Restricted cortical termination fields of the midline and intralaminar thalamic nuclei in the rat

Surg Neurol 183 1991;35:183-8
Quantification of Midline Following Head Injury
Shift as a Predictor of Poor Outcome
Keith B. Quattrocchi, M.D., Praveen Prasad, M.D., Neil H. Willits, Ph.D.,
and Franklin C. Wagner, Jr., M.D. Departments of Neurological Surgery and Statistics, University of California, Davis, School of Medicine, Sacramento, California
Quattrocchi KB, Prasad P, Willits NH, Wagner FC. Quantification of midline shift as a predictor of poor outcome following head injury. Surg Neurol 1991;35:183-8.
A retrospective study of patient outcome, based on admis- sion computed tomography, was carried out in 75 consecu- tive patients with head injury. Computed tomography data collected included the type and extent of intracranial hemorrhage, the extent of midline shift, and the ratio of midline shift compared with the extent of intracranial hemorrhage. Midline shift was considered to be out of proportion to intracranial hemorrhage when the midline shift of the septum pellucidum exceeded the extent of the hemorrhage as measured radially from the inner table of the skull. When computed tomography data were analyzed by logistic regression, significant predictive factors for poor outcome were intracranial hemorrhage (34%), intra- cranial hemorrhage with midline shift (61%), and midline shift out of proportion to the extent of intracranial hemor- rhage (88%). When patient outcome and mortality rates are considered, our study indicates that midline shift out of proportion to the extent of intracranial hemorrhage is a highly useful predictor of poor patient outcome following head injury.
KEY WORDS: Head injury; Computed tomography; Outcome
A variety of methods have been employed in order to predict better the clinical course and outcome following closed head injury. A number of studies have utilized clinical data, such as the Glasgow Coma Scale (GCS), somatosensory evoked potentials, and biochemical markers as predictors of poor patient outcome [2,6,8, 9 ,13,19,30-32,35,38,40] . The relationship between the type of injury, as determined by computed tomography (CT), and patient outcome has been described pre-
Address reprint requests to: Keith B. Quattrocchi, M.D., Department of Neurological Surgery, University of California, Davis, School of Medicine, 2516 Stockton Boulevard, Suite 254, Sacramento, Califor- nia 95816.
Received December 1, 1989; accepted August 16, 1990.
viously [7,11,22,26,30,38]. For example, the presence of intracranial hemorrhage and midline shift on the ad- mission CT scan has been found to correlate with poor outcome following severe head injury. In contrast, the association between the quantitative extent o f midline shift and patient outcome has not been as well defined [2,4,11,12,29,30,37]. Although several studies have ex- amined the relationship between the quantitative extent of midline shift and both low admission GCS score and high intracranial pressure, the extent of midline shift was not compared with patient outcome in these studies [7, 26,30,38,40]. Other studies, which have demonstrated a relationship between the presence of midline shift or intracerebral swelling and poor patient outcome, have not defined the relationship between the quantitative extent of midline shift and patient outcome [23-25] .
The purpose of this study was to determine if more specific CT criteria could be developed to predict patient outcome following closed head injury. Specifically, the effect of midline shift out of proport ion to the extent of intracranial hemorrhage was compared with patient outcome. Midline shift was considered to be out of pro- portion to the extent of intracranial hemorrhage when the shift of the septum pellucidum from the midline exceeded the extent of intracranial hemorrhage, as mea- sured radially from the inner table of the skull [25]. Although the use of volumetric methods to measure the extent of intracranial hemorrhage has been shown to be a more precise method for determining mass effect, simple radial and midline measurements were chosen for this study as these measurements are easily obtain- able and do not require special computations [2,25 ]. We hypothesized that midline shift out of proportion to the extent of intracranial hemorrhage would occur in associ- ation with severe hemispheric injury and would there- fore select for a group of patients with poor prognosis. The results of this study indicate that the finding of midline shift out of proport ion to the extent of intracran- ial hemorrhage on the admission CT scan is a highly predictive and previously undescribed indicator of poor outcome following closed head injury.
