Resting heart rate and risk of incident heart failure: three prospective cohort studies and a...
21
Resting Heart Rate and Risk of Incident Heart Failure: Three Prospective Cohort Studies and a Systematic Meta-Analysis Hassan Khan, MD, PhD; Setor Kunutsor, MD; Andreas P. Kalogeropoulos, MD, PhD; Vasiliki V. Georgiopoulou, MD; Anne B. Newman, MD, MPH; Tamara B. Harris, MD, MS; Kirsten Bibbins-Domingo, MD, PhD; Jussi Kauhanen, PhD; Mihai Gheorghiade, MD; Gregg C. Fonarow, MD; Stephen B. Kritchevsky, PhD; Jari A. Laukkanen, MD, PhD; Javed Butler, MD, MPH Background-—The relationship between resting heart rate (RHR) and incident heart failure (HF) has been questioned. Methods and Results- —RHR was assessed at baseline in 7073 participants in 3 prospective cohorts (Cardiovascular Health Study, Health ABC study and Kuopio Ischemic Heart Disease Study) that recorded 1189 incident HF outcomes during 92 702 person- years of follow-up. Mean age of participants was 67 (9.9) years and mean RHR was 64.6 (11.1) bpm. Baseline RHR correlated (P<0.001) positively with body mass index (r=0.10), fasting glucose (r=0.18), and C-reactive protein (r=0.20); and inversely with serum creatinine (r= 0.05) and albumin (r= 0.05). Baseline RHR was non-linearly associated with HF risk. The age and sex- adjusted hazard ratio for HF comparing the top (>72 bpm) versus the bottom (<57 bpm) quartile of baseline RHR was 1.48 (95% confidence interval [CI] 1.26 to 1.74) and was modestly attenuated (1.30, 95% CI 1.10 to 1.53) with further adjustment for body mass index, history of diabetes, hypertension, smoking status, serum creatinine, and left ventricular hypertrophy. These findings remained consistent in analyses accounting for incident coronary heart disease, excluding individuals with prior cardiovascular events, or those taking beta-blockers; and in subgroups defined by several individual participant characteristics. In a pooled random effects meta-analysis of 7 population-based studies (43 051 participants and 3476 HF events), the overall hazard ratio comparing top versus bottom fourth of RHR was 1.40 (95% CI: 1.19 to 1.64). Conclusions-—There is a non-linear association between RHR and incident HF. Further research is needed to understand the physiologic foundations of this association. ( J Am Heart Assoc. 2015;4:e001364 doi: 10.1161/JAHA.114.001364) Key Words: heart failure • heart rate • risk factor A ging of the population, worsening risk factor profile, and improved care of acute cardiovascular disease (CVD) have all led to an increase in the prevalence of heart failure (HF). 1 Heart failure is associated with an unacceptably high morbidity and mortality 2 and imposes a significant economic burden, underscoring the need to identify high-risk individuals in order to tailor preventive and therapeutic measures. Resting heart rate (RHR) is independently associated with prognosis among patients with prevalent HF and RHR lowering has been demonstrated to benefit patients with HF and reduced ejection fraction. 3–5 Whereas, some studies have suggested a positive association between baseline RHR and incident HF risk, 6,7 others have only shown a sex-differenti- ated association, 8 with uncertainties remaining about the From the Department of Medicine, Emory University, Atlanta, GA (H.K., A.P.K., V.V.G.); Department of Public Health and Primary Care, University of Cambridge, Cambridge, UK (S.K.); Department of Epidemiology and Medicine, University of Pittsburgh, Pittsburgh, PA (A.B.N.); Intramural Research Program, Laboratory of Epidemiology and Population Sciences, National Institute on Aging, Bethesda, MD (T.B.H.); Departments of Medicine and Epidemiology & Biostatistics, University of California, San Francisco, CA (K.B.-D.); Institute of Public Health, School and Clinical Nutrition, University of Eastern Finland, Kuopio, Finland (J.K., J.A.L.); Center for Cardiovascular Innovation, Northwestern Feinberg School of Medicine, Chicago, IL (M.G.); Cardiology Division, University of California Los Angeles, Los Angeles, CA (G.C.F.); Section of Gerontology and Geriatric Medicine, Wake Forest School of Medicine, Winston Salem, NC (S.B.K.); Division of Cardiology, Health Sciences Center, Stony Brook University, SUNY at Stony Brook, NY (J.B.). Accompanying Appendices S1 and S2 are available at http://jaha.ahajournals.org/content/4/1/e001364/suppl/DC1 This manuscript was prepared using CHS data obtained from the NHLBI Biologic Specimen and Data Repository Information Coordinating Center and does not necessarily reflect the opinions or views of the CHS study or the NHLBI. Correspondence to: Javed Butler, MD, MPH, Division of Cardiology, Health Sciences Center, Stony Brook University, T-16, Room 080, SUNY at Stony Brook, NY 11794. E-mail: [email protected] Received September 22, 2014; accepted December 11, 2014. ª 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell. This is an open access article under the terms of the Creative Commons Attribution-NonCommercial License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes. DOI: 10.1161/JAHA.114.001364 Journal of the American Heart Association 1 ORIGINAL RESEARCH by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from by guest on June 20, 2016 http://jaha.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Resting heart rate and risk of incident heart failure: three prospective cohort studies and a...

Resting Heart Rate and Risk of Incident Heart Failure: ThreeProspective Cohort Studies and a Systematic Meta-AnalysisHassan Khan, MD, PhD; Setor Kunutsor, MD; Andreas P. Kalogeropoulos, MD, PhD; Vasiliki V. Georgiopoulou, MD; Anne B. Newman, MD,MPH; Tamara B. Harris, MD, MS; Kirsten Bibbins-Domingo, MD, PhD; Jussi Kauhanen, PhD; Mihai Gheorghiade, MD; Gregg C. Fonarow, MD;Stephen B. Kritchevsky, PhD; Jari A. Laukkanen, MD, PhD; Javed Butler, MD, MPH
Background-—The relationship between resting heart rate (RHR) and incident heart failure (HF) has been questioned.
Methods and Results-—RHR was assessed at baseline in 7073 participants in 3 prospective cohorts (Cardiovascular Health Study,Health ABC study and Kuopio Ischemic Heart Disease Study) that recorded 1189 incident HF outcomes during 92 702 person-years of follow-up. Mean age of participants was 67 (9.9) years and mean RHR was 64.6 (11.1) bpm. Baseline RHR correlated(P<0.001) positively with body mass index (r=0.10), fasting glucose (r=0.18), and C-reactive protein (r=0.20); and inversely withserum creatinine (r=�0.05) and albumin (r=�0.05). Baseline RHR was non-linearly associated with HF risk. The age and sex-adjusted hazard ratio for HF comparing the top (>72 bpm) versus the bottom (<57 bpm) quartile of baseline RHR was 1.48 (95%confidence interval [CI] 1.26 to 1.74) and was modestly attenuated (1.30, 95% CI 1.10 to 1.53) with further adjustment for bodymass index, history of diabetes, hypertension, smoking status, serum creatinine, and left ventricular hypertrophy. These findingsremained consistent in analyses accounting for incident coronary heart disease, excluding individuals with prior cardiovascularevents, or those taking beta-blockers; and in subgroups defined by several individual participant characteristics. In a pooledrandom effects meta-analysis of 7 population-based studies (43 051 participants and 3476 HF events), the overall hazard ratiocomparing top versus bottom fourth of RHR was 1.40 (95% CI: 1.19 to 1.64).
Conclusions-—There is a non-linear association between RHR and incident HF. Further research is needed to understand thephysiologic foundations of this association. ( J Am Heart Assoc. 2015;4:e001364 doi: 10.1161/JAHA.114.001364)
Key Words: heart failure • heart rate • risk factor
A ging of the population, worsening risk factor profile, andimproved care of acute cardiovascular disease (CVD)
have all led to an increase in the prevalence of heart failure(HF).1 Heart failure is associated with an unacceptably highmorbidity and mortality2 and imposes a significant economicburden, underscoring the need to identify high-risk individualsin order to tailor preventive and therapeutic measures.
Resting heart rate (RHR) is independently associated withprognosis among patients with prevalent HF and RHRlowering has been demonstrated to benefit patients with HFand reduced ejection fraction.3–5 Whereas, some studies havesuggested a positive association between baseline RHR andincident HF risk,6,7 others have only shown a sex-differenti-ated association,8 with uncertainties remaining about the
FromtheDepartmentofMedicine,EmoryUniversity,Atlanta,GA (H.K.,A.P.K., V.V.G.);DepartmentofPublicHealthandPrimaryCare,University ofCambridge,Cambridge,UK(S.K.); Department of Epidemiology andMedicine, University of Pittsburgh, Pittsburgh, PA (A.B.N.); Intramural Research Program, Laboratory of Epidemiology and PopulationSciences, National Institute on Aging, Bethesda, MD (T.B.H.); Departments of Medicine and Epidemiology & Biostatistics, University of California, San Francisco, CA(K.B.-D.); Institute of Public Health, School and Clinical Nutrition, University of Eastern Finland, Kuopio, Finland (J.K., J.A.L.); Center for Cardiovascular Innovation,Northwestern FeinbergSchool ofMedicine,Chicago, IL (M.G.); CardiologyDivision,University ofCalifornia LosAngeles, Los Angeles,CA (G.C.F.); Section ofGerontology andGeriatric Medicine, Wake Forest School of Medicine, Winston Salem, NC (S.B.K.); Division of Cardiology, Health Sciences Center, Stony Brook University, SUNY at StonyBrook, NY (J.B.).
Accompanying Appendices S1 and S2 are available at http://jaha.ahajournals.org/content/4/1/e001364/suppl/DC1This manuscript was prepared using CHS data obtained from the NHLBI Biologic Specimen and Data Repository Information Coordinating Center and does notnecessarily reflect the opinions or views of the CHS study or the NHLBI.
Correspondence to: Javed Butler, MD, MPH, Division of Cardiology, Health Sciences Center, Stony Brook University, T-16, Room 080, SUNY at Stony Brook, NY11794. E-mail: [email protected]
Received September 22, 2014; accepted December 11, 2014.
ª 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell. This is an open access article under the terms of the CreativeCommons Attribution-NonCommercial License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited and isnot used for commercial purposes.
DOI: 10.1161/JAHA.114.001364 Journal of the American Heart Association 1
ORIGINAL RESEARCH
by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from

shape of this association due to the small size of the priorinvestigations. Most studies have included individuals fromselect population9 or patients with pre-existing disease3 orusing drugs that modify heart rate.10 It is important to assessthe association of RHR with risk of HF prospectively in orderto also avoid the potential bias of reverse causality. In thisstudy, we sought to assess the association between RHR andincident HF in 3 population-based cohort studies by perform-ing an individual participant meta-analysis of these cohorts.To contextualize our findings, we also performed a systematicreview and meta-analysis of the published prospectiveevidence on the association of RHR and risk of incident HF.
