
Prevalence and Correlates of Left Ventricular Hypertrophy in the African American Study of Kidney...
13
Prevalence and Correlates of Left Ventricular Hypertrophy in the African American Study of Kidney Disease Cohort Study Gail E. Peterson, Tine de Backer, Avril Gabriel,* Vladimir Ilic, Tudor Vagaonescu, Lawrence J. Appel, Gabriel Contreras, Cindy Kendrick, Stephen Rostand, Robert A. Phillips; for the African American Study of Kidney Disease Investigators Abstract—African Americans with hypertensive renal disease represent a high-risk population for cardiovascular events. Although left ventricular hypertrophy is a strong predictor of adverse cardiac outcome, the prevalence and associated factors of left ventricular hypertrophy in this patient population are not well described. The African American Study of Kidney Disease Cohort Study is a prospective, observational study that is an extension of the African American Study of Kidney Disease randomized clinical trial that was conducted from 1994 to 2001 in African Americans with hypertension and mild-to-moderate renal dysfunction. Echocardiograms and 24-hour ambulatory blood pressure monitoring were performed at the baseline visit of the cohort. Of 691 patients enrolled in the cohort study, 599 patients had interpretable baseline echocardiograms and ambulatory blood pressure data. Left ventricular hypertrophy was defined using a cut point for left ventricular mass index 49.2 g/m 2.7 in men and 46.7 m/m 2.7 in women. The majority of patients had left ventricular hypertrophy (66.7% of men and 73.9% of women). In a multiple regression analysis, higher average day and nighttime systolic blood pressure, younger age, and lower predicted glomerular filtration rate were associated with left ventricular hypertrophy, but albuminuria was not. These data demonstrate a striking prevalence of left ventricular hypertrophy in the African American Study of Kidney Disease Cohort and identify potential targets for prevention and therapeutic intervention in this high-risk patient population. (Hypertension. 2007;50:1033-1039.) Key Words: hypertension hypertrophy left ventricular echocardiography African Americans kidney failure chronic blood pressure monitoring ambulatory A frican Americans with hypertension are at increased risk of cardiovascular morbidity and mortality and have more frequent progression to end-stage renal disease com- pared with other ethnic groups in the United States. 1–5 In addition, those patients who develop chronic kidney disease are at even greater risk for cardiovascular mortality. 6 Why African Americans are a particularly high-risk group is not fully understood. Left ventricular hypertrophy (LVH) is a strong independent predictor of adverse cardiovascular events, and several studies have found a higher prevalence for LVH in African Americans compared with whites. 7–9 The African American Study of Kidney disease (AASK) cohort involves African American patients with nondiabetic, hypertensive renal disease. The prevalence and associated factors of target-organ damage, such as LVH, in this patient population have not been well described previously. In addition, echocardiographic data in this patient population are virtually nonexistent; to our knowledge only 1 other study has specifically assessed echocardiographic findings in a small number of African Americans with hypertensive renal dis- ease. 10 Because this population is at high risk for cardiovas- cular events, the AASK cohort is an ideal group of patients in which to evaluate to identify the frequency and correlates of LVH to help target those patients who may benefit from aggressive therapy for risk reduction. Methods Study Population The AASK Cohort Study is a prospective, observational study that is an extension of the AASK, which tested the effects of 3 medications used as initial antihypertensive therapy (ramipril, metoprolol, and amlodipine) and usual (mean arterial pressure of 102 to 107 mm Hg) Received March 7, 2007; first decision April 16, 2007; revision accepted September 26, 2007. From the Division of Cardiology (G.E.P.), University of Texas Southwestern Medical Center, Dallas; Cardiovascular Research Foundation (T.d.B., V.I., T.V.), New York, NY; Lenox Hill Hospital (A.G.), New York, NY; University of Medicine and Dentistry, New Jersey-Robert Wood Johnson Medical School (T.V.), New Brunswick, NJ; Johns Hopkins (L.J.A.), Baltimore, Md; University of Miami (G.C.), Fla; Biostatistics and Epidemiology (C.K.), Cleveland Clinic, Ohio; University of Alabama (S.R.), Birmingham; and the University of Massachusetts Memorial Medical Center and Medical School (R.A.P.), Worcester. *Deceased. Correspondence to Gail E. Peterson, Division of Cardiology, University of Texas Southwestern Medical Center, 5909 Harry Hines Blvd, HA9.133, Dallas, TX 75235-9047. E-mail [email protected] © 2007 American Heart Association, Inc. Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.107.090613 1033 Heart by guest on December 11, 2014 http://hyper.ahajournals.org/ Downloaded from by guest on December 11, 2014 http://hyper.ahajournals.org/ Downloaded from by guest on December 11, 2014 http://hyper.ahajournals.org/ Downloaded from by guest on December 11, 2014 http://hyper.ahajournals.org/ Downloaded from by guest on December 11, 2014 http://hyper.ahajournals.org/ Downloaded from by guest on December 11, 2014 http://hyper.ahajournals.org/ Downloaded from by guest on December 11, 2014 http://hyper.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Prevalence and Correlates of Left Ventricular Hypertrophy in the African American Study of Kidney...

Prevalence and Correlates of Left Ventricular Hypertrophyin the African American Study of Kidney Disease
Cohort StudyGail E. Peterson, Tine de Backer, Avril Gabriel,* Vladimir Ilic, Tudor Vagaonescu, Lawrence J. Appel,
Gabriel Contreras, Cindy Kendrick, Stephen Rostand, Robert A. Phillips; for the African AmericanStudy of Kidney Disease Investigators
Abstract—African Americans with hypertensive renal disease represent a high-risk population for cardiovascular events.Although left ventricular hypertrophy is a strong predictor of adverse cardiac outcome, the prevalence and associatedfactors of left ventricular hypertrophy in this patient population are not well described. The African American Study ofKidney Disease Cohort Study is a prospective, observational study that is an extension of the African American Studyof Kidney Disease randomized clinical trial that was conducted from 1994 to 2001 in African Americans withhypertension and mild-to-moderate renal dysfunction. Echocardiograms and 24-hour ambulatory blood pressuremonitoring were performed at the baseline visit of the cohort. Of 691 patients enrolled in the cohort study, 599 patientshad interpretable baseline echocardiograms and ambulatory blood pressure data. Left ventricular hypertrophy wasdefined using a cut point for left ventricular mass index �49.2 g/m2.7 in men and �46.7 m/m2.7 in women. The majorityof patients had left ventricular hypertrophy (66.7% of men and 73.9% of women). In a multiple regression analysis,higher average day and nighttime systolic blood pressure, younger age, and lower predicted glomerular filtration ratewere associated with left ventricular hypertrophy, but albuminuria was not. These data demonstrate a striking prevalenceof left ventricular hypertrophy in the African American Study of Kidney Disease Cohort and identify potential targetsfor prevention and therapeutic intervention in this high-risk patient population. (Hypertension. 2007;50:1033-1039.)
Key Words: hypertension � hypertrophy � left ventricular � echocardiography � African Americans� kidney failure � chronic � blood pressure monitoring � ambulatory
African Americans with hypertension are at increased riskof cardiovascular morbidity and mortality and have
more frequent progression to end-stage renal disease com-pared with other ethnic groups in the United States.1–5 Inaddition, those patients who develop chronic kidney diseaseare at even greater risk for cardiovascular mortality.6 WhyAfrican Americans are a particularly high-risk group is notfully understood. Left ventricular hypertrophy (LVH) is astrong independent predictor of adverse cardiovascularevents, and several studies have found a higher prevalence forLVH in African Americans compared with whites.7–9
The African American Study of Kidney disease (AASK)cohort involves African American patients with nondiabetic,hypertensive renal disease. The prevalence and associatedfactors of target-organ damage, such as LVH, in this patientpopulation have not been well described previously. In
addition, echocardiographic data in this patient population arevirtually nonexistent; to our knowledge only 1 other study hasspecifically assessed echocardiographic findings in a smallnumber of African Americans with hypertensive renal dis-ease.10 Because this population is at high risk for cardiovas-cular events, the AASK cohort is an ideal group of patients inwhich to evaluate to identify the frequency and correlates ofLVH to help target those patients who may benefit fromaggressive therapy for risk reduction.
