Mathematical biomarkers for the autonomic regulation of cardiovascular system
Upload
independentCategory
view
2download
0
Revisiting the James versus Cannon debate onemotion: startle and autonomic modulation in
patients with spinal cord injuries
Pilar Cobos a,*, Marıa Sanchez b, Carmen Garcıa c,Marıa Nieves Vera b, Jaime Vila b
a Departamento de Personalidad, Evaluacion y Tratamiento Psicologico, Facultad de Psicologıa, Universidad
de Malaga, Malaga, Spainb Departamento de Personalidad, Evaluacion y Tratamiento Psicologıca, Facultad de Psicologı, Universidad
de Granada, Granada, Spainc Departamento de Tecnologıa Electronica de la E. T. Superior de Telecomunicacion, Universidad de Malaga,
Malaga, Spain
Abstract
James’ hypothesis that impaired peripheral physiology in patients with spinal cord injuries
(SCI) impairs emotional processing, as manifested in the modulation of physiological
responses and in the subjective component of emotions, was examined in the present study.
A pilot study confirmed the utility of Lang’s picture viewing paradigm in a group of 78
students using the Spanish norms of the International Affective Picture System. In the main
study, 19 patients with SCI and 19 well controls matched for sex, age and education were
examined. Results showed: (1) no differences between SCI and control participants in the
valence and arousal ratings of the pictures; (2) similar heart rate modulation in both groups,
i.e. the unpleasant pictures produced greater deceleration than the pleasant ones; and (3) no
decrease in emotional experience in the SCI group compared with the control group. The
implications of the results for the James versus Cannon controversy on the theory of emotions
are discussed.
# 2002 Elsevier Science B.V. All rights reserved.
Keywords: Emotions; Spinal cord injuries; Startle; Heart rate; Skin conductance
* Corresponding author
E-mail addresses: [email protected] (P. Cobos), [email protected] (J. Vila).
Biological Psychology 61 (2002) 251�/269
www.elsevier.com/locate/biopsycho
0301-0511/02/$ - see front matter # 2002 Elsevier Science B.V. All rights reserved.
PII: S 0 3 0 1 - 0 5 1 1 ( 0 2 ) 0 0 0 6 1 - 3
1. Introduction
Psychologists have repeatedly debated the implication of peripheral bodily
responses in the experience and expression of emotions. The old debate between
supporters of the James (James, 1884, 1890, 1894) and Cannon (Cannon 1914, 1927,
1929) theories established the coordinates from which later theories have evolved:
peripheralism versus centralism, bodily responses versus cognition, and specificityversus dimensionality. These dichotomous perspectives have remained present
throughout the history of psychology, the emphasis varying according to the
dominant paradigm*/behaviorist versus cognitive*/with few attempts being made
at integration.
One of these attempts is that proposed by Lang in the context of his
bioinformational and hierarchical theory of emotions (Birbaumer and Ohman,
1993; Bradley, 2000; Lang, 1979, 1994, 1995; Lang et al., 1997, 2000). Basically,
Lang’s model understands human emotions as action dispositions that aredetermined by the activation of specific brain circuits. These circuits are located in
deep cortical and subcortical structures, being closely related to two primary
motivational systems: the appetitive and the defensive. When these circuits are
activated, the physiological, behavioral and subjective manifestations of emotions
arise, exerting a modulatory effect on the brain’s other processing operations,
including the potentiation or inhibition of simple exteroceptive reflexes. Lang’s
model assumes that the functional architecture of emotion is hierarchically organized
along elements that are both specific and dimensional, physiological and cognitive,and peripheral and central, providing a new theoretical context in which the old
James�/Cannon debate can be tested. Research data supporting Lang’s model have
mainly been obtained using two paradigms: mental imagery and picture viewing
(Lang, 1985, 1995).
A line of research specifically designed to investigate the James�/Cannon
controversy on emotion, yet to be studied under Lang’s paradigms, is that examining
patients with spinal cord injuries (SCI). Ever since the seminal paper by James
(1884), patients with different degrees of reduction in their peripheral feedback havebeen considered ideal participants for testing these theories. Studies on emotions in
participants with spinal cord lesions have almost exclusively used self-report
measures (Dana, 1921; Hohmann, 1966; Richards et al., 1982; Lowe and Carroll,
1985; Chwalisz et al., 1988; Bermond et al., 1991), with their associated
methodological biases, including investigator bias due to social desirability and
demand characteristics. Indeed, the results of these studies do not all point in the
same direction and have been criticized for methodological flaws (Chwalisz et al.,
1988; Trieschmann, 1980; Tucker, 1980; Reisenzein, 1983; Richards et al., 1982), forabsence of a complete lesion (Fehr and Stern, 1970), or for failures to control for
medication and other relevant variables (Chwalisz et al., 1988).
The aim of the present study was to examine the emotional modulation of
psychophysiological responses in patients with SCI using Lang’s picture viewing
paradigm. This paradigm combines the visualization of affective pictures with the
presentation of a brief burst of white noise to elicit the startle reflex. In addition to
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269252
the subjective assessments, this paradigm can provide uncontaminated evidence
against or in favor of the role of peripheral bodily responses in the processing of
emotional experience and expression, helping to clarify the old controversies. Lang’s
paradigm was recently used to study completely paralyzed patients with amiotrophic
lateral sclerosis (ALS), and yielded evidence against the idea of impaired emotional
processing in patients with severely impaired peripheral physiology (Birbaumer,
2001). ALS is a severe neurological disease that progressively destroys motorneurons, leading to a total loss of voluntary muscular responses. Communication
with this type of completely paralyzed locked-in patients is possible using techniques
such as the thought-translation-device developed by Birbaumer et al. (1999), and
based on the recording and self-regulation of slow cortical potentials, or the brain�/
computer Interface technology developed by Wolpaw et al. (2000)), and based on the
recording and self-regulation of spontaneous EEG activity (for a description of
alternative brain�/computer interfaces, see Kubler et al., 2001). Using the thought-
translation-device, Birbaumer has reported normal reactivity of ALS patients in thepicture viewing paradigm as indicated by EMG, heart rate, and subjective ratings of
affective pictures.
The startle reflex is a chained series of rapid flexor movements prompted by any
abrupt sensory stimulation. In humans, the first and most reliable component of the
reflex is a rapid eyeblink. Eyeblink startle has been considered a defensive reflex that
serves a protective function, helping to avoid organ injury (Pavlov, 1927; Landis &
Hunt, 1939) and acting as a behavioral interrupt that clears the processor to deal
with a possible threat (Graham, 1979; Lang, 1995). In the picture viewing paradigm,eyeblink magnitude is consistently potentiated when participants view unpleasant
pictures and inhibited when they view pleasant pictures (Lang, 1995; Bradley, 2000).
