Protein oxidation and proteasome: New aspects for clinical approaches
218
CLINICAL AND EXPERIMENTAL MEDICAL JOURNAL Official Journal of Markusovszky Lajos Foundation based on the Orvosi Hetilap, established by Markusovszky Lajos in 1857, as an International Edition Established by János Fehér (2006) Founding Editor-in-Chief ■ JÁNOS FEHÉR (Budapest) Coeditor-in-Chief ■ NEVEN ŽARKOVIĆ (Zagreb) Deputy Editors-in-Chief ■ ERZSÉBET FEHÉR (Budapest), MAMUN-AL-MAHTAB (Bangladesh), KÁROLY RÁCZ (Budapest) Senior Editors ■ MAURIZIO BATTINO (Ancona), KRISZTINA HAGYMÁSI (Budapest), GABRIELLA LENGYEL (Budapest), ALAJOS PÁR (Pécs), ÁRPÁD SZÁLLÁSI (Esztergom) Editors ■ A. BLÁZOVICS (Budapest), H. BODÁNSZKY (Budapest), E. DINYA (Budapest), G. FIRNEISZ (Budapest), P. IGAZ (Budapest), Z. LANGMÁR (Budapest), V. NAGY (Budapest), G. PÁR (Pécs), Á. PUSZTAY (Budapest) Column care coworkers ■ Cs. BALÁZS (Budapest), J. GERVAIN (Székesfehérvár), L. GULÁCSI (Budapest), B. HUNYADY (Pécs), Gy. JERMENDY (Budapest), L. KALABAY (Budapest), A. KISS (Budapest), I. KISS (Budapest), J. OSZTOVITS (Budapest), K. SIMON (Siófok), A. WIMMER (Budapest), G. WINKLER (Budapest) Editorial Board President ■ M. PALKOVITS (Budapest) G. ÁCS (New York), M. BANACH (Lodz), G. BARTOSZ (Lodz), A. BERG (Berlin), J. BETKÓ (Budapest), F. BIASI (Italy), A. BIGNAMINI (Milan), A. BISHAYEE (Rootstown, Ohio, USA), H. E. BLUM (Freiburg), G. BROOSER (Budapest), M. CLASSEN (Munich), G. CSOMÓS (Hamburg), I. CZURIGA (Debrecen), A. DOBOZY (Szeged), S. ECKHARDT (Budapest), P. ECKL (Salzburg), Z. ENGLERT (Budapest), A. FALUS (Budapest), P. FERENCI (Vienna), P. G. FORBATH (Toronto), I. FORGÁCS (Budapest), S. GARDÓ (Győr), B. GÖMÖR (Budapest), M. R. GRACZYNSKI (Warsaw), T. GRUNE (Düsseldorf), F. GUERAUD (Toulouse), M. HAHN (Erlangen), J. HANKISS (Budapest), L. IFFY (New Jersey), F. JAKAB (Budapest), Zs. JAKAB (Stockholm) J. KAPPELMAYER (Debrecen), É. KELLER (Budapest), M. KELTAI (Budapest), J. KISS (Budapest), Y. KITA (Tokyo), L. KOPPER (Budapest), L. LAKNER (Szombathely), L. LAMPÉ (Debrecen), A. LUGASI (Budapest), N. J. LYGIDAKIS (Athens), M. MACEK (Prague), N. McINTYRE (London), K. MEYER zum BÜSCHENFELDE (Mainz), A. MOGYORÓSI (Richmond), J. MOLNÁR (Szeged), P. MOLNÁR (Debrecen), G. NAGY (Sydney), I. NÁSZ (Budapest), A.-E. NEGRE-SALVAYRE (Toulouse), L. OKOLICSANYI (Padova), É. OLÁH (Debrecen), M. P. OTIN (Spain), T. PAÁL (Budapest), Z. PAPP (Budapest), S. PENA (Amsterdam), P. PETRUSZ (Chapel Hill), G. POLI (Torino), I. RÁCZ (Győr), O. RÁCZ (Košice), G. RAMADORI (Goettingen), J. REICHEN (Bern), O. RIBÁRI (Budapest), I. ROMICS (Budapest), L. ROMICS (Budapest), Zs. SCHAFF (Budapest), P. SCHMIDT (Győr), W. G. SIEMS (Bad Harzburg), P. SÓTONYI (Budapest), I. SÜVEGES (Budapest), F. SZALAY (Budapest), F. TATZBER (Vienna), H. THALER (Vienna), E. TOLNAY (Budapest), T. TSUJI (Okayama), Zs. TULASSAY (Budapest), K. UCHIDA (Nagoya), L. VASAS (Budapest), L. VÉCSEI (Szeged), L. VÉRTES (Budapest), J. VESELY (Olomouc), J. VINA (Valencia), G. WEBER (Indianapolis), A. C. YOGESH (Washington, D.C.), K. ŽARKOVIĆ (Zagreb), E. ZSIGMOND (Chicago) AKADÉMIAI KIADÓ, BUDAPEST
Transcript of Protein oxidation and proteasome: New aspects for clinical approaches
CLINICAL AND EXPERIMENTAL MEDICAL JOURNAL
Offi cial Journal of Markusovszky Lajos Foundationbased on the Orvosi Hetilap, established by Markusovszky Lajos
in 1857, as an International Edition
Established by János Fehér (2006)
Founding Editor-in-Chief ■ JÁNOS FEHÉR (Budapest)
Coeditor-in-Chief ■ NEVEN ŽARKOVIĆ (Zagreb)
Deputy Editors-in-Chief ■ ERZSÉBET FEHÉR (Budapest), MAMUN-AL-MAHTAB (Bangladesh),KÁROLY RÁCZ (Budapest)
Senior Editors ■ MAURIZIO BATTINO (Ancona), KRISZTINA HAGYMÁSI (Budapest),GABRIELLA LENGYEL (Budapest), ALAJOS PÁR (Pécs),
ÁRPÁD SZÁLLÁSI (Esztergom)
Editors ■ A. BLÁZOVICS (Budapest), H. BODÁNSZKY (Budapest), E. DINYA (Budapest), G. FIRNEISZ (Budapest),P. IGAZ (Budapest), Z. LANGMÁR (Budapest), V. NAGY (Budapest), G. PÁR (Pécs), Á. PUSZTAY (Budapest)
Column care coworkers ■ Cs. BALÁZS (Budapest), J. GERVAIN (Székesfehérvár),L. GULÁCSI (Budapest), B. HUNYADY (Pécs), Gy. JERMENDY (Budapest),
L. KALABAY (Budapest), A. KISS (Budapest), I. KISS (Budapest), J. OSZTOVITS (Budapest),K. SIMON (Siófok), A. WIMMER (Budapest), G. WINKLER (Budapest)
Editorial Board
President ■ M. PALKOVITS (Budapest)
G. ÁCS (New York), M. BANACH (Lodz), G. BARTOSZ (Lodz), A. BERG (Berlin), J. BETKÓ (Budapest),F. BIASI (Italy), A. BIGNAMINI (Milan), A. BISHAYEE (Rootstown, Ohio, USA), H. E. BLUM (Freiburg),G. BROOSER (Budapest), M. CLASSEN (Munich), G. CSOMÓS (Hamburg), I. CZURIGA (Debrecen),
A. DOBOZY (Szeged), S. ECKHARDT (Budapest), P. ECKL (Salzburg), Z. ENGLERT (Budapest),A. FALUS (Budapest), P. FERENCI (Vienna), P. G. FORBATH (Toronto), I. FORGÁCS (Budapest),
S. GARDÓ (Győr), B. GÖMÖR (Budapest), M. R. GRACZYNSKI (Warsaw), T. GRUNE (Düsseldorf),F. GUERAUD (Toulouse), M. HAHN (Erlangen), J. HANKISS (Budapest), L. IFFY (New Jersey),
F. JAKAB (Budapest), Zs. JAKAB (Stockholm) J. KAPPELMAYER (Debrecen), É. KELLER (Budapest),M. KELTAI (Budapest), J. KISS (Budapest), Y. KITA (Tokyo), L. KOPPER (Budapest),
L. LAKNER (Szombathely), L. LAMPÉ (Debrecen), A. LUGASI (Budapest), N. J. LYGIDAKIS (Athens),M. MACEK (Prague), N. McINTYRE (London), K. MEYER zum BÜSCHENFELDE (Mainz),
A. MOGYORÓSI (Richmond), J. MOLNÁR (Szeged), P. MOLNÁR (Debrecen), G. NAGY (Sydney),I. NÁSZ (Budapest), A.-E. NEGRE-SALVAYRE (Toulouse), L. OKOLICSANYI (Padova), É. OLÁH (Debrecen),
M. P. OTIN (Spain), T. PAÁL (Budapest), Z. PAPP (Budapest), S. PENA (Amsterdam), P. PETRUSZ (Chapel Hill),G. POLI (Torino), I. RÁCZ (Győr), O. RÁCZ (Košice), G. RAMADORI (Goettingen), J. REICHEN (Bern),
O. RIBÁRI (Budapest), I. ROMICS (Budapest), L. ROMICS (Budapest), Zs. SCHAFF (Budapest), P. SCHMIDT (Győr),W. G. SIEMS (Bad Harzburg), P. SÓTONYI (Budapest), I. SÜVEGES (Budapest), F. SZALAY (Budapest),
F. TATZBER (Vienna), H. THALER (Vienna), E. TOLNAY (Budapest), T. TSUJI (Okayama),Zs. TULASSAY (Budapest), K. UCHIDA (Nagoya), L. VASAS (Budapest), L. VÉCSEI (Szeged),L. VÉRTES (Budapest), J. VESELY (Olomouc), J. VINA (Valencia), G. WEBER (Indianapolis),
A. C. YOGESH (Washington, D.C.), K. ŽARKOVIĆ (Zagreb), E. ZSIGMOND (Chicago)
AKADÉMIAI KIADÓ, BUDAPEST

REVIEWS7
Protein Oxidation and Proteasome: New Aspects for Clinical ApproachesBETUL CATALGOL, NESRIN KARTAL OZER, TILMAN GRUNE
15Compliance and Persistence with Medications
for Chronic Obstructive Pulmonary DiseaseTAMÁS ÁGH, ÁGNES MÉSZÁROS
23Associations of Autoimmune Endocrine Diseases
CSABA BALÁZS, JÁNOS FEHÉR
39The Pulmonological Manifestations of Rheumatoid Arthritis
GYÖRGY BERNSCHERER, CSABA KARABÉLYOS, ZSOLT TARJÁN
49The Mechanism of the Development of Pain Perception. New Results in the
Neurophysiology of Pain Relating to NeuroscienceJUDIT GYULAHÁZI
65The Evaluation of Therapeutic Modalities in the Treatment
of Palmary and Axillary HyperhydrosisKÁROLY VINCZE, LÁSZLÓ HERKE, JÓZSEF FERENCZY, ISTVÁN SEFFER, ZSUZSANNA LELOVICS
ORIGINAL PAPERS73
In Vitro Model of Bone Regeneration with Bioactive Glass and Lipid PeroxidationLIDIJA MRAKOVCIC, MARINA CINDRIC, NEVEN ZARKOVIC, SUZANA BOROVIC SUNJIC,
ANDREA MOGUS MILANKOVIC, RENATE WILDBURGER
79Intermittent Haemodialysis-Induced Oxidative Stress and the Effect
on Infl ammatory Parameters in Critically Ill PatientsKARL-HEINZ SMOLLE, PETER KAUFMANN, VANESSA STADLBAUER, FRANZ TATZBER, BRIGITTE M. WINKLHOFER-ROOB, REINGARD AIGNER, GHOLAMALI KHOSCHSORUR,
WILLIBALD WONISCH
CONTENTS
3
89Serum Total Peroxides Are Increased in Patients with Stage IV Compared
to Stage IIb Peripheral Arterial Disease: Percutaneous Transluminal Angioplasty May Generate Epitopes for Autoantibodies Against Oxidized
Low Density LipoproteinMARTIN TRINKER, KARL-HEINZ SMOLLE, STEFAN SCHEIDL, FRANZ TATZBER,
MEINRAD LINDSCHINGER, WILLIBALD WONISCH
99The Effect of Perceptual Characteristics of Tablets upon Patient’s Choice
FERENC KÖTELES, ILDIKÓ KOMSA, GYÖRGY BÁRDOS
105The “HÍVÁS” Club: Social Support in Post Cancer Recovery
KORNÉLIA ROZÁLIA LAZÁNYI, PÉTER MOLNÁR, ANTAL BUGÁN, LÁSZLÓ DAMJANOVICH, ZOLTÁN GARAMI, BALÁZS FÜLÖP, KORNÉLIA SZLUHA
115Gastric Ulcer Protective Activity of Hibiscus sabdariffa: An Experimental,
Biochemical and Histological StudySALEH ALQASOUMI, MOHAMMED AL-DOSARI, MOHAMMED AL-SOHAIBANI,
TAWFEQ AL-HOWIRINY, MOHAMMED AL-YAHYA, SYED RAFATULLAH
129Antioxidant and Protective Effects of Spinach (Spinacia oleracea L.)
Leaves Against Carbon Tetrachloride-Induced Liver InjuryMOHAMMED S. AL-DOSARI
CLINICAL STUDIES141
Effects of Oligofructose Containing Diet in Obese PersonsMAGDA ANTAL, SZABOLCS PÉTER, ANDREA REGÖLY-MÉREI, LAJOS BIRÓ, GYÖRGYI ARATÓ,
JUDIT SCHMIDT, KATALIN NAGY, ERIKA GREINER, NATÁLIA LÁSZTITY, CSABA SZABÓ, ÉVA MARTOS
153Endoscopic Management of Post-Operative Biliary Tract Injuries
ZOLTÁN VÖLGYI, TÜNDE FISCHER, MÁRIA SZENES, BEÁTA GASZTONYI
4
CONTENTS
163Patients with Syphilis and Gonorrhoea: Analysis of Cases Based
on Data (2005–2008) of the National Sexually Transmitted Disease Centre, Department of Dermatology, Venereology and Dermatologic Oncology,
Semmelweis UniversityKATINKA PÓNYAI, MÁRTA MARSCHALKÓ, MÁRIA SCHÖFFLER-ACKERMAN,
ESZTER OSTORHÁZI, FERENC ROZGONYI, VIKTÓRIA VÁRKONYI, SAROLTA KÁRPÁTI
CASE REPORTS175
Whipple’s Disease: Do We Think of It Enough?TÜNDE FISCHER, MÁRTA TIBOLY, PÉTER TÓTH, MÁRIA SZENES, ZOLTÁN VÖLGYI,
OTÍLIA BALI, BEÁTA GASZTONYI
187A Case of Primary Biliary Cirrhosis: First Report from Bangladesh
MAMUN-AL-MAHTAB, KABIR UDDIN, SALIMUR RAHMAN, MOBIN KHAN, KAMAL, MONIRUZZAMAN BHUIYAN, GULZAR HUSSAIN
193Anaphylactoid Reaction Following Forest Fly (Hippobosca Equina) Bite:
A Human CaseALICE DECASTELLO, ROBERT FARKAS
199Ciprofl oxacin-Induced Stevens–Johnson Syndrome: First Report from Bangladesh
MAMUN-AL-MAHTAB, SALIMUR RAHMAN, AKMAT ALI, ANANTA SHRESTHA,
JAHANGIR SARKAR, MOBIN KHAN
203Primary Adenocarcinoma of the
Rectovaginal Septum Without Associated EndometriosisZOLTÁN LANGMÁR, MIKLÓS NÉMETH, TAMÁS MÁTRAI , KÁLMÁN IVÁNYI, LÁSZLÓ HARSÁNYI,
MAGDOLNA DANK, ESZTER SZÉKELY, ZOLTÁN KAZY
207Pitfalls in Management of Chronic Hepatitis B: Report of Four Cases
from BangladeshMD. FAZAL KARIM, MAMUN AL-MAHTAB, SALIMUR RAHMAN, MOBIN KHAN
CONTENTS
5
211Acute Pancreatitis in a Pregnant Female with Peripartum Cardiomyopathy
PANKAJ JAIN
GUIDE TO THE AUTHORS215
6
CONTENTS

Protein Oxidation and Proteasome: New Aspects for Clinical Approaches
BETUL CATALGOL1, NESRIN KARTAL OZER1, TILMAN GRUNE2
1Department of Biochemistry, Faculty of Medicine, Marmara University, 34668 Haydarpasa, Istanbul, Turkey
2Institute of Biological Chemistry and Nutrition, University Hohenheim, Stuttgart, Germany
Oxidative stress is an inevitable process during aerobic life. Proteins as the most abundant macromolecules in organ-isms are damaged during oxidative stress and in the following living cells try to rescue defective polypeptides and restore their function. For this purpose several repair and removal systems are activated. The main proteolysis sys-tem for the removal of oxidized proteins is the proteasomal system. Protein oxidation products and the impairment in the repair and removal systems are reported to play important roles in the progress of various diseases and aging. This review describes the protein oxidation in detail and the role of this process in several diseases. We propose that management of protein oxidation will be benefi cial for clinical trials in the prevention and therapy of the diseases.
Keywords: oxidative stress, protein oxidation, aging, disease
Abbreviations
Aβ = amyloid beta; AD = Alzheimer’s disease; AGE = advanced glycation end products; HNE = 4-hydroxynonenal; LDL = low density lipoprotein; MDA = malondialdehyde; NFT = neurofi brillary tangles; 8-OHdG = 8-hydroxy-2′-deoxyguanosine; RAGE = receptor for advanced glycation end products; ROOH = peroxide; ROS = reactive oxygen species; RS = reactive species; SP = senile plaques; NADPH = reduced nicotinamide adenine dinucleotide phos-phate
IntroductionRS are generated by diverse mechanisms and include several reactive oxygen and nitrogen species. These atoms or molecules are called RS since they are highly reactive, take place in oxidation reactions easily and cause denaturation and inactivation of biomolecules. Several cellular systems exist to minimize the oxidizing effects of RS. Oxidative stress, which is defi ned as an imbalance between RS formation and corresponding antioxidant defense mech-anisms, produces damage by multiple pathways. Increased proliferation, adaptation by up-regulating of defense systems, cell injury with increased burden of oxidatively damaged macromolecules like lipids, DNA, proteins and carbohydrates, or senescence and cell death take place in consequences of oxidative stress [1].
Among the other effects of oxidative stress, damage to proteins is crucial since proteins are important parts of cellular structures and have important functions as receptors, anti-
Corresponding address: Tilman Grune MD, Institute of Biological Chemistry and Nutrition, University Hohenheim, Garbenstrasse 28, 70593 Stuttgart, Germany. E-mail: [email protected]
1.1
REVIEWS
REVIEWS
DOI: 10.1556/CEMED.4.2010. 7 2010 ▪ Volume 4, Number 1 ▪ 7–13.

bodies, transport proteins and enzymes. Oxidative protein modifi cations might be classifi ed in several ways and detections of various products are used as indicators of oxidation. Protein damage may be caused by direct attack of RS or by secondary damage involving attack by products of lipid peroxidation, such as isoketals, MDA and HNE [2].
In another classifi cation, protein damage may be divided by site specifi city such as pro-tein backbone and side chains. Polypeptide chain fragmentation is one of the important mod-ifi cations of protein backbones that results in peptide fragments with derivatized terminal amino acids. This fragmentation begins with the formation of an α-carbon-centered radical that reacts with oxygen to form a peroxyl species fi rst and then a hydroperoxide. Following the decomposition of α-carbon hydroperoxides, peptide chain is cleaved and ketoacyl/amide derivatives of the carboxy and amino-terminal amino acids are formed [3].
Amino acid side chains mainly of the sulfur-containing amino acids such as methionine and cysteine are known to be highly susceptible to the free radical damage, but other amino acids are also susceptible to damage. Several products are formed such as cystine, methion-ine sulfoxide, aspartate, 3,4-dihydroxphenylalanine, hydroxyleucine, and N-formylkynure-nine following the oxidation of different side chains. Aromatic amino acids like tyrosine, phenylalanine and tryptophan are also targets of free radical attack. Oxidation of lysine, argi-nine, proline or threonine residues results in carbonyl-containing products. These carbonyl derivatives are frequently determined as biomarkers of protein oxidation because of their relative early formation and stability [4, 5].
Another late product of protein oxidation is the formation of protein aggregates. Insolu-ble aggregates are formed by covalent cross-linking of the carbon-centered radicals of amino acid side chains, for example 2-2′-biphenyl cross-link formed by two tyrosyl radicals. Non-covalent interactions like hydrophobic as well as electrostatic interactions between oxidized residues may also be reasons for aggregate formation. Large aggregates are often poor sub-strates for proteases and their accumulation is known to be toxic to cells. Such an aggregate accumulation has been reported for many experimental models, especially age-related dis-eases, as measured by several markers. Also in aging models, insoluble fl uorescence materi-als called lipofuscin, ceroid and AGE (advanced glycation end product)-like fl uorophores are used as indicators of protein aggregation [6].
Living cells try to recover from defective polypeptides. For this purpose they contain several repair and removal systems. Repair systems are generally limited and specifi c for the modifi cations. Disulfi de bonds and methionine sulfoxide can be repaired by protein disulfi de isomerase, methionine sulfoxide reductase and thioredoxin reductase. Heat shock or stress proteins also have the ability to reconstitute the native structure of proteins following oxida-tive damage [7, 8].
The degradation of proteins is a physiological process required to maintain normal cel-lular function. Therefore, cells have developed highly regulated intracellular proteolytic sys-tems responsible for the removal of such nonfunctional proteins before they start to aggre-gate. Mammalian cells contain several pathways for general protein breakdown, comprising membrane proteases, lysosomal cathepsins, calcium-activated calpains, caspases, mitochon-drial proteases and the proteasomal system. Besides all proteolytic systems, the major prote-olytic system responsible for the removal of oxidized cytosolic and nuclear proteins is the proteasomal system. The proteasome, known to be localized in the cytosol and in the nuclei of mammalian cells and furthermore attached to the endoplasmic reticulum and the cell
2010 ▪ Volume 4, Number 1 8 CEMED
REVIEWS

membrane, is mainly composed of 20S core proteasome. This core complex degrades the oxidized proteins in a ubiquitin- and ATP-independent manner [9].
Experimental evidence from several studies shows that many of the alterations during aging and the progression of certain diseases are the result of the occurrence of protein oxida-tion products and decrease in the degradation of oxidized proteins.
The Proteasome in Aging and Diseases
Aging
The aging process is characterized by changes in cellular functions and decline in repair mechanisms against several damages. There are hundreds of theories to explain the mecha-nisms of aging, including the mainly accepted free radical theory of aging fi rst published by Harman [10]. This theory suggests a leading role of oxidative modifi cations during the aging process and the decrease in the antioxidative capacity of the cell. In this regard, the protea-somal system is one of the systems that declines with aging. Decrease in the proteasomal activity with age has been shown in several cell lines by different groups such as human lymphocytes and keratinocytes [11–13], rat spinal cords [14] and rat brain [15].
It was proposed that the functional decline of the proteasome is due to inhibition by ag-gregates of nondegraded oxidized proteins. Age pigments such as lipofuscin, ceroid or AGE-pigment like fl uorophores are main protein aggregates accumulating during the aging pro-cess. Lipofuscin contains conjugates of MDA and protein thiol groups deduced from its fl uorescence character and it was recently shown by several groups that the presence of such material infl uences proteasomal activity [16]. This aggregated cross-linked material will be autophagozytosed resulting in a major accumulation of this material in lysosomes. The ob-served age-related accumulation of oxidized cross-linked material may be the result of both increased protein oxidation followed by aggregation and/or decline in protein breakdown and a malfunction of the proteasomal system [17].
Aging leads to the development of related neurodegenerative, cardiovascular diseases and cancer. In these diseases, the role of protein oxidation, protein turnover and proteasome has been extensively studied. It seems that the oxidative processes in the brain are facilitated by the high oxygen consumption of this organ [18].
Alzheimer’s Disease
AD is an important age-related disease, the most common form of adult-onset dementia. The major alterations in this disease are SP and NFT representing an accumulation of intran-euronal and extracellular fi lamentous protein aggregates. The major proteins in these forma-tions are hyperphosphorylated tau in NFT and Aβ peptide, derived from amyloid precursor protein in SP [19]. Protein aggregate formation seems to be related to oxidative stress and mainly to the protein oxidation process. Oxidative damage found in AD includes the forma-tion of AGE [20], nitration [21], lipid peroxidation adduction products [22], carbonyl-modi-fi ed neurofi lament protein and free carbonyls [23]. Oxidized proteins (protein carbonyls) were found to be increased in frontal pole and occipital pole in AD patients compared with controls [23]. Mishto et al. found a decrease in the trypsin-like activity of proteasome emerged
REVIEWS
CEMED 9 2010 ▪ Volume 4, Number 1

in the hippocampus and cerebellum of AD patients [24]. Lovell et al. found elevated levels of free and protein-bound HNE in the ventricular fl uids of AD patients [25]. Iron in a redox-active state, thought to play an important role in free radical production in AD, was shown to be increased in NFT as well as Aβ deposits [26]. Iron catalyzes the formation of hydroxyl radical from H2O2 and also the formation of AGE. Aβ itself has been directly implicated in ROS formation through peptidyl radicals [27]. Additionally, AGE and Aβ activate specifi c receptors, such as the RAGE and the class A scavenger-receptor, to increase reactive oxygen production [28].
Parkinson’s Disease
Parkinson’s disease is a second common neurodegenerative disorder. Common clinical symptoms are mainly caused by the degeneration of nigrostriatal dopaminergic neurons found in the substantia nigra pars compacta [29]. Intracellular cytosolic formation of Lewy bodies formed by polyubiquitinated α-synuclein is the main histological marker of this dis-ease [30]. Parkin that normally functions as an E3-ligase of the ubiquitin proteasome system is another protein forming aggregates [31]. There are several studies of the role of oxidative damage in Parkinson’s disease. In dopaminergic cells, dopamine is decomposed by a reaction catalyzed by transition metals – superoxide anions are released during this reaction [32]. Peroxynitrite, hydrogen peroxide, protein carbonyls, 3-nitrotyrosine modifi cations, MDA, HNE, and 8-OHdG are also known to occur in Parkinson lesions. Interestingly, McNaught et al. [33] have shown a decrease in the amount of α-subunits of the proteasome in dopamin-ergic neurons of Parkinson’s disease brains. All these fi ndings indicate the role of oxidative stress.
Atherosclerosis
Hypercholesterolemia is a major risk factor for coronary artery diseases. Hypercholester-olemia was reported to increase the levels of RS through stimulation of polymorphonuclear leukocytes and RS have been implicated in the development of hypercholesterolemic athero-sclerosis [34]. In the development of atherosclerosis, RS are produced by endothelial cells, smooth muscle cells and macrophages, which oxidize LDL in the subendothelial space at the sites of endothelial damage, initiating, therefore, events that culminate in the formation of a fi brous plaque. Rupture of fi brous plaque leads to thrombus formation and occlusion of the vessel. Prasad et al. showed that cholesterol feeding of rabbits caused an increase in MDA levels and glutathione peroxidase activities and a decrease in superoxide dismutase activity in the myocardium [35]. High cholesterol was also suggested to play a role in AD. Patients with elevated cholesterol may have increased susceptibility to AD in addition to coronary artery disease and hypertension [36]. Cholesterol may initiate Aβ formation, an already men-tioned potent source of oxidative stress and irreversible protein aggregation. We showed the possible role of high cholesterol in AD in an experimental approach feeding rabbits a high-cholesterol diet and were able to demonstrate an increase in serum cholesterol and MDA levels [37, 38]. Additionally, moderate increase in HNE-proteins, 3-nitrotyrosinated proteins and protein carbonyls was observed in the hippocampus area of the rabbits [37].
2010 ▪ Volume 4, Number 1 10 CEMED
REVIEWS

Diabetes Type I and II
Diabetes is a constantly rising disease all over the world. In the pathology of diabetes, in-creased amounts of hyperglycemia-induced oxidative stress, especially in diabetic neuropa-thies and atherosclerosis, play the most important role. Oxidative damage in hyperglycemia is induced by the autooxidation of glucose, enhanced activity of aldose reductase, the forma-tion of AGEs, an increased activity of protein kinase C and a mitochondrial overproduction of superoxide anions [39]. Increased ROOH, oxidized low-density proteins and 8-OHdG levels have been shown to be elevated in humans in types 1 and 2 diabetes patients [40, 41] compared to an age-matched control. Protein oxidation was also increased, detected by the use of protein carbonyls and nitrotyrosine, both in plasma and intracellularly [42]. Addition-ally a chronic decrease of the cellular antioxidative capacity in diabetes has been shown: the important antioxidant glutathione [43] and the vitamins C and E are reduced [44] and a cel-lular depletion of NADPH [45] has been reported. Also the proteasomal activity and there-fore, the ability to degrade oxidatively damaged proteins seem to be reduced [46].
Proteasomal System in Cancer and Cancer Therapy
The proteasomal system plays a key role in several molecular pathways via degradation of the bulk of proteins and controls the amount and activity of oncogene and tumor suppressor gene products, transcription factors and other signaling molecules. Additionally proteasomal system induces tumorigenesis by the degradation of tumor suppressor p53, and p27Kip1 in-hibitor of cyclin-dependent kinases. Tumor cells generally have higher proteasome amounts and activity compared to normal differentiated cells [47].
Considering the roles of the proteasomal system in cellular events, proteasomal inhibi-tors have been developed and serve as promising agents for cancer therapy. Adams et al. [48] designed highly specifi c boronic acid derivatives as proteasome inhibitors. Bortezomib (Vel-cade™) is the fi rst dipeptidyl boronate compound in clinical trials, mainly in applications for multiple myeloma [49]. Besides direct effects of bortezomib in cancer therapy, it has also been used in patients developing chemotherapy and radiotherapy resistance [50].
ConclusionProtein oxidation and the proteasomal system have important roles in the pathogenesis of several diseases and in the aging process. Due to the involvement of the proteasome in many cellular processes, it has now become an important target in therapeutic approaches.
AcknowledgmentNKO and TG were supported by COST B35 Action.
REVIEWS
CEMED 11 2010 ▪ Volume 4, Number 1

ReferencesHalliwell, B., Gutteridge, J. M. C.:[1] Cellular responses to oxidative stress: adaptation, damage, repair, senes-cence and death. In: Halliwell, B., Gutteridge, J. M. C. (eds): Free Radicals in Biology and Medicine. Oxford University Press, New York, 2007, pp. 187–267.Davies, M. J.:[2] Singlet-oxygen mediated damage to proteins and its consequences. Biochem. Biophys. Res. Commun., 2003, 305, 761–770.Davies, K. J. A.:[3] Protein damage and degradation by oxygen radicals I. General aspects. J. Biol. Chem., 1987, 262, 9895–9901.Berlett, B. S., Stadtman, E. R.:[4] Protein oxidation in aging, disease, and oxidative stress. J. Biol. Chem., 1997, 272, 20313–20316.Grune, T., Reinheckel, T., Davies, K. J. A.:[5] Degradation of oxidized proteins in mammalian cells. FASEB J., 1997, 11, 526–534.Grune, T., Jung, T., Merker, K. et al.:[6] Decreased proteolysis caused by protein aggregates, inclusion bodies, plaques, lipofuscin, ceroid, and ‘aggresomes’ during oxidative stress, aging, and disease. Int. J. Biochem. Cell. Biol., 2004, 36, 2519–2530.Puig, A., Gilbert, H. F.:[7] Protein disulfi de isomerase exhibits chaperone and anti-chaperone activity in the oxi-dative refolding of lysozyme. J. Biol. Chem., 1994, 269, 7764–7771.Noonan, E. J., Place, R. F., Giardina, C. et al.:[8] HSP70B regulation and function. Cell Stress Chap., 2007, 12, 393–402.Grune, T., Merker, K., Sandig, G. et al.:[9] Selective degradation of oxidatively modifi ed protein substrates by the proteasome. Biochem. Biophys. Res. Commun., 2003, 305, 709–718.Harman, D.:[10] Aging: a theory based on free radical and radiation chemistry. J. Gerontol., 1956, 11, 298–300.Petropoulos, I., Conconi, M., Wang, X. et al.:[11] Increase of oxidatively modifi ed protein is associated with a decrease of proteasome activity and content in aging epidermal cells. J. Gerontol. A Biol. Sci. Med. Sci., 2000, 55, B220–B227.Sitte, N., Merker, K., von Zglinicki, T. et al.:[12] Protein oxidation and degradation during cellular senescence of human BJ fi broblasts: part I – effects of proliferative senescence. FASEB J., 2000, 14, 2495–2502.Hwang, J. S., Hwang, J. S., Chang, I. et al.:[13] Age-associated decrease in proteasome content and activities in human dermal fi broblasts: restoration of normal level of proteasome subunits reduces aging markers in fi broblasts from elderly persons. J. Gerontol. A Biol. Sci. Med. Sci., 2007, 62, 490–499.Keller, J. N., Huang, F. F., Markesbery, W. R.:[14] Decreased levels of proteasome activity and proteasome expres-sion in aging spinal cord. Neuroscience, 2000, 98, 149–156.Zeng, B. Y., Medhurst, A. D., Jackson, M. et al.:[15] Proteasomal activity in brain differs between species and brain regions and changes with age. Mech. Ageing Dev., 2005, 126, 760–766.Sitte, N., Huber, M., Grune, T. et al.:[16] Proteasome inhibition by lipofuscin/ceroid during postmitotic aging of fi broblasts. FASEB J., 2000, 14, 1490–1498.Jung, T., Bader, N., Grune, T.:[17] Lipofuscin: formation, distribution, and metabolic consequences. Ann. N. Y. Acad. Sci., 2007, 1119, 97–111.Boveris, A., Chance, B.:[18] The mitochondrial generation of hydrogen peroxide. General properties and effect of hyperbaric oxygen. Biochem. J., 1973, 134, 707–716.Markesbery, W. R.:[19] Oxidative stress hypothesis in Alzheimer’s disease. Free Radic. Biol. Med., 1997, 23, 137–147.Smith, M. A., Taneda, S., Richey, P. L. et al.: [20] Advanced Maillard reaction end products are associated with Alzheimer disease pathology. Proc. Natl. Acad. Sci. U.S.A., 1994, 91, 5710–5714.Good, P. F., Werner, P., Hsu, A. et al.:[21] Evidence of neuronal oxidative damage in Alzheimer’s disease. Am. J. Pathol., 1996, 149, 21–28.Sayre, L. M., Zelasko, D. A., Haris, P. L. et al.:[22] 4-Hydroxynonenal-derived advanced lipid peroxidation end products are increased in Alzheimer’s disease. J. Neurochem., 1997, 68, 2092–2097.Smith, C. D., Carney, J. M., Starke-Reed, P. E. et al.: [23] Excess brain protein oxidation and enzyme dysfunc-tion in normal aging and in Alzheimer disease. Proc. Natl. Acad. Sci. U.S.A., 1991, 88, 10540–10543.Mishto, M., Belavista, E., Santoro, A. et al.:[24] Immunoproteasome and LMP2 polymorphism in aged and Alzheimer’s disease brains. Neurobiol. Aging, 2006, 27, 54–66.
2010 ▪ Volume 4, Number 1 12 CEMED
REVIEWS

Lovell, M. A., Ehmann, W. D., Markesbery, W. R.:[25] Elevated 4-hydroxynonenal in ventricular fl uid in Alzheimer’s disease. Neurobiol. Aging, 1997, 18, 457–461.Smith, M. A., Haris, P. L. R., Sayre, L. M. et al.:[26] Iron accumulation in Alzheimer disease is a source of redox-generated free radicals. Proc. Natl. Acad. Sci. U.S.A., 1997, 94, 9866–9868.Hensley, K., Carney, J. M., Mattson, M. P. et al.:[27] A model for beta-amyloid aggregation and neurotoxicity based on free radical generation by the peptide: relevance to Alzheimer disease. Proc. Natl. Acad. Sci. U.S.A., 1994, 91, 3270–3274.Yan, S. D., Chen, X., Fu, J. et al.: [28] RAGE and amyloid-beta peptide neurotoxicity in Alzheimer’s disease. Nature, 1996, 382, 685–691.Bernheimer, H., Birkmayer, W., Hornykiewicz, O. et al.: [29] Brain dopamine and the syndromes of Parkinson and Huntington. Clinical, morphological and neurochemical correlations. J. Neurol. Sci., 1973, 20, 415–455.Kawahara, K., Hashimoto, M., Bar-On, P. et al.:[30] alpha-Synuclein aggregates interfere with parkin solubility and distribution: role in the pathogenesis of Parkinson disease. J. Biol. Chem., 2008, 283, 6979–6987.Sakata, E., Yamaguchi, Y., Kurimoto, E. et al.:[31] Parkin binds the Rpn10 subunit of 26S proteasomes through its ubiquitin-like domain. EMBO Rep., 2003, 4, 301–306.Jenner, P., Olanow, C. W.:[32] Oxidative stress and the pathogenesis of Parkinson’s disease. Neurology, 1996, 47, S161–S170.McNaught, K. S., Belizaire, R., Jenner, P. et al.:[33] Selective loss of 20S proteasome alpha-subunits in the sub-stantia nigra pars compacta in Parkinson’s disease. Neurosci. Lett., 2002, 326, 155–158.Stokes, K. Y., Cooper, D., Tailor, A. et al.: [34] Hypercholesterolemia promotes infl ammation and microvascular dysfunction: role of nitric oxide and superoxide. Free Radic. Biol. Med., 2002, 33, 1026–1036.Prasad, K., Mantha, S., Kalra, J. et al.:[35] Hypercholesterolemia-induced oxidative stress in heart and its pre-vention by vitamin E. Int. J. Angiol., 1997, 6, 13–17.Pappolla, M. A., Bryant-Thomas, T. K., Herbert, D. et al.: [36] Mild hypercholesterolemia is an early risk factor for the development of Alzheimer amyloid pathology. Neurology, 2003, 61, 199–205.Aytan, N., Jung, T., Tamturk, F. et al.:[37] Oxidative stress related changes in the brain of hypercholesterolemic rabbits. Biofactors, 2008, 33, 225–236.Ozer, N. K., Negis, Y., Aytan, N. et al.:[38] Vitamin E inhibits CD36 scavenger receptor expression in hypercho-lesterolemic rabbits. Atherosclerosis, 2006, 184, 15–20.Mullarkey, C. J., Edelstein, D., Brownlee, M.: [39] Free radical generation by early glycation products: a mecha-nism for accelerated atherogenesis in diabetes. Biochem. Biophys. Res. Commun., 1990, 173, 932–939.Dandona, P., Thusu, K., Cook, S. et al.:[40] Oxidative damage to DNA in diabetes mellitus. Lancet, 1996, 347, 444–445.Hussein, O. A., Gefen, Y., Zidan, J. M. et al.:[41] LDL oxidation is associated with increased blood hemoglobin A1c levels in diabetic patients. Clin. Chim. Acta, 2007, 377, 114–118.Telci, A., Cakatay, U., Salman, S. et al.:[42] Oxidative protein damage in early stage type 1 diabetic patients. Dia-betes Res. Clin. Pract., 2000, 50, 213–223.Likidlilid, A., Patchanans, N., Poldee, S. et al.:[43] Glutathione and glutathione peroxidase in type 1 diabetic patients. J. Med. Assoc. Thai., 2007, 90, 1759–1767.Vincent, A. M., Russell, J. W., Low, P. et al.:[44] Oxidative stress in the pathogenesis of diabetic neuropathy. Endocr. Rev., 2004, 25, 612–628.Greene, D. A., Stevens, M. J., Obrosova, I. et al.:[45] Glucose-induced oxidative stress and programmed cell death in diabetic neuropathy. Eur. J. Pharmacol., 1999, 375, 217–223.Xu, J., Wu, Y., Song, P. et al.:[46] Proteasome-dependent degradation of guanosine 50-triphosphate cyclohydro-lase I causes tetrahydrobiopterin defi ciency in diabetes mellitus. Circulation, 2007, 116, 944–953.Coux, O., Tanaka, K., Goldberg, A. L.:[47] Structure and functions of the 20S and 26S proteasomes. Annu. Rev. Biochem., 1996, 65, 801–847.Adams, J., Palombella, V. J., Sausville, E. A. et al.:[48] Proteasome inhibitors: a novel class of potent and effec-tive antitumor agents. Cancer Res., 1999, 59, 2615–2622.Adams, J.:[49] Development of the proteasome inhibitor PS-341. Oncologist, 2002, 7, 9–16.Badros, A., Gahres, N.:[50] Bortezomib, thalidomide, and dexamethasone for relapsed multiple myeloma: add it up and wait. Clin. Adv. Hematol. Oncol., 2005, 3, 916–917.
REVIEWS
CEMED 13 2010 ▪ Volume 4, Number 1


Compliance and Persistence with Medications for Chronic Obstructive Pulmonary Disease
TAMÁS ÁGH, ÁGNES MÉSZÁROS
University Pharmacy Department of Pharmacy Administration, Semmelweis University, Budapest, Hungary
Non-compliance and non-persistence with medication represent a signifi cant problem of realizing the optimal dis-ease management in chronic obstructive pulmonary disease (COPD). Underuse and overuse are both important factors of inadequate therapy. Poor compliance increases the frequency of exacerbations, the number of hospitaliza-tions, results in higher mortality and reduced quality of life. When prescribing medication, besides patient character-istics, the expected compliance and persistence should also be considered. Patient education and a better clinician–patient relationship should increase the effectiveness of treatments.
Keywords: adherence, compliance, persistence, COPD
Abbreviations
AC = anticholinergics; COPD = chronic obstructive pulmonary disease; ICS = inhaled corticosteroids; LABA = long-acting beta-agonists; LABA + ICS = fi xed combination of long-acting beta-agonists and inhaled corticosteroids; MPR = medication possession ratio; MTX = methylxantines
The number of registered COPD patients in Hungary is 110,000; however, the estimated in-cidence reaches 500,000 persons [1]. Both prevalence and mortality fi gures show a continu-ous rise in the developed, industrialized countries. COPD is the fourth leading cause of death and is anticipated to be the third most common cause of death in Europe and in the world by 2020 [2]. The annual per capita health care expenditure on people with COPD is more than two times higher than that spent on people without obstructive pulmonary disease [3]. Ac-cording to the WHO forecast, a notable rise of the burden of the disease is expected: COPD was the 12th most common disease in 1990, and it is projected to be the 5th by 2020.
Because of the chronic progress of COPD, patient adherence plays an important role in improving clinical outcomes and quality of life [4]. Medication non-compliance signifi cantly increases the frequency of exacerbations, the number of hospitalizations, and mortality [5, 6]. Frequent acute exacerbations reduce patients’ quality of life remarkably [7].
There is a gap between effi cacy (works under experimental conditions) and effective-ness (performs in the real world) of a given treatment [8]. One reason for this difference is the non-compliance with medication regimens. Unfortunately, the full clinical benefi t of the therapy cannot be realized with poor patient compliance [9]. Thus, clinical and economic impact of non-compliance plays an important role as explained in Fig. 1 [10].
Corresponding address: Tamás Ágh MD, Kossuth L. u. 12., H-2510 Dorog, Hungary.E-mail: [email protected]
28691
REVIEWS
DOI: 10.1556/CEMED.4.2010. 15 2010 ▪ Volume 4, Number 1 ▪ 15–22.

Defi nitions: Compliance and PersistenceThe defi nitions of patient co-operation are not similar. This causes many diffi culties when comparing the results of the studies. The ISPOR (International Society of Pharmacoeconom-ics and Outcomes Research) classifi cation is the most acceptable one. Compliance and per-sistence, the two most important aspects of a patient’s drug-taking behaviour, are defi ned on the basis of this classifi cation (Fig. 2) as follows.
Fig. 1 Pharmacoeconomic impact of non-compliance and non-persistence
Fig. 2 Defi nitions of compliance and persistence
Compliance
Medication compliance refers to the degree of conformity to the medical treatment. It exhib-its the extent to which a patient acts in accordance with the prescribed duration and dose of
2010 ▪ Volume 4, Number 1 16 CEMED
REVIEWS

a dosing regimen. Compliance is an index-number, which is added in percentage and refers to a specifi ed time interval [11].Models for measuring compliance [12]:– MPR: number of days of medication supplied within the refi ll interval/number of days
in refi ll interval.– Continuous measure of adherence: MPR is calculated across multiple refi lls.– Continuous measure of medication gaps: the sum of the number of days in the gaps be-
tween refi lls in the observation period/time between the fi rst and last fi lls.– Proportion of days covered: the number of days with drug on-hand/the number of days in
the observation interval.Patients with compliance over 80% (MPR) can be called co-operating.
Persistence
The persistence refers to the act of continuing the treatment for the prescribed duration. It is the time dimension-index of the quality of drug therapy. Mostly it is counted in days, but it can also be measured in months or years [11].There are many methods for measuring persistence [12].– The duration of time from the initiation (or at chronic disease from an optional date) to the
discontinuation of drug therapy.– Monitoring the medication prescriptions and the prescription fi lls within an added time-
interval. Usually prescription refi lls of 12 months are monitored. This method can also be used in cases of seasonal diseases, which do not need a permanent drug therapy.
– The percentage of the number of treated patients in a defi ned period.In the studies pertaining to persistence, a time interval is defi ned as the so-called permissible gap. It is reported as the maximum allowable period of the refi ll interval without discontinu-ation of the therapy.
Compliance and Persistence with Medications for COPDThere are many causes of non-compliance and non-persistence: lack of prescription refi lls, incorrect use of the medication (incorrect inhalation technique) or premature discontinuation of the therapy.
Not in all cases do the patients fi ll their prescribed medication. Kennedy et al. [13] asked 14,500 Medicare benefi ciaries about their prescription fi lling habits. The estimated rate of lack of fi llings at least one prescription in 1 year among all participants was 4.4%. Failure-to-fi ll rates were signifi cantly higher among patients with psychiatric conditions (8%), obstruc-tive pulmonary disease (6.6%), cardiovascular disease (5.2%) and arthritis (5.2%). Drug costs and side-effects are the most common reasons for failing to fi ll a prescription. Patients often believe that the prescribed medication is useless.
In a retrospective study, Breekveldt-Postma et al. [14] examined the prescription refi lls rate with ICS therapy in a cohort of 2,000 COPD patients. The 1-year persistence with ICS therapy was found to be only 25%.
Similarly, Jung et al. [15] obtained a low patient co-operation in their trial. They exam-ined the medication compliance and persistence in COPD patients during their last year of
REVIEWS
CEMED 17 2010 ▪ Volume 4, Number 1

Table 1 Medication possession ratios for COPD medication users
MPR (over 12 months)
ICS 0.35
LABA 0.34
MTX 0.52
AC 0.38
AC – anticholinergics, ICS – inhaled corticosteroids, LABA – long-acting beta-agonists, MTX – methylxantines, MPR – medication possession ratio.Jung, E., Pickard, A. S., Salmon, J. W. et al.: Medication adherence and persistence in the last year of life in COPD patients. Respir. Med., 2009, 103, 525–534.
life. The compliance of the complex therapy was 44% (MPR) and the persistence was 30%. Comparison of these results with the data of other common chronic diseases points out that the compliance with COPD therapy is remarkably low. The 1-year-compliance of hyperten-sion, dyslipidaemia and diabetes mellitus is on average 72% (MPR: 67–76%), and the persis-tence is 63% [16]. Jung et al. found signifi cant differences in patient co-operation between drug classes (Table 1). MPRs generally did not reach 0.80 for any studied medication regi-men. The medication’s sub-optimal clinical benefi ts are expected only over this rate. At low-er compliance levels, only minimal health gains can be obtained and the cost-effectiveness of the therapy sinks remarkably. One reason for the higher MPRs of MTX is that elderly veter-ans have more diffi culty using inhaled medications, therefore they prefer oral drugs. How-ever, a 90-day supply was allowed for MTX while inhaled medications were dispensed for 30 days. Persistence with LABA was the lowest (21%), while MTX therapy had the highest (44%) result. Under the examined inhaled drug classes, AC showed the highest compliance and persistence.
In a further study by Breekveldt-Postma et al. [17], persistence was assessed during the fi rst year of the medical treatment with retrospective analysis of prescription refi lls data. Tiotropium, ipratropium, LABA and a fi xed combination of LABA and ICS (LABA + ICS) were monitored. The persistence was the highest, 37% with tiotropium. The patients’ drug-taking behaviour was found to be signifi cantly lower with other inhaled drugs (ipratropium: 14%, LABA: 13%, LABA + ICS: 17%). The effect of hospitalization on patient co-operation was also studied. As a result of prior hospitalization, the 1-year persistence rates were in-creased by 2–3 times (tiotropium: 61%, ipratropium: 37%, LABA: 41%, LABA + ICS: 33%) in the fi rst year of the medical treatment. Once-daily dosing of tiotropium compared with other studied drugs may have led to enhanced persistence.
Cramer et al. [18] recruited the enhanced persistence with tiotropium. They monitored 31,368 Canadian COPD patients’ refi lls data of ipratropium, ipratropium + salbutamol, for-moterol, formoterol + budesonide, salmeterol, salmeterol + fl uticason and tiotropium therapy. The 12-month persistence was signifi cantly higher with tiotropium – 53% – compared with the other inhaled drugs where persistence was between 7% and 30%.
2010 ▪ Volume 4, Number 1 18 CEMED
REVIEWS

Non-compliance does not only mean underuse of the prescribed medication, overuse is also a common problem [6, 19]. Krigsman et al. [20] found that 59% of COPD patients un-deruse and 12% overuse the ICS. Another study by Krigsman et al. [21] monitored the drug-taking behaviour of asthma and COPD patients with retrospective analysis evaluating repeat prescription data. The obtained results indicate that 53% of the patients had undersupply and 18% oversupply.
Eighty-four percent of the COPD patients have one or more co-morbidity [22]. The question is obvious: is the COPD patients’ compliance also low with other medication therapy? Over a period of 3 years Krigsman et al. [23] analysed the refi ll prescription data of COPD patients, who suffered also from diabetes. Medication compliance for diabetes drugs was 68% and for COPD drugs it was 42%.
Corden et al. [24] analysed the association between medication compliance and quality of life between nebulizer using COPD patients. Data were obtained from 82 patients with microprocessor-equipped nebulizers over a period of 4 weeks. Quality of life was measured with St. George’s Respiratory Questionnaire. The medication compliance was 57%. Compli-ance was signifi cantly negatively correlated with quality of life.
Reasons of Non-Compliance and Non-PersistenceThe reasons for the low compliance obtained by patients are: medical, psychological, social-economic problems; barriers to access medication; understanding the perception of the ill-ness and the goal of the drug therapy; previous negative experiences with the medication; side-effects of the drug; comfort criteria or just forgetfulness [8, 25].
The complex therapy of COPD requires compliant medication regimens as well as be-haviour and lifestyle changes (such as: smoking cessation). Adequate medication compliance can improve quality of life and reduce exacerbations, but cannot fully reverse disease symp-toms [26]. These all can be at the background of non-compliance. Depression is a common co-morbidity of COPD and it is also a known factor for inadequate drug-taking behaviour [27]. When depression is diagnosed, it is necessary to establish a good patient co-operation. Inadequate inhaler technique can also issue non-compliance among COPD patients. It occurs mainly among elderly veterans. The recognition of individual demands and their consider-ation by the therapy are the responsibilities of the therapist. Confusion with side-effects is acutely obtained with ICS therapy. The prescribed drug doses are often reduced purposely by the patients to decrease the probability of the side-effects [28]. The most common reason that patients cite for not using their medication is the belief that it does not do any good so they no longer need it [29]. Patients misunderstand or forget soon the clinician’s instructions. Immediately after the consultation they recall less then 50% of the information conveyed by the physician [30]. Compliant drug behaviour is not to be hoped for by such lack of knowl-edge.
Compliance-Enhancing InterventionsMany studies have been published about strategies to improve compliance with therapy; few of these have focused on obstructive pulmonary disease. Patient education, self-monitoring
REVIEWS
CEMED 19 2010 ▪ Volume 4, Number 1
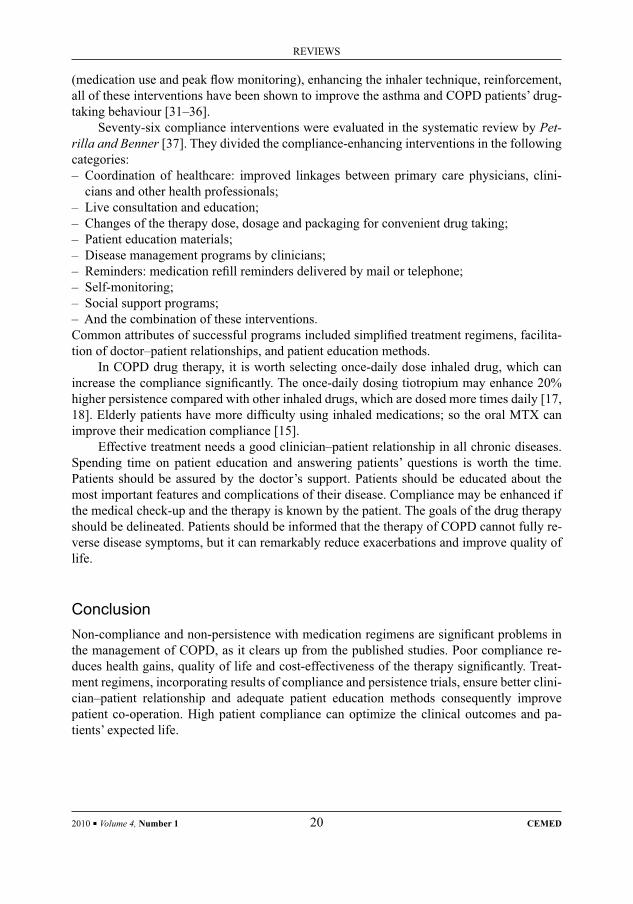
(medication use and peak fl ow monitoring), enhancing the inhaler technique, reinforcement, all of these interventions have been shown to improve the asthma and COPD patients’ drug-taking behaviour [31–36].
Seventy-six compliance interventions were evaluated in the systematic review by Pet-rilla and Benner [37]. They divided the compliance-enhancing interventions in the following categories:– Coordination of healthcare: improved linkages between primary care physicians, clini-
cians and other health professionals;– Live consultation and education;– Changes of the therapy dose, dosage and packaging for convenient drug taking;– Patient education materials;– Disease management programs by clinicians;– Reminders: medication refi ll reminders delivered by mail or telephone;– Self-monitoring;– Social support programs;– And the combination of these interventions.Common attributes of successful programs included simplifi ed treatment regimens, facilita-tion of doctor–patient relationships, and patient education methods.
In COPD drug therapy, it is worth selecting once-daily dose inhaled drug, which can increase the compliance signifi cantly. The once-daily dosing tiotropium may enhance 20% higher persistence compared with other inhaled drugs, which are dosed more times daily [17, 18]. Elderly patients have more diffi culty using inhaled medications; so the oral MTX can improve their medication compliance [15].
Effective treatment needs a good clinician–patient relationship in all chronic diseases. Spending time on patient education and answering patients’ questions is worth the time. Patients should be assured by the doctor’s support. Patients should be educated about the most important features and complications of their disease. Compliance may be enhanced if the medical check-up and the therapy is known by the patient. The goals of the drug therapy should be delineated. Patients should be informed that the therapy of COPD cannot fully re-verse disease symptoms, but it can remarkably reduce exacerbations and improve quality of life.
ConclusionNon-compliance and non-persistence with medication regimens are signifi cant problems in the management of COPD, as it clears up from the published studies. Poor compliance re-duces health gains, quality of life and cost-effectiveness of the therapy signifi cantly. Treat-ment regimens, incorporating results of compliance and persistence trials, ensure better clini-cian–patient relationship and adequate patient education methods consequently improve patient co-operation. High patient compliance can optimize the clinical outcomes and pa-tients’ expected life.
2010 ▪ Volume 4, Number 1 20 CEMED
REVIEWS
ReferencesJonas, J.:[1] Epidemiological data of pulmonary diseases in Hungary (In Hungarian). Korányi National Institute of Tuberculosis and Pulmonology, 2008.Holguin, F., Folch, E., Redd, S. C. et al.:[2] Comorbidity and mortality in COPD-related hospitalizations in the United States 1979–2001. Chest, 2005, 128, 2005–2011.Rabe, K. F., Hurd, S., Anzueto, A. et al.:[3] Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am. J. Respir. Crit. Care Med., 2007, 176, 532–555.WHO:[4] Adherence to Long-Term Therapies: Evidence for Action. World Health Organization, 2003, pp. 1–59.Regueiro, C. R., Hamel, M. B., Davis, R. B. et al.:[5] A comparison of generalist and pulmonologist care for pa-tients hospitalized with severe chronic obstructive pulmonary disease: resource intensity, hospital costs, and survival. Am. J. Med., 1998, 105, 366–372.Bourbeau, J., Bartlett, S. J.:[6] Patient adherence in COPD. Thorax, 2008, 63, 831–838.Seemungal, T. A. R., Donaldson, G. C., Paul, E. A. et al.:[7] Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med., 1998, 157, 1418–1422.Gulácsi, L.:[8] Health Economics (In Hungarian). Medicina Press, Budapest, 2005.Haynes, R. B., Montague, P., Oliver, T. et al.:[9] Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst. Rev., 2000, 2. CD000011.Cleemput, I., Kesteloot, K., DeGeest, S.:[10] A review of the literature on the economics of noncompliance. Room for methodological improvement. Health Policy, 2002, 59, 65–94.Cramer, J. A., Roy, A., Burrell, A. et al.:[11] Medication compliance and persistence: terminology and defi nitions. Value Health, 2008, 11, 44–47.Peterson, A. M., Nau, D. P., Cramer, J. A. et al.:[12] A checklist for medication compliance and persistence studies using retrospective databases. Value Health, 2007, 10, 3–12.Kennedy, J., Tuleu, I., Mackay, K.:[13] Unfi lled prescriptions of medicare benefi ciaries: prevalence, reasons, and types of medicines prescribed. J. Manag. Care Pharm., 2008, 14, 553–560.Breekveldt-Postma, N. S., Gerrits, C. M. J. M., Lammers, J. W. J. et al.:[14] Persistence with inhaled corticosteroid therapy in daily practice. Respir. Med., 2004, 98, 752–759.Jung, E., Pickard, A. S., Salmon, J. W. et al.:[15] Medication adherence and persistence in the last year of life in COPD patients. Respir. Med., 2009, 103, 525–534.Cramer, J. A., Benedict, A., Muszbek, N. et al.:[16] The signifi cance of compliance and persistence in the treatment of diabetes, hypertension and dyslipidaemia: a review. Int. J. Clin. Pract., 2008, 62, 76–87.Breekveldt-Postma, N. S., Koerselman, J., Erkens, J. A. et al.:[17] Enhanced persistence with tiotropium com-pared with other respiratory drugs in COPD. Respir. Med., 2007, 101, 1398–1405.Cramer, J. A., Bradley-Kennedy, C., Scalera, A.:[18] Treatment persistence and compliance with medications for chronic obstructive pulmonary disease. Can. Respir. J., 2007, 14, 25–29.Restrepo, R. D., Alvarez, M. T., Wittnebel, L. D. et al.:[19] Medication adherence issues in patients treated for COPD. Int. J. COPD, 2008, 3, 371–384.Krigsman, K., Moen, J., Nilsson, J. L. G. et al.:[20] Refi ll adherence by the elderly for asthma/chronic obstructive pulmonary disease drugs dispensed over a 10-year period. J. Clin. Pharm. Ther., 2007, 32, 603–611.Krigsman, K., Nilsson, J. L. G., Ring, L.:[21] Refi ll adherence for patients with asthma and COPD: comparison of a pharmacy record database with manually collected repeat prescriptions. Pharmacoepidemiol. Drug Saf., 2007, 16, 441–448.Yeo, J., Karimova, G., Bansal, S.:[22] Co-morbidity in older patients with COPD – its impact on health service utilisation and quality of life, a community study. Age Ageing, 2006, 35, 33–37.Krigsman, K., Nilsson, J. L. G., Ring, L.:[23] Adherence to multiple drug therapies: refi ll adherence to concomi-tant use of diabetes and asthma/COPD medication. Pharmacoepidemiol. Drug Saf., 2007, 16, 1120–1128.Corden, Z. M., Bosley, C. M., Rees, P. J. et al.:[24] Home nebulized therapy for patients with COPD: patient compliance with treatment and its relation to quality of life. Chest, 1997, 112, 1278–1282.George, J., Kong, D. C. M., Thoman, R. et al.:[25] Factors associated with medication nonadherence in patients with COPD. Chest, 2005, 128, 3198–3204.Rand, C. S.:[26] Patient adherence with COPD therapy. Eur. Respir. Rev., 2005, 14, 97–101.
REVIEWS
CEMED 21 2010 ▪ Volume 4, Number 1

Van Manen, J. G., Bindels, P. J. E., Dekker, F. W. et al.:[27] Risk of depression in patients with chronic obstruc-tive pulmonary disease and its determinants. Thorax, 2002, 57, 412–416.Apter, A. J., Reisine, S. T., Affl eck, G. et al.:[28] Adherence with twice-daily dosing of inhaled steroids: socioeco-nomic and health-belief differences. Am. J. Respir. Crit. Care Med., 1998, 157, 1810–1817.Chambers, C. V., Markson, L., Diamond, J. J. et al.:[29] Health beliefs and compliance with inhaled corticoster-oids by asthmatic patients in primary care practices. Respir. Med., 1999, 93, 88–94.Dimatteo, M. R.:[30] Psychology of Health Illness and Medical Care: An Individual Perspective. Thomson Brooks/Cole, California, 1991.Onyirimba, F., Apter, A., Reisine, S. et al.:[31] Direct clinician-to-patient feedback discussion of inhaled steroid use: its effect on adherence. Ann. Allergy Asthma Immunol., 2003, 90, 411–415.Bailey, W. C., Richards, J. M., Brooks, C. M. et al.:[32] A randomized trial to improve self-management practices of adults with asthma. Arch. Intern. Med., 1990, 150, 1664–1668.Put, C., Van den Bergh, O., Lemaigre, V. et al.:[33] Evaluation of an individualised asthma programme directed at behavioural change. Eur. Respir. J., 2003, 21, 109–115.Hesselink, A. E., Penninx, B. W. J. H., Van Der Windt, D. A. W. M. et al.:[34] Effectiveness of an education pro-gramme by a general practice assistant for asthma and COPD patients: results from a randomised con-trolled trial. Patient Educ. Couns., 2004, 55, 121–128.Gallefoss, F.:[35] The effects of patient education in COPD in a 1-year follow-up randomised, controlled trial. Patient Educ. Couns., 2004, 52, 259–266.Worth, H., Dhein, Y.:[36] Does patient education modify behaviour in the management of COPD? Patient Educ. Couns., 2004, 52, 267–270.Petrilla, A. A., Benner, J. S.:[37] Critical evaluation of interventions to enhance patient compliance with chronic medications. Value Health, 2003, 6, 200.
2010 ▪ Volume 4, Number 1 22 CEMED
REVIEWS

Associations of Autoimmune Endocrine DiseasesCSABA BALÁZS1, JÁNOS FEHÉR2
1Department of Medicine, Hospital of the Order of Charity in Buda, Budapest, Hungary22nd Department of Medicine, Semmelweis University Medical School, Budapest, Hungary
Recently, an increasing amount of data on the connection between neuro-endocrine and immune systems has been gathered. Results of molecular genetic research have provided evidence for a common language of these systems including neurotransmitters, hormones and cytokines. It has been proved that the immune system is capable of pro-ducing neurotransmitters and hormones and even the endocrine system can prepare cytokines. This integrative (ho-listic) approach makes possible the investigation of physiological and pathological events as interactions of psycho-neuro-endocrine-immune systems. The associations of autoimmune diseases and the autoimmune polyendocrine syndromes constitute a heterogeneous group of disorders characterised by decreased or lost immune tolerance against self-antigens. Molecular genetic research has explored the mechanism of the associations of diseases that are called organ-specifi c. Autoimmune polyendocrine syndrome type 1 is characterised by the presence of at least two of the three cardinal diseases: Addison’s disease, autoimmune hypoparathyroidism and mucocutaneous candidiasis. This rare autosomal recessive syndrome is induced by mutations of the autoimmune regulator (AIRE) gene. Autoim-mune polyendocrine syndrome type 2 that occurs at a much higher frequency is observed and defi ned as the coexis-tence of Addison’s disease, autoimmune thyroid disease and/or type 1 diabetes mellitus. Autoimmune polyendocrine syndrome type 3 is characterised by an association of autoimmune thyroid disease and type 1 diabetes mellitus. In contrast to autoimmune polyendocrine syndrome type 1, HLA and other antigens have proved to be important in types 2 and 3 of the syndrome. Identifi cation of genetic factors predisposing to these syndromes contributes to our understanding of the common mechanisms involved in autoimmunity and offers a possibility for early treatment and prevention as well.
Keywords: immunoendocrine diseases, associations of autoimmune diseases, immunoendocrine regulation, inte-grative medicine, polyendocrine autoimmune diseases
Abbreviations
ACTH = adrenocorticotrophic hormone; AIRE = autoimmune regulator gene; APECED = autoimmune poly-endo-crinopathy, candidiasis, ectodermic dystrophy; APS = autoimmune polyendocrine syndrome; AT = autoimmune thyroiditis; CTLA-4 = cytotoxic T lymphocyte antigen 4; DC = dendritic cell; EMG = electromyogram; IBD = in-fl ammatory bowel disease; IDDM = type 1 diabetes mellitus; ITP = idiopathic thrombocytopenic purpura; LATS = long acting thyroid stimulator; MCTD = mixed connective tissue disease; MHC = major histocompatibility complex; OS = obese strain (chicken); POEMS = polyneuropathy, organomegaly, endocrinopathy, M-protein, skin lesions; RA = rheumatoid arthritis; SLE = systemic lupus erythematosus; SNP = single nucleotide polymorphism; TAD = thyroid-associated disease; Tg = thyroglobulin; TNF = tumour necrosis factor; TPO = thyroid peroxidase enzyme; TRAIL = TNF-related apoptosis-inducing ligands; TSH = thyroid stimulating hormone
The discovery of autoimmunity can be ranked among the most signifi cant results of medi-cine in the last 50 years. Clinical observations and experiments have shown that a whole series of diseases previously thought as having no known origin (“idiopathic”) can be traced back to the abnormal function of the immune system. In 1956, Roitt et al. fi rst demonstrated
Corresponding address: Csaba Balázs MD, Department of Medicine, Hospital of the Order of Charity in Buda, Frankel L. str. 4, Budapest, Hungary. E-mail: [email protected]
28706
REVIEWS
DOI: 10.1556/CEMED.4.2010. 23 2010 ▪ Volume 4, Number 1 ▪ 23–38.

antibodies in the sera of patients with Hashimoto’s thyroiditis which reacted with the thyroid gland [1]. Later, a disease similar to Hashimoto’s thyroiditis could be induced in rabbits by administration of a thyroid extract. A new development in the study of Graves–Basedow disease was the discovery of an immune globulin, LATS, which later proved to be an anti-body against the TSH receptor and responsible for the hyperfunction of the thyroid [2–6]. In 1957 Witebsky et al. formulated the criteria for autoimmune diseases [5] (Table 1).
Table 1 Classifi cation of APS
• APS-1: candidiasis, hypoparathyroidism, Addison’s disease
• APS-2: Addison’s disease + autoimmune thyroid disease and/or type 1 diabetes mellitus
• APS-3: autoimmune thyroid disease + one of the above mentioned diseases
A better knowledge of immune regulation and immune genetics promoted a better un-derstanding of the pathomechanism of autoimmune diseases. The immune system is consti-tuted by a complicated network of cells linked to each other via multiple connections. Rec-ognition of antigens is performed by monocytes, macrophages and DC. This recognition is a complex process including breakdown of substances taken up by the cells, analysis of the epitomes of cleaved compounds and transfer of information obtained about them. In recogni-tion and transfer (“presentation”) of antigens, molecules of the MHC have an important func-tion. They forward the recognised information to thymus- and bursa-dependent cells (T and B lymphocytes). The former can also be divided into two subgroups: the Th1 (T helper-1) cells are responsible for the cellular immune reactions, while T2 (T helper-2) cells direct the humoral immune processes. T cells undergo division, so-called blastic transformation in the presence of activating substances (mitogens) and antigens. During this process, they produce biologically active substances, some of which may be cytotoxic. B lymphocytes exert their effect via antibodies that are different both in their structure and in their function. Some of the antibodies bind to own individual immunoglobulins (idiotype) and create the so-called idiotype-anti-idiotype network that has an important role in the main task of the immune system, preservation of individual integrity. Some of them may be cytotoxic or may enhance or inhibit the function of the cells [6–11]. Due to the pathologic immune regulation, the cells of the immune system recognise self-cells or parts with differing antigenicity (“epitopes”) as foreign. Depending on the extent of sharing of the epitopes by the individual organs, sys-temic or organ-specifi c autoimmune diseases may develop [11–13]. The most recent results of molecular biological research have also revealed that these shared epitopes are present in different organs to varying extent. This can explain the clinical experience showing that SLE is often associated with other diseases formerly thought to be organ-specifi c. In the develop-ment of autoimmune processes, regulating T cells (Treg) have a determinant role [12, 14–16]. Peripheral CD4+ cells are known to express in 5–10% also Foxp3+, CTLA-4 (cytostatic T-lymphocyte antigen 4), and GITR (glucocorticoid-induced tumour necrosis factor receptor family-related receptor) molecules. It has been demonstrated by a growing number of studies
2010 ▪ Volume 4, Number 1 24 CEMED
REVIEWS
that the pathological functioning of CD4+ CD25+ Treg cells play a role in the development of a whole series of autoimmune diseases (SLE, AT, type 1A diabetes mellitus and autoimmune bowel diseases) [15, 17, 18]. It is also known that CD4+ CD25+ Treg cells Foxp3+ Treg are of decisive importance in the maintenance of the immunological tolerance of the organism and in the prevention of autoimmune diseases [12, 18–20]. Thanks to genetic research it has been elucidated that several genes may play a role in the inheritance of autoimmune diseases. Of these the role of MHC genes was discovered at fi rst, and the recent studies also demonstrated the importance of genes located in various chromosomes including HLA II (6p), CTLA-4 (2q), Foxp3 (10p) and AIRE (21p) [21–24]. However, epidemiological studies and observa-tions on twins indicate that in addition to the genetic factors, both epigenetic and environ-mental factors are also decisive in the impairment of immune regulation and in the develop-ment of autoimmune diseases. A detailed analysis of these factors, however, would extend beyond the scope of this paper’s subject matter, and therefore we refer to literary data relating to it [25–28]. A biological recognition of great importance of the last decade showed that the psycho-neuro-endocrine system and the immune system not only interact with each other but also use common biochemical signals. The solution of this common “language” has be-come possible with the help of the most recent advances of molecular biology and genetics. At present , we do not know yet all the details of this multifaceted interaction, but our current knowledge is enough for declaring that not separated systems but an integrated psycho-neu-ro-endocrine-immune system is responsible for the preservation of the organism’s homeosta-sis [29–31]. The interactions of the immune system were attributed to substances produced by it, the lymphokines. In recent years, however, it turned out that lymphokines are pro-duced not only by the cells of the immune system but also by the cells of the neuro-endocrine system, and therefore today these information-forwarding substances are called cytokines. Cytokines are polypeptide type molecules which specifi cally bind to the receptors on the cells’ surface and modify their function. In contrast to the hormones, cytokines exert their effects mostly by a paracrine or autocrine way. It should be mentioned, however, that some-times there are overlaps in the effects of hormones and cytokines. This means that cytokines can be detected in the peripheral circulation and they may behave like hormones (e.g. inter-leukin 6 stimulates the hypothalamo-pituitary axis most intensively), on the other hand there are hormones (e.g. prolactin, ACTH and TSH) that may act as cytokines in the tissues. The basic approach of holistic medicine means that it studies the physiological and patho-logical mechanisms of the organism as an integral whole. By solving the code of a language that integrates regulation in the human body, research has opened a new direction in medi-cine. Numerous examples for interactions between systems previously thought to be auto-nomic can be mentioned from everyday practice. Hormones (steroids, prolactin and hor-mones of the thyroid gland) infl uence the physiological and pathological function of the immune system, and monoclonal antibodies against cytokines are suitable for curing endo-crine diseases of autoimmune pathomechanism in the daily praxis [22]. The most recent re-sults show that various parts in the brain co-ordinate in different ways the maturation and functioning of immune cells, and the “homunculus” model created on the basis of this indi-cates which cerebral areas direct the maturation and activation of the immune system [25, 29, 30] (Fig. 1).
REVIEWS
CEMED 25 2010 ▪ Volume 4, Number 1

Fig. 1 Major sites of regulation of the immune system in the central nervous system
1
2
3
4
5
6
1
2
345
6
Theoretical and Clinical Fundamentals of the Association of Organ-Specifi c Autoimmune Endocrine DiseasesHashimoto’s thyroiditis is a chronic infl ammation in which the destructive autoimmune (hu-moral and cellular) process injures the acinar cells of the thyroid and may result in the devel-opment of hypothyroidism. The disease is a typical form of organ-specifi c autoimmune en-docrinopathies in which the presence of autoantibodies was fi rst demonstrated. It is important to understand the pathomechanism of the disease because it may serve as a basis for under-standing the development of other endocrinopathies of autoimmune origin. AT can be elicited not only experimentally, but it also occurs spontaneously. This model helped to obtain knowl-edge of immunologic and immunogenetic factors that are signifi cant in the evolution of the disease. It succeeded to breed a strain from the Cornell chicken, the OS in which an illness similar to Hashimoto’s thyroiditis develops at the age of 8–10 weeks; the titre of anti-thyroid antibodies also increases and the animals become hypothyroid. In these animals, the develop-ment of the symptoms of thyroiditis was hindered by neonatal bursectomy or administration of androgen hormone, and it was made earlier and more severe by thymectomy. It has also been revealed that the evolution of the disease is infl uenced by genetic factors as well. Locus B which codes the tissue antigens in chicken is determinant in the development of the disease as in animals of B1B1 and B1B4 genotype the lymphocytic infi ltration of the thyroid is marked at the age of 6–10 weeks, and there is a concomitant elevation in the titre of anti-Tg antibodies. Animals with the B4B4 genotype, however, get the illness less frequently. In hu-man AT, it has been demonstrated that the damage of thyrocytes is a complex process consist-ing of several steps wherein, in addition to the immunologic, immunogenetic factors, epige-netic and environmental factors also play a role [6, 7] (Fig. 2).
2010 ▪ Volume 4, Number 1 26 CEMED
REVIEWS

