
Value of transesophageal echocardiography during repair of congenital heart defects
Upload
independentCategory
view
1download
0
Prognostic value of left atrial volume in patients whounderwent dobutamine stress echocardiography forknown or suspected coronary artery diseaseJeane Mike Tsutsui, MD,a, Paulo M. M. Dourado, MD,a Abdou Elhendy, MD,b Sandra N. R. S. Falcao, MD,a
Renise M. Goes, MD,a Antonio C. P. Chagas, MD,a Protasio L. da Luz, MD,a Jose A. F. Ramires, MD,a
and Wilson Mathias, Jr, MDa São Paulo, Brazil; and Marshfield, WI
Background Left atrial volume indexed (LAVI) has been reported as a predictor of cardiovascular events. Wesought to determine the prognostic value of LAVI for predicting the outcome of patients who underwent dobutamine stressechocardiography (DSE) for known or suspected coronary artery disease (CAD).
Methods From January 2000 to July 2005, we studied 981 patients who underwent DSE and off-line measurementsof LAVI. The value of DSE over clinical and LAVI data was examined using a stepwise log-rank test.
Results During a median follow-up of 24 months, 56 (6%) events occurred. By univariate analysis, predictors of eventswere male sex, diabetes mellitus, previous myocardial infarction, left ventricular ejection fraction (LVEF), left atrial diameterindexed, LAVI, and abnormal DSE. By multivariate analysis, independent predictors were LVEF (relative risk [RR] = 0.98, 95%CI0.95-1.00), LAVI (RR = 1.04, 95% CI 1.02-1.05), and abnormal DSE (RR = 2.70, 95% CI 1.28-5.69). In an incrementalmultivariate model, LAVI was additional to clinical data for predicting events (χ2 36.8, P b .001). The addition of DSE to clinicaland LAVI yielded incremental information (χ2 55.3, P b .001). The 3-year event-free survival in patients with normal DSE and LAVI≤33 mL/m2 was 96%; with abnormal DSE and LAVI ≤33 mL/m2, 91%; with normal DSE and LAVI N34 mL/m2, 83%; and withabnormal DSE and LAVI N34 mL/m2, 51%.
Conclusion Left atrial volume indexed provides independent prognostic information in patients who underwent DSEfor known or suspected CAD. Among patients with normal DSE, those with larger LAVI had worse outcome, and amongpatients with abnormal DSE, LAVI was still predictive. (Am Heart J 2008;156:1110-6.)
Dobutamine stress echocardiography (DSE) is a widelyused technique for diagnosis and prognostic evaluation ofpatients with known or suspected coronary artery disease(CAD).1-5 The detection of ischemia during DSE has beenbased on the assessment of transient segmental wallmotion abnormalities (WMAs). Other manifestations ofmyocardial ischemia include diastolic dysfunction, whichmay result in chronic pressure burden to left atrium.6,7
Left atrial volume is an accurate measurement of left atrialsize8,9 and reflects the chronicity and magnitude of theincreased left ventricular filling pressure. Left atrialvolume indexed (LAVI) by body surface area has been
From the aHeart Institute (InCor)-University of São Paulo Medical School, São Paulo, Braziand bDepartment of Cardiology-Marshfield Clinic, Marshfield, WI.This study was supported by FAPESP- Fundação de Amparo à Pesquisa do Estado de SãoPaulo, São Paulo, Brazil.Submitted December 16, 2007; accepted July 21, 2008.Reprint requests: Jeane Mike Tsutsui, MD, Heart Institute (InCor)-University of SãoPaulo Medical School, Avenida Dr, Enéas Carvalho de Aguiar, 44, Sao PauloCEP:05403-000, Brazil.E-mails: [email protected], [email protected]/$ - see front matter© 2008, Mosby, Inc. All rights reserved.doi:10.1016/j.ahj.2008.07.015
l,
associated with cardiovascular risk burden and has beenshown to provide prognostic information additional toclinical risk factors in different patient populations.10-14
Other risk factors of CAD such as hypertension, age, anddiabetes may result in decreased myocardial complianceand increased filling pressure, with subsequent leftatrial enlargement.Recently, normal resting LAVI has been shown to be
associated with a normal stress echocardiogram, sug-gesting that this would be a simple means of identifyingpatients with low probability of ischemia and lowlikelihood of severe CAD.15 The long-term prognosticvalue of left atrial volume measurements in patients whounderwent DSE is unknown. Therefore, we aimed tostudy the prognostic value of LAVI and DSE results forpredicting death and nonfatal myocardial infarction (MI)in patients with known or suspected CAD.
MethodsPatientsFrom January 2000 to July 2005, we studied 1,219 consecutive
patients from our institutional databank who were referred for

Tsutsui et al 1111American Heart JournalVolume 156, Number 6
DSE because of known or suspected CAD. Exclusion criteriawere age b18 years, nondiagnostic DSE, treatment with pace-maker implantation, hypertrophic cardiomyopathy, significantmitral valve disease (stenosis or regurgitation more thanmoderate), severe aortic stenosis, and resting 2-dimensionalimages not appropriate for retrospective off-line measurementsof left atrial size.Diabetes mellitus was defined as a fasting glucose level
≥120 mg/dL or the need for insulin or oral hypoglycemic agents.Hyperlipidemia was defined as a total cholesterol ≥200 mg/dLor treatment with lipid-lowering medications. Hypertensionwas defined as blood pressure ≥140/90 mm Hg or use ofantihypertensive medication. Antiischemic therapy wasdefined as chronic use of nitrates, β-blockers, or calcium-channel blockers. The study was approved by the InstitutionalReview Board of the University of São Paulo Medical School (SãoPaulo, Brazil), and written informed consent was obtained fromall patients.
