
Prevention of Legg-Calvé-Perthes disease
11
Prevention of LeggCalvéPerthes disease. Transphyseal NeckHead Drilling. Nuno Craveiro Lopes and Carolina Escalda. Orthopedic and Traumatologic Department, Pediatric Orthopedic Unit, Garcia de Orta Hospital, Almada, Portugal Published at Rev. Port. Ortop. Traum., 19:3, 223238, 2011 ABSTRACT Purpose It is well documented that multiple factors are involved in the pathogenesis of LeggCalvéPerthes disease (LCPD) and that several fractional and sequential ischemic episodes are necessary and that a specific sequence of chained events is needed to trigger the disease in a susceptible child. Within this context, the reinforcement of the arterial blood flow and of the venous drainage of the epiphyseal femoral head could constitute a way of avoiding the repetition of ischemic episodes thus preventing the onset of LCPD. To determine the effects of transphyseal neckhead drilling (TNHD), we have developed an experimental study and reviewed data from the cases where the procedure was used clinically. Methods Fortyfour, White New Zealand rabbits, were used. Drills from 2 to 3.5mm in diameter were used along with a specially made guide, in order to minimize trauma. There were 4 study groups: Group I – hips not operated on, used as a control. Group II – Drilling of <10% of the total growth plate area. Group III Drilling of >10% of the total growth plate area. Group IV – Metaphyseal drilling, without reaching the growth plate. Clinically, we have been using TNHD for 30 years. We reviewed 205 TNHD procedures done in 96 cases of ischemic disease of the growing hip (IDGH) and 117 cases of LeggCalvéPerthes disease (LCPD). Results We found that TNHD with the perforation of less than 10% of the growth plate area didn’t interfere with the growth of the proximal femur and induces a marked increase of epiphyseal microvascularisation, due to the formation of anastomosis between metaphyseal and epiphyseal circulation. Clinically, from the 96 IDGH patients treated with TNHD, 55 have already reached the end of growth. None have progressed to LCPD and no growth disturbances of the affected femur where observed. Studies done with Gadolinium enhanced MRI, showed patent anastomosis between the metaphyseal and epiphyseal circulations. From a group of 20 IDGH patients not subjected to TNHD, 5 on stage III, all developed LCPD, and from 15 on stage II, 3 developed LCPD. Conclusions Epidemiological data from the area of influence of our unit, comparing the incidence of LCPD before and after the implementation of the IDGH detection protocol and LCPD prevention with TNHD, have shown a decrease of LCPD cases from 8.5/100.000 to 1.8/100.000 per year, on the population less than 16 years of age. Significance We confirmed clinically what we have found experimentally: TNHD induces anastomosis of small blood vessels between metaphysis and epiphysis, thus supplementing the epiphyseal unstable supply, preventing new ischemic episodes on a IDGH patient and aborting the evolution to LCPD. INTRODUCTION The multifactorial origin of LeggCalvéPerthes disease (LCPD) is well documented [6,7,8,20,21,22,23,24,26,27,37,43]. The same is true for the existence of two or more ischemic episodes preceding the onset of the disease [3,4,7,10,21,25,38,41,43,44,49]. After more than 30 years of experimental and clinical data analysis about the initial stage of LCPD [9,10,11,12,13,14], the senior Author (NCL) verified that these episodes are symptomatic. Patients complain of pain and transient limping, and it is possible to detect those ischemic episodes with imaging techniques. The same Author has also found that those episodes represent an autonomous disease, which, if some enchained factors are present, can evolve to LCPD. The Author named this preLCPD situation, Ischemic Disease of the Growing Hip (IDGH)[15,16,17,18,19]. To clarify the pathogenesis of LCPD, the senior Author developed an animal model and analysed the data of patients treated with Transphyseal NeckHead Drilling (TNHD), in the stage of sequential ischemic episodes and initial necrosis [15,16]. Within this context, the reinforcement of the arterial blood flow and of the venous drainage of the
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Prevention of Legg-Calvé-Perthes disease

Prevention of LeggCalvéPerthes disease.Transphyseal NeckHead Drilling.Nuno Craveiro Lopes and Carolina Escalda.Orthopedic and Traumatologic Department, Pediatric Orthopedic Unit,Garcia de Orta Hospital, Almada, Portugal
Published at Rev. Port. Ortop. Traum., 19:3, 223238, 2011
ABSTRACTPurpose It is well documented that multiple factors are involved in the pathogenesis of
LeggCalvéPerthes disease (LCPD) and that several fractional and sequential ischemic episodes arenecessary and that a specific sequence of chained events is needed to trigger the disease in a susceptiblechild. Within this context, the reinforcement of the arterial blood flow and of the venous drainage of theepiphyseal femoral head could constitute a way of avoiding the repetition of ischemic episodes thuspreventing the onset of LCPD. To determine the effects of transphyseal neckhead drilling (TNHD), wehave developed an experimental study and reviewed data from the cases where the procedure was usedclinically.
Methods Fortyfour, White New Zealand rabbits, were used. Drills from 2 to 3.5mm in diameterwere used along with a specially made guide, in order to minimize trauma. There were 4 study groups:Group I – hips not operated on, used as a control. Group II – Drilling of <10% of the total growth platearea. Group III Drilling of >10% of the total growth plate area. Group IV – Metaphyseal drilling,without reaching the growth plate. Clinically, we have been using TNHD for 30 years. We reviewed205 TNHD procedures done in 96 cases of ischemic disease of the growing hip (IDGH) and 117 casesof LeggCalvéPerthes disease (LCPD).
