Incorporating Predictive Maintenance Practices into Marine ...
Upload
independentCategory
view
2download
0
REVIEW
Predictive biomarkers for cancer therapy with PARP inhibitorsJ Michels1,2,3, I Vitale4,5, M Saparbaev2,3,6, M Castedo1,2,3,11 and G Kroemer1,2,3,7,8,9,10,11
Poly(ADP-ribose) polymerase (PARP) inhibitors have raised high expectations for the treatment of multiple malignancies. PARPinhibitors, which can be used as monotherapies or in combination with DNA-damaging agents, are particularly efficientagainst tumors with defects in DNA repair mechanisms, in particular the homologous recombination pathway, for instance due toBRCA mutations. Thus, deficient DNA repair provides a framework for the success of PARP inhibitors in medical oncology. Here,we review encouraging results obtained in recent clinical trials investigating the safety and efficacy of PARP inhibitors as anti-cancer agents. We discuss emerging mechanisms of regulation of homologous recombination and how inhibition of DNA repairmight be used in cancer therapy. We surmise that the identification of patients that are likely to benefit from PARP inhibitionwill improve the clinical use of PARP inhibitors in a defined target population. Thus, we will place special emphasis on biomarkerdiscovery.
Oncogene advance online publication, 16 September 2013; doi:10.1038/onc.2013.352
Keywords: PAR; base excision repair; homologous recombination; BRCAness; synthetic lethality
INTRODUCTIONThe superfamily of poly(ADP-ribose) (PAR) polymerases (PARPs),1
whose discovery dates back to the early 1960s, nowadays en-compasses 17 distinct members that participate in a wide arrayof cell functions, including DNA transcription, DNA repair,genomic stability maintenance, cell cycle regulation as well asnon-apoptotic cell death (Table 1).2–5
PARP1, a multifunctional enzyme of 113 kDa, is the mostabundant, ubiquitously expressed and best-characterized memberof the superfamily.6 PARP1 has a highly conserved structural andfunctional organization including: an N-terminal double zinc fingerDNA-binding domain, a central auto-regulation domain and aC-terminal catalytic domain that binds oxidized nicotinamideadenine dinucleotide (NADþ ).7 PARP1 is a DNA nick sensor thatutilizes NADþ as a substrate to catalyze the covalent attachmentof ADP-ribose units to the g-carboxyl group of Glu residues of awide array of target proteins. This post-translational modificationknown as poly-ADP-ribosylation or PARylation increases morethan 500-fold in the presence of DNA-strand breaks.8 AlthoughPARP1 accounts for the vast majority (B85%) of PAR polymersynthesis, five other members have catalytic activity of PARylation,namely PARP2, PARP3, PARP4 and PARP5A/B (also known astankyrase1/2).9 Recently, Hottiger reported a new classification forthe ADP-ribosyl transferases grouping the PARP family membersand distinguishing proteins with mono or poly(ADP)ribosylationactivity.9
Here, we provide an overview on the roles of PARP1, focusingon its involvement in cellular stress management, and thepossibility to target PARP1 for the treatment of cancer. We willdevote special attention to the discovery of predictive biomarkersthat may improve patient selection.
PARP1 IN PHYSIOLOGICAL AND PATHOLOGICAL RESPONSESPARP1 is historically known as a sensor of DNA nicks, contributingto the single-strand break repair, the orchestration of the DNAdamage response (DDR) and the maintenance of genomicstability.10,11 Nevertheless, several recent studies have led to theidentification of a plethora of novel roles for PARP1, placing itsactivity at the center of the cellular stress response network.
PARP1� /� knockout mice exhibit (i) increased genetic instabilityas measured by the frequency of micronuclei, sister chromatidexchanges and other chromosome aberrations as well as (ii) majorDNA repair defects coupled to hypersensitivity to alkylating agentsand g-radiation.12 Nonetheless, the inhibition of PARP is not lethalfor mammals,13 and Parp1� /� mice are viable and fertile, eventhough they manifest accelerated aging and exhibit a higherincidence of spontaneous or carcinogen-induced tumors thanwild-type controls.14 However, the simultaneous loss of PARP1 andPARP2 is lethal at the onset of gastrulation, suggesting that the twoPARP proteins have redundant roles in embryogenesis.15
PARP1 and the DDRDue to the continuous exposure to endogenous and exogenousDNA-damaging insults, cells experience DNA lesions such as SSBsand double-strand breaks (DSBs) that require continuous activa-tion of DNA repair pathways (Box 1).
