Quantitative analysis of peristalsis in the guinea-pig small intestine using spatio-temporal maps
16
Transcript of Quantitative analysis of peristalsis in the guinea-pig small intestine using spatio-temporal maps

The controlled progression of contents along the gastro-intestinal tract is an essential part of digestion. Differentpatterns of intestinal movements are involved in thephysiological progression of contents along the digestive tractand are the result of the interplay between spontaneousactivity of intestinal smooth muscle and enteric neuralcircuits (Costa & Furness, 1982; Huizinga et al. 1998).Almost one hundred years ago, Bayliss and Starling (1899)revealed the presence of polarized reflex pathways in theintestine and suggested that they were responsible for thepropulsion of contents. The analysis of intestinal propulsionwas significantly advanced by Trendelenburg in 1917 whoshowed that reproducible propulsive motor patterns could betriggered in isolated segments of guinea-pig ileum by liquiddistension. This form of intestinal peristalsis elicited in
vitro is dependent on the activation of enteric circuits asmany investigators have demonstrated (Kosterlitz, 1968;Tonini et al. 1981; Waterman et al. 1994b).
Slow distension of isolated segments of guinea-pig intestineby liquid infusion produces a neurally-mediated shorteningof the longitudinal muscle (Kosterlitz & Robinson, 1959)and an increase in diameter coinciding with an inhibitoryreflex mechanism involving nitric oxide (intestinalaccommodation; Waterman et al. 1994a). This initialresponse to liquid distension has been named the‘preparatory phase’ (Trendelenburg, 1917; Kosterlitz, 1968).At a threshold volume or intraluminal pressure, a contractionof the circular muscle occurs at the oral end and propagatesaborally to empty the segment. This propulsive event iscalled the ‘emptying phase’ and involves the activation ofdifferent enteric neural pathways (Waterman & Costa, 1994;Waterman et al. 1994b).
Despite the common description of this motor behaviour asthe ‘peristaltic reflex’ (Kosterlitz, 1968), it has becomeapparent that there is a sequential activation of neural
Journal of Physiology (1999), 517.2, pp.575—590 575
Quantitative analysis of peristalsis in the guinea-pig smallintestine using spatio-temporal maps
G. W. Hennig, M. Costa, B. N. Chen and S. J. H. Brookes
Department of Human Physiology and Centre for Neuroscience, Flinders University
of South Australia, GPO Box 2100, Adelaide 5001, South Australia, Australia
(Received 14 August 1998; accepted after revision 24 February 1999)
1. Peristalsis was evoked in guinea-pig small intestine by slow fluid infusion and recorded ontovideo and digitized. Spatio-temporal maps of diameter and longitudinal movement wereconstructed and parameters of motion were calculated.
2. During the filling of the isolated segments of intestine, rhythmic local longitudinalmovements were observed at several points along the preparation. These phasic longitudinalmuscle contractions were associated with small but significant local increases in diameter andprobably reflect a passive mechanical coupling by connective tissue in the gut wall. Inaddition, occasional synchronized longitudinal muscle contractions caused net shortening ofthe preparation and always preceded the onset of peristaltic emptying.
3. Peristaltic emptying was characterized by a contraction of the circular muscle which usuallystarted at the oral end of the preparation, that propagated aborally, propelling the contents.However, in 19% of trials, the first circular muscle contraction occurred in the aboral half ofthe preparation.
4. The propagation of peristalsis consisted of separate sequential circular muscle contractionsseveral centimetres long, particularly in the oral half of the preparation, giving a ‘step-like’appearance to the spatio-temporal map. The gut was transiently distended aboral to thepropagating circular muscle contraction due to the propulsion of contents.
5. At each point in the preparation, the longitudinal muscle remained contracted during thepropulsive part of the circular muscle contraction. Only when the circular muscle contractionbecame lumen occlusive did lengthening of the longitudinal muscle take place.
6. Spatio-temporal maps are a powerful tool to visualize and analyse the complexity of gastro-intestinal motility patterns.
8636

pathways. Thus, peristalsis should not be regarded as asimple reflex, but rather as a motor pattern, similar to someco-ordinated locomotor patterns (Tonini et al. 1996).
In order to analyse the components of this motor pattern,we have developed a simple method of constructing spatio-temporal maps of changes in diameter and longitudinalmuscle length from video recordings. Using this method, wehave analysed quantitatively the dynamics of peristalsis inthe guinea-pig small intestine and have revealed newpatterns of motor activity. Some of these results have beencommunicated previously (Hennig et al. 1998).
METHODSTissue preparation
Guinea-pigs (IMVS coloured) of either sex, weighing 250—400 gwere killed by cervical dislocation, followed by bleeding from thecarotid arteries (protocol approved by the Animal WelfareCommittee of Flinders University). A ventral midline incision wasmade to expose the peritoneal cavity and a segment of ileum(6—8 cm long) was removed 10 cm oral to the ileo-caecal junction.The segment was flushed clean, cannulated at the oral and aboralends, and placed in a heated organ bath containing Krebs solution ofthe following composition (mÒ): NaCl, 118; KCl, 4·7; NaHµPOÚ, 1·0;NaHCO×, 25; MgSOÚ, 1·2; ª_glucose, 11·0; and CaClµ, 2·5; pH 7·4.
G. W. Hennig, M. Costa, B. N. Chen and S. J. H. Brookes J. Physiol. 517.2576
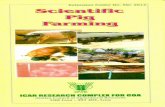
Figure 1. Experimental arrangements used to study peristalsis
A segment of ileum (black), cannulated at each end, was placed in oxygenated warmed Krebs solution.Intraluminal pressure was monitored with a pressure transducer (P) and Krebs solution was infused via theoral cannula by a syringe pump. Movements of the preparation were recorded onto S-VHS video tape. Thepreparations emptied their luminal contents via the aboral cannula, through a one-way valve or into avertical tube. In A, both ends of the preparation were fixed to prevent the overall shortening of the segmentand the height of the outflow was adjusted to control outflow resistance. In B, the preparation was able toshorten during filling as the outflow cannula was mounted on a flexible tube. In C, the preparation emptiedvia the aboral cannula into a large diameter tube, thus maintaining intraluminal pressure constant. Fluidflowed back into the intestine after emptying.

