
Quality of attachment relationships and peer relationship dysfunction among late adolescents with...
9
Journal of Anxiety Disorders 27 (2013) 116–124 Contents lists available at SciVerse ScienceDirect Journal of Anxiety Disorders Quality of attachment relationships and peer relationship dysfunction among late adolescents with and without anxiety disorders Laura E. Brumariu ∗ , Ingrid Obsuth, Karlen Lyons-Ruth Harvard Medical School, Cambridge Hospital, 1493 Cambridge Street, Cambridge, MA 02139, United States a r t i c l e i n f o Article history: Received 14 September 2011 Received in revised form 8 August 2012 Accepted 7 September 2012 Keywords: Attachment disorganization Social dysfunction Anxiety disorders Late adolescents a b s t r a c t Little is known about the links between anxiety disorders and parent–child attachment disorganization and quality of peer relationships in late adolescence. This study examined the quality of attachment and peer relationships among adolescents with and without anxiety disorders in a sample of 109 low- to moderate-income families. Psychopathology was assessed with the SCID-I. Attachment disorganization and dysfunction in peer relationships were measured using semi-structured interviews and behav- ioral observations. Adolescents with anxiety disorders and comorbid conditions showed higher levels of attachment disorganization across three measurement approaches, as well as higher levels of dys- function in peer relationships than those with no Axis I diagnosis. Adolescents without anxiety disorders but with other Axis I disorders differed only in the quality of school relationships from those with no diagnoses. The pattern of results suggests that pathological anxiety, in the context of other comorbidities, may be a marker for more pervasive levels of social impairment. © 2012 Elsevier Ltd. All rights reserved. 1. Introduction Anxiety disorders consist of a diverse group of psychological difficulties with varied intensities and clinical presentations. All anxiety disorders, however, share a basic component, which is intense fear and anxiety (Rapee & Barlow, 2001). Although transi- tory fears are part of typical development, the intense anxiety that reaches the level of an anxiety disorder is associated with internal distress, low self-esteem, deficits in emotion regulation, and high levels of life interference (Rapee, Schniering, & Hudson, 2009). Correlates of disorders occurring during adolescence have received less attention compared to disorders of childhood and adulthood (Irwin, Burg, & Cart, 2002). Adolescence is a critical time of transition from a position of dependence on the family to more autonomous functioning in the larger community (Allen & Hauser, 1996; Sroufe, Egeland, Carlson, & Collins, 2005). Adolescence is also marked by rapid developmental changes including physical mat- uration, alterations in the neural and neurotransmitter systems underlying affect regulation, emerging increased intimacy in rela- tionships, and growing peer influence (Spear, 2000; Sroufe et al., This study was supported by a Clinical Research Training Fellowships through NIMH Grant T32 MH 16259-32 to Laura E. Brumariu, by NIMH Grant R01MH062030 to Karlen Lyons-Ruth, and by a Social Sciences and Humanities Research Council of Canada Postdoctoral Research Fellowship to Ingrid Obsuth. ∗ Corresponding author. Tel.: +1 617 503 8467; fax: +1 617 503 8470. E-mail addresses: [email protected], [email protected] (L.E. Brumariu). 2005). Not surprisingly, anxiety disorders are prevalent during this period (see Kendall, Hedtke, & Aschenbrand, 2006 for a review). Thus, it is important to investigate how the presence of anxiety dis- orders is related to social functioning in adolescence in both family relationships and in peer relationships including school, friendship, and romantic relationships. The purpose of the present study was to examine the social relationship correlates of anxiety disorders among late adolescents from low- to moderate-income families. Both the disorganization in primary attachment relationships and social dysfunction in broader relationship domains were of interest. 1.1. Anxiety disorders and mother–child attachment 1.1.1. Attachment theory and anxiety Parental regulation of the child’s fear and anxiety lies at the heart of attachment theory. Bowlby (1973) proposed that, when a child is confident that the attachment figure will fulfill the secure base and safe haven roles (i.e., is securely attached), s/he will be less prone to develop anxiety in response to life stressors. By contrast, when a child is unable to predict the attachment figure’s availabil- ity when experiencing disturbing situations, s/he will respond with fear and anxiety. Thus, Bowlby suggested that securely attached children will experience less anxiety than insecurely attached children. Although disorganized attachment is the attachment pattern most associated with the development of psychopathology (DeKlyen & Greenberg, 2008; Lyons-Ruth & Jacobvitz, 2008), there has been little discussion in the literature regarding the potential 0887-6185/$ – see front matter © 2012 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.janxdis.2012.09.002
Transcript of Quality of attachment relationships and peer relationship dysfunction among late adolescents with...
Ql
LH
a
ARRA
KASAL
1
daitrdl
raoa1muut
NtC
(
0h
Journal of Anxiety Disorders 27 (2013) 116– 124
Contents lists available at SciVerse ScienceDirect
Journal of Anxiety Disorders
uality of attachment relationships and peer relationship dysfunction amongate adolescents with and without anxiety disorders�
aura E. Brumariu ∗, Ingrid Obsuth, Karlen Lyons-Rutharvard Medical School, Cambridge Hospital, 1493 Cambridge Street, Cambridge, MA 02139, United States
r t i c l e i n f o
rticle history:eceived 14 September 2011eceived in revised form 8 August 2012ccepted 7 September 2012
eywords:
a b s t r a c t
Little is known about the links between anxiety disorders and parent–child attachment disorganizationand quality of peer relationships in late adolescence. This study examined the quality of attachment andpeer relationships among adolescents with and without anxiety disorders in a sample of 109 low- tomoderate-income families. Psychopathology was assessed with the SCID-I. Attachment disorganizationand dysfunction in peer relationships were measured using semi-structured interviews and behav-
ttachment disorganizationocial dysfunctionnxiety disordersate adolescents
ioral observations. Adolescents with anxiety disorders and comorbid conditions showed higher levelsof attachment disorganization across three measurement approaches, as well as higher levels of dys-function in peer relationships than those with no Axis I diagnosis. Adolescents without anxiety disordersbut with other Axis I disorders differed only in the quality of school relationships from those with nodiagnoses. The pattern of results suggests that pathological anxiety, in the context of other comorbidities,may be a marker for more pervasive levels of social impairment.
. Introduction
Anxiety disorders consist of a diverse group of psychologicalifficulties with varied intensities and clinical presentations. Allnxiety disorders, however, share a basic component, which isntense fear and anxiety (Rapee & Barlow, 2001). Although transi-ory fears are part of typical development, the intense anxiety thateaches the level of an anxiety disorder is associated with internalistress, low self-esteem, deficits in emotion regulation, and high
evels of life interference (Rapee, Schniering, & Hudson, 2009).Correlates of disorders occurring during adolescence have
eceived less attention compared to disorders of childhood anddulthood (Irwin, Burg, & Cart, 2002). Adolescence is a critical timef transition from a position of dependence on the family to moreutonomous functioning in the larger community (Allen & Hauser,996; Sroufe, Egeland, Carlson, & Collins, 2005). Adolescence is alsoarked by rapid developmental changes including physical mat-
ration, alterations in the neural and neurotransmitter systemsnderlying affect regulation, emerging increased intimacy in rela-ionships, and growing peer influence (Spear, 2000; Sroufe et al.,
� This study was supported by a Clinical Research Training Fellowships throughIMH Grant T32 MH 16259-32 to Laura E. Brumariu, by NIMH Grant R01MH062030
o Karlen Lyons-Ruth, and by a Social Sciences and Humanities Research Council ofanada Postdoctoral Research Fellowship to Ingrid Obsuth.∗ Corresponding author. Tel.: +1 617 503 8467; fax: +1 617 503 8470.
E-mail addresses: [email protected], [email protected]. Brumariu).
887-6185/$ – see front matter © 2012 Elsevier Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.janxdis.2012.09.002
© 2012 Elsevier Ltd. All rights reserved.
2005). Not surprisingly, anxiety disorders are prevalent during thisperiod (see Kendall, Hedtke, & Aschenbrand, 2006 for a review).Thus, it is important to investigate how the presence of anxiety dis-orders is related to social functioning in adolescence in both familyrelationships and in peer relationships including school, friendship,and romantic relationships.
The purpose of the present study was to examine the socialrelationship correlates of anxiety disorders among late adolescentsfrom low- to moderate-income families. Both the disorganization inprimary attachment relationships and social dysfunction in broaderrelationship domains were of interest.
