
Effect of Benincasa hispida fruits on testosterone-induced prostatic hypertrophy in albino rats
Upload
independentCategory
view
1download
0
1 23
European Archives of Oto-Rhino-Laryngologyand Head & Neck ISSN 0937-4477Volume 271Number 8 Eur Arch Otorhinolaryngol (2014)271:2311-2316DOI 10.1007/s00405-014-2978-6
Grade 4 tonsillar hypertrophy associatedwith decreased retronasal olfactoryfunction: a pilot study
Melih Cayonu, Murat Salihoglu, AytugAltundag, Hakan Tekeli & GürkanKayabasoglu

1 23
Your article is protected by copyright and
all rights are held exclusively by Springer-
Verlag Berlin Heidelberg. This e-offprint is
for personal use only and shall not be self-
archived in electronic repositories. If you wish
to self-archive your article, please use the
accepted manuscript version for posting on
your own website. You may further deposit
the accepted manuscript version in any
repository, provided it is only made publicly
available 12 months after official publication
or later and provided acknowledgement is
given to the original source of publication
and a link is inserted to the published article
on Springer's website. The link must be
accompanied by the following text: "The final
publication is available at link.springer.com”.

1 3
Eur Arch Otorhinolaryngol (2014) 271:2311–2316DOI 10.1007/s00405-014-2978-6
MIscEllAnEOus
Grade 4 tonsillar hypertrophy associated with decreased retronasal olfactory function: a pilot study
Melih Cayonu · Murat Salihoglu · Aytug Altundag · Hakan Tekeli · Gürkan Kayabasoglu
Received: 16 January 2014 / Accepted: 20 February 2014 / Published online: 9 March 2014 © springer-Verlag Berlin Heidelberg 2014
consumption. In addition, there was no difference between the groups in terms of “sniffin’ sticks” subtests and TDI scores. It was determined that the retronasal olfactory scores of the participants with grade 4 tonsil size were significantly lower than the retronasal olfactory scores of the participants with grade 1 tonsil size. The current investigation demon-strates that grade 4 tonsillar hypertrophy has significant negative effects on the retronasal route of olfactory sensing, when compared with grade 1 tonsillar hypertrophy.
Keywords Tonsillar hypertrophy · Retronasal · Orthonasal · Olfaction
Introduction
While some people are born with naturally enlarged ton-sil tissues, the causes of tonsillar hypertrophy are usu-ally related to infections in the tonsils or adjacent tissues. severe cases of this condition can lead to the blockage and obstruction of the oral airway, which can make breathing and swallowing difficult (Fig. 1). Tonsillar hypertrophy is more common in children with adenoid hypertrophy, but it can also be present in adults without adenoid hypertro-phy. Patients with severe tonsillar hypertrophy may be prone to snoring, and difficult and painful swallowing due to the enlarged tissues of the tonsils, which can result in a decreased taste perception or appetite.
Research shows that odorants travel to the olfactory receptors by two routes. “sniffing” brings odorants through the nostrils into the nasal cavity (orthonasal olfaction), and chewing and swallowing force odorants emitted by foods upward, behind the palate, into the nasal cavity from the rear of the mouth (retronasal olfaction). There are clear differences between orthonasal and retronasal olfaction in
Abstract Tonsillar hypertrophy is common in children, but it can also be present in adults. Enlarged tonsils, a significant anatomical barrier, may affect the flow of odor molecules from the oral cavity to the nasal passages, which has not yet been studied. Thus, we aimed to investigate the mass effect of palatine tonsillar hypertrophy on retronasal olfaction. This study was carried out in 146 subjects, with a mean age of 22.1 ± 2.2 years, ranging 20–29 years. An oropharyngeal examination of the participants was completed, and tonsil-lar hypertrophy was graded according to the subjective ton-sil size scale. The participants were divided into four groups according to their tonsil size grading; then, each subject’s orthonasal olfactory and retronasal olfactory functions were assessed using “sniffin’ sticks” and retronasal olfactory testing. There were no differences observed between the groups in terms of age, gender, cigarette smoking, or alcohol
M. cayonu (*) Department of Otorhinolaryngology, Amasya university Training and Research Hospital, Kirazlıdere, Amasya 05100, Turkeye-mail: [email protected]
M. salihoglu Department of Otorhinolaryngology, Gulhane Military Medical Academy Haydarpasa Training Hospital, uskudar, Istanbul 34668, Turkey
A. Altundag Division of Otorhinolaryngology, Istanbul surgery Hospital, sisli, Istanbul 34365, Turkey
H. Tekeli Department of neurology, Gulhane Military Medical Academy Haydarpasa Training Hospital, uskudar, Istanbul 34668, Turkey
G. Kayabasoglu Department of Otorhinolaryngology, sakarya university Training and Research Hospital, Adapazarı, Turkey
Author's personal copy

2312 Eur Arch Otorhinolaryngol (2014) 271:2311–2316
1 3
neuronal processing and perception, so that these two path-ways convey two distinct sensory signals [1–7]. Taste per-ception consists mainly of the interaction between retrona-sal olfaction and gustatory stimuli [8].
