Application of a circulating antigen detection immunoassay for laboratory diagnosis of...
9
Application of a circulating antigen detection immunoassay for laboratory diagnosis of extra-pulmonary and pulmonary tuberculosis Abdelfattah M. Attallah a, * , Sanaa Osman b , Amr Saad b , Mohamed Omran a , Hisham Ismail a , Gellan Ibrahim a , Ahmed Abo-Naglla c a R&D Department, Biotechnology Research Center, P.O. Box 14, 23 July St., Industrial Zone, 34517 New Damietta City, Egypt b Faculty of Science, Cairo University, Giza, Egypt c Faculty of Medicine, Al-Azhar University, Cairo, Egypt Received 18 October 2004; received in revised form 29 November 2004; accepted 29 November 2004 Abstract Background: Diagnosis of extra-pulmonary tuberculosis is often difficult to establish using standard methods. Recently, a 55- kDa mycobacterial antigen was identified in sera of individuals with pulmonary TB using a simple and rapid dot-ELISA based on monoclonal antibody (TB-55 mAb). Here, we have evaluated the application of the dot-ELISA for the detection of target antigen in sera of individuals with extra-pulmonary TB. Methods: The Western blot and indirect immunoperoxidase staining was used to identify the target TB antigen using the TB-55 mAb. The dot-ELISA was used to detect the target antigen in serum samples. Results: The target antigen was identified at 55-kDa molecular weight in serum, ascitic fluid and CSF samples from individuals with extra-pulmonary TB. The purified antigen from these samples showed similar biochemical properties to the previously described antigen. The target antigen was localized in areas without caseous necrosis in lymph tissues. The dot-ELISA detected the target antigen in 90% sera of individuals with extra-pulmonary TB and in 87% sera of individuals with pulmonary TB with a specificity of 97% among control individuals. Conclusion: The detection of the 55-kDa antigen using dot-ELISA can be routinely employed to support clinical diagnosis of extra-pulmonary TB and pulmonary TB. D 2005 Elsevier B.V. All rights reserved. Keywords: Tuberculosis; Extra-pulmonary; Diagnosis; 55-kDa; Circulating antigen; Serum enzyme immunoassay; dot-ELISA 1. Introduction Tuberculosis (TB) remains a leading infectious cause of death and a leading public health priority in 0009-8981/$ - see front matter D 2005 Elsevier B.V. All rights reserved. doi:10.1016/j.cccn.2004.11.036 * Corresponding author. Tel.: +20 57 402889, 20 57 403889, 20 57 404889; fax: +20 57 401889. E-mail address: [email protected] (A.M. Attallah). Clinica Chimica Acta 356 (2005) 58 – 66 www.elsevier.com/locate/clinchim
Transcript of Application of a circulating antigen detection immunoassay for laboratory diagnosis of...
www.elsevier.com/locate/clinchim
Clinica Chimica Acta
Application of a circulating antigen detection immunoassay for
laboratory diagnosis of extra-pulmonary and
pulmonary tuberculosis
Abdelfattah M. Attallaha,*, Sanaa Osmanb, Amr Saadb, Mohamed Omrana,
Hisham Ismaila, Gellan Ibrahima, Ahmed Abo-Nagllac
aR&D Department, Biotechnology Research Center, P.O. Box 14, 23 July St., Industrial Zone, 34517 New Damietta City, EgyptbFaculty of Science, Cairo University, Giza, Egypt
cFaculty of Medicine, Al-Azhar University, Cairo, Egypt
Received 18 October 2004; received in revised form 29 November 2004; accepted 29 November 2004
Abstract
Background: Diagnosis of extra-pulmonary tuberculosis is often difficult to establish using standard methods. Recently, a 55-
kDa mycobacterial antigen was identified in sera of individuals with pulmonary TB using a simple and rapid dot-ELISA based
on monoclonal antibody (TB-55 mAb). Here, we have evaluated the application of the dot-ELISA for the detection of target
antigen in sera of individuals with extra-pulmonary TB.
Methods: The Western blot and indirect immunoperoxidase staining was used to identify the target TB antigen using the TB-55
mAb. The dot-ELISA was used to detect the target antigen in serum samples.
Results: The target antigen was identified at 55-kDa molecular weight in serum, ascitic fluid and CSF samples from individuals
with extra-pulmonary TB. The purified antigen from these samples showed similar biochemical properties to the previously
described antigen. The target antigen was localized in areas without caseous necrosis in lymph tissues. The dot-ELISA detected
the target antigen in 90% sera of individuals with extra-pulmonary TB and in 87% sera of individuals with pulmonary TB with a
specificity of 97% among control individuals.
Conclusion: The detection of the 55-kDa antigen using dot-ELISA can be routinely employed to support clinical diagnosis of
extra-pulmonary TB and pulmonary TB.
