Preliminary results from a controlled evaluation of thermal biofeedback as a treatment for essential...
25
Biofeedback and Self-Regulation, Vol. 9, No. 4, 1984 Preliminary Results from a Controlled Evaluation of Thermal Biofeedback as a Treatment for Essential Hypertension 1 Edward B. Blanchard 2 State University o/New York at Albany Guy C. McCoy Albany Medical College Frank Andrasik, Maryrose Acerra, Thomas P. Pallmeyer, Robert Gerardi, Mindy Halpern, and Alison Musso State University of New York at Albany In a controlled trial, thermal biofeedback (n = 20) and abbreviated progressive relaxation (n = 22) were compared in the treatment of mild to moderate hypertensive patients whose blood pressures (BP) were initially controlled on two medications. For the clinical end point of maintaining control of BP on a single drug after treatment, biofeedback was superior to relaxation training (at 3 months, 47% success for biofeedback versus 23~o for relaxation). This same result tended to be true for patient-measured home BPs. BPs from laboratory psychophysiological testing showed no consistent advantage for one treatment over the other. Descriptor Key Wards: hypertension; thermal biofeedback; relaxation training; cardiovascular reactivity. For the past few years there has been much discussion at biofeedback meetings of the use of thermal biofeedback as a treatment for hypertension; however, only very limited published reports on this procedure have thus far appeared. Green, Green, and Norris (1979) presented preliminary data ~This research was supported by a grant from NHLBI, HL-27622. 2Address all correspondence to Dr. Edward B. Blanchard, Center for Stress and Anxiety Disorders, 1535 Western Avenue, Albany, New York 12203. 471 0363 3586/84/1200 0471503.50/0 © 1984 Plenum Publishing Corporation
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Preliminary results from a controlled evaluation of thermal biofeedback as a treatment for essential...
Biofeedback and Self-Regulation, Vol. 9, No. 4, 1984
Preliminary Results from a Control led Evaluat ion
of Thermal Biofeedback as a Treatment for
Essential Hypertension 1
Edward B. Blanchard 2 State University o/New York at Albany
Guy C. McCoy Albany Medical College
Frank Andrasik, Maryrose Acerra, Thomas P. Pallmeyer, Robert Gerardi, Mindy Halpern, and Alison Musso State University of New York at Albany
In a controlled trial, thermal biofeedback (n = 20) and abbreviated progressive relaxation (n = 22) were compared in the treatment o f mild to moderate hypertensive patients whose blood pressures (BP) were initially controlled on two medications. For the clinical end point o f maintaining control o f B P on a single drug after treatment, biofeedback was superior to relaxation training (at 3 months, 47% success f o r biofeedback versus 23~o f o r relaxation). This same result tended to be true f o r patient-measured home BPs. BPs f r o m laboratory psychophysiological testing showed no consistent advantage f o r one treatment over the other.
Descriptor Key Wards: hypertension; thermal biofeedback; relaxation training; cardiovascular reactivity.
F o r the past few years there has been much discuss ion at b io f eedback
meet ings o f the use o f t he rma l b i o f e e d b a c k as a t r ea tmen t fo r hyper tens ion ; however , on ly very l imi ted pub l i shed repor t s on this p r o c e d u r e have thus far a p p e a r e d . Green , Green , and Nor r i s (1979) p resen ted p r e l im ina ry d a t a
~This research was supported by a grant from NHLBI, HL-27622. 2Address all correspondence to Dr. Edward B. Blanchard, Center for Stress and Anxiety Disorders, 1535 Western Avenue, Albany, New York 12203.
471
0363 3586/84/1200 0471503.50/0 © 1984 Plenum Publishing Corporation

4"/2 Blanchard, McCoy, Andrasik, Acerra, Pallmeyer, Gerardi, Halpern, and Musso
on 12 patients seen at the Menninger Foundation: Seven of the 12 had clinically meaningful decreases in either systolic blood pressure (SBP) or diastolic blood pressure (DBP) while all 7 of the patients who started the training program on antihypertensive medication were able to decrease the dosage, and 6 were medication-free. Bertilson, Bartz, and Zimmerman (1979) reported on the treatment of 8 college males with borderline (3) or high normal (5) BP with a combination of relaxation training and thermal biofeedback. Statistically significant reductions in SBP were found within sessions as well as from the beginning of training to the end of session 14.
We ourselves have presented data from our ongoing evaluation of thermal biofeedback at meetings of the Biofeedback Society of America (Blanchard et al., 1983, 1984). In this manuscript we present preliminary results from the ongoing research project.
M E T H O D
Overview
In our research on the nonpharmacological treatment of hyperten- sion, we have targeted a very specific subset of the total hypertensive population, those patients who require at least two drugs to maintain adequate control of their blood pressure (BP). This subpopulation was targeted for two overlapping reasons: While the annual costs of typical doses of diuretics is approximately $50 to $100 per year, when one adds a typical second-stage drug, costs of usual doses increase by approximately $300 to $1,000 per year (McCoy, unpublished data, 1982). Moreover, one adds a significant increment in side effects when the second stage drug is added to the regimen (Physician "s Desk Reference, 1984). Thus, our overall goal has been to evaluate whether patients whose BP was well-controlled on two drugs can be adequately maintained on only a diuretic after completing a course of one of two nonpharmacological therapies.
Since this is a preliminary report, we are presenting short-term data from patients in two conditions--our experimental condition: thermal biofeedback training, and the comparison condition: abbreviated pro- gressive relaxation training. This latter condition has been established in other controlled studies (e.g., Taylor, Farquhar, Nelson, & Agras, 1977; Agras, Southam, & Taylor, 1983) to be an effective nonpharmacological treatment for hypertension. More detailed reports from our comprehensive assessment and follow-up procedures will follow in years to come.