© 1991 by Elsevier Science Publishing Co., Inc. 0090-3019/91/$3.50
184 Surg Neurol Quattrocchi et al 1991;35:183-8
M a t e r i a l s a n d M e t h o d s
Between January 1, 1987, and June 30, 1987, a total of 455 patients were admitted to the University of California, Davis Medical Center, with the diagnosis of closed head injury. Of these, 82 patients were admitted with the diagnosis of closed head injury and intracranial hemorrhage, with complete records available for 56 patients. During this same period 20 patients with closed head injury and normal admission CT scans were randomly selected for purposes of comparison. Of these 20 patients with normal CT scans, complete records were available in 19 cases. All patients were examined within 6 hours of injury and CT scans were obtained within 1 hour of admission. Admission clinical data collected included the mode of injury, the admission GCS score, the use of a seat belt or helmet, the patient's age and sex, reported posttraumatic grand mal seizure activity, the presence of severe systemic injury, and the results of various laboratory studies, such as arterial blood gases and alcohol levels. Severe systemic injury was considered to be present when either intraabdominal injury, pul- monary contusion, pelvic fractures, or multiple long bone fractures were present in association with closed head injury. Acidosis was defined by an admission pH of less than 7.25 and hypoxia was considered to be present when the admission PO2 was less than 50 torr. Hypotension was defined by an admission systolic blood pressure of less than 90 mm Hg.
Those patients with findings suggestive of an intra- cranial mass lesion and all comatose patients were intu- bated for hyperventilation, received 1 g/kg of intrave- nous mannitol, and were taken immediately for CT scanning. From the CT scanner, all patients who had significant mass lesions were taken to the operating room. All comatose patients had an intracranial pressure monitoring device placed. Before and after surgery, all patients were treated aggressively in order to control intracranial pressure. Postoperatively, pentobarbital-in- duced coma was utilized for those patients with intra- cranial pressure sustained over 25 mm Hg despite dehy- dration and hyperventilation. Although all patients were admitted to the study irrespective of their admission GCS score, the data were analyzed differentially for all patients and for all patients admitted with a GCS score of 8 or less. Midline shift was calculated by determining the degree of displacement of the septum pellucidum from the midline. The extent of mass effect from hemor- rhage was determined by measuring the extent of hemor- rhage radially from the inner table. Patient outcome was measured by the Glasgow Outcome Scale (GOS) at 6 weeks, 3 months, 6 months, and 1 year. Logistic regres- sion and Fischer's exact test were utilized in all data analyses.
