
A Pragmatic Neurological Screen for Patients With Suspected Cord Compressive Myelopathy
12
doi: 10.2522/ptj.20060150 Originally published online July 17, 2007 2007; 87:1233-1242. PHYS THER. Adam Goode Chad E Cook, Eric Hegedus, Ricardo Pietrobon and Suspected Cord Compressive Myelopathy A Pragmatic Neurological Screen for Patients With http://ptjournal.apta.org/content/87/9/1233 found online at: The online version of this article, along with updated information and services, can be Collections Tests and Measurements Spinal Cord Injuries Perspectives in the following collection(s): This article, along with others on similar topics, appears e-Letters "Responses" in the online version of this article. "Submit a response" in the right-hand menu under or click on here To submit an e-Letter on this article, click E-mail alerts to receive free e-mail alerts here Sign up by guest on May 18, 2015 http://ptjournal.apta.org/ Downloaded from by guest on May 18, 2015 http://ptjournal.apta.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of A Pragmatic Neurological Screen for Patients With Suspected Cord Compressive Myelopathy
doi: 10.2522/ptj.20060150Originally published online July 17, 2007
2007; 87:1233-1242.PHYS THER. Adam GoodeChad E Cook, Eric Hegedus, Ricardo Pietrobon andSuspected Cord Compressive MyelopathyA Pragmatic Neurological Screen for Patients With
http://ptjournal.apta.org/content/87/9/1233found online at: The online version of this article, along with updated information and services, can be
Collections
Tests and Measurements Spinal Cord Injuries
Perspectives in the following collection(s): This article, along with others on similar topics, appears
e-Letters
"Responses" in the online version of this article. "Submit a response" in the right-hand menu under
or click onhere To submit an e-Letter on this article, click
E-mail alerts to receive free e-mail alerts hereSign up
by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from
A Pragmatic Neurological Screen forPatients With Suspected CordCompressive MyelopathyChad E Cook, Eric Hegedus, Ricardo Pietrobon, Adam Goode
Physical therapists commonly use screening tests to identify upper motoneuronlesions such as cord compressive myelopathy (CCM), the presence of which neces-sitates appropriate medical referral. Signs and symptoms of CCM include sensory andataxic changes of the lower extremities, poorly coordinated gait, weakness, tetraspas-ticity, clumsiness, spasticity, hyperreflexia, and primitive reflexes. Clinical tests andmeasures such as Hoffmann sign, clonus, Lhermitte sign, the grip and release test, thefinger escape sign, the Babinski test, and the inverted supinator sign have historicallybeen used as screens for CCM. For effectiveness as a screen, a clinical test or measureshould demonstrate high sensitivity. Diagnostic accuracy studies have shown thatclinical tests and measures for CCM often display low sensitivity, indicating that anegative finding may falsely suggest the absence of a condition or disease that actuallyis present. To counter the low levels of sensitivity, screening should include acombination of a thorough patient history, recognition of and appropriate referral forcauda equina symptoms, and clusters of any pertinent contributory tests andmeasures.
CE Cook, PT, PhD, MBA, OCS,FAAOMPT, is Assistant Professor,Department of Community andFamily Medicine, and Director ofOutcomes Measures, Departmentof Surgery, Center for Excellence inSurgical Outcomes, Duke Univer-sity, Durham, NC 27710 (USA). Ad-dress all correspondence to DrCook at: [email protected].
E Hegedus, PT, DPT, MS, OCS, isAssistant Professor, Department ofCommunity and Family Medicine,Duke University.
R Pietrobon, MD, PhD, MBA, isAssociate Professor, Departmentof Surgery, Center for Excellencein Surgical Outcomes, DukeUniversity.
A Goode, PT, DPT, is Assistant Pro-fessor, Department of Communityand Family Medicine, DukeUniversity.
[Cook CE, Hegedus E, Pietrobon R,Goode A. A pragmatic neuro-logical screen for patients withsuspected cord compressivemyelopathy. Phys Ther. 2007;87:1233–1242.]
© 2007 American Physical TherapyAssociation
Perspective
Post a Rapid Response orfind The Bottom Line:www.ptjournal.org
September 2007 Volume 87 Number 9 Physical Therapy f 1233 by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from

Physical therapists examine pa-tients with neurological symp-toms in which accurate and ef-
fective differentiation is necessary.Neurological disorders can be classi-fied into lower motoneuron (LMN)lesions resulting from damage tothe alpha motoneuron, which mayoccur with spinal cord compres-sion, or upper motoneuron (UMN)lesions resulting from damage tothe descending inputs on the alphamotoneuron.1 Both LMN and UMNlesions typically are present in con-cert. Radiculopathy and myelopathyare examples of LMN and UMN le-sions that present similar signs andsymptoms. Radiculopathy is consid-ered a LMN lesion in which chemicalor nerve root compression causesnerve root pain.2 Myelopathy is aUMN lesion resulting from sagittalnarrowing of the spinal canal.3
Because findings of myelopathy fre-quently overlap with radiculopathy,conscientious attention and appro-priate testing is paramount.4,5 Care-ful examination and evaluation arenecessary to rule out a disorder sothat appropriate physical therapy in-tervention may begin. The purposeof this perspective is to recommendthe use of selective combinations ofscreening tools to identify patienthistory, demographics, and appro-priate symptoms of cord compres-sive myelopathy (CCM).
Spinal cord pathologies such as CCMdiffer depending on the form andlocation of the lesion. Multiple scle-rosis (MS) and amyotrophic lateralsclerosis (ALS) are 2 conditions thatpresent competing signs and symp-toms with CCM but differ in a num-ber of ways. Individuals with MS of-ten will exhibit abnormal cranialnerve testing and a positive jaw re-flex, whereas individuals with CCMwill exhibit neither.6 Amyotrophiclateral sclerosis affects both theUMNs and LMNs and demonstratesno changes in sensation.3 Cervical,
thoracic, and lumbar CCM secondaryto chronic degenerative changes aremuch more common forms of dys-function, present in 90% of peopleby the seventh decade of life.7 Theexact prevalence or incidence ofprogression from degenerativechanges to myelopathy is unknown,7
although cervical CCM is the mostcommon form of spinal cord dys-function in a person over the age of55 years.6
Clarification of the form of spinalcord lesion is essential because sur-gical treatment has been shown toretard the effects of CCM when it isdiagnosed in an expeditious man-ner.8,9 Failure to accurately and effi-ciently identify patients with CCMcan result in progression of symp-toms that are no longer effectivelytreated with conservative or surgicalinterventions.10 Additionally, failureto recognize CCM may result in treat-ment approaches that are contraindi-cated and may place the patient atfurther risk of disease progression.10
Physical therapists commonly use aneurological screen (NS), oftentermed an “upper-quarter screen” ora “lower-quarter screen,” as a com-ponent of a physical therapist exam-ination. The NS is a method used tounderstand the source of a patient’ssymptoms, to differentiate betweenUMNs and LMNs,4,5,11,12 and to deter-mine whether a patient is appro-priate for physical therapy manage-ment.11 Generally, tests and measuresused during an NS are performed atthe beginning of the physical exami-nation as a screening test.13
Screening tests should be inexpen-sive and relatively accurate andshould cause little morbidity duringapplication.14 Screening tests are de-signed to assist the clinician in rulingout selected diagnoses or impair-ments, should demonstrate high sen-sitivity during preclinical stages, andshould be used with disorders that
have high prevalence.14–16 When atest demonstrates high sensitivity,the likelihood of a false negative islow because the test demonstratesthe ability to identify accuratelythose who truly have the disease orimpairment, thus demonstrating theability to “rule out” a condition.16
The low rate of false negatives mini-mizes the mistake by the clinician ofidentifying a patient as “normal”when the patient may indeed havethe pathology—in this case, CCM.Tests with high sensitivity correctlyidentify those who truly have the dis-ease by providing a measurementvalue exclusive to this population.