Thermal Biofeedback for Hypertension 473
Subjects
As noted above, patients were randomly assigned to one of two treatment conditions: thermal biofeedback or abbreviated progressive relaxation. The characteristics of the two samples, on an individual patient by patient basis, are presented in Table I.
A summary of the data in Table I reveals that the sample consisted of 42 patients (23 male, 19 female), average age 48.6 years, who had been on antihypertensive medication for an average of 10.0 years. There were no significant differences between the two treatment groups on sex, age, or length of time on medication. The home BP values are from the week of home monitoring during which the pretreatment assessment took place. As such they represent the values from at least the 4th week of home monitoring.
In 5 cases (2 biofeedback, 3 relaxation) the patient entered the study on only a single second-stage drug.
All patients gave written, informed consent for each aspect of the study.
Procedure
Approximately 6007o of patients were self-referred on the basis of local media coverage of the project while the other 40°70 were referred by physicians. All participants entered the study through the physician at Albany Medical College (GCM). At an initial visit, a brief history of the patient's hypertension was taken, medical records were sent for, and the patient was taught to take his own BP at home using a dual stethoscope sphygmomanometer. Thereafter, the patient took his own BP daily and mailed the results back to the research team on a weekly basis.
More precisely, the patient was asked to take and record four BPs at home: in the morning, .after resting in a supine position for 3 minutes (AM-supine) and then after standing for 30 seconds (AM-standing). These same conditions were to be repeated in the evening (PM-supine and PM-standing).
If the patient's BP was not well controlled, as indicated by home BP records and office BP's, medication was adjusted by the study physician until control was obtained. Then baseline home BP recordings were begun.
After 4 weeks of home BPs had been obtained, the patient was scheduled for detailed physical, biochemical, psychological, and psycho-

474 Blanchard, McCoy, Andrasik, Acerra, Pallmeyer, Gerardi, Halpem, and Musso
%
010 ~" ~ ~

T h e r m a l B i o f e e d b a c k f o r H y p e r t e n s i o n 4 7 5
_ _ _ ~ ~ ~ ~
N
N
O ~'~
II II
rr ©
O
~E
©
II
. . rl II
476 Bianchard, McCoy, Andrasik, Acerra, Pallmeyer, Gerardi, Halpern, and Musso
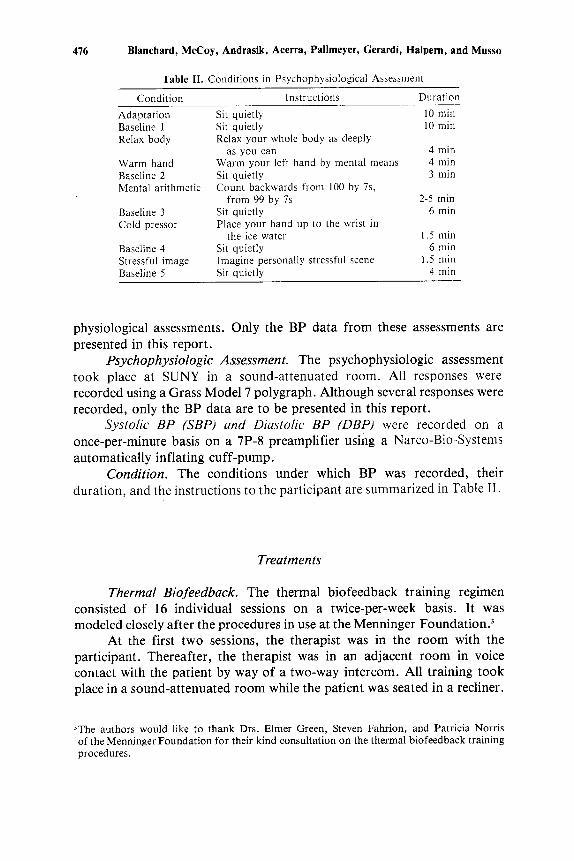
Table II. Conditions in Psychophysiological Assessment
Condit ion Instructions Duration
Adaptat ion Sit quietly 10 rain Baseline 1 Sit quietly 10 min Relax body Relax your whole body as deeply
as you can 4 min Warm hand Warm your left hand by mental means 4 rain Baseline 2 Sit quietly 3 rain Mental arithmetic Count backwards from 100 by 7s,
f rom 99 by 7s 2-5 rain Baseline 3 Sit quietly 6 rain Cold pressor Place your hand up to the wrist in
the ice water 1.5 min Baseline 4 Sit quietly 6 rain Stressful image Imagine personally stressful scene 1.5 rain Baseline 5 Sit quietly 4 rain
physiological assessments. Only the BP data from these assessments are presented in this report.
Psychophysiologic Assessment. The psychophysiologic assessment took place at SUNY in a sound-a t t enua ted room. All responses were
recorded using a Grass Model 7 polygraph. Although several responses were recorded, only the BP data are to be presented in this report.
Systolic BP (SBP) and Diastolic BP (DBP) were recorded on a
once-per-minute basis on a 7P-8 preamplifier using a Narco-Bio-Systems
automatically inflating cuff-pump. Condition. The conditions under which BP was recorded, their
duration, and the instructions to the participant are summarized in Table II.
Treatments
Thermal Biofeedback. The thermal biofeedback training regimen consisted of 16 individual sessions on a twice-per-week basis. It was modeled closely after the procedures in use at the Menninger Foundation?
At the first two sessions, the therapist was in the room with the participant. Thereafter, the therapist was in an adjacent room in voice contact with the patient by way of a two-way intercom. All training took place in a sound-attenuated room while the patient was seated in a recliner.
3The authors would like to thank Drs. Elmer Green, Steven Fahrion, and Patricia Norris of the Menninger Foundation for their kind consultation on the thermal biofeedback training procedures.

