
Preclinical and clinical aspects of biomodulation of 5-fluorouracil
39
Cancer Treatment Reviews (1994) 20, 11-49 ANTITUMOUR TREATMENT Preclinical and clinical aspects of biomodulation of 5-fluorouracil George A. Sotos, Liam Grogan, Carmen J. Allegra” NCI-Navy Medical Oncology Branch, National Cancer Institute, Bethesda, MD 20889-5101, U.S.A. Introduction Since its introduction into clinical oncology in 1958, 5-fluorouracil (5-FU) has remained the mainstay of therapy for advanced colorectal and gastrointestinal malignancies. Unfortunately, it achieves response rates of only 1 O&20% when used as a single agent and little if any additional benefit is gained when combined with other cytotoxic chemotherapeutic agents. Hence, single agent 5-FU has remained the standard therapy for metastatic colorectal cancer. The low response rates and the lack of clinically effective synergistic combination regimens justify new investigations to improve the efficacy of 5-FU. One such strategy, commonly known as biomodulation, is an attempt to manipulate the metabolism of 5-FU and consequently its interaction with its target end-points within an individual cell (1, 2). Biomodulation differs from the underlying principle of combination chemotherapy regimens in which each of the component single agents has activity and may or may not affect the activity of the other agents. Knowledge of 5-FU metabolism and understanding mechanisms of chemotherapeutic resistance serve as the foundation for the clinical development of 5-FU biomodulation. 5-FU is metabolized by a number of enzymes along several pathways (Figure 1). Pyrimidine nucleoside phosphorylase converts 5-FU to fluorodeoxyuridine (FdUrd) and thymidine kinase phosphorylates FdUrd to fluorodeoxyuridine monophosphate (FdUMP), an active metabolite. FdUMP forms a stable covalent bond with ‘To whom correspondence should be addressed at: NCI-Navy Medical Oncology Branch, Naval Hospital Bethesda, 8901 Wisconsin Ave., Bldg. 8, Rm. 5101, Bethesda, MD 20889-5105 0305-7372/94/010011+39 $08.00/O 11 @ 1994 W. B. Saunders
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Preclinical and clinical aspects of biomodulation of 5-fluorouracil
Cancer Treatment Reviews (1994) 20, 11-49
ANTITUMOUR TREATMENT
Preclinical and clinical aspects of biomodulation of 5-fluorouracil
George A. Sotos, Liam Grogan, Carmen J. Allegra”
NCI-Navy Medical Oncology Branch, National Cancer Institute, Bethesda, MD 20889-5101, U.S.A.
Introduction
Since its introduction into clinical oncology in 1958, 5-fluorouracil (5-FU) has remained the mainstay of therapy for advanced colorectal and gastrointestinal malignancies. Unfortunately, it achieves response rates of only 1 O&20% when used as a single agent and little if any additional benefit is gained when combined with other cytotoxic chemotherapeutic agents. Hence, single agent 5-FU has remained the standard therapy for metastatic colorectal cancer. The low response rates and the lack of clinically effective synergistic combination regimens justify new investigations to improve the efficacy of 5-FU. One such strategy, commonly known as biomodulation, is an attempt to manipulate the metabolism of 5-FU and consequently its interaction with its target end-points within an individual cell (1, 2). Biomodulation differs from the underlying principle of combination chemotherapy regimens in which each of the component single agents has activity and may or may not affect the activity of the other agents. Knowledge of 5-FU metabolism and understanding mechanisms of chemotherapeutic resistance serve as the foundation for the clinical development of 5-FU biomodulation.
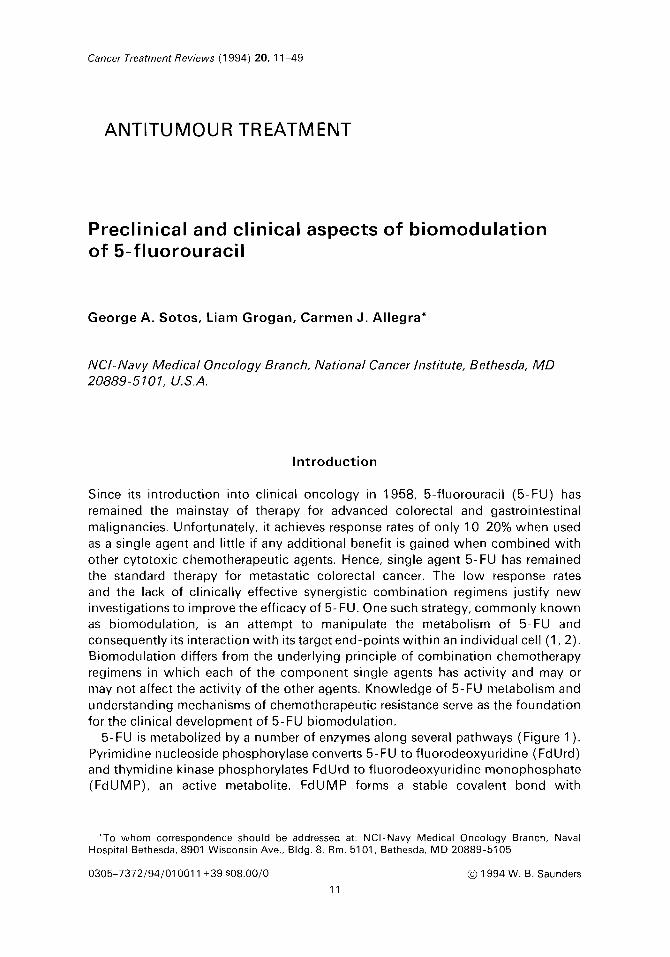
5-FU is metabolized by a number of enzymes along several pathways (Figure 1). Pyrimidine nucleoside phosphorylase converts 5-FU to fluorodeoxyuridine (FdUrd) and thymidine kinase phosphorylates FdUrd to fluorodeoxyuridine monophosphate (FdUMP), an active metabolite. FdUMP forms a stable covalent bond with
‘To whom correspondence should be addressed at: NCI-Navy Medical Oncology Branch, Naval Hospital Bethesda, 8901 Wisconsin Ave., Bldg. 8, Rm. 5101, Bethesda, MD 20889-5105
0305-7372/94/010011+39 $08.00/O
11
@ 1994 W. B. Saunders

12 G. A. SOTOS ET AL
de now purine synthesis
LV
- MTX(Glu)n
Cisplatin
IFN-a duMp- dTMP- - d’I”TP
\u
FdUTP f FdUrd - FdUMP -FdUDP -
i+ DNA
+ IdUrd
DH-FU 4
Aspartate +
Carbamoyl
PRPP PPi
T;p Orotate u - UMP - UDP +
RNA
Phosphate E
T
I-
a PALA s e
FUTP
UTP’ + Urd
Figure 1. 5-FU metabolism and biomodulator sites of action (see text for abbreviations)
thymidylate synthase (TS), a central enzyme in de novo synthesis of thymidylate, and the reduced folate 5,10-methylene tetrahydrofolate. This ternary complex inhibits TS and consequently DNA synthesis and repair. FdUMP can be further phosphorylated and incorporated into DNA as FdUTP. 5-FU is also metabolized to FUMP, either directly or indirectly, and incorporated into RNA as the triphosphate FUTP. By affecting one or multiple enzymes or natural substrates involved in either 5-FU metabolism or in normal purine or pyrimidine biosynthesis with which 5-FU competes, intracellular conditions can be changed to favor 5-FU metabolism.
Although the mechanisms of action of biomodulating agents may overlap or not be completely understood, they can be grouped based on their ability to augment 5-FU interference with DNA or RNA synthesis, either indirectly through metabolic effects on the biosynthesis of nucleic acids or by direct effects on the nucleic acids themselves (Table 1). Many of the clinically promising biomodulators studied appear to affect DNA synthesis. Leucovorin (LV) does so indirectly by modulating

BIOMODULATION OF 5-FLUOROURACIL
Table 1. Biochemical modulators of 5-FluorouraciP
13
Primary nucleic acid target Modulator
DNA-Indirect Leucovorin
Interferon-r
Interferon-y
DNA-Direct Cisplatrn
AZT
IdUrd
RNA Methotrexate
Trimetrexate
PALA
Uridine
BAU/BBAU
Known or presumed Mechanism of Action
Increased TS inhibition
? Increased 5-FU anaboiism
Decreased TS induction
DNA repair inhibition Increased TS inhrbition
Increased AZT incorporation Into DNA
Increased IdUrd incorporation into DNA
Purrne synthesis inhrbrtion Increased PRPP levels Increased 5-FU incorporation into RNA
Purine synthesis inhibition Increased PRPP levels Increased 5-FU incorporation into RNA
Pyrimidine biosynthesis inhibition Increased 5-FU incorporation into RNA
? Selective decreased 5- FU incorporation into RNA
Uridine phosphorylase (pyrimidine biosynthesis) inhibition Increased 5-FU anabolism
“See text for abbreviations
TS activity. lnterferons (IFN) may have multiple effects but are postulated to involve 5-FU anabolism directly and to affect DNA synthesis. Agents which affect DNA synthesis more directly are cisplatin, azidothymidine (AZT) and iododeoxyuridine (IdUrd). Biomodulators affecting RNA synthesis primarily include the antifolates such as methotrexate (MTX), N-(phosphonacetyl)L-aspartate (PALA), uridine, benzylacyclouridine (BAU), and benzyloxybenzylacyclouridine (BBAU).
Agents affecting DNA indirectly
L euco vorin
Leucovorin is one of the most extensively studied and thus far the most clinically successful attempts at improving the activity of 5-FU. Leucovorin (5-for- myltetrahydrofolate, citrovorum factor) is a reduced folate which is metabolized in

14 G. A. SOTOS ET Al
the cell to various forms of tetrahydrofolate including 5,l O-methylenetetra- hydrofolate. 5,10-methylenetetrahydrofolate acts as the methyl donor in the TS reaction. In this reaction FdUMP binds to TS, a central enzyme in the de nova synthesis of thymidylate and a key element in the synthesis and repair of DNA (Figure 1). The stability of the interaction between FdUMP and TS is directly related to the intracellular folate concentration and investigators found that inhibition of TS by FdUMP could be enhanced by high intracellular folate levels (3, 4). The addition of exogenous folate in the form of the stable, reduced folate was capable of expanding intracellular folate pools with resultant enhanced cytotoxicity of 5-FU in preclinical in vitro systems, particularly in cells whose intracellular folate concentrations were adequate for growth but suboptimal for enzymatic inhibition by the fluoropyrimidines (5, 6).
Ullman and co-workers were one of the first groups to study the effect of leucovorin on 5FU growth inhibition in L1210 leukemia cells in culture and found that leucovorin concentrations in excess of 0.5 ,uM could enhance the growth inhibition of 5-FU by fivefold in these cells (5). In this study they used a concentration of leucovorin between IO-20 times the concentration of folate required for optimal cell growth. They also demonstrated that the combination of 5-FU/LV was better at stabilizing the ternary complex of FdUMP/TS/folates than 5-FU alone in intact cells. A number of other investigators found similar synergy in a variety of human and non-human cell lines exposed to various concentrations and schedules of both 5-FU and leucovorin (5-l 0). The concentration of leucovorin required to achieve optimal growth inhibition in vitro was generally found to be I-10 ,uM. Preclinical in vitro and in viva studies analysing the effect of leucovorin timing with respect to 5-FU found that leucovorin was an effective modulator in vitro when given prior to or simultaneously with 5-FU. An analysis of exposure duration with various concentrations of combined 5-FU/LV on human colorectal (WiDr) and bladder cancer (T-24) cell lines noted maximal cytotoxic effect as the concentration of leucovorin approached 10 ,uM. These investigators also noted greater activity with more prolonged exposures up to 72 h. They concluded that an extended duration of exposure to both 5-FU and leucovorin may substantially improve the therapeutic efficacy of this combination (11).
A study of human colon cancer xenografts in immune deficient mice found that response to 5-FU did not correlate with intracellular concentration of the drug, concentration of free FdUMP or incorporation into total RNA (12, 13). The investigators found that in relatively insensitive tumors only 40-50% of the available TS was bound by FdUMP in the absence of exogenous folate co-factor and in these tumors it was necessary to add exogenous folate to achieve maximal binding of FdUMP for complete inhibition of TS. In responsive tumors complete inhibition of TS occurred without the addition of exogenous folate. This study suggested that exogenous folates are necessary to maximize TS inhibition in some but not all human colon cancers (6, 14). The in vitro and in vivo data suggested that certain cell lines and tumors had levels of endogenous folates adequate to support cell growth but suboptimal for TS inhibition and it was postulated that differences in sensitivity to 5-FU may be explained by differences in the levels of endogenous folates (6, 14).
Leucovorin is transported into the cell by a transmembrane carrier and is then metabolized to 5,10-methylenetetrahydrofolate. Commercially available leucovorin

BIOMODULATION OF 5-FLUOROURACIL 15
possesses a terminal glutamic acid moiety which becomes polyglutamated upon entering the cell. The polyglutamated state of the folate is a critical determinant in the ability of 5,10-methylenetetrahydrofolate to interact with TS and FdUMP. Polyglutamation involves the enzymatic addition of up to five or six glutamic acid moieties to the parent compound and results in enhanced affinity of these folates for their respective enzyme targets. Higher polyglutamates of 5,l O-methyl- enetetrahydrofolate are approximately 50 to IOO-fold more potent in stabilizing ternary complex formation with TS and FdUMP when compared with the mono and diglutamate forms (15, 16). Furthermore the additional glutamic acid moieties are charged and this leads to prolonged intracellular retention resulting in prolonged TS inhibition.
Preclinical investigations in in vitro and in vivo model systems have attempted to define the rate, extent, and effect of 5,10-methylenetetrahydrofolate formation and polyglutamation. In human colon (HCT-116) and breast (MCF-7) carcinoma cell lines Boarman and colleagues found a IO-fold increase in 5,10-methyl- enetetrahydrofolate intracellular pools with increasing leucovorin exposures from 0.1 to 50 PM. In this study there was also a sixfold increase in total intracellular folate pools predominantly due to expansion of tetrahydrofolate and IO-formyl- tetrahydrofolate (17). In a human colon xenograft model in immune-deprived mice the critical tetrahydrofolate and 5,10-methylenetetrahydrofolate intracellular pools could be increased fourfold using prolonged (24 h) infusions of leucovorin at doses ranging from 20 to 1000 mg/m’ (18). Leucovorin appeared to have a dose dependent effect on intratumor 5,10-methylenetetrahydrofolate levels that varied with each in vivo human xenograft studied (18). By comparing iv bolus, 4 h or 24 h leucovorin infusion schedules using constant doses of leucovorin and 5-FU, the effects of variations in schedule on 5,10-methylenetetrahydrofolate levels in human colon cancer xenografts in immune deficient mice were determined (19). Inter- estingly, all three schedules increased intratumor levels of folates between 3.5 and 7-fold with the greatest increase seen with the 24 h schedule. With equivalent doses of leucovorin the maximal sustained elevation of 5,l O-methylenetetra- hydrofolate levels was associated with longer infusions consistent with saturable cellular transport of leucovorin.
Polyglutamation is associated with an exponential increase in intracellular reten- tion such that the pentaglutamated folate forms have an intracellular half-life of approximately 20 h compared to 1 h for the monoglutamate forms (17). Investigators found that duration of exposure appears to be the most important factor in metabolism to the higher polyglutamate forms. In the human colon cancer cell line (HCT-116) exposure to high concentrations of leucovorin (10 pM) results in a greater intracellular concentration of the lower polyglutamate forms when compared with exposure to low concentrations (1 FM) regardless of time of exposure (17). In contrast, duration of exposure did affect intracellular concentration of the higher polyglutamate forms. The intracellular amounts of the higher polyglutamates in cells exposed to high concentrations of leucovorin (10 ,uM) were not significantly different from cells treated with lower concentrations (1 ,uM) provided the cells were exposed for 24 h. Of importance, prolonged exposure (24 h) to a low concentration of leucovorin (1 ,u~) resulted in a substantially greater intracellular accumulation of higher polyglutamates when compared to brief exposures (2 h) to even a 10 ,uM concentration of leucovorin. These data suggest that the duration of

16 G. A. SOTOS HAL
exposure to leucovorin appears to be the principal factor in the formation of the higher folate polyglutamates. The importance of folate polyglutamation was demonstrated further in a study by Romanini and colleagues which illustrated that cells incapable of polyglutamating exogenously administered folates did not share the enhanced cytotoxicity of simultaneously administered 5-FU with cells that were capable of polyglutamation (20). Collectively the data from these in vitro and in vivo experiments suggest that duration of exposure is a critical component in the optimal clinical use of leucovorin. The optimal means of expanding the 5,10- methylenetetrahydrofolate polyglutamate pool as determined by the preclinical data supports the use of continuous or multiple repetitive dosing schedules of exogenous leucovorin.
There are a small number of studies which have attempted to evaluate human tumor metabolism following 5-FU in the presence of leucovorin. In a study of patients with metastatic breast cancer treated with high dose leucovorin (500 mg/m’) and 5-FU, the median TS inhibition in tumor tissue following 5-FU alone was 31% compared to 87% in tumors treated with 5-FU and leucovorin (21). Higher degrees of TS inhibition were associated with clinical response in this study. In serial biopsies of five patients with colorectal tumors treated with 5-FU/LV, Rustum and co-workers demonstrated similar findings (22). These data suggest that persistent in vivo TS inhibition is associated with clinical response and supports the importance of TS as a clinical target for anticancer therapy.
Leucovorin is commercially available as a racemic mixture of an inactive R leucovorin isomer and an active S isomer. Bertrand and colleagues demonstrated that R leucovorin was capable of competing for cellular uptake with S leucovorin (23). However, these authors were unable to demonstrate that the addition of the inactive isomer diminished the ability of the active isomer to enhance the cytotoxicity of 5-FU in a human lymphoblastic leukemia cell line (CCRF-CEM). Boarman and co-workers found that the addition of ratios of up to 2O:l inactive to active stereoisomers of leucovorin did not alter the intracellular metabolism of the active isomer to either the various intracellular folate forms or to the higher polyglutamate states during 24 h leucovorin exposures in a human colon carcinoma cell line (HCT- 116) (17). In uncontrolled clinical studies using the pure biologically active form of leucovorin in patients with advanced gastrointestinal malignancy, investigators found that the toxicity and response rate associated with the use of this form of leucovorin were not substantially different from those previously reported by these same investigators using the commercially available racemic leucovorin mixture (24, 25).
A large number of uncontrolled and controlled clinical studies using a variety of doses and schedules of 5-FU/LV principally in patients with gastrointestinal tumors has been completed. In randomized studies in colorectal cancer the mean response rate of patients treated with 5-FU/LV was 23% (range 16-48%, eight studies, 668 patients) which was significantly better (p < 0.001) than the 11% (range 7-l 7%, eight studies, 525 patients) noted with an equivalent dose of 5-FU alone (26). While similar response rates were obtained weekly and daily for 5-day schedules, differences were observed within each schedule with regard to the effect of various doses on response.
Using a weekly schedule, patients were randomized to receive identical doses of 5-FU by intravenous bolus with leucovorin given either as a 25 mg/m’ 15-min