Fig. 2 Outline of the pathomechanism of autoimmune thyroiditis
In addition to Tg, several thyroidal antigens are known as having relevance in autoim-mune pathomechanism. TPO, sodium iodine symporter (NIS) and anti-deiodinase antibodies also play a role in the infl ammatory processes. Of the autoantibodies, anti-Tg antibodies are known to impair thyrocytes via their antibody-dependent cytotoxicity and anti-TPO antibod-ies are known to bind complement and have direct toxicity, while some of them are also ca-pable of inhibiting the TPO enzyme. The role of apoptosis induced by the autoimmune proc-esses (Fas–Fas ligand) and biological mediators belonging to the TNF cytokine family and substances which bind them (ligands) (TRAIL = TNF-related apoptosis-inducing ligands) has been supported by a growing number of experimental data [31–34]. The importance of genetic factors in AT has been underlined by data of literature demonstrating the familial ac-cumulation of the disease [20]. Investigation of HLA antigens confi rmed that ATs form groups that are also genetically different. Increases in the frequencies of HLA DR3 or HLA DR5 were found in Hashimoto’s thyroiditis or in post partum thyroiditis (PPT) and atrophic thy-roiditis, respectively. It has been demonstrated that DR3 and DQ8 alleles are susceptible while DR2, DR4 and DQ6 alleles are resistant to the disease. The CTLA-4 is known to be important in the development of immune tolerance as the CTLA-4 molecule inhibits T cell proliferation. Some alleles of the CTLA-4 gene (G49) indicate an increased susceptibility to the disease; however, the question why AT is the autoimmune disease that develops cannot be answered yet. Therefore, in addition to the “common genes” responsible for autoimmu-nity, thyroid-specifi c genes are sought for, of which primarily the Tg-specifi c ones seem to be important. The investigation succeeded in fi nding the gene of susceptibility to AT in the vi-cinity (8q24) of the locus of Tg gene (chromosome 8) and it also turned out that individual point mutations of Tg (SNPs) increase susceptibility to the disease to varying extents. In ad-
REVIEWS
CEMED 27 2010 ▪ Volume 4, Number 1

dition to the genetic background, the so-called epigenetic factors have an increasingly strong reason for demonstrating that hereditary mechanisms not coded in DNA sequences are also responsible for the particular autoimmune diseases that will develop in a given patient [10, 16, 22, 24, 25]. On the basis of most recent observations on twins, we can accept as demon-strated that also environmental factors have a determinant role in the genesis of AT, i.e. in identical, monozygotic twins, the genetic disposition was estimated to be only 46–89% [20, 21]. Of the environmental factors, iodine has a determinant role, and as it has also been demonstrated by the program of WHO against iodine defi ciency, iodine supplementation has led not only to the prevention of congenital iodine-defi cient state but also to an increase in the number of patients with AT. The thyroiditis-provoking effect of increased iodine intake was related partly to the elicited changes in the antigenicity of autoantigens (e.g. Tg), partly with an increased expression of autoantigens and antigen transfer. Viral and bacterial infections are supposed to be able to induce the disease, but this could not be demonstrated so far [21, 32]. Observations demonstrating the association between the individual diseases of au-toimmune pathogenesis are important both from theoretical and practical aspects. The impor-tance of the issue lies in the fact that until now only the abnormal functioning of the “immune response genes” was thought to be responsible for the development of autoimmune diseases. The study of autoimmune polyendocrine syndrome type 1 (APS-1) revealed the existence of the so-called AIRE, the mutation or alleles of which are responsible for the specifi c associa-tion of the diseases. This discovery started a trend in genomic research which looks for po-tential mutations also in the evolution of individual endocrinopathies. The previous opinion that autoimmune diseases were limited to one organ each has become outdated. Particular associations of systemic autoimmune diseases and organ-specifi c forms occur frequently, causing variety, diversity of diseases. Research on this group of diseases bears special practi-cal signifi cance because it calls the attention of the clinicians to the often different associa-tions of individual diseases and by this way it makes the frequently thorny path to diagnosis and therapy easier. It is a characteristic example of the association of autoimmune diseases when AT is either accompanied or followed by autoimmune gastritis, pernicious anaemia, IDDM, Addison’s disease or hypadrenia [32–35].
Clinical Forms of APSAPS means the association of several endocrine diseases of autoimmune pathogenesis. Accordingly, the following classifi cation has been accepted (Table 1).
The fi rst APS was described very probably by Addison in 1855, although he did not know that he found a specifi c group of diseases. Later, after the description of the individual entities, the current classifi cation was recommended by Neufeld et al. in 1980 [35–37]. These diseases were considered previously as “idiopathic” and the present classifi cation could only be created after the recognition of autoimmunity. Elaboration and use of the criteria of Witeb-sky et al. and then of Rose and Bona to endocrine diseases of autoimmune origin were fun-damental for a better understanding of the condition’s nature [5–7, 38–42] (Table 2).
Recognition of the endocrine background provided new information not only on the evolution of diseases but also on the causes of associations. Common cellular and humoral mechanisms against the shared epitopes are responsible for the more frequent associated oc-currence of certain conditions.
2010 ▪ Volume 4, Number 1 28 CEMED
REVIEWS
APS-1Defi nition: it means the association of at least two of the three diseases mentioned below (Table 3).
Table 2 Evidences of autoimmune disease
• Direct evidence(s): passive transfer of the disease with autoantibodies or autoreactive T cells
• Indirect evidence: reproduction of the disease under experimental conditions
• Secondary evidence(s): lymphocytic infi ltration in the target organ, association with another autoimmune dis-ease, correlation with HLA antigens, benefi cial therapeutic effect of immunoregulation
Table 3 Major components of APS-1
• Chronic mucocutaneous candidiasis (manifesting at the age of about 5 years)
• Chronic hypoparathyroidism (paraesthesia, Chvostek–Trousseau signs, EMG signs, dry skin, nail deformities)
• Addison’s disease (at the age between 6 month and 40 years, mean: 14.6 years) (hyperpigmentation, hypoglycae-mia, weight loss, adynamia, hypotonia, diarrhoea, nausea – coma)
The disease also had other known names previously. Of those the most frequently used was APECED, or Whitaker’s syndrome. The disease begins in childhood; its fi rst sign is chronic candidiasis followed by the signs of hypoparathyroidism and then Addison’s disease [35, 37, 42, 43]. In addition to the major symptoms, minor symptoms (vitiligo, alopecia areata, coeliac disease, autoimmune hepatitis, hypogonadism, malabsorption, diabetes mel-litus, AT and chronic atrophic gastritis) appear after the age of 20 years and form the very colourful spectrum of the disease [42, 43].
Epidemiology
APS-1 is a rare disease. Its prevalence is extremely varying; it is 1:9,000 among Iranian Jews, 1:14,000 in Finland, 1:25,000 in Sardinia, 1:80,000 in Norway and 1:200,000 in Northern Italy; the female/male ratio is 1.0:2.4 [35, 37, 44] (Table 4).
Table 4 Immunological background of major APS-1 symptoms
• Candidiasis: primary T cell immunodefi ciency
• Hypoparathyroidism: anti-parathyroid antibodies, anti Ca sensor antibodies
• Addison’s disease: anti-adrenal cortex antibodies (ACA), anti-21 hydroxylase antibodies
REVIEWS
CEMED 29 2010 ▪ Volume 4, Number 1

Symptoms
In almost 100% of cases, mucocutaneous chronic candidiasis (CC), poorly responding to treatment, can be detected and it presents itself in childhood (Fig. 3).
Importantly, APS-1 underlies ~45% of cases of CC occurring in childhood. Tetany/ hypoparathyroidism and Addison’s disease can be detected in 79% and 72%, respectively. Other organ-specifi c conditions (gonadal hypofunction, vitiligo, pernicious anaemia, enamel hypoplasia, nail dystrophy and alopecia) are associated with the disease considerably less frequently. In forms with hypoparathyroidism, malabsorption should also be thought of. The infl ammation of oesophagus may be painful and it causes cicatrisation in some cases or it may induce an increase in the number of epithelial neoplasms. Chronic hypoparathyroidism manifests itself later, averagely in the age of 3 months to 15 years. The most characteristic clinical symptoms include neuromuscular disorders, signs of tetany, paraesthesia, hypotonia and malabsorption. Chvostek’s sign (spasms at the area innervated by the facial nerve, the angle of the mouth is drawn aside and the eyelid contracts) can be elicited and the Trousseau sign (contraction of tetany occurring upon strangulation of the arm for ~3–5 min) is positive. Latent tetany can be revealed by EMG. Also further signs of hypocalcaemia (dry skin, thin hair and deformities of the nails) can be observed. The signs and symptoms of Addison’s disease present themselves in the postnatal age from 6 months to 40 years and show no dif-ference in comparison with the so-called monosystemic form that is independent of APS. The marked weakness, weight loss, hypotonia, fl uid depletion and hypocalcaemic episodes are striking. Upon the effect of infection or physical and mental overload, the patient may come to a crisis. The most frequent gastrointestinal symptoms include diarrhoea, abdominal pain, nausea and vomiting. Increased pigmentation of the skin and mucous membranes (gingiva, mouth) can be observed (Fig. 4).
Fig. 3 Signs of mucocutaneous candidiasis on the oral mucosa of a patient with APS-1
2010 ▪ Volume 4, Number 1 30 CEMED
REVIEWS
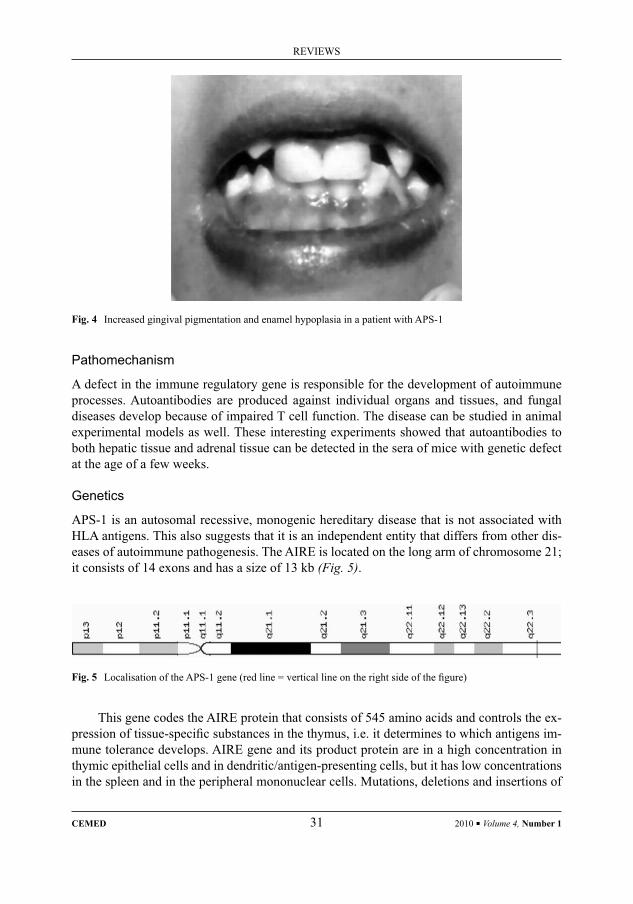
Pathomechanism
A defect in the immune regulatory gene is responsible for the development of autoimmune processes. Autoantibodies are produced against individual organs and tissues, and fungal diseases develop because of impaired T cell function. The disease can be studied in animal experimental models as well. These interesting experiments showed that autoantibodies to both hepatic tissue and adrenal tissue can be detected in the sera of mice with genetic defect at the age of a few weeks.
Genetics
APS-1 is an autosomal recessive, monogenic hereditary disease that is not associated with HLA antigens. This also suggests that it is an independent entity that differs from other dis-eases of autoimmune pathogenesis. The AIRE is located on the long arm of chromosome 21; it consists of 14 exons and has a size of 13 kb (Fig. 5).
Fig. 4 Increased gingival pigmentation and enamel hypoplasia in a patient with APS-1
Fig. 5 Localisation of the APS-1 gene (red line = vertical line on the right side of the fi gure)
This gene codes the AIRE protein that consists of 545 amino acids and controls the ex-pression of tissue-specifi c substances in the thymus, i.e. it determines to which antigens im-mune tolerance develops. AIRE gene and its product protein are in a high concentration in thymic epithelial cells and in dendritic/antigen-presenting cells, but it has low concentrations in the spleen and in the peripheral mononuclear cells. Mutations, deletions and insertions of
REVIEWS
CEMED 31 2010 ▪ Volume 4, Number 1
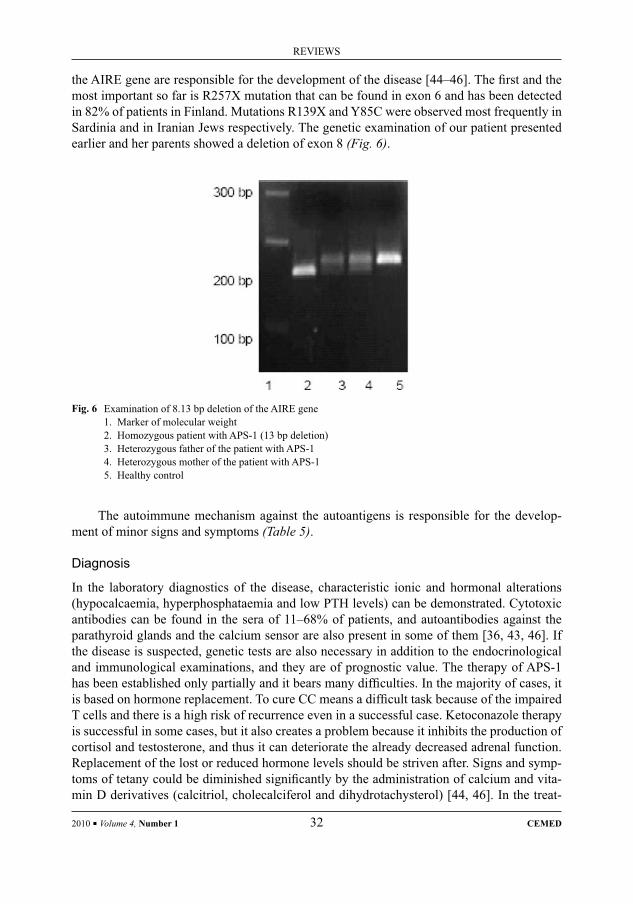
the AIRE gene are responsible for the development of the disease [44–46]. The fi rst and the most important so far is R257X mutation that can be found in exon 6 and has been detected in 82% of patients in Finland. Mutations R139X and Y85C were observed most frequently in Sardinia and in Iranian Jews respectively. The genetic examination of our patient presented earlier and her parents showed a deletion of exon 8 (Fig. 6).
Fig. 6 Examination of 8.13 bp deletion of the AIRE gene1. Marker of molecular weight2. Homozygous patient with APS-1 (13 bp deletion)3. Heterozygous father of the patient with APS-14. Heterozygous mother of the patient with APS-15. Healthy control
The autoimmune mechanism against the autoantigens is responsible for the develop-ment of minor signs and symptoms (Table 5).
Diagnosis
In the laboratory diagnostics of the disease, characteristic ionic and hormonal alterations (hypocalcaemia, hyperphosphataemia and low PTH levels) can be demonstrated. Cytotoxic antibodies can be found in the sera of 11–68% of patients, and autoantibodies against the parathyroid glands and the calcium sensor are also present in some of them [36, 43, 46]. If the disease is suspected, genetic tests are also necessary in addition to the endocrinological and immunological examinations, and they are of prognostic value. The therapy of APS-1 has been established only partially and it bears many diffi culties. In the majority of cases, it is based on hormone replacement. To cure CC means a diffi cult task because of the impaired T cells and there is a high risk of recurrence even in a successful case. Ketoconazole therapy is successful in some cases, but it also creates a problem because it inhibits the production of cortisol and testosterone, and thus it can deteriorate the already decreased adrenal function. Replacement of the lost or reduced hormone levels should be striven after. Signs and symp-toms of tetany could be diminished signifi cantly by the administration of calcium and vita-min D derivatives (calcitriol, cholecalciferol and dihydrotachysterol) [44, 46]. In the treat-
2010 ▪ Volume 4, Number 1 32 CEMED
REVIEWS

Table 5 Minor APS-1 symptoms and antibodies against autoantigens responsible for its development
• Vitiligo
Melanocyte antigen
• Coeliac disease
Reticulin, endomysium antigen
• Hypogonadism
Steroid-producing cells
17-hydroxylase enzyme antigen
P450 scc antigen
• Autoimmune hepatitis
L-K microsomal antigen
• Type 1 diabetes mellitus
ICA (islet cell antigen)
GAD (glutamate decarboxylase enzyme)
IA2 antigen
• Autoimmune thyroiditis
TPO (thyroid peroxydase enzyme)
Tg (thyroglobulin)
• Chronic atrophic gastritis
Parietal cells
H/K ATP-ase enzyme
Intrinsic factor
• Alopecia areata
Tyrosine hydroxylase
• Malabsorption
Tryptophan
ment of autoimmune hepatitis, prednisolone and azathioprine are used, but their use is considerably limited by the immune defi cient state. Until now the immunostimulant products have not normalised the impaired immune response (IR). Studies with stem cells, although they show promise, are currently in an experimental stage.
REVIEWS
CEMED 33 2010 ▪ Volume 4, Number 1

Table 6 The most important differences between APS-1 and APS-2
APS-1 APS-2
Beginning in childhood Beginning in adulthood
AIRE gene mutation detectable No AIRE gene mutation
No association with HLA Associated with HLA DR3/4
Immune defi ciency detectable No evidence of immune defi ciency
Mucocutaneous candidiasis No mucocutaneous candidiasis
APS-2The disease, previously designated by the name of Schmidt’s syndrome, is characterised by the association of Addison’s disease and IDDM/or autoimmune thyroid disease. The com-mon symptom of the condition (present in 100% of patients) is Addison’s disease, while AT (or Graves–Basedow disease) and IDDM can be found in 70% and 52% of patients, respec-tively. The association of the leading two diseases can be modulated by other illnesses. The disease is 2-3 times more common in women [31]. The disease manifests itself at the age of 30–40 years. The clinical signs and symptoms are identical with those of the individual-asso-ciated diseases.
Epidemiology
The prevalence of the disease depends on the association of the conditions examined. IDDM is associated with thyroid disease of autoimmune pathogenesis, pernicious anaemia or Ad-dison’s disease in 5.7%, 0.5% and 0.1%, respectively. At the same time, IDDM could be di-agnosed in 8–20% of patients with Addison’s disease. The incidence of APS-2 increases with advancing age [21, 35, 38, 40].
Genetics
The disease is of autosomal dominant inheritance with incomplete penetrance. Research of recent years has made it clear that in contrast to APS-1, HLA antigens and their related IR genes are decisive in this disease. This disease is signifi cantly more common in people with a haplotype of HLA-DR3/HLA-DR4 [30]. Certain HLA haplotypes (DR3 DQA1*0501 DQB1*0202 DRB1*0301 and DR4 DQA1*0301 DQB1*0302 DRB1*0401) signifi cantly increase the risk of the disease, while others (HLA DR6 DQA1*DQB1*0503 DRB1*1401) have a protective effect [10, 30]. TNF and cytotoxic T-lymphocyte 4 (CTLA-4) genes, which are associated with HLA genes, have been shown to be important in the development and inheritance of the disease [31, 32]. The substantial differences between APS-1 and APS-2 are summarised in Table 6.
2010 ▪ Volume 4, Number 1 34 CEMED
REVIEWS
APS-3This disease was originally defi ned by Neufeld as an association of Hashimoto’s thyroiditis, Graves–Basedow disease, Graves’ orbitopathy, praetibial myxoedema and one of the follow-ing autoimmune diseases [37]:– IDDM– Atrophic gastritis– Pernicious anaemia– Vitiligo– Alopecia– Myasthenia gravisIt turned out, however, that this group of diseases is considerably more complex, as the auto-immune disease of the thyroid TAD was associated with other autoimmune conditions in 28%, including Sjögren’s disease, coeliac disease, myasthenia or SLE. It has been observed that several autoimmune diseases were present in an incomplete form in more than half of patients with TAD. As patients with TAD amount to 7-8% of the population, a new classifi ca-tion was made with the essentials that it is suitable for classifying both overt and subclinical diseases [28, 32, 35, 37, 47] (Table 7).
Table 7 Classifi cation of the diseases associated with autoimmune thyroid diseases (TAD)
Autoimmune diseases of the thyroid (TAD)(Hashimoto’s thyroiditis, Graves–Basedow disease, Graves’ orbitopathy)
IDDM Autoimmune gastritis Vitiligo MCTD
Hirata disease Pernicious anaemia Alopecia areata RA
Hypophysitis IBD ITP SLE
Addison’s disease Autoimmune hepatitis Myasthenia gravis Sjögren’s disease
Hypoparathyroidism Primary biliary cirrhosis Multiple sclerosis Vasculitis
TAD-3/A(endocrine)
TAD-3/B(gastrointestinal)
TAD-3/C(haematological/dermal/neural)
TAD-3/D(systemic-collagen)
Differential Diagnosis of APSRegarding the different associations of entities observed in the individual forms of APS, dif-fi culties may emerge in differential diagnosis. Of the diseases of chromosomal origin, Turner syndrome may cause a diagnostic problem, as AT (in 30%) and other endocrinopathies may also occur in this disease. In Kearns–Sayre syndrome hypoparathyroidism, primary hypogo-nadism, IDDM and hypopituitarism can be observed as well; however, myopathy is in the foreground of the disease. Wolfram syndrome (diabetes mellitus, diabetes insipidus, optic atrophy and neural hearing loss) is a rare congenital disease that begins in childhood. POEMS syndrome may cause diagnostic diffi culty in adults. The abnormity of plasma cells and the appearance of M gradient may help in the diagnosis [47].
REVIEWS
CEMED 35 2010 ▪ Volume 4, Number 1

Diagnostic ProtocolClinical picture/course is determinant in diagnostics. Laboratory data, however, may help in the early recognition of the diseases. The following tests are recommended: TPO, Tg, TSH-R GAD65, 17-hydroxylase and 21-hydroxylase antibodies. The presence of M gradient or the absence of IgA may be detected by quantitative immunoelectrophoresis. Determination and follow-up of the levels of target organ hormones are essential not only for the diagnosis but also for monitoring the appropriateness of therapy.
Therapy and CareThe treatment is founded on infl uencing the abnormal function of immune system, improving the impaired functions and replacing the defi cient hormones. On the basis of pathomecha-nism, we should (possibly) strive for the termination of autoimmunity. This problem has been solved only in part yet. By the intake of hormones (e.g. thyroid hormones, insulin), we reduce the expression of HLA-DR molecules on the surface of target organs’ cells and mitigate the autoimmune process. The essence of this so-called isohormonal therapy can be understood best during the treatment of AT. TSH can enhance the expression of HLA-DR molecules, and thus the timely T4 and T3 therapy not only means, by reducing TSH levels, replacement of the hormones but also inhibits the autoimmune process. Products inhibiting thyroid function not only play a role in the development of euthyroidism, but by inhibiting the autoantigens, they also inhibit the autoimmune process. Timely insulin therapy also inhibits the expression of HLA-DR beta cells and restrains the destruction of the cells. For the other part of hormone replacement therapies, no immunomodulating effects have been demonstrated (e.g. increased intake of vitamin D used in hypoparathyroidism). The importance of patient care and preven-tion follows from the foregoing.
Life expectancies of patients may improve by appropriate and life-long care, and one of the main elements of this is informing the patients about the nature of their disease and that the administered medication has to be modifi ed inevitably in certain stressful situations. With an appropriate hormonal therapy women who were previously infertile can give birth to chil-dren; however, closer supervision is required during pregnancy and after delivery. The objec-tive and at the same time result of care implies that patients’ life expectancies should not worsen, but on the other hand, their quality of life should allow them, after having chosen an appropriate work, to live a life of full value [47].
ReferencesRoitt, I. M., Doniach, D., Cambell, P. N. et al.:[1] Autoantibodies in Hashimoto’s thyroiditis. Lancet, 1956, 2, 820–824.Rose, N. R., Witebsky, E.:[2] Studies in organ specifi city. Changes in the thyroid glands of rabbits following active immunization with rabbit thyroid extracts. J. Immunol., 1956, 76, 417–427.Adams, D. D., Purves, H. D.:[3] Abnormal response in the assay of thyrotropin. Proc. Univ. Otago Med. Sch., 1956, 32, 11–12.Kriss, J. P.:[4] Inactivation of long-acting thyroid stimulator (LATS) by anti-kappa, anti-lambda antisera. Clin. Endocrinol., 1968, 28, 1440–1444.
2010 ▪ Volume 4, Number 1 36 CEMED
REVIEWS

Witebsky, E., Rose, N. R., Terplan, K. et al.:[5] Chronic thyroiditis in autoimmunization. JAMA, 1957, 164, 1439–1447.Witebsky, E., Kite, J. H., Wick, G.:[6] Spontaneous thyroiditis in the obese strain chickens. Demonstration of circulating antibodies. J. Immunol., 1970, 103, 708–712.Wick, G., Kite, J. H., Witebsky, E.:[7] Spontaneous thyroiditis in the obese strain of chickens. The effect of thymectomy and thymoburesectomy on the development of the disease. J. Immunol., 1970, 104, 54–59.Kaczur, V., Vereb, Gy., Balázs, Cs. et al.:[8] Effect of anti-thyroid peroxidase (TPO) antibodies on TPO activity measured by chemiluminescence assay. Clin. Chem., 1997, 43, 1392–1399.Kifor, O., McElduff, A., Leboff, M. S. et al.:[9] Activating antibodies to the calcium-sensing receptor in two patients with autoimmune hypoparathyroidism. J. Endocrinol. Metab., 2004, 89, 548–556.Ludgate, M.:[10] The molecular genetics of three thyroid autoantigens: thyroglobulin, thyroid peroxidase and thyrotropin receptor. Autoimmunity, 1990, 7, 201–205.Mayer, A., Ploix, C., Orgazzi, J. et al.:[11] Calcium-sensing receptor autoantibodies are relevant markers of acquired hypoparathyroidism. J. Clin. Endocrinol. Metab., 2004, 89, 4484–4488.Zhang, B., Sun, Ch., Qu, Y. et al.:[12] Defi ciency of mouse CD4+ CD25+ Foxp3+ regulatory T cells in xenoge-neic pig thymus-grafted nude mice suffering from autoimmune diseases. Cell. Mol. Immunol., 2008, 5, 325–332.Wang, P. W., Liu, R. T., Hank, S. H. et al.:[13] Cytotoxic T lymphocyte-associated molecule-4 polymorphism and relapse of Graves’ hyperthyroidism after antithyroid withdrawal. J. Clin. Endocrinol. Metab., 2004, 89, 169–173.Fountoulakis, S., Vartolomantos, G., Kolaitis, N. et al.:[14] HLA-DR expressing peripheral T regulatory cells in newly diagnosed patients with different forms of autoimmune thyroid disease. Thyroid, 2008, 11, 1–6.Grimm, M., Spiecker, M., Cartina, R. et al.:[15] Inhibition of major histocompatibility complex (MHC) class II gene transcription by nitric oxide and antioxidants. J. Biol. Chem., 2002, 277, 26460–26467.Adrian, L., Daniel, H. D., Lesage, S. et al.:[16] Gene dosage-limiting role of AIRE in thymic expression, clonal deletion, and organ-specifi c autoimmunity. J. Exp. Med., 2004, 200, 1015–1026.Villiano, M. J. B., Huber, A. K., Greenberg, D. A. et al.:[17] Autoimmune thyroiditis and diabetes: dissecting the joint genetic susceptibility in a large cohort of multiplex families. J. Clin. Endocrinol. Metab., doi:10.1210, 2008–2193.Fountoulakis, S., Vartolomantos, G., Kolaitis, N. et al.:[18] HLA-DR expressing peripheral T regulatory cells in newly diagnosed patients with different forms of autoimmune thyroid disease. Thyroid, 2008, 11, 1–6.Bednarczuk, T., Gopinath, B., Ploski, R. et al.:[19] Susceptibility genes in Graves’ ophthalmopathy: searching for needle in a haystack? Clin. Endocrinol., 2007, 67, 3–19.Aust, G., Krohn, K., Morgenthaler, N. G. et al.:[20] Graves’ disease and Hashimoto’s thyroiditis in monozygotic twins: case study as well as transcriptomic and immunohistological analysis of thyroid tissues. Eur. J. Endo-crinol., 2006, 154, 13–20.Betterle, C., Lazzaratto, F., Presotto, F.:[21] Autoimmune polyglandular syndrome type 2: the tip of an iceberg? Clin. Exp. Immunol., 2004, 137, 225–233.Eisenbarth, G. S., Jackson, R. A.:[22] Immunogenetics of polyglandular failure and related disease. In: Farid, N. R. (ed): HLA in Endocrine and Metabolic Disorders. Academic Press, New York, 1984, pp. 235–264.Elfström, P., Montgomery, S. M., Kampe, O. et al.:[23] Risk of primary adrenal insuffi ciency in patients with celiac disease. J. Clin. Endocrinol. Metab., 2007, 92, 3595–3598.Yarman, S., Oguz, F., Carin, M.:[24] HLA-DRB1*03 is a susceptibility gene in patients with Graves’ disease with and without ophthalmopathy. Int. J. Immunogenet., 2007, 34, 23–25.Ogren, M. P., Lombroso, P. J.:[25] Epigenetics: behavioral infl uences on gene function, Part II: molecular mecha-nism. J. Am. Acad. Child Adolesc. Psychiatry, 2008, 48, 374–378.Esteller, M.:[26] Epigenetics in cancer. N. Engl. J. Med., 2008, 13, 1148–1158.Adrian, L., Daniel, H. D., Lesage, S. et al.:[27] Gene dosage-limiting role of AIRE in thymic expression, clonal deletion, and organ-specifi c autoimmunity. J. Exp. Med., 2004, 200, 1015–1026.Klecha, A. J., Barreiro-Arcos, M. L., Frick, L. et al.:[28] Immuno-endocrine interactions in autoimmune thyroid diseases. Neuroimmunomodulation, 2008, 15, 68–75.Silverma, M. N., Sternberg, E. M.:[29] Neuroendocrine-immune interactions in rheumatoid arthritis: mecha-nism of glucocorticoid resistance. Neuroimmunomodulation, 2008, 15, 19–28.Kadioglu, P., Acbay, O., Demir, G. et al.:[30] The effect of prolactin and bromocriptine on human peripheral im-mune status. J. Endocrinol. Invest., 2001, 24, 147–151.
REVIEWS
CEMED 37 2010 ▪ Volume 4, Number 1
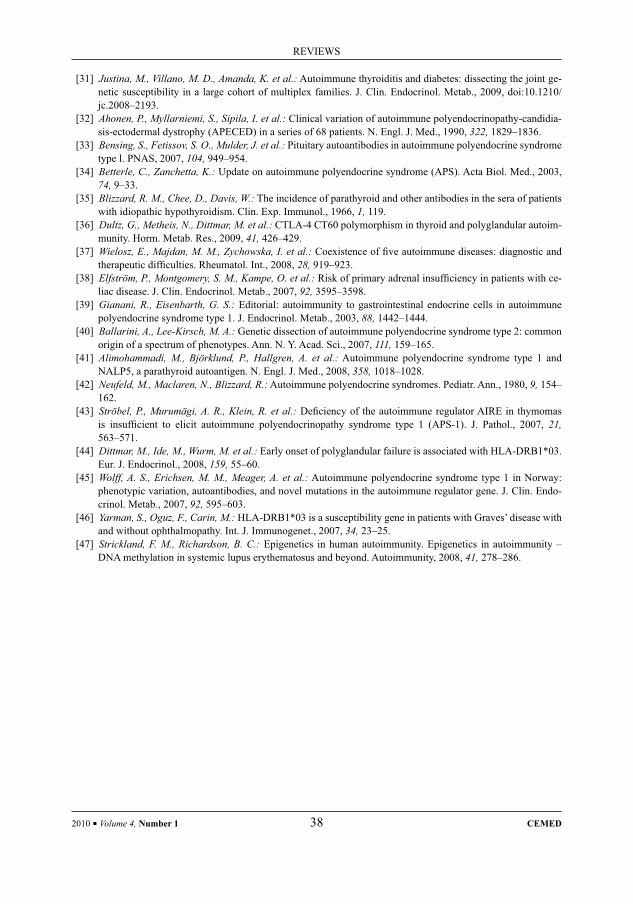
Justina, M., Villano, M. D., Amanda, K. et al.:[31] Autoimmune thyroiditis and diabetes: dissecting the joint ge-netic susceptibility in a large cohort of multiplex families. J. Clin. Endocrinol. Metab., 2009, doi:10.1210/jc.2008–2193.Ahonen, P., Myllarniemi, S., Sipila, I. et al.:[32] Clinical variation of autoimmune polyendocrinopathy-candidia-sis-ectodermal dystrophy (APECED) in a series of 68 patients. N. Engl. J. Med., 1990, 322, 1829–1836.Bensing, S., Fetissov, S. O., Mulder, J. et al.:[33] Pituitary autoantibodies in autoimmune polyendocrine syndrome type l. PNAS, 2007, 104, 949–954.Betterle, C., Zanchetta, K.:[34] Update on autoimmune polyendocrine syndrome (APS). Acta Biol. Med., 2003, 74, 9–33.Blizzard, R. M., Chee, D., Davis, W.:[35] The incidence of parathyroid and other antibodies in the sera of patients with idiopathic hypothyroidism. Clin. Exp. Immunol., 1966, 1, 119.Dultz, G., Metheis, N., Dittmar, M. et al.:[36] CTLA-4 CT60 polymorphism in thyroid and polyglandular autoim-munity. Horm. Metab. Res., 2009, 41, 426–429.Wielosz, E., Majdan, M. M., Zychowska, I. et al.:[37] Coexistence of fi ve autoimmune diseases: diagnostic and therapeutic diffi culties. Rheumatol. Int., 2008, 28, 919–923.Elfström, P., Montgomery, S. M., Kampe, O. et al.:[38] Risk of primary adrenal insuffi ciency in patients with ce-liac disease. J. Clin. Endocrinol. Metab., 2007, 92, 3595–3598.Gianani, R., Eisenbarth, G. S.:[39] Editorial: autoimmunity to gastrointestinal endocrine cells in autoimmune polyendocrine syndrome type 1. J. Endocrinol. Metab., 2003, 88, 1442–1444.Ballarini, A., Lee-Kirsch, M. A.:[40] Genetic dissection of autoimmune polyendocrine syndrome type 2: common origin of a spectrum of phenotypes. Ann. N. Y. Acad. Sci., 2007, 111, 159–165.Alimohammadi, M., Björklund, P., Hallgren, A. et al.:[41] Autoimmune polyendocrine syndrome type 1 and NALP5, a parathyroid autoantigen. N. Engl. J. Med., 2008, 358, 1018–1028.Neufeld, M., Maclaren, N., Blizzard, R.:[42] Autoimmune polyendocrine syndromes. Pediatr. Ann., 1980, 9, 154–162.Ströbel, P., Murumägi, A. R., Klein, R. et al.:[43] Defi ciency of the autoimmune regulator AIRE in thymomas is insuffi cient to elicit autoimmune polyendocrinopathy syndrome type 1 (APS-1). J. Pathol., 2007, 21, 563–571.Dittmar, M., Ide, M., Wurm, M. et al.:[44] Early onset of polyglandular failure is associated with HLA-DRB1*03. Eur. J. Endocrinol., 2008, 159, 55–60.Wolff, A. S., Erichsen, M. M., Meager, A. et al.:[45] Autoimmune polyendocrine syndrome type 1 in Norway: phenotypic variation, autoantibodies, and novel mutations in the autoimmune regulator gene. J. Clin. Endo-crinol. Metab., 2007, 92, 595–603.Yarman, S., Oguz, F., Carin, M.:[46] HLA-DRB1*03 is a susceptibility gene in patients with Graves’ disease with and without ophthalmopathy. Int. J. Immunogenet., 2007, 34, 23–25.Strickland, F. M., Richardson, B. C.:[47] Epigenetics in human autoimmunity. Epigenetics in autoimmunity – DNA methylation in systemic lupus erythematosus and beyond. Autoimmunity, 2008, 41, 278–286.
2010 ▪ Volume 4, Number 1 38 CEMED
REVIEWS

The Pulmonological Manifestations of Rheumatoid Arthritis
GYÖRGY BERNSCHERER1, CSABA KARABÉLYOS2, ZSOLT TARJÁN3
1Bernscherer és Tsa. Bt., Budapest, Hungary2Biotest Hungaria Kft., Törökbálint, Hungary
3Raditec Kft., Budapest, Hungary
In their review article, the authors overview the primary and secondary pulmonary complications of rheumatoid arthritis (RA) with the help of bibliographic data. They emphasize the pulmonological complications of disease-modifying antirheumatic drugs (DMARDs) used for the pharmaceutical therapy of RA, of which they discuss the methotrexate-induced pulmonary diseases. Methotrexate is used in nearly all additive double and triple – O’Dell-scheme – combined DMARDs therapy, because of which the early detection of drug-induced pulmonological com-plications is important. For rheumatologists, the treatment of methotrexate-resistant RA is proving to be a great challenge. The biological therapeutical drugs act as cytokine antagonists by blocking the TNF-α and, compared to DMARDs, they can more effectively inhibit the progression of the disease. These are the biological response modi-fi ers. Their main representatives are infl iximab, adalimumab, and etanercept. At the end, the authors discuss the bio-logical response modifi ers caused secondary pulmonary complications, e.g. the biological response modifi ers asso-ciated pulmonary tuberculosis, bacterial tracheobronchitis, bacterial pneumonia, bronchiectasia, pulmonary oedema, rapid fi brotising alveolitis, and coccidiomycosis. At 3% of the biological response modifi ers treated RA patients living in Arizona, California, Nevada, the pulmonary and disseminated mycosis – coccidiomycosis can appear with a 15% mortality. As a consequence of frequent earthquakes, the spores rising from the ground into the air infect the biological response modifi ers treated immunosuppressed patients. The authors are attentive to the fact that patients who travel to the aforementioned endemic or earthquake-active regions while receiving biological therapy are at potentially higher risk, and because of this, their consulting a doctor is indispensable. Studies and use of newer groups of biological response modifi ers medicines are awaited in the near future for RA. Nowadays in patients who are nonreactive for TNF-α inhibitor treatment, the use of B-lymphocyte inhibitor rituximab, characteristic in non-Hodgkin lymphoma therapy, is possible. The pulmonary complications of RA therapy of cytokine are not yet known. Antirheumatic therapy nowadays causes a signifi cant improvement in the quality of patients’ lives, while an increas-ing number of modern therapeutical methods cause more complications.
Keywords: rheumatoid arthritis, primary pulmonological complication, secondary pulmonologic manifestation, disease-modifying antirheumatic drugs, biologic response modifi ers, TNF-α inhibitor, infl iximab, adalimumab, etanercept, rituximab, coccidiomycosis, earthquake
Abbreviations
AM = articular manifestation; BAL = bronchoalveolar lavage; BRM = biologic response modifi ers; BOOP = bron-chiolitis obliterans organizing pneumonia; DILD = diffuse interstitial lung disease; DLST = drug lymphocyte stimu-lation test; DMARD = disease-modifying antirheumatic drug; EAM = extra-articular manifestation; FA = fi brosing alveolitis; HRCT = high-resolution CT; ILD = interstitial lung disease; IPP = interstitial plasmocytic pneumonia; LIP = lymphoid interstitial pneumonia; MAC = mycobacterium avium complex; MTX = methotrexate; NSIP = non-specifi c interstitial pneumonia; RA = rheumatoid arthritis; RF = rheuma factor; TBB = transbronchial lung biopsy; UIP = usual interstitial pneumonia
Corresponding address: György Bernscherer MD, Bernscherer és Tsa. Bt., Budapest, Hungary.E-mail: [email protected]
28385
REVIEWS
DOI: 10.1556/CEMED.4.2010. 39 2010 ▪ Volume 4, Number 1 ▪ 39–47.

IntroductionRA is prevalent in 1% of the whole population. Almost 40% of the patients experience some EAM. The second most common EAM in 5% of all patients is pulmonary disease. The prev-alence of EAM in different geographical areas and ethnic groups is highly variable, but the frequency of incidents is almost constant (Table 1) [1].
Table 1 Extra-articular manifestations in order of prevalence
Sjögren’s syndrome 11%
Pulmonary manifestation 5%
Raynaud’s phenomenon 3%
Livedo reticularis 5%
Carpal tunnel syndrome 3%
Vasculitis 1%
Amyloidosis 1%
Felty’s syndrome 0.3%
AM is usually associated with the presence of IgM RF isotype. However, EAM is more common in RF positive patients; its occurrence can be attributed to IgA RF isotype [2]. The presence of IgA isotype in patients with EAM induces excess mortality, which is increased by smoking – irrespective of the pulmonary status of the patient [3]. In some cases, at fi rst the patient experiences EAM, especially interstitial pneumonia, not AM.
A biopsy made in this early stage produces the histopathologic fi nding of UIP. This early diagnosis can only be altered later when the autoimmune disorders become more evi-dent. This way, the patient will be labeled with the specifi c diagnosis of RA associated inter-stitial pneumonia from the group of NSIP, and adequate treatment will be available. The histological classifi cation of interstitial pneumonia with an unknown reason is best described in the comprehensive publication of Miklos Zsiray [4].
Primary Pulmonary Complications of Rheumatoid ArthritisPrimary pulmonary complications can be suspected when non-productive cough and effort dyspnoea are observed. As a result of inability to move and avoidance of physical activity, dyspnoea is usually not detected. Table 2 lists the primary pulmonary complications of RA. Pleuritis is described in clinically active patients with high titer of RF, mostly without fever. Five percent of patients have usually unilateral exudative thoracic effusion with lymphocyte dominance. The titer of RF in thoracic punctate is almost equivalent with the titer of RF in serum.
2010 ▪ Volume 4, Number 1 40 CEMED
REVIEWS
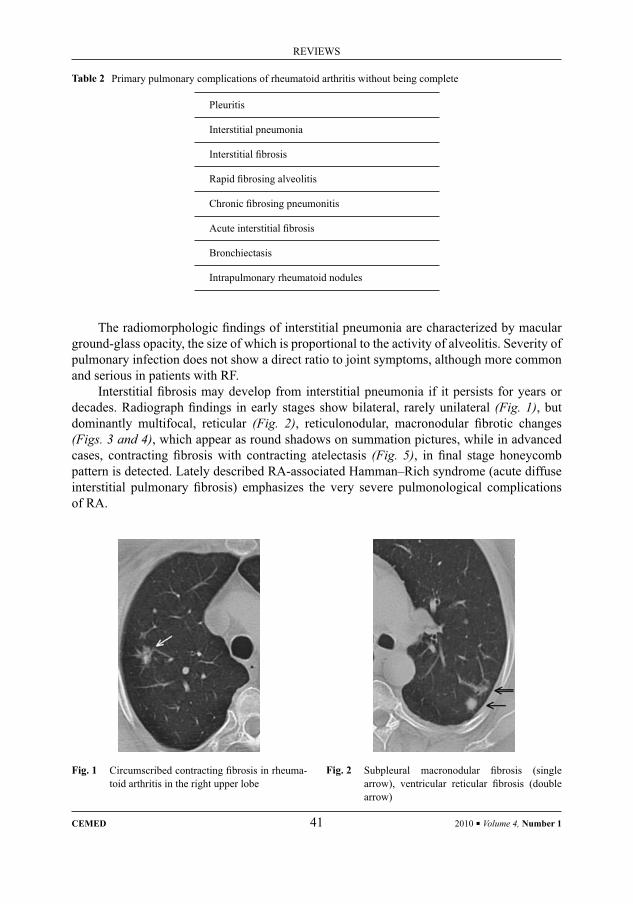
The radiomorphologic fi ndings of interstitial pneumonia are characterized by macular ground-glass opacity, the size of which is proportional to the activity of alveolitis. Severity of pulmonary infection does not show a direct ratio to joint symptoms, although more common and serious in patients with RF.
Interstitial fi brosis may develop from interstitial pneumonia if it persists for years or decades. Radiograph fi ndings in early stages show bilateral, rarely unilateral (Fig. 1), but dominantly multifocal, reticular (Fig. 2), reticulonodular, macronodular fi brotic changes (Figs. 3 and 4), which appear as round shadows on summation pictures, while in advanced cases, contracting fi brosis with contracting atelectasis (Fig. 5), in fi nal stage honeycomb pattern is detected. Lately described RA-associated Hamman–Rich syndrome (acute diffuse interstitial pulmonary fi brosis) emphasizes the very severe pulmonological complications of RA.
Table 2 Primary pulmonary complications of rheumatoid arthritis without being complete
Pleuritis
Interstitial pneumonia
Interstitial fi brosis
Rapid fi brosing alveolitis
Chronic fi brosing pneumonitis
Acute interstitial fi brosis
Bronchiectasis
Intrapulmonary rheumatoid nodules
Fig. 1 Circumscribed contracting fi brosis in rheuma-toid arthritis in the right upper lobe
Fig. 2 Subpleural macronodular fi brosis (single arrow), ventricular reticular fi brosis (double arrow)
REVIEWS
CEMED 41 2010 ▪ Volume 4, Number 1

Fig. 3 Round shadow imitating but diffuse macronodular fi brosis
Fig. 4 Macronodular fi brosis Fig. 5 Severe, contracting fi b-rosis with contracting at-electasis
Intrapulmonary rheumatoid nodules are benign, with rare changes, which is problem-atic from a differential diagnostic aspect. Rheumatoid nodules may persist for years or de-cades. They can be spontaneously absorbed, while in some cases, only their central part is absorbed, and becoming cavernous, they again cause differential diagnostic problems. Bron-chiolitis obliterans is a rare pulmonary manifestation of RA, causing progressive, irreversible airway obstruction. HRCT of the lungs shows scattered centrilobular micronodules with mu-coid impaction and hyperinfl ation [5].
Secondary Pulmonary Complications, Occurring on the Basis of Primary Pulmonary ChangesMycobacteriosis can develop when RA associated interstitial pneumonia is superinfected with MAC. Manifestation is due to the decrease of the local pulmonary defence mechanism, and as a result, the originally nonpathogenic mycobacterium evokes disease, with secondary nonproductive cough, dyspnoea, and haemoptoe. The radiomorphologic pattern shows infi l-trative shadow with cavity [6]. Secondary amyloidosis can accompany RA, during which a liver-produced acute protein or fi brous protein named amyloid-A will deposit in the paren-chyma of the lung. This is the so-called diffuse alveolar-septal amyloidosis, with a signifi cant reticulonodular pattern. In some cases, the amyloid plaques provoke local bronchial stenosis and bronchiectasis accompanied by secondary haemoptoe in the submucosal area of the tra-cheobronchial system. Amyloid cancer, which sometimes causes haemoptoe, can appear as a multiplex and solitary round shadow, leading to differential diagnostical diffi culty. Cells ob-tained from biopsy, after Congo red staining, under polarizing microscope show the signifi -cant green birefringence of amyloid. Only RA-patients with genetically-impaired amyloid-A metabolism suffer from secondary amyloidosis.
2010 ▪ Volume 4, Number 1 42 CEMED
REVIEWS

In case of Caplan syndrome (rheumatoid pneumoconiosis), silicosis leads to more se-vere pulmonary changes in patients with RA. Prevalence of RF in patients with silicosis is higher than average. Radiological feature of rheumatoid pneumoconiosis is characterized by multiplex centrally necrotizing pulmonary round shadows with a diameter of 0.5–5 cm. Al-most all of the mentioned secondary pulmonary complications are accompanied by haemop-toe. So in treating haemoptoe in patients with RA, these clinical features should be consid-ered, too. Secondary pulmonary complications developed on the basis of primary pulmonary changes are summarized in Table 3.
Table 3 Secondary pulmonary complications, occurring on the basis of primary pulmonary changes without being complete
RA associated interstitial pneumonia superinfected with MAC
RA associated pulmonary amyloidosis
RA associated bronchiectasis
RA associated pulmonary vasculitis with secondary hypertension in pulmonary circulation
Rheumatoid pneumoconiosis
Bronchiolitis obliterans
Secondary Pulmonary Complications as the Results of Drug Treatment of Rheumatoid ArthritisIn the last few years, a considerable change of attitude can be observed in treating RA with drugs as structural joint destruction is detectable even in the very early stage. DMARDs should be given intensively as soon as the diagnosis of RA is certain. The commonly used conventional DMARDs are listed in Table 4. Intensive treatment includes administration of
Table 4 Conventional DMARDs
Methotrexate
Lefl unomide
Chloroquine
Sulfasalazine
Cyclosporine-A
Azathioprine
Cyclophosphamide
Aurothiomalate
REVIEWS
CEMED 43 2010 ▪ Volume 4, Number 1
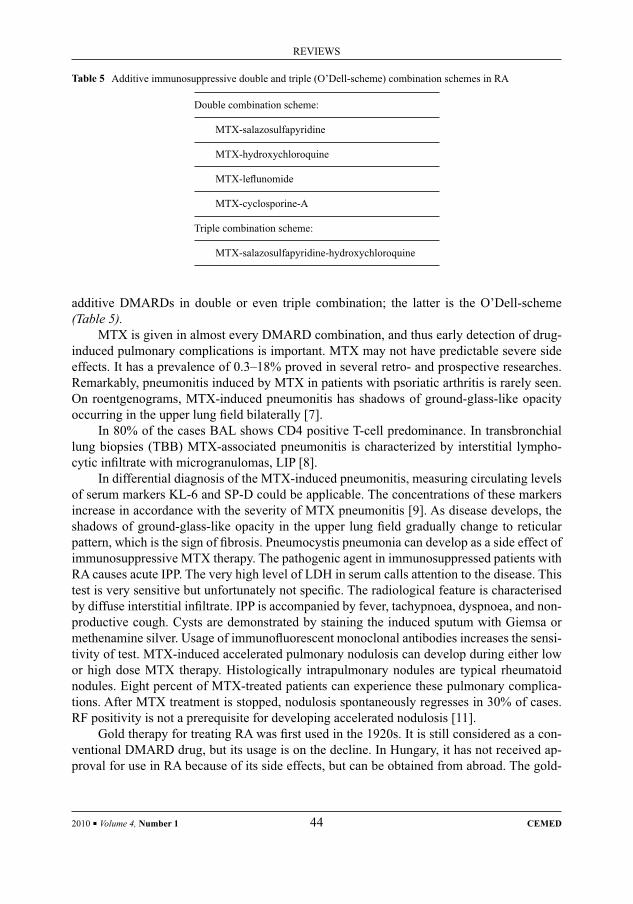
Table 5 Additive immunosuppressive double and triple (O’Dell-scheme) combination schemes in RA
Double combination scheme:
MTX-salazosulfapyridine
MTX-hydroxychloroquine
MTX-lefl unomide
MTX-cyclosporine-A
Triple combination scheme:
MTX-salazosulfapyridine-hydroxychloroquine
additive DMARDs in double or even triple combination; the latter is the O’Dell-scheme (Table 5).
MTX is given in almost every DMARD combination, and thus early detection of drug-induced pulmonary complications is important. MTX may not have predictable severe side effects. It has a prevalence of 0.3–18% proved in several retro- and prospective researches. Remarkably, pneumonitis induced by MTX in patients with psoriatic arthritis is rarely seen. On roentgenograms, MTX-induced pneumonitis has shadows of ground-glass-like opacity occurring in the upper lung fi eld bilaterally [7].
In 80% of the cases BAL shows CD4 positive T-cell predominance. In transbronchial lung biopsies (TBB) MTX-associated pneumonitis is characterized by interstitial lympho-cytic infi ltrate with microgranulomas, LIP [8].
In differential diagnosis of the MTX-induced pneumonitis, measuring circulating levels of serum markers KL-6 and SP-D could be applicable. The concentrations of these markers increase in accordance with the severity of MTX pneumonitis [9]. As disease develops, the shadows of ground-glass-like opacity in the upper lung fi eld gradually change to reticular pattern, which is the sign of fi brosis. Pneumocystis pneumonia can develop as a side effect of immunosuppressive MTX therapy. The pathogenic agent in immunosuppressed patients with RA causes acute IPP. The very high level of LDH in serum calls attention to the disease. This test is very sensitive but unfortunately not specifi c. The radiological feature is characterised by diffuse interstitial infi ltrate. IPP is accompanied by fever, tachypnoea, dyspnoea, and non-productive cough. Cysts are demonstrated by staining the induced sputum with Giemsa or methenamine silver. Usage of immunofl uorescent monoclonal antibodies increases the sensi-tivity of test. MTX-induced accelerated pulmonary nodulosis can develop during either low or high dose MTX therapy. Histologically intrapulmonary nodules are typical rheumatoid nodules. Eight percent of MTX-treated patients can experience these pulmonary complica-tions. After MTX treatment is stopped, nodulosis spontaneously regresses in 30% of cases. RF positivity is not a prerequisite for developing accelerated nodulosis [11].
Gold therapy for treating RA was fi rst used in the 1920s. It is still considered as a con-ventional DMARD drug, but its usage is on the decline. In Hungary, it has not received ap-proval for use in RA because of its side effects, but can be obtained from abroad. The gold-
2010 ▪ Volume 4, Number 1 44 CEMED
REVIEWS
Table 6 Secondary pulmonary complications caused by conventional DMARDs
Methotrexate-induced pneumonitis
Methotrexate-induced pulmonary fi brosis
Methotrexate-induced pneumocystis pneumonia
Methotrexate-induced accelerated pulmonary nodulosis
Gold-induced bacterial pneumonia
Gold-induced pulmonary fi brosis
Gold-induced bacterial pneumonia
Gold-induced pulmonary oedema
Cyclosporine-A-induced pneumocystis pneumonia
induced risk of parenchymal complications is higher in HLA-DR3 antigen positive patients [12]. The radiological morphology of gold-induced pneumonitis and gold lung is character-ized by diffuse small nodular and reticular shadows. To confi rm the diagnosis, sometimes DLSTs are necessary [13]. Gold-induced hypogammaglobulinaemia can cause prolonged bacterial pneumonia and pulmonary oedema [14].
Table 6 shows the secondary pulmonary complications of conventional DMARDs. Rheumatologists face the growing challenge in treating RA patients resistant to MTX. The use of biologic therapeutical drugs acting as cytokine antagonists led to unexpected success. These drugs slow down the progression of RA more effectively than conventional DMARDs. In Hungary, at the time of going to press, four BRM are available, which are effective by blocking TNF-α.
In the near future, new cytokine antagonists will become available. When resistance to MTX is observed, infl iximab is the fi rst to be used. Paradoxically, infl iximab added simulta-neously with MTX minimizes the synthesis of antibodies against infl iximab. When therapeu-tical response is not adequate due to synthesis of antibodies, adalimumab or etanercept can be administered. BRM therapy can reactivate latent tuberculosis infection, and so screening is compulsory before the initiation of treatment, which includes the Koch tests of direct and cultured sputum, tuberculin skin test and chest X-rays as well.
At 3% of RA patients treated with BRM living in Arizona, California, and Nevada pulmonary and disseminated mycosis – coccidiomycosis – can appear with a 15% of mortal-ity. As a consequence of frequent earthquakes, the spores rising from the soil into the air in-fect the BRM treated immunosuppressed patients. In these areas, beside chest X-ray exami-nation and tuberculin skin test, serologic testing of coccidiomycosis is necessary prior to the therapy. Seropositivity means contraindication for therapy. BRM treated patients travelling to endemic regions are at high risk, so their consulting a doctor is indispensable.
Recurrent bacterial infections of the airways experienced in patients treated with BRM may lead to susceptibility to bronchiectasis. BRM treatment is not appropriate for patients
REVIEWS
CEMED 45 2010 ▪ Volume 4, Number 1
Table 7 Secondary pulmonary complications caused by biologic response modifi ers (BRM)
BRM associated pulmonary tuberculosis
BRM associated bacterial tracheobronchitis
BRM associated bacterial pneumonia
BRM associated bronchiectasis
BRM associated pulmonary oedema
BRM associated rapid progressive fi brosing pneumonitis
BRM associated coccidiomycosis
with bronchiectasis and RA. BRM therapy may aggravate the already existing congestive heart failure, and therefore is not recommended for patients in stages III, IV of NYHA. The pulmonary complications of BRM therapy are summarised in Table 7.
In the near future, new members of BRM will be tested and applied for treating RA.At the moment, in patients who are nonreactive for TNF-α inhibitor treatment, ritux-
imab – a monoclonal antibody against B cell CD20 antigen, commonly used for treating non-Hodgkin’s lymphomas – can be effective. The pulmonary complications of this cytokine are not yet known. The advanced antirheumatic therapies can signifi cantly improve the pa-tients’ quality of life; however, practitioners encounter the pulmonary complications of these modern medications. By tracing the history of the patient, important conclusions can be drawn concerning the primary and secondary pulmonary complications of RA. Examinations should include not only conventional chest radiography and laboratory tests but HRCT, BAL, transthoracal, and surgical lung biopsies as well.
ConclusionsThe summary did not aim to cover all aspects of this extensive topic or deal with treatments of diseases and their complications. It only wanted to give assistance to the differential diag-nosis of the pulmonary complications caused by RA.
AcknowledgmentsThe authors would like to express their gratitude to the general practitioners working in the XVIIIth district of Budapest for sending the patients to their institute/National Health Service XVIIIth district, T.B. clinic, as well as to the colleagues at the Institute, Sági Péterné and Ludvig Istvánné, because without their help this review would not have been possible.
2010 ▪ Volume 4, Number 1 46 CEMED
REVIEWS
ReferencesCalgüneri, M., Ureten, K., Akif Oztürk, M.:[1] Extra-articular manifestations of rheumatoid arthritis: results of a university hospital of 526 patients in Turkey. Clin. Exp. Rheumatol., 2006, 24, 305–308.Jónsson, T., Arinbjarnarson, S., Thorsteinsson, J.:[2] Raised IgA rheumatoid factor (RF) but not IgM RF or IgG RF is associated with extra-articular manifestations in rheumatoid arthritis. Scand. J. Rheumatol., 1995, 24, 372–375.Turesson, C., Jacobsson, L. T.:[3] Epidemiology of extra-articular manifestations in rheumatoid arthritis. Scand. J. Rheumatol., 2004, 33, 65–72.Zsiray, M.:[4] Classifi cation of lung fi broses. Clinical evaluation of histological identifi cations of interstitial pneumonias with unknown reason. LAM, 2003, 13, 427–432.Kase, C., Okubo, M., Yamasaki, M.:[5] Minocycline for the treatment of bronchiolitis obliterans associated with rheumatoid arthritis. Ryumachi, 2001, 41, 745–750.Kobashi, Y., Miyashita, N., Niki, Y.:[6] A case of pulmonary mycobacterium avium complex disease complicat-ed by interstitial pneumonia with collagen vascular disease. Kekkaku, 2003, 78, 487–490.Miwa, Y., Kaga, S., Hanaoka, R.:[7] A case of rheumatoid arthritis complicated with a pneumonitis during con-comitant treatment with methotrexate and bucillamine. Ryumachi, 2002, 42, 70–75.Leduc, D., De Vuyst, P., Lheureux, P.:[8] Pneumonitis complicating low-dose methotrexate therapy for rheuma-toid arthritis. Discrepancies between lung biopsy and bronchoalveolar lavage fi ndings. Chest, 1993, 104, 1620–1623.Miyata, M., Sakuma, F., Fukaya, E.:[9] Detection and monitoring of methotrexate-associated lung injury using serum markers KL-6 and SP-D in rheumatoid arthritis. Intern. Med., 2002, 41, 467–473.Tierney, Jr. L. M., McPhee, S. J., Papadakis, M. A.:[10] Current Medical Diagnosis and Treatment, 5th Hungarian Edition. Melania Publishing Ltd., 2003, pp. 1485–1487.Kerstens, P. J., Boerbooms, A. M., Jeurissen, M. E.:[11] Accelerated nodulosis during low dose methotrexate therapy for rheumatoid arthritis. An analysis of ten cases. J. Rheumatol., 1992, 19, 867–871.Berkow, R., Fletcher, A. J.:[12] MSD Medical Handbook (The Merck Manual). Melania Publishing Ltd., 1994, pp. 1309–1310.Bando, M., Takishita, Y., Bando, H.:[13] A case of gold-induced pneumonitis showing a positive reaction in the drug lymphocyte stimulation test (DLST) for gold. Nihon Kyobu Shikkan Gakkai Zasshi, 1992, 30, 128–132.Takahashi, S., Fujita, M., Saga, T.:[14] A case of rheumatoid arthritis complicated with prolonged pneumonia and pulmonary oedema possibly caused by gold sodium thiomalate-induced hypogammaglobulinaemia. Nippon Naika Gakkai Zasshi, 1988, 77, 1040–1045.
REVIEWS
CEMED 47 2010 ▪ Volume 4, Number 1

The Mechanism of the Development of Pain Perception
New Results in the Neurophysiology of Pain Relating to Neuroscience
JUDIT GYULAHÁZI1, 2
1Department of Anaesthesiology and Intensive Therapy, Medical School and Health Science Center, University of Debrecen, Debrecen, Hungary
2The Doctors’ Training School, Eötvös Loránd University, Budapest, Hungary
Pain, as a subjective content of consciousness, is an essential attention-calling sign that helps to survive. It is oblig-atory for every physician to relieve pain, but pain is different in each individual, which makes analgesia diffi cult to carry out. Improving neuroimaging techniques have made it possible for us to have a better understanding of the neural processes accompanying the development of pain perception. On the basis of 24 articles found as a result of the search on PubMed for keywords “pain” and “neuroimaging”, here we review the various parts of the pain neuron matrix, their tasks and the assumed mechanism of the shaping of acute pain perception. The shaping of individual pain perception is regulated by the modular function of the medial part of the pain matrix, cognitive regulation in-cluding attention, preliminary expectations, re-evaluation, and by affective regulation. Experimental results of em-phatic pain suggest that pain perception may also occur without a real, tissue-damaging stimulus. In case of chronic pain, the induction of nociception, due to a steady, tangible conversion of the pain neuron matrix as well as due to its changed function, the induction of the perception of the pain will modify.
Keywords: pain sensation, neuroimaging, pain network, empathy, chronic pain
Abbreviations
ACC = anterior cingulate cortex; A = amygdala; HIP = hippocampus; 5-HT = serotonin; IC = insular cortex; NMDA = N-methil-d-aspartat; PAG = periaqueductal grey; S1 = primary somatosensory cortex; PFC = prefrontal cortex; M1 = primary motor cortex; RVMG = rostro-ventral medullar grey; S2 = secondary somatosensory cortex; SMA = supplementary motor area
Pain is an unpleasant experience incidental to actual or potential tissue damage. It manifests a subjective content of consciousness possessing sensory, cognitive and affective compo-nents. In spite of its being an unpleasant experience, its role is indispensable for survival because by giving us notice of circumstances dangerous for us, it makes it possible to defend ourselves or ask for help. After pain has fulfi lled its role of calling attention, it becomes im-portant to relieve it because pain is not only a source of a lot of suffering but the stress reac-tion aroused by pain overstrains both the human body and soul. The assuagement of pain constitutes a fundamental task for every physician. The task is not easy because the same
Corresponding address: Judit Gyulaházi MD, Department of Anaesthesiology and Intensive Therapy, Medical School, Medical and Health Centre, University of Debrecen, Debrecen, Hungary. E-mail: [email protected]
28715
REVIEWS
DOI: 10.1556/CEMED.4.2010. 49 2010 ▪ Volume 4, Number 1 ▪ 49–63.
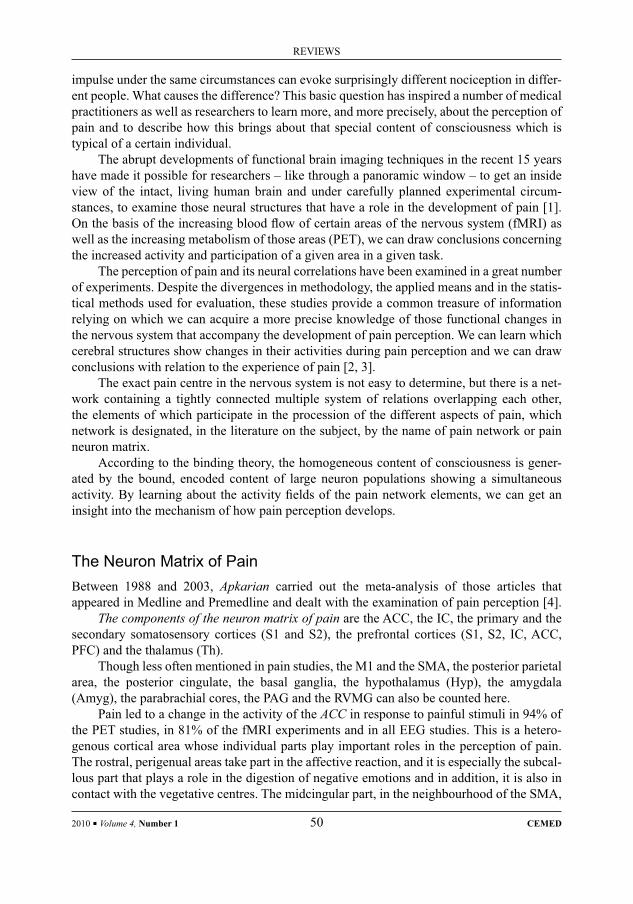
impulse under the same circumstances can evoke surprisingly different nociception in differ-ent people. What causes the difference? This basic question has inspired a number of medical practitioners as well as researchers to learn more, and more precisely, about the perception of pain and to describe how this brings about that special content of consciousness which is typical of a certain individual.
The abrupt developments of functional brain imaging techniques in the recent 15 years have made it possible for researchers – like through a panoramic window – to get an inside view of the intact, living human brain and under carefully planned experimental circum-stances, to examine those neural structures that have a role in the development of pain [1]. On the basis of the increasing blood fl ow of certain areas of the nervous system (fMRI) as well as the increasing metabolism of those areas (PET), we can draw conclusions concerning the increased activity and participation of a given area in a given task.
The perception of pain and its neural correlations have been examined in a great number of experiments. Despite the divergences in methodology, the applied means and in the statis-tical methods used for evaluation, these studies provide a common treasure of information relying on which we can acquire a more precise knowledge of those functional changes in the nervous system that accompany the development of pain perception. We can learn which cerebral structures show changes in their activities during pain perception and we can draw conclusions with relation to the experience of pain [2, 3].
The exact pain centre in the nervous system is not easy to determine, but there is a net-work containing a tightly connected multiple system of relations overlapping each other, the elements of which participate in the procession of the different aspects of pain, which network is designated, in the literature on the subject, by the name of pain network or pain neuron matrix.
According to the binding theory, the homogeneous content of consciousness is gener-ated by the bound, encoded content of large neuron populations showing a simultaneous activity. By learning about the activity fi elds of the pain network elements, we can get an insight into the mechanism of how pain perception develops.
The Neuron Matrix of PainBetween 1988 and 2003, Apkarian carried out the meta-analysis of those articles that appeared in Medline and Premedline and dealt with the examination of pain perception [4].
The components of the neuron matrix of pain are the ACC, the IC, the primary and the secondary somatosensory cortices (S1 and S2), the prefrontal cortices (S1, S2, IC, ACC, PFC) and the thalamus (Th).
Though less often mentioned in pain studies, the M1 and the SMA, the posterior parietal area, the posterior cingulate, the basal ganglia, the hypothalamus (Hyp), the amygdala (Amyg), the parabrachial cores, the PAG and the RVMG can also be counted here.
Pain led to a change in the activity of the ACC in response to painful stimuli in 94% of the PET studies, in 81% of the fMRI experiments and in all EEG studies. This is a hetero-genous cortical area whose individual parts play important roles in the perception of pain. The rostral, perigenual areas take part in the affective reaction, and it is especially the subcal-lous part that plays a role in the digestion of negative emotions and in addition, it is also in contact with the vegetative centres. The midcingular part, in the neighbourhood of the SMA,
2010 ▪ Volume 4, Number 1 50 CEMED
REVIEWS

is responsible for the regulation of the cognitive developments. The caudal, motorial part controls the arrangement of the aversive motor response.
The IC is also a heterogenous cortical area showing changes of activity in painful situa-tions according to 94% of the studies. The prefrontal lobe can probably be connected with memory and cognitive regulation through the intervention of its relations with the PFC, but it also has its role in the perception of emphatic pain [5]. The posterior part performs the func-tion of the sensory aspects of personal pain. The medial part has connection with the motor ganglions, thus taking part in the organization of aversive behaviour. The right side insula is the place for visceral response representation related to inner vigilance and emotive situa-tions which provides the substratum for cognitive evaluations.
The parts of the PFC – in a close interaction with each other, of course – constitute im-portant factors of the cognitive regulation of pain. Through their connections they infl uence sensory and affective digestion and the motor and the autonomous response.
The ventrolateral part plays a role in the re-evaluation of the expectations related to pain, in reality control, while the dorsolateral part, together with the ACC and with the I, plays a role in the modulation of attention.
The S1 and the S2 perform the sensory part of pain perception, the identifi cation of the pain stimulus, its intensity and the localization of its place. Somatothopy S2, similar to that occurring in response to a tactile stimulus can be detected in the region – though different in the facial situation – (the position of the face in the S2 is anterior compared with the position of the foot).
The Th behaves as a switching-board for all the runways of the sensory modality.The SMA takes part in the organization of the motor response.The association centres of the posterior part of the parietal cortex play an important role
in situation analysis.The nucleus accumbens is part of the reward network activated during the assuaging of
pain.The HIP is the place of the memory of pain, this is responsible for the remembrance of
previously endured pain experiences.The amygdala plays an important part in the modulation of the pain-fear-memory.The diencephalic periaqueductal grey is the source of the descending inhibitory pain
modulating path.The RVMG is the source of the descending facilitating path.
The Information-Processing Mechanism of Acute PainThe process of pain perception takes place in parallelly running, but with each other con-nected, hierarchic matrices [6].
The lateral part of the pain matrix is the network carrying out the sensory-discrimina-tive function.
The sensory transmission of the nociceptive stimulus: the tenesmus spreads via the A deltoid and the C fi bres to the sensory neurons situated in the dorsal horn of the spinal cord; from here, via the brain stem and the tractus spinothalamicus, it arrives at the fi rst switch-over place, to the specifi c medial neurons of the Th, and then the tenesmus is conducted to S1 and S2, where the spatial and temporal discrimination as well as the recognition of the
REVIEWS
CEMED 51 2010 ▪ Volume 4, Number 1
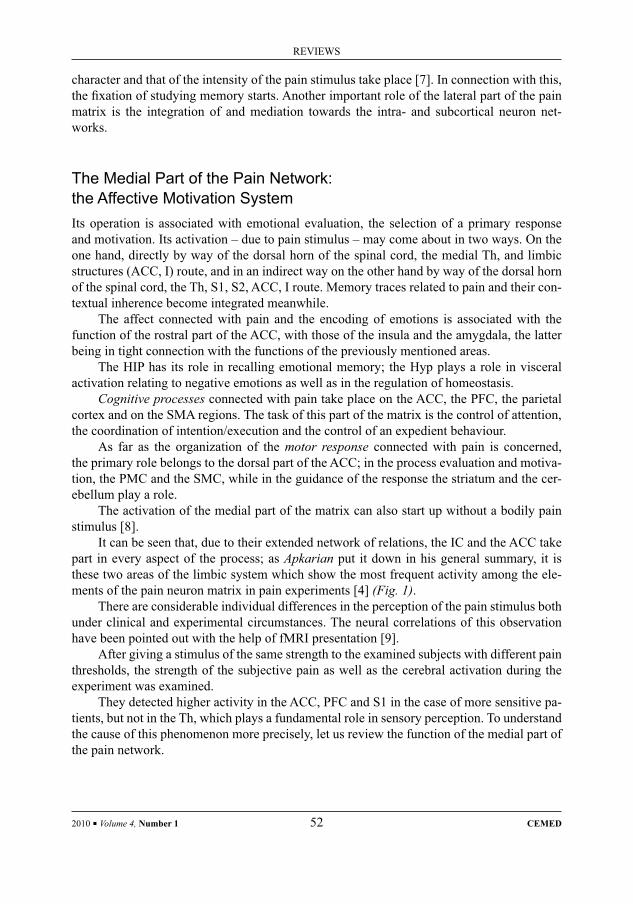
character and that of the intensity of the pain stimulus take place [7]. In connection with this, the fi xation of studying memory starts. Another important role of the lateral part of the pain matrix is the integration of and mediation towards the intra- and subcortical neuron net-works.
The Medial Part of the Pain Network:the Affective Motivation SystemIts operation is associated with emotional evaluation, the selection of a primary response and motivation. Its activation – due to pain stimulus – may come about in two ways. On the one hand, directly by way of the dorsal horn of the spinal cord, the medial Th, and limbic structures (ACC, I) route, and in an indirect way on the other hand by way of the dorsal horn of the spinal cord, the Th, S1, S2, ACC, I route. Memory traces related to pain and their con-textual inherence become integrated meanwhile.
The affect connected with pain and the encoding of emotions is associated with the function of the rostral part of the ACC, with those of the insula and the amygdala, the latter being in tight connection with the functions of the previously mentioned areas.
The HIP has its role in recalling emotional memory; the Hyp plays a role in visceral activation relating to negative emotions as well as in the regulation of homeostasis.
Cognitive processes connected with pain take place on the ACC, the PFC, the parietal cortex and on the SMA regions. The task of this part of the matrix is the control of attention, the coordination of intention/execution and the control of an expedient behaviour.
As far as the organization of the motor response connected with pain is concerned, the primary role belongs to the dorsal part of the ACC; in the process evaluation and motiva-tion, the PMC and the SMC, while in the guidance of the response the striatum and the cer-ebellum play a role.
The activation of the medial part of the matrix can also start up without a bodily pain stimulus [8].
It can be seen that, due to their extended network of relations, the IC and the ACC take part in every aspect of the process; as Apkarian put it down in his general summary, it is these two areas of the limbic system which show the most frequent activity among the ele-ments of the pain neuron matrix in pain experiments [4] (Fig. 1).
There are considerable individual differences in the perception of the pain stimulus both under clinical and experimental circumstances. The neural correlations of this observation have been pointed out with the help of fMRI presentation [9].
After giving a stimulus of the same strength to the examined subjects with different pain thresholds, the strength of the subjective pain as well as the cerebral activation during the experiment was examined.
They detected higher activity in the ACC, PFC and S1 in the case of more sensitive pa-tients, but not in the Th, which plays a fundamental role in sensory perception. To understand the cause of this phenomenon more precisely, let us review the function of the medial part of the pain network.
2010 ▪ Volume 4, Number 1 52 CEMED
REVIEWS
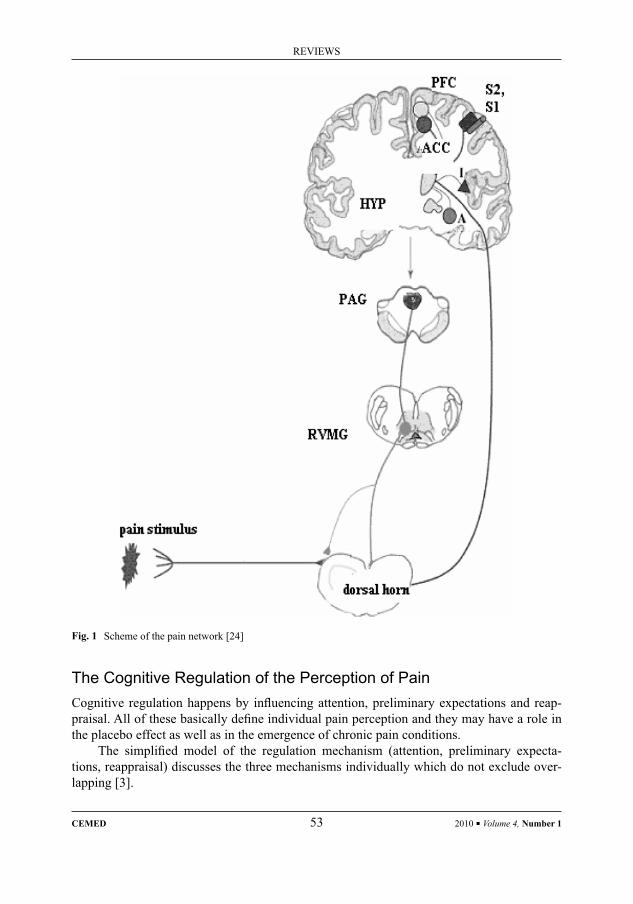
The Cognitive Regulation of the Perception of PainCognitive regulation happens by infl uencing attention, preliminary expectations and reap-praisal. All of these basically defi ne individual pain perception and they may have a role in the placebo effect as well as in the emergence of chronic pain conditions.
The simplifi ed model of the regulation mechanism (attention, preliminary expecta-tions, reappraisal) discusses the three mechanisms individually which do not exclude over-lapping [3].
Fig. 1 Scheme of the pain network [24]
REVIEWS
CEMED 53 2010 ▪ Volume 4, Number 1

Attention
Attention, by defi ning sources of stimuli coming from the outside or inside environment, modulates perception and cognition [10, 11]. It infl uences the spatial localization of pain as well as its sensory and affective functions.
Attention increases activation in the pain network and facilitates the functional connec-tion of the key areas of the network during pain perception. Studies examining the effects of distracting attention on the sensation of pain concluded that – within the pain network – in the Th, the ACC, the IC, the S1 and S2, decreased activation was experienced if the patient was given a distracting stimulus in addition to the pain stimulus [10, 11]. As a result of the interactive analysis of distracting tasks, it was found that simultaneously with the modifying infl uence exerted on pain perception by distraction, the most signifi cant activity increase could be detected in the PFC, the ACC and in the PAG [12].
The PFC, the ACC and the IC, being in mutual interaction, adaptively, perhaps maladap-tively, are supposed to modulate the perception of pain with other members of the pain matrix via the descending activation system [13].
Preliminary Expectations
Our preliminary expectations related to the given context, having developed as a result of the synthesis of our experiences in the course of our personal development, may infl uence our pain sensation. Our concepts, created with reference to a certain happening, make it possible for our sensory, motor and cognitive systems to prepare for giving an adequate response under given circumstances.
In response to the signal indicating pain – prior to the appearance of the stimulus – an increase of activity can be detected in the pain network: in the medial PFC, the ACC, IC an-terior and in the PMC of the opposite side [14].
Preliminary expectations basically infl uence the extent of pain sensation independently of the intensity of the pain stimulus. In the case of a lower expectation, the subjects of the examination showed a lower intensity of pain than in the case of a higher expectation, even if the stimulus was of the same strength. On the other hand, if pain of a lower intensity was expected, even a strong stimulus resulted in experiencing stimulus of a weaker intensity.
On a neural level, the activation of the pain matrix is correlated with a subjective ap-praisal. This identifi es how the neural mechanism, corresponding to preliminary expecta-tions, infl uences perception.
Our preliminary expectations are necessary to be properly prepared for the events to come, but their collation with the real events and their subsequent revision is also very important for an adequate accommodation. Ploghaus was the fi rst to correlate the mecha-nism of appraisal and learning as related to pain with the activity of the HIP, the gyrus frontal superior, the posterior parietal cortex and with that of the cerebellum [15].
Reappraisal
Pain is a threatening signal. The extent of being threatened also depends on how dangerous the individual himself/herself considers the situation to be as well as on the estimation of his/her means at his/her disposal for facing the situation. If he/she regards the latter as suffi cient, pain will be controllable and the person will fi ght with all his/her might. Otherwise he/she
2010 ▪ Volume 4, Number 1 54 CEMED
REVIEWS

will withdraw and will become passive. In so far as there is more possibility for control, the extent of the danger can be reappraised, and thus the experience of pain may alter.
If the patient was allowed to control the pain stimulus himself/herself, the intensity of his/her pain sensation would decrease. As a neural correlation, a decreased activity was found in the ACC, the IC, and in the S2, while on the right side, in the ventrolateral part of the PFC, an increase of activity could be seen [16].
The PFC is the key role player in the cognitive regulation of pain perception. It has extended connections and gains information from all sensory modalities. It is in connec-tion with limbic structures (ACC, IC, HYP, A) regulating affects, vegetative functions and motivation as well as with cerebral regions regulating motor function, and consequently, it is able to regulate behaviour.
The Role of Affects to Infl uence Pain PerceptionThe relationship between mood and pain perception has been comprehensively examined under both clinical and laboratory circumstances.
It has been proved, under experimental conditions, that bad mood infl uences pain per-ception. Villemure and his colleagues examined how bad and pleasant odour infl uence the perception of pain. They found that a change in the mood modifi ed the extent of the unpleas-ant character of the perceived pain; however, it did not infl uence its intensity. It has been found, in addition, that mood is the best predictive sign concerning the discomfort of pain to be felt later, more predictive than the level of tension [11].
The obtained results have been confi rmed by Loggia et al. [17]. He was examining, to-gether with his colleagues, how pain perception of the subjects of the experiment changed when their mood was infl uenced by being shown video recordings of natural catastrophes or neutral cityscapes to them. The experimenters measured the extent of the unpleasant charac-ter of the pain (affective component) and the intensity of the pain (sensory component), and also examined the change of mood as well as the level of tension or tranquillity. It was found that disaster scenes generated bad mood and increased tension and the unpleasant character of the applied heat pain stimulus, but not its intensity. The video of a neutral cityscape did not bring about any change. The results confi rm clinical experiences.
The examination of the pain perception of depressed patients with an extremely nega-tive mood serves with an instructive result [18]. It was examined with fMRI what kind of cerebral activity change there was in response to painful and non-painful heat stimulus in patients with major depression compared with healthy ones. It was found that those with depression, in anticipating pain, produced an increased activity on the right side IC, in the dorsal part of the ACC and on the right side A compared with healthy people. This was so when they anticipated a painful stimulus but not when they anticipated a painless one. During painful stimulus, an increased activation could be observed in depressed patients on the right side A, and a decreased activation in the rostral ACC, in the PAG and in the PFC, compared to the application of a painless stimulus. Results show that depressed patients have an in-creased reaction in anticipating pain, which is able to infl uence the perception of the pain to occur.
Catastrophizing pain is a condition in which experiencing pain is of an ever increasing interest for the patient. To describe pain, the patient uses the most extremely negative attri-
REVIEWS
CEMED 55 2010 ▪ Volume 4, Number 1
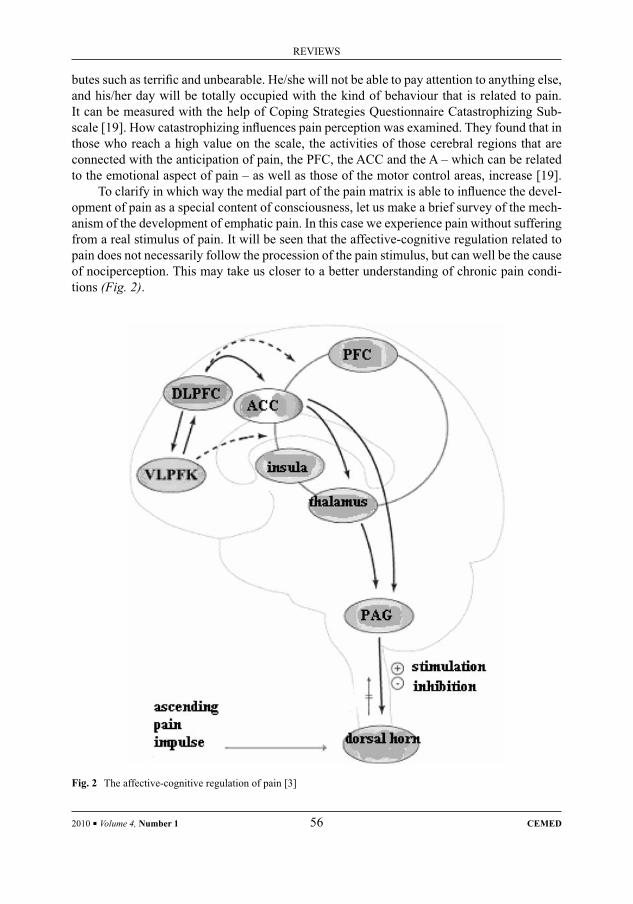
butes such as terrifi c and unbearable. He/she will not be able to pay attention to anything else, and his/her day will be totally occupied with the kind of behaviour that is related to pain. It can be measured with the help of Coping Strategies Questionnaire Catastrophizing Sub-scale [19]. How catastrophizing infl uences pain perception was examined. They found that in those who reach a high value on the scale, the activities of those cerebral regions that are connected with the anticipation of pain, the PFC, the ACC and the A – which can be related to the emotional aspect of pain – as well as those of the motor control areas, increase [19].
To clarify in which way the medial part of the pain matrix is able to infl uence the devel-opment of pain as a special content of consciousness, let us make a brief survey of the mech-anism of the development of emphatic pain. In this case we experience pain without suffering from a real stimulus of pain. It will be seen that the affective-cognitive regulation related to pain does not necessarily follow the procession of the pain stimulus, but can well be the cause of nociperception. This may take us closer to a better understanding of chronic pain condi-tions (Fig. 2).
Fig. 2 The affective-cognitive regulation of pain [3]
2010 ▪ Volume 4, Number 1 56 CEMED
REVIEWS