Experimental set-ups
Two experimental arrangements based on Tonini et al. (1981) andWaterman et al. (1994b) were used to study peristalsis elicited byslow intraluminal infusion of Krebs solution (Fig. 1A and B). Adifferent experimental arrangement was used to study spontaneousperistalsis when intraluminal volume was held at a constant level(Fig. 1C).
The oral end of a segment of small intestine was cannulated toallow slow infusion of Krebs solution into the lumen. The aboralend was cannulated and fitted with a one-way valve to preventback flow of Krebs solution. Intraluminal pressure was measured ateach end using pressure transducers (Statham P23X) connected toa MacLab data acquisition system (AD Instruments, Sydney,Australia). Both the oral and aboral ends were fixed to preventshortening of the segment in the longitudinal direction (Fig. 1A).
Krebs solution was infused via the oral cannula at a constant rate(4·25 ìl s¢) until a propagated peristaltic contraction occurred(emptying phase). At the beginning of the circular musclecontraction, the infusion was stopped and the segment was allowedto empty by the propagated peristaltic contraction. Cycles ofperistalsis were repeated every 5 min.
In a second variation of the above preparation, the aboral end wascannulated and fitted with a one-way valve connected to a longpiece of silastic tubing that was free to move in the longitudinaldirection. Surface markers (black silk knots) were tied onto themesentery approximately every 10—15 mm to monitor the motionof the longitudinal muscle layer (Fig. 1B). This arrangementpermitted the changes in the longitudinal direction along thesegment to be better investigated.
In a third variation, the aboral end was connected to a verticalopen tube with no valve and was free to move in the longitudinaldirection. Intraluminal pressure was set by varying the height ofthe column of Krebs solution in the aboral cannula by slowlyinfusing Krebs solution to a sub-threshold volume for the triggeringof peristalsis (approximately 60%). In these experiments, surfacemarkers were fixed as described above (Fig. 1C).
Image acquisition
A video camera (Panasonic WV-CL504) was positioned above theileum (Fig. 1) to record intestinal motor patterns on a highresolution S-VHS video recorder (Panasonic AG-7355) in PALformat at 25 frames per second (frames s¢). Frames of motion weredigitized on an Apple Power Macintosh (7600Ï132) from video
Mapping intestinal movementsJ. Physiol. 517.2 577
Figure 2. Construction of spatio-temporal map of intestinal diameter (DMaps)
A single frame of a video recording of the intestine (A) was subjected to the threshold procedure (seeMethods) and converted into a binary image (B). The number of black pixels in each column (correspondingto diameter of the intestine at each point along its length) was converted into a grey scale pixel (bar abovepreparation, in B). Multiple frames were treated in this way to produce a diameter map (C), showing thediameter at each point from the oral end of the preparation to the aboral end: the preparation was 55 mmlong. In this map, the minimum diameter was 2·1 mm (represented by white pixels) and the maximum was7·5 mm (black pixels) and the map represents a time period of approximately 18 s. Time starts at the top ofthe diameter map. The white dotted line corresponds to the frame shown in A and B. Using the diametermap, the profile of the intestine could be reconstructed at any moment (D).

using a modified version of the image analysis software developedby the National Institute of Health (NIH Image 1.62), at25 frames s¢.
The maximum resolution achievable using S-VHS video tape isapproximately 400—410 columns by 625 rows. Depending on thefinal magnification (approximately ² 2·5), this corresponded to avertical resolution of 0·15—0·25 mm and horizontal resolution of0·2—0·3 mm. To achieve a workable balance between the capturerate and the size of the digitized image, a half sized capture screenwas used (384 ² 256 pixels) which enabled the video stream to becaptured at video rate (25 frames s¢). The temporal accuracy ofcapture from the S-VHS video recorder onto the computer was verystable, with time discrepancies of less than 1 s h¢. The correlationbetween the video and the pressure recordings was established byusing visual markers synchronized to time points in the pressurerecording.
Construction of spatio-temporal maps of intestinal motion
The movement of the intestinal wall was portrayed by mappingchanges in diameter (diameter map or DMap) and changes in lengthbetween marked points along the intestinal segment (longitudinalmap or LMap) over time.
Diameter maps (Fig. 2)
A threshold procedure was applied to video frames (Fig. 2A) todefine the edges of the gut. Images were converted to binary(1bitÏblack or white) with black representing the intestinal wall and
white the background (Fig. 2B). The diameter of the preparationat every pixel column along the length of the segment wasdetermined by the number black pixels in each column. Thesediameters were represented as single grey-scale pixels with thesmallest diameter coded as white and largest diameter as black(Fig. 2B). Intermediate diameters were assigned a proportionallevel of grey. The grey-scale coded pixels from each frame of themovie were used to construct a single row. Sequential rows wereplaced underneath each other in a separate image to produce aspatio-temporal map of intestinal diameters (diameter map; DMap:Fig. 2C). The vertical displacement of the preparation from the topof the video image was measured by calculating the position of thefirst black pixel, and was stored in a separate image (not shown).The vertical displacement information was used in conjunction withthe diameter map to reconstruct gut profiles (Fig. 2D).
Longitudinal maps (Fig. 3)
In preparations with surface markers attached at regular intervalsalong the preparation (Fig. 3A), a diameter map was constructed asdescribed above. In these maps, the longitudinal markers appearedas vertically oriented white lines (Fig. 3B). The movement of thelongitudinal markers over time was extracted from the DMap usingtracking algorithms within NIH Image 1.62 (Fig. 3C; black lines).The distance between the markers was calculated and encoded as agrey-scale value between each pair of markers (Fig. 3C; grey lines).A linear interpolation routine was applied to each row (representinga single time frame), resulting in a smooth transition of grey-scale
G. W. Hennig, M. Costa, B. N. Chen and S. J. H. Brookes J. Physiol. 517.2578
Figure 3. Construction of spatio-temporal maps of longitudinal motion (LMaps)
A single frame of a video recording shows five black surface markers along the length of the preparation (A).A DMap, constructed from 20 s of recording (B) shows the movements of the surface markers as vertical,pale, wavy bands — the black dotted line represents the frame shown in A. A tracking routine was used todefine the positions of the surface markers (black wavy lines, C) and the midpoint between each band wasdetermined (grey lines, C). The distance between adjacent surface marker lines was then determined andrepresented as a grey scale pixel, at the calculated midpoint. Linear interpolation of grey scales was used tofill in the areas between the midpoints (D). The resulting LMap shows local shortening of the preparation,compared with resting conditions (prior to Krebs infusion) as pale grey. Local lengthening of thepreparation is shown as dark grey. The right hand end of the LMap (D) represents the net shortening of thepreparation in each video frame.

