Prevention of recurrent variceal bleeding
6
Available online at www.sciencedirect.com Digestive and Liver Disease 40 (2008) 337–342 Mini-Symposium Prevention of recurrent variceal bleeding A. Berzigotti, J.C. Garc´ ıa-Pag´ an ∗ Hepatic Hemodynamic Laboratory, Liver Unit, IMD, Hospital Clinic, IDIBAPS and Ciberehd, University of Barcelona, C. Villarroel 170, 08036 Barcelona, Spain Received 3 December 2007; accepted 4 December 2007 Available online 4 March 2008 Abstract Patients surviving a first episode of variceal bleeding have a risk of over 60% of experiencing recurrent haemorrhages within 1 year from the index episode. Because of this, all patients surviving a variceal bleeding should receive active treatments for the prevention of rebleeding. -Blockers ± isosorbide-5-mononitrate and band ligation are effective in preventing recurrent bleeding and both can be used. Combination of -blockers ± isosorbide-5-mononitrate and band ligation may be the best treatment to prevent rebleeding but more studies are needed to confirm this issue. In patients with recurrent variceal bleeding despite appropriate medical and endoscopic treatment, transjugular intrahepatic porto-systemic shunt is highly effective in controlling bleeding. The efficacy is not significantly different from that of shunt surgery (distal splenorenal shunt or 8 mm H-graft shunt), especially since the introduction of polytetrafluoroethylene-covered stents. Therefore, in this situation, transjugular intrahepatic porto-systemic shunt using polytetrafluoroethylene stents should be the treatment of choice. © 2008 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All rights reserved. Keywords: -blockers; Endoscopic bandi ligation; Transjugular intrahepatic porto-systemic shunt; Variceal rebleeding Patients surviving a first episode of variceal bleeding have a risk of over 60% of experiencing recurrent haemorrhages within 1 year from the index episode. Because of this, all patients surviving a variceal bleeding should receive active treatments for the prevention of rebleeding [1]. Available treatments for preventing variceal rebleeding include pharmacological therapy, endoscopic therapy, TIPS and surgical shunting. 1. Pharmacological treatment Pharmacological therapy is aimed at reducing portal pres- sure, which is the main pathophysiologic factor determining variceal bleeding. Portal pressure can be reduced either by reducing porto-collateral blood flow, or by reducing intra- hepatic resistance, or both. Non-selective -blockers are the first line pharmacologi- cal therapy for the prevention of rebleeding [1]. They decrease portal pressure by decreasing porto-collateral blood-flow, ∗ Corresponding author. Fax: +34 93 227 9856. E-mail address: [email protected] (J.C. Garc´ ıa-Pag´ an). through a blockade of cardiac -1 receptors, leading to a decrease of cardiac output, and of vascular -2 receptors, which induces splanchnic vasoconstriction. Several meta-analyses have consistently found a marked benefit of -blockers showing a reduction in rebleeding rate from 63% in controls to 42% in treated patients [2]. Notably, -blockers also induce a significant decrease of overall mor- tality from 27% to 20% [2] and of mortality from bleeding [3]. According to the available data, the number needed to be treated (NNT) to prevent an episode of rebleeding by -blockers is 5 and the NNT to avoid a death is 14 [2]. -Blockers have been compared with endoscopic variceal sclerotherapy in the prevention of rebleeding. No significant differences were found either for rebleeding or for mortality but side effects were significantly less frequent and severe with -blockers [2]. The combination of propranolol or nadolol plus isosorbide-5-mononitrate (IMN) enhances the reduction of portal pressure induced by non-selective -blockers [4]. There are only two studies comparing IMN associated with propranolol [5] or nadolol [6] vs. the corresponding -blocker alone, in the prevention of rebleeding. One of these studies showed significant benefit of the pharmacological associa- 1590-8658/$34 © 2008 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.dld.2007.12.003
Transcript of Prevention of recurrent variceal bleeding

A
t�ocpss©
K
awpt
ia
1
svrh
cp
1d
Available online at www.sciencedirect.com
Digestive and Liver Disease 40 (2008) 337–342
Mini-Symposium
Prevention of recurrent variceal bleedingA. Berzigotti, J.C. Garcıa-Pagan ∗
Hepatic Hemodynamic Laboratory, Liver Unit, IMD, Hospital Clinic, IDIBAPS and Ciberehd,University of Barcelona, C. Villarroel 170, 08036 Barcelona, Spain
Received 3 December 2007; accepted 4 December 2007Available online 4 March 2008
bstract
Patients surviving a first episode of variceal bleeding have a risk of over 60% of experiencing recurrent haemorrhages within 1 year fromhe index episode. Because of this, all patients surviving a variceal bleeding should receive active treatments for the prevention of rebleeding.-Blockers ± isosorbide-5-mononitrate and band ligation are effective in preventing recurrent bleeding and both can be used. Combinationf �-blockers ± isosorbide-5-mononitrate and band ligation may be the best treatment to prevent rebleeding but more studies are needed toonfirm this issue. In patients with recurrent variceal bleeding despite appropriate medical and endoscopic treatment, transjugular intrahepatic
orto-systemic shunt is highly effective in controlling bleeding. The efficacy is not significantly different from that of shunt surgery (distalplenorenal shunt or 8 mm H-graft shunt), especially since the introduction of polytetrafluoroethylene-covered stents. Therefore, in thisituation, transjugular intrahepatic porto-systemic shunt using polytetrafluoroethylene stents should be the treatment of choice.2008 Editrice Gastroenterologica Italiana S.r.l. Published by Elsevier Ltd. All rights reserved.