Methods
Study PopulationsThe 3 cohort studies that were included were the Heath Agingand Body Composition (Health ABC) study, the CardiovascularHealth Study (CHS), and the Kuopio Ischemic Heart Disease(KIHD) study. The Health ABC Study is a community-basedcohort of 3075 individuals aged 70 to 79 years at incep-tion.11,12 Participants were identified from a random sampleof white Medicare beneficiaries and all age-eligible blackresidents in designated zip codes surrounding Pittsburgh, PAand Memphis, TN. To be eligible, participants had to report nodifficulty walking one-quarter of a mile or climbing 10 stairswithout resting. Exclusion criteria included difficulties withactivities of daily living, obvious cognitive impairment, orintention of moving within 3 years. Baseline data werecollected in 1997–1998.11,12 The design and rationale ofCHS has been previously published.13 Briefly, non-institution-alized individuals 65 to 100 years old were recruited fromMedicare eligibility lists and examined at 4 field centres inForsyth County, NC; Sacramento County, CA; AlleghenyCounty, PA; and Washington County, MD). An original cohortof 5201 participants was recruited in 1989–1990 and asecond cohort of 687 black participants was recruited in1992–1993 (total, 5888 participants; 2495 men, 3393women). KIHD study is a population-based study, represen-tative of men living in the city of Kuopio and its surroundingrural communities in Eastern Finland.18 The men were 42 to61 years of age during baseline examinations performedbetween March 20, 1984 and December 5, 1989. Of 3235potentially randomly selected eligible men, 2682 (83%)volunteered to participate in this study, 186 did not respondto the invitation, and 367 declined to give informed consent.18
Each cohort study was approved by its Institutional ResearchEthics Committee, and each participant gave written informedconsent.11,12,18
For the current analysis, we created an individual-levelpooled dataset from CHS, Health ABC study, and KIHD study
for participants without prevalent HF who did not have anymajor electrocardiographic abnormalities at baseline (ventric-ular conduction defect, major Q-wave abnormality, isolatedST-T wave abnormalities, atrial fibrillation, or atrio-ventricularblocks). Prevalent HF was adjudicated on the basis of self-report, medications, and review of medical records. From the5888 CHS participants we excluded those with prevalent HF(n=275) and individuals with major ECG abnormalities(N=1550). From the 3075 Health ABC participants, weexcluded those with prevalent HF (n=95) or inadequate datato adjudicate HF (n=45) and those with major ECG abnor-malities (n=1102) at baseline. From KIHD we excluded thosewith prevalent HF (n=194) and those with major ECGabnormalities (n=164). The final cohort for this analysiscomprised 7073 participants with non-missing data atbaseline on several HF risk factors including age, sex, bodymass index, diabetes status, history of hypertension, leftventricular hypertrophy, and serum creatinine levels.
Study OutcomesWe used 10 plus-year adjudicated outcomes from all 3prospective studies for this analysis. In the Health ABC andCHS studies, all participants were asked to report anyhospitalizations every 6 months and were asked directquestions about interim events. Medical records for over-night hospitalizations were reviewed at each site. All firstadmissions with an overnight stay that was confirmed asrelated to HF were classified as incident HF. Heart failurediagnosis was adjudicated based on symptoms, signs, chestradiograph results, and echocardiographic findings.13 Thecriteria required at least HF diagnosis from a physician andtreatment for HF.12 In addition, data on left ventricularejection fraction during the index HF hospitalization wasavailable in a subset of HF cases. All deaths were reviewedby each study’s diagnosis and disease ascertainmentcommittee and underlying causes of death were determinedby central adjudication. In the KIHD study, participants areunder continuous surveillance for the development of newCVD events, including new incident HF cases18. The sourcesof information on HF were based on hospital records andmedico-legal reports. The diagnostic classification of HFcases were coded according to the International Classifica-tion of Disease, Tenth Revision (ICD-10) codes (I00 to I99)and (I50.0 to I50.9, I11, I42.0 to I42.9). The diagnosis of HFwas based on a previous history of heart disease, physicalexamination by a doctor, laboratory investigations includingthe determination of natriuretic peptides, echocardiography,as well as electrocardiographic findings. Data on incidentacute coronary events and deaths were obtained bycomputer linkage to the national hospital discharge anddeath certificate registers.9
DOI: 10.1161/JAHA.114.001364 Journal of the American Heart Association 2
Resting Heart Rate and Risk of Heart Failure Khan et alORIG
INALRESEARCH
by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from
Study DefinitionsResting heart rate (bpm) was automatically measured from a12-lead electrocardiogram recorded in the morning as part ofthe baseline enrollment visit, along with fasting venous bloodsample collection. Race was self-reported. Hypertension wasdefined as self-reported history of physician diagnosis accom-panied by use of antihypertensive medications. Diabetesmellitus was considered present if the participant reported ahistory of diabetes mellitus or use of anti-hyperglycemicmedication. Smoking was defined as current, past (≥100lifetime cigarettes), or never. Left ventricular hypertrophy wasdiagnosed based on the following criteria; R amplitude >26 mmin either V5 or V6, or >20 mm in any of leads I, II, III, aVF, or>12 mm in lead aVL or R in V5 or V6 plus S amplitude in V1>35 mm. Prevalent HF was based on hospital records andmedico-legal reports. Prevalent coronary artery disease (CAD)was defined as: (1) history of surgical or percutaneousrevascularization; or (2) electrocardiographic evidence ofmyocardial infarction; or (3) self-reported history of myocardialinfarction or angina accompanied by use of anti-anginalmedications. Incident CAD was defined as hospitalization formyocardial infarction or angina pectoris, or elective revascu-larization. Prevalent vascular disease was defined as prevalent:(1) CAD; (2) cerebrovascular disease (history of stroke,transient ischemic attack, or carotid endarterectomy); or (3)PVD (history of intermittent claudication or vascular bypassor angioplasty).14,15 Incident vascular disease was defined asincident (1) CAD; (2) cerebro-vascular disease (stroke, tran-sient ischemic attack, or symptomatic carotid artery disease);(3) PVD; or (4) death due to cardiovascular causes.
Statistical AnalysisThe principal analyses were pre-specified to exclude partic-ipants with a history of HF and major ECG abnormalities atbaseline. Cross-sectional associations of RHR with variousrisk factors were assessed using linear regression modelsadjusted for cohort, age, and sex. The primary outcome wasincident HF, defined as first-ever nonfatal hospital admissionfor HF. Participants contributed only follow-up time torecorded first HF outcome. Time-to-event analyses wereconducted using Cox proportional hazard models, stratified bycohort and sex. The proportional hazards assumptions weretested as previously described and satisfied.16 To characterizeshapes of associations, multivariate fractional polynomialmodels were fitted to data. In secondary analyses of theindividual studies, the hazards were further adjusted forseveral potential confounders, including glucose, loge trigly-cerides, cholesterol, HDL-c, albumin, loge C-reactive protein(CRP). Subgroup analyses were conducted using interactiontests to assess statistical evidence of any differences inhazards across levels of pre-specified individual level charac-
teristics, including age at survey, smoking, history of diabetesmellitus, history of hypertension, history of cardiovasculardisease, left ventricular hypertrophy, history of anti-hyperten-sive medication use, body mass index, and systolic bloodpressure.
Meta-AnalysisA systematic review was conducted using a predefinedprotocol and in accordance with the PRISMA and MOOSEguidelines17,18 (Appendices S1 and S2). Prospective (cohortor nested case-control) studies of the association betweenresting heart rate and incident heart failure that werepublished up to March 2014 were sought using computer-based databases (MEDLINE, EMBASE, and Science CitationIndex). We crossed the term “heart rate” (and similar) with HF,left ventricular dysfunction (and similar terms) without anylanguage restrictions. Reference lists of the retrieved articleswere searched for additional articles. Studies were eligible forinclusion if they had at least 1 year of follow-up and hadrecruited participants from approximately general populations(ie, did not select participants on the basis of pre-existingdisease at baseline). Hazard ratios and risk ratios wereassumed to approximate the same underlying measure ofrelative risk (RR),19 henceforth referred to as risk ratios (RRs).Reported study-specific RRs were converted to a consistentcomparison as described previously.20 Note the log risk ratiofor a 1 SD change is equivalent to the log risk ratio for acomparison of extreme quarters divided by 2.54 assuming anormal distribution or that a transformation of the explanatoryvariable for which the risk ratio is based was normallydistributed. Risk estimates were transformed and pooled toinvolve comparisons between the top fourth and bottomfourth of the baseline levels of RHR. Study-specific RRs werecombined using a random-effects meta-analysis (subsidiaryanalyses used a fixed effect meta-analysis). Standard errors ofthe log risk estimates were calculated using publishedconfidence limits and were standardized in the same way.Consistency of findings among studies was assessed byCochran’s Q statistic (v2 test) and the I2 statistic.21,22 Severalstudy-level characteristics were pre-specified as characteris-tics for assessment of heterogeneity, which was conductedusing stratified analyses and random effects meta-regres-sion.22 All statistical analyses were conducted using Stataversion 13 (Stata Corp, College Station, TX).
Results
Study PopulationTable 1 summarizes baseline characteristics of the 4095participants in the CHS, 1269 participants in Health ABC
DOI: 10.1161/JAHA.114.001364 Journal of the American Heart Association 3
Resting Heart Rate and Risk of Heart Failure Khan et alORIG
INALRESEARCH
by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from
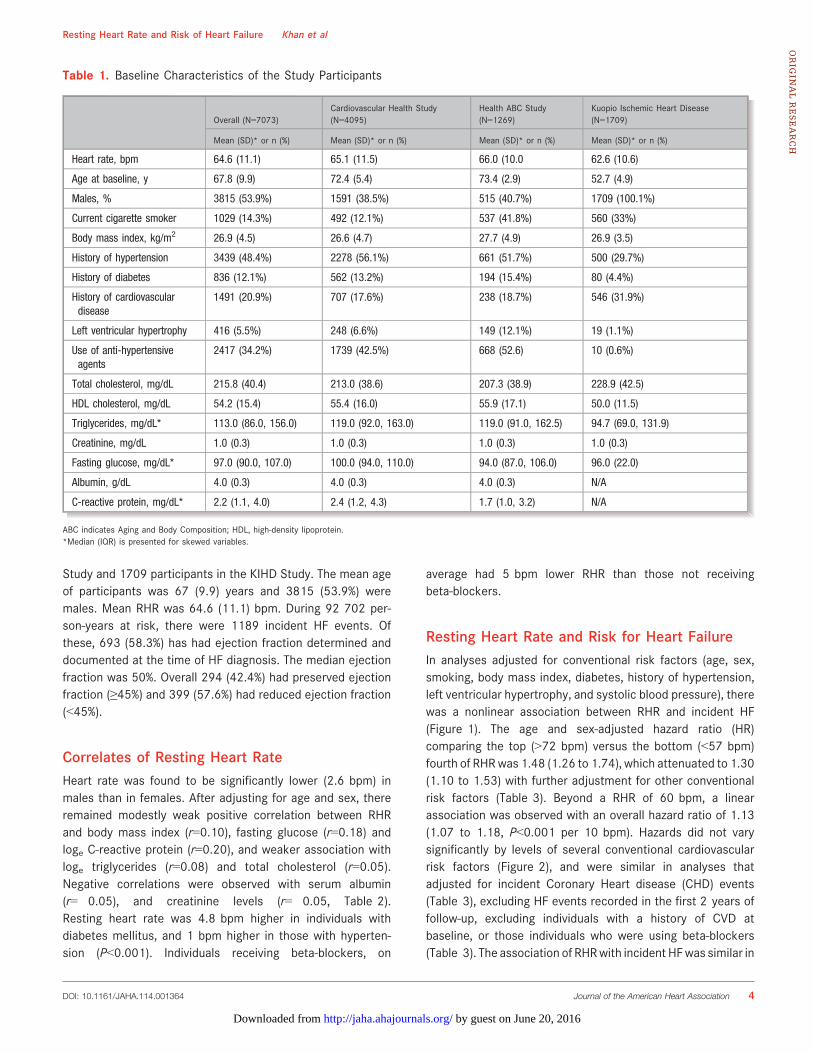
Study and 1709 participants in the KIHD Study. The mean ageof participants was 67 (9.9) years and 3815 (53.9%) weremales. Mean RHR was 64.6 (11.1) bpm. During 92 702 per-son-years at risk, there were 1189 incident HF events. Ofthese, 693 (58.3%) has had ejection fraction determined anddocumented at the time of HF diagnosis. The median ejectionfraction was 50%. Overall 294 (42.4%) had preserved ejectionfraction (≥45%) and 399 (57.6%) had reduced ejection fraction(<45%).