This emotional modulation of the startle reflex is explained by Lang and colleagues
as a motivational priming effect: unconditioned reflexes are primed that are linked to
appetitive or defensive motivational systems. Thus, activation of the defensive
motivational system by viewing unpleasant pictures should prime defensive reflexes,
whereas activation of the appetitive motivational system by viewing pleasant pictures
should lead to inhibition of defensive responding (Bradley, 2000).In the context of the picture viewing paradigm, other physiological responses have
also shown consistent covariations with subjective ratings of picture-elicited valence
and arousal: heart rate, skin conductance, facial EMG, and event-related potentials.
Heart rate and skin conductance are two autonomic physiological responses of
special interest for our research, because they are presumably impaired in SCI
patients. Heart rate shows a consistent pattern of decelerative changes during the 6 s
of picture viewing: an initial deceleration during seconds 1�/2, a subsequent
acceleration during seconds 3�/4, and a final greater deceleration during seconds5�/6. The decelerative pattern is significantly greater when viewing unpleasant
pictures versus pleasant ones, while the neutral pictures elicit an intermediate
pattern. Skin conductance also shows a consistent pattern, characterized by a slow
increase after the first 2 s that does not recover within the 6 s picture presentation.
The increase is significantly greater when viewing both pleasant and unpleasant
pictures than when viewing neutral pictures.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269 253

The present study tested the specific hypothesis that impaired peripheral
physiology in patients with SCI impairs emotional processing, as manifested in
modulation of physiological responses (eyeblink startle, heart rate and skin
conductance) as well as in the subjective component of emotions. Regarding the
subjective component, the study by Hohmann (1966) was taken as the classic
methodological reference for the study of emotions in people who have suffered
spinal cord lesions. In addition to the emotions and affects studied by Hohmann(fear, anger, sadness, and sentimentalism), our study included scales to evaluate
changes in other emotions (joy and love). The study was preceded by a pilot study to
test the picture viewing task in students, using the Spanish norms of the international
affective picture system (Molto et al., 1999; Vila et al., 2001) and the data acquisition
and experimental control software developed in our lab in the context of the present
research (Garcıa et al., 1997).
2. Pilot study
2.1. Participants
A total of 78 undergraduate volunteer students (66 females, 12 males) participated
in the study (age range�/20�/23 years). None of the participants reported being
under pharmacological or psychiatric treatment and none had cardiac disorders or
auditory or visual deficiencies.
2.2. Design
A within-subjects design was employed, with valence as a repeated measure factor
with three levels: pleasant, neutral, and unpleasant.
2.3. Task
Thirty pictures, consisting of 10 pleasant, 10 neutral, and 10 unpleasant pictures,were selected from the IAPS on the basis of their valence ratings (scale 1�/9)
according to Spanish norms (Molto et al., 1999). Pleasant pictures were within the
7.86�/8.3 range, neutral pictures within the 4.06�/4.97 range, and unpleasant pictures
within the 1.38�/2.14 range. Participants saw the 30 pictures in a random order with
the following limitations: each block of 10 pictures included at least 2 pictures of
each valence category, and no more than 3 pictures belonging to the same category
were presented consecutively. Each picture was presented for 6 s with an inter-trial
interval of 24 s. The acoustic startle probe was randomly delivered between seconds 2and 4 during half of the pictures in each category. The task was preceded by a 5-min
non-stimulation period and finished 1 min after the last picture. IAPS identification
number of the pictures used are: (pleasant) 2080, 2360, 2070, 1710, 2170, 2540, 8490,
7330, 1750, 1920; (neutral) 6150, 5920, 1310, 9270, 2230, 1390, 7700, 1120, 7560,
3250; (unpleasant) 3180, 3010, 2710, 3230, 9400, 9420, 3170, 9410, 2800, 3000.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269254

2.4. Apparatus
The following apparatus was used: (1) a Letica polygraph (Model 4006) to record
integrated EMG through the 905 EMG amplifier. Recording was done using a band
filter of 10�/1000 Hz. Rectification and contour-following-integration was set at 150
ms time constant, with a sensitivity of between 100 and 200 mV/full scale; (2) a
Reflecta (model MC 150) slide projector to display the slides; and (3) a Letica (modelLE 150) auditory stimulator to generate white noise. The sounds were presented
through earphones (model telephonics) and the intensity was calibrated with a Bruel
and Kjaer sonometer (model 2235) using an artificial ear (model 4153).
Data acquisition and stimulus control were monitored by the BioLab program,
software specifically developed by the Department of Telecommunication Engineer-
ing of Malaga University for this research (see Cobos, 1999). It uses a 12-bit PCL-
812PG Advantech card on a PC Pentium and MS-DOS together with some
LabWindows libraries. The physiological variable was recorded at a voltage rangeof �/5 to �/5 V and a sampling rate of 1000 Hz, starting 1 s before picture onset and
finishing 3 s after picture offset.
2.5. Dependent variables
The eyeblink component of the startle response was measured by recording
integrated EMG activity from the orbicularis oculi muscle beneath the left eye, usingsmall Sensormedic electrodes filled with electrolyte paste. Eyeblink magnitude was
scored as the maximum increase in microvolts occurring between 20 and 120 ms after
noise onset. In addition, valence and arousal ratings for each picture were obtained
by using the self-assessment-manikin (SAM) scale (Lang et al., 1988) to evaluate the
pleasantness and arousal of each picture after the task. This scale ranges from 1 to 9
points.
2.6. Procedure
Each participant underwent a single session at the laboratory. After completing
the informed consent form, the participant reclined in a comfortable chair and the
EMG sensors were attached. The participant was then instructed to view each
picture for the entire time it was on the screen. In addition, he/she was told that
occasional noises would be heard through the headphones and could be ignored.
After checking the physiological recording, the beginning of the test was signaled by
turning down the lighting in the participant’s room to a pre-established subduedlevel. After the picture series was finished, the sensors were removed and the same
picture series was presented again in the same order, with an inter-picture interval of
12 s, in order to evaluate the pleasantness and arousal of each picture using the SAM
scale. Finally, the participant was debriefed and given the academic credit for his/her
participation.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269 255
2.7. Data analysis
Analysis of variance for repeated measures was applied to the average eyeblink
magnitude in the five probe trials within each valence category. The Greenhouse
Geisser epsilon correction was applied for the adjustment of the degrees of freedom.
Results are reported with the original degrees of freedom and the corrected P -values.
Post-hoc comparisons were performed using the Tukey test. The subjective variableswere analyzed using the Friedman test (x2).
2.8. Results
2.8.1. Subjective ratings
Average valence ratings were: pleasant (7.74, S.D.�/1.33), neutral (4.32, S.D.�/
1.34), and unpleasant (1.78, S.D.�/1.08). Results of the Friedman test showed
significant differences between the valence ratings (x2(2, 78)�/155.51, PB/ 0.0001).