c porto-
tdw
bf�t[b�
sdbw
eywords: �-blockers; Endoscopic bandi ligation; Transjugular intrahepati
Patients surviving a first episode of variceal bleeding haverisk of over 60% of experiencing recurrent haemorrhagesithin 1 year from the index episode. Because of this, allatients surviving a variceal bleeding should receive activereatments for the prevention of rebleeding [1].
Available treatments for preventing variceal rebleedingnclude pharmacological therapy, endoscopic therapy, TIPSnd surgical shunting.
. Pharmacological treatment
Pharmacological therapy is aimed at reducing portal pres-ure, which is the main pathophysiologic factor determiningariceal bleeding. Portal pressure can be reduced either byeducing porto-collateral blood flow, or by reducing intra-epatic resistance, or both.
Non-selective �-blockers are the first line pharmacologi-al therapy for the prevention of rebleeding [1]. They decreaseortal pressure by decreasing porto-collateral blood-flow,
∗ Corresponding author. Fax: +34 93 227 9856.E-mail address: [email protected] (J.C. Garcıa-Pagan).
ipTpas
590-8658/$34 © 2008 Editrice Gastroenterologica Italiana S.r.l. Published by Elseoi:10.1016/j.dld.2007.12.003
systemic shunt; Variceal rebleeding
hrough a blockade of cardiac �-1 receptors, leading to aecrease of cardiac output, and of vascular �-2 receptors,hich induces splanchnic vasoconstriction.Several meta-analyses have consistently found a marked
enefit of �-blockers showing a reduction in rebleeding raterom 63% in controls to 42% in treated patients [2]. Notably,-blockers also induce a significant decrease of overall mor-
ality from 27% to 20% [2] and of mortality from bleeding3]. According to the available data, the number needed toe treated (NNT) to prevent an episode of rebleeding by-blockers is 5 and the NNT to avoid a death is 14 [2].
�-Blockers have been compared with endoscopic varicealclerotherapy in the prevention of rebleeding. No significantifferences were found either for rebleeding or for mortalityut side effects were significantly less frequent and severeith �-blockers [2].The combination of propranolol or nadolol plus
sosorbide-5-mononitrate (IMN) enhances the reduction ofortal pressure induced by non-selective �-blockers [4].
here are only two studies comparing IMN associated withropranolol [5] or nadolol [6] vs. the corresponding �-blockerlone, in the prevention of rebleeding. One of these studieshowed significant benefit of the pharmacological associa-vier Ltd. All rights reserved.