Experiencing Others’ Pain, EmpathyEmpathy is one of our faculties that develop in early childhood. Being able to assess other people’s sensory and emotional experiences helps us establish successful relationships with our fellow-men. We are not only able to understand the experience of others, but also to get into a similar emotional condition, that is, we are able to feel pain experienced by other people. Empathy is not an “all or nothing” phenomenon, and it is infl uenced, to a great extent, by contextual as well as by intra- and interpersonal factors. The technical development of the last decade has made it possible to examine the neural correlations of emphatic pain.
In their experiment, Singer and his colleagues pointed out, with the help of fMRI, the increase of activity in the pain matrix of patients, who either experienced pain themselves, or experienced pain caused to a close relation of theirs [8]. They could only see the hand of their partner without seeing their emotional reactions during the examination. Different colours of fl ashes of light provided information about the intensity of pain. While, in the case of fi rst hand experiences the whole of the pain network became activated, in the case of pain caused to a close relation, it was only the left side anterior IC and the rostral ACC where an increase of the activity could be detected. Its extent correlated with the level surveyed in the empathy-questionnaire. On the basis of this, Singer comes to the conclusion that the ground of experiencing others’s pain is the activation of that part of the pain matrix which is respon-sible for the affective function. The absence of the activation of the lateral part of the matrix shows that practically no actual stimulus befell the person taking part in the examination.
Lamm and his colleagues also examined the question of experiencing others’s pain, but they found the same neural activity in the case when the person underwent the pain experi-ence himself, and thus they found activation – in addition to those of the ACC and the ante-rior IC – also in PEG, S2 and in the SMC. The activity change of both components of the pain matrix can be caused by the context in which the pain developed as well as by the conclu-sions drawn by the observer [5].
On the basis of the results of Gu and Han, the perception of somebody else’s pain is not a process without the will of one’s own, and we have to pay our attention not only to the body of the other person but also to his pain, otherwise the activation of the cerebral regions (ACC, IC, PMC) serving as the basis for the ground of emphatic pain, in other words, the activation of places of both cognitive and affective functions will fail to come about. In addition, if the situation does not fully agree with the real facts, the activation will weaken in the ACC and fails to occur in IC and in the putamen altogether [20].
On the basis of the results of empathy examinations, it can be concluded that the activa-tion of the medial part of the neuron matrix of pain, in other words, the affective-cognitive processes can bring about pain experience without any painful stimulus hitting the body. All this may be of great help to us in understanding the conditions of chronic pain. Due to the limits of the decomposing ability of the imaging processes related to time as well as because of the divergent experimental arrangements and of the statistical analyses, it is diffi cult to reconcile contradictions. Further examinations are necessary for a proper understanding of a precise mechanism of function.
REVIEWS
CEMED 57 2010 ▪ Volume 4, Number 1
Chronic PainWhile acute pain is of vital importance from the point of view of survival, it is diffi cult to identify the adaptive function of conditions accompanying chronic pain which often exists for years. It is a source of a lot of suffering for the sick person and imposes a big burden on the family, the therapeutic staff and the society.
In chronic pain there is a disproportion between the intensity of the injurious stimulus, its location and its nature, and between the pain experience. Its forms are: hypersensitivity, when the receptive fi eld grows so extensive that even the stimulation of areas distant from the place of the injury produces pain and allodynia, when an innocuous stimulus evokes a painful reaction. Assuaging chronic pain is a great challenge every physician must face and for the sake of overcoming this challenge, we are to understand the mechanism of its assumed devel-opment [21, 22]. On the basis of the research results of recent years, its development can be explained with the modifi ed structure and function of its pain neuron matrix rather than with the injury of the peripheral tissues [23, 24].
The development of acute pain experience is a process that has been studied extensively. In acute pain studies, in the course of well-planned examinations of homogeneous groups of patients, several aspects of pain perception could be examined. Because of the many kinds of case records, the great variety of sickness, accompanied psychic disturbances and because of the different accounts of the individual patients, the research of chronic pain is far more com-plicated. It is not easy to set up homogeneous groups suffering from the same disease. Sepa-rating the neural correlations of pain-relieving treatments of different length from those of accompanied psychic disturbances is also rather intricate.
The neuron imaging methods providing great help in the research of acute pain have made it possible to see the changes in the activity of the neuron network. However, the sepa-ration of the stimulating and that of the inhibitory cell groups within the matrix is not possi-ble by these methods. Due to these causes, the results obtained with patients suffering from chronic pain are rather contradictory.
Examinations concerning acute pain stimulus have been carried out on patients suffer-ing from chronic pain [25]. In patients with allodynia, while applying tactile stimulus, an increase of activity could be observed in the IC and in the S2, while there was a decrease of activity in the ACC. In case of heat stimulus, an increase of activity was proved in the S1, the IC and in the PFC.
Activity changes brought about by chronic pain were also examined. In the meta-analy-sis of studies of neuropathic patients, Moisset found that in the case of spontaneous pain the activity of the ACC, that of the IC, the S1 and S2 as well as that of the PFC increased [26].
In case of cluster headache, regional blood fl ood increase was detected in the dorsal and in the medial brainstem structures as well as in the FPC and in the cerebellum [27].
2010 ▪ Volume 4, Number 1 58 CEMED
REVIEWS

The Mechanism of the Enduring Plastic Change of the Pain NetworkOn the basis of the latest research results, we have reasons to believe that the development of chronic pain is supraspinally commanded [23, 24].
Within the pain matrix the even function of the stimulating and that of the inhibitory neuron population lose balance, and the pathways taking part in the pain perception of certain parts of the body grow stronger. In accordance with certain assumptions, chronic pain is a process regulated downwards from above.
On its development, in consequence of tissular injury, an enduring plastic change of the nerve tissue occurs in the dorsal horn of the spinal cord, in the ACC and in the IC, both play-ing a central role in the pain matrix. The enduring stimulus, the continuously existing de-crease of the inhibition and the changed function of the descending, modulating bi-phase pathway bring about structural and functional changes.
The development of hypersensitization, according to Zhuo, can be divided into three phases [24]. In the phase of rapid change, which starts from the very fi rst moments following the injury and lasts for a few hours, the extent of stimulation, due to the change in the quan-tity of the outfl owing mediators as well as that of the post-synaptic modulation, increases. In addition, the decrease in local inhibition cannot be excluded. In the second phase, which is enduring and can last from some hours up to some days, the translation mechanisms also contribute to its development. The quantity of proteins playing a key role in the transmission of signs, such as the quantity of the NMDA (glutamate) receptors, increases. Trophic and other factors, playing a role in the promotion of growth, also contribute to long-lasting trans-formation. Because of the increased quantity of materials that have their parts in the transmis-sion of signs, the possibility of the development of positive intracortical feed back loops also occurs. In the third, persisting phase the aforementioned structural changes will enduringly be maintained, a reorganization of cortical neuron networks will come into being, new rela-tions will be established among areas within the cortex. In the background of structural changes, potentially, a loss of cells in the population of inhibitory cells may also have a role.
The balance of the descending stimulating/inhibitory pathways will change in condi-tions of chronic pain. The balance shifts, following the activation of the ACC, towards the activation of the stimulating pathway originating in the RVM. At the same time, the activity of the inhibitory path connected with the endogenic opioid mechanism originating in the PAG decreases.
In patients with laesio in the ACC, following the inhibition of the NMDA receptors of the ACC and following the laesio of the RVM which is the starting point of the descending stimulation path, and while antagonizing 5-HT which is the mediator of the descending stim-ulation in the spinal cord, analgesia was observed in patients suffering from chronic pain. This supports the hypothesis that in chronic pain conditions the path of the descending stim-ulation may have a key role in the development of pain [23, 24]. This, however, conveys the suggestion that the activation of the pain matrix is not brought about by the pain stimulus affecting the body. There exists a possibility that it is the part of the pain matrix carrying out the affective-cognitive regulation that sets the process in action. The healing strategies of chronic pain conditions cannot leave therapeutic means involving affective-cognitive regula-tion out of consideration (Fig. 3).
REVIEWS
CEMED 59 2010 ▪ Volume 4, Number 1

DiscussionAcute pain is an unpleasant experience that develops as a consequence of actual or potential tissue injury. It is an important sign that is indispensable for survival, and helps us to avoid aversive situations and urges us to ask for help. Depending on the individual and on indi-vidual contexts, people give accounts of very different experiences caused by the same stim-ulus [9]. An outline of the development of pain as a special content of the consciousness renders help for the sometimes very diffi cult task of assuaging pain.
Fig. 3 Descending bi-phase modulation [24]
2010 ▪ Volume 4, Number 1 60 CEMED
REVIEWS
The functional imaging procedures of recent decades have made it possible to study pain perception, the development of the pain experience and those neural connections that are in the background of these, by way of experiences providing information about the develop-ment of acute pain [1, 2, 4].
It has become obvious that there is no single pain centre existing. The development of pain, as a special content of the consciousness, is brought about by an impulse caused by si-multaneously evolved and connected neuron cell populations.
Cerebral regions that play roles in the development of pain are called, in the correspond-ing literature, the neuron matrix or the network of pain. The parts of this pain network are: the ACC, the IC, the PEG, the S2, the PFC and the Th [4]. Though less often mentioned in pain studies, the SMA and the primary motor cortex (PMC), the posterior parietal area, the posterior cingulate, the basal ganglia, the Hyp, the amygdala (A), the parabrachial cores, the PAG and the RVMG can also be counted here.
The development of the pain experience is, to a large extent, the result of the simultane-ous activation of the closely cooperating networks with the lateral sensory and those of the medial cognitive-affective functions [6]. The function of the lateral part of the pain network covers the identifi cation of the stimulus, its spatial and chronological discrimination and the judgement of its intensity. The medial part of the pain matrix modulates, basically through cognitive and affective regulation, the individual nature of pain [3]. Cognitive regulation in-fl uences the quality of the pain experience through attention, the formation of preliminary expectations, and the mechanisms of reassessment. It is the affects, the enduringly main-tained negative emotional conditions, that predict the unpleasant nature of pain well but do not predict its intensity [17, 18]. Strigo and his colleagues found, during the examination of acute pain development in patients suffering from depression, that in this lastingly negative mood the patients produced an increased reaction in anticipating pain [18].
To examine how the medial part of the pain matrix is able to infl uence the development of pain regarded as a special content of consciousness, we surveyed the development of the mechanism of emphatic pain. Empathy is that faculty of ours with the help of which we are able to experience the emotions and the pain of others. Its neural correlations can be depicted with the help of various functional imaging procedures [5, 8, 20]. On the basis of the results of empathy examinations, it can be said that when observing the pain of others, the medial part of the neuron matrix of pain will be activated and the affective-cognitive processes may give rise to the emergence of pain experience in the observer even without being excited by a direct stimulus.
The treatment of chronic pain conditions constitutes one of the greatest challenges for public health service in our days. The limited success of the applied relieving processes causes a lot of suffering for both the patient and his/her environment; it imposes a consider-able fi nancial burden on society and as far as the medical staff is concerned, for them it is a source of frustration. The understanding of the development of chronic pain may lead us to the establishment of more effi cient pain-relieving strategies.
The basis of the development of chronic pain is a long-lasting, plastic change in those neural structures that play a role in pain perception [23, 24].
According to the examinations of Zhuo, the process is infl uenced from upwards de-scending downwards. In addition to the spinal cord, the enduring, plastic transformation of the ACC and that of the IC can also be well detected, both playing a central role in the pain
REVIEWS
CEMED 61 2010 ▪ Volume 4, Number 1

matrix. Hypersensitization can be divided into three phases: the rapid, the enduring and the persisting ones. In consequence of these processes, a structural transformation will come into being between certain cortical areas as well as between the neural populations of the different cortical layers. The balance of stimulation and inhibition will upset within the pain network. Continuous stimulation will be transferred, via the descending stimulating path originating in the RVM, to spinal structures.
Chronic pain conditions provide a good example of the fact that physical and psychical processes cannot be separated from each other and they bring about, with close connection with each other, that special content of consciousness that we call pain and that, in the given context, is characteristic of human beings only.
A better understanding of the development of the pain experience is of great help for every medical person to be able to relieve the pain of their patients as effi ciently as pos-sible.
The relief of pain must be performed, in every single case, on the basis of individual strategy and in close cooperation with the patient. The intensity of the pain experience as well as the level of its unpleasantness indicates the size of the pain neuron matrix activity. Its measure will have an infl uence over the applied pain-relieving demands.
The means that help to infl uence the affective and the cognitive components of pain perception are at the disposal of not only psychotherapists but all medical people. The fol-lowing things can be rated here: the improvement of the patient’s mood, the decrease of his/her fear and stress, the distraction of his/her attention from the painful part of his/her body or from that of the painful situation. The appraisal of the situation, the infl uencing of the pre-liminary expectations concerning the oncoming pain and last but not least, the modifi cation of the reappraisal of the painful situation can be assured by providing a possibility to control as well as by providing the necessary means for facing and overcoming the situation.
The aforementioned can contribute to the effi ciency of our pain-relieving activity and most importantly, it can make our patients’ lives easier.
ReferencesStephenson, D. T., Arneric, S. P.:[1] Neuroimaging of pain: advances and future prospects. J. Pain, 2008, 9, 567–579.Tracey, I.:[2] Imaging pain. Br. J. Anaesth., 2008, 101, 32–39.Wiech, K., Ploner, M., Tracey, I.:[3] Neurocognitive aspects of pain perception. Trends Cogn. Sci., 2008, 12, 306–313.Apkarian, V. A., Bushnell, C. M., Treede, R. et al.:[4] Human brain mechanisms of pain perception and regula-tion in health and disease. Eur. J. Pain, 2005, 9, 463–484.Lamm, C., Nusbaum, H. C., Meltzoff, A. N. et al.:[5] What are you feeling? Using functional magnetic resonance imaging to assess the modulation of sensory and affective responses during empathy for pain. PLoS ONE, 2007, 2, e1292.Chen, C. A.:[6] Pain perception and its genesis in the human brain. Acta Physiol. Sin., 2008, 60, 677–685.Murányi, M., Radák, Z.:[7] Fájdalom és ópioidok. Orv. Hetil., 2008, 149, 2363–2370.Singer, T., Seymour, B., O’Doherty, J. et al.:[8] Empathy for pain involves the affective but not sensory compo-nents of pain. Science, 2004, 303, 1157–1162.Coghil, R. C., McHaffi e, J. G., Yen, Y. F.:[9] Neural correlates of interindividual differences in the subjective experience of pain. PNAS, 2003, 100, 8538–8542.Bantick, S. J., Wise, R. G., Ploghaus, A. et al.:[10] Imaging how attention modulates pain in humans using func-tional MRI. Brain, 2002, 125, 310–319.
2010 ▪ Volume 4, Number 1 62 CEMED
REVIEWS

Frankenstein, U. N., Richter, W., McIntyre, M. C. et al.:[11] Distraction modulates anterior cingulate gyrus activa-tions during the cold pressor test. Neuroimage, 2001, 14, 827–836.Villemure, C., Slotnick, B. M., Bushnell, M. C.:[12] Effects of odors on pain perception: deciphering the roles of emotion and attention. Pain, 2003, 106, 101–108.Fields, H. L., Basbaum, A.:[13] Central nervous system mechanisms of pain modulation. In: McMahon, S. B., Koltzenburg, M. (eds): Textbook of Pain. Elsevier, London, 2006, pp. 125–142.Porro, C. A., Baraldi, P., Pagnono, G. et al.:[14] Does anticipation of pain affect cortical nociceptive systems? J. Neurosci., 2002, 22, 3206–3214.Ploghaus, A.:[15] Learning about pain: the neural substrate of the prediction error for aversive events. Proc. Natl. Acad. Sci. U.S.A., 2000, 97, 9281–9286.Salomon, T. V., Johnstone, T., Backonja, M. M. et al.:[16] Individual differences in the effects of perceived control-lability on pain perception: critical role of the prefrontal cortex. J. Cogn. Neurosci., 2007, 19, 993–1003.Loggia, M. L., Jeffrey, S., Mogil, M. et al.:[17] Experimentally induced mood changes preferentially affect pain unpleasantness. J. Pain, 2008, 9, 784–791.Strigo, I. A., Simmons, A. N., Matthews, S. C. et al.:[18] Association of major depressive disorder with altered functional brain response during anticipation and processing of heat pain. Arch. Gen. Psychiatry, 2008, 65, 1275–1284.Gracely, R. H., Geisser, M. E., Giesecke, T. et al.:[19] Pain catastrophizing and neural responses to pain among persons with fi bromyalgia. Brain, 2004, 127, 835–843.Gu, X., Han, S.:[20] Attention and reality constraints on the neural processes of empathy for pain. Neuroimage, 2007, 36, 256–267.Kehlet, H., Jensen, T. S., Wool, C. J.:[21] Persistent postsurgical pain: risk factors and prevention. Lancet, 2006, 367, 1618–1625.Carrasquillo, Y., Gereau, R. W.:[22] Pain sensitization. Learn. Mem., 2008, 4, 65–90.Ko, S., Zhuo, M.:[23] Central plasticity and persistent pain. Drug discovery today. Dis. Model., 2004, 1, 101–106.Zhuo, M.:[24] Cortical excitation and chronic pain. Trends Neurosci., 2008, 31, 199–207.Lorenz, J., Cross, D. J., Minoshima, S. et al.:[25] A unique representation of heat allodynia in the human brain. Neuron, 2002, 35, 383–393.Moisset, X., Bouhassira, D.:[26] Brain imaging of neuropathic pain. Neuroimage, 2007, 37 (Suppl. 1), S80–S88.Weiller, C., May, A., Limmroth, V. et al.:[27] Brain stem activation in spontaneous human migraine attacks. Nat. Med., 1995, 1, 658–660.
REVIEWS
CEMED 63 2010 ▪ Volume 4, Number 1


The Evaluation of Therapeutic Modalitiesin the Treatment of Palmary and Axillary Hyperhydrosis
KÁROLY VINCZE1, LÁSZLÓ HERKE1, JÓZSEF FERENCZY2, ISTVÁN SEFFER2, ZSUZSANNA LELOVICS3
1Department of General Vascular and Thoracic Surgery, Kaposi Mór Teaching Hospital, Kaposvár, Hungary2Seffer–Renner Private Clinic, Kaposvár, Hungary
3Faculty of Health Sciences, University of Pécs, Pécs, Hungary
The authors summarize their therapeutic methods of palmary and axillary hyperhydrosis (HH). They discuss the characteristics, frequency of upper limb and patho-anatomical features of chronic sweating. Therapeutic measures, treatment methods, technological improvements, recent knowledge and relevant literature are used to summarize an almost 40 years’ experience. Open thoracotomic desympathisation applied at the beginning was gradually replaced by a minimally invasive VATS-sympathectomy (video-assisted thoracoscopic surgery). The possibilities of conser-vative treatment and local excision methods will also be discussed, as well as the application and effi ciency of Botox®-treatments used in plastic surgery. The mean frequency of 0.1–1.0% described in the literature is indicative of a signifi cant number of unresolved cases, which thus requires more effi cient diagnostic measures and patient orientation practices. The authors’ past experiences suggest that the most effi cient treatment of upper limb HH is thoracic sympathectomy (ramicotomy and the relevant T2–T3 or T4 ganglia) according to the Smithwick procedure and it has been modifi ed by others. If necessary, one-stage bilateral VATS-surgery may be applied. Another effective conservative treatment regimen is the Botox® therapy, which was applied individually at the Department of Plastic Surgery. No signifi cant complications or compensatory HH could be observed.
Keywords: hyperhydrosis, thoracic sympathectomy, VATS, botulinum toxin-A
IntroductionPrimary (local) hyperhydrosis (HH) is excessive sweating due to the activation of the vegeta-tive sympathetic system irrespective of the environmental temperature [1, 2]. The disease can greatly infl uence lifestyle, work, socialisation of the individuals and can be the cause of psy-chological disorders [1, 2]. Despite the extensive interest refl ected in the international litera-ture, national publications about prevalence, clinical features and treatment possibilities are missing [3, 4]. The prevalence of HH is around 0.1–1.0% [1, 2, 4, 5], and thus probably its incidence is higher than public opinion suggests.
The aim of reviewing nearly 40 years’ experience in the treatment of HH was to show the results achieved in the mirror of the changes in surgical techniques. Our standard surgical procedure was thoracic sympathectomy (TS) (Smithwick developed) [6], which we performed as axillar thoracotomy at the beginning and then with VATS (video-assisted thoracoscopic surgery). In addition, this study is meant to present experiences in Botulinum toxin (Botox) (Vistabel/Allergan/, active substance: 50 units A-type Clostridium botulinum toxin) produced
Corresponding address: Zsuzsanna Lelovics MD, Vörösmarty Mihály u. 4, 7621 Pécs, Hungary.E-mail: [email protected]
28618
REVIEWS
DOI: 10.1556/CEMED.4.2010. 65 2010 ▪ Volume 4, Number 1 ▪ 65–71.
by the Clostridium botulinum treatment. This was based on individual decision. Botox ther-apy began to spread in domestic plastic surgery in the 1990s as the primary therapy for HH affecting the axillary region [7–10].
BackgroundThe fi rst surgery, as a therapy (curing epilepsy), was performed on the sympathetic nervous system by Alexander [11]. Leriche (in 1913), and later Brüning (1923), suggested cutting the sympathetic nerves to solve atherosclerotic vascular problems [12, 13]. Kotzareff performed his fi rst TS to cure HH in 1920 [14]. Smithwick published his suggestions concerning the technique of thoracic sympathectomy in 1938. This is supposed to be used even today [6]. Hughes in 1942, and Goetz and Marr in South Africa in 1944 performed TS with thoraco-scopic technique independently [15, 16]. Kux reported results of 1,400 cases of thoraco-scopic sympathectomy in 1954 (he had performed thoracoscopic sympathectomy as early as 1937, but he published his fi ndings only later [17]). In 1990, Kao presented the fi rst TS per-formed using VATS technique [18].
Kiss (related to his research done in the Anatomy Institute at Pécs University, and pub-lished as his dissertation in 1957) clarifi ed the segmental origin of preganglionic neurons of the thoracic and lumbal sympathetic chain [19]. Papp and Winter reported sympathectomy performed by way of thoracic surgery [20], while Kulka and Fazekas published the results of bilateral (extrapleural) TS done at the same time [21]. These surgeries were done because of ischemic syndrome as those done later by Csengődy and Fauszt as a TS solution related to thoracic outlet syndrome (TOS) [22].
Nagy and his co-worker published the fi rst Hungarian videoendoscopic TS [23]. TS performed using VATS technique by Fazekas and his co-workers aimed to solve ischemic problems, and they did not perform TS to treat HH [23, 24].
Lőke performed the fi rst TS from axillary thoracotomy as a therapeutic measure for HH in 1971 [3]. This was the fi rst surgery performed to cure HH in Hungary. TS was suggested as a therapy for HH in the handbook of thoracic surgery published in Hungary in 2006 [4].
Several papers concerning the techniques and effectiveness of TS in the treatment of HH have been published [2, 9, 25–29]. There are data on extending the T2–T3 ganglia excision to T4 suggested by Smithwick, its positive role in axillary HH [26], and the use of clips instead of ganglionectomy that can be transferred or removed if needed [9]. In other cases, e.g. palmar HH dominancy, there is a difference in therapeutic effects between the sympathectomy or re-section of the affected section and ganglia [30]. Most of the reports agree that TS performed with any kind of surgical technique is almost 100% effective (HH disappears) [9, 25, 28, 30, 31]. Lin reported the results of 1,360 TS performed for treating HH: HH disappeared in 99% of the cases, and the ratio was similar on the follow-up examination 28 months later [32].
Introduction of the VATS technique decreased the complications of TS signifi cantly, and several authors confi rmed the advantages of the method [28, 30, 32]. Our relatively small number of VATS surgeries also confi rms this. The most common complication is compensatory HH (Kestenholz showed it to be 4–48%) [33], (others found it around 60%) [9, 26, 27, 29, 32]. In our patient population, this could not be confi rmed. Postoperative dilata-
2010 ▪ Volume 4, Number 1 66 CEMED
REVIEWS

tion disturbances occurred in 2.0–2.5% [32, 34, 35]; the Horner triad – usually transient – occurred in 2–5% [9, 28, 29, 32].
Ueyama reviewed TS done by VATS technique (50 Japanese institutions, 7,017 operated HH) and observed intraoperative bleeding in 0.3% and Horner triad in 2–5% [28]. Ojimba registered the occurrence of Horner symptom to be 1% and that of pneumothorax to be 2% in a British statistics [34]. Others documented the decrease of complications on using VATS technique [9, 35].
Clinical Data and MethodsFor the methods used in different periods and their results and complications see Table 1.
The data processing was based on the surgical and out-patient documentation. The long-term (>1 year) follow up was done partly by way of written communication, partly on per-sonal interviews. The mean age of the patients was 31.1 years (SD: 9.8, range: 12–56 years). One hundred and three females and only four males were included in the study.
We performed the Smithwick type TS from axillary thoracotomy in the fi rst 19 years. The rate of complications was not signifi cant; the main problem was intercostal neuralgia lasting for months in two cases (Table 1).
In the second period, we performed TS from a “mini” thoracotomy. Although the sample was relatively small, the patients were satisfi ed, complications were rare and HH disappeared completely. We managed to shorten the duration of hospitalisation.
Not only did the introduction of the VATS technique at our department in 1998 reduce the time of hospitalization from more than 8 days to one-third, but there were also no com-plications (we performed bilateral TS, working with three ports). We did not use CO2-insuf-fl ation in the thoracic cavity, but we kept apart the lungs with the “fan” introduced through the 3rd port.
Botox therapy was done in the Seffer–Renner Private Clinic. The treated area was the surface covered with hirci; the therapeutical effectivity was measured with iodine-starch test. Generally, patients got 100 NE Botox injection. It was necessary to repeat the treatment be-cause of the recurrence of HH after 6–8 months. No severe complications were detected.
DiscussionHH is an excessive perspiration, more intense than necessary for thermoregulation. It can be focal (primary, local) or general (secondary) [36]. The focal appearance can be found on the palms, axilla, face and feet. The 4–5 millions of sweat glands are more densely distrib-uted on the skin surfaces of these body regions. The density of sweat glands can even be 500–700 cm−2 on the palms and axilla [31, 36].
Although the exact pathogenesis of HH is unknown, the local appearance in half of the cases is determined genetically; the autosomal dominant inheritance is proved [7, 25, 37]. The rate of primary HH is 0.1–1.0% [5–7, 25, 31, 36, 37]. Around half (58 patients) of the individuals treated were from our medical attendance area, while the others came from dif-
REVIEWS
CEMED 67 2010 ▪ Volume 4, Number 1

Table 1 The clinical data of our patients
Period Number of patients Methods
Length of hospital
stay
ComplicationsResults
No. Type
1971–1990 46
(axill. HH:18, palm.10, both 18)
Axill. thoracothomy+ Smithwicktype TS resection of T2–3 ganglia and sympathectomy
8.3 days 6 2 neuralgia1 pneumonia1 bleeding1 Horner triad1 wound healing
problem
HH disappeared in 100% Patient satisfaction > 90% Comp. HH = 0
1990–1998 18
(axill. 6,palm. 5,both 7)
„Mini” axill. thoracothomy+ thoracic symp. (TS)
6 days 3 1 expansion disorder1 postoperative
pleuritis1 wound healing
problem (wound edge necrosis)
HH disappeared in 100% Patient satisfaction > 95% Comp. HH = 0
1998– 16
(axill. 4,palm. 6,both 6)
VATS-TS 3.5 days 0 HH disappeared in 100Patient satisfaction 100%Comp. HH = 0
Since 2003 27
(ax. HH)
Clostr. Botulinum-A toxin inj. (Botox)Intradermal application 100 NE in multiple phases (as out-patients)25 bilateral therapiesIn 8 cases 2×,in 3 cases 3×,in 2 patient unilateral therapy
Effect was 100%, but after 8–10 months declines and disappears.The injection is painful, the application is costly.
Altogether 107
ferent parts of the country. There are no Hungarian data on the incidence of HH. The inci-dence of HH is 1.0% in the UK [8]; a survey among 150,000 people showed a 2.8% fre-quency in the United States in 2003 [31], and this means an incidence higher than 8% in he whole population. According to the survey by Adar (in Israel), the incidence of severe HH is 0.15–0.25%, which affects mainly the young [5].
2010 ▪ Volume 4, Number 1 68 CEMED
REVIEWS

HH is the most frequent among women and between ages 20 and 45 [1, 2, 9, 36]. One-third of the sufferers of HH have only axillary, while 25–29% of them only palmar excessive sweating [26, 27, 31, 36]. The abnormal sweating appears in childhood in 75% of the cases [27], which manifests in young adulthood [1, 5, 31]. Those who suffer from different HH rarely require therapy. The mild and moderate sweating is a factor in everyday life [1], and only severe HH requires medical attendance [7, 9, 28, 29].
The conservative therapeutical possibilities cover a wide range, although they are inef-fective in severe cases [2, 7, 31, 36]. In the fi rst line anticholinergic drugs, local astringents, glutaraldehide powder, iontophoresis and sedatives are used [7, 9, 31, 38]. The alcoholic so-lution of 20% aluminium-chlorate hexahydrate can help in mild or medium HH [31, 37].
Botox therapy was performed in the Seffer–Renner Private Outpatient Clinic in Kapos-vár, Hungary. The Botox injection made from A serotype of C. botulinum was used primarily to cure the axillary HH since the beginning of the 1990s [39, 40]. It was used individually after detailed information was provided for the patients. Following the assessment of distri-bution of the sweat glands in the axillary region, Botox was administered as injection in doses stated earlier. The therapy was effective through 6–8 months. Our results were similar to those published in the literature [2, 7, 36].
We did not perform local excision in cases of axillary HH. We did not try this in HH because of predictable disadvantages despite the high number of supportive reports [41–43]. Excision techniques used by Breach [41] and Hafner [43] and the fat suction method by Shenaq [44] were also missing from our practice. Thoracic sympathectomy became the “gold standard” of the HH therapy in the middle of the last century [4, 7, 9, 28, 29].
ConclusionOur results and experiences in curing HH with VATS sympathectomy suggest that further efforts should be made to continue it. In the case of bilateral HH, the benefi ts of bilateral solution were described by others simultaneously [45]. Instead of several ineffective conser-vative solutions, the Botox injection therapy is available for those who do not want the sur-gery [7, 10, 38, 40, 46], ensuring a reassuring result for 6–8 months. Surgical TS preferably performed with VAT technique could provide a long-lasting, reliable result along the negli-gible proportion of complications. More effective discovery, diagnosis of HH patients and admitting them to specialized institutes would provide help in treatment of their abnormal sweating in many more cases.
AcknowledgmentsThe authors thank all the colleagues, especially Dezső Embey-Isztin MD, for referring their patients with hyperhydrosis to our department.
REVIEWS
CEMED 69 2010 ▪ Volume 4, Number 1

ReferencesTelaranta, T.:[1] Treatment of social phobia by endoscopic thoracic sympathicotomy. Eur. J. Surg. Suppl., 1998, 580, 27–32.Stolman, L. P.:[2] Treatment of hyperhidrosis. Dermatol. Clin., 1998, 16, 863–869.Lőke, M.:[3] A felső végtag transthoracalis desympathizálása [= Transthoracal sympathectomy of the upper limb]. Somogyi Orv. Szle., 1975, 15, 99–103.Vadász, P. (ed.):[4] Az általános mellkassebészet tankönyve [= Manual of General Thoracic Surgery]. Semmel-weis, Budapest, 2006, pp. 99–100.Adar, R.:[5] Surgical treatment of palmar hyperhidrosis before thoracoscopy: experience with 475 patients. Eur. J. Surg. Suppl., 1994, 572, 9–11.Smithwick, R. H.:[6] Modifi ed dorsal sympathectomy for vascular spasm (Raynaud’s disease) of the upper extremity: a preliminary report. Ann. Surg., 1936, 104, 339–350.Amin, K. A.:[7] Primary focal hyperhidrosis. Dermatol. Rev. J., 2007, 2, 1–9.Collin, J., Whatling, P.:[8] Treating hyperhidrosis. Surgery and botulinum toxin are treatments of choice in severe cases. Br. Med. J., 2000, 320, 1221–1222.Reisfeld, R.:[9] Sympathectomy for hyperhidrosis: should we place the clamps at T2–T3 or T3–T4? Clin. Auton. Res., 2006, 16, 384–389.Glogau, R. G.:[10] Botulinum A neurotoxin for axillary hyperhidrosis. No sweat Botox. Dermatol. Surg., 1998, 24, 817–819.Alexander, W.:[11] The Treatment of Epilepsy. Y. J. Pentland, Edinburgh, 1889, p. 228.Leriche, R.:[12] De l’èlongation et de la section des nerfs pèrivasculaires daus certains syndromes dou-loureux d’origine artèrielle et daus quelques troubles trophiques. Lyon Chir., 1913, 10, 378–382.Brüning, F.:[13] Zur Technik der kombinierten Resektionsmethode sämtlicher sympatischen Nervenbahnen am Halse. Tbl. für Chir., 1923, 51, 1056–1059.Kotzareff, A.:[14] Rèsection partielle du tronc sympathique cervical droit pour hyperhydrose unilatèrale (re-gious) faciale, cervicale, thoraque et brachiale droites. Rev. Med. Suisse Rom., 1920, 40, 111–113.Hughes, J.:[15] Endothoracic sympathectomy. Proc. R. Soc. Med., 1942, 35, 585–586.Goetz, R. H., Marr, J. A. S.:[16] The importance of the second thoracic ganglion for the sympathetic supply of the upper extremities. Clin. Proc. (Cape Town), 1944, 3, 102–114.Kux, E.:[17] Thorakoskopische Eingriffe am Nervensystem. Georg Thieme, Stuttgart, 1954.Kao, M. C., Lin, J. Y., Chen, Y. L. et al.:[18] Minimally invasive surgery: video endoscopic thoracic sympathec-tomy for palmar hyperhidrosis. Ann. Acad. Med. Singapore, 1996, 25, 673–678.Kiss, T.:[19] Adatok a lumbális sympathectomia sebészi bonctanához, patológiájához és klinikumához [= Data for surgical anatomy, pathology and clinical course of lumbal sympathectomy]. Kandidátusi értekezés [= PhD thesis]. Pécs, 1957.Papp, S., Winter, L.:[20] A mellkasi behatolással végzett thoracalis sympathetomiákról [= Thoracic sympathecto-mies from thoracotomy]. Magy. Seb., 1968, 11, 120–127.Kulka, F., Fazekas, S.:[21] Egy ülésben végzett kétoldali thoracalis sympathectomia [= Simultaneous bilateral thoracic sympathectomy]. Magy. Seb., 1967, 20, 233–234.Csengődy, J., Fauszt, J.:[22] Befolyásolja-e a thoracalis sympathectomia a mellkas-vállövi kompressziós syn-droma műtéti eredményeit? [= Does thoracic sympathectomy infl uence the surgical result of thoracic outlet syndrome?] Magy. Seb., 1985, 38, 226–231.Nagy, A., Guba, Á., Szabados, Gy. et al.:[23] Endoscopos thoracalis sympathectomia. Magy. Seb., 1993, 46, 235–238.Fazekas, T., Sebestény, M., Bátorfy, J. et al.:[24] Videoendoscopos thoracalis sympathectomia. Magy. Seb., 1996, 49, 203–209.Ro, K. M., Cantor, R. M., Lange, K. L. et al.:[25] Palmar hyperhidrosis: evidence of genetic transmission. J. Vasc. Surg., 2002, 35, 382–386.Licht, P. B., Jørgensen, O. D., Ladegaard, L. et al.:[26] Thoracoscopic sympathectomy for axillary hyperhidrosis: the infl uence of T4. Ann. Thorac. Surg., 2005, 80, 455–460.Lin, C. C., Mo, L. R., Lee, L. S. et al.:[27] Thoracoscopic T2-sympathetic block by clipping – a better and revers-ible operation for treatment of hyperhidrosis palmaris: experience with 326 cases. Eur. J. Surg. Suppl., 1998, 580, 13–16.
2010 ▪ Volume 4, Number 1 70 CEMED
REVIEWS

Ueyama, T., Matsumoto, Y., Abe, Y. et al.:[28] Endoscopic thoracic sympathicotomy in Japan. Ann. Chir. Gynaecol., 2001, 90, 200–202.Yamamoto, H., Kanehira, A., Kawamura, M. et al.:[29] Needlescopic surgery for palmar hyperhidrosis. J. Thorac. Cardiovasc. Surg., 2000, 120, 276–279.Assalia, A., Bahouth, H., Ilivitzki, A. et al.:[30] Thoracoscopic sympathectomy for primary palmar hyperhidrosis: resection versus transection – a prospective trial. World J. Surg., 2007, 31, 1976–1981.Strutton, D. R., Kowalski, J. W., Glaser, D. A. et al.:[31] US prevalence of hyperhidrosis and impact on indivi-duals with axillary hyperhidrosis: results from a national survey. J. Am. Acad. Dermatol., 2004, 51, 241–248.Lin, T. S., Fang, H. Y.:[32] Transthoracic endoscopic sympathectomy in the treatment of palmar hyperhidrosis – with emphasis on perioperative management (1360 case analyses). Surg. Neurol., 1999, 52, 453–457.Kestenholz, P. B., Weder, W.:[33] Thoracic sympathectomy. Curr. Probl. Dermatol., 2002, 30, 64–76.Ojimba, T. A., Cameron, A. E.:[34] Drawbacks of endoscopic thoracic sympathectomy. Br. J. Surg., 2004, 91, 264–269.Zacherl, J., Imhof, M., Huber, E. R. et al.:[35] Video assistance reduces complication rate of thoracoscopic sympathicotomy for hyperhidrosis. Ann. Thorac. Surg., 1999, 68, 1177–1181.Haider, A., Solish, N.:[36] Focal hyperhidrosis: diagnosis and management. CMAJ, 2005, 172, 69–75.Kaufmann, H., Saadia, D., Polin, C. et al.:[37] Primary hyperhidrosis – evidence for autosomal dominant inheri-tance. Clin. Auton. Res., 2003, 13, 96–98.Atkins, J. L., Butler, P. E.:[38] Hyperhidrosis: a review of current management. Plast. Reconstr. Surg., 2002, 110, 222–228.Naumann, M., Flachenecker, P., Bröcker, E. B. et al.:[39] Botulinum toxin for palmar hyperhidrosis. Lancet, 1997, 349, 252.Heckmann, M., Ceballos-Baumann, A. O., Plewig, G. et al.:[40] Botulinum toxin A for axillary hyperhidrosis (excessive sweating). N. Engl. J. Med., 2001, 344, 488–493.Breach, N. M.:[41] Axillary hyperhidrosis: surgical cure with aesthetic scars. Ann. R. Coll. Surg. Engl., 1979, 61, 295–297.Tung, T. C., Wie, F. C.:[42] Excision of subcutaneous tissue for the treatment of axillary osmidrosis. Br. J. Plast. Surg., 1997, 50, 61–66.Hafner, J., Beer, G. M.:[43] Axillary sweat gland excision. Curr. Probl. Dermatol., 2002, 30, 57–63.Shenaq, S. M., Spira, M., Christ, J.:[44] Treatment of bilateral axillary hyperhidrosis by suction-assisted lipoly-sis technique. Ann. Plast. Surg., 1987, 19, 548–551.Elia, S., Guggino, G., Mineo, D. et al.:[45] Awake one stage bilateral thoracoscopic sympathectomy for pal-mar hyperhidrosis: a safe outpatient procedure. Eur. J. Cardiothorac. Surg., 2005, 28, 312–317.Moran, K. T., Brady, M. P.:[46] Surgical management of primary hyperhidrosis. Br. J. Surg., 1991, 78, 279–283.
REVIEWS
CEMED 71 2010 ▪ Volume 4, Number 1


In Vitro Model of Bone Regeneration with Bioactive Glass and Lipid PeroxidationLIDIJA MRAKOVCIC1, MARINA CINDRIC2, NEVEN ZARKOVIC1, SUZANA BOROVIC SUNJIC1, ANDREA MOGUS MILANKOVIC3,
RENATE WILDBURGER4
1Division of Molecular Medicine, Rudjer Boskovic Institute, Zagreb, Croatia2Department of Pathology, School of Medicine, University of Zagreb,
University Hospital Centre, Zagreb, Croatia3NMR Center, Rudjer Boskovic Institute, Zagreb, Croatia
4Universitätsklinik für Unfallchirurgie, Medizinische Universität Graz, Graz, Austria
Tissue regeneration is a complex biological process of vital importance since it allows renewal of damaged cells and organs. The healing of long bones and large joints is often extended or incomplete primarily in elderly people or in polytraumatized patients. Various attempts are made to solve this severe medical and social problem by developing novel bioactive materials, among which bioactive glass is the most attractive because of its osteoconductive and osteostimulative properties. Lipid peroxidation is defi ned as an important parameter of systematic stress response in patients with traumatic brain injuries and bone fractures. The major bioactive marker and fi nal product of lipid per-oxidation, 4-hydroxynonenal (HNE), is a particularly interesting biomolecule because it regulates differentiation, proliferation and apoptosis of cells and might therefore play an important role in regulating the regeneration of dam-aged tissue such as bone. Therefore, in this study, we investigated the concept of using bioactive glass functionalized with HNE as an in vitro model of bone regeneration.
Keywords: bone regeneration, bioactive glass, 4-hydroxynonenal
Abbreviations
HNE = 4-hydroxynonenal; bFGF = basic fi broblast growth factor; IGF-1 = insulin like growth factor type 1; BSA = bovine serum albumin; HOS = human osteosarcoma cell line; DMEM = Dulbecco’s modifi ed eagle medium; FCS = fetal calf serum
IntroductionFractures of long bones or large joints are often not followed by successful recovery, in par-ticular in elderly patients, in patients who suffer from multi-fragmentary bone fractures or in polytraumatized patients. Because these fractures cause severe pain and long-lasting invalid-ity, they represent not only a diffi cult medical disorder but also a serious social and eco-nomic problem. In a large number of cases, the resulting skeletal defi ciencies require surgical intervention and repair [1]. An important problem in orthopaedic surgery is the choice be-tween a transplanted viable tissue and an implanted synthetic material. While the use of au-tografts has been the most widely recommended approach, it does have its drawbacks, in-
Corresponding address: Lidija Mrakovcic MD, Division of Molecular Medicine, Laboratory for Oxidative Stress, Rudjer Boskovic Institute, Bijenicka 54, Zagreb, Croatia. E-mail: [email protected]
1.7
ORIGINAL PAPERS
ORIGINAL PAPERS
DOI: 10.1556/CEMED.4.2010. 73 2010 ▪ Volume 4, Number 1 ▪ 73–78.
cluding donor site morbidity, limited donor bone supply as well as different anatomic and structural problems. On the other hand, rejection phenomena and the risk of viral transmis-sion with allogenic and xenogenic grafts lead to reduced usage of these materials for the transplantation of living tissues in reconstructive surgery [2–4]. Research on bone-substitute materials has been conducted to overcome this problem. Ideally, a bone graft should be bio-compatible, able to support abundant bone formation (osteoconductive), able to induce bone formation (osteoinductive), able to form a continuous interface with surrounding bone tissue (osteointegrative), able to support angiogenesis and able to be structurally and mechanically compatible with bone tissue. Bioactive material is by defi nition “one that elicits a specifi c biological response at the interface of the material that results in the formation of a bond between the tissues and the material” [5]. There is a wide range of calcium phosphate ceram-ics (Ca–P), bioactive glasses (BG) and bioactive glass-ceramics currently available in the market [6, 7]. These materials generate a carbonated hydroxyapatite layer that is chemically and structurally equivalent to the biological mineral of bone. This is known to be the deter-mining step for biointegration [8]. Furthermore, it was found that BG with a composition of less than 55% SiO2 not only exhibit osteoconductivity, but are also responsible for osteopro-duction by stimulating proliferation and differentiation of osteoprogenitor cells [9]. These glasses have been widely used in a variety of clinical applications, from middle ear ossicular prosthesis in otological surgery to bone grafting material in the fi elds of maxillofacial surgery and dentistry [10, 11]. Major bone-bioactive material known to date is 45S5 bioactive glass [4]. In addition to being osteointegrative, the biocompatible, osteoconductive and osteoin-ductive nature of 45S5 bioactive glass has been well documented [4, 12–18]. Nevertheless, synthetic materials typically cannot replace all the functions of a host tissue and are incapable of adapting to the changing requirements of the body over time. Because of these limitations, the search for new alternative strategies for repairing bone defects has been focused on tissue engineering.
On the other hand, the phenomenon of enhanced osteogenesis in patients with traumatic brain injury that exert very short period of bone healing followed by heterotopic ossifi cation or hypertrophic callus formation has been found to be connected with stress response that involves hormonal imbalance associated with the change of growth factor activities, in par-ticular bFGF and IGF-1, together with oxidative stress and lipid peroxidation [19–23]. Thus, lipid peroxidation was defi ned as an important parameter of systemic response in patients with traumatic brain injuries and with bone fractures. Recent results have shown that the end product of lipid peroxidation, 4-hydroxynonenal (HNE), acts as a growth-regulating factor interfering with the activity of cytokines and may affect the growth of cultured human bone cells [24, 25]. HNE is known as a major bioactive marker of lipid peroxidation that acts as a second messenger of free radicals and a signaling molecule and is a particularly interesting biomolecule because it regulates differentiation, proliferation and apoptosis of cells and might therefore play an important role in regulating the regeneration of damaged tissue such as bone [26–31]. HNE has already been successfully used to functionally activate carbon nanotubes, thus stimulating in vitro neuronal growth [32]. However, similar approach has not been applied until now for bioactive glass and bone tissue. In this study, we investigated the concept of using functionalized BG 45S5 and 19–93 with HNE as an in vitro model of bone regeneration.
2010 ▪ Volume 4, Number 1 74 CEMED
ORIGINAL PAPERS
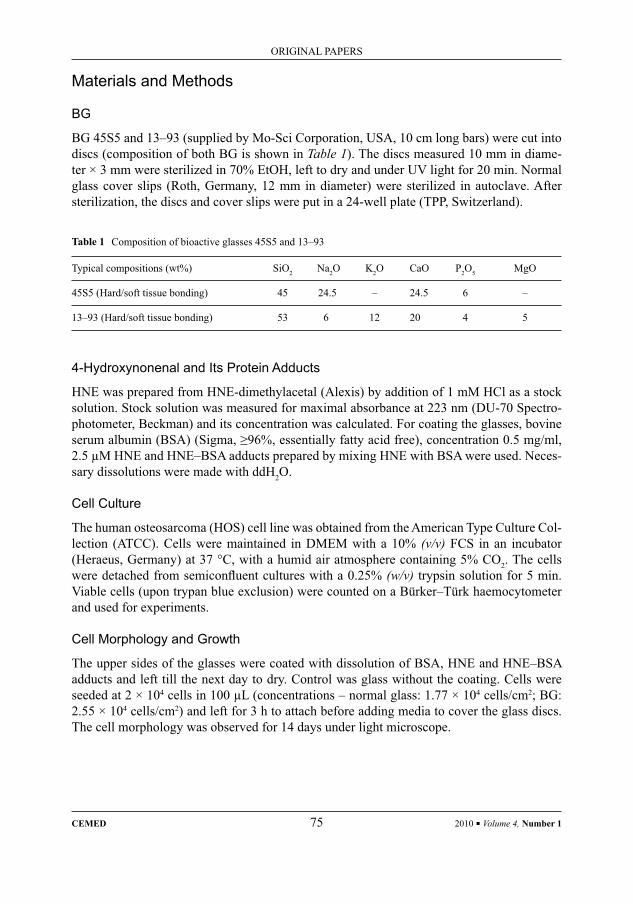
Materials and Methods
BG
BG 45S5 and 13–93 (supplied by Mo-Sci Corporation, USA, 10 cm long bars) were cut into discs (composition of both BG is shown in Table 1). The discs measured 10 mm in diame-ter × 3 mm were sterilized in 70% EtOH, left to dry and under UV light for 20 min. Normal glass cover slips (Roth, Germany, 12 mm in diameter) were sterilized in autoclave. After sterilization, the discs and cover slips were put in a 24-well plate (TPP, Switzerland).
Table 1 Composition of bioactive glasses 45S5 and 13–93
Typical compositions (wt%) SiO2 Na2O K2O CaO P2O5 MgO
45S5 (Hard/soft tissue bonding) 45 24.5 – 24.5 6 –
13–93 (Hard/soft tissue bonding) 53 6 12 20 4 5
4-Hydroxynonenal and Its Protein Adducts
HNE was prepared from HNE-dimethylacetal (Alexis) by addition of 1 mM HCl as a stock solution. Stock solution was measured for maximal absorbance at 223 nm (DU-70 Spectro-photometer, Beckman) and its concentration was calculated. For coating the glasses, bovine serum albumin (BSA) (Sigma, ≥96%, essentially fatty acid free), concentration 0.5 mg/ml, 2.5 μM HNE and HNE–BSA adducts prepared by mixing HNE with BSA were used. Neces-sary dissolutions were made with ddH2O.
Cell Culture
The human osteosarcoma (HOS) cell line was obtained from the American Type Culture Col-lection (ATCC). Cells were maintained in DMEM with a 10% (v/v) FCS in an incubator (Heraeus, Germany) at 37 °C, with a humid air atmosphere containing 5% CO2. The cells were detached from semiconfl uent cultures with a 0.25% (w/v) trypsin solution for 5 min. Viable cells (upon trypan blue exclusion) were counted on a Bürker–Türk haemocytometer and used for experiments.
Cell Morphology and Growth
The upper sides of the glasses were coated with dissolution of BSA, HNE and HNE–BSA adducts and left till the next day to dry. Control was glass without the coating. Cells were seeded at 2 × 104 cells in 100 μL (concentrations – normal glass: 1.77 × 104 cells/cm2; BG: 2.55 × 104 cells/cm2) and left for 3 h to attach before adding media to cover the glass discs. The cell morphology was observed for 14 days under light microscope.
ORIGINAL PAPERS
CEMED 75 2010 ▪ Volume 4, Number 1
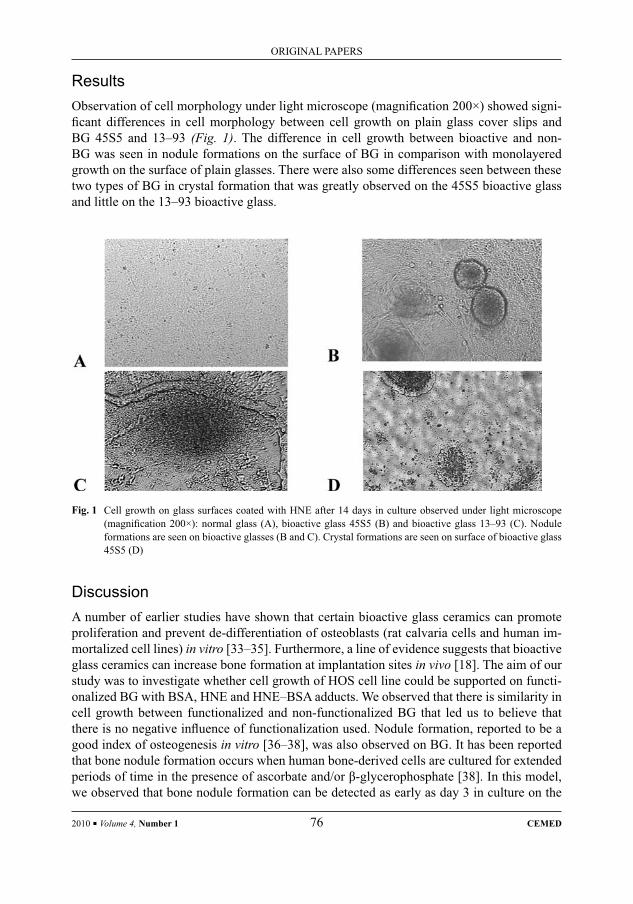
ResultsObservation of cell morphology under light microscope (magnifi cation 200×) showed signi-fi cant differences in cell morphology between cell growth on plain glass cover slips and BG 45S5 and 13–93 (Fig. 1). The difference in cell growth between bioactive and non-BG was seen in nodule formations on the surface of BG in comparison with monolayered growth on the surface of plain glasses. There were also some differences seen between these two types of BG in crystal formation that was greatly observed on the 45S5 bioactive glass and little on the 13–93 bioactive glass.
Fig. 1 Cell growth on glass surfaces coated with HNE after 14 days in culture observed under light microscope (magnifi cation 200×): normal glass (A), bioactive glass 45S5 (B) and bioactive glass 13–93 (C). Nodule formations are seen on bioactive glasses (B and C). Crystal formations are seen on surface of bioactive glass 45S5 (D)
DiscussionA number of earlier studies have shown that certain bioactive glass ceramics can promote proliferation and prevent de-differentiation of osteoblasts (rat calvaria cells and human im-mortalized cell lines) in vitro [33–35]. Furthermore, a line of evidence suggests that bioactive glass ceramics can increase bone formation at implantation sites in vivo [18]. The aim of our study was to investigate whether cell growth of HOS cell line could be supported on functi-onalized BG with BSA, HNE and HNE–BSA adducts. We observed that there is similarity in cell growth between functionalized and non-functionalized BG that led us to believe that there is no negative infl uence of functionalization used. Nodule formation, reported to be a good index of osteogenesis in vitro [36–38], was also observed on BG. It has been reported that bone nodule formation occurs when human bone-derived cells are cultured for extended periods of time in the presence of ascorbate and/or β-glycerophosphate [38]. In this model, we observed that bone nodule formation can be detected as early as day 3 in culture on the
2010 ▪ Volume 4, Number 1 76 CEMED
ORIGINAL PAPERS

bioactive glass, without either of the supplements mentioned earlier in the culture medium. Crystal formation was observed greatly on the surface of bioactive glass 45S5, while on BG 13–93 it was little to not present on the surface of the plain glass. This suggests the possible presence of the carbonated hydroxyapatite layer that is equivalent chemically and structur-ally to the biological mineral of bone, and thus needed for bone regeneration.
All our current fi ndings give us promising results that this could be an in vitro model for the investigation of osteogenesis, but to get more clear answers, some additional experiments need to be done.
AcknowledgmentsThis research is supported by the Croatian Ministry of Science, Education and Sport, by the Austrian National Bank Jubilaeums Fund and by COST Action B35.
ReferencesDamien, J. C., Parson, J. R.:[1] Bone graft and bone graft substitutes: a review of current technology and applications. J. Appl. Biomater., 1991, 2, 187–208.Kitsugi, T., Yamamuro, T., Nakamura, T. et al.:[2] Four calcium phosphate ceramics as bone substitute for non-weight-bearing. Biomaterials, 1993, 14, 216–224.Daculsi, G., Leberos, R. Z., Nery, E. et al.:[3] Transformation of biphasic calcium phosphate ceramics in vivo, ultrastructural and physico-chemical characterization. J. Biomed. Mater. Res., 1989, 23, 883–894.Hench, L. L.:[4] Bioceramics: from concept to clinic. J. Am. Ceram. Soc., 1991, 74, 1487–1510.Hench, L. L., Splinter, R. J., Allen, W. C. et al.:[5] Bonding mechanism at the interface of ceramic prosthetic materials. Part 1. J. Biomed. Mater. Res. Symp., 1971, 2, 117–141.Hench, L. L., West, J. K.:[6] Biological applications of bioactive glasses. Life Chem. Rep., 1996, 13, 187–241.Kokubo, T., Ito, S., Huang, T. et al.:[7] Ca, P-rich layer formed on high strength bioactive glass ceramic A-W. J. Biomed. Mater. Res., 1990, 24, 331–343.Kitsugi, T., Nakamura, T., Yamamura, T. et al.:[8] SEM EPMA observation of three types of apatite containing glass ceramics implanted in bone: the variance of a Ca–P rich layer. J. Biomed. Mater. Res., 1987, 21, 1255–1271.Oghushi, H., Dohi, Y., Yoshikawa, T. et al.:[9] Osteogenic differentiation of cultured marrow stem cells on the surface of bioactive glass ceramic. J. Biomed. Mater. Res., 1996, 32, 341–348.Kinnunen, I., Aitasalo, K., Pollonen, M. et al.:[10] Reconstruction of orbital fl oor fractures using bioactive glass. J. Craniomaxillofac. Surg., 2000, 28, 229–234.Park, J. S., Suh, J. J., Choi, S. H. et al.:[11] Effects of pretreatment clinical parameters on bioactive glass implan-tation in intrabony periodontal defects. J. Periodontol., 2001, 72, 730–740.Ducheyne, P.:[12] Bioceramics: material characteristics versus in vivo behavior. J. Biomed. Mater. Res., 1987, 21, 219–236.Oonishi, H., Kushitani, S., Yasukawa, E. et al.:[13] Particulate bioglass compared with hydroxyapatite as a bone graft substitute. Clin. Orthop., 1997, 334, 316–325.Davies, J. E., Baldan, N.:[14] Scanning electron microscopy of the bone-bioactive implant interface. J. Biomed. Mater. Res., 1997, 36, 429–440.Gatti, A. M., Valdre, G., Andersson O. H.:[15] Analysis of the in vivo reactions of a bioactive glass in soft and hard tissue. Biomaterials, 1994, 15, 208–212.Hattar, S., Berdal, A., Asselin, A. et al.:[16] Behaviour of moderately differentiated osteoblast-like cells cultured in contact with bioactive glasses. Eur. Cells Mater., 2002, 4, 61–69.Hench, L. L.:[17] The story of bioglass. J. Mater. Sci.: Mater. Med., 2006, 17, 967–978.Vogel, M., Voigt, C., Gross, U. et al.:[18] In vivo comparison of bioactive glass particles in rabbits. Biomaterials, 2001, 22, 357–362.
ORIGINAL PAPERS
CEMED 77 2010 ▪ Volume 4, Number 1

Wildburger, R., Zarkovic, N., Egger, G. et al.:[19] Basic fi broblast growth factor (bFGF) immunoreactivity as a possible link between head injury and impaired bone fracture healing. Bone Miner., 1994, 27, 183–192.Wildburger, R., Zarkovic, N., Egger, G. et al.:[20] Comparison of the values of basic fi broblast growth factor de-termined by an immunoassay in the sera of patients with traumatic brain injury and enhanced osteogenesis and the effects of the same sera on the fi broblast growth in vitro. Eur. J. Clin. Chem. Clin. Biochem., 1995, 33, 693–698.Wildburger, R., Zarkovic, N., Leb, G. et al.:[21] Post-traumatic changes of insulin like growth factor type 1 and growth hormone in patients with bone fractures and traumatic brain injury. Wien. Klin. Wochenschr., 2001, 113, 119–126.Wildburger, R., Zarkovic, N., Tatzber, F. et al.:[22] Post-traumatic dynamic changes of the titer of auto antibodies oxidized low-density lipoproteins; unspecifi c or organ-specifi c consequences of injury. Biofactors, 1997, 6, 292–293.Wildburger, R., Borovic, S., Zarkovic, N. et al.:[23] Post-traumatic dynamic changes of the antibody titer against oxidized low-density lipoproteins. Wien. Klin. Wochenschr., 2000, 112, 798–803.Borovic Sunjic, S., Cipak, A., Rabuzin, F. et al.:[24] The infl uence of 4-hydroxy-2-nonenal on proliferation, dif-ferentiation and apoptosis of human osteosarcoma cells. Biofactors, 2005, 24, 141–148.Borovic, S., Cipak, A., Meinitzer, A. et al.:[25] Differential sensitivity to 4-hydroxynonenal for normal and malig-nant mesenchymal cells. Redox Rep., 2007, 12, 50–54.Zarkovic, N., Ilic, Z., Jurin, M. et al.:[26] Stimulation of HeLa cell growth by physiological concentrations of 4-hydroxynonenal. Cell Biochem. Funct., 1993, 11, 279–286.Zarkovic, N., Schaur, R. J., Puhl, H. et al.:[27] Mutual dependence of growth modifying effects of 4-hydroxy-nonenal and fetal calf serum in vitro. Free Radic. Biol. Med., 1994, 16, 877–884.Kreuzer, T. H., Grube, R., Zarkovic, N. et al.:[28] 4-Hydroxynonenal modifi es the effects of serum growth factors on the expression of c-fos proto-oncogene and the proliferation of HeLa carcinoma cells. Free Radic. Biol. Med., 1998, 25, 42–49.Zarkovic, N., Zarkovic, K., Schaur, R. J. et al.:[29] 4-Hydroxynonenal as a second messenger of free radicals and growth modifying factor. Life Sci., 1999, 65, 1901–1904.Biasi, F., Vizio, B., Mascia, C. et al.:[30] JNK up-regulation as a key event in the pro-apoptotic interaction be-tween TGF-β1 and 4-hydroxynonenal in colon mucosa. Free Radic. Biol. Med., 2006, 40, 443–454.Zarkovic, N.:[31] 4-Hydroxynonenal as a bioactive marker of pathopysiological processes. Mol. Aspects Med., 2003, 24, 281–291.Mattson, M. P., Haddon, R. C., Rao, A. M.:[32] Molecular functionalization of carbon nanotubes and use as substrates for neuronal growth. J. Mol. Neurosci., 2000, 14, 175–182.Matsuda, T., Davies, J. E.:[33] The in vitro response of osteoblasts to bioactive glass. Biomaterials, 1987, 8, 275–284.Vrouwenvelder, W. C. A., Groot, C. G., de Groot, K.:[34] Behaviour of fetal rat osteoblasts cultured in vitro on bioactive glass and nonreactive glasses. Biomaterials, 1992, 13, 382–392.Price, N., Bendall, S. P., Frondosa, C. et al.:[35] Human osteoblast-like cells (MG63) proliferate on a bioactive glass surface. J. Biomed. Mater. Res., 1997, 37, 394–400.Gough, J. E., Jones, J. R., Hench, L. L.:[36] Nodule formation and mineralisation of human primary osteoblasts cultured on a porous bioactive glass scaffold. Biomaterials, 2004, 25, 2039–2046.Malaval, L., Modrowski, D., Gupta, A. K. et al.:[37] Cellular expression of bone-related proteins during the in vitro osteogenesis in rat bone marrow stromal cell cultures. J. Cell Physiol., 1994, 158, 555–572.Beresford, J. N., Graves, S. E., Smoothy, C. A.:[38] Formation of mineralised nodules by bone-derived cells in vitro: a model of bone formation? Am. J. Med. Genet., 1993, 45, 163–178.
2010 ▪ Volume 4, Number 1 78 CEMED
ORIGINAL PAPERS

Intermittent Haemodialysis-Induced Oxidative Stress and the Effect
on Infl ammatory Parameters in Critically Ill PatientsKARL-HEINZ SMOLLE1, PETER KAUFMANN1, VANESSA STADLBAUER1,
FRANZ TATZBER2, BRIGITTE M. WINKLHOFER-ROOB3, REINGARD AIGNER4, GHOLAMALI KHOSCHSORUR5, WILLIBALD WONISCH5, 6
1Department of Internal Medicine, Medical University, Graz, Austria2Institute of Nuclear Medicine, University Medical Center, Vienna, Austria
3Human Nutrition & Metabolism Research and Training Center, Institute of Molecular Biosciences, Karl-Franzens University, Graz, Austria
4Department of Nuclear Medicine, Medical University, Graz, Austria5Clinical Institute of Medical and Chemical Laboratory Diagnostics, Medical University, Graz, Austria
6Institute of Physiological Chemistry, Center for Physiological Medicine, Medical University, Graz, Austria
In this study, we evaluated the impact of intermittent haemodialysis (IHD) on different indices of infl ammation [elastase, procalcitonin (PCT) and neopterin] and on oxidative stress biomarkers [total peroxides (TOC), autoanti-bodies against oxidized LDL (oLAb), malondialdehyde (MDA)] in eight mechanically ventilated, critically ill pa-tients with acute oliguric renal failure. IHD decreased the neopterin levels (113 ± 74 vs. 81 ± 46 nmol/L, p = 0.003) in contrast to elastase concentrations, which increased in plasma during this procedure (100 ± 45 vs. 184 ± 73 μg/L, p = 0.002). The membrane passage increased the generation of total peroxides (247 ± 232 vs. 342 ± 253 μmol/L, p = 0.028), whereas PCT, MDA and oLAb were not affected. These results indicate that infl ammatory parameters are signifi cantly affected by renal replacement therapy and that membrane passage causes peroxide generation. Therefore, these markers should be interpreted with caution to avoid misinterpretation if used as clinical prognostic markers in critically ill patients undergoing renal replacement therapy.
Keywords: critical illness, infl ammation, reactive oxygen species, intensive care
IntroductionTreatment of sepsis is still challenging. With invasive infection or severe trauma, excessive amounts of pro-infl ammatory cytokines such as tumour necrosis factor (TNF), interleukin-1 (IL-1) and interleukin-6 (IL-6) are released into the systemic circulation. The severity of sepsis and the mortality rate correlate signifi cantly with serum concentrations of different infl ammatory mediators. Numerous studies in critically ill patients aimed to remove pro-in-fl ammatory mediators with continuous hemofi ltration, but any blood-membrane interaction also generates cytokines [1–8]. Most of these studies demonstrated the presence of such me-diators in the ultrafi ltrate, though decreases in plasma concentrations were either marginal or non-existent [9, 10].
Corresponding address: Karl-Heinz Smolle MD, Department of Internal Medicine, Intensive Care Unit, Medical University, Auenbruggerplatz 15, A-8036 Graz, Austria. E-mail: [email protected]
1.8
ORIGINAL PAPERS
DOI: 10.1556/CEMED.4.2010. 79 2010 ▪ Volume 4, Number 1 ▪ 79–88.