D 2005 Elsevier B.V. All rights reserved.
Keywords: Tuberculosis; Extra-pulmonary; Diagnosis; 55-kDa; Circulating antigen; Serum enzyme immunoassay; dot-ELISA
0009-8981/$ - see front matter D 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.cccn.2004.11.036
* Corresponding author. Tel.: +20 57 402889, 20 57 403889, 20
57 404889; fax: +20 57 401889.
E-mail address: [email protected] (A.M. Attallah).
1. Introduction
Tuberculosis (TB) remains a leading infectious
cause of death and a leading public health priority in
356 (2005) 58–66

A.M. Attallah et al. / Clinica Chimica Acta 356 (2005) 58–66 59
the world [1]. The World Health Organization (WHO)
estimates that there are more than 8 million new cases
of TB each year, and that one-third of the world
population is infected with the bacterium Mycobacte-
rium tuberculosis and at risk for active disease [2].
Although the lung is the primary site of disease in 80–
84% of TB cases, extra-pulmonary TB has become
more common with the advent of HIV infection [3,4].
The most commonly reported extra-pulmonary sites
of the disease are the lymph nodes [5], pleura [6] and
bones or joints [7,8]. Other sites include the genito-
urinary system [9], the central nervous system [10,11],
the abdomen [12,13] and in rare cases, virtually any
other organ [14]. Extra-pulmonary TB remains an
important diagnostic and therapeutic problem. Efforts
to control the disease are currently hampered by the
lack of effective tools for the detection of infected
individuals, although new diagnostic tests are being
developed [15]. Bacteria in extra-pulmonary TB cases
can be present in low numbers at inaccessible sites
[3]. Despite rapid advances in molecular genetics for
detection of M. tuberculosis, it is clear that interest in
serodiagnosis remains high, especially for those
situations in which a specimen may not contain the
infecting agent [16]. Extensive efforts to devise a
sensitive and specific immunodiagnostic test for the
detection of M. tuberculosis-circulating antigen have
been made by several investigators [17,18]. Recently,
Attallah et al. [19] developed a simple and rapid dot-
ELISA based on IgG monoclonal antibody (TB-55
mAb) specific for a 55-kDa mycobacterial antigen and
evaluated its performance in the diagnosis of pulmo-
nary TB. In the present study, we have investigated
the presence of the target TB antigen in serum as well
as ascitic fluid, cerebrospinal fluid and lymph node
tissues of patients with extra-pulmonary TB and
evaluated the application of the developed dot-ELISA
for the detection of the target antigen in sera of
patients with extra-pulmonary and pulmonary TB.
2. Materials and methods
2.1. Samples
2.1.1. Serum samples
Serum samples of 506 individuals (383 males, 123
females; age 14–58 year) screened by radiograph at
the Department of Chest Diseases at Sayd Galal
University Hospital, Al-Azhar University, Cairo,
Egypt that approved the study were recruited. Patients
with extra-pulmonary TB (n=93) were diagnosed by
clinical symptoms, radiographic evidence and ultra-
sound, or a combination of these techniques, depend-
ing on the location of the infection in each patient.
The sites of extra-pulmonary TB include peritonitis
(n=25), meningitis (n=22), lymphadenitis (n=14),
genitourinary tract (n=19), Pott’s disease (n=5),
arthritis (n=3), sinusitis (n=3) and miliary (n=2).
None of extra-pulmonary TB patients had clinical or
radiological evidence of concurrent active pulmonary
TB. Patients with pulmonary TB (n=296) were
diagnosed by sputum smear for acid-fast bacilli
(AFB) or by culture for M. tuberculosis and all had
no prior clinical history of TB. In addition, selected
patients admitted to the hospital for a defined acute or
chronic non-TB diseases (n=69) including asthma
(n=10), ischemic heart disease (n=10), chronic
obstructive pulmonary disease (n=30), pneumonia
(n=5), bronchitis (n=5), lung cancer (n=5) and lung
infection (n=4) as well as 48 healthy volunteers (age
10–56) with no signs of clinical impairment and
normal chest radiographs were included as controls.
2.1.2. Ascitic fluid
Ascites were obtained from the 25 tuberculous
peritonitis patients (20 males, 5 females; age 45–58)
and centrifuged at 4000 rpm for 10 min. The deposits
were examined microscopically for AFB by Ziehl-
Neelsen (ZN) staining. Supernatants were coded and
used for the detection of antigen. Five patients with
non-tuberculous ascites (4 transudative and 1 exuda-
tive) negative for M. tuberculosis by smear were used
as controls.