338 A. Berzigotti, J.C. Garcıa-Pagan / Digestive and Liver Disease 40 (2008) 337–342
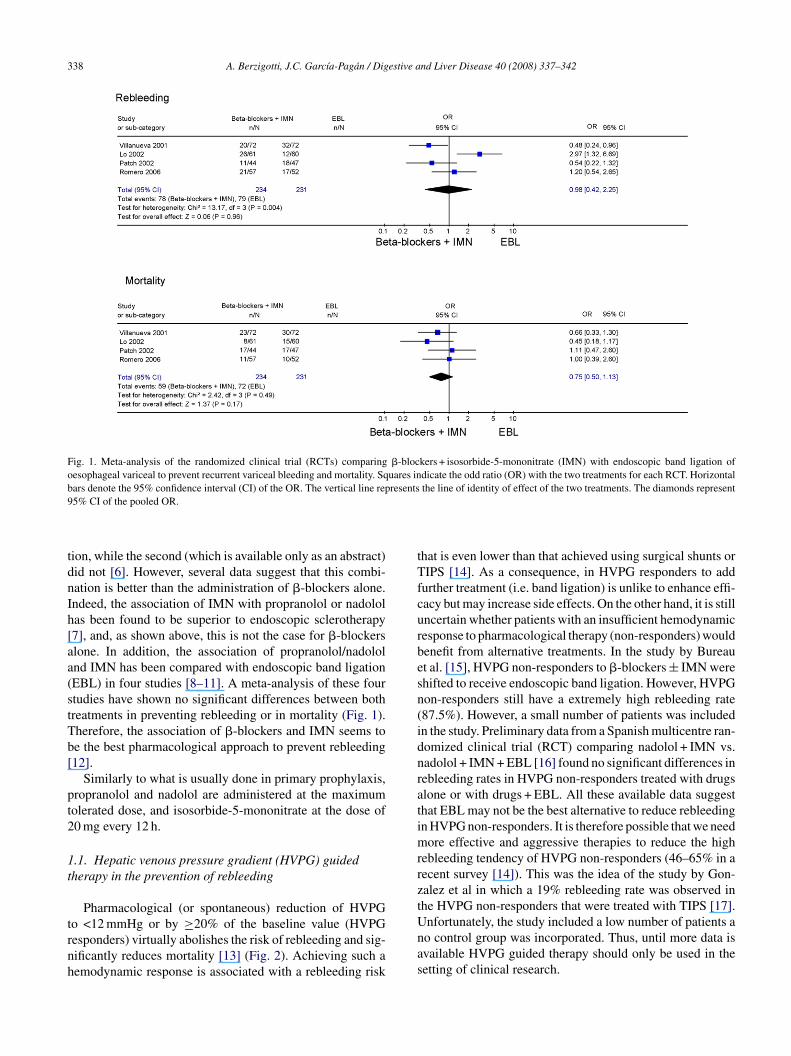
Fig. 1. Meta-analysis of the randomized clinical trial (RCTs) comparing �-blockers + isosorbide-5-mononitrate (IMN) with endoscopic band ligation ofoesophageal variceal to prevent recurrent variceal bleeding and mortality. Squares indicate the odd ratio (OR) with the two treatments for each RCT. Horizontalb resents9
tdnIh[aa(stTb[
pt2
1t
trnh
tTfcurbesn(idnratimrrzt
ars denote the 95% confidence interval (CI) of the OR. The vertical line rep5% CI of the pooled OR.
ion, while the second (which is available only as an abstract)id not [6]. However, several data suggest that this combi-ation is better than the administration of �-blockers alone.ndeed, the association of IMN with propranolol or nadololas been found to be superior to endoscopic sclerotherapy7], and, as shown above, this is not the case for �-blockerslone. In addition, the association of propranolol/nadololnd IMN has been compared with endoscopic band ligationEBL) in four studies [8–11]. A meta-analysis of these fourtudies have shown no significant differences between bothreatments in preventing rebleeding or in mortality (Fig. 1).herefore, the association of �-blockers and IMN seems toe the best pharmacological approach to prevent rebleeding12].
Similarly to what is usually done in primary prophylaxis,ropranolol and nadolol are administered at the maximumolerated dose, and isosorbide-5-mononitrate at the dose of0 mg every 12 h.