Left atrial size parametersParameters of left atrial size were left atrial anteroposterior
diameter, left atrial volume, left atrial diameter indexed by bodysurface area (LADI), and LAVI. Measurements were performedoff-line from baseline echocardiographic views, obtainedbefore the stress test, by one observer who had no knowledge ofstress test results and prognostic data. The anteroposteriordiameter of the left atrium was measured by 2-dimensionalimaging, and left atrial volume was estimated using area-lengthformula according to recommendations of the American Societyof Echocardiography.9 Single-plane left atrial area was measuredat end-ventricular systole, ensuring that there was no fore-shortening of the atrium. The area was planimetered with theinferior left atrium border defined as the plane of the mitralannulus, excluding the confluence of the pulmonary veins andthe left atrial appendage. Left atrial length was obtained from themiddle of the plane of the mitral annulus to the root of leftatrium. In patients with atrial fibrillation, it was considered theaverage of 3 measurements. Interobserver variability of LADIand LAVI measurements were assessed in 30 randomly assignedsubjects by 2 independent observers. Intraobserver variability ofLADI and LAVI measurements were assessed in 30 randomlyassigned subjects by the same observer at least 6 months apart.Left atrial volume indexed was defined as normal when it was≤28 mL/m2, mildly abnormal when it was 29 to 33 mL/m2,moderately abnormal when it was 34 to 39 mL/m2, and severelyabnormal when it was ≥40 mL/m2. On the other hand, leftatrium was considered normal when LADI was ≤23 mm/m2,mildly abnormal when it was 24 to 26 mm/m2, moderatelyabnormal when it was 27 to 29 mm/m2, and severely abnormalwhen it was ≥30 mm/m2.9
Dobutamine stress protocolAll patients underwent DSE with early injection of atropine
protocol as previously described.16 Left ventricular ejectionfraction (LVEF) was measured using modified Simpson's rule.End points of the tests were achievement of 85% of themaximum predicted heart rate, defined as 220 — age in years,detection of severe or extensive WMA by echocardiography, STelevation N0.1 mV at an interval of 80 milliseconds after the Jpoint in patients without a previous MI, sustained arrhythmias,
severe angina, or intolerable side effects.17 Blood pressure, heartrate, and 12-lead electrocardiogram were monitored at eachstage of dobutamine infusion. The test was considereddiagnostic if the target heart rate was achieved and/or ischemiawas detected. The test was considered nondiagnostic when itwas prematurely interrupted because of significant adverseeffect or did not achieve 85% of the maximum predicted heartrate at the end of protocol without inducible ischemia.17
The stress tests were defined as abnormal if they had newor preexisting WMA in ≥2 contiguous segments. Patients withnormal wall motion both at baseline and at peak stress wereclassified as having a normal DSE. Patients with WMA atbaseline without extension observed at peak dobutaminestress were classified as having an abnormal DSE with fixedWMA. Patients with normal wall motion at baseline whodeveloped new WMA with stress, patients with resting WMAwith new WMA in other segments, and patients whodeveloped biphasic response were characterized as havingabnormal DSE with inducible WMA. The results of DSE weremade available to the referring physicians.
Follow-upFollow-up was obtained from review of the patient's
hospital chart, electronic records, and telephone interviewwith the patient. End points of the study were death andnonfatal MI. Cardiac death was defined as death associatedwith known or suspected MI, life-threatening arrhythmia, orpulmonary edema. Sudden unexpected death occurring with-out another explanation was included as cardiac death. Non-fatal MI was defined by means of a serial increase in cardiacspecific enzymes and/or development of new electrocardio-graphic changes. Patients who underwent coronary arterybypass grafting surgery or percutaneous coronary interventionwere censored at the time of the revascularization. Follow-upwas completed in March 2007.