MethodsStudy PopulationThe AASK Cohort Study is a prospective, observational study that isan extension of the AASK, which tested the effects of 3 medicationsused as initial antihypertensive therapy (ramipril, metoprolol, andamlodipine) and usual (mean arterial pressure of 102 to 107 mm Hg)
Received March 7, 2007; first decision April 16, 2007; revision accepted September 26, 2007.From the Division of Cardiology (G.E.P.), University of Texas Southwestern Medical Center, Dallas; Cardiovascular Research Foundation (T.d.B.,
V.I., T.V.), New York, NY; Lenox Hill Hospital (A.G.), New York, NY; University of Medicine and Dentistry, New Jersey-Robert Wood JohnsonMedical School (T.V.), New Brunswick, NJ; Johns Hopkins (L.J.A.), Baltimore, Md; University of Miami (G.C.), Fla; Biostatistics and Epidemiology(C.K.), Cleveland Clinic, Ohio; University of Alabama (S.R.), Birmingham; and the University of Massachusetts Memorial Medical Center and MedicalSchool (R.A.P.), Worcester.
*Deceased.Correspondence to Gail E. Peterson, Division of Cardiology, University of Texas Southwestern Medical Center, 5909 Harry Hines Blvd, HA9.133,
Dallas, TX 75235-9047. E-mail [email protected]© 2007 American Heart Association, Inc.
Hypertension is available at http://hyper.ahajournals.org DOI: 10.1161/HYPERTENSIONAHA.107.090613
1033
Heart
by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from

or lower (mean arterial pressure �93 mm Hg) blood pressure (BP)control. Eligible patients enrolled in the AASK were AfricanAmerican men and women with hypertension, between the ages of18 and 70, diastolic BP of �95 mm Hg, with a glomerular filtrationrate (GFR) of 20 to 65 mL/min per 1.73 m2 and no apparent cause ofrenal insufficiency other than hypertension. The clinical compositeoutcome was reduction in GFR by 50% from baseline, the develop-ment of end-stage renal disease, or death. During the trial, mean BPwas 128/89 mm Hg (�12/8 mm Hg) in the lower BP group and141/85 mm Hg (�12/7 mm Hg) in the usual BP group. There was nodifference in the progression of kidney disease or in the clinicalcomposite outcome between the 2 BP groups. The ramipril grouphad a significant reduction in the composite outcome compared withthe metoprolol and amlodipine groups. Based on the results, in theabsence of contraindications, patients in the cohort phase weretreated with an angiotensin-converting enzyme inhibitor.
All participants in the AASK who had not died or reachedend-stage renal disease were invited to enroll in the cohort study. Thestudy was approved by the institutional review committee at eachparticipating site and adhered to the principles of the Declaration ofHelsinki and Title 45, US Code of Federal Regulations, Part 46,Protection of Human Subjects. All of the subjects gave informedconsent, and procedures followed were in accordance with institu-tional guidelines. Patients enrolled in the AASK Cohort Study hadexcellent BP control during the trial. The average mean BP of cohortparticipants during the trial was 98 mm Hg (�8 mm Hg;93�7 mm Hg in the lower BP group and 104�5 mm Hg in the usualBP group). Details of the study design and inclusion/exclusioncriteria have been reported elsewhere.11
EchocardiographyPatients enrolled in the cohort had an echocardiogram performed attheir baseline visit. M-mode, 2D, and Doppler echocardiographyexaminations were performed at each of the 21 enrolling centersusing commercially available equipment. To ensure data quality,echocardiograms were obtained by trained technologists using astandardized protocol and read centrally at the AASK CardiovascularCore Laboratory. At the core laboratory, echocardiographic tracingswere coded, digitized, and interpreted blindly using the DigiViewDigital/Video System(s), Model DV-DVRS-100 (Digisonics, Inc).An average of 3 measurements was made of each variable. Theend-diastolic (LVIDds) and end-systolic LV internal diameters(LVIDs), interventricular septal thickness, and the posterior wallthickness (PWT) were measured from 2D guided M-mode tracings,according to the American Society of Echocardiography guide-lines.12 When optimal orientation was not possible, measurementswere made using 2D views.13 Left ventricular mass (LVM) wascalculated using an anatomically validated formula14 and normalizedto allometric height.15 LVH as defined according to gender-specificcriterion as LVM index �49.2 g/m2.7 in men and �46.7 g/m2.7
in women.
MethodsRelative wall thickness (RWT) was calculated using the formula(2 PWT)/LVIDd. A concentric remodeling pattern was defined asan RWT � 0.44.16 Left ventricular systolic function was assessedby endocardial fractional shortening [(LVIDd�LVIDDs)/LVIDd]. Echocardiograms were read by 1 of 5 echocardio-graphers. Intraclass correlation statistics showed good agreementbetween measurements (M-mode LVM: 0.72; mitral E wave to Awave ratio: 0.93). Likewise, there was good intrarater variability(eg, mean difference in M-mode LVM was 17.35 g [SD: 27.81],and mean difference of mitral E/A ratio was 0.03 [SD: 0.08]).
BP MeasurementsOffice BP was measured in a standardized method by trained andcertified observers using the Tycos Classic handheld Aneroid device.Two BP measurements were obtained in the seated position and 1 inthe upright position. Patients were encouraged to have their BPmanaged by the AASK cohort staff based as outlined previously.11
Ambulatory BP monitoring (ABPM) was performed over a24-hour period, using the SpaceLabs 90217 Ultralite or SpaceLabs90207 devices. During each 24-hour recording, measurements wereobtained every 30 minutes from which awake and asleep averageswere calculated, along with dipping status. Nighttime BP wasdefined as 12:00 AM to 6:00 AM. A blunted BP at night, the so-callednondipping pattern, was defined as �10% fall in average systolicBP (SBP).
Other MeasurementsUrinary albumin excretion was determined by measuring 24-houralbumin and creatinine levels. A urine albumin: creatinine ratio of�0.22 was used to define albuminuria.
Estimated GFR (eGFR) was calculated from serum creatinine usingan equation developed from baseline data in the AASK trial.17 Specif-ically, eGFR�329�(serum creatinine)�1.096�(age)�0.294�(0.736 forwomen).
Statistical AnalysisBaseline characteristics were summarized as means and SDs forcontinuous variables and as frequencies and percentages for categor-ical variables and were compared between those with and withoutLVH using a 2-sample t test or �2 test, as appropriate. Multiple linearregression analysis was used to relate LVM to the followingprespecified predictor variables: average daytime SBP, averagenighttime SBP, eGFR, age, hematocrit (%), gender, and the log-transformed urine albumin:creatinine ratio. Results of all of thestatistical tests are reported as 2-sided P values, without adjustmentfor multiple comparisons.
ResultsStudy ParticipantsOf the 1094 participants in the AASK, 787 patients were aliveand not on dialysis, and 691 individuals agreed to enrollmentin the cohort study. Baseline echocardiograms were obtainedin 649 patients, of whom 41 lacked ABPM data and 8 lackedmeasurable LVM. Therefore, 599 patients were evaluated forthis report.
