
Prevalence and management of hypertension in primary care in Portugal. Insights from the VALSIM...
25
2ECEBIDO PARA PUBLICA»ºO 3ETEMBRO DE r !CEITE PARA PUBLICA»ºO *ANEIRO DE 2ECEIVED FOR PUBLICATION 3EPTEMBER r !CCEPTED FOR PUBLICATION *ANUARY 2%35-/ Introdução: A hipertensão arterial (HTA) é o factor de risco cardiovascular corrigível mais frequente, e o seu tratamento e controlo assume importância central nas estratégias preventivas. No entanto, não são conhecidos os padrões de tratamento antihipertensor (aHT) mais frequentes em Portugal. Objectivo: Determinar a prevalência da HTA e caracterizar o seu tratamento nos utentes adultos dos Cuidados de Saúde Primários #30 IDENTIkCANDO OS FµRMACOS MAIS UTILIZADOS E SUA VARIA»ºO DEMOGRµkCA Método: Estudo descritivo transversal nos CSP envolvendo 719 médicos de família segundo distribuição proporcional à densidade populacional de cada região do continente e ilhas – Estudo VALSIM. Os primeiros 2 utentes adultos de cada dia de consulta foram convidados a participar, independentemente do motivo de consulta. Após consentimento informado, foi utilizado um inquérito para RECOLHA DE DADOS SÅCIODEMOGRµkCOS CLÀNICOS e laboratoriais. A medição da pressão arterial (PA) foi realizada 2 vezes, após 5 minutos de repouso na posição sentada, considerando-se A M¼DIA DAS MEDI»ÉES ! (4! FOI DEkNIDA por pressão arterial medida superior a 140/90mmHg ou abaixo desse limiar sob terapêutica aHT. Resultados: Foram observados 16.856 indivíduos (58,1±15,1 anos; 61,3% mulheres). !"342!#4 0REVALENCE AND MANAGEMENT OF HYPER TENSION IN PRIMARY CARE IN 0ORTUGAL )NSIGHTS FROM THE 6!,3)- STUDY Introduction: Hypertension (HT) is the MOST COMMON MODIkABLE RISK FACTOR FOR cardiovascular disease, and HT management and control is of major importance in preventive strategies. However, patterns of antihypertensive (AHT) treatment have never been evaluated in Portugal. Objective: To estimate the prevalence of HT and to characterize its management in a primary care setting, identifying the most frequently used drugs and evaluating regional variations in treatment patterns. Methods: The VALSIM study is a descriptive cross-sectional study performed in a primary care setting, involving 719 general practitioners (GPs) and representative of all REGIONS OF 0ORTUGAL 4HE kRST TWO PATIENTS AGED t18 years consulting their GP on each day were asked to participate, irrespective of the reason for the consultation. After informed consent was obtained, a questionnaire was used to collect sociodemographic, clinical and laboratory data. Two blood pressure (BP) measurements were taken after a 5-minute rest PERIOD IN A SEATED POSITION (4 WAS DEkNED as BP higher than 140/90 mmHg or use of antihypertensive medication. 0REVAL½NCIA E 0ADRÉES DE 4RATAMENTO DA (IPERTENS»O !RTERIAL NOS #UIDADOS DE 3AÊDE 0RIM¶RIOS EM 0ORTUGAL 2ESULTADOS DO %STUDO 6!,3)- ;= NUNO CORTEZ-DIAS, SUSANA MARTINS, ADRIANA BELO, MANUELA FIUZA EM NOME DOS INVESTIGADORES DO ESTUDO VALSIM Serviço de Cardiologia do Hospital de Santa Maria, Lisboa, Portugal Faculdade de Medicina de Lisboa, Lisboa, Portugal Centro Nacional de Colecção de Dados em Cardiologia da Sociedade Portuguesa de Cardiologia, Delegação de Coimbra, Coimbra, Portugal 2EV 0ORT #ARDIOL ARTIGOS ORIGINAIS
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Prevalence and management of hypertension in primary care in Portugal. Insights from the VALSIM...

Introdução: A hipertensão arterial (HTA) é o factor de risco cardiovascular corrigível
mais frequente, e o seu tratamento e controlo assume importância central nas estratégias
preventivas. No entanto, não são conhecidos os padrões de tratamento antihipertensor (aHT)
mais frequentes em Portugal.Objectivo: Determinar a prevalência da HTA
e caracterizar o seu tratamento nos utentes adultos dos Cuidados de Saúde Primários
Método: Estudo descritivo transversal nos CSP envolvendo 719 médicos de família
segundo distribuição proporcional à densidade populacional de cada região do continente e ilhas – Estudo VALSIM. Os primeiros 2
utentes adultos de cada dia de consulta foram convidados a participar, independentemente do motivo de consulta. Após consentimento
informado, foi utilizado um inquérito para
e laboratoriais. A medição da pressão arterial (PA) foi realizada 2 vezes, após 5 minutos de repouso na posição sentada, considerando-se
por pressão arterial medida superior a 140/90mmHg ou abaixo desse limiar sob
terapêutica aHT.Resultados: Foram observados 16.856
indivíduos (58,1±15,1 anos; 61,3% mulheres).
Introduction: Hypertension (HT) is the
cardiovascular disease, and HT management and control is of major importance in preventive strategies. However, patterns of antihypertensive (AHT) treatment have never been evaluated in Portugal.Objective: To estimate the prevalence of HT and to characterize its management in a primary care setting, identifying the most frequently used drugs and evaluating regional variations in treatment patterns.Methods: The VALSIM study is a descriptive cross-sectional study performed in a primary care setting, involving 719 general practitioners (GPs) and representative of all
18 years consulting their GP on each day were asked to participate, irrespective of the reason for the consultation. After informed consent was obtained, a questionnaire was used to collect sociodemographic, clinical and laboratory data. Two blood pressure (BP) measurements were taken after a 5-minute rest
as BP higher than 140/90 mmHg or use of antihypertensive medication.
NUNO CORTEZ-DIAS, SUSANA MARTINS, ADRIANA BELO, MANUELA FIUZA EM NOME DOS INVESTIGADORES DO ESTUDO VALSIM
Serviço de Cardiologia do Hospital de Santa Maria, Lisboa, Portugal
Faculdade de Medicina de Lisboa, Lisboa, Portugal
Centro Nacional de Colecção de Dados em Cardiologia da Sociedade Portuguesa de Cardiologia,
Delegação de Coimbra, Coimbra, Portugal
ARTIGOS ORIGINAIS
A prevalência de HTA ajustada ao sexo, idade e dimensão das regiões foi de 42,62%
(homens: 43,09%; mulheres: 42,19%). Entre os 9 189 indivíduos sob tratamento aHT, 47,62% foram tratados em monoterapia,
36,16% estavam medicados com duas classes aHT e 16,22% com três ou mais classes.
As classes mais frequentemente instituídas em monoterapia foram os antagonistas dos
receptores da angiotensina (ARA 16,9% dos hipertensos), inibidores da enzima conversora
da angiotensina (IECA 14,41%) e os diuréticos (D 5,85%). As associações de dois aHT mais frequentes foram ARA-D (11,82%), IECA-D
(11,79%), IECA-antagonista dos canais de cálcio (ACC 2%), ACC-D (1,81%) e ARA-
ACC (1,53%). Globalmente, os aHT mais usados foram os D (47,4%), ARA (43,0%) e IECA (39,2%). Os ACC só foram instituídos
em 18,9% dos hipertensos e os bloqueadores -adrenérgicos em 16,2%. Detectou-se
variação do método de tratamento em função do sexo, idade e região. Os D foram mais utilizados nos idosos, nas mulheres, nos
Açores (61,9%) e Alentejo (58,3%). Os ARA foram utilizados nos indivíduos de meia-idade,
nos homens e mais prescritos na região Norte (48,6%).
Conclusões: Os padrões de tratamento da HTA exibem elevada variabilidade regional. A proporção de hipertensos sob monoterapia
é ainda muito elevada, impondo-se uma utilização mais frequente de associações
do controlo tensional. Além disso, o incremento do recurso aos ACC será também
provavelmente útil, já que a frequência de utilização actual é inferior à prevista tendo em
conta a realidade de outros países europeus.
Palavras-Chave
Hipertensão; Prevalência; Tratamento; Antihipertensores;
Cuidados de saúde primários; Portugal.
AbreviaturasaSIR: ajustada ao sexo, idade e dimensão das regiões; ACC:
antagonistas dos canais de cálcio; ARA: antagonistas dos receptores da angiotensina II; aHT: antihipertensores; AVC:
CSP: Cuidados de Saúde Primários; HTA: hipertensão arterial; IECA: inibidores da enzima conversora da angiotensina; NA:
não aplicável; PNA: prevalência não ajustada; VALSIM: Estudo Epidemiológico de Prevalência da Síndrome Metabólica na
População Portuguesa.
Results: A total of 16,856 subjects were evaluated (mean age 58.1±15.1 years; 61.3% women). The prevalence of HT adjusted for age and gender was 42.62% (males: 43.09%, females: 42.19%). Of the 9,189 hypertensive patients under treatment, the proportion receiving one, two or three or more drug classes was 47.62%, 36.16% and 16.22% respectively. The classes most frequently used in monotherapy were angiotensin receptor blockers (ARBs, 16.9%), angiotensin-converting enzyme inhibitors (ACEIs, 14.41%) and diuretics (5.85%). The most common associations of two classes were ARB-diuretic (11.82%), ACEI-diuretic (11.79%), ACEI-calcium channel blocker (CCB, 2%), CCB-diuretic (1.81%) and ARB-CCB (1.53%). The most frequently used AHT drugs were diuretics (47.4%), ARBs (43%) and ACEIs (39.2%). CCBs were used in 18.9% and beta-blockers in 16.2% only. Different patterns of
age and region of residence. Diuretics were used more in the elderly, women, and in the Azores (61.9%) and the Alentejo (58.3%). ARBs were used preferentially in middle-aged patients, men and in the Northern region (48.6%).Conclusions: There is considerable regional variation in treatment patterns. The proportion of hypertensive patients under monotherapy is still very high. Increasing the use of combination antihypertensive therapy would probably improve HT control in the population. Furthermore, increased use of CCBs would probably also be useful, as they are used less than would be expected, compared to other European countries.
Key words
Hypertension; Prevalence; Treatment; Antihypertensives;
Primary care; Portugal.
AbbreviationsACEIs: angiotensin-converting enzyme inhibitors; AGAR: adjusted for gender, age and region size; AHT: antihypertensive; ARBs: angiotensin receptor blockers; BBs: beta-blockers; CAD: coronary artery disease; CCBs: calcium channel blockers; CV: cardiovascular; HT: hypertension; MS: metabolic syndrome; PHC: primary health care; VALSIM: Epidemiological Study of the Prevalence of the Metabolic Syndrome in the Portuguese Population.

Cardiovascular (CV) disease is the cause of death in at least 34.1% of the Portuguese
population, mainly due to stroke (15.1%) and coronary artery disease (CAD) (8%)(1). Various
link between hypertension (HT) and CAD, stroke and renal failure. HT is the most common
management and control is of major importance in preventive strategies.
A study by Wolf-Maier et al. analyzed the population aged between 35 and 64 years in six European countries (Finland, Sweden, England, Germany, Spain and Italy), Canada and the US(2). Mean HT prevalence in the European countries
and Canada were 28% and 27% respectively(2). The higher prevalence of HT in Europe is
of treatment and control. In the US and Canada, 23% of hypertensives are controlled, while the percentage drops to 8% (5-9%) in the European countries(2). HT prevalence in the adult Portu-guese population is estimated at 42.1%, with only 39.0% of patients under antihypertensive (AHT) therapy and 11.2% controlled(3).
Innovations in therapy have led to changes in treatment patterns. In England, the proportion of patients prescribed two or more AHT drugs rose from 40% to 56% between 1998(4) and 2003(5), the most frequently used drugs being diuretics (30±1.61%), beta-blockers (BBs, 27±1.56%), calcium channel blockers (CCBs, 22±1.45%) and angiotensin-converting enzyme inhibitors (ACEIs, 18±1.35%).
In order to plan preventive strategies aimed at improving diagnosis, treatment and control of HT in Portugal, it is important to characterize the most common treatment patterns and to identify
public health measures.The aim of the present subanalysis of the
VALSIM study (Epidemiological Study of the Prevalence of the Metabolic Syndrome in the Portuguese Population) is to estimate the prevalence of HT in adult users of primary health care (PHC) and to characterize the most frequently used treatment regimes at the national and regional level.
As doenças cardiovasculares são a causa de mortalidade de pelo menos 34,1% da
população portuguesa, fundamentalmente como consequência do acidente vascular cerebral (AVC, 15,1%) e da doença coronária (8%)(1). Diversos estudos epidemiológicos provaram a relevante associação da hipertensão arterial
renal. Efectivamente, a HTA é o factor de risco
seu tratamento e controlo assume importância central nas estratégias preventivas.
A prevalência média de HTA na Europa é de 44% (38-55%), enquanto nos Estados Unidos da América (EUA) e Canadá se situa nos 28% e 27%, respectivamente(2). Nesse estudo, Wolf-Maier et al restringiram a análise à população com idade compreendida entre os 35 e os 64 anos e avaliaram 6 países europeus (Finlândia, Suécia, Inglaterra, Alemanha, Espanha e Itália)(2). Este excesso de prevalência de HTA na Europa
na taxa de tratamento e controlo. Nos EUA e Canadá, 23% dos hipertensos estão controlados, proporção que desce para 8% (5-9%) nos países europeus(2). Estima-se que a prevalência de HTA na população adulta portuguesa será 42,1%, estando apenas 39,0% dos doentes hipertensos medicados com fármacos antihipertensores (aHT) e 11,2% estarão controlados(3).
As inovações na terapêutica da HTA têm
mento. Em Inglaterra, a proporção de doentes medicados com 2 ou mais fármacos aHT subiu de 40% para 56% entre 1998(4) e 2003(5) e os fármacos mais utilizados foram os diuréticos (30±1,61%), os bloqueadores -adrenérgicos (BB, 27±1,56%), os antagonistas dos canais de cálcio (ACC, 22±1,45%) e os inibidores da enzima conversora da angiotensina (IECA 18±1,35%).
Para o planeamento das estratégias preven-tivas, destinadas a melhorar o diagnóstico, tratamento e controlo da HTA, será relevante a caracterização dos padrões de tratamento aHT
eventuais lacunas e alvos de actuação em termos de saúde pública.
A presente subanálise do Estudo VALSIM (Estudo Epidemiológico de PreVALência da SIndrome Metabólica na População Portuguesa)