Correlates of Resting Heart RateHeart rate was found to be significantly lower (2.6 bpm) inmales than in females. After adjusting for age and sex, thereremained modestly weak positive correlation between RHRand body mass index (r=0.10), fasting glucose (r=0.18) andloge C-reactive protein (r=0.20), and weaker association withloge triglycerides (r=0.08) and total cholesterol (r=0.05).Negative correlations were observed with serum albumin(r=�0.05), and creatinine levels (r=�0.05, Table 2).Resting heart rate was 4.8 bpm higher in individuals withdiabetes mellitus, and 1 bpm higher in those with hyperten-sion (P<0.001). Individuals receiving beta-blockers, on
average had 5 bpm lower RHR than those not receivingbeta-blockers.
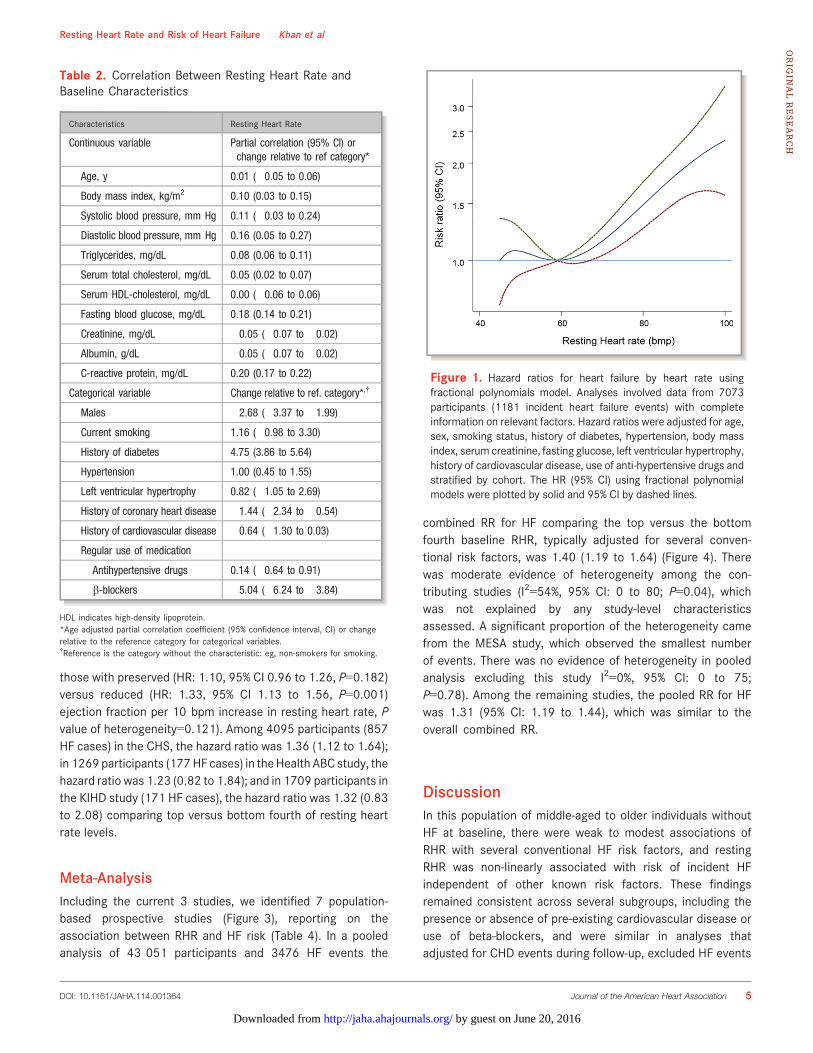
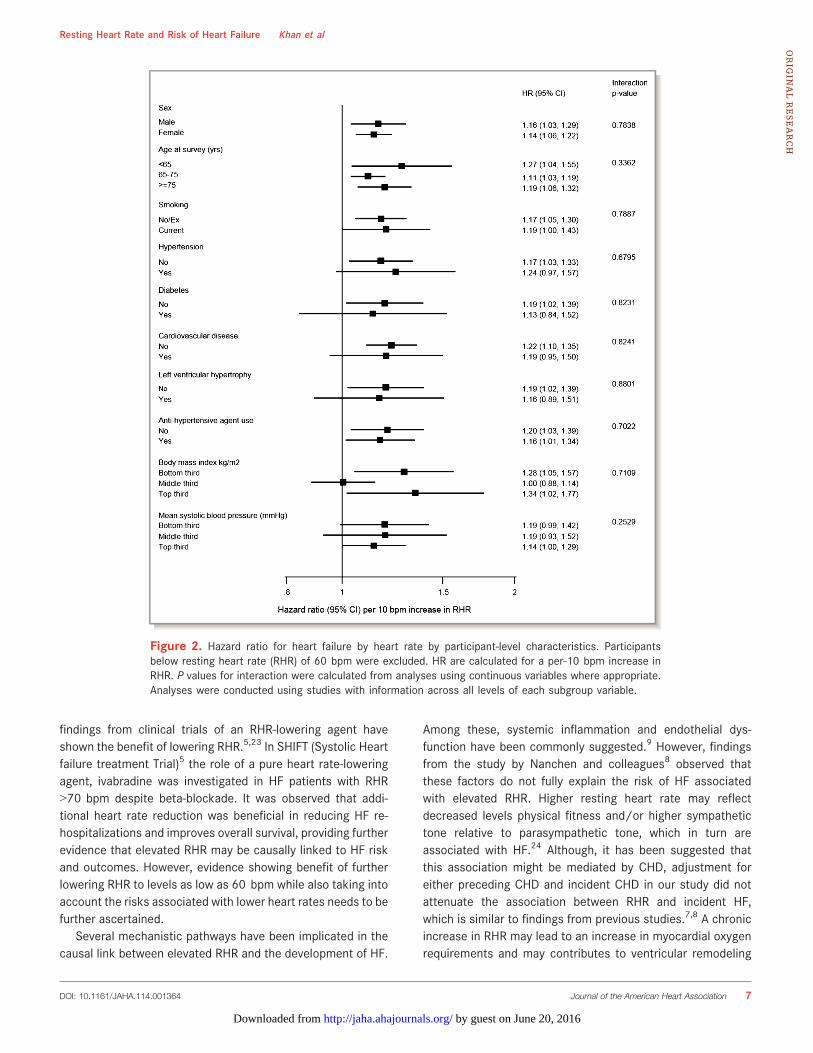
Resting Heart Rate and Risk for Heart FailureIn analyses adjusted for conventional risk factors (age, sex,smoking, body mass index, diabetes, history of hypertension,left ventricular hypertrophy, and systolic blood pressure), therewas a nonlinear association between RHR and incident HF(Figure 1). The age and sex-adjusted hazard ratio (HR)comparing the top (>72 bpm) versus the bottom (<57 bpm)fourth of RHRwas 1.48 (1.26 to 1.74), which attenuated to 1.30(1.10 to 1.53) with further adjustment for other conventionalrisk factors (Table 3). Beyond a RHR of 60 bpm, a linearassociation was observed with an overall hazard ratio of 1.13(1.07 to 1.18, P<0.001 per 10 bpm). Hazards did not varysignificantly by levels of several conventional cardiovascularrisk factors (Figure 2), and were similar in analyses thatadjusted for incident Coronary Heart disease (CHD) events(Table 3), excluding HF events recorded in the first 2 years offollow-up, excluding individuals with a history of CVD atbaseline, or those individuals who were using beta-blockers(Table 3). The association of RHRwith incident HFwas similar in
Table 1. Baseline Characteristics of the Study Participants
Overall (N=7073)Cardiovascular Health Study(N=4095)
Health ABC Study(N=1269)
Kuopio Ischemic Heart Disease(N=1709)
Mean (SD)* or n (%) Mean (SD)* or n (%) Mean (SD)* or n (%) Mean (SD)* or n (%)
Heart rate, bpm 64.6 (11.1) 65.1 (11.5) 66.0 (10.0 62.6 (10.6)
Age at baseline, y 67.8 (9.9) 72.4 (5.4) 73.4 (2.9) 52.7 (4.9)
Males, % 3815 (53.9%) 1591 (38.5%) 515 (40.7%) 1709 (100.1%)
Current cigarette smoker 1029 (14.3%) 492 (12.1%) 537 (41.8%) 560 (33%)
Body mass index, kg/m2 26.9 (4.5) 26.6 (4.7) 27.7 (4.9) 26.9 (3.5)
History of hypertension 3439 (48.4%) 2278 (56.1%) 661 (51.7%) 500 (29.7%)
History of diabetes 836 (12.1%) 562 (13.2%) 194 (15.4%) 80 (4.4%)
History of cardiovasculardisease
1491 (20.9%) 707 (17.6%) 238 (18.7%) 546 (31.9%)
Left ventricular hypertrophy 416 (5.5%) 248 (6.6%) 149 (12.1%) 19 (1.1%)
Use of anti-hypertensiveagents
2417 (34.2%) 1739 (42.5%) 668 (52.6) 10 (0.6%)
Total cholesterol, mg/dL 215.8 (40.4) 213.0 (38.6) 207.3 (38.9) 228.9 (42.5)
HDL cholesterol, mg/dL 54.2 (15.4) 55.4 (16.0) 55.9 (17.1) 50.0 (11.5)
Triglycerides, mg/dL* 113.0 (86.0, 156.0) 119.0 (92.0, 163.0) 119.0 (91.0, 162.5) 94.7 (69.0, 131.9)
Creatinine, mg/dL 1.0 (0.3) 1.0 (0.3) 1.0 (0.3) 1.0 (0.3)
Fasting glucose, mg/dL* 97.0 (90.0, 107.0) 100.0 (94.0, 110.0) 94.0 (87.0, 106.0) 96.0 (22.0)
Albumin, g/dL 4.0 (0.3) 4.0 (0.3) 4.0 (0.3) N/A
C-reactive protein, mg/dL* 2.2 (1.1, 4.0) 2.4 (1.2, 4.3) 1.7 (1.0, 3.2) N/A
ABC indicates Aging and Body Composition; HDL, high-density lipoprotein.*Median (IQR) is presented for skewed variables.
DOI: 10.1161/JAHA.114.001364 Journal of the American Heart Association 4
Resting Heart Rate and Risk of Heart Failure Khan et alORIG
INALRESEARCH
by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from
those with preserved (HR: 1.10, 95% CI 0.96 to 1.26, P=0.182)versus reduced (HR: 1.33, 95% CI 1.13 to 1.56, P=0.001)ejection fraction per 10 bpm increase in resting heart rate, Pvalue of heterogeneity=0.121). Among 4095 participants (857HF cases) in the CHS, the hazard ratio was 1.36 (1.12 to 1.64);in 1269 participants (177HF cases) in theHealth ABC study, thehazard ratio was 1.23 (0.82 to 1.84); and in 1709 participants inthe KIHD study (171 HF cases), the hazard ratio was 1.32 (0.83to 2.08) comparing top versus bottom fourth of resting heartrate levels.