A significant number of patients complain of a reduction in their sense of smell, so it becomes important to reveal the factors that can influence retronasal olfaction as well as orthonasal olfaction [9–11]. Despite this, retronasal smell-ing, so far, has received far less attention than its orthona-sal counterpart. There are numerous studies about the nasal pathologies causing conductive orthonasal olfaction; how-ever, there is little data about the factors preventing retro-nasal odors from reaching the olfactory mucosa [1, 12–17].
Oral conditions, mouth movements, mastication, swal-lowing, and the presence of adenoid hypertrophy are known to influence the perception of retronasal stimuli [18–20]. However, to the best of our knowledge there was no other study about the effects of tonsillar hypertrophy on retronasal olfaction in the literature. Therefore, the aim of this study was to evaluate the mass effect of hypertrophic palatine ton-sils, lateral border of oropharyngeal isthmus between the oral cavity and oropharynx, on retronasal olfaction.
Materials and methods
study design
This study was approved by the clinical Research Eth-ics committee of Istanbul cerrahpasa Medical Faculty (10.05.13-83045809/11277). The study was conducted at the otolaryngology clinics of Gulhane Military Medical Academy Haydarpasa Training Hospital and Istanbul sur-gery Hospital, and informed consent was obtained from all participating subjects.
The volunteers were evaluated using flexible naso-pharyngeal endoscopy and subjects with no signs of nasal polyposis, nasopharyngeal pathologies, or rhinosinusitis were included in the study. Individuals with a history of subjective olfactory dysfunction, tonsillectomy, or other oropharyngeal surgeries, such as adenoidectomy or palatal surgery were excluded from the study. Also, volunteers with class 3 and 4 mallampati score according to the modified mallampati classification, were excluded from the study [21, 22]. Only volunteers with class 1 and 2 mallampati score were included in the study to minimize tissue effect of tongue and soft palate. In addition, volunteers with asym-metrical tonsil hypertrophy were not included in the study.
After completing the oropharyngeal examinations of the participants, tonsillar hypertrophy was graded according to the subjective tonsil size scale [23]. Tonsil size was graded from 1 to 4: grade 1 tonsil size implied tonsils hidden within the pillars; in grade 2, the tonsil was in the tonsillar fossa, and extended to the posterior pillar; a grade 3 tonsil was out of the tonsillar fossa, but did not extend across the midline between the posterior pillar and midpoint of the soft palate; and in grade 4, the tonsil extended to the midline or touched the other tonsil at the midline. After grading the palatine ton-sil sizes, the “sniffin’ sticks” olfactory test and retronasal olfactory testing were performed. All the participants com-pleted the olfactory testing process and nobody was excluded from the study due to his/her olfactory testing results.
Orthonasal olfactory testing
Psychophysical testing of olfactory function was performed using the validated “sniffin’ sticks” test, where odorants were presented in commercially available felt-tip pens (“sniffin’ sticks”, Burghart GmbH, Wedel, Germany) [24, 25]. For odor presentation, the pen’s cap was removed by the experimenter for ~3 s, and the tip of the pen was placed ~1.0–2.0 cm in front of the nostrils. The test consists of one threshold and two suprathreshold subtests, namely a test for olfactory thresholds of n-butanol, a test for odor discrimination (16 tri-plets with two different odors) and one for odor identification (16 common odors, presented in a four-alternative, forced-choice procedure). The maximum score of each subtest was 16, resulting in a maximum composite score of 48 [threshold, discrimination, and identification (TDI) score] [26]. The nor-mal values for the TDI composite score are >30.3, with a cut-off between anosmia and hyposmia at 16.5 [27].