Tables 1 to 3 present characteristics of participants overalland stratified by LVH. Overall, the mean age of participantswas 60.1�10.1 years), and 38.4% were women. Averagebody mass index was 31.2�6.98 kg/m2. The mean hematocritwas 38.4�5.3%. eGFR averaged 44.2�16.5 mL/min per 1.73m2, and average serum creatinine was 2.25�1.35 mg/dL.Albuminuria was present in 12.6% of patients. Additionalcharacteristics are shown in Table S1 (please see http://hyper.ahajournals.org).
BP measurements are displayed in Table 2. Average clinicBP was 135�21.5/80�12.4 mm Hg. Average ambulatorydaytime SBP was 138�17 mm Hg, and average nighttimeSBP was 134�21 mm Hg. Average 24-hour pulse pressurewas 56.1�12.5 mm Hg.
Echocardiographic characteristics are shown in Table 3.The majority of patients had normal left ventricular systolicfunction as measured by fractional shortening (average:38�10%). A high proportion of patients had evidence fordiastolic dysfunction, with a median E wave to A wave ratioof 0.92�0.38. Left atrial size was enlarged (mean area:19.2�5.12 cm2. Concentric remodeling was common in thispopulation (mean RWT: 0.53�0.13). Of the patient popula-tion, 69.4% had LVH (66.7% of men and 73.9% of women).The mean LVM index was 60.9�21.6 g/m2.7 overall;60.5�21.0 g/m2.7 in men, and 61.7�22.5 g/m2.7 in women.
1034 Hypertension December 2007
by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from

Factors Associated With LVHVariables predictive of LVH were younger age, greater bodymass index, the presence of albuminuria, higher average dayand average nighttime SBP, and higher 24-hour pulse pres-sure. Table 2 shows the correlations between LVH and clinicand ABPM values. Average 24-hour SBP, average day SBP,and average night SBP were all highly predictive of LVH.The difference between daytime and nighttime BP was notsignificantly associated with LVH.
Echocardiographic characteristics associated with the pres-ence of LVH (Table 3) include greater internal diastolic andsystolic dimensions, greater wall thicknesses, larger aorticroot diameter and left atrial size, higher RWT, and higherDoppler stroke volume. Patients with LVH had lower heartrates but a similar cardiac index and fractional shortening.
The Figure shows the joint relationship of daytime andnighttime SBP by quartiles with mean LVM. Independentrelationships were observed between the degree of LVH andprogressive increases in both BP indices as fixed levels of theother index.
Multivariable AssociationsOn multiple regression analysis (adjusted R2�0.10), greateraverage nighttime and daytime SBP, lower estimated eGFR,
and younger age were independent correlates of LVH (Table4). Hematocrit and the presence of microalbuminuria werenot independently associated with LVH.
DiscussionThis study represents the first comprehensive systematicexamination of the prevalence and correlates of LVH inAfrican American patients with hypertensive kidney dysfunc-tion, a population at very high risk for cardiovascular disease.Despite adequate BP control over 5 years before evaluation,there was an extraordinarily high prevalence of LVH in theAASK cohort. In most series, only �30% of patients withhypertension have LVH18 compared with �70% in theAASK Cohort Study.
Our findings point to both direct and potentially indirecteffects of BP on LVH. In particular, ABPM values werehighly correlated with LVH. We found that the most predic-tive value for LVH in this patient population was averagedaytime SBP based on ABPM. Our finding is consistent withother studies that have shown a direct relationship betweenLVH and SBP as measured either by ABPM or office BPaveraged over a 30-year period.19–21 In the Framinghampopulation, a continuous association between SBP and LVH
Table 1. Demographic and Clinical Data: Comparison Between Patients With and Without LVH
VariableAll Patients
(n�599)LVH
(n�416)No LVH(n�183) P
Age, mean�SD 60.1�10.1 59.4�10.1 61.9�10.0 0.0055
Gender, n (%), % female 230.0 (38.4) 170.0 (40.9) 60.0 (32.8) 0.0611
Body mass index, mean�SD, kg/m2 31.2�6.98 32.6�7.09 27.9�5.48 0.0001
Smoking status, n (%) 0.2107
Never smoked 244.0 (40.8) 176.0 (42.4) 68.0 (37.2)
Currently smoking 105.0 (17.6) 76.0 (18.3) 29.0 (15.8)
Past smoker 249.0 (41.6) 163.0 (39.3) 86.0 (47.0)
Hematocrit, mean�SD, % 38.4�5.27 38.2�5.12 38.9�5.59 0.193
eGFR, mean�SD, mL/min/1.73 m2 44.2�16.5 43.4�16.3 46.1�17.0 0.0734
Serum creatinine, mean�SD, mg/dL 2.25�1.35 2.30�1.48 2.14�1.00 0.1164
Serum cholesterol, mean�SD, mg/dL 201.0�45.5 202.0�45.8 199.0�44.7 0.3787
Albuminuria, n (%), UACR �0.22 75.0 (12.6) 66.0 (15.9) 9.0 (4.9) 0.0002
UACR indicates urinary albumin:creatinine ratio.
Table 2. Association of BP Measurements with LVH
Variable, mm HgAll Patients (n�599),
Mean�SDLVH (n�416),
Mean�SDNo LVH (n�183),
Mean�SD P
Baseline clinic SBP 135.0�21.5 138.0�21.1 131.0�21.6 0.0003
Baseline clinic DBP 80.7�12.4 81.6�12.8 78.8�11.3 0.0068
Baseline clinic pulse pressure 54.6�16.6 55.9�16.5 51.8�16.7 0.0057
24-h pulse pressure 56.1�12.5 58.0�12.5 51.6�11.4 0.0001
24-h average SBP 136.0�18.0 139.0�18.0 130.0�16.6 0.0001
24-h average DBP 80.0�11.2 80.7�11.5 78.3�10.3 0.0126
Average day SBP 138.0�17.0 140.0�16.8 132.0�16.2 0.0001
Average day DBP 82.6�10.8 83.2�10.9 81.3�10.5 0.0388
Average night SBP 134.0�21.0 137.0�21.1 128.0�19.2 0.0001
Average night DBP 77.3�13.0 78.2�13.6 75.4�11.6 0.01
Average day-night SBP 3.26�12.8 2.80�12.9 4.31�12.7 0.1818
Peterson et al Left Ventricular Hypertrophy in African Americans 1035
by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from

was found even at BP levels considered to be in the normal ornear-reference range.22 Most investigators have found thatSBP is better correlated with LVH than diastolic BP19,20 andthat ABPM is a better predictor of LVH than clinic BP.20
Average nighttime SBP was also strongly predictive ofLVH. Although average daytime SBP was reasonably wellcontrolled in our population, average nighttime SBP waselevated. In other studies, African Americans have beenshown to have higher nighttime BP than whites despitesimilar daytime BP.23,24 The majority of patients with uncom-plicated hypertension experience a fall in their nighttime BPof �10% of the daytime mean arterial BP. The absence of afall in nocturnal BP has been linked to target organ damage,such as carotid artery structural alterations and LVH in somestudies25–29 but not others.30,31 Observational studies haveshown that hypertensive patients with elevated nighttime BPare at greater risk for experiencing cardiovascular outcomesand stroke compared with hypertensive patients with anormal decrease in nocturnal BP.25,32 In our patient popula-
tion there was an additive relationship between nighttime anddaytime SBP, with the greater LVM occurring in patient inthe upper quartiles of both night and day SBP.
