Prognostic significance of DNA ploidy in patients with stage II and stage III colon carcinoma
11
49 Prognostic Significance of DNA Ploidy in Patients with Stage II and Stage III Colon Carcinoma A Prospective Flow Cytometric Study BACKGROUND. The prognostic value of flow cytometric DNA ploidy in colorectal Giovanni Lanza, M.D. 1 carcinoma has not been defined clearly. Most previous studies were conducted Roberta Gafa `, M.D. 1 retrospectively using archival formalin fixed, paraffin embedded tumor samples. Alessandra Santini, M.D. 2 Conversely, few data on prospective studies employing fresh or frozen tissue speci- Iva Maestri, M.Sc. 1 mens are available. There is general agreement that fresh/frozen material is more Alessandra Dubini, M.D. 1 reliable than paraffin embedded tissue for DNA ploidy analysis by flow cytometry. Giuseppe Gilli 3 METHODS. In the current investigation we evaluated the prognostic significance of Luigi Cavazzini, M.D. 1 nuclear DNA content in a prospective series of 191 patients with curatively resected TNM Stage II (n Å 107) or Stage III (n Å 84) sporadic colon carcinomas. DNA 1 Dipartimento di Medicina Sperimentale e Diag- ploidy status was assessed by flow cytometry utilizing multiple frozen tumor sam- nostica, Sezione di Anatomia, Istologia e Cito- ples. Mean follow-up in surviving patients was 48.5 months (median, 46.9 months; logia Patologica, Universita ` di Ferrara, Ferrara, range, 29 – 77 months). The Cox proportional hazards model was used to adjust Italy. for several clinical and pathologic covariates. 2 Oncologia Medica, Azienda Ospedaliera Ar- RESULTS. Of the 191 carcinomas examined, 47 (24.6%) were classified as DNA cispedale S. Anna, Ferrara, Italy. diploid and 144 (75.4%) as DNA aneuploid. DNA ploidy pattern was significantly 3 Servizio di Fisica Sanitaria, Azienda Ospeda- related to tumor site (P õ 0.0001), histologic type (P Å 0.0002), and grade of liera Arcispedale S. Anna, Ferrara, Italy. differentiation (P Å 0.009), but not to other clinical and pathologic variables. Pa- tients with DNA diploid tumors showed a better disease free (P Å 0.013) and overall survival (P Å 0.021) than patients with DNA aneuploid adenocarcinomas. In particular, patients with Stage II DNA diploid tumors (n Å 30) had an excellent clinical outcome, with an overall 5-year survival rate of 97%. When patients were analyzed according to the anatomic site of the tumor, a significant relationship between DNA ploidy status and disease free and overall survival was observed in the group of patients with carcinomas of the proximal colon (n Å 84) (P Å 0.004 and P Å 0.002, respectively), but not among patients whose tumors were sited distally to the splenic flexure (n Å 107). In multivariate analysis, nuclear DNA content was demonstrated to be an independent prognostic variable for both disease free and overall survival. Furthermore, in the group of patients with tumors of the proximal colon, DNA ploidy pattern was the single most important prognos- tic factor. CONCLUSIONS. Our results confirm that flow cytometric DNA ploidy status is a Supported in part by Grants from the Italian significant and independent prognostic factor in patients with colon carcinoma. Ministry of the University (MURST, funds These findings may have clinical implications for the management of affected ‘‘60%’’ and ‘‘40%’’). patients, especially those with Stage II disease. Cancer 1998; 82:49 – 59. q 1997 American Cancer Society. Address for reprints: Dr. Giovanni Lanza, Dipar- timento di Medicina Sperimentale e Diagnostica, Sezione di Anatomia, Istologia e Citologia Pato- KEYWORDS: colon carcinoma, DNA ploidy, flow cytometry, prognosis, proximal and logica, Universita ` di Ferrara, Via Fossato di Mor- distal colon. tara 64/b, 44100 Ferrara, Italy. T Received March 12, 1997; revision received June 26, 1997; accepted June 26, 1997. he prognostic value of flow cytometric DNA ploidy in patients with colorectal carcinoma has not been defined clearly. Most investiga- q 1998 American Cancer Society / 7b9a$$1510 12-17-97 13:59:24 cana W: Cancer
-
Upload
independent -
Category
Documents
-
view
8 -
download
0
Transcript of Prognostic significance of DNA ploidy in patients with stage II and stage III colon carcinoma

49
Prognostic Significance of DNA Ploidy in Patientswith Stage II and Stage III Colon CarcinomaA Prospective Flow Cytometric Study
BACKGROUND. The prognostic value of flow cytometric DNA ploidy in colorectalGiovanni Lanza, M.D.1
carcinoma has not been defined clearly. Most previous studies were conductedRoberta Gafa, M.D.1
retrospectively using archival formalin fixed, paraffin embedded tumor samples.Alessandra Santini, M.D.2
Conversely, few data on prospective studies employing fresh or frozen tissue speci-Iva Maestri, M.Sc.1
mens are available. There is general agreement that fresh/frozen material is moreAlessandra Dubini, M.D.1
reliable than paraffin embedded tissue for DNA ploidy analysis by flow cytometry.Giuseppe Gilli3METHODS. In the current investigation we evaluated the prognostic significance ofLuigi Cavazzini, M.D.1
nuclear DNA content in a prospective series of 191 patients with curatively resected
TNM Stage II (n Å 107) or Stage III (n Å 84) sporadic colon carcinomas. DNA1 Dipartimento di Medicina Sperimentale e Diag-
ploidy status was assessed by flow cytometry utilizing multiple frozen tumor sam-nostica, Sezione di Anatomia, Istologia e Cito-ples. Mean follow-up in surviving patients was 48.5 months (median, 46.9 months;logia Patologica, Universita di Ferrara, Ferrara,range, 29–77 months). The Cox proportional hazards model was used to adjustItaly.for several clinical and pathologic covariates.
2 Oncologia Medica, Azienda Ospedaliera Ar-RESULTS. Of the 191 carcinomas examined, 47 (24.6%) were classified as DNAcispedale S. Anna, Ferrara, Italy.diploid and 144 (75.4%) as DNA aneuploid. DNA ploidy pattern was significantly
3 Servizio di Fisica Sanitaria, Azienda Ospeda- related to tumor site (P õ 0.0001), histologic type (P Å 0.0002), and grade ofliera Arcispedale S. Anna, Ferrara, Italy. differentiation (P Å 0.009), but not to other clinical and pathologic variables. Pa-
tients with DNA diploid tumors showed a better disease free (P Å 0.013) and
overall survival (P Å 0.021) than patients with DNA aneuploid adenocarcinomas.