The VALSIM study is a cross-sectional study of a representative sample of adults resident in mainland Portugal and the islands of Madeira and the Azores treated at PHC centers, with the aim of characterizing CV risk factors and in particular metabolic syndrome (MS). The study involved
and proportional distribution by district and
(Nomenclature of Territorial Units for Statistics) regions of mainland Portugal (Northern, Central, Lisbon and Tagus Valley, Alentejo and Algarve) and the autonomous regions of Madeira and the Azores. The study was carried out between April 2006 and November 2007.
an appointment on a given day were invited to participate, irrespective of the reason for the consultation and of the presence of CV risk factors. The inclusion criterion was the existence of laboratory results for HDL cholesterol, triglycerides and fasting glucose performed up to one year prior to the consultation; the exclusion criterion was the presence of clinical conditions that could affect a diagnosis of MS, such as thyroid dysfunction. After informed consent was obtained, a questionnaire was applied to characterize sociodemographic and anthropometric variables, clinical (previous diagnosis of HT, diabetes, CAD, stroke or antihypertensive therapy) and laboratory data from the 12 months prior to the consultation, diet, sedentarism and smoking. Blood pressure (BP) was measured in a seated position after
sphygmomanometer or semi-automatic device, the mean of two consecutive measurements
140/90 mmHg or lower if the patient was under AHT therapy.
Categorical variables were analyzed to determine absolute and relative frequencies,
rates were standardized, with adjustment for gender and age, by the total probability theorem, taking into account the demographic composition of the adult population resident in Portugal,
pretendeu estimar a prevalência de HTA nos utentes adultos dos Cuidados de Saúde Primários (CSP) e caracterizar os regimes terapêuticos aHT mais utilizados a nível nacional e regional.
O estudo VALSIM foi um estudo epidemioló-gico transversal, de uma amostra representativa dos adultos residentes em Portugal continental e ilhas seguidos nos CSP, para caracterização dos factores de risco CV e em particular de síndrome metabólica. Participaram no estudo 719 médicos de família, segundo distribuição
NUTS (Nomenclatura de Unidades Territoriais
(Norte, Centro, Lisboa e Vale do Tejo, Alentejo e Algarve) e das regiões autónomas da Madeira e Açores. O estudo decorreu entre Abril de 2006 e Novembro de 2007.
Os primeiros dois utentes adultos de cada dia de consulta, independentemente do motivo de consulta e independentemente da presença de factores de risco CV, foram convidados a participar no estudo. Constituiu critério de inclusão a presença de resultados analíticos de co lesterol-HDL, triglicéridos e glicémia em je jum efectuados nos 12 meses precedentes à consulta; e critério de exclusão a presença de situações
síndrome metabólica, como disfunção tiroideia. Após consentimento informado, foi aplicado um questionário para caracterização de variáveis
clínicos (diagnóstico prévio de HTA, diabetes mellitus tipo II, DC, AVC, terapêutica aHT), parâmetros analíticos referentes aos 12 meses precedentes à consulta, hábitos nutricionais, sedentarismo e hábitos tabágicos. A pressão arterial (PA) foi medida na posição sentada após um período de repouso de 5 minutos, utilizando-
semi-automático. Foi registada a média de duas determinações consecutivas. A HTA foi
a 140/90mmHg ou abaixo desse limiar sob terapêutica AHT.

by district and region, in 2000 (2001 Census, National Institute of Statistics [INE]). Categorical variables were compared using the chi-square test. Numerical variables were analyzed based on the number of observations, mean, standard deviation, median, maximum and minimum values, standard error and analysis of variance by Levene’s test. Numerical variables with a normal distribution (as assessed by the Kolmogorov-Smirnov test) were compared using the Student’s t test for means and Levene’s test for variance, and those with a non-normal distribution were compared using non-parametric tests (Kruskal-Wallis). The statistical analysis was performed
used in comparative analyses (p<0.05).
The study included 16,856 individuals, of whom the majority were women (61.62%). The age of those surveyed ranged between 18 and 96 years, with a mean of 58.1±15.1 and a median of 60. The mean age of the men was 58.1±14.6 years and of the women 57.5±15.3 years. The age difference between the sexes, although
The sample population was considered statistically representative of individuals treated at PHC centers in all regions. Differences from the general population in terms of distribution by gender, age and region were determined and taken into account in estimating prevalence. Based on a theoretical HT prevalence in the adult Portuguese population of 42.1%, 49.5% for men and 38.9% for women (PAP study estimates(3))
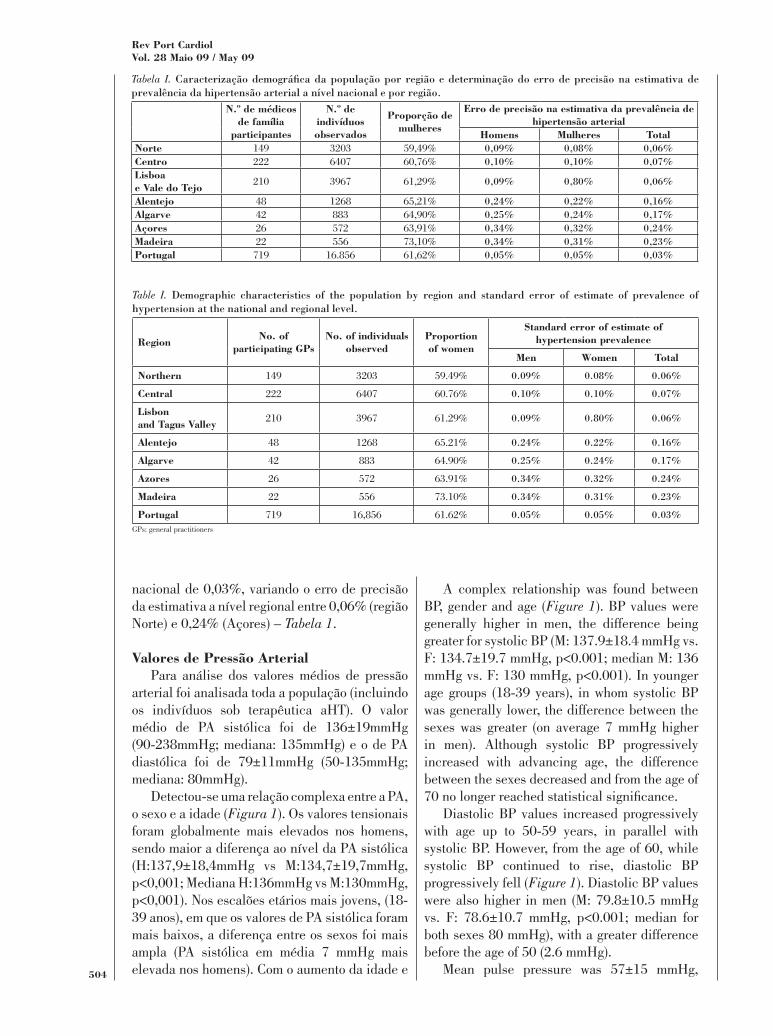
error of estimate of HT prevalence among adult users of PHC centers was 0.03% at the national level, ranging at the regional level from 0.06% in the Northern region to 0.24% in the Azores (Table I).
To determine mean values, BP was analyzed for the whole population, including those under AHT therapy. Mean systolic BP was 136±19 mmHg (90-238 mmHg; median 135 mmHg) and diastolic BP was 79±11 mmHg (50-135 mmHg; median 80 mmHg).
As variáveis categóricas foram avaliadas com determinação da frequência absoluta e da
a 95% (IC95%). Na estimativa das prevalências, procedeu-se à padronização das taxas com cor-recção para o sexo e idade através do teorema da probabilidade total, tendo em conta a composição
em Portugal, por distrito e região, no ano 2000 (CENSUS 2001, INE). As variáveis categóricas foram comparadas com o teste do qui-quadrado. Em relação às variáveis numéricas, calculou-se o número de observações (N), média, desvio padrão, mediana, valores máximo, mínimo, erro padrão e análise de variância (teste de Levene). As variáveis numéricas com distribuição normal (avaliada pelo teste de Kolmogorov-Smirnov) foram comparadas utilizando-se os testes t-Student no que respeita à média e teste de Levene no que respeita à variância, e as variáveis com distribuição não normal foram comparadas mediante testes não paramétricos (Kruskal-Wallis). A análise estatística foi efectuada em
de 5% nas análises comparativas (p <0,05).
Foram avaliados 16.856 indivíduos, com predomínio do sexo feminino (61,62%). A idade dos inquiridos variou entre os 18 e os 96 anos, com idade média de 58,1±15,1 anos e mediana de 60 anos. A idade média dos homens foi de 58,1±14,6 anos e a das mulheres foi de 57,5±15,3 anos. Apesar de a diferença etária entre os sexos
(p<0,001). A amostra incluída foi considerada estatisticamente representativa da população de indivíduos seguidos nos CSP em todas as regiões. As diferenças quanto à distribuição por sexo, idade e região relativamente à população em geral foram determinadas e consideradas na estimativa da prevalência. Considerando a prevalência teórica de HTA na população adulta portuguesa de 42,1%, 49,5% no sexo masculino e 38,9% no sexo feminino (valores estimados no estudo PAP(3)
erro de precisão da estimativa da prevalência de HTA entre os utentes adultos dos CSP foi a nível
A complex relationship was found between BP, gender and age (Figure 1). BP values were generally higher in men, the difference being greater for systolic BP (M: 137.9±18.4 mmHg vs. F: 134.7±19.7 mmHg, p<0.001; median M: 136 mmHg vs. F: 130 mmHg, p<0.001). In younger age groups (18-39 years), in whom systolic BP was generally lower, the difference between the sexes was greater (on average 7 mmHg higher in men). Although systolic BP progressively increased with advancing age, the difference between the sexes decreased and from the age of
Diastolic BP values increased progressively with age up to 50-59 years, in parallel with systolic BP. However, from the age of 60, while systolic BP continued to rise, diastolic BP progressively fell (Figure 1). Diastolic BP values were also higher in men (M: 79.8±10.5 mmHg vs. F: 78.6±10.7 mmHg, p<0.001; median for both sexes 80 mmHg), with a greater difference before the age of 50 (2.6 mmHg).
Mean pulse pressure was 57±15 mmHg,
nacional de 0,03%, variando o erro de precisão da estimativa a nível regional entre 0,06% (região Norte) e 0,24% (Açores) – Tabela 1.
Para análise dos valores médios de pressão arterial foi analisada toda a população (incluindo os indivíduos sob terapêutica aHT). O valor médio de PA sistólica foi de 136±19mmHg (90-238mmHg; mediana: 135mmHg) e o de PA diastólica foi de 79±11mmHg (50-135mmHg; mediana: 80mmHg).
Detectou-se uma relação complexa entre a PA, o sexo e a idade (Figura 1). Os valores tensionais foram globalmente mais elevados nos homens, sendo maior a diferença ao nível da PA sistólica (H:137,9±18,4mmHg vs M:134,7±19,7mmHg, p<0,001; Mediana H:136mmHg vs M:130mmHg, p<0,001). Nos escalões etários mais jovens, (18-39 anos), em que os valores de PA sistólica foram mais baixos, a diferença entre os sexos foi mais ampla (PA sistólica em média 7 mmHg mais elevada nos homens). Com o aumento da idade e
Tabela I.
149 3203 59,49% 0,09% 0,08% 0,06%222 6407 60,76% 0,10% 0,10% 0,07%
210 3967 61,29% 0,09% 0,80% 0,06%
48 1268 65,21% 0,24% 0,22% 0,16%42 883 64,90% 0,25% 0,24% 0,17%26 572 63,91% 0,34% 0,32% 0,24%22 556 73,10% 0,34% 0,31% 0,23%719 16.856 61,62% 0,05% 0,05% 0,03%
Table I.
149 3203 59.49%
222 6407 60.76%
210 3967 61.29%
48 1268 65.21%
42 883 64.90%
26 572 63.91%
22 556 73.10%
719 16,856 61.62%GPs: general practitioners
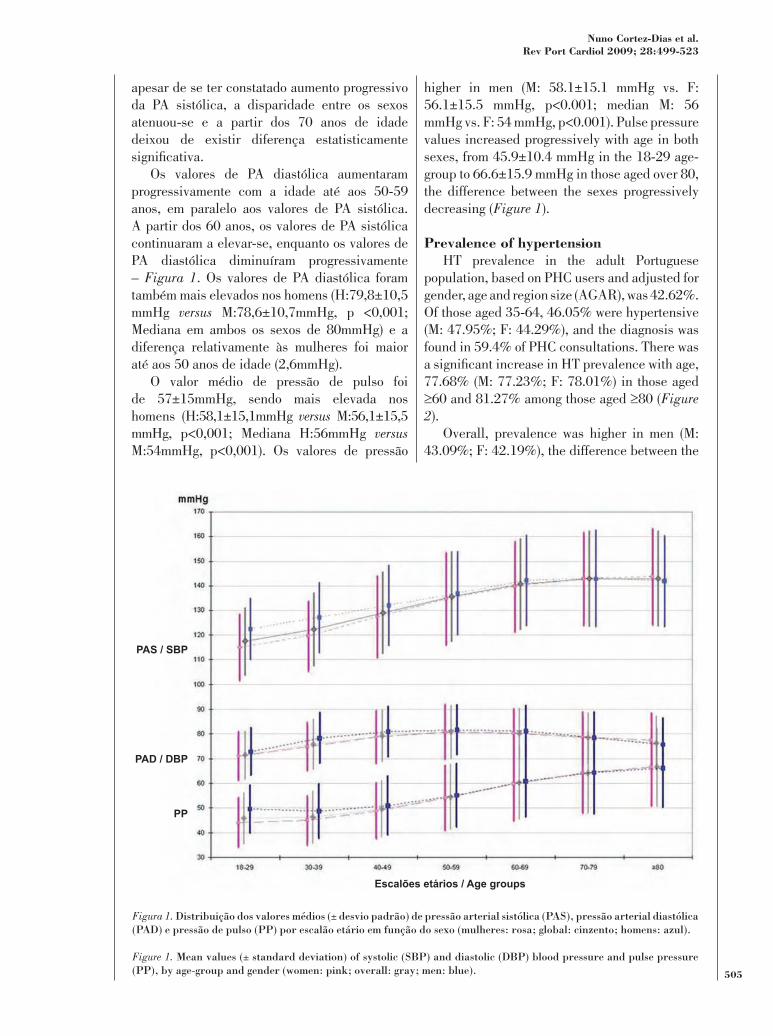
higher in men (M: 58.1±15.1 mmHg vs. F: 56.1±15.5 mmHg, p<0.001; median M: 56 mmHg vs. F: 54 mmHg, p<0.001). Pulse pressure values increased progressively with age in both sexes, from 45.9±10.4 mmHg in the 18-29 age-group to 66.6±15.9 mmHg in those aged over 80, the difference between the sexes progressively decreasing (Figure 1).
HT prevalence in the adult Portuguese population, based on PHC users and adjusted for gender, age and region size (AGAR), was 42.62%. Of those aged 35-64, 46.05% were hypertensive (M: 47.95%; F: 44.29%), and the diagnosis was found in 59.4% of PHC consultations. There was
77.68% (M: 77.23%; F: 78.01%) in those aged 60 and 81.27% among those aged 80 (Figure
2).Overall, prevalence was higher in men (M:
43.09%; F: 42.19%), the difference between the
apesar de se ter constatado aumento progressivo da PA sistólica, a disparidade entre os sexos atenuou-se e a partir dos 70 anos de idade deixou de existir diferença estatisticamente
Os valores de PA diastólica aumentaram progressivamente com a idade até aos 50-59 anos, em paralelo aos valores de PA sistólica. A partir dos 60 anos, os valores de PA sistólica continuaram a elevar-se, enquanto os valores de PA diastólica diminuíram progressivamente – Figura 1. Os valores de PA diastólica foram também mais elevados nos homens (H:79,8±10,5 mmHg versus M:78,6±10,7mmHg, p <0,001; Mediana em ambos os sexos de 80mmHg) e a diferença relativamente às mulheres foi maior até aos 50 anos de idade (2,6mmHg).
O valor médio de pressão de pulso foi de 57±15mmHg, sendo mais elevada nos homens (H:58,1±15,1mmHg versus M:56,1±15,5 mmHg, p<0,001; Mediana H:56mmHg versus M:54mmHg, p<0,001). Os valores de pressão
Escalões etários / Age groups
PAS / SBP
PAD / DBP
PP
Figura 1.
Figure 1.