Results We found that TNHD with the perforation of less than 10% of the growth plate areadidn’t interfere with the growth of the proximal femur and induces a marked increase of epiphysealmicrovascularisation, due to the formation of anastomosis between metaphyseal and epiphysealcirculation. Clinically, from the 96 IDGH patients treated with TNHD, 55 have already reached the endof growth. None have progressed to LCPD and no growth disturbances of the affected femur whereobserved. Studies done with Gadolinium enhanced MRI, showed patent anastomosis between themetaphyseal and epiphyseal circulations. From a group of 20 IDGH patients not subjected to TNHD, 5on stage III, all developed LCPD, and from 15 on stage II, 3 developed LCPD.
Conclusions Epidemiological data from the area of influence of our unit, comparing theincidence of LCPD before and after the implementation of the IDGH detection protocol and LCPDprevention with TNHD, have shown a decrease of LCPD cases from 8.5/100.000 to 1.8/100.000 peryear, on the population less than 16 years of age.
Significance We confirmed clinically what we have found experimentally: TNHD inducesanastomosis of small blood vessels between metaphysis and epiphysis, thus supplementing theepiphyseal unstable supply, preventing new ischemic episodes on a IDGH patient and aborting theevolution to LCPD.
INTRODUCTIONThe multifactorial origin of LeggCalvéPerthes disease (LCPD) is well documented
[6,7,8,20,21,22,23,24,26,27,37,43]. The same is true for the existence of two or more ischemic episodespreceding the onset of the disease [3,4,7,10,21,25,38,41,43,44,49]. After more than 30 years ofexperimental and clinical data analysis about the initial stage of LCPD [9,10,11,12,13,14], the seniorAuthor (NCL) verified that these episodes are symptomatic. Patients complain of pain and transientlimping, and it is possible to detect those ischemic episodes with imaging techniques. The same Authorhas also found that those episodes represent an autonomous disease, which, if some enchained factorsare present, can evolve to LCPD. The Author named this preLCPD situation, Ischemic Disease of theGrowing Hip (IDGH)[15,16,17,18,19].
To clarify the pathogenesis of LCPD, the senior Author developed an animal model and analysedthe data of patients treated with Transphyseal NeckHead Drilling (TNHD), in the stage of sequentialischemic episodes and initial necrosis [15,16].
Within this context, the reinforcement of the arterial blood flow and of the venous drainage of the

epiphyseal femoral head, independent from the reticular network, could constitute a way of avoiding therepetition of ischemic episodes thus preventing the onset of LCPD. The idea of supplementing theunstable epiphyseal blood flow trough the growth plate was attractive but controversial.
To determine the effects of neckhead drilling across the physeal growth plate, namely the possiblereinforcement of the epiphyseal blood flow and the repercussion on the growth of the proximal femur,the Authors have developed a second experimental study [18,19], and latter established a preventionprotocol of LCPD based on the early detection of IDGH and its treatment by TNHD.
MATERIAL AND METHODFor the first experimental model, 27 White New Zealand rabbits, seven to eight weeks old, were
used. This growth stage of the rabbit is equivalent to that of a 56 year old child. To try to reproduce themorphologic, radiological and histological aspects of LCPD, a no invasive method was used, consistingon the use of flexible splints to place the legs of the rabbits in extension and internal rotation for 6hours, promoting an effusion and secondary collapse of the retinacular vessels, without causing theirdestruction [2]. In the following day microtrauma was produced on the right hip only, using a vibratorymotor for a period of 30 seconds. This sequence was repeated twice a week [15,16].
The image data and histological examinations from 19 patients who presented signs and symptomscompatible with the existence of IDGH under risk of development of LCPD, and 17 patients withLCPD in the initial stage were analysed. These patients were treated between 1995 and 2006 withTNHD, and had samples for histological examination.
For the second experimental study to determine the effect of neckhead drilling across the physealgrowth plate, the Authors used fortyfour White New Zealand rabbits, aged between 6 and 12 weeks.Drills from 2 to 3.5mm in diameter were used along with a specially made guide, in order to minimizetrauma [18,19].
There were 4 study groups:Group I – 44 left hips. Not operated on, used as a control.Group II – 30 right hips. Drilling of <10% of the growth plate. Single drilling with 2 and 2.5mm
drills, using as an entry point the trochanter, crossing the neckhead growth plate thru the epiphysis. Theperforated area ranged in size from 6% to 10% of the total growth plate area, depending on the rabbit’sage.
Group III 7 right hips. Drilling of >10% of the growth plate. Single drilling with 3 and 3.5mmdrills, using the same technique. The perforated area ranged in size from 12% to 20% of the totalgrowth plate area.
Group IV – 7 right hips. Metaphyseal drilling. Single drilling with 2.5mm drills on the metaphysealarea of the trochanter and neck of the femur, without reaching the growth plate.