Cuprophane membranes used in intermittent haemodialysis (IHD) stimulate the infl am-matory system. TNF-α-inducing activity increased with regenerated cellulose, cellulose tri-acetate and polyacrylonitrile-membranes. It did not increase with polysulfone or polyamide dialyzers [11].
In contrast to numerous studies which investigated the impact of IHD on cytokines, which are not yet available for routine diagnosis, our study focused on the effect of IHD on infl ammatory parameters, such as procalcitonin (PCT), neopterin and polymorphnuclear elastase (PMN elastase), which are used as diagnostic and prognostic tools in critically ill patients.
PCT, a polypeptide of 116 amino acids with a MW of 13 kDa, is produced by mononu-clear cells after stimulation with lipopolysaccharide (LPS) or cytokines. Plasma levels of PCT correlate not only with the extent and the activity of the infl ammation process but also with the clinical course and have the potential to assess treatment effi cacy as well [12–17].
PMN elastase, a glycoprotein of 218 amino acids with a molecular weight (MW) of 30 kDa, is released from peripheral polymorphonuclear leukocytes (PMN) after being activated by infection, trauma or injury. Blood PMN elastase concentrations are used both as a prog-nostic infl ammatory parameter and as a predictive marker for post-surgical and post-traumat-ic complications [18, 19]. Granulocytes are activated and PMN elastase is released as well if these cells contact dialyzer membranes [20–22]. Neopterin, with a MW of 253 D, is a useful biomarker of infl ammation involving monocyte/macrophage activation and has been found to be elevated in several diseases, for example, pancreatitis, where neopterin levels also refl ect the severity of the disease [23]. Serum neopterin might also be a useful marker for the early identifi cation of patients at risk of multiple organ dysfunction syndrome or in the manage-ment of septicemic patients in intensive care units [15, 24, 25]. In addition to that, Neopterin was reported to indicate the degree and prognosis of the disease in critically ill patients [26].
Release of granular enzymes from polymorphonuclear leukocytes and generation of reactive oxygen species (ROS) causing lipid peroxidation have been reported in patients treated by IHD [27, 28]. MDA is a lipid peroxidation end-product and can, therefore, be used as a biomarker of oxidative stress, which is believed to play a key role in atherogenesis [29]. Lipid hydroperoxides are generated through the attack of ROS on polyunsaturated fatty acids (PUFAs). The emerging carbon-centred lipid radical reacts quickly with molecular oxygen, resulting in a lipid peroxyl radical, which further abstracts a hydrogen atom from an adjacent PUFA, yielding a lipid hydroperoxide [30]. This oxidative stress biomarker, which is associ-ated with the clinical situation [31], signifi cantly correlates with infl ammation markers [32, 33]. Autoantibodies against oxidized low density lipoprotein (oLAb) are inversely re-lated to the initima-media thickness of the carotid arteries [34] and the determination of these antibodies was reported to be a useful biological marker of in vivo LDL oxidation for screen-ing and follow-up studies [35].
Renal replacement procedures can potentially remove markers of infl ammation from the systemic circulation, depending on the biocompatibility and the membrane performance. On the contrary, this procedure increases oxidative stress. We, therefore, hypothesized that IHD signifi cantly affects infl ammatory mediators, especially if they are of low MW, poten-tially causing problems in the interpretation of these biomarkers when patients are under re-nal replacement therapy. Moreover, an increase of ROS might affect the fettle of patients undergoing IHD. The present study prospectively examined the effects of IHD on infl amma-
2010 ▪ Volume 4, Number 1 80 CEMED
ORIGINAL PAPERS

tory mediators and oxidative stress biomarkers in critically ill patients with acute oliguric renal failure and who were mechanically ventilated.
Materials and Methods
Samples
Eight critically ill patients (three males, mean age 57.6 ± 22.8 years and fi ve females, mean age 57.6 ± 22.8 years) with SIRS or sepsis, as defi ned by the ACCP/SCCM Consensus Con-ference and mechanically ventilated, were studied during the fi rst 240 min of IHD (Table 1). The study protocol was approved by the local ethics committee. Written, informed consent was obtained from the next of kin of each patient. Serum and ultrafi ltrate samples were fro-zen at −70 °C until assayed.The clinical indications for initiating IHD were:1. Signifi cant azotemia (initial BUN levels between 60 and 100 mg/dL)2. Life-threatening fl uid overload3. Severe electrolyte imbalanceAll patients were oliguric, with less than 200 mL of urine per day.
Table 1 Clinical features of patients
Age/sex Diagnosis SAPSII/TISS score
68/f Intoxication, diabetes mellitus, acute heart failure 64/32
78/f Bacterial meningitis 78/29
33/m Acute heart failure, hypertensive crisis, pulmonary edema 80/27
88/m Acute heart failure, prostate cancer, urosepsis 46/42
52/m Diabetes mellitus, necrotizing fasciitis sepsis 68/36
61/f Acute pyelonephritis, acute heart failure, pulmonary edema 81/37
48/f Ethanol intoxication, rhabdomyolysis 56/42
76/f Pneumonia, septic shock 91/37
IHD Procedure
For IHD, a conventional circuit (Gambro, Lund and Sweden) with a low fl ux, polysulfone membrane (F8 HPS, Fresenius Medical Care, Bad Homburg, Germany) was used for 4 h. The blood fl ow was 200–250 mL/min, dialysate fl ow 500 mL/min and the net ultrafi ltration was 500–800 mL/h to achieve negative fl uid balance.
Blood samples were taken afferent port, prior to the infusion of pre-dilution, represent-ing the patient’s systemic level and from the efferent port of the extracorporal circuit at the
ORIGINAL PAPERS
CEMED 81 2010 ▪ Volume 4, Number 1
start of hemofi ltration at 0, 10, 60 and 240 min. Ultrafi ltrate was not collected due to the low cut-off of the membrane used.
Biomarkers
PCT was measured using the Lumitest® PCT supplied by B.R.A.H.M.S.-Diagnostica GmbH (Berlin, Germany).
PMN elastase was measured using the Ecoline® Immunoassay supplied by Merck (Darmstadt, Germany).
Neopterin was measured using the commercial Neopterin Radio-Immuno-Assay (RIA) supplied by IBL (Hamburg, Germany).
MDA was determined with a high-performance liquid chromatographic (HPLC) method with spectrofl uorimetric detection as described by Khoschsorur et al. [36]. Plasma was mixed with H3PO4 (0.44M), aqueous TBA (42 mM) and bidistilled water. The mixture was heated in a boiling-water bath for 60 min, it was then cooled on ice and alkaline methanol was added (1:1). After a centrifugation step, the neutralized reaction mixture was chromato-graphed on a 150 mm 4.6 mm LiChrosorb RP18 column using phosphate buffer/methanol (40:60) as mobile phase. The fl ow rate was 0.8 mL min−1 and the fl uorimetric detection was performed with excitation at 527 nm and emission at 551 nm. Calibration was done with a TEP standard solution processed in exactly the same way as the plasma samples.
Serum total peroxide concentrations were determined by a rapid enzymatic in vitro di-agnostic assay supplied by LDN (Nordhorn, Germany), as described elsewhere [37].
Autoantibodies against oxidized LDL (oLAb) were measured in serum with the com-mercial enzyme immunoassay supplied by Biomedica (Vienna, Austria), according to the method of Tatzber and Esterbauer [29].
Statistics
Statistical analysis was performed using the Sigma-Stat 3.1 and Sigma-Plot 9.0 package (SPSS, Erkrath, Germany). Treatment groups were compared using the paired t-test. One-Way Repeated Measures ANOVA was used to analyse changes over time. When normality testing failed, the Wilcoxon Signed-Rank Test and the Friedman Repeated Measures ANOVA on Ranks, respectively, were used.
ResultsDemographic data, including diagnosis and SAPSII/TISS scores, are shown in Table 1.
Indices of Infl ammation in the Course of IHD
Procalcitonin (PCT)
We observed a signifi cant increase in PCT concentrations over time for post-membrane sam-ples. However, there were no signifi cant changes in PCT levels in the IHD group after the membrane passage or in the time course of pre-membrane samples. The results are listed in Table 2.
2010 ▪ Volume 4, Number 1 82 CEMED
ORIGINAL PAPERS
Table 2 Membrane effects on infl ammatory parameters (Elastase, Neopterin and Procalcitonin) and oxidative stress biomarkers during IHD procedure
Infl ammation parameters
Parameter: Elastase (mU/mL) Neopterin (nmol/L) Procalcitonin (ng/mL)
Time (min)
Pre-IHD Post-IHD P1 Pre-IHD Post-IHD P1 Pre-IHD Post-IHD P1
T0 100 ± 45 125 ± 72 0.031 113 ± 74 33 ± 25 0.005 20 ± 37 22 ± 46 0.195
T10 125 ± 76 145 ± 72 0.010 107 ± 64 41 ± 23 0.008 20 ± 37 21 ± 39 1.000
T60 177 ± 84 204 ± 81 0.031 88 ± 51 26 ± 17 0.002 20 ± 38 23 ± 47 0.219
T240 184 ± 73 217 ± 65 0.005 81 ± 46 26 ± 18 0.003 22 ± 42 26 ± 53 0.383
P2 0.002 0.002 0.003 0.034 0.112 0.001
P1: Paired t-test P1: Paired t-test P1: Wilcoxon Signed-Rank Test
P2: One-Way Repeated Measures P2: One-Way Repeated Measures P2: Friedman Repeated Measures
ANOVA ANOVA ANOVA on ranks
Oxidative stress biomarkers
Parameter: Total peroxides (AU) MDA (μmol/L) oLAb (mU/mL)
Time (min)
Pre-IHD Post-IHD P1 Pre-IHD Post-IHD P1 Pre-IHD Post-IHD P1
T0 108 ± 137 247 ± 232 0.030 1.46 ± 0.6 1.07 ± 0.7 0.070 315 ± 204 377 ± 373 0.844
T10 138 ± 177 267 ± 242 0.012 1.60 ± 0.8 1.63 ± 0.9 0.844 288 ± 168 391 ± 376 0.219
T60 134 ± 179 316 ± 260 0.010 1.47 ± 0.7 1.41 ± 0.8 0.798 392 ± 315 420 ± 379 0.469
T240 188 ± 206 342 ± 253 0.004 1.32 ± 0.5 1.24 ± 0.5 0.391 422 ± 376 442 ± 372 0.056
P2 0.059 0.028 0.583 0.170 0.279 0.159
P1: Paired t-test P1: Paired t-test P1: Wilcoxon Signed-Rank Test
P2: One-Way Repeated Measures P2: Friedman Repeated Measures P2: Friedman Repeated Measures
ANOVA ANOVA on ranks ANOVA on ranks
Elastase
Elastase levels in IHD patients increased signifi cantly not only from pre- to post-membrane but also continuously over time after the onset of haemodialysis.
ORIGINAL PAPERS
CEMED 83 2010 ▪ Volume 4, Number 1

Neopterin
Neopterin was signifi cantly lower in post-membrane samples compared to pre-membrane samples and there was also a signifi cant decrease in the time course of neopterin levels for pre-membrane and post-membrane samples.
Oxidative Stress Biomarkers in the Course of IHD
Malondialdehyde (MDA)
We observed no signifi cant differences in the MDA level, neither between pre- and post-membrane samples nor in the course of the treatment.
Total Peroxides
Peroxide concentrations in IHD patients signifi cantly increased after membrane passage as well as in the time course of post-membrane samples and barely failed to become signifi cant in the time course of pre-membrane samples.
Autoantibodies Against Oxidized LDL (oLAb)
There were no signifi cant differences in the oLAB titer in the IHD group.
DiscussionSeveral studies evaluated the effects of haemodialysis on the elimination of different kinds of cytokines, complement factors and endotoxins, but little is known about infl ammatory and oxidative stress parameters. The rationale of this study was to evaluate the effects of IHD on frequently used infl ammatory parameters and oxidative stress biomarkers in critically ill patients.
PCT plasma levels did not change during IHD treatment, although we observed in-creased post-membrane PCT concentrations. These results are in accordance with Herget-Rosenthal et al. [38], who found unchanged PCT concentrations during IHD with low-fl ux membranes but a decrease in PCT levels by 17% with high fl ux haemodialysis. Thus, the elimination of PCT in substantial amounts is solely possible with convective or diffusive procedures with adequate rates of blood fl ow and ultrafi ltration, and highly permeable mem-branes. The increase of PMN elastase after membrane passage in IHD indicated a non-spe-cifi c activation of granulocytes. This is consistent with the results of Hörl et al. [20], who reported increases in PMN elastase complexes with different dialysis membranes, refl ecting their biocompatibility. Compared to high fl ux cellulose acetate membranes, high fl ux PMMA membranes cause greater leukocyte stimulation, as demonstrated by the greater release of PMN elastase during haemodialysis [39, 40].
Strohmaier [24] and Pacher [25] reported increased neopterin levels in patients who became septic in the course of their illness in contrast to those who did not, as well as in subjects with a fatal outcome in comparison to survivors. A decrease in neopterin levels nor-mally indicates an improvement during the course of disease. We observed a dramatic de-
2010 ▪ Volume 4, Number 1 84 CEMED
ORIGINAL PAPERS

crease in neopterin concentrations after membrane passage in IHD patients, as neopterin was quickly removed from circulation into the ultrafi ltrate due to its low MW.
Water- and lipid-soluble antioxidants are metabolized during the course of dialysis. Moreover, oxidative stress exceeds the antioxidative capacity in patients on haemodialysis, as indicated by increased production of peroxides, depending on the membrane material [41, 42]. Cellulose membranes, in particular, are associated with a signifi cant increase in resting and stimulated peroxide production. This was observed to a lesser extent with synthetic membranes such as polymethylmethacrylate and polysulfone. In addition, increased oxidized plasma protein products may also refl ect decreased antioxidant defence. This is also in agree-ment with the report of Gonzalez-Diez et al. [43] which indicated a decreased total antioxi-dant status as well as decreased activities of antioxidant enzymes and glutathione levels in chronic renal failure patients undergoing chronic dialysis treatment. In addition, these pa-tients exhibited increased levels of oxidative stress in lymphocytes, that is, thiobarbituric-acid-reactive substances (TBARS) and 8-hydroxy-2-deoxyguanosine, whereas these oxida-tive stress markers were unaltered in plasma. The latter coincides with the unchanged levels for MDA in plasma and oLAb in serum in the present study, which are middle- to long-term oxidative stress biomarkers. The fi ndings of Himmelfarb and McMonagle showed that albu-min may be an important defence against oxidative stress [44]. This result is supported by the fi nding of Soejima et al. that patients with hypoalbuminaemia demonstrate a greater degree of lipid peroxidation [45]. Serum total peroxides, representing a short-term oxidative stress biomarker, increased signifi cantly in IHD after membrane passage. In addition to it, there was also a continuous increase in post-membrane peroxide concentrations over the observation period. Increased oxidative stress in dialysis patients is caused by diverse effects, fi rst, there is loss of low-molecular-weight antioxidants, secondly, dialysis systems could be hemoincompatible and thirdly, pro-oxidant uremic toxins might also contribute to a dete-riorated balance between pro- and antioxidants. Incipient stages using hemodiafi ltration with on-line regeneration of the ultrafi ltrate (HFR) were shown to be preferential to polysul-fone membranes with respect to attenuated oxidative stress [43, 46]. Furthermore, the treat-ment with antioxidants was reported to improve oxidative stress in dialysis patients signifi -cantly [47].
Conclusions
This study showed that renal replacement therapy was associated with an unspecifi c activa-tion of granulocytes, as indicated by increased PMN elastase levels after membrane passage, contributing to the activation of cells of the immune system and, as a possible consequence, to oxidative stress. We observed a decrease of neopterin concentrations in the IHD group, because they passed from circulation into the ultrafi ltrate. The membrane passage in the IHD group increased the production of total peroxides, indicating a consumption of antioxidants. Unlike peroxides, the other oxidative stress biomarkers, that is, MDA and oLAb, were not modifi ed in the course of membrane passage. Although, this study has some limitations due to a small and highly heterogeneous population, these results indicate that infl ammatory pa-rameters are greatly altered by renal replacement therapy and that membrane passage causes the generation of peroxides.
ORIGINAL PAPERS
CEMED 85 2010 ▪ Volume 4, Number 1
From these data, we conclude that haemodialysis procedure, to some extent, affects routinely used parameters for the estimation of the clinical state of intensive care patients and, therefore, they should be interpreted with caution.
Competing InterestsThe authors have no competing interests to declare.
Authors’ contributionsKHS, PK, WW and FT designed the study, acquired, analysed and interpreted the data; RA, VS, GK and WW studied the infl ammatory and oxidative stress parameters; BMW and WW performed the statistical analysis.
AcknowledgmentsThe authors gratefully acknowledge Günther Jürgens for making his laboratory available for the determination of oxidative stress biomarkers and the excellent technical assistance of the medical and nursing staff of the Intensive Care Unit, University Hospital, Graz, for their co-operation and support. This study was supported by the COST Action B35.
ReferencesTonnesen, E., Hansen, M.-B., Hahndorf, K. et al.:[1] Cytokines in plasma and ultrafi ltrate during continuous arteriovenous haemofi ltration. Anaesth. Intens. Care, 1993, 21, 752–758.Bellomo, R., Tipping, P., Boyce, N.:[2] Continuous venovenous hemofi ltration with dialysis removes cyto-kines from the circulation of septic patients. Crit. Care Med., 1993, 21, 522–526.Andreasson, S., Göthberg, S., Berggren, H. et al.:[3] Hemofi ltration modifi es complement activation after extra-corporeal circulation in infants. Ann. Thorac. Surg., 1993, 56, 1515–1517.Bellomo, R., Tipping, P., Boyce, N.:[4] Interleukin-6 and interleukin-8 extraction during continuous veno-venous hemodiafi ltration in septic acute renal failure. Ren. Fail., 1995, 17, 457–466.Hoffman, J.-N., Hartl, W.-H., Deppisch, R. et al.:[5] Hemofi ltration in human sepsis: evidence for elimination of immunomodulatory substances. Kidney Int., 1995, 48, 1563–1570.Sander, A., Armbruster, W., Sander, B. et al.:[6] Hemofi ltration increases IL-6 clearance in early systemic infl am-matory response syndrome but does not alter IL-6 and TNFα plasma concentrations. Intens. Care Med., 1997, 23, 878–884.Kellum, J.-A., Johnson, J.-P., Kramer, D. et al.:[7] Diffuse vs convective therapy: effects on mediators of infl am-mation in patients with severe systemic infl ammatory response syndrome. Crit. Care Med., 1998, 26, 1995–2000.De Vriese, A.-S., Colardyn, F.-A., Philippe, J.-J. et al.:[8] Cytokine removal during continuous hemofi ltration in septic patients. J. Am. Soc. Nephrol., 1999, 10, 846–853.Wakabayashi, Y., Kamijou, Y., Soma, K. et al.:[9] Removal of circulating cytokines by continuous hemofi ltra-tion in patients with systemic infl ammatory response syndrome of multiple organ dysfunction syndrome. Br. J. Surg., 1996, 83, 393–394.Van Bommel, E.-F., Hesse, C.-J., Jutte, N.-H. et al.:[10] Cytokine kinetics (TNF-alpha, IL-1beta, IL-6) during continuous hemofi ltration: a laboratory and clinical study. Contrib. Nephrol., 1995, 116, 62–75.
2010 ▪ Volume 4, Number 1 86 CEMED
ORIGINAL PAPERS
Lonnemann, G., Behme, T.-C., Lenzner, B. et al.:[11] Permeability of dialyzer membranes to TNF alpha-inducing substances derived from water bacteria. Kidney Int., 1992, 42, 61–68.Oberhoffer, M., Karzai, W., Meier-Hellmann, A. et al.:[12] Sensitivity and specifi city of various markers of infl am-mation for the prediction of tumor necrosis factor-alpha and interleukin-6 in patients with sepsis. Crit. Care Med., 1999, 27, 1814–1818.Assicot, M., Grendel, D., Carsin, H. et al.:[13] High serum procalcitonin concentration in patients with sepsis and infection. Lancet, 1993, 341, 515–518.Giamarellos-Bourboulis, E.-J., Grecka, P., Poulakou, G. et al.:[14] Assessment of procalcitonin as a diagnostic marker of underlying infection in patients with febrile neutropenia. Clin. Infect. Dis., 2001, 32, 1718–1725.Ruokonen, E., Ilkka, L., Niskanen, M. et al.:[15] Procalcitonin and neopterin as indicators of infection in critically ill patients. Acta Anaesthesiol. Scand., 2002, 46, 398–404.Meisner, M., Tschaikowsky, K., Palmaers, T. et al.:[16] Comparison of procalcitonin (PCT) and C-reactive protein (CRP) plasma concentrations at different SOFA scores during the course of sepsis and MODS. Crit. Care, 1999, 3, 45–55.Meisner, M., Adina, H., Schmidt, J.: [17] Correlation of procalcitonin and C-reactive protein to infl ammation, complications, and outcome during the intensive care unit course of multiple-trauma patients. Crit. Care, 2006, 10, 1–10.Lee, W.-L., Downey, G.-P.:[18] Leukocyte elastase: physiological functions and role in acute lung injury. Am. J. Respir. Crit. Care Med., 2001, 164, 896–904.Ikei, S., Ogawa, M., Yamaguchi, Y.:[19] Blood concentrations of polymorphonuclear leucocyte elastase and inter-leukin-6 indicators for the occurrence of multiple organ failures at the early stage of acute pancreatitis. J. Gastro enterol. Hepatol., 1998, 13, 1274–1283.Hörl, W.-H., Steinhauer, H.-B., Schollmeyer, P.:[20] Plasma levels of granulocyte elastase during haemodialysis: effects of different dialyzer membranes. Kidney Int., 1985, 28, 791–796.Irvine, L., Travers, M., Simpson, K. et al.:[21] Infl uence of haemodialysis membranes on the release of granulo-cyte elastase. Int. J. Artif. Organs, 1989, 12, 502–504.Haag-Weber, M., Hörl, W.-H.:[22] Effect of biocompatible membranes on neutrophil function and metabolism. Clin. Nephrol., 1994, 42 (Suppl. 1), S31–S36.Wachter, H., Fuchs, D., Hausen, A. et al.:[23] Neopterin: Biochemistry, Methods, Clinical Application. De Gruyter, Berlin, New York, 1992.Strohmaier, W., Redl, H., Schlag, G. et al.:[24] D-erythro-neopterin plasma levels in intensive care patients with and without septic complications. Crit. Care Med., 1987, 15, 757–760.Pacher, R., Redl, H., Frass, M. et al.:[25] Relationship between neopterin and granulocyte elastase plasma levels and the severity of multiple organ failure. Crit. Care Med., 1989, 17, 221–226.Baydar, T., Yuksel, O., Sahin, T.-T. et al.:[26] Neopterin as a prognostic biomarker in intensive care unit patients. J. Crit. Care, 2009, 24, 318–321.Rosenkranz, A.-R., Templ, E., Traindl, O. et al.:[27] Reactive oxygen product formation by human neutrophils as an early marker for biocompatibility of dialysis membranes. Clin. Exp. Immunol., 1994, 98, 300–305.Daschner, M., Lenhartz, H., Botticher, D. et al.:[28] Infl uence of dialysis on plasma lipid peroxidation products and antioxidant levels. Kidney Int., 1996, 50, 1268–1272.Tatzber, F., Esterbauer, H.:[29] Free radicals, lipoprotein oxidation and atherosclerosis. In: Bellomo, G., Finardi, G., Maggi, E., Rice-Evans, C. (Eds): The Richelieu Press, London, 1995, pp. 245–262.Esterbauer, H., Gieseg, S., Giessauf, A. et al.:[30] Free radicals and oxidative modifi cation of LDL: role of natural antioxidants. In: Woodford, F. P., Davignon, J., Sniderman, A. (Eds): Elsevier Science, 1995, pp. 203–208.Lindschinger, M., Nadlinger, K., Adelwöhrer, N. et al.:[31] Oxidative stress: potential of distinct peroxide determi-nation systems. Clin. Chem. Lab. Med., 2004, 42, 907–914.Resch, U., Tatzber, F., Budinsky, A. et al.:[32] Reduction of oxidative stress and modulation of autoantibodies against modifi ed low-density lipoprotein after rosuvastatin therapy. Br. J. Clin. Pharmacol., 2006, 61, 262–274.Nikolic-Heitzler, V., Rabuzin, F., Tatzber, F. et al.:[33] Persistent oxidative stress after myocardial infarction treat-ed by percutaneous coronary intervention. Tohoku J. Exp. Med., 2006, 210, 247–255.Fukumoto, M., Shoji, T., Emoto, M. et al.:[34] Antibodies against oxidized LDL and carotid artery intima-media thickness in a healthy population. Arterioscler. Thromb. Vasc. Biol., 2000, 20, 703–707.Chiesa, R., Melissano, G., Castellano, R. et al.:[35] In search of biological markers of high-risk carotid artery atherosclerotic plaque: enhanced LDL oxidation. Ann. Vasc. Surg., 1998, 12, 1–9.
ORIGINAL PAPERS
CEMED 87 2010 ▪ Volume 4, Number 1
Khoschsorur, G.-A., Winklhofer-Roob, B.-M., Rabl, H. et al.: [36] Evaluation of a sensitive HPLC method for the determination of malondialdehyde, and application of the method to different biological materials. Chro-matographia, 2000, 52, 181–184.Tatzber, F., Griebenow, S., Wonisch, W. et al.:[37] Dual method for the determination of peroxidase activity and total peroxides – iodide leads to a signifi cant increase of peroxidase activity in human sera. Anal. Biochem., 2003, 316, 147–153.Herget-Rosenthal, S., Marggraf, G., Pietruck, F. et al.:[38] Procalcitonin for accurate detection of infection in haemodialysis. Nephrol. Dial. Transplant., 2001, 16, 975–979.Irvine, L., Travers, M., Simpson, K. et al.:[39] Infl uence of haemodialysis membranes on the release of granulo-cyte elastase. Int. J. Artif. Organs, 1989, 12, 502–504.Fuchs, D., Hausen, A., Reibnegger, G. et al.:[40] Neopterin levels in long-term hemodialysis. Clin. Nephrol., 1988, 30, 220–224.Himmelfarb, J., McMonagle, E., McMenamin, E.:[41] Plasma protein thiol oxidation and carbonyl formation in chronic renal failure. Kidney Int., 2000, 58, 2571–2578.Ward, R.-A., Ouseph, R., McLeish, K.-R.:[42] Effects of high-fl ux hemodialysis on oxidant stress. Kidney Int., 2003, 63, 353–359.Gonzalez-Diez, B., Cavia, M., Torres, G. et al.:[43] Effect of a hemodiafi ltration session with on-line regenera-tion of the ultrafi ltrate on oxidative stress. Blood Purif., 2008, 26, 505–510.Himmelfarb, J., McMonagle, E.:[44] Albumin is the major plasma protein target of oxidant stress in uremia. Kidney Int., 2001, 60, 358–363.Soejima, A., Matsuzawa, N., Miyake, N. et al.:[45] Hypoalbuminemia accelerates erythrocyte membrane lipid peroxidation in chronic hemodialysis patients. Clin. Nephrol., 1999, 51, 92–97.Calo, L.-A., Naso, A., Carraro, G. et al.:[46] Effect of haemodiafi ltration with online regeneration of ultrafi l-trate on oxidative stress in dialysis patients. Nephrol. Dial. Transplant., 2007, 22, 1413–1419.Roob, J.-M., Khoschsorur, G., Tiran, A. et al.:[47] Vitamin E attenuates oxidative stress induced by intravenous iron in patients on hemodialysis. J. Am. Soc. Nephrol., 2000, 11, 539–549.
2010 ▪ Volume 4, Number 1 88 CEMED
ORIGINAL PAPERS
Serum Total Peroxides Are Increased in Patients with Stage IV Compared to Stage IIb Peripheral Arterial Disease: Percutaneous Transluminal Angioplasty May
Generate Epitopes for Autoantibodies Against Oxidized Low Density Lipoprotein
MARTIN TRINKER1, KARL-HEINZ SMOLLE2, STEFAN SCHEIDL2, FRANZ TATZBER3, MEINRAD LINDSCHINGER4, WILLIBALD WONISCH5, 6
1Department of Internal Rehabilitation, Klinikum Bad Gleichenberg, Styria, Austria2Department Institute of Internal Medicine, Medical University, Graz, Austria
3Institute of Biochemical Engineering, University of Applied Sciences, Höchstädtplatz 5, Technikum Vienna, Vienna, Austria
4Institute of Nutritional and Metabolic Diseases, Schwarzl Outpatient Clinic, Laßnitzhöhe, Austria5Clinical Institute of Medical and Chemical Laboratory Diagnostics, Medical University, Graz, Austria
6Institute of Physiological Chemistry, Center for Physiological Medicine, Medical University, Graz, Austria
Reactive oxygen species are involved, among others, in peripheral arterial disease (PAD). During percutane-ous transluminal angioplasty (PTA) vascular walls become damaged, which fi nally leads to ischemia/reperfusion injury. In PAD patients with Fontaine stage IIb (11 males and 6 females) and with Fontaine stage IV (7 males and 3 females) undergoing revascularisation, we correlated oxidative stress biomarkers, i.e. serum total peroxides and autoantibodies against oxidized LDL (oLAb), with the stage of PAD. Subjects with stage IV disease had signifi -cantly higher peroxide levels at baseline compared to stage IIb (510 ± 360 AU vs. 150 ± 220 AU, p < 0.05). Revas-cularisation was associated with a signifi cant decrease in the oLAb titer (314 ± 240 vs. 251 ± 190 mU/mL, p < 0.05). Total peroxides may indicate the severity of PAD and the time course of oLAb titers could be used as a biomarker for revascularisation.
Keywords: peripheral arterial disease, antibodies against oxidized LDL, peroxides, percutaneous transluminal an-gioplasty, oxidative stress
IntroductionAtherosclerosis is a generalized disease that affects more than half of the population in indus-trialised countries [1]. Three major phenomena may contribute signifi cantly to the character-istics of the atherosclerotic lesion: smooth muscle cell proliferation, the formation of abun-dant connective tissue matrix, and the accumulation of intra- and extracellular lipids [2]. Experimental and clinical investigations have shown that oxidation of low-density lipopro-tein (LDL) may represent a key event in the development and progression of atherosclerosis [3]. Early atherosclerosis is characterized by massive accumulation of monocytes and chole-
Corresponding address: Martin Trinker MD, Department of Internal Rehabilitation, Klinikum Bad Gleichenberg, 8344 Bad Gleichenberg, Styria, Austria. E-mail: [email protected]
1.9
ORIGINAL PAPERS
DOI: 10.1556/CEMED.4.2010. 89 2010 ▪ Volume 4, Number 1 ▪ 89–97.
sterol-containing lipid-loaded foam cells, derived from monocyte macrophages in the suben-dothelial space. These oxidative modifi cations of LDL generate molecular epitopes that are more atherogenic than native LDL [4]. It was demonstrated that oxidized low-density lipo-protein (oLDL) could be recognized and endocytozed via the scavenger receptor pathway of macrophages [3] and it was discovered that the modifi cation of LDL by endothelial cells in-volves lipid peroxidation and degradation of LDL phospholipids [5].
Such epitopes typical of oLDL were demonstrated in human atherosclerotic lesions [6]. The immunogenicity of oLDL provides the basis for the formation of antibodies that are be-lieved to mirror the extent of LDL oxidation occurring in vivo. All these investigations led to the introduction of the LDL oxidation hypothesis for the development of atherosclerosis [7–9]. Membrane systems in mammalian cells are rich in polyunsaturated fatty acids, and therefore highly susceptible to oxidative stress, defi ned as a disturbance in the prooxidant–antioxidant balance [10].
Its clinical manifestation tends to be focal and is mostly associated with complicated atherosclerotic lesions. Morbidity mainly becomes apparent as cerebrovascular, cardiovascu-lar or peripheral arterial disease (PAD). From a clinical perspective, PAD is mostly classifi ed into four stages according to the Fontaine classifi cation [11, 12].
Percutaneous transluminal angioplasty (PTA) is a technique for recanalisation of oc-cluded vascular segments. The mechanism of transluminal dilatation of stenotic arteries in-volves stretching the vessel wall, leading to longitudinal splits and fractures of the intima, often including the medial layer [13].
Peroxides, which are primary products of the lipid peroxidation cascade, mirror the damaging effect of free radicals, and therefore, total peroxides in serum were used as an in-dicator of the extent of ongoing lipid peroxidation in PAD.
It was shown that the titer of antibodies against oLDL (oLAB) was an independent pre-dictor of progression of carotid atherosclerosis in a group of Finnish men [14]. Therefore, we investigated baseline and time course of oLAb titers in patients undergoing PTA.
Materials and Methods
Patients
Twenty-seven consecutive patients suffering from PAD with Fontaine classifi cation IIb or IV, who were admitted for diagnosis or treatment, were included in this study. The diagnosis of PAD was established clinically and confi rmed by measurements of hemodynamics via ultra-sound. Stages were selected because of clear clinical differentiation and justifi cation for in-vasive procedures. All patients had at least diagnostic angiographies and mostly percutane-ous transluminal angioplasties. Calculating the ankle brachial index before and the day after the procedure estimated the success of angioplasty.
Patients were separated into two groups according to the stage of their disease: 17 were classifi ed as stage IIb disease (11 males and 6 females), complaining of intermittent claudica-tion after walking less than 200 m. Ten suffering from necrosis and/or gangrene were classi-fi ed as stage IV (7 males and 3 females). After informed consent, routine blood samples were used to measure and compare basic levels of peroxides and oLAb titers.
2010 ▪ Volume 4, Number 1 90 CEMED
ORIGINAL PAPERS

The patients were then separated into two further groups: the fi rst group included pa-tients with successful revascularisation. The second group comprised patients without reper-fusion, either because angioplasty had failed or because angiography alone was performed.
Blood Sampling and Preparation
Blood samples were taken before (t0), 1 h after (t1), and the day after (t2) the procedure from a separate cannula in the forearm. Samples were centrifuged 30 min after collection at 1,500 × g for 10 min. Serum was stored at −70 °C for not more than 2 weeks until use.
Measurement of Lipid Peroxidation Parameters
Peroxides and autoantibodies against oLDL were determined simultaneously. For each as-say only one and the same batch was used. The same patients’ samples were analyzed on the same plate in duplicate.
Determination of Peroxides
Serum total peroxides (TOC®) were determined by a rapid enzymatic in vitro diagnostic as-say (Labor Diagnostic Nord, LDN, Nordhorn, Germany) as described previously [15, 16]. The test system is based on a peroxide/peroxidase reaction using 3,5,3′,5′-tetramethylbenzi-dine (TMB) as chromogenic substrate. Results were calculated from the linear standard curve. Peroxide levels were specifi ed as μmol/L.
Determination of Autoantibodies Against Oxidized LDL
Titers of oLAb were measured in serum with a commercial enzyme immunoassay (Biomed-ica, Vienna, Austria) [17]. The assay is based on the binding reaction of the 1:50 diluted samples to the previously oxidized LDL (by cupric ions) bound to the microtiter wells. De-tection was done by binding a secondary, peroxidase-coupled anti-IgG antibody, which per-mitted colorimetric detection of this enzyme with TMB as substrate. Results were expressed as mU/mL.
Statistical Analyses
The SPSS Advanced Model package was used for statistical analysis. Actual measured data were compared regarding different stages of PAD, whereas changes over time were com-pared in case of the two treatment groups.
Normality testing was done using the Shapiro–Wilk model. T-test was used to compare different groups. In case of failed normality testing, the nonparametric Mann–Whitney test was used. Values with p < 0.05 were considered statistically signifi cant.
ResultsPatients suffering from PAD clinical stage IIb were slightly younger (67 ± 8 years) than those with stage IV disease (73 ± 8 years). Gender distribution was similar in both groups,
ORIGINAL PAPERS
CEMED 91 2010 ▪ Volume 4, Number 1
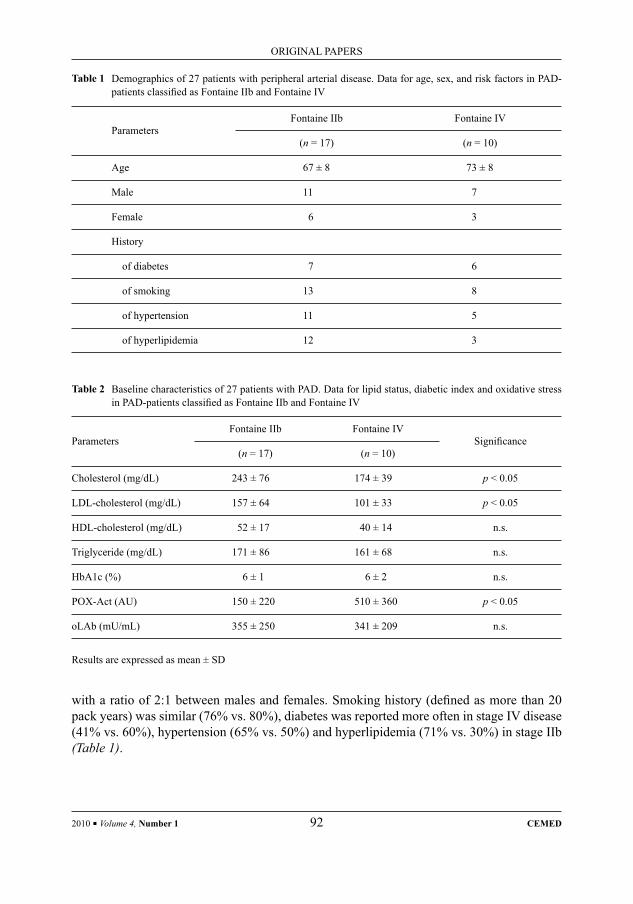
with a ratio of 2:1 between males and females. Smoking history (defi ned as more than 20 pack years) was similar (76% vs. 80%), diabetes was reported more often in stage IV disease (41% vs. 60%), hypertension (65% vs. 50%) and hyperlipidemia (71% vs. 30%) in stage IIb (Table 1).
Table 1 Demographics of 27 patients with peripheral arterial disease. Data for age, sex, and risk factors in PAD-patients classifi ed as Fontaine IIb and Fontaine IV
ParametersFontaine IIb Fontaine IV
(n = 17) (n = 10)
Age 67 ± 8 73 ± 8
Male 11 7
Female 6 3
History
of diabetes 7 6
of smoking 13 8
of hypertension 11 5
of hyperlipidemia 12 3
Table 2 Baseline characteristics of 27 patients with PAD. Data for lipid status, diabetic index and oxidative stress in PAD-patients classifi ed as Fontaine IIb and Fontaine IV
ParametersFontaine IIb Fontaine IV
Signifi cance(n = 17) (n = 10)
Cholesterol (mg/dL) 243 ± 76 174 ± 39 p < 0.05
LDL-cholesterol (mg/dL) 157 ± 64 101 ± 33 p < 0.05
HDL-cholesterol (mg/dL) 52 ± 17 40 ± 14 n.s.
Triglyceride (mg/dL) 171 ± 86 161 ± 68 n.s.
HbA1c (%) 6 ± 1 6 ± 2 n.s.
POX-Act (AU) 150 ± 220 510 ± 360 p < 0.05
oLAb (mU/mL) 355 ± 250 341 ± 209 n.s.
Results are expressed as mean ± SD
2010 ▪ Volume 4, Number 1 92 CEMED
ORIGINAL PAPERS

Lipid and Glucose Profi le
Cholesterol and LDL-cholesterol levels were signifi cantly higher in stage IIb PAD patients (Table 2). On the other hand, triglycerides, high-density lipoproteins (HDL) and hemoglobin A1c were in the same range in both groups.
Oxidative Stress
Long-standing PAD, as is the case in stage IV disease, was associated with signifi cantly in-creased peroxide levels (510 ± 360 AU vs. 150 ± 220 AU, p < 0.05, Table 2, Fig. 1). Nonethe-less, the antibody titer against oLDL was similar at baseline in both groups (Fig. 2), while there was a signifi cant decrease in oLAb titers after revascularisation (Fig. 3), independent of the stage of disease (IIb and IV). This effect started immediately (1 h, t1) after revascularisa-tion and was signifi cantly pronounced over the next 24 h (t2). These changes in the oLAb
Fig. 3 Change of oLAb titers in accordance with revas-cularisation
Fig. 4 Change of POX in accordance with revascula-risation
Fig. 1 Peroxide baseline levels of 27 patients with pe-ripheral arterial disease according to the stage of disease
Fig. 2 Baseline oLAb titers of 27 patients with periph-eral arterial disease according to the stage of disease
ORIGINAL PAPERS
CEMED 93 2010 ▪ Volume 4, Number 1

titer were not observed in the PTA control group, which included all patients without revas-cularisation, either because angioplasty failed or because angiography alone was performed (Table 3).
In contrast to oLAb titers, there was no change in the time course for total peroxide levels (Fig. 4), neither in the revascularized artery nor in the PTA control group.
DiscussionSignifi cantly higher peroxide levels in advanced disease mirror the increased radical forma-tion in long-lasting disease, which supports the hypothesis that lipid peroxidation contributes to PAD. This is of particular relevance because increased peroxide levels emerged in spite of lower levels of LDL cholesterol in these subjects, which refl ects most probably the rigorous treatment of patients suffering from rest pain. Therefore, these peroxides may stimulate the persistent oxidation of intra- and extracellular lipids in the course of the lipid peroxidation chain reaction and may therefore exacerbate the disease. This is consistent with previous re-ports indicating increased peroxide levels in patients with advanced arteriosclerotic disease in those with diabetes mellitus, and in smokers [18]. Moreover, increased peroxide levels
Table 3 Oxidative stress biomarkers in Fontaine IIb and Fontaine IV PAD patients with respect to the classifi cation “PTA-successful versus PTA-failed”
ParametersPTA-successful PTA-failed
(n = 18) Signifi cance (n = 9) Signifi cance
Fontaine IIb 11 6
Fontaine IV 7 3
POX-Act (AU) t0 339 ± 374 172 ± 165
POX_D1 −1.3 n.s. 0.8 n.s.
POX-Act (AU) t1 340 ± 388 171 ± 170
POX_D2 −1.1 n.s. −10.6 n.s.
POX-Act (AU) t2 340 ± 375 182 ± 152
oLAb (mU/mL) t0 314 ± 240 422 ± 207
oLAb_D1 46 n.s. 26 n.s.
oLAb (mU/mL) t1 268 ± 217 396 ± 189
oLAb_D2 63 p < 0.05 −2.6 n.s.
oLAb (mU/mL) t2 251 ± 190 425 ± 231
D1 describes changes from baseline to t1 (t0–t1)D2 from baseline to t2 (t0–t2). Results are expressed as mean ± SD
2010 ▪ Volume 4, Number 1 94 CEMED
ORIGINAL PAPERS

facilitate platelet activation and lead to the release of vascular endothelial growth factor [19], and in a recent publication [20], the authors report improved oxidative stress in those patients with stable coronary artery disease who received sirolimus-eluting stents, as compared to those who received bare metal stents, which contributes to the difference in the restenosis rate between these different types of stents.
The oLAb titer was shown to correlate inversely with the intima-media thickness of the carotid arteries and with plasma oxidized LDL in healthy subjects [21, 22]. This underlines the protective action of antibodies directed against oxidized LDL. Although top athletes often exhibit high oLAb titers [23, 24], these antibodies were reported to be consumed in the course of a competition season as a result of excess peroxides generating epitopes for these antibodies, which consequently decrease through binding to these epitopes [25]. In this con-text, we found a signifi cant decrease in oLAb titers after revascularisation. This is in accor-dance with previous reports of transient reductions in oLAb titers [26] after immediate reper-fusion and after acute myocardial infarction. Furthermore, a decrease in oLAb titers was also shown in myocardial infarction patients treated by percutaneous coronary intervention [27]. Recently it was reported that oLAb titers correlated to a greater extent with myocardial dam-age than with severity of coronary atherosclerosis and lipid profi les [28]. All these fi ndings indicate the formation of reactive oxygen species, which is associated with the oxidation of LDL and might cause vascular damage. In contrast to previous studies [14], we could not correlate the oLAb titers with disease progression, although we found a trend towards lower levels in advanced disease (stage IV), indicating increased consumption. Furthermore, it should be noted that the use of several oxidative stress biomarkers is in favour of a single determination [20] and improves the validity of the evaluated data.
Our results suggest that total peroxides indicate the severity of PAD and that the con-sumption of autoantibodies against oxidized LDL in the time course of PTA may be used as a biomarker for successful revascularisation.
Antioxidants have been demonstrated to be effective in lowering lipid peroxidation [29, 30] and may have a positive impact on the course of disease progression to reduce the risk of re-stenosis in humans and non-human primates [31–33].
Because initial and long-term success of PTA varies widely [34], it should be investi-gated if PAD patients undergoing a PTA may benefi t from supplementation with antioxi-dants.
AcknowledgmentsThe authors gratefully acknowledge Günther Jürgens for making his laboratory available for the determination of oxidative stress biomarkers at the Institute of Physiological Chemistry, Medical University Graz. This study was supported by the COST Action B35.
ReferencesWorld Health Organization Study Group:[1] Classifi cation of atherosclerotic lesions: report of a study group. WHO Tech. Rep. Ser., 1958, 143, 1–20.Ross, R.: [2] The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature, 1993, 362, 801–809.
ORIGINAL PAPERS
CEMED 95 2010 ▪ Volume 4, Number 1
Steinberg, D., Parthasarathy, S., Carew, T. E. et al.:[3] Beyond cholesterol. Modifi cations of low-density lipo-protein that increase its atherogenecity. NEJM, 1989, 320, 915–924.Jürgens, G., Lang, J., Esterbauer, H.:[4] Modifi cations of human low-density lipoprotein by the lipid peroxida-tion product 4-hydroxy nonenal. Biochim. Biophys. Acta, 1986, 875, 103–114.Steinbrecher, U. P., Parthasarathy, S., Leake, D. S. et al.:[5] Modifi cation of low density lipoprotein by endothe-lial cells involves lipid peroxidation and degradation of low density lipoprotein phospholipids. Proc. Natl. Acad. Sci. U.S.A., 1984, 81, 3883–3887.Jürgens, G., Chen, Q., Esterbauer, H. et al.:[6] Immunostaining of human autopsy aortas with antibodies to modifi ed apolipoprotein B and apoprotein(a). Arterioscler. Thromb., 1993, 13, 1689–1699.Witztum, J. L.:[7] The oxidation hypothesis of atherosclerosis. Lancet, 1994, 344, 793–795.Esterbauer, H., Ramos, P.:[8] Chemistry and pathophysiology of oxidation of LDL. Rev. Physiol. Biochem. Pharmacol., 1995, 127, 31–64.Berliner, J. A., Navab, M., Fogelman, A. M. et al.:[9] Atherosclerosis: basic mechanism, oxidation, infl ammation, and genetics. Circulation, 1995, 91, 2488–2496.Sies, H.:[10] Oxidative Stress: Oxidants and Antioxidants. Academic Press, London, 1993.Fontaine, R., Kim, M., Kieny, R.:[11] Die chirurgische Behandlung der peripheren Durchblutungsstörungen. Helv. Chir. Acta, 1954, 5/6, 199–233.Salvatore, N.:[12] Classifi cation, epidemiology, risk factors, and natural history of peripheral arterial disease. Diabetes Obes. Metab., 2002, 4(Suppl. 2), S1–S6.Isner, J. M., Rosenfi eld, K.:[13] Redefi ning the treatment of peripheral artery disease. Role of percutaneous revas-cularisation. Circulation, 1993, 88, 1534–1557.Salonen, J. T., Yla-Herttuala, S., Yamamoto, R. et al.:[14] Autoantibody against oxidised LDL and progression of carotid atherosclerosis. Lancet, 1992, 339, 883–887.Tatzber, F., Griebenow, S., Wonisch, W. et al.:[15] Dual method for the determination of peroxidase activity and total peroxides – iodide leads to a signifi cant increase of peroxidase activity in human sera. Anal. Bio-chem., 2003, 316(2), 147–153.Roob, J. M., Khoschsorur, G., Tiran, A. et al.:[16] Attenuates oxidative stress induced by intravenous iron in patients on hemodialysis. J. Am. Soc. Nephrol., 2000, 11, 539–549.Tatzber, F., Esterbauer, H.:[17] Autoantibodies to oxidized low density lipoprotein. In: Bellomo, G., Finardi, G., Maggi, E., Rice-Evans, C. (eds): Atherosclerosis – IX. Richelieu Press, London, 1995, pp. 245–262.Roller, R. E., Nimmrichter, V., Trinker, M. et al.:[18] Oxidative stress during peripheral angioplasty. Implication for late restenosis? Int. Angiol., 2001, 20, 131–135.Roller, R. E., Renner, W., Dorr, A. et al.: [19] Oxidative stress and increase of vascular endothelial growth factor in plasma of patients with peripheral arterial occlusive disease. Thromb. Haemost., 2001, 85, 368.Kochiadakis, G. E., Arfanakis, D. A., Marketou, M. E. et al.:[20] Oxidative stress changes after stent implantation: a randomized comparative study of sirolimus-eluting and bare metal stents. Int. J. Cardiol., 2009, in press.Fukumoto, M., Shoji, T., Emoto, M. et al.:[21] Antibodies against oxidized LDL and carotid artery intima-media thickness in a healthy population. Arterioscler. Thromb. Vasc. Biol., 2000, 20, 703–707.Shoji, T., Nishizawa, Y., Fukumoto, M. et al.:[22] Inverse relationship between circulating oxidized low density lipoprotein (oxLDL) and anti-oxLDL antibody levels in healthy subjects. Atherosclerosis, 2000, 148, 171–177.Pincemail, J., Lecomte, J., Castiau, J. P. et al.:[23] Evaluation of autoantibodies against oxidized LDL and anti-obidant status in top soccer and basketball players after 4 months of competition. Free Radic. Biol. Med., 2000, 28, 559–565.Schippinger, G., Wonisch, W., Abuja, P. M. et al.:[24] Lipid peroxidation and antioxidant status in professional American football players during competition. Eur. J. Clin. Invest., 2002, 32, 686–692.Schippinger, G., Fankhauser, F., Abuja, P. M. et al.:[25] Competitive and seasonal oxidative stress in elite alpine ski racers. Scand. J. Med. Sci. Sports, 2009, 19, 206–212.Schumacher, M., Eber, B., Tatzber, F. et al.:[26] Transient reduction of autoantibodies against oxidized LDL in patients with acute myocardial infarction. Free Radic. Biol. Med., 1995, 18, 1087–1091.Nikolic-Heitzler, V., Rabuzin, F., Tatzber, F. et al.:[27] Persistent oxidative stress after myocardial infarction treat-ed by percutaneous coronary intervention. Tohoku J. Exp. Med., 2006, 210, 247–255.Tsai, W. C., Li, Y. H., Chao, T. H. et al.:[28] Relation between antibody against oxidized low-density lipoprotein and extent of coronary atherosclerosis. J. Formos. Med. Assoc., 2002, 101, 681–684.
2010 ▪ Volume 4, Number 1 96 CEMED
ORIGINAL PAPERS
Jialal, I., Fuller, C. J., Huet, B. A.:[29] Effect of α-tocopherol supplementation on LDL oxidation: a dose-re-sponse study. Arterioscler. Thromb. Vasc. Biol., 1995, 15, 190–198.Kaikkonen, J., Porkkala-Sarataho, E., Morrow, J. D. et al.:[30] Supplementation with vitamin E but not with vitamin C lowers lipid peroxidation in vivo in mildly hypercholesterolemic men. Free Radic. Res., 2001, 35, 967–978.Sasahara, M., Raines, E. W., Chait, A. et al.:[31] Inhibition of hypercholesterolaemia-induced atherosclerosis in the nonhuman primate by probucol. I. Is the extent of atherosclerosis related to the resistance of LDL to oxidation? J. Clin. Invest., 1994, 94, 155–164.Fang, J. C., Kinlay, S., Beltrame, J. et al.:[32] Effect of vitamins C and E on progression of transplant-associated arteriosclerosis: a randomized trial. Lancet, 2002, 359, 1108–1113.Wonisch, W., Uhl, K., Schimetta, W. et al.:[33] Pre-operative delivery of a vitamin cocktail diminished oxidative stress after vascular surgery in PAD patients – a pilot investigation. Biofactors, 2005, 24, 299–303.Johnston, K. W., Rae, M., Hogg-Johnston, S. A. et al.:[34] 5-year results of a prospective study of percutaneous transluminal angioplasty. Ann. Surg., 1987, 206, 403–413.
ORIGINAL PAPERS
CEMED 97 2010 ▪ Volume 4, Number 1
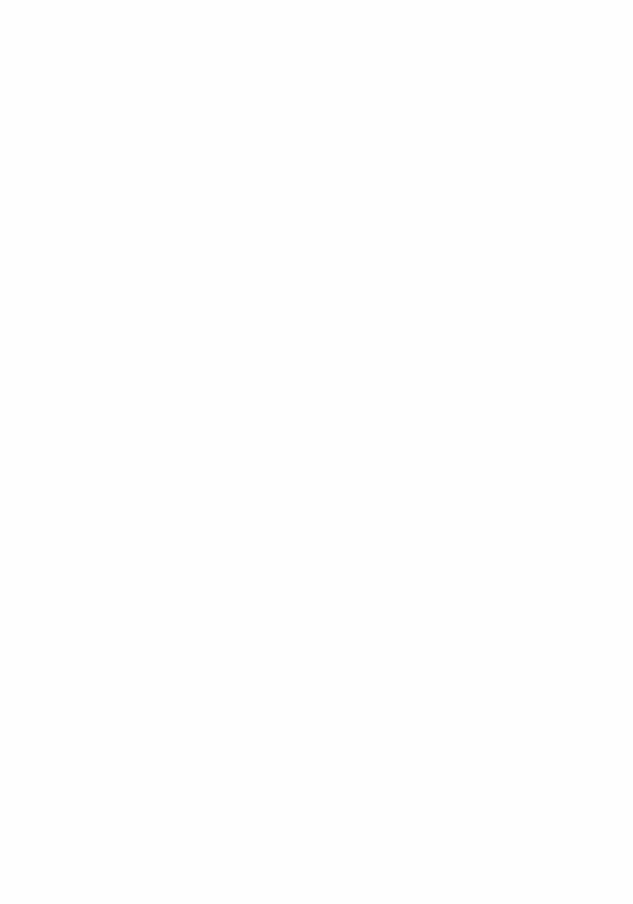

The Effect of Perceptual Characteristics of Tablets upon Patient’s Choice
FERENC KÖTELES1, ILDIKÓ KOMSA2, GYÖRGY BÁRDOS2, 3
1Department of Personality and Health Psychology, Institute of Psychology2Department of Physiology and Neurobiology, Institute of Biology
3Group of Behavioural Sciences, Institute for Health Promotion and Sport Sciences Eötvös Loránd University, Budapest, Hungary
Perceptual characteristics of curatives can have an impact on their expected effectiveness. The hypotheses of the present work were that differences can be found among preferences of different looking tablets and these prefer-ences are determined by the combination of the effect, colour and shape/size of tablets. In the paper-and-pencil study, the estimated probabilities of choice for tablets with different perceptual characteristics were rated in three effect groups on fi ve-grade Likert scales by 181 university students (mean age: 19.8 years, 37.9% males). Signifi cant differences were found among the ratings of tablets within every effect group. White tablets were generally preferred in the analgesic–antipyretic group. Small, round, white and blue tablets proved to be the most attractive in the seda-tive–hypnotic group and small, round, red and yellow tablets in the spasmolytic group. Considering tablets with a given pharmaceutic effect, patient’s choice is infl uenced by the combination of colour and shape/size. Discrepancies between the expected and the actual perceptual characteristics of medicines might infl uence their overall effective-ness and patient’s adherence to treatment.
Keywords: tablet colour and shape, perceptual characteristics, placebo, compliance
IntroductionThe overall effect and effectiveness of a curative is the result of the interaction of so-called specifi c (i.e. biochemical-pharmacological) and non-specifi c (or placebo) effects. This termi-nology is a bit confusing, as non-specifi c effects can be very specifi c in terms of the affected body parts or organs or of their direction of action (e.g. stimulant/sedative) [1]. Often men-tioned sources of non-specifi c effects are doctor–patient relationship, needs and expectations of the patient, suggestions and information given by the doctor, personality and psychologi-cal state of the doctor and of the patient, context of treatment and properties of medication [2]. The most important properties of medication are the route of administration (e.g. percu-taneous or oral), and the perceptual characteristics of curatives (size, shape, colour). Accord-ing to the generally accepted view, patients consider injections more powerful than oral application forms in some cultures [3, 4], and capsules are regarded to be slightly more effec-tive than tablets [5–7]. We have no good empirical evidence regarding the psychological ef-fects of the size of tablets. Early authors recommended the use of very small and very large tablets, as a bigger one is more impressive, while small size indicates more powerful ingre-
Corresponding address: György Bárdos MD, Department of Physiology and Neurobiology, Pázmány Péter sétány 1/C, H-1117 Budapest, Hungary. E-mail: [email protected]
1.10
ORIGINAL PAPERS
DOI: 10.1556/CEMED.4.2010. 99 2010 ▪ Volume 4, Number 1 ▪ 99–104.

dients [3, 8]. It is worth emphasizing, however, that the size and the shape of a tablet are not separable from each other: round tablets over a given size (volume) are diffi cult to swallow, thus in this case the industry prefers to produce the oblong form [9].
Previous research on psychological effects of tablet colours have generally focused on the attractiveness of colours [9–11] and on the associations between colours and drug effects or organ systems [7, 12–15]. The result of these studies were, as summarised by the review of de Craen and his colleagues [16], that warm (red, yellow and orange) colours evoke stimulant, whereas white and cold colours (blue and green) evoke tranquillant-sedative ex-pectations.
The usual design of empirical studies in this area was the following: participants were shown differently coloured tablets or capsules, and they had to choose the effects that in their opinion were the most closely associated with the presented items. Using this design, detailed information has been collected about associations among perceptual characteristics of tablets and capsules and their expected effects [15, 17]. A better model of the real life situation is, however, when one has a given symptom (e.g. pain), considers his or her possibilities (differ-ent available painkillers) and chooses one that seems to suit him or her the best. Using this new design, previously demonstrated associations should (re)appear as differences in per-ceived attractivity of different looking tablets.
Based on the above reasoning, the main hypothesis of the present study was that sig-nifi cant differences can be shown in perceived attractiveness of different looking tablets. In addition, we hypothesized that preferences are determined not only by the colours of tab-lets, but by the combination of their effect, colour, and size/shape.
Methods
Participants
One hundred eighty-one university students (Eötvös Loránd University, Budapest, Hungary) between 18 and 25 years of age (mean age 19.8 years, SD = 1.44; 37.9% males) participated in the study. People studying medicine or pharmaceutics were excluded. Volunteers have not received any fi nancial or educational reward for their participation.
Materials
Three widely used effect groups (analgesic–antipyretic, sedative–hypnotic, and spasmolytic) were selected. Five pictures of different tablets in their original size and colour were shown to the participants within each effect group. Every group contained two tablets that were most frequently chosen in the previous studies [15, 17] and three more that differed only in one feature (colour or shape) from the fi rst two. For example, in the spasmolytic group, primary tablets were small round red (SR) and small round yellow (SY), and additional tablets were (1) medium round yellow (MY; differed from SY only in size), (2) oblong red (OR; differed from SR in shape) and (3) small round blue (SB; differed from both SR and SY in colour). Table 1 summarizes the perceptual characteristics of the tablets within each group. The pictures of the tablets within each effect group were randomly arranged and presented on a single sheet.
2010 ▪ Volume 4, Number 1 100 CEMED
ORIGINAL PAPERS

Procedure
Participants were asked to imagine a situation where they needed a medicine with the given effect and to rate the estimated probability of choice for every tablet on a fi ve-grade Likert-scale. No problems or diffi culties were reported about the questionnaire.
ResultsDescriptive statistics of ratings are summarised in Table 1. To examine our fi rst hypothesis, repeated measure ANOVAs were completed for every effect group. Signifi cant (p < 0.001) main effects were found in all three cases. In the analgesic–antipyretic group, all three white
Table 1 The perceptual characteristics of the tablets within the effect groups (small round: diameter = 6 mm; me-dium round: diameter = 13 mm; oblong: length = 18 mm), the descriptive statistics of rated probabilities of choice, and the statistically signifi cant (p < 0.01) preferences
Effect group Tablet look-and-feel Mean (95% CIs) Signifi cant preference in post hoc test
Analgesic–antipyretic 1. Medium round white 3.94 (3.879–4.101) Yes (to 2, 3, 4, 5)
2. Oblong green 2.40 (2.234–2.573) No
3. Small round white 3.46 (3.290–3.638) Yes (to 2, 4, 5)
4. Medium round red 2.33 (2.171–2.492) No
5. Oblong white 3.04 (2.877–3.211) Yes (to 2, 4)
Sedative–hypnotic 1. Small round white 3.88 (3.717–4.040) Yes (to 2, 3, 4, 5)
2. Medium round blue 2.42 (2.251–2.589) No
3. Small round red 2.57 (2.404–2.745) No
4. Oblong white 2.79 (2.619–2.962) No
5. Small round blue 2.94 (2.769–3.120) Yes (to 2, 3)
Spasmolytic 1. Medium round yellow 2.52 (2.364–2.674) No
2. Small round red 3.25 (3.087–3.410) Yes (to 1, 3, 4)
3. Oblong red 2.47 (2.296–2.643) No
4. Small round red 2.91 (2.754–3.069) No
5. Small round yellow 3.25 (3.076–3.421) Yes (to 1, 3, 4)
Preferred tablets from a previous study are marked in italic
ORIGINAL PAPERS
CEMED 101 2010 ▪ Volume 4, Number 1
Fig. 3 Mean attractiveness ratings (estimated probability of use) for the fi ve tablets within the spasmolytic group. Error bars show 95% confi dence intervals of means. MY = medium round yellow; SR = small round red; OR = oblong red; SB = small round blue; SY = small round yellow
Fig. 1 Mean attractiveness ratings (estimated probabil-ity of use) for the fi ve tablets within the analge-sic–antipyretic (NSAID) group. Error bars show 95% confi dence intervals of means. MW = me-dium round white; OG = oblong green; SW = small round white; MR = medium round red; OW = oblong white
Fig. 2 Mean attractiveness ratings (estimated probabil-ity of use) for the fi ve tablets within the seda-tive–hypnotic group. Error bars show 95% con-fi dence intervals of means. SW = small round white; MB = medium round blue; SR = small round red; OW = oblong white; SB = small round blue
tablets were preferred to the other two, although signifi cant differences among the three white tablets were also found (medium round > small round > oblong; Fig. 1). In the seda-
2010 ▪ Volume 4, Number 1 102 CEMED
ORIGINAL PAPERS

tive–hypnotic group, small round white tablets were preferred to all others, and SB ones were preferred to two other combinations (small round red and medium round blue; Fig. 2). In the spasmolytic group, small round red and yellow tablets were preferred to the three other pos-sibilities (Fig. 3).
DiscussionSignifi cant differences in the estimated probabilities of choice for different looking tablets were found within every investigated effect group. Five out of the six tablets preferred in our previous studies were clearly preferred in the present study, too. Since the task used in this study was closer to a real life situation (one needs a curative with a given effect and makes a choice from among the available tablets), the results are much more valid than those of the previous studies (participants usually had to choose a tablet with a given look-and-feel for a desired effect). According to our results, the perceptual characteristics of the tablets can play a role in the selection process (at least when the choice is really free, e.g. OTC medicines).
The second hypothesis of the present study has also been confi rmed. While the colour played the most important role within the NSAID group (all three white tablets were pre-ferred over the coloured ones), it infl uenced preferences in the other groups only in interac-tion with the shape/size of the tablets. In the sedative–hypnotic group, the small round white tablet was more attractive than the other white and/or small round tablets and both small round red and yellow tablets were preferred to medium yellow and OR ones among spasmo-lytics. Therefore, it cannot be simply stated that white colour is associated with sedative ef-fect or yellow with spasmolytic effect in people’s mind, because it is true only for given colour/size/shape combinations. The relationship between analgesic–antipyretic effects and white colour seems to be more general. Moreover, tablets with the same perceptual charac-teristics were rated differently in different effect groups (e.g. SR tablets were preferred as spasmolytics and rejected as sedatives). In summary, participants’ preferences usually de-pended on the combination of three features (effect, colour, shape/size) of the tablets. The origin of these preferences may be in part inherited (general colour preferences) [18] and in part culturally mediated [4, 14], but evidence of personal learning has also been found [17].
The perceived associations between perceptual characteristics of tablets and their effects can have at least two therapeutic implications: they can (1) increase or decrease the overall effectiveness of curatives (e.g. via non-specifi c effects) and (2) can infl uence patients’ com-pliance (adherence). It is well known that the effectiveness of hypnotic and especially anal-gesic drugs can easily be enhanced by non-specifi c interventions, typically suggestions [19, 20]. While there is only weak empirical evidence regarding the physiological effects generated by look-and-feel of medicines [16], this possibility seems to be acceptable from a theoretical point of view. Concerning the underlying mechanisms, both expectations gener-ated by and conditioned responses based on look-and-feel of medicines previously used can elicit psychophysiological effects [1]. According to the direction of previous (personal and/or cultural) learning, these non-specifi c effects can be benefi cial (placebo) or harmful (nocebo) as well. As for compliance, the cognitive dissonance evoked by the discrepancy between expected and actual look-and-feel of medicines can be mainly harmful, as it can result in quitting the therapy [21, 22].
ORIGINAL PAPERS
CEMED 103 2010 ▪ Volume 4, Number 1

ConclusionsConsidering tablets with a given effect, patient’s choice is infl uenced by the combination of colour and shape/size. Discrepancies between the expected and the actual perceptual charac-teristics of medicines can infl uence their overall effectiveness and patient’s adherence to the treatment.
ReferencesKirsch, I.:[1] Specifying nonspecifi cs: psychological mechanisms of placebo effects. In: Harrington, A. (ed): The Placebo Effect. An Interdisciplinary Exploration. Harvard University Press, Cambridge, 1997, pp. 166–186.Ross, S., Buckalew, L. W.:[2] Placebo agentry: assessment of drug and placebo effects. In: White, L., Tursky, B., Schwartz, G. E. (eds): Placebo – Theory, Research, and Mechanisms. Guilford, New York, 1985, pp. 67–82.Leslie, A.:[3] Ethics and practice of placebo therapy. Am. J. Med., 1954, 16, 854–862.Moerman, D. E.:[4] Explanatory mechanisms for placebo effects: cultural infl uences and the meaning re-sponse. In: Guess, H. A., Kleinman, A., Kusek, J. W., Engel, L. W. (eds): The Science of the Placebo. Toward an Interdisciplinary Research Agenda. BMJ Books, London, 2002, pp. 77–107.Nash, H.: [5] Psychologic effects of amphetamines and barbiturates. J. Nerv. Ment. Dis., 1962, 134, 203–217.Hussain, M. Z.:[6] Effect of shape of medication in treatment of anxiety states. Br. J. Psychiatry, 1972, 120, 507–509.Buckalew, L. W., Ross, S.:[7] Medication property effects on expectations of action. Drug Dev. Res., 1991, 23, 101–108.Lasagna, L.:[8] Placebos. Sci. Am., 1955, 193, 68–71.Overgaard, A. B., Møllerdash Sonnergaard, J., Christrup, L. L. et al.:[9] Patients’ evaluation of shape, size and colour of solid dosage forms. Pharm. World Sci., 2001, 23, 185–188.Sallis, R. E., Buckalew, L. W.:[10] Relation of capsule color and perceived potency. Percept. Mot. Skills, 1984, 58, 897–898.Coffi eld, K. E., Buckalew, L. W.:[11] A study for color preferences of drugs and implications for compliance and drug-taking. J. Alcohol Drug Educ., 1988, 34, 28–36.Jacobs, K. W., Nordan, F. M.:[12] Classifi cation of placebo drugs: effect of color. Percept. Mot. Skills, 1979, 49, 367–372.Buckalew, L. W., Coffi eld, K. E.:[13] An investigation of drug expectancy as a function of capsule colour, size, and preparation form. J. Clin. Psychopharmacol., 1982, 2, 245–248.Buckalew, L. W., Coffi eld, K. E.:[14] Drug expectations associated with perceptual characteristics: ethnic fac-tors. Percept. Mot. Skills, 1982, 55, 915–918.Köteles, F., Bárdos, Gy.:[15] Expectations of drug effects based on colours and sizes of tablets. Mentálhig. Pszichoszom., 2007, 8, 277–290 (in Hungarian with English abstract).de Craen, A. J., Roos, P. J., Leonard de Vries, A. et al.:[16] Effect of colour of drugs: systematic review of perceived effect of drugs and of their effectiveness. Br. Med. J., 1996, 313, 1624–1626.Köteles, F., Fodor, D., Cziboly, Á. et al.:[17] Expectations of drug effects based on colours and sizes – the impor-tance of learning. Clin. Exp. Med. J., 2009, 3, 99–107.Adams, F. M., Osgood, C. E.:[18] A cross-cultural study of the affective meanings of color. J. Cross Cult. Psychol., 1973, 4, 135–156.Geers, A. L., Kosbab, K., Helfer, S. G. et al.:[19] Further evidence for individual differences in placebo respond-ing: an interactionist perspective. J. Psychosom. Res., 2007, 62, 563–570.Benedetti, F., Amanzio, M., Vighetti, S. et al.:[20] The biochemical and neuroendocrine bases of the hyperalge-sic nocebo effect. J. Neurosci., 2006, 26, 12014–12022.Buckalew, L. W.:[21] A cognitive dissonance perspective on the patient compliance problem. Psychol. Bull., 1982, 3, 28–33.Buckalew, L. W., Sallis, R. E.:[22] Patient compliance and medication perception. J. Clin. Psychol., 1986, 42, 49–53.
2010 ▪ Volume 4, Number 1 104 CEMED
ORIGINAL PAPERS

The “HÍVÁS” Club: Social Support in Post Cancer Recovery
KORNÉLIA ROZÁLIA LAZÁNYI1, PÉTER MOLNÁR1, ANTAL BUGÁN1, LÁSZLÓ DAMJANOVICH3, ZOLTÁN GARAMI3,
BALÁZS FÜLÖP3, KORNÉLIA SZLUHA2
1Institute of Behavioural Sciences2Department of Radiotherapy
3Department of Surgery,Medical and Health Science Center, University of Debrecen, Hungary
The mental and emotional state of the individuals have a strong effect on the course of their illnesses as well as the speed of recovery. Adequate quantity and quality of information and social support are a prerequisite for mental, and often for physical well-being. In our investigation at the DE OEC, we gathered data on the psychological and physical states of 100 breast cancer patients in order to reveal the role of a helping atmosphere in the recovery phase of their illness. The results suggested that patients attending the HÍVÁS support group could cope with their disease and its side effects better, and experienced a higher level of well-being.
Keywords: social support, support groups, breast cancer, post cancer recovery
IntroductionThe mental consequences of suffering from cancer are numerous. It has been proven, how-ever, by many that the mental state of the patient also has effects on the formation and the course of the cancer itself. According to data from the literature, strong personal distress, acute stress events, depression, deception, and the loss of hope are strongly correlated with the frequency of cancer turnout [1–6]. The complex process of coping also largely infl uences the disease and its treatment [7]. While positive thoughts are associated with increased sub-jective well-being, negative thoughts and emotions are not only destructive in mental, but also in a direct biological sense. Improved (more positive and less negative) affective states are associated with changes in immune functioning, which are thought to enhance one’s abil-ity to fi ght off infectious agents. According to Rabin [8], the appropriate mood infl uences immunity by altering circulating levels of hormones (primarily epinephrine, norepinephrine, and cortisol) that regulate the immune response [9]. According to Koh and Lee [6], and Her-bert and Cohen [5], a negative personal equation impedes the resilient processes of the self and of coping by means of a diminished functioning of the immune system.
Mental factors infl uencing the coping process were thoroughly examined in numerous scientifi c studies. The topics most often considered are the following: adjustment, intrusive thoughts, information needs, body integrity and social support. (A short summary of these topics will be provided in the following section).
Corresponding address: Kornélia Rozália Lazányi MD, Bogár u. 29/e, 1022 Budapest, Hungary.E-mail: [email protected]
1.11
ORIGINAL PAPERS
DOI: 10.1556/CEMED.4.2010. 105 2010 ▪ Volume 4, Number 1 ▪ 105–113.

Adjustment
Anxiety or worry is the most widespread form of distress in cancer patients [10, 11]. The fi rst possible incident of maladjustment is the moment of the diagnosis. Besides, the highest anx-iety levels due to cancer can be measured at the end of the primary treatment, when the duty of checking for symptoms falls back onto the patient, in the case of recurrences or when a bad prognosis is disclosed. The incidence of the following risk factors also impedes optimal adjustment [12]:– Inability to accept physical changes caused by the disease or treatment,– Lack of support from family members and/or friends,– Lack of involvement in satisfying activities,– Previous bad experience of cancer in the family,– Low expectations with regard to the effectivity of the treatment.Adjustment is especially diffi cult when the patient is young at the time of the diagnosis or already has a psychiatric history [13].
Opening up to one’s spouse, family members or close friends, or engaging in activities such as journal writing or artistic expression, can have a signifi cant positive effect on how a patient copes with breast cancer [14, 15]. It can decrease the number of the visits to the doctor and can help in achieving improved overall health.
Intrusive Thoughts
Intrusive thoughts constitute one of the re-experiencing symptoms in post-traumatic stress disorder. They cause intermittent depression and slow down the process of recovery [16]. Cancer survivors frequently report distressing, cancer-related recollections. Matsuoka et al. [17] suggest that disturbing feelings are predictors of the continuous presence of psychologi-cal distress in cancer survivors. Their somatic consequences can be seen in non-cancer pa-tients as well [18, 19]. There are reports about psychological treatments that not only wipe out intrusive thoughts, but positively alter the immune system as well. For example, Bakke [20] record that hypnotic-guided imagery in the form of an 8-week imagery training caused positive changes in psychological well-being and decreased the prevalence of intrusive thoughts.
Experienced Insecurity
Nothing is certain in the life of cancer patients. The cancer diagnosis transfers them into a previously unfamiliar world. Most patients are desperately seeking information to fi nd their way (out). Jahraus et al. [21] found that the majority of breast cancer patients desire as much information as possible (good and bad), in as many details as possible, and are willing to participate in decision-making. Information-seeking activities and the acquisition of all avail-able knowledge concerning cancer are essential parts of the coping process for women facing increased stress because of breast cancer diagnosis [22]. Golant [23] reported signifi cant decreases in ambiguity resulting from a half-day patient education conference. Participants indicated that the education materials and the specifi c mind–body techniques reinforcing the importance of side effect management were useful in everyday problems with work or in other daily activities.
2010 ▪ Volume 4, Number 1 106 CEMED
ORIGINAL PAPERS
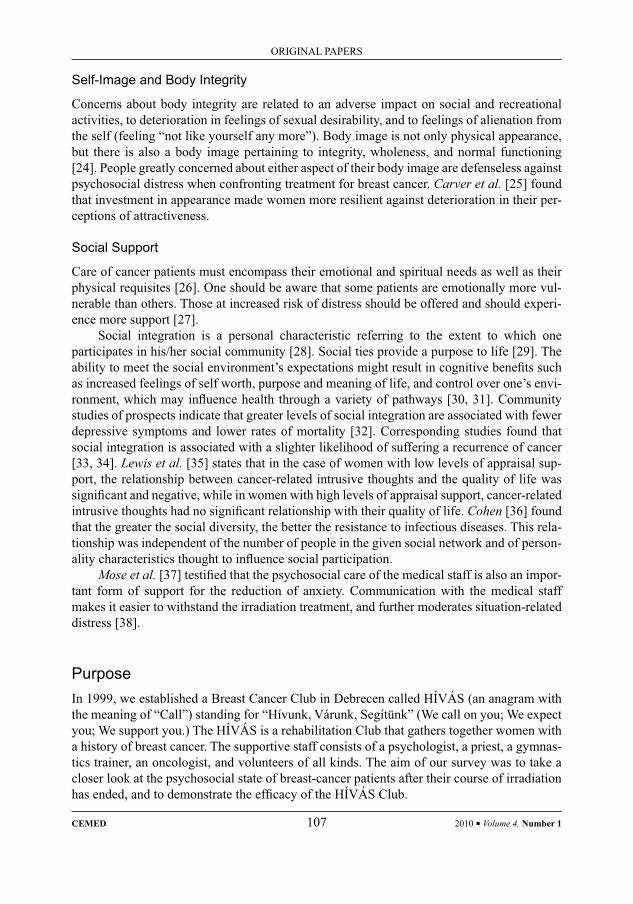
Self-Image and Body Integrity
Concerns about body integrity are related to an adverse impact on social and recreational activities, to deterioration in feelings of sexual desirability, and to feelings of alienation from the self (feeling “not like yourself any more”). Body image is not only physical appearance, but there is also a body image pertaining to integrity, wholeness, and normal functioning [24]. People greatly concerned about either aspect of their body image are defenseless against psychosocial distress when confronting treatment for breast cancer. Carver et al. [25] found that investment in appearance made women more resilient against deterioration in their per-ceptions of attractiveness.
Social Support
Care of cancer patients must encompass their emotional and spiritual needs as well as their physical requisites [26]. One should be aware that some patients are emotionally more vul-nerable than others. Those at increased risk of distress should be offered and should experi-ence more support [27].
Social integration is a personal characteristic referring to the extent to which one participates in his/her social community [28]. Social ties provide a purpose to life [29]. The ability to meet the social environment’s expectations might result in cognitive benefi ts such as increased feelings of self worth, purpose and meaning of life, and control over one’s envi-ronment, which may infl uence health through a variety of pathways [30, 31]. Community studies of prospects indicate that greater levels of social integration are associated with fewer depressive symptoms and lower rates of mortality [32]. Corresponding studies found that social integration is associated with a slighter likelihood of suffering a recurrence of cancer [33, 34]. Lewis et al. [35] states that in the case of women with low levels of appraisal sup-port, the relationship between cancer-related intrusive thoughts and the quality of life was signifi cant and negative, while in women with high levels of appraisal support, cancer-related intrusive thoughts had no signifi cant relationship with their quality of life. Cohen [36] found that the greater the social diversity, the better the resistance to infectious diseases. This rela-tionship was independent of the number of people in the given social network and of person-ality characteristics thought to infl uence social participation.
Mose et al. [37] testifi ed that the psychosocial care of the medical staff is also an impor-tant form of support for the reduction of anxiety. Communication with the medical staff makes it easier to withstand the irradiation treatment, and further moderates situation-related distress [38].
PurposeIn 1999, we established a Breast Cancer Club in Debrecen called HÍVÁS (an anagram with the meaning of “Call”) standing for “Hívunk, Várunk, Segítünk” (We call on you; We expect you; We support you.) The HÍVÁS is a rehabilitation Club that gathers together women with a history of breast cancer. The supportive staff consists of a psychologist, a priest, a gymnas-tics trainer, an oncologist, and volunteers of all kinds. The aim of our survey was to take a closer look at the psychosocial state of breast-cancer patients after their course of irradiation has ended, and to demonstrate the effi cacy of the HÍVÁS Club.
ORIGINAL PAPERS
CEMED 107 2010 ▪ Volume 4, Number 1

Participants of the Survey, MethodsFor our study, 100 breast cancer patients fi lled in our questionnaire, on a voluntary basis. The following two departments of the Medical and Health Science Center at the University of Debrecen (DE OEC) participated in our survey:– Department of Radiotherapy,– Department of Surgery I.The members of the research group were female patients all receiving radiotherapy. Our sample was representative in comparison with other treatment methods applied in the wake of other forms of cancer treatment such as chemotherapy and surgery. Some of the partici-pants of this study attended the HÍVÁS Club, while others did not. The relative ratio of the two groups of patients (37/63) is appropriate for average breast cancer patients at the Univer-sity of Debrecen.The questionnaire contained items on the following particulars:– Personal data,– Factors that might induce breast-cancer according to data from the literature,– Clinical anamnesis,– Somatic side effects,– Psychological factors,– “Services” supplied by the physician,– Devices and products that promote recovery.
ResultsThe average age of the volunteers was 55.4. There was no signifi cant difference between the average age of HÍVÁS members and non-members. Forty-nine percent of the HÍVÁS members (N1 = 18) had a previous anamnesis of cancer among the female ancestry, and 60% of them (N2 = 22) had breast cancer patient(s) among their close (relatives). The non-mem-bers had a much better family anamnesis (N1 = 22, that is 35% and N2 = 2, that is only 3%). The most probable explanation for this ratio of support group membership for those with bad family anamnesis is that those with preliminary experiences with cancer are more likely to ask for and are not ashamed of receiving help from others needing guidance and assistance.
In some aspects, we could not detect any signifi cant difference between the HÍVÁS members and non-members. For example, in both groups, patients with higher than second-ary education sensed psychical complaints more vividly than others with primary or second-ary education. Patients with lower education were the most concerned about the alteration of their body image. Most of the patients were devastated by their altered body image and the decreased sense of femininity. Almost 85% of the patients were at the postmenopausal age. Patients above 50 reported a lower level of mental confusion than the younger members of our sample. They could more easily adapt to the altered body image, to decreased self-regard, to intrusive thoughts, and a decreased sense of femininity.
In other fi elds, the impact of the HÍVÁS Club was well measurable. Somatic and psy-chological complaints, for example, decreased signifi cantly, due to support group member-ship. They were the least frequent in the group of irradiated breast cancer patients. The other
2010 ▪ Volume 4, Number 1 108 CEMED
ORIGINAL PAPERS
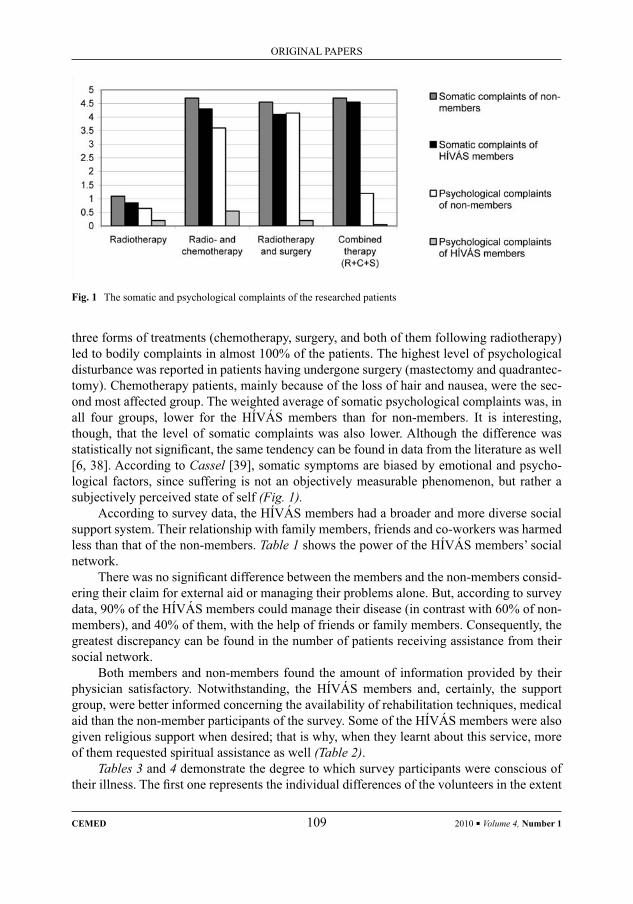
Fig. 1 The somatic and psychological complaints of the researched patients
three forms of treatments (chemotherapy, surgery, and both of them following radiotherapy) led to bodily complaints in almost 100% of the patients. The highest level of psychological disturbance was reported in patients having undergone surgery (mastectomy and quadrantec-tomy). Chemotherapy patients, mainly because of the loss of hair and nausea, were the sec-ond most affected group. The weighted average of somatic psychological complaints was, in all four groups, lower for the HÍVÁS members than for non-members. It is interesting, though, that the level of somatic complaints was also lower. Although the difference was statistically not signifi cant, the same tendency can be found in data from the literature as well [6, 38]. According to Cassel [39], somatic symptoms are biased by emotional and psycho-logical factors, since suffering is not an objectively measurable phenomenon, but rather a subjectively perceived state of self (Fig. 1).
According to survey data, the HÍVÁS members had a broader and more diverse social support system. Their relationship with family members, friends and co-workers was harmed less than that of the non-members. Table 1 shows the power of the HÍVÁS members’ social network.
There was no signifi cant difference between the members and the non-members consid-ering their claim for external aid or managing their problems alone. But, according to survey data, 90% of the HÍVÁS members could manage their disease (in contrast with 60% of non-members), and 40% of them, with the help of friends or family members. Consequently, the greatest discrepancy can be found in the number of patients receiving assistance from their social network.
Both members and non-members found the amount of information provided by their physician satisfactory. Notwithstanding, the HÍVÁS members and, certainly, the support group, were better informed concerning the availability of rehabilitation techniques, medical aid than the non-member participants of the survey. Some of the HÍVÁS members were also given religious support when desired; that is why, when they learnt about this service, more of them requested spiritual assistance as well (Table 2).
Tables 3 and 4 demonstrate the degree to which survey participants were conscious of their illness. The fi rst one represents the individual differences of the volunteers in the extent
ORIGINAL PAPERS
CEMED 109 2010 ▪ Volume 4, Number 1
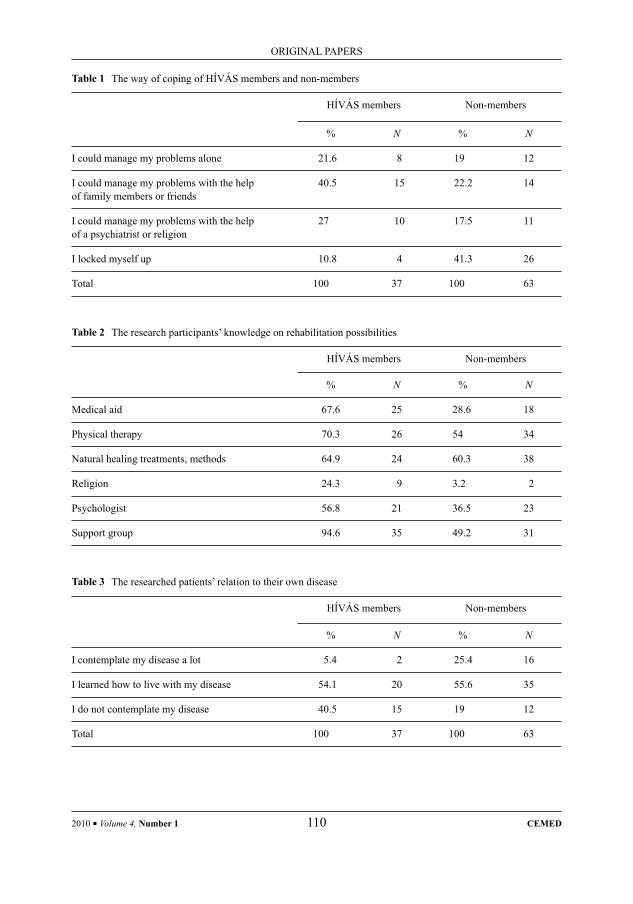
Table 1 The way of coping of HÍVÁS members and non-members
HÍVÁS members Non-members
% N % N
I could manage my problems alone 21.6 8 19 12
I could manage my problems with the help of family members or friends
40.5 15 22.2 14
I could manage my problems with the help of a psychiatrist or religion
27 10 17.5 11
I locked myself up 10.8 4 41.3 26
Total 100 37 100 63
Table 2 The research participants’ knowledge on rehabilitation possibilities
HÍVÁS members Non-members
% N % N
Medical aid 67.6 25 28.6 18
Physical therapy 70.3 26 54 34
Natural healing treatments, methods 64.9 24 60.3 38
Religion 24.3 9 3.2 2
Psychologist 56.8 21 36.5 23
Support group 94.6 35 49.2 31
Table 3 The researched patients’ relation to their own disease
HÍVÁS members Non-members
% N % N
I contemplate my disease a lot 5.4 2 25.4 16
I learned how to live with my disease 54.1 20 55.6 35
I do not contemplate my disease 40.5 15 19 12
Total 100 37 100 63
2010 ▪ Volume 4, Number 1 110 CEMED
ORIGINAL PAPERS

to which they dealt with their breast cancer, while the second one contrasts the lack of so-matic manifestations with the feeling of being a healthy person.
These survey data suggest that the members of the HÍVÁS Club have learnt how to live with their breast cancer anamnesis to the same degree as the non-members. The difference lies in the coping mechanism. While 25.4% of the non-members contemplate their disease day after day, most HÍVÁS members do not have permanent concerns about breast cancer.
The last table shows that although the ratio of cured patients (without recurrence and metastases) is almost the same in both groups, 28.6% (three times more) of the non-members do not consider themselves as cured.
ConclusionsWe have arrived at the conclusion that social support affects the patients’ attitude towards their disease, in a number of ways. We have also found that the social context of the breast cancer patients largely infl uences their sense of disease and the results of their treatment. Besides talking to family members or close friends, joining a cancer support group has proved the best possibility for participation in a broad social network. As we have seen, affi liation to support groups helps the patients cognitively reframe their situation. It also teaches them how to reframe their need for depending on others as a form of return on the emotional investment they made in the relationship over the years.
As we have also learnt, 37% of general breast cancer patients at the University of Debrecen are members of the HÍVÁS Club. The HÍVÁS members not only sense somatic and psychological spillovers less intensely, but can also live with their disease more easily. Our results show that patients attending the support group could more easily adapt to cancer and its side effects. Members of the HÍVÁS Club had better relationships with family mem-bers, friends or co-workers. Also, being among companions in distress helped them tolerate their altered body image better. On the whole, we can conclude that breast cancer has less effect on these patients’ social ties, body image, sexual life, self respect and self reliance.
Table 4 Comparison of the HÍVÁS members’ and non-members’ sense of illness
HÍVÁS members Non-members
% N % N
I have recurrence 5.4 2 4.8 3
I have metastases 5.4 2 6.3 4
I have neither recurrence nor metastases 10.8 4 28.6 18
I consider myself healthy 78.4 29 60.3 38
Total 100 37 100 63
ORIGINAL PAPERS
CEMED 111 2010 ▪ Volume 4, Number 1