.1. Hepatic venous pressure gradient (HVPG) guidedherapy in the prevention of rebleeding
Pharmacological (or spontaneous) reduction of HVPG
o <12 mmHg or by ≥20% of the baseline value (HVPGesponders) virtually abolishes the risk of rebleeding and sig-ificantly reduces mortality [13] (Fig. 2). Achieving such aemodynamic response is associated with a rebleeding riskUnas
the line of identity of effect of the two treatments. The diamonds represent
hat is even lower than that achieved using surgical shunts orIPS [14]. As a consequence, in HVPG responders to add
urther treatment (i.e. band ligation) is unlike to enhance effi-acy but may increase side effects. On the other hand, it is stillncertain whether patients with an insufficient hemodynamicesponse to pharmacological therapy (non-responders) wouldenefit from alternative treatments. In the study by Bureaut al. [15], HVPG non-responders to �-blockers ± IMN werehifted to receive endoscopic band ligation. However, HVPGon-responders still have a extremely high rebleeding rate87.5%). However, a small number of patients was includedn the study. Preliminary data from a Spanish multicentre ran-omized clinical trial (RCT) comparing nadolol + IMN vs.adolol + IMN + EBL [16] found no significant differences inebleeding rates in HVPG non-responders treated with drugslone or with drugs + EBL. All these available data suggesthat EBL may not be the best alternative to reduce rebleedingn HVPG non-responders. It is therefore possible that we need
ore effective and aggressive therapies to reduce the highebleeding tendency of HVPG non-responders (46–65% in aecent survey [14]). This was the idea of the study by Gon-alez et al in which a 19% rebleeding rate was observed inhe HVPG non-responders that were treated with TIPS [17].
nfortunately, the study included a low number of patients ao control group was incorporated. Thus, until more data isvailable HVPG guided therapy should only be used in theetting of clinical research.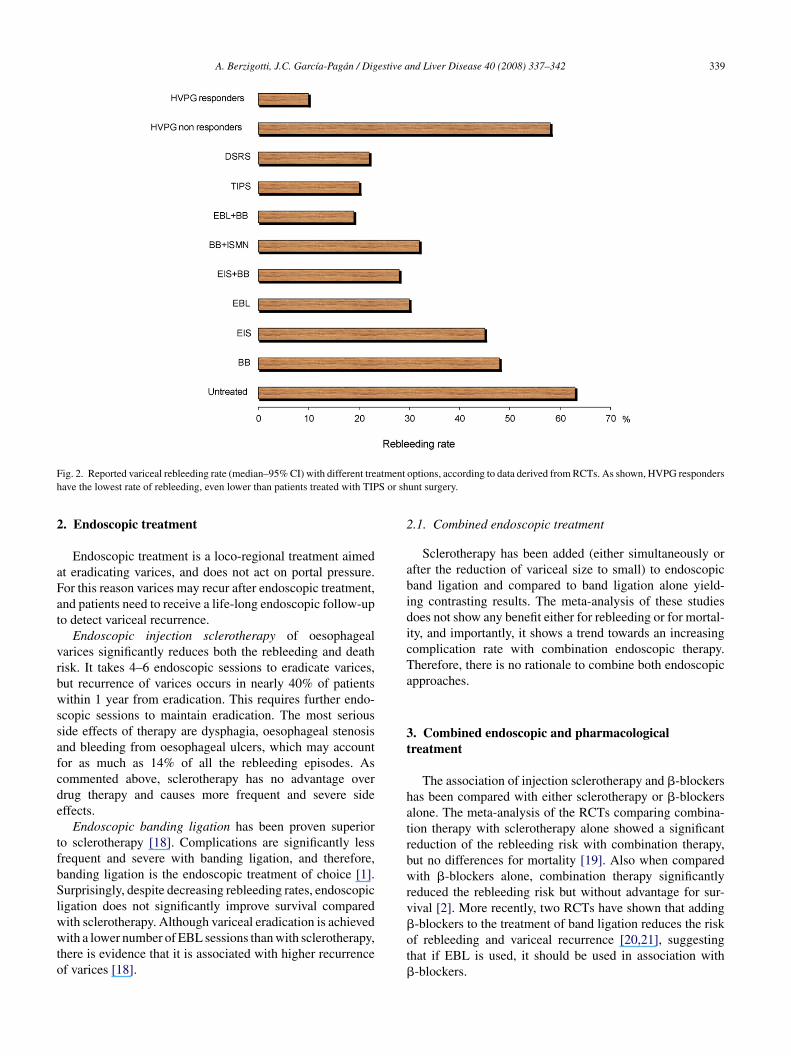
A. Berzigotti, J.C. Garcıa-Pagan / Digestive and Liver Disease 40 (2008) 337–342 339
F atmenth S or sh
2
aFat
vrbwssafcde
tfbSlwwto
2
abidicTa
3t
hatrbwrv
ig. 2. Reported variceal rebleeding rate (median–95% CI) with different treave the lowest rate of rebleeding, even lower than patients treated with TIP
. Endoscopic treatment
Endoscopic treatment is a loco-regional treatment aimedt eradicating varices, and does not act on portal pressure.or this reason varices may recur after endoscopic treatment,nd patients need to receive a life-long endoscopic follow-upo detect variceal recurrence.