Statistical analysisContinuous variables normally distributed were expressed as
mean and SD and categorical variables as proportions.Correlation of LAVI and LADI was evaluated using Pearson'scoefficient. Comparisons between groups were performedwith standard t test, χ2, or analysis of variance, asappropriated. Interobserver agreement was assessed by linearregression. Kaplan-Meier curves were used to estimate thedistribution of time to the end point of interest. The Coxmodel was used to estimate the relative risk of events for eachvariable. Differences between time-to-event curves werecompared with the log-rank test. The Cox hazard model wasused to estimate the relative risk (RR) with respective 95% CIsof the combined end points of death and nonfatal MI for eachvariable including clinical and echocardiographic character-istics. Left atrial size parameters and LVEF were analyzed asquantitative variables, whereas DSE results were analyzed as aqualitative variable (normal or abnormal). The incrementalvalue of LAVI over clinical and echocardiographic data wasassessed in 3 modeling steps. The first step consisted of fittinga multivariate model of only clinical data. Left atrial volumeindexed was then added to this model, followed by DSEresults (normal vs abnormal). The significance of addingadditional variables to previous modeling steps was based on
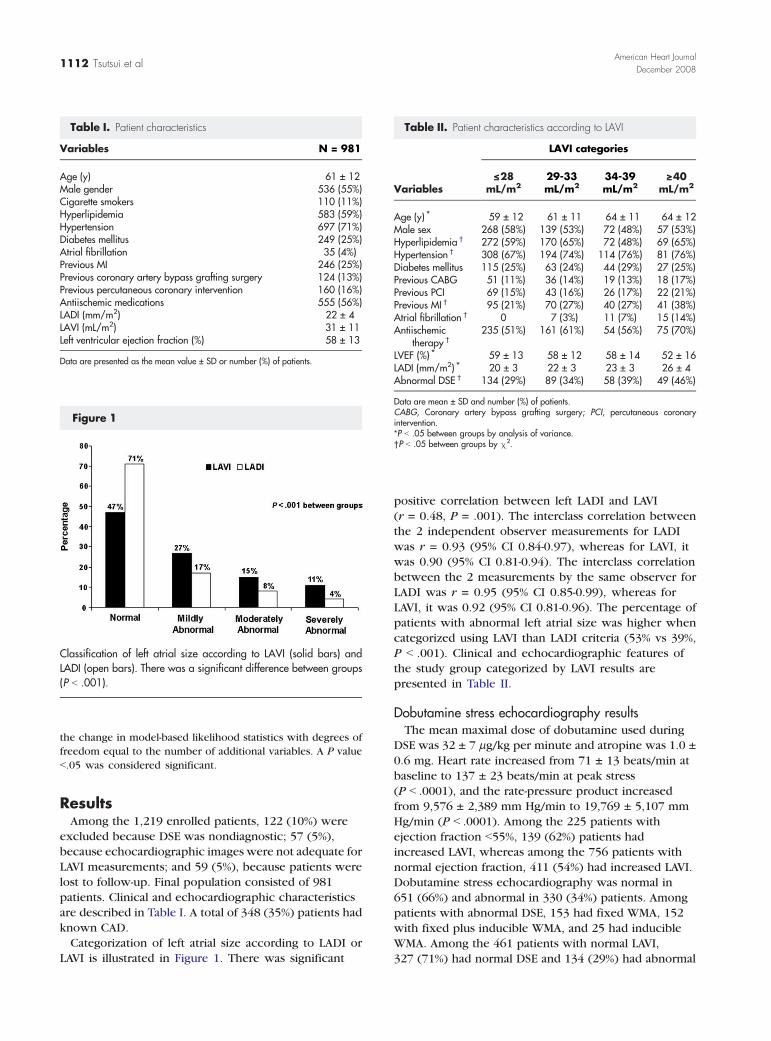
Table I. Patient characteristics
Variables N = 981
Age (y) 61 ± 12Male gender 536 (55%)Cigarette smokers 110 (11%)Hyperlipidemia 583 (59%)Hypertension 697 (71%)Diabetes mellitus 249 (25%)Atrial fibrillation 35 (4%)Previous MI 246 (25%)Previous coronary artery bypass grafting surgery 124 (13%)Previous percutaneous coronary intervention 160 (16%)Antiischemic medications 555 (56%)LADI (mm/m2) 22 ± 4LAVI (mL/m2) 31 ± 11Left ventricular ejection fraction (%) 58 ± 13
Data are presented as the mean value ± SD or number (%) of patients.
Figure 1
Classification of left atrial size according to LAVI (solid bars) andLADI (open bars). There was a significant difference between groups(P b .001).
Table II. Patient characteristics according to LAVI
Variables
LAVI categories
<__28mL/m2
29-33mL/m2
34-39mL/m2
>__40mL/m2
Age (y) ⁎ 59 ± 12 61 ± 11 64 ± 11 64 ± 12Male sex 268 (58%) 139 (53%) 72 (48%) 57 (53%)Hyperlipidemia † 272 (59%) 170 (65%) 72 (48%) 69 (65%)Hypertension † 308 (67%) 194 (74%) 114 (76%) 81 (76%)Diabetes mellitus 115 (25%) 63 (24%) 44 (29%) 27 (25%)Previous CABG 51 (11%) 36 (14%) 19 (13%) 18 (17%)Previous PCI 69 (15%) 43 (16%) 26 (17%) 22 (21%)Previous MI † 95 (21%) 70 (27%) 40 (27%) 41 (38%)Atrial fibrillation † 0 7 (3%) 11 (7%) 15 (14%)Antiischemic
therapy †235 (51%) 161 (61%) 54 (56%) 75 (70%)
LVEF (%) ⁎ 59 ± 13 58 ± 12 58 ± 14 52 ± 16LADI (mm/m2) ⁎ 20 ± 3 22 ± 3 23 ± 3 26 ± 4Abnormal DSE † 134 (29%) 89 (34%) 58 (39%) 49 (46%)
Data are mean ± SD and number (%) of patients.CABG, Coronary artery bypass grafting surgery; PCI, percutaneous coronaryintervention.⁎P b .05 between groups by analysis of variance.†P b .05 between groups by χ2.