On the basis of our data, we can state that support group membership helps diminish the number of patients who withdraw into themselves, while it helps increase the number of those who consider themselves cured and do not contemplate breast cancer each day, any more.
ReferencesPaget, J.:[1] On disease of the mammary areola preceding cancer of the mammary gland. St. Bartholomew Hosp. Rep., 1874, 10, 87–89.Parker, S. L., Davis, K. J., Wingo, P. A. et al.:[2] Cancer statistics by race and ethnicity. CA Cancer J. Clin., 1998, 48, 31–48.LeShan, L.:[3] Psychological states as factors in the development of malignant disease: a critical review. J. Natl. Cancer Inst., 1959, 22, 1–18.Grossarth-Maticek, R., Schmidt, P., Vetter, H. et al.:[4] Psychotherapy research in oncology. In: Steptoe, A., Mathews, A. (eds): Health Care and Human Behavior. Academic Press, London, 1984, pp. 325–341.Herbert, T. B., Cohen, S.:[5] Depression and immunity: a meta-analytic review. Psychol. Bull., 1993, 113, 472–486.Koh, K. B., Lee, B. K.:[6] Reduced lymphocyte proliferation and interleukin-2 production in anxiety disor-ders. Psychosom. Med., 1998, 60, 479–483.Davidson, L., Strauss, J. S.:[7] Beyond the biopsychosocial model: integrating disorder, health and recovery. Psychiatry, 1995, 58, 44–55.Rabin, B. S.:[8] Stress, Immune Function and Health: The Connection. John Wiley & Sons, New York, 1999.Sklar, L. S., Anisman, H.:[9] Stress and cancer. Psychol. Bull., 1981, 89, 369–406.Sklar, L. S., Anisman, H.:[10] Stress and coping factors infl uence tumour growth. Science, 1979, 205, 513–515.Schwarger, R., Leppin, A.:[11] Social support and health: a meta-analysis. Psychol. Health, 1989, 3, 1–15.Carr, J. E.:[12] Stress and illness. In: Wedding, D. (ed): Behavior and Medicine. Hogrefe and Huber, Bern, 2001, pp. 231–245.Spiegel, D., Bloom, J. R., Kraemer, H. C. et al.:[13] Effect of psychosocial treatment on survival of patients with metastatic breast cancer. Lancet, 1989, 2, 901–918.Stoll, B. A.:[14] Psychosomatic aspects of cancer. In: Christine, M. J., Mellett, P. G. (eds): The Psychosomatic Approach Contemporary Practice of Whole-Person Care. Wiley, New York, 1986, pp. 395–423.Kopp, M.:[15] A reménytelenség szerepe a betegségek létrejöttében. (In Hungarian) Kórház, 1997, 4, 4–9.Matsuoka, Y., Nakano, T., Inagaki, M. et al.:[16] Cancer-related intrusive thoughts as an indicator of poor psycho-logical adjustment at 3 or more years after breast surgery: a preliminary study. Breast Cancer Res. Treat., 2002, 2, 117–124.Glaser, R., Rice, J., Sheridan, J. et al.:[17] Stress related immune suppression: health implications. Brain Behav. Immun., 1987, 1, 7–20.Cohen, M., Klein, E., Kuten, A. et al.:[18] Increased emotional distress in daughters of breast cancer patients is associated with decreased natural cytotoxic activity, elevated levels of stress hormones and decreased secre-tion of Th1 eytokines. Int. J. Cancer, 2002, 3, 347–354.Bakke, A. C., Purtzer, M. Z., Newton, P.:[19] The effect of hypnotic-guided imagery on psychological well- being and immune function in patients with prior breast cancer. J. Psychosom. Res., 2002, 6, 1131–1137.Jahraus, D., Sokolsky, S., Thurston, N. et al.:[20] Evaluation of an education program for patients with breast cancer receiving radiation therapy. Cancer Nurs., 2002, 3, 231–245.Blechman, E. A., Brownell, K. D.:[21] Behavioral Medicine and Women. Guilford Press, New York, 1997.Golant, M., Altman, T., Martin, C.: [22] Managing cancer side effects to improve quality of life: a cancer psycho education program. Cancer Nurs., 2003, 1, 37–44.Fava, G. A.:[23] Behavioral treatment of altered brain-gut mechanisms. In: Corazziari, E. (ed): Neuro Gastroen-terology. Walter de Gruyter, Berlin, 1996, pp. 109–113.Carver, C. S., Pozo-Kaderman, C., Price, A. A. et al.:[24] Concern about aspects of body image and adjustment to early stage breast cancer. Psychosom. Med., 1998, 2, 168–174.
2010 ▪ Volume 4, Number 1 112 CEMED
ORIGINAL PAPERS

Drossman, D. A.:[25] Irritable bowel syndrome: the role of psychosocial factors. Stress Med., 1994, 10, 49–55.Dunbar, J. M., Marshall, G. D., Howell, M. F.:[26] Behavioral strategies for improving compliance. In: Haynes, D. W., Sackett, D. L. (eds): Compliance in Health Care. Johns Hopkins University Press, Baltimore, 1979, pp. 174–190.Blaser, D.:[27] Social support and mortality in an elderly community population. Am. J. Epidemiol., 1982, 115, 684–694.Kawachi, I., Berkman, L. F.:[28] Social cohesion, social capital and health. In: Berkman, L. F., Kawachi, I. (eds): Social Epidemiology. Oxford University Press, New York, 2000, pp. 174–190.Caldwell, R. A., Pearson, J. L., Chin, J. R.:[29] Stress moderating effects: social support in the context of gender and locus of control. Pers. Soc. Psychol. Bull., 1987, 13, 5–17.Sarason, B. R., Sarason, I. G., Pierce, G. R.:[30] Social Support: An Interactional View. Wiley, New York, 1990.Berkman, L. F.:[31] The role of social relations in health promotion. Psychosom. Med., 1995, 57, 245–254.Helgeson, V. S., Cohen, S., Fritz, H. L.:[32] Social ties and the onset and progression of cancer. In: Holland, J. (ed): Textbook of Psycho-Oncology. Oxford University Press, New York, 1998, pp. 99–109.Caserta, M., Lund, D.:[33] Intrapersonal resources and the effectiveness of self-help groups of bereaved older adults. Gerontologist, 1993, 33, 619–629.Lewis, J. A., Manne, S. L., Duttamel, K. N. et al.:[34] Social support, intrusive thoughts, and quality of life in breast cancer survivors. J. Behav. Med., 2001, 3, 231–245.Cohen, S., Wills, T. A.:[35] Stress, social support, and the buffering hypothesis. Psychol. Bull., 1985, 98, 310–357.Mose, S., Rahn, A. N., Budischewski, K. M. et al.:[36] The effect of adjuvant radiotherapy on the mental health of female patients with breast- conserving operated breast carcinoma. Strahlenther. Onkol., 1999, 3, 112–118.Knight, C., Barthel, H.:[37] Quality Hospice Care. A Hospice Staff Training Manual. Embi, Texas, 1993.Cohen, J. J.:[38] Individual variability and immunity. Brain Behav. Immun., 1999, 13, 76–79.Cassel, J.:[39] Psychosocial processes and “stress”: theoretical formulation. Int. J. Health Serv., 1974, 4, 471–482.
ORIGINAL PAPERS
CEMED 113 2010 ▪ Volume 4, Number 1


Gastric Ulcer Protective Activity of Hibiscus sabdariffa: An Experimental,
Biochemical and Histological StudySALEH ALQASOUMI1, 2, MOHAMMED AL-DOSARI1,
MOHAMMED AL-SOHAIBANI3, TAWFEQ AL-HOWIRINY1, MOHAMMED AL-YAHYA1, SYED RAFATULLAH2
1Department of Pharmacognosy, College of Pharmacy, P.O. Box 2457, King Saud University, Riyadh 11451, Saudi Arabia
2Medicinal, Aromatic and Poisonous Plants Research Center, College of Pharmacy, P.O. Box 2457, King Saud University, Riyadh 11451, Saudi Arabia
3Department of Pathology, P.O. Box 2925, King Khalid University Hospital, King Saud University, Riyadh 11461, Saudi Arabia
Hibiscus sabdariffa L. (Roselle) is a vegetable known to possess various therapeutic properties. We evaluated the anti-ulcerogenic property of ethanolic extract of dried calyces (EEHS) in different ulcer models in Wistar albino rats. The extract at 250 and 500 mg/kg body weight, orally has a signifi cant effect in cold restraint stress, pylorus ligation, necrotizing agents (80% ethanol, 0.2 M NaOH and 25% NaCl) and indomethacin-induced gastric ulcer models. The extract showed an ability to signifi cantly protect against gastric mucosal injury in all models used. Furthermore, EEHS has signifi cantly decreased the basal gastric acid secretion, as well as signifi cantly increased gastric wall mucus secretion (GWM) and non-protein sulfhydryl (NP-SH) concentrations in gastric tissue. Whereas, the extract signifi cantly reduced the ethanol-induced elevated levels of malondialdehyde (MDA) in the rat stomach. These pharmacological and biochemical fi ndings were further supported by the histological assessment of the stomach. The phytochemical constituents present in the H. sabdariffa calyces may contribute to its anti-ulcer activity through one or more mechanism(s), including the antisecretory and antioxidant nature of the extract.
Keywords: Hibiscus sabdariffa, Roselle, gastric anti-ulcer, cytoprotection, antioxidant
Abbreviations
EEHS = ethanolic extract of Hibiscus sabdariffa; GWM = gastric wall mucus; NP-SH = non-protein sulfhydryl; MDA = malondialdehyde
The consumption of a variety of herbs and vegetables by people is thought to contribute a great deal to the improvement of human health with regard to prevention and/or cure of dis-eases because plants have long served as useful and rational source of therapeutic agents [1]. Natural sources such as plants present promise of cure as they have been the raw materials for the synthesis of drugs and important source of new therapeutic agents [2]. Various phy-tochemical constituents have been identifi ed from herbal ingredients with anti-ulcer activity [3]. In recent years, attention has been focused on anti-ulcer properties of edible plants, as an important source for the prevention of diseases.
Corresponding address: Syed Rafatulah MD, Medicinal, Aromatic and Poisonous Plants Research Center (MAP-PRC), College of Pharmacy, P.O. Box 2457, King Saud University, Riyadh 11451, Saudi Arabia.E-mail: [email protected]; [email protected]
1.12
ORIGINAL PAPERS
DOI: 10.1556/CEMED.4.2010. 115 2010 ▪ Volume 4, Number 1 ▪ 115–127.

Hibiscus sabdariffa L. is a genesis of the Malvaceae family. It is called by different local names in various countries. In Saudi Arabia, it is called Karkade. In English-speaking coun-tries and in India, it is named Roselle or Red Sorrel and Lal Ambada, respectively. As a tra-ditional medicine, it is claimed to possess various therapeutic and pharmacological activities. The calyces are used to make beverages and have been used in Arab traditional and Unani medicines as diuretic, stomachic, aphrodisiac, cholagogue, digestive, laxative, and as a rem-edy for heart ailment, hypertension and for thinning the blood viscosity [4]. Moreover, the calyx of Roselle is reported to have antioxidant properties [5]. A clinical trial on hypertensive patients revealed the antihypertensive effect of H. sabdariffa aqueous extract [6]. It is also used as an anticancer [7], anticlastogenic [8], antispasmodic [9], antistress [10], and antidi-arrheal [11, 12] agent, and as a diuretic and hypolipidemic [13, 14] agent in traditional medi-cine of various countries.
The Roselle contains a number of phytochemical constituents including quercetin, an-thocyanin, L-ascorbic acid and protocatechuic acid [15]. It also contains anisaldehyde, arachidic acid, β-carotene, β-sitosterol, delphinidin, gossypetin and hibiscetin [16]. In the current study, we investigated the gastroprotective effects of ethanolic extract of the calyces of H. sabdariffa (EEHS) by employing hypothermic resistant stress- and various chemical-induced gastric ulcer models alongside biochemical and histological assessment of gastric tissue in rats.
Material and Methods
Plant Material and Preparation of Extract
Dried calyces of H. sabdariffa were purchased from a local vegetable market in Riyadh, and the identity of these calyces was confi rmed by an expert taxonomist of the Department of Pharmacognosy, where a voucher specimen (no. 6709) of the plant has been kept in the Her-barium of the College of Pharmacy, KSU, Riyadh. The dried, coarsely pulverized calyces of H. sabdariffa were placed in a glass percolator with ethanol and were allowed to stand at room temperature for about 72 h. The percolate was collected and dried under reduced pres-sure in vacuo. The extract obtained was later used and dissolved in distilled water for evalu-ation of anti-ulcer activity.
Animals and Dosing
The animal study protocol was approved by the Research and Ethics Committee of the Ex-perimental Animal Care Society, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia. Albino Wistar rats of either sex, approximately of the same age, weighing 150–200 g and fed on a diet of standard chow were used in this study. They were randomly divided into experimental groups of six rats each. Aqueous solutions of ulcerogens and EEHS were fresh-ly prepared before administration. EEHS at doses of 250 and 500 mg/kg were given orally in the anti-ulcer studies and intraperitoneally for gastric secretion evaluation. The rats were sacrifi ced and the stomachs removed and opened along the greater curvature. After washing with saline, the gastric lesions were quantifi ed by a person unaware of the treatments.
2010 ▪ Volume 4, Number 1 116 CEMED
ORIGINAL PAPERS

Hypothermic Restraint Stress-Induced Ulcers
The method described by Senay and Levine [17] was adopted with slight modifi cations. Ani-mals were fasted for 36 h but had access to water ad libitum. Thirty minutes after the oral administration of EEHS (250 and 500 mg/kg), the rats were immobilized in restraint cages and placed inside a ventilated refrigerator maintained at 3 ± 1 °C for 3 h. The animals were then sacrifi ced and the stomachs were excised. They were examined for ulceration and the severity of intraluminal bleeding according to the following arbitrary scale described by Chiu et al. [18]. 0 = no blood detectable; 1 = thin blood follows the rugae; 2 = thick blood follows the rugae; 3 = thick blood follows the rugae with blood clots in certain areas; and 4 = exten-sive covering of the whole gastric mucosal surface with thick blood.
Pylorus-Ligated (Shay) Rats (Anti-Secretory Studies)
Rats were fasted for 36 h with access to water ad libitum before pylorus ligation. Care was taken not to cause bleeding or to occlude blood vessels [19]. EEHS was administered intra-peritoneally immediately after pylorus ligation (Shay). The rats were sacrifi ced at 6 h after pylorus ligation. The stomachs were removed; the contents were collected, volumes mea-sured, centrifuged and analyzed for titratable acidity against 0.01 mol/L NaOH at pH 7.
Gastric Lesions Induced by Necrotizing Agents (Cytoprotection)
Each rat was administered 1 mL of a necrotizing agent (80% ethanol, 0.2 mol/L NaOH or 25% NaCl). EEHS was given 30 min before the administration of necrotizing agents. One hour after the administration of ethanol and the alkalis, the rats were sacrifi ced and examined for stomach lesions. The scoring of stomach lesions was as follows: patchy lesions of the stomach induced by ethanol were scored according to the method described by Robert et al. [20] using the following scale: 0 = normal mucosa; 1 = hyperemic mucosa or up to three small patches; 2 = from four to ten small patches; 3 = more than ten small or up to three medium-sized patches; 4 = from four to six medium-sized patches; 5 = more than six medi-um-sized or up to three large patches; 6 = from four to six large patches; 7 = from seven to ten large patches; 8 = more than ten large patches or extensive necrotic zones. “Small” was defi ned as up to 2 mm across (max. diameter), “medium-sized” between 2 and 4 mm across and “large” more than 4 mm across.
Determination of Gastric Wall Mucus (GWM)
GWM was determined according to the modifi ed procedure of Crone et al. [21]. The glandu-lar segment of the stomach was separated from the rumen of the stomach, weighed, and transferred immediately to 10 mL of 0.1% w/v Alcian blue solution (in 0.16 mmol/L sucrose solution buffered with 0.05 mL sodium acetate at pH 5). Tissue was stained for 2 h in Alcian blue and excess dye was removed by two successive rinses with 10 mL of 0.25 mmol/L su-crose, fi rst after 15 min and then after 45 min. Dye complexed with the GWM was extracted with 10 mL of 0.5 mmol/L magnesium chloride, which was intermittently shaken for 1 min at 30 min intervals for 2 h. Four milliliters of blue extract were then vigorously shaken with an equal volume of diethyl ether. The resulting emulsion was centrifuged at 4,000 r/min for
ORIGINAL PAPERS
CEMED 117 2010 ▪ Volume 4, Number 1
10 min and the absorbance of the aqueous layer was recorded at 580 nm. The quantity of Al-cian blue extracted per gram of wet glandular tissue was then calculated.
Gastric Lesions Induced by Indomethacin
Indomethacin was suspended in 1.0% carboxy-methylcellulose (CMC) in water (6 mg/mL) and administered orally to the 36 h fasted rats at a dose of 30 mg/kg body weight. Control rats were treated similarly with an equivalent amount of vehicle [22]. The H. sabdariffa extract was given 30 min prior to indomethacin administration at a dose of 250 and 500 mg/kg. The animals were sacrifi ced 6 h after treatment. The stomachs were excised, rinsed with normal saline and examined for ulceration.
Determination of Total Protein (TP)
TP was estimated by the kit method, supplied by Crescent Diagnostics, Jeddah, Saudi Arabia.
Estimation of Non-Protein Sulfhydryls (NP-SH)
Gastric mucosal NP-SH were measured according to the method of Sedlak and Lindsay [23]. The glandular part of the stomach was homogenized in ice-cold 0.02 mmol/L ethylenedi-aminetetraacetic acid (EDTA). Aliquots of 5 mL of the homogenates were mixed in 15 mL test tubes with 4 mL of distilled water and 1 ml of 50% trichloroacetic acid (TCA). The tubes were shaken intermittently for 10 min and centrifuged at 3,000 r/min. Two milliliters of su-pernatant were mixed with 4 mL of 0.4 mol/L Tris buffer at pH 8.9. 0.1 mL of 5,5´-dithio-bis(2-nitrobenzoic acid) (DTNB) was added and the sample was shaken. The absorbance was measured within 5 min of DTNB addition at 412 nm against a reagent blank.
Determination of Malondialdehyde (MDA)
The method reported by Utley et al. [24] was followed. The animals were killed 1 h after ethanol administration. The stomachs were removed and each was homogenized in 0.15 mol/L KCl (at 4 °C) in a Potter–Elvehjem type C homogenizer to give a 10% w/v homoge-nate. Aliquots of homogenate 1 mL in volume were incubated at 37 °C for 3 h in a metabolic shaker. Then 1 mL of 10% aqueous TCA was added and mixed. The mixture was then centri-fuged at 800 g for 10 min. One milliliter of the supernatant was removed and mixed with 1 mL of 0.67% w-thiobarbituric acid in water and placed in a boiling water bath for 10 min. The mixture was cooled and diluted with 1 mL distilled water. The absorbance of the solution was then read at 535 nm. The content of MDA (nmol/g wet tissue) [index of the magnitude of lipid peroxidation (LPO)] was then calculated by reference to a standard curve of MDA solution.
Histopathological Evaluation
Gastric tissue samples were fi xed in neutral buffered formalin for 24 h. Sections of gastric tissue were histopathologically examined to study the ulcerogenic and/or anti-ulcerogenic activity of EEHS. The tissues were fi xed in 10% buffered formalin and processed using a VIP
2010 ▪ Volume 4, Number 1 118 CEMED
ORIGINAL PAPERS

tissue processor. The processed tissues were embedded in paraffi n blocks and sections about 5 μm thick were cut using an American optical rotary microtome. These sections were stained with haematoxylin and eosin using routine procedures [25]. The slides were examined micro-scopically for pathomorphological changes such as congestion, hemorrhage, necrosis, edema, and erosions using an arbitrary scale for severity assessment of these changes.
Statistical Analysis
Values in tables and fi gures are given as means ± SE. Data were analyzed by using one-way analysis of variance (ANOVA) followed by Student’s t-test.
Results
Effect of EEHS on Hypothermic Restraint Stress-Induced Gastric Mucosal Lesions
Table 1 shows that EEHS at a doses of 250 and 500 mg/kg body weight signifi cantly inhib-ited intraluminal bleeding and ulcer formation induced by hypothermic restraint stress. Al-though the ulcer index was reduced at a dose of 250 mg/kg body weight, this reduction was not found to be statistically signifi cant.
Table 1 Effect of ethanolic extract of EEHS on hypothermic restrain stress-induced intraluminal bleeding and gastric lesions in rats (mean ± SE)
Group serial Treatment Dose (mg/kg, i.g.)
Intraluminal bleeding Gastric lesion
Score Ulcer index
1 Control (distilled water) – 2.50 ± 0.83 20.66 ± 5.27
2 EEHS 250 00 ± 00 10.33 ± 3.72
3 EEHS 500 00 ± 00 5.83 ± 2.04*
Six rats were used in each group*P < 0.05 vs. control (distilled water) group, student’s t-test
Effect of EEHS on Gastric Secretions in 6 h Pylorus-Ligated Rats
In the gastric secretion determination model, using ligated pylorus for 6 h, the treatment with EEHS at both doses (250 and 500 mg/kg) signifi cantly reduced the volume of basal gastric secretion, titratable acidity and ulceration in comparison with the control group (Table 2).
Effect of EEHS on Necrotizing Agents-Induced Gastric Lesions
The treatment of rats with 80% ethanol, 0.2 mol/L NaOH and 25% NaCl produced extensive gastric lesions in the glandular mucosa of the stomach in all the control rats. Pretreatment
ORIGINAL PAPERS
CEMED 119 2010 ▪ Volume 4, Number 1
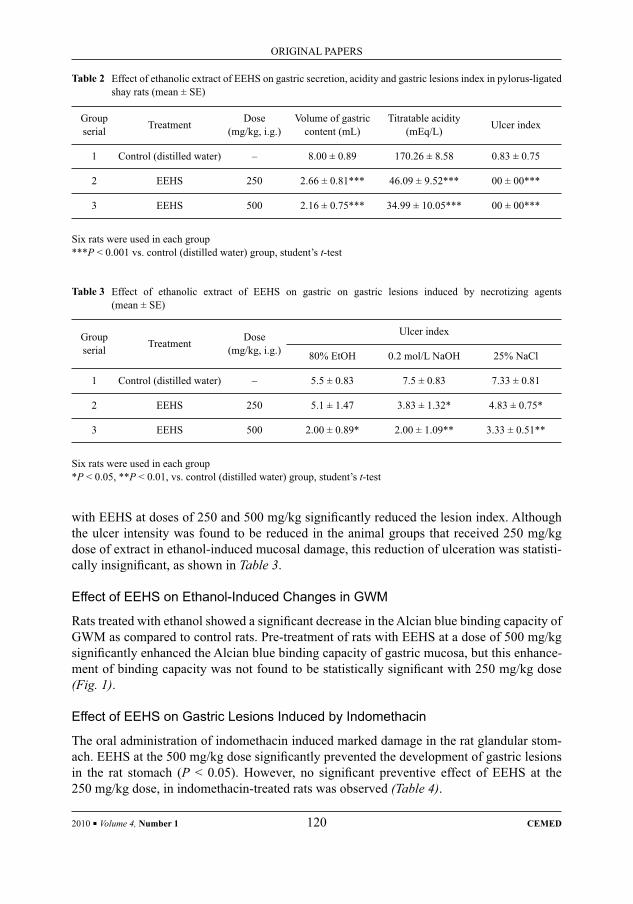
with EEHS at doses of 250 and 500 mg/kg signifi cantly reduced the lesion index. Although the ulcer intensity was found to be reduced in the animal groups that received 250 mg/kg dose of extract in ethanol-induced mucosal damage, this reduction of ulceration was statisti-cally insignifi cant, as shown in Table 3.
Effect of EEHS on Ethanol-Induced Changes in GWM
Rats treated with ethanol showed a signifi cant decrease in the Alcian blue binding capacity of GWM as compared to control rats. Pre-treatment of rats with EEHS at a dose of 500 mg/kg signifi cantly enhanced the Alcian blue binding capacity of gastric mucosa, but this enhance-ment of binding capacity was not found to be statistically signifi cant with 250 mg/kg dose (Fig. 1).
Effect of EEHS on Gastric Lesions Induced by Indomethacin
The oral administration of indomethacin induced marked damage in the rat glandular stom-ach. EEHS at the 500 mg/kg dose signifi cantly prevented the development of gastric lesions in the rat stomach (P < 0.05). However, no signifi cant preventive effect of EEHS at the 250 mg/kg dose, in indomethacin-treated rats was observed (Table 4).
Table 2 Effect of ethanolic extract of EEHS on gastric secretion, acidity and gastric lesions index in pylorus-ligated shay rats (mean ± SE)
Group serial Treatment Dose
(mg/kg, i.g.)Volume of gastric
content (mL)Titratable acidity
(mEq/L) Ulcer index
1 Control (distilled water) – 8.00 ± 0.89 170.26 ± 8.58 0.83 ± 0.75
2 EEHS 250 2.66 ± 0.81*** 46.09 ± 9.52*** 00 ± 00***
3 EEHS 500 2.16 ± 0.75*** 34.99 ± 10.05*** 00 ± 00***
Six rats were used in each group***P < 0.001 vs. control (distilled water) group, student’s t-test
Table 3 Effect of ethanolic extract of EEHS on gastric on gastric lesions induced by necrotizing agents (mean ± SE)
Group serial Treatment Dose
(mg/kg, i.g.)
Ulcer index
80% EtOH 0.2 mol/L NaOH 25% NaCl
1 Control (distilled water) – 5.5 ± 0.83 7.5 ± 0.83 7.33 ± 0.81
2 EEHS 250 5.1 ± 1.47 3.83 ± 1.32* 4.83 ± 0.75*
3 EEHS 500 2.00 ± 0.89* 2.00 ± 1.09** 3.33 ± 0.51**
Six rats were used in each group*P < 0.05, **P < 0.01, vs. control (distilled water) group, student’s t-test
2010 ▪ Volume 4, Number 1 120 CEMED
ORIGINAL PAPERS
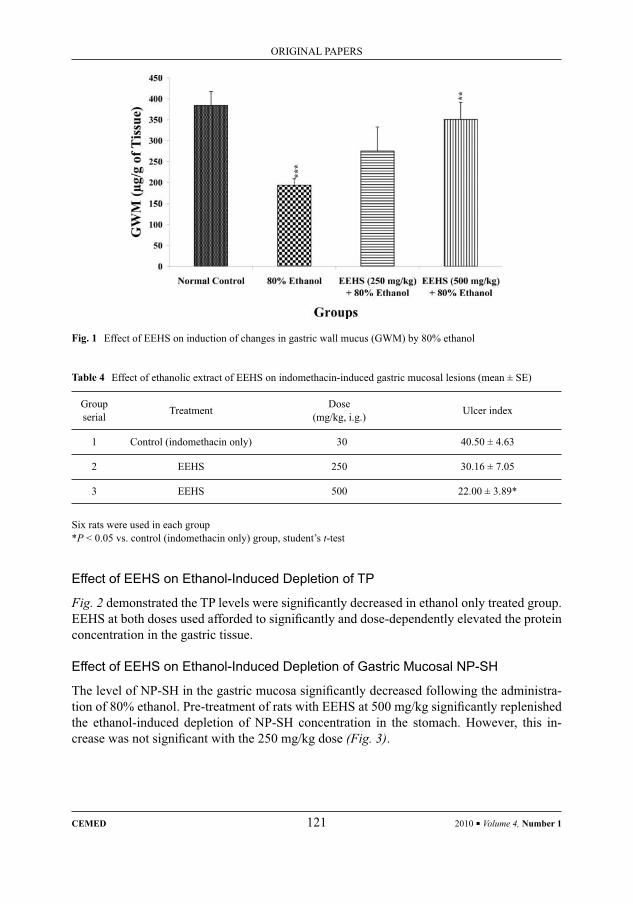
Table 4 Effect of ethanolic extract of EEHS on indomethacin-induced gastric mucosal lesions (mean ± SE)
Group serial Treatment Dose
(mg/kg, i.g.) Ulcer index
1 Control (indomethacin only) 30 40.50 ± 4.63
2 EEHS 250 30.16 ± 7.05
3 EEHS 500 22.00 ± 3.89*
Six rats were used in each group*P < 0.05 vs. control (indomethacin only) group, student’s t-test
Fig. 1 Effect of EEHS on induction of changes in gastric wall mucus (GWM) by 80% ethanol
Effect of EEHS on Ethanol-Induced Depletion of TP
Fig. 2 demonstrated the TP levels were signifi cantly decreased in ethanol only treated group. EEHS at both doses used afforded to signifi cantly and dose-dependently elevated the protein concentration in the gastric tissue.
Effect of EEHS on Ethanol-Induced Depletion of Gastric Mucosal NP-SH
The level of NP-SH in the gastric mucosa signifi cantly decreased following the administra-tion of 80% ethanol. Pre-treatment of rats with EEHS at 500 mg/kg signifi cantly replenished the ethanol-induced depletion of NP-SH concentration in the stomach. However, this in-crease was not signifi cant with the 250 mg/kg dose (Fig. 3).
ORIGINAL PAPERS
CEMED 121 2010 ▪ Volume 4, Number 1

Effect of EEHS on Ethanol-Induced Increase in MDA
As depicted in Fig. 4, MDA levels in the gastric mucosa were signifi cantly higher in the ethanol treated group than in the untreated control group. On the other hand, EEHS at 500 mg/kg dose signifi cantly decreased the MDA content. The lower dose (250 mg/kg), how-ever, decreased the MDA content, but insignifi cantly.
Fig. 2 Effect of EEHS on TP concentration in gastric ulcer induced by 80% ethanol
Fig. 3 Effect of EEHS on NP-SH concentration in gastric ulcer induced by 80% ethanol
2010 ▪ Volume 4, Number 1 122 CEMED
ORIGINAL PAPERS
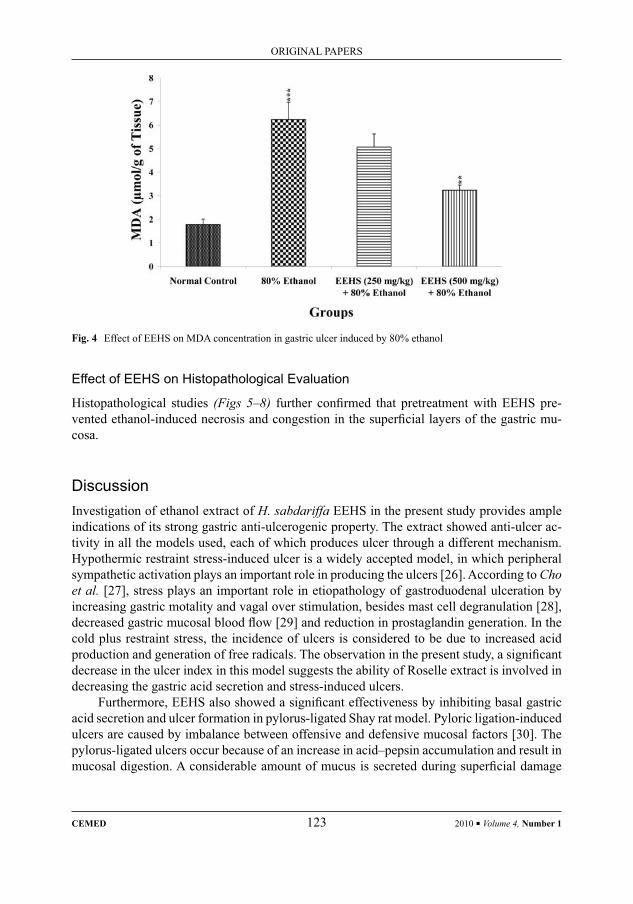
Fig. 4 Effect of EEHS on MDA concentration in gastric ulcer induced by 80% ethanol
Effect of EEHS on Histopathological Evaluation
Histopathological studies (Figs 5–8) further confi rmed that pretreatment with EEHS pre-vented ethanol-induced necrosis and congestion in the superfi cial layers of the gastric mu-cosa.
DiscussionInvestigation of ethanol extract of H. sabdariffa EEHS in the present study provides ample indications of its strong gastric anti-ulcerogenic property. The extract showed anti-ulcer ac-tivity in all the models used, each of which produces ulcer through a different mechanism. Hypothermic restraint stress-induced ulcer is a widely accepted model, in which peripheral sympathetic activation plays an important role in producing the ulcers [26]. According to Cho et al. [27], stress plays an important role in etiopathology of gastroduodenal ulceration by increasing gastric motality and vagal over stimulation, besides mast cell degranulation [28], decreased gastric mucosal blood fl ow [29] and reduction in prostaglandin generation. In the cold plus restraint stress, the incidence of ulcers is considered to be due to increased acid production and generation of free radicals. The observation in the present study, a signifi cant decrease in the ulcer index in this model suggests the ability of Roselle extract is involved in decreasing the gastric acid secretion and stress-induced ulcers.
Furthermore, EEHS also showed a signifi cant effectiveness by inhibiting basal gastric acid secretion and ulcer formation in pylorus-ligated Shay rat model. Pyloric ligation-induced ulcers are caused by imbalance between offensive and defensive mucosal factors [30]. The pylorus-ligated ulcers occur because of an increase in acid–pepsin accumulation and result in mucosal digestion. A considerable amount of mucus is secreted during superfi cial damage
ORIGINAL PAPERS
CEMED 123 2010 ▪ Volume 4, Number 1
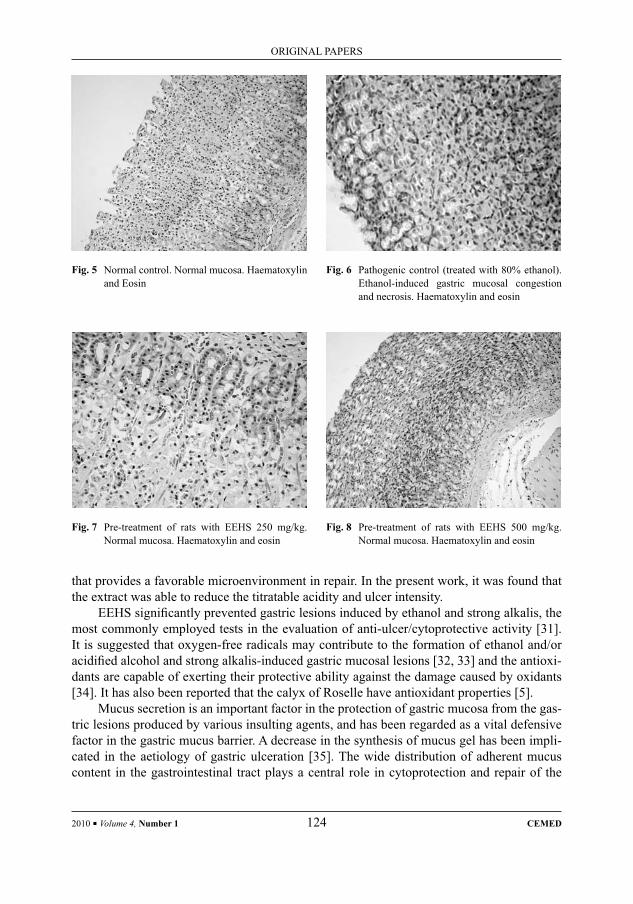
that provides a favorable microenvironment in repair. In the present work, it was found that the extract was able to reduce the titratable acidity and ulcer intensity.
EEHS signifi cantly prevented gastric lesions induced by ethanol and strong alkalis, the most commonly employed tests in the evaluation of anti-ulcer/cytoprotective activity [31]. It is suggested that oxygen-free radicals may contribute to the formation of ethanol and/or acidifi ed alcohol and strong alkalis-induced gastric mucosal lesions [32, 33] and the antioxi-dants are capable of exerting their protective ability against the damage caused by oxidants [34]. It has also been reported that the calyx of Roselle have antioxidant properties [5].
Mucus secretion is an important factor in the protection of gastric mucosa from the gas-tric lesions produced by various insulting agents, and has been regarded as a vital defensive factor in the gastric mucus barrier. A decrease in the synthesis of mucus gel has been impli-cated in the aetiology of gastric ulceration [35]. The wide distribution of adherent mucus content in the gastrointestinal tract plays a central role in cytoprotection and repair of the
Fig. 8 Pre-treatment of rats with EEHS 500 mg/kg. Normal mucosa. Haematoxylin and eosin
Fig. 7 Pre-treatment of rats with EEHS 250 mg/kg. Normal mucosa. Haematoxylin and eosin
Fig. 5 Normal control. Normal mucosa. Haematoxylin and Eosin
Fig. 6 Pathogenic control (treated with 80% ethanol). Ethanol-induced gastric mucosal congestion and necrosis. Haematoxylin and eosin
2010 ▪ Volume 4, Number 1 124 CEMED
ORIGINAL PAPERS

gastric mucosa [36, 37]. The replenishment of GWM in the present study by EEHS indicates its cytoprotective action on experimentally induced gastric ulcers.
On the other hand, EEHS blocks the indomethacin-induced gastric lesions, due to the ability of indomethacin, the most commonly used non-steroidal anti-infl ammatory drug (NSAID) which causes gastrointestinal ulceration, to suppress prostaglandin biosynthesis [38], resulting in overproduction of leukotrienes and other products of 5-lipoxygenase path-way [39]. These agents break the mucosal barrier, provoking an increase in gastric mucosal permeability to H+ and Na+ ions, and decrease in the transmucosal potential difference caus-ing the erosion and ulcers [40]. It seems that EEHS may possibly increase and/or generate synthesis of cytoprotective prostaglandin and inhibition of leukotrienes.
Administration of HSEE also increased the NP-SH and protein content of the gastric mucosa of alcohol treated animals. It is well documented that increase in sulfhydryl com-pounds [41] and protein [42] contribute to protecting the stomach from ethanol injury. A large part of NP-SH present in rat gastric mucosal tissue [43]. GSH has been shown to protect gastric tissues against oxidative stress [44]. Besides, the extract of Roselle signifi cantly re-duced the MDA concentration in gastric tissue when challenged with ethanol. MDA is one of the end products of LPO. LPO is the oxidative deterioration of polyunsaturated lipids. LPO in vivo has been said to be of basic importance in aging, in damage to cells by air pollution, in some phases of atherosclerosis, in some forms of liver and other tissue injury, and in oxy-gen toxicity [45]. The effectiveness of the extract helps in alleviating the chemically induced oxidative stress-induced ulcer with marked depletion in LPO and enhancement in NP-SH and protein levels, suggesting decrease in oxidative damage. This could be due to restoration of balance of free radical scavenging enzyme NP-SH in the gastric mucosa by effectively coun-teracting the free radicals generation.
The ulcer protecting action of the EEHS was further supported by the histological fi nd-ings with regard to gastric tissue.
In conclusion, the present fi ndings demonstrate the anti-ulcer activity of the EEHS may be due to its antisecretory and antioxidant nature by which it ultimately provides pre-domi-nantly mucosal defensive factors.
AcknowledgmentsThe authors are grateful to Dr. Mohd Nazam Ansari and Mr. Malik Sawood Ahmed for their technical assistance.
ReferencesRoberts, J. E., Tyler, V. E.:[1] Tyler’s Herbs of Choice. The Therapeutic Use of Phytomedicinals. The Haworth Herbal Press, New York, 1999, p. 11.Andreo, M. A., Ballsteros, K. V. R., Hiruma-Lima, C. A. et al.:[2] Effects of Mouriri pusa extracts on experimen-tally induced gastric lesions in rodents: role of endogenous sulfhydryls and nitric oxide in gastroprotection. J. Ethanopharmacol., 2006, 107, 431–441.Lewis, D. A., Hanson, P. J.:[3] Antiulcer drugs of plant origin. Prog. Med. Chem., 1991, 28, 201–231.Chopra, R. N., Neyar, S. L., Chopra, I. C.:[4] Glossary of Indian Medicinal Plants. Council of Scientifi c & Indus-trial Research, New Delhi, 1956, p. 133.
ORIGINAL PAPERS
CEMED 125 2010 ▪ Volume 4, Number 1
Hirumpanich, V., Utaipat, A., Morales, N. P. et al.:[5] Antioxidant effects of aqueous extracts from dried calyx of Hibiscus sabdariffa Linn. (Roselle) in vitro using rat low-density lipoprotein (LDL). Biol. Pharm. Bull., 2005, 28, 481–484.Mozaffari-Khosravi, H., Jalali-Khanabadi, B. A., Afkhami-Ardekani, M. et al.:[6] The effects of sour tea (Hibis-cus sabdariffa) on hypertension in patients with type II diabetes. J. Hum. Hypertens., 2009, 23, 48–54.Lin, H. H., Huang, H. P., Huang, C. C. et al.:[7] Hibiscus polyphenol-rich extract induces apoptosis in human gastric carcinoma cells via p53 phosphorylation and p38 MAPK/FasL cascade pathway. Mol. Carcinog., 2005, 43, 86–99.Adetutu, A., Odunola, O. A., Owoade, O. A. et al.: [8] Anticlastogenic effects of Hibiscus sabdariffa fruits against sodium arsenite-induced micronuclei formation in erythrocytes in mouse bone marrow. Phytother. Res., 2004, 18, 862–864.Ali, M. B., Salih, W. M., Mohamed, A. H. et al.:[9] Investigation of the antispasmodic potential of Hibiscus sab-dariffa calyces. J. Ethnopharmacol., 1991, 31, 249–257.Ali, B. H., Mousa, H. M., El-Mougy, S.:[10] The effect of a water extract and anthocyanins of Hibiscus sabdariffa L. on paracetamol-induced hepatoxicity in rats. Phytother. Res., 2003, 17, 56–59.Salah, A. M., Gathumbi, J., Vierling, W.:[11] Inhibition of intestinal motility by methanol extracts of Hibiscus sabdariffa L. (Malvaceae) in rats. Phytother. Res., 2002, 16, 283–285.Herrera-Arellano, A., Flores-Romero, S., Chavez-Soto, M. A. et al.:[12] Effectiveness and tolerability of a stan-dardized extract from Hibiscus sabdariffa in patients with mild to moderate hypertension: a controlled and randomized clinical trial. Phytomedicine, 2004, 11, 375–382.Mojiminiyi, B. O., Adegunloye, B. J., Egbeniyi, Y. A. et al.:[13] An investigation of the diuretic effect of an aqueous extract of the petals of Hibiscus sabdariffa. J. Med. Sci., 2000, 2, 77–80.Chen, C. C., Hsu, J. D., Wang, S. F. et al.:[14] Hibiscus sabdariffa extract inhibits the development of atheroscle-rosis in cholesterol-fed rabbits. J. Agric. Food Chem., 2003, 51, 5472–5477.Hirunpanich, V., Utaipat, A., Morales, N. P. et al.:[15] Hypocholes-terolemic and antioxidant effects of aqueous extracts from the dried calyx of Hibiscus sabdariffa L. in hypercholesterolemic rats. J. Ethnopharmacol., 2006, 103, 252–260.Gaet, N.:[16] Hibiscus sabdariffa L. In: Iva, A. (ed.) Medicinal Plants of the World. Human Press, New York, 1999, pp. 165–170.Senay, E. C., Levine, R. L.:[17] Synergism between cold and restraint for rapid production of stress ulcer in rats. Proc. Soc. Exp. Biol. Med., 1967, 124, 1221–1231.Chiu, P. J. S., Gerhart, C., Brown, A. D. et al.:[18] Effects of a gastric antisecretory cytoprotectant 2-methyl-8-(phenylmethoxy)imidazo (1,2-a)-pyridine-3-acetonitrile (Sch 28080) on cysteamine, reserpine and stress ulcers in rats. Arzneim. Forsch., 1984, 34, 783.Shay, H., Komarov, S. A., Fels, S. S. et al.:[19] A simple method for the uniform production of gastric ulcer-ation in the rat. Gastroenterology, 1945, 5, 43–61.Robert, A., Nezamis, J. E., Lancaster, C. et al.:[20] Mild irritants prevent gastric necrosis through adaptive cyto-protection mediated by prostaglandins. Am. J. Physiol., 1983, 245, G113.Crone, S. J., Morrissey, S. M., Woods, R. J.:[21] A method for the quantitative estimation of gastric barrier mucus. J. Physiol., 1974, 242, 116–117.Bhargawa, K. P., Gupta, M. B., Tangri, K. K.:[22] Mechanism of ulcerogenic activity of indomethacin and oxy-phenbutazone. Eur. J. Pharmacol., 1973, 22, 191–195.Sedlak, J., Lindsay, R. H.:[23] Estimation of total protein bound and nonprotein sulfhydryl group in tissue with Ellman’s reagents. Anal. Biochem., 1968, 25, 192–205.Utley, H. G., Bernheim, F., Hochstein, P.:[24] Effect of sulfhydryl reagents on peroxidation in microsomes. Arch. Biochem. Biophys., 1967, 118, 29–32.Culling, C. F.:[25] Handbook of Histopathological and Histochemical Techniques. 3rd edn., London, Butterworth and Co., 1974, p. 37.Djahanguiri, B., Taubin, H. L., Landsburg, L.:[26] Increased sympathetic activity in the pathogenesis of restraint ulcer in rats. J. Pharmacol. Exp. Ther., 1973, 184, 163–168.Cho, C. H., Ogle, C. W., Dai, S.:[27] Acute gastric ulcer formation response to electrical vagal stimulation in rats. Eur. J. Pharmacol., 1976, 35, 215–219.Cho, C. H., Ogle, C. W.:[28] Cholinergic-mediated gastric mast cell degranulation with subsequent histamine H1 and H2-receptor activation in stress ulceration in rats. Eur. J. Pharmacol., 1979, 55, 23–33.
2010 ▪ Volume 4, Number 1 126 CEMED
ORIGINAL PAPERS
Hase, T., Moss, B. J.:[29] Microvascular changes of gastric mucosa in the development of stress ulcer in rats. Gastroenterology, 1973, 65, 224–234.Goel, R. K., Bhattacharya, S. K.:[30] Gastroduodenal mucosal defense and mucosal protective agents. Indian J. Exp. Biol., 1991, 29, 701–714.Schmeda-Hirschmann, G., Rodriguez, J., Astudillo, L.:[31] Gastroprotective activity of the diterpene solidag-enone and its derivatives on experimentally induced gastric lesions in mice. J. Ethnopharmacol., 2002, 81, 111–115.Trier, J. S., Szabo, S., Allan, C. H.:[32] Ethanol-induced damage to mucosal capillaries of rat stomach. Ultra-structural features and effects of prostaglandin E2 and cysteamine. Gastroenterology, 1987, 92, 13–22.Matsumoto, T., Moriguchi, R., Yamada, H.:[33] Role of polymorphonuclear leucocytes and oxygen-derived free radicals in the formation of gastric lesions induced by HCl/ethanol, and a possible mechanism of protection by antiulcer polysaccharide. J. Pharm. Pharmacol., 1992, 45, 535–539.Farina, C., Pinza, M., Pifferi, G.:[34] Synthesis and anti-ulcer activity of new derivatives of glycyrrhetic, oleano-lic and ursolic acids. Il Farmaco, 1998, 53, 22–32.Jainu, M. K., Mohan, V., Devi, C. S. S.:[35] Gastroprotective effect of Cissus quadrangularis extract in rats with experimentally induced ulcer. Indian J. Med. Res., 2006, 123, 799–806.Younau, F., Person, J., Allen, A. et al.:[36] Changes in the structure of the mucus gel in the mucosal surface of the stomach in association with peptic ulcer disease. Gastroenterology, 1982, 82, 827–831.Sanyal, A. K., Mitra, P. K., Goel, R. K.:[37] A modifi ed method to estimate dissolved mucosubstance in gastric juice. Indian J. Exp. Biol., 1983, 21, 78–80.Wallace, J.:[38] Mechanisms of protection and healing: current knowledge and future research. Am. J. Med., 2001, 110, 19S–22S.Rainsford, K. D.:[39] The effects of 5-lipoxygenase inhibitors and leukotriene antagonists on the development of gastric lesions induced by non-steroidal anti-infl ammatory drugs. Agents Actions, 1987, 21, 316–319.Whittle, B. J.:[40] Temporal relationship between cycloxygenase inhibition, as measured by prostacyclin biosyn-thesis, and the gastrointestinal damage induced by indomethacin in rat. Gastroenterology, 1981, 80, 94–98.Szabo, S., Trier, J. S., Frankel, P. W.:[41] Sulfhydral compounds may mediate gastric cytoprotection. Science, 1981, 214, 200–202.Alqasoumi, S., Al-Sohaibani, M., Al-Howiriny, T. et al.:[42] Rocket ‘Eruca sativa’: a salad herb with potential gastric anti-ulcer activity. World J. Gastroenterol., 2009, 15, 1958–1965.Boyd, S. C., Sasame, H. A., Boyd, M. R.:[43] High concentrations of glutathione in glandular stomachs. Possible implication for carcinogenesis. Science, 1979, 205, 1010–1012.Stein, H. J., Hinder, R. A., Oosthuizeu, M. M. J.:[44] Gastric mucosal injury caused hemorrhagic shock and reper-fusion: protective role of the antioxidant glutathione. Surgery, 1990, 108, 467–474.Kwicien, S., Brzozowski, T., Konturek, S. J.:[45] Effects of reactive oxygen species action on gastric mucosa in various models of mucosal injury. J. Physiol. Pharmacol., 2002, 53, 39–50.
ORIGINAL PAPERS
CEMED 127 2010 ▪ Volume 4, Number 1

Antioxidant and Protective Effects of Spinach (Spinacia oleracea L.) Leaves Against Carbon
Tetrachloride-Induced Liver InjuryMOHAMMED S. AL-DOSARI
Department of Pharmacognosy, College of Pharmacy, King Saud University, Riyadh 11451, Saudi Arabia
Spinach, (Spinacia oleracea L.) is a popular vegetable. The hepatoprotective activity of the ethanolic extract of the leaves of spinach (EESO) was studied against carbon tetrachloride (CCl4)-induced oxidative stress (OS) and liver injury in rats. Pretreatment of rats with EESO, at 250 and 500 mg/kg body weight for 21 consecutive days signifi -cantly prevented the CCl4-induced hepatic damage as indicated by the serum marker enzymes (SGOT, SGPT, ALP and GGT) and bilirubin levels. Parallel to these changes, the leaves extract also prevented CCl4-induced OS in rat liver by inhibiting lipid peroxidation (LPO) and restoring the levels of antioxidant non-enzymatic biomarker, such as total protein (TP) and non-protein sulfhydryl (NP-SH) in liver tissue. The biochemical changes were consistent with the histological fi ndings of the liver tissue suggesting marked hepatoprotective effect of the leaves extract in a dose-dependent manner, besides, a signifi cant reduction was also observed in pentobarbital-induced sleeping time in mice. The results of spinach extract were comparable to that of silymarin. The protective effect of the EESO against CCl4-induced acute hepatotoxicity could be attributed to the potent antioxidant constituents of the spinach.
Keywords: spinach, Spinacia oleracea L., hepatoprotection, carbon tetrachloride, antioxidant
Abbreviations
EESO = ethanolic extract of Spinacia oleracea; SGOT = serum glutamate oxalate transaminase; SGPT = serum glutamate pyruvate transaminase; ALP = alkaline phosphatase; GGT = gamma-glutamyl transferase; TP = total pro-tein; NP-SH = non-protein sulfhydryl; MDA = malondialdehyde; CCl4 = carbon tetrachloride
Chronic liver diseases represent a major global health concern and the cirrhosis of liver be-ing the ninth leading cause of death in the USA [1]. Alcoholic liver disease, non-alcoholic fatty liver disease, chronic viral hepatitis B and C and carcinoma of liver are the major enti-ties. The treatment of these diseases by applying conventional medicine therapies are often limited in effi cacy and carry the risk of undesirable and/or side effects [2]. Therefore, the treatment of liver diseases with herbal medicinal ingredients seems highly attractive. Con-sumption of vegetables and fruits is associated with a lower risk of various diseases, includ-ing cancer and cardiovascular diseases. This benefi cial effect has been ascribed in part to the antioxidant contents in plant-based foods [3].
Spinach, (Spinacia oleracea L.) belonging to the family Chenopodiaceae, locally known as Ispanakh, is a vegetable plant with deep green leaves used as an aperient food and a sooth-ing medicament in cystitis and gastroenteritis. The fresh leaves are cooked and taken as food
Corresponding address: Mohammed S. Al-Dosari MD, Department of Pharmacognosy, College of Pharmacy, P.O. Box 2457, King Saud University, Riyadh 11451, Saudi Arabia. E-mail: [email protected]
1.13
ORIGINAL PAPERS
DOI: 10.1556/CEMED.4.2010. 129 2010 ▪ Volume 4, Number 1 ▪ 129–140.

[4]. In South-East Asia, spinach is regarded as carminative, laxative and as a drug that stimu-lates digestive secretions [5]. Fresh leaf juice of spinach increases breast milk and is used in anemia, jaundice, cirrhosis of the liver and in conditions of general weakness. The juice of leaves is cooling and very nutritive [6]. A decoction of the plant is prescribed in febrile affec-tions, in lithiasis and infl ammation of the lungs and bowels. The juice of the leaves is also used as a diuretic and as a gargle in sore-throat. Poultices of the leaves or boiled seeds are applied to soften tumors and promote the maturation of boils [7–9]. Very recently, it was sug-gested that the glycoglycerolipid fraction isolated from spinach is a safe and effective anti-cancer bioactive agent and/or food material [10]. Bhatia and Jain have reported the protec-tive effect of methanolic extract of S. oleracea against radiation-induced oxidative stress (OS) [11].
Spinach leaves have been shown to contain fl avonoids and p-coumaric acid derivatives as antioxidant components to combat effectively oxidative damage [12, 13]. Considering their therapeutic usefulness in traditional medicine and their reported antioxidant chemical constituents, the present study was undertaken to evaluate the protective effect of an ethano-lic extract of spinach (S. oleracea) (EESO) leaves on carbon tetrachloride (CCL4)-induced hepatotoxicity; additionally, the antioxidant activity of EESO in liver-injured rats was also investigated.
Material and Methods
Plant Material and Preparation of Dosage Form
Fresh leaves of spinach were purchased from the vegetable market of Riyadh and identifi ed at the Department of Pharmacognosy, College of Pharmacy, King Saud University, Riyadh. A voucher specimen (#6609) was deposited in the Herbarium of the Department of Pharma-cognosy.
Shade-dried leaves of spinach (500 g) were submitted to maceration in ethanol (96%) for 72 h at room temperature (26 ± 2 °C). Thereafter, the extract was fi ltered and then con-centrated under reduced pressure (at approximately 4 °C). The maceration was repeated three times and a green solid and dry ethanolic crude extract was obtained (6.1% w/w yield). The dried extract was dissolved in distilled water and used in two doses of 250 and 500 mg/kg body weight in all experiments.
Animals
Male Wistar albino rats, weighing 150–170 g, obtained from the Experimental Animal Care Center, College of Pharmacy, King Saud University, Riyadh, were used in the experiment. Swiss albino mice (25–30 g) were used for studies of sleeping time and acute toxicity test. The animals were kept at a constant temperature (22 ± 2 °C), humidity (55%) and light–dark conditions (12/12 h light/dark ratio). The animals were provided with Purina chow diet and drinking water ad libitum. The conduct of experiments and the procedure of sacrifi ce (using ether) were approved by the Ethics Committee of the Experimental Animal Care Society, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia.
2010 ▪ Volume 4, Number 1 130 CEMED
ORIGINAL PAPERS
Phytochemical Screening
A phytochemical analysis of spinach leaves was conducted for the detection of alkaloids, cardiac glycosides, fl avonoids, tannins, anthraquinones, saponins, volatile oils, cyanogenic glycosides, coumarins, sterols and/or triterpenes and sulphur-containing compounds [14].
Acute Toxicity Test
The acute toxicity of the ethanolic extract of spinach leaves was evaluated in mice using the up-and-down procedure [15].
Six female rats (weight: 200–250 g) received EESO starting at 2 g/kg orally by gav-age. The animals were observed for toxic symptoms continuously for the fi rst 4 h after dos-ing. Finally, the number of survivors was noted after 24 h and these animals were then main-tained for a further 13 days with daily observations [15].
CCL4-Induced Liver Toxicity
Rats were divided into fi ve groups (I–V) (N = 6 animals/group). Group I was kept as a con-trol. Group II–V received CCl4 in liquid paraffi n (1:1) 1.25 mL/kg body weight intraperitone-ally [16]. Groups III and IV were administered with spinach extract 250 and 500 mg/kg, body weight per day orally for 21 days; group V was treated with silymarin 10 mg/kg per day body weight for the same period. Spinach and silymarin treatment was started 21 days prior to CCl4 administration and continued until the end of the experiment. After 48 h, following CCl4 administration, blood was collected by heart puncture, allowed to clot and serum was sepa-rated for biochemical estimations. After blood collection, all groups of animals were sacri-fi ced using anaesthetic ether and their livers were dissected for biochemical and histopatho-logical assessment.
Estimation of Marker Enzymes and BilirubinSerum glutamate oxaloacetate transaminase (SGOT) [17], serum glutamate pyruvate transam-inase (SGPT) [17], alkaline phosphatase (ALP) [18], γ-glutamyl transferase (GGT) [19] and bilirubin [20] were determined using Refl otron® Plus Analyzer and Roche kits.
Lipid Peroxidation (LPO) Determination
The method reported by Utley et al. [21] was followed. The liver tissue was homogenized in 0.15 M KCl (at 4 °C, Potter–Elvehjem type C homogenizer) to give a 10% w/v homogenate. Aliquots of homogenate (1 mL) were incubated at 37 °C for 3 h in a metabolic shaker. Then, 1 mL of 10% aqueous trichloroacetic acid (TCA) was added and mixed. The mixture was then centrifuged at 800g for 10 min. Then, supernatant (1 mL) was mixed with 1 mL of 0.67% w-thiobarbituric acid and placed in a boiling water bath for 10 min. The mixture was cooled and diluted with 1 mL distilled water. The absorbance of the solution was then read using spectrophotometer (UVmini-1240, Shimadzu Italia, Milano) at 535 nm. The content of malondialdehyde (MDA) (nmol/g wet tissue) was then calculated, by reference to a standard curve of MDA solution.
ORIGINAL PAPERS
CEMED 131 2010 ▪ Volume 4, Number 1
Estimation of Non-Protein Sulfhydryl Groups (NP-SH)
Hepatic NP-SH was measured according to the method of Sedlak and Lindsay [22]. The liver was homogenized in ice-cold 0.02 M ethylene diamine tetraacetic acid (EDTA). Aliquots of 5 mL of the homogenates were mixed in 15 mL test tubes with 4 mL of distilled water and 1 mL of 50% TCA. The tubes were shaken intermittently for 10 min and centrifuged at 3,000 rpm. Two milliliters of supernatant were mixed with 4 mL Tris buffer (0.4 mol/L, pH 8.9) and 0.1 mL of 5,5´-dithio-bis(2-nitrobenzoic acid) (DTNB) and the sample was shaken. The absorbance was read using spectrophotometer (UVmini-1240, Shimadzu Italia, Milano) within 5 min of addition of DTNB at 412 nm against a reagent blank.
Determination of Total Protein (TP)
The TP was estimated by the kit method, supplied by Crescent Diagnostics, Jeddah, Saudi Arabia.
Histopathological Studies
The liver tissues were fi xed in 10% buffered formalin and processed using a VIP tissue pro-cessor. The processed tissues were then embedded in paraffi n blocks and sections of about 5 μm thickness were cut by employing an American optical rotary microtome. These sections were stained with haematoxylin and eosin using routine procedures [23]. The slides were examined for pathomorphological changes under a research microscope by a person who was not aware of experimental protocols.
Measurement of Pentobarbital Sleeping Time
The sleeping time in mice was measured using pentobarbital. Mice were divided into four groups of ten animals each. Group I received the vehicle (0.3 mL of saline), group II received CCl4 only, and groups III and IV received spinach extract (250 and 500 mg/kg body weight). Thirty minutes later, the animals of groups II–IV were treated with sodium pentobarbital (50 mg/kg, intraperitoneally). The time interval between the onset and the regaining of the righting refl ex was measured as the sleeping time [24].
Statistical Analysis
Values are given as arithmetic means ± standard error of the mean (SEM). The data were statistically analysed by using a one-way analysis of variance (ANOVA), followed by Dun-nett’s t-test.
Results
Phytochemical Screening
The preliminary qualitative phytochemical screening of spinach leaves revealed the presence of fl avonoid, tannins, sterols and/or triterpenes.
2010 ▪ Volume 4, Number 1 132 CEMED
ORIGINAL PAPERS
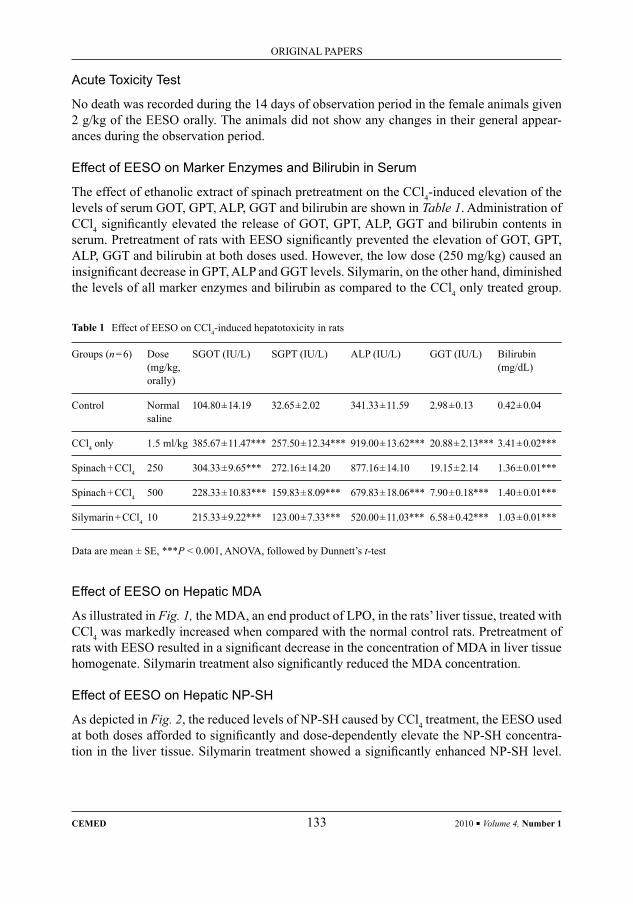
Table 1 Effect of EESO on CCl4-induced hepatotoxicity in rats
Groups (n = 6) Dose (mg/kg, orally)
SGOT (IU/L) SGPT (IU/L) ALP (IU/L) GGT (IU/L) Bilirubin (mg/dL)
Control Normal saline
104.80 ± 14.19 32.65 ± 2.02 341.33 ± 11.59 2.98 ± 0.13 0.42 ± 0.04
CCl4 only 1.5 ml/kg 385.67 ± 11.47*** 257.50 ± 12.34*** 919.00 ± 13.62*** 20.88 ± 2.13*** 3.41 ± 0.02***
Spinach + CCl4 250 304.33 ± 9.65*** 272.16 ± 14.20 877.16 ± 14.10 19.15 ± 2.14 1.36 ± 0.01***
Spinach + CCl4 500 228.33 ± 10.83*** 159.83 ± 8.09*** 679.83 ± 18.06*** 7.90 ± 0.18*** 1.40 ± 0.01***
Silymarin + CCl4 10 215.33 ± 9.22*** 123.00 ± 7.33*** 520.00 ± 11.03*** 6.58 ± 0.42*** 1.03 ± 0.01***
Data are mean ± SE, ***P < 0.001, ANOVA, followed by Dunnett’s t-test
Acute Toxicity Test
No death was recorded during the 14 days of observation period in the female animals given 2 g/kg of the EESO orally. The animals did not show any changes in their general appear-ances during the observation period.
Effect of EESO on Marker Enzymes and Bilirubin in Serum
The effect of ethanolic extract of spinach pretreatment on the CCl4-induced elevation of the levels of serum GOT, GPT, ALP, GGT and bilirubin are shown in Table 1. Administration of CCl4 signifi cantly elevated the release of GOT, GPT, ALP, GGT and bilirubin contents in serum. Pretreatment of rats with EESO signifi cantly prevented the elevation of GOT, GPT, ALP, GGT and bilirubin at both doses used. However, the low dose (250 mg/kg) caused an insignifi cant decrease in GPT, ALP and GGT levels. Silymarin, on the other hand, diminished the levels of all marker enzymes and bilirubin as compared to the CCl4 only treated group.
Effect of EESO on Hepatic MDA
As illustrated in Fig. 1, the MDA, an end product of LPO, in the rats’ liver tissue, treated with CCl4 was markedly increased when compared with the normal control rats. Pretreatment of rats with EESO resulted in a signifi cant decrease in the concentration of MDA in liver tissue homogenate. Silymarin treatment also signifi cantly reduced the MDA concentration.
Effect of EESO on Hepatic NP-SH
As depicted in Fig. 2, the reduced levels of NP-SH caused by CCl4 treatment, the EESO used at both doses afforded to signifi cantly and dose-dependently elevate the NP-SH concentra-tion in the liver tissue. Silymarin treatment showed a signifi cantly enhanced NP-SH level.
ORIGINAL PAPERS
CEMED 133 2010 ▪ Volume 4, Number 1
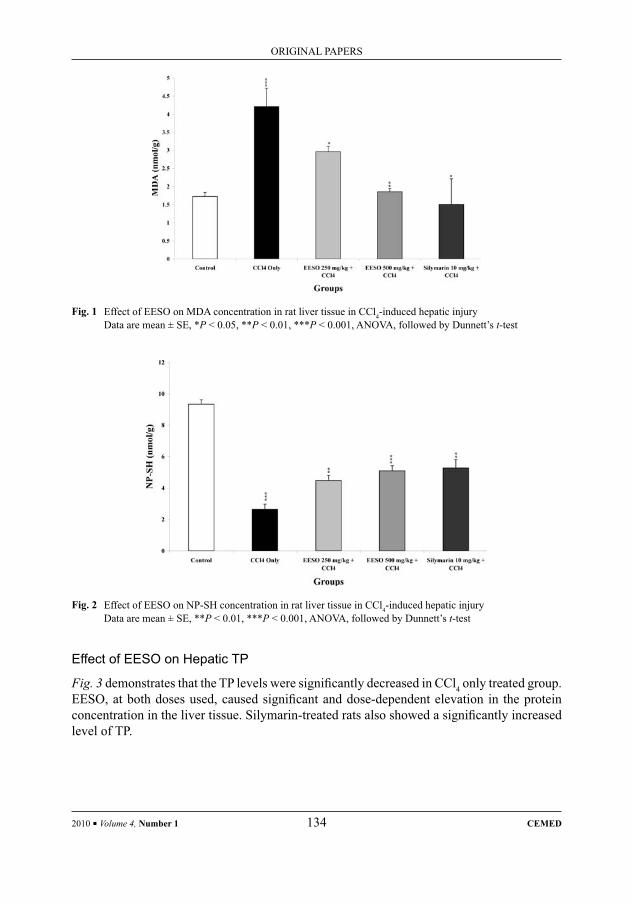
Effect of EESO on Hepatic TP
Fig. 3 demonstrates that the TP levels were signifi cantly decreased in CCl4 only treated group. EESO, at both doses used, caused signifi cant and dose-dependent elevation in the protein concentration in the liver tissue. Silymarin-treated rats also showed a signifi cantly increased level of TP.
Fig. 2 Effect of EESO on NP-SH concentration in rat liver tissue in CCl4-induced hepatic injuryData are mean ± SE, **P < 0.01, ***P < 0.001, ANOVA, followed by Dunnett’s t-test
Fig. 1 Effect of EESO on MDA concentration in rat liver tissue in CCl4-induced hepatic injuryData are mean ± SE, *P < 0.05, **P < 0.01, ***P < 0.001, ANOVA, followed by Dunnett’s t-test
2010 ▪ Volume 4, Number 1 134 CEMED
ORIGINAL PAPERS
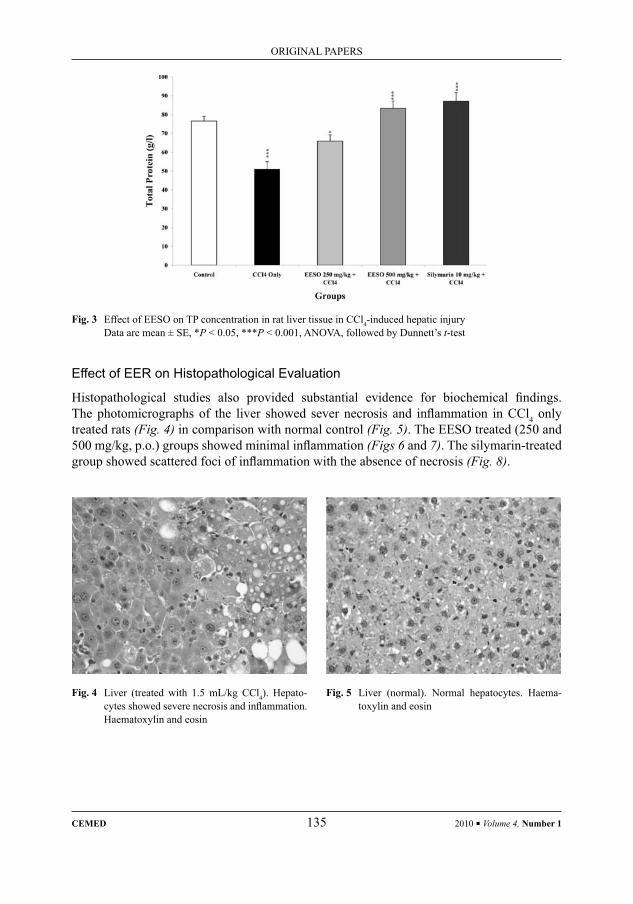
Fig. 3 Effect of EESO on TP concentration in rat liver tissue in CCl4-induced hepatic injuryData are mean ± SE, *P < 0.05, ***P < 0.001, ANOVA, followed by Dunnett’s t-test
Effect of EER on Histopathological Evaluation
Histopathological studies also provided substantial evidence for biochemical fi ndings. The photomicrographs of the liver showed sever necrosis and infl ammation in CCl4 only treated rats (Fig. 4) in comparison with normal control (Fig. 5). The EESO treated (250 and 500 mg/kg, p.o.) groups showed minimal infl ammation (Figs 6 and 7). The silymarin-treated group showed scattered foci of infl ammation with the absence of necrosis (Fig. 8).
Fig. 4 Liver (treated with 1.5 mL/kg CCl4). Hepato-cytes showed severe necrosis and infl ammation. Haematoxylin and eosin
Fig. 5 Liver (normal). Normal hepatocytes. Haema-toxylin and eosin
ORIGINAL PAPERS
CEMED 135 2010 ▪ Volume 4, Number 1
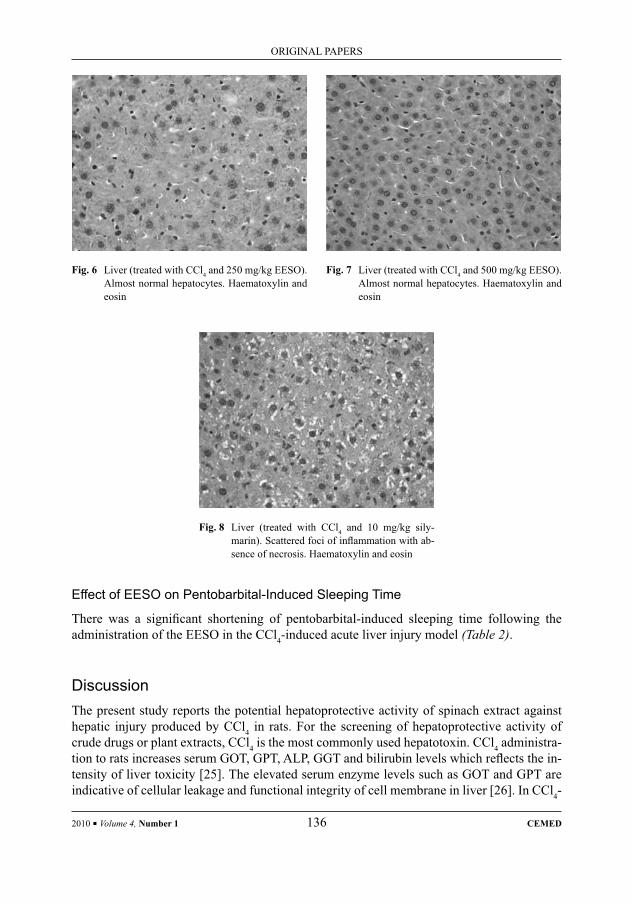
Effect of EESO on Pentobarbital-Induced Sleeping Time
There was a signifi cant shortening of pentobarbital-induced sleeping time following the administration of the EESO in the CCl4-induced acute liver injury model (Table 2).
DiscussionThe present study reports the potential hepatoprotective activity of spinach extract against hepatic injury produced by CCl4 in rats. For the screening of hepatoprotective activity of crude drugs or plant extracts, CCl4 is the most commonly used hepatotoxin. CCl4 administra-tion to rats increases serum GOT, GPT, ALP, GGT and bilirubin levels which refl ects the in-tensity of liver toxicity [25]. The elevated serum enzyme levels such as GOT and GPT are indicative of cellular leakage and functional integrity of cell membrane in liver [26]. In CCl4-
Fig. 8 Liver (treated with CCl4 and 10 mg/kg sily-marin). Scattered foci of infl ammation with ab-sence of necrosis. Haematoxylin and eosin
Fig. 6 Liver (treated with CCl4 and 250 mg/kg EESO). Almost normal hepatocytes. Haematoxylin and eosin
Fig. 7 Liver (treated with CCl4 and 500 mg/kg EESO). Almost normal hepatocytes. Haematoxylin and eosin
2010 ▪ Volume 4, Number 1 136 CEMED
ORIGINAL PAPERS
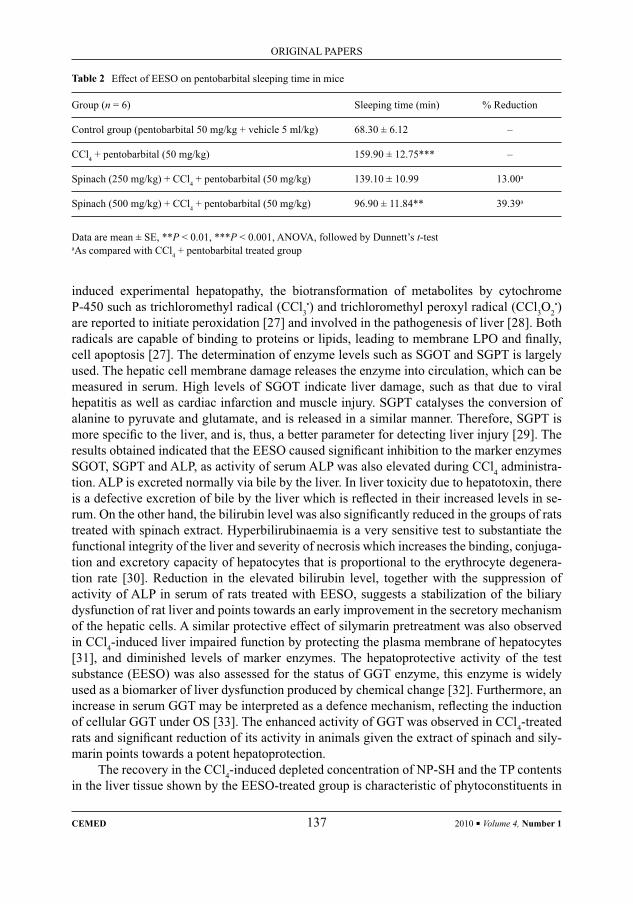
Table 2 Effect of EESO on pentobarbital sleeping time in mice
Group (n = 6) Sleeping time (min) % Reduction
Control group (pentobarbital 50 mg/kg + vehicle 5 ml/kg) 68.30 ± 6.12 –
CCl4 + pentobarbital (50 mg/kg) 159.90 ± 12.75*** –
Spinach (250 mg/kg) + CCl4 + pentobarbital (50 mg/kg) 139.10 ± 10.99 13.00a
Spinach (500 mg/kg) + CCl4 + pentobarbital (50 mg/kg) 96.90 ± 11.84** 39.39a
Data are mean ± SE, **P < 0.01, ***P < 0.001, ANOVA, followed by Dunnett’s t-testaAs compared with CCl4 + pentobarbital treated group
induced experimental hepatopathy, the biotransformation of metabolites by cytochrome P-450 such as trichloromethyl radical (CCl3
•) and trichloromethyl peroxyl radical (CCl3O2•)
are reported to initiate peroxidation [27] and involved in the pathogenesis of liver [28]. Both radicals are capable of binding to proteins or lipids, leading to membrane LPO and fi nally, cell apoptosis [27]. The determination of enzyme levels such as SGOT and SGPT is largely used. The hepatic cell membrane damage releases the enzyme into circulation, which can be measured in serum. High levels of SGOT indicate liver damage, such as that due to viral hepatitis as well as cardiac infarction and muscle injury. SGPT catalyses the conversion of alanine to pyruvate and glutamate, and is released in a similar manner. Therefore, SGPT is more specifi c to the liver, and is, thus, a better parameter for detecting liver injury [29]. The results obtained indicated that the EESO caused signifi cant inhibition to the marker enzymes SGOT, SGPT and ALP, as activity of serum ALP was also elevated during CCl4 administra-tion. ALP is excreted normally via bile by the liver. In liver toxicity due to hepatotoxin, there is a defective excretion of bile by the liver which is refl ected in their increased levels in se-rum. On the other hand, the bilirubin level was also signifi cantly reduced in the groups of rats treated with spinach extract. Hyperbilirubinaemia is a very sensitive test to substantiate the functional integrity of the liver and severity of necrosis which increases the binding, conjuga-tion and excretory capacity of hepatocytes that is proportional to the erythrocyte degenera-tion rate [30]. Reduction in the elevated bilirubin level, together with the suppression of activity of ALP in serum of rats treated with EESO, suggests a stabilization of the biliary dysfunction of rat liver and points towards an early improvement in the secretory mechanism of the hepatic cells. A similar protective effect of silymarin pretreatment was also observed in CCl4-induced liver impaired function by protecting the plasma membrane of hepatocytes [31], and diminished levels of marker enzymes. The hepatoprotective activity of the test substance (EESO) was also assessed for the status of GGT enzyme, this enzyme is widely used as a biomarker of liver dysfunction produced by chemical change [32]. Furthermore, an increase in serum GGT may be interpreted as a defence mechanism, refl ecting the induction of cellular GGT under OS [33]. The enhanced activity of GGT was observed in CCl4-treated rats and signifi cant reduction of its activity in animals given the extract of spinach and sily-marin points towards a potent hepatoprotection.
The recovery in the CCl4-induced depleted concentration of NP-SH and the TP contents in the liver tissue shown by the EESO-treated group is characteristic of phytoconstituents in
ORIGINAL PAPERS
CEMED 137 2010 ▪ Volume 4, Number 1

