
Preparation and preclinical evaluation of 177Lu-nimotuzumab targeting epidermal growth factor...
11
Preparation and preclinical evaluation of 177 Lu-nimotuzumab targeting epidermal growth factor receptor overexpressing tumors ☆,☆☆ Denis R. Beckford Vera ⁎ , Sebastian Eigner, Katerina Eigner Henke, Ondrej Lebeda, Frantisek Melichar, Milos Beran Department of Radiopharmaceuticals, Nuclear Physics Institute of the Academy of Sciences of the Czech Republic, Husinec-Rez 130, CZ-250 68, Husinec-Rez, Czech Republic Received 6 April 2011; received in revised form 30 June 2011; accepted 3 July 2011 Abstract Objectives: Nimotuzumab (h-R3) is a humanized monoclonal antibody (mAb) which recognizes the external domain of the epidermal growth factor receptor (EGFR) with high specificity. It was demonstrated that h-R3 has a unique clinical profile for immunotherapy of adult gliomas and pediatric pontine gliomas. The aim of this work was to evaluate the conjugate 177 Lu-h-R3 as a potential radioimmunoconjugate for radioimmunotherapy (RIT) of tumors overexpressing EGFR. Methods: h-R3 was modified with the macrocylcic ligand S-2-(4-isothiocyanatobenzyl)-1,4,7,10-tetraazacyclododecane tetraacetic acid (p- SCN-Bn-DOTA) and the acyclic ligand S-2-(4-Isothiocyanatobenzyl)-diethylenetriamine pentaacetic acid (p-SCN-Bn-DTPA); the immunoconjugates were labeled with no-carried added 177 Lu. Specificity and affinity were tested using radioimmunoassays in a cell line overexpressing EGFR. Biodistribution in mice, healthy or bearing A431 epithelial carcinoma xenografts, was performed for 11 days. Tumor uptake, the influence of the nature of the chelate and the way of administration were studied. Absorbed dose in tumor and selected organs was calculated using the OLINDA/EXM software; the data from the animals was extrapolated to humans. Results: 177 Lu-h-R3 conjugates were obtained with specific activity up to 915 MBq/mg without significant loss of immunoreactivity. The binding of 177 Lu-h-R3 conjugates to A431 cells showed to be EGFR specific, and the affinity was similar to native h-R3. Tumor uptake reached a maximum value of 22.4±3.1 %ID/g at 72 h and remained ∼20% ID/g over 1 week. Locoregional application showed better tumor/ nontumor ratios than intravenous application. Conclusions: 177 Lu-h-R3 should be considered for further evaluations as a potential radiopharmaceutical for RIT of tumors overexpressing EGFR. © 2012 Elsevier Inc. All rights reserved. Keywords: Radioimmunotherapy; Nimotuzumab; 177 Lu; Monoclonal antibody 1. Introduction Radioimmunotherapy (RIT) is a therapeutic modality that involves the use of monoclonal antibodies (mAb) to deliver the energy of beta- or alpha particles to targeted cells. Even when this technique is approved, it is still in the early stages of development [1]. Relevant results have been obtained in the treatment of refractory non-Hodgkin's lymphoma (NHL) employing ibritumomab tiuxetan (Zevalin) and/or iodine ( 131 I) tositumomab (Bexxar), the first radioimmunoconju- gates (RIC) approved by the US Food and Drug Adminis- tration (FDA) in 2002 and 2003, respectively. Nevertheless, the treatment of solid tumors using this modality remains to be thoroughly investigated. Discrete advances have been achieved in the treatment of minimal residual disease, locoregional applications, pretargeted RIT and as a combi- nation of therapies [2,3]. Epidermal growth factor receptor (EGFR) is a target of anticancer therapies due to its overexpression in a variety of malignant epithelial tumors and it is associated with a poor Available online at www.sciencedirect.com Nuclear Medicine and Biology 39 (2012) 3 – 13 www.elsevier.com/locate/nucmedbio ☆ This research was supported by EUREKA Grant No. E08018 and Project NPVII 2B06165 from the Czech Ministry of Education, Youth and Sports. ☆☆ Conflicts of interest statement: The authors declare that they have no conflicts of interest. ⁎ Corresponding author. Tel.: +420 266 172 207; fax: +420 220 940 151. E-mail addresses: [email protected], [email protected] (D.R. Beckford Vera). 0969-8051/$ – see front matter © 2012 Elsevier Inc. All rights reserved. doi:10.1016/j.nucmedbio.2011.07.001
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Preparation and preclinical evaluation of 177Lu-nimotuzumab targeting epidermal growth factor...

Available online at www.sciencedirect.com
Nuclear Medicine and Biology 39 (2012) 3–13www.elsevier.com/locate/nucmedbio
Preparation and preclinical evaluation of 177Lu-nimotuzumab targetingepidermal growth factor receptor overexpressing tumors☆,☆☆
Denis R. Beckford Vera⁎, Sebastian Eigner, Katerina Eigner Henke, Ondrej Lebeda,Frantisek Melichar, Milos Beran
Department of Radiopharmaceuticals, Nuclear Physics Institute of the Academy of Sciences of the Czech Republic, Husinec-Rez 130, CZ-250 68,Husinec-Rez, Czech Republic
Received 6 April 2011; received in revised form 30 June 2011; accepted 3 July 2011
Abstract
Objectives: Nimotuzumab (h-R3) is a humanized monoclonal antibody (mAb) which recognizes the external domain of the epidermalgrowth factor receptor (EGFR) with high specificity. It was demonstrated that h-R3 has a unique clinical profile for immunotherapy of adultgliomas and pediatric pontine gliomas. The aim of this work was to evaluate the conjugate 177Lu-h-R3 as a potential radioimmunoconjugatefor radioimmunotherapy (RIT) of tumors overexpressing EGFR.Methods: h-R3 was modified with the macrocylcic ligand S-2-(4-isothiocyanatobenzyl)-1,4,7,10-tetraazacyclododecane tetraacetic acid (p-SCN-Bn-DOTA) and the acyclic ligand S-2-(4-Isothiocyanatobenzyl)-diethylenetriamine pentaacetic acid (p-SCN-Bn-DTPA); theimmunoconjugates were labeled with no-carried added 177Lu. Specificity and affinity were tested using radioimmunoassays in a cell lineoverexpressing EGFR. Biodistribution in mice, healthy or bearing A431 epithelial carcinoma xenografts, was performed for 11 days. Tumoruptake, the influence of the nature of the chelate and the way of administration were studied. Absorbed dose in tumor and selected organs wascalculated using the OLINDA/EXM software; the data from the animals was extrapolated to humans.Results: 177Lu-h-R3 conjugates were obtained with specific activity up to 915 MBq/mg without significant loss of immunoreactivity. Thebinding of 177Lu-h-R3 conjugates to A431 cells showed to be EGFR specific, and the affinity was similar to native h-R3. Tumor uptakereached a maximum value of 22.4±3.1 %ID/g at 72 h and remained ∼20% ID/g over 1 week. Locoregional application showed better tumor/nontumor ratios than intravenous application.Conclusions: 177Lu-h-R3 should be considered for further evaluations as a potential radiopharmaceutical for RIT of tumorsoverexpressing EGFR.© 2012 Elsevier Inc. All rights reserved.
Keywords: Radioimmunotherapy; Nimotuzumab; 177Lu; Monoclonal antibody
1. Introduction
Radioimmunotherapy (RIT) is a therapeutic modality thatinvolves the use of monoclonal antibodies (mAb) to deliverthe energy of beta- or alpha particles to targeted cells. Evenwhen this technique is approved, it is still in the early stages
☆ This research was supported by EUREKA Grant No. E08018 andProject NPVII 2B06165 from the Czech Ministry of Education, Youth andSports.
☆☆ Conflicts of interest statement: The authors declare that they haveno conflicts of interest.
⁎ Corresponding author. Tel.: +420 266 172 207; fax: +420 220 940 151.E-mail addresses: [email protected], [email protected]
(D.R. Beckford Vera).
0969-8051/$ – see front matter © 2012 Elsevier Inc. All rights reserved.doi:10.1016/j.nucmedbio.2011.07.001
of development [1]. Relevant results have been obtained inthe treatment of refractory non-Hodgkin's lymphoma (NHL)employing ibritumomab tiuxetan (Zevalin) and/or iodine(131I) tositumomab (Bexxar), the first radioimmunoconju-gates (RIC) approved by the US Food and Drug Adminis-tration (FDA) in 2002 and 2003, respectively. Nevertheless,the treatment of solid tumors using this modality remains tobe thoroughly investigated. Discrete advances have beenachieved in the treatment of minimal residual disease,locoregional applications, pretargeted RIT and as a combi-nation of therapies [2,3].