Thermal Biofeedback for Hypertension 477
For all sessions, a thermistor was attached to the index finger of the nondominant hand. Temperature was measured continuously using a Med Associates ANL-410. Both auditory and visual feedback of temperature were available continuously and the patient sampled both. Over 80O7o of patients chose the visual feedback: a large meter, approximately 25 cm wide, on which the pen could move approximately 150 degrees. Sensitivity varied with a full-scale deflection representing from 2°F to 20°F.
At the first session, no feedback was available to the patient. Instead, after the rationale for the treatment was fully explained, the therapist went through a list of autogenic phrases that the patient was to repeat to himself while trying to experience what he was saying. The feedback display was visible to the therapist, who gave periodic verbal feedback and encouragement. The actual training portion of the session was about 20 minutes. At the conclusion the patient was given a small alcohol-in-glass thermometer to use for home practice and was asked to practice the hand-warming and autogenic phrases at least once per day and to record reactions and results on sheets provided.
At the second session, the feedback display was positioned so that it was visible to both the patient and the therapist. Again the therapist went through the list of autogenic phrases. The home practice record was reviewed and instructions were renewed.
Beginning at the third session, the patient was left alone with the feedback display. All sessions had the following format:
Discussion of home practice problems while attaching thermistor 5-10 rain
Adaptation (T out of room) 10 rain In-session baseline 5 rain Self-control 1 (Patient asked to warm hands with
no feedback available) 5 min Feedback training 20 rain Self-control 2 (Patient again asked to warm hands
with no feedback available) 5 rain Discussion while disconnecting thermistor 5 rain
Total 60 rain
Patients were cautioned "not to try too hard, but instead to let your hands become warm." They were also told to experiment with whatever ideas and images seemed to help them, including, but not limited to, the autogenic phrases.
For patients who started the session with warm hands (around 93-95°F in baseline), it was suggested that they try cooling and then warming the hands to gain control of peripheral vasodilation.

478 Blanchard, McCoy, Andrasik, Acerra, Pallmeyer, Gerardi, Halpern, and Musso
If patients became extremely proficient at hand warming, they were tried on foot warming. The thermistor is attached to the bottom of the big toe. This occurred with only two patients.
Relaxation Training. The relaxation training regimen was modeled after one we have previously used with headache patients (Blanchard et al., 1982) and was adapted from the work of Bernstein and Borkovec (1973) and Jacobson (1938). It consisted of eight sessions spread over 8 weeks with content as described in Table III. It was administered live on an individual basis.
At the first session, the patient was given an audiocasette of the full 16 muscle group procedures to assist him in his home practice. Patients were strongly urged to practice the relaxation exercises at least once per day for at least 20 minutes. Frequent reminders were made of the importance of regular home practice.
There is thus a deliberate confound in the two training procedures in that the patients receiving thermal biofeedback were seen 16 times while those receiving relaxation training were seen only 8 times. The number of contacts was based on expert opinion as to how much contact was necessary to give a patient receiving either treatment "an adequate dose" of that treatment. Thus, treatments were equated in terms of adequacy of contacts for the particular treatment rather than actual number of contacts. This is analogous to equating two drug regimens by giving therapeutic doses of each rather than equating number of pills or number of milligrams of the drug.
Table Ill. Relaxation Training Regimen
Week no. Session no, Content
1 1
1. 2
2 3
3 4
4 5
5 6
6 7
7 No session 8 8
Introduction and rationale; training with 16 muscle groups; instruction on home practice
Discuss home practice; training with 16 muscle groups; introduce imagery
Discuss home practice; training with 16 muscle groups; continue imagery
Discuss home practice; training with 8 muscle groups
Discuss home practice; training with 4 muscle groups; encourage use of relaxa- tion in stressful situations
Discuss home practice; training with 4 muscle groups; relaxation by recall; instructions in breathing
Discuss home practice; training with 4 muscle groups; cue-controlled relaxation
Patient practices at home Check progress; cue-controlled relaxation
Thermal Biofeedback for Hypertension 479
Treatment Credibility
Treatment credibility was assessed on approximately 60°70 of each treatment group at the first session, after an explanation and description of the treatment, but before either relaxation or biofeedback was begun.
Posttreatment Assessment
At the conclusion of treatment, the patient was reassessed, while still on two drugs, by both the study physician and with the psycho- physiological procedure described earlier.
Drug Withdrawal
At the completion of the posttreatment assessment, the patient was given a schedule for tapering the second-stage drug. This took from 8 to 40 days, depending on the drug and the initial dosage. The patient continued to take his BP at home daily and to report these and medications to the study physician on a weekly basis.
Once the patient had fully discontinued the second-stage drug (in our terms was "drug-free"), a 4-week period began. The patient continued to practice his self-regulatory exercise and to send in home BPs.
Post-Drug- Withdrawal Assessment
After the 4-week drug-free phase, the patient was again reassessed both by the study physician and with the psychophysiological testing. The actual interval between becoming drug-free and completing reassessment averaged 6 weeks (range: 4-14 weeks).
Follow-Up
Following the post-drug-withdrawal assessment, the patient entered a follow-up phase of up to 1 year. He was seen by the study physician approximately once every 3 months and continued to report home BPs. Data from this phase will be reported in a later communication?
4"Process data" such as the temperature reached in the various phases of the biofeedback training, degree of relaxation achieved in the relaxation training, and home practice data are still undergoing analysis and will be the subject of a later report.