Unlike previous studies, we found that younger age wasassociated with greater LVM in this cohort population. TheAASK cohort population is derived from a high-risk, olderpopulation followed through the 5-year AASK and is com-posed of survivors who had not died or reached end-stagerenal disease. Therefore, this unexpected finding may representa survival bias; those patients who were older with lower LVMand those who were younger (with or without high LVM) mayhave been less likely to reach an outcome in the trial, and,therefore, were eligible for enrollment in the cohort study.
We did not find an independent relationship between thepresence of albuminuria and LVH. This observation contrastswith some33,34 but not other35,36 studies where albuminuriacorrelated with LVM. Many of these studies measured clinicrather than ambulatory BP.33 ABPM values (particularlyambulatory SBP) have been shown to have a closer associa-tion with LVM compared with office measurements.35,37–39
The use of ABPM data in our analysis may be one reason forthe lack of an independent association between urinaryalbumin excretion and LVH. Other studies using ABPM intheir analysis have also found a lack of independent associ-ation between albuminuria and LVH.35,36 Unlike other studiesevaluating albuminuria, the vast majority of patients (75%) inthe AASK cohort were treated with angiotensin-convertingenzyme inhibitors. Increased renin-angiotensin activity hasbeen associated with the presence of microalbuminuria andtarget organ damage,40 and it is possible that the widespreaduse of angiotensin-converting enzyme inhibitors in our pa-tient population accounted in part for the lack of associationin our study. Previous studies also excluded patients withrenal insufficiency,33–35 whereas all of the AASK cohortpatients had established hypertensive renal dysfunction.
Table 3. Echocardiographic Data: Comparison Between Patients With and Without LVH
Variable All Patients (n�599) LVH (n�416) No LVH (n�183) P
LVIDd, mean�SD, mm 48.4�6.70 50.1�6.49 44.3�5.30 0.0001
LVIDs, mean�SD, mm 28.8�6.85 30.1�7.04 25.8�5.34 0.0001
IVST, mean�SD, mm 13.4�2.91 14.2�2.81 11.6�2.30 0.0001
PWT, mean�SD, mm 12.7�2.46 13.4�2.39 11.1�1.81 0.0001
Aortic root diameter, mean�SD, mm 34.2�5.10 34.8�5.04 33.0�5.03 0.0001
Left atrium diameter, mean�SD, mm 41.2�6.95 43.0�6.55 37.2�6.08 0.0001
Left atrial area, mean�SD, cm2 19.2�5.12 20.4�5.21 16.6�3.72 0.0001
LV mass index, mean�SD, g/m2.7 60.9�21.6 70.0�19.6 40.2�6.07 0.0001
RWT, mean�SD 0.53�0.13 0.55�0.14 0.51�0.11 0.0003
RWT�0.44, n (%) 467.0 (78.0) 329.0 (79.1) 138.0 (75.4) 0.3173
Fractional shortening, mean�SD, % 0.38�0.10 0.38�0.10 0.38�0.10 0.8899
Doppler SV, mean�SD, mL 98.9�58.9 103.0�60.2 89.8�55.0 0.0124
Doppler cardiac index, mean�SD, L/min/m2 3.03�1.67 3.08�1.72 2.92�1.54 0.3413
SV/PP ratio, mean�SD 1.72�1.12 1.73�1.12 1.69�1.14 0.6902
SV/PP ratio, mean�SD, 24-h pulse pressure 1.83�1.14 1.84�1.12 1.81�1.17 0.7632
Heart rate, mean�SD 67.0�13.4 66.1�13.0 69.5�13.9 0.0117
IVST indicates intraventricular wall thickness; PWT, posterior wall thickness; SV, stroke volume; SV/PP ratio, stroke volume:pulsepressure ratio.
0
50
100
150
200
250
300
Day SBP>149
Day SBP136-149
Day SBP126-136
Day SBP< 126
Night SBP < 120
Night SBP 120-133
Night SBP 133-147
Night SBP > 147
Figure. Joint association of mean LVM with quartiles of day andnight SBP.
1036 Hypertension December 2007
by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from
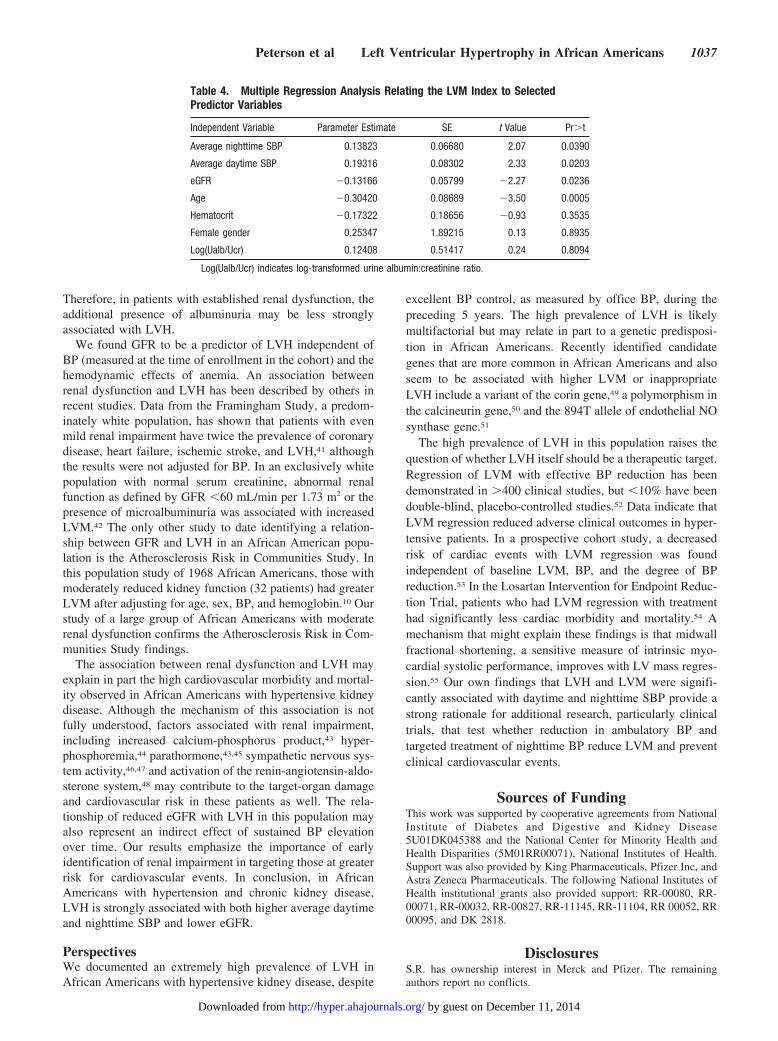
Therefore, in patients with established renal dysfunction, theadditional presence of albuminuria may be less stronglyassociated with LVH.
We found GFR to be a predictor of LVH independent ofBP (measured at the time of enrollment in the cohort) and thehemodynamic effects of anemia. An association betweenrenal dysfunction and LVH has been described by others inrecent studies. Data from the Framingham Study, a predom-inately white population, has shown that patients with evenmild renal impairment have twice the prevalence of coronarydisease, heart failure, ischemic stroke, and LVH,41 althoughthe results were not adjusted for BP. In an exclusively whitepopulation with normal serum creatinine, abnormal renalfunction as defined by GFR �60 mL/min per 1.73 m2 or thepresence of microalbuminuria was associated with increasedLVM.42 The only other study to date identifying a relation-ship between GFR and LVH in an African American popu-lation is the Atherosclerosis Risk in Communities Study. Inthis population study of 1968 African Americans, those withmoderately reduced kidney function (32 patients) had greaterLVM after adjusting for age, sex, BP, and hemoglobin.10 Ourstudy of a large group of African Americans with moderaterenal dysfunction confirms the Atherosclerosis Risk in Com-munities Study findings.