BIOMODULATION OF 5-FLUOROURACIL 17
infusion or a 2 h 500 mg/m’ infusion once weekly for 6 weeks out of an 8-week cycle on a Gastrointestinal Tumor Study Group (GITSG) trial (27). There was a 30% response rate associated with the higher dose leucovorin which was sig- nificantly better than the 10% response rate in the 5-FU alone arm (p < 0.01). The 19% response rate associated with the lower leucovorin dose was not statistically different from the response rate in the 5-FU alone arm. This study demonstrated a dose response effect with the addition of leucovorin to this weekly schedule which is consistent with a dose response effect found with bolus administration in in vitro and in vivo preclinical studies.
The North Central Cancer Treatment Group (NCCTG) using the schedule of 5-FU and leucovorin daily for 5 days every month randomized patients with colo- rectal cancer to receive a low dose leucovorin (20 mg/m*/day), a higher dose leuco- vorin (200 mg/m’/day) or 5-FU alone (28, 29). Patients received 370 mg/m2 of 5-FU with 200 mg/m’ of leucovorin daily for 5 days every 4-5 weeks or 5-FU at a dose of 425 mg/m’ and a leucovorin dose of 20 mg/m’. Patients on the low dose leucovorin arm received 15% more 5-FU which may partially account for the observed differences in response rates. The low dose leucovorin arm was associated with the most significant difference in response rate, 43%, compared to 10% for patients treated with 5-FU alone. Both groups receiving high and low dose leucovorin achieved similar statistically significant improvements in survival (median survival of 12.2 months and 12.0 months, respectively) compared to patients on the control arm (median survival 7.7 months) treated with 5-FU alone. An explanation why repetitive lower dose leucovorin was as effective as higher dose leucovorin in this study may be surmized from the preclinical data. Whereas the absolute dose of leucovorin may be critical in short-term exposures, repetitive or continuous infusion schedules can maintain an active level of leucovorin inde- pendent of dose for prolonged periods and this has been shown to be optimal for intracellular metabolism to higher folate polyglutamates with associated potentiation of TS inhibition.
Only one of nine published randomized studies has shown an improvement in survival for patients with advanced colorectal cancer receiving 5-FU/LV (26-36). In the NCCTG study, this survival benefit was confined to the 47% of patients on the high and low dose leucovorin arms who did not have measurable disease (28). A recent meta analysis of over 1300 patients in the eight other randomized trials found no benefit in survival for patients treated with 5-FU/LV (26). These data suggest, not unexpectedly, that modulation of 5-FU with leucovorin may maximally benefit those patients with less advanced disease. As a consequence, leucovorin modulation of 5-FU may have its greatest impact in the adjuvant setting and several large co-operative groups are currently testing this hypothesis.
Leucovorin modulation of 5-FU has been studied in preclinical systems and in a large number of clinical trials using various doses and schedules of both agents. Collectively the clinical and preclinical information concerning the dose, timing, and duration of leucovorin exposure supports the use of continuous infusion or repetitive low dose schedules. These schedules appear to be the most effective in the generation of the higher polyglutamates of 5,10-methylenetetrahydrofolate, the most efficient intracellular folate metabolite for ternary complex formation and TS inhibition. While much has been learned, additional preclinical and clinical investigations are required to elucidate more fully the optimal dose and schedu!e of

18 G. A. SOTOS ET AL
leucovorin. These investigations should include studies addressing the dosing interval between leucovorin and 5-FU. Oral administration may serve as a convenient mechanism for prolonging exposure to adequate levels of leucovorin in clinical practice. In the future, constant infusion schedules using various doses of leucovorin need to be explored and the potential value of alternative folates such as 5-methyltetrahydrofolate and 5,10-methylenetetrahydrofolate in modulating the activity of the fluoropyrimidines deserves further examination.
Interferon
The interferons are a family of glycoproteins with diverse functions. The three main types are alpha, beta, and gamma interferon and are characterized by their acid stability, cell surface receptors and primary sequences. Their use as antineoplastic agents stems from early studies demonstrating in vitro antiproliferative effects and augmentation of immune parameters such as NK cell activity and antibody- dependent cell-mediated immunity. Clinical trials have demonstrated, however, that their use as single agents is essentially limited to relatively uncommon hematologic malignancies such as hairy cell leukemia and is ineffective against the majority of solid tumors (37).
Combination therapy with interferons appears more promising and they have been shown to modulate the bioactivity of more than 20 chemotherapeutic agents (37). Biomodulation of 5-FU by interferon was first demonstrated by Namba et al. in mice with subcutaneously implanted human cervical cancer HeLa cells using a beta-IFN preparation (37). Interpreting early experiments is complicated, however, due to the use of partially purified preparations with combinations of different types of IFN.
Studies with purified recombinant IFN preparations have allowed better char- acterization of the activity of individual IFN types, and have also confirmed in vitro synergy. Table 2 lists a number of experiments using each of the three IFN types combined with 5-FU which show activity against a number of hematologic and solid malignancies (37). Elias and Crissman demonstrated enhanced inhibition of proliferation by murine gamma and alpha/beta-IFN against murine colon adenocarcinoma (MCA 38) cells. They also demonstrated improved inhibition of proliferation of l-IL-60 human leukemia cell lines by recombinant alpha-IFN (38). Recombinant alpha-2a-IFN has been shown to augment inhibition of proliferation in HT-29 human colon cancer cells (37). Gamma-IFN has been demonstrated to enhance 5-FU cytolysis of HT-29 cells and improve growth inhibition of DF-48 pancreatic cancer cells (37) and H630 human colon carcinoma cells (40). Wadler et a/. demonstrated augmented cytotoxicity of 5-FU against HT-29 and SW-480 human colon adenocarcinoma cells by recombinant alpha and beta-IFN at all doses tested, and by gamma-IFN at the highest dose level tested (41). In addition, studies by Stolfi (42) and Ligo (43) have shown that polyl-polyC, an inducer of IFN, can diminish the toxicity of 5-FU in both normal and L1210 tumor bearing mice.
The mechanism of this synergy remains speculative and may differ for each type of IFN. Most experiments have investigated the activity of alpha-IFN. Elias et al. showed that synergy of alpha-IFN was greatest with FdUrd, an intermediate in FdUMP synthesis, compared to 5-FU and fluorouridine (FUrd), a precursor of FUTP, in HL-60 cells, and that it was abrogated with the addition of thymidine. They

BIOMODULATION OF 5-FLUOROURACIL 19
Table 2. Preclinical synergy of IFN/5-FUa
I FN Specres Assay Cell line Cell type Ref
murine IFN-alpha/beta murine IFN-gamma
rlFN-alpha” rlFN-alpha rlFN-gamma rlFN-gamma
rlFN-gamma
rlFN-alpha rlFN-beta rl FN-gamma
proliferation proliferation
proliferation proliferation proliferation proliferation
cytolysis
cloning cloning clonmg
MCA-38 murine colon CA” MCA-38 murine colon CA
HT-29 HL-60 DF-48 H630
human colon CA human leukemia pancreatic CA human colon CA
HT-29 human colon CA
HT-29,SW-480 HT-29,SW-480 HT-29,SW-480
human colon CA human colon CA human colon CA
38 38
37 38 37 40
39
41 41 41
“Adapted from: Wadler, S. & Schwartz, E. L. (1990) Cancer Res. 50: 3473-3486 “CA-carcinoma “r-recombinant
postulated that this reflected interference with DNA through FdUMP stabilization of TS, rather than interference with RNA synthesis as the mechanism of synergy (38). They also showed that alpha-IFN treatment resulted in a 1 O-fold increase in FdUMP (39). Other investigators demonstrated that alpha-IFN produced an approximately 2.5-fold increase in FdUMP after a 24-h exposure in HT-29 colon carcinoma cells (44). This was accompanied by a ninefold increase in pyrimidine nucleoside (thymidine) phosphorylase, the enzyme responsible for conversion of 5-FU to FdUrd, but no increase in the activity of thymidine kinase, responsible for the conversion of FdUrd to FdUMP. While a twofold increase in the activity of uridine phosphorylase was noted, this was not accompanied by an increase in FUTP or FU incorporation into RNA. These data are compatible with those of Elias and colleagues and suggest that pyrimidine nucleoside phosphorylase may be a target for the biomodulating activity of alpha-IFN.
Other potential mechanisms may also be involved. Grem et al. demonstrated that alpha-IFN decreased clearance, increased half-life, and increased concentrations of 5-FU in patients in a phase I trial treated with alpha-IFN, 5-FU and LV (45, 46). A subsequent phase II trial demonstrated decreased catabolism of 5-FU to dihy- drofluorouracil in peripheral blood mononuclear cells after treatment and suggests a mechanism for the decreased 5-FU clearance (47, 48). Similar results were obtained by Danhauser et al. who observed a significant dose-independent 20-35% decrease in clearance, and increase in steady-state concentrations of 5-FU after treatment with 5-FU and IFN without LV (49). Schuller et al. studied the pharmacokinetics of 5-FU in the presence of both IFN and LV. They observed a significant decrease in the clearance of 5-FU with 5-FU/IFN compared to both 5-FU alone and to 5-FU/IFN/LV, but no significant difference between 5-FU/IFN/LV and 5-FU alone suggesting a relative negative influence of LV on the combination (50). In addition, immune effects such as enhanced NK activity and host protective effects have been postulated as potential mechanisms of synergy (37).

20 G. A. SOTOS ET AL
Chu et al., using gamma-IFN and 5-FU, demonstrated synergistic growth inhibition in the relatively 5-FU resistant H630 human colon cancer cell line. This was abolished with thymidine, again implying DNA synthesis via TS inhibition as the target of synergy. TS levels were measured and found to be increased 3 to 5- fold in the cells treated with single agent 5-FU compared to baseline levels, but this was not observed with the 5-FU/gamma-IFN combination. The acute overexpression of TS was not observed in more sensitive cell lines suggesting that the acute induction of TS may be a mechanism for resistance of colon cell lines. There was no effect of gamma-IFN on concentrations of 5-FU metabolites, FdUMP and FUTP, nor on DNA or RNA 5-FU incorporation, suggesting that the ability of gamma-IFN to inhibit TS overexpression is its mechanism of synergy with 5-FU in this model system (40). Similar increases in TS have been identified 24 h after 5-FU exposure in the tumors of patients with breast cancer and have been postulated to represent a clinically important mechanism of resistance to 5-FU (21).
A number of clinical trials have been conducted based on the preclinical evidence of synergy between 5-FU and IFN. Wadler et al. studied alpha-2a-IFN and 5-FU in 32 previously untreated patients with advanced colorectal cancer. Using 750 mg/m’ of 5-FU as a continuous infusion for 5 days, then weekly by IV bolus and recombinant alpha-IFN-2a million units (MU) subcutaneously 3 times per week, they observed an overall partial response rate of 63% (51). Several additional trials utilized the same doses and schedules also in previously untreated patients with advanced colorectal cancer. Kemeny et al, noted a partial response in 26% of 34 patients (52), and Pazdur et al. reported responses in 35% of 52 patients (53). Only one complete response was described among the 118 patients in these three studies. Other trials using alpha-IFN have noted comparable response rates between 31 and 39% (54, 116), and 2527% in two studies in patients with esophageal cancer (55). Kemeny et a/. and Pazdur et a/. reported overall median survivals of 13 and 16 months respectively. Preliminary results of two multicenter randomized phase III trials have recently been reported. Both utilized weekly 5-FU with two times weekly IFN and compared it either to 5-FU alone (56) or to 5-FU/LV (57). No significant differences in response rates or survival were demonstrated in either trial.
Although the reported response rates are encouraging, the toxicity of the regimen is considerable. Wadler et al. reported three toxic deaths (41). Kemeny et al. described prominent stomatitis, diarrhea and neurotoxicity occurring in 33-50% of the patients and requiring dose reduction of IFN in 84% and of 5-FU in 63% of the patients (52). Pazdur and colleagues noted grade 4 toxicity in 25% of patients and grade 3 in 82%, including one treatment-related death. They also noted a high incidence of granulocytopenia and mucositis, as well as diarrhea and neurotoxicity requiring dose reductions (53).
Because of the apparent DNA-directed mechanism of action of IFN it has been postulated that the combination of I FN and LV may achieve greater potentiation of 5-FU activity than with either agent alone. Preclinical work by Houghton et a/. has demonstrated potentiation by IFN of the 5-FU/LV combination as well as 5-FU alone (58). They exposed two human colon adenocarcinoma cell lines to 5-FU, LV and alpha-IFN in different combinations for 72 h. They showed that both LV and IFN potentiated 5-FU cytotoxicity by approximately threefold when added individually to 5-FU, and by approximately 10 to 14-fold when all three drugs were

BIOMODULATION OF 5-FLUOROURACIL 21
combined. This was evident using non-cytotoxic concentrations of 5-FU and with clinically achievable levels of both IFN and LV, and supports independent mechanisms of action for LV and IFN. They also observed that the potentiation of 5-FU and 5-FU/LV cytotoxicity by IFN was only partially reversible by the addition of thymidine, suggesting a mechanism independent of TS.
A number of clinical trials attempting double biomodulation of 5-FU have been conducted in relatively small numbers of patients using a variety of doses, schedules and routes of administration of all three agents. Response rates range from 9 to 50% with the majority falling in the 25-37% range with few complete responses described (59-62, 116). Recently, in a pilot study by Grem and colleagues, patients with gastrointestinal adenocarcinomas were treated with 5-FU 375-425 mg/m’, LV 500 mg/m’, and alpha-IFN 5510 MU/m* day (46). In 22 patients previously untreated with 5-FU, there were three complete and seven partial responses for an overall response rate of 45%. While there was increased dose-limiting mucositis and diarrhea, and a significantly lower median platelet nadir when compared to matched cycles without IFN, the promising clinical responses prompted a phase II study. Alpha-IFN 5 MU/m2 subcutaneously on days 1-7 with 5-FU 370 mg/m2 and LV 500 mg/m* intravenously on days 2-6 were administered to 46 patients with previously untreated advanced colorectal carcinoma with good performance status. Of 44 assessable patients, there were four complete and 20 partial responses for an overall response rate of 54% (48).
Biomodulation of 5-FU by IFN appears to have interesting clinical activity. The further elucidation of the mechanism(s) of synergy of IFNs alpha and gamma is critical, and should lead to additional studies to determine how to achieve optimal IFN biomodulation of 5-FU alone and with other modulatory agents.
Agents affecting DNA directly
Cispla tin
Cisplatin and 5-FU as single agents have significant activity in head and neck, gastrointestinal and a variety of other epithelial malignancies (63). Preclinical rationale for combining these agents was provided by Schabel and co-workers who demonstrated synergistic cytotoxicity in L1210 leukemia cell tumors grown in mice with concurrent infusions of both 5-FU and cisplatin when compared to either agent alone (64). Subsequent clinical data confirmed higher response rates in patients treated with combination therapy. Scanlon and colleagues investigated 1 h exposures of either 5-FU or cisplatin, or 30 min exposures to both drugs in sequence in the human ovarian cancer cell line A2780 (65). They observed less than 14% cytotoxicity for either agent alone compared to 76% for the sequence of cisplatin followed by 5-FU and 59% for the reverse sequence. They also were able to demonstrate a modest 2.5-fold increase in intracellular pools of 5,10- methylenetetrahydrofolate and tetrahydrofolate, and a similar increase in ternary complex formation when the cells were pretreated with cisplatin (65). These data are consistent with the postulate that cisplatin modulates 5-FU inhibition of TS as

22 G. A. SOTOS ETAL
the mechanism of achieving synergistic cytotoxicity. The majority of clinical studies utilize this rationale and employ a schedule of cisplatin followed by 5-FU.
However, there are contrasting preclinical data to suggest that the optimal interaction between these two agents utilizes a schedule of administration where 5-FU precedes cisplatin and in which there is an interval of 24-48 h between the agents. Johnston and colleagues demonstrated a greater than additive effect on growth inhibition of a human colon cancer cell line (H-548) with the schedule of 5-FU followed by cisplatin and only additive cytotoxicity using the reverse schedule (66). While no differences were observed in catalytic activity of TS or the fraction of bound enzyme with either schedule when compared to either drug alone, the combination of 5-FU followed by cisplatin demonstrated a greater degree of DNA damage. Esaki and colleagues found similar results using the human squamous carcinoma cell line HST-1 (67). These investigators compared exposure to either drug alone and in combination using different schedules and found a greater than additive cytotoxic effect when the 5-FU infusion preceded cisplatin and an attenuated effect with the opposite schedule. They found this synergism to be maximal when the interval between 5-FU and cisplatin was greater than 24 h. Essentially identical results were noted in an immune deprived murine model (68). Thymidine had no effect on the 5-FU/cisplatin interaction, in contrast to what one would expect if inhibition of TS was the principal mechanism of synergy (67). Utilizing an alkaline elution technique to evaluate the removal of DNA intrastrand cross-links these authors showed a significant reduction of adduct removal in cells exposed to 5-FU followed by cisplatin with a 48 h drug-free interval (67). Pratesi and co-workers found that the two drugs delivered in the sequence 5-FU followed by cisplatin significantly reduced the tumor number and the total tumor burden in chemically induced colon cancers in CF-1 mice compared to untreated mice. Interestingly the opposite schedule did not have a significant effect on these parameters (69). As a group these preclinical investigations suggest that the optimal schedule of these agents may be 5-FU followed by cisplatin with 5-FU modulating cisplatin cytotoxicity by interfering with DNA adduct repair.
To date the issue of schedule dependence on clinical effectiveness has not been well studied in patients. Almost all the studies of combination 5-FU and cisplatin use a schedule of cisplatin followed by 5-FU or less commonly concurrent infusions of both drugs. In colorectal cancer initial promising results with the combination of 5-FU and cisplatin were not confirmed by a number of randomized studies. There is a suggestion from uncontrolled studies that this combination may be more effective in rectal carcinoma (average response rate, 37%, five studies, 51 patients) than colon cancer (average response rate, 15%, five studies, 174 patients) (63). The only randomized study to show a significant difference in response rates between combination therapy and 5-FU alone utilized a regimen of cisplatin given at 20 mg/m’/day for 5 days with a concurrent 5-day infusion of 5-FU (1000 mg/m’/day). In this study the response rate in the cisplatin/5-FU arm was 35% compared to only 7% in the 5-FU alone arm; however, there was no improvement in survival (70).
In head and neck cancer the single agent activity of both cisplatin and 5-FU is higher (average 20-30%) when compared to the activity of these agents in colorectal cancer. Kish and colleagues reported a 70% response rate with 27% complete responders in 30 patients treated with cisplatin followed by a 96-h infusion of 5-