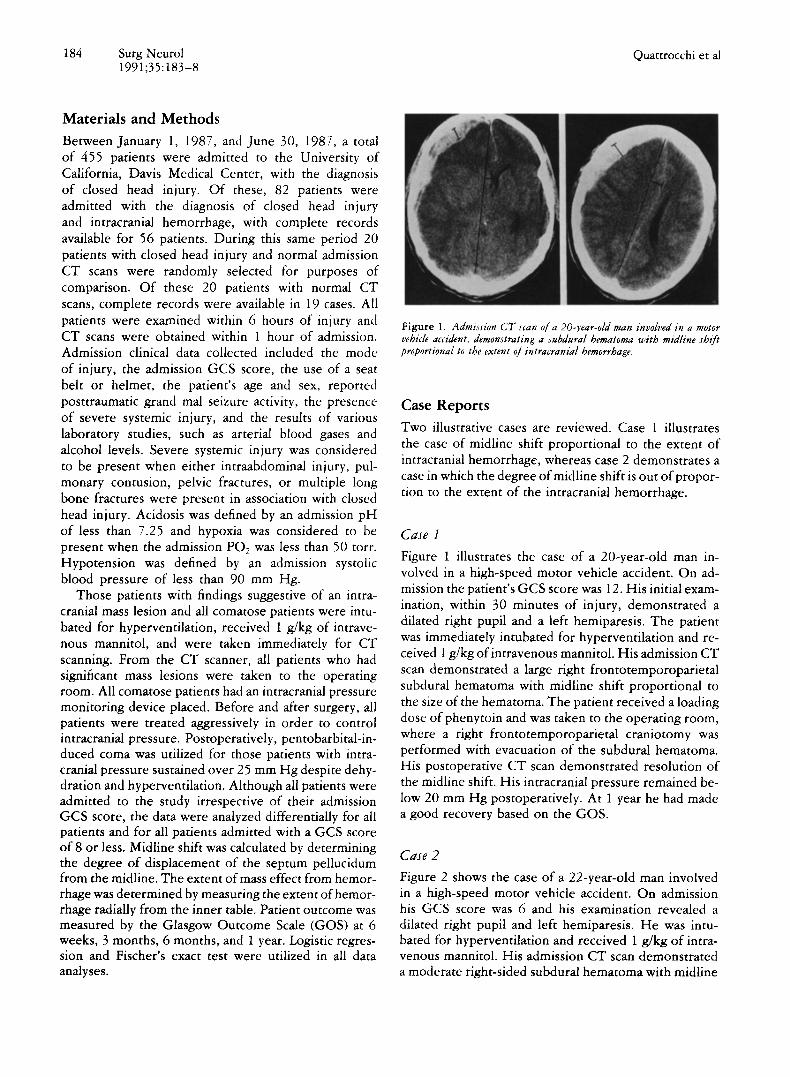
Figure 1. Admission CT scan of a 20-year-old man involved in a motor vehicle accident, demonstrating a subdural hematoma with midline shift proportional to the extent of intracranial hemorrhage.
Case Reports Two illustrative cases are reviewed. Case 1 illustrates the case of midline shift proportional to the extent of intracranial hemorrhage, whereas case 2 demonstrates a case in which the degree of midline shift is out of propor- tion to the extent of the intracranial hemorrhage.
C a s e 1
Figure 1 illustrates the case of a 20-year-old man in- volved in a high-speed motor vehicle accident. On ad- mission the patient's GCS score was 12. His initial exam- ination, within 30 minutes of injury, demonstrated a dilated right pupil and a left hemiparesis. The patient was immediately intubated for hyperventilation and re- ceived 1 g/kg of intravenous mannitol. His admission CT scan demonstrated a large right frontotemporoparietal subdural hematoma with midline shift proportional to the size of the hematoma. The patient received a loading dose ofphenyto in and was taken to the operating room, where a right frontotemporoparietal craniotomy was performed with evacuation of the subdural hematoma. His postoperative CT scan demonstrated resolution of the midline shift. His intracranial pressure remained be- low 20 mm Hg postoperatively. At 1 year he had made a good recovery based on the GOS.
C a s e 2
Figure 2 shows the case of a 22-year-old man involved in a high-speed motor vehicle accident. On admission his GCS score was 6 and his examination revealed a dilated right pupil and left hemiparesis. He was intu- bated for hyperventilation and received 1 g/kg of intra- venous mannitol. His admission CT scan demonstrated a moderate right-sided subdural hematoma with midline

CT and Head Injury Outcome Surg Neurol 185 1991;35:183-8
F i g u r e 2. Admission C T scan of a 22-year-old man involved in a high- speed motor vehicle accident, demonstrating a subdural hematoma with midline shift out of proportion to the extent of intracranial hemorrhage.
shift out of proport ion to the extent of hemorrhage. The patient received a loading dose of phenytoin and was taken to the operating room, where a right frontotem- poroparietal craniotomy was performed with evacuation of the subdural hematoma. In addition, a right anterior temporal lobectomy was performed. A postoperative CT scan revealed severe right hemispheric swelling with increased midline shift despite evacuation of the hema- toma. Postoperatively, the patient's intracranial pressure remained under 20 mm Hg and the patient survived to a vegetative state 1 year following his injury.
