
PROCESS EVALUATION OF QUALITY IN THE DIAGNOSIS AND TREATMENT OF TUBERCULOSIS AT KERSA DISTRICT,...
77
i | Page PROCESS EVALUATION OF QUALITY IN THE DIAGNOSIS AND TREATMENT OF TUBERCULOSIS AT KERSA DISTRICT, JIMMA ZONE BY DESALEGN DABARO THESIS SUBMITTED TO DEPARTMENT OF HEALTH PLANNING AND HEALTH SERVICES MANAGEMENT, MONITORING AND EVALUATION UNIT, AS PARTIAL FULFILLMENT OF MASTERS DEGREE IN HEALTH MONITORING AND EVALUATION. JIMMA UNIVERSITY OCTOBER, 2012
Transcript of PROCESS EVALUATION OF QUALITY IN THE DIAGNOSIS AND TREATMENT OF TUBERCULOSIS AT KERSA DISTRICT,...
i | P a g e
PROCESS EVALUATION OF QUALITY IN THE DIAGNOSIS AND
TREATMENT OF TUBERCULOSIS AT KERSA DISTRICT, JIMMA
ZONE
BY
DESALEGN DABARO
THESIS SUBMITTED TO DEPARTMENT OF HEALTH PLANNING AND
HEALTH SERVICES MANAGEMENT, MONITORING AND EVALUATION
UNIT, AS PARTIAL FULFILLMENT OF MASTERS DEGREE IN HEALTH
MONITORING AND EVALUATION.
JIMMA UNIVERSITY
OCTOBER, 2012
ii | P a g e
PROCESS EVALUATION OF QUALITY OF CARE IN DIAGNOSIS
AND TREATMENT OF TUBERCULOSIS AT KERSA DISTRICT,
JIMMA ZONE
THESIS SUBMITTED TO DEPARTMENT OF HEALTH
PLANNING AND HEALTH SERVICES MANAGEMENT,
MONITORING AND EVALUATION UNIT, AS PARTIAL
FULFILLMENT OF MASTERS DEGREE IN HEALTH
MONITORING AND EVALUATION.
BY
DESALEGN DABARO (BSC)
ADVISORS
1. MR. YOHANNES EJIGU (MSC in HME)
2. MR. WAJU BEYENE (MPH)
JIMMA UNIVERSITY
OCTOBER, 2012

iii | P a g e
Abstract
Background: Even though Ethiopia has implemented the DOTS service for long time, the
national targets of TB control were not achieved yet. Like the country wide, the kersa
district shares the same problem, and also TB control program has never been evaluated in
this district. Hence, the aim of this evaluation is to assess the quality of service provided in
the diagnosis and treatment of TB at Kersa district from June 25 to July 19, 2012
Method: Facility based case study design involving both qualitative and a quantitative
method was used. Reviewing the records of TB patients registered for one year
(october1/2010 to september30/2011), consecutive reviewing of individual patient folders
of 384 patients aged 15 years or more, exit interview of 61 patients aged 15 or more, and
interviewing 14 experts, resource inventory and observation of laboratory practice and
patient-provider interaction were the methods of data collection. Quantitative data was
analyzed using SPSS 16.0 software and the findings were presented in figures, mean,
proportion and frequency table. Expert interview result was summarized and analyzed in
major thematic areas and supplemented the quantitative finding.
Results: The availability dimension was judged as fair based on preset judgment criteria.
There were no pediatric dose of TB drug and revised TB register in all HCs and no
separate TB treatment unit in two of HCs. The compliance of HCWs with the guideline of
the program was judged as poor. From 384 TB suspects 249 (64.8%) were requested for
AFB examination, 4.4% of them were smear positive. Diagnosis of all smears positive PTB
patients was correct. While cure rate of smear positive PTB was 64.6%, treatment success
rate of all forms TB was 98%. All patients were satisfied with the majority of satisfaction
items, but relatively high (29.5%) patients were dissatisfied with the convenience of HCs to
their home and 31.1% were dissatisfied with the daily visiting of HCs for TB treatment.
Conclusion and recommendation: The overall quality of the service was fair. The absence
of pediatric dose of anti-TB drugs, absence of separate TB units in two of HCs, absence of
TB register, weak supervision mechanisms, poor screening of TB suspects and poor
recording mechanisms were main constraints of service. It is recommended that there
should be adequate and continuous supply of TB drugs, all HCWs should screen TB
suspects based on the NTP guideline, planed and regular supervision mechanisms of the
service should be strengthened and there should be new (revised) TB register.
iv | P a g e
Acknowledgement
I would like to express my deep appreciation and sincerely thanks to my advisor Mr.
Yohannes Ejigu and Mr. Waju Beyene for their constructive comments from the beginning
of this study.
It is also my pleasure to extend my deep gratitude to all of monitoring and evaluation
department instructors for their great roles of teaching to shape me as an evaluator.
I am also grateful to health office managers, tuberculosis prevention and control program
expert and health care providers in Kersa district for their kindly support throughout this
study.
I am also grateful to Jimma University for provision of financial support to conduct this
study.
Glory to my God for He has made everything beautiful in its time.

v | P a g e
Table of Contents
Abstract ........................................................................................................................................ iii
Acknowledgement ........................................................................................................................ iv
Chapter 1: Introduction .................................................................................................................. 1
1.1: Background ............................................................................................................. 1
1.2: Statement of the problem ......................................................................................... 2
1.3: Purpose of the evaluation ......................................................................................... 3
Chapter 2: Program description ...................................................................................................... 4
2.1: Stakeholder identification ........................................................................................ 4
2.2: Objective of the TB program ................................................................................... 6
2.3: Major strategies ....................................................................................................... 6
2.4: Resources and activities of the program ................................................................... 6
2.5: Stage of program development................................................................................. 9
Chapter 3: Literature review ..........................................................................................................11
3.1: Quality of care in TB program ............................................................................... 11
Chapter 4: Questions and objectives of evaluation .........................................................................14
4.1: Evaluation questions .............................................................................................. 14
4.2: Objective of evaluation .......................................................................................... 14
Chapter 5: Methods of evaluation ..................................................................................................15
5.1: Study area and period ............................................................................................ 15
5.2: Theoretical framework of the evaluation ................................................................ 15
5.3: Focus and approach of evaluation .......................................................................... 17
5.4: Evaluation design .................................................................................................. 17
5.5: Dimensions of evaluation....................................................................................... 17
5.6: Population and sampling ........................................................................................ 19
5.7: Sample size and Sampling technique ..................................................................... 19
5.8: Inclusion and exclusion criteria .............................................................................. 21
5.9: Data collection ....................................................................................................... 21
5.9.1: Development of tools ...................................................................................... 21
5.9.2: Data collectors ................................................................................................ 22
5.9.3: Data quality management ................................................................................ 22
5.10: Data analysis........................................................................................................ 22
5.11: Matrix of analysis and judgment .......................................................................... 23
5.12: Ethical consideration ............................................................................................ 23
5.13: Dissemination plan .............................................................................................. 24
Chapter 6: RESULT ......................................................................................................................25
6.1: Availability dimension ........................................................................................... 25
6.2: Compliance dimension........................................................................................... 28
6.2.1: Diagnosis of tuberculosis ................................................................................ 28
6.2.2: Treatment of tuberculosis ................................................................................ 30
6.2.3: Treatment monitoring ..................................................................................... 31
6.3: Patient satisfaction survey ...................................................................................... 35

vi | P a g e
6.4: Summary of dimension .......................................................................................... 40
Chapter 7: Discussion ...................................................................................................................41
Chapter 8: Conclusion and recommendation ..................................................................................45
8.1: Conclusion............................................................................................................. 45
8.2: Recommendation ................................................................................................... 45
Chapter 9: Meta evaluation ...........................................................................................................46
9.1: Accuracy standard ................................................................................................. 46
9.2: Utility standard ...................................................................................................... 46
9.3: Feasibility standard ................................................................................................ 46
9.4: Propriety standard .................................................................................................. 47
Chapter 10: References .................................................................................................................47
Chapter 11: Annex ........................................................................................................................51
11.1: Consent forms ...................................................................................................... 51
11.2: Tools of data collection ........................................................................................ 53
List of tables and figure
Table 1: Stakeholder analysis and description ................................................................................. 5
Table 2: Summary of sample size, data source and sampling technique .........................................21
Table 3: Judgment analysis matrix of diagnosis and treatment of TB at Kersa district, 2012...........23
Table 4: Judgment matrix of availability dimension of diagnosis and treatment of TB at Kersa
district, 2012 .................................................................................................................................27
Table 5: Number of smear positive PTB patients received sputum follow up test at Kersa district,
2012..............................................................................................................................................31
Table 6: Compliance dimension of diagnosis and treatment of tuberculosis at Kersa district, 2012 .34
Table 7: Socio-demographic characteristics of TB patients at Kersa district, 2012. ........................35
Table 8: The satisfaction level of patients with the DOTS service at Kersa district, 2012 (N=61) ...38
Table 9: Summary indicators of client satisfaction level at Kersa district .......................................39
Table 10: Summary dimensions of quality in the diagnosis and measurement of tuberculosis at
Kersa district, 2012 .......................................................................................................................40
Figure 1: Logic model of diagnosis and treatment of tuberculosis at kersa district, 2012 ................. 8
Figure 2: Conceptual framework of diagnosis and treatment of tuberculosis at Kersa District, 2012
.....................................................................................................................................................16

vii | P a g e
Abbreviations
AFB Acid-Fast Bacilli
CDR Case Detection Rate
DOTS Directly Observed Treatment Strategy
EPTB Extra pulmonary Tuberculosis
HC Health Center
HBCs High Burden Countries
HIV Human Immunodeficiency Virus
HCWs Health Care Workers
NTP National Tuberculosis Control Programme
PTB Positive Pulmonary Tuberculosis
TB Tuberculosis
WHO World Health Organization

1 | P a g e
Chapter 1: Introduction
1.1: Background
Tuberculosis (TB) is an infectious disease caused by the bacillus Mycobacterium
tuberculosis. It is a major global health problem. Each year, there are around 9 million
new cases of TB, and close to 2 million people die from the disease. All countries are
affected, but most cases occur in Africa and Asia. Globally there are 22 high-burden
countries (HBCs) that account for about 80% of the world‟s TB cases (1, 2).
According to latest estimates, Ethiopia stands 7th in the list of HBCs for TB. According
to ministry of health hospital statistics data, tuberculosis is the leading cause of
morbidity, the third cause of hospital admission next to deliveries and malaria, and the
second cause of death next to malaria (3).
In Ethiopia the incidence of TB of all forms and smear positive TB stand at 341 and 152
per 100,000 populations, respectively. The prevalence and mortality of Tuberculosis of
all forms is estimated to be 546 and 73 per 100,000 populations respectively. In the year
2006/7 Ethiopia registered 129,743 cases of TB (3).
Global efforts to control TB were strengthened in 1991, when a World Health Assembly
resolution recognized TB as a major global public health problem. Two targets for TB
control such as 70% of case detection rate and 85% of cure rate were established as the
part of this resolution. Eventually these two targets were embedded within the DOTS
strategy launched by WHO in 1994, and subsequently endorsed by the WHO STOP TB
Strategy in 2006 (3).
The effort of TB control began in Ethiopia in the early 1960s with the establishment of
TB centers and sanatoriums in three major urban areas in the country. Now a day
Ethiopia has adopted the global targets for TB control by implementing both DOTS and
STOP TB Strategy (3).

2 | P a g e
1.2: Statement of the problem
Without treatment, individuals with active TB will infect an average of 10-15 people
each year and can ultimately die from the disease. The increasing burden of TB is due to
many factors, including; poor management of programs; the spread of HIV; poverty;
population growth; and rapid, uncontrolled urbanization (4).
Despite widespread acceptance of the principles of DOTS, most developing countries
have been unable to expand DOTS as rapidly as needed and have failed to achieve the
global targets. The quality and population coverage of DOTS are still low in most
countries. The TB laboratory service network is poor and also there were insufficient
resources and shortage of trained staff to provide essential service (5, 6).
In 1992 a standardized TB prevention and control programme, incorporating DOTS, was
started as a pilot in Arsi and Bale zone, Oromia Region of Ethiopia. The current DOTS
geographic coverage reaches 90%, whereas the Health Facility coverage is 75% (3).
Though the country has implemented the DOTS service for long time, the national
targets of TB control were not achieved yet. Currently case notification and treatment
success rate were 46% and 84%, respectively (1, 6).
Jimma zone in general and kersa district particularly share the same problems of
achievement. According to zonal health department report the case detection rate of
Jimma zone was 24.4% and 31.7% for smear positive and all form of TB respectively
(7). In the same year the kersa district and Jimma zone health department annual
performance report shows that the case detection rate of kersa district is low and even
far below from national and zonal report too, and it was 15.4% and 26.4% for smear
positive and all form of TB respectively (7, 8).

3 | P a g e
In addition to this poor achievement, TB program has never been evaluated before at
Kersa district. Hence the aim of this study is to evaluate the quality of diagnosis and
treatment of TB at Kersa district.
1.3: Purpose of the evaluation
The finding of this study will help programme coordinators, service providers and all
those concerned by providing information to create a better basis for health care
planning and management to improve TB program.
The study also serves as a base line for other studies and used as a bench mark for
continuous quality improvement in the district particular and in the zone, region and
country in general.