1112 Tsutsui et alAmerican Heart Journal
December 2008
the change in model-based likelihood statistics with degrees offreedom equal to the number of additional variables. A P valueb.05 was considered significant.
ResultsAmong the 1,219 enrolled patients, 122 (10%) were
excluded because DSE was nondiagnostic; 57 (5%),because echocardiographic images were not adequate forLAVI measurements; and 59 (5%), because patients werelost to follow-up. Final population consisted of 981patients. Clinical and echocardiographic characteristicsare described in Table I. A total of 348 (35%) patients hadknown CAD.Categorization of left atrial size according to LADI or
LAVI is illustrated in Figure 1. There was significant
positive correlation between left LADI and LAVI(r = 0.48, P = .001). The interclass correlation betweenthe 2 independent observer measurements for LADIwas r = 0.93 (95% CI 0.84-0.97), whereas for LAVI, itwas 0.90 (95% CI 0.81-0.94). The interclass correlationbetween the 2 measurements by the same observer forLADI was r = 0.95 (95% CI 0.85-0.99), whereas forLAVI, it was 0.92 (95% CI 0.81-0.96). The percentage ofpatients with abnormal left atrial size was higher whencategorized using LAVI than LADI criteria (53% vs 39%,P b .001). Clinical and echocardiographic features ofthe study group categorized by LAVI results arepresented in Table II.
Dobutamine stress echocardiography resultsThe mean maximal dose of dobutamine used during
DSE was 32 ± 7 μg/kg per minute and atropine was 1.0 ±0.6 mg. Heart rate increased from 71 ± 13 beats/min atbaseline to 137 ± 23 beats/min at peak stress(P b .0001), and the rate-pressure product increasedfrom 9,576 ± 2,389 mm Hg/min to 19,769 ± 5,107 mmHg/min (P b .0001). Among the 225 patients withejection fraction b55%, 139 (62%) patients hadincreased LAVI, whereas among the 756 patients withnormal ejection fraction, 411 (54%) had increased LAVI.Dobutamine stress echocardiography was normal in651 (66%) and abnormal in 330 (34%) patients. Amongpatients with abnormal DSE, 153 had fixed WMA, 152with fixed plus inducible WMA, and 25 had inducibleWMA. Among the 461 patients with normal LAVI,327 (71%) had normal DSE and 134 (29%) had abnormal
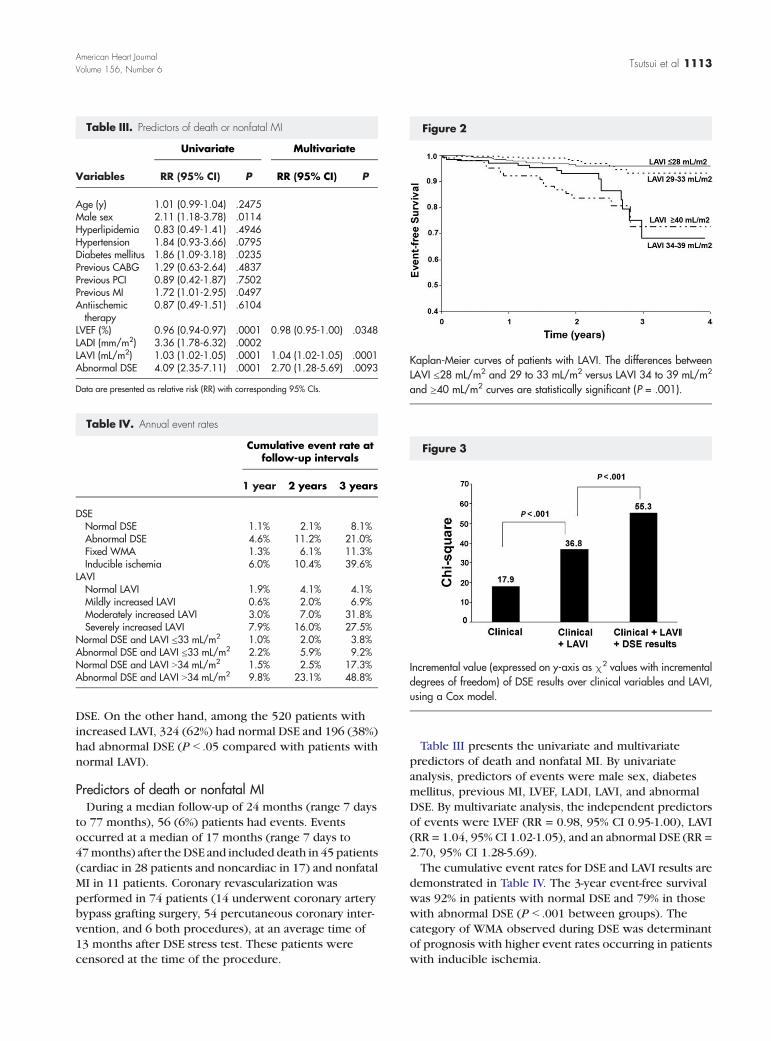
Table III. Predictors of death or nonfatal MI
Variables
Univariate Multivariate
RR (95% CI) P RR (95% CI) P
Age (y) 1.01 (0.99-1.04) .2475Male sex 2.11 (1.18-3.78) .0114Hyperlipidemia 0.83 (0.49-1.41) .4946Hypertension 1.84 (0.93-3.66) .0795Diabetes mellitus 1.86 (1.09-3.18) .0235Previous CABG 1.29 (0.63-2.64) .4837Previous PCI 0.89 (0.42-1.87) .7502Previous MI 1.72 (1.01-2.95) .0497Antiischemictherapy
0.87 (0.49-1.51) .6104
LVEF (%) 0.96 (0.94-0.97) .0001 0.98 (0.95-1.00) .0348LADI (mm/m2) 3.36 (1.78-6.32) .0002LAVI (mL/m2) 1.03 (1.02-1.05) .0001 1.04 (1.02-1.05) .0001Abnormal DSE 4.09 (2.35-7.11) .0001 2.70 (1.28-5.69) .0093
Data are presented as relative risk (RR) with corresponding 95% CIs.