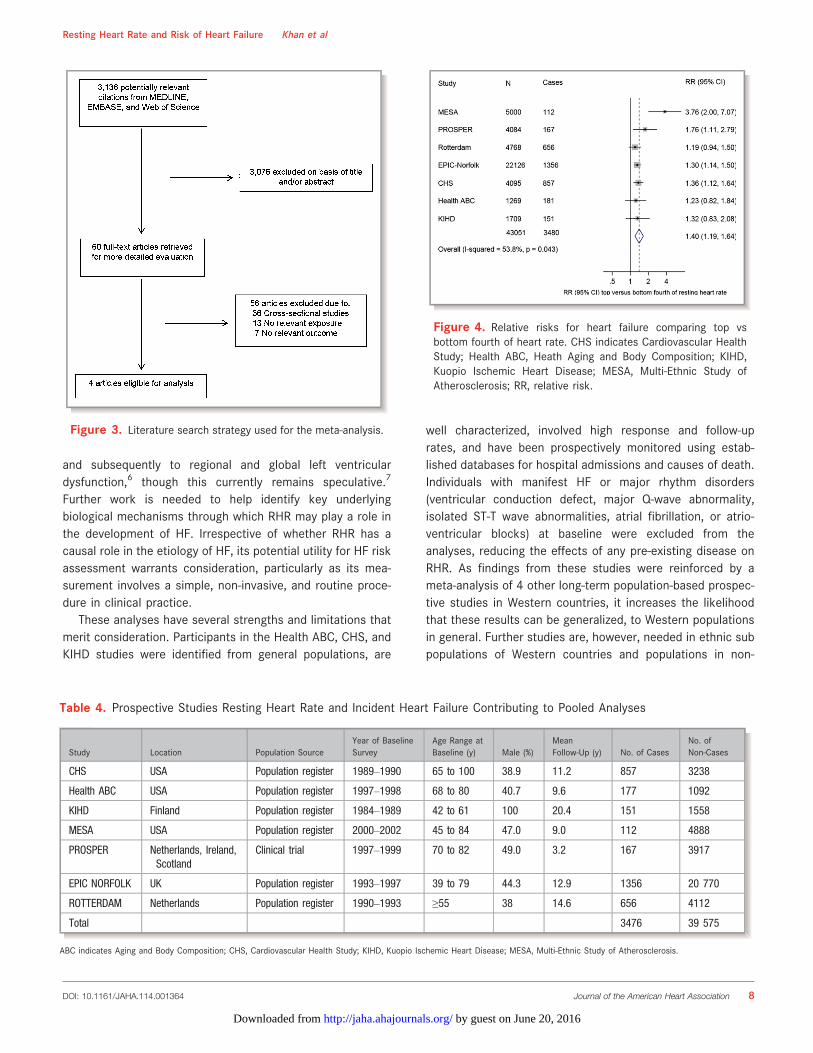
Meta-AnalysisIncluding the current 3 studies, we identified 7 population-based prospective studies (Figure 3), reporting on theassociation between RHR and HF risk (Table 4). In a pooledanalysis of 43 051 participants and 3476 HF events the
combined RR for HF comparing the top versus the bottomfourth baseline RHR, typically adjusted for several conven-tional risk factors, was 1.40 (1.19 to 1.64) (Figure 4). Therewas moderate evidence of heterogeneity among the con-tributing studies (I2=54%, 95% CI: 0 to 80; P=0.04), whichwas not explained by any study-level characteristicsassessed. A significant proportion of the heterogeneity camefrom the MESA study, which observed the smallest numberof events. There was no evidence of heterogeneity in pooledanalysis excluding this study I2=0%, 95% CI: 0 to 75;P=0.78). Among the remaining studies, the pooled RR for HFwas 1.31 (95% CI: 1.19 to 1.44), which was similar to theoverall combined RR.
DiscussionIn this population of middle-aged to older individuals withoutHF at baseline, there were weak to modest associations ofRHR with several conventional HF risk factors, and restingRHR was non-linearly associated with risk of incident HFindependent of other known risk factors. These findingsremained consistent across several subgroups, including thepresence or absence of pre-existing cardiovascular disease oruse of beta-blockers, and were similar in analyses thatadjusted for CHD events during follow-up, excluded HF events
Table 2. Correlation Between Resting Heart Rate andBaseline Characteristics
Characteristics Resting Heart Rate
Continuous variable Partial correlation (95% CI) orchange relative to ref category*
Age, y 0.01 (�0.05 to 0.06)
Body mass index, kg/m2 0.10 (0.03 to 0.15)
Systolic blood pressure, mm Hg 0.11 (�0.03 to 0.24)
Diastolic blood pressure, mm Hg 0.16 (0.05 to 0.27)
Triglycerides, mg/dL 0.08 (0.06 to 0.11)
Serum total cholesterol, mg/dL 0.05 (0.02 to 0.07)
Serum HDL-cholesterol, mg/dL 0.00 (�0.06 to 0.06)
Fasting blood glucose, mg/dL 0.18 (0.14 to 0.21)
Creatinine, mg/dL �0.05 (�0.07 to �0.02)
Albumin, g/dL �0.05 (�0.07 to �0.02)
C-reactive protein, mg/dL 0.20 (0.17 to 0.22)
Categorical variable Change relative to ref. category*,†
Males �2.68 (�3.37 to �1.99)
Current smoking 1.16 (�0.98 to 3.30)
History of diabetes 4.75 (3.86 to 5.64)
Hypertension 1.00 (0.45 to 1.55)
Left ventricular hypertrophy 0.82 (�1.05 to 2.69)
History of coronary heart disease �1.44 (�2.34 to �0.54)
History of cardiovascular disease �0.64 (�1.30 to 0.03)
Regular use of medication
Antihypertensive drugs 0.14 (�0.64 to 0.91)
b-blockers �5.04 (�6.24 to �3.84)
HDL indicates high-density lipoprotein.*Age adjusted partial correlation coefficient (95% confidence interval, CI) or changerelative to the reference category for categorical variables.†Reference is the category without the characteristic: eg, non-smokers for smoking.
Figure 1. Hazard ratios for heart failure by heart rate usingfractional polynomials model. Analyses involved data from 7073participants (1181 incident heart failure events) with completeinformation on relevant factors. Hazard ratios were adjusted for age,sex, smoking status, history of diabetes, hypertension, body massindex, serum creatinine, fasting glucose, left ventricular hypertrophy,history of cardiovascular disease, use of anti-hypertensive drugs andstratified by cohort. The HR (95% CI) using fractional polynomialmodels were plotted by solid and 95% CI by dashed lines.
DOI: 10.1161/JAHA.114.001364 Journal of the American Heart Association 5
Resting Heart Rate and Risk of Heart Failure Khan et alORIG
INALRESEARCH
by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from
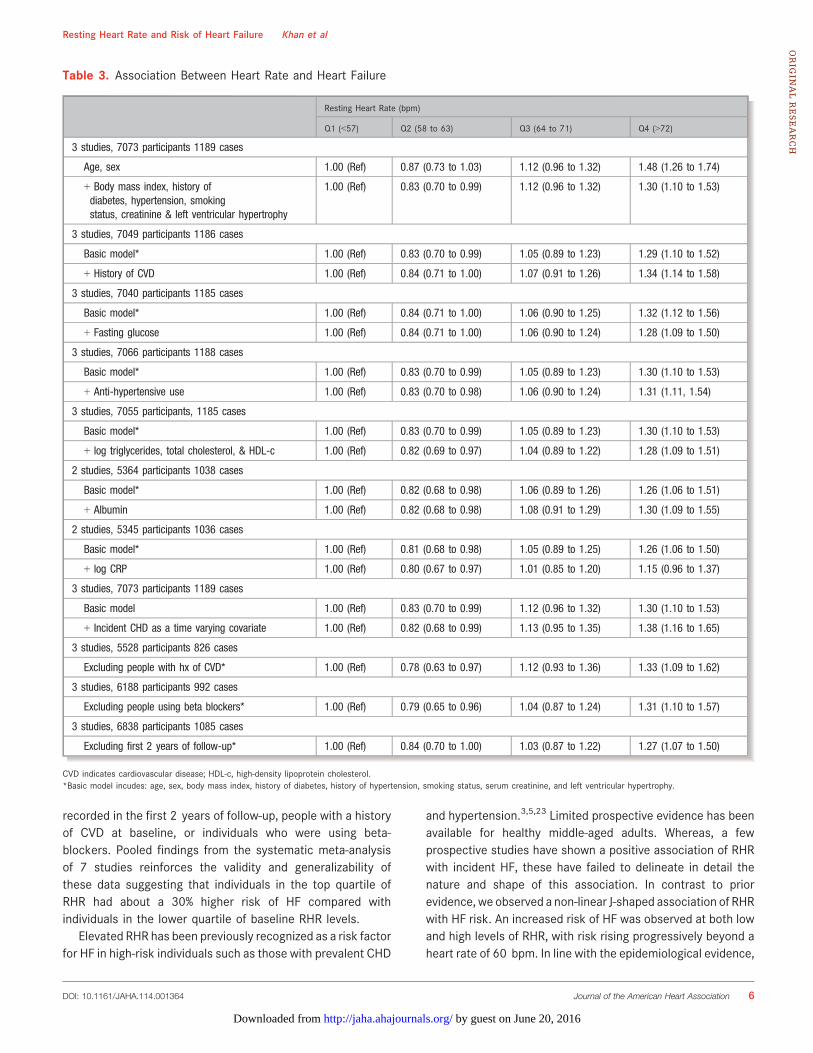
recorded in the first 2 years of follow-up, people with a historyof CVD at baseline, or individuals who were using beta-blockers. Pooled findings from the systematic meta-analysisof 7 studies reinforces the validity and generalizability ofthese data suggesting that individuals in the top quartile ofRHR had about a 30% higher risk of HF compared withindividuals in the lower quartile of baseline RHR levels.
Elevated RHR has been previously recognized as a risk factorfor HF in high-risk individuals such as those with prevalent CHD
and hypertension.3,5,23 Limited prospective evidence has beenavailable for healthy middle-aged adults. Whereas, a fewprospective studies have shown a positive association of RHRwith incident HF, these have failed to delineate in detail thenature and shape of this association. In contrast to priorevidence, we observed a non-linear J-shaped association of RHRwith HF risk. An increased risk of HF was observed at both lowand high levels of RHR, with risk rising progressively beyond aheart rate of 60 bpm. In line with the epidemiological evidence,
Table 3. Association Between Heart Rate and Heart Failure
Resting Heart Rate (bpm)
Q1 (<57) Q2 (58 to 63) Q3 (64 to 71) Q4 (>72)
3 studies, 7073 participants 1189 cases
Age, sex 1.00 (Ref) 0.87 (0.73 to 1.03) 1.12 (0.96 to 1.32) 1.48 (1.26 to 1.74)
+ Body mass index, history ofdiabetes, hypertension, smokingstatus, creatinine & left ventricular hypertrophy
1.00 (Ref) 0.83 (0.70 to 0.99) 1.12 (0.96 to 1.32) 1.30 (1.10 to 1.53)
3 studies, 7049 participants 1186 cases
Basic model* 1.00 (Ref) 0.83 (0.70 to 0.99) 1.05 (0.89 to 1.23) 1.29 (1.10 to 1.52)
+ History of CVD 1.00 (Ref) 0.84 (0.71 to 1.00) 1.07 (0.91 to 1.26) 1.34 (1.14 to 1.58)
3 studies, 7040 participants 1185 cases
Basic model* 1.00 (Ref) 0.84 (0.71 to 1.00) 1.06 (0.90 to 1.25) 1.32 (1.12 to 1.56)
+ Fasting glucose 1.00 (Ref) 0.84 (0.71 to 1.00) 1.06 (0.90 to 1.24) 1.28 (1.09 to 1.50)
3 studies, 7066 participants 1188 cases
Basic model* 1.00 (Ref) 0.83 (0.70 to 0.99) 1.05 (0.89 to 1.23) 1.30 (1.10 to 1.53)
+ Anti-hypertensive use 1.00 (Ref) 0.83 (0.70 to 0.98) 1.06 (0.90 to 1.24) 1.31 (1.11, 1.54)
3 studies, 7055 participants, 1185 cases
Basic model* 1.00 (Ref) 0.83 (0.70 to 0.99) 1.05 (0.89 to 1.23) 1.30 (1.10 to 1.53)
+ log triglycerides, total cholesterol, & HDL-c 1.00 (Ref) 0.82 (0.69 to 0.97) 1.04 (0.89 to 1.22) 1.28 (1.09 to 1.51)
2 studies, 5364 participants 1038 cases
Basic model* 1.00 (Ref) 0.82 (0.68 to 0.98) 1.06 (0.89 to 1.26) 1.26 (1.06 to 1.51)
+ Albumin 1.00 (Ref) 0.82 (0.68 to 0.98) 1.08 (0.91 to 1.29) 1.30 (1.09 to 1.55)
2 studies, 5345 participants 1036 cases
Basic model* 1.00 (Ref) 0.81 (0.68 to 0.98) 1.05 (0.89 to 1.25) 1.26 (1.06 to 1.50)
+ log CRP 1.00 (Ref) 0.80 (0.67 to 0.97) 1.01 (0.85 to 1.20) 1.15 (0.96 to 1.37)
3 studies, 7073 participants 1189 cases
Basic model 1.00 (Ref) 0.83 (0.70 to 0.99) 1.12 (0.96 to 1.32) 1.30 (1.10 to 1.53)
+ Incident CHD as a time varying covariate 1.00 (Ref) 0.82 (0.68 to 0.99) 1.13 (0.95 to 1.35) 1.38 (1.16 to 1.65)
3 studies, 5528 participants 826 cases
Excluding people with hx of CVD* 1.00 (Ref) 0.78 (0.63 to 0.97) 1.12 (0.93 to 1.36) 1.33 (1.09 to 1.62)
3 studies, 6188 participants 992 cases
Excluding people using beta blockers* 1.00 (Ref) 0.79 (0.65 to 0.96) 1.04 (0.87 to 1.24) 1.31 (1.10 to 1.57)
3 studies, 6838 participants 1085 cases
Excluding first 2 years of follow-up* 1.00 (Ref) 0.84 (0.70 to 1.00) 1.03 (0.87 to 1.22) 1.27 (1.07 to 1.50)
CVD indicates cardiovascular disease; HDL-c, high-density lipoprotein cholesterol.*Basic model incudes: age, sex, body mass index, history of diabetes, history of hypertension, smoking status, serum creatinine, and left ventricular hypertrophy.