4 | P a g e
Chapter 2: Program description
2.1: Stakeholder identification
The major stakeholders of the program included were the Jimma University, program
managers at Jimma zone health department and Kersa district health office and health
care providers. These stakeholders identified during evaluability assessment which were
conducted before evaluation.
Stakeholders provided the general information of the program performance, decided on
the readiness of TB program for evaluation, identified the areas of the program to be
evaluated and participated in evaluation question development. Likewise they have
participated on developing indicators and setting the matrix of analysis for program
judgment.
There was one day meeting with stakeholders before starting the evaluation to agree on
the evaluation parameters. During the whole process of evaluation they were kept
informed regarding progress of the evaluation. Finally there is evaluation result
dissemination plan to all stakeholders to communicate the findings and lessons learned
included in the report.
The finding of the evaluation report was provided to the program stakeholders. The
findings expected to be used for planning, capacity building program, raising awareness,
adjust plan, share experiences from lessons learnt, strengthening and developing/revising
strategies, and taking corrective measures. The following table summarizes about
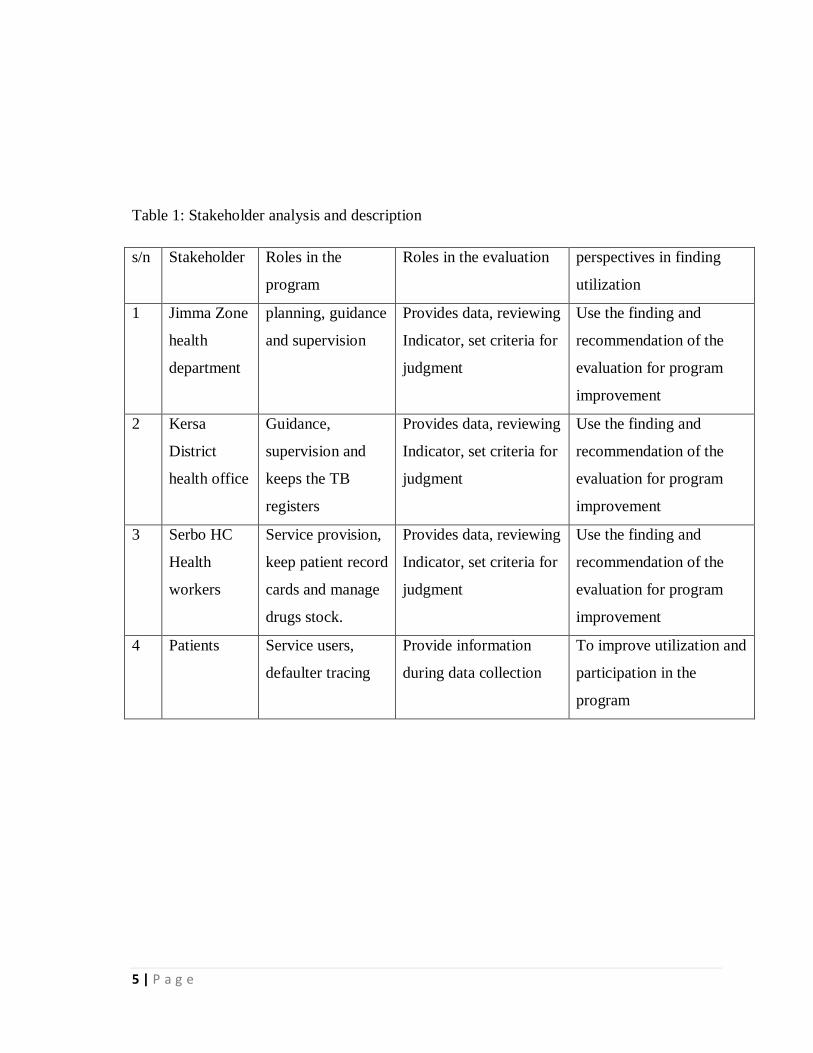
stakeholders‟ engagement along with their interests and perspectives. (Table 1)
5 | P a g e
Table 1: Stakeholder analysis and description
s/n Stakeholder Roles in the
program
Roles in the evaluation perspectives in finding
utilization
1 Jimma Zone
health
department
planning, guidance
and supervision
Provides data, reviewing
Indicator, set criteria for
judgment
Use the finding and
recommendation of the
evaluation for program
improvement
2 Kersa
District
health office
Guidance,
supervision and
keeps the TB
registers
Provides data, reviewing
Indicator, set criteria for
judgment
Use the finding and
recommendation of the
evaluation for program
improvement
3 Serbo HC
Health
workers
Service provision,
keep patient record
cards and manage
drugs stock.
Provides data, reviewing
Indicator, set criteria for
judgment
Use the finding and
recommendation of the
evaluation for program
improvement
4 Patients Service users,
defaulter tracing
Provide information
during data collection
To improve utilization and
participation in the
program

6 | P a g e
2.2: Objective of the TB program
The general objectives of NTP are interrupting transmission of the infections; reducing
morbidity, mortality and disability; preventing emergence and spread of drug resistance;
reduce burden of TB among people living with HIV; and reducing HIV burden among TB
patients (3).
2.3: Major strategies
Major strategies in reaching the objectives include early case detection, adequate
chemotherapy, and provision of comprehensive and standard patient care, enhanced case
management, community participation, accurate monitoring and evaluation of program
performance (3).
National targets of NTP: Two national targets of NTP are achieving and maintaining the
detection of at least 70% of new sputum smear positive TB cases, and the cure rate of at
least 85% among these detected cases (3).
The objective TB program at Kersa district were to increase smear-positive TB cases
detection rate from 15 % to 40% and to increase treatment success rate from 80% to 90%
at the end of 2011/12 (8).
2.4: Resources and activities of the program
The resources and activities of the program were identified from the NTP guideline of
Ethiopia (3).
Identified resources include the presence of trained providers, separate TB unit, adequate
and uninterrupted supply of TB drugs, AFB reagents and other laboratory consumables
(slides, sputum cup, immersion oil), equipment (microscopy and weighing scales), health
7 | P a g e
education materials, manuals and guidelines supply of registers and formats (AFB request
paper, performance report form ,referral forms and standard supervision checklist)
Patient management activities were mainly carried out by general HCWs at the health
centers include case detection, contact examination, case treatment, patient education, HIV
counseling and testing and recording and reporting.
Programme management activities which were mainly carried out by separate TB units
were planning, training, and monitoring and evaluation (supportive supervision, review
meetings) and resource mobilization
The indicators of treatment outcomes were collected from a review TB register. Treatment
adherence rate, cure rate of smear positive PTB, treatment complete rate of smear negative
PTB, EPTB and overall treatment success rate were some of the outcome indicators
reviewed. In addition to this, the perspective of patients with the DOTS service was also
surveyed.

8 | P a g e
Inputs Activities Outputs Outcomes Impacts
Diagnosis &
treatment
Training of HCWs
Distribution of drug, reagent, guidelines, register, standard formats,
microscopes, weighing scales and other medical
supplies
Drugs, reagents, guidelines, microscopes, standard formats & other
medical supplies
# Patients
diagnosed & treated
# HCWs trained
Improved CDR, TSR
& Health status
Increased patient
satisfaction
Reduction in
TB morbidity
& mortality
Reduced Incidence &
Prevalence of TB
Improved Rx.
adherence
Increased patient
knowledge
# Patients received HE
Provision of HE
Human a resource, Infrastructure
HE materials
Improved HCWs‟ knowledge
Supervision checklist Supervision
Recording and reporting materials
Recording & reporting
# Supervision conducted
# Reports submitted
# Drugs, Reagents, and
guidelines, registers,
standard formats
microscopes, weighing
scales and other supplies
distributed
Regular supply of resources & improved surveillance system
Figure 1: Logic model of diagnosis and treatment of tuberculosis at kersa district, 2012

9 | P a g e
2.5: Stage of program development
History of TB control started from attempts of treating unidentified cause to treating cases
infected with the bacilli, from no remedy to effective treatment, from compulsory isolation
to chemical isolation (treating infectious cases with anti-TB drugs), and from vertical to
integrated approach where the service delivery was progressively decentralized to
peripheral health institutions in the communities (9).
After the introduction of effective treatment, TB control was organized as a vertical
program staffed with health workers particularly assigned to run the program. This reduced
the annual risk of infection by 5 -13% in developed countries due to the available resources
and improved general living conditions (9).
However, similar results were not achieved in developing countries due to the associated
high cost. Hence, TB control was integrated into general health service to ensure effective
and efficient use of resources. However, lack of technical efficiency by the general health
workers, neglect of TB control activities, health sector reform and resurgence of TB due to
human immunodeficiency syndrome epidemic weakened the TB control efforts. This was
also complicated by socioeconomic deterioration: increased poverty, malnutrition and
overcrowding (9).
The affordability of rifampicin, poor treatment adherence and high TB burden paved way to
the introduction of DOTS strategy. DOTS strategy aims to detect 70% of new smear-
positive cases and to cure 85% of them. However, its effectiveness was limited in settings
with low health service coverage. To improve TB control efforts, the Stop TB partnership
further envisioned eliminating TB as a public health problem and, ultimately, to achieve a
world free of TB (9).
In Ethiopia the TB program becomes the today‟s situation through the different
developmental hierarchy like, in 1960s TB sanatoria established, , in 1976 NTP established,
in 1992 TB DOTS first piloted, in 1994 central office of NTP combined the tuberculosis
and leprosy program and tuberculosis and tuberculosis team established, In 1995 Planning

10 | P a g e
and programming department for 1996-2000 designed, in 1996 tripartite- tripartite
agreement signed: FMHO, WHO, KNCV to implement DOTS strategy all over the country,
in 1997 Planning and Programming Department implemented, in 1997 TB and Leprosy
program is integrated in to the general health services, in 2001 TBL control program fully
integrated and in 2004 TB/HIV collaborative activities were initially rolled out. In the study
area, kersa district, TB Control program implementation has started since 1996. Four HCs
and 8 health posts provide the DOTS service and only three HCs provide AFB examination
service (3, 9)
Government is the main source of the fund. However, there was one nongovernmental
organization called „heal TB‟, that work with the government on TB control program. The
main contribution of this organization was provision of in-service training to HCWs and
supervision of the service at both health facility and community level (8).
11 | P a g e
Chapter 3: Literature review
3.1: Quality of care in TB program
One component of the DOTS strategy is regular, uninterrupted supply of all essential anti-
tuberculosis drugs and laboratory supplies, in line with this NTP guideline of Ethiopia
recommended that every health unit involved in the prevention, diagnosis and treatment of
Tuberculosis should have an adequate and uninterrupted supply of drugs, laboratory
reagents and equipment in order to achieve sustainable program implementation. But
different study findings showed that not all health facilities have adequate resource as
recommended by NTP as well as WHO, this could be one of the important factors which
made the program not to met the intended target; 70% of case detection rate and 85% of
cure rate by DOTS (3).
Study in southern nation and nationalities region of Ethiopia revealed that only 9 of 13
diagnostic centers have reagents for Acid-fast stain, this indicates as there was scarcity of
reagents for AFB staining (10). Similarly, study in Jimma zone showed that only 60.0% of
the study health facilities had sufficient laboratory reagents and slides for sputum smear
microscopy. The same study showed that TB drugs were available on weekends in only
10% of the study health facilities, and only 50% of the study health facilities had a copy of
NTP manual and teaching material (flip charts) on TB (11).
Developing human resource is one of the integral components of the Stop TB Strategy,
because expanding access to TB care relies heavily on the availability of well-trained health
workers within the primary health care system( 2). But different studies showed the scarcity
and inadequate training of HCWs in DOTS service. Qualitative study of barriers to
tuberculosis care among Somali pastoralists in Ethiopia showed that there were lack of
access to formal health services and high staff turnover (12). In addition to this, study done
in Tigray region showed that TB care providers were not trained in 44% of study facilities
(13).
12 | P a g e
As Donabedian described, the quality of care is the product of applying science and
technology in actual practice and this becomes true when the application is based on preset
recommended standards of program (14). However, studies in different settings showed that
due to different reasons, some providers do not use standards of operation, and this has a
negative impact in the program achievement.
According to the study finding in Tigray region, TB diagnosis was considered as incorrect
in 9 of 42 smear positive PTB (13). In public-private mix Hospitals of Indonesia 4-18% of
sputum smear positive Tuberculosis cases were not managed with standardized diagnosis
and treatment (15); and study in Gambia showed that the proper implementation of
fundamental DOTS-elements, particularly follow up and sputum review were undermined
due high workload (16).
Study findings in Jimma zone showed that address of patients and name of contact person
were not registered in 23% and 18% of cases, respectively, and also the proper number of
smear was performed for only 38.3% cases. (11) Study in Tigray region showed that only
39% TB focal persons were able to manage adverse effects (13).
According to study finding in southern region of Ethiopia, from 2209 slides collected from
peripheral laboratories for external quality assurance overall, false reading was 3.2% (17).
Study in Jimma zone showed, the proportion of smear positive patients successfully
completing the minimum of 8 months of treatment was 69.2%. The treatment defaulters
rate was 10% and above in 3(30%) of the health facilities. The overall treatment completion
rate was 74%, while default and death rates were 22% and 3.8%, respectively (13)
Regarding the knowledge of patients about the tuberculosis, the same study revealed that
only 29 (12%) of the 237 patients mentioned bacteria as a cause of TB. Exposure to cold
was mentioned by 92 (39%) respondents. Even though 186 (79%) stated that they could
potentially transmit TB to others, only 39% knew the correct means of transmission. Over
half knew neither the side effects nor the indications for stopping their medication. Of the
237 patients, 34% encountered problems during the continuation phase, and 30% were
worried that someone might know about their illness (13).

13 | P a g e
Similar to this, study conducted in Gilgile gibe field research area of west Ethiopia showed
that among 476 TB suspects 395 (83%) ever heard of TB( have awareness ), and regarding
the perception about the TB 50.4%, 33.7% and 15.9% perceived as evil eye, germs and
Satan and witchcraft respectively (18). Study conducted in Sudan showed that only 36.2%
of respondents had satisfactory knowledge about tuberculosis and its treatment (19). study
on Women‟s Perspectives on Pathway to Diagnosis of Pulmonary Tuberculosis identified
many barriers that could prevent women from getting a proper diagnosis, including lack of
knowledge, lack of financial resources, lack of power, male supremacy in decision-making,
perceived corruption in healthcare facilities, fear of stigma and this fear heavily boosted by
the idea that PTB equates HIV/AIDS (20).

14 | P a g e
Chapter 4: Questions and objectives of evaluation
4.1: Evaluation questions
1. Are the required resources available for diagnosis and treatment of TB? If not, why?
2. Is the diagnosis and treatment of TB being implemented according to the NTP guideline?
If not, why?
3. Are the TB patients satisfied by the services provided? If not, why?
4.2: Objective of evaluation
General objective
To evaluate the quality of care provided in the diagnosis and treatment of Tuberculosis in
Kersa district from June 25-July19/2012
Specific objective
1. To assess the availability of resources for the diagnosis and treatment of TB.
2. To assess the compliance of Tuberculosis diagnosis and treatment with the NTP
guideline.
3. To assess the satisfaction level of TB patients with service received.

15 | P a g e
Chapter 5: Methods of evaluation
5.1: Study area and period
Kersa is one of the 17districts in the Jimma zone. It is located at 22km to the North Eastern
part of Jimma town. Its total area is 978.6km2. It is bounded by Limu Kossa and Tiro Afeta
districts in the north, Ommo Nada districts in the East , Manna district and Jimma town in
the South, Dedo district in the West. The altitude ranges from 1600-2400 above sea levels.
Temperature rang is 240c-28oc. Annual average rainfall is 1586.6mm. There are 35 Kebele
in the district, and the total population of the district is 188268.
Health facilities of the district include five HCs, 35 health posts, one drug store and 12 drug
vendors, and total human resource workings under health office are 76 technical staff, 70
HEWs, and 30administrative/ supportive staff (8).
This study was conducted from June 25 to July 19, 2012
5.2: Theoretical framework of the evaluation
The Donabedian model of health care quality assessment was used. This model consists of
three approaches of health care quality measurement, such as structure, process and
outcome. (14)

16 | P a g e
Compliance
Clinicians screen TB suspects
and order AFB test
AFB test performed by
laboratory technicians
Clinicians interpreted the
laboratory result and enrolled
to TB treatment
Figure 2: Conceptual framework of diagnosis and treatment of tuberculosis at Kersa District,
2012
(Adapted from Avedis Donabedian, 2003 edition with few modification)
* Laboratory consumables: slides, sputum cup, immersion oil,
*standard formats: AFB request form, referral form, report form
Sat
isfi
ed
pat
ients
Structure Process Outcome
Availability of:
Infrastructure, Qualified
health care providers,
Medical equipments, TB
drugs, AFB reagents and
laboratory consumables
*, guidelines, register
books Standard formats
and guideline
Improved
health status
Amenities of care: a
properly functioning
appointment system,
pleasant and
comfortable
surroundings, privacy
etc Increased treatment
adherence

17 | P a g e
5.3: Focus and approach of evaluation
Both formative and participatory approaches of program evaluation were used. Formative
approach was used because it provides information for the program improvement, and this
was also the main purpose of this evaluation. This means that the evaluation information
would indicate how things are going by highlighting problems related to program activities
and would also indicate whether the activities being conducted in a proper manner or not.
(21). Participatory approach was used to engage and enable stakeholders to take role from
the beginning of evaluation as described in chapter 2, section 2.1.
The focus of this evaluation was the process of the service, and some outcome indicators,
such as case detection rate, treatment success rate, and patient satisfaction were also
assessed.
5.4: Evaluation design
Facility based case study design involving both quantitative and qualitative methods were
used. This design was used because it investigates a contemporary phenomenon in depth
and within its real-life context; relies on multiple sources of evidence, with data needing to
converge in a triangulating fashion and benefits from the prior development of theoretical
propositions to guide data collection and analysis (22).
5.5: Dimensions of evaluation
Availability of infrastructure and resources for diagnosis, compliance of HCWs to NTP
guideline and client satisfaction were the main dimensions of this evaluation.
This study assessed the availability and adequacy of infrastructure, trained health workers,
medical equipments, anti-TB drugs, AFB staining reagents and consumables (slides,
immersion oil, sputum cup etc), standard formats (AFB request paper, referral forms, and
report forms), TB register and laboratory register.
Client satisfaction was assessed with four component dimensions of access, such as
availability, accommodation, accessibility and acceptability (23).
18 | P a g e
Operational definition of terms:
Quality: - means the provision of health care service that is known to be safe, effective and
satisfy the needs of clients.
Availability: Is the presence of required resources for diagnosis and treatment of TB as per
guideline.
Adequacy: Is the degree of fit between the volume and type of existing services and
resources to the client volume and types of needs.
Compliance: is the occurrence of diagnosis and treatment activities based on national
guideline recommendations.
Client satisfaction: is the measure of clients‟ perceived quality of care in the services
provided.
Accessibility: Is the relationship between the location of supply and the location of clients,
taking account of client transportation resources and travel time and distance.
Accommodation: Is the relationships between the manners in which the supply resources
are organized
Acceptability: Is the relationship of clients' attitudes about personal and practice of
providers to the actual characteristics of existing providers.
Structure: Refers the conditions under which care is provided.
Process: Is the activities that constitute health care including diagnosis, treatment and
patient education which usually carried out by professional personnel, but also including
other contributions to care, particularly by patients and their families.
Outcome: Is the changes (desirable or undesirable) in individuals and populations that can
be attributed to health care.

