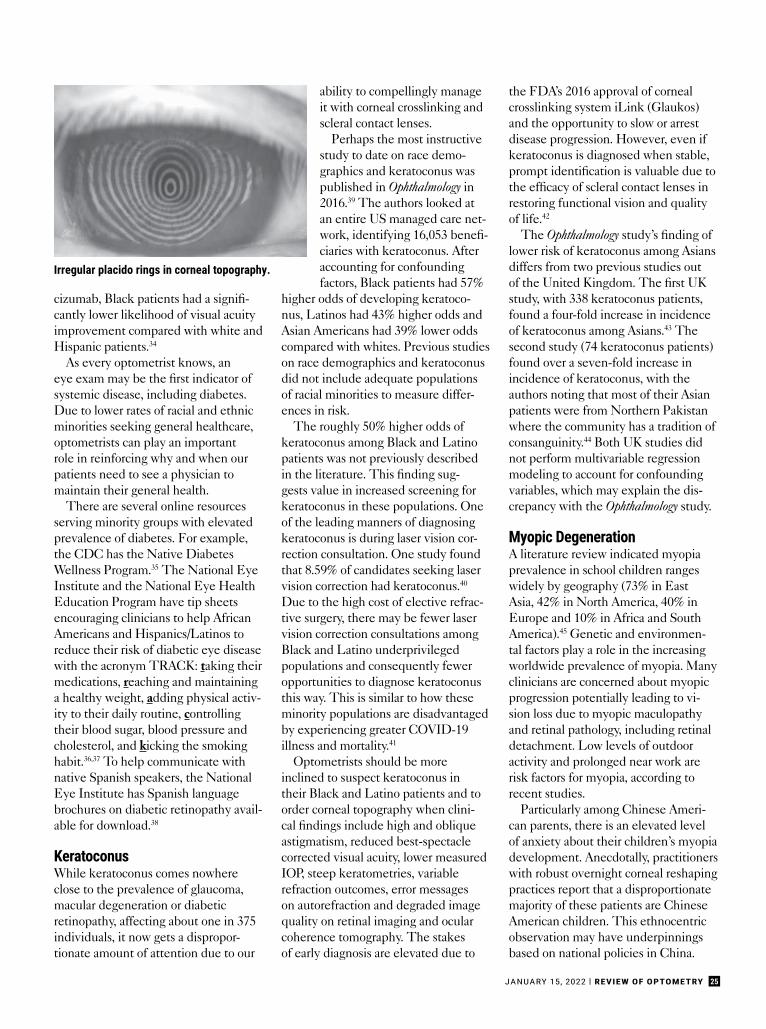
KeratoconusWhile keratoconus comes nowhere close to the prevalence of glaucoma, macular degeneration or diabetic retinopathy, affecting about one in 375 individuals, it now gets a dispropor-tionate amount of attention due to our
ability to compellingly manage it with corneal crosslinking and scleral contact lenses.
Perhaps the most instructive study to date on race demo-graphics and keratoconus was published in Ophthalmology in 2016.39 The authors looked at an entire US managed care net-work, identifying 16,053 benefi-ciaries with keratoconus. After accounting for confounding factors, Black patients had 57%
higher odds of developing keratoco-nus, Latinos had 43% higher odds and Asian Americans had 39% lower odds compared with whites. Previous studies on race demographics and keratoconus did not include adequate populations of racial minorities to measure differ-ences in risk.
The roughly 50% higher odds of keratoconus among Black and Latino patients was not previously described in the literature. This finding sug-gests value in increased screening for keratoconus in these populations. One of the leading manners of diagnosing keratoconus is during laser vision cor-rection consultation. One study found that 8.59% of candidates seeking laser vision correction had keratoconus.40
Due to the high cost of elective refrac-tive surgery, there may be fewer laser vision correction consultations among Black and Latino underprivileged populations and consequently fewer opportunities to diagnose keratoconus this way. This is similar to how these minority populations are disadvantaged by experiencing greater COVID-19 illness and mortality.41
Optometrists should be more inclined to suspect keratoconus in their Black and Latino patients and to order corneal topography when clini-cal findings include high and oblique astigmatism, reduced best-spectacle corrected visual acuity, lower measured IOP, steep keratometries, variable refraction outcomes, error messages on autorefraction and degraded image quality on retinal imaging and ocular coherence tomography. The stakes of early diagnosis are elevated due to
the FDA’s 2016 approval of corneal crosslinking system iLink (Glaukos) and the opportunity to slow or arrest disease progression. However, even if keratoconus is diagnosed when stable, prompt identification is valuable due to the efficacy of scleral contact lenses in restoring functional vision and quality of life.42
The Ophthalmology study’s finding of lower risk of keratoconus among Asians differs from two previous studies out of the United Kingdom. The first UK study, with 338 keratoconus patients, found a four-fold increase in incidence of keratoconus among Asians.43 The second study (74 keratoconus patients) found over a seven-fold increase in incidence of keratoconus, with the authors noting that most of their Asian patients were from Northern Pakistan where the community has a tradition of consanguinity.44 Both UK studies did not perform multivariable regression modeling to account for confounding variables, which may explain the dis-crepancy with the Ophthalmology study.
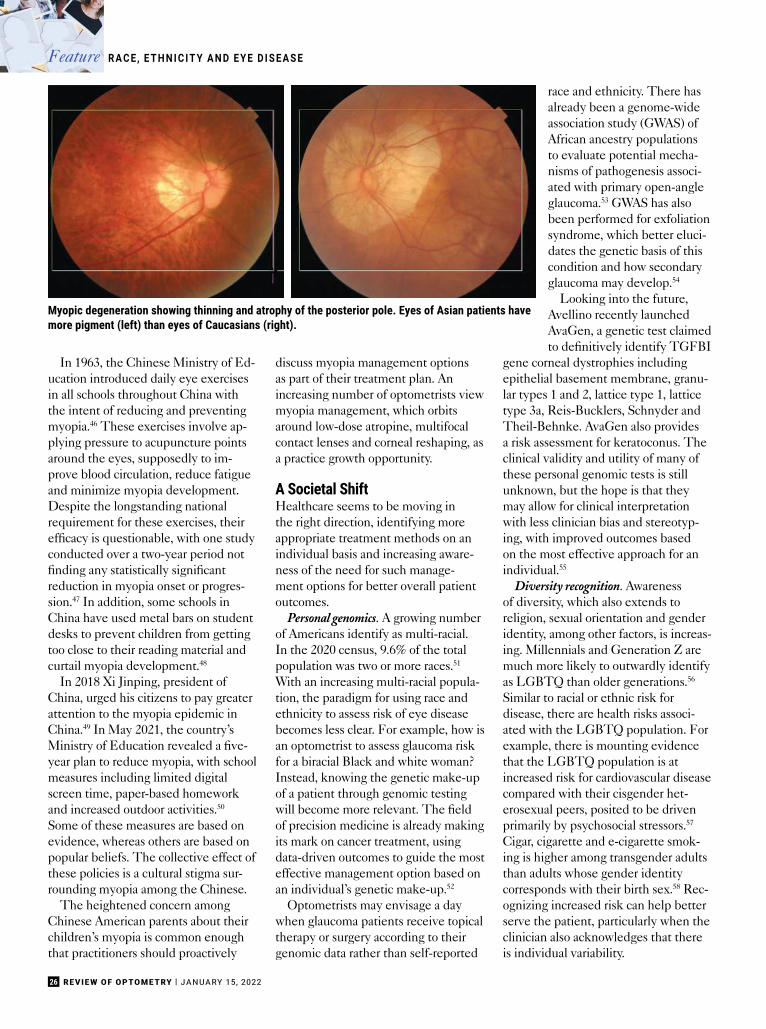
Myopic DegenerationA literature review indicated myopia prevalence in school children ranges widely by geography (73% in East Asia, 42% in North America, 40% in Europe and 10% in Africa and South America).45 Genetic and environmen-tal factors play a role in the increasing worldwide prevalence of myopia. Many clinicians are concerned about myopic progression potentially leading to vi-sion loss due to myopic maculopathy and retinal pathology, including retinal detachment. Low levels of outdoor activity and prolonged near work are risk factors for myopia, according to recent studies.
Particularly among Chinese Ameri-can parents, there is an elevated level of anxiety about their children’s myopia development. Anecdotally, practitioners with robust overnight corneal reshaping practices report that a disproportionate majority of these patients are Chinese American children. This ethnocentric observation may have underpinnings based on national policies in China.
Irregular placido rings in corneal topography.
25JANUARY 15, 2022 | REVIEW OF OPTOMETRY
In 1963, the Chinese Ministry of Ed-ucation introduced daily eye exercisesin all schools throughout China withthe intent of reducing and preventingmyopia.46 These exercises involve ap-plying pressure to acupuncture pointsaround the eyes, supposedly to im-prove blood circulation, reduce fatigueand minimize myopia development.Despite the longstanding nationalrequirement for these exercises, theirefficacy is questionable, with one studyconducted over a two-year period notfinding any statistically significantreduction in myopia onset or progres-sion.47 In addition, some schools inChina have used metal bars on studentdesks to prevent children from gettingtoo close to their reading material andcurtail myopia development.48
In 2018 Xi Jinping, president ofChina, urged his citizens to pay greaterattention to the myopia epidemic inChina.49 In May 2021, the country’sMinistry of Education revealed a five-year plan to reduce myopia, with schoolmeasures including limited digitalscreen time, paper-based homeworkand increased outdoor activities.50
Some of these measures are based onevidence, whereas others are based onpopular beliefs. The collective effect ofthese policies is a cultural stigma sur-rounding myopia among the Chinese.
The heightened concern amongChinese American parents about theirchildren’s myopia is common enoughthat practitioners should proactively
discuss myopia management optionsas part of their treatment plan. Anincreasing number of optometrists viewmyopia management, which orbitsaround low-dose atropine, multifocalcontact lenses and corneal reshaping, asa practice growth opportunity.
A Societal ShiftHealthcare seems to be moving inthe right direction, identifying moreappropriate treatment methods on anindividual basis and increasing aware-ness of the need for such manage-ment options for better overall patientoutcomes.
Personal genomics. A growing numberof Americans identify as multi-racial.In the 2020 census, 9.6% of the totalpopulation was two or more races.51
With an increasing multi-racial popula-tion, the paradigm for using race andethnicity to assess risk of eye diseasebecomes less clear. For example, how isan optometrist to assess glaucoma riskfor a biracial Black and white woman?Instead, knowing the genetic make-upof a patient through genomic testingwill become more relevant. The fieldof precision medicine is already makingits mark on cancer treatment, usingdata-driven outcomes to guide the mosteffective management option based onan individual’s genetic make-up.52
Optometrists may envisage a daywhen glaucoma patients receive topicaltherapy or surgery according to theirgenomic data rather than self-reported
race and ethnicity. There hasalready been a genome-wideassociation study (GWAS) ofAfrican ancestry populationsto evaluate potential mecha-nisms of pathogenesis associ-ated with primary open-angleglaucoma.53 GWAS has alsobeen performed for exfoliationsyndrome, which better eluci-dates the genetic basis of thiscondition and how secondaryglaucoma may develop.54
Looking into the future,Avellino recently launchedAvaGen, a genetic test claimedto definitively identify TGFBI
gene corneal dystrophies includingepithelial basement membrane, granu-lar types 1 and 2, lattice type 1, latticetype 3a, Reis-Bucklers, Schnyder andTheil-Behnke. AvaGen also providesa risk assessment for keratoconus. Theclinical validity and utility of many ofthese personal genomic tests is stillunknown, but the hope is that theymay allow for clinical interpretationwith less clinician bias and stereotyp-ing, with improved outcomes basedon the most effective approach for anindividual.55
Diversity recognition. Awarenessof diversity, which also extends toreligion, sexual orientation and genderidentity, among other factors, is increas-ing. Millennials and Generation Z aremuch more likely to outwardly identifyas LGBTQ than older generations.56
Similar to racial or ethnic risk fordisease, there are health risks associ-ated with the LGBTQ population. Forexample, there is mounting evidencethat the LGBTQ population is atincreased risk for cardiovascular diseasecompared with their cisgender het-erosexual peers, posited to be drivenprimarily by psychosocial stressors.57
Cigar, cigarette and e-cigarette smok-ing is higher among transgender adultsthan adults whose gender identitycorresponds with their birth sex.58 Rec-ognizing increased risk can help betterserve the patient, particularly when theclinician also acknowledges that thereis individual variability.
Myopic degeneration showing thinning and atrophy of the posterior pole. Eyes of Asian patients havemore pigment (left) than eyes of Caucasians (right).
26 REVIEW OF OPTOMETRY | JANUARY 15, 2022
R A C E, E T H N I C I T Y A N D E Y E D I S E A S EFeature
27JANUARY 15, 2022 | REVIEW OF OPTOMETRY
Just like how an 80-year-old womanmay wonder how a 25-year-old maleoptometrist can relate to her eye careneeds, a similar dynamic may occurwhen a Black woman is examined bya white optometrist. The same canbe said about other disparate charac-teristics between the patient and theclinician. Self-awareness is a good firststep, but this doesn’t mean calling outobvious differences and making theman emphasis of the relationship.
Another key is recognizing thatgood care transcends racial and ethnicdifferences, language barriers, socioeco-nomic status and age. In each of thesesituations, human connection and trustcan develop over shared emotions andfeelings. Ultimately, humans are morein harmony with one another than weare different. We can still relate to eachother based on commonalities whilealso celebrating our differences and thevariety that they bring. ■
1. Gross ER, Zambelli VO, Small BA, et al. A personalized medicineapproach for Asian Americans with the aldehyde dehydrogenase 2*2variant. Annu Rev Pharmacol Toxicol. 2015;55:107-27.2. Hoffman KM, Trawalter S, Axt JR, Oliver MN. Racial bias in painassessment and treatment recommendations, and false beliefsabout biological differences between blacks and whites. PNAS.2016;113(16):4296-301.3. Godoy M. KQED. Is it time for a race reckoning in kidney medicine?December 28, 2020. www.kqed.org/news/11852910/is-it-time-for-a-race-reckoning-in-kidney-medicine. Accessed December 9, 2021.4. Richter R, Best J. Stanford Medicine. How accounting for racesabotages health treatment. May 10, 2021. stanmed.stanford.edu/2021issue1/race-based-medicine-sabotages-care.html. AccessedDecember 9, 2021.5. Golden SH. Johns Hopkins Medicine. Coronavirus in African Ameri-cans and other people of color. April 20, 2020. hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/covid19-racial-disparities.Accessed December 9, 2021.6. Ways and Means Committee. Ways and Means Committee issuesrequest for information on the misuse of race within clinical care.September 17, 2020. waysandmeans.house.gov/media-center/press-releases/ways-and-means-committee-issues-request-information-misuse-race-within. Accessed December 9, 2021.7. Vyas DA, Eisenstein LG, Jones DS. Hidden in plain sight — reconsider-ing the use of race correction in clinical algorithms. N Engl J Med.2020;383:874-82.8. Javitt JC, McBean AM, Nicholson GA, et al. Undertreatment of glau-coma among Black Americans. N Engl J Med. 1991;325:1418-22.9. Muñoz B, West SK, Rubin GS, et al. Causes of blindness and visualimpairment in a population of older Americans: the Salisbury Eye Evalua-tion Study. Arch Ophthamol. 2000;118(6):819-25.10. Tielsch JM, Sommer A, Katz J, et al. Racial variations in the preva-lence of primary open-angle glaucoma. The Baltimore Eye Survey. JAMAOphthamol. 1991;266(3):369-74.11. Varma R, Ying-Lai M, Francis BA, et al. Prevalence of open-angleglaucoma and ocular hypertension in Latinos: the Los Angeles LatinoEye Study. Ophthalmology. 2004;111(8):1439-48.12. Vajaranant TS, Wu S, Torres M, et al. The changing face of primaryopen-angle glaucoma in the United States: demographic and geographicchanges from 2011 to 2050. Am J Ophthamol. 2012;154(2):303-14.13. Majithia S, Tham YC, Chun Yuen CC, et al. Retinal nerve fiber layer thickness and rim area profiles in asians: pooled analysis from the Asian Eye Epidemiology Consortium. Ophthalmology. November 29, 2021.[Epub ahead of print].14. Halawa OA, Kolli A, Oh G, et al. Racial and socioeconomic differencesin eye care utilization among Medicare beneficiaries with glaucoma. Ophthalmology. October 6, 2021. [Epub ahead of print].15. Cheng BT, Tanna AP. Association of race and ethnicity with thefrequency of outpatient glaucoma care. Ophthalmology. December 10,2021. [Epub ahead of print].
16. Nguyen N, Mora JS, Gaffney MM, et al. A high prevalence ofoccludable angles in a Vietnamese population. Ophthalmology.1996;103(9):1426-31.17. Pekmezci M, Vo B, Lim AK, et al. The characteristics of glaucoma inJapanese Americans. Arch Ophthalmol. 2009;127(2):167-71.18. Arnarsson A, Damji KF, Sverrisson T, et al. Pseudoexfoliation in theReykjavik Eye Study: prevalence and related ophthalmological variables.Acta Ophthalmol Scand, 2007;85(8):822-7.19. Winkler NS, Fautsch MP. Effects of prostaglandin analogues onaqueous humor outflow pathways. J Ocul Pharmacol Ther. 2014;30(2-3):102-9.20. Whitson JT. Travoprost--a new prostaglandin analogue for the treat-ment of glaucoma. Expert Opin Pharmacother. 2002;3(7):965-77.21. Broadway D, Grierson I, Hitchings R. Racial differences in the resultsof glaucoma filtration surgery: are racial differences in the conjunctival cell profile important? Br J Ophthalmol. 1994;78(6):466-75.22. CDC. Learn about age-related macular degeneration. www.cdc.gov/visionhealth/resources/features/macular-degeneration.html. AccessedDecember 9, 2021.23. NIH. Age-related macular degeneration (AMD) data and statistics.www.nei.nih.gov/learn-about-eye-health/outreach-campaigns-and-resources/eye-health-data-and-statistics/age-related-macular-degenera-tion-amd-data-and-statistics. Accessed December 9, 2021.24. The Eye Diseases Prevalence Research Group. Prevalence of age-related macular degeneration in the United States. Arch Ophthalmol.2004;122(4):564-72.25. Frank RN, Puklin JE, Stock C, Canter LA. Race, iris color, and age-re-lated macular degeneration. Trans Am Ophthalmol Soc. 2000;98:109-15.26. Chakravarthy U, Wong TY, Fletcher A, et al. Clinical risk factorsfor age-related macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol. 2010;10:31.27. Age-related Eye Disease Study Research Group. Risk factors associ-ated with age-related macular degeneration. A case-control study in theage-related eye disease study: Age-Related Eye Disease Study ReportNumber 3. Ophthalmology. 2000;107(12):2224-32.28. Sloan FA, Brown DS, Carlisle ES, et al. Monitoring visual status: whypatients do or do not comply with practice guidelines. Health Serv Res.2004;39(5):1429-48.29. CDC. National Diabetes Statistics Report 2020. Estimates ofdiabetes and its burden in the United States. www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf. AccessedDecember 9, 2021.30. Golden SH, Brown A, Cauley JA, et al. Health disparities in endocrinedisorders: biological, clinical, and nonclinical factors–an Endocrine Soci-ety scientific statement. J Clin Endocrinol Metab. 2012;97(9):E1579-639.31. Fonda SJ, Bursell SE, Lewis DG, et al. Prevalence of diabetic eyediseases in American Indians and Alaska Natives (AI/AN) as identified by the Indian Health Service’s National Teleophthalmology Program usingultrawide field imaging (UWFI). Ophthalmic Epidemiol. 2021;1-9.32. Emanuele N, Sacks J, Klein R, et al. Ethnicity, race, and baselineretinopathy correlates in the Veterans Affairs Diabetes Trial. DiabetesCare. 2005;28(8):1954-8.33. Bancks MP, Kershaw K, Carson AP, et al. Association of modifiable risk factors in young adulthood with racial disparity in incident type 2 dia-betes during middle adulthood. JAMA Ophthalmol. 2017;318(24):2457-65.34. Osathanugrah P, Sanjiv N, Siegel NH, et al. The impact of race onshort-term treatment response to bevacizumab in diabetic macularedema. Am J Ophthalmol. 2021;222:310-7.35. CDC. Native Diabetes Wellness Program. www.cdc.gov/diabetes/ndwp/index.html. Accessed December 9, 2021.36. NIH. Educating African Americans about diabetic eye disease. www.nei.nih.gov/sites/default/files/nehep-pdfs/NEHEP_DED_AAI_TipSheet.pdf. Accessed December 9, 2021.37. NIH. Educating Hispanics/Latinos about diabetic eye disease. www.nei.nih.gov/sites/default/files/nehep-pdfs/NEHEP_DED_HispanicLati-nos_TipSheet.pdf. Accessed December 9, 2021.
38. NIH. Diabetic retinopathy: what you should know. www.nei.nih.gov/learn-about-eye-health/resources-for-health-educators/outreach-materials/la-retinopatia-diabetica-lo-que-usted-debe-saber-diabetic-retinopathy-what-you-should-know. Accessed December 9, 2021.39. Woodward MA, Blachley TS, Stein JD. The association between so-ciodemographic factors, common systemic diseases, and keratoconus:an analysis of a nationwide healthcare claims database. Ophthalmology.2016;123(3):457-65.40. Althomali TA, Al-Qurashi IM, Al-Thagafi SM, et al. Prevalence of keratoconus among patients seeking laser vision correction in Taif areaof Saudi Arabia. Saudi J Ophthalmol. 2018;32(2):114-8.41. Alcendor DJ. Racial disparities-associated COVID-19 mortalityamong minority populations in the US. J Clin Med. 2020;9(8):2442.42. Bergmanson JPG, Walker MK, Johnson LA. Assessing scleralcontact lens satisfaction in a keratoconus population. Optom Vis Sci.2016;93(8):855-60.43. Pearson AR, Soneji B, Sarvananthan N, Sandford-Smith JH. Doesethnic origin influence the incidence or severity of keratoconus? Eye (Lond). 2000;14(Pt 4):625-8.44. Georgiou, Funnell CL, Cassels-Brown A, O-Conor R. Influence of eth-nic origin on the incidence of keratoconus and associated atopic diseasein Asians and white patients. Eye(Lond). 2004;18(4):379-83.45. Grzybowski A, Kanclerz P, Tsubota K, et al. A review on theepidemiology of myopia in school children worldwide. BMC Ophthalmol.2020;20(1):27.46. Wang H, Qian Y, Congdon N, et al. Effect of Chinese eye exerciseson change in visual acuity and eyeglasses wear among school-agedchildren in rural China: a propensity-score-matched cohort study. BMCComplement Med Ther. 2020;82:20.47. Kang MT, Li SM, Peng X, et al. Chinese eye exercises and myopiadevelopment in school age children: a nested case-control study. SciRep. 2016;6:28531.48. Inventor Spot. Anti-myopia school desks “bar” Chinese students fromnearsightedness. inventorspot.com/articles/antimyopia_school_desks_bar_chinese_students_nearsightedness. Accessed December 9, 2021.49. Binagwaho A. CNN. How lessons from Rwanda could help China fix its myopia crisis. November 15, 2018. edition.cnn.com/2018/11/14/health/china-myopia-rwanda-africa-intl/index.html. Accessed December9, 2021.50. Gov.cn. China launches 5-year campaign against youth myopia. May11, 2021. english.www.gov.cn/statecouncil/ministries/202105/11/con-tent_WS609a1cc4c6d0df57f98d9565.html. Accessed December 9, 2021.51. United States Census Bureau. data.census.gov/cedsci/table?q=United%20States&tid=DECENNIALPL2020.P1. AccessedDecember 9, 2021.52. NIH. Cancer genomics overview. www.cancer.gov/about-nci/organi-zation/ccg/cancer-genomics-overview. Accessed December 9, 2021.53. Hauser MA, Allingham RR, Aung T, et al. Association of genetic vari-ants with primary open-angle glaucoma among individuals with AfricanAncestry. JAMA Ophthalmol. 2019;322(17):1682-91.54. Aung T, Ozaki M, Lee MC, et al. Genetic association study of exfolia-tion syndrome identifies a protective rare variant at LOXL1 and five new susceptibility loci. Nat Genet. 2017;49(7):993-1004.55. NIH. Regulation of genetic tests. www.genome.gov/about-genomics/policy-issues/Regulation-of-Genetic-Tests. Accessed December 9, 2021.56. HuffPost. Sieczkowski. 20% Of millennials identify as LGBTQ, accord-ing to new GLAAD study. March 30, 2017. www.huffpost.com/entry/20-percent-millennials-lgbtq-glaad-study_n_58dd140be4b05eae031d8f9c.Accessed December 9, 2021.57. Caceres BA, Streed Jr CG, Corliss HL, et al. Assessing and address-ing cardiovascular health in LGBTQ adults: a scientific statement from the American Heart Association. Circulation. 2020;142(19):e321-32.58. Buchting FO, Emory KT, Scout, et al. Transgender use of cigarettes,cigars, and e-cigarettes in a national study. AJPM. 2017;53(1):e1-7.59. Pivnick EK, Rivas ML, Tolley EA, et al. Interpupillary distance in anormal Black population. Clin Genet. 1999;55(3):182-91.
frame selectionOptical dispensaries can cater to their practice’s racial and ethnic demographics. For example, a practicewith primarily Asian patients may find that European style eyewear does not accommodate flatter Asiannoses. An “Asian-fit” frame line, TC Charton, is designed so that their eyewear does not slide down the noseand impact the cheeks. Other frame lines such as Oakley offer an Asian style nose bridge in most of theirpopular designs.
An optical serving a largely Black community may find it helpful to skew their frame selection to includeframes for larger interpupillary distances (IPD) that are customary of this patient demographic. One studyfound that the adult Black male has an average IPD of 70mm vs. the adult white male who has an averageIPD of 62mm, while the adult Black female has an average IPD of 66mm vs. the adult white female who hasan average IPD of 60mm.59
There are new technologies to assist in frame selection according to individual facial anatomy, includingTopology Eyewear, which uses an iPhone or iPad with depth sensor technology to scan a patient’s face. Theresulting scan and app allow the optician to either select the best frames from stock to accommodate thepatient’s facial anatomy or, alternatively, to design custom-made eyewear specific to the patient.

28 REVIEW OF OPTOMETRY | JANUARY 15, 2022
Connecting across cultures:how to reach out to Hispanics
This burgeoning group offers an ideal example of the need to develop “cultural competence” in the clinic. Otherdistinct communities are profiled here as well.
The face of America is changing.By 2050, more than 50% of thepopulation will be comprised ofminority groups, which can cause
unease for some who feel the chang-ing demographics are also altering thecharacter of the United States.1 Buthopefully, this demographic inevita-bility will be an impetus for optom-etrists to better understand the needs,attitudes and interpersonal dynamicsof individuals with backgrounds thatdiffer from their own.
Hispanic growth is particularlyastounding. This group alone con-tributed more than 50% of the USpopulation growth in the last decade.The 2020 Census revealed that thereare now 62 million Hispanic individu-als in the US.2 By 2040, one of everyfour Americans will be Hispanic.*
Who are they? The Census definesLatinos as people descended from
Cuban, Mexican, Puerto Rican, Cen-tral/South American or other Spanishcultures. Mexican Americans repre-sent almost two-thirds of all Hispan-ics. This is not surprising since a great
deal of the Southwest was once partof Mexico. Also, millions of Mexicanshave worked in the United States formany decades, including the agricul-tural fields. Puerto Ricans, who areAmerican citizens by birth, are one ofevery 11 US Hispanics; outside of theisland, they usually live in enclavesin the Northeast and Central Florida.One of every 30 US Hispanics areCuban, and most reside in Floridaand the Northeast. Hispanics alsoinclude many other groups from Cen-tral America, South America and theSpanish-speaking Caribbean.
Hispanic people are descendants ofthree groups: European (mainly fromSpain and Portugal), Indigenous andAfrican. Latinos may have more orless of each component, dependingon their country or region of origin.For example, I was born in PuertoRico. I have 79% European, 12% In-digenous and 6% African ancestry. Itis clear that it makes no sense to labelLatinos into any traditional racialcategories.
Dr. Santiago, a fellow of the American Academy of Optometry (AAO), is a diplomate in the AAO’s Public Health and Environmental Section. He is also vicepresident of VOSH International, chair of the Public Health Committee of the Latin American Association of Optometry and Optics, and a professor anddirector of research at the Inter American University of Puerto Rico (IAUPR) School of Optometry. Previously, he was he was dean of IAUPR School ofOptometry, founding dean of Midwestern University Arizona College of Optometry and president of the Association of Schools and Colleges of Optometry(ASCO). He was also a member of ASCO’s Cultural Competence Guidelines Committee. Dr. Santiago has no financial interests to disclosure.
Aboutthe author
By Hector C. Santiago, od, phDBayamón, Puerto Rico
Optometrists who can make Hispanicpatients feel welcome will engender trustand loyalty among this growing population.
Photo: Getty Images
C U LT U R A L C O M P E T E N C YFeature
* In this article, the terms Hispanic and Latino are used as synonyms. Both are used here to refer to people of Latin American culture of any gender. Nowadays,the term Latinx is also used by a growing number of academics and indivudals.
PEER REVIEWED

29JANUARY 15, 2022 | REVIEW OF OPTOMETRY
Latinos are younger (median ageclose to 30 years) than the US popula-tion (median age nearly 39 years).This fact means that you are morelikely to see younger families. It is anopportunity to be the optometrist ofseveral generations of them.
These individuals tend to havelarger households: 26% live in five-person families or more, about twicethat of other groups. This implies thatcaring for one family member is morelikely to be known and appreciated byother members of their families.
Latinos represent over 10% of thenation’s buying power ($1.7 trillion).In just nine years (2000 to 2009), His-panic buying power increased 69%,compared to 48% for other groups.This implies that you have great op-portunities to provide quality eye careservices and eyewear to them.
What is CulturallyCompetent Care?The notion of cultural competenceimplies developing the knowledge,skills and attitudes that allow us tounderstand, become aware and adapt
our care to the patient’s needs and ex-pectations. The purpose is to reducehealthcare disparities that arise fromcultural barriers, improving outcomesand the patient’s sense of receiv-ing empathic care.3 It has also beendefined as “the ability of systems toprovide care to patients with diversevalues, beliefs, and behaviors, includ-ing tailoring delivery to meet patients’social, cultural and linguistic needs.”4
The Association of Schools and Col-leges of Optometry (ASCO) cites sixcritical reasons for ODs to developskills in this area (Table 1). Some USstates already require optometrists tofulfill an annual continuing educationrequirement in cultural competency,and others are likely to follow.
Becoming culturally competentimplies cultural humility, which hasbeen described as “a lifelong processof self-reflection and self-critiquewhereby the individual not onlylearns about another’s culture, butone starts with an examination of her/his own beliefs and cultural identi-ties.”5 For instance, even aside fromour family backgrounds and cultural
identities, we optometrists all practiceand espouse medical culture, a data-driven and pro-treatment mindsetthat can be at odds with patients whovalue their personal or spiritual beliefsat least as highly.
Of course, some skeptics brush allthis off as another form of politicalcorrectness, arguing that it is the taskof US citizens from other cultures toassimilate into mainstream Americansociety. I feel that attitude createsblind spots in the way one approacheseye care, reduces our effectivenessand limits the growth of our practices.
Opinions and willingness to pursuecultural competency will differ, butadopting this approach takes less ef-fort than you may realize. Some practi-tioners believe that becoming cultur-ally competent is a complicated task. Ioften tell them that most of us alreadypractice some form of cultural compe-tence. For example, when we exam-ine children, we adapt our language,gestures, equipment and examinationto their needs. When we examine theelderly, we may modify the speed ofour exam, lighting, contrast and toneof voice. It is no different when weexamine patients of different ethnici-ties, values, ages, religions or nationalorigins: we adapt our methods anddemeanor to serve their needs betterand achieve better outcomes.
Eyecare professionals who wantto serve Hispanics and prosper as aresult of their growth must becomeculturally competent. We all havecultural eyeglasses that filter ourperceptions and judge other groups’judgements. As Huff and Kline haveexpressed, to provide culturallycompetent care, one must “examineour own perceptions, stereotypes and
Editor’s note: To augment Dr. Santiago’scommentary about Hispanic Americans,we have asked several optometrists whosee other distinct population groups toshare their experiences. Look for thesecontributions in a series of sidebarsthroughout this article. For an in-depthdiscussion of the Black experience inoptometry, see the article by Dr. EssenceJohnson that follows this one.
TABLE 1. SIX REASONS TO PURSUE CULTURAL COMPETENCE 3
1. Meet regulatory mandates.
2. Respond to demographic changes in the United States.
3. Address longstanding health and healthcare disparities.
4. Improve the quality of health care and health outcomes.
5. Gain a competitive edge.
6. Decrease likelihood of liability/malpractice claims.
Hispanic families can be large. Try to accommodate the inclusion of relatives in the clinicwhen feasible and desired by the patient; for example, to assist with translation.
Photo: Getty Images