sexes varying with age and region of residence. In the younger age-groups, prevalence was
42% higher among men aged under 50 compared to women in the same age-group (OR: 1.42; 95% CI: 1.23-1.63; p<0.001). After the age of 60, HT prevalence was similar for both sexes, but slightly higher in women in the very elderly ( 80 years) (M: 78.93%; F: 82.54%). There was
de pulso aumentaram progressivamente com a idade em ambos os sexos, de 45,9± 10,4mmHg no grupo etário 18-29 anos para 66,6±15,9mmHg nos indivíduos com idade superior a 80 anos, com atenuação progressiva da diferença entre os sexos (Figura 1).
A prevalência de HTA na população adulta portuguesa, estimada a partir dos utentes dos CSP [mediante ajustamento ao sexo, idade e dimensão das regiões (aSIR)] foi de 42,62%. Cerca de 46,05% dos indivíduos com 35-64 anos eram hipertensos (H:47,95%; M:44,29%), e esse diagnóstico esteve presente em 59,4% das consultas nos CSP. Detectou-se aumento
sendo nos indivíduos com idade 60 anos de 77,68% (H: 77,23%; M: 78,01%) e entre aqueles com idade 80 anos atingiu 81,27% – Figura 2.
Em termos globais, a prevalência foi mais elevada nos homens (H: 43,09%; M: 42,19%), variando a proporção entre os sexos em função da faixa etária e da região de residência. Nos grupos etários mais jovens, a prevalência foi claramente superior entre os homens (p <0,001), sendo o risco de HTA 42% maior entre os homens com idade inferior a 50 anos, comparativamente às mulheres da mesma faixa etária (OR:1,42; IC95%:1,23-1,63; p<0,001). Após os 60 anos de
Idade (anos) / Age (years)
Prev
alên
cia
(%) /
Pre
vale
nce
(%)
Homens / Men
Mulheres / Women
Figura 2.
Figure 2.
Figura 3.
Figure 3.