19 | P a g e
5.6: Population and sampling
All adult patients diagnosed at outpatient department, all TB patients and all HCWs involved in
DOTS service at Kersa district were target population for this study. All individual patient
folders with cough of two or more weeks, TB unit register, all TB patients who have been
following TB treatment and all HCWs who involved in DOTs service were source population.
5.7: Sample size and Sampling technique
For health facilities: To maximize the source of information all functional HCs (4HCs) were
included.
Record review: At TB diagnosis unit level
The sample size for chart (individual patient folder) audit was determined using single
population proportion formula. The assumptions: Level of confidence 95%, 5% margin of error,
and P is the proportion of compliance of HWs to national TB guideline to diagnose TB, but since
there is no study done on compliance of HCWs on national TB guideline on study area, p =50%
was taken to have maximum sample size. Based on these assumptions the actual sample size for
the study was computed using the formula for single population proportion
n = (Z α/2)2 P (1-p)
d2
Where, n= sample size, Z α/2= Critical value=1.96, P= compliance of HCWs to national
guideline, d= precision (marginal error) =0.05,
Then n = (1.96)2 (0.5*0.5) =384
(0.05)2
TB register review: All one year records of new TB patients registered for treatment from
october1/2010 to september30/2011, which were 154 were reviewed.

20 | P a g e
Sample size for observation:
The sample size for observation of laboratory practice and patient-providers interaction was
determined based on the saturation of information. The sample size for laboratory practice was
12 and for providers-patient interaction was 20.
Sampling techniques:
The sample size (N=384) of individual patient folders proportionally allocated to three HCs,
which provide the AFB examination service. Proportional allocation was based on the average
number of adult patients (>15years old) visiting the HCs. From OPD abstract register, in average
230 adult patients visit Serbo HC, 130 visits Bala Wajo and 125 visit Bulbul HC per week.
Hence, 182 patient folders selected from Serbo HC, 103 from Bala Wajo and 99 from Bulbul
HC. Then, consecutive patient folders selected retrospectively from study period backward until
the required sample size was obtained.
TB register: All one year records of new TB patients registered from October1/2010 to
september30/2011, which were 154, were reviewed to have adequate sample size.
Expert interview: Fourteen experts was interviewed purposely: Three clinicians who work at
adult OPD, three laboratory technicians, three TB service providers, and four heads of health
centers. In addition to this the expert of the program at the district was interviewed to have more
details of the program. Consecutive patients who full fill the inclusion criterion (age 15 years or
older) were included in patient exit interview.
Observation: Both laboratory practice and provider-patient interaction was conducted with
consecutive patients.

21 | P a g e
Table 2: Summary of sample size, data source and sampling technique
Study unit Sample size Sampling technique
HCs 4 Purposive
Individual patient folder 384 Consecutive
TB unit register 154 Census
Expert interview 14 Purposive
TB patients 61 All TB patients
Laboratory practice observation 12 Consecutive
Provider – patient interaction observation 20 Consecutive
5.8: Inclusion and exclusion criteria
Inclusion criteria:
HCs which provide both diagnosis and treatment service were included. Individual patient folder
of adult patients aged 15 or more years and experiencing persistent cough for two or more weeks
were eligible. Cough was accompanied by one or more of TB symptoms were Weight loss, Chest
pain, Shortness of breath, intermittent fever, and Night sweats, loss of appetite, fatigue and malaise.
The records of all new patients registered for one year was eligible for TB unit register review.
Clinicians, health officers in this case, laboratory technicians, TB unit focal person, and heads of
HCs and TB program expert of the district health office were participants of this study. In
addition to this, all TB patients who were following their treatment at study HCs during the study
period were eligible. All patients were 15 or more years of old. All study subjects who did not
met the above criteria and also TB patients who were critically ill to respond were ineligible.
5.9: Data collection
5.9.1: Development of tools
The tools were developed after reviewing NTP guideline and WHO standards. Checklists for TB
resource inventory and health center, laboratory practice and provider-patient interaction
observation were prepared with the consideration NTP guideline and WHO standards.
22 | P a g e
Semi-structured questioner was developed after preliminary analysis of both quantitative and
qualitative data for expert interview. Questioner for client interview adapted with little
modification from standard client satisfaction questionnaire (23)
5.9.2: Data collectors
Individual patient folders and TB registers were reviewed by three nurses; resource inventory
was done by one nurse, three nurses conducted provider-patient observation and patient exit
interview and one laboratory technician observed laboratory practice. Expert interview was
conducted by principal investigator. Data collectors have been supervised by one health officer.
Therefore, the evaluation team consisted of nine data collectors, including principal investigator
and one supervisor. All the data collectors and supervisor were trained about the data collection
for two days. However, orientation was given to the supervisor separately on how to supervise
the data collectors.
5.9.3: Data quality management
Client interview questionnaire was translated into Afan Oromo and back translated into English
to check its consistency. Tools used in the study were pre-tested in one HC with population
having similar socio- demographic status which was not included in the study and correction was
done accordingly. Data collectors and supervisor were trained on how to collect data and how to
supervise data collectors, respectively. During data collection, regular supervision was conducted
daily. Field notes changed in to fair notes on daily basis.
5.10: Data analysis
Quantitative data was checked for completeness, edited, coded, entered and analyzed using SPSS
version 16.0. Descriptive summery was done using tables, proportion and figures. Qualitative
data was categorized thematically and supplemented the quantitative findings. Finally the
dimensions of quality in the diagnosis and treatment of TB was judged based on the pre- set
judgment matrix.

23 | P a g e
5.11: Matrix of analysis and judgment
The weight of dimensions and the respective indicators was given depending on their level of
relevance to the program. In each evaluation dimension detailed indicators that used to decide
the performance of the diagnosis and treatment of TB were listed. The indicators were given
weight and the value of dimensions was the sum of respective indicators, then the sum of all
dimension attributed to the quality of the service. The judgment criteria and standards of each
dimension and respective indicators were summarized in the following table; and more
description was presented in result section. (See chapter 6)
Table 3: Judgment analysis matrix of diagnosis and treatment of TB at Kersa district, 2012
Dimension
Rec
om
men
ded
(%)
Obse
rved
(%
)
Indic
ators
Wei
ght
(%)
Res
ult
(%
)
Judgment criteria of each dimension and their
respective indicators (%)
Availability 100 10 40 >90 v. good, 81-90 good, 70-80 fair, < 70 poor
Compliance 100 10 40 >90 v. good, 81-90 good, 70-80 fair, < 70 poor
satisfaction 100 13 20 >90 v. good, 81 -90 good, 70-80 fair, < 70 poor
Overall quality of the service 33 100 >90 v. good, 81 -90 good, 70-80 fair, < 70 poor
5.12: Ethical consideration
Ethical clearance was obtained from the ethical committee of public health and medical science
college of Jimma University. Permission was obtained from Kersa district health office.
For all participants‟ information sheet and consent form which can introduce about the study,
respondents right, autonomy and willingness to participate in the study was prepared and given
or read to participants and willingness was obtained from the study participants prior to each
interview. Names and other personal information which can violate the confidentiality of the
respondents was not taken or recorded. Any information was kept confidential and only used for
evaluation purpose. During data collection privacy of respondents was kept, free to withdrawal
from the interview at any time.

24 | P a g e
5.13: Dissemination plan
The finding was presented to the Jimma University scientific community and submitted to the
department of health service management, unit of monitoring and evaluation of College of Public
health and Medical sciences. It was also communicated to concerned stakeholders of Kersa
district health office to enable them to make informed decision in their managerial activities.

25 | P a g e
Chapter 6: RESULT
6.1: Availability of resources
This evaluation was conducted in four HCs which provide the general medical service including
DOTS service. All HCs provide DOTS service, but there was no AFB examination service in
one of HCs (Kusay Beru). Treatment provided throughout the week and also AFB examination
service provided throughout the week except weekends.
In all HCs there was adequate amount of adult dose of TB drugs and AFB staining reagents,
however there was no pediatric dose of drug in all HCs. In each HC there were one functional
microscopy and weighing scale. One of HCs (Kusay Beru) was equipped with solar microscopy,
because there was no electricity.
According to the HCWs response the reason for the absence of pediatric dose TB drug in all HCs
was the absence of it at district health office, Jimma zone health department and even at Oromia
region health bureau. Even though the HC which did not have electricity was equipped with solar
microscopy, there was no AFB examination service. According to HCWs opinion solar
microscopy is not appropriate for AFB examination and the result is not reliable.
There were two providers in one of HCs (Serbo) and the rest three each has one provider who
have received in service training about TB care. However, in one of HCs (Kusay Beru) TB
treatment has been provided by not trained provider. The reason for this was the provider of TB
care was at the same time the head of the HC; thus overburdened by HC administrative work and
can‟t provide TB treatment for full time. One of HCs (Serbo) has two health officers and the rest
each three HC has one. Similar to this there were two laboratory technicians in Serbo HC and the
rest three each has one. Except in Kusay Beru HC, where AFB examination service was not
provided, all laboratory technicians in the rest HCs have received in service training on AFB
microscopic examination.
The reason for successful provision of in service training was the presence of partner called „heal
TB‟ who provide in service training and supervision of health facilities. Experts expressed the
necessity of having additional provider in TB treatment because when one is out off work due to
26 | P a g e
illness or annual leave the additional health worker will be replaced so the work will not be
interrupted.
There was no separate TB treatment unit two of HCs (Bala Wajo and Kusay Beru). According to
the experts‟ response there were no free rooms to separate for TB treatment. However, all
participants agreed on the necessity of having the separate TB clinics and explained that it will
be established for the future. Similarly, there was no separate room for AFB examination, thus
the AFB was integrated with other routine laboratory services. There were also no separate
sputum specimen collection areas in all HCs.
In all HCs there were IEC materials in different language (Afan Oromo, Amharic and English)
posted in waiting areas and different units of services. TB suspects screening procedures was
posited in OPD room in all HCs, but there was no NTP guideline at OPD room in all HCs. The
guideline of the program was available in two of HCs (Serbo and Bulbul) which also have
separate TB treatment unit. Guideline was available only in TB units. There was TB treatment
algorism in all HCs, whether it was separate TB clinic or not. In all HCs there were standard
formats (AFB request paper, referral and report forms) and laboratory AFB register, but there
was no standard TB register in all HCs.
27 | P a g e
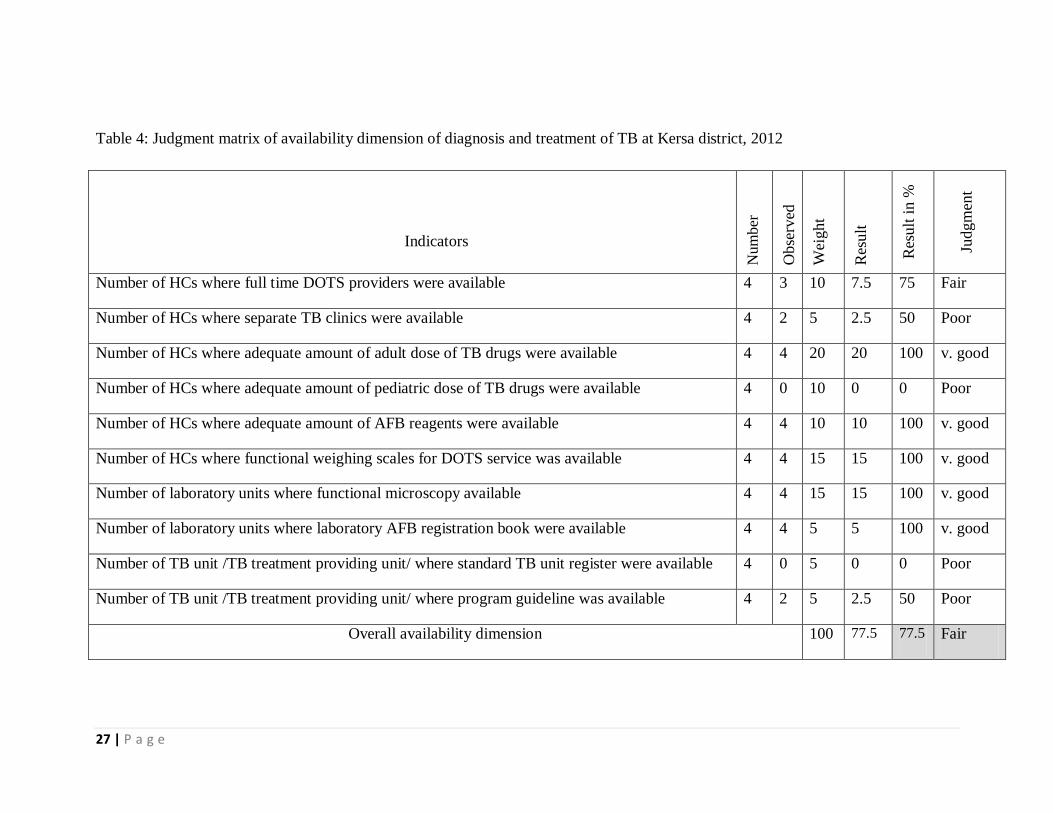
Table 4: Judgment matrix of availability dimension of diagnosis and treatment of TB at Kersa district, 2012
Indicators
Nu
mb
er
Obse
rved
Wei
ght
Res
ult
Res
ult
in %
Judgm
ent
Number of HCs where full time DOTS providers were available 4 3 10 7.5 75 Fair
Number of HCs where separate TB clinics were available 4 2 5 2.5 50 Poor
Number of HCs where adequate amount of adult dose of TB drugs were available 4 4 20 20 100 v. good
Number of HCs where adequate amount of pediatric dose of TB drugs were available 4 0 10 0 0 Poor
Number of HCs where adequate amount of AFB reagents were available 4 4 10 10 100 v. good
Number of HCs where functional weighing scales for DOTS service was available 4 4 15 15 100 v. good
Number of laboratory units where functional microscopy available 4 4 15 15 100 v. good
Number of laboratory units where laboratory AFB registration book were available 4 4 5 5 100 v. good
Number of TB unit /TB treatment providing unit/ where standard TB unit register were available 4 0 5 0 0 Poor
Number of TB unit /TB treatment providing unit/ where program guideline was available 4 2 5 2.5 50 Poor
Overall availability dimension 100 77.5 77.5 Fair

28 | P a g e
6.2: Compliance dimension
6.2.1: Diagnosis of tuberculosis
Individual patient folder of 384 TB suspects (patients with cough of > 2weeks) diagnosed at
three HCs (Serbo, Bulbul and Bala Wajo) were reviewed to make sure that whether TB suspects
were requested for AFB examination service or not. One eighty two (47.4%) of them were
diagnosed at Serbo HC, 103 (26.8%) at Bulbul HC and 99 (25.8%) at Bala Wajo HC. The age of
all patients was 15 year and above, the mean age was 36.80 (SD +/- 16.14). One hundred eighty
three (47.7%) of patients were males and 201(52.3%) were females.
AFB examination was ordered for only 249 (64.8%) of 384 patients. Experts mentioned that the
reason for not ordering all the TB suspects for AFB examination could be the negligence of
HCWs. One of heads of HCs said, “if the clinicians are alert to screen TB suspects accordingly,
the procedure is very easy to do so and nothing makes them to miss the case.”
The test result of 21(8.4%) patients was not recorded in both individual patient folders and in the
laboratory AFB register, so they were assumed not had received AFB examination service.
Therefore AFB performed only for 228 (59.4%) of TB suspects. Ten (4.4%) of which were
smear positive, and thus diagnosed as smear positive PTB. This diagnosis was considered as
correct because the laboratory register review showed that all patients had three initial smears
positive for AFB.
Regarding low case detection, experts suggested that requesting all TB suspects for AFB test and also
strengthening referral linkage of TB suspects from community could increase smear positive case
detection.