1.1. Anxiety disorders and mother–child attachment
1.1.1. Attachment theory and anxietyParental regulation of the child’s fear and anxiety lies at the
heart of attachment theory. Bowlby (1973) proposed that, when achild is confident that the attachment figure will fulfill the securebase and safe haven roles (i.e., is securely attached), s/he will be lessprone to develop anxiety in response to life stressors. By contrast,when a child is unable to predict the attachment figure’s availabil-ity when experiencing disturbing situations, s/he will respond withfear and anxiety. Thus, Bowlby suggested that securely attachedchildren will experience less anxiety than insecurely attached
children. Although disorganized attachment is the attachmentpattern most associated with the development of psychopathology(DeKlyen & Greenberg, 2008; Lyons-Ruth & Jacobvitz, 2008), therehas been little discussion in the literature regarding the potential
nxiet
aadmsaaJtaofrpg
auba
1
AAutctsat
a(Rsiwtua
al2CodepRMmclotsinnaptc
L.E. Brumariu et al. / Journal of A
ssociation between the disorganized pattern of attachment andnxiety disorders specifically. Theoretically, individuals withisorganized attachments are thought to perceive their attach-ent figures as unable to protect them. In addition, developmental
tudies have established that parents of children with disorganizedttachments are more likely to engage in frightening, frightened ortypical behavior when interacting with the child (Lyons-Ruth &acobvitz, 2008). At the behavioral level, attachment disorganiza-ion leads to difficulties in organizing a consistent strategy of eitherpproaching or avoiding the caregiver when under stress. The lackf a consistent strategy to deal with distress would then leave theearful arousal unresolved for those with disorganized attachmentelationships, increasing the likelihood that anxiety would reachathological levels. Thus, one would expect that those with disor-anized attachments would be vulnerable to anxiety disorders.
As this summary indicates, disorganized attachment behaviorsre defined as behaviors exhibited in relation to attachment fig-res (Lyons-Ruth & Jacobvitz, 2008). Thus, they are not expected toe general features of social interaction but to appear at times ofttachment stress in relation to the need for comfort and security.
.1.2. Measuring attachment disorganization in adolescenceMost studies of adolescent attachment have used the Adult
ttachment Interview (AAI; George, Kaplan, & Main, 1996). TheAI is a semi-structured interview designed to assess an individ-al’s current state of mind about past parent–child experienceshat leads to an overall classification of secure/autonomous, inse-ure/dismissing, insecure/preoccupied, or unresolved with respecto experience of loss or abuse (George et al., 1996). The Unre-olved classification indexes disorganization on the AAI. However,n important conceptual and methodological problem arises whenhere has been no serious loss or abuse to inquire about on the AAI.
Another approach to assessing disorganization on the AAI is tossess the presence of a pervasively unintegrated hostile–helplessHH) state of mind in regard to attachment relationships (Lyons-uth, Yellin, Melnick, & Atwood, 2005). The hostile–helpless codingystem indexes pervasively unintegrated and affectively polar-zed evaluations of attachment relationships across the interview,
hether or not experiences of loss or abuse have occurred. Thus,he HH coding system complements the traditional coding ofnresolved states of mind regarding loss or trauma in assessingttachment disorganization.
The first observational assessment has been recently developednd validated for parent–child attachment disorganization in ado-escence (Hennighausen, Bureau, David, Holmes, & Lyons-Ruth,011). Specifically, the Goal-Corrected Partnership in Adolescenceoding System (GPACS) was designed to assess observed formsf disorganized attachment, including subtypes of adolescentisorganization (punitive, caregiving/role confused, and disori-nted) that parallel the subpatterns of disorganization observed inreschool and middle childhood (Bureau, Easterbrooks, & Lyons-uth, 2009; O’Connor, Bureau, McCartney, & Lyons-Ruth, 2011;ain & Cassidy, 1988). These controlling behavioral strategies areanifested either in a caregiving or a punitive fashion. Specifically,
aregiving/role-confused interactions are characterized by the ado-escent’s efforts to maintain the parent’s well-being (i.e., directing,rganizing, and entertaining the parent) such as giving directiveso the parent, taking the lead to assure the flow of the discus-ion, and telling jokes that engage and amuse the parent. Punitiventeractions are characterized by overt and covert expressions ofegative affect by the adolescent and/or by the parent (i.e., domi-ating and humiliating behavior). Finally, disoriented interactions
re marked by odd, out-of-context behaviors (i.e., rapid and inap-ropriate shifts in affect or behavior, “freezing”, wandering aroundhe room during discussion, unusual shifts away from topic of dis-ussion), as seen in both verbal and physical interaction. These oddy Disorders 27 (2013) 116– 124 117
behaviors are analogous to the disorganized behaviors observedin infancy, though by adolescence they occur more often in oddfeatures of verbal discourse (Hennighausen et al., 2011). In sum-mary, each attachment measure for adolescents captures distinctand complimentary aspects of attachment disorganization.
1.1.3. Empirical links between anxiety disorders and attachmentRecent reviews of the literature suggest that secure attach-
ment is indeed linked to lower levels of anxiety symptoms inchildhood and adolescence (for reviews, see Brumariu & Kerns,2010a; DeKlyen & Greenberg, 2008). There is also some evi-dence suggesting that ambivalent attachment rather than avoidantattachment is associated with higher levels of anxiety and internal-izing problems in preadolescence/adolescence, based on studieswhich included secure, avoidant, and ambivalent classifications,but not the disorganized classification (Brumariu & Kerns, 2010a;Colonnesi et al., 2011). When disorganization was also assessed,disorganization rather than ambivalence was related to generalinternalizing symptoms in childhood/adolescence (Brumariu &Kerns, 2010a). However, Brumariu and Kerns (2010a) cautionedthat few studies assessed the insecure patterns, and most of thesestudies examined internalizing symptoms rather than specificallyanxiety. Recent studies further demonstrated that disorganizedattachment is significantly related to higher levels of anxietysymptoms in childhood (Borelli, David, Crowley, & Mayes, 2010;Brumariu & Kerns, 2010b; Brumariu, Kerns, & Seibert, 2012; Mosset al., 2006). Importantly, with one exception (Warren, Huston,Egeland, & Sroufe, 1997), none of the studies reviewed in Brumariuand Kerns (2010a) examined the presence of anxiety disorders ascompared to symptoms of anxiety, and none of the studies of ado-lescents measured disorganization of attachment strategies. In amore recent study of adolescents, however, Ivarsson, Granqvist,Gillberg, and Broberg (2010) showed that both the dismissing and“the cannot classify” classifications on the AAI increased the like-lihood of obsessive–compulsive disorder (OCD). Unexpectedly, theunresolved category decreased the likelihood of OCD. OCD patientswith or without comorbid depressive disorders had a higher pro-portion of dismissing states of mind than patients with depressivedisorders only or controls.
Even in the literature on adults there are few studies assessingthe relation between attachment disorganization and anxiety dis-orders. Manassis, Bradley, Goldberg, Hood, and Swinson (1994)found that 78% of the 18 women with anxiety disorders (panic,OCD and Generalized Anxiety Disorder [GAD]) in their sample wereclassified as unresolved on the AAI. Fonagy et al. (1996) also founda significant relation between an unresolved classification and adiagnosis of anxiety disorder (GAD, OCD, phobias, and somato-form/stress disorder). Based on the Adult Attachment Projective,Buchheim and George (2011) also reported that individuals withanxiety disorders displayed significantly higher levels of unre-solved attachment than controls. In contrast, in a sample of 80inpatients, Riggs et al. (2007) found that secure patients were morelikely, and dismissing patients were less likely, to have an anxi-ety diagnosis than other attachment groups. van Emmichoven, vanIJzendoorn, de Ruiter, and Brosschot (2003) reported that, com-pared to a control group, there were fewer secure participants inthe anxiety disordered group in their sample. There were no dif-ferences in the distribution of the unresolved attachment betweenthe controls and participants with anxiety disorders.
Several additional studies have explored the relation betweenattachment disorganization and the presence of specific anxietydisorders in adulthood. The unresolved classification was associ-
ated with the presence of a PTSD diagnosis in a sample of Dutchveterans (Harari et al., 2009), as well as with a greater likelihoodof comorbid anxiety and PTSD in a sample of Vietnam combat vet-erans (Nye et al., 2008). Finally, among women with a history of
1 Anxiet
cmaInaToto
1
a1crftcmsrhs(Krras
1
c(KsdsMop&idc
1
trclIs
ia(ob2
(n = 28) and 7.3% were Hispanic (n = 8). Fifty-nine adolescents lived
18 L.E. Brumariu et al. / Journal of
hildhood abuse, unresolved states of mind were associated withore comorbid anxiety disorders and with increased likelihood of
PTSD diagnosis, specifically (Stovall-McClough & Cloitre, 2006).n sum, in contrast to the adult literature, previous literature hasot thoroughly explored the relation between anxiety disordersnd disorganization in attachment relationships in adolescence.herefore, very little is known about the link between anxiety dis-rders and attachment disorganization in late adolescence, duringhis critical period of transition to more autonomous functioningutside the family.