480 Blanchard, McCoy, Andrasik, Acerra, Pailmeyer, Gerardi, Halpern, and Musso
Clinical End Point and Declaration of Failure
As the patient began to discontinue his second-stage medication, extra care was taken in monitoring his home BP records. The following criteria were established by which to judge if a patient had been successfully withdrawn from the second-stage medication. These criteria were, we believe, conservative and biased in the direction of calling the patient a "failure at drug withdrawal" when perhaps he had not been. These criteria are listed below:
1. Office BP > 140/90. Average BP measured in physician's office in seated position was the ultimate criterion for BP control. Average sitting BP must be < 140/90, regardless of home BPs, for the patient to be considered successful and not restarted on second- stage medication.
2. Onset o f symptoms. Patient was told to call the physician if any new symptoms developed, regardless of home BP level. With new symptoms, patient is seen promptly in the office for evaluation of BP and symptoms. If the physician does not believe the symptoms are significant, and if the patient agrees, and if office BP does not exceed highest weekly BP average prior to drug tapering by 15/15, tapering continues or patient remains off medication.
3. Excessive ,(> 20 mm Hg) lqse in home BP. Patient is also told to call the physician if two consecutive home BP readings exceed the highest weekly average baseline BP prior to drug tapering by 20 mm Hg. Decision is made at the point as to whether the patient should be seen in office or not.
4. Failure to achieve baseline home BP levels. If, after drug with- drawal, the patient's home BP weekly average is not at or below the home BP weekly average for the last week of baseline, the patient is declared a failure.
5. Patient's personal physician believes the patient should resume sec- ond-stage medication.
Dependent Measures
There are three different sets of dependent variables in this study: (1) clinical endpoint, as described above- tha t is, whether the patient was able to remain off a second-stage drug with BP still controlled; (2) home BPs, measured by the patient at home as described above. The weekly averages of these values from end of baseline, end of treatment, and 4 weeks after drug withdrawal, were analyzed; (3)psychophysiological testing BPs,