The Necessity of ScreeningDespite the importance of screeningfor conditions such as CCM, recentevidence suggests that less than 5%of primary care physicians routinelyexamine for these findings duringtheir initial screen.17 Even when pro-vided with guidelines for manage-ment of patients with acute spinepain, physicians demonstrate poorconcordance toward examinationusing guideline-recommended ap-proaches.18,19 In a review of 6 differ-ent international guidelines for man-agement of spine pain, all guidelinesrecommended a specific screen fordetection of “red flags” such asCCM.20 Although the 6 internationalguidelines did not agree specificallyon what constituted an appropriatescreen, all of them suggested the im-portance of specific historical char-acteristics, laboratory findings, andoutcomes from physical testing in-cluding neurological testing.20
As entry-point providers, physicaltherapists are increasingly placed ina position to initially screen for CCM.We know of no studies that haveoutlined the frequency in whichphysical therapists routinely screenfor CCM, although conservative in-terventions are well document-ed21–23 as is treatment specifically byphysical therapists.24 At present,
Neurological Screening for Suspected Cord Compressive Myelopathy
1234 f Physical Therapy Volume 87 Number 9 September 2007 by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from

clinical tests and measures for CCMby physical therapists and physicianslack sensitivity, a necessary elementin an effective initial screen.21,25
Signs and Symptoms ofCCMIn contrast to radiculopathy and so-matic referred pain, CCM involvesspinal cord compression or injuryand is considered a serious finding.The most commonly encounteredform involves cervical spondyloticcord compressive myelopathy (cervi-cal CCM).6,26 Cervical CCM is associ-ated with physiological narrowingof the sagittal diameter of the spinalcanal secondary to congenital ordegenerative changes.26
The compression associated withcervical CCM may progress to spinalcord ischemia, leading to histopatho-logical changes of the spinal cord,often termed “myelomalacia.”27 Ini-tial symptoms in milder cases canstart with hand clumsiness or numb-ness, which may be unilateral atfirst, before gait abnormalities arenoted.6,28–34 Hand clumsiness ornumbness involves less sensory lossthan motor dysfunction and is, in es-sence, an apraxia of the distal upperextremities and hands.30
Additional signs and symptoms ofcervical CCM manifest as pain inthe cervical, upper-quarter region orshoulder; widespread numbness; par-esthesia; and sensory and ataxicchanges of the lower extremities.3 Ad-ditional findings may include weak-ness, tetraspasticity,4 gait-related clum-siness,4 spasticity, hyperreflexia,35 andthe presence of primitive reflexes.36
Other clinical findings indicative ofprogressive decline include acquiredspastic paraparesis,6 tetraparesis, orparaparesis.27 Because the signs andsymptoms often are sequential, weak-ness and stiffness of the legs37,38 typi-cally precede pain and the occasionalfindings of bowel and bladderchanges.39,40
Thoracic and lumbar CCM also canlead to serious complications.41
Within the thoracic region, myelo-pathic compression occurs fromcompression fractures,42 metastaticcancers,43 tuberculosis,43 and rheu-matoid arthritis.44 A disk herniationis a possible, but rare, contributor tomyelopathy in the thoracic spine.45
Because the spinal cord terminates atL1 or L2, CCM in the lumbar spine isregionally associated with spinalcord compression at the upper lum-bar segments. Disk herniations arethe most common contributor toCCM; nonetheless, the prevalence inthe upper lumbar spine is rare, ac-counting for less than 2% to 3% of allherniations in the lumbar spine.46
Lower thoracic and upper lumbarsigns and symptoms are similar tothose found in cervical CCM. Find-ings may include progressive asym-metric weakness in both legs andfoot drop with difficulty walking.45
Muscle fasciculations, musclecramps, and multilevel muscle weak-ness also are prevalent.45 Generally,sensation changes fluctuate overtime (no problems early, with pro-gressive sensation loss over time),and reflexes provide variableinformation.43,45
At the conus medullaris, concurrentsymptoms associated with UMN andLMN damage are possible.40 Damageto the peripheral nerves of the caudaequina, or the conus medullaris, canresult in cauda equina syndrome(CES). The incidence of CES rangesfrom 1% to 5%, depending on theorigin (ie, disk herniation, tumor) ofthe injurious event.40 Cauda equinasyndrome involves compression ordamage to the nerves of the caudaequina and may result in sciatica,low back pain, saddle and perianalhypesthesia or analgesia, reflexchanges, sexual dysfunction, lower-extremity weakness, and bowel andbladder dysfunction.47 Because pa-thology of the lumbar spine can dam-
age parasympathetic supply to thebowel and bladder and sensorynerves to the perineum,46 lumbarCCM can frequently demonstratesymptoms comparable to those ofCES, including changes in motorfunction in the lower extremitiesand pelvis.35 Distinguishing betweenthe 2 conditions is less essential be-cause both conditions warrant addi-tional medical workup and are con-sidered serious red flag findings.