29 | P a g e
The finding of laboratory practice observation
Twelve laboratory practice observation was conducted. Each patient submitted 3 specimens,
therefore the total number of sputum specimen submitted were (12X3=36). Observation
conducted from collection of sputum up to recording and dispatching of the result.
All of the patients observed were new for AFB examination. In all HCs the laboratory
technicians were responsible for specimen collection. Clinicians sent the TB suspects with the
AFB request paper to the laboratory unit. The common information filled in the request paper
was the name, age, sex, the purpose of the AFB request (whether for diagnosis or follow up).
Only for two patients did HCWs wrote the name of the health center where diagnosis performed.
Laboratory technicians instructed all patients to produce the suitable sputum specimen. For all
specimens (specimen number=36) new sputum container and new frosted slides were used. In all
laboratories the applicator stick was used for smearing and Bunsen burner for fixing the smear.
All laboratories did not filter both carbon fuchsin and methyline blue. In all cases the staining
procedures was undertaken in the recommended AFB staining procedures (five minutes for
carbon fuchsin, three minutes for acid alcohol and one minute for methyline blue).
Time spent to examine each slide was observed. It takes 1-5minutes to examine each slide with
the mean time of 3.2 minutes. All technicians stored AFB slides accordingly for external quality
control; all negative and positive slides in separate boxes.
Laboratory technicians described that though they stored AFB slides for rechecking, they have
never sent to regional laboratory. TB focal person at the district is responsible to collect and take
AFB slides from the diagnostic units to regional laboratory. But the district TB focal person was
even did not supervisees each HC in the last six months prior to the study period.
Diagnoses from TB register review
Forty nine of 154 TB patients were smear positive, 14 of which were diagnosed at study HCs.
Laboratory register review showed that, 12 of those 14 smears positive PTB patients diagnosed
at study HCs had three, and the rest two patients had two initial smears positive for AFB. Therefore,
diagnosis was considered as correct for all smear positive PTB patients diagnosed at study HCs.

30 | P a g e
Experts described that smear negative PTB and EPTB were diagnosed at Jimma specialized
Hospital. Therefore, the compliance of diagnosis for smear negative and EPTB were not
assessed.
6.2.2: Treatment of tuberculosis
Records of 154 all forms of new TB patients registered in four HCs for one year october1/2010
to september30/2011, was reviewed. One hundred twelve (72.7%) were registered at Serbo HC,
19 (12.3%) at Bulbul HC, 23 (14.9%) at Bala Wajo HC. Forty nine (31.8%) of patients were
smear positive PTB, 36 (23.4%) smear negative PTB and 69 (44.8%) were EPTB. one hundred
one (66%) of patients were treated by RH and 52 (34%) were by EH. Seventy three (47.4%)
were males and 81 (52.6%) were females. Twenty one of patients aged below five year, and
majority of patients, 133 were in age category of 15-45 years.
Except one all patients finished intensive phase of treatment. While 31 (64.6%) of 48 smears
positive PTB patients claimed as cured, 120 of all forms of cases completed the treatment. One
patient died at the midst of intensive phase, one has default the treatment and the result of one
was not recorded. Therefore, in general the treatment success rate including cured and treatment
completed was 98%.
According to HCWs response the reasons for such high success rate were: treatment service has
never been interrupted in any particular time, the number of patients was small to follow up and
patients have good awareness regarding the consequence of treatment interruption. In addition
to these there was good provider- patient interaction, which could strengthen the treatment
compliance. The reason for relatively low cure rate was some patients could not produce
appropriate sputum for follow up AFB test, therefore follow 5th
/7th
month sputum were not
performed.

31 | P a g e
6.2.3: Treatment monitoring
The weight of the patients was used to determine the dose of the drug. There was no pediatric
dose of the drug, so the dose and regimen of the drug that such patients had received was not
assessed.
The weight of all patients under intensive phase of treatment was recorded at the beginning of
treatment. One hundred twenty one (91%) of 133 patients received the right dose of drug under
intensive phase. Eight patients received under the recommended doses and four patients received
above the recommended dose.
The weight of 110 patients was measured at the beginning of continuation phase (end of
intensive phase), and the rest 23 patients were not. From those 110 patient, 58 (52.7%) received
the right dose, 47 (42.7%) received below and five (4.5%) patients received above the
recommended dose. All patients received the right regimen under both phases of treatment.
From TB register, 106 (62.3%) of 153 intensive phase patients received the observed treatment
for the recommended 56 days while the rest treated for less than 56 days (mean=43 days).
Seventeen (32.7%) of 52 continuation phase patients treated by EH visited HCs in regular interval
of one month to receive TB drugs and the remaining 35 patients missed at least one monthly
appointment (mean=2.48). The adherence rate of patients treated with RH was not assessed, because
there was no revised TB register in all HCs.
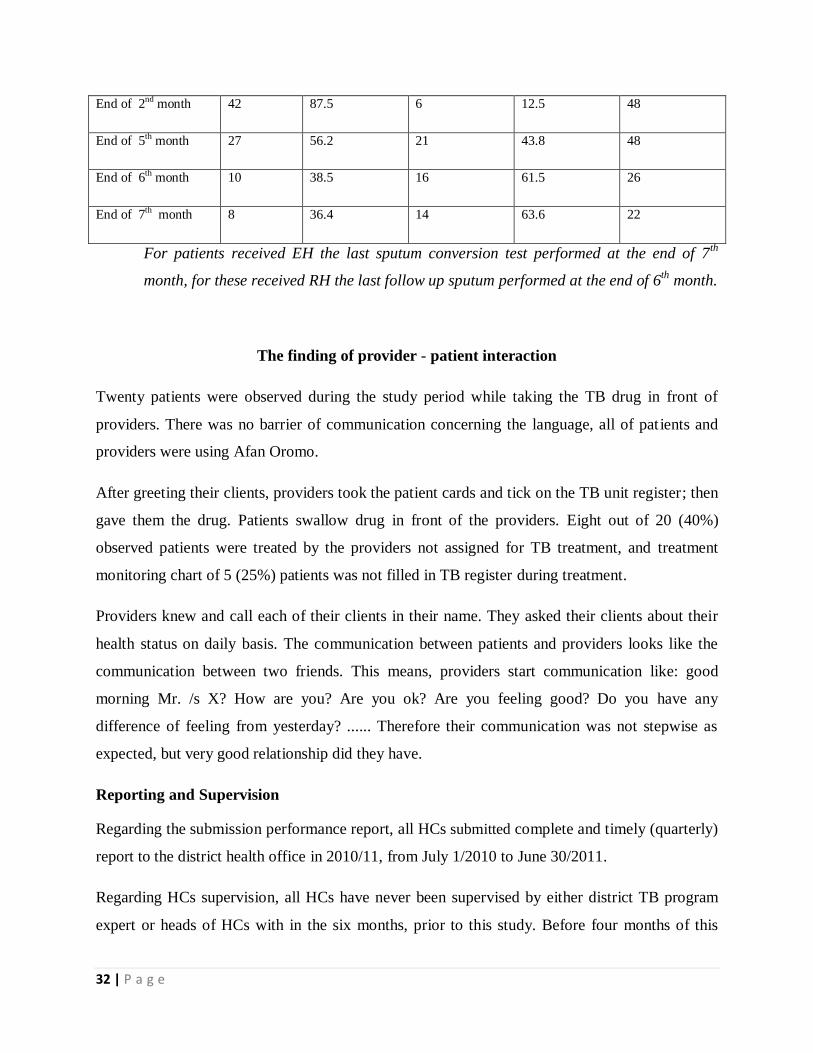
The application of recommended sputum examination of smear positive PTB patients at the end
of 2nd
, 5th, 6th/7
th months of treatment was checked from TB unit register review. Forty eight
smear positive PTB patients finished both intensive and continuation phase of treatment and their
sputum follow up test presented in the following table. (Table 5)
Table 5: Number of smear positive PTB patients received sputum follow up test at Kersa district,
2012.
AFB test Performed Not performed Number
Frequency Percent Frequency Percent
32 | P a g e
End of 2nd month 42 87.5 6 12.5 48
End of 5th month 27 56.2 21 43.8 48
End of 6th month 10 38.5 16 61.5 26
End of 7th month 8 36.4 14 63.6 22
For patients received EH the last sputum conversion test performed at the end of 7th
month, for these received RH the last follow up sputum performed at the end of 6th
month.
The finding of provider - patient interaction
Twenty patients were observed during the study period while taking the TB drug in front of
providers. There was no barrier of communication concerning the language, all of patients and
providers were using Afan Oromo.
After greeting their clients, providers took the patient cards and tick on the TB unit register; then
gave them the drug. Patients swallow drug in front of the providers. Eight out of 20 (40%)
observed patients were treated by the providers not assigned for TB treatment, and treatment
monitoring chart of 5 (25%) patients was not filled in TB register during treatment.
Providers knew and call each of their clients in their name. They asked their clients about their
health status on daily basis. The communication between patients and providers looks like the
communication between two friends. This means, providers start communication like: good
morning Mr. /s X? How are you? Are you ok? Are you feeling good? Do you have any
difference of feeling from yesterday? ...... Therefore their communication was not stepwise as
expected, but very good relationship did they have.
Reporting and Supervision
Regarding the submission performance report, all HCs submitted complete and timely (quarterly)
report to the district health office in 2010/11, from July 1/2010 to June 30/2011.
Regarding HCs supervision, all HCs have never been supervised by either district TB program
expert or heads of HCs with in the six months, prior to this study. Before four months of this
33 | P a g e
study, all HCs were supervised by Jimma zone health department TB program expert, but did not
provided the written feedback. As the providers mentioned, the experts of the program have
provided only the oral feedback of the supervision.
However, all HCs have been supervised by heal TB staffs (NGO) at least once within the six
months; and one of the HCs (Bulbul) received the written feed back of the supervision during
study period. They have supervised not only TB unit but also the laboratory unit and OPD
(clinicians‟ practice).

34 | P a g e
Table 6: Compliance dimension of diagnosis and treatment of tuberculosis at Kersa district, 2012
Indicators Number Observed weight Result Result
in %
Judgment
Proportion of patients with > 2 weeks of cough for who smear test ordered. 384 249 15 9.7 64.6 Poor
Treatment adherence rate under intensive phase 153 106 15 10.4 69.3 Poor
Proportion of patients under intensive phase of treatment who enrolled in correct dose of treatment 133 121 15 13.6 90.6 Good
Proportion of patients under continuation phase who enrolled in correct dose of treatment 109 64 10 2.9 29 Poor
Proportion of SM + ve PTB for who sputum follow up performed at the end of 2nd month of Rx 48 42 10 8.7 87 Good
Proportion of SM + ve PTB for who sputum follow up performed at the end of 5th month of Rx 48 27 5 2.8 28 Poor
Proportion of SM + ve PTB for who sputum follow up performed at the end of 6/7th month of Rx 48 18 5 1.8 18 Poor
Treatment success rate 153 150 15 14.7 98 v. good
Number of complete reports submitted timely to district health office in 2011/12 4 4 5 5 100 v. good
Number of supervision conducted by district TB program expert in the last six months. 16 0 5 0 0 Poor
Over all compliance dimension 100 69.6 69.6 Poor

35 | P a g e
6.3: Patient satisfaction survey
From total 72 TB patients at Kersa district during data collection period, 12 were not participated
in this study, because 4 were below 15 years old and 7 were referred to health posts. Therefore
exit interview was conducted with only 61 TB patients, of which 16 (26.2%) were under
intensive phase and 45 (73.8%) were under continuation phase of treatment. Thirty nine (63.9%)
patients were following their treatment at Serbo HC, 8 (13.15) at Bulbul HC, 9 (14.8%) at Bala
Wajo HC and 5 (8.2%) at Kusay Beru HC.
Table 7: Socio-demographic characteristics of TB patients at Kersa district, 2012.
Sex Number Percent
male 29 47.5
female 32 52.5
Age Number Percent
15-24 30 49.2
25-44 31 50.8
Ethnicity Number Percent
Oromo 52 85.2
Amhara 3 4.9
Kefa 3 4.9
Silte 2 3.3
Yem 1 1.6
Religion Number Percent
Muslim 51 83.6

36 | P a g e
orthodox 10 16.4
Marital status Number Percent
married 42 68.9
not married 19 31.1
Occupation Number Percent
farmer 26 42.6
house wife 18 29.5
student 8 13.1
merchant 6 9.8
government employees 3 4.9
Educational status Number Percent
illiterate 27 44.3
1-4 20 32.8
5-8 10 16.4
>9 4 6.5
Residence Number Percent
rural 51 83.6
urban 10 16.4
Only two patients use public transport, car, and one patient uses horse as means of transportation,
and the rest 58 (95.1%) patients visit HCs on foot. The distance of their home to HCs was
assessed in terms of the time that they spend for one trip to HC. The mean time it takes is