In particular, patients with Stage II DNA diploid tumors (n Å 30) had an excellent
clinical outcome, with an overall 5-year survival rate of 97%. When patients were
analyzed according to the anatomic site of the tumor, a significant relationship
between DNA ploidy status and disease free and overall survival was observed in
the group of patients with carcinomas of the proximal colon (n Å 84) (P Å 0.004
and P Å 0.002, respectively), but not among patients whose tumors were sited
distally to the splenic flexure (n Å 107). In multivariate analysis, nuclear DNA
content was demonstrated to be an independent prognostic variable for both
disease free and overall survival. Furthermore, in the group of patients with tumors
of the proximal colon, DNA ploidy pattern was the single most important prognos-
tic factor.
CONCLUSIONS. Our results confirm that flow cytometric DNA ploidy status is aSupported in part by Grants from the Italian
significant and independent prognostic factor in patients with colon carcinoma.Ministry of the University (MURST, fundsThese findings may have clinical implications for the management of affected‘‘60%’’ and ‘‘40%’’).patients, especially those with Stage II disease. Cancer 1998;82:49–59.
q 1997 American Cancer Society.Address for reprints: Dr. Giovanni Lanza, Dipar-timento di Medicina Sperimentale e Diagnostica,Sezione di Anatomia, Istologia e Citologia Pato- KEYWORDS: colon carcinoma, DNA ploidy, flow cytometry, prognosis, proximal andlogica, Universita di Ferrara, Via Fossato di Mor-
distal colon.tara 64/b, 44100 Ferrara, Italy.
TReceived March 12, 1997; revision receivedJune 26, 1997; accepted June 26, 1997.
he prognostic value of flow cytometric DNA ploidy in patients withcolorectal carcinoma has not been defined clearly. Most investiga-
q 1998 American Cancer Society
/ 7b9a$$1510 12-17-97 13:59:24 cana W: Cancer

50 CANCER January 1, 1998 / Volume 82 / Number 1
tors agree that presence of aneuploid cell populations gram, abdominal computed tomography scan and ul-trasonography, and abdominal exploration at laparot-by flow cytometry is associated with reduced patient
survival.1–8 However, only in a limited number of stud- omy. Patients with idiopathic inflammatory bowel dis-ease or familial adenomatous polyposis, those withies was DNA ploidy status demonstrated to be an inde-
pendent prognostic variable by multivariate analysis evidence of hereditary nonpolyposis colorectal carci-noma syndrome (according to the Amsterdam crite-including traditional prognostic parameters.9–14 More-
over, other investigations have been unable to show ria), or those with a malignant tumor detected outsidethe colon within the previous 5 years were not in-any significant relation between clinical outcome and
tumor DNA content.15–18 Several factors probably ac- cluded in the study. Three patients had synchronouscolonic adenocarcinomas and were classified ac-count for these contradictory results. Marked varia-
tions in findings can be ascribed to differences in study cording to the tumor with the most advanced stage.Twenty-six patients with Stage III disease and 20 pa-size, patient selection, tumor sampling, methods of
tissue disaggregation, use of archival or fresh/frozen tients with Stage II disease received postoperative ad-juvant chemotherapy. No patient received preopera-material, and data analysis. In this respect, it is im-
portant to note that most flow cytometric studies re- tive radiation or chemotherapy.Information regarding clinical outcome was ob-garding the prognostic relevance of DNA ploidy in pa-
tients with colorectal carcinoma have been performed tained from hospital chart review or direct telephoneinterview with the patients’ personal physicians. Peri-retrospectively using archival formalin fixed, paraffin
embedded tissue specimens, whereas only a few anal- odic controls included a clinical examination, bloodtest (comprising serum carcinoembryonic antigen),yses employed fresh or frozen tumor samples. As also
recently stated, fresh/frozen material is preferable to endoscopy, abdominal ultrasonography, and radiogra-phy of the thorax. Computed tomography and mag-paraffin embedded tissue for DNA analysis by flow
cytometry.19 In addition, patients with colonic and rec- netic resonance imaging also were performed in casesof suspected tumor recurrence. During the observa-tal adenocarcinomas should be analyzed separately,
due to the differences in the pattern of tumor recur- tion period, 41 patients (21.5%; 14 with Stage II and27 with Stage III disease) developed tumor recurrencerence and therapeutic intervention between these
sites. (36 with distant metastasis and 5 with local recur-rence) and 33 of these patients (11 with Stage II andWe reported previously the relationship between
nuclear DNA content and several clinical and patho- 22 with Stage III disease) died of recurrent disease.Eleven patients (7 with Stage II and 4 with Stage IIIlogic variables as well as with p53 protein expression
in colorectal adenocarcinomas.20,21 In the current in- disease) died of causes unrelated to colon carcinomawithout clinical evidence of disease. The mean follow-vestigation we evaluated the prognostic significance
of DNA ploidy (as determined by flow cytometry using up in surviving patients was 48.5 months (median, 46.9months; range, 29–77 months).frozen tumor samples) in a large series of patients
with Stage II and Stage III colon carcinoma who hadundergone curative surgical resection. Histopathologic Evaluation
Morphologic analysis was performed by one author(G.L.) on hematoxylin and eosin and periodic acid-MATERIAL AND METHODS
The study included 191 prospectively collected pa- Schiff stained sections. Three to 13 tissue blocks of thetumor were examined in each case.tients with International Union Against Cancer TNM22
Stage II (nÅ 107) or Stage III (nÅ 84) colon carcinoma Histologic type (adenocarcinoma or mucinouscarcinoma) was determined following the criteria ofwho underwent curative surgical resection between
January 1990 and December 1993. Ninety-five patients the World Health Organization.23 Grade of differentia-tion was evaluated according to Jass et al.,24 as pre-were men and 96 were women, with a mean age of 66.7
years (range, 41–87 years). Forty-eight tumors were viously reported.21,25 Tissue sections also were care-fully examined for the presence of extramural venouslocated in the right colon (cecum and ascending co-
lon), 36 in the transverse colon (including both flex- invasion. This was recorded as being present onlywhen the findings were considered to be unequivocal.ures), 24 in the descending colon, and 83 in the sig-
moid colon. Tumors were subdivided further into twoanatomic subgroups: carcinomas of the proximal co- Flow Cytometric DNA Analysis
Flow cytometric DNA ploidy analysis was performedlon (right and transverse colon) and carcinomas of thedistal colon (descending and sigmoid colon). as reported previously.20,21 All specimens were col-
lected in the operating room immediately after resec-Tumor stage was based on pathologic and clinicalevaluation, which included preoperative chest radio- tion and rapidly processed. Multiple (from 2–5) non-
/ 7b9a$$1510 12-17-97 13:59:24 cana W: Cancer

DNA Ploidy and Prognosis in Colon Carcinoma/Lanza et al. 51
necrotic representative tissue samples (approximately G2 / M fractions of DNA diploid stemlines when thepercentage of tetraploid cells amounted to ú15% and0.8 cm 1 0.8 cm 1 0.2 cm) were taken from different
areas at the periphery of each tumor, snap frozen and there was evidence of an associated S-phase and G2 /M (octaploid) peak. Multiploid tumors were classifiedstored at 075 7C until use. In each case samples of
normal-appearing mucosa also were taken at a dis- according to the aneuploid cell population with thehighest DI value.tance of at least 5 cm from the tumor burden.