(adjusted for the gender and age distribution of each region), the lowest being in the Azores. Of the mainland regions, prevalence was lowest in the Northern region and highest in the Alentejo, where it reached 51.5% (Figure 3).
Of the total number of hypertensive individuals assessed (n=9964), AHT therapy was begun or continued in 89.72% (AGAR), with a higher percentage of women (M: 87.54%; F: 91.73%). In patients aged under 60, the decision to begin therapy was often delayed, even in the presence
was not prescribed in 57.78% of hypertensives aged under 30, and the likelihood of not being prescribed therapy in this age-group was greater among women (M: 40.53% versus F: 43.93%, p<0.001). After the age of 60, as HT prevalence increased, the diagnosis almost always led to the institution of drug therapy, only 5.36% of this group not being prescribed medication at PHC consultations. The probability that detection of elevated BP values would lead to a decision to initiate or maintain AHT therapy varied according to region, being lower in Madeira (84.55%), the Northern region (85.34%), the Algarve (85.46%) and the Central region (86.18%), and higher in the Alentejo (93.58%), Lisbon and Tagus Valley (96%) and the Azores (97.67%).
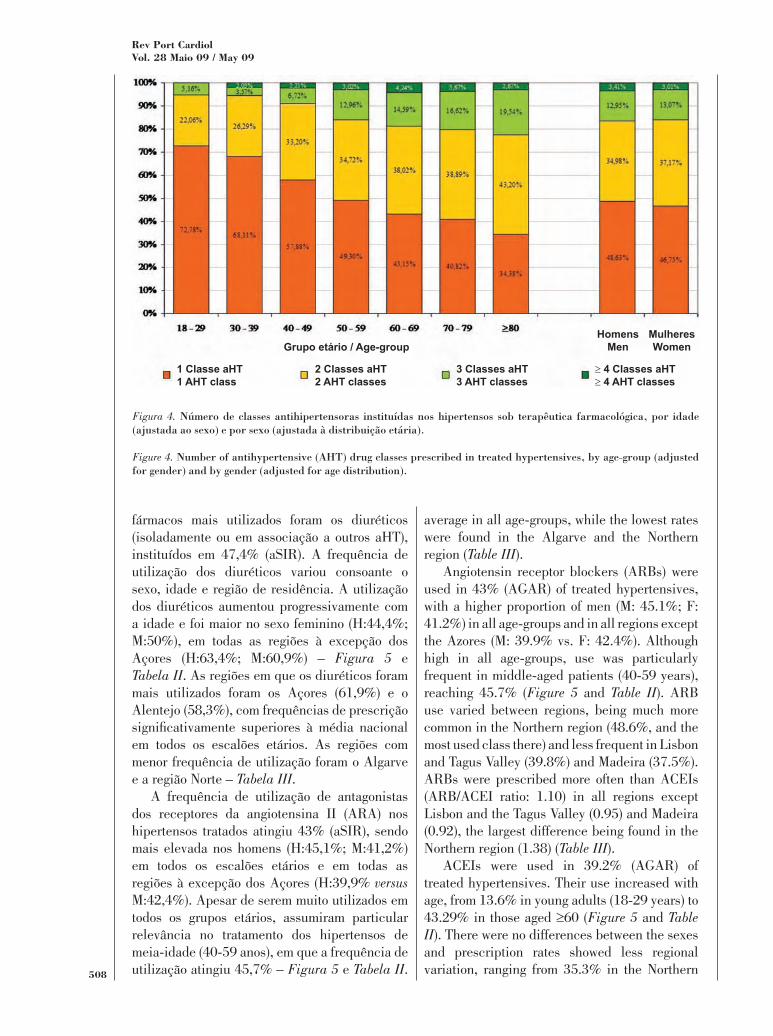
The proportion of treated hypertensives under monotherapy was 47.62% (AGAR), higher in men (M: 48.63%; F: 46.75%), and decreased with age, from 72.78% in the 18-29 age-group to 34.38% in those aged over 80 (Figure 4). The percentages for hypertensives medicated with two, three or more classes of drugs were 36.16%, 13.02% and 3.20% respectively.
The most commonly used drugs among the 9189 treated hypertensives were diuretics, prescribed in 47.4% (AGAR), either alone or in association with other classes. Use of diuretics varied according to gender, age and region of residence, rising progressively with age and higher in women (M: 44.4%; F: 50%), in all regions except the Azores (M: 63.4%; F: 60.9%) (Figure 5 and Table II). The regions with the highest use of diuretics were the Azores (61.9%)
higher prescription rates than the national
idade, a prevalência de HTA foi similar em ambos os sexos, havendo mesmo ligeiro predomínio do sexo feminino entre os indivíduos muito idosos ( 80 anos) (H: 78,93%; M: 82,54%). Detectou-
por sexo e idade da região), sendo mais baixa no arquipélago dos Açores. Entre as regiões do continente a prevalência foi menor no Norte e mais elevada no Alentejo, onde atingiu 51,5% – Figura 3.
Do total de indivíduos hipertensos avaliados (N=9964), foi instituída ou mantida terapêutica aHT em 89,72% (aSIR), sendo a proporção maior entre as mulheres (H:87,54%; M:91,73%). Até aos 60 anos de idade, a decisão de instituir terapêutica aHT foi frequentemente protelada,
dos valores tensionais. Efectivamente, não foi iniciada terapêutica farmacológica em 57,78% dos hipertensos com idade inferior a 30 anos. Nessa faixa etária, a probabilidade de não ser iniciada terapêutica aHT foi maior no sexo fe-minino (H:40,53% versus M:43,93%, p<0,001). Depois dos 60 anos, e em paralelo com o aumento da prevalência de HTA, o diagnóstico conduziu, quase sempre, à instituição de terapêutica farmacológica, sendo apenas de 5,36% o grupo de hipertensos avaliados nos CSP a quem não foi proposta terapêutica aHT. Finalmente, a probabilidade de a detecção de valores tensionais aumentados conduzir à decisão de iniciar ou manter terapêutica aHT exibiu variação regional, sendo menor na Madeira (84,55%), Norte (85,34%), Algarve (85,46%) e Centro (86,18%) e maior no Alentejo (93,58%), Lisboa e Vale do Tejo (96%) e Açores (97,67%).
A proporção de hipertensos tratados que estavam sob monoterapia foi de 47,62% (aSIR), sendo maior no sexo masculino (H:48,63%; M:46,75%) e diminuiu com a idade, de 72,78% no grupo etário 18-29 anos para 34,38% de-pois dos 80 anos – Figura 4. As proporções de hipertensos sob terapêutica com 2, 3 ou mais do que 3 classes hipertensoras foram 36,16%, 13,02% e 3,20%, respectivamente.
Entre os 9189 hipertensos tratados, os
average in all age-groups, while the lowest rates were found in the Algarve and the Northern region (Table III).
Angiotensin receptor blockers (ARBs) were used in 43% (AGAR) of treated hypertensives, with a higher proportion of men (M: 45.1%; F: 41.2%) in all age-groups and in all regions except the Azores (M: 39.9% vs. F: 42.4%). Although high in all age-groups, use was particularly frequent in middle-aged patients (40-59 years), reaching 45.7% (Figure 5 and Table II). ARB use varied between regions, being much more common in the Northern region (48.6%, and the most used class there) and less frequent in Lisbon and Tagus Valley (39.8%) and Madeira (37.5%). ARBs were prescribed more often than ACEIs (ARB/ACEI ratio: 1.10) in all regions except Lisbon and the Tagus Valley (0.95) and Madeira (0.92), the largest difference being found in the Northern region (1.38) (Table III).
ACEIs were used in 39.2% (AGAR) of treated hypertensives. Their use increased with age, from 13.6% in young adults (18-29 years) to 43.29% in those aged 60 (Figure 5 and Table II). There were no differences between the sexes and prescription rates showed less regional variation, ranging from 35.3% in the Northern
fármacos mais utilizados foram os diuréticos (isoladamente ou em associação a outros aHT), instituídos em 47,4% (aSIR). A frequência de utilização dos diuréticos variou consoante o sexo, idade e região de residência. A utilização dos diuréticos aumentou progressivamente com a idade e foi maior no sexo feminino (H:44,4%; M:50%), em todas as regiões à excepção dos Açores (H:63,4%; M:60,9%) – Figura 5 e Tabela II. As regiões em que os diuréticos foram mais utilizados foram os Açores (61,9%) e o Alentejo (58,3%), com frequências de prescrição
em todos os escalões etários. As regiões com menor frequência de utilização foram o Algarve e a região Norte – Tabela III.
A frequência de utilização de antagonistas dos receptores da angiotensina II (ARA) nos hipertensos tratados atingiu 43% (aSIR), sendo mais elevada nos homens (H:45,1%; M:41,2%) em todos os escalões etários e em todas as regiões à excepção dos Açores (H:39,9% versus M:42,4%). Apesar de serem muito utilizados em todos os grupos etários, assumiram particular relevância no tratamento dos hipertensos de meia-idade (40-59 anos), em que a frequência de utilização atingiu 45,7% – Figura 5 e Tabela II.
Grupo etário / Age-group
1 Classe aHT1 AHT class
2 Classes aHT2 AHT classes
3 Classes aHT3 AHT classes
4 Classes aHT 4 AHT classes
HomensMen
MulheresWomen
Figura 4.
Figure 4.
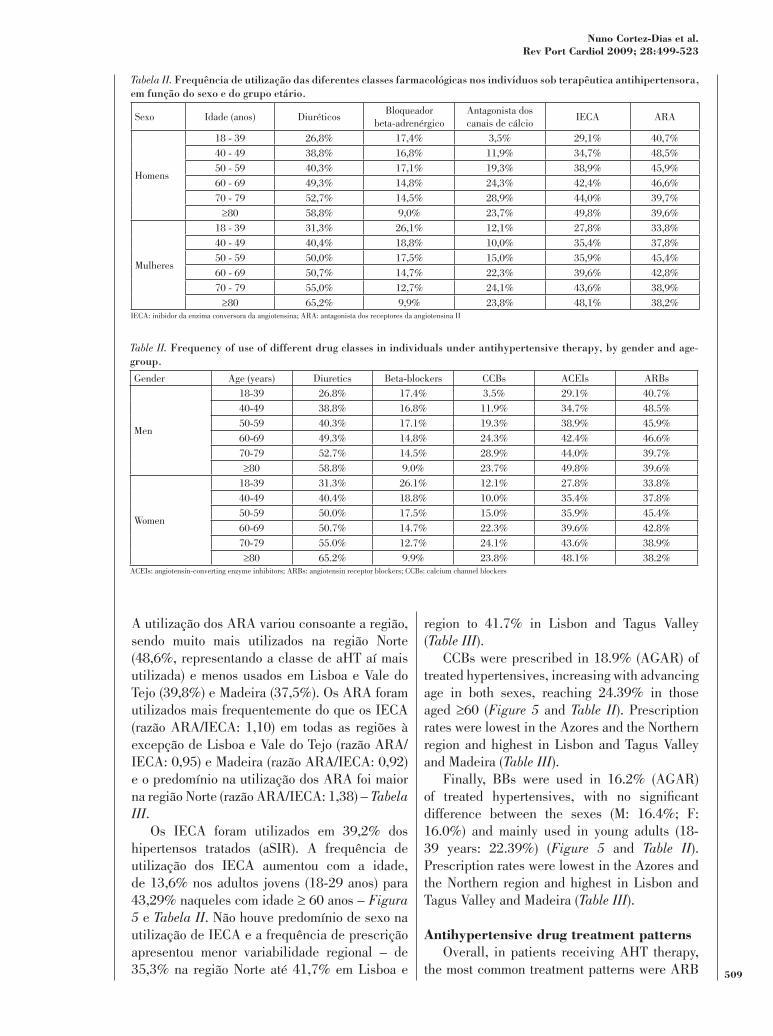
region to 41.7% in Lisbon and Tagus Valley (Table III).
CCBs were prescribed in 18.9% (AGAR) of treated hypertensives, increasing with advancing age in both sexes, reaching 24.39% in those aged 60 (Figure 5 and Table II). Prescription rates were lowest in the Azores and the Northern region and highest in Lisbon and Tagus Valley and Madeira (Table III).
Finally, BBs were used in 16.2% (AGAR)
difference between the sexes (M: 16.4%; F: 16.0%) and mainly used in young adults (18-39 years: 22.39%) (Figure 5 and Table II). Prescription rates were lowest in the Azores and the Northern region and highest in Lisbon and Tagus Valley and Madeira (Table III).
Overall, in patients receiving AHT therapy, the most common treatment patterns were ARB
A utilização dos ARA variou consoante a região, sendo muito mais utilizados na região Norte (48,6%, representando a classe de aHT aí mais utilizada) e menos usados em Lisboa e Vale do Tejo (39,8%) e Madeira (37,5%). Os ARA foram utilizados mais frequentemente do que os IECA (razão ARA/IECA: 1,10) em todas as regiões à excepção de Lisboa e Vale do Tejo (razão ARA/IECA: 0,95) e Madeira (razão ARA/IECA: 0,92) e o predomínio na utilização dos ARA foi maior na região Norte (razão ARA/IECA: 1,38) – Tabela III.
Os IECA foram utilizados em 39,2% dos hipertensos tratados (aSIR). A frequência de utilização dos IECA aumentou com a idade, de 13,6% nos adultos jovens (18-29 anos) para 43,29% naqueles com idade 60 anos – Figura 5 e Tabela II. Não houve predomínio de sexo na utilização de IECA e a frequência de prescrição apresentou menor variabilidade regional – de 35,3% na região Norte até 41,7% em Lisboa e
Tabela II.
Sexo Idade (anos) DiuréticosBloqueador
beta-adrenérgicoAntagonista dos canais de cálcio
IECA ARA
Homens
18 - 39 26,8% 17,4% 3,5% 29,1% 40,7%
40 - 49 38,8% 16,8% 11,9% 34,7% 48,5%
50 - 59 40,3% 17,1% 19,3% 38,9% 45,9%
60 - 69 49,3% 14,8% 24,3% 42,4% 46,6%
70 - 79 52,7% 14,5% 28,9% 44,0% 39,7%
80 58,8% 9,0% 23,7% 49,8% 39,6%
Mulheres
18 - 39 31,3% 26,1% 12,1% 27,8% 33,8%
40 - 49 40,4% 18,8% 10,0% 35,4% 37,8%
50 - 59 50,0% 17,5% 15,0% 35,9% 45,4%
60 - 69 50,7% 14,7% 22,3% 39,6% 42,8%
70 - 79 55,0% 12,7% 24,1% 43,6% 38,9%
80 65,2% 9,9% 23,8% 48,1% 38,2%IECA: inibidor da enzima conversora da angiotensina; ARA: antagonista dos receptores da angiotensina II
Table II.
Gender Age (years) Diuretics Beta-blockers CCBs ACEIs ARBs
Men
18-39 26.8% 17.4% 3.5% 29.1% 40.7%
40-49 38.8% 16.8% 11.9% 34.7% 48.5%
50-59 40.3% 17.1% 19.3% 38.9% 45.9%
60-69 49.3% 14.8% 24.3% 42.4% 46.6%
70-79 52.7% 14.5% 28.9% 44.0% 39.7%
80 58.8% 9.0% 23.7% 49.8% 39.6%
Women
18-39 31.3% 26.1% 12.1% 27.8% 33.8%
40-49 40.4% 18.8% 10.0% 35.4% 37.8%
50-59 50.0% 17.5% 15.0% 35.9% 45.4%
60-69 50.7% 14.7% 22.3% 39.6% 42.8%
70-79 55.0% 12.7% 24.1% 43.6% 38.9%
80 65.2% 9.9% 23.8% 48.1% 38.2%ACEIs: angiotensin-converting enzyme inhibitors; ARBs: angiotensin receptor blockers; CCBs: calcium channel blockers

(16.9%) or ACEI (14.41%) as monotherapy, and ARB-diuretic (11.8%) or ACEI-diuretic (11.8%) combinations (Table IV).
Among patients treated with monotherapy (47.62%), the most prescribed classes were ARBs (35.5%; M: 38.14%; F: 33.12%) and ACEIs (30.27%; M: 31.19%; F: 29.48%), with less frequent use of diuretics (12.29%; M: 9.22%; F: 15.08%), BBs (8.96%; M: 8.17%; F: 9.56%) and CCBs (6.55%; M: 6.14%; F: 6.94%). There were differences in the age distribution of patients under monotherapy (Table IV): individuals medicated with BBs tended to be younger (mean age 58.5±12.2 years), while those medicated with CCBs or diuretics tended to be older (66.0±10.3 and 65.0±11.2 years respectively).
Of treated hypertensives, 52.38% were prescribed at least two classes (M: 51.34%; F: 53.25%). In those treated with two classes
dose combination, the most common associations were ARB-diuretic (32.68%; M: 33.95%; F: 31.66%), ACEI-diuretic (32.60%; M: 29.84%; F: 34.81%), ACEI-CCB (5.52%; M: 6.13%; F: 5.01%), CCB-diuretic (4.99%; M: 4.19%; F: 5.66%) and ARB-CCB (4.24%; M: 4.52%; F: 4.08%), although the frequency of each
Vale do Tejo (Tabela III).Os ACC foram utilizados em 18,9% dos
hipertensos tratados (aSIR), sendo a utilização crescente com a idade em ambos os sexos e atingindo 24,39 % nos indivíduos 60 anos – Figura 5 e Tabela II. A frequência de utilização dos ACC foi menor nos Açores e região Norte e mais elevada em Lisboa e Vale do Tejo e na Madeira – Tabela III.
Finalmente, os BB foram prescritos em 16,2% dos hipertensos tratados (aSIR), sem diferença
M:16,0%) e predominando a sua utilização nos adultos jovens (18-39 anos: 22,39%) – Figura 5 e Tabela II. A frequência de utilização dos BB foi menor nos Açores e região Norte e mais elevada em Lisboa e Vale do Tejo e Madeira – Tabela III.
Em termos globais, entre os doentes submetidos a terapêutica aHT, os padrões de tratamento mais frequentes foram a administração de ARA em monoterapia (16,9%), IECA em monoterapia (14,41%), associação ARA-diurético (11,8%) e associação IECA-diurético (11,8%) – Tabela IV.
Entre os doentes tratados em monoterapia
Tabela III.
43,1% 13,0% 15,5% 35,3% 48,6%
46,7% 12,7% 20,1% 39,7% 40,9%
49,7% 21,2% 21,1% 41,7% 39,8%
58,3% 14,0% 17,3% 41,6% 47,0%
35,4% 15,1% 19,0% 37,4% 41,4%
61,9% 12,1% 9,6% 39,9% 41,3%
52,3% 21,2% 26,5% 40,6% 37,5%
47,4% 16,2% 18,9% 39,2% 43,0%IECA: inibidor da enzima conversora da angiotensina; ARA: antagonista dos receptores da angiotensina II
Table III.
43.1% 13.0% 15.5% 35.3% 48.6%
46.7% 12.7% 20.1% 39.7% 40.9%
49.7% 21.2% 21.1% 41.7% 39.8%
58.3% 14.0% 17.3% 41.6% 47.0%
35.4% 15.1% 19.0% 37.4% 41.4%
61.9% 12.1% 9.6% 39.9% 41.3%
52.3% 21.2% 26.5% 40.6% 37.5%
47.4% 16.2% 18.9% 39.2% 43.0%ACEIs: angiotensin-converting enzyme inhibitors; ARBs: angiotensin receptor blockers; CCBs: calcium channel blockers