The differences were significant between the three valence categories. Average
arousal ratings were: pleasant (3.34, S.D.�/1.55), neutral (3.35, S.D.�/1.14), and
unpleasant (6.83, S.D.�/1.25). Results of the Friedman test also showed significant
differences between the arousal ratings (x2(2, 78)�/117.62, PB/ 0.0001). In this case,
the difference were significant only between the unpleasant and the other twocategories; no significant differences was observed between the neutral and pleasant
categories.
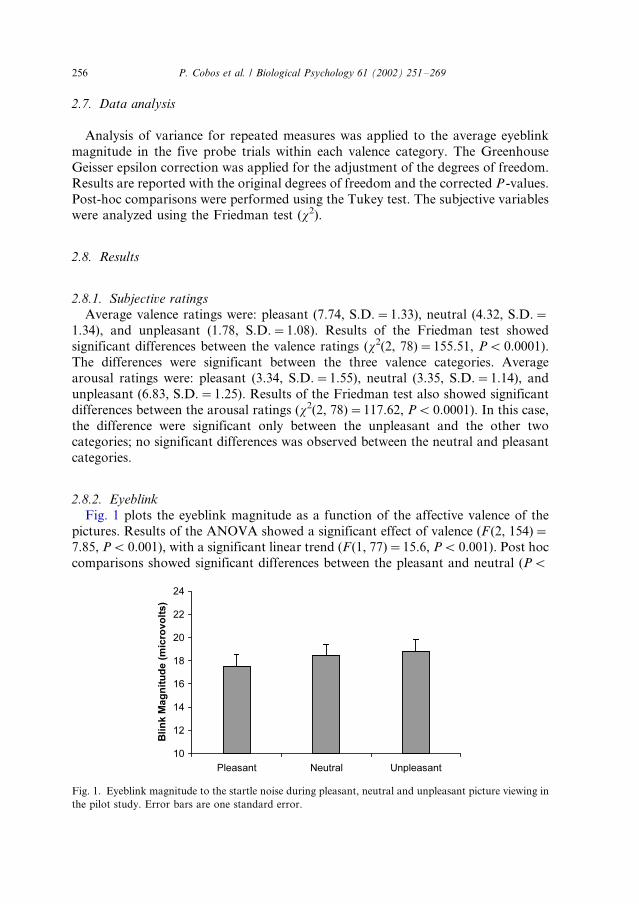
2.8.2. Eyeblink
Fig. 1 plots the eyeblink magnitude as a function of the affective valence of the
pictures. Results of the ANOVA showed a significant effect of valence (F (2, 154)�/
7.85, PB/ 0.001), with a significant linear trend (F(1, 77)�/15.6, PB/ 0.001). Post hoc
comparisons showed significant differences between the pleasant and neutral (PB/
Fig. 1. Eyeblink magnitude to the startle noise during pleasant, neutral and unpleasant picture viewing in
the pilot study. Error bars are one standard error.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269256

0.05), and between the pleasant and unpleasant (PB/ 0.001) categories; no significant
difference was observed between the neutral and unpleasant categories.
2.9. Discussion
The startle results reproduced the expected valence effect reported by Lang and
colleagues. The magnitude of the startle response to the probe was greater when
participants were viewing the unpleasant pictures than when viewing the pleasant
ones, with the neutral pictures producing an intermediate magnitude. Results of thesubjective ratings confirmed the a priori selection of the pictures based on the
Spanish norms of the International Affective Picture System. As expected, the
participants rated the pleasant pictures as significantly more pleasant than the
neutral and unpleasant ones, and the neutral pictures as significantly less unpleasant
than the unpleasant ones. The arousal ratings showed significant differences between
the unpleasant and neutral categories and between the unpleasant and pleasant ones.
However, the arousal ratings of the pleasant pictures were not significantly different
from those of the neutral ones. The latter result is not uncommon when the selectionof pictures is based only on valence ratings, because both American and Spanish
students consistently rate unpleasant materials as more arousing than pleasant ones
(Bradley, 2000; Molto et al., 1999; Vila et al., 2001). In general, the results of the
pilot study were considered adequate to extend the same methodology to test our
main hypothesis, which addressed the emotional modulation of eyeblink startle and
other physiological responses in SCI patients.
3. Main study
3.1. Participants
The study included 19 participants with SCI, 7 women (aged 21�/53 years) and 12
men (aged 24�/57 years); and 19 control participants, 7 women and 12 men, matched
for age and education. The physical and health status of the patients was good,
within the obvious limits imposed by their lesions, and they had no psychiatric
problems or dependence on drugs or alcohol. None of the participants had received
any psychological or psychiatric therapy after their lesion, the duration of which
ranged from 22 months to 28 years. The characteristics of the lesions and the age,sex, duration of the lesion, marital status, and education of the patients are shown in
Table 1. The inclusion criterion for the patient group was a minimum 18-month
history of complete or incomplete traumatic or surgical spinal cord injury. Exclusion
criteria were: any degree of mental handicap, severe visual or auditory deficit, and/or
higher nervous system involvement.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269 257

3.2. Design
The physiological variables were compared between injured and noninjured
participants using a factorial design with two independent groups and several
repeated measures factors, as specified below. The subjective variables were
compared as follows: first, by using a general two group design (patients and
controls); second, by dividing the 19 SCI patients into three groups, according to the
level of their lesion: High lesions (the six with highest lesions), Middle lesions (theseven with lesions at an intermediate level), and Low lesions (the six with the lowest
lesions); third, by dividing the 19 SCI patients into two groups according to the
extent of their lesion: complete lesion (12 patients with complete section of the spinal
cord) and incomplete lesion (7 patients with a partial section of the spinal cord); and
fourth, by dividing the patients into two groups according to the duration of the
lesion: 10 patients with duration B/10 years and 9 patients with duration E/10 years.
3.3. Task
The task was the same as in the pilot study.
Table 1
Lesion and socio-demographic characteristics of the SCI patients
Level and extent of the injury Age (years/month) Years since lesion Education Marital status
Men
C1-2a 24.05 7 Se S
C4a 39.01 21 Su S
T4a 40.08 26 Se S/P
T6a,c 48.04 23 Su S/P
T6a 30 1.11 Se M
T6b 24 4 Pri S
T7a 31.10 16 Pri S/P
T8b,c 33.04 10 Se S/P
T8-9b 40.06 5 Pri M
T10a,c 52 27 Pri M
T11a 57.10 28 Pri D
L1-4b 34 4 Se M
Women
C3b 23.04 7 Se S/P
C6b 21.11 6 Se S/P
T5a 44.10 1.10 Se M
T7a,c 53 6 Pri M
T9a 38.08 20 Se S
T10b,c 39.01 3 Pri D
T12a 41.11 19 Pri M
Pri, primary; Se, secondary; Su, superior; S, single; M, married; D, divorced; S/P, single with partner.a Extent of the injury: complete.b Extent of the injury: incomplete.c Incomplete sensory loss.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269258
3.4. Apparatus
The apparatus was that used in the pilot study. In addition, a Letica GSR-200
amplifier and a Letica CAR-300 amplifier were used to record skin conductance and
heart rate, respectively.
