
RAD Croatian Academy of Sciences and Arts
108
RAD Croatian Academy of Sciences and Arts - Medical Sciences Editorial Board Uredništvo Vol 540 = 48-49 (2019) knjiga 540, svezak 48-49 Editor in Chief Glavni i odgovorni urednik Marko Pećina Deputy Editor Zamjenica glavnog urednika Vida Demarin Assistant Editors Urednici Ivana Čepelak Iva Dekaris Alemka Markotić Josip Madić Mirna Šitum Zrinka Tarle Editorial Board Secretary Tajnik uredništva Filip Đerke Advisory Board Savjet Željko Cvetnić Ivo Čikeš Dragan Dekaris Hedvig Hricak Vjekoslav Jerolimov Ivica Kostović Zvonko Kusić Dražen Matičić Davor Miličić Steven Živko Pavletić Željko Reiner Daniel Rukavina Miroslav Samaržija Nenad Šestan Slobodan Vukičević Editor in Chief Glavni i odgovorni urednik Marko Pećina Publisher Izdavač Croatian Academy of Sciences and Arts Department of Medical Sciences Hrvatska akademija znanosti i umjetnosti Razred za medicinske znanosti For the Publisher Za izdavača Dario Vretenar Web Editor / Web urednik Filip Đerke Edition / Naklada 200 DOI numbers / DOI brojevi Kristina Polak Bobić Redaction address: Trg Nikole Šubića Zrinskog 11, Zagreb [email protected] DISCLAIMER e statements, opinions and data contained in this publication are solely those of the individual authors and contributors and not of the Publisher and the Edi- tor-In-Chief. e appearance of advertisements in the Journal is not the warranty, endorsement, or approval of the products or service advertised or of their effec- tiveness, quality or safety. e publisher and the Editor-In-Chief disclaim respon- sibility for any ideas, methods, instructions or products referred to in the content or advertisements. RAD CASA was founded by the Croatian Academy of Sciences and Arts in 1867, the Journal: RAD CASA - MEDICAL SCIENCES was founded by the Academy’s Department of Medical Sciences in 1951. e articles are categorized according to “Guidelines for Authors” available at the RAD CASA Medical Sciences webpage: www.rad-med.com RAD CASA Medical Sciences is published twice a year as a double issue. doi 10.21857/y6zolb3l1m issn 1848-641x (online) issn: 1330-5301 (print) DRUG DOSAGE e authors and the publisher have extended every effort to ensure that drug selec- tion and dosage set forth in this text are in accord with current recommendations and practice at the time of publication. However, in view of ongoing research, changes in government regulations, and the constant flow of information relating to drug therapy and drug reactions, the reader is urged to check the package insert for each drug for any change in indications and dosage and for added warnings and precautions. is is particularly important when the recommended agent is a new and/or infrequently employed drug. RAD CASA Medical Sciences is included in / indexed by: Printed with support of the Foundation of the Croatian Academy of Sciences and Arts impressum
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of RAD Croatian Academy of Sciences and Arts

RAD Croatian Academy of Sciences and Arts -
Medical Sciences
Editorial BoardUredništvo Vol 540 = 48-49 (2019)
knjiga 540, svezak 48-49
Editor in ChiefGlavni i odgovorni urednik
Marko Pećina
Deputy EditorZamjenica glavnog urednika
Vida Demarin
Assistant EditorsUrednici
Ivana ČepelakIva DekarisAlemka MarkotićJosip MadićMirna ŠitumZrinka Tarle
Editorial Board SecretaryTajnik uredništva
Filip Đerke
Advisory BoardSavjet Željko CvetnićIvo ČikešDragan DekarisHedvig HricakVjekoslav JerolimovIvica KostovićZvonko KusićDražen MatičićDavor MiličićSteven Živko PavletićŽeljko ReinerDaniel RukavinaMiroslav SamaržijaNenad ŠestanSlobodan Vukičević
Editor in ChiefGlavni i odgovorni urednik
Marko Pećina
PublisherIzdavačCroatian Academy of Sciences and ArtsDepartment of Medical SciencesHrvatska akademija znanosti i umjetnostiRazred za medicinske znanosti
For the PublisherZa izdavača
Dario Vretenar
Web Editor / Web urednik
Filip Đerke
Edition / Naklada
200
DOI numbers / DOI brojevi
Kristina Polak Bobić
Redaction address: Trg Nikole Šubića Zrinskog 11, [email protected]
Disclaimer
The statements, opinions and data contained in this publication are solely those of the individual authors and contributors and not of the Publisher and the Edi-tor-In-Chief. The appearance of advertisements in the Journal is not the warranty, endorsement, or approval of the products or service advertised or of their effec-tiveness, quality or safety. The publisher and the Editor-In-Chief disclaim respon-sibility for any ideas, methods, instructions or products referred to in the content or advertisements.
RAD CASA was founded by the Croatian Academy of Sciences and Arts in 1867, the Journal: raD casa - meDical sciences was founded by the Academy’s Department of Medical Sciences in 1951.
The articles are categorized according to “Guidelines for Authors” available at the RAD CASA Medical Sciences webpage: www.rad-med.com
RAD CASA Medical Sciences is published twice a year as a double issue.
doi 10.21857/y6zolb3l1missn 1848-641x (online) issn: 1330-5301 (print)
Drug Dosage
The authors and the publisher have extended every effort to ensure that drug selec-tion and dosage set forth in this text are in accord with current recommendations and practice at the time of publication. However, in view of ongoing research, changes in government regulations, and the constant flow of information relating to drug therapy and drug reactions, the reader is urged to check the package insert for each drug for any change in indications and dosage and for added warnings and precautions. This is particularly important when the recommended agent is a new and/or infrequently employed drug.
RAD CASA Medical Sciences is included in / indexed by:
Printed with support of the Foundation of the Croatian Academy of Sciences and Arts
impressum

raD casa - meDical sciences is an international peer-reviewed medical journal open to physicians and scientists from the field of biomedicine. It accepts contributions in the form of original article, review, short review, case report, letter to the editor, short communication, and correspondence.
Plagiarism detection
Manuscripts are checked for text similarity and manually verified by the research integrity editor. We use CrossRef Similarity Check software and deal with manuscripts suspected on plagiarism following the COPE flowcharts and ICMJE guidelines.
ethical aPProval and informed consent
When reporting trials on human subjects, authors should indicate whether the procedures were follow-ing the ethical standards set by the responsible hu-man experimentation committee (institutional and national) and the latest version of the Declaration of Helsinki given by World Medical Association. Eth-ical approval (institutional or national) should be obtained for every study that includes the collection of an additional patient sample of any biological material (more than those required for the medical evaluation). Regardless of the preserved anonymity, patients presented in case report articles should always sign informed consent. Case reports without patients’ consent are not eligible for publication in Rad.
language
Rad is published exclusively in English. It is the author’s responsibility to ensure that the English language is thoroughly revised before submitting the work for publication. Note that the Editorial Board reserves the right to reject a manuscript if the use of language is deemed too poor. The Abstract should be written in both English and Croatian if it is possible (if not, the proofreader will translate it to Croatian).
article-Processing charges
Manuscript submission, article processing and publishing are free of charge.
article tyPes
Contributions to the Journal are classified into the categories listed in the table below. The maximum word count does NOT include the title, authors and affiliations, abstract, keywords, subheadings, table and figure legends, and references. However, it does include the text in the tables, if any.
authorshiP
Rad follows the guidelines for authorship set forth by the International Committee of Medical Journal Editors (ICMJE) Each author should meet all four criteria as follows: 1. substantial contributions to conception and design, acquisition of data, or analysis and interpre-
tation of data 2. drafting the article or revising it critically for important intellectual content 3. final approval of the version to be published 4. agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.According to ICMJE: “In addition to being accountable for the parts of the work the author has done, an author should be able to identify which co-authors are responsible for specific other parts of the work. Also, the authors should have confidence in the integrity of the contributions of their co-au-thors. All those designated as authors should meet all four criteria for authorship, and all who meet the four criteria should be identified as authors.“Rad adopted the system by which each author is identified with his/her unique identification num-ber, ORCID, thus ensuring transparency in author-ship and personal identification. It is available for free at http://orcid.org/. It is recommended for each author to provide his/her ORCID number.
manuscriPt submission
During the manuscript, submission process corre-sponding author is asked to provide his ORCID ID number. The corresponding author is responsible to fill in the Submission form on behalf of all co-au-thors. Manuscript Submission form consists of the following sections: authorship statement, statement of originality, conflict of interest disclosure, protec-tion of research participants, and copyright transfer and publication license.Instructions for authors comply with the “Recom-mendations for the Conduct, Reporting, Editing, and Publication of Scholarly work in Medical Jour-nals” (http://www.icmje.org/recommendations/, updated in 2016). Editors hold the right to make all the necessary changes to the language and style of the original manuscript to adhere to the uniform standards of the Journal.
manuscriPt PreParation
The manuscript should be written in English and uploaded via the online submission system available at Journal website (www.rad-med.com)The following should be submitted:• Cover letter• Title page• Manuscript (without authors and affiliations)• Figure (optional)• Supplementary material (optional).Please note that a Manuscript file should not contain any information on the authors and their affiliation. Also, the Manuscript file name should not contain any reference to the author’s name. This is important because all manuscripts are sent for blind peer review.All pages of the manuscript (except for the cover letter and title page, which are attached separately) should be within a single document. Original man-uscripts should be structured as follows: Abstract, Keywords, Introduction, Materials and Methods, Results, Discussion, Acknowledgments, Tables and Figures, and References.abstract All types of manuscripts should contain an abstract. An abstract of 350 words maximum should be provided on a separate page in the Manuscript file (abstract only, without authors and affiliation). The abstract of an original article should be structured into four headings: Introduction, Materials and Methods, Results, and Conclusions. For other article types, abstracts do not have to be structured.
Keywords Please whenever possible, provide 3-5 keywords from MeSH database)introduction In the Introduction section, the authors should point out new information in the manuscript, the hypothesis, and the aim of their work. The Introduction section should not contain results and conclusions.materials and methods The Materials and meth-ods section should only include information that was available at the time the study was planned. All information obtained during the study should be provided in the Result section. The detailed instruc-tions for writing materials and methods are available at the Journal website (www.rad-med.com). results State the main or most important finding first. The data presented in the tables or figures should not be repeated in the text. Graphs should be used as an alternative to tables with many entries. discussion Emphasize the new and important conclusion based on the study results in the context of the best available evidence. Do not repeat the data presented in the Introduction or Results sec-tion. Clearly, state the limitations of the study.acKnowledgements All contributors who do not meet the authorship criteria should be listed in the Acknowledgments section. These persons must give verbal permission to be acknowledged. Authors should provide that statement during the manuscript submission process. Financial and material support should also be acknowledged and reported in the conflict of interest disclosure during the manuscript submission process.references Authors are responsible for verifying the accuracy of the references by using an electronic bibliographic source, such as PubMed, or printed original articles. References must not refer to the retracted article except if the authors want to refer to the particular retraction.Rad applies the Vancouver referencing style. Litera-ture citation should conform to the standards avail-able at NLM’s International Committee of Medical Journal Editors (ICMJE) Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals (examples are available at Journal website (www.rad-med.com)References should be numbered consecutively, using Arabic numerals in parentheses, in the order of appearance in the text.
conflict of interest
According to the International Committee of Med-ical Journal Editors (ICMJE): “Conflict of interest exists when an author (or the author’s institution) has financial (employment, consultancies, stock ownership, honoraria and paid expert testimony) or personal relationship, academic competition or intellectual passion that inappropriately influences his actions.”
other Possible conflicts of interest
All reviewers, editors, section editors, Editorial Board members, included in the publication process will also be asked to disclose any potential conflict of interest regarding the manuscript they are asked to review (primarily relationships with the pharma-ceutical industry; incorporated into our submission system).
For more detailed information and instructions for authors, we suggest visiting the Journals’ official
webpage: www.rad-med.com
Type Max. word count
Max. numberof refernces
Letter to theeditor 1000 5
Review 5000 100Short review 3500 50Original article 5000 30
Short communication 1500 10
Case report 1500 20
Correspondence 1000 7
Editorial Policies and Guidelines for Authors

Contents
RAD Croatian Academy of Sciences and Arts -
Medical SciencesVol 540 = 48-49 (2019)
knjiga 540, svezak 48-49
1 Editorial Where We Are Indexed or Where We Are Visible Marko Pećina, Filip Đerke, Vida Demarin
3 Original Article: Triple Class HIV-1 Drug Resistance in Croatia: the First Report Ana Planinić, Maja Oroz, Snježana Židovec Lepej
8 Original Article: Arteriovenous Fistula After Kidney Transplantation in University Hospital Centre Osijek Anton Jurić, Lada Zibar
15 Original Article: Connection Between Body Position During Sleep and Findings from Full-Night Polysomnography in Patients with Obstructive Sleep Apnea Alen Juginović, Renata Pecotić
27 Review Article: Hallux Sesamoiditis - Radiological Diagnostics and Conservative Management Igor Borić, Marko Pećina, Maja Mirković, Tatjana Cicvara Pećina, Damir Matoković, Mihovil Plečko, Ivo Dumić-Čule
33 Review Article: Comprehensive Medication Management Services as a Solution to Medication Mismanagement: A European Perspective Iva Mucalo, Andrea Brajković, Ivona Jukic, Danijela Jonjić, Dagmar Radin, Djenane Ramalho de Oliveira
41 Review Article: Aging, Calorie Restriction and Calorie Restriction Mimetics Ivana Čepelak, Slavica Dodig, Daniela Čepelak Dodig
51 Review Article: Air Pollution: a New Risk Factor for Developing Stroke Vida Demarin, Sandra Morović, Filip Đerke
58 Original Article: High-fat Diet Induced Dysbiosis & Amelioration by Astaxanthin Kyle Haasbroek, Wakako Takabe, Masayuki Yagi, Yoshikazu Yonei
67 Case Report: Third Degree Atrioventricular Block in Children Vinko Vrdoljak, Matej Šapina, Suzana Bitanga, Matej Katavić
71 Case Report: Upper Respiratory Infection Followed by Concurrent Sweet’s Syndrome and Erythema Nodosum Alemka Markotić, Ivana Puškarić, Tomislava Skuhala
75 Case Report: Inguinal Hernia Containing an Incarcerated Ureter of a Transplanted Kidney Luka Filipović-Grčić, Neva Coce

78 Essay: Cooperation in the Field of Public Health and Medicine: Instances of Expert and Knowledge Mobility between Vienna, Zagreb and the Far East Željko Dugac
86 Essay: War Invalids and Disabled Soldiers in the Habsburg Army: The Case of the Đurđevac Regiment in 1860/61 Ivana Horbec, Dubravko Habek
93 Book Review: Sports Medicine Marko Pećina et al.
94 Book Review: Restorative Dental Medicine Zrinka Tarle et al.
95 Book Review: Neurodegenerative Diseases – Dementias Vladimira Vuletić, Daniel Rukavina
96 News & Education: Vida Demarin - Laureate of the Croatian Academy of Medical Sciences Filip Đerke
97 News & Education: The 3rd Rijeka Forum on Neurodegenerative Diseases: Diagnosis and Treatment in Early Stage of Disease Vladimira Vuletić, Daniel Rukavina
99 News & Education: Heart and Brain - Risk Factors and Prevention Petra Črnac Žuna, Hrvoje Budinčević, Edvard Galić, Vida Demarin
100 News & Education: 11th International Professional-educational Symposium: Štampar Days Ivan Vukoja, Jakov Ivković
101 Author Index101 Keyword Index

Sadržaj
RAD Hrvatske akademije znanosti i umjetnosti
Medicinske znanostiVol 540 = 48-49 (2019)
knjiga 540, svezak 48-49
1 Uvodnik Gdje smo indeksirani ili gdje smo sve vidljivi? Marko Pećina, Filip Đerke, Vida Demarin
3 Izvorni rad: Rezistencija HIV1 virusa na 3 klase lijekova: prvi slučaj Ana Planinić, Maja Oroz, Snježana Židovec Lepej
8 Izvorni rad: Arterijskovenska fistula nakon bubrežnog presađivanja u Kliničkom bolničkom centru Osijek Anton Jurić, Lada Zibar
15 Izvorni rad: Povezanost položaja tijela tijekom spavanja s nalazima cjelonoćne polisomnografije u pacijenata s opstrukcijskom apnejom Alen Juginović, Renata Pecotić
27 Pregledni rad: Sezamoiditis - radiološka dijagnostika i konzervativno liječenje Igor Borić, Marko Pećina, Maja Mirković, Tatjana Cicvara Pećina, Damir Matoković, Mihovil Plečko, Ivo Dumić-Čule
33 Pregledni rad: Sveobuhvatna usluga upravljanja farmakoterapijom kao rješenje za propuste u propisivanju lijekova: europska perspektiva Iva Mucalo, Andrea Brajković, Ivona Jukic, Danijela Jonjić, Dagmar Radin, Djenane Ramalho de Oliveira
41 Pregledni rad: Starenje, kalorijske restrikcije i kalorijsko restrikcijska mimetrika Ivana Čepelak, Slavica Dodig, Daniela Čepelak Dodig
51 Pregledni rad: Zagađenje zraka: novootkriveni faktor rizika u razvoju moždanog udara Vida Demarin, Sandra Morović, Filip Đerke
58 Izvorni rad: Disbioza inducirana dijetom bogatom mastima & Amelioracija pomoću astaksantina Kyle Haasbroek, Wakako Takabe, Masayuki Yagi, Yoshikazu Yonei
67 Prikaz slučaja: Atrioventrikularni blok srca trećeg stupnja u djece Vinko Vrdoljak, Matej Šapina, Suzana Bitanga, Matej Katavić
71 Prikaz slučaja: Respiratorna infekcija gornjig dišnih putova praćena istovremeno Sweetovim sindromom i nodoznim eritemom Alemka Markotić, Ivana Puškarić, Tomislava Skuhala
75 Prikaz slučaja: Ingvinalna hernija koja sadrži inkarcerirani ureter transplantiranog bubrega Luka Filipović-Grčić, Neva Coce

78 Esej: Suradnja u području javnog zdravlja i medicine: primjeri transera znanja i stručnjaka između Beča, Zagreba i Dalekog istoka Željko Dugac
86 Esej: Ratni invalidi i vojnici s invaliditetom u Habsburškoj vojsci: prikaz Đurđevačke pukovnije 1860/61. Ivana Horbec, Dubravko Habek
93 Prikaz knjige: Sportska medicina Marko Pećina i suradnici
94 Prikaz knjige: Restaurativna dentalna medicina Zrinka Tarle i suradnici
95 Prikaz knjige: Neurodegenerativne bolesti - Demencije Vladimira Vuletić, Daniel Rukavina
96 Novosti & Edukacija: Vida Demarin - Laureat Akademije medicinskih znanosti Hrvatske Filip Đerke
97 Novosti & Edukacija: 3. riječki forum o neurodegenerativnim bolestima: dijagnosticiranje i liječenje u ranim stadijima bolesti Vladimira Vuletić, Daniel Rukavina
99 Novosti & Edukacija: Srce i mozak - rizični faktori i prevencija Petra Črnac Žuna, Hrvoje Budinčević, Edvard Galić, Vida Demarin
100 Novosti & Edukacija: 11. Međunarodni profesionalno-edukacijski simpozij: Štamparovi dani Ivan Vukoja, Jakov Ivković
101 Indeks autora101 Indeks ključnih riječi

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com1
Editorial
he changes in the format and layout of our pre-vious double issue of the RAD Medical Sciences 537 = 46-47 have been led the great attention and received general approval in our communi-ty. The high interest in our journal is the best reflected in the frequent calls and emails with
the most common question of where RAD Medical Sciences is indexed or in which citation databases are we represented. The interest in potential article submission has come mainly from the members of the academic community and, of course, primarily from younger colleagues, mostly those in postgrad-uate studies. It is a well-known fact that there is a certain ob-session in the scientific community, and especially at universi-ties, in applying quantitative metric indicators of the scientific researches relevant to the ranking of universities on the world rankings, or the value of an institution, or individual in the context of an allocation for some funding, professional scien-tific advancement, etc., etc.To avoid metrics becoming a goal rather than an instrument of scientific evaluation, scientists, their associations, and sci-entists in the field of scientometric have warned several in-ternational initiatives and declarations about the inconsistent and arbitrary application of metrics and the dangers that re-sult, as it stands out, as wrote Professor Jelka Petrak in an article titled “Not all quotes” and published in the journal of the Faculty of Medicine, University of Zagreb (mef.hr 38 (1): 102, 2019.)It always goes beyond the scope of this Editorial de-bate on the importance of citation for the evaluation of a journal, and it would be too potent for us to en-gage in this discussion based on the achievements of this small Journal so far, but in accordance with our efforts in further development of our Journal, we will cite our ed-
itor-in-chief Marko Pećina, published in the internationally renowned journal International Orthopedics (in which M. Pećina is the Editor-Emeritus):“A journalist’s contribution to the scientific literature and its im-pact on the scientific community is reflected by its citations. Spe-cifically, the acknowledgement that one article gives is another citation, whereas the acknowledgement that the referenced article receives is a citation. Citation counts vary considerably by re-search area and databases. The Internet has dramatically changed the way of sharing and the speed of medical information flow. In general, Google Scholar shows a greater number of citations, followed by Scopus® and then Web of Science®. Currently, web platforms and professional sites provide specific information on defined fields of science, and social media is allowed for inputs from the general public. These are changing the scene of the pub-lishing industry from the concept of the impact factor to alterna-tive metrics (known as the Altmetrics) that measure the impact of a paper-based on social media attention including the number of downloads, reads, views, clicks, likes, hits and tweets. Sourced from the Web, altmetrics can measure how often papers and other scholarly outputs like datasets are discussed and used around the world. For example, a paper published in 2017 received 2-3 ci-tations in JCR, but more than 1500 reads and downloads in the same period. Therefore, it is important to consider altmetrics in the evaluation of scientific papers. ” Int Orthop 42(11):2499-2505, 2018..
Pećina and colleagues in the Editorial of the already men-tioned journal Int. Orthop 39(8):1459-1464, 2015. states, among other things, that “social and professional media have
WHERE WE ARE INDEXED OR WHERE WE ARE VISIBLE
T
1-2
9.29
5
36.7
40
26.7
07
52.3
15
8.68
0 13.9
85
13.7
16
42.4
63
9.86
8
5.18
8
17.7
74
10.3
08
5.44
0
7.50
1
4.17
3
598
0
10000
20000
30000
40000
50000
60000
30(2006.)
31(2007.)
33(2009.)
34(2010.)
35(2010.)
36(2011.)
37(2012.)
38(2012.)
39(2013.)
40(2014.)
41(2015.)
42(2015.)
43(2016.)
44(2017.)
45(2018.)
46-47(2019.)
Online Reach in Hits for Each Issue of the RAD since 2006
Marko Pećina, Filip Đerke, Vida Demarin

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com2
57. ttps://dx.doi.org/10.21857/mzvkptz3n98. Haasbroek K, Takabe W, Yagi M and Yoshikazu Y. High-fat diet induced dysbiosis & amelioration by astaxanthin RAD CASA - Medical Sciences. 540=48-49 (2019): 58-66. https://dx.doi.org/10.21857/9xn31crexy9. Vrdoljak V, Šapina M, Bitanga S and Katavić M. Third Degree Atrio-ventricular Block in Children. RAD CASA- Medical Sciences. 540=48-49 (2019): 67-70. https://dx.doi.org/10.21857/m3v76t6o3y10. Markotić M, Puškarić I and Skuhala T. Upper Respiratory Infection Followed by Concurrent Sweet’s Syndrome and Erythema Nodosum. RAD CASA- Medical Sciences. 540=48-49 (2019): 71-74. https://dx.doi.org/10.21857/mwo1vczw1y11. Filipović-Grčić L and Coce N. Inguinal hernia containing an incarcerat-ed ureter of a transplanted kidney. RAD CASA - Medical Sciences. 540=48-49 (2019): 75-77. https://dx.doi.org/10.21857/yk3jwhrq3912. Dugac Ž. Cooperation in the Field of Public Health and Medicine: In-stances of Expert and Knowledge Mobility between Vienna, Zagreb and the Far East. RAD CASA - Medical Sciences. 540=48-49 (2019): 78-85. https://dx.doi.org/10.21857/y7v64t56ny13. Hrobec I and Habek D. War Invalids and Disabled Soldiers in the Habsburg Army: The Case of the Djurdjevac Regiment in 1860/61. RAD CASA - Medical Sciences. 540=48-49 (2019): 86-91. https://dx.doi.org/10.21857/yl4okf3209
challenged the traditional, acknowledged or past metrics for academic and scientific impact. In scholarly and scientific publishing, altmetrics are non-traditional metrics proposed as alternatives to more traditional citation impact metrics, such as IF. The term altmetrics was proposed in 2010 as a general-ization of article-level metrics. Although altmetrics are often thought of as metrics about articles, they can be applied to people, journals, books, data sets, presentations, videos, source code repositories, web pages, etc. Altmetrics cover not just ci-tation counts, but also other aspects of the impact of a work, such as how many data and knowledge bases refer to it, arti-cle views, downloads or mentions in social media and news media. Altmetrics is a very broad group of metrics, capturing various parts of impact paper or work can have. “Following the above, we will show the visibility of RAD of Medical Science on the portal of Croatian scientific and pro-fessional journals HRČAK (“hamster”), on which RAD has been since November 11th, 2007.
Now, the RAD CASA Medical Sciences is included in the fol-lowing databases: EBSCO (www.ebsco.com), Google Scholar (scholar.google.com), Scholar (www.scholar.com), HRČAK (Portal of Croatian Scientific and Professional Journals) and DiZbi (the Digital Collection of the Croatian Academy of Sci-ences and Arts: DiZbi.HAZU). All articles published in the
Journal have valid DOI number and are stored in the Croatian Web Archive (HAW). Our efforts are focused on the mission that RAD CASA Medical sciences will be included in other international databases such as Medline and Scopus soon. The actual double issue 48-49 includes three original papers1-3, five review articles4-8, three case reports9-11. We would partic-ularly like to point out two essays we accepted in this issue. Each has a specific and interesting approach to the topic, in the first essay author present the transfer of knowledge and ex-perts between Vienna, Zagreb, inter-war China and the USSR about public health and medicine. In the second one, authors present the research about health conditions and most repre-sented illnesses of Frontiersmen in the second part of the 19th century based on the Austrian State Archives12,13. We always continue informing our readers about the events held at the scientific symposia or congresses organised or spon-sored by the Department of Medical Sciences and we are also pleased to present book review published by the members of our Department.To sum up, in this editorial we would like to point out a little about journal evaluation indicators, but also the fact that we all need to be aware of the meaning of applying metric indi-cators. In that spirit, we conclude: „From the Editors’ point of view, we do feel concerned about the citation of published papers and the visibility of our Journal.“
literature:1. Planinc A, Oroz M and Zidovec Lepej S. Triple class HIV-1 drug resis-tance in Croatia: the first report. RAD CASA - Medical Sciences. 540=48-49 (2019): 3-7. https://dx.doi.org/10.21857/m16wjc6l692. Juric A and Zibar L. Arteriovenous Fistula After Kidney Transplantation in Clinical Hospital Centre Osijek. RAD CASA - Medical Sciences. 540=48-49 (2019): 16-24. https://dx.doi.org/10.21857/yrvgqtkdp93. Juginović A, Pecotić R. Connection Between Body Position During Sleep and Findings from Full-Night Polysomnography in Patients with Obstructive Sleep Apnea. RAD CASA - Medical Sciences. 540=48-49 (2019): 15-26. https://dx.doi.org/10.21857/ydkx2crgw94. Borić I, Pećina M, Mirković M et al. Hallux Sesamoiditis- Radiological Diagnostics and Conservative Management. RAD CASA - Medical Sciences. 540=48-49 (2019): 27-32. https://dx.doi.org/10.21857/m8vqrtzxg95. Mucalo I, Brajković A, Jukić I, Jonjić D, Radin D, de Oliveira DR. Com-prehensive Medication Management Services as a Solution to Medication Mismanagement: A European Perspective. RAD CASA - Medical Sciences. 540=48-49 (2019): 33-40. https://dx.doi.org/10.21857/90836cwv2y6. Čepelak I, Dodig S and Čepelak Dodig D. Aging, calorie restriction and calorie restriction mimetics. RAD CASA - Medical Sciences. 540=48-49 (2019): 41-50. https://dx.doi.org/10.21857/9e31lhnddm7. Demarin V, Morovic S and Derke F. Air Pollution: a New Risk Factor for Developing Stroke. RAD CASA - Medical Sciences. 540=48-49 (2019): 51-
Editorial
1-2

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com3
Triple Class HIV-1 Drug Resistance in Croatia: the First Report
Ana Planinić1, Maja Oroz2, Snježana Židovec Lepej1
1 Department of Immunological and Molecular Diagnostics, University Hospital for Infectious Diseases ‘‘Dr. Fran Mihalje-vic’’, Zagreb, Croatia2 University of Zagreb School of Medicine, Zagreb, Croatia
abstract:Resistance of Human Immunodeficiency Virus (HIV) to antiretroviral drugs is an important limitation in achieving complete suppression of viral replication and therefore represents an important clinical issue. It refers especially to therapy-naive individuals infected with resistant HIV strains, e.g. individuals with transmitted drug resistance (TDR). Transmitted drug resistance mutations (TDRMs) are clinically relevant and may reduce the efficacy of antiretroviral therapy. In this paper, we report the first case of HIV-1 transmitted triple-class drug resistance in Croatia. The aim of this study was to characterize drug resistance patterns and TDRMs in the newly diagnosed, treatment-naive HIV-1 patient with such a complex resistance pattern. Sanger sequencing (SS) of the sample showed four reverse transcriptase inhibitor (RTI) resistance mutations (E44D, T215E, K103N, L100I) affecting two drug classes and two protease inhibitor resistance mutations (V32I, I47V). To characterize HIV-1 minority drug resistance variants below the detection limit of SS, deep sequencing (DS) analysis was performed. DS analysis identified the same triple class resis-tance pattern that was identified by SS with addition of several other RTI mutations. The patient described in this report is the first patient with HIV-1 triple-class resistance in Croatia and further studies will be directed toward analysing possible local onward transmission of this resistant virus.
Keywords: HIV; Transmitted drug resistance (TDR); Sanger sequencing (SS); Deep sequencing (DS)
Sažetak:rezistencija HiV1 Virusa na 3 klase lijekoVa: prVi slučaj
Rezistencija virusa humane imunodeficijencije (HIV) na antiretrovirusne lijekove sprječava supresiju virusne replikacije te predstavlja značajan izazov u kliničkoj medicini. Posebno valja istaknuti problem primarne rezistencije (engl. transmitted drug resistance, TDR) koja se odnosi na prethodno neliječene osobe koje su zaražene rezistentnim sojevima HIV-a. Mutacije koje su pov-ezane s primarnom rezistencijom (engl. transmitted drug resistant mutations, TDRM) su klinički značajne i mogu nepovoljno djelovati na učinkovitost antiretrovirusnog liječenja. U ovom je radu opisana prva osoba s primarnom rezistencijom HIV-a na 3 klase antiretrovirusnih lijekova u Hr-vatskoj. Cilj ovog istraživanja bio je analizirati obrasce primarne rezistencije i TDRM u novodi-jagnosticiranog i neliječenog HIV-om zaraženog pojedinca. Primjenom Sangerovog sekvenciranja (SS) dokazali smo četiri mutacije povezane s rezistencijom na inhibitore reverzne transkriptaze (E44D, T215E, K103N, L100I) koje smanjuju osjetljivost na dvije klase lijekova (nukleozidne analoge inhibitore reverzne transkriptaze i nenukleozidne inhibitore reverzne transkriptaze) kao i dvije mutacije (V32I, I47V) povezane s rezistencijom na inhibitore proteaze. U svrhu identifikacije mogućeg postojanja manjinskih rezistentnih varijante ispod granice detekcije SS-a, provedena je analiza dubinskim sekvenciranjem (DS). DS analiza identificirala je isti obrazac rezistencije na 3 klase antiretrovirusnih lijekova identificiran s SS uz nekoliko dodatnih mutacija. U ovom je radu opisan prvi slučaj primarne rezistencije HIV-a na 3 klase antiretrovirusnih lijekova, a buduća istraživanja analizirat će moguće putove transmisije ovog rezistentnog virusa u Hrvatskoj.
ključne riječi: HIV; primarna rezistencija; Sanger sekvenciranje (SS); dubinsko sekvenciranje (DS)
OPEN ACCESS
Correspondence: Ana Planinić, PhD
This article was submitted to RAD CASA - Medical Sciences as the
original article
Conflict of Interest Statement: The authors declare that the
research was conducted in the absence of any commercial or
financial relationships that could be construed as a potential conflict of
interest.
Received: 03 November 2019Accepted: 28 November 2019Published: 17 December 2019
Citation:Planinc A, Oroz M and Zidovec Lepej S. Triple class HIV-1 drug resistance
in Croatia: the first report. RAD CASA - Medical Sciences. 540=48-
49 (2019): 3-7. https://dx.doi.org/10.21857/m16wjc6l69
Copyright (C) 2019 Planinc, Oroz and Zidovec. This is an open-ac-cess article distributed under the terms of the Creative Commons Attribution License (CC BY). The
use, distribution or reproduction in other forums is permitted, provided
the original author(s) and the copyright owners(s) are credited
and that the original publication in this journal is cited, in accordance whit accepted adacemic practice.
No use, distribution or reproduction is permitted which does not comply
with these terms.
Original Article
3-7

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com4
introduction
Highly active antiretroviral therapy (HAART) has had a tremendous impact on many individuals infected with Human Immunodeficiency Virus (HIV) and is the most important achievement in the history of HIV-therapy so far1. Despite the wide use and benefit of antiretroviral drugs, the efficacy of HAART can be compromised by the emergence of drug resistance2.Resistance occurs as a result of mutations in the pol region of HIV genome coding for viral enzymes, reverse transcriptase, protease and integrase, that represent molecular targets of antiretroviral drugs3. Resistance of HIV to antiretroviral drugs is an important limitation to the suppression of viral replication and therefore represents an important clinical issue4. This issue refers especially to therapy-naive individuals infected with resistant HIV strains (transmitted drug re-sistance, TDR). Transmitted-drug resistance mutations (TDRMs) can persist significantly longer than acquired DRMs in infected persons, even in the absence of drug pressure5. That goes in favor of hypothesis that TDR is driven mainly by onward transmission from ART-naive individuals rather than from patients with a history of ART6-8. TDRMs may reduce the efficacy of antiretroviral therapy (ART), but genotypic resistance testing, performed before initiating treatment or after virologic failure, helps clinicians in choosing the right regimen and improves the efficacy of ART2.To achieve the subsequent long-term treatment success, the resistance must be held under control by monitoring in both routine diagnostic setting and clinical research1,9.Sanger sequencing has been the golden standard for characterization of HIV resistance so far, but with the development of new ˝deep sequencing˝ technologies and their increased sensitivity for detection of minor mutations, many clinical laboratories and research groups begun to implement it in their research10-14. With Sanger sequencing it is possible to detect viral quasispecies present in 15-20% of the total viral population while viral variants present in lower frequency will not be detected. On the other hand, deep sequencing allows analysis of viral minor variants represented in <1% of the total population, which provides a new insight on pathogenesis of HIV-1 infection. The advantages of such sequencing are of exceptional importance because deep sequencing can help monitor the resistance while minor resistant variants are still in development and do not dominated the viral popu-lation10-14. The following groups of antiretroviral drugs are used for treatment of HIV-infection: nucleoside (NRTI) and non-nucleoside reverse transcriptase inhibitors (NNRTIs), protease inhibitors (PIs) and integrase inhibitors (INSTI). First-line ART consists of three or more antiretroviral drugs, usually two NRTIs in combination with one integrase inhibitor (recommended by the International AIDS Society-USA Guidelines, IAS-USA)2.Croatia has a centralized system of care and universal free access to an-tiretroviral drugs for all HIV infected persons15. HAART is available since 1998 while the resistance testing is performed since 200516.In this paper we report the first sampled case of transmitted tri-ple-class, drug-resistant HIV-1 in Croatia in a treatment-naive newly-diagnosed patient.
materials and methods
HIV-1 genotypingViral RNA was isolated from patient plasma using the QIAamp MinElute Virus Spin Kit (Qiagen, Hilden, Germany). HIV-1 geno-typing was performed using an in-house HIV-1 genotyping assay with
the BigDye Terminator v3.1 Cycle Sequencing Kit (Thermo Fisher Scientific, Dreieich, Germany) covering the protease (PR) and a part of reverse transcriptase (RT). Sequence analysis was performed on an ABI Prism 3500 capillary sequencer (Thermo Fisher Scientific, Germany). Vector NTI software (Thermo Fisher Scientific, Waltham, MA) was used to generate the consensus sequence and compare it with the reference strain HIV-1LAV-1 (GenBank number K02013). HIV-1 subtypes was assessed with the REGA HIV-1subtyping tool Version 3.0.Primary resistance to antiretroviral drugs was defined as the presence of ≥1 mutation placed on the WHO surveillance for drug resistance mutations (SDRM) list17. Clinically relevant resistance to Nucleoside Reverse Transcriptase Inhibitors (NRTI), Non-Nucleoside Reverse Transcripase Inhibitors (NNRTI) or Protease Inhibitors (PI) was eval-uated with IAS Drug Resistance Mutation list and Stanford Univer-sity HIV Drug Resistance Database (HIVdb), Genotypic Resistance Interpretation Algorithm version 8.82,18
In addition, drug resistance result of HIVdb was compared to those of 2 other algorithms: Rega Institute and Agence Nationale de Re-cherches sur le SIDA (ANRS).
Deep sequencing analysisTo characterize HIV-1 minority drug resistance variants present at frequencies (<10%) below the detection limit of Sanger sequencing, deep sequencing analysis was performed on the sample. The whole HIV-1 protease region and part of the reverse transcriptase region were sequenced with Illumina Miniseq (California, USA). After extraction, HIV-1 RNA was reverse transcribed with SuperScript® III First-Strand Synthesis System for RT-PCR (Invitrogen, Carlsbad, CA) and UNINEF primer55. Amplification of the target region was done in 4 separate multiplex PCR reactions using ALLinTM Taq DNA Polymerase (highQu GmbH, UK). Viral DNA libraries were prepared for deep sequencing with NEBNext® UltraTM II DNA Library Prep Kit for Illumina (New England BioLabs, MA, USA), according to the manufacturer’s instructions. Sequencing was performed using MiniS-eq MID output 300 cycles reagent kit (paired-end; 150+150). The se-quencing data were further analysed with HyDRA Web (Government of Canada, Ottawa, Canada) with a 5% sensitivity threshold19.
results
Patient characteristicsIn 2017, a 26 year old man was diganosed with HIV at the chronic stage of infection. HIV-1 subtyping showed that the patient was infected with subtype B. The route of HIV-transmission was sex with men. The patient had no previous exposure to therapy. Viral load at the time of diagnosis was 27 400 HIV-1 RNA copies/ml of plasma.
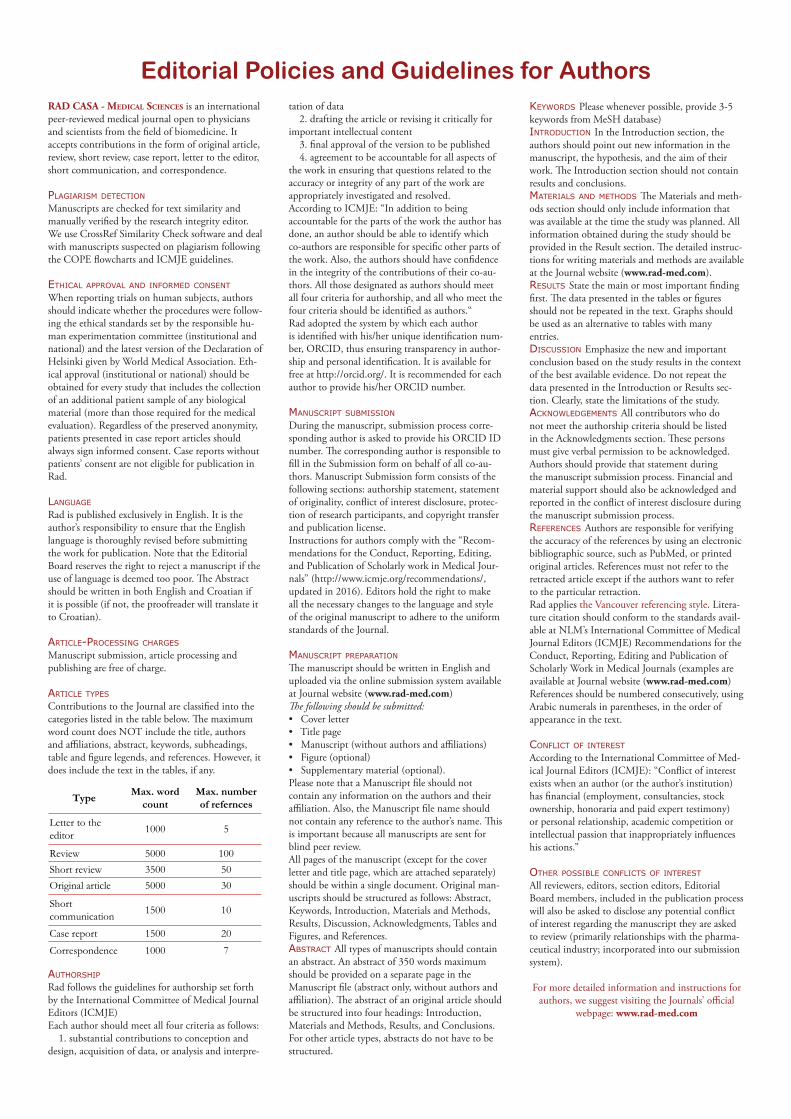
Sanger sequencing (SS)Sanger sequencing of the sample showed four RTI resistance mu-tations (E44D, T215E, K103N, L100I) affecting two drug classes (NRTI, NNRTI) and two PI resistance mutations (V32I, I47V) (Table 1).When interpreting the results of genotipic resistance using three different algorithms, three levels of resistance were used: ˝S˝ (suscepti-ble), ˝R˝ (resistant), and ˝I˝ (intermediate).The results were considered consistent if all algorithms assigned the same level of resistance for the same drug. Complete divergence in the interpretation of the results was related to the case when one
Original Article
3-7
RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com5
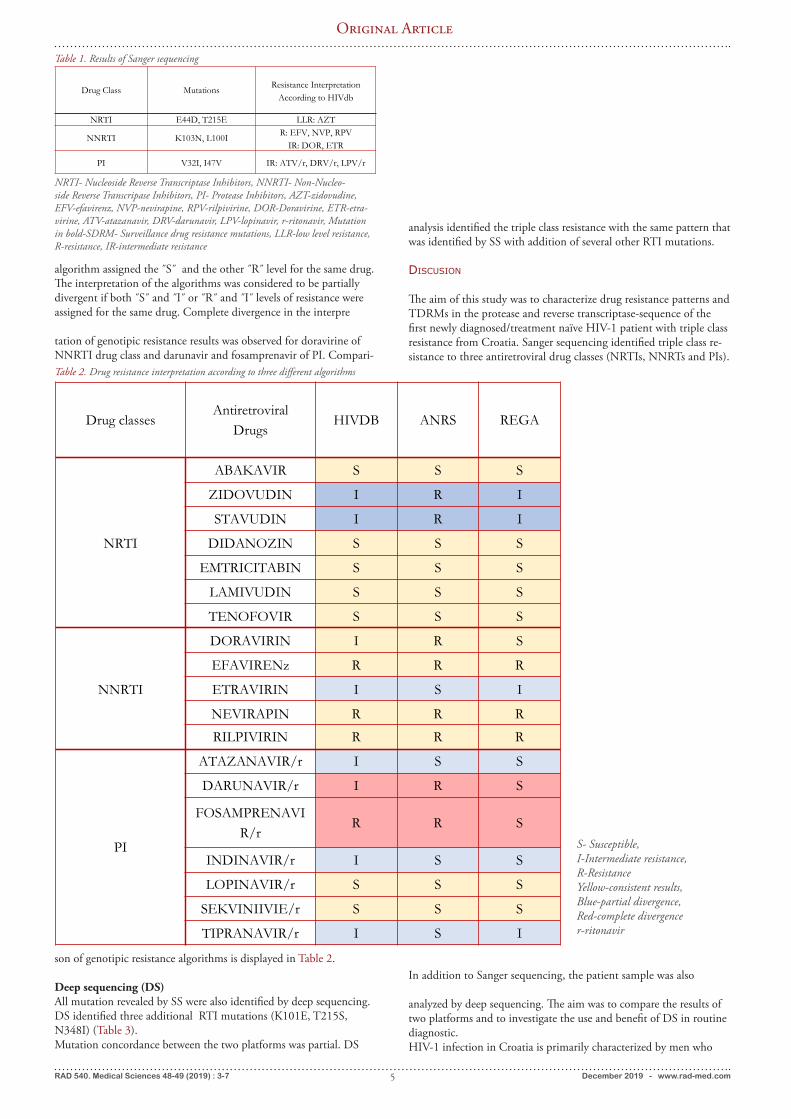
algorithm assigned the ˝S˝ and the other ˝R˝ level for the same drug. The interpretation of the algorithms was considered to be partially divergent if both ˝S˝ and ˝I˝ or ˝R˝ and ˝I˝ levels of resistance were assigned for the same drug. Complete divergence in the interpre
tation of genotipic resistance results was observed for doravirine of NNRTI drug class and darunavir and fosamprenavir of PI. Compari-
son of genotipic resistance algorithms is displayed in Table 2.
Deep sequencing (DS)All mutation revealed by SS were also identified by deep sequencing. DS identified three additional RTI mutations (K101E, T215S, N348I) (Table 3).Mutation concordance between the two platforms was partial. DS
analysis identified the triple class resistance with the same pattern that was identified by SS with addition of several other RTI mutations.
discusion
The aim of this study was to characterize drug resistance patterns and TDRMs in the protease and reverse transcriptase-sequence of the first newly diagnosed/treatment naïve HIV-1 patient with triple class resistance from Croatia. Sanger sequencing identified triple class re-sistance to three antiretroviral drug classes (NRTIs, NNRTs and PIs).
Drug Class Mutations Resistance InterpretationAccording to HIVdb
NRTI E44D, T215E LLR: AZT
NNRTI K103N, L100I R: EFV, NVP, RPVIR: DOR, ETR
PI V32I, I47V IR: ATV/r, DRV/r, LPV/r
Table 1. Results of Sanger sequencing
NRTI- Nucleoside Reverse Transcriptase Inhibitors, NNRTI- Non-Nucleo-side Reverse Transcripase Inhibitors, PI- Protease Inhibitors, AZT-zidovudine, EFV-efavirenz, NVP-nevirapine, RPV-rilpivirine, DOR-Doravirine, ETR-etra-virine, ATV-atazanavir, DRV-darunavir, LPV-lopinavir, r-ritonavir, Mutation in bold-SDRM- Surveillance drug resistance mutations, LLR-low level resistance, R-resistance, IR-intermediate resistance
Drug classesAntiretroviral
DrugsHIVDB ANRS REGA
NRTI
ABAKAVIR S S S
ZIDOVUDIN I R I
STAVUDIN I R I
DIDANOZIN S S S
EMTRICITABIN S S S
LAMIVUDIN S S S
TENOFOVIR S S S
NNRTI
DORAVIRIN I R S
EFAVIRENz R R R
ETRAVIRIN I S I
NEVIRAPIN R R R
RILPIVIRIN R R R
PI
ATAZANAVIR/r I S S
DARUNAVIR/r I R S
FOSAMPRENAVIR/r
R R S
INDINAVIR/r I S S
LOPINAVIR/r S S S
SEKVINIIVIE/r S S S
TIPRANAVIR/r I S I
Table 2. Drug resistance interpretation according to three different algorithms
S- Susceptible, I-Intermediate resistance, R-ResistanceYellow-consistent results, Blue-partial divergence, Red-complete divergencer-ritonavir
In addition to Sanger sequencing, the patient sample was also
analyzed by deep sequencing. The aim was to compare the results of two platforms and to investigate the use and benefit of DS in routine diagnostic. HIV-1 infection in Croatia is primarily characterized by men who
Original Article
3-7

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com6
have sex with men (MSM) who are mainly infected in Croatia20-21. Currently, HIV-infected persons are entering clinical care at early stages of infection (including acute and recent), but substantial pro-portion of patients are still enrolled into clinical care at the symptom-atic stage of HIV-disease (late presenters). The patient described in this paper classifies as a late presenter to clinical care. The prevalence of TDR in treatment-naive individuals remains stable in most developed countries and the prevalence of acquired drug resistance is decreasing22-29. This implies that further transmission of HIV-1 with TDRMs is occurring in ART-naive individuals6-8. The European SPREAD study, which included data for 25 European countries and Israel, showed an overall primary resistance prevalence of 8.4% (study period 2008 to 2010)30.The prevalence of primary HIV resistance to RT inhibitors in Croatia was one of the highest in the world (22%) for the period 2006-2008 and was associated with a local cluster of MSM caring SDRM T215S31. While NNRTI associated mutations were present at low frequency, no primary resistance mutations related to PI were found during this period31. Results of a more recent study focusing on the period 2014-2017, showed the emergence of SDRM to NNRTI and PI as well as high overall prevalence of primary resistance (around 17%)32.Besides T215 revertants (T215S being the most frequent) that are found common in untreated persons in Croatia, recent data suggested that triple class resistance patterns also contribute to the spread of resistant strains in Croatia as well. Triple class resistant variants, sim-ilar to those that have been described in the patient presented in this
study, have been found to participate actively in the further spread of infection and primary resistance both locally and globally32. Results of DS analysis partialy matched the results of Sanger se-quencing. In addition, DS identified low-abundant viral variants with frequencies <10% which were not detected by SS.DS analysis showed that resistant variants responsible for initial infection could have gone under the radar of standard detection (<15%) in late-presenters diagnosed in chronic stage of infection. The implementation of new tehnologies with already existing ones is especially usefull when dealing with complex clinical issues like this patient. This gives a new perspective and inside when choosing first-line treatment options.Availability of more antiretroviral drugs as well as new drug classes has led to virological success even in patients with resistance but indi-viduals with triple class resistance have been associated with a higher risk of disease progression and death34-36. Therefore, the management of such patients is extremely challenging and the issue raises public health concerns because the resistant virus is likely to be spread widely. Early diagnosis and antiretroviral treat-ment of HIV-1 infections are therefore required to prevent the spread of drug-resistant HIV-1.
author contributions:All authors listed have made a substantial, direct and intellectu-al contribution to the work, and approved it for publication.
Sample Mutation concordance
SSSDRM
DSSDRM
Frequency, n (%)
Coverage, number of reads
1378 partial V32I, I47VL100I
K103NT215E
V32II47VL100I
K103NK101ET215ET215SN348I
6.343.132.032.64.638.34.723.6
94728868568272651745147236
Table 3. Comparison of SDRM detected with Sanger (SS) and deep sequencing (DS)
SDRM-Surveillance drug resistance mutations
literature:1. Volberding PA, Deeks SG. Antiretroviral therapy and manage-ment of HIV infection. Lancet. 2010; 376:49-62.2. Günthard HF, Calvez V, Paredes R, Pillay D, Shafer RW, Wens-ing AM, Jacobsen DM, Richman DD. Human Immunodeficiency Virus Drug Resistance: 2018 recommendations of the internation-al antiviral society-USA Panel. Clin Infect Dis. 2018.3. TenoRes Study Group. Global epidemiology of drug resistance after failure of WHO recommended first-line regimens for adult HIV-1 infection: a multicentre retrospective cohort study. Lancet Infect Dis. 2016; 16:565-75. 4. De Luca A. The impact of resistance on viral fitness and its clin-ical implications. In: Geretti AM, editor. Antiretroviral Resistance in Clinical Practice. London. 2006.5. Machnowska P, Meixenberger K, Schmidt D, IJessen H, Hillen-brand H, Gunsenheimer-Bartmeyer B, Hamouda O, Kucherer C, Bannert N, the German HIV-1 Seroconverter Study Group. Prev-alence and persistence of transmitted drug resistance mutations in the German HIV-1 Seroconverter Study Cohort. PLOS ONE, 2019; https://doi.org/10.1371/journal.pone.0209605.6. Pouran Yousef K, Meixenberger K, Smith MR, Somogyi S, Gromoller S, Schmidt D, et al. Inferring HIV-1 Transmission Dy-
namics in Germany From Recently Transmitted Viruses. J Acquir Immune Defic Syndr. 2016; 73(3):356-63. 7. Hauser A, Hofmann A, Hanke K, Bremer V, Bartmeyer B, Kuecherer C, et al. National molecular surveillance of recently acquired HIV infections in Germany, 2013 to 2014. Euro Surveill. 2017; 22(2). 8. De Luca A, Zazzi M. Interplay Between Transmitted and Ac-quired HIV Type 1 Drug Resistance: Reasons for a Disconnect. J Infect Dis. 2015; 212(1):5-7. 9. Cossarini F, Spagnuolo V, Gianotti N, Carbone A, Lazzarin A, Castagna A. Management of HIV infection after triple class failure.. New Microbiologica. 2012; 36: 23-39.10. Messiaen P, Verhofstede C, Vandenbroucke I, Dinakis S, Van Eygen V, Thys K, Winters B, Aerssens J, Vogelaers D, Stuyver LJ, Vandekerckhove L. Ultra-deep sequencing of HIV-1 reverse transcriptase before start of an NNRTI-based regimen in treat-ment-naive patients. Virology. 2012; 426(1):7-11.11. Ekici H, Rao SD, Sönnerborg A, Ramprasad VL, Gupta R, Neogi U. Cost-efficient HIV-1 drug resistance surveillance using multiplexed high-throughput amplicon sequencing: implica-tions for use in low- and middle-income countries. J Antimicrob
Original Article
3-7

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com7
Chemother. 2014; 69(12):3349-55.12. Kijak GH, Sanders-Buell E, Harbolick EA, Pham P, Chenine AL, Eller LA, Rono K, Robb ML, Michael NL, Kim JH, Tovanab-utra S. Targeted deep sequencing of HIV-1 using the IonTorrent-PGM platform. J Virol Methods. 2014; 205:7-16. 13. Casadellà M, Paredes R. Deep sequencing for HIV-1 clinical management. Virus Res. 2017 Jul 2. Alidjinou EK, Deldalle J, Hallaert C, Robineau O, Ajana F, Choisy P, Hober D, Bocket L. RNA and DNA Sanger sequencing versus next-generation sequencing for HIV-1 drug resistance testing in treatment-naive patients. J Antimicrob Chemother. 2017; 72(10):2823-2830.14. Trabaud MA, Icard V, Ramière C, Tardy JC, Scholtes C, André P. Comparison of HIV-1 drug-resistance genotyping by ul-tra-deep sequencing and sanger sequencing using clinical samples. J Med Virol. 2017; 89(11):1912-1919.15. Croatian National Institute of Public Health. (http://www.hzjz.hr/epidemiologija/hiv.htm) (Accessed October 2019)16. Begovac J, Zekan A, Skoko-Poljak D. Twenty years of human immunodeficiency virus infection in Croatia-an epidemic that is still in an early stage. Coll Antropol 2006; 30:17-23.17. Bennett, DE et al. Drug resistance mutations for surveillance of transmitted HIV-1 drug-resistance: 2009 update. PLoS One. 2009; 4: e4724. DOI: 10.1371/journal.pone.0004724, 18. Stanford University HIV Drug Resistance Database. Available at, http://hivdb.stanford.edu/DR/ (Accessed, October, 2019).19. HyDRA Web. Analyze Next Generation Sequencing data for HIV Drug Resistance. Available at, https://hydra.canada.ca/pages/home?lang=en-CA, (Accessed, June 2019). 20. Bozicevic, I, Begovac, J. The emerging HIV epidemic among men who have sex with men in southeastern Europe. Expert. Rev. Anti. Infect. Ther. 8, 2010; 1351-1358.21. Bozicevic, I et al. Prevalence of HIV and sexually transmitted infections and patterns of recent HIV testing among men who have sex with men in Zagreb, Croatia. Sex. Transm. Infect. 2012; 88:539-544. 22. Pineda-Pena AC, Schrooten Y, Vinken L, Ferreira F, Li G, Tro-vao NS, et al. Trends and predictors of transmitted drug resistance (TDR) and clusters with TDR in a local Belgian HIV-1 epidemic. PLoS One. 2014; 9(7):e101738. 23. Yang WL, Kouyos R, Scherrer AU, Boni J, Shah C, Yerly S, et al. Assessing the Paradox Between Transmitted and Acquired HIV Type 1 Drug Resistance Mutations in the Swiss HIV Cohort Study From 1998 to 2012. J Infect Dis. 2015; 212(1):28-38. 24. Mourad R, Chevennet F, Dunn DT, Fearnhill E, Delpech V, Asboe D, et al. A phylotype-based analysis highlights the role of drug-naive HIV-positive individuals in the transmission of an-tiretroviral resistance in the UK. AIDS. 2015; 29(15):1917-25. 25. Parczewski M, Leszczyszyn-Pynka M, Witak-Jedra M, Maciejewska K, Rymer W, Szymczak A, et al. Transmitted HIV drug resistance in antiretroviral-treatment-naive patients from Poland differs by transmission category and subtype. J Antimicrob Chemother. 2015; 70(1):233-42. 26. Ambrosioni J, Sued O, Nicolas D, Parera M, Lopez-Dieguez
M, Romero A, et al. Trends in Transmission of Drug Resistance and Prevalence of Non-B Subtypes in Patients with Acute or Re-cent HIV-1 Infection in Barcelona in the Last 16 Years (1997–2012). PLoS One. 2015; 10(6):e0125837. 27. Schmidt D, Kollan C, Fatkenheuer G, Schulter E, Stellbrink HJ, Noah C, et al. Estimating trends in the proportion of trans-mitted and acquired HIV drug resistance in a long term observa-tional cohort in Germany. PLoS One. 2014; 9(8):e1044728. Paraskevis D, Kostaki E, Magiorkinis G, Gargalianos P, Xylomenos G, Magiorkinis E, et al. Prevalence of drug resistance among HIV-1 treatment-naive patients in Greece during 2003–2015: Transmitted drug resistance is due to onward transmissions. Infect Genet Evol. 2017; 54:183-91.29. Bezemer D, van Sighem A, Lukashov VV, van der Hoek L, Back N, Schuurman R, et al. Transmission networks of HIV-1 among men having sex with men in the Netherlands. AIDS. 2010; 24(2):271-82. 30. Vercauteren J, Wensing AM, van de Vijver DA, Albert J, Balotta C, Hamouda O, Kucherer C, Struck D, Schmit JC, Asjo B, Bruckova M, Camacho RJ, Clotet B, Coughlan S, Grossman Z, Horban A, Korn K, Kostrikis L, Nielsen C, Paraskevis D, Poljak M, Puchhammer-Stockl E, Riva C, Ruiz L, Salminen M, Schuur-man R, Sonnerborg A, Stanekova D, Stanojevic M, Vandamme AM, Boucher CA. Transmission of drug-resistant HIV-1 is stabi-lizing in Europe. J Infect Dis. 2009; 200:1503-1508.31. Grgic I, Zidovec Lepej S, Lunar MM, Poljak M, Vince A, Vrakela IB, Planinic A, Seme K, Begovac J. The prevalence of transmitted drug resistance in newly diagnosed HIV-infected in-dividuals in Croatia: the role of transmission clusters of men who have sex with men carrying the T215S surveillance drug resistance mutation. AIDS Res Hum Retroviruses. 2013; 29:329-336.32. Oroz M, Planinic A, Begovac J, Židovec-Lepej S. High preva-lence of transmitted HIV drug resistance mutations in a cohort of newly diagnosed HIV-infected patients at entrance to care in the period from 201 to 2015: The Croatian data. Abstract presented at 16th European Meeting on HIV & Hepatitis 2018, May 30- June 1, Rome, Italy. 33. Zaccarelli M, Tozzi V, Lorenzini P, Trotta MP, Forbici F, Vis-co-Comandini U, Gori C, et al.Multiple drug class-wide resistance associated with poorer survival after treatment failure in a cohort of HIV-infected patients. AIDS (London, England). 2005;19 (10):1081-1089.34. Grover D, Copas A, Green H, Edwards SG, Dunn DT, Sabin C, Phillips A, Allen E, Pillay D and UK collaborative group on hiv drug resistanceand uk collaborative hiv cohort study. What is the risk of mortality following diagnosis of multidrug-resis-tant HIV-1? The Journal of Antimicrobial Chemotherapy. 2008; 61(3):705-713.35. Di Giambenedetto S, Colafigli M, Pinnetti C, Bacarelli A, Cingolani A, Tamburrini E, Cauda R, De Luca A. Genotypic resistance profile and clinical progression of treatment-experi-enced HIV type 1-infected patients with virological failure. AIDS Research and Human Retroviruses. 2008; 24(2):149-154.
Original Article
3-7

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com8
Arteriovenous Fistula After Kidney Transplantation in University Hospital
Centre OsijekAnton Jurić1 , Lada Zibar2,3
1 University Hospital Centre Osijek, Department of Diagnostic and Interventional Radiology, Osijek, Croatia2University Hospital Merkur, Department of Internal medicine, Division of Nephrology, Zagreb, Croatia
3 School of Medicine, University J. J. Strossmayer, Osijek, Croatia
abstract:Aims: To examine the proportion of patients with thrombosis or surgical ligation of arteriovenous fistula (AVF) after kidney transplantation (TX) and to explore the time passed after the TX until the loss of AVF function.Patients and methods: The study design was historical cohort study. The study included all 123 patients (57.7 % men, median age 58 years, from 34 to 79) that underwent kidney TX in the University Hospi-tal Centre Osijek during the first 10 years of practicing that kind of surgery in the hospital. The data on AVF function, thrombosis or ligation were undertaken from medical records, along with demographics (age, gender, time after TX). The data were presented descriptively and after statistical analysis that was performed using SPSS (version 17.0).Results: FunctionalAVF immediately prior to TX was found in 78 % of the patients. The AVF was still functional in 39.84 % of all patients for 3 years (median, interquartile range, IQR 0 – 3) after TX. AVF thrombosis happened in 17.89 %, while surgical ligation was performed in 20.33 % of all patients. The most common reason for ligation was increased risk of heart failure (in 75 % of the ligations), followed by aneurysmatic dilatation and arm swelling. Median time after TX to thrombosis or ligation of AVF was 2 years, IQR 0 – 3. Thrombosis or ligations were significantly more frequent in women. The outcome of AVF after kidney TX was not related to the patient’s age.Conclusion: AVF after kidney TX often became nonfunctional, either after spontaneous thrombosis or after surgical ligation, which was required for increased heart failure risk in the majority of the cases.
Keywords: arteriovenous fistula; kidney transplantation; thrombosis; ligation; heart failure
Sažetak: Arterijskovenska fistula nakon bubrežnog presađivanja u Kliničkom bolničkom centru OsijekCilj: Istražiti udio ispitanika u kojih je nakon bubrežnog presađivanja (transplantacije, TX) došlo do tromboze ili ligacije arterijskovenske fistule (AVF) te istražiti vrijeme nakon TX-a u kojemu je došlo do gubitka funkcije AVF-a.Ispitanici i postupci: Istraživanje je ustrojeno kao kohortno povijesno istraživanje.Uključeno je svih 123 bolesnika (57,7 % muških, medijana dobi 58 godina, od 34 do 79) kojima je bubrežni presadak trans-plantiran u Kliničkom bolničkom centru Osijek tijekom prvih 10 godina otkako se u toj bolnici vrši bubrežni TX. Iz medicinskih zapisa preuzeti su podaci o funkciji AVF-a, trombozama i ligacijama, kao i demografski podatci (dob, spol, vrijeme nakon TX-a). Podaci su prikazani deskriptivno i analitički, a statistički obrađeni pomoću SPSS-a (inačica 17.0).Rezultati: AVF neposredno prije TX-a imalo je 78 % bolesnika. Još uvijek funkcionira u 39,84 % svih ispitanika, 3 godine (medijan, interkvartilni raspon, IQR od 0 do 3) nakon TX-a. Tromboza AVF-a je nastupila u njih 17,89 %, a ligacija je izvedena u 20,33 % svih ispitanika. Najčešći razlog ligacije AVF-a u našem istraživanju bio je srčano opterećenje (u 75 % ligacija), zatim aneurizmatična dilatacija AVF-a te otok ruke. Vrijeme nakon TX-a do tromboze ili ligacije bilo je medijana 2 godine (IQR 0 – 3). Trom-boza ili ligacija bili su značajno češći u žena. Sudbina AVF-a nakon bubrežnog TX-a nije bila povezana s dobi bolesnika.Zaključak: AVF nakon bubrežnog TX-a često postaje nefunkcionalna, nakon spontane tromboze ili kirurške ligacije, a koja je najčešće indicirana zbog srčanog opterećenja.
ključne riječi: arterijskovenska fistula; bubrežna transplantacija; tromboza; ligacija; srčano zatajenje;
OPEN ACCESS
Correspondence: Anton Jurić [email protected]/0000-001-8770-7268
This article was submitted to RAD CASA - Medical Sciences as the original article
Conflict of Interest State-ment: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Received: 28 August 2019Accepted: 17 October 2019Published: 27 December 2019
Citation:Juric A and Zibar L. Arteriovenous Fistula After Kidney Transplantation in Clinical Hospital Centre Osijek. RAD CASA - Medical Sciences. 540=48-49 (2019): 8-14. https://dx.doi.org/10.21857/yrvgqtkdp9
Copyright (C) 2019 Juric and Zibar. This is an open-access article distributed under the terms of the Creative Commons Attribution Li-cense (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original au-thor(s) and the copyright owners(s) are credited and that the original publication in this journal is cited, in accordance whit accepted adacemic practice. No use, distribution or re-production is permitted which does not comply with these terms.
Original Article
8-14