spinach with a protective role against CCl4 [34]. As sulfhydryls are known to play an impor-tant physiological function in the human body as an antitoxic agent, NP-SH may act directly through a conjugative reaction with CCl4 or its metabolites, leading to inhibition of its hepa-totoxic action [35, 36]. However, NP-SH also acts as a non-enzymatic antioxidant that re-duces H2O2, hydroperoxides (ROOH) and xenobiotic poisoning [37].
OS is a state of imbalance between the generation of reactive oxygen species (ROS) and the level of antioxidant defence system. Nutritional antioxidant defi ciency may also lead to OS [38]. In this study, elevation in the level of the end product of LPO in the liver of rat treated with CCl4 was observed. LPO by free radical derivatives of CCl4-induced liver injury [39] and increase in the MDA level by CCl4 intoxication in liver suggest enhanced LPO, lead-ing to tissue damage and failure of the antioxidant defence mechanism to prevent the forma-tion of excessive free radicals [40]. Spinach ethanolic extract pretreatment at both doses signifi cantly reversed these changes due to its reportedly strong antioxidant effects, which were comparable with that of the silymarin-treated group. The present fi nding is in accor-dance, as earlier reports described a very effective LPO preventative activity of spinach in vivo and in vitro systems [41]. The screening of phytochemical constituents from spinach leaves showed the presence of fl avonoids, tannins, sterols and/or triterpenes.
Previously, it was reported that the fl avonoids are typical phenolic compounds and powerful chain-breaking antioxidants [11]. It was also reported that LPO can be inhibited by fl avonoids, possibly through their activity as strong scavengers [42]. A large number of naturally occurring fl avonoids have been reported to have antioxidant properties which scav-enge free radicals [43]. Additionally, the pretreatment of EESO exhibited its capacity to stimulate hepatic drug metabolizing enzymes by causing a signifi cant reduction in the time of pentobarbital-induced narcosis. It is now accepted that hepatic damage prolongs the loss of righting refl ex induced by short-acting barbiturates, such as pentobarbital, which is a mea-sure of the function of the capacity of liver drug metabolizing enzymes. Prior treatment of animals with the drugs that stimulate liver drug metabolizing enzymes considerably shortens the duration of barbiturates-induced narcolepsy [44]. The ability of spinach extract to protect the liver from toxic challenge was further confi rmed by the histopathological assessment of the liver tissue, which basically supported the results from the serum enzymatic assays.
In summary, the present data indicate the effi ciency of the ethanolic extract of S. olera-cea leaves in protecting and/or attenuating CCl4-induced liver toxicity as shown by the reduc-tion of serum hepatic specifi c enzymes activity and enhanced antioxidant defence. The pro-tecting of hepatic enzymes leakage was comparable to that demonstrated by the reference standard substance, silymarin.
ReferencesKim, W. R., Brown, R. S., Terrault, N. A. et al.:[1] Burden of liver disease in the United States: summary of work-shop. Hepatology, 2002, 36, 227–242.Stickel, F., Schuppan, D.:[2] Herbal medicine in the treatment of liver diseases. Dig. Liver Dis., 2007, 39, 293–304.Nicolle, C., Cardinault, N., Gueux, E. et al.:[3] Health effect of vegetable-based diet: lettuce consumption im-proves cholesterol metabolism and antioxidant status in the rat. Clin. Nutr., 2004, 23, 605–614.Kamal, H.:[4] Encyclopaedia of Islamic Medicine. General Egyptian Book Organization, Cairo, p. 598, 1975.
2010 ▪ Volume 4, Number 1 138 CEMED
ORIGINAL PAPERS
Perry, L. M.:[5] Medicinal Plants of East and Southeast Asia: Attributed Properties and Uses. The MIT Press, Cambridge, p. 78, 1986.Yusuf, M., Chowdhury, J. U., Wahab, M. A., et al.:[6] Medicinal Plants of Bangladesh. Bangladesh Council of Scientifi c and Industrial Research, Dhaka 1205, Bangladesh, p. 231, 1994.Chopra, R. N., Nayar, S. L., Chopra, I. C.:[7] Glossary of Indian Medicinal Plants. Council of Scientifi c and In-dustrial Research, New Delhi, p. 232, 1956.Dymock, W., Warden, C. J. H., Hooper, D.:[8] Pharmacographia Indica; A History of the Principal Drugs of Vegetable Origin, Met with in British India. Education Society’s Press, Byculla, Bombay, p. 367, 1890.Aman, M.:[9] Medicinal Secrets of Your Food. 2nd edn., Indo-American Hospital, Mysore, India, pp. 430–432, 1969.Maeda, N., Kokai, Y., Ohtan, S. et al.:[10] Inhibitory effects of preventive and curative orally administered spin-ach glycoglycero-lipid fraction on the tumor growth of sarcoma and colon in mouse graft models. Food Chem., 2009, 112, 205–210.Bhatia, A. L., Jain, M.:[11] Spinacia oleracea L. protects against gamma radiations: a study on glutathione and lipid peroxidation in mouse liver. Phytomedicine, 2004, 11, 607–615.Bergman, M., Varshavsky, L., Gottlieb, H. E. et al.:[12] The antioxidant activity of aqueous spinach extract: chemical identifi cation of active fraction. Phytochemistry, 2001, 58, 143–152.Bergman, M., Perelman, A., Dubinsky, Z. et al.:[13] Scavenging of reactive oxygen species by a novel glucuroni-dated fl avonoid antioxidant isolated and purifi ed from spinach. Phytochemistry, 2003, 63, 753–762.Fransworth, N. R.:[14] Biological and phytochemical screening of plants. J. Pharm. Sci., 1966, 55, 225–272.The Organization of Economic Co-operation Development (OECD):[15] The OECD Guideline for Testing of Chemical: 420 Acute Oral Toxicity. OECD, Paris, pp. 1–14, 2001.Rafatullah, S., Al-Sheikh, A., Alqasoumi, S. et al.:[16] Protective effect of fresh radish juice (Raphanus sativus L.) against carbon tetrachloride-induced hepatotoxicity. Int. J. Pharmacol., 2008, 4, 130–134.Reitman, S., Frankel, A.:[17] A colorimetric method for the determination of serum glutamic oxaloacetic acid and glutamic pyruvic transaminases. Am. J. Clin. Pathol., 1957, 28, 56–63.King, E. J., Armstrong, A. R.:[18] Calcium, phosphorus and phosphate. In: Varley, H. (ed.): Practical Clinical Biochemistry. CBS Publishers, New Delhi, 1988, p. 458.Fiala, S., Fiala, A. E., Dixon, B.:[19] Gamma glutamyl transpeptidase in transplantable chemically induced rat hepatomas and spontaneous mouse hepatomas. J. Natl. Cancer Inst., 1972, 48, 1393–1409.Stiehl, A.:[20] Hyperbilirubinämie bei Lebererkrankungen. Fortschr. Med., 1982, 100, 842–845.Utley, H. G., Bernheim, F., Hochstein, P.:[21] Effect of sulfhydryl reagents on peroxidation in microsomes. Arch. Biochem. Biophys., 1967, 118, 29–32.Sedlak, J., Lindasy, R. H.:[22] Estimation of total protein bound and nonprotein sulfhydryl group in tissue with Ellman’s reagents. Anal. Biochem., 1968, 25, 192–205.Culling, C. F.:[23] Handbook of Histopathological and Histochemical Techniques. 3rd edn., Butterworth and Co., London, p. 37, 1974.Dandiya, P. C., Collumbine, H.:[24] Studies on Acorus calamus: pharmacological actions of essential oil. J. Phar-macol. Exp. Ther., 1959, 125, 353–359.Srivastava, A., Shivanandappa, T.:[25] Hepatoprotective effect of the root extract of Decalepis hamiltonii against carbon tetrachloride-induced oxidative stress in rats. Food Chem., 2010, 118, 411–417.Kumar, S. S., Kumar, B. R., Mohan, G. K.:[26] Hepatoprotective effect of Trichosanthes cucumerina var. cuc-umerina L. on carbon tetrachloride induced liver damage in rats. J. Ethnopharmacol., 2009, 123, 347–350.Recknagel, R. O., Glende, E. A. Jr., Dolak, J. A. et al.: [27] Mechanisms of carbon tetrachloride toxicity. Pharma-col. Ther., 1989, 43, 139–154.Recknagel, R. O.:[28] Carbon tetrachloride hepatotoxicity. Pharmacol. Rev., 1967, 19, 145–208.Gupta, M., Mazumdar, U. K., Kumar, T. S. et al.:[29] Antioxidant and hepatoprotective effects of Bauhinia race-mosa against paracetamol and carbon tetrachloride induced liver damage in rats. Iran. J. Pharmacol. Ther., 2004, 3, 12–20.Sreelatha, S., Padma, P. R., Umadevi, M.:[30] Protective effects of Coriandrum sativum extracts on carbon tetra-chloride-induced hepatotoxicity in rats. Food Chem. Toxicol., 2009, 47, 702–708.Ramellini, G., Meldolesi, J.:[31] Liver protection by silymarin. In vitro effect on dissociated rat hepatocytes. Arzneim. Forsch. (Drug Res.), 1976, 26, 69–73.Vodela, J. K., Dalvi, R. R.:[32] Effect of chlorpyrifos on hepatic γ-glutamyl transferase, serum cholinesterase and xenobiotic metabolizing enzyme activities in rats. Bull. Environ. Contam. Toxicol., 1997, 57, 796–801.
ORIGINAL PAPERS
CEMED 139 2010 ▪ Volume 4, Number 1

Lee, D. H., Blomhoff, R., Jacobs, D. R. Jr.:[33] Is serum γ-glutamyltransferase a marker of oxidative stress? Free Radic. Res., 2004, 38, 535–539.Moon, J. O., Park, S. K., Nagano, T.:[34] Hepatoprotective effect of Fe-TPEN on carbon tetrachloride induced liver injury in rats. Biol. Pharm. Bull., 1998, 21, 284–288.Kumar, S.:[35] Studies on radioprotectors in mammals and their possible use in radiotherapy. Radiobiol. Radio-ther., 1985, 26, 359–365.Sakr, S. A., Abdel-Aal, W. E., Boulos, M. N. et al.:[36] Prevention by thiola of histological alteration in rat liver induced by carbon tetrachloride. J. Egypt. Soc. Pathol., 1994, 14, 451–458.Kadiska, M. B., Gladen, B. C., Baird, D. D. et al.:[37] Biomarkers of oxidative stress study: are plasma antioxi-dants markers of CCl4 poisoning? J. Free Radic. Biol. Med., 2000, 28, 838–845.Gutteridge, J. M. C., Halliwell, B.:[38] Antioxidants in Nutrition Health and Disease. Oxford University Press, Oxford, 1994.Hsu, Y. W., Tsai, C. F., Chang, W. H. et al.:[39] Protective effects of Dunaiella salina – a carotenoids-rich alga, against carbon tetrachloride-induced hepatoxicity in mice. Food Chem. Toxicol., 2008, 46, 3311–3317.Naik, S. R.:[40] Antioxidants and their role in biological functions: an overview. Indian Drugs, 2003, 40, 501–516.Lomnitski, L., Nyaska, A., Ben-Shaul, V. et al.:[41] Effects of antioxidants apocyanin and the natural water-soluble antioxidant from spinach on cellular damage induced by lipopolysaccharide in rats. Toxicol. Pathol., 2000, 287, 580–587.Baumann, J., Wurm, J., von Bruchhausen, F.:[42] Prostaglandin synthetase inhibition by fl avonoids and pheno-lic compounds in relation to their O2-scavenging properties. Arch. Pharm. (Weiheim), 1980, 313, 330–337.Castenmiller, J. J. M., Linssen, J. P. H., Heinonen, I. M. et al.:[43] Antioxidant properties of differently pro-cessed spinach products. Nahrung, 2002, 46, 290–293.Sreedevi, C. D., Latha, P. G., Ancy, P. et al.:[44] Hepatoprotective studies on Sida acuta Burm. f. J. Ethanophar-macol., 2009, 124, 171–175.
2010 ▪ Volume 4, Number 1 140 CEMED
ORIGINAL PAPERS

Effects of Oligofructose Containing Diet in Obese Persons
MAGDA ANTAL1, SZABOLCS PÉTER1, ANDREA REGÖLY-MÉREI1, LAJOS BIRÓ1, GYÖRGYI ARATÓ1,
JUDIT SCHMIDT1, KATALIN NAGY1, ERIKA GREINER1, NATÁLIA LÁSZTITY2, CSABA SZABÓ1, ÉVA MARTOS1
1National Institute for Food and Nutrition Science, Budapest, Hungary2Heim Pál Children’s Hospital – Outpatient Clinic, Budapest, Hungary
In the treatment of obesity, the introduction of a low-calorie diet is a fundamental requirement. The enhancement of the fi ber content of food causing satiety may contribute to the observation of dietary prescriptions. Oligofructoses belong to the group of dietary fi bers. Aim: To study the effects of the consumption of a low-energy diet (2,000 kcal/day) completed with Jerusalem artichoke concentrate in obese adolescents and adults. Methods: 12 obese students (6 boys and 6 girls) and 6 obese women were put on a low-calorie regimen for 12 weeks, whereas 16 obese students (10 boys and 6 girls) and 17 obese women consumed the same low-calorie diet also completed with Jerusalem arti-choke concentrate containing 14 g/day oligofructose. The sensation of fullness was estimated. In addition to anthro-pometric parameters, serum biomarkers of lipid and carbohydrate metabolism and adipokines were determined. Results: The consumption of the low-calorie diet completed with Jerusalem artichoke concentrate resulted in a di-minished sensation of hunger. The body mass index and body fat percentage decreased signifi cantly. In girls and women, the serum levels of triglyceride also signifi cantly reduced and the rate of insulin resistance (IR) estimated on the basis of homeostasis model assessment also improved. Conclusions: The results of this pilot study appear to demonstrate that the Jerusalem artichoke concentrate produced by a new technology can be a promising component of future diet therapy.
Keywords: obesity, adolescents, adults, oligofructose
Abbreviations
BMI = body mass index; BF% = body fat percentage; HOMAIR = homeostasis model assessment of insulin resis-tance
The big challenge of the twenty-fi rst century is to change the trend of nutrition to ensure optimal physiological functions to each individual, opening the door at the same time to dis-ease risk’s reduction to a minimum. In the spirit of this conception arose the functional food products, and one of their candidates is the Jerusalem artichoke concentrate containing olig-ofructose, prepared with the help of a new technology from an improved variety of arti-choke.
Oligofructose is derived from the inulin content of artichoke. Considering its chemical structure, inulin is a linear polyfructosane containing on an average 10–30 fructose units in β-1,2 binding. The structure and biological properties of oligofructose are similar to inulin,
Corresponding address: Magda Antal MD, National Institute for Food and Nutrition Science, Budapest, Hungary.E-mail: [email protected]
28387
CLINICAL STUDIES
CLINICAL STUDIES
DOI: 10.1556/CEMED.4.2010. 141 2010 ▪ Volume 4, Number 1 ▪ 141–152.

however, it contains only fi ve fructose molecules. The glycoside binding of fructose mole-cules cannot be decomposed by the enzymes of the small intestine. Colon bacteria produce short chain fatty acids, such as lactate, acetate, propionate, and butyrate from them by releas-ing H2, CO2, and CH4. Inulin and oligofructose come under the category of dietary fi bers. In their capacity as dietary fi bers, they foster the sensation of fullness and favorably infl uence colon microfl ora, therefore, they are classifi ed as prebiotics. According to certain scientifi c investigations, they decrease the serum levels of cholesterol and triglyceride and reduce the risk of colon tumor development in animals. Thus, their actions can be promising in dieto-therapy. Fructo-oligosaccharides found in nature and produced industrially can be consumed safely and do not have any side effects, even by an intake of 2,170 mg/kg/day [1–4].
The prevalence of overweight and obesity is growing year by year, not only in the adult population but also among children. It is known that childhood obesity is a major risk factor of obesity in adulthood. Obesity is regarded as a signifi cant risk factor of cardiovascular diseases and type 2 diabetes [5]. About 17 million people die worldwide every year due to cardiovascular diseases; one of the most important etiologic factors of these conditions is diabetes mellitus. A considerable part of this disease can be prevented through the elimina-tion of primary risk factors, that is, change in lifestyle [6, 7].
One of the most fundamental steps in obesity prevention and treatment is adoption of a proper diet [8, 9]. In the case of overweight or obese adults, dietary intervention is declared clinically signifi cant if it results in at least 5% loss in body weight, but in obese children, there is no uniform consensus in this respect [10]. Regarding the composition of low-energy (1,200–1,500 kcal) diet recommended for adults, fat-, carbohydrate- and protein contents in energy% are <30, 55, and 15, respectively. A moderate low-energy diet (−300, −500 kcal) is recommended in childhood obesity, with a fat-, carbohydrate- and protein ratio of 25–30, 55–60, and 15 energy%, respectively [8, 9].
Results of both national and international studies appear to indicate that adjustment of an effective weight loss diet is more complicated in obese children than in adults. The key issue in the observation of rules of a low-energy diet is how to overcome the increased sen-sation of hunger. The favorable properties of oligofructoses may hopefully contribute to the success of obese persons’ dietotherapy by including Jerusalem artichoke-derived products.
The aim of our study was to investigate the effect of a diet supplemented with Jerusalem artichoke concentrate containing oligofructose, used in the dietotherapy of obese adolescents and adults. In the present survey, we wished to fi nd out whether the effects of a dietotherapy of 12-week duration introduced to obese persons judged by body fat percent (BF%) are im-proved by supplementation with Jerusalem artichoke concentrate containing oligofructose, as compared to the actions of an identically composed dietary regimen, but without Jerusa-lem artichoke concentrate.
MethodsThe investigations were carried out in two metropolitan elementary schools, starting in Sep-tember 2007.
2010 ▪ Volume 4, Number 1 142 CEMED
CLINICAL STUDIES
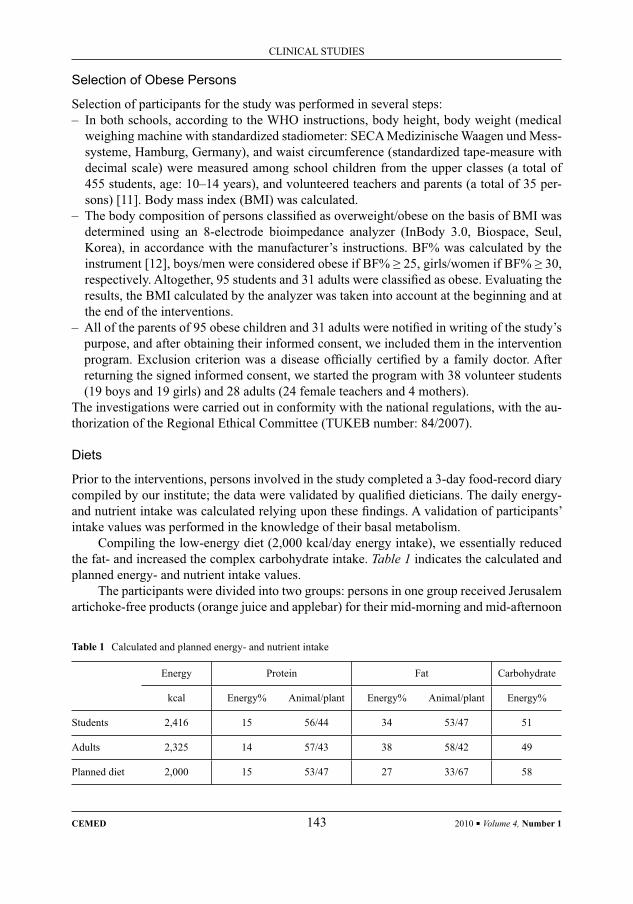
Selection of Obese Persons
Selection of participants for the study was performed in several steps:– In both schools, according to the WHO instructions, body height, body weight (medical
weighing machine with standardized stadiometer: SECA Medizinische Waagen und Mess-systeme, Hamburg, Germany), and waist circumference (standardized tape-measure with decimal scale) were measured among school children from the upper classes (a total of 455 students, age: 10–14 years), and volunteered teachers and parents (a total of 35 per-sons) [11]. Body mass index (BMI) was calculated.
– The body composition of persons classifi ed as overweight/obese on the basis of BMI was determined using an 8-electrode bioimpedance analyzer (InBody 3.0, Biospace, Seul, Korea), in accordance with the manufacturer’s instructions. BF% was calculated by the instrument [12], boys/men were considered obese if BF% ≥ 25, girls/women if BF% ≥ 30, respectively. Altogether, 95 students and 31 adults were classifi ed as obese. Evaluating the results, the BMI calculated by the analyzer was taken into account at the beginning and at the end of the interventions.
– All of the parents of 95 obese children and 31 adults were notifi ed in writing of the study’s purpose, and after obtaining their informed consent, we included them in the intervention program. Exclusion criterion was a disease offi cially certifi ed by a family doctor. After returning the signed informed consent, we started the program with 38 volunteer students (19 boys and 19 girls) and 28 adults (24 female teachers and 4 mothers).
The investigations were carried out in conformity with the national regulations, with the au-thorization of the Regional Ethical Committee (TUKEB number: 84/2007).
Diets
Prior to the interventions, persons involved in the study completed a 3-day food-record diary compiled by our institute; the data were validated by qualifi ed dieticians. The daily energy- and nutrient intake was calculated relying upon these fi ndings. A validation of participants’ intake values was performed in the knowledge of their basal metabolism.
Compiling the low-energy diet (2,000 kcal/day energy intake), we essentially reduced the fat- and increased the complex carbohydrate intake. Table 1 indicates the calculated and planned energy- and nutrient intake values.
The participants were divided into two groups: persons in one group received Jerusalem artichoke-free products (orange juice and applebar) for their mid-morning and mid-afternoon
Table 1 Calculated and planned energy- and nutrient intake
Energy Protein Fat Carbohydrate
kcal Energy% Animal/plant Energy% Animal/plant Energy%
Students 2,416 15 56/44 34 53/47 51
Adults 2,325 14 57/43 38 58/42 49
Planned diet 2,000 15 53/47 27 33/67 58
CLINICAL STUDIES
CEMED 143 2010 ▪ Volume 4, Number 1

snacks, whereas the subjects in the other group consumed identical products, but supple-mented with Jerusalem artichoke-concentrate. Consumption of supplemented products im-plied 14 g/day oligofructose intake. The two kinds of orange juice and applebar were pro-vided by Rauch Hungaria Ltd. and the Göböljárás plant of ChokiBank Ltd., respectively.
Breakfast (300 kcal), dinner (400 kcal), and lunch during school break (800 kcal) could be chosen by obese participants from the 30-day mosaic dietary guideline.
Satiety was verifi ed with the help of a Hunger/Satiety Scale compiled on the basis of literature data (www2.oprah.com/health/bob/bestlife/diet/basics_scale.jhtml).
Laboratory Analyses
Blood was collected in a closed system (Becton–Dickinson vacutainer), transportation was carried out cooled, according to the rules of clinical chemistry laboratories.
The serum levels of glucose (Randox test, GL-2623), triglycerides (Randox test, TR-210), total cholesterol, HDL-cholesterol, and LDL-cholesterol (Randox test, CH-200; CH-2652; CH-2657) were determined using a chemical analyzer (Daytona Olympos). The deter-mination of serum insulin-, leptin-, resistin-, and adiponectin levels was performed using ELISA method (INS-EASIA Biosource, Human Leptin ELISA BioVendor, Human Resistin ELISA BioVendor, Human Adiponectin ELISA BioCat).
Pathological values: total cholesterol: >5.2 mmol/L; HDL-cholesterol: male: <0.9 mmol/L, female: <1.2 mmol/L; LDL-cholesterol: >3.4 mmol/L; triglyceride: child: >1.50 mmol/L, adult: >1.71 mmol/L; serum glucose: >6.4 mmol/L; insulin: >20.0 μIU/mL. Normal values based on our own measurements: leptin: male: 3.0 ng/mL, female: 12.0 ng/mL; resis-tin: 5.5 ng/mL; adiponectin: male: 10.0 μg/mL, female: 13.0 μg/mL.
The degree of IR was determined on the basis of HOMA model: HOMAIR = (noctur-nal insulin value μIU/mL × nocturnal glucose value mmol/L)/22.5. It is to be noted that cur-rently there is no accepted value for the establishment of childhood IR, therefore, in our case, HOMAIR = 4.0 was regarded as a limiting value in both children and adults [13, 14].
Verifi cation
Dieticians visited schools once or twice per week, if needed, and inquired about the results achieved, and discussed emerging issues. During the consultations, they also touched upon the children’s satisfaction with their diet, with special regard to the sensation of hunger. The body weight was controlled bi-weekly.
Clinicians were in regular touch with the participants.Anthropometric and laboratory analyses performed for the fi rst time were repeated at
the end of the intervention.
Statistical Evaluation
Personal and survey data were recorded on ready-made surveying sheets on the site, and later they were fed in the Access database manager as personal records. The Students’ paired t-test was used for the statistical evaluation of data between the beginning and the end of the study. The tables indicate means ± SD and the level of signifi cance (p < 0.05).
2010 ▪ Volume 4, Number 1 144 CEMED
CLINICAL STUDIES
ResultsNineteen volunteered students (8 boys and 11 girls aged 10–14) and 8 teachers were involved in the consumption of low-energy diet. The 12-week dietary protocol was completed by 12 students (6 boys and 6 girls) and 6 teachers, and the drop-out rate was 37 and 25%, respec-tively. The cause for the premature termination of the diet was either indiscipline (regular overconsumption) or the fear of venipuncture.
Consumption of low-energy diet supplemented with Jerusalem artichoke concentrate was started with 19 volunteered students (11 boys and 8 girls aged 10–14) and 19 adults (15 teachers and 4 mothers). The 12-week dietary protocol was completed by 16 students (10 boys and 6 girls) and 17 adults (14 teachers and 3 mothers), and the drop-out rate was 16 and 11%, respectively. It is to be noted that one teacher, who discontinued the diet on the third week of the survey, complained about gastrointestinal symptoms caused by the consumption of Jerusalem artichoke. Other participants did not complain about any side effects of Jerusa-lem artichoke. Those who stayed out of the protocol were one parent and her daughter due to a bout of infl uenza, one boy without any argument, and one girl due to fear of venipuncture.
Satiety
Fifty percent of participants on the low-energy diet and 75% of participants on the low-ener-gy diet supplemented with Jerusalem artichoke concentrate indicated pleasant satiety or that they have eaten till repletion during the interventions.
Energy- and Nutrient Intake
Major dietary defi ciencies were also revealed among participants on low-energy diet during the course of weekly interviews. These were corrected by dieticians during consultation. In participants consuming low-energy diet supplemented with Jerusalem artichoke concen-trate, only minor complaints occurred and these could be attributed to the sensation of full-ness caused by Jerusalem artichoke.
Anthropometric Parameters
BMI, BF%, and waist circumference did not change in either group consuming low-energy diet. BMI and BF% decreased signifi cantly, waist circumference was diminished slightly in each group consuming the low-energy diet supplemented with Jerusalem artichoke (Table 2).
Lipid Parameters
Total cholesterol, HDL-cholesterol, LDL-cholesterol, and triglyceride values of participants consuming low-energy diet were within the normal range both at the beginning and at the termination of the diet. Lipid parameters of boys and girls on diet supplemented with Jerusa-lem artichoke concentrate were within the normal range. It is to be mentioned that in girls, the triglyceride level signifi cantly decreased till the end of the survey. In female participants, the total cholesterol and LDL-cholesterol levels were within the moderately pathological range either at the introduction or the terminatin of the diet. The signifi cant decrease of trig-lyceride level should be considered a positive fi nding (Table 3).
CLINICAL STUDIES
CEMED 145 2010 ▪ Volume 4, Number 1

Carbohydrate Metabolism
In both boys and girls consuming low-energy diet, a suspicion of IR based on HOMAIR existed both at the beginning and at the end of the interventions. In females, the serum levels of insulin decreased considerably, and as a corollary, the mean value of HOMAIR also de-clined till the end of the dietotherapy. HOMAIR values of participants consuming the diet supplemented with Jerusalem artichoke concentrate indicated IR in both boys and girls at the beginning, and the mean values were within the normal range till the end of the dietotherapy. HOMAIR values also decreased in females, although within the normal range (Table 4).
Adipokines
Out of the adipokines (leptin, resistin, and adiponectin), resistin signifi cantly decreased in boys due to low-energy diet. The concentrations of the examined biomarkers in the other groups did not change before and after the diet (Table 5).
Table 2 Effect of dietotherapy on certain anthropometric parameters
Age (years)Body mass index (kg/m2) Body fat (%) Waist circumference (cm)
1 2 1 2 1 2
Subjects consuming low-energy diet
Boys 12.7 29.0 28.8 36.4 35.7 93.1 92.8
n = 6 ±1.21 ±5.11 ±4.90 ±6.87 ±6.49 ±10.55 ±9.85
Girls 12.2 28.3 28.2 39.2 38.2 85.2 85.3
n = 6 ±1.17 ±4.47 ±4.27 ±5.87 ±5.71 ±8.58 ±9.86
Women 40.3 28.1 28.1 32.3 32.3 86.2 87.2
n = 6 ±8.89 ±3.48 ±3.34 ±4.28 ±4.77 ±6.23 ±8.62
Subjects consuming low-energy diet supplemented with Jerusalem artichoke concentrate
Boys 12.0 25.7 24.9** 34.0 31.4** 87.2 86.2
n = 10 ±1.41 ±3.21 ±3.27 ±4.20 ±6.40 ±9.10 ±9.15
Girls 11.0 25.6 24.9* 36.7 34.3* 81.9 80.5
n = 6 ±0.63 ±4.02 ±4.16 ±6.23 ±6.80 ±12.04 ±9.05
Women 53.0 29.3 28.8* 36.9 35.1** 92.2 91.6
n = 17 ±7.62 ±5.11 ±4.81 ±5.44 ±3.87 ±11.04 ±9.87
1: starting value; 2: after 12-week dietotherapy*p < 0.05; **p < 0.01
2010 ▪ Volume 4, Number 1 146 CEMED
CLINICAL STUDIES

Table 3 Effect of dietotherapy on serum lipid biomarkers
Total cholesterol(mmol/L)
HDL-cholesterol (mmol/L)
LDL-cholesterol (mmol/L)
Triglycerides(mmol/L)
1 2 1 2 1 2 1 2
Subjects consuming low-energy diet
Boys 4.2 4.1 1.0 1.0 2.8 2.8 1.2 0.9
±0.48 ±0.16 ±0.14 ±0.21 ±0.39 ±0.18 ±0.32 ±0.34
Girls 4.1 4.1 1.0 1.1 2.6 2.5 1.2 1.1
±0.68 ±0.67 ±0.10 ±0.08 ±0.62 ±0.64 ±0.41 ±0.36
Women 5.3 5.2 1.4 1.4 3.3 3.3 1.4 1.0
±1.14 ±1.03 ±0.23 ±0.18 ±1.01 ±1.05 ±0.71 ±0.23
Subjects consuming low-energy diet supplemented with Jerusalem artichoke concentrate
Boys 4.1 4.4 1.1 1.2 2.5 2.8 1.0 1.0
±1.05 ±0.98 ±0.23 ±0.25 ±0.91 ±0.81 ±0.54 ±0.68
Girls 4.2 4.4 1.1 1.2 2.6 2.7 1.2 0.8*
±0.37 ±0.61 ±0.21 ±0.28 ±0.46 ±0.55 ±0.56 ±0.33
Women 6.1 5.9 1.4 1.4 3.9 3.8 1.7 1.4*
±1.15 ±1.00 ±0.35 ±0.35 ±0.98 ±0.56 ±0.56 ±0.72
1: starting values; 2: after 12-week dietotherapy*p < 0.05
DiscussionWhile compiling low-energy diet, we set out from energy- and nutrient intake of obese par-ticipants, and relying upon these fi ndings, compiled their diet: the total fat-, carbohydrate- and protein intake amounted to 27, 58, and 15% of the total energy. In addition, we substan-tially decreased the ratio of fats of animal–plant origin and neared the ratio of animal to plant protein (Table 1). Beyond this, the diet supplemented with Jerusalem artichoke concentrate contained 14 g oligosaccharide as well. In the knowledge of the fact that adults and children in a free-living community should perform their duties as usual, we made efforts to promote their satiety as much as possible. Although, we did not reduce the energy value of the diet to the recommended level, adults consuming low-energy diet still regularly complained about sensation of hunger. Half of the students reported hunger sensation; this could be the reason for the frequent consumption of snacks and also the drop-out rate of 25% of teachers and 37% of students. Adults and children consuming low-energy diet supplemented with Jerusa-lem artichoke concentrate received the offered diet much favorably and, accordingly, the
CLINICAL STUDIES
CEMED 147 2010 ▪ Volume 4, Number 1
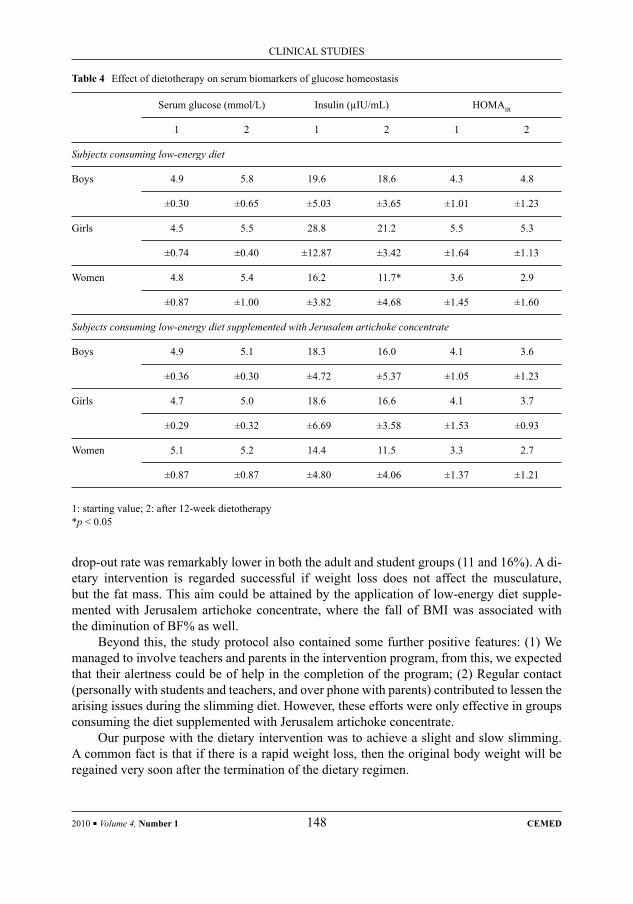
drop-out rate was remarkably lower in both the adult and student groups (11 and 16%). A di-etary intervention is regarded successful if weight loss does not affect the musculature, but the fat mass. This aim could be attained by the application of low-energy diet supple-mented with Jerusalem artichoke concentrate, where the fall of BMI was associated with the diminution of BF% as well.
Beyond this, the study protocol also contained some further positive features: (1) We managed to involve teachers and parents in the intervention program, from this, we expected that their alertness could be of help in the completion of the program; (2) Regular contact (personally with students and teachers, and over phone with parents) contributed to lessen the arising issues during the slimming diet. However, these efforts were only effective in groups consuming the diet supplemented with Jerusalem artichoke concentrate.
Our purpose with the dietary intervention was to achieve a slight and slow slimming. A common fact is that if there is a rapid weight loss, then the original body weight will be regained very soon after the termination of the dietary regimen.
Table 4 Effect of dietotherapy on serum biomarkers of glucose homeostasis
Serum glucose (mmol/L) Insulin (μIU/mL) HOMAIR
1 2 1 2 1 2
Subjects consuming low-energy diet
Boys 4.9 5.8 19.6 18.6 4.3 4.8
±0.30 ±0.65 ±5.03 ±3.65 ±1.01 ±1.23
Girls 4.5 5.5 28.8 21.2 5.5 5.3
±0.74 ±0.40 ±12.87 ±3.42 ±1.64 ±1.13
Women 4.8 5.4 16.2 11.7* 3.6 2.9
±0.87 ±1.00 ±3.82 ±4.68 ±1.45 ±1.60
Subjects consuming low-energy diet supplemented with Jerusalem artichoke concentrate
Boys 4.9 5.1 18.3 16.0 4.1 3.6
±0.36 ±0.30 ±4.72 ±5.37 ±1.05 ±1.23
Girls 4.7 5.0 18.6 16.6 4.1 3.7
±0.29 ±0.32 ±6.69 ±3.58 ±1.53 ±0.93
Women 5.1 5.2 14.4 11.5 3.3 2.7
±0.87 ±0.87 ±4.80 ±4.06 ±1.37 ±1.21
1: starting value; 2: after 12-week dietotherapy*p < 0.05
2010 ▪ Volume 4, Number 1 148 CEMED
CLINICAL STUDIES
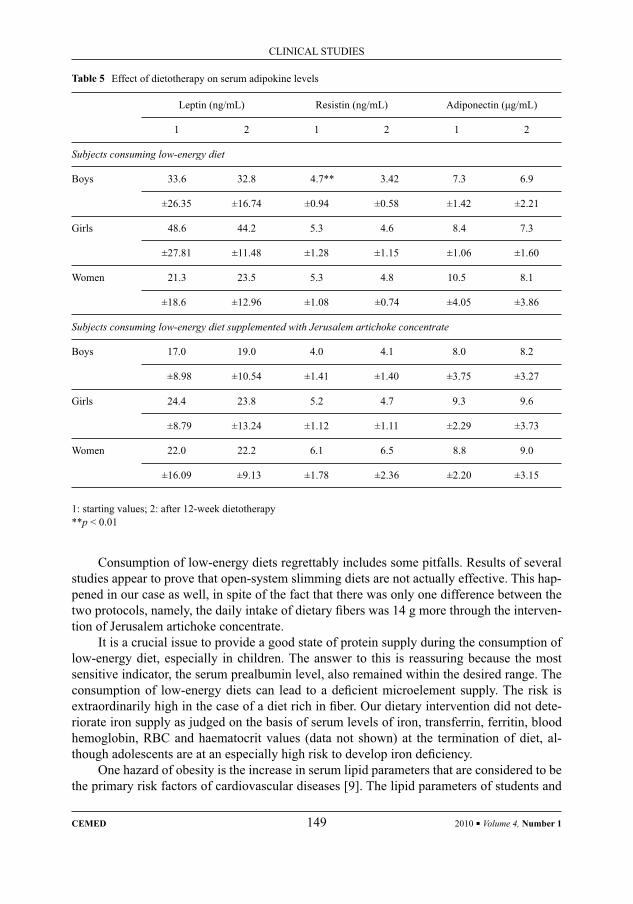
Consumption of low-energy diets regrettably includes some pitfalls. Results of several studies appear to prove that open-system slimming diets are not actually effective. This hap-pened in our case as well, in spite of the fact that there was only one difference between the two protocols, namely, the daily intake of dietary fi bers was 14 g more through the interven-tion of Jerusalem artichoke concentrate.
It is a crucial issue to provide a good state of protein supply during the consumption of low-energy diet, especially in children. The answer to this is reassuring because the most sensitive indicator, the serum prealbumin level, also remained within the desired range. The consumption of low-energy diets can lead to a defi cient microelement supply. The risk is extraordinarily high in the case of a diet rich in fi ber. Our dietary intervention did not dete-riorate iron supply as judged on the basis of serum levels of iron, transferrin, ferritin, blood hemoglobin, RBC and haematocrit values (data not shown) at the termination of diet, al-though adolescents are at an especially high risk to develop iron defi ciency.
One hazard of obesity is the increase in serum lipid parameters that are considered to be the primary risk factors of cardiovascular diseases [9]. The lipid parameters of students and
Table 5 Effect of dietotherapy on serum adipokine levels
Leptin (ng/mL) Resistin (ng/mL) Adiponectin (μg/mL)
1 2 1 2 1 2
Subjects consuming low-energy diet
Boys 33.6 32.8 4.7** 3.42 7.3 6.9
±26.35 ±16.74 ±0.94 ±0.58 ±1.42 ±2.21
Girls 48.6 44.2 5.3 4.6 8.4 7.3
±27.81 ±11.48 ±1.28 ±1.15 ±1.06 ±1.60
Women 21.3 23.5 5.3 4.8 10.5 8.1
±18.6 ±12.96 ±1.08 ±0.74 ±4.05 ±3.86
Subjects consuming low-energy diet supplemented with Jerusalem artichoke concentrate
Boys 17.0 19.0 4.0 4.1 8.0 8.2
±8.98 ±10.54 ±1.41 ±1.40 ±3.75 ±3.27
Girls 24.4 23.8 5.2 4.7 9.3 9.6
±8.79 ±13.24 ±1.12 ±1.11 ±2.29 ±3.73
Women 22.0 22.2 6.1 6.5 8.8 9.0
±16.09 ±9.13 ±1.78 ±2.36 ±2.20 ±3.15
1: starting values; 2: after 12-week dietotherapy**p < 0.01
CLINICAL STUDIES
CEMED 149 2010 ▪ Volume 4, Number 1

teachers consuming low-energy diet were within the normal range before and after the diet treatments. Strasser et al. reported on similar results, namely: the lipid parameters of per-sons with normal body weight and moderately obese patients did not change by restricted energy intake [15]. According to Ditschuneit et al. [16], low-energy diet treatment of obese persons did not infl uence even pathological total cholesterol, LDL-cholesterol, and triglycer-ide values. In the female group consuming low-energy diet supplemented with Jerusalem artichoke concentrate, the total cholesterol and LDL-cholesterol values were within the path-ological range before and after the treatment, whereas the serum triglyceride values decreased in both the female and girl groups as a result of the diet treatment. At present, it is unani-mously accepted that increased serum triglyceride concentration is a risk factor of cardiovas-cular diseases [17, 18]; therefore, a signifi cant reduction of serum triglyceride concentration is benefi cial in this respect. In humans, the effect of oligofructose on serum lipids is contro-versial. Luo [19] and Pedersen [20] could not prove any lipid-lowering effect, while others [21] reported a decrease in triglyceride levels after inulin intake. The effect was attributed to propionates evolved during inulin’s fermentation [22]. In animal studies, propionate evolved from inulin and from other oligosaccharides yield the modifi cation of lipogenic enzymes’ gene expression that is evidenced by a decrease in mRNS concentration of fatty acid syn-thetase [23, 24]. Although, diminution of serum triglyceride levels was published by several authors, it is noteworthy that in such case, the effect is not detectable in everyone, and there is no essential change in about 25% of persons consuming inulin [25, 26].
IR exists when the physiological blood glucose level is still maintained with the help of insulin overproduction. The homoeostasis model (HOMAIR) is used to ascertain this state. HOMAIR basal values indicated IR, except in females. Due to low-energy diet, teach-ers’ HOMAIR value decreased within the normal range; in case of students, no appreciable change occurred. Due to low-energy diet supplemented with Jerusalem artichoke concen-trate, HOMAIR values improved in both students and females.
In a study by Yamashita et al., fructans decreased fasting blood glucose levels in dia-betic patients, whereas other authors could not confi rm this fi nding [27, 28]. Luo et al. could not prove the benefi cial actions of fructo-oligosaccharides on the insulin-stimulated glucose metabolism, even in healthy adults [19]. We suggest in our study that the cause of the im-provement in HOMAIR value could be the sequel of the decrease in BF%.
Polypeptide hormones produced by adipose tissue, adipokines, such as leptin, adiponec-tin, and resistin, play a role in energy homeostasis, glucose and lipid metabolism, and exert actions on the immune- and neuroendocrine system [29]. It is generally accepted that in obese persons plasma concentrations of leptin and resistin increase, adiponectin decreases, whereas after weight loss a reversion follows. Nevertheless, subsequent data revealed that this effect depends on the extent of weight loss, that is if the weight loss does not exceed 5%, neither the concentration of leptin nor that of adiponectin changes signifi cantly [30]. In the present study, weight loss was inconsiderable, thus, this can explain the stagnation of leptin and adiponectin concentration.
Limitations of the Study
Dietotherapy of obese persons was performed in free-living population during school time. This was partly advantageous because in this manner participants received a group treat-ment, at the same time the infl uential role of classmates was inevitable. Due to the moderate
2010 ▪ Volume 4, Number 1 150 CEMED
CLINICAL STUDIES

number of partcipants, we consider the present investigations to be a promising preliminary study that is to be repeated in a larger community. If the reiteration will be performed in a free-living population, participants must be selected in advance from a more populous com-munity, since from 95 obese students, 38 students volunteered, and the study was completed by 28; the situation was slightly better in adults.
In summary, the results of the present study show that in the group of students consum-ing low-energy diet supplemented with Jerusalem artichoke concentrate, about 25% more students reported satiety than in the group consuming the same diet but not containing Jeru-salem artichoke concentrate; BMI and BF% decreased signifi cantly; the serum levels of trig-lyceride in girls and females decreased signifi cantly; and HOMAIR values improved at the end of the dietotherapy.
On the basis of all these, we suggest that the use of low-energy diet supplemented with Jerusalem artichoke concentrate containing oligofructose can be promising in the dietothera-py of obese persons of a free-living population.
This study was performed within the framework of the NKF (41002/2004) project.
ReferencesRoberfroid, M. B., Delzenne N.M.: [1] Dietary fructans. Ann. Rev. Nutr., 1998, 18, 117–143.Mahan, K. L., Escott-Stumps, S.[2] (eds) Krause’s Food, Nutrition, Diet Therapy. WB Saunders, Philadelphia, 1996, pp. 42, 47.Crow, D.: [3] Inulin – a comprehensive scientifi c review. 2000, http://members.shaw.ca/duncancrow/inulin_ review.html.Antal, M.: [4] Assessment of importance of fructans in food-hygiene (in Hungarian). Sport és Egészségtudomány, 2004, 3 (Suppl. 1), 14–17.Report of Joint WHO/FAO Expert Consultation:[5] Diet, nutrition and the prevention of chronic diseases. WHO Technical Report Series No. 916, Geneva, 2003, 77, 88.Fehér, J., Lengyel, G.: [6] Nutrition and cardiovascular mortality (in Hungarian). Orv. Hetil., 2006, 147, 1491–1496.Fehér, J., Lengyel G.: [7] Clinical utilization of combined rosiglitazone and glimepiride in the treatment of type 2 diabetes mellitus (in Hungarian). Orv. Hetil., 2007, 148, 2331–2335.Pados, G.: [8] Treatment of obesity (in Hungarian). Orv. Hetil., 2006, 145, 1765–1767.Juhász, A., Katona, E., Csongrádi, É. et al.: [9] Practicing physician’s view on obesity (in Hungarian). Orv. Hetil., 2006, 147, 579–590.Kalavainen, M.P., Korppi, M.O., Nuutinen, O.M.: [10] Clinical effi cacy of group-based treatment for childhood obesity compared with routinely given individual counseling. Int. J. Obes., 2007, 31, 1500–1508.WHO:[11] Physical status, the use and interpretation of anthropometry. WHO Technical Report Series No. 854, Geneva, 1995, 263–311, 445.Antal, M., Biró, L., Regöly-Mérei, A. et al.: [12] Methods in the assessment of adolescent obesity in epidemiologic study (in Hungarian). Orv. Hetil., 2008, 149, 51–57.Monzillo, L. U., Hamdy, O.: [13] Evaluation of insulin sensitivity in clinical practice and in research settings. Nutr. Rev., 2003, 61, 397–412.Dhuper, S., Cohen, H. W., Daniel, J. et al.: [14] Utility of modifi ed ATP III defi ned metabolic syndrome and severe obesity as predictors of insulin resistance in overweight children and adolescents: a cross-sectional study. Cardiovasc. Diabetol., 2007, 6, 1186–1195.Strasser, B., Spreitzer, A., Haber, P.: [15] Fat loss depends on energy defi cit only, independently of the method for weight loss. Ann. Nutr. Metab., 2007, 51, 428–432.Ditschuneit, H. H., Frier, H. I., Flechtner-Mors, M.: [16] Lipoprotein responses to weight loss and weight mainte-nance in high-risk obese subjects. Eur. J. Clin. Nutr., 2002, 56, 264–270.
CLINICAL STUDIES
CEMED 151 2010 ▪ Volume 4, Number 1
Assmann, G., Schulte, H., Funke, H. et al.: [17] The emergency of triglycerides as a signifi cant independent risk factor in coronary artery disease. Eur. Heart. J., 1998, 19 (Suppl. M), M8–M14.Asia Pacifi c Cohort Studies Collaboration: [18] Serum triglycerides as a risk factor for cardiovascular diseases in the Asia-Pacifi c region. Circulation, 2004, 110, 2678–2686.Luo, J., Rizkalla, S. W., Alamowitch, C. et al.: [19] Chronic consumption of short-chain fructooligosaccharides by healthy subjects decreased basal hepatic glucose production but had no effect on insulin-stimulated glucose metabolism. Am. J. Clin. Nutr., 1996, 63, 939–945.Pedersen, A., Sandstrom, B., Van Amelsvoort, J. M. M.: [20] The effect of ingestion of inulin on blood lipids and gastrointestinal symptoms in healthy females. Br. J. Nutr., 1997, 78, 215–222.Jackson, K. G., Taylor, G. R. J., Clohessy, A. M. et al.: [21] The effect of the daily intake of inulin on fasting lipid, insulin and glucose concentrations in middle aged men and women. Br. J. Nutr., 1999, 82, 23–30.Letexier, D., Diraison, F., Beylot, M.: [22] Addition of inulin to moderately high-carbohydrate diet reduces hepatic lipogenesis and plasma triacylglycerol concentrations in humans. Am. J. Clin. Nutr., 2003, 77, 559–564.Roberfroid, M. B.: [23] Prebiotics and probiotics: are they functional foods? Am. J. Clin. Nutr., 2000, 71, 1682S–1687S.Delzenne, N. M., Daubioul, C., Neyrinck, A. et al.: [24] Inulin and oligofructose modulate lipid metabolism in animals: review of biochemical events and future prospects. Br. J. Nutr., 2002, 87, S255–S259.Williams, C. M.: [25] Effects of inulin on lipid parameters in humans. J. Nutr., 1999, 129, 1471S–1473S.Balcázar-Muñoz, B. R., Martínez-Abundis, E., Gonzáles-Ortiz, M.: [26] Effect of oral inulin administration on lipid profi le and insulin sensitivity in subjects with obesity and dyslipidemia. Rev. Med. Chil., 2003, 131, 597–604.Yamashita, K., Kawai, K., Itakura, J.: [27] Effects of fructo-oligosaccharides on blood glucose and serum lipids in diabetic subjects. Nutr. Res., 1984, 4, 961–966.Alles, M. S., de Roos, N. M., Bakx, J. C. et al.: [28] Consumption of fructooligosaccharides does not favourably affect blood glucose and serum lipid concentration in patients with type II diabetes. Am. J. Clin. Nutr., 1999, 69, 64–69.Ahima, R. S., Lazar, M. A.: [29] Adipokines and the peripheral and neural control of energy balance. Mol. Edo-crinol., 2008, Jan 17, doi:10./me.2007-0529.Valsamakis, G., McTernan, P. G., Chetty, R. et al.: [30] Modest weight loss and reduction in waist circumfer-ence after medical treatment are associated with favorable changes in serum adipocytokines. Metabolism, 2004, 53, 430–434.
2010 ▪ Volume 4, Number 1 152 CEMED
CLINICAL STUDIES

Endoscopic Management of Post-Operative Biliary Tract Injuries
ZOLTÁN VÖLGYI, TÜNDE FISCHER, MÁRIA SZENES, BEÁTA GASZTONYI
Department of Medicine, Hospital of Zala County, Zalaegerszeg, Hungary
Post-operative biliary tract injuries have traditionally been treated by surgery; since the 1990s, however, this was replaced by endoscopic methods. These complications occur most frequently after laparoscopic surgery. Whenever biliary leakage is suspected, a close cooperation between endoscopists and surgeons is essential. Immediate visuali-sation of the biliary tract by endoscopic retrograde cholangio-pancreatography (ERCP) is mandatory to confi rm the diagnosis and locate the exact site of the lesion. Various endoscopic techniques have proven to be effective in the treatment of post-cholecystectomy biliary leaks. The crucial point is to equalise duodenal and biliary tract pressures so that bile fl ow into the duodenum is ensured and healing of the lesion is facilitated. This can be achieved by endo-scopic sphincterotomy either alone or in combination with subsequent implantation of a plastic stent. These methods seem to be equally suitable; for greater lesions, however, insertion of a stent is advisable. For biliary tract strictures, multiple stenting is recommended, the results of which are promising in the long run as well.
Keywords: post-operative biliary complications, ERCP, EST, biliary endoprosthesis
Abbreviations
ERCP = endoscopic retrograde cholangio-pancreatography; EST = endoscopic sphincterotomy; HG = high grade; LC = laparoscopic cholecystectomy; LG = low grade
IntroductionIn recent decades, the ever increasing amount of knowledge and technical progress have compelled medical practitioners to specialise within their profession. On the one hand, it promo ted professional pursuance of the sub-disciplines concerned, but on the other hand, it made a general overview of medical science more diffi cult. As a logical consequence, inter(sub)disciplinary cooperation has gained even more emphasis in the specialising health care, in the everyday praxis of medical treatment. A perfect example for this mutual depen-dency is the collaboration between surgeons and physicians that has great traditions and is acquiring new dimensions these days, as well as, in our case, the cooperation between surgeons and gastroenterologists. Recent technical progress has made the performance of several interventions possible on the endoscopic route, which could previously have been performed only by a surgeon as open operations (Table 1). At the same time, pre- and intra-operative endoscopy can often be helpful for surgeons (e.g. localisation of polyps, early tu-mours, or sources of haemorrhage; intraoperative ERCP coupled with LC for the removal of choledocholiths). However, the availability of a trained surgical team is a reassurance to en-
Corresponding address: Zoltán Völgyi MD, Department of Medicine, County Hospital Zala, Zrínyi Miklós str. 1, H-8900 Zalaegerszeg, Hungary. E-mail: [email protected]
28767
CLINICAL STUDIES
DOI: 10.1556/CEMED.4.2010. 153 2010 ▪ Volume 4, Number 1 ▪ 153–162.
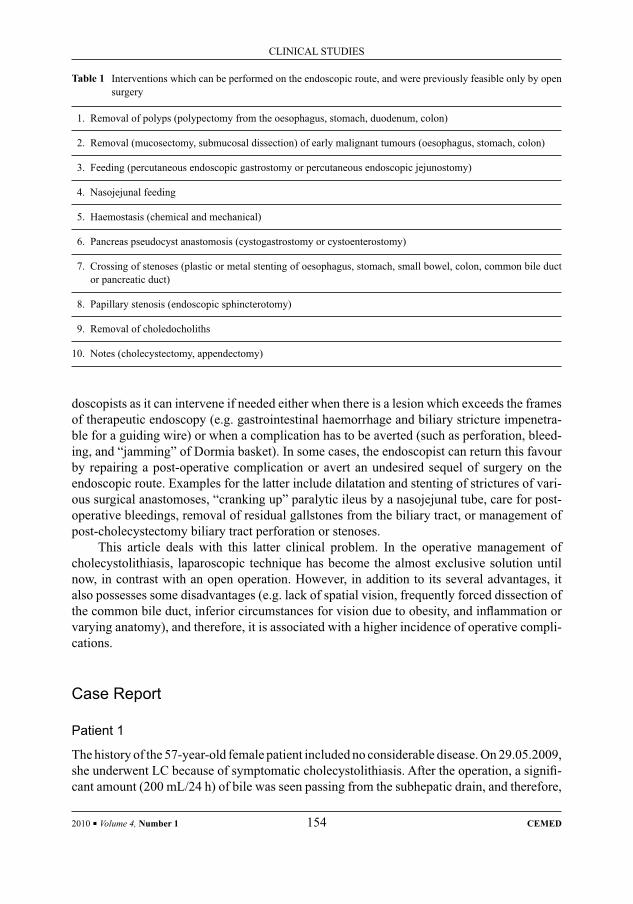
doscopists as it can intervene if needed either when there is a lesion which exceeds the frames of therapeutic endoscopy (e.g. gastrointestinal haemorrhage and biliary stricture impenetra-ble for a guiding wire) or when a complication has to be averted (such as perforation, bleed-ing, and “jamming” of Dormia basket). In some cases, the endoscopist can return this favour by repairing a post-operative complication or avert an undesired sequel of surgery on the endoscopic route. Examples for the latter include dilatation and stenting of strictures of vari-ous surgical anastomoses, “cranking up” paralytic ileus by a nasojejunal tube, care for post-operative bleedings, removal of residual gallstones from the biliary tract, or management of post-cholecystectomy biliary tract perforation or stenoses.
This article deals with this latter clinical problem. In the operative management of cholecystolithiasis, laparoscopic technique has become the almost exclusive solution until now, in contrast with an open operation. However, in addition to its several advantages, it also possesses some disadvantages (e.g. lack of spatial vision, frequently forced dissection of the common bile duct, inferior circumstances for vision due to obesity, and infl ammation or varying anatomy), and therefore, it is associated with a higher incidence of operative compli-cations.
Case Report
Patient 1
The history of the 57-year-old female patient included no considerable disease. On 29.05.2009, she underwent LC because of symptomatic cholecystolithiasis. After the operation, a signifi -cant amount (200 mL/24 h) of bile was seen passing from the subhepatic drain, and therefore,
Table 1 Interventions which can be performed on the endoscopic route, and were previously feasible only by open surgery
1. Removal of polyps (polypectomy from the oesophagus, stomach, duodenum, colon)
2. Removal (mucosectomy, submucosal dissection) of early malignant tumours (oesophagus, stomach, colon)
3. Feeding (percutaneous endoscopic gastrostomy or percutaneous endoscopic jejunostomy)
4. Nasojejunal feeding
5. Haemostasis (chemical and mechanical)
6. Pancreas pseudocyst anastomosis (cystogastrostomy or cystoenterostomy)
7. Crossing of stenoses (plastic or metal stenting of oesophagus, stomach, small bowel, colon, common bile duct or pancreatic duct)
8. Papillary stenosis (endoscopic sphincterotomy)
9. Removal of choledocholiths
10. Notes (cholecystectomy, appendectomy)
2010 ▪ Volume 4, Number 1 154 CEMED
CLINICAL STUDIES

we performed ERCP (30.05.2009). During this, after having opened the common bile duct, we fi lled the biliary tract with contrast material and observed extravasation at the level of the cystic duct’s stump. Then, we inserted a 10-cm long and 11.5-Fr wide plastic stent. Mild pancreatitis developed after the intervention; however, the output of the abdominal drain decreased from day to day. On 06.06.2009, the drain was removed, and soon the patient was discharged free of complaints. On 14.07.2009, we performed elective stent removal and observed a negative pancreatogram during the examination.
Patient 2
The history of the 58-year-old patient included no considerable disease. On 13.01.2009, he underwent LC because of cholecystolithiasis. On post-operative day 2, bilious discharge be-gan through his sub-hepatic drain, and therefore we performed ERCP, during which we saw a common bile duct with even path and normal width; however, outfl ow of contrast material as wide as a pencil-point could be observed at the level of the cystic duct and it went on in a caudal direction (Fig. 1). Then we made an incision of 1.5 cm as sphincterotomy in the direc-tion of the common bile duct, which was followed by an abundant fl ow of bile into the duo-denum. When probing the common bile duct with Dormia basket, we found no lithiasis of the biliary tract. Four days after the ERCP, the patient was discharged free of symptoms.
Fig. 1 ERCP picture (patient 2). An arrow indicates the site of contrast material extravasation
CLINICAL STUDIES
CEMED 155 2010 ▪ Volume 4, Number 1

Patient 3
On 13.08.2009, the 78-year-old female patient underwent anterior resection according to Dixon because of a tumour of the sigmoid, and cholecystectomy was performed at the same session because of a tense gallbladder fi lled with gallstones. As the common bile duct opened during the separation of the cholecyst, a Kehr T-tube was inserted. From the post-operative day 7 onwards, a signifi cant amount of bile (500 mL/day) appeared through the abdominal drain; therefore, we performed ERCP on 27.08.2009. During this, after having opened the common bile duct, we experienced stoppage of the contrast material at the place of the cystic duct’s orifi ce; however, when injected through the Kehr tube, it showed immediate extravasa-tion into a pool adjacent to the common bile duct (Fig. 2). As we did not succeed in getting over the stenosis even by a guiding wire, there was no feasible endoscopic solution, so that repeated laparotomy followed. During this, a malpositioned clip could be seen that was placed at the earlier surgery and caused strangulation of the common bile duct, the continuity of which ceased above it. After having the lesion repaired and a Kehr tube inserted, the state of the patient normalised.
Fig. 2 ERCP picture (patient 3). The pool, indicated by an arrow, suggests extravasation of contrast material
Patient 4
The 79-year-old male patient, who underwent LC 5 years prior to his admission, was hos-pitalised because of mechanical jaundice. During the ERCP, we observed a uniformly dilated common bile duct of ~8 mm that was fi lled homogeneously and had a sharp contour and a regular path. At the level of the cystic duct’s stump that was closed by clips, we observed a stop of semilunar contour at the transition of the common hepatic duct – the common bile duct, which could be penetrated neither by a contrast material nor by a guiding wire (Fig. 3a). Upon repeated attempts, we could pass the guiding wire. Then a stricture of a pencil-point’s width could be visualised at the full length of the hepatic duct (~3 cm long), with the fi lling of regular but dilated intrahepatic bile ducts above it. With a little forcing, a Soehendra biliary dilation catheter could be inserted through the stricture, and then we spanned it with a 12-cm long plastic stent with a diameter of 8 Fr (Fig. 3b). On day 3 after the intervention, the patient was discharged free of complaints.
2010 ▪ Volume 4, Number 1 156 CEMED
CLINICAL STUDIES

Occurrence of Biliary Tract InjuriesThere are two types of post-operative biliary tract injuries which may also combine with each other. Owing to a discontinuity that occurs at various levels of bile ducts, bilious fl uid accumulations develop in the immediate post-operative period, while the formation of stric-tures is to be expected in the later post-operative period.
Most commonly, the injuries affect the stump of the cystic duct; they may be of diather-mic origin, they may arise from a malpositioned clip, or they may be based on ischemia due to damaged blood supply. The second most common site is an aberrant branch of the right hepatic bile duct (Luschka’s duct), the injury of which usually occurs during separation of the infl amed cholecyst from the liver. Less frequently, it may develop at a site where an intra-operatively inserted Kehr tube has slipped out. Sometimes, a distal obstruction, which in-duced or maintained the process (choledocholithiasis, stenosis of the Vater papilla), can also be detected.
Usually 0.8%–1.7% of LCs is followed by a leakage of bile, although data signifi cantly vary and a considerable part of cases remain latent due to a lack of clinical symptoms. According to a retrospective Italian survey (1998–2000) of 56,591 operations, 235 biliary tract injuries (0.42%) occurred, and 80% of it in patients with no risk factors (e.g. obesity, previous abdominal surgery, or hepatic cirrhosis) at all [1]. In their prospective material, surgeons in Stockholm observed a total of 1.5% (25/1,568) biliary tract injuries [2]. A Japa-nese workgroup’s series of similar magnitude (1,365 LCs) showed a rate of 1.7% for post-operative biliary leakage [3]. Interestingly, the complication usually follows easy LCs, done
Fig. 3 ERCP picture (patient 4). (a) Stricture located at the proximal part of the common bile duct (arrow). (b) The above stricture after fi lling of the intrahepatic bile ducts
(a) (b)
CLINICAL STUDIES
CEMED 157 2010 ▪ Volume 4, Number 1

by not inexperienced surgeons, and it is caused by an unnecessarily early dissection of the cystic duct.
DiagnosisA diagnosis is usually made in the days following the operation, less frequently, the injury is observed already during surgery. An excessive amount of bile passing through the abdominal drain calls attention to the abnormity, but the patient’s complaints (pain, fever, jaundice, and distension) may also contribute to early diagnosis; however, asymptomatic cases may occur as well. Also, after removal of the abdominal drain, a biloma, peritonitis, or an abdominal abscess may indicate the condition. A prolonged loss of bile may be associated with sys-temic undesired events such as hyponatraemia or renal failure.
Since the 1990s, the previously exclusive operative methods have been replaced by en-doscopic techniques, of course keeping in mind that best results can be attained by immediate reconstruction, a prerequisite of which is, however, intraoperative detection of the complica-tion. Post-operative diagnostic possibilities include transabdominal and endoscopic ultra-sonography, percutaneous transhepatic cholangiography, magnetic resonance cholangiopan-creatography, and ERCP. The latter has a clear priority as it serves not only diagnostic purposes but also offers therapeutic possibilities. If there is suspicion, early ERCP has to be sought for, as by this means, the lesion can be localised, its severity can be revealed, and in the decisive majority of cases (85–100%), it also offers a defi nitive solution with a low rate of complications.
Classifi cationPreviously, biliary tract injuries were classifi ed according to Bismuth who differentiated them based on the highest level of injury. This had the disadvantage of not including the in-juries of collateral branches. Following the advent of laparoscopic technique, other types of injuries have come into prominence, which in 1995 brought into being a new classifi cation (Strasberg) (Fig. 4) that could describe a wider scale of injuries. The latter classifi cation in-cludes that of Bismuth, too (Type E 1–5 means Bismuth 1–5) and it also helps therapeutic decisions, as milder lesions (A–C) can certainly be treated by the endoscopic route, while the most severe ones (Type E) always require surgical operation.
Possibilities of Endoscopic TherapyThere is no clear-cut recommendation on which endoscopic therapeutic process is to be pre-ferred, but there is a common principle: the area of the lesion must be relieved by equalising duodenal and biliary pressures that promotes healing. One of the possibilities is EST; another includes insertion of a stent with or without EST. A higher rate of haemorrhagic com-plications may be a disadvantage of EST, while stenting alone may be associated with an increased number of pancreatitis cases. It is also debated if a lesion should be spanned by the stent, but probably, an increase of length (“crossing stent”) may bring no further benefi ts (the
2010 ▪ Volume 4, Number 1 158 CEMED
CLINICAL STUDIES
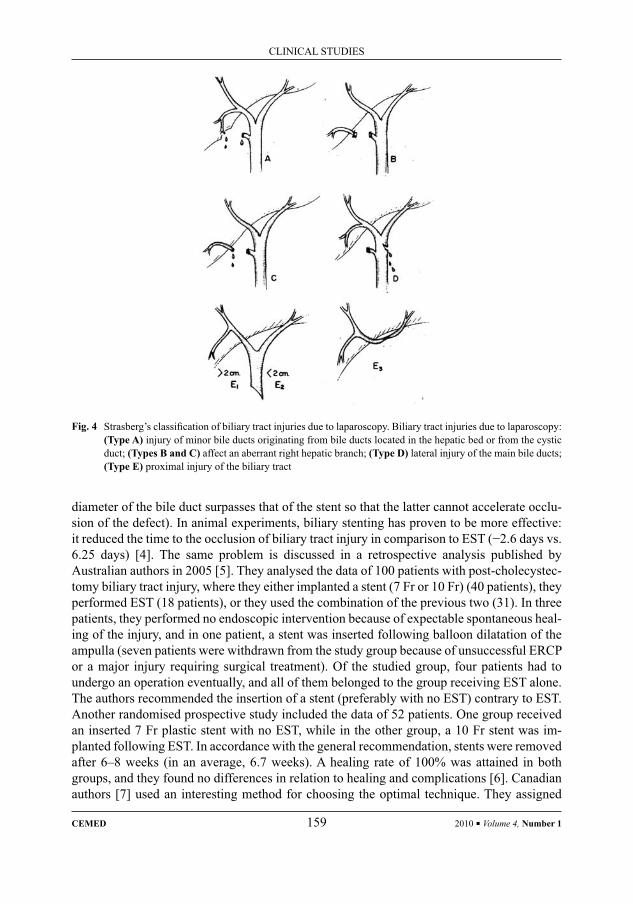
diameter of the bile duct surpasses that of the stent so that the latter cannot accelerate occlu-sion of the defect). In animal experiments, biliary stenting has proven to be more effective: it reduced the time to the occlusion of biliary tract injury in comparison to EST (−2.6 days vs. 6.25 days) [4]. The same problem is discussed in a retrospective analysis published by Australian authors in 2005 [5]. They analysed the data of 100 patients with post-cholecystec-tomy biliary tract injury, where they either implanted a stent (7 Fr or 10 Fr) (40 patients), they performed EST (18 patients), or they used the combination of the previous two (31). In three patients, they performed no endoscopic intervention because of expectable spontaneous heal-ing of the injury, and in one patient, a stent was inserted following balloon dilatation of the ampulla (seven patients were withdrawn from the study group because of unsuccessful ERCP or a major injury requiring surgical treatment). Of the studied group, four patients had to undergo an operation eventually, and all of them belonged to the group receiving EST alone. The authors recommended the insertion of a stent (preferably with no EST) contrary to EST. Another randomised prospective study included the data of 52 patients. One group received an inserted 7 Fr plastic stent with no EST, while in the other group, a 10 Fr stent was im-planted following EST. In accordance with the general recommendation, stents were removed after 6–8 weeks (in an average, 6.7 weeks). A healing rate of 100% was attained in both groups, and they found no differences in relation to healing and complications [6]. Canadian authors [7] used an interesting method for choosing the optimal technique. They assigned
Fig. 4 Strasberg’s classifi cation of biliary tract injuries due to laparoscopy. Biliary tract injuries due to laparoscopy: (Type A) injury of minor bile ducts originating from bile ducts located in the hepatic bed or from the cystic duct; (Types B and C) affect an aberrant right hepatic branch; (Type D) lateral injury of the main bile ducts; (Type E) proximal injury of the biliary tract
CLINICAL STUDIES
CEMED 159 2010 ▪ Volume 4, Number 1

patients with post-operative biliary tract injury into two groups, and they chose the used technique depending on that. The group of LG injuries included cases where the extravasa-tion of contrast material during ERCP could be seen only when the intrahepatic bile ducts were also fi lled, in contrast to the high-grade lesions (HG), where the site of the lesion also became obvious already prior to the fi lling of the intrahepatic bile ducts. Then, they per-formed EST alone in the LG group, when there was no other indication for stenting (stricture) and there was no contraindication of sphincterotomy (e.g. hypoprothrombinaemia), and stent implantation, with or without EST, in the HG group. In the former group, they observed 91% (68/75) healing in 75 patients who underwent EST and had LG lesion, and the remaining seven patients recovered after stent insertion (6) or surgery (1). The latter group consisted of 100 patients. In three cases, immediate operation was performed because of the size of the lesion, whereas of the remaining 97 patients, 94 recovered and 3 were cured after a further insertion of a stent. Summing up, it can be concluded that this simple classifi cation has proven to be suitable for selecting the optimal endoscopic technique.
Transient administration of metal stents for biliary leaking is a new procedure. Ameri-can authors published their results relating to the temporary use of metal stents in patients with biliary leaking fi rst in 2007 [8]. While they had an adequate effi cacy, the signifi cant rate of stent migrations and the diffi cult removal due to mucosal hyperplasia that developed at both ends of the stents prompted them to improve the technique. The results of this were published in their most recent paper on a series of 13 patients where they used self-expanding covered metal stents with anchors at both ends which averted migration and a special (poly-tetrafl uoroethylene and fl uorinated ethylene–propylene) coating which prevented mucosal hypertrophy. These patients had biliary tract injuries that showed no regression upon the conventional endoscopic techniques (EST, stent), and therefore, the above stents were im-planted temporarily for an average of 103 days. Not including the two patients who died in the meantime due to complications of non-biliary nature, all the remaining 11 patients have recovered and had no biliary leaking also during the follow-up period (in an average, 318 days). Setbacks of the new technique included the development of new strictures of the bile ducts (2/11) and the formation of choledocholiths (10/11). They recommend it for the treatment of patients where biliary leaking persists despite conventional endoscopic tech-niques [9].
Also, other alternative therapeutic modalities have been published, including topical administration of nitroglycerine, which decreases Oddi sphincter tone [10], closure of the injury with n-butyl-2-cyanoacrylate [11], and botulinum toxin that was used successfully in an animal model [12].
Post-Operative Strictures of the Biliary TractAlthough this paper is focusing mainly on post-operative biliary leakage, it is important to mention the other type of post-operative biliary tract complications, namely, bile duct stric-tures. Stenoses may develop either directly by complete or partial clipping or ligating of a main or secondary bile duct, or secondarily due to ischemic or thermal damage. A diagnosis is made in the former cases usually during surgery or in the immediate post-operative period, whereas in the latter cases, months, perhaps years elapse after the operation until diagnosis. Early signs and symptoms include pain, fever, and jaundice, while recurring cholangitis,
2010 ▪ Volume 4, Number 1 160 CEMED
CLINICAL STUDIES

lithiasis of the bile ducts, or secondary biliary cirrhosis belong to the late ones. Contrary to the former exclusively surgical management, endoscopy has gained a signifi cant role also in the therapy of stenoses. Following balloon dilatation of the stricture, Costamagna et al. used to place a biliary duct stent with the largest possible diameter into the common bile duct and then change it every 3 months and increase their number until the stenosis is dilated. Of their published 45 patients, 40 (89%) were free of symptoms in the 49-month follow-up period (laboratory and ultrasound fi ndings also showed recovery) [13]. The average treatment dura-tion was 12.1 month (±5.3 month).
DiscussionA decisive part of post-operative biliary injuries can be treated by the endoscopic route. The possibilities of this include EST performed during ERCP, stent insertion, or a combina-tion of these. In case of LG lesions or in the presence of choledocholithiasis, stenosis of the Vater papilla, primarily EST, is to be preferred, whereas stent implantation is recommended for HG lesions when strictures are present or there is a risk of their development. There is no agreement regarding the size of the stent. Some consider a short, 5-cm long, 7–10-Fr wide biliary endoprosthesis suffi cient to equalise the pressures on both sides of the Oddi sphincter, whereas others are of the opinion that using a thick (11.5 Fr) stent is reasonable as it spans the lesion, and this way it provides a tamponade and promotes healing. According to current international consensus, the stent is left in place for 6–8 weeks. ERCP is also suitable for the elimination of factors that hinder the healing of the lesion, including the removal of choledo-choliths or termination of the Vater papilla stricture. Transitory application of metal stents is a new procedure for biliary tract leakage, which resisted the above methods or when the problem seems more serious from the very beginning. Its use is limited by the relatively high number of complications (stenosis and choledocholiths). During the later follow-up of pa-tients, attention should be paid to the recognition of biliary tract stenoses, and it is expedient to reverse the process by appropriate, timely stenting, yet before its fi brotic transformation.
ConclusionsThe authors aimed at calling attention to the endoscopic possibilities in the management of bilious leakage following biliary tract surgery, underlining that – with the exclusion of the most severe cases (e.g. complete clipping of the common bile duct and transection of a major bile duct) – there is no need for patients to undergo a repeated operation, as endoscopic meth-ods are also prominently suitable for the treatment of this group of patients.
ReferencesNuzzo, G., Giuliante, F., Giovannini, I. et al.: [1] Bile duct injury during laparoscopic cholecystectomy. Arch. Surg., 2005, 140, 986–992.Söderlund, C., Frozanpor, F., Linder, S.:[2] Bile duct injuries at laparoscopic cholecystectomy: a single institu-tion prospective study. Acute cholecystitis indicates an increased risk. World J. Surg., 2005, 29, 987–993.
CLINICAL STUDIES
CEMED 161 2010 ▪ Volume 4, Number 1
Kimura, T., Suzuki, K., Umehara, Y. et al.: [3] Features and management of bile leaks after laparoscopic chole-cystectomy. J. Hepatobil. Pancreat. Surg., 2005, 12, 61–64.Marks, J. M., Ponsky, J. L., Shillingstad, R. B. et al.: [4] Biliary stenting is more effective than sphincterotomy in resolution biliary leaks. Surg. Endosc., 1998, 12, 327–330.Kaffes, A. J., Hourigan, L., de Luca, N. et al.: [5] Impact of endoscopic intervention in 100 patients with sus-pected postcholecystectomy bile leak. Gastrointest. Endosc., 2005, 61, 269–275.Mavrogiannis, C., Liatsos, C., Papanikolaou, I. S. et al.: [6] Biliary stenting versus biliary stenting plus sphinc-terotomy for the treatment of post laparoscopic cholecystectomy biliary leaks: a prospective randomized study. Eur. J. Gastroenterol. Hepatol., 2006, 18, 405–409.Gurpal, S., Sandha, M. B., Bourke, M. J. et al.: [7] Endoscopic therapy for bile leak based on a new classifi ca-tion: results in 207 patients. Gastrointest. Endosc., 2004, 60, 567–574.Kahaleh, M., Sundaram, V., Condron, S. L. et al.: [8] Temporary placement of covered self-expandable metal-lic stents in patients with biliary leak: midterm evaluation of a pilot study. Gastrointest. Endosc., 2007, 66, 52–59.Wang, A. Y., Ellen, K., Berg, C. L.:[9] Fully covered self-expandable metallic stents in the management of com-plex biliary leaks: preliminary data – a case series. Endoscopy, 2009, 41, 781–786.Pala, F. X., Mendez, E. X., Gomez, P. S. et al.: [10] Topical nitroglycerin: an alternative in conservative treat-ment of biliary fi stula. Rev. Esp. Enferm. Dig., 1996, 88, 877–879.Seewald, S., Groth, S., Sriram, P. V. et al.: [11] Endoscopic treatment of biliary leakage with n-butil-2 cyanoacry-late. Gastrointest. Endosc., 2002, 56, 916–919.Brodyska, J. A., Marks, J. M., Malm, J. A. et al.: [12] Sphincter of Oddi injection with botulinum toxin is as effec-tive as endobiliary stent in resolving cystic duct leaks in canine model. Gastrointest. Endosc., 2002, 56, 849–851.Costamagna, G., Pandolfi , M., Mutignani, M. et al.: [13] Long-term results of endoscopic management of post-operative bile duct strictures with increasing numbers of stents. Gastrointest. Endosc., 2001, 54, 162–168.
2010 ▪ Volume 4, Number 1 162 CEMED
CLINICAL STUDIES
Patients with Syphilis and Gonorrhoea: Analysis of Cases Based on Data (2005–2008)
of the National Sexually Transmitted Disease Centre, Department of Dermatology, Venereology
and Dermatologic Oncology, Semmelweis UniversityKATINKA PÓNYAI, MÁRTA MARSCHALKÓ,
MÁRIA SCHÖFFLER-ACKERMAN, ESZTER OSTORHÁZI, FERENC ROZGONYI, VIKTÓRIA VÁRKONYI, SAROLTA KÁRPÁTI
Department of Dermatology, Venereology and Dermatologic Oncology, Semmelweis University Medical School, Budapest, Hungary
In the STD Centre of Hungary at our department, we have been providing care for patients with syphilis, gonorrhoea and other STD infections since 2004. Our STD centre includes a screening station where we perform anonymous screening for HIV and syphilis. Between the 1st of January 2005 and the 31st of December 2008, there were a total of 42,114 patient–doctor encounters. We performed 25,362 screening examinations for HIV and syphilis, in associa-tion with a medical visit (HIV: 12,337; syphilis: 13,025). Voluntary screening examinations were performed in 18,883 cases (HIV: 16,614; syphilis: 2,269). During the 4 years, we diagnosed 600 and 339 new cases of syphilis and gonorrhoea, respectively. The obligatory HIV screening of STI patients resulted in a total of 47 new HIV infec-tions, and we diagnosed 63 new infections of syphilis or gonorrhoea among the known HIV-seropositive patients under care. By including the network of care providers in the whole country, we performed successful contact trac-ing for syphilis and gonorrhoea on 400 and 150–200 occasions per year, respectively. We present our statistical data in order to call attention to the renaissance of syphilis and gonorrhoea, and the importance of STD co-infections.
Keywords: STI, syphilis, gonorrhoea, epidemiology, Hungary
Abbreviations
Go = gonorrhoea; HIV = human immunodefi ciency virus; OBNI = National Institute of Dermatology and Venereol-ogy (in Hungary, previously); RPR = rapid plasma reagin; STD = sexually transmitted disease; STI = sexually trans-mitted infection; Sy = syphilis; TP-PA = treponema pallidum particle agglutination; TP ELISA = treponema pal-lidum enzyme-linked immunosorbent assay; TPHA = treponema pallidum haemagglutination; VDRL = venereal disease research laboratory
IntroductionThanks to the introduction of antibiotic therapy, syphilis (sy) and gonorrhoea (go) have be-come curable diseases. In December 1954, Ernő Kálmán MD trustingly wrote in his paper published in the Népegészségügy (National Health): “Based on the results up to now, one
Corresponding address: Katinka Pónyai MD, Mária str. 41, H-1085 Budapest, Hungary.E-mail: [email protected]
28697
CLINICAL STUDIES
DOI: 10.1556/CEMED.4.2010. 163 2010 ▪ Volume 4, Number 1 ▪ 163–174.