30 REVIEW OF OPTOMETRY | JANUARY 15, 2022
prejudices toward the target groupand be willing to suspend judgments(where they exist) in favor of learningwho these people really are ratherthan who or what you might thinkthey are.”6
Beware of Generalization,Stereotyping and ChauvinismThere are barriers to the goal ofbecoming culturally competent. Aswe approach our patients, we formhypotheses about them.
Consider: Mrs. Maria Rodriguezfrom Brownsville, TX, with a Spanishaccent, comes to my office. I wonderif she is Mexican American, a devoutCatholic with a large extended fam-ily. This statement is a hypothesis or
The Asian American group is a growing minor-ity.1 However, the population is far from
homogenous and more nuanced than statisticsdepict. Though they (or their ancestors) are fromthe same continent, most do not share the samelanguage, beliefs, customs or history. Grouping thispopulation into a single entity masks meaningfuldistinctions. Nevertheless, we will attempt to elu-cidate some beliefs based on the limited researchavailable.
Asians have immigrated to North Americafor myriad reasons. Some came for educationalopportunities, while others immigrated because ofoccupational shortages. Some Asian groups mayhave entered the United States via refugee status.Hence, the history and socioeconomic status ofeach group is vastly different; their understandingof US culture and the English language also variesconsiderably.
Some commonalities include respect for author-ity, value of education, providing for one’s familyabove all else and a stigma related to mental healthissues. When caring for an Asian American patient,providers must have cultural considerations inmind, such as the patient’s belief regarding etiologyof illnesses, unfamiliarity of Western medicine andmethods, and language barriers.2-3 While diverseAsian ethnic groups share some commonalitiesregarding healthcare beliefs, it’s important to notethat each group also has unique cultural beliefsabout health and illness. These may also be furtherinfluenced by religious dogma. There are also situa-tions to consider within the context of multigenera-tional households. For example, a patient is likelymaking their medical decisions collectively withtheir family members instead of by themselves.
Understanding an Asian American patient’shealth beliefs and perception of present illness isimportant to care for them effectively. For example,improper diet and stress as causation of illness androutine exercise as illness prevention are consistentbeliefs across many Asian American subgroups.The Chinese perspective is influenced by traditionalChinese medicine, which is rooted in maintaininga balance between yin and yang. An imbalance inthese forces, it is believed, may result in illness.4
A traditional Vietnamese belief is that thereis a balance of hot or cold wind in one’s body,better known as “hơi”, and “giác” is a remedy to balance the elements in which heated glasses areplaced onto the skin to draw out the bad wind.This treatment leaves a round, red mark that has
led to Vietnamese parents being prosecuted forchild abuse. Nowadays, this is better known by themass media as “cupping” after it was popularized by athletes like Olympic swimmer Michael Phelpsas a way to heal faster. Despite the popularity ofalternative medicine such as cupping, healthcareproviders have limited knowledge of traditionalAsian interventions, which impacts outcomesfor Asian Americans. Patients may not take theirmedicine for a variety of reasons. It is the provider’sresponsibility to find out why. They may be usingalternative traditional treatments. Spending timeto understand these practices will aid the providerto negotiate the best ways to manage the patient’socular conditions.
Studies indicate both Western and non-Westernpatients prefer a partnership style of communi-cation when discussing their health care, but apaternalistic communication style prevails amongAsian American families. This is likely in part due toSoutheastern Asians adhering to a social hierarchy,even in the context of their health care. Doctorsare generally accepted to be higher on the socialhierarchy and respect must be given to people ofthis high status; patients will defer to the doctorand their medical recommendations out of respect.Subsequently, a partnership communication stylemay not be the most appropriate in the culturalcontext of many Asian American patients. If mutualmedical decision making is desired, doctors mustovercome the patient’s default to deference andpoliteness and encourage them to become moreactive participants in their health care.5
It is especially challenging to provide care fora patient who does not speak your language, andinitially, our Asian American patients may appearto be agreeable to the prescribed treatment planif some communication is lost in translation.Many will use their children to interpret, but that
adds other challenges, since the child isnot equipped to handle diagnoses that arevision- and life-threatening. To overcomethis, it is recommended to use certifiedmedical interpreters who understand thecultural context and can act as a liaison forboth cultures. Offering interpretation relievesanxiety because the patient’s concerns andcomplaints will be addressed and engendersa trusting relationship between doctor andpatient.
It is also important to remember thatthere will be various subcultures within anAsian American family. Keep in mind the
culture of the family’s origin, the culture of theimmigrant family moving to North America andthe culture of their children—who may feel they donot belong to their culture of origin or the cultureof North America. Noting these struggles andproviding compassion to these challenges will aidthe provider in navigating how one may approachthe delivery of care. For example, a parent maynot want their child to wear soft contact lensesbecause of cost but their child may want contactlenses to fit in at school.
Each Asian American group faces vastly differ-ent challenges, and their understanding of US cul-ture and English varies widely. Caring for a patientwho speaks a different primary language requiresthought and skill, and a cooperative approach willappeal to the preferred partnership style of com-munication and keep family members involved.Even though many Asian American groups holdsome common beliefs regarding health care, eachsubgroup holds its own cultural views about healthand illness. Understanding these perspectives willhelp the provider effectively to manage the patient’socular conditions.
1. Pew Research Center. Key facts about Asian Americans, adiverse and growing population. Accessed November 29, 2021.www.pewresearch.org/fact-tank/2021/04/29/key-facts- about-asian-americans.2. Louie, KB. Cultural considerations: Asian-Americans andPacific Islanders. Imprint. 1995; 42(5):41-44.3. Uba L. Cultural barriers to health care for Southeast Asianrefugees. Public Health Rep. 1992;107(5):544-48.4. Zhao M, Esposito N, Wang K. Cultural beliefs and attitudestoward health and health care among Asian-born womenin the United States. J Obstet Gynecol Neonatal Nurs.2010;39(4):370-385.5. Claramita M, Utarini A, Soebono H, Van Dalen J, Van derVleuten C. Doctor-patient communication in a Southeast Asiansetting: the conflict between ideal and reality. Adv Health SciEduc Theory Pract. 2011;16(1):69-80.
C U LT U R A L C O M P E T E N C YFeature
The ASIAN population: diverse unto itselfBy Mary Hoang, OD, Memphis, and Gary Chu, OD, BostonDr. Hoang is an assistant professor at SCO. Dr. Chu is vice president of professional affairs at NECO.
Photo: Getty Images
31JANUARY 15, 2022 | REVIEW OF OPTOMETRY
generalization that I am willing to testduring my conversation with her. I amopen to other alternatives and willingto suspend my judgment until I findout. On the other hand, if based onthe same facts, I conclude that she isMexican American, devout Catholicwith a large extended family, and I amnot willing to test this hypothesis, I amstereotyping her—a barrier in the roadto becoming culturally competent.
Chauvinism—the belief that one’sgroup, nation or culture is superior toothers—is often a barrier to acceptingothers. Each of us may feel that “our”way of life seems normal and right,while others may appear abnormal,irrational or inferior. Chauvinism mayshow in our interactions with ourpatients. For example, we may ignoretheir explanation of their illnesses. Wemay belittle or even prohibit the useof traditional remedies. This behavioris a sure way to lose the confidence ofyour Hispanic patient.
Hispanic Cultural ValuesThe patient’s habits and beliefs areoften the best guides to culturallycompetent care. Each cultural valuewill guide our behavior toward eachgroup. Here we must walk a fine line:it is essential to treat each person asan individual and not assume thattheir membership in a particulargroup necessarily means they willbehave in a certain way. However, Iwould like to articulate several tradi-tional core values of Hispanics thatmay be present in your patient:
Respeto. This means the consid-eration and deference each persondeserves as a human being, but alsoas a function of their age, education,reputation and achievements.
Implications: As an eye care profes-sional with a high level of education,optometrists receive respeto fromtheir patients. By the same token, thepatients expect respeto from theirdoctors. One of the most commonfaux-pas of non-Hispanic optometristsis to greet the patient with their firstname on their first encounter (“Goodmorning, Pedro”) as a way to seem
friendly and put them at ease. Youshould instead refer to the patientwith their surname (“Welcome, Mr.Rodriguez” or “Señor Rodriguez”).It may be acceptable to use their firstname as you get to know them overtime.
The patient may be using comple-mentary medicine (such as herbs) andeven consulting a folk healer (curand-ero). It’s essential to push back againstyour own bias toward medical cultureand instead respect the patient’s cul-
tural traditions while still counselingthem on what you consider the bestcourse of care, without expressingdisdain or ridicule.
Some older Hispanic patients mayavoid direct eye contact. You maymisinterpret this behavior as a lack ofinterest in your conversation. Avoid-ance of eye contact from the patientis a sign of respect to you as a doctorand an authority figure. Accept thatand maintain your eye contact withthe patient.
Optometry inside the arctic circleBy Gregory Black, OD, Ft. Lauderdale, FLAssistant professor at Nova Southeastern University
On Alaska’s northwesterncoastline near the Bering
Strait, 33 miles north of theArctic Circle, lies the village ofKotzebue. There, Maniilaq EyeClinic is the sole provider foran area the size of the state ofIndiana. Dr. Meagan Lincoln,who was born and raised inKotzebue, established the cur-rent optometry and opticianryprograms within the hospital in2016, and I have been involvedin village travel since 2017.There are 11 villages within the Maniilaq service area, with Kotzebue as the regional hub. Among thepopulation, 83% of the 8,623 residents are Inupiat.
As with every population, there are subtle and not-so-subtle differences. With a population densityof 0.20 per square mile, it is understandable that patients will have a larger personal space bubblethan elsewhere in the US. In this isolated area, patients are more independent in most aspects of life.In the optometry clinic, for instance, they prefer to insert and remove their contact lenses themselves.Discussion of the impact of birth control pills and hormone replacement therapy for dry eye and LASIKconsiderations is a more delicate conversation in Kotzebue than it is in South Florida. Accustomed toa good deal of personal space, patients need to be warned that they will be tilted back for BIO priorto the procedure rather than while I tilt them back, otherwise they will flinch. These were learned veryquickly due to the reactions experienced, and my approached changed.
The use of nonverbal communication is more common in this region; for example, kids will use anupward eyebrow movement to signal yes and scrunch their nose to signal no. I no longer ask a yes/noquestion if a child is behind the phoropter or I have my back to them.
A couple of characteristics of the population have made refraction and drop instillation significantlyeasier. Patients actually know which is better one or two and will even volunteer “same” withoutprompting. The vast majority of pediatric patients accept drops if it is explained that it will only stingfor 30 to 45 seconds. The pediatric patients have a bravery that I have not seen in other populations.In speaking with nurse practitioners and dental colleagues, they report a similar response to injectionsand dental procedures.
As a provider who has cared for many different cultures, races and religions in both South Floridaand now rural Alaska, I have learned that by displaying respect, concern and compassion for yourpatients, you will be seen as a trusted provider. You will make mistakes, but learn from them. Look forclues of discomfort, which are usually going to be nonverbal. Listen when a patient gives you advice.Also remember that everyone is an individual; just because something is common in a populationdoesn’t mean that it applies to everyone. If at all possible, seek out advice from an optometrist repre-sentative of the population you are serving. Dr. Lincoln is extremely helpful in that regard for me.
Caring for Indigenous populations may not be an everyday experience for many optometrists; whenit arises, knowing some basic characteristics of the group will help you build a rapport one-on-one.
KOTZEBUE•
Photo: Getty Images

32 REVIEW OF OPTOMETRY | JANUARY 15, 2022
Familismo. This cultural valueimplies that the family is the pillarof society, and there is a strong senseof worth associated with belong-ing to a family. The family typicallyincludes the father, mother, siblings,grandparents, nieces, nephews andgodparents.
Implications: Hispanics may comewith family members to the appoint-ment. Consider a larger waiting roomif you practice in a neighborhoodwhere many Hispanics visit youroffice. Be willing to allow a familymember inside the exam room if thepatient desires.
Family members usually assist oth-ers when they need help with theircare. For example, they may helpdispense eye drop medications to anelderly relative as required. They maybe the ones to remind their familymembers of their medical appoint-ments. Therefore, it is practical andhelpful if that family member accom-panies the patient to the exam room.
Also, be aware that many decisionsabout eye care and eyewear are madewith the counseling and assistance ofother family members. Although thepatient has the ultimate voice, youand your staff should allow the familymember’s involvement in the decisionprocess.
Personalismo. This value relates tothe importance of developing sincere,authentic and caring relationshipsamong human beings above otherpriorities.
Implications: Get to know your His-panic patient’s interests, hobbies andclose family members. Before initiat-ing your examination, devote time tochat about personal matters.
Sit closer (less than one meter),lean forward and provide handshakesas needed. This behavior will helpyou obtain confianza—your patient’strust—to envisage you as someonewho cares about them. Gaining confi-anza will allow you to be not only theoptometrist for the patient but morelikely the optometrist that other fam-ily members will choose and prefer.
The Concept of TimeMany Americans display the charac-teristics of what can be described asa linear-active culture—they performtasks one at a time, sequentially, andpunctuality is considered very impor-tant. On the other hand, many Latinosdisplay the characteristics of a multi-active culture. They may performdifferent tasks almost simultaneously.Human relations and transactions areconsidered more important than fol-lowing a schedule.
You may find that some of yourLatino patients may not show on timeand you may be irritated by this, pos-
C U LT U R A L C O M P E T E N C YFeature
Things to consider during muslim patient encountersBy Mawada Osman OD, MS, Columbus, OHAssistant professor of clinical practice and outreach coordinator at OSU College of Optometry
The Islamic faith encompasses alargely diverse group of people from
many different ethnicities, cultures andbackgrounds. In the United States, themajority of Muslims are immigrantsfrom Middle Eastern/North African andSouth Asian countries, which makeup about 30+ nations. Although thediverse cultural and ethnic backgroundis intertwined with an individual’s reli-gious beliefs, there are certain aspectsthat are unique to the Islamic religion that may have an impact on health behaviors and overall health-care experiences and outcomes.
In Islam, both men and women are required to behave and dress modestly. This includes wearingloose-fitting clothing for both genders and wearing a head covering known as a “hijab” for women.As modest behavior is highly recommended in Islam, you may find some patients reluctant to shakehands with a provider of the opposite gender. This should not be taken personally or interpreted asoffensive. Instead, you could greet your patient with a head nod and raising your hand to your chest asa way of showing respect and understanding. Patients may also prefer and request to have a providerof the same gender. When possible, these services should be provided to the patient. However, if notpossible, especially with smaller clinics, it is important to request permission from the patient when-ever performing clinical examination/procedures that require direct touch of the patient—for example,lifting the eyelids. Wearing medical gloves would also be preferred.
One aspect that we do not think much about as optometrists is a patient’s dietary requirements.Pork consumption is prohibited in Islam. We need to keep this in mind when prescribing oral medica-tions such as antibiotics that come in capsule form. The capsules are made of pig-based gelatin andsome patients might feel uncomfortable consuming such medications. Another medication we tend toprescribe as optometrists are AREDS2 supplements. Most come in softgel form, which also containsgelatin. Alternatives should be used when possible.
Family plays an integral role in the Muslim community. Family members, both nuclear and extended,are consulted regarding important medical decisions, especially surgical procedures. Communicatingand building trust with family members should be as much of a priority as it is with the patient—espe-cially those family members that come in with the patient.
Creating a welcoming environment in your office space allows your patients to feel more comfort-able and included. This can be done by displaying images of a diverse group of people on your officewalls and website. You can take the extra step and reflect that interest by hiring a diverse group ofindividuals to be a part of your office team. A very important aspect in delivering culturally competentcare to your Muslim patients is just getting to know them. Muslims are multi-ethnic and make up thesecond largest religion in the world. Have a conversation with your patient expressing your interest inlearning more.
The main holidays celebrated by Muslims are Eid Al-Fitr, which is celebrated after the holy month ofRamadan (a time of fasting and spiritual connection), and Eid Al-Adha, which is celebrated on the 10thto the 13th of the twelfth Islamic month (lunar calendar). Extending a simple “Happy Eid” greeting toyour patient (or if you want to try the Islamic/Arabic greeting, you can also say “Eid Mubarak,” whichtranslates to “blessed Eid”) reflects your appreciation for their culture and belief system. At the end ofthe day, the goal of cultural competence is to create a connection between you and your patient thatallows for open communication, building of trust and ultimately providing excellent care.
For a more detailed guide on the delivery of culturally competent care for Muslim patients, see“A Health Care Provider’s Guide To Islamic Religious Practices” by the Council on American-IslamicRelations.
Photo: Getty Images

33JANUARY 15, 2022 | REVIEW OF OPTOMETRY
sibly coloring your impression of thisindividual. To avoid such an outcome,prepare yourself for at least the pos-sibility of this. You may want to askthem to arrive earlier than expected tomake sure you keep your schedule, oryou may decide to have some flexibleappointments where they are exam-ined in the order they come to youroffice.
The Concept of SpaceThe Latino distance of comfort forinteraction is about 80cm (roughly 2.5ft.)—closer than the typical American.Hugging, handshakes and kissing onthe cheek among Hispanic women areacceptable.
As you examine your patient, learnto sit closer to them and expressfriendship through handshakes.Distancing yourself is a sure way to beperceived as a cold, unfriendly doctor.
The Language BarrierOne of the biggest obstacles tooptimal care is the language barrier,especially for older Hispanics. Theideal solution is learning basic conver-sational Spanish by the optometrist.The second best is hiring caring bilin-gual staff members who may serve asinterpreters.
If you do this, make sure they aretrained and understand the rules ofinterpretation. They must not add oromit any words nor hold side conver-sations with the patient. The first-person approach is recommended—ifthe patient says, “I have pain in myright eye,” the interpreter should sayand interpret it as “I have pain in myright eye.” The doctor must alwayslook and address the patient duringthe interview, not the interpreter.Possibly the best positioning is theinterpreter sitting beside and slightlybehind the patient, facing the doctor.Alternatively, you may use telephoneor video interpreting services.
You should also provide printedinformation in the native language ofthe patient. You may acquire educa-tional materials in Spanish printed bythe American Optometric Association.
You may use or refer the patient towebsites and YouTube videos with in-formation on eye diseases; just makesure that the information is accurateand up to date.
Health Care NeedsHispanics have the second-highestprevalence of adult obesity (45%) andhypertension (44%) after Black indi-viduals.8,9 They also have the second-
highest prevalence of diabetes (17%)after Hawaiians/Pacific Islanders.10
However, for some Latinos, chubbi-ness is seen as a sign of healthiness.You should be comfortable counsel-ing them with sensitivity and respectabout weight, blood glucose controland healthier lifestyles.
About one-third of Hispanic indi-viduals with diabetes have diabeticretinopathy.11 This high prevalence
caring for orthodox Jewish communitiesBy Daniella Rutner, OD, New York CityAssociate clinical professor and chief of vision rehabilitation at SUNY College of Optometry
Judaism is an ethno-religion (i.e., con-ferred both through birth and through
conversion) comprised of the beliefs andpractices of the Jewish people as recordedin their several-millennia-old scriptures(chiefly, the Torah) and oral traditions(compiled in the Talmud). Since roughly themid 19th century, it has consisted of threemajor denominations: Reform, Conservativeand Orthodox. The latter, OrthodoxJudaism—which counts itself historicallythe oldest of the three traditions—is strictest in practice, most recognizable in dress and, by intention,the least integrated into mainstream American culture. Notable examples of strict practice are dietaryrestriction (“keeping kosher”) and refraining one day per week from work-related activities (Sabbathobservance every Saturday). Perhaps the most universally notable example of recognizable dress isthe male head covering.
The “Orthodox” umbrella is quite wide, including within it “Ultra-Orthodox” subgroups such asHasidic, Chabad and Yeshiva. A clinician treating patients from these Ultra-Orthodox subpopulationsshould be sensitive to some potential sources of cultural friction:
Language. The more stringent Orthodox denominations (Hasidic and Yeshivish) are inclined to liveand work in communities that proactively foster cultural insularity, and that reality may present theclinicians with some language barriers. Often, English is not the primary language spoken at home somuch as Yiddish or Hebrew. Frequently, women moving within these subpopulations are more fluent inspoken and written English than their husbands or male relatives.
Education. Adult educational levels vary greatly among the Orthodox Jewish population, spanninganywhere from advanced degrees to the equivalent of middle grade-school. It should be noted that inthe more stringent yeshivas (schools), the English alphabet is not introduced until age 6 or 7.
Physical modesty: touch. Typically, Orthodox Jews will avoid any form of touch with membersof the opposite gender outside immediate family, often preferring to avoid even shaking hands.Accordingly, the physical examiner should minimize touch and attempt to educate the patient prior totouching. Gloves are advised, as they naturally work to emphasize the clinical nature of the interaction.
Physical modesty: dress. Modesty is also reflected in Orthodox Jewish attire, extending even to thetypes of frames the young male patient might be permitted to adorn himself with in school or withinhis social milieu.
General propriety: speech. Many Orthodox Jews actively work to ethically monitor their own con-versation, purging from their habits of speech aggressive commentary such as sarcasm and even, insome cases, needless discussion of trivialities. As a result, they may well be more sensitized to certainforms of “casual” or quasi-intimate conversation, with discussions that tread on private or personalmatters very possibly making them uncomfortable.
General propriety: physicality. A male and female ought not to be alone in a room with a closeddoor. If there are no cameras in the clinician’s room or window panels on the door, leaving the doorslightly ajar will assist the patient’s general sense of propriety, as will having another person in theroom (with the patient’s permission). Finally, it is important to note that eye contact is understood tobelong to the realm of potentially intimate interactions and is best minimized by members of the oppo-site gender. The same is true of physical space; the clinician should try to avoid standing invasivelyclose to the Orthodox Jewish patient.
Photo: Getty Images
34 REVIEW OF OPTOMETRY | JANUARY 15, 2022
C U LT U R A L C O M P E T E N C YFeature
The people of Appalachia have beenunfairly stereotyped by Hollywood as
uneducated and backwards in just aboutevery way. Having practiced in Newport,TN (population: 6,868) for the last 26years, I’ve seen this unfair bias againstrural America disproven time and timeagain.
Yes, a significant percentage of thiscommunity typically does not pursuehigher education. In the 2020 census, only12% of Newport residents reported havinga college degree. But this affects theirearning potential more than anything else.The median household income of $24,124is well below the national average of$67,521 and the poverty rate here is 42.9%(vs. 11.4% nationally). However, this tight-knit, hardworking community takes care of one another andis part of the reason we also have an extremely low cost of living.
While 90% of the population may be white, I don’t see this manifest as a bias against other races,although I’m sure that many of my patients would feel like a fish out of water in Los Angeles or NewYork. It is interesting to note that two of our last three city mayors have been African American.
This is a devoutly Christian community, and in fact, one of the things I enjoy doing with my patientsafter giving bad news is praying. Most of our patients love that. I always pray with them when I amreferring them for cataract surgery and especially for a sight-threatening issue. Sometimes we evenpray just if they are having some bad times in life. That might be something different we do here thatmay not be done in other areas of the country.
This strong religious conviction does not, however, mean my patients are opposed to heeding medi-cal advice—another stereotype out there. As a matter of fact, as someone who’s been a member of asmall rural community for so many years, I feel the trust our patients have in us is unmatched in anyother geographical area. These are people I go to church with, see at the grocery store and encounterin all walks of life. They know me, they respect me and they listen to me.
Financially, there are definite hardships to address without sacrificing quality of care. We often haveto work with our cataract surgeon and/or retina surgeon to allow flexible payments when a patientrequires tertiary care. We have to get creative on charging. For anyone without insurance, we charge aflat fee per year that covers not only that emergency visit but all follow-ups and a full exam with a pairof single vision glasses.
Also, being in a small town, we can often barter with patients for our services. For the first cornealforeign body I removed, I was reimbursed four jars of moonshine!
In terms of eye disease prevalence, we see lots of diabetic retinopathy, as people in rural Appalachiacertainly have dietary staples that are not the best. Also, we have lots of welders and see a fair amountof foreign body cases from local medical providers. We are also in an area that sees more retinitispigmentosa than most ODs would.
I think it’s safe to say most optometrists in the US don’t have much experience with rural life. It’sdefinitely different than what we see happening in the rest of the country. I certainly have no complaintof an “overabundance” of optometrists, and we serve on staff at our local hospital. We get all referralsfrom local medical facilities, and it makes for a very interesting and varied career. I love my communityand cannot imagine practicing anywhere else.
optometry in appalachia: challenge your assumptionsBy Kurt Steele, OD, Newport, TNPrivate practitioner at Vision Source of Newport
Newport•
implies that all Hispanics must have acomprehensive dilated fundus exami-nation at every visit.
About one-fourth of Latinos lacka primary health care provider.11 Youmay maintain a list of primary physi-cians that you deem are more likelyto be Latino-friendly to refer yourpatient as needed. One of every fi ve
Latinos may lack health insurance.12
However, many are willing to pay out-of-pocket if they value their doctorand eye care services.
Caveats and TakeawaysIn this article, we have expressedgeneralizations about Hispanics andother groups. Avoid stereotyping your
patients. Be aware that some of thesegeneralizations may not apply to yourpatient. Be open-minded and bewilling to learn about the patient youhave in front of you.
Latino presence is here to stay.Their numbers are growing fast, andwithin 20 years, the group will fullyconstitute one-quarter of Americansociety. Their buying power is also in-creasing at a rapid pace. The demandfor eye care services will dramaticallyincrease during the coming decades.Understanding Latino cultural valuesand becoming culturally competentcan serve them better and promotethe growth of our practices.
1. Colby, SL, Ortman, JM. Projections of the size and compo-sition of the US population: 2014 to 2060. US Department ofCommerce Economics and Statistics Administration, US Cen-sus Bureau (2015). Available at www.census.gov/content/dam/census/library/publications/2015/demo/p25-1143.pdf.2. 2020 census results. US Census Bureau US Departmentof Commerce Economics and Statistics Administration,US Census Bureau (2021). Available at www.census.gov/programs-surveys/decennial-census/decade/2020/2020-census-main.html.3. ASCO Guidelines for culturally competent eye and visioncare. Diversity task force, Association of Schools and Col-leges of Optometry. Released June 2008. Available at www.optometriceducation.org/fi les/guidelines_culturallycompe-tenteyeandvisioncare.pdf.4. Betancourt, J., Green, A., Carrillo, E. (2002). Cultural com-petence in health care: Emerging frameworks and practicalapproaches. The Commonwealth Fund. Available at www.commonwealthfund.org.5. Tervalon M, Murray-Garcia J. Cultural humility versus cul-tural competence: A critical distinction in defi ning physician training outcomes in multicultural education. J Health Carefor the Poor and Underserved.1998;9(2):117-125.6. Huff RM, Kline MV. Health Promotion in MulticulturalPopulations: A Handbook for Practitioners and Students, 3rdedition. Sage Publications (2007).7. Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalenceof obesity and severe obesity among adults: United States,2017-18. National Center for Health Statistics Data Brief No.360 (2020).8. Ostchega Y, Fryar CD, Nwanko T, Nguyen DD. Hypertensionprevalence among adults aged 18 and over: United States,2017-2018. National Center for Health Statistics Data BriefNo. 364 (2020).9. Centers for Disease Control and Prevention (2021):Hispanic/Latino Americans and Type 2 Diabetes. Available atwww.cdc.gov/diabetes/library/features/hispanic-diabetes.html. Accessed Jan 4, 2022.10. Mora N, Kempen JH, Sobrin L, Lucia. Diabetic retinopathyin Hispanics: a perspective on 11. Disease Burden. Amer JOphthalm. 2018(196):xviii–xxiv.11. Livingston G, Minushkin S, Cohn D. Hispanics and HealthCare in the United States. In Pew Research Center’s HispanicTrends Project (2008). Available at www.pewresearch.org/hispanic/2008/08/13/hispanics-and-health-care-in-the-united-states-access-information-and-knowledge.12. Offi ce of Health Policy. Health insurance coverage and access to care among Latinos: recent trends and challenges(2021). Issue Brief #HP-2021. Department of Healtn anmdHuman Services. Available at: https://aspe.hhs.gov/sites/default/fi les/documents/68c78e2fb15209dd191cf9b0b1380fb8/aspe_latino_health_coverage_ib.pdf.
Photo: Getty Images

ForeseeHome is a registered trademark, and the ForeseeHome AMD Monitoring Program and logo and the Notal Vision logo are trademarks of Notal Vision. © 2020 Notal Vision, Inc. All rights reserved.
References: 1. Rao P et al. Ophthalmology. 2018;125(4):522-528. 2. Domalpally A, Clemons TE, Bressler SB, et al. Ophthalmol Retina. 2019;3(4):326-335.
See website for FDA Indication for Use.
Prevent AMD Vision Loss with Digital Healthcare
GET STARTED TODAY
1-855-600-3112 Mon-Fri, 8 AM to 6 PM EST
www.foreseehome.com/doctor
20/83 VA Average at wet AMD diagnosis according to IRIS Registry real-world data1
≥20/40 VAAverage at wet AMD diagnosis
with ForeseeHome2
Monitoring Center
Benefits Verification & Authorization
Practice Workflow Implementation
Early Detection Helps Preserve VisionForeseeHome is a remote monitoring program for at-risk dry AMD patients that helps detect wet AMD earlier and alerts you of changes.
Remote patient monitoring leads to better outcomes and stronger optometric practices
HOME STUDY
IRIS REGISTRY
Engagement & Education
Continuous Monitoring
Vision Alert Management
Remote Patient Management
Solidify long-term relationships with your patients
No cost to your practicePlug and play digital health solution for your patients
Strengthen your referral relationships with qualified wet AMD referralsFDA ClearedFDA Medicare CoveredMedicare
The Key to Successful Home MonitoringNOTAL VISION MONITORING CENTER
SM-169.2
creo