Endoscopic injection sclerotherapy of oesophagealarices significantly reduces both the rebleeding and deathisk. It takes 4–6 endoscopic sessions to eradicate varices,ut recurrence of varices occurs in nearly 40% of patientsithin 1 year from eradication. This requires further endo-
copic sessions to maintain eradication. The most seriouside effects of therapy are dysphagia, oesophageal stenosisnd bleeding from oesophageal ulcers, which may accountor as much as 14% of all the rebleeding episodes. Asommented above, sclerotherapy has no advantage overrug therapy and causes more frequent and severe sideffects.
Endoscopic banding ligation has been proven superioro sclerotherapy [18]. Complications are significantly lessrequent and severe with banding ligation, and therefore,anding ligation is the endoscopic treatment of choice [1].urprisingly, despite decreasing rebleeding rates, endoscopic
igation does not significantly improve survival compared
ith sclerotherapy. Although variceal eradication is achievedith a lower number of EBL sessions than with sclerotherapy,here is evidence that it is associated with higher recurrencef varices [18].
�ot�
options, according to data derived from RCTs. As shown, HVPG respondersunt surgery.
.1. Combined endoscopic treatment
Sclerotherapy has been added (either simultaneously orfter the reduction of variceal size to small) to endoscopicand ligation and compared to band ligation alone yield-ng contrasting results. The meta-analysis of these studiesoes not show any benefit either for rebleeding or for mortal-ty, and importantly, it shows a trend towards an increasingomplication rate with combination endoscopic therapy.herefore, there is no rationale to combine both endoscopicpproaches.
. Combined endoscopic and pharmacologicalreatment
The association of injection sclerotherapy and �-blockersas been compared with either sclerotherapy or �-blockerslone. The meta-analysis of the RCTs comparing combina-ion therapy with sclerotherapy alone showed a significanteduction of the rebleeding risk with combination therapy,ut no differences for mortality [19]. Also when comparedith �-blockers alone, combination therapy significantly
educed the rebleeding risk but without advantage for sur-ival [2]. More recently, two RCTs have shown that adding
-blockers to the treatment of band ligation reduces the riskf rebleeding and variceal recurrence [20,21], suggestinghat if EBL is used, it should be used in association with-blockers.
3 estive a
htatrctaw
omc
4(
swtiTif
tebeswmp
[HfrcciswCeilwttrtt
otsss
oc
5s
5
iistba(ivogNorpp
a
ulpvTwi
crra
5
b
40 A. Berzigotti, J.C. Garcıa-Pagan / Dig
More recently, a RCT, still published as an abstract [16],as evaluated whether EBL may improve the efficacy ofhe combined administration of nadolol + IMN. In this study,lthough adding band ligation to nadolol plus IMN was showno be superior to nadolol + IMN alone in preventing varicealebleeding, no significant differences were observed whenonsidering rebleeding episodes of any cause. This was dueo a greater number of ulcer-related bleeding in the treatmentrm including banding. In addition, no difference in survivalas observed.Altogether these results emphasize that the combination
f the best endoscopic treatment (EBL) and the best phar-acological treatment (�-blockers + IMN) may be the best
hoice, but this should be further evaluated.
. Transjugular intrahepatic porto-systemic shuntTIPS) and surgical shunts
TIPS has evolved as an means of decompressing portalystem alternative to shunt surgery. TIPS has been comparedith sclerotherapy and with banding ligation in several RCT
o prevent variceal rebleeding [22]; the results of the major-ty of published studies show rebleeding rates of 9–23% forIPS and of 21–66% for endoscopic treatment, demonstrat-
ng consistently that TIPS is superior to endoscopic therapyor the prevention of rebleeding.