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com9
introduction
The Arteriovenous Fistula (AVF) is a permanent vascular approach for patients with chronic kidney disease (CKD) in the form of a direct (subcutaneous compound between the radial artery and the cephalic vein on the forearm, but may be used and the blood vessels more proximal than the carpal joint or under the elbows) or of the indirect AVF (a compound between the artery and vein which is usually formed by a syntethic vascular implant), so-called. polytetrafluoro-ethylene graft (PTFE). The central venous catheter (CVC) is used in those patients who have exhausted other possibilities of permanent vascular access1-4. CKD is defined as a reduction of renal glomerular filtration <60 ml / min / 1.73 m2 of body surface area for three or more months. Diabetic and hypertensive nephropathy, glomerulonephritis, and autosomal dominant polycystic kidney disease are the main causes of CKD appearing in developed countries such as the United States, but also in many underdeveloped countries5,6. Clinical symptoms of the disease appear in the damage more than 80% of kidney function, or from the third stage of a disease. It manifests as anemia, weakness, fatigue, loss of appetite and nocturia. The final stage of the CKD is in fifth grade. Then there are various organic complications such as cardiovascular, digestive, neurological, hematological, endocrinolog-ical, etc. At this stage, life is unsustainable without replacing renal function by dialysis through previously created AVF or transplanta-tion (TX)7-10.
rePlacement of renal function
Dialysis is the process of eliminating waste metabolites and excess water from the body. There are two methods of dialysis: hemodialy-sis (HD) and peritoneal dialysis (PD)10. HD is a procedure that re-moves blood from the body, and purified through a filter out of the body, called dialyzer, and require repeated access to the bloodstream. HD-blood of the patient flowing through the tube connected AVF and through a dialyzer. During HD, heparin is used, a medication that prevents blood clotting inside the dialyser. Inside the dialyzer, a porous membrane made of separated blood fluid (dialysate) which is chemically similar to normal body fluids. The pressure side of the membrane where the dialysate is less than that on the side of the blood, allowing the liquid, and waste products harmful compounds in the blood cross the (filtered) through the membrane into the dialysate. Blood cells and large proteins are too large to pass through the small membrane cavities. The dialyzed (purified) blood returns to the patient's body 10.PD uses the peritoneum as a semipermeable membrane for the ex-change of matter. It is based on pouring a solution containing elec-trolytes and glucose or icodextrin as the osmotic substances in the abdominal cavity, typically by gravity. Uremic toxins from the blood passes into the dialysate concentration gradient down the diffusion process, while the osmolality of dialysate determines migration of water. The tip of the catheter with numerous perforations is placed in a small pelvis and the outer part remains outside the abdominal cavity1-4.TX is the best method of repleacing the renal function in the treatment of CKD. Often, a regular exacerbated renal function is achieved so that one transplanted kidney can completely replace the lost function of its own kidneys. Dialysis is usally necessary for the appropriate treatment and preparation of patients for TX and sub-sequent immunosuppression therapy, although TX can also be done
without prior dialysis - so-called. preemptivni TX. Due to constant immune response to allograft kidney, lifetime is performed immuno-suppressive therapy to prevent graft rejection11-17.There are several chiral access options for HD: AVF, then AV graft or CVC18,19. In a study evaluating the quality of life in patients with AVF or AV graft, it was concluded that he was equal to or moderate20. However, due to the blood flow of about 400 ml / min required for high quality dialysis, high passage and low incidence of infection, AVF is a better choice compared to AV graft or CVC18,19. It is most commonly used when kidney glomerular filtration is <15 ml / min / 1.73 m2 of body surface21. It is created by a short joining of the arteries with the vein located mostly on the proximal part of the upper arm (cervical vein and radial artery or basal vein and ulnar artery)18,19. The maturity for successfully performing subcutaneous AVF puncture is reached when arterial venous arterialization occurs due to the constant artery blood vessel. The vein grows and becomes visible on the skin22. The AVF's maturity can also be stimulated by compressing the rubber ball. Then it becomes large enough to accept a large blood flow of about 400 ml / min required for successful dialysis. AVF, as such, becomes mature for its basic function23.
avf comPlications
In recent years ischemic lesions that were caused by arterial phe-nomenon of "steal", have become more common in the elderly population with high morbidity accompanying vascular disease and diabetes patients. There are two forms of this phenomenon. The first is associated with the rapid flow in which AVF with very low resistance begins to "suck" the blood from the palmar arch and ulnar artery, creating a critical ischemia of the fingers. In theory, this type of lesion is relatively easily corrected by limiting the size of anastomosis and reducing the flow of fistula24,25. Since resistance goes with the fourth potency of the radius according to Poiseuill's law, only a drastic reduction of the lumen of the fistula will be effec-tive. However, creating an effective and safe lumen is difficult and it poses a risk of low flow and possible thrombosis.Harder, but unfortunately increasing frequency, is another form of the "steal" phenomenom and that in patients with low blood flow through the AVF. This form is primarily a result of stenosis of peripheral arteries, so even normal blood flow through the fistula will create a critical ischemia in the distal vascular pool. Preoperative monitoring helps to predict the risk of a potential low flow "steal" phenomena from the limited vasodilation of the palmar arch arter-ies, which is manifested by abnormally low postishemic diastolic flow after fingers pressing. There are several treatment options to eliminate this problem. One is to close the fistula and use CVC, and the alternative procedure was originally proposed by Schanzer et al. and has recently been renamed DRIL (distal revascularization-inter-val ligation, closure of distal part of revascularization)26,27.Cardiovascular diseases are the main cause of death in dialysis patients or patients with kidney transplants. In the case of renal TX, the AVF is left open because it is unknown how long it will take for a satisfactory kidney function to last. It is closed by ligation only in the case of cardiac failure, rapid blood flow through the fistula, complications at the entrance to the fistula itself or in case of aesthetic reasons. In the case of ligation, fistula loss occurs and can not be re-opened in case of repeated HD needs. Ligation is more common with fistulas on the upper arm because of the faster blood flow. Fast flow through AVF, greater than 2200 ml/min results in
Original Article
8-14

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com10
increased cardiac output, followed by cardiac failure, hypertrophy or left ventricular dilatation, increased diastolic pressure, pulmonary hypertension, cardiomegaly, distal ischemia, aneurysmatic enlarge-ment etc.28-37. Rapid blood flow leads to damage to the AVF's blood vessel endothelium, which favors the development of inflammatory activity. This results in the accumulation of inflammatory mediators such as interleukin 2, interleukin 6, tumor necrosis factor alpha and C-reactive protein. They exacerbate the onset of heart failure and lead to an increase in mortality in hemodialysis patients 38-44.AVF aneurysms usually result from the destruction of the blood vessels wall and the replacement of the biophysically less valuable collagen tissue. Once aneurysm occurs, Laplace's law predicts a spontaneous tendency of progression, because pressure applied to the walls of blood vessels becomes larger with an increased diameter of the aneurysm. The prerequisite for creating aneurysm is usually stenosis and prolonged increase in blood flow pressure. The main complications of aneurysm are rupture, infection (resulting from intraaneurysmatic thrombi), and in rare cases anterograde or retro-grade emboli45.In addition to the AVF's surgical closure, spontaneous occlusion or thrombosis may occur in the arteries, anastomoses themselves, or usually veins. The most common cause of AVF occlusion is the diameter of the cephalic vein and radial artery. The smaller it is, the greater the risk of occlusion. In addition, high blood pressure and high levels of parathyroid hormone also increase the risk of occlusion. Occlusion can also be due to intimal hyperplasia of blood vessels during the anastomotic surgical procedure46,47. Thrombosis can be caused by stenosis itself, wearing inappropriate clothing, and aneurysmatic enlargement, causing turbulent blood flow, arterial blood supply and arterial hypotension. Pathophysiology based on stenosis is a blood flow turbulence that activates platelets and endo-thelial cells. In this context, the role of platelet growth factor48 was also determined. The final trigger that causes thrombosis is critical reduction of blood flow through the fistula. Many studies prove that low flow through AVF best predictor of thrombosis. The critical flow rate is different in PTFE grafts and AV fistulas. Fistulas that are most susceptible to thrombosis are those with a flow rate <200 ml / min. This is far less than what is needed for optimal blood flow during dialysis. As a result of low blood flow, dialysis will become ineffective and will result in recirculation49. Several procedures help identify critical low blood flow and upcoming stenosis: auscultation (high frequency noise at the site of stenosis), hand lift examination (col-lapse of poststenotic vein segment and permanent congestion of the prestenotic segment), prolonged bleeding after removal of the needle from the injection site and increased pressure in the venous supply during HD, particularly over a number of consecutive dialysis50.Central venous stenosis may be clinically asymptomatic before the creation of vascular access and become symptomatic only when the flow increases. If critical stenosis can not accommodate the increased flow rate, the result will be a run-off hands and cyanosis, as well as the creation of collateral in the wall of the chest. Stenosis of the cen-tral vein is typically the result of previous subclavian catheter, or may be the result of incorporation of a pacemaker and its wire, then pri-mary thrombosis in patients with antiphospholipid antibodies and coagulation disorders, tumors pressure etc. One therapeutic option is to ligate anastomosis and use a second arm after a corresponding X-ray image to exclude bilateral stenosis51-56.
hyPothesis and aim
The hypothesis reads: „Arteriovenous fistula after renal transplanta-tion often become non-functional or require ligation.“ The aims of this study are to investigate the proportion of kidney transplanted subjects with spontaneous thrombosis, planar "closure" of AVF (liga-tion) after TX, and the remaining proportion of AVFs still function-al. Then investigate time after TX where there was a possible loss of AVF function, and finally determine the relationship between these outcomes of AVF with demographic characteristics of respondents (age, sex, time after TX).
methods
The study is structured as a cohort historical research. The study was conducted at the Department of Nephrology, Department of Internal Medicine, Clinical Hospital Center Osijek April-May 2018, with the approval of the Department and the approval of the Ethics Com-mittee for Research Faculty of Medicine Osijek at the University of Osijek.The study included all patients transplanted into KBC Osijek in the first 10 years of kidney TX (2007 - 2017) at this hospital. Of the 123 patients, 57.7% were men. The median age of all patients at the time the study was 58 years, ranging from 34-79 years.AVF function data and events related to AVF (thrombosis, "closure" or ligation), as well as demographic characteristics (age characteristics, sex, time after TX) are taken from medical records.
statistical Procedures
The data are presented descriptively and processed analytically. Nominal data are presented using absolute and relative frequencies. The numerical data are presented as medians and interquartile range. The distribution normality was tested by Kolmogorov-Smirnov test. Frequency differences were measured by the hi-squared test in the numerical variables of the asymmetric distribution with the Kruskal-Wallis test. Statistical significance was accepted at P <0.05. Statistical analysis was performed using SPSS software (version 17.0).
results
The study was conducted on 123 patients, of whom 71 (57.7%) were men and 52 (42.3%) women. Functional AVF, just before TX, had 96 (78%) patients, 77 (80.2%) on the left hand. AVF after TX is currently functioning in 49 patients (39.8% of all and 51% of patients with functional AVF just prior to TX) (median follow-up 3 years, interquartile range (IQR) 1-5, from 0 to 10). AVF thrombosis had, at some point after TX, 22 (17.9% of all) patients (21.9% of those with functional AVF immediately before TX), and 25 (20.3 % of all, or 26% of those who had functional AVF just prior to TX). The most common cause of ligation was (for 18 patients, 75% who had ligation) cardiac overload (Table 1).Glomerulonephritis and autosomal dominant polycystic kidney dis-ease were the two most common causes of renal failure in transplant patients. These are followed by interstitial nephritis, diabetes, arterial hypertension and others (malignant disease, urinary abnormali-ties, vasculitis) (Table 2)The time to thrombosis or ligation of AVF was median 2 years (IQR 0 - 3). The median age at TX was 52 years (IQR 47-58) ranging from 27 to 70 years (Table 3). The median age of all patients was 58 years, ranging from 34 to 79. Twelve patients (9.8%) had 2 or more renal TX-a. AVF is curently functioning
Original Article
8-14

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com11
in 49 (39.84 %) patients (Picture 1). In the post-transplant period until the time of this study, 13 (10.6%) respondents died, most often due to a heart attack (4 patients, 3.3%). Graft works or the patient died with a functioning graft in 107 (87%) patients. Graft does not work or the patient died with graft by failed in 16 (13%) patients. The patient is alive and graft works in 96 (78%) patients. The patient is not alive or is not functioning graft in 27 (22%) patients. (Table 4).The fate of AVF significantly differed between men and wom-en, so women had more often AVF thrombosis or ligation (χ2 = 7,948, P = 0.047). In most women who had a func-tional AVF (36 out of 52) immediately before TX, there was
Number (%) of respondents
GenderMales 71 (57,7)Females 52 (42,3)
AVF* before transplantationYes 96 (78)No 27 (22)Total 123 (100)
AVF* considering the handRight arm 19 (19,8)Left arm 77 (80,2)Total 96 (100)
The reason for the ligationAneurysmatic dilatation 5 (21)Cardiac overload 18 (75)Hand oedema 1 (4)
Total 24 (100)*arteriovenous fistula
Table 1. Characteristics of the patient
Basic kidney diseaseNumber (%) of
respondentsGlomerulonephritis 56 (45,5)Autosomal dominant polycystic kidney disease 22 (17,9)Diabetes 13 (10,6)Arterial hypertension 6 (4,9)Interstitial nephritis 14 (11,4)Others 12 (9,8)
Table 2. Cause of renal function failure (N = 123)
Median(interquartile range)
Minimum –maximum
Time after TX to thrombosis or ligation of AVF (year)(n = 47)
2 (0 – 3) 0 - 7
Time after TX to AVF Thrombosis (months) in thefirst year after TX (n = 12)
1 (1 – 3) 1 - 9
Time on dialysis (years) 3 (1 – 5) 0 - 14Follow-up after TX (years) 3 (1 – 5) 0 - 9Age at TX (years)Age at TX (years) 52 (47 – 58) 27 - 70
Table 3. Age of transplantation patients (TX), time to thrombosis or arterial fistula ligation (AVF), dialysis time and duration of TX
without AVF, before TX-a
22%
in function40%
tromosis18%
ligation20%
without AVF, before TX-a
in function
tromosis
ligation
Picture 1. Distribution of patients with fate of arterial fistula (AVF) after renal transplantation (TX). AVF patients did not have functional AVF just before TX. Number provided below indicates the percentage of the absolute number of patients in the group.
a thrombosis (in 9) or AVF was ligated (in 13). In 60 out of 71 men AVF was functional just before TX, 13 of them was thrombosed and in 12 was ligated. Patients did not differ in age from AVF fate (P = 0.76, Kruskal-Wallis test).
discussion
In our study of 123 patients with kidney transplant, AVF is currently functioning in 39.84% of patients (median follow-up 3 years), AVF thrombosis at some point after TX had 17.89% of patients, and their ligation 20.33%. The most common cause of AVF ligation in our study was heart over-load, for 18 patients (75% of those who had a ligation). AVF after the renal TX has, therefore, often become dysfunctional, spontaneous or surgically closed.In the research of Schier et al. there were 113 patients involved. In most patients it was necessary to close the AVF because of the onset of symptoms of heart overload, which corresponds to our results, which, in their study were caused by the rapid flow of blood through the AVF59. Since the blood flow is faster through the AVF, which are on the upper arms but the forearms60, so is the “closure” of AVF in the research of Schier et al. more often in those patients with AVFs on the upper arms.We do not have information on the exact localiza-tion of the AVF on hand for our patients and no data on the flow rate through the AVF. Vascular surgeons did not want to do the AVF ligation if there were no pathological findings in echocardiography in these patients, and the most common pathological findings on echocardiography were pulmonary hypertension and right ventricular dilatation59. Echocar-diographic data for our patients were also not available.The assessment of cardiac load was mostly clinical. This and our research shows that the need to close AVF in patients with kidney stones is not uncommon59. Furthermore, studies by Unger and Van Dujnhover indicate that closure of the AVF ligation has a positive impact on the weight and diameter of the left ventricle57,58. Thus, AVF ligation in our patients due to cardiac overload is justified.However, the published reports are not unambiguous. Unger et al. in 17 transplant patients demonstrated that rapid blood flow through AVF favors the development of cardiac failure and death of the patient57.
Original Article
8-14

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com12
Contrary to De Lima et al. and Meeus et al. show different results and claim that cardiac failure does not appear to be an AVF complication and that rapid blood flow through AVF for a longer period has a weak influence on morphology and heart function.They find that cardiac failure only occurs in those pa-tients who already suffer from heart disease. It should be noted however that their studies were conducted on relatively young patients in the range of 33.4 ± 12.5 years who were generally in good condition without heart failure and had not been sub-jected to TX33,36. However, De Lima et al., comparing echocar-diographic features in 39 transplanted patients with functional AVF and 21 patients with “closed” AVF, proved that “open” AVF can cause cardiac overload33. In the research conducted by Manca et al. in 365 transplanted patients with AVF, 42 (11.5%) had AVF ligation due to aneurysmatic dilation, steal phenom-ena, infection, edema or aesthetic reasons28. A special case was described by Clarkson et al. in which AVF was the cause of high pulmonary arterial pressure and early decompensation of the right ventricle30. In our study of other reasons for the closure of AVF, except cardiac overload were aneurysmatic dilatation in 21% of them and hand oedema in 4% of patients, while in re-search conducted by Schier et al. only two ligation were related to flow, but one was due to aesthetic reasons and the other due to infection59.Our study included all 123 patients who received a kidney transplant transplant in KBCO since in that hospital performs kidney TX (over a ten year period). The median age of all patients at the time of the study was 58 years, ranging from 34 to 79 years. In Leeja et al. the median age of all patients was 64 years, and 47% of them were older than 65 years. According to their study, no link was found between the age of patients over 65 and the number of AVF closures (ligations)61. Neither in our study of AVF fate after TX was not related to the age of the patient.Miller et al. have shown that the incidence of thrombosis and other technical complications of AVF are more apparent in women than in men which is in line with our study in which AVF thrombosis or ligation was more common in women. Otherwise, this phenomenon that occurs more frequently in female patients in Miller et al., is not fully understood, but is considered to be related to the diameter of the blood vessels and the difficulty of expanding the veins under the pressure of the
blood coming from the artery62.In our study, the median time spent on dialysis was 3 years and 9.8% of patients had two or more TXs. In a study by Schier et al. the median time spent on dialysis was 3 years and 6 months, and 21.2% of patients had two or more TXs. Accordingly, no correlation was found between the number of TXs in patients and the number of AVF ligation, as well as a correlation be-tween the time spent on dialysis and the need for AVF closure59. In our study, such a thesis was not proven. Among other things, Schier et al. consider that there is a link between faster need for “closure” of AVF with faster flow rate and reduced need for “closur” of AVF with slower blood flow59. In our study, as noted above, no data were available on the rate of blood flow through the AVF.The median time to AVF thrombosis or ligation in our par-ticipants was 2 years, while in 12 patients who experienced thrombosis during the first year, AVF usually stopped function-ing as early as the first month. In a study by Schier et al., the median time to thrombosis or ligation of AVF was 2 years and 6 months, consistent with our result59.Previous studies on the fate of AVF have been in the form of case reports or have been conducted in a small number of patients. This study, as well as the study conducted by Schier et al., may show success in the closure or ligation of AVF to pre-vent the development of cardiac overload, especially in individ-uals with rapid blood flow through AVF. An individual decision to close or not to close AVF must include all relevant factors, especially the function of the transplanted kidney, as well as the ability to create a new vascular approach in the event of graft re-jection. Diseases such as anemia and hypertension can mask the symptoms of heart failure, therefore echocardiographic moni-toring as well as other non-invasive procedures may be useful for timely intervention in the event of a potential development of cardiac overload caused by rapid flow through AVF59. In our patients, the assessment of heart overload caused by AVF has not been echocardiographically demonstrated.
conclusion
Based on the results of the study, the following conclusions can be drawn: AVF before TX had 78% of patients, AVF is currently functioning in 39.84% of patients, and AVF was ligated or thrombosed in 38.22% of patients. Furthermore, the most common cause of AVF ligation in our study was cardiac overload, the time to thrombosis or ligation was median 2 years after TX, and if thrombosis occurred in the first posttransplant year, then it occurred at the median time 1 month after TX. And finally, AVF thrombosis or ligation was more common in women, and the fate of AVF after renal TX was not related to patient age. In conclusion, AVF after renal TX often becomes dysfunctional, following spontaneous thrombosis or surgical ligation most commonly indicated by cardiac overload.
Number (%) of respondents
The outcomeAlive 110 (89,4)Died 13 (10,6)
The cause of deathHeart attack 4 (3,3)Kidney carcinoma 1 (0,8)Cytomegaloviral disease 1 (0,8)Cardiac failure 1 (0,8)Cholecystitis with sepsis 2 (1,6)Unknown cause 1 (0,8)Pulmonary embolism 1 (0,8)Sepsis 2 (1,6)
Graft works or the patient died with a functioning graftYES 107 (87)NO 16 (13)
Graft works and the patient is aliveNO 27 (22)YES 96 (78)Total 123 (100)
Table 4. The outcome of the treatment
Original Article
8-14

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com13
author contributions:All authors listed have made a substantial, direct and intellec-tual contribution to the work, and approved it for publication.
literature:1. Kes, P.;Bašić Jukić, N.; Jurić I. 2006. Liječenje željezom bolesnika na dijalizi. Acta Medica Croatica. 60-4572. Davidson, AM (ur.); Cameron, JS.; Grünfeld, JP.; Ponticelli, C.; Ritz, E.; Winearls, C.G. i sur. 2005. Oxford Textbook of Clinical Nephrology. III. izd. Oxford University Press. Oxford. 3. Jacobs, C.;, Kjellstrand, CM.; Koch, KM.; Winchester, JF. 1996. Replacement of Renal Function by Dialysis. IV. izd. Kluwer Academic Pubs. Dordrecht – Boston – London.4. Kes, P. i sur. 2006. Regulacija krvnog tlaka u bolesnika na dijalizi. Liječ Vjesn. 128-3685. Levey, A.; Eckardt, K.; Tsukamoto, Y.; Levin, A.; Coresh, J.; Rossert, J. i sur. 2005. Definition and classification of chronic kidney disease: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney International. 67(6):2089-2100.6. Webster, AC.; Bagler, E.V.; Morton, R. L.; Masson, P. 2017.Chron-ic kidney disease. Lancet. 389(10075):1238–1252.7. Skorecki, K. i sur. 2005. Chronic renal failure. U: Kaspar, D.L. i sur. (ur.) Harrison’s Principles of Internal Medicine. 15. Izd. Mc-Graw-Hill.New York. 1653.8. Kumar, P.; Clark, M. 2005.Clinical Medicine. 6. Izd. Elsevi-er-Saunders, Edinburgh. 665.9. Levey ,A.S. i sur. 2005.National Kidney Foundation Practice Guidelines for Chronic Kidney Disease: Evaluation, Clasification. And Stratification. Ann Intern Med. 139-137.10. Ivančević, Željko; Rumboldt, Zvonko; Bergovec, Mijo; Silobrčić, Vlatko. 2010. MSD (THE MERCK MANUAL OF DIAGNOSIS AND THERAPY) - priručnik dijagnostike i terapije. 2.hrvatsko izdanje.Split: PLACEBO.11. Nankivell, B.J.; Chapman, J.R. 2006. Chronic allograft nephropa-thy: Current concepts and future directions. Transplatation. 81-64312. Sollecito, T.P. 2006. Transplatacijska medicina. U: MS Green-berg. Ur. Glick, M. Burketova Oralna medicina. 10. Izd. Medicinska naklada. Zagreb. 503.13. Referentni centar Ministarstva zdravstva i socijalne skrbi Repub-like Hrvatske za tipizaciju tkiva. Godišnje izvješće za 2005. godinu, lipanj 2006.14. Ministarstvo zdravstva i socijalne skrbi RH. Projekti i programi: Transplatacijski program; Legislativa (2004): Nacionalne smjernice za transplataciju bubrega (2005).15. Cohen, B.; Smits, J.; Haase, B.; Persijn, G.; Vanrenterghem, Y.; Frei, U. 2004. Expanding the donor pool to increase renal transplan-tation. Nephrology Dialysis Transplantation. 20(1)-34-41.16. Danovitch, G.M. (ur.). 2005. Handbook of kidney transplatation. 4. Izd. Lipinccott, Williams and Wilkins Philadelphia.1.17. Kes, P. i sur. 2005. Određivanje srčanožilnog rizika prije trans-platacije bubrega. Liječ Vjesn. 127-330.18. Macrae, J.M.; Pandeya, S; Humen, D.P;, Krivitski, N.; Lindsay, R.M. 2004. Arteriovenous fistula-associated high-output cardiac failure: a review of mechanism. Am J Kidney Dis. 43-17.19. Clarkson, M.R.; Giblin, L.; Brown, A.; Little, D.; Donohoe, J.
2002. Reversal of pulmonary hypertension after ligation of a brachio-cephalic arteriovenous fistula. Am J Kidney Dis.40-E8.20. Swaroop, D.; Dimple, M. 2015. Comparative study to assess healthrelated quality of life among chronic kidney disease patients undergoing hemodialysis having arteriovenous fistula and venovenous vascular access. BFUNJ. 8(1).21. Moist, L.M.; Lok, C.E.; Vachharajani, T.J.; Xi, W.; Al Jaishi, A.; Polkinghorne, K.R. i sur. 2012.Optimal vascular access in theelderly patient. Seminars in Dialysis. 25(6),640-648. 22. National Kidney Foundation (NKF). 2006. KDOQI clinical practice guidelines and clinical practice recommendations for 2006 updates: Vascular access.American Journal of Kidney Diseases. 48(Suppl. 1).S176 S322.23. Besarab, A. 2004.Vascular access: Issues and management.Contri-butions to Nephrology.142:29-46.24. Burrows, L.; Kwun, K.; Schanzer, H.; Haimov, M. 1979.Hae-modynamicdangers of high flow arteriovenous fistulas. Proc Eur Dial Transplant Assoc. 16:686–687.25. Kinnaert, P.; Struyven, J.; Mathieu, J.; Vereerstaeten, P.; Toussaint, C.; Van Gerrstruyden, J. 1980.Intermittent claudication of the hand after creation of an arteriovenous fistula in the forearm. Am J Surg. 139:838–843.26. Schanzer, H.; Schwartz, M.; Harrington, E.; Haimov, M. 1988.Treatment of ischaemia due to “steal” by arteriovenous fistula with distal artery ligation and revascularization. J Vasc Surg. 7:770–773.27. Knox, R.C.; Berman, S.S.; Hughes, J.D.; Gentile, A.T.; Mills, J.L. 2002.Distal revascularization-interval ligation: A durable and effective treatment for ischemic steal syndrome after hemodialysis access. J Vasc Surg. 36:250–256.28. Manca, O.; Pisano, O.L. 2005. Carta P et al. The management of hemodialysis arteriovenous fistulas in well functioning renal trans-planted patients: many doubts, few certainties. J Vasc Access. 6-182.29. Macrae, J.M.; Pandeya, S.; Humen, D.P.; Krivitski, N.; Lindsay, R.M. 2004. Arteriovenous fistula-associated high-output cardiac failure: a review of mechanism. Am J Kidney Dis. 43-17.30. Clarkson, M.R.; Giblin, L.; Brown, A.; Little, D.; Donohoe, J. 2002. Reversal of pulmonary hypertension after ligation of a brachio-cephalic arteriovenous fistula. Am J Kidney Dis.40-E8.31. Kramar, R.; Oberbauer, R. 2010. Austrian Dialysis and Trans-plantation Registry (OEDTR). Annual Report. Austrian Society of Nephrology.32. Al-ghonaim, M.; Manns, B.J.; Hirsch, D.J.; Gao, Z.; Tonelli, M. 2008. Relation between access blood flow and mortality in chronic hemodialysis patients. Clin J Am Soc Nephrol. 3-387.33. De lima, J.J.G.; Campos Vieira, M.L.; Molnar, LJ.;Medeiros, C.J.; Ianhez, L.E.; Krieger, E.M. 1999. Cardiac effects of persistent hemodialysis arteriovenous access in recipients of renal allograft. Cardiology. 92-236.34. Movilli, E.; Viola, B.F.; Brunori, G et al. 2010. Long-term effects of arteriovenous fistula closure on echocardiographic functional and
Original Article
8-14

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com14
structural findings in hemodialysis patients: a prospective study. Am J Kidney Dis. 55-682.35. Acharya, S.; Banerjee, D.; Fronek, J.; Fossati, N.; Chemla, E.S. 2009. High-output cardiac failure following insertion of right femoral artery to left femoral vein ptfe graft for haemodialysis: a case report. Semin Dial. 22-462.36. Meeus F, Kourilsky O, Guerin AP, Gaudry C, Marchais SJ, Lon-don GM. 2000. Pathophysiology of cardiovascular disease in hemodi-alysis patients. Kidney Int. 76S:140.37. Santoro D, Savica V, Bellinghieri G. 2010. Vascular access for hemodialysis and cardiovascular complications. Minerva Urol Nefrol. 62: 81.38. III. NKF-K/DOQI Clinical Practice Guidelines for Vascular Access: update 2000. American journal of kidney diseases: the official journal of the National Kidney Foundation. 2001.; 37(1 Suppl 1):S137±81.39. Owen, W.F.; Lowrie, E.G. 1998. C-reactive protein as an outcome predictor for maintenance hemodialysis patients. Kidney international. 1998.;54(2):627±36. 40. Kaysen GA. 2001. The microinflammatory state in uremia: causes and potential consequences. Journal of the American Society of Ne-phrology: JASN. 12(7):1549±57. 41. Schomig, M.; Eisenhardt, A.; Ritz, E. 2000. The microinflamma-tory state of uremia. Blood purification. 18 (4):327±32. 42. Rao, M.; Guo, D.; Perianayagam, M.C.; Tighiouart, H.; Jaber, B.L.; Pereira, B.J. et al. 2005. Plasma interleukin-6 predicts cardiovas-cular mortality in hemodialysis patients. American journal of kidney diseases: the official journal of the National Kidney Foundation. 45(2):324±33.43. Hoshi, T.; Kitagawa, K.; Yamagami, H.; Furukado, S.; Hougaku, H.; Hori, M. 2005. Relations of serum high-sensitivity C-reactive protein and interleukin-6 levels with silent brain infarction. Stroke; a journal of cerebral circulation. 36(4):768±72.44. Kobayashi, S.; Nagino, M.; Komatsu, S.; Naruse, K.; Nimura, Y.; Nakanishi, M. et al. 2003. Stretch-induced IL-6 secretion from endo-thelial cells requires NF-kappaB activation. Biochemical and biophysi-cal research communications. 308(2):306±12.45. Klaus Konner, K.;, Nonnast-Daniel, B.;Ritz, E. 2003.The Arterio-venous Fistula. JASN June 1, 2003 vol. 14 no. 61669-168046. Maga, P.; Krzanowski, M.; Kaczmarczyk, P.; Koscielniak, J.; Par-tyka, L.; Belowski, A et al. 2017. Endovascular treatment of dysfunc-tional arteriovenous fistula in hemodialyzed patients — the results of one year follow-up. Acta Angiologica. 22(4):143-14947. Hong, Ding; Di, Gao. 2016. Analysis of arteriovenous fistula fail-ure in hemodialysis patients. Biomedical Research. 27(2):396-400.48. De Marchi, S.; Falleti, E.; Giacomello, R.; Stel, G.; Cecchin, E.; Sepiacci, G.; Bortolotti, N.; Zanello, F.; Gonano, F.; Bartoli, E. 1996. Risk factors for vascular disease and arteriovenous fistula dysfunction in hemodialysis patients. J Am Soc Nephrol. 7:1169–1177.49. Tonelli, M., Hirsch, D.; Clark, T.W.I.; Wile, C.; Mossop, P.;
Marryatt, J.; Jindal, K. 2002. Access flow monitoring of patients with native vessel arteriovenous fistulae and previous angioplasty. J Am Soc Nephrol. 13:2969–2973.50. Turmel-Rodrigues, L.; Pengloan, J.; Rodrige, H.; Brillet, G.; Lataste, A.; Pierre, D.; Jourdan, J-L.; Blanchard, D. 2000. Treatment of failed native arteriovenous fistulae for hemodialysis by intervention-al radiology. Kidney Int. 57: 1124–1140.51. Schwab, S.J.; Quarles, L.D.; Middleton, J.P.; Cohan, R.H.; Saeed, M.; Dennis,V.W. 1988. Hemodialysis-associated subclavian vein ste-nosis. Kidney Int 33: 1156–1159.52. Schillinger, F.; Schillinger, D.; Montagnac, R.; Milcent, T. 1991. Post catheterization vein stenosis in haemodialysis: Comparative angiographic study of 50 subclavian and 50 internal jugular accesses. Nephrol Dial Transpl. 1991.;6: 722–724.53. Konner, K,.;Vorwerk, D. 1997.Permanent pacemaker wires causing subclavian vein stenosis in presence of AV fistula-Is it ever wrong to try angioplasty and stenting ? Nephrol Dial Transplant. 12: 1735–1738.54. Kovalik, E.C.; Newman, G.E.; Suhocki, P.; Knelson, M.; Schwab, S.J. 1994. Correction of central venous stenoses: Use of angioplasty and vascular Wallstents. Kidney Int 45. 1177–1181.55. Vorwerk, D.; Guenther, R.W.; Mann, H.; Bohndorf, K.; Keulers, P.; Alzen, G.; Sohn, M.; Kistler, D.1995. Venous stenosis and occlu-sion in hemodialysis shunts: Follow-up results of stent placement in 65 patients. Radiology 195. 140–146.56. Duncan, J.M.; Baldwin, R.T.; Caralis, J.P.; Cooley, D.A. 1991. Subclavian vein-to-right atrial bypass for symptomatic venous hyper-tension. Ann Thorac Surg 52. 1342–1343.57. Unger, P.; Wissing, K.M.; De pauw L.; Neubauer, J.; Van de borne P. 2002. Reduction of left ventricular diameter and mass after surgical closure in renal transplant recipients. Transplantation. 74-73.58. Van Duijnhoven ECM, Cheriex ECM, Tordoir JHM, Kooman JP, Van hooff JP. 2001. Effect of closure of the arteriovenous fistula on left ventricular dimensions in renal transplant patients. Nephrol Dial Transplant. 16-368.59. Schier, T.; Gobel, G.; Bosmüller, C.; Gruber, I.; Tiefenthaler, M. 2013. Incidence of arteriovenous fistula closure due to high-out-put cardiac failure in kidney-transplanted patients. Clin Transplant. 27:858–865.60. Huijbregts, H.J.; Bots, M.L.; Wittens, C.H.; Schrama, Y.C.; Blankestijn, P.J. 2009. Access blood flow and the risk of complications in mature forearm and upper arm arteriovenous fistulas. Blood Purif. 27-212.61. Lee, K.G.; Chong, T.T.; Goh, N.; Achudan, S.; Tan, Y.L.; Tan, R.Y.; Choong, H.L.; Tan, C.S. 2017. Outcomes of arteriovenous fistu-la creation, effect of preoperativevein mapping and predictors of fistula success in incidenthaemodialysis patients: A single-centre experience.Nephrology 22. 382–387.62. Miller, C.D.; Robbin, M.L.; Allon, M. 2003. Gender differences in outcomes of arteriovenous fistulas in hemodialysis patients. Kidney Int. 63:346–52.
Original Article
8-14

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com15
Connection Between Body Position During Sleep and Findings from Full-Night Polysomnography in Patients with Obstructive Sleep ApneaAlen Juginović1,2 , Renata Pecotić1
1 University of Split School of Medicine, Split, Croatia2 St. Catherine Specialty Hospital, Zabok, Croatia
abstract:Aim: The aim of our study was to determine the association between body position during sleep and OSA severity in patients with newly diagnosed OSA after full-length polysomnography.Subjects and Methods: We conducted a cross-sectional and clinical study involving 414 subjects (281 men and 133 women) older than 18 whose median age was 55 years. In 2017, subjects came to the Center for Sleep Medicine at UHC Split and the Split School of Medicine and their dana was taken from the archives of the same center. All patients did a full-night polysomnography after which the severity of OSA was estimated with the help of AHI in accordance with the OSA diagnosis guidelines prescribed by the American Academy of Sleep Medicine (AASM) and European Sleep Research Society (ESRS). Excessive daily sleepiness has been estimated by the Epworth Sleepiness Scale (ESS). Results: Statistical analysis showed that patients had spent more time on the back (189.9±118.4min) than on the left (113.3±90.9min) or right side (80.6±90.6min) during sleep and had the most sleep apneas on their back (AHI = 31.1±31.9). Patients with diagnosed OSA (AHI≥5) also had higher AHI values on the back (39.1±31.9) than on the left (23.8±25.2) or right side (18.5±25.6) during sleep. Patients with diagnosed OSA in comparison to patients without OSA diagnosis had statistically significantly higher BMI (29.5±4.6kg/m2 vs. 25.3±4.1kg/m2, P<0.001) and neck circumference (42.0±4.4cm vs 37.4±3.9cm, P<0.001). Overall, considering the whole sample, men were taller (180.8±7.4cm than 165.9±6.7cm, P<0.001), had higher BMI (29.4±4.5kg/m2 compared to 26.8±4.9kg/m2, P<0.001 ) and bigger neck circumference (43.2±3.5cm vs. 36.2±3.4cm, P=0.002), as well as a larger ESS sum (7.6±4.7 compared to 6.3±4.8, P=0.021). Using the Pearson Correlation Coefficient, we showed a negative correlation of AHI with sleep time on the right side (r=-0.178, P=0.005) in OSA patients, while positive correlation was found in sleep on the left side (r=0.003, P=0.959) and back (r=0.183, P=0.002). Conclusion: Our research showed that patients sleep the most time n their back and that AHI ist the highest in that sleep position in comparison to other sleep position which worsens sleep quality in the long term.
Keywords: Sleep; Body position; Polysomnography; Obstrucitve Sleep Apnea
Sažetak:poVezanost položaja tijela tijekom spaVanja s nalazima cjelonoćne polisomnografije u pacije-nata s opstrukcijskom apnejom
Cilj: Cilj našeg istraživanja je utvrditi povezanost položaja tijela tijekom spavanja sa stupnjem OSA-e u pacijenata s novodijagnosticiranom OSA-om nakon cjelonoćne polisomnografije.Ispitanici i metode: Proveli smo presječno i kliničko istraživanje koje je uključivalo 414 ispitanika (281 muškarac i 133 žene) starijih od 18 godina čiji je medijan starosti bio 55 godina. Ispitanici su 2017. godine došli na dijagnos-tičku obradu u Centar za medicinu spavanja KBC-a Split i Medicinskog fakulteta u Splitu te su njihovi podatci uzeti iz arhive istog centra. Svim pacijentima napravljena je cjelonoćna polisomnografija nakon koje je s pomoću AHI-ja procijenjena težina OSA-e u skladu sa smjernicama za dijagnostiku OSA-e koje su propisane od strane Američke akademije za medicinu spavanja (engl. American Academy of Sleep Medicine, AASM) i Europskog društva za istraživanje spavanja (engl. European Sleep Research Society, ESRS). Prekomjerna dnevna pospanost procijenjena je Epworthovom ljestvicom pospanosti (engl. Epworth Sleepiness Scale, ESS). Rezultati: Statistička analiza pokazala je da su pacijenti prosječno više vremena proveli spavajući na leđima (189.9±118.4min) nego na lijevom (113.3±90.9min) ili desnom boku (80.6±90.6min) te da su imali najviše apneja tijekom spavanja na leđima (AHI=31.1±31.9). Pacijenti s dijagnosticiranom OSA-om (AHI≥5) također su imali veću AHI vrijednost na leđima (39.1±31.9) nego na lijevom (23.8±25.2) ili desnom boku (18.5±25.6). Pacijenti s dijagnosticiranom OSA-om u odnosu na pacijente bez dijagnoze OSA-e imali su statistički značajno veći ITM (29.5±4.6kg/m2 vs 25.3±4.1kg/m2, P<0.001) i opseg vrata (42.0±4.4cm vs 37.4±3.9cm, P<0.001). Ukupno gledajući cijeli uzorak, muškarci su bili viši (180.8±7.4cm u odnosu na 165.9±6.7cm, P<0.001), imali veći ITM (29.4±4.5kg/m2 u odnosu na 26.8±4.9kg/m2, P<0.001) i opseg vrata (43.2±3.5cm u odnosu na 36.2±3.4cm, P=0.002), kao i veći ESS zbroj (7.6±4.7 u odnosu na 6.3±4.8, P=0.021). Koristeći Pearsonov koeficijent korelacije, uočili smo nega-tivnu korelaciju AHI-ja s vremenom spavanja na desnom boku (r=-0.178, P=0.005) u pacijenata s OSA-om, dok je pozitivna korelacija pronađena kod spavanja ne lijevom boku (r=0.003, P=0.959) i leđima (r=0.183, P=0.002).Zaključak: Naše istraživanje pokazalo je da pacijenti najviše vremena provode spavajući na leđima te da je AHI vrijednost upravo u tom položaju veća u odnosu na druge položaje tijela što dugoročno narušava kvalitetu spav-anja.
ključne riječi: Spavanje; Položaj tijela; Polisomnografija; Opstruktivna apneja
OPEN ACCESS
Correspondence: Alen Juginović MD
[email protected]/0000-0003-4871-1963
This article was submitted to RAD CASA - Medical Sciences as the
original article
Conflict of Interest State-ment: The authors declare that the research was conducted in
the absence of any commercial or financial relationships that could be construed as a potential conflict of
interest.
Received: 17 July 2019Accepted: 1 December 2019
Published: 17 December 2019
Citation:Juginović A, Pecotić R. Connec-
tion Between Body Position During Sleep and Findings from Full-Night Polysomnography in Patients with
Obstructive Sleep Apnea. RAD CASA - Medical Sciences. 540=48-49 (2019): 15-26. https://dx.doi.
org/10.21857/ydkx2crgw9
Copyright (C) 2019 Juginović and Pecotić. This is an open-access
article distributed under the terms of the Creative Commons Attri-
bution License (CC BY). The use, distribution or reproduction in other
forums is permitted, provided the original author(s) and the copyright owners(s) are credited and that the original publication in this journal is cited, in accordance whit accepted adacemic practice. No use, distri-
bution or reproduction is permitted which does not comply with these
terms.
Original Article
15-26

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com16
what is sleeP?Up until the 1950s, many people thought of sleep as a passive part of our life although we spend almost a third of our life sleeping. Today we know for sure that our brain is very active during sleep and that some of its parts are even more active than when awake. Though not easy to define it, sleep is considered a natural state of altered coun-ciousness which is characterized by relative inhibition of sensory activ-ity, inhibition of almost all voluntary (skeletal, striated) muscles and reduced interaction with the environment1. The optimal number of hours of sleep ranges from 7 to 9 for people between 18 and 65 years of age. For older people the optimal number of hours of sleep is a bit less, for younger ones a bit more, while babies under the age of 1 need 12 to 17 hours (Figure 1) 2,3. For good sleep quality, sleep hygiene is very important. It includes various habits or exercises that not only assure a comfortable night, but high concetration and apention levels during the day. Some parts of good sleep hygiene are: • No caffeine, alcohol or other stimuli right before sleep • No fapy/heavy food right before sleep • Active lifestyle during the day • Sleeping on a quality mapress and pillow in a dark envi ronment with adequate and comfortable room temperature • Consistent rhythm and hours of sleep in regards to age • No usage of computers, smartphones and other electronic devices before sleep that emit blue light etc.Sleep can be split into two phases which interchange, non-REM (non-Rapid Eye Movement) and REM (Rapid Eye Movement) phase. Non-REM phase consists of three sleep stages (stage N1, N2, and N3), while REM phase includes only REM sleep stage. During sleep, most people go through several (4-5) cycles of sleep (Figure 2), de-pending on how much time they sleep. One sleep cycle lasts roughly 90 to 110 minutes and is defined as a period in which a person goes through the aforementioned stages of non-REM and REM sleep. Most healthy adults begin their sleep cycle in stage N1 right after they fall asleep. Next, they go into stage N2 which is the longest sleep stage, then to stage N3 and afterwards back to one of the shallower stages like stage N1 or N2. The last stage is REM sleep stage which concludes the sleep cycle. A new cycle begins after the person goes into stage N1 or N2 after they leave the REM sleep stage in the previ-ous sleep cycle and then the classic papern continues: stage N1 – stage N2 – stage N3 – stage N1 or N2 – REM stage – new sleep cycle. Interestingly, mammals (dogs, cats etc.) have been found to have a very similar fundamental sleep cycle to humans5.
the circadian rhythm
Circadian rhythm (Latin “circa“ = around; Latin “diem“ = day) is an endogenous cyclic rhythm with a periodicity of around 24 hours which regulates the sleep/wake cycle. This rhythm is controled by the circadian or biological or circadian clock1. It is extremely important because many biochemical and physiological processes depend on it functioning well. A branch in biology which studies periodic phenom-ena in living beings is called chronobiology (Greek “chronos“ = time). In 2017, The Nobel Prize in Physiology or Medicine was awarded to three scientists from the USA for discovering the molecular mecha-nisms controlling the circadian rhythm of the fruit fly6,7.Almost 300 years ago, De Mairan proved the existence of an endog-enous rhythm in plants by studying the folding of leaves of a specific plant in the evening hours. He noticed that the plant was folding its leaves in the evening even when it was kept constantly in the dark the
whole day. He described this as though “the plant felt the presence of the sun without seeing it“8. From seaweed to mammals, almost all animals adjusted their circadian clock to the 24 hour cycle which strongly depends on the presence of light.In humans, the central circadian clock (circadian pacemaker, master clock) in located in the hypothalamus, i.e. in its suprachiasmatic nucleus (Latin “nucleus suprachiasmaticus“, SCN) which is located, as the name suggests, above the optic chiasm.The function of the circadian clock depends a lot on the day/night cycle. Light (not only daylight, but also light emitted from screens of smartphones, TVs, computers etc.) is, along with drugs, temperature, physical activity and other, one of the examples of so called “zeitge-
ber“ (German for “time giver“) , i.e. external factors which affect the circadian clock. Light enters the eye through the pupil and falls on the retina which is made up of 10 histological layers. After the activa-tion of the first-order neurons (photoreceptors: rods, cones) of the visual pathway, the signals go to the bipolar (second-order neurons) and ganglion cells (third-order neurons) whose axons make up the optic nerve. They end up in the thalamic lateral geniculate body
Figure 1. Duration of Sleep Stages During Life. Note how slow-wave sleep, i.e. deep sleep reduces in time as people get older. Furthermore, older people sleep up to 36% less than 5-year-old children4.
Stage N1 (5%)
New cycle, stage N1 or N2
REM stage (25%)Stage N2 - longest
stage (45%)
Stage N1 or N2
Stage N3 (25%)
Figure 2. Healthy Adult Sleep Cycle – orange rectangles represent non-REM phase, green REM phase. The percentage in the brackets represents the share of each sleep stage in optimal total sleep time. After stage N3, the induvidual goes shortly to stage N1 or N2 before going to REM. After REM stage, a new sleep cycle begins with either stage N1 or stage N2.
Original Article
15-26

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com17
(fourth-order neuron) and from there the signals go to the cortex of the occipital brain lobe where the picture gets to the conscious level. For the circadian clock, though, first-order neurons are important. Apart from rods (night sight) and cones (colour differentiation), a new small population of cells has been discovered in the retina. These cells called intrinsically photosensitive Retinal Ganglion Cells (ipRGCs) are also photoreceptors. IpRGCs contain light-sensitive photopigment melanopsin which is responsible for their photosensi-tivity9. When exposed to light for longer and because of melanopsin activation, calcium ions enter the ipRCGs and activate them via membrane depolarization through various physiological processes10. The formed electrical impulse (action potential) travels through the axons of ipRGCs directly via the optic nerve right to the hypothalam-ic suprachiasmatic nucleus (SCN) which is activated by the release of glutamate from the nerve endings. SCN then “knows“ that there is light in the environment and “concludes“ it is day outside. Remem-ber, the light which activates the ipRGCs can be from computers, smartphones, home lighting etc. and not only sunlight. This is how we can easily deregulate during night the SCN and many physi-ological processes this nucleus controls in the body. The pathway that connects the ipRGCs to the SCN is called retinohypothalamic pathway because it connects the ipRGCs in the retina to the SCN in the hypothalamus. It is key in the regulation of the circadian clock and therefore the circadian rhythm11.Along with the central circadian clock in the SCN, there are periph-eral circadian clocks in various organs (heart, lungs, liver) and systems (endocrine) which the SCN controls, along with the physiological processes.
breathing related sleeP disorders: sleeP aPnea
Sleep apnea is the most common breathing related sleep disorders and one of the most common sleep disorders in general. It is defined as a total cessation of breathing during sleep which lasts at least 10 seconds and is accompanied by desaturation of at least 3%. Cessation of breathing that does not meet these criteria is not classified as sleep apnea. Sleep apnea can be divided in three groups: obstructive apnea (most common), central apnea and mixed apnea. Another significant clinical entitiy is hypopnea, i.e. shallow breathing. It is defined as a reduction in breathing depht by 30% compared to normal breathing and lasts at least 10 seconds, usually accompanied by desaturation of 3% or more.
risK factors and Prevalence
Obstructive sleep apnea represents a major public health issue. According to a 2017 study, the prevalence of sleep apnea in the general population varies from 9% to as much as 38% and mostly affects middle aged and older men and significantly less women and children 12. The most common type of sleep apnea by far is obstruc-tive sleep apnea, followed by mixed and then central apnea. In the United States, at least 25 million adults suffer from sleep apnea, and the number is constantly rising13. Risk factors for sleep apnea include: body mass index above 25, narrowed airway, broad neck (> 43cm for men, > 38cm for women), male sex, age (> 40 years), family history of sleep apnea, alcohol, smoking, intake of sedatives, nasal septum deviation, nasal congestion, stroke (for central apnea). Because of all the risk factors, it is important that people have an active and healthy lifestyle in order to reduce the risk of getting sleep apnea, as well as many other diseases14.
tyPes and symPtoms of sleeP aPnea
Sleep apnea is divided in three types: obstructive (most common), central and mixed apnea. It is important to remember that all three types share the same basic traits: total cessation of breathing for at least 10 seconds and desaturation of at least 3%. Obstructive sleep apnea (OSA) is a repetitive breathing cessation during sleep which is caused by partial or complete collapse of the upper airway which blocks or significantly reduces the airflow to the lungs. Primarily, the collapse happens at the level of velopharynx (from the begin-ning of the soft palate to the uvula) and oropharynx (from the tip of the uvula to the top of the epiglottis). The affected person tries to breathe with thoracic (intercostal muscles) and/or abdominal muscles (diaphragm) but cannot because of the airway obstruction. Causes of the collapse are not yet clarified, but neuromuscular factors probably play a role. Significantly reduced muscle tone of muscles important for maintaining the stability of the upper airway (tensor veli palatini and genioglossus muscles) is an important cause15. Muscle tone in normally lower during sleep, but here it is exaggerated. In overweight people, peripharyngeal fat tissue narrows the airway are increases the risk of its collapse, therefore inducing sleep apnea16,17. The most common mechanical obstacle to airflow when lying flat is when the base of the tongue falls backwards, thus covering the airway. This can happen together with the collapse of the soft palate and other nearby muscles which alltogether block the airway (Figure 3). Significantly reduced muscle tone (muscle hypotonia) which occurs during sleep and causes the pharyngeal and soft pallet muscle collapse plays a big role in preventing air going to the lungs. In children, enlarged tonsils and/or adenoids (lymphoid tissue) can cause OSA. If so, they can be surgically removed with good outcomes.The main difference between central sleep apnea (CSA) and obstruc-tive sleep apnea is that in CSA signals from the respiratory centers in the medulla are not reaching the respiratory muscles and the patient in not even trying to breathe because of that. Central apnea is rare, and its causes are not yet fully understood. There are two subtypes of CSA: primary (idiopathic) and secondary. Primary, i.e. idiopathic CSA is of unknown cause, rare and is diagnosed by excluding other potential causes. Secondary CSA can be associated with Cheyne-Stokes respiration, opioid consumption, CSA on high altitude and CSA as a secondary manifestation of certain diseases18.Secondary, CSA may be caused by some neurological disorders in-cluding neuromuscular diseases which either significantly weaken or disable breathing due to weakening of the respiratory muscles in one of the phases of the diesase. Some examples are myasthenia gravis, amyotrophic lateral sclerosis (ALS) and others. Due to the inability to breathe, hypercapnia (elevated levels of CO2 in the blood) occurs. Tumors and other lesions in the brainstem can weaken the signal going to the respiratory muscles which is especially noticeable in sleep and can cause hypercapnia.Secondary CSA also includes the hereditary disease called congenital central hypoventilation syndrome, also known as Ondine’s curse. For genetic reasons and without an anatomical and pathological substrate, alveolar hypoventilation occurs during sleep and causes hypercapnia and hypoxemia (20). Primarily central chemoreceptors in the brainstem react to hypercapnia (peripheral chemoreceptors in the aortic and carotide body react too). They “notice“ the change in pH in the cerebrospinal fluid, i.e. blood which becomes acidic (aci-dosis). Chemoreceptors react to hypercapnia with hyperventilation to get excess CO2 out of the blood. People who have “overly sensitive“
Original Article
15-26

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com18
chemoreceptors or some underlying diseases may exhibit unnecessarily long hyperventilation periods which lead to the reduction of PaCO2 (partial pressure of CO2 in arterial blood) on a level significantly lower than normal, below the so called CO2 apenic threshold and there-fore breathing cessation occurs. Reduction of PaCO2 below the CO2 apenic threshold during sleep leads to breathing cessation, i.e. central sleep apnea. In summary, in Ondine’s curse, reduction of PaCO2 due to hyperventilation below the apenic threshold which is located just below the normal level od CO2, leads to hypoventilation and breath-ing cessation during sleep without breathing muscle contractions, i.e. leads to central sleep apnea20.Central sleep apnea with characteristics of Cheyne-Stokes respira-tion is described as irregular crescendo/decrescendo breathing which oscilates between hypopnea, hyperpnea and then hypopnea and finally apnea. The person takes shallow breaths followed by deep ones and then shallow ones again up to the point of total breathing cessation (Figure 4).Cheyne-Stokes respiration cycle lasts 60-90 seconds22. The cause of it lies in the increase of CO2 in the blood, i.e. hypercapnia which leads to compensation in the form of hyperventilation which leads
to hypocapnia and finally apnea to “build up“ the reduced CO2. An especially important cause of CSA with Cheyne-Stokes respiration paperns is heart failure in as many as 60% of cases. Due to prolonged circulatory time in heart failure patients, CO2 needs more time to reach the central chemoreceptors which causes constant “overshoot-ing“ of the adequate CO2 level and more than needed longevity of hyperventilation which leades to hypocapnia and the reduction of PaCO2 below the CO2 apneic threshold and the occurrence of cen-tral apnea23. This type of respiration can be found in renal failure and other neurological disorders.CSA is connected with long-term opioid use (morphine, heroin, codeine and other) because they suppress breathing by acting on μ-opioid receptor sin the medulla24,25. Furthermore, high altitudes, especially above 7600 meters but lower as well, can cause hypopnea and apnea during sleep26.Mixed sleep apnea (MSA) has features both of central and obstruc-tive sleep apnea. During the same apneic period, the person tries to breathe by contracting abdominal/thoracic muscles (just like in OSA) in one part of the apneic period, while in the other part doesn’t have muscle contractions (just like CSA). It is possible and not rare that patients experience episodes of central, obstructive and mixed apnea during the same night.Common sleep apnea symptoms include snoring, breathing cessa-tions, feeling of suffocatiing during the night, daytime tiredness, sleep during the day, reduced level of enthusiasm and concentration, morn-ing headaches, dry mouth, etc.27. Snoring occurs due the relaxation of the uvula and soft palete which party block the airflow thus causing irregular flow of air and the unpleasant sound.
diagnosis and treatment
The gold standard for diagnosing sleep apnea in full-night poly-somnography in a Center for Sleep Medicine under supervision of qualified personnel. Full-night polygraphy is also a valuable method, especially because the patients can sleep at home, but it doens not include the supervision of qualified personnel nor EEG which means
Figure 3. Obstructive Sleep Apnea – soft palate and tongue fall backwards due to significant muscle hypotonia and block the airflow (19).
Figure 4. Central Sleep Apnea with Cheyne-Stokes Respiration Papern. Note the repetitive crescendo/decrescendo breathing papern (hypopnea-hyperpnea-hypopnea-apnea) during stage N2 non- REM sleep (circled). AOer each apnea there is a period of desaturation (SpO2 graph which is second to last on the picture). The rectangle represents the apnea, i.e. no breathing period. Note that only two out of five of Cheyne-Stokes breathing paperns are circled, one for the movement of abdominal muscles (upper row with circle) and the other for thoracic muscles (lower row with circle) 21.
Original Article
15-26

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com19
it cannot record sleep stages and sleep architecture disorders which can be of potentially great value. For the assesment of the risk of sleep apnea, patient fill out different questionnaires before potentially going to polysomnography/polygraphy recordings. Some examples of questionnaires are: Berlin Questionaire, STOP BANG, Pipsburgh Sleep Quality Index and others which are composed of questions regarding the symptoms of sleep apnea. STOP BANG is commonly used and is an abbreviation for: Snoring, Tiredness, Observed apnea, Pressure (arterial hypertension), BMI (risk for apnea above 35), Age (risk for apnea above 50), Neck (circumference above 40 cm at increased risk), Gender (male sex at more risk). Epworth Sleepiness Scale is an important scale which asseses the level of sleepiness while doing routine daily activities (watching TV, reading, etc.) because dytime tiredness is associated with sleep apnea28. For the assesment of risk of sleep apnea, the Mallampati score can also be used, althouth its primary purpose is the risk assesment of intubation in anesthesia. This simple test is performed in a way that the patient opens his/her mouth wide and the doctor asseses the visibility of the soft palete, tonsils, uvula and palatal arches. It has four categories, from category one (everything visable) to four (only hard palate visable). Higher Mallampati scores are associated with higher AHI (apnea-hypopnea index; the average number of apneas and/or hypopneas per hour of sleep) although some research questions the test’s clinical value29,30.Sleep apnea can be diagnosed both with polygraphy and polysom-nography. The main criteria for diagnosing sleep apnea is total breath-ing cessation of at least 10 seconds (oronasal airflow sensor) followed by desaturation of at least 3% (pulse oximeter). For distinguishing the types of apnea, the upper and lower belt are key. If at least one of the belts detects muscle contractions (movement of the thorax and/or abdomen) and there is no breathing for at least 10 seconds followed by desaturation of 3% or more, we conclude the existence of obstruc-tive sleep apnea because the person is trying to breathe, but cannot due to a mechanical obstruction in the airway. If none of the belts detect any muscle contractions, along with more than 10 seconds of breathing cessation and desaturation of at least 3%, we conclude that this is central sleep apnea. Therefore, the key difference is that in obstructive apnea there are muscle contractions, whereas in central apnea there are not (Figure 5 and Figure 6). Furthermore, the severity of apnea is important to ass-es so we can treat it properly. The severity of apnea is indicated with the index called AHI (Apnea – Hypopnea Index). This index is calcu-lated in a way that all apenas (all types) and hypopneas during sleep are added together and then divided with the number of hours spent sleeping. The end result (AHI) signifies the average number of apneas and/or hypopneas per hour of sleep. AHI below 5 is a state without sleep apnea. This means that the person that has less than 5 apneas and/or hypopneas per hour of sleep does not have a diagnosis of sleep apnea, but just sporadic episodes of apnea/hypopnea. AHI from 5 to 14.9 indicates mild sleep apnea, 15 to 29.9 moderate, while a result
of more than 30 severe sleep apnea. In comparison, in children, AHI from 1 to 4.9 is classified as mild sleep apnea, 5 to 9.9 moderate and 10 and above severe31. There is another way of classifying sleep apnea and it is called RDI (Respiratory Disturbance Index). It is very similar to AHI, but apart from apneas and hypopneas, it also adds together phenomena called RERA (Respiratory Effort Related Arousal) and then divides all that with the number of hours of sleep. Values for diagnosis of mild, moderate and severe sleep apnea are the same as for AHI. RERA is a state which is characterized by obstruc-tion (doesn’t have to be complete) of the upper airways for at least 10 seconds and results in increased effort when trying to breathe but does not meet the criteria for apnea or hypopnea. The increased effort of breathing causes arousals and changes in EEG recordings to alpha waves. Therefore, that person goes to a state of relaxed wakefulness without being conscious of it32. Apnea, in most cases, cannot be cured as such, but can be successfully treated and kept under control throughout life. Before the actual treatment, it is important to emphasize that a healthy and active lifestyle can greatly help decrease the risk for apnea and many other diseases. Sleeping with the upper body raised by 30%, as well as sleeping on the side give more stability to the airway and significant-ly reduces the risk for sleep apnea33. The gold standard for treating any type of sleep apnea and drastically reducing the potential apnea complications is a device called CPAP (Continuous Positive Airway Pressure)34. CPAP has a flexible tube and a mask on the end of it which is put on the nose and/or mouth depending on the model and is used only during sleep time (Figure 7). It blows air in the airway and lungs under positive pressure of 5-15 cm of water. During the whole period of sleep CPAP blows air in the upper airway under minimal and constant pressure after the pressure has been adjusted for each patient (process called titration). Therefore, from the evening when it is turned on, till the morning when it is turned off, CPAP constantly blows air under the same pressure into the airway, regard-less if the person is exhaling or inhaling. Even after titration, some people find it difficult to exhale against the CPAP pressure and they are advised to try BiPAP (Bilevel Positive Airway Pressure). BiPAP is almost identical to CPAP but has two pressure levels, one when the patient is inhaling and one when exhaling (lower pressure) making it easier to breathe. APAP (Automatic Positive Airway Pressure) is similar to CPAP but instead of one or two levels of pressure, it automatically adjusts the pressure during the night to suit the patient. In summary, PAP (Positive Airway Pressure) devices blow air into the airway like an invert vacuum cleaner, thus keeping the airway opened and free of potential obstructions (tongue that falls back, hypotonia of soft palate and pharynx muscles)35. Also, when the patient is not breathing without any obstructions (central sleep apnea) they blow air inside the lungs eliminating apnea. PAP devices do not stop the hypotonia of the pharynx and soft palate muscles as such, but they do stop them from becoming an obstacle in the airway in case of
Figure 5. Polysomnographic Recording of Obstructive Sleep Apnea. Note the red rectangle in the “Flow“ field and the flat line inside it indicating breath-ing cessation. “THO“ and “ABD“ fields below it indicate that there is contraction of the thoracic and ab-dominal muscles (waves in the picture) because the person is trying to breathe but cannot due to the obstruction of the airflow (recording taken with permission from the Center for Sleep Medicine of the University of Split School of Medicine and University Hospital Split).
Original Article
15-26