The Authors apply a TNHD procedure if there are probability of evolution to LCPD. As a guide ofthe probability of evolution to LCPD, the Authors had developed a classification of IDGH considering3 stages: Stage I, (Fig.1) represents a hip where one can identify sequel of an old ischemic episode; ithas a low probability of evolution to LCPD. Stage II, (Fig.2) shows sequel of an old episode with a newischemic episode in evolution; it is considered to have a moderate probability of evolution. Finally,stage III, (Fig.3) presenting signs of a recent episode with a new one in evolution, situation that isconsidered to have almost 100% of probability to evolve to LeggCalvéPerthes disease.
Indication for TNHD, includes a child over 5 years old presenting an ischemic episode on the MRI(IDGH Stage II or III) or a Perthes lesion on the necrotic or early fragmentation stage (Fig.4). Anotherindication for TNHD is the identification of a IDGH stage I in the opposite hip of a more than 5 yearsold patient with Perthes disease in one of the hips.
TNHD is performed with image intensifier control, with a 5mm trephine (perforated areacorrespond to less than 5% of the growth plate), over a wire guide centred on the ischemic or necroticarea. It is a low risk, 10minute procedure (Fig.5 and 6).
To identify the ischemic episodes and to detect the cases of IDGH at risk of evolution to LCPD, theAuthors have developed a screening protocol. All pediatricians and general doctors of the area ofinfluence of the hospital have been informed of the protocol and advised to send all children whopresented hip, thigh or knee pain and limping for more than one day of evolution to the emergency unit.

Fig.5 Procedure for TNHT with a 5mm trephine
Fig.6 – Sequence of the procedure. a) Wire guide positioning b)Introduction of the trephine over the wire guide reaching the subchondralbone. c) image control of the position of the trephine with flectionabdution
of the lower limb.
From January 1993 to December 1995 when we begun the implementation of the prevention
Fig.1IDGH Stage I
Irregular contour(a)Synovitis(b), thick
cartilage(c).No actual ischemia (d)
Fig.2IDGH Stage IIIrregular contour(a)
Synovitis witheffusion(b), Subchond.
ischemia(c)
Fig.3IDGH Stage III
Porosis (weakening)(a)Synovitis witheffusion(b)
Subchond. ischemia(c)
Fig.4LCPD Stage I
Dense, subchond. Fr.(a)Synovitis witheffusion(b)
Extensive necrosis(c)

protocol, the Authors have observed 123 children, with ages between 3 and 12 years, presenting apainful syndrome of the hip. The Authors did a second prospective comparative study between January1996 and December 1998, after the implementation of the preventive protocol, including 110 childrenof the same age. The study protocol included a standard clinical, radiological and laboratorialexamination to detect other diagnosis as epiphisiolysis, septic arthritis, rheuma, trauma, LCPD andother causes and on the remaining cases, it included also a first ultrasound screening to determine theexistence of criteria of probability of IDGH and a second screening using a nuclear magnetic resonanceon those cases, to detected an ischemic episode characteristic of IDGH stage II and III.
RESULTSOn the first animal model [15,16] we observed that the prolonged and repeated positioning of the
legs of the rabbit induced an intra articular pressure level sufficient to produce an ischemic episode atthe proximal femoral epiphysis. After this episode, we observed a process of rapid revascularization ofthe preserved vascular canals with repositioning of myeloid and osteoid tissues by differentiation ofendothelial cells in mesenchymal progenitor cells, without distortion of the epiphyseal structure or lossof its mechanical resistance. When a new ischemic episode was produced later on after the completionof the repairing process, all the reparative sequence was repeated again, without loss of the mechanicalresistance of the epiphysis (Fig.7). However, the repetition of an ischemic episode during thereconstruction of a previous episode, lead to an alteration of the reparative response, with osteoclastichyperactivity in the subchondral zone and formation of a distorted bone structure in the epiphysis byosteoblastic hyperactivity and creeping substitution, which leads to a mechanically weak bone structure,similar to that described in LCPD as "woven bone". In these conditions, the existence of trauma ormicrotrauma on the right hip, lead to the appearance of a subchondral pathological fracture andcollapse of the structure of the epiphysis, with formation of a true bone sequestum on that side only.This represents the initial stage of LCPD (Fig.8).
Fig.7 Experimental Model two week IDGHSubchondral weakening(a), double layerlamellae(b), normal myeloid tissue(c)
Fig.8 Experimental Model five weeks – LCPD.Subchondral fracture(a), woven bone(b) and
fibrous tissue proliferation(c)
The analysis of the image data and histological examinations from the patients has shown thatpatients where IDGH was detected presented histological signals of a recent ischemic event on theosteoid and myeloid or recent ischemia over a remodelled anterior ischemic event (Fig.9). In all the
cases where the bone samples showed profuse “woven bone” and total substitution of the myeloid byfibrous, progressed into LCPD (Fig.10). Such biopsies were consistent with failure of immediaterevascularization, as the vascular canals had collapsed.