R e s u l t s
Patient Profile
Of the 56 patients with intracranial hemorrhage, 46 were male and 10 were female. Of the 19 patients with closed head injury and normal CT scans, 14 were male and five female. The median age of all patients was 30 years, with
a range of 1 to 78 years of age. When analyzed by logistic regression, the best clinical predictor of poor outcome was the GCS (p = 0.0002). Other clinical and laboratory data predictive of poor outcome included the presence of acidosis (p -- 0.0054), an admission blood alcohol level of greater than 100 mg/100 mL (p = 0.0330), the presence of intracranial pressure greater than 20 mm Hg (p = 0.0050), the absence of seat belts (p = 0.0016), and the presence of serious systemic injury (p = 0.007). The presence of hypotension on admission ( p - - 0.3705), the admission hematocrit (p -- 0.4600), and the presence of posttraumatic seizures (p = 0.4788) were not found to correlate with poor outcome. The absence of a helmet was suggestive of poor outcome following motorcycle accidents; however, because of the small sample size, a significant correlation was not found (p = 0.0820).
Computed Tomography
Patient outcome, as related to the admission CT scan, is summarized in Table 1. Good outcome was judged to occur when patients had good recovery or moderate disability, as based on the GOS. Poor outcome was judged to occur when patient outcome at 1 year was severe disability, vegetative state, or death. When CT findings were analyzed by logistic regression, significant factors for poor outcome included the presence of intra- cranial hemorrhage (p -- 0.0100), intracranial hemor- rhage in the presence ofmidl ine shift (p = 0.0125), and midline shift out of proport ion to intracranial hemor- rhage (p = 0.0165). The mortality rates for closed head injury without intracranial hemorrhage (1/19), with in- tracranial hemorrhage (14/56), with intracranial hemor- rhage and midline shift (11/28), and with midline shift out of proportion to intracranial hemorrhage (6/8) were 5%, 25%, 39%, and 75%, respectively (p < 0.05).
Table 1. Outcome as Related to the Admission CT Scan
Average No. of Extent of Extent of Percent poor CT scan GCS patients hemorrhage a shift a Ratio S/M b outcome
Normal 12 19 NA N A N A 6%
Contusion 11 13 3 -+ 2 0.5 -+ 1.6 0.05 -+ 0.18 7%
EDH 15 3 19 -+ 14 10 -+ 11 0.38 + 0.36 0% ICH 10 11 13 + 11 6 +- 9 0.28 _+ 0.31 22%
SDH 9 20 5 - 3 6 + 5 1 -+ 0.83 82% DAI 3 3 1.7 _+ 2 NA N A 100% IVH 6 1 NA NA N A 0%
SAH 10 2 NA N A N A 0% BIH 8 3 9 -+ 6 0.74 +- 1.4 0.74 + 0.14 100%
Abbreviations: BIH, bilateral intracerebral hemorrhages; CT, computed tomography; DAI, diffuse axonal injury; EDH, epidural hematoma; GCS, Glasgow Coma Scale; ICH, intracerebral hemorrhage; IVH, intraventricular hemorrhage; NA, not applicable; SAH, subarachnoid hemorrhage; SDH, subdural hematoma.
Data presented as millimeters of shift or hemorrhage + 1 standard deviation. b Ratio of midline shift to extent of intracranial hemorrhage.

186 Surg Neurol 1991;35:183-8
Quattrocchi et al
Table 2. Outcome as Related to the Presence or Absence of Midline Shift
Shift Shift Normal present absent CT
Poor outcome 14 (50%) 4 (14%) 1 (5%)
Good outcome 14 (50%) 24 (86%) 18 (95%)
Total 28 (100%) 28 (100%) 19 (100%)
Abbreviation: CT, computed tomography.
These differences were also significant when considering only those patients admitted with a GCS of 8 or less.