Epidermal growth factor receptor (EGFR) is a target ofanticancer therapies due to its overexpression in a variety ofmalignant epithelial tumors and it is associated with a poor

4 D.R. Beckford Vera et al. / Nuclear Medicine and Biology 39 (2012) 3–13
prognosis [4,5]. In fibroblasts cells, the expression of EGFRranges from 40,000 to 100,000 receptors per cell [6,7]. Incontrast, EGFR is overexpressed in the majority of solidtumors, including breast and ovarian cancer, colon cancer,head-and-neck cancer and non–small cell lung cancer(NSCLC), with some breast cancers expressing up to2×106 EGFR receptors per cell [8]. Several approacheshave been used to inhibit the EGFR-associated signaltransduction cascade. Monoclonal antibodies bound to aspecific region of EGFR have been successfully used toinhibit its dimerization and autophosphorylation [5,9,10].
Nimotuzumab (TheraCIM, CIMher, Theraloc) is a human-ized mAb (IgG1) obtained by transplanting the complemen-tary determining regions of the murine monoclonal antibodyior-egf/r3 to human framework which recognizes the externaldomain of EGFRwith high specificity [11,12]. Unlike most ofthe drugs against the EGFR, h-R3 does not show severeadverse effects in the clinic; for example, no serious skin rasheshave been reported [13]. h-R3 has demonstrated veryencouraging results in pediatric pontine (brainstem) andadult gliomas [14]. It is undergoing clinical trials in non–small cell lung cancer and a Phase II monotherapy trial inEurope in patients with advanced metastatic pancreatic cancer[15]. 188Re-labeled h-R3 showed promising results in a Phase Itrial for the radiation treatment of gliomas via an in-dwellingcatheter into the postoperative cavity following resection [16].
Beta radiation radionuclide emitters such as 131I (t1/2=8.0days; β−=0.6 MeV and Eγ=0.364 MeV) and 90Y (t1/2=2.67days; β−=2.28 MeV) have been successfully used in RIT.Residualizing radionuclides, such as 90Y and 177Lu, arepotentially more suitable radionuclides for RIT [17]. 177Lu(t1/2=6.7 days, Eγ=0.208 MeV, β−=0.497 MeV, max rangein tissue penetration=2.0 mm) is being strongly consideredfor RIT since it combines the advantages of both 90Y and 131Iand the ability to form stable complexes with macrocyclicand acyclic ligands [18–21]. Its half-life is appropriate forpreparation, transport and successful delivery of therapeuticdoses to the tumor by radioimmunoconjugates such asmonoclonal antibodies. In addition, 177Lu emits two low-energy γ lines with energy of 113 and 208 keV that aresuitable for imaging and assessment of delivered doses.
The aim of this work was to evaluate the RIC177Lu-nimotuzumab (177Lu-h-R3), in a model of humanepithelial carcinoma, as a potential radioimmunoconjugatefor RIT of tumors overexpressing EGFR. The effects of thenature of the bifunctional chelate used for 177Lu labeling andthe administration approach, intravenous vs. locoregional,were also studied.
2. Materials and methods
2.1. Reagents and equipment
177Lu no-carrier added (nca in 0.05 mol/L HCl), producedindirectly via the 176Yb(n,γ)177Yb→(β−)→177Lu reaction,was generously donated by Isotope Technologies Garching
(ITG, Munich, Germany). 90YCl3 (555 MBq in 22 μl of 0.05M HCl) was purchased from PerkinElmer. Bifunctionalchelators, p-SCN-Bn-DOTA and p-SCN-Bn-DTPA werepurchased from Macrocyclics (Dallas, TX, USA). Nimotuzu-mab was purchased in 10-ml vials (5.0 mg/ml in phosphate-buffered saline) from Oncoscience AG (Wedel, Germany).Chelex 100 in sodium form was purchased from Sigma(Steinheim, Germany). All other reagents were purchasedfrom Merck (Darmstadt, Germany) or Fluka (Steinhelm,Germany) with the highest purity available. Ultrapure water(Aquatec Water Systems, California, USA) was used for allprocedures. To avoid metal contamination, all the solutionsused in conjugation and radiolabeling reactions were passedthrough a Chelex 100 column (1×10 cm), and all glasswarewas washed with 2 M HCl and ultrapure water.
Size-exclusion high-performance liquid chromatography(SE-HPLC) was performed at room temperature on an Agilent1200 series chromatographic system (Agilent, Waldbronn,Germany) equipped with a Rheodyne injector (Milford, USA)and an online γ-ray detector (Raytest, Straubenhardt,Germany). The Gina Start version 4.07 software (Strauben-hardt, Germany) was used for data processing. UV measure-ments were performed on a Spectronic Unicam, Heλios-αspectrophotometer (ThermoSpectronic, Cambridge, UK)using a 1-cm sample cell. Radiation counting of TLC plateswas performed with a Cyclone Plus Storage PhosphorSystem (PerkinElmer, USA) or miniGITA (Raytest). TheVivaspin 6 and 20 centrifugal devices (molecular weightcutoff 30 kDa) were purchased from Sartorius (StedimBiotech, Goettingen, Germany).
2.2. Conjugation of nimotuzumab with p-SCN-Bn-DOTA
The original solution of h-R3 was concentrated to 10 mg/mlby ultrafiltration using Vivaspin 20. Concentrations of mAbwere determined by UV spectrophotometry at 280 nm. Tenmilligrams of humanized mAb h-R3 in 0.01 mol/L phosphatebuffer (pH 7.2) was mixed with p-SCN-Bn-DOTA (20- or 50-fold molar excess) or p-SCN-Bn-DTPA (20-fold molar excess)previously dissolved in phosphate buffer (pH 8.5) and final pHwas adjusted to 8.5 with NaOH 1 mol/L. Afterwards, thereaction mixture was incubated overnight at 4°C. Theimmunoconjugates were purified by ultrafiltration on Vivaspin6 until the absorbance in the ultrafiltrate at 280 nm was nearlyzero. Protein concentration was determined by Bradford assay.Conjugates were stored at 4°C for further use. Immunoconju-gates were characterized by SE-HPLC. About 20 μl of theconjugatewas injected onto aTSK-Gel SW3000 (7.5×300mm,10μm,TosoHass) columnusing 0.9%NaCl/0.05%NaN3 as themobile phase. The flow ratewasmaintained at 1ml/min, and theelution was monitored by UV spectrophotometer at 280 nm.
2.3. Determination of the average number of chelates perantibody molecule (L/P)
The average number of chelates linked to an antibodymolecule was determined using 90Y by a radioactive method

5D.R. Beckford Vera et al. / Nuclear Medicine and Biology 39 (2012) 3–13
previously described [22]. Briefly, 49 μg (10 μl) of theconjugates was added to 30–50 μl of NH4OAc 0.5 mol/L(pH 7.0). Afterwards, 10, 20 or 30 μl (3.33×10−4 mol/L) of astandardized YCl3 solution spiked with 90Y was added. Thereaction mixture was incubated at 42°C for 3 h, then 1/9 ofthe reaction volume of DTPA (0.01 mol/L, pH 6.0) wasadded and the reaction mixture was incubated at roomtemperature for another 15 min. An aliquot of 2 μl of thereaction mixture was developed on SG-ITLC plates using a10% (0.4 mol/L) solution of ammonium acetate andmethanol (1:1) as the mobile phase. The number of chelatesper antibody molecule was calculated from the ratio ofcounts remaining at the origin to the total number of countsmultiplied by the mole ratio of metal (Y3+)/mole ofconjugate.
2.4. 177Lu Radiolabeling
Aliquots of 177LuCl3 (15–185 MBq, 1–25 μl) were addedto 25–50 μl of 0.5 mol/L NH4OAc buffer at pH 7.0,followed by 50–100 μl (0.200–0.540 mg) of conjugates.Afterwards, the reaction mixture was incubated at 42°C for1.5 h. In order to scavenge any free radiometal for furtherquality control, a solution of DTPA or EDTA (7–17 μl, 0.01mol/L, pH 6.0) was added to the reaction vial and the mixturewas incubated for 15 min at room temperature. In theseconditions, the radioimmunoconjugates remain at the origin,while radiometal-DTPA/EDTA complexes migrate to Rf
0.4–0.8. The effect of the number of chelate per antibodymolecule and the nature of the chelate on the radiolabelingefficiency and specific activity were studied.