The levels of PARP1 protein increase in response to DNAdamage,16 and PARP1 contributes to both SSB and DSB repair.PARP1 associates with persisting SSBs or DSBs where it becomesactivated and catalyzes the PARylation of multiple nuclear acceptorproteins adjacent to the DNA break including that of PARP1 itself,histones, DNA repair proteins, chromatin regulators and transcriptionfactors.7,17 PARylation facilitates the chromatin decondensation,
1INSERM, U848, Villejuif, France; 2Institut Gustave Roussy, Villejuif, France; 3Universite de Paris Sud, Villejuif, France; 4Regina Elena National Cancer Institute, Roma, Italy; 5NationalInstitute of Health, Rome, Italy; 6CNRS UMR8200, Villejuif, France; 7Metabolomics Platform, Institut Gustave Roussy, Villejuif, France; 8Centre de Recherche des Cordeliers, Paris,France; 9Pole de Biologie, Hopital Europeen Georges Pompidou, AP-HP, Paris, France and 10Faculty of Medicine, Universite Paris Descartes, Paris, France. Correspondence:Dr M Castedo or Professor G Kroemer, INSERM U848, Institut Gustave Roussy, 114 rue Edouard Vaillant, F-94805 Villejuif, France.E-mail: [email protected] or [email protected] authors share senior co-authorship.Received 17 June 2013; revised 9 July 2013; accepted 12 July 2013
Oncogene (2013), 1–14& 2013 Macmillan Publishers Limited All rights reserved 0950-9232/13
www.nature.com/onc

thereby rendering DNA lesions accessible to the repair machinery. Inaddition, PARP1 may favor the assembly of protein complexesinvolved in DDR.18,19 Although controversial,20,21 PARP1 may operatein base excision repair (BER) by detecting the presence of SSBs, aswell as by recruiting and modulating the activity of repair proteinssuch as X-ray cross-complementing gene 1 (XRCC1), DNA ligase IIIand 8-oxoguanine-DNA glycosylase.11,22
PARP1 may contribute to nucleotide excision repair, assuggested by the finding that ultraviolet radiation-induced directDNA lesions including thymine dimers—which are removed bythe nucleotide excision repair machinery—activate PARP1.23
PARP1 operates in nucleotide excision repair by stabilizingdamaged DNA-binding protein 224,25 or by associating withXeroderma Pigmentosum Complementation Group A.26
PARP1 is believed to promote the repair and restart of stalledreplication forks during homologous recombinational repair (HRR)by attracting MRE11, a component of the MRN (Mre11-Rad50-Nbs1) complex, to collapsed replication forks.27 The combinedaction of PARP1 and BRCA2 may also protect stalled replicationforks from Mre11-mediated degradation.28,29 Moreover, PARP1activates HRR by antagonizing the suppressive impact of theKU70–KU80 heterodimer and/or ligase IV—two key players ofnon-homologous end joining (NHEJ)—on HRR.30–32
PARP1 is essential to accomplish alternative (A) NHEJ.33,34
Moreover, PARP1 may cooperate with DNA-PKcs in the initiatingstep of canonical (C) NHEJ.35 However, the precise contribution of
Table 1. Multiple PARP functions
Actor Function Reference
DNA repair XRCC1 BER 11,22
DDB2, XPA NER 24–26
MRE11 HRR 27
DNA-PKC NHEJ 35
Genomicstability
Topoisomerase I Genomicmaintenance
88
Telomereendings
Genomic stability 199
Mitotic spindlepoles
Mitosis 199
DNAtranscription
Histone H1 Decondensation ofthe double DNAhelix
200
Cell cycleprogression
c-Fos, c-Myc G0-G1 transition 201
Inflammation TNF-a, NF-kB,HMGB1
Acute and chronicinflammation
62
Cellmetabolism
NADþ Mitochondrialrespiration
66
Cell death/survival
AIF Parthanatos 47
ROS Apoptosis 202
Glycolysisinhibition, NADþ
depletion
Necrosis 66,202
AMPK activation Autophagy 52
Abbreviations: AIF, apoptosis-inducing factor; AMPK, AMP kinase; ATM,ataxia-telangiectasia mutated; BER, base excision repair; DDB2, damagedDNA-binding protein; DNA-PKc, DNA-dependant protein kinase; HRR,homologous recombinational repair; NADþ , nicotinamide adenine dinu-cleotide; NER, nucleotide excision repair; NHEJ, non-homologous endjoining; PARP, poly-(ADP-ribose) polymerase; ROS, reactive oxygen species;TNF-a, tumor necrosis factor a; XPA, xeroderma pigmentosum comple-mentary group A; XRCC1, X-ray repair cross-complementing 1.
Box 1 DNA repair pathways
� Base excision repair (BER) is a DNA repair pathway thatremoves non-bulky base lesions in form of the free bases, asthey occur after spontaneous, oxidative and alkylating DNAdamage.181 BER includes different effectors acting at distinctsteps. In human cells DNA glycosylases (for example,8-oxoguanine-DNA glycosylase (OGG1), alkyl-N-purine-DNAglycosylase (ANPG), endonuclease III DNA glycosylase hNTH1)retrieve the damaged bases182–185 generating abasic sites thatthen are cleaved by AP endonuclease 1, APE1, inducing single-strand breaks (SSBs).186 PARP1 and PARP2 attract differentrepair enzymes to the DNA lesion site (for example, X-raycross-complementing factor 1 XRCC1, polymerase b, pro-liferating cell nuclear antigen (PCNA), ligase 3).37
� Nucleotide excision repair (NER) is a pluripotent pathwayfor recognition and removal of bulky helix disturbing DNAlesions generated by UV irradiation and anticancer agentssuch as cisplatin (CDDP). NER involves dual incisions thatbracket lesion site and release of the 24–32 nucleotide-longoligomer containing damaged residues. Two sub-pathwaysare identified, (i) the transcription-coupled repair (TC-NER) intranscriptionally active genes and (ii) the global genomicrepair (GG-NER) operating on the entire genome.187 RNApolymerase II is stalled at the DNA lesions are sensed bycockayne syndrome WD repeat proteins (CSA and CSB) in TC-NER and by Xeroderma pigmentosum (XPC) in GG-NER.188 Inboth pathways, the lesions are excised by endonucleases (forexample, XPG and ERCC1-XPF) and resulting DNA gap is thenfilled and sealed by DNA polymerases d, e and ligase III,respectively. NER also contributes to repair intra andinterstrand crosslinks (ICL) and oxidative DNA damage.