2.1.3. Cerebrospinal fluid (CSF)
CSF samples were obtained from 22 tuberculous
meningitis patients (15 males, 7 females; age 36–50)
before antibiotic therapy. They were considered likely
to have meningitis on the basis of clinical features,
such as neck rigidity, positive Kernig’s sign and
compatible CSF biochemical parameters, e.g., ele-
vated protein levels (60–400 mg%, mean 98 mg%),
low glucose concentration (8–30 mg%, mean 23
mg%) and pleocytosis (30–700 cells/cm3) in their
CSF specimens. These patients had neither manifes-

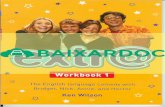
Fig. 2. Identification of the TB-55 mAb target antigen in ascitic
fluids of patients with peritonitis tuberculosis using Western blot
Lanes 1, 2: Two patients with transudative and exudative non-
tuberculous respectively as negative controls; lanes 3, 4: two
patients with peritonitis tuberculosis. The TB-55 mAb identified a
reactive band at 55-kDa molecular weight only in the ascites and
serum samples of the patients with peritonitis tuberculosis
Molecular weight markers were not shown but indicated by arrows
A.M. Attallah et al. / Clinica Chimica Acta 356 (2005) 58–6660
tations of pulmonary TB nor had received chemo-
therapy for TB in the recent past. The CSF specimens
were collected from all patients under aseptic con-
ditions and were centrifuged at 5000�g for 30 min.
The deposits were examined by ZN staining.
2.1.4. Lymph node tissues
Paraffin sections of lymph node tissues from
patients of tuberculous lymphadenitis (n=14) were
processed for routine histological and immunohisto-
chemical examinations. Hematoxylin and Eosin
(H&E) staining was done to evaluate morphological
features (granuloma formation and caseation) and ZN
staining was done to look for AFB.
2.2. SDS–PAGE and Western immunoblotting assays
Serum, CSF, ascitic fluid and BCG (Egyptian
Organization for Biological Products and Vaccines,
Dokki, Giza, Egypt), at 30 Ag/lane were separated by
sodium dodecyl sulfate–polyacrylamide gel electro-
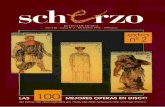
Fig. 1. Identification of the TB-55 mAb target antigen in sera of
patients with different types of extra-pulmonary tuberculosis using
Western blot. Lanes 1, 2: Sera from 2 healthy individuals as
negative controls. Lanes 3, 4: BCG vaccine and serum sample from
a patient with pulmonary tuberculosis; respectively as positive
controls. Lanes 5–10: Sera of 6 patients with extra-pulmonary
tuberculosis including: lymphadenitis tuberculosis (lane 5), genito-
urinary tract tuberculosis (lane 6), Pott’s disease (lane 7), arthritis
tuberculosis (lane 8), sinusitis tuberculosis (lane 9), miliary tuber-
culosis (lane 10). The TB-55 mAb identified two reactive bands at
82-kDa and 55-kDa molecular weights in BCG and one band at 55-
kDa molecular weight in serum samples of infected individuals.
Molecular weight markers (not shown but indicated by arrows)
include Phosphorylase B (97.4-kDa), Bovine serum albumin (66.2-
kDa), Glutamate dehydrogenase (55.0-kDa), Ovalbumin (42.7-
kDa), Aldolase (40-kDa), Carbonic anhydrase (31-kDa), Soya bean
trypsin inhibitor (21.5-kDa).
Fig. 3. Identification of the TB-55 mAb target antigen in
cerebrospinal fluids of patients with tuberculous meningitis using
Western blot. Lanes 1, 2: Two patients with non-tuberculous
meningitis as negative controls; lanes 3, 4: two patients with
tuberculous meningitis. The TB-55 mAb identified a reactive band
at 55-kDa molecular weight only in the CSF and serum samples of
the patients with tuberculous meningitis. Molecular weight markers
were not shown but indicated by arrows.
.
.
.
phoresis (SDS–PAGE) and immunostained using the
TB-55 mAb as previously described by Attallah et al.
[19].
2.3. Isolation and partial characterization of the 55-
kDa antigen from different sources
The 55-kDa antigen was purified from ascitic
fluids, CSF and serum samples of patients with

A.M. Attallah et al. / Clinica Chimica Acta 356 (2005) 58–66 61
extra-pulmonary TB by preparative gel electroelution.
To determine some characteristics of purified anti-
gens, samples of antigen fractions were treated with
protease and several other chemical reagents and
tested in dot-ELISA according to Attallah et al. [19].