Table IV. Annual event rates
Cumulative event rate atfollow-up intervals
1 year 2 years 3 years
DSENormal DSE 1.1% 2.1% 8.1%Abnormal DSE 4.6% 11.2% 21.0%Fixed WMA 1.3% 6.1% 11.3%Inducible ischemia 6.0% 10.4% 39.6%
LAVINormal LAVI 1.9% 4.1% 4.1%Mildly increased LAVI 0.6% 2.0% 6.9%Moderately increased LAVI 3.0% 7.0% 31.8%Severely increased LAVI 7.9% 16.0% 27.5%
Normal DSE and LAVI ≤33 mL/m2 1.0% 2.0% 3.8%Abnormal DSE and LAVI ≤33 mL/m2 2.2% 5.9% 9.2%Normal DSE and LAVI N34 mL/m2 1.5% 2.5% 17.3%Abnormal DSE and LAVI N34 mL/m2 9.8% 23.1% 48.8%
Figure 2
Kaplan-Meier curves of patients with LAVI. The differences betweenLAVI ≤28 mL/m2 and 29 to 33 mL/m2 versus LAVI 34 to 39 mL/m2
and ≥40 mL/m2 curves are statistically significant (P = .001).
Figure 3
Incremental value (expressed on y-axis as χ2 values with incrementaldegrees of freedom) of DSE results over clinical variables and LAVI,using a Cox model.
Tsutsui et al 1113American Heart JournalVolume 156, Number 6
DSE. On the other hand, among the 520 patients withincreased LAVI, 324 (62%) had normal DSE and 196 (38%)had abnormal DSE (P b .05 compared with patients withnormal LAVI).
Predictors of death or nonfatal MIDuring a median follow-up of 24 months (range 7 days
to 77 months), 56 (6%) patients had events. Eventsoccurred at a median of 17 months (range 7 days to47months) after theDSE and included death in 45 patients(cardiac in 28 patients and noncardiac in 17) and nonfatalMI in 11 patients. Coronary revascularization wasperformed in 74 patients (14 underwent coronary arterybypass grafting surgery, 54 percutaneous coronary inter-vention, and 6 both procedures), at an average time of13 months after DSE stress test. These patients werecensored at the time of the procedure.
Table III presents the univariate and multivariatepredictors of death and nonfatal MI. By univariateanalysis, predictors of events were male sex, diabetesmellitus, previous MI, LVEF, LADI, LAVI, and abnormalDSE. By multivariate analysis, the independent predictorsof events were LVEF (RR = 0.98, 95% CI 0.95-1.00), LAVI(RR = 1.04, 95% CI 1.02-1.05), and an abnormal DSE (RR =2.70, 95% CI 1.28-5.69).The cumulative event rates for DSE and LAVI results are
demonstrated in Table IV. The 3-year event-free survivalwas 92% in patients with normal DSE and 79% in thosewith abnormal DSE (P b .001 between groups). Thecategory of WMA observed during DSE was determinantof prognosis with higher event rates occurring in patientswith inducible ischemia.