BIOMODULATION OF 5-FLUOROURACIL 23
FU (71). These and other promising studies prompted the evaluation of this combination in a number of randomized studies comparing activity with single agent methotrexate, cisplatin or 5- FU. To date despite significantly different response rates favoring combination therapy these studies have failed to show a survival advantage (72, 73).
A recent study in unresectable head and neck cancer comparing alternating chemotherapy (5.FU and cisplatin) and radiotherapy with radiotherapy alone found a statistically significant increase in median survival for patients treated with combined modality therapy and a twofold increase in the probability of survival at 3 years compared to patients treated with radiotherapy alone. In this study the schedule differed from the usual cisplatin followed by 5-FU (74). These investigators used both 5-FU (200 mg/m’/day) and cisplatin (20 mg/m’/day) as a bolus infusion daily for 5 days in each cycle. Although this study was designed to answer the question as to whether alternating chemoradiotherapy was better than radiotherapy alone in unresectable head and neck cancer, the improvement in overall survival suggests a potential benefit to the alternate schedule of cisplatin and 5-FU.
Palmeri and co-workers tested an alternate schedule in an uncontrolled trial of leucovorin 500 mg/m2/week plus 5-FU 400 mg/m2/week on day 1 and cisplatin 20 mg/m2/week on day 2 in 40 patients with metastatic colon cancer (75). The overall response rate was 24% with five partial responders in 12 patients pretreated with 5-FU. Unfortunately the dose of cisplatin used in this study was low leaving open the possibility that a higher dose may have been even more effective.
Recently Carey and colleagues reported interesting long-term follow-up in patients with esophageal carcinoma treated with neoadjuvant chemotherapy consisting of two cycles of 5-FU (1000 mg/m2) given by continuous infusion days l-4 and cisplatin (100 mg/m’) administered on day 4 followed by surgery and local radiotherapy (76). The overall complete clinical response rate was 41% with 7% of patients having no pathological evidence of tumor at surgery. The actuarial 5-year survival was 31% for all patients comparing favorably with the 21% 5-year survival reported for historical controls in the same institution.
Despite significant improvements in response rates the benefit of combining 5-FU and cisplatin has not translated into consistently prolonged survival in any patient group studied to date. The preclinical data suggest that a schedule in which 5-FU precedes cisplatin with a 24-48 h drug free interval may be optimal. Unfortunately there appears to have been very little clinical interest in assessing the schedule dependence of 5-FU/cisplatin. Of 23 phase 2 and 3 trials currently listed as active in the Physicians Data Query which include at least one 5-FU/cisplatin combination arm, only two studies assess any schedule other than cisplatin followed by 5-FU (77). It would seem reasonable, particularly in head and neck cancer where the combination of 5-FU/cisplatin has yielded impressive response rates, to assess the schedules of drug administration which preclinical data suggest may be optimal.
Azido th ymidine
Over the past several years, there has been growing interest in the combination of 5-FU and AZT (zidovudine) for the treatment of patients with epithelial tumors, particularly those of the gastrointestinal tract. AZT is an approved therapy for the

24 G. A. SOTOS ET AL
treatment of patients with human immunodeficiency virus (HIV) infection. AZT produces cytotoxicity by incorporation of its triphosphate into DNA after anabolism through a series of kinase reactions that result in phosphorylation of the nucleoside to the triphosphate form. Several investigative groups have demonstrated that AZT is synergistic with both methotrexate and 5-FU in a variety of cell lines including the human colon carcinoma cell lines HCT-8 and HCT-29, hepatoma 3924A cells, and ovarian and pancreatic carcinoma cell lines (78-82). Darnowski and colleagues have also demonstrated synergy between AZT and 5-FU in vivo in immune deficient mice implanted with the HCT-8 carcinoma cells and found that AZT was capable of enhancing the cytotoxicity of 5-FU by approximately 2 to 3-fold (79). AZT is a competitive inhibitor of mammalian thymidine kinase with inhibition constants in the l-2 pM range with thymidine as the variable substrate (78, 80). Because of this interaction, Weber and co-workers postulated that AZT is capable of enhancing the cytotoxic activity of 5-FU by decreasing the ability of malignant cells to salvage thymidine; thus, enhancing the thymidine-less state resulting from 5-FU (80-82). However, AZT does not affect the efficiency with which 5-FU inhibits thymidylate synthase or its incorporation into nucleic acids, thus suggesting that the effect of AZT on thymidine kinase has a relatively minor role in the synergistic interaction between 5-FU and AZT. In support of this conclusion is the finding that thymidine did not alter the cytotoxicity induced by AZT and, when used alone, AZT did not result in alterations in intracellular thymidine triphosphate pools (78, 79). Rather than AZT resulting in alteration of 5-FU cytotoxicity, 5-FU appears to be modulating the activity of AZT.
Co-administration of 5-FU with AZT increases the incorporation of AZT into DNA by up to 50% in in vitro models and up to twofold in in vivo tumor models consistent with the postulate that the cytotoxicity of the AZT/5-FU combination is directly attributable to the degree of AZT incorporation into DNA. Of interest is the finding that while methotrexate did not affect AZT triphosphate pools, the addition of methotrexate did increase DNA incorporation by up to threefold and was shown to synergise with AZT in cytotoxicity assays (78). Presumably, the mechanism of increased AZT incorporation in DNA is the result of decreases in intracellular thymidine triphosphate pools induced by either methotrexate or 5-FU. In general, the preclinical data provide strong evidence that it is the antimetabolites, through their effects on intracellular thymidine triphosphate pools, that are responsible for modulating DNA incorporation and hence cytotoxicity of AZT. Since AZT is not a particularly active agent for the treatment of solid tumors, it remains to be seen whether its activity can be modulated adequately to effect a meaningful clinical response in patients with solid tumors.
The AZT/5-FU combination has been tested in preliminary clinical investigations. A report by Posner and colleagues tested high dose oral AZT (maximum tolerated dose 7.5 g/m*/dayx3) in combination with a 72 h continuous infusion of 5-FU and oral LV in a dose escalating Phase I investigation (83). Intractable nausea and vomiting were dose-limiting. Eighteen patients with prior therapy were treated on the trial; however, no responses were noted. A second trial was undertaken by the same group using a continuous 48-h infusion of AZT (2-20 g/m*/d) beginning 24 h after the start of continuous infusion 5-FU (800 mg/m*/dx72 h) and oral leucovorin (84). No responses were noted in 18 previously treated patients. Despite finding a dose-dependent increase in DNA strand breaks in peripheral blood cells,

BIOMODULATION OF 5-FLUOROURACIL 25
it was concluded that more rapid infusion schedules that would result in higher plasma levels of AZT would be required for anticancer activity. However, the plasma concentrations achieved with oral and intravenous dosing on the schedules investigated were approximately 1 O-30 ,uM and 130 pM respectively. The preclinical models and the dose-dependent DNA fragmentation in patients suggest that the achieved plasma concentrations in man are adequate for interaction with 5-FU, although peak levels achieved in murine models with bolus administration of AZT were somewhat higher (fivefold). The combination of 5-FU and AZT is based on sound preclinical evidence of a greater than additive interaction between these compounds. Available clinical data suggest that the combination is feasible in patients. The ultimate utility of this combination will await further clinical inves- tigations in a homogeneous group of untreated patients treated with maximum tolerated doses of both AZT and 5-FU.
lododeoxyuridine
lododeoxyuridine is a halogenated pyrimidine analogue of thymidine that is capable of producing cytotoxicity in a variety of carcinoma cell lines. The major mechanism by which IdUrd produces its cytotoxicity is by incorporation into DNA after phosphorylation to the triphosphate level (Figure 1). Albeit much less potent than fluorodeoxyuridine, IdUrd is also an inhibitor of thymidylate synthase and can undergo dehalogenation to deoxyuridylate via this enzyme (85). IdUrd has most commonly been employed as a radiation sensitizer, an effect that presumably results from its ability to be incorporated into DNA. Investigators have demonstrated that the percentage of thymidine replaced by IdUrd may be directly correlated with the degree of radiation sensitivity and the frequency of DNA strand breaks (86-91). In addition to enhanced incorporation in DNA, the combination of fluoropyrimidines with IdUrd increases radiosensitization by redistributing cells into S phase, pre- sumably resulting from intracellular thymidine depletion that accompanies fluo- ropyrimidine exposure (89, 92).
Using a human bladder cancer cell line (T24), Benson and colleagues dem- onstrated that the addition of either fluorouracil or fluorodeoxyuridine to IdUrd resulted in a greater than additive cytotoxic interaction (93). This enhanced cytotoxicity was attributed to increased incorporation of IdUrd triphosphate into DNA as a result of decreased competition from the physiologic nucleotide thymidine triphosphate and diminished dehalogenation of IdUrd. Both of these events resulted from inhibition of thymidylate synthase by the fluoropyrimidines.
Using human colon carcinoma cell lines (HuTu80 and HT29), investigators from the University of Michigan demonstrated that both 5-FU and fluorodeoxyuridine were capable of increasing the amount of IdUrd incorporation into DNA in a dose dependent fashion over the range of 0.1 to 100 pM and 1 to 100 nM for fluorouracil and fluorodeoxyuridine respectively (86, 88, 89). The use of IdUrd alone resulted in a dose dependent (up to 30 PM) increase in the level of IdUrd incorporation into DNA. Using clinically achievable concentrations of IdUrd and fluorouracil (3 pM
and 1 pM respectively), these investigators demonstrated that the combination resulted in approximately 16% replacement of thymidine in DNA by IdUrd or approximately 3.5-fold more replacement than was achieved using IdUrd in the

26 G. A. SOTOS ET AL
absence of fluorouracil in the HT29 human colon cancer cell line. The combination of fluorodeoxyuridine with IdUrd resulted in approximately a 2.5-fold increase in IdUrd incorporation compared to exposures with IdUrd alone. The enhanced incorporation of IdUrd by the fluoropyrimidines resulted in enhanced radiation sensitivity and also enhanced cytotoxicity commensurate with the increases in DNA thymidine replacement.
Investigations using the HT29 human colon cancer cell line were extended to experiments using a tumor bearing immune-deprived murine model. Lawrence and colleagues found that infusion of fluorodeoxyuridine resulted in a 3.5fold increase in thymidine replacement in the tumor when compared with infusions of IdUrd alone (86). Unfortunately, incorporation of IdUrd into the DNA of normal tissues including bone marrow and gastrointestinal tract were also increased to a similar extent as that in tumor. However, the toxicity associated with the combined use of fluorodeoxyuridine and IdUrd was less than what was appreciated with higher doses of IdUrd alone that resulted in similar thymidine replacement levels in normal tissues but only half as much replacement in the tumor. These studies provide evidence that the combination of fluorodeoxyuridine and IdUrd may result in a selective increase in IdUrd incorporation into the DNA of tumor, as opposed to normal tissues, when compared with IdUrd alone.
More recent investigations suggest that a second halogenated pyrimidine, bro- modeoxyuridine, may hold more clinical promise owing to greater tumor DNA incorporation and a more acceptable toxicity profile (88, 90). However, while theoretically advantageous, a trial directly comparing IdUrd with bromodeoxyuridine assessing tumor growth in an in vivo model has not been reported. Using a rabbit model with an implanted VX2 rabbit anaplastic squamous cell carcinoma, Stetson and colleagues found that fluorodeoxyuridine, but not fluorouracil, was capable of increasing the incorporation of bromodeoxyuridine into the DNA of the VX2 tumor in preference to incorporation into normal tissues of the bone marrow and intestinal mucosa (87). Fluorouracil, on the other hand, appeared to increase incorporation into the normal tissues to a much greater extent than that into the VX2 tumor cells. Conversely, the use of either fluorodeoxyuridine or fluorouracil significantly increased the incorporation of IdUrd into the DNA of the VX2 tumor. While fluorouracil had little effect on the incorporation of IdUrd into normal tissues, fluorodeoxyuridine significantly enhanced the incorporation of iododeoxyuridine into normal tissues. These data suggest that fluoropyrimidine/halopyrimidine com- binations are biomodulatory. However, since the in viva animal data appear to be model specific, the precise role, degree of selectivity and best combination of these agents awaits clinical investigations.
Given the positive interactions between LV and 5-FU, it is interesting to note that LV enhances the cytotoxicity of IdUrd in several in vitro cell systems including the HT29 human colon carcinoma cell line and the MCF-7 human breast carcinoma cell line (85). The addition of LV to IdUrd diminished the dehalogenation of IdUrd by thymidylate synthase resulting in a threefold increase in intracellular IdUrd triphosphate and up to a twofold increase in DNA incorporation. While IdUrd monophosphate was found to be a relatively weak inhibitor of thymidylate synthase compared to fluorodeoxyuridine monophosphate, the addition of LV to IdUrd resulted in an enhanced inhibition of this enzyme and presumably accounts for the diminished dehalogenation of IdUrd. Since LV markedly enhances the cytotoxicity

BIOMODULATION OF 5-FLUOROURACIL 27
of IdUrd it should be considered in regimens using IdUrd alone or in combination with fluoropyrimidines.
While malignant tissues frequently become resistant to the effects of chem- otherapeutic agents, normal tissues rarely achieve such resistance. Investigators at the Cancer Research Campaign Laboratories investigated an interesting approach for enhancing the specificity of IdUrd for tumor versus normal tissues (94). Using a nude mouse model bearing human xenografts of choriocarcinoma or colonic carcinoma that were resistant to the effects of hydroxyurea, they demonstrated that hydroxyurea was capable of markedly inhibiting the incorporation of IdUrd into normal tissues that retained their sensitivity to hydroxyurea while not affecting the incorporation of IdUrd into tumor tissues that were resistant to the effects of hydroxyurea. This selective effect could be further enhanced by the addition of a fluoropyrimidine to the combination of hydroxyurea and IdUrd suggesting a further potential means for enhancing the selectivity of the biomodulatory interaction between IdUrd and fluoropyrimidines.
In contrast to most efforts in biochemical modulation, the investigative groups interested in the fluoropyrimidine-iododeoxyuridine combination have attempted to demonstrate the presumed mechanisms of interaction between these agents in the tumor and normal tissues of patients as a part of their clinical investigations, Using the DNA of granulocytesfrom patients undergoing therapy with 9914 day continuous infusions of IdUrd (1000 mg/m2/day), Belanger and colleagues found that the maximum incorporation of IdUrd into DNA occurred at the end of the infusion and accounted for a 7 to 17% substitution of thymidinefor IdUrd (95). Thrombocytopenia was the dose-limiting toxicity for patients on this trial and the investigators were able to demonstrate that the percentage substitution of granulocyte DNA was directly correlated with the degree of thrombocytopenia and neutropenia incurred by the patients. Of interest, co-administration of fluorodeoxyuridine did not significantly enhance the degree of IdUrd incorporation into the DNA of granulocytes consistent with a possible selective effect of fluorodeoxyuridine on IdUrd incor- poration. Unfortunately, a true measure of selectivity could not be ascertained from this investigation since there were no data available for the incorporation of IdUrd into the DNA of tumor or the effect of the fluoropyrimidine on this incorporation. However, in a companion study performed in patients with hepatic metastases treated with 3-day infusions of either systemic IdUrd or intrahepatic artery IdUrd, IdUrd replaced between 2-4.5% of the tumor DNA thymidine using intravenous infusions and approximately twice that amount when using the intra-arterial route (96-98). There was a trend towards increased IdUrd incorporation in the tumor tissue with the addition of fluorodeoxyuridine while less than 1% of the thymidine in normal liver DNA was replaced by IdUrd. These data demonstrate that IdUrd is selectively incorporated into tumor DNA compared to normal liver and suggest that fluorodeoxyuridine may enhance the incorporation in tumor but not in normal tissues. Using the intrahepatic artery route of delivery, one partial response and four minor responses out of 11 patients were noted. Since no responses were noted in three patients treated with intravenous route therapy, it is possible that regional has an added advantage over systemic therapy.
Additional data concerning the rate of replacement of IdUrd in the tumor DNA of patients with sarcomas, head and neck tumors, and gliomas, identified sarcomas and head and neck tumors as having relatively high replacement indices (up to