Retronasal olfactory testing
For retronasal olfactory testing, a standardized validated test was used [18]. The test is based on identification of odorized powders or granules presented to the oral cavity (e.g., spices, instant drinks, and instant soups; Table 1). The
Fig. 1 Grade 4 tonsil hypertrophy
Author's personal copy

2313Eur Arch Otorhinolaryngol (2014) 271:2311–2316
1 3
substances were applied to the midline of the tongue on fenestrated plastic sticks. subjects were free to sample as much stimulant as needed for identification. This approach also minimized the problem of standardizing the area of stimulation, differences in tongue, or oral cavity size. In a typical trial, the experimenter placed ~0.05 g on the mid-dle of the tongue inside the oral cavity. nostrils were not closed during the application of powders on the tongue. After administration of each powder, participants rinsed their mouths with tap water. The procedure was self-timed. Each substance was identified by means of a closed set with four verbal items using a forced-choice procedure. The test result was a sum score of the correctly identified stimuli.
statistical analysis
Data analyses were performed using sPss 21.0 (statisti-cal Package for social sciences, sPss Inc., chicago, Il, usA). The normal distribution of the considered variables was first evaluated using the shapiro–Wilk test. The data were shown as the mean ± standard deviation for the con-tinuous variables, and the number of cases was used for the categorical ones. The differences between the groups were analyzed by the analysis of variance (AnOVA) or chi square, as appropriate. Post-hoc Tukey’s tests were also performed to identify the differences among the groups. correlational analyses were calculated according to the Pearson’s test, and the level of significance was set at 0.05.
Results
This study was carried out in 146 subjects, with a mean age of 22.1 ± 2.2 years, ranging from 20 to 29 years. The participants were divided into four groups according to their tonsil size grading, and the groups were named appropriately with the tonsil size grades. Table 2 gives the descriptive statistics of each of the variables of the study groups. There was no difference between the groups in terms of age, gender, cigarette smoking, or alcohol consumption.
The differences in the retronasal olfaction scores were significant among the four groups (p = 0.035). When the post-hoc tests were performed, it was determined that the retronasal olfactory scores of the participants with grade 4 tonsil size were significantly lower than the retronasal olfactory scores of the participants with grade 1 tonsil size (p = 0.03). no significant decrease was detected in group 4, when compared to groups 2 and 3, and there was no sig-nificant difference among groups 1, 2, and 3. In addition, the effect of tonsil hypertrophy on retronasal olfaction was evaluated with linear regression model. Our data showed that the tonsil hypertrophy had a slightly negative effect on retronasal olfaction (p = 0.003, r = 0.24).
There was no difference among the groups in terms of the “sniffin’ sticks” subtests and TDI scores; whereas, there was a significant correlation between the TDI scores and retronasal test olfactory scores (p < 0.001, r = 0.82).