.2. Anxiety disorders and dysfunction in peer relationships
Given that adolescence is a developmental period when youthssert their autonomy away from their family (e.g., Allen & Hauser,996), an additional question of interest is whether late adoles-ents with anxiety disorders have relationship difficulties in socialelationships outside the family, including school relationships,riendships, and romantic relationships. In adolescence, peer rela-ionships begin to supplement family relationships, thus, they areritical to adolescent well-being (Sroufe et al., 2005). By age 16,any adolescents report being engaged in a romantic relation-
hip (Carver, Joyner, & Udry, 2003), and by emerging adulthood,omantic relationships become increasingly important. Studiesave shown that children and adolescents who experience anxietyymptoms are more likely to experience poor peer relationshipse.g., low peer competence, peer rejection or victimization; seeingery, Erdley, Marshall, Whitaker, & Reuter, 2010, for a review). Aelatively limited number of studies, however, have assessed peerelationships in clinically anxious youth, and thus little is knownbout how anxiety disordered late adolescents function in specificocial domains (Kingery et al., 2010).
.3. Anxiety disorders and comorbidity
Anxiety disorders are highly comorbid with depression in bothhildhood and adulthood and with substance abuse in adulthoodAngold, Costello, & Erkanli, 1999; Costello, Egger, & Angold, 2005;essler, Chiu, Demler, & Walters, 2005; Merikangas et al., 1998;ee also Rapee et al., 2009). Although comorbidity of anxiety disor-ers with other disorders is the norm, many studies have relied onamples that include individuals with anxiety disorders only (e.g.,anassis et al., 1994) or did not examine associations of anxiety dis-
rders in the context of comorbidity with other conditions whenarticipants met criteria for other diagnoses (e.g., Stovall-McClough
Cloitre, 2006). Yet to draw conclusions with meaningful clinicalmplications, it is important to explore the links between anxietyisorders and social functioning in the context of other comorbidonditions.
.4. Goals of the current study
The primary goal of this study was to assess the relation betweenhe presence of anxiety disorders and the quality adolescent socialelationships, in the context of other comorbidities. Thus, weompared late adolescents with no Axis I diagnosis to (a) late ado-escents with one or more anxiety disorders and comorbid Axis
conditions, and to (b) those without anxiety disorders but withimilar comorbid Axis I diagnoses.
We employed a multi-method approach to measuring the qual-ty of primary attachment relationships by using three measures ofttachment disorganization: unresolved loss or trauma on the AAI
Main, Goldwyn, & Hesse, 2003), hostile–helpless representationsn the AAI (Lyons-Ruth et al., 2005), and disorganized/controllingehaviors in observed interactions (GPACS, Hennighausen et al.,011). We hypothesized that late adolescents with anxietyy Disorders 27 (2013) 116– 124
disorders would have higher levels of both unresolved states ofmind regarding loss or trauma and higher levels of hostile–helplessrepresentations of attachment relationships compared to thosewith no Axis I diagnosis. We expected that compared to those withno Axis I diagnosis, late adolescents with anxiety disorders wouldhave higher levels of disorganized interaction patterns character-ized by caregiving/role confusion or disorientation, but not higherlevels of punitive control, which has been related to externalizingbehavior at earlier ages (Moss, Cyr, & Dubois-Comtois, 2004).
Secondly, we evaluated the quality of peer relationships in threespecific social domains: friendships, romantic relationships, andschool relationships. We hypothesized that late adolescents withanxiety disorders would experience higher dysfunction in all threesocial domains compared to those with no Axis I diagnosis.
Since we expected that late adolescents with anxiety disorderswould have other Axis I diagnoses, we also examined whether thosewith other Axis I diagnoses but no anxiety disorders would showelevated levels of dysfunction across the same social domains.
2. Method
2.1. Participants
The sample included 109 late adolescents (66 females and 43males) and their mothers, with low to moderate family incomes inan urban area in Northeastern US. The 109 adolescents includedall those from a larger study sample of 120 participants whohad complete diagnostic data on the Structured Clinical Inter-view for DSM-IV AXIS I (SCID-I, First, Spitzer, Gibbon, & Williams,1997). Mothers reported the income of the family of originby checking one of seven income categories, with the lowestcategory including 5000–10,000/yr and the highest category refer-ring to more than $60,000/yr (mean range of family of originincome = $30,000–$40,000/yr). In the larger study of 120 families,sixty-four families were first seen in adolescence; 56 families hadbeen followed longitudinally since infancy. The 64 families seenonly in adolescence were matched to longitudinal families on ado-lescent age and ethnicity. The 56 longitudinally studied familieswere part of a cohort of 76 low-income families recruited duringthe first 18 months of the child’s life, yielding a longitudinal reten-tion rate of 74% (14% could not be located; 9% refused; and 3% livedoverseas). Attrition was unrelated to eight socioeconomic indicesin infancy as well as to all outcome assessments in infancy (effectsizes ϕ or � = −.14 through .13). Half of the families seen in infancywere referred to the study by social service providers due to theirconcerns about the quality of care provided to the infant; otherfamilies seen in infancy did not exhibit problems in infant care(for additional description, see Lyons-Ruth, Connell, Grunebaum,& Botein, 1990). Exclusion criteria for recruitment in infancy werepremature birth or physical problems in the first year of life. Nospecific exclusion criteria were employed for families first seen inadolescence. Families first seen in adolescence were recruited fromthe same communities through advertisements and they reportedno referrals for parenting help in infancy. Thus, sample compositionensured a range of caregiving risk within the sample.
All mothers were biological mothers, except one mother, whowas the child’s aunt but had raised the child from age 3 monthsdue to the biological mother’s death. The mean age for adolescentswas 19.9 (SD = 1.45, range 19–23 years). Sixty-seven percent of theadolescents were Caucasian (n = 73), 35.7% were African-American
with their families of origin, six adolescents lived with relatives,eight adolescents lived with significant others, 35 adolescentslived with roommates in apartments or in dorms, and one was injail.

nxiet
2
RpirpACtttmtptttcvth
2
2F
erpwthSfi
2
attwipaeho
2eSptfiAiwwr2dc
L.E. Brumariu et al. / Journal of A
.2. Procedure
All procedures were approved by the Hospital Institutionaleview Board. Written informed consent was obtained from botharent and adolescent. Adolescents and their mothers participated
n a 60- to 90-min laboratory visit. They were taken to sepa-ate rooms to complete interviews and questionnaires assessingsychopathology and their relationships with parents and peers.dolescents and their mothers also separately completed an Issueshecklist on which they rated sources of disagreement in their rela-ionship. Parent and adolescent could also add their own topics tohe suggested list. After both checklists were completed, a topichat was present on both checklists and was highly rated by both
other and adolescent was selected for discussion by a lab assis-ant and the young adult taped a 1-min statement of his or herosition. The parent and adolescent were then reunited for an ini-ial 5-min unstructured reunion period, followed by the playing ofhe taped young adult statement and a 10-min discussion of theopic of disagreement. All interactions were videotaped and lateroded as described below. Different coders coded each type of inter-iew or interaction task, and coders were naive to all other data inhe study, including the adolescent’s diagnostic status, and mainypotheses.
.3. Measures
.3.1. Structured Clinical Interview for DSM-IV AXIS I (SCID-I,irst et al., 1997)
The Structured Clinical Interview for DSM-IV AXIS I (SCID-I, Firstt al., 1997), indicating whether or not participants meet crite-ia for DSM-IV AXIS I diagnoses, was administered to adolescentarticipants in the laboratory by an experienced trained clinicianith 20 years of mental health clinical practice who received addi-
ional training in SCID administration. Including this study, sheas conducted over 300 SCID interviews for research studies. TheCID yields reliability kappa’s of .61 for current diagnosis and .68or lifetime diagnoses, comparable to other structured diagnosticnterviews (First et al., 1997).
.3.2. Adult Attachment Interview (AAI, George et al., 1996)Adult Attachment Interviews (AAI, George et al., 1996) were also
dministered to the adolescent participants prior to the interactionask. The AAI is a semi-structured interview designed to elicit a par-icipant’s current state of mind regarding attachment experiencesith parents and other significant caregivers during childhood. The
nterviewer asks about the quality of childhood experiences witharents, the participant’s responses to experiences of rejection, sep-ration, loss, and trauma during childhood, and the participant’svaluation of the effects of those childhood experiences on his orer current functioning. In this study, the participants’ current statef mind in relation to their parents was assessed.