� Mismatch repair (MMR) is a system that recognizes andrepairs DNA replication and recombination errors, such asmismatched bases, deletions and insertions. In human cellstwo major heterodimers: Msh2/Msh6 (MutSa), and Msh2/Msh3 (MutSb) recognize DNA mismatches and trigger theirremoval by recruiting MutLa (MLH1/PMS2) and MutLb(MLH1/PMS1) complexes.
� Direct repair (DR) is the direct reversal of a damaged base toits native state without excision and de novo DNA synthesis.At present, there are three types of DNA damage known tobe repaired by chemical reversion including: photoreactiva-tion process by photolyases, O-methylation (in O6-Guanine,O4-Thymine and phosphates) is directly reversed by theprotein O6-methylguanine DNA methyltransferase (MGMT)and oxidative demethylation of N-methyl groups by AlkBfamily proteins. MGMT transfers the methyl/alkyl groupsfrom mutagenic DNA base lesions O6-meG and O4-meTgenerated by chemotherapeutic agents like dacarbazine andTMZ onto one of its nucleophilic cysteine residues situated inthe protein active site. Importantly, the cysteine acceptor siteis not regenerated after the transfer, and therefore theseproteins are not true enzymes. The self-methylated DNA-methyltransferases are referred to as suicidal DNA repairproteins, as they are irreversibly inactivated during thisstoichiometric repair reaction.73,189
� Homologous recombination (HR) is a prominent DNAhomology-directed double-strand break (DSB) repair pathwaythat in general proceeds in error-free manner. In HR repairpathway, Rad51 protein catalyzes DNA-strand exchangebetween similar or identical DNA molecules. DSB is repairedusing the homologous non-damaged sister chromatid orhomologous chromosome as a template. In human cells, HRrequires BRCA1 and BRCA2, RAD51 and FANC proteins. HRonly acts during the S and G2 phases of the cell cycle.190
Anticancer profile of PARP inhibitorsJ Michels et al
2
Oncogene (2013) 1 – 14 & 2013 Macmillan Publishers Limited

PARP1 to C-NHEJ—at least in human cells—remains to beestablished24, and a role of PARP3, rather than PARP1, inpromoting the DSB repair during C-NHEJ has recently beenproposed.36
Given its multiple roles in DDR, pharmacological inhibitors ofthe enzymatic activity of PARP are considered as promising agentsfor anticancer therapy (see below). PARP inhibitors subvert SSBrepair, thereby inducing the formation of stalled replication forksand/or suppress DSB repair. Alternatively, PARP inhibitors may actby trapping PARP1 at the SSB intermediate formed during BER,thus impairing the access of BER proteins to the DNA lesion andprovoking the obstruction of replicative forks.37 PARP inhibitorsare particularly effective against BRCA1- and BRCA2-defectivetumors by provoking synthetic lethality.16 In this context, a currentmodel suggests that, in conditions of HRR deficiency (HRD), whichmay result from loss-of-function mutations in BRCA1/2, DNAdamage sensors (NBS1, ataxia-telangiectasia mutated (ATM), ATR,CHK1 and CHK2) or RAD51, the inhibition of PARP would triggerthe error-prone NHEJ mechanism, resulting in genetic instabilityand/or cell death.38 Consistent with this hypothesis, HRR-deficientcells become insensitive to PARP inhibitors when NHEJ is disabledby DNA-PKcs inhibitors.38
PARP1 as a modulator of cell survival and deathPARP1 is believed to have key functions in the modulation of thecellular response to several stressors.19 Upon exposure to DNA-damaging agents or endogenous oxidative stress, PARP1 becomesactive and generates signals that either favor adaptation to stressor stimulate cell death. The cell’s ultimate fate depends on thenature of the stimulus, the severity of the damage, the cellularcontext and the balance between the activation versus inhibitionof PARP.
Uncontrolled PARP1 activation may result in the induction of celldeath. Upon extensive DNA damage that saturates the DNA repairmachinery, prolonged PARP activation can result in the depletion ofNADþ and subsequently of ATP pools, thus inducing necrotic celldeath.39–41 Moreover, PARP1 may act downstream of the kinasesRIPK1 and RIPK3 in TRAIL-induced necroptosis.42 As compared withwild-type controls, Parp1� /� mice are more resistant to severalparadigms of injury-induced tissue degeneration, reinforcing thenotion that PARP1 contributes to the execution of regulatednecrosis.43 Although the cleavage and inactivation of PARP1 bycaspases is a well-recognized byproduct of apoptosis,5 theimplication of PARP1 in cell death is controversial and limited (formore details see Virag et al.44). Nevertheless, PARP overactivationseems to trigger a peculiar form of cell death called ‘parthanatos’that is dependent from apoptosis-inducing factor but independentfrom caspases. According to one proposed model, the activation ofPARP1 and the translocation of PAR polymers from the nucleus to
the mitochondria would lead to the mitochondrial release ofapoptosis-inducing factor, which then translocates to the nucleusand participates in chromatin degradation.45,46 The binding ofapoptosis-inducing factor to PAR may be important for theactivation of parthanatos.47
In striking contrast with its role in the execution of cell death,PARP1 also has a pivotal function in cell survival processes. Indeed,PARP1 activity is required for the maintenance of genomicstability, and PARylation is implicated in both DNA repair (seeabove) and mitosis.48 Moreover, growing evidence suggests thatPARP1 activation might be involved in the decision of cells toinduce a cytoprotective autophagic response, thereby avoidingcell death.49–51 Reportedly, PARP1 may mediate autophagyinduction through the activation of AMP kinase.52–54