The association between renal dysfunction and LVH mayexplain in part the high cardiovascular morbidity and mortal-ity observed in African Americans with hypertensive kidneydisease. Although the mechanism of this association is notfully understood, factors associated with renal impairment,including increased calcium-phosphorus product,43 hyper-phosphoremia,44 parathormone,43,45 sympathetic nervous sys-tem activity,46,47 and activation of the renin-angiotensin-aldo-sterone system,48 may contribute to the target-organ damageand cardiovascular risk in these patients as well. The rela-tionship of reduced eGFR with LVH in this population mayalso represent an indirect effect of sustained BP elevationover time. Our results emphasize the importance of earlyidentification of renal impairment in targeting those at greaterrisk for cardiovascular events. In conclusion, in AfricanAmericans with hypertension and chronic kidney disease,LVH is strongly associated with both higher average daytimeand nighttime SBP and lower eGFR.
PerspectivesWe documented an extremely high prevalence of LVH inAfrican Americans with hypertensive kidney disease, despite
excellent BP control, as measured by office BP, during thepreceding 5 years. The high prevalence of LVH is likelymultifactorial but may relate in part to a genetic predisposi-tion in African Americans. Recently identified candidategenes that are more common in African Americans and alsoseem to be associated with higher LVM or inappropriateLVH include a variant of the corin gene,49 a polymorphism inthe calcineurin gene,50 and the 894T allele of endothelial NOsynthase gene.51
The high prevalence of LVH in this population raises thequestion of whether LVH itself should be a therapeutic target.Regression of LVM with effective BP reduction has beendemonstrated in �400 clinical studies, but �10% have beendouble-blind, placebo-controlled studies.52 Data indicate thatLVM regression reduced adverse clinical outcomes in hyper-tensive patients. In a prospective cohort study, a decreasedrisk of cardiac events with LVM regression was foundindependent of baseline LVM, BP, and the degree of BPreduction.53 In the Losartan Intervention for Endpoint Reduc-tion Trial, patients who had LVM regression with treatmenthad significantly less cardiac morbidity and mortality.54 Amechanism that might explain these findings is that midwallfractional shortening, a sensitive measure of intrinsic myo-cardial systolic performance, improves with LV mass regres-sion.55 Our own findings that LVH and LVM were signifi-cantly associated with daytime and nighttime SBP provide astrong rationale for additional research, particularly clinicaltrials, that test whether reduction in ambulatory BP andtargeted treatment of nighttime BP reduce LVM and preventclinical cardiovascular events.
Sources of FundingThis work was supported by cooperative agreements from NationalInstitute of Diabetes and Digestive and Kidney Disease5U01DK045388 and the National Center for Minority Health andHealth Disparities (5M01RR00071), National Institutes of Health.Support was also provided by King Pharmaceuticals, Pfizer Inc, andAstra Zeneca Pharmaceuticals. The following National Institutes ofHealth institutional grants also provided support: RR-00080, RR-00071, RR-00032, RR-00827, RR-11145, RR-11104, RR 00052, RR00095, and DK 2818.
DisclosuresS.R. has ownership interest in Merck and Pfizer. The remainingauthors report no conflicts.
Table 4. Multiple Regression Analysis Relating the LVM Index to SelectedPredictor Variables
Independent Variable Parameter Estimate SE t Value Pr�t
Average nighttime SBP 0.13823 0.06680 2.07 0.0390
Average daytime SBP 0.19316 0.08302 2.33 0.0203
eGFR �0.13166 0.05799 �2.27 0.0236
Age �0.30420 0.08689 �3.50 0.0005
Hematocrit �0.17322 0.18656 �0.93 0.3535
Female gender 0.25347 1.89215 0.13 0.8935
Log(Ualb/Ucr) 0.12408 0.51417 0.24 0.8094
Log(Ualb/Ucr) indicates log-transformed urine albumin:creatinine ratio.
Peterson et al Left Ventricular Hypertrophy in African Americans 1037
by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from

References1. Kaplan NM. Ethnic aspects of hypertension. Lancet. 1994;344:450–452.2. Francis CK. Hypertension, cardiac disease, and compliance in minority
patients. Am J Med. 1991;91:29S–36S.3. Gillum RF. The epidemiology of cardiovascular disease in black
Americans. N Engl J Med. 1996;335:1597–1599.4. Cooper RS, Rotimi CN, Ward R. The puzzle of hypertension in African-
Americans. Sci Am. 1999;280:56–63.5. Saunders E. Tailoring treatment to minority patients. Am J Med. 1990;
88:21S–23S.6. Levey AS, Beto JA, Coronado BE, Eknoyan G, Foley RN, Kasiske BL,
Klag MJ, Mailloux LU, Manske CL, Meyer KB, Parfrey PS, Pfeffer MA,Wenger NK, Wilson PW, Wright JT Jr. Controlling the epidemic ofcardiovascular disease in chronic renal disease: what do we know? Whatdo we need to learn? Where do we go from here? National KidneyFoundation Task Force on Cardiovascular Disease. Am J Kidney Dis.1998;32:853–906.
7. Kizer JR, Arnett DK, Bella JN, Paranicas M, Rao DC, Province MA,Oberman A, Kitzman DW, Hopkins PN, Liu JE, Devereux RB. Dif-ferences in left ventricular structure between black and white hyper-tensive adults: the Hypertension Genetic Epidemiology Network study.Hypertension. 2004;43:1182–1188.
8. Arnett DK, Strogatz DS, Ephross SA, Hames CG, Tyroler HA. Greaterincidence of electrocardiographic left ventricular hypertrophy in blackmen than in white men in Evans County, Georgia. Ethn Dis. 1992;2:10–17.
9. Drazner MH, Dries DL, Peshock RM, Cooper RS, Klassen C, Kazi F,Willett D, Victor RG. Left ventricular hypertrophy is more prevalent inblacks than whites in the general population: the Dallas Heart Study.Hypertension. 2005;46:124–129.
10. Astor BC, Arnett DK, Brown A, Coresh J. Association of kidney functionand hemoglobin with left ventricular morphology among African Amer-icans: the Atherosclerosis Risk in Communities (ARIC) study. Am JKidney Dis. 2004;43:836–845.
11. Appel LJ, Middleton J, Miller ER 3rd, Lipkowitz M, Norris K, AgodoaLY, Bakris G, Douglas JG, Charleston J, Gassman J, Greene T, JamersonK, Kusek JW, Lewis JA, Phillips RA, Rostand SG, Wright JT. Therationale and design of the AASK cohort study. J Am Soc Nephrol.2003;14:S166–S172.
12. Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendations regardingquantitation in M-mode echocardiography: results of a survey of echo-cardiographic measurements. Circulation. 1978;58:1072–1083.
13. Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R,Feigenbaum H, Gutgesell H, Reichek N, Sahn D, Schnittger I, SilvermanNH, Tajik AJ. Recommendations for quantitation of the left ventricle bytwo-dimensional echocardiography. American Society of Echocardiogra-phy Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J Am Soc Echocardiogr. 1989;2:358–367.
14. Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I,Reichek N. Echocardiographic assessment of left ventricular hypertrophy:comparison to necropsy findings. Am J Cardiol. 1986;57:450–458.
15. de Simone G, Daniels SR, Devereux RB, Meyer RA, Roman MJ, deDivitiis O, Alderman MH. Left ventricular mass and body size in nor-motensive children and adults: assessment of allometric relations andimpact of overweight. J Am Coll Cardiol. 1992;20:1251–1260.