.3.2.1. The Adult Attachment Scoring and Classification System (Maint al., 2003). The Adult Attachment Scoring and Classificationystem (Main et al., 2003) was used to assign autonomous, preoccu-ied, dismissing, unresolved, and cannot classify classifications onhe AAI. AAIs were coded by two coders who were trained and certi-ed as reliable through the standard Main et al. training procedures.
subset of 15 interviews were coded by both coders to establishnter-rater reliability on the present sample (kappa = .62). Coders
ere naïve to all other data. For data analysis, the AAI classificationsere grouped into a three-level variable indexing overall insecu-
ity/disorganization of attachment [1 = autonomous/secure, n = 43; = organized insecure (i.e., dismissing or preoccupied), n = 45 (nismissing = 35 and n preoccupied = 10); 3 = unresolved or cannotlassify, n = 21]. The Adult Attachment Scoring and Classification
y Disorders 27 (2013) 116– 124 119
System for the AAI has good stability over time, good validity inrelation to measures of psychopathology, measures of parenting,and quality of infant attachment, and discriminant validity hasbeen demonstrated with respect to memory, intelligence, cognitivecomplexity, and social adjustment (see Hesse, 2008 for a review).
2.3.2.2. Hostile/helpless representations of attachment relationships.The AAI was also coded using the hostile–helpless (HH) codingsystem (Lyons-Ruth et al., 2005), which assesses pervasively unin-tegrated positive and negative evaluations of childhood attachmentrelationships on a 1–9 scale [1 = no evidence of HH, 9 = high lev-els of HH, M(SD) = 4.69 (1.64)]. Transcripts coded higher on thehostile–helpless scale are characterized by evidence of opposingevaluations of primary attachment relationships occurring acrossthe interview that are neither discussed nor reconciled by the par-ticipant, e.g., “We were friends. . .We were enemies.” The intraclasscorrelation on 15 randomly selected transcripts was .83. Validityhas been established in relation to childhood trauma, disruptedparenting, and disorganized infant attachment. Additional detailis available elsewhere describing coding criteria and detailing howthis coding system differs from and extends the Main et al. (2003)coding system for the AAI (Lyons-Ruth, Yellin, Melnick, & Atwood,2003; Lyons-Ruth et al., 2005).
2.3.3. Goal-Corrected Partnership in Adolescence Coding System(GPACS)
Videotaped interactions were coded using the GPACS(Hennighausen et al., 2011). The GPACS includes ten scales asfollows: Collaborative Communication indexing cooperativegoal-corrected partnership; Caregiver Validation of Adolescent’sVoice that indexes the caregiver’s support for the adolescent’sself-expression; and eight scales that index three major subtypesof disorganized interaction, including punitive, caregiving/role-confused, and disoriented behavior. These eight scales are: (1)parental punitive behavior (e.g., mother making angry, hurtful, ormocking comments about the adolescent), (2) adolescent punitivebehavior (e.g., adolescent making angry, critical, or mockingcomments about the parent; sharply dictating how the parentshould behave), (3) adolescent disoriented/distracted behavior(e.g., assuming a trance-like posture or expression (“freezing”);pausing abruptly in mid-sentence; closing eyes for prolongedperiods), (4) parental disoriented/distracted behavior (e.g., sameas adolescent disoriented behavior), (5) adolescent odd, out-ofcontext behavior (e.g., using a forced, high-pitched, or childish toneof voice; chanting or making repetitive comments; shifting intounusual, fantasy-based topics; stiff, stilted, or mistimed gestures),(6) parental odd, out-of-context behavior (e.g., using a forced, high-pitched, or childish tone of voice; wandering aimlessly around theroom; unusual shifts away from the topic; stiff, stilted, or mistimedgestures), (7) adolescent caregiving (e.g., attempting to manage,take care of, and/or appease the parent by offering guidance, orga-nizing the task, and/or providing entertainment such as silly jokes;coy/flirtatious behaviors), and (8) parental role-confusion (e.g.,making comments about feeling inadequate, uncertain, or helpless;asking for advice on topics more typically discussed with partneror other adult (personal relationships, discipline of siblings).Intraclass correlations between two coders, naïve to all other data,ranged between .75 and .96 (n = 16). Confirmatory factor analysesof the ten scales confirmed a four-factor model: a factor indexingcollaboration in interactions and three factors indexing typesof disorganization including punitive, caregiving/role -confused,and disoriented behavior, CFI = .969; TLI = .942; RMSEA = .060, 90%
CI (.065–.076) (Obsuth, Hennighausen, Brumariu, & Lyons-Ruth,submitted for publication). Only the three factors indexing dis-organization were used in this study [Ms (SDs) = 3.29 (1.26), 4.41(1.64) and 3.24 (1.53) for punitive, disoriented and caregiving/role
1 Anxiety Disorders 27 (2013) 116– 124
ctcse
2H
1twvrpfrAsOiHed(It
2
fGrtmwsiw(ssto
3
3
(oIcgg
r(gosdom
Table 1Other Axis I diagnoses among participants with and without anxiety disorders.
Diagnoses Anxiety disordersn = 44
Other Axis I diagnosesn = 35
Depressive disorders 20 (45%) 15 (43%)Bipolar disorder 3 (7%) 5 (14%)Substance abuse disorders 23 (52%) 19 (54%)
20 L.E. Brumariu et al. / Journal of
onfused, respectively]. The GPACS has shown validity in relationo disorganized attachment classification in infancy, to attachmentlassification on the AAI at age 25, and to parent and adolescentelf-reports of role-confusion (Hennighausen et al., 2011; Obsutht al., submitted for publication).
.3.4. Adult Personality Functioning Assessment (APFA; Hill,arrington, Fudge, Rutter, & Pickles, 1989)
The Adult Personality Functioning Assessment (APFA; Hill et al.,989) is a semi-structured interview which inquires about func-ioning over four to six-year time periods in the domains ofork/school, romantic relationships, and friendships. The inter-
iewer uses flexible questioning to obtain information and makeatings on the basis of detailed rating rules, a dictionary of exam-les, and training. Ratings are made for each domain on scalesrom 1 to 6 where “1” reflects a high level of adaptation and “6”eflects very poor functioning. Scoring was conducted using thedolescence to Adult Personality Functioning (ADAPFA) scoringystem which has been designed for late adolescence (Naughton,ppenheim, & Hill, 1996). The APFA has good inter-rater reliabil-
ty and subject-informant agreement (Hill et al., 1989; Hill, Fudge,arrington, Pickles, & Rutter, 1995). In this study, interviews cov-red the period from 14 to 19 years of age and three distinctomains: friendships (M = 3.29, SD = 1.05), romantic relationshipsM = 4.25, SD = 1.23), and school relationships (M = 3.75, SD = 1.42).ntraclass correlations among coders ranged from .80 to 1.00 (napes = 12).
.4. Missing data on social functioning variables
In the present sample, the rate of missing information on socialunctioning variables ranged from 0% to 4.6%. Specifically, thePACS variables had a 4.6% rate of missing data, and APFA had
ates of 2.8% for the quality of romantic relationships and 1.8% forhe quality of friendships and school relationships. These data were
issing due to technical difficulties or participants becoming tiredith the protocol. For a rate of missing information of 4.6%, five data
ets were generated, yielding excellent efficiency to detect a signif-cant effect of 99% according to Rubin’s (1987) guidelines. The data
ere imputed through the Markov Chain Monte Carlo procedureMCMC; Gilks, Richardson, & Spiegelhalter, 1995), using SPSS ver-ion 19 software. Results with missing and imputed data yieldedimilar results. Power analysis using G*Power program indicatedhat based on a sample of 109 participants, there is 97% power tobtain an effect size of .4 (Faul, Erdfelder, Lang, & Buchner, 2007).
. Results
.1. Descriptive data
Thirty participants did not meet criteria for any Axis I disorders30% male), 44 participants met criteria for at least one anxiety dis-rder (48% male), and 35 participants met criteria for other Axis
disorders, but not for an anxiety disorder (37% male). Thus, out-omes were assessed for these three groups: the no Axis I diagnosesroup, the other Axis I diagnoses group, and the Anxiety disordersroup.