3.5. Physiological variables
Eyeblink Magnitude was recorded as in the pilot study. Heart rate was derived
from the blood pulse amplitude recorded at the distal phalanx of the right index
finger, using a Letica photoelectric sensor at a sensitivity of 1�/10 mV/full scale. The
inter-beat interval was measured in milliseconds and transformed into average heart
rate every half-second using a weighted averaging procedure (Reyes del Paso and
Vila, 1998). The heart rate response was expressed as change in heart rate from
baseline (before each picture) every half-second during the 6 s picture presentation.Skin resistance was measured from the second phalanx of the index and middle
fingers of the left hand, using standard Sensormedic electrodes filled with isotonic
electrolyte paste (0.29 g NaCl per 100 ml water). The amplifier used a constant
current of 10 A. Recording was done at a sensitivity of 100�/200 kV/full scale. Skin
resistance was transformed into skin conductance units and expressed as change in
conductance from stimulus onset to maximum increase during the 6 s slide
presentation.
3.6. Subjective measures
Valence and arousal ratings of the pictures were obtained using the SAM as in the
pilot study.
3.6.1. Structured interview
This interview included questions related to the following emotions: joy, love,
sentimentalism, fear, anger, and sadness. Participants were asked to search formemories of important and intense experiences in their past (always before the lesion
in the patient group) and present. Using the scale employed by Hohmann, they were
asked if they perceived each emotion less (1), the same (2), or more (3) than in the
past. For the analysis, the emotions of joy, love, and sentimentalism were grouped
into the category of ‘positive emotions’, whereas the emotions of fear, anger, and
sadness were grouped into the category of ‘negative emotions’.
3.7. Procedure
Recruitment of the spinal cord injury patients for the study was made by
contacting the Base Center for the Disabled of the province of Malaga (Spain) and
all the local Disabled Associations in the same province. The control participants
were selected from members of the staff of the faculty of psychology or from
contacts fulfilling the necessary requirements. In all cases, the laboratory session and
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269 259
the interview were conducted by the first author, who waited for the participants at
the entrance to the faculty to take them to the laboratory. The atmosphere for the
session was always relaxed and unhurried, with no objections being raised by any
participant at any point, the patients collaborating fully. After completing the
informed consent form, the participant reclined in a comfortable chair and the
physiological sensors were attached. The instructions given to the participants were
the same as in the pilot study. Finally, after finishing the task and evaluating thepictures using the SAM, the participant completed the structured interview.
3.8. Data analysis
Analysis of variance was applied to the physiological variables using a factorial
design consisting of the group factor and the following repeated measures factors:
valence of the pictures (pleasant, neutral and unpleasant) and, when applicable,
noise (pictures with noise versus pictures with no-noise), and form of the response
(the physiological values within the 6 s picture presentation). As in the pilot study,
the Greenhouse Geisser epsilon correction was applied to the repeated measure
factors. Subjective variables were analyzed using the Friedman test (x2) for within-subject comparisons and the Student’s t-test or analysis of variance for between-
group comparisons. In addition, in order to directly compare our results with those
of Hohmann, an analysis was also undertaken of the frequency of patients reporting
decrement, no change, or increment in each emotional scale.
4. Results
4.1. Subjective ratings (SAM)
Ratings of valence and arousal showed significant differences between pleasant,
neutral, and unpleasant pictures for both SCI and control participants: valence in
SCI (x2(2, 19)�/38, PB/ 0.0001); valence in control ((x2(2, 19)�/38, PB/ 0.0001);arousal in SCI (x2(2, 19)�/26.6, PB/ 0.0001); arousal in control (x2(2, 19)�/22.92,
PB/ 0.0001). Average valence ratings were in line with the a priori selection of the
pictures: pleasant (SCI�/7.51, S.D.�/0.86; control�/7.83, S.D.�/0.6), neutral
(SCI�/4.45, S.D.�/0.75; control�/4.51, S.D.�/0.43), and unpleasant (SCI�/1.63,
S.D.�/0.59; control�/1.66, S.D.�/0.66). No significant differences were found
between the SCI and control participants. Average arousal ratings did not
significantly differ between the groups: pleasant (SCI�/4.85, S.D.�/2.01; con-
trol�/3.89, S.D.�/2.51), neutral (SCI�/3.67, S.D.�/1.74; control�/3.62, S.D.�/
1.52), and unpleasant (SCI�/7.37, S.D.�/1.31; control�/7.32, S.D.�/1.37). As in
the pilot study, the valence ratings showed significant differences between the three
valence categories whereas the arousal ratings showed significant differences only
between the unpleasant and the other two categories and not between the pleasant
and neutral ones.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269260
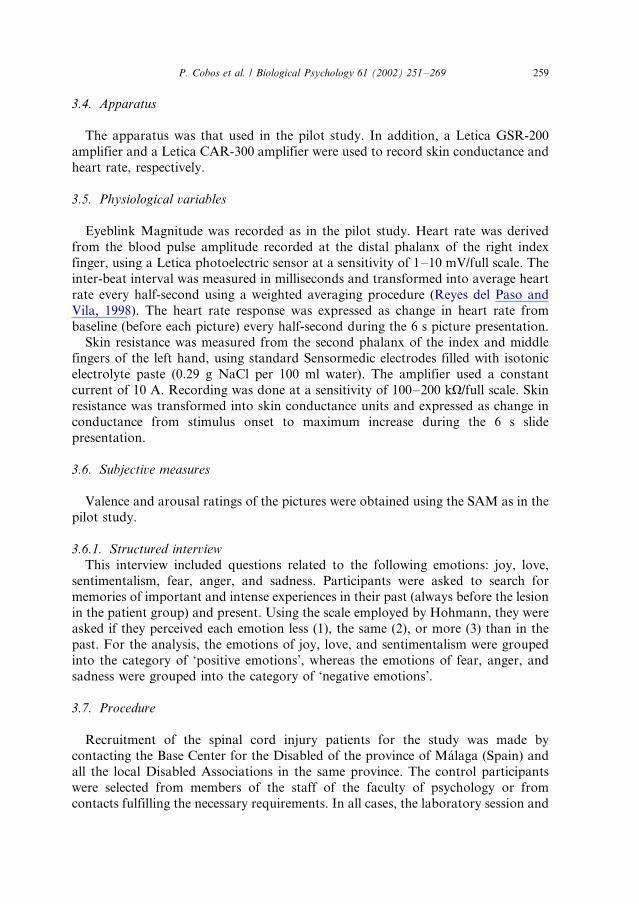
4.2. Eyeblink
Fig. 2 plots the eyeblink magnitude as a function of the groups and of the affective
valence of the pictures. Results of the 2�/(3) ANOVA (Group�/Valence) showed no
significant effects of the two main factors or of their interaction. As illustrated in Fig.