Similarly, TIPS has also been shown to be superior tohe combination of IMN and propranolol [23]. However, asxpected, the very high effectiveness in preventing recurrentleeding is associated with a marked increase in the risk ofncephalopathy, and no benefit on survival. For these rea-ons, TIPS is regarded as a salvage therapy for those patientsho bleed despite adequate medical and endoscopic treat-ent. Surgery is the other possible alternative to treat these
atients.TIPS has been compared with surgical shunts in two RCTs
24,25]. In the first it was compared with 8 mm portocaval-graft shunt [24]. A significantly lower rebleeding rate was
ound with the surgical shunt. Significantly more patientsequired liver transplant in the TIPS group than in the surgi-al shunt group. There was no difference in mortality. Theomposite endpoint of “failures” which included rebleed-ng, shunt thrombosis, deaths, and need for transplant, wasignificantly higher for the TIPS. In the second trial TIPSas compared with the distal splenorenal shunt (DSRS) inhild’s class A and B patients [25]. No significant differ-nces in rebleeding rate (5.5% in the DSRS group, and 9%n the TIPS group), incidence of hepatic encephalopathy,iver transplantation or mortality was found. These resultsere obtained with a significant higher reintervention rate in
he TIPS group (82%), that was performed with bare stents,
han in the DSRS group (11%). However, a multicentre RCTeported much lower obstruction and reintervention rates withhe use of polytetrafluoroethylene (PTFE)-covered stents,hat was associated with lower rates of recurrent bleedingfpiR
nd Liver Disease 40 (2008) 337–342
r ascites without increased the incidence of encephalopa-hy, than with the use of bare stents [26]. These resultsuggest that the small disadvantage of TIPS vs. surgicalhunt would be overcome by the use of PTFE-coveredtents.
We recommend TIPS using PTFE stents as the treatmentf choice for medical and endoscopic failure in patients withirrhosis.
. Prevention of rebleeding from portal hypertensiveources other than oesophageal varices
.1. Gastric varices
The best treatment to prevent gastric variceal rebleed-ng is not well defined, since this condition has a lowncidence. Type 1 gastric varices (GOV 1) are an exten-ion of oesophageal varices along the lesser curvature ofhe stomach, and consequently, their management shoulde the same as for oesophageal varices. Very few datare available on the treatment of isolated gastric varicesIGV1) and fundal gastro-oesophageal varices (GOV 2). Its accepted that when IGV 1 are due to isolated splenicein thrombosis splenectomy should be performed. In allther situations, evidence is poor. For acute bleeding fromastric varices, endoscopic variceal obturation (EVO) with-butyl-cyanoacrylate, isobutyl-2-cyanoacrylate (bucrylate)r thrombin has been shown to be more effective than scle-otherapy or EBL both for the control of bleeding and for therevention of rebleeding [27–29]. Therefore, these agents arereferred in the endoscopic therapy of fundal varices.
In clinical practice, non-selective �-blockers are usuallydded to EVO for the prevention of rebleeding.
Several papers demonstrated the effectiveness of TIPS inncontrolled bleeding from gastric varices. In a recently pub-ished RCT [30], TIPS proved more effective than EVO inreventing rebleeding from gastric varices with similar sur-ival and frequency of complications, despite the fact thatIPS stents were uncovered, and rebleeding rate after TIPSas much higher than previously reported, suggesting an
naccurate TIPS follow-up.Recent AASLD practice guidelines [12] advise that PTFE-
overed TIPS can be recommended for the prevention of theebleeding from gastric varices in patients in whom bleedingecurs despite endoscopic and pharmacological therapy, evenfter a single failure has occurred.
.2. Portal hypertensive gastropathy (PHG)
Prevention of recurrent bleeding from PHG should beased on non-selective �-blockers, at the same dosage as
or treating oesophageal varices [31]. Adequate iron sup-lementation may be useful to prevent or correct chronicron-deficient anaemia in patients with severe PHG [31].are patients that have repeated severe bleeding from
estive a
Penhc
CN
A
IM
R
[
[
[
[
[
[
[
[
[
[
A. Berzigotti, J.C. Garcıa-Pagan / Dig
HG despite pharmacological therapy, may benefit fromndoscopic ablation, either by argon plasma coagulation,eodymium:yttrium-aluminum-garnet (Nd:YAG) laser, oreater probe. If this is not feasible or fails, TIPS may beonsidered as an alternative therapy.
Practice points
• All patients surviving a bleeding episodeshould be treated to prevent rebleeding.
• �-Blockers ± IMN, band ligation or bothshould be used for prevention of recurrentbleeding.
• In patients who rebleed from oesophagealor gastric varices despite optimal medicaland/or endoscopic secondary prophylaxis,TIPS using PTFE-covered stents is highlyeffective.
Research agenda
• Further evaluation of the role of the combina-tion of �-blockers ± IMN plus EBL preventingvariceal rebleeding.