From each tumor sample a frozen section was cut The coefficient of variation (CV) for the G0/G1
peaks was calculated by means of the incorporatedand stained with hematoxylin and eosin to ascertainby histologic examination the presence of adequate software using the RFIT model, which estimates the
percent CV by determining the peak width at the in-neoplastic material (ú50% of tumor cells). When pres-ent, regions with a high content of nonneoplastic cells flection point (60% of peak height). The mean CV of
the diploid G0/G1 peaks of all the tumor samples exam-were removed from the frozen block with a scalpel.For the analysis, tissue samples were thawed at room ined was 3.2% (range, 2.1–5.1%).temperature and minced with scalpels in phosphate-buffered saline (PBS). The nuclei suspensions ob- Statistical Analysis
The association between DNA ploidy and the differenttained were filtered through a 160-mm nylon mesh toremove large cell clumps and debris. The nuclei con- clinical and pathologic variables was examined by the
chi-square test. Disease free and overall survivalcentration was then adjusted to approximately 1 1106/mL. Tumor samples were run in duplicate, and in curves were generated using the Kaplan-Meier method
and were compared by the log rank test. Patients whoone sample nuclei of normal colonic mucosa of thesame patient were mixed before staining as an internal died of causes unrelated to colon carcinoma were cen-
sored from further analysis at the time of death. Multi-individual specific and tissue specific diploid refer-ence. Samples were stained for 30 minutes at 4 7C in variate analysis was performed with the Cox propor-
tional hazards model. All data were analyzed using thethe dark with propidium iodide (50 mg/mL) in PBScontaining RNase (50 mg/mL) and Nonidet P40 (BDH SYSTAT statistical package including the SURVIVAL
supplementary module (Systat Inc., Evanston, IL).Chemicals Ltd, Poole, England) (0.05%). Immediatelybefore flow cytometric analysis, the suspensions were Probability values of õ 0.05 were considered signifi-
cant. All P values reported are two-sided.passed through a 52-mm nylon mesh. The DNA con-tent in the suspensions of nuclei was measured bymeans of a FACScan flow cytometer (Becton Dickin- RESULTS
DNA Ploidy and Clinicopathologic Featuresson Immunocytometry Systems, San Jose, CA), usingthe CellFIT (version 2.0) (Becton Dickinson) software Of the 191 carcinomas examined, 47 (24.6%) were clas-
sified as DNA diploid and 144 (75.4%) as DNA aneu-package for data acquisition and analysis. Propidiumiodide stained chicken erythrocyte nuclei and calf thy- ploid. Among the aneuploid tumors, 26 had a DI °
1.20 and 13 were tetraploid. Twenty-one carcinomasmocyte nuclei, prepared as described in the DNAQuality Control Particle Kit (Becton Dickinson), were (11%) showed multiple aneuploid cell populations.
The mean DI of aneuploid tumors was 1.65 (range,used as daily biologic calibrators for instrument set-up and for quality control of instrument performance. 0.93–2.99).
No relationship was found between DNA ploidyFor each sample, a minimum of 25,000 events wasevaluated. pattern and patient age and gender, tumor stage, ex-
tent of lymph node involvement, and extramural ve-According to international convention,26 adeno-carcinomas with a single G0/G1 peak were classified as nous invasion (Table 1). As reported previously,20,21
nuclear DNA content was related closely to the ana-DNA diploid. Only tumors with at least two separateG0/G1 peaks were considered to be DNA aneuploid. tomic site and the histologic type of the tumor (Table
1). Tumors of the right and transverse colon more fre-Carcinomas were designated multiploid if two or moredistinct aneuploid G0/G1 peaks could be identified. quently were DNA diploid than those located distally
to the splenic flexure (36 of 84 [42.9%] vs. 11 of 107The degree of DNA aneuploidy was expressed by theDNA index (DI), defined as the ratio of the modal [10.3%]; Põ 0.0001). Furthermore, aneuploid cell pop-
ulations were detected more often in nonmucinouschannel position of the G0/G1 peak of the aneuploidcell population divided by the modal channel position tumors than in mucinous tumors (134 of 168 [79.8%]
vs. 10 of 23 [43.5%]; P Å 0.0002). A significant relation-of the G0/G1 peak of the diploid reference cells. Bydefinition, DNA diploid tumors have a DI of 1.00. G0/ ship also could be demonstrated between DNA ploidy
status and grade of differentiation, with poorly differ-G1 aneuploid populations with a tetraploid DNA con-tent (DI Å 2.00 { 0.10) were discriminated from the entiated tumors more frequently showing a diploid
/ 7b9a$$1510 12-17-97 13:59:24 cana W: Cancer

52 CANCER January 1, 1998 / Volume 82 / Number 1
TABLE 1DNA Ploidy Pattern in Relation to Clinical and Pathologic Variables
Variable No. of patients (%) Diploid (%) Aneuploid (%) P valuea
GenderMale 95 (49.7) 23 (24.2) 72 (75.8)Female 96 (50.3) 24 (25.0) 72 (75.0) 0.8992
Age (yrs)õ 60 45 (23.6) 12 (26.7) 33 (73.3)¢ 60 146 (76.4) 35 (24.0) 111 (76.0) 0.1967
Tumor siteProximal colon 84 (44.0) 36 (42.9) 48 (57.1)Distal colon 107 (56.0) 11 (10.3) 96 (89.7) õ 0.0001
Tumor stage (TNM)II 107 (56.0) 30 (28.0) 77 (72.0)III 84 (44.0) 17 (20.2) 67 (79.8) 0.2142
Lymph node involvement (TNM)N0 107 (56.0) 30 (28.0) 77 (72.0)N1 55 (28.8) 10 (18.2) 45 (81.8)N2–3 29 (15.2) 7 (24.1) 22 (75.9) 0.3856
Histologic type (WHO)Adenocarcinoma 168 (88.0) 34 (20.2) 134 (79.8)Mucinous carcinoma 23 (12.0) 13 (56.5) 10 (43.5) 0.0002
Degree of differentiationWell/moderate 148 (77.5) 30 (20.3) 118 (79.7)Poor 43 (22.5) 17 (39.5) 26 (60.5) 0.0098
Venous invasionAbsent 166 (86.9) 43 (25.9) 123 (74.1)Present 25 (13.1) 4 (16.0) 21 (84.0) 0.2838
Total 191 47 (24.6) 144 (75.4)
WHO: World Health Organization.a Chi-square test.