28 G. A. SOTOS ET AL
26%) when compared to gliomas (O-4%) (99). Presumably, the rate of replacement may be used to identify tumors most susceptible to combination regimens using IdUrd and fluorouracil.
Phase I clinical investigations combining 5-FU with IdUrd have also identified a pharmacokinetic interaction between these agents providing an additional mech- anism for the observed interactions between these drugs. Remick and colleagues using intrahepatic arterial infusions of IdUrd and 5-FU, noted that plasma levels of fluorouracil were significantly elevated during concurrent intrahepatic arterial administration of IdUrd (100). This interaction is further supported by canine experiments in which 5-FU was given as a bolus administration at the mid-point of a 6-h continuous infusion of either bromodeoxyuridine or IdUrd where a similar interaction was identified (101). However, this observation has not been consistently found. In studies by Speth and colleagues using intravenous IdUrd and fluo- rodeoxyuridine, no pharmacokinetic interaction was identified (102).
Investigators at the University of Wisconsin studied 18 patients with hepatic metastases treated with intrahepatic artery infusions of 5-FU and IdUrd (100). These investigators found hepatotoxicity to be dose limiting and identified a single partial response in 17 evaluable patients. Using concurrent continuous intravenous infusions of IdUrd and 5-FU for 5 consecutive days in a Phase I trial, Benson and colleagues identified myelotoxicity and gastrointestinal toxicity as dose limiting. While three minor responses were reported in 23 patients, there were no other responses (103). A recent investigation demonstrated the feasibility of combining infusional IdUrd with LV modulated 5-FU given on a weekly (Roswell Park) schedule (104). These investigators found the maximum tolerated dose of IdUrd given over a 24 h period by constant intravenous infusion to be 1 g/m’. Seventeen of the 24 patients entered onto the study had no prior chemotherapy. Of these patients, three demonstrated partial remissions.
These studies demonstrate the feasibility of combining IdUrd with 5-FU and LV modulated 5-FU. Further clinical investigations will be required to delineate the potential role of IdUrd in fluorouracil containing regimens.
Agents affecting RNA
Methotrexate
Methotrexate (MTX) is a folic acid analogue that competitively inhibits dihydrofolate reductase (DH FR), the enzyme responsible for regeneration of reduced folates from dihydrofolate (Figure 1). DHFR inhibition results in metabolic inhibition by a multifactorial mechanism that includes partial reduced folate depletion and direct enzymatic inhibition of folate-requiring enzymes of de not~o purine and pyrimidine synthesis by MTX and dihydrofolate polyglutamates (15, 105, 106). Thus, in the presence of MTX, dTMP synthesis, which is a rate-limiting step in DNA synthesis, is interrupted. As a consequence of TS inhibition, intracellular dUMP concentrations rise. In the presence of decreased dTMP concentrations, the activity of deoxy- cytidylate deaminase, responsible for converting dCMP to dUMP, is enhanced and results in further increases in dUMP concentrations. Excess dUMP can be

BIOMODULATION OF 5-FLUOROURACIL 29
misincorporated as dUTP into DNA and result in DNA fragmentation and/or miscoding (107).
A property of MTX important in its function is its ability to be polyglutamated. MTX is actively transported into the cell by a system which normally transports reduced folates. Once inside the cell, MTX can efflux unchanged or become polyglutamated. The anionic charges of glutamate residues prevent efflux and thereby maintain high intracellular concentrations of MTX (107). The poly- glutamated forms are also capable of inhibiting a number of enzymes including DHFR, TS, and enzymes involved in de nova purine synthesis (15, 106).
Early preclinical studies with combination MTX and 5-FU by Kline et al. in mice with subcutaneous L1210 murine leukemia tumors demonstrated improved survival after treatment with MTX and 5-FU compared to MTX alone (107). Moreover, as shown in a number of in vitro and in viva studies, there appears to be increased synergy with an increased interval between MTX and 5-FU administration. Bareham et al. and Dilarenzo et al. observed sequence-dependent synergy of MTX and 5-FU in inhibition of humoral immunity in mice. In 1977, Lee & Khwaja used combination MTX/5-FU as adjuvant therapy in mice with murine mammary carcinoma. A reduction in metastases and a prolonged survival were noted when MTX was given before 5-FU, but not when the sequence was reversed. Similarly, Bertino et al. demonstrated a 20% increased survival in CD-l mice with murine S-l 80 sarcomas when treated with MTX followed by 5-FU, but not when 5-FU was given simultaneously with or before MTX (108). These early studies stimulated further research into mechanisms of synergy and the importance of drug sequence (107, 109).
The interaction of MTX with 5-FU is complex and theoretical models for both antagonism and synergy have been postulated. Methotrexate, by altering reduced folate pools involved in ternary complex formation may be expected to hinder 5-FU inhibition of TS (110, 111). By inhibiting de nova purine synthesis, there is also less nucleic acid synthesis available for fluoropyrimidine nucleotide incorporation. However, the net balance of potential negative and positive effects appears to favor synergy. Phosphoribosylpyrophosphate (PRPP), an intermediate needed in de now purine synthesis, accumulates in the cell when de now purine synthesis is inhibited. It also serves as the donor of phosphoribose in the first step of 5-FU activation (Figure 1); thus, elevated PRPP concentrations favor increased 5-FU anabolism. The consequent increased levels of fluorinated nucleotides result in both increased incorporation into RNA and enhanced TS inhibition (111). Support for this mechanism was proposed by Cadman et a/. who demonstrated that PRPP levels increased in a dose-dependent fashion with increasing MTX exposure in L1210 cells treated with 5-FU (112). MTX also resulted in dose-dependent increases in FUMP and FUTP levels. The findings by Kemeny et a/. of a statistically significant increase in PRPP concentrations over pretreatment levels in biopsied tumor tissue from two patients treated with sequential MTX/5-FU are consistent with this mechanism (113). Another potential mechanism of synergy is dTTP depletion leading to false incorporation of FdUTP into DNA. The most plausible mechanism, however, appears to be through increased levels of PRPP resulting from inhibition of purine synthesis (107).
Additional preclinical studies have evaluated the importance of the MTX pre- treatment interval. Using human colon adenocarcinoma (HCT-8) and breast car-

30 G. A. SOTOS ET AL
cinema cell lines (47-DN), Benz et a/. demonstrated synergistic growth inhibition which increased as the interval between MTX pretreatment and 5-FU increased from zero to 24 h (114). Mini et al, also showed sequence specific synergy using colony survival in the human leukemia CCRF-CEM cell line. The reverse sequence of 5-FU pretreatment followed by MTX yielded antagonistic cytotoxic effects (109).
Clinical trials combining MTX and 5-FU have been conducted using a variety of doses and schedules. Most have employed MTX pretreatment with time intervals ranging from 1 to 24 h. Marsh et a/. compared 24 h (arm A) to 1 h (arm B) pretreatment with MTX 200 mg/m’ and 5-FU 600 mg/m’ in 159 patients with advanced untreated colorectal cancer. Both arms received leucovorin rescue 24 h after MTX. Arm A patients had significantly improved overall response rates of 29% compared to 14.5% for arm B patients, (p = 0.026), and improved median survival of 15.3 vs. 11.4 months, (p = 0.003) (115). Although both arms received LV rescue it is possible that the LV contributed to the differences as it was given 23 h after 5-FU in arm B and at the same time as 5-FU in arm A. Despite this, it appears that the interval between MTX and 5-FU is an important response variable. Several reviews have summarized response rates according to interval of MTX pretreatment and have found, in general, that regimens employing longer time intervals (20-24 h) achieve slightly higher response rates than those using intervals less than or equal to 7 h (107, 115, 116). Response rates from phase II trials of MTX/5- FU using a 4-7 h interval range from 15542% and those using a 20-24 h interval range from 20-50% (113, 116). Historically, 5-FU alone has a reponse rate of 1 O-20%. Phase III studies directly comparing combination therapy with single agent therapy have been conducted, also utilizing different dosing intervals. Four randomized studies utilizing pretreatment intervals of 4-7 h yielded conflicting results complicated further by small numbers of patients, widely varying 5-FU doses, and the variable use of LV (28, 31, 116). Of four trials utilizing tolerable doses of 5-FU and pretreatment intervals greater than 20 h, three demonstrated significantly improved response rates, and one showed a significantly improved median survival (Table 3) (28, 116, 117).
The Nordic group trial compared MTX 200 mg/m’ IV over 2 h and 5-FU 500
Table 3. Clinical trials of MTX/5-FU vs. 5-FU employing MTX pretreatment intervals of 20+ hours”
Trial MTX 5-FU Response
(mg/m*) (mg/m’) LV @) Survival
(months) Fief
Nordic 200 500 + 24p < 0.01 8.5~ < 0.02 117 600 - 3 6
Machiavelli 200 1200 + 28p<O.O5 8 116 1200 - 12 8.3
Poon 40 700 26p=O.O4 8 28 500 - 10 8
“See text for abbreviations

BIOMODULATION OF 5-FLUOROURACIL 31
mg/m2 followed by LV rescue to 5-FU alone 600 mg/m2 in 249 patients with advanced untreated colorectal cancer. The 5-FU was administered twice, at 3 and 21 h after MTX in the combination arm. Response rates were 24% and 3% and overall median survival was 8.5 and 6 months for the combination vs. single agent group, respectively. Both endpoints achieved statistical significance (117). Machiavelli et a/. treated 118 patients with MTX 200 mg/m2 followed 20 h later by 5-FU 1200 mg/m2 and LV or 5-FU 1200 mg/m2 alone. A statistically significant difference in response rates, 28% and 12%, for the combination treatment and 5-FU alone respectively, were noted (116). Poon et al. performed a multi-arm phase III trial comparing low dose MTX 40 mg/m2 or high dose MTX 200 mg/m2 plus 5-FU 700 mg/m2 with 5-FU 500 mg/m2 alone in patients with advanced colorectal cancer previously untreated by chemotherapy (28). Low dose MTX was given 24 h before 5-FU without LV rescue and high dose MTX was given 7 h before 5-FU with LV rescue given 24 h after MTX. Response rates were 26%, 21% and 10% for the low dose, high dose, and no MTX groups respectively, achieving statistical significance only for the low dose MTX arm vs. 5-FU alone.
Again, however, the possible biomodulatory effects of leucovorin when given as rescue therapy for MTX impedes interpretation. Both the Nordic group trial and the study by Macchiavelli et al, included LV rescue with the MTX arms and achieved total response rates comparable to the 23% published for 5-FU/LV phase Ill studies (116, 117). In the trial by Poon et al. the low dose MTX without LV achieved response rates comparable to the high dose MTX with LV rescue, but the pretreatment time interval was also different and may contribute to the difference. Other arms of the Poon trial included 5-FU with high or low dose leucovorin. Response rates were greatest for the low dose LV regimen at 43% compared to 26% for both the high dose LV and low dose MTX arms. Both LV arms and the low dose MTX arm achieved statistical significance over 5-FU alone. Direct comparisons among the regimens is difficult, however, because doses of 5-FU varied among the three arms. Statistically significant improvement in survival was achieved with both leucovorin regimens, but was only suggested with the high dose MTX regimen when results were corrected for performance status, tumor-related symptoms, and degree of tumor anaplasia (28).
These results suggest that there does appear to be improved response to MTX followed by 5-FU when compared to single agent 5-FU. Pretreatment intervals of 20 to 24 h appear superior to intervals of zero to 1 h, and may be minimally better than intervals of 3 to 7 h (107, 116). Response rates of the best MTX/5-FU regimens seem comparable to 5-FU/LV regimens but a survival advantage compared to 5-FU alone is not clear, achieving statistical significance only in the Nordic group trial. Given the evidence supporting use of low dose LV and the potential importance of the sequence of LV administration, the contribution of rescue LV to the clinical activity should be considered in future trials of MTX biomodulation.
Trimetrexate
Although interpretation of efficacy of MTX/5-FU regimens can be clouded by the use of LV rescue, the combination of these three drugs in preclinical studies has not been shown to improve cytotoxicity over two drug combinations (118). It has been postulated that this lack of synergy may stem from competition between MTX

32 G. A. SOTOS ETAL
and LV for the cell membrane transport system, for polyglutamation, and because LV rescues the cell from the metabolic effects of MTX. Trimetrexate (TMTX), is another antifolate inhibitor of DHFR. However, it is not polyglutamated and does not compete directly with LV for cellular transport. Romanini et al. measured PRPP levels and assessed cytotoxicity of various combinations of 5-FU/LV with and without TMTX or MTX in human CCRF-CEM leukemia cells (118). When cells were exposed for 20 h to the same concentrations of MTX and TMTX alone, intracellular PRPP concentrations increased similarly by approximately fivefold over baseline. Cytotoxicity of 5- FU/LV combined with either MTX or TMTX was increased compared to 5- FU/LV. When 10 ,uM LV was added to iso-effective concentrations of MTX and TMTX each in combination with 5-FU, there was a significant increase in cytotoxicity for TMTX/5-FU, but not for MTX/5-FU. Also, intracellular concentrations of LV were measured after exposure to 1 pM LV with 10 pM MTX or TMTX, and were found to be significantly higher with TMTX and significantly lower with MTX compared to exposure to LV alone. These data demonstrate enhanced cytotoxicity of TMTX/5-FU/LV compared to MTX/5-FU/LV and 5-FU/LV combinations and suggest a competitive negative interaction between MTX and LV. Based on this study, Conti et al. conducted a phase I trial of sequential TMTX, 5-FU, and high dose LV in previously treated patients with gastrointestinal carcinomas (119). Patients were treated with TMTX 20-I 10 mg/m’ followed 24 h later by 500 mg/m’ 5-FU and LV rescue. In 19 patients, peripheral blood mononuclear cell PRPP levels were increased almost sixfold with TMTX doses of 50-I 10 mg/m’ while tumor cells obtained from two patients demonstrated increases of approximately twofold. Toxicity was comparable to 5-FU/LV regimens and there was a 19% partial reponse rate in patients with previously treated colon carcinoma. The optimal TMTX dose and the precise mechanism of synergy remain to be determined but the evidence for in situ biochemical activity and clinical activity serve as impetus for further study.
PALA
N-(Phosphonacetyl)-L-aspartate (PALA) was synthesized in 1978 as an inhibitor of aspartate transcarbamylase (ACTase), an early enzyme in de novo pyrimidine synthesis (Figure 1). Preclinical studies demonstrated activity against a number of murine leukemia and solid tumor cell lines and against transplanted human MX-1 mammary and LX-l lung tumors. Biochemical studies in vitro and in vivo showed that treatment with PALA indeed inhibited ACTase activity and diminished intra- cellular levels of UTP and CTP in both normal and tumor tissue. Data from phase I clinical trials confirmed both inhibition of ACTase and decreased concentrations of UTP in patients’ tumor tissue. Although several minor responses were noted in the phase I studies, multiple phase II trials of PALA given as a single agent in a variety of doses, schedules and routes of administration yielded disappointing response rates of O-l 2% (120).
Combining PALA with 5-FU derives logically from the known mechanisms of action of each agent (Figure 1). 5-FU, through competition of its metabolites with uridine nucleotide derivatives, interferes with both DNA and RNA synthesis. FUTP can be incorporated directly into RNA thereby disrupting its function, and FdUMP forms a stable ternary complex with thymidylate synthase and inhibits normal DNA

BIOMODULATION OF 5-FLUOROURACIL 33
synthesis. PALA reduces uridine nucleotide pools and creates a more favorable ratio for the FU metabolites with which they compete. Decreased UTP concentration allows increased incorporation of FUTP into RNA. PALA inhibition of ACTase also results in underutilization and therefore elevated levels of PRPP, which then favors synthesis of FUMP and consequently increased incorporation of FUTP into RNA (121). Inhibition of pyrimidine synthesis also causes decreased dUMP con- centrations and therefore decreased competition with FdUMP for TS binding.
These biochemical interactions affecting both RNA and DNA synthesis have been shown to occur in vitro. In human MDA mammary cancer cells exposed to both 5-FU and PALA, UTP depletion led to increased incorporation of FUTP into RNA and synergistic growth inhibition (122). Treatment of MCF-7 breast cancer cells with PALA and 5-FU resulted in a threefold increase in PRPP and a 59% decrease in clonogenic survival compared to treatment with 5-FU alone (123). In Sarcoma 180 cells (S-180), PALA pretreatment resulted in higher levels of free FdUMP and enhanced formation of the TS ternary complex (124). Similar biochemical data exists from in vivo models. Studies in rats with intraperitoneally implanted hepatoma ascites cell line AS-30D (125) and in CDF81 mice with syngeneic spontaneously metastasizing breast carcinoma (126), both documented increased incorporation of fluorouracil nucleotides into tumor RNA after treatment with PALA/5-FU, as well as enhanced antitumor activity, when compared to 5-FU alone.
Other preclinical experiments were done which demonstrated that the sequence of drug administration and the interval between the drugs was important for biomodulation. Liang et al. used S-180 cells to demonstrate that synergy was greater when PALA was given 12 h or more before 5-FU compared to 6 h or less (124). Martin et al. showed that synergy was evident when PALA was given 24 h prior to 5-FU in CD8Fl mice (126).
The preclinical evidence for enhanced antitumor activity combining PALA with 5-FU led to a series of clinical trials. Data from phase I clinical trials suggested that PALA as a single agent may have activity at high doses, and studies in murine animal models demonstrated that high dose PALA with low dose 5-FU was as effective as low dose PALA with high dose 5-FU with regard to anticancer activity (127). Therefore, early phase I clinical trials of combination PALA and 5-FU generally utilized high-dose PALA. Partial responses were noted, primarily in patients with colorectal cancer, and phase II studies were conducted. However, at the high doses tested, toxicity was unacceptable and led to a reduction in dose of 5-FU to levels that markedly compromised its clinical activity (127). Thus, clinical efficacy, defined in terms of response rates, of the combined therapy in phase II trials using high dose PALA with the lower doses of 5-FU was no better than historical controls treated with higher doses of 5-FU alone.
Additional preclinical studies provided a rationale for using lower doses of PALA in clinical trials that would not compromise the higher, more effective doses of 5-FU. Martin et al. studied the effects in vivo of different doses of PALA on sensitive murine CD8Fl breast cancer cells, intestinal epithelial cells, and bone marrow (126). They found that 100 mg/kg of PALA selectively increased incorporation of FU into RNA in tumor cells while not affecting intestinal epithelial cells. PALA doses greater than or equal to 200 mg/kg affected FU-RNA incorporation essentially equally in both tumor and intestine. The bone marrow was unaffected at all doses tested. In mice treated with either placebo, the MTD of 5-FU or low dose PALA