Participants in the anxiety disorders group met diagnostic crite-ia for one or more anxiety disorders, including panic disordern = 4), social phobia (n = 16), obsessive–compulsive disorder (n = 2),eneralized anxiety disorder (n = 10), post-traumatic stress dis-rder (n = 3), agoraphobia (n = 2), anxiety disorder not otherwise
pecified (n = 8), and specific phobia (n = 15). Ten participants metiagnostic criteria for only one anxiety disorder, and did not havether comorbid Axis I diagnoses. Ten participants experiencedore than one anxiety disorder and these 10 participants also hadEating disorder 2 (5%) 2 (6%)Somatoform disorder 1 (2%) 1 (3%)
other Axis I comorbid diagnoses. In total, thirty-four participantswith anxiety disorders also met criteria for other comorbid AxisI disorders. Other Axis I diagnoses among participants with anxi-ety disorders and without anxiety disorders are shown in Table 1.Given the low-income nature of this sample, as well as the over-sampling of caregiving risk in the longitudinal cohort, it is notsurprising that the rates of anxiety disorders, as well as those ofother Axis I diagnoses, are higher than those reported in epidemio-logical studies (see Kendall et al., 2006; Rudolph, Hammen, & Daley,2006 for reviews). For example, in epidemiological studies, preva-lence rates for panic disorder, obsessive–compulsive disorder, andposttraumatic stress disorder range from <1% to 2%, and preva-lence rates for generalized anxiety disorder are about 1% (Kendallet al., 2006), which are lower than those found here (i.e., in thissample, prevalence rates were 3.67% for panic disorder, 2.75% forposttraumatic stress disorder, and 9.17% for generalized anxietydisorder). Consistent with epidemiological studies, the rate forobsessive–compulsive disorder in this sample was 1.84%. In agree-ment with our data, studies show phobias to be the most commonanxiety disorder in adolescence (Kendall et al., 2006).
3.2. Preliminary analyses
Preliminary analyses investigated whether the adolescent’s age,gender, ethnicity, or family income were related to the attachment,social domain dysfunction, or anxiety disorder variables. None ofthe demographic variables (adolescent’s age, gender, and ethnicityor family income) were related to the presence of anxiety dis-orders [i.e., diagnostic status; for adolescent age, F(2, 106) = .16,p > .05; for family income, F(2, 106) = 40, p > .05; for ethnicityand gender, �2(2) = 4.35 and �2(2) = 2.46, respectively, p > .05]. Inregard to the relation between age and social functioning variables,we found only two significant relations for attachment: partici-pants who were older were rated less punitive and disorientedin their interactions with their mothers on the GPACS (r = −.25,p < .01, and r = −.21, p < .05). Age was not related to dysfunction inpeer relationship variables (rs ranged between −.07 and −.11, allps > .05). Males had more difficulties in school relationships thanfemales (Ms = 4.07 and 3.51, respectively, t(107) = −2.19, p < .05),but no other comparisons were significant. Family income wasrelated to several variables: overall insecurity/disorganization onthe AAI (r = −.41, p < .001), the extent of hostile/helpless represen-tations on the AAI (r = −.21, p < .05), disorientation in interactionon the GPACS (r = −.31, p < .01), role confusion in interaction onthe GPACS (r = −.21, p < .05), friendship dysfunction on the APFA(r = −.27, p < .01) and school relationships dysfunction on the APFA(r = −.37, p < .001). Ethnicity was unrelated to study variables. Alldemographic variables related significantly to social functioningvariables were controlled in relevant analyses.
Table 2 includes zero-order correlations among attachmentvariables and zero-order correlations between the attachment and
peer relationships variables. Indices of disorganization were mod-estly correlated, suggesting that they measure somewhat differentaspects of disorganization and complement one another. Associa-tions between measures of attachment disorganization in relation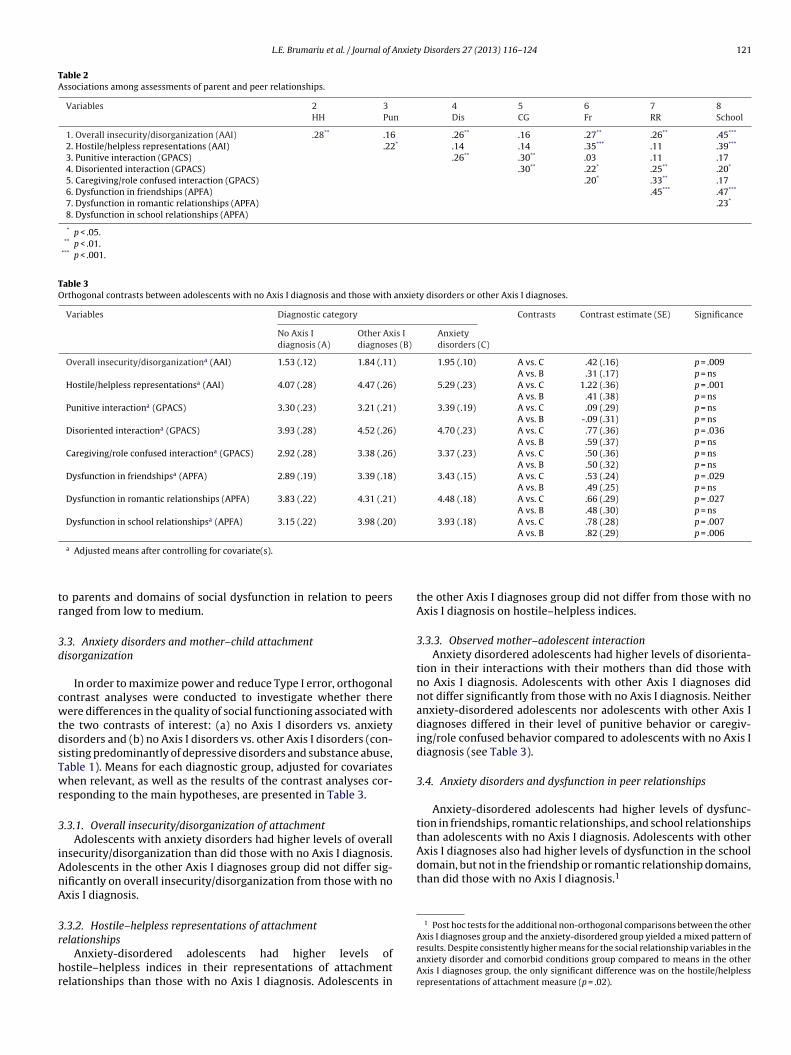
L.E. Brumariu et al. / Journal of Anxiety Disorders 27 (2013) 116– 124 121
Table 2Associations among assessments of parent and peer relationships.
Variables 2 3 4 5 6 7 8HH Pun Dis CG Fr RR School
1. Overall insecurity/disorganization (AAI) .28** .16 .26** .16 .27** .26** .45***
2. Hostile/helpless representations (AAI) .22* .14 .14 .35*** .11 .39***
3. Punitive interaction (GPACS) .26** .30** .03 .11 .174. Disoriented interaction (GPACS) .30** .22* .25** .20*
5. Caregiving/role confused interaction (GPACS) .20* .33** .176. Dysfunction in friendships (APFA) .45*** .47***
7. Dysfunction in romantic relationships (APFA) .23*
8. Dysfunction in school relationships (APFA)
* p < .05.** p < .01.
*** p < .001.
Table 3Orthogonal contrasts between adolescents with no Axis I diagnosis and those with anxiety disorders or other Axis I diagnoses.
Variables Diagnostic category Contrasts Contrast estimate (SE) Significance
No Axis Idiagnosis (A)
Other Axis Idiagnoses (B)
Anxietydisorders (C)
Overall insecurity/disorganizationa (AAI) 1.53 (.12) 1.84 (.11) 1.95 (.10) A vs. C .42 (.16) p = .009A vs. B .31 (.17) p = ns
Hostile/helpless representationsa (AAI) 4.07 (.28) 4.47 (.26) 5.29 (.23) A vs. C 1.22 (.36) p = .001A vs. B .41 (.38) p = ns
Punitive interactiona (GPACS) 3.30 (.23) 3.21 (.21) 3.39 (.19) A vs. C .09 (.29) p = nsA vs. B -.09 (.31) p = ns
Disoriented interactiona (GPACS) 3.93 (.28) 4.52 (.26) 4.70 (.23) A vs. C .77 (.36) p = .036A vs. B .59 (.37) p = ns
Caregiving/role confused interactiona (GPACS) 2.92 (.28) 3.38 (.26) 3.37 (.23) A vs. C .50 (.36) p = nsA vs. B .50 (.32) p = ns
Dysfunction in friendshipsa (APFA) 2.89 (.19) 3.39 (.18) 3.43 (.15) A vs. C .53 (.24) p = .029A vs. B .49 (.25) p = ns
Dysfunction in romantic relationships (APFA) 3.83 (.22) 4.31 (.21) 4.48 (.18) A vs. C .66 (.29) p = .027A vs. B .48 (.30) p = ns
Dysfunction in school relationshipsa (APFA) 3.15 (.22) 3.98 (.20) 3.93 (.18) A vs. C .78 (.28) p = .007A vs. B .82 (.29) p = .006
tr
3d
cwtdsTwr
3
iAnA
3r
hr
domain, but not in the friendship or romantic relationship domains,than did those with no Axis I diagnosis.1
1 Post hoc tests for the additional non-orthogonal comparisons between the other
a Adjusted means after controlling for covariate(s).
o parents and domains of social dysfunction in relation to peersanged from low to medium.