• Identify patients with a high risk of medicaland endoscopic treatment failure to evalu-ate the efficacy of applying more aggressiveapproaches (i.e. TIPS) before failure.
• Evaluate the role of targeting treatmentsaccording with baseline HVPG or its responseto pharmacological treatments.
onflict of interest statementone declared.
cknowledgments
This work was supported in part by grants from thenstituto de Salud Carlos III (PI 04/0655, PI 06/0623) and
inisterio de Educacion y Ciencia (SAF n◦ 07/61298).
eferences
[1] de Franchis R. Evolving consensus in portal hypertension report ofthe baveno IV consensus workshop on methodology of diagnosis andtherapy in portal hypertension. J Hepatol 2005;1:167–76.
[
nd Liver Disease 40 (2008) 337–342 341
[2] D’Amico G, Pagliaro L, Bosch J. Pharmacological treatment ofportal hypertension: an evidence-based approach. Semin Liver Dis1999;4:475–505.
[3] Bernard B, Lebrec D, Mathurin P, Opolon P, Poynard T. Beta-adrenergicantagonists in the prevention of gastrointestinal rebleeding in patientswith cirrhosis: a meta-analysis. Hepatology 1997;1:63–70.
[4] Garcia-Pagan JC, Feu F, Bosch J, Rodes J. Propranolol comparedwith propranolol plus isosorbide-5-mononitrate for portal hyperten-sion in cirrhosis. A randomized controlled study. Ann Intern Med1991;10:869–73.
[5] Gournay J, Masliah C, Martin T, Perrin D, Galmiche JP. Isosorbidemononitrate and propranolol compared with propranolol alone for theprevention of variceal rebleeding. Hepatology 2000;6:1239–45.
[6] Rosalia P, Pasta L, D’Amico G, Politi F, Vizzini G, Traina M, et al.Isosorbide mononitrate with nadolol compared to nadolol alone forprevention of recurrent bleeding in cirrhosis. A double blind placebocontrolled randomized trial. Final report. J Hepatol 2001:63A.
[7] Villanueva C, Balanzo J, Novella MT, Soriano G, Sainz S, TorrasX, et al. Nadolol plus isosorbide mononitrate compared with scle-rotherapy for the prevention of variceal rebleeding. N Engl J Med1996;25:1624–9.
[8] Villanueva C, Minana J, Ortiz J, Gallego A, Soriano G, Torras X, et al.Endoscopic ligation compared with combined treatment with nadololand isosorbide mononitrate to prevent recurrent variceal bleeding. NEngl J Med 2001;9:647–55.
[9] Patch D, Sabin CA, Goulis J, Gerunda G, Greenslade L, Merkel C,et al. A randomized, controlled trial of medical therapy versus endo-scopic ligation for the prevention of variceal rebleeding in patients withcirrhosis. Gastroenterology 2002;4:1013–9.
10] Lo GH, Chen WC, Chen MH, Hsu PI, Lin CK, Tsai WL, et al. Bandingligation versus nadolol and isosorbide mononitrate for the preven-tion of esophageal variceal rebleeding. Gastroenterology 2002;3:728–34.
11] Romero G, Kravetz D, Argonz J, Vulcano C, Suarez A, Fassio E, etal. Comparative study between nadolol and 5-isosorbide mononitratevs. endoscopic band ligation plus sclerotherapy in the prevention ofvariceal rebleeding in cirrhotic patients: a randomized controlled trial.Aliment Pharmacol Ther 2006;4:601–11.
12] Garcia-Tsao G, Sanyal AJ, Grace ND, Carey WD. Prevention andmanagement of gastroesophageal varices and variceal hemorrhage incirrhosis. Am J Gastroenterol 2007;9:2086–102.
13] D’Amico G, Garcia-Pagan JC, Luca A, Bosch J. Hepatic vein pressuregradient reduction and prevention of variceal bleeding in cirrhosis: asystematic review. Gastroenterology 2006;5:1611–24.
14] Bosch J, Garcia-Pagan J. Prevention of variceal rebleeding. Lancet2003;9361:952–4.
15] Bureau C, Peron JM, Alric L, Morales J, Sanchez J, Barange K, et al.“A la carte” treatment of portal hypertension: adapting medical therapyto hemodynamic response for the prevention of bleeding. Hepatology2002:1361–6.