Diagnosis of MyelopathyDiagnostic criteria for CCM have in-cluded evidence of spinal cord ab-normality based on magnetic reso-nance imaging (MRI) findings anddedicated clinical testing procedures.3
Magnetic resonance imaging is con-sidered the best imaging method be-cause it expresses the amount of com-pression placed on the spinal cord48
and demonstrates relatively highlevels of sensitivity (79%–95%) andspecificity (82%–88%) (positive likeli-hood ratio�4.39–7.92, negative like-lihood ratio�0.06–0.27) in identify-ing selected abnormalities such asspace-occupying tumors,8,49,50 diskherniation,51,52 and ligamentous ossi-fication.53 The MRI provides the abil-ity to rule out a tumor or syrinx(fluid-filled cavity that develops inthe spinal cord)3 and provides de-tailed views of the spinal cord, inter-vertebral disk, vertebral osteophytes,and ligaments—all structures that po-tentially compress the spinal cord.26
Furthermore, MRI findings havebeen shown to correlate with preop-erative severity of cervical compres-sive myelopathy and prognosis aftersurgery.8,49,54–56 Patients with ad-vanced spinal cord changes oftendemonstrate poor outcomes aftersurgery, and those with only minorcompression tend to demonstratefair recovery or retardation of pro-gression of symptoms.10
Nonetheless, MRI findings are notconclusively indicative of CCM.57
Spinal cord-related changes and sub-
Neurological Screening for Suspected Cord Compressive Myelopathy
September 2007 Volume 87 Number 9 Physical Therapy f 1235 by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from

sequent symptoms from CCM over-lap other types of intrinsic myelopa-thy, such as MS, syrinx, or ALS.Careful screening of the MRI, includ-ing the presence of T2-weightedchanges, is crucial to show clear,relevant, spinal cord compres-sion.22,58–61 False positives are com-mon because spinal cord compres-sion alone does not directly equateto clinical signs and symptoms.59,61
Diagnosis usually is made from a de-tailed history of progressive patientsymptoms, weakness and hyper-reflexia on examination, and clearcompression of the spinal cord at anappropriate symptomatic level onthe MRI scan, with or without T2-weighted changes. Because T2-weighted MRI changes usually donot abate with surgery,62 thesechanges are more indicative of dam-age than of reversible ischemia. Be-cause a dedicated criterion standard,such as the singular use of an MRIscan to determine myelopathy, doesnot exist, tests designed to measurethe presence of CCM always are in-vestigated in the presence ofuncertainty.63
Aside from MRI, a neuromusculartest, such as an electromyogram(EMG) or an electroneurogram, of-ten is used to differentiate cervicalCCM from carpal tunnel syndromeor other peripheral nerve problems.Because cervical CCM is a UNM syn-drome, the EMG is expected to dis-play a normal finding unless thereare intervening root or peripheralnerve problems. Kang and Fan64 re-ported normal EMG results in 100%of patients diagnosed with cervicalCCM. Evoked potentials have dem-onstrated the greatest assistancewith the diagnosis of cervical CCM.Motor evoked potentials have a re-ported 70% sensitivity in the upper-extremity muscles and 95% sensi-tivity for muscles of the lowerextremity for the diagnosis of cervi-cal CCM.65 From an electrodiagnos-tic standpoint, the use of sensory
evoked potentials (SEP) has demon-strated superior diagnostic ability, asKang and Fan64 reported abnormalSEP in 19 of 20 patients diagnosedwith cervical CCM.
As physical therapists increase theirexposure as entry-point providers,the opportunity to identify the pres-ence of CCM will increase, yet theuse of MRI to identify CCM is stilluncommon within physical therapistpractice. Magnetic resonance imag-ing is a sensitive instrument to detectCCM, whereas we will demonstratethat most clinical tests and measuresdesigned to screen for CCM lack sen-sitivity. Physical therapists require ef-fective tests and measures that dem-onstrate high sensitivity to properlyrule out signs and symptoms of CCM.
Patient History and ClinicalTests and Measures forMyelopathyAlthough patient history is routinelyused during diagnosis of CCM,66 weknow of no studies that have mea-sured the sensitivity of patient his-tory in diagnosing myelopathy. None-theless, careful attention to the patienthistory may provide useful informa-tion when combined with other phys-ical findings. Patients with CCM maycomplain of little to no neck pain67
or of paresthesia in a nondermatomalpattern and frequently do not ap-preciate the underlying weaknessthat is present.9 Subtle changes in gaitare often the first clue of the presenceof CCM.9 As CCM progresses, pa-tients may report balance distur-bances, variable degrees of weaknessor paralysis, and proximal muscleweaknesses.9 Findings of bowel andbladder changes39,40 associated withsevere CCM should be addressedimmediately.
There are a number of clinical testsand measures purportedly designedto screen for UMN lesions such asCCM. Clinical tests and measures
such as Hoffmann sign, clonus, Lher-mitte sign, the Babinski sign, the fin-ger escape sign, the grip and releasetest, and the inverted supinator re-flex9,27,68 are used traditionally torule out the presence of CCM. Ofthese tests, the grip and release test,clonus, and the inverted supinatorreflex have not been studied fordiagnostic accuracy. The finger es-cape sign has been inadequatelymeasured.
Finger Escape SignHand dysfunction has been recog-nized as a specific sign of cervicalmyelopathy.69 A commonly used testfor hand dysfunction is the fingerescape sign, which involves the in-voluntary flexion and abductionwithin 1 minute of extended and ad-ducted fingers when held statically.9
We are aware of one study70 thatexamined the sensitivity of the fingerescape sign, identifying a sensitivityof 55% in a sample of 36 subjectswith myelopathy.
Grip and Release TestThe grip and release test is recog-nized by the inability to grip and re-lease the fist rapidly upon request.9
Although the test is considered to bea specific finding for myelopathy andhas been used to rule in myelopathyfor research purposes,69 we are un-aware of any studies that have exam-ined sensitivity.
ClonusClonus is considered a UMN lesionthat appears several weeks after thepresence or onset of a lesion.71 Apositive clonus finding is more than2 repetitive beats during wrist orankle dorsiflexion movements andmay be the result of a number ofcauses, including cerebral hemi-spheric or spinal cord damage.72 Weknow of no studies that have mea-sured the sensitivity of clonus in rul-ing out CCM.
Neurological Screening for Suspected Cord Compressive Myelopathy
1236 f Physical Therapy Volume 87 Number 9 September 2007 by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from
Inverted Supinator ReflexFor the inverted supinator reflex, apositive test is identified as fingerflexion or triceps muscle extensionduring brachioradialis muscle reflextesting.68,73 A positive finding is con-sidered a sign of an LMN lesion at thespinal level of reflex testing and of aUMN lesion such as CCM below thespinal level of testing.73 We know ofno studies that have investigated thediagnostic accuracy of the invertedsupinator reflex test.
The Hoffmann sign, the Lhermittesign, and the Babinski sign have beenstudied for diagnostic accuracy, withvarying levels of methodologicalquality, which may affect the diag-nostic accuracy results. For example,Berger and Fannin74 reported a sen-sitivity of 80% in subjects with neu-rological dysfunction other thanCCM but failed to blind test adminis-trators to the condition of the patientor to standardize the reference usedto qualify the origin of the myelopa-thy for comparison. Ghosh andPradhan75 found slightly lower sensi-tivity values and demonstrated thestrongest study design, which did in-clude subjects with suspected CCMand appropriate blinding. Conse-quently, the strength of the designduring study origination suggeststhat Ghosh and Pradhan’s findingsexhibited stronger internal and ex-ternal validity. Other investiga-tors76,77 found dramatically lowersensitivity values and used a studydesign that allowed examiner bias orused subjects who are not com-monly tested using the Babinski sign.Use of diagnostic accuracy valuesmay have limited generalizability ifthe spectrums of patients used forthe study are not similar to thosewho would receive the test in clini-cal practice, also known as “spec-trum bias.”78
Babinski SignThe Babinski sign is a commonlyused clinical test for CCM and other
forms of UMN lesions. A positive testis associated with a pyramidal defectand is earmarked by great toe exten-sion, and sometimes adduction,79
during stimulus and fanning of thedigits 2 through 5. Babinski sign find-ings are frequently used in concertwith imaging to detect the presenceof a UMN lesion. Findings associatedwith the Babinski sign are variable,and the use of this test recently hasbeen questioned for effectiveness asa screening tool.80 Some authors81,82
have argued that the Babinski sign isdifficult to differentiate from upgo-ing toe movement that occurs duringa flexion synergy of the leg and sug-gested that examination of the entireleg is imperative. Failure to differen-tiate may result in artificially higherlevels of sensitivity.