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com20
their collapse. The successful use of CPAP together with an active and healthy lifestyle increases concentration and effectiveness, reduces daily tiredness, snoring, risk for diabetes and cardiovascular diseases and other complications of untreated apnea36-39. PAP devices are not an apnea cure because apnea quickly returns if the person stops using them. In Croatia, patients receive CPAP free of charge if their AHI is higher than 30 (severe apnea) or rarely in the event of moderate apnea if the patient fulfils at least three of the following additional criteria: obesity, daytime sleepiness, resistent arterial hypertension, unregulated diabetes and acute events like stroke or myocardial infarction. If none of the PAP devices are useful for the patient, ASV (Adaptive Ser-vo-Ventilation) can be recommended. It looks similar to PAP devices, but it focuses more on the volume of air rather than pressure which is blown into the airway. This way, it broadens the airway and the patient can breathe.Other methods for treating sleep apnea include: surgery, positional therapy and using the oral appliance (Figure 8). Surgical methods are useful in removing anatomical abnormalities in the upper airways. The most used method is uvulapalatopharyngoplasty (UPPP, UP3) where the adeonides and tonsils (lymphoid tissue) are removed, and the uvula, soft palate and the pharynx are corrected. It can usually help with snoring. Positional therapy is easier to execute. It consists of not sleeping on the back, but rather on the side due to the connection of sleeping on back with increased AHI40. There are many methods for avoiding sleeping on the back and one of the most innovative is stiching a tennis ball on the back side of the pajamas so every time the person turns on his/her back it will be uncomfortable and will immediately turn of to the side41. Sometimes the discomfort caused by the tennis ball wakes the patient up which reduces sleep quality.
Figure 6. Polygraphic Recording With Central Sleep Apnea. Nothe the red rectange and the flat line inside it that represents breathing cessation. The field marked “Abdomen“ below it shows an almost totally flat line indicating no contraction of abdominal muscles because the signal from the brain doesn’t reach them. Desaturation occurs after the apneic period in the “SpO2“ field marked by a falling line with desaturation values. Also note there are no EEG resordings because this is not a polysomnographic, but polygraphic recording (recording taken with permission from the Center for Sleep Medicine of the University of Split School of Medicine and University Hospital Split).
The oral appliance is put on the teeth only during sleep and protrudes the mandible forward, thus reducing the risk of the tongue falling backward. It also broadens the airway42. It is the treatment of choice for mild and moderate apneas when the patient cannot adapt to PAP devices. In Croatia, the patient has to pay for the appliance in full be-cause it is not covered by health insurance43. An interesting treatment for moderate apnea is the use of the musical instrument didgeridoo. In this research, patients practiced playing the instrument six times a week and AHI, as well as daily tiredness reduced significantly. As the didgeridoo is a wind instrument, the underlying improvements are probably based on the strenghtening of oropharingeal muscles by blowing in the instrument and therefore reducing the risk of their collapse44. Another relatively new method of treating apnea is the stimulation of the 12th cranial nerve (hypoglossal nerve) which innervates almost all tongue muscles (geniglossal, hypoglossal and other muscles). In a surgical method, a stimulator is implanted and connected to the nerve and by constant stimulation, it reduces the risk of airway collapse45. This method is still in its beginnings.
long-term comPlications of untreated sleeP aPnea
There are numerous complications that untreated sleep apnea can lead to. One of the dangerous ones is daytime fatigue and sleepiness, especially in professional drivers of buses, trucks and dangerous goods where it can increase the risk of having a road traffic accident by up to five times46. The conncection between obesity and the risk of sleep apnea has been evaluated many times in the past, but recent research shows that in the early age of adolescence neurocognitive problems can be a result of sleep apnea47,48. In older people who suffer from breathing related sleep disorders, the onset of mild cognitive impair-ment, which can lead to Alzheimer’s disease, can be 10 to 11 years
Figure 7. CPAP Device on a Model Patient. The device is used just during sleep. Usually there is a small water container in the device so air can be humidified before being blown in the airway. Otherwise, the unhumidified air can dry out the mouth and irritate the nasal mucosa. Patients need to get used to all PAP devices which may cause sneezing, dry mouth, irritation of nasal mucosa and other. A small number of patients cannot get used to PAP devices and they are advised to lose weight if obese, use oral appliances and surgery.
Figure 8. Oral Appliance – note that the use of the oral appliance prevents the tongue falling back and keeps the airway open. It is used in mild and moderate apneas (27).
Original Article
15-26

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com21
earlier in comparison to healthy population and that the use of PAP devices neutralizes that earlier onset49. An important complication of untreated apnea is the increased risk of cardiovascular diseases (myo-cardial infarction, atrial fibrillation, arterial hypertension), diabetes type 2, stroke, metabolic syndrome (obesity, elevated triglycerides, lipids, glucose and arterial pressure), liver disease (non-alcoholic fapy liver disease) and other50,51. One of the proposed connections between sleep apnea and cardiovascular disease is the occurrence of systemic inflammation and elevated inflammatory markers which decrease with apnea treatment. Furthermore, intermipent hypoxia, i.e. the exchange of normoxia (when there is no apnea) and hypoxia (apneic event), can induce an inflammatory reaction which can negatively impact the cardiovascular system52. Because of oxygen reduction, and CO2 increase during and following the apneic event, the sympathetic nervous system is activated. Peripheral chemoreceptors in the carotid and aortal body activate it primarily because of hypoxia (but because of hypercapnia as well). The result is vasoconstriction which increases arterial pressure and the load on the heart until the levels of O2 and CO2 in the blood normalize. The normalization usually comes aOer the apneic event. The next apnea causes the same sympathetic activa-tion again and the repetition of the described papern. This is repeated tens of hundreds of times during just one night, let alone for weeks, months, years and decades if apnea is leO untreated. This causes severe changes in the organism in the form of arterial hypertension, cardiovascular diseases and sympathetic dysfunction. If the person had been diagnosed with arterial hypertension prior to apnea, it can worsen53. Elevated sympathetic activity leads to significantly increased peripheral insulin resistance, which together with repetitive periods of hypoxia during apnea and the shortened sleep time, increase the risk of diabetes type 2 54. Daily tiredness and lowered concentration levels in drivers reduce the likelihood of appropriate driving manners and increase the risk of road traffic accidents which can have fatal consequences. The underlying cause of daily tiredness are so called micro-awakenings which occur frequently after the apneic events. While the patient is going through an apneic episode, the body fights to breathe and the muscles contract in OSA. The resulting hypoxia and hypercapnia right after the apnea cause a series of very deep and powerful breaths to normalize the concentration of blood gases which
Apnea
(9-38% ofpopulation)
PolyspmnographyPolygraphy
Questionnaires (Berlin, STOP
BANG) AHI(apneas +
hypopneas/number of hours of
sleep)
Risk factors: obesity, broad neck, smoking, male sex, age
Obstructive (muscle
contractions,obstruction)
Central (no muscle
contractions)Mixed
Older men
Desaturation at least 3%
Breathing cessation for at least 10 seconds
Complications: arterial
hypertension, diabetes,
cardiovascular diseases, daily
tiredness (drivers)
Treatment:CPAP
Oral applianceHealthy and
active lifestyle
“wake up“ the patient (EEG alpha waves) without him/her ever being conscious of it. If the patient exhibits numerous micro-awakening during the night, sleep architecture and quality will become disrupted because constant transition to alpha waves (constant apneas and micro-awakenings) from whichever sleep stage prevents patients from spending sufficient time in deep sleep stages which are extremely im-portant for rest. If this is the case, the patient will feel tired, lacklustre and with poor energy and concentration during the day.
aim and hyPothesis
The aim of this research is to find a connection between body posi-tion during sleep and severity of obstructive sleep apnea (OSA) in pa-tients with newly diagnosed OSA after full-night polysomnography. Regarding on written, the hypothesis reads: „The severity of OSA will be significantly higher while sleeping on the back in comparison to sleeping on the left or right side.“
subjects and merhods
This research is a cross-sectional and clinical research. 414 patients (281 male and 133 female) who came in 2017 for diagnostic purpos-es to the School of Medicine and University Hospital Split Center for Sleep Medicine were included in the research. Demographic data of the patients was taked from the archive of the Center for Sleep Medicine. All patients underwent full-night polysomnography with the device Alice 5LE, Philips Respironics, Eindhoven, The Neth-erlands. The diagnosis, as well as the severity of the sleep disorder, was evaluated with AHI after the full-night polysomnography, all in accordance with the American Academy of Sleep Medicine (AASM) and European Sleep Research Society (ESRS) guidelines for OSA diagnosis. Patients under 18 years of age and patients who underwent full-night polygraphy were not included in the study.
Questionnaires All patients who undergo full-night polysomnography in the Center for Sleep Medicine in Split, Croatia fill out a few questionnaires which are frequently used to asses risk for OSA, as well as daytime sleepiness.Epworth Sleepiness ScaleEpworth Sleepiness Scale which is validated in Croatian was used to
Figure 9. Fundamentals of Sleep Apnea
Original Article
15-26
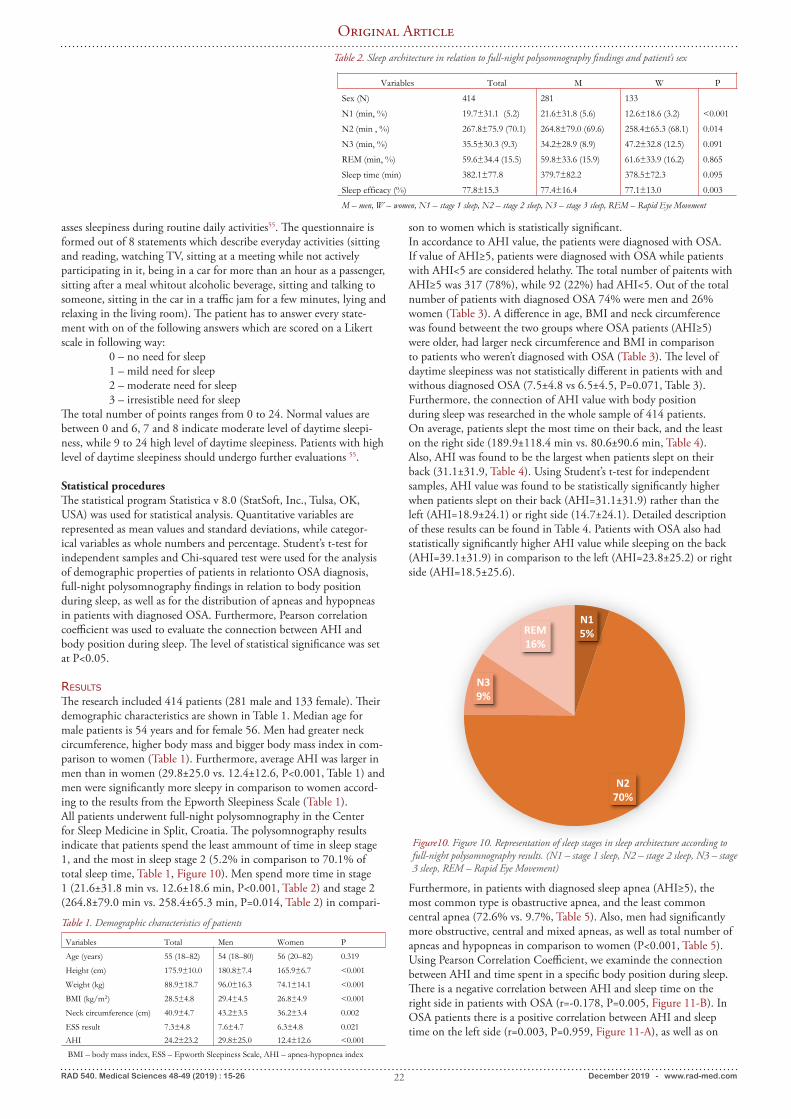
RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com22
asses sleepiness during routine daily activities55. The questionnaire is formed out of 8 statements which describe everyday activities (sitting and reading, watching TV, sitting at a meeting while not actively participating in it, being in a car for more than an hour as a passenger, sitting after a meal whitout alcoholic beverage, sitting and talking to someone, sitting in the car in a traffic jam for a few minutes, lying and relaxing in the living room). The patient has to answer every state-ment with on of the following answers which are scored on a Likert scale in following way: 0 – no need for sleep 1 – mild need for sleep 2 – moderate need for sleep 3 – irresistible need for sleepThe total number of points ranges from 0 to 24. Normal values are between 0 and 6, 7 and 8 indicate moderate level of daytime sleepi-ness, while 9 to 24 high level of daytime sleepiness. Patients with high level of daytime sleepiness should undergo further evaluations 55.
Statistical proceduresThe statistical program Statistica v 8.0 (StatSoft, Inc., Tulsa, OK, USA) was used for statistical analysis. Quantitative variables are represented as mean values and standard deviations, while categor-ical variables as whole numbers and percentage. Student’s t-test for independent samples and Chi-squared test were used for the analysis of demographic properties of patients in relationto OSA diagnosis, full-night polysomnography findings in relation to body position during sleep, as well as for the distribution of apneas and hypopneas in patients with diagnosed OSA. Furthermore, Pearson correlation coefficient was used to evaluate the connection between AHI and body position during sleep. The level of statistical significance was set at P<0.05.
results
The research included 414 patients (281 male and 133 female). Their demographic characteristics are shown in Table 1. Median age for male patients is 54 years and for female 56. Men had greater neck circumference, higher body mass and bigger body mass index in com-parison to women (Table 1). Furthermore, average AHI was larger in men than in women (29.8±25.0 vs. 12.4±12.6, P<0.001, Table 1) and men were significantly more sleepy in comparison to women accord-ing to the results from the Epworth Sleepiness Scale (Table 1).All patients underwent full-night polysomnography in the Center for Sleep Medicine in Split, Croatia. The polysomnography results indicate that patients spend the least ammount of time in sleep stage 1, and the most in sleep stage 2 (5.2% in comparison to 70.1% of total sleep time, Table 1, Figure 10). Men spend more time in stage 1 (21.6±31.8 min vs. 12.6±18.6 min, P<0.001, Table 2) and stage 2 (264.8±79.0 min vs. 258.4±65.3 min, P=0.014, Table 2) in compari-
son to women which is statistically significant. In accordance to AHI value, the patients were diagnosed with OSA. If value of AHI≥5, patients were diagnosed with OSA while patients with AHI<5 are considered helathy. The total number of paitents with AHI≥5 was 317 (78%), while 92 (22%) had AHI<5. Out of the total number of patients with diagnosed OSA 74% were men and 26% women (Table 3). A difference in age, BMI and neck circumference was found betweent the two groups where OSA patients (AHI≥5) were older, had larger neck circumference and BMI in comparison to patients who weren’t diagnosed with OSA (Table 3). The level of daytime sleepiness was not statistically different in patients with and withous diagnosed OSA (7.5±4.8 vs 6.5±4.5, P=0.071, Table 3).Furthermore, the connection of AHI value with body position during sleep was researched in the whole sample of 414 patients. On average, patients slept the most time on their back, and the least on the right side (189.9±118.4 min vs. 80.6±90.6 min, Table 4). Also, AHI was found to be the largest when patients slept on their back (31.1±31.9, Table 4). Using Student’s t-test for independent samples, AHI value was found to be statistically significantly higher when patients slept on their back (AHI=31.1±31.9) rather than the left (AHI=18.9±24.1) or right side (14.7±24.1). Detailed description of these results can be found in Table 4. Patients with OSA also had statistically significantly higher AHI value while sleeping on the back (AHI=39.1±31.9) in comparison to the left (AHI=23.8±25.2) or right side (AHI=18.5±25.6).
Furthermore, in patients with diagnosed sleep apnea (AHI≥5), the most common type is obastructive apnea, and the least common central apnea (72.6% vs. 9.7%, Table 5). Also, men had significantly more obstructive, central and mixed apneas, as well as total number of apneas and hypopneas in comparison to women (P<0.001, Table 5).Using Pearson Correlation Coefficient, we examinde the connection between AHI and time spent in a specific body position during sleep. There is a negative correlation between AHI and sleep time on the right side in patients with OSA (r=-0.178, P=0.005, Figure 11-B). In OSA patients there is a positive correlation between AHI and sleep time on the left side (r=0.003, P=0.959, Figure 11-A), as well as on
Variables Total Men Women P
Age (years) 55 (18–82) 54 (18–80) 56 (20–82) 0.319
Height (cm) 175.9±10.0 180.8±7.4 165.9±6.7 <0.001
Weight (kg) 88.9±18.7 96.0±16.3 74.1±14.1 <0.001
BMI (kg/m2) 28.5±4.8 29.4±4.5 26.8±4.9 <0.001
Neck circumference (cm) 40.9±4.7 43.2±3.5 36.2±3.4 0.002
ESS result 7.3±4.8 7.6±4.7 6.3±4.8 0.021AHI 24.2±23.2 29.8±25.0 12.4±12.6 <0.001
BMI – body mass index, ESS – Epworth Sleepiness Scale, AHI – apnea-hypopnea index
Table 1. Demographic characteristics of patients
Variables Total M W P
Sex (N) 414 281 133
N1 (min, %) 19.7±31.1 (5.2) 21.6±31.8 (5.6) 12.6±18.6 (3.2) <0.001
N2 (min , %) 267.8±75.9 (70.1) 264.8±79.0 (69.6) 258.4±65.3 (68.1) 0.014
N3 (min, %) 35.5±30.3 (9.3) 34.2±28.9 (8.9) 47.2±32.8 (12.5) 0.091
REM (min, %) 59.6±34.4 (15.5) 59.8±33.6 (15.9) 61.6±33.9 (16.2) 0.865
Sleep time (min) 382.1±77.8 379.7±82.2 378.5±72.3 0.095
Sleep efficacy (%) 77.8±15.3 77.4±16.4 77.1±13.0 0.003
M – men, W – women, N1 – stage 1 sleep, N2 – stage 2 sleep, N3 – stage 3 sleep, REM – Rapid Eye Movement
Table 2. Sleep architecture in relation to full-night polysomnography findings and patient’s sex
N15%
N270%
N39%
REM16%
Figure10. Figure 10. Representation of sleep stages in sleep architecture according to full-night polysomnography results. (N1 – stage 1 sleep, N2 – stage 2 sleep, N3 – stage 3 sleep, REM – Rapid Eye Movement)
Original Article
15-26

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com23
the back (r=0.183, P=0.002, Figure 11-C).
discussion
The results of the research show that patients who underwent full-night polysomnography in the Center for Sleep Medicine in Split, Croatia spend the most time on their back during sleep. In this position, they have significantly higher AHI value in comparison to sleeping on left or right side. At the same time, AHI positively cor-relates with the time spent sleeping on the back and left side, while negatively with sleeping on the right side. Previous research show that sleeping on the back increases the risk of upper airway collapse56. Also, avoiding sleeping on the back contrib-utes to reduction of the number and duration of repeated episodes of upper airway obstruction, especially in patients with mild and moderate apneas57,58. According to some research, it is estimated that almost 60% of OSA patients, that diagnosis has to do with sleeping on the back59. Furthermore, in an article by Menon and Kumar about the influence of body position during sleep on OSA, patients with di-agnosed OSA can be classified in two groups: positional and nonposi-tional OSA60. Positional OSA group is the one in which the RDI (Re-spiratory Disturbance Index) value is more than twice as large on the
Variables*AHI<5 AHI≥5
PN=92 N=317
Sex (N, %) M 43 (15.5) 234 (84.5)<0.001*
W 49 (37.1) 83 (62.9)
Age (godine) 45 (18–72) 56 (20–82) <0.001**
BMW (kg/m2) 25.3±4.1 29.5±4.6 <0.001**
Neck circumference
(cm)
37.4±3.9 42.0±4.4 <0.001**
ESS result 6.5±4.5 7.5±4.8 0.071**M – men, W – women, BMI – body mass index, ESS – Epworth Sleepiness Scale
* χ2 test ; ** Student's t-test for independent samples
Table 3. Demographic characteristics of patients in relation to OSA. AHI<5 doesn’t have OSA, AHI≥5 has OSA.
Variables Total – all bodypositions Left side Back Right side
1. Sleep time (min) 1. 379.8±78.6 1. 113.3±90.9
1. 189.9±118.4
1. 80.6±90.6
1. AHI 1. 24.2±23.2 1. 18.9±24.1
1. 31.1±31.9*
1. 14.7±24.1
1. AHI≥5 1. 30.8±22.4 1. 23.8±25.2
1. 39.1±31.9
1. 18.5±25.6
AHI – apnea-hypopnea indeks; *One Way ANOVA (P<0.001)
Variables* Total M W PObstructive apnea (N,%)
74.2±93.1(72.6)
73.9±98.2(71.9)
20.9±34.8(76.0)
<0.001
Central apnea (N, %) 9.9±17.6 (9.7) 9.8±17.8 (9.6) 3.7±9.3 (13.5) <0.001Mixed apneja (N, %) 18.3±38.8
(17.9)19.4±40.8(18.9)
2.9±5.6 (10.6) <0.001
Total apneas (N) 102.2±122.9 102.8±130.2 27.5±41.0 <0.001Hypopnea (N) 97.2±66.3 89.6±71.7 50.8±53.5 <0.001* M – men, W – women; Student's t-test for independent samples
Table 4. Full-night polysomnography findings in regard to body position during sleep
Table 5. Representation of apneas and hypopneas in patients with diagnosed sleep apnea (AHI≥5) according to full-night polysomnpgraphy.
0 20 40 60 80 100 120
AHI
0,0
33,5
67,5
102,9
138,6
172,8
209,9
245,4
284,1
318,4
364,8
L_sl
eep
AHI:L_sleep: r = 0,0031; p = 0,9588
0 20 40 60 80 100 120
AHI
-200
0
200
400
600
800
1000
1200
R_sl
eep
AHI:R_sleep: r = -0,1778; p = 0,0049
0 20 40 60 80 100 120
AHI
-100
0
100
200
300
400
500
600
S_s
leep
AHI:S_sleep: r = 0,1828; p = 0,0018
Figure 11. Correlation (Pearson Correlation Coefficient) between Apnea-Hypopnea Indeks (AHI) and time spent in specific body position during sleep; position on left side (L_sleep, A), right side (R_sleep, B) and back (S_sleep, C) during sleep in patients who are diagnosed with obstructive sleep apnea (AHI≥5).
back position in comparison to the left and right side. Nonpositional OSA group is defined as the group where OSA patients have the RDI value less than twice as large on the back in comparison to the right or left side. Frank et al. define positional OSA with the AHI or ODI (oxygen desaturation index) ratio in the back position in comparison to other body positions while speeping in the ratio ≥2 ili >2 (61, 62). A very important variable which is being discussed in literature is the effect of the diagnostic procedure on the level of OSA considering that more than 50% of time during full-night polysomnography patients spend sleeping on their back because of the equipment and electrodes to which they are connected which is not the case when
Original Article
15-26

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com24
sleeping at home in a natural environment63,64. Therefore, there is a possibility of overestimating the level of OSA in diagnostic procedures because of more time spent on the back position which can also be a limiting factor to our study too. Furthermore the influence of body position on OSA severity is being discussed in terms of treatment options. Research show indicate posture-control devices as a method of treating OSA as they are significantly more sophisticated than their usual therapeutic approach such as sewing a tennis ball to the back of the pajamas or applying various improvised equipment to avoid sleep on the back position65. Previous research show that positional therapy is useful in treating patients with mild moderately severe OSA58,59,65. Results from our research show that patients spend significantly more time during sleep on their back in comparison to side positions which is in accordance to the published research about full-night polysom-nography in Center for Sleep Medicine conditions. Also, AHI value is larger when sleeping on the back in comparison to side positions up in patients with diagnosed OSA (AHI≥5).The effects of body position on certain sleep stages show that body position differently affects REM and non-REM sleep in a way that the increase in AHI while sleeping on the back is more emphasized during non-REM sleep stage66. According to our research, non-REM sleep stages take up around 84% and REM stage 16% of total sleep time. Stage 2 non-REM sleep is the longest (70%) and stage 1 the shortest (5%) in total sleep time.It is a well known fact that BMI and older age affect time being spent on sleeping on the back64. Our research show that our patients are middle to older aged (age median is 55 years) who have higher BMI (28.5±4.8kg/m2) with the average AHI of 24.2±23.2. When sex is taken into account, men were significantly taller, had higher BMI and neck circumference in comparison to women. Similar results were found in studies from Huand et al. in regard to BMI and Dancey et al. in regard to neck circumference67,68. Furthermore, Epworth Sleep-iness Scale score was significantly higher in men in comparison to women which suggests higher daytime sleepiness. Daytime sleepiness is also negatively affected by the significantly higher AHI value in men which is expected if we take into consideration the well known fact that the higher level of OSA negatively affect sleep quality, impairs sleep integrity and architecture, and causes frequent microarousals and awakenings.Our research shows that the male sex is a significant risk factor for OSA. This result was confirmed by the research done by Senaratna et al. where they concluded that the prevalence of OSA among people older that 18 is between 9% and 38%. In men, the prevalence was between 13% and 33%, while in women 6% to 19%12,69. According to Cairns et al., the middle age is a good predictor for OSA, especially in women70. Heizner et al. show that the prevalence of sleep apnea in men aged between 40 and 60 is significantly higher than in women
(79.6% in comparison to 46.7%)71. Namely, OSA is associated with a whole series of cardiometabolic disorders and the increase in total morbidity and mortality in the population72. Timely intervention and treatment of OSA can not only improve quality of life, but also many hemodynamic and metabolic parameters which can in the end lead to reduced risk for various diseases.This research has its limitations in the sense that it included only patients who underwent full-night polysomnography so the results cannot be applicable to the whole OSA population because a certain number od patients undergo full-night polygraphy in the patient’s home. Also, it is shown in literature that the accuracy of determining body position during sleep with specific sensors is a variable worth thinkong about. Namely, watching the patient’s body position with a camera in the room which is done by qualified presonnel gives more realistic data about body position73. Our research relied on sensors which can be a limiting factor. Results of our research confirmed the hypothesis that the level of severity of OSA will be significantly higher when sleeping on the back position in comparison to the left or right side. What is left to research is the effect of positional therapy and/or reduction of weight on the severity of OSA in our patient population. Finally, further research is needed to more precisely determine the mechanisms undelying positional and nonpositional OSA and to create algorithms which would clearly define the course of action to determine diagnosis and choose the method of treatment for OSA patients associated with body position during sleep.
conclusion
Men with diagnosed OSA have larger neck cirmumference, weight and body mass indeks in comparison to women. Furthermore, men with diagnosed OSA have higher AHI value, as well as Epworth Sleepiness Scale score in comparison to women. Regarding sleep architecture, stage 1 and stage 2 non-REM sleep was longer in men than in women with OSA. OSA patients spent the most time sleeping on their back and AHI value was statistically higher (39.1±31.9) in that position than on the left (23.8±25.2) or right (18.5±25.6) side. The total number of obstructive, mixed and central apneas, as well as hypopneas was higher in men that in women with OSA which is statistically significant. A positive correlation was found between AHI value and sleeping on the left side and back, while a negative one between AHI value and sleeping on the right side.
author contributions:All authors listed have made a substantial, direct and intellectu-al contribution to the work, and approved it for publication.
literature:1. Zee PC, Attarian H, Videnovic A. Circadian rhythm abnormalities. Continuum (Minneap Minn). 2013;19(1 Sleep Disorders):132-47. doi:10.1212/01.2. Bassetti CL, Dogas Z, Peigneux P. Sleep Medicine Textbook. Singa-pore: Wiley; 2014.3. Hirshkowitz M, Whiton K, Albert SM, Alessi C, Bruni O, DonCarlos L, et al. National Sleep Foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health.
2015;1(1):40-3. doi: 10.1016/j.sleh.2014.12.010.4. Ohayon MM, Carskadon MA, Guilleminault C, Vitiello MV. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: developing normative sleep values across the human lifespan. Sleep. 2004;27(7):1255-73. doi: 10.1093/sleep/27.7.1255.5. Foundation NS: Animals’ Sleep: Is There a Human Connection? [Internet]. Available from: https://www.sleepfoundation.org/sleep-
Original Article
15-26

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com25
news/animals-sleep-there-human-connection [cited 2019 Jul 27].6. Sehgal A. Physiology Flies with Time. Cell. 2017;171(6):1232-5. doi: 10.1016/j.cell.2017.11.028.7. Sehgal A, Mignot E. Genetics of sleep and sleep disorders. Cell. 2011;146(2):194-207. doi: 10.1016/j.cell.2011.07.004.8. JJO dM. Observation botanique. Histoire de l’Academie Royale des Sciences. 1729:35-6.9. Pickard GE, Sollars PJ. Intrinsically photosensitive retinal gan-glion cells. Rev Physiol Biochem Pharmacol. 2012;162:59-90. doi: 10.1007/112_2011_4.10. Graham DM, Wong KY, Shapiro P, Frederick C, Pattabiraman K, Berson DM. Melanopsin ganglion cells use a membrane-asso-ciated rhabdomeric phototransduction cascade. J Neurophysiol. 2008;99(5):2522-32. doi: 10.1152/jn.01066.2007.11. Kofuji P, Mure LS, Massman LJ, Purrier N, Panda S, Engeland WC. Intrinsically Photosensitive Retinal Ganglion Cells (ipRGCs) Are Necessary for Light Entrainment of Peripheral Clocks. PLoS One. 2016;11(12):e0168651. doi: 10.1371/journal.pone.0168651.12. Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC, et al. Prevalence of obstructive sleep apnea in the gen-eral population: A systematic review. Sleep Med Rev. 2017;34:70-81. doi: 10.1016/j.smrv.2016.07.002.13. Association AS: Sleep and Sleep Disorder Statistics [Internet]. Available from: https://www.sleepassociation.org/sleep/sleep-statistics/ [cited 2019 Jul 27].14. Health NIo: Sleep Apnea [Internet]. Available from: http://www.nhlbi.nih.gov/health/health-topics/topics/sleepapnea/ [cited 2019 Jul 27].15. Patil SP, Schneider H, Schwartz AR, Smith PL. Adult obstructive sleep apnea: pathophysiology and diagnosis. Chest. 2007;132(1):325-37. doi: 10.1378/chest.07-004016. Schwab RJ, Gupta KB, Geser WB, Metzger LJ, Hoffman EA, Pack AI. Upper airway and sos tissue anatomy in normal subjects and patients with sleep-disordered breathing. Significance of the lateral pharyngeal walls. Am J Respir Crit Care Med. 1995;152(5 Pt 1):1673-89. doi:10.1164/ajrccm.152.5.758231317. Davies RJ, Stradling JR. The relationship between neck circum-ference, radiographic pharyngeal anatomy, and the obstructive sleep apnoea syndrome. Eur Respir J. 1990;3(5):509- 14. 18. Sateia JM. International Classification of Sleep Disorders-Third Edition. Chest. 2014;146(5):1387-1394. doi: 10.1378/chest.14-0970.19. Clinic M: Obstructive sleep apnea 2018 [Internet]. Available from: http://www.mayoclinic.org/diseases-conditions/obstruc-tive-sleep-apnea/home/ovc-20205684 [cited 2019 Jul 27].20. Eckert DJ, Jordan AS, Merchia P, Malhotra A. Central sleep apnea: Pathophysiology and treatment. Chest. 2007;131(2):595-607. doi: 10.1378/chest.06.2287.21. Pedrosa RP, Drager LF, Antunes MO, Arteaga E, Lorenzi-Filho G. Cheyne-stokes respiration associated with hypertrophic cardiomyop-athy and normal les ventricular ejection fraction. Clinics (Sao Paulo). 2010;65(9):927-9. doi: 0.1590/S1807-59322010000900017.22. Muza RT. Central sleep apnoea-a clinical review. J Thorac Dis. 2015;7(5):930-7. doi: 10.3978/j.issn.2072-1439.2015.04.45.23. Advisor C: Central Sleep Apnea Syndrome [Internet]. Available from: https://www.clinicaladvisor.com/pulmonary-medicine/cen-tral-sleep-apnea-syndrome- idiopathic-csa-cheyne-stokes-respiration-csa-due-to-a-drug-or-substance-high-altitude- periodic-breathing-csa-due-to-a-medical-condition-other-than-cheyne-stokes/article/625213/ [cited 2019 Jul 27].24. Javaheri S, Patel S. Opioids Cause Central and Complex Sleep Apnea in Humans and Reversal With Discontinuation: A Plea for Detoxification. J Clin Sleep Med. 2017;13(6):829-33. doi: 10.5664/
jcsm.6628.25. Alattar MA, Scharf SM. Opioid-associated central sleep apnea: a case series. Sleep Breath. 2009;13(2):201-6. doi: 10.1007/s11325-008-0221-7.26. Thorpy MJ. Classification of sleep disorders. Neurotherapeutics. 2012;9(4):687-701. doi: 10.1007/s13311-012-0145-627. Clinic M: Obstructive sleep apnea 2018 [Internet]. Available from: http://www.mayoclinic.org/diseases-conditions/obstruc-tive-sleep-apnea/diagnosis- treatment/treatment/txc-20206034) [cited 2019 Jul 27].28. Corlateanu A, Pylchenko S, Sircu V, Botnaru V. Predictors of day-time sleepiness in patients with obstructive sleep apnea. Pneumologia. 2015;64(4):21-5. doi: 10.13075/ijomeh.1896.00360.29. Yagi H, Nakata S, Tsuge H, Yasuma F, Noda A, Morinaga M, et al. Morphological examination of upper airway in obstructive sleep apnea. Auris Nasus Larynx. 2009;36(4):444-9. doi: 10.1016/j.anl.2008.11.003.30. Hukins C. Mallampati class is not useful in the clinical assessment of sleep clinic patients. J Clin Sleep Med. 2010;6(6):545-9. 31. Tan HL, Gozal D, Ramirez HM, Bandla HP, Kheirandish-Gozal L. Overnight polysomnography versus respiratory polygraphy in the diagnosis of pediatric obstructive sleep apnea. Sleep. 2014;37(2):255-60. doi:10.5665/sleep.3392.32. Tsara V, Amfilochiou A, Papagrigorakis MJ, Georgopoulos D, Liolios E. Guidelines for diagnosis and treatment of sleep-related breathing disorders in adults and children. Definition and classifica-tion of sleep related breathing disorders in adults: different types and indications for sleep studies (Part 1). Hippokratia. 2009;13(3):187-91. 33. Neill AM, Angus SM, Sajkov D, McEvoy RD. Effects of sleep posture on upper airway stability in patients with obstructive sleep apnea. Am J Respir Crit Care Med. 1997;155(1):199- 204. doi: 10.1164/ajrccm.155.1.9001312.34. Sullivan CE, Issa FG, Berthon-Jones M, Eves L. Reversal of ob-structive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet. 1981;1(8225):862-5. doi: 10.1016/s0140-6736(81)92140-1.35. Center ASE: What is the Difference Between CPAP and BiPAP Therapy? [Internet]. Available from: http://www.alaskasleep.com/blog/what-is-bipap-therapy-machine-bilevel- positive-airway-pressure [cited 2019 Jul 27].36. Tregear S, Reston J, Schoelles K, Phillips B. Continuous positive airway pressure reduces risk of motor vehicle crash among drivers with obstructive sleep apnea: systematic review and meta-analysis. Sleep. 2010;33(10):1373-80. doi: 10.1093/sleep/33.10.1373.37. Bradley TD, Floras JS. Obstructive sleep apnoea and its cardio-vascular consequences. Lancet. 2009;373(9657):82-93. doi: 10.1016/S0140-6736(08)61622-0.38. Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardio-vascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046-53. doi: 10.1016/S0140-6736(05)71141-7.39. Spicuzza L, Caruso D, Di Maria G. Obstructive sleep apnoea syn-drome and its management. Ther Adv Chronic Dis. 2015;6(5):273-85. doi: 10.1177/2040622315590318.40. Bidarian-Moniri A, Nilsson M, Rasmusson L, Attia J, Ejnell H. The effect of the prone sleeping position on obstruc-tive sleep apnoea. Acta Otolaryngol. 2015;135(1):79-84. doi: 10.3109/00016489.2014.962183.41. Eijsvogel MM, Ubbink R, Dekker J, Oppersma E, de Jongh FH, van der Palen J, et al. Sleep position trainer versus tennis ball
Original Article
15-26
RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com26
technique in positional obstructive sleep apnea syndrome. J Clin Sleep Med. 2015;11(2):139-47. doi: 10.5664/jcsm.4460.42. Chan AS, Sutherland K, Schwab RJ, Zeng B, Petocz P, Lee RW, et al. The effect of mandibular advancement on upper airway structure in obstructive sleep apnoea. Thorax. 2010;65(8):726-32. doi: 10.1136/thx.2009.131094.43. HZZO: Medicinski proizvodi [Internet]. Available from: http://www.hzzo.hr/zdravstveni- sustav-rh/medicinski-proizvodi/ [cited 2019 Jul 27].44. Puhan MA, Suarez A, Lo Cascio C, Zahn A, Heitz M, Braend-li O. Didgeridoo playing as alternative treatment for obstruc-tive sleep apnoea syndrome: randomised controlled trial. BMJ. 2006;332(7536):266-70. doi:10.1136/bmj.38705.470590.55.45. Hong SO, Chen YF, Jung J, Kwon YD, Liu SYC. Hypoglossal nerve stimulation for treatment of obstructive sleep apnea (OSA): a primer for oral and maxillofacial surgeons. Maxillofac Plast Reconstr Surg. 2017;39(1):27. doi: 10.1186/s40902-017-0126-0.46. Tregear S, Reston J, Schoelles K, Phillips B. Obstructive sleep ap-nea and risk of motor vehicle crash: systematic review and meta-analy-sis. J Clin Sleep Med. 2009;5(6):573-81. 47. Schwartz AR, Patil SP, Laffan AM, Polotsky V, Schneider H, Smith PL. Obesity and obstructive sleep apnea: pathogenic mechanisms and therapeutic approaches. Proc Am Thorac Soc. 2008;5(2):185-92. doi: 10.1513/pats.200708-137MG.48. Frye SS, Fernandez-Mendoza J, Calhoun SL, Gaines J, Sawyer MD, He F, et al. Neurocognitive and behavioral functioning in adoles-cents with sleep-disordered breathing: a population-based, dual-energy X-ray absorptiometry study. Int J Obes (Lond). 2018;42(1):95-101. doi: 10.1038/ijo.2017.229.49. Osorio RS, Gumb T, Pirraglia E, Varga AW, Lu SE, Lim J, et al. Sleep-disordered breathing advances cognitive decline in the elderly. Neurology. 2015;84(19):1964-71. doi: 10.1212/WNL.0000000000001566.50. Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. Lancet. 2014;383(9918):736-47. doi: 10.1016/S0140-6736(13)60734-5.51. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353(19):2034-41. doi: 10.1056/NEJ-Moa043104.52. Unnikrishnan D, Jun J, Polotsky V. Inflammation in sleep ap-nea: an update. Rev Endocr Metab Disord. 2015;16(1):25-34. doi: 10.1007/s11154-014-9304-x.53. Narkiewicz K, Somers VK. The sympathetic nervous system and obstructive sleep apnea: implications for hypertension. J Hypertens. 1997;15(12 Pt 2):1613-9. doi: 10.1097/00004872-199715120-00062.54. Tasali E, Mokhlesi B, Van Cauter E. Obstructive sleep apnea and type 2 diabetes: interacting epidemics. Chest. 2008;133(2):496-506. doi: 10.1378/chest.07-0828.55. Pecotic R, Dodig IP, Valic M, Ivkovic N, Dogas Z. The evaluation of the Croatian version of the Epworth sleepiness scale and STOP questionnaire as screening tools for obstructive sleep apnea syndrome. Sleep Breath. 2012;16(3):793-802. doi:10.1007/s11325-011-0578-x.56. Neill AM, Angus SM, Sajkov D, McEvoy RD. Effects of sleep pos-ture on upper airway stability in patients with obstructive sleep apnea. Am J Respir Crit Care Med. 1997;155(1):199-204. doi: 10.1164/ajrccm.155.1.9001312.57. Cartwright RD. Effect of sleep position on sleep apnea severity. Sleep. 1984;7(2):110-4. doi: 10.1093/sleep/7.2.110
58. Cartwright RD, Lloyd S, Lilie J, Kravitz H. Sleep position training as treatment for sleep apnea syndrome: a preliminary study. Sleep. 1985;8(2):87-94. doi:10.1093/sleep/8.2.87 59. Oksenberg A, Silverberg DS. The effect of body posture on sleep-related breathing disorders: facts and therapeutic implications. Sleep Med Rev. 1998;2(3):139-62. 60. Oksenberg A, Khamaysi I, Silverberg DS, Tarasiuk A. Association of body position with severity of apneic events in patients with severe nonpositional obstructive sleep apnea. Chest. 2000;118(4):1018-24. doi: 10.1378/chest.118.4.1018.61. Cartwright RD, Diaz F, Lloyd S. The effects of sleep posture and sleep stage on apnea frequency. Sleep. 1991;14(4):351-3. doi: 10.1093/sleep/14.4.351.62. Frank MH, Ravesloot MJ, van Maanen JP, Verhagen E, de Lange J, de Vries N. Positional OSA part 1: Towards a clinical classification system for position-dependent obstructive sleep apnoea. Sleep Breath. 2015;19(2):473-80. doi: 10.1007/s11325-014-1022-9.63. Metersky ML, Castriotta RJ. The effect of polysomnography on sleep position: possible implications on the diagnosis of po-sitional obstructive sleep apnea. Respiration. 1996;63(5):283-7. doi:10.1159/000196561. 64. Menon A, Kumar M. Influence of body position on severity of obstructive sleep apnea: a systematic review. ISRN Otolaryngol. 2013;2013:670381. doi: 10.1155/2013/670381.65. Levendowski DJ, Seagraves S, Popovic D, Westbrook PR. Assess-ment of a neck-based treatment and monitoring device for positional obstructive sleep apnea. J Clin Sleep Med. 2014;10(8):863-71. doi: 10.5664/jcsm.3956.66. Oksenberg A, Silverberg DS, Arons E, Radwan H. Positional vs nonpositional obstructive sleep apnea patients: anthropomorphic, noc-turnal polysomnographic, and multiple sleep latency test data. Chest. 1997;112(3):629-39. doi:10.1378/chest.112.3.629.67. Huang KT, Chin CH, Tseng CC, Chang HC, Chen YC, Wang CC, i sur. The influence of obesity on different genders in pa-tients with obstructive sleep apnea. The Scientific World Journal. 2014;2014:487215. doi:10.1155/2014/48721568. Dancey DR, Hanly PJ, Soong C, Lee B, Shepard J, Jr., Hoffstein V. Gender differences in sleep apnea: the role of neck circumference. Chest. 2003;123(5):1544-50. doi: 10.1378/chest.123.5.1544.69. Wahner-Roedler DL, Olson EJ, Narayanan S, Sood R, Hanson AC, Loehrer LL, i sur. Gender-specific differences in a patient popu-lation with obstructive sleep apnea-hypopnea syndrome. Gend Med. 2007;4(4):329-38. 70. Cairns A, Poulos G, Bogan R. Sex differences in sleep apnea predictors and outcomes from home sleep apnea testing. Nat Sci Sleep. 2016;8:197-205. doi: 10.2147/NSS.S101186.71. Heinzer R, Vat S, Marques-Vidal P, Marti-Soler H, Andries D, Tobback N, i sur. Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. Lancet Respir Med. 2015;3(4):310-8. doi: 10.1016/S2213-2600(15)00043-0.72. Drager LF, Togeiro SM, Polotsky VY, Lorenzi-Filho G. Obstruc-tive sleep apnea: a cardiometabolic risk in obesity and the metabolic syndrome. J Am Coll Cardiol. 2013;62(7):569-76. doi: 10.1016/j.jacc.2013.05.045.73. Mador MJ, Kufel TJ, Magalang UJ, Rajesh SK, Watwe V, Grant BJ. Prevalence of positional sleep apnea in patients undergo-ing polysomnography. Chest. 2005;128(4):2130-7. doi:10.1378/chest.128.4.2130
Original Article
15-26

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com27
Hallux Sesamoiditis - Radiological Diagnostics and Conservative Management
Igor Borić1, Marko Pećina2, Maja Mirković3, Tatjana Cicvara Pećina4, Damir Matoković5, Mihovil Plečko6 , Ivo Dumić-Čule4
1 St. Catherine Specialty Hospital, Zabok2 Department for Orthopedics, School of Medicine, University of Zagreb, Zagreb3 Polyclinic for orthopedics, physical medicine and rehabilitation “Kinematika”, Zagreb4 Department of diagnostic and interventional radiology, University Hospital “Dubrava”, Zagreb5 County General Hospital Požega, Požega6 Department for Orthopedics, University Hospital Center Zagreb, Zagreb
abstract:Sesamoid bones play an essential role in first metatarsophalangeal (MTP) joint biomechanics, together with other articular surfaces, joint capsule, plantar fascia, ligaments and tendons. They are prone to different acute and chronic injuries, such as acute fracture, stress fractures, chondromalacia, avascular necrosis, bursitis degenerative changes, inflammation etc., all of which clinically manifest as a painful condition and are often diagnosed under a broad term called sesamoiditis. The mechanism of injury is most commonly associated with overuse of the anterior part of the sole of the foot accompanied by excessive dorsiflexion of the great toe. Sesamoiditis presents with pain and localized swelling in the projection of the tibial sesamoid bone, which is affected more frequently than the fibular one. Diagnostic radiology plays a key role in determination of etiology of the disease, as well as in planning of it’s treatment. Typical radiological examination includes weight-bearing dorsoplantar, lateral, oblique medial and oblique lateral radiographs of the foot, together with a direct axial radiograph of sesamoid bones. Computerized tomography is used for distinction of acute fractures and early stage of stress fractures from other pathological conditions. Magnetic resonance imaging allows differentiation between bony pathology and soft tissue conditions. Sesamoiditis management is primarily conservative and it depends on duration and severity of the condition. Orthotic insoles customized according to pedobarographic findings may be useful for solving biomechanical deformities that could have led to development of sesamoiditis. Specific pads placed under the first MTP joint in order to prevent the great toe from dorsiflexion proved to be a very effective conservative treatment option. Surgical treatment is considered if conservative methods fail to provide sufficient management of the condition.
Keywords: sesamoid bones; hallux; sesamoiditis; diagnostic radiology; sesamoiditis treatment;
Sažetak:sezamoiDitis - raDiološka Dijagnostika i konzerVatiVno liječenje
Sezamske kosti u području metatarzofalangealnog zgloba nožnog palca (hallux) dio su anatomsko-biomehaničkog kompleksa kojeg čine zglobna tijela, čahura, plantarna fascija, sveze i tetive mišića. U sklopu navedenog komplek-sa sezamske kosti podložne su raznim akutnim i kroničnim oštećenjima u smislu prijeloma, stres prijeloma, hon-dromalacije, avaskularne nekroze, burzitisa, degenerativnih promjena, upala itd., a što se sve klinički očituje kao bolno stanje i sve se podvodi pod široki pojam sesamoiditisa. Mehanizam koji dovodi do sesamoiditisa najčešće je vezan uz prenaprezanje prednjeg dijela stopala praćenog ekscesivnom dorzifleksijom nožnog palca. U kliničkoj sli-ci sesamoiditisa najčešći simptom je bol i lokalizirana oteklina i to u području tibijalne sezamske kosti koja je dale-ko češće zahvaćena u odnosu na fibularnu sezamsku kost. Radiološka dijagnostika je značajna kako u otkrivanju etiologije tako i u planiranju liječenja sesamoiditisa. Standardna radiološka pretraga obuhvaća antero-posteriornu snimku pod opterećenjem stopala, lateralnu snimku, kose snimke te aksijalnu snimku sezamskih kostiju. Komp-juterizirana tomografija pokazala se korisnom za razlikovanje akutnog prijeloma i ranog stadija stres prijeloma sezamske kosti od drugih patologija koje mogu zahvatiti sezamske kosti. MRI omogućuje diferencijaciju između koštanih promjena i promjena na mekom tkivu. Liječenje sezamoiditisa je prvenstveno konzervativno i uvelike ovisno o uznapredovalosti promjena u području cijelog metatarzofalangealnog kompleksa. Ortopedski ulošci nakon pedobarografske analize opterećenja stopala mogu otkloniti biomehaničke deformacije koje su potencijalno pridonijele razvoju sesamoiditisa. Posebni podlošci ispod metatarzofalangealnog zgloba palca u smislu sprečavanja dorzifleksije palca su vrlo korisni i efikasni u konzervativnom liječenju sesamoiditisa. Kirurško liječenje može biti preporučeno nakon neuspjelog konzervativnog liječenja.
ključne riječi: sezamske kosti; nožni palac; sesamoiditis; radiološka dijagnostika; liječenje sesa-moiditisa;
OPEN ACCESS
Correspondence: Mihovil Plečko MD
[email protected]/0000-0001-6569-9287
This article was submitted to RAD CASA - Medical Sciences as the
review article
Conflict of Interest Statement: The authors declare that the
research was conducted in the absence of any commercial or
financial relationships that could be construed as a potential conflict of
interest.
Received: 13 October 2019Accepted: 28 November 2019Published: 10 December 2019
Citation:Borić I, Pećina M, Mirković M et
al. Hallux Sesamoiditis- Radiolog-ical Diagnostics and Conservative
Management. RAD CASA - Medical Sciences. 540=48-49 (2019): 27-32. https://dx.doi.org/10.21857/
m8vqrtzxg9
Copyright (C) 2019 Borić, Pećina, Mirković et al. This is an open-ac-cess article distributed under the terms of the Creative Commons Attribution License (CC BY). The
use, distribution or reproduction in other forums is permitted, provided
the original author(s) and the copyright owners(s) are credited
and that the original publication in this journal is cited, in accordance whit accepted adacemic practice.
No use, distribution or reproduction is permitted which does not comply
with these terms.
Review Article
27-32

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com28
introduction
Sesamoid bones (ossa sesamoidea) were first described by Galen in the second century, who compared them with sesame seeds. Sesamoid bones are inserted into tendons of certain muscles, usually where the tendon is passing over a joint, such as in first metacarpo-phalangeal and first metatarsophalangeal (MTP) joints. They can less often be found in areas of interphalangeal joints both in the foot and in the hand. Also, this type of bones can be found in the lower extremity, located in tendons of triceps surae muscle, tibialis posterior muscle and peroneus longus muscle. The largest sesamoid bone is the patella, inserted into the tendon of the quadriceps muscle. Sesamoid bones can also be embedded into joint capsules or be divided by a synovial bursa from the underlying bone, wherein both cases the articular surface of the sesamoid bone is covered by hyaline cartilage. They play an essential part in first MTP joint biomechanics, together with other articular surfaces, joint capsule, plantar fascia, ligaments and tendon1-6 In this complex we find two sesamoid bones, tibial (medial) sesamoid bone embedded into the medial head of the flexor hallucis brevis muscle (FHB) and fibular (lateral) sesamoid bone embedded into the lateral head of FHB. Both of these bones are located under the head of the first metatarsal bone, with the tibial sesamoid being placed distally in comparison to the fibular sesamoid. A crest is located on the plantar surface of the first metatarsal bone, dividing two sesamoid bones and forming two joints: medial and lateral metatarsosesamoid joints. Their function is to distribute and ease the pressure produced during gait that affects the head of the first metatarsal bone, to lower the friction on the flexor hallucis longus muscle which passes between these two bones, as well as to act as a fulcrum for FHB. Sesamoid bones of the great toe ossify at age of 8-9 in girls and at age of 11-13 in boys. During the ossification process the tibial sesamoid bone can be divided into two or more parts, thus forming a bipartite or multipartite bone. Studies show that a bipartite tibial sesamoid bone has an incidence of 10% - 30%, where in fibular sesamoid bone partition rarely occurs. In 25% of the cases bipartite tibial sesamoid bone is present bilaterally.
etiology
As a part of the first MTP joint complex, sesamoid bones are prone to different acute and chronic injuries, such as acute fracture caused by trauma7, stress fractures8,9,10, chondromalacia, osteocartilaginous injury11, avascular necrosis12, osteochondritis13, bursitis, degenera-tive changes, inflammation, developmental anomalies14-18, all of which is clinically diagnosed under a broad term called sesamoid-itis. The mechanism of injury is most commonly associated with overuse of the anterior part of the sole of the foot accompanied by excessive dorsiflexion of the great toe19. This usually occurs in sports that involve running and jumping, especially in the initial phase of running and during sprinting. Moreover, ballet dancers often use “relevé” position of the sole of the foot, thus putting a great amount of load on the head of the first metatarsal bone20. Furthermore, deformities such as pes cavus, conditions like a rigid sole of the foot and hard surfaces where different sports are played can facilitate development of sesamoiditis, often colloquially called turf toe in such cases21-27. Injury of plantar structures of the first MTP joint in American football players were first described by Bowers and Martin in 1976. and Rodeo et al. reported that 45% of American football players have suffered from turf toe during their sports career18.
clinical Presentation
Sesamoiditis presents with pain and localized swelling in the projec-tion of the tibial sesamoid bone, which is affected more frequently than the fibular one. Pain can occur acutely after trauma, or it can develop chronically, in a subtler way, which happens in most cases. Putting static load on the first MTP joint area and wearing certain rigid types of footwear intensifies the pain, while running could be impeded. In the later phase of the disease, pain can occur on the lateral part of the foot, as patient inverts his foot while walking to avoid putting pressure to the great toe. During dorsiflexion of the great toe sesamoid bones move distally, as well as the area painful to palpation on the affected great toe (Figure 1). Swelling is often overlooked, due to the presence of adipose tissue in this area. Passive movements in the first MTP joint can be painless. On the other hand, projection of the sesamoid bones is painful to palpation, as well as plantar flexion against resistance in the first MTP joint, thus being classical symptoms of sesamoiditis28.
diagnostics
Diagnostic radiology plays a key role in determination of etiology of the disease, as well as in planning of it’s treatment15,29,30,31. Typical radiological examination of sesamoid bones include weight-bearing
Figure1. The passive axial compression test (PACT). A) The sesamoid bones are under the first metatarsal head. B) Maximal dorsal flexion of the hallux produces distal migration of the sesamoids. C) Applying compression proximal to the sesamoids stabilizes them in their most distal position. D) Test is positive if passive plantar flexion in the metatarsophalangeal joint produces pain.
Review Article
27-32

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com29
dorsoplantar, lateral, oblique medial and oblique lateral radiographs (dorsoplantar radiograph with the foot angled 40 degrees medially/laterally) of the foot, together with a direct axial radiograph of sesamoid bones. For the axial sesamoid projection patient’s foot is in maximal dorsiflexion with toes pulled back towards the patient, with the tangential X-ray being directed from the anterior part of the foot towards the posterior part, providing a profile image of sesamoid bones at the first MTP joint. Radiographs may show malposition, bi-/multi-partition of sesamoid bones, hallmarks of
osteoarthritis of the first MTP joint, fractures, osteonecrosis, stress fractures, translation and proximal retraction of sesamoid bones, infection etc. Distinction of fracture from bipartite sesamoid bones could be done by taking radiographs of both foot, as the bipartite sesamoid bones often present bilaterally. Fractures of sesamoids typ-ically present on radiographs as communitive puzzle-like fragments, with displacement and sharp, irregular edges. Formation of callus in follow-up radiographs may confirm fracture diagnosis. Bipartite ses-amoid bone is usually bigger than the undivided bone with smooth
Figure2. Weight-bearing dorsoplantar radiographs of the foot shows: A) and B) bipartite tibial sesamoid bone in two different patients (arrow): bipartite bones are bigger than the undivided bone, divided fragments have smooth, round and sclerotic edges; C) fracture of the fibular sesamoid (arrow): sharp oblique fracture line.
Figure3. Direct axial radiograph of sesamoid bones shows sclerotic and fragmented fibular sesamoid bone as a sign of osteonecrosis (arrow).
Review Article
27-32
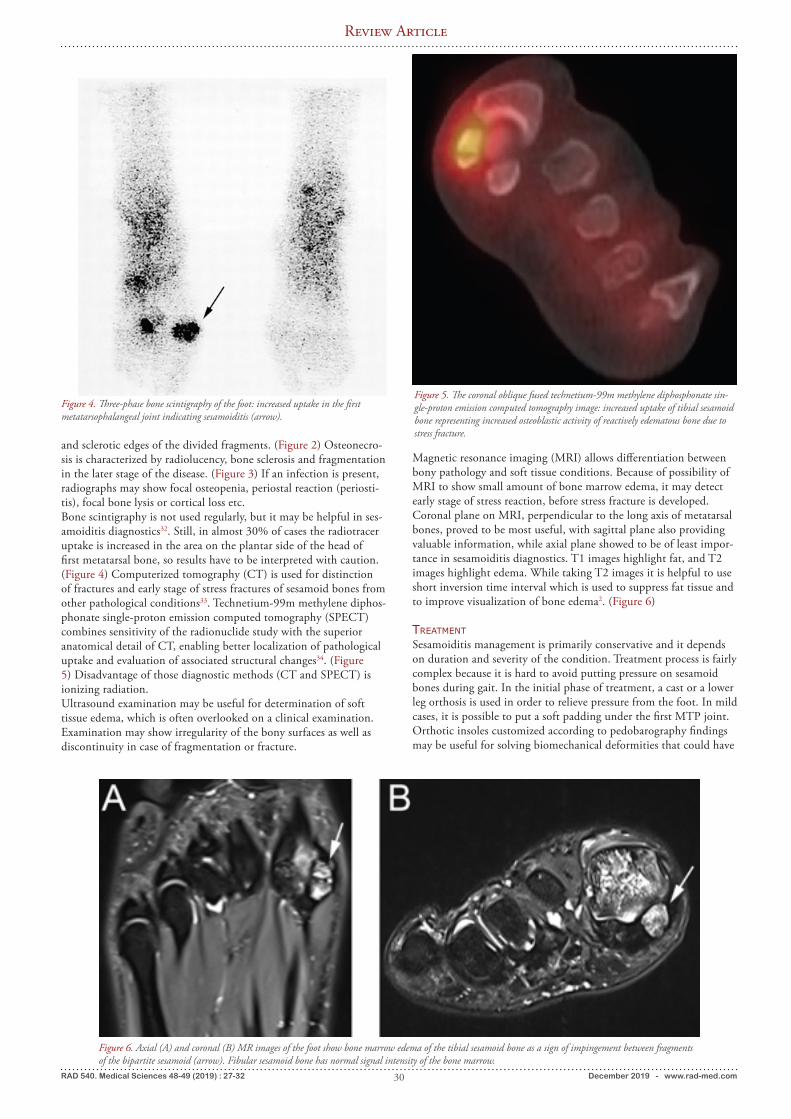
RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com30
and sclerotic edges of the divided fragments. (Figure 2) Osteonecro-sis is characterized by radiolucency, bone sclerosis and fragmentation in the later stage of the disease. (Figure 3) If an infection is present, radiographs may show focal osteopenia, periostal reaction (periosti-tis), focal bone lysis or cortical loss etc. Bone scintigraphy is not used regularly, but it may be helpful in ses-amoiditis diagnostics32. Still, in almost 30% of cases the radiotracer uptake is increased in the area on the plantar side of the head of first metatarsal bone, so results have to be interpreted with caution. (Figure 4) Computerized tomography (CT) is used for distinction of fractures and early stage of stress fractures of sesamoid bones from other pathological conditions33. Technetium-99m methylene diphos-phonate single-proton emission computed tomography (SPECT) combines sensitivity of the radionuclide study with the superior anatomical detail of CT, enabling better localization of pathological uptake and evaluation of associated structural changes34. (Figure 5) Disadvantage of those diagnostic methods (CT and SPECT) is ionizing radiation. Ultrasound examination may be useful for determination of soft tissue edema, which is often overlooked on a clinical examination. Examination may show irregularity of the bony surfaces as well as discontinuity in case of fragmentation or fracture.
Figure 4. Three-phase bone scintigraphy of the foot: increased uptake in the first metatarsophalangeal joint indicating sesamoiditis (arrow).
Figure 5. The coronal oblique fused technetium-99m methylene diphosphonate sin-gle-proton emission computed tomography image: increased uptake of tibial sesamoid bone representing increased osteoblastic activity of reactively edematous bone due to stress fracture.
Figure 6. Axial (A) and coronal (B) MR images of the foot show bone marrow edema of the tibial sesamoid bone as a sign of impingement between fragments of the bipartite sesamoid (arrow). Fibular sesamoid bone has normal signal intensity of the bone marrow.
Magnetic resonance imaging (MRI) allows differentiation between bony pathology and soft tissue conditions. Because of possibility of MRI to show small amount of bone marrow edema, it may detect early stage of stress reaction, before stress fracture is developed. Coronal plane on MRI, perpendicular to the long axis of metatarsal bones, proved to be most useful, with sagittal plane also providing valuable information, while axial plane showed to be of least impor-tance in sesamoiditis diagnostics. T1 images highlight fat, and T2 images highlight edema. While taking T2 images it is helpful to use short inversion time interval which is used to suppress fat tissue and to improve visualization of bone edema2. (Figure 6)
treatment
Sesamoiditis management is primarily conservative and it depends on duration and severity of the condition. Treatment process is fairly complex because it is hard to avoid putting pressure on sesamoid bones during gait. In the initial phase of treatment, a cast or a lower leg orthosis is used in order to relieve pressure from the foot. In mild cases, it is possible to put a soft padding under the first MTP joint. Orthotic insoles customized according to pedobarography findings may be useful for solving biomechanical deformities that could have
Review Article
27-32

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com31
Figure 7. Pedobarogram of an athlete suffering from sesamoiditis: A) three dimensional demonstration of pedobarogram (increased plantar pressure in the area of sesamoid bones, concave form of foot - pes cavus); B) plantar pressures measured in shoes; C) plantar pressure measured in shoes after applying CAD/CAM insole (decreased pressure in the area of sesamoid bones; increased contact area)
literature:1. Srinivasan R. The hallucal-sesamoid complex:normal anatomy, im-aging and pathology.Semin Musculoskelet Radiol. 2016;20:224-232. doi: 10.1055/s-0036-15811212. Cohen BE. Hallux sesamoid disorders. Foot Ankle Clin. 2009;14(1):91-104. doi: 10.1016/j.fcl.2008.11.0033. Scranton PE Jr, Rutkowski R. Anatomic variations in the first ray: Part II. Disorders of the sesamoids. Clin Orthop Relat Res. 1980;(151):256-64.4. Kadakia AR, Molloy A. Current concepts review: traumatic dis-orders of the first metatarsophalangeal joint and sesamoid complex. Foot Ankle Int. 2011;32(8):834-9. Boike A, Schnirring-Judge M,
McMillin S. Sesamoid disorders of the first metatarsophalangeal joint. Clin Podiatr Med Surg. 2011;28(2):269-85. doi: 10.3113/FAI.2011.08345. Boike A, Schnirring-Judge M, McMillin S. Sesamoid disorders of the first metatarsophalangeal joint. Clin Podiatr Med Surg. 2011;28(2):269-85. doi: 10.1016/j.cpm.2011.03.0066. Nwawka OK, Hayashi D, Diaz LE, Goud AR, Arndt WF 3rd, Ro-emer FW, Malguria N, Guermazi A. Sesamoids and accessory ossicles of the foot: anatomical variability and related pathology. Insights Imaging. 2013;4(5):581-93. doi: 10.1007/s13244-013-0277-1.7. Lee SYS, Tan TJ, Yan YY. Fracture of a Bipartite Medial Hallux Sesamoid Masquerading as a Tripartite Variant: A Case Report and
led to development of sesamoiditis. (Figure 7) Specific pads placed under the first MTP joint in order to prevent the great toe from dorsiflexion proved to be a very effective conservative treatment option. Nonsteroidal anti-inflammatory drugs can be used for pain relief, while the use of corticosteroid injections showed relief of symp-toms, but is discussable because of its side effects, especially when used repeatedly. Saxena A. et al. described positive effect of radial soundwaves for sesamoidopathy in athletes35. Surgical treatment is considered if conservative methods fail to provide sufficient management of the condition. It should be considered with caution regarding the role that sesamoid bones play in the great toe biome-chanics. Sesamoidectomy may be performed after failed conserva-tive management of different pathological conditions, ie. non-union or stress fractures, osteonecrosis, chondromalacia, infections etc. Studies show that this operation proved to be satisfying with 94.4% of patients returning to sports, of which 90.0% returning to level of activity they had prior to acquiring sesamoiditis. However, overall complication rate was 22.5% and the revision rate was 3.0%36,37,38,39. Nevertheless, in some cases surgery is inevitable. Nowadays, it is possible to perform minimally invasive surgery in
terms of arthroscopic sesamoidectomy, using different portals for approaching to either tibial or fibular sesamoid bone.
conclusion
As the modern technologies are evolving and thus providing the possibility to diagnose etiology of injuries and other conditions that affect sesamoid bones, it is becoming obsolete to use the clinical diagnosis of sesamoiditis. Nevertheless, most of this conditions are still treated in the same manner. Novel concepts of treatment provide good results, with most of patients being able to return to the previous level of activity they had before acquiring any of above mentioned conditions.
author contributions:All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Review Article
27-32