Beyond its inhibitory action on the DDR, PARP inactivation maybe cytotoxic for additional reasons. Thus, PARP inhibition may(i) elicit a cell cycle arrest in the G2/M phase;16 (ii) increase the levelof genomic instability, including a hyperrecombinant phenotype,55
telomere shortening56,57 and chromosome aberrations (forexample, chromosome fusion, sister chromatid exchange, micro-nuclei and aneu-/tetraploidization);13,58 and (iii) activate theintrinsic pathway of apoptosis, as recently demonstrated by ourgroup on a panel of CDDP-resistant NSCLC cell lines.59
Other functions of PARP1Apart from its contribution in recovering from DNA damage and inregulating cell death, PARP has an important role in inflammatoryprocesses and in ischemia-reperfusion injury.60,61 PARP1 actsduring acute and chronic inflammation by (i) stimulating thesecretion of pro-inflammatory mediators (for example, TNFa,NF-kB and HMGB1), (ii) regulating the differentiation of T cells and(iii) controlling the maturation of B lymphocytes.62 In line withthese observations, some preclinical studies demonstrated thatthe inhibition of PARP has antidiabetic effects and confers cardio-protection and neuroprotection in vascular diseases.63–65
Both PARP1 and PARP2 have been implicated in the regulationof bioenergetic metabolism.66 Through yet ill-defined mechanisms,PARP1 hyperactivation may also contribute to the pathogenesis ofAlzheimer’s disease.67,68 Finally, PARP activation downregulatesmitochondrial respiration and oxidative metabolism, therebyenhancing age-related diseases (for example, diabetes andobesity). This effect could be ascribed to three different mecha-nisms, namely (i) direct PARylation of some metabolic enzymespotentially affecting their catalytic activity, (ii) effects onmetabolism-relevant transcription factors and (iii) alteration ofcellular NADþ concentrations.66 In this context, PARP1 inhibitorshave been evaluated as agents that may avoid excessive necrosisafter cardiac or brain ischemia.
PARP INHIBITORS—PRECLINICAL DATASeveral distinct PARP inhibitors may synergize with conventionalDNA-damaging agents, such as ionizing radiation and chemothera-peutics, in increasing their in vitro and in vivo effectivenessagainst tumor cells. This applies to investigational agents such as3-aminobenzamide, NU1025 (8-hydroxy-2-methylquinazolin-4-(3H)one), NU1085 (2-(4-hydroxyphenyl)benzamidazole-4-carboxa-mide), PJ34 (phenanthridinone), as well as to recently developedPARP inhibitors including ABT888 (also known as Veliparib),AG014699 (also known as Rucaparib, AG14447 or PF-01367338),CEP8983 (a 4-methoxy-carbazole derivate), E7016, GPI 15427 andolaparib (also known as AZD2281 or KU-0059436).
Inhibition of PARP1 by olaparib or similar agents increases theradiosensitivity of glioblastoma69,70 and non-small-cell lungcarcinoma,71 both in vitro and in vivo. The underlying mecha-nism of olaparib-mediated radiosensitization was found to involveDNA replication-generating DSBs.70
� Translesion synthesis (TLS) is a DNA damage tolerancepathway that allows the DNA replication machinery toreplicate past DNA lesions by switching on the specializedtranslesion DNA polymerases (for example, Y-family poly-merase H and A-family polymerase Q), which is oftenoveractivated in cancer cells. TLS operates if the S-phasehas been initiated in spite of DNA damage.
� Non-homologous end joining (NHEJ) is a pathway thatrepairs double-strand breaks generated by closel-spacednicks on the complementary strands. In NHEJ DSB is ligatedwithout need for a homologous template this processinvolves KU70 (also known as XRCC6), KU80 (also known asXRCC5), DNA-dependant protein kinase catalytic subunit(DNA-PKcs), artemis, ligase 4 and XRCC4-XPF. NHEJ is cellcycle independent and rapid though highly error-prone.191
Anticancer profile of PARP inhibitorsJ Michels et al
3
& 2013 Macmillan Publishers Limited Oncogene (2013) 1 – 14

Temozolomide (TMZ) is an alkylating agent currently used forthe treatment of malignant glioma and metastatic melanoma thatleads to the formation of a wide spectrum of methyl DNA adducts,including O-methyl adducts, which are repaired by the DRpathway,72 and N-methyl adducts, which are removed by DNAglycosylase-initiated BER and by the AlkB family of oxidative DNAdemethylases during DR.73 To date, TMZ resistance is believed toarise from two distinct mechanisms, namely (i) the increasedactivity of the O6-methylguanine DNA methyltransferase thateliminates the O-methyl adducts or (ii) a deficiency in MMR, whichresults in microsatellite instability, and, consequently, in the lack ofrepair of—and increased tolerance to—O-methyl adducts.74,75
Inhibition of PARP with consequent defective BER enhances thecytotoxicity of TMZ, correlating with an increase in TMZ-inducedN-methyl adducts.76 Such synergistic effects were observed indifferent cell types responding to TMZ, namely (i) in melanomaand cervical carcinoma cells, if combined with the pharmaco-logical PARP inhibitor GPI 15427 or small interfering RNAs for thedepletion of PARP1 and PARP2, (ii) in neuroblastoma cells, ifcombined with AG014699, both in vitro and in vivo, in xenograftedtumor models,77,78 and (iii) in a other tumor types, including thosea priori non-responsive to TMZ, if combined with ABT888.79
Remarkably, in leukemia cells, the combination between ABT888and TMZ inhibited the growth of MMR-deficient and MMR-proficient cells regardless of the O6-methylguanine DNA methyl-transferase level.80 Intriguingly enough, GPI 15427 enhanced thein vivo antitumor effects of TMZ even against PARP1-depletedcells.78 This finding indicates that GPI 1542 might act on otherPARP isoforms than PARP1 or might have yet-to-be-elucidatedoff-target effects.