36 REVIEW OF OPTOMETRY | JANUARY 15, 2022
breaking down barriers: theblack experience in optometry
How to establish trust and provide effective communication to create a stronger connectionbetween optometrists and the Black community.
Let’s be reminded of the oath wetook when becoming a doctorof optometry. When we recitedthe optometric oath, we affirmed
that the health of our patients will beour first consideration; we will pro-vide professional care for the diversepopulations that seek our services withconcern, compassion and due regardfor their human rights and dignity; wewill work to expand access to qualitycare and improve health equity for allcommunities; we will place the treat-ment of those who seek our care abovepersonal gain and strive to see thatnone shall lack for proper care; and wewill do the utmost to serve our commu-nities, our country and humankind as acitizen as well as a doctor of optometry.1
When you take a minute to reflecton certain aspects of the optometricoath, it is a mighty task that nearly46,000 optometrists have committedto assume the care of the eyes of over331 million individuals in the UnitedStates. The population of Blacks or
African Americans alone or in combina-tion with other racial groups totals 46.9million people.2 Providing eye care tothis demographic is a formidable taskfor all providers. Relegating the careof the entire Black community to the
1.8% of optometrists that look likethem proves to be an even more daunt-ing task.3
Studies show minority physicians aremore likely to practice in underservedareas and have patient populations
Dr. Johnson received her doctorate of optometry from the Pennsylvania College of Optometry at Salus University and is a community and correctionalhealth optometrist who practices at Southeast Dallas COPC. She is also the chief visionary officer of Black EyeCare Perspective, co-advisor and co-founder of the Black EyeCare Perspective Pre-Optometry Club and the National Optometric Association Region IV Trustee. She is a consultant for Johnson & Johnson Vision Care and is a member of the Transitions Optical diversity advisory board.
Aboutthe author
By ESSENCE JOHNSON, oddallas
Adam Ramsey, OD, co-founder of Black EyeCare Perspective (BEP), treats a patient at hispractice in West Palm Beach, FL.
Photo: Adam Ram
sey, ODB L A C K E X P E R I E N C E I N O P TO M E T RYFeature
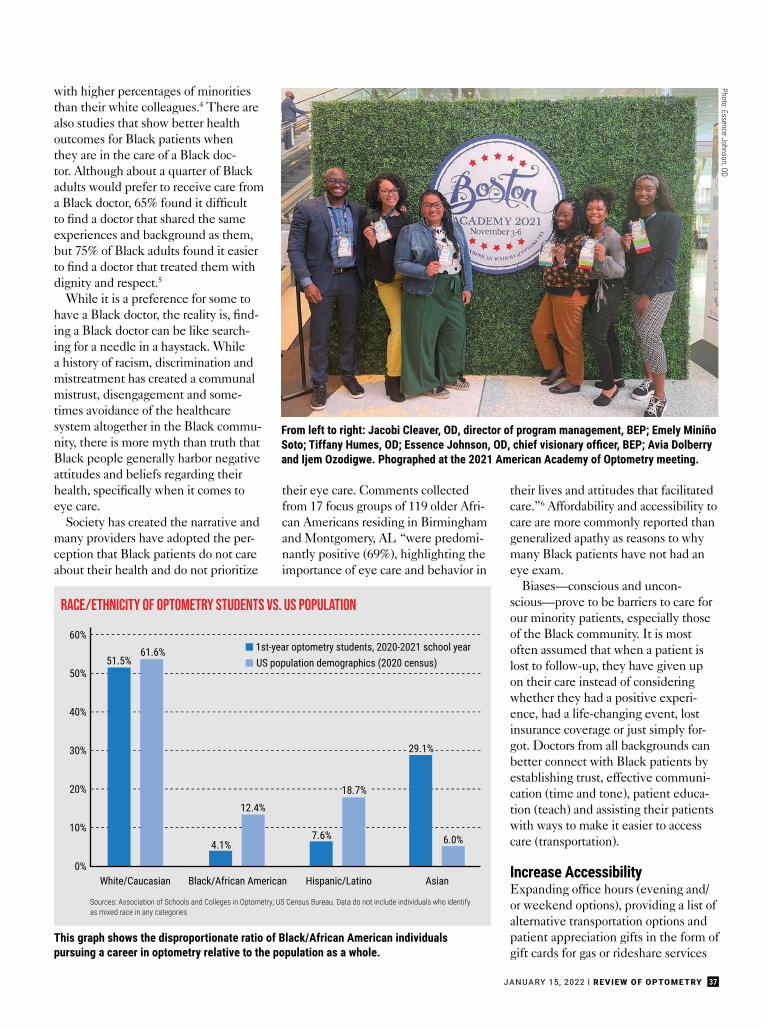
37JANUARY 15, 2022 | REVIEW OF OPTOMETRY
Photo: Essence Johnson, OD
with higher percentages of minoritiesthan their white colleagues.4 There arealso studies that show better healthoutcomes for Black patients whenthey are in the care of a Black doc-tor. Although about a quarter of Blackadults would prefer to receive care froma Black doctor, 65% found it difficultto find a doctor that shared the sameexperiences and background as them,but 75% of Black adults found it easierto find a doctor that treated them withdignity and respect.5
While it is a preference for some tohave a Black doctor, the reality is, find-ing a Black doctor can be like search-ing for a needle in a haystack. Whilea history of racism, discrimination andmistreatment has created a communalmistrust, disengagement and some-times avoidance of the healthcaresystem altogether in the Black commu-nity, there is more myth than truth thatBlack people generally harbor negativeattitudes and beliefs regarding theirhealth, specifically when it comes toeye care.
Society has created the narrative andmany providers have adopted the per-ception that Black patients do not careabout their health and do not prioritize
their eye care. Comments collectedfrom 17 focus groups of 119 older Afri-can Americans residing in Birminghamand Montgomery, AL “were predomi-nantly positive (69%), highlighting theimportance of eye care and behavior in
their lives and attitudes that facilitatedcare.”6 Affordability and accessibility tocare are more commonly reported thangeneralized apathy as reasons to whymany Black patients have not had aneye exam.
Biases—conscious and uncon-scious—prove to be barriers to care forour minority patients, especially thoseof the Black community. It is mostoften assumed that when a patient islost to follow-up, they have given upon their care instead of consideringwhether they had a positive experi-ence, had a life-changing event, lostinsurance coverage or just simply for-got. Doctors from all backgrounds canbetter connect with Black patients byestablishing trust, effective communi-cation (time and tone), patient educa-tion (teach) and assisting their patientswith ways to make it easier to accesscare (transportation).
Increase AccessibilityExpanding office hours (evening and/or weekend options), providing a list ofalternative transportation options andpatient appreciation gifts in the form ofgift cards for gas or rideshare services
From left to right: Jacobi Cleaver, OD, director of program management, BEP; Emely MiniñoSoto; Tiffany Humes, OD; Essence Johnson, OD, chief visionary officer, BEP; Avia Dolberry and Ijem Ozodigwe. Phographed at the 2021 American Academy of Optometry meeting.
This graph shows the disproportionate ratio of Black/African American individualspursuing a career in optometry relative to the population as a whole.
Race/Ethnicity of Optometry students vs. us population
60%
50%
40%
30%
20%
10%
0%White/Caucasian Black/African American Hispanic/Latino Asian
51.5%
4.1%
n 1st-year optometry students, 2020-2021 school yearn US population demographics (2020 census)
7.6% 6.0%
12.4%
61.6%
29.1%
18.7%
Sources: Association of Schools and Colleges in Optometry; US Census Bureau. Data do not include individuals who identifyas mixed race in any categories
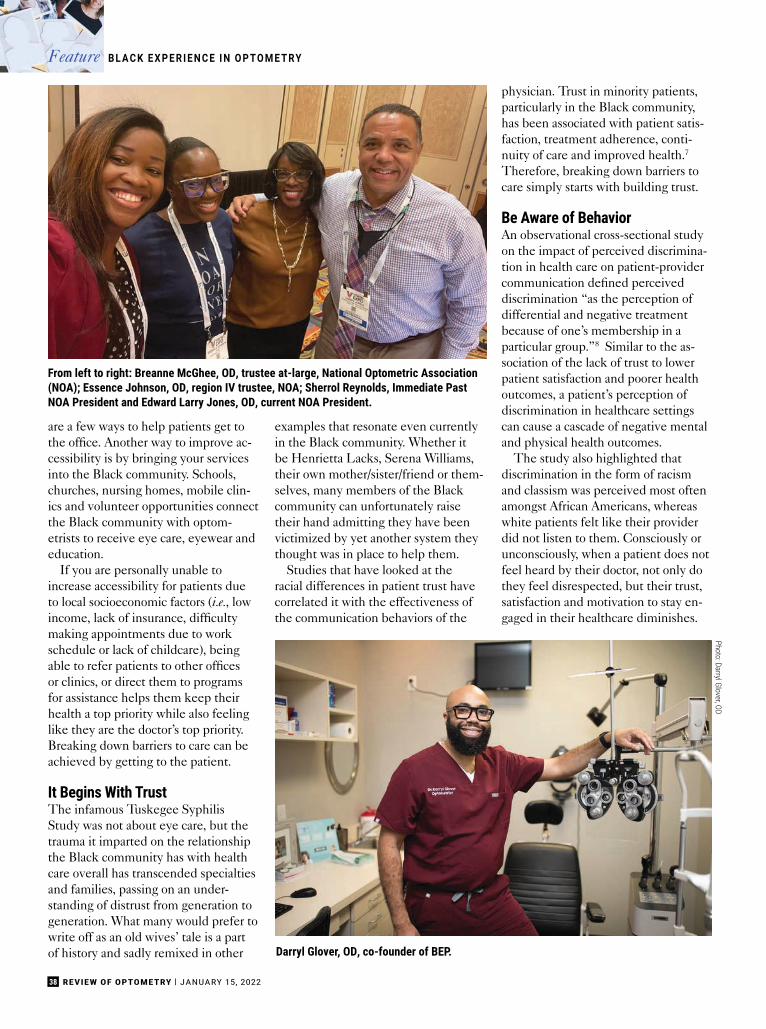
38 REVIEW OF OPTOMETRY | JANUARY 15, 2022
are a few ways to help patients get tothe office. Another way to improve ac-cessibility is by bringing your servicesinto the Black community. Schools,churches, nursing homes, mobile clin-ics and volunteer opportunities connectthe Black community with optom-etrists to receive eye care, eyewear andeducation.
If you are personally unable toincrease accessibility for patients dueto local socioeconomic factors (i.e., lowincome, lack of insurance, difficultymaking appointments due to workschedule or lack of childcare), beingable to refer patients to other officesor clinics, or direct them to programsfor assistance helps them keep theirhealth a top priority while also feelinglike they are the doctor’s top priority.Breaking down barriers to care can beachieved by getting to the patient.
It Begins With TrustThe infamous Tuskegee SyphilisStudy was not about eye care, but thetrauma it imparted on the relationshipthe Black community has with healthcare overall has transcended specialtiesand families, passing on an under-standing of distrust from generation togeneration. What many would prefer towrite off as an old wives’ tale is a partof history and sadly remixed in other
examples that resonate even currentlyin the Black community. Whether itbe Henrietta Lacks, Serena Williams,their own mother/sister/friend or them-selves, many members of the Blackcommunity can unfortunately raisetheir hand admitting they have beenvictimized by yet another system theythought was in place to help them.
Studies that have looked at theracial differences in patient trust havecorrelated it with the effectiveness ofthe communication behaviors of the
physician. Trust in minority patients,particularly in the Black community,has been associated with patient satis-faction, treatment adherence, conti-nuity of care and improved health.7
Therefore, breaking down barriers tocare simply starts with building trust.
Be Aware of BehaviorAn observational cross-sectional studyon the impact of perceived discrimina-tion in health care on patient-providercommunication defined perceiveddiscrimination “as the perception ofdifferential and negative treatmentbecause of one’s membership in aparticular group.”8 Similar to the as-sociation of the lack of trust to lowerpatient satisfaction and poorer healthoutcomes, a patient’s perception ofdiscrimination in healthcare settingscan cause a cascade of negative mentaland physical health outcomes.
The study also highlighted thatdiscrimination in the form of racismand classism was perceived most oftenamongst African Americans, whereaswhite patients felt like their providerdid not listen to them. Consciously orunconsciously, when a patient does notfeel heard by their doctor, not only dothey feel disrespected, but their trust,satisfaction and motivation to stay en-gaged in their healthcare diminishes.
From left to right: Breanne McGhee, OD, trustee at-large, National Optometric Association(NOA); Essence Johnson, OD, region IV trustee, NOA; Sherrol Reynolds, Immediate PastNOA President and Edward Larry Jones, OD, current NOA President.
B L A C K E X P E R I E N C E I N O P TO M E T RYFeature
Darryl Glover, OD, co-founder of BEP.
Photo: Darryl Glover, OD
39JANUARY 15, 2022 | REVIEW OF OPTOMETRY
When doctors communicate withpatients, it is important to be aware ofboth informational and affective be-haviors. Informational behaviors, suchas data collecting, had a lesser effect ontrust in Black patients when comparedto affective or partnership buildingbehaviors. Doctors are not dictatorsgiving commands, but the doctor-patient relationship is an ever-evolvingpartnership where together theycollaborate coming up with treatmentplans and learning from one another.Creating a positive rapport helps re-move barriers to care especially in theBlack community, although it takestime to establish. Physicians can moni-tor their affective behavior by knowingthese aspects of rapport building:7
• positive (compliments, laughter)• emotional (empathetic or concern
statements)• negative (criticism, disagree-
ments).• social (small talk)• understanding (paraphrasing or
repetition)Remember, it is not only what you
say but how you say it or do not say it.Verbal as well as nonverbal communi-cation can equally convey a tone. Evenwith a mask on, people can tell if youare speaking to them with a smile andit takes self-awareness and practice tonot mirror a patient’s negative affect.Similar to how imagery is used to helpcombat jitters before speaking in frontof a crowd, picture your patient as amember of your own family and askyourself if that was your parent/grand-parent/sibling, how would you likethem to be treated?
Be mindful of pronouns andwhether or not a patient prefers tobe addressed by their first and/orlast name. If you are unsure how topronounce someone’s name, simplyask them to say it for you so you don’tmispronounce it. Breaking down barri-ers to care can be achieved by talkingto patients with a positive tone.
Take Time With Each PatientWith patients scheduled 10, 20 or even30 minutes, the goal is to see each one
as effectively and eq-uitably as possible. Bemindful of how it maylook from a patient’sperspective: How longare they in the office?How many patients arethey witnessing beingseen before them? Notevery patient can un-derstand the complex-ity of each individual’scase. Creating astandardized approachto every patient willcreate a cadence androutine patients willbecome familiar withover time, and theywill grow to under-stand the elements ofan exam and base theirvisits on quality overquantity.
An element of theexam that is oftenshort-changed ispatient education.Economic factors aside, the averagehealth literacy in the Black communityis perceived to be low. Quite frankly,in general people “don’t know whatthey don’t know.” They may not knowtheir family’s health history due tocomplex family dynamics or a familialhierarchy. At least once in an optom-etrist’s career they will meet a patientwith a “stigma” or “cadillacs.” This isanother opportunity to break a barrierand bridge a gap through educatingthe Black community on astigma-tism and cataracts, as well as the topdiseases that cause blindness in racialand ethnic minorities—the “threesilent killers:” diabetes, hypertensionand glaucoma. Breaking down barriers
to care can be achieved by spendingmore time with patients and makingpatient education a priority.
Are We There Yet?It is not uncommon in the Blackcommunity to take on a “do as I say”and not “as I do” mentality. Surveysshow that four out of five Black peopleacknowledge eye exams should occurevery year, but year after year lessthan half of the people in the Blackcommunity get their eyes examined.9
The same plan employed to get moreBlack people to the polls or to get theCOVID-19 vaccine should also beemployed for eye care with the samelevel of excitement and societal and
Darryl Glover, OD, and future optometrist Emely Miniño Soto.
Ways to Support national organizationsThe National Optometric Foundation (NOF) and Diversity Perspective are the philanthropic andcharitable arms of the National Optometric Association (NOA) and Black EyeCare Perspective (BEP),respectively. All tax-deductible donations go toward advancing their missions. Individuals and cor-porations can make donations by selecting the NOF when shopping at Kroger or AmazonSmile, or atwww.nationaloptometricassociationdonations.square.site. Donations can also be made to DiversityPerspective at www.paypal.com/paypalme/13promise by choosing Diversity Perspective when makingqualifying purchases using AmazonSmile.
Photo: Essence Johnson, OD

40 REVIEW OF OPTOMETRY | JANUARY 15, 2022
political support. When asked, afford-ability and accessibility rank high onbarriers to receiving eye care. On a na-tional level, inadequate transportationoptions continue to have a negativeimpact on the health and well-being,particularly of the elderly in the Blackcommunity.6
Support National OrganizationsWhile research currently supportspatients of the Black communitythat may be treated by non-minoritydoctors are at higher risk of adversemedical outcomes, it was the recom-mendations from American educatorAbraham Flexner’s 1910 report thathas negatively impacted Black doc-tors, and patients and the ramificationsare still felt centuries later. Flexner’sfindings resulted in the closing of allbut two of the seven historically blackmedical schools that educated Blackdoctors at the time—Meharry MedicalCollege and Howard University—andinfected society with the belief thatBlack doctors should only treat Blackpatients, but if not properly trainedand treated, the Black communitywould be a health threat to affluentwhite communities.
Preceding the release of the Flexnerreport, what is now known as the Na-tional Medical Association (NMA) wasfounded in 1895 by a group of physi-cians who were denied membershipinto other professional organizationsand societies, like the American Medi-
cal Association which was foundedin 1847.10 The American OptometricAssociation was founded in 1898; forsome of the same reasons the NMAwas established, 25 African Ameri-can optometrists gathered with thepurpose to establish a nationally recog-nized optometric association com-prised of Black doctors. That meetingtook place in the spring of 1969 andwas the first of many for the NationalOptometric Association (NOA).11
With the mission of “Advancingthe Visual Health of Minority Popula-tions,” membership into NOA is opento all ODs with diverse backgroundswilling to make an investment in thefuture of optometry and eye health,and passionate about supportingNOA’s purpose to recruit minoritystudents into the schools and collegesof optometry and placement into ap-propriate practice settings upon gradu-ation, in addition to educating andcaring for the community to eliminate
barriers and disparities in eye health.To become a member of NOA and
help advance its mission, please visitnationaloptometricassociation.com.
Black EyeCare PerspectiveIt is in part from the network createdby the NOA and its student organiza-tion (the National Optometric StudentAssociation) and various summer pro-grams (Texas Optometry Careers Op-portunity Program at the Universityof Houston College of Optometry andthe Pennsylvania College of Optom-etry’s Summer Enrichment Program),that optometrists Adam Ramsey, Dar-ryl Glover, Jacobi Cleaver and myselfwere brought together. Collectively,we are working to redefine the colorof the eyecare industry 1% at timethrough an organization called theBlack EyeCare Perspective (BEP).
BEP was designed and created tocultivate and foster lifelong relation-ships between African American eyecare professionals and the eyecareindustry. BEP believes one must beunited in their efforts and intentionalin their impact to truly see the per-centage of Black optometrists increaseand reflect that of the Census-reportedpopulation (1.8% vs. 13%).
In 2020, BEP launched its 13%Promise initiative to encourage com-mitment and action among individualsand corporations to increase Black andAfrican American representation ineyecare to align with the US Censusfor better health outcomes of under-represented communities. Industrypartnerships and targeted program-ming help support the vision of the
Ways to Support Black EyeCare Perspective• Join the 13% Promise by committing to a monthly or annual donation of $130, $1,300, $13,000 or
more. All donations are tax-deductible and support scholarships, programs and initiatives.
• Refer a future optometrist or volunteer to speak at a Black EyeCare Perspective Pre-OptometryClub meeting held on the 13th of every month.
• Save the date for Black EyeCare Perspective Pre-Optometry Club’s second annual Signing Day inSpring 2022. All students entering into a school or college of optometry in the fall are invited toparticipate. Follow @beppoc on Facebook and Instagram for more information.
• Purchase merchandise at the BEP Store: www.blackeyecareperspective.myspreadshop.com.
• Share the Black EyeCare Professional locator on www.blackeyecareperspective.com. To be addedto the locator, email [email protected].
B L A C K E X P E R I E N C E I N O P TO M E T RYFeature
Nwamaka Ngoddy, OD, practices in Atlanta and is also the creator of Anwuli Eyewear, a lineof frames specifically to fit the facial features of the Black and African American community.
Photo: Nicole Brody

41JANUARY 15, 2022 | REVIEW OF OPTOMETRY
13% Promise: to create a pipelinefor Black students into optometry,connect communities with Black eyecare professionals and Black eye carebusinesses and cultivate relationshipsbetween Black optometrists and op-portunities in the eye care industry.
BEP is also creating brave spacesand facilitating courageous conversa-tions within the eyecare communitythrough diversity, equity and inclusioninitiatives and influencing the mind-set of the next generation of eyecareprofessionals to raise awareness andimpact the industry in ways we haveyet to see.
Black Eye Care PerspectivePre-Optometry ClubThe Black EyeCare PerspectivePre-Optometry Club (BEPPOC),established in 2020, is the first pre-optometry club nationally recognizedby the Associations of the Schoolsand Colleges of Optometry to ensurenot a single potential Black or AfricanAmerican student or optometrist isignored, discouraged or disadvan-taged. Nearing a membership of 100Black future optometrists represent-ing 54 undergraduate institutions—15being Historically Black Colleges andUniversities—membership is free andmeetings are held on the 13th of everymonth. BEPPOC is an integral part ofthe pipeline for increasing the numberBlack students entering the eyecareprofession.
Minding our “T”sBlack Americans, Asian Americans,Hispanic Americans, white Ameri-cans—we all are all a part of thisnation and the term American shouldring synonymously with people fromall backgrounds, not exclusively withjust one group and independent ofany other identifying or classifying fac-tors. The health of our patients whoare from diverse populations is ourfirst priority. We all should continue towork to expand access to quality careand improve health equity for all com-munities and strive to see that no onelacks proper care.
The secret to creating a strongerconnection between ODs and theBlack community? Stop creating andaccepting as inevitable a self-fulfillingprophecy that there are disparities inhealthcare that disproportionately affectminority communities but there is noth-ing that can be done now to start break-ing down the barriers that should’venever been placed centuries ago.
By minding our “T”s—trust, time,tone, teaching and transportation—wecan break down a few of those barriersto care for patients in the Black com-munity. Together, we can do the smallthings that make a great impact notjust in connecting with the Black com-munity, but in enriching healthcare,advancing eye care and strengtheningevery doctor-patient relationship. ■
1. American Optometric Association. www.aoa.org/about-the-aoa/ethics-and-values. Accessed December 27, 2021.2. United States Census Bureau. www.census.gov/library/stories/2021/08/improved-race-ethnicity-measures-reveal-
united-states-population-much-more-multiracial.html. 2021.Accessed December 27, 2021.3. Black EyeCare Perspective. www.blackeyecareperspective.com/the-13-promise. Accessed December 27, 2021.4. Smedley BD, Stith AY, Colburn L, et al. The Right Thing toDo, The Smart Thing to Do: Enhancing Diversity in the HealthProfessions. Institute of Medicine. National Academies Press.2001.5. Washington, J. New poll shows Black Americans put far lesstrust in doctors and hospitals than white people. www.theun-defeated.com/features/new-poll-shows-black-americans-put-far-less-trust-in-doctors-and-hospitals-than-white-people.2021. Accessed December 27, 2021.6. Owsley C, McGwin G, Scilley K, et al. Perceived barriers tocare and attitude about vision and eye care: focus groups witholder African Americans and eye care providers. InvestigativeOphthalmology & Visual Science. 2006;47:2797-802.7. Martin KD, Roter DL, Beach MC, et al. Physician communica-tion behaviors and trust among Black and white patients withhypertension. Med Care. 2013;51(2):151-7.8. Hausmann LRM, Hannon MJ, Kresevic DM, et al. Impactof perceived discrimination in health care on patient-providercommunication. Med Care. 2011;49(7):626-33.9. African-Americans need to make vision care a priority.www.ophthalmologymanagement.com/issues/2008/novem-ber-2008/stat-tracker. Ophthalmology Management. 2008.Accessed December 27, 2021.10. Mitchell EP. The National Medical Association 1895-2020:struggle for healthcare equity in the United States of America.J Natl Med Assoc. 2020;112(4):331-2.11. National Optometric Association. www.nationaloptomet-ricassociation.com/about-us/our-history. Accessed December27, 2021.
how to broach difficult discussions on raceLast November at the AAO meeting in Boston, the Plenary session was devoted to conversations aboutrace—in society and in the clinic. Beverly Daniel Tatum, PhD, an expert on the psychology of racism andrace relations and best-selling author of Why Are All Black Kids Sitting Together in the Cafeteria?, wasthe featured speaker. In a “fireside chat” with Academy president-elect Susan Cotter, OD, Dr. Tatumdove into issues of prejudice and racism, describing how they impact health care as a system and eyecare specifically. The objective of this session was to have a better understanding of what racism isand how it impacts optometry and healthcare and patients.
Dr. Tatum talked about how hard it is to have conversations about race, but noted that everyone hassome experience in this topic—whether they’ve talked about it or not. “We learn early on, in this countryat least, that you’re not supposed to talk about some things,” she said. “Thus, an adult’s first instinct isto shush and not talk about sensitive things.”
She explained that when we don’t have these types of conversations, we are learning and reinforc-ing the idea that we’re supposed to ignore what we can all see happening around one another. That initself is part of the problem, she argues, and it inevitably bleeds into our professional lives.
Getting rid of stereotypes is also part of the challenge. Here’s three ways Dr. Tatum suggested youcan turn conversation into action to limit stereotypes and help you breakdown barriers in your practice:
Interact. Counteract with positive images. If you have limited experience with a particular groupand you only know the stereotype, getting to know people in that group in some ways can minimize theimpact of stereotypes. Come to understand they are an exception.
Educate Early. Expose children to a wide range of people to help prevent stereotypes from gettingdrilled in their head. Today, there are several children’s books with diverse images and positive storiesof children of all backgrounds that can help this.
Engage. Start engaging with people different from yourself. If you have that skill, you’ll be success-ful. If not, you’re going to be increasingly isolated, Dr. Tatum noted.
Edward Larry Jones, OD, was part of a group discussion panel following the initial discussion. Someof the things that transpired included him driving home how important it is to make his patients ofcolor feel comfortable. He starts his exams by associating the patient with someone he personallyknows and says out loud that he is going to treat him/her just like they are family or a friend, which canput not just the patient more at ease, but himself as well.
He also continued Dr. Tatum’s previous point, saying that by ignoring what’s right in front of you, youbecome ignorant.
“All of us are educators,” he said. “We can’t walk away from that knowledge. According to theresearch, 74,000 Black people a year are dying from health disparities. That’s a travesty. We can’tignore that or walk away from that.”
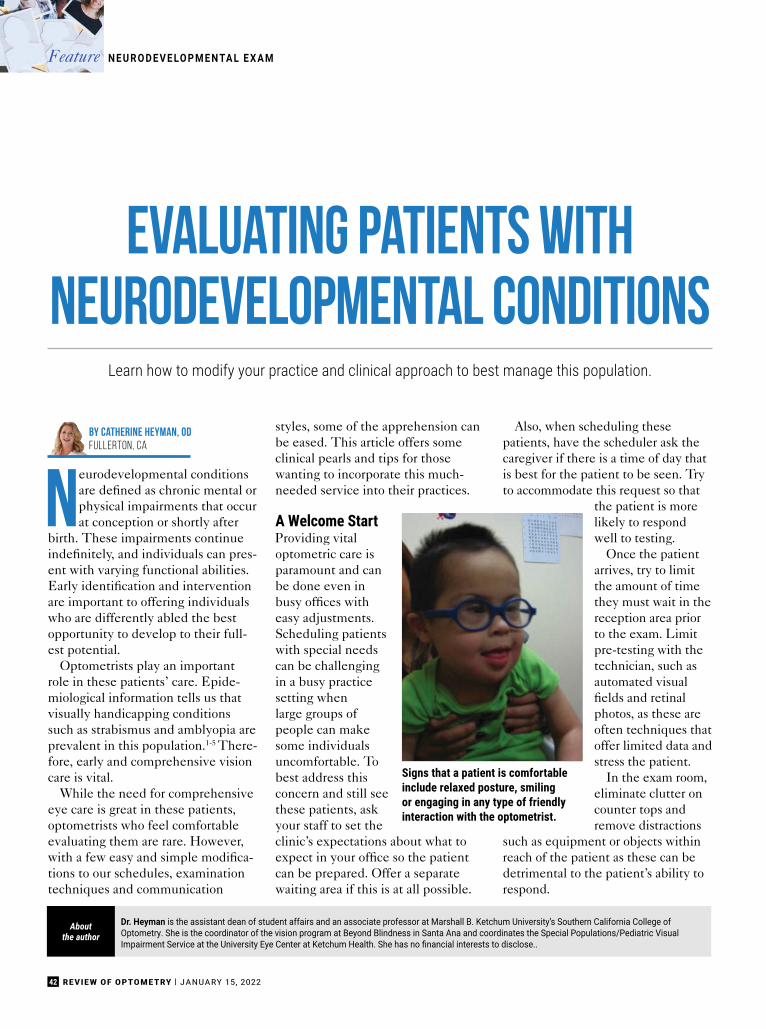
42 REVIEW OF OPTOMETRY | JANUARY 15, 2022
Evaluating Patients withNeurodevelopmental Conditions
Learn how to modify your practice and clinical approach to best manage this population.
Neurodevelopmental conditionsare defined as chronic mental orphysical impairments that occurat conception or shortly after
birth. These impairments continueindefinitely, and individuals can pres-ent with varying functional abilities.Early identification and interventionare important to offering individualswho are differently abled the bestopportunity to develop to their full-est potential.
Optometrists play an importantrole in these patients’ care. Epide-miological information tells us thatvisually handicapping conditionssuch as strabismus and amblyopia areprevalent in this population.1-5 There-fore, early and comprehensive visioncare is vital.
While the need for comprehensiveeye care is great in these patients,optometrists who feel comfortableevaluating them are rare. However,with a few easy and simple modifica-tions to our schedules, examinationtechniques and communication
styles, some of the apprehension canbe eased. This article offers someclinical pearls and tips for thosewanting to incorporate this much-needed service into their practices.
A Welcome StartProviding vitaloptometric care isparamount and canbe done even inbusy offices witheasy adjustments.Scheduling patientswith special needscan be challengingin a busy practicesetting whenlarge groups ofpeople can makesome individualsuncomfortable. Tobest address thisconcern and still seethese patients, askyour staff to set theclinic’s expectations about what toexpect in your office so the patientcan be prepared. Offer a separatewaiting area if this is at all possible.
Also, when scheduling thesepatients, have the scheduler ask thecaregiver if there is a time of day thatis best for the patient to be seen. Tryto accommodate this request so that
the patient is morelikely to respondwell to testing.
Once the patientarrives, try to limitthe amount of timethey must wait in thereception area priorto the exam. Limitpre-testing with thetechnician, such asautomated visualfields and retinalphotos, as these areoften techniques thatoffer limited data andstress the patient.
In the exam room,eliminate clutter oncounter tops andremove distractions
such as equipment or objects withinreach of the patient as these can bedetrimental to the patient’s ability torespond.
By catherine Heyman, ODFullerton, CA
Dr. Heyman is the assistant dean of student affairs and an associate professor at Marshall B. Ketchum University’s Southern California College ofOptometry. She is the coordinator of the vision program at Beyond Blindness in Santa Ana and coordinates the Special Populations/Pediatric VisualImpairment Service at the University Eye Center at Ketchum Health. She has no financial interests to disclose..
Aboutthe author
Signs that a patient is comfortableinclude relaxed posture, smilingor engaging in any type of friendlyinteraction with the optometrist.
N E U R O D E V E LO P M E N TA L E X A MFeature

43JANUARY 15, 2022 | REVIEW OF OPTOMETRY
Carefully consider the best posi-tioning for each individual patient.This can include leaving the patientin a comfortable wheelchair and hav-ing the patient sit on the caregiver’slap or laying on a mat on the floor.Choose the position that will allowthe patient to be most comfortableand allow them to respond to testingwithout expending muscle energy tohold up their head or sit upright if thisis difficult for them.
Remember that first and foremostpatients with special needs are people.Don’t define these patients by theircondition. When communicating, usepeople-first language: “a child withautism,” not “an autistic child” or,worse, “an autistic.”6 Never put thediagnosis before the person. Alwaysaddress case history questions withthe patient first and allow them toanswer as they are able. The caregivercan fill in the blanks. To the extentpossible, have your office staff collectas much case history as possible priorto the patient arriving at the office.This can be done though a web-based
secure historyform or overthe phone onceconfirmation of thecaregiver’s identityis established.
Extended casehistory during theexam can causeanxiety for thepatient, so keepthis brief. Duringthe exam, speak inshort, declarativesentences andvisually supportwhat you say withpointing. Match
your facial expressions to your wordsand avoid speaking loudly, usingsarcasm or repeating instructionsover and over. Often, there is a delayin auditory processing; count to fivebefore you repeat yourself as yourpatient is likely to respond duringthat time once they have completedprocessing your instruction.
Adjust Your TechniqueTechniques to gain the patient’scooperation during the exam areimportant. Offering choices allowsthe patient to decide to participate.Would the patient like towatch Elmo or Mickey Mousewhile retinoscopy is be-ing done? Talking your waythrough the exam also helps.Explain what is going tohappen and help the patientanticipate a transition to thenext task by giving them fore-warning. Let them know youhave one more minute withthis activity and then you willdo something else.
Ask the caregiver for bestpractices when working witha patient to motivate themand make them feel com-fortable. Does this patientrespond well to clapping aftera task is successfully com-pleted? Are they motived bystickers or food?
Have the caregiver share thetechniques they use with the patientto best motivate this individual. Thecaregiver can also give the optom-etrist insight into whether the patientuses sign language to communicateand can show you a few signs thatwill help throughout the exam.Singing songs during the exam andplaying the patient’s favorite musicor video on a phone or tablet can alsohelp improve cooperation.
Many patients with special needshave sensory issues, such as tactiledefensiveness, or an aversion totouch or being touched. Be consid-erate of this and inform the patientof the need to touch them prior toperforming a technique that requirestouch or holding an object near thepatient’s face, such as during a covertest, lens rack retinoscopy or binocu-lar indirect ophthalmoscopy (BIO).Demonstrate the technique with thecaregiver or a stuffed animal to helpacclimate the patient. Start by touch-ing the patient away from their faceand slowly work up to there.
Recognize that behavior is com-munication. If the patient is becom-ing tense or beginning to performself-stimulating behaviors, allow thethem to take a break. Stimulation
Use a 20D lens and transilluminator for an ocular healthevaluation.
Explain what is going to happenand help the patient anticipatea transition to the next task bygiving them forewarning.
Consider the best positioning for each patient, suchas leaving them in a comfortable wheelchair. Choosethe position that will allow them to respond to testingwithout expending muscle energy to hold up theirhead or sit upright if this is difficult for them.