Table 1 Odorized powder or granules used for retronasal olfactory testing
Target item Distracter items Brand name (distributor name and city location)
Ginger Mustard, paprika,curry Zencefil (Dogasal®, Ankara)
Grapefruit lemon, sour cherry, red currant Grapefruit (Firmenich®, Istanbul)
Bread sauerkraut, pizza, garlic Rusk bread (Etimek®, Bilecik)
Milk Vanilla, banana, coconut süttozu (Pınar®, Istanbul)
strawberry Apple, red currant, tangerine Çilek (Ori®, Istanbul)
Vanilla cherry, banana, honey Vanilin (Dr. Oetker®, Izmir)
Orange Raspberry, strawberry, cherry Portakal (Ori®, Istanbul)
Onion chives, salami, smoked ham sogan (Arifoglu®, Istanbul)
cocoa caramel, muscat, juniper Kakao (Dr. Oetker®, Izmir)
celery chives, parsley, carrots Kereviz kök granül (Kurucum®Isparta)
Mushrooms Bread, fish, white wine Mushrooms (Firmenich®, Istanbul)
Paprika Ginger, curry, mustard Karabiber (Bagdat®, Ankara)
coffee cinnamon, muscat, cocoa Türk Kahvesi (Ülker®, Izmir)
smoked ham Fish, bread, chives smoked ham (Firmenich®, Istanbul)
cloves Anise, caraway, dill Karanfil (Arifoglu®, Istanbul)
Garlic Ham, chives, celery sarımsak Granül (Bagdat®, Ankara)
Muscat cinnamon, coffee, cocoa Muscat (Firmenich®, Istanbul)
curry Mustard, cheese, cucumber Köri (Bagdat®, Ankara)
cinnamon Honey, caramel, cocoa Tarçın (Dogasal®, Ankara)
Raspberry Peach, pineapple, white grapes Raspberry (Firmenich®, Istanbul)
Author's personal copy
2314 Eur Arch Otorhinolaryngol (2014) 271:2311–2316
1 3
The overall percentage of participants with smoking habits was 55.5 %. Due to this high rate of smoking, when we compared the results of the olfactory tests between the smokers and non-smokers, it was detected that the smok-ers had significantly decreased retronasal olfactory scores (p < 0.001, r = 0.36). In addition, significant negative effects of smoking on odor threshold, odor discrimination, and odor identification scores were detected (p = 0.12, r = 0.2; p = 0.001, r = 0.27; and p = 0.001, r = 0.28, respectively).
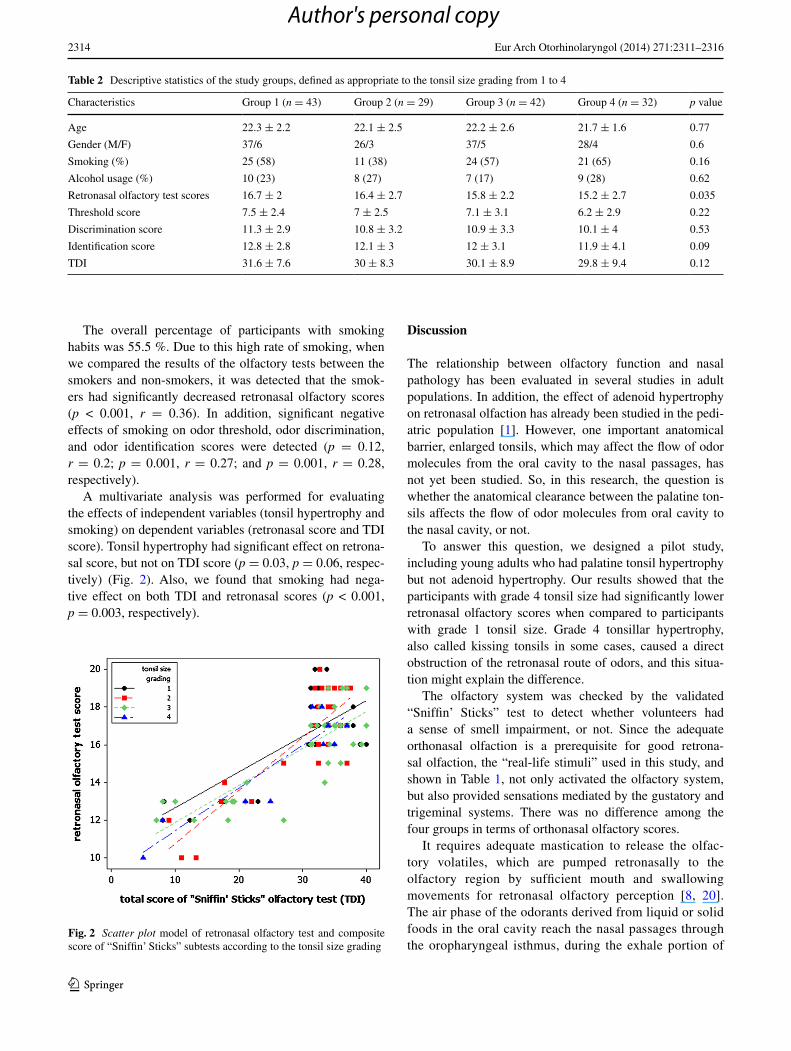
A multivariate analysis was performed for evaluating the effects of independent variables (tonsil hypertrophy and smoking) on dependent variables (retronasal score and TDI score). Tonsil hypertrophy had significant effect on retrona-sal score, but not on TDI score (p = 0.03, p = 0.06, respec-tively) (Fig. 2). Also, we found that smoking had nega-tive effect on both TDI and retronasal scores (p < 0.001, p = 0.003, respectively).