The relationship between the presence or absence of midline shift on the admission CT scan and patient outcome is summarized in Table 2. The presence of midline shift was associated with poor outcome in 50% of cases, whereas the absence of midline shift was associ- ated with poor outcome in only 14% of cases (p ~ 0.05).
The effect of midline shift out of proportion to the extent of intracranial hemorrhage, as it relates to patient outcome, is reviewed in Table 3. Patients with intracra- nial hemorrhage proportional to the extent of midline shift had poor outcome in 40% of the cases. Patients with midline shift out of proportion to the size of the intracranial hemorrhage had poor outcome in 88% of cases. There was no significant difference in the size of the intracranial hemorrhage or in the incidence of surgi- cal decompression between these two groups of patients. As shown in Table 4, there was no significant difference in the extent ofintracranial hemorrhage when comparing those patients with midline shift proportional to the extent of intracranial hemorrhage with patients with midline shift out of proportion to the extent of intra- cranial hemorrhage. Therefore, the extent of intracra- nial hemorrhage alone does not account for the lower admission GCS score and the higher morbidity and mortality among those patients with shift out of propor- tion to the extent of midline hemorrhage. Analysis by logistic regression demonstrates that the presence of midline shift out of proportion to the extent of intra- cranial hemorrhage is predictive of poor outcome (p = 0.0165).
T a b l e 3. Outcome as Related to the Presence of Midline Shift Out of Proportion to the Size of Intracranial Hemorrhage
Shift > mass" Shift = mass b
Poor outcome 7 (88%) 8 (40%) Good outcome 1 (12%) 12 (60%) Total 8 (100%) 20 (100%)
" Midline shift out of proportion to the extent of intracranial hemorrhage. b Midline shift equal to the extent of intracranial hemorrhage.
Table 4. Comparison of Admission CT and GCS Data for Patients with Midline Shift Proportional to the Extent of Midline Shift and Out of Proportion to the Extent of Midline Shift
Shift > mass" Shift = mass b p'
Extent of hemorrhage a 7 + 3 12 -+ 10 0.1157
Extent of shift 12 -+ 4 8 -+ 6 0.0737
Ratio of S/M' 1.9 -+ 5 0.62 -+ 0.2 <0.001
Average admission GCS 5 +- 2 8 -+ 4 0.0313
Abbreviations: CT, computed tomography; GCS, Glasgow Coma Scale. ° Midline shift out of proportion to the extent of intracranial hemorrhage. b Midline shift equal to the size of the hemorrhage. ' Analysis of variance with multiple comparisons; significance set at 95%.
Data presented as millimeters of hemorrhage or midline shift -+ 1 standard deviation.
Ratio of midline shift to extent of intracranial hemorrhage.
Discussion
Head injury is a significant national health problem, with approximately 500,000 new cases occurring each year in the United States. For those patients with severe head injury, representing nearly 50,000 cases each year, the mortality rate has been estimated to be 40%, with sig- nificant disability occurring in the majority of survivors [ 10]. In response to the tremendous economic and man- power costs created by this problem, numerous studies have investigated the relationship between outcome and admission, clinical laboratory and radiographic studies. These studies have shown that the type of injury, as defined by the admission CT scan, does correlate with patient outcome. Specifically, the presence of intracra- nial hemorrhage, midline shift, and cerebral swelling has been shown to correlate with poor outcome following severe closed head injury [7,11,12,24,30]. Recently, several studies have investigated the relationship be- tween the quantitative extent of midline shift, the admis- sion GCS score, and intracranial pressure following head injury. These studies have shown that significant midline shift correlates with high intracranial pressure, abnormal posturing, and low admission GCS score. Although the presence of midline shift and cerebral swelling has been shown to correlate with poor outcome following head injury, the relationship between the quantitative extent ofmidline shift and patient outcome has not been as well defined [23-25,38,40].