44 REVIEW OF OPTOMETRY | JANUARY 15, 2022
of large muscle groups is calming,and you can have the patient take amoment to stretch or walk aroundthe room, if they are able. Addition-ally, ask the caregiver if the patientcan have a snack or bottle as way of abreak during the exam. A weightedblanket can calm a patient who isupset.
Establish a rapport with the patientto make them feel comfortable withthe optometric exam and with you.Watch for signs that the patient iscomfortable such as relaxed posture,smiling or engaging in any type offriendly interaction with the optom-etrist. Have a battery of differentlighted toys and high contrast toys,i.e., black and white. Employ the“one toy, one look strategy” whendeciding on the number of toys thatyou will need. If the patient has seenit, grab a new toy to hold their inter-est.
Begin the exam with versions,gross visual fields and near point ofconvergence prior to visual acuitiesto help the patient become comfort-able. These allow optometrists tomake initial observations about thepatient’s overall visual functioningthat will help guide the rest of theexamination. The gestalt of the over-all visual function will be developedonce the examination is complete.
Testing should be done to thehighest level possible, i.e., using asclose to standard techniques as thepatient can handle and moving downthe level of complexity as neededto meet the needs of the individualpatient.
The exam will often be primar-ily comprised of objective testing.Clinicians will need to be open tousing forced choice or preferentiallooking types of visual acuity testingif the patient cannot perform Snellenacuity, cycloplegic retinoscopy usinglens bars, and use a 20D lens andtransilluminator for an ocular healthevaluation.4 Use your observationalskills, ability to adapt testing to meetthe developmental needs of thepatient and your knowledge of whatto expect for the patient’s particularcondition to fill in the data. Limittesting to those data points that pro-vide the most bang for your buck, i.e.,look for any amblyogenic factors ortreatable disease first and foremost.
The evaluation of a patient withspecial needs should be efficient: getin, get it done, get out. Set a goal oflimiting data collection to a total of30 minutes in the chair at the most.
Perhaps more than any otherpopulation, working with patientswith special needs brings with itsome unique psychological chal-
lenges. This includes understandingwhere patients stand with medicalprocedures they have previously hadto endure. One thing that can causeanxiety in these patients is the whitecoat. Do not wear one when seeingthis population.
Other common triggers of anxietyinclude unexpected or explainedprocedures and, of course, drop in-stallation. To help with the anxiety ofdrop installation, be sure to make itquick with limited or no prior discus-sion. Ask the caregiver to help holdthe patient and have an extremelyinteresting toy to distract the patientonce the drops are instilled. Once thedrops are instilled, allow the patientto exit the exam room and take abreak, have a snack or some othersoothing experience.
Let the caregiver know that lesspatient response is required for thesubsequent techniques (retinos-copy and BIO) and that very youngpatients can actually be asleep duringthe completion of the examination.
To triage these patients, be familiarwith common eye conditions associ-ated with the patient’s specific neu-rodevelopmental condition to helpprioritize the most important aspectsof the optometric examination.2,3
Resources and Care TeamOptometrists are uniquely able toprovide resources for families ofpatients with special needs. Becausevision plays a primary role in learning,the link between optometric servicesand education is strong. Parents of
Be considerate and inform the patient ofthe need to touch them before performinga technique that requires contact.
Don’t rush, but be efficient. Set a goal of limiting data collection to a total of 30 minutes in the chair at the most.
Testing should be done to thehighest level possible, i.e., usingas close to standard techniquesas the patient can handle andmoving down the level ofcomplexity as needed to meetthe needs of the individualpatient.
N E U R O D E V E LO P M E N TA L E X A MFeature

Apellis is exploring the role of complement in Geographic Atrophy1
C3 is the linchpin of complement overactivation in GA.2-7
All three complement pathways converge at C3 and it drives
multiple downstream effects — inflammation, opsonization, and
formation of the membrane attack complex — all of which can
ultimately lead to retinal cell death. Increased levels of complement
activity have been found not just in the lesion itself, but also in the
area just outside the lesion, known as the pre-lesion.2-9
1. Katschke KJ Jr, et al. Sci Rep. 2018;8(1):13055. 2. Mastellos DC, et al. Trends Immunol. 2017;38(6):383-394. 3. Ricklin D, et al. Immunol Rev. 2016;274(1):33-58. 4. Heesterbeek TJ, et al. Opthalmol Vis Sci. 2020;61(3):18. 5. Seddon JM, et al. Nat
Genet. 2013;45:1266-1370. 6. Yates JRW, et al. N Engl J Med. 2007;357(6):553-561. 7. Smailhodzic D, et al. Ophthalmology. 2012;119(2):339-346. 8. Boyer DS, et al. Retina. 2017;37:819-835. 9. Park DH, et al. Front Immunol. 2019;10:1007.
© 2021 Apellis Pharmaceuticals, Inc. All rights reserved. 07/21 US-GA-2100016 v1.0
Scan the code to explore new territory with us at pre-lesion.com
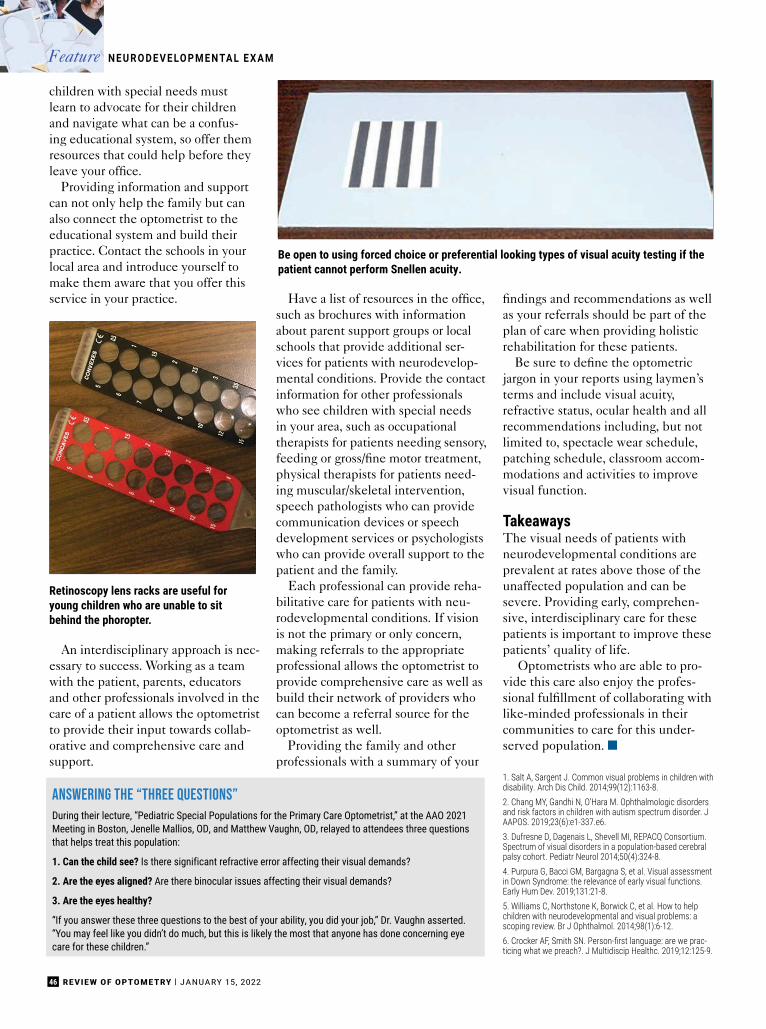
46 REVIEW OF OPTOMETRY | JANUARY 15, 2022
children with special needs mustlearn to advocate for their childrenand navigate what can be a confus-ing educational system, so offer themresources that could help before theyleave your office.
Providing information and supportcan not only help the family but canalso connect the optometrist to theeducational system and build theirpractice. Contact the schools in yourlocal area and introduce yourself tomake them aware that you offer thisservice in your practice.
An interdisciplinary approach is nec-essary to success. Working as a teamwith the patient, parents, educatorsand other professionals involved in thecare of a patient allows the optometristto provide their input towards collab-orative and comprehensive care andsupport.
Have a list of resources in the office,such as brochures with informationabout parent support groups or localschools that provide additional ser-vices for patients with neurodevelop-mental conditions. Provide the contactinformation for other professionalswho see children with special needsin your area, such as occupationaltherapists for patients needing sensory,feeding or gross/fine motor treatment,physical therapists for patients need-ing muscular/skeletal intervention,speech pathologists who can providecommunication devices or speechdevelopment services or psychologistswho can provide overall support to thepatient and the family.
Each professional can provide reha-bilitative care for patients with neu-rodevelopmental conditions. If visionis not the primary or only concern,making referrals to the appropriateprofessional allows the optometrist toprovide comprehensive care as well asbuild their network of providers whocan become a referral source for theoptometrist as well.
Providing the family and otherprofessionals with a summary of your
findings and recommendations as wellas your referrals should be part of theplan of care when providing holisticrehabilitation for these patients.
Be sure to define the optometricjargon in your reports using laymen’sterms and include visual acuity,refractive status, ocular health and allrecommendations including, but notlimited to, spectacle wear schedule,patching schedule, classroom accom-modations and activities to improvevisual function.
TakeawaysThe visual needs of patients withneurodevelopmental conditions areprevalent at rates above those of theunaffected population and can besevere. Providing early, comprehen-sive, interdisciplinary care for thesepatients is important to improve thesepatients’ quality of life.
Optometrists who are able to pro-vide this care also enjoy the profes-sional fulfillment of collaborating withlike-minded professionals in theircommunities to care for this under-served population. ■
1. Salt A, Sargent J. Common visual problems in children withdisability. Arch Dis Child. 2014;99(12):1163-8.2. Chang MY, Gandhi N, O’Hara M. Ophthalmologic disordersand risk factors in children with autism spectrum disorder. JAAPOS. 2019;23(6):e1-337.e6.3. Dufresne D, Dagenais L, Shevell MI, REPACQ Consortium.Spectrum of visual disorders in a population-based cerebralpalsy cohort. Pediatr Neurol 2014;50(4):324-8.4. Purpura G, Bacci GM, Bargagna S, et al. Visual assessmentin Down Syndrome: the relevance of early visual functions.Early Hum Dev. 2019;131:21-8.5. Williams C, Northstone K, Borwick C, et al. How to helpchildren with neurodevelopmental and visual problems: ascoping review. Br J Ophthalmol. 2014;98(1):6-12.6. Crocker AF, Smith SN. Person-first language: are we prac-ticing what we preach?. J Multidiscip Healthc. 2019;12:125-9.
Retinoscopy lens racks are useful foryoung children who are unable to sitbehind the phoropter.
ANSWERING THE “THREE QUESTIONS”During their lecture, “Pediatric Special Populations for the Primary Care Optometrist,” at the AAO 2021Meeting in Boston, Jenelle Mallios, OD, and Matthew Vaughn, OD, relayed to attendees three questionsthat helps treat this population:
1. Can the child see? Is there significant refractive error affecting their visual demands?
2. Are the eyes aligned? Are there binocular issues affecting their visual demands?
3. Are the eyes healthy?
“If you answer these three questions to the best of your ability, you did your job,” Dr. Vaughn asserted.“You may feel like you didn’t do much, but this is likely the most that anyone has done concerning eyecare for these children.”
Be open to using forced choice or preferential looking types of visual acuity testing if thepatient cannot perform Snellen acuity.
N E U R O D E V E LO P M E N TA L E X A MFeature

MARCH 9-13NEW ORLEANS
ERNEST N. MORIAL CONVENTION CENTER
REGISTER TODAY ATattendseco.com
Get a first look at the research, technology, and techniques thatare evolving patient care and propelling the optometric
profession forward. Whether you are looking for the latest inclinical advancements or business management solutions, you
will find the speakers, education, solutions, and connections youneed to stay on the cutting edge.
48 REVIEW OF OPTOMETRY | JANUARY 15, 2022
How to Offer Inclusive Carefor LGBTQ+ Patients
Recognize inherent biases in practices and implement more supportive behaviorto interact with members of this community respectfully.
Being an optometrist has been arewarding job. However, whenI (Dr. Roberts) graduated fromschool 15 years ago, I was not
sure if patients would accept me forbeing different. I was from a smallrural town where diversity was scarceand discussions of diversity andinclusion were not mainstream inculture—let alone in the optometrycurriculum. At the time, I was closeted(meaning I hadn’t told anyone aboutmy sexuality) and scared to deaththat my future would crumble shouldpeople know the truth about who I amand who I love. At graduation, I wasjust coming to grips with who I trulywas, but being a part of the lesbian,gay, bisexual, transgender or queer/questioning (LGBTQ+) communityfrightened me. I certainly did not feelsafe enough to trust a medical profes-sional with knowing my hidden truth.
BackgroundNow I can look back at how far I havecome: I am out, married to the loveof my life, have an adopted son anda great job within the Departmentof Veteran Affairs. I have also beenappointed the LGBTQ+ Veteran carecoordinator due to my advocacy forLGBTQ+ veterans for our facility andsmaller out-patient clinics. Never ina million years did I feel that I wouldbe this embraced. Hopefully, thisarticle will allow you as a provider tofeel more comfortable with LGBTQ+patients in your office and to enhancetheir experience as patients and hu-man beings.
I will never forget having that first,honest discussion with friends, thenfamily, then finally the medical com-munity (in that order). Unfortunately,due to past experiences, this is thecase for most people in the LGBTQ+community.1 Most, at some point,have felt the stigma of being differentin society, experienced discriminationand have psychological insult from
being denied civil and human rights.Further, many have lacked family andpersonal acceptance of their true self.3
We have come so far in a shortperiod of time with the legalization ofgay marriage, but, like human rightsmovements of the past, there is stillprogress that needs to be made toreduce disparities and achieve fullequality. The largest thing to know isthat being LGBTQ+ is not a disease.However, it was only in 1987 that“homosexuality” was removed fromthe Diagnostic and Statistical Manual ofMental Disorders.1
In reality, the LGBTQ+ communi-ty “consists of a cross-cultural, broadrange of community members thatincludes all races, ethnic and religiousbackgrounds, as well as a range ofsocioeconomic status.”1 Therefore,it is so important to become awareof unconscious biases as clinicians toprovide the best possible care to pa-tients. As the most recent optometricoath states, “I will provide profes-sional care for the diverse populations
By Matthew J. Roberts, OD,and Paula McDowell, ODKalamazoo, MI; Big Rapids, MI
Dr. Roberts practices at the VA Battle Creek Medical Center, where he is the team lead of the Low Vision Clinic and the LGBTQ+ Veteran Care Coordinator.He also practices at the Unified Clinics at Western Michigan University in Kalamazoo, MI, where he is also an adjunct professor, a fellow of the American Academy of Optometry and chair of the Michigan Optometric Association’s Continuing Education Committee. He has no financial disclosures.
Dr. McDowell is chief of pediatrics, pediatric residency supervisor and professor at Michigan College of Optometry at Ferris State University in Big Rapids, MI. She is a fellow of the American Academy of Optometry, an investigator for the Pediatric Eye Disease Investigator Group and chair of the Michigan Optometric Association’s Children’s Vision Care Committee. She has no financial disclosures.
Aboutthe authors
L G BT Q+ C A R EFeature

49JANUARY 15, 2022 | REVIEW OF OPTOMETRY
who seek my services, with concern,with compassion and with due regardfor their human rights and dignity.”2
The most recent updates also state,“I will work to expand access to qual-ity care and improve health equity forall communities.”2
The three main ways that a pro-vider can help improve the patientexperience are to understand and useappropriate terminology, understandbarriers to care for this population anduse gender-inclusive practices withinthe office. In this article, Dr. McDow-ell and I will discuss how to increaseyour awareness and best enact thesechanges.
Using Appropriate TermsUnderstanding terminology can helpbuild rapport with patients. Thiscan be difficult, as terminology sur-rounding LGBTQ+ individuals andidentity, in particular, is constantlyevolving. However, both the optom-etrist and staff need to know what isderogatory and what is not; when indoubt, following the patient’s lead isoften safe.1
Previous literature frequently citesout-of-date, derogatory or inaccurateterminology, but the good news isthat there is an abundance of recentliterature surrounding this topic. Thefollowing is a very brief list of someterminology that is prominent withinthe LGBTQ+ community that allclinicians should be aware of:1
• Ally: a heterosexual and cisgen-der person who supports equal civilrights, gender equality and LGBTQ+social movements, challenging ho-mophobia, biphobia and transphobia.
• Bisexual: Individuals that are at-tracted to both males and females.
• Cisgender: Denoting or relating toa person whose sense of gender iden-tity corresponds with their assignedsex at birth.
• Coming out: Sharing gender orsexual identity publicly.
• FTM (female to male): Assignedfemale sex at birth but identifiesas male, sometimes referred to as atransgender male.
• Gender: A person’s internal senseof being male, female or somewherein between, often self-identified byage six or earlier.
• Gender non-conforming (GNC) ornon-binary (NB): Gender behaviorsthat do not strictly align with femi-nine or masculine binaries.
• Intersex: Individuals born withanatomical sexual characteristicsthat are not typical of male or femalebinary notions.
• MTF (male to female): Assignedmale sex at birth but identifies asfemale, sometimes referred to as atransgender female.
• Queer: A general term that refersto lesbian, gay, bisexual, transgenderand queer individuals (sometimesconsidered derogatory but oftenthought to have been reclaimed bythose in the LGBTQ+ community).
• Questioning: Individuals uncertainof their gender identity and/or sexualorientation.
• Sex assigned at birth: Sex assignedbased on infant’s external genitalia,chromosomal make-up and/or hormoneprevalence.
• Sexual iden-tity: An individual’sdescription of theirown sexuality.
• Sexual orienta-tion: An individual’ssexual identity con-cerning their genderattraction.
• Transgender:Individuals whosegender identity isdifferent than theirsex assigned at birth.
• Transition: Anindividual’s psy-chological, medicalor social processof transitioningfrom one gender toanother. This is indi-vidualized and mayinclude one, some,all or none of thesetransitions.
Barriers to CareOptometrists are often on the front-line of healthcare. By being more cul-turally competent with the LGBTQ+population, we can improve healthoutcomes by eliminating disparitiesthis population often faces. The fol-lowing includes a list of challengesin this population, with each of thesestatistics higher and more prominentin racial minority groups:3
• LGBTQ+ youth are more likelyto be homeless and are two to threetimes more likely to commit suicide.
• Lesbians and bisexual females aremore likely to be overweight or obese.
• Gay men are at a higher risk ofHIV and other sexually transmittedinfections (STIs), especially amongcommunities of color.
• Transgender individuals have ahigh prevalence of HIV/STIs, vic-timization, mental health conditions,higher risk of suicide and are lesslikely to have health insurance thanheterosexual or cisgender members ofthe LGBTQ+ community.
Intake forms with marital status might include “significant other” or “partner” to show inclusiveness. For children, optionsfor legal guardian(s) or caregiver(s) are more inclusive than aspecific space for a mother and father.

50 REVIEW OF OPTOMETRY | JANUARY 15, 2022
• Elderly LGBTQ+ individuals faceadditional barriers to health becauseof isolation and lack of social servicesand culturally competent providers.
• LGBTQ+ populations have thehighest rates of tobacco, alcohol andother drug use.
While none of the above are in-herent to being an LGBTQ+ indi-vidual, the frequent abuse and riskof discrimination of “coming out”contributes to the astounding rates ofdepression and suicide. As providers,we can ask if the patient has accessto appropriate mental health services,and be aware of local support groupsand inclusive primary care providers.
An Inclusive PracticeIn practice, patient paperwork andforms need to reflect an inclusiveenvironment, since paperwork is oneof the first things that a patient seesupon entering the office. For all pa-tients, providing space for legal nameand nickname or preferred name iscommon, and still appropriate for theLGBTQ+ population. Sex shouldbe listed as male, female or other. Amore complete option is to have bothbirth sex and self-identified genderidentity, with options for pronouns.
Intake forms with marital statusmight include terminology suchas “significant other” or “partner”(instead of husband/wife) to showa practice’s inclusiveness. For chil-
dren, options for legal guardian(s) orcaregiver(s) are more inclusive than aspecific space for a mother and father.
One of the smallest steps to im-prove inclusivity, while yet making alarge impact, is the use of pronounsthat match the patient’s identity. Tomost heterosexual cisgender individu-als, this may seem like an unnecessarystep. However, to the transgender andGNC/NB community, using appropri-ate pronouns validates who they are.
When a person is misgendered, itadds to the challenges and burdensthat they already face. Worst of all,it brings up feelings of dysphoria,anxiety, stigmatization, lowered self-esteem and embarrassment. Simplyusing gender-af-firming pronounslowers rates ofsuicide and is aneasy way to havea hugely positiveimpact on yourpatients’ life.4
In sharingpronouns, it isalso becomingcommon practicein group introduc-tions to includepronouns. Thisshows anyone inthe group thatmay be GNCthat they will
not be the only ones to reveal theirpronouns. This creates a supportiveenvironment for employees that willalso extend to improved patient care.To show patients this inclusivity, in-clude pronouns on both websites andbusiness cards. There are also stickersand pins readily available to attach toa clinic badge or white coat to keepyour pronouns visible and remindyour patient that you have a gender-inclusive practice.
One frequent question we get is,“How do we use pronouns in theexam room?” Your pronoun can beadded as part of your introduction.An example to the patient could be,“Hello, I’m Dr. Matthew Roberts,your optometrist, and my pronounsare he/him/his,” or, “Hello, I’m Dr.Paula McDowell, and my pronounsare she/her/hers.”As the leader in theclinic, it is our job to start the meetingproperly, even in one-on-one inter-views.
If there is someone that identi-fies as GNC, this shows that personthey are in a safe environment. Also,if a patient has marked that they areGNC on their form, as their optom-etrist it is acceptable and encour-aged to ask directly, “What are yourpronouns?” Of course, it is always ap-propriate to use a patient’s preferredname or nickname in a face-to-facesetting as well.
Within your practice, consider including literature or symbols that are pertinent to theLGBTQ+ community in the waiting room. The Pride Progress Flag’s design is inclusive ofmarginalized racial communities as well as the transgender community.
Being more culturally competent with the LGBTQ+ population canimprove health outcomes by eliminating disparities this populationoften faces.
Photo: Getty Images
Photo: Getty Images
L G BT Q+ C A R EFeature

51JANUARY 15, 2022 | REVIEW OF OPTOMETRY
There are some challenges withpreferred names in that the patient’scurrent name may not match withlegal paperwork or their previousname recorded in the office. An in-clusive practice will use the patient’snickname or preferred name and besure not to use a name linked to anidentity that the patient no longeridentifies with.
To use the old, or dead, name isan offensive practice called “dead-naming,” which should be avoidedwhenever possible. However, while anickname should be easy to record inthe chart and use in patient conversa-tions, the legal paperwork may stillhave to use the previous name forinsurance submissions. It is useful toinform patients of this discrepancy sothat they are aware that paperworkfrom the insurance company may usethe old name, and make sure thatdocumentation is clear in the chart forstaff as well.
Within the practice, include lit-erature or symbols that are pertinentto the LGBTQ+ community in thewaiting room. Common symbols in-clude the equal sign from the HumanRights Campaign, or the rainbow flag,which has been redesigned itself to bemore inclusive as the Progress Flag.
The smallest symbol will be noticedby patients without needing to have alarge-sized display. Also, ensure thatthere is racial diversity within displaysand include both transgender andsame-sex couples.1
InteractionsAlthough an optometrist may beaware of their own biases, it is im-portant to educate your staff aboutappropriate interactions and language.As they often interact with patientsmore frequently than the doctor, whatyour staff says and does places a largeimpact on the practice. Encouragethem to practice in becoming comfort-able discussing gender identity, andinclude periodic trainings, tutorials orrole-play to help increase comfort.2
Other strategies may not be asobvious to implement but can stillenhance inclusivity. First and fore-most, be aware. If there is derogatorylanguage occurring in the practice (byeither staff or patients), do not esca-late, but educate. Correcting attitudestakes time and it can be difficult beingaware of what one’s biases are.
Second, be an ally to your staff andyour patients. By taking into consider-ation the steps listed here, an optom-etrist can help build a better commu-
nity and improve health outcomes.Third, ask questions to those within
the LGBTQ+ community to becomemore aware of their needs. Thosewithin the community do not takeoffense to someone trying to betterunderstand.
Fourth, make a list of internal bias-es you may have. This is the best wayto try to work through them to ensureequal care is given to each patient, nomatter the background.5
Finally, get involved in your com-munity. If the community you servehas a Pride event, support it bygetting a booth, for example. Thishelps the practice show its stance asan ally for the community. The visioninformation that you can provide isinvaluable and knowing that there isa safe eye care practice for LGBTQ+individuals to visit when needed isone way to reduce barriers to care.4
TakeawaysThe diversity within the LGBTQ+community is part of what makes it sounique. Being more aware of internalimplicit biases makes a better clini-cian. Even as an individual within theLGBTQ+ community, I (Dr. Roberts)have become aware of my own biases,but continuing to educate and nowproviding education to others hasmade me a better clinician and a bet-ter father. As the two of us have seenoptometry become more diverse, allof us need to meet that challenge withopen arms. ■
1. Bass B, Nagy H. Cultural competence in the care ofLGBTQ patients. StatPearls. www.ncbi.nlm.nih.gov/books/NBK563176/. October 9, 2021. Accessed November 12,2021.2. American Optometric Association. Ethics & values. www.aoa.org/about-the-aoa/ethics-and-values. Accessed Novem-ber 12, 2021.3. Office of Disease Prevention and Health Promotion. Les-bian, gay, bisexual and transgender health. Healthy People2020. www.healthypeople.gov/2020/topics-objectives/topic/lesbian-gay-bisexual-and-transgender-health. Last updatedOctober 27, 2021. Accessed November 12, 2021.4. Gelpi M, Fidas D, Perrou M, et al. What’s your pronoun? strategies for inclusion in the Workplace. Out & Equal. out-andequal.org/whats-your-pronoun-strategies-for-inclusion/.May 2020. Accessed November 12, 2021.5. Heistad K. Unconscious bias challenge. Culture CoachInternational. qstream.com/wp-content/uploads/2020/03/Unconscious-Bias-Challenge.669cf2af4ed44a81d7f97bff3ddbb66a.pdf. August 9, 2019. Accessed November 12, 2021.
One of the smallest steps to improve inclusivity while yet making a large impact is theuse of pronouns; for example, in staff badges. Have stickers and pins readily available toattach to a clinic badge or white coat to keep your pronouns visible and remind patientsthat you have a gender-inclusive practice.
52 REVIEW OF OPTOMETRY | JANUARY 15, 2022
How to Defuse aDifficult Patient
Whatever the trigger, take a deep breath and adopt an empathetic approach to calm the situation.
Afew years ago, optometrist IanWhipple of Ogden, UT, exam-ined a patient with the mostadvanced keratoconus he had
ever seen. Dr. Whipple managed toquickly convince the patient that spe-cialty contact lenses would be the bestsolution after sharing that many of hisother advanced keratoconus patientsexperienced improved quality of lifewith specialty lenses.
The process went smoothly untila staff member tried to authorize thepatient’s insurance coverage and it wasdenied. Hearing the bad news, thepatient marched over to Dr. Whipple’sbilling manager and launched into atirade.
“The patient wasn’t ready to pay forthe lenses out of pocket, so he tookhis frustration out on my staff,” Dr.Whipple recounts.
Whether you’ve been in practice forone year or 40, every optometrist willface a difficult patient at some point intheir career. In fact, it’s estimated that15% of patient encounters are on themore challenging side.1
In today’s world, where feelingsof isolation are common due to thepandemic and opinions differ stronglyon how COVID-19 protocols should be
handled, emotionsmay be more height-ened, which can leadto an environmentthat’s ripe for difficultpatient encounters,says Patricia Poma,OD, of Bloomfield,MI.
“Difficult pa-tients are a part ofdoing business,”adds Highland, CA,optometrist PamelaMiller. “You needto recognize thefact that people can be difficult, andyou don’t know what’s going on in apatient’s life.”
The Cost-Triggered PatientWhen a patient is disgruntled, educa-tion and communication are essen-tial, Dr. Poma says. For example, ifa patient is upset because the officebilled their exam as a medical visitinstead of billing their vision plan, it’snot appropriate to say, “Your insurancedeductible wasn’t met, and that’s howthe doctor decided to bill your exam, sotherefore you owe us money,” she adds.
Instead, she suggests the conversa-tion should take an informative angleand sound something like this, “Thedoctor noticed that you have some
spots near your macula and thereforespent a little more time examiningyour eyes. To make sure your condi-tion won’t progress, further testing wasdone with the latest technology thefield offers, which we use to providethe best outcomes for our patients.Unfortunately, this isn’t covered byyour vision insurance, but we will workwith you to ensure optimal vision andcreate a plan for the resulting financesmoving forward.”
When Dr. Whipple’s advancedkeratoconus patient became furiousafter insurance wouldn’t cover the costof the specialty lenses, Dr. Whipplechanged course and imagined what itwould be like to be in the other man’sshoes.
By Jane ColeContributing Editor
Photo: Ian Whipple, OD
At Dr. Whipple’s practice, a staff member discusses costs witheach patient before their eye exam.
D I F F I C U LT PAT I E N T SFeature

53JANUARY 15, 2022 | REVIEW OF OPTOMETRY
“It was an intense situation,” henotes. “The patient couldn’t see, andwe had a solution for him, but insur-ance wouldn’t cover it. If I were him,I’d be frustrated too. When I recog-nized that, I could feel empathy.”
In this case, the empathetic approachworked. The patient returned a fewdays later and was fit in a specialty lens,which he paid for out of pocket. “He’sbeen on his best behavior ever since,and today, he’s the nicest guy and agreat patient,” Dr. Whipple says. “Andhe’s since gotten insurance that coversthe cost of his specialty lenses.”
Transparency is key in defusingangry patient encounters, Dr. Whipplesuggests. At his practice, each patient isbriefed by a staff member about pricingand insurance coverage before theyever step foot in the exam room.
The Denial PatientVincent Zingaro, OD, of ChesterSprings, PA, recently diagnosed apatient with macular degeneration.The woman, however, kept insistingshe just needed a new pair of glasses toimprove her vision.
“I explained there wasn’t a changein her glasses prescription and that sheneeded treatment from a retina special-ist for wet macular degeneration. Shebecame angry and told me there wasn’tanything the specialist could do,” Dr.Zingaro recalls. “I explained the treat-ment options, and I was frustrated toosince she didn’t accept my findings ortake my advice.”
After a somewhat argumentativeconversation, the patient demandedher prescription and left the office, de-clining Dr. Zingaro’s offer to schedulethe referral appointment for her.
A few weeks later, the patientreturned with a new pair of glasses thatshe had purchased at a different office.In the middle of the crowded receptionarea, the woman began yelling at Dr.Zingaro’s optician, complaining that shecouldn’t see out of her new glasses.
Dr. Zingaro immediately escortedthe woman away from his other pa-tients and took her to an open examroom, where he calmly told her that theproblem wasn’t with the glasses butinstead with her retina, and that sheneeded to see a specialist.
“I made the mistake of dismiss-ing the patient initially when shedidn’t accept my diagnosis. I think it’simportant for doctors to have empathyfor the patient. We don’t always knowwhat each patient is going through intheir life, and it’s easy to want to rushthrough to the next patient when ourschedules are busy. Stepping back andacknowledging the patient’s fears cango a long way in minimizing unpleasantpatient interactions,” he says.
This time, the woman accepted herdiagnosis from Dr. Zingaro, who sched-uled the specialist appointment for her.
When dealing with a patient indenial, sometimes a doctor may have tothink outside of the box. Dr. Whipplerecently diagnosed a new patient withmoderate glaucoma, and the woman
was not only upsetabout the news, but alsowouldn’t accept it.
“The patient wasfamiliar with the HarryPotter series, so I usedthe example of the char-acter Voldemort, who isknown in the books as,‘He who must not benamed,’” Dr. Whipplesays. “I asked her, ‘Howcan we know what tofight if we can’t evenname it?’ We need totalk about it and come
up with a treatment plan. I know it’sdisappointing news, but what’s evenworse is having a condition and notdoing anything about it. Your glaucomais only moderate now, but it could getworse if we don’t treat it.”
The Fretful PatientIt’s always important to be open andhonest about the diagnosis and long-term impacts of a severe or threateningeye condition, even though it may be adifficult conversation to have with thepatient, Dr. Poma says.
The staff and doctor need to be veryconfident and compassionate with pa-tients who are worried, she adds. “Thegoal is to ensure that we are capableand caring. Eye contact is especiallycrucial, along with words of encourage-ment and a smile. I sometimes willmake casual conversation with the pa-tient while I’m working so that they’redistracted from what I’m doing.”
When breaking the news about apotentially troubling diagnosis, doctorsshould keep the initial informationsimple and avoid using technical, medi-cal language that might be confusing, astudy suggests.2
Optometrist Andrew Fischer ofJasper, IN, adopts the “KISS” mindsetwhen he describes a new or changingdiagnosis to a patient and keeps hisexplanation simple.
“Explaining a medical condition canbe both intimidating and confusing toa patient,” Dr. Fischer says. “I clearlyand briefly explain the diagnosis andwhenever possible, use photos, imag-ing or other visuals to help the patientunderstand what exactly I’m seeing.”
Dr. Fischer also takes the time todescribe the potential visual, systemicand lifestyle impacts the conditioncould have, and then he reviews theplan to mitigate any progression of thecondition, all of which can help ease aworried patient’s concerns.
The Busy PatientDr. Fischer recently treated a two-year-old who had recurrent styes. Atfirst, Dr. Fischer prescribed at-hometreatments, but the issue persisted.
Transparency among all the staff of a practice is key inreducing the chances of a difficult patient encounter.
Photo: Ian Whipple, OD
A subsequent dose of oral antibioticscleared the lid; however, a few monthslater, the mother brought the tod-dler back to the practice with a largechalazion. After discussing his findingswith the mother and breaking the newsthat the child would need the chalazionsurgically removed, Dr. Fischer referredthe patient to the only pediatric special-ist who accepted the family’s insurance.The problem was that the specialist waslocated about 2.5 hours away.
A few weeks later, the patient’s fathershowed up at Dr. Fischer’s practice,irate and frustrated with the front deskstaff. The father was yelling so loudlythat Dr. Fischer could hear him fromthe other side of the office. Dr. Fischer,who was in the middle of an eye examwith a patient, excused himself to es-cort the father to an empty room wherehe could vent.
“He was very upset that his son’s ap-pointment was so far away that he hadto take time off work,” Dr. Fischer says.“When he’d said his piece, he did calmdown enough for us to discuss why Ireferred his son.”
Dr. Fisher explained to the fatherthat other offices in their area that ac-cept the family’s insurance don’t treatpediatric patients.
“I also made sure he understood thatI appreciated the strain the appoint-ment put on his work schedule. I reallydidn’t do anything more than listen tohim, but sometimes that’s all it takes toresolve a difficult situation,” Dr. Fischer
says. “I think it is important to remem-ber to approach any situation where apatient is difficult or upset with empa-thy. Give the patient time to addresstheir concerns, make it clear that youhear them and understand the situationand then do everything that is withinreason to rectify the situation.”
The Language Barrier PatientSometimes difficult patient encountersmay be the result of limited Englishproficiency.
Dr. Fischer has a large populationof Spanish-speaking patients in hiscommunity, which he says can createan opportunity for a difficult exam. “Iknow and understand a fair amount ofSpanish—enough to get through anexam easily—until there is a medicalcondition to explain,” he says. In thesecases, he relies on five of his staff mem-bers who are fluent or nearly fluent inSpanish.
Additionally, if a deaf patient comesin for an office visit, he will contractwith an American Sign Languageinterpreter. “Otherwise, in these cases,we will write back and forth on a padof paper, which is slower but also worksvery well,” he says.
In the case of a patient who has lim-ited English proficiency, Dr. Whipplewill ask the individual to bring someonethey know who speaks English to in-terpret during the office visit. “If we’rehaving a hard time understanding eachother on the phone, we ask the patient
to bring an inter-preter.”
When a trans-lator accompa-nies a patient tothe exam, Dr.Miller will pullher chair backand addressboth individuals,making a pointnot to focus allher attentionon the transla-tor, which couldmake the patientfeel devalued.
While hiring a translator may be acostly prospect, remote interpretingservices are available. When she findsherself in a pinch, Dr. Poma will some-times resort to Google Translate.
COVID-19 Mandate FrustrationsWe would be remiss to not take intoaccount how COVID has heightenedpatient tensions. Depending on howthe virus has affected your region, maskmandates may vary. Almost two yearsinto the pandemic, mask wear andother COVID-related safety restrictionsremain a flashpoint for some.
In fact, the American Psychiatric As-sociation’s recent Stress in America reportfound that eight out of 10 Americanssaid the pandemic has created signifi-cant stress in their life.3
So, how should an OD dial down thetension when a patient is fired up aboutmasking up?
Dr. Zingaro’s practice implementeda mask mandate, regardless of vaccina-tion status, based on recommendationsfrom his state’s optometric association.
“On occasion, we get a patient whorefuses to wear a mask, and we just tellthem that we can’t see them withoutone,” Dr. Zingaro says. “They typicallyturn around and leave without sayinganything. Luckily, this is rare and hasonly happened five or six times in thelast 18 months or so. I think it’s hard tofind a healthcare facility at the momentthat will allow you to go in unmasked.This will change eventually, but this isour current reality.”
Drawing a line in the sand aboutmask wear is essential for practices, Dr.Zingaro suggests. “I feel if we let thatslide, it could get ugly pretty quick,” headds.
During the onset and height of thepandemic, Dr. Fischer asked all his pa-tients to wear a mask during the exam,and the policy had minimal pushback,he says.
Over the course of the pandemic,mask guidelines changed, and Dr.Fischer’s office followed suit. Currently,vaccinated patients aren’t required towear a mask during their exam. How-ever, when mask mandates were in full
54 REVIEW OF OPTOMETRY | JANUARY 15, 2022
tips to turn down the heatWhen a patient loses their cool, it’s critical for the doctor to keep theirs intact,Dr. Miller says. She offers several suggestions on how to turn a negative patientencounter around:• Stand back, take a deep breath and don’t downplay the patient’s issue. “It’s
important to remember that not all people are as wonderful as you are,” shesays with a laugh.
• Employ a good bedside manner and empathy. Sometimes, the patient justneeds to hear the words, “I understand,” Dr. Miller explains.
• Repeat the patient’s problem back to them. In addition to saying, “What canI do to take care of this for you?” she also suggests taking responsibility if aproblem does arise. For example, if a patient is unhappy that their spectaclelens Rx isn’t correct, Dr. Miller says to fall on your sword and not blame thelab. “It’s best to say, ‘I made a mistake. Let me see what I can do to fix it.’”
• Talk “with” the patient and not “at” the patient.• Ask, “Did I answer all your questions?” at the end of the exam.
D I F F I C U LT PAT I E N T SFeature