2.5. Quality control
Radiolabeled conjugates were purified from unboundradiometal, when needed, by size exclusion chromatographyon PD-10 columns (GE Healthcare, Buckinghamshire, UK)eluted with phosphate buffered saline at 0.01 mol/L.Radiometal labeling efficiency and radiochemical puritywere determined by thin-layer chromatography performedon SG-ITLC plates (Pall Corporation, USA), using 10% (w/v) ammonium acetate/methanol (1:1) as the mobile phase.SE-HPLC was also employed using a TSK-Gel SW 3000(7.5×300 mm, 10 μm, TosoHass) column, with an isocraticmobile phase of 0.9% NaCl/0.05% NaN3 and a flow rate of1.0 ml/min.
2.6. Cell culture
The human squamous carcinoma cell line A431 (CLR1555; American Type Culture Collection) was used in all cellexperiments. The A431 cell line was cultured in DMEMhigh-glucose medium. Media were supplemented with 10%fetal calf serum (FCS) and penicillin/streptomycin (penicillin100 IU/ml and streptomycin 100 μg/ml). All media,supplements, antibiotics and buffers used in cell culturewere purchased from PAA The Cell Culture Company(Pasching, Austria). During cell culture and cell experiments
(unless otherwise stated), cells were grown at 37°C inincubators with humidified air, equilibrated with 5% CO2.
2.7. Saturation binding experiment
For the saturation binding experiment, A431 cells werecultured ∼2×105cells/well on 12-well plates (BD Falcon,Becton-Dickinson, UK) in 1 ml of medium for 48 h prior tothe studies. Cells were treated with solutions of differentconcentrations (100 μl/well, 3.0–120.0 nmol/L) of 177Lu-DOTA-h-R3 or 177Lu-DTPA-h-R3 and incubated for 3 h at4°C. The nonspecific background binding was studied byadding a 100 times excess of native nimotuzumab to somewells. Triplicate cell dishes were used for each measuringpoint. After incubation, the medium was discarded and cellswere washed with ice-cold phosphate buffer solution (PBS).Cells were lysed using 0.5 ml of 0.5 M NaOH containing 5%SDS, and the radioactivity was measured in a γ-counter(Wizard 3″, Wallac, Turku, Finland). Dissociation constants(Kd) were estimated from the nonlinear fitted curves usingGraphPad Prism software (GraphPad Software, California,USA). For cell counting, a representative parallel samplefrom the experiments was trypsinized for about 15 min andthe cells were counted using a fully automated cell analyzingsystem (CASY TT, Roche Innovatis, Germany). The meanwas used as a cell number for all wells.
2.8. Competitive binding experiment and immunoreactivity
Biological activities of the 177Lu-h-R3 conjugates wereestimated by competitive inhibition experiments againstnative nimotuzumab. Therefore A431 cells were cultured asdescribed above. The cells were treated with 177Lu-h-R3conjugates (100 μl/well, 50 ng, ∼75000 cpm/well) premixedwith different concentrations of native h-R3 in cell culturemedium and incubated for 3 h at 4°C. Afterwards, the cellswere treated as described above. Concentration values thatcaused 50% of inhibition (IC50) of
177Lu-h-R3 to its receptorwere estimated from the nonlinear fitted curves using theGraphPad Prism software. The immunoreactive fraction ofthe 177Lu-h-R3 conjugates was determined using the methoddescribed by Konishi et al. [23] based on competitivebinding assay using a fixed cell concentration and differentdilutions of radioimmunoconjugate. Normalized cell boundradioactivity was plotted as a function of h-R3 concentration,and the immunoreactivity fraction was estimated by fittingthe data to the equation previously described [21].
2.9. Animal experiments
Male Balb/c nu/nu mice, 6 weeks old, purchased fromCharles River Laboratories (Sulzfeld, Germany) were usedfor in vivo experiments. All animal experiments wereperformed according to the Animals Ethics Committee ofthe Institute of Nuclear Research, Rez, Czech Republic. Forbiodistribution studies in a human tumor model over-expressing EGFR, subcutaneous xenografts were establishedfrom the A431 human epithelial carcinoma cell line by

Fig. 1. Typical instant thin layer chromatography profile of 177Lu-DOTA-h-R3 (top) and 177Lu-DTPA-h-R3 (bottom).
6 D.R. Beckford Vera et al. / Nuclear Medicine and Biology 39 (2012) 3–13
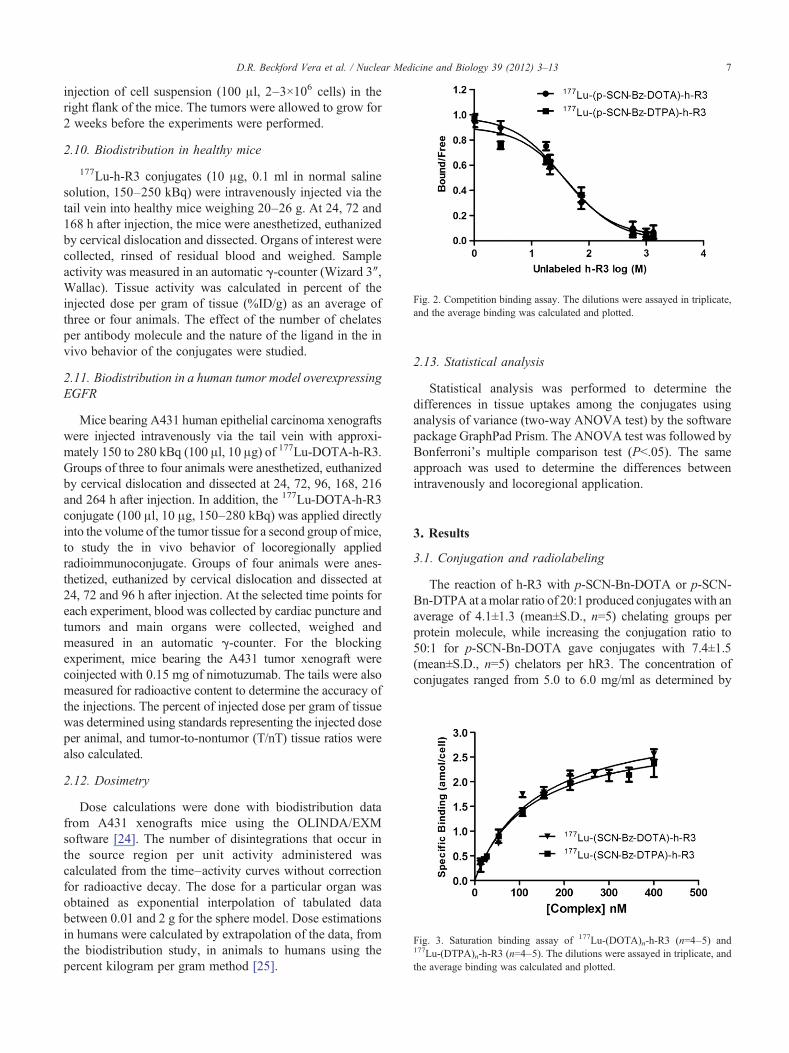
ig. 2. Competition binding assay. The dilutions were assayed in triplicate,nd the average binding was calculated and plotted.
