A controlled comparison of thermal biofeedback and relaxation training in the treatment of essential...
14
Biofeedback and Self-Regulation, Vol. 12, No. 3, 1987 A Controlled Comparison of Thermal Biofeedback and Relaxation Training in the Treatment of Essential Hypertension: III. Psychological Changes Accompany- ing Treatment 1 Edward B. Blanchard, 2 Robert J. McCaffrey, Alison Musso, and Maryrose A. Gerardi The University of Albany, State University of New York Guy C. McCoy Albany Medical College Eighty-seven medicated essential hypertensives received either thermal bi- ofeedback (TBF) or progressive muscle relaxation (PMR) training as a sub- stitute for their second-stage antihypertensive medication. The psychological changes accompanying the treatments were obtained at pretreatment, at post- treatment and at the 3- and 6-month follow-up. Few psychological changes were noted, owing in part to the absence of psychopathological elevations at pretreatment. Short-term psychological changes were greater in patients who were withdrawn from their second-stage antihypertensive medication and then treated compared with those treated and then withdrawn from their medication. This finding may reflect the presence of antihypertensive medi- cation side effects involving psychological factors. In general, TBF patients were more Type B at long-term follow-up compared with PMR patients, who tended toward greater Type A characteristics. Descriptor Key Words: thermal biofeedback; progressive muscle relaxation; essential hyper- tension; Type A; trait anger; psychological changes. 1This research was supported by a grant from NHLBI, HL-27622. 2Address all correspondence to Dr. Edward B. Blanchard, Center for Stress and Anxiety Dis- orders, 1535 Western Avenue, Albany, New York 12203. 227 0363-3586/87/0900-0227505.00/0 © 1987PlenumPublishing Corporation
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of A controlled comparison of thermal biofeedback and relaxation training in the treatment of essential...

Biofeedback and Self-Regulation, Vol. 12, No. 3, 1987
A Controlled Comparison of Thermal Biofeedback and Relaxation Training in the Treatment of Essential
Hypertension: III. Psychological Changes Accompany-
ing Treatment 1
Edward B. Blanchard, 2 Robert J. McCaffrey, Alison Musso, and Maryrose A. Gerardi The University o f Albany, State University of New York
Guy C. McCoy Albany Medical College
Eighty-seven medicated essential hypertensives received either thermal bi- ofeedback (TBF) or progressive muscle relaxation (PMR) training as a sub- stitute for their second-stage antihypertensive medication. The psychological changes accompanying the treatments were obtained at pretreatment, at post- treatment and at the 3- and 6-month follow-up. Few psychological changes were noted, owing in part to the absence o f psychopathological elevations at pretreatment. Short-term psychological changes were greater in patients who were withdrawn from their second-stage antihypertensive medication and then treated compared with those treated and then withdrawn from their medication. This finding may reflect the presence o f antihypertensive medi- cation side effects involving psychological factors. In general, TBF patients were more Type B at long-term follow-up compared with PMR patients, who tended toward greater Type A characteristics.
Descriptor Key Words: thermal biofeedback; progressive muscle relaxation; essential hyper- tension; Type A; trait anger; psychological changes.
1This research was supported by a grant from NHLBI, HL-27622. 2Address all correspondence to Dr. Edward B. Blanchard, Center for Stress and Anxiety Dis- orders, 1535 Western Avenue, Albany, New York 12203.
227
0363-3586/87/0900-0227505.00/0 © 1987 Plenum Publishing Corporation
228 Blanchard, McCaffrey, Musso, Gerardi, and McCoy
In the treatment of psychophysiologic disorders with self-regulatory treat- ments such as relaxation and thermal biofeedback, the usual target or goal is the change in some physiological response, such as blood pressure (BP) in the treatment of hypertension, or in some symptom, such as report of head pain in chronic headache. In a recent report from our center (Blan- chard, Andrasik, et al., 1986), we noted the significant reductions in trait anxiety and depression that accompanied self-regulatory treatment of ten- sion, migraine, and combined migraine and tension headache. These posi- tive psychological changes, or side effects, appeared regardless of whether there was significant headache relief or not. This finding has led us to exa- mine whether there are similar positive side effects of self-regulatory treat- ment when the target is essential hypertension.