2, the expected valence effect was not observed. There was a non-significant tendency
for the SCI group to produce greater eyeblink magnitudes to all pictures compared
with the control group (F (1, 36)�/1.74, P �/0.10).
In order to test whether the absence of affective startle modulation in both groups
was due to the low arousal rating of the pleasant pictures, we reanalyzed the EMG
data and included only the three most arousing pleasant pictures, the three least
arousing neutral pictures, and the three most arousing unpleasant pictures. There
was a very slight tendency to show greater startle magnitude to the unpleasant
pictures than to the pleasant ones in both groups, but these differences did not
approach statistical significance (F (2, 36)�/0.95, P�/ 0.25).
4.3. Heart rate
4.3.1. Baseline level
Heart rate at baseline, before starting the pictures, was higher for SCI patients(80.99 bpm) than for control participants (75.24 bpm), although the difference did
not reach significance (F (1, 36)�/2.49, P�/ 0.10).
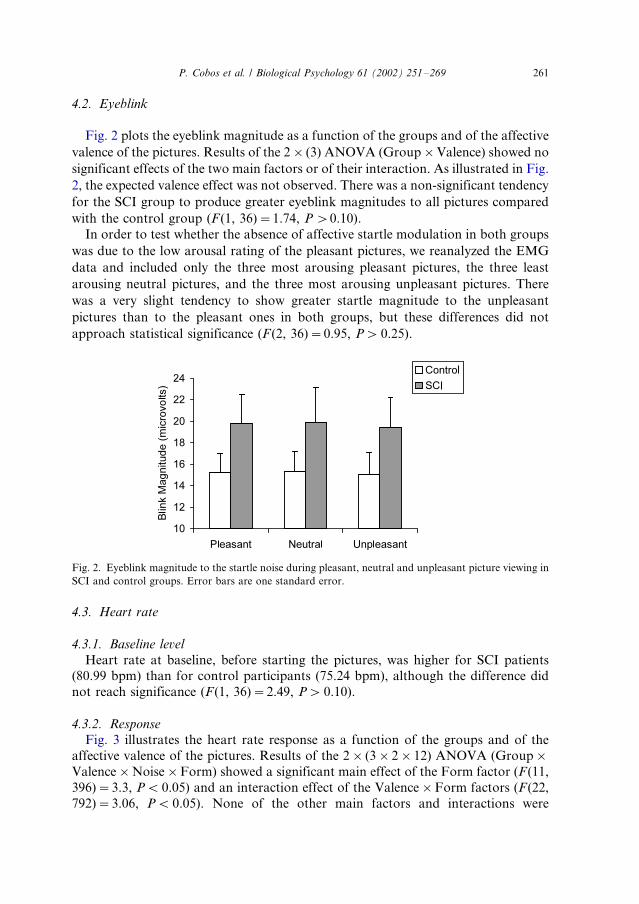
4.3.2. Response
Fig. 3 illustrates the heart rate response as a function of the groups and of the
affective valence of the pictures. Results of the 2�/(3�/2�/12) ANOVA (Group�/
Valence�/Noise�/Form) showed a significant main effect of the Form factor (F (11,
396)�/3.3, PB/ 0.05) and an interaction effect of the Valence�/Form factors (F (22,
792)�/3.06, PB/ 0.05). None of the other main factors and interactions were
Fig. 2. Eyeblink magnitude to the startle noise during pleasant, neutral and unpleasant picture viewing in
SCI and control groups. Error bars are one standard error.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269 261
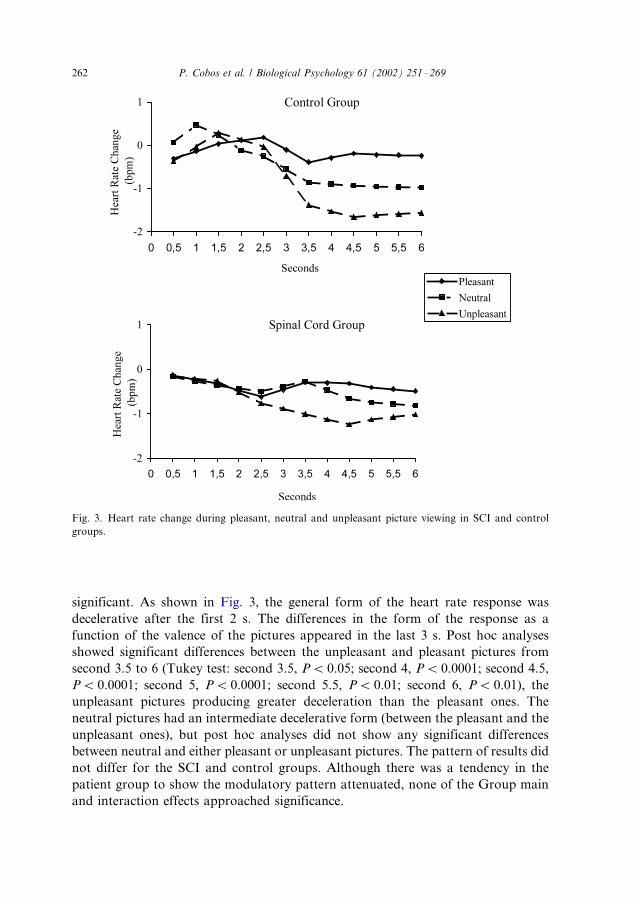
significant. As shown in Fig. 3, the general form of the heart rate response was
decelerative after the first 2 s. The differences in the form of the response as a
function of the valence of the pictures appeared in the last 3 s. Post hoc analyses
showed significant differences between the unpleasant and pleasant pictures from
second 3.5 to 6 (Tukey test: second 3.5, PB/ 0.05; second 4, PB/ 0.0001; second 4.5,
PB/ 0.0001; second 5, PB/ 0.0001; second 5.5, PB/ 0.01; second 6, PB/ 0.01), the
unpleasant pictures producing greater deceleration than the pleasant ones. The
neutral pictures had an intermediate decelerative form (between the pleasant and the
unpleasant ones), but post hoc analyses did not show any significant differences
between neutral and either pleasant or unpleasant pictures. The pattern of results did
not differ for the SCI and control groups. Although there was a tendency in the
patient group to show the modulatory pattern attenuated, none of the Group main
and interaction effects approached significance.
Fig. 3. Heart rate change during pleasant, neutral and unpleasant picture viewing in SCI and control
groups.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269262
4.4. Skin conductance
4.4.1. Baseline level
Skin conductance at baseline was lower for SCI patients (6.67 microsiemens) than
for control participants (9.07 microsiemens), although the difference did not reach
statistical significance (F (1, 36)�/2.90, PB/ 0.10).