Idade (anos) / Age (years)
Diuréticos
Diuretics
Beta-blockers
Bloqueador beta-adrenérgico
Antagonista doscanais de cálcio
Calcium channelblockers
Inibidor da enzima conversora da angiotensina
Angiotensin-converting enzyme inhibitors
Antagonista dos receptores de angiotensina II
Angiotensin receptor blockers
Figura 5.
Figure 5.
Diuréticos / Diuretic
ACC / CCB
IECA / ACEI
IECA-ACC / ACEI-CCB
ARA-ACC / ARB-CCB
ARA / ARB
1 Classe aHT - outra 1 AHT class - other
2 Classes aHT - outras 2 AHT classes - others
3 Classes aHT - outras 3 AHT classes - others
4 Classes aHT4 AHT classes
IECA-diurético-ACCACEI-diuretic-CCB
IECA-diurético / ACEI-diuretic
IECA-diurético-ACCACEI-diuretic-CCB
ACC - diurético / CCB-diuretic
ARA - diurético / ARB-diuretic
Beta-bloqueador / Beta-blocker
Figura 6.
Figure 6.
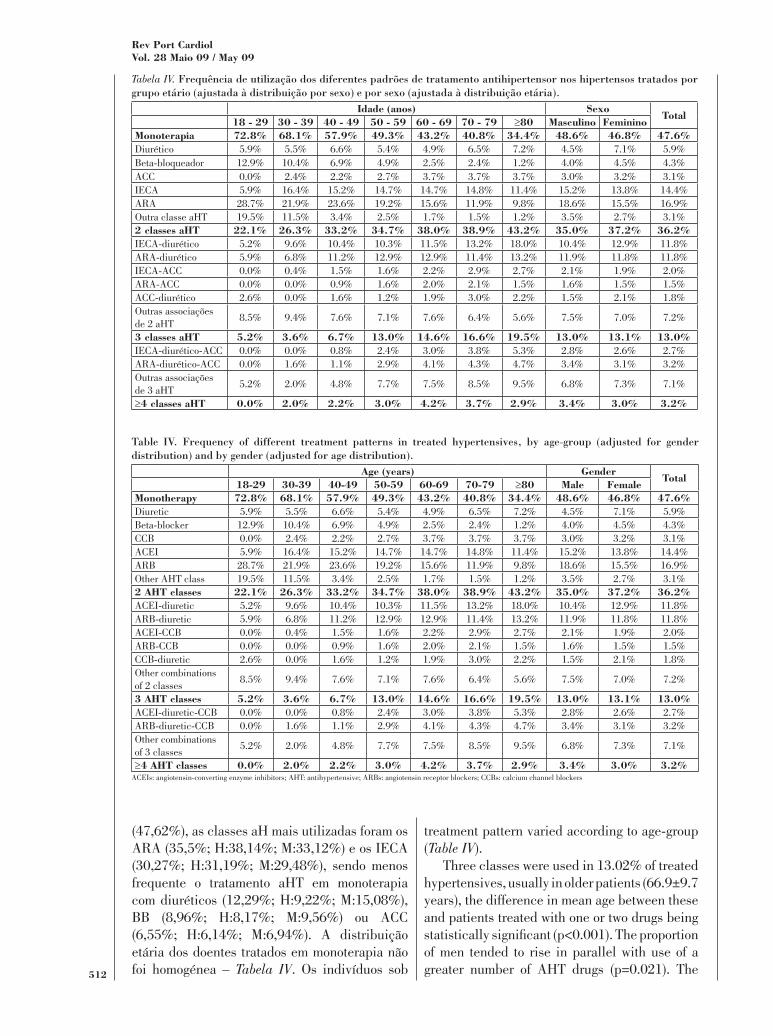
treatment pattern varied according to age-group (Table IV).
Three classes were used in 13.02% of treated hypertensives, usually in older patients (66.9±9.7 years), the difference in mean age between these and patients treated with one or two drugs being
of men tended to rise in parallel with use of a greater number of AHT drugs (p=0.021). The
(47,62%), as classes aH mais utilizadas foram os ARA (35,5%; H:38,14%; M:33,12%) e os IECA (30,27%; H:31,19%; M:29,48%), sendo menos frequente o tratamento aHT em monoterapia com diuréticos (12,29%; H:9,22%; M:15,08%), BB (8,96%; H:8,17%; M:9,56%) ou ACC (6,55%; H:6,14%; M:6,94%). A distribuição etária dos doentes tratados em monoterapia não foi homogénea – Tabela IV. Os indivíduos sob
Tabela IV.
Sexo
Diurético 5.9% 5.5% 6.6% 5.4% 4.9% 6.5% 7.2% 4.5% 7.1% 5.9%Beta-bloqueador 12.9% 10.4% 6.9% 4.9% 2.5% 2.4% 1.2% 4.0% 4.5% 4.3%ACC 0.0% 2.4% 2.2% 2.7% 3.7% 3.7% 3.7% 3.0% 3.2% 3.1%IECA 5.9% 16.4% 15.2% 14.7% 14.7% 14.8% 11.4% 15.2% 13.8% 14.4%ARA 28.7% 21.9% 23.6% 19.2% 15.6% 11.9% 9.8% 18.6% 15.5% 16.9%Outra classe aHT 19.5% 11.5% 3.4% 2.5% 1.7% 1.5% 1.2% 3.5% 2.7% 3.1%
IECA-diurético 5.2% 9.6% 10.4% 10.3% 11.5% 13.2% 18.0% 10.4% 12.9% 11.8%ARA-diurético 5.9% 6.8% 11.2% 12.9% 12.9% 11.4% 13.2% 11.9% 11.8% 11.8%IECA-ACC 0.0% 0.4% 1.5% 1.6% 2.2% 2.9% 2.7% 2.1% 1.9% 2.0%ARA-ACC 0.0% 0.0% 0.9% 1.6% 2.0% 2.1% 1.5% 1.6% 1.5% 1.5%ACC-diurético 2.6% 0.0% 1.6% 1.2% 1.9% 3.0% 2.2% 1.5% 2.1% 1.8%Outras associações de 2 aHT
8.5% 9.4% 7.6% 7.1% 7.6% 6.4% 5.6% 7.5% 7.0% 7.2%
IECA-diurético-ACC 0.0% 0.0% 0.8% 2.4% 3.0% 3.8% 5.3% 2.8% 2.6% 2.7%ARA-diurético-ACC 0.0% 1.6% 1.1% 2.9% 4.1% 4.3% 4.7% 3.4% 3.1% 3.2%Outras associações de 3 aHT
5.2% 2.0% 4.8% 7.7% 7.5% 8.5% 9.5% 6.8% 7.3% 7.1%
Diuretic 5.9% 5.5% 6.6% 5.4% 4.9% 6.5% 7.2% 4.5% 7.1% 5.9%Beta-blocker 12.9% 10.4% 6.9% 4.9% 2.5% 2.4% 1.2% 4.0% 4.5% 4.3%CCB 0.0% 2.4% 2.2% 2.7% 3.7% 3.7% 3.7% 3.0% 3.2% 3.1%ACEI 5.9% 16.4% 15.2% 14.7% 14.7% 14.8% 11.4% 15.2% 13.8% 14.4%ARB 28.7% 21.9% 23.6% 19.2% 15.6% 11.9% 9.8% 18.6% 15.5% 16.9%Other AHT class 19.5% 11.5% 3.4% 2.5% 1.7% 1.5% 1.2% 3.5% 2.7% 3.1%
ACEI-diuretic 5.2% 9.6% 10.4% 10.3% 11.5% 13.2% 18.0% 10.4% 12.9% 11.8%ARB-diuretic 5.9% 6.8% 11.2% 12.9% 12.9% 11.4% 13.2% 11.9% 11.8% 11.8%ACEI-CCB 0.0% 0.4% 1.5% 1.6% 2.2% 2.9% 2.7% 2.1% 1.9% 2.0%ARB-CCB 0.0% 0.0% 0.9% 1.6% 2.0% 2.1% 1.5% 1.6% 1.5% 1.5%CCB-diuretic 2.6% 0.0% 1.6% 1.2% 1.9% 3.0% 2.2% 1.5% 2.1% 1.8%Other combinations of 2 classes
8.5% 9.4% 7.6% 7.1% 7.6% 6.4% 5.6% 7.5% 7.0% 7.2%
ACEI-diuretic-CCB 0.0% 0.0% 0.8% 2.4% 3.0% 3.8% 5.3% 2.8% 2.6% 2.7%ARB-diuretic-CCB 0.0% 1.6% 1.1% 2.9% 4.1% 4.3% 4.7% 3.4% 3.1% 3.2%Other combinations of 3 classes
5.2% 2.0% 4.8% 7.7% 7.5% 8.5% 9.5% 6.8% 7.3% 7.1%
ACEIs: angiotensin-converting enzyme inhibitors; AHT: antihypertensive; ARBs: angiotensin receptor blockers; CCBs: calcium channel blockers

most common combinations of three AHT classes were ARB-diuretic-CCB and ACEI-diuretic-CCB. Four or more drug classes were prescribed in 3.2% of treated hypertensives, mainly middle-aged or elderly patients (Table IV).
cardiovascular risk factor, and is responsible for an estimated 6% of deaths worldwide(6). Advances in treatment in the second half of the 20th century led to a progressive decrease in mortality due to stroke and CAD in most developed countries(7). Stroke mortality in Portugal also fell in the last quarter of the 20th century, but it remains one of the highest in the world, at 125.9/100,000 men and 99.6/100,000 women(8). Thus, assessing the effectiveness of HT treatment and identifying problems in detection and treatment in PHC are of major importance in planning preventive strategies aimed at modifying the overall CV risk of the population. The present study set out to identify possible targets for improving blood pressure control by characterizing antihypertensive drug treatment patterns. Espiga de Macedo et al. reported that only 11.2% of hypertensives in Portugal had adequately controlled BP values, and that the percentage among those undergoing therapy was only 28.9%(3). It is therefore urgent to implement public health measures that will improve the epidemiological situation in Portugal.
The VALSIM study analyzed PHC users, and so its results and conclusions should only
not aimed at determining the prevalence of CV risk factors in the general population. However, it is worth presenting estimates of prevalence in the general population based on standardized results from the VALSIM study, since comparison with the results from published reference population-based studies will strengthen the external validity of the study and the consistency of the results presented. According to our study’s results, estimated HT prevalence in the population resident in mainland Portugal and the
to that reported by Espiga de Macedo et al.(3) in the mainland population (42.1±1.2%). Most studies comparing HT prevalence in different
terapêutica com BB foram tendencialmente mais jovens (idade média 58.5±12.2 anos) enquanto aqueles tratados com ACC ou com diuréticos foram tendencialmente mais idosos (66.0±10.3 e 65.0±11.2 anos, respectivamente).
Cerca de 52,38% dos hipertensos tratados estavam medicados com pelo menos duas classes aHT (H:51,34%; M:53,25%). Entre os hiper-tensos tratados com duas classes aHT (36,16%), em administração separada ou como associação
ARA-diurético (32,68%; H:33,95%; M:31,66%), IECA-diurético (32,60%; H:29,84%; M:34,81%), IECA-ACC (5,52%; H:6,13%; M:5,01%), ACC-diurético (4,99%; H:4,19%; M:5,66%) e ARA-ACC (4,24%; H:4,52%; M:4,08%), embora a frequência de utilização de cada padrão de tratamento tenha variado com a faixa etária – Tabela IV.
Foram utilizadas 3 classes de aHT em 13,02% dos hipertensos tratados, tendencial-mente mais idosos (66,9±9,7anos, sendo a dife-rença rela tivamente à idade média dos doentes tratados com 1 ou 2 fármacos estatisticamente
para o aumento da proporção de doentes do sexo masculino com o aumento do número de aHT utilizados (p=0,021). Entre as combinações de 3 classes aHT, destacaram-se as associações ARA-diurético-ACC e IECA-diurético-ACC. Em 3,2% dos hipertensos tratados, foram utilizadas 4 ou mais classes de aHT, tratando- -se predominantemente de hipertensos de meia- -idade ou idosos – Tabela IV.
tratamento mais frequente, estimando-se que seja responsável por 6% das mortes a nível mundial(6). Os avanços no tratamento da HTA na segunda metade do século XX conduziram à diminuição progressiva da mortalidade por AVC e doença coronária na maioria dos países desenvolvidos(7). A mortalidade por AVC também diminuiu em Portugal durante o último quartel do século XX, mas continua a ser uma das taxas mais elevadas em todo o mundo, de 125,9/100.000 homens e de 99,6/100.000 mulheres(8). Consequentemente, a avaliação da efectividade do tratamento da HTA