DOI: 10.1161/JAHA.114.001364 Journal of the American Heart Association 6
Resting Heart Rate and Risk of Heart Failure Khan et alORIG
INALRESEARCH
by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from
findings from clinical trials of an RHR-lowering agent haveshown the benefit of lowering RHR.5,23 In SHIFT (Systolic Heartfailure treatment Trial)5 the role of a pure heart rate-loweringagent, ivabradine was investigated in HF patients with RHR>70 bpm despite beta-blockade. It was observed that addi-tional heart rate reduction was beneficial in reducing HF re-hospitalizations and improves overall survival, providing furtherevidence that elevated RHR may be causally linked to HF riskand outcomes. However, evidence showing benefit of furtherlowering RHR to levels as low as 60 bpm while also taking intoaccount the risks associated with lower heart rates needs to befurther ascertained.
Several mechanistic pathways have been implicated in thecausal link between elevated RHR and the development of HF.
Among these, systemic inflammation and endothelial dys-function have been commonly suggested.9 However, findingsfrom the study by Nanchen and colleagues8 observed thatthese factors do not fully explain the risk of HF associatedwith elevated RHR. Higher resting heart rate may reflectdecreased levels physical fitness and/or higher sympathetictone relative to parasympathetic tone, which in turn areassociated with HF.24 Although, it has been suggested thatthis association might be mediated by CHD, adjustment foreither preceding CHD and incident CHD in our study did notattenuate the association between RHR and incident HF,which is similar to findings from previous studies.7,8 A chronicincrease in RHR may lead to an increase in myocardial oxygenrequirements and may contributes to ventricular remodeling
Figure 2. Hazard ratio for heart failure by heart rate by participant-level characteristics. Participantsbelow resting heart rate (RHR) of 60 bpm were excluded. HR are calculated for a per-10 bpm increase inRHR. P values for interaction were calculated from analyses using continuous variables where appropriate.Analyses were conducted using studies with information across all levels of each subgroup variable.
DOI: 10.1161/JAHA.114.001364 Journal of the American Heart Association 7
Resting Heart Rate and Risk of Heart Failure Khan et alORIG
INALRESEARCH
by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from
and subsequently to regional and global left ventriculardysfunction,6 though this currently remains speculative.7
Further work is needed to help identify key underlyingbiological mechanisms through which RHR may play a role inthe development of HF. Irrespective of whether RHR has acausal role in the etiology of HF, its potential utility for HF riskassessment warrants consideration, particularly as its mea-surement involves a simple, non-invasive, and routine proce-dure in clinical practice.
These analyses have several strengths and limitations thatmerit consideration. Participants in the Health ABC, CHS, andKIHD studies were identified from general populations, are
well characterized, involved high response and follow-uprates, and have been prospectively monitored using estab-lished databases for hospital admissions and causes of death.Individuals with manifest HF or major rhythm disorders(ventricular conduction defect, major Q-wave abnormality,isolated ST-T wave abnormalities, atrial fibrillation, or atrio-ventricular blocks) at baseline were excluded from theanalyses, reducing the effects of any pre-existing disease onRHR. As findings from these studies were reinforced by ameta-analysis of 4 other long-term population-based prospec-tive studies in Western countries, it increases the likelihoodthat these results can be generalized, to Western populationsin general. Further studies are, however, needed in ethnic subpopulations of Western countries and populations in non-
Figure 3. Literature search strategy used for the meta-analysis.
Table 4. Prospective Studies Resting Heart Rate and Incident Heart Failure Contributing to Pooled Analyses
Study Location Population SourceYear of BaselineSurvey
Age Range atBaseline (y) Male (%)
MeanFollow-Up (y) No. of Cases
No. ofNon-Cases
CHS USA Population register 1989–1990 65 to 100 38.9 11.2 857 3238
Health ABC USA Population register 1997–1998 68 to 80 40.7 9.6 177 1092
KIHD Finland Population register 1984–1989 42 to 61 100 20.4 151 1558
MESA USA Population register 2000–2002 45 to 84 47.0 9.0 112 4888
PROSPER Netherlands, Ireland,Scotland
Clinical trial 1997–1999 70 to 82 49.0 3.2 167 3917
EPIC NORFOLK UK Population register 1993–1997 39 to 79 44.3 12.9 1356 20 770
ROTTERDAM Netherlands Population register 1990–1993 ≥55 38 14.6 656 4112
Total 3476 39 575
ABC indicates Aging and Body Composition; CHS, Cardiovascular Health Study; KIHD, Kuopio Ischemic Heart Disease; MESA, Multi-Ethnic Study of Atherosclerosis.
Figure 4. Relative risks for heart failure comparing top vsbottom fourth of heart rate. CHS indicates Cardiovascular HealthStudy; Health ABC, Heath Aging and Body Composition; KIHD,Kuopio Ischemic Heart Disease; MESA, Multi-Ethnic Study ofAtherosclerosis; RR, relative risk.
Resting Heart Rate and Risk of Heart Failure Khan et al
DOI: 10.1161/JAHA.114.001364 Journal of the American Heart Association 8
by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from

Western countries. Repeat measurements of RHR were notavailable, preventing the quantification of the extent of within-person variability in RHR measurements. Also, individualpatient-level data was only available for 3 of the 7 cohorts,further limiting the participant-level analysis that could beshown across all cohorts.
In conclusion, in Western populations there is a non-linearassociation between resting heart rate and risk of incident HF,which is independent of conventional HF risk factors. Furtherassessment of the possible role of RHR reduction in HFprevention is warranted.
Author ContributionsDr(s) Butler and Khan had full access to all of the data inthe study and take responsibility for the integrity of the dataand the accuracy of the data analysis. Study concept anddesign: Khan, Kalogeropoulos, Laukkanen, Butler. Acquisi-tion of data: Butler, Harris, Kritchevsky, Khan, Kunutsor,Laukkanen. Analysis and interpretation of data: Kalogeropo-ulos, Kunutsor, Khan, Laukkanen, Butler. Drafting of themanuscript: Butler, Khan, Kunutsor. Critical revision of themanuscript for important intellectual content: Bibbins-Domingo,Butler, Fonarow, Gheorghiade, Georgiopoulou, Harris, Kalogero-poulos, Kauhanen, Khan, Kunutsor, Laukkanen, Newman.Statistical analysis: Khan. Obtained funding: Butler, Kritchevsky,Laukkanen. Study supervision: Butler, Laukkanen.
Sources of FundingCardiovascular Health Study: This research was supported bycontract numbers N01-HC-85079 through N01-HC-85086,N01-HC-35129, N01 HC-15103, N01 HC-55222, N01-HC-75150, N01-HC-45133, grant U01 HL080295 from theNational Heart, Lung, and Blood Institute, with additionalcontribution from the National Institute of NeurologicalDisorders and Stroke. A full list of the Cardiovascular HealthStudy investigators and institutions can be found at http://www.chs-nhlbi.org/pi.htm. Health ABC study: This researchwas supported by National Institute on Aging (NIA) ContractsN01-AG-6-2101; N01-AG-6-2103; N01-AG-6-2106; NIA grantR01-AG028050, NINR grant R01-NR012459 and supported inpart by the Intramural Research Program of the NIH, NationalInstitute on Aging. Kuopio Ischemic Heart Disease study(KIHD): This research was supported by Academy of Finland,Helsinki, Finland; City of Kuopio, Kuopio, Finland; FinnishMedical Foundation, Helsinki, Finland, and Finnish CulturalFoundation, Helsinki, Finland https://www.uef.fi/en/nutri-tionepidemiologists/kihd. The contents of this paper aresolely the responsibility of the authors and do not representthe views of the Sponsors. The sponsors did not participate in
the design and conduct of the study; collection, management,analysis, and interpretation of the data; or preparation of themanuscript.
DisclosuresNone.
References1. Heidenreich PA, Trogdon JG, Khavjou OA, Butler J, Dracup K, Ezekowitz MD,
Finkelstein EA, Hong Y, Johnston SC, Khera A, Lloyd-Jones DM, Nelson SA,Nichol G, Orenstein D, Wilson PWF, Woo YJ. Forecasting the future ofcardiovascular disease in the United States: a policy statement from theAmerican Heart Association. Circulation. 2011;123:933–944.
2. Bleumink GS, Knetsch AM, Sturkenboom MCJM, Straus SMJM, Hofman A,Deckers JW, Witteman JCM, Stricker BHC. Quantifying the heart failureepidemic: prevalence, incidence rate, lifetime risk and prognosis of heartfailure The Rotterdam Study. Eur Heart J. 2004;25:1614–1619.
3. Butler J, Kalogeropoulos A, Georgiopoulou V, Belue R, Rodondi N, Garcia M,Bauer DC, Satterfield S, Smith AL, Vaccarino V, Newman AB, Harris TB, WilsonPWF, Kritchevsky SB. Incident heart failure prediction in the elderly: the HealthABC Heart Failure Score. Circ Heart Fail. 2008;1:125–133.
4. Ferrari R. The story of the heartbeat, I: part I—heart rate: the rhythm of life.Eur Heart J. 2012;33:4–5.
5. B€ohm M, Swedberg K, Komajda M, Borer JS, Ford I, Dubost-Brama A,Lerebours G, Tavazzi L; SHIFT Investigators. Heart rate as a risk factor inchronic heart failure (SHIFT): the association between heart rate and outcomesin a randomised placebo-controlled trial. Lancet. 2010;376:886–894.