Discussion
The relationship between olfactory function and nasal pathology has been evaluated in several studies in adult populations. In addition, the effect of adenoid hypertrophy on retronasal olfaction has already been studied in the pedi-atric population [1]. However, one important anatomical barrier, enlarged tonsils, which may affect the flow of odor molecules from the oral cavity to the nasal passages, has not yet been studied. so, in this research, the question is whether the anatomical clearance between the palatine ton-sils affects the flow of odor molecules from oral cavity to the nasal cavity, or not.
To answer this question, we designed a pilot study, including young adults who had palatine tonsil hypertrophy but not adenoid hypertrophy. Our results showed that the participants with grade 4 tonsil size had significantly lower retronasal olfactory scores when compared to participants with grade 1 tonsil size. Grade 4 tonsillar hypertrophy, also called kissing tonsils in some cases, caused a direct obstruction of the retronasal route of odors, and this situa-tion might explain the difference.
The olfactory system was checked by the validated “sniffin’ sticks” test to detect whether volunteers had a sense of smell impairment, or not. since the adequate orthonasal olfaction is a prerequisite for good retrona-sal olfaction, the “real-life stimuli” used in this study, and shown in Table 1, not only activated the olfactory system, but also provided sensations mediated by the gustatory and trigeminal systems. There was no difference among the four groups in terms of orthonasal olfactory scores.
It requires adequate mastication to release the olfac-tory volatiles, which are pumped retronasally to the olfactory region by sufficient mouth and swallowing movements for retronasal olfactory perception [8, 20]. The air phase of the odorants derived from liquid or solid foods in the oral cavity reach the nasal passages through the oropharyngeal isthmus, during the exhale portion of
Table 2 Descriptive statistics of the study groups, defined as appropriate to the tonsil size grading from 1 to 4
characteristics Group 1 (n = 43) Group 2 (n = 29) Group 3 (n = 42) Group 4 (n = 32) p value
Age 22.3 ± 2.2 22.1 ± 2.5 22.2 ± 2.6 21.7 ± 1.6 0.77
Gender (M/F) 37/6 26/3 37/5 28/4 0.6
smoking (%) 25 (58) 11 (38) 24 (57) 21 (65) 0.16
Alcohol usage (%) 10 (23) 8 (27) 7 (17) 9 (28) 0.62
Retronasal olfactory test scores 16.7 ± 2 16.4 ± 2.7 15.8 ± 2.2 15.2 ± 2.7 0.035
Threshold score 7.5 ± 2.4 7 ± 2.5 7.1 ± 3.1 6.2 ± 2.9 0.22
Discrimination score 11.3 ± 2.9 10.8 ± 3.2 10.9 ± 3.3 10.1 ± 4 0.53
Identification score 12.8 ± 2.8 12.1 ± 3 12 ± 3.1 11.9 ± 4.1 0.09
TDI 31.6 ± 7.6 30 ± 8.3 30.1 ± 8.9 29.8 ± 9.4 0.12
Fig. 2 Scatter plot model of retronasal olfactory test and composite score of “sniffin’ sticks” subtests according to the tonsil size grading
Author's personal copy

2315Eur Arch Otorhinolaryngol (2014) 271:2311–2316
1 3
each natural breathing cycle that occurs during lip clo-sure, and normal lingual manipulation or dental chewing of the food [28].
The oral cavity is a three-dimensional place where taste perception starts. This anatomical cavity in healthy adults is generally connected to the nasal passages whenever the person is not speaking, swallowing, or choosing to produce a velopharyngeal closure [29]. The oropharyngeal isthmus lies between the soft palate and the dorsum of the tongue, and is bounded on both sides by the palatoglossal arches. Posteriorly to the oropharyngeal isthmus, the palatine ton-sils are placed between the palatoglossal and glossopharyn-geal plica, narrowing the isthmus in people with tonsillar hypertrophy.