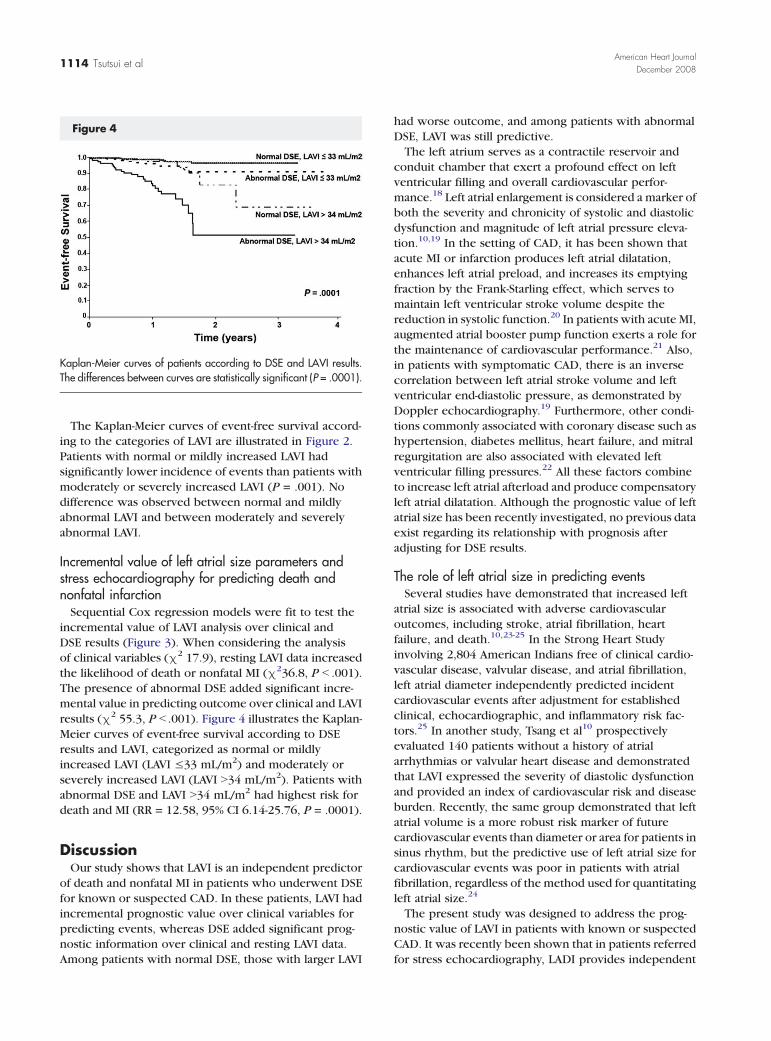
Figure 4
Kaplan-Meier curves of patients according to DSE and LAVI results.The differences between curves are statistically significant (P = .0001).
1114 Tsutsui et alAmerican Heart Journal
December 2008
The Kaplan-Meier curves of event-free survival accord-ing to the categories of LAVI are illustrated in Figure 2.Patients with normal or mildly increased LAVI hadsignificantly lower incidence of events than patients withmoderately or severely increased LAVI (P = .001). Nodifference was observed between normal and mildlyabnormal LAVI and between moderately and severelyabnormal LAVI.
Incremental value of left atrial size parameters andstress echocardiography for predicting death andnonfatal infarctionSequential Cox regression models were fit to test the
incremental value of LAVI analysis over clinical andDSE results (Figure 3). When considering the analysisof clinical variables (χ2 17.9), resting LAVI data increasedthe likelihood of death or nonfatal MI (χ236.8, P b .001).The presence of abnormal DSE added significant incre-mental value in predicting outcome over clinical and LAVIresults (χ2 55.3, P b .001). Figure 4 illustrates the Kaplan-Meier curves of event-free survival according to DSEresults and LAVI, categorized as normal or mildlyincreased LAVI (LAVI ≤33 mL/m2) and moderately orseverely increased LAVI (LAVI N34 mL/m2). Patients withabnormal DSE and LAVI N34 mL/m2 had highest risk fordeath and MI (RR = 12.58, 95% CI 6.14-25.76, P = .0001).
DiscussionOur study shows that LAVI is an independent predictor
of death and nonfatal MI in patients who underwent DSEfor known or suspected CAD. In these patients, LAVI hadincremental prognostic value over clinical variables forpredicting events, whereas DSE added significant prog-nostic information over clinical and resting LAVI data.Among patients with normal DSE, those with larger LAVI
had worse outcome, and among patients with abnormalDSE, LAVI was still predictive.The left atrium serves as a contractile reservoir and
conduit chamber that exert a profound effect on leftventricular filling and overall cardiovascular perfor-mance.18 Left atrial enlargement is considered a marker ofboth the severity and chronicity of systolic and diastolicdysfunction and magnitude of left atrial pressure eleva-tion.10,19 In the setting of CAD, it has been shown thatacute MI or infarction produces left atrial dilatation,enhances left atrial preload, and increases its emptyingfraction by the Frank-Starling effect, which serves tomaintain left ventricular stroke volume despite thereduction in systolic function.20 In patients with acute MI,augmented atrial booster pump function exerts a role forthe maintenance of cardiovascular performance.21 Also,in patients with symptomatic CAD, there is an inversecorrelation between left atrial stroke volume and leftventricular end-diastolic pressure, as demonstrated byDoppler echocardiography.19 Furthermore, other condi-tions commonly associated with coronary disease such ashypertension, diabetes mellitus, heart failure, and mitralregurgitation are also associated with elevated leftventricular filling pressures.22 All these factors combineto increase left atrial afterload and produce compensatoryleft atrial dilatation. Although the prognostic value of leftatrial size has been recently investigated, no previous dataexist regarding its relationship with prognosis afteradjusting for DSE results.