The association of PARP inhibitors with cisplatin (CDDP) showedadditive or hyperadditive effects on cervical cancer, liver cancerand testicular germ cell tumor cell lines.81–83 Moreover, whenadded to NSCLC cells, CDDP synergizes with PJ34, CEP8983 orPARP1-depleting small interfering RNAs with regard to theinhibition of cell proliferation, induction of DNA damage fociand activation of the intrinsic apoptotic pathway.84 BRCA1-/2-mutated breast cancer xenografts were also more sensitive to thecombination of AG014699 and carboplatin (which is chemicallyrelated to CDDP) than to each drug alone.85
Topoisomerases I and II have pivotal roles in DNA replicationand transcription, in thus far that they ‘unwind’ the double DNAhelix.86 Topoisomerase inhibitors act by stabilizing this unwindedform of the DNA helix, thus causing the subsequent conversionof transient SSBs into permanent DSBs during DNA replication.87
PARP1 interferes with the DNA relaxation activity of topo-isomerase I either through direct protein–protein interaction orthrough PARylation.88 Importantly, PARP inactivation potentiatesthe cytotoxicity of topoisomerase I inhibitors (for example,camptothecin and topotecan) on neuroblastoma, colorectal lung,breast and ovary human cancer cells,77,89,90 as well as that oftopoisomerase II inhibitors (for example doxorubicin, C-1305) onliver, ovarian and BRCA1-positive breast cancer cells.91–93
Targeting DNA repair deficienciesPARP inhibitors given as standalone therapies have been shown tomediate some degree of cytotoxicity against human cancer celllines grown in vitro,16 as well as in a few in vivo human and murinetumor models.85 PARP inhibitors are particularly toxic when theyare administered to BRCA-deficient cells, suggesting that PARPinhibition and HR defects might be synthetically lethal for cancercells.94 Thus, pharmacological or genetic inactivation of eitherPARP1, BRCA1 or BRCA2 alone is compatible with cell survival,whereas their simultaneous inhibition is not.16 This discoveryraised the possibility to exploit PARP inhibitors for the treatmentof breast or ovarian cancers with defects in BRCA1 or BRCA2.95 Ofnote, HR-deficient cells susceptible to PARP inhibitors present
constitutive PARP hyperactivation96 leading to an increase in theintracellular PAR levels without any consistent increase in the levelof PARP protein expression.97 As a result, increased levels of PARmay predict responsiveness to PARP inhibitors.
Apart from BRCA mutations, constitutive modifications of theexpression of other DDR effectors may induce HRD, a conditionthat has been referred to ‘BRCAness’ and that may be efficientlytargeted by PARP inhibitors (Box 2). In this context, Aurora Aoverexpression and MRE11 downregulation may be explored assurrogate markers of BRCAness. Aurora A is a mitotic kinase withessential roles in cell cycle control and mitosis.98,99 Aurora A isoverexpressed in multiple cancers, and this deregulation has beencausally linked to tumorigenesis.100 The overexpression of AuroraA may affect DSB repair by preventing the recruitment of RAD51to DNA DSBs by a mechanism that would require the inhibition ofthe checkpoint kinase CHK1.101 As a result, DSB repair by HR isimpaired and cells become susceptible to PARP inhibitors. AuroraA overexpression is a candidate predictive biomarker of PARPinhibitor sensitivity.
The phosphatase and tensin homolog (PTEN) is a tumorsuppressor gene that inhibits the oncogenic phosphoinositide3-kinase (PI3K)–AKT–mTOR pathway downstream of epidermalgrowth factor receptor (EGFR) signaling. Loss of PTEN is most
Box 2 BRCAness
Germline-transmitted inactivating mutations of the BRCA1 orBRCA2 genes compromise. HR proficiency, predispose tofemale breast (85% lifetime risk), ovarian (10–40%), malebreast, pancreatic and prostate cancer.192 Sporadic tumorsmay display ‘BRCAness’, that is, HR defects without mutationsin BRCA1 or BRCA2.171,193 BRCAness can be explained byepigenetic inactivation (for instance due to promotermethylation) of BRCA1 or BRCA2, (epi)mutations in othergenes, post-translational protein modifications, as well aspharmaclogical inhibitors that inactivate HR-dependent repair:
� Sporadic ovarian (5–31%) (55% of high-grade serous ovariancarcinoma) and breast cancers (11–14%) (in particular TNBC)present an epigenetic silencing of BRCA1 by methylation ofit’s promoter.171,194
� ATM and MRE11195 mutations in lymphocytic leukemia causedefects in the early steps of the HR pathway.