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com32
Review of the Literature. J Foot Ankle Surg. 2019;58(5):980-983. doi: 10.1053/j.jfas.2018.12.0198. Alexa O, Popia I. Stress fracture of the internal sesamoid bone of the first metatarsophalangeal joint. Case report. Rev Med Chir Soc Med Nat Iasi. 2005;109(4):822-4. (in Romanian) 9. Van Hal, M. E., Keene, J. S., and Lange, T. A., Stress fractures of the great toe sesamoids. Am. J. Sports Med. 1982;10:122-128. doi: 10.1177/03635465820100021210. Robertson GAJ, Goffin JS, Wood AM. Return to sport following stress fractures of the great toe sesamoids: a systematic review. Br Med Bull. 2017;122(1):135-149. doi: 10.1093/bmb/ldx01011. Coughlin MJ, Kemp TJ, Hirose CB. Turf toe: soft tissue and osteocartilaginous injury to the first metatarsophalangeal joint. Phys Sportsmed. 2010;38(1):91-100. doi: 10.3810/psm.2010.04.176612. Bartosiak K, McCormick JJ. Avascular Necrosis of the Sesamoids. Foot Ankle Clin. 2019;24(1):57-67. doi: 10.1016/j.fcl.2018.09.00413. Garrido IM, Bosch MN, González MS, Carsí VV. Osteochondritis of the hallux sesamoid bones. Foot Ankle Surg. 2008;14(4):175-9. doi: 10.1016/j.fas.2008.02.00414. Frankel, J. P. and Harrington, J. Symptomatic bipartite sesamoids. J. Foot Surg. 1990;29:318-323.15. Favinger JL, Porrino JA, Richardson ML, Mulcahy H, Chew FS, Brage ME. Epidemiology and imaging appearance of the normal Bi-/multipartite hallux sesamoid bone. Foot Ankle Int. 2015;36(2):197-202. doi: 10.1177/107110071455248416. Kumar S, Kadavigere R, Puppala R, Ayachit A, Singh R. Sub-hallucal Interphalangeal Sesamoiditis: A Rare Cause of Chronic Great Toe Pain. J Clin Diagn Res. 2015;9(5):TD01-2. doi: 10.7860/JCDR/2015/13210.587017. Kanatli U, Ozturk AM, Ercan NG, Ozalay M, Daglar B, Yetkin H. Absence of the medial sesamoid bone associated with metatarsophalan-geal pain. Clin Anat. 2006;19(7):634-9. doi: 10.1002/ca.2028218. Rodeo SA, Warren RF, O’Brien SJ, Pavlov H, Barnes R, Hanks GA. Diastasis of bipartite sesamoids of the first meta-tarsophalangeal joint. Foot Ankle. 1993;14(8):425-34. doi: 10.1177/10711007930140080119. Pećina M, Bojanić I. Overuse Injuries of the Musculoskeletal System, Second Edition, CRC Press, Boca Raton-London-New York-Washington,D.C. 2004; pp 296-298.20. Hardaker, W. T., Jr. Foot and ankle injuries in classical ballet danc-ers. Orthop. Clin. Am. 1989;20:621-627.21. McBryde, A. M. and Anderson, R. B. Sesamoid foot problems in the athlete. Clin. Sports Med. 1988;7:51-60.22. Schein AJ, Skalski MR, Patel DB, White EA, Lundquist R, Gottse-gen CJ, Forrester DM, Matcuk GR Jr. Turf toe and sesamoiditis: what the radiologist needs to know. Clin Imaging. 2015;39(3):380-9. doi: 10.1016/j.clinimag.2014.11.01123. Mason LW, Molloy AP. Turf Toe and Disorders of the Sesamoid Complex. Clin Sports Med. 2015;34(4):725-39. doi: 10.1016/j.csm.2015.06.00824. Brophy RH, Gamradt SC, Ellis SJ, Barnes RP, Rodeo SA, Warren RF, Hillstrom H. Effect of turf toe on foot contact pressures in profes-sional American football players. Foot Ankle Int. 2009;30(5):405-9. doi: 10.3113/FAI-2009-0405
25. George E, Harris AH, Dragoo JL, Hunt KJ. Incidence and risk factors for turf toe injuries in intercollegiate football: data from the national collegiate athletic association injury surveillance system. Foot Ankle Int. 2014;35(2):108-15. doi: 10.1177/107110071351403826. McCormick JJ, Anderson RB. The great toe: failed turf toe, chronic turf toe, and complicated sesamoid injuries. Foot Ankle Clin. 2009;14(2):135-50. doi: 10.1016/j.fcl.2009.01.00127. Hotfiel T, Carl HD, Jendrissek A, Swoboda B, Barg A, Engel-hardt M. [Die Turf-Toe-Verletzung – ein Hyperextensionstrauma der Großzehe]. Sportverletz Sportschaden. 2014;28(3):139-45. doi: 10.1055/s-0034-1366873 (in German) 28. Allen MA, Casillas MM. The passive axial compression (PAC) test: a new adjunctive provocative maneuver for the clinical diagno-sis of hallucal sesamoiditis. Foot Ankle Int. 2001;22(4):345-6. doi: 10.1177/10711007010220041429. Sanders TG, Rathur SK. Imaging of painful conditions of the hallucal sesamoid complex and plantar capsular structures of the first metatarsophalangeal joint. Radiol Clin North Am. 2008;46(6):1079-92. doi: 10.1016/j.rcl.2008.09.00130. Waldrop NE 3rd, Zirker CA, Wijdicks CA, Laprade RF, Clan-ton TO. Radiographic evaluation of plantar plate injury: an in vitro biomechanical study. Foot Ankle Int. 2013;34(3):403-8. doi: 10.1177/107110071246495331. Yildirim Y, Cabukoglu C, Erol B, Esemenli T. Effect of meta-tarsophalangeal joint position on the reliability of the tangential sesamoid view in determining sesamoid position. Foot Ankle Int. 2005;26(3):247-50. doi: 10.1177/10711007050260031132. Yang RH, Chu YK. Hallucal sesamoiditis manifested on bone scan. Clin Nucl Med. 2013;38(12):1019-21.33. Welck MJ, Singh D, Cullen N, Goldberg A. Evaluation of the 1st metatarso-sesamoid joint using standing CT - The Stanmore classification. Foot Ankle Surg. 2018;24(4):314-319. doi: 10.1016/j.fas.2017.03.00534. Sharma P, Singh H, Agarwal KK, Sudhir KS, Khangembam BC, Bal C, Malhotra A, Kumar R. Utility of (99m)Tc-MDP SPECT-CT for the diagnosis of sesamoiditis as cause of metatarsalgia. Indian J Nucl Med. 2012;27(1):45-7. doi: 10.4103/0972-3919.10886535. Saxena A, Yun A, Patel R, Gerdesmeyer L, Maffulli N. Radial Soundwave for Sesamoidopathy in Athletes: A Pilot Study. J Foot Ankle Surg. 2016;55(6):1333-1335. doi: 10.1053/j.jfas.2016.07.02436. Shimozono Y, Hurley ET, Brown AJ, Kennedy JG. Sesamoidecto-my for Hallux Sesamoid Disorders: A Systematic Review. J Foot Ankle Surg. 2018;57(6):1186-1190. doi: 10.1053/j.jfas.2018.03.04437. Taylor CF, Butler M, Parsons SW. Problems associated with the excision of the hallux sesamoids. Foot Ankle Clin. 2014;19(3):425-36. doi: 10.1016/j.fcl.2014.06.01438. Alshouli MT, Lin A, Kadakia AR. Simultaneous first metatar-sophalangeal joint arthrodesis and sesamoidectomy with a single dorsomedial incision. Foot Ankle Spec. 2014;7(5):403-8 doi: 10.1177/193864001454521739. Ford SE, Adair CR, Cohen BE, Davis WH, Ellington JK, Jones CP, Anderson RB. Efficacy, Outcomes, and Alignment Following Iso-lated Fibular Sesamoidectomy via a Plantar Approach. Foot Ankle Int. 2019;1071100719 doi: 10.1177/1071100719868734
Review Article
27-32

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com33
Comprehensive Medication Management Services as a Solution to Medication Mismanagement: A European PerspectiveIva Mucalo1 , Andrea Brajković1, Ivona Jukic2, Danijela Jonjić1, Dagmar Radin3, Djenane Ramalho de Oliveira4
1 University of Zagreb Faculty of Pharmacy and Biochemistry, A. Kovacica 1, Zagreb, Croatia2 Community pharmacy Mandis Pharm, Branimirova ulica 65, Zagreb, Croatia3 University of Zagreb Faculty of Political Science, Lepusiceva 6, Zagreb, Croatia4 Centre for Pharmaceutical Care Studies (Centro de Estudos Atencao Farmaceutica), Federal University of Minas Gerais, Belo Horizonte, MG, Brazil
abstract:Due to an increase in the prevalence of chronic diseases, medication use and their cost is rising rapidly. This scenario render chronic patients at an increased risk of experiencing drug therapy problems, subsequently leading to unfavourable clinical and economic outcomes. Thus, to ensure patients’ optimal medication use and improve their clinical outcomes, a comprehensive and systematic management of medications is deemed crucial. Hence, Comprehensive Medication Management (CMM) services offered by trained pharmacists can fill this gap by decreasing the unnecessary and often harmful use of medicines and consequent resulting complications. Collaborative practice between pharmacists and gen-eral practitioners, together with patients’ active participation in the definition of treatment regimens, plays an important role in the effectiveness of CMM services. CMM services is defined as the standard of care that ensures each patient’s medications (prescription, non-prescription, alternative, traditional, vitamins, or nutritional supplements) are individ-ually assessed to determine that each medication is appropriate for the patient, effective for the medical condition, safe given the comorbidities and other medications taken, and that the patient is able to take them as intended. It includes an individualized care plan that achieves the intended goals of therapy with appropriate follow-up to determine actual patient outcomes.Apart from the USA, several countries (e.g. Australia, Canada and Brazil) have managed to integrate CMM services into their existing health care system at the primary care level. However, in Europe, in spite of the widespread recog-nition of the need for medication management services, initiation and implementation of CMM services are lagging behind. Hence, for CMM services to become a reality in Europe and elsewhere, numerous prerequisites need to be accomplished, including policies and legal regulations supporting the provision of CMM services on a much larger scale, clearly defined and standardized professional practice and common language shared among the pharmacists, and well trained and experienced practitioners providing full-time, direct patient care.
Keywords: medication management; comprehensive medication management services; chronic diseases; pharmaceutical care;
Sažetak:sVeobuHVatna usluga upraVljanja farmakoterapijom kao rješenje za propuste u propisiVanju
lijekoVa: europska perspektiVaZbog porasta prevalencije kroničnih bolesti, potrošnja lijekova ubrzano raste. Uslijed toga, kronični bolesnici su izloženi povećanom riziku pojave terapijskih problema što dovodi do nepovoljnih kliničkih i ekonomskih ishoda liječenja. Stoga se smatra da je sveobuhvatno i sustavno upravljanje farmakoterapijom ključno za osiguranje optimalne uporabe lijekova kao i za poboljšanje kliničkih ishoda liječenja. Sveobuhvatna usluga upravljanja farmakoterapijom (engl. Comprehensive Med-ication Management Services, CMM services) koju provode posebno educirani ljekarnici može ponuditi rješenje za ovaj problem, smanjujući nepotrebnu, a često i štetnu primjenu lijekova te njene posljedične komplikacije. Kolaborativna prak-sa ljekarnika i liječnika obiteljske medicine, koja uključuje i aktivno sudjelovanje pacijenata u kreiranju terapijskih režima, važan je čimbenik koji doprinosi učinkovitosti CMM usluge. CMM usluga se definira kao standard skrbi koji osigurava da se svakom pacijentu pojedinačno procjenjuju svi lijekovi (u receptnom ili bezreceptnom režimu, biljni, tradicionalni), vitamini ili dodaci prehrani koje uzima, kako bi se za svaki od njih utvrdilo je li prikladan za pacijenta, je li učinkovit za pacijentovo zdravstveno stanje, je li siguran s obzirom na komorbiditete i druge lijekove koje pacijent uzima, te je li pacijent sposoban i u mogućnosti uzimati lijekove kako treba. Usluga sadrži individualizirani plan skrbi kojim se postižu predviđeni ciljevi terapije kao i odgovarajuće praćenje (follow-up) kako bi se utvrdili stvarni ishodi liječenja. Pored SAD-a, nekoliko je drugih zemalja (Australija, Kanada i Brazil) uspjelo integrirati CMM uslugu u svoje postojeće sustave primarne zdravstvene zaštite. Međutim, u Europi, unatoč raširenosti spoznaje o potrebi za upravljanjem farmakoterapijom, razvoj i implementacija CMM usluge zaostaje. Kako bi se CMM usluge realizirale u Europi i ostalim zemljama, potrebno je ispuniti brojne preduvjete, uključujući donošenje politika i zakonskih propisa koji podržavaju pružanje CMM usluga u mnogo većem obimu, ostvarivanje jasno definirane i standardizirane profesionalne prakse i zajedničkog jezika ljekarnika, te stvaranje dobro educiranih i iskusnih ljekarnika koji u punom radnom vremenu pružaju izravnu skrb pacijentima.
ključne riječi: upravljanje farmakoterapijom; sveobuhvatna usluga upravljanja farmakoterapijom; kronične bolesti; ljekarnička skrb;
OPEN ACCESS
Correspondence: Iva Mucalo MPharm, PhD
PG Dip Pharm [email protected]
orcid.org/0000-0002-5566-9356
This article was submitted to RAD CASA - Medical Sciences as the
review article
Conflict of Interest State-ment: The authors declare that the research was conducted in
the absence of any commercial or financial relationships that could be construed as a potential conflict of
interest.
Received: 5 October 2019Accepted: 20 November 2019Published: 17 December 2019
Citation:Mucalo I, Brajković A, Jukić I, Jonjić D, Radin D, de Oliveira
DR. Comprehensive Medication Management Services as a Solution to Medication Mismanagement: A
European Perspective. RAD CASA - Medical Sciences. 540=48-49 (2019): 33-40. https://dx.doi.
org/10.21857/90836cwv2y
Copyright (C) 2019 Mucalo, Bra-jković, Jukić, Jonjić, Radin and de
Oliveira. This is an open-access article distributed under the terms
of the Creative Commons Attri-bution License (CC BY). The use,
distribution or reproduction in other forums is permitted, provided the
original author(s) and the copyright owners(s) are credited and that the original publication in this journal is cited, in accordance whit accepted adacemic practice. No use, distri-
bution or reproduction is permitted which does not comply with these
terms.
Review Article
33-40

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com34
introduction
According to the 2018 World Health Organization Country Profiles, noncommunicable diseases are the leading cause of death globally, and one of the major health challenges of the 21st century1. In 2016, they were responsible for 71% (41 million) of the deaths globally, with cardiovascular diseases, cancers, chronic respiratory diseases and diabetes being the major causes1. Due to an increase in the prevalence of chronic illnesses, the number of prescriptions as well as their cost is rising rapidly2,3. The latest OECD publication “Health at a Glance: Europe 2018” states that pharmaceuticals expenditure represents the third largest item of health care spending in the European Union (EU), with Croatia having one of the highest expenditures on medical goods (mainly pharmaceuticals) among the EU Member States4. Moreover, an ample evidence base suggests that patients are often inadequately treated or not offered therapies that are likely to bring benefit4,5. Consequently, patients are at an increased risk of experi-encing drug therapy problems (DTPs) which, if not resolved, have substantial unfavourable clinical repercussions and add substantial costs to the health care system6-8. One way to address these issues is by improving the health-care system delivery and medication management. This includes, but is not lim-ited to, the use of multidisciplinary care teams to provide coordinated care and ensure safe and effective pharmacotherapy to patients9. Comprehensive Medication Management (CMM) services offered by trained pharmacists can fill this gap by decreasing the unnecessary and often harmful use of medicines and consequent resulting complica-tions2,10-13. Today there is a widely accepted notion that a patient care process must involve a professional who is capable of applying a logical, standardized and reproducible process to pharmacotherapy decisions 14. When medications were fewer in number, less complicated and more manageable, physicians were able to fulfil this responsibility. However, this is no longer true. CMM services are supported by a vast evidence-based literature6,10-13,15 and grounded in the practice of phar-maceutical care, as proposed by Cipolle, Strand and Morley14,16,17. It is also promoted by several organizations such as the American College of Clinical Pharmacy18,19, Get the Medications Right Institute20, and Patient-Centered Primary Care Collaborative, which includes more than 500 organisations, all active stakeholders in the health-care sys-tem2. Thus, this service has a scientific and clinical base that attempts to systematize the work of the clinical pharmacist with the patient and in collaboration with other providers, in order to optimize the use of medications in individuals’ daily lives.
the need for medication management services
Over the past few decades, the use of medications has undergone significant changes ranging from increases in prescription numbers, increases in the number and type of practitioners with prescribing rights, rising costs of new medications, to the rise in the increasing-ly complex new and emerging therapies. Another important factor worth mentioning is the continued lack of a structured, systematic decision-making process for drug selection and dosing14.Existing evidence suggests that as much as one-fifth of all health spending is wasteful and could be reduced, or eliminated, without undermining health system performance21. In fact, after inpatient and outpatient care, pharmaceuticals (excluding those used in hospitals) represented the third largest health care expense, accounting for one sixth of all health expenditure in the EU in 2016. The total retail
pharmaceutical bill across the EU was more than EUR 210 billion in 2016, representing an increase of approximately 5% (in nominal terms) since 2010. In Croatia, prescription medications accounted for 87 - 90% of all medications financial costs from 2012 to 2016, grow-ing about 3.5% annually, and reaching its peak of 10.2% in 2016 (22). These trends indicate a need to manage the use of prescription medications more efficiently. Inadequate medication management has other consequences, such as increased levels of drug-related morbidity and mortality, which are directly responsible for health care costs, and call for health-care system reform14. According to the latest data, more than 1.2 million people in EU countries died in 2015 from diseases and injuries that could have been avoided either through stronger public health policies or more effective and timely health care4. Additionally, potentially avoidable hospital admissions for some chronic conditions, out of which diabe-tes, hypertension, heart failure, chronic obstructive pulmonary disease (COPD) and bronchiectasis and asthma stand out, consume over 37 million bed days each year23. Over 4.6 million admissions were made for these five conditions in 2015, amounting to 5.6% of all admis-sions which might have been avoided4. The estimated annual cost of drug-related morbidity and mortality resulting from nonoptimized medication therapy in the United States (US) was $528.4 billion, equivalent to 16% of total US health care expenditures in 20166. Thus, governments and health plans pay for poor adherence to treat-ment, the lack of control of chronic diseases, and the development of complications in the long term. Additionally, in cases of multiple comorbidities, visits to different medical specialists concurrently, and without coordination or communication among them, often contrib-ute to the worsening of medication related problems.Hence, the expansion of CMM programs led by clinical pharmacists in collaboration with physicians and other licensed prescribers has been recommended in the United States as an effective and scalable approach to mitigate these avoidable costs and improve patient outcomes6.
medication management services as a solution to the Problem
A definition of medication management servicesComprehensive medication management services is defined as the standard of care that ensures each patient’s medications (whether they are prescription, nonprescription, alternative, traditional, vitamins, or nutritional supplements) are individually assessed to determine that each medication is appropriate for the patient, effective for the medical condition, safe given the comorbidities and other medications taken, and that the patient is able to take them as intended2. The con-cept and definition of the service has evolved over the years. In 2003, the Center for Medicare and Medicaid Services recommended the provision of medication therapy management services as an additional new service required for patients receiving Medicare Part D bene-fits2,24. There are a number of definitions for medication management services available, but today we rely on the definitions proposed by the Patient Centered Primary Care Collaborative2, American Medical Association25, and the Minnesota State Legislature26.CMM services is an evidence-based and patient-centered clinical prac-tice, provided by pharmacist with an aim of preventing, identifying and resolving DTPs to optimize patients’ medication experience and
Review Article
33-40

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com35
clinical outcomes. Through this rational and standardized process, the pharmacist reviews the medications used by the patient and identifies possible problems associated with the indication, effectiveness, safety and compliance with the pharmacotherapy treatment. In addition to the comprehensive assessment of patient’s drug-related needs, CMM includes the development of an individualized care plan to determine desired goals of therapy with the patient, as well as appropriate fol-low-up to evaluate actual patient outcomes that result from the care plan. All of this occurs because the patient understands, agrees with, and actively participates in the treatment regimen, thus optimizing each patient’s medication experience and clinical outcomes. The CMM services delivered in a health centre has the following five elements in common: a) the service needs to be delivered directly to a specific patient (as opposed to performing a prescription review without seeing the patient); b) it must include an assessment of the patient’s medication-related needs, followed by an individualized care plan and follow up; c) the care must be comprehensive, i.e. pharma-ceutical care practitioner assesses all of the patient’s medications (pre-scribed, over-the-counter, supplements, herbal remedies etc.), since medications interact with other medications and impact all medical conditions; d) the work of pharmacists needs to be coordinated with physicians and other team members: and e) the service is expected to add unique value to the care of the patient.The interventions proposed within the CMM services are grounded in the philosophy and ethics of the professional practice of pharma-ceutical care and delivered according to the standards of practice for the patient care process described by the practice14. Pharmaceutical care was defined in 1990 as a practice in which a pharmacist-prac-titioner is held responsible for patient’s drug related needs and accountable for this commitment, providing rational drug therapy with the purpose of achieving positive patient outcomes27.
how is cmm delivered?CMM is a patient-centred clinical service offered by pharmacists spe-cially trained to do so. The pharmacist works directly with the patient in collaboration with physicians and other members of the multi-disciplinary health care team. Care is coordinated among providers and across systems of care as patients transition in and out of various settings. Detailed description of steps and activities that need to be completed in order to carry out complete CMM services, including the patient care process, is presented in Table 1. The three steps of the patient care process include a) the assessment of the patient, his or her medical problems, and drug therapies leading to the DTP identification, b) care plan development and c) follow-up evaluations. These steps are highly dependent upon each other, and the fulfilment of all steps is necessary to practice pharmaceutical care and to have positive impact on patient’s medication experience. The assessment step in the patient care process is the most important of the three as it influences all other components of the patient care pro-cess. The primary purpose of the assessment is to determine to what extent the patient’s drug-related needs are being met and if any DTPs are present, while the goal of the care plan development is to deter-mine how to manage patients’ medical conditions favourably with pharmacotherapy. Finally, follow-up evaluation aims to determine the actual outcomes of drug therapy for the patient, compare these results with the intended goals of therapy, determine the effectiveness and safety of pharmacotherapy, evaluate patient adherence, and establish the current status of the patient’s medical conditions being managed
with drug therapy14. All the steps in the care process of the CMM ser-vices must be documented in a manner that adds unique value to the care of the patient, and contain information about the patient, the clinical pharmacist’s interventions and decisions, as well as the results achieved in the management of pharmacotherapy.
As all patient care providers need a structured, rational thought process for sound clinical decision retrieval, the Pharmacotherapy Workup was developed and adopted as a systematic problem-solving process, specific to the practice of pharmaceutical care. This pro-cess represents the cognitive work, taking place in the mind of the practitioner, and is used to identify, resolve, and prevent drug therapy problems (DTPs), establish therapy goals, select interventions and evaluate outcomes. As highlighted by Cipolle et al14, what makes a practitioner qualified to do her/his work is the application of a unique knowledge base and set of clinical skills by using a system-atic thought process, and in the case of the pharmaceutical care practitioner, this unique knowledge base focuses on pharmacology, pharmacotherapy, and pharmaceutical care practice.
the value of medication management services
The benefits of CMM services are numerous and include improved clinical outcomes11,12,15,28-32, decreased medical costs17,32-34, better access to health care services, time-savings to other health care provid-ers, reduced adverse drug events, as well as significant impact on the appropriateness, effectiveness, safety and compliance with medica-tions18.The ability of CMM to improve patient outcomes and provide system-wide benefits has been well documented35. Early results from a high-risk population involving 1651 patients, seen during 4453 en-counters, show positive results: the percentage of medical conditions at goal changed from 54% at baseline to 80% with the introduction of the service33. Furthermore, in a Medicare group of 706 patients, 28% were found to have ten or more DTPs. As these DTPs were identified and resolved, significant improvements in blood pressure control and cholesterol were documented with an average cost savings of over 1750$ per patient2.Various studies have demonstrated the positive impact of pharma-cists’ interventions in the management of chronic diseases, such as cardiovascular diseases (CVD) and diabetes, and improvement in patient care when pharmacists are located in primary care ambulatory clinics working side by side the physicians and nurses17. Particularly, the greatest improvement in patient’s clinical outcomes receiving CMM services has been observed in patients with medical conditions that are extremely costly and are associated with the use of multiple medications (hypertension, diabetes, CVD, COPD)12,36,37. Hence, patients with these comorbidities are considered as great candidates to receive the service. According to the largest database published until now14, the total number of 88,556 DTPs was identified and resolved in 22,694 patients receiving CMM services in a 4-year period. Out of 18,866 patients’ medical conditions that were not at goal at their first visit to pharmaceutical care practitioner, 74% of conditions improved or remained the same after receiving CMM services (14). In a retrospective study from 2004, pharmaceutical care practitioners identified 3,407 DTPs in 2,985 patients during their patients’ first assessment, out of which 61% had one or more DTPs identified and resolved. As a result of pharmaceutical care provision, in one third of patients, medical conditions improved17. Ramalho de Oliveira et
Review Article
33-40

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com36
al 12 showed that pharmacists identified and addressed 38,631 DTPs among 9,068 patients during a 10-year period, whereof 80% of DTPs were directly resolved with patients, without consulting physicians. More than a half of DTPs necessitated inclusion of a new medication or dosage increase, while only 16.5% were associated with non-adher-ence. Rao et al 38 showed that 81% of patients’ DTPs were resolved or well managed by pharmacists, while Borges et al 39 resolved 62.7% of DTPs in patients with type 2 diabetes. Moreover, CMM services have shown the positive impact on individual CV risk factors: blood pressure (12,28,31,40), glycated hemoglobin (HbA1c) (30,31,39) and LDL cholesterol12,30,40. Furthermore, studies have demonstrated the economic and social welfare of CMM services17,32,34,41. Patients receiving face-to-face CMM services had lower total health expenditures, with the reduction in total annual health expenditures exceeding the cost of providing CMM services by as high as 12:1, and with the average ratio of 3:1 to 5:1 (return on investment, ROI )33. A report reviewing the team-based medication therapy management system in four clinics revealed that spending growth was 11% less in innovation clinics (team-based care that incorporates comprehensive medication therapy management) than that in 38 non-innovation clinics42. Furthermore, the median monthly health care costs per member, measured at five intervals over a 15-month period, were significantly lower in innovation than in non-innovation sites42. The Ashville project, involving community pharmacy based practitioners specially trained to address issues in patients with diabetes, asthma, CVD and depression, demonstrated a 4:1 ROI and a decrease in direct yearly average medical costs between $1200 and $1872 per patient 32,43,44.
The value of this service has been recognized by patients who had the opportunity to use it as well as by physicians and other health care professionals, health plans, employers and payers. Firstly, it is worth mentioning that patients benefit not only from improved clinical outcomes, but also from having health care professionals who are willing and capable to understand their unique medication experi-ence. Physicians profit by having pharmacotherapy experts managing complex therapies side by side, thus enabling them to have more time for diagnostics and quality medical care provision33,45. Finally, insurers pay only for medications that are appropriate, effective and safe for the patient, and are used as intended.
current situation of cmm services across euroPe Health systems across Europe have achieved remarkable progress in treating life-threatening diseases, yet more effective healthcare interventions are needed if we are to improve management of health problems in the community. While disparities in healthcare systems between the European countries persist, patient-centred practices, in which pharmacists are held accountable for patients’ clinical out-comes, are still underdeveloped and lack inclusion at the primary care level. In Europe, in spite of the widespread recognition of the need for medication management services, initiation and implementation of CMM services are lagging behind. Limited published data on CMM services implementation46 confirms that this service has not been developed or recognized in Europe, as it has been in the Anglo-Saxon countries especially USA and Australia18,47,48. Although supported by relevant laws, it seems that governments have not taken an active interest in promoting a movement toward pharmacists playing a major role in primary health care. The following text will not provide
an in-depth description of the current situation regarding the status of medication management services in Europe, as this has been fully described elsewhere14, but rather shed a light on recent advancements that have occurred across European countries.
Integration of clinical pharmacist into general practitioner (GP) services in Great Britain began in 2015 when the National Health Service (NHS) England instigated the initiative and partly funded over 400 clinical pharmacists to provide support to almost 700 GP surgeries and more than seven million patients 49. To date, over 1,000 full time equivalent clinical pharmacists provide the service across the country with a further 1,500 pharmacist roles planned by 2020 50,51. This far-sighted initiative came in response to considerations about general practice workforce capacity, where concerns about shortfalls in GP numbers have been raised 52. However, it is unclear whether the patient care process proposed by Cipolle et al 14,53 is used as the theoretical framework to take care of the patients.Very recent publications from Iceland and Netherlands highlight the importance of developing pharmaceutical care practice separately from the dispensing process and in close cooperation with physicians, at the primary care level48,54. Netherlands is an interesting example of community pharmacy having a leading role in pharmaceutical care provision, with reimbursements for pharmaceutical care services being covered by the Dutch government and health insurance companies14. Although it appears that the prerequisites for the implementation of medication management services are in place, at present the em-ployment of CMM services in primary care is suboptimal, if any54. Namely, pharmacists lack access to patient information, they are short of clinical knowledge and skills, and the working processes of phar-macists and general practitioners match poorly. Nevertheless, attempts have been made to integrate a non-dispensing pharmacist in general practice and the results demonstrated favourable outcomes. Albeit, the process of care they employed did not follow the patient care process proposed by Cipolle et al 14,53. Although Iceland undoubtedly embraced the concept of pharmaceuti-cal care, medication management services are still limited, and serious efforts will need to be invested before further development can oc-cur14. General practitioners are not familiar with pharmaceutical care and additionally no such service is offered in pharmacies or primary care settings. Efforts have been made to introduce pharmacist-led pharmaceutical care into primary care clinics in Iceland in collabora-tion with GPs, and results showed that GPs would now like to have access to a pharmacist on a daily basis48.In Slovenia, consultations delivered by non-dispensing pharmacists as a part of medication review clinics started in 2012, and today they are running in over 30 health centres (altogether over 50 clinics available, however not running full time)55. However, lack of published data on clinical outcomes of this service limits us in making comparisons and conclusions on its effectiveness. Spain has made progress towards the provision of clinical services mainly in community pharmacies. Considering the lack of published literature, pharmacists do not seem to be involved in direct patient care in ambulatory clinics or in the provision of CMM services. However, some very important initiatives have been made to prepare pharmacists to provide CMM services and to foster these services. The “Universidad de San Jorge” in Zaragoza offers a master program in which students are trained to care for real patients in collabora-tion with other members of the care team, which creatively includes
Review Article
33-40

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com37
STEPS AND ACTIVITIES HEALTH PROFESSIONAL
PATIENT REFERRAL AND RECRUITMENT
Ø Identify patients who benefit most from the service:a) Patients who have not reached their therapeutic goalb) Patients taking very complex dosage regimensc) Patients who are frequently readmitted to the hospitald) Patients experiencing adverse drug reactionse) Patients needing prevention therapyf) Patients who are having difficulty to understand and follow their
medication regimen.
General practitioners, medical specialists, pharmacists, self-referral, other (nurses, family/friend recommendation)
THE PATIENT CARE PROCESS
Pharmaceutical-carepractitioner
Assessment of the patient’s drug related
needs
Ø Meet the patient and uncover patient's medication experience(preferences, expectations and beliefs).
Ø Collect patient specific information: demographic information, socialhistory (alcohol, tobacco, caffeine) and clinical information (relevantmedical history, medication history, current medication list includingprescription and over-the-counter medications, herbal remedies,supplements and medications used for a limited period of time, andrelevant laboratory values) including allergies, side-effects andimmunizations.
Ø Prioritize patients’ active medical conditions and medication-relatedneeds.
Identification of drug-related problems
Ø Determine that all the patient’s medications are properly indicated, themost effective available, the safest possible, and that the patient is ableand willing to take the medication as intended.
Ø Analyse the assessment data to determine if any drug therapy problemsare present.
Care plan development Ø Identify goals of therapy for each indication managed with drug therapy.Ø Develop a care plan that includes interventions to resolve current drug
therapy problems, prevent potential drug therapy problems and achievegoals of therapy.
Ø Discuss and negotiate the care plan with the patient and his prescriber,ensure patient's and prescriber's understanding and agreement with theplan, and schedule follow-up evaluation.
Ø Document the care plan which includes all the steps and clinical statusdetermined for every patient's medical condition.
Follow-up evaluation Ø Make follow-up evaluation for each patient to reassess whether any newdrug therapy problems have developed, monitor patient’s progresstoward the achievement of the goals of therapy, and refine the care planto ensure therapy goals are achieved and medication therapy isoptimized.
CARE COORDINATION BY ALL TEAM MEMBERS –REPEATING PROCESS-CARE
Ø Collaborate and integrate with other health care providers such asprescribers, medical specialists, pharmacists, care managers, and others,with the purpose of achieving optimal care for the patient and assuringall goals of therapy are understood by all team members.
Pharmaceutical-care practitioner, general practitioner, medical specialists and other (e.g. nurses)
Table 1. Steps and activities that need to be accomplished to provide effective CMM services
Review Article
33-40

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com38
a psychologist, a philosopher and an anthropologist. Moreover, in 2012 the “Sociedad Española de Optimización de la Farmacoterapia (SEDOF)” was founded in Andalucía with the goal to congregate pharmacists interested in developing CMM services56. SEDOF pro-motes the “Escuela de optimización de la farmacoterapia”, which is in its 14th version. These courses include discussions on patient cases and reflect on specific aspects of patient care within the framework of CMM services.Croatia is one of the countries where the implementation of com-prehensive medication management services started only recently. Although Croatia embraces the concept of pharmaceutical care prac-tice, policies and legal regulations supporting the provision of CMM services on a much larger scale, still need to be developed. Accord-ing to the Law on Pharmacy57, Croatian pharmacists are obligated to provide pharmaceutical care in cooperation with other health care workers. However, the same Law ties pharmaceutical activities exclusively to community and hospital pharmacies, and precludes pharmacists from providing care at locations where their expertise is indispensable, such as nursery homes, health care centres and hospital wards. The abovementioned is only one of the existing legal obstacles that needs to be addressed prior to CMM services implementation. Nevertheless, pharmacy graduates in Croatia are competent in pro-viding clinical services more than ever before, mainly due to the cur-riculum reform that has commenced in the academic year 2005/2006 due to which the focus has shifted from more chemically oriented pharmaceutical sciences toward clinically based and patient-focused courses. In order to harmonize our study programme with the EU Directive 2005/36/EC, Faculty of Pharmacy and Biochemistry University of Zagreb (UoZ) introduced an obligatory six-month traineeship and new modules (e.g. Pharmacotherapy and Clinical Pharmacy, Pharmaceutical Care, Consultation Skills, Health legisla-tion, Sociology in Pharmacy etc.) in the academic year 2011/2012 (58). Furthermore, since the academic year 2010/2011, the postgrad-uate specialist study program “Clinical pharmacy” has been offered at the Faculty of Pharmacy and Biochemistry UoZ, and it precedes the 3-year Specialization in Clinical Pharmacy assigned from the Ministry of Health. All of these changes equipped Croatian pharma-cists with clinical knowledge and skills needed for engaging in clinical activities. Nevertheless, up until now the government did not provide any standardized and legal framework allowing for the development of strategies to broaden pharmacists’ responsibilities and expand those into the integrated health care system. Hence, pharmacists’ educa-tional requirements for CMM services provision in Croatia still need to be defined within the profession itself and subsequently legalized.On the bright side, a small group of younger pharmacists in Croatia is currently taking the lead and creating new services. The CMM
services are piloted by two pharmacists from the UoZ Faculty of Pharmacy and Biochemistry at the primary care clinic, Health Centre Zagreb Centre, since January 201846. Until now, this is the only county health centre providing CMM services at the primary care level in Croatia. This positive development, even if it is small, holds promise for the further progression of medication management services in Croatia.The examples of the abovementioned countries showcase that a process of comprehensively and rationally managing patients’ medi-cations is not systematically implemented across European countries and that the countries are struggling to find the best solution in that endeavour. Due to disparate standing points, resulting from different cultural, sociolegal and ethical backgrounds, one cannot foresee a direction countries will take and the rate at which the change will be occurring. In conclusion, for CMM services to become a reality in Europe and elsewhere, it is of paramount importance that pharmacists who will provide these services have one professional practice as their theoretical and ethical foundation. Thus, we will be able to teach to this practice and pharmacists will be able to communicate between themselves and to others what they do for patients. In addition, only then we will be able to evaluate the results of what we do, compare between ourselves and improve upon that. That is how all other members of the healthcare team work, which reflects the rules of patient care worldwide. Moreover, we will need policy to support the development and implementation of these services in a manner that can be reimbursed, reproducible and sustainable over time. What we really need are governments and health plans willing to support clinical pharmacists, namely professionals willing and capable to provide this service, as it will only live its full potential when we have well trained and experienced practitioners. To achieve this, clinical pharmacists need not only to expand their clinical knowledge by having experience with lots of patients, but also to reflect upon and assess these experiences. We will not have clinical experts until we have pharmacists that can provide direct patient care as a full-time job, caring for as many patients as possible. Only then will they gain expertise and exert their full potential. Consequently, we will know what this service is able to produce in terms of clinical outcomes and healthcare cost reduction. We cannot emphasize enough that the pol-icy piece is key here. We need innovators, forward thinkers to support clinical pharmacists as they work on building their clinical practices and expertise. In the end, that is what patients deserve from us.
author contributions:All authors listed have made a substantial, direct and intellec-tual contribution to the work, and approved it for publication.
literature:1. World Health Organization. Noncommunicable diseases key facts. 2018. Available at: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases. Accessed September 11th 2019. 2. McInnis T, Strand L, Webb CE. Integrating Comprehensive Med-ication Management to Optimize Patient Outcomes. Resour Guid. 2012;A-26. 3. Institute of Medicine. Informing the Future: Critical Issues in Health: Fourth Edition. Washington DC: The National Academies
Press, 2007.4. OECD/EU. Health at a Glance: Europe 2018: State of Health in the EU Cycle. Paris: OECD Publishing, 2018. doi: 10.1787/health_glance_eur-2018-en.5. Levine DM, Linder JA, Landon BE. The quality of outpatient care delivered to adults in the United States, 2002 to 2013. JAMA Intern Med. 2016; 176(12):1778–90. doi:10.1001/jamaint-ernmed.2016.6217.6. Watanabe JH, McInnis T, Hirsch JD. Cost of Prescription
Review Article
33-40

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com39
Drug–Related Morbidity and Mortality. Ann Pharmacother. 2018;52(9):829–37. doi: 10.1177/1060028018765159.7. Ernst FR, Grizzle AJ. Drug-related morbidity and mortality: Updating the cost-of-illness model. J Am Pharm Assoc (Wash). 2001;41(2):192-9. doi: 10.1016/S1086-5802(16)31229-3.8. Johnson JA, Bootman JL. Drug-related morbidity and mortality and the economic impact of pharmaceutical care. Am J Heal Pharm. 1997;54(5):554-8. doi: 10.1093/ajhp/54.5.554.9. Wiedenmayer K, Summers RS, Mackie CA, Gous AGS, Everard M, Tromp D. Developing pharmacy practice - A focus on patient care. World Health Organization, International Pharmaceutical Federation, 2006. 10. Butler A, Dehner M, Gates RJ, Shane P, Chu M, DeMartini L, et al. Comprehensive Medication Management programs: 2015 status in Southern California. Res Soc Adm Pharm. 2017;13(1):63–87. doi: 10.1016/j.sapharm.2016.02.003.11. Santos BD, Gonzaga do Nascimento MM, Batista de Oliveira GC, Nascimento YA, Mambrini JVM, Cid AS, et al. Clinical Impact of a Comprehensive Medication Management Service in Prima-ry Health Care. J Pharm Pract. 2019;18:897190019866309. doi: 10.1177/0897190019866309. [cited 2019 Sep 23]. [Epub ahead of print].12. Ramalho de Oliveira D, Brummel AR, Miller DB. Medication therapy management: 10 years of experience in a large integrated health care system. J Manag Care Pharm. 2010;16(3):185–95. doi: 10.18553/jmcp.2010.16.3.185.13. Australian Medical Association. Analysis of non-dispensing phar-macists in general practice clinics. Sydney: Deloitte Access Econom-ics, 2015. 14. Cipolle RJ, Strand LM, Morley PC. Pharmaceutical care practice: the patient-centered approach to medication management. 3rd ed. New York: McGraw-Hill, 2012. 15. Mendonça SAM, Melo AC, Pereira GCC, Serio dos Santos DMS, Grossi EB, Boas Sousa MCV, et al. Clinical outcomes of medication therapy management services in primary health care. Brazilian J Pharm Sci. 2016;52(3):365–73. doi: 10.1590/s1984-82502016000300002.16. Cipolle RJ, Strand LM, Morley PC. Pharmaceutical Care Practice. New York: McGraw- Hill, 1998. 17. Strand LM, Cipolle RJ, Morley PC, Frakes MJ. The impact of pharmaceutical care practice on the practitioner and the patient in the ambulatory practice setting: twenty-five years of experience. Curr Pharm Des. 2004;10:3987–4001. doi: 10.2174/1381612043382576. 18. McBane SE, Dopp AL, Abe A, Benavides S, Chester EA, Dixon DL, et al. Collaborative drug therapy management and comprehen-sive medication management - 2015. Pharmacotherapy. 2015;35:e39–50. doi:10.1002/phar.1563.19. American College of Clinical Pharmacy. Comprehensive Medi-cation Management in Team-Based Care. 2017. Available at: https://www.accp.com/docs/positions/misc/CMM%20Brief.pdf. Accessed September 12th 2019.20. GTMR Institute. Get the medications right. 2019. Available at: https://gtmr.org/. Accessed September 12th 2019.21. OECD. Tackling Wasteful Spending on Health. Par-is: OECD Publishing, 2017. Available at: https://doi.org/10.1787/9789264266414-en. Accessed September 12th 2019.22. Draganić P, Škribulja M, Oštarčević S. Potrošnja lijekova u Hrvatskoj 2012. - 2016. Agencija za lijekove i medicinske proizvode - HALMED. Available at: http://www.halmed.hr/fdsak3jnFsk1Kfa/publikacije/Potrosnja-lijekova-u-RH_2012-2016.pdf. Accessed Sep-tember 12th 2019.23. Purdy S, Griffin T, Salisbury C, Sharp D. Ambulatory care
sensitive conditions: terminology and disease coding need to be more specific to aid policy makers and clinicians. Public Health. 2009;123(2):169-73. doi: 10.1016/j.puhe.2008.11.001.24. Public Law 108–173—DEC. 8, 2003, The Medicare Prescription Drug, Improvement, and Modernization Act of 2003. 2003. Available at: https://www.govinfo.gov/app/details/PLAW-108publ173. Accessed September 12th 2019.25. American Medical Association. Current Procedural Terminology. Available at: https://www.ama-assn.org/amaone/cpt-current-procedur-al-terminology. Accessed September 12th 2019.26. Minnesota statute 256B.0625 subd. 13h, 2005. Available at: https://www.revisor.mn.gov/statutes/ ?id=256B.0625. Accessed Sep-tember 12th 2019.27. Hepler CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47(3):533–43. 28. Planas LG, Crosby KM, Mitchell KD, Farmer KC. Evaluation of a hypertension medication therapy management program in patients with diabetes. J Am Pharm Assoc (2003) [Internet]. 2009;49(2):164–70. doi: 10.1331/JAPhA.2009.08164. 29. Neves CM, Gonzaga do Nascimento MM, Silva DÁM, Ramal-ho de Oliveira D. Clinical Results of Comprehensive Medication Management Services in Primary Care in Belo Horizonte. Pharmacy (Basel). 2019;7(2):58. doi: 10.3390/pharmacy7020058.30. Obreli-Neto PR, Guidoni CM, de Oliveira Baldoni A, Pilger D, Cruciol-Souza JM, Gaeti-Franco WP, et al. Effect of a 36-month phar-maceutical care program on pharmacotherapy adherence in elderly diabetic and hypertensive patients. Int J Clin Pharm. 2011;33(4):642-9. doi: 10.1007/s11096-011-9518-x.31. Mourão AO, Ferreira WR, Martins MA, Reis AM, Carrillo MR, Guimarães AG, et al. Pharmaceutical care program for type 2 diabetes patients in Brazil: a randomised controlled trial. Int J Clin Pharm. 2013;35(1):79–86. doi: 10.1007/s11096-012-9710-7.32. Cranor CW, Bunting BA, Christensen DB. The Asheville Project: Long-term clinical and economic outcomes of a community pharmacy diabetes care program. J Am Pharm Assoc (Wash). 2003;43:173–84. doi: 10.1331/108658003321480713.33. Isetts BJ, Schondelmeyer SW, Artz MB, Lenarz LA, Heaton AH, Wadd WB, et al. Clinical and economic outcomes of medication therapy management services: the Minnesota experience. J Am Pharm Assoc (2003). 2008;48(2):203-11. doi: 10.1331/JAPhA.2008.07108.34. Obreli-Neto PR, Marusic S, Guidoni CM, Baldoni Ade O, Renovato RD, Pilger D, et al. Economic evaluation of a pharma-ceutical care program for elderly diabetic and hypertensive patients in primary health care: a 36-month randomized controlled clinical trial. J Manag Care Spec Pharm. 2015;21(1):66–75. doi: /10.18553/jmcp.2015.21.1.66.35. Giberson S, Yoder S, Lee MP. Improving Patient and Health System Outcomes through Advanced Pharmacy Practice. A Report to the U.S. Surgeon General. Office of the Chief Pharmacist. U.S. Public Health Service, 2011.36. Detoni KB, Oliveira IV, Gonzaga do Nascimento MM, Caux TR, Alves MR, Ramalho de Oliveira D. Impact of a medication therapy management service on the clinical status of patients with chronic obstructive pulmonary disease. Int J Clin Pharm. 2017;39(1):95-103. doi: 10.1007/s11096-016-0402-6.37. Rodis JL, Sevin A, Awad MH, Porter B, Glasgow K, Horn-beck Fox C, et al. Improving Chronic Disease Outcomes Through Medication Therapy Management in Federally Qualified Health Centers. J Prim Care Community Health. 2017;8(4):324-31. doi: 10.1177/2150131917701797.38. Rao D, Gilbert A, Strand LM, Cipolle RJ. Drug therapy problems found in ambulatory patient populations in Minnesota and South
Review Article
33-40

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com40
Australia. Pharm World Sci. 2007;29(6):647–54. doi: 10.1007/s11096-007-9123-1.39. Borges AP, Guidoni CM, Ferreira LD, de Freitas O, Pereira LR. The pharmaceutical care of patients with type 2 diabetes mellitus. Pharm World Sci. 32(6):730-6. doi: 10.1007/s11096-010-9428-3.40. Bunting BA, Smith BH, Sutherland SE. The Asheville Project: Clinical and economic outcomes of a community-based long-term medication therapy management program for hypertension and dyslip-idemia. J Am Pharm Assoc (2003). 2008;48(1):23-31. doi: 10.1331/JAPhA.2008.07140.41. Schultz H, Westberg SM, Ramalho de Oliveira D, Brummel A. Patient-perceived value of Medication Therapy Management (MTM) services : a series of focus groups. Inov Pharm. 2012;3(4):Article 96. doi: 10.24926/iip.v3i4.278.42. Isetts BJ, Brummel AR, Ramalho de Oliveira D, Moen D. Man-aging Drug-related Morbidity and Mortality in the Patient-centered Medical Home. Medical Care. 2012;50(11):997–1001. doi: 10.1097/MLR.0b013e31826ecf9a. 43. Cranor CW, Christensen DB. The Asheville Project: Factors Associated With Outcomes of a Community Pharmacy Diabe-tes Care Program. J Am Pharm Assoc. 2003;43(2):160-72. doi: 10.1331/108658003321480704. 44. Cranor CW, Christensen DB. The Asheville Project: Short-term outcomes of a community pharmacy diabetes care program. J Am Pharm Assoc. 2003;43(2):149–59. Available from: doi: 10.1331/108658003321480696.45. Funk KA, Pestka DL, Roth McClurg MT, Carroll JK, Sorensen TD. Primary Care Providers Believe That Comprehensive Medica-tion Management Improves Their Work-Life. J Am Board Fam Med. 2019;32(4):462-73. doi: 10.3122/jabfm.2019.04.180376.46. Brajković A, Mucalo I, Vidović T, Gonzaga do Nascimento MM, Balenović A, Protrka I, et al. Implementation of medication man-agement services at the primary healthcare level – a pilot study. Acta Pharm. 2019;69:585–606. 47. Butler A, Dehner M, Gates RJ, Shane P, Chu M, DeMartini L, et al. Comprehensive Medication Management Programs : 2015 Status in Southern California. 2016;13(1):63-87. doi: 10.1016/j.sapharm.2016.02.003.48. Blondal AB, Sporrong SK, Almarsdottir AB. Introducing Pharma-
ceutical Care to Primary Care in Iceland—An Action Research Study. Pharmacy. 2017;5(2):23. doi: 10.3390/pharmacy5020023.49. Torjesen I. More than 400 pharmacists will be recruited to GP sur-geries by next year. BMJ. 2015;351:h6167. doi: 10.1136/bmj.h6167.50. Sims L, Campbell J. Ills, pills, and skills: developing the clin-ical skills of pharmacists in general practice. Br J Gen Pract. 2017;67(662):417–18. doi:10.3399/bjgp17X692453.51. Langran T, Nanda N, Bataveljic A, Gonzalez-Durio J. Supporting the management of type 2 diabetes with pharmacist-led reviews: An observational analysis. BMJ Open. 2017;7:e013451. doi: 10.1136/bmjopen-2016-013451.52. Centre for Workforce Intelligence. In-depth review of the general practitioner workforce. London: Centre for Workforce Intelligence. 2014.53. Haines ST, Kliethermes M, Sorensen TD. The Patient Care Pro-cess. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. eds. Pharmacotherapy: A Pathophysiologic Approach, 10th ed. New York: Mc-Graw-Hill, 2016. Available at: http://accesspharmacy.mhmedical.com/content.aspx?bookid=1861§ionid=174720532. Accessed September 12th 2019.54. Hazen ACM, Wal AW, Sloeserwij VM, Zwart DLM, Gier JJ, Wit NJ, et al. Controversy and consensus on a clinical pharmacist in pri-mary care in the Netherlands. Int J Clin Pharm. 2016;38(5):1250–60. doi: 10.1007/s11096-016-0360-z.55. Zavod za zdravstveno zavarovanje Sloveniji. Recept, Bilten o zdravilih iz obveznega zdravstvenega zavarovanja. 2017;Letnik 14/ št.1. Accessed September 12th 2019. from http://www.zzzs.si/ZZZS/info/egradiva.nsf/0/ba51d225d7c16f2dc12581d9003c992e/$FILE/bilten%20Recept_23.11.2017.pdf56. Sociedad Española de Optimización de la Farmacoterapia. Avail-able at: http://www.sedof.es. Accessed September 12th 2019.57. The Constitution of the Republic of Croatia, The Official Gazette, Law on Pharmacy No 121/03, 142/06, 35/08, 117/08. 2003. Available at: https://www.zakon.hr/z/409/Zakon-o-ljekarni%C5%A1tvu. Ac-cessed September 12th 2019.58. Brajković A, Hadžiabdić MO, Mucalo I, Bach-Rojecky L, Pepić I, Vanić Ž, et al. Uvođenje Stručnog osposobljavanja za ljekarnike (SO) u studij Farmacije na Farmaceutsko-biokemijskom fakultetu Sveučiliš-ta u Zagrebu. Farm Glas. 2017;73:869-79.
Review Article
33-40

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com41
Aging, Calorie Restriction and Calorie Restriction Mimetics
Ivana Čepelak1 , Slavica Dodig1, Daniela Čepelak Dodig2
1 Department of Medical Biochemistry and Hematology, School of Pharmacy and Biochemistry, University of Zagreb, Croatia2 Croatian Institute of Public Health-Department for Toxicology, Zagreb, Croatia
abstract:In line with the increase in the number of older people in the world, the focus of scientists is directed at examining mechanisms of the aging process as well as establishing strategies/interventions in order to slow down aging and achieve longevity. On preclinical testing models, the most effective strategy for this purpose, as well as for the purpose of delaying age-related diseases, nutritional interven-tion- restriction of calorie (CR) has been demonstrated, but also some alternative forms of calorie restriction. Possible undesirable effects of restriction are still in the testing phase, and it is known that it is generally difficult to implement in humans. Therefore, the new area of research in gerontology has become the discovery and examination of the effects of compounds that mimic the effects of caloric restriction, so called caloric restriction mimetics (CRM). These compounds include numerous compounds of natural origin but also approved medicaments with certain indications. This overview summarizes the latest data on known mechanisms of caloric restriction and more familiar caloric restriction mimetics.
Keywords: aging; caloric restriction; caloric restriction mimetics; sirtuins; resveratrol;
Sažetak:Starenje, kalorijske restrikcije i kalorijsko restrikcijska mimetrikaU skladu s povećanjem broja starijih ljudi u svijetu, fokus znanstvenika usmjeren je na ispitivanje me-hanizama procesa starenja kao i na uspostavljanje strategija / intervencija kako bi se usporilo starenje i postigla dugovječnost. Na predkliničkim modelima ispitivanja, najučinkovitija strategija za ovu svrhu, kao i za odgađanje bolesti povezanih s dobi, pokazana je prehrambena intervencija - ograničenje kalo-rija, ali i neki alternativni oblici ograničavanja kalorija. Mogući neželjeni učinci restrikcije još su u fazi ispitivanja, a poznato je da je to općenito teško provesti kod ljudi. Stoga je novo područje istraživanja u gerontologiji postalo otkriće i ispitivanje učinaka spojeva koji oponašaju učinke kalorijske restrikci-je, takozvane mimetike kalorijske restrikcije. Ti spojevi uključuju brojne spojeve prirodnog podrijetla, ali i odobrene lijekove s određenim indikacijama. Ovaj pregled sažima najnovije podatke o poznatim mehanizmima kalorijskog ograničenja i poznatijim mimeticima za ograničenje kalorija.
ključne riječi: starenje; kalorijska restrikcija; kalorijsko restrikcijska mimetrika; sirtuini; resveratrol;
OPEN ACCESS
Correspondence: Prof. Ivana Čepelak, PhD
[email protected]/0000-0001-7934-599X
This article was submitted to RAD CASA - Medical Sciences
as the review article
Conflict of Interest Statement: The authors declare that the re-
search was conducted in the absence of any commercial or financial rela-
tionships that could be construed as a potential conflict of interest.
Received: 4 October 2019Accepted: 25 November 2019Published: 17 December 2019
Citation:Čepelak I, Dodig S and Čepelak
Dodig D. Aging, calorie restriction and calorie restriction mimetics. RAD
CASA - Medical Sciences. 540=48-49 (2019): 41-50. https://
dx.doi.org/10.21857/9e31lhnddm
Copyright (C) 2019 Čepelak, Dodig and Čepelak Dodig. This is an
open-access article distributed under the terms of the Creative Commons
Attribution License (CC BY). The use, distribution or reproduction in other
forums is permitted, provided the original author(s) and the copyright owners(s) are credited and that the original publication in this journal is cited, in accordance whit accepted adacemic practice. No use, distri-
bution or reproduction is permitted which does not comply with these
terms.
Review Article
41-50

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com42
introduction
Aging is an inexorable, complex and progressive but natural process that results in persistent worsening of the functioning of the body and increased morbidity and mortality. As a result of improved health care, the rate of the elderly population is steadily rising in most developed countries and is one of the biggest social challenges of today. Among other things, the process is associated with cellular senescence, short-ening telomeres, genomic instability, epigenetic changes, intercellu-lar communication changes, mitochondrial dysfunction, stem cell depletion, chronic inflammation, loss of protease and the like1. Figure 1 shows some of the factors contributing to aging progression and age-related diseases. All these changes also increase the tendency of the elderly toward various pathological conditions, which are most commonly associated with persistent chronic inflammation3. Therefore, the primary focus of modern medicine is the treatment of specific age-related diseases. In the scientific community, more than 300 theory of aging processes are discussed, and the theory of oxidative stress seems to be the most comprehensive4. According to the Blagosklonny and Hall propos-als, aging can be understood, for example, as “a type of unregulated continuation of normal developmental processes and related cellular programs with special emphasis on growth”5, and this theory is com-plemented by inflammatory aging theory6. Inflammation occurring in older people is defined as subclinical, chronic and sterile one, with the accumulation of senescent cells, characterized by pro-inflammatory secretory phenotype7.However, prolonged life expectancy does not yet imply a healthy life span since aging is associated with a number of chronic diseases, such as diabetes, cancer, cardiovascular and neurodegenerative diseases8. Furthermore, the greater prevalence of age-related diseases is necessari-ly reflected in the cost of health care. Therefore, the scientific commu-nity around the world makes significant efforts to discover strategies for achieving so-called healthy, but also active aging. The term “Active Aging” includes the optimization of various opportunities for health, participation in life processes and the necessary security, all to improve the Quality of Life of older individuals9. Research in the field of aging is largely carried out on laboratory models and is directed towards various genetic and pharmacological interventions in the aging process itself10. Although they have been going on for decades, the translating of the obtained results into the human population is still questionable.Interventions for the purpose of healthy aging and longevity should include the attenuation or deceleration of some, if not all, already mentioned molecular-cellular changes, which include the aging pro-cess, the processes of inducing pathology associated with aging, and in particular, processes of deregulated sensing of nutrients or energy1. It has been shown that various interventions, including genetic manipu-lation, some drugs implementation and calorie limitation, extend the lifespan of several experimental models11. The superiority of some of these strategies in extending life expectancy has not been known until recently. However, the meta analysis of the published studies with Caenorhabditis and Drosophila, using the appropriate algorithm, emphasized the overall advantage of calorie (or energy) restriction
(CR) in slowing down the aging process and prolonging the lifespan12. It is therefore considered that more acceptable, anti-aging strategies, are those strategies that include environmental factors, to reduce the number of risk factors of bad health13. Accordingly, one of the leading concepts of gerontology is a non-genetic, non-pharmacological CR strategy or a reduction in food intake, but without undernutrition, i.e. CR with optimal nutrition. The concept is not new, as through the history numerous communities promoted health benefits of dietary restrictions, including the ancient Greeks and Romans. Numerous studies, mainly on various model organisms, have shown that CR slows aging, prolongs the period of healthy life, postpones the onset of various age-related diseases and prolongs life expectancy14,15. CR as the idea of encouraging longevity originates from 1917 by Osborne et al. (16), who noticed after restriction of food in the rats, a reduced growth but extended life span. Later, this association was experimen-tally verified and confirmed by numerous research groups on animal models ranging from fungi to mammals17,18. Research results on non-human primates19 are consistent with other models.Because of the ethical limitations there are a small number of studies on the human sample (mostly epidemiological studies are conducted. Results of one of the few researches on the human sample, Compre-hensive Assessment of Long Term Effects of Reducing Caloric Intake Energy Research (CALERIE)20, confirmed the results of Biosphere 2 21, i.e. a previously conducted two-year study of some anti-aging ef-fects22. However, some undesirable effects of CR have been identified in this and other studies23,24. Given the possibility of the unwanted effects of long-lasting CR, questionable adhering to CR regime throughout life or for a long time, newer research as an alternative strategy involves the detection and development of CR mimetics (CRMs). This concept was first introduced by Lane et al. in 1998, proposing 2-deoxy-D-glucose (2DG) as CRM25.The data selected for this review were collected by searching the PubMed database, by the use of the following terms: lifespan, aging, healthspan, caloric restriction, dietary restriction, CR-mimetics. The focus of this paper is the possible CR mechanisms and the more familiar CRM. Additional searches were made in accordance with the names of specific pathways and pharmacological agents. Arti-cles published in English between 2000 and 2019 were included. A limited number of selected articles and reviews is in accordance with the guidelines of the journal. We apologize to the authors of other ex-cellent review articles that are not included in the text for this reason.
calorie restriction
Calorie restriction (or energy restriction) means reduced caloric intake, less than 20% (mild CR) and 50% (severe CR) than the body needs26 or reduced intake of food but without malnutrition. Nu-
Figure 1. Some features that contribute to aging prosess and age-related diseases. Modified according to reference (2).
Review Article
41-50

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com43
merous studies have shown that CR induces pleiotropic, favorable changes in terms of longevity and extension of healthy life span, or postponement of the beginning of age-related diseases, regardless of whether CR is short or long-term practice. These include postpone-ment of sarcopenia, brain atrophy, protection from arthritis and cardiovascular disease, prevention of age-related diabetes, reduction of incidence and progression of cancer, protection of colon health, maintenance of cognitive functions, etc.27 Also, CR includes changes such as: modulation of important regulatory pathways through ex-pression and stimulation the activity of key enzymes of metabolism, decreased oxidative damage of important biomolecules, increased an-tioxidative defense, modulation of mitochondrial activity, enhanced clearance of degraded biomolecules, reduction of chronic inflamma-tion, control of cell repair mechanisms on molecular (eg. DNA re-pair, protein repair, membrane lipid repair), subcellular (autophagy), cellular and tissue levels (apoptosis) etc.28
Generally practiced CR methods include reduced consumption of food, change of nutritional ingredients, digestion inhibition and ab-sorption of nutritional ingredients, inhibition of appetite and satiety and CRMs28. The implementation of the CR regime in the general human population is bad and may be unsafe for some persons, depending on their age or body weight. Long-lasting CR can, in fact, result in malnutrition, so the effects of CR variants, eg. Intermittent Fasting Diatery restriction (IF-DR), or occasionally starvation (every other day) are also tested. Due to the occasional nature of fasting, IF-DR approach seems to relieve the constant hunger effect, experienced by CR practitioners 29. Some studies show that reduced intake of protein sources without calorie change30 or even restriction of certain amino acids, such as methionine or tryptophan31, has a similar effect as CR. This has in some ways set the CR intervention questionable, because these interventions include restrictions on nutrition, but not in calories. More recently, the term dietary restriction - DR32, which can, as mentioned above, includes various feeding regimes (alternate starvation day, intermittent starvation, change in dietary intake). A large number of studies, on the other hand, are also aimed at assess-ing the efficacy of natural and/or pharmacological compounds that mimic the effects of CR, i.e. CRM.
mechanisms of calorie restriction
The cellular energy balance, essential for normal functioning of the organism, is associated with several key energy and nutritional pathways. They are also involved in the emergence of physiological dysfunction that occurs with aging. CR promotes already men-tioned life-sustaining processes, and CR effects mechanisms include nutrient and energy status sensors, enzymes from the group of kinase and deacetylase, involved in post-translational modifications, signal cascades/pathways and transcription factors and coactivators necessary for the metabolic balance maintenance process. In many experimental models, several nutrient-sensing signaling pathways are described, such as insulin-like growth factor-1, IGF-1:, mechanistic Target-of-Rapamycin, mTOR; Adenosine Monophosphate-Activated Protein Kinase, AMPK; and some Sirtuin (SIRT) family members
(especially SIRT-1) are cosidered essential for CR27. The core features of these factors are briefly listed in this section. At certain process levels there are interactions of these signal pathways, sharing many downstream targets that regulate cellular processes associated with aging, but also with CR33.Mechanistic (or mammalian) Target of Rapamycin is a serine/threonine protein kinase involved in various physiological processes (cell metabolism, cell survival, cell growth, autophagy), an activity that can be inhibited by the immunosuppressive drug rapamycin34. It is also a key regulator of cell growth and metabolism that integrates multiple signal pathways linked, among other things to cellular energy, nutrient availability and stress35. There are two structurally and functionally different protein mTOR-complexes: mTORC1 and mTORC2 36 that are linked to protein synthesis, autophagy, lipid metabolism. mTORC1 is the primary modulator of protein, lipid and nucleotide synthesis, autophagy, mitochondrial metabolism and is largely regulated by the availability of nutrients, growth factors, energy, and stress levels. It seems that mTORC1 activation in higher organisms also requires the presence of insulin and IGF-137. The most well-known downstream goals of mTOR are ribosomal protein S6 ki-nase 1 (S6K1), and eucariotic translation initiation factor, 4E-binding protein 1 (4EBP1)38. Although mTOR is not a direct transcription regulator, it regulates a number of transcription factors, eg. NF-χB (inflammation), peroxisome proliferator-activated receptor-χ, PPARχ (adipogenesis), transcription factor EB (TFEB, autophagy) and oth-ers39. mTORC2 is involved in metabolism modulation, cytoskeletal dynamics, cell survival control, but its regulation is less known40.Harrison et al. were the first who discovered the association of inhib-itory activity of rapamycin on mTOR and prolongation of lifespan of genetic heterogeneous mice41, as confirmed by further studies. Detailed explanation of the mechanisms of this connection still does not exist, but it is assumed to include these downstream effectors of mTOR such as S6K1 and 4E-BP42 and, for example, autophagy acti-vation43, self-regeneration of some stem cells44, resistance to different types of stress and suppression of inflammatory cytokine secretion from the senescent cell45. Inhibition of mTOR signaling, with rapamycin or nutritional inter-ventions, thus protects against metabolic dysfunction, neurodegener-ation and cancer, and leads to an increase in lifespan in various model organisms (yeasts, flies and C. elegans), while increased mTOR signaling is included in pathogenesis of several age-related diseases, such as type 2 diabetes mellitus and cancer46. Unlike other signaling pathways (AMPK and SIRT-1) as an energy sensors, mTOR activity is therefore inhibited by reducing the availability of nutrients in order to preserve energy reserves.AMP-activated protein kinase. The cells provide energy by degra-dation of adenosine triphosphate (ATP) into adenosine diphosphate (ADP) and inorganic phosphate in mitochondria, whereby the rate of synthesis and ATP consumption coincides with the maintenance of the energy balance required for normal cellular processes. With this goal, during a low energy availability period, cells are rapidly replenishing ATP storage by enzymatic coupling of two ADPs, with
Review Article
41-50
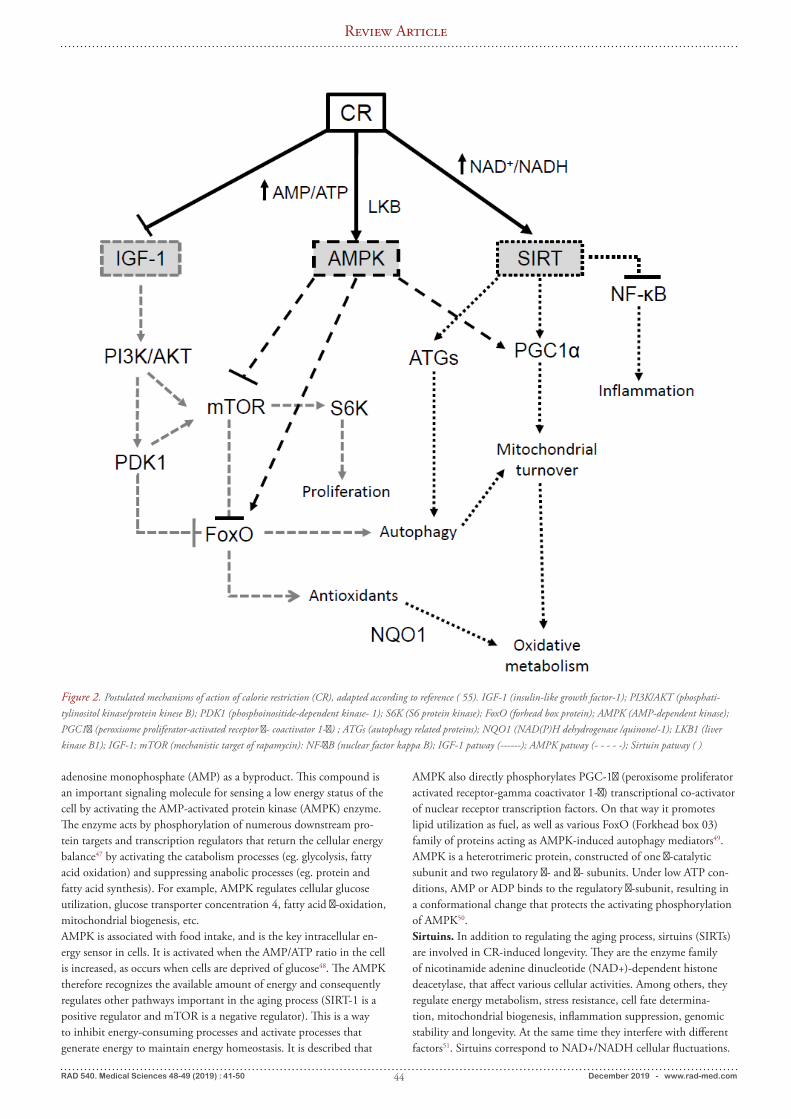
RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com44
adenosine monophosphate (AMP) as a byproduct. This compound is an important signaling molecule for sensing a low energy status of the cell by activating the AMP-activated protein kinase (AMPK) enzyme. The enzyme acts by phosphorylation of numerous downstream pro-tein targets and transcription regulators that return the cellular energy balance47 by activating the catabolism processes (eg. glycolysis, fatty acid oxidation) and suppressing anabolic processes (eg. protein and fatty acid synthesis). For example, AMPK regulates cellular glucose utilization, glucose transporter concentration 4, fatty acid χ-oxidation, mitochondrial biogenesis, etc.AMPK is associated with food intake, and is the key intracellular en-ergy sensor in cells. It is activated when the AMP/ATP ratio in the cell is increased, as occurs when cells are deprived of glucose48. The AMPK therefore recognizes the available amount of energy and consequently regulates other pathways important in the aging process (SIRT-1 is a positive regulator and mTOR is a negative regulator). This is a way to inhibit energy-consuming processes and activate processes that generate energy to maintain energy homeostasis. It is described that
AMPK also directly phosphorylates PGC-1χ (peroxisome proliferator activated receptor-gamma coactivator 1-χ) transcriptional co-activator of nuclear receptor transcription factors. On that way it promotes lipid utilization as fuel, as well as various FoxO (Forkhead box 03) family of proteins acting as AMPK-induced autophagy mediators49. AMPK is a heterotrimeric protein, constructed of one χ-catalytic subunit and two regulatory χ- and χ- subunits. Under low ATP con-ditions, AMP or ADP binds to the regulatory χ-subunit, resulting in a conformational change that protects the activating phosphorylation of AMPK50.Sirtuins. In addition to regulating the aging process, sirtuins (SIRTs) are involved in CR-induced longevity. They are the enzyme family of nicotinamide adenine dinucleotide (NAD+)-dependent histone deacetylase, that affect various cellular activities. Among others, they regulate energy metabolism, stress resistance, cell fate determina-tion, mitochondrial biogenesis, inflammation suppression, genomic stability and longevity. At the same time they interfere with different factors51. Sirtuins correspond to NAD+/NADH cellular fluctuations.
Figure 2. Postulated mechanisms of action of calorie restriction (CR), adapted according to reference ( 55). IGF-1 (insulin-like growth factor-1); PI3K/AKT (phosphati-tylinositol kinase/protein kinese B); PDK1 (phosphoinositide-dependent kinase- 1); S6K (S6 protein kinase); FoxO (forhead box protein); AMPK (AMP-dependent kinase); PGC1α (peroxisome proliferator-activated receptor α- coactivator 1-α) ; ATGs (autophagy related proteins); NQO1 (NAD(P)H dehydrogenase /quinone/-1); LKB1 (liver kinase B1); IGF-1; mTOR (mechanistic target of rapamycin): NF-αB (nuclear factor kappa B); IGF-1 patway (------); AMPK patway (- - - - -); Sirtuin patway ( )
Review Article
41-50