Differences in relation to the perception of stimuli, either orthonasally or retronasally, are, to a certain degree, due to the differences in airflow pattern. It is known that mild changes in nasal anatomy may produce large differ-ences in the perception of odors [15, 16]. likewise, the ret-ronasal odor pathway has been shown to be affected from the pathologies preventing the airflow, oral cavity to olfac-tory cleft. unlike from conductive orthonasal dysfunction, which is affected from mild changes in the nasal anatomy, the retronasal olfaction can be affected from severe ana-tomical changes, which occurs through the way of retrona-sal route, such as grade 4 tonsillar hypertrophy.
As known, females have better olfactory abilities than males, that is why the low number of female participants is the limitation of this study [27]. Further studies with adequate female and male participants are needed to inves-tigate the preoperative and postoperative (after tonsillec-tomy) retronasal olfactory scores of patients with tonsillar hypertrophy, which will allow us to better understand of palatine tonsil’s effect on retronasal olfaction.
Conclusion
The perception of foods is based on the interaction between ortho and retronasal smell, taste, trigeminal acti-vation and texture, so it is difficult to investigate one of these factors in isolation. That is why retronasal olfaction has received less attention than the orthonasal olfaction, until recently. Technical problems excluded retronasal olfactory testing from routine clinical practice. The cur-rent investigation demonstrates that grade 4 tonsillar hypertrophy has significant negative effects on retronasal olfactory scores when compared with grade 1 tonsillar hypertrophy.
Conflict of interest The authors state that they had no funding, financial relationships, or conflicts of interest in the completion of this research.
References
1. Konstantinidis I, Triaridis s, Triaridis A, Petropoulos I, Karagi-annidis K, Kontzoglou G (2005) How do children with adenoid hypertrophy smell and taste? clinical assessment of olfactory function pre- and post-adenoidectomy. Int J Pediatr Otorhi-nolaryngol 69(10):1343–1349
2. landis Bn, Frasnelli J, Reden J, lacroix Js, Hummel T (2005) Differences between orthonasal and retronasal olfactory func-tions in patients with loss of the sense of smell. Arch Otolaryngol Head neck surg 131(11):977–981
3. Pfaar O, landis Bn, Frasnelli J, Hüttenbrink KB, Hummel T (2006) Mechanical obstruction of the olfactory cleft reveals dif-ferences between orthonasal and retronasal olfactory functions. chem senses 31(1):27–31
4. Rombaux P, Mouraux A, Bertrand B, nicolas G, Duprez T, Hum-mel T (2006) Retronasal and orthonasal olfactory function in relation to olfactory bulb volume in patients with posttraumatic loss of smell. laryngoscope 116(6):901–905
5. Rombaux P, Bertrand B, Keller T, Mouraux A (2007) clini-cal significance of olfactory event-related potentials related to orthonasal and retronasal olfactory testing. laryngoscope 117(6):1096–1101
6. Bojanowski V, Hummel T (2012) Retronasal perception of odors. Physiol Behav 107(4):484–487
7. Frasnelli J, van Ruth s, Kriukova I, Hummel T (2005) Intrana-sal concentrations of orally administered flavors. chem senses 30(7):575–582
8. Welge-lüssen A, Husner A, Wolfensberger M, Hummel T (2009) Influence of simultaneous gustatory stimuli on orthonasal and ret-ronasal olfaction. neurosci lett 454(2):124–128
9. Murphy c, schubert cR, cruickshanks KJ, Klein BE, Klein R, nondahl DM (2002) Prevalence of olfactory impairment in older adults. JAMA 288(18):2307–2312
10. Vennemann MM, Hummel T, Berger K (2008) The association between smoking and smell and taste impairment in the general population. J neurol 255(8):1121–1126