34 G. A. SOTOS ET AL
with 5-FU, tumor regression occurred in 0%, 7%, and 31% respectively, with no difference in mortality. These preclinical data demonstrated both tumor selective bioactivity ot low dose PALA and synergistic cytotoxicity with high dose 5-FU. While this represents interesting data and prompted additional clinical trials, it is important to consider that the selectivity may be tumor and/or species specific.
Casper et al. conducted a phase I trial using PALA at doses ranging from 250 mg/m* to 2 g/m* with varying doses of 5-FU, and measured the effect of PALA on total body normal tissue c/e nova pyrimidine synthesis with an indirect assay. They found that the lowest PALA dose was as effective as the highest in inhibiting de nova pyrimidine synthesis in normal tissues (128). This served as rationale for utilizing low modulatory doses of PALA in clinical trials. In a subsequent phase l/II trial, Ardalan et al. compared weekly PALA 250 mg/m* intravenously followed 24 h later by a 24-h infusion of 5-FU 750-2600 mg/m* administered to 28 patients to 5-FU alone in the same dose and schedule given to a randomized group of 19 patients all with advanced untreated gastrointestinal malignancies. Although the number of patients was small, they observed a 39% response rate with two complete responses in the combination group compared to a 21% response rate in the 5-FU alone group (129). O’Dwyer and colleagues used the same combination and schedule to treat 39 chemotherapy naive patients with colorectal cancer, and achieved a total response rate of 43% including three complete responses (130). Kemeny and colleagues used the same low dose of PALA combined with 600,700, or 800 mg/m* of 5-FU given as a bolus infusion. They noted one complete response and an overall response rate of 35% (131).
Projected mean survival reported by O’Dwyer et a/. and overall median survival from Kemeny et al. were 17 and 18 months, respectively. By comparison, in the North Central Cancer Treatment Group study comparing 5-FU with and without low and high dose LV, reported median survivals were 12 months for the LV treated patients and 7 months for those receiving 5-FU alone (28). Obviously, patient selection may play a major role in these differences. Dose limiting toxicities were similar in the three trials and were primarily gastrointestinal and myelosuppression. A syndrome of ascites, hyperbilirubinemia, hypoalbuminemia, and elevated trans- aminases was reported by Kemeny et al. occurring in part or in whole in 15 of the 17 patients who responded to PALA/5-FU combination therapy (132).
Biochemical data from clinical studies are limited. However, recent investigations suggest that the 250 mg/m’ dose of PALA may be too low to produce consistent inhibition of ACTase. Ardalan et al. noted decreased peripheral leukocyte ACTase activity of only 10% in four patients treated with a 5-day continuous infusion of PALA 940 mg/m’/day and 5-FU (133). Grem et al, in a phase I study using the PALA/5-FU/LV regimen, noted a similar modest decrease in peripheral blood mononuclear cell ACTase activity (9%) using a PALA dose of 250 mg/m*, but with increasing doses observed a dose-dependent enhanced inhibition of ACTase (134). Smith and colleagues measured leukocyte ACTase activity in patients receiving PALA/5-FU/dipyridamole and found that the 250 mg/m* dose of PALA resulted in little ACTase inhibition (135).
Given the promising response rates of PALA/5-FU, it seems logical to add other biomodulators to this regimen to try further to improve efficacy. A recent phase I trial conducted by Grem et al. determined the MTD for single dose PALA combined with a 72-h infusion of 5-FU and LV (134). The first phase of the study determined

BIOMODULATION OF 5-FLUOROURACIL 35
the MTD for 5-FU to be 2300 mg/m’when combined with LV 500 mg/m’as a 72-h continuous infusion. In the second portion of the trial, new patients were treated with escalating single doses of PALA followed by 5-FU 2000 mg/m2 and LV 500 mg/m’to determine the maximum dose of PALA achievable without compromising the dose of 5-FU. Biochemical assays on ACTase inhibition were also performed and demonstrated a dose-dependent inhibition. A PALA dose of 1266 mg/m* was recommended as it was the highest dose achievable without compromising the dose intensity of 5-FU. These studies provide a rationale for using higher, more consistently biochemically active doses of PALA that do not result in a compromise of 5-FU dose since the sensitivity of tumors to PALA would be expected to vary and may be substantially less sensitive than both normal tissues and relatively sensitive preclinical models.
While the low dose PALA, high dose 5-FU combination trials are promising in terms of overall response rates, especially for patients with colorectal cancer, additional biochemical studies and larger phase III trials are needed to optimize and compare this combination with regimens of other 5-FU modulators,
Uridine
In addition to enhancing the cytotoxic activity of 5-FU through nucleic acid incorporation or enzyme inhibition, attempts have been made to modulate the activity of 5-FU by altering selectivity through the use of uridine rescue (136). Using intermittent uridine doses beginning 2 h after fluorouracil, Martin and colleagues described a 1.5 to 3-fold increase in MTD of 5-FU in mice bearing advanced murine colon tumor 26 as assessed by changes in white blood cell count and body weight (137). These levels of uridine exposure have been found to result in approximately a twofold increase in intracellular UTP pools in a variety of human colon and leukemia cell lines (138). Subsequent preclinical investigations demonstrated that uridine rescue was able to reduce 5-FU induced host-toxicity without significant alteration of anti-tumor activity (137, 139). The enhanced selectivity afforded by uridine rescue has been attributed to an accelerated clearance of fluorouracil metabolites from the RNA of normal KY. malignant tissue. Since uridine appears to be actively concentrated in normal tissues through an energy requiring transport system that appears to be defective in a number of neoplastic cell lines, transport inhibitors have been suggested as a potential means for further enhancing the selectivity of uridine rescue (140). Uridine markedly improved the selectivity of a regimen that included 5-FU with the addition of PALA and MMPR given 24 h prior to the dose of fluorouracil in a tumor bearing murine model (137). In a separate set of experiments using an in vivo breast tumor model, uridine rescue was shown to enhance the selectivity of a sequenced regimen consisting of PALA plus high dose MTX, followed by 5-FU and rescue with both LV and uridine (139). These results were echoed by a series of investigations demonstrating the ability of delayed uridine rescue to permit the use of higher doses of 5-FU with resultant improved antitumor activity in a relatively chemoresistant colon 26 murine car- cinoma but not in the more 5-FU sensitive murine colon 38 (141, 142). Using an identical high-dose intermittent uridine rescue schedule reported by Martin and colleagues, Peters and co-workers demonstrated the ability of uridine rescue to enhance the therapeutic activity of 5-FU. In particular, these investigators found a

36 G. A. SOTOS ET AL
striking ability of uridine to rescue colon 26 tumored mice from the toxicity of LV modulated 5-FU without altering the potent anti-tumor activity of this regimen.
These resultssupport the concept that the use of double modulation of fluorouracil with both LV and uridine rescue may be more efficacious than either single modulation alone and should be considered for further clinical investigation. The high doses of uridine used in these investigations resulted in peak plasma uridine concentrations of up to 6 mM with sustained levels greater than 1 mM for up to 6 h after uridine injection. However, in vitro investigations using a human colonic carcinoma cell line WiDr demonstrated that the use of as little as 100 pM uridine concentrations were effective in reversing the growth inhibitory effects of a 24-h exposure to 3 pM fluorouracil (142).
In addition to its use as a rescue agent for the fluoropyrimidines, uridine has also been used to enhance fluoropyrimidine cytotoxicity by simultaneous administration (143-l 45). Investigations by Parker and colleagues using an in vitro murine T-cell lymphoma cell line (S-49), demonstrated that the simultaneous use of low dose uridine (10 FM) along with 5-FU, resulted in a twofold increase in cytotoxicity (143, 144). The basis for the enhanced cytotoxicity appeared to be due to increased anabolism of 5-FU resulting in increased RNA incorporation of fluorouracil metabolites. In addition to the inhibitory effects of uridine on c/e novo pyrimidine synthesis, uridine was also found to be a potent noncompetitive inhibitor of dihydropyrimidine dehydrogenase (Ki = 0.71 FM), an enzyme responsible for the catabolic deactivation of 5-FU (146). These investigators postulate that, at least in part, the enhanced cytotoxicity associated with the simultaneous use of uridine and 5-FU may be explained by decreases in the catabolism of 5-FU and suggests that the simultaneous use of these agents may prove beneficial in achieving clinical responses.
Uridine diphosphoglucose has been investigated as a potential alternative to uridine as a rescue agent for the fluoropyrimidines. Uridine diphosphoglucose was shown to be capable of expanding the intracellular UTP pools in normal tissues, but not tumor tissues, by up to twofold (147). The use of this agent resulted in an increase in the maximum tolerated dose of 5-FU by approximately 50% and this translated into enhanced antitumor activity in murine models. Uridine diphos- phoglucose appears to be as effective as uridine for the modulation of 5-FU and may not be associated with dose limiting diarrhea although uridine diphosphoglucose has not yet been administered in man.
A series of investigations performed in the Netherlands by van Groeningen and colleagues have established the toxicities and maximum tolerated doses of uridine when used intravenously and orally in patients (148-153). These investigators defined 12 g/m2 as the MTD for a single intravenous injection. Transient shivering appeared to be the major dose limiting toxicity associated with this schedule of uridine. While not conclusive, the use of high dose intravenous uridine on 1 or 2 days following 5-FU in two patients did not appear to prevent the myelosuppression and gastrointestinal toxicity associated with 5-FU. The authors concluded that the use of a single, high-dose injection of uridine would not have been expected to alleviate 5-FU associated toxicity given the preclinical data suggesting that a more prolonged exposure to uridine would be required to rescue normal cells from 5-FU toxicity. Given this realization, these authors also investigated constant infusion schedules and intermittent (3 h on, 3 h off), infusions of uridine. Since constant

BIOMODULATION OF 5-FLUOROURACIL 37
infusions were associated with the frequent development of high fevers, the intermittent schedule was preferentially investigated in seven patients. The devel- opment of fever was not a problem using the intermittent infusion schedule; however, phlebitis was a common occurrence for all intravenous schedules neces- sitating inpatient administration of uridine via central venous access device.
These phase I investigations demonstrated that uridine could be safely admin- istered for prolonged periods of time using 3 g/m’/h over 3 h alternating with a 3-h treatment-free interval, and result in peak plasma uridine levels in the millimolar range and trough levels during the treatment-free period between 138 and 670 pM
(pretreatment plasma uridine concentrations = 3-8 PM). The half-life of intrav- enously administered uridine was approximately 2 h. The preclinical data support these levels as adequate to effect rescue from 5-FU. While phlebitis was a persistent problem with the use of intermittent infusions of uridine, fevers were far less common and not dose limiting. In nine patients who were treated with weekly 5-FU, the use of intermittent 3-h infusions of uridine over a 72-h period at a dose of 2 g/m*/h was capable of reversing the myelosuppression but not the throm- bocytopenia associated with 5-FU. Of interest, was the finding that a single 72-h period of intermittent infusions of uridine resulted in protection from 5-FU myelosuppression for up to five additional weekly doses of 5-FU without additional uridine rescue. Using a similar intermittent dosing schedule for uridine rescue, Seiter and colleagues found that use of uridine permitted a 25% dose increase in 5-FU when used in conjunction with PALA and MTX each given 24 h prior to fluorouracil and leucovorin rescue (154). These investigators found a high rate of central venous catheter complications (24%) and grade 3 or 4 gastrointestinal toxicity in approximately 30% of patients treated at the 700 and 750 mg/m’ dose of 5-FU. Myelotoxicity was rare even at the highest doses of fluorouracil tested. While 90% of patients developed grade 2 fevers with the uridine infusions, this was not felt to be dose limiting. Similar to the experience in the Netherlands, the peak plasma uridine levels were found to be approximately 1 mM while the trough levels during the 3-h off period had a median level of approximately 350 ,uM. Since 72% of the 27 patients who were evaluable for response had been previously treated with prior chemotherapy, no definitive statements can be made with regard to the efficacy of the tested regimen; however, no responses were seen in these patients.
Because of the need for central vascular access and complications associated with the use of intravenous uridine, the use of orally administered uridine has been investigated in phase I trials (148, 153). The bioavailability of oral uridine in both mice and man is approximately 7-10%. Using multiple dose administrations every 6 h for 3 days, van Groeningen and colleagues identified 5 mg/m’ as the MTD with diarrhea being dose limiting. The steady-state plasma uridine levels achieved with this dosing scheme at the MTD was approximately 50 pM. Using oral uridine 5 gm/m2 every 6 h for 3 days beginning 3 h after a weekly treatment with 5-FU, these investigators found that oral uridine was able to reverse 5-FU induced myelosuppression but not thrombocytopenia in a manner similar to intermittent intravenous uridine. Identical to that observed after 3 days of intermittent intravenous uridine, the oral schedule also protected against 5-FU associated myelosuppression for up to 3 additional weekly doses of 5-FU. These data suggest that despite the relatively low bioavailability of uridine and the low plasma levels achieved, oral uridine affords similar protection to host tissues compared with intravenous uridine.

38 G. A. SOTOS ET AL
Using oral uridine in conjunction with a PALA modulated 5-FU combination, Kemeny and colleagues reported a marked ability of uridine to alleviate the hematologic and gastrointestinal toxicities associated with the fluorouracil regimen consistent with the studies reported by van Groeningen and colleagues (155). In 25 patients with untreated advanced colorectal carcinoma who were evaluable for response, only a single partial response was observed. A subsequent investigation in patients with advanced gastric carcinoma tested the ability of uridine to permit dose intensification of a regimen utilizing MTX, 5-FU and adriamycin (FAMTX). The authors altered the ‘standard’ FAMTX regimen by increasing the interval between MTX and 5-FU to 24 h and increasing the frequency of administration of MTX and 5-FU to every 2 weeks with adriamycin given every 28 days (156). Uridine was administered orally at a dose of 8 gm/m’ every 6 h for 12 doses and this was begun 12 h following the administration of 5-FU. The authors found little toxicity with this regimen; however, there were also no responses noted in the initial 12 patients treated. Because of this experience, an additional 25 patients were treated with the uridine interval increased to 24 h following the 5-FU dose. While this change resulted in a response rate similar to that previously reported for FAMTX and an ability to give the 5-FU and MTX every 2 weeks, the role of uridine protection in this regimen cannot be discerned. These data, while preliminary, suggest that while uridine can ameliorate 5-FU toxicity, it may also result in ablation of the cytotoxic effects of fluorouracil on the tumor.
Clearly, the use of uridine as a rescue agent for the host toxicities associated with 5-FU is an interesting and apparently clinically achievable goal given the current state of clinical investigations. The oral use of uridine appears to be the simplest route of administration and appears at least as efficacious as intravenously administered uridine. The critical question that awaits additional clinical information is whether uridine will reverse the cytotoxic effects of fluorouracil on tumors as well as host tissue and whether gastrointestinal toxicities associated with the use of LV modulated 5-FU will also be relieved by the use of uridine. Some of the most impressive examples of enhanced selectivity for 5-FU in the preclinical literature are in those investigations using multiple modulations of 5-FU such as uridine with LV or PALA. It will be of great interest to understand the potential role of uridine in regimens utilizing multiple fluorouracil modulations.
Benzylacyclouridine and Benzyloxybenzylacyclouridine
The pyrimidine acyclonucleosides BAU and BBAU were first synthesized by Chu, Niedzwicki, and colleagues and found to be potent and specific inhibitors of the enzyme uridine phosphorylase with inhibition constants for the mammalian enzyme of 0.1-0.2 ,uM and 0.03 ,uM for BAU and BBAU, respectively (157-159). Uridine phosphorylase is responsible for the reversible conversion of pyrimidine ribosides to their respective base forms. Since uridine phosphorylase appeared to be a major route by which neoplastic cells catabolize the fluoropyrimidine ribosides to their less potent base forms, it was hypothesized that the use of uridine phosphorylase inhibitors would selectively inhibit catabolism of fluoropyrimidine ribosides in malignant vs. normal tissues which preserve the ability to degrade these compounds via thymidine phosphorylase. Chu and colleagues were the first investigators to demonstrate that the co-administration of BAU or BBAU was able to potentiate

BIOMODULATION OF 5-FLUOROURACIL 39
the cytotoxic activity of fluorodeoxyuridine in human pancreas (DAN) and lung (LX-l) carcinoma cell lines (160, 161). The more potent inhibitor BBAU was found to be more effective than BAU in its ability to potentiate the activity of fluorodeoxyuridine. BBAU also markedly enhanced the ability of fluorodeoxyuridine to produce tumor shrinkage of the human pancreatic carcinoma cell line in the immunocompromised murine model without enhancing host-toxicity, thus demonstrating a selective ability to modulate the cytotoxic activity of fluo- rodeoxyuridine in tumor versus normal tissues. This observation was further strengthened by a demonstration of the ability of both BAU and BBAU to protect animals against lethal doses of fluorodeoxyuridine with co-administration (162).
Because of its ability to inhibit hepatic uridine phosphorylase, BAU delays plasma disappearance of administered uridine and causes a marked expansion of plasma and tissue uridine even in the absence of exogenously administered uridine (162- 165). In the murine model, BAU results in 5 to IO-fold increase in plasma and tissue levels of uridine. The administration of BAU 1 h prior to the exogenous administration of uridine in mice results in an up to IOO-fold expansion of tissue uridine pools for up to 4 h. The use of both BAU and uridine is capable of selective modulation of fluorouracil cytotoxicity in mice bearing colon tumor 38 transplants by increasing the LD-50 of 5-FU by 50% while enhancing the growth inhibitory effects of fluorouracil on colon tumor 38 transplants. Martin and colleagues demonstrated that the use of BAU allowed for a 50% dose reduction in the amount of oral uridine required for protection from the 5-FU induced toxicity while preserving the antitumor activity of the fluorouracil containing regimen in mice bearing spontaneous mammary carcinomas (165).
The pharmacokinetics of BAU were investigated by Davis and colleagues in several animal models (166). The plasma half-life of BAU was found to be approximately 30 min in the cynomolgus monkey and its oral bioavailability was found to be approximately 60-70% in murine and rodent models (163, 166). While these authors also found that BAU administration led to increases in plasma uridine concentrations in mice and to a lesser extent in rats, BAU had no effect on plasma uridine concentrations in cynomolgus monkeys despite having a similar ability to inhibit the uridine phosphorylase in this species and the achievement of high plasma levels. In the monkey, BAU appeared to undergo extensive metabolism to a glucuronide. These data are important in that they intimate that the murine models used to test the uridine phosphorylase inhibitors may not be an accurate reflection of the ultimate utility of these compounds in man. BAU is currently undergoing phase I testing in man and the ultimate clinical use of this compound will await the outcome of trials demonstrating the ability of BAU to alter plasma uridine levels in man.
Summary
Although single agent 5-FU has for many years been the standard therapy fat advanced colorectal malignancies, a number of recent clinical trials show higher response rates with biomodulation of 5-FU by several different agents. In general, trials of leucovorin, methotrexate, interferon, and PALA given in biomodulatory doses and sequences with 5- FU have demonstrated comparable response rates over