Thermal Biofeedback for Hypertension 481
measured and recorded automatically, during each phase of the psychophysiological assessment.
RESULTS
Patient Flow and Clinical End Point
In Table IV are presented the data on patient flow through the study and, most important, the results on the dependent variable of primary clinical concern, whether patients could, after treatment, successfully be maintained on a single antihypertensive drug.
One patient in each condition dropped out after completing treatment but before the posttreatment assessment.
A comparison of initially successful versus unsuccessful (either could not be withdrawn from second-stage medication or relapsed within 4 weeks of being drug-free) reveals an advantage for the Biofeedback treatment (x 2 -- 3.58, p = .06). At a 1-month (approximately 3 months after second- stage drug was completely discontinued) follow-up, there is still a trend (x 2 = 2.68,p = .10) for the biofeedback-treated patients to do better (47°7o vs. 23070 for Relaxation still drug-free).
For each of the BP measures to be presented below, there are two sets of analyses: The first involves comparison of the patients in the two treatments who completed the posttreatment assessment in 2(Groups) X 2(pre/post) repeated-measures ANOVAS. The second set of analyses involves comparisons of the patients who completed the post-drug-with-
Table IV. Patient Flow Frequency and Clinical End Point Results
Treatments
Thermal Relaxation Stage of project biofeedback training
Started treatment 20 22 Dropped out in treatment 0 0 Completed posttreatment
assessment 19 21 Unable to be withdrawn from second-stage drug or maintained off drug 6 12
Completed post-drug-withdrawal assessment 13 9
Successful at 1-month follow-up 9 5
482 Blanchard, McCoy, Andrasik, Acerra, Pallmeyer, Gerardi, Halpern, and Musso
drawal assessment in 2(Groups) x 3(Pre-, Posttreatment, Post-Drug-With- drawal) repeated-measures ANOVAS. These latter analyses are on fewer subjects because of failure to be successfully withdrawn and are somewhat biased in favor of the relaxation training because of this condition's differential rate of failure to withdraw from second-stage drug. The repeated-measures ANOVA program used in these analyses, BMDP P2V (Dixon & Brown, 1979), utilizes the unweighted means procedure to correct for unequal cell sizes.
Home Blood Pressures
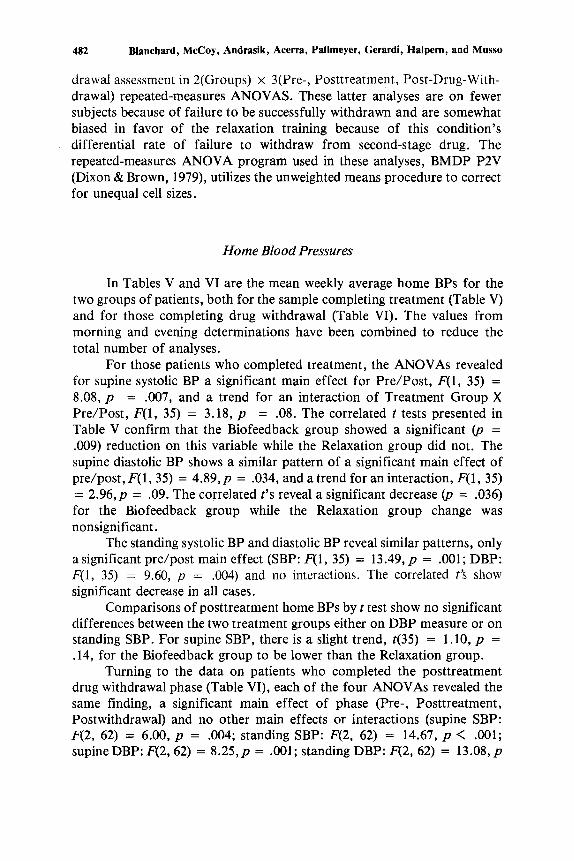
In Tables V and VI are the mean weekly average home BPs for the two groups of patients, both for the sample completing treatment (Table V) and for those completing drug withdrawal (Table VI). The values from morning and evening determinations have been combined to reduce the total number of analyses.
For those patients who completed treatment, the ANOVAs revealed for supine systolic BP a significant main effect for Pre /Pos t , F(1, 35) = 8.08, p = .007, and a trend for an interaction of Treatment Group X Pre/Post , F(1, 35) = 3.18, p = .08. The correlated t tests presented in Table V confirm that the Biofeedback group showed a significant (p = .009) reduction on this variable while the Relaxation group did not. The supine diastolic BP shows a similar pattern of a significant main effect of pre/post , F(1, 35) = 4.89, p = .034, and a trend for an interaction, F(1, 35) = 2.96, p = .09. The correlated t's reveal a significant decrease (p = .036) for the Biofeedback group while the Relaxation group change was nonsignificant.
The standing systolic BP and diastolic BP reveal similar patterns, only a significant pre/post main effect (SBP: F(1, 35) = 13.49, p = .001; DBP: F(1, 35) = 9.60, p = .004) and no interactions. The correlated t's show significant decrease in all cases.
Comparisons of posttreatment home BPs by t test show no significant differences between the two treatment groups either on DBP measure or on standing SBP. For supine SBP, there is a slight trend, t(35) = 1.10, p = .14, for the Biofeedback group to be lower than the Relaxation group.
Turning to the data on patients who completed the posttreatment drug withdrawal phase (Table VI), each of the four ANOVAs revealed the same finding, a significant main effect of phase (Pre-, Posttreatment, Postwithdrawal) and no other main effects or interactions (supine SBP: F(2, 62) = 6.00, p = .004; standing SBP: F(2, 62) = 14.67, p < .001; supine DBP: F(2, 62) = 8 .25,p = .001; standing DBP: F(2, 62) = 13.08, p

Thermal Biofeedback for Hypertension 483
8
¢%
© ©
o
o o o q o .
II ~ Jl II II ~ II II
~ 6 6 6 6 ~ 0 0 0 0 0 0 0 0
m ~ m ~ E E
ca
. o ~ o ~ . o o-~

484 Blanchard, McCoy, Andrasik, Acerra, Pailmeyer, Gerardi, Halpern, and Musso
8
0
a,,,
© o a3
o ~ ~ = ~ ' ~ ' ~ = ~
~ 9 6 d d d
~0000
©
i . ~ ~ . ~ . ~
. ~ o ~ . £ ~ . £ ~