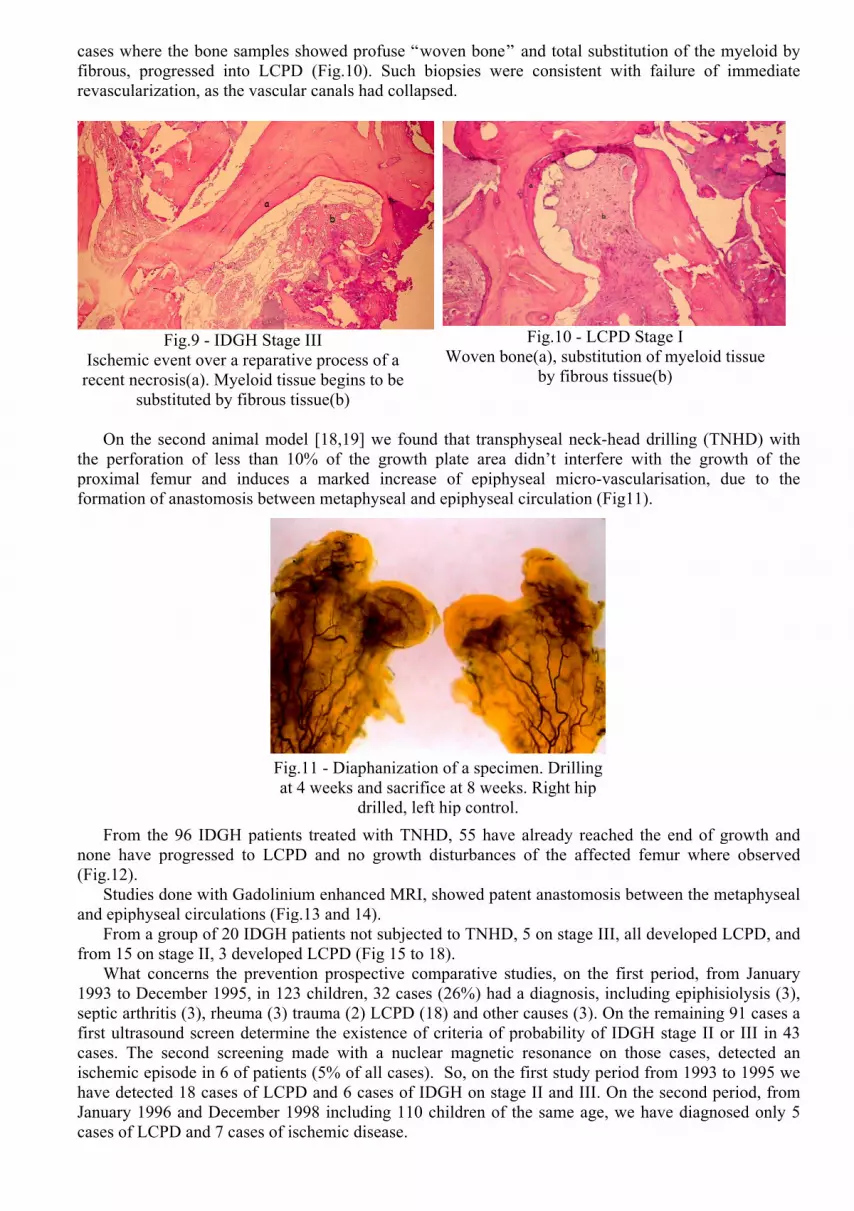
On the second animal model [18,19] we found that transphyseal neckhead drilling (TNHD) withthe perforation of less than 10% of the growth plate area didn’t interfere with the growth of theproximal femur and induces a marked increase of epiphyseal microvascularisation, due to theformation of anastomosis between metaphyseal and epiphyseal circulation (Fig11).
From the 96 IDGH patients treated with TNHD, 55 have already reached the end of growth andnone have progressed to LCPD and no growth disturbances of the affected femur where observed(Fig.12).
Studies done with Gadolinium enhanced MRI, showed patent anastomosis between the metaphysealand epiphyseal circulations (Fig.13 and 14).
From a group of 20 IDGH patients not subjected to TNHD, 5 on stage III, all developed LCPD, andfrom 15 on stage II, 3 developed LCPD (Fig 15 to 18).
What concerns the prevention prospective comparative studies, on the first period, from January1993 to December 1995, in 123 children, 32 cases (26%) had a diagnosis, including epiphisiolysis (3),septic arthritis (3), rheuma (3) trauma (2) LCPD (18) and other causes (3). On the remaining 91 cases afirst ultrasound screen determine the existence of criteria of probability of IDGH stage II or III in 43cases. The second screening made with a nuclear magnetic resonance on those cases, detected anischemic episode in 6 of patients (5% of all cases). So, on the first study period from 1993 to 1995 wehave detected 18 cases of LCPD and 6 cases of IDGH on stage II and III. On the second period, fromJanuary 1996 and December 1998 including 110 children of the same age, we have diagnosed only 5cases of LCPD and 7 cases of ischemic disease.
Fig.9 IDGH Stage IIIIschemic event over a reparative process of arecent necrosis(a). Myeloid tissue begins to be
substituted by fibrous tissue(b)
Fig.10 LCPD Stage IWoven bone(a), substitution of myeloid tissue
by fibrous tissue(b)
Fig.11 Diaphanization of a specimen. Drillingat 4 weeks and sacrifice at 8 weeks. Right hip
drilled, left hip control.