� Aurora A, a mitotic kinase, overexpressed in a diverse array ofcancers may inhibit the recruitment of RAD51 at the DNAdamage site.101
� Fanconi gene promoter methylation has been reported inlung, cervical and ovarian cancer.196–198
� The amplification of EMSY a protein capable of silencingBRCA2 is observed in sporadic breast (13%) and high-gradeovarian cancer (17%).172
� ETS transcription factors are aberrantly expressed in differentcancers and may repress BRCA1/2 and subsequently impairHRR.140
� PARP1 binding protein PARPBP (also known as PARI orCI2orf48) may inhibit HR by interacting with RAD51 atreplication forks.177 PARPBP is overexpressed in pancreaticductal carcinoma and positively regulate the poly(ADP-ribosyl)ation activity of PARP1.175,176
� Pharmacological inhibitors of the HR are being developed forcancer therapy. In particular, specific inhibitors of ataxia-telangiectasia mutated (ATM) kinase, cyclin-dependentkinase 1 (CDK1), epidermal growth factor receptor (EGFR),heat-shock protein of 90 KDa (HSP90), histone deacetylases(HDAC), phosphoinositide 3-kinase (PI3K) pathway andBCR-ABL (imatinib) may compromise HR (see main text).
Anticancer profile of PARP inhibitorsJ Michels et al
4
Oncogene (2013) 1 – 14 & 2013 Macmillan Publishers Limited

frequently found in glioblastoma, NSCLC, as well as endometrial(up to 80% of cases), breast and prostate cancers.102 The impact ofPTEN loss on DSBs repair is controversial.103–105 Some authorsreported that the absence of PTEN sensitized cancer cells tothe inhibition of PARP, presumably by downregulating RAD51and consequently impairing HR.106,107 Accordingly, KU0058948selectively killed endometrioid endometrial cancer cells displayingPTEN loss and HR deficiency.108 Nevertheless, a recent studyperformed on primary prostate cancers has weakened thisconclusion, as the authors failed to observe a significantcorrelation between, on one hand, the PTEN status and, on theother hand: (i) RAD51 expression levels, (ii) sensitivity to PARPinhibitors and (iii) the expression of genes associated to syntheticlethality, such as RAD51, ATM, PRKDC, BRCA1, BRCA2, MRE11, CDK6and MSH2.105 Instead, PARP I sensitivity was associated with adefect in MRE11 expression coupled to PARP hyperactivation.105
MRE11 is a key component of the MRN complex (Mre11-Rad50-Nbs1) that promotes the restart of stalled replication forks andinduces HRR by recruiting and activating the ATM kinase.27,109,110
Thus, MRE11 deficiency may be a more accurate predictive markerfor PARP inhibition sensitivity than PTEN deficiency.
PARP inhibitors can kill cells lacking DDR pathways other thanHRR. Thus, HRR-proficient human mesothelioma, NSCL, epithelialovarian and cervix cancer cell lines that had acquired CDDPresistance due to prolonged culture in the presence of the drug,upregulated the activity of PARP (and hence promoted PARylationof cellular, mostly nuclear proteins).59 When exposed to PARPinhibitors, these cells increased the number of BRCA1 and RAD51foci, which are both surrogate markers of HRR activation.111
Although these cells were proficient in the initiation of BER,they were deficient in XRCC1 and polymerase b.59 Intriguingly,synthetic lethality has been observed for Chinese hamster ovariancells and human ovarian, breast and cervix cancer cells when theywere first XRCC1-depleted and then treated with either PARP orDSB inhibitors (for example, ATM and DNA PKC inhibitors).21,112
These results suggest that the absence of XRCC1 expression mayconstitute a biomarker that predicts sensitivity to PARP inhibitors.
Manipulating HRR for sensitization to PARP inhibitorsOne approach to extend the indications of PARP inhibitors to HRR-proficient cancers might consist in combining them with chemicalinhibitors of HRR. Prospective targets related to the HRR pathwayinclude ATM, the cyclin-dependent kinase 1 (CDK1), EGFR, heat-shock protein of 90 KDa, histone deacetylase and the PI3Kpathway (see below). Moreover, gimeracil has been discoveredas a drug that inhibits the early steps of HRR.113
The combined inhibition of PARP1 and ATM is incompatiblewith embryogenesis, as revealed by the phenotype of doubleknockout mice.114 ATM, a kinase triggered by DNA damage (thatis, DSB), induces DDR (that is, HRR and NHEJ) and cell cyclecheckpoint activation that is often dysregulated in cancer.115 PARPinhibitors are extremely efficient against cancer cells bearing ATMdefects, as shown in the context of Mantle cell lymphoma.116–118
PARP-inhibited cells were also found to be sensitive to theinhibition of the DNA-PK variant involved in NHEJ.32,119,120 Notabledifferences exist between different proteins involved in NHEJ.This applies to DNA-PK and KU80 in the sense that Parp1� /�
DNA-PK� /�mice are viable, while Parp1� /� KU80� /� mice arenot.121 Of note, the association of DNA-PK and ATM inhibitors wasunable to kill PARP1-deficient cells more efficiently than ATMinhibitors alone.121 The synergistic effect of PARP inhibitors andATM inhibitors is encouraging and warrants further investigation.
Another downstream target of DNA-PK is the non-receptorprotein kinase c-ABL that phosphorylates RAD51.122,123 c-ABL isspecifically targeted by imatinib mesylate, a tyrosine kinaseinhibitor that transformed the prognosis of patients with gastro-intestinal stromal tumors and chronic myeloid leukemia.124,125
Imatinib downregulates the HRR and renders human prostate andpancreatic cancer cell lines susceptible to radiotherapy andchemotherapy (that is, gemcitabine and mitomycine C).126 As aresult, it may be worthwhile to explore the association of imatinibwith PARP inhibition.