55JANUARY 15, 2022 | REVIEW OF OPTOMETRY
effect, if a patient refused wear, Dr.Fischer asked them to reschedule to alater date, in hopes that the guidelineswould eventually change.
During the early days of the pan-demic, his practice also adjusted itsschedule to include fewer patientappointments throughout the day. Thisnew approach limited contact betweenpatients, gave staff the opportunity todeep clean rooms between exams andprovided patients ample space in theoptical for frame selection, Dr. Fischerexplains.
Dr. Poma has experienced bothends of the spectrum of COVID-19protocols, and she’s found that on manyoccasions, it’s difficult to make eitherside happy.
“We decided to have a discussionamong the doctors and made protocolsand procedures based on OSHA, CDCand local health department recom-mendations,” Dr. Poma says.
She and the other doctors at her prac-tice even role-played different scenar-ios with staff based on potential issuesthat might arise among patients due toCOVID and her practice’s associatedsafety requirements.
“Whenever a patient comes indemanding service that is beyond ourprotocols, we calmly tell them thatwe aren’t able to accommodate theirrequest but that we would be very sadto lose their business,” Dr. Poma says.
When appropriate, she will remind apatient that it’s her job to follow CDC/
OSHA guidelines,even if they don’t wantto wear a mask.
On the other hand,she has also dealt withpeople who demandto be seen when thereare no other patientsin the office. There arethose who have evenrequested that Dr.Poma and her staff bedressed in hazmat gear.
“We simply tellthem that our protocolsare well established,ensuring safety. We
inform them that we have spent over$10,000 in air scrubbers, but if theyaren’t comfortable, we can see themonce the COVID numbers decline inour state,” she says.
To tamp down any disgruntled pa-tient encounters due to your practice’sCOVID-19 guidelines, experts suggestit’s best to spell out your requirementsprior to the visit, which may be com-municated during the initial schedul-ing call, and reinforce them with textor e-mail appointment reminders andsignage throughout the office.4
When to Set BoundariesDr. Poma and her staff make an effortto help each patient unless the indi-vidual becomes irrational, belligerent orthreatening. In these cases, the patientis told, “You’re more than welcome totake your happiness elsewhere,” shesays. The patient is then sent a letter,stating their relationship with the prac-tice has been terminated, and a shortlist of other eye care offices in the area.
“We also have a code word withinour office that’s a signal for others to call911. We use a name of a frame line thatwe don’t carry. It is a security blanketfor ‘just in case,’” she says.
To ensure office safety, Dr. Miller hasmirrors throughout her clinic and doorsare left ajar, even during the exam, soshe can remove herself from a situationif one arises and so staff have easy ac-cess to her as needed.
While violent patient outbursts might
seem rare, workplace violence is mostcommon in the medical setting, and itfrequently involves a patient or familymember threatening physicians orpractice staff.5 In one such incident in2013, a disgruntled former patient useda fake name to make an appointmentand shot to death a Newport Beach,CA, doctor after the doctor entered theexam room.6
Practices need to set boundaries andshouldn’t tolerate certain behaviors,Dr. Whipple explains. “I’ve had to let ahandful of patients go through the yearsfor inappropriate behavior, especiallywhen employees felt uncomfortable,including one time when a patient tooka photo of a tech when she wasn’t look-ing. That’s not okay. If a staff membertells me a patient is really difficult andisn’t a right fit for our practice, I’ll trustmy staff’s judgement and we’ll removethe patient. You need to stand by yourteam,” Dr. Whipple says.
Final ThoughtsWhen a difficult patient encounterarises, Dr. Poma suggests the best thingto do is to simply listen.
“Most people want to air their griev-ances and just be heard,” she says.“Stay calm and don’t interrupt. Manytimes, a patient is just upset aboutsomething in their lives, and they taketheir emotions out on staff or manage-ment. When the patient is finishedexpressing, I simply ask, ‘What can I doto make you happy?’ or, ‘How wouldyou like me to fix this problem?’ Mostof the time, they’re speechless and real-ize they were overreacting.” ■
1. Jackson JL, Kroenke K. Difficult patient encounters in the ambulatory clinic: clinical predictors and outcomes. Arch Intern Med. 1999;159:1069-75.
2. Hardavella G, Aamli-Gaagnat A, Frille A, et al. Top tips to deal with challenging situations: doctor–patient interactions. Breathe (Sheff). 2017;13(2):129-35.
3. Stress in America 2020. APA. www.apa.org/news/press/releases/stress/2020/report-october. October 2020. Accessed December 15, 2021.
4. Cole J. How to calm patients’ nerves about COVID. www.reviewofoptometry.com/article/how-to-calm-patients-nerves-about-covid. June 3, 2020. Accessed December 15, 2021.
5. Cheng KS. How to prepare for and survive a violent patient encounter. Fam Pract Manag. 2018;25(6):5-10.
6. Fry H. Retired barber who murdered Newport Beach doctor was sane during the 2013 killing, jury finds. Los Angeles Times. www.latimes.com/local/lanow/la-me-newport-murder-20170828-story.html. August 28, 2017. Accessed December 7, 2021.
Clinics have adapted protocols to ensure safety during COVID.
Photo: Ian Whipple, OD

56 REVIEW OF OPTOMETRY | JANUARY 15, 2022
Making your practicekid-friendly
How to simplify exams and make them fun while minimizing stress for you, the pediatric patients and their parents.
Working with pediatric patients can be intimidating,but is the most fun and rewarding experience. Itcan be somewhat daunting from the get-go whena child and parent enter an optometrist’s office
due to parents not knowing what to expect and not exactlylooking forward to receiving potentially life-changingnews about their child’s condition. When it comes to thekid patients, they can at times be undisciplined, may havetrouble sitting still and have to be engaged from the mo-ment they walk through the door.
For a pediatric exam, we ultimately need the sameinformation that we collect during an adult exam; we justuse creativity and varied methods to obtain that same basedata set. Simplifying the initial approach down to the ba-sics of an eye exam can make a pediatric work-up protocolsignificantly more approachable for both doctors and staff.
In this article—the first of a four-part series on pediat-ric care—we will talk about specific ways to add fun andlightness to a sometimes intimidating experience for thepatient and their parent, and discuss the best ways to per-form an exam on the youngest of patients.
Exam EarlyOver the last few years, I have seen a significant increasein the number of patients referred for formal evaluationfrom both doctors’ offices and school districts. This islargely because of an increase in availability and accuracy
of photo-screener technology, and also possibly because ofan increase in technology use in classrooms.
In the absence of a photo-screener alert from apediatrician or school, children may benefit from having abaseline dilated eye exam by age three. This ensures thatas they are exposed to visual language, they can interprettheir visual world as accurately as possible and we can treatamblyopia if amblyopic factors are found.
This is also an important age for dilated fundusevaluation for potentially life-threatening diseases such asretinoblastoma. In your local community, communicatingwith pediatricians, alerting daycares and schools and
Dr. Galt practices pediatric optometry at The Eye Center of Northern Colorado. She fell in love with caring for the pediatric patient population while at theUniversity of Houston College of Optometry and specialized through the University of Alabama at Birmingham School of Optometry Pediatrics Residencyprogram. She has no financial disclosures.
Aboutthe author
By sarah galt, odfort collins, co
PEER REVIEWED
An optometrist is making this eye exam fun for a young patient.
P E D I AT R I C E X A M SFeature
57JANUARY 15, 2022 | REVIEW OF OPTOMETRY
talking with peers can increase the number of childrenwho receive eye care.
Interactive ItemsWaiting rooms are our patient’s initial impression of whatwill be happening to them, if their parent hasn’t primedthem with a description of their eye exam.
Right now, our office does not have toys out, as theseare high-touch items that encourage movement and thatwe cannot effectively disinfect at this time. In an idealworld, and maybe again in the future, pediatric patientsare greeted by colorful, interactive toys to help them stayrelaxed and enjoy their experience.
How to Perform an ExamThe challenge of a pediatric exam comes from obtainingnecessary data in a way that minimizes frustration of thepatient and the staff member. Doctors and staff must beready to see pediatric patients, both in terms of equipmentand mindset. All you technically need is a retinoscope anda BIO, but additional tools and forethought can providecooperation and comfort of your patient and their parentsignificantly.
Some offices I travel to are not equipped with a full arrayof peds tools. In those cases, we have a “peds bucket,”which typically includes stickers, a spinning light, adhesivepatches, stereo booklet and glasses, loose prisms and atalking Elmo doll. Any of these items or substitutes can befound easily and kept around the office to set you up forsuccess in maintaining pediatric patients’ attention.
Pre-testing: Stickers, spinning light toys and small toyscan transform the success of your data acquisition withpediatric patients. A child is far more likely to follow a funlight when you ask them, “What colors do you see?” or tofixate on a sticker when you can say, “Does this look likea happy elephant?” than to follow our typical adult script.Having toys and stickers allows you to connect with thepatient and can decrease the harshness of being at thedoctor’s office.
Acuity: We aim to test visual acuity with as advanced atechnique as the patient is capable of; that does not meanthe patient has to be able to read the chart. The hierarchyranges from Snellen with our verbal patients who knowletters, to Lea symbol charts and matching, to central,stead and maintained; to blink to light and an optoki-netic nystagmus drum. We operate with a majority of ourpre- or non-verbal patients getting an allocation of centralsteady and maintained or central steady and fixated visualacuities. Teller acuities, used in research and academicsettings, aren’t as functional for your high-volume clinicsetting.
Dilation: I cannot pretend to be the expert in this topic,as I rarely dilate a patient on my own. In most circum-stances, my wonderful technicians dilate my patients toreduce the possibility of a breakdown when I re-enterthe room for retinoscopy. When my technicians are kind
enough to play the “bad guy” and administer drops, theygenerally agree that speed is on their side. They do a greatjob of reading the room and determining the patient’s levelof anxiety surrounding the drop administration process.
In the case of a very alert child who may have sensorysensitivities, further explanation may be helpful. In other
Having colorful, interactive items and toys in your waiting room willkeep pediatric patients engaged and relaxed as they wait for theirappointment.
A young patient during a pediatric eye exam.
58 REVIEW OF OPTOMETRY | JANUARY 15, 2022
cases, asking the patient if they want cherry or apple fla-vored eye drops—and administering quickly—may be themost effective, rather than drawing out the process with anexplanation.
In all circumstances, we respect the patient’s bodilyautonomy, but there are times that a big hug by the parentto prevent scratching and kicking makes our drop deliverymore successful.
Once dilated, the provider performs retinoscopy andposterior segment exam (BIO) on all patients, and slitlamp exam is typically performed for patients four yearsold and above (we can manage slit lamp on infants if thepatient’s caregiver is willing and we deem it important).
Retinoscopy: In our office we use loose lens retinoscopywith sphere and cylinder lens combinations for neutraliza-tion. During retinoscopy, I tend to sing a song with or tothe patient to maintain their gaze. My counterpart is lessprone to singing, so he will make “mouse noises” behindthe retinoscope or have a technician hold up a spinninglight or Elmo doll beside his head to maintain fixationlong enough to find an accurate neutralization of refractiveerror.
You will inevitably find yourself performing retinoscopyon a screaming, inconsolable toddler at some point, buthaving these tools and an ability to not take yourself tooseriously to sing nursery rhymes can reduce that likelihoodsignificantly.
I do not prescribe a final glasses prescription withoutretinoscopy obtained after a dilating agent. When new
patient parents come into our office not wanting their chil-dren dilated, our technicians are well-versed in respectfulways to discuss why we encourage it. When necessary, Iwill enter the conversation and emphasize that we cannot:
(1) accurately assess refractive error, and therefore how itaffects binocular vision;
(2) fully evaluate posterior segment health, withoutdilating agents.
We do respect when parents feel dilation is not thebest option for their child after they have heard all of therelevant reasons for our suggesting it. For these patients, Ihave frequent follow-ups and make every effort to obtaina non-dilated view of the optic nerve at their initial visit.I would rather be managing patients in my office thanhave them walk away and possibly not be cared for at all.Parents typically respond well to this, and when I reach alevel of concern about prescribing that I bring up dilationagain, it is better received. I recommend dilating yourpediatric patients whenever possible.
Effective CommunicationThe challenge of a pediatric exam comes from obtainingthe above data in a non-traditional way. The same goesfor communication with our pediatric patients duringtheir exams and after when discussing the outcomes andthe future of their children’s ophthalmic care. During anyexamination, technicians, doctors, patients and parentsbenefit from extensive description of what is going tohappen, what is happening and what results we get fromeach exam element.
We find metaphors very helpful when communicatingwith both the patient and parent. I follow my colleague’slead, as he has his metaphors very finely tuned, so a fewthat I cannot take credit for are below:
keeping kids engagedCooperation by the patient and trust by the parent are improved whenyou keep discussion open throughtout.
Below are a few “scripts” that I find give patients and parents an ideaof the next steps without alienating myself or my process. This includesgiving optometry instruments fun names which can keep kids engagedand asking them questions about different objects in the room. Thesecan be adjusted to your patient’s age, as nine-year-olds may be offendedif you ask them to sing their ABCs.
• “I am going to use this spoon (cover paddle) and I will cover up eacheye; you just get to sit and chat with me about the silly sticker on mymask—who is that? What about that airplane across the room—howmany windows does it have?”
• “You have already done so much hard work! We only have three stepsleft and then you’re all done. We will use our wiggle flashlight (reti-noscope), my crazy hat (BIO) and the bicycle (slit lamp, which hashandlebars).”
• “Can you tell me what secret color is at the top of my spinning light?”
• “Is your mom making a silly face behind me?”
A parent keeps a young patient still by feeding them a bottle duringan eye exam.
P E D I AT R I C E X A M SFeature

59JANUARY 15, 2022 | REVIEW OF OPTOMETRY
Amblyopia:“Right now, John-ny’s right eye hasBlu-ray qualityvision. Becauseof his differencein prescriptionin the left eye,that eye has VHSquality vision, butwe have a lot oftools to help usupgrade so thatboth eyes seeespecially well.”
Contact lenses:“Glasses are likea T-shirt; contactsare like a tuxedo.
You have to take extra special care and a little more timeat the beginning and end of the day to clean and take careof your contact lenses.”
Compliance: “The fi rst few days you may not like theseglasses; you may think that we didn’t get things right thistime! But you gave me really good attention and I feelgood about the prescription. Sometimes I like to call them‘breakfast glasses’ because if we have them on for break-fast, we are more likely to wear them all day. It’s okay ifyou need to build-up wear over the week, too.”
Follow-up: “You’ve got special eyeballs, they’re veryinteresting. Because of your special eyeballs, we are goingto be good friends.” I then set the expectation for howoften I plan to see the patient. For example, I may sayevery three to four months, only dilating annually unlessneeded otherwise.
Keeping open communication by talking throughoutthe exam, even if it is a one-sided conversation, can calmyour nerves as well as the patient’s. If you are able toconnect with your patient, the exam will be smoother andparents will often feel much more confi dent in your examresults.
I also like to inform parents and patients that dilationmay last longer in children than they have experiencedfrom their adult exams. If the patient has noted that nearhas blur, I reassure them with, “I know your hands looka little funny, the phone might, too. I promise that’s notforever, that will just be for today. You may enjoy far awayactivities more than up close activities today, and the nicepeople who check you out will have some groovy sun-glasses for you.”
Our offi ce sees patients of all ages, but I like to thinkthat the front desk does enjoy greeting our pediatric pa-tients. Big smiles (behind masks) from them upon arrivaland departure are the icing on the cake to patient andparent experiences in our offi ce.
A pediatric patient has a toy to keep herengaged during her exam.
Follow us on Instagram at @revoptomfor striking clinical images, news
headlines, issue previews and greatcontent from the magazine—all
formatted for mobile.
A NEW WAYTO EXPERIENCE
REVIEW OF OPTOMETRY
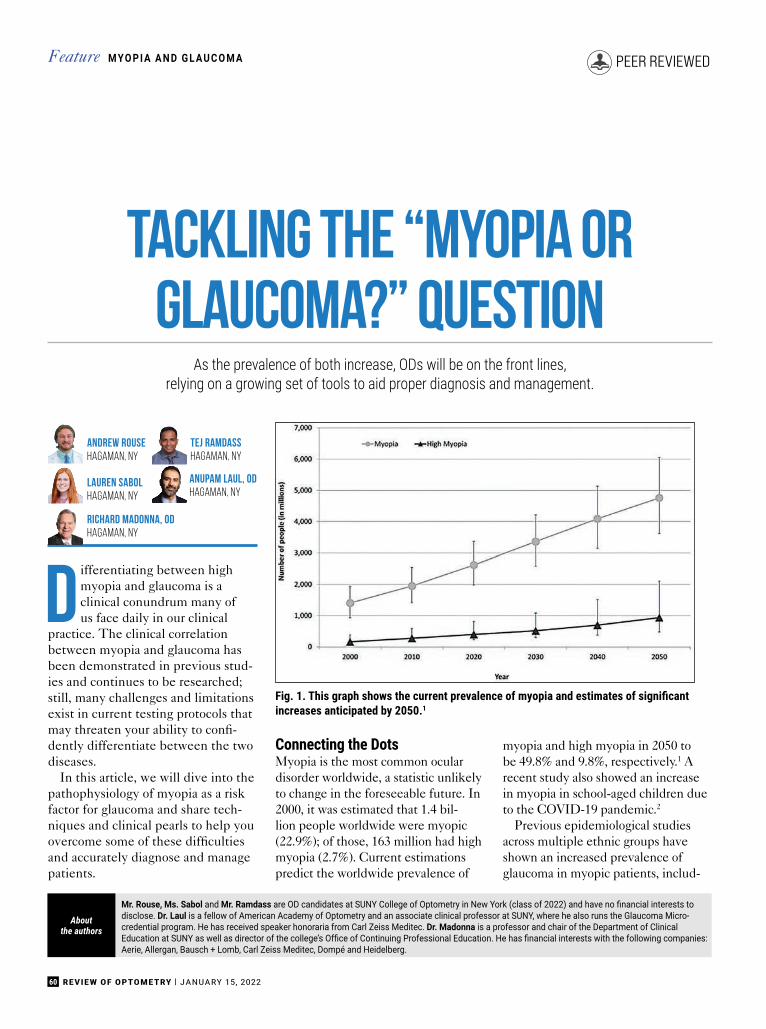
60 REVIEW OF OPTOMETRY | JANUARY 15, 2022
Tackling the “Myopia orGlaucoma?” Question
As the prevalence of both increase, ODs will be on the front lines,relying on a growing set of tools to aid proper diagnosis and management.
Differentiating between highmyopia and glaucoma is aclinical conundrum many ofus face daily in our clinical
practice. The clinical correlationbetween myopia and glaucoma hasbeen demonstrated in previous stud-ies and continues to be researched;still, many challenges and limitationsexist in current testing protocols thatmay threaten your ability to confi-dently differentiate between the twodiseases.
In this article, we will dive into thepathophysiology of myopia as a riskfactor for glaucoma and share tech-niques and clinical pearls to help youovercome some of these difficultiesand accurately diagnose and managepatients.
Connecting the DotsMyopia is the most common oculardisorder worldwide, a statistic unlikelyto change in the foreseeable future. In2000, it was estimated that 1.4 bil-lion people worldwide were myopic(22.9%); of those, 163 million had highmyopia (2.7%). Current estimationspredict the worldwide prevalence of
myopia and high myopia in 2050 tobe 49.8% and 9.8%, respectively.1 Arecent study also showed an increasein myopia in school-aged children dueto the COVID-19 pandemic.2
Previous epidemiological studiesacross multiple ethnic groups haveshown an increased prevalence ofglaucoma in myopic patients, includ-
M YO P I A A N D G L A U C O M AFeature
Mr. Rouse, Ms. Sabol and Mr. Ramdass are OD candidates at SUNY College of Optometry in New York (class of 2022) and have no financial interests to disclose. Dr. Laul is a fellow of American Academy of Optometry and an associate clinical professor at SUNY, where he also runs the Glaucoma Micro-credential program. He has received speaker honoraria from Carl Zeiss Meditec. Dr. Madonna is a professor and chair of the Department of ClinicalEducation at SUNY as well as director of the college’s Office of Continuing Professional Education. He has financial interests with the following companies: Aerie, Allergan, Bausch + Lomb, Carl Zeiss Meditec, Dompé and Heidelberg.
Aboutthe authors
Andrew RouseHagaman, NY
Tej RamdassHagaman, NY
Lauren SabolHagaman, NY
Anupam Laul, ODHagaman, NY
Richard Madonna, ODHagaman, NY
PEER REVIEWED
Fig. 1. This graph shows the current prevalence of myopia and estimates of significant increases anticipated by 2050.1

61JANUARY 15, 2022 | REVIEW OF OPTOMETRY
ing the Blue Mountain Eye study,Barbados Eye Study, Beaver Dam EyeStudy, Singapore Malay Eye Study,Beijing Eye Study and Latino EyeStudy. Another recent meta-analysis bydetermined that for each 1.0D increaseof myopia, glaucoma risk increasedby 20%, shown to accelerate around-6.0D of myopia and further at -8.0D,demonstrating a correlation betweendegenerative myopia and increasedglaucoma risk.3
It is currently unknown how myopiaincreases the risk of glaucoma, butthere are several hypotheses. One isthat the tilting of the optic nerve oftenseen in myopia may lead to a directinsult or a shearing effect to the gan-glion cell axons. Another hypothesis isthat the effects of intraocular pressure(IOP) can be more pronounced inmyopes due to thinning of the retinalnerve fi ber layer (RNFL), laminacribrosa and sclera.4
In glaucoma, the primary site foraxonal injury is the lamina cribrosa. Asmentioned previously, the tilting of theoptic nerve can have a direct effect onthe retinal ganglion cell axons. Thismay be due to the increased stretchingof the lamina cribrosa, particularly onthe temporal side, and increased scleralbend due to the tilting of the opticnerve commonly seen in myopia.
The increase in axial length (AL)in myopia also causes a stretching andthinning of the lamina cribrosa. Thethinning not only makes the retinalganglion cell axons more susceptibleto increased IOP, but it also alters thetranslaminar pressure gradient. Thetranslaminar pressure gradient is thedifference between the outward pres-sure on the optic nerve by IOP andinward pressure from the cerebrospinalfl uid. In some studies, the translaminarpressure gradient has a better correla-tion with the degree of glaucomatousoptic neuropathy.5 The lamina cribrosais composed of a collagen matrix simi-lar to that of the cornea.
The Ocular Response Analyzer(ORA) is a relatively new device thatmeasures the biomechanical propertiesof the cornea. It uses a bidirectional
applanation process to assess the vis-coelastic properties of the cornea. Al-though it’s not fully understood, somestudies link the viscoelastic propertiesof the cornea to those of the laminacribrosa.6 Corneal hysteresis (CH) isa measurement of the cornea’s abilityto dampen the effects of eye pressureand has been shown to be an indepen-dent risk factor for glaucoma progres-sion.7 Several studies have shown thatmyopic eyes tend to have a lower CH,suggesting that those eyes are moreprone to stretching and axonal injuryin comparison to emmetropic andhyperopic eyes.8 Using CH can helpyou determine the risk of glaucomaor progression. A patient with a lowerCH (<8mm Hg) is more at risk than apatient with higher CH (>12mm Hg).9
Another useful measurement ofthe ORA is the corneal-compensatedIOP (IOPcc). IOP obtained by thetraditional Goldmann applanationtechnique can be inaccurate sincecorneal properties tend to differ inmyopic patients either via the naturaldifferences in collagen compositionand/or arrangement in the cornealstroma. This measure compensates forthe corneal properties and may offera more accurate measure of the IOP.Although research is still active, usingthe ORA to obtain corneal hysteresisvalues and IOPcc may be a useful toolto determine IOP and gauge the abil-ity of the eye to resist its increase.
Traditional methods of diagnosingglaucoma include direct observa-tion of the optic nerve to determine
TABLE 1. CORNEAL HYSTERESIS NORMS
Low CH <8mm Hg
Medium CH 8-12mm Hg
High CH >12mm Hg
This table shows the normative values for corneal hysteresis. To assess risk in glaucoma,the lower the CH, the greater the risk for glaucoma or glaucoma progression.9
Fig. 2. Traditional fundus photography shows anomalous optic nerve insertion, tilting andtorsion and posterior staphyloma in a highly myopic patient (top). Below is the same imageof the optic nerves using red-free fundus photography to visualize the extent of thinningmore easily (bottom).