The role of left atrial size in predicting eventsSeveral studies have demonstrated that increased left
atrial size is associated with adverse cardiovascularoutcomes, including stroke, atrial fibrillation, heartfailure, and death.10,23-25 In the Strong Heart Studyinvolving 2,804 American Indians free of clinical cardio-vascular disease, valvular disease, and atrial fibrillation,left atrial diameter independently predicted incidentcardiovascular events after adjustment for establishedclinical, echocardiographic, and inflammatory risk fac-tors.25 In another study, Tsang et al10 prospectivelyevaluated 140 patients without a history of atrialarrhythmias or valvular heart disease and demonstratedthat LAVI expressed the severity of diastolic dysfunctionand provided an index of cardiovascular risk and diseaseburden. Recently, the same group demonstrated that leftatrial volume is a more robust risk marker of futurecardiovascular events than diameter or area for patients insinus rhythm, but the predictive use of left atrial size forcardiovascular events was poor in patients with atrialfibrillation, regardless of the method used for quantitatingleft atrial size.24
The present study was designed to address the prog-nostic value of LAVI in patients with known or suspectedCAD. It was recently been shown that in patients referredfor stress echocardiography, LADI provides independent
Tsutsui et al 1115American Heart JournalVolume 156, Number 6
value for predicting death and MI.25 Bangalore et al25
demonstrated in a large group of patients that LADI≥24 mm/m2 was a significant predictor of eventsindependent of left ventricular systolic dysfunction andischemia. Anteroposterior diameter of the left atrium iseasier to acquire and universally used in clinical practiceand research, but its validity has recently been chal-lenged.8 Because of the asymmetrical conformation ofthis cavity, left atrial size is more accurately reflected bymeasurement of volume rather than linear dimension.24
In our study, we observed a significant positive correla-tion between LADI and LAVI. However, a higherpercentage of patients were classified as having increasedleft atrial size using LAVI parameter than LADI. Left atrialdiameter indexed was predictor of hard events inunivariate analysis but no longer had prognostic valuewhen considering LAVI in multivariate model. Risk wasmostly observed with moderate to severe as compared tomild enlargement or normal volume.Although the prognostic value of DSE considering only
the wall motion analysis over clinical variables isestablished in different patient groups, normal wallmotion responses to dobutamine were associated withannualized mortality rates up to 8%, and cardiac eventrates up to 3.6%.2,5,26-29 Our results are in accordancewith previous descriptions, in such a way that DSE resultswas a strong independent predictor of hard events.However, patients with normal DSE had a 3-year eventrate of 8.1%. On the other hand, patients with normal DSEand normal LAVI had a 3-year event rate of 3.8%. Left atrialvolume indexed was also an independent predictor as acontinuous variable demonstrating that the bigger the leftatrial volume is, the higher the probability of the patientsto have a future event. The addition of LAVI informationsignificantly increased the prognostic value of DSE forpredicting death and MI. The LAVI volume indexprovided better stratification within each category ofstress test results.
Limitations of the studyAlthough the percentage of patients with atrial fibrilla-
tion at the time of DSE in our population was low (4%),we have to consider that this could be a possible cause oferror in predicting prognosis. Because the history ofintermittent atrial fibrillation was not included in thedatabank, it was not considered as a clinical variablebecause of the difficulties in determining this dataretrospectively. With the relatively small number ofevents, the multivariable model may be unstable and thusvalidation of these findings in another dataset would addstrength to the conclusions.
ConclusionsLeft atrial volume indexed provides independent
prognostic information for predicting death and nonfatal
MI in patients who underwent DSE for known orsuspected CAD. Among patients with normal DSE, thosewith larger LAVI had worse outcome, and among patientswith abnormal DSE, LAVI was still predictive.
References1. Picano E, Mathias Jr W, Pingitore A, et al. Safety and tolerability of
dobutamine-atropine stress echocardiography: a prospective, multi-centre study. Echo Dobutamine International Cooperative StudyGroup. Lancet 1994;344:1190-2.
2. Marwick TH, Case C, Sawada S, et al. Prediction of mortality usingdobutamine echocardiography. J Am Coll Cardiol 2001;37:754-60.
3. Picano E, Sicari R, Landi P, et al. Prognostic value of myocardialviability in medically treated patients with global left ventriculardysfunction early after an acute uncomplicated myocardial infarction:a dobutamine stress echocardiographic study. Circulation 1998;98:1078-84.
4. Cornel JH, Balk AH, Boersma E, et al. Safety and feasibility ofdobutamine-atropine stress echocardiography in patients withischemic left ventricular dysfunction. J Am Soc Echocardiogr 1996;9:27-32.
5. Elhendy A, Schinkel AF, Bax JJ, et al. Prognostic value of dobutaminestress echocardiography in patients with normal left ventricularsystolic function. J Am Soc Echocardiogr 2004;17:739-43.
6. Apstein CS, Grossman W. Opposite initial effects of supply anddemand ischemia on left ventricular diastolic compliance: theischemia-diastolic paradox. J Mol Cell Cardiol 1987;19:119-28.
7. Bonow RO, Kent KM, Rosing DR, et al. Improved left ventriculardiastolic filling in patients with coronary artery disease afterpercutaneous transluminal coronary angioplasty. Circulation 1982;66:1159-67.
8. Lester SJ, Ryan EW, Schiller NB, et al. Best method in clinical practiceand in research studies to determine left atrial size. Am J Cardiol1999;84:829-32.