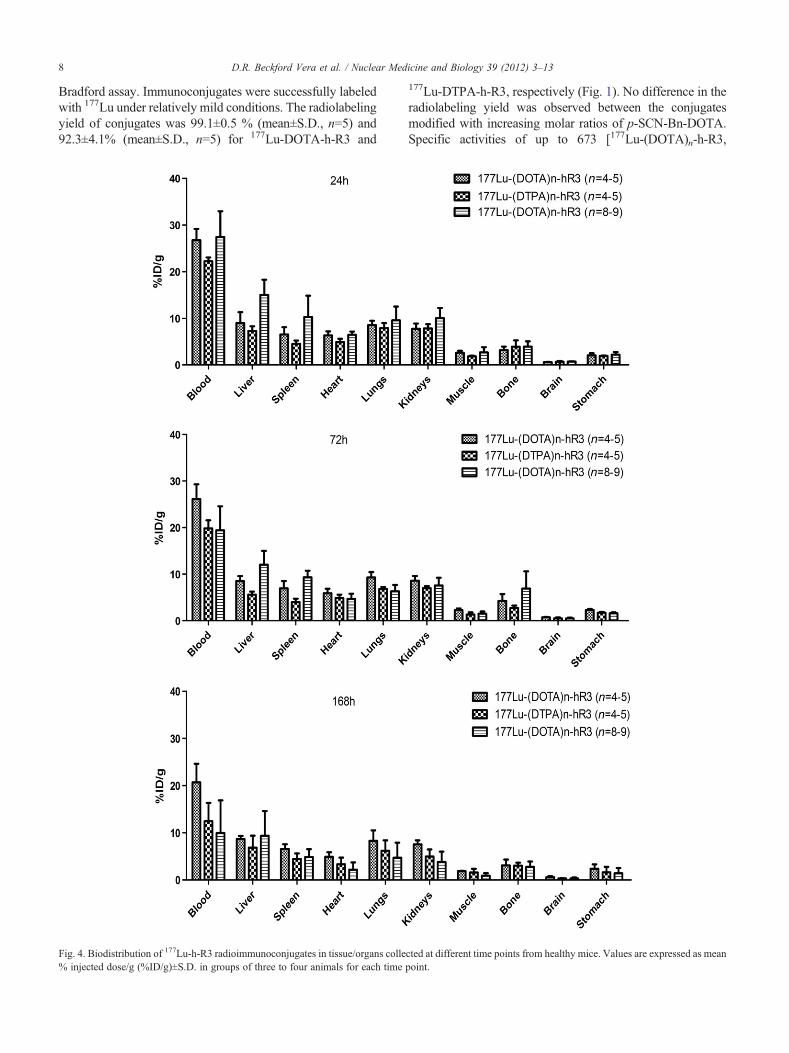
ig. 3. Saturation binding assay of 177Lu-(DOTA)n-h-R3 (n=4–5) and7Lu-(DTPA)n-h-R3 (n=4–5). The dilutions were assayed in triplicate, ande average binding was calculated and plotted.
7D.R. Beckford Vera et al. / Nuclear Medicine and Biology 39 (2012) 3–13
injection of cell suspension (100 μl, 2–3×106 cells) in theright flank of the mice. The tumors were allowed to grow for2 weeks before the experiments were performed.
2.10. Biodistribution in healthy mice
177Lu-h-R3 conjugates (10 μg, 0.1 ml in normal salinesolution, 150–250 kBq) were intravenously injected via thetail vein into healthy mice weighing 20–26 g. At 24, 72 and168 h after injection, the mice were anesthetized, euthanizedby cervical dislocation and dissected. Organs of interest werecollected, rinsed of residual blood and weighed. Sampleactivity was measured in an automatic γ-counter (Wizard 3″,Wallac). Tissue activity was calculated in percent of theinjected dose per gram of tissue (%ID/g) as an average ofthree or four animals. The effect of the number of chelatesper antibody molecule and the nature of the ligand in the invivo behavior of the conjugates were studied.
2.11. Biodistribution in a human tumor model overexpressingEGFR
Mice bearing A431 human epithelial carcinoma xenograftswere injected intravenously via the tail vein with approxi-mately 150 to 280 kBq (100 μl, 10 μg) of 177Lu-DOTA-h-R3.Groups of three to four animals were anesthetized, euthanizedby cervical dislocation and dissected at 24, 72, 96, 168, 216and 264 h after injection. In addition, the 177Lu-DOTA-h-R3conjugate (100 μl, 10 μg, 150–280 kBq) was applied directlyinto the volume of the tumor tissue for a second group of mice,to study the in vivo behavior of locoregionally appliedradioimmunoconjugate. Groups of four animals were anes-thetized, euthanized by cervical dislocation and dissected at24, 72 and 96 h after injection. At the selected time points foreach experiment, blood was collected by cardiac puncture andtumors and main organs were collected, weighed andmeasured in an automatic γ-counter. For the blockingexperiment, mice bearing the A431 tumor xenograft werecoinjected with 0.15 mg of nimotuzumab. The tails were alsomeasured for radioactive content to determine the accuracy ofthe injections. The percent of injected dose per gram of tissuewas determined using standards representing the injected doseper animal, and tumor-to-nontumor (T/nT) tissue ratios werealso calculated.
2.12. Dosimetry
Dose calculations were done with biodistribution datafrom A431 xenografts mice using the OLINDA/EXMsoftware [24]. The number of disintegrations that occur inthe source region per unit activity administered wascalculated from the time–activity curves without correctionfor radioactive decay. The dose for a particular organ wasobtained as exponential interpolation of tabulated databetween 0.01 and 2 g for the sphere model. Dose estimationsin humans were calculated by extrapolation of the data, fromthe biodistribution study, in animals to humans using thepercent kilogram per gram method [25].
Fa
2.13. Statistical analysis
Statistical analysis was performed to determine thedifferences in tissue uptakes among the conjugates usinganalysis of variance (two-way ANOVA test) by the softwarepackage GraphPad Prism. The ANOVA test was followed byBonferroni's multiple comparison test (Pb.05). The sameapproach was used to determine the differences betweenintravenously and locoregional application.
3. Results
3.1. Conjugation and radiolabeling
The reaction of h-R3 with p-SCN-Bn-DOTA or p-SCN-Bn-DTPA at amolar ratio of 20:1 produced conjugates with anaverage of 4.1±1.3 (mean±S.D., n=5) chelating groups perprotein molecule, while increasing the conjugation ratio to50:1 for p-SCN-Bn-DOTA gave conjugates with 7.4±1.5(mean±S.D., n=5) chelators per hR3. The concentration ofconjugates ranged from 5.0 to 6.0 mg/ml as determined by
F17
th
8 D.R. Beckford Vera et al. / Nuclear Medicine and Biology 39 (2012) 3–13
Bradford assay. Immunoconjugates were successfully labeledwith 177Lu under relatively mild conditions. The radiolabelingyield of conjugates was 99.1±0.5 % (mean±S.D., n=5) and92.3±4.1% (mean±S.D., n=5) for 177Lu-DOTA-h-R3 and
Fig. 4. Biodistribution of 177Lu-h-R3 radioimmunoconjugates in tissue/organs colle% injected dose/g (%ID/g)±S.D. in groups of three to four animals for each time
177Lu-DTPA-h-R3, respectively (Fig. 1). No difference in theradiolabeling yield was observed between the conjugatesmodified with increasing molar ratios of p-SCN-Bn-DOTA.Specific activities of up to 673 [177Lu-(DOTA)n-h-R3,
cted at different time points from healthy mice. Values are expressed as meanpoint.

9D.R. Beckford Vera et al. / Nuclear Medicine and Biology 39 (2012) 3–13
n=4–5], 915 [177Lu-(DOTA)n-h-R3, n=7–9] and 478[177Lu-(DTPA)n-h-R3, n=4–5] MBq/mg were obtained.When purification was applied, the radiochemical puritywas greater than 98%.
3.2. Saturation and competitive binding experiments
The immunoreactive fractions were 94.5±3.1% and88.3±4.6% (mean immunoreactivity±S.E.) for 177Lu-DOTA-h-R3 and 177Lu-DTPA-h-R3, respectively. Theresults from the binding competitive experiments showeda sigmoid curve. The binding of 177Lu-hR3 conjugates toA431 cell lines showed to be epidermal growth factorreceptor specific (Fig. 2). Fifty percent displacements(mean IC50±S.D., n=3) were achieved at 34.9±2.7 and44.3±5.1 nmol/L of unmodified h-R3 for 177Lu-DOTA-h-R3 and 177Lu-DTPA-h-R3, respectively. The Kd deter-mined by saturation binding experiment of the radiolabeledh-R3 was 13.8±1.9×10−8 and 12.2±1.3×10−8 mol/L for177Lu-DOTA-h-R3 and 177Lu-DTPA-h-R3, respectively.The number of binding sites per cell was ∼2×106
calculated from the Bmax value (Fig. 3).
3.3. Biodistribution in healthy animals
The biodistribution study in healthy animals wasperformed in order to compare the behavior of 177Lu-h-R3conjugates, mainly in blood, liver, spleen, lung and bone.The results are summarized in Fig. 4. At 24 h, significantlyhigher concentration in blood of 177Lu-DOTA-h-R3 thanthat of 177Lu-DTPA-h-R3 (Pb.05) was observed. Statisti-cally, no significant differences were observed in bloodconcentration between 177Lu-DOTA-h-R3 conjugates pre-pared with increasing conjugation ratios, but the liver uptakewas significantly higher for the 177Lu-DOTA-h-R3 conju-
Fig. 5. Biodistribution of the 177Lu-(DOTA)n-h-R3 (n=4–5) radioimmunoconjugatmice. Values are expressed as mean %ID/g±S.D. in groups of three to four anima
gate with the higher DOTA/h-R3 ratio (Pb.01). At the72- and 168-h time points, the concentration in blood of177Lu-(DOTA)n-hR3 (n=4–5) was significantly higherthan that of 177Lu-(DTPA)n-hR3 (n=4–5) and 177Lu-(DOTA)n-hR3 (n=7–9) conjugates (72 h, Pb.01 and 168 h,Pb.001). No significant differences in lungs, kidneys, heart,brain, stomach and bone uptakes among the 177Lu-h-R3conjugates (PN.05) could be observed in the whole study.Statistical analysis showed that there was no significantdifference in tissue-to-blood ratios for 177Lu-(DOTA)n-h-R3(n=4–5) until 168 h (PN.05). The liver-to-blood ratiosincreased with time for 177Lu-(DOTA)n-h-R3 (n=7–9,Pb.001) and for 177Lu-(DTPA)n-h-R3 (n=4–5, Pb.05). Forall preparations, bone-to-blood ratios remained constant overtime (PN.05).