nuclear DNA content than well and moderately differ- ately aneuploid tumors (DI ° 1.20) showed a betterrecurrence free and overall survival than those withentiated tumors (17 of 43 [39.5%] vs. 30 of 148 [20.3%];
P Å 0.0098) (Table 1). To a great extent this relation- the other aneuploid tumors, but this difference failedto reach statistical significance.ship was determined by tumor site. In fact the majority
of poorly differentiated tumors (30 of 43, 69.8%) were As expected, tumor stage was a strong prognosticpredictor of disease free and overall survival in the 191localized in the proximal colon, and ú50% were DNA
diploid (16 of 30, 53.3%). In contrast, 12 of the 13 patients included in the study (P Å 0.001 and P Å0.007, respectively). When patients were stratified bypoorly differentiated tumors located distally to the
splenic flexure were DNA aneuploid. tumor stage, a survival advantage for patients withDNA diploid tumors was observed in Stage II as wellas in Stage III disease (Fig. 2), although the differencesDNA Ploidy and Survival
Patients with DNA diploid tumors showed a better did not reach statistical significance. In particular, pa-tients with Stage II DNA diploid tumors had an excel-disease free (PÅ 0.013) and overall survival (PÅ 0.021)
than patients with DNA aneuploid tumors (Fig. 1). Of lent clinical outcome, with an overall 5-year survivalrate of 97%. The 5-year survival rate of patients withthe 47 patients with DNA diploid tumors, only 4 (8.5%)
developed tumor recurrence and 3 of these patients Stage III DNA diploid tumors was similar to the 5-yearsurvival rate of patients with Stage II DNA aneuploid(6.4%) died of colon carcinoma. Conversely, 37 of the
144 patients with DNA aneuploid tumors (25.7%) de- tumors (81% and 78%, respectively), whereas the 5-year survival rate of patients with Stage III DNA aneu-veloped tumor recurrence, and 30 of these patients
(20.8%) died of recurrent disease. There were no sig- ploid tumors was only 60%. Similar results were ob-tained when tumors were subdivided according to anificant differences in disease free and overall survival
between patients with single and multiple aneuploid DI ° 1.10 and ú1.10 or ° 1.20 and ú1.20 (data notshown).cell populations. Patients with tetraploid and moder-
/ 7b9a$$1510 12-17-97 13:59:24 cana W: Cancer

DNA Ploidy and Prognosis in Colon Carcinoma/Lanza et al. 53
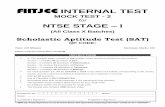
FIGURE 1. (A) Disease free survival and (B) overall survival of patients with colon carcinoma according to flow cytometric DNA ploidy status.
FIGURE 2. (A) Disease free survival and (B) overall survival of patients with colon carcinoma according to both TNM stage and DNA ploidy pattern.
Twenty patients with Stage II tumors (6 DNA dip- veloped tumor recurrence. In contrast, 11 of the 22patients with Stage III DNA aneuploid tumors of theloid and 14 DNA aneuploid tumors) and 26 patients
with Stage III tumors (4 DNA diploid and 22 DNA right and transverse colon (50%) developed tumor re-currence and 10 of these patients (45.5%) died of re-aneuploid tumors) received adjuvant chemotherapy.
When these patients were excluded from the analyses, current disease during the observation period.DNA ploidy status remained significantly related todisease free (P Å 0.020) and overall survival (P Å DNA Ploidy and Other Prognostic Factors
In addition to tumor stage and DNA ploidy status,0.028).When patients were analyzed according to the an- other histopathologic variables were related to the dis-
ease outcome in the series of patients examined (Tableatomic site of the tumor, a significant relationship be-tween DNA ploidy status and disease free and overall 2). Extramural venous invasion (P Å 0.001) and extent
of lymph node involvement (P Å 0.001) were signifi-survival could be observed in the group of patientswith tumors of the proximal colon (P Å 0.004 and P cant predictors of disease free survival. Extent of
lymph node involvement (P Å 0.003), degree of differ-Å 0.002, respectively), but not among patients whosetumors were localized distally to the splenic flexure entiation (P Å 0.035), and venous invasion (Põ 0.001)
were significant predictive factors for overall survival.(Fig. 3). In the proximal colon, the difference in clinicaloutcome between patients with DNA diploid and an- Conversely, patient age and gender, tumor site, histo-
logic type, and adjuvant therapy were not related sig-euploid tumors was particularly evident among thosewith Stage III disease (disease free survival, P Å 0.005; nificantly to recurrence free and overall survival.
The results of multivariate analysis according tooverall survival, P Å 0.003) (Fig. 4). Only 1 of the 15patients with Stage III DNA diploid tumors (6.7%) de- the Cox proportional hazards model are summarized
/ 7b9a$$1510 12-17-97 13:59:24 cana W: Cancer

54 CANCER January 1, 1998 / Volume 82 / Number 1
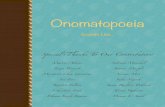
FIGURE 3. Disease free survival of patients with tumors of the (A) proximal colon and (B) distal colon according to DNA ploidy pattern. A significantrelationship between nuclear DNA content and clinical outcome could be demonstrated in patients with tumors of the right and transverse colon (P Å0.004), but not in patients with tumors localized distally to the splenic flexure. NS: not significant.
involvement and other clinical and pathologic vari-ables.
A multivariate analysis also was performed to eval-uate the prognostic role of DNA ploidy in the groupof patients with tumors localized proximally to thesplenic flexure. In this analysis DNA ploidy status,TNM stage, and patient age and gender were includedas covariates to be assessed. As shown in Table 4, DNAploidy was the most significant prognostic factor forboth recurrence (P Å 0.009) and survival (P Å 0.015).