The purpose of this study was to see if more specific CT criteria could be defined that would be predictive of poor outcome following closed head injury. In this retrospective study of 75 consecutive patients with se- vere closed head injury, the degree of midline shift was quantified by considering midline shift to be out of pro- portion to the extent of hemorrhage when the degree of midline septum pellucidum shift exceeded the extent of intracranial hemorrhage, as measured radially from the

CT and Head Injury O u t c o m e Surg Neurol 187 1991;35:183-8
inner table of the skull. The results of this study indicate that the presence of a midline shift out of proportion to the extent of intracranial hemorrhage is a highly pre- dictive indicator of poor patient outcome that has not been previously described. The poor outcome rate for patients with midline shift out of proportion to the ex- tent of intracranial hemorrhage was 88% as compared with 40% when considering midline shift proportional to the extent of hemorrhage (p = 0.0165). These results remained significant when only those patients with se- vere head injury, as defined by an admission GCS score of less than 8, were selected. Therefore, both patient outcome and patient mortality rates are adversely af- fected by the presence of midline shift out of proportion to intracranial hemorrhage following closed head injury. The mortality rate for patients with intracranial hemor- rhage without midline shift (25%) and without intracra- nial hemorrhage (5%) was significantly less than that for patients with intracranial hemorrhage and midline shift (39%) or for patients with midline shift out of propor- tion to the extent of intracranial hemorrhage (75 %). The majority of patients with midline shift out of proportion to the extent of intracranial hemorrhage demonstrated subdural hematoma on their admission CT scan. This finding is consistent with previous studies of intracranial hemorrhage following closed head injury, which have found the highest mortality rates among patients with subdural hemorrhage [7,11,22,26,30,38]. When com- paring either the extent of intracranial hemorrhage or the degree of midline shift alone in those patients with shift proportional to the extent of hemorrhage, as op- posed to those with midline shift out of proportion to the extent of hemorrhage, no statistical difference was found (Table 4). Neither of these factors alone ac- counted for the significant difference in admission GCS and GOS scores between these two groups of patients. Therefore, the extent of initial injury as judged by the size of the hemorrhage or extent of shift alone did not appear to correlate with poor outcome.
There is no single factor that can accurately predict patient outcome following closed head injury. The best results have utilized clinical data, somatosensory evoked potentials, intracranial pressure, and CT scanning in a multifactorial approach [22,38,42]. The advantages of CT scanning include the relative ease by which the CT scan can be obtained and interpreted and the anatomical basis by which CT scanning can be utilized in predicting outcome following closed head injury. The qualitative presence of intracranial hemorrhage and midline shift has been shown to correlate with poor patient outcome [23-25] . The results of the study indicate that the pres- ence of midline shift out of proportion to the extent of intracranial hemorrhage is highly predictive of poor outcome following closed head injury.
References
1. Albercio AM, Ward JD, Choi SC. Outcome after head injury. J Neurosurg 1987;67:648-56.
2. Alexander E, Marshall RB, Laster DW. Subtemporal decompres- sion: radiological observations and current surgical experience. Br J NS 1987;1:427-33.
3. Becker DP, Vries JK, Young HF. Controlled cerebral perfusion pressure and ventilation in human mechanical brain injury: pre- vention of progressive brain swelling. In: Lundberg N, Ponte "n U, Brock M, eds. Intracranial pressure 2. New York: Springer, 1975:480-4.
4. Bowers SA, Marshall LF. Outcome in 200 consecutive cases of severe head injury treated in San Diego county: a prospective study. Neurosurgery 1980;6:237-42.
5. Braakman R, Gelpke GJ, HabbemaJDF, et al. Systemic selection of prognostic features in patients with severe head injury. Neuro- surgery 1980;6:362-70.
6. Cant BR, Shaw NA. Monitoring by compressed spectral array in prolonged coma. Neurology 1984;34:35-9.
7. Clifton GL, Grossman RG, Makela ME, Miner ME, Handel S, Sadhu V. Neurological course and correlated computerized to- mography findings after severe closed head injury. J Neurosurg 1980;52:611-24.