3.4. Biodistribution in xenograft-bearing mice
The biodistribution studies of 177Lu-(DOTA)n-h-R3(n=4–5) were conducted in A431 human epidermalcarcinoma xenografts in Balb/c nude mice. For intravenousapplication, the biodistribution study was performed over aperiod of 264 h and for the locoregional application at 24-,72- and 96-h time points. Uptakes in the tumor and majororgans of interest over time are shown in Fig. 5.Tumoruptake reached a maximum value of 22.4±3.1 %ID/g at 72h. From 72 to 216 h, the average tumor uptake was 18.3±0.3 %ID/g. Tumor uptake decreased to 12.6±2.8 %ID/gfrom 216 to 264 h. Normal tissue uptakes were lower than9 %ID/g in all tissues and they decreased over time, exceptfor bone and spleen whose values remain approximatelyconstant throughout the whole study. Bone uptake was lowwith a maximum value of 2.7±1.1 %ID/g at 24 h and anaverage of 1.6±0.5 from 72 to 264 h. At 168 h, T/nT tissue
e in tissue/organs collected at different time points from A431 tumor-bearingls for each time point.
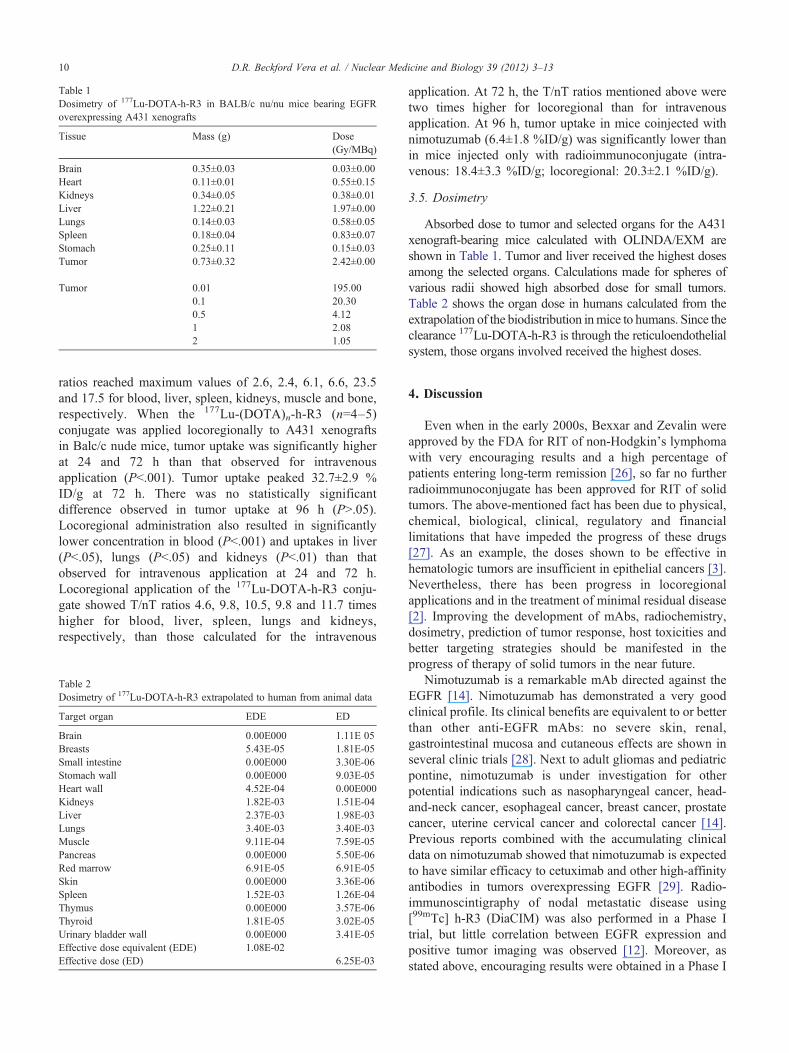
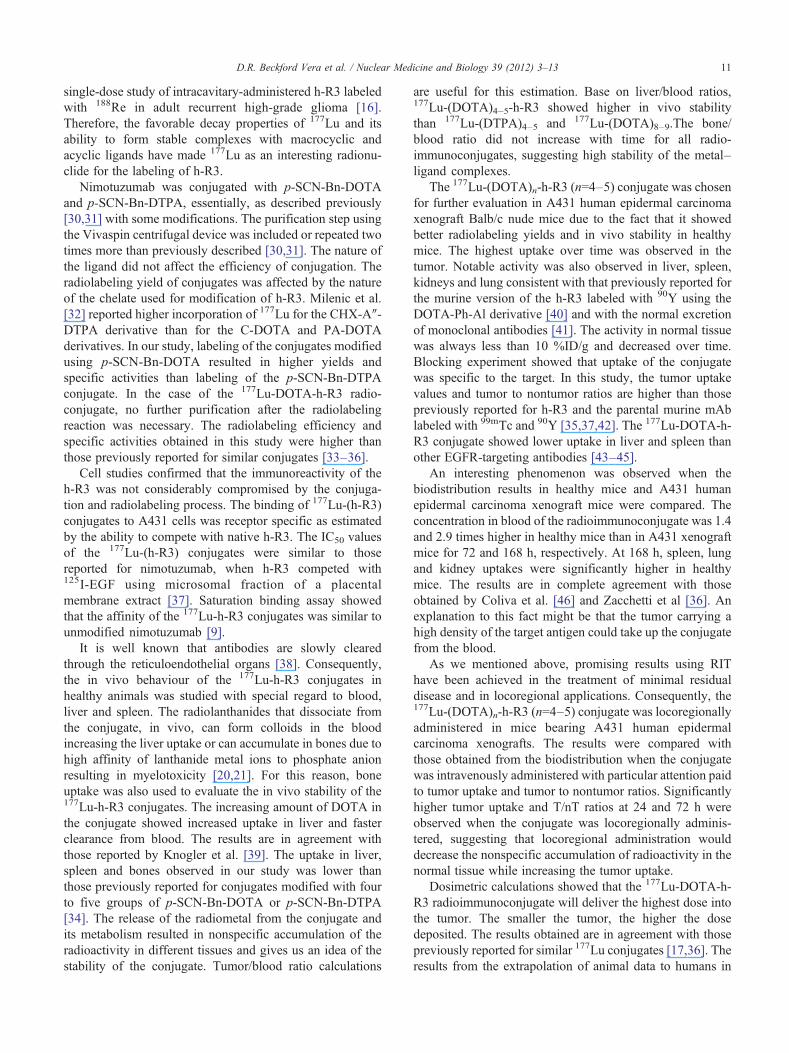
Table 1Dosimetry of 177Lu-DOTA-h-R3 in BALB/c nu/nu mice bearing EGFRoverexpressing A431 xenografts
Tissue Mass (g) Dose(Gy/MBq)
Brain 0.35±0.03 0.03±0.00Heart 0.11±0.01 0.55±0.15Kidneys 0.34±0.05 0.38±0.01Liver 1.22±0.21 1.97±0.00Lungs 0.14±0.03 0.58±0.05Spleen 0.18±0.04 0.83±0.07Stomach 0.25±0.11 0.15±0.03Tumor 0.73±0.32 2.42±0.00
Tumor 0.01 195.000.1 20.300.5 4.121 2.082 1.05
10 D.R. Beckford Vera et al. / Nuclear Medicine and Biology 39 (2012) 3–13
ratios reached maximum values of 2.6, 2.4, 6.1, 6.6, 23.5and 17.5 for blood, liver, spleen, kidneys, muscle and bone,respectively. When the 177Lu-(DOTA)n-h-R3 (n=4–5)conjugate was applied locoregionally to A431 xenograftsin Balc/c nude mice, tumor uptake was significantly higherat 24 and 72 h than that observed for intravenousapplication (Pb.001). Tumor uptake peaked 32.7±2.9 %ID/g at 72 h. There was no statistically significantdifference observed in tumor uptake at 96 h (PN.05).Locoregional administration also resulted in significantlylower concentration in blood (Pb.001) and uptakes in liver(Pb.05), lungs (Pb.05) and kidneys (Pb.01) than thatobserved for intravenous application at 24 and 72 h.Locoregional application of the 177Lu-DOTA-h-R3 conju-gate showed T/nT ratios 4.6, 9.8, 10.5, 9.8 and 11.7 timeshigher for blood, liver, spleen, lungs and kidneys,respectively, than those calculated for the intravenous
Table 2Dosimetry of 177Lu-DOTA-h-R3 extrapolated to human from animal data
Target organ EDE ED
Brain 0.00E000 1.11E 05Breasts 5.43E-05 1.81E-05Small intestine 0.00E000 3.30E-06Stomach wall 0.00E000 9.03E-05Heart wall 4.52E-04 0.00E000Kidneys 1.82E-03 1.51E-04Liver 2.37E-03 1.98E-03Lungs 3.40E-03 3.40E-03Muscle 9.11E-04 7.59E-05Pancreas 0.00E000 5.50E-06Red marrow 6.91E-05 6.91E-05Skin 0.00E000 3.36E-06Spleen 1.52E-03 1.26E-04Thymus 0.00E000 3.57E-06Thyroid 1.81E-05 3.02E-05Urinary bladder wall 0.00E000 3.41E-05Effective dose equivalent (EDE) 1.08E-02Effective dose (ED) 6.25E-03
application. At 72 h, the T/nT ratios mentioned above weretwo times higher for locoregional than for intravenousapplication. At 96 h, tumor uptake in mice coinjected withnimotuzumab (6.4±1.8 %ID/g) was significantly lower thanin mice injected only with radioimmunoconjugate (intra-venous: 18.4±3.3 %ID/g; locoregional: 20.3±2.1 %ID/g).