Kumar and Ramasubramanian81 de-scribed the crossed upgoing toe signand the Allen-Cleckley sign as varia-tions of the Babinski sign. Thecrossed upgoing toe sign involves re-sisted flexion of the opposite hipwith the knee in full extension anddetection of an upgoing toe on thecontralateral foot. The test appearsto be specific and not sensitive. TheAllen-Cleckley sign appears to be amoderately sensitive test and in-volves flicking the second digit ofthe foot into extension or pressureof the distal phalange of the second
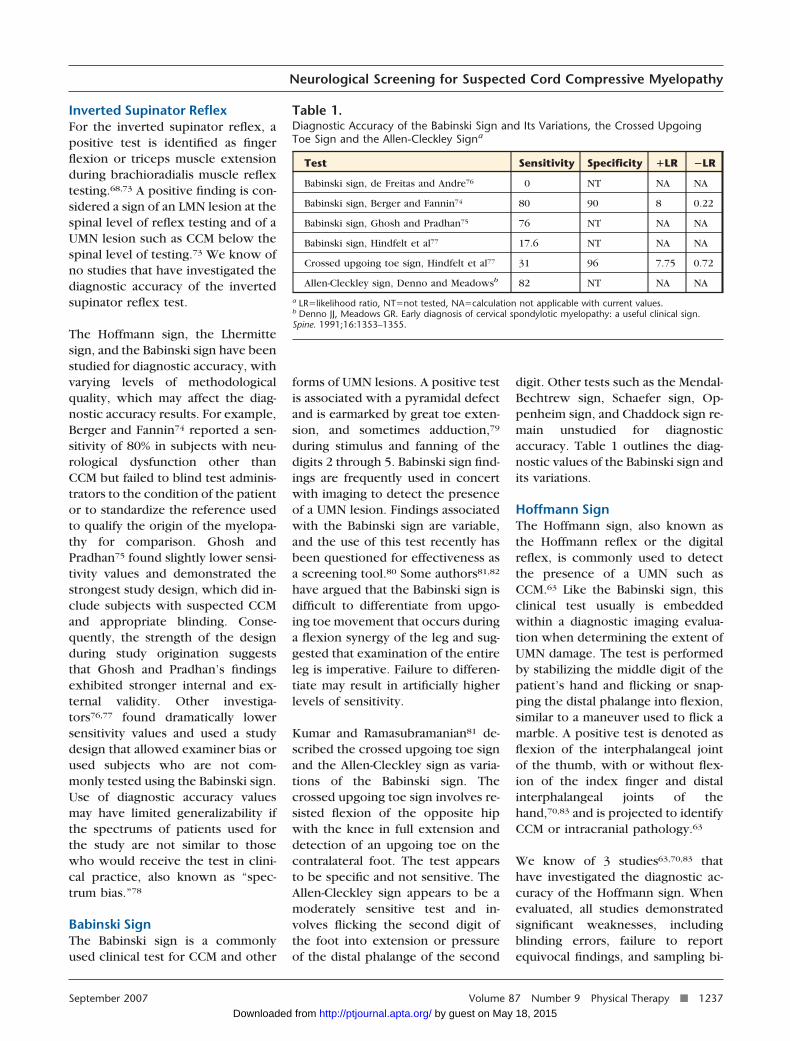
digit. Other tests such as the Mendal-Bechtrew sign, Schaefer sign, Op-penheim sign, and Chaddock sign re-main unstudied for diagnosticaccuracy. Table 1 outlines the diag-nostic values of the Babinski sign andits variations.
Hoffmann SignThe Hoffmann sign, also known asthe Hoffmann reflex or the digitalreflex, is commonly used to detectthe presence of a UMN such asCCM.63 Like the Babinski sign, thisclinical test usually is embeddedwithin a diagnostic imaging evalua-tion when determining the extent ofUMN damage. The test is performedby stabilizing the middle digit of thepatient’s hand and flicking or snap-ping the distal phalange into flexion,similar to a maneuver used to flick amarble. A positive test is denoted asflexion of the interphalangeal jointof the thumb, with or without flex-ion of the index finger and distalinterphalangeal joints of thehand,70,83 and is projected to identifyCCM or intracranial pathology.63
We know of 3 studies63,70,83 thathave investigated the diagnostic ac-curacy of the Hoffmann sign. Whenevaluated, all studies demonstratedsignificant weaknesses, includingblinding errors, failure to reportequivocal findings, and sampling bi-
Table 1.Diagnostic Accuracy of the Babinski Sign and Its Variations, the Crossed UpgoingToe Sign and the Allen-Cleckley Signa
Test Sensitivity Specificity �LR �LR
Babinski sign, de Freitas and Andre76 0 NT NA NA
Babinski sign, Berger and Fannin74 80 90 8 0.22
Babinski sign, Ghosh and Pradhan75 76 NT NA NA
Babinski sign, Hindfelt et al77 17.6 NT NA NA
Crossed upgoing toe sign, Hindfelt et al77 31 96 7.75 0.72
Allen-Cleckley sign, Denno and Meadowsb 82 NT NA NA
a LR�likelihood ratio, NT�not tested, NA�calculation not applicable with current values.b Denno JJ, Meadows GR. Early diagnosis of cervical spondylotic myelopathy: a useful clinical sign.Spine. 1991;16:1353–1355.
Neurological Screening for Suspected Cord Compressive Myelopathy
September 2007 Volume 87 Number 9 Physical Therapy f 1237 by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from

ases. Sung and Wang63 reported asensitivity of 94%, and Wong et al70
reported a sensitivity of 82% usingthe Hoffmann sign during assess-ment of patients with cervical spinedisorders. Wong et al70 tested onlypatients with demonstrable evidenceof a UMN lesion using MRI, and Sungand Wang63 incorporated the Hoff-mann sign within the diagnostic ref-erence and did not blind investiga-tors to the subjects’ conditions.Blinding apparently plays a signifi-cant role in the determination ofHoffmann sign, as Glaser et al83 re-ported a sensitivity of 58% when theinvestigators were unblinded toother clinical findings such as patienthistory and additional tests and mea-sures and a sensitivity of only 28%when the investigators were blinded.This dramatic change in sensitivitybased on blinding of investigatorsseems to suggest that a positive or anegative finding is influenced heavilyby other findings within the examina-tion. Glaser et al83 did report specific-ity values of 74% (unblinded) and71% (blinded) (positive likelihoodratio�0.97–2.23, negative likelihoodratio�0.57–1.01), suggesting that thetest is more specific than sensitive.
Table 2 outlines the diagnostic accu-racy of the Hoffmann sign.