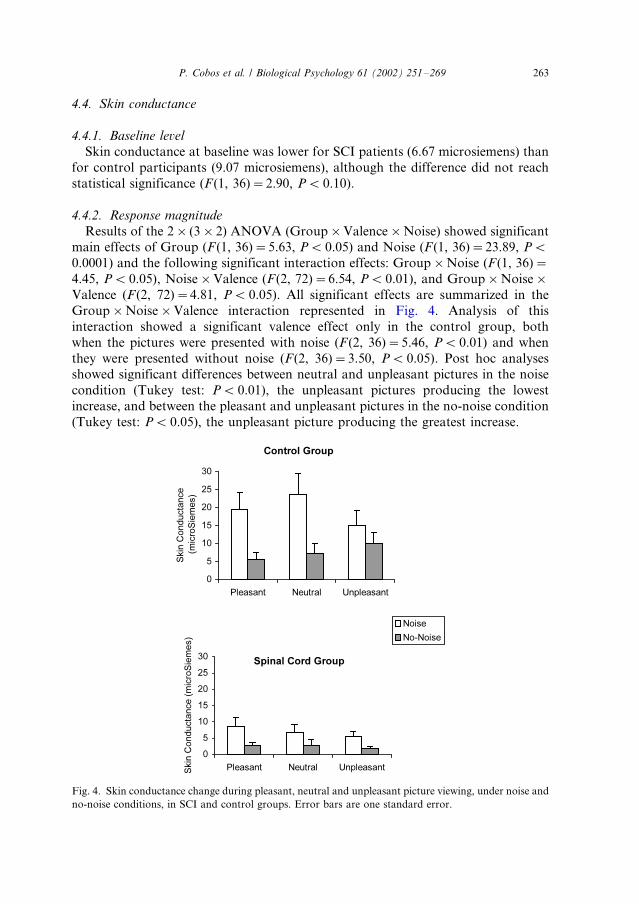
4.4.2. Response magnitude
Results of the 2�/(3�/2) ANOVA (Group�/Valence�/Noise) showed significantmain effects of Group (F (1, 36)�/5.63, PB/ 0.05) and Noise (F (1, 36)�/23.89, PB/
0.0001) and the following significant interaction effects: Group�/Noise (F (1, 36)�/
4.45, PB/ 0.05), Noise�/Valence (F (2, 72)�/6.54, PB/ 0.01), and Group�/Noise�/
Valence (F (2, 72)�/4.81, PB/ 0.05). All significant effects are summarized in the
Group�/Noise�/Valence interaction represented in Fig. 4. Analysis of this
interaction showed a significant valence effect only in the control group, both
when the pictures were presented with noise (F (2, 36)�/5.46, PB/ 0.01) and when
they were presented without noise (F (2, 36)�/3.50, PB/ 0.05). Post hoc analysesshowed significant differences between neutral and unpleasant pictures in the noise
condition (Tukey test: PB/ 0.01), the unpleasant pictures producing the lowest
increase, and between the pleasant and unpleasant pictures in the no-noise condition
(Tukey test: PB/ 0.05), the unpleasant picture producing the greatest increase.
Fig. 4. Skin conductance change during pleasant, neutral and unpleasant picture viewing, under noise and
no-noise conditions, in SCI and control groups. Error bars are one standard error.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269 263

4.5. Self-reported emotions
Most patients noticed either no change or an increase in their emotions, with just a
few feeling they had decreased. Some participants were unable to compare, and their
responses were considered as missing values in the analysis. When only the patient
group is considered (as in the Hohmann study), significant differences appear in the
scales of anger (decrease�/0; no change�/8; increase�/8; x2�/8.01, PB/ 0.05) andsadness (decrease�/1; no change�/5; increase�/11; x2�/8.95, PB/ 0.05), always in
the direction of increment. When compared with the control group, significant
differences appeared only in the sadness scale (t (1, 34)�/2.14, PB/ 0.05), with the
patient group showing a greater increment.
To determine the existence of differences in emotion assessments between the
subgroups of patients with high, middle or low lesions, the corresponding statistical
analyses were carried out. There was a general tendency in the group with middle
lesions to score higher for both pleasant and unpleasant emotions, although in nocase did these attain statistical significance.
The scores of patients with spinal cord lesions were compared according to the
extent of the lesion. There was a tendency for the group with incomplete lesions to
have higher scores in joy, love, and sentimentalism, and lower scores in anger, fear,
and sadness, although these were not statistically significant.
Finally, patient scores were compared according to the duration of the lesion.
There was a tendency for the group with longer duration to have lower scores in joy,
love, and fear, and higher scores in sentimentalism, anger, and sadness, althoughstatistical significance was not reached.
5. Discussion
In the present study, the subjective valence and arousal ratings of the pictures were
similar among SCI patients and control participants. They did not differ from the
normative ratings based on Spanish student samples (Molto et al., 1999). Thus, noevidence of reduced subjective experience to affective visual pictures was found in the
patient group. In addition, the patients and controls showed a similar affective
modulation of heart rate: both groups showed a significantly greater heart rate
deceleration while viewing unpleasant pictures than while viewing pleasant pictures,
with the neutral pictures producing intermediate heart rate responses. No evidence of
startle modulation was found in either group. However, evidence of skin
conductance modulation was found in control participants in interaction with the
noise condition: when the pictures were presented without noise, the unpleasant(most arousing) pictures produced greater skin conductance responses than the
pleasant and neutral ones, and the opposite was observed for picture�/noise
presentations. In general, these results are in agreement with those found by
Birbaumer (2001) in completely paralyzed ALS-patients using the picture viewing
together with the thought-translation-device for communication with the patients.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269264

Both physiological (heart rate and eyeblink startle) and subjective measures showed
no significant differences between patients and well controls.
The group with spinal cord injury scored higher than the control group in self-
reports of negative emotions, significantly so in report of sadness. Comparison
within the spinal cord injury group, according to the level, extension, and duration of
the lesion, provided no evidence for a decreased affective experience in patients with
greater peripheral loss. In general, these results are in agreement with those found by
Lowe and Carroll (1985), Chwalisz et al. (1988) and Bermond et al. (1991) in SCI
patients using Hohmann’s methodology. These three studies reported either no
change or an increase in emotional experience after the lesion, failing to replicate
Hohmann’s data. In general, these results clearly contradict James’ theory (1884)
and the so-called strong and weak forms of the feedback arousal theory (Chwalisz et
al., 1988; Reisenzein, 1983). According to the latter theory, peripheral physiological
feedback is either absolutely necessary for the emotional experience (strong form) or
is a contributing factor enhancing the intensity of this experience (weak form).