Fig.13 IDGH Stage III7 months after TNHT
Fig.14 Gadolinium enhancedMRI. Vascular anastomosis
metaphysisepiphysis
Fig.15 04/1995 IDGH Stage IIIPorosis, wider medial space
Fig.16 04/1995 IDGH Stage IIISubchondral ischemia
Fig.17 10/1995 – Lost from followup.6 months later LCPD Stage I
Fig.18 10/1995 – LCPD Stage IExtensive necrosis
Fig.12 – Evolution of a case of IDGH after TNHD. a) 10/1989 – 6 years old IDGH stage III. b)11/1989 – 6 years old, one month after TNHD. c) 9/1993 – 10 years old, 4 years after TNHD. d)04/2002 – 19 years old, 13 years after TNHD.

DISCUSSIONThe first signs on the importance of multiple ischemic episodes were brought up in experimental
research performed in dogs by Freeman [4], on rabbits by Sanchis [41] and later by Bencano[1]. Theywere able to simulate the disease through repeated, total surgical section of the vascular network to thefemoral head.
Vegter [54] through the use of intraarticular injection of serum under pressure on the hip of arabbit, demonstrated the importance of the repeated fractional necrosis, provoked by the increase ofintraarticular pressure on the onset of the disease, indicating that the probable cause of the deformity ofthe head, is a reduction of its mechanical resistance due to superposing new necrotic episodes over areconstruction process in progress.
Eyring [22], SotoHall [46], Kallio [32], Vegter [55] and Schoenecker [45]demonstrated that the invivo positioning of lower limbs in prolonged and repeated medial rotation and extension, is sufficient toincrease the joint pressure on the hip and that it reached values superior to the systolic pressure whenthere was a simultaneous intraarticular effusion, even if small.
Mckibbin [33], Inoue [33] and Catterall [7] presented histological studies performed on femoralheads of patients with LCPD. These patients revealed images of necrosis superposed to zones of boneregeneration of a prior ischemic insult, confirming the theory of the repetitive ischemic episodes in theorigin of LCPD.
Our experimental research on the hips subject to repeated posture in medial rotation and extensionshowed us that the first signs of simple necrosis to the epiphyseal nucleus appeared after repeatedpositioning on both hips and signs of LCPD only on the hips subjected to micro trauma. Those findingswhich are in accordance with the mentioned Authors, seems to confirm that the repeated ischemicevents weakens the epiphyseal bone structure and that a trauma or micro trauma is necessary to developthe subchondral fracture that begins LCPD.
Our clinical data confirmed the repetitive ischemic episode theory proposed by the mentionedAuthors, namely that there are a period of fractional and sequential ischemic episodes before the onsetof Perthes disease that leads to the fragility of the epiphyseal structure by subchondral osteoclastichyperactivity and epiphyseal abnormal osteoblastic hyperactivity; Then if a trauma or micro traumaoccurs, a subchondral fracture and epiphyseal collapse begins LCPD.
What concerns the TNHD procedure, The effect of the surgical perforation of the growth plate,have been studied by several authors in the past.[5,24,28,31,35,40,46],
These researchers observed that multiple pin hole perforations or single perforations of smalldiameter did not cause alterations of bone growth, however, the perforations of larger diameter caused asignificant delay or a complete growth arrest through the formation of a rigid bone bridge.
In our present research, we were able to determine that the central perforation of an area less than10% of the femoral neckhead growth plate area does not hinder growth. This conclusion is based onthe direct and the radiological examinations and on the statistical evaluation of the numerousparameters measured. By those data, we may even deduce that with that perforation, there was anincrease in the sphericity of the head of the femur.
The histological examination of these specimens showed normal growth plate thickness andorganization, except immediately next to the perforated area.
In agreement with other authors [5,24,54]. We observed in the histological specimens, signs that asmall caliber perforation creates a bone bridge, whose tensile strength is inferior to the mechanicalgrowth forces of the unperforated portion of the growth plate. This fact permits the progressiveelongation of the bone bridge, with a dragging and thinning effect over the borders of the growth platein the direction of the metaphysis.
Also, in agreement with such authors, we observed that the perforation of larger dimensions, leadsto a distortion of the proximal femur, such as, a shorter neck with a prominent trochanter, a verticaltilting of the neckhead growth plate and flattening of the epiphyseal nucleus.
These alterations were accompanied by a decrease in the thickness of the growth plate and a moreor less marked structural disorganization.
We noted still that the resulting growth delay and deformity was bigger when a larger perforationwas performed in younger rabbits (younger than 9 weeks of age), corresponding to a less than 5 yearold child [14,29].
The idea of improving the vascular conditions in the epiphyseal nucleus via the perforation of thefemoral neckhead growth plate is not new. Harris’s research [29], using rabbits, confirmed

histologically the penetration of cancellous bone through the perforations in the growth plate and afaster bone regeneration in the epiphyseal nucleus after bone necrosis provoked by surgical vascularsection.
Siffert’s research [45], showed histological preparation of femoral hips of rabbits, where heobserved the vascular and bone trabecular continuity between the metaphysis and the epiphysis after theperforation of the growth plate.
In our work, besides the histological confirmation of the observations performed by other Authors,we demonstrated the existence of an accentuated and constant increase of small blood vessels in theepiphysis of the head of the femur after perforation of the growth plate, which was maintained until theend of the bone growth in rabbits (26 weeks). This result was not accomplished when only themetaphyseal zone of the neck of the femur was perforated.