countries are based on the 35-64 age-group. On this basis, the estimated prevalence in our study was 46.05% (M: 47.95%; F: 44.29%), which is considerably higher than found in the US(9) (28%), Canada(10) (27%), Sweden(11,12) (38%) and Italy(2) (38%), similar to those reported for England(4,5) (42%) and Spain(13) (47%), and lower than in Germany(14) (55%). HT prevalence
mainland Portugal, the highest prevalence was in the Alentejo (51.54%) and the lowest in the Northern region (41.62%), similar results to those reported by Espiga de Macedo et al.(3). These regional differences are to a large extent explained by differences in the age structure of each region, since HT prevalence increases
There was a progressive and parallel increase in systolic and diastolic BP values up to the age of 50-59 years, after which systolic values continued to rise while diastolic values stabilized and then slightly fell in the oldest groups. These age-related changes in BP are similar to those reported in other populations. Systolic BP values were around 5 mmHg higher than those in the US(9) and Canadian(10) populations for all age-groups. Values of systolic BP for each age-
reported in Italy(2), Spain(13), England(4,5) and Finland(2), and were around 10 mmHg lower from the age of 60 than those in Germany(14) and Sweden(11,12). Diastolic BP values in those aged
in the US population(9), but were similar to those reported in other European populations(2,15). Finally, the mean systolic (136±19 mmHg) and diastolic (79±11 mmHg) BP values observed in the VALSIM study are close to those reported by Espiga de Macedo et al. (135±21 mmHg and 81±11 mmHg respectively)(3).
Various clinical trials have shown that monotherapy with any class of AHT drug provides adequate BP control in less than 20-30% of hypertensives, except for those with grade 1 HT (BP 140-159/90-99 mmHg)(16,17), and in a recent clinical trial of hypertensives with high CV risk, only 1 in 10 patients attained BP values below 140/90 mmHg with monotherapy(18). The guidelines for HT treatment
detecção e tratamento assumirá grande relevância no planeamento das estratégias preventivas nos CSP, tendo em vista a intervenção sobre o risco CV global da população. Ao caracterizar os padrões de tratamento farmacológico da HTA, o presente estudo pretende contribuir para a
actuação, que possibilitem a melhoria da taxa de controlo tensional. Efectivamente, Espiga de Macedo et al documentaram que apenas 11,2% dos hipertensos em Portugal apresentam valores tensionais controlados, sendo a taxa de controlo tensionais entre aqueles submetidos a terapêutica aHT de apenas 28,9%(3), pelo que é urgente a implementação de medidas de saúde pública que melhorem a realidade epidemiológica nacional.
O Estudo VALSIM analisou a população utente dos CSP, sendo os seus resultados e con-clusões apenas aplicáveis a essa população que
não sendo um estudo populacional da população geral, não pretende determinar a prevalência de factores de risco CV nessa população que não avaliou directamente. No entanto, é útil a apresentação das estimativas de prevalência na população geral decorrentes da padronização dos resultados do Estudo VALSIM, já que a sua comparação com os resultados dos estudos populacionais de referência já publicados contribui para a avaliação da validade externa do estudo e da consistência dos demais resultados apresentados. Assim, de acordo com os presentes resultados, a prevalência estimada de HTA na população residente em Portugal continental e regiões autónomas é de 42,62%, valor que é similar àquele previamente estimado por Espiga de Macedo et col(3), referente ao território continental (42,1±1,2%). Na maioria dos estudos, a comparação das prevalências de HTA entre países faz-se com base na prevalência no grupo etário 35-64 anos. Aplicando esse critério, a prevalência estimada no nosso estudo foi de 46,05% (H:47,95%; M:44,29%), valor que é substancialmente superior aos observados nos Estados Unidos da América(9) (EUA) (28%), Canadá(10) (27%), Suécia(11,12) (38%) e Itália(2) (38%), encontrando-se ao nível daqueles registados em Inglaterra(4,5) (42%) e Espanha(13) (47%), e sendo inferior ao observado na Alemanha(14) (55%). Além disso, a prevalência de
Portugal continental, detectou-se a prevalência
placed increasing emphasis on combinations of
therapy. Thus, the 2007 guidelines of the European Society of Hypertension and the European Society of Cardiology recommend
patients with marked HT and high or very high CV risk and those in whom stricter control of BP is required such as patients with diabetes, renal failure, proteinuria, or a history of stroke or myocardial infarction(19). The proportion of hypertensives treated with monotherapy is thus
in PHC, and reducing this proportion through public health strategies is likely to improve BP control rates in the population.
The majority of hypertensive patients in PHC in Portugal (52.38%) were medicated with two or more drugs, but the percentage under monotherapy was still very high (47.62%). This situation is unsatisfactory, the proportion being higher than in recent studies in other European countries(5) and similar to the US (47%(20)). Moreover, observational studies have shown that the percentage of patients under monotherapy in
falling, and is therefore probably by now even lower. For example, Primatesta et al. found that the rate of monotherapy in England fell from 60% in 1998(4) to 44% in 2003(5).
In addition, the proportion of patients under combination therapy was markedly lower than that reported in tertiary health care in Portugal, where virtually all patients receive such treatment(21).
In patients under monotherapy, the most frequently prescribed classes in PHC centers in Portugal were ARBs (35.5%), ACEIs (30.3%) and
the patterns found in other European countries. The most common drugs used as monotherapy in England were diuretics (30±1.61%), BBs (27±1.56%), CCBs (22±1.45%) and ACEIs (18±1.35%), while Godley et al.(20) found that those most commonly used in the US were ACEIs (27.3%), diuretics (26.6%), BBs (23.4%) and CCBs (15.4%). Deciding which AHT drug to use initially as monotherapy, while the subject of disagreement, is becoming less important in the light of evidence that most hypertensives will
mais elevada no Alentejo (51,54%) e a mais reduzida na região Norte (41,62%), resultados que estão em linha com os determinados por Espiga de Macedo et al(3). Estas diferenças a nível
pelas diferenças ao nível da estrutura etária de cada região, já que a prevalência da HTA aumenta decisivamente com a idade.
Detectou-se elevação progressiva e em para-lelo dos valores de PA sistólica e diastólica até ao 50-59 anos, após o que os valores tensionais sistólicos continuaram a progredir, enquanto os diastólicos estabilizaram, para diminuir ligeiramente nos grupos mais idosos. Na comparação dos valores tensionais observados com aqueles determinados noutras populações, destaca-se que a evolução tensional com a idade é sobreponível. Os valores de PA sistólica foram cerca de 5mmHg superiores aos documentados na população norte-americana(9) e canadiana(10), em todos os escalões etários. Não existem di-fe renças assinaláveis quanto aos valores de PA sistólica determinados por grupo etário e aqueles registados em Itália(2), Espanha(13), Inglaterra(4,5)
ou Finlândia(2), sendo inclusivamente a partir dos 60 anos cerca de 10mmHg inferiores aos registados na Alemanha(14) ou Suécia(11,12). Rela tivamente aos valores de PA diastólica, foram a partir dos
aos observados na população norte-americana(9). No entanto, acompanharam os valores tensionais diastólicos medidos nas restantes populações europeias(2,15). Finalmente, os valores tensionais documentados nos Estudo VALSIM, referentes à PA sistólica (136±19mmHg) e à PA diastólica (79±11mmHg) são coincidentes com os registados por Espiga de Macedo et al, 135±21mmHg e 81±11mmHg, respectivamente(3).
Diversos ensaios clínicos têm mostrado que a monoterapia com qualquer classe aHT só possibilita o adequado controlo tensional em menos de 20-30% da população hipertensa, exceptuando-se os doentes com HTA grau 1 (PA 140-159/90-99 mmHg)(16,17). Além disso, num ensaio clínico recente em hipertensos de alto risco CV, apenas 1 em cada 10 doentes atingiram PA inferior a 140/90 mmHg sob monoterapia(18). Por isso, as orientações das diferentes sociedades
in fact need combination therapy(19). The choice
in patients with mild BP elevation and low to moderate CV risk, should be made according
presence of MS, diabetes, or cardiovascular or renal disease), comorbidities that limit the use of certain drug classes, possible drug interactions, drug tolerability and cost(19). The most frequently prescribed drugs for monotherapy in PHC in Portugal are appropriate for the probable risk
to European guidelines, with the tolerability of ARBs being preferred over the lower cost of
and protection of the individual patient(19). Nevertheless, in view of the demonstrated CV protection of ACEIs, which is at least as good as ARBs, their cost and the rate of adverse side effects (notably cough, which leads to suspension of the drug in up to 20% of patients(22)), proportionately greater use of ACEIs in monotherapy would have been expected.
The most common combinations in the present study in patients treated with two classes were ARB-diuretic (32.7%) and ACEI-diuretic (32.6%), with much lower percentages for ACEI-CCB (5.5%), CCB-diuretic (5%) and ARB-CCB (4.2%). The associations used are in accordance with European practice guidelines for hypertension, combining classes with good tolerability and complementary mechanisms of action, the antihypertensive effect of the combination being greater than that of its components in isolation(19). By way of comparison, the most common combinations of two classes in England were ACEI-diuretic (27±2.1%), CCB-diuretic (21±2.1%) and BB-diuretic (21± 1.93%)(4)
less favorable than that found in PHC in Portugal, particularly with regard to the BB-diuretic association. Although this combination has been used successfully in various clinical trials, it has also been shown to have adverse metabolic effects. The incidence of diabetes was found to be higher in patients treated with diuretics (often in association with BBs) in the Systolic Hypertension in the Elderly Program (SHEP)(23) and Medical Research Council (MRC)(24) trials. Thus, while a valid combination, it should be avoided in patients at increased risk
atribuído importância crescente à combinação de classes farmacológicas, incluindo sob a forma de
recomendações de 2007 da Sociedade Europeia de Hipertensão e da Sociedade Europeia de Cardiologia defendem que se deve optar pela instituição desde o início do tratamento de 2 classes aHT em baixa dose nos doentes com elevação tensional marcada, risco CV alto ou muito alto e naqueles em quem sejam necessá-rios níveis de controlo tensional mais exigentes (diabéticos, disfunção renal, proteinúria, his-tória de AVC ou enfarte do miocárdio)(19). Assim, a proporção de hipertensos tratados em
tratamento da HTA nos CSP, já que a sua redução mediante estratégias planeadas de saúde pública previsivelmente irá melhorar a taxa de controlo tensional da população.
Nos CSP em Portugal, a maioria dos hiperten-sos (52,38%) estava medicada com dois ou mais fármacos aHT, mas a proporção de doentes sob monoterapia permanecia ainda muito elevada (47,62%). Esta proporção é insatisfatória, sendo superior à observada em estudos recentes noutros países europeus(5) e em linha com aquela registada nos EUA (47%(20)). Além disso, os estudos observacionais têm mostrado que a proporção de doentes sob monoterapia nesses países têm vindo
pelo que neste momento serão provavelmente ainda menores. Por exemplo, Primatesta et al. constatou que a taxa de tratamento com monoterapia em Inglaterra diminuiu de 60% em 1998(4) para 44% em 2003(5).
Além disso, a proporção de doentes sob terapêutica combinada foi notoriamente inferior à descrita nos Cuidados de Saúde Terciários em Portugal, onde praticamente todos os doentes são tratados com conjugação de classes aHT (21).
Entre os doentes sob monoterapia, as classes mais utilizadas nos CSP em Portugal foram os ARA (35,5%), os IECA (30,3%) e os diuréticos (12,3%). A proporção de utilização das diferentes classes aHT nos doentes sob monoterapia foi
noutros países europeus. Em Inglaterra, os fármacos mais utilizados em monoterapia foram os diuréticos (30±1,61%), os BB (27±1,56%), os