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com45
If there is not enough supply with nutrients, especially glucose, NAD+ will accumulate and then SIRTs will be activated. Deacetyl-ation activity or removal of acetyl residues on numerous proteins, enzymes and transcription factors involved in key aspects of cellular physiology is related to NAD+ as a co-substrate. However, other activities of these enzymes, such as desukcinylation, demalonylation and depropionylation are also described. Seven sirtuin enzymes members (SIRT-1 to SIRT-7) were identi-fied among the mammals, which are localized in different cellular compartmetns13,52. Sirtuin-1 is largely localized in the nucleus and, to a lesser extent, in the cytoplasm. It is most closely associated with mechanisms involved in aging and longevity, by deacetylating the main regulator of biogenesis PGC-1χ and transcriptional FoxO fac-tor53. FoxO proteins are capable of increasing longevity by ensuring resistance to oxidative stress, protecting protein structures and pro-moting lipid metabolism and autophagy15. Also, SIRT-1 deacetylates some glycolytic enzymes and transcription inducer hypoxia-inducible factor 1 thereby reducing the glycolysis process54.Insulin-like growth factor. Insulin/IGF-1 pathway (IIS) of cellular signaling is hormone-regulated, and includes insulin, insulin-like peptides, receptor substrates and numerous downstream effectors33. Increased serum glucose concentration after food intake stimulate secretion of insulin hormones that activates IIS signaling. This signal-ing pathway is also involved in modulating the aging process but also there are significant differences in this pathway depending on model organisms and mammalian species33,35. Activation or suppression of various dowstream effectors such as PI3/AKT/Ras (phosphatidyli-nositol 3-kinase/protein kinase B/Ras), mTOR, S6K and transcrip-tional FoxO and etc. are also involved in signaling this pathway during the CR regime33. CR, diet modulation, appropriate protein : carbohydrate ratio in diet, and reduced growth hormone contraction reduce the activity of IIS signaling, which is associated with health improvement and longevity of various species including human34,56. Due to reduced food intake during CR, signaling of this pathway is decreased, due to reduced insulin secretion and consequently the repression of FoxO factor13. The result is a more efficient response to stress because the transcription factor FoxO as an important target of the IIS pathway is involved in the induction of some stress response genes33,57.In addition to the aforementioned main regulators of signaling pathways, some factors are also described which are also, at certain levels, associated with the participants of said signaling paths during CR. These are, for example, a) neuropeptide (NP) mediated by CR-induced autophagy process 57; b) PGC-1χ, a member of the transcription cluster family, participates in the process of mitochon-drial biogenesis58; c) nuclear factor (erythroid-derived 2)-like 2 (Nrf2) 59, which participates in increasing the expression of mitochondrial and cellular antioxidants; d) fibroblast growth factor 21 (FGF21) as an endocrine signal associated with metabolic control, whose value changes after low protein or methionine intake60. The described regulators and pathways of cellular energy and sensi-tivity to nutrients can in particular modulate life expectancy, but as
mentioned above, they are not exclusive to each other. They actually act synergistically in detecting changes in calorie/energy status in order to maintain cell homeostasis. For example, decreased availabil-ity of macronutrients is one of the most common activators for the acivation of autophagy, partly by activating AMPK and SIRT-1, and by inhibiting mTOR signaling61. Figure 2 shows the simplified main regulators and network of CR participants.Under CR conditions, the ratio of ATP/AMP is changed and the AMPK is activated. Cell metabolism changes, resulting in the accumulation of NAD+, which will lead to activation of SIRT-1. An antagonistic response involves inhibition of anabolic pathways mTOR and insulin/IGF1. Downstream factors/mediators can pro-duce redundant effects that are reflected in processes such as prolifera-tion balanced cell growth, increased autophagy/mitophagy, improved mitochondrial biogenesis, enhanced antioxidative defense, decreased inflammation, resulting in improved healthy and prolonged lifespan.
caloric restriction mimetics
In model organisms of rodents and nonhuman primates, it has been shown that diet regimes in the form of dietary adaptation such as CR, have favorable effects on health and extend life62. Also, results on a human samples, eg. CALERIE, Biosphere 2 Study21, CRON Study62, show that moderate CR improves human health and reduces various metabolic factors associated with pathogenesis of chronic diseases. Serious or severe CR slows down the accumulation of mo-lecular damage and thus maintains key physiological functions63. Still existing incompatibility of the results of the long-term studies of lon-gevity has been attributed to differently designed examinations as well as to the composition and breeding of food64. In addition to the CR as a strategy for beneficial effects on health and thus the aging process of model organisms, alternative life-style strategies that mimic CR, as occasional and intermitent starvation, limitation of some amino acids or protein intake, etc.8 are described and discussion of the practicali-ties and effects of such approaches are ongoing.Despite the potential benefits of CR to improve physiological func-tions in the aging process, most people are noncompliant to practice CR, or change nutritional routine for a long time. In other words, maintenance of CR with optimal nutrition is difficult to enforce in humans13. Furthermore, continuous CR represents a potential risk for older adults with normal weight who are already prone to loss of bone density and muscle mass. It is also described that reducing energy intake is aggravated by loss of skeletal muscle mass in older adults24, and adverse reactions such as sensitivity to cold, anemia, and depression62,65,66 are also reported in younger subjects. In restriktively fed animals, disorders in healing skin wounds67 and susceptibility to infections68 were observed.In order to limit the risks of adverse effects of CR and take advantage of positive effects, over the past decade, significant attention has been paid to establishing more feasible approaches. The effects of com-pounds and interventions that “mimic CR or starvation” are detected and tested, that is, without real CR regime. These are: a) pharma-cological and nutritional compounds, CRM and b) CR mimicking
Review Article
41-50

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com46
lifestyle (behavioural) approaches to lifestyle change69,70. According to Ingram et al., CRMs are considered compounds or ap-proaches/procedures, that mimic the metabolic, hormonal and physi-ological effects of CR, activate stress response paths that correspond to the level during CR (known under the term hormesis), enhance stress protection, produce CR-like effects on longevity, reduce the incidence of aging-related illnesses, maintain youth functions, and not reduce significantly, at least in the short run, food intake69. It is assumed that administration of mimetics that fulfill all or at least part of these criteria could have a positive impact on healthy life expectancy and longevity. In defining their effects, an important role will be to detect more reliable biomarkers of the aging process itself, since the existing ones still do not meet the criteria of an ideal biomarker71.CR mimetics are classified according to mechanisms of action such as AMPK, SIRTs (NAD-boosting compounds included herein), autophagy activators and mTOR inhibitors. Of the already discovered compounds that have the potential to imitate CR effects, some in hu-mans have clinical use with other indications. These are, for example, rapamycin (mTOR inhibitor), metformin (AMPK activator), and polyphenolic compound - resveratrol (AMPK and SIRT-1 activators) whose various properties are also frequently tested in human popu-lations. Other compounds referred to as CRM potential compounds are: D-glucosamine glycosaminoglycan precursor and hexokinase enzyme inhibitor used to prevent osteoarthritis72, some antilipolylic compounds as nicotinic acid derivatives - acipimox73, and fibrates (ac-tivate PGC174; melatonin75, SRT1-720 and SRT-2104-direct activa-tors of SIRT-1; pegvisomant, growth hormone receptor antagonist33; AZD8055/INK128, a direct mTOR kinase inhibitor33, tiazolidinedi-ones agonists PPARs) used in diabetes therapy and obesity13, a lipoic acid thiol compound with strong antioxidant properties76 and others. Table 1 lists some CRMs and their mechanism of action.As previously described, CR acts on multiple intracellular signal pathways. CR mimetics on the other hand partially induce some of these mechanisms. For example, 2DG inhibits glycolysis, thus favor-ing AMPK and SIRT signaling activity; metformin amplifies AMPK signaling, which indirectly leads to autophagy and amplification of
the mitochondrial turnover, resveratrol increases the activity of SIRT and AMPK, etc.77 The likelihood that some compound will stimulate all the mechanisms is small and therefore the CRM-„cocktail“ effects will be tested, which would have an optimum synergistic effect on life expectancy.
Below are the main features of the most famous compounds with CRM potential.Metformin (N,N-dimethylimidocarbonimide diamide), a member of the biguanide group, has been using for several decades in type 2 diabetes mellitus therapy since it inhibits the gluconeogenesis process and decreases insulin level78. It has been established that metformin has the ability to imitate most CR mechanisms and is presumed to be the main target of metformin AMPK79. AMPK activation leads to suppressive insulin/IGF-1 and mTOR signaling and activation of SIRT-127. It is also considered that alterations in cell signaling occur secondary after inhibition of complex I mitochondrial respirato-ry chain resulting in ATP concentration decrease80. The increased AMP/ATP ratio, furthermore, activates AMPK, and consequently the transcription factors and the metabolic enzyme of said signaling pathways, in order to restore energy to the cells. Hence, they influence the processes associated with longevity such as mitochondrial turnover autophagy, stress defense, protein synthesis and inflammation81.The results of metformin research as CRM, are now controversial, i.e. effects on longevity are not observed in all species investigated82. Controversial results and the possibility of occurrence of lactic acidosis with chronic administration of metformin83 point to caution and the need to determine optimal metformin dose for the purpose of healthy aging and longevity. The results of a human pattern study entitled “Targeting Aging with Metformin”, which are underway, should form a pattern or paradigm for assessing pharmacological approaches to delay or slowdown of aging81.2-deoxy D-glucose, glucose analog and glycolysis inhibitor, is one of the first compounds considered as CRM25. It inhibits the activity of the glycolytic enzyme phosphoglucose isomerase thereby preventing the conversion of glucose-6-phosphate into fructose-6-phosphate. The
Mimetic CR (category of compound) Mechanisms of acting
Metformin(biguanide)
Inhibition of mitochondrial complex I; activation of PI3/AKT cascade; activation of AMPK
2-deoxy-D-glucose (glycolytic inhibitor)
Inhibition of phosphoglucose isomerase
Rapamycin (mTOR inhibitor) and rapalogs Inhibition of mTOR leading to autophagy
Resveratrol(sirtuin activating compound)
Activation of SIRT-1
Nicotinamide riboside NAD precursorSpermidine (polyamine) Activation of autophagy
Neuropeptide Y(neuropeptide)
Stimulation of autophagy
Table 1. Calorie restriction mimetics
Review Article
41-50

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com47
result is the energy supply limit in the form of ATP, and the AMP/ATP ratio increases. Next, activation of AMPK pathway is followed. Thereafter, activation of SIRTs and autophagy (84) occur. It is con-sidered that 2DG causes delay of age-related dysfunction, and shows effects similar to CR85. On some organisms it has been shown that 2DG can stimulate stress response proteins and heat shock protein 7086. However, the attitudes of 2DG effect on life extensions differ, which is probably the result of differently designed research. A favor-able effect was generally observed at lower concentrations of 2DG, while with increased concentration this compound had a cardiotoxic effect in rats87.Rapamycin [23,27-epoxy-3H-pyrido(2,1-c)(1,4) oxazacyclohentri-acontine] is a macrolide antibiotic (also known as Sirolimus) with immunosuppressive and antiproliferative properties, most commonly used in organ transplantation88. The effect of promoting rapamy-cin’s longevity was first discovered in yeast and later confirmed on numerous other organisms, while human-based examinations are still to be carried out. Rapamycin has low bioavailability, and in order to achieve higher solubility and stability, the authors emphasize the need for the development of rapamycin analogues89. Additional reasons for the analogs are also the immunosuppressive properties of rapamycin and the consequent possibility to develop viral and bacterial diseases. In this respect, investigations of the most effective dose of rapamycin for healthy aging and longevity are being conducted.The mechanism by which rapamycin exerts its effect involves inhi-bition of mTOR signaling90. It is assumed that rapamycin forms a heterotrimeric complex with two proteins, FK506 binding protein (FKBP)-type peptidyl-prolyl cis-trans-isomerase and the FKBP-rapa-mycin-associated protein. This heterotrimer can be complexed with mTOR and thus inhibit the formation of mTORC1 complexes and consequently cell growth and proliferation. Activating of autopha-gy-related protein 1 (ATG1) can stimulate activation of the autoph-agy process77. Rapamycin reduces inhibition of SIRT-1 by decreasing NF-χB mediated inflammation91.Resveratrol (3,4,5-trihydroxystilbene) is a natural, vegetable polyphe-nol compound of the stilbene subgroup, with antioxidant activity being most common in grape and red wine92. In 2003, the in vitro NIA (National Institute for Aging) screening program confirmed the resveratrol property to activate SIRT-1, and model systems demon-strated that this activation was followed by autophagy93. Significant number of articles show that resveratrol prolongs the life of different species, but there are opposite opinions94,95. Among others, it has been described that resveratrol reduces insulin secretion, increas-es insulin sensitivity, decreases body fat, increases mitochondrial biogenesis and oxidative phosphorylation, increases AMPK activity, autophagy and mitophagy, and also NAD/NADH ratio, which activates SIRT-155. Although the exact mechanism of action is not entirely clear, resveratrol binds to the regulatory N-terminal subunit of SIRT-1, leading to conformational change, which in turn results in increased deacetylation activity of SIRT-196. Unwanted effects of resveratrol have not yet been recorded except for extremely high
concentrations97.Spermidine. The polyamine compound, spermidine is also included in CRMs. Studies of the anti-aging effects of spermidine are still ongoing and are not quite clear, but seem to be partly related to the induction of autophagy98. Spermidine acts as an inhibitor of acetyltransferase EP300, endogenous autophagy inhibitor, which acts by acetylation of lysine residues within various proteins. Compounds used in traditional medicine, for example anacardic acid, curcumin, garcinol and epigallocatchin-3-gallate, also inhibit EP30098. In addi-tion, spermidine exhibits various pleiotropic effects including antioxi-dative and anti-inflammatory activity, improvement of mitochondrial metabolic activity, and improvement of the proteostasis process. The undesirable effect of polyamines, including spermidine, is the ability to stimulate tumor progression at high concentrations99.CR-mimicking lifestyle (behavioral) strategies include the limitation of macro- or micronutrients (eg. protein or amino acids), periodic starvation (including, for example, feeding ad libitum 5 days a week and starvation or limiting food intake for two days), intermittent starvation (change of day of normal feeding and day of complete re-striction of food, or minimum food intake) with different recommen-dations, i.e. restricted feeding and habitual exercise. As it is assumed it will not be possible to find a drug that will include all pathways/mechanisms of CR without undesirable effects, the results of testing of the combination of different CRMs, CRM com-binations with a specific CR level or other combinations of types will be interesting due to balancing the detrimental effects of chronic CR regime on one side, and the unwanted CRM effects on the other89,100.
conclusion
The aging process is an inevitable process that is additionally adverse-ly affected by the development of age-related diseases. In the area of geroscience, great efforts have been made to detect the causes and mechanisms of this process in order to establish appropriate genetic or nutritional/pharmacological interventions for the purpose of healthy aging and longevity. This does not seem easy, since the mech-anisms are networked, ie., there are mutual activating or suppressing actions.The CR has now proved to be a promising intervention in achieving that goal. CR promotes life-prolonging processes such as autophagy, mitochondrial biogenesis, and ATP production. Although the ideal calorie intake is currently unknown and is likely to be different for each person, the results of CR research on various model systems and types have provided insights into the main signaling pathways of healthy aging and longevity.Some of these pathways have become the main goals or candidates for CRM development that could be used for the purpose of healthi-er aging or postponement of aging-related illnesses. Besides examina-tions of individual, potential CRM compounds, but also investiga-tions with their combinations and combinations of CRM and other imitation CR strategies are performed. Alternative CR strategies occasional starvation, modulation of nutritional input/balanced input
Review Article
41-50

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com48
of macronutrients, and other effects to be explored in future research. It is assumed that different strategies will also have different effects on complex pathway signaling participants. It is to be expected, that the real direction will be given interdisciplinary research that will define the most optimal type of strategy. Undoubtedly, the implementation of omics-based approaches such as genomics, transcriptomics, metab-olomics and proteomics will be of great help.Discussion about aging as a) normal/partially normal or natural or b) partial pathological process is ongoing, and the latest developments in gerontology reveal the molecular link between aging and pathological conditions. However, many open questions remain about the aging
process at the molecular level. Generally, it is necessary to try, if pos-sible, to define more clearly processes that induce aging, ie “natural” aging and age-related diseases. The application of CRM on a human beings for the purpose of achieving longevity, will only be enabled and justified after researches has been carried out on a number of non-hu-man primate models, which for now have a small number, and after considering ethical, economic and social implications.
author contributions:All authors listed have made a substantial, direct and intellectu-al contribution to the work, and approved it for publication.
literature:1. López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G., The hallmarks of aging. Cell. 2013;153:1194-1217.2. Singh AK, Singh S, Rizvi SI. Autophagy induction: A promising antiaging strategy. In: Rizvi SI, Çakatay U, Editors. Molecular basis and emerging strategies for anti-aging interventions. Springer Nature Singapore Pte Ltd. 2018; pp 161-174.3. Kennedy BK, Berger SL, Brunet A, Campisi J, Cuervo AM, Epel ES, et al. Geroscience: linking aging to chronic disease. Cell 2014;159(4):709-13. 4. Harman D. Aging: a theory based on free radical and radiation chemistry. J Gerontol. 1956;11:298-3009 . 5. Blagosklonny MV, Hall MN. Growth and aging: a common molec-ular mechanism. Aging (Albany NY) 2009;1(4):357-62.6. Franceschi C, Bonafè M, Valensin S, Olivieri F, De Luca M, Ottavi-ani E, et al. Inflamm-aging. An evolutionary perspective on immu-nosenescence. Ann N Y Acad Sci. 2000; 908:244-54.7. Coppé JP, Desprez PY, Krtolica A, Campisi J. The senescence-asso-ciated secretory phenotype: the dark side of tumor suppression. Annu Rev Pathol 2010;5:99-118.8. Cavallini G, Donati A, Gori Z, Bergamini E. Towards an under-standing of the anti-aging mechanism of caloric restriction. Curr Aging Sci. 2008;1:4-9.9. World Health Organization: Active Ageing: A Policy Framework. Geneva: 2002 http://whqlibdoc.who.int/hq/2002/who_nmh_nph_02.8.pdf3]. 10. Partridge L. Intervening in ageing to prevent the diseases of age-ing. Trends in Endocrinol and Metab. 2014;25:555-557.11. Gillespie ZE, Pickering J, Eskiw JH. Better living through chemistry: Caloric restriction (CR) and CR mimetics alter genome function to promote increased health and lifespan. Front Genet. 2016;7(142):1-21.12. Liang Y, Liu C, Lu M, Dong Q, Wang Z, Wang Z, et al. Calorie restriction is the most reasonable anti-ageing intervention: a me-ta-analysis of survival curves. Sci Rep. 2018;8:1-9.13. Testa G. Calorie Restriction and dietary restriction mimetics: A strategy for improving healthy aging and longevity. Curr Pharm Des. 2016;20(9):1-28.14. Yu BP. Aging and oxidative stress: Modulation by dietary restric-tion. Free Radic Biol Med. 1996;21:651–668. 15. Fontana L, Partridge L, Longo VD. Extending healthy life span--from yeast to humans. Science 2010; 328:321–326.
16. Osborne TB, Mendel LB, Ferry EL. The effect of retardation of growth upon the breeding period and duration of life of rats. Science 1917;45:294-295.17. Robertson T B, Ray L A. Experimental studies on growth: XV. On the growth of relatively long lived compared with that of relatively short lived animals. J Biol Chem. 1920;42:71-107.18. McCay CM, Maynard LA, Sperling G, Barnes LL. Retarded growth, lifespan, ultimate body size and age changes in the albino rat after feeding diets restricted in calories. J Nutr 1939;18:1-13.19. Mattison JA, Roth GS, Beasley TM, Tilmont EM, Handy AM, Herbert RL, et al. Impact of caloric restriction on health and survival in rhesus monkeys from the NIA study. Nature 2012;489:318-321. 20. Rickman AD, Williamson DA, Martin CK, Gilhooly CH, Stein RI, Bales CW, et al. The CALERIE Study: design and methods of an innovative 25% caloric restriction intervention. Contemp Clin Trials. 2011;32:874-881.21. Walford RL, Weber L, Panov S. Caloric restriction and aging as viewed from Biosphere 2. Receptor. 1995;5:29–33.22. Meydani M, Das S, Band, M Epstein, S, Roberts S. The effect of caloric restriction and glycemic load on measures of oxidative stress and antioxidants in humans: results from the CALERIE trial of human caloric restriction. J Nutr Health Aging. 2011;15:456-460.23. Villareal DT, Fontana L, Das SK, Redman L, Smith SR, Saltzman E, et al. CALERIE Study Group. Effect of two-year caloric restriction on bone metabolism and bone mineral density in non-obese younger adults: A randomized clinical trial. J Bone Miner Res. 2016;31:40-51. 24. Miller SL, Wolfe RR. The danger of weight loss in the elderly. J Nutr Health Aging. 2008;12:487-491.25. Lane MA, Ingram DK, Roth GS. 2-Deoxy-D-glucose feeding in rats mimics physiological effects of calorie restriction. J Anti Aging Med. 1998;1:327-337. 26. Mattson MP, Duan W, Guo Z. Meal size and frequency affect neuronal plasticity and vulnerability to disease: cellular and molecular mechanisms. J Neurochem. 2003;84:417-431.27. Balasubramanian P Howell PR, Anderson RM. Aging and caloric restriction research: Biological perspective with translational potential. EbioMedicine. 2017;21:37-44.28. Lushcak O, Gospodaryov D. Mimetics of caloric restriction. In: Antiaging drugs: From basic research to clinical practice. Ed. Vaiser-man A. The Royal Society of Chemistry; 2017; pp 231-297.29. Horne BD, Muhlestein JB, Anderson JL. Health effects of inter-mittent fasting: hormesis or harm? A systematic review. Am J Clin
Review Article
41-50

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com49
Nutr 2015;102:464-470.30. Fontana L, Weiss EP, Villareal DT, Klein S, Holloszy JO. Long-term effects of calorie or protein restriction on serum IGF-1 and IGFBP-3 concentration in humans. Aging Cell. 2008;7:681-687.31. Orentreich N, Matias, JR, DeFelice A, Zimmerman JA. Low methionine ingestion by rats extends life span. J Nutr. 1993;123:269-274.32. Gems D, Partridge L. Genetics of longevity in model organisms: debates and paradigm shifts. Annu Rev Physiol. 2013; 75;621-644.33. Pan H, Finkel T. Key proteins and pathways that regulate lifespan. J Biol Chem. 2017;292(16):6452-6460.34. Solon-Biet SM, J. Mitchell SJ, de Cabo R, Raubenheimer D, Le Couteur DG, Simpson SJ. Macronutrients and caloric intake in health and longevity. J Endocrinol. 2015; 226(1): R17–R28.35. Stanfel MN, Shamieh LS, Kaeberlein M, Kennedy BK. The TOR pathway comes of age. Biochim Biophys Acta 2009;1790:1067-1074. 36. Ming X, Montani J & Yang Z. Perspectives of targeting mTORC1-S6K1 in cardiovascular aging. Front Physiol 2012;3(5):1-11.37. Xu S, Cai Y, Wei Y. mTOR signaling from cellular senescence to organismal aging. Aging Dis. 2014;5:263-273.38. Yoon MS. The Role of mammalian target of rapamycin (mTOR) in insulin signaling. Nutrients 2017;9:1-17.39. Kennedy BK, Lamming DW. The mechanistic target of rapamy-cin: the grand ConducTOR of metabolism and aging. Cell Metab. 2016;23:990-1003.40. Shimobayashi M, Hall MN. Making new contacts: the mTOR network in metabolism and signalling crosstalk. Nat Rev Mol Cell Biol. 2014;15:155-162. 41. Harrison DE, Strong R, Sharp ZD, Nelson JF, Astle CM, Flurkey K, et al. Rapamycin fed late in life extends lifespan in genetically heterogeneous mice. Nature 2009;460:392-395.42. Mieulet V, Roceri M, Espeillac C, Sotiropoulos A, Ohanna M, Oorschot V, et al. S6 kinase inactivation impairs growth and translational target phosphorylation in muscle cells maintaining proper regulation of protein turnover. Am J Physiol Cell Physiol. 20017;293:C712-C722. 43. Hansen M, Chandra A, Mitic LL, Onken B, Driscoll M, Kenyon C. A role for autophagy in the extension of lifespan by dietary restric-tion in C. elegans. PLoS Genet. 2008;4(2):1-14. 44. Yilmaz ÖH, Katajisto P, Lamming DW, Gültekin Y, Bauer-Rowe KE, Sengupta S, et al. mTORC1 in the Paneth cell niche couples intestinal stem-cell function to calorie intake. Nature 2012;486:490-495.45. Laberge RM, Sun Y, Orjalo AV, Patil CK, Freund A, Zhou L, et al. MTOR regulates the pro-tumorigenic senescence-associated secretory phenotype by promoting IL1A translation. Nat Cell Biol. 2015;171049-1061.46. Zoncu R, Efeyan A, Sabatini DM. mTOR: From growth signal integration to cancer, diabetes and ageing. Nat Rev Mol Cell Biol. 2011;12:21-35.47. Cantó C, Auwerx J. Calorie restriction: is AMPK a key sensor and effector? Physiology (Bethesda) 2011;26(4):214-24.48. Hardie DG. Sensing of energy and nutrients by AMP-activated protein kinase. Am J Clin Nutr. 2011;93891S-896S.49. Nakashima K, Yakabe Y. AMPK activation stimulates myofibril-lar protein degradation and expression of atrophy-related ubiquitin ligases by increasing FOXO transcription factors in C2C12 myotubes. Biosci Biotechnol Biochem. 2007;71(7):1650-1656.50. Mihaylova MM, Shaw RJ. The AMP-activated protein kinase (AMPK) signaling pathway coordinates cell growth, autophagy, & metabolism. Nat Cell Biol. 2011;13(9):1016-23.
51. Watroba M, Szukiewicz D. The role of sirtuins in aging and age-related diseases. Adv Med Sci. 2016;61:52-62.52. Guarente L. Calorie restriction and sirtuins revisited. Genes Dev 2013;27(19):2072-2085. 53. Amigo I, Kowaltowski AJ. Dietary restriction in cerebral bioener-getics and redox state. Redox Biol. 2014;2:296-304.54. Kitada M, Koya D. - The use of calorie restriction mimetics to study aging. Methods Mol Biol. 2013;1048:95-107.55. Lopez-Lluch G, Navas P. Calorie restriction as an intervention in ageing. J Physiol. 2016;594(8):2043-60. 56. Laron Z. The GH-IGF1 axis and longevity. The paradigm of IGF1 deficiency. Hormones 2008;7(1):24-27.57. Efeyan A, Comb WC, Sabatini DM. Nutrient-sensing mecha-nisms and pathways. Nature 2015;517:302-310.58. Allard JS, Perez E, Zou S, de Cabo R. Dietary activators of Sirt1. Mol Cell Endocrinol. 2009;299:58-63.59. Picca A, Pesce V, Lezza AMS. Does eating less make you live longer and better? An update on calorie restriction. Clin Interv Aging 2017:12 1887-1902.60. Chau MD, Gao J, Yang Q, Wu Z, Gromada J. Fibroblast growth factor 21 regulates energy metabolism by activating the AMPK-SIRT1-PGC-1alpha pathway. Proc Natl Acad Sci. 2010;107:12553-12558.61. Rubinsztein DC, Marino G, Kroemer G. Autophagy and aging. Cell 2011;146:682-695.62. Most J, Tosti V, Redman LM, Fontana L. Calorie restriction in humans: an update. Ageing Res Rev. 2017;39:36-45.63. Yang L, Licastro D, Cava E, Veronese N, Spelta F, Rizza W, et al. Long-term calorie restriction enhances cellular quality-control pro-cesses in human skeletal muscle. Cell reports 2016;14:422-428.64. Cava E, Fontana L. Will calorie restriction work in humans? Aging 2013;5:507-514.65. Martin CK, Bhapkar M, Pittas AG, Pieper CF, Das SK, William-son DA, et al. Effect of calorie restriction on mood, quality of life, sleep, and sexual function in healthy nonobese adults: The CALERIE 2 Randomized Clinical Trial. JAMA Intern Med. 2016;176(6):743-52.66. Romashkan SV, Das SK, Villareal DT, Ravussin E, Redman LM, Rochon J, et al. Safety of two-year caloric restriction in non-obese healthy individuals. Oncotarget. 2016;7(15):19124-19133.67. Hunt ND, Li GD, Zhu M, Levette A, Chachich ME, Spangler EL, et al. Effect of calorie restriction and refeeding on skin wound healing in the rat. Age (Dordr). 2012;34(6):1453-1458. 68. Goldberg EL, Romero-Aleshire MJ, Renkema KR, Ventevogel MS, Chew WM, Uhrlaub JL, et al. Lifespan-extending caloric restric-tion or mTOR inhibition impair adaptive immunity of old mice by distinct mechanisms. Aging Cell 2015;14:130-138.69. Ingram DK, Zhu M, Mamczarz J, Zou SG, Lane MA, Roth GS, et al. Calorie restriction mimetics: An emerging research field. Aging Cell 2006;5:97-108. 70. Mattson MP, Allison DB, Fontana L, Harvie M, Longo VD, Mal-aisse WJ, et al. Meal frequency and timing in health and disease. Proc Natl Acad Sci. USA 2014;111:16647-16653.71. Dodig S, Čepelak I, Pavić I. Hallmarks of senescence and aging. Biochem Med. 2019;29(3):030501.72. Weimer S, Priebs J, Kuhlow D, Groth M, Priebe S, Mansfeld J, et al. D-Glucosamine supplementation extends life span of nematodes and of ageing mice. Nat Comm 2014;5:1-12.73. Donati A, Cavallini G, Carresi C, Gori Z, Parentini I, Berga-mini E. Anti-aging effects of anti-lipolytic drugs. Exp Gerontol. 2004;39:1061-1067.74. Brandstädt S, Schmeisser K, Zarse K, Ristow M. Lipid-lowering
Review Article
41-50

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com50
fibrates extend C. elegans lifespan in a NHR-49/PPARalpha-depen-dent manner. Aging (Albany NY) 2013;5(4):270-275.75. Navarro-Alarcón M, Ruiz-Ojeda FJ, Blanca-Herrera RM, A-Serra-no MM, Acuña-Castroviejo D, Fernández-Vázquez G, et al. Melatonin and metabolic regulation: a review. Food Funct 2014;5:2806-2832.76. Merry BJ, Kirk AJ, Goyns MH. Dietary lipoic acid supplementa-tion can mimic or block the effect of dietary restriction on life span. Mech Ageing Dev. 2008;129;341-348.77. Nikolai S, Pallauf K, Huebbe P, Rimbach G. Energy restric-tion and potential energy restriction mimetics. Nutr Res Rev. 2015;28(2):100-120.78. Hundal RS, Krssak M, Dufour S, Laurent D, Lebon V, Chan-dramouli V, et al. Mechanism by which metformin reduces glucose production in type 2 diabetes. Diabetes 2000;49:2063-2069. 79. Lu J, Shi J, Li M, Gui B, Fu R, Yao G, et al. Activation of AMPK by metformin inhibits TGF-χ-induced collagen production in mouse renal fibroblasts. Life Sci. 2015;127:59-65.80. Foretz, M., Guigas, B., Bertrand, L., Pollak, M., Viollet, B. Metformin: from mechanisms of action to therapies. Cell Metab. 2014;20:953-966.81. Barzilai N, Crandall JP, Kritchevsky SB, Espeland MA.. Met-formin as a tool to target aging. Cell Metab. 2016;23(6):1060-1065.82. Slack C, Foley A, Partridge L. Activation of AMPK by the putative dietary restriction mimetic metformin is insufficient to extend life span in Drosophila. PloS ONE 2012;7(10):1-7. 83. Holst H, Eldrup E, Guldstad NH, Bülow HH, Christensen HR. Metformin associated with lactic acidosis in treatment of type 2 diabe-tes. Ugeskr Laeger. 2012;174:1598-1602.84. Cantó C, Gerhart-Hines Z, Feige JN, Lagouge M, Noriega L, Milne JC, et al. AMPK regulates energy expenditure by modulating NAD+ metabolism and SIRT1 activi. Nature 2009;458:1056-1060.85. Shintani H, Shintani T, Ashida H, Sato M. Celorie restriction Mimetics: Upstream-Type Compounds for Modulating Glucose Me-tabolism. Nutrients 2018;10(12):1-17.86. Lee J, Bruce-Keller AJ, Kruman Y, Chan SL, Mattson MP. 2-De-oxy-D-glucose protects hippocampal neurons against excitotoxic and oxidative injury: evidence for the involvement of stress proteins. J Neurosci Res. 1999;57(1):48-61. 87. Minor RK, Smith DL, Sossong AM, Kaushik S, Poosala S, Span-
gler EL, et al. Chronic ingestion of 2-deoxy-d-glucose induces cardiac vacuolization and increases mortality in rats. Toxicol Appl Pharmacol. 2010;243:332-339. 88. Dumont FJ, Su Q. Mechanism of action of the immunosuppres-sant rapamycin. Life Sci. 1996;58:373–395. 89. Blagosklonny MV. From rapalogs to anti-aging formula. Oncotar-get 2017;8(22): 35492-35507.90. Heitman J, Movva NR, Hall MN. Targets for cell cycle arrest by the immunosupresant rapamycin in yeast. Science 1991;253:905-909.91. Takeda-Watanabe A, Kitada M, Kanasaki K, Koya D. SIRT1 inactivation induces inflammation through the dysregulation of autophagy in human THP-1 cells. Biochem Biophys Res Commun. 2012;427:191-196.92. Siemann EH, Creasy LL. Concentration of the phytoalexin resver-atrol in wine. Am J Enol Vitic. 1992;43:49-52.93. Morselli E, Galluzzi L, Kepp O, Criollo A, Maiuri MC, Tav-ernarakis N, et al. Autophagy mediates pharmacological lifespan exten-sion by spermidine and resveratrol. Aging 2009;1(12):961-970.94. Chen W, Rezaizadehnajafi L, Wink M. Influence of resveratrol on oxidative stress resistance and life span in Caenorhabditis elegans. J Pharm Pharmacol. 2013;65:682-688. 95. Staats S, Wagner AE, Kowalewski B, Rieck FT, Soukup ST, Kulling SE, et al. Dietary resveratrol does not affect life span, body composition, stress response, and longevity-related gene expression in Drosophila melanogaster. Int J Mol Sci. 2018;19(1):1-15.96. Howitz KT, Bitterman KJ, Cohen HY, Lamming DW, Lavu S, Wood JG, et al. Small molecule activators of sirtuins extend Saccharo-myces cerevisiae lifespan. Nature 2003;425:191-196.97. Crowell JA, Korytko PJ, Morrissey RL, Booth TD, Levine BS. Resveratrol-associated renal toxicity. Toxicol Sci. 2004;82:614–619. 98. Madeo F. Carmona-Gutierrez D, Keep O, Kroemer G. Spermi-dine delays aging in humans. Aging (Albany NY) 2018;10(8):2209–2211.99. Madeo F, Eisenberg T, Pietrocola F, Kroemer G. Spermidine in health and disease. Science 2018;359(6374):1-12.100. Pifferi F, Terrien J, Perret M, Epelbaum J, Blanc S, Picq JL, Dhenain M, Aujard F. Promoting healthspan and lifespan with caloric restriction in primates. Communications Biology 2019;2:1-3.
Review Article
41-50

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com51
Air Pollution: a New Risk Factor for Developing Stroke
Vida Demarin1 , Sandra Morović2, Filip Đerke3
1 International Institute for Brain Health, Zagreb, Croatia2 Aviva Medical Center, Zagreb, Croatia3 Department of Neurology, Clinical Hospital Dubrava, Zagreb, Croatia
abstract:Many years scientist try to explore the connection between air pollution and its influence on human health and after numerous conducted researches they came up with the clear evidence that air pollution has a significant impact on overall health and especially on stroke. In the Global Burden of Disease Study, it has emerged as a significant contributor to the global stroke burden, especially in low- and middle-income countries.Furthermore, these and some other researches have suggested a closer link between air pollution and ischemic stroke, due to huge diversity of the results of numerous other studies, for drawing definitive conclusions, fur-ther research is still needed.Due to the complexity of stroke with its types and subtypes, the results of their reaction to air pollution dif-fer. Some studies have shown the link between cardioembolic stroke and AP, others with SAH but not with intracerebral haemorrhage. There was a suggestion that nitrogen dioxide exposure might be associated with stroke caused by small vessel disease, while other studies are not reporting any association of AP and the risk of ischemic stroke. In some studies, AP was more affecting young adults and in some, it was more pronounced in women. Some studies reported a more clear link between AP and recent stroke in patients with other risk factors like diabetes and previous stroke. Studies have varied by the concentration and types of pollutants studied, which vary geographically, as well as by duration to AP exposure being short- or long-term, and in some studies being present only during warm seasons.Regulations have improved air quality in many countries in Europe and the United States, resulting in greater life expectancy, which highlights the continued importance of further efforts in that direction.
Keywords: Air pollution; Stroke risk factors; Pollutant concentration; Exposure duration.
Sažetak:zagađenje zraka: noVootkriVeni faktor rizika u razVoju možDanog uDara
Već nekoliko godina znanstvenici pokušavaju istražiti povezanost zagađenja zraka i njegovog utjecaja na zdravlje ljudi, a nakon brojnih provedenih istraživanja došli su do jasnih dokaza da zagađenje zraka ima značajan utjecaj na cjelokupno zdravlje, s posebnim naglaskom na ravoj moždanog udara. U “Global Bourden of Disease” (szo)pokazalo se da zagađeni zrak značajno doprinosi globalnom opterećenju od moždanog udara, posebno u zemljama s niskim i srednjim dohotkom.Nadalje, ova i neka druga istraživanja sugeriraju blisku povezanost zagađenja zraka i ishemijskim moždanim udarom, dok zbog raznolikosti rezultata brojnih drugih studija, za donošenje konačnih zaključaka, potrebna su još daljnja istraživanja.Zbog složenosti moždanog udara s njegovim tipovima i podvrstama, rezultati njihove reakcije na onečišćenje zraka razlikuju se. Neke studije pokazuju vezu između kardioemboličkog moždanog udara i zagađenog zraka, druge sa subarahnoidalnim krvarenjem, ali ne i intracerebralnog krvarenjem. Bilo je nagovještaja i da je izlag-anje dušičnom dioksidu povezano s moždanim udarom uzrokovanim bolešću malih žila, dok druge studije ne opisuju tu povezanost sa rizikom od ishemijskog moždanog udara. U nekim je istraživanjima zagađeni zrak više utjecao na mlade odrasle osobe, a u nekim je bio izraženiji i kod žena. Neke studije izvijestile su očitiju vezu između zagađenja zraka i nedavnog moždanog udara u bolesnika s drugim faktorima rizika poput dijabe-tesa i prethodnog moždanog udara.Studije su varirale o koncentraciji i vrstama ispitivanih onečišćujućih tvari, koje se razlikuju geografski, kao i po trajanju kratkoročnog ili dugoročnog izlaganja onečišćenom zraku a u nekim su studijama uzročne pov-ezanosti prisutne samo tijekom toplih doba godine. U mnogim zemljama Europe i SAD-u su na snazi propisi kojima se potiče poboljšanje kvalitete sraka, što je, između ostalog, rezultiralo dužim životnim vijekom, a što ukazuje na trajnu važnost daljnjih napora istaživanju utjecaja onečišćenog zraka na ljudsko zdravlje.
ključne riječi: Zagađenje zraka; Rizični faktori za moždani udar; Koncentracija zagađivača; Duljina izloženosti;
OPEN ACCESS
Correspondence: Vida Demarin MD PhD
[email protected]/0000-0003-4942-259X
This article was submitted to RAD CASA - Medical Sciences
as the review article
Conflict of Interest Statement: The authors declare that the re-
search was conducted in the absence of any commercial or financial rela-
tionships that could be construed as a potential conflict of interest.
Received: 11 October 2019Accepted: 29 October 2019
Published: 17 December 2019
Citation:Demarin V, Morovic S and Derke F. Air Pollution: a New Risk Factor for
Developing Stroke. RAD CASA - Medical Sciences.
540=48-49 (2019):51-57. https://dx.doi.org/10.21857/mzvkptz3n9
Copyright (C) 2019 Demarin, Morovic and Derke. This is an open-access
article distributed under the terms of the Creative Commons Attribution Li-cense (CC BY). The use, distribution
or reproduction in other forums is permitted, provided the original au-thor(s) and the copyright owners(s)
are credited and that the original publication in this journal is cited, in accordance whit accepted adacemic
practice. No use, distribution or reproduction is permitted which does
not comply with these terms.
Review Article
51-57

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com52
introduction
Airborne chemical contamination is a major environmental risk factor worldwide and contributes significantly to many diseases, including neurologic diseases.At the XXIV World Congress of Neurology (WCN) in Dubai this year, a session on the environment and neurology explored the link between environmental contamination and neurologic disorders. En-vironmental pollution is considered the third greatest contributor to disability-adjusted life years (DALYs) due to stroke, as supported by observations of seasonal, diurnal, and geographic variations in stroke incidence. Strokes track very closely with and soon after increases in conjunction with levels of carbon monoxide, sulfur dioxide, nitrogen dioxide, and fine particulate matter (≤2.5 μm).Air pollution causes 7.6% of all deaths making it the the fifth cause of death globally and this figure is expected to increase by 50% by 20501.The impact of air pollution on overall health and especially on stroke has been the matter of investigation for many years. In the Global Burden of Disease Study, it has emerged as a significant contribu-tor to global stroke burden, especially in low- and middle-income countries2.In January 2019, the World Health Organization recognized air pollution as “the greatest environmental risk to health.”3. Microscop-ic pollutants — including airborne particulate matter (PM), ozone, sulphur dioxide, carbon monoxide, nitrogen dioxide, and nitrogen oxide — represent the greatest risk to human health4.Crucially, air pollution differs from other modifiable risk factors for cardiovascular disease because exposure to air pollution, for the large majority of people, is unavoidable. Even though the individual risk estimates for exposure to air pollution are relatively small compared to other cardiovascular risk factors…the overall population attribut-able risk and the subsequent burden are significant4.Air pollution is an expansive term consisting of a complex mixture of thousands of components from a wide range of different sources. The main pollutants currently recognised to pose the risk to health include airborne particulate matter (PM) and gaseous pollutants such as ozone (O3), sulphur dioxide (SO2), carbon monoxide (CO), and nitrogen oxides including nitrogen dioxide (NO2) and nitrogen oxide (NOx)4.Particulate matter causes endothelial dysfunction and induces thrombosis by altering reactive oxygen species, nitric oxide, insulin resistance and lipid levels, as well as transiently increasing blood coagulability and plaque rupture1.A study review by Genc S et al5 found that air pollution affects the central nervous system through a variety of cellular, molecular, and inflammatory pathways that damage brain structures or predis-pose those who are exposed to neurological diseases. Fine PM and nanoparticles trigger the release of soluble inflammatory mediators within the body, which then rapidly enter the circulatory system and have the potential to directly affect the vascular system. A number of studies, published since 2002. were reviewed to assess
the relation between air pollution and stroke with age, geographical location, particulate and gaseous matter type, duration of exposure, previous stroke, and comorbidities. It remains to be defined if air pollution has pathophysiological effects that preferentially predispose individuals to ischemic or hemorrhagic stroke. There is ample evi-dence showing an association between acute and chronic exposure to PM2.5 or gaseous pollutants with stroke. This potentially avoidable scenario and its dramatic consequences are heavily under-recognized by health professionals and the wider public. Preventive measures in people at high vascular risk are warranted1.Even though some research has suggested a link between air pollution and ischemic stroke, drawing definitive conclusions has proven elu-sive and many authors still suggest further research.Study Short-term changes in ambient particulate matter and risk of stroke: a systematic review and a meta-analysis,6 provided a com-prehensive review of all observational human studies (January 1966 to January 2014) on the association between short-term changes in ambient PM levels and cerebrovascular events. They also performed meta-analyses to evaluate the evidence for an association between each PM size fraction (PM2.5, PM10, PM2.5-10) and each outcome (total cerebrovascular disease, ischemic stroke/transient ischemic attack, hemorrhagic stroke) separately for mortality and hospital ad-mission. They used a random-effects model to estimate the summary per cent change in relative risk of the outcome per 10-μg/m3 increase in PM3.It was found that PM2.5 and PM10 are associated with a 1.4% (95% CI 0.9% to 1.9%) and 0.5% (95% CI 0.3% to 0.7%) higher total cerebrovascular disease mortality, respectively, with evidence of inconsistent, nonsignificant associations for hospital admission for total cerebrovascular disease or ischemic or hemorrhagic stroke. Currently, limited evidence does not suggest an association between PM2.5-10 and cerebrovascular mortality or morbidity. The authors discussed the potential sources of variability in results across studies highlighted some observations, and identified gaps in the literature and made recommendations for future studies.Shah et al.7 performed a meta-analysis of the association between air pollution, stroke admissions, and death from stroke. From 2748 articles, 238 were reviewed in-depth with 103 satisfying the inclusion criteria and 94 contributing to our meta-estimates. This provided a total of 6.2 million events across 28 countries. Admission to hospital for stroke or mortality from stroke was associated with an increase in concentrations of carbon monoxide (relative risk 1.015 per 1 ppm, 95% confidence interval 1.004 to 1.026), sulphur dioxide (1.019 per 10 ppb, 1.011 to 1.027), and nitrogen dioxide (1.014 per 10 ppb, 1.009 to 1.019). Increases in PM2.5 and PM10 concentration were also associated with admission and mortality (1.011 per 10 μg/m3 (1.011 to 1.012) and 1.003 per 10 μg/m3 (1.002 to 1.004), respectively). The weakest association was seen with ozone (1.001 per 10 ppb, 1.000 to 1.002). Strongest associations were observed on the day of exposure with more persistent effects observed for PM2·5. It was shown that gaseous and particulate air pollutants have a marked and close temporal association with admissions to hospital for stroke
Review Article
51-57

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com53
or mortality from stroke. Public and environmental health policies to reduce air pollution could reduce the burden of stroke.Although a small proportion of studies originated in low- and mid-dle-income countries, these countries showed the greatest proportion of stroke burden associated with pollution. Since both stable pollu-tion levels and rapid changes (over a period of hours) in pollutant concentrations correlate with vascular events, it is important to consider the date of onset of symptoms (not the date of hospital ad-mission or death) to correctly assess causal exposure to pollution (8).In Air pollution and subtypes, severity and vulnerability of ischemic stroke – A population-based case-crossover study9 authors analyzed stroke cases from the South London Stroke Register to identify patients with first-time strokes in a geographically-defined area. They used the Oxford Clinical and Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria to classify stroke subtype. To classify stroke severity, they used a clinical classification system. Data on air pollution concentrations and exposures came from air pollution monitoring stations linked to postal codes. Researchers also evaluated lags in air pollutant effects ranging from zero to six days.They studied the following pollutants: particulate matter less than 10 microns in diameter (PM10), NO2, ozone (O3), carbon monoxide (CO), and sulfur dioxide (SO2). Overall… there was no the consistent pattern between short term exposure and increased risk of ischemic stroke subtypes or severity. The possible exception was the suggestion that NO2 (nitrogen diox-ide) exposure might be associated with stroke caused by cerebrovas-cular small vessel disease Between 1995-2006, 2590 cases of ischemic stroke occurred (mean age 71.7 years, 49.7% female, 75.6% white), 62.5% had pre-existing hypertension, 59.9% had a past transient ischemic attack, nearly one-fifth had preexisting coronary heart disease, atrial fibrillation, or diabetes. No clear link between ischemic stroke and pollutants, in relation to pre-existing risk factors, including lifestyle, pre-existing medical conditions, and sociodemographic factors.Some positive links between several pollutants at various lag times, but no overall consistent pattern between pollutants and risk of ischemic stroke subtypes or severity with possible exception - the risk of stroke from small vessel disease increased with increasing exposure to NO2: 3-day lag: OR 1.21 (1.00–1.46), 5-day lag: 1.21 (1.01–1.45), 6-day lag: 1.26 (1.05–1.52), average over 6 days: OR 1.51 (1.12–2.02).In the study Fine Particulate Air Pollution (PM2.5) and the Risk of Acute Ischemic Stroke10, the authors analyzed data from 9202 patients hospitalized with acute ischemic stroke, having a docu-mented date and time of stroke onset, and residing within 50 km of a PM2.5 monitor in 8 cities in Ontario, Canada. Results do not support the hypothesis that short-term increases in PM2.5 levels are associated with ischemic stroke risk overall. However, specific patient subgroups may be at increased risk of particulate-related ischemic strokes. In conclusion, data from this perspective, the multicenter study suggest that short-term elevations of ambient fine particulate
matter are associated with increased risk of ischemic stroke onset among patients with diabetes mellitus and those hospitalized with noncardioembolic strokes. The authors suggest that additional research is required to confirm these findings in larger cohorts of patients with detailed information.To assess the relationship between short-term exposure to outdoor ambient air pollutants – fine particulate matter (PM2.5) and black carbon (BC) and ischemic stroke (IS) and its different subtypes, and the potential modifying effect of neighbourhood greenspace and noise, the authors11 analyzed 2742 cases with known onset date and time, living in the study area, from BASICMAR 2005-2014. stroke registry. Overall, no association was found between PM2.5 and BC (black carbon) exposure and acute IS risk. By stroke subtype, a large-artery atherosclerotic stroke could be triggered by daily increas-es in BC, a diesel fuel-related pollutant in the study area.Data from Dijon Stroke Register between March 1994 and Decem-ber 2004.12 with 2078 strokes analyzed pollutant concentrations (SO2, CO, NO2, O3 and PM10), which were measured hourly. The only positive finding was an association between O3 and ischemic stroke at a 1-day lag – only significant in men, over 40 years of age and only for large vessel disease (p=0,02) and for TIA (p=0,01). There were no significant associations for haemorrhagic stroke. They found an increase in association in men with several cardiovascular risk factors (smoker, dyslipidemia and hypertension).All members of the largest health maintenance organization in Israel, who were admitted to a local hospital with stroke between 2005 and 2012.13 were analyzed. A number of 4837 stroke cases were identified 89.4% being ischemic stroke). The interquartile range of PM <10 and <2.5 μm was 36.3 to 54.7 and 16.7 to 23.3 μg/m3, respectively. Higher risk for ischemic stroke associated with PM among young adults was observed. The authors pointed out that this finding can be explained by the inflammatory mechanism, linking air pollution and stroke.To assess who is the most vulnerable to stroke, during the short-term exposure to ambient air pollution the authors analyzed this association during the year14. They observed positive associations between ischemic stroke and air pollution during the ‘warm’ season (April through September).There were no statistically significant associations with any of the other pollutants after adjusting for NO2 concentrations. Associations with ischemic stroke were stronger for those with a history of stroke (OR=2.31; 95% CI: 1.39, 3.83), heart disease (OR=1.99; 95% CI: 1.20, 3.28), and taking medication for diabetes (OR=2.03; 95% CI: 1.14, 3.59). The temperature was inversely associated with ischemic stroke during the ‘warm’ season, but no associations were evident with the other stroke subtypes. Air pollution was not associated with hemorrhagic stroke or transient ischemic attacks. The findings suggest that specific patient characteristics modify associations between air pollution and ischemic stroke.Levels of particulate and gaseous air pollution were measured from 1998 to 2004 at central outdoor monitoring sites in Helsinki. Associations between daily levels of air pollutants and deaths caused
Review Article
51-57

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com54
by stroke among persons aged 65 years or older were evaluated in warm and cold seasons using Poisson regression. Results suggest that especially PM2.5, but also ultrafine particles and carbon monoxide, are associated with increased risk of fatal stroke, but only during the warm season. The effect of the season might be attributable to seasonal differences in exposure or air pollution mixture15. In the cohort study, analyzing stroke and long.term exposure to out-door air pollution from nitrogen dioxide, the authors found the new evidence that long-term exposure to traffic-related air pollution in adult life may be a risk factor for ischemic stroke but not hemorrhag-ic stroke. Fatal ischemic strokes, likely denoting admissions for more severe strokes, were most strongly associated with NO2
16.Data obtained from the Takashima Stroke and AMI Registry, which covers a population of approximately 55,000 in Takashima County in central Japan were analyzed17. There were 2,038 first-ever strokes (1,083 men, 955 women) and 429 first-ever AMI cases (281 men, 148 women) during 1988-2004. The mean pollutant levels were as follows: SPM 26.9 μg/m3; SO2 3.9 ppb; NO2 16.0 ppb, and Ox 28.4 ppb. In single-pollutant and two-pollutant models, SO2 was associated with the risk of a cerebral haemorrhage. Other stroke subtypes and AMI were not associated with air pollutant levels.Association between hemorrhagic stroke occurrence and meteoro-logical factors and pollutants were analyzed18, and findings showed the relationship between hemorrhagic stroke and meteorological parameters and pollutants under similar weather and environmental conditions in a small area. Among meteorological and pollutant variables, only higher particulate matter concentrations correlated independently with intracerebral haemorrhage occurrence, while only ozone was independently associated with subarachnoid haemorrhage occurrence. These findings suggest the possibility that there are pathogenic associations between hemorrhagic stroke and meteorolog-ical factors and pollutants. In another study, the same authors19 studied monthly variations in aneurysmal subarachnoid haemorrhage incidence and mortality and eventual correlation with weather and pollution. There was a trend toward lower SAH occurrence in the summer and higher SAH occurrence in January and during the change of seasons. These trends were significantly associated with the mean monthly temperature and diurnal temperature range. However, no correlation was observed between SAH mortality and meteorological/air pollution parame-ters. These findings suggest that meteorological factors may play an important role in monthly variations in the occurrence of aneurysmal SAH, although aneurysm rupture itself is likely to be multifactorial.A recent study20 analyzed long – term exposure to air pollution and survival after ischemic stroke in China National Stroke Registry Co-hort. This first national hospital-based prospective registry cohort of stroke in China included 12 291 ischemic stroke patients who visited hospitals from 2007 to 2008. All patients were followed for 1-year post-stroke. Deaths during the follow-up period were recorded. Participants’ 3-year pre-stroke exposures to ambient PM1, PM2.5, PM10 (particulate matter with aerodynamic diameters ≤1, ≤2.5, and ≤10 μm, respectively) and NO2 ( nitrogen dioxide) were estimated
by machine learning algorithms with satellite remote sensing, land use information, and meteorological data. Cox proportional hazards models were used to examine the association between air pollu-tion and survival after ischemic stroke. In total, 1649 deaths were identified during the 1-year follow-up period. After controlling for potential confounders, significant associations were observed between exposure to PM1 and PM2.5 and incident fatal ischemic stroke, showing that pre-stroke exposure to PM1 and PM2.5 was associated with increased incident fatal ischemic stroke in the year following an ischemic stroke in China. Improved air quality may be beneficial for people to recover from stroke. In the cohort of post-menopausal women across the US, the authors found little evidence to support the hypothesis that transient eleva-tions in ambient PM2.5, PM10, SO2, or O3 were associated with higher relative risk of total stroke, ischemic stroke, or hemorrhagic stroke. Daily levels of NO2 and NOx were likewise not associated with the relative risk of total stroke or ischemic stroke, although we did find that transient changes in NO2 and NOx were associated with higher risk of hemorrhagic stroke with the strongest association observed with a 3-day moving average prior to stroke hospitalization. Additional studies are still needed to conclusively establish or refute the hypothesis that short-term changes in ambient air pollution levels are associated with a higher risk of stroke21. Recent review describes clinical and epidemiological studies examin-ing the adverse effects of urban air pollution on the central nervous system (CNS). Air pollution and particulate matter (PM) are associ-ated with neuroinflammation and reactive oxygen species (ROS) and these processes affect multiple CNS pathways. Exposures to air pollu-tion impact cognitive function, stroke risk, and carotid artery disease. Pediatric and elderly populations are highly vulnerable due to CNS development and ageing processes. Compiling and contextualizing current evidence should provoke thought and future investigations focused on improving health outcomes22.The acute effect of air pollutants on ischaemic stroke (IS) and IS-related death in five urban districts in Changzhou, China was investigated between 9 January 2015 and 31 December 2016. A total of 32 840 IS cases and 4028 IS deaths were enrolled. The results sug-gested that short-term exposure to ambient NO2 was associated with increased IS risk. In addition, SO2 was associated with increased IS counts and deaths. These findings may have significant public health implications for the prevention of IS and IS-related deaths. The authors recommended further studies to validate their research23.In the study related to short-term exposure to ambient fine particu-late matter (PM2,5 and PM10) and the risk of heart rhythm abnor-malities and stroke, in case of stroke the authors found a stronger correlation between the number of hospitalizations and death cases and exposure to fine dust for ischaemic stroke than for haemorrhagic stroke. In addition, a the significantly more harmful impact of the exposure to ultra particles (particles of aerodynamic diameter below 2,5 μm) has been confirmed. Among important mechanisms respon-
Review Article
51-57

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com55
sible for the observed health impact of particulate matter there are induction and intensification of inflammation, increased oxidative stress increased autonomic nervous system activity, vasoconstriction, rheological changes and endothelial dysfunction. Among people of higher susceptibility to fine dust negative health impact are: elderly (over 65 years old), obese people, patients with respiratory and cardiovascular diseases, patients with diabetes and those with coagulation disorders24.In another study of short-term exposures to ambient air pollution and risk of recurrent ischemic stroke in order to investigate the association between short-term changes in ambient pollution (par-ticulate matter <2.5μm in aerodynamic diameter (PM2.5) and ozone (O3)) and the risk of recurrent ischemic stroke among individuals living in a bi-ethnic community, there were no evidence of associa-tions between previous-day air pollution levels and recurrent isch-emic stroke. The authors pointed out that research on the influence of air pollutants on risk of stroke recurrence is still in its infancy, and more research is necessary for studies that are adequately powered to understand the relation25.In the Japanese study authors analyzed data for 6885 ischemic stroke patients from a multicenter hospital-based stroke registry in Japan who were previously independent and hospitalized within 24 hours of stroke onset. Time of symptom onset was confirmed, and the association between PM (suspended PM and PM2.5) and the occurrence of ischemic stroke was analyzed by time stratified case-crossover analysis.Ambient PM2.5 and suspended PM at lag days 0 to 1 were associat-ed with subsequent the occurrence of ischemic stroke (ambient tem-perature–adjusted odds ratio [95% confidence interval] per 10 μg/m3: suspended PM, 1.02 [1.00–1.05]; PM2.5, 1.03 [1.00–1.06]). In contrast, ambient suspended PM and PM2.5 at lag days 2 to 3 or 4 to 6 showed no significant association with stroke occurrence. The association between PM2.5 at lag days 0 to 1 and ischemic stroke was maintained after adjusting for other air pollutants (nitrogen dioxide, photochemical oxidants or sulfur dioxide) or influenza epidemics and was evident in the cold season. These findings suggest that short-term exposure to PM2.5 within 1 day before onset is associated with the subsequent occurrence of ischemic stroke26.
In another study27 authors reviewed the medical records of 1705 Boston area patients hospitalized with neurologist confirmed ischemic stroke and abstracted data on the timeof symptom onset and clinical characteristics. The PM2.5 concentrations were mea-sured at a central monitoring station. They used the time-stratified case-crossover study design to assess the association between the risk of ischemic stroke onset and PM2.5 levels in the hours and days preceding each event. They examined whether the association with PM2.5 levels differed by presumed ischemic stroke pathophysiologic mechanism and patient characteristics.The increase in risk was greatest within 12 to 14 hours of expo-sure to PM2.5 and was most strongly associated with markers of traffic-related pollution suggesting that exposure to PM2.5 levels
considered generally safe by the US EPA increase the risk of ischemic stroke onset within hours of exposure.As evidence from epidemiological studies has demonstrated that outdoor air pollution is now a well-known major problem of public health, mainly in low and middle income countries, but contrasting with myocardial infarction, there are few data on the association of air pollution and stroke, the authors proposed a narrative literature review of the effects and the underlying biological mechanisms of short- and long-term exposure to air pollutants on stroke risk and mortality, using data from Dijon Stroke Registry with the following key-words: stroke, cerebrovascular events, ischemic and haemorrhage stroke, transient ischaemic attack, mortality, air pollution and air pollutants. Twenty-one papers were selected. Air pollution, of which whose small particulate matter are the most toxic, contributes to about one-third of the global burden of stroke. They could identify vulnerable patients with classical neuro-vascular risk factors or a prior history of stroke or transient ischemic attack or persons living in low-income countries. Biological mechanisms of this new morbid association are discussed. Air pollution should be recognized as a silent killer inducing stroke whose mortality rates remain elevated by its role as a new modifiable neurovascular risk factor, needing public health policies28.As some subpopulations may be particularly vulnerable to PM pol-lution, in this review focus was on one subgroup, long-term stroke survivors, and the emerging evidence suggesting that survivors of a stroke may be at a higher risk from the deleterious effects of PM pol-lution. While the mechanisms for mortality are still under debate, long-term stroke survivors may be vulnerable to similar mechanisms that underlie the well-established association between PM pollution and cardiovascular disease. The fact that long-term stroke survivors of ischemic, but not hemorrhagic, strokes appear to be more vulner-able to the risk of death from higher PM pollution may also bolster the connection to ischemic heart disease. Survivors of an ischemic stroke may be more vulnerable to dying from higher concentrations of PM pollution than the general population. The clinical impli-cations of this association suggest that reduced exposure to PM pollution may result in fewer deaths amongst stroke survivors29.
The World Health Organization (WHO) has estimated that 90% of the world’s population breathes air that exceeds WHO contami-nation limits. The Global Burden of Diseases study 2015 estimated that 898,100 cerebrovascular disease deaths and 19.2 million DALYs were attributable to ambient particulate matter air pollution30. Air pollution accounts for nearly 30% of global stroke burden, with the greatest effects in low- and middle-income countries. In these countries, much of the pollution is within households as a result of incomplete combustion of fuels for cooking and heating.Long-term exposure to airborne contaminants results in accelerated carotid atherosclerosis, damage to vascular endothelium, increased sympathetic nervous system activity, vasoconstriction, increased blood pressure, and thrombosis. Acute exposures affect cerebrovas-cular hemodynamics and vascular resistance, with reduced blood
Review Article
51-57