6. Opdahl A, Ambale Venkatesh B, Fernandes VRS, Wu CO, Nasir K, Choi E-Y,Almeida ALC, Rosen B, Carvalho B, Edvardsen T, Bluemke DA, Lima JAC.Resting heart rate as predictor for left ventricular dysfunction and heart failure:MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll Cardiol.2014;63:1182–1189.
7. Pfister R, Michels G, Sharp SJ, Luben R, Wareham NJ, Khaw K-T. Resting heartrate and incident heart failure in apparently healthy men and women in theEPIC-Norfolk study. Eur J Heart Fail. 2012;14:1163–1170.
8. Nanchen D, Leening MJG, Locatelli I, Cornuz J, Kors JA, Heeringa J, Deckers JW,Hofman A, Franco OH, Stricker BHC, Witteman JCM, Dehghan A. Resting heartrate and the risk of heart failure in healthy adults: the Rotterdam Study. CircHeart Fail. 2013;6:403–410.
9. Diaz A, Bourassa MG, Guertin M-C, Tardif J-C. Long-term prognostic value ofresting heart rate in patients with suspected or proven coronary arterydisease. Eur Heart J. 2005;26:967–974.
10. Rautaharju PM, Prineas RJ, Wood J, Zhang Z-M, Crow R, Heiss G. Electrocar-diographic predictors of new-onset heart failure in men and in women free ofcoronary heart disease (from the Atherosclerosis in Communities [ARIC]Study). Am J Cardiol. 2007;100:1437–1441.
11. Kalogeropoulos A, Georgiopoulou V, Kritchevsky SB, Psaty BM, Smith NL,Newman AB, Rodondi N, Satterfield S, Bauer DC, Bibbins-Domingo K, SmithAL, Wilson PWF, Vasan RS, Harris TB, Butler J. Epidemiology of incident heartfailure in a contemporary elderly cohort: the Health, Aging, and BodyComposition study. Arch Intern Med. 2009;169:708–715.
12. Rodondi N, Newman AB, Vittinghoff E, de Rekeneire N, Satterfield S, HarrisTB, Bauer DC. Subclinical hypothyroidism and the risk of heart failure,other cardiovascular events, and death. Arch Intern Med. 2005;165:2460–2466.
13. Fried LP, Borhani NO, Enright P, Furberg CD, Gardin JM, Kronmal RA, Kuller LH,Manolio TA, Mittelmark MB, Newman A. The Cardiovascular Health Study:design and rationale. Ann Epidemiol. 1991;1:263–276.
14. Cesari M, Penninx BWJH, Newman AB, Kritchevsky SB, Nicklas BJ, Sutton-Tyrrell K, Tracy RP, Rubin SM, Harris TB, Pahor M. Inflammatory markers andcardiovascular disease (The Health, Aging and Body Composition [Health ABC]Study). Am J Cardiol. 2003;92:522–528.
15. Newman AB, Simonsick EM, Naydeck BL, Boudreau RM, Kritchevsky SB,Nevitt MC, Pahor M, Satterfield S, Brach JS, Studenski SA, Harris TB.Association of long-distance corridor walk performance with mortality,cardiovascular disease, mobility limitation, and disability. JAMA. 2006;295:2018–2026.
16. Thompson S, Kaptoge S, White I, Wood A, Perry P, Danesh J. Statistical meth-ods for the time-to-event analysis of individual participant data from multipleepidemiological studies. Int J Epidemiol. 2010;39:1345–1359.
DOI: 10.1161/JAHA.114.001364 Journal of the American Heart Association 9
Resting Heart Rate and Risk of Heart Failure Khan et alORIG
INALRESEARCH
by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from

17. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items forsystematic reviews and meta-analyses: the PRISMA statement. BMJ.2009;339:b2535.
18. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, Moher D,Becker BJ, Sipe TA, Thacker SB. Meta-analysis of observational studies inepidemiology: a proposal for reporting. Meta-analysis Of Observational Studiesin Epidemiology (MOOSE) group. JAMA. 2000;283:2008–2012.
19. Symons MJ, Moore DT. Hazard rate ratio and prospective epidemiologicalstudies. J Clin Epidemiol. 2002;55:893–899.
20. Chene G, Thompson SG. Methods for summarizing the risk associations ofquantitative variables in epidemiologic studies in a consistent form. Am JEpidemiol. 1996;144:610–621.
21. Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency inmeta-analyses. BMJ. 2003;327:557–560.
22. Thompson SG, Sharp SJ. Explaining heterogeneity in meta-analysis: acomparison of methods. Stat Med. 1999;18:2693–2708.
23. Fox K, Ford I, Steg PG, Tendera M, Robertson M, Ferrari R; BEAUTIFULinvestigators. Heart rate as a prognostic risk factor in patients with coronaryartery disease and left-ventricular systolic dysfunction (BEAUTIFUL): asubgroup analysis of a randomised controlled trial. Lancet. 2008;372:817–821.
24. Fox K, Borer JS, Camm AJ, Danchin N, Ferrari R, Lopez Sendon JL, Steg PG,Tardif J-C, Tavazzi L, Tendera M; Heart Rate Working Group. Resting heart ratein cardiovascular disease. J Am Coll Cardiol. 2007;50:823–830.
DOI: 10.1161/JAHA.114.001364 Journal of the American Heart Association 10
Resting Heart Rate and Risk of Heart Failure Khan et alORIG
INALRESEARCH
by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from
SUPPLEMENTAL MATERIAL

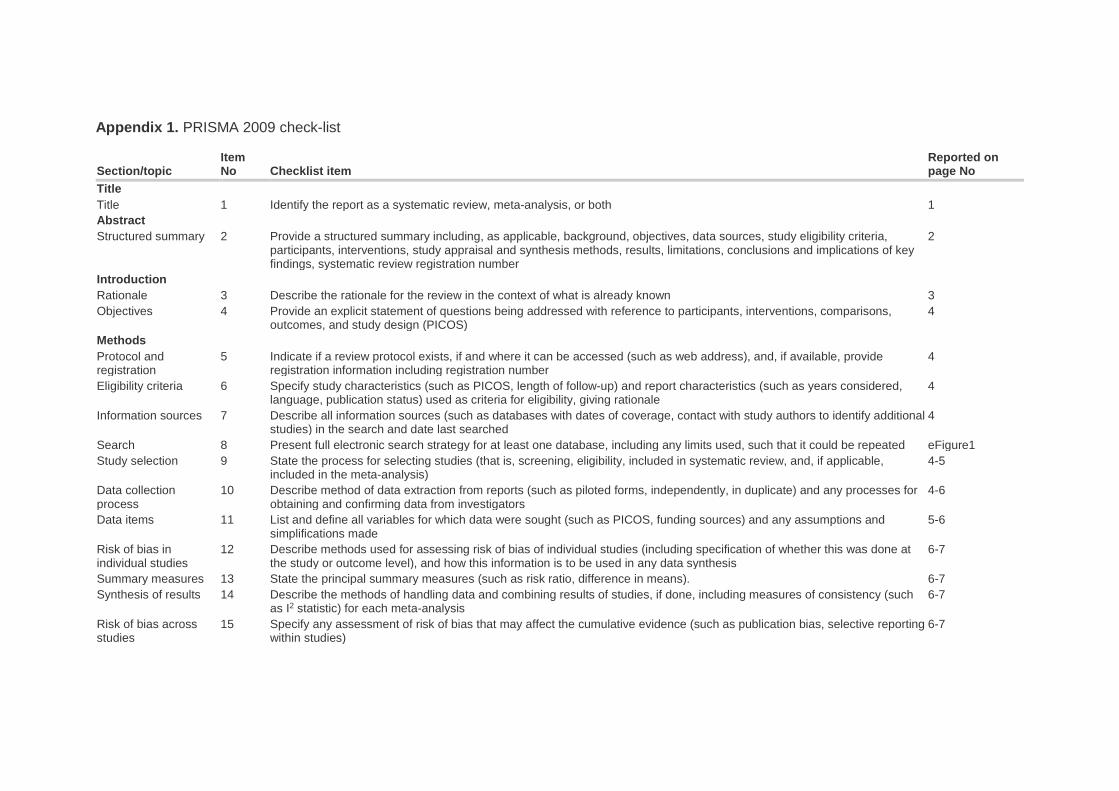
Appendix 1. PRISMA 2009 check-list
Section/topic Item No Checklist item
Reported on page No
Title Title 1 Identify the report as a systematic review, meta-analysis, or both 1 Abstract Structured summary 2 Provide a structured summary including, as applicable, background, objectives, data sources, study eligibility criteria,
participants, interventions, study appraisal and synthesis methods, results, limitations, conclusions and implications of key findings, systematic review registration number
2
Introduction Rationale 3 Describe the rationale for the review in the context of what is already known 3 Objectives 4 Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons,
outcomes, and study design (PICOS) 4
Methods Protocol and registration
5 Indicate if a review protocol exists, if and where it can be accessed (such as web address), and, if available, provide registration information including registration number
4
Eligibility criteria 6 Specify study characteristics (such as PICOS, length of follow-up) and report characteristics (such as years considered, language, publication status) used as criteria for eligibility, giving rationale
4
Information sources 7 Describe all information sources (such as databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched
4
Search 8 Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated eFigure1 Study selection 9 State the process for selecting studies (that is, screening, eligibility, included in systematic review, and, if applicable,