37 | P a g e
83.46minutes with the SD of 59.3. The walk time of 12 patients was less than 30 minutes; it
takes 30-60 minutes for 17 patients, 61-120 minutes for 25 patients and the rest spent above 120
minutes to reach HCs.
Among the total interviewed, 12 of the patients claimed the presence of other family members
suffering from cough for two and more than two weeks. Out of those 10 (83.3%) visited HCs for
AFB examination, and the rest were not. Similarly 32 participants claimed for the presence of
children below five years of age in their house, out of which 24 (75%) brought to HCs and got
diagnosis for TB.
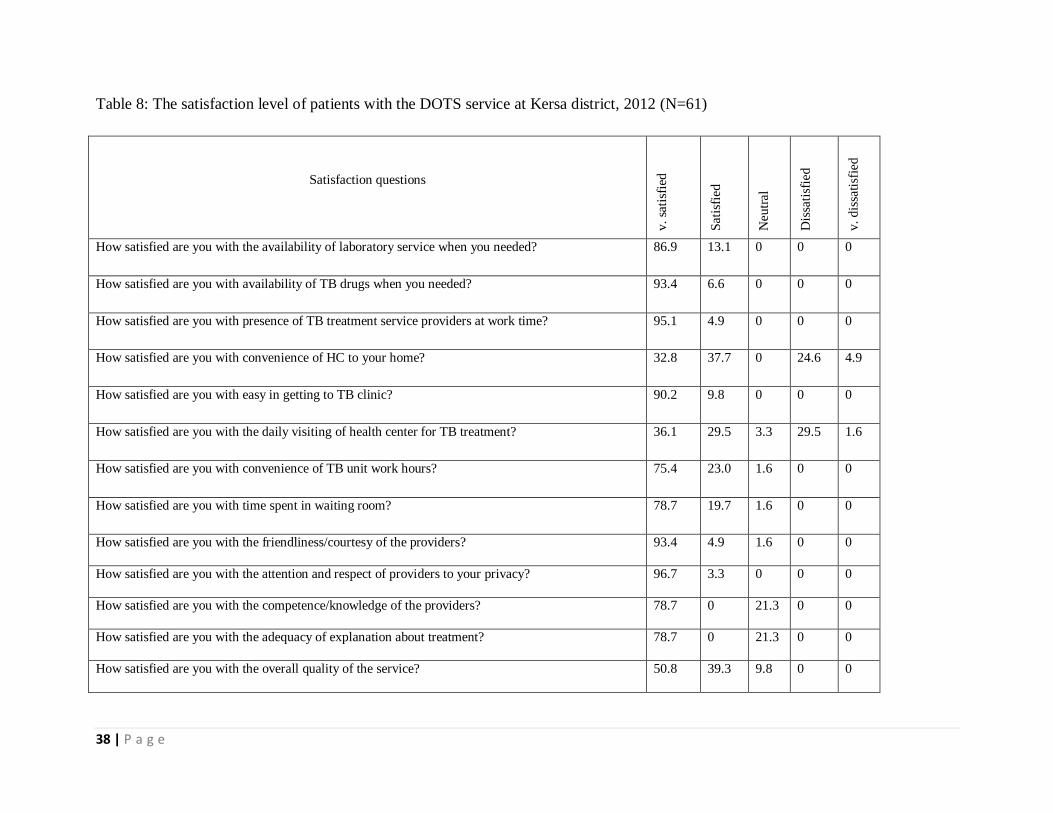
Patient satisfaction level
Client satisfaction was assessed using 13 likert scale items. The responses of client were
dichotomized in to satisfied and dissatisfied; those who were very satisfied and satisfied were
categorized as „satisfied‟ and very dissatisfied and dissatisfied were categorized as „dissatisfied‟.
In general, the majority of patients were satisfied with all items. All participants were satisfied
with items which indicate the availability of providers, availability of TB treatment and
laboratory service, convenience of TB clinic to get easy. More than 90% of patients were
satisfied with convenience of TB clinic working hour, waiting time, attention and respect of
providers, friendless with the providers and overall service quality.
However, 29.5 % of patients were dissatisfied with the convenience of HC to their home; and
31.1% were dissatisfied with the daily visiting of HC for TB treatment. In addition to this, 21.3%
were neither satisfied nor dissatisfied with the competency of providers and adequacy of
explanation about the treatment. (Table 8)
38 | P a g e
Table 8: The satisfaction level of patients with the DOTS service at Kersa district, 2012 (N=61)
Satisfaction questions
v.
sati
sfie
d
Sat
isfi
ed
Neu
tral
Dis
sati
sfie
d
v. d
issa
tisf
ied
How satisfied are you with the availability of laboratory service when you needed? 86.9 13.1 0 0 0
How satisfied are you with availability of TB drugs when you needed? 93.4 6.6 0 0 0
How satisfied are you with presence of TB treatment service providers at work time? 95.1 4.9 0 0 0
How satisfied are you with convenience of HC to your home? 32.8 37.7 0 24.6 4.9
How satisfied are you with easy in getting to TB clinic? 90.2 9.8 0 0 0
How satisfied are you with the daily visiting of health center for TB treatment? 36.1 29.5 3.3 29.5 1.6
How satisfied are you with convenience of TB unit work hours? 75.4 23.0 1.6 0 0
How satisfied are you with time spent in waiting room? 78.7 19.7 1.6 0 0
How satisfied are you with the friendliness/courtesy of the providers? 93.4 4.9 1.6 0 0
How satisfied are you with the attention and respect of providers to your privacy? 96.7 3.3 0 0 0
How satisfied are you with the competence/knowledge of the providers? 78.7 0 21.3 0 0
How satisfied are you with the adequacy of explanation about treatment? 78.7 0 21.3 0 0
How satisfied are you with the overall quality of the service? 50.8 39.3 9.8 0 0

39 | P a g e
Table 9: Summary indicators of client satisfaction level at Kersa district
s/n Indicators % Observed Weight Result
Result
in %
Judgment
1 Proportion of patients satisfied with the availability of laboratory services when needed 100 100 5 5 100 v. good
2 Proportion of patients satisfied with the availability of drugs when needed 100 100 10 10 100 v. good
3 Proportion of patients satisfied with the availability of providers in TB clinic 100 100 10 10 100 v. good
4 Proportion of patients satisfied with the convenience of HC to their home 100 70.5 5 3.5 70.5 Poor
5 Proportion of patients satisfied with the simplicity/convenience to get TB clinic at HC 100 100 5 5 100 v. good
6 Proportion of patients satisfied with the daily visiting of HC for TB treatment? 100 65.6 10 6.6 65.6 Poor
7 Proportion of patients satisfied with the convenience of TB unit work hours 100 100 5 5 100 v. good
8 Proportion of patients satisfied with the time spent while waiting for providers. 100 98.4 10 9.8 98.4 v. good
9 Proportion of patients satisfied with the attention and respect of providers to their
privacy.
100 100 10 10 100 v. good
10 Proportion of patients satisfied with the competence/knowledge of the providers 100 78.8 5 3.9 78.8 Poor
11 Proportion of patients satisfied with the adequacy of explanation about the treatment 100 78.8 5 3.9 78.7 Poor
12 Proportion of patents satisfied with the overall quality of the service 100 90.2 20 18 90 v. good

40 | P a g e
6.4: Summary of dimension
The quality of the service was measured through 33 indicators of the different respective
dimension as presented in the following table. (Table 10)
Table 10: Summary dimensions of quality in the diagnosis and measurement of tuberculosis
at Kersa district, 2012
s/n Dimension Expected Observed # Indicators Weigh Result Judgment
1 Availability 100% 77.5% 10 40% 31% Fair
2 Compliance 100% 69.6% 10 40% 27.8% Poor
3 satisfaction 100% 90% 13 20% 18% Good
Overall quality of the service 33 100% 77% Fair
41 | P a g e
Chapter 7: Discussion
All HCs have been providing TB treatment, but one of which did not have AFB
examination service due to the absence electricity. This mean there were only three
diagnostic units for 188,268 population of the district. From this account the diagnostic unit
(microscopic unit) to population ratio is 1:62,756, this is lower than the WHO
recommendation for developing countries, which is 1:50,000 (24).
All HCs have at least one nurse who has received in service training on TB care, however
in one of HCs there was no full time assigned TB treatment provider. Therefore, in three of
four HCs (75%) TB care was provided by trained TB focal persons, which is better when
compared with the study finding at Tigray where only in 57% of TB clinics TB care run by
trained TB focal person. Based on the study finding of health workforce crisis in TB control
of 22 HBCs, there was the shortage of staffs at district health facility level in two countries
and 14 at central level. However the same the same study revealed that there was no
apparent association between reported staff numbers and the country's TB burden or current
case detection rates (25).
From TB register review the cure rate of smear positive PTB was 64.6% and treatment
success rate was 98%. When compared with the study finding at south India, the present
study revealed relatively low cure rate and high treatment success rate, which were 84.2%
and 83.4% respectively (26). The treatment success rate is also far better than the national
target (85%) for treatment success (3).
From TB register review 5.8% of patients under intensive phase received below the
recommended dose and 2.9% above the recommended dose. Similarly, 40.6% patients
under continuation phase of treatment received below the recommended dose and 4.7%
above the recommended dose. In addition to this 21 children received the adult dose of drug
due to the absence of pediatric dose in all HCs. This contrasts the NTP as well as WHO
standards; and also could cause drug side effect, hepatotoxicity (27).
42 | P a g e
The adherence rate of intensive phase patients was 62.3%; and 32.7% of continuation phase
patients did not miss their monthly appointment. This is the better adherence rate when
compared with the study finding in Tigray region where only 5% of patients received
observed treatment for recommended 56 days of intensive phase and only 16% attended
health facilities on monthly basis to collect TB drug (14).
However, this finding is against the recommendation of both NTP guideline and WHO
standards of TB treatment. According to this recommendation, all intensive phase patients
must take TB treatment on daily basis, followed by 6 months of self-administered treatment
with a monthly visit to health facility to receive the drugs. (3, 6)
From total 48 smear positive PTB patients, 87.5%, 56.2% and 37.5% have got smear follow
up test at the end of 2nd
,5th and 6/7
th months of treatment, respectively. This contrasts the
NTP guideline, which recommends that all sputum-positive patients on TB treatment must
have one sputum specimen follow test at the end of 2nd, 5th and 7th „month (3). The
proportion of patients got the sputum follow- up test at the end of 2nd
month was relatively
high, 87.5%. However, this is lower than the study finding at Burkina Faso, which is
92.1%. (28)
Only 64.8% of patients with persistent cough for two or more weeks were ordered for AFB.
However the NTP and WHO standards recommended 100% of such patients should have
AFB examination (3).
The major reasons that providers mentioned regarding this poor diagnosis was negligence
of HCWs to screen TB suspects. The similar finding was obtained from the study at China,
where the failure of doctors to recognize TB symptoms and being not very alert to TB-
related symptoms were reasons that the experts described for the purpose of poor diagnosis
(29).
Smear positive case detection rate was 4.4%, this contrasts the recommended smear
positive case detection for developing countries, that is 10% (24); and also relatively lower

43 | P a g e
than the study finding at Tanzania, where it was 6.1% (30). It is also too far lower than the
study finding in India where 27 %o, (31), SNNPR where it was 25%. (32), and Rwanda,
where, 17.3% of TB suspects were smear positive (33).
Limited access or utilization of health facilities, insufficient clinical suspicion and referral
of TB suspects for diagnosis, inadequate use or functioning of smear microscopy services
were some of the reasons for low smear positive case detection (24). Similarly, low
availability of TB diagnosis units (only 3AFB examination service providing HCs), low
requesting of TB suspects for AFB examination and absence of laboratory quality control
system were the contributing factors for low smear positive case detection (4.4%).
There was poor supervision system in all HCs. All HCs have never been supervised by
district TB focal person within six months, prior to study period. However, NTP guideline
and WHO recommends planned and regular supervision of TB program. According to NTP
guideline district TB focal person should supervise health facilities once per month (3).
All patients were satisfied with the majority of satisfaction items. The overall satisfaction
level was 90%. This is higher than the study findings in Jimma specialized Hospital, which
were 57.1% and 77%, (34), and 77% (35) and Saud Arabia, which was 66.1% (36).
The difference could be due the context of service provision. This study was conducted in
HCs where patients experienced long time relationship with the providers, but the studies
presented above were conducted in Hospital level and did not have such long time
relationship with the providers.
However certain number of patients became dissatisfied with the convenience of HC to
their home and visiting the HC on daily basis for TB treatment. This might be due to the
distance of HCs to the location of patients. Because the travel time of 15 of 18 patients
dissatisfied with the HCs convenience and 10 of 19 patients dissatisfied with the daily
visiting of HCs was 1hr or more (mean time= 84.4 minutes). This is relatively similar with
the study finding (82.4 minutes) at West Shoa Zone, Central Ethiopia (37).

44 | P a g e
Major limitations considered were respondent bias for client exit interview and also during
the patient- provider observation HCWs may act as required because of the observer is
there. In addition to this, the possible limitations include the medical records which were
the source of information for this study might not be documented well.
As presented in the above table, the structural aspect (availability) of service was fair; the
process aspect (compliance) was poor and the outcome of the service (client satisfaction)
was good. This finding was against the conceptual framework of the service.
However, the structure-process-outcome model is only a servant, not a master. It should be
remembered that the relations postulated to exist between adjacent pairs in the structure-
process-outcome model are not certainties. The general assumptions behind the
Donabedians model (Structure-process-outcome) of health care quality measurement were
(14).
If appropriate resources are available, the likelihood of their appropriate use and
then achieving attainable outcomes is high.
Resources availability doesn‟t guarantee quality of service. However, processes of
care cannot be implemented in the absence of adequate resources
If healthcare is provided in compliance with standard guideline, potentially
attainable outcomes will be achieved.
If clients are satisfied with the service provided, then they tend to be loyal.
And if they‟re loyal they not only utilize the service more, but also refer other
clients. However client satisfaction doesn‟t guarantee the quality of service.

45 | P a g e
Chapter 8: Conclusion and recommendation
8.1: Conclusion
The overall quality of the service was fair. However there were certain constraints in the
provision of quality TB care. Absence of pediatric dose of TB drugs, absence of separate
TB units in two of HCs and absence of TB register were some of the constraints from
structural aspects of quality. Likewise, prescribing incorrect dose of drug, low treatment
adherence rate for both phases, not requesting all TB suspects for AFB examination and
poor supervision trends were some of the constraints from process aspects of quality.
Though all patients were satisfied with majority of satisfaction items, relatively high
proportion, 31.1% were dissatisfied with daily visiting of HCs and 29.5% were dissatisfied
with the convenience of HCs to their home.
8.2: Recommendation
There should be regular and continuous supply of TB drug (pediatric dose)
Heads of HCs should supervise the performance of the HCWs regularly (preferably
once per week).
District health office should facilitate refresher in-service training for HCWs
working at diagnosis units by using the NTP guideline.
TB focal person should carry out specific supportive supervisions visits in HCs
monthly on a regular basis.
Both internal and external laboratory quality control system should be strengthened.
All HCs should decentralize DOTS service to health posts.
46 | P a g e
Chapter 9: Meta evaluation
Meta evaluation standards such as utility, feasibility, propriety, and accuracy were used to
determine the effectiveness of evaluation. The quality of this study was evaluated based on
the Meta evaluation standards by using program evaluation models Meta evaluation
checklist set by Daniel L. Stufflebeam (38).
9.1: Accuracy standard
All the data collection, analysis, and presentation techniques were carried out based on
scientific methods. Quality control strategies were formulated well. Data was collected
from multiple sources using multiple methods and triangulation was employed to reach a
valid conclusion by program document review, and expert interview to maximize accuracy.
9.2: Utility standard
The evaluation protocol considers the information needs of major intended users by
involving them starting from the evaluability assessment to the implementation of
evaluation. The evaluation questions were the needs of the stakeholders about the program.
Thus, there was a high likelihood of addressing information needs and values of
stakeholders that ensure utilization of the evaluation findings for program improvement.
9.3: Feasibility standard
TB control program by using the DOTS and other strategy is a well-established program
with national guideline that makes certain the availability of adequate data for the
evaluation. The cost considered the presence of limited resources and the resources which
were used are justifiable for benefits of program improvement.