values along the intestinal segment (Fig. 3D). Whiter areas in theLMap indicate regions between surface markers that were closertogether with darker areas indicating regions that were furtherapart. The absolute movement between each pair of markers wasscaled so that white represents the minimum distance, and blackthe maximum distance.
Reconstruction of intestinal profiles
Single profiles of an intestinal segment could be reconstructed fromany row of the diameter map. Diameter values from a row wereconverted into pixel columns of corresponding diameter (Fig. 2D)with the vertical displacement providing the start position for eachpixel column. Movies of reconstructed profiles could be producedthat were indistinguishable from the original binary movie, providedthat the outline of the intestine was free from specular noise.
The changes of diameter over time at a particular point along theintestine could be plotted as a time plot by converting grey-scalecoded pixels at a particular position along the segment into verticalco-ordinates (Fig. 4, CM). To ensure that the diameter values weretaken from the same point along the segment, the trajectories ofthe surface markers (Fig. 4) were used as guides from whichdiameter values were extracted. This time plot is equivalent to anisotonic recording from one point along the intestinal segment. Thedistance between two surface markers could be converted into atime plot using a similar technique (Fig. 4, LM). Smoothing routineswere applied to reduce excessive pixellation of the time plots (3 or 5point running means).
Analysis of motion from maps
The maximum and minimum diameter and rate of contractionduring peristalsis were averaged over a 5 mm region at oral andaboral ends, at least 5 mm away from the edge of the cannulae. Thevelocity of propagation was calculated by fitting a least squaresregression line to the mid-diameter level during the peristalticcontraction. To compare preparations in which the aboral end movedfreely with those in which the aboral end was fixed, the DMaps thatwere free to move, were artificially ‘stretched’ by using nearestneighbour interpolation at each time point along the preparation,to maintain a fixed resting length. In differentiated maps, the rateof change of diameter was calculated using 0·2 s intervals.
Shortening of the longitudinal muscle was expressed as a percentageof the resting length.
Statistics
Statistical comparisons were made using factorial ANOVA, withFisher’s PLSD post hoc tests. A probability of less than 0·05 wasconsidered significant.
RESULTSPeristalsis elicited by slow liquid distension
Slow infusion of Krebs solution into isolated segments ofguinea-pig small intestine evoked peristalsis in a similarmanner to that described in numerous previous studies(Trendelenburg, 1917; Tonini et al. 1981; Waterman & Costa,1994). Notably, there was a graded longitudinal shorteningof the preparation during the preparatory phase ofperistalsis (Trendelenburg, 1917; Kosterlitz & Lees, 1964),then at a threshold volume, there was an abrupt contractionof the circular muscle at the oral end which propagatedaborally, expelling intraluminal contents and correlatedwith a large transient increase in intraluminal pressure
(Fig. 4, Pressure). These changes in the dimensions ofpreparation were apparent in spatio-temporal maps (Fig. 4,DMap). During the preparatory phase, there was an overalldarkening of the DMap over time, reflecting the increase indiameter evoked by distension. This increase in diameter wasalso apparent in the diameter trace (Fig. 4; CM, dilatationindicated by a rightward deflection) extracted from betweenthe arrowheads in the DMap. In parallel with this, thepreparation shortened as demonstrated by the gradedlightening of the LMap in Fig. 4 and in the longitudinalmuscle trace (Fig. 4; LM, shortening indicated by arightward deflection).
The LMap also revealed patterns of longitudinal motoractivity along the length of the intestine during thepreparatory phase. These patterns consist of oblique stripesand are due to delays of rhythmic longitudinal muscleoscillations along the preparation. The slope of the stripesindicate the direction and speed of propagation oflongitudinal muscle contractions (see legend of Fig. 4). Ateach measured point along the intestine, the longitudinalmuscle oscillated rhythmically at about 37 cycles min¢. Thislongitudinal muscle motor activity had little effect on theoverall length of the preparation. Close to the threshold forperistaltic emptying, the preparation shortened substantially(Fig. 4, indentations on right edge of the LMap).
At the beginning of the emptying phase, there was acontraction of the circular muscle at the oral end, whichpropagated aborally, invading the entire segment. Thisappears as the diagonal white streak in the DMap (Fig. 4,DMap). After emptying, the intestine often flattened andtwisted significantly, causing artefacts in DMaps. For thisreason, no analysis was performed in this period.
Circular muscle during the preparatory phase
The DMaps show a gradual darkening during the infusionof fluid, reflecting an overall increase in diameter of thepreparation as it accommodated the increasing volume. Theaboral end of preparations was distended more rapidlythan the oral end. The mean rate of diameter change wasdetermined throughout the preparatory phase for the oral,middle and aboral ends of preparations which were free toshorten (Fig. 5). The diameter at the aboral end increasedmore quickly than at the oral end during slow filling,suggesting that the tissue aborally was more compliant.
Relationship between longitudinal and circularmuscle layers during the preparatory phase
Before the threshold volume for peristalsis had beenreached, DMaps often showed small changes in diameter(11Ï19 animals) that resembled the patterns of activity inthe longitudinal muscle (Fig. 6A and B). These oblique dark‘bands’ became more evident with greater distensionvolumes and appeared to propagate orally. Small changes indiameter also occurred when preparations were held at aconstant volume (approximately 60% of the thresholdvolume) although the direction of propagation of the smalldiameter changes was more variable. In order to establish
Mapping intestinal movementsJ. Physiol. 517.2 579

G. W. Hennig, M. Costa, B. N. Chen and S. J. H. Brookes J. Physiol. 517.2580
Figure 4. Example of peristalsis evoked by slow liquid infusion at 4·25 ìl s¢
Infused fluid volume is shown schematically on the left as a black ramp. Time starts at the top of the figure.Intraluminal pressure is represented in the adjacent trace, showing a large, abrupt increase in pressureduring peristaltic emptying. The diameter map (DMap) of the same period shows a gradual darkeningduring the course of the infusion, reflecting the gradual increase in diameter (see circular muscle diameter

whether these small diameter changes were correlated withlongitudinal muscle activity, DMaps and LMaps werecompared (see Figs 6 and 9). As the longitudinal muscleshortened locally, there was a significantly correlated increasein diameter (darkening) in the corresponding DMap(correlation coefficient r = 0·95 at LM oscillations between4—5 mm) measured in the middle of the preparation. Forevery 5 mm of longitudinal muscle shortening between twosurface markers (12—14 mm apart) there was approximately1 mm increase in diameter. This indicates that mechanicalinteractions occur between the muscle layers in isolatedtubular preparations and that these interactions can berestricted to small localized regions.
If the aboral end of the preparation was free to move, therewas always a shortening of the preparation prior to initiationof the emptying phase by 10·8 ± 0·8 mm, corresponding to achange in length of approximately 19% (n = 4, 17 samples).A progressive shortening of the longitudinal muscle occurredduring the entire period of filling at 0·1 ± 0·002 mm s¢.Just prior to the emptying phase, the rate of longitudinalshortening increased to 1·63 ± 0·17 mm s¢. This shorteningis visible in Fig. 7C as a horizontal shift of the aboral endand in Fig. 4 as a whitening in the LMap.
Circular muscle movements during the emptyingphase of peristalsis
The contraction of the circular muscle usually started at theoral end and propagated aborally. The circular muscle at theoral end remained contracted for the entire emptying phasewhich lasted 1·83 ± 0·09 s. It should be noted that the liquidinfusion was switched off at the beginning of the emptyingphase to prevent fluid from refilling the preparation. Aboralto the advancing circular muscle contraction, the intestinerapidly increased in diameter, as revealed by the markeddarkening in the DMap (Fig. 7A).
A number of parameters of motions of the circular muscleduring the emptying phase were calculated and are shownin Table 1.
To visualize and analyse the dynamics of the propagatedcircular muscle contraction more clearly, DMaps weredifferentiated with respect to time. In such maps, high ratesof circular muscle shortening are shown in white, while high
rates of dilatation are shown in black (Fig. 7B). DMaps andtheir differentiated versions, revealed a number of featuresnot previously recognized. The propagated peristalticcontractions often had a ‘step-like’ appearance, rather thanappearing as a smooth wave of contraction. In these cases,peristalsis was equally effective in emptying the segment andconsisted of a series of sequential, more separate localizedcontractions (Fig. 8B top and bottom; 8C top and 8Dbottom). These contractions, in some cases, occurred almostsimultaneously over a significant length of the segment(Fig. 8C and D both middle) and thus no measurement ofthe speed of propagation of the separate contractions wasattempted. In all cases the mean speed of propagation ofthe peristaltic contraction was calculated as described inMethods, by fitting a least squares regression line to themid-diameter level during the peristaltic contraction (Table 1).
Mapping intestinal movementsJ. Physiol. 517.2 581
trace, CM). The arrowheads on the DMap show the point of the intestine at which circular muscle (CM) andlongitudinal muscle (LM) traces were generated. Longitudinal muscle activity also increased during thepreparatory phase (shown by the overall shortening of the preparation in the DMap and by the trace oflongitudinal muscle activity, LM). The longitudinal map of the same period (right hand part of figure,LMap) shows a gradual shortening of the segment of intestine during the infusion (revealed as a graduallightening of the map). The pattern of oblique stripes in the LMap during the preparatory phasecorresponds to phasic changes in longitudinal muscle length (at approximately 37 c.p.m.) that occur withsome delay along the length of the preparation, suggesting that the longitudinal muscle contractionspropagate sometimes orally (sloping to the left) and at other times aborally (sloping to the right). There is asudden net shortening of the longitudinal muscle just prior to the onset of peristalsis (visible in both theDMap and LMap). The circular muscle initially lengthens at the start of peristaltic emptying, then rapidlyshortens (leftward deflection on CM trace). In contrast the longitudinal muscle, at the same point in theintestine, shortens prior to emptying (rightward deflection on LM trace).
Figure 5. Rate of change of diameter varied along theintestine during slow filling
Measurements of circular muscle diameter at the oral, middleand aboral ends of 5 preparations were used to calculate themean rate of increase of diameter during slow filling. The oralend distended significantly more slowly during infusion thanthe aboral end (P < 0·05), indicating that the oral end is lessdistensible. This probably reflects greater inhibitory neuronalinput to the circular muscle at the aboral end during filling.