2.4. Immunohistochemical staining
Paraffin sections (4-Am) of lymph node tissue were
stained by indirect immunoperoxidase to demonstrate
the presence of Mycobacterium antigens. Sections
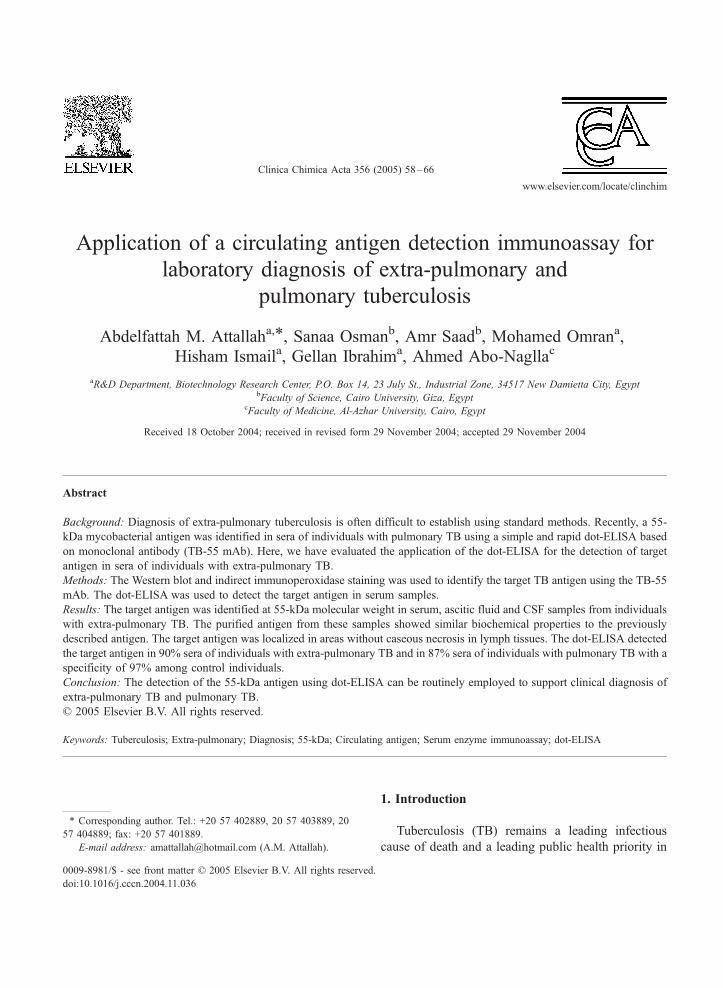
Fig. 4. SDS–PAGE and capillary zone electrophoresis (CZE) analyses of th
extra-pulmonary tuberculosis. A. SDS–PAGE analyses. Lane 1: Sample
resolved proteins were Coomassie blue stained. A single band was s
electropherogram of the purified antigen from CSF. The purified antigen (2
buffer, pH 8.3, on a 65-cm�75-Am capillary, 30 kV, at 20 8C and UV de
were washed several times with 0.05 M Tris-buffered
saline with Tween 20, pH 7.6, TBS-T. Smears were
then treated with 3% H2O2 for 5 min and washed, then
TB-55mAb antibody diluted in 0.01MTBSwas added
and incubated for 30 min. Subsequently, horseradish
peroxidase conjugated goat antibody to mouse IgG
diluted 1:500 in 1.5% BSA in TBS was added and
incubated for 60 min. After that, the sections were
washed then incubated for 10 min at room temperature
in a diaminobenzidine tetrachloride substrate. Finally,
the sections were counterstained with Harris hematox-
e 55-kDa antigen purified from different body fluids of patients with
from ascites, CSF or serum; lane 2: purified antigen fraction. The
hown at 55-kDa molecular weight in purified fraction. B. CZE
5 Ag per 1 ml of distilled water) was separated with 100-mM Borate
tection at 200 nm. A single peak was shown at 11 min.

A.M. Attallah et al. / Clinica Chimica Acta 356 (2005) 58–6662
ylin, dehydrated, cleared in xylene, mounted in
Permount (Sigma) and visualized under a microscope.
Specimens of tuberculous lymphadenitis with omission
of TB-55 mAb were used as negative controls.
2.5. Dot-enzyme linked immunosorbent assay
(dot-ELISA)
The dot-ELISA as a simple and rapid assay was
used for screening of TB antigen in serum using
specific IgG TB-55 mAb according to Attallah et al.
[19]. In brief, all the assay steps run out on the surface
of nitrocellulose membrane filter fixed in a plastic
cartilage. Tested samples (500 Ag/dot) were added
onto the membrane surface. After washing, the TB-55
mAb antibody diluted in 0.01M PBS was added. The
alkaline phosphatase conjugated goat antibody diluted
in 0.05 M Tris buffer was added onto the membrane
surface. The NBT/BCIP substrate solution was used
to develop the color within 2 min. The reaction was
then stopped and the result was evaluated.