62 REVIEW OF OPTOMETRY | JANUARY 15, 2022
M YO P I A A N D G L A U C O M AFeature
rim thinning, measuring IOP withGoldmann tonometry, using opti-cal coherence tomography (OCT) tomeasure the thickness of the RNFLand performing a visual field test todetermine any functional vision loss asa result of glaucoma. However, thesetraditional measures may be difficultto use due to anatomical changes inhighly myopic eyes that make it chal-lenging to determine if a glaucoma-tous process is occurring.
Optic NerveTo diagnose glaucoma, cliniciansassess the optic nerve with a fundusexam to determine if there is neuro-retinal rim thinning, particularly inthe superior-temporal and inferior-temporal quadrants that are mostvulnerable to glaucomatous damage.10
In degenerative myopia, tilting of theoptic nerve and posterior staphylomasmake this assessment challenging and,in some cases, impossible.
How would you describe the opticnerve head appearance in Figure 2?This is a difficult question to answer,and many optometrists may describeor document this patient’s optic nerve
in different ways. To helpdetermine the extent of rimthinning, red-free fundusphotos should be capturedwhich facilitate the visualiza-tion and delineation of theneuroretinal rim and opticcup. Other technologiessuch as OCT can be used toquantify the thickness of theRNFL.
OCTSince entering optometricpractice in the late 1990s,this imaging modality has be-come a versatile tool used toexamine the clinical mani-festations of a variety of dis-eases—glaucoma included.When spectral-domain OCTbecame commercially avail-able in 2007, it revolution-ized the ability to diagnoseglaucoma.
OCT takes structural measure-ments of the RNFL thickness and candetect change over time. Dependingon the device, the OCT will take a4.5x4.5mm circular scan around theoptic nerve. It then measures wherethe Bruch’s membrane opening is todetermine the edge of the optic nerveand measures the thickness of the rimtissue by taking the shortest distance
to the edge of the internal limitingmembrane.
In degenerative myopic patients,tilting of the optic nerve, posteriorstaphylomas and RNFL thinning inmyopia generally result in abnormalOCT scans or incorrect segmentation.Other changes seen in myopic pa-tients on OCT is the temporalizationof the RNFL bundles. Studies haveshown that as the degree of myopia isincreased (both increases in AL andspherical equivalent), the greater thetemporalization of the RNFL bundles(Figure 3).11 Abnormal OCT scans aresometimes flagged as red and may hintthat there might be a glaucomatousprocess occurring.
Myopia is a common cause of “reddisease,” which indicates a falsepositive of glaucoma (Figure 4).12
Clinicians may see this and initiateglaucoma treatment; however, it’s im-portant to recognize that the abnormalthinning is secondary to the myopicchanges and not a true glaucomatousprocess.
Within the OCT programming,each scan is compared to a normativeor reference database created basedon studies performed by each com-pany. This helps clinicians deter-mine whether the measured RNFLthickness is statistically normal orabnormal. The inclusion and exclu-
Fig. 3. Above are the RNFL thickness maps (left panel)and RNFL thickness deviation maps (right panel) oftwo myopic eyes with AL of (top) 27.26mm (sphericalerror: -6.75D) and (bottom) 26.61mm (spherical error:-2.00D). The RNFL distribution angles were 103.38(top) and 137.58 (bottom) showing the increasedtemporalization of the RNFL bundles.11
Fig. 4. This abnormal OCT shows poor segmentation in both the heat maps and tomogramsin a high myope. The statistical analysis shows “red,” meaning abnormal thinning; however,this isn’t due to glaucoma but rather is from poor segmentation caused by high myopia.
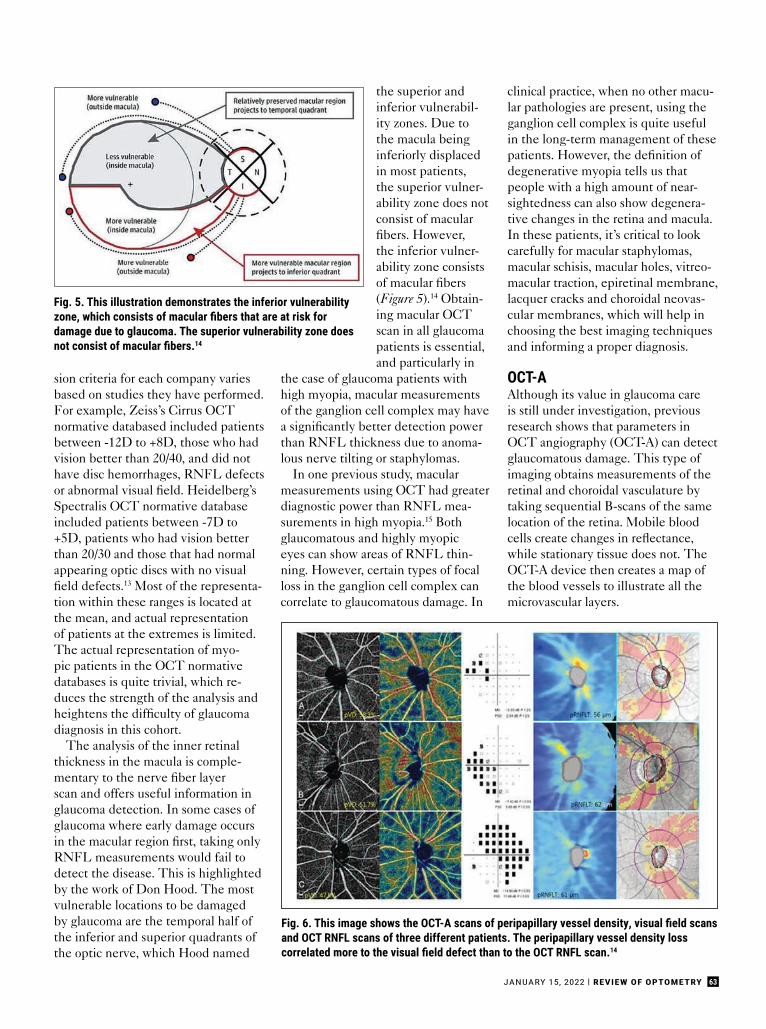
63JANUARY 15, 2022 | REVIEW OF OPTOMETRY
sion criteria for each company variesbased on studies they have performed.For example, Zeiss’s Cirrus OCTnormative databased included patientsbetween -12D to +8D, those who hadvision better than 20/40, and did nothave disc hemorrhages, RNFL defectsor abnormal visual field. Heidelberg’sSpectralis OCT normative databaseincluded patients between -7D to+5D, patients who had vision betterthan 20/30 and those that had normalappearing optic discs with no visualfield defects.13 Most of the representa-tion within these ranges is located atthe mean, and actual representationof patients at the extremes is limited.The actual representation of myo-pic patients in the OCT normativedatabases is quite trivial, which re-duces the strength of the analysis andheightens the difficulty of glaucomadiagnosis in this cohort.
The analysis of the inner retinalthickness in the macula is comple-mentary to the nerve fiber layerscan and offers useful information inglaucoma detection. In some cases ofglaucoma where early damage occursin the macular region first, taking onlyRNFL measurements would fail todetect the disease. This is highlightedby the work of Don Hood. The mostvulnerable locations to be damagedby glaucoma are the temporal half ofthe inferior and superior quadrants ofthe optic nerve, which Hood named
the superior andinferior vulnerabil-ity zones. Due tothe macula beinginferiorly displacedin most patients,the superior vulner-ability zone does notconsist of macularfibers. However,the inferior vulner-ability zone consistsof macular fibers(Figure 5).14 Obtain-ing macular OCTscan in all glaucomapatients is essential,and particularly in
the case of glaucoma patients withhigh myopia, macular measurementsof the ganglion cell complex may havea significantly better detection powerthan RNFL thickness due to anoma-lous nerve tilting or staphylomas.
In one previous study, macularmeasurements using OCT had greaterdiagnostic power than RNFL mea-surements in high myopia.15 Bothglaucomatous and highly myopiceyes can show areas of RNFL thin-ning. However, certain types of focalloss in the ganglion cell complex cancorrelate to glaucomatous damage. In
clinical practice, when no other macu-lar pathologies are present, using theganglion cell complex is quite usefulin the long-term management of thesepatients. However, the definition ofdegenerative myopia tells us thatpeople with a high amount of near-sightedness can also show degenera-tive changes in the retina and macula.In these patients, it’s critical to lookcarefully for macular staphylomas,macular schisis, macular holes, vitreo-macular traction, epiretinal membrane,lacquer cracks and choroidal neovas-cular membranes, which will help inchoosing the best imaging techniquesand informing a proper diagnosis.
OCT-AAlthough its value in glaucoma careis still under investigation, previousresearch shows that parameters inOCT angiography (OCT-A) can detectglaucomatous damage. This type ofimaging obtains measurements of theretinal and choroidal vasculature bytaking sequential B-scans of the samelocation of the retina. Mobile bloodcells create changes in reflectance,while stationary tissue does not. TheOCT-A device then creates a map ofthe blood vessels to illustrate all themicrovascular layers.
Fig. 6. This image shows the OCT-A scans of peripapillary vessel density, visual field scans and OCT RNFL scans of three different patients. The peripapillary vessel density losscorrelated more to the visual field defect than to the OCT RNFL scan.14
Fig. 5. This illustration demonstrates the inferior vulnerabilityzone, which consists of macular fibers that are at risk for damage due to glaucoma. The superior vulnerability zone doesnot consist of macular fibers.14
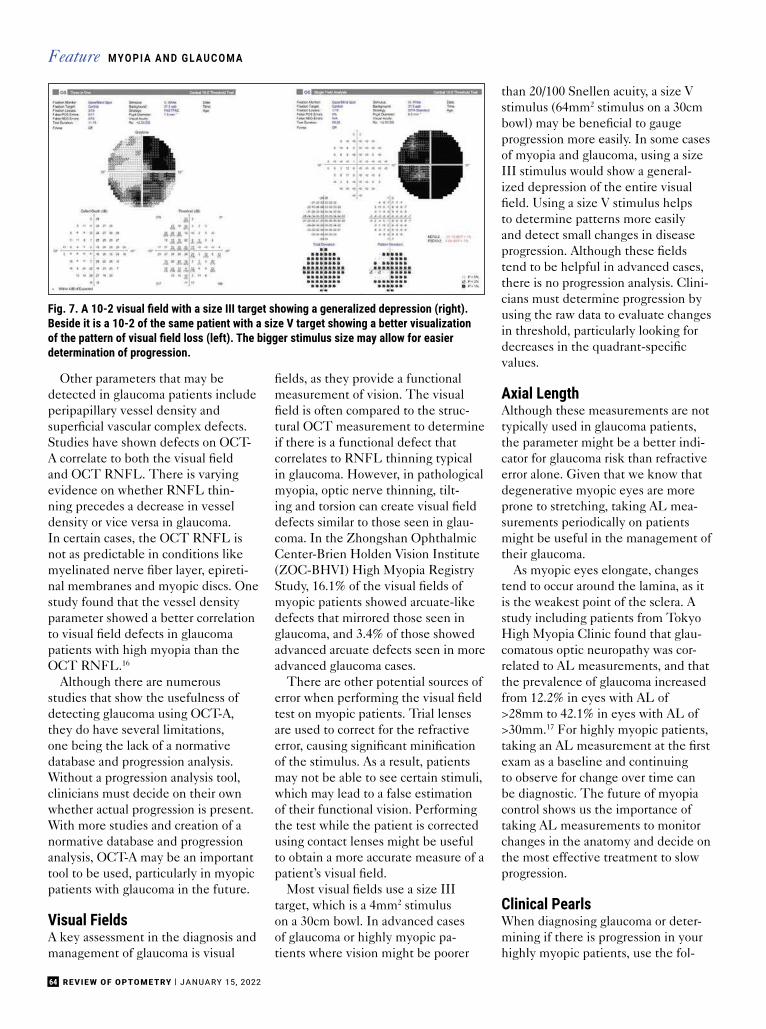
64 REVIEW OF OPTOMETRY | JANUARY 15, 2022
Other parameters that may bedetected in glaucoma patients includeperipapillary vessel density andsuperfi cial vascular complex defects.Studies have shown defects on OCT-A correlate to both the visual fi eldand OCT RNFL. There is varyingevidence on whether RNFL thin-ning precedes a decrease in vesseldensity or vice versa in glaucoma.In certain cases, the OCT RNFL isnot as predictable in conditions likemyelinated nerve fi ber layer, epireti-nal membranes and myopic discs. Onestudy found that the vessel densityparameter showed a better correlationto visual fi eld defects in glaucomapatients with high myopia than theOCT RNFL.16
Although there are numerousstudies that show the usefulness ofdetecting glaucoma using OCT-A,they do have several limitations,one being the lack of a normativedatabase and progression analysis.Without a progression analysis tool,clinicians must decide on their ownwhether actual progression is present.With more studies and creation of anormative database and progressionanalysis, OCT-A may be an importanttool to be used, particularly in myopicpatients with glaucoma in the future.
Visual FieldsA key assessment in the diagnosis andmanagement of glaucoma is visual
fi elds, as they provide a functionalmeasurement of vision. The visualfi eld is often compared to the struc-tural OCT measurement to determineif there is a functional defect thatcorrelates to RNFL thinning typicalin glaucoma. However, in pathologicalmyopia, optic nerve thinning, tilt-ing and torsion can create visual fi elddefects similar to those seen in glau-coma. In the Zhongshan OphthalmicCenter-Brien Holden Vision Institute(ZOC-BHVI) High Myopia RegistryStudy, 16.1% of the visual fi elds ofmyopic patients showed arcuate-likedefects that mirrored those seen inglaucoma, and 3.4% of those showedadvanced arcuate defects seen in moreadvanced glaucoma cases.
There are other potential sources oferror when performing the visual fi eldtest on myopic patients. Trial lensesare used to correct for the refractiveerror, causing signifi cant minifi cationof the stimulus. As a result, patientsmay not be able to see certain stimuli,which may lead to a false estimationof their functional vision. Performingthe test while the patient is correctedusing contact lenses might be usefulto obtain a more accurate measure of apatient’s visual fi eld.
Most visual fi elds use a size IIItarget, which is a 4mm2 stimuluson a 30cm bowl. In advanced casesof glaucoma or highly myopic pa-tients where vision might be poorer
than 20/100 Snellen acuity, a size Vstimulus (64mm2 stimulus on a 30cmbowl) may be benefi cial to gaugeprogression more easily. In some casesof myopia and glaucoma, using a sizeIII stimulus would show a general-ized depression of the entire visualfi eld. Using a size V stimulus helpsto determine patterns more easilyand detect small changes in diseaseprogression. Although these fi eldstend to be helpful in advanced cases,there is no progression analysis. Clini-cians must determine progression byusing the raw data to evaluate changesin threshold, particularly looking fordecreases in the quadrant-specifi cvalues.
Axial LengthAlthough these measurements are nottypically used in glaucoma patients,the parameter might be a better indi-cator for glaucoma risk than refractiveerror alone. Given that we know thatdegenerative myopic eyes are moreprone to stretching, taking AL mea-surements periodically on patientsmight be useful in the management oftheir glaucoma.
As myopic eyes elongate, changestend to occur around the lamina, as itis the weakest point of the sclera. Astudy including patients from TokyoHigh Myopia Clinic found that glau-comatous optic neuropathy was cor-related to AL measurements, and thatthe prevalence of glaucoma increasedfrom 12.2% in eyes with AL of>28mm to 42.1% in eyes with AL of>30mm.17 For highly myopic patients,taking an AL measurement at the fi rstexam as a baseline and continuingto observe for change over time canbe diagnostic. The future of myopiacontrol shows us the importance oftaking AL measurements to monitorchanges in the anatomy and decide onthe most effective treatment to slowprogression.
Clinical PearlsWhen diagnosing glaucoma or deter-mining if there is progression in yourhighly myopic patients, use the fol-
M YO P I A A N D G L A U C O M AFeature
Fig. 7. A 10-2 visual fi eld with a size III target showing a generalized depression (right). Beside it is a 10-2 of the same patient with a size V target showing a better visualization of the pattern of visual fi eld loss (left). The bigger stimulus size may allow for easier determination of progression.
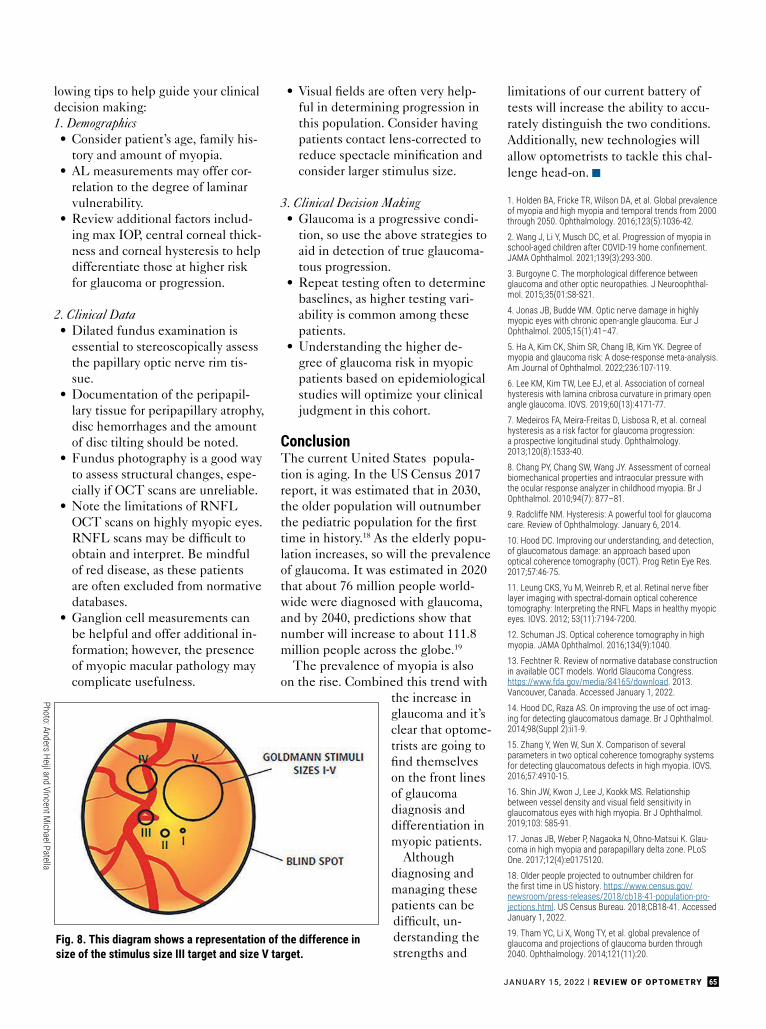
65JANUARY 15, 2022 | REVIEW OF OPTOMETRY
lowing tips to help guide your clinicaldecision making:1. Demographics• Consider patient’s age, family his-
tory and amount of myopia.• AL measurements may offer cor-
relation to the degree of laminarvulnerability.
• Review additional factors includ-ing max IOP, central corneal thick-ness and corneal hysteresis to helpdifferentiate those at higher riskfor glaucoma or progression.
2. Clinical Data• Dilated fundus examination is
essential to stereoscopically assessthe papillary optic nerve rim tis-sue.
• Documentation of the peripapil-lary tissue for peripapillary atrophy,disc hemorrhages and the amountof disc tilting should be noted.
• Fundus photography is a good wayto assess structural changes, espe-cially if OCT scans are unreliable.
• Note the limitations of RNFLOCT scans on highly myopic eyes.RNFL scans may be difficult toobtain and interpret. Be mindfulof red disease, as these patientsare often excluded from normativedatabases.
• Ganglion cell measurements canbe helpful and offer additional in-formation; however, the presenceof myopic macular pathology maycomplicate usefulness.
• Visual fields are often very help-ful in determining progression inthis population. Consider havingpatients contact lens-corrected toreduce spectacle minification andconsider larger stimulus size.
3. Clinical Decision Making• Glaucoma is a progressive condi-
tion, so use the above strategies toaid in detection of true glaucoma-tous progression.
• Repeat testing often to determinebaselines, as higher testing vari-ability is common among thesepatients.
• Understanding the higher de-gree of glaucoma risk in myopicpatients based on epidemiologicalstudies will optimize your clinicaljudgment in this cohort.
ConclusionThe current United States popula-tion is aging. In the US Census 2017report, it was estimated that in 2030,the older population will outnumberthe pediatric population for the firsttime in history.18 As the elderly popu-lation increases, so will the prevalenceof glaucoma. It was estimated in 2020that about 76 million people world-wide were diagnosed with glaucoma,and by 2040, predictions show thatnumber will increase to about 111.8million people across the globe.19
The prevalence of myopia is alsoon the rise. Combined this trend with
the increase inglaucoma and it’sclear that optome-trists are going tofind themselveson the front linesof glaucomadiagnosis anddifferentiation inmyopic patients.
Althoughdiagnosing andmanaging thesepatients can bedifficult, un-derstanding thestrengths and
limitations of our current battery oftests will increase the ability to accu-rately distinguish the two conditions.Additionally, new technologies willallow optometrists to tackle this chal-lenge head-on. g
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalenceof myopia and high myopia and temporal trends from 2000through 2050. Ophthalmology. 2016;123(5):1036-42.
2. Wang J, Li Y, Musch DC, et al. Progression of myopia inschool-aged children after COVID-19 home confinement. JAMA Ophthalmol. 2021;139(3):293-300.
3. Burgoyne C. The morphological difference betweenglaucoma and other optic neuropathies. J Neuroophthal-mol. 2015;35(01:S8-S21.
4. Jonas JB, Budde WM. Optic nerve damage in highlymyopic eyes with chronic open-angle glaucoma. Eur JOphthalmol. 2005;15(1):41–47.
5. Ha A, Kim CK, Shim SR, Chang IB, Kim YK. Degree ofmyopia and glaucoma risk: A dose-response meta-analysis.Am Journal of Ophthalmol. 2022;236:107-119.
6. Lee KM, Kim TW, Lee EJ, et al. Association of cornealhysteresis with lamina cribrosa curvature in primary openangle glaucoma. IOVS. 2019;60(13):4171-77.
7. Medeiros FA, Meira-Freitas D, Lisbosa R, et al. cornealhysteresis as a risk factor for glaucoma progression:a prospective longitudinal study. Ophthalmology.2013;120(8):1533-40.
8. Chang PY, Chang SW, Wang JY. Assessment of cornealbiomechanical properties and intraocular pressure withthe ocular response analyzer in childhood myopia. Br JOphthalmol. 2010;94(7): 877–81.
9. Radcliffe NM. Hysteresis: A powerful tool for glaucomacare. Review of Ophthalmology. January 6, 2014.
10. Hood DC. Improving our understanding, and detection,of glaucomatous damage: an approach based uponoptical coherence tomography (OCT). Prog Retin Eye Res.2017;57:46-75.
11. Leung CKS, Yu M, Weinreb R, et al. Retinal nerve fiber layer imaging with spectral-domain optical coherencetomography: Interpreting the RNFL Maps in healthy myopiceyes. IOVS. 2012; 53(11):7194-7200.
12. Schuman JS. Optical coherence tomography in highmyopia. JAMA Ophthalmol. 2016;134(9):1040.
13. Fechtner R. Review of normative database constructionin available OCT models. World Glaucoma Congress.https://www.fda.gov/media/84165/download. 2013.Vancouver, Canada. Accessed January 1, 2022.
14. Hood DC, Raza AS. On improving the use of oct imag-ing for detecting glaucomatous damage. Br J Ophthalmol.2014;98(Suppl 2):ii1-9.
15. Zhang Y, Wen W, Sun X. Comparison of severalparameters in two optical coherence tomography systemsfor detecting glaucomatous defects in high myopia. IOVS.2016;57:4910-15.
16. Shin JW, Kwon J, Lee J, Kookk MS. Relationshipbetween vessel density and visual field sensitivity in glaucomatous eyes with high myopia. Br J Ophthalmol.2019;103: 585-91.
17. Jonas JB, Weber P, Nagaoka N, Ohno-Matsui K. Glau-coma in high myopia and parapapillary delta zone. PLoSOne. 2017;12(4):e0175120.
18. Older people projected to outnumber children forthe first time in US history. https://www.census.gov/newsroom/press-releases/2018/cb18-41-population-pro-jections.html. US Census Bureau. 2018;CB18-41. Accessed January 1, 2022.
19. Tham YC, Li X, Wong TY, et al. global prevalence ofglaucoma and projections of glaucoma burden through2040. Ophthalmology. 2014;121(11):20.
Fig. 8. This diagram shows a representation of the difference insize of the stimulus size III target and size V target.
Photo: Anders Heijl and Vincent Michael Patella
REVIEW OF OPTOMETRY | JANUARY 15, 202266
With significant increases in dai-ly screen time, the impact ofsuch exposure on eye health,and from blue light exposure
in particular, has gained increasedinterest in recent years. Numerousquestions surround the potentialimplications of digital device use oneye health. In this article, the effectsof digital device use specific to the eyewill be discussed, as well as the role ofthe optometrist in educating patientson the risks of digital device exposureand mitigation strategies.
How Much ScreenTime Are We Getting?Digital devices are increasingly usedby children and adults for education,gaming, social interaction and otherdaily activities, such as shopping. Itwas estimated that adults 18 yearsand older spent an average of 12
hours and 21 minutes per day usingscreens in the first quarter of 2020(Figure 1).1 Children ages 10 to 18years spent 12 hours per day on aver-age using electronic devices duringthe 2021 school year.2 In the UnitedStates, 44% of children use mobiledevices before the age of one, and byage four, 75% have their own mobiledevice.3
What is Blue Light?Before discussing blue light in thecontext of digital devices, let’s discusslight as electromagnetic radiation(Figure 2). Light that is perceivedby the human eye is termed “vis-ible light,” which ranges fromapproximately 400nm to 700nm.Wavelengths from 400nm to 500nmare generally perceived as “blue,”medium wavelengths from 500nm to600nm are perceived as “green” andlonger wavelengths from 600nm to700nm are perceived as “red.” Short-wavelength blue light has higher en-ergy than long-wavelength red light.
Ultraviolet (UV) light includeswavelengths that are shorter than vis-ible light, ranging from approximately10nm to 400nm, and infrared lightincludes wavelengths that are longerthan visible light, from approximately700nm to 1mm. The majority of UVlight that reaches the eye is absorbedby the cornea, which absorbs UV-C,and the crystalline lens, which absorbsUV-A, -B and -C, and therefore doesnot reach the retina.
An additional protection from lightdamage is the macular pigment, con-sisting of zeaxanthin and lutein, whichabsorbs approximately 40% of high-energy blue light with an absorptionspectrum peaking at 460nm.4
The spectral output (i.e., wavelengthcomposition) is comprised of variousnatural and artificial sources of light(Figure 3). The highest intensity lightthat humans are exposed to is sunlight,which can be as high as 150,000 luxon a bright sunny day. Indoor roomilluminance generally ranges from30 to 600 lux, and illuminance from
10 Questions on Digital Devicesand Eye Health—Answered!
With screen time rising in children and adults, ODs must understand the potential impact.
Dr. Ostrin is an associate professor at the University of Houston College of Optometry, where she received her optometry degree and PhD. She teaches in the optometry andvision science programs, covering topics such as gross anatomy, ocular anatomy, eye growth and accommodation. She is a fellow of the American Academy of Optometryand a gold fellow of the Association for Research in Vision and Ophthalmology. She has no relevant financial interests to disclose.
About theauthor
Earn 2 CE Credits(COPE APPROVED)
By lisa ostrin, od, phdhouston
PEER REVIEWEDOptometric Study Center B LU E L I G HT O C U L A R E F F E CT S
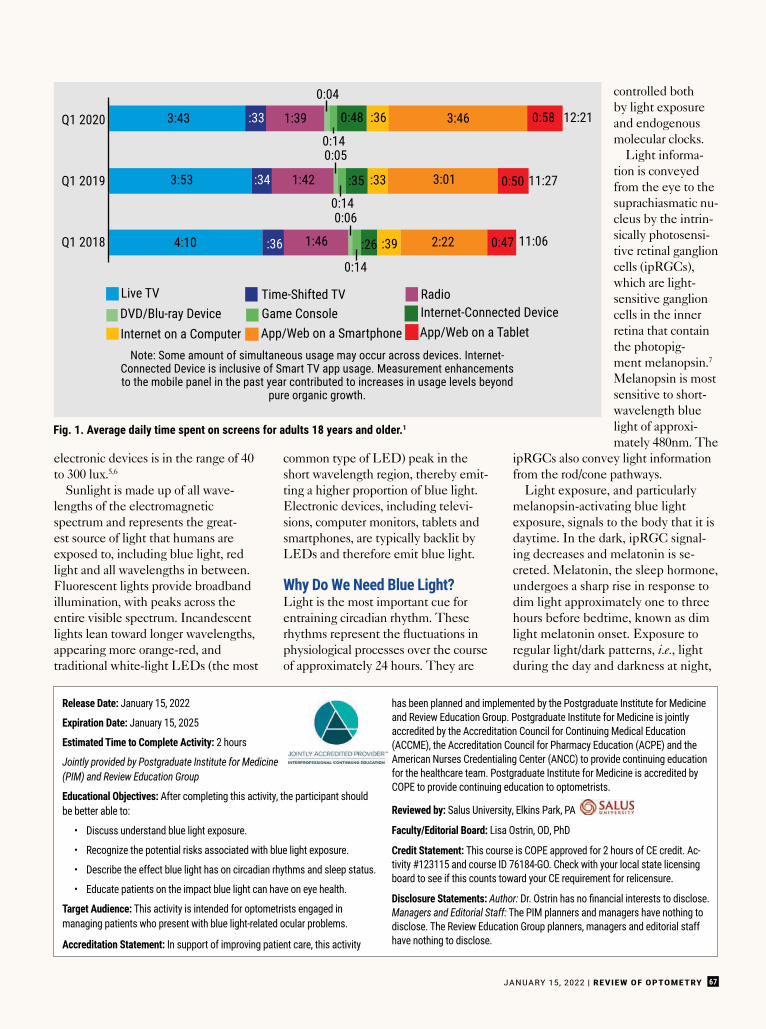
JANUARY 15, 2022 | REVIEW OF OPTOMETRY 67
Release Date: January 15, 2022
Expiration Date: January 15, 2025
Estimated Time to Complete Activity: 2 hours
Jointly provided by Postgraduate Institute for Medicine(PIM) and Review Education Group
Educational Objectives: After completing this activity, the participant shouldbe better able to:
• Discuss understand blue light exposure.
• Recognize the potential risks associated with blue light exposure.
• Describe the effect blue light has on circadian rhythms and sleep status.
• Educate patients on the impact blue light can have on eye health.
Target Audience: This activity is intended for optometrists engaged inmanaging patients who present with blue light-related ocular problems.
Accreditation Statement: In support of improving patient care, this activity
has been planned and implemented by the Postgraduate Institute for Medicineand Review Education Group. Postgraduate Institute for Medicine is jointlyaccredited by the Accreditation Council for Continuing Medical Education(ACCME), the Accreditation Council for Pharmacy Education (ACPE) and theAmerican Nurses Credentialing Center (ANCC) to provide continuing educationfor the healthcare team. Postgraduate Institute for Medicine is accredited byCOPE to provide continuing education to optometrists.
Reviewed by: Salus University, Elkins Park, PA
Faculty/Editorial Board: Lisa Ostrin, OD, PhD
Credit Statement: This course is COPE approved for 2 hours of CE credit. Ac-tivity #123115 and course ID 76184-GO. Check with your local state licensingboard to see if this counts toward your CE requirement for relicensure.
Disclosure Statements: Author: Dr. Ostrin has no fi nancial interests to disclose. Managers and Editorial Staff: The PIM planners and managers have nothing todisclose. The Review Education Group planners, managers and editorial staffhave nothing to disclose.
Q1 2020
Q1 2019
Q1 2018
3:43 1:39 3:46
0:04
0:140:05
0:140:06
:26
0:14
:35 3:01
2:22
0:48 0:58
0:50
0:47
12:21
11:27
11:06
1:42
1:46
:33 :36
:33
:39
:34
:36
3:53
4:10
Live TVDVD/Blu-ray DeviceInternet on a Computer
Time-Shifted TVGame ConsoleApp/Web on a Smartphone
Note: Some amount of simultaneous usage may occur across devices. Internet-Connected Device is inclusive of Smart TV app usage. Measurement enhancementsto the mobile panel in the past year contributed to increases in usage levels beyond
pure organic growth.
RadioInternet-Connected DeviceApp/Web on a Tablet
electronic devices is in the range of 40to 300 lux.5,6
Sunlight is made up of all wave-lengths of the electromagneticspectrum and represents the great-est source of light that humans areexposed to, including blue light, redlight and all wavelengths in between.Fluorescent lights provide broadbandillumination, with peaks across theentire visible spectrum. Incandescentlights lean toward longer wavelengths,appearing more orange-red, andtraditional white-light LEDs (the most
common type of LED) peak in theshort wavelength region, thereby emit-ting a higher proportion of blue light.Electronic devices, including televi-sions, computer monitors, tablets andsmartphones, are typically backlit byLEDs and therefore emit blue light.
Why Do We Need Blue Light?Light is the most important cue forentraining circadian rhythm. Theserhythms represent the fl uctuations inphysiological processes over the courseof approximately 24 hours. They are
controlled bothby light exposureand endogenousmolecular clocks.
Light informa-tion is conveyedfrom the eye to thesuprachiasmatic nu-cleus by the intrin-sically photosensi-tive retinal ganglioncells (ipRGCs),which are light-sensitive ganglioncells in the innerretina that containthe photopig-ment melanopsin.7
Melanopsin is mostsensitive to short-wavelength bluelight of approxi-mately 480nm. The
ipRGCs also convey light informationfrom the rod/cone pathways.
Light exposure, and particularlymelanopsin-activating blue lightexposure, signals to the body that it isdaytime. In the dark, ipRGC signal-ing decreases and melatonin is se-creted. Melatonin, the sleep hormone,undergoes a sharp rise in response todim light approximately one to threehours before bedtime, known as dimlight melatonin onset. Exposure toregular light/dark patterns, i.e., lightduring the day and darkness at night,
Fig. 1. Average daily time spent on screens for adults 18 years and older.1
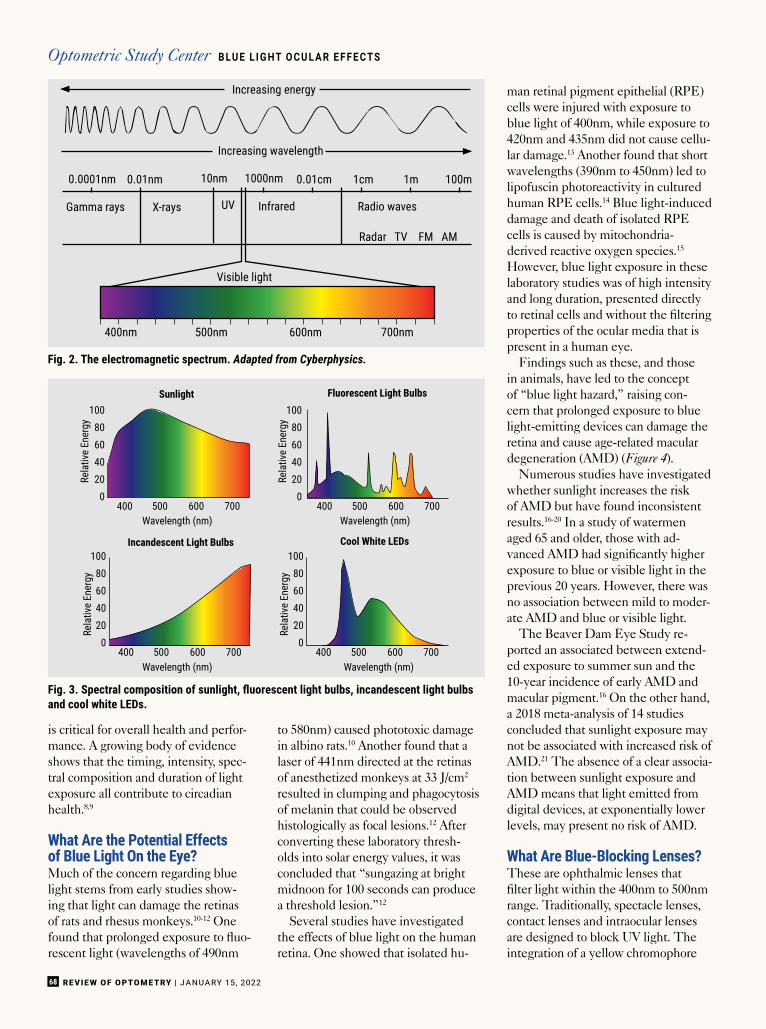
REVIEW OF OPTOMETRY | JANUARY 15, 202268
Increasing energy
0.0001nm
Gamma rays X-rays UV Infrared
Visible light
400nm 500nm 600nm 700nm
Radio waves
Radar TV FM AM
0.01nm 0.01cm 1cm 1m 100m10nm 1000nm
Increasing wavelength
10080604020
0
10080604020
0
10080604020
0
10080604020
0400
400 400
400
Rela
tive
Ener
gyRe
lativ
e En
ergy
Rela
tive
Ener
gyRe
lativ
e En
ergy
Wavelength (nm)
Wavelength (nm) Wavelength (nm)
Wavelength (nm)
Sunlight
Incandescent Light Bulbs
Fluorescent Light Bulbs
Cool White LEDs
500
500 500
500600
600 600
600700
700 700
700
is critical for overall health and perfor-mance. A growing body of evidenceshows that the timing, intensity, spec-tral composition and duration of lightexposure all contribute to circadianhealth.8,9
What Are the Potential Effectsof Blue Light On the Eye?Much of the concern regarding bluelight stems from early studies show-ing that light can damage the retinasof rats and rhesus monkeys.10-12 Onefound that prolonged exposure to fluo-rescent light (wavelengths of 490nm
to 580nm) caused phototoxic damagein albino rats.10 Another found that alaser of 441nm directed at the retinasof anesthetized monkeys at 33 J/cm2
resulted in clumping and phagocytosisof melanin that could be observedhistologically as focal lesions.12 Afterconverting these laboratory thresh-olds into solar energy values, it wasconcluded that “sungazing at brightmidnoon for 100 seconds can producea threshold lesion.”12
Several studies have investigatedthe effects of blue light on the humanretina. One showed that isolated hu-
man retinal pigment epithelial (RPE)cells were injured with exposure toblue light of 400nm, while exposure to420nm and 435nm did not cause cellu-lar damage.13 Another found that shortwavelengths (390nm to 450nm) led tolipofuscin photoreactivity in culturedhuman RPE cells.14 Blue light-induceddamage and death of isolated RPEcells is caused by mitochondria-derived reactive oxygen species.15
However, blue light exposure in theselaboratory studies was of high intensityand long duration, presented directlyto retinal cells and without the filteringproperties of the ocular media that ispresent in a human eye.
Findings such as these, and thosein animals, have led to the conceptof “blue light hazard,” raising con-cern that prolonged exposure to bluelight-emitting devices can damage theretina and cause age-related maculardegeneration (AMD) (Figure 4).
Numerous studies have investigatedwhether sunlight increases the riskof AMD but have found inconsistentresults.16-20 In a study of watermenaged 65 and older, those with ad-vanced AMD had significantly higherexposure to blue or visible light in theprevious 20 years. However, there wasno association between mild to moder-ate AMD and blue or visible light.
The Beaver Dam Eye Study re-ported an associated between extend-ed exposure to summer sun and the10-year incidence of early AMD andmacular pigment.16 On the other hand,a 2018 meta-analysis of 14 studiesconcluded that sunlight exposure maynot be associated with increased risk ofAMD.21 The absence of a clear associa-tion between sunlight exposure andAMD means that light emitted fromdigital devices, at exponentially lowerlevels, may present no risk of AMD.
What Are Blue-Blocking Lenses?These are ophthalmic lenses thatfilter light within the 400nm to 500nmrange. Traditionally, spectacle lenses,contact lenses and intraocular lensesare designed to block UV light. Theintegration of a yellow chromophore
Fig. 2. The electromagnetic spectrum. Adapted from Cyberphysics.
Fig. 3. Spectral composition of sunlight, fluorescent light bulbs, incandescent light bulbs and cool white LEDs.
Optometric Study Center B LU E L I G HT O C U L A R E F F E CT S
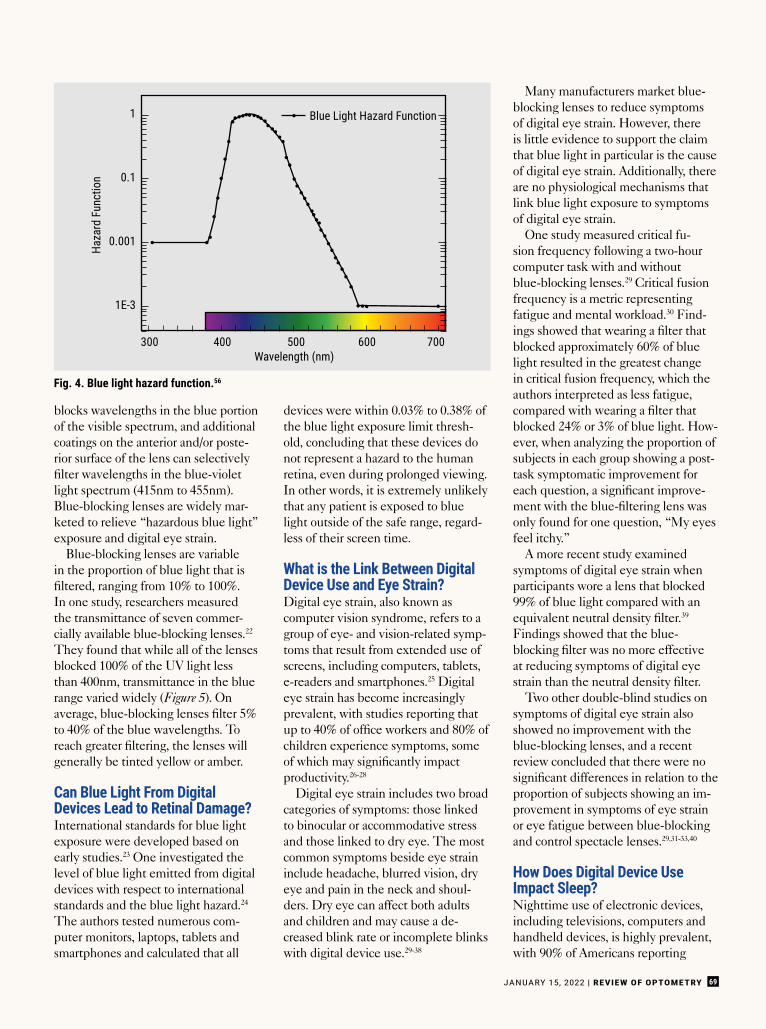
JANUARY 15, 2022 | REVIEW OF OPTOMETRY 69
blocks wavelengths in the blue portionof the visible spectrum, and additionalcoatings on the anterior and/or poste-rior surface of the lens can selectivelyfilter wavelengths in the blue-violetlight spectrum (415nm to 455nm).Blue-blocking lenses are widely mar-keted to relieve “hazardous blue light”exposure and digital eye strain.
Blue-blocking lenses are variablein the proportion of blue light that isfiltered, ranging from 10% to 100%.In one study, researchers measuredthe transmittance of seven commer-cially available blue-blocking lenses.22
They found that while all of the lensesblocked 100% of the UV light lessthan 400nm, transmittance in the bluerange varied widely (Figure 5). Onaverage, blue-blocking lenses filter 5%to 40% of the blue wavelengths. Toreach greater filtering, the lenses willgenerally be tinted yellow or amber.
Can Blue Light From DigitalDevices Lead to Retinal Damage?International standards for blue lightexposure were developed based onearly studies.23 One investigated thelevel of blue light emitted from digitaldevices with respect to internationalstandards and the blue light hazard.24
The authors tested numerous com-puter monitors, laptops, tablets andsmartphones and calculated that all
devices were within 0.03% to 0.38% ofthe blue light exposure limit thresh-old, concluding that these devices donot represent a hazard to the humanretina, even during prolonged viewing.In other words, it is extremely unlikelythat any patient is exposed to bluelight outside of the safe range, regard-less of their screen time.
What is the Link Between DigitalDevice Use and Eye Strain?Digital eye strain, also known ascomputer vision syndrome, refers to agroup of eye- and vision-related symp-toms that result from extended use ofscreens, including computers, tablets,e-readers and smartphones.25 Digitaleye strain has become increasinglyprevalent, with studies reporting thatup to 40% of office workers and 80% ofchildren experience symptoms, someof which may significantly impactproductivity.26-28
Digital eye strain includes two broadcategories of symptoms: those linkedto binocular or accommodative stressand those linked to dry eye. The mostcommon symptoms beside eye straininclude headache, blurred vision, dryeye and pain in the neck and shoul-ders. Dry eye can affect both adultsand children and may cause a de-creased blink rate or incomplete blinkswith digital device use.29-38
Many manufacturers market blue-blocking lenses to reduce symptomsof digital eye strain. However, thereis little evidence to support the claimthat blue light in particular is the causeof digital eye strain. Additionally, thereare no physiological mechanisms thatlink blue light exposure to symptomsof digital eye strain.
One study measured critical fu-sion frequency following a two-hourcomputer task with and withoutblue-blocking lenses.29 Critical fusionfrequency is a metric representingfatigue and mental workload.30 Find-ings showed that wearing a filter thatblocked approximately 60% of bluelight resulted in the greatest changein critical fusion frequency, which theauthors interpreted as less fatigue,compared with wearing a filter thatblocked 24% or 3% of blue light. How-ever, when analyzing the proportion ofsubjects in each group showing a post-task symptomatic improvement foreach question, a significant improve-ment with the blue-filtering lens wasonly found for one question, “My eyesfeel itchy.”
A more recent study examinedsymptoms of digital eye strain whenparticipants wore a lens that blocked99% of blue light compared with anequivalent neutral density filter.39
Findings showed that the blue-blocking filter was no more effectiveat reducing symptoms of digital eyestrain than the neutral density filter.
Two other double-blind studies onsymptoms of digital eye strain alsoshowed no improvement with theblue-blocking lenses, and a recentreview concluded that there were nosignificant differences in relation to theproportion of subjects showing an im-provement in symptoms of eye strainor eye fatigue between blue-blockingand control spectacle lenses.29,31-33,40
How Does Digital Device UseImpact Sleep?Nighttime use of electronic devices,including televisions, computers andhandheld devices, is highly prevalent,with 90% of Americans reporting
Haza
rd F
unct
ion
Wavelength (nm)
Blue Light Hazard Function
300 400 500 600 700
1
0.1
0.001
1E-3
Fig. 4. Blue light hazard function.56
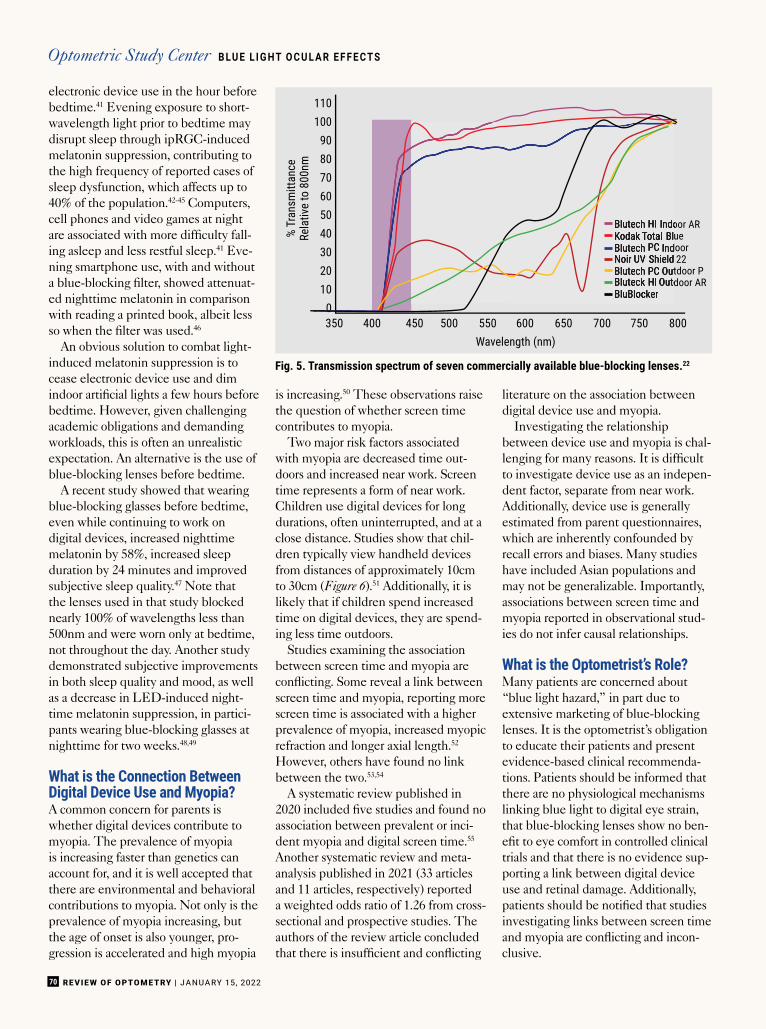
REVIEW OF OPTOMETRY | JANUARY 15, 202270
electronic device use in the hour beforebedtime.41 Evening exposure to short-wavelength light prior to bedtime maydisrupt sleep through ipRGC-inducedmelatonin suppression, contributing tothe high frequency of reported cases ofsleep dysfunction, which affects up to40% of the population.42-45 Computers,cell phones and video games at nightare associated with more difficulty fall-ing asleep and less restful sleep.41 Eve-ning smartphone use, with and withouta blue-blocking filter, showed attenuat-ed nighttime melatonin in comparisonwith reading a printed book, albeit lessso when the filter was used.46
An obvious solution to combat light-induced melatonin suppression is tocease electronic device use and dimindoor artificial lights a few hours beforebedtime. However, given challengingacademic obligations and demandingworkloads, this is often an unrealisticexpectation. An alternative is the use ofblue-blocking lenses before bedtime.
A recent study showed that wearingblue-blocking glasses before bedtime,even while continuing to work ondigital devices, increased nighttimemelatonin by 58%, increased sleepduration by 24 minutes and improvedsubjective sleep quality.47 Note thatthe lenses used in that study blockednearly 100% of wavelengths less than500nm and were worn only at bedtime,not throughout the day. Another studydemonstrated subjective improvementsin both sleep quality and mood, as wellas a decrease in LED-induced night-time melatonin suppression, in partici-pants wearing blue-blocking glasses atnighttime for two weeks.48,49
What is the Connection BetweenDigital Device Use and Myopia?A common concern for parents iswhether digital devices contribute tomyopia. The prevalence of myopiais increasing faster than genetics canaccount for, and it is well accepted thatthere are environmental and behavioralcontributions to myopia. Not only is theprevalence of myopia increasing, butthe age of onset is also younger, pro-gression is accelerated and high myopia
is increasing.50 These observations raisethe question of whether screen timecontributes to myopia.
Two major risk factors associatedwith myopia are decreased time out-doors and increased near work. Screentime represents a form of near work.Children use digital devices for longdurations, often uninterrupted, and at aclose distance. Studies show that chil-dren typically view handheld devicesfrom distances of approximately 10cmto 30cm (Figure 6).51 Additionally, it islikely that if children spend increasedtime on digital devices, they are spend-ing less time outdoors.
Studies examining the associationbetween screen time and myopia areconflicting. Some reveal a link betweenscreen time and myopia, reporting morescreen time is associated with a higherprevalence of myopia, increased myopicrefraction and longer axial length.52
However, others have found no linkbetween the two.53,54
A systematic review published in2020 included five studies and found noassociation between prevalent or inci-dent myopia and digital screen time.55
Another systematic review and meta-analysis published in 2021 (33 articlesand 11 articles, respectively) reporteda weighted odds ratio of 1.26 from cross-sectional and prospective studies. Theauthors of the review article concludedthat there is insufficient and conflicting
literature on the association betweendigital device use and myopia.
Investigating the relationshipbetween device use and myopia is chal-lenging for many reasons. It is difficultto investigate device use as an indepen-dent factor, separate from near work.Additionally, device use is generallyestimated from parent questionnaires,which are inherently confounded byrecall errors and biases. Many studieshave included Asian populations andmay not be generalizable. Importantly,associations between screen time andmyopia reported in observational stud-ies do not infer causal relationships.
What is the Optometrist’s Role?Many patients are concerned about“blue light hazard,” in part due toextensive marketing of blue-blockinglenses. It is the optometrist’s obligationto educate their patients and presentevidence-based clinical recommenda-tions. Patients should be informed thatthere are no physiological mechanismslinking blue light to digital eye strain,that blue-blocking lenses show no ben-efit to eye comfort in controlled clinicaltrials and that there is no evidence sup-porting a link between digital deviceuse and retinal damage. Additionally,patients should be notified that studiesinvestigating links between screen timeand myopia are conflicting and incon-clusive.
% Tr
ansm
ittan
ceRe
lativ
e to
800
nm
110100
908070605040302010
0350 400 450 500 550 600 650 700 750 800
Wavelength (nm)
Blutech HI Indoor ARKodak Total BlueBlutech PC IndoorNoir UV Shield 22Blutech PC Outdoor PBluteck HI Outdoor ARBluBlocker
Blutech HI IndoorKodak Total BlueBlutech PC IndoorNoir UV Shield 22Blutech PC OutdoorBluteck HI OutdoorBluBlocker
0
Fig. 5. Transmission spectrum of seven commercially available blue-blocking lenses.22
Optometric Study Center B LU E L I G HT O C U L A R E F F E CT S