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com56
flow and atrial arrhythmia. Not only are these exposures important risk factors for neurodegenerative diseases, but they also play a role in neurodevelopmental disorders.Even solid particles in the environment can affect the nervous system. It has been documented that solid plastic nanoparticles work their way up the food chain; they are ingested by algae, which are eaten by daphnia, then spread to fish, disrupting the function of ecosystems all along the way. Eventually these particles end up at the top of the food chain, including humans. They are small enough to cross the blood-brain barrier.
concluding remarKs:Due to huge diversity of results of numerous studies, for drawing definitive conclusions, further research is still needed.Studies have varied by the concentration and types of pollutants studied, which vary geographically, as well as by duration to AP ex-posure, being acute, short or long, and in some studies being present only during the warm season.
Due to the complexity of stroke with its types and subtypes, the results of their reaction to air pollution differ. Who is more suscepti-ble to getting an ischemic stroke, or eventually haemorrhagic? Is the combination with other risk factors important, and especially with which of them? Also, there is a possible publication bias as negative studies are less likely to be published.Nevertheless, regulations have improved air quality in many countries in Europe and the United States, resulting in greater life expectancy, which highlights the continued importance of further efforts in that direction.
author contributions:All authors listed have made a substantial, direct and intellec-tual contribution to the work, and approved it for publication.
literature:1. Estol CJ. Is breathing our polluted air a risk factor for stroke? International Journal of Stroke. 0(0) 1–11. Article reuse guidelines: sagepub.com/journals-permissions DOI: 10.1177/1747493019832999 journals.sagepub.com/home/wso2. Feigin VL, Roth GA, Naghavi M, et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 2016;15:913–24.3.World Health Organization. Ten threats to global health in 2019. https://www.who.int/emergencies/ten-threats-to-global-health-in-2019. 4. Lee KK, Miller MR, Shah ASV. Air pollution and stroke. Stroke. 2018;20(1):2-11.5.Genc S, Zadeoglulari Z, Fuss SH, et al. The adverse effects of air pollution on the nervous system. J Toxicol. 201. Article ID:782462.6. Wang Y, Eliot MN, Wellenius GA. Short-term changes in ambient particulate matter and risk of stroke: a systematic review and me-ta-analysis. J Am Heart Assoc. 2014;3(4). pii: e000983. doi: 10.1161/JAHA.114.000983.7. Shah AS, Lee KK, McAllister DA, et al. Short term exposure to air pollution and stroke: systematic review and meta-analysis. BMJ. 2015;350:h1295.8. Rasche M, Walther M, Schiffner R, et al. Rapid increases in nitrogen oxides are associated with acute myocardial infarction: a case-crossover study. Eur J Prev Cardiol. 2018;25:1707–1716.9. Maheswaran R, Pearson T, Beevers SD, et al. Air pollution and subtypes, severity and vulnerability to ischemic stroke – a population based case-crossover study. PloS One 2016;11:e0158556.10. O’Donnell MJ, Fang J, Mittleman MA, et al. Fine particulate air pollution (PM2.5) and the risk of acute ischemic stroke. Epidemiolo-gy. 2011;22:422–431.11. Vivanco-Hidalgo RM, Avellaneda-Gómez C, Dadvand P, et al. Association of residential air pollution, noise, and greenspace with initial ischemic stroke severity. Environ Res. 2019;179(Pt A):108725. doi: 10.1016/j.envres.2019.108725. [Epub ahead of print]
12. Henrotin JB, Besancenot JP, Bejot Y, et al. Short-term effects of ozone air pollution on ischaemic stroke occurrence: a case-crossover analysis from a 10-year population-based study in Dijon, France. Occup Environ Med 2007;64: 439–445.13. Sade MY, Novack V, Ifergane G, et al. Air pollution and ischemic stroke among young adults. Stroke. 2015;46:3348–3353.14. Villeneuve PJ, Johnson JYM, Pasichnyk D, et al. Shortterm effects of ambient air pollution on stroke: who is most vulnerable? Sci Total Environ. 2012;430:193–201.15. Kettunen J, Lanki T, Tiittanen P, et al. Associations of fine and ultrafine particulate air pollution with stroke mortality in an area of low air pollution levels. Stroke. 2007;38:918–922.16. Andersen ZJ, Kristiansen LC, Andersen KK, et al. Stroke and Long-Term Exposure to Outdoor Air Pollution From Nitrogen Dioxide. A Cohort Study. Stroke. 2012;43(2):320-5. doi: 10.1161/STROKEAHA.111.629246.17. Turin TC, Kita Y, Rumana N, et al. Short-Term Exposure to Air Pollution and Incidence of Stroke and Acute Myocardial Infarction in a Japanese Population. Neuroepidemiology 2012;38:84-92. https://doi.org/10.1159/000335654. 18. Han MH, Yi HJ, Ko Y, et al. Association between hemorrhagic stroke occurrence and meteorological factors and pollutants. BMC Neurol. 2016;16:59. doi: 10.1186/s12883-016-0579-2.19. Han MH, Kim J, Choi KS, et al. Monthly variations in aneurys-mal subarachnoid hemorrhage incidence and mortality: Correlation with weather and pollution. . PLoS ONE 12(10): e0186973. https://doi. org/10.1371/journal.pone.0186973.20. Chen G, Wang A, Li S, et al. Long-Term Exposure to Air Pollution and Survival After Ischemic Stroke. The China National Stroke Reg-istry Cohort. Stroke. 2019;50:563-570. DOI: 10.1161/STROKEA-HA.118.023264.21. Sun S, Stewart JD, Eliot MN, et al. Short-term exposure to air pollution and incidence of stroke in the Women’s Health Initiative. Environment International. 2019;132, ID 105065. https://doi.org/10.1016/j.envint.2019.105065.22. Babadjouni RM, Hodis DM, Radwanski R, et al. Clinical effects of
Review Article
51-57

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com57
air pollution on the central nervous system; a review. J Clin Neurosci. 2017;43:16–24. 23. Dong H, Yu Y, Yao S, et al. Acute effects of air pollution on ischaemic stroke onset and deaths: a time-series study in Chang-zhou, China. BMJ Open. 2018;8:e020425. doi:10.1136/bmjop-en-2017-020425.24. Kowalska M, Kocot K. Short-term exposure to ambient fine particulate matter (PM2,5 and PM10) and the risk of heart rhythm abnormalities and stroke. Postepy Hig Med Dosw (Online). 2016 Sep 28;70(0):1017-1025.25. Wing JJ, Adar S, Sanches B, et al. Short-Term Exposures to Ambi-ent Air Pollution and Risk of Recurrent Ischemic Stroke. Environ Res. 2017;152:304–307. 26. Matuso R, Michikawa T, Ueda K, et al. Short-Term Exposure to Fine Particulate Matter and Risk of Ischemic Stroke. Stroke. 2016;47:3032-3034. doi:10.1161/STROKEAHA.116.015303.27. Wellenius GA, Burger RM, Coull, BA; Schwartz, J; Suh, HH; Koutrakis, P; Schlaug, G; Gold, DR; Murray A. Ambient Air Pollu-tion and the Risk of Acute Ischemic Stroke, Arch Intern Med. 2012;172(3):229-23428. Graber M, Mohr S, Baptiste L, Duloquin G, Blanc-Labarre C, Mariet AS, Giroud M, Béjot Y. Air pollution and stroke. A new mod-
ifiable risk factor is in the air. Rev Neurol (Paris). 2019 May 29. pii: S0035-3787(18)30976-7. doi: 10.1016/j.neurol.2019.03.003. 29. Desikan A. Outdoor air pollution as a possible modifiable risk fac-tor to reduce mortality in post-stroke population. Neural Regen Res. 2017 Mar;12(3):351-353. doi: 10.4103/1673-5374.202917.30. Cohen AJ et al.Estimates and 25-year trends of the Global Burden of Disease attributable to ambient air pollution:ananalysis of data from the Global burden of disease study 2015. The Lancet. 2017,389:1907-1918 doi:10.1016/S0140-6736(17)30505-631. Béjot, Y., Reis, J., Giroud, M., & Feigin, V. (2018). A review of epidemiological research on stroke and dementia and exposure to air pollution. International Journal of Stroke, 13(7), 687–695. https://doi.org/10.1177/174749301877280032. Zhang, R., Liu, G., Jiang, Y., Li, G., Pan, Y., Wang, Y., … Wang, Y. (2018). Acute Effects of Particulate Air Pollution on Ischemic Stroke and Hemorrhagic Stroke Mortality. Frontiers in Neurology, 9. https://doi.org/10.3389/fneur.2018.0082733. Tian, Y., Liu, H., Zhao, Z., Xiang, X., Li, M., Juan, J., … Gao, P. (2018). Association between ambient air pollution and daily hospital admissions for ischemic stroke: A nationwide time-series analysis. PLOS Medicine, 15(10), e1002668. https://doi.org/10.1371/journal.pmed.1002668
Review Article
51-57
RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com58
High-fat Diet Induced Dysbiosis & Amelioration by Astaxanthin
Kyle Haasbroek1, Wakako Takabe1, Masayuki Yagi1, Yoshikazu Yonei1 .
1 Anti-Aging Medical Research Center and Glycation Stress Research Center, Graduate School of Life and Medical Sciences, Doshisha University, Japan
abstract:Astaxanthin is a carotenoid that is present in high quantities in the meat of fish like salmon and the shells of shrimp and crab. It exhibits free radical scavenging antioxidant activity when consumed di-etarily. Astaxanthin is absorbed by the small intestine before exerting its antioxidant effect; however, a portion of dietary intake remains unabsorbed in the digestive tract and reaches the large intes-tines . We hypothesized that astaxanthin may exert its antioxidant action in the large intestine to influence the gut microbiota. In this review we introduce the results of two studies of astaxanthin. Firstly, a clinical trial targeting post-menopausal women screened for high oxidative stress burden. Astaxanthin was administered orally for eight weeks in order to examine its effects and safety, and subjects were surveyed for any changes in subjective symptoms. Secondly, in a mouse model, real time PCR (polymerase chain reaction) was used to examine the ability of astaxanthin to prevent changes in the enteric flora induced by a high-fat diet. When fat intake increases due to changes in diet, the equilibrium between the various species that constitute the intestinal flora is altered. As a result, degenerative changes in lifestyle-related disease and aging of the host are promoted. Here we find that the intake of astaxanthin was able to inhibit these changes in the gut microbiota of mice induced by a high-fat diet. Even in humans, it is highly probably that the unabsorbed astaxanthin that remains in the intestinal tract exerts a positive effect against disturbance of the intestinal flora caused by a high-fat diet.
Keywords: Astaxanthin; Gut microbiota; Antioxidant; High fat diet; Dysbiosis
Sažetak:Disbioza inducirana dijetom bogatom mastima & Amelioracija pomoću astaksantinaAstaksantin je karotenoid prisutan u velikom količinama u mesu riba poput lososa i oklopima kozica i rakova. Kada se uzima kao hrana ispoljava svoju sposobnost hvatanja slobodnih radikala i antioksidativnog djelovanja. Prije no što započne svoje antioksidativno djelovanje apsorbira se preko tankog crijeva, međutim , dio ostaje neapsorbiran i dospijeva u debelo crijevo. Razmatrali smo mogućnost da astaksantin pomoću svojih antioksidativnih svojstava može utjecati na crijevnu mikrobiotu. U okviru ovog preglednog rada osvrnut ćemo se na rezultate dvaju istraživanja. Prvo je kliničko ispitivanje usmjereno na postmenopauzalne žene koje su prošle screening na opterećenost oksidativnim stresom. Astaksantin su dobivale oralno kroz 8 tjedana kako bi se procijenili njegovi učinci i sigurnost, a ispitanice su anketirane vezano za promjene u subjektivnim simptomima. Dru-gi, mišji model, koristio je PCR (Lančanu reakciju polimeraze) u pravom vremenu kako bi ispitao potencijal astaksantina u sprječavanju promjena u crijevnoj flori induciranih dijetom bogatom mas-tima. Pri dijeti bogatoj mastima povećava se unos masti što narušava ravnotežu raznih vrsta koje sačinjavaju intestinalnu floru. Posljedična neravnoteža rezultira degenerativnim promjenama i boles-tima vezanima za način života. U ovom istraživanju nalazimo da unos astaksantina može spriječiti promjena u mikrobioti miševa izazvane prehranom bogatom mastima. Čak i u ljudi je za vjerovati da neapsorbirani astaksantin koji ostaje u debelom crijevu ima pozitivan učinak protiv poremećaja uzrokovanih prehranom bogatom mastima.
ključne riječi: Astaksantin; Crijevna mikrobiota; Antioksidans; Prehrana bogata mastima; Disbioza
OPEN ACCESS
Correspondence: Yoshikazu Yonei [email protected]/0000-0002-2682-752X
This article was submitted to RAD CASA - Medical Sciences as the Original Article
Conflict of Interest Statement: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Received: 17 October 2019Accepted: 24 November 2019Published: 17 December 2019
Citation:Haasbroek K, Takabe W, Yagi M and Yoshikazu Y. High-fat diet induced dysbiosis & amelioration by astaxan-thin RAD CASA - Medical Sciences. 540=48-49 (2019): 58-66. https://dx.doi.org/10.21857/9xn31crexy
Copyright (C) 2019 Haasbroek, Takabe, Yagi and Yoshikazu. Fran-ceschi, Buljan and Situm.This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owners(s) are credited and that the original publication in this journal is cited, in accordance whit accepted ad-acemic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
Original Article
58-66
RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com59
introduction
Astaxanthin is a carotenoid that is present in high quantities in the meat of fish like salmon and the shells of shrimp and crab1. It has attracted much attention in the field of preventative medicine for its effects against various lifestyle-related illnesses, its anti-fatigue action, and general health improving properties2. Astaxanthin is also garner-ing attention as an ingredient in supplements, for which it is natural-ly produced by the microalgae Haematococcus pluvialis. Astaxanthin exhibits free radical scavenging antioxidant activity when consumed dietarily3,4. Previously we performed an open-label non-controlled study examining the safety and efficacy of eight-week oral astaxan-thin intake in post-menopausal women with high oxidative stress burden, demonstrating increased antioxidant capacity, lower blood pressure, and improvement of constipation and menopause symp-toms5. Astaxanthin is absorbed by the small intestine before exerting its antioxidant effect; however, a portion of dietary intake remains unabsorbed in the digestive tract and reaches the large intestines6-8. We hypothesized that astaxanthin may exert its antioxidant action in the large intestine to influence the gut microbiota (enteric flora), and are continuing research into the phenomenon.The enteric flora changes with age and lifestyle/environment9,10, and is associated with overall health and the incidence of carcinogenesis. Every individual’s intestinal tract is inhabited by a characteristic ecosystem of bacteria that collectively forms the gut microbiome. Normally there is equilibrium between the gut microbiota and host, as well as between bacterial species. When this balance is disrupted, dysbiosis11 and opportunistic infections occur, greatly influencing aging12, nutrition13, the efficacy of medication14,15, physiological func-tion16, immune function17, and carcinogenesis18-20 of the host.In this review we introduce the results of two studies of astaxanthin. Firstly, a clinical trial5 targeting post-menopausal women screened for high oxidative stress burden. Astaxanthin was administered orally for eight weeks in order to examine its effects and safety, and subjects were surveyed for any changes in subjective symptoms. Secondly, in a mouse model, real time PCR (polymerase chain reaction)21-23 was used to examine the ability of astaxanthin to prevent changes in the enteric flora induced by a high-fat diet24.
clinical study methods
In this study, participants were screened in order to select those with high oxidative stress. The screening test measured diacron-reactive oxygen metabolites (d-ROM) as an indicator of the intensity of oxi-dative stress burden. From an initial group of 35 healthy post-meno-pausal women (d-ROM = 362.3 ± 51.4 CARR U), 14 with low d-ROM scores were excluded, and the remaining group of 21 partic-ipants (d-ROM = 387.4 ± 32.4 CARR U) with high oxidative stress burden comprised the participants of this study. Participants took two 6 mg astaxanthin soft capsules ([AstaReal ACT] Fuji Chemical Industry Co.) per day for 8 weeks.For the evaluation, symptoms were divided into “physical symptoms” and “psychological symptoms” in the Anti-Aging QOL Common Questionnaire 25). Participants were asked to rank their severity on a
scale of one to five. Of the 34 surveyed physical symptoms, eight symptoms significantly improved after 8 weeks of taking the supplement: “eye fatigue,” “stiff shoulders,” “weight gain,” “skin problems,” “constipation,” “hair loss,” “grey hair,” and “cold sensitivity” (Table 1). Of 21 psychological symptoms, “difficulty falling asleep” improved significantly after 8 weeks. There was no significant change in the lifestyle habits of the participants. Improving “constipation” is one of the known benefits of astaxanthin, and is commonly reported in post marketing surveillance. Astaxan-thin also relieves loose stool and diarrhea associated with abnormal intestinal fermentation. Its bioavailability is low at 2~5%, with the greater majority remaining and acting within the digestive tract. Astaxanthin may be exerting antioxidant action, clearing free radicals derived from bacterial toxins produced by non-beneficial species, im-proving the intestinal environment and increasing motility as a result.
exPerimental animal study methods
The experimental method is as follows24. 20 4-week-old ICR mice were raised in individual cages for one week and acclimatized. After acclimatization, the mice were weighed and sorted into the following 4 groups consisting of 5 mice each: ordinary diet (Group C), ordi-nary diet + astaxanthin (Group CA), high-fat diet (Group H), high fat diet + astaxanthin (Group HA).Labo MR Stock (Nosan Corporation) was used for the ordinary diet, and HFD-60 Oriental Yeast Co.) for the high-fat diet. Both types of feed were prepared with added astaxanthin (Fuji Chemical Industry Co., Ltd.) to achieve a final concentration of 0.02%. The nutri-tional contents of the ordinary diet consisted of 3.9% fat, 18.8% protein, 54.7% carbohydrates, and 6.6% dietary fiber; the high fat diet contained 35% fat, 23% protein, 25.3% carbohydrates, and 6.6% dietary fiber. Feces were collected over 24 hours on the final acclimatization day, hereafter designated Day 0. The collected feces were stored at −20 °C.Fecal bacteria were tested using real-time PCR as follows. Feces collected on Days 0, 14, and 28 were thawed and weighed before drying overnight at room temperature. The following day, dry mass was weighed and samples were powderized. Approximately 100 mg of each powdered sample was weighed into a microtest tube, and DNA was extracted using the QIAamp® DNA Stool Mini Kit (Qiagen). DNA solutions were prepared and DNA concentration was measured using NanoDrop. DNA solutions for total bacteria, Lactobacillus, Streptococcus, Clostridium coccoides group, and Clostridium leptum were diluted 100 times; other targets were adjusted to a final concentration of 20 μg/μL. Primer sequences were determined in accordance with the protocol for the LightCycler® 480 SYBR Green I Master (Roche Di-agnostics), and real-time PCR analysis was performed following the
Baseline Week 8(Physical Symptoms)
Eye Fatigue 3.1±0.8 2.4±0.8 **Stiff Shoulders 3.4±1.0 2.9±1.1 **Weight Gain 2.9±1.4 2.5±1.4 *
Skin Problems 2.5±0.8 2.1±0.8 **Constipation 2.4±1.2 2.0±1.0 *
Hair Loss 2.3±0.9 1.9±0.8 *Gray Hair 3.6±0.9 3.1±0.9 *
Cold Sensitivity 2.8±1.0 2.3±1.1 **(Psychological Symptoms)
Difficulty Falling Asleep 2.1±0.89 1.8±0.8 *Symptom Score: 1 not at all, 2 a little, 3 moderately, 4 quite a lot, 5 very much.* p < 0.05, ** p < 0.01 vs. baseline score, paired t-test. Cited from reference 5).
Table 1. Symptom Scores from Anti-Aging QOL Common Questionnaire
Original Article
58-66

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com60
methods of Matsuki et al. or Endo et al.21-23 Bacteroides, Bifidobacte-rium, Prevotella, Lactobacillus, Clostridium Coccoides, and Clostrid-ium leptum were targeted for analysis alongside two phyla, Firmicutes and Bacteroidetes, as well as total bacteria. The copy numbers of the targets were standardized as a percentage of total bacterial copies.
results of the exPerimental study
Change in body weight, feces color and quantityMice administered the high-fat diet demonstrated a significant increase in weight (p < 0.05) compared to ordinary diet groups (comparing H to C, HA to CA). No significant difference in weight was detected in the astaxanthin fed groups. The color of feces changed to a grayish white in the high-fat diet group mice, and became a wine red after the addition of astaxanthin. The amount of feces collected from the high-fat diet groups on Day 28 was significantly reduced (p < 0.001).
Fecal DNA ContentThe amounts of DNA recovered from feces as measured by Nano-Drop (mean of Day 0, 14, 28) were: Group C: 89.8 ± 21.5 ng/μL; Group CA: 102.7 ± 28.5 ng/μL; Group H: 70.2 ± 21.2 ng/μL; Group HA: 66.9 ± 28.4 ng/μL. When compared to the ordinary diet groups (Group C and Group CA), the high-fat diet groups (Group H and Group HA) tended to have less DNA content (p = 0.001).
Genus Streptococcus (lactic acid bacteria)Streptococcus comprised less than 16% of the total bacterial count (Figure 1). The number of bacteria increased substantially in the ordi-nary diet, but the change was minor in the high-fat diet (p = 0.028). Compared to the ordinary diet, the increase in bacteria in the high-fat diet group was extremely small (p = 0.008). With the addition of astaxanthin, the bacterial count of Group HA returned to the same level as the ordinary diet groups (Groups C and CA) on Day 28. The difference with and without astaxanthin in the high-fat diet groups was significant (p = 0.044).The genus Streptococcus is comprised of a variety of gram-positive and generally facultative anaerobic bacteria which belongs to the order Lactobacillales (lactic acid bacteria). While Streptococcus pneumoniae is a well-known pathogenic species (the leading cause of pneumonia), many other species are members of the salivary and gut microbiomes. At the genus level, depletion of Streptococcus has been observed in obese teenagers with high fructose intake26 and in children with celiac disease27. Conversely, Streptococcus is reported to increase in abundance in the guts of infants with a genetic predisposition for type 1 diabetes28 as well as in colorectal cancer patients29. The seemingly contradictory implications of these different shifts in abundance may be due to the specific species which are falling out of balance in each situation. On the species level, several bacteria are noted in the literature as potential probiotics. Streptococcus salivarius is an inhabitant of both the oral cavity and the gut: it has been demonstrated to possess anti-inflammatory and immuno-regulatory effects30,31. Streptococcus
thermophilus, another probiotic species, may help to reduce uremic toxins caused by dysbiosis in the colon of patients with chronic kidney diseases32. As part of a probiotic cocktail together with other lactic acid bacteria (IRT5), S. thermophilus has shown efficacity in modulating auto-immunity33-35. By increasing the abundance of Streptococcus species, astaxanthin may contribute to maintaining the microbiome’s homeostasis by promoting the proliferation of these beneficial bacteria.
Genus Lactobacillus (lactic acid bacteria)Lactobacillus comprised less than 3% of total bacterial copy numbers (Figure 2). Bacterial count was increased significantly in the high-fat diet group (p = 0.004). The ordinary meal groups (groups C and CA) also showed a trend of increasing bacterial count on days 14 and 28. There was no significant difference in the rate of bacterial count increase between the ordinary and high fat diets (p = 0.069). The rate of increase of bacterial count was shown to significantly increase with the addition of astaxanthin (p = 0.031).The genus Lactobacillus is widely known as a prominent member of the lactic acid bacteria and a common source of probiotics. As such, a large amount of research has focused on the beneficial effects of Lactobacillus species on gut health. In the early days of research into the human microbiomes, Lactobacillus was easily cultured from feces and mistakenly thought to constitute a majority of the gut microbi-ome36. With the advent of genomic techniques to detect the countless species that are not easily cultivated in the lab (many of which are anaerobic), it was realized that Lactobacillus species are in actuality a small minority of the total biological diversity of the human gut, and many species are only transitory inhabitants that do not maintain a permanent presence in the intestinal tract. Despite this, the health effects of various Lactobacillus species have been heavily studied and numerous benefits have been reported. Lactobacillus sakei has demonstrated efficacy in ameliorating obesity
0,02,04,06,08,0
10,012,014,016,0
Day 0 Day 14 Day 28
Genus Streptococcus
C
CA
H
HA
Figure 1. Putative copy numbers of the genus StreptococcusResults shown as percent of total bacterial copy number, mean ± standard devia-tion. C: ordinary diet group, CA: ordinary diet + astaxanthin group, H: high-fat diet group, HA: high-fat diet + astaxanthin group, (n = 5 each). The addition of astaxanthin increased bacterial count in the high-fat diet group (indicated by arrows, p < 0.05). Groups compared using Tukey’s multiple comparison test. Cited from reference 24).
Original Article
58-66

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com61
caused by a high-fat diet in mouse models37,38. Mice fed L. sakei as a probiotic show reduced weight gain and lower serum levels of choles-terol, triglycerides, and leptin. Serum and fecal levels of short chain fatty acids are also increased after ingestion of L. sakei, counteracting the reduction seen in high-fat diets.Lactobacillus plantarum has also been studied in mice fed high-fat diets39. When fed the probiotic, mice consuming a high-fat diet again experienced reduced weight gain and lower plasma levels of leptin, cholesterol, and triglycerides. It is also able to mitigate liver damage and weakened intestinal permeability of the intestines caused by obesity. Additionally, L. plantarum has been reported to increase the diversity of the enteric flora39,40, reduce the severity of colitis41,42, and it has also demonstrated anti-tumor effects43. Lactobacillus rhamnosus has been shown to decrease the amount of colon aberrant crypt foci and reduce pro-carcinogenic biomarkers in a rat model44, lower cholesterol45, and improve insulin resistance and obesity induced by high-fat diet46.Lactobacillus casei has demonstrated immunoregulatory activity, reducing colorectal cancer46 and breast tumors48 in mice models.Finally, Lactobacillus acidophilus has many reported beneficial effects. It has been found to improve gut dysbiosis, intestinal barrier function, and liver pathology in non-alcoholic fatty liver disease49. Like several of the previous species, it reduces high-fat diet induced obesity and improves insulin resistance46. It also demonstrates an anti-inflammatory effect, protecting mice from induced colitis50,51. In humans, L. acidophilus has been observed to be significantly reduced in the feces of type 2 diabetics52.
Clostridium coccoides GroupThe Clostridium coccoides group contributed less than 1.4% of the total bacterial count (Figure 3). Bacterial count significantly increased from the high-fat diet (p = 0.016). The increase was greater in the high-fat diet than the ordinary diet (p = 0.012). The addition of astaxanthin was revealed to significantly lower the increase of bacteria
in the high-fat diet (p = 0.029).Clostridium is a major genus of anaerobic endo-spore forming bacteria53. Several species in the genus are known pathogens, such as Clostridium botulinum (the causative pathogen of botulism), Clostridium tetani (tetanus) and former member Clostridium difficile (now Clostridioides difficile). Conversely, the Clostridium coccoides group also contains many bacteria that inhabit the human gut and play a considerable role in the intestinal ecosystem by fermenting dietary plant polysaccharides. As a group, Clostridium has been reported to shift with age, becom-ing less abundant in the elderly53. This diminishing of Clostridium is associated with complications of aging such as frailty, hospitalization, and antibiotic treatment. However, Clostridium is also found to be elevated in the gut of children with type-1 diabetes, and its abun-dance is positively correlated with plasma glucose levels54. Clostrid-ium coccoides group is also significantly increased in the stool of obese individuals with metabolic syndrome and its abundance is correlated with higher serum levels of triglycerides55. Much like the genus Streptococcus, the effects of these shifts in abundance may differ depending on the specific species involved. At the species level, Clostridium asparagiforme, Clostridium scin-dens, and Clostridium hylemonae are reported at high frequency in the elderly53. C. scindens and C. hylemonae exhibit bile-acid 7-dehydroxylating activity, producing secondary bile acids which are associated with the risk of developing gallstones and colon cancer.The Clostridium coccoides group also includes other anaerobic endo-spore forming bacteria of the human microbiome that are not necessarily taxonomically related to the genus Clostridium. Some Eubacterium species are also lumped into this group. These are com-monly probiotic bacteria that are known for producing short-chain fatty acids such as butyrate, which exhibit anti-inflammatory and immuno-regulatory activity. Generally, Eubacterium abundance fol-lows the opposite trend of the previously named Clostridium species,
Figure 2. Putative copy numbers of the genus LactobacillusResults shown as percent of total bacterial copy number, mean ± standard devia-tion. C: ordinary diet group, CA: ordinary diet + astaxanthin group, H: high-fat diet group, HA: high-fat diet + astaxanthin group, (n = 5 each). Addition of astaxanthin raised bacterial count (indicated by arrows, p < 0.05). Groups com-pared using Tukey’s multiple comparison test. Cited from reference 24).
Figure 3. Putative copy numbers of the Clostridium coccoides groupResults shown as percent of total bacterial copy number, mean ± standard devia-tion. C: ordinary diet group, CA: ordinary diet + astaxanthin group, H: high-fat diet group, HA: high-fat diet + astaxanthin group, (n = 5 each). High-fat diet increased the rate of growth of bacterial count, (indicated by dotted lines), and addition of astaxanthin reduced it (indicated by arrows, p < 0.05). Groups com-pared using Tukey’s multiple comparison test, rate of change by diet compared using Mann-Whitney’s U test. Cited from reference 24).
Original Article
58-66

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com62
being reduced in abundance in the elderly53. Depending on which species are involved, the results of changes in Clostridium abundance could be either beneficial or harmful. In the present study, Clostridium was found to increase during the high-fat diet, and was reduced toward normal levels by treatment with astaxan-thin. Thus, the specific species affected may be those associated with dysbiosis caused by high fat intake, and not necessarily the beneficial varieties.
Genus BifidobacteriumBifidobacterium made up an extremely small amount of the total bacterial at less than 0.000006% (Figure 4). There was no significant difference between groups or before and after astaxanthin treatment. Since the standard deviation among individuals was so large, this result is only included for reference purposes.Bifidobacterium is a genus of gram-positive anaerobic bacteria that is the first major colonizer of the human gastrointestinal tract and plays a significant role in maintaining intestinal health by preventing constipation, diarrhea, and colorectal cancer56. An abundance of the genus is closely correlated with the aging process57. Bifidobacterium colonizes newborns from birth and makes up a majority of infant microbiomes during their breast-feeding years, with species such as Bifidobacterium longum, B. breve, and B. bifidum being the most abundant. Their abundance falls to lower levels by adulthood (2-14% of total bacteria), and is significantly reduced in the elderly. Low levels of Bifidobacterium are associated with obesity and diabetes (types 1 and 2)54,57.Bifidobacterium species have demonstrated numerous positive health effects and see common use as probiotics. B. longum and B. breve have both shown anti-obesity effects in a high-fat diet mouse model 58): oral intake of both species resulted in a reduction in weight gain, reduced triglyceride accumulation in the liver, and increased cecal abundance of lactic acid bacteria; B. longum intake additionally reduced serum triglycerides. Similar effects are seen in B. bifidum59 as well as various other strains60. B. animalis subsp. lactis (AKA B. lactis), in addition to reducing weight gain, glycemic response, and fasting insulin levels in a high-fat diet mouse model, is also reported to reduce inflammation by down-regulating tumor-necrosis factor expression in adipose and hepatic tissues61. B. lactis also mediates the effects of metabolic syndrome by improving glucose sensitivity, modulating the enteric flora, and producing a high amount of the short chain fatty-acid acetate62.Bifidobacterium may also impact anxiety and stress (via the gut-brain axis). In a mouse model of chronic stress, mice that were resistant to social stress from exposure to aggression had a higher abundance of Bifidobacterium, and intake of a probiotic containing B. longum and B. infantis increased resilience to stress and mitigated its symptoms63. B. bifidum has also been reported to reduce signs of stress in a ma-ternal separation mouse model: mice ingesting the probiotic showed significantly reduced susceptibility to stress, with lower serum corti-costerone and improved intestinal permeability64.The lack of any observed change from astaxanthin intake in contrast
to the other genera examined may simply be due to the very low initial abundance, or perhaps indicate that a difference in metabolic pathways of Bifidobacterium prevents the positive effect of the carot-enoid on its physiology.
Other bacteria: Bacteroides, Prevotella, Clostridium leptumOf the total bacterial, Bacteroides comprised less than 0.003%, a very small amount. The count was significantly increased by the high fat diet (p = 0.006). Addition of astaxanthin resulted in no significant difference.Prevotella copies were also few, at 0.06%. The high fat diet markedly reduced bacterial count (p < 0.001). There was no significant change with the addition of astaxanthin.Clostridium leptum copies comprised less than 1.6% of the total bacteria. It was significantly increased by the high fat diet (p = 0.017). There was no significant difference with astaxanthin.
Phylum level analysisThe results of phylum level analysis are represented as the ratios of Firmicutes, Bacteroidetes, and other copy numbers, as shown in Figure 5.Firmicutes accounted for 20% of total copies on Day 0, but increased to 40% on both Day 14 and Day 28 in the high-fat diet group (p < 0.001, Figure 6). There was no difference with the addi-tion of astaxanthin. Bacteroidetes made up 45~50% of total copies on Day 0, but fell to 20% on both Day 14 and Day 28 (p < 0.001 (Figure 7). There was no difference with the addition of astaxanthin.
changes in enteric flora due to ingestion of high-fat diet
Consumption of a high-fat diet increases the secretion of bile acids65, and causes various changes to the intestinal microbiota66. These changes are more pronounced in the large intestine than the small in-testine67. High-fat diets weaken intestinal immunity, disrupt mucosal barrier function, and cause abnormal fermentation to occur in the intestines68. As a result, carcinogenesis is also increased69.
0,000000
0,000001
0,000002
0,000003
0,000004
0,000005
0,000006
Day 0 Day 14 Day 28
Bifidobacterium
C
CA
HHA
(%)
Figure 4. Putative copy numbers of the genus BifidobacteriumResults shown as percent of total bacterial copy number, mean ± standard devia-tion. C: ordinary diet group, CA: ordinary diet + astaxanthin group, H: high-fat diet group, HA: high-fat diet + astaxanthin group, (n = 5 each). Cited from reference 24).
Original Article
58-66

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com63
Results pertaining to changes in gut microbiota caused by a high-fat diet have been reported in both animal and human studies. In a mouse model of type 2 diabetes (KK-Ay) Bacteroides is reduced and Clostridium coccoides tends to increase in the cecum70. In a mouse model of high-fat diet induced obesity, Bifidobacterium abundance in the cecum and feces was decreased71. In rats, Bacteroides and Prevotella were increased72. In humans, it has been reported that obese subjects likely consuming a high-fat diet carry a reduced amount of Bacteroides73. At the phylum level, Firmicutes have been
found to increase while Bacteroidetes decrease73-75.In this study, the results of the phylum level analysis generally agreed with those previously reported73-75. Due to the high-fat diet (Group H), Bacteroides, Clostridium coccoides, and Clostridium leptum amounts increased, while Streptococcus (lactic acid bacteria) decreased. The difference in the change of Bacteroides may be due to differences between host animal (rat vs. mouse), or perhaps dif-ferences in testing methodology. However, Bacteroides species have previously been considered non-beneficial bacteria, so the results of the present study seem reliable.
effects of astaxanthin on enteric flora
The following results regarding the effectiveness of astaxanthin were obtained from the animal study. First, astaxanthin can be expected to
inhibit the short-term increase of Bacteroides (gram negative bacteria) caused by high-fat diet. Interestingly, the addition of astaxanthin increased the amount of Lactobacillus (lactic acid bacteria). Similarly, Streptococcus (lactic acid bacteria) was also increased by astaxan-thin in the high fat diet. These results suggest that administering astaxanthin may improve enteric flora (inhibiting the overgrowth of gram-negative bacteria, increasing lactic acid bacteria).For this experiment, astaxanthin was not administered via tube feed-ing, but instead a fixed amount (0.02% astaxanthin) was mixed into
the mice’s feed. While tube feeding would have allowed for more con-sistency in dosage, the resulting damage to the upper gastrointestinal tract and increased stress on the mice would likely affect the intestinal microbiota. Individual differences were also increased: with mixed feed the dosage of astaxanthin depends on feed intake and is not a fixed quantity, however there is little stress on the mice.Astaxanthin intake was estimated from the feed intake of the mice (mean body weight at 8 weeks: Group C 38~41 g, Group H 44~48 g). The feed intake of Group C mice was about 3 g/day, consisting of 0.2 g/day of fat, 0.9 g/day of protein, and 1.0 mg/day of astaxan-thin per mouse. The group H mice received about 5 g/day of feed consisting of 1.1 g/day of fat, 0.7 g/day of protein, and 0.6 mg/day of astaxanthin. The equivalent intake of astaxanthin for a human (average body weight 60 kg) would be 1,500 mg/day for group CA
0%10%
20%
30%
40%
50%
60%
70%
80%90%
100%
C CA H HA C CA H HA C CA H HA
Day0 Day14 Day28
Others
Bacteroidetes
Firmicutes
Bacteroidetes
Firmicutes
Others
Figure 5. Phylum Level AnalysisRatios of bacterial abundance of the phyla Bacte-roidetes, Firmicutes, and others, relative to total primer measurement for all bacteria. C: ordinary diet group, CA: ordinary diet + astaxanthin group, H: high-fat diet group, HA: high-fat diet + astaxanthin group, (n = 5 each). Cited from reference 24).
0,0
10,0
20,0
30,0
40,0
50,0
60,0
Day 0 Day 14 Day 28
Firmicutes
C
CA
H
HA
*** p < 0.001# p < 0.001
#
*** *** ** **
Figure 6. Putative copy number of the phylum FirmicutesResults shown as percent of total bacterial copy number, mean ± standard devia-tion. C: ordinary diet group, CA: ordinary diet + astaxanthin group, H: high-fat diet group, HA: high-fat diet + astaxanthin group, (n = 5 each). Groups compared using Tukey’s multiple comparison test (*** vs. Day 0), rate of change by diet com-pared using Mann-Whitney’s U test (#, dotted lines). Cited from reference 24).
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
Day 0 Day 14 Day 28
Bacteroidetes
C
CA
H
HA
#
*** p < 0.001# p < 0.01
*****
******
(%)
Figure 7. Putative copy numbers of the phylum BacteroidetesResults shown as percent of total bacterial copy number, mean ± standard devia-tion. C: ordinary diet group, CA: ordinary diet + astaxanthin group, H: high-fat diet group, HA: high-fat diet + astaxanthin group, (n = 5 each). Groups compared using Tukey’s multiple comparison test (*** vs. Day 0), rate of change by diet com-pared using Mann-Whitney’s U test (#, dotted lines). Cited from reference 24).
Original Article
58-66

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com64
and 800 mg/day for group HA, significantly higher than the typical supplement amounts of 6-24 mg/day. Thus, from this experiment it is not clear whether such an amount is suitable for human intake.Approximately 95% of the astaxanthin remains in the intestinal tract unabsorbed. Less than 5% is absorbed and enters systemic circula-tion, only some of which reaches the digestive tract again. Therefore, the majority of the astaxanthin likely acts directly on the intestinal microbiota. Any action by the astaxanthin on the intestinal tract or intestinal immunity has not yet been reported.
conclusion
The various bacterial cells that live in the human gut and form the intestinal microbiome number in the range of 600 trillion, 10 times the number of native cells that make up the human body itself. The makeup of the enteric flora shifts not only with age, but also due to diet, exercise, alcohol intake, smoking, and other lifestyle/environ-mental factors. These changes play a role in health, contributing to things such as obesity, skin conditions, atopy, allergies, and carcino-genesis. In order to maintain a youthful and healthy body, it is crucial to protect the health and stability of the enteric flora. Modern diets have led to an increase in the consumption of fats in recent years, and the resulting changes to the intestinal microbiota have been report-ed70,71,76,77. Mitigating these changes is of great importance.The mechanism by which astaxanthin prevented changes to the bacterial flora from a high-fat diet could not be determined within the scope of the presented studies. However, the following potential mechanisms are proposed: 1. It is possible that the antioxidant action of astaxanthin exerted a
beneficial effect on the enteric flora. The change in bacterial com-position induced by the high-fat diet, particularly the growth of gram-negative bacteria, created higher levels of oxidative stress. As astaxanthin intake improved the enteric flora, the increased oxidative stress may have been mitigated. This needs to be confirmed. 2. Astaxanthin may be degraded by bacteria, producing low molecular weight substances which may then be responsible for the beneficial changes to the enteric flora in high-fat diets. It is necessary to examine the metabolic pathways of astaxanthin in the intestinal tract. 3. Astaxanthin or its metabolites may have an effect on intestinal immunity. Markers related to intestinal immunity (e.g. IgA, defensin) need to be examined.The intestinal tract of every individual is inhabited by an assortment of characteristic bacteria, which collectively form the enteric microbi-ome. When fat intake increases due to changes in diet, the equilib-rium between the various species that constitute the intestinal flora is altered. As a result, degenerative changes in lifestyle-related disease and aging of the host are promoted. Here we find that the intake of astaxanthin was able to inhibit these changes in the gut microbiota of mice induced by a high-fat diet. Even in humans, it is highly probably that the unabsorbed astaxanthin that remains in the intestinal tract exerts a positive effect against disturbance of the intestinal flora caused by a high-fat diet.
author contributions:All authors listed have made a substantial, direct and intellectu-al contribution to the work, and approved it for publication.
literature:1. Ambati RR, Phang SM, Ravi S, et al. Astaxanthin: Sources, extraction, stability, biological activities and its commercial appli-cations: A review. Mar Drugs. 2014;12(1):128-152. doi: 10.3390/md12010128.2. Yuan JP, Peng J, Yin K, et al. Potential health-promoting effects of astaxanthin: A high-value carotenoid mostly from microalgae. Mol Nutr Food Res. 2011;55(1):150-165. doi: 10.1002/mnfr.201000414.3. Wolf AM, Asoh S, Hiranuma H, et al. Astaxanthin protects mitochondrial redox state and functional integrity against oxidative stress. J Nutr Biochem. 2010;21(5):381-389. doi: 10.1016/j.jnut-bio.2009.01.011.4. Naguib YM. Antioxidant activities of astaxanthin and related carot-enoids. J Agric Food Chem. 2000;48(4):1150-1154.5. Iwabayashi M, Fujioka N, Nomoto K, et al. Efficacy and safety of eight-week treatment with astaxanthin in individuals screened for increased oxidative stress burden. Anti-Aging Med. 2009;6(4):15-21. doi: 10.3793/jaam.6.15. 6. Odeberg JM, Lignell Å, Pettersson A, et al. Oral bioavailability of the antioxidant astaxanthin in humans is enhanced by incorporation of lipid based formulations. Eur J Pharm Sci. 2003;19:299-304. doi: 10.1016/S0928-0987(03)00135-0.7. Okada Y, Ishikura M, Maoka T. Bioavailability of astaxanthin in
Haematococcus algal extract: The effects of timing of diet and smoking habits. Biosci Biotechnol Biochem. 2009;73(9):1928-1932.8. Meor Mohd Affandi MMR, Julianto T, Majeed ABA. Enhanced oral bioavailability of astaxanthin with droplet size reduction. Food Sci. Technol. Res. 2012;18(4):549-554.9. Nagpal R, Mainali R, Ahmadi S, et al. Gut microbiome and aging: Physiological and mechanistic insights. Nutr Healthy Aging. 2018;4(4):267-285. doi: 10.3233/NHA-170030.10. Odamaki T, Kato K, Sugahara H, et al. Age-related changes in gut microbiota composition from newborn to centenarian: A cross-section-al study. BMC Microbiology. 2016;16(90).11. DeGruttola AK, Low D, Mizoguchi A, et al. Current un-derstanding of dysbiosis in disease in human and animal mod-els. Inflamm Bowel Dis. 2016;22(5):1137-1150. doi:10.1097/MIB.0000000000000750.12. Bodogai M, O’Connell J, Kim K, et al. Commensal bacteria contribute to insulin resistance in aging by activating innate B1a cells. Sci Transl Med. 2018;10(467):eaat4271. doi:10.1126/scitranslmed.aat4271.13. Gentile CL, Weir TL. The gut microbiota at the intersection of diet and human health. Science. 2018;362(6416):776-780. doi: 10.1126/science.aau5812.14. Wilson ID, Nicholson JK. Gut microbiome interactions with drug
Original Article
58-66

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com65
metabolism, efficacy, and toxicity. Transl Res. 2017;179:204-222. doi: 10.1016/j.trsl.2016.08.002.15. Zimmermann M, Zimmermann-Kogadeeva M, Wegmann R, et al. Mapping human microbiome drug metabolism by gut bacteria and their genes. Nature. 2019;570(7762):462-467. doi: 10.1038/s41586-019-1291-3.16. Gérard C, Vidal H. Impact of gut microbiota on host glycemic control. Front Endocrinol (Lausanne). 2019;10:29. doi: 10.3389/fendo.2019.00029.17. Lazar V, Ditu LM, Pircalabioru GG, et al. Aspects of gut microbi-ota and immune system interactions in infectious diseases, immuno-pathology, and cancer. Front Immunol. 2018;9:1830. doi: 10.3389/fimmu.2018.01830.18. Alexander JL, Scott AJ, Pouncey AL, et al. Colorectal carcinogen-esis: An archetype of gut microbiota-host interaction. Ecancermedi-calscience. 2018;12:865. doi: 10.3332/ecancer.2018.865.19. Rea D, Coppola G, Palma G, et al. Microbiota effects on cancer: From risks to therapies. Oncotarget. 2018;9(25):17915–17927. doi: 10.18632/oncotarget.2468120. Vivarelli S, Salemi R, Candido S, et al. Gut microbiota and cancer: From pathogenesis to therapy. Cancers (Basel). 2019;11(1):38. doi: 10.3390/cancers1101003821. Matsuki T, Watanabe K, Fujimoto J, et al. Use of 16S rRNA gene-targeted group-specific primers for real-time PCR analysis of predominant bacteria in human feces. Appl Environ Micro-biol. 2004;70(12):7220-7228. doi: 10.1128/AEM.70.12.7220-7228.2004. 22. Matsuki T, Watanabe K, Fujimoto J, et al. Development of 16S rRNA-gene-targeted group-specific primers for the detection and identification of predominant bacteria in human feces. Appl Environ Microbiol. 2002;68(11):5445-5451. doi: 10.1128/aem.68.11.5445-5451.2002 .23. Endo A, Okada S, Morita H. Molecular profiling of Lactobacillus, Streptococcus, and Bifidobacterium species in feces of active racehors-es. J Gen Appl Microbiol. 2007;53(3):191-200. 24. Yonei Y, Yagi M, Nakamura M, et al. Effects of astaxanthin on intestinal microflora in mice fed a high-fat diet. Anti-Aging Med. 2013;10(4):77-91.25. Oguma Y, Iida K, Yonei Y, et al. Significance evaluation of Anti-Aging QOL Common Questionnaire. Glycative Stress Res. 2016;3(3):177-185. doi: 10.24659/gsr.3.3_17726. Jones RB, Alderete TL, Kim JS, et al. High intake of dietary fructose in overweight/obese teenagers associated with depletion of Eubacterium and Streptococcus in gut microbiome. Gut Microbes. 2019:1-8. doi: 10.1080/19490976.2019.1592420.27. Sánchez E, Donat E, Ribes-Koninckx C, et al. Duodenal-mucosal bacteria associated with celiac disease in children. Appl Environ Mi-crobiol. 2013;79(18):5472-5479. doi: 10.1128/AEM.00869-13.28. Kostic AD, Gevers D, Siljander H, et al. The dynamics of the human infant gut microbiome in development and in progression toward type 1 diabetes. Cell Host Microbe. 2015;17(2):260-273. doi: 10.1016/j.chom.2015.01.001.29. Wang T, Cai G, Qiu Y, et al. Structural segregation of gut micro-biota between colorectal cancer patients and healthy volunteers. ISME J. 2012;6(2):320-329. doi: 10.1038/ismej.2011.109.30. Cosseau C, Devine DA, Dullaghan E, et al. The commensal Strep-tococcus salivarius K12 downregulates the innate immune responses of human epithelial cells and promotes host-microbe homeostasis. Infect Immun. 2008;76(9):4163-4175. doi: 10.1128/IAI.00188-08.31. Kaci G, Goudercourt D, Dennin V, et al. Anti-inflammato-ry properties of Streptococcus salivarius, a commensal bacterium of the oral cavity and digestive tract. Appl Environ Microbiol.
2014;80(3):928-934. doi: 10.1128/AEM.03133-13.32. Vitetta L, Llewellyn H, Oldfield D. Gut dysbiosis and the intestinal microbiome: Streptococcus thermophilus, a key probiotic for reducing uremia. Microorganisms. 2019;7(8):228. doi: 10.3390/microorganisms7080228.33. Chae CS, Kwon HK, Hwang JS, et al. Prophylactic effect of probiotics on the development of experimental autoimmune myas-thenia gravis. PLoS One. 2012;7(12):e52119. doi: 10.1371/journal.pone.0052119.34. Kim J, Choi SH, Kim YJ, et al. Clinical effect of IRT-5 probiotics on immune modulation of autoimmunity or alloimmunity in the eye. Nutrients. 2017;9(11):1166. doi: 10.3390/nu911116635. Kwon HK, Kim GC, Kim Y, et al. Amelioration of experimen-tal autoimmune encephalomyelitis by probiotic mixture is medi-ated by a shift in T helper cell immune response. Clin Immunol. 2013;146(3):217-227. doi: 10.1016/j.clim.2013.01.001. 36. Walter J. Ecological role of lactobacilli in the gastrointestinal tract: Implications for fundamental and biomedical research. Appl En-viron Microbiol. 2008;74(16):4985-4996. doi: 10.1128/AEM.00753-08.37. Jang HM, Han SK, Kim JK, et al. Lactobacillus sakei allevi-ates high-fat-diet-induced obesity and anxiety in mice by inducing AMPK activation and SIRT1 expression and inhibiting gut mi-crobiota-mediated NF-χB activation. Mol Nutr Food Res. 2019 Mar;63(6):e1800978. doi: 10.1002/mnfr.201800978. 38. Ji Y, Park S, Chung Y, et al. Amelioration of obesity-related biomarkers by Lactobacillus sakei CJLS03 in a high-fat diet-induced obese murine model. Sci Rep. 2019;9(1):6821. doi: 10.1038/s41598-019-43092-y.39. Wu CC, Weng WL, Lai WL, et al. Effect of Lactobacillus planta-rum strain K21 on high-fat diet-fed obese mice. Evid Based Comple-ment Alternat Med. 2015;2015:391767. doi: 10.1155/2015/39176740. Linninge C, Xu J, Bahl MI, et al. Lactobacillus fermentum and Lactobacillus plantarum increased gut microbiota diversity and func-tionality, and mitigated Enterobacteriaceae, in a mouse model. Benef Microbes. 2019;10(4):413-424. doi: 10.3920/BM2018.0074.41. Zhang F, Li Y, Wang X, et al. The impact of Lactobacillus planta-rum on the gut microbiota of mice with DSS-induced colitis. Biomed Res Int. 2019;2019:3921315. doi: 10.1155/2019/392131542. Trabelsi I, Ktari N, Ben Slima S, et al. Effect of a probiotic Lactobacillus plantarum TN8 strain on trinitrobenzene sulphon-ic acid-induced colitis in rats. J Anim Physiol Anim Nutr (Berl). 2017;101(2):311-319. doi: 10.1111/jpn.1253643. Hu J, Wang C, Ye L, et al. Anti-tumour immune effect of oral administration of Lactobacillus plantarum to CT26 tumour-bearing mice. J Biosci. 2015;40(2):269-79.44. Gamallat Y, Ren X, Wallana W, et al. Probiotic Lactobacillus rhamnosus modulates the gut microbiome composition attenuates preneoplastic colorectal Aberrant crypt foci. Journal of Functional Foods. 2019;53:146-156. doi: 10.1016/j.jff.2018.12.018.45. Park S, Kang J, Choi S, et al. Cholesterol-lowering effect of Lactobacillus rhamnosus BFE5264 and its influence on the gut microbiome and propionate level in a murine model. PLoS One. 2018;13(8):e0203150. doi: 10.1371/journal.pone.0203150.46. Bagarolli RA, Tobar N, Oliveira AG, et al. Probiotics modulate gut microbiota and improve insulin sensitivity in DIO mice. J Nutr Biochem. 2017;50:16-25. doi: 10.1016/j.jnutbio.2017.08.00647. Lenoir M, Del Carmen S, Cortes-Perez NG, et al. Lactobacillus casei BL23 regulates Treg and Th17 T-cell populations and reduces DMH-associated colorectal cancer. J Gastroenterol. 2016;51(9):862-873. doi: 10.1007/s00535-015-1158-9.48. Aragón F, Carino S, Perdigón G, et al. The administration of
Original Article
58-66

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com66
milk fermented by the probiotic Lactobacillus casei CRL 431 exerts an immunomodulatory effect against a breast tumour in a mouse model. Immunobiology. 2014;219(6):457-64. doi: 10.1016/j.im-bio.2014.02.005.49. Xue L, He J, Gao N, et al. Probiotics may delay the progression of nonalcoholic fatty liver disease by restoring the gut microbiota struc-ture and improving intestinal endotoxemia. Sci Rep. 2017;7:45176. doi: 10.1038/srep45176.50. Chen L, Zou Y, Peng J, et al. Lactobacillus acidophilus suppresses colitis-associated activation of the IL-23/Th17 axis. J Immunol Res. 2015;2015:909514. doi: 10.1155/2015/909514.51. Park JS, Choi JW, Jhun J, et al. Lactobacillus acidophilus improves intestinal inflammation in an acute colitis mouse model by regulation of Th17 and Treg cell balance and fibrosis development. J Med Food. 2018;21(3):215-224. doi: 10.1089/jmf.2017.3990.52. Halawa MR, El-Salam MA, Mostafa BM, et al. The gut microbi-ome, Lactobacillus acidophilus; Relation with type 2 diabetes mellitus. Curr Diabetes Rev. 2019;15(6):480-485. doi: 10.2174/1573399815666190206162143.53. Kurakawa T, Ogata K, Matsuda K, et al. Diversity of intesti-nal Clostridium coccoides group in the Japanese population, as demonstrated by reverse transcription-quantitative PCR. PLoS One. 2015;10(5):e0126226. doi: 10.1371/journal.pone.0126226.54. Murri M, Leiva I, Gomez-Zumaquero JM, et al. Gut microbiota in children with type 1 diabetes differs from that in healthy children: A case-control study. BMC Med. 2013;11:46. doi:10.1186/1741-7015-11-46.55. Jamar G, Santamarina AB, Dias GC, et al. Relationship between fatty acids intake and Clostridium coccoides in obese individuals with metabolic syndrome. Food Res Int. 2018;113:86-92.N.D. 56. O’Callaghan A, van Sinderen D. Bifidobacteria and their role as members of the human gut microbiota. Front Microbiol. 2016;7:925. doi: 10.3389/fmicb.2016.00925.57. Arboleya S, Watkins C, Stanton C, et al. Gut Bifidobacteria pop-ulations in human health and aging. Front Microbiol. 2016;7:1204. doi: 10.3389/fmicb.2016.01204.58. Alsharafani M, Roderfeld M, Roeb E, et al. Bifidobacterium breve M4A and Bifidobacterium longum subsps. longum FA1 reduced weight gain and hepatic lipid droplets in young mice fed high-fat. J Prob Health. 2016;4:3. doi: 10.4172/2329-8901.1000152.59. Li Z, Jin H, Oh SY, et al. Anti-obese effects of two Lactobacilli and two Bifidobacteria on ICR mice fed on a high fat diet. Bio-chem Biophys Res Commun. 2016;480(2):222-227. doi: 10.1016/j.bbrc.2016.10.031.60. Yin YN, Yu QF, Fu N, et al. Effects of four Bifidobacteria on obesity in high-fat diet induced rats. World J Gastroenterol. 2010;16(27):3394-3401. doi: 10.3748/wjg.v16.i27.3394.61. Wang J, Tang H, Zhang C, et al. Modulation of gut microbiota during probiotic-mediated attenuation of metabolic syndrome in high fat diet-fed mice. ISME J. 2015;9:1-15. doi: 10.1038/ismej.2014.99.62. Aoki R, Kamikado K, Suda W, et al. A proliferative probiotic Bifidobacterium strain in the gut ameliorates progression of metabolic disorders via microbiota modulation and acetate elevation. Sci Rep. 2017;7:43522. doi: 10.1038/srep43522.
63. Yang C, Fujita Y, Ren Q, et al. Bifidobacterium in the gut micro-biota confer resilience to chronic social defeat stress in mice. Sci Rep. 2017;7:45942. doi: 10.1038/srep45942.64. Fukui H, Oshima T, Tanaka Y, et al. Effect of probiotic Bifido-bacterium bifidum G9-1 on the relationship between gut microbiota profile and stress sensitivity in maternally separated rats. Sci Rep. 2018;8:12384. doi: 10.1038/s41598-018-30943-3.65. Nigro ND, Campbell RL, Singh DV, et al. Effect of diet high in beef fat on the composition of fecal bile acids during intestinal car-cinogenesis in the rat. J Natl Cancer Inst. 1976;57(4):883-888.66. Cani PD, Delzenne NM, Amar J, et al. Role of gut microflora in the development of obesity and insulin resistance following high-fat diet feeding. Pathol Biol (Paris). 2008;56(5):305-309. doi: 10.1016/j.patbio.2007.09.008. 67. Steegenga WT, de Wit NJ, Boekschoten MV, et al. Structur-al, functional and molecular analysis of the effects of aging in the small intestine and colon of C57BL/6J mice. BMC Med Genomics. 2012;5:38. doi: 10.1186/1755-8794-5-3868. Okazaki Y, Tomotake H, Tsujimoto K, et al. Consumption of a resistant protein, sericin, elevates fecal immunoglobulin A, mu-cins, and cecal organic acids in rats fed a high-fat diet. J Nutr. 2011 Nov;141(11):1975-1981. doi: 10.3945/jn.111.144246. 69. Cummings JH, Wiggins HS, Jenkins DJ, et al. Influence of diets high and low in animal fat on bowel habit, gastrointestinal transit time, fecal microflora, bile acid, and fat excretion. J Clin Invest. 1978;61(4):953-963.70. Kitano Y, Murazumi K, Duan J, et al. Effect of dietary porphyran from the red alga, Porphyra yezoensis, on glucose metabolism in diabetic KK-Ay mice. J Nutr Sci Vitaminol (Tokyo). 2012;58(1):14-19. 71. Kondo S, Xiao JZ, Satoh T, et al. Antiobesity effects of Bifido-bacterium breve strain B-3 supplementation in a mouse model with high-fat diet-induced obesity. Biosci Biotechnol Biochem. 2010;74(8):1656-1661.72. Mozes S, Bujnáková D, Sefcíková Z, et al. Developmental changes of gut microflora and enzyme activity in rat pups exposed to fat-rich diet. Obesity (Silver Spring). 2008 Dec;16(12):2610-2615. doi: 10.1038/oby.2008.435. 73. DiBaise JK, Zhang H, Crowell MD, et al. Gut microbiota and its possible relationship with obesity. Mayo Clin Proc. 2008;83(4):460-469. doi: 10.4065/83.4.460.74. Sefcíková Z, Kmet V, Bujnáková D, et al. Development of gut microflora in obese and lean rats. Folia Microbiol (Praha). 2010;55(4):373-375. doi: 10.1007/s12223-010-0061-2.75. Kim KA, Gu W, Lee IA, et al. High fat diet-induced gut micro-biota exacerbates inflammation and obesity in mice via the TLR4 signaling pathway. PLoS One. 2012;7(10):e47713. doi: 10.1371/jour-nal.pone.0047713. 76. Macfarlane GT, Macfarlane S. Diet and metabolism of the intestinal flora. Bioscience Microflora: Bioscience and Microflora. 2002;21(4):199-208. doi: 10.12938/bifidus1996.21.199.77. Yokota A, Fukiya S, Islam KB, et al. Is bile acid a determinant of the gut microbiota on a high-fat diet? Gut Microbes. 2012;3(5):455-459.
Original Article
58-66