This increase in epiphyseal blood circulation was due to the reinforcement of the vascular networkformed through the perforation of the growth plate and not due to the hemodynamic changes on theretinacular vessels, which was not changed when compared with the Control Group.
The perforation of the femoral neckhead growth plate was first performed by Ferguson [23], as atreatment for severe LeggCalvePerthes disease in children. Those cases were done in an advancedfragmentation stage when the author did not get good responses using traditional treatment methods.The perforation of the neckhead growth plate technique, had its advocates, but was dropped when newtechniques, such as, the recentring osteotomies were developed which had better results.
The current research indicates that the neckhead drilling could be essential in the prevention ofLeggCalvePerthes Disease (LCPD) if this technique is used in the preradiological ischemic stageindicated by repetitive hip pain that can be detected through a cold spot on the nuclide or MRI bonescan [3,21,38,44,49].
In this stage, under the hemodynamic point of view, this condition is comparable to the coronaryischemic heart disease with repetitive angina that precedes a myocardial infarction [7,10,43] and theintent of the tunnelling procedure is to create a reinforcement of the blood flow similar to the onecreated in coronary bypass surgery.
Drilling can also be useful in the early treatment of the LCPD, when at the initial necrotic(condensed) stage, where it will speed up the evolution to fragmentation, as it permits penetration ofblood flow to the center of the necrotic zone and reabsorption of the sequestum by the cutting conesfrom inside to outside, as it has also been verified by the first users of this method [23]. After thefragmentation stage has started, this method is no longer useful.
The Authors have 96 patients where TNHD was applied with the diagnosis of IDGH stage II andIII, 55 of them have already reached the end of growth and no one progressed to Perthes disease orshowed growth disturbance of the proximal femur. No other complications as fractures, infections etc,was reported on those cases. Control of patency of the anastomosis using a MRI in T1 sequence withGadolinium, comproved that the anastomosis induced by the drilling procedure is a long lasting one.
A control group of 20 patients diagnosed as ischemic disease, which was not subjected to thedrilling procedure, 3 cases in 15 of Stage II developed Perthers disease (20%), and 5 cases of stage III,all developed Perthes disease.
Epidemiological data from the area of influence of our unit, comparing the incidence of LCPDbefore and after the implementation of the IDGH detection protocol and LCPD prevention with TNHD,have shown a decrease of LCPD cases from 8.5/100.000 to 1.8/100.000 per year, on the population lessthan 16 years of age.
CONCLUSIONSThe results of the first experimental model suggests the existence of a pathologic entity, prior to
LCPD, characterized by the existence of successive ischemic events at the level of the femoral proximalepiphysis, that in certain circumstances can develop into LCPD. We call this entity Ischemic Disease ofthe Growing Hip (IDGH).
The clinical study confirmed the existence of a period of fractional and sequential ischemic episodesbefore the onset of LCPD. These ischemic events lead to weakening of the epiphyseal bone structure attwo levels: subchondral cortical bone weakening by osteoclastic hyperactivity and epiphysealcancellous bone weakening by osteoblastic hyperactivity and woven bone formation. If a trauma ormicro trauma happens at that timing, then a pathologic subchondral fracture triggers the beginning ofLeggCalvéPerthes disease.

The second experimental model have shown that TNHD induces a increase ofmicrovascularization, on the epiphisis due to the formation of a bone bridge trough the growth plate,and with it, vascular structures transverse from the methaphysis to the epiphysis, creating ananastomosis between the two networks. We found that growth arrest or slowing due to the drillingprocedure is a matter of dimension; when less than 10% of the area of the growth plate is drilled, theresistance of the formed bone bridge is much less than the growth force of the remaining growth plateand growth continues normally. When the drilled area is bigger than 20%, the resistance of the bonebridge is higher than the force of the remaining growth plate and there is an arrest. In between those twonumbers some slowing of growth happens.
The Authors conclude that it is possible to identify the fractional and transitory ischemic events thatprecede the beginning of LeggCalvéPerthes disease, and to define a group of cases at risk of evolutionto LCPD. On those cases, TNHD induces anastomosis of small blood vessels between metaphysis andepiphysis, thus supplementing the epiphyseal unstable supply, preventing new ischemic episodes on aIDGH patient and aborting the evolution to LCPD.
Bibliography
1 BENCANO, A.C.; RUEDA, F.S.L.; PADRON, J.R.: Enfermedad de Perthes: MecanismoPatogenético Experimental. Rev. Ortop. Traum. 33 IB: 428433, 1989.
2 BORGSMILLER, W.K. and Cols.: The Effect of Hydrostatic Pressure in the Hip Joint onProximal Femoral Epiphyseal and metaphyseal Blood Flow. Trans. Orthop. Res. Soc., 5: 23, 1980.
3 CALVER, R.: Radionuclide Scanning in the Early Diagnosis of Perthes Disease. J. Bone JointSurg., 63B: 379, 1981.
4 CALVERT, P.T. and Cols.: Effects of Vascular Occlusion on the Femoral Head in GrowingRabbits. acta Orthop. Scand., 55: 526530, 1984.
5 CAMPBELL, C,J. and Cols.: The Effect Produced in the Cartilaginous Epiphyseal Plate ofImmature Dogs by Experimental Surgical Traumata. J. Bone Joint Surg., 41A: 12211242, 1959.