8. Cooper PR, Chalif DJ, RamseyJF, Moore RJ. Radioimmunoassay of the brain type isoenzyme of creatine phosphokinase (CD-BB): a new diagnostic tool in the evaluation of patients with head injury. Neurosurgery 1983;12:536-41.
9. Deutschman CS, Konstantinides FN, Raup S, Cerra FB. Physio- logical metabolic response to isolated closed-head injury, part 1. J Neurosurg 1986;64:89-98.
10. Frankowski RF, Annegers JF, Whitman S. Epidemiological and descriptive studies part 1: the descriptive epidemiology of head trauma in the United States. In: Becker DP, Polvishock JT, eds. Central nervous system trauma status report. 1985:33-51.
11. Gennarelli TA, Spielman GM, Langfitt TW, Gildenberg PL, Har- ington T, Jane JA, Marshall LF, Miller JD, Pitt LH. Influence of the type ofintracranial lesion on outcome from severe head injury. J Neurosurg 1982;56:26-32.
12. Gudeman SK, Kishore PRS, Miller JD, Girevedulis AK, Maurice H, Lipper MB, Becker DP. The genesis and significance of delayed traumatic intracerebral hematoma. Neurosurgery 1979;5: 309-13.
13. Hamill RW, Woolf PD, McDonald JV, Lee LA, Kelly M. Cate- cholamines predict outcome in traumatic brain injury. Ann Neurol 1987;21:438-43.
14. Hans P, Born JD, Chapelle J-P, Milbouw G. Creatinine kinase isoenzymes in severe head injury. J Neurosurg 1983;58:689-92.
15. Jamieson KG, Yelland JD. Surgically treated traumatic subdural hematomas. J Neurosurg 1972;37:137-49.
16. Jennett BJ, Teasdale G, Braakman R, Minderhound J, Heiden J, Kurze T. Prognosis of patients with severe head injury. Neurosur- gery 1979;4:283-9.
17. Johnston IH, Johnston JA, Jennett B. Intracranial-pressure changes following head injury. Lancet 1970;2:433-6.
18. Karnaze DS, Marshall LF, Bickford RG. EEG monitoring of clini- cal coma: the compressed spectral array. Neurology (NY) 1982; 32:289-92.
19. Kaste M, Hernesniemi J, Somer X, Hillbomm M, Konttinen A. Creatinine kinase isoenzymes in acute brain injury. J Neurosurg 1981;55:511-5.
20. Langfitt TW. Measuring the outcome from head injuries.J Neuro- surg 1978;48:673-8.
21. Langfitt TW, Gennarelli TA, Obrist WD. Prospects for the future in the diagnosis and management of head injury: pathophysiology,

188 Surg Neuro l Quat t rocchi et al 1991;35:183-8
brain imaging and population-based studies. Clinical neurosur- gery. Baltimore: Williams and Wilkins, 1981:353-75.
22. Langfitt TW, Obrist WD, Alavi A, Grossman RI, Zimmerman R, Jaggi J, Uzzell B, Reivich M, Patton DR. Computerized tomogra- phy, magnetic resonance imaging and positron emission tomogra- phy in the study of brain trauma. J Neurosurg 1986;64:760-7.
23. Lobato RD, Cordobes F, RivasJJ, Fuente M, Montero A, Barcena A, Perez C, Cabrera A, Lamas E. Outcome from severe head injury related to the type of intracranial lesion: a computerized tomography study. J Neurosurg 1983;59:762-74.
24. Lobato RD, Juan JR, Cordobes F, Aired E, Perez C, Sababia R, Cabrera A, Diez I, Gomez P, Lamas E. Acute epidural hematoma: an analysis of factors infuencing the outcome of patients undergo- ing surgery in coma. J Neurosurg 1988;68:48-57.
25. Lobato RD, Sarabia R, Cordobes F, Rivas JJ, Adrados A, Cabrera A, Gomez P, Madera A, Lamas E. Posttraumatic cerebral hemi- spheric swelling: analysis of 55 case studies with computerized tomography. J Neurosurg 1988;68:417-23.