In 3 of 12 preparations a localized contraction of the circularmuscle occurred at the aboral end, preceding the oralinitiation of peristalsis contraction (Fig. 8B middle; 19% ofall trials from 12 preparations). This was a consistentfeature in 1 of 12 preparations.
The differentiated DMaps also revealed that the maximumrate of contraction of the circular muscle was greatertowards the aboral end of the segment during peristalsis(Table 1), perhaps because the starting diameter was greater,due to fluid displaced aborally by the propagating circular
G. W. Hennig, M. Costa, B. N. Chen and S. J. H. Brookes J. Physiol. 517.2582
Figure 6. Relationship between longitudinal and circular muscle during the preparatory phase
During slow filling of the intestine, the longitudinal muscle showed characteristic phasic contractions thatappeared to propagate orally (LMap in B). These correlated with small phasic increases in overall diameterof the preparation revealed in DMaps (see dark bands in A). This suggests that localized longitudinal muscleshortening may cause a localized small increase in diameter.
––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––Table 1. Parameters of motion
––––––––––––––––––––––––––––––––––––––––––––––Fixed Free Significance
Means ± s.e.m. Means ± s.e.m. P
––––––––––––––––––––––––––––––––––––––––––––––Threshold diameter oral (mm) 4·9 ± 0·05 5·6 ± 0·09 *< 0·001Maximum diameter aboral (mm) 5·9 ± 0·1 6·5 ± 0·07 *< 0·001Empty diameter oral (mm) 2·7 ± 0·06 3·2 ± 0·09 *< 0·01Empty diameter aboral (mm) 2·5 ± 0·6 3·2 ± 0·08 *< 0·001
Rate of CM contraction oral (mm s¢) 2·2 ± 0·6 2·2 ± 0·6 > 0·05Rate of CM contraction aboral (mm s¢) 3·3 ± 0·09 2·5 ± 0·06 *< 0·001Propagation velocity of CM contraction (mm s¢) 30·2 ± 0·9 29·6 ± 1·5 >0·05––––––––––––––––––––––––––––––––––––––––––––––Parameters of motion calculated during the emptying phase of peristalysis in preparations that were fixedat each end (Fixed, n = 21; 4 animals) or free to move at the aboreal end (Free, n = 31; 5 animals). CM,circular motion.––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––

muscle contraction. The parameters of peristalsis analysedin preparations in which the aboral end was free to move(permitting net shortening of the intestinal segment) werecompared with preparations in which the aboral end wasfixed. DMaps from freely contracting preparations wereartificially stretched as described in Methods, to permitdirect comparison with fixed preparations (Fig. 7C and D).The threshold diameter at which peristalsis was evoked at theoral end was significantly greater in preparations that werefree to shorten (Table 1). Similarly, the maximum diameterreached during peristalsis was greater in preparations thatwere free to shorten. The minimum diameter after emptyingwas greater in preparations that were free to shorten, atboth oral and aboral ends. The mean rate of circular musclecontraction in preparations of fixed length was greateraborally than orally. The mean rate of propagation of the
circular muscle contraction did not differ significantly aftercorrecting for the overall change in length of freelyshortening preparations (Table 1).
Relationship between longitudinal and circularmuscle during the emptying phase of peristalsis
As described above, the contraction of the circular muscleusually occurred first at the oral end and subsequentlypropagated aborally. In the middle and aboral ends thecontraction was preceded by a distension due to thedisplacement of fluid from further orally. The relationshipbetween longitudinal and circular shortening at the oral,middle and aboral ends of the preparation were determinedby plotting local changes in length and diameter versus
each other (Fig. 9). During the preparatory phase (Fig. 9,from points a to b) there were phasic contractions of thelongitudinal muscle which correlated closely with small
Mapping intestinal movementsJ. Physiol. 517.2 583
Figure 7. Comparison of peristaltic emptying in preparations that were either fixed at both endsor free to move at the aboral end
A DMap of a preparation in which both oral and aboral ends were attached to fixed cannulae (A) shows anabrupt start to the emptying phase. The same map differentiated, to show the dynamic changes in circularmuscle length (B), reveals that the emptying occurred as a sequence of three contractions at various pointsalong its length, giving rise to ‘step-like’ propagation. In C, the aboral end of the preparation was attachedto a freely moving cannula (see Fig. 1B) and surface markers were used to map the local shortening of thepreparation. A pronounced shortening of the preparation occurred prior to the initial contraction of thecircular muscle and the preparation lengthened during the ensuing emptying phase. The DMap wassubsequently processed to maintain a constant overall length (D), making it possible to compare directly theemptying phase of fixed preparations (A) and preparations that were free to shorten (D), revealing that therate of propagation of circular muscle contraction was not affected by shortening of the longitudinal muscle.

G. W. Hennig, M. Costa, B. N. Chen and S. J. H. Brookes J. Physiol. 517.2584
Figure 8. Dynamics of peristaltic emptying in preparations maintained at a fixed length
Three differentiated diameter maps from each of four animals (A, B, C and D) show features ofpropagation of the circular muscle contraction during the emptying phase. Most examples show a ‘step-like’activation of the circular muscle contraction as it propagated aborally (B top and bottom, C top andD bottom). The initial circular muscle contraction usually occupied a small region at the oral end of thesegment; however, occasionally the contraction occurred in a large region simultaneously (C and D middle).

increases in diameter. After the threshold for peristalsis(point b), there was a rapid decrease in diameter but thelength remained constant (between points b and c). Thisindicates that the longitudinal muscle remained activeduring the circular muscle contraction. The longitudinalmuscle at the oral end of the segment remained active for0·89 ± 0·04 s (n = 5; 31 samples) during the circular musclecontraction before noticable elongation occurred. Thiscorresponds to 48% of the duration of the circular musclecontraction to its peak. The corresponding figures at theanal end were 1·00 ± 0·03 s (47% of duration circular musclecontraction). Lengthening of the longitudinal muscleoccurred when the diameter approached a minimum (point c)and is probably due to passive elongation due to the ongoingcircular muscle shortening.
Spontaneous peristalsis in partially distendedpreparations
In order to study patterns of activity during the fillingphase, four preparations that were free to shorten weremaintained at a constant volume distension, correspondingto approximately 60% of the threshold volume for peristaltic
emptying. In all these preparations there were patternedoscillations of longitudinal muscle shortening (meanfrequency, 32 cycles min¢) and periodic larger shorteningsof the entire preparation by 11·7 ± 2·2% occurring at3·5—4 cycles min. Interestingly, after considerable delays,peristaltic emptying occurred without further fluid infusion,at mean intervals of 8·0 ± 0·7 min (29 bouts of emptying).This indicates that there is considerable variation in thethreshold for peristalsis when the gut is partially distendedfor long periods. Each bout of peristaltic emptying waspreceded by a larger-than-average shortening of thepreparation by 23·1 ± 2·9% of resting length (n = 17; from 4animals). Measurement of parameters of peristaltic emptyingrevealed no differences from preparations distended tothreshold which were free to shorten, with one exception.The rate of propagation of the circular muscle contractionwas significantly slower than in preparations distendedusing a ramp distension (22·0 ± 2·3 mm s¢; P < 0·01,n = 19; from 4 animals). This suggests that the volume ofintraluminal contents may play a significant role in the rateof propagation of peristalsis along the intestine.
Mapping intestinal movementsJ. Physiol. 517.2 585
Figure 9. Relationship between circular and longitudinal shortening during the emptying phase
Local changes in diameter and length (calculated from surface markers) were plotted for the oral, middleand aboral regions of a preparation during the preparatory and emptying phases of peristalsis. Values werecalculated at intervals of 40 ms (each represented by a single dot). During filling, there were phasiccontractions of the longitudinal muscle which correlated with phasic increases in diameter (between pointsa and b). At the onset of peristaltic emptying (point b), there was a sudden decrease in diameter, initiallywithout lengthening, indicating that the longitudinal muscle did not relax during the initiation ofperistalsis. Lengthening only commenced during the later stages of the circular muscle contraction(point c). Similarly, in the middle and aboral regions, there was no significant localized lengthening duringthe circular muscle contraction. However, particularly at the aboral end of the preparation there was asignificant increase in diameter just prior to the circular muscle contraction due to fluid displaced from thecontraction further orally.
Occasionally, a circular muscle contraction occurred aborally before the peristaltic contraction was initiatedat the oral end (B middle). The dark bands after the peristaltic contraction (B) are artefacts due to excessivebending caused by longitudinal muscle movement in a fixed preparation.