.3. Anxiety disorders and mother–child attachmentisorganization
In order to maximize power and reduce Type I error, orthogonalontrast analyses were conducted to investigate whether thereere differences in the quality of social functioning associated with
he two contrasts of interest: (a) no Axis I disorders vs. anxietyisorders and (b) no Axis I disorders vs. other Axis I disorders (con-isting predominantly of depressive disorders and substance abuse,able 1). Means for each diagnostic group, adjusted for covariateshen relevant, as well as the results of the contrast analyses cor-
esponding to the main hypotheses, are presented in Table 3.
.3.1. Overall insecurity/disorganization of attachmentAdolescents with anxiety disorders had higher levels of overall
nsecurity/disorganization than did those with no Axis I diagnosis.dolescents in the other Axis I diagnoses group did not differ sig-ificantly on overall insecurity/disorganization from those with noxis I diagnosis.
.3.2. Hostile–helpless representations of attachment
elationshipsAnxiety-disordered adolescents had higher levels ofostile–helpless indices in their representations of attachmentelationships than those with no Axis I diagnosis. Adolescents in
the other Axis I diagnoses group did not differ from those with noAxis I diagnosis on hostile–helpless indices.
3.3.3. Observed mother–adolescent interactionAnxiety disordered adolescents had higher levels of disorienta-
tion in their interactions with their mothers than did those withno Axis I diagnosis. Adolescents with other Axis I diagnoses didnot differ significantly from those with no Axis I diagnosis. Neitheranxiety-disordered adolescents nor adolescents with other Axis Idiagnoses differed in their level of punitive behavior or caregiv-ing/role confused behavior compared to adolescents with no Axis Idiagnosis (see Table 3).
3.4. Anxiety disorders and dysfunction in peer relationships
Anxiety-disordered adolescents had higher levels of dysfunc-tion in friendships, romantic relationships, and school relationshipsthan adolescents with no Axis I diagnosis. Adolescents with otherAxis I diagnoses also had higher levels of dysfunction in the school
Axis I diagnoses group and the anxiety-disordered group yielded a mixed pattern ofresults. Despite consistently higher means for the social relationship variables in theanxiety disorder and comorbid conditions group compared to means in the otherAxis I diagnoses group, the only significant difference was on the hostile/helplessrepresentations of attachment measure (p = .02).

1 Anxiet
4
tao&ipiambsewtrac2
crwrsMcbsio
iaiAeAetaosmfita
hrtsytdptctppwpi
22 L.E. Brumariu et al. / Journal of
. Discussion
Theory suggests a close link between anxiety disorders andhe quality of attachment relationships (Bowlby, 1973), but only
few studies have addressed the relation between the presencef anxiety disorders and attachment disorganization (Brumariu
Kerns, 2010a). The current report represents a step forwardn filling this gap in the literature. This study expands uponrevious research by examining whether the presence of anx-
ety disorders is associated with the quality of mother–childttachment disorganization in a sample of late adolescents, usingulti-method assessments that capture both representations and
ehaviors central to attachment disorganization. Peer relation-hips are also of critical importance in late adolescence (Sroufet al., 2005), and this study adds to the literature by investigatinghether adolescents with anxiety disorders experience dysfunc-
ion in three peer domains: friendships, school relationships, andomantic relationships. Further, we addressed these questions in
sample in which anxiety disorders co-occurred with other psy-hiatric diagnoses, as is typical for these diagnoses (Costello et al.,005).
As predicted, late adolescents with anxiety disorders andomorbid conditions had higher levels of overall insecu-ity/disorganization and hostile–helpless states of mind than thoseith no Axis I diagnosis. These findings extend previous literature
eporting an association between anxiety disorders and unresolvedtates of mind on the AAI in older samples (Fonagy et al., 1996;anassis et al., 1994) by investigating these relations in late adoles-
ence. In addition, hostile–helpless indicators have not previouslyeen assessed in relation to anxiety disorders and results demon-trate that adolescents with anxiety disorders are also showingncreased difficulty integrating positive and negative evaluationsf attachment figures.
Also unique to this study is the incorporation of a behav-oral measure of parent–adolescent attachment disorganization,ssessing three patterns of disturbed interaction with the parentn the context of a discussion of a conflict in their relationship.nxiety-disordered adolescents exhibited higher levels of disori-ntation in those discussions compared to adolescents with noxis I diagnosis. The disoriented and odd, out-of-context behaviorsxhibited by these adolescents are analogous to the contradic-ory and out-of-context behaviors characteristic of disorganizedttachment in infancy (Hennighausen et al., 2011). In infancy, dis-rganized behavior is thought to arise because the caregiver, whohould be the source of comfort, is unable to provide comfort anday even be a source of fear (Lyons-Ruth & Jacobvitz, 2008). These
ndings indicate that adolescents with anxiety disorders are unableo organize their behaviors effectively in interactions with theirttachment figures.
We also found that adolescents with anxiety disorders hadigher levels of dysfunction in the peer domains of friendshipelationships, romantic relationships, and school relationshipshan those with no Axis I diagnosis. A relatively small number oftudies have evaluated the peer relationships of clinically anxiousouth (see Kingery et al., 2010, for a review) and our study addso this scarce literature. In addition, our study is one of the first toifferentiate the quality of functioning in three specific domains ofeer relationships. Our findings converge with previous researchhat has demonstrated that anxious youths are more likely thanontrols to anticipate negative outcomes for social situations ando show more negative social cognitions during interactions witheers (Kingery et al., 2010). Given the concomitant difficulty in
rimary attachment relationships found in this study, adolescentsith anxiety disorders might be expected to be less equipped toarticipate in close social relationships involving trust and confid-ng, thus being at a particular disadvantage in developing intimate
y Disorders 27 (2013) 116– 124
peer friendships and romantic relationships (Booth-LaForce &Kerns, 2008).
We also examined whether adolescents in the other Axis I diag-noses group, who predominantly exhibited substance abuse anddepression, would also show lower quality of mother–adolescentand peer relationships than adolescents with no Axis I diagnosis. Nosignificant differences between these two groups emerged on anyof the attachment disorganization variables. In relation to peers,the only domain in which adolescents in the other Axis I diagnosesgroup exhibited higher levels of dysfunction than those with noAxis I diagnosis was in the domain of school relationships.
Although we did not find differences in attachment disorgani-zation between adolescents in the other Axis I diagnoses group andthose with no Axis I diagnosis, it will be important to clarify fur-ther the complex relations between attachment in adolescence andother Axis I psychopathology, an underdeveloped area in the liter-ature. Diagnoses in this group were varied, so that studies focusingon individual diagnosis might yield different results. In addition,the relations found in the current study between anxiety disordersand quality of attachment and peer relationships do not rule outother influences on anxiety disorders (Brumariu & Kerns, 2010a).Future studies should evaluate the relations between anxiety dis-orders and relationship quality in the context of other potentiallyimportant factors, including temperament and genetic factors.
Although not the main focus of this study, the modest linksbetween quality of functioning in parent and peer relationshipsdeserve comment. There were a number of significant but generallysmall to medium associations among the indicators of function-ing in parent–child and peer relationships, suggesting that theseare not redundant assessments. To capture the overall quality ofsocial functioning associated with anxiety disorders, it is importantto include assessments of multiple social domains. Interestingly,we did not find gender differences in anxiety disorders in thishigher-risk cohort. Although previous studies have shown that girlsare more likely than boys to experience an anxiety disorder, theliterature is not entirely consistent (Costello et al., 2005). In addi-tion, our nonsignificant results may be due to our smaller samplesize.