47 | P a g e
9.4: Propriety standard
There was no procedure that affects the privacy, dignity, confidentiality, and rights of
participants. Ethical Issues of the evaluation protocol are well respected. This ensures that
the evaluation fulfills the propriety standards.
Chapter 10: References
1. World Health Organization. WHO report 2011. Global tuberculosis control:
WHO/HTM/TB/2011.16. Geneva, Switzerland: WHO, 2011
2. World Health Organization. The Global Plan To Stop TB 2011-15: Transforming
the fight toward elimination of tuberculosis. Geneva, Switzerland: WHO, 2011
3. Federal Ministry of Health Ethiopia: Tuberculosis, Leprosy and TB/HIV Prevention
and Control Programme Manual Fourth Edition. Addis Ababa, Ethiopia: FMOH,
2008
4. Kendall, A.E. U.S. Response to the Global Threat of Tuberculosis: Basic Facts.
2012
5. Makombe, R. Special Summit of African Union on HIV/AIDS, Tuberculosis and
Malaria (ATM). SP/Ex.CL/ATM/4 (I) .Abuja, Nigeria: AU, 2–4 may, 2006
6. World Health Organization. WHO report 2010. Global tuberculosis control:
WHO/HTM/TB/2010.7. Geneva, Switzerland: WHO, 2010
7. Kersa district health office. DHO report 2010/11. District Tuberculosis control:
Serbo, Kersa: DHO, 2010/11
8. Jimma zone health department. Zonal performance report 2010/11. Jimma zone
Tuberculosis control: Jimma: Jimma, 2010/11
9. Good practice guidance on HIV/AIDS, TB and malaria final report, July 2008
10. Shargie E, & Lindtjorn, B. DOTS improves treatment outcomes and service
coverage for Tuberculosis in South Ethiopia: A retrospective trend analysis. BMC
Public Health, 2005
11. Taddese Geremew, C. J. Assessment of quality of care delivered for infectious
pulmonary tuberculosis patients. Ethiop J Health Sci. , Vol. 1, No. 1. Jimma Zone
Health Office, Ministry of Health, August,2011

48 | P a g e
12. Qian Long, Y. L. (2 October 2008). Barriers to tuberculosis care: a qualitative study
among Somali pastoralists in Ethiopia. BMC Health Services Research, 2008
13. M Mesfin, J. N. Quality of tuberculosis care and its association with patient
adherence to treatment in eight Ethiopian districts. Oxford University Press, (2009)
14. Donabedian, A. Introduction to Quality Assurance in Health Care. First edition,
Oxford University, 2003
15. Ari Probandari, L. L. –K. Missed opportunity for standardized diagnosis and
treatment among adult Tuberculosis patients in hospitals involved in Public-Private
Mix for Directly Observed Treatment Short-Course strategy in Indonesia: a cross-
sectional study: BMC health service research, 2010
16. Sanneh AFNS, P. J. Comparison of Pulmonary TB DOTS clinic medication before
and after the introduction of daily DOTS treatment and attitudes of treatment
defaulters in the Western Division of the Gambia. African Health Sciences Vol 10
No 2 ., June 2010
17. Shargie E, M. A. (2005).Quality control of sputum microscopic examinations for
acid fast bacilli in southern Ethiopia. Ethiop.J.Health Dev.2005;19(2):104-108]
18. Gemeda Abebe, A.L. Awareness, healthcare seeking behavior and perceived stigma
towards tuberculosis among tuberculosis suspects in a rural community in southwest
Ethiopia. (Unpublished) 2007
19. Mohamed A.I, M.Pharm, Y. M. (anuary 2007,). Knowledge of Tuberculosis: A
Survey among Tuberculosis Patients in Omdurman, Sudan: Khartoum, Sudan.
Sudanese Journal of Public Health: January 2007
20. Wikström, G. Women‟s Perspectives on Pathway to Diagnosis of Pulmonary
Tuberculosis Women Voices from Community Level in Uganda. Nordic School of
Public Health, 2011
21. Alkin, Marvin C. Evaluation essentials from A to Z. New York, USA: The Guilford
Press, 2011
22. Yin, Robert K. Case study research: Design and methods. Reve Beverly Hills,
California: Sage; 2009
23. Roy P, Thomas WJ. The concept of access. Medical Care. Vol. XIX, No. 2 .J.B.
Lippincott. co.; February 1981. P. 128-131

49 | P a g e
24. World Health Organization. Compendium of Indicators for Monitoring and
Evaluating National Tuberculosis Programs. WHO/HTM/TB/2004.344.Geneva,
Switzerland: WHO, 2004
25. José Figueroa-Munoz1, Karen Palmer1, Mario R Dal Poz2, Leopold Blanc1,Karin
Bergström1 and Mario Raviglione1. 24 February 2005. The health workforce crisis
in TB control: a report from high-burden countries.: World Health Organization :
Geneva, Switzerland , 24 February 2005
26. K. Jaggarajamma, G. Sudha, V. Chandrasekaran, C. Nirupa, A. Thomas, T. Santha,
M. Muniyandi and P.R. Narayanan. reasons for non-compliance among patients
treated under revised national tuberculosis control programme (rNTP), tiruvallur
district, south INDIA. Indian J Tuberc 2007; 54:130-135
27. Jussi J. Saukkonen, David L. Cohn, etal… An Official ATS Statement:
Hepatotoxicity of Antituberculosis Therapy. American Thoracic Society
Documents. Vol 174. pp 935–952, 2006 (Internet address: www.atsjournals.org
28. S. M. Dembele, H. Z. Ouedraogo, A. Combary, N. Saleri, J. Macq, B. Dujardin.
Conversion rates at two-month follow-up of smear-positive tuberculosis patients in
Burkina Faso. The International Journal of Tuberculosis and Lung Disease .INT J
TUBERC LUNG DIS 11(12):1339–1344, 2007
29. B. Xua,b, G. Fochsen b, Y. Xiua, A. Thorson b, J.R. Kempc, Q.W. Jiang.
Perceptions and experiences of health care seeking and access to TB care.
Departments of Epidemiology, School of Public Health. Fudan University:
Shanghai, China. Health Policy 69 (2004) 139–149
30. Jeremiah S., Benson R., Emmanuel O., et al. Low sputum smear positive
tuberculosis among pulmonary tuberculosis suspects in a tertiary hospital in
Mwanza, Tanzania. Tanzania Journal of Health Research Volume 14, Number 2,
April 201
31. Mohammad Tahir, S.K. Sharma, Duncan-smith Rohrberg, Deepak Gupta, U.B.
Singh and P.K. Sinha. DOTS at a tertiary care center in northern India: Indian J
Med Res 123, May 2006, pp 702-706
50 | P a g e
32. Mohammed A. Yassin1 and Luis E. Cuevas2. How many sputum smears are
necessary for case finding in pulmonary tuberculosis? Tropical Medicine and
International Health, volume 8 no 10 pp 927–932 October 2003
33. Muvunyi et al. Prevalence and diagnostic aspects of sputum smear positive
tuberculosis cases at a tertiary care institution in Rwanda. African Journal of
Microbiology Research Vol. 4(1) pp. 088-091 January, 2010
34. Lemessa olijira, Solomon Gebreselassie. Satisfaction with outpatient health services
at Jimma Hospital, south Western Ethiopia. (Ethiop. J. Health Dev. 2001;15(3):179-
184)
35. Fekadu A. et al. Assessment of clients‟ satisfaction with health service deliveries at
Jimma University specialized hospital. Ethiop J Health Sci. Vol. 21, No. 2 July
2011
36. Alzolibani.A. Patient satisfaction and expectations of the quality of service of
University affiliated dermatology clinics. Journal of Public Health and
Epidemiology Vol. 3(2), pp. 61-67, February 2011
37. Birhanu et al. Determinants of satisfaction with health care provider interactions at
health centers in central Ethiopia: BMC Health Services Research 2010, 10:78
38. Stufflebeam LD. Evaluation models, new directions for Evaluation American
Evaluation Associations, San Francisco, Jossy-bass, November 2001
51 | P a g e
Chapter 11: Annex
11.1: Consent forms
Consent forms for all TB DOTS service providers at _______________________ HC
Dear sir/ madam
My name is ______________________________________________________ I came
from Jimma University. I am a conducting the process evaluation of quality in the diagnosis
and treatment of tuberculosis. The purpose of the study is to find ways of improving the
quality of diagnosis and treatment of tuberculosis. I am interested to know your experiences
so far in providing TB DOTS services. May I ask you some questions about this? Please be
assured that this discussion is strictly confidential and your name will not be recorded.
Also, you are not obliged to answer any question you don‟t want to, and you may withdraw
from the interview at any time.
Do I have your permission to continue? Yes ____________No________________
Name and signature of the data collector: _________________________________
Name and signature of the supervisor: ___________________________________

52 | P a g e
Consent forms for TB patients at _________________________________ HC
Dear sir/ madam
My name is _______________________________________________________ I came
from _________________________________________ I am a member of an evaluation
team of process evaluation of quality in the diagnosis and treatment of tuberculosis at kersa
district. It is believed that provision of quality tuberculosis diagnosis and treatment
increases clients' satisfaction, which contributes to increase good treatment outcome. The
purpose of this study is to evaluate the quality of diagnosis and treatment service provided
in health center and level of satisfaction of Tuberculosis patients, and finally to give
important comment that will help to strengthen and improve quality of service. To do this,
your information is very important. I would like to ask you a few questions about your visit
to the health facility to find out your experience today. I would be very grateful if you could
spend a few minutes to answer questions related to the service. I will not put your name or
registration number in the format. All the information you give will be kept strictly
confidential. Your participation is voluntary and you are not obliged to answer any
questions you don't want. But your honest participation will contribute to generate
information that can be used to improve the quality of diagnosis and treatment of
tuberculosis.
Do I have your permission to continue? Yes _____ No________________________
Name and signature of the data collector: __________________________________
Name and signature of the supervisor: _____________________________________
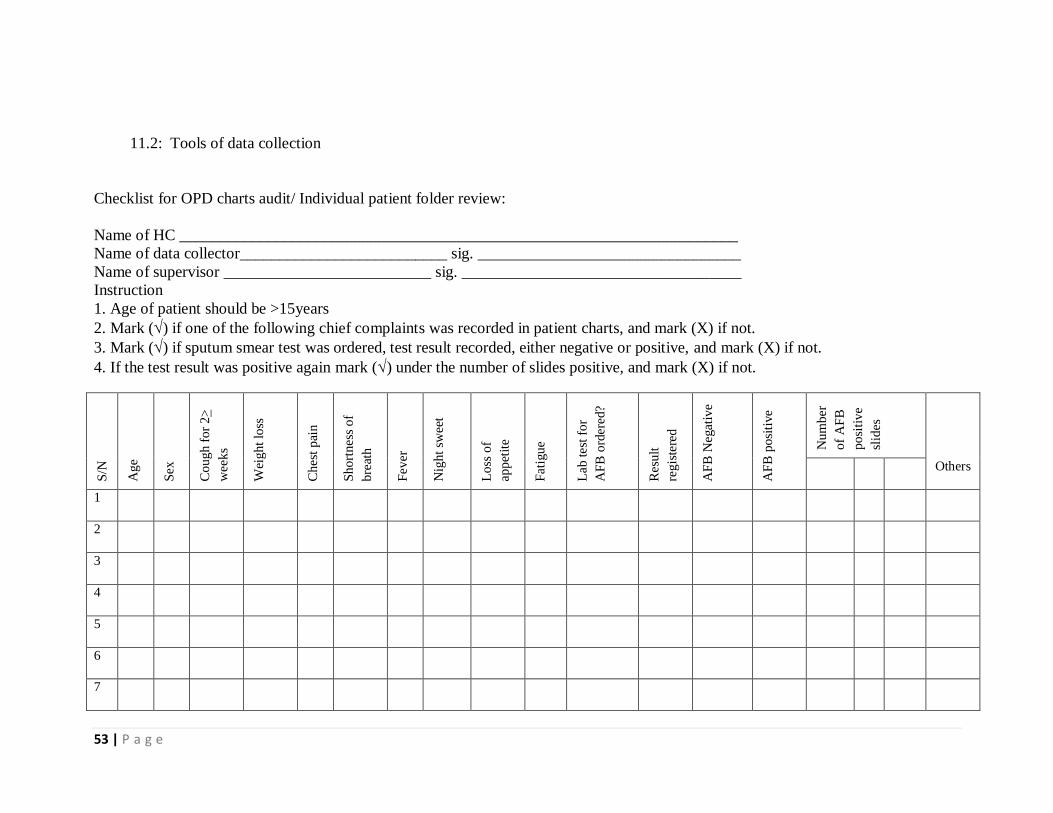
53 | P a g e
11.2: Tools of data collection
Checklist for OPD charts audit/ Individual patient folder review:
Name of HC ______________________________________________________________________
Name of data collector__________________________ sig. _________________________________
Name of supervisor __________________________ sig. ___________________________________
Instruction
1. Age of patient should be >15years
2. Mark () if one of the following chief complaints was recorded in patient charts, and mark (X) if not.
3. Mark () if sputum smear test was ordered, test result recorded, either negative or positive, and mark (X) if not.
4. If the test result was positive again mark () under the number of slides positive, and mark (X) if not.
S/N
Ag
e
Sex
Co
ug
h f
or
2>
wee
ks
Wei
gh
t lo
ss
Ch
est
pai
n
Sh
ort
nes
s o
f
bre
ath
Fev
er
Nig
ht
swee
t
Lo
ss o
f
app
etit
e
Fat
igu
e
Lab
tes
t fo
r
AF
B o
rder
ed?
Res
ult
reg
iste
red
AF
B N
egat
ive
AF
B p
osi
tive
Nu
mb
er
of
AF
B
po
siti
ve
slid
es
Others
1
2
3
4
5
6
7

54 | P a g e
TB unit register review checklist:
Name of HC ______________________________________________________________________
Name of data collector__________________________ sig. _________________________________
Name of supervisor __________________________ sig. _________________________________
Instruction: Mark () if the following evidences were recorded in TB patient chart, and mark (X) if not.
S/N
MR
N
Un
it T
B
Pat
ien
t n
ame
Pat
ien
t ad
dre
ss
Sex
Co
nta
ct n
ame
Co
nta
ct a
dd
ress
Ag
e
Sm
ear
resu
lt
Lab
no
.
Wei
gh
t
Cat
ego
ry
P/P
os
P/n
eg.
EP
TB
In
ten
siv
e p
has
e
DA
TE
RX
sta
rted
Mo
nth
RX
sta
rted
No
. d
ays
RX
in
terr
up
ted
HIV
tes
t o
ffer
ed
HIV
res
ult
Sputum follow up
in months
Co
nti
nu
atio
n p
has
e
No
. d
ays
RX
in
terr
up
ted
Treatment outcome
Oth
ers
Cu
red
Co
mp
lete
d
Die
d
Fai
lure
Def
ault
Tra
nsf
erre
d o
ut
Dru
g
Do
se
2nd
3rd
5th
6th
Oth
ers
Dru
g
Do
se