Although there have been numerous studies of the self-regulatory treat- ment of hypertension (see McCaffrey & Blanchard, 1985, for a recent review), very few studies have assessed possible psychological changes accompany- ing treatment. Bali (1979) compared a combination of relaxation procedures to supportive psychotherapy in the treatment of hypertension. The psy- chotherapy group later received relaxation training. Bali reported significant within-group decreases in Taylor Manifest Anxiety Scale (Taylor, 1953) scores accompanying the relaxation training. No between-group comparisons were reported.
Seer and Raeburn (1980) compared two variants of meditation to a no- treatment control. Although the SCL-90 (DeRogatis, 1975) and STAI (Spiel- berger, Gorsuch, & Lushene, 1970) were given, no results were reported. Fi- nally, Hafner (1982) compared meditation with and without biofeedback to a no-treatment control. The Rathus Assertiveness Scale (Rathus, 1973) and Middlesex Questionnaire showed no changes for treated subjects. Treated females, but not males, showed decrease in hostility and extra punitiveness.
In the course of conducting a moderate-size comparison of two self- regulatory treatments for essential hypertension (Blanchard et al, 1984; Blan- chard, McCoy, et al., 1986), progressive muscle relaxation (PMR), and ther- mal biofeedback (TBF), we have investigated the psychological changes that accompany treatment. From these data we sought to determine whether there are differential psychological changes associated with PMR and TBF.
M E T H O D
Overview of Experimental Design and Clinical Outcome
The details of the experimental design and clinical outcome with regard to blood pressure (BP) and medication reduction have been presented else-

Psychological Changes 229
where (Blanchard et al., 1984; Blanchard, McCoy, et al., 1986). To briefly summarize, patients entered the study with BP controlled on two antihyper- tensive medications, with the goal (and clinical end point) being elimination of the second-stage antihypertensive medication while BP remained under control. Half of the patients were randomized to receive PMR while the other half were to receive TBF. Within each of these treatment conditions, an attempt was made to taper half of the patients of f the second-stage drug pri- or to treatment while the other half were treated before drug withdrawal. Patients whose medications could not be discontinued were restabilized and treated in the same condition. The details of this are shown schematically in Figure 1.
As can be seen, patients received psychological assessment at three points: prior to treatment or tapering, at the end of their first phase (at ap- proximately 3 months), and then at the end of their second phase (approxi- mately 3 months later).
Patients
A total of 86 patients (52 males, 34 females) with an average age of 49.5 years were initially randomized to the four primary treatment condi- tions. The mean duration of antihypertensive medication usage was 8.1 years. All of the patients had been diagnosed both by their personal physician and by the study physician (G.C.M.) as having essential hypertension. All pa- tients entered the study with their BP controlled (SBP less than 140 mm Hg and DBP less than 90 mm Hg) on at least two drugs, usually a diuretic and a sympathetically active drug. The mean BPs at pretreatment were 136.1/85.5.
All patients underwent a thorough physical and laboratory examination prior to entering the study in order to rule out any obvious end organ damage or other serious medical disorder. In addition, all patients were screened through clinical interview for the presence of any major psychiatric disorder (e.g., schizophrenia, bipolar affective disorder, organic brain syndrome).
All patients provided written informed consent for each stage of their participation in the study. Data on the demographic characteristics of the patients in the four primary conditions have been reported elsewhere (Blan- chard, McCoy, et al., 1986) and revealed no significant differences across the four conditions.
Dependent Variables
Clinical End Point. The principal dependent variable in this study was the "clinical end point." Specifically, patients were termed a success if their

230 Blanchard, McCaffrey, Musso, Gerardi, and McCoy
Four Week Baseline [ Pts. monitor [
ASSESSMENT #i Pre-Treatment (n=78)
R e l a x a t i o n I ~ h e r m a l B i o l e e d b a e ~
!