16] Study group Spanish Cooperative Variceal Rebleeding. MulticenterRCT comparing drug therapy vs the combination of drug therapy plusendoscopic band ligation in the prevention of rebleeding in patientswith cirrhosis. Hepatology 2007:202A.
17] Gonzalez A, Augustin S, Perez M, Dot J, Saperas E, TomaselloA, et al. Hemodynamic response-guided therapy for prevention ofvariceal rebleeding: an uncontrolled pilot study. Hepatology 2006;4:806–12.
18] Garcia-Pagan JC, Bosch J. Endoscopic band ligation in the treat-ment of portal hypertension. Nat Clin Pract Gastroenterol Hepatol2005;11:526–35.
19] D’Amico G, Pagliaro L, Bosch J. The treatment of portal hypertension:
a meta-analytic review. Hepatology 1995;1:332–54.20] Lo GH, Lai KH, Cheng JS, Chen MH, Huang HC, Hsu PI, et al.Endoscopic variceal ligation plus nadolol and sucralfate compared withligation alone for the prevention of variceal rebleeding: a prospective,randomized trial. Hepatology 2000;3:461–5.
3 estive a
[
[
[
[
[
[
[
[
[
[
42 A. Berzigotti, J.C. Garcıa-Pagan / Dig
21] de la PJ, Brullet E, Sanchez-Hernandez E, Rivero M, Vergara M,Martin-Lorente JL, et al. Variceal ligation plus nadolol compared withligation for prophylaxis of variceal rebleeding: a multicenter trial. Hep-atology 2005;3:572–8.
22] Burroughs AK, Vangeli M. Transjugular intrahepatic portosystemicshunt versus endoscopic therapy: randomized trials for secondaryprophylaxis of variceal bleeding: an updated meta-analysis. Scand JGastroenterol 2002;3:249–52.
23] Escorsell A, Banares R, Garcia-Pagan JC, Gilabert R, Moitinho E,Piqueras B, et al. TIPS versus drug therapy in preventing varicealrebleeding in advanced cirrhosis: a randomized controlled trial. Hepa-tology 2002;2:385–92.
24] Rosemurgy AS, Serafini FM, Zweibel BR, Black TJ, Kudryk BT,Nord HJ, et al. Transjugular intrahepatic portosystemic shunt vs.small-diameter prosthetic H-graft portacaval shunt: extended follow-up of an expanded randomized prospective trial. J Gastrointest Surg2000;6:589–97.
25] Henderson JM, Boyer TD, Kutner MH, Rikkers L, Jeffers L, Abu-Elmagd K. DSRS vs TIPS for refractory variceal bleeding: a prospectiverandomized controlled trial. Hepatology 2004:725A.
26] Bureau C, Garcia-Pagan JC, Otal P, Pomier-Layrargues G, Chab-bert V, Cortez C, et al. Improved clinical outcome using
[
nd Liver Disease 40 (2008) 337–342
polytetrafluoroethylene-coated stents for tips: results of a randomizedstudy. Gastroenterology 2004;2:469–75.
27] Lo GH, Lai KH, Cheng JS, Chen MH, Chiang HT. A prospective,randomized trial of butyl cyanoacrylate injection versus band ligation inthe management of bleeding gastric varices. Hepatology 2001;5:1060–4.
28] Sarin SK, Jain AK, Jain M, Gupta R. A randomized controlled trial ofcyanoacrylate versus alcohol injection in patients with isolated fundicvarices. Am J Gastroenterol 2002;4:1010–5.
29] Tan PC, Hou MC, Lin HC, Liu TT, Lee FY, Chang FY, et al. A random-ized trial of endoscopic treatment of acute gastric variceal hemorrhage:N-butyl-2-cyanoacrylate injection versus band ligation. Hepatology2006;4:690–7.
30] Lo GH, Liang HL, Chen WC, Chen MH, Lai KH, Hsu PI,et al. A prospective, randomized controlled trial of transjugularintrahepatic portosystemic shunt versus cyanoacrylate injection inthe prevention of gastric variceal rebleeding. Endoscopy 2007;8:
679–85.31] Perez-Ayuso RM, Pique JM, Bosch J, Panes J, Gonzalez A, PerezR, et al. Propranolol in prevention of recurrent bleeding fromsevere portal hypertensive gastropathy in cirrhosis. Lancet 1991;8755:1431–4.