JANUARY 15, 2022 | REVIEW OF OPTOMETRY 71
Optometrists should educate parentsthat nighttime screen time and artifi-cial light can lead to sleep disruptions.They can also convey general recom-mendations for screen use in childrenby referring parents to guidelines set bythe American Academy of Pediatriciansand World Health Organization.
How can the OD help relieve digitaleye strain? Note that it is a diagnosisof exclusion. Refractive status must becomprehensively examined, consider-ing objective and subjective as wellas non-cyclopleged and cycloplegedmeasures. A careful assessment ofbinocular vision should be performed,as binocular vision conditions can oftenpresent with the same symptoms asdigital eye strain. A patient’s individualviewing needs should be discussed,which will vary based on academic orwork demands and leisure screen time.Patients who are presbyopic or near-ing presbyopia, or those with reducedaccommodative amplitude and facility,may benefit from computer glasses toreduce accommodative demand at theirhabitual computer-viewing distance.
Physical attributes, such as bodyheight and arm length, should be con-sidered. For both children and adults,workstations should be set up withideal ergonomics that take into accountviewing distance, angle and height.Glare, brightness, contrast and font sizeare also important factors for comfortduring extended screen time. Dry eyesymptoms related to digital devices canbe addressed by teaching the patientto blink during screen time, usinglubricating drops and employing other
traditional treatments for dry eye. Acommon clinical recommendation is the20-20-20 rule. For every 20 minutes ofnear work, look at objects further than20 feet away for at least 20 seconds.This general rule-of-thumb may helpremind patients to blink and intermit-tently relax their eyes.
Based on studies demonstrating theattenuating effects of blue light on mel-atonin, screen time and artificial lightexposure should be decreased one totwo hours before bedtime.46,47 This canalso be accomplished through the useof amber-tinted lenses before bedtime.Lenses with the ability to block closeto 100% of shorter wavelengths are themost effective. Other options includeusing apps and installing home lightingthat both aim to reduce blue light. g
1. Staying PUT: consumers forced indoors during crisis spend more timeon media. 2020. www.nielsen.com/us/en/insights/article/2020/staying-put-consumers-forced-indoors-during-crisis-spend-more-time-on-media.Accessed November 20, 2021.2. Bhandari K, Shukla D, Mirhajianmoghadam H, et al. Objectively measuredhabitual viewing behaviors in schoolchildren. Optom Vis Sci Suppl. 2021;E-Abstract 215133.3. Kabali HK, Irigoyen MM, Nunez-Davis R, et al. Exposure and use of mobilemedia devices by young children. Pediatrics. 2015;136(6):1044-50.4. Loane E, Kelliher C, Beatty S, et al. The rationale and evidence base fora protective role of macular pigment in age-related maculopathy. Br JOphthalmol. 2008;92(9):1163-8.5. Gringas P, Middleton B, Skene D, et al. Bigger, brighter, bluer-better?Current light-emitting devices-adverse sleep properties and preventativestrategies. Front Public Health. 2015;3:233.6. Ostrin LA. Objectively measured light exposure in emmetropic and myopicadults. Optom Vis Sci. 2017;94(2):229-38.7. Sollars PJ, Smeraski CA, Kaufman JD, et al. Melanopsin and non-melanopsin expressing retinal ganglion cells innervate the hypothalamicsuprachiasmatic nucleus. Vis Neurosci. 2003;20(6):601-10.8. Bumgarner JR, Nelson RJ. Light at night and disrupted circadian rhythmsalter physiology and behavior. Integr Comp Biol. 2021;61(3):1160-9.9. Xiao H, Cai H, Li X. Non-visual effects of indoor light environment onhumans: a review. Physiol Behav. 2021;228:113195.10. Noell WK, Walker VS, Kang BS, et al. Retinal damage by light in rats.Invest Ophthalmol. 1966;5(5):450-73.11. Ham WT Jr., Ruffolo JJ Jr., Mueller HA, et al. Histologic analysis ofphotochemical lesions produced in rhesus retina by short-wave-length light.Invest Ophthalmol Vis Sci. 1978;17(10):1029-35.12. Ham WT Jr., Mueller HA, Sliney DH. Retinal sensitivity to damage fromshort wavelength light. Nature. 1976;260(5547):153-5.13. Youn HY, Chou BR, Cullen AP, et al. Effects of 400 nm, 420 nm, and435.8 nm radiations on cultured human retinal pigment epithelial cells. JPhotochem Photobiol B. 2009;95(1):64-70.14. Davies S, Elliott MH, Floor E, et al. Photocytotoxicity of lipofuscin in hu-man retinal pigment epithelial cells. Free Radic Biol Med. 2001;31(2):256-65.15. King A, Gottlieb E, Brooks DG, et al. Mitochondria-derived reactive oxygenspecies mediate blue light-induced death of retinal pigment epithelial cells.Photochem Photobiol. 2004;79(5):470-5.16. Tomany SC, Cruickshanks KJ, Klein R, et al. Sunlight and the 10-yearincidence of age-related maculopathy: the Beaver Dam Eye Study. ArchOphthalmol. 2004;122(5):750-7.17. Taylor HR, West S, Munoz B, et al. The long-term effects of visible light onthe eye. Arch Ophthalmol. 1992;110(1):99-104.18. Darzins P, Mitchell P, Heller RF. Sun exposure and age-relatedmacular degeneration. An Australian case-control study. Ophthalmology.1997;104(5):770-6.19. Mitchell P, Smith W, Wang JJ. Iris color, skin sun sensitivity, andage-related maculopathy. The Blue Mountains Eye Study. Ophthalmology.1998;105(8):1359-63.20. Delcourt C, Carriere I, Ponton-Sanchez A, et al. Light exposure and therisk of age-related macular degeneration: the Pathologies Oculaires Liees al’Age (POLA) study. Arch Ophthalmol. 2001;119(10):1463-8.21. Zhou H, Zhang H, Yu A, et al. Association between sunlight exposure andrisk of age-related macular degeneration: a meta-analysis. BMC Ophthalmol.2018;18(1):331.
22. Giannos SA, Kraft ER, Lyons LJ, et al. Spectral evaluation of eyeglassblocking efficiency of ultraviolet/high-energy visible blue light for ocular protection. Optom Vis Sci. 2019;96(7):513-22.
23. Protection ICoN-IR. ICNIRP guidelines on limits of exposure to incoherentvisible and infrared radiation. Health Physics. 2013;105:23.
24. O’Hagan JB, Khazova M, Price LL. Low-energy light bulbs, computers,tablets and the blue light hazard. Eye. 2016;30(2):230-3.
25. Rosenfield M. Computer vision syndrome: a review of ocular causes and potential treatments. Ophthalmic Physiol Opt. 2011;31(5):502-15.
26. Portello JK, Rosenfield M, Bababekova Y, et al. Computer-related visual symptoms in office workers. Ophthalmic Physiol Opt. 2012;32(5):375-82.
27. The 21st Century Eye: Three Ways to Protect Your Vision [press release].aoa.org. 2015.
28. Daum KM, Clore KA, Simms SS, et al. Productivity associated with visualstatus of computer users. Optometry. 2004;75(1):33-47.
29. Lin JB, Gerratt BW, Bassi CJ, et al. Short-wavelength light-blockingeyeglasses attenuate symptoms of eye fatigue. Invest Ophthalmol Vis Sci.2017;58(1):442-7.
30. Luczak A, Sobolewski A. Longitudinal changes in critical flicker fusion fre-quency: an indicator of human workload. Ergonomics. 2005;48(15):1770-92.
31. Singh S, Downie LE, Anderson AJ. Do blue-blocking lenses reduce eyestrain from extended screen time? A double-masked randomized controlledtrial. Am J Ophthalmol. 2021;226:243-51.
32. Rosenfield M, Li RT, Kirsch NT. A double-blind test of blue-blocking filters on symptoms of digital eye strain. Work. 2020;65(2):343-8.
33. Leung TW, Li RW, Kee CS. Blue-light filtering spectacle lenses: optical and clinical performances. PloS one. 2017;12(1):e0169114.
34. Courtin R, Pereira B, Naughton G, et al. Prevalence of dry eye disease invisual display terminal workers: a systematic review and meta-analysis. BMJOpen. 2016;6(1):e009675.
35. Moon JH, Lee MY, Moon NJ. Association between video display terminaluse and dry eye disease in school children. J Ped Ophthalmol Strab.2014;51(2):87-92.
36. Patel S, Henderson R, Bradley L, et al. Effect of visual display unit use onblink rate and tear stability. Optom Vis Sci. 1991;68(11):888-92.
37. Tsubota K, Nakamori K. Dry eyes and video display terminals. N Engl JMed. 1993;328(8):584.
38. Chu CA, Rosenfield M, Portello JK. Blink patterns: reading from a com-puter screen versus hard copy. Optom Vis Sci. 2014;91(3):297-302.
39. Palavets T, Rosenfield M. Blue-blocking filters and digital eyestrain. Optom Vis Sci. 2019;96(1):48-54.
40. Lawrenson JG, Hull CC, Downie LE. The effect of blue-light blockingspectacle lenses on visual performance, macular health and the sleep-wake cycle: a systematic review of the literature. Ophthalmic Physiol Opt.2017;37(6):644-54.
41. Gradisar M, Wolfson AR, Harvey AG, et al. The sleep and technology useof Americans: findings from the National Sleep Foundation’s 2011 Sleep in America poll. J Clin Sleep Med. 2013;9(12):1291-9.
42. Vartanian GV, Li BY, Chervenak AP, et al. Melatonin suppression by lightin humans is more sensitive than previously reported. J Biol Rhythms.30(4):351-4.
43. Brainard GC, Hanifin JP, Warfield B, et al. Short-wavelength enrichment of polychromatic light enhances human melatonin suppression potency. JPineal Res. 2015;58(3):352-61.
44. Mai E, Buysse DJ. Insomnia: prevalence, impact, pathogenesis, differen-tial diagnosis, and evaluation. Sleep Med Clin. 2008;3(2):167-74.
45. Mottram AR, Svenson JE. Rhythm disturbances. Emerg Med Clin NorthAm. 2011;29(4):729-46.
46. Schmid SR, Hohn C, Bothe K, et al. How smart is it to go to bed with thephone? The impact of short-wavelength light and affective states on sleepand circadian rhythms. Clocks Sleep. 2021;3(4):558-80.
47. Ostrin LA, Abbott KS, Queener HM. Attenuation of short wavelengthsalters sleep and the ipRGC pupil response. Ophthalmic Physiol Opt.2017;37(4):440-50.
48. Burkhart K, Phelps JR. Amber lenses to block blue light and improvesleep: a randomized trial. Chronobiol Int. 2009;26(8):1602-12.
49. van der Lely S, Frey S, Garbazza C, et al. Blue blocker glasses as acountermeasure for alerting effects of evening light-emitting diode screenexposure in male teenagers. J Adolesc Health. 2015;56(1):113-9.
50. Chua SY, Sabanayagam C, Cheung YB, et al. Age of onset of myopiapredicts risk of high myopia in later childhood in myopic Singapore children.Ophthalmic Physiol Opt. 2016;36(4):388-94.
51. Bhandari KR, Ostrin LA. Objective measures of viewing behaviour inchildren during near tasks. Clin Exp Optom. 2021:1-8.
52. Hansen MH, Laigaard PP, Olsen EM, et al. Low physical activity andhigher use of screen devices are associated with myopia at the age of 16-17years in the CCC2000 Eye Study. Acta Ophthalmol. 2020;98(3):315-21.
53. Hagen LA, Gjelle JVB, Arnegard S, et al. Prevalence and Possible Factorsof Myopia in Norwegian Adolescents. Sci Rep. 2018;8(1):13479.
54. Toh SH, Coenen P, Howie EK, et al. A prospective longitudinal study ofmobile touch screen device use and musculoskeletal symptoms and visualhealth in adolescents. Appl Ergon. 2020;85:103028.
55. Lanca C, Saw SM. The association between digital screen time andmyopia: a systematic review. Ophthalmic Physiol Opt. 2020;40(2):216-29.
56. Price RB, Labrie D, Bruzell EM, et al. The dental curing light: a potentialhealth risk. J Occup Environ Hyg. 2016;13(8):639-46.
Fig. 6. Screen exposure may have a negativeeffect on ocular surface health.
Photo: Getty Images
REVIEW OF OPTOMETRY | JANUARY 15, 202272
O P TO M E T R I C S T U D Y C E N T E R Q U I Z
To obtain continuing education credit through the Optometric Study Center, complete the test form on the following page and return it with the$35 fee to: Jobson Healthcare Information, LLC, Attn.: CE Processing, 395 Hudson Street, 3rd Floor New York, New York 10014. To be eligible,please return the card within three years of publication. You can also access the test form and submit your answers and payment via credit card
online at revieweducationgroup.com. You must achieve a score of 70 or higher to receive credit. Allow four weeks for processing. For each Optomet-ric Study Center course you pass, you earn 2 hours of credit. Please check with your state licensing board to see if this approval counts toward your CErequirement for relicensure.
1. Which range of electromagnetic radiationrepresents the visible spectrum?
a. 100nm-400nm.b. 400nm-700nm.c. 700nm-900nm.d. 900nm-2mm.
2. Which effect does ipRGC stimulation fromblue light have on melatonin secretion andsleep?
a. ipRGC stimulation promotes melatoninsecretion and increases sleepiness.
b. ipRGC stimulation promotes melatoninsecretion and decreases sleepiness.
c. ipRGC stimulation suppresses melatoninsecretion and increases sleepiness.
d. ipRGC stimulation suppresses melatoninsecretion and decreases sleepiness.
3. Which is the greatest source of blue lightexposure?
a. The sun.b. LEDs.c. Fluorescent light bulbs.d. Incandescent light bulbs.
4. Recent reports show that adults spend howmuch time per day viewing digital devices?
a. 2-4 hours.b. 6-8 hours.c. 10-12 hours.d. 14-16 hours.
5. Compared with red light, blue light haswhich?
a. Shorter wavelength and higher energy.b. Shorter wavelength and lower energy.c. Longer wavelength and higher energy.d. Longer wavelength and lower energy.
6. Which of the following ocular structuresdoes not help to filter out UV and/or blue light?
a. Cornea.b. Lens.c. Vitreous.d. Macular pigment.
7. Which of the following best describes thespectral output of cool white LEDs?
a. Constant energy across the entire visiblespectrum.
b. Individual peaks with equal energy acrossthe entire visible spectrum.
c. Greater output in the red region of the visiblespectrum.
d. Greater output in the blue region of thevisible spectrum.
8. Daytime blue light exposure is important forwhich of the following?
a. Alertness.b. Improving mood.c. Regulating circadian rhythm.d. All of the above.
9. Digital eye strain refers to which of thefollowing?
a. Macular damage from digital devices.b. A group of eye- and vision-related symptoms
that result from extended use of screens.c. Decrease in ocular motility with extended
use of screens.d. Perception of phosphenes when viewing
devices.
10. Retinal damage from blue light has beendemonstrated in which?
a. Isolated human RPE cells.b. Children who display extensive digital device
use.c. Adults with computer-related occupations.d. Teens who have transitioned to virtual
learning during COVID-19.
11. Wearing 100% blue-blocking glasses beforebedtime has been shown to do what?
a. Decrease sleep duration.b. Decrease sleep quality.c. Increase nighttime melatonin.d. Decrease nighttime melatonin.
12. Which of the following is important for theoptometrist to assess in patients suspectedof having digital eye strain?
a. Workstation ergonomics.b. Comprehensive refraction.c. Binocular vision assessment.d. All of the above.
13. In the United States, which percentage of children use mobile devices before the ageof one?
a. 21%.b. 44%.c. 75%.d. 50%.
14. Studies investigating links between digital device use and refractive error in childrenshow that screen time does what?
a.Significantly increases the risk of myopia. b. Significantly decreases the risk of myopia.
c. Has inconclusive effects on the risk ofmyopia.
d. Significantly increases the risk of hyperopia.
15. Which of the following is not a symptom ofdigital eye strain?
a. AMD.b. Dry eye.c. Asthenopia.d. Blurred vision.
16. All of the following are considered evidence-based treatment options for digital eyestrain except for which?
a. Lubricating eye drops.b. Viewing breaks.c. Blue-blocking lenses.d. Plus-powered computer glasses for
presbyopes.
17. The illuminance of sunlight can range upto 150,000 lux. Illuminance from digitaldevices is in the range of which of thefollowing?
a. 1-30 lux.b. 40-300 lux.c. 1,000-3,000 lux.d. Greater than 3,000 lux.
18. Critical flicker fusion frequency is often assessed as a measure of which?
a. Eye fatigue.b. Dry eye.c. Contrast sensitivity.d. Macular damage.
19. To improve sleep quality, blue light should be eliminated from screens at which point?
a. At all times.b. In the morning after waking.c. At midday.d. At night before bedtime.
20. The 20-20-20 rule refers to which of thefollowing?
a. Reading at a 20cm viewing distance for 20minutes.
b. Performing 20 eye exercises of viewing from20 feet to 20cm.
c. Sleeping for 20 minutes for every 20 minutesof digital device use.
d. Viewing 20 feet away for 20 seconds every20 minutes of digital device use.
Optometric Study Center B LU E L I G HT O C U L A R E F F E CT S
JANUARY 15, 2022 | REVIEW OF OPTOMETRY 73
Please retain a copy for your records. Please print clearly.
First Name
Last Name
The following is your: Home Address Business Address
Business Name
Address
City State
ZIP
Telephone # - -
Fax # - -
OE Tracker Number
Answers to CE exam:1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Examination Answer Sheet10 Questions on Digital Devices and Eye Health—Answered!Valid for credit through January 15, 2025
Online: This exam can be taken online at revieweducationgroup.com. Upon passingthe exam, you can view your results immediately and download a real-time CEcertificate. You can also view your test history at any time from the website.
Directions: Select one answer for each question in the exam and completely darkenthe appropriate circle. A minimum score of 70% is required to earn credit.
Mail to: Jobson Healthcare Information, LLC, Attn.: CE Processing, 395 HudsonStreet, 3rd Floor New York, New York 10014
Payment: Remit $35 with this exam. Make check payable to Jobson HealthcareInformation, LLC.
Credit: This course is COPE approved for 2 hours of CE credit. Course ID is 76184-GO.
Processing: There is a four-week processing time for this exam.
Jointly provided by Postgraduate Institute for Medicine and Review Education Group.Salus University has sponsored the review and approval of this activity.
31. The content was evidence-based.
32. The content was balanced and free of bias.
33. The presentation was clear and effective.
Rate the quality of the material provided:
1=Strongly disagree, 2=Somewhat disagree,3=Neutral, 4=Somewhat agree, 5=Strongly agree
1 2 3 4 5
1 2 3 4 5
By submitting this answer sheet, I certify that I have read the lesson in its entirety and completed the self-assessment exam personally based on the material presented.I have not obtained the answers to this exam by any fraudulent or improper means.
Signature Date Lesson 122302 RO-OSC-0122
Post-activity evaluation questions:
Rate how well the activity supported your achievement of these learning objectives. 1=Poor, 2=Fair, 3=Neutral, 4=Good, 5=Excellent
21. Discuss understand blue light exposure.
22. Recognize the potential risks associated with blue light exposure.
23. Describe the effect blue light has on circadian rhythms and sleep status.
24. Educate patients on the impact blue light can have on eye health.
25. Based upon your participation in this activity, do you intend to change your practice behavior? (Choose only one of the following options.) A I do plan to implement changes in my practice based on the information presented. B My current practice has been reinforced by the information presented. C I need more information before I will change my practice.
26. Thinking about how your participation in this activity will influence your patient care, how many of your patients are likely to benefit?(please use a number):
27. If you plan to change your practice behavior, what type of changes do you plan to implement? (Check all that apply.)
28. How confident are you that you will be able to make your intended changes? A Very confident B Somewhat confident C Unsure D Not confident
29. Which of the following do you anticipate will be the primary barrier to implementing these changes?
30. Additional comments on this course:_______________________________________________________________________________________________________
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
A Formulary restrictions B Time constraints C System constraints
D Insurance/financial issues E Lack of interprofessional team support F Treatment related adverse events
G Patient adherence/compliance H Other, please specify:____________________________________________
A Apply latest guidelines B Change in diagnostic methods C Choice of management approach
D Change in current practice for referral E Change in vision correction offerings F Change in differential diagnosis
G More active monitoring and counseling H Other, please specify: _______________________________________________________________
1 2 3 4 5
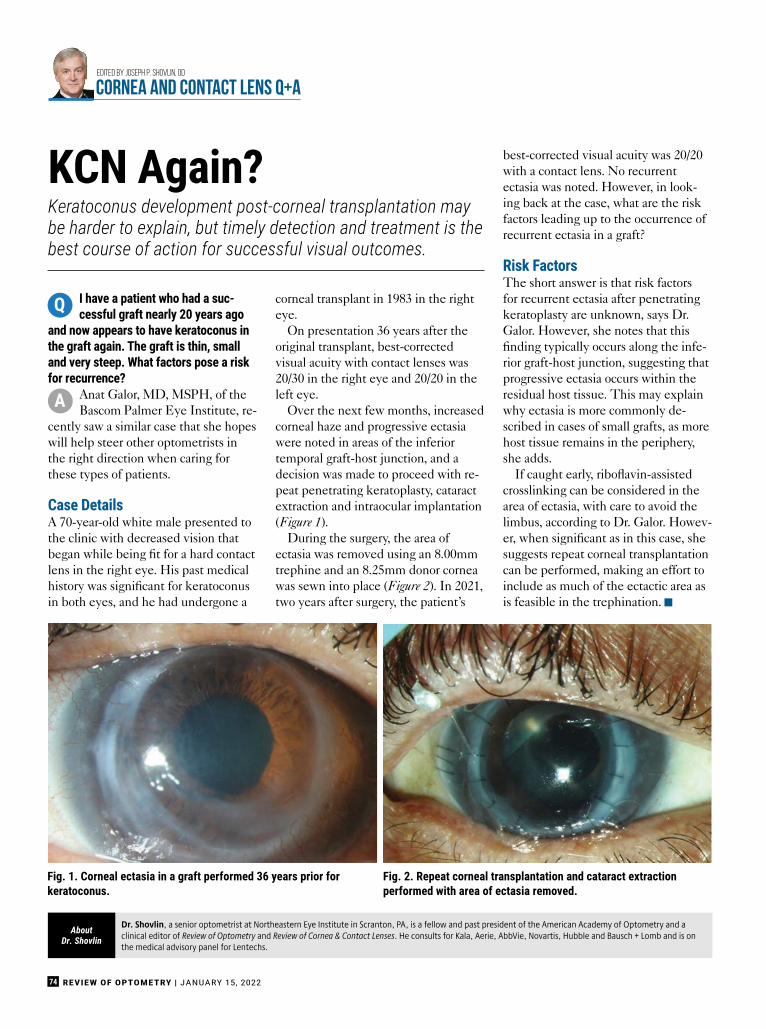
I have a patient who had a suc-cessful graft nearly 20 years ago
and now appears to have keratoconus inthe graft again. The graft is thin, smalland very steep. What factors pose a riskfor recurrence?
Anat Galor, MD, MSPH, of theBascom Palmer Eye Institute, re-
cently saw a similar case that she hopeswill help steer other optometrists inthe right direction when caring forthese types of patients.
Case DetailsA 70-year-old white male presented tothe clinic with decreased vision thatbegan while being fit for a hard contactlens in the right eye. His past medicalhistory was significant for keratoconusin both eyes, and he had undergone a
corneal transplant in 1983 in the righteye.
On presentation 36 years after theoriginal transplant, best-correctedvisual acuity with contact lenses was20/30 in the right eye and 20/20 in theleft eye.
Over the next few months, increasedcorneal haze and progressive ectasiawere noted in areas of the inferiortemporal graft-host junction, and adecision was made to proceed with re-peat penetrating keratoplasty, cataractextraction and intraocular implantation(Figure 1).
During the surgery, the area ofectasia was removed using an 8.00mmtrephine and an 8.25mm donor corneawas sewn into place (Figure 2). In 2021,two years after surgery, the patient’s
best-corrected visual acuity was 20/20with a contact lens. No recurrentectasia was noted. However, in look-ing back at the case, what are the riskfactors leading up to the occurrence ofrecurrent ectasia in a graft?
Risk FactorsThe short answer is that risk factorsfor recurrent ectasia after penetratingkeratoplasty are unknown, says Dr.Galor. However, she notes that thisfinding typically occurs along the infe-rior graft-host junction, suggesting thatprogressive ectasia occurs within theresidual host tissue. This may explainwhy ectasia is more commonly de-scribed in cases of small grafts, as morehost tissue remains in the periphery,she adds.
If caught early, riboflavin-assistedcrosslinking can be considered in thearea of ectasia, with care to avoid thelimbus, according to Dr. Galor. Howev-er, when significant as in this case, shesuggests repeat corneal transplantationcan be performed, making an effort toinclude as much of the ectactic area asis feasible in the trephination. g
REVIEW OF OPTOMETRY | JANUARY 15, 202274
Edited by Joseph P. Shovlin, OD
CORNEA and CONTACT LENS Q+A
Dr. Shovlin, a senior optometrist at Northeastern Eye Institute in Scranton, PA, is a fellow and past president of the American Academy of Optometry and aclinical editor of Review of Optometry and Review of Cornea & Contact Lenses. He consults for Kala, Aerie, AbbVie, Novartis, Hubble and Bausch + Lomb and is onthe medical advisory panel for Lentechs.
AboutDr. Shovlin
Fig. 1. Corneal ectasia in a graft performed 36 years prior forkeratoconus.
Keratoconus development post-corneal transplantation maybe harder to explain, but timely detection and treatment is thebest course of action for successful visual outcomes.
KCN Again?
Q
A
Fig. 2. Repeat corneal transplantation and cataract extractionperformed with area of ectasia removed.