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com67
Third Degree Atrioventricular Block in ChildrenVinko Vrdoljak1 , Matej Šapina2, Suzana Bitanga1, Matej Katavić1
1 Department of Pediatrics, University Hospital Center Sestre Milosrdnice, Zagreb, Croatia2 Department of Pediatrics, University Hospital Center Osijek, Osijek, Croatia
abstract:Atrioventricular (AV) block is defined as a delay or interruption in the transmission of an impulse from the atria to the ventricles due to an anatomical or functional impairment in the conduction system. The conduction disturbance can be transient or permanent. In third degree AV block, also referred to as complete heart block, there is complete dissociation of the atrial and ventricular activity. Atrioventricular block is considered to be “congenital” when it occurs spontaneously in a fetus or young child. In children, the most common cause of permanent acquired complete AV block is surgery for congenital heart disease. Injury to fetal conduction tissues caused by transpla-cental exposure to maternal autoantibodies related to systemic lupus erythematosus or Sjogren’s syndrome is responsible for 60 to 90 percent of cases of congenital CHB overall1-3. As many as 40 percent of cases of congenital CHB do not present until later in childhood (mean age five to six years). Only rarely do these patients (5 percent) have proven autoimmune etiology. The increased risk of sudden death is associated with the onset of deep bradycardia or ventricular arrhythmia. A routine electrocardiogram is sufficient to diagnose the disease. A 15-year-old girl has been examined at the emergency pediatric outpatient clinic of the University Hospital Centre “Sestre Milosrdnice” for recurrent episodes of presyncope. Physical examination revealed no major devia-tions other than bradycardia. Her vital signs were within the reference range, with the exception of a pulse of about 44 beats per minute. The electrocardiogram showed atrioventricular dissociation consistent with third degree atrioventricular block. The echocardiogram showed a structurally normal heart except for sinus bradycardia. The girl underwent permanent epicardial pacemaker implantation after which there were no symptoms.
Keywords: complete heart block, CHB, complete atrioventricular block, third degree atrioven-tricular block, congenital atrioventricular block, acquired atrioventrikular block, children, brady-cardia
Sažetak:atrioVentrikularni blok srca trećeg stupnja u Djece
Atrioventrikularni (AV) blok je definiran kao kašnjenje ili prekid u prijenosu impulsa iz atrija u ven-trikule zbog anatomskih ili funkcionalnih oštećenja u provodnom sustavu srca. Poremećaj provodl-jivosti može biti prolazan ili trajan. U AV bloku trećeg stupnja, koji se još naziva i kompletni srčani blok, dolazi do potpune disocijacije atrijske i ventrikularne aktivnosti. Atrioventrikularni blok se smatra “kongenitalnim” kada se pojavljuje spontano kod fetusa ili malog djeteta. Stečeni permanent-ni kompletni AV blok kod djece najčešće je posljedica kirurške korekcije prirođenih srčanih grešaka. Ozljeda fetalnog provodnog srčanog tkiva uzrokovana transplacentarnom izloženošću majčinim autoantitijelama povezanim sa sistemskim eritematoznim lupusom ili Sjogrenovim sindromom odgovorna je za 60 do 90 posto slučajeva kongenitalnog srčanog bloka1-3. Čak 40 posto slučajeva kongenitalnog srčanog bloka se javlja kasnije u djetinjstvu (prosječna dob od pet do šest godina). Od navedenih samo rijetki pacijenti (5 posto) imaju dokazanu autoimunu etiologiju. Povećan rizik iznenadne smrti se veže uz nastup duboke bradikardije ili ventrikulske aritmije. Za dijagnozu bolesti je dovoljan rutinski elektrokardiogram. Djevojčica od 15 godina je pregledana u hitnoj pedijatrijskoj ambulanti kliničkog bolničkog centra “Sestre Milosrdnice”, zbog ponavljajućih epizoda presinkopa. Tjelesnim pregledom se nije utvrdilo većih odstupanja, osim bradikardije. Njeni vitalni znakovi su bili unutar referentnog raspona, s izuzetkom pulsa koji je iznosio oko 44 otkucaja u minuti. Elektro-kardiogram je pokazao atrioventrikularnu disocijaciju u skladu s atrioventrikularnim blokom trećeg stupnja. Ehokardiogram je izuzev sinusne bradikardije pokazao strukturno normalno srce. Djevojka je podvrgnuta ugradnji trajnog epikardijalnog pacmakera nakon čega više nije imala simptoma i tegoba u budućnosti.
ključne riječi: kompletni srčani blok, kompletni atrioventrikularni blok, atrioventrikularni blok 3. stupnja, kongenitalni atrioventrikularni blok, stečeni atrioventrikularni blok, djeca, bradikardija
OPEN ACCESS
Correspondence: Vinko Vrdoljak MD
[email protected]/0000-0002-7321-8057
This article was submitted to RAD CASA - Medical Sciences
as the Case Report
Conflict of Interest Statement: The authors declare that the re-
search was conducted in the absence of any commercial or financial rela-
tionships that could be construed as a potential conflict of interest.
Received: 11 November 2019Accepted: 5 December 2019
Published: 17 December 2019
Citation:Vrdoljak V, Šapina M, Bitanga S and
Katavić M. Third Degree Atrio-ventricular Block in Children. RAD CASA- Medical Sciences. 540=48-49 (2019): 67-70. https://dx.doi.
org/10.21857/m3v76t6o3y
Copyright (C) 2019. Vrdoljak, Šapi-na, Bitanga and Katavić. This is an
open-access article distributed under the terms of the Creative Commons
Attribution License (CC BY). The use, distribution or reproduction in other
forums is permitted, provided the original author(s) and the copyright owners(s) are credited and that the original publication in this journal is cited, in accordance whit accepted adacemic practice. No use, distri-
bution or reproduction is permitted which does not comply with these
terms.
Case Report
67-70

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com68
case Presentation
A 15-year-old girl was referred to pediatric emergency department outpatient clinic of the University Hospital Centre “Sestre Milosrd-nice” due to a recurrence of an episode of presyncope back in 3 days. For the past 11 months, there has been a daily feeling of shortness of breath. Three days before admission, she felt weak, flushed before her eyes, faded. The day before her admission, her eyes turned black again at school and she collapsed. There were no convulsive elements and she did not lose consciousness. After the examination, her vital signs were within the reference range. The heart action was brady-cardic, a systolic murmur 1/6 heard over Erb’s point was observed. The heart rate received was a bio variable and ranged from 42-60/min. The electrocardiogram showed atrioventricular dissociation consistent with third degree atrioventricular block. A 24-h holter was made, recording an average rhythm of 44/min (daily 51/min, night 36/min). The minimum rhythm was reduced by 28/min, the maximum by 109/min. RR breaks of up to 3.5 s with rare isolated VES were noted. An echocardiographically discontinuation of the continuous interatrial septum at the level of the oval fossa 2 mm with an L-R flow of 1.06 m/s, hemodynamically insignificant. Spi-rometry was neat, salbutamol test negative. She had normal electro-lytes, renal and liver function, full blood count and random blood sugar test results. Anti-SSA/Ro and anti-SSB/La, anti-double-strand-ed deoxyribonucleic acid (dsDNA), antinuclear antibodies (ANA) and antineutrophil cytoplasmic antibodies (ANCA) autoantibodies. were negative. There were no heart diseases in the family. The child underwent implantation of a permanent epicardial pacemaker after there were no symptoms.
discussion
The atrioventricular (AV) block is defined as the interruption or de-lay in the transfer of impulses from the atrium to the ventricles due to an anatomical or functional disorder in the conduction cardiac system. The atrioventricular block is considered “congenital” when it occurs spontaneously in a fetus or child. Congenital complete heart block (CHB) was first described in 1901 by Morquio, who also noted familial occurrence and association with Stokes-Adams attacks and death4. The presence of fetal bradycardia (40 to 80 beats per minute) as a manifestation of CHB was first noted in 1921 and is the initial sign of this disorder in many cases5. The incidence of congenital CHB is estimated from 1 in 15,000 to 1 and 22,000 newborns6,7. In children, the most common cause of permanently acquired complete AV block is surgery for congenital heart disease. Fetal conduction injury caused by transplacental transfer of ma-ternal antibodies to patients with systemic lupus erythematosus or Sjogren’s syndrome is thought to be responsible for 60-90 percent of the cause of congenital CHB.1-3 Among women with anti-Ro / SSA and / or anti-La / SSB antibodies, fetal / neonatal CHB occurs in approximately 2 percent of pregnancies8,9. 40 percent of all congenital heart block cases are not clinically presented until later in childhood (average between 5 and 7 years)3. Only rarely do these patients (5 percent) have proven autoimmune etiology
3. The etiology of complete heart block in children includes the following: autoimmune diseases, structural abnormalities due to congenital heart defects (eg congenitally corrected transposition of large blood vessels, defects of endocardial pads), idiopathic familial congenital complete heart block, or the consequence of overfeeding myocardial myocardial surgery10. Congenitally impaired AV nodal function may also be observed in some simple cases of atrial septal defect among patients with Holt-Oram syndrome, an autosomal dominant disorder causing cardiac and upper-limb abnormalities that causes a mutation on the TBX5 gene11. The manifestation of congenital CHB varies depending on the age of presentation, causes, ventricular frequency, and ventricular function. Patients with autoimmune etiology present earlier than those with other causes of CHB12. Clinically, CHB is presented differently at a certain age. Regarding neonatal age, the primary presentation of infants with congenital heart block is a slow heart rate below 100 beats per minute. Such newborns may appear pale due to decreased cardiac output. Signs of congestive heart failure (eg, crackles on lung exam-ination, elevated jugular venous pulsations, peripheral edema, etc) may also occur. First or second degree AV block found in infants at birth can progress to CHB and should be followed carefully13,-16. 40 percent of patients with congenital CHB present later in childhood. The primary finding in these children is a slow heart rate with or without symptoms, including poorer effort tolerance, presyncope or syncope (Stokes-Adams seizures). Sudden death has also been rarely described17-19. A routine electrocardiogram is sufficient to diagnose the disease and echocardiography reveals an associated structural heart failure or cardiomyopathy. Holter monitoring and load tests assess the basal frequency of the downstream rhythm of the conductor and the possibility of its increase in various physiological requirements, tendency for deep bradycardia and arrhythmias. The therapeutic approach for prenatal diagnosed congenital CHB is largely expect-ant. If fetal hydrops or other signs of fetal distress develop, there is a possibility of early delivery or emergency pacing. If CHB diagnosed in utero is caused by transplacental transfer of maternal antibodies to patients with systemic lupus erythematosus or Sjogren’s syn-drome, corticosteroid therapy should be considered depending on the time of diagnosis. If the heart block is already complete and has been present for more than three weeks, it is considered that an attempt at reversing this complete heart block is futile, and therefore serial echocardiographic and obstetrical follow-up, but no therapy is recommended. If, however, the third degree heart block has been recently diagnosed, a therapeutic course of dexamethasone 4 mg. orally once a day for a period of six weeks may be attempted. For in-fants and children who are presented later, the therapeutic approach depends on the presence or absence of symptoms. Patients with adequate ventricular frequency and no symptoms may be followed, while symptomatic patients (usually those with a slower ventricular rhythm) need a permanent pacemaker20. Pacemaker implantation was recommended (class I) or felt to be reasonable (class IIa) for patients with congenital CHB and the following characteristics:
Case Report
67-70

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com69
symptomatic bradycardia or low cardiac output (class I), wide QRS escape rhythm, complex ventricular ectopy, or ventricular dys-function (class I), infants with normal anatomy and a ventricular rate of less than 55 beats per minute (class I), infants with other structural congenital heart disease and a ventricular rate of less than 70 beats per minute (class I), children beyond the first year of life with an average heart rate of less than 50 beats per minute, or abrupt pauses two to three times the basic RR cycle length (class IIa). CHB, which is presented prenatally, and is mainly due to maternal antibodies, is associated with a higher mortality rate10,21,22. The outcome of patients diagnosed in the infant is better than the outcome of those diagnosed in utero. Children with CHB who are asymptomatic generally remain asymptomatic until later childhood, adolescence, or adulthood6,23. Prognosis is generally excellent among infants and those diagnosed later in childhood10. However, exercise limitation and even mortality in childhood are not negligible24-26. Even patients who have been asymptomatic throughout childhood are at increased risk of sudden death. In a review of 102 patients who were without symptoms through age 15, 27 (26 percent) had a subsequent syncopal episode, eight of which were fatal18. The ventricular rate tends to fall slowly with age18. To compensate for the slow heart rate, the heart enlarges to produce a higher stroke volume; in some cases, this may lead to voltage criteria for left ventricular enlargement and nonspecific ST-T wave changes27 as
well as to heart failure28,29. In general, the prognosis of the following pacemaker implantation is excellent15,30,31. However, a significant number of patients (5 to 11 percent) develop heart failure over the long term, even if a pacemaker is inserted28,29.
conclusion
The most common etiologies of CHB include the following: idio-pathic familial congenital CHB, autoimmune antibodies, structural heart abnormalities due to congenital heart disease (eg, congenitally corrected transposition of the great arteries, endocardial cushion defects), consequence of myocarditis or mechanical trauma from surgical or transcatheter interventions. Symptoms of children with complete AV block and structurally normal heart range from unbearable physical exertion, syncope to complete absence of symp-toms. Treatment of patients with low cardiac output syndrome or at risk of sudden death is performed by installing a permanent elec-trostimulator. Despite its infrequency and life-threatening potential, patients with congenital complete heart block have an excellent survival rate with timely diagnosis and intervention.
author contributions:All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
literature:1. Johansen AS, Herlin T. [Neonatal lupus syndrome. Association with complete congenital atrioventricular block]. Ugeskr Laeger 1998; 160:2521.2. Ross BA. Congenital complete atrioventricular block. Pediatr Clin North Am 1990; 37:69.3. Jaeggi ET, Hamilton RM, Silverman ED, et al. Outcome of chil-dren with fetal, neonatal or childhood diagnosis of isolated congenital atrioventricular block. A single institution’s experience of 30 years. J Am Coll Cardiol 2002; 39:130.4. Morquio, L . Sur une maladie infantile et familiale characterisée par des modifications permanentes du pouls, des attaques syncopales et epileptiforme et la mort subite. Arch Méd d’Enfants 1901; 4:467.5. White, P, Eustis, R . Congenital heart block. Am J Dis Child 1921; 22:299.6. Michaëlsson M, Engle MA. Congenital complete heart block: an international study of the natural history. Cardiovasc Clin 1972; 4:85.7. Brito-Zerón P, Izmirly PM, Ramos-Casals M, et al. The clinical spectrum of autoimmune congenital heart block. Nat Rev Rheumatol 2015; 11:301.8. Brucato A, Frassi M, Franceschini F, et al. Risk of congenital com-plete heart block in newborns of mothers with anti-Ro/SSA antibod-ies detected by counterimmunoelectrophoresis: a prospective study of 100 women. Arthritis Rheum 2001; 44:1832.9. Buyon JP, Kim MY, Copel JA, Friedman DM. Anti-Ro/SSA antibodies and congenital heart block: necessary but not sufficient. Arthritis Rheum 2001; 44:1723.10. Brito-Zerón P, Izmirly PM, Ramos-Casals M, et al. Autoimmune congenital heart block: complex and unusual situations. Lupus 2016; 25:116.
11. Mori AD, Bruneau BG. TBX5 mutations and congenital heart disease: Holt-Oram syndrome revealed. Curr Opin Cardiol 2004; 19:211.12. Cruz RB, Viana VS, Nishioka SA, et al. Is isolated congenital heart block associated to neonatal lupus requiring pacemaker a dis-tinct cardiac syndrome? Pacing Clin Electrophysiol 2004; 27:615.13. Askanase AD, Friedman DM, Copel J, et al. Spectrum and pro-gression of conduction abnormalities in infants born to mothers with anti-SSA/Ro-SSB/La antibodies. Lupus 2002; 11:145.14. Nield LE, Silverman ED, Taylor GP, et al. Maternal anti-Ro and anti-La antibody-associated endocardial fibroelastosis. Circulation 2002; 105:843.15. Eliasson H, Sonesson SE, Salomonsson S, et al. Outcome in young patients with isolated complete atrioventricular block and permanent pacemaker treatment: A nationwide study of 127 patients. Heart Rhythm 2015; 12:2278.16. Waltuck J, Buyon JP. Autoantibody-associated congenital heart block: outcome in mothers and children. Ann Intern Med 1994; 120:544.17. Sholler GF, Walsh EP. Congenital complete heart block in patients without anatomic cardiac defects. Am Heart J 1989; 118:1193.18. Michaëlsson M, Jonzon A, Riesenfeld T. Isolated congenital complete atrioventricular block in adult life. A prospective study. Circulation 1995; 92:442.19. Karpawich PP, Gillette PC, Garson A Jr, et al. Congenital com-plete atrioventricular block: clinical and electrophysiologic predictors of need for pacemaker insertion. Am J Cardiol 1981; 48:1098.20. Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients
Case Report
67-70

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com70
With Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2019; 74:e51.
21. Izmirly PM, Saxena A, Kim MY, et al. Maternal and fetal factors associated with mortality and morbidity in a multi-racial/ethnic registry of anti-SSA/Ro-associated cardiac neonatal lupus. Circulation 2011; 124:1927.22. Levesque K, Morel N, Maltret A, et al. Description of 214 cases of autoimmune congenital heart block: Results of the French neonatal lupus syndrome. Autoimmun Rev 2015; 14:1154.23. McHenry MM. Factors influencing longevity in adults with con-genital complete heart block. Am J Cardiol 1972; 29:416.24. Dewey RC, Capeless MA, Levy AM. Use of ambulatory electrocar-diographic monitoring to identify high-risk patients with congenital complete heart block. N Engl J Med 1987; 316:835.25. Reybrouck T, Vanden Eynde B, Dumoulin M, Van der Hauwaert LG. Cardiorespiratory response to exercise in congenital complete
atrioventricular block. Am J Cardiol 1989; 64:896.ž26. Motonaga KS, Punn R, Axelrod DM, et al. Diminished exercise capacity and chronotropic incompetence in pediatric patients with congenital complete heart block and chronic right ventricular pacing. Heart Rhythm 2015; 12:560.27. Kertesz NJ, Friedman RA, Colan SD, et al. Left ventricular me-chanics and geometry in patients with congenital complete atrioven-tricular block. Circulation 1997; 96:3430.28. Moak JP, Barron KS, Hougen TJ, et al. Congenital heart block: development of late-onset cardiomyopathy, a previously underappreci-ated sequela. J Am Coll Cardiol 2001; 37:238.29. Udink ten Cate FE, Breur JM, Cohen MI, et al. Dilated cardio-myopathy in isolated congenital complete atrioventricular block: early and long-term risk in children. J Am Coll Cardiol 2001; 37:1129.30. Pordon CM, Moodie DS. Adults with congenital complete heart block: 25-year follow-up. Cleve Clin J Med 1992; 59:587.31. Groves AM, Allan LD, Rosenthal E. Outcome of isolated congeni-tal complete heart block diagnosed in utero. Heart 1996; 75:190.
Case Report
67-70

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com71
Upper Respiratory Infection Followed by Concurrent Sweet’s Syndrome and Erythema Nodosum
Alemka Markotić1,2,3 , Ivana Puškarić1, Tomislava Skuhala1,4
1 University Hospital for Infectious Diseases „Dr. Fran Mihaljević“, Zagreb, Croatia2 School of Medicine, University of Rijeka, Rijeka, Croatia3 Catholic University of Croatia, Zagreb, Croatia4 School of Dental Medicine, University of Zagreb, Zagreb, Croatia
abstract:Sweet’s syndrome (SS) is a rare inflammatory condition presented with fever, leukocytosis, ery-thematous, tender plaques and histology evidence of dense neutrophilic infiltration in the dermis. It appears mostly in women between age 30-60 years. Erythema nodosum (EN), a form of pan-niculitis, is manifested as erythematous painful rounded lumps and occurs 3-5 times more often in female patients in all age groups, but mostly between the second and the fourth decades of life. Although rare, concurrent occurrence of Sweet’s syndrome and erythema nodosum is described and may be associated with autoimmune disorders, certain malignancies, gastrointestinal disease or upper respiratory tract infections. Here, we described 34-year-old saleswoman who developed con-current Sweet’s syndrome and erythema nodosum seven days after upper respiratory tract infection onset. During upper respiratory infection, she was treated with three-days azithromycin therapy, together with ibuprofen and paracetamol. Later, when she developed concurrent SS and EN, she was treated initially with clindamycin and prednisone 40 mg, followed by 60 mg of prednisone after which the patient becomes afebrile with gradual rash regression. There is limited knowledge on concurrent SS and EN, their etiopathogenesis and association with different diseases, infections and /or medications. Concurrent SS and EN in our patient was probably triggered by the upper respiratory tract infection. Although, there is no evidence that azithromycin may induce SS or EN or both, it could be considered as a possible trigger alone or together with the upper respiratory tract infection.
Keywords: upper respiratory infection, pharyngitis, Sweet’s syndrome, erythema nodosum, azith-romycin
Sažetak:respiratorna infekcija gornjiH DišniH putoVa praćena istoVremeno sweetoVim sinDromom i noDoznim eritemom
Sweetov sindrom (SS) rijetko je upalno stanje koje se manifestira vrućicom, leukocitozom, eritem-atoznim, nježnim plakovima i histološkim dokazom guste neutrofilne infiltracije u dermisu. Pojavl-juje se uglavnom u žena u dobi od 30-60 godina. Nodozni eritem (EN), oblik panikulitisa, očituje se bolnim, eritematoznim, zaobljenim potkožnim čvorovima i javlja se 3-5 puta češće u bolesnica u svim dobnim skupinama, ali uglavnom između drugog i četvrtog desetljeća života. Iako je rijetka, istodobna pojava Sweet-ovog sindroma i nodoznog eritema opisana je i može biti povezana s autoi-munim poremećajima, određenim malignim bolestima, gastrointestinalnom bolešću ili infekcijama gornjih dišnih putova. Ovdje smo opisali 34-godišnju prodavačicu koja je razvila istodobni Sweetov sindrom i nodozni eritem sedam dana nakon početka infekcije gornjih dišnih putova. Tijekom infek-cije gornjih dišnih puteva, liječena je trodnevnom terapijom azitromicinom, zajedno s ibuprofenom i paracetamolom. Kasnije, kad je razvila istodobno SS i EN, liječena je u početku klindamicinom i prednizonom od 40 mg, a zatim sa 60 mg prednizona, nakon čega bolesnica postaje afebrilna s pos-tupnom regresijom osipa. Malo se zna o istodobnom SS i EN, njihovoj etiopatogenezi i povezanosti s različitim bolestima, infekcijama i / ili lijekovima. Istodobni SS i EN u naše bolesnice vjerojatno je potaknut infekcijom gornjih dišnih puteva. Iako nema dokaza da azitromicin može izazvati SS ili EN ili oboje, moglo bi se pretpostaviti da bi mogao biti okidač sam ili zajedno s infekcijom gornjih dišnih puteva.
ključne riječi: infekcija gornjih dišnih puteva, faringitis, Sweetov sindrom, nodozni eritem, azitromicin
OPEN ACCESS
Correspondence: Prof. Alemka Markotić MD PhD
[email protected]/0000-0003-4104-7940
This article was submitted to RAD CASA - Medical Sciences
as the Case report
Conflict of Interest Statement: The authors declare that the research was conducted in the absence of any commercial or financial relationships
that could be construed as a potential conflict of interest.
Received: 5 November 2019Accepted: 10 December 2019
Published: 17 December 2019
Citation:Markotić M, Puškarić I and Skuhala T. Upper Respiratory Infection Followed
by Concurrent Sweet’s Syndrome and Erythema Nodosum.
RAD CASA- Medical Sciences. 540=48-49 (2019): 71-74. https://dx.doi.org/10.21857/mwo1vczw1y
Copyright (C) 2019 Markotić, Puškarić, Skuhala. This is an
open-access article distributed under the terms of the Creative Commons
Attribution License (CC BY). The use, distribution or reproduction in other
forums is permitted, provided the original author(s) and the copyright owners(s) are credited and that the original publication in this journal is cited, in accordance whit accepted adacemic practice. No use, distri-
bution or reproduction is permitted which does not comply with these
terms.
Case Report
71-74

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com72
introduction
Upper respiratory tract infections (URI) include the infection in nose, sinuses, pharynx, larynx, and the large airways and are leading cause of morbidity. Usually, they are caused by different viruses, mostly rhinoviruses, but also the influenza virus, adenovirus, entero-virus, and respiratory syncytial virus. Bacterial infections are also common and often pharyngitis could be caused by Streptococcus pyogenes, a Group A streptococcus1,2. Sweet’s syndrome (SS) is a rare inflammatory condition presented with fever, leukocytosis erythematous, tender plaques and histology evidence of dense neutrophilic infiltration in the dermis. Different diseases, including infectious diseases, malignancies and medications are associated with SS. It appears mostly in women between age 30-60 years3-5. There are major and minor criteria for diagnosis of SS (Figure 1)6,7. For the treatment of patients with Sweet’s syn-drome systemic corticosteroids have been considered the primary option, but iodide or colchicine can also result in rapid resolution symptoms and lesions. In case that corticosteroids are contraindi-cated, indomethacin, clofazimine, dapsone, and cyclosporine can be administered3,4.Erythema nodosum (EN), a form of panniculitis, is manifested as erythematous painful rounded lumps, 1-6 cm in diameter and occurs 3-5 times more often in female patients in all age groups,
but mostly between the second and the fourth decades of life. EN is usually located symmetrically on the anterior surface of the lower extremities, but can also spread to the upper extremities and neck. It does not ulcerate and resolves without scarring. Streptococcal phar-yngitis is the most common trigger of EN, which appears 2–3 weeks after infection resolution. Mycoplasma, Chlamydia, Mycobacteri-um, Yersinia spp., Coccidioides and Histoplasma caused infections could be followed by EN as well. Other medical conditions, which could be linked to EN development are: sarcoidosis, medication including antibiotics, inflammatory bowel diseases and sometimes pregnancy. If an infectious agent triggered EN, antibiotic therapy can be administered and non-steroidal anti-inflammatory agents are usually given. In case that some medication was responsible for the occurrence of EN, it should be stopped. The most common drugs that cause erythema nodosum are: oral contraceptives, sulfonamides and penicillin. However, despite investigation, no underlying cause is found in most erythema nodosum patients8.Although rare, concurrent occurrence of Sweet’s syndrome and erythema nodosum is described and may be associated with auto-immune disorders, certain malignancies, gastrointestinal disease. A case of a young male with a recent streptococcal infection was also described9-16.
Major criteria
erythematous, tender plaques
histopathologic evidence of dense neutrophilic infiltration in the
dermis
Minor criteria
fever >38 ℃
inflammatory or infectious diseases (upper respiratory or gastrointestinal) vaccination or pregnancy
succes on systemic glucocorticosteroid therapy or potassium iodide
abnormal clinical laboratory values (three of four):1. erythrocyte sedimentation rate >20 mm/h
2. elevated C-reactive protein3. >8000 leukocytes/µl4. >70% neutrophils
Figure 1. Figure 1. Major and minor diagnostic criteria for classic Sweet’s syndrome based on fulfilling both major and two of the four minor criteria6,7.
Case Report
71-74

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com73
case rePort
In 34-year-old saleswoman, the disease began eight days before admission to the hospital with a sore throat that lasted for the five days. On the sixth day after the upper respiratory tract symptoms onset, she became febrile up to 40 °C with chills and shivering. Next day she noticed a rash on the body and hands with mild pain and she was admitted to the hospital day after. Two days before admission she completed her three-days azithromycin therapy, taking ibuprofen and paracetamol as well. In childhood, she had contracted varicella and had lung tuberculosis at the age of 12. She had no chronic illnesses and was not taking therapy for chronic illnesses. Her daughter had a respiratory, possibly viral infection a week ago. She stated that she was allergic to amoxicillin clavulanic acid. On admission, she is conscious, febrile (38.5 C), normotensive (110/70 mmHg), with neat pulse and respiratory frequency. Round-ed lumps, suggestive of erythema nodosum were observed on the skin of the lower legs of the patient, together with the annular plaques and pustules (0.5-1 cm in diameter) developed on the skin of patient’s forearm (Figure 2 A, C) and very few at the trunk and neck. The conjunctival injection is recorded on both sides. Later, during the day, she became highly febrile up to 41 C.She had high sedimentation rate (70 mm/h) and C-reactive protein (CRP) was 197 mg/l, with 8.800 leukocytes/μl. Chest X-ray was
normal and a slightly enlarged liver and polyp in the gallbladder were recorded on an abdominal ultrasound. On the second day of hospitalization, a skin biopsy was taken from the annular papule on the forearm and histopathologic evidence of neutrophilic infiltration in the dermis was confirmed later on. Initially, she was treated with clindamycin, and prednisone 40 mg. Three days later, sedimentation rate was 40 mm/h and CRP was 70 mg/l. Five days after admission, the patient was still febrile up to 38.5 χ and the prednisone dose was increased to 60 mg, after which the patient becomes afebrile with gradual rash regression (Figure 2 B, D).
discussion
Although etiology of SS or EN are not known, both syndromes could be triggered with upper respiratory infections or medications and associated with autoimmune or malignant diseases. Both are also reactive dermatoses with some similar clinical manifestations and histopathological findings, which could be successfully solved with corticosteroid therapy 3-5. Concurrent SS and EN are rare, but are described in the literature in connection with autoimmune or malignant diseases and also some respiratory, mostly streptococcal infections9-13.Here we presented concurrent SS and EN in 34-years old, previous-ly healthy woman with preceding upper respiratory tract infection
Figure 2. Rounded lumps (erythema nodosum) on the skin of the patient’s lower leg, three (A) and ten days after the rash onset (B); Annular plaques and pustules developed on the skin of patient’s forearm three (C) and ten days after the rash onset (D).
A B
C D
Case Report
71-74

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com74
treated with azithromycin. We presumed that concurrent SS and EN in our patient was triggered with respiratory infection, but there is also possibility to be induced by antibiotic therapy. There is evidence in the literature that SS or EN are associated with some respiratory or gastrointestinal infections, including recent description of 29-year old Mexican who developed concurrent SS and EN possibly after the upper respiratory tract infection9-13. So far, there is no evidence in the literature that SS or EN could be induced by ibuprofen or parac-etamol, which our patient took during the upper respiratory infection. Recent publication, however, described SS induced by an oral acet-aminophen-codeine suspension and tablets, following repair of a facial fracture17. Also, no azithromycin therapy was associated with SS or/and EN so far and here we have no proof that this could be the case in our patient as well. Previously it was stated that tetracycline, minocy-cline, or clindamycin may be associated with SS18,19. The therapy with oral prednisone was successful in our patient and skin rash was almost completely gone in three weeks of follow up.
conclusion
There is limited knowledge on concurrent SS and EN, their etio-pathogenesis and association with different diseases, infections and /or medications. Here, we presented a concurrent SS and EN in 34-years old women, which was probably triggered by the upper respiratory tract infection. Although, there is no evidence that azithromycin may induce SS or EN or both, it could be considered as a possible trigger alone or together with the upper respiratory tract infection.
author contributions: All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
literature:1. Zeng L, Zhang L, Hu Z, Ehle EA, Chen Y, Liu L, Chen M. Sys-tematic review of evidence-based guidelines on medication therapy for upper respiratory tract infection in children with AGREE instrument. PLoS One. 2014;9(2):e87711.2. Civljak R, Tot T, Falsey AR, Huljev E, Vranes J, Ljubin-Sternak S. Viral pathogens associated with acute respiratory illness in hospitalized adults and elderly from Zagreb, Croatia, 2016 to 2018. J Med Virol. 2019;91(7):1202-1209.3. Heath MS, Ortega-Loayza AG. Insights Into the Pathogenesis of Sweet’s Syndrome. Front Immunol. 2019;10:414. doi: 10.3389/fim-mu.2019.00414. eCollection 2019.4. Marzano AV, Borghi A, Wallach D, Cugno M. A Comprehen-sive Review of Neutrophilic Diseases. Clin Rev Allergy Immunol. 2018;54(1):114-130.5. Volpe M. Sweet Syndrome Associated with Upper Respiratory Infection and Amoxicillin Use. Cureus. 2016;8(4):e568.6. Su WP, Liu HN. Diagnostic criteria for Sweet’s syndrome. Cu-tis.1986;37:167–74.7. Nofal A, Abdelmaksoud A, Amer H, Nofal E, Yosef A, Gharib K, Albalat W, Eldesouky F, Ebrahim HM, Abdelshafy AS, Fayed H. Sweet’s syndrome: diagnostic criteria revisited. J Dtsch Dermatol Ges. 2017;15(11):1081-1088. 8. Schwartz RA, Nervi SJ. Erythema nodosum: a sign of systemic disease. Am Fam Physician. 2007;75(5):695-700.9. Moreau E, Peiffert D, Schmutz JL, Granel-Brocard F, Bursztejn AC. Sweet syndrome and erythema nodosum in a case of anal canal cancer during concomitant radiochemotherapy. Eur J Dermatol. 2019. doi: 10.1684/ejd.2019.3628.10. Cohen PR, Holder WR, Rapini RP. Concurrent Sweet’s syndrome and erythema
nodosum: a report, world literature review and mechanism of patho-genesis. J Rheumatol. 1992;19(5):814-20.11. Wilkinson SM, Heagerty AH, English JS. Acute febrile neutrophil-ic dermatosis in association with erythema nodosum and sarcoidosis. Clin Exp Dermatol. 1993;18(1):47-9.12. Gillott TJ, Whallett AJ, Struthers GR, Ilchyshyn A. Concurrent Sweet’s syndrome (acute febrile neutrophilic dermatosis), erythema nodosum and sarcoidosis. Clin Exp Dermatol. 1997;22(1):54-6.13. Wasson S, Govindarajan G, Folzenlogen D. Concurrent occurrence of Sweet’s syndrome and erythema nodosum: an overlap in the spectrum of reactive dermatoses. Clin Rheumatol. 2006;25(2):268-72. 14. Harris T, Henderson MC. Concurrent Sweet’s syndrome and ery-thema nodosum. J Gen Intern Med. 2011;26(2):214-5.15. Qiao J, Wang Y, Bai J, Wu Y, Fang H. Concurrence of Sweet’s syndrome, pathergy phenomenon and erythema nodosum-like lesions. An Bras Dermatol. 2015;90(2):237-9.16. Muscardin LM, Paolino G, Cota C, Didona D, Panetta C, Donati P. Concurrent Sweet’s Syndrome and erythema nodosum in a patient with bilio-pancreatic diversion. G Ital Dermatol Venereol. 2017;152(4):392-394. 17. Bradley LM, Higgins SP, Thomas MM, Rodney IJ, Halder RM. Sweet syndrome induced by oral acetaminophen-codeine following repair of a facial fracture. Cutis. 2017;100(3):E20-E23.18. Corazza M, Lauriola MM, Borghi A, et al. Sweet’s syndrome: A retrospective clinical, histopathological and immunohistochemical analysis of 11 cases. Acta Derm Venereol 2008;88(6):601-6.19. Contrucci RB, Martin DB. Sweet syndrome: A case report and review of the literature. Ear Nose Throat J. 2015;94(7):282-4.
Case Report
71-74

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com75
Inguinal hernia containing an incarcerated ureter of a transplanted kidney
Luka Filipović-Grčić1,2 , Neva Coce2
1 Department of Radiology, University Hospital Centre Zagreb, Zagreb, Croatia2 School of Medicine, University of Zagreb, Zagreb, Croatia
abstract:We presented a case of an inguinal hernia containing an incarcerated ureter in a patient with trans-planted kidney. A 60-year-old man was admitted to hospital with elevated creatinine levels and trans-abdominal ultrasound recognised hydronephrosis. An unenhanced CT scan revealed an in-carcerated ureter in the inguinal hernia sac. The imaging confirmed hydronephrosis of the enlarged kidney with dilated pyelon and calyces. Later control examinations reported no change of grade of hydronephrosis and kidney function, probably due to the intermittent nature of ureteral incarcer-ation. We present this case in light of the recent increase in reporting of ureteroinguinal hernias and as a reminder to radiologists always to check the course of the ureters when they encounter or suspect inguinal hernia.
Keywords: inguinal hernia, CT scan, ureteroinguinal hernia, incarcerated ureter, hydronephrosis
Sažetak:Ingvinalna hernija koja sadrži inkarcerirani ureter transplantiranog bubregaU ovom radu prikazujemo slučaj pacijenta s transplantiranim bubregom koji je razvio ingvinalnu herniju sa inkarceriranim ureterom. Muškarac u dobi od 60 godina primljen je u bolnicu s povišenim kreatininom te transabdominalnim ultrazvukom otkrivenom hidronefrozom. Nativni CT pregled pokazao je inkarcerirani ureter u vreći ingvinalne hernije. Potvrđena je i hidronefroza uvećanog bubrega s dilatiranim pijelonom i kaliksima. Kasniji kontrolni pregledi utvrdili su stacionarnu hidronefrozu trećeg stupnja te očuvanu bubrežnu funkciju, vjerojatno uslijed intermitentne prirode inkarceracije. Ovaj prikaz donosimo potaknuti sve učestalijim prijavljivanjem slučajeva uretero-ingvinalnih hernija posljednjih godina. Također, nadamo se da će ovaj rad poslužiti kao podsjetnik radiolozima da uvijek provjere tijek uretera pri pregledu ili sumnji na ingvinalnu herniju.
ključne riječi: ingvinalna hernija, CT, ureteroingvinalna hernija, inkarcerirani ureter, hidrone-froza
OPEN ACCESS
Correspondence: Luka Filipovic-Grcic MD
[email protected]/0000-0003-0024-8359
This article was submitted to RAD CASA - Medical Sciences
as the Case Report
Conflict of Interest Statement: The authors declare that the re-
search was conducted in the absence of any commercial or financial rela-
tionships that could be construed as a potential conflict of interest.
Received: 11 September 2019Accepted: 25 October 2019
Published: 17 December 2019
Citation:Filipović-Grčić L and Coce N. Inguinal
hernia containing an incarcerated ureter of a transplanted kidney. RAD
CASA - Medical Sciences. 540=48-49 (2019): 75-77. https://
dx.doi.org/10.21857/yk3jwhrq39
Copyright (C) 2019 Filipović-Grčić and Coce. This is an open-access
article distributed under the terms of the Creative Commons Attribution Li-cense (CC BY). The use, distribution
or reproduction in other forums is permitted, provided the original au-thor(s) and the copyright owners(s)
are credited and that the original publication in this journal is cited, in accordance whit accepted adacemic
practice. No use, distribution or reproduction is permitted which does
not comply with these terms.
Case Report
75-77

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com76
bacKground
Inguinal hernia is a relatively common medical condition where the contents of the abdominal cavity protrude through the inguinal canal. The prevalence of abdominal wall hernias for all ages is around 1.7%, with inguinal hernias accounting for 75% of the cases1. Only 66% of these cases are symptomatic, usually involving pain and discomfort, particularly associated with strenuous activities, a unilateral bugle may appear, depending on the size of the hernia and the constitution of the patient2. Most patients are men, indeed, they are 25 times more likely to develop an inguinal hernia than women. This has traditionally been attributed to the fact that men have a larger inguinal canal that facili-tated the descent of the testes in the prenatal period.
case Presentation
A 60 year old male patient with a history of kidney transplantation, recently elevated creatinine levels and suspected hydronephrosis, was admitted for a CT urography. Due to the elevated creatinine level (152 μmol/L) unenhanced CT scan was performed (Figure 1 and Figure 2). The enlarged transplant (13 cm long) was re-lived in the right iliac fossa, with dilated pyelon and calyxes, with-out parenchymal reduction, thus establishing the diagnosis of grade III (moderate) hydronephrosis. A dilated proximal ureter was ob-served, incarcerated and folded within inguinal hernia. In the distal portion of the ureter only filiform flow was detected. The pa-tient did not report any symptoms regarding inguinal hernia. He was treated with hemodialysis 7 years prior the transplantation 9 years ago due to the endemic nephrop-athy. Additionally, he suffers from stable angina, hypertension and prostate hypertrophy. He also underwent parathyroidectomy 8 years ago and had coronary artery bypass graft after an infarction 6 years ago. Subsequent laboratory findings were in accordance with imaging results: C-reactive protein was 1.4 mg/L, urea was elevated to 11.5 mmol/L and creatinine 152 μmol/L. The rest of the findings were inconspicuous. Surgical treatment was proposed to the patient, how-ever, he was disinclined. Later control examinations reported stable grade of hydronephrosis and preserved kidney function probably due to the intermittent nature of ureteral incarceration.
discussion
Inguinal hernias usually contain small intestine and omentum, howev-er, other organs and organ parts, such as appendix, sigmoid colon, ce-cum, ovaries and urinary bladder may also be seen. The most frequent representative of the urinary tract is the bladder, present in 1-4% of all inguinal hernias, mostly direct ones3. Ureter, on the other hand, is a rare finding, described in only about 140 cases in the last 140 years. It is possible that it is underreported as it usually causes no symptoms and presents as an incidental finding. The condition is more common in transplanted patients, particularly if the grafted ureter is too long, or if it crosses over, rather than under the spermatic cord4,5. The ure-ter may be involved in femoral hernia as well, although two times less
likely than in inguinal hernias. Just as regular inguinal hernias, uret-eroinguinal hernias occur mostly in overweight men over 50 years of age. They are usually indirect (80%) and on the right side6. The main reason for this is the fascia of Toldt, which secures and fixes the ureter in the retroperitoneum on the left. There are two types of ureteroinguinal hernia: paraperitoneal and extraperitoneal. The first, associated with kidney transplants, is believed to be acquired, due to the adhesions which attach ureter to the peritoneum that then drags it into herni-al sac5. Extraperitoneal type is less common and presumably a result of congenital defect due to failed separation of ureteric bud from the Wolffian duct which leads to their joint migration to the scrotum. This kind of developmental anomaly is often associated with other anoma-
Figure 1. CT scan in coronal plane showing incarcerated ureter inside hernia sac on the right.
Case Report
75-77

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com77
lies and, if detected, it should prompt the search for other anomalies and vice versa4. The importance of proper diagnosis of ureteroinguinal hernias lies in their ability to cause hydronephrosis and in the possibility of ureteral injury during surgical treatment of hernia with overlooked ureter. The rate of reporting ureteroinguinal hernias has improved in the last years and many new cases provide interesting insights into this matter. One such case reported a bilateral obstructive uropathy caused by extrinsic inguinal hernia compressing both ureters without their involvement in the hernial sac itself7. The other described potentially useful hint for quick assessment of the probability of abnormalities in ureteral course on CT scans; namely, if the mid portion of the ureter lies anterior to the psoas muscle by more than 1 cm at the level of L4, the chances are there is something unusual in the distal portion8.
Figure 2. CT scan in sagittal plane showing incarcerated ureter and enlarged kidney with third grade hydronephrosis of the transplanted kidney.
conclusion
To conclude, we would like to remind our colleges to look for ure-troinguinal hernias in overweight men, especially with transplanted kidneys, developing hydronephrosis. Also, it is necessary to exclude the involvement of the ureter in every inguinal hernia destined for operation.
author contributions: All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
literature:
1. Jenkins JT, O’Dwyer PJ. Inguinal hernias. BMJ. 2008;336(7638):269–272. doi:10.1136/bmj.39450.428275.AD2. Fitzgibbons RJ Jr. Forse, RA. Groin hernias in adults. The New England Journal of Medicine. 19 February 2015. 372 (8): 756–63. doi:10.1056/NEJMcp14040683. Khan K, Chaudhry A, Feinman MB. Inguinoscrotal her-nia containing the urinary bladder. BMJ Case Reports 2016;2016:bcr2016217408.4. Epps JC, Close TP. Extraperitoneal herniation of the ureter. Ap-plied Radiology. March-April 2019. (43-45)5. Yahya Z, Al-habbal Y, Hassen S. Ureteral inguinal hernia:
an uncommon trap for general surgeons. BMJ Case Reports 2017;2017:bcr2017219288.6. Sidiqi MM, Menezes G. Asymptomatic herniation of ureter in the routine inguinal hernia: A dangerous trap for general surgeons. Int J Surg Case Rep. 2018;49:244–246. doi:10.1016/j.ijscr.2018.07.0137. Grice PT, Nkwam N. Inguinal hernia causing extrinsic com-pression of bilateral ureters leading to chronic obstructive uropathy, Journal of Surgical Case Reports, Volume 2018, Issue 4, April 2018, rjy062, https://doi.org/10.1093/jscr/rjy0628. Allam ES, Johnson DY, Grewal SG, Johnson FE. Inguinoscrotal herniation of the ureter: Description of five cases. International Jour-nal of Surgery Case Reports. Volume 14, 2015, Pages 160-163
Case Report
75-77

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com78
Cooperation in the Field of Public Health and Medicine: Instances of
Expert and Knowledge Mobility between Vienna, Zagreb and the Far East
Željko Dugac1 .
1 Croatian Academy of Arts and Sciences, Divison for the History and Philosophy of Science,
Department of Philosophy of Science, Ante Kovačića 5, Zagrebabstract:In this essay the transfer of knowledge and experts between Vienna, Zagreb, inter-war China and the USSR will be analysed through the collaboration between two well-known interwar public health reformers, Aus-trian Julius Tandler and Croat Andrija Štampar. In the 1930s, they worked in China under the auspices of the League of Nations Health Organization and developed intensive cooperation in the field of public health. Based on the diary records of Andrija Štampar and the preserved archival correspondence, their personal and professional contacts were analysed. The main interest was the exchange of experiences and opinions, as well as their observations about the people and ideas they encountered and the situations in which they found themselves. This essay also tries to shed some light on the milieu in which the notions of public health and social medicine advanced, as well as the multiple external factors which influenced those developments. However, the opportunities for constructive work in the field of public health grew increasingly slim in the political constellation of the time. The League of Nations was losing its power and its health organisation followed suit. The local resistance to foreign influences in China was becoming progressively intense. The ever more severe unrest led the world into World War II and pushed the establishment of an international public health order to the margins for some time to come. However, what remained in memory was a flow of ideas and experiences which was formed in Central and Southeastern Europe and which subsequently tried to make their way far to the East and develop not only local but also general and international qualities. Many of these ideas became the basis for a new world-wide public health system that developed after World War II.
Keywords: Julius Tandler, Andrija Štampar, China, interwar period, history of medicine, history of public health
Sažetak:Suradnja u području javnog zdravlja i medicine: primjeri transera znanja i stručnjaka između Beča, Zagreba i Dalekog istokaU ovom su radu predstavljeni transfer znanja i stručnjaka između Beča, Zagreba, međuratne Kine i SSSR-a kroz suradnju dvaju poznatih međuratnih reformatora javnog zdravstva, Austrijanca Juliusa Tandlera i Hrvata Andrije Štampara. Ta su dva javnozdravstvena stručnjaka 1930-tih radili u Kini pod pokroviteljstvom Zdravstvene organizacije Lige naroda i razvijali intenzivnu suradnju u području javnog zdravstva i medicinske nastave. Na temelju dnevničkih zapisa Andrije Štampara i sačuvane arhivske korespondencije analizirani su njihovi osobni i profesionalni kontakti. Glavno zanimanje ovog rada se veže uz razmjenu njihovih iskustava i mišljenja, kao i njihova zapažanja o ljudima i idejama s kojima su se susreli te situacijama u kojima su se našli. Ovaj rad također pokušava osvijetliti milje u kojem su se javno zdravstvene i socijalno medicinske ideje razvijale kao i vanjske čimbenika, nevezane uz samu struku, koji su utjecali na njih. Krajem 30-tih godina 20. stoljeća prilike za konstruktivan rad na području javnog zdravstva postajale su sve slabije a pod utjecajem tadašnje političke konstelacije i gubita utjecaja Lige naroda. Lokalni otpor stranim utjecajima u Kini postajao je sve intenzivniji. Sve oštriji nemiri vodili su svijet u Drugi svjetski rat i gurnuli uspostavljanje međunarod-nog javnozdravstvenog poretka u posve drugi plan. Međutim, ono što je ostalo u naslijeđe je bio protok ideja i iskustava koji je zahvatio ne samo lokalno područje Srednje i Jugoistočne Europe već se proširio sve do područja Dalekog istoka. Mnoge od tih ideja postale su temelj novog svjetskog javnog zdravstvenog sustava koji se razvio nakon Drugog svjetskog rata.
ključne riječi: Julius Tandler, Andrija Štampar, Kina, međuratno razdoblje, povijest medicine, povijest javnog zdravstva
OPEN ACCESS
Correspondence: Prof Željko Dugac [email protected] This article was submitted to RAD CASA - Medical Sciences as the Essay
Conflict of Interest Statement: The author declare that the research was conducted in the absence of any commercial or financial relation-ships that could be construed as a potential conflict of interest.
Received: 10 November 2019Accepted: 24 November 2019Published: 17 December 2019
Citation:Dugac Ž. Cooperation in the Field of Public Health and Medicine: Instanc-es of Expert and Knowledge Mobility between Vienna, Zagreb and the Far East. RAD CASA - Medical Sciences. 540=48-49 (2019): 78-85. https://dx.doi.org/10.21857/y7v64t56ny
Copyright (C) 2019 Dugac.This is an open-access article distributed un-der the terms of the Creative Com-mons Attribution License (CC BY). The use, distribution or reproduc-tion in other forums is permitted, provided the original author(s) and the copyright owners(s) are credited and that the original publication in this journal is cited, in accordance whit accepted adacemic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
Essay
78-85

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com79
introduction
Cooperation in the field of public health and medicine is a case in point of the mobility of intellectuals and expertise in Central and Southeastern Europe in the first decades of the 20th century which al-lows us to take stock of its manifold features. In this essay, I am going to address a lesser-known and under-researched issue – the transfer of knowledge and experts between Vienna, Zagreb, inter-war China and the USSR.I would thus like to bring to light some of the details concerning the cooperation and mutual contact between two widely-known public health reformers, Austrian Julius Tandler and Croat Andrija Štampar. In the 1920s, the former worked on public health reform in Austria, while the latter acted in the Kingdom of Yugoslavia, following which both transferred their knowledge and experience to China in the 1930s, with Tandler attempting to do so in the USSR, as well. Julius Tandler’s cooperation with the USSR health administration, which had started in February 1936, ended because of Tandler’s death in August 1936. Andrija Štampar paid a study visit to the country the same year. Therefore, rather than constituting any actual type of cooperation, which can only be questionable, this could be described as a merely conceptual exchange of ideas and a scan of the situation and the possibilities at hand.
Štampar was a student of Tandler’s at the Faculty of Medicine in Vienna. The two went on to become colleagues in the area of public health work in their respective home countries and subsequently found themselves working as university professors and medical experts in China and the USSR in the 1930s. Both Štampar and Tandler were employed by the Chinese administration and were also members of an expert team brought together by the Health Section of the League of Nations to provide support in the training of staff and the standardization of both medical education and health service provision in line with Western standards and the international norms of the day.1,2,3 In this chapter, my intention will not be to reflect in greater detail on Štampar’s and Tandler’s work in China and the USSR, considering the fact that that part of their life stories has already been expounded upon to a fair extent, particularly as far as Štampar is concerned. I am rather going to principally focus on their mutual exchange and interactions 4. In other words, my concern will be their exchange of experiences and opinions, as well as their observations about the people and ideas they encountered and the sit-uations in which they found themselves. By looking more closely into this, I will try to shed some light on the milieu in which the notions of public health and social medicine advanced, as well as the multiple external factors which influenced those developments. For this analysis, I have largely relied on the writings of Andrija Štam-par found in his personal journal, which he kept from 1931 to 1938, during a period of intensive international activity and frequent travel on his part. In addition to this, my analysis has benefitted greatly from the written correspondence between Tandler and Štampar, which is kept in the archives of the Josephinum Institute for the History of Medicine in Vienna. For this essay I also used archival
material kept at the University Archives in Vienna and parts of the Andrija Štampar’s diary published in 2008. a meeting between student and Professor, colleagues and friends
Tandler’s and Štampar’s relationship transformed from one between student and professor at university to one between colleagues, as well as friends in later years. In the 1930s, many European intellectuals and public health reformers were forced to leave their academic and administrative posts because of the rise of political extremism which finally led to the emergence of fascism. In 1931, Štampar was compelled to unwillingly retire from his position in the Kingdom of Yugoslavia, which led him to pursue the only possible opportunity to continue with constructive public health work – at the League of Na-tions Health Organisation (LNHO). The LNHO was an organisation which was trying to sustain an international reformist environment among its members and was therefore used as an assembly forum by experts who had suddenly become ideologically unsound after the political changes in their home countries. Štampar and Tandler were merely two in a line of other experts with similar life stories, such as the German professionals who fled fascism. In a note found in one of Štampar’s letters to Tandler in 1933, one sees that Štampar was using personal contact to learn about people who had found themselves in trouble in order to transfer them to a new place of employment. In Štampar’s words: “I am certainly travelling to Germany. I hope to see you in Vienna. Could you recommend me any candidates for an anatomy and physiology professorship in Nanjing and send me their names forthwith to Zemun?5 The Italian-Spanish public health reformer and malariologist Gustavo Pittaluga faced much the same, as he was also forced to leave Spain during the period.6
Julius Tandler was born in 1869 in Jihlava in the the Czech region of Moravia. He was an Austrian physician, a professor of anatomy at the University of Vienna, a Social Democratic politician and a public health reformer. He graduated at the Faculty of Medicine in Vienna on 27 July 1895. 7 He was first employed at the same Faculty as a member of the teaching staff in 1910. From 1914 to 1917, during World War I, Tandler was also dean of the faculty. Though known as an anatomist, Tandler was extraordinarily involved in the field of public health and social medicine. After the end of World War I, he became health advisor at the Viennese Department of Health, where he made exceptional advancements with respect to public health and social development. In addition to this, in 1930 Tandler took on the position of advisor to the League of Nations Health Organisation. With the ascent of fascism in Austria, Tandler leaves his post and emigrates from the country to China and later to the former Soviet Union.8
Andrija Štampar was born in 1888 in the small town of Drenovci in the Croatian region of Slavonija. Having graduated from high school in the city of Vinkovci in 1906, he followed in the footsteps of his many other young Croatian compatriots to study medicine in Vien-
Essay
78-85

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com80
na, the capital of the Austro-Hungarian Monarchy. At the time, the University of Vienna was home to numerous distinguished professors and scholars such as Carl Toldt, Julius Wagner-Jauregg, Hans Chiari and others, some of whom later became Nobel laureates. However, the lectures which impressed Štampar the most were not held by such lofty luminaries but by lecturers who spoke of an inceptive science which had still not had gained enough supporters – social medicine. It is an undeniable fact, which stems from Štampar’s later work, that his development was to a significant degree influenced by Ludwig Teleky9, a socially oriented lecturer at the Faculty of Medicine in Vienna, whose courses in social medicine were taken by Štampar in the 9th semester of his studies (academic year 1910/1911).10 Besides taking social medicine classes at the Faculty of Medicine, Štampar also attended Julius Tandler’s lectures on topics concerning social medicine at Vienna’s Open University. This marked the beginning of a long-lasting and deep professional connection, a sharing of common views on social medicine and finally of a personal friendship.
Having graduated from his medical studies in Vienna and upon the award of his diploma on the 23rd of December 1911, Andrija Štampar returns to Croatia.11 In 1919, soon after the establishment of the Kingdom of Serbs, Croats and Slovenes, Štampar is given an important position in the country’s health administration, becom-ing the Head of the Department of Hygiene at the newly formed Ministry of Public Health. He occupied the post until his retirement in 1931, during which time he accomplished the tremendous task of raising public health standards in an economically and hygienically underdeveloped country laden with war-caused deprivation and rife with epidemics. Enthusiastic about the ideas of social medicine, Štampar undertakes the effort of building a completely new kind of public health system by establishing a series of health institutions for social medicine and preventive healthcare. Štampar raised the public healthcare services to a level hitherto unknown not only in Central and Southeastern Europe but also beyond. In addition to this, he instituted education programs for a wide variety of medical person-nel and developed additional professional training for physicians, as well as an entire range of health education and promotion campaigns which reached even the most remote rural parts of the country. Štam-par is joined in his work by a line of progressive young physicians, medical nurses, engineers, artists, writers and painters, each acting in their respective field to promote and disseminate new scientific insights, new forms of public healthcare and hygiene practices, as well as a novel culture of life at large. All this took place with the goal of suppressing the spread of transmittable diseases which had at the time been the principal cause of morbidity and mortality amongst the population.12
The latter activities were most comprehensively carried out by the School of Public Health in Zagreb. The school was established in 1926 and its new grounds opened a year later, in 1927, with the fi-nancial support of the Rockefeller Foundation. It was at that time that the School of Public Health became the central institution responsible
for the implementation of new and complex forms of public health-care work. In addition to this, Štampar initiated a range of organised activities aimed at establishing various laboratories with educated staff who procured the technology needed for the production of different immunological and serological preparations, which were in turn the precondition for the fabrication of diverse vaccines for the popula-tion. With the financial assistance of the Rockefeller Foundation in Zagreb, the laboratory established at the School of Public Health set up the technological equipment for the production of Neosalvarzan, a particular type of drug against syphilis. By doing so, the laboratory joined the ranks of only a small number of other institutions in 1930s Europe which had been producing a completely modern kind of medication.13
When the political environment changed at the beginning of the 1930s, Štampar was forced to leave the country and find work abroad, which marked the beginning of what would be a very rich interna-tional career under the auspices of the League of Nations Health Organisations. In 1932, he comes to China as an LNHO expert to occupy the post of healthcare advisor to Chiang Kai-shek’s govern-ment. From 1932 to 1936, Štampar visits China on three separate occasions, each taking an extended period of time, as his journal shows in great detail. During his stays in China, Štampar addressed many issues of public health, trying to organise healthcare services in this vast country much like he had previously done in the Kingdom of Yugoslavia. In the process, he took part in organising and promoting Western-style education among Chinese physicians, medical nurses and midwives. Working in such a large and populous country, which was moreover constantly ridden with war and tumult, was not an easy task. In his endeavours, Štampar encountered numerous problems which, among other things, often concerned ideological differences. As is widely known, he was congenial to social ideas which had at the time seemed quite radical. However, Štampar also found many associates and like-minded professionals among his Chinese peers, in addition to a number of Westerners who had come to China to find employment.4 One of his colleagues in this business was his former professor and old friend Julius Tandler. tandler and ŠtamPar in and around china and the ussrThe possibility of establishing Tandler in China while also making use of his expertise stirred correspondence between Štampar and Tandler concerning the manner in which such a possibility might be materialized. By 1933, Štampar had already travelled to China on one occasion and was preparing for another visit to the country and the continuation of his work there. That was why, in a letter to Štampar, Tandler discusses the possibility of going to China, writing: Surely you remember our last conversations about China! I just received an invitation from Mr. Yen to spend a few months in Shanghai and also hold lectures in anatomy there. I have already tentatively given him my consent and am currently handling the matter of how to bring this journey about. I should need to make my way there at the end of Au-gust. Naturally, provided that the political situation allows this. None-
Essay
78-85

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com81
theless, it would be of particular importance for me to know how the League of Nations sees this matter, although it does not concern the organisation directly. I imagine that the League of Nations may task me with a mission of its own, too, but I find it equally imagin-able that it might be better for me not to inform the Committee for Hygiene about my plans at all, considering the differing opinions of the Committee and myself about the training of physicians in China. It might come to pass that the Chinese government burdens me with this problem at once! And you know that I am a bad representative of diplomatic medicine! Seeing as we have already spoken of this issue several times, as well as expressed our common desire to travel to China together, I am informing you of all this and asking you for your opinion and advice. You might possibly – should you find it the right thing to do, of course – inform e.g. Reichmann in whichever way suits you that you have learned about my intention. I leave that all to you.14
In his reply to the letter, Štampar writes: During the time of the recent events in your country, I thought of you very often and was quite worried about your exceptional work… From your letter I have learned that the Faculty of Medicine in Shanghai had invited you to stay in China for a few months. I am acquainted with most of the gentlemen at the Faculty of Medicine in Shanghai and I believe the school to be the finest in China. Dr Yen, the dean of the faculty, is a remarkable man who managed to acquire funding for his institution during the gravest financial crisis. I think he is currently taking efforts to continue with institution building. Dr Bume is there, too. In my opinion, you were right in accepting the invitation. With the support of the League of Nations, numerous scholars have previously been invited to those faculties and, during my travels in China, I have met many foreign lecturers at institutions of higher education who had been invited there by the Chinese authorities. I have not had the opportunity to talk about these matters with Reichmann and I do not know what he thinks about them. One thing is certain: not everything needs to be executed through the League of Nations. I do not believe that the political situation in China will add difficulty to your journey. In today’s circumstances, various developments are bound to take place in such a large country, which is merely a part of the common flow of things. However, in my opinion, in no other country than China can so much can be seen, learned and done today. I am deeply convinced that you will see and find extraordi-nary things, considering your knowledge and experiences…Seeing as you have received an invitation from a Chinese university, I find that the Committee for Hygiene could have done well to entrust you with some sort of mission; it seems to me that diverse opinions of well-known experts on various issues should be collected in a country such as China; only that way will we come to a somewhat appropriate institution building programme; I do not know if Reichmann shares my opinion or how strong his wish to do so is; however, I will not miss the chance to discuss the matter with him. In any case, I will inform Reichmann about the invitation you received…15
As planned, Tandler was thereupon sent to China, which encour-aged discussion about plans for the autumn of 1933. In one letter dating from October of that year, Štampar says: I was very happy to hear from Dr Liu, the director of the Health Service, that he had invited you to Jiangsu and Nanjing. As per the itinerary, we are going to meet on our journey to Jiangsu and spend three days travelling together. Upon your return from Jiangsu Province, you are going to come to Nanjing.16 Dr Liu J. Heng was a surgeon who was respon-sible for the health sector as member of Chian Kai-shek’s regime, while also acting as the director of many significant institutions in China: he was the Director of the Nanjing Hospital and the Institute of Hygiene in Nanjing, the country’s capital at the time, the Head of the Army Medical Corps, Chair of the Committee for Opium Abuse Prevention, Director of the Faculty of Medicine in Beijing etc.
Štampar’s journal offers much greater insight into their encounters and the situational contexts in which they found themselves working. In his journal, for example, Štampar states: This evening, I am vis-iting Professor Tandler, who arrived to hold anatomy lectures at the Chinese medical school two weeks ago. I felt sorry when I saw him because I suddenly realized this man’s tragedy: he had dedicated his entire life to the advancement of his country and used his position as chief of health care in Vienna to create one of the world’s best health organisations, only to be forced to flee the circumstances in Austria, for which he neither has the propensity nor the aptitude, and to spend his old days in the Far East among foreign folk who cannot un-derstand him, let alone comprehend the tragedy of his soul. He told me that his impressions of the country were at first utterly unfavour-able; however, the other day he had witnessed the presentation of a new city building in the Chinese part of town which had been torn down last year. The Chinese youth whom he’d seen at the event made him convinced that white people had no business here in 30 years. We parted by agreeing on a schedule for our future meetings; for instance, we agreed that he would soon come to Nanjing and that we would go to Beijing together around Christmas.6
Štampar also dedicates a special chapter in his journal to Tandler, titling it “My Teacher Professor Tandler”. In it, he writes: As if he had sensed how future events would unfold, despite his now old age, Professor Tandler accepted an invitation from the Faculty of Medi-cine in Shanghai to teach a course in anatomy in the winter semester. I had met with him several times and was not able to convince him surely enough how things in Austria would unravel. In fact, not many shared my predictions, which later developments sadly showed to be correct. When I spoke about the matter with Rajchmann, Salter, Monnet and Bogomolov, the Soviet representative, at the local office of the League of Nations in Nanjing eight days before the events in Austria took place, nobody agreed with my view of things. When Tandler was returning from Beijing, I met him at the train station and informed him of the events in Austria. It was difficult for me to see the astonishment and tears in the eyes of this superb man, whose way of managing social welfare and public healthcare matters
Essay
78-85

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com82
in the city had been an exemplary model for the rest of the world. Nobody could understand the pain and the feelings he felt in those moments as well as me. I understood him when he read about how they were shooting canons to tear down the very workers’ housing whose construction he had commissioned for the health wellbeing of the common folk; I understood him when I saw him reading the news about the destruction of his organisation, about the dismissal of people he had raised to perform real health work. How much tragedy at the end of one’s life: the fruit of long and carefully planned labour was now a thing of the past.
In Štampar’s journal we also find the following mention of Tandler: During my stay in Shanghai, I was also visited by some other people, acquaintances with whom I had previously worked or with whom I had been in connection. Amongst the Europeans, the one I was most fond of was Professor Tandler, who had also come to China the previous year in order to do something in his life at a very unfavour-able time. We all know Tandler as a great anatomist and healthcare policy expert, who had taught anatomy at the University of Vienna for no less than 40 years. For the past 12 years, he was a member of the Vienna city administration, the best and most successful of all socialist administrations, whose merits nevertheless could not save it from falling prey to the reactionary forces which triumphed across Europe. It so came to pass that the 65-year-old Professor Tandler came to see the institutions he had created grow derelict and become absorbed by a new spirit, he saw workers’ housing bombed and wit-nessed the suffering of his associates and political leaders. At the first news he received about the events in Vienna, he hurried there by the fastest route, although he knew that what waited for him there was imprisonment and humiliation by the reactionary forces. However, in this regard as well as in others, the situation in Vienna was different to other countries where reactionary forces had gained a foothold. He was met at the border and told that he would be arrested. When he showed up at the Vienna train station, he was once more informed of the exact time when he would be picked up at his residence. At the station, he saw some acquaintances, some of whom avoided him just to stop him from coming near. Having come home, he got ready and took a bath and then later in the evening he was taken to prison. He was not told why he had been imprisoned until they finally fabricat-ed a story according to which he had been involved in planning the upheaval in Vienna in February of the previous year. It is interesting that foreigners stood by Tandler, most of all the American Medical Association who sent a telegram to Dollfuß, asking him about the reasons for Tandler’s imprisonment, to which Dollfuß failed to reply. When he later asked journalists, i.e. the representatives of the interna-tional press, to visit him and inform him of the authorities’ intentions, the main representative of the foreign press refused to come until the Chancellor answered the American Medical Association’s inquiry. After 12 days in prison, Tandler was released. The people of Vienna, particularly the common folk for whom he had worked so hard, loved and still love Tandler. Whenever he would show his face on the street, he was cordially greeted. As things always go, his experiences with
intellectuals were bad. Everybody avoided him, none of the active university professors so much as asked about him, let alone stood by him. Only Professor Eiselberg and Wagner Jauregg, who had retired long ago, inquired about his destiny. His immediate associates had been relieved of duty. The Jews had all been laid off. It was impos-sible for him to stay in Vienna, every step he took reminded him of the recent past and his activities: the decay of institutions and their spirit, into which he had invested so much of himself, the suffering of common folk, workers with whom he had grown close and whom he could not help in his present circumstances – all of this had such an effect on the old professor and social worker that he left Vienna last summer and fared off into the world in his old age simply to forget about his sorrow, should that prove to be possible. There is no doubt that Tandler would have found pleasure in new and constructive work once more and that the events in Vienna would have at least faded from his memory if it were not so difficult at his age to adapt to new circumstances and problems, which require different solutions than the problems he faced in Vienna. There is also another kind of trouble which meets such men of action and authority: Tandler was a member of a powerful party which wielded exclusive power in a large city with a competent local administration. He had an authority which nobody could oppose. He was always in his communication and quite galling in his criticism. His direct and dominating manner consequently caused him great difficulties in China, because he forgot that form is more important than the substance of the work done there. It was very hard for me to observe Tandler’s psychological distress as he made preparations to once again return to Austria, this time because the government refused to continue paying him his pension if he stayed abroad. This time he arrived to China through America, where he had been invited by the New York University Medical School to hold a se-ries of special lectures in anatomy. He had spent the past two months in Hunan, where he assessed the local medical school and set up an institute for anatomy with the help of his assistant. He had also stayed in Xi’an at the invitation of the Tongji University from Shanghai, who had asked him to look into the possibility of moving the university from Shanghai to Xi’an: he was thrilled with the idea and showed a strong intention to come back here and take part in the establishment of a new medical school on the principles he considered optimal. He asked me to take an interest in the matter and to make some arrangements concerning his arrival. We spent a few days in Shanghai together and this man, whom I found to be exquisite in every regard, made a deep impression on me at all times. Despite his mature age, he believed that he would live to see his ideals triumph. The actions of his political opponents in Vienna had made him very bitter and ev-erything I saw made me realize that he had a keen desire for revenge. What hurt him the most was the destruction of institutions which he had founded and which were without doubt among the best ones established in Europe during the past decade. When I escorted him to the shore one foggy morning, I felt a kind of ache in my heart to see my teacher waving his wide hat at me on the deck of a small boat carrying him down the river, where he was to board an ocean ship.6 Working in China was not easy and many obstacles came in one’s
Essay
78-85