26. Lobato RD, Sarabia R, RivasJJ, Cordobes F, Castro S, Munoz MJ, Cabrera A, Barcena A, Lamas E. Normal computerized tomogra- phy scans in severe head injury: prognostic and clinical manage- ment implications. J Neurosurg 1986;65: 784-9.
27. Lundberg N, Troupp H, Lorin H. Continuous recording of the ventricular-fluid pressure in patients with severe acute traumatic brain injury: a preliminary report. J Neurosurg 1965;22:581-90.
28. MillerJD, Becker DP, WardJD, Sullivan HG, Adams WE, Rosner MJ. Significance of intracranial hypertension in severe head injury. J Neurosurg 1977;47:503-16.
29. Miller JD, ButterworthJF, Gudeman SK, Faulkner JE, Choi SC, Selbhorst JB, Horbison JW, Lutz HA, Young HF, Becker DP. Further experience in the management of severe head injury. J Neurosurg 1981;54:289-99.
30. Narayan RK, Greenberg RP, Miller JD, Enas GG, Choi SC, Kishore PR, Selhorst JB, Lutz HA, Becker DP. Improved confi- dence of outcome prediction in severe head injury: a comparative analysis of the clinical examination, multimodality evoked poten- tials, CT scanning and intracranial pressure. J Neurosurg 1981; 54:751-62.
31. Rabow L, DeSalles AA, Becker DP, Yang M, Kontos HA, Ward JD, Moulton RJ, Clifton G, Gruemer HD, Muizelaar JP. CSF brain creatine kinase levels and lactic acidosis in severe head injury. J Neurosurg 1986;65:625-9.
32. Rao CJ, Shukla PK, Mohanty SR. Predictive value of serum lactate dehydrogenase in head injury. J Neurol Neurosurg Psychiatry 1978;41:948-53.
33. Richards T, HoffT. Factors affecting survival from acute subdural hematoma. Surgery 1974;75:253-8.
34. Rossanda M, Collice M, Porta M. Intracranial hypertension in head injury, clinical significance and relation to respiration. In: Lundberg N, Ponte "n U, Brock M, eds. Intracranial pressure 2. New York: Springer, 1975:475-9.
35. Rumpl E, Prugger M, Gerstenbrand F, Hackl JM, Pallau A. Cen- tral somatosensory conduction time and short latency somatosen- sory evoked potential in post-traumatic coma. Electroencephalogr Clin Neurophysiol 1983;56:583-96.
36. Sahuquillo-BarrisJ, Lamarca-CiuroJ, Vilalta-CastanJ, Rubio-Gar- cia E, Rodriquiz-Pazas M. Acute subdural hematoma and diffuse axonal injury after severe head injury. J Neurosurg 1988;68: 894-900.
37. Sweet RC, Miller JD, Lipper M, Kishore PR, Becker DP. The significance of bilateral abnormalities on the CT scan in patients with severe head injury. Neurosurgery 1987;3:16-21.
38. Teasdale E, Cardoso E, Galbraith S, Teasdale G. CT scan in severe diffuse head injury: physiological and clinical correlations. J Neu- rol Neurosurg Psychiatry 1984;47:600-3.
39. Thomas DGT, Hioyle NR, Seeldrayers P. Myelin basic protein immunoreactivity in serum of neurosurgical patients. J Neurol Neurosurg Psychiatry 1984;47:173-5.
40. Toutant SM, Klauber MR, Marshall LF, Toole BM, Bower SA, Seelig JM, Varnell JB. Absent or compressed basal cisterns on first CT scan: ominous predictors of outcome in severe head injury. J Neurosurg 1984;61:691-4.
41. Troupp H. Intraventricular pressure in patients with severe brain injuries. J Trauma 1965;5:373-8.
42. Vapalahiti M, Troupp H. Prognosis for patients with severe brain injuries. Br Med J 1971;3:404-7.
Copyright © 2022 FDOKUMEN