Some recent results indicate that BRCA1 is functional only uponphosphorylation by CDK1, a core component of the cell cyclemachinery.127 The depletion of CDK1 by means of a doxycyclineinducible shRNA compromises the ability of H1299 NSCLC cells toform RAD51 foci in response to g-irradiation.128 Accordingly, thesimultaneous inhibition of CDK1 and PARP synergistically inhibitedthe growth of human NSCLC xenografts and of transgene-inducedlung adenocarcinomas.128
EGFR inhibitors, namely tyrosine kinase inhibitors (that is,erlotinib and gefitinib), and monoclonal antibodies (for example,cetuximab) are effective treatments in EGFR mutated NSCLC andKRAS wild-type colorectal cancers respectively.129,130 Intriguingly,EGFR inhibitors attenuate the repair of DSBs by HR (that is, bydownregulation of BRCA1) and NHEJ (that is, by inhibiting thephosphorylation and translocation of DNA-PK to thenucleus),131,132 conferring susceptibility to PARP inhibition. It willbe interesting to learn whether these preclinical results can beconfirmed in vivo, in suitable xenograft models.
Inhibitors of the chaperone heat-shock protein 90 such asallylamino-17-demethoxygeldanamycin 17-AAG—a compoundthat is currently under clinical investigation133,134—may inhibitHR by provoking the degradation of some proteins such as BRCA2and RAD51.135 Consistent with this notion, 17-AAG exacerbatesthe cytotoxic effects of both irradiation and olaparib onglioblastoma multiforme.136 Along similar lines, histonedeacetylase inhibitors can affect the DDR by modifying theexpression of proteins involved in HR.137 Indeed, the histonedeacetylase inhibitor suberoylanilide hydroxamic acid efficientlyinhibits the growth of hepatocellular carcinoma cells whenassociated with olaparib.138 These findings are encouraging, butneed further confirmation.
ETS gene fusions are found in a wide array of cancers, includingEwing’s sarcoma, acute myeloid leukemia and prostate cancer.139
PARP inhibition suppresses the growth of ETS gene fusion-positivebut not ETS gene fusion-negative xenografts, along with theaccumulation of double-strand DNA lesions.140 ETS was recentlyidentified as the transcription factor with the highest number ofBRCA1/2 binding motifs.141 ETS may repress the BRCA promoterupon its activation by the mitogen-activated protein kinasepathway.142,143 PI3K inhibitors have been reported to stimulateERK-dependent ETS1 activity and subsequent HR impairment dueto decreased expression of BRCA1/2 and concomitant upregulationof PAR levels indicative of increased PARP activity.141,144 As a result,triple-negative breast cancer (TNBC) BRCA-proficient cellssuccumbed to the combined pharmacological inhibition of PI3Kand PARP.141 These results indicate that the presence of ETS genefusions predict sensitivity to PARP inhibitors. Furthermore, theysuggest that therapeutic measures that upregulate ETS1 functionmay synergize with PARP inhibitors.
HER2 as a modulator of the response to PARP inhibitorsHER2 overexpressing (HER2þ ) human breast cancer cell lines aresusceptible to PARP inhibition by ABT888 and AZD2281 regardlessof their HR status. HER2 knockdown abrogated their PARPhypersensitivity.145 Of note, one third of human breast cancersare HER2þ , and the overexpression of HER is a negativeprognostic factor.146 HER2 overexpression has been linked tothe activation of NF-kB.147 Given the fact that PARP is a co-activator of NF-kB,148 it is well possible that the susceptibility ofHER2þ breast cancer cells to PARP inhibition can be explained bytheir dependence on the NF-kB signaling pathway.145 As a result,HER2 overexpression might predict the response of breast cancercells to PARP inhibition.
Anticancer profile of PARP inhibitorsJ Michels et al
5
& 2013 Macmillan Publishers Limited Oncogene (2013) 1 – 14

53BP1 and acquired PARP resistanceUpon long-term exposure to PARP inhibitors, BRCA-deficienttumors develop an acquired resistance to these compoundsthrough a mechanism that often implies the restoration of HRproficiency.149 Thus, pancreatic cancer cells carrying a BRCA2mutation became resistant to PARP inhibition due to intragenicdeletions restoring the open-reading frame of BRCA2.150,151 Alongsimilar lines, loss of 53BP1 (a DNA damage-responsive intranuclearprotein involved in HR and NHEJ), an event that restores HR, canrender BRCA1-deficient cells resistant to PARP inhibitors152 andother DNA-damaging agents such as CDDP.153 Thus, 53BP1expression levels (or functionality) may constitute an interestingbiomarker to identify HR-deficient tumors that would respond toPARP inhibitors.
CLINICAL EVALUATION OF PARP INHIBITORSCurrent clinical trials involve multiple PARP inhibitors, such asAZD2461 and olaparib (also known as AZD2281 or KU-0059436)from AstraZeneca (Cambridge, UK), veliparib (also known asABT888) from Abbott (Green Oaks, IL, USA), CEP9722 fromCephalon (Frazer, PA, USA), rucaparib (also known as AG014699,AG14447 or PF-01367338) from Clovis Oncology Inc. (Boulder, CO,USA) Pfizer, GPI-21016 from Eisai/MGI Pharma (Tokyo, Japan), MK-4827 from Merck (Whitehouse Station, NJ, USA), INO-1001 fromInotek/Genentech (San Francisco, CA, USA), BMN-673 fromBioMarin Pharmaceutical Inc. (Novato, CA, USA) and E7449 fromEisai Inc., (Woodcliff Lake, NJ, USA) (http://www.clinicaltrials.gov/).All these compounds are administered orally. We will not discussthe highly deceptive clinical evaluation of iniparib (also known asBSI-201 or SAR240550) from BiPar/Sanofi-Aventis (Paris, France)that was erroneously considered as a PARP inhibitor, yet lacks anyspecific activity at this level.154
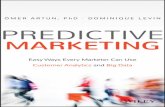
PARP inhibitors are being evaluated in oncology either asmonotherapeutic agents or in combination with other anticancertherapies, seeking higher efficiency (Figure 1). In only one quarterof clinical trials, patients were selected based on the presence of
confirmed or clinically suspected HRR deficiencies (BRCA muta-tions, basal-like or TNBC, high-grade EOC with platinum sensitivity),and rather few studies included biomarker analyses (Tables 2–3).