Lhermitte SignThe Lhermitte sign involves lowercervical flexion in sitting or standingand production of an electrical“type” response or a “pins and nee-dles” sensation near the end range offlexion.84 Although the test was de-signed to measure spinal cord com-pression, it is commonly associatedwith screening for multiple sclerosisand is considered a moderately accu-rate tool for differentiation of spinalcord and spinal nerve trauma. Weknow of 2 studies35,84 that measuredthe diagnostic accuracy of the Lher-mitte sign, and the sensitivity ismarkedly low (Tab. 3).
Unfortunately, all of these studiesdemonstrated several procedural bi-ases that may vary the diagnosticaccuracy values. Uniformly, mosttests demonstrated poor-to-moderatesensitivity, which can reduce theodds of appropriately screening formyelopathy in the absence of highprevalence. These poor sensitivityresults suggest that using an individ-ual test in isolation is likely a poor
selection as a screen when usedearly in an examination.
DiscussionAlthough the clinical tests and mea-sures for CCM are designed asscreens and are frequently used earlyin an examination to “rule out” thepresence of CCM, there are signifi-cant risks for misleading results.79
None of the tests described in thisarticle is overtly sensitive to “ruleout” CCM; thus, the presence of anegative finding should not comfortthe clinician that the condition isabsent.27,79,81 Many of the tests re-main unstudied for diagnostic effec-tiveness or were tested in the pres-ence of spectrum bias. Spectrumbias limits the usefulness of the find-ings because the patients who weretested are not likely to represent apopulation seen in traditional prac-tice. A majority of studies are ham-pered by examiner bias, and the test-ing methods used within the studieslack differentiation from other neu-rological dysfunctions such as cere-bral hemispheric damage.
An additional complication is thatthe natural history of myelopathy ispoorly characterized.31,34,85,86 Thereare many situations in which boththe patient examination and the MRIscan are indistinct or ubiquitous, inthat it may be unclear on examina-tion whether the patient has mildmyelopathy and only mild-to-moderate spinal cord compressionwithout changes on the T2-weightedMRI. Conversely, many patients dem-onstrate significant compression onMRI but are relatively asymptomat-ic.9,59,61,87 In addition, several factorsassociated with disease progressionin myelopathy (eg, patient age, de-gree of spinal cord compression, pre-operative function, duration ofsymptoms, severity of osteoarthritis,number of affected levels) have allbeen associated with outcome, buthave not proven to be a predictor inall studies.88,89
Table 2.Diagnostic Accuracy of the Hoffmann Signa
Authors Sensitivity Specificity �LR �LR
Sung and Wang63 94 NT NA NA
Wong et al70 82 NT NA NA
Glaser et al,83 investigators unblinded 58 74 2.23 0.57
Glaser et al,83 investigators blinded 28 71 0.97 1.01
a LR�likelihood ratio, NT�not tested, NA�calculation not applicable with current values.
Table 3.Diagnostic Accuracy of Lhermitte Signa
Authors Sensitivity Specificity �LR �LR
Uchihara et al84 3 97 1 1
Crandall and Batzdorf35 17 NT NA NA
a LR�likelihood ratio, NT�not tested, NA�calculation not applicable with current values.
Neurological Screening for Suspected Cord Compressive Myelopathy
1238 f Physical Therapy Volume 87 Number 9 September 2007 by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from

Furthermore, there is uncertainty re-garding which tests and measuresare most important in ruling outCCM.66,90 Traditionally, screeningfor a neurologically based pathologyhas involved the combination of der-matome, myotome, deep tendonreflex, and pathological reflex (eg,Babinski, Hoffman) testing in theform of an upper- or lower-quarterscreen.12,91–95 The presence ofpathologic reflexes, hypertonic deeptendon reflexes, and sensation defi-cits in a nondermatomal patternshould necessitate further medicalexamination or imaging. Nonethe-less, it is likely that clinical findingswill provide inconsistent screeningresults, as the majority of clinicaltests for CCM lack sensitivity, havebeen poorly tested, or involve ambi-guity when tested independently ofother findings. Ambiguity is likely as-sociated with the complexity of thedisorder and the weaknesses of thetests and study designs.
A pragmatic examination could re-duce the risk of examination errorbased solely on the limitations of thetests and measures and could im-prove the sensitivity of the test dur-ing the early and middle portions ofthe natural history of myelopathy.We suggest following 3 examinationguidelines during screening:
(1) Perform a comprehensive pa-tient history.
(2) Rule out analogous symptoms as-sociated with CES so that physi-cal therapist examination, evalu-ation, and intervention maybegin.
(3) Use a battery of clinical tests toimprove the sensitivity of rulingout CCM with full recognitionthat a negative finding mayfalsely suggest the absence of acondition or disease that actuallyis present.
Perform a ComprehensivePatient HistoryBecause CCM is diagnosed usingclinical tests and measures, patienthistory, and the explicitly sensitiveuse of MRI, we recommend a carefuland detailed patient history once thepatient reaches the age of 55 years.The patient history should involvethe use of standard questions, includ-ing gait-related queries and questionsregarding other clinical findings as-sociated with CCM. Thoracic spineCCM generally is associated withtrauma, metastasis, or tuberculosis,and, although rare, CCM in the lum-bar spine usually is associated with aherniated disk. Cervical CCM in-volves signs and symptoms such aslower-extremity spasticity,35 motorweakness,3,35 gait difficulties,3 andsensory changes often occurringlater than motor changes.3,35 Any po-tentially positive finding should war-rant further diagnostic workup usingMRI.
Rule Out Analogous SymptomsAssociated With CESCauda equina signs and symptomsoften will overlap those of CCM. It isnot uncommon to find sphincter dis-turbances,35 radicular pain,35 andbowel and bladder problems withboth conditions.46 Moreover, be-cause CES causing bowel and blad-der dysfunction is considered anemergency that benefits from earlysurgical decompression,43 any asso-ciative symptoms found during thescreen should prompt immediatemedical referral.
Use a Battery of Clinical Tests toImprove the Sensitivity of RulingOut CCMBecause the clinical tests and mea-sures for CCM lack sensitivity, wesuggest that they should not be usedsingularly and should never be usedin the absence of a complete patienthistory. When sensitivity is poor foreach given clinical test and measure,combining tests with the Boolean
operator “OR” improves sensitivity.Previous authors have used a similarapproach during the development ofscreening tools to reduce unneces-sary use of radiographs. The OttawaAnkle Rules96 and the CanadianC-spine Rule for the cervical spine97
involve guidelines during the screen-ing examination that earmark thatpatient for a radiological screen (ad-ditional workup). The Ottawa rulefor an ankle fracture states that aradiograph series is necessary onlywhen there is pain near the malleoliand one or more of the followingfindings: (1) patient age 55 years orgreater, (2) unable to bear weight for4 steps both immediately and in theemergency room, or (3) pain withpalpation of the posterior edge or tipof either malleolus. Similarly, the Ca-nadian C-spine Rule98 makes judi-cious use of the Boolean operator“OR” to increase sensitivity. Bothrules demonstrate high sensitivity,which effectively identifies those pa-tients who most likely will not ben-efit from a radiograph series. It isworth noting that the low sensitivityvalues may be partially associatedwith the difficulty in diagnosingCCM and the ambiguity in assess-ment of the patient’s signs and symp-toms and MRI findings that make upa diagnosis.