40 G. A. SOTOS ET AL
a broad range. However, in the absence of controlled direct comparative phase III trials, final judgement on clinical superiority of a particular regimen must be reserved. Nevertheless, on the basis of current data, certain approaches appear promising and warrant further investigation. Compared to single agent 5-FU, survival benefit has been demonstrated with both low and high dose leucovorin/5-FU regimens and response rates in the 20-50% range appear reproducibly higher than those of 5-FU alone. Low dose and either continuous infusion or repetitive dosing of leucovorin, as well as the effect of treatment sequence and intervals between drugs, require additional investigation. When given 20-24 h before 5-FU, methotrexate achieves response rates similar to leucovorin modulated 5-FU, but the potential role of rescue leucovorin used in many of the trials makes definitive interpretation difficult. interferon/5-FU regimens attaining response rates of 30-40% are promising but need to be carefully and rationally designed. Low dose PALA with effective doses of 5-FU achieving responses in 35-45% of patients represent a marked improvement in earlier trials of high dose PALA, but additional studies with higher doses not compromising 5-FU dose intensity should be considered.
Certainly, the concomitant use of multiple modulating agents also needs further investigation. While many such trials already performed attained results no better than single agent biomodulation, the preliminary results obtained by Grem and colleagues with IFN/LV/5-FU in untreated patients, and by Conti et al. using TMTX/LV/5-FU in previously treated patients are encouraging. Further under- standing of the mechanisms of action and interaction of modulating agents should allow additional rational combinations to be explored clinically.
Cisplatin biomodulation of 5-FU has been studied in gastrointestinal and head and neck malignancies achieving excellent results in the latter group. Preclinical evidence exists which suggests, however, that 5-FU modulation of cisplatin may be more effective, especially when 5-FU is administered 24 h or more before cisplatin. Clinical investigation of this sequence is currently lacking. Data to support the clinical promise of AZT, IdUrd, uridine, and the benzylacyclouridines are not yet available, although preclinical and preliminary clinical studies are promising.
References
I. Allegra, C. J. (1991) Biochemical modulation: A modality that has come of therapeutic age. J. Clin. Oncol. 9: 1723-l 726.
2. Rustum, Y. M. & Campbell, J. F. (1988) Metabolic modulation of fluorouracil by leucovorin: Biochemical rationale and clinical implications. In: Erlichman, C. (ed) Pharmanual, Leucovorin:An Expanding Role in Chemotherapy, 3-14. Montreal: PharmaLibri.
3. Santi, D. V., McHenry, C. S. & Sommer, H. (1974) Mechanisms of interaction of thymidylate synthetase with 5-fluorouridylate. Biochemistry 13: 471-480.
4. Danenberg, P. V. & Danenberg, K. D. (1978) Effect of 5,10-methylenetetrahydrofolate on the dissociation of 5-fluoro-2’-deoxyuridylate from thymidylate synthetase: Evidence for an ordered mechanism. Biochemistry 17: 4018-4024.
5. Ullman, B., Lee, M., Martin, Jr., D. W. & Santi, D. V. (1978) Cytotoxicity of 5-fluoro-2’. deoxyuridine: Requirement for reduced folate cofactors and antagonism by methotrexate. Proc. Nat1 Acad. Sci. USA 75: 980-983.
6. Evans, R. M., Laskin, J. D., Hakala, M. T. (1981) Effect of excess of folates and deoxyinosine on
the activity and site of actron of 5-fluorouracil. Cancer Res. 41: 3288-3295.

BIOMODULATION OF 5-FLUOROURACIL 41
7. Waxman, S. & Bruckner, H. (1982) The enhancement of 5-fluorouracil antimetabolic activity by leucovorin, menadione and a-Tocopherol. fur. J. Cancer C/in. Oncol. 18: 685-692.
8. Keyomarsi, K. & Moran, R. G. (1986) Folinic acid augmentation of the effects of fluoropyrimidrnes on munne and human leukemic cells. Cancer Res. 46: 5229-5235.
9. Mini, E., Moroson, B. A. & Bertino, J. R. (1987) Cytotoxicity of floxuridine and 5-fluorouracrl in human T-lymphoblast leukemia cells: Enhancement by leucovorin. Cancer Treat. Rep. 71: 381-
389. 10. Park, J. G., Collins, J. M., Gazdar, A. F., Allegra, C. J., Steinberg, S. M., Greene, R. F. & Kramer, B.
S. (1988) Enhancement of fluorinated pyrimidine-induced cytotoxicity by leucovorm in human colorectal carcinoma cell lines. J. Nat/ Cancer inst. 80: 1560-I 564.
11. Moran, R. G. & Scanlon, K. L. (1991) Schedule-dependent enhancement of the cytotoxrcity of
fluoropyrimidrnes to human carcinoma cells in the presence of folinic acid. Cancer Res. 51: 4618-
4623. 12. Houghton, J. A., Maroda, S. J., Phillips, J. 0. & Houghton, P. J. (1981) Biochemical determinants
of responsiveness to 5-fluorouracil and its derivatives in xenografts of human colorectal aden- ocarcrnomas in mice. Cancer Res. 41: 144-l 49.
13. Houghton, J. A. & Houghton, P. J. (1980) On the mechanism of cytotoxicity of fluorinated pyrimidines in four human colon adenocarcinoma xenografts maintained in immune-deprived mice.
Cancer 45: 1159-l 167. 14. Yin, M. B., Zakrzewski, S. F. & Hakala, M. T. (1982) Relationship of cellular folate cofactor pools
to the activity of 5-fluorouracil. Mol. Pharmacol. 23: 190-l 97. 15. Allegra, C. J., Chabner, B. A., Drake, J. C., Lutz, R., Rodbard, D. & Jolivet, J. (1985) Enhanced
inhibition of thymidylate synthase by methotrexate polyglutamates. J. Biol. Chem. 260: 9720-
9726.
16. Radparvar, S., Houghton, P. J. & Houghton, J. A. (1989) Effect of polyglutamylation of 5,10-
methylenetetrahydrofolate on the binding of 5-fluoro-2’.deoxyuridylate to thymidylate synthase purified from a human colon adenocarcinoma xenograft. Biochem. Pharmacol. 38: 335-342.
17. Boarman, D. M. & Allegra, C. J. (1992) Intracellular metabolrsm of 5-formyl tetrahydrofolate rn human breast and colon cell lines. Cancer Res. 52: 36-44.
18. Houghton, J. A., Williams, L. G., Cheshire, P. J. Wainer, I. W., Jadaud, P. & Houghton, P. J. (1990) Influence of dose of [6 RS] leucovorin in reduced folate pools and 5-fluorouracil-mediated thymrdylate synthase inhibition in human colon adenocarcinoma xenografts. Cancer Res. 50: 3940-
3946.
19. Houghton, J. A., Williams, L. G., de Graaf, S. S. N. Cheshire, P. J., Rdoman, J. H., Maneval, D. C., Wainer, I. W., Jadaud, P. & Houghton, P. J. (1990) Relationship between dose rate of
[6RS] leucovorin administration, plasma concentrations of reduced folates, and pools of 5,10-
methylenetetrahydrofolates and tetrahydrofolates in human colon adenocarcinoma xenografts. Cancer Res. 50: 3493-3502.
20. Romanini, A., Lin, J. T., Niedzwiecki, D. Bunni, M., Priest, D. G. & Bertino, J. R. (1991) Role of
folypolyglutamates m biochemical modulation of fluoropyrimidines by leucovorin. Cancer Res. 51: 789-793.
21. Swain, S. M., Lippman, M. E., Egan, E. F., Drake, J. C., Steinberg, S. M. & Allegra, C. J. (1989) 5-
fluorouracil and high-dose leucovorin In previously treated patients with metastatic breast cancer. J. Clin. Oncol. 7: 890-899.
22. Rustum, Y., M., Madajewicz, S., Campbell, J., Zakrzewskr, S. F., Petrelli, N., Herrera, L. O.,
Mittelman, A. R. & Creaven, P. J. (1984) The current status of 5-fluorouracil-leucovorin calcium combination, 77-82. New York, Projects in Medicine, Division of Park Row Publishers, Inc.
23. Bertrand, R. & Jolivet, J. (1989) Lack of interference by the unnatural isomer of 5-for-
myltetrahydrofolate with the effects of the natural isomer in leucovorin preparations. J. Nat/ Cancer Inst. 81: 1175-I 178.
24. Machover, D., Grison, X., Goldschmidt, E., Zittoun, J., Lotz, J. P., Metzger, G., Hannoun, L., Guillot,
T., Salmon, R., Mauban, S., Part, R. & Izrael, V. (1992) 5-fluorouracil (5-FU) combined with the [6S] stereoisomer of folinic acid ([6S]- FA) in high doses for treatment of patients with advanced
colorectal carcinoma (CRC). International Symposium on Novel Approachesto SelectiveTreatments of Human Solid Tumors: Laboratory and Clinical Correlation, Roswell Park Cancer Institute, New
York, 33, September 9-12. 25. Erlichman, C., Fine, S., Kerr, I., Hoffman, W. & Gorg, C. (1992) A phase II trial of 5-fluorouracil

42 G. A. SOTOS ET AL
and L-leucovorin-a multicentre experience. international Symposium on Novel Approaches to
Selective Treatments of Human Solid Tumors: Laboratory and Clinical Correlation, Roswell Park Cancer Institute, 30-32, New York, September 9-l 2.
26. Piedbois, P., Buyse, M., Rustum, Y., Machover, D., Erlichman, C., Carlson, Ft. W., Valone, F., Labianca, R., Doroshow, J. H. & Petrelli, N. (1992) Modulation of fluorouracil by leucovorin in
patients with advanced colorectal cancer: Evidence in terms of response rate. J. C/in. Oncol. 10: 896-903.
27. Petrelli, N., Douglass, H. O., Herrera, L., Russell, D., Stablein, D. M., Bruckner, H. W., Mayer, R. J.,
Schinella, R.. Green, M. D., Muggia, F. M., Megibow, A., Greenwald, E. S., Bukowski, R. M., Harris, J., Levin, B., Gaynor, E., Loutfi, A., Kalser, M. H., Barkin, J. S., Benedetto, P., Woolley, P. V., Nauta, R., Weaver, D. W. & Leichman, L. P. (1989) The modulation of fluorouracil with
leucovorin in metastatic colorectal carcinoma: A prospective randomized phase III trial. J. C/in. Oncol. 7: 1419-I 426.
28. Poon, M. A., O’Connell, M. J., Moertel, C. G., Wieand, H. S., Cullinan. S. A., Everson, L. K., Krook,
J. E., Mailliard, J. A., Laurie, J. A., Tschetter, L. K. & Wiesenfeld, M. (1989) Biochemical modulation of fluorouracil: Evidence of significant improvement of survival and quality of life in patients with advanced colorectal carcinoma. J. C/in. Oncol. 7: 1407-I 417.
29. Poon, M. A., O’Connell, M. J., Wieand, H. S. Krook, J. E., Gerstner, J. B., Tschetter, L. K., Levitt,
R., Kardinal, C. G. & Mailliard, J. A. (1991) Biochemical modulation of fluorouracil with leucovorin: Confirmatory evidence of improved therapeutic efficacy in advanced colorectal cancer. J. C/in. Oncol. 9: 1967-l 972.
30. Erlichman, C., Fine, S., Wong, A. & Elhakim. T. (1988) A randomized trial of fluorouracil and folinic
acid in patients with metastatic colorectal carcinoma. ./. C/in. Oncol. 6: 469-475. 31. Petrelli, N., Herrara, L., Rustum, Y., Burke, P., Creaven, P., Stulc, J., Emrich, L. J. 81 Mittelman, A.
(1987) A prospective randomized trial of 5-fluorouracil versus 5.fluorouracil and high-dose leucovorin versus 5-fluorouracil and methotrexate in previously untreated patients with advanced colorectal carcinoma. J. C/in. Oncol. 5: 1559-l 565.
32. Nobile, M. T., Rossa, R., Sertoli, M. R., Rubagotti, A., Vidili, M. G., Guglielmi, A., Venturini. M., Canobbio, L., Fassio, T., Gallo, L., Galligioni, E., Gallotti, P., Bruzzi, P. & Sobrero, A. (1992) Randomized comparison of weekly bolus 5-fluorouracil with or without leucovorin in metastatic
colorectal carcinoma. Eur. J. Cancer 28A: 1823-l 827. 33. Doroshow, J. H., Multhauf, P., Leong, L., Margolin, K., Litchfield, T., Akman, S., Carr, B., Mertrand,
M., Goldberg, D., Blayney, D., Odujinrin, 0.. DeLap, R., Shuster, J. & Newman, E. (1990) Prospective randomized comparison of fluorouracil versus fluorouracil and high-dose continuous infusion leucovorin calcium for the treatment of advanced measurable colorectal cancer in patients previously unexposed to chemotherapy. .I. C/in. Oncol. 8: 491-501.
34. Di Costanzo, F., Bartolucci, R., Calabresi, F., Sofra, M., Marzola, M., Belsanti, V., Boni, C. & Bacchi, M. (1992) Fluorouracil-alone versus high-dose folinic acid and fluorouracil in advanced colorectal cancer: A randomized trial of the Italian Oncology Group for Clinical Research (GOIRC). Ann. Oncol. 3: 371-376.
35. Valone, F. H., Friedman, M. A., Wittlinger, P. S. Drakes, T., Eisenberg, P. D., Malec, M., Hannigan,
J. F. & Brown, Jr, B. W. (1989) Treatment of patients with advanced colorectal carcinomas with fluorouracil alone, high-dose leucovorin plus fluorouracil, or sequential methotrexate, fluorouracrl, and leucovorin: A randomized trial of the Northern California Oncology Group. J. C/in. Oncol. 7: 1427-I 436.
36. Labianca, R., Pancera, G., Aitini, E., Barni, S., Beretta, A., Beretta, G. D., Cesana, B., Comella, G., Cozzaglio, L., Cristoni, M., Spagnolli, P., Frontini, L., Gottardi, O., Martignoni, G., Scapaticci, R.,
Smerieri, F., Vinci, M., Zadro, A., Zaniboni, A. & Luporini G. (1991) Folinic acid+5-fluorouracil (5.FU) versus equidose 5-FU in advanced colorectal cancer. Phase III study of ‘GISCAD’ (Italian Group for the Study of Digestive Tract Cancer). Ann. Oncol. 2: 673-379.
37. Wadler, S. & Schwartz, E. L. (1990) Antineoplastic activity of the combination of interferon and
cytotoxic agents against experimental and human malignancies: A review. Cancer Res. 50: 3473- 3486.
38. Elias, L. & Crissman, H. A. (1988) Interferon effects upon the adenocarcinoma 38 and HL-60 cell lines: Antiproliferative responses and synergistic interactions with halogenated pyrimrdine antimetabolites. Cancer Res. 48: 4868-4873.
39. Elias, I. & Sandoval, J. M. (1989) Interferon effects upon fluorouracil metabolism by HL-60 cells. Biochem. Biophys. Res. Commun 163: 867-874.