I. Withdraw from / 2nd Stg. Drug [
i
i
i i
i i
i . . . .
H . Relaxation Training
(n=26)
M. Withdraw from 2nd Stg. Drug
i . . . .
IV. Thermal Biofeedback
(n=Z4)
Phase 1 (8 wke)
I . Relaxation Training
(n=8)
ASSESS)~ENT #2 Mid-Treatment (n=71)
[
IT. Withdraw from 2nd Stg. Drug
~(O~of study)
HI. Thermal Biofeedback
(n=13)
IV. Withdraw from 2rid Stg. Drug Phase 2
~ ( O u t of study)
ASSESSMENT #3 Post-Treatment (n=45)
(Relaxat~ion) ~ d b a c k )
(n=7) ~ ( n = l o ) J
S~_ ASSESSMENT #4 Month Follow-up (n~2S)
(n=5) (n=14)
ASSESSMENT #5 8-Month Follow-up (n=19)
(Failures out of Study)
(Failures out of Study)
Fig, 1. Patient flow chart through protocol.

Psychological Changes 231
blood pressure remained under control (i.e., BP < 140/90) on a single drug (diuretic) and their overall medical status remained satisfactory. Patients were classified as a failure if they had to be returned to the second-stage antihyper- tensive drug (see Blanchard et al., 1984; Blanchard, McCoy, et al., 1986, for complete description of criteria for declaring patient a failure).
The clinical end point data (Blanchard, McCoy, et al., 1986) showed a significant advantage in the short-term (approximately 2 months postdrug withdrawal, p < .001) and in the long-term (13 months posttreatment, p < .05) for TBF over PMR.
Psychological Variables. The psychological variables consisted of the SCL-90 (DeRogatis, 1975), Beck Depression Inventory (Beck, Ward, Men- delson, Mock, & Erbaugh, 1961), State-Trait Anxiety Inventory (Spielberg- er et al., 1970), State-Trait Anger Scales (Spielberger, 1980), Rathus Assertiveness Inventory (Rathus, 1973), Holmes and Rahe Life Events Scale (Homes & Rahe, 1967), Buss-Durkee Hostility Scale (Buss & Durkee, 1957), and Jenkins Activity Survey (Jenkins, Zyzanski, & Roseman, 1965).
As noted in Figure 1, the psychological data were obtained at pretreat- ment assessment, midtreatment assessment, and posttreatment assessment, and during 3- and 6-month follow-up. The short-term psychological changes for patients in Conditions I and III, who were withdrawn from their second- stage drug and then treated with either PMR (I) or TBF (III), are based on the post-drug withdrawal, midtreatment assessment, and the posttreatment assessment. The short-term psychological changes for patients in Condition II and IV are based on the pretreatment assessment and midtreatment psy- chological assessment. The long-term psychological data were analyzed us- ing the pretreatment and the two follow-up assessments (i.e., 3 and 6 months).
Description of Treatment
Thermal Biofeedback Training. This regimen consisted of 16 individu- al sessions on a twice-per-week basis and was modeled closely after the proce- dure used at the Meninger Foundation (Green, Green, & Norris, 1979), where it was developed.
The actual biofeedback training sessions were approximately 50 minutes long. They included, after an adaptation period, a 5-minute in-session base- line, 20 minutes of actual feedback training, and a 5-minute self-control phase before and after the feedback training. Deep diaphragmatic breathing was taught early in the session.
Patients were given a small (about 10 cm) alcohol-in-glass thermome- ter to assist home practice. Patients were asked to practice warming their hands for about 20 minutes daily on their own. See Blanchard, McCoy, et al. (1986) for a more detailed description of the TBF training.

232 Blanchard, McCaffrey, Musso, Gerardi, and McCoy
Progressive Muscle Relaxation Training. PMR training consisted of a total of eight sessions spread over 8 weeks. Patients were seen twice in the 1st week and then once weekly for the next 7 weeks, except for no session at week 7. The regimen followed closely Bernstein and Borkovec's (1973) adaptation of Jacobson's (t938) progressive muscle relaxation.