3.5. Dosimetry
Absorbed dose to tumor and selected organs for the A431xenograft-bearing mice calculated with OLINDA/EXM areshown in Table 1. Tumor and liver received the highest dosesamong the selected organs. Calculations made for spheres ofvarious radii showed high absorbed dose for small tumors.Table 2 shows the organ dose in humans calculated from theextrapolation of the biodistribution inmice to humans. Since theclearance 177Lu-DOTA-h-R3 is through the reticuloendothelialsystem, those organs involved received the highest doses.
4. Discussion
Even when in the early 2000s, Bexxar and Zevalin wereapproved by the FDA for RIT of non-Hodgkin's lymphomawith very encouraging results and a high percentage ofpatients entering long-term remission [26], so far no furtherradioimmunoconjugate has been approved for RIT of solidtumors. The above-mentioned fact has been due to physical,chemical, biological, clinical, regulatory and financiallimitations that have impeded the progress of these drugs[27]. As an example, the doses shown to be effective inhematologic tumors are insufficient in epithelial cancers [3].Nevertheless, there has been progress in locoregionalapplications and in the treatment of minimal residual disease[2]. Improving the development of mAbs, radiochemistry,dosimetry, prediction of tumor response, host toxicities andbetter targeting strategies should be manifested in theprogress of therapy of solid tumors in the near future.
Nimotuzumab is a remarkable mAb directed against theEGFR [14]. Nimotuzumab has demonstrated a very goodclinical profile. Its clinical benefits are equivalent to or betterthan other anti-EGFR mAbs: no severe skin, renal,gastrointestinal mucosa and cutaneous effects are shown inseveral clinic trials [28]. Next to adult gliomas and pediatricpontine, nimotuzumab is under investigation for otherpotential indications such as nasopharyngeal cancer, head-and-neck cancer, esophageal cancer, breast cancer, prostatecancer, uterine cervical cancer and colorectal cancer [14].Previous reports combined with the accumulating clinicaldata on nimotuzumab showed that nimotuzumab is expectedto have similar efficacy to cetuximab and other high-affinityantibodies in tumors overexpressing EGFR [29]. Radio-immunoscintigraphy of nodal metastatic disease using[99mTc] h-R3 (DiaCIM) was also performed in a Phase Itrial, but little correlation between EGFR expression andpositive tumor imaging was observed [12]. Moreover, asstated above, encouraging results were obtained in a Phase I
11D.R. Beckford Vera et al. / Nuclear Medicine and Biology 39 (2012) 3–13
single-dose study of intracavitary-administered h-R3 labeledwith 188Re in adult recurrent high-grade glioma [16].Therefore, the favorable decay properties of 177Lu and itsability to form stable complexes with macrocyclic andacyclic ligands have made 177Lu as an interesting radionu-clide for the labeling of h-R3.
Nimotuzumab was conjugated with p-SCN-Bn-DOTAand p-SCN-Bn-DTPA, essentially, as described previously[30,31] with some modifications. The purification step usingthe Vivaspin centrifugal device was included or repeated twotimes more than previously described [30,31]. The nature ofthe ligand did not affect the efficiency of conjugation. Theradiolabeling yield of conjugates was affected by the natureof the chelate used for modification of h-R3. Milenic et al.[32] reported higher incorporation of 177Lu for the CHX-A″-DTPA derivative than for the C-DOTA and PA-DOTAderivatives. In our study, labeling of the conjugates modifiedusing p-SCN-Bn-DOTA resulted in higher yields andspecific activities than labeling of the p-SCN-Bn-DTPAconjugate. In the case of the 177Lu-DOTA-h-R3 radio-conjugate, no further purification after the radiolabelingreaction was necessary. The radiolabeling efficiency andspecific activities obtained in this study were higher thanthose previously reported for similar conjugates [33–36].
Cell studies confirmed that the immunoreactivity of theh-R3 was not considerably compromised by the conjuga-tion and radiolabeling process. The binding of 177Lu-(h-R3)conjugates to A431 cells was receptor specific as estimatedby the ability to compete with native h-R3. The IC50 valuesof the 177Lu-(h-R3) conjugates were similar to thosereported for nimotuzumab, when h-R3 competed with125I-EGF using microsomal fraction of a placentalmembrane extract [37]. Saturation binding assay showedthat the affinity of the 177Lu-h-R3 conjugates was similar tounmodified nimotuzumab [9].
It is well known that antibodies are slowly clearedthrough the reticuloendothelial organs [38]. Consequently,the in vivo behaviour of the 177Lu-h-R3 conjugates inhealthy animals was studied with special regard to blood,liver and spleen. The radiolanthanides that dissociate fromthe conjugate, in vivo, can form colloids in the bloodincreasing the liver uptake or can accumulate in bones due tohigh affinity of lanthanide metal ions to phosphate anionresulting in myelotoxicity [20,21]. For this reason, boneuptake was also used to evaluate the in vivo stability of the177Lu-h-R3 conjugates. The increasing amount of DOTA inthe conjugate showed increased uptake in liver and fasterclearance from blood. The results are in agreement withthose reported by Knogler et al. [39]. The uptake in liver,spleen and bones observed in our study was lower thanthose previously reported for conjugates modified with fourto five groups of p-SCN-Bn-DOTA or p-SCN-Bn-DTPA[34]. The release of the radiometal from the conjugate andits metabolism resulted in nonspecific accumulation of theradioactivity in different tissues and gives us an idea of thestability of the conjugate. Tumor/blood ratio calculations
are useful for this estimation. Base on liver/blood ratios,177Lu-(DOTA)4–5-h-R3 showed higher in vivo stabilitythan 177Lu-(DTPA)4–5 and 177Lu-(DOTA)8–9.The bone/blood ratio did not increase with time for all radio-immunoconjugates, suggesting high stability of the metal–ligand complexes.
The 177Lu-(DOTA)n-h-R3 (n=4–5) conjugate was chosenfor further evaluation in A431 human epidermal carcinomaxenograft Balb/c nude mice due to the fact that it showedbetter radiolabeling yields and in vivo stability in healthymice. The highest uptake over time was observed in thetumor. Notable activity was also observed in liver, spleen,kidneys and lung consistent with that previously reported forthe murine version of the h-R3 labeled with 90Y using theDOTA-Ph-Al derivative [40] and with the normal excretionof monoclonal antibodies [41]. The activity in normal tissuewas always less than 10 %ID/g and decreased over time.Blocking experiment showed that uptake of the conjugatewas specific to the target. In this study, the tumor uptakevalues and tumor to nontumor ratios are higher than thosepreviously reported for h-R3 and the parental murine mAblabeled with 99mTc and 90Y [35,37,42]. The 177Lu-DOTA-h-R3 conjugate showed lower uptake in liver and spleen thanother EGFR-targeting antibodies [43–45].