included in the meta-analysis) 4-5
Data collection process
10 Describe method of data extraction from reports (such as piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators
4-6
Data items 11 List and define all variables for which data were sought (such as PICOS, funding sources) and any assumptions and simplifications made
5-6
Risk of bias in individual studies
12 Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis
6-7
Summary measures 13 State the principal summary measures (such as risk ratio, difference in means). 6-7 Synthesis of results 14 Describe the methods of handling data and combining results of studies, if done, including measures of consistency (such
as I2 statistic) for each meta-analysis 6-7
Risk of bias across studies
15 Specify any assessment of risk of bias that may affect the cumulative evidence (such as publication bias, selective reporting within studies)
6-7
Section/topic Item No Checklist item
Reported on page No
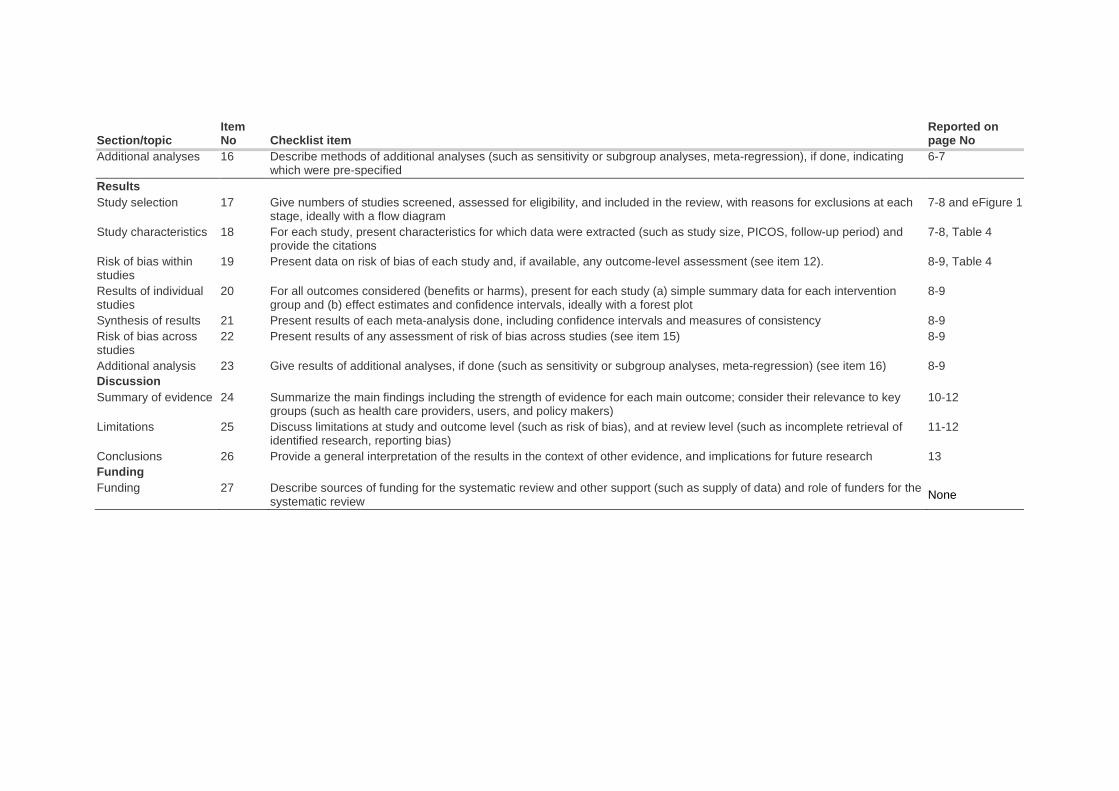
Additional analyses 16 Describe methods of additional analyses (such as sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified
6-7
Results Study selection 17 Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each
stage, ideally with a flow diagram 7-8 and eFigure 1
Study characteristics 18 For each study, present characteristics for which data were extracted (such as study size, PICOS, follow-up period) and provide the citations
7-8, Table 4
Risk of bias within studies
19 Present data on risk of bias of each study and, if available, any outcome-level assessment (see item 12). 8-9, Table 4
Results of individual studies
20 For all outcomes considered (benefits or harms), present for each study (a) simple summary data for each intervention group and (b) effect estimates and confidence intervals, ideally with a forest plot
8-9
Synthesis of results 21 Present results of each meta-analysis done, including confidence intervals and measures of consistency 8-9 Risk of bias across studies
22 Present results of any assessment of risk of bias across studies (see item 15) 8-9
Additional analysis 23 Give results of additional analyses, if done (such as sensitivity or subgroup analyses, meta-regression) (see item 16) 8-9 Discussion Summary of evidence 24 Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key
groups (such as health care providers, users, and policy makers) 10-12
Limitations 25 Discuss limitations at study and outcome level (such as risk of bias), and at review level (such as incomplete retrieval of identified research, reporting bias)
11-12
Conclusions 26 Provide a general interpretation of the results in the context of other evidence, and implications for future research 13 Funding Funding 27 Describe sources of funding for the systematic review and other support (such as supply of data) and role of funders for the
systematic review None
Appendix 2. MOOSE checklist Criteria Brief description of how the criteria were handled
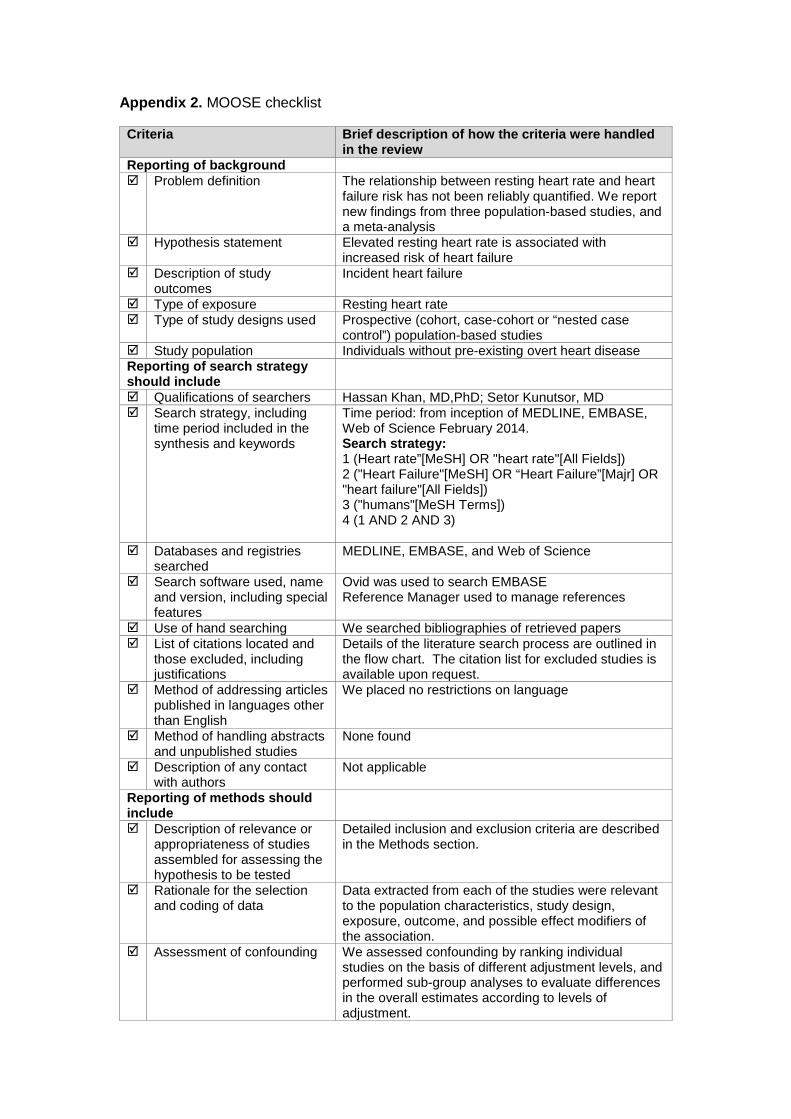
in the review Reporting of background Problem definition The relationship between resting heart rate and heart
failure risk has not been reliably quantified. We report new findings from three population-based studies, and a meta-analysis
Hypothesis statement Elevated resting heart rate is associated with increased risk of heart failure
Description of study outcomes
Incident heart failure
Type of exposure Resting heart rate Type of study designs used Prospective (cohort, case-cohort or “nested case
control”) population-based studies Study population Individuals without pre-existing overt heart disease Reporting of search strategy should include
Qualifications of searchers Hassan Khan, MD,PhD; Setor Kunutsor, MD Search strategy, including
time period included in the synthesis and keywords
Time period: from inception of MEDLINE, EMBASE, Web of Science February 2014. Search strategy: 1 (Heart rate”[MeSH] OR "heart rate"[All Fields]) 2 ("Heart Failure"[MeSH] OR “Heart Failure”[Majr] OR "heart failure"[All Fields]) 3 ("humans"[MeSH Terms]) 4 (1 AND 2 AND 3)
Databases and registries searched
MEDLINE, EMBASE, and Web of Science
Search software used, name and version, including special features
Ovid was used to search EMBASE Reference Manager used to manage references
Use of hand searching We searched bibliographies of retrieved papers List of citations located and
those excluded, including justifications
Details of the literature search process are outlined in the flow chart. The citation list for excluded studies is available upon request.
Method of addressing articles published in languages other than English
We placed no restrictions on language
Method of handling abstracts and unpublished studies
None found
Description of any contact with authors
Not applicable
Reporting of methods should include
Description of relevance or appropriateness of studies assembled for assessing the hypothesis to be tested
Detailed inclusion and exclusion criteria are described in the Methods section.
Rationale for the selection and coding of data
Data extracted from each of the studies were relevant to the population characteristics, study design, exposure, outcome, and possible effect modifiers of the association.
Assessment of confounding We assessed confounding by ranking individual studies on the basis of different adjustment levels, and performed sub-group analyses to evaluate differences in the overall estimates according to levels of adjustment.
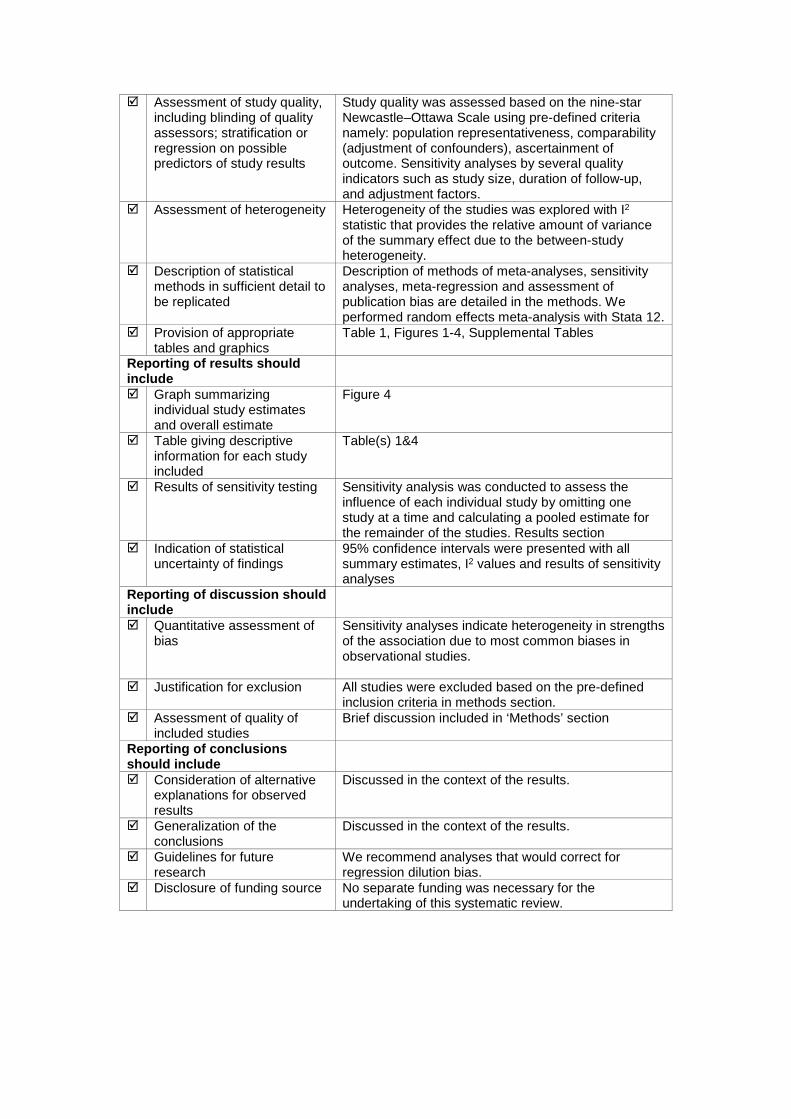
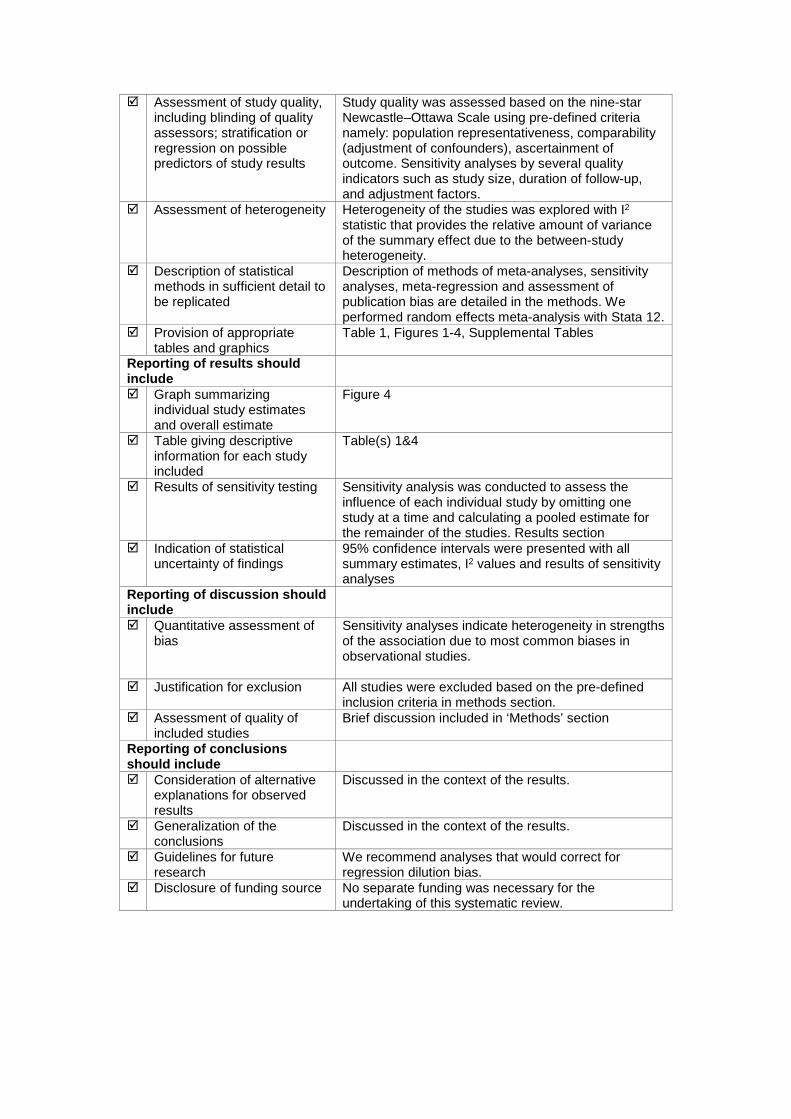
Assessment of study quality, including blinding of quality assessors; stratification or regression on possible predictors of study results
Study quality was assessed based on the nine-star Newcastle–Ottawa Scale using pre-defined criteria namely: population representativeness, comparability (adjustment of confounders), ascertainment of outcome. Sensitivity analyses by several quality indicators such as study size, duration of follow-up, and adjustment factors.