3. Results
3.1. Identification of the TB-55 mAb target antigen in
body fluids
The target antigen of the TB-55 mAb was
identified by the Western blot at 55-kDa in serum
Fig. 5. Localization of the TB-55 mAb target antigen of lymph tissue usin
(indicated by arrows) lymph tissue stained with the TB-55 mAb (�400
necrosis, was seen as solid, beaded or fragmented rods, within phagocyte
seen on ZN staining. Diffuse staining in the form of antigenic dust was
immunostaining lymph tissue (�400).
samples (Fig. 1), ascites (Fig. 2) and CSF samples
(Fig. 3) from patients with extra-pulmonary TB. In
addition to 55-kDa, a high molecular weight reactive
epitope was identified at 82-kDa in BCG vaccine, Fig.
1. The 55-kDa target antigen was purified from these
body fluids using electroelution from preparative
polyacrylamide slab gels. The antigen fractions
purified either from serum, ascites and CSF of extra-
pulmonary TB patients showed a single band at 55-
kDa in Coomassie blue stained SDS–PAGE (Fig. 4A)
and one peak when analyzed by CZE at 11 min (Fig.
4B). The reactive epitope on the purified antigens was
sensitive (i.e. showing negative result using dot-
ELISA; colorless dot) to acid and base hydrolysis,
mercaptoethanol, protease and pepsin treatments. The
purified antigens were precipitated with TCA, and the
reconstituted precipitates showed high reactivity (i.e.
showing positive result using dot-ELISA; colored dot)
toward the TB-55 mAb. In contrast, the supernatants
of purified antigens showed no reactivity. Periodate
oxidation did not affect the reactivity of the target
epitope on the purified antigens.
3.2. Localization of the target antigen of TB-55 mAb
using indirect immunoperoxidase staining
The target antigen of the TB-55 mAb was seen in
areas without caseous necrosis as solid, beaded or
fragmented rods within phagocyte cytoplasm, some of
which were similar in size and shape to AFB as seen
g indirect immunoperoxidase staining. A. Positive immunostaining
). The target antigen of the TB-55 mAb, in areas without caseous
cytoplasm, some of which were similar in size and shape to AFB as
also seen in giant cells and epithelioid cell cytoplasm. B. Negative

Table 1
Validation of dot-ELISA test for diagnosis of extra-pulmonary
tuberculosis
Group No. dot-ELISAa % Positive
Positive Negative
Extra-pulmonary tuberculosis 93 84 9 90%
Controls 117 4 113 3%
Non-tuberculous disease 69 2 67 3%
Healthy individuals 48 2 46 4%
a Rapid detection of the 55-kDa circulating antigen in serum.
A.M. Attallah et al. / Clinica Chimica Acta 356 (2005) 58–66 63
on ZN staining. Their distribution in these areas was
microanatomically similar to the distribution of AFB
as seen on ZN staining. Diffuse staining in the form of
antigenic dust was also seen in giant cells and
epithelioid cell cytoplasm (Fig. 5A). Specimens of
tuberculous lymphadenitis with omission of the TB-
55 mAb were used as negative controls (Fig. 5B).
3.3. Rapid detection of the 55-kDa circulating antigen
in sera using dot-ELISA
The performance characteristics of dot-ELISA for
the detection of the 55-kDa antigen in sera of patients
with extra-pulmonary TB are shown in Table 1. The
55-kDa circulating antigen was detected in 90% sera
of extra-pulmonary TB. Only 3% of 69 non-TB
patients and 4% of 48 healthy controls had a false-
positive antigen showing a total specificity of 97%. In
a large number of individuals with pulmonary TB
(n=296), the target antigen was detected using dot-
ELISA in 87% of their sera. All samples showing
false-negative results using the dot-ELISAwere tested
using the more sensitive Western blot and the 55-kDa
antigen was detected in all (100%) false-negative
samples.
4. Discussion
Extra-pulmonary TB is often difficult to diagnose
because of its diverse clinical presentations [15,20].