55 | P a g e
Record review checklist for TB patient charts
Name of HC ______________________________________________________________________
Name of data collector__________________________ sig. _________________________________
Name of supervisor __________________________ sig. _________________________________
Instruction: Mark () if the following evidences were recorded in TB patient chart, and mark (X) if not.
X-R
AY
res
ult
if p
erfo
rmed
cult
ure
res
ult
if p
erfo
rmed
His
to -
pat
ho
log
ical
evid
ence
fro
m a
bio
psy
( F
NA
tes
t) i
f C
lin
ical
evid
ence
con
sist
ent
wit
h
acti
ve
EP
TB
T
reat
men
t
wit
h b
road
-
spec
tru
m
anti
bio
tics
AF
B r
esu
lt i
f
per
form
ed
afte
r
anti
bio
tic
trea
tmen
t
Disease
Classification
Others
S/N
Ag
e
Sex
3sl
ide
2 s
lid
es
1 s
lid
e
Su
gg
esti
ve
for
TB
N
ot
Su
gg
esti
ve
for
TB
Po
siti
ve
Neg
ativ
e
Po
siti
ve
Neg
ativ
e
Yes
No
Yes
No
Po
siti
ve
Neg
ativ
e
SM
-ve
PT
B
SM
+v
e
PT
B
EP
TB
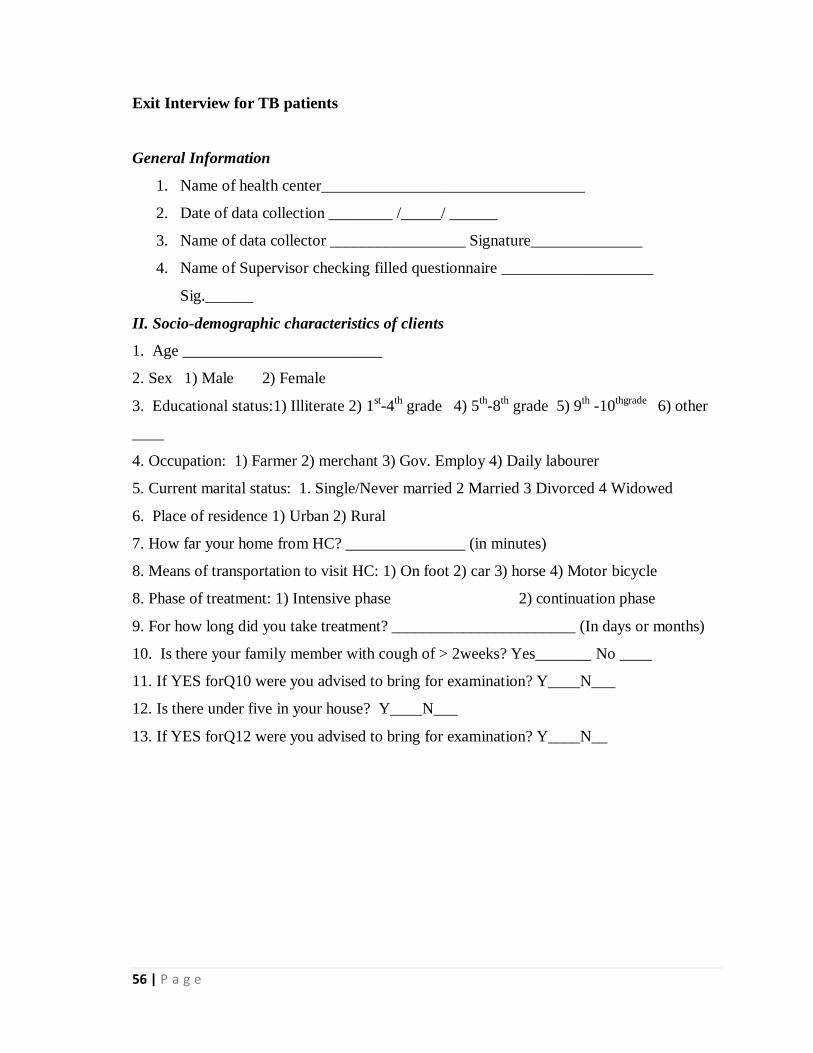
56 | P a g e
Exit Interview for TB patients
General Information
1. Name of health center_________________________________
2. Date of data collection ________ /_____/ ______
3. Name of data collector _________________ Signature______________
4. Name of Supervisor checking filled questionnaire ___________________
Sig.______
II. Socio-demographic characteristics of clients
1. Age _________________________
2. Sex 1) Male 2) Female
3. Educational status:1) Illiterate 2) 1st-4
th grade 4) 5
th-8
th grade 5) 9
th -10
thgrade 6) other
____
4. Occupation: 1) Farmer 2) merchant 3) Gov. Employ 4) Daily labourer
5. Current marital status: 1. Single/Never married 2 Married 3 Divorced 4 Widowed
6. Place of residence 1) Urban 2) Rural
7. How far your home from HC? _______________ (in minutes)
8. Means of transportation to visit HC: 1) On foot 2) car 3) horse 4) Motor bicycle
8. Phase of treatment: 1) Intensive phase 2) continuation phase
9. For how long did you take treatment? _______________________ (In days or months)
10. Is there your family member with cough of > 2weeks? Yes_______ No ____
11. If YES forQ10 were you advised to bring for examination? Y____N___
12. Is there under five in your house? Y____N___
13. If YES forQ12 were you advised to bring for examination? Y____N__
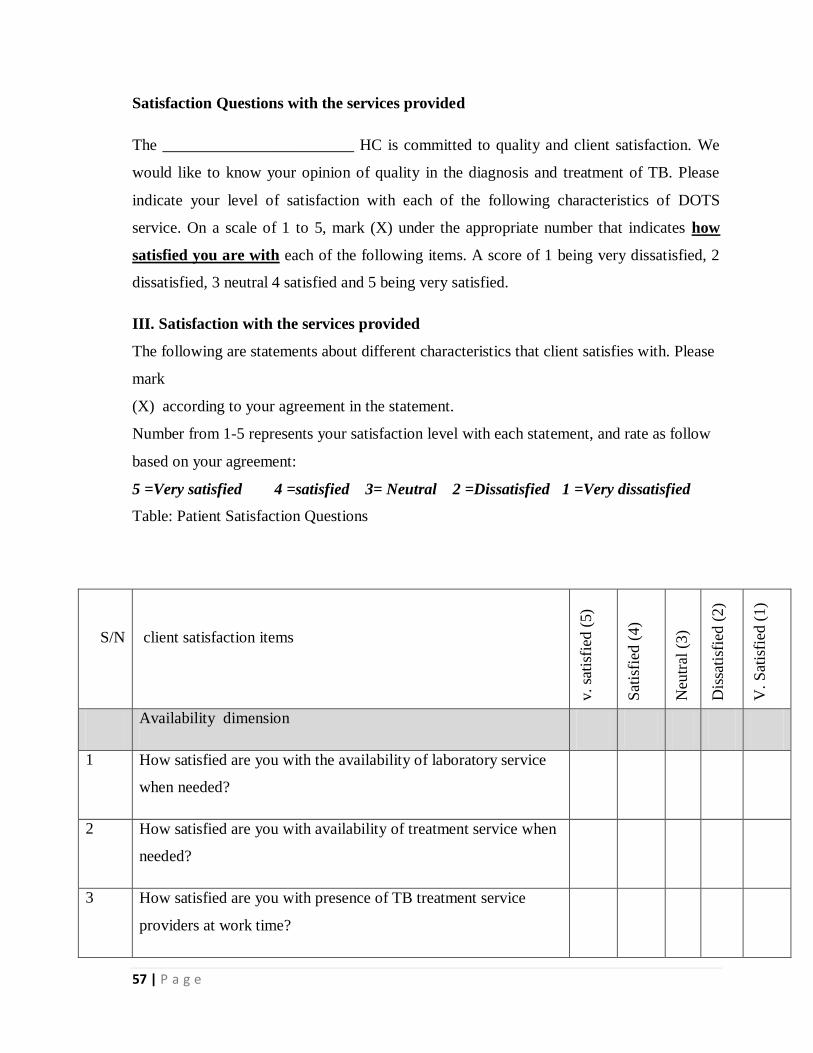
57 | P a g e
Satisfaction Questions with the services provided
The ________________________ HC is committed to quality and client satisfaction. We
would like to know your opinion of quality in the diagnosis and treatment of TB. Please
indicate your level of satisfaction with each of the following characteristics of DOTS
service. On a scale of 1 to 5, mark (X) under the appropriate number that indicates how
satisfied you are with each of the following items. A score of 1 being very dissatisfied, 2
dissatisfied, 3 neutral 4 satisfied and 5 being very satisfied.
III. Satisfaction with the services provided
The following are statements about different characteristics that client satisfies with. Please
mark
(X) according to your agreement in the statement.
Number from 1-5 represents your satisfaction level with each statement, and rate as follow
based on your agreement:
5 =Very satisfied 4 =satisfied 3= Neutral 2 =Dissatisfied 1 =Very dissatisfied
Table: Patient Satisfaction Questions
S/N client satisfaction items
v.
sati
sfie
d (
5)
Sat
isfi
ed (
4)
Neu
tral
(3)
Dis
sati
sfie
d (
2)
V.
Sat
isfi
ed (
1)
Availability dimension
1 How satisfied are you with the availability of laboratory service
when needed?
2 How satisfied are you with availability of treatment service when
needed?
3 How satisfied are you with presence of TB treatment service
providers at work time?

58 | P a g e
Accessibility dimension
1 How satisfied are you with convenience of HC to your home?
2 How satisfied are you with easy in getting to TB clinic?
Accommodation dimension
1 How satisfied are you with the daily visiting of health center for
TB treatment?
2 How satisfied are you with convenience of TB unit work hours?
3 How satisfied are you with time spent in waiting room?
Acceptability dimension
1 How satisfied are you with the friendliness/courtesy of the
providers?
2 How satisfied are you with the attention and respect of providers
to your privacy?
3 How satisfied are you with the competence/knowledge of the
providers?
4 How satisfied are you with the adequacy of explanation about
treatment?
5 How satisfied are you with overall quality of service?
Have you any other comments that you would like to share?

59 | P a g e
Gaaffiiwwan hammam akka tajaajila kennamutti gammadaniif qophaa’e.
Buufatni fayyaa____________________________________________ tajaajila qulqulluu fi
fayyadamtoota gammachiisuuf kan dhabbatee dha. Amma wanti nuti barbaannu yaada isin
qulqullina tajaajila fi yaalii dhukkuba daranyoo sombaaf kennamu irratti qabdan
baruudhaaf. Mee adaraa sadarkaa gammachuu isin tokko tokko tajaajila daranyoo sombaaf
kennamu irratti qabdan nuf ibsaa. Sadarkaa 1 hamma 5 jiru irratti hammam akka itti
gammadan mallattoo (X) kennuun agarsiisaa. Tokkoon tokkoon gaffiichaa madaalli 1 kan
baay‟ee itti hin gammaneef, 2 itti hin gammanneef, 3 yaada hin qabuuf, 4 itti gamadeeraaf,
5 baay‟ee itti gamadeeraaf kan qophaa‟ee dha.
Lakk. Gaaffiwwan hammam akka itti gammadani
Baa
y‟e
e gam
mad
eera
(5)
Itti
gam
mad
eera
(4)
Yaa
da
hin
qab
u(3
)
Itti
hin
gam
man
ne(
2)
Baa
y‟e
e hin
gam
man
ne(
1)
Jiraachuu tajaajilaa
1 Yeroo barbaaddanitti jiraachuu tajaajila laaboratoriitti hammam
gammadan?
2 Yeroo barbaddanitti jiraachuu yaalii daranyoo sombaa argachuutti
hammam gammadan?
3 Hojeetaan fayyaa kilinika qorichi daranyoo sombaa guyyaa
guyyaan kennamuutti argamuu isaanitti hammam gammadan?
Salphina tajaajila
1 Buufatni fayyaa fageenyi inni mana keessan irraa qabutti
hammam gammadan?
2 Akka salphaatti kilinika daranyoon sombaa itti yaalamu jiru
argachuutti hammam gammadan?
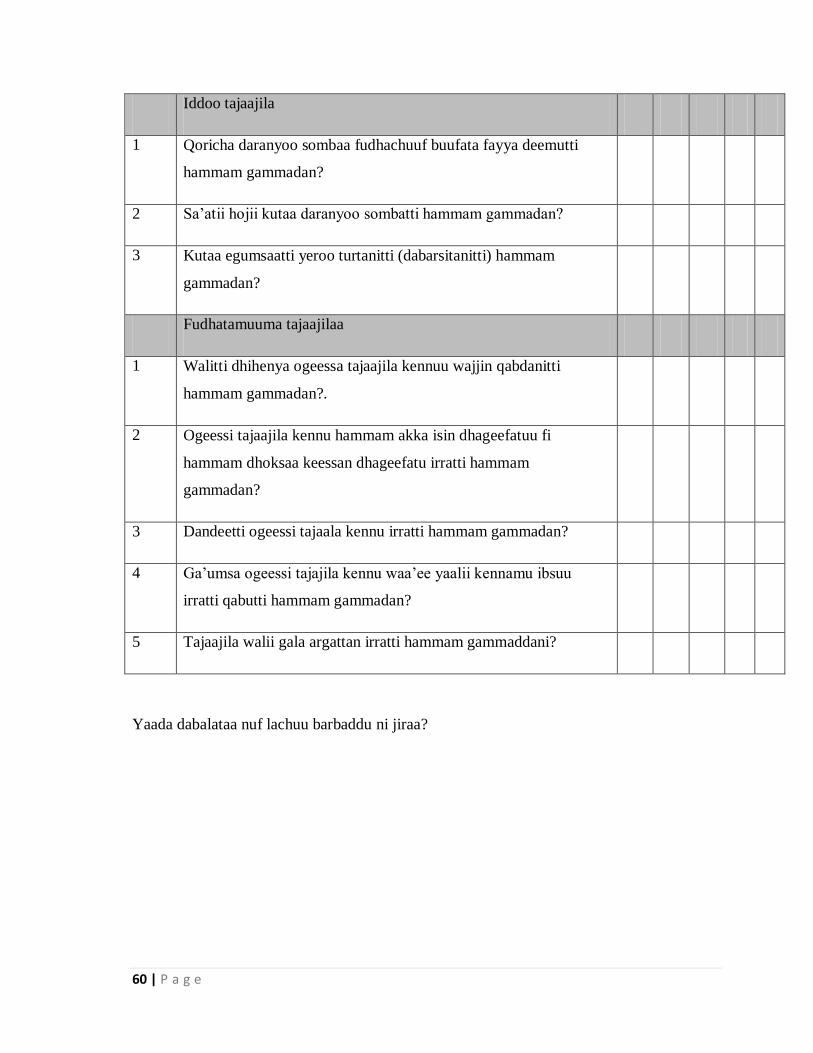
60 | P a g e
Iddoo tajaajila
1 Qoricha daranyoo sombaa fudhachuuf buufata fayya deemutti
hammam gammadan?
2 Sa‟atii hojii kutaa daranyoo sombatti hammam gammadan?
3 Kutaa egumsaatti yeroo turtanitti (dabarsitanitti) hammam
gammadan?
Fudhatamuuma tajaajilaa
1 Walitti dhihenya ogeessa tajaajila kennuu wajjin qabdanitti
hammam gammadan?.
2 Ogeessi tajaajila kennu hammam akka isin dhageefatuu fi
hammam dhoksaa keessan dhageefatu irratti hammam
gammadan?
3 Dandeetti ogeessi tajaala kennu irratti hammam gammadan?
4 Ga‟umsa ogeessi tajajila kennu waa‟ee yaalii kennamu ibsuu
irratti qabutti hammam gammadan?
5 Tajaajila walii gala argattan irratti hammam gammaddani?
Yaada dabalataa nuf lachuu barbaddu ni jiraa?
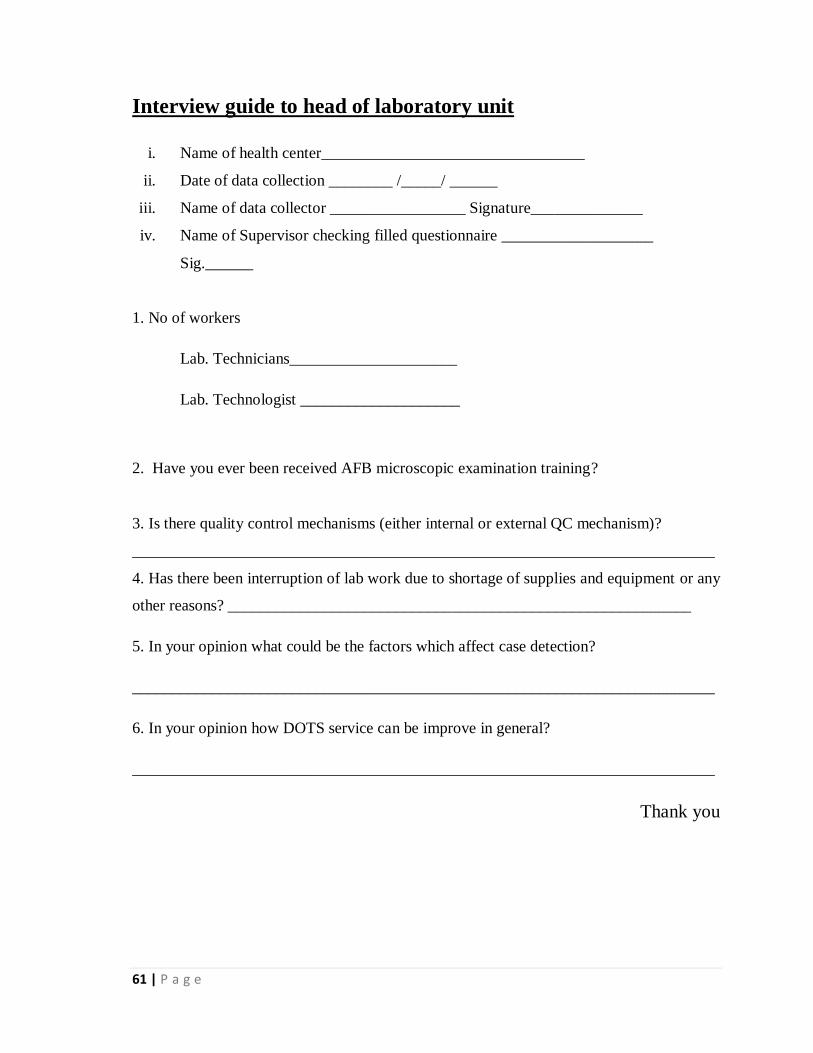
61 | P a g e
Interview guide to head of laboratory unit
i. Name of health center_________________________________
ii. Date of data collection ________ /_____/ ______
iii. Name of data collector _________________ Signature______________
iv. Name of Supervisor checking filled questionnaire ___________________
Sig.______
1. No of workers
Lab. Technicians_____________________
Lab. Technologist ____________________
2. Have you ever been received AFB microscopic examination training?
3. Is there quality control mechanisms (either internal or external QC mechanism)?
_________________________________________________________________________
4. Has there been interruption of lab work due to shortage of supplies and equipment or any
other reasons? __________________________________________________________
5. In your opinion what could be the factors which affect case detection?
_________________________________________________________________________
6. In your opinion how DOTS service can be improve in general?
_________________________________________________________________________
Thank you