for diabetes, particularly those with MS(19).
Several clinical trials and meta-analyses suggest that the differences between classes in terms of CV morbidity and mortality are small for similar reductions in BP, and hence the most important point is achievement of adequate BP control and not the drug class used to attain that goal(25-27). Nevertheless, certain drug classes
lowering effect, although these are proportionally (19). Data from a recent
meta-analysis involving 68,000 patients(28) and the results of the ASCOT trial(18) suggest that CCBs provide slightly better protection from stroke than the other drug classes, but less protection against progression to heart failure(28,29). Furthermore, a recent meta-analysis(31) including the ASCOT(18) and LIFE(30) trials found that BBs provide less protection from stroke that other AHT classes, probably because they induce a smaller reduction in central blood pressure(32). The guidelines for HT management in PHC in the United Kingdom therefore recommend that BBs be considered as fourth-line therapy only(33).
According to the VALSIM study results, the most frequently used class overall was diuretics
were prescribed in 47.4% of cases, particularly in older and female patients. Prescription rates for ARBs and ACEIs were similar (43.0% and 39.2% respectively), but ARBs tended to be prescribed more in men, particularly middle-aged individuals (40-59 years), while use of ACEIs increased with age. The rates for CCBs
(18.9% and 16.2% respectively), although they were prescribed in patients from different age-groups – CCBs mainly in older patients and BBs in young adults.
It is also useful to compare the results from PHC with the situation in tertiary centers, as assessed by Quitéria Rato et al.(21). They found a similar rate of use of diuretics (48%), lower
prescription rates of the other therapeutic classes, including ACEIs (48%), BBs (40%) and CCBs (40%).
The overall prescription pattern of different AHT classes in PHC in Portugal reveals underuse of CCBs, particularly among older patients, in
ACC (22±1,45%) e os IECA (18±1,35%). Pelo contrário, Godley et al(20) demonstrou que os aHT mais utilizados em monoterapia nos EUA são os IECA (27,3%), diuréticos (26,6%), BB (23,4%) e
aHT a ser utilizada em monoterapia, apesar de controversa, tem merecido cada vez menor relevância face à evidência de que a grande maioria dos hipertensos irá necessitar na realida-de da associação de múltiplas classes aHT(19). A
com elevação ligeira da PA e risco CV baixo ou moderado, deve suscitar a escolha de uma
(idade, raça, presença de síndrome metabólica, diabetes mellitus, doença cardiovascular ou doença renal), presença de comorbilidades que limitem a utilização de determinadas classes farmacológicas, possibilidade de interacções medicamentosas, tolerabilidade e custo da terapêutica(19). As classes mais utilizadas em monoterapia nos CSP em Portugal estão de
doentes candidatos a monoterapia segundo as recomendações europeias e parecem previlegiar a tolerabilidade dos ARA em detrimento do menor custo médio de outras classes aHT. Efectiva -
protecção individual do doente(19). No entanto, em
IECA, que será no mínimo similar ao dos ARA, ao seu custo médio e atendendo à frequência dos efeitos adversos associados (nomeadamente da tosse, que conduzirá à suspensão do fármaco em até 20% dos doentes(22)), seria previsível que a utilização dos IECA’s em monoterapia fosse proporcionalmente superior.
No presente estudo, as associações mais utilizadas nos doentes tratados com duas classes aHT foram ARA-diurético (32,7%) e IECA-diurético (32,6%), e numa proporção muito inferior as associações IECA-ACC (5,5%), ACC-diurético (5%) e ARA-ACC (4,2%). As diferentes associações utilizadas estão de acordo com as recomendações europeias para o tratamento da
tolerabilidade favorável e mecanismos de acção complementar, sendo o efeito antihipertensor da combinação superior ao de cada um dos seus componentes(19). Em termos comparativos, destaca-se que as associações de duas classes

CCBs compared to placebo in elderly patients with systolic and diastolic(34) or isolated systolic HT(35,36), providing at least as good CV protection as diuretics, ACEIs and ARBs(19). Moreover, in view of the additional protection of CCBs against stroke(28), their use in Portugal should be higher than in other countries.
the use of different classes. In the Northern region, ARBs were the most frequently prescribed, the rates for the other classes being lower than the national average. Lisbon and Tagus Valley was the only region in which prescription of ACEIs was higher than for ARBs, and it also had the highest rates for BBs and CCBs. Use of diuretics was highest in the Alentejo, and was also high in the Azores, with lower rates for CCBs and BBs than the national average.
The results of the present study suggest that public health strategies should aim to promote more effective, rational and evidence-based treatment patterns, taking into account the
prove blood pressure control, it is recommended that the proportion of hypertensives treated with combinations of various AHT classes
particularly useful in this context. Although regional variations in AHT prescription patterns should be borne in mind, the overall results showed underuse of CCBs in hypertensives treated in PHC in Portugal. This is of particular
stroke prevention(28).
The present study was carried out in PHC centers, since in population studies this is a reliable way of recruiting large numbers of indi-viduals who are representative of the different regions of a country. However, the method of
appointment on a given day), while intended to be random, may have been affected by limited access to PHC. The sample analyzed in the VALSIM study has a gender and age distribution
and thus differs from the distribution found in the general population. Since the study was not
aHT mais utilizadas em Inglaterra foram IECA-diurético (27±2,1%), ACC-diurético (21±2,1%) e BB-diurético (21±1,93%)(4)
favorável do que aquele documentado nos CSP em Portugal, nomeadamente no que concerne à associação BB-diurético. Apesar dessa combinação ter sido utilizada com sucesso em diferentes ensaios clínicos, tem sido também demonstrado que possui efeitos dismetabólicos. Efectivamente, a incidência de diabetes mellitus foi maior nos doentes tratados com diurético (frequentemente em associação com BB) nos ensaios clínicos SHEP(23) e MRC(24). Assim, apesar de ser uma associação válida, deve ser evitada nos doentes com risco aumentado de diabetes mellitus, particularmente naqueles com síndrome metabólica(19).
Os diferentes ensaios clínicos e metanálises sugerem que para reduções similares da PA, as diferenças entre as diferentes classes aHT no que respeita à morbilidade e mortalidade CV são reduzidas, pelo que o mais importante é a obtenção de adequado controlo tensional e não a classe far macológica com que o mesmo é atingido(25-27).
independentes da descida tensional produzida, muito embora sejam proporcionalmente menos
(19). Assim, os dados de uma metanálise recente envolvendo mais de 68.000 doentes(28) e ainda os resultados do estudo ASCOT(18) sugerem que os ACC possibilitaram protecção relativamente ao AVC discretamente superior aos restantes grupos farmacológicos, e por outro lado, menor protecção relativamente
(28,29). Além disso, os resultados do estudo ASCOT(18)
e do estudo LIFE(30) foram considerados numa metanálise recente(31) de acordo com a qual os BB induzem menor protecção relativamente ao AVC do que as demais classes aHT, provavelmente por induzirem menor descida da PA central(32). Consequentemente, as recomendações para o tratamento da HTA nos CSP no Reino Unido propõem que os BB sejam considerados apenas fármacos aHT de 4ª linha(33).
De acordo com os presentes resultados, os aHT globalmente mais utilizados foram os diuréticos (particularmente no âmbito de associações de

nos hipertensos mais idosos e no sexo feminino. A frequência de utilização dos ARA e IECA foi próxima (43,0% e 39,2%, respectivamente), mas a prescrição de ARA exibiu predomínio do sexo masculino, particularmente em indivíduos de meia-idade (40-59 anos), enquanto a utilização dos IECA aumentou com a idade. A frequência
menor e relativamente próxima entre si (18,9% e 16,2%, respectivamente), muito embora tenham
oposto – o ACC em hipertensos tendencialmente mais idosos, e os BB em adultos jovens.
Torna-se também relevante a comparação dos presentes resultados referentes aos CSP com a realidade dos Cuidados de Saúde Terciários, avaliada por Quitéria Rato et al(21). Nesse estudo foi encontrada uma frequência similar de utilização dos diuréticos (48%), menor frequência de recurso aos ARA (20%) e frequências
restantes classes terapêuticas, incluindo IECA (48%), BB (40%) e ACC (40%).
O padrão global de utilização das diferentes classes aHT nos CSP em Portugal denota subutilização dos ACC, particularmente nos indivíduos mais idosos em que têm grande utilidade. Efectivamente, vários ensaios clínicos provaram o benefício dos ACC relativamente ao placebo em doentes idosos com HTA sisto--diastólica(34) ou HTA sistólica isolada(35,36), possibilitando protecção CV pelo menos similar à dos diuréticos, IECA ou ARA(19). Além disso, tendo em consideração a protecção adicional dos ACC relativamente ao AVC(28), seria desejável que a sua utilização em Portugal fosse maior do que nos outros países.
utilização das diferentes classes aHT. Na região Norte, os ARA foram os aHT mais utilizados, sendo a utilização das restantes classes inferior à média nacional. A região de Lisboa e Vale do Tejo foi a única em que a utilização dos IECA excedeu a prescrição de ARA, sendo também a região com maior frequência de recurso aos BB e ACC. No Alentejo, a utilização de diuréticos foi mais frequente do que nas restantes regiões. Nos Açores, houve uma maior frequência de utilização de diuréticos, sendo o recurso aos ACC e BB inferior à média nacional.
based on the general population, it was not aimed at determining the overall prevalence of CV risk factors directly. However, given the very large number of individuals analyzed, the sample is representative of both sexes, all regions and all age-groups. The representativeness of the sample is clear from analysis of the standard error of estimate of overall HT prevalence, by gender and region of residence (Table I). In view of the representativeness of each of the subgroups, the results can be standardized through adjustment for gender, age and region of residence using the total probability theorem (with correction for missing data). This minimizes any bias resulting from the fact that these variables are independent risk factors for HT, and is designed to enable comparison between our estimates of prevalence and those of reference population studies. The estimated prevalence of HT in the present study is similar to that reported in the largest study to date in the Portuguese population(3), which supports the consistency of the results and strengthens its external validity. Nevertheless, considerable caution is required in extrapolating the results to the population as a whole, as there
individuals using PHC centers and those who do not seek medical attention and may have
to estimate directly the level of awareness, treatment and control in the population, since hypertensives who consult their general practitioner (GP), for whatever reason, are more likely to be aware of the diagnosis, to have begun therapy and to have a scheduled follow-up.
The study design was aimed mainly at analyzing the response of PHC to detection of elevated BP and assessing treatment patterns in Portugal, since under the National Health Service the majority of hypertensive patients consult their GP regularly to renew their prescriptions. The data on clinical variables for each patient (previous diagnosis of diabetes, CAD, stroke, HT and current therapy) was recorded by the GP to ensure the quality of the information provided. However, no details of the active ingredient, dosage or treatment duration of each antihypertensive drug were recorded, which would be important in any assessment of the effectiveness of therapy based on treatment patterns.

Blood pressure was measured by the GP, two measurements being taken during a single consultation, with no evaluation of intra- or interobserver variability. Despite its limitations, this methodology has been used in most epidemiological studies, and produces acceptable results in terms of the rate of false positives (generally higher) and false negatives (usually very low). In addition, in view of the HT
140/90 mmHg – the effect of
NHANES III survey, HT prevalence decreased by
Finally, mercury sphygmomanometers or semi-automatic devices were used depending on the resources available in each PHC center, which is another variable to be taken into account.
HT prevalence in the Portuguese mainland and autonomous regions, estimated on the basis of observation of adult users of PHC centers, was 42.62%. Most hypertensives (52.38%) are medicated with two or more drugs. Among the 47.62% under monotherapy, the most frequently used classes in Portugal are ARBs (16.9%), ACEIs (14.41%) and diuretics (5.85%). Overall, the most common AHT drugs used are diuretics (47.4%), ARBs (43%) and ACEIs (39.2%), with CCBs (18,9%) and BBs (16.2%) being less
the frequency of prescription of each drug class, according not only to gender and age but also to region of residence.
Public health strategies should also address the need to reduce the proportion of patients under monotherapy. In addition, the present results reveal underuse of CCBs in hypertensives treated in PHC. Greater use of this drug class is likely to improve BP control and is of particular importance in Portugal due to the additional
from the Portuguese Society of Cardiology, the Directorate-General of Health, and the Portuguese Association of General Practice Physicians, and was funded by an unrestricted
Os presentes resultados sugerem que a
deverá ter em conta a promoção de padrões
clínico de cada doente. Para a melhoria do controlo tensional, será recomendável aumentar a proporção de hipertensos tratados com combinações de várias classes aHT, e para esse efeito são particularmente úteis as associações
embora se tenha demonstrado variabilidade regional dos padrões de tratamento aHT, que deverá ser tida em consideração, os resultados globais revelam subutilização dos ACC nos hipertensos seguidos nos CSP em Portugal. Tal facto parece ser particularmente relevante, dada
tensional e o seu benefício adicional potencial na prevenção do AVC(28).
O presente estudo foi realizado no contexto dos CSP, uma vez que em estudos populacionais,
número de indivíduos, representativos das várias regiões de um país. Porém, o método de selecção (os primeiros 2 utentes de cada dia de consulta), pretendendo-se aleatório, poderá ser afectado pelas limitações no acesso aos CSP. A amostra de indivíduos analisada no Estudo VALSIM tem uma distribuição por sexo e idade que corresponde à da população utente dos CSP, sendo necessariamente diferente da distribuição observada na população geral. Assim, não sendo um estudo populacional da população geral, não pretende determinar a prevalência de factores de risco CV nessa população que não avaliou directamente. No entanto, dado que o número de indivíduos analisados foi muito grande, as amostras são representativas da população de ambos os sexos, de todas as
A representatividade das amostras é evidente na análise do erro de precisão da estimativa de prevalência de HTA global, por sexo e por região de residência – Tabela 1. Atendendo à representatividade da amostra em cada um dos subgrupos, é possível padronizar os resultados mediante ajustamento para essas variáveis e a metodologia estatística empregue corresponde ao teorema da probabilidade total (com correcção