Although this study contributes to the further understanding ofthe relations between anxiety disorders and functioning in closerelationships, limitations should also be noted. We assessed con-structs of interest at a single time point, so the direction of causalitycannot be determined. While Bowlby (1973) proposed that attach-ment relationships might play an etiological role in generating highlevels of anxiety, it is also likely that higher levels of anxiety willhave a negative effect on both parent–child relationships and peerrelationships. Longitudinal studies and randomized interventiondesigns are necessary to disentangle possible bidirectional effects.While this study focused on attachment disorganization, there issome evidence that ambivalent attachment might be related toanxiety and internalizing problems (Brumariu & Kerns, 2010a;Colonnesi et al., 2011). The examination of the relation betweenambivalent attachment and anxiety disorders was hampered inthis study, as in other studies, by the low rate of ambivalentattachment in Western societies (Bakermans-Kranenburg & vanIJzendoorn, 2009). It will be important to investigate this relationin late adolescence in future studies. In addition, although the AAIprovides information regarding the current state of mind in rela-tion to both parents, the GPACS scores reflect attachment withmothers only, and future studies should address this issue by inves-tigating father–adolescent attachment as well. Literature suggeststhat quality of attachment influences the quality of peer relation-
ships (Booth-LaForce & Kerns, 2008), and future studies shouldevaluate whether anxiety-disordered adolescents have poorer peerrelationships due to poor quality of attachment with parents. Fur-ther, the adolescents with anxiety disorders studied here had other
nxiet
cdwvinaaadoefpsaArgafqatm
ldlaefifrioth
mirfdisti
A
gec
R
A
A
B
L.E. Brumariu et al. / Journal of A
omorbid Axis I conditions. While this is the norm among anxiety-isordered individuals (e.g., Costello et al., 2005), the literatureould also benefit from comparing the relationship quality of indi-
iduals with anxiety disorders only to the relationship quality ofndividuals with anxiety disorders and comorbid conditions. Theumber of participants in our sample meeting diagnostic criteria forn anxiety disorder only was small and precluded such analyses. Inddition, studies with larger sample sizes should investigate if therere consistent differences between participants with anxiety disor-ers and comorbid conditions and those with other Axis I disordersnly. For example, it would be important to investigate whetherxperiencing anxiety disorders is more specifically related to dys-unctions in attachment-like peer relationships (friends, romanticartners), while quality of less intimate school-related relation-hips is linked to a more diverse array of disorders, includingnxiety disorders as well as depression, substance abuse, and otherxis I conditions. Finally, our anxiety disorders group included aange of anxiety disorder diagnoses. Future studies should investi-ate whether the relations found here between anxiety disordersnd attachment disorganization or peer dysfunction are differentor different types of anxiety disorders. For example, given the pooruality of interpersonal relationships found in samples of sociallynxious children (Kingery et al., 2010), there is a possibility thathe presence of social phobia rather than other anxiety disorders
ight be more relevant for attachment and peer relationships.Our results have implications for treatment programs for ado-
escents with anxiety disorders. While few treatments have beenesigned solely for the adolescent period (Kendall et al., 2006), the
iterature provides empirical support for cognitive behavioral ther-py (Chorpita, Daleiden, Ebesutani, Young, & Becker, 2011; Rapeet al., 2009; Silverman, Pina, & Viswesvaran, 2008). Despite thesendings, a significant proportion of adolescents do not improve
ollowing state-of-the-art treatments (Rapee et al., 2009). Ouresults support the importance of investigating whether target-ng dysfunctions in close relationships and enhancing the qualityf relationships of youth experiencing anxiety disorders improvesreatment outcome, particularly when included in therapies thatave received empirical support.
In summary, across three independent and well-validatedeasures of attachment disorganization, late adolescents with anx-
ety disorders showed higher levels of disorganized attachmentepresentations and behaviors, as well as poorer functioning in peerriendships and romantic relationships than those with no Axis Iiagnosis. Among adolescents with other Axis I diagnoses, consist-
ng predominantly of depressive disorders and substance abuse,uch differences did not emerge. Thus, the present results suggesthat adolescents with anxiety disorders may be especially prone tompairments in attachment and peer relationships.
cknowledgements
We would like to thank the families who have so generouslyiven their time to this study. We would also like to acknowl-dge the invaluable contributions of Nancy Hall Brooks, the studyoordinator, to the conduct of the study.
eferences
llen, J. P., & Hauser, S. T. (1996). Autonomy and relatedness in adolescent–familyinteractions as predictors of young adults’ states of mind regarding attachment.Developmental and Psychopathology, 8, 793–809.
ngold, A., Costello, E. J., & Erkanli, A. (1999). Comorbidity. Journal of Child Psychologyand Psychiatry, 40, 57–87.
akermans-Kranenburg, M. J., & van IJzendoorn, M. H. (2009). The first 10,000 adultattachment interviews: Distributions of adult attachment representations innonclinical and clinical groups. Attachment & Human Development, 11, 223–263.
y Disorders 27 (2013) 116– 124 123
Borelli, J. L., David, D. H., Crowley, M. J., & Mayes, L. C. (2010). Links between disorga-nized attachment classification and clinical symptoms in school-aged children.Journal of Child and Family Studies, 19, 243–256.
Booth-LaForce, C. L., & Kerns, K. A. (2008). Child–parent attachment relationships,peer relationships, and peer-group functioning. In: K. H. Rubin, W. M. Bukowski,& B. Laursen (Eds.), Handbook of peer interactions, relationships, and groups (pp.490–507). New York: Guildford Press.
Bowlby, J. (1973). Attachment and loss. Separation. Anxiety and danger New York:Basic Books.
Brumariu, L. E., & Kerns, K. A. (2010a). Parent–child attachment and internalizingsymptoms in childhood and adolescence: A review of empirical findings andfuture directions. Development and Psychopathology, 22, 177–203.
Brumariu, L. E., & Kerns, K. A. (2010b). Mother–child attachment patterns and dif-ferent types of anxiety symptoms in middle childhood: Is there specificity ofrelations? Child Psychiatry and Human Development, 41, 663–674.
Brumariu, L. E., Kerns, K. A., & Seibert, A. (2012). Mother-child attachment, emotionregulation, and anxiety symptoms in middle childhood. Personal Relationships,19, 569–585.
Buchheim, A., & George, C. (2011). Attachment disorganization and borderlinepersonality disorder and anxiety disorder. In: J. Solomon, & C. George (Eds.), Dis-organized attachment and caregiving (pp. 343–382). New York: Guildford Press.
Bureau, J.-F., Easterbrooks, A., & Lyons-Ruth, K. (2009). Attachment disorganiza-tion and role-reversal in middle childhood: Maternal and child precursors andcorrelates. Attachment & Human Development, 11, 265–284.
Carver, K., Joyner, K., & Udry, R. J. (2003). National estimates of adolescent roman-tic relationships. In: P. Florsheim (Ed.), Adolescent romantic relations and sexualbehavior: Theory, research, and practical implications (pp. 23–56). Mahwah, NJ:Lawrence Erlbaum Associates.
Chorpita, B. F., Daleiden, E. L., Ebesutani, C., Young, J., Becker, K. D., Nakamura, B.J., et al. (2011). Evidence-based treatments for children and adolescents: Anupdated review of indicators of efficacy and effectiveness. Clinical Psychology:Science and Practice, 18, 153–171.
Colonnesi, C., Draijer, E. M., Stams, G. J. J. M., Van der Bruggen, C. O., Bögels, S. M., &Noom, M. J. (2011). The relation between insecure attachment and child anxiety:A meta-analytic review. Journal of Clinical Child and Adolescent Psychology, 40(4),630–645.
Costello, E. J., Egger, H., & Angold, L. A. (2005). The developmental epidemiologyof anxiety disorders: Phenomenology, prevalence, and comorbidity. Child andAdolescent Psychiatric Clinics of North America, 14, 631–648.
DeKlyen, M., & Greenberg, M. T. (2008). Attachment and psychopathology in child-hood. In: J. Cassidy, & P. R. Shaver (Eds.), Handbook of attachment, theory, researchand clinical applications (2nd ed., Vol. 2, pp. 637–666). New York: Guilford Press.
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statisti-cal power analysis program for the social, behavioral, and biomedical sciences.Behavior Research Methods, 39, 175–191.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1997). Structured clinicalinterview for DSM-IV Axis I disorders – clinical version (SCID-CV). Washington, DC:American Psychiatric Press.
Fonagy, P., Leigh, T., Steele, M., Steele, H., Kennedy, R., Mattoon, G., et al. (1996).The relation of attachment status, psychiatric classification, and response topsychotherapy. Journal of Consulting and Clinical Psychology, 64, 22–31.
George, C., Kaplan, N., & Main, M. (1996). Adult attachment interview protocol (3rded). Unpublished manuscript. University of California at Berkley.
Gilks, W. R., Richardson, S., & Spiegelhalter, D. J. (1995). Markov chain Monte Carlo inpractice. New York: Chapman and Hall.
Harari, D., Bakermans-Kranenburg, M. J., de Kloet, C. S., Geuze, E., Vermetten,E., Westenberg, H. G. M., et al. (2009). Attachment representations in Dutchveterans with and without deployment-related PTSD. Attachment & HumanDevelopment, 11, 515–536.