Thermal Biofeedback for Hypertension 485
= .7
i
L~

486 Blanchard, McCoy, Andrasik, Acerra, Pallmeyer, Gerardi, Haipern, and Musso
< .001). Despite the lack of significant interactions, we have calculated a series of correlated t tests to examine the changes of each treatment condition across the experimental phases. In particular, we are interested in whether the postwithdrawal BPs remain significantly lower than the pretreatment BPs or not. The values of the t tests are summarized in Table VII.
If one adopts a relatively conservative alpha level of .02, then all of the postwithdrawal BPs for the Biofeedback group are significantly lower than the pretreatment values (and, in fact, there are n o m e a n r i s e s in any home BP for the Biofeedback group as a result of withdrawing the second-stage drug), while only the standing DBP for the Relaxation group is significantly lower.
We might also note that the home BPs confirm that these patients at pretreatment were well controlled on their medications.
Comparisons of the postwithdrawal BPs by t test reveal no significant differences between home DBPs, and only slight trends (p = .15) for the
16oN Reaxat°n PreTreat 2Drugs n 20 Relaxation: Post-Treat. (2 Drugs) • - - - -u Biofeedback: Pre-Treat. (2 Drugs) (n = 12) n--- -D Biofeedback: Post-Treat. (2 Drugs)
* / / • \ \ \
/ / ix ///; " \ / \ / ~ , \ '/ \',/// li:'/\ "
/ 't ~0
Base- Re'lax Warm Balee - Mental Base- Cold Base- Stress. Base- line-1 Body Hand line-2 Arith, line-3 Press. line-4 Image. line-5
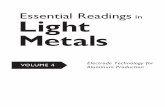
Fig. 1. Systolic BP at each condition of the psychophysiological test for each treatment con- dition at pretreatment and posttreatment. (Patients on two drugs at both tests).

Thermal Biofeedback for Hypertension 487
home SBPs o f the Biofeedback group to be lower than those of the Relaxation group.
Psychophysiological Assessment Blood Pressures
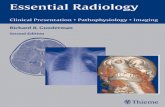
In Figures 1 and 2 are presented the mean SBP and DBP values, respectively, for each treatment group, for each condition, at the pretreatment and post t reatment physiological assessments.
The A N O V A on the data in Figure 1 (SBP) revealed a significant Pre/Post main effect, F(1, 30) = 9.36, p = .005, a significant Conditions main effect, F(9, 270) = 3 8 . 5 , p < .001, a significant Condition X P re /Pos t interaction, F(9, 270) = 2.13, p = .027, and a trend for there to be a Group X Pre /Pos t interaction, F(1, 30) = 2.48, p = .12. These indicate that, overall, posttreatment SBPs are lower than pretreatment SBPs and that the var- ious experimental conditions have differential effects on SBP.
Since the port ion of these data of most interest is in whether there is differential change between the two groups f rom pretreatment to posttreatment, we have calculated a series of two-way ANOVAs (Group x Pre /Pos t ) on the data for each experimental condition. In each of these the term of most interest is the interaction. The values of the Fs and their
A A Relaxation: Pre÷Treat (2 Drugs) n = 17 110. ~ Relaxation: Pest-Treat (2 Drugs) n = 17
- - I I Biofeedback: Pre-Treat. (2 Drugs) n = 12 [3 - - - -£ ] Biofeedback: Post-Treat (2 Drugs) n = 12
80 c ~ - ~ _ _ - - ~ , " ' D " , , , u , - , " - o
Base- Relax W a r m Base- Menta l Base- Co ld Base- Stress, Base- line-1 Body H a n d l ine-2 Ar i th. l ine-3 Press. l ine-4 Image . l ine-5
Condi t ion
Fig. 2. Diastolic BP at each condition of the psychophysiological test for each treatment con- dition at pretreatment and posttreatment. (Patients on two drugs at both tests.)
I
E E v 100-
g
r l
g e n
. o 9 0 -

488 Blancbard, McCoy, Andrasik, Acerra, Pallmeyer, Gerardi, Halpem, and Musso
_o ©
0
©
©
. o. o. o. o. o.
?
. o o o ~ o

Thermal Biofeedback for Hypertension 489
probability levels for the interactions that approached significance are listed in Table VIII. Also listed are the values for the correlated t's on the two groups of patients to indicate whether the SBPs for that group at that test condition were lower at posttreatment than at pretreatment.
From the results in Table VIII, one can see that most of the differential psychophysiological testing effects are in the relaxation and return-to-baseline conditions. The Biofeedback treated group tends to show significantly lower SBPs in these conditions at posttreatment than they had at pretreatment, while the within-group decreases for the Relaxation-treated group are not significant.
Neither group shows a significant decrease in SBP to Mental Arithmetic or the Cold Pressor, while both show significantly less responsiveness to the Stressful Imagery at posttreatment.
Turning next to the data on DBP shown in Figure 2, there is only an Experimental Condition main effect, F(9, 243) = 41.5, p < .001, but no Group or Pre/Post main effects or interactions. Correlated t tests confirm the lack of significant within-group change in DBP for either group at any condition.
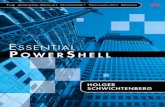
In Figures 3 and 4 are the mean SBP and DBP values, respectively, for each condition for those patients successfully withdrawn from the second-stage drug at each of the three psychophysiological assessments. (Missing data have appreciably reduced the sample sizes in this case.)
For the data in Figure 3 (SBP) the ANOVA revealed a significant main effect of Experimental Condition, F(9, 108) = 33.0, p < .001, and a significant main effect of Time Assessment, F(2, 24) = 7.82, p = .002, and no other main effects or interactions. For Time of Assessment, the average pressure across all experimental conditions was significantly higher at post-drug-withdrawal than at posttreatment (p < .01), with the pretreatment levels in between the two other values and not different from either of them. This means that the values of SBP at the various conditions were not significantly higher after treatment, and after the second-stage drug was withdrawn, than they were at pretreatment. Separate two-way ANOVAs at each experimental condition failed to reveal any differential effects of the two treatment conditions across assessment times.
For DBP (Figure 4) the overall ANOVA yielded the expected main effect of Condition, F(9, 108) = 22.8, p < .001, a main effect of Time of Assessment, F(2, 24) = 3.35, p = .052, and interactions of Condition X Time of Assessment,/7(18,216) = 2.30,p = .003, and Group X Condition X Time of Assessment, F(18, 216) = 1.96, p = .013. Further analyses reveal trends for differential responding of the two treatment groups across assessments for these conditions: initial baseline (p = .10), the third