An interesting phenomenon was observed when thebiodistribution results in healthy mice and A431 humanepidermal carcinoma xenograft mice were compared. Theconcentration in blood of the radioimmunoconjugate was 1.4and 2.9 times higher in healthy mice than in A431 xenograftmice for 72 and 168 h, respectively. At 168 h, spleen, lungand kidney uptakes were significantly higher in healthymice. The results are in complete agreement with thoseobtained by Coliva et al. [46] and Zacchetti et al [36]. Anexplanation to this fact might be that the tumor carrying ahigh density of the target antigen could take up the conjugatefrom the blood.
As we mentioned above, promising results using RIThave been achieved in the treatment of minimal residualdisease and in locoregional applications. Consequently, the177Lu-(DOTA)n-h-R3 (n=4–5) conjugate was locoregionallyadministered in mice bearing A431 human epidermalcarcinoma xenografts. The results were compared withthose obtained from the biodistribution when the conjugatewas intravenously administered with particular attention paidto tumor uptake and tumor to nontumor ratios. Significantlyhigher tumor uptake and T/nT ratios at 24 and 72 h wereobserved when the conjugate was locoregionally adminis-tered, suggesting that locoregional administration woulddecrease the nonspecific accumulation of radioactivity in thenormal tissue while increasing the tumor uptake.
Dosimetric calculations showed that the 177Lu-DOTA-h-R3 radioimmunoconjugate will deliver the highest dose intothe tumor. The smaller the tumor, the higher the dosedeposited. The results obtained are in agreement with thosepreviously reported for similar 177Lu conjugates [17,36]. Theresults from the extrapolation of animal data to humans in

12 D.R. Beckford Vera et al. / Nuclear Medicine and Biology 39 (2012) 3–13
this study showed doses to normal organs lower than thosereported by Iznaga-Escobar et al. [47] for 99mTc-h-R3. It isnecessary to mention that, in the extrapolation of the animaldata obtained in this study to humans, cross-reactivity ofnimotuzumab is not taken into account. In this respect,locoregional anti-EGFR RIT might be a more promisingoption. Biodistribution and internal dosimetry, in patientswith malignant gliomas, after locoregional administration of188Re-nimotuzumab were studied [48]. In this study, thenormal organs which received the highest absorbed doses, indecreasing order, were the kidneys, liver and urinary bladder.Even when mean absorbed dose in tumor regions was higherfor patients treated with 555 MBq, adverse events wereobserved. Nevertheless, locoregional single dose of 188Re-nimotuzumab of 370 MBq was safely used in the routinetreatment of patients [16,48]. The demonstrated necessity ofhigh EGFR expression for stable binding of nimotuzumab tothe receptor suggests that nimotuzumab would preferentiallytarget tissues overexpressing the target antigen whileminimizing toxicity [9,49–51]. This fact led us to thinkthat, due to the nuclear properties of 177Lu, the tumor-targeting properties and the stability of 177Lu-nimotuzumab,the use of this radioimmunoconjugate could improve thetherapy outcome and the absorbed dose in normal tissue.
5. Conclusions
According to the results presented above, 177Lu-DOTA-h-R3 could be obtained with high specific activity withoutsignificant loss of immunoreactivity and it specificallyaccumulated in EGFR overexpressing tumors. Consequent-ly, 177Lu-DOTA-h-R3 seems to have a potential for furtherevaluations as a radiopharmaceutical for RIT of EGFRoverexpressing tumors. The results presented in this reportcould be of use for future preclinical and clinical studiesusing this radioimmunoconjugate. Further optimization ofthe radioimmunoconjugate, such as reduction of its size inorder to reduce even more the uptake in normal tissues andthe use of 90Y for RIT of larger-size tumors, is ongoing.
Acknowledgments
We gratefully acknowledge Dr. Mark Harfensteller andIsotope Technologies Garching (ITG, Munich, Germany),for providing the n.c.a.177Lu. The authors would like tothank Ing. Aliona Frai for her support in the animal study.We thank Lenka Maresova and Ludmila Jandova from theDepartment of Radiopharmacy, Institute of Nuclear Re-search, Husinec-Rez, Czech Republic, for outstandingsupport during the biodistribution studies.
References
[1] Schaefer NG, Ma J, Huang P, Buchanan J, Wahl RL. Radio-immunotherapy in non-Hodgkin lymphoma: opinions of U.S. medicaloncologists and hematologists. J Nucl Med 2010;51(6):987–94.
[2] Sharkey RM, Goldenberg DM. Perspectives on cancer therapy withradiolabeled monoclonal antibodies. J Nucl Med 2005;46(Suppl1):115S–27S.
[3] Govindan SVG, David M. Immunoconjugate anticancer therapeutics.Discovery 2010:371–92.
[4] Mendelsohn J, Baselga J. Epidermal growth factor receptor targeting incancer. Semin Oncol 2006;33(4):369–85.
[5] Rocha-Lima CM, Soares HP, Raez LE, Singal R. EGFR targeting ofsolid tumors. Cancer Control 2007;14(3):295–304.
[6] Carpenter G, Cohen S. Epidermal growth factor. Annu Rev Biochem1979;48:193–216.
[7] Real FX, Rettig WJ, Chesa PG, Melamed MR, Old LJ, Mendelsohn J.Expression of epidermal growth factor receptor in human cultured cellsand tissues: relationship to cell lineage and stage of differentiation.Cancer Res 1986;46(9):4726–31.
[8] Herbst RS, Langer CJ. Epidermal growth factor receptors as a target forcancer treatment: the emerging role of IMC-C225 in the treatment oflung and head and neck cancers. Semin Oncol 2002;29(1 Suppl4):27–36.
[9] Talavera A, Friemann R, Gomez-Puerta S, Martinez-Fleites C, GarridoG, Rabasa A, et al. Nimotuzumab, an antitumor antibody that targetsthe epidermal growth factor receptor, blocks ligand binding whilepermitting the active receptor conformation. Cancer Res 2009;69(14):5851–9.
[10] Martinelli E, De Palma R, Orditura M, De Vita F, Ciardiello F. Anti-epidermal growth factor receptor monoclonal antibodies in cancertherapy. Clin Exp Immunol 2009;158(1):1–9.
[11] Mateo C, Moreno E, Amour K, Lombardero J, Harris W, Perez R.Humanization of a mouse monoclonal antibody that blocks theepidermal growth factor receptor: recovery of antagonistic activity.Immunotechnology 1997;3(1):71–81.
[12] Vallis KA, Reilly RM, Chen P, Oza A, Hendler A, Cameron R, et al. Aphase I study of 99mTc-hR3 (DiaCIM), a humanized immunoconjugatedirected towards the epidermal growth factor receptor. Nucl MedCommun 2002;23(12):1155–64.
[13] Allan DG. Nimotuzumab: evidence of clinical benefit without rash.Oncologist 2005;10(9):760–1.
[14] Spicer J. Technology evaluation: nimotuzumab, the Center ofMolecular Immunology/YM BioSciences/Oncoscience. Curr OpinMol Ther 2005;7(2):182–91.
[15] Bayes M, Rabasseda X, Prous JR. Gateways to clinical trials. MethodsFind Exp Clin Pharmacol 2007;29(7):467–509.
[16] Casaco A, Lopez G, Garcia I, Rodriguez JA, Fernandez R, Figueredo J,et al. Phase I single-dose study of intracavitary-administerednimotuzumab labeled with 188Re in adult recurrent high-grade glioma.Cancer Biol Ther 2008;7(3):333–9.
[17] Brouwers AH, van Eerd JE, Frielink C, Oosterwijk E, Oyen WJ,Corstens FH, et al. Optimization of radioimmunotherapy of renal cellcarcinoma: labeling of monoclonal antibody cG250 with 131I, 90Y,177Lu, or 186Re. J Nucl Med 2004;45(2):327–37.
[18] Ehrhardt GJ, Ketring AR, Ayers LM. Reactor-produced radionuclidesat the University of Missouri Research Reactor. Appl Radiat Isot1998;49(4):295–7.
[19] Mausner LF, Srivastava SC. Selection of radionuclides for radio-immunotherapy. Med Phys 1993;20(2 Pt 2):503–9.
[20] Liu S. Bifunctional coupling agents for radiolabeling of biomoleculesand target-specific delivery of metallic radionuclides. Adv Drug DelivRev 2008;60(12):1347–70.
[21] Liu S, Edwards DS. Bifunctional chelators for therapeutic lanthanideradiopharmaceuticals. Bioconjug Chem 2001;12(1):7–34.