para os missing data). Este ajustamento minimiza o enviesamento que resultaria do facto de o sexo, idade e região de residência serem factores de risco independentes associados à ocorrência de HTA, e visa apenas a comparação das estimativas de prevalência com os resultados dos estudos populacionais de referência já publicados. O facto de a estimativa de prevalência de HTA decorrente do presente estudo ser sobreponível à do maior estudo previamente realizado na população portuguesa(3) sugere a consistência dos resultados e reforça a sua validade externa, mas a sua interpretação deve ser sempre cuidadosa. Efectivamente, é necessária grande precaução na extrapolação dos resultados para a realidade populacional global, já que existirão previsivelmente diferenças relevantes entre os indivíduos seguidos nos CSP e os indivíduos que não procuram assistência médica e que poderão ter HTA não diagnosticada. Em particular, não deve ser utilizado para estimar directamente o nível de conhecimento, tratamento e controlo na população, já que os hipertensos que recorrem ao médico de família, independentemente do motivo da consulta, terão maior probabilidade de reconhecimento do diagnóstico, instituição de terapêutica e planeamento do seguimento.
O desenho do estudo torna-o sobretudo adequado para analisar a resposta dos CSP face à detecção de PA aumentada e avaliar os padrões de tratamento aHT utilizados em Portugal, já que de acordo com a organização do Serviço Nacional de Saúde, a grande maioria dos doentes hipertensos recorre ao seu médico de família periodicamente para a manutenção da terapêutica. O inquérito individual relativo a cada doente com avaliação das variáveis clínicas (diagnóstico prévio de diabetes mellitus, doença coronária, AVC, HTA e terapêutica em curso) foi preenchido pelo médico assistente, o que reforça a qualidade da informação apurada. No entanto, no que respeita à terapêutica aHT, não foi descriminado o princípio activo instituído, a sua posologia e duração do tratamento com cada fármaco, o que seria relevante para a avaliação da efectividade do tratamento em função do padrão farmacológico aHT instituído.
A medição da pressão arterial foi efectuada pelo médico assistente, com realização de duas medições em apenas uma visita, sem que tenha sido avaliada a variabilidade intra- ou interobservador na medição da PA. Apesar das
grant to the Portuguese Society of Cardiology from Laboratório Novartis.
The investigators again express their thanks
their contribution to this study. We also thank the National Cardiology Data Collection Center (CNCDC) of the Portuguese Society of Cardiology for their invaluable support, particularly Dr. Sandra Corker for her help with administration.
A complete list of the VALSIM study invest-igators appears in a previous publication(37).

ACC entre os hipertensos seguidos nos CSP. A maior utilização dos ACC será provavelmente útil para a melhoria do controlo tensional e será particularmente relevante em Portugal atendendo aos potenciais benefícios acrescidos dessa classe aHT na prevenção do AVC.
O Estudo Valsim recebeu o patrocínio cientí-
da Direcção Geral de Saúde e da Associação Portuguesa de Médicos de Clínica Geral e foi suportado por uma bolsa atribuída, sem restrições, à Sociedade Portuguesa de Cardiologia pelo Laboratório Novartis.
Os investigadores renovam o agradecimento
seu empenho na concretização deste estudo. Agradecem também ao Centro Nacional de Colecção de Dados de Cardiologia (CNCDC) da Sociedade Portuguesa de Cardiologia pelo valioso apoio dispensado, e em particular à Dr.ª Sandra Corker pelo secretariado.
A lista completa dos investigadores do Estudo VALSIM foi apresentada em publicação prévia(37).
Pedido de Separatas para:Address for reprints:
NUNO CORTEZ-DIAS
Rua Prof. Moisés Amzalak, nº14, 7º Fte1600-648 Lisboae-mail: [email protected]
limitações intrín secas, esta metodologia tem sido utilizada na maioria dos estudos epidemiológicos, conduzindo a resultados aceitáveis no que respeita à taxa de falsos positivos (geralmente maior) e de falsos negativos (usualmente muito reduzida). De facto, considerando o limiar de PA
é reduzido. Por exemplo, no estudo NHANES III, a prevalência de HTA diminuiu em apenas 2% da primeira para a segunda visita. Finalmente,
ou aparelhos semi-automáticos conforme disponível no Centro de Saúde, o que constitui também um factor de variação.
A prevalência de HTA na população residente em Portugal continental e regiões autónomas estimada a partir das observações nos utentes adultos dos CSP atinge 42,62%. A maioria dos hipertensos (52,38%) está medicada com 2 ou mais fármacos aHT. Entre os 47,62% sob monoterapia, as classes mais utilizadas são os ARA (16,9%), os IECA (14,41%) e os diuréticos (5,85%). Globalmente, os aHT mais utilizados em Portugal são os diuréticos (47,4%), ARA (43%), IECA (39,2%), sendo menos utilizados
de cada classe não apenas com o sexo e idade, mas também consoante a região de residência.
O planeamento das estratégias de saúde pública deverá ter em conta a necessidade de reduzir adicionalmente a proporção de doentes tratados em monoterapia. Além disso, os presentes resultados revelam subutilização dos
(1) Direcção-Geral da Saúde. Direcção de Serviços de Epidemiologia e Estatísticas de Saúde. Divisão de Estatísticas de Saúde. Elementos Estatísticos: Informação Geral: Saúde 2005 / Direcção-Geral da Saúde. Direcção-Geral da Saúde, editor. 58-60. 2007. Divisão de Estatísticas de Saúde.
(2) Wolf-Maier K, Cooper RS, Banegas JR et al. Hypertension prevalence and blood pressure levels in 6 European countries, Canada, and the United States. JAMA 2003; 289(18):2363-2369.
(3) De Macedo ME, Lima MJ, Silva AO, Alcantara P, Ramalhinho V, Carmona J. Prevalence, awareness, treatment and control of hypertension in Portugal. The PAP study. Rev Port Cardiol 2007; 26(1):21-39.
(4) Primatesta P, Brookes M, Poulter NR. Improved hypertension management and control: results from the Health Survey for England 1998. Hypertension 2001; 38(4):827-832.
(5) Primatesta P, Poulter NR. Improvement in hypertension management in England: results from the Health Survey for England 2003. J Hypertens 2006; 24(6):1187-1192.
(6) Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: Global Burden of Disease Study. Lancet 1997; 349(9063):1436-1442.
from the Director of the National Heart, Lung, and Blood Institute.

Arch Intern Med 2002; 162(2):131-132.
(8) Moon L, Pierre M, Jacobzone S, ARD-Stroke Experts Group. Stroke Care in OECD Countries: A Comparison of Treatment, Costs and Outcomes in 17 Countries. OECD Health Working Papers [5], 12-103. 6-6-2003. Organisation for Economic Co-operation and Development.
(9) Burt VL, Whelton P, Roccella EJ et al. Prevalence of hypertension in the US adult population. Results from the Third National Health and Nutrition Examination Survey, 1988-1991. Hypertension 1995; 25(3):305-313.
(10) Joffres MR, Ghadirian P, Fodor JG, Petrasovits A, Chockalingam A, Hamet P. Awareness, treatment, and control of hypertension in Canada. Am J Hypertens 1997; 10(10 Pt 1):1097-1102.
(11) Stegmayr B, Harmsen P, Rajakangas A et al. Stroke around the Baltic Sea: incidence, case fatality and population risk factors in Denmark, Finland, Sweden and Lithuania. Cerebrovasc Dis 1990; 6:80-88.
(12) Persson M, Carlberg B, Mjorndal T, Asplund K, Bohlin J, Lindholm L. 1999 WHO/ISH Guidelines applied to a 1999 MONICA sample from northern Sweden. J Hypertens 2002; 20(1):29-35.
(13) Banegas JR, Rodriguez-Artalejo F, de la Cruz Troca JJ, Guallar-Castillon P, del Rey CJ. Blood pressure in Spain:
average pressure. Hypertension 1998; 32(6):998-1002.
(14) Thamm M. [Blood pressure in Germany--current status and trends]. Gesundheitswesen 1999; 61 Spec No:S90-3.:S90-S93.
(15) Wolf-Maier K, Cooper RS, Kramer H et al. Hypertension
United States. Hypertension 2004; 43(1):10-17.
(16) Morgan TO, Anderson AI, MacInnis RJ. ACE inhibitors, beta-blockers, calcium blockers, and diuretics for the control of systolic hypertension. Am J Hypertens 2001; 14(3):241-247.
(17) Dickerson JE, Hingorani AD, Ashby MJ, Palmer CR, Brown MJ. Optimisation of antihypertensive treatment by crossover rotation of four major classes. Lancet 1999; 353(9169):2008-2013.
(18) Dahlof B, Sever PS, Poulter NR et al. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding
Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet 2005; 366(9489):895-906.
(19) Mancia G, De Backer G, Dominiczak A et al. 2007 ESH-ESC Practice Guidelines for the Management of Arterial Hypertension: ESH-ESC Task Force on the Management of Arterial Hypertension. J Hypertens 2007; 25(9):1751-1762.
(20) Godley P, Nguyen A, Yokoyama K, Rohack J, Woodward B, Chiang T. Improving hypertension care in a large group-model MCO. Am J Health Syst Pharm 2003; 60(6):554-564.
(21) Rato Q, Cardoso AA. Retrospective review of the medical records of cardiology hospital outpatient clinics with the aim of determining the therapeutic approach to patients suffering from high blood pressure and/or dyslipidemia. Rev Port Cardiol 2006; 25(10):889-905.
(22) Yusuf S, Teo K, Anderson C et al. Effects of the angiotensin-receptor blocker telmisartan on cardiovascular events in high-risk patients intolerant to angiotensin-converting enzyme inhibitors: a randomised controlled trial. Lancet 2008; 372(9644):1174-1183.
(23) Kostis JB, Wilson AC, Freudenberger RS, Cosgrove NM, Pressel SL, Davis BR. Long-term effect of diuretic-based therapy on fatal outcomes in subjects with isolated systolic hypertension with and without diabetes. Am J Cardiol 2005; 95(1):29-35.
(24) Medical Research Council trial of treatment of hypertension in older adults: principal results. MRC Working Party. BMJ 1992; 304(6824):405-412.
(25) Neal B, MacMahon S, Chapman N. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: results of prospectively designed overviews of randomised trials. Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet 2000; 356(9246):1955-1964.
(26) Verdecchia P, Reboldi G, Angeli F et al. Angiotensin-converting enzyme inhibitors and calcium channel blockers for coronary heart disease and stroke prevention. Hypertension 2005; 46(2):386-392.
(27) Turnbull F, Neal B, Pfeffer M et al. Blood pressure-dependent and independent effects of agents that inhibit the renin-angiotensin system. J Hypertens 2007; 25(5):951-958.
(28) Turnbull F. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet 2003; 362(9395):1527-1535.
(29) Turnbull F, Neal B, Algert C et al. Effects of different blood pressure-lowering regimens on major cardiovascular events in individuals with and without diabetes mellitus: results of prospectively designed overviews of randomized trials. Arch Intern Med 2005; 165(12):1410-1419.
(30) Dahlof B, Devereux RB, Kjeldsen SE et al. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002; 359(9311):995-1003.
(31) Lindholm LH, Carlberg B, Samuelsson O. Should beta-blockers
meta-analysis. Lancet 2005; 366(9496):1545-1553.
(32) Williams B, Lacy PS, Thom SM et al. Differential impact of blood pressure-lowering drugs on central aortic pressure and clinical outcomes: principal results of the Conduit Artery Function Evaluation (CAFE) study. Circulation 2006; 113(9):1213-1225.
(33) Williams B, Poulter NR, Brown MJ et al. British Hypertension Society guidelines for hypertension management 2004 (BHS-IV): summary. BMJ 2004; 328(7440):634-640.
(34) Gong L, Zhang W, Zhu Y et al. Shanghai trial of nifedipine in the elderly (STONE). J Hypertens 1996; 14(10):1237-1245.
(35) Staessen JA, Fagard R, Thijs L et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet 1997; 350(9080):757-764.
(36) Liu L, Wang JG, Gong L, Liu G, Staessen JA. Comparison of active treatment and placebo in older Chinese patients with isolated systolic hypertension. Systolic Hypertension in China (Syst-China) Collaborative Group. J Hypertens 1998; 16(12 Pt 1):1823-1829.
(37) Fiuza M, Cortez-Dias N, Martins S, Belo A. Metabolic Syndrome in Portugal: Prevalence and Implications for Cardiovascular Risk - Results from the VALSIM Study. Rev Port Cardiol 2008; 27(12):1495-1529.




