490 Blanchard, McCoy, Andrasik, Acerra, Pallmeyer, Gerardi, Halpern, and Musso
155
145
"I-
E E
O.. 135
g m
1 2 5
115
Relaxation: Pre-Treat. (2 Drugs) (n =6) O ~ O Relaxation: Post-Treat. (2 Drugs)
Relaxation: Post-Withdraw. {1 Drug) I - - I Biofeedback: Pre-Treat (2 Drugs) (n =8) El---r1 Biofeedback: Post-Treat (2 Drugs) A . - A Biofeedback: Post-Withdraw. (1 Drug)
/ /
ix / \
/ / \ \ /
" " D . . . . . . . . . . 1:3" . . . . . . . . . . .
/ /
A
/ \
/ \ /
\
\ \ \
\ , ~ 'A
" ' U
Base- Relax Warm Base- Mental Base- Coid Base- Stress. Base- line-1 Body Hand line-2 Arith. line-3 Press. line-4 Image. line-5
Fig. 3. Systolic BP at each condition of the psychophysiological test for each treatment condi- tion at pretreatment, posttreatment, and post-drug-withdrawal (Patients on two drugs at first two tests and on one drug at post-drug-withdrawal.)
baseline, after mental arithmetic (p = .06), and for the cold pressor (p = .13).
To examine the possible differential effects of the two treatment conditions further, a series of correlated t tests were calculated for patients in each treatment conditions for whom data were available for these three experimental conditions at all three psychophysiological assessments. These results are summarized in Table IX.
From Table IX two things are clear; first, the Biofeedback-treated patients show significantly higher DBPs after withdrawal of the second-stage drug than they had at posttreatment or at p re t rea tmen t . Thus, they were significantly worse on these measures after treatment and drug withdrawal. For the Relaxation-treated patients, the rise in DBP from

Thermal Biofeedback for Hypertension 491
105
-v-
E g
g 95
"0 0 o
o 0
.~ 85 121
75
Relaxation: Pre-Treat. (2 Drugs) (n = 5) Relaxation: Post-Treat• (2 Drugs) Relaxation: Post-Withdraw (1 Drug)
O--m Biofeedback:Pre-Treat.(2Drugs)(n=9} ] £3---m Biofeedback: Post-Treat. (2 Drugs) / Zh - -A Biofeedback: Post-Withdraw (1 Drug) / t / / /
, , /
/ / \ \ /
I" \ \ \ tl III
I I I , '
1
r r , , ~ i i , , ,
Base- Relax Warm Base- Mental Base- Cold Base- Stress. Base- line-1 Body Hand line-2 Arith. line-3 Press. line-4 Image. line-5
Fig. 4. Diastolic BP at each condition of the psychophysiological test for each treatment con- dition at pretreatment, posttreatment, and post-drug-withdrawal. (Patients on two drugs at first two tests and on one drug at post-drug-withdrawal.)
posttreatment to postwithdrawal is nonsignificant. More important, the DBPs at postwithdrawal, when patients are on one drug, were not significantly different from the DBPs at pretreatment, when the patient is on two drugs (and were even arithmetically lower).
Treatment Credibility
Table X presents the mean value ratings made by each treatment group on the six treatment rationale questions administered at pretreatment. Each question was rated on a 0 (most negative) through 9 (most positive) point scale.
The data reveal no differences between the two groups concerning expectancy for outcome. However, there was a trend indicating that the relaxation group expected to reach a higher level of mastery of treatment skills by the end of their training.

492 Blanchard, McCoy, Andrasik, Acerra, Pallmeyer, Gerardi, Halpem, and Musso
._=
"i "i . 2
o "T.
2
b E E
o3

Thermal Biofeedback for Hypertension
Table X. Mean Ratings of Pretreatment Rationale
493
Biofeedback Relaxation l tem (n = 12) (n = 12) t d f p
1. How logical does this type of therapy seem to you for helping people control high blood pressure 7.83 8.00 .28 22 .784 How confident are you that this training will be successful in help- ing you to control your blood pres- sure as a substitute for your medica- tion? 6.50 7.33 1.20 22 .243 How important do you think it is that we make this treatment available to others with hypertension? 7.83 8.08 .35 22 .732 How successful do you think this training would be in decreasing other problems involving tension like anxiety, insomnia, headaches, etc.? 7.66 8.16 1.22 22 .237 Please rate the level of mastery of treatment skills you believe you will obtain by the end of the last therapy session. 7.50 8.4I 1.93 22 .067 How confident would you be in recommending this training to a friend who has hypertension? 6.83 7.83 1.24 22 .227
2.
3.
4.
5.
6.
DISCUSSION
The somewhat lengthy set of results seem to support one primary conclusion: Thermal biofeedback shows both a clinical and a statistical advantage over relaxation training in the treatment of hypertensive patients who require two drugs to control their blood pressure. This conclusion is supported by our clinical end point data on the ability of the patient to discontinue the second-stage antihypertensive medication while maintaining control of blood pressure and holds up (47°7o success for BF vs. 23°7o success for Relax) at a 3-month follow-up.
The home BP results are consistent with this conclusion, with the bio- feedback-treated group showing consistent significant reductions in BP after treatment and also significantly lower BPs after withdrawal of the second-stage drug in comparison to pretreatment levels. The relaxation- treated patients, on the other hand, generally did not show significant lowering of home BPs at posttreatment; at post-drug-withdrawal their BPs were generally equal to the pretreatment levels. This last finding seems to indicate that the relaxation training had "substituted," more or less, for the second-stage drug in these patients.