creo
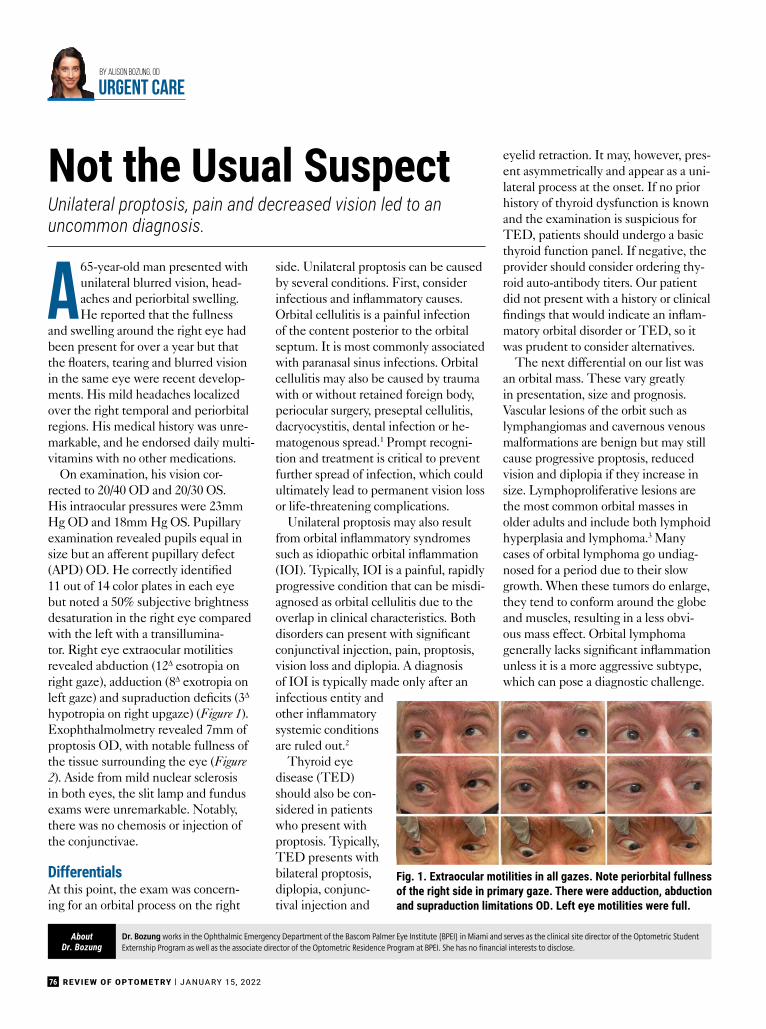
76 REVIEW OF OPTOMETRY | JANUARY 15, 2022
by alison bozung, oD
URGENT CARE
A65-year-old man presented withunilateral blurred vision, head-aches and periorbital swelling.He reported that the fullness
and swelling around the right eye hadbeen present for over a year but thatthe floaters, tearing and blurred visionin the same eye were recent develop-ments. His mild headaches localizedover the right temporal and periorbitalregions. His medical history was unre-markable, and he endorsed daily multi-vitamins with no other medications.
On examination, his vision cor-rected to 20/40 OD and 20/30 OS.His intraocular pressures were 23mmHg OD and 18mm Hg OS. Pupillaryexamination revealed pupils equal insize but an afferent pupillary defect(APD) OD. He correctly identified11 out of 14 color plates in each eyebut noted a 50% subjective brightnessdesaturation in the right eye comparedwith the left with a transillumina-tor. Right eye extraocular motilitiesrevealed abduction (12∆ esotropia onright gaze), adduction (8∆ exotropia onleft gaze) and supraduction deficits (3∆
hypotropia on right upgaze) (Figure 1).Exophthalmolmetry revealed 7mm ofproptosis OD, with notable fullness ofthe tissue surrounding the eye (Figure2). Aside from mild nuclear sclerosisin both eyes, the slit lamp and fundusexams were unremarkable. Notably,there was no chemosis or injection ofthe conjunctivae.
DifferentialsAt this point, the exam was concern-ing for an orbital process on the right
side. Unilateral proptosis can be causedby several conditions. First, considerinfectious and inflammatory causes.Orbital cellulitis is a painful infectionof the content posterior to the orbitalseptum. It is most commonly associatedwith paranasal sinus infections. Orbitalcellulitis may also be caused by traumawith or without retained foreign body,periocular surgery, preseptal cellulitis,dacryocystitis, dental infection or he-matogenous spread.1 Prompt recogni-tion and treatment is critical to preventfurther spread of infection, which couldultimately lead to permanent vision lossor life-threatening complications.
Unilateral proptosis may also resultfrom orbital inflammatory syndromessuch as idiopathic orbital inflammation(IOI). Typically, IOI is a painful, rapidlyprogressive condition that can be misdi-agnosed as orbital cellulitis due to theoverlap in clinical characteristics. Bothdisorders can present with significantconjunctival injection, pain, proptosis,vision loss and diplopia. A diagnosisof IOI is typically made only after aninfectious entity andother inflammatorysystemic conditionsare ruled out.2
Thyroid eyedisease (TED)should also be con-sidered in patientswho present withproptosis. Typically,TED presents withbilateral proptosis,diplopia, conjunc-tival injection and
eyelid retraction. It may, however, pres-ent asymmetrically and appear as a uni-lateral process at the onset. If no priorhistory of thyroid dysfunction is knownand the examination is suspicious forTED, patients should undergo a basicthyroid function panel. If negative, theprovider should consider ordering thy-roid auto-antibody titers. Our patientdid not present with a history or clinicalfindings that would indicate an inflam-matory orbital disorder or TED, so itwas prudent to consider alternatives.
The next differential on our list wasan orbital mass. These vary greatlyin presentation, size and prognosis.Vascular lesions of the orbit such aslymphangiomas and cavernous venousmalformations are benign but may stillcause progressive proptosis, reducedvision and diplopia if they increase insize. Lymphoproliferative lesions arethe most common orbital masses inolder adults and include both lymphoidhyperplasia and lymphoma.3 Manycases of orbital lymphoma go undiag-nosed for a period due to their slowgrowth. When these tumors do enlarge,they tend to conform around the globeand muscles, resulting in a less obvi-ous mass effect. Orbital lymphomagenerally lacks significant inflammationunless it is a more aggressive subtype,which can pose a diagnostic challenge.
Unilateral proptosis, pain and decreased vision led to anuncommon diagnosis.
Not the Usual Suspect
Dr. Bozung works in the Ophthalmic Emergency Department of the Bascom Palmer Eye Institute (BPEI) in Miami and serves as the clinical site director of the Optometric StudentExternship Program as well as the associate director of the Optometric Residence Program at BPEI. She has no financial interests to disclose.
AboutDr. Bozung
Fig. 1. Extraocular motilities in all gazes. Note periorbital fullnessof the right side in primary gaze. There were adduction, abductionand supraduction limitations OD. Left eye motilities were full.
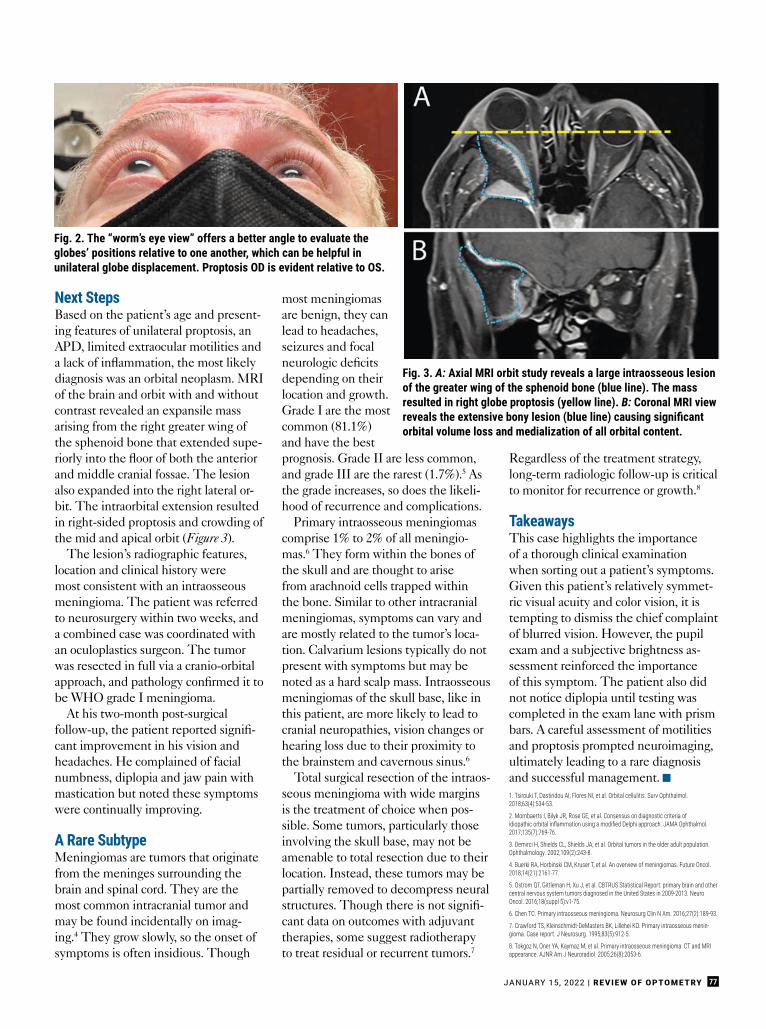
JANUARY 15, 2022 | REVIEW OF OPTOMETRY 77
Next StepsBased on the patient’s age and present-ing features of unilateral proptosis, anAPD, limited extraocular motilities anda lack of inflammation, the most likelydiagnosis was an orbital neoplasm. MRIof the brain and orbit with and withoutcontrast revealed an expansile massarising from the right greater wing ofthe sphenoid bone that extended supe-riorly into the floor of both the anteriorand middle cranial fossae. The lesionalso expanded into the right lateral or-bit. The intraorbital extension resultedin right-sided proptosis and crowding ofthe mid and apical orbit (Figure 3).
The lesion’s radiographic features,location and clinical history weremost consistent with an intraosseousmeningioma. The patient was referredto neurosurgery within two weeks, anda combined case was coordinated withan oculoplastics surgeon. The tumorwas resected in full via a cranio-orbitalapproach, and pathology confirmed it tobe WHO grade I meningioma.
At his two-month post-surgicalfollow-up, the patient reported signifi-cant improvement in his vision andheadaches. He complained of facialnumbness, diplopia and jaw pain withmastication but noted these symptomswere continually improving.
A Rare SubtypeMeningiomas are tumors that originatefrom the meninges surrounding thebrain and spinal cord. They are themost common intracranial tumor andmay be found incidentally on imag-ing.4 They grow slowly, so the onset ofsymptoms is often insidious. Though
most meningiomasare benign, they canlead to headaches,seizures and focalneurologic deficitsdepending on theirlocation and growth.Grade I are the mostcommon (81.1%)and have the bestprognosis. Grade II are less common,and grade III are the rarest (1.7%).5 Asthe grade increases, so does the likeli-hood of recurrence and complications.
Primary intraosseous meningiomascomprise 1% to 2% of all meningio-mas.6 They form within the bones ofthe skull and are thought to arisefrom arachnoid cells trapped withinthe bone. Similar to other intracranialmeningiomas, symptoms can vary andare mostly related to the tumor’s loca-tion. Calvarium lesions typically do notpresent with symptoms but may benoted as a hard scalp mass. Intraosseousmeningiomas of the skull base, like inthis patient, are more likely to lead tocranial neuropathies, vision changes orhearing loss due to their proximity tothe brainstem and cavernous sinus.6
Total surgical resection of the intraos-seous meningioma with wide marginsis the treatment of choice when pos-sible. Some tumors, particularly thoseinvolving the skull base, may not beamenable to total resection due to theirlocation. Instead, these tumors may bepartially removed to decompress neuralstructures. Though there is not signifi-cant data on outcomes with adjuvanttherapies, some suggest radiotherapyto treat residual or recurrent tumors.7
Regardless of the treatment strategy,long-term radiologic follow-up is criticalto monitor for recurrence or growth.8
TakeawaysThis case highlights the importanceof a thorough clinical examinationwhen sorting out a patient’s symptoms.Given this patient’s relatively symmet-ric visual acuity and color vision, it istempting to dismiss the chief complaintof blurred vision. However, the pupilexam and a subjective brightness as-sessment reinforced the importanceof this symptom. The patient also didnot notice diplopia until testing wascompleted in the exam lane with prismbars. A careful assessment of motilitiesand proptosis prompted neuroimaging,ultimately leading to a rare diagnosisand successful management. g1. Tsirouki T, Dastiridou AI, Flores NI, et al. Orbital cellulitis. Surv Ophthalmol.2018;63(4):534-53.
2. Mombaerts I, Bilyk JR, Rose GE, et al. Consensus on diagnostic criteria ofidiopathic orbital inflammation using a modified Delphi approach. JAMA Ophthalmol. 2017;135(7):769-76.
3. Demirci H, Shields CL, Shields JA, et al. Orbital tumors in the older adult population.Ophthalmology. 2002;109(2):243-8.
4. Buerki RA, Horbinski CM, Kruser T, et al. An overview of meningiomas. Future Oncol.2018;14(21):2161-77.
5. Ostrom QT, Gittleman H, Xu J, et al. CBTRUS Statistical Report: primary brain and othercentral nervous system tumors diagnosed in the United States in 2009-2013. NeuroOncol. 2016;18(suppl 5):v1-75.
6. Chen TC. Primary intraosseous meningioma. Neurosurg Clin N Am. 2016;27(2):189-93.
7. Crawford TS, Kleinschmidt-DeMasters BK, Lillehei KO. Primary intraosseous menin-gioma. Case report. J Neurosurg. 1995;83(5):912-5.
8. Tokgoz N, Oner YA, Kaymaz M, et al. Primary intraosseous meningioma: CT and MRIappearance. AJNR Am J Neuroradiol. 2005;26(8):2053-6.
Fig. 2. The “worm’s eye view” offers a better angle to evaluate theglobes’ positions relative to one another, which can be helpful inunilateral globe displacement. Proptosis OD is evident relative to OS.
Fig. 3. A: Axial MRI orbit study reveals a large intraosseous lesionof the greater wing of the sphenoid bone (blue line). The massresulted in right globe proptosis (yellow line). B: Coronal MRI viewreveals the extensive bony lesion (blue line) causing significant orbital volume loss and medialization of all orbital content.
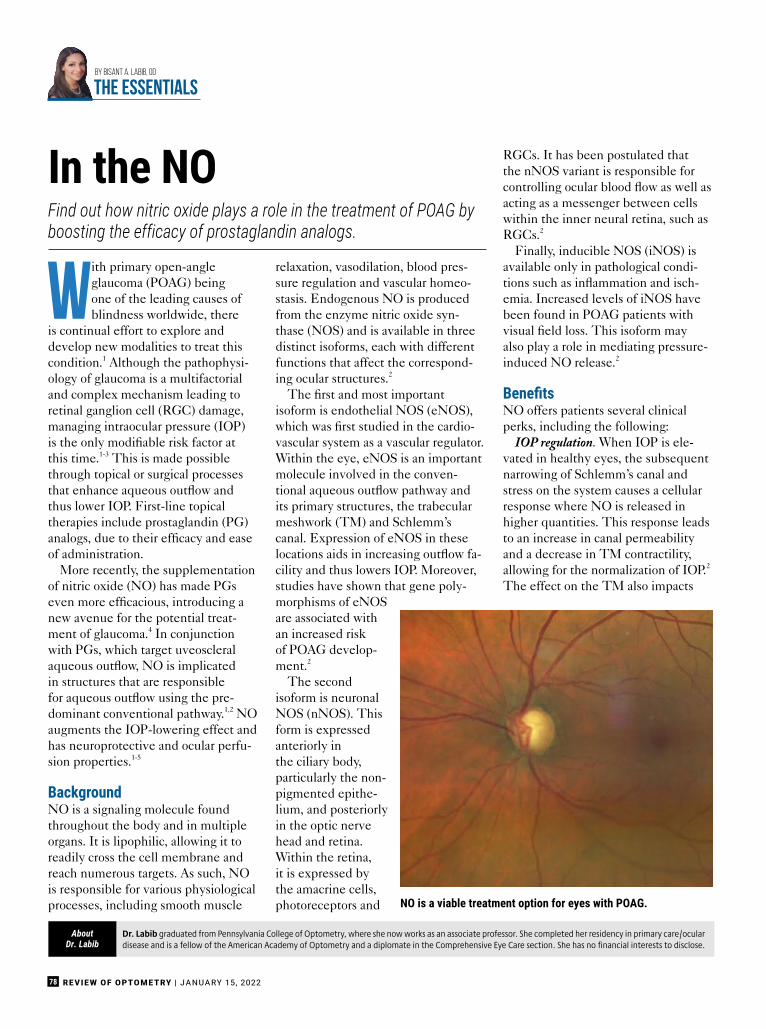
REVIEW OF OPTOMETRY | JANUARY 15, 202278
Dr. Labib graduated from Pennsylvania College of Optometry, where she now works as an associate professor. She completed her residency in primary care/oculardisease and is a fellow of the American Academy of Optometry and a diplomate in the Comprehensive Eye Care section. She has no financial interests to disclose.
AboutDr. Labib
With primary open-angleglaucoma (POAG) beingone of the leading causes ofblindness worldwide, there
is continual effort to explore anddevelop new modalities to treat thiscondition.1 Although the pathophysi-ology of glaucoma is a multifactorialand complex mechanism leading toretinal ganglion cell (RGC) damage,managing intraocular pressure (IOP)is the only modifiable risk factor atthis time.1-3 This is made possiblethrough topical or surgical processesthat enhance aqueous outflow andthus lower IOP. First-line topicaltherapies include prostaglandin (PG)analogs, due to their efficacy and easeof administration.
More recently, the supplementationof nitric oxide (NO) has made PGseven more efficacious, introducing anew avenue for the potential treat-ment of glaucoma.4 In conjunctionwith PGs, which target uveoscleralaqueous outflow, NO is implicatedin structures that are responsiblefor aqueous outflow using the pre-dominant conventional pathway.1,2 NOaugments the IOP-lowering effect andhas neuroprotective and ocular perfu-sion properties.1-5
BackgroundNO is a signaling molecule foundthroughout the body and in multipleorgans. It is lipophilic, allowing it toreadily cross the cell membrane andreach numerous targets. As such, NOis responsible for various physiologicalprocesses, including smooth muscle
relaxation, vasodilation, blood pres-sure regulation and vascular homeo-stasis. Endogenous NO is producedfrom the enzyme nitric oxide syn-thase (NOS) and is available in threedistinct isoforms, each with differentfunctions that affect the correspond-ing ocular structures.2
The first and most importantisoform is endothelial NOS (eNOS),which was first studied in the cardio-vascular system as a vascular regulator.Within the eye, eNOS is an importantmolecule involved in the conven-tional aqueous outflow pathway andits primary structures, the trabecularmeshwork (TM) and Schlemm’scanal. Expression of eNOS in theselocations aids in increasing outflow fa-cility and thus lowers IOP. Moreover,studies have shown that gene poly-morphisms of eNOSare associated withan increased riskof POAG develop-ment.2
The secondisoform is neuronalNOS (nNOS). Thisform is expressedanteriorly inthe ciliary body,particularly the non-pigmented epithe-lium, and posteriorlyin the optic nervehead and retina.Within the retina,it is expressed bythe amacrine cells,photoreceptors and
RGCs. It has been postulated thatthe nNOS variant is responsible forcontrolling ocular blood flow as well asacting as a messenger between cellswithin the inner neural retina, such asRGCs.2
Finally, inducible NOS (iNOS) isavailable only in pathological condi-tions such as inflammation and isch-emia. Increased levels of iNOS havebeen found in POAG patients withvisual field loss. This isoform mayalso play a role in mediating pressure-induced NO release.2
BenefitsNO offers patients several clinicalperks, including the following:
IOP regulation. When IOP is ele-vated in healthy eyes, the subsequentnarrowing of Schlemm’s canal andstress on the system causes a cellularresponse where NO is released inhigher quantities. This response leadsto an increase in canal permeabilityand a decrease in TM contractility,allowing for the normalization of IOP.2
The effect on the TM also impacts
Find out how nitric oxide plays a role in the treatment of POAG byboosting the efficacy of prostaglandin analogs.
In the NO
B
By Bisant A. Labib, OD
THE ESSENTIALS
NO is a viable treatment option for eyes with POAG.
JANUARY 15, 2022 | REVIEW OF OPTOMETRY 79
diurnal IOP fluctuations, which aredampened with a healthy TM.1 Inpatients with ocular hypertensionor POAG, this response to IOP andstress is absent, highlighting the roleof NO inhibition in glaucomatouspathology.2
Ocular perfusion. In addition to theeffect on aqueous outflow dynam-ics, NO has been implicated in opticnerve head perfusion. NOS inhibitionhas been found to impair blood flowto the optic nerve in POAG patientscompared with healthy controls.2 Thismechanism of glaucomatous dam-age due to vascular dysregulation iswell-established and can be, in part,explained by NO. The molecule isa vasoactive factor that is producedby the vascular endothelium and isimportant for maintaining basal flowwithin the retina and optic nervehead. In cases of elevated IOP, NOaids in autoregulation, which mayexplain its role in the development orexacerbation of POAG.2
Neuroprotection. NO has beenshown to exhibit both neurotoxic andneuroprotective properties. While
elevated levels have been implicatedin diseases such as Alzheimer’s andeven in RGC degeneration, activa-tion of NO has also been shown as aninhibitor of apoptotic cell death. Inanimal models, NO donor compoundshave elicited potential neuroprotec-tive properties.2 The ocular perfusionproperties of NOS promote vasodila-tion and vascular permeability, con-tributing to possible neuroprotection.5
TreatmentCurrently, the only FDA-approvedtopical agent for the treatment ofglaucoma that makes use of NOis Vyzulta (latanoprostene bunod0.024%, Bausch + Lomb). The drug isa NO-donating derivative of latano-prost. Clinical trials demonstratedclear superiority of this agent com-pared with PGs alone, as well as withother topical treatments. This shouldcome as no surprise, as the combina-tion of ingredients acts on both routesof aqueous outflow.4 Furthermore,studies have demonstrated that evenhigh dietary nitrate intake was associ-ated with up to a 21% reduced risk of
incident POAG. This includes NOsources from dark, leafy green vegeta-bles (lettuce, kale, broccoli, spinach),celery, potatoes and onions.3,6
TakeawaysAppropriately managing patients withPOAG is imperative to preservingvisual function. With IOP remainingthe only modifiable risk factor, it isimportant to familiarize yourself withnewly available options, research andfactors in determining treatment ef-ficacy. g
1. Aliancy J, Stamer WD, Wirostko B. A review of nitric oxidefor the treatment of glaucomatous disease. OphthalmolTher. 2017;6(2):221-32.2. Wareham LK, Buys ES, Sappington RM. The nitric oxide-guanylate cyclase pathway and glaucoma. Nitric Oxide.2018;77:75-87.3. Reina-Torres E, De Ieso ML, Pasquale LR, et al. The vitalrole for nitric oxide in intraocular pressure homeostasis.Prog Retin Eye Res. 2021;83:100922.4. Impagnatiello F, Bastia E, Almirante N, et al. Prostaglan-din analogues and nitric oxide contribution in the treatmentof ocular hypertension and glaucoma. Br J Pharmacol.2019;176(8):1079-89.5. Galassi F, Renieri G, Sodi A, et al. Nitric oxide proxies andocular perfusion pressure in primary open angle glaucoma.Br J Ophthalmol. 2004;88(6):757-60.6. Ramdas WD. The relation between dietary intakeand glaucoma: a systematic review. Acta Ophthalmol.2018;96(6):550-6.
Akorn ............................................................................................................................................ 9........................................................................................................................................................www.acellfx.com
Alcon Laboratories ............................................................................................................Cover Tip
Allergan, Inc. ................................................................................................................................10........................................................................................................................................................... (833) REF-SMPL.....................................................................................................................................................www.allergan.com
Allergan, Inc. ................................................................................................................................. 2.....................................................................................................................................................www.vuitypro.com
Apellis ......................................................................................................................................... 45.................................................................................................................................................www.pre-lesion.com
Bruder..........................................................................................................................................19............................................................................................................................................................(888) 827-8337......................................................................................................................................................eyes@bruder.com........................................................................................................................................................www.bruder.com
CooperVision ............................................................................................................................... 83............................................................................................................................................www.coopervision.com
Haag-Streit USA............................................................................................................................. 5........................................................................................................................................................... (800) 787-5426.........................................................................................................................................www.lenstarmyopia.com
Keeler Instruments ....................................................................................................................... 7...........................................................................................................................................................(800) 523-5620.........................................................................................................................customerservice@keelerusa.com..................................................................................................................................................www.keelerusa.com
MacuLogix....................................................................................................................................17...................................................................................................................................www.maculogix.com/ebook
MacuHealth................................................................................................................................. 75..............................................................................................................................................www.macuhealth.com
Menicon America..........................................................................................................................15.....................................................................................................................................www.meniconamerica.com
Nanodropper ............................................................................................................................... 84........................................................................................................................................................... (507) 405-5676....................................................................................................................................support@nanodropper.com............................................................................................................................................www.nanodropper.com
Notal Vision ................................................................................................................................. 35............................................................................................................................................................ (855) 600-3112.............................................................................................................................www.foreseehome.com/doctor
Reichert Technologies..................................................................................................................13.............................................................................................................................................www.reichert.com/vrx
VTI................................................................................................................................................21...........................................................................................................................................................(844) 884-5367.............................................................................................................................................dbenoti@vtivision.com....................................................................................................................................................www.vtivision.com
This index is published as a convenience and not as part of the advertisingcontract. Every care will be taken to index correctly. No allowance will bemade for errors due to spelling, incorrect page number, or failure to insert.
ADVERTISER INDEX

REVIEW OF OPTOMETRY JANUARY 15, 2022
Review Classifi eds
Practice For Sale
Opportunitiescurrently available in:CA, CT, DC, DE, FL,MD, MO, NJ, NY, OH,PA, RI, TN, VA.
To find out more or tosubmit your resume go to:sightrite.com/careers
Set your ownschedule
Never work evenings orweekends again. We have plenty of flexible, part-time,and full-time positions available.
Work less,earn more
The average SightRiteoptometrist worksapproximately 5 hours a daywhile earning more than mostdoctors make in an 8-10 hourday. Looking to earn even more?Simply increase your patientload to increase your salary.
25
FLEXIBILITY.FREEDOM.
CAREER GROWTH.With SightRite, there's a better way
to practice optometry.
Email/call:[email protected] ext 223www.sightrite.com
We will be exhibiting at
VISION EXPO EASTCome visit us atBOOTH #F5051
Career Opportunities

REVIEW OF OPTOMETRY JANUARY 15, 2022
Review Classifi eds
Targeting Optometrists?CLASSIFIED ADVERTISING WORKS
• JOB OPENINGS • CME PROGRAMS• PRODUCTS & SERVICES • AND MORE. . .
Contact us today for classified advertising:Toll free: 888-498-1460
E-mail: [email protected]
:
.
a)
Faculty
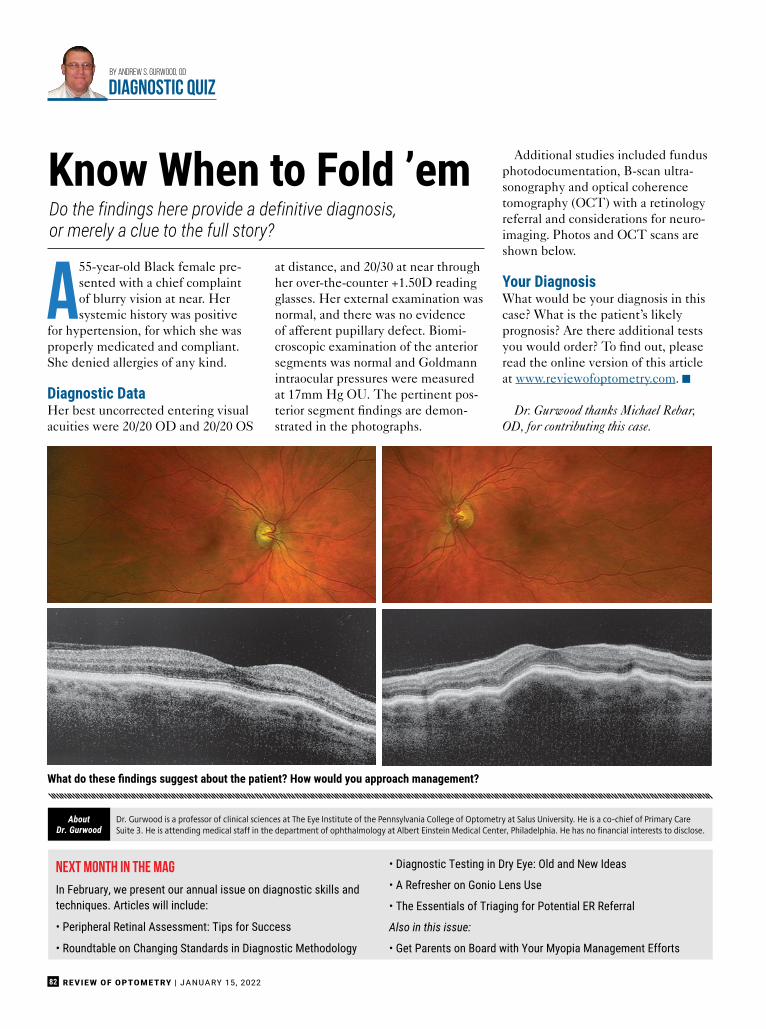
82 REVIEW OF OPTOMETRY | JANUARY 15, 2022
A55-year-old Black female pre-sented with a chief complaintof blurry vision at near. Hersystemic history was positive
for hypertension, for which she wasproperly medicated and compliant.She denied allergies of any kind.
Diagnostic DataHer best uncorrected entering visualacuities were 20/20 OD and 20/20 OS
at distance, and 20/30 at near throughher over-the-counter +1.50D readingglasses. Her external examination wasnormal, and there was no evidenceof afferent pupillary defect. Biomi-croscopic examination of the anteriorsegments was normal and Goldmannintraocular pressures were measuredat 17mm Hg OU. The pertinent pos-terior segment findings are demon-strated in the photographs.
Additional studies included fundusphotodocumentation, B-scan ultra-sonography and optical coherencetomography (OCT) with a retinologyreferral and considerations for neuro-imaging. Photos and OCT scans areshown below.
Your DiagnosisWhat would be your diagnosis in thiscase? What is the patient’s likelyprognosis? Are there additional testsyou would order? To find out, pleaseread the online version of this articleat www.reviewofoptometry.com. g
Dr. Gurwood thanks Michael Rebar,OD, for contributing this case.
Do the findings here provide a definitive diagnosis,or merely a clue to the full story?
Know When to Fold ’em
By Andrew S. Gurwood, OD
diagnostic quiz
What do these findings suggest about the patient? How would you approach management?
Next Month in the Mag
In February, we present our annual issue on diagnostic skills andtechniques. Articles will include:
• Peripheral Retinal Assessment: Tips for Success
• Roundtable on Changing Standards in Diagnostic Methodology
• Diagnostic Testing in Dry Eye: Old and New Ideas
• A Refresher on Gonio Lens Use
• The Essentials of Triaging for Potential ER Referral
Also in this issue:
• Get Parents on Board with Your Myopia Management Efforts
Dr. Gurwood is a professor of clinical sciences at The Eye Institute of the Pennsylvania College of Optometry at Salus University. He is a co-chief of Primary CareSuite 3. He is attending medical staff in the department of ophthalmology at Albert Einstein Medical Center, Philadelphia. He has no financial interests to disclose.
AboutDr. Gurwood
GGEE TT II NN TT HH EE GG AA MM
EE
GGEE
TT II NN TT HH EE GG AA
MMEE

95% of ODs say Bigger is NOT Beeer*
Ask us how less is more for your paaents...and your clinic's booom line
www.nanodropper.com | [email protected] | (507) 405-5676
*According to a survey conducted by Nanodropper in April 2021 out of the 300+ ODs,more than 95% said their paaents would benefit from smaller eyedrops.
Use discount code REVIEWOPTO10 for 10% off your first order!
SIZE MATTERS




