may reasonably expect that the practical elimination of new infections with syphilis will be-come a reality within 1-2 years.” This optimistic vision of the future has not come true, as sexually transmitted diseases which are reckoned to be classical show an increasing trend worldwide, in spite of the successful antibiotic therapies available [1, 2].
Also, in Hungary, no “practical elimination of fresh syphilis” occurred, and even the number of infected people shows an increasing trend again in recent years. Go and sy are classical sexually transmitted diseases, their diagnosis and therapy are important tasks for all physicians because of their severe epidemiologic and chronic complications.
As the National Institute of Dermatology and Venereology in Hungary (OBNI) ceased to exist in 2004, the network of care providers for STD patients remained without a central organisational unit. At the same time, our STD centre was established at the Department of Dermatology, Venereology and Dermatologic Oncology of Semmelweis University and it assumed the task of OBNI, the provision of further care for STD patients.
The current paper is aimed at calling attention, by demonstrating data of the STD Cen-tre, Department of Dermatology, Venereology and Dermatologic Oncology of Semmelweis University, to the often forgotten classical STDs. Our clinical data allow one to draw practi-cal conclusions for the situation in the country and for the assessment of future agenda. Data of our patients treated with diagnoses of sy and go in the period between 2005 and 2008 are analysed in our paper.
PatientsAs legal successors of the OBNI, the STD centre of our department has been providing care for patients with sy, go and other STD infections since 2004. Our STD centre includes a screening station where we perform anonymous screening for HIV and sy. Between the 1st of January 2005 and the 31st of December 2008, there were a total of 42,114 patient–doctor encounters. We performed 25,362 screening examinations for HIV and sy, in association with a medical visit (HIV: 12,337; syphilis: 13,025). Voluntary screening examinations were per-formed in 18,883 patients (HIV: 16,614; syphilis: 2,269) (Table 1).
Table 1 Patients attending our STD centre between 2005 and 2008, and numbers of patients with syphilis or gonor-rhoea
2005 2006 2007 2008 Total
Patients examined 7,987 11,255 12,254 10,618 42,114
Syphilis 128 1.6% 159 1.41% 105 0.85% 208 1.96% 600 1.42%
Gonorrhoea 66 0.82% 100 0.88% 103 0.84% 70 0.66% 339 0.8%
2010 ▪ Volume 4, Number 1 164 CEMED
CLINICAL STUDIES
Methods
Sy Diagnostics
We use dark fi eld microscopy for direct detection of pathogens from a primary affection or a wet secondary cutaneous lesion.
Serological tests include: RPR test (IMMUTREP® RPR Ref. OD051/OD061), VDRL (IMMUTREP® RPR Ref. OD051/OD061). Specifi c tests: TPHA (IMMUTREP® TPHA Ref. OD211/OD071/OD081), TP ELISA (DiaSorin® – ETI – Treponema plus Ref. NO148/Ref.NO149 – Biomedica Hungary Kft.), Western blot IgG and IgM (EcoLine® recombinant – Genzyme VIROTECH GmbH – Biomedica Hungary Kft.), or TP-PA (Serodia® TP-PA MAST Diagnostica).
Establishment of the diagnosis: direct detection of pathogens, results of serological tests and the clinical picture served as a basis for establishing a diagnosis. In early seronega-tive, symptomatic period, our diagnosis was based on clinical picture and direct detection of the pathogen, whereas in early seropositive, symptomatic stage, on the positive result of se-rological tests and the clinical picture.
In case of recent latent sy, the diagnosis is established on the basis of positive results of the screening and the confi rming test (RPR, TPHA, TP ELISA). Latent tardive sy may occur at negative RPR/VDRL as well.
Biological aspecifi c positivity (BAP) means positive result of a non-specifi c lipoid test occurring at negativity of the specifi c tests.
Go Diagnostics
Samples have been taken for culture from urethra, cervix, anus and pharynx, and have under-gone Gram staining as well. Cultures took place on Thayer Martin agar and in parallel on vancomycin-free chocolate agar (at 37 °C for 72 h). In case of a positive result of culture, biochemical identifi cation was done by oxidase reaction, API 20NE® (BioMerieux, Diagnos-ticum Zrt.). Antibiogram was obtained on Chocolate agar plus PolyViteX® (BioMerieux Di-agnosticum Zrt.) medium with OXOID® (Diagnosticum Zrt.) antibiotic discs. Minimal in-hibitory concentration (MIC) was determined by E-Test® (Frank Diagnosticum Zrt.).
For screening of symptom-free contact persons, we used the PCR technique (Roche Cobas Amplicor).
Establishment of the diagnosis: in men with typical clinical picture (profuse purulent discharge with acute onset), detectability of Gram-negative intracellular diplococci in the fl uor is of diagnostic value. In women, the result of cervical smear should always be evalu-ated together with culture results.
Contact Tracing Methods
Contact tracing is aimed at terminating the chain of infections by treating the contact per-sons. For this purpose, the fi rst step is to obtain usable information on the contacts, which is not an easy task, it is feasible only after having gained full confi dence of the patient. Maximal consideration of patients’ rights is compulsory, while recognising that the patient cannot be forced to give information on his/her sexual partners and practices.
CLINICAL STUDIES
CEMED 165 2010 ▪ Volume 4, Number 1
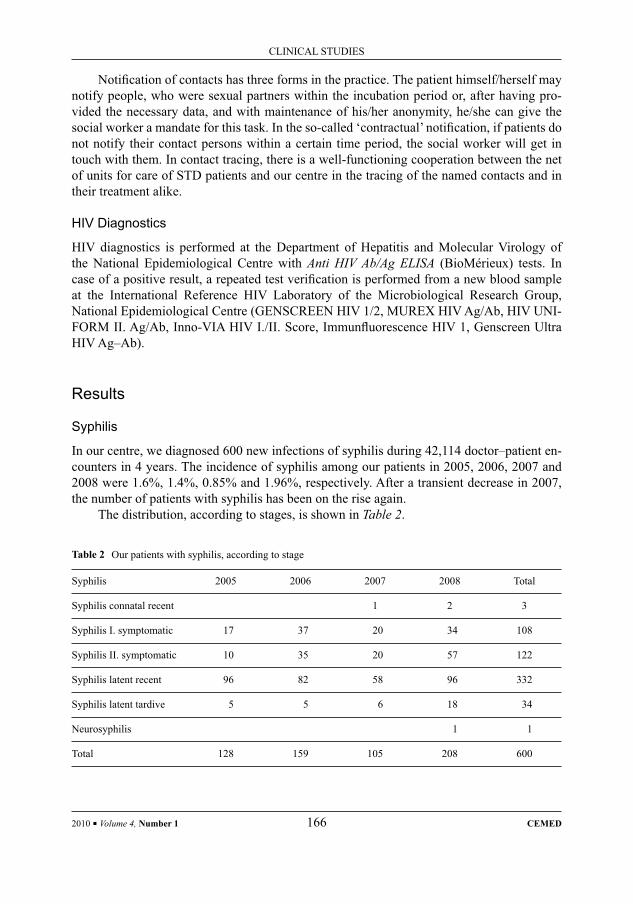
Notifi cation of contacts has three forms in the practice. The patient himself/herself may notify people, who were sexual partners within the incubation period or, after having pro-vided the necessary data, and with maintenance of his/her anonymity, he/she can give the social worker a mandate for this task. In the so-called ‘contractual’ notifi cation, if patients do not notify their contact persons within a certain time period, the social worker will get in touch with them. In contact tracing, there is a well-functioning cooperation between the net of units for care of STD patients and our centre in the tracing of the named contacts and in their treatment alike.
HIV Diagnostics
HIV diagnostics is performed at the Department of Hepatitis and Molecular Virology of the National Epidemiological Centre with Anti HIV Ab/Ag ELISA (BioMérieux) tests. In case of a positive result, a repeated test verifi cation is performed from a new blood sample at the International Reference HIV Laboratory of the Microbiological Research Group, National Epidemiological Centre (GENSCREEN HIV 1/2, MUREX HIV Ag/Ab, HIV UNI-FORM II. Ag/Ab, Inno-VIA HIV I./II. Score, Immunfl uorescence HIV 1, Genscreen Ultra HIV Ag–Ab).
Results
Syphilis
In our centre, we diagnosed 600 new infections of syphilis during 42,114 doctor–patient en-counters in 4 years. The incidence of syphilis among our patients in 2005, 2006, 2007 and 2008 were 1.6%, 1.4%, 0.85% and 1.96%, respectively. After a transient decrease in 2007, the number of patients with syphilis has been on the rise again.
The distribution, according to stages, is shown in Table 2.
Table 2 Our patients with syphilis, according to stage
Syphilis 2005 2006 2007 2008 Total
Syphilis connatal recent 1 2 3
Syphilis I. symptomatic 17 37 20 34 108
Syphilis II. symptomatic 10 35 20 57 122
Syphilis latent recent 96 82 58 96 332
Syphilis latent tardive 5 5 6 18 34
Neurosyphilis 1 1
Total 128 159 105 208 600
2010 ▪ Volume 4, Number 1 166 CEMED
CLINICAL STUDIES

Ninety-fi ve percent of patients were diagnosed in early, infectious stage during all 4 years; however, the number of those screened in early symptomatic stage varied, it was 21%, 45.3%, 38.1% and again 43.75% in 2005, 2006, 2007 and 2008, respectively. Of pa-tients with late syphilis, acquired more than 2 years earlier, we diagnosed 5 cases in 2005 and 2006 each, 6 cases in 2007 and 18 cases in 2008. We diagnosed one case of neurosyphilis in 2008 and no case affecting other internal organ systems or the cardiovascular system was seen during these 4 years.
We observed one patient with congenital syphilis in 2007 and two patients in 2008. During the 4 years, we screened no patient with congenital syphilis.
Table 3 shows the changes in the number of infections diagnosed during pregnancy and the number of safety treatments in pregnant women who had an infection of syphilis earlier and received appropriate treatment: we treated nine and eight pregnant women under hospital conditions in 2007 and 2008, respectively. Safety treatment was provided to seven and ten patients in 2007 and 2008, respectively.
In 2005 and 2006, merely a tenth of HIV screening examinations was constituted by those who applied for a voluntary screening; however, this rate increased to 16% and then 23% in 2007 and 2008 (Table 4).
Table 3 Patients diagnosed with syphilis during pregnancy; safety therapies
2007 2008
Safety therapy 7 10
Syphilis diagnosed during pregnancy 9 8
Table 4 Numbers of serological screening examinations performed at our STD centre from 2005 to 2008
2005 2006 2007 2008 Total
Recommended by a doctor
HIV 2,631 3,042 3,226 3,438 12,337
Syphilis 2,923 2,994 3,176 3,932 13,025
Total 5,554 6,036 6,402 7,370 25,362
Voluntary
HIV 4,835 4,523 4,251 3,005 16,614
Syphilis 437 469 679 684 2,269
Total 5,272 4,992 4,930 3,689 18,883
Total 10,826 11,028 11,332 11,059 44,245
CLINICAL STUDIES
CEMED 167 2010 ▪ Volume 4, Number 1
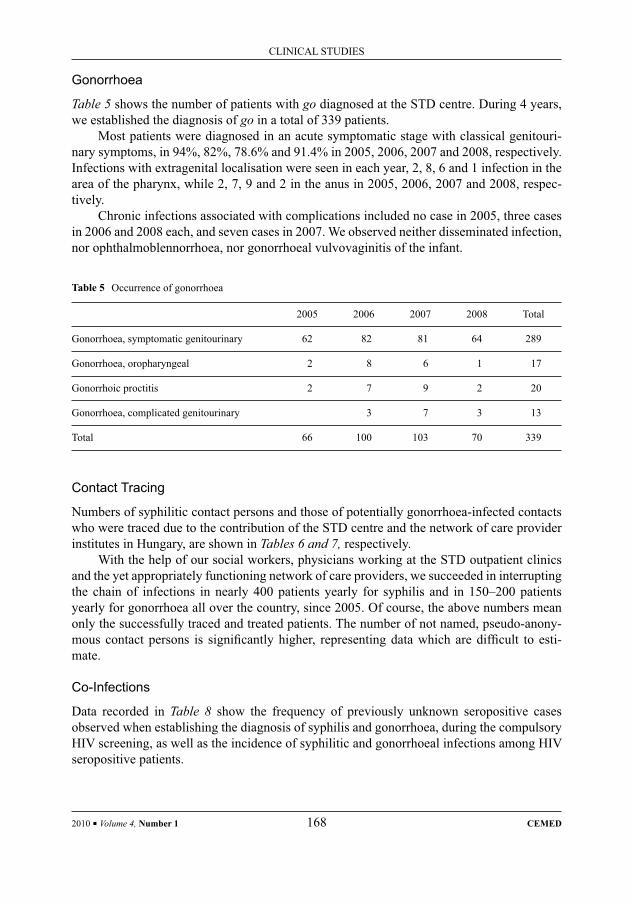
Gonorrhoea
Table 5 shows the number of patients with go diagnosed at the STD centre. During 4 years, we established the diagnosis of go in a total of 339 patients.
Most patients were diagnosed in an acute symptomatic stage with classical genitouri-nary symptoms, in 94%, 82%, 78.6% and 91.4% in 2005, 2006, 2007 and 2008, respectively. Infections with extragenital localisation were seen in each year, 2, 8, 6 and 1 infection in the area of the pharynx, while 2, 7, 9 and 2 in the anus in 2005, 2006, 2007 and 2008, respec-tively.
Chronic infections associated with complications included no case in 2005, three cases in 2006 and 2008 each, and seven cases in 2007. We observed neither disseminated infection, nor ophthalmoblennorrhoea, nor gonorrhoeal vulvovaginitis of the infant.
Table 5 Occurrence of gonorrhoea
2005 2006 2007 2008 Total
Gonorrhoea, symptomatic genitourinary 62 82 81 64 289
Gonorrhoea, oropharyngeal 2 8 6 1 17
Gonorrhoic proctitis 2 7 9 2 20
Gonorrhoea, complicated genitourinary 3 7 3 13
Total 66 100 103 70 339
Contact Tracing
Numbers of syphilitic contact persons and those of potentially gonorrhoea-infected contacts who were traced due to the contribution of the STD centre and the network of care provider institutes in Hungary, are shown in Tables 6 and 7, respectively.
With the help of our social workers, physicians working at the STD outpatient clinics and the yet appropriately functioning network of care providers, we succeeded in interrupting the chain of infections in nearly 400 patients yearly for syphilis and in 150–200 patients yearly for gonorrhoea all over the country, since 2005. Of course, the above numbers mean only the successfully traced and treated patients. The number of not named, pseudo-anony-mous contact persons is signifi cantly higher, representing data which are diffi cult to esti-mate.
Co-Infections
Data recorded in Table 8 show the frequency of previously unknown seropositive cases observed when establishing the diagnosis of syphilis and gonorrhoea, during the compulsory HIV screening, as well as the incidence of syphilitic and gonorrhoeal infections among HIV seropositive patients.
2010 ▪ Volume 4, Number 1 168 CEMED
CLINICAL STUDIES
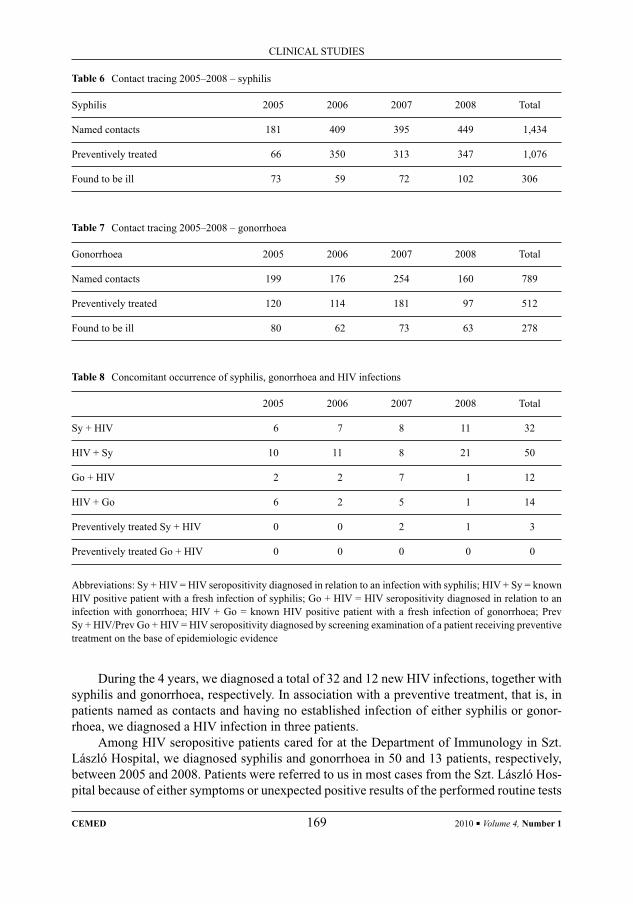
Table 6 Contact tracing 2005–2008 – syphilis
Syphilis 2005 2006 2007 2008 Total
Named contacts 181 409 395 449 1,434
Preventively treated 66 350 313 347 1,076
Found to be ill 73 59 72 102 306
Table 7 Contact tracing 2005–2008 – gonorrhoea
Gonorrhoea 2005 2006 2007 2008 Total
Named contacts 199 176 254 160 789
Preventively treated 120 114 181 97 512
Found to be ill 80 62 73 63 278
Table 8 Concomitant occurrence of syphilis, gonorrhoea and HIV infections
2005 2006 2007 2008 Total
Sy + HIV 6 7 8 11 32
HIV + Sy 10 11 8 21 50
Go + HIV 2 2 7 1 12
HIV + Go 6 2 5 1 14
Preventively treated Sy + HIV 0 0 2 1 3
Preventively treated Go + HIV 0 0 0 0 0
Abbreviations: Sy + HIV = HIV seropositivity diagnosed in relation to an infection with syphilis; HIV + Sy = known HIV positive patient with a fresh infection of syphilis; Go + HIV = HIV seropositivity diagnosed in relation to an infection with gonorrhoea; HIV + Go = known HIV positive patient with a fresh infection of gonorrhoea; Prev Sy + HIV/Prev Go + HIV = HIV seropositivity diagnosed by screening examination of a patient receiving preventive treatment on the base of epidemiologic evidence
During the 4 years, we diagnosed a total of 32 and 12 new HIV infections, together with syphilis and gonorrhoea, respectively. In association with a preventive treatment, that is, in patients named as contacts and having no established infection of either syphilis or gonor-rhoea, we diagnosed a HIV infection in three patients.
Among HIV seropositive patients cared for at the Department of Immunology in Szt. László Hospital, we diagnosed syphilis and gonorrhoea in 50 and 13 patients, respectively, between 2005 and 2008. Patients were referred to us in most cases from the Szt. László Hos-pital because of either symptoms or unexpected positive results of the performed routine tests
CLINICAL STUDIES
CEMED 169 2010 ▪ Volume 4, Number 1
of syphilis serology. (A single patient could acquire syphilis/gonorrhoea during the period of his/her care on more than one occasion so that the data show the incidence of syphilis and not the number of patients!)
DiscussionSyphilis and gonorrhoea are sexually transmitted diseases; any other means of their propaga-tion are rare. Risk factors for their acquisition include promiscuity, neglect of the barrier methods of protection, use of drugs, prostitution, or sexual contact with partners belonging to a risk group [1, 3, 4, 5].
Data on STD are very heterogeneous all over the world. The incidence of major bacte-rial and viral STIs is estimated to 125 million infections worldwide. In the United States of America, reported patients amount to 50–60% of the factual number of patients, and this rate is probably even worse in developing countries due to defi ciencies in screening system, care and data handling [1, 2, 6].
In developing countries, sexually transmitted infections are counted upon as one of the fi rst ten most frequent diseases in young men, while they attain the second place in young women. Although they represent only 25% of the sexually active population, young adults (the age group between 15 and 24 years) add up to approximately 50% of STD patients. Based on some data, approximately 1–5% of newborns in developing countries have a chance to develop neonatal ophthalmoblennorhoea complicated with subsequent blindness, and con-genital syphilis is the cause in 25% of the total perinatal mortality [3, 7].
The incidence of syphilis and gonorrhoea, together with other STDs, shows an increas-ing trend worldwide, particularly in the developing countries. In the developed countries, the incidence of both diseases decreased after World War II up to the end of the 50s, and after a transient elevation (60s and 70s), it decreased again just until recently [1, 7].
Among men, there were 3.8/100,000 and 5.1/100,000 cases of syphilis, whereas in women, the corresponding numbers were 1.1/100,000 and 0.9/100,000 in 2002 and 2005, respectively, all over the world. In general, 12 million new infections are diagnosed yearly worldwide [7].
At the beginning of the 90s, syphilis epidemic started practically from the area of the former member states of the Soviet Union and then it spread slowly towards Western Europe. In Russia, the prevalence of syphilis in 1996 was 61 times higher than in 1989, corresponding to the prevalence after World War II. In Romania and Bulgaria, the number of syphilis cases, including the number of cases of congenital syphilis, has seen an explosive [1, 7, 8, 9] in-crease.
The epidemic reached Western Europe after 1995. In this year – with the exception of Germany – only a total of 300 infections were reported, and even these were mostly imported from countries outside the European Union. Since 1996, however, the incidence of syphilis has shown a gradual rise both in Northern and Western European countries [3].
In the United States, the incidence of syphilis continuously decreased until the end of the 90s, the lowest number of cases reported ever (since 1941) was observed in 2000. From 2001, however, a rise was observed again, mostly among young men, but also in women [1, 6, 8].
2010 ▪ Volume 4, Number 1 170 CEMED
CLINICAL STUDIES

In Hungary, the number of syphilis cases signifi cantly decreased up to the end of the 80s as a result of the epidemiological measures taken in the 1950s and the introduction of com-pulsory penicillin treatment. The number of patients with syphilis was less than 100 per year between 1955 and 1964, and below 10 per year between 1959 and 1963 (except 1961). 1989 was the last year with fewer than 100 cases observed. From 1990 onwards, the incidence of syphilis infections has shown a gradual increase: in 1992, the number of reported infections was already 205. After a transient fall in 1993 (142 cases), a slow rise could be observed from 1994 onwards (1994: more than 200, 1997: more than 300 cases) [8].
From the end of the 90s, the Hungarian data refl ect the trend observed worldwide. We could see a slow decrease until 2004 and stagnation since 2005 in the data of syphilis: with the exception of 2007, more than 500 fresh infections were diagnosed in the whole country in each year. In 2008, the number of cases at the outpatient clinics of our department has doubled, but – in spite of the expectations – this was not followed by a parallel rise in the number of cases concerning the whole country (Table 9) [8–10].
Table 9 Number of patients with syphilis in Hungary compared to the number of patients seen at our STD centre
2005 2006 2007 2008 Total
Hungary, total 545 561 405 560 2,052
STD centre 128 159 105 208 600
% 45 31 26 38.5
Patients with syphilis in early symptomatic state attend the outpatient clinics of our de-partment in large numbers. On the one hand, this indicates an improvement of both the screening system and the cooperation and awareness of the profession and the associate pro-fessions, and even the patients, and on the other hand, it results in an early interruption of the chain of infections.
In parallel with the above, the number of voluntarily requested screening examinations has also increased, indicating that the potential risk of syphilis infection became a part of common knowledge.
Together with the rising number of patients with syphilis, also an increase of cases diag-nosed during pregnancy, as well as newborns with congenital syphilis, is to be expected. Congenital syphilis is considered as one of the best epidemiological indicators of the disease. According to WHO data, syphilis affects approximately 1 million pregnancies per year worldwide. This means practically 270,000 cases of congenital syphilis, 460,000 abortions or perinatal deaths and 270,000 premature births or newborns with low birth weight [1, 7, 11].
In Hungary, there was no congenital syphilis from 1978 until 1994. Both in 1994 and 1996, three early cases of congenital syphilis each were observed, all in foreigners and from pregnancies without prenatal care. Since 1994, however, almost in every year, a case was observed in Hungary. In 2007 and 2008, we observed 1 and 2 cases, respectively, at our out-patient clinics [8].
CLINICAL STUDIES
CEMED 171 2010 ▪ Volume 4, Number 1

Table 10 Incidence of gonorrhoea in Hungary compared to the number of patients seen at our STD centre
2005 2006 2007 2008
Hungary 851 916 1,042 928
STD centre 68 100 103 70
% 8 11 10 7.5
Performance of screening examinations within prenatal care in order to prevent cases with syphilis is compulsory only in the fi rst trimester of pregnancy. Later during the preg-nancy, however, the mother may acquire a fresh infection of syphilis, or the non-specifi c screening examination performed in a patient with very recent infection may yet be negative indicating no infection [11].
Based on the data of our STD centre, neither the number of congenital syphilis cases nor that of cases during pregnancy showed an increase in spite of the growing number of infec-tions, representing excellent data from an epidemiological aspect.
The worldwide incidence of go was 123/100,000 in 1997 and 115.6/100,000 in 2005. In Europe, the incidence of the infection began to rise at the end of the 90s: in the countries of Western Europe, in Great Britain and in Austria, the number of reported cases doubled between 1996 and 2001. In Ireland, the number of reported patients increased by 320% dur-ing that time [9]. In the United States, approximately, 600,000 new infections per year have been diagnosed; the prevalence of the disease showed a decrease of 74% between 1975 and 1997; since 2005, the prevalence is slowly growing and the male–female ratio is slowly shift-ing in favour of women [1, 6].
Concomitantly with the spreading of go, a new problem has come to the fore, namely, the appearance of Neisseria gonorrhoea strains resistant to quinolones and azithromycin. Identifi cation of these constitutes one of the bases for eliminating the disease.
In Hungary, a continuous decrease was seen from 1952. The morbidity of go calculated to 100,000 inhabitants was 43.2 in 1989 and 12.3 in 1999 [9]. Since 2005, the incidence of go in Hungary, including also at our STD centre, shows stagnation; a maximum of 1,000 cases per year have been reported all over the country (Table 10). When reviewing the pa-tients of our STD centre, we see that we continued to succeed in diagnosing most of them in an early symptomatic stage. Acquisition of the disease may occur via only extragenital co-itus; this way of transmission was seen in 20% of our cases yearly. Nevertheless, we diag-nosed no haematogenic dissemination and only a small number of chronic infections [10].
One of the bases for interrupting the chain of infections is a successful tracing of contact persons. The sexual partners of the so-called index patient who became infected with an STD include, in part, the so-termed source of infection transmitting the disease, and, in part, po-tentially infected individuals, the so-called at-risk contacts. We reveal them, summon them to appear and provide them with either a complete therapy or – those with an asymptomatic clinical picture – a preventive treatment. This process is essential for the interruption of the
2010 ▪ Volume 4, Number 1 172 CEMED
CLINICAL STUDIES
chain of infections. Information and education of persons involved in contact tracing, that is, primary prevention, also plays an important role [2, 4, 12].
Contact tracing is a special activity which requires great empathy and a multifaceted professional knowledge. Patients often feel compelled to conceal the truth due to human frailty, fear of being stigmatised and becoming an outcast or because they are concerned about their family, job or social status. We can break through the strong social and moral bar-riers very diffi cultly only by personal persuasion and prolonged counselling [12, 13]. With the help of our social workers, physicians working at the STD outpatient clinics and the yet appropriately functioning network of care providers, we succeeded in interrupting the chain of infections in nearly 400 patients yearly for syphilis and in 150–200 patients yearly for gonorrhoea all over the country, since 2005.
An estimated 60% of patients with STD also carry another sexually transmitted infec-tion concomitantly. The association of HIV with other STIs has a special signifi cance, as they may mutually affect the outcome of the diseases. In recent years, a strikingly increased num-ber of concomitant syphilis and HIV infections could be observed among our patients as well [1, 14].
The behavioural disease characteristics of STIs are readily demonstrated by the acquisi-tion of fresh syphilis/gonorrhoea in known and treated HIV-positive patients in 63 cases. This calls the attention to the fact that these patients continue their promiscuous lifestyle and omit the use of barrier methods of protection [2, 13]. Based on the currently valid guidelines, the performance of HIV screening examination is compulsorily recommended in patients with freshly diagnosed syphilis or gonorrhoea and in their contacts. Thanks to the routinely per-formed screening examination, we observed HIV seropositivity in 44 cases at our outpatient clinics between 2005 and 2008 [15].
ConclusionSTD diseases have special signifi cance not only from the point of view of health care but also from social aspects. In addition to their epidemiological importance, their late sequels and complications have to be underlined. Early complications include infertility, abortion, prema-ture delivery and chronic infections, but the development of tumours (HPV, HSV) observed as late complications and the occurrence of incurable neurological and ophthalmologic com-plications or systemic symptoms affecting other organ systems, bear the same importance.
Diagnostics and therapy of the classical sexually transmitted diseases was solved at the beginning of the twenty-fi rst century. In spite of this development, the number of STIs shows an increasing trend not only in Hungary but also worldwide. The developing complications could all be prevented and treated; nevertheless, we will expectedly see them in an increasing number, not only we, specialists of dermatology and venereology, but also professionals be-longing to any of the other medical specialities.
Through this paper, we would like to call attention to the fact that the problem of ve-nereological diseases, long forgotten and thought to be solved, is continuing to be actual and it may even expectedly be more prominent in the future.
CLINICAL STUDIES
CEMED 173 2010 ▪ Volume 4, Number 1
ReferencesDa Ros, C. T., Schmitt, S.: [1] Global epidemiology of sexually transmitted diseases. Asian J. Androl., 2008, 10, 110–114.Kálmán, E., Király, K., Kovács, L.: [2] The problematic of antivenereal fi ght (in Hungarian). Népegészségügy, 1954, 12, 309–320.Fenton, K., Breban, R., Vardavas, R. et al.: [3] Infectious syphilis in high income settings in the 21st century. Lancet Infect. Dis., 2008, 8, 244–253.Várkonyi, V., Tisza, T., Podányi, B. et al.: [4] The variable manifestations of syphilis (in Hungarian). Bőrgyógy. Venerol. Szle., 1999, 75, 61–67.Együd, K., Varga, V.: [5] Syphilitis infection of children in the consequence of mother milk nutrition (in Hun-garian). Gyermekek STD Gen. Infekt., 2008, 2, 11–18.Weinstock, H., Berman, S., Cates, W. Jr.: [6] Sexually transmitted diseases among American youth: incidence and prevalence estimates, 2000. Perspect. Sex. Reprod. Health, 2004, 36, 6–10.Adler, M.: [7] Sexually transmitted diseases control in developing countries. Genitourin. Med., 1996, 72, 83–88.Berecz, M., Várkonyi, V., Horváth, A.: [8] The epidemiological trends of syphilis in Hungary on the basis of mor-bidity in 1997 (in Hungarian). Magy. Venerol. Arch., 1998, 2, 95–103.Várkonyi, V., Dudás, M., Kaszás, K. et al.: [9] Sexually transmitted diseases after the turn of millennium in Hun-gary (2000–2007) (in Hungarian). STD Gen. Infekt., 2008, 4, 158–166.EPINFO, Epidem. Inform. Weekly (in Hungarian), 2009, [10] 16, 3–13.Walker, J. A.: [11] A continuing but neglected problem. Semin. Fetal Neonatal. Med., 2007, 12, 198–206.Trelle, S., Shang, A., Nartey, L. et al.: [12] Improved effectiveness of partner notifi cation for patients with sexually transmitted infections: systematic review. Br. Med. J., 2007, 334, 354.Karp, G., Schlaeffer, F., Jotkowitz, A. et al.: [13] Syphilis and HIV co-infection. Eur. J. Intern. Med., 2009, 20, 9–13.Várkonyi, V.: [14] STD atlas to the medical praxis (in Hungarian). Medicina Könyvkiadó Zrt., Budapest, 2006.Guideline for the investigation and treatment in sexually transmitted infections (in Hungarian). Egészségügyi [15] Köz löny, 2002, 52, 1509–1518.
2010 ▪ Volume 4, Number 1 174 CEMED
CLINICAL STUDIES

Whipple’s Disease: Do We Think of It Enough?TÜNDE FISCHER1, MÁRTA TIBOLY1, PÉTER TÓTH1, MÁRIA SZENES1,
ZOLTÁN VÖLGYI1, OTÍLIA BALI2, BEÁTA GASZTONYI1
1Department of Medicine, Hospital of Zala County, Zalaegerszeg, Hungary2Department of Pathology, Hospital of Zala County, Zalaegerszeg, Hungary
Whipple’s disease is a chronic, systemic, relapsing bacterial illness, which always has a fatal outcome without treat-ment. It represents a signifi cant diagnostic challenge for both clinicians and pathologists. In 80% of cases, the dis-ease affects middle-aged white men belonging to the Caucasian race. Case report: The authors present three cases and review the aetiology, clinical features, presumed pathomechanism and the possibilities of treatment. Conclu-sion: Several immunologic mechanisms underlying Whipple’s disease have emerged, but their primary or secondary nature has not yet been elucidated. First of all, this is a gastrointestinal disease; however, extraintestinal symptoms may often precede fi nal diagnosis by several years. The histological hallmark for the diagnosis is the presence of numerous macrophages in the duodenal mucosa showing periodic acid – Schiff (PAS)-positive inclusions as well as polymerase chain reaction. The choice of antibiotics and the duration of therapy are empirical, but in most cases, there is an immediate response to the treatment. Relapses are common, particularly in patients with central nervous system involvement.
Keywords: Whipple’s disease, malabsorption syndromes, lymph node enlargement, positive PAS stain
Abbreviations
AIDS = acquired immunodefi ciency syndrome; CNS = central nervous system; CRP = C-reactive protein; CT = com-puter tomography; ESR = erythrocyte sedimentation rate; IFN = interferon; IL = interleukin; ITP = idiopathic throm-bocytopenic purpura; PAS = periodic acid – Schiff; PCR = polymerase chain reaction; pro-BNP = N-terminal pro-hormone brain natriuretic peptide; Plt = platelet; TNF = tumour necrosis factor; US = ultrasound
Whipple’s disease is a chronic, systemic illness caused by the Tropheryma whipplei bacteri-um. Typically, it presents itself in the form of diarrhoea, weight loss and abdominal pain, but in 80% of patients, it begins with recurring arthropathy, lymph node enlargement, fever and hyperpigmentation of the areas exposed to sunlight. The latter symptoms may precede the establishment of diagnosis by even a decade. The clinical picture may be modulated further by the infl ammation of serous membranes as well as peripheral and central nervous system (CNS) disorders [1]. On account of the non-specifi c, far-fl ung symptoms, the diagnosis may be extremely diffi cult. Classical hallmarks for the diagnosis include periodic acid – Schiff (PAS) staining of samples obtained by intestinal biopsy as well as demonstration of the pathogen by polymerase chain reaction (PCR). Its therapy is empirical, and usually, there is an immediate response to the treatment. In this article, we present the cases of three patients and a review on the epidemiology, various symptoms and pathomechanism of Whipple’s disease, on the maze of establishing the diagnosis and the possibilities of treatment.
Corresponding address: Tünde Fischer MD, Zrínyi M. str. 1, H-8900 Zalaegerszeg, Hungary.E-mail: fi [email protected]
28668
CASE REPORTS
CASE REPORTS
DOI: 10.1556/CEMED.4.2010. 175 2010 ▪ Volume 4, Number 1 ▪ 175–185.

Case Reports
Case 1
The history of the 58-year-old male patient includes diabetes mellitus controlled by oral hy-poglycaemic agents and hypertension. In January 2007, his examination began in another institute because of diarrhoea, weight loss of 15 kg in 6 months and anorexia. The laboratory tests showed moderate microcytic, hypochromic anaemia and thrombocytosis, and the ab-dominal ultrasonography showed a negative result. The thoracic X-ray examination demon-strated moderate cardiomegaly as well as some pleural fl uid in the left sinus. The performed gastroscopy and colonoscopy described duodenitis and diverticulosis, respectively. In Febru-ary 2007, the performed abdominal computer tomography (CT) showed splenomegaly, ab-normal retroperitoneal, mesenteric, and bilateral inguinal lymph nodes. No lymphadenom-egaly was depicted by the thoracic CT.
After that, the patient was admitted to the haematological unit of our department with the above fi ndings, in a prostrate condition. Examinations performed in order to clear up the origin of lymphadenomegaly – CT-directed abdominal core biopsy, axillary lymphadenec-tomy – have demonstrated epitheloid cell granuloma. Iliac crest biopsy was performed; no abnormality could be observed in the bone marrow by evaluation of fl ow cytometry and bone cylinder; and the chromosome analysis produced a negative result. Serologic tests for toxoplasma, Epstein–Barr virus and cytomegalovirus and immuno-serological examinations (anti-nuclear factor, double-stranded DNA) revealed no alteration. In the meantime, a febrile state developed, the thoracic X-ray examination described an underlying pneumonia, and in addition to the above, an elevated erythrocyte sedimentation rate, hypalbuminaemia, an ele-vated C-reactive protein (CRP) level, severe hypocalcaemia and moderate azotaemia could be observed. His fever ceased upon antibiotic therapy. We were compelled to give a transfu-sion because of the developing signifi cant anaemia, and to administer parenteral potassium supplementation for the severe potassium defi ciency of the patient who had become cachec-tic. The patient’s condition and laboratory results showed a transient improvement, and, therefore, we decided for his further observation.
In November 2007, after almost a year of tribulations, we took a stand in favour of a repeated gastroscopy with regard to the deteriorating general condition and the renewed, in-creasing anaemia of the patient. During the examination, we saw islet-like atrophy and hae-morrhagic imbibition of the mucous membrane in the segments of the bulb and the descend-ing part of the duodenum that could be examined. The histological examination showed in the lamina propria, in addition to infl ammatory infi ltration, a great number of macro-phages with foamy cytoplasm which, placed next to each other, fi lled the lamina propria in an almost cobblestone-like way (Fig. 1A). After having consulted with the pathologist, we gave the opinion on the case as Whipple’s disease, and initiated prolonged sulfamethoxazole–trimethoprim therapy.
In January 2008, colonoscopy was performed in order to complete the examinations and it showed terminal ileitis (histology: chronic non-specifi c infl ammation) and proctosig-moiditis. No abnormity suggesting any neurological manifestation was found during exami-nation by a specialist of neurology. A specialist of psychiatry described no demential process; however, the possibility of organic cerebral affection emerged because of a discrepancy be-tween the results of the verbal and performance parts of the tests. In order to elucidate the
2010 ▪ Volume 4, Number 1 176 CEMED
CASE REPORTS
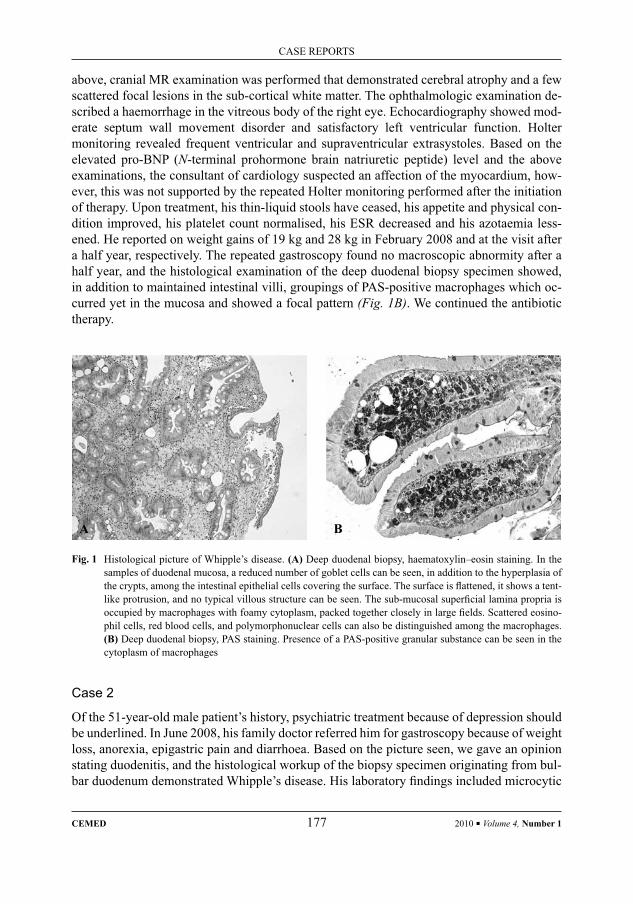
above, cranial MR examination was performed that demonstrated cerebral atrophy and a few scattered focal lesions in the sub-cortical white matter. The ophthalmologic examination de-scribed a haemorrhage in the vitreous body of the right eye. Echocardiography showed mod-erate septum wall movement disorder and satisfactory left ventricular function. Holter monitoring revealed frequent ventricular and supraventricular extrasystoles. Based on the elevated pro-BNP (N-terminal prohormone brain natriuretic peptide) level and the above examinations, the consultant of cardiology suspected an affection of the myocardium, how-ever, this was not supported by the repeated Holter monitoring performed after the initiation of therapy. Upon treatment, his thin-liquid stools have ceased, his appetite and physical con-dition improved, his platelet count normalised, his ESR decreased and his azotaemia less-ened. He reported on weight gains of 19 kg and 28 kg in February 2008 and at the visit after a half year, respectively. The repeated gastroscopy found no macroscopic abnormity after a half year, and the histological examination of the deep duodenal biopsy specimen showed, in addition to maintained intestinal villi, groupings of PAS-positive macrophages which oc-curred yet in the mucosa and showed a focal pattern (Fig. 1B). We continued the antibiotic therapy.
Case 2
Of the 51-year-old male patient’s history, psychiatric treatment because of depression should be underlined. In June 2008, his family doctor referred him for gastroscopy because of weight loss, anorexia, epigastric pain and diarrhoea. Based on the picture seen, we gave an opinion stating duodenitis, and the histological workup of the biopsy specimen originating from bul-bar duodenum demonstrated Whipple’s disease. His laboratory fi ndings included microcytic
Fig. 1 Histological picture of Whipple’s disease. (A) Deep duodenal biopsy, haematoxylin–eosin staining. In the samples of duodenal mucosa, a reduced number of goblet cells can be seen, in addition to the hyperplasia of the crypts, among the intestinal epithelial cells covering the surface. The surface is fl attened, it shows a tent-like protrusion, and no typical villous structure can be seen. The sub-mucosal superfi cial lamina propria is occupied by macrophages with foamy cytoplasm, packed together closely in large fi elds. Scattered eosino-phil cells, red blood cells, and polymorphonuclear cells can also be distinguished among the macrophages. (B) Deep duodenal biopsy, PAS staining. Presence of a PAS-positive granular substance can be seen in the cytoplasm of macrophages
A B
CASE REPORTS
CEMED 177 2010 ▪ Volume 4, Number 1

anaemia; the thoracic X-ray examination described a discrete pleural callus in the apex of the right lung and the abdominal ultrasonography showed hepatosplenomegaly and a little amount of ascites. We began treating the patient with sulfamethoxazole–trimethoprim and started the examinations for extraintestinal manifestations. The patient did not show up for the recommended follow-up examination even after being summoned.
Case 3
The 59-year-old female patient was under haematological care because of idiopathic throm-bocytopenic purpura since 1996, and she received rheumatologic treatment because of recur-ring complaints related to her joints for years. She lost 27 kg since 2005. In April 2008, her examination began because of increased swelling of her joints, epigastric pain of a burning nature and loose stools. Her laboratory results showed leucocytosis as well as thrombocyto-sis; practically no autoimmune disease underlying her articular complaints was demonstrat-ed. Her abdominal ultrasound examination found no organic abnormity, and the patient gave no consent to the recommended gastroscopy. Hyperacidity and gastro-oesophageal refl ux disease was thought to underlie her complaints, and they introduced H2 receptor blocker therapy. In October 2008, she was hospitalised because of profuse diarrhoea. Supposing in-fectious origin against the background of her complaints, they started ex iuvantibus cipro-fl oxacin treatment, but the faecal culture produced a negative result. After a transient im-provement, her condition deteriorated again. Her laboratory results showed hypalbuminaemia, elevated CRP, differential blood count shifted to the left, microcytic anaemia and severe iron defi ciency. Regarding that the patient later gave her consent to being examined endoscopi-cally only under general anaesthesia, we performed these examinations in November 2008. Oedema, patchy erosions and atrophy of the duodenal mucosa could be seen during gastro-duodenoscopy (Fig. 2), and the histology demonstrated Whipple’s disease. We began treating the patient with sulfamethoxazole–trimethoprim (Fig. 3), and started the examinations for extraintestinal manifestations. Abdominal ultrasonography, thoracic X-ray examination, echocardiography as well as neurological specialist examination demonstrated no substantial alteration, and the ophthalmologic examination showed no abnormity.
DiscussionWhipple’s disease is a chronic, systemic, relapsing bacterial illness. References to its signs and symptoms can be found already in publications from the end of the nineteenth century (Allchim and Kebb, 1895). In 1907, George Whipple described the case of a 36-year-old physician who suffered from diarrhoea, arthralgia and bronchitis for more than 5 years, until his death. During the autopsy, Whipple found an infi ltration by foamy macrophages and ap-position of fatty drops in the duodenal mucosa, and he supposed a probable disorder of lipid metabolism underlying the disease. He named the disease intestinal lipodystrophy. In the subsequent 50 years, the diagnosis was based on clinical features, and then, PAS-positivity of the macrophages has become a histological criterion since 1949. The bacterial origin of the disease was clearly demonstrated by an electron microscopic examination in 1960. Attempts to culture the bacterium were unsuccessful for years, and fi nally, the pathogen was isolated initially from a cardiac valve in 1997. Its culture was accomplished in the cells of anterior
2010 ▪ Volume 4, Number 1 178 CEMED
CASE REPORTS

pituitary a few years later, in 2000. The complete gene structure has been described in 2003 [2]. In Hungary, the role of the following should be emphasised: Tamás Beró reported the fi rst diagnosed human case, Zsolt Barta gathered immunopathological knowledge on the disease, and János Gaál collected its musculoskeletal aspects [3].
Characteristics of the Bacterium
The disease is caused by a Gram-positive bacterium, T. whipplei. The pathogen has an atypi-cal morphology, it becomes incorporated in the macrophages, but it can be found in an extra-cellular localisation as well. Its shape reminds to a short rod, it is 0.3 μm wide and 2 μm long. It gives a positive reaction with PAS staining. The latter also constitutes a base for the diag-nosis. In vitro, the bacterium’s multiplication takes place in an acidic medium (pH 5) that may reduce the effi cacy of treatment by inhibiting the effect of certain antibiotics. The bacte-rium shows genetic heterogeneity. Genetic variants are bound to the habitat of patients and show geographic differences. No relationship between genotypes of different variants and symptoms of illnesses caused by them has been elucidated as yet. Some of them are not pathogenic; others cause typical Whipple’s disease, while some genotypes may induce an
Fig. 2 Endoscopic picture of Whipple’s disease. Islet-like atrophy and haemorrhagic imbibition of the postbulbar duodenal mucosa can be seen macroscopically
Fig. 3 Post-treatment macroscopic picture of Whipple’s disease
CASE REPORTS
CEMED 179 2010 ▪ Volume 4, Number 1

atypical clinical picture such as endocarditis. Although there is no known source of the infec-tion, the bacterium seems to be ubiquitous. It has already been detected from sewage-water and human faeces which may imply that the bacterium gets to the environment with human stool and then returns to the body with the drinking water. However, the role of humans as host could neither be proven nor excluded. The bacterium’s DNA has been detected from the saliva (in 35%), gastric juice (in 11.4%) and duodenal mucosa (in 4.8%) of symptom-free individuals. It is questionable whether we may consider such cases as refl ecting the non-pathogen variant of the bacterium, symptom-free carrier or early stage of the disease [4].
Incidence
The disease affects primarily white, Caucasian, rural men, and the average age is 50 years. Its incidence is less than 0.1% [5], it occurs in men eight times more frequently than in women. Each year, 0–12 cases are published in the international literature, and the known reported cases amount to less than 1,000. It occurs in childhood sporadically. In spite of the ubiquitous nature of the bacterium, the disease is quite rare. An explanation for this should be sought for in the impairment of cellular and humoral immunity. Several alterations of the immune sys-tem can be observed in patients with Whipple’s disease, but whether these changes are pri-mary or they can be considered as consequences of the already existing infection, has not yet been elucidated. Nevertheless, it is presumed that immune defects predispose to the develop-ment of the disease, and these are probably specifi c to the pathogen T. whipplei, as these pa-tients show no increased susceptibility to other diseases in comparison to the general popula-tion. The differences in distribution according to geographic location, ethnic status and gender as well as the more frequent presence of HLA-B27 antigen in patients suffering from the disease (it can be detected in 8% of the general population and in 26% of Whipple pa-tients) suggest congenital or acquired defi ciency of cellular and humoral defence. However, the pattern of age distribution, the lack of other infections and the absence of familial accu-mulation are inconsistent with the role of an immunologic disorder [4].
Immunologic MechanismThe primary site for the pathogen to colonize is in the small bowel what makes an oral route of infection likely. From the intestinal lumen, the bacteria migrate to the epithelial cells and then into the basal layer of the mucosa, they cross the basal membrane and activate the mac-rophages. According to some studies, cutaneous anergy and decreased macrophage function can be observed in the infected patients. The latter means a disorder affecting both phagocy-tosis and breakdown of the organism that underwent phagocytosis. The number of circulating cells expressing CD 11b decreases in both active and inactive infections. This molecule pro-motes phagocytosis of microbes, it plays a role in antigen processing and it mediates the in-tracellular killing processes induced by interferon (IFN)-γ. The decreased expression of CD 11b is accompanied by a decreased production of interleukin (IL)-12, IL-2 and IFN-γ at an increasing production of IL-4 and IL-10. Finally, the process results in pathological phagocy-tosis and intracellular degradation of T. whipplei [6]. A presumed role of immunological fac-tors in the development of the disease is also supported by cases where patients receive im-munosuppressive therapy because of their years-long arthralgia, and in a short time (within
2010 ▪ Volume 4, Number 1 180 CEMED
CASE REPORTS

2–4 months), the treatment is followed by diarrhoea and the disease shows rapid progression. The phenomenon cannot be observed in patients who receive no treatment for their arthralgia or are treated with non-steroidal anti-infl ammatory drugs (NSAIDs). In patients receiving immunosuppressive therapy, an endoscopic examination is performed usually in a short time because of severe diarrhoea and soon it may lead the treating physician to a diagnosis [6]. In patients whose arthralgia was treated with no immunosuppressive drugs, usually 63–86 months elapse between the appearance of joint pains and the diagnosis of Whipple’s disease. Of the different immunosuppressive drugs, corticosteroids cause the most rapid deterioration in patients’ condition; diarrhoea presents itself after an average of 2 months. The mechanism is not known exactly, but there is probably an increased translocation of bacteria from the lumen into the sub-mucosa due to the immunosuppressive therapy, eliciting an infl ammatory response and diarrhoea [6]. A role for immunological factors can also be deduced from the report of Kneitz et al. who presented a case where the patient received infl iximab therapy because his long-lasting, febrile, chronic arthropathy was thought to be Still’s disease. The treatment caused a rapid deterioration in the patient’s condition, and abrupt weight loss, ery-thema nodosum, diarrhoea, progressive lymphadenomegaly and sigmoido-vesical fi stula de-veloped. The treatment against tumour necrosis factor (TNF)-α accelerated the natural course of the disease extremely and it made possible the rapid propagation of T. whipplei in the pa-tient’s body. The authors recommended the examination of intestinal biopsies for T. whipplei in all cases where TNF-α inhibitor therapy would be planned because of a rheumatic disease or Crohn’s disease [7].
Clinical Course
General Features
The clinical appearance of the disease is non-specifi c, it is characterised by a multiplicity of affected organs. Suspicion of the disease may emerge because of the symptom triad of weight loss, chronic diarrhoea and arthralgia. Its probability is particularly high in a patient with prolonged, intermittent fever associated with lymphadenopathy. In addition to the above signs and symptoms, abdominal pain, neurological disorders and pigmentation of the skin may also occur. Impairment of enterocytes is responsible for symptoms of malabsorption. The frequently observed anaemia can be traced back to disordered vitamin B12 and iron ab-sorption, occult gastrointestinal haemorrhages and chronic infl ammation. Thrombocytosis or thrombocytopenia may occur alike. Diseased bowels and lymphatic vessels cause protein loss, hypalbuminaemia and oedema. Low cholesterol levels and defi ciency of vitamins (B12, D, K and folic acid) are characteristic; non-specifi c alterations may include an elevated CRP level and lymphocytopenia. Eosinophilia and abnormities of serum immunoglobulin levels have also been reported [6]. Initially, the clinical picture resembles chronic intestinal infl ammation with colicky abdominal pain and occult intestinal haemorrhage. In addition to the intestinal one, oesophageal, gastric, colic and hepatic affection can also be observed [4] rarely. Bacteria and infl ammatory cells, primarily macrophages, infi ltrate the mucosa and cause obstruction in mesenteric lymph nodes. The enlarged abdominal lymph nodes may also raise the suspicion of a neoplasm. Weight loss is gradual, 5–15 kg in a year. Cachexia devel-ops in untreated cases [4].
CASE REPORTS
CEMED 181 2010 ▪ Volume 4, Number 1
Affected Organs
Arthropathy
Intermittent fever and arthralgia are the most common symptoms (in 73%) preceding the di-agnosis [8]. Prior to the appearance of diarrhoea, patients often receive rheumatologic treat-ment for years. The infl ammatory nature of the affection of joints is typical. The arthralgic complaints follow an intermittent, migrating pattern; they cause no deformation and affect mostly the great joints with no radiological alteration. Complaints relating to the joints usu-ally recede after the appearance of gastrointestinal symptoms. PAS-positive macrophages and bacteria can be detected from the synovial fl uid [4].
Signs and Symptoms Relating to the Skin
Pigmentation at skin areas exposed to sunlight occurs in some patients.
CNS
In Whipple’s disease, the CNS is affected by 5–50%. The typical triad of CNS manifestation includes progressive dementia, myoclonus and ophthalmoplegia. This triad can be observed in 10% of patients. The picture may be modifi ed by decreased cognitive function, disordered consciousness, disordered eye movements, nystagmus, ataxia, polydipsia, hyperphagia, al-tered libido and disordered sleep. The latter symptoms suggest hypothalamic affection that occurs in 31% of patients with CNS manifestations. Sleep disorders may also persist for months after a successful therapy. Based on the report of Papadopoulou, treatment with 600 mg/day carbamazepine may be effective [9]. Nervous system symptoms may occur al-ready at the beginning of the disease, but more frequently, they appear during or after therapy, in the period of clinical relapse. Progressive nervous system disease occurring after success-ful treatment of intestinal symptoms usually has a fatal outcome. According to some publica-tions, Whipple’s disease may increase the risk of stroke, primarily in consequence of the fi -brosis induced in arteries and arterioles. It deserves attention, however, that the occurrence of stroke usually coincides with the period of generalisation of the disease. Systemic infl amma-tion probably impairs complement production, affects the coagulation cascade and signifi -cantly increases the risk of thrombosis. The bacteria, after having entered the brain via the circulating blood, cause vasculitis which also increases the possibility of an ischemic or hae-morrhagic infarction [5]. If an antibiotic that cannot penetrate the blood–brain barrier is used in patients with CNS manifestations, viable bacteria may survive in the cerebrospinal fl uid, causing relapse of the disease [6].
Ocular Symptoms
Uveitis, vitreitis, keratitis, retinitis and retrobulbar neuritis are rare manifestations of the disease. They are usually associated with enteral and CNS disease and may cause consequen-tial retinal haemorrhage and oedema of the optic disc.
2010 ▪ Volume 4, Number 1 182 CEMED
CASE REPORTS

Cardiovascular System
Cardiovascular manifestations occur in a third of patients with Whipple’s disease. Endocardi-tis, myocarditis or pericarditis may appear relatively rarely. Myocardial affection may mani-fest itself clinically in the form of cardiac failure usually caused by regurgitation due to a defect of cardiac valves. In general, it shows the clinical picture of an endocarditis of non-infectious origin (thickening and deformation of mitral and aortic valves), but it may cause adhesive pericarditis, myocardial fi brosis and aspecifi c electrocardiographic alterations as well.
Pulmonary Lesions
Pulmonary manifestations may appear in 13% of patients with dry cough and signs of pleural irritation. The radiological picture shows pulmonary infi ltration or development of pleural fl uid. Enlargement of peripheral and mesenteral lymph nodes is common in patients with Whipple’s disease; the mediastinal lymphoid region is rarely affected. The lymphadenom-egaly cannot be differentiated from other reactive processes and infl ammatory diseases, sar-coidosis or lymphomas by physical or imaging examination. The common hydrothorax is a consequence of the infl ammation of serous membranes.
DiagnosisIn case of clinical suspicion, gastroscopy is the examination of fi rst choice. Endoscopy has an important role both in establishing the diagnosis and in the follow-up. In accordance with the recommendations in the literature, samples should be taken by biopsy from the proximal and distal duodenum as well as from the proximal jejunum. Macroscopically, yellowish white, occasionally erythematous erosions, plaques can be seen on the intestinal mucosa. As a result of antibiotic therapy, these lesions disappear in weeks or months, but the PAS-positive reac-tion may remain for several months [6]. Despite the characteristic endoscopic picture, sample taking is mandatory because the diagnosis is based on the histological examination. By light microscope fatty drops, lymphangiectasia and infi ltration by macrophages can be seen. The cytoplasm of macrophages seems foamy by haematoxylin–eosin staining, and PAS staining makes the granules visible. The reaction detects the glycoprotein content of T. whipplei. As PAS-positive inclusions seen in the macrophages may also suggest other infections (My-cobacterium avium, Rhodococcus equi, Bacillus cereus, Corynebacterium, Histoplasma, or fungi), it is recommended to confi rm the diagnosis also by another method (electron micro-scope, immunohistochemy, or PCR) [10]. Not only intracellular but also extracellular patho-gens can be detected by electron microscopy. The PCR examination can be used for quantita-tive assessment of the pathogen, for the test samples should be taken from duodenum, synovial fl uid, lymph node, cardiac valve and cerebrospinal fl uid [6]. Diagnosis and monitor-ing, however, are currently based on clinical and laboratory fi ndings and histopathological follow-up. There were also attempts to use immunohistochemical methods (detection of polyclonal antibodies produced against T. whipplei) for diagnosing Whipple’s disease, but cross-reactions were observed with certain other bacteria (Shigella and Streptococcus aga-lactiae-specifi c) so that the method has not yet spread in the practice [2].
CASE REPORTS
CEMED 183 2010 ▪ Volume 4, Number 1

Differential Diagnosis
The clinical symptoms are aspecifi c and, therefore, several problems of differential diagnosis may crop up. Other gastrointestinal, rheumatologic, neurological, psychiatric or ophthalmo-logic diseases may emerge, but there is no other disease which would cause similar histo-logical lesions in the small bowel [3]. As for differential diagnosis, Crohn’s disease, celiac disease, amyloidosis, macroglobulinaemia, histoplasmosis, non-tuberculotic mycobacterial infections of patients with acquired immunodefi ciency syndrome (AIDS) as well as lympho-mas affecting the gastrointestinal system or the region of abdominal lymph nodes may also arise.
TherapySeveral antibiotics have been used for the treatment of Whipple’s disease in monotherapy or in a combined form. In lack of controlled trials, no optimal way of treatment could be estab-lished, and susceptibility of the bacterium to drugs is also unknown. Upon empirical antibi-otic therapy, the symptoms cease in a few weeks, and the molecular biological tests turn to negative. Histological alterations in the affected organ(s), however, remain detectable for years. Therapy is aimed at eradication of the bacterium and prevention of relapse. Approxi-mately, 20% of patients give no appropriate response to the treatment, and a relapse can be observed in about 40% of cases. Relapse can be seen mostly in patients with affected CNS when drugs are used which do not cross the blood–brain barrier or the treatment is continued for an inappropriate time. The average time for relapse is 4.2 years [4]. Results show that post-treatment progression or relapse is caused by the same species as the original infection, thus, there is no new infection. Chloramphenicol that was used often initially is now rarely used because of its side effects. After that, the tetracyclines became the basic pillars of ther-apy until comprehensive studies revealed a high (35%) rate of relapse. These observations led to the currently recommended therapy consisting of the intravenous administration of 2 g/day ceftriaxone or 1 g/day meropenem for 2 weeks, followed by daily 160/800 mg oral co-trimoxazole for more than a year. In patients with hypersensitivity to sulphonamides, medicines of penicillin, tetracycline, fl uoroquinolone or cephalosporine content can be taken into consideration [6]. The treatment should be continued for a year, at least, even if the pa-tient is free of symptoms. Clinical improvement is usually accompanied by improving labo-ratory results and regenerating the villous structure. Follow-up biopsies are recommended at 6 and 12 months from diagnosis. After initiation of treatment, diarrhoea is discontinued in days and arthralgia ceases in weeks. Weight gain starts within a few months.
ConclusionsWhipple’s disease may underlie diarrhoea, development of anaemia and symptoms of malab-sorption probably more frequently than the cases where this entity is diagnosed. These symp-toms suggest already an advanced stage and often raise the suspicion of malignancy. In such cases, upper panendoscopy, performed as a part of the examinations searching for a tumour, may fi nally lead to defi nite diagnosis. In the fi rst few years or even a decade of the disease,
2010 ▪ Volume 4, Number 1 184 CEMED
CASE REPORTS

the leading symptom is intermittent arthropathy that does not respond to conventional rheu-matologic treatment. Recognition of the disease is made more diffi cult also by the fact that patients often receive antibiotic treatment because of the symptoms for shorter or longer pe-riods. An antibiotic treatment with inappropriate dose and duration, however, only results in transient improvement, altering the clinical presentation of the disease and delaying the es-tablishment of the diagnosis. The pathomechanism of the disease is yet only partially known, but immunologic processes certainly play a role in its development.
When reporting our cases, our objective was to emphasise that Whipple’s disease, which is fatal without treatment, is considerably more frequent than it is thought of in clinical prac-tice.
ReferencesTulassay, Zs.:[1] The Basis of Internal Medicine (in Hungarian). Medicina, Budapest, 2007, pp. 898–899.Kneitz, C., Suerbaum, S., Beer, M. et al.:[2] Exacerbation of Whipple’s disease associated with infl iximab treat-ment. Scand. J. Rheumatol., 2005, 34, 148–151.Sun, D. F., Fang, J.:[3] Two common reason of malabsorption syndromes: celiac disease and Whipple’s disease. Digestion, 2006, 74, 174–183.Famularo, G., Minisola, G., de Simone, C.:[4] A patient with cerebral Whipple’s disease and a stroke-like syn-drome. Scand. J. Gastroenterol., 2005, 40, 607–609.Tousimis, A. J.:[5] Whipple’s disease: an electron microscopical study of the small intestinal biopsies. Microsc. Microanal., 2007, 13, 334–335.Deriban, G., Marth, T.:[6] Current concepts of immunopathogenesis, diagnosis and therapy in Whipple’s dis-ease. Curr. Med. Chem., 2005, 13, 2921–2926.Finzi, G., Franzi, F., Mastaglio, C. et al.:[7] Ultrastructural evidence of Tropheryma whipplei in PAS-negative granulomatosus lymph nodes. Ultrastruct. Pathol., 2007, 31, 169–172.Papadopoulou, M., Rentzos, M., Vagiakis E. et al.:[8] An unusual case of insomnia associated with Whipple encephalopathy: fi rst case reported from Greece. Neurol. Sci., 2005, 26, 174–177.Muir-Padilla, J., Myers, J. B.:[9] Whipple disease. A case report and review of the literature. Arch. Pathol. Lab. Med., 2005, 129, 933–936.Somogyi, Á., Szabó, T., Pál, K. et al.:[10] Successful treatment of Whipple disease. The history of a patient with lymphnode enlargement (in Hungarian). LAM, 2004, 14, 676–682.
CASE REPORTS
CEMED 185 2010 ▪ Volume 4, Number 1


A Case of Primary Biliary Cirrhosis: First Report from Bangladesh
MAMUN-AL-MAHTAB1, KABIR UDDIN2, SALIMUR RAHMAN1, MOBIN KHAN1, KAMAL3, MONIRUZZAMAN BHUIYAN4, GULZAR HUSSAIN5
1Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh2Combined Military Hospital, Dhaka, Bangladesh
3Department of Pathology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh4Holy Family Red Crescent Medical College Hospital, Dhaka, Bangladesh
5Ayesha Memorial Hospital, Dhaka, Bangladesh
Primary biliary cirrhosis (PBC) is a rare autoimmune liver disease, not infrequent in the West, but hardly reported from the East. We report a case of PBC for the fi rst time from Bangladesh. The patient was an elderly woman pre-senting with vague complaints. The diagnosis was confi rmed by antibody testing and histopathology, whereas other possible causes of cirrhosis were also excluded.
Keywords: PBC, autoimmune liver disease, cirrhosis
IntroductionPrimary biliary cirrhosis (PBC) is an autoimmune liver disease characterized by progressive destruction of intra-hepatic bile ducts. The disease was fi rst described in 1851 by Addison and Gull [1]. The disease shows family clustering, with mothers and daughters showing the highest prevalence [2]. Patients are 90% females, usually between 40 and 60 years of age, although patients can be as young as 20 years old or as old as 80 [3]. Cases have been re-ported among Asians, Caucasians and also in blacks, although the incidence is higher in Caucasians. A large number of cases are being diagnosed due to physician awareness and the availability of better diagnostic modalities.
Case ReportThe patient, an elderly female coming from a middle-class socio-economic background, pre-sented with easy fatigability and itching for the past 2 years. She had no history of jaundice.
On clinical examination, she was found to be mildly icteric and had spleenomegaly. No stigmata of cirrhosis of liver was found. We investigated her extensively. A routine blood test revealed Hb 9.6 g/dL, ESR 55 mm in fi rst hour, total count of WBC 3.5 × 109/L, neutrophils 56%, lymphocytes 40%, eosinophils 2% and monocytes 2%. Her liver profi le showed serum bilirubin 0.6 mg/dL, serum ALT 29 U/L, serum AST 21 U/L and serum alkaline phosphatase 398 U/L, prothrombin time 12 s (control 12 s) (INR 1.0) and serum albumin 3.9 g/dL. She
Corresponding address: Mamun-Al-Mahtab MD, Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh. E-mail: [email protected]
1.18
CASE REPORTS
DOI: 10.1556/CEMED.4.2010. 187 2010 ▪ Volume 4, Number 1 ▪ 187–191.

tested negative for anti-HEV IgM, anti-HAV IgM, HBsAg, anti-HBc total and anti-HCV. HBV DNA was undetectable by PCR (Amplicon HBV Monitor Assay, RT-PCR, Roche Mo-lecular Systems, California). Anti-nuclear antibody and liver–kidney-microsomal antibodies were also negative. Other investigations showed serum ceruloplasmin 43.5 mg/dL. The patient tested positive for anti-mitochondrial (M2) antibody. All ELISA were done by an ELISA kit manufactured by Orgentec Diagnostika GmbH, Germany.
An ultrasonography of the whole abdomen revealed spleenomegaly. Liver was unre-markable. Endoscopy of the upper gastrointestinal tract revealed that she had erosive antral gastritis and duodenitis. We also did a diagnostic ERCP to exclude any co-existent obstruc-tive aetiology, and found normal cholangio-pancreatogram.
A liver biopsy was done percutaneously under local anesthesia with full aseptic precau-tions. A core of the liver tissue was obtained and sent for histopathology to a histopathologist who was unaware of the clinical and laboratory fi ndings of the patient. Histopathology showed normal hepatic architecture replaced by regenerating nodules separated by fi brous tissue. The relationship between the central vein and the portal triad was lost. The portal triad showed a dense infi ltration of chronic infl ammatory cells. Histopathology fi ndings were con-sistent with cirrhosis of liver.
We, thus, concluded that the patient is suffering from PBC. The patient is now receiving symptomatic treatment with cholestyramine, ursodeoxycholic acid (UDCA), probiotics, lactulose and anti-ulcer drugs.
DiscussionIn PBC, bile duct destruction results from immunological disturbance [4]. There is an infi ltra-tion of the bile duct epithelium with T cells [5]. These produce cytokines that contribute to hepato-cellular damage [6]. Suppressor T cells are reduced in number and function [7]. Epi-theloid granuloma develops, suggesting delayed type hypersensitivity [8].
There is a suggestion that infections may trigger PBC [9] and Escherichia coli [10], Mycobacterium gordonae [11] and retroviruses [12] have all been implicated.
Non-organ and non-species specifi c circulating anti-mitochondrial antibodies are found in almost 100% of patients with PBC [13]. Target antigens are localized on the inner-mito-chondrial membrane [14]. The antigenic component specifi c for PBC is M2. ELISA for anti-M2 is 88% sensitive and 96% specifi c for PBC [15]. Increased incidence of C4A-QO allele has been reported in PBC patients [16]. This particular allele is associated with many autoim-mune diseases. PBC patients may have autoimmune, genetic susceptibility evidenced by the presence of HLA-B8, DR3 and DR4 [17]. It has been suggested that immunogenetic back-ground, familial predisposition and environmental factors, all interplay in the development of PBC.
The onset of PBC is insidious and most frequently as pruritus without jaundice. The lat-ter may never develop, but usually appears 6 months to 2 years following the onset of pruri-tus. Jaundice preceding pruritus is extremely unusual and jaundice without pruritus at any time is very rare.
On examination, patients may be mildly anaemic, with fi rm hepatomegaly and just pal-pable spleen. PBC may be associated with a number of diseases, in particular, autoimmune
2010 ▪ Volume 4, Number 1 188 CEMED
CASE REPORTS

diseases such as rheumatoid arthritis, dermatomyositis, mixed connective tissue disease and systemic lupus erythomatosus [18]. Autoimmune thyroiditis has been reported in 20% PBC patients. Coeliac disease is co-existent in 3% and ulcerative colitis is another rare association [19]. Patients may also have autoimmune thrombocytopenia and autoimmune haemolytic anaemia [20]. Thirty-nine percent PBC patients develop gall stones. Besides, pulmonary abnormalities [21] and renal abnormalities [22] have all been described. There is a small increase in overall cancer risk and mortality in PBC patients [23].
Liver biochemistry shows serum bilirubin and serum AST about twice normal, serum alkaline phosphatase about four times and normal serum albumin. Serum GGT may also be raised. Serum IgM is usually raised. ERCP is performed in confusing cases and reveals nor-mal intra-hepatic biliary tree.
Characteristic histopathological appearance in PBC is injury to septal and/or inter-lobu-lar bile ducts. However, surgical liver biopsy is superior to needle liver biopsy in identifying such lesions. Histopathological appearance in PBC has been divided into four stages, namely, stage I, where there is fl orid bile duct lesions, stage II characterized by ductular proliferation, stage III with septal fi brosis and bridging known as “scarring” and fi nally, stage IV, where patients develop cirrhosis [24].
Differential diagnosis of PBC includes primary sclerosing cholangitis, autoimmune cholangiopathy and cholestatic drug reactions.
Management is supportive. It is important to maintain the nutritional status of patients as well as the replacement of fat soluble vitamins. Vitamin D and calcium supplements are given for correction of osteomalacia, whereas pruritus is usually helped by cholestyramine. UDCA has been shown to be benefi cial for PBC patients in studies from France [25]. Multi-centre studies have subsequently confi rmed that UDCA reduces the need for transplantation and death in PBC patients [26]. Indeed, recent studies show that patients with early PBC who respond to UDCA (i.e. 40% reduction of ALT at 1 year on treatment) have a normal lifespan [27]. Even those who do not respond to UDCA have a better lifespan [28]. Immunosuppres-sive agents such as azathioprine, D-penicillamine, chlorambucil and cylosporin A and corti-costeroids have all been tried, but the results are inconclusive. However, more recent studies suggest that PBC does respond to steroids, and budesonide, fi brates and farnesoid X-receptor antagonists may be the options for UDCA non-responders [29–31].
Liver transplantation is indicated in PBC patients with intractable pruritus and hepato-cellular failure. Patients should be considered for transplantation when serum bilirubin is >150 μmol/L. One-year survival post-transplantation is 85–90%, whereas 5-year survival is 60–70% [32].
The clinical course of PBC is variable. In some, the disease remains steady, whereas in others, the clinical course may be progressively downhill. When serum bilirubin is >100 μmol/L, survival beyond 2 years is unlikely. Other factors predicting poor survival in PBC include increased symptoms, advanced age, hepato-spleenomegaly, ascites and serum albu-min <3 g/dL. Hepato-cellular carcinoma is less frequent in PBC compared to other chronic hepatitis, but is very much a possibility, unlike what was assumed previously [33].
The causes of death in PBC include variceal haemorrhage, encephalopathy and Gram-negative septicaemia.
CASE REPORTS
CEMED 189 2010 ▪ Volume 4, Number 1