62 | P a g e
Interview guide to clinicians and DOTS providers
1. What are the general problems related to TB diagnosis? What are the likelihood
solutions?
_________________________________________________________________________
2. What are the general problems related to TB treatment? What are the likelihood
solutions?
_________________________________________________________________________
3. In your opinion how could case detection be improved?
________________________________________________________________________
4. In your opinion how could treatment adherence improved?
Thank you

63 | P a g e
Interview guide to district program expert
1. Would you please describe your profession and experience in NTP in the district?
________________________________________________________________________
________________________________________________________________________
2. What are the general problems related to TB diagnosis? What are the likelihood
solutions?
_________________________________________________________________________
_________________________________________________________________________
3. What are the general problems related to TB treatment? What are the likelihood
solutions?
_________________________________________________________________________
_________________________________________________________________________
4. In your opinion how could case detection be improved?
________________________________________________________________________________
________________________________________________________________________________
5. In your opinion how DOTS service can be improve in general?
_________________________________________________________________________
_________________________________________________________________________
6. Describe the availability of health workers involved in TB diagnosis and treatment in the
district?
_________________________________________________________________
7. Describe the adequacy of drugs and reagents? Is there an occasion of interruption and
why? Which items? What measures were taken for interruption or shortage and your
suggestion to improve?
_________________________________________________________________
8. Describe if any other comments you would like to share?
____________________________________________________________
Thank you
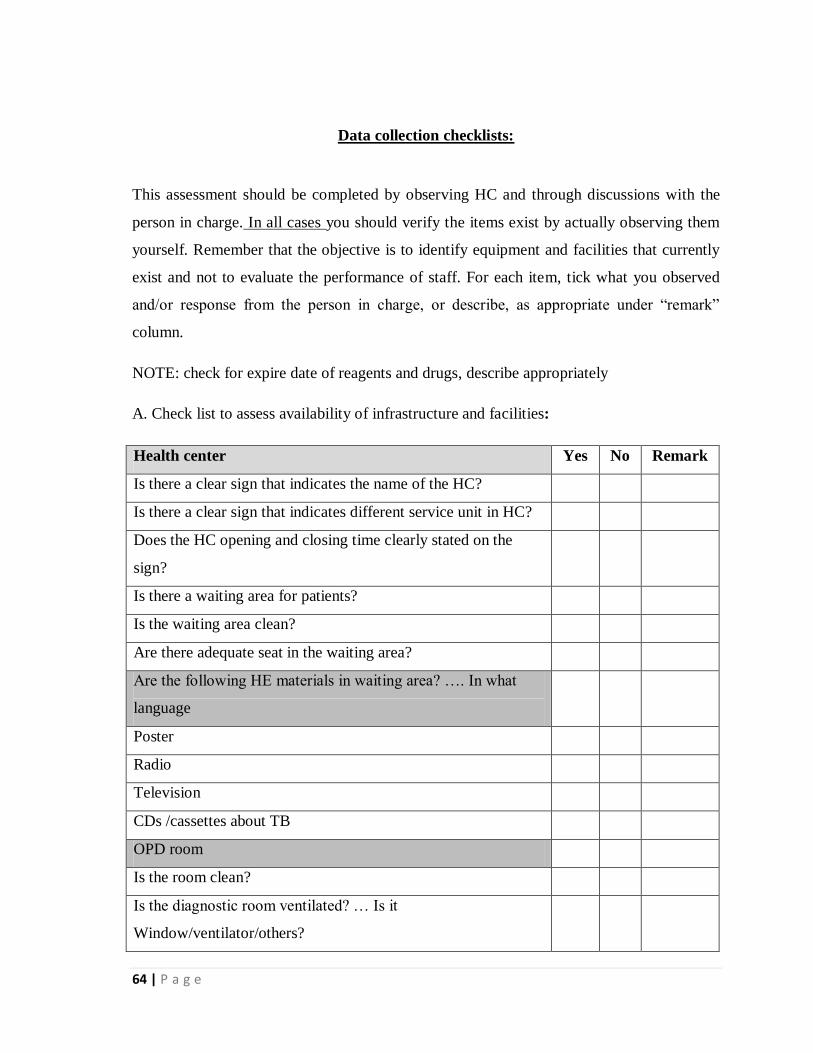
64 | P a g e
Data collection checklists:
This assessment should be completed by observing HC and through discussions with the
person in charge. In all cases you should verify the items exist by actually observing them
yourself. Remember that the objective is to identify equipment and facilities that currently
exist and not to evaluate the performance of staff. For each item, tick what you observed
and/or response from the person in charge, or describe, as appropriate under “remark”
column.
NOTE: check for expire date of reagents and drugs, describe appropriately
A. Check list to assess availability of infrastructure and facilities:
Health center Yes No Remark
Is there a clear sign that indicates the name of the HC?
Is there a clear sign that indicates different service unit in HC?
Does the HC opening and closing time clearly stated on the
sign?
Is there a waiting area for patients?
Is the waiting area clean?
Are there adequate seat in the waiting area?
Are the following HE materials in waiting area? …. In what
language
Poster
Radio
Television
CDs /cassettes about TB
OPD room
Is the room clean?
Is the diagnostic room ventilated? … Is it
Window/ventilator/others?

65 | P a g e
Does HC have light?
Are the following facilities/items in the room?
HE material posted in OPD room at visible place.....In what
language?
NTP guideline
Lab. AFB request paper
Drug prescription paper
Patient referral form
Laboratory layout and equipment
Does lab. Unit clean?
Does lab unit has the following standards
NTP guideline
Quality control standards
Standard operating procedures( posted on staining area)
Health education material posted on visible place (in what
language?)
Laboratory arrangement….Does lab unit has the following
work areas?
Separate area/room for specimen reception
Separate area/room for preparing and staining smears
Separate area/room for smear examination
Separate area/room for registration
Benches or tables….does lab unit has benches or tables for
Specimen reception, slide storage and laboratory registers
Smear-preparation
Staining
Microscopic examination
List of laboratory materials……are the following materials
available?
Microscope

66 | P a g e
Immersion oil with a dropper
Lens tissue
Glove
Slides
Wire loop / wooden applicator
Bunsen burner or spirit lamp burner
Forceps for holding slide and fixing
Sink with running water
Basin if there is no sink
Water filter can if no running water
Waste receptacle
Disinfectant ( either 5% phenol or 10% sodium hypo chloride)
Sputum cups
Slide holder
Slide rack
Alarm clock
Bucket for water
Box for keeping examined slides
List of the reagents used in Ziehl Nelson staining technique
Carbon fuchsine
Acid alcohol
Methylene blue
Is there posted AFB sops in the laboratory at visible spaces?
Is TB unit clean?
Is TB unit ventilated?
Does health education material posted in TB unit at visible
spaces?
Is there NTP manual in TB unit?
Is there TB unit register?

67 | P a g e
Is there functional weighting scale in TB unit?
Others
TB Unit
Is the TB unit clean?
Check availability of following items in TB unit
TB unit register
NTP guideline
RH Eligibility and Dosage Flow Chart
Health education material posted on visible place (in what
language?)
RHZE
RH
Functional weighing scale
Pharmacy unit STORE…check availability of
RHZE
RH
Sputum cup
Slides
Carbol fuchsine
Methyline blue
Immersion oil
Review stock card for either
RHZE Stock out for the last three months
RH Stock out for the last three months
Sputum cup Stock out for the last three months
Slides Stock out for the last three months
Carbol fuchsine Stock out for the last three months
Methyline blue Stock out for the last three months
Immersion oil Stock out for the last three months
Check availability of buffer stock for at least one month

68 | P a g e
RHZE
RH
Sputum cup
Slides
Carbol fuchsine
Methyline blue
Immersion oil
Laboratory activity observation checklist
This assessment should be completed by observing lab unit. In all cases you should verify
each activity by actually observing on site. Note that this is not to evaluate the performance
lab personnel; to observe the routine aspects of sputum smear examination. For each tick
Yes/No based on what you observed and/or describe, as appropriate under “remark”
column.
Pre analytic phase Yes No Remark
Equipment and materials arranged before starting smear
preparation
Ask the name of patients, match it with the name on the request
paper
Use new sputum cup to collect specimen
Write the same number on the body of container and request
paper
Demonstrating the patient to bring quality sputum specimen
Evaluating the quality and volume of specimen
Cross check the number of the request form and sputum container
Analytic phase
Use new slides
Use filtered carbol- fuchsine
Use filtered methyline blue
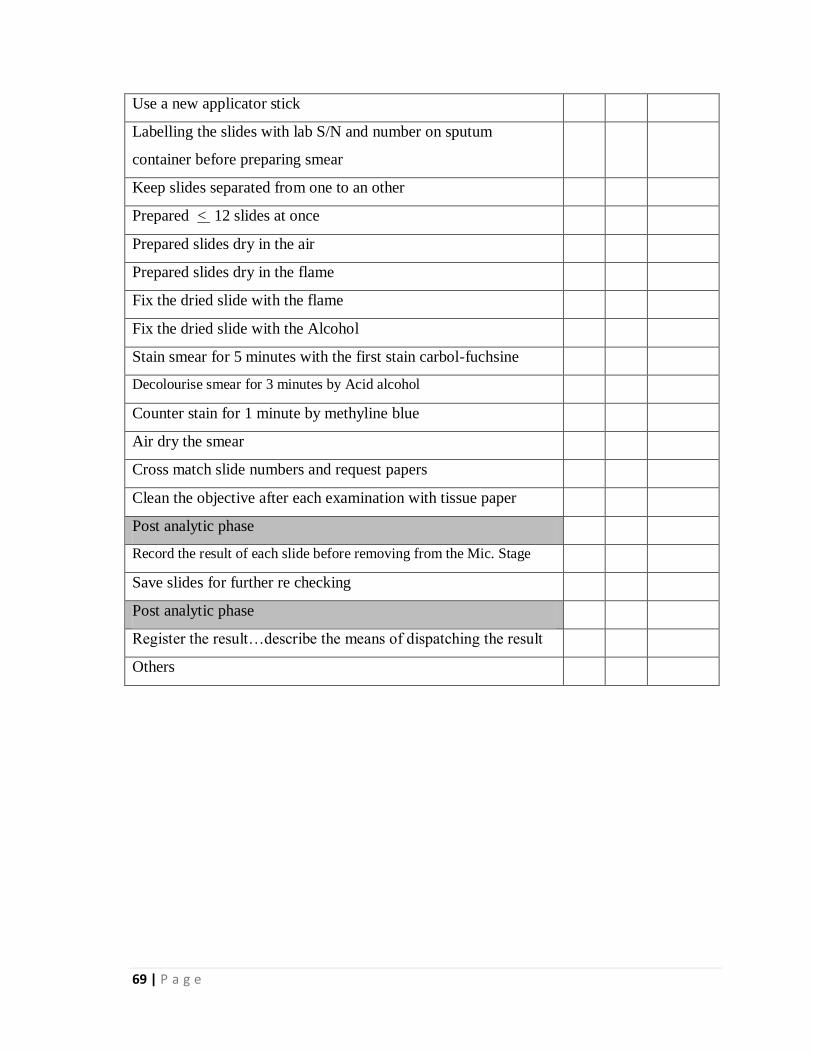
69 | P a g e
Use a new applicator stick
Labelling the slides with lab S/N and number on sputum
container before preparing smear
Keep slides separated from one to an other
Prepared < 12 slides at once
Prepared slides dry in the air
Prepared slides dry in the flame
Fix the dried slide with the flame
Fix the dried slide with the Alcohol
Stain smear for 5 minutes with the first stain carbol-fuchsine
Decolourise smear for 3 minutes by Acid alcohol
Counter stain for 1 minute by methyline blue
Air dry the smear
Cross match slide numbers and request papers
Clean the objective after each examination with tissue paper
Post analytic phase
Record the result of each slide before removing from the Mic. Stage
Save slides for further re checking
Post analytic phase
Register the result…describe the means of dispatching the result
Others

70 | P a g e
Provider-patient interaction observation checklist
S/N Provider-patient interaction Yes No
1. While discussing with the patient, did the provider use clear language
that patient understand simply…if possible local language
2. Before the treatment, did the provider measure patient weight?
3. Did the health worker provide correct drug based on the weight of patient?
4. Did the treatment provider observe the patient while swallowing the
drugs?
5. Did the provider remind the patient of the schedule of the next
sputum examination?
6. Did provider provided health education?
7. Did the provider let the patient ask any questions the patient may
have?
8. Did the provider respond to patient‟s questions?
9. Did the provider stress very well about the problem of defaulting&
explain the method they can be easily traced
10. Did the health worker record on the unit register immediately after
consultation of every patient?




