Assessment of heterogeneity Heterogeneity of the studies was explored with I2 statistic that provides the relative amount of variance of the summary effect due to the between-study heterogeneity.
Description of statistical methods in sufficient detail to be replicated
Description of methods of meta-analyses, sensitivity analyses, meta-regression and assessment of publication bias are detailed in the methods. We performed random effects meta-analysis with Stata 12.
Provision of appropriate tables and graphics
Table 1, Figures 1-4, Supplemental Tables
Reporting of results should include
Graph summarizing individual study estimates and overall estimate
Figure 4
Table giving descriptive information for each study included
Table(s) 1&4
Results of sensitivity testing
Sensitivity analysis was conducted to assess the influence of each individual study by omitting one study at a time and calculating a pooled estimate for the remainder of the studies. Results section
Indication of statistical uncertainty of findings
95% confidence intervals were presented with all summary estimates, I2 values and results of sensitivity analyses
Reporting of discussion should include
Quantitative assessment of bias
Sensitivity analyses indicate heterogeneity in strengths of the association due to most common biases in observational studies.
Justification for exclusion All studies were excluded based on the pre-defined inclusion criteria in methods section.
Assessment of quality of included studies
Brief discussion included in ‘Methods’ section
Reporting of conclusions should include
Consideration of alternative explanations for observed results
Discussed in the context of the results.
Generalization of the conclusions
Discussed in the context of the results.
Guidelines for future research
We recommend analyses that would correct for regression dilution bias.
Disclosure of funding source No separate funding was necessary for the undertaking of this systematic review.
C. Fonarow, Stephen B. Kritchevsky, Jari A. Laukkanen and Javed ButlerNewman, Tamara B. Harris, Kirsten Bibbins-Domingo, Jussi Kauhanen, Mihai Gheorghiade, Gregg
Hassan Khan, Setor Kunutsor, Andreas P. Kalogeropoulos, Vasiliki V. Georgiopoulou, Anne B.Analysis−Systematic Meta
Resting Heart Rate and Risk of Incident Heart Failure: Three Prospective Cohort Studies and a
Online ISSN: 2047-9980 Dallas, TX 75231
is published by the American Heart Association, 7272 Greenville Avenue,Journal of the American Heart AssociationThe doi: 10.1161/JAHA.114.001364
2015;4:e001364; originally published January 14, 2015;J Am Heart Assoc.
http://jaha.ahajournals.org/content/4/1/e001364World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://jaha.ahajournals.org/content/suppl/2015/01/27/jah3812.DC1.htmlData Supplement (unedited) at:
for more information. http://jaha.ahajournals.orgAccess publication. Visit the Journal at
is an online only OpenJournal of the American Heart AssociationSubscriptions, Permissions, and Reprints: The
by guest on June 20, 2016http://jaha.ahajournals.org/Downloaded from

SUPPLEMENTAL MATERIAL
Appendix 1. PRISMA 2009 check-list
Section/topic Item No Checklist item
Reported on page No
Title Title 1 Identify the report as a systematic review, meta-analysis, or both 1 Abstract Structured summary 2 Provide a structured summary including, as applicable, background, objectives, data sources, study eligibility criteria,
participants, interventions, study appraisal and synthesis methods, results, limitations, conclusions and implications of key findings, systematic review registration number
2
Introduction Rationale 3 Describe the rationale for the review in the context of what is already known 3 Objectives 4 Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons,
outcomes, and study design (PICOS) 4
Methods Protocol and registration
5 Indicate if a review protocol exists, if and where it can be accessed (such as web address), and, if available, provide registration information including registration number
4
Eligibility criteria 6 Specify study characteristics (such as PICOS, length of follow-up) and report characteristics (such as years considered, language, publication status) used as criteria for eligibility, giving rationale
4
Information sources 7 Describe all information sources (such as databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched
4
Search 8 Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated eFigure1 Study selection 9 State the process for selecting studies (that is, screening, eligibility, included in systematic review, and, if applicable,
included in the meta-analysis) 4-5
Data collection process
10 Describe method of data extraction from reports (such as piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators
4-6
Data items 11 List and define all variables for which data were sought (such as PICOS, funding sources) and any assumptions and simplifications made
5-6
Risk of bias in individual studies
12 Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis
6-7
Summary measures 13 State the principal summary measures (such as risk ratio, difference in means). 6-7 Synthesis of results 14 Describe the methods of handling data and combining results of studies, if done, including measures of consistency (such
as I2 statistic) for each meta-analysis 6-7
Risk of bias across studies
15 Specify any assessment of risk of bias that may affect the cumulative evidence (such as publication bias, selective reporting within studies)
6-7

Section/topic Item No Checklist item
Reported on page No
Additional analyses 16 Describe methods of additional analyses (such as sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified
6-7
Results Study selection 17 Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each
stage, ideally with a flow diagram 7-8 and eFigure 1
Study characteristics 18 For each study, present characteristics for which data were extracted (such as study size, PICOS, follow-up period) and provide the citations
7-8, Table 4
Risk of bias within studies
19 Present data on risk of bias of each study and, if available, any outcome-level assessment (see item 12). 8-9, Table 4
Results of individual studies
20 For all outcomes considered (benefits or harms), present for each study (a) simple summary data for each intervention group and (b) effect estimates and confidence intervals, ideally with a forest plot
8-9
Synthesis of results 21 Present results of each meta-analysis done, including confidence intervals and measures of consistency 8-9 Risk of bias across studies
22 Present results of any assessment of risk of bias across studies (see item 15) 8-9
Additional analysis 23 Give results of additional analyses, if done (such as sensitivity or subgroup analyses, meta-regression) (see item 16) 8-9 Discussion Summary of evidence 24 Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key
groups (such as health care providers, users, and policy makers) 10-12
Limitations 25 Discuss limitations at study and outcome level (such as risk of bias), and at review level (such as incomplete retrieval of identified research, reporting bias)
11-12
Conclusions 26 Provide a general interpretation of the results in the context of other evidence, and implications for future research 13 Funding Funding 27 Describe sources of funding for the systematic review and other support (such as supply of data) and role of funders for the
systematic review None

Appendix 2. MOOSE checklist Criteria Brief description of how the criteria were handled
in the review Reporting of background Problem definition The relationship between resting heart rate and heart
failure risk has not been reliably quantified. We report new findings from three population-based studies, and a meta-analysis
Hypothesis statement Elevated resting heart rate is associated with increased risk of heart failure
Description of study outcomes
Incident heart failure
Type of exposure Resting heart rate Type of study designs used Prospective (cohort, case-cohort or “nested case
control”) population-based studies Study population Individuals without pre-existing overt heart disease Reporting of search strategy should include
Qualifications of searchers Hassan Khan, MD,PhD; Setor Kunutsor, MD Search strategy, including
time period included in the synthesis and keywords
Time period: from inception of MEDLINE, EMBASE, Web of Science February 2014. Search strategy: 1 (Heart rate”[MeSH] OR "heart rate"[All Fields]) 2 ("Heart Failure"[MeSH] OR “Heart Failure”[Majr] OR "heart failure"[All Fields]) 3 ("humans"[MeSH Terms]) 4 (1 AND 2 AND 3)
Databases and registries searched
MEDLINE, EMBASE, and Web of Science
Search software used, name and version, including special features
Ovid was used to search EMBASE Reference Manager used to manage references
Use of hand searching We searched bibliographies of retrieved papers List of citations located and
those excluded, including justifications
Details of the literature search process are outlined in the flow chart. The citation list for excluded studies is available upon request.
Method of addressing articles published in languages other than English
We placed no restrictions on language
Method of handling abstracts and unpublished studies
None found
Description of any contact with authors
Not applicable
Reporting of methods should include
Description of relevance or appropriateness of studies assembled for assessing the hypothesis to be tested
Detailed inclusion and exclusion criteria are described in the Methods section.
Rationale for the selection and coding of data
Data extracted from each of the studies were relevant to the population characteristics, study design, exposure, outcome, and possible effect modifiers of the association.
Assessment of confounding We assessed confounding by ranking individual studies on the basis of different adjustment levels, and performed sub-group analyses to evaluate differences in the overall estimates according to levels of adjustment.
Assessment of study quality, including blinding of quality assessors; stratification or regression on possible predictors of study results
Study quality was assessed based on the nine-star Newcastle–Ottawa Scale using pre-defined criteria namely: population representativeness, comparability (adjustment of confounders), ascertainment of outcome. Sensitivity analyses by several quality indicators such as study size, duration of follow-up, and adjustment factors.
Assessment of heterogeneity Heterogeneity of the studies was explored with I2 statistic that provides the relative amount of variance of the summary effect due to the between-study heterogeneity.
Description of statistical methods in sufficient detail to be replicated
Description of methods of meta-analyses, sensitivity analyses, meta-regression and assessment of publication bias are detailed in the methods. We performed random effects meta-analysis with Stata 12.
Provision of appropriate tables and graphics
Table 1, Figures 1-4, Supplemental Tables
Reporting of results should include
Graph summarizing individual study estimates and overall estimate
Figure 4
Table giving descriptive information for each study included
Table(s) 1&4
Results of sensitivity testing
Sensitivity analysis was conducted to assess the influence of each individual study by omitting one study at a time and calculating a pooled estimate for the remainder of the studies. Results section
Indication of statistical uncertainty of findings
95% confidence intervals were presented with all summary estimates, I2 values and results of sensitivity analyses
Reporting of discussion should include
Quantitative assessment of bias
Sensitivity analyses indicate heterogeneity in strengths of the association due to most common biases in observational studies.
Justification for exclusion All studies were excluded based on the pre-defined inclusion criteria in methods section.
Assessment of quality of included studies
Brief discussion included in ‘Methods’ section
Reporting of conclusions should include
Consideration of alternative explanations for observed results
Discussed in the context of the results.
Generalization of the conclusions
Discussed in the context of the results.
Guidelines for future research
We recommend analyses that would correct for regression dilution bias.
Disclosure of funding source No separate funding was necessary for the undertaking of this systematic review.