The most affordable diagnostic methods for the
clinical setting are the immunoassays, since it is rapid,
easy to perform and require simple reagents. Many
serological assays have been developed for specific
antibody detection in TB patients [17,18,21]. How-
ever, people in the tropical areas are in contact with
various pathogens and developed cross-reacting anti-
bodies responsible for poor specificity [22]. Moreover,
the sensitivity of antibody detection tests is much
lower in HIV seropositive patients coinfected with
tuberculosis [23]. In addition, changes in antigen
conformation that may occur as a result of passive
coating of the antigens to solid supports may cause
technical artifacts resulting in false-positive and false-
negative reactions [24]. Recently, more efforts are
directed toward developing reliable, and less costly
immunoassays based on the detection of mycobacte-
rial antigens in different body fluids using specific
antibodies. Such tests could be useful for the diagnosis
and follow-up of TB patients [25]. Several M. tuber-
culosis antigens were detected in different body fluids
of infected individuals, e.g., 30-kDa antigen and 31-
kDa antigen in serum [26,27], 43-kDa antigen in
ascitic fluid [28], 43-kDa antigen, antigen 5, and 14-
kDa antigen in CSF [29–31]. It is possible that such
antigens could be shed directly into the infected area
or may arise from sequestered Mycobacterium in
tissues. Moreover, the diagnostic potential of Myco-
bacterium antigen detection has been evaluated in
serum [26,32,33], ascitic fluid [28] and CSF [34,35],
with sensitivity rates of 41–93% and specificity rate of
86–100%. However, none of these tests to detect
mycobacterial antigens has become available for
clinical utility nor achieved widespread use for the
diagnosis of TB. Recently, a 55-kDa circulating
Mycobacterium antigen was identified in sera of
individuals with pulmonary TB using specific mono-
clonal antibody designated TB-55 mAb [19]. In the
present work, the 55-kDa antigen was identified in
serum, ascitic fluid and CSF samples of patients with
extra-pulmonary TB. However, it is of interest that an
antigen with similar size; 55-kDa; has not been
previously reported in serum samples of patients with
extra-pulmonary TB. The 55-kDa target antigen was
purified from serum, ascites and CSF samples of
extra-pulmonary TB patients. The protein nature of
the reactive epitope was confirmed by several experi-
ments. These purified antigens showed the same
biochemical characteristics as the previously
described 55-kDa antigen purified from sera of
pulmonary TB patients [19]. In addition to the 55-
kDa reactive epitope, a higher molecular weight
epitope was identified at 82-kDa in BCG vaccine
suggesting that the 55-kDa serum antigen may be the

A.M. Attallah et al. / Clinica Chimica Acta 356 (2005) 58–6664
stable degradation product from the higher molecular
weight antigen. However, further molecular study is
required for confirmation. Earlier studies of immuno-
histochemical staining have shown the utility of
polyclonal and monoclonal antibodies to identify M.
tuberculosis antigens in the lung, brain and lymph
node and joint specimens of tuberculous patients [34].
The distribution of the 55-kDa target antigen in areas
without caseous necrosis of lymph node tissues was as
described for other mycobacterial antigens [36].
Regardless of the mechanism by which the antigen
appears in body fluids, the detection of the 55-kDa
circulating antigen in ascitic fluid, CSF and the
presence of this antigen in serum samples of extra-
pulmonary TB will make it easier for diagnosis.
Although the ELISA system is very practical and
sensitive, the testing equipment required is not always
available in areas where tuberculosis is endemic. An
alternative to ELISA could be the dot blot method,
which uses only a paper matrix onto which the antigen
is spotted, and the development of the antigen–
antibody reaction is done by an enzyme or the use
of a colloidal gold conjugate [37]. We previously
demonstrated the use of a simple and rapid dot-ELISA
based on the TB-55 mAb for the direct detection of a
circulating Mycobacterium antigen in sera of pulmo-
nary TB [19]. The technical aspects of the dot-ELISA
can be performed very simply and the staff of a single
laboratory can easily handle large number of serum
specimens. In addition, the reagents used in the assay
have shelf life of more than 2 years, and more
importantly, the assay is reproducible. The test can
be used for the initial diagnosis of extra-pulmonary
TB such as tuberculous peritonitis, meningitis, lym-
phadenitis, genitourinary tract, Pott’s disease, arthritis
and miliary TB. In the present study, we evaluated the
sensitivity and specificity of the dot-ELISA in patients
with extra-pulmonary TB and in a large number of
patients with pulmonary TB. The reported overall high
degree of sensitivity (88%) was similar to that
reported in our previous study [19]. Moreover, all
samples showing false-negative results using the dot-
ELISA were tested using the more sensitive Western
blot and the 55-kDa antigen was detected in all
(100%) false-negative samples. The dot-ELISA test
showed few false-positive results among healthy
individuals (4%) and the selected control group of
patients with non-tuberculous diseases (3%) resulting
in a high degree of specificity (97%). This degree of
specificity was slightly higher than that (93%)
previously reported of the test [19]. The false-positive
reactions in countries where TB is endemic will
diminish the utility of any assay. Any new test should
have a specificity of N90%, otherwise there will be
significant over-treatment [24]. It is clear that our
assay can be used in populations characterized by a
high prevalence of TB. As all selected patients with
non-tuberculous diseases in our study were sputum
negative, only radiographs and clinical symptoms
were used for their diagnosis. Therefore, it is possible
that a concurrent TB infection could also be present in
some of these patients, diagnosed with circulating
antigen detection, i.e., showing false positives. How-
ever, a large number of different controls still required
ascertaining the specificity of the test. Hopefully the
high degree of specificity of the test will not be
changed. In conclusion, we have identified of the TB-
55 mAb target antigen in ascitic fluid, CSF, serum and
lymph node tissue specimens. Mycobacterium antigen
detection using dot-ELISA is sensitive, specific, rapid
and cost effective, and could find practical application
for laboratory diagnosis of pulmonary and extra-
pulmonary TB, even in the laboratories with limited
resources and limited technical expertise. Hence, we
recommend this method as a routine test for the early
and rapid diagnosis of TB in populations characterized
by a high prevalence of TB. Further studies regarding
the detection of the TB circulating antigen before and
after treatment of extra-pulmonary TB infected
patients will be performed.