[22] Meares CF, McCall MJ, Reardan DT, Goodwin DA, Diamanti CI,McTigue M. Conjugation of antibodies with bifunctional chelatingagents: isothiocyanate and bromoacetamide reagents, methods ofanalysis, and subsequent addition of metal ions. Anal Biochem1984;142(1):68–78.
[23] Konishi S, Hamacher K, Vallabhajosula S, Kothari P, Bastidas D,Bander N, et al. Determination of immunoreactive fraction of
13D.R. Beckford Vera et al. / Nuclear Medicine and Biology 39 (2012) 3–13
radiolabeled monoclonal antibodies: what is an appropriate method?Cancer Biother Radiopharm 2004;19(6):706–15.
[24] Stabin MG, Sparks RB, Crowe E. OLINDA/EXM: the second-generation personal computer software for internal dose assessment innuclear medicine. J Nucl Med 2005;46(6):1023–7.
[25] Kirschner AIR, Beierwalters W. Radiation dosimetry of 131I-19-iodocholesterol: the pitfalls of using tissue concentration data, theauthor's reply. J Nucl Med 1975;16:248–9.
[26] Delbeke D. Reaching out with radioimmunotherapy. J Nucl Med2010;51(11):16N.
[27] Boswell CA, Brechbiel MW. Development of radioimmunotherapeuticand diagnostic antibodies: an inside-out view. Nucl Med Biol 2007;34(7):757–78.
[28] Ramakrishnan MS, Eswaraiah A, Crombet T, Piedra P, Saurez G, IyerH, et al. Nimotuzumab, a promising therapeutic monoclonal fortreatment of tumors of epithelial origin. MAbs 2009;1(1):41–8.
[29] Greta Garrido AR, Elias Gracia, Ilia Tikhomirov and Rolando Perez.Binding properties of the anti-EGFR monoclonal antibody, nimotuzu-mab, limit interaction with the EGFR in renal and epidermal cells.100th AACR Annual Meeting; Apr 18-22. Denver, CO: In: Proc AmAssoc Cancer Res; 2009. p. Abstract nr 2763.
[30] Beckford DR, Xiques CA, Leyva MR, Pérez MM, Casanova EG,Zamora BM. New radioimmunoconjugate 90Y-DOTA-h-R3. Synthesisand radiolabeling. Nucleus 2007;41:3–8.
[31] Castillo AX, Olive KI, Gonzalez EC, Beckford D, Montaña RL,Alvarez AM, et al. An adapted purification procedure to improvethe quality of 90Y for clinical use. Radiochim Acta 2009;97(97):739–46.
[32] Milenic DE, Garmestani K, Chappell LL, Dadachova E, Yordanov A,Ma D, et al. In vivo comparison of macrocyclic and acyclic ligands forradiolabeling of monoclonal antibodies with 177Lu for radioimmu-notherapeutic applications. Nucl Med Biol 2002;29(4):431–42.
[33] Rasaneh S, Rajabi H, Babaei MH, Daha FJ. 177Lu labeling of Herceptinand preclinical validation as a new radiopharmaceutical for radio-immunotherapy of breast cancer. Nucl Med Biol 2010;37(8):949–55.
[34] Mohsin H, Fitzsimmons J, Shelton T, Hoffman TJ, Cutler CS, LewisMR, et al. Preparation and biological evaluation of 111In-, 177Lu- and90Y-labeled DOTA analogues conjugated to B72.3. Nucl Med Biol2007;34(5):493–502.
[35] Almqvist Y, Steffen AC, Tolmachev V, Divgi CR, Sundin A. In vitroand in vivo characterization of 177Lu-huA33: a radioimmunoconjugateagainst colorectal cancer. Nucl Med Biol 2006;33(8):991–8.
[36] Zacchetti A, Coliva A, Luison E, Seregni E, Bombardieri E, GiussaniA, et al. (177)Lu- labeled MOv18 as compared to (131)I- or (90)Y-labeled MOv18 has the better therapeutic effect in eradication of alphafolate receptor-expressing tumor xenografts. Nucl Med Biol 2009;36(7):759–70.
[37] Morales-Morales A, Duconge J, Caballero-Torres I, Nunez-GandolffG, Fernandez E, Iznaga-Escobar N. Biodistribution of 99mTc-labeledanti-human epidermal growth factor receptor (EGF-R) humanizedmonoclonal antibody h-R3 in a xenograft model of human lungadenocarcinoma. Nucl Med Biol 1999;26(3):275–9.
[38] Tabrizi M, Tseng C, Roskos L. Elimination mechanisms of therapeuticmonoclonal antibodies. Drug Discov Today 2006;11(1-2):81–8.
[39] Knogler K, Grunberg J, Novak-Hofer I, Zimmermann K, SchubigerPA. Evaluation of 177Lu-DOTA-labeled aglycosylated monoclonalanti-L1-CAM antibody chCE7: influence of the number of chelators onthe in vitro and in vivo properties. Nucl Med Biol 2006;33(7):883–9.
[40] Pnwar P, Iznaga-Escobar N, Mishra P, Srivastava V, Sharma RK,Chandra R, et al. Radiolabeling and biological evaluation of DOTA-Ph-Al derivative conjugated to anti-EGFR antibody ior egf/r3 for targetedtumor imaging and therapy. Cancer Biol Ther 2005;4(8):854–60.
[41] Griffiths GL, Govindan SV, Sharkey RM, Fisher DR, Goldenberg DM.90Y-DOTA-hLL2: an agent for radioimmunotherapy of non-Hodg-kin's lymphoma. J Nucl Med 2003;44(1):77–84.
[42] Morales AA, Duconge J, Alvarez-Ruiz D, Becquer-Viart ML, Nunez-Gandolff G, Fernandez E, et al. Humanized versus murine anti-humanepidermal growth factor receptor monoclonal antibodies for immu-noscintigraphic studies. Nucl Med Biol 2000;27(2):199–206.
[43] Reilly RM, Kiarash R, Sandhu J, Lee YW, Cameron RG, Hendler A, etal. A comparison of EGF and MAb 528 labeled with 111In for imaginghuman breast cancer. J Nucl Med 2000;41(5):903–11.
[44] Wen X, Wu QP, Ke S, Ellis L, Charnsangavej C, Delpassand AS, et al.Conjugation with (111)In-DTPA-poly(ethylene glycol) improvesimaging of anti-EGF receptor antibody C225. J Nucl Med 2001;42(10):1530–7.
[45] Liu Z, Liu Y, Jia B, Zhao H, Jin X, Li F, et al. Epidermal growth factorreceptor-targeted radioimmunotherapy of human head and neck cancerxenografts using 90Y-labeled fully human antibody panitumumab. MolCancer Ther 2010;9(8):2297–308.
[46] Coliva A, Zacchetti A, Luison E, Tomassetti A, Bongarzone I, SeregniE, et al. 90Y Labeling of monoclonal antibody MOv18 and preclinicalvalidation for radioimmunotherapy of human ovarian carcinomas.Cancer Immunol Immunother 2005;54(12):1200–13.
[47] Iznaga Escobar N, Morales AM, Duconge J, Torres IC, Fernandez E,Gomez JA. Pharmacokinetics, biodistribution and dosimetry of 99mTc-labeled anti-human epidermal growth factor receptor humanizedmonoclonal antibody R3 in rats. Nucl Med Biol 1998;25(1):17–23.
[48] Torres LA, Coca MA, Batista JF, Casaco A, Lopez G, Garcia I, et al.Biodistribution and internal dosimetry of the 188Re-labelled humanizedmonoclonal antibody anti-epidemal growth factor receptor, nimotuzu-mab, in the locoregional treatment of malignant gliomas. Nucl MedCommun 2008;29(1):66–75.
[49] Zuckier LS, Berkowitz EZ, Sattenberg RJ, Zhao QH, Deng HF, ScharffMD. Influence of affinity and antigen density on antibody localizationin a modifiable tumor targeting model. Cancer Res 2000;60(24):7008–13.
[50] Boland WK, Bebb G. Nimotuzumab: a novel anti-EGFR monoclonalantibody that retains anti-EGFR activity while minimizing skintoxicity. Expert Opin Biol Ther 2009;9(9):1199–206.
[51] Garrido G, Tikhomirov IA, Rabasa A, Yang E, Gracia E, Iznaga N, etal. Bivalent binding by intermediate affinity of nimotuzumab: acontribution to explain antibody clinical profile. Cancer Biol Ther2011;11(4):373–82.




