9. Lang RM, Bierig M, Devereux RB, et al. Recommendations forchamber quantification: a report from the American Society ofEchocardiography's Guidelines and Standards Committee and theChamber Quantification Writing Group, developed in conjunctionwith the European Association of Echocardiography, a branch of theEuropean Society of Cardiology. J Am Soc Echocardiogr 2005;18:1440-63.
10. Tsang TS, Barnes ME, Gersh BJ, et al. Left atrial volume as a morpho-physiologic expression of left ventricular diastolic dysfunction andrelation to cardiovascular risk burden. Am J Cardiol 2002;90:1284-9.
11. Moller JE, Hillis GS, Oh JK, et al. Left atrial volume: a powerfulpredictor of survival after acute myocardial infarction. Circulation2003;107:2207-12.
12. Barnes ME, Miyasaka Y, Seward JB, et al. Left atrial volume in theprediction of first ischemic stroke in an elderly cohort without atrialfibrillation. Mayo Clin Proc 2004;79:1008-14.
13. Beinart R, Boyko V, Schwammenthal E, et al. Long-term prognosticsignificance of left atrial volume in acute myocardial infarction. J AmColl Cardiol 2004;44:327-34.
14. Di Tullio MR, Sacco RL, Sciacca RR, et al. Left atrial size and the risk ofischemic stroke in an ethnically mixed population. Stroke 1999;30:2019-24.
15. Alsaileek AA, Osranek M, Fatema K, et al. Predictive value of normalleft atrial volume in stress echocardiography. J Am Coll Cardiol 2006;47:1024-8.
16. Tsutsui JM, Osorio AF, Lario FA, et al. Comparison of safety andefficacy of the early injection of atropine during dobutamine stress
1116 Tsutsui et alAmerican Heart Journal
December 2008
echocardiography with the conventional protocol. Am J Cardiol2004;94:1367-72.
17. Armstrong WF, Zoghbi WA. Stress echocardiography: currentmethodology and clinical applications. J Am Coll Cardiol 2005;45:1739-47.
18. Pagel PS, Kehl F, Gare M, et al. Mechanical function of the left atrium:new insights based on analysis of pressure-volume relations andDoppler echocardiography. Anesthesiology 2003;98:975-94.
19. Appleton CP, Galloway JM, Gonzalez MS, et al. Estimation of leftventricular filling pressures using two-dimensional and Dopplerechocardiography in adult patients with cardiac disease. Additionalvalue of analyzing left atrial size, left atrial ejection fraction and thedifference in duration of pulmonary venous and mitral flow velocity atatrial contraction. J Am Coll Cardiol 1993;22:1972-82.
20. Sigwart U, Grbic M, Goy JJ, et al. Left atrial function in acute transientleft ventricular ischemia produced during percutaneous transluminalcoronary angioplasty of the left anterior descending coronary artery.Am J Cardiol 1990;65:282-6.
21. Rahimtoola SH, Ehsani A, Sinno MZ, et al. Left atrial transportfunction in myocardial infarction. Importance of its booster pumpfunction. Am J Med 1975;59:686-94.
22. Matsuda Y, Toma Y, Moritani K, et al. Assessment of left atrialfunction in patients with hypertensive heart disease. Hypertension1986;8:779-85.
AVAILABILITY OF JOU
As a service to our subscribers, copies of back issues of the Ameand are available for purchase from Elsevier until inventory isService, 11380 Westline Industrial Drive, St. Louis, MO 63146on availability and prices of particular issues.
23. Tsang TS, Gersh BJ, Appleton CP, et al. Left ventricular diastolicdysfunction as a predictor of the first diagnosed nonvalvular atrialfibrillation in 840 elderly men and women. J Am Coll Cardiol 2002;40:1636-44.
24. Tsang TS, Abhayaratna WP, Barnes ME, et al. Prediction ofcardiovascular outcomes with left atrial size: is volume superior toarea or diameter? J Am Coll Cardiol 2006;47:1018-23.
25. Bangalore S, Yao SS, Chaudhry FA. Role of left atrial size in riskstratification and prognosis of patients undergoing stress echocar-diography. J Am Coll Cardiol 2007;50:1254-62.
26. Poldermans D, Arnese M, Fioretti PM, et al. Improved cardiacrisk stratification in major vascular surgery with dobutamine-atropine stress echocardiography. J Am Coll Cardiol 1995;26:648-53.
27. Chuah SC, Pellikka PA, Roger VL, et al. Role of dobutamine stressechocardiography in predicting outcome in 860 patients withknown or suspected coronary artery disease. Circulation 1998;97:1474-80.
28. Biagini E, Elhendy A, Bax JJ, et al. Seven-year follow-up afterdobutamine stress echocardiography: impact of gender on prog-nosis. J Am Coll Cardiol 2005;45:93-7.
29. Tsutsui JM, Elhendy A, Anderson JR, et al. Prognostic value ofdobutamine stress myocardial contrast perfusion echocardiography.Circulation 2005;112:1444-50.
RNAL BACK ISSUES
rican Heart Journal for the preceding 2 years are maintaineddepleted. Please write to Elsevier Subscription Customer
, or call 800-654-2452 or 314-453-7041 for information
Copyright © 2022 FDOKUMEN




