Acknowledgement
The authors would like to thank Dr. Khaled Zalata,
Pathology Department, Faculty of Medicine, Man-
soura University for his kind assistance.
References
[1] Philip Wand BS. Laboratory role in tuberculosis control. Wisc
Med J 2003;102:31–4.
[2] Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC.
Consensus statement. Global burden of tuberculosis: estimated
incidence, prevalence, and mortality. WHO Global Surveil-
lance and Monitoring Project. JAMA 1999;282:677–86.

A.M. Attallah et al. / Clinica Chimica Acta 356 (2005) 58–66 65
[3] Martin EM, Sandra MA, Inger B, Ottenhoff HM, Peter A. Use
of ESAT-6 and CFP-10 antigens for diagnosis of extra-
pulmonary tuberculosis. J Infect Dis 2001;183:175–6.
[4] Liberato IR, de Albuquerque MF, Campelo AR, de Melo HR.
Characteristics of pulmonary tuberculosis in HIV seropositive
and seronegative patients in a Northeastern region of Brazil.
Rev Soc Bras Med Trop 2004;37:46–50.
[5] Kidane D, Olobo JO, Habte A, Negesse Y, Aseffa A, Abate G,
et al. Identification of the causative organism of tuberculous
lymphadenitis in Ethiopia by PCR. J Clin Microbiol 2002;
40:4230–4.
[6] Hiraki A, Aoe K, Eda R, Maeda T, Murakami T, Sugi K, et al.
Comparison of six biological markers for the diagnosis of
tuberculous pleuritis. Chest 2004;125:987–9.
[7] Marmor M, Parnes N, Dekel S. Tuberculosis infection
complicating total knee arthroplasty: report of 3 cases and
review of the literature. J Arthroplasty 2004;19:397–400.
[8] N’dri Oka D, Varlet G, Cowppli-Bony P, Haidara A, Ba Zeze
V. Diagnosis and treatment of extensive vertebral tuberculosis.
Rev Neurol 2004;160:419–23.
[9] Chavhan GB, Hira P, Rathod K, Zacharia TT, Chawla A,
Badhe P, et al. Female genital tuberculosis: hysterosalpingo-
graphic appearances. Br J Radiol 2004;77:164–9.
[10] Sutlas PN, Unal A, Forta H, Senol S, Kirbas D. Tuberculous
meningitis in adults: review of 61 cases. Infection 2003;
31:387–91.
[11] Thwaites GE, Chau TT, Farrar JJ. Improving the bacterio-
logical diagnosis of tuberculous meningitis. J Clin Microbiol
2004;42:378–9.
[12] Vardareli E, Kebapci M, Saricam T, Pasaoglu O, Acikalin M.
Tuberculous peritonitis of the wet ascitic type: clinical features
and diagnostic value of image-guided peritoneal biopsy. Dig
Liver Dis 2004;36:199–204.
[13] Sabetay C, Enache D, Plesea E, Zaharia B, Stoica A, Rosca A,
et al. Intestinal tuberculosis in children: differential diagnosis
and treatment. Chirurgia 2000;95:179–91.
[14] Gqlgqn EM, Bqlent AM, Gqlden AM, Mehtap TM. Imaging
of extrapulmonary tuberculosis. Radiographics 2000;20:
471–88.
[15] Walsh A, McNerney R. Guidelines for establishing trials of
new tests to diagnose tuberculosis in endemic countries. Int J
Tuberc Lung Dis 2004;8:609–13.
[16] Banerjee S, Gupta S, Kumar S, Shrikhande AV, Reddy MV,
Harinath BC. Seroreactivity of 31 kDa and 41 kDa Myco-
bacterial secretory proteins isolated from culture filtrate in
extra pulmonary tuberculosis. Indian J Pathol Microbiol
2003;46:261–4.
[17] Khomenko AG, Bayensky AV, Chernousova LN, Kulikov-
skaya NV, Demianenko NV, Litvinov VI. Serodiagnosis of
tuberculosis: detection of Mycobacterial antibodies and anti-
gens. Tuberc Lung Dis 1996;77:510–5.
[18] Stavri H, Moldovan O, Mihaltanm F, Banica D, Doyle RJ.
Rapid dot sputum and serum assay in pulmonary tuberculosis.