Our physiological data, however, showed differential effects that require
individual consideration. Our heart rate data replicate prior findings in well
participants: a greater final deceleration during the 6-s unpleasant pictures compared
with pleasant and neutral pictures (Bradley et al., 1993; Lang et al., 1993; Hare, 1973;
Klorman et al., 1977). This greater decelerative pattern to unpleasant visual stimuli
was interpreted by Lang and colleagues as indicative of a vagally mediated aversive
bradycardia similar to that found in passive aversive conditioning (LeDoux, 1990;
Obrist, 1981). The similarity between our two groups in the pattern of heart rate
affective modulation supports this interpretation, given that the vagal control of the
heart is not affected by the spinal lesion, whereas the sympathetic control (depending
on the level and extent of the lesion) is. Although there were nonsignificant group
effects in heart rate, the tendency to show an attenuated modulatory pattern in the
patient group might reflect this reduction in autonomic nervous system control on
the heart via the sympathetic branch. An alternative explanation would point to the
reduced number of participants in the study. A larger sample of both patients and
controls might have increased statistical power and the observed tendency would
have reached statistical significance.
The absence of affective eyeblink modulation in the main study, may have
multiple causes, including, among others, the age or type of the participants, or
inadequate startle trials or picture selection. The age of our participants in the main
study was considerably higher than in the pilot study, where affective modulation
was detected using the same task. The heterogeneity of our patients and control
participants regarding age and other characteristics might have contributed to
obscure the expected effect. Moreover, our task used a reduced number of trials (five
per affective category) and the pictures were selected exclusively on the basis of
valence ratings. Post hoc analyses showed that our selected pleasant pictures were
rated significantly lower in arousal than the unpleasant ones and that there were no
differences in arousal between the pleasant and the neutral pictures. Because the
modulation augments with increases in arousal for both pleasant and unpleasant
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269 265

pictures (Cuthbert et al., 1996), the low arousal of the pleasant pictures might have
contributed to the absence of eyeblink modulation in our main study.
The skin conductance response to the pictures showed a significant reduction in
the patient group, with no evidence of affective modulation, which was only
observed in the control participants and in interaction with the noise condition. The
expected skin conductance modulation is a greater response to the most arousing
pictures, both pleasant and unpleasant (Lang, 1995; Bradley, 2000). The greaterresponse, under no-noise presentation, to the unpleasant pictures in our study,
compared to the neutral and pleasant ones, can be explained by the arousal ratings
of our pictures, which were significantly lower for the neutral and pleasant pictures.
The opposite effect for picture�/noise presentation is difficult to explain on the basis
of published results. Nevertheless, the strongest effect was the significant reduction
in the skin conductance response of the patient group. Because skin conductance is
exclusively mediated by the sympathetic branch of the autonomic nervous system,
which is affected by spinal cord lesion, we can speculate that the differences inaffective modulation observed between heart rate and skin conductance are
exclusively due to vagal influences. If this is so, our skin conductance data indirectly
support the above-mentioned interpretation of the greater decelerative heart rate
response to unpleasant pictures as a vagally mediated aversive bradycardia.
A theoretical problem in the interpretation of the physiological data is to what
extent the neural lesion in the patient group prevents any demonstration (against or
in favor) of central emotional processing using peripheral physiological measures
that are potentially affected by the lesion. Is the lack of affective modulation in thephysiological response an index of reduced emotional processing or just an index of
the peripheral lesion itself? In our study, this problem is especially relevant in the
skin conductance data, because the patient group showed a significant reduction in
this physiological response. Given the heart rate results, we are inclined to interpret
the skin conductance data as a direct consequence of the lesion rather than as an
absence of modulation. A related issue is to what extent different physiological
responses can show different patterns of modulation to the same affective stimuli.
Can eyeblink, heart rate, and skin conductance show different patterns ofmodulation? It should be noted that the physiological mechanisms of somatic
reflexes are quite different from those of autonomic responses. Moreover, within
autonomic responses, the mechanisms of heart rate are quite different from those of
skin conductance. Given these considerations, different patterns of modulation to
the same perceptual stimuli can be expected when different physiological indices are
used.
Finally, we would like to comment on some potential implications of our results
for traditional theories of emotion, in particular for the peripheralism versuscentralism controversy. On one hand, our self-report data suggest that emotions are
the results of central processes activated in the brain and that the subjective
component is probably independent of peripheral physiology. On the other hand,
some peripheral physiology, in particular heart rate, can index central emotional
processing, even in people with impaired somatic and autonomic physiology. Given
the modest correlations normally found between physiological and subjective
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269266
measures of emotions (Lang, 1995), peripheral physiological evidence that corrobo-
rates the normal affective reports of patients is not only a further argument against
the idea of impaired emotional processing in participants with impaired peripheral
physiology, but also an argument against the idea of emotion as a cognitive process
totally unrelated to bodily responses. The heart rate data in our study, like the
eyeblink response in Birbaumer’s study, clearly show a specific physiological
response pattern that covariates with self-reported emotion, even in people withsevere peripheral restriction. As Lang’s theory implies, an integrative approach to
emotion, which considers that emotion involves processes that are simultaneously
central and peripheral, seems more appropriate than the traditional dichotomous
approach of peripheralism versus centralism.
Acknowledgements
Support for this research was provided by the Spanish Ministry of Education
(research project PB97-0841) and Junta de Andalucıa (research group HUM 388).
References
Bermond, B., Nieuwenhuyse, B., Fasotti, L., Schuerman, J., 1991. Spinal cord lesions, peripheral
feedback, and intensities of emotional feelings. Cognition and Emotion 5, 201�/220.
Birbaumer, N, 2001. Emotion, brain activation and complete paralysis: fMRI and EEG as communication
devices. Abstracts of the II International Workshop on Emotion and the Brain. Universidad de las
Islas Baleares.
Birbaumer, N., Ohman, A. (Eds.), The Structure of Emotion: Psychophysiological, Cognitive, and Clinical
Aspects. Hogrefe & Huber, Seatle 1993.
Birbaumer, N., Ghanayim, N., Hinterberger, T., Iversen, I., Kotchoubey, B., Kubler, A., Perlmouter, J.,
Taub, E., Flor, H., 1999. A spelling device for the paralysed. Nature 398, 297�/298.
Bradley, M.M., 2000. Emotion and motivation. In: Cacciopo, J.T., Tassinary, L.G., Berntson, G.G.
(Eds.), Handbook of Psychophysiology. Cambridge University, New York, pp. 602�/642.
Bradley, M.M., Lang, P.J., Cuthbert, B.N., 1993. Emotion, novelty, and the startle reflex: habituation in
humans. Behavioral Neuroscience 107, 970�/980.
Cannon, W.B., 1914. The interrelations of emotions as suggested by recent psychological researches.
American Journal of Psychology 25, 256�/282.
Cannon, W.B., 1927. The James�/Lange theory of emotion: a critical examination and an alternative
theory. American Journal of Psychology 39, 106�/124.