DISCUSSIONIn this paper, a simple method was developed to generatespatio-temporal maps of patterns of movement in theisolated guinea-pig ileum similar to that used by (Benard et
al. 1997). These maps were used to quantify changes in thelength and diameter of the intestine during peristalsis evokedby slow fluid infusion, with high spatial and temporalresolution. From such detailed analysis, organized patternsof longitudinal muscle contractility became apparent duringthe preparatory or filling phase. It was also clear that thelongitudinal muscle contracts in synchrony with the circularmuscle during the propagating wave of circular musclecontraction, as suggested by some authors (Bayliss & Starling,1899; Yokoyama & Ozaki, 1990; Smith & Robertson, 1998)rather than relaxing as others have suggested (Kottegoda,1969). In addition, the emptying phase of peristalsis wasshown to consist, in many preparations, of a ‘step-wise’sequential activation of separate circular muscle contractionsat different points along the intestine, rather than as asmooth propagating wave of contraction.
The longitudinal muscle in the preparatory phase ofperistalsis
The gradual shortening of the intestine during thepreparatory phase, together with superimposed longitudinaloscillations has been previously described (Trendelenburg,1917; Hukuhara et al. 1969; Tsuchiya, 1972; Yokoyama &North, 1983). Oscillations of the longitudinal muscle, withoutcircular muscle activity have been reported in isolatedpreparations of intestine from other laboratory animals(Cannon, 1912; Gonella, 1971; Cheung & Daniel, 1980). Thesmall longitudinal muscle oscillations, which occurred atfrequencies of 32—37 cycles min¢, may well be caused byslow waves with superimposed smooth muscle actionpotentials. Slow waves accompanied by bursts of actionpotentials have been recorded from longitudinal muscle indifferent species, including the guinea-pig (Yokoyama &North, 1983; Szurszewski, 1987; Bolton, 1989). With thismethod, combined with electrophysiological recordings fromsmooth muscle cells, it will be possible to investigate thespatio-temporal patterns of these longitudinal muscleoscillations, and their relation with slow waves.
The rhythmic longitudinal oscillations probably correspondto the pendular movements of the intestine described lastcentury. Krishnan (1932) observed pendular movements incats and concluded that they were solely due to longitudinalmuscle activity and produced a to and fro movement of thecontents, with an associated small passive dilatation of thecircular muscle.
Our results support this interpretation. We calculated thatfor every 5 mm of longitudinal shortening between twosurface markers there was an associated increase in diameterof 1 mm. This increase in diameter is likely to be due topassive mechanical interactions between the longitudinal andcircular dimensions of the intestine that have been describedpreviously (Gregory & Bentley, 1968; Wood & Perkins,
1970). Indeed, Hukuhara & Fukuda (1965) demonstratedthat fluid distension of tubes made of inert material cancause significant shortening. It has been suggested thatlongitudinal muscle movements are likely to result in effectivemixing of the intestinal contents (Melville et al. 1975).
The progressive shortening of the preparation during thefilling in the preparatory phase is generally considered as areflex contraction of the longitudinal muscle and has beenreported to be sensitive to both hexamethonium and atropine(Baur, 1928; Kosterlitz & Robinson, 1959; Kosterlitz, 1968;Tsuchiya, 1972) although it has also been suggested thatpassive mechanisms may contribute (Hukuhara & Fukuda,1965).
The rapid oscillations in local longitudinal muscle correlatedwith small changes of length of the entire preparation.However, in all preparations in which one end was free tomove, considerably larger phasic shortenings occurredoccasionally (up to 4 min¢) at higher levels of distensionand the onset of the emptying phase was always precededby a large contraction. The LMaps showed that this was dueto synchronous shortening of the longitudinal muscle atmany points along the length of the preparation, whichoverrode the rhythmicity of the local contractions. Sincelongitudinal muscle layer of the guinea-pig ileum isinnervated by motor neurons with short projections, 2—3 mmlong (Brookes et al. 1992), it seems likely that a burst offiring in interneuronal pathways must synchronize activityin longitudinal muscle motor neurons along the preparationto cause these large contractions. At least three descendinginterneuronal pathways and one orally projecting pathwayare known to exist in the guinea-pig ileum (Costa et al.
1996). Which of these neuronal pathways leads to theshortening of the entire segment remains to be established.
The circular muscle in the preparatory phase ofperistalsis
In contrast to the longitudinal muscle, which showedconsiderable contractile activity during the preparatoryphase, the circular muscle showed very little activity. Thediameter of the gut increased gradually with distension,revealed as a graded darkening of DMaps, but essentially nomotor activity was detected in the circular muscle until thethreshold for peristalsis was reached. However, any changein diameter of less than 0·25 mm would not be detectedwith the present system (see Methods). There are a numberof possible reasons for the differences in activation of theexternal muscle layers. It is likely that the circular muscle isrelatively less excitable (or more inhibited) and requiresconsiderable excitatory motor input to reach the thresholdfor contraction, whereas the longitudinal muscle layer isnormally very close to threshold, judged by the presence ofspontaneous contractions. This difference in state could bedue to a preferential inhibition of circular muscle, but notlongitudinal muscle, by prostaglandins released fromdamaged tissue (Bennett et al. 1976; Maggi et al. 1994).Another possibility is that the circular muscle, but not the
G. W. Hennig, M. Costa, B. N. Chen and S. J. H. Brookes J. Physiol. 517.2586