J Microbiol Methods 2003;52:285–96.
[19] Attallah AM, Abdel Malak CA, Ismail H, El-Saggan AH,
Omran MM, Tabll AA. Rapid and simple detection of a
Mycobacterium tuberculosis circulating antigen in serum
using dot-ELISA for field diagnosis of pulmonary tuber-
culosis. J Immunoassay Immunochem 2003;24:73–87.
[20] Singh KK, Muralidhar M, Kumar A, Chattopadhyaya TK,
Kapila K, Singh MK, et al. Comparison of in house
polymerase chain reaction with conventional techniques for
the detection of Mycobacterium tuberculosis DNA in
granulomatous lymphadenopathy. J Clin Pathol 2000;
53:355–61.
[21] Pottumarthy S, Wells VC, Morris AJ. A comparison of seven
tests for serological diagnosis of tuberculosis. J Clin Microbiol
2000;38:2227–31.
[22] Rasolofo V, Chanteau S. Field evaluation of rapid tests for
tuberculosis diagnosis. J Clin Microbiol 1999;37:4201.
[23] Ratanasuwan W, Kreiss JK, Nolan CM, Schaeffler BA,
Suwanagool S, Tunsupasawasdikul S, et al. Evaluation of
the MycoDot test for the diagnosis of tuberculosis in HIV
seropositive and seronegative patients. Int J Tuberc Lung Dis
1997;1:259–64.
[24] Pereira Arias-Bouda LM, Kuijper S, van Deutekom H, van
Gijlswijk R, Pekel I, Jansen HM, et al. Enzyme-linked
immunosorbent assays using immune complexes for the
diagnosis of tuberculosis. J Immunol Methods 2003;283:
115–24.
[25] Pereira Arias-Bouda LM, Nguyen LN, Ho LM, Kuijper S,
Jansen HM, Kolk AHJ. Development of antigen detection
assay for diagnosis of tuberculosis using sputum samples.
J Clin Microbiol 2000;38:2278–83.
[26] Ng TT, Strang JI, Wilkins EG. Serodiagnosis of pericardial
tuberculosis. Q J Med 1995;88:317–20.
[27] Nair ER, Banerjee S, Kumar S, Reddy MV, Harinath BC.
Purification and characterization of a 31-kDa Mycobacterial
excretory-secretory antigenic protein with a diagnostic poten-
tial in pulmonary TB. Indian J Chest Dis Allied Sci 2001;
43:81–90.
[28] Wadee AA, Boting L, Reddy SG. Antigen capture assay for
detection of a 43-Kilodalton Mycobacterium tuberculosis
antigen. J Clin Microbiol 1990;28:2786–91.
[29] Radhakrishnan VV, Mathai AA. Dot-immunobinding assay for
the laboratory diagnosis of tuberculous meningitis and its
comparison with enzyme-linked immunosorbent assay. J Appl
Bacteriol 1991;71:428–33.
[30] Sumi MG, Mathai A, Sarada C, Radhakrishnan VV. Rapid
diagnosis of tuberculous meningitis by a dot-immunobinding
assay to detect Mycobacterial antigen in cerebrospinal fluid
specimens. J Clin Microbiol 1999;37:3925–7.
[31] Aggarwal P, Wali JP, Singh S, Handa R, Wig N, Biswas A. A
clinico-bacteriological study of peripheral tuberculous lym-
phadenitis. J Assoc Physicians India 2001;49:808–12.
[32] Ashok M, Neelam K, Beena KR. Immunohistochemical
detection of Mycobacterial antigen in tuberculous lymphade-
nitis. Indian J Tuberc 2002;49:213–6.
[33] Lenka MP, Lan NN, Ly MH, Sjoukje K, Henk MJ, Arend HK.
Development of antigen detection assay for diagnosis of
tuberculosis using sputum samples. J Clin Microbiol 2000;
38:2278–83.
[34] Srivastava KL, Bansal M, Gupta S, Srivastava R, Kapoor RK,
Wakhlu I, et al. Diagnosis of tuberculous meningitis by
A.M. Attallah et al. / Clinica Chimica Acta 356 (2005) 58–6666
detection of antigen and antibodies in CSF and sera. Indian
Pediatr 1998;35:841–50.
[35] Mathai A, Radhakrishnan VV, Sarada C, George SM.
Detection of heat stable Mycobacterial antigen in cerebrospi-
nal fluid by dot-immunobinding assay. Neurol India 2003;
51:52–4.
[36] Sood J, Gupta OP, Narang P, Cheirmaraj K, Reddy MV,
Harinath BC. Penicillinase ELISA for detection of
tubercular antigen in tuberculosis. J Commun Dis 1991;
23:173–7.
[37] Stott DI. Immunoblotting and dot blotting. J Immunol
Methods 1989;119:153–87.