The relaxation regimen began with systematic tensing and relaxing of 16 muscle groups, was reduced then to 8 groups, and then to 4 groups. Relax- aion by recall, in which muscles are passively relaxed by matching the memory of the relaxed state, was next introduced, followed by cue-controlled relaxa- tion. Attention to the value of deep diaphragmatic breating was stressed throughout.
All training was done live on an individual basis, with the patient com- fortably seated in an upholstered recliner. At the first session the patients were given an audiocassette of the instructions for the full 16 muscle group relaxation program and were instructed to practice relaxing on their own for at least 20 minutes daily. From the middle of training on, some discussion was held with patients on how to apply the relaxation to everyday stressful situations.
R E S U L T S
Pretreatment Psychological Characteristics
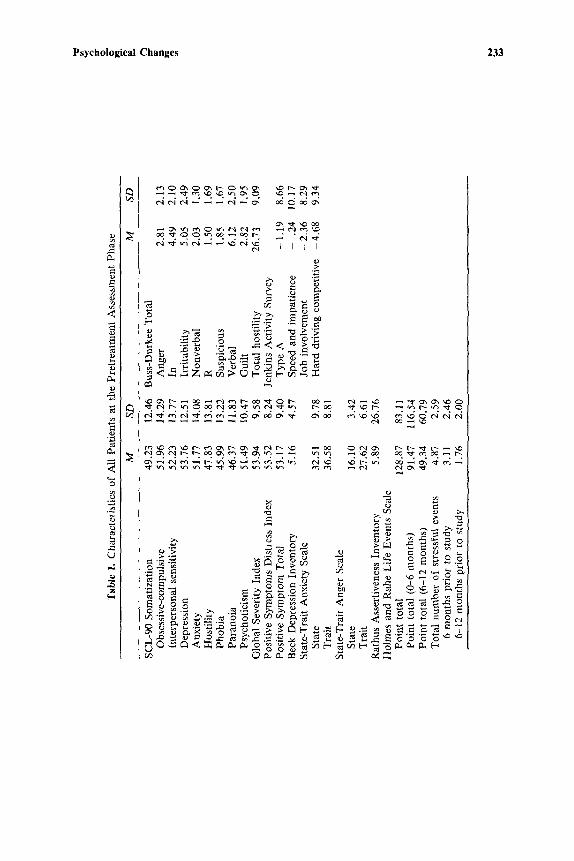
The psychological characteristics of all the patients who began the study are presented in Table I. As indicated in Table I, the sample of essential hyper- tensives as a whole revealed few psychopathological characteristics.
Short-Term Psychological Changes
The short-term psychological changes were examined in patients who were treated with either PMR or TBF while on their antihypertensive medi- cation and then withdrawn from their antihypertensive medication (Condi- tions II and IV), Separate 2 x 2 ANOVAs (treatment groups x time (pre/post assessment)) were performed on each of the psychological varia- bles. Correlated t tests were also performed, as warranted, on the pre- to posttreatment changes within specific treatment condition. Of the several vari- ables studied, only the State-Trait Anger Scale revealed significant effects, and interaction of Group X Phase on both state and trait anger. Table II presents the significant findings for these analyses. As demonstrated in Ta- ble II, the PMR patients showed a reduction in state and trait anger from
Psychological Changes 233
<
('~1 '~- u'~ e~ ~ ,-.~ ~ ¢~ ~ I I [ I
~ ",~
" ~ " ~ o ~ ~ c~ ~ ' ~ ~ "~ ~
e d ' 4 M e . i ~ e d d . . . ; @ ~ d d ' 4 d d
~ . ~ , ~ . . ~ ~ . ~ ~ ~ . ,
. ~ c~
~ < ~ . ~ o ~ ~ -~

234 Blanchard, McCaffrey, Musso, Gerardi, and McCoy
o~
° ~
L~
i
~" V
II rl
6
A~
Psychological Changes 235
pre- to posttreatment, while the TBF patients tended to demonstrate slightly greater state and trait anger from pretreatment to posttreatment. Only the reduction of trait anger for the PMR patients reached significance (p < .05).