longitudinal muscle, is actively inhibited by enteric inhibitorymotor neurones. There is a substantial innervation of thecircular muscle by inhibitory motor neurones (Brookes et al.1991) whereas the longitudinal muscle is innervated nearlyexclusively by excitatory motor neurons in the guinea-pigileum (Brookes et al. 1992). There is ample evidence forongoing inhibitory neural activity in the circular muscle ofisolated segments of intestine (Wood, 1972; Biber & Fara,1973; Tonini et al. 1974), including the guinea-pig ileumcircular muscle (Smith, 1989). This inhibitory activity resultsin maximal muscle relaxation during the accommodatoryreflex in the guinea-pig small intestine during slow distension(Waterman et al. 1994b).
The initiation of peristaltic emptying
Based on visual monitoring, the start of the emptyingphase of peristalsis has long been considered to be due to anabrupt, large amplitude contraction of the circular muscle atthe oral end of the preparation. This is confirmed by theDMaps where the initiation of emptying is shown as asudden whitening at the oral end of the map. However, in19% of trials, contractions of the circular muscle occurredfirst in the aboral half of the preparation (e.g. Fig. 8B),revealing some variability in the patterning of circularmuscle contraction. The occurrence of an abrupt start to thecontraction of the circular muscle is not because the circularmuscle is incapable of generating graded responses; it is wellestablished that the ascending excitatory reflex, evoked byrapid distension (usually with an intraluminal balloon), isgraded with stimulus intensity (Bayliss & Starling, 1899;Costa & Furness, 1976; Smith et al. 1990; Tonini et al.
1996). Additional mechanisms may be involved that areresponsible for its abrupt start (Tonini et al. 1996). Thelarger shortening of the preparation that always precedesthe peristaltic contraction may contribute to the initiation ofperistalsis as suggested by Kottegoda (1969). As discussedabove, the shortening of the intestine results in an increasein diameter due to the mechanical interaction between thetwo muscle layers. This increase in diameter would furtheractivate the excitatory reflex activity of the circular musclemotor neurons. A burst of activity of these excitatory motorneurons releasing acetylcholine onto the circular musclewould initiate the peristaltic contraction. However, theoverall shortening of the segment is not a prerequisite forthe initiation of the emptying phase, as anchoring both endsof the preparation did not prevent peristaltic emptying(Kosterlitz et al. 1956).
Propagation of the circular muscle contraction duringperistaltic emptying
The spatio-temporal maps clearly show the emptying phaseof peristalsis as an oblique white streak preceded by adarker dilated area. Detailed analysis of differentiatedDMaps revealed that the circular muscle often contractedsimultaneously over several centimetres of intestine so thatthe propagation actually consisted of a series of separate‘step-like’ contractions along the segment. Interestingly, inmost cases, these ‘steps’ were clearest in the oral half of the
preparation. At the beginning of the emptying phase,relatively little fluid was displaced by the circular musclecontraction which was restricted to the oral end. As emptyingproceeded, the propelled contents accumulated, causing awave of dilatation that preceded the contraction (Alvarez &Zimmermann, 1927). This dilatation was most marked inthe aboral half of the preparation and may explain thesmoother propagation of the peristaltic contraction in thisregion. From the apparent smoothness of the pressure waverecorded at the aboral end of the preparation, themechanical consequence of the ‘step-like’ progression of thecircular muscle contraction may be minimal. The averagespeed of propagation of the peristalsic contraction,calculated by ignoring the ‘step-like’ progression of thecontractions, was approximately 30 mm s¢. This speed wasnot different in preparations which were allowed to shortenduring emptying, indicating that longitudinal muscleactivity does not influence the speed of propagation of thecircular muscle contraction. Interestingly, when preparationswere held at a constant volume (60% of threshold) forextended periods of time, the average speed of propagationof circular muscle contraction was reduced to approximately20 mm s¢. This suggests that there is some flexibility in thepropulsive peristaltic contraction and reinforces oursuggestion that peristalsis should be regarded as a motorpattern rather than as a simple reflex.
Relation between longitudinal and circular musclelayers during the emptying phase
There has long been uncertainty about the exact timing oflongitudinal and circular muscle activities during peristalticemptying although evidence that they can contract togetherhas been provided (Bayliss & Starling, 1899; Yokoyama &Ozaki, 1990; Smith & Robertson, 1998). Our method hasprovided an accurate description of these events at multiplepoints along a preparation. By plotting length againstdiameter for restricted regions at the oral, middle and aboralends of the preparation, it was possible to correlate theactivity of the circular and longitudinal muscle layers duringperistaltic emptying (Fig. 6).
As the emptying phase commenced, there was an abruptshortening of the circular muscle, suggesting that there isa switching from a prevailing effect of inhibitory motorneurons, responsible for the accommodation in thepreparatory phase (Waterman et al. 1994a), to a suddenrecruitment of circular muscle excitatory motor neurons.The plots in Fig. 9 (between points b and c) clearly showthat the longitudinal muscle does not relax during thisperiod. This would indicate that both longitudinal andcircular muscle excitatory motor neurons are active duringthe first half of the circular muscle contraction. It alsoindicates that excitatory motor neurons to both musclelayers are active over half the duration of the propagation ofthe peristaltic contraction. These observations support theconclusion that the longitudinal muscle contraction persistedduring the circular muscle contraction (Tsuchiya, 1972).
Mapping intestinal movementsJ. Physiol. 517.2 587

In the later part of the circular muscle contraction, there is aconsiderable elongation of the longitudinal muscle (Fig. 9,after point C). This elongation appears to occur when theparticular segment of intestine has emptied its contents. Thisincrease in length may simply reflect mechanical interactionof the two layers as suggested by Wood & Perkins (1970). Itis unlikely that it is due to a reciprocal inhibition of thelongitudinal muscle as proposed by Kottegoda (1969), sincethe longitudinal muscle layer receives a very sparseinnervation by inhibitory motor neurons (Brookes et al.
1992). At some point during the emptying phase the driveto longitudinal muscle motor neurons must be switched offsince the preparation returns to its resting length afteremptying is completed.
Physiological recordings of peristalsis
The movements of the gut involve simultaneous contractionsand relaxations of both circular and longitudinal smoothmuscle layers at every point along its length. The resultingvisual and numerical complexity has been a major hindranceto the analysis of the physiological mechanisms thatunderlie gut motility. Initially, recording methods aimed atsimplifying this complexity by recording accurately fromjust one or a few sites. Mechanical recordings of physiologicalevents can be traced back to the kymographic methodinvented by Carl Ludwig in 1847 (quoted in Holmes &Olesko, 1995). This was developed further by Bayliss &Starling (1899) with the development of the ‘enterograph’which allowed them to record, via a system of levers,movements of the gut wall at several sites simultaneously.Mechanical recordings at several sites along segments of guthave subsequently been made, both in vivo and in vitro, bymany workers, allowing some analysis of propagatingcontractions (Costa & Furness, 1976; Schemann & Ehrlein,1986; Huizinga et al. 1998).
An alternative strategy to document gut motility has beento use image analysis of whole segments of gut. This wasfirst developed by Cannon (1902) who recorded the motionsof radio-opaque material in the lumen of the intestine ofcats. Since then, many workers have analysed radiographicimages in vivo and cinematographic images in situ or inisolated preparations (Fleisch & Wyss, 1923; Alvarez &Zimmermann, 1927; Baur, 1928; Hukuhara, 1931; Schulze-Delrieu et al. 1991; Waterman et al. 1994b). The manualanalysis of such images is very labour intensive. Theseobservations have led to the recognition of some patterns ofmotility including peristalsis, but description of morecomplex patterns and activity over protracted periods hasnot been forthcoming.
The method that we developed here, combines these twomethodological approaches and is based on the production ofspatio-temporal maps of intestinal activity in which eitherthe diameter (DMap) or the longitudinal length (LMap) ofevery segment of gut is portrayed as a grey scale, asdescribed by Benard et al. (1997). This allows a completerecord of many minutes of activity to be compressed into one
or two small maps, giving a visual immediacy that allows thedetection of subtle patterns that are not obvious in frame-by-frame analysis. Since the maps are made up of quantifieddiameter measurements, movements at any particular sitecan be readily extracted, providing traces which are theequivalent of isotonic recordings at any point in thepreparation. Thus, to some extent, spatio-temporal maps canbridge the gap between image analysis of entire preparationsand physiological recording at a restricted number of sites.
Limitations of spatio-temporal maps
The spatial resolution of spatio-temporal maps is determinedonly by pixel density and the magnification used: in thisstudy one pixel corresponded to approximately 0·2—0·3 mm.The images were thus equivalent to approximately 300isotonic transducers attached along a 7 cm segment ofintestine, without the interference that would be causedby physical attachment. The spatial resolution couldtheoretically be increased by using higher magnification ofsmaller pieces of tissue, or by combining images frommultiple video cameras. The temporal resolution of thesystem was determined by the 25 frames s¢ sampling rateof the PAL recording format. The information stored in thespatio-temporal maps could be used to reconstruct thesilhouette of the segment of intestine, and thus representsan efficient way to store images of motility. Indeed, we havecalculated that with appropriate compression routines, 95 hof intestinal motion could be stored as spatio-temporal mapson a single CD_ROM (21 h uncompressed).
The most striking benefit of this type of image analysis isthat extended periods of spatially complex movements canbe displayed in a single plot, allowing subtle patterns to bereadily recognized. In frame-by-frame analysis of video orcinematographic images, the constant updating of the imagesmakes detailed pattern recognition nearly impossible, evenwhen viewed in slow motion. The ability to extractquantitative data from spatio-temporal maps has been usedby Benard et al. (1997) who recently published a methodbased on similar principles for constructing diameter mapsto investigate motor behaviour of isolated rat intestine.However, their method did not include analysis oflongitudinal muscle contractions and their system capturedimages at a lower rate (6 frames s¢ versus 25). This type ofmethodology will be applicable in many areas where highcontrast images can be obtained. We expect that the use ofradio-opaque markers may allow similar analysis of motilityin vivo and perhaps allow analysis of the propulsion ofcontents. The potential value of combining this approachwith other recording methods is also apparent. For exampleit will be possible to monitor the activity of significantlengths of intestine while at the same time recordingspontaneous or physiologically evoked muscle electricalactivity (Gonella, 1971; Tsuchiya, 1972; Yokoyama & North,1983; Lammers et al. 1993). It should also be possible tocombine spatio-temporal maps with monitoring of intra-cellular Ca¥, intracellular recordings from neurons, multipleluminal manometry or strain gauges (Summers & Dusdieker,
G. W. Hennig, M. Costa, B. N. Chen and S. J. H. Brookes J. Physiol. 517.2588