16. Ganau A, Devereux RB, Roman MJ, de Simone G, Pickering TG, SabaPS, Vargiu P, Simongini I, Laragh JH. Patterns of left ventricular hyper-trophy and geometric remodeling in essential hypertension. J Am CollCardiol. 1992;19:1550–1558.
17. Lewis J, Agodoa L, Cheek D, Greene T, Middleton J, O’Connor D, OjoA, Phillips R, Sika M, Wright J Jr. Comparison of cross-sectional renalfunction measurements in African Americans with hypertensive nephro-sclerosis and of primary formulas to estimate glomerular filtration rate.Am J Kidney Dis. 2001;38:744–753.
18. Korner PI, Jennings GL. Assessment of prevalence of left ventricularhypertrophy in hypertension. J Hypertens. 1998;16:715–723.
19. Verdecchia P, Schillaci G, Guerrieri M, Gatteschi C, Benemio G, BoldriniF, Porcellati C. Circadian blood pressure changes and left ventricularhypertrophy in essential hypertension. Circulation. 1990;81:528–536.
20. Mancia G, Zanchetti A, Agabiti-Rosei E, Benemio G, De Cesaris R,Fogari R, Pessina A, Porcellati C, Rappelli A, Salvetti A, Trimarco B.Ambulatory blood pressure is superior to clinic blood pressure in pre-dicting treatment-induced regression of left ventricular hypertrophy.
SAMPLE Study Group. Study on Ambulatory Monitoring of BloodPressure and Lisinopril Evaluation. Circulation. 1997;95:1464–1470.
21. Lauer MS, Anderson KM, Levy D. Influence of contemporary versus30-year blood pressure levels on left ventricular mass and geometry: theFramingham Heart Study. J Am Coll Cardiol. 1991;18:1287–1294.
22. Levy D, Anderson KM, Savage DD, Kannel WB, Christiansen JC,Castelli WP. Echocardiographically detected left ventricular hypertrophy:prevalence and risk factors. The Framingham Heart Study. Ann InternMed. 1988;108:7–13.
23. Harshfield GA, Treiber FA, Wilson ME, Kapuku GK, Davis HC. Alongitudinal study of ethnic differences in ambulatory blood pressurepatterns in youth. Am J Hypertens. 2002;15:525–530.
24. Fumo MT, Teeger S, Lang RM, Bednarz J, Sareli P, Murphy MB. Diurnalblood pressure variation and cardiac mass in Am blacks and whites andSouth African blacks. Am J Hypertens. 1992;5:111–116.
25. Verdecchia P, Porcellati C, Schillaci G, Borgioni C, Ciucci A, BattistelliM, Guerrieri M, Gatteschi C, Zampi I, Santucci A, Santucci C, Reboldi G.Ambulatory blood pressure. An independent predictor of prognosis inessential hypertension. Hypertension. 1994;24:793–801.
26. Cuspidi C, Meani S, Salerno M, Valerio C, Fusi V, Severgnini B, LonatiL, Magrini F, Zanchetti A. Cardiovascular target organ damage inessential hypertensives with or without reproducible nocturnal fall inblood pressure. J Hypertens. 2004;22:273–280.
27. Fagard R, Staessen J, Thijs L, Amery A. Multiple standardized clinicblood pressures may predict left ventricular mass as well as ambulatorymonitoring. A metaanalysis of comparative studies. Am J Hypertens.1995;8:533–540.
28. Toprak A, Koc M, Tezcan H, Ozener IC, Oktay A, Akoglu E. Night-timeblood pressure load is associated with higher left ventricular mass indexin renal transplant recipients. J Hum Hypertens. 2003;17:239–244.
29. Verdecchia P, Schillaci G, Guerrieri M, Boldrini F, Gatteschi C, BenemioG, Porcellati C. Prevalence and determinants of left ventricular diastolicfilling abnormalities in an unselected hypertensive population. EurHeart J. 1990;11:679–691.
30. Grandi AM, Broggi R, Jessula A, Laurita E, Cassinerio E, Piperno F,Bertolini A, Guasti L, Venco A. Relation of extent of nocturnal bloodpressure decrease to cardiovascular remodeling in never-treated patientswith essential hypertension. Am J Cardiol. 2002;89:1193–1196.
31. Bjorklund K, Lind L, Andren B, Lithell H. The majority of nondippingmen do not have increased cardiovascular risk: a population-based study.J Hypertens. 2002;20:1501–1506.
32. Shimada K, Kawamoto A, Matsubayashi K, Nishinaga M, Kimura S,Ozawa T. Diurnal blood pressure variations and silent cerebrovasculardamage in elderly patients with hypertension. J Hypertens. 1992;10:875–878.
33. Wachtell K, Palmieri V, Olsen MH, Bella JN, Aalto T, Dahlof B, GerdtsE, Wright JT Jr, Papademetriou V, Mogensen CE, Borch-Johnsen K,Ibsen H, Devereux RB. Urine albumin/creatinine ratio and echocardio-graphic left ventricular structure and function in hypertensive patientswith electrocardiographic left ventricular hypertrophy: the LIFE study.Losartan Intervention for Endpoint Reduction. Am Heart J. 2002;143:319–326.
34. Pontremoli R, Nicolella C, Viazzi F, Ravera M, Sofia A, Berruti V,Bezante GP, Del Sette M, Martinoli C, Sacchi G, Deferrari G. Microal-buminuria is an early marker of target organ damage in essential hyper-tension. Am J Hypertens. 1998;11:430–438.
35. Wiinberg N, Bang LE, Wachtell K, Larsen J, Olsen MH, Tuxen C,Hildebrandt PR, Rokkedal J, Ibsen H, Devereux RB. 24-h Ambulatoryblood pressure in patients with ECG-determined left ventricular hyper-trophy: left ventricular geometry and urinary albumin excretion-a LIFEsubstudy. J Hum Hypertens. 2004;18:391–396.
36. Palatini P, Graniero GR, Canali C, Santonastaso M, Mos L, Piccolo D,D’Este D, Berton G, Zanata G, De Venuto G. Relationship betweenalbumin excretion rate, ambulatory blood pressure and left ventricularhypertrophy in mild hypertension. J Hypertens. 1995;13:1796–1800.
37. Redon J, Liao Y, Lozano JV, Miralles A, Pascual JM, Cooper RS.Ambulatory blood pressure and microalbuminuria in essential hyper-tension: role of circadian variability. J Hypertens. 1994;12:947–953.
38. White WB, Schulman P, McCabe EJ, Dey HM. Average daily bloodpressure, not office blood pressure, determines cardiac function inpatients with hypertension. JAMA. 1989;261:873–877.
39. Bianchi S, Bigazzi R, Baldari G, Sgherri G, Campese VM. Diurnalvariations of blood pressure and microalbuminuria in essential hyper-tension. Am J Hypertens. 1994;7:23–29.
1038 Hypertension December 2007
by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from

40. Erley CM, Holzer M, Kramer BK, Riesler T. Renal hemodynamics andorgan damage in oung hypertensive patients with different plasma reninactivities after ACE-inhibition. Nephrol Dial Transplant. 1992;7:216–220.
41. Culleton BF, Larson MG, Wilson PW, Evans JC, Parfrey PS, Levy D.Cardiovascular disease and mortality in a community-based cohort withmild renal insufficiency. Kidney Int. 1999;56:2214–2219.