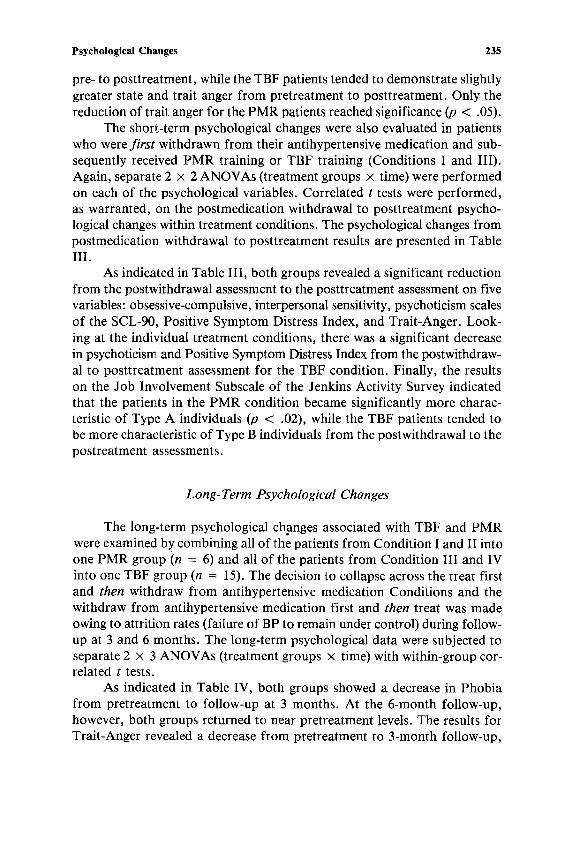
The short-term psychological changes were also evaluated in patients who were first withdrawn from their antihypertensive medication and sub- sequently received PMR training or TBF training (Conditions I and III). Again, separate 2 × 2 ANOVAs (treatment groups × time) were performed on each of the psychological variables. Correlated t tests were performed, as warranted, on the postmedication withdrawal to posttreatment psycho- logical changes within treatment conditions. The psychological changes from postmedication withdrawal to posttreatment results are presented in Table III.
As indicated in Table III, both groups revealed a significant reduction from the postwithdrawal assessment to the posttreatment assessment on five variables: obsessive-compulsive, interpersonal sensitivity, psychoticism scales of the SCL-90, Positive Symptom Distress Index, and Trait-Anger. Look- ing at the individual treatment conditions, there was a significant decrease in psychoticism and Positive Symptom Distress Index from the postwithdraw- al to posttreatment assessment for the TBF condition. Finally, the results on the Job Involvement Subscale of the Jenkins Activity Survey indicated that the patients in the PMR condition became significantly more charac- teristic of Type A individuals (p < .02), while the TBF patients tended to be more characteristic of Type B individuals from the postwithdrawal to the postreatment assessments.
Long-Term Psychological Changes
The long-term psychological changes associated with TBF and PMR were examined by combining all of the patients from Condition I and II into one PMR group (n = 6) and all of the patients from Condition III and IV into one TBF group (n = 15). The decision to collapse across the treat first and then withdraw from antihypertensive medication Conditions and the withdraw from antihypertensive medication first and then treat was made owing to attrition rates (failure of BP to remain under control) during follow- up at 3 and 6 months. The long-term psychological data were subjected to separate 2 × 3 ANOVAs (treatment groups x time) with within-group cor- related t tests.