1981; Bercik et al. 1994; Huizinga et al. 1998) and intra-luminal flow (Bertuzzi et al. 1978; Macagno & Christensen,1980) to improve the understanding of the biomechanicalbasis of intestinal motor function.
The major limitations of the technique relate to the need forhigh contrast images with well defined edges, which maylimit its use in vivo. Movements of the wall can be causedeither by localized muscle activity acting on the contents orby forces produced some distance away and coupled bypassive physical means, via connective tissue or by theintraluminal contents. This means that analysis of themechanisms that cause intestinal motility has to beapproached with caution.
Despite its limitations, we are confident that combiningfocal mechanical or electrical recordings with spatio-temporalmapping will help unravel the mechanisms that underlie theapparent complexity of intestinal motility.
Alvarez, W. C. & Zimmermann, A. (1927). The absence of inhibitionahead of peristaltic rushes. American Journal of Physiology 83,52—59.
Baur, M. (1928). Die Peristaltik des isolierten Meerschwein-chendunndarms im Filmversuch. Archives of ExperimentalPathology and Pharmacology 133, 69—83.
Bayliss, W. M. & Starling, E. H. (1899). The movements andinnervation of the small intestine. Journal of Physiology 24,99—143.
Benard, T., Bouchoucha, M., Dupres, M. & Cugnenc, P. H. (1997).In vitro analysis of rat intestinal wall movements at rest and duringpropagated contraction — a new method. American Journal ofPhysiology 36, 776—784.
Bennett, A., Eley, K. G. & Stockley, H. L. (1976). Inhibition ofperistalsis in guinea-pig isolated ileum and colon by drugs thatblock prostaglandin synthesis. British Journal of Pharmacology 57,335—340.
Bercik, P., Armstrong, D., Fraser, R., Dutoit, P., Emde, C.,Primi, M. P., Blum, A. L. & Kucera, P. (1994). Origins of motilitypatterns in isolated arterially perfused rat intestine.Gastroenterology 106, 649—657.
Bertuzzi, A., Mancinelli, R., Ronzoni, G. & Salinari, S. (1978).A mathematical model of intestinal motor activity. Journal ofBiomechanics 11, 41—47.
Biber, B. & Fara, J. (1973). Intestinal motility increased bytetrodotoxin, lidocaine and procaine. Experientia 29, 551—552.
Bolton, T. B. (1989). Electrophysiology of the intestinal musculature.In Handbook of Physiology, section 1, The Gastrointestinal System,vol. I, ed. Schultz, S. G., Wood, J. D. & Rauner, B. B., pp.217—250. American Physiological Society, Bethesda, MD, USA.
Brookes, S. J. H., Song, Z. M., Steele, P. A. & Costa, M. (1992).Identification of motor neurons to the longitudinal muscle of theguinea pig ileum. Gastroenterology 103, 961—973.
Brookes, S. J. H., Steele, P. A. & Costa, M. (1991). Identificationand immunohistochemistry of cholinergic and non-cholinergiccircular muscle motor neurons in the guinea-pig small intestine.Neuroscience 42, 863—878.
Cannon, W. B. (1902). The movements of the intestines studied bymeans of the roentgen rays. American Journal of Physiology 6,251—277.
Cannon, W. B. (1912). Peristalsis, segmentation and the myentericreflex. American Journal of Physiology 30, 114—128.
Cheung, D. W. & Daniel, E. E. (1980). Comparative study of thesmooth muscle layers of the rabbit duodenum. Journal ofPhysiology 309, 13—27.
Costa, M., Brookes, S. J. H., Steele, P. A., Gibbins, I. L.,
Burcher, E. & Kandiah, C. J. (1996). Neurochemical classificationof myenteric neurons in the guinea-pig ileum. Neuroscience 75,949—967.
Costa, M. & Furness, J. B. (1976). The peristaltic reflex: an analysisof the nerve pathways and their pharmacology.Naunyn—Schmiedeberg’s Archives of Pharmacology 294, 47—60.
Costa, M. & Furness, J. B. (1982). Nervous control of intestinalmotility. In Mediators and Drugs in Gastrointestinal Motility I.Morphological Basis and Neurophysiological Control, 59ÏI, ed.Bertacchini, A., pp. 279—382. Springer—Verlag, Berlin.
Fleisch, A. & Wyss, W. H. (1923). Zur Kenntnis der visceralenTiefensensibilitat. Pfl�ugers Archiv 200, 291—314.
Gonella, J. (1971). Etude electromyographique des contractionssegmentaires et peristaltiques du duodenum de Lapin. Pfl�ugersArchiv 322, 217—234.
Gregory, J. E. & Bentley, G. A. (1968). The peristaltic reflex in theisolated guinea pig ileum during drug-induced spasm of thelongitudinal muscle. Australian Journal of Experimental Biologyand Medical Science 46, 1—16.
Hennig, G. W., Costa, M. & Brookes, S. J. H. (1998). Relationshipbetween circular and longitudinal muscle motor activity in theguinea-pig small intestine. Neurogastroenterology and Motility 10,75.
Holmes, F. L. & Olesko, K. M. (1995). The images of precision. InThe Values of Precision, ed. Wise, M. N., pp. 198—221. PrincetonUniversity Press, Princeton, New Jersey.
Huizinga, J. D., Ambrous, K. & Der-Silaphet, T. (1998). Co-operation between neural and myogenic mechanisms in the controlof distension-induced peristalsis in the mouse small intestine.Journal of Physiology 506, 843—856.
Hukuhara, T. (1931). Die normale Dunndarmbewegung. Pfl�ugersArchiv 226, 518—542.
Hukuhara, T. & Fukuda, H. (1965). The motility of the isolatedguinea-pig small intestine. Japanese Journal of Physiology 15,125—139.
Hukuhara, T., Neya, T. & Tsuchiya, K. (1969). The effect of theintrinsic mucosal reflex upon the propagation of intestinalcontractions. Japanese Journal of Physiology 19, 824—833.
Kosterlitz, H. W. (1968). Intrinsic and extrinsic nervous control ofmotility of the stomach and the intestines. In Handbook ofPhysiology, section 6, vol. IV, ed. Code, C. F., pp. 2147—2171.American Physiological Society, Washington.
Kosterlitz, H. W. & Lees, G. M. (1964). Pharmacological analysis ofintrinsic intestinal reflexes. Pharmacology Review 16, 301—339.
Kosterlitz, H. W., Pirie, V. W. & Robinson, J. A. (1956). Themechanism of the peristaltic reflex in the isolated guinea-pig ileum.Journal of Physiology 133, 681—694.
Kosterlitz, H. W. & Robinson, J. A. (1959). Reflex contractions ofthe longitudinal muscle coat of the isolated guinea-pig ileum.Journal of Physiology 146, 369—379.
Kottegoda, S. R. (1969). An analysis of possible nervous mechanismsinvolved in the peristaltic reflex. Journal of Physiology 200,687—712.
Mapping intestinal movementsJ. Physiol. 517.2 589