DISCUSSIONMost previous flow cytometric studies regarding the
FIGURE 4. Disease free survival of patients with Stage III tumors of the relationship between DNA ploidy and survival in pa-proximal colon according to DNA ploidy pattern. tients with colorectal carcinoma were conducted ret-
rospectively using archival formalin fixed, paraffin em-bedded tumor samples. In the majority of these inves-tigations patients with DNA diploid tumors had ain Table 3. In Model 1 only tumor stage, patient age
and gender, tumor site, and DNA ploidy pattern were better survival compared with patients with aneuploidtumors.1–7,9,10,13,14 However, the extent of this relation-included as covariates. Model 2 included tumor type,
grade of differentiation, and venous invasion in addi- ship was quite variable and some authors failed toshow any relation between nuclear DNA content andtion to the covariates in Model 1. In Model 3 the extent
of lymph node involvement was employed as covariate clinical outcome.15,16,18 Conversely, only a few data onprospective studies employing fresh or frozen tissuerather than the TNM stage and in Model 4 adjuvant
therapy (none vs. chemotherapy) was added to the specimens are currently available. There is generalagreement that fresh/frozen material is more reliablecovariates in Model 2. In all the analyses DNA ploidy
pattern was a significant independent prognostic fac- than paraffin embedded tissue for DNA ploidy analysisby flow cytometry.19 The results of the current studytor for both tumor recurrence and survival. Only in
the analysis of overall survival with Model 3 was the are in accordance with those previously obtained inother prospective flow cytometric studies employingP value for DNA ploidy status of borderline signifi-
cance (P Å 0.057). It is noteworthy that in patients fresh or frozen colorectal tumor samples.11,12,27 In par-ticular, Kouri et al.11 and Rognum et al.12 showed thatwith DNA aneuploid tumors the risk of recurrence and
cancer-related death was more than three times higher DNA ploidy status allows to discriminate patients withdifferent risk of recurrence and cancer-related deaththan in patients with DNA diploid tumors, even after
adjustment for TNM stage or extent of lymph node within Dukes Stage B and Stage C disease. Moreover,
/ 7b9a$$1510 12-17-97 13:59:24 cana W: Cancer

DNA Ploidy and Prognosis in Colon Carcinoma/Lanza et al. 55
TABLE 2Disease Free and Overall Survival in Relation to Clinicopathologic Features and DNA Ploidy Pattern
Disease free survival Overall survival
No. of Patients with recurrent Patients dyingVariable patients disease (%) P valuea of disease (%) P valuea
GenderMale 95 26 (27.4) 18 (18.9)Female 96 15 (15.6) 0.060 15 (15.6) 0.516
Age (yrs)õ 60 45 9 (20.0) 8 (17.8)¢ 60 146 32 (21.9) 0.844 25 (17.1) 0.932
Tumor siteProximal colon 84 17 (20.2) 15 (17.9)Distal colon 107 24 (22.4) 0.768 18 (16.8) 0.917
Tumor stage (TNM)II 107 14 (13.1) 11 (10.3)III 84 27 (32.1) 0.001 22 (26.2) 0.007
Lymph node involvement (TNM)N0 107 14 (13.1) 11 (10.3)N1 55 15 (27.3) 11 (20.0)N2–3 29 12 (41.4) 0.001b 11 (37.9) 0.003b
Histologic type (WHO)Adenocarcinoma 168 39 (23.2) 31 (18.5)Mucinous carcinoma 23 2 (8.7) 0.087 2 (8.7) 0.173
Degree of differentiationWell/moderate 148 29 (19.6) 21 (14.2)Poor 43 12 (27.9) 0.155 12 (27.9) 0.035
Venous invasionAbsent 166 30 (18.1) 23 (13.9)Present 25 11 (44.0) 0.001 10 (40.0) 0.001
Adjuvant therapyNone 145 31 (21.4) 24 (16.6)Chemotherapy 46 10 (21.7) 0.592 9 (19.6) 0.222
DNA ploidyDiploid 47 4 (8.5) 3 (6.4)Aneuploid 144 37 (25.7) 0.013 30 (20.8) 0.021
WHO: World Health Organization.a Log rank test.b Globally significant.
in both these studies DNA ploidy was an independent studies utilizing fresh or frozen tissue specimens thenumber of colonic Dukes Stage B and C tumors exam-prognostic variable in multivariate survival analysis.
More recently, Chapman et al.8 reported a significant ined generally was much smaller than in the currentseries and that a separate analysis of colonic and rectalrelationship between DNA ploidy status (as measured
from fresh and paraffin embedded tissues) and long tumors has not been performed.In agreement with other studies,7,20,21,30–32 weterm survival only in patients with Dukes Stage B colo-
rectal carcinoma. In another study the probability of found a close relation between nuclear DNA contentand anatomic site. Tumors of the right and transverserecurrence and death was significantly higher for pa-
tients with multiploid tumors than for patients with colon more frequently were DNA diploid than thoselocalized distally to the splenic flexure (42.9% vs.diploid or single aneuploid tumors grouped together,
whereas no difference in survival was observed be- 10.3%; P õ 0.0001). When tumors of the proximal anddistal colon were analyzed independently, the survivaltween DNA diploid and overall DNA aneuploid tu-
mors.28 However, no relation between DNA ploidy sta- advantage conferred by a diploid tumor appeared tobe confined to patients with tumors located proximallytus and clinical outcome was demonstrated in other
investigations in which similar analytic procedures to the splenic flexure (disease free survival, P Å 0.004;overall survival, P Å 0.002). The lack of correlationwere employed.17,29 It is important to note that in these
/ 7b9a$$1510 12-17-97 13:59:24 cana W: Cancer

56 CANCER January 1, 1998 / Volume 82 / Number 1
TABLE 3Multivariate Analysis of Prognostic Factors for Disease Free and Overall Survival
Disease free survival Overall survival
Hazard HazardVariable Category ratio 95% CI P value ratio 95% CI P value
Model 1TNM stage III vs. II 2.702 1.406–5.191 0.003 2.630 1.264–5.474 0.010DNA ploidy Aneuploid vs. diploid 3.487 1.170–10.392 0.025 3.983 1.087–14.600 0.038
Model 2TNM stage III vs. II 2.259 1.124–4.540 0.022 1.956 0.879–4.354 0.099DNA ploidy Aneuploid vs. diploid 3.367 1.104–10.268 0.033 3.869 1.095–13.667 0.036Venous invasion Present vs. absent 1.846 0.860–3.963 0.116 2.356 1.000–5.551 0.050
Model 3N status N2–3 vs. N0 3.633 1.537–8.585 0.003 3.238 1.292–8.117 0.012
N1 vs. N0 1.786 0.825–3.865 0.142 1.379 0.551–3.449 0.490DNA ploidy Aneuploid vs. diploid 3.294 1.076–10.085 0.037 3.394 0.961–11.989 0.057Venous invasion Present vs. absent 2.006 0.916–4.393 0.082 2.801 1.148–6.835 0.024
Model 4TNM stage III vs. II 2.261 1.125–4.545 0.022 1.972 0.888–4.380 0.095DNA ploidy Aneuploid vs. diploid 3.340 1.093–10.206 0.034 3.777 1.063–13.423 0.040Venous invasion Present vs. absent 1.811 0.835–3.927 0.134 2.197 0.920–5.244 0.077
Cl: confidence interval.