6 CATTERALL, A. and Cols.: LeggCalvéPerthe's Disease. Current Problems in Orthopaedics.Churchill Livingstone, London, 1982.
7 CATTERALL, A. and Cols.: Perthes Disease: Is the Epiphyseal Infarction Complete ? A Study ofthe Morphology in two Cases. J. Bone Joint Surg., 64B: 276281, 1982.
8 CHUNG, S.M.K.: The Arterial Supply of the Developing Proximal End of the Human Femur. J.Bone Joint Surg., 58A: 961970, 1976.
9 CRAVEIRO LOPES, N.; BETTENCOURT, P.: Doença de LeggCalvéPerthes. Novos ConceitosDiagnósticos e Terapéuticos. Rev. Ortop. Traum. IB., 11P: 3147, 1985.
10 CRAVEIRO LOPES, N.; BETTENCOURT, P.: Doença de LeggCalvéPerthes. EvoluçãoNatural de 9 Parâmetros Radiológicos em Ancas Assintomáticas e Sintomáticas. Rev. Ortop.Traum. IB., 12P: 153164, 1986.
11 CRAVEIRO LOPES, N.; BETTENCOURT, P.: Resultados do tratamento conservador nas ancascom menos de 50% do núcleo lesado e sem sinais de cabeça em risco. Rev. Ortop. Traum. IB.,13P: 3540, 1987.
12 CRAVEIRO LOPES, N.; BETTENCOURT, P.: Doença de LeggCalvéPerthes. Resultados dotratamento cirúrgico com osteotomia intertrocantérica de tríplo efeitos em ancas com sinais de“cabeça em risco”. Rev. Ortop. Traum. IB., 13P: 95105, 1987.
13 CRAVEIRO LOPES, N.; BETTENCOURT, P.: Doença de LeggCalvéPerthes. Resultado dotratamento cirúrgico com a tunelização transfisária cervicocefálica nas ancas com mais de 50%de envolvimento e sem sinais de “cabeça em risco”. Rev. Ortop. Traum. IB., 14P: 3946, 1988.
14 CRAVEIRO LOPES, N.; VASCONCELOS, F.P.; AMARAL, S.: Goniometria da anca normal.Estudo radiográfico na Criança Portuguesa. Rev. Ortop. Traum IB, 15P: 1124, 1989.
15 CRAVEIRO LOPES, N.: Modelo experimental básico para o estudo da patologia do crescimentona extremidade superior do fémur. Rev. Port. Ortop. Traum., 1:2, 199213, 1993.
16 CRAVEIRO LOPES, N.:LeggCalvéPerthes Disease after repeated extensioninternal rotationposture of the hip followed by micro trauma. An experimental study in the growing rabbit. J BoneJoint Surg [Br] Supp II; 75164, 1993.
17 CRAVEIRO LOPES, N.: Doença de LeggCalvéPerthes. Current Concept Review. Rev. Port.Ortop. Traum.,; 2:1,7579, 1994.

18 CRAVEIRO LOPES, N.: Etiopatogenia da doença de LeggCalvéPerthes. Modelo experimentalno coelho White New Zealand em crescimento. Rev Port Ortop Traum., 2:1, 8193, 1994.
19 CRAVEIRO LOPES, N.: Estudo dos efeitos da tunelização transfisária cervicocefálica do fémurcomo método para prevenir a doença de LeggCalvéPerthes. Modelo experimental no coelhoWhite New Zealand em crescimento. Ver. Port. Ortop. Traum., 2:4, 395404, 1994.
20 CROCK, H.V.: The Blood Supply of the Lower Limb Bones in Man. Ed. Livingstone Ltd,London, 1967.
21 DANIGELIS, J.A. and Cols.: 99mTcpolyphosphate Bone Imaging in LeggPerthes Disease.Radiology, 115: 407, 1975.
22 EYRING, E.J.; MURRAY, W. R.: The Effect of Joint Position oon the Pressure of intraarticularEffusion. J. Bone Joint Surg., 46A: 12351241, 1964.
23 FERGUSON, A.B.; HOWORTH, M. B.: Coxa Plana and Related Conditions at Hip. J. Bone JointSurg., 16: 781803, 1934.
24 FORD, L.T.; KEY, J.A.: A Study of Experimental Trauma to the Distal Femoral Epiphysis inRabbits. J. Bone Joint Surg., 38A: 8492, 1956.
25 FREEMAN, M.A.R.; ENGLAND, J.P.S.: Experimental Infarction of the immature canine femoralhead. Proc. R. Soc. Med., 62, 431433, 1969.
26 GAGE, J.R.; WINTER, R.B.: Avascular Necrosis of the Capital Femoral Epiphysis as aComplication of Closed Reduction of Congenital Dislocation of the Hip. J. Bone Joint Surg., 54A:373388, 1972.
27 GORE, D.R.: Iatrogenic Avascular Necrosis of the Hip in Young Children. A Review of SixCases. J. Bone Joint Surg., 56A: 493502, 1974.
28 HAAS, S.L.: Restriction of Bone Growth by Pins through the Epiphyseal Cartilaginous Plate. J.Bone Joint Surg., 32A: 338343, 1950.