As indicated in Table IV, both groups showed a decrease in Phobia from pretreatment to follow-up at 3 months. At the 6-month follow-up, however, both groups returned to near pretreatment levels. The results for Trait-Anger revealed a decrease from pretreatment to 3-month follow-up,

236 Blanchard, McCaffrey, Musso, Gerardi, and McCoy
<
8
0
P~
off
r,
0
N
o ~
v v
II II ' II ~ . II ~ V ~V ,-.V ~V ,~
II ~ v
V
II " ~ V
,.2
e~
~Q ~O
~ ' "N "N
.~ ? -
E o -
' , ~ ' 0
L ~
r ~
< ~ "~ ~ - ~ - . g o ~
r ~
~ v
~ o , ~ - v ~
"O
O
=~. 0 0
¢'-1 ~,D
o<-=
I [
I I

Psychological Changes 23"/
..=
v~
O
[-
o
J e~
v
II II •
v ~ v
v
~ v
H ~ V ¢",1
I I I I I
..=

238 Blanchard, McCaffrey, Musso, Gerardi, and McCoy
which continued to the 6-month follow-up. There was also a statiscally sig- nificant decrease in Trait-Anger from 3- to 6-month follow-up for the TBF group. The Speed and Impatience scale of the Jenkins Activity Survey rev- ealed an increase in Type B characteristics in both treatment groups during follow-up but no differential between-group effects. Finally, the Job Involve- ment Subscale revealed that the PMR group became more characteristic of Type A individuals during follow-up while the TBF group showed the oppo- site effect (i.e., TBF patients were more characteristic of Type B individu- als) during follow-up.
DISCUSSION
The present study indicates that there are both short-term and long- term psychological changes in patients receiving PMR or TBF as an adjunct to antihypertensive medication for the control of BP in essential hyperten- sion. It is interesting to note that there are a greater number of short-term psychological changes in patients who are withdrawn from their second-stage, sympathetically active, antihypertensive medication and then treated, com- pared with patients who are treated with either PMR or TBF and then with- drawn from their second-stage drug. One factor that may contribute to the "appearance" of greater psychological improvement in the withdrawal from medication then treat conditions is the alleviation of biobehavioral sequelae associated with the therapeutic use of adrenergic-inhibiting antihypertensive agents, such as metoprolol (for a review of this literature see Rosen & Kos- tis, 1985). Thus, the greater number of short-term psychological changes in this group may reflect an interaction betweeen PMR or TBF treatment with a concomitant reduction in CNS side effects due to the cessation of the pa- tients' second-stage antihypertensive medication. This hypothesis certainly warrants further investigation and in absence of any differential treatment outcome may be a preferable procedure for administering treatments.
The long-term pyschological changes (i.e., out to 6-month posttreat- ment follow-up) revealed that changes in two of the four variables (i.e., Trait- Anger, and Job Involvement Subscale) present at the short-term outcome continued to be present at follow-up. Interestingly, two other variables emerged as statistically significant during long-term follow-up (i.e., Phobia, and Speed and Impatience).
The issue of differential psychological changes attributable to either PMR or TBF in patients who were treated first and then withdrawn from their second-stage medication reveals that PMR patients showed less state and trait anger from pre- to posttreatment (time) while the TBF patients demonstrated an increase in both variables. The precise reasons for this are
Psyhcological Changes 239
unclear. There were, however, differences in the number of office sessions for each condition (8 for PMR vs. 16 for TBF). In addition, the therapist was present for all PMR sessions but for only the first two sessions for TBF. Finally, only patients with the PMR condition were given instructions for breathing and transfer of training. Nonetheless, it is interesting to note that both treatment conditions showed reduction in Trait Anger at 3- and 6-month follow-up assessments. Similarly, the short-term differences on the Job In- volvement Scale indicating an increase in Type A characteristics among PMR patients at the short-term evaluation continued during long-term follow-up.
In general, the psychological changes obtained in the present study with a population of essential hypertensives were modest compared with those reported for anxiety and depression in headache (Blanchard, Andrasik, et al., 1986) and irritable bowel syndrome populations (Blanchard, Radnitz, Schwarz, Neff, & Gerardi, 1987). The lack of changes in anxiety and depres- sion in the present study probably reflects the absence of elevations on these variables at pretreatment. In fact, the population of essential hypertensives in the study were basically psychologically normal at the pretreatment as- sessment. Given this state of affairs, the absence of dramatic changes reported to occur at posttreatment with other psychophysiological disorders is not sur- prising. It remains to be determined if the psychological characteristics of the present population of essential hypertensives are representative of essen- tial hypertension generally.