TABLE 4 ever, due to the small percentage of tumors showingMultivariate Analysis of Prognostic Factors for Disease Free and a diploid nuclear DNA content, we can assume thatOverall Survival (84 Patients with Tumors Located in the Proximal the prognostic impact of DNA ploidy status would beColon)
quite limited in tumors located in this site.In the last few years, several investigations dem-Hazard
Variable (category) ratio 95% CI P value onstrated the existence of important biologic differ-ences between tumors of the proximal and distal co-
Disease free survivallon.33,34 In particular, tumors of the left colon and rec-DNA ploidytum are characterized by a higher incidence of allelic(aneuploid vs.
diploid) 7.396 1.655–33.049 0.009 losses, especially allelic deletions of 17p and 18q, thanTNM stage (III vs. II) 3.347 1.168–9.593 0.024 tumors arising in the proximal colon.30–32,35,36 p53 gene
Overall survival mutations also were found to be more prevalent inDNA ploidy
tumors of the distal colon.37 In contrast, microsatellite(aneuploid vs.instability was detected mainly in tumors of the rightdiploid) 12.629 1.642–97.125 0.015
TNM stage (III vs. II) 2.479 0.832–7.389 0.103 and transverse colon.38,39 A relationship between mo-lecular genetic alterations and DNA ploidy pattern also
Cl: confidence interval.has been shown. In fact, 17p and 18q allelic deletionsand p53 gene mutations were demonstrated to bemore frequent in DNA aneuploid than in DNA diploidcolorectal tumors,30–32,40,41 whereas in the vast majoritybetween DNA ploidy status and survival in the groupof cases tumors with microsatellite instability are char-of patients with tumors of the distal colon was pro-acterized by a diploid nuclear DNA content.38,42 Allduced mainly by the unfavorable clinical behavior ofthese data appear to support the suggestion that DNAStage III diploid tumors. In fact, none of the nine pa-ploidy, as measured by flow cytometry, at least in parttients with Stage II DNA diploid tumors of the distalreflects distinct genetic pathways of carcinogenesiscolon developed tumor recurrence. Conversely, bothoperating in the proximal and in the distal colon.patients with DNA diploid Stage III left-sided tumors
Recently, specific genetic alterations have beendied of recurrent disease. On the basis of these data,shown to correlate with unfavorable disease outcomewe cannot define precisely the predictive value of DNA
ploidy in patients with distal colon carcinoma. How- in patients with colorectal carcinoma.31,35–37,43–45 Cyto-
/ 7b9a$$1510 12-17-97 13:59:24 cana W: Cancer

DNA Ploidy and Prognosis in Colon Carcinoma/Lanza et al. 57
genetic studies indicate that aneuploidy reflects the strated to be of benefit.51,52 Moreover, nearly 80%of these patients will be cured with surgery alone.presence of cell populations with numeric chromo-
somal abnormalities, but the precise mechanisms It should be especially important to identify subsetsof patients with different risks of disease recurrenceleading to aneuploidy are not well understood. The
association with the genetic alterations mentioned and cancer-related death within this population. Inthe current study we demonstrated that patientsearlier or with other as yet unidentified genetic
changes might explain the different clinical outcome with Stage II DNA diploid colon tumors have anexcellent clinical outcome. Only 1 of the 30 patientsof patients with DNA diploid and aneuploid colorectal
tumors observed in the current study as well as in with DNA diploid tumors (3.3%) developed tumorrecurrence and died of disease during the observa-several other studies. The relationship between DNA
ploidy and genetic changes also might explain our tion period. Conversely, 13 of the 77 patients withaneuploid Stage II tumors (16.9%) developed tumorfinding that DNA ploidy is a more powerful prognostic
indicator than tumor stage for tumors of the proximal recurrence and 10 of these patients (13%) died ofrecurrent disease. On the basis of these data we cancolon.
Most aneuploid large bowel tumors are charac- speculate that patients with DNA diploid Stage IIcolon tumors might not require postoperative che-terized by the presence of abnormal cell popula-
tions in the near-triploid or hypotetraploid regions. motherapy.Approximately 25% of the patients included inConversely, tumors with a moderate increase of
DNA content represent only a small percentage of the study received adjuvant chemotherapy. How-ever, the prognostic importance of nuclear DNAaneuploid colorectal carcinomas.32,46 Previously, we
demonstrated that, as DNA diploid tumors, aneu- content was not affected significantly by this factor.The results of the current study confirm thatploid tumors with a DI ° 1.20 are more frequent
in the proximal colon than in the left colon and flow cytometric DNA ploidy status is a significantand independent prognostic factor in patients withrectum.20,21 Moreover, DNA diploid and aneuploid
tumors with a DI° 1.20 showed similar frequencies colon carcinoma. These findings may have clinicalimplications for the management of affected pa-of p53 overexpression, whereas a significantly
higher prevalence of p53 overexpression was ob- tients, in particular those with Stage II disease.served in aneuploid tumors with a DIú1.20.21 Otherstudies showed biologic and clinical similarities be- REFERENCES
1. Quirke P, Dixon MF, Clayden AD, Durdey P, Dyson JED,tween DNA diploid and moderately aneuploid colo-Williams NS, et al. Prognostic significance of DNA aneu-rectal tumors.30,32,47 – 49 A consensus review of theploidy and cell proliferation in rectal adenocarcinomas. J
clinical utility of DNA flow cytometry in colorectal Pathol 1987;151:285–91.carcinoma stated that near-diploid DNA aneuploid 2. Schutte B, Reynders MMJ, Wiggers T, Arends JW, Volovics
L, Bosman FT, et al. Retrospective analysis of the prognostictumors (0.8 õ DNA index õ 1.2) should be catego-significance of DNA content and proliferative activity inrized and reported separately.19 Tetraploid tumorslarge bowel carcinoma. Cancer Res 1987;47:5494–6.also should be analyzed separately from the other
3. Jones DJ, Moore M, Schofield PF. Refining the prognosticaneuploid tumors, because the clinical significance significance of DNA ploidy status in colorectal cancer: aof DNA tetraploidy in colorectal carcinoma is not prospective flow cytometric study. Int J Cancer 1988;41:206–
10.clear.11,19 In the current study we found that moder-4. Jass JR, Mukawa K, Goh HS, Love SB, Capellaro D. Clinicalately aneuploid (DI ° 1.20) and tetraploid tumors
importance of DNA content in rectal cancer measured byhad more favorable clinical behavior comparedflow cytometry. J Clin Pathol 1989;42:254–9.