The pharmacokinetic and pharmacodynamic characteristics ofolaparib have first been evaluated in a phase I trial on 60 patientswith solid tumors (including ovarian, breast and prostate cancer),22 of whom carried BRCA1 or BRCA2 mutations.95 Importantly,objective tumor responses were observed only among BRCAcarriers with 63% clinical benefit rate. Encouraged by these results,a supplemental cohort of 50 ovarian patients bearing BRCA1 orBRCA2 mutations was included. Among them, 13 were platinum-refractory (progressive disease, PD, during previous platinum-based chemotherapy), 24 were platinum-resistant (PD o6 monthsafter previous platinum-based chemotherapy) and 13 wereplatinum sensitive (PD 46 months after previous platinum-based chemotherapy). These patients exhibited a response rate(according to RECIST criteria or reduction in the circulating levelsof the ovarian cancer-associated marker CA-125) of 23%, 45% and69%, respectively.155 The effectiveness of olaparib correlated withBRCA mutation and platinum sensitivity.
The aim of a subsequent phase II trial was to determine theefficacy of olaparib in BRCA1 or BRCA2 mutation carriers withadvanced refractory breast cancer (54 patients) or epithelialovarian cancer (EOC, 57 patients). For two cohorts receiving 400or 100 mg olaparib per day, the ORR was 41% and 21%(clinical benefit rate 52% and 26%) in breast cancer and theORR was 33% and 13% (clinical benefit rate 66% and 42%) inEOC, respectively.156,157 In a recent non randomized phase IIstudy, women with advanced recurrent high-grade serous orundifferentiated ovarian carcinoma or TNBC (63 patients) werestratified according to the presence of BRCA1 or BRCA2 mutationsand treated with olaparib 400 mg twice daily. ORR was 41% forBRCA-mutated patients and surprisingly high—24%—for non-mutated patients.158 Thus, a fraction of ovarian and breast cancersthat lack BRCA mutations can respond to PARP inhibitors.
A randomized study has compared Olaparib monotherapy (200or 400 mg bid) with pegylated liposomal doxorubicin (50 mg/m2)both given for 28 days, in heavily pretreated EOC with confirmed
Figure 1. Clinical trials with PARP inhibitors. The figure illustrates 93 oncological trials involving PARP listed in the US National Institute ofHealth registry of Clinical Trials (http://www.clinicaltrials.gov). (a) Distribution according to the study phase. (b) Distribution according totumor types: non-specified solid tumors (30%), ovarian cancer (22%), breast cancer (17%), hematological malignancies (9%), lung cancer (3%),cerebral tumors (3%) and other cancers (16%). (c) In most trials (61%) patients were not selected according to predictive features for theresponse to PARP inhibition. However, a minority of trials focused on patients with BRCA mutations (18%) or clinical features of presumed‘BRCAness’ (21%) (e.g., high serous epithelial ovarian cancers, triple-negative breast cancers). (d) Distribution according to therapeuticstrategies: monotherapy (28%) combination therapy with chemotherapy (63%), targeted therapies (7%) or radiotherapy (2%). (e) Combinationtherapies with conventional chemotherapy included platinum compounds (42%), temozolomide (28%), topotecan (7%), anthracyclines (4%)or others (19%).
Anticancer profile of PARP inhibitorsJ Michels et al
6
Oncogene (2013) 1 – 14 & 2013 Macmillan Publishers Limited

BRCA1/2 mutation and a platinum-free interval shorter than12 months (reflecting platinum resistance or intermediateresponses). The ORR of 31% for the group receiving 400 mgolaparib was consistent with previous studies.155,156 However, thetrial failed to reveal significant differences in progression-freesurvival (PFS) or ORR between the groups,159 with the particularitythat PFS for pegylated liposomal doxorubicin was rather highcompared with prior studies in EOC.160 There are indications thatBRCA1/2-mutated tumors are more anthracycline-sensitive thannon-mutated tumors,111 and this might explain the high efficacyof pegylated liposomal doxorubicin in this study, which onlyenrolled BRCA1/2-mutated patients. However, the patients in thisstudy were poor responders to CDDP and hence belonged to asubgroup of patients that reportedly exhibit low responses toPARP inhibitors.155
PARP inhibitors have been evaluated in NSCLC (Oza, ASCO 2012,abstract 5001) and EOC as a maintenance therapy after platinumtreatment.161 PFS was significantly longer in patients withplatinum-sensitive high-grade serous EOC treated with 400 mgbid olaparib compared to placebo after two or more platinum-based regimens (median, 8.4 months vs 4.8 months; HzR, 0.35;95% CI, 0.25–0.49; Po0.001). The study groups were well balancedwith 22% of BRCA mutations, and subgroup analyses led to theconclusion that all patient groups profited from olaparibindependently from the BRCA mutational status, age, ethnicorigin or the baseline response to platinum. However, an interimanalysis of OS revealed no significant improvement (HzR, 0.94;95% CI, 0.63–1