42. Leoncini G, Viazzi F, Parodi D, Vettoretti S, Ratto E, Ravera M,Tomolillo C, Del Sette M, Bezante GP, Deferrari G, Pontremoli R. Mildrenal dysfunction and subclinical cardiovascular damage in primaryhypertension. Hypertension. 2003;42:14–18.
43. Mitsnefes MM, Kimball TR, Kartal J, Witt SA, Glascock BJ, Khoury PR,Daniels SR. Cardiac and vascular adaptation in pediatric patients withchronic kidney disease: role of calcium-phosphorus metabolism. J AmSoc Nephrol. 2005;16:2796–2803.
44. Strozecki P, Adamowicz A, Nartowicz E, Odrowaz-Sypniewska G,Wlodarczyk Z, Manitius J. Parathormon, calcium, phosphorus, andleft ventricular structure and function in normotensive hemodialysispatients. Ren Fail. 2001;23:115–126.
45. Stack AG, Saran R. Clinical correlates and mortality impact of leftventricular hypertrophy among new ESRD patients in the United States.Am J Kidney Dis. 2002;40:1202–1210.
46. Zoccali C, Mallamaci F, Tripepi G, Parlongo S, Cutrupi S, Benedetto FA,Cataliotti A, Malatino LS. Norepinephrine and concentric hypertrophy inpatients with end-stage renal disease. Hypertension. 2002;40:41–46.
47. Converse RL Jr, Jacobsen TN, Toto RD, Jost CM, Cosentino F, Fouad-Tarazi F, Victor RG. Sympathetic overactivity in patients with chronicrenal failure. N Engl J Med. 1992;327:1912–1918.
48. Vlahakos DV, Hahalis G, Vassilakos P, Marathias KP, Geroulanos S.Relationship between left ventricular hypertrophy and plasma renin
activity in chronic hemodialysis patients. J Am Soc Nephrol. 1997;8:1764–1770.
49. Rame JE, Drazner MH, Post W, Peshock R, Lima J, Cooper RS, DriesDL. Corin I555(P568) allele is associated with enhanced cardiac hyper-trophic response to increased systemic afterload. Hypertension. 2007;49:857–864.
50. Tang W, Arnett DK, Devereux RB, Panagiotou D, Province MA, MillerMB, de Simone G, Gu C, Ferrell RE. Identification of a novel 5-base pairdeletion in calcineurin B (PPP3R1) promoter region and its associationwith left ventricular hypertrophy. Am Heart J. 2005;150:845–851.
51. Lapu-Bula R, Quarshie A, Lyn D, Oduwole A, Pack C, Morgan J,Nkemdiche S, Igho-Pemu P, Onwuanyi A, Li R, Ofili E. The 894T alleleof endothelial nitric oxide synthase gene is related to left ventricular massin African Americans with high-normal blood pressure. J Natl MedAssoc. 2005;97:197–205.
52. Schmieder RE. Reversal of left ventricular hypertrophy: Analysis of 412published studies. Am J Hypertens. 1994;7:25A. Abstract.
53. Verdecchia P, Schillaci G, Borgioni C, Ciucci A, Gattobigio R, ZampiI, Reboldi G, Porcellati C. Prognostic significance of serial changes inleft ventricular mass in essential hypertension. Circulation. 1998;97:48 –54.
54. Devereux RB, Wachtell K, Gerdts E, Boman K, Nieminen MS,Papademetriou V, Rokkedal J, Harris K, Aurup P, Dahlof B. Prog-nostic significance of left ventricular mass change during treatment ofhypertension. JAMA. 2004;292:2350 –2356.
55. Schussheim AE, Diamond JA, Phillips RA. Left ventricular midwallfunction improves with antihypertensive therapy and regression of leftventricular hypertrophy in patients with asymptomatic hypertension. Am JCardiol. 2001;87:61–65.
Peterson et al Left Ventricular Hypertrophy in African Americans 1039
by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from

Prevalence and Correlates of Left Ventricular Hypertrophy in the African American Study of Kidney Disease Cohort Study
Gail E. Peterson, MD1, Tine de Backer, MD2, Avril Gabriel*3, Vladimir Ilic, MD2, Tudor
Vagaonescu, MD2,4, Lawrence J Appel, MD, MPH5, Gabriel Contreras, MD, MPH6,
Cindy Kendrick7, Stephen Rostand, MD8, and Robert A. Phillips, MD, PhD9, for the
AASK investigators.
1 UT Southwestern Medical Center, Dallas, TX; 2Cardiovascular Research Foundation, New York, NY; 3Lenox Hill Hospital, New York, NY; 4UMDNJ-Robert Wood Johnson Medical School, New Brunswick, NJ; 5Johns Hopkins, Baltimore, MD; 6University of Miami, Miami, FL; 7Biostatistics and Epidemiology, Cleveland Clinic, Cleveland, OH; 8University of Alabama, Birmingham, AB, 9UMASS Memorial Medical Center and Medical School, Worcester, MA.
*deceased Word Count: Abstract 233 words, Manuscript 5988 words. Corresponding author: Gail Peterson, MD
Division of Cardiology
University of Texas Southwestern Medical Center
5909 Harry Hines Blvd, HA9.133
Dallas,Texas 75235-9047
214-645-7500
Fax 214-645-7501
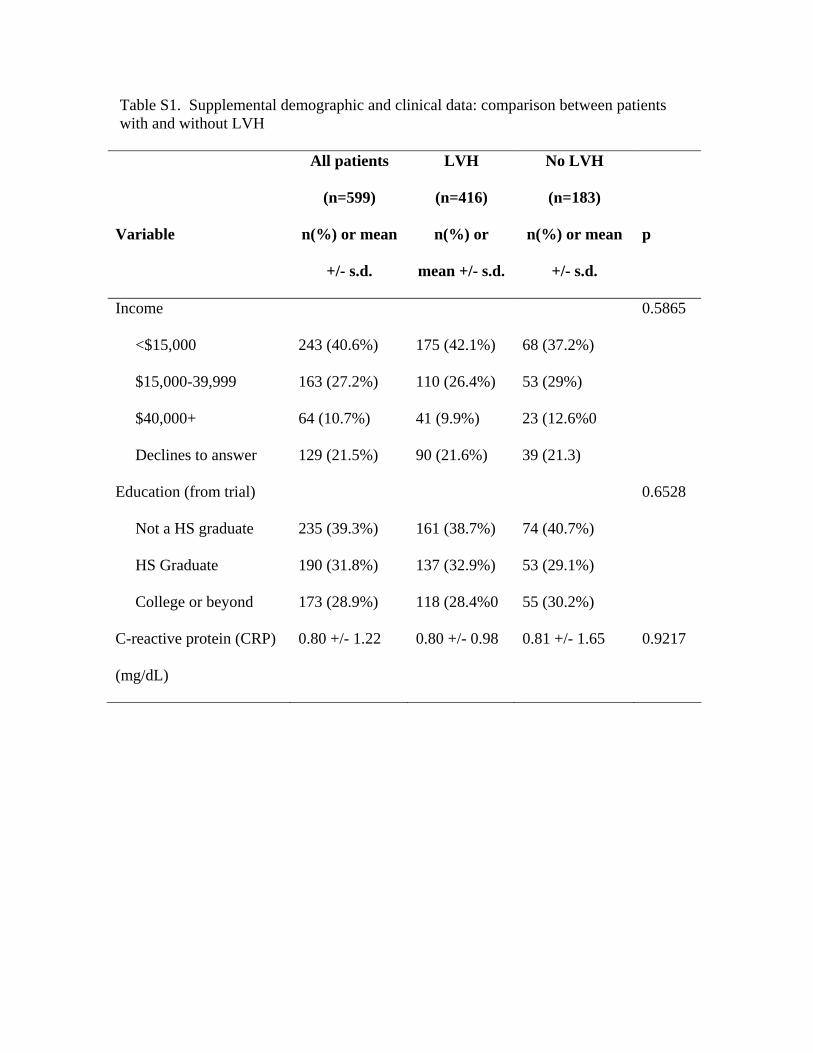
Table S1. Supplemental demographic and clinical data: comparison between patients with and without LVH
All patients
(n=599)
LVH
(n=416)
No LVH
(n=183)
Variable n(%) or mean
+/- s.d.