with other aneuploid tumors, but the difference was 5. Halvorsen TB, Johannesen E. DNA ploidy, tumor site, andnot statistically significant. Additional studies per- prognosis in colorectal cancer. A flow cytometric study of
paraffin-embedded tissue. Scand J Gastroenterol 1990;formed on larger series of patients are needed to25:141–8.evaluate the predictive value of DI subclasses in
6. Baretton G, Gille J, Oevermann E, Lohrs U. Flow-cytometriccolorectal carcinoma.analysis of the DNA-content in paraffin-embedded tissue
Recent clinical trials have established substan- from colorectal carcinomas and its prognostic significance.tial therapeutic advances of adjuvant chemother- Virchows Arch B Cell Pathol Inc Mol Pathol 1991;60:123–31.
7. Bosari S, Lee AKC, Wiley BD, Heatley GJ, Silverman ML.apy in Stage III colon carcinoma. Fluorouracil plusFlow cytometric and image analyses of colorectal adenocar-levamisole currently is considered the standard ofcinomas: a comparative study with clinical correlations. Amcare for the postoperative treatment of patientsJ Clin Pathol 1993;99:187–94.
with Stage III colon carcinoma.50,51 For patients 8. Chapman MAS, Hardcastle JD, Armitage NCM. Five-yearwith surgically resected Stage II colon carcinoma, prospective study of DNA tumor ploidy and colorectal can-
cer survival. Cancer 1995;76:383–7.adjuvant therapy has not been clearly demon-
/ 7b9a$$1510 12-17-97 13:59:24 cana W: Cancer

58 CANCER January 1, 1998 / Volume 82 / Number 1
9. CJ, Leif RC, et al. Convention on nomenclature for DNAScott NA, Wieand HS, Moertel CG, Cha SS, Beart RW, Liebercytometry. Cancer Genet Cytogenet 1984;13:181–3.MM. Colorectal cancer: Dukes’ stage, tumor site, preopera-
tive plasma CEA level, and patient prognosis related to tu- 27. Wirsching RP, Lamerz R, Wiebecke B, Demmel N, Liewaldmor DNA ploidy pattern. Arch Surg 1987;122:1375–9. F, Valet G. Flow cytometric evaluation of colorectal carci-
noma as completion of conventional tumor examination. J10. Kokal WA, Gardine RL, Sheibani K, Morris PL, Prager E, ZakExp Clin Cancer Res 1987;6:117–28.IW, et al. Tumor DNA content in resectable, primary colo-
rectal carcinoma. Ann Surg 1989;209:188–93. 28. Silvestrini R, D’Agnano I, Faranda A, Costa A, Zupi G, Cosi-melli M, et al. Flow cytometric analysis of ploidy in colorectal11. Kouri M, Pyrhonen S, Mecklin J-P, Jarvinen H, Laasonen A,cancer: a multicentric experience. Br J Cancer 1993;67:1042–Franssila K, et al. The prognostic value of DNA-ploidy in6.colorectal carcinoma: a prospective study. Br J Cancer
1990;62:976–81. 29. Sciallero S, Bonelli L, Geido E, Lettieri L, Zeraschi E, BruzziP, et al. Lack of prognostic value of flow cytometric DNA12. Rognum TO, Lund E, Meling GI, Langmark F. Near diploidcontent analysis in colorectal adenocarcinomas. Eur J Can-large bowel carcinomas have better five-year survival thancer 1994;30A:569.aneuploid ones. Cancer 1991;68:1077–81.
30. Delattre O, Olschwang S, Law DJ, Melot T, Remvikos Y,13. Witzig TE, Loprinzi CL, Gonchoroff NJ, Reiman HM, Cha SS,Salmon RJ, et al. Multiple genetic alterations in distal andWieand HS, et al. DNA ploidy and cell kinetic measurementsproximal colorectal cancer. Lancet 1989;ii:353–6.as predictors of recurrence and survival in stages B2 and C
colorectal adenocarcinoma. Cancer 1991;68:879–88. 31. Offerhaus GJA, De Feyter EP, Cornelisse CJ, Tersmette KWF,Floyd J, Kern SE, et al. The relationship of DNA aneuploidy14. Tsuchiya A, Ando Y, Ishii Y, Yoshida T, Abe R. Flow cytome-to molecular genetic alterations in colorectal carcinoma.tric DNA analysis in Japanese colorectal cancer. A multivari-Gastroenterology 1992;102:1612–9.ate analysis. Eur J Surg Oncol 1992;18:585–90.
32. Meling GI, Lothe RA, Borresen A-L, Graue C, Hauge S,15. Fisher ER, Siderits RH, Sass R, Fisher B. Value of assessmentClausen OPF, et al. The TP53 tumour suppressor gene inof ploidy in rectal cancers. Arch Pathol Lab Medcolorectal carcinomas. II. Relation to DNA ploidy pattern1989;113:525–8.and clinicopathological variables. Br J Cancer 1993;67:93–8.16. Visscher DW, Zarbo RJ, Ma CK, Sakr WA, Crissman JD. Flow
33. Bufill JA. Colorectal cancer: evidence for distinct genetic cat-cytometric DNA and clinicopathologic analysis of Dukes’egories based on proximal or distal tumor location. AnnA & B colonic adenocarcinomas: a retrospective study. ModIntern Med 1990;113:779–88.Pathol 1990;3:709–12.
34. Pocard M, Salmon RJ, Muleris M, Remvikos Y, Bara J, Dutril-17. Enker WE, Kimmel M, Cibas ES, Cranor ML, Melamed MR.laux B, et al. Deux colons—deux cancers? AdenocarcinomesDNA/RNA content and proliferative fractions of colorectalcoliques proximal ou distal: arguments en faveur d’une can-carcinomas: a five-year prospective study relating flow cy-cerogenese distincte. Bull Cancer (Paris) 1995;82:10–21.tometry to survival. J Natl Cancer Inst 1991;83:701–7.