ConclusionWith regard to CCM, how can theprimary care clinician use the best-available evidence to rule out the di-agnosis so that appropriate physicaltherapy intervention can begin? Wesuggest that a careful, judiciousscreen involving any positive or un-clear finding should prompt a refer-ral for an MRI or equivalent imagingmethod. Acceptance of any positiveor unclear finding will reduce therisk of late diagnosis and subsequentprogression of symptoms. We havedemonstrated that current clinicalexamination tests and measures havepoor sensitivity, suggesting that anegative finding may falsely rule out
Neurological Screening for Suspected Cord Compressive Myelopathy
September 2007 Volume 87 Number 9 Physical Therapy f 1239 by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from

CCM in patients who actually haveCCM. Furthermore, such a diagnos-tic mistake may have devastatingconsequences to the “missed” pa-tient who may have received effec-tive and timely surgical intervention.To our knowledge, this judiciousscreening method is not commonlyimplemented in medical practice.26
Future studies should investigatethe diagnostic accuracy of clus-tered findings and focus on im-provements in methods. In addi-tion, additional diagnostic accuracystudies with improved study de-signs could further identify thetests and measures that are appro-priate screening tools, and suchstudies are warranted.
Dr Cook provided concept/idea/project de-sign, project management, institutional liai-sons, and clerical support. Dr Cook and DrHegedus provided data collection and anal-ysis. All authors provided writing and con-sultation (including review of manuscriptbefore submission).
This article was received June 1, 2006, and wasaccepted April 26, 2007.
DOI: 10.2522/ptj.20060150
References1 Purves D, Augustine G, Fitzpatrick D, et al.
Neuroscience. 2nd ed. Sunderland, Mass:Sinauer Associates Inc; 2001.
2 Cook CE. Orthopedic Manual Therapy:An Evidence-Based Approach. Upper Sad-dle River, NJ: Prentice Hall; 2007.
3 McCormick WE, Steinmetz MP, Benzel EC.Cervical spondylotic myelopathy: makethe difficult diagnosis, then refer for sur-gery. Cleve Clin J Med. 2003;70:899–904.
4 Dvorak J. Epidemiology, physical examina-tion, and neurodiagnostics. Spine. 1998;23:2663–2673.
5 Manifold SG, McCann PD. Cervical radicu-litis and shoulder disorders. Clin OrthopRelat Res. 1999:105–113.
6 Montgomery DM, Brower RS. Cervicalspondylotic myelopathy: clinical syn-drome and natural history. Orthop ClinNorth Am. 1992;23:487–493.
7 Dvorak J, Sutter M, Herdmann J. Cervicalmyelopathy: clinical and neurophysiologi-cal evaluation. Eur Spine J. 2003;12(suppl2):S181–S187.
8 Fujiwara K, Yonenobu K, Ebara S, et al.The prognosis of surgery for cervical com-pression myelopathy: an analysis of thefactors involved. J Bone Joint Surg Br.1989;71:393–398.
9 Emery SE. Cervical spondylotic myelopa-thy: diagnosis and treatment. J Am AcadOrthop Surg. 2001;9:376–388.
10 Yoshimatsu H, Nagata K, Goto H, et al.Conservative treatment for cervical spon-dylotic myelopathy. prediction of treat-ment effects by multivariate analysis.Spine J. 2001;1:269–273.
11 Govind J. Lumbar radicular pain. AustFam Physician. 2004;33:409–412.
12 Wainner RS, Gill H. Diagnosis and nonop-erative management of cervical radiculop-athy. J Orthop Sports Phys Ther. 2000;30:728–744.
13 Woolf AD. How to assess musculoskeletalconditions: history and physical examina-tion. Best Pract Res Clin Rheumatol.2003;17:381–402.
14 Obuchowski NA, Graham RJ, Baker ME,Powell KA. Ten criteria for effectivescreening: their application to multisliceCT screening for pulmonary and colorec-tal cancers. AJR Am J Roentgenol. 2001;176:1357–1362.
15 Grimes DA, Schulz KF. Uses and abuses ofscreening tests. Lancet. 2002;359:881–884.
16 Sackett D, Richardson W, Rosenberg W,Haynes R. Evidence-Based Medicine: Howto Practice and Teach EBM. New York,NY: Churchill Livingstone Inc; 1997.
17 Bishop PB, Wing PC. Knowledge transferin family physicians managing patientswith acute low back pain: a prospectiverandomized control trial. Spine J. 2006;6:282–288.
18 Bishop PB, Wing PC. Compliance withclinical practice guidelines in family phy-sicians managing worker’s compensationboard patients with acute lower backpain. Spine J. 2003;3:442–450.
19 Gonzalez-Urzelai V, Palacio-Elua L, Lopez-de-Munain J. Routine primary care man-agement of acute low back pain: adher-ence to clinical guidelines. Eur Spine J.2003;12:589–594.
20 Staal JB, Hlobil H, van Tulder MW, et al.Occupational health guidelines for themanagement of low back pain: an interna-tional comparison. Occup Environ Med.2003;60:618–626.
21 Boyce RH, Wang JC. Evaluation of neckpain, radiculopathy, and myelopathy: im-aging, conservative treatment, and surgi-cal indications. Instr Course Lect. 2003;52:489–495.
22 Matsumoto M, Toyama Y, Ishikawa M,et al. Increased signal intensity of the spi-nal cord on magnetic resonance images incervical compressive myelopathy: Does itpredict the outcome of conservative treat-ment? Spine. 2000;25:677–682.
23 Nakamura K, Kurokawa T, Hoshino Y,et al. Conservative treatment for cervicalspondylotic myelopathy: achievement andsustainability of a level of “no disability.”J Spinal Disord. 1998;11:175–179.
24 Browder DA, Erhard RE, Piva SR. Intermit-tent cervical traction and thoracic manip-ulation for management of mild cervicalcompressive myelopathy attributed to cer-vical herniated disc: a case series. J OrthopSports Phys Ther. 2004;34:701–712.
25 Davis DP, Wold RM, Patel RJ, et al. Theclinical presentation and impact of diag-nostic delays on emergency departmentpatients with spinal epidural abscess.J Emerg Med. 2004;26:285–291.
26 Gross J, Benzel E. Dorsal surgical approachfor cervical spondylotic myelopathy. In:Camins MD, ed. Techniques in Neurosur-gery. Philadelphia, Pa: Lippincott Williams& Wilkins; 1999:162–176.
27 Young WF. Cervical spondylotic myelopa-thy: a common cause of spinal cord dys-function in older persons. Am FamPhysician. 2000;62:1064–1070, 1073.
28 Chiles BW III, Leonard MA, Choudhri HF,Cooper PR. Cervical spondylotic myelop-athy: patterns of neurological deficit andrecovery after anterior cervical decompres-sion. Neurosurgery. 1999;44:762–769; dis-cussion 769–770.
29 Clark CA, Barker GJ, Tofts PS. Magneticresonance diffusion imaging of the humancervical spinal cord in vivo. Magn ResonMed. 1999;41:1269–1273.