29 HEIKEL, H,V,A.: On Ossification and Growth of Certain Bones of Rabbit and Man. Acta Orthop.Scand., 29: 171184, (16), 1960.
30 HENARD, D.C.; CALANDRUCCIO, R.A.: Experimental Production of Roentgenoprophic andHistological Changes in the Capital Femoral Epiphysis Following Abduction, Extension andInternal Rotation of the Hip. J. Bone Joint Surg., 52A: 600, 1970.
31 IMBERT, R.: Pathologie Expérimentale de l'appareil de croissance des os longs. Marseille Chir.,3: 581599, 1951.
32 INOUE, A. et Cols.: The pathogenesis of Perthes disease. J. Bone Joint Surg., 58B, 453461, 1976.33 KALLIO, P.: Transient Synovitis and Perthes Disease is there an Aetiological Connection?. J.
Bone Joint Surg., 68B: 808811, 1986.34 KEMP, H.B.S.: Perthes Disease in Rabbits and Puppies. Clin. Orthop. and Rel. Res., 209: 139159,
1986.35 – KLEINBERG, S.; BOCHMAN, J.: The Operative versus the Manipulative Treatment of Slipped
Epiphysis. Journal of the American Medical Association, 107, 1, 154, 1936.36 KOHLER, R. and Cols.: La Scintigraphie Osseuse dans la Maladie de LeggPerthesCalvé.
Technique, Resultats, Indications. Rev. Chir. Orthop., 70: 114, 1984.37 McKIBBIN, B.; RALIS, Z.: Pathological changes in a case of Perthes' disease. J. Bone Joint Surg.,
56B: 438447, 1974.38 MENDONÇA, J. and Cols.: Detecção Cintigráfica Precoce da Doença de Perthes na Sinovite da
Anca. Rev. Ortop. Traum. IB., 10P: 153161, 1984.39 OGDEN, J.A.: Changing Patterns of Proximal Femoral Vascularity. J. Bone Joint Surg., 56A:
941950, 1974.40 OLLIER, L.: Traité Expérimental et Clinique de la Régénération des Os et de la Production
Artificielle du Tissu Osseux. Vol.1, pp. 236238, 386392. Paris, Masson et Fils, 1867.41 PATERSON, D.; SAVAGE, J.P.: The Nuclide Bone Scan in the Diagnosis of Perthes' Disease.
Clin. Orth. and Rel. Res., 209: 2329, 1986.42 RATLIFF, A.H.C.: Fractures of the Neck of the Femur in Children. J. Bone Joint Surg., 44B:
528542, 1962.43 SALTER, R.B. and Cols.: LeggCalvéPerthes Disease. The Prognostic Significance of the
Subchondral Fracture and a TwoGroup Classification of the Femoral Head Involvement. J. BoneJoint Surg., 66A: 479489, 1984.
44 SANCHIS, M. and Cols.: Sinovitis Transitoria de la Cadera. Su Relacion con la Enfermedad de

Perthes. Estudio Gammagráfico. Rev. Esp. Cir. Osteoart., 21:273, 1986.45 SCOENECKER, P.L.; BITZ, O.M.; WHITESIDE, L.A.: The Acute Effect of Position of
Immobilization on Capital Femoral Epiphyseal blood flow. A Quantitative Study Using theHydrogen Washout Technique. J. Bone Joint Surg. 60A: 899904, 1978
46 SIFFERT, R.S.: The Effect of Staples and Longitudinal Wires on Epiphyseal Growth. J. Bone JointSurg., 38A: 10771088, 1956.
47 SOTTOHALL, R. et Cols.: Variations in the intraarticular pressure of the hip joint in injury anddisease. J. Bone Joint Surg., 46A, 509517, 1964.
48 STULBERG, S.D., COOPERMAN, D.R., WALLENSTEIN, D.R.: The natural history ofLegg–Calve–Perthes disease. J Bone Joint Surg Am, 7, 1095–1108, 1981.
49 SUTHERLAND, A.D. and Cols.: The Diagnosis and Management of Perthes Disease. J. BoneJoint Surg., 62B: 300, 1980.
50 TACHDJIAN, M.O. and GRANA, L.: Response of the Hip Joint to Increased IntraarticularHydrostatic Pressure. Clin. Orthop. Rel. Res., 61: 199212, 1968.
51 TRUETA, J.: The Normal Vascular Anatomy of the Human Femoral Head during Growth. J. BoneJoint Surg., 39B: 358394, 1957.
52 WINGSTRAND, H. and Cols.: Sonography and Joint Pressure in Synovitis of the Hip. J. BoneJoint Surg., 69B: 254256, 1987.
53 WOODHOUSE, C.F.: Dynamic Influences of Vascular Occlusion Affecting the Development ofAvascular Necrosis of the Femoral Head. Clin. Orthop. Rel. Res., 32: 119129, 1964.
54 VEGTER, J.: Fractional Necrosis of the Femoral Head Epiphysis after Transient Increase in JointPressure. An Experimental Study in Juvenile Rabbits. J. Bone Joint Surg., 69B: 530535, 1987.
55 VEGTER, J.: The Influence of Joint Posture on Intraarticular Pressure. A Study of TransientSynovitis and Perthes' Disease. J. Bone Joint Surg., 69B: 7174, 1987.




