Hennighausen, K. H., Bureau, J. F., David, D. H., Holmes, B. M., & Lyons-Ruth, K. (2011).Disorganized attachment behavior observed in adolescence: validation in rela-tion to Adult Attachment Interview Classifications at age 25. In: J. Solomon, & C.George (Eds.), Disorganized attachment and caregiving (pp. 207–244). New York:Guildford Press.
Hesse, E. (2008). The adult attachment interview: protocol, method of analysis andempirical studies. In: J. Cassidy, & P. Shaver (Eds.), Handbook of attachment: the-ory, research, and clinical applications (2nd ed., pp. 552–598). New York: GuilfordPress.
Hill, J., Fudge, H., Harrington, R., Pickles, A., & Rutter, M. (1995). The Adult PersonalityFunctioning Assessment (APFA): Factors influencing agreement between subjectand informant. Psychological Medicine, 25, 263–275.
Hill, J., Harrington, R., Fudge, H., Rutter, M., & Pickles, A. (1989). Adult PersonalityFunctioning Assessment (APFA). An investigator-based standardized interview.British Journal of Psychiatry, 155, 24–35.
Irwin, C. E., Burg, S. J., & Cart, C. U. (2002). America’s adolescents: Where have webeen, where are we going? Journal of Adolescent Health, 31, 91–121.
Ivarsson, T., Granqvist, P., Gillberg, C., & Broberg, A. G. (2010). Attachment statesof mind in adolescents with obsessive compulsive disorder and/or depres-sive disorders: A controlled study. European Child and Adolescent Psychiatry, 19,845–853.
Kendall, P. C., Hedtke, K. A., & Aschenbrand, S. G. (2006). Anxiety disorders. In: D.
A. Wolfe, & E. J. Mash (Eds.), Behavioral and emotional disorders in adolescents:nature, assessment, and treatment (pp. 259–299). New York: Guilford Press.Kessler, R. C., Chiu, W. T., Demler, O., & Walters, E. E. (2005). Prevalence, severity, andcomorbidity of 12-month DSM-IV disorders in the National Comorbidity Surveyreplication. Archives of General Psychiatry, 62, 617–627.
1 Anxiet
K
L
L
L
L
M
M
M
M
M
M
N
24 L.E. Brumariu et al. / Journal of
ingery, J. N., Erdley, C. A., Marshall, K. C., Whitaker, K. G., & Reuter, T. R. (2010). Peerexperiences of anxious and socially withdrawn youth: An integrative review ofthe developmental and clinical literature. Clinical Child and Family PsychologyReview, 13, 91–128.
yons-Ruth, K., & Jacobvitz, D. (2008). Disorganized attachment. Genetic factors, par-enting, contexts, and developmental transformation from infancy to adulthood.In: J. Cassidy, & P. R. Shaver (Eds.), Handbook of attachment: theory, research, andclinical applications (2nd ed., pp. 666–697). New York: Guilford.
yons-Ruth, K., Connell, D., Grunebaum, H., & Botein, D. (1990). Infants atsocial risk: Maternal depression and family support services as media-tors of infant development and security of attachment. Child Dev, 61,85–98.
yons-Ruth, K., Yellin, C., Melnick, S., & Atwood, G. (2003). Childhood experi-ences of trauma and loss have different relations to maternal unresolved andhostile–helpless states of mind on the AAI. Attachment & Human Development,5, 330–352.
yons-Ruth, K., Yellin, C., Melnick, S., & Atwood, G. (2005). Expanding the con-cept of unresolved mental states: Hostile/helpless states of mind on the adultattachment interview are associated with atypical maternal behavior and infantdisorganization. Developmental Psychopathology, 17, 1–23.
ain, M., & Cassidy, J. (1988). Categories of response to reunion with the parent at age6: Predictable from infant attachment classifications and stable over 1-monthperiod. Developmental Psychology, 24, 415–426.
ain, M., Goldwyn, R., & Hesse, E. (2003). Adult attachment scoring and classificationsystem Version 7.2. Unpublished manuscript. University of California at Berkley.
anassis, K., Bradley, S., Goldberg, S., Hood, J., & Swinson, R. P. (1994). Attachmentin mothers with anxiety disorders and their children. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 33, 1106–1113.
erikangas, K. R., Mehta, R. L., Molnar, B. E., Walters, E. E., Swendsen, J. D., Aguilar-Gaziola, S., et al. (1998). Comorbidities of substance use disorders with moodand anxiety disorders: Results of the international consortium in psychiatricepidemiology. Addictive Behaviors, 23, 893–907.
oss, E., Cyr, C., & Dubois-Comtois, K. (2004). Attachment at early school ageand developmental risk: Examining family context and behavior problemsof controlling-caregiving, controlling-punitive, and behaviorally disorganizedchildren. Developmental Psychology, 40, 519–532.
oss, E., Smolla, N., Cyr, C., Dubois-Comtois, K., Mazzarello, T., & Berthi-aume, C. (2006). Attachment and behavior problems in middle childhood as
reported by adult and child informants. Development and Psychopathology, 18,425–444.aughton, M., Oppenheim, A., & Hill, J. (1996). Assessment of personality function-ing in the transition from adolescent to adult life: Preliminary findings. BritishJournal of Psychiatry, 168, 33–37.
y Disorders 27 (2013) 116– 124
Nye, E. C., Katzman, J., Bell, J. B., Kilpatrick, J., Brainard, M., & Haaland, K. Y. (2008).Attachment organization in Vietnam combat veterans with posttraumatic stressdisorder. Attachment & Human Development, 10, 41–57.
Obsuth, I., Hennighausen, K., Brumariu, L. E., & Lyons-Ruth, K. Disorganized Behaviorin Adolescent-Parent Interactions: Relations to Attachment State of Mind, PartnerAbuse, and Psychopathology, submitted for publication.
O’Connor, E., Bureau, J. F., McCartney, K., & Lyons-Ruth, K. Risks and outcomes asso-ciated with disorganized/controlling patterns of attachment at age three in theNICHD study of early child care and youth development. Infant Mental HealthJournal, 2011.
Rapee, R. M., & Barlow, D. H. (2001). Generalized anxiety disorders, panic disorders,and phobias. In: P. B. Sutker, & H. E. Adams (Eds.), Comprehensive handbook ofpsychopathology (3rd ed., pp. 131–154). New York: Kluwer Academic/PlenumPublishers.
Rapee, R. M., Schniering, C. A., & Hudson, J. L. (2009). Anxiety disorders during,childhood and adolescence: Origins and treatment. Annual Review of ClinicalPsychology, 5, 311–341.
Riggs, S. A., Paulson, A., Tunnell, E., Sahl, G., Atkinson, H., & Ross, C. A. (2007). Attach-ment, personality, and psychopathology among adults inpatients. Self-reportedromantic attachment style versus Adult Attachment Interview states of mind.Development and Psychopathology, 19, 263–291.
Rubin, D. B. (1987). Multiple imputation for nonresponse surveys. New York: Wiley.Rudolph, K. D., Hammen, C., & Daley, S. E. (2006). Mood disorders. In: D. A. Wolfe,
& E. J. Mash (Eds.), Behavioral and emotional disorders in adolescents: nature,assessment, and treatment (pp. 300–342). New York: Guilford Press.
Silverman, W. K., Pina, A. A., & Viswesvaran, C. (2008). Evidence-based psychosocialtreatments for phobic and anxiety disorders in children and adolescents. Journalof Clinical Child and Adolescent Psychology, 37, 105–130.
Spear, L. P. (2000). The adolescent brain and age-related behavioural manifestations.Neuroscience and Biobehavioral Reviews, 24, 417–463.
Sroufe, L. A., Egeland, B., Carlson, E. A., & Collins, W. A. (2005). The development of theperson: the Minnesota study of risk and adaptation from birth through adulthood.New York: Guilford Press.
Stovall-McClough, K. C., & Cloitre, M. (2006). Unresolved attachment, PTSD and dis-sociation in women with childhood abuse histories. Journal of Consulting andClinical Psychology, 74, 219–228.
van Emmichoven, I. A. Z., van IJzendoorn, M. H., de Ruiter, C., & Brosschot, J. F.(2003). Selective processing of threatening information: Effects of attachment
representation and anxiety disorder on attention and memory. Development andPsychopathology, 15, 219–237.Warren, S. L., Huston, L., Egeland, B., & Sroufe, L. A. (1997). Child and adolescentanxiety disorders and early attachment. Journal of the American Academy of Childand Adolescent Psychiatry, 36, 637–644.




