30 Good DC, Couch JR, Wacaser L. “Numb,clumsy hands” and high cervical spondy-losis. Surg Neurol. 1984;22:285–291.
31 Kadanka Z, Bednarik J, Vohanka S, et al.Conservative treatment versus surgery inspondylotic cervical myelopathy: a pro-spective randomised study. Eur Spine J.2000;9:538–544.
32 MacFadyen DJ. Posterior column dysfunc-tion in cervical spondylotic myelopathy.Can J Neurol Sci. 1984;11:365–370.
33 Nurick S. The natural history and the re-sults of surgical treatment of the spinalcord disorder associated with cervicalspondylosis. Brain. 1972;95:101–108.
34 Rowland LP. Surgical treatment of cervicalspondylotic myelopathy: time for a con-trolled trial. Neurology. 1992;42:5–13.
35 Crandall PH, Batzdorf U. Cervical spondy-lotic myelopathy. J Neurosurg. 1966;25:57–66.
36 Hawkes C. Smart handles and red flags inneurological diagnosis. Hosp Med. 2002;63:732–742.
37 Adams RD, Victor M. Diseases of the spinalcord, peripheral nerve and muscle. In:Adam RD, Victor M, eds. Principles ofNeurology. 5th ed. New York, NY:McGraw-Hill Inc; 1993:1100–1101.
38 Brain WR, Northfield D, Wilkinson M. Theneurological manifestations of cervicalspondylosis. Brain. 1952;75:187–225.
39 Cohen DB. Infectious origins of caudaequina syndrome. Neurosurg Focus. 2004;16:e2.
40 Thongtrangan I, Le H, Park J, Kim DH.Cauda equina syndrome in patients withlow lumbar fractures. Neurosurg Focus.2004;16:e6.
Neurological Screening for Suspected Cord Compressive Myelopathy
1240 f Physical Therapy Volume 87 Number 9 September 2007 by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from
41 Arafat QW, Jackowski A, Chavda SV, WestRJ. Case report: ossification of the thoracicligamenta flava in a Caucasian—a rarecause of myelopathy. Br J Radiol. 1993;66:1193–1196.
42 Muto M, Muto E, Izzo R, et al. Vertebro-plasty in the treatment of back pain.Radiol Med (Torino). 2005;109:208–219.
43 Arce D, Sass P, Abul-Khoudoud H. Recog-nizing spinal cord emergencies. Am FamPhysician. 2001;64:631–638.
44 Nakamura C, Kawaguchi Y, Ishihara H,et al. Upper thoracic myelopathy causedby vertebral collapse and subluxation inrheumatoid arthritis: report of two cases.J Orthop Sci. 2004;9:629–634.
45 Kleopa KA, Zamba-Papanicolaou E, Kyri-akides T. Compressive lumbar myelopathypresenting as segmental motor neuron dis-ease. Muscle Nerve. 2003;28:69–73.
46 Kostuik JP. Medicolegal consequences ofcauda equina syndrome: an overview.Neurosurg Focus. 2004;16:e8.
47 Bagley CA, Gokaslan ZL. Cauda equinasyndrome caused by primary and meta-static neoplasms. Neurosurg Focus. 2004;16:e3.
48 Batzdorf U, Flannigan BD. Surgical decom-pressive procedures for cervical spondy-lotic myelopathy: a study using magneticresonance imaging. Spine. 1991;16:123–127.
49 Fukushima T, Ikata T, Taoka Y, Takata S.Magnetic resonance imaging study on spi-nal cord plasticity in patients with cervicalcompression myelopathy. Spine. 1991;16:S534–S538.
50 Ono K. Cervical myelopathy secondary tomultiple spondylotic protrusions: a clini-copathologic study. Spine. 1977;2:125.
51 Yousem DM, Atlas SW, Hackney DB. Cervi-cal spine disk herniation: comparison of CTand 3DFT gradient echo MR scans.J Comput Assist Tomogr. 1992;16:345–351.
52 Pui MH, Husen YA. Value of magneticresonance myelography in the diagnosisof disc herniation and spinal stenosis.Australas Radiol. 2000;44:281–284.
53 Mizuno J, Nakagawa H, Hashizume Y.Analysis of hypertrophy of the posteriorlongitudinal ligament of the cervical spine,on the basis of clinical and experimentalstudies. Neurosurgery. 2001;49:1091–1097;discussion 1097–1098.
54 Ogino H, Tada K, Okada K, et al. Canaldiameter, anteroposterior compression ra-tio, and spondylotic myelopathy of thecervical spine. Spine. 1983;8:1–15.
55 Ono K, Ebara S, Fuji T, et al. Myelopathyhand: new clinical signs of cervical corddamage. J Bone Joint Surg Br. 1987;69:215–219.
56 Zeidman SM, Ducker TB, Raycroft J.Trends and complications in cervicalspine surgery: 1989–1993. J SpinalDisord. 1997;10:523–526.
57 Bednarik J, Kadanka Z, Dusek L, et al.Presymptomatic spondylotic cervical cordcompression. Spine. 2004;29:2260–2269.
58 Al-Mefty O, Harkey LH, Middleton TH,et al. Myelopathic cervical spondylotic le-sions demonstrated by magnetic reso-nance imaging. J Neurosurg. 1988;68:217–222.
59 Chen CJ, Lyu RK, Lee ST, et al. Intramed-ullary high signal intensity on T2-weightedMR images in cervical spondylotic myelop-athy: prediction of prognosis with type ofintensity. Radiology. 2001;221:789–794.
60 Kumar VG, Rea GL, Mervis LJ, McGregorJM. Cervical spondylotic myelopathy:functional and radiographic long-term out-come after laminectomy and posterior fu-sion. Neurosurgery. 1999;44:771–777;discussion 777–778.
61 Matsuda Y, Miyazaki K, Tada K, et al. In-creased MR signal intensity due to cervicalmyelopathy: analysis of 29 surgical cases.J Neurosurg. 1991;74:887–892.
62 Wada E, Yonenobu K, Suzuki S, et al. Canintramedullary signal change on magneticresonance imaging predict surgical out-come in cervical spondylotic myelopathy?Spine. 1999;24:455–461; discussion 462.
63 Sung RD, Wang JC. Correlation between apositive Hoffmann’s reflex and cervical pa-thology in asymptomatic individuals.Spine. 2001;26:67–70.
64 Kang DX, Fan DS. The electrophysiologi-cal study of differential diagnosis betweenamyotrophic lateral sclerosis and cervicalspondylotic myelopathy. ElectromyogrClin Neurophysiol. 1995;35:231–238.
65 De Mattei M, Paschero B, Sciarretta A,et al. Usefulness of motor evoked poten-tials in compressive myelopathy. Electro-myogr Clin Neurophysiol. 1993;33:205–216.
66 Singh A, Gnanalingham KK, Casey AT,Crockard A. Use of quantitative assess-ment scales in cervical spondylotic my-elopathy: survey of clinician’s attitudes.Acta Neurochir (Wien). 2005;147:1235–1238; discussion 1238.