11. landis Bn, Hummel T (2006) new evidence for high occur-rence of olfactory dysfunctions within the population. Am J Med 119(1):91–92
12. simopoulos E, Katotomichelakis M, Gouveris H, Tripsianis G, livaditis M, Danielides V (2012) Olfaction-associated quality of life in chronic rhinosinusitis: adaptation and validation of an olfaction-specific questionnaire. laryngoscope 122(7):1450–1454
13. Becker s, Pflugbeil c, Gröger M, canis M, ledderose GJ, Kramer MF (2012) Olfactory dysfunction in seasonal and peren-nial allergic rhinitis. Acta Otolaryngol 132(7):763–768
14. schriever VA, Gupta n, Pade J, szewczynska M, Hummel T (2013) Olfactory function following nasal surgery: a 1-year fol-low-up. Eur Arch Otorhinolaryngol 270(1):107–111
15. nguyen DT, nguyen-Thi Pl, Jankowski R (2012) How does measured olfactory function correlate with self-ratings of the sense of smell in patients with nasal polyposis? laryngoscope 122(5):947–952
16. Garzaro M, Pezzoli M, landolfo V, Defilippi s, Giordano c, Pec-orari G (2012) Radiofrequency inferior turbinate reduction: long-term olfactory and functional outcomes. Otolaryngol Head neck surg 146(1):146–150
17. Haxel BR, Fuchs c, Fruth K, Mann WJ, lippert BM (2011) Eval-uation of the efficacy of the ‘nasal airflow-inducing manoeuvre’ for smell rehabilitation in laryngectomies by means of the snif-fin’ sticks test. clin Otolaryngol 36(1):17–23
18. Heilmann s, strehle G, Rosenheim K, Damm M, Hummel T (2002) clinical assessment of retronasal olfactory function. Arch Otolaryngol Head neck surg 128:414–418
Author's personal copy

2316 Eur Arch Otorhinolaryngol (2014) 271:2311–2316
1 3
19. Welge-lüssen A, Ebnöther M, Wolfensberger M, Hummel T (2009) swallowing is differentially influenced by retronasal com-pared with orthonasal stimulation in combination with gustatory stimuli. chem senses 34(6):499–502
20. Hummel T (2008) Retronasal perception of odors. chem Biodiv-ers 5(6):853–861
21. Mallampati sR, Gatt sP, Gugino lD, Desai sP, Waraksa B, Freiberger D, liu Pl (1985) A clinical sign to predict difficult tracheal intubation: a prospective study. can Anaesth soc J 32(4):429–434
22. samsoon Gl, Young JR (1987) Difficult tracheal intubation: a retrospective study. Anaesthesia 42:487–490
23. Friedman M, Tanyeri H, la Rosa M, landsberg R, Vaidyanathan K, Pieri s, caldarelli D (1999) clinical predictors of obstructive sleep apnea. laryngoscope 109(12):1901–1907
24. Hummel T, sekinger B, Wolf s, Pauli E, Kobal G (1997) “sniffin’ sticks”: olfactory performance assessed by the combined testing of odor identification, odor discrimination and olfactory thresh-old. chem senses 22(1):39–52
25. Kobal G, Klimek l, Wolfensberger M et al (2000) Multicenter investigation of 1,036 subjects using a standardized method for
the assessment of olfactory function combining tests of odor identification, odor discrimination, and olfactory thresholds. Eur Arch Otorhinolaryngol 257(4):205–211
26. Wolfensberger M, schnieper I, Welge-lussen A (2000) “snif-fin’ sticks”: a new olfactory test battery. Acta Otolaryngol 120(2):303–306
27. Hummel T, Kobal G, Gudziol H et al (2007) normative data for the ‘‘sniffin’ sticks’’ including tests of odor identification, odor discrimination, and olfactory thresholds: an upgrade based on a group of more than 3,000 subjects. Eur Arch Otorhinolaryngol 264(3):237–243
28. Deibler KD, lavin EH, linforth Rs, Taylor AJ, Acree TE (2001) Verification of a mouth simulator by in vivo measurements. J Agric Food chem 49(3):1388–1393
29. Buettner A, Beer A, Hannig c, settles M (2001) Observation of the swallowing process by application of videofluoroscopy and real-time magnetic resonance imaging-consequences for retrona-sal aroma stimulation. chem senses 26(9):1211–1219
Author's personal copy
Copyright © 2022 FDOKUMEN




