ConclusionPBC is a rare cause of cirrhosis of liver; however, with strong clinical suspicion and the avail-ability of investigative modalities, it is possible to diagnose patients with PBC. Early diagno-sis and appropriate management improve the quality of life of patients and also probably, prolong survival. It is, therefore, important to recognize such patients early.
ReferencesAddison, T., Gull, W.:[1] On a certain affection of the skin – vitiligoidea – α plana, β tuberose. Guy’s Hosp. Rep., 1851, 7, 265.Jones, D. E. J., Watt, F. E., Metcalf, J. V. et al.:[2] Familial primary biliary cirrhosis revisited: a geographically based population study. J. Hepatol., 1999, 30, 402.Mistry, P., Seymour, C. A.:[3] Primary biliary cirrhosis – from Thomas Addison to the 1990s. Q. J. Med., 1992, 82, 185.Gershwin, M. E., Mackay, I. R.:[4] Primary biliary cirrhosis: paradigm or paradox for autoimmunity. Gastroen-terology, 1991, 100, 822.Yamada, G., Hodo, I., Tobe, K. et al.:[5] Ultrastructural immunocytochemical analysis of lymphocytes infi ltrat-ing bile duct epithelia in primary biliary cirrhosis. Hepatology, 1990, 12, 98.Martinez, O. M., Villanueva, J. C., Gershwin, E. et al.:[6] Cytokine patterns and cytotoxic mediators in primary biliary cirrhosis. Hepatology, 1995, 31, 113.Ballardini, G., Mirakian, R., Bianchi, F. B. et al.:[7] Aberrant expression of HLA-DR antigens on bile duct epi-thelium in primary biliary cirrhosis: relevance to pathogenesis. Lancet, 1984, ii, 1009.Lee, R. G., Epstein, O., Jauregui, H. et al.:[8] Granulomas in primary biliary cirrhosis: a prognostic feature. Gastroenterology, 1981, 81, 983.Haydon, G. H., Neuberger, J.:[9] PBC: an infectious disease? Gut, 2000, 47, 586.Buttler, P., Valle, F., Hamilton-Miller, J. M. T. et al.:[10] M2 mitochondrial antibodies and urinary rough mutant bacteria in patients with primary biliary cirrhosis and in patients with recurrent bacteriuria. J. Hepatol., 1993, 17, 408.Vialgut, I., Villa, J., Pares, A. et al.:[11] Mycobacterium gordonae DNA in liver tissue in patients with primary biliary cirrhosis. J. Hepatol., 1994, 21, 87.Mason, A. L., Lizhe, X., Guo, L. et al.:[12] Detection of retroviral antibodies in primary biliary cirrhosis and other idiopathic biliary disorders. Lancet, 1998, 351, 1620.Bruguera, M., Llach, J., Rodes J.:[13] Nonsyndromic paucity of intrahepatic bile ducts in infancy and idiopathic ductopenia in adulthood: the same syndrome? Hepatology, 1992, 15, 830.Surh, C. D., Roche, T. E., Danner, D. J. et al.:[14] Antimitochondrial antibodies in primary biliary cirrhosis rec-ognize cross-reactive epitope(s) on protein X and dihydrolipoamide acetyltransferase of pyruvate dehydroge-nase complex. Hepatology, 1898, 10, 127.Teoh, K-L., Rowley, M. J., Zafi rakis, H. et al.:[15] Enzyme inhibitory autoantibodies to pyruvate dehydrogenase complex in primary biliary cirrhosis: applications of a semiautomated assay. Hepatology, 1984, 20, 1220.Manns, M. P., Bremm, A., Schneider, P. M. et al.:[16] HLA DRw8 and complement C4 defi ciency as risk factors in primary biliary cirrhosis. Gastroenterology, 1991, 101, 1367.Lohse, A. W., Meyer, G. V. M., Buschenfelde, K-H. et al.:[17] Characterization of the overlap syndrome of primary biliary cirrhosis (PBC) and autoimmune hepatitis: evidence for it being a hepatic form of PBC in genetically susceptible individuals. Hepatology, 1999, 29, 1078.Hall, S., Axelsen, P. H., Larson, D. E. et al.:[18] Systemic lupus erythromatosus developing in patients with pri-mary biliary cirrhosis. Ann. Intern. Med., 1984, 100, 308.Bush, A., Mitchison, H., Walt, R. et al.:[19] Primary biliary cirrhosis and ulcerative colitis. Gastroenterology, 1987, 92, 2009.Chen, C-Y., Lu, C-L., Chiu, C-F. et al.:[20] Primary biliary cirrhosis associated with mixed type autoimmune haemolytic anaemia and sicca syndrome: a case report and review of the literature. Am. J. Gastroenterol., 1997, 92, 1547.
2010 ▪ Volume 4, Number 1 190 CEMED
CASE REPORTS
Weissman, E., Becker, N. H.:[21] Interstitial lung disease in primary biliary cirrhosis. Am. J. Med. Sci., 1983, 285, 21.Burroughs, A. K., Rosentein, I. J., Epstein, O. et al.:[22] Bacteriuria and primary biliary cirrhosis. Gut, 1984, 25, 133.Howel, D., Metcalf, J. V., Gray, J. et al.:[23] Cancer risk in primary biliary cirrhosis: a study in northern England. Gut, 1999, 45, 756.Scheuer, P. J.:[24] Primary biliary cirrhosis. Proc. R. Soc. Med., 1967, 60, 1257.Poupon, R. E., Poupon, R., Balkau, B. et al.:[25] Ursodiol for the long-term treatment of primary biliary cirrhosis. N. Engl. J. Med., 1994, 330, 1342.Poupon, R. E., Lindor, K. D., Cauch-Dudek, K. et al.:[26] Combined analysis of randomized control trials of ursodeoxycholic acid in primary biliary cirrhosis. Gastroenterology, 1997, 113, 884.Kumagi, T., Alswat, K., Hirschfi eld, G. M. et al.:[27] New insights into autoimmune liver disease. Hepatol. Res., 2008, 1–17.Pares, A., Caballeria, L., Rodes, J.:[28] Excellent long-term survival in patients with primary biliary cirrhosis and biochemical response to ursodeoxycholic acid. Gastroenterology, 2006, 130, 715–720.Rautianen, H., Karkkainen, P., Karvonen, A. et al.:[29] Budesonide combined with UDCA to improve liver histology in primary biliary cirrhosis: a three-year randomized trial. Hepatology, 2005, 41, 747–752.Ohmoto, K., Yoshioka, N., Yamamoto, S.:[30] Long-term effect of bezafybrateon parameters of hepatic fi brosis in primary biliary cirrhosis. J. Gastroenterol., 2006, 41, 502–503.Fiorucci, S., Rizzo, G., Donini, A. et al.:[31] Targeting farnesoid X receptor for liver and metabolic disorders. Trends Mol. Med., 2007, 13, 298–309.Tzakis, A. G., Carcassonne, C., Todo, S. et al.:[32] Liver transplantation for primary biliary cirrhosis. Semin. Liver Dis., 1989, 9, 144.Krasner, N., Johnson, P. J., Portman, B. et al.:[33] Hepatocellular carcinoma in primary biliary cirrhosis: report of 4 cases. Gut, 1979, 20, 255–258.
CASE REPORTS
CEMED 191 2010 ▪ Volume 4, Number 1


Anaphylactic Reaction Following Forest Fly(Hippobosca equina) Bite: A Human Case
ALICE DECASTELLO1, ROBERT FARKAS2
1Department of Family Medicine, Semmelweis University, Budapest, Hungary2Department of Parasitology and Zoology, Faculty of Veterinary Science,
Szent István University, Budapest, Hungary
The authors report the case of a 46-year-old female patient, who experienced an anaphylactic reaction with a lucky outcome following an insect bite. Within a short time, a hard swelling of 15-cm diameter, covered by a serous crust, appeared at the border of her forehead and hairy scalp, with oedema on her forehead. Soon thereafter, erythema and itching developed locally and all over her body, with oedema of her hands, face and lips, later accompanied by shivering, nausea and vomiting. Based on identifi cation with the help of a taxonomic key, the captured insect proved to be a forest fl y (Hippobosca equina). As far as we know, this is the fi rst published case of anaphylaxis induced by the bite of this species in Hungary. Forest fl ies are present all over the world; they have been known in Hungary for a long time; they suck blood several times a day mostly from horses, donkeys or cattle kept on pastures or in stables and cowsheds, and occasionally also from other animal species. As vectors, they transmit various pathogens. By reporting our case, we wish to call the attention of family doctors and clinicians to horse tick bite and the clinical signs and symptoms caused by it, since they have no specifi c experience required for the diagnosis of such insect bites.
Keywords: forest fl y, Hippobosca equina, anaphylaxis
Several animal species, including snakes, scorpions, jellyfi shes, fl eas, bees, wasps, mosqui-toes, gadfl ies, spiders, ants and ticks, are known to inject substances into humans with their bite, which may elicit mild or serious and even fatal consequences. Worldwide, there are several hundreds of victims every year due to anaphylactic reaction induced by various in-sect bites, mostly, the stings of bees and wasps belonging to the order of Hymenoptera [1–4]. The crotoxin-containing venom of bees or a greater amount of hornet venom immitted into the body may cause death in susceptible people. If a quick and effi cient help is not forthcom-ing, most deaths occur in the fi rst hour. Insect bite allergies are caused by IgE antibodies produced against protein-type substances of insect venom. In mild forms, only cutaneous symptoms occur at the site of the bite, including itching, pain, hives and oedema. In severe cases, generalised symptoms due to anaphylactic reaction may also develop, possibly even within a few minutes, or sometimes after several hours, causing shortness of breath, tachy-cardia, hypotension, vomiting and diarrhoea. Fortunately, the number of cases where anaphy-lactic shock causes loss of consciousness and death due to cardiac arrest within minutes is very small.
Although most problems are caused by bees and wasps, sporadically, other insects, in-cluding forest fl ies, can also elicit allergic reactions in humans.
Forest fl y (Hippobosca equina) (Diptera: Hippoboscidae) is a 3–9-mm long fl y species having a compact, dorsoventrally fl attened body in reddish brown colour. On account of its
Corresponding address: Alice Decastello MD, Wesselényi u. 11, 1077 Budapest, Hungary.E-mail: [email protected]
1.19
CASE REPORTS
DOI: 10.1556/CEMED.4.2010. 193 2010 ▪ Volume 4, Number 1 ▪ 193–198.
shape, it is also named, together with other species belonging to the family, louse fl ies [5]. The imagoes of both genders have a blood-sucking mouthpart, which is directed forwards. Their palps, which consist of three segments, are seated in a deep socket. Their antennae encircle the mouth organ like a sheath. It has a pair of well-developed wings that extend be-yond the skin-like abdomen, and in a resting posture, they are placed on each other in a scissor-like way (Fig. 1). They are present all over the world [6–11]. In Hungary, they have been known for a long time, and they were captured at several places in the country [5, 12–14]. They suck blood several times a day, mostly from the rumps of horses and donkeys, which are kept in stables or on grazing grounds, from parts between their hind limbs where the skin is thinner, but sometimes also from other parts of their body [15]. They may often feed on cattle, and also occasionally on other animal species such as dogs or wild ruminants [16, 17]. Although they are good fl yers, they usually remain in the vicinity of animals. As all species belonging to the family of Hippoboscidae, their females are also larviparous. They lay third instar larvae which are ready to enter the pupa state, and they are also called improp-erly “pupiparous fl ies” [12]. The females often lay the mature larvae into the environment, on a soil which is rich in humus, roots of plants, where the imagos will hatch after a period of pupa time which lasts for several weeks or months, depending on environmental temperature [6]. They can be found in the highest numbers during the warm summer months in July and August [18]. Their lifespan is approximately 6–10 weeks.
By their blood-sucking, they make animals restless, and occasionally, they may cause signifi cant blood loss, as well as milder or more serious dermatitis. As blood-sucking insects, forest fl ies can transmit various pathogens (e.g. piroplasms and rickettsiae). An American study showed that 71% of 17 H. equina collected from cattle were infected with Bartonella [19].
Occasionally, they can suck blood from humans who live or stay mostly in the vicinity of horses and do not belong to the normal hosts of horse ticks. Their signifi cance for public health depends on individual sensitivity as well. Some people do not even notice that they have been bitten by a forest fl y. At the site of the bite, however, a swelling with reddish colour develops that may cause intense itching, and persists for 2–3 weeks. Sometimes, urgent med-ical intervention may be needed, because the secretion of the salivary glands of the imagoes, when entering the human body, elicits an IgE-mediated anaphylactic reaction [20]. As a re-sult of the lack of appropriate history data, this reaction can be exactly diagnosed or differen-tiated from allergic reactions caused by other insect species only by in vivo (cutaneous test-ing) or in vitro (ELISA, immunoblot) methods [21]. It is worth mentioning that deer ked (Lipoptena cervi), another blood-sucking species belonging to the family of Hippoboscidae and also widespread in Hungary, may also cause inconvenience to humans. The deer ked is a parasite on wild ruminants, and its peculiarity is that after dwelling on its hosts, its imagoes lose their wings. In a Russian publication, Chistyakov [22] reports on cases of dermatitis caused by these ectoparasites occurring in more than 300 people living in the St. Petersburg district, during the period of August–September when the imagoes of this species have swarmed in large numbers. Reunala et al. [23] observed that they suck blood most often on the head and on the upper part of the back of humans. Rhinoconjunctival allergy caused by this species has been demonstrated in Finland [24].
A need for protection against horse ticks emerge very rarely in practice. When neces-sary, they can be easily eliminated by various anti-arthropod products.
2010 ▪ Volume 4, Number 1 194 CEMED
CASE REPORTS

Fig. 2 Oedema of the forehead, erythema and swell-ing covered by serous crust on the hairy scalp, caused by a forest fl y
Fig. 1 Forest fl y (Hippobosca equina)
Case ReportThe history of a 46-year-old female patient who lives in the countryside, includes oesopha-geal ulcer and rheumatologic treatment for pain in her left hip. Hypersensitivity to medicines: Algopyrin (metamizole sodium). Her medication: Noacid (pantoprazole) and Motilium (domperidone).
She recalls that on 10.06.2009, at about 18:00, she noticed on her forehead – no bite, only the moving of an insect. Her husband removed the insect from her hair and put it into a small vial. Then, after approximately 15 min, the patient’s lips and palms started to itch, and she felt an increasingly frequent and intense throbbing in her ears. Her face turned red and swelling developed in the middle of her forehead at the border of the hairy scalp. After a few minutes, her face became puffy, her fi ngers swelled and she felt swelling in her throat. This phenomenon was accompanied by very intense and frequent palpitation that was almost pain-ful; a high degree of weakness and headache developed. Her blood pressure decreased (106/56 mmHg) and her heart rate was 110/min. At 18:20, after the intake of a Calcium San-doz effervescent tablet (calcium carbonate, calcium lactate gluconate), she felt that her heart began to beat slower, but the intensity of its “pounding” remained unchanged. She experi-enced extreme weakness, and her headache intensifi ed further. This state lasted for about an hour, and then, her heart rate began to decrease very slowly, and – in parallel with this – her blood pressure increased; at 20:00 her HR and BP were 86/min and 120/82 mmHg, respec-tively. In the meantime, she noticed that her entire body became red and her limbs swelled. At 21:30, she shivered, felt nausea and vomited once. The vomiting caused no alleviation; the malaise remained and the headache attacked her in vigorous waves. She did not have a good night’s sleep, and the malaise persisted for a long time; fortunately, the anaphylactic reaction receded. When she woke up in the morning, she felt very weak and broken. Her forehead was puffy, and a hard swelling of a 15-cm diameter developed in the area of the bite; it caused no pain but only mild itching, and a serous crust was formed. After 2 days, the patient visited her family doctor with the insect put into the vial. The physician found an itching and hard swell-ing covered by serous crust and oedema of the forehead (Fig. 2). Her heartbeat was rhythmic, 78/min, and her blood pressure was 125/82 mmHg. Antihistamine and antibiotic treatment
CASE REPORTS
CEMED 195 2010 ▪ Volume 4, Number 1

was initiated immediately, which was also approved by a specialist consultation of a derma-tologist (she took Loratadine 10 mg once a day and Amoxicillin 1,000 mg twice a day for 7 days). The hard swelling on her head, covered by serous crust, and the oedema on her fore-head healed after 10 days.
Based on a taxonomic key [12], the insect has been identifi ed as a forest fl y (H. equina).
DiscussionForest fl ies are present all over the world. They are found in large numbers at several places in Hungary, especially where horses, donkeys or cattle are kept. H. equina lives in stables and kennels, it lays its eggs into fodder or litter and it requires the presence of animals in the places of its habitat [20]. Our patient lives in the countryside; her neighbour is in the business of horse-keeping and ride-hiring; another neighbour keeps cattle.
The insect which bit her came to the surroundings of the patient probably from the nearby horses or the cattle stables. The local and generalised cutaneous symptoms that oc-curred soon after the forest fl y bite were followed by systemic symptoms characteristic of an anaphylactic reaction. Occasionally, immediate medical help may be required, as the secre-tion of the salivary glands of the forest fl y entering the human body may elicit an IgE-medi-ated anaphylactic reaction [20, 21]. This process also occurred in this patient’s case; fortu-nately, it did not make such a rapid progress, so no corticosteroids were required for her care. We performed no specifi c examinations, but – based on identifi cation of the insect and the symptoms which appeared soon after its bite – it can be stated that the anaphylactic reac-tion was elicited by allergens from the saliva of H. equina which entered the patient’s body during its blood-sucking. However, we could not rely on the examination of specifi c IgE, as no appropriate extract is available for determining the allergy caused by this species. A ques-tion may arise as to why this kind of reaction occurred in the patient, as no such reaction may develop after the fi rst bite. There may be two explanations for this. The patient might have been bitten by an imago of this species on an earlier occasion, but she might not have noticed the bite then. The other explanation is that the anaphylactic reaction occurred because of a previous alteration caused by another insect species, this assumes the possibility of a cross-reaction between the venoms of H. equina and another, unknown insect species; however, no reference to this can be found in the literature. The family doctor has called the patient’s attention to the fact that she should take special care for the eradication of blood-sucking forest fl ies in her environment, as in the event of another bite, an even more serious reaction is to be expected, warranting immediate medical attention. In foreign literature, there are al-ready reports on a few similar cases, in one of them, the course – although in a more severe form – weirdly resembles the case discussed by us [20, 21]. If identifi cation of the insect is not possible, then an examination of antibodies produced in the body against the venoms of wasp, bee and, if feasible, other arthropods should be performed. During cutaneous tests, a reaction completely similar to that after a bite occurs; therefore, we use these tests only after a negative blood test, and exclusively with the availability of inpatient care. The bite of this species may be important also because it can – as a vector – propagate the pathogens of various diseases (e.g. rickettsiosis, toxoplasmosis and tularaemia) with the secretion of its salivary gland [5].
2010 ▪ Volume 4, Number 1 196 CEMED
CASE REPORTS

We have considered reporting on this case as important, because neither clinicians nor family doctors possess the necessary knowledge for diagnosing insect bites, particularly when their praxis is located in big towns. The attention of children and adults staying in the vicinity of horses should also be called to the dangers which may be caused by this species.
In Hungarian literature, there have been publications on stings of jellyfi sh [25], tungiasis caused by imported human chigoe (Tunga penetrans) [26], human ehrlichiosis that devel-oped after a tick bite [27], as well as on stings in general [28, 29]. As far as we know, no such case has yet been reported in Hungary, and we hope that we succeeded in completing the domestic literature on diseases caused by bites.
ReferencesIncorvaia, C., Mauro, M., Pastorello, E. A.:[1] Hymenoptera stings in conscripts. Allergy, 1997, 52, 680–681.De Maat-Bleeker, F., van Bronswijk, E. M. H.:[2] Allergic reaction caused by bites from blood-sucking insects of the Tabanidae family, species Haematopota pluvialis (L). Allergy, 1995, 50, 388.Freye, H. B., Litwin, C.:[3] Coexistent anaphylaxis to Diptera and Hymenoptera. Ann. Allergy Asthma Immu-nol., 1996, 76, 270–272.Hemmer, W., Focke, M., Vieluf, D. et al.:[4] Anaphylaxis induced by horsefl y bites: identifi cation of a 69 kd IgE-binding salivary gland protein from Chrysops spp (Diptera Tabanidae) by Western blot analysis. J. Allergy Clin. Immunol., 1998, 101, 134.Májer, J.:[5] The catalogue of insects in County Somogy (In Hungarian) (Diptera: Hippoboscidae). Nat. Somogy., 2001, 1, 425–426.Hafez, M., Hilali, M., Fouda, M.:[6] Biological studies on Hippobosca equina (L.) (Diptera: Hipposboscidae) infesting domestic animals in Egypt. Z. Angew. Entomol., 1977, 83, 426–441.Beaucournu, J. C., Beaucournu-Saguez, F., Guiguen, C.:[7] Nouvelles données sur les diptères pupipares (Hip-poboscidae et Streblidae) de la sous-région méditerranéenne occidentale. Ann. Parasitol. Hum. Comp., 1985, 60, 311–327.Romaniuk, K.:[8] Outbreaks of diptera in cows and primitive Polish horses maintained in pastures. Medycyna Wet., 2005, 61, 332–334.Kazimierczak, K.:[9] Louse-fl ies (Hippoboscidae, Diptera) in Poland – their biology and importance. Ż ycie Wet., 2007, 82, 51–52.Romaniuk, K., Gad, K., Kiszka, W.:[10] Estimating Hippobosca equina occurrence in primitive Polish horses. Medycyna Wet., 2007, 63, 1100–1101.Trilari, T., Krčmar, S.:[11] Contribution to the knowledge of louse fl ies of Croatia (Diptera: Hippoboscidae). Nat. Croat., 2005, 14, 131–140.Soós, Á.:[12] Bábtojó legyek. Muscidae pupirarae. Magyarország Állatvilága XV/17. Akadémiai Kiadó, Buda-pest, 1955, p. 64.Soós, Á., Húrka, K.:[13] Family Hippoboscidae. In: Soós, Á., Papp, L. (eds): Catalogue of Palearctic Diptera, vol. 11, Scathophagidae – Hypodermatidae. Akadémiai Kiadó, Budapest, 1986, pp. 215–227.Papp, L., Kaufman, G.:[14] Scatopsidae, Lauxaniidae, Diastatidae and Hippoboscidae (Diptera) of the Kiskunság National Park, Hungary. Fólia Ent. Hung., 1989, 50, 111–117.Hafez, M., Hilali, M., Fouda, M.:[15] Ecological studies on Hippobosca equina (Linnaeus, 1758) (Diptera: Hip-posboscidae) infesting domestic animals in Egypt. Z. Angew. Entomol., 1979, 87, 327–335.García-Romero, C.:[16] A contribution to the study of parasites of red deer (Cervus elaphus) in the provinces of Toledo and Ciudad Real (Castille-La Mancha, Spain). Ecología (Madrid), 2000, 14, 235–249.Wallach, A. D.:[17] Ectoparasites on reintroduced roe deer Capreolus capreolus in Israel. Wildl. Dis., 2008, 44, 693–696.Romaniuk, K., Gad, K., Kiszka, W.:[18] Occurrence of Hippobosca equina invasion in primitive Polish horses during the grazing period. Medycyna Wet., 2008, 64, 1155–1156.Halos, L., Jamal, T., Maillard, R. et al.:[19] Role of Hippoboscidae fl ies as potential vectors of Bartonella spp. infecting wild and domestic ruminants. Appl. Environ. Microbiol., 2004, 70, 6302–6305.
CASE REPORTS
CEMED 197 2010 ▪ Volume 4, Number 1
Quercia, O., Emiliani, F., Foschi, F. G. et al.:[20] Anaphylactic reaction after Hippobosca equina bite. Alergol. Inmunol. Clin., 2005, 20, 31–33.Vidal, C., Armisén, M., Bartolomé, B. et al.:[21] Anaphylaxis to Hippobosca equina (louse fl y). Ann. Allergy Asthma Immunol., 2007, 99, 284–286.Chistyakov, A. F.:[22] Skin lesions in people due to bite of Lipoptena cervi. Vestn. Dermatol. Venerol., 1968, 42, 59–62.Reunala, T., Rantanen, T., Vuojolahti, P. et al.:[23] Deer ked dermatitis. Duodecim,1980, 96, 897–902.Laukkanen, A., Ruoppi, P., Mäkinen-Kiljunen, S.:[24] Deer ked-induced occupational allergic rhinoconjunctivitis. Ann. Allergy Asthma Immunol., 2005, 94, 604–608.Tamás, I., Veres, I., Remenyik, É.:[25] About bite of medusa. Demonstration of one case (in Hungarian). Orv. Hetil., 2008, 149, 35–41.Kucsera, I., Vincze, I., Danka, J. et al.:[26] Human tungiasis imported to Hungary (in Hungarian). Orv. Hetil., 2007, 148, 2003–2005.Nemes, Zs., Péterfi , Z.:[27] Human erlichiosis. A newer disease mediated by insects (in Hungarian). Praxis, 1998, 7, 56–56.Dobozy, E.:[28] About bites and light injuries (in Hungarian). Praxis, 2004, 13, 5–9.Nagy, A., Mikola, I.:[29] The role of environmental factors in the widespread of zoonotic diseases (in Hungarian). Budapesti Közegészségügy, 2000, 4, 343–347.
2010 ▪ Volume 4, Number 1 198 CEMED
CASE REPORTS

Ciprofl oxacin-Induced Stevens–Johnson Syndrome: First Report from Bangladesh
MAMUN-AL-MAHTAB, SALIMUR RAHMAN, AKMAT ALI, ANANTA SHRESTHA, JAHANGIR SARKAR, MOBIN KHAN
Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh
Stevens–Johnson syndrome, otherwise known as erythema multiforme majus, was fi rst described in 1922 by Stevens and Johnson as a febrile illness with stomatitis, purulent conjunctivitis, and skin lesions. Case report: We report a 28-year-old married woman who presented with fever and was advised ciprofl oxacin tablet. After taking two doses of the tablet, she developed papulo-vesicular rash involving the trunk and the upper and lower limbs, including mucous membranes. She also developed a painful red eye. She eventually developed jaundice and her case was ul-timately diagnosed as ciprofl oxacin-induced Stevens–Johnson syndrome. Discussion: Medications appear to be the most common cause of Stevens–Johnson syndrome. It commonly affects multiple organs. Treatment for Stevens–Johnson syndrome is as diverse as the symptoms and it should be begun by withdrawing any offending agent identi-fi ed. Conclusion: Stevens–Johnson syndrome is a potentially fatal multiorgan disease. This aspect of the condition is best addressed by early involvement of medical specialists.
Keywords: ciprofl oxacin, Stevens–Johnson syndrome, multiorgan disease
IntroductionStevens–Johnson syndrome (SJS), otherwise known as erythema multiforme majus, is thought to represent a continuum of disease, the most benign type of which is erythema mul-tiforme, whereas toxic epidural necrolysis is the most severe [1]. The syndrome is generally described as vesiculobullous erythema multiforme of the skin, mouth, eyes, and genitals [2]. The condition was fi rst described in 1922 by Stevens and Johnson as a febrile illness with stomatitis, purulent conjunctivitis, and skin lesions [3].
Because SJS is a rare condition, estimates of its incidence and prevalence are challeng-ing. Hospital record reviews have provided the most useful information. The records of pa-tients hospitalized between 1972 and 1986 with a diagnosis of EM-minor, SJS, and TEN, from a large urban area in the United States, were reviewed and the incidence of hospitaliza-tion for one of these conditions was 4.2 per 106 person-year [4]. Incidence ranges from 1.2 to 6 cases per million per year; the condition is fatal in 5% of treated cases and in 15% of un-treated cases.
Case ReportA 28-year-old married woman presented with fever. For this complaint, she took paracetamol with no satisfactory improvement. Four days later, she visited a physician and was advised
Corresponding address: Mamun-Al-Mahtab MD, Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh. E-mail: [email protected]
1.20
CASE REPORTS
DOI: 10.1556/CEMED.4.2010. 199 2010 ▪ Volume 4, Number 1 ▪ 199–202.

ciprofl oxacin tablet. After taking two doses of the tablet, she developed papulo-vesicular rash involving the trunk and upper and lower limbs, including mucous membranes. She also de-veloped a painful red eye. Initially, this rash was diagnosed as chicken pox and she was re-ferred to an infectious disease hospital and treated accordingly. But, as her rash gradually became larger and ruptured and she developed jaundice, she consulted another physician, as well as an ophthalmologist and a hepatologist. On this background, they diagnosed her case as ciprofl oxacin-induced Stevens–Johnson syndrome. As her condition deteriorated, she was admitted to the intensive care unit and treated with IVIG along with meropenum, topical and systemic steroids, and other supportive measures.
After a few weeks, her condition improved along with a reduction in the amino trans-ferases and serum bilirubin level. She had no recent history of taking other medicines, includ-ing a contraceptive agent.
Her investigations revealed HBsAg, anti-HCV, anti-HAV IgM, and anti-HEV IgM neg-ative. Prothrombin time was 14.5 s (control 12 s), haemoglobin 12.4 g/dL, platelet count 200,000/cmm, and WBC 4,000/cmm. Neutrophil was 79%, lymphocyte 16%, and eosinophil 3%. PBF was anisochromic, anisocytic. Urine R/E showed albumin ++, RBC 30–35/HPF, pus cell 6–8/HPF; serum bilirubin 35 mg/dL, SGPT 445U/L, serum ALP 131U/L, serum electrolytes normal, serum creatinine 187 μmol/L, serum albumin 2.2 g/dL; serum calcium and serum magnesium were normal. Urine culture showed no growth. ANA and Coomb’s test were negative. Reticulocyte count was 12%, γGT 880 U/L, and haemoglobin electrophoresis was normal. AMA and ASMA were negative. Ultrasonogram of the abdomen revealed mild hepatomegaly with hypoechoic liver parenchyma.
DiscussionMedications appear to be the most common cause of Stevens–Johnson syndrome and have been implicated in as many of 60% of cases studied [5].
Short courses of sulfonamide, aminopenicillin, quinolone, and cephalosporin drugs all increase the risk of Stevens–Johnson syndrome. Longer-term therapy with anticonvulsant agents, oxicam, nonsteroidal antiinfl ammatory drugs (NSAIDs), or allopurinol has also been identifi ed as a possible cause of Stevens–Johnson syndrome [6]. This syndrome has also been linked to herpes simplex virus, mycoplasma bacterial species, and measles vaccine [7]. It can be preceded by a prodrome consisting of fever, malaise, sore throat, nausea, vomiting, arth-ralgias, and myalgias [5]. This prodrome is followed within 14 days by conjunctivitis and by bullae on the skin and on the mucosal membranes of the mouth, nares, pharynx, esophagus, urethra, and vulvovaginal as well as anal regions.
Stevens–Johnson syndrome commonly affects multiple organs, and esophageal stric-tures develop in some patients [8]. Ocular complications occur in about 70% of patients with Stevens–Johnson syndrome [9]. Photophobia and a purulent form of conjunctivitis may be present initially, but corneal ulcerations and anterior uveitis can develop. Secondary infec-tion, corneal opacity, and blindness can follow [5].
Affected patients and their fi rst-degree relatives should be instructed to avoid any identi-fi ed drug or chemical that may be responsible. However, extensive skin involvement requires the staffi ng provided by a major burn unit. Treatment consists of warming the environment, increasing caloric intake, preventing superinfection and sepsis, and correcting electrolyte
2010 ▪ Volume 4, Number 1 200 CEMED
CASE REPORTS

disturbance [10]. The treatment for Stevens–Johnson syndrome is as diverse as the symptoms and it should be begin by withdrawing any offending agent identifi ed. Many skin lesions can be treated with any of various topical mixtures, such as wet Burrow’s compresses [11]. Oral or intravenous use of steroid agents has been a matter of controversy. Many studies showed the benefi cial effects of using steroid agents in adults [12, 13].
Mild to moderate disease can be managed with corticosteroid agents on an outpatient basis [14].
Twenty-seven to fi fty percent patients have been found to progress to severe ocular dis-ease. The treatment of ocular disease usually begins with an aggressive lubrication of the ocular surface. As infl ammation and cicatricial changes ensue, topical steroids, symblepha-ron lysis, and topical retinoid therapy may be employed. Maintenance of ocular integrity can be achieved through the use of adhesive glues, lamellar grafts, and penetrating keratoplasty. Visual rehabilitation can be considered once the eye has been quiet for at least 3 months. Long-term management frequently involves treatment of trichitic lashes and eyelid margin repair for distichiasis, entropion, and ectropion. Scleral contact lenses, mucosal membrane grafts, limbal stem cell transplants, and amniotic membrane grafting may be required. Im-munomodulating therapy may halt the immunologic dysregulation and result in infl amma-tory consequences. Recent reports suggest that IV-Ig may provide an alternative therapeutic modality, with or without the use of systemic steroids.
Although mild forms of erythema multiforme majus may resolve in 2–3 weeks, recov-ery from Stevens–Johnson syndrome may require 2–3 months, depending on the number of organs affected and the severity of disease [2].
ConclusionStevens–Johnson syndrome is a potentially fatal multiorgan disease with a strong etiologic link to some medications. Physicians must, therefore, consider this syndrome as a potential complication of treatment, especially when the use of medication is questionable. The mul-tiorgan aspect of the condition is best addressed by early involvement of medical specialists. Treatment with steroid agents may be helpful, but this option remains controversial. Affected patients and their fi rst-degree relatives should be instructed to avoid any identifi ed drugs or chemicals that may be responsible for causing the condition.
ReferencesWilkins, J., Morrison, L., White, C. R. Jr.:[1] Oculocutaneous manifestations of the erythema multiforme/Ste-vens–Johnson syndrome/toxic epidermal necrolysis spectrum. Dermatol. Clin., 1992, 10, 571–582.Habif, T. P.:[2] Clinical Dermatology, 3rd edn. Mosby-Year Book, St Louis, 1996, pp. 570–572.Stevens, A. M., Johnson, F. C.:[3] A new eruptive fever associated with stomatitis and ophthalmia: report of two cases in children. Am. J. Dis. Child., 1922, 24, 526–533.Chan, H., Stern, R. S., Arndt, K. A. et al.:[4] The incidence of erythema multiforme, Stevens–Johnson syn-drome and toxic epidermal necrolysis. Arch. Dermatol., 1990, 126, 43–47.Fritsch, P. O., Ruiz-Maldonado, R.:[5] Stevens–Johnson syndrome toxic epidermal necrolysis. In: Freedberg, I. M., Eisen, A. Z., Wolff, K. et al. (eds): Fitzpatrick’s Dermatology in General Medicine, vol. 1, 5th edn. McGraw-Hill, New York, 1999, pp. 644–654.
CASE REPORTS
CEMED 201 2010 ▪ Volume 4, Number 1

Roujeau, J-C, Kelly, J. P., Naldi, L. et al.:[6] Medication use and the risk of Stevens–Johnson syndrome or toxic epidermal necrolysis. N. Engl. J. Med., 1995, 333, 1600–1607.Hazir, T., Saleem, M., Abbas, K. A.:[7] Stevens–Johnson syndrome following measles vaccination. J. Pak. Med. Assoc., 1997, 47, 264–265.Tan, Y. M., Goh, K. L.:[8] Esophageal stricture as a late complication of Stevens–Johnson syndrome. Gastroin-test. Endosc., 1999, 50, 566–568.
Power, W. J., Ghoraishi, M., Merayo-Lloves, J. et al.:[9] Analysis of the acute ophthalmic manifestations of the erythema multiforme/Stevens–Johnson syndrome/toxic epidermal necrolysis disease spectrum. Ophthal-mology, 1995, 102, 1669–1676.Roujeau, J. C.:[10] Treatment of severe drug eruptions. J. Dermatol., 1999, 26, 718–722.Kazmierowski, J. A., Wuepper, K. D.:[11] Erythema multiforme. In: Provost, T. T., Farmer, E. R. (eds): Current Therapy in Dermatology, vol. 2. BC Decker, Philadelphia, 1988, pp. 47–48.Patterson, R., Miller, M., Kaplan, M. et al.:[12] Effectiveness of early therapy with corticosteroids in Stevens–Johnson syndrome: experience with 41 cases and a hypothesis regarding pathogenesis. Ann. Allergy, 1994, 73, 27–34.Patterson, R., Grammer, L. C., Greenberger, P. A. et al.:[13] Stevens–Johnson syndrome (SJS): effectiveness of corticosteroids in management and recurrent SJS. Allergy Proc., 1992, 13, 89–95.Noskin, G. A., Patterson, R.:[14] Outpatient management of Stevens–Johnson syndrome: a report of four cases and management strategy. Allergy Asthma Proc., 1997, 18, 29–32.
2010 ▪ Volume 4, Number 1 202 CEMED
CASE REPORTS

Primary Adenocarcinoma of the Rectovaginal Septum Without Associated Endometriosis
ZOLTÁN LANGMÁR1, 5, MIKLÓS NÉMETH2, TAMÁS MÁTRAI3, KÁLMÁN IVÁNYI1, LÁSZLÓ HARSÁNYI4, MAGDOLNA DANK5,
ESZTER SZÉKELY6, ZOLTÁN KAZY1
12nd Department of Obstetrics and Gynecology, Faculty of Medicine, Semmelweis University, Budapest, Hungary
2Department of Obstetrics, Gynecology and Gynecologic Oncology, St. Stephan Hospital, Budapest, Hungary
3Department of General and Chest Surgery, National Institute of Oncology, Budapest, Hungary41st Department of Surgery, Faculty of Medicine, Semmelweis University, Budapest, Hungary
5Department of Diagnostic Radiology and Oncotherapy, Faculty of Medicine, Semmelweis University, Budapest, Hungary
62nd Department of Pathology, Faculty of Medicine, Semmelweis University, Budapest, Hungary
Primary adenocarcinoma of the rectovaginal septum is a rare clinical entity that arises most often from endometriosis. The authors report a successfully treated case of primary adenocarcinoma of the rec-tovaginal septum without associated endometriosis in a 68-year-old woman. Diagnostic and treatment modalities were reviewed by the authors emphasizing that early diagnosis is diffi cult and that the only curative method is primary surgical therapy.
Keywords: adenocarcinoma, rectovaginal septum, endometriosis, therapy
Primary adenocarcinoma of the rectovaginal septum is a rare clinical entity that arises most often from endometriosis [1–7]. Regarding this issue, there are only a few relevant publica-tions in international literature. Associated endometriosis was confi rmed in most cases [8]. Adenocarcinoma of the rectovaginal septum can be asymptomatic for a considerable time. According to the literature, early diagnosis is possible only by physical and radiologic ex-aminations performed for other reasons [2, 8–10]. The authors present a case of a primary rectovaginal adenocarcinoma without associated endometriosis successfully treated with pri-mary surgical resection and combined chemotherapy. The patient is under regular follow-up and so far no recurrence has been confi rmed.
Case ReportThe 68-year-old female patient with a suspected vaginal tumour was referred to our depart-ment from an outpatient gynaecology clinic on 2nd October 2006. The patient complained of vague pressure from the anus. Her obstetrical history was unexceptional (one vaginal birth without complications and one spontaneous abortion). She had her last regular period at the age of 45. She had not received any hormone replacement therapy and had never been on
Corresponding address: Zoltán Langmár MD, 2nd Department of Obstetrics and Gynecology, Semmelweis Univer-sity, Üllői út 78/A, H-1082 Budapest, Hungary. E-mail: [email protected]
28442
CASE REPORTS
DOI: 10.1556/CEMED.4.2010. 203 2010 ▪ Volume 4, Number 1 ▪ 203–206.
contraceptive pills. Major items of her general anamnesis were the medically balanced hy-pertension and gastroesophageal refl ux disease.
Physical Findings
The outer genitalia were normal for her age. A compact, moderately sensitive tumour was palpable on the back vaginal wall expanding in the direction of the rectovaginal space. The uterus was normal and the surrounding area was slightly sensitive on both sides without pal-pable mass. Tissue above the vaginal tumour appeared macroscopically intact during colpos-copy.
Vaginal and Abdominal Ultrasonography
There was cystic formation (31 mm × 37 mm) with irregular shape on the right side of the uterus and increased vascularisation around the edges of the tumour but without fl ow param-eters inactive of malignity.
Based on the fi ndings, our attempt was to excise the tumour vaginally. The resection was performed under intra-venous narcosis. Considering intra-operatively that a wide excision of the tumour has a risk of intestinal injury due to the proximity of the rectum, only a punch-biopsy was done. Histopathological examination revealed a necrotic adenocarcinoma which may have originated from the vaginal glands (Dr. Németh–Dr. Járay). Based on this result, an abdominal operation was planned. The second operation was performed by a multi-speciality team (abdominal surgeon, general gynaecologist and gynaecologic oncologist) at the 1st De-partment of Surgery under intra-tracheal narcosis. The exploration was done through a lower midline laparotomy. Following isolation of the bowels, the greenish, walnut-sized, smooth-surfaced tumour was observed to be unseparated from the ovaries. No other pathological changes were observed in the abdominal cavity. During the operation, hysterectomy and bi-lateral salpingo-oophorectomy was performed. Owing to the proximity of the vagina and the rectum, the upper third of the vagina and an ampullar part of the rectum were also resected. The rectovaginal lesion was removed in this block. Subsequently, an end-to-end anastomosis of the rectum was performed. After repeated evaluation of the entire abdominal cavity and the omentum, no pathological changes were observed. The post-operational course was un-eventful and the patient was discharged from the hospital on the eighth day with normal in-testinal function. Based on the histopathological fi ndings (adenocarcinoma of the vagina, endometrioid subtype, ovarian metastasis), the patient was recommended to be given adju-vant oncotherapy. Since the patient refused radiotherapy, she was given six cycles of com-bined paclitaxel–carboplatin chemotherapy. The patient is currently symptom and complaint free and serial radiologic examinations have not detected any tumour recurrence so far.
Hystopathological Summary (Dr Székely)
Based on the histological and immunohistochemical evaluation, the origin of the papillary endometroid carcinoma may have been the rectovaginal septum (according to the literature, this is possible on the basis of endometriosis). The tumour expanded through the parametri-um into the right ovary and the surface of the rectum. FIGO stage: IVB.
2010 ▪ Volume 4, Number 1 204 CEMED
CASE REPORTS

DiscussionPrimary adenocarcinoma of the rectovaginal septum is a rare clinical entity that arises in most of the cases from endometriosis [3, 4]. Adenocarcinoma without associated endometri-osis was confi rmed in only three cases. The age of the patients ranged between 32 and 54 years. The fi rst symptoms of the disease were urinary retention, aspecifi c pain, excessive vaginal discharge, abdominal discomfort and rectal or vaginal bleeding [4, 6–11]. Diagnosis is diffi cult and often delayed because of the location of the tumour. Correspondingly, only unspecifi c symptoms and complaints caused by an advanced clinical condition call attention to the malignant tumour. The average diameter of the diagnosed primary tumours is 3.5 cm (1–6 cm). According to the publications, the only curative therapy is primary surgical re-moval [2, 8–11]. Advanced tumours, however, require intestinal surgery and may potentially necessitate complete removal of the rectum and the application of colostoma. In our case total removal of the tumour was possible by a partial resection of the rectum and by perform-ing an end-to-end anastomosis. Histological evaluation of the published cases verifi ed the existence of papillary adenocarcinoma, adenoacanthoma or clear cell adenocarcinoma [3–6, 8–11]. Despite the data that the formation of the tumour is linked to the existence of endo-metriosis and its “malignisation theory”, there is little data to prove this unequivocally. Ma-lignant transformation has been verifi ed only in 1% of the endometriosis cases [5]. We have not diagnosed a co-existence of endometriosis either. This may have several reasons accord-ing to the literature: (1) regression of endometriosis after the menopause; (2) the expanding tumour destroys the endometriotic nodules; (3) the tumour originates primarily from the glands of the vagina or the rectum independently from endometriosis (in our case this process can be excluded); (4) in the rectovaginal septum, endometriosis forms by a mechanism dif-ferent from that formed in other areas of the body (metaplasia of the Müllerian-duct rem-nants) and thus makes it diffi cult to evaluate histological picture [12]. Evidence for the latter may be that the endometric nodules located here do not respond to usual drug treatment either. There are no conclusive opinions regarding the therapy of this clinical entity because of the rarity of the disease; however, each author emphasizes the importance of primary surgical treatment. Several authors recommend post-operative radiotherapy with or without chemotherapy [1–4, 9, 13, 14]. Since our patient refused radiotherapy unequivocally, and taking into consideration the request of the patient as a follow-up treatment, she was given six cycles of combined paclitaxel–carboplatin chemotherapy, which proved to be effi cient. Our intention of presenting this rare case is to call attention to the diffi culties of the early diagnosis of the tumours originating from the rectovaginal septum and the exact evaluation of non-specifi c symptoms potentially related to malignant tumours.
ReferencesHernádi, Z.:[1] Carcinoma vaginae. In: Hernádi, Z. (ed): Nőgyógyászati onkológia. Therapia Kiadó, Budapest, 2004, pp. 66–73.Slomovitz, B. M., Coleman, R. L.:[2] Invasive cancer of the vagina and the urethra. In: DiSaia, P. J., Creasman, W. T. (eds): Clinical Gynecologic Oncology. Mosby-Elsevier, St. Louis, 2007, pp. 265–276.Yazbeck, C., Poncelet, C., Chosidow, D. et al.:[3] Primary adenocarcinoma arising from endometriosis of the rectovaginal septum: a case report. Int. J. Gynecol. Cancer, 2005, 15, 1203–1205.
CASE REPORTS
CEMED 205 2010 ▪ Volume 4, Number 1
Dockerty, M. B., Pratt, J. H., Decker, D. J.:[4] Primary adenocarcinoma of the rectovaginal septum probably arising from endometriosis. Report of two cases. Cancer, 1954, 7, 893–898.Ferreira, H. P., Clayton, S. G.:[5] Three cases of malignant change in endometriosis, including two cases arising in the rectovaginal septum. J. Obstet. Gynaecol. Br. Emp., 1958, 54, 41–44.Lash, S. R., Rubenstone, A. I.:[6] Adenocarcinoma of the rectovaginal septum probably arising from endometrio-sis. Am. J. Obstet. Gynecol., 1959, 78, 299–302.Han, A. C., Hiovenden, S., Rosenblum, N. G. et al.:[7] Adenocarcinoma arising in extragonadal endometriosis. Cancer, 1998, 83, 1163–1168.Berger, A., Rouzier, R., Carnot, F. et al.:[8] Primary adenocarcinoma of the rectovaginal septum: a report and literature review. Eur. J. Obstet. Gynecol. Reprod. Biol., 2001, 95, 111–113.Ulrich, U., Rhiem, K., Kaminski, M. et al.:[9] Parametrial and rectovaginal adenocarcinoma arising from en-dometriosis. Int. J. Gynecol. Cancer, 2005, 15, 1206–1209.Davis, J. M.:[10] Carcinoma of the rectovaginal septum. Proc. R. Soc., 1967, 60, 24.Young, E. E., Gamble, C. N.:[11] Primary adenocarcinoma of the rectovaginal septum arising from endometriosis. Cancer, 1969, 24, 597–601.Nisolle, M., Donnez, J.:[12] Peritoneal endometriosis, ovarian endometriosis, and adenomyotic nodules of the rectovaginal septum are three different entities. Fertil. Steril., 1997, 68, 585–596.Poller, I.:[13] A hüvely. In: Németh, Gy. (ed): Sugárterápia. Springer, Berlin, 2001, pp. 347–350.Harrison, M. M., Marx, G. M., Hacker, N. F. et al.:[14] Cytotoxic drug treatment of vulval and vaginal cancer. In: Bősze, P., Markman, M. (eds): What Gynecologic Oncologists Should Know About Chemotherapy. NOK Press, Budapest, 2005, pp. 184–185.
2010 ▪ Volume 4, Number 1 206 CEMED
CASE REPORTS

Pitfalls in Management of Chronic Hepatitis B: Report of Four Cases from Bangladesh
MD. FAZAL KARIM1, MAMUN AL-MAHTAB2, SALIMUR RAHMAN2, MOBIN KHAN2
1Department of Hepatology, Dhaka Medical College, Dhaka, Bangladesh2Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh
Treatment of chronic hepatitis B has changed much since the introduction of interferon. Nucleosides have come to replace interferon in some situations like decompensated states. However, there is no clear cut guideline in many fi elds. Even end of treatment response is low in conventional treatments. This study describes a few scenarios where diffi culties were faced. Unresolved questions in the management of chronic hepatitis B involve ‘who to treat, when to treat, how to treat?’ These should be clearly addressed.
Keywords: chronic hepatitis B, management, pitfalls
IntroductionManagement of chronic hepatitis B is ever evolving. Many issues are still unresolved or par-tially solved. New information on the clinical management of chronic hepatitis B is emerging rapidly, requiring that physicians be alert to updated treatment recommendations. Hepatolo-gists, in many issues, consult among themselves about how to proceed. Resistance to nucleo-side and nucleotide analogs is becoming an increasingly common clinical problem. HBV DNA titer for management has been lowered to encompass more patients and to avoid com-plication of disease. Current anti-viral agents are not suffi cient to effect viral control. The ideal drug that will eradicate the HBV has yet to be developed [1].
Two major groups of anti-viral therapies are currently in use. These are interferon-α [IFN-α (or pegylated interferon-α, PEG IFN-α)] and nucleoside or nucleotide analogues. There are new nucleoside and nucleotides in the pipeline. Clearance of infected hepatocytes occurs in only a small proportion of patients. The continued use of single nucleotides in se-quence may lead to the emergence of multidrug resistant hepatitis B [2].
Corresponding address: Mamun Al-Mahtab MD, Department of Hepatology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh. E-mail: [email protected]
1.22
CASE REPORTS
DOI: 10.1556/CEMED.4.2010. 207 2010 ▪ Volume 4, Number 1 ▪ 207–210.
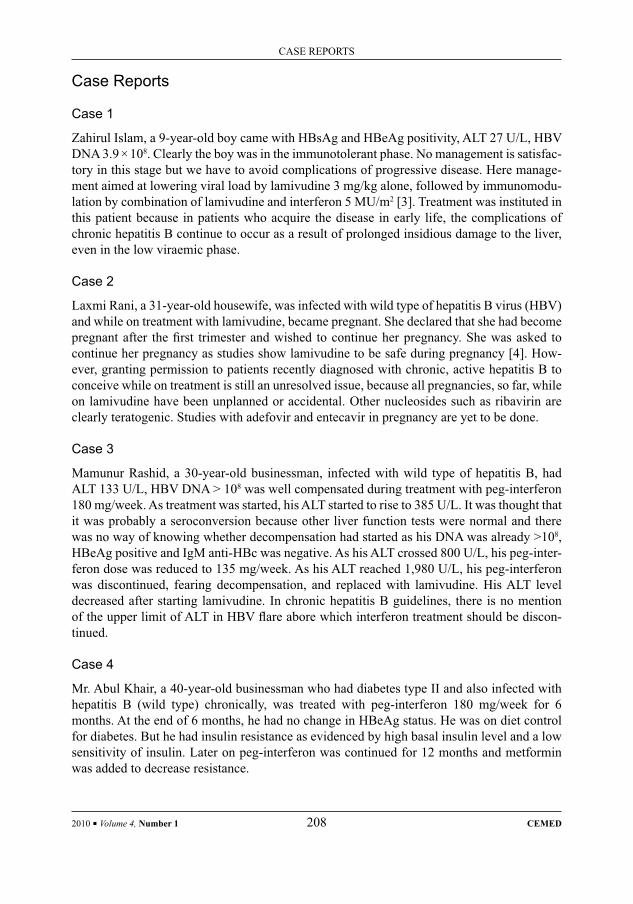
Case Reports
Case 1
Zahirul Islam, a 9-year-old boy came with HBsAg and HBeAg positivity, ALT 27 U/L, HBV DNA 3.9 × 108. Clearly the boy was in the immunotolerant phase. No management is satisfac-tory in this stage but we have to avoid complications of progressive disease. Here manage-ment aimed at lowering viral load by lamivudine 3 mg/kg alone, followed by immunomodu-lation by combination of lamivudine and interferon 5 MU/m2 [3]. Treatment was instituted in this patient because in patients who acquire the disease in early life, the complications of chronic hepatitis B continue to occur as a result of prolonged insidious damage to the liver, even in the low viraemic phase.
Case 2
Laxmi Rani, a 31-year-old housewife, was infected with wild type of hepatitis B virus (HBV) and while on treatment with lamivudine, became pregnant. She declared that she had become pregnant after the fi rst trimester and wished to continue her pregnancy. She was asked to continue her pregnancy as studies show lamivudine to be safe during pregnancy [4]. How-ever, granting permission to patients recently diagnosed with chronic, active hepatitis B to conceive while on treatment is still an unresolved issue, because all pregnancies, so far, while on lamivudine have been unplanned or accidental. Other nucleosides such as ribavirin are clearly teratogenic. Studies with adefovir and entecavir in pregnancy are yet to be done.
Case 3
Mamunur Rashid, a 30-year-old businessman, infected with wild type of hepatitis B, had ALT 133 U/L, HBV DNA > 108 was well compensated during treatment with peg-interferon 180 mg/week. As treatment was started, his ALT started to rise to 385 U/L. It was thought that it was probably a seroconversion because other liver function tests were normal and there was no way of knowing whether decompensation had started as his DNA was already >108, HBeAg positive and IgM anti-HBc was negative. As his ALT crossed 800 U/L, his peg-inter-feron dose was reduced to 135 mg/week. As his ALT reached 1,980 U/L, his peg-interferon was discontinued, fearing decompensation, and replaced with lamivudine. His ALT level decreased after starting lamivudine. In chronic hepatitis B guidelines, there is no mention of the upper limit of ALT in HBV fl are abore which interferon treatment should be discon-tinued.
Case 4
Mr. Abul Khair, a 40-year-old businessman who had diabetes type II and also infected with hepatitis B (wild type) chronically, was treated with peg-interferon 180 mg/week for 6 months. At the end of 6 months, he had no change in HBeAg status. He was on diet control for diabetes. But he had insulin resistance as evidenced by high basal insulin level and a low sensitivity of insulin. Later on peg-interferon was continued for 12 months and metformin was added to decrease resistance.
2010 ▪ Volume 4, Number 1 208 CEMED
CASE REPORTS
DiscussionUnresolved questions in management of chronic hepatitis B involve “who to treat, when to treat, how to treat” [5]. Although various drugs are available for the treatment of chronic hepatitis B, emergence of the hepatitis B e antigen (HBeAg)-negative mutant variant, spe-cifi cally in Asia, the Middle East and southern Europe, is creating a new challenge as this variant is less responsive to available treatments. HBeAg-negative chronic hepatitis B rap-idly progresses to cirrhosis and its related complications [6]. The end points of treatment are not clearly defi ned, and differ in HBeAg positive versus negative disease [2].
Issues that remain controversial or need to be studied further are the necessity of a base-line liver biopsy, the HBV DNA and ALT thresholds for initiation of therapy, the optimal duration of anti-viral therapy, selection of one agent over another, and the role of combination therapy [7].
Clear guidelines regarding treatment of special groups are lacking. Management of spe-cial populations, including patients with normal alanine aminotransferase levels, children and adolescents, women planning pregnancy or already pregnant, patients undergoing che-motherapy or other forms of immunosuppression, patients with HBV and human immunode-fi ciency virus co-infection, and those undergoing liver transplantation, present further chal-lenges [8].
There is no non-invasive technique of knowing the underlying necro-infl ammatory or fi brosis stage. So many cases are missed in which patients do not wish to do biopsy or where biopsy is relatively or absolutely contraindicated. Also, there is no guideline regarding treat-ment of chronic hepatitis B in patients with insulin resistance.
There are situations where patients are having decompensated liver disease related to chronic hepatitis B. Here we prefer to use nucleoside analog, particularly lamivudine, without considering HBeAg status or HBV DNA level as the patient will ultimately deterio-rate. Here adefovir is not a good choice as these patients usually or ultimately develop hepa-torenal syndrome where adefovir is contraindicated. The combination of lamivudine and adefovir is a preferred agent where close monitoring of renal function is undertaken.
If we stop lamivudine in the face of resistance where patient has good immune status, there is no harm, as continuing treatment will add to resistance. Addition of adefovir is a good alternative. In treatment of naïve wild chronic HBV infection, sequential therapy with lami-vudine followed by IFN-α seems to have better sustained virologic response [9]. In precore mutants lamivudine is associated with the risk of developing viral mutants and, after therapy discontinuation, with high rate of relapse. In relapsing patients, severe acute recurrence of hepatitis B may occur [10].
Despite the emergence of multidrug-resistant strains of HBV and previous success with combination therapy for other chronic viral infections, we are still using sequential mono-therapy for chronic HBV infection. There is now an emerging body of data suggesting that combination therapy can decrease anti-viral resistance in HBV infection [11].
There are many case reports of hepatic decompensation after administration of inter-feron as a fi rst line anti-viral agent. Then switch to nucleoside analog is undertaken. If we calculate the tolerance of the patient to interferon from the beginning, we can avoid decom-pensation.
If we measure the HBV DNA level in acute hepatitis B and start lamivudine depending on DNA level, then we can avoid fulminant hepatic failure.
CASE REPORTS
CEMED 209 2010 ▪ Volume 4, Number 1

ConclusionTreatment of chronic hepatitis B is still in development. Many questions will arise until a potent anti-viral and immunomodulatory option is established. Funding: none.
ReferencesArosemena, L. R., Cortes, R. A., Servin, L. et al.:[1] Current and future treatment of chronic hepatitis B. Minerva Gastroenterol. Dietol., 2005, 51, 77–93, PMID: 15756148.Dusheiko, G., Antonakopoulos, N.:[2] Treatment of hepatitis B. Gut, published 14 May 2007, DOI 10.1136/gut.2005.077891, PMID: 17502343.D’Antiga, L., Marion, Aw., Atkins, M. et al.:[3] Combined lamivudine/interferon-α treatment in ‘immunotoler-ant’ children perinatally infected with hepatitis B: a pilot study. J. Pediatr., 2006, 148, 228–233, PMID: 16492434.Su, G. G., Pan, K. H., Zhao, N. F. et al.:[4] Effi cacy and safety of lamivudine treatment for chronic hepatitis B in pregnancy. World J. Gastroenterol., 2004, 10, 910–912, PMID: 15040044.Hoofnagle, J. H., Doo, E., Liang, T. J. et al.:[5] Management of hepatitis B: summary of a clinical research workshop. Hepatology, 2007, 45, 1056–1075, PMID: 17393513.Saikia, N., Talukdar, R., Mazumder, S. et al.:[6] Management of patients with HBeAg-negative chronic hepatitis B. Postgrad. Med. J., 2007, 83, 32–39, PMID: 17267676.Morgan, M., Park, W., Keeffe, E. B.:[7] Diagnosis and treatment of chronic hepatitis B: an update. Minerva Gastroenterol. Dietol., 2007, 53, 25–41, PMID: 17415343.Dore, G. J., Guan, R., Wasim Jafri, S. M. et al.:[8] Management of chronic hepatitis B in challenging patient populations. Liver Int., 2006, 26 (Suppl. 2), 38–46, PMID: 17087768.Yuen, M. F., Lai, C. L.:[9] Combination therapy for chronic hepatitis B: simultaneous or sequential? Am. J. Gas-troenterol., 2007, 102, 105–106, PMID: 17266690.Ascione, A., Ascione, T., Lanza, A. G. et al.:[10] Factors infl uencing outcome of lamivudine in anti-HBe-positive chronic hepatitis B. Hepatogastroenterology, 2006, 53, 919–923, PMID: 17153453.Sasadeusz, J. J., Locarnini, S. L., Macdonald, G.:[11] Why do we not yet have combination chemotherapy for chronic hepatitis B? Med. J. Aust., 2007, 186, 204–206, PMID: 17309424.
2010 ▪ Volume 4, Number 1 210 CEMED
CASE REPORTS

Acute Pancreatitis in a Pregnant Female with Peripartum Cardiomyopathy
PANKAJ JAIN
Department of Gastroenterology, Apollo Modi Hospital, Kota, India
Acute pancreatitis (AP) and peripartum cardiomyopathy (PPC) are rare complications during pregnancy and can lead to high maternal mortality and fetal loss. We report a case of a 34-year-old multigravida at 36 weeks gestation diagnosed to have AP who delivered a cyanosed fetus. Subsequently, she developed PPC and recovered on conserva-tive treatment.
Keywords: acute pancreatitis, pregnancy, peripartum cardiomyopathy
Acute pancreatitis (AP) is a rare complication during pregnancy and can lead to high mater-nal mortality and fetal loss [1]. We report a case of a 34-year-old multigravida with 36 weeks gestation diagnosed to have AP who delivered a cyanosed child who was revived with resus-citative measures. Subsequently, she developed peripartum cardiomyopathy (PPC) and re-covered on conservative treatment.
CaseA 34-year-old gravid three, para one, abortion one with one live issue, with 36 weeks preg-nancy, was admitted for 1 day with pain in the abdomen and vomiting. The pain was in the epigastrium, radiating to the back and associated with vomiting the food she had taken. There was no history of alcohol or any other drug intake. She had past history of eclampsia in the fi rst pregnancy. On examination, she had pallor with pulse rate of 84/min and blood pressure 120/70 mmHg. On examination, uterine fundal height was 36 weeks with fetal heart sound present, tenderness in epigastric region and bowel sound absent. Investigation revealed hemoglobin of 11.3 g/dL (normal 12–16 g/dL), total leucocyte count 10.4 × 103/mm3 (normal 4–10 × 103/mm3), neutrophilic leucocytosis, a normal platelet count, bilirubin, serum alanine aminotransferase, serum aspartate aminotransferase, urea, creatinine, sodium, potassium and random blood sugar were normal. Her serum amylase was 1,880 U/L, serum lipase 520 U/L, serum alkaline phosphatase 530 U/L, serum LDH 278 IU/L, serum triglycerides 308 mg/dL (normal < 170 mg/dL), serum calcium 9.4 mg/dL (normal 9–11 mg/dL) and serum albumin 3.1 g/dL. Urine examination revealed no albumin.
Ultrasonography revealed bulky pancreas with peripancreatic fl uid (Fig. 1), gall bladder fi lled with sludge (Fig. 2), a live fetus of 36 weeks. So, she was diagnosed to have AP. She was managed conservatively with nil per mouth, continuous nasogastric suction via nasogas-
Corresponding address: Pankaj Jain MD, Department of Gastroenterology, Apollo Modi Hospital, Kota, India.E-mail: [email protected]
1.23
CASE REPORTS
DOI: 10.1556/CEMED.4.2010. 211 2010 ▪ Volume 4, Number 1 ▪ 211–214.
Fig. 1 Ultrasound of abdomen shows enlarged pancreas and peripancreatic lymph node
Fig. 2 Ultrasound of abdomen shows gall bladder sludge
2010 ▪ Volume 4, Number 1 212 CEMED
CASE REPORTS
tric tube, intravenous fl uid, antibiotic and analgesics. Fetus monitoring was done by daily fetal heart sound auscultation and ultrasound for liquor.
On the second day, ultrasound for fetus showed absent liquor. She underwent cesarean section, delivered a cyanosed child with an Apgar score of 4. The child was revived with re-suscitation measures.
Postoperative, she developed sudden onset dyspnea, hypertension, with chest ausculta-tion showing bilateral crepitation and echocardiography revealed an ejection fraction of 30%, with all the four chambers dilated. Her electrocardiogram showed ventricular tachycardia, but blood pressure was normal. She was intubated, put on ventilator and managed with oxygen, diuretics, amiodarone and antibiotics. She was extubated next day and was hemody-namically stable. She was started orally on the fourth day on a low fat diet and tolerated it. She was discharged on the tenth day on diuretics, amiodarone and low fat diet. She under-went laparoscopically cholecystectomy 4 weeks later. Her repeat echocardiography done 3 months later showed an improvement in ejection fraction to 50%.
DiscussionBiliary sludge and gallstones (GS) form in up to 31% and 3% of pregnant women, respec-tively, although sludge frequently resolves postpartum [2]. The index case had epigastric pain and elevated serum amylase and lipase levels consistent with AP, which occurs in approxi-mately one in 1,000–3,300 pregnancies [1]. Pancreatitis during pregnancy occurs in 72% of multiparous females who had pancreatitis and 52% occurs in the third trimester [1]. GS dis-ease is the most common cause of pancreatitis and occurs in 67–100% of cases during preg-nancy [1].
The development of biliary tract complication during pregnancy has implications for maternal and fetal morbidity. Eddy et al. [3] in their 10-year study of 101 patients of AP in 305,101 deliveries reported 3.6% perinatal mortality but no maternal deaths. Although GS were not diagnosed at any stage, biliary sludge is considered to be a precursor of GS and can be a cause of AP. Pregnancy increases serum cholesterol and triglyceride levels, increases bile stasis due to high progesterone levels and thus may induce GS formation. The changes in hepatic bile that occurs in the last trimester of pregnancy is due to high estrogen levels [4]. Pancreatitis in pregnancy is also proposed due to refl ux of gastrointestinal contents into am-pulla of vater, mutations in the cystic fi brosis transmembrane conductance regulator gene and immunological interactions between mother and child.
Management of AP during pregnancy should initially be similar to management in non-pregnant patients, with fl uid resuscitation, narcotic pain control and nutritional supplementa-tion. The fetus should be carefully monitored by external heart rate monitoring. Cholecystec-tomy should be delayed until after delivery if pancreatitis develops in the third trimester.
Cardiac complications associated with severe AP are congestive heart failure, myocar-dial infarction, cardiac arrhythmia, and cardiogenic shock. Myocardial depression and shock are thought to be secondary to vasoactive peptides and a myocardial depressant factor. There is an increase in cardiac index and a decrease in total peripheral resistance, which usually respond to infusion of crystalloids. Intravenous dopamine can be started in those patients in whom hypotension persists despite fl uid resuscitation to maintain the systemic blood pres-sure.
CASE REPORTS
CEMED 213 2010 ▪ Volume 4, Number 1

PPC is a rare form of heart failure of unknown cause with an incidence of one in 3,000 live births, onset between last month of pregnancy up to 5 months postpartum with a reported high maternal morbidity and mortality of 20–50% [5]. Early diagnosis and treatment of PPC are essential for a favorable outcome. Poor prognostic factors are high parity, twin gestation, age greater than 30 years, and a late onset of symptoms after delivery [6]. Patients with PPC should receive standard heart failure therapy. Therapy regimens include diuretics to diminish volume overload, afterload reduction with angiotensin-converting enzyme inhibitors and β-blockers after signs and symptoms of congestion improve. Anticoagulation therapy can be given to patients postpartum if symptoms are persistent or ventricular function is mark-edly decreased, as such individuals have a high risk of systemic and pulmonary embolism. Our patient had high parity and age greater than 30 years, but prompt accurate diagnosis and therapy led to her recovery.
So, biliary tract disease should be considered in any pregnant woman with abdominal pain.
ReferencesRamin, K. D., Ramin, S. M., Richey, S. D. et al.:[1] Acute pancreatitis in pregnancy. Am. J. Obstet. Gynecol., 1995, 173, 187–191.Ko, C. W.:[2] Incidence, natural history, and risk factors for biliary sludge and stones during pregnancy. Hepatol-ogy, 2005, 41, 359–365.Eddy, J. J., Gideonsen, M. D., Song, J. Y. et al.:[3] Pancreatitis in pregnancy. Obstet. Gynecol., 2008, 112, 1075–1081.Lynn, J., Williams, L., O Brien, J.:[4] Effects of estrogen upon bile: implication with respect to gallstone forma-tion. Ann. Surg., 1973, 178, 514–524.Veille, J. C., Zaccaro, D.:[5] Peripartum cardiomyopathy: summary of an international survey on peripartum cardiomyopathy. Am. J. Obstet. Gynecol., 1999, 181, 315–319.Ravikishore, A. G., Kaul, U. A., Sethi, K. K. et al.:[6] Peripartum cardiomyopathy: prognostic variables at initial evaluation. Int. J. Cardiol., 1991, 32, 377–380.
2010 ▪ Volume 4, Number 1 214 CEMED
CASE REPORTS

Submission of PapersAll manuscripts for Clinical and Experimental Medical Journal (CEMED) should be submit-ted online via the Editorial Manager system (see NOTE below). This is the preferred method of submission, and facilitates processing of your manuscript. Only in exceptional cases where the authors have no electronic facilities, the author should submit one original copy of the manuscript, plus two photocopies and a copy on disk, to the following address:
Editor-in-Chief: Professor János Fehér, 2nd Department of Medicine, Medical Faculty, Semmelweis University, Szentkirályi u. 46, H-1088 Budapest. Phone/fax: +36 1 317 4548.
Authors are required to submit, with their manuscripts, the names and full contact de-tails (including e-mail address) of 3 potential referees (who should not come from the same institute).
It is the author’s responsibility to ensure that papers are written in clear and comprehen-sible English. Authors whose native language is not English are strongly advised to have their manuscripts checked by an English-speaking colleague prior to submission.
Submission of a paper implies that it has not been published previously (except in the form of an abstract or as part of a published lecture or academic thesis), that it is not under consideration for publication elsewhere, that its publication is approved by all authors and tacitly or explicitly by the responsible authorities where the work was carried out, and that, if accepted, it will not be published elsewhere in the same form, in English or in any other lan-guage, without the written consent of the Publisher.
NOTE: We are pleased to announce that the online manuscript submission and peer review system EditorialManager has been introduced for the submission of manuscripts to the Clin-ical and Experimental Medical Journal. Details are available online at: www.edmgr.com/cemed.
Types of ContributionsOriginal research papers; review articles; rapid communications; short communications; viewpoints; letters to the Editor; book reviews.1. Research papers – original full-length research papers which have not been published
previously, except in a preliminary form, and should not exceed 8500 words (including allowance for no more than 6 tables and illustrations).
2. Review articles – will be accepted in areas of topical interest, will normally focus on lit-erature published over the previous fi ve years, and should not exceed 12,000 words (in-cluding allowance for no more than 6 tables and illustrations).
3. Rapid communications – an original research paper reporting a major scientifi c result or fi nding with signifi cant implications for the research community, designated by the Editor.
4. Short communications – Short communications of up to 3500 words, describing work that may be of a preliminary nature but which merits immediate publication.
1.24
GUIDE TO THE AUTHORS
GUIDE TO THE AUTHORS
DOI: 10.1556/CEMED.4.2010. 215 2010 ▪ Volume 4, Number 1 ▪ 215–217.

5. Viewpoints – Authors may submit viewpoints of about 1500 words on any subject cov-ered by the Aims and Scope.
6. Letters to the Editor – Letters are published from time to time on matters of topical inter-est.
7. Book reviews.
Manuscript PreparationGeneral: Manuscripts must be typewritten, double-spaced with wide margins on one side of white paper. Each page must be numbered, and lines must be consecutively numbered from the start to the end of the manuscript. Good quality printouts with a font size of 12 or 10 pt are required. The corresponding author should be identifi ed (include a fax number and an e-mail address). Full postal addresses must be given for all co-authors. Authors should consult a recent issue of the journal for style if possible. An electronic copy of the paper should ac-company the fi nal version. The Editors reserve the right to adjust style to certain standards of uniformity. Authors should retain a copy of their manuscript since we cannot accept respon-sibility for damage or loss of papers. Original manuscripts are discarded one month after publication unless the Publisher is asked to return original material after use.
Abstracts: Each paper should be provided with an abstract of 100–150 words, reporting concisely on the purpose and results of the paper.
Keywords: 3–5 characteristic words of the manuscript.Text: Follow this order when typing manuscripts: Title, Authors, Affi liations, Abstract,
Keywords, Abbreviations, Main text, Acknowledgments, Appendix, References, Figure Cap-tions and then Tables. Do not import the Figures or Tables into your text. The corresponding author should be identifi ed with an asterisk and footnote. All other footnotes (except for table footnotes) should be identifi ed with superscript Arabic numbers. The title of the paper should unambiguously refl ect its contents. Where the title exceeds 80 characters, a suggestion for an abbreviated running title should be given.
Units: The SI system should be used for all scientifi c and laboratory data; if, in certain instances, it is necessary to quote other units, these should be added in parentheses. Tem-peratures should be given in degrees Celsius. The unit ‘billion’ (109 in America, 1012 in Eu-rope) is ambiguous and should not be used.
Symbols: Abbreviations for units should follow the suggestions of the British Standards publication BS 1991. The full stop should not be included in abbreviations, e.g. m (not m.), ppm (not p.p.m.), % and ‘/ ’ should be used in preference to ‘per cent’ and ‘per’. Where ab-breviations are likely to cause ambiguity or may not be readily understood by an interna-tional readership, units should be put in full.
Current recognised chemical nomenclature should be used, although commonly accept-ed trivial names may be used where there is no risk of ambiguity.
The use of proprietary names should be avoided. Papers essentially of an advertising nature will not be accepted.
References: All publications cited in the text should be presented in a list of referenc-es following the text of the manuscript with reference members in square brackets ([ ]). No more than 50 references should be cited in your manuscript. In the text refer to the num-
2010 ▪ Volume 4, Number 1 216 CEMED
GUIDE TO THE AUTHORS

ber cited in square brackets ([ ]) or the author’s name (without initials). The list of references should be arranged according to the citation by authors’ names and should be as full as pos-sible, listing all authors, the full title of articles and journals, publisher and year.
References should be given in the following form:
Finglas, P. M., Wigertz, K., Vahteristo, L. et al.: [1] Standardisation of HPLC techniques for the determination of naturally-occurring folates in food. Food Chem., 1999, 64, 245–255.Marasas, W. F. O.: [2] Fumonisins: History, worldwide occurrence and impact. In: L. S. Jackson, J.W. DeVries, L. B. Bullerman (eds): Fumonisins in Food, Advances in Experimental Medicine and Biology, Vol. 392. Ple-num Press, New York, 1996, pp. 1–18.Feher, J., Csomos, G., Vereckei, A.: [3] Free Radicals in Biology and Medicine. Springer Verlag, Berlin–Heidel-berg–NewYork–London–Paris–Tokyo, 1987.Noel, S., Collin, S.: [4] Trans-2-nonenal degradation products during mashing. In Proceedings of the 25th Euro-pean brewery convention congress. IRL Press, Oxford, 1995, pp. 483–490.
Figures and captions: When placing several fi gures in the manuscript, please strive for uniformity. The fi gures should be placed together, after the text, just like an enclosure. Intro-duction of the online version of CEMED removes restrictions on colour images. We encour-age authors to send high-resolution colour images – all these will remain in colour in the online version. The charge for publishing colour images in the printed version is 40 EUR (60 USD) + VAT per colour image.
Please submit fi gures in electronic form, as JPG or TIFF fi les, with a minimum of 300 dpi. Figure captions should be typed double-spaced on a separate page. The location of the fi gures in the text should also be clearly indicated.
Open Access articles for a moderate publishing fee. Clinical and Experimental Medical Journal is an Open Access journal. Authors of accepted manuscripts are requested to pay an article processing charge of 450 EUR or 620 USD (+ VAT where applicable) to cover the publishing costs of their paper. A limited number of waivers may be granted, particularly for authors from developing countries (contact the Editor-in-Chief for details).
Open Access policy of Clinical and Experimental Medical Journal includes the free and unrestricted self-archiving of the fi nal published version of papers on the Author’s webpage or on the Author’s institutional repository with open or restricted access. When self-archiving or communicating a paper via e-mail, the Author should quote the correct citation and en-close a link to the published article (http://dx.doi.org/[DOI of the Article without brackets]).
Offprints and/or PDF fi les of the CEMED papers can be ordered at [email protected] http://www.akkrt.hu/offprint for details and rates.
Editor-in-Chief: Prof. János FehérMD, DScSzentkirályi u. 46, H-1088 Budapest, HungaryInternet: www.akademiai.com/content/121436Phone/fax: +36 1 317 4548; E-mail: [email protected]émiai KiadóPrielle Kornélia u. 19/d, H-1117 Budapest, HungarySubmission of manuscripts: www.edmgr.com/cemed
GUIDE TO THE AUTHORS
CEMED 217 2010 ▪ Volume 4, Number 1