n(%) or
mean +/- s.d.
n(%) or mean
+/- s.d.
p
Income 0.5865
<$15,000 243 (40.6%) 175 (42.1%) 68 (37.2%)
$15,000-39,999 163 (27.2%) 110 (26.4%) 53 (29%)
$40,000+ 64 (10.7%) 41 (9.9%) 23 (12.6%0
Declines to answer 129 (21.5%) 90 (21.6%) 39 (21.3)
Education (from trial) 0.6528
Not a HS graduate 235 (39.3%) 161 (38.7%) 74 (40.7%)
HS Graduate 190 (31.8%) 137 (32.9%) 53 (29.1%)
College or beyond 173 (28.9%) 118 (28.4%0 55 (30.2%)
C-reactive protein (CRP)
(mg/dL)
0.80 +/- 1.22 0.80 +/- 0.98 0.81 +/- 1.65 0.9217
Appendix. African American Study of Kidney Disease Cohort Investigators
Case Western Reserve University: Principal Investigators – Jackson T. Wright, Jr.,
Mahboob Rahman, Study Coordinator - Renee Dancie, Louise Strauss. Emory
University: Principal Investigator - Janice Lea, Study Coordinators - Beth Wilkening,
Arlene Chapman and Diane Watkins. Harbor-UCLA Medical Center: Principal
Investigator - Joel D. Kopple, Study Coordinators - Linda Miladinovich, Jooree Choi,
and Patricia Oleskie, Connie Secules. Harlem Hospital Center: Principal Investigator -
Velvie Pogue, Study Coordinators - Donna Dowie, Herman Anderson, Leroy Herbert,
Robeta Locko, Hazeline Nurse, Jen-Tse. Cheng, G Darkwa, Victoria Dowdy, Beverly
Nicholas. Howard University: Principal Investigators - Otelio Randall, Tamrat Retta,
Study Coordinators - Shichen Xu, Muluemebet Ketete, Debra Ordor, Carl Tilghman.
Johns Hopkins University: Principal Investigators - Edgar Miller, Brad Astor,
Study Coordinators - Charalett Diggs, Jeanne Charleston, Charles Harris, Thomas
Shields. Charles R. Drew University: Principal Investigators - Keith Norris, David
Martins, Study Coordinators - Melba Miller, Holly Howell, Laurice Pitts.
Medical University of South Carolina: Principal Investigator - DeAnna Cheek, Study
Coordinator - Deborah Brooks. Meharry Medical College: Principal Investigators -
Marquetta Faulkner, Olufemi Adeyele, Study Coordinators - Karen Phillips, Ginger
Sanford, Cynthia Weaver. Morehouse School of Medicine: Principal Investigatos -
William Cleveland, Kimberly Chapman, Study Coordinators - Winifred Smith, Sherald
Glover. Mount Sinai School of Medicine and University of Massachusetts: Principal
Investigators - Robert Phillips, Michael Lipkowitz, Mohammed Rafey Study
Coordinators - Avril Gabriel, Eileen Condren, Natasha Coke. Ohio State University:
Principal Investigators - Lee Hebert, Ganesh Shidham, Study Coordinators - Leena
Hiremath, Stephanie Justice. University of Chicago, Chicago: Principal Investigators -
George Bakris, James Lash, Study Coordinators - Linda Fondren, Louise Bagnuolo,
Janet Cohan, Anne Frydrych. University of Alabama, Birmingham: Principal
Investigators - Stephen Rostand, Denyse Thornley-Brown, Study Coordinator - Beverly
Key. University of California, San Diego: Principal Investigators - Francis B. Gabbai,
Daniel T. O'Connor; Study Coordinator - Brenda Thomas. University of Florida:
Principal Investigators - C. Craig Tisher, Geraldine Bichier, Study Coordinators -
Cipriano Sarmiento, Amado Diaz, Carol Gordon. University of Miami: Principal
Investigators - Gabriel Contreras, Jacques Bourgoignie, Dollie Florence-Green, Study
Coordinator - Jorge Junco, Jacqueline Vassallo. University of Michigan: Principal
Investigators - Kenneth Jamerson, Akinlou Ojo, Tonya Corbin, Study Coordinators -
Denise Cornish-Zirker, Tanya Graham, Wendy Bloembergen. University of Southern
California: Principal Investigators - Shaul Massry, Miroslav Smogorzewski, Study
Coordinators - Annie Richardson, Laurice Pitts. University of Texas Southwestern
Medical Center, Dallas: Principal Investigators - Robert Toto, Gail Peterson, Ramesh
Saxena, Study Coordinators - Tammy Lightfoot, Sherry-Ann Blackstone, Carlos Loreto.
Vanderbilt University: Principal Investigators - Julie Lewis, Gerald Schulman, Study
Coordinators - Mo Sika, Sandy McLeroy. National Institute of Diabetes and Digestive
and Kidney Diseases: Lawrence. Y. Agodoa, Josephine. P. Briggs, John. W. Kusek;
Steering Committee Chair - Lawrence. Appel. Data Coordinating Center (Cleveland
Clinic Foundation): Jennifer Gassman, Gerald Beck, Tom Greene, Bo Hu, Study

Coordinators – Karen Brittain, Susan Sherer, Laurie Tuason, Cynthia Kendrick, Sharon
Bi, Harvey Litowitz, Xianyou Liu, Xuelei Wang, Kimberly Wiggins, Cheryl A. Tatum.
Central Biochemistry Laboratory: Frederick Van Lente, Joan Waletzky, Cathy
O'Laughlin, LaChauna Burton. External Advisory Committee: William McClellan,
Lucile Adams-Campbell, Kathy Faber-Langendoen, Bryce Kiberd, Elisa Lee, Timothy
Meyer, David Nathan, John Stokes, Herman Taylor, Peter W. Wilson. Cardiovascular
Research Foundation: Tine deBacker, Alexandra Lansky, Steve Slack.

for the African American Study of Kidney Disease InvestigatorsAppel, Gabriel Contreras, Cindy Kendrick, Stephen Rostand and Robert A. Phillips
Gail E. Peterson, Tine de Backer, Avril Gabriel, Vladimir Ilic, Tudor Vagaonescu, Lawrence J.Study of Kidney Disease Cohort Study
Prevalence and Correlates of Left Ventricular Hypertrophy in the African American
Print ISSN: 0194-911X. Online ISSN: 1524-4563 Copyright © 2007 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Hypertension doi: 10.1161/HYPERTENSIONAHA.107.090613
2007;50:1033-1039; originally published online October 29, 2007;Hypertension.
http://hyper.ahajournals.org/content/50/6/1033World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://hyper.ahajournals.org/content/suppl/2007/10/05/HYPERTENSIONAHA.107.090613.DC1.htmlData Supplement (unedited) at:
http://hyper.ahajournals.org//subscriptions/
is online at: Hypertension Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialHypertensionin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on December 11, 2014http://hyper.ahajournals.org/Downloaded from




