BIOMODULATION OF 5-FLUOROURACIL 43
40. Chu, E., Zinn, S., Boarman, D. & Allegra, C. J. (1990) interaction of 7 interferon and 5-fluorouracil in the H630 human colon carcinoma cell line. Cancer Res. 50: 5834-5840.
41. Wadler, S., Wersto, R., Weinberg, V., Thompson, D. & Schwartz, E. L. (1990) Interactron of
fluorouracil and interferon in human colon cancer cell lines: cytotoxic and cytokinetic effects. Cancer Res. 50: 5735-5739.
42. Stolfi, R. L., Martin, D. S., Sawyer, R. C. & Spiegelman, S. (1983) Modulation of 5-fluorouracrl- induced toxicity in mice with Interferon or with the Interferon inducer, polyrnosinic-polycytidylic acid. Cancer Res. 43: 561-566.
43. Ligo, M., Chapekar, M. S. & Glazer, R. I. (1985) Synergistic antitumor effect of fluoropyrimidrnes
and polyinosinrc-polycytidylic acid against L1210 leukemia. Cancer Res. 45: 4039-4042. 44. Schwartz, E. L., Hoffman, M., O’Connor, C. J. & Wadler, S. (1992) Stimulation of 5-fluorouracil
metabolic activation by interferon- 2 in human colon carcinoma cells. Biochem. Biophys. Res.
Commun. 182: 1232-l 239. 45. Grem, J. L., Chu, E., Boarman, D., Balis, F. M., Murphy, R. F., McAtee, N. & Allegra, C. J. (1992)
Biochemical modulation of fluorouracil with leucovorin and interferon: Preclinical and clinical
investigations. Semi. Oncol. 19: 36-44. 46. Grem, J. L., McAtee, N., Murphy, R. F., Balls, F. M., Steinberg, S. M., Hamilton, J. M., Sorensen,
J. M., Sartor, 0.. Kramer, B. S., Goldstern, L. J., Gay, L. M., Caubo, K. M., Goldspiel, B. & Allegra, C. J. (1991) A pilot study of Interferon alfa-2a in combination with fluorouracil plus high-dose
leucovorin in metastatic gastrointestinal carcinoma. J. C/in. Oncol. 9: 181 l-l 820. 47. Yee, L. K., Allegra, C. J., Steinberg, S. M. & Grem, J. L. (1992) Decreased catabolism of fluorouracil
rn peripheral blood mononuclear cells during combination therapy with fluorouracil, leucovorin,
and interferon r-2a. J. Natl Cancer Inst. 84: 1820-I 825. 48. Grem, J., Jordan, E., Robson, M., Binder, R., Yee, L., Hamilton, J. M., Arbuck, S., Steinberg, S.,
McAtee, N. & Allegra C. (1993) A Phase II study of interferon x-2a (IFN X) in combination with
5-fluorouracil (5.FU) and leucovorin (LCV) in advanced colorectal cancer. Proc. ASCO 12: 600. 49. Danhauser, L. L., Freimann. Jr., J. H., Gilchrist, T. L., Gutterman, J. U., Hunter, C. Y., Yeomans, A.
C. & Markowitz, A. B. (1993) Phase I and plasma pharmacokrnetic study of infusional fluorouracil combined with recombinant interferon alfa-2b in patients with advanced cancer. J. C/in. Oncol.
11: 751-761.
50. Schuller, J., Czejka, M., Miksche M., Fogl, U. & Schernthaner, G. (1991) Influence of interferon x 2b (IFN) & leucovorin (LV) on pharmacokinetics (PK) of 5-fluorouracil. froc. ASCO 10: 263.
51. Wadler, S. & Wiernik P. H. (1990) Clinical update on the role of fluorouracil and recombinant Interferon alfa-2a in the treatment of colorectal carcinoma. Semin Oncol. 17: 16-21.
52. Kemeny, N. & Younes, A. (1992) Alfa-2A interferon and 5-fluorouracil for advanced colorectal carcinoma: The Memorial Sloan- Kettering experience. Semin. Oncol. 19: 171-I 75.
53. Pazdur, R., Moore, Jr., D. F. & Bready, B. (1992) Modulation of fluorouracil with recombinant alfa Interferon: M. D. Anderson clinical trial. Semin. Oncol 19: 176-I 79.
54. Weh, H. J., Platz, D., Braumann. D., Guggisch, P., Schmiegel, W. H., Drescher, S., Kleeberg, U. R.,
Mullerleile, U., Crone-Munzebrock, W., Hoffmann, R., Muller, P., Klapdor, R.. Pompecki, R., Erdmann, H., Reichel, L., Hoffmann, L., Mainzer, K. & Hossfeld, D. K. (1992) Treatment of metastatic
colorectal carcinoma wrth a combinatron of fluorouracil and recombinant interferon alfa-2b:
Preliminary data of a phase II study. Semin. Oncol. 19: 180-I 84. 55. Wadler, S., Fell, S., Haynes, H., Katz, H. J., Rozenblit, A., Kaleya, R. & Wiernik, P. H. (1993)
Treatment of carcinoma of the esophagus with 5-fluorouracil and recombinant alfa-2a-interferon. Cancer 71: 1726-l 730.
56. York, M., Greco. F. A., Figltn, R. A. & Einhorn, L. (1993) A randomized phase III trial comparing
5-FU wrth or without interferon alfa 2a for advanced colorectal cancer. Proc. ASCO 12: 590.
57. Kocha, W. (1993) 5-Fluorouracrl (5-FU) plus interferon alfa-2a (Roferon-A) versus 5-fluorouracil plus leucovorin (LV) in metastatrc colorectal cancer-results of a multicentre, multinational phase III study. Proc. ASCO 12: 562.
58. Houghton, J. A., Adkins, D. A., Rahman, A. & Houghton, P. J. (1991) Interaction between 5-fluorouracil, [6RS] leucovorin, and recombinant human interferon- 22a in cultured colon
adenocarcinoma cells. Cancer Common. 3: 225-231. 59. Preiss, J. (1992) Fluorouracil plus interferon + folinic acid in regional and systemic therapy in
colorectal cancer. Semin. Oncol. 19: 220-224.
60. Kreuser, E-D., Hilgenfeld, R. U., Matthias, M., Hoksch, B., Boewer, C., Oldenkott, B., Knauf, W.

44 G. A. SOTOS ET AL
U., B-L., J., Schalhorn, A., Zeitz, M. & Thiel, E. (1992) A phase I trial of interferon x-2b with folinrc acid and 5-fluorouracil administered by 4-hour infusion in metastatic colorectal carcinoma. Semin. Oncol. 19: 197-203.
61. Bernhard, H., Klein, O., zum Buschenfelde, K-H. & Knuth, A. (1992) Treatment of refractory colorectal carcinomas with fluorouracil, folinic acid, and interferon alfa-2a. Semin. Oncol. 19: 204- 207.
62. Punt, C. J. A., de Mulder, P. H. M., Burghouts, J. Th. M. & Wagener, D. J. Th. (1992) Fluorouracil continuous infusion plus alfa interferon plus oral folinic acid in advanced colorectal cancer. Semin.
Oncol. 19: 208-210.
63. Madafewicz, S. & Avvento, L. (1990) Clinical trials with 5.fluorouracil, folinic acid and cisplatin in patients with gastrointestinal malignancies, J. Chemother. 2: 33-37.
64. Schabel, Jr., F. M., Trader, M. W., Laster, Jr., W. Ft., Corbett, T. H. & Griswold, Jr., D. P. (1979) cis-Dichlorodiammineplatinum (II): Combination chemotherapy and cross-resistance studies with tumors in mice. Cancer Treat. Rep. 63: 1459-l 473.
65. Scanlon, K. J., Newman, E. M. & Priest, D. G. (1986) Biochemical basis for cisplatin and 5- fluorouracil synergrsm in human ovarian carcinoma cells. Proc. /Vat/. Acad. Sci. USA 83: 8923- 8925.
66. Johnston, P. & Allegra, C. (1990) The interaction of 5-fluorouracil and cisplatin in human colon carcinoma cells. Proc. AACR 31: 2497.
67. Esaki, T., Kanano, S., Tatsumoto, T., Kuroki-Migita, M., Mrtsugi, K., Nakamura, M. & Niho, Y. (1992) Inhibition by 5-fluorouracil of cis diamminedichloroplatinum(ll)-induced DNA interstrand
cross-link removal in a HST-1 human squamous carcinoma cell line, Cancer Res. 52: 6501-6506. 68. Kuroki, M., Kanano, S., Mitsugi, K., Ichinose, I., Anzai, K., Nakamura, M., Nagafuchi, S. & Niho, Y.
(1992) In vivo comparative therapeutic study of optimal administration of 5-fluorouracil and cisplatin using a newly established HST-1 human squamous-carcinoma cell line. CancerChemother.
Pharmacol. 29: 273-276. 69. Pratesi, G., Gianni, L., Manzotti, C. & Zunino, F. (1988) Sequence dependence of the antitumor
and toxic effects of 5-fluorouracil and cis-diamminedichloroplatinum combination on primary colon tumors in mice. Cancer Chemother. Pharmacol. 21: 237-240.
70. Kemeny, N., Israel, K., Niedzwiecki, D., Chapman, D., Botet, J., Minsky, B., Vinciguerra, V.,
Rosenbluth, R., Bosselli, B., Cochran, C. & Sheehan, K. (1990) Randomized study of continuous infusion fluorouracil versus fluorouracil plus cisplatin in patients with metastatic colorectal cancer. J. Clin. Oncol. 8: 313-318.
71. Kish, J. A., Weaver, A., Jacobs, J., Cummings, G. & Al-Sarraf, M. (1984) Cisplatin and 5-
fluorouracil infusion in patients with recurrent and disseminated epidermoid cancer of the head and neck. Cancer 53: 1819-I 824.
72. Forastiere, A. A., Metch, B., Schuller, D. E., Ensley, J. F., Hutchins, L. F., Triozzi, P., Kish, J. A.,
McClure, S., VonFeldt, E., Williamson, S. K. & Von Hoff, D. D. (1992) Randomized comparison of cisplatin plus fluorouracil and carboplatin plus fluorouracil versus methotrexate in advanced
squamous-cell carcinoma of the head and neck: A Southwest Oncology Group Study. ./. C/in. Oncol. 10: 1245-l 251.
73. Jacobs, C., Lyman, G., Velez-Garcia, E., Sridhar, K., Knrght, W., Hochster, H., Goodnough, L. T.,
Mortimer, J. E., Einhorn, L. H., Schacter, L., Cherng, N., Dalton, T., Burroughs, J. & Rozencweig, M. (1992) A phase III randomized study comparing cisplatin and fluorouracil as single agents and In combination for advanced squamous cell carcinoma of the head and neck. J. C/in. Oncol. 10: 257-263.
74. Merlano, M., Vitale, V., Rosso. R., Benasso, M., Corvo, R., Cavallari, M., Sangurneti, G., Bacigalupo, A., Badellmo, F., Margarino, G., Brema, F., Pastorino, G., Marziano, C., Grimaldi, A., Scasso, F., Sperati, G., Pallestrini, E., Garaventa, G., Accomando, E., Cordone, G., Comella, G., Daponte, A., Rubagotti, A., Bruzzi, P. & Santi, L. (1992) Treatment of advanced squamous-cell carcinoma of
the head and neck with alternating chemotherapy and radiotherapy. N. Engl. J. Med. 327: 1 115- 1121.
75. Palmeri, S., Gebbia, V., Russo, A., Gebbia, N., Rustum, Y. & Rausa, L. (1992) Cisplatinum in combination with 5-fluorouracil and citrovorum factor in the treatment of advanced colorectal carcinoma. Cancer Invest. 19(6): 497-504.
76. Carey, R. W., Hilgenberg, A. D., Wilkins, Jr, E. W., Choi, N. C., Mathisen, D. J., Grillo, H. C., Wain, J. C., Logan, D. L. & Bromberg, C. (1993) Long-term follow-up of neoadjuvant chemotherapy with 5-fluorouracil and cisplatin with surgical resection and possible postoperative radiotherapy

BIOMODULATION OF 5-FLUOROURACIL 45
and/or chemotherapy In squamous cell carcinoma of the esophagus. Cancer Invest. ll(2): 99- 105
77. PDQ. Physicians Data Query, National Cancer Institute, May 1993. 78. Tosi, P., Calabresi, D., Goulette, F. A., Renaud, C. A., & Darnowski, J. W. (1992) Azrdothymidine-
induced cytotoxicity and incorporation into DNA in the human colon tumor cell line HCT-8 is enhanced by methotrexate in vitro and in vivo.
79. Brunette, I., Falcone, A., Calabresi, P., Goulette, F. A. & Darnowski, J. W. (1990) 5-Fluorouracil
enhances azidothymidine cytotoxicity: In vitro, in VIVO, and biochemical studies. Cancer Res. 50: 4026-4031.
80. Weber, G., Nagai, M., Prajda, N., Nakamura, H., Szekeres, T. & Olah, E. (1991) AZT: A biochemical response modifier of methotrexate and 5-fluorouracil cytotoxicity rn human ovarian and pancreatic carcinoma cells. Cancer Comm. 3 (4): 127-l 32.
81. Weber, G., Ichikawa, S., Nagai, M. & Natsumeda, Y. (1990) Azidothymidtne inhibition of thymidine krnase and synergistic cytotoxicrty with methotrexate and 5-fluorouracil in rat hematoma and
human colon cancer cells. Cancer Comm. 2 (4): 129-l 33.
82. Zhen, Y.-S., Taniki, T. & Weber, G. (1992) Azidothymidine and dipyridamole as biochemical response modifiers: Synergism with methotrexate and 5-fluorouracil in human colon and pancreatic
carcinoma cells. Oncol. Res. 4 (2): 73-78. 83. Posner, M. R., Darnowski, J. W., Calabresi, P., Brunetti, I,, Corvese, D., Curt, G., Cummings, F. J.,
Clark, J., Browne, M. J., Beitz, J. & Weitberg, A. B. (1990) Oral zidovudine, continuous-infusion fluorouracrl, and oral leucovorin calcium: A phase I study. J. Nat/ Cancer Inst. 82: 171 O-1 714.
84. Posner, M. R., Darnowski, J. W., Weitberg, A. B., Dudley, M. N., Corvese, D., Cummings, F. J.,
Clark, J., Murray, C., Clendennin, Bigley, J. & Calabresi, P. (1992) High-dose intravenous
zidovudine with 5-fluorouracil and leucovorin. Cancer 70: 2929-2934.
85. Greene, R. F. & Collins, J. M. (1990) Effects of leucovorin on idoxuridine cytotoxicity and DNA incorporation. Cancer Res. 50: 6652-6656.
86. Lawrence, T. S., Davis, M. A., McKeever, P. E., Maybaum, J., Stetson, P. L., Normolle, D. P. &
Ensminger, W. D. (1991) Fluorodeoxyuridine-mediated modulation of iododeoxyuridine incor- poration and radiosensitization in human colon cancer cells in vitro and in VIVO. Cancer Res. 5:
3900-3905.
87. Stetson, P. L., Normolle, D. P., Knol, J. A., Johnson, N. J., Yang, Z., Sakmar, E., Prieskorn, D., Terrio, P., Knutsen, C. A. & Ensminger, W. D. (1991) Biochemical modulation of 5-bromo-2’-
deoxyuridine and 5-iodo-2’.deoxyuridine incorporatron into DNA in VX2 tumor-bearing rabbits. J. Nat1 Cancer Inst. 83 (22): 1659-l 667.
88. Maybaum, J., Burton, E. C.. Shelton, D. A., Jing, H. -W., Dusenbury. C. E., Ensminger, W. D. &
Stetson, P. L. (1991) Divergent patterns of rncorporation of bromodeoxyuridine and iodo- deoxyuridine in human colorectal tumor cell lines. Biochem. Pharmacol. 42: 131-I 37.
89. Lawrence, T. S., Davis, M. A., Maybaum, J., Stetson, P. L. & Ensminger, W. D. (1992) Modulation
of iododeoxyuridine-mediated radiosensitization by 5.fluorouracil in human colon cancer cells. lnt. J. Radiat. Oncol. Biol. Phys. 2 (3): 449-503.
90. Lawrence, T. S., Davis, M. A., Maybaum, J., Mukhopadhyay, S. K., Stetson, P. L., Normolle, D. P.,
McKeever, P. E. & Ensmrnger W. D. (1992) The potential superiority of bromodeoxyuridine to
rododeoxyuridine as a radiation sensitizer in the treatment of colorectal cancer. Cancer Res. 52: 3698-3704.
91. Kinsella, T. J., Dobson, P. 0.. Mrtchell. J. B. & Fornace, A. J. (1987) Enhancement of X ray induced
DNA damage by pre-treatment with halogenated pyrimidine analogs, lnt. J. Radiat. Oncol. B/o/.
Phys. 13 (5): 733-739. 92. Hall, E. J. (1988) Radiobiology for the Radiologist, 3rd edrtron. Philadelphia: J. B. Lrppincott.
93. Benson, A. B., Trump, D. L., Cummings, K. B. & Fischer, P. H. (1985) Modulation of 5-IODO-2’. deoxyuridine metabolism and cytotoxicity in human bladder cancer cells by fluoropyrimidines. Biochem. Pharmacol. 34 (21): 3925-3931.
94. Bagshawe, K. D., Sharma, S. K., Southall, P. J. Boden, J. A., Boxer, G. M., Patridge, T. A., Antoniw, P. & Pedley, R. B. (1991 ) Selective uptake of toxic nucleoside (125 IUdr) by resistant cancer. Br. J.
Radioi. 64: 37-44. 95. Belanger, K., Klecker, R. W., Rowland, J., Kinsella, T. J. & Collins, J. M. (1986) Incorporation of
iododeoxyuridine into DNA of granulocytes In patients. Cancer Res. 46: 6509-6512.
96. Speth, P. A. J., Kinsella, T. J., Chang, A. E., Klecker, R. W., Belanger, K. & Collins, J. M. (1988)