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com83
way, especially for an elderly professor who could not easily sever his relations with his old homeland, his family and the work he had previously done. In a letter from 1935 sent to Tandler’s address in Vienna, Štampar explains to him once more the current situation in China in connection to a new offer for cooperation sent to Tandler: …in the meantime, you must have received the invitation. It was my wish to expressly let you know my opinion on this…The people in Nanjing have the best intention to establish a good medical school; they have invited you based on that outlook, although those same people did not treat you very nicely last year; naturally, we also need to take into account the Chinese character to be able to better un-derstand many things; however, of course, we are never going to have full disclosure of the forces which were in play then; let us leave those things to the past. First, I will tell you something about the invitation sent to you. From that invitation you may see that you will actually have two missions, one at the Military Medical School and the other at the Central University School; both sides will contribute the same amount of money for your remuneration; although it thus seems at first sight that you will have to serve two masters, that is only formally the case, in my opinion, because both schools are actually supervised by Dr Liu; thanks to his influence, Dr Cheer has been ap-pointed dean of the medical school at the Central University, seeing as he belongs to its staff; that means that you will in reality mostly deal with Dr Liu. It would not make much sense for me to write to you about Dr Liu, as you already know him very well; he is very alien to our ideology and that is something we must come to grips with; his wish is to do something good for China and the matter is one of a personal rather than a Chinese nature for him; in his heart of hearts he has a dislike of foreigners, especially those with stronger personalities; he prefers the foreigners which belong to his circle; I do not believe that he could be changed; he is the way he is and will stay that way. These are the things you need to bear in mind before you make your decision; nevertheless, I trust you will not have any moral difficulties if you only dedicate yourself to the task assigned to you; I believe that you will receive the funding necessary for the implemen-tation of your programme despite the difficult financial situation…Another thing concerning my situation; despite Dr Liu’s objections, I have managed to make certain progress in the provinces; I am now travelling southwest at the invitation of the provincial governments; it seems that the work in the west has taken root and I have very friendly relations to the people working there. I hope to have similar success on this journey, as well. However, the organisation of local activities by the League of Nations is so dismal that the value of all my success eventually and ultimately declines to a terrific degree; we are here to do something but we neither have a real mission nor any contact with the other branches of the League of Nations, like some forgotten children in a distant land; we receive excessive salaries but we mostly do little work; you must surely know how I feel and with whom my sympathies in China lie – not with the authorities but with the repressed people; however, all my activity completely depends on some individuals who are as fickle as the weather. I have not received any answer to my requests from Geneva for months,
yet without intellectual engagement in one’s work it is impossible to do good things and have lasting success; because of my ideological inclination, with which Dr Liu is well familiar, I have been having many difficulties with him; as you know, my work is not limited to one particular part of our profession but is rather of a general nature and in this sort of situation many difficulties arise…On the whole, there are still various possibilities for useful work here; however, only those who not only have great experience but also the moral strength to overcome many extraordinary difficulties are capable of performing the tasks ahead while still maintaining a fresh spirit and never sinking into pessimism. You possess those wonderful qualities; I told you all there is to say the way my conscience deemed it proper; think about it, my dear teacher, and decide upon it to the best of your knowledge and feeling.17
Tandler also receives correspondence concerning his repeated en-gagement in China from Berislav Borčić, Štampar’s closest associate, director of the School of Public Health in Zagreb and LNHO expert who also worked in China, where he once led the Nanjing Institute of Hygiene. In 1935, Borčić writes to Tandler in Vienna: I have been infomed that you have in principle agreed to take up a position at the Faculty of Medicine in Nanjing. I hope that you will give your definite consent and spend some years working in Nanjing. As I have learned, the gentlemen in Nanjing would be singularly pleased if you were to accept the offer and are ready to help you not only in the im-plementation of anatomy courses but also in the general work on the organization of the new faculty. Štampar is also very much looking forward to your arrival, although he does also have certain concerns, just like I do, because we know how difficult it is to cope with our Chinese friends. Štampar will stay in Nanjing most likely until March or April 1936, which would mean that you will still be able to meet him there, should you go to China. I will stay in Zagreb for some time, although I have received invitations from Nanjing and Geneva to return to Nanjing.18
Štampar writes about the possibility of Tandler’s return to China in his journal, stating the following: Professor Tandler has got in touch with me, too. He has once again been invited to Nanjing to spend two years organizing the Department of Anatomy at the newly established medical school, as well as at the Military Medical School in Nanjing. In his letter to me, he tells me that he must go abroad despite his old age because he cannot stand the mood in the city where he had so successfully worked for a number of good years. I was impressed by the content of the letter and I spent a long time thinking about my teacher, whose fate I share myself. Everything tells me that Tandler will accept the invitation sent to him because he still wants to create something in the autumn of his life. By the measure of his enthusiasm and optimism, he is still a young man, though he is now well into his sixties. He has received several offers to work in foreign parts but it seems to me that he likes the Far East because of its potential, even in the darkest of times, and that he expects to find some possibilities for useful work here.6
Essay
78-85

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com84
This offer to work in foreign parts, as will soon become clear, had ar-rived from the USSR, where Štampar himself travelled to, as well, just before the summer of 1936, leaving from Manchuria by Trans-Siberi-an Railway on his way to Moscow. He had done so at the invitation of the Commissariat for Public Health Protection of the USSR, in con-nection to the issue of hygiene standards in rural areas. A meeting of experts working for the League of Nations was scheduled to take place on the 15th of July 1936 in Moscow and was attended by many other public health experts from abroad, as well, such as Jacques Parisot and Ludwik Rajchmann as the director of the LNHO. The participants of the meeting were also temporarily joined by Selskar Gunn, a member of the staff of the Rockefeller Foundation. Of course, Tandler found himself in Moscow, too, having come there in February 1936 at the invitation of the Soviet government.
Štampar does not fail to record the following in his journal: …I had particularly been looking forward to dear Tandler, who came to the train station to welcome me but could not wait until the small hours of the night for my train, which had been running very late. Nevertheless, I met him the following morning and we could not get enough of our conversation. He had come to Moscow in February at the invitation of the Soviet government and, from what I saw, he was well-received. He was commissioned with overseeing the development of plans for a vast construction programme by the Commissariat for Public Health. He is staying at a hotel and does still not have his own office. He is thrilled with the reconstruction work being done by the Soviet Union but he complained to me about the bureaucracy stifling many things. According to his view of things, there are still some remnants of the imperial bureaucratic system left in the administra-tion and it will take a long time for the administration to be cleansed of that spirit. He told me that was how things had gone for them in Austria, too: they had had extraordinary plans but the Austrian impe-rial bureaucracy ruined many things. There are not many foreigners in the health service, at least in the headquarters, because the experiences they had with foreigners had reportedly been unfavourable. Seeing as Tandler had entered office in the Soviet administration, the Austrian
government renounced his right to a pension, which is why he is now pondering how to bring his family here, because it was hard for him on his own. He has a two-year contract with a monthly salary of 2000 roubles, while his apartment at the hotel is paid for from the office budget. According to his words, this salary is enough for him as a foreigner… 6
Štampar writes that, during the two days of his stay in Moscow, he had the opportunity to see the city and the immediate surroundings. The good Tandler took me for a ride outside the city in the evening. We were both amazed by the tremendous amount of activity in all directions… 6 Štampar and Tandler spent time together in the USSR in June and July 1936, while only a month later, in August 1936, Tandler passed away. Writing about Tandler in his journal with great nostalgia for his friend, Štampar says: and I was left without him in a large country to roam, to work, to cry and to laugh.6 conclusion
Štampar indeed continued to work and stand for the ideas which had shared with his professor Julius Tandler. However, the opportunities for constructive work in the field of public health grew increasingly slim in the political constellation of the time. The League of Nations was losing its power and its health organisation followed suit. The local resistance to foreign influences in China was becoming progres-sively intense. The ever more severe unrest led the world into World War II and pushed the establishment of an international public health order to the margins for some time to come. However, what remained in memory was a flow of ideas and experiences which had been formed in Central and Southeastern Europe and which subsequently tried to make their way far to the East and develop not only local but also general and international qualities. Many of these ideas became the basis for a new world-wide public health system that developed after World War II.
This research emerged as part of a project funded by the Croatian Science Foundation, Nr 5974, Transition of Croatian Elites form the
Habsburg Monarchy to the Yugoslav State, led by Iskra Iveljić.
literature:1. Hiller S.M, Jewell J.A., Health Care and Traditional Medicine in China 1800–1982, London, Routledge, 1983.2. Yip K., Health and National Reconstruction in Nationalist China, Michigan, Association for Asian Studies, 1995. 3. Borowy I. (ed.), Uneasy Encounters: The Politics of Medicine and Health in China 1900–1937, Frankfurt am Main, Peter Lang, 2009.4. Dugac Ž., Public health experiences from interwar Croatia (Yugo-slavia) and making Western medicine in the 1930s China. Acta Med Hist Adriat 2018; 16(1); pp. 75–106.5. Letter, Štampar to Tandler, Geneva, 26 July 1933, correspondence between Tandler and Štampar, archive of the Institut für Geschichte der Medizin–Josephinum, Vienna (AIGM).6. Dugac Ž. – Pećina M. (eds.), Andrija Štampar: Dnevnik s putovanja 1931–1938, Zagreb, HAZU, Srednja Europa, Škola narodnog zdravlja Andrija Štampar, 2008, pp. 734–735; 193-194; 266–267; 444–446;
512; 670-671; 676; 267.7. Julius Tandler, Archiv der Universität Wien, Vienna (AUW), 27 July 1895, Promotionsprotokoll M.33.6-33.9., p. 571.8. Sablik K., Julius Tandler: Mediziner und Sozialreformer: eine Biog-raphie, Vienna, A. Schendl, 1983.9. Hubensdorf, M. & Ludwig Teleky. Unpublished manuscript in preparation, kindly provided by the authors.10. Andrija Štampar, AUW, Nationale. Mediziner-Winter-Semester 1910–11, (S).0.11. Andrija Štampar, AUW, 23. Dezember 1911, Promotionspro-tokoll M.33.6–33.9., p. 571.12. Dugac Ž., Andrija Štampar (1888–1958): Resolute Fighter for Health and Social Justice. In: Borowy I., Hardy A. (ed.), Of Medicine and Men: Biographies and Ideas in European Social Medicine be-tween the World Wars, Frankfurt am Main, Peter Lang, 2008.13. Dugac Ž., Protiv bolesti i neznanja: Rockefellerova fondacija u
Essay
78-85

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com85
međuratnoj Jugoslaviji. Zagreb: Srednja Europa, 2015.14. Letter, Tandler to Štampar, Vienna, 9 May 1933, Correspondence between Tandler and Štampar, AIGM.15. Letter, Štampar to Tandler, Zemun, 20 May 1933, Correspon-dence between Tandler and Štampar, AIGM. Letter, Štampar to Tandler, Zemun, 20 May 1933, Correspondence between Tandler and Štampar, AIGM.16. Letter, Štampar to Tandler, Nanjing, 28 October 1933, Corre-spondence between Tandler and Štampar, AIGM.17. Letter, Tandler to Štampar, Hong Kong, 2 October 1935, Corre-spondence between Tandler and Štampar, AIGM.18. Letter, Borčić to Štampar, Zagreb, 21 October 1935, Correspon-dence between Tandler and Štampar, AIGM.
Essay
78-85

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com86
War Invalids and Disabled Soldiers in the Habsburg Army: The Case of the
Djurdjevac Regiment in 1860/61
Ivana Horbec1 , Dubravko Habek2,3
1 Croatian Institute of History, Zagreb, Croatia2 University Department of Obstetrics and Gynecology Clinical Hospital “Sveti Duh”, Zagreb,
3 Croatian Catholic University, Zagreb, Croatia
abstract:Soldiers of the Military Frontier fought numerous wars for the Habsburg Monarchy from the 16th to the 19th century. By the nature of their service they were susceptible to injuries and health difficulties that limited their ability to perform the service. The aim of this research was to analyse health conditions and most represented illnesses of Frontiersmen in the second part of the 19th century, as well as the Habsburg policy towards disabled soldiers and war invalids. The analysis is based on the case report and findings of the General Arbitration Commission of the Varaždin gen-eral command for the Đurđevac regiment in the military year 1860/61, kept in the Austrian State Archives.
Keywords: Invalids, Habsburgs Army, Military Frontier, medicine, medicohistoriography
Sažetak:Ratni invalidi i vojnici s invaliditetom u Habsburškoj vojsci: prikaz Đurđevačke pukovnije 1860/61.Vojnici Vojne krajine borili su se za Habsburšku Monarhiju u brojnim ratovima od 16. do 19. stoljeća. Po prirodi svoje službe bili su podložni ozljedama i zdravstvenim tegobama koje su ograničavale njihovo ispunjavanje službe. Cilj ovog istraživanja bila je analiza zdravstvenog stanja i najzastupljenijih bolesti u Graničara u drugoj polovici 19. stoljeća te habsburšku politiku prema vojnim invalidima i onesposobljenim vojnicima. Analiza se temelji na prikazima slučajeva i nalazi-ma Generalne arbitrarne komisije varaždinske generalkomande za Đurđevačku regimentu u vojnoj godini 1860./61., koji se čuvaju u Austrijskom državnom arhivu.
ključne riječi: Invalidi, Habsbruška vojska, Vojna krajina, Medicina, Medicinska historiografija
OPEN ACCESS
Correspondence: Ivana Horbec [email protected]/0000-0002-4898-2555
This article was submitted to RAD CASA - Medical Sciences as the Essay
Conflict of Interest State-ment: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Received: 28 August 2019Accepted: 27 October 2019Published: 17 December 2019
Citation:Hrobec I and Habek D. War Inva-lids and Disabled Soldiers in the Habsburg Army: The Case of the Djurdjevac Regiment in 1860/61.RAD CASA - Medical Sciences. 540=48-49 (2019): 86-91. https://dx.doi.org/10.21857/yl4okf3209
Copyright (C) 2019 Horbec and Habek.This is an open-access article distributed under the terms of the Creative Commons Attribution Li-cense (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original au-thor(s) and the copyright owners(s) are credited and that the original publication in this journal is cited, in accordance whit accepted adacemic practice. No use, distribution or re-production is permitted which does not comply with these terms.
Essay
86-91

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com87
introduction: the habsburg monarchy and its frontiers-men
The Military Frontier (Military Border, Germ. Militärgrenze) acted as a special military region along the eastern borders of the Habsburg Monarchy with the Ottoman Empire throughout the Early Modern Period up until its abolition in 1873/1881. As a territory with its own administrative, judicial and financial structure, the Frontier was cru-cial for the subsistence of the Habsburg Monarchy, as well as for the continuous existence of a stable military force. The population of the Military Frontier – known as the Frontiersmen (Germ. Grenzer) – undertook to defend the Monarchy in return for the land they were granted by the Habsburgs. Every grown man was therefore subject to military service for the Monarchy.
Governed directly from the Court of Vienna, i.e. the Viennese Court War Council (Hofkriegsrat), the Frontier was constantly reorganised and subject to numerous ordinances so as to keep the functionality in line with contemporary principles of warfare and public administration. At the end of the 17th century, following the Treaty of Karlowitz (1699) between the Habsburg Monarchy and the Ottoman Empire, the territory of the Military Frontier expanded towards the East and settled along the rivers of Danube and Sava, as well as in the eastern parts of the Banat of Temeswar so as to include parts of present-day Croatia, Serbia, Romania and Hungary. In the mid-18th century the Military Frontier was finally modelled after the regular regiments of the Habsburg army, with the difference that the Frontier’s general commands and regiments also served as administrative units until the second part of the 19th century. In Croatian lands under the Habsburg rule, the Frontier consisted of four general-commands (for Slavonia, Varaždin area, Ban’s Frontier and Karlovac area), subdivided into altogether 11 regiments. The Slavonian general command consisted of three regiments (Gradiška, Brod, Petrovaradin); General command of the Varaždin area of two regiments (Đurđevac, Križevci); Ban’s Frontier also of two regiments (Glina, Petrinja) and Karlovac general command of four regiments (Gospić, Lika, Otočac, Slunj)1-7 (for administrative division of the land cf. Map 1).
The Grenzers fought numerous wars led by the Habsburgs from the 16th to the 19th century – not only the Ottoman wars at the eastern borders of the Monarchy, but also, especially from the 18th century on, the European wars Habsburgs led with Prussia, France or Russia. Since the Thirty Years’ War (1618-1648) they gained a significant reputation in contemporary warfare8,9. However, the Grenzers were by the nature of their service also susceptible to health difficulties in performing the service. War invalids and disabled soldiers were so common in the Military Frontier that the Habsburg administration had taken a particular account on how to register or treat and reward these subjects, or even to restrict the burden they created to the society. This paper aims to illustrate the Vienna Court’s policy towards the disabled soldiers of the Military Frontier in the second half of the
19th century – in a time when a solid structure of the Frontier was set and the policy towards the disabled soldiers was firmly adopted. Our research relates to 348 disabled soldiers from a regiment of Đurđevac in Varaždin general command during the military year 1860/61. Relating to the overall policy of the Court of Vienna to-wards the disabled soldiers in the Habsburg Monarchy since 1750s, the procedures adopted by the Habsburg army will be analysed, as well as the health condition of the soldiers in relation to their age and service time in the army. The paper also aims to contribute to the knowledge of the major illnesses that affected the soldiers of the Military Frontier in the second half of the 19th century, as well as to the understanding of the state-controlled treatment of such individuals.
measures of state care towards disabled soldiers in the habsburg monarchy Since the second half of the 18th century, supported by the ideas of the Enlightenment, significant progress was achieved in the Habsburg Monarchy in the development of the public health care system10. Habsburg rulers and political centres of power in Vienna turned their attention to the social role of the state: active partic-ipation of the ruler and his institutions in regulating major social systems – as was the public health care – was defined as his duty, and an object of the state’s field of interest (political issue, or politicum). That resulted with designing a stable, (proto)modern system of a public health care in all provinces of the Habsburg Monarchy11, as well as with the foundation for all future regulations respecting current trends in the institutional approach to the public health care system. One of the major turning points in designing a stable, proto-modern system of public health care was the 1770 General Norm in Health Care Issues, the basic piece of legislation regulating the public health care system in the Habsburg Monarchy (Sanitäts- und Kontumazordnung; Generale normativum in re sanitatis)11,12. With this ordinance, a network of institutions was set up dedicated to the health care, with the new health care system being subordi-nated to the Habsburg ruler and exempt from the local spheres of influences. The expansion of the network of medical educational in-stitutions – from the Medical School of the University of Vienna to the specialized institutions, as was the Josephinum, a non-university academy primarily designed for training of military surgeons – had the decisive influence on the improvement of medical services and the further professionalization of medical professions10,11,13. Educated medical practitioners were granted the exclusive right to practice medicine, replacing all other competing providers of health care services (as clergy, quacks, herbalists and others): they became public servants, subject to state regulations.
Directly controlled by the Court of Vienna, the Military Frontier was a front-runner in implementing new health care standards and state ordinances. As early as the 1730s a Sanitary cordon was estab-lished as part of the Military Frontier on the eastern borders of the Monarchy, whose purpose was permanent anti-epidemic protection
Essay
86-91

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com88
of both of the Monarchy and entire Central Europe11,14. The number of medical personnel in the Frontier was much higher in comparison to the civil parts of the Monarchy (with only exception of the bigger cities). Every regiment of the Frontier had medical stationaries with military hospitals, pharmacies, several physicians and a dozen of military surgeons and midwives entrusted with the health care in companies. According to the Systematic regulation from 1800 (Sys-temalverordnung), each regiment had to have a physician in charge for the health care in the regiment (Regimentsartzt), two senior physicians (Oberartzt), four senior military surgeons (Oberwundar-tzt) and a major number of lower physicians and military surgeons, employed at the companies. The supreme control over the health care in the Frontier was exercised by the main military physician stationed in the headquarters in Zagreb15. This medical team was also responsible for detecting disabled soldiers and estimating their health conditions. It also provided an expert opinion on further treatment of these individuals.
An existence of a systematic state care for military invalids and disabled soldiers could be traced to the mid-18th century, when first institutional infrastructure aimed at facilitating self-sustainability of military invalids and disabled soldiers could be found, followed by a series of state ordinances and provisions of the Court War Council. The foundation of the Court Commission for the Invalids (Invalid-enhofkommission) in 1750/51 as an independent Court institution could be singled out as a turning point in making of the ruler’s strategy towards the military invalids and disabled soldiers16. The Commission consisted of representatives from several institutions – from the already mentioned Court War Council, then the General War Commissariat (Generalkriegskommissariat), which was techni-cally a sub-department of a General War Council responsible for the economics of the Habsburg military organisations, a Directorium in
publicis and cameralibus, a massive executive body of the supreme state administration in that period, Chancelleries of specific lands of the Monarchy etc. The Commission for the Invalids joined the Directorium in 1757 and the General War Commissariat in 1762, and was re-established as an independent Court institution under the name Department for Invalids (Invalidenamt). It was abolished in 1803, handing its agenda to the Court War Council. In larger cities the “Houses for military invalids” (Militärinvalidenhaus) were build aimed to take care for the war veterans and serving as almshouses. Also the legislation went in line with the institutional establish-ment: for example, it was ordained on August 5th 1750 that disabled individuals should have priority in gaining the apprenticeships at craftsmen17, and in 1759 the continuous financial help from military financial offices for disabled soldiers not admitted to the Invaliden-haus was established18. Since the second half of the 18th century, the donations to the foundation for the disabled soldiers were also encouraged19. On the other hand, disabled soldiers faced significant constrains in their public life: for example, the beggary was forbidden to them and military authority were obliged to keep the record of the soldiers who started such practice and to direct them to the Houses for military invalids17, and they were allowed to marry only under the condition the marriage would be approved by the Department for Invalids as a means of improving their condition – because their eventual offspring was estimated by the legislator as “more damaging than useful to the state”.
According to the 1807 General Law of the Military Border (Grund-gesetze für die Carldstädter, Warasdiner, Banal-, Slawonische und Banatische Militärgrenze) all military invalids were exempt from labour services21. The substantial care for the military invalids was encouraged by the local authorities too: for example, the Croatian Parliament asked from the Court of Vienna to grant more appro-
Map 1. The administrative division of the Croatian lands in the 18th
century. The Military Frontier along the Ottoman border is marked in dark
grey. Author of the map: Tomislav Kaniški.
Essay
86-91

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com89
priate support for the disabled Grenzers “that have long served”23. The establishment of foundations for financial support of disabled soldiers and their families is also mentioned in 19th-century sources: one foundation was, for example, established by the Administrative Commission in Vienna after the wars against the Napoleon in 1815, aiming to help the wounded soldiers of the Đurđevac regiment. This foundation was additionally confirmed by the “Statute of Governor Jelačić’s Foundation for invalid soldiers” on 24. November 185024. Towards, and during the 19th century, the Court War Council issued a number of ordinances related to the ascertaining of the disability of such subjects, as well as their treatment and classification. As the most important for 19th-century practice, the ordinances of March 29th and June 23rd 1777 and the provisions of November 11th 1800, December 26st 1801 and November 15th 1808 could be singled out25. Special revisions made by the corps of officers and brigadiers were also established, in order to inspect the health conditions of Grenzers in military units and determine their capacity for military service. The General Arbitration Commissions (Superarbitrierungs-commission), that existed at every general command, inspected their findings and proposed the treatment and classification to the Court War Council. They were empowered for the inspection only of the military personnel serving in the regiments under their jurisdiction.
a „nominal liSt“ of diSabled SoldierS for the ĐurĐevac regiment in the military year 1860/61The number of war invalids and disabled soldiers depended, of course, on activity of the Habsburg army and the Grenzers’ partic-ipation in war operations. During the wars their share in the adult male population of the Frontier could rise up to 75%, with “full invalids” building up to the 31% of the adult male population3. According to Karl Bernard von Hietzinger and his “Statistics of the Military Frontier” from 1817-1823, every 16th soldier from the Ban’s general command was found temporary disabled for military service due to his health conditions, as well as every 14th soldier of the Karlovac general command or every 17th soldier from Varaždin general command27.
Disabled soldiers and military invalids were classified by the Gen-eral Arbitration Commissions as the “full invalids” (Realinvalid), “half-invalids” (Halbinvalid) and “temporary disabled” (Zeitinvalid). According to the agreed classification, “full invalids” were individuals with incurable health issues, who were permanently incapable of military service, yet still capable of “light” services, as, for example, in military hospitals. The classification “half-invalids” related to the Grenzers who were, due to their health issues, permanently incapa-ble for warfare, but were still capable of other services in the Military Frontier. “Temporary disabled” were individuals who were tempo-rarily unfit for military service due to their health conditions, but could eventually be healed and again capable for military service25. Such list of disabled Grenzers were prepared by the corps of officers and brigadiers, and served for the General Arbitration Commission to organize a check-up and to provide an opinion for the Court War
Council on the classification of the individual soldier, his health con-ditions and future assignments in the Military Frontier. Some of the rare preserved sources could point to the extent on how these regulations were adapted in practice. Our research was focused on the case report made by the General Arbitration Commission for soldiers serving in the Regiment of Đurđevac in Varaždin General Command in the military year 1860/6128. The report was signed by Dr Matzner, head physician of the Varaždin General Command. According to the command of the Court War Council from May 2nd 1862, the Regiment of Đurđevac conducted a record of health conditions of all active soldiers serving in the regiment. The total of 348 soldiers were found unfit for the military service and were demobilised in the military year 1860/61. That number related to proximately 5% of the adult male population of the regiment. The results of the investigation were submitted to the General Arbitra-tion Commission of the Varaždin general command in May 1862. The Commission called all of the 348 men for a check-up and made a report on the Court War Council, suggesting the classification and treatment of these subjects. 24 of them were found fitting for the military service again. Nine of them were classified as “temporary
Diagnosis Nr. of soldiersAmputations and wounds
with neurological and
orthopedic sequelae
60
Chronic respiratory
obstructive diseases
51
Orthopaedic deformities and
anomalies
39
Tuberculosis 23Hernia, hydrocele 20
Eye diseases 18
Weakness 18Skin diseases 16
Rheumatism 12
Spleen diseases 11Ear diseases 10
Psychiatric diseases 8
Gout 7Goiter 3
Epilepsy 2
Baldness 1Tooth decay 1
Scorbut 1
Table 1. The illnesses of the soldiers diagnosed in the regiment of Đurđevac in Varaždin general command in the military year 1860/61
Essay
86-91

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com90
disabled”, whose recovery was soon to be expected. 22 men were classified as “half-invalids”, and four men were sent to a health resort of Topusko in the Ban’s general command for recovery. One man was sent to the hospital for further check-up, and altogether 21 men did not respond to the call due to their illness or other reasons. Seven people died during the process. Others (248 men) were proclaimed “full invalids” and not capable for further military service. The disabled soldiers were 20 to 34 years old and served in the mil-itary from 5 months to 16 years until their disability. According to the findings of the General Arbitration Commission of the Varaždin general command, most of the disabled soldiers (60 cases) were diag-nosed with conditions from amputations and wounds with neurolog-ical and orthopedic sequelae (neuralgia, paresis, limb shortening or amputees). In 39 cases orthopaedic deformities and anomalies were diagnosed. Chronic respiratory obstructive diseases (asthma, emphy-sema) were reported in 51 patients, while tuberculosis was diagnosed for 23 patients. 20 soldiers were diagnosed with hernia and hydro-cele, while poor eyesight and other eye diseases (trachoma) was found in 18 examined soldiers. Probably due to malnutrition, 18 inspected soldiers were diagnosed with weakness and infirmity. Furthermore, skin diseases (scrofula, ulcer) were diagnosed for 16 examined soldiers, rheumatism for 12 soldiers, heart and spleen diseases for 11 soldiers, deafness and ear diseases for 10 soldiers, psychiatric diseases for eight soldiers. Finally, seven of the examined soldiers had gout, two epilepsy, three goiter, one baldness, one tooth decay and one scorbut (Table 1).
The beginning of the second half of the 19th century was an era of then-incurable infectious diseases, such as tuberculosis, which had a natural course but with high morbidity and complications, up to high mortality. Only then will infectious agents of infectious diseases slowly begin to be discovered and disinfection and antisepsis put into operation, still far from the discovery of chemotherapeutics and antibiotics.
The above diagnoses and the morbidity among the male population are typical for the pathology for the time. The results could be com-pared to the data of hospitalized patients at the Zagreb Foundation Hospital in 1839, presented by Lujo Thaller29. Mostly the infectious diseases were diagnosed: recurrent fever and sexually transmitted diseases (lues, gonorrhea), as well as diarrhea, itch and tuberculosis, followed by chronic dementia, gout or meningitis. According to our own research of the hospitalized patients in the military hospital (Garnisonsspital) in Bjelovar in the beginning of the second half of the 19th century, the most common cause of death was tuberculosis in 19.7%, hydrops in 16.4%, pneumonia 10.5%, typhus 5.9% and febris nervosa in 4.8%30.
literature:1. Moačanin F, Valentić V. Vojna Krajina u Hrvatskoj, Zagreb: Po-vijesni muzej Hrvatske, 1981.2. Valentić V. Vojna krajina i pitanje njezina sjedinjenja s Hrvatskom, Zagreb, 1981.3. Roksandić D. Vojna Hrvatska – La Croatie Militaire. Krajiško društvo u Francuskom carstvu, sv. 1, Zagreb: Školska knjiga, 1988.4. Buczynski A. Gradovi Vojne krajine, II vols, Zagreb, 1997.5. Kaser K. Freier Bauer und Soldat: die Militarisierung der agrar-ischen Gesellschaft an der kroatisch-slawonischen Militärgrenze (1535-1881), Wien-Köln-Weimar: Böhlau, 1997.6. Štefanec N. Država ili ne. Ustroj Vojne krajine 1578. godine i hr-vatsko-slavonski staleži u regionalnoj obrani i politici, Srednja Europa, Zagreb 2011.7. Roksandić D, Milković Šarić K (eds.), Vojna krajina u suvremenoj historiografiji, Zagreb, FF Press, 2012.8. Brnardić V. Imperial Armies of the Thirty Year’s War: Infantry and Artillery. Oxford: Osprey Publishing, 2009.9. Brnardić V. Imperial Armies of the Thirty Year’s War: Cavarly. Ox-ford: Osprey Publishing, 2010.10. Spary EC. “Introduction: Centre and periphery in the eigh-teenth-century Habsburg ‘medical empire’”, Studies in History and Philosophy of Biological and Biomedical Sciences 43 (2012), 684-690.11. Horbec I. Zdravlje naroda – bogatstvo države. Prosvijećeni apsolu-tizam i počeci sustava javnoga zdravstva u Hrvatskoj. Zagreb, 2015.12. Supplementum Codicis Austriaci, oder Chronologische Sam-
mlung aller vom 1ten Jänner 1759 bis letzten Dezember 1770 […] erlassenen Generalien, Patenten, Satzordnungen, Rescriptem, Resolutionen, dann Landesobrichkeitlichen Edikten, Mandaten und Dekreten, part VI., Vienna 1777, pp. 1247-1298. 13. Broman TH. The Transformation of German Academic Medicine, Cambridge University Press, 1996.14. Vodopija J (ed.), Sanitarni kordon nekad i danas. Zbornik radova Simpozija odr#anog u povodu 250-te obljetnice Sanitarnog kordona. Zagreb: Interpublic, 1978.15. Bazala V. Poviestni razvoj medicine u hrvatskim zemljama, Za-greb, 1943.16. Walter F. Die österreichische Zentralverwaltung, Vol II: Von der Vereinigung der Österreichischen und Böhmischen Hofkanzlei bis zur Errichtung der Ministerialverfassung (1749-1848). Part I/I: Die Geschichte der österreichischen Zentralverwaltung in der Zeit Maria Theresias (1740-1780). Wien, 1938.17. Joseph Kropatschek, ed.] Sammlung aller k. k. Verordnungen und Gesetze vom Jahre 1740 bis 1780 […], Vol. I. Wien 1786.18. Joseph Kropatschek, ed.] Sammlung aller k. k. Verordnungen und Gesetze vom Jahre 1740 bis 1780 […], Vol. III. Wien 1786.19. Joseph Kropatschek, ed.] Sammlung aller k. k. Verordnungen und Gesetze vom Jahre 1740 bis 1780 […], Vol. VII. Wien 1787.20. Joseph Kropatschek, ed.] Sammlung aller k. k. Verordnungen und Gesetze vom Jahre 1740 bis 1780 […], Vol. VI. Wien 1786.21. Milković K. “Položaj časnika prema zakonskoj regulativi za Vojnu krajinu: Krajiška prava (1754.) i Osnovni krajiški zakon (1807.),
Essay
86-91

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com91
Povijesni prilozi 31 (2006), pp. 161.-182. 22. Roksandić D. Vojna Hrvatska – La Croatie Militaire. Krajiško društvo u Francuskom carstvu, sv. 1, Zagreb: Školska knjiga, 1988.23. Čepulo D, Krešić M, Hlavacka M, Reiter I (eds.) Croatian, Slove-nian and Czech Constitutional Documents 1818-1849. Berlin, New York: De Gruyter, 2010.24. Statuten des Ban Jellačić-Invalides Fondes. Agram, National Buchdruckerei des Dr. Ljudevit Gaj, 1850. Croatian State Archives in Zagreb (Hrvatski državni arhiv Zagreb), holdings Zagreb General Command (Zagrebačka Generalkomanda), box 12, R 6-1850.25. von Bundschuh C (ed.), Uibersicht das bey der k. k. österre-ichischen Armee bestehenden Militär-Oeconomie-Systems und aller sich darauf beziehenden Gesetze, III. Supplement. Prag 1817.26. von Bundschuh K. Zusammenstellung derjenigen Diestespflicht-en […]. Prag, 1826.27. von Hietzinger CB. Statistik der Militärgrenze des österre-ichischen Kaiserthums. Ein Versuch. Vol.1, Wien 1817.28. The Austrian State Archives (Österreichisches Staatsarchiv], War Archives (Kriegsarchiv), Court War Council (Hofkriegsrat), 1862-8-15-2/10.29. Thaller L. Povijest medicine u Hrvatskoj Slavoniji od godine 1770. do 1850. Karlovac: Dionička štamparija d.d.,1927.30. Habek D. Iz povijesti zdravstva Bjelovara. Zavod za znanstvenois-traživački i umjetnički rad u Bjelovaru. Zagreb, Bjelovar: Hrvatska akademija znanosti i umjetnosti, 2015.
Essay
86-91


RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com93
author: Filip Đerke
In the today’s highly civilised society, sports and recreational sports are generally present phenomena. Sports medicine follows the track of their development as well. It is not exclusively in-tended for top class sportspeople. It rather stands in service of every individual and the whole community – from childhood to old age.This is the reason why knowledge regarding the achievements of sports medicine are of importance for the wide circle of medical experts, healthcare and sports workers, kinesiologists, coaches, and – naturally – sportspeople and persons engaging in recre-ational sports. It is important that all who engage in sports and recreational sports have at their disposal an available source of information from the domain of sports medicine, compiled by specialists in individual fields.The book tackles the following issues included in the scope of activities covered by sports medicine: physiology of sports and exercise; pre-participation screening; theory and methodology of training; sports nutrition, doping, traumatology; problems related to the female sex and age; sports cardiology; biomechan-ics; regenerative medicine; injuries in individual sports. Separate chapters are dedicated to analysing the possibilities of protection against injuries of the orofacial area, the head and the brain. Ma-jor attention is furthermore paid to the syndromes of overuse injuries of the musculoskeletal system, considering their ever in-creasing frequency related both to the population in general and to sportspeople and persons engaging in recreational sports in particular.The book contains tributes by 59 authors of various specialities. This reflects the state of the today’s sports medicine (medicine in the sports), which uses the knowledge from diverse professions in scientific and everyday practical work. The interdisciplinarity in-deed is the greatest value of this textbook. The book was written based on the yearlong rich experience of the chief author, and on the enthusiasm of his younger co-authors – well-renowned both in Croatia and abroad.Divided in 39 chapters, on 406 pages, the book includes 412
Book Review
figures and drawings (mainly in colour), 55 tables, and 380 ref-erences.
Book PromotioOn Wednesday, November 27, 2019, a solemn presentation of the book Sports Medicine, authored by academician Marko Peć and associates, took place at the HAZU Palace.In front of the crowded HAZU Hall, the book was initially ad-dressed by the academic Miličić as a host in front of the HAZU, and in front of the School of Medicine, University of Zagreb Prof. Marijan Klarica, then on behalf of the University of Applied Health as a co-publisher of this valuable work and as co-author of the work Dean Prof. Krešimir Rotim, and reviewers of the work. The speakers emphasized the significant contribution of many co-authors who, as authors of individual chapters, actively con-tributed to the high quality of the book. The book Sports Medi-cine is a capital issue in the field of Sports Medicine, co-published by the University of Applied Health, the School of Medicine, University of Zagreb and the Publisher “Medicinska naklada”. The textbook itself is a modern teaching material that shows the wealth of knowledge and experience that the authors want to share with all doctors, especially specialists in occupational med-icine and sports, physical medicine and rehabilitation, orthopae-dics, traumatology, kinesiology, but also students of postgraduate doctoral and specialist studies.
SPORTS MEDICINE Medicinska naklada, Zagreb 2019
From left to right: Krešimir Rotim, Anđa Raič, Boris Labar, Domagoj Delimar Marko Pećina

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com94
Book Review
author: Vjekoslav Jerolimov
The book was presented on 4 July 2019 in the Revival Stateroom of the Croatian Academy of Sciences and Arts (Zagreb, Opatička 18). The beginning of the presentation was marked by opening words given by academician Zvonko Kusić, president of the Foundation of the Croatian Academy of Sciences and Arts, prof. Damir Boras, PhD, rector of the University of Zagreb, and academician Vida De-marin, secretary of the Department of Medical Sciences of the Cro-atian Academy of Sciences and Arts. The book was then presented by book reviewers prof. Goranka Prpić Mehičić, PhD, prof. Hrvoje Brkić, PhD, and academician Vjekoslav Jerolimov. At the end of the promotion the public was addressed by prof. Zrinka Tarle, PhD, book editor and Dean of the School of Dental Medicine, University of Zagreb, and prof. Anđa Raič on behalf of the publishing house Medicinska naklada from Zagreb.The authors of this university textbook are Marko Jakovac, Bernard Janković, Eva Klarić Sever, Danijela Marović, Vlatko Pandurić, Katica Prskalo and Zrinka Tarle from the School of Dental Med-icine, University of Zagreb and Alena Knežević Čizmić from the Herman Ostrow School of Dentistry, University of Southern Cal-ifornia, Los Angeles, USA. This textbook presents an important and indispensable piece of lit-erature for a successful mastering of subjects in graduate and post-graduate studies of dental medicine, approved by the University of Zagreb in the series Manualia universitatis studiorum Zagrabiensis. The textbook is completely compatible with clinical courses Restor-ative Dental Medicine I and Restorative Dental Medicine II, as well as with the preclinical course Preclinical Dental Medicine, which are fundamental study courses at the School of Dental medicine in Zagreb. The book completely covers implementation plans of these courses at the 4th and 5th year of the study of dental medicine, and will be useful not only for students of integrated undergraduate and graduate study, but also for students of postgraduate doctoral and specialist studies.This university textbook is a comprehensive reading piece which contains all the segments important for understanding both the theoretical and the practical level of restorative dental medicine. It is divided into 18 chapters which cover anatomical and biological
properties of dental tissues, case history and diagnostic procedures in restorative dental medicine, developmental tooth anomalies, as-sessment of the condition of hard tooth tissues, tooth caries, dental trauma, dental instruments and dry work field, minimally invasive preparations, pulp protection, glass-ionomer cements, dental amal-gams, making of amalgam fillings, adhesive systems, composite ma-terials, polymerisation, making of direct composite fillings, indirect restorations, ceramic materials, post endodontic tooth restoration and tooth bleaching.
This extremely valuable study material – a textbook, the first of its kind in Croatia when it comes to range and value, will greatly fa-cilitate mastering the afore-mentioned study parts of graduate and postgraduate studies in dental medicine. The book is methodically and extremely appropriately conceived, and it contains a large num-ber of pictures and charts, which will greatly alleviate acquiring the course matter and enrich the textual part of the textbook. The au-thors have used the most relevant world literature, as well as citations based on their own extensive research, which shows their great com-petence for writing this university teaching material. The originality of this textbook can also be seen in its contemporary approach to pathological manifestations and diagnostic, therapeutic and preven-tive procedures in restorative dental medicine, which are often not recognised enough or on time in everyday dental practice. Simply said, this is an extremely important educational material of the mod-ern study of dental medicine.
Promotion of the book „Restorative Dental Medicine“, Zrinka Tarle and col. at the Croatian Academy of Sciences and Arts in Zagreb

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com95
Book Review
authors: Vladimira VuletićDaniel Rukavina
The promotion of the book “Neurodegenerative Diseases – Demen-tias” took place at the University of Rijeka campus on 17th of Sep-tember 2019, as part of the 34th Symposium of the Department of Biomedical Sciences in Rijeka of the Croatian Academy of Sciences and Arts. The title of the symposium was “A modern approach to diagnosis and prevention of dementias”. The book is published by the Croatian Academy of Sciences and Arts, with main editors Ac-ademician Daniel Rukavina and Ass. Prof. Vladimira Vuletić. The promotion and symposium were very well attended, with approx-imately 70 participants. Welcome words were given by the editors and two reviewers, Prof. Emerit. Juraj Sepčić, and Academician Vida Demarin, on behalf of Academician Zvonko Kusić, who could not attend the meeting.Both reviewers congratulated and remarked on the extraordinary quality of the book proceedings, as well as the timing of the main topic, as dementias become a greater issue to the older general popu-lation in the developed world. The articles published in this book are contributions of invited speakers attending the 2nd Forum on Neu-rodegenerative Diseases which was held in Rijeka on October 17th, 2018. Co-organizers of the Forum were the Clinical Hospital Center in Rijeka, the University of Rijeka Faculty of Medicine, and the Cro-atian Medical Association – Branch office Rijeka. The symposium was endorsed by the European Association of Neurology (EAN) and was held under the auspices of the University of Rijeka, which cele-brated its 45th year of the foundation of modern University and 385 years of the University of Rijeka’s establishment by the Jesuits. The meeting aimed to introduce to all those interested on what hap-pens when a person loses the guaranteed wealth of his most isolated organ - the brain, by the devastating effects of chronic diseases. From that meeting, a book was created, that covered the topics spoken about at the meeting and primarily covers the clinical face of neuro-degenerative diseases with dementia: Parkinson’s disease, Lewy body dementia, vascular pathology of the brain, prion diseases, cognitive issues in multiple sclerosis, neuroimaging diagnostics and pathology, as well as pharmacological therapy and prevention options.In the articles presented in the first part of the book some basic mechanisms were discussed. Professor Hardy gave an overview of genomic analyses of neurodegenerative diseases identifying many genes involved in their pathogenesis. Professor Revesz presented from the neuropathologists perspective and professors Manganotti and Babić from neurophysiological and neuropharmacological as-pects. Professor Vida Demarin gave a focus on approaches for pre-vention. Clinical aspects and pathophysiological mechanisms were in the focus of presentations of Professors Bogdanović, Padovani, Pirtošek and Vuletić. Cognitive problems in the field of demye-linating diseases of the central nervous system were highlighted by Professor Fredrikson and other clinical aspects were in the focus of articles of Professors Borovečki and Klepac. We are delighted with the contribution of Professor Eric Smeets who gave an overview on clinical management of the very rare disease called Rett syndrome. The reviewers remarked that neuroscience attracts clinicians and
researchers from various scientific disciplines and many, including some of those present, consider it one of the most challenging fron-tiers of science. It is no coincidence that the “brain decade”, which ended in the last century, is followed by the “century of the mind”. The progress made in recent decades in understanding the biology of the nervous system is remarkable; however, the results of contin-uous research are still insufficient to resolve the many unknowns in understanding the etiopathogenetic mechanisms of numerous nerve disorders, especially those that lead to progressive and irreversible brain failure - dementia.With this book, the readers have been given a valuable, pluri-dimen-sional book. The very well documented chapters combine the funda-mental and clinical aspects of dementia in neurodegenerative diseas-es. Attention has also been paid to health and social programs aimed at improving the prognosis of dementia, previously considered fa-tal. This book will, of course, have a primary educational function. According to reviewers opinion it will serve healthcare profession-als (and associated professions) by enriching their professional bio-medical culture, improving their day-to-day work and the services they provide to such patients; discussions will stimulate researchers with ideas for new projects and stimulate all of us, professionals and laypeople, to change our “lifestyles” and preserve the health of our brains. There is no health without brain health!The book before us is a contribution to a better knowledge of the chronic diseases of the central nervous system that affect our exis-tence, take it and open it; on its pages, among the multitude of para-graphs and facts, each of us will find sentences written for him.
The promotion of the book “Neurodegenerative Diseases – Dementias” at the Campus of the University of Rijeka in Rijeka

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com96
News & Education
author: Filip Đerke
On December 11, 2019, held the “Dies Academicus” of the Croatian Academy of Medical Sciences (CAMS) at which on behalf of the Academy the president of the Academy Professor Jasna Lipozenčić and the Chairman of the Academy’s Commit-tee on awards and acknowledgements Professor Šime Mihatov have awarded Professor Vida Demarin as the title Laureate of the Academy for the year 2018. The ceremony venue was the main hall of the Croatian Medical Association. According to the Academy’s protocol, every year they can award one outstanding member. Professor Demarin has been the full member of the CAMS since 1994, in some terms, she had been an active mem-ber of Academy Committees and in her professional work, she contributed to the reputation of the Academy in Croatian and international society.
Professor Demarin is not only the reputable researcher, also the Deputy editor in the RAD CASA Medical sciences and Pres-ident of the Department of Medical Scieces at the Croatian Academy of Sciences and Arts, is the full professor with tenure at the University of Zagreb. Her main areas of research studying are vascular disorders of the brain, the cerebral autoregulation and cerebral vasoreactivity. She is a pioneer in s Doppler Diag-nostics in Croatia and in Central and Southeastern Europe, and her work has significantly advanced the noninvasive diagnosis of cerebrovascular disorders in primary prevention of stroke. She has published more than 400 scientific papers, 59 papers and 59 books and educational texts. She has given more than 150 invited lectures at international and 50 national conferences on. There are more than 4000 citations in the SCI. She is the editor and also a member of several editorial boards of medical jour-nals. Professor Demarin is successfully organizing several na-tional and international congresses, symposia and courses. Since 2002 she is organizing conferences on evidence based medicine, and since 2003 is leading conferences on brain disorders, orga-nized by the Department of Medical Sciences of the Croatian
Professor Vida Demarin - the Laureate of the Croatian Academy of Medical Sciences
Academy of Arts and Sciences. She was a principal researcher in many completed projects of the Ministry of Science, Edu-cation and Sports, Head of the Croatian branch of four inter-national projects, Principal researcher in several international neuropharmacological researches. She is President of the Board or a member of several international scientific societies and was elected a member of the American Academy of Neurologists, the American Society for Heart and Stroke and the European Society for stroke.Professor Vida Demarin is one of the pioneers of preventive ac-tion in the prevention of cerebrovascular disease and improving the quality of life. She was among the founders of the Croatian Neurological Society and CMA, and was its president, then the Croatian Society for Stroke Prevention and the Croatian Soci-ety for Neurovascular Disorders of the CMA. She is a member of the Croatian Academy of Medical Sciences since 1994. Pro-fessor Demarin affirmed in the country and abroad, and her scientific and professional work has significantly influenced the development of neuroscience in Croatia and worldwide.
Prof.Vida Demarin, MD, PhD, Full member of CASA, Head of the Department of Medical Sciences CASA

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com97
News & Education
authors: Vladimira VuletićDaniel Rukavina
The symposium „3rd Rijeka Forum on Neurodegenerative Diseases: Diagnosis and Treatment in Early Stage of Dis-ease“ was held in Rijeka in the campus of the University of Rijeka (October 17-18, 2019) under the patronage of the Department of Biomedical Sciences in Rijeka of the Croa-tian Academy of Sciences and Arts. Medical Faculty of the University of Rijeka, the Croatian Neurological Society and the Rijeka branch of the Croatian Medical Association were co-organizers.Three years ago, in discussions with Dr. Vladimira Vuletić, Chairman of the Department of Neurology at the Clinical Hospital Center in Rijeka, we came to the idea of organiz-ing meetings in Rijeka, on the topic of neurodegenerative diseases. The idea was to organize meetings on an annual ba-sis, each year bringing new aspects, approaches, and break-throughs in this flourishing clinical and scientific field, set to be held under the auspices of the Croatian Academy of Sciences and Arts. Our intention was that meetings (called as Rijeka Forum) follow translational approach in the field of neuroscience. This is the same approach we used as the main idea and one of the principal goals of all meetings held in Rijeka in the last six years in the organization of Depart-ment of biomedical sciences in Rijeka of the Croatian Acad-emy of Sciences and Arts. The 3rd Rijeka Forum is showing that we already established the tradition.This year 17 lecturers from 5 countries, experts in the field of neurodegenerative diseases, delivered riveting lectures fo-cusing on the aspects of early diagnosis and treatment, as well as prevention of the debilitating chronic neurological diseases. The symposium had free attendance and attracted a wide audience, from graduate and postgraduate students, to basic and clinical medicine scientists.The symposium was opened with introductory talks of the president of the Scientific committee, Daniel Rukavina, full member of Croatian Academy and the Head of the De-partment of Biomedical Sciences in Rijeka and Vladimira Vuletić, president of the Organizing committee and head of the Department of Neurology at the Faculty of Medicine Rijeka and head of the Clinic of Neurology at the Clinical Hospital Center Rijeka. Furthermore, welcome addresses were given by Zdravka Poljaković, President of the Croa-tian Neurological Society, Davor Štimac, Head of the Clin-ical Hospital Center Rijeka, Tomislav Rukavina, Dean of the Medical Faculty of the University of Rijeka and Vida Demarin, Secretary of the Department of Medical Sciences and full member of the Croatian Academy of Sciences and Arts.The symposium was split into three main topics, first en-
compassed the genetic, cerebrospinal fluid and pathological determinants of neurodegenerative diseases. This was fol-lowed by the early diagnostic and prevention, while the last topic was the clinical aspect and treatment of neurodegener-ative diseases. The opening lecture of the first topic was held by the esteemed professor John Hardy, of the UCL Institute of Neurology (London,UK), who spoke about the genomics of neurodegeneration and enlightened the rapid progress in understanding the genetic background of these diseases that happened in the last ten years. He was followed by Borut Peterlin (University Clinical Center Ljubljana, Slovenia), who spoke about a personalized approach to patients with Parkinson’s disease based on their genetic background. A focus on finding the right biomarkers and connecting early preclinical research in degenerative diseases were the focus of lectures given by Kaj Blennow (Gothenburg University) and Tamas Revesz (University College London).The second topic, focused on diagnostics and prevention, was opened by Vida Demarin (International Institute for
The 3rd Rijeka Forum on Neurodegenerative Diseases: Diagnosis and Treatment in Early Stage of Disease

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com98
News & Education
Brain Health, Zagreb), who has given an interesting and im-portant overview of lifestyle factors in prevention of cogni-tive decline. This was followed by a lecture from Paolo Man-ganotti (University of Trieste), who focused on the clinical neurophysiology measures in neurodegenerative disorders. The next lecture was given by Alessandro Padovani (Univer-sity of Brescia, Italy), who explained the emerging findings from TMS and DATSCAN in enlightening the early alter-ations in cholinergic and dopamergic systems in Alzheimer’s disease. The penultimate lecture of the first day was given Maja Trošt (University Medical Center Ljubljana), who pre-sented the latest findings in using PET FDG as a biomarker of early stages in neurodegenerative diseases. Finally, the day was closed by Lea Dolenc Grošelj (University Clinical Cen-ter Ljubljana. Slovenia), who spoke about sleep as an early marker for neurodegenerative diseases.The second day of the symposium was focused to the lec-tures covering the clinical aspects and treatments of neuro-degenerative diseases. The opening lecture by Sten Fredrik-son (Karolinska Institute, Stockholm, Sweden) covered the early detection of multiple sclerosis, with some new insights on when the disease really starts. The differences, and similarities, of dementia in Alzheimer’s disease and Lewy Body dementia was the topic of the lecture by Nenad Bogdanović (Karolinska Institute, Stockholm, Sweden), who was followed by Fran Borovečki (University Hospital
Centre Zagreb) with his lecture on the early diagnosis of Fronto-Temporal Dementia. Furthermore, Nataša Klepac (University Hospital Centre Zagreb) spoke about the early diagnosis of the Corticobasal Syndrome and Progressive Su-pranuclear Palsy, while Darko Chudy (University Hospital Centre Dubrava, Zagreb) presented his work on early deep brain stimulation in various movement disorders. Vladimira Vuletić (Clinical Hospital Center Rijeka) presented a thor-ough overview of the possible biomarkers in early Parkin-son’s disease. The final topic of the symposium was closed by two lectures focusing on Rett syndrome, which were given by two experts, Leopold M.G. Curfs and Eric Smeets, from the Rett Expertise Center in Maastricht, Netherland. They spoke on the Rett syndrome in general within an European context, while also focusing on the developmental regression aspects of the disease.Overall, this international symposium had truly magnificent lectures, which were interesting for all participants. Impor-tantly, it presented as a great occasion for young students and researchers to discuss these important topics with the leading international experts. The Fourth Rijeka Forum will be held next year, in a similar time and at the same venue of the new University Campus in Rijeka. This is a clear sign that Rijeka Forums on neurodegenerative diseases have es-tablished both tradition and international recognition.

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com99
News & Education
authors: Petra Črnac ŽunaHrvoje BudinčevićEdvard GalićVida Demarin
The 18th Scientific Conference on Brain Disorders was held on October 25th 2019 at the Library of the Croatian Academy of Sciences and Arts, entitled: Heart and Brain - Risk Factors and Prevention.The main organizer of the event was the Medical Sciences De-partment of the Croatian Academy of Sciences and Arts, co-or-ganized by the International Institutefor Brain Health, the Cro-atian Stroke Society and the Hypertension, Infarction & Stroke Prevention Association.The event was held on the occasion of World Stroke Day, cele-brated on October 29th, thus contributing to the propagation of the importance of a mutidisciplinary approach in the preven-tion and treatment of risk factors for cerebrovascular disease.The event was conceived as a series of interdisciplinary lectures and an interactive section. It attracted approximately 100 par-ticipants and significant interest from the media and the general public. The lectures have been held by 11 distinguished lectur-ers, experts in the fields of neuropsychiatry, neurology, nephrol-ogy, endocrinology and cardiology.Prof. Vida Demarin gave a lecture about the importance of the prevention of modifiable risk factors for heart and brain dis-eases, focused primarily on the importance of lifestyle, nutri-tion and physical activity. Prof Bojan Jelaković spoke about the practical approach in the treatment of arterial hypertension and presented many new findings and guidelines for daily clinical practice. Prof Zdravka Poljaković interpreted the management of arterial hypertension in acute stroke. Ass Prof Edvard Galić talked about new options in the treatment of dyslipidemia. Prof Tomislav Breitenfeld gave a lecture about hyperlipidemia and stroke. Ass Prof Miro Bakula spoke about the impact of obe-sity on diseases of the cardiovascular system. Ass Prof Sandra Morović gave a lecture on how obesity affects the brain. Prof Diana Delić Brkljačić talked about the timing and individual-ization of anticoagulant therapy before stroke. Ass Prof Hrvoje
Budinčević gave a lecture about the timing and approach of anticoagulant therapy introduction after stroke. Ass Prof Dario Rahelić spoke about the impact of diabetes on cardiovascular disease. Ass Prof Vladimira Vuletić gave a lecture about type 3 diabetes – Alzheimer’s disease.
In conclusion, cardiovascular and cerebrovascular disease are a significant public health issue causing not only physical disabil-ity and inability to perform daily activities, but it is also one of the major contributing factors for the development of vascular cognitive impairment and vascular dementia. It is estimated that approximately 90% of strokes and 35% of dementias are preventable. Therefore, it is crucial to approach to this signif-icant public health challenge with structured prevention and treatment programs and to raise awareness among healthcare professionals, as well as among the general population, that the course of cerebrovascular disease can be modified and its pro-gression can be prevented.
Heart and Brain - Risk Factors and Prevention
Auditorium in Library of CASA Auditorium in Library of CASA

RAD 540. Medical Sciences 48-49 (2019) : December 2019 - www.rad-med.com100
News & Education
authors: Ivan VukojaJakov Ivković
The ŠTAMPAR DAYS - International professional-educational symposium has been held in the birthplace of Andrija Štampar, Brodski Drenovac, since 2009. This year Symposium was held from December 5th to 8th, 2019. The Symposium has been organized by the „Andrija Štampar“ – Association of Peoples’s Health, Medical Faculty University of Zagreb, Faculty of Food and Technology Osijek, Medical Faculty University of Osijek, Clinical Hospital Center Osijek, County Hospital Požega, EHEDG, Pannonian Institute for People’s Health, Society for Nutrition and Dietetics with Food to Health, and co-organized by other domestic and foreign partners. The meetings are ac-credited according to the Regulations of the Croatian Medical Chamber and Croatian Nursing Chamber, with the endorse-ment of the Department of Medical Sciences of the Croatian Academy of Sciences and Arts. In order to promote public health aspirations and principles of Andrija Štampar, Štampar days turned into an unavoidable annual event which has three parts. The first part consists of blood pressure and glucose mea-surements for the citizens of Pozega County, the second one is the preventive program of bullying “Be cool, do not be bully”. The third part of Štampar days is the symposiums, international symposium Healthy Lifestyles and domestic symposium Chal-lenges and Opportunities of Endosonography. The symposium Challenges and Opportunities of Endosonogra-phy were held in December 6th in County Hospital Požega. The main topic of the symposium was the application of the FNA technique in a general hospital. The symposium was opened by prof. Grgurević, Vice President of the Croatian Gastroenterolo-gy Society and Iveković, President of the Endoscopic Section of the Croatian Gastroenterology Society. 4 plenary lectures were held, prof. Nadan Rustemović regarding FNA in pancreatic cys-tic lesions, asst.prof. Tajana Pavić regarding FNA vs FNB appli-cation, asst.prof. Neven Baršić regarding FNA in subendothelial lesions and asst.prof. Tajana Štoos Veić regarding cytology. Local experts Zvonimir Gugić and Ivan Vukoja lectured about vague endosonographic cases with the introduction offered by Milan
Gojo. At the round table with discussion and solutions in un-clear cases, the place was taken by asst.prof. Nikola Gotovac and Goran Šantak, prof. Ivica Grgurević and Hrvoje Iveković.
The symposium Healthy Lifestyles was held on December 7th – 8th in Pleternica library, and was organized through 5 expert sessions focusing on the prevention of chronic non-communi-cable diseases while emphasizing healthy lifestyles. The session of cardio and cerebrovascular diseases was opened by plenary lectures of prof. Ines Banjari and asst. prof. Hrvoje Budinčević, followed by lectures of prof. Vida Demarin, prof. Midhat Jašić and Hrvoje Tiljak, asst. prof. Marinko Dikanović and local pub-lic health expert Jasmina Kovačević. A session of kinesiology and physiotherapy was opened with plenary lectures by asst. prof. Cvita Gregov and Tatjana Trošt Bobić, followed by lectures of prof. Jasminka Milas Ahic, Zdravko Lovric and Vedrana Von-drak. The session of infant obesity was opened with a plena-ry lecture by prof. Andrijana Včeva and followed by lectures of Ivana Markota, prof. Maja Miškulin, prof. Nizama Salihe-fendić, prof. Senada Selmanović, asst. prof. Vera Musil and Dal-ibor Divković. The symposium was continued with a session of Health Economics, where plenary lectures were given by Ivan Lukovnjak and Boris Lukovnjak, and lectures by prof. Ivan Miškulin, asst. prof. Mate Car, prof. Mirjana Kujundžić Tiljak, prof. Dubravka Mahaček, prof. Vatroslav Zovko and asst.prof. Željko Zubčić. The symposium concluded with a Bioethics Ses-sion. The plenary lecture was given by prof. Muharem Zildžić, and invited lectures by prof. Jadranka Božikov, prof. Đurđica Ačkar, asst. prof. Mile Marinčić, prof. Brankica Svitlica, Ivan Vukoja and Maja Živković. There has also been 34 poster pre-sentation, special edition od journal With food to health regard-ing 11th Štampar day was edited with 104 pages, 30 abstracts and 9 full papers. More than 300 participants from Croatia, Bosnia and Herzegovina, Serbia, Austria and China have been registered at the symposiums.The next 12th Štampar days will be held from December 10th – 13th, 2020, in Brodski Drenovac, Croatia. More information will be available on our web site: www.unzas.hr.
11th International Professional-Educational Symposium:Štampar Days

RAD CASA - Medical Sciences - www.rad-med.com December 2019 - Vol 540 = 48-49
Author index
RAD Croatian Academy of Sciences and Arts -
Medical Sciences
Keyword index
Bitanga, Suzana 67Borić, Igor 27Brajković, Andrea 33Budinčević, Hrvoje 99Čepelak Dodig, Daniela 41Čepelak, Ivana 41Cicvara Pećina, Tatjana 27Coce, Neva 75Črnac Žuna, Petra 99Demarin, Vida 1, 51, 99Đerke, Filip 1, 51, 93, 96Dodig, Slavica 41Dugac, Željko 78Dumić-Čule, Ivo 27Filipović-Grčić, Luka 75Galić, Edvard 99Haasbroek, Kyle 58Habek, Dubravko 86Horbec, Ivana 86Jerolimov, Vjekoslav 94Jonjić, Danijela 33
Juginović, Alen 15 Jukic, Ivona 33Jurić, Anron 8Katavić, Matej 67Markotić, Alemka 71Matoković, Damir 27Mirković, Maja 27Morović, Sandra 51Mucalo, Iva 33Oroz, Maja 3Pecotić, Renata 15Pećina, Marko 1, 27, 93Planinić, Ana 3Plečko, Mihovil 27Puškarić, Ivana 71Radin, Dagmar 33Ramalho de Oliveira, Djenane 33Rukavina, Daniel 95, 97Šapina, Matej 67Skuhala, Tomislava 71Takabe, Wakako 58
Acquired atrioventricular block, 67Aging, 41Air pollution, 51Andrija Štampar, 78Antioxidant, 58Arteriovenous fistula, 8Astaxanthin, 58Azithromycin, 71Body position, 15Bradycardia, 67Caloric restriction mimetics, 41Caloric restriction, 41Children, 67China, 78Chronic diseases, 33Complete atrioventricular block, 67Complete heart block, 67Comprehensive medication management services, 33Congenital atrioventricular block, 67CT scan, 75Deep sequencing, 3
Diagnostic radiology, 27Dysbiosis, 58Erythema nodosum, 71Exposure duration, 51Gut microbiota, 58Habsburgs Army, 86Hallux, 27Heart failure, 8High fat diet, 58History of medicine, 78History of public health, 78HIV, 3Hydronephrosis, 75Incarcerated ureter, 75Inguinal hernia, 75Interwar period, 78Invalids, 86Julius Tandler, 78Kidney transplantation, 8Ligation, 8Medication management, 33Medicine, 86
Medicohistoriography, 86Military Frontier, 86Obstrucitve Sleep Apnea, 15Pharmaceutical care, 33Pharyngitis, 71Pollutant concentration, 51Polysomnography, 15Resveratrol, 41Sanger sequencing, 3Sesamoid bones, 27Sesamoiditis treatment, 27Sesamoiditis, 27Sirtuins, 41 Sleep, 15Stroke risk factors, 51Sweet’s syndrome, 71Third degree atrioventricular block, 67Thrombosis, 8Transmitted drug resistance , 3Upper respiratory infection, 71Ureteroinguinal hernia, 75
Vrdoljak, Vinko 67Vuletić, Vladimira 95, 97Yagi, Masayuki 58Yonei, Yoshikazu 58Zibar, Lada 8Židovec Lepej, Snježana 3




