494 Blanchard, McCoy, Andrasik, Acerra, Pallmeyer, Gerardi, Halpern, and Musso
Specific comparisons of posttreatment and postwithdrawal home BPs do not, however, show a statistical advantage for thermal biofeedback over relaxation training.
The data from the psychophysiological testing were inconsistent: While the Biofeedback conditions showed some significant lowering of systolic BP at posttreatment (vs. pretreatment), particularly under baseline and relaxation conditions, the Relaxation condition did not. When examining the psychophysiological test results at post-drug-withdrawal, a different result is found: The BP values for the biofeedback treatment patients are arithmetically worse than the pretreatment levels; these results are statistically significant in three instances. For the Relaxation-treated patients, the postwithdrawal BPs tend to be essentially the same as the pretreatment levels, again indicating that relaxation had "subst i tu ted" for the second-stage drug.
Thus, at post-drug-withdrawal there is a trend for an advantage of relaxation over biofeedback on the psychophysiological testing data. This conclusion is limited by the very limited amount of data available at post-drug-withdrawal.
Our primary conclusions must be conditioned by four points: (1) The biofeedback patients received twice as many treatment contacts (over the same time interval) as the relaxation patients. It could thus be that success is merely a function of frequency of contact with the trainer, not the procedure, per se. (2) One particular relaxation regimen was used; others might yield different or better results. However, our regimen is very similar to the one successfully used by Agras and Taylor (Agras, personal communication, September 1983). (3) The results are short-term, approximately 4 months post-drug-withdrawal. Longer-term follow-up is ongoing and could show a different outcome. (4) These results are for a very specific patient population: patients whose BPs were well controlled on a two-drug regimen. Whether comparable results would be found with mild or borderline hypertension is not known. (5) We do not have data on what would happen to comparable patients who received no treatment but whose second-stage drug was discontinued for up to 4 months.
RESULTS
Agras, W. S., Southam, M. A., & Taylor, C. B. (1983). Long-term persistence of relaxation induced blood pressure lowering during the working day. Journal of Consulting and Clinical PSychology, 51, 792-794.
Bernstein, D. A., & Borkovec, T. D. (1973). Progressive relaxation training. Champaign, Illinois: Research Press...

Thermal Biofeedback for Hypertension 495
Bertilson, H. S., Bartz, A. E., & Zimmerman, A. D. (1979). Treatment program for border- line hypertension among college students: Relaxation, finger temperature biofeedback and generalization. Psychological Reports, 44, 107-114.
Blanchard, E. B., Andrasik, F., McCoy, G. C. Acerra, M., Pallmeyer, T. P., Gerardi, R. J., & Halpern, M. (1984, March). A controlled comparison of thermal biofeedback and progressive relaxation in the treatment of moderate hypertension. Proceedings of the 15th annual meeting, Biofeedback Society of America, (pp. 40-43). Wheat Ridge, Colorado: Biofeedback Society of America.
Blanchard, E. B., Andrasik, F., Neff, D. F., Arena, J. G., Ahles, T. .A., Jurish, S. E., Pallmeyer, T. P., Saunders, N. L., Teders, S. J., Barron, K. D., & Rodichok, L. D. (1982). Biofeedback and relaxation training with three kinds of headache: Treatment effects and their prediction. Journal of Consulting and Clinical Psychology~ 50, 562- 575.
Blanchard, E. B., McCoy, G. C., Andrasik, F., Pallmeyer, T. P., Saunders, N. L., Gerardi, R. J., & Acerra, M. C. (1983, March). A preliminary report on the controlled com- parison of thermal biofeedback and relaxation training in the treatment of moderate to severe essential hypertension. In Proceedings of the 14th Annual Meeting of Biofeed- back Society of America (pp. 45-46). Wheat Ridge, Colorado: Biofeedback Society of America.
Dixon, W. J., & Brown, M. B. (Eds.). (1979). Biomedical computer progress P-series (pp. 540-580). Berkeley: University of California Press.
Green, E. E., Green, A. N., & Norris, P. A. (1979). Preliminary observations on the new non-drug method for control of hypertension. Journal of the South Carolina Medical Association, 75, 575-586.
Jacobson, E. (1938). Progressive relaxation. Chicago: University of Chicago Press. Taylor, C. B., Farquhar, J. W., Nelson, E., & Agras, W. S. (1977). Relaxation therapy and
high blood pressure. Archives of General Psychiatry, 34, 339-343.