35. Kern SE, Fearon ER, Tersmette KWF, Enterline JP, Leppert18. Tang R, Ho Y-S, You YT, Hsu KC, Chen JS, Changchien CR,M, Nakamura Y, et al. Allelic loss in colorectal carcinoma.et al. Prognostic evaluation of DNA flow cytometric and his-JAMA 1989;261:3099–103.topathologic parameters of colorectal cancer. Cancer
1995;76:1724–30. 36. Jen J, Kim H, Piantadosi S, Liu Z-F, Levitt RC, Sistonen P, etal. Allelic loss of chromosome 18q and prognosis in colo-19. Bauer KD, Bagwell CB, Giaretti W, Melamed M, Zarbo RJ,rectal cancer. N Engl J Med 1994;331:213–21.Witzig TE, et al. Consensus review of the clinical utility of
DNA flow cytometry in colorectal cancer. Cytometry 37. Hamelin R, Laurent-Puig P, Olschwang S, Jego N, Asselain1993;14:486–91. B, Remvikos Y, et al. Association of p53 mutations with short
survival in colorectal cancer. Gastroenterology 1994;106:42–20. Lanza G Jr., Maestri I, Ballotta MR, Dubini A, Cavazzini L.8.Relationship of nuclear DNA content to clinicopathologic
features in colorectal cancer. Mod Pathol 1994;7:161–5. 38. Lothe RA, Peltomaki P, Meling GI, Aaltonen LA, Nystrom-21. Lanza G Jr., Maestri I, Dubini A, Gafa R, Santini A, Ferretti Lahti M, Pylkkanen L, et al. Genomic instability in colorectal
cancer: relationship to clinicopathological variables andS, et al. p53 expression in colorectal cancer: relation to tumortype, DNA ploidy pattern, and short-term survival. Am J Clin family history. Cancer Res 1993;53:5849–52.Pathol 1996;105:604–12. 39. Kim H, Jen J, Vogelstein B, Hamilton SR. Clinical and patho-
22. Hermanek P, Sobin LH, editors. UICC TNM Classification logical characteristics of sporadic colorectal carcinomaswith DNA replication errors in microsatellite sequences. Amof malignant tumours. 4th edition. Berlin: Springer-Verlag,
1987:47–9. J Pathol 1994;145:148–56.40.23. Jass JR, Sobin LH. Histological typing of intestinal tumours. Goh H-S, Chan C-S, Khine K, Smith DR. p53 and behaviour
of colorectal cancer. Lancet 1994;344:233–4.In: World Health Organization. International histologicalclassification of tumours. 2nd edition. Berlin: Springer-Ver- 41. Campo E, Miquel R, Jares P, Bosch F, Juan M, Leone A, etlag, 1989:32–3. al. Prognostic significance of the loss of heterozygosity of
24. Jass JR, Atkin WS, Cuzick J, Bussey HJR, Morson BC, Nor- Nm23-H1 and p53 genes in human colorectal carcinomas.Cancer 1994;73:2913–21.thover JMA, et al. The grading of rectal cancer: historical
perspectives and a multivariate analysis of 447 cases. Histo- 42. Bocker T, Schlegel J, Kullmann F, Stumm G, Zirngibl H, Ep-pathology 1986;10:437–59. plen JT, et al. Genomic instability in colorectal carcinomas:
25. Lanza G Jr., Cavazzini L, Borghi L, Ferretti S, Buccoliero comparison of different evaluation methods and their bio-logical significance. J Pathol 1996;179:15–9.F, Rubbini M. Immunohistochemical assessment of growth
fractions in colorectal adenocarcinomas with monoclonal 43. Laurent-Puig P, Olschwang S, Delattre O, Remvikos Y, Assel-antibody Ki-67. Relation to clinical and pathological vari- ain B, Melot T, et al. Survival and acquired genetic alter-ables. Pathol Res Pract 1990;186:608–18. ations in colorectal cancer. Gastroenterology 1992;102:1136–
26. Hiddemann W, Schumann J, Andreef M, Barlogie B, Herman 41.
/ 7b9a$$1510 12-17-97 13:59:24 cana W: Cancer

DNA Ploidy and Prognosis in Colon Carcinoma/Lanza et al. 59
44. O’Connell MJ, Schaid DJ, Ganju V, Cunningham J, Kovach 49. Harlow SP, Eriksen BL, Poggensee L, Chmiel JS, ScarpelliDG, Murad T, et al. Prognostic implications of prolifera-JS, Thibodeau SN. Current status of adjuvant chemotherapy
for colorectal cancer: can molecular markers play a role in tive activity and DNA aneuploidy in Astler-Coller Dukesstage C colonic adenocarcinomas. Cancer Res 1991;predicting prognosis? Cancer 1992;70:1732–9.
45. Goh H-S, Yao J, Smith DR. p53 point mutation and survival 51:2403 – 9.50. Moertel CG, Fleming TR, Macdonald JS, Haller DG, Lauriein colorectal cancer patients. Cancer Res 1995;55:5217–21.
46. Giaretti W, Santi L. Tumor progression by DNA flow cytometry JA, Tangen CM, et al. Fluorouracil plus levamisole as effec-tive adjuvant therapy after resection of stage III colon carci-in human colorectal cancer. Int J Cancer 1990;45:597–603.
47. Bauer KD, Lincoln ST, Vera-Roman JM, Wallemark CB, noma: a final report. Ann Intern Med 1995;122:321–6.51. Shulman K, Schilsky R. Adjuvant therapy of colon cancer.Chmiel JS, Madurski ML, et al. Prognostic implications of
proliferative activity and DNA aneuploidy in colonic adeno- Semin Oncol 1995;22:600–10.52. Moertel CG, Fleming TR, Macdonald JS, Haller DG, Lauriecarcinomas. Lab Invest 1987;57:329–35.
48. Giaretti W, Danova M, Geido E, Mazzini G, Sciallero S, Aste JA, Tangen CM, et al. Intergroup study of fluorouracil pluslevamisole as adjuvant therapy for stage II/Dukes’ B2 colonH, et al. Flow cytometric DNA index in the prognosis of
colorectal cancer. Cancer 1991;67:1921–7. cancer. J Clin Oncol 1995;13:2936–43.
/ 7b9a$$1510 12-17-97 13:59:24 cana W: Cancer