Cannon, W.B., 1929. Bodily Changes in Pain, Hunger, Fear and Rage. Appleton, New York.
Cuthbert, B.N., Bradley, M.M., Lang, P.J., 1996. Probing picture perception: activation and emotion.
Psychophysiology 33, 103�/111.
Chwalisz, K., Diener, E., Gallagher, D., 1988. Autonomic arousal feedback and emotional experience:
evidence from the spinal cord injured. Journal of Personality and Social Psychology 54, 820�/828.
Cobos, P. (1999): Estados emocionales y patrones psicofisiologicos en la discapacidad: Lesion Medular.
Malaga (Spain): Servicio de Publicaciones de la Universidad de Malaga.
Dana, C.L., 1921. The anatomic seat of the emotions: a discussion of the James�/Lange theory. Archives
of Neurology and Psychiatry 6, 634�/639.
Fehr, F.S., Stern, J.A., 1970. Peripheral physiological variables and emotion: The James�/Lange theory
revisited. Psychological Bulletin 74, 411�/424.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269 267
Garcıa, C., Jimenez, F., Cobos, M.P., Valero, L., 1997. BioLab: un programa informatico para la
adquicision de senales fisiologicas. Psicologica 18, 139�/151.
Graham, F.K., 1979. Distinguishing among orienting, defense and startle reflexes. In: Kimmel, H.D., Van
Olst, E.H., Orlebeke, J.F. (Eds.), The Orienting Reflex in Humans. Erlbaum, New Jersey.
Hare, R.D., 1973. Orienting and defensive responses to visual stimuli. Psychophysiology 10, 453�/463.
Hohmann, G.W., 1966. Some effects of spinal cord lesion on experienced emotional feelings.
Psychophysiology 3, 526�/534.
James, W., 1884. What is an emotion? Mind 9, 188�/205.
James, W., 1890. The Principles of Psychology. Holt, New York.
James, W., 1894. The physical basis of emotion. Psychological Review 1, 516�/529.
Klorman, R., Weissbert, R.P., Wiessenfeld, A.R., 1977. Individual differences in fear and autonomic
reactions to affective stimulation. Psychophysiology 14, 45�/51.
Kubler, A., Kotchoubey, B., Kaiser, J., Wolpaw, J., Birbaumer, N., 2001. Brain�/computer communica-
tion: unlocking the locked in. Psychological Bulletin 127, 358�/375.
Landis, C., Hunt, W.A., 1939. The Startle Pattern. Farrar, New York.
Lang, P.J., 1979. A bio-informational theory of emotional imagery. Psychophysiology 16, 495�/512.
Lang, P.J., 1985. The cognitive psychophysiology of emotion: fear and anxiety. In: Tuma, A.H., Maser, J.
(Eds.), Anxiety and the Anxiety Disorders. Erlbaum, Hillsdale, NJ.
Lang, P.J., 1994. The motivational organization of emotion: Affect-reflex connections. In: VanGoozen, S.,
Van de Poll, N.E., Sergeant, J.A. (Eds.), Emotions: Essays on Current Issues in the Field of Emotion
Theory. Erlbaum, Hillsdale, NJ.
Lang, P.J., 1995. The emotion probe: studies of motivation and attention. American Psychologist 50, 372�/
385.
Lang, P.J., Bradley, M.M., Cuthbert, B.N., 1997. Motivated attention: affect, activation and action. In:
Lang, P.J., Simons, F.R., Balaban, M.T. (Eds.), Attention and Orienting: Sensory and Motivational
Processes. Erlbaum, Hillsdale, NJ.
Lang, P.J., Davis, M., .Ohman, A., 2000. Fear and anxiety: animal models and human cognitive
psychophysiology. Journal of Affective Disorders 61, 137�/159.
Lang, P.J., Greenwald, M.K., Bradley, M.M., Hamm, A.O., 1993. Looking at pictures: affective, facial,
visceral, and behavioral reactions. Psychophysiology 30, 261�/273.
Lang, P.J., .Ohman, A., Vaitl, D., 1988. The international affective picture system (Photographic slides).
University of Florida, Center for Research in Psychophysiology, Gainesville, FL.
LeDoux, J.E., 1990. Information flow from sensation to emotion plasticity in the neural computation of
stimulus value. In: Gabriel, M., Moore, J. (Eds.), Learning and Computational Neuroscience,
Foundations of Adaptive Network. Bradford Books, Cambridge.
Lowe, J., Carroll, D., 1985. The effects of spinal injury on the intensity of emotional experience. British
Journal of Clinical Psychology 24, 135�/136.
Molto, J., Montanes, S., Poy, R., Segarra, P., Pastor, M.C., Tormo, M.P., Ramırez, I., Hernandez, M.A.,
Sanchez, M., Fernandez, M.C., Vila, J., 1999. Un nuevo metodo para el estudio experimental de las
emociones: El International Affective Picture System (IAPS). Adaptacion espanola. Revista de
Psicologıa General y Aplicada 52, 55�/87.
Obrist, P.A., 1981. Cardiovascular Psychophysiology: A perspective. Plenum, New York.
Pavlov, I.P., 1927. Conditioned Reflexes. Dover Publications, New York.
Reisenzein, R., 1983. The Schachter theory of emotion: two decades later. Psychological Bulletin 94, 239�/
264.
Reyes del Paso, G., Vila, J., 1998. The continuing problem of incorrect heart rate estimation in
psychophysiological studies: An off-line solution for cardiotachometer users. Biological Psychology 48,
269�/279.
Richards, J.S., Hirt, M.J.S., Melamed, L., 1982. Spinal cord injury: a sensory restriction perspective.
Archives of Physical Medicine and Rehabilitation 63, 195�/200.
Trieschmann, R.B., 1980. Spinal Cord Injuries: Psychological, Social and Vocational Adjustment.
Pergamon Press, New York.
Tucker, S.J., 1980. The psychology of spinal cord injury: Patient-staff interaction. Rehabilitation
Literature 41, 114�/121.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269268

Vila, J., Sanchez, M., Ramırez, I., Fernandez, M.C., Cobos, P., Rodrıguez, S., Munoz, M.A., Tormo,
M.P., Herrero, M., Segarra, P., Pastor, M.C., Montanes, S., Poy, R., Molto, J., 2001. El Sistema
Internacional de Imagenes Afectivas (IAPS): Adaptacion Espanola. Segunda parte. Revista de
Psicologıa General y Aplicada 54, 635�/657.
Wolpaw, J.R., McFarland, D.J., Vaughan, T.M., 2000. Brain computer research at the Wadsworth
Center. IEEE Transactions on Rehabilitation Engineering 8, 222�/226.
P. Cobos et al. / Biological Psychology 61 (2002) 251�/269 269
Copyright © 2022 FDOKUMEN