Krishnan, B. T. (1932). Studies on the function of the intestinalmusculature: The normal movements of the small intestine and therelations between the action of the longitudinal and circular musclefibres in those movements. Quarterly Journal of Experimentation 22,57—63.
Lammers, W. J. E. P., Al-Kais, A., Singh, S., Arafat, K. & El-
Sharkawy, T. Y. (1993). Multielectrode mapping of slow-waveactivity in the isolated rabbit duodenum. American Journal ofPhysiology 74, 1454—1461.
Macagno, E. O. & Christensen, J. (1980). Fluid mechanics of theduodenum. Annual Review of Fluid Mechanics 12, 139—158.
Maggi, C. A., Patacchini, R., Meini, S. & Giuliani, S. (1994). Effectof longitudinal muscle-myenteric plexus removal and indomethacinon the response to tachykinin NK-2 and NK-3 receptor agonists inthe circular muscle of the guinea-pig ileum. Journal of AutonomicPharmacology 14, 49—60.
Melville, J., Macagno, E. & Christensen, J. (1975). Longitudinalcontractions in the duodenum: their fluid-mechanical function.American Journal of Physiology 228, 1887—1892.
Schemann, M. & Ehrlein, H. J. (1986). Postprandial patterns ofcanine jejunal motility and transit of luminal content.Gastroenterology 90, 991—1000.
Schulze-Delrieu, K., Brown, B. P. & Custer-Hagen, T. (1991).Contraction and accommodation of guinea-pig duodenum in vitro.American Journal of Physiology 261, G364—372.
Smith, T. K. (1989). Spontaneous junction potentials and slow wavesin the circular muscle of isolated segments of guinea-pig ileum.Journal of the Autonomic Nervous System 27, 147—154.
Smith, T. K., Bornstein, J. C. & Furness, J. B. (1990). Distension-evoked ascending and descending reflexes in the circular muscle ofguinea-pig ileum: an intracellular study. Journal of the AutonomicNervous System 29, 203—217.
Smith, T. K. & Robertson, W. J. (1998). Synchronous movements ofthe longitudinal and circular muscle during peristalsis in theisolated guinea-pig colon. Journal of Physiology 506, 563—577.
Summers, R. W. & Dusdieker, N. S. (1981). Patterns of spike burstspread and flow in the canine small intestine. Gastroenterology 81,742—750.
Szurszewski, J. H. (1987). Electrical basis for gastrointestinalmotility. In Physiology of the Gastrointestinal Tract, ed. Johnson,L. R., pp. 383—422. Raven Press, New York.
Tonini, M., Costa, M., Brookes, S. J. H. & Humphreys, C. M. S.
(1996). Dissociation of the ascending excitatory reflex fromperistalsis in the guinea-pig small intestine. Neuroscience 73,287—297.
Tonini, M., Frigo, G., Lecchini, S., D’Angelo, L. & Crema, A.
(1981). Hyoscine-resistant peristalsis in guinea-pig ileum. EuropeanJournal of Pharmacology 71, 375—381.
Tonini, M., Lecchini, S., Frigo, G. & Crema, A. (1974). Action oftetrodotoxin on spontaneous electrical activity of some smoothmuscle preparations. European Journal of Pharmacology 29,236—240.
Trendelenburg, P. (1917). Physiologische und pharmakologischeVersuche Uber die Dunndarmperistaltik. Naunyn—Schmiedeberg’sArchives of Pharmacology 81, 55—129.
Tsuchiya, K. (1972). Electrical and mechanical activities of thelongitudinal muscle in the peristaltic wave elicited by the intra-luminal pressure raising. Rendic Gastroenterology 4, 115—125.
Waterman, S. A. & Costa, M. (1994). The role of enteric inhibitorymotoneurones in peristalsis in the isolated guinea-pig smallintestine. Journal of Physiology 477, 459—468.
Waterman, S. A., Costa, M. & Tonini, M. (1994a). Accommodationmediated by enteric inhibitory reflexes in the isolated guinea-pigsmall intestine. Journal of Physiology 474, 539—546.
Waterman, S. A., Tonini, M. & Costa, M. (1994b). The role ofascending excitatory and descending inhibitory pathways inperistalsis in the isolated guinea-pig small intestine. Journal ofPhysiology 481, 223—232.
Wood, J. D. (1972). Excitation of intestinal muscle by atropine,tetrodotoxin and xylocaine. American Journal of Physiology 222,118—125.
Wood, J. D. & Perkins, W. E. (1970). Mechanical interaction betwenlongitudinal and circular axes of the small intestine. AmericanJournal of Physiology 281, 762—768.
Yokoyama, S. & North, R. A. (1983). Electrical activity oflongitudinal and circular muscle during peristalsis. AmericanJournal of Physiology 244, G83—88.
Yokoyama, S. & Ozaki, T. (1990). Contractions of the longitudinaland circular muscle of the small intestine. Progress in Clinical andBiological Research 327, 483—492.
Acknowledgements
This work has been funded by the National Health and MedicalResearch Council of Australia and the Flinders Medical CentreFoundation. S. J.H.B. was supported, for part of this study, by aSenior Research Fellowship in Digestive Science of theGastroenterological Society of Australia. G.W.H. was supported forpart of this study by a Biomedical Research Scholarship from theGastroenterological Society of Australia.
Corresponding author
M. Costa: Professor of Neurophysiology, Department of Physiology,School of Medicine, Flinders University, GPO Box 2100, Adelaide5001, South Australia, Australia.
Email: [email protected]
.
G. W. Hennig, M. Costa, B. N. Chen and S. J. H. Brookes J. Physiol. 517.2590