46 G. A. SOTOS ETAL
Selective incorporation of iododeoxyundine into DNA of hepatic metastases versus normal human liver. Clin. Pharmacol. Ther. 44: 369-375.
97. Speth, P. A., Kinsella, T. J., Chang, A. E., Klecker, R. W., Belanger, K., Smith, R., Rowland, J.,
Cupp, J. E. & Collins, J. M. (1989) lododeoxyuridine (IDURD) incorporation into DNA of human hematopoietic cells, normal liver and hepatic metastases in man: As a radiosensitizer and as a
marker for cell kinetic studies, lnt. J. Radiat. Oncol. Biol. Phys. 16 (5): 1247-l 250. 98. Chang, A. E., Collins, J. M., Speth, P. A. J., Smith, R., Rowland, J. B., Walton, L., Begley, M. G.,
Glatstein, E., Kinsella, T. J. (1989) A phase I study of intraarterial iododeoxyuridine in patients with colorectal liver metastases. ./. C/in. Oncol. 7: 662-668.
99. Cook, J. A., Glass, J., Lebovics, R., Bobo, H., Pass, H., DeLaney, T. F., Oldfreld, E. H., Mitchell, J. B., Glatstem, E. & Goffman, T. E. (1992) Measurement of thymidine replacement in patients with
high grade gliomas, head and neck tumors, and high grade sarcomas after continuous intravenous
infusions of 5-iododeoxyuridine. Cancer Res. 52: 719-725. 100. Remick, S. C., Benson, A. B., Weese, J. L., Willson, J. K. V., Ramirez, G., Wirtanen, G. W., Alberti,
D. B., Nieting, L. M., Tutsch, K. D., Fischer, P. H. & Trump, D. L. (1989) Phase I trial of hepatic artery infusion of 5-iodo-2’.deoxyuridine and 5-fluorouracil in patients with advanced hepatic
malignancy: Biochemically based combination chemotherapy. Cancer Res. 49: 6437-6442. 101. Brenner, D. E., Knutsen, C., Deremer, S., Terrio, P., Vaerten, M., Stetson, P., Smith, D. E. & Ensminger,
W. D. (1992) 5-Fluorouracil (5.FU) pharmacokinetic interactions with iododeoxyuridine (IURD) and bromodeoxyuridine (BURD). Proc. AACR 33: A3256.
102. Speth, P. A. J., Kinsella, T. J., Belanger. K., Klecker, R. W., Smith, R., Rowland, J. B. & Collins, J.
M. (1988) Fluorodeoxyuridine modulation of the incorporation of iododeoxyuridine into DNA of
granulocytes: A phase I and clinical pharmacological study. Cancer Res. 48: 2933-2937. 103. Benson, A., Locker, G., McDunn, S., Sheehan, T., Kram, J., Strond, W., Prachand, S., Carro, G.,
Gordon, L. & Knop, R. (1991 ) Phase I study and pharmacokinetics of continuous-infusion 5-
fluorouracil (5FU) and 5-IODU-2’-deoxyuridine (IDURD) Proc. ASCO 10: A349. 104. Delap, R., Marshall, J., Woolley, P., Richmond, E., Bodurian & King, D. (1993) Leucovorin,
fluorouracil, and iododeoxyuridine (LIF): A phase I study in patients with advanced cancer. Proc. ASCO 12: 676.
105. Bertino, J. R. (1993) Ode to methotrexate. J. C/in. Oncol. 11: 5-I 4. 106. Allegra, C. J., Drake, J. C., Jolivet, J., Chabner, B. A. (1985) Inhibitron of pho-
sphoribosylamrnoimidazolecarboxamide transformylase by methotrexate and dihydrofolic acid
polyglutamates. Proc. NatlAcad. Sci. USA 82: 4881-4885.
107. Damon, L. E., Cadman, E. & Benz, C. (1989) Enhancement of 5.fluorouracil antitumor effects by the prior administration of methotrexate. Pharmac. Ther. 43: 155-I 85.
108. Bertino, J. R., Sawicki, W. L., Lindquist, C. A. & Gupta, V. S. (1977) Schedule-dependent antitumor
effects of methotrexate and 5-fluorouracil. Cancer Res. 37: 327-328.
109. Mini, E. & Bertino, J. Ft. (1982) Time and dose relationships for methotrexate (MTX), fluorouracil (FUra) and combinations of these drugs for maximum cell kill in human CCRF-CEM cells. Proc.
AACR 23: 712. 110. Doroshow, J. H. & Newman, E. M. (1991 ) Fluoropyrimidine brochemical modulation in colon
cancer: Pharmacology relevant in both the laboratory and the clinic. J. C/in. Oncol 9: 365-367.
111. Bertino, J. R., Mini, E. & Fernandes, D. J. (1983) Sequential methotrexate and 5-fluorouracil: Mechanisms of synergy. Semin. Oncol. 10: 2-5.
112. Cadman, E., Heimer, R. & Davrs L. (1979) Enhanced 5-fluorouracil nucleotide formation after
methotrexate administration: explanation for drug synergism. Science 205: 1135-l 137. 113. Kemeny, N. E., Ahmed, T., Michaelson, R. A., Harper, H. D. &Yip, L. C. (1984) Activity of sequential
low-dose methotrexate and fluorouracil in advanced colorectal carcinoma: Attempt at correlation with tissue and blood levels of phosphoribosylpyrophosphate. J. C/in. Oncol 2: 31 I-31 5.
114. Benz, C., Schoenberg, M., Choti, M. & Cadman, E. (1980) Schedule-dependent cytotoxicity of methotrexate and 5-fluorouracrl in human colon and breast tumor cell lines. J. C/in. Invest. 66:
1162-l 165.
115. Marsh, J. C., Bertino, J. R., Katz, K. H., Davis, C. A., Durivage, H. J., Rome, L. S., Richards, F., Capizzi, R. L., Farber, L. R., Pasquale, D. N., Stuart, R., Koletsky, A. J., Makuch, R. & O’Hollaren, K. (1981) The influence of drug interval on the effect of methotrexate and fluorouracil in the treatment of advanced colorectal cancer. J. C/in. Oncol. 9: 371-380.
116. Kohne-Wompner, C-H., Schmoll, H-J, Harstrick, A. & Rustum, Y. M. (1992) Chemotherapeutic

BIOMODULATION OF 5-FLUOROURACIL 47
strategies In metastatic colorectal cancer: An overview of current clrnical trials. Semin. Oncol. 19:
105-I 25. 117. Nordic Gastrointestinal Tumor Adjuvant Therapy Group (1989) Superiority of sequential metho-
trexate, fluorouracil, and leucovorin to fluorouracil alone m advanced symptomatic colorectal carcinoma: A randomized trial. J. C/in. Oncol. 7: 1437-l 446.
118. Romanini, A., Li, W. W., Coloftore, J. R. & Bertino, J. R. (1992) Leucovorin enhances cytotoxicrty of trimetrexate/fluorouracil, but not methotrexate/fluorouracil, in CCRF-CEM cells. J. Nat/ Cancer
Inst. 84: 1033-l 038. 119. Conti, J. A., Kemeny, N., Goker, E., Tong, W., Colofiore, J., Andre, M., Ragusa, K., Bertino, J. R.
(1993) A phase I trial of sequential trimetrexate, fluorouracil and high-dose leucovorin in previously treated patients with gastrointestinal carcinoma. froc. ASCO: 12: 567.
120. Grem, J. L., King, S. A., O’Dwyer, P. J. & Leyland-Jones, B. (1988) Biochemistry and clinical
activity of N-( Phosphonacetyl))L-aspartate: A review. Cancer Rex 48: 4441-4454.
121. Martin, D. S. & Kemeny, N. E. (1992) Modulation of fluorouracil by N-(Phosphonacetyl)-L- asparate: A review. Semin. Oncol. 19: 49-55.
122. Ardalan, B., Glazer, R. I., Kensler, T. W., Jayaram, H. N., Pham, T. V., MacDonald, J. S. & Cooney,
D.A. (1981 ) Synergistic effect of 5-fluorouracil and N-(phosphonacetyl)-L-asparate on cell growth and ribonucleic acid synthesis in human mammary carcinoma. Biochem. Pharmacol. 30: 2045-
2049.
123. Major, P. P., Egan, E. M., Sargent, L. & Kufe, D. W. (1982) Modulation of 5-FU metabolism in human MCF-7 breast carcinoma cells. Cancer Chemother. Pharmacol. 8: 87-91.
124. Liang, C-M., Donehower, R. C. & Chabner, B. A. (1981) Biochemical interactions between N-
(Phosphonacetyl)-L-aspartate and 5-fluorouracil. Mol. Parmacol. 21: 224-230. 125. Anukarahanonta, T., Holstege, A. & Keppler, D. 0. R. (1980) Selective enhancement of 5-
fluorouridine uptake and action in rat hepatomas in vivo following pretreatment with D-galac-
tosamine and 6-azauridine or N-(phosphonacetyl))L-aspartate. Eur. J. Cancer 16: 1171~1180.
126. Martin, D. S., Stolfi, R. L., Sawyer, R. C., Spiegelman, S., Casper, E. S. & Young, C. W. (1983) Therapeutrc utility of utilizing low doses of N-(Phosphonacetyl))L-aspartic acid in combination
with 5-fluorouracil: A murine study with clinical relevance. Cancer Res. 43: 2317-2321. 127. Martin, D. S. & Kemeny, N. E. (1992) Overview of N-(Phosphonacetyl)-L-asparate + fluorouracil
in clinical trials. Semin. Oncol 19: 228-233.
128. Casper, E. S., Vale, K., Williams, L. J., Martrn, D. S. & Young, C. W. (1983) Phase I and clrnical
pharmacological evaluation of biochemrcal modulation of 5-fluorouracil with N-(Phosphonacetyl)- L-aspartic acid. Cancer Res. 43: 2324-2329.
129. Ardalan, B., Singh, G. & Silberman, H. (1988) A randomized phase I and II study of short-term Infusion of high-dose fluorouracil with or without N-(Phosphonacetyl)-L-aspartic acid in patients
with advanced pancreatic and colorectal cancers. J. C/in. Oncol. 6: 1053-I 058. 130. O’Dwyer, P. J., Paul, A. R., Walczak, J., Weiner, L. M., Litwrn, S. & Comis, R. L. (1990) Phase II
study of biochemical modulation of fluorouracil by low-dose PALA In patients with colorectal cancer. J. Clin. Oncol 8: 1497-l 503.
131. Kemeny, N., Conti, J. A., Seiter, K., Niedzwreckr, D., Botet, J., Martin, D., Costa, P., Wiseberg, J. & McCulloch, W. (1992) Brochemical modulation of bolus fluorouracil by PALA in patients with
advanced colorectal cancer. J. C/in. Oncol. 10: 747-752.
132. Kemeny, N., Seiter, K., Martin, D., Urmacher, C., Niedzwieckr, D., Kurtz, R. C., Costa, P. & Murray, M. (1991) A new syndrome: Ascites, hyperbilirubinemia, and hypoalbuminemia after biochemical
modulation of fluorouracil with N-phosphonacetyl-L-aspartate (PALA). Ann. lntern. Med. 115:
946-951. 133. Ardalan, B., Jasmin, D., Jayaram, H. N. & Presant, C. A. (1984) Phase I study of continuous-
infusion PALA and 5-FU. Cancer Treat. Rep. 68: 531-534. 134. Grem, J., McAtee, N., Murphy, R., Balis, F., Drake, J., Hamilton, J., Goldstein, L., Sorensen, J.,
Setser, A., Jordan, E. & Allegra, C. (1992) Phase I study of continuous IV infusion (Cl) 5.FU and leucovorin (LV) plus N-(phosphonacetyl)-L-asparate (PALA) in advanced GI cancer. Proc. ASCO 11: 271.
135. Smith, S., Capizzi, R., Richards, F., Homesley, H., Fernandes, D., Case, D., Barbery, R., Rhinehardt, D., Lovelace, J., Barrett, R., Cruz, J.. Cooper, M. R., Muss, H. & Whrte, D. (1992) Randomized phase I and clinical pharmacologic trial of pals/5-FU*dipyridamole in patients with advanced
cancer. froc. ASCO 11: 315.

48 G. A. SOTOS ET AL
136. Klubes, P. & Cerna, I. (1983) Use of uridine rescue to enhance the antitumor selectivity of 5. fluorouracil. Cancer Res. 43: 3182-3186.
137. Martin, D. S., Stolfi, R. L., Sawyer, R. C., Spiegelman, S. & Young, C. W. (1982) High-dose 5- fluorouracil with delayed uridine ‘rescue’ in mice. Cancer Res. 42: 3964-3970.
138. Leyva, A. & Wetmore, L. A. (1990) Uridine modulation of UTP pool in human tumor cell Irnes,
relevant to uridine rescue of 5-fluorouracil toxicity. Proc. AACR 31: A251 3. 139. Martin, D. S., Stolfi, Ft. L., Sawyer, Ft. C., Spiegelman, S. & Young, C. W. (1983) Improved
therapeutic index with sequential N-phosphonacetyl-L-aspartate plus high-dose methotrexate plus
high-dose 5-fluorouracil and appropriate rescue. Cancer Res. 43: 4653-4661. 140. Darnowski, J. W. & Handschumacher, R. E. (1989) Enhancement of fluorouracil therapy by the
manipulation of tissue uridine pools. fharmacol. Ther. 41 (1 -2) 381-392.
141. Nadal, J. C., van Groeningen, C. J., Pinedo, H. M. & Peters, G. J. (1989) Schedule-dependency
of in vivo modulation of 5-fluorouracil by leucovorin and uridine in murine colon carcinoma. Invest. Mew Drugs 7: 163-I 72.
142. Peters, G. J., van Dijk, J., Laurensse, E., van Groeningen, C. J., Lankelma, J., Leyva, A., Nadal, J. C. & Pinedo, H. M. (1988) In vitro biochemical and in vivo biological studies of the uridine ‘rescue’
of 5-fluorouracil. Br. J. Cancer 57: 259-265. 143. Parker, W. B. & Klubes, P. (1985) Enhancement by uridine of the anabolism of 5-fluorouracil in
mouse T-lymphoma (S-49) cells. Cancer Res. 45: 42494256.
144. Parker, W. B., Kennedy, K. A. & Klubes, P. (1987) Dissociation of 5.fluorouracil-induced DNA fragmentation from either its rncorporation into DNA or its cytotoxicity in murine T-lymphoma (S- 49) cells. Cancer Res. 47: 979-982.
145. Hartmann, H. R. & Bollag, W. (1986) Modulation of the effects of fluoropyrimidines on toxicity and tumor inhibition in rodents by uridine and thymidine. Med. Oncol. Tumor Pharmacother. 3
(2): 111~118. 146. Tuchman, M., Ramnaraine, M. L. R. & O’Dea, R. F. (1985) Effects of uridine and thymidine on the
degradation of 5-fluorouracil, uracil, and thymine by rat liver dihydropyrimidine dehydrogenase. Cancer Res. 45: 5553-5556.
147. Colofiore, J. R., Stolfi, R. L. & Martin, D. S. (1991) Uridinediphosphoglucose (UDPG) as an alternative to free uridine (UR) for the rescue from 5-fluorouracil (FU)-associated toxicity. Proc.
AACR 32: A201 6. 148. van Groeningen, C. J., Peters, G. J. & Pinedo, H. M. (1993) Reversal of 5-fluorouracil-Induced
toxicity by oral administratron of uridine. Ann. Oncol. 4: 317-320. 149. van Groemngen, C. J., Peters, G. J. & Pinedo, H. M. (1992) Modulation of fluorouracil toxicity
with uridine. Semin. Oncol. 19: (2) (Suppl. 3): 148-I 54. 150. Peters, G. J., Lankelma, J. & Pinedo, H. M. (1984) Phase I and pharmacokinetic studres of hrgh-
dose uridine intended for rescue from 5-fluorouracil toxicity. Cancer Res. 44: 5928-5933. 151. van Groeningen, C. J., Leyva, A., Kraal, I., Peters, G. J. & Pinedo, H. M. (1986) Clinical and
pharmacokinetic study of prolonged administration of high-dose uridine intended for rescue from 5-fluorouracil toxicity. Cancer Treat. Rep. 70: 7455750.
152. van Groeningen, C. J., Peters, G. J., Leyva, A., Laurensse, E. J. & Pinedo, H. M. (1989) Reversal of 5-fluorouracil-induced myelosuppression by prolonged administration of high-dose uridine. J. Nat1 Cancer Inst. 81: 157-l 62.
153. van Groeningen, C. J., Peters, G. J., Nadal, J. C., Laurensse, E. J. & Pinedo, H. M. (in press) Clinical and pharmacological study of orally administered uridine. J. Nat/. Cancer Inst.
154. Seiter, K, Kemeny, N., Martin, D., Schneider, A., Williams, L., Colofiore, J. & Sawyer, R. (1993) Uridrne allows dose escalation of 5-fluorouracil when given with N-phosphonacetyl-L-aspartate, methotrexate, and leucovorin. Cancer 71: 1875-l 881.
155. Kemeny, N., Conti, J., Martin, D., Seiter, K., Costa, P., Sawicki, E. & Weisberg, J. (1992) Oral uridine (UR) protects from 5-fluorouracil (FU) toxicity in metastatic colorectal carcinoma: Phase l/II trial of phosphonacetyl-L-aspartic acid (PALA) + FU with UR as a rescue agent. Proc. ASCO 11: 498.
156. Christman, K., Schwartz, G., Saltz, L., Dougherty, J., Casper, E., Yao, T., Toomasi, F., Friedrich, C., Martin, D., Bertino, J. & Kelsen D. (1993) Uridine (Urd) allows dose-intensification of FAMTX (5.fluorouracil (FU), adriamycin (A), methotrexate (MTX) Proc. AX0 12: 589.
157. Niedzwicki, J. G., el Kouni, M. H., Chu, S. H. & Cha, S. (1981) Pyrimidine acyclonucleosides. Inhibitors of uridine phosphorylase. Biochem. Pharmacol. 30 (15): 2097p2101.
158. Niedzwicki, J. G., Chu, S. H., el Kouni, M. H., Rowe, E. C. & Cha, S. (1982) 5-Benzylacycloundine

BIOMODULATION OF 5-FLUOROURACIL 49
and 5-benzyloxybenzylacyclouridine, potent inhibitors of uridine phosphorylase. Biochem. Phar- macol. 31 (10): 1857-1861.
159. Niedzwicki, J. G., el Kouni, M. H., Chu, S. H. & Cha, S. (1983) Structure-activity relationship of
ligands of the pyrimidine nucleoside phosphorylases. Biochem. Pharmacol. 32 (3): 399-415. 160. Chu, M. Y. W., Naguib, F. N. M., Iltzsch, M. H., el Kouni, M. H., Chu, S. H. & Cha, S. (1984)
Potentiation of 5-fluoro-2’.deoxyuridine antineoplastic activity by the uridine phosphorylase
inhibrtors benzylacyclouridine and benzyloxybenzylacyclouridine. Cancer Res. 44: 1852-l 856. 161. Chu, S. H.. Wiemann, M. C., Chu, M. Y. & Calabresi, P. (1987) Mono- and di-benzyl analogs of
acyclouridine (BAU and BBAU) potentiate the antitumor activity of FUdR against the pancreatic DAN, lung LX-l and colon HCT-8 human carcinoma cell lines. Proc. Am. Assoc. Cancer Res. 28:
410. 162. Darnowski, J. W. & Handschumacher, R. E. (1985) Tissue-specific enhancement of uridine
utilization and 5-fluorouracil therapy in mice by benzylacyclourrdine. Cancer Res. 45: 5364-5368. 163. Darnowski, J. W. & Handschumacher, R. E. (1988) Benzylacyclouridine-pharmacokinetics, metab-
olism and biochemical effects in mice. Biochem. Pharmacol. 37 (13): 2613-2618. 164. Darnowski, J. W., Handschumacher, R. E., Wiegand, R. A., Goulette, F. A. & Calabresi, P. (1991)
Tissue-specific expansion of uridine pools in mice. Effects of benzylacyclouridine, dipyridamole and exogenous urrdine. Biochem. Pharmacol. 41 (12): 2031-2036.
165. Martin, D. S., Stolfi, R. L. & Sawyer, R. C. (1989) Utility of oral uridine to substitute for parenteral
uridine rescue of 5-fluorouracil therapy, with and without a uridine phosporylase inhibitor (5. benzylacyclouridine). Cancer Chemofher. Pharmacol. 24: 9-l 4.
166. Davis, S. T., Joyner, S. S., Chandrasurin, P. & Baccanari, D. P. (1993) Species-dependent differences
in the biochemical effects and metabolism of 5-benzylacyclouridine. Biochem. Pharmacol 45 (1): 173-181.




