REFEERENCES
Bali, L. R. (1979). Long-term effect of relaxation on blood pressure and anxiety levels of essen- tial hypertensive males: A controlled study. Psychosomatic Medicine, 41(8), 637-646.
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J., & Erbaugh, J. (1961). An inventory for measuring depression. Archives of General Psychiatry, 5, 561-571.
Bernstein, D. A., & Borkovec, T. D. (1973). Progressive relaxation training. Champaign, Il- linois: Research Press.
Blanchard, E. B., Andrasik, F., Appelbaum, K. A., Evans, D. D., Myers, P., & Barton, K. D. (1986). Three studies of the psychological changes in chronic headache patients as- sociated with biofeedback and relaxation therapies. Psychosomatic Medicine, 48, 73-83.
Blanchard, E. B., McCoy, G. C~, Andrasik, F., Acerra, M. Pallmeyer, T. P., Gerardi, R., Hal- pern, M., & Musso, A. (1984). Preliminary results from a controlled evaluation of ther- mal biofeedback as a treatment for essential hypertension. Biofeedback and Self-Regulation, 9, 471-495.
Blanchard, E. B., McCoy, G. C., Musso, A., Gerardi, M. A., Pallmeyer, T. P., Gerardi, R. J., Cotch, P. A., Siracusa. K., & Andrasik, F. (1986). A controlled comparison of thermal biofeedback and relaxation training in the treatment of essential hypertension: I. Short- term and long-term outcome. Behavior Therapy, 17, 563-579.
Blanchard, E. B., Radnitz, C., Schwarz, S. P., Neff, D. F., & Gerardi, M. A. (1987). Psycho- logical changes associated with self-regulatory treatment of irritable bowel syndrome. Biofeedback and Self-Regulation, 12, 31-38.

240 Blanchard, McCaffrey, Musso, Gerardi, and McCoy
Buss, A. H., & Durkee, A. (1957). An inventory for assessing different kinds of hostility. Jour- nal of Consulting Psychology, 21, 243-248.
DeRogatis, L. (1975). The SCL-9OR. 1228 Wine Spring Lane, Baltimore,, Maryland. Green, E. E., Green, A. N., & Norris, P. A. (1979). Preliminary observations on the new non-
drug method for control of hypertension. Journal of the South Carolina Medical As- sociation, 75, 575-586.
Hafner, R. J. (1982). Psychological treatment of essential hypertension: A controlled compari- son of medication and meditation plus biofeedback. Biofeedback and Self-Regulation, 7, 305-316.
Holmes, T. H., & Rahe, R. H. (1967). The social readjusment rating scale. Journal of Psy- chosomatic Research, 11, 213-218.
Jacobson, E. (1938). Progressive relaxation. Chicago: University of Chicago Press. Jenkins, C. D., Zyzanski, S. J., & Rosenman, R. H. (1965). Jenkins Activity Survey. New York:
Psychological Corp. McCaffrey, R. J., & Blanchard, E. B., (1985). Stress management approaches to the treatment
of essential hypertension. Annals of Behavioral Medicine, 7, 5-12. Rathus, S. A. (1973). A 30-item schedule for assessing assertive behavior. Behavior Therapy,
4, 398-406. Rosen, R. C., & Kostis, J. B. (1985). Biobehavioral sequelae associated with adrenergic-inhibiting
antihypertensive agents: A critical review. Health Psychology, 4, 579-604. Seer, P., & Raeburn, J. N. (1980). Meditation training and essential hypertension: A methodo-
logical study. Journal of Behavioral Medicine, 3, 59-71. Spielberger, C. D. (1980). Preliminary manual for the State-Trait Anger Scale (STAS). Tampa,
Florida: University of South Florida. Spielberger, C. D., Gorsuch, R. L., & Lusbene, R. E. (1970). STAI manual for the State-Trait
Anxiety Inventory. Palo Alto: Consulting Psychologists Press. Taylor, J. A. (1953). A personality scale of manifest anxiety. Journal of Abnormal and Social
Psychology, 48, 285-290.
(Revision received June 8, 1987)




