67 Emery SE, Bohlman HH, Bolesta MJ, JonesPK. Anterior cervical decompression andarthrodesis for the treatment of cervicalspondylotic myelopathy: two- toseventeen-year follow-up. J Bone JointSurg Am. 1998;80:941–951.
68 Estanol BV, Marin OS. Mechanism of theinverted supinator reflex: a clinical andneurophysiological study. J Neurol Neuro-surg Psychiatry. 1976;39:905–908.
69 Sakai N. Finger motion analysis of the pa-tients with cervical myelopathy. Spine.2005;30:2777–2782.
70 Wong TM, Leung HB, Wong WC. Correla-tion between magnetic resonance imagingand radiographic measurement of cervicalspine in cervical myelopathic patients.J Orthop Surg (Hong Kong). 2004;12:239–242.
71 Deveci M, Bozkurt M, Sengezer M. Clonus:an unusual delayed neurological complica-tion in electrical burn injury. Burns. 2001;27:647–651.
72 Mayer NH. Clinicophysiologic concepts ofspasticity and motor dysfunction in adultswith an upper motoneuron lesion. MuscleNerve Suppl. 1997;6:S1–S13.
73 Boyle RS, Shakir RA, Weir AI, McInnes A.Inverted knee jerk: a neglected localisingsign in spinal cord disease. J Neurol Neu-rosurg Psychiatry. 1979;42:1005–1007.
74 Berger JR, Fannin M. The “bedsheet” Ba-binski. South Med J. 2002;95:1178–1179.
75 Ghosh D, Pradhan S. “Extensor toe sign”by various methods in spastic childrenwith cerebral palsy. J Child Neurol. 1998;13:216–220.
76 de Freitas GR, Andre C. Absence of theBabinski sign in brain death: a prospectivestudy of 144 cases. J Neurol. 2005;252:106–107.
77 Hindfelt B, Rosen I, Hanko J. The signifi-cance of a crossed extensor hallucis re-sponse in neurologic disorders: a compar-ison with the Babinski sign. Acta NeurolScand. 1976;53:241–250.
78 Whiting P, Rutjes AW, Dinnes J, et al. De-velopment and validation of methods forassessing the quality of diagnostic accu-racy studies. Health Technol Assess. 2004;8:iii, 1–234.
79 Smith MS. Babinski’s sign: abduction alsocounts. JAMA. 1979;242:1849–1850.
80 Glick TH, Workman TP, Gaufberg SV. Spi-nal cord emergencies: false reassurancefrom reflexes. Acad Emerg Med. 1998;5:1041–1043.
81 Kumar SP, Ramasubramanian D. The Ba-binski sign: a reappraisal. Neurol India.2000;48:314–318.
82 van Gijn J. The Babinski reflex. PostgradMed J. 1995;71:645–648.
83 Glaser JA, Cure JK, Bailey KL, Morrow DL.Cervical spinal cord compression and theHoffmann sign. Iowa Orthop J. 2001;21:49–52.
84 Uchihara T, Furukawa T, Tsukagoshi H.Compression of brachial plexus as a diag-nostic test of cervical cord lesion. Spine.1994;19:2170–2173.
85 Fouyas IP, Statham PF, Sandercock PA.Cochrane review on the role of surgery incervical spondylotic radiculomyelopathy.Spine. 2002;27:736–747.
86 Matsumoto M, Chiba K, Ishikawa M, et al.Relationships between outcomes of con-servative treatment and magnetic reso-nance imaging findings in patients withmild cervical myelopathy caused by soft discherniations. Spine. 2001;26:1592–1598.
87 Nakanishi T, Shimada Y, Toyokura Y. So-matosensory evoked responses to me-chanical stimulation in normal subjectsand in patients with neurological disor-ders. J Neurol Sci. 1974;21:289–298.
88 Ebersold MJ, Pare MC, Quast LM. Surgicaltreatment for cervical spondylitic myelop-athy. J Neurosurg. 1995;82:745–751.
89 Kato Y, Iwasaki M, Fuji T, et al. Long-termfollow-up results of laminectomy for cer-vical myelopathy caused by ossification ofthe posterior longitudinal ligament.J Neurosurg. 1998;89:217–223.
90 McCormack BM, Weinstein PR. Cervicalspondylosis: an update. West J Med. 1996;165:43–51.
Neurological Screening for Suspected Cord Compressive Myelopathy
September 2007 Volume 87 Number 9 Physical Therapy f 1241 by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from

91 Cyriax J. Textbook of Orthopedic Medi-cine. Vol 1. 8th ed. London, United King-dom: Bailliere Tindall; 1982.
92 Hoppenfeld S. Physical Examination ofthe Spine and Extremities. Norwalk,Conn: Appleton & Lange; 1976.
93 Magee DJ. Orthopedic Physical Assess-ment. 3rd ed. Philadelphia, Pa: WB Saun-ders Co; 1997.
94 Winkel D, Vleeming A. Diagnosis andTreatment of the Spine. Gaithersburg, Md:Aspen Publishers; 1996.
95 Yoss RE, Corbin KB, Maccarty CS, LoveJG. Significance of symptoms and signsin localization of involved root in cervi-cal disk protrusion. Neurology. 1957;7:673– 683.
96 Stiell IG, Greenberg GH, McKnight RD,et al. A study to develop clinical decisionrules for the use of radiography in acuteankle injuries. Ann Emerg Med. 1992;21:384–390.
97 Hoffman JR, Schriger DL, Mower W, et al.Low-risk criteria for cervical-spine ra-diography in blunt trauma: a prospec-tive study. Ann Emerg Med. 1992;21:1454–1460.
98 Stiell IG, Wells GA, Vandemheen KL, et al.The Canadian C-spine Rule for radiogra-phy in alert and stable trauma patients.JAMA. 2001;286:1841–1848.
Neurological Screening for Suspected Cord Compressive Myelopathy
1242 f Physical Therapy Volume 87 Number 9 September 2007 by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from

doi: 10.2522/ptj.20060150Originally published online July 17, 2007
2007; 87:1233-1242.PHYS THER. Adam GoodeChad E Cook, Eric Hegedus, Ricardo Pietrobon andSuspected Cord Compressive MyelopathyA Pragmatic Neurological Screen for Patients With
References
http://ptjournal.apta.org/content/87/9/1233#BIBLfor free at: This article cites 88 articles, 12 of which you can access
Cited by
http://ptjournal.apta.org/content/87/9/1233#otherarticles
This article has been cited by 2 HighWire-hosted articles:
Information Subscription http://ptjournal.apta.org/subscriptions/
Permissions and Reprints http://ptjournal.apta.org/site/misc/terms.xhtml
Information for Authors http://ptjournal.apta.org/site/misc/ifora.xhtml
by guest on May 18, 2015http://ptjournal.apta.org/Downloaded from














![[Colorectal Carcinoma with Suspected Lynch Syndrome: A Multidisciplinary Algorithm.]](https://static.fdokumen.com/doc/165x107/6335f98064d291d2a302b343/colorectal-carcinoma-with-suspected-lynch-syndrome-a-multidisciplinary-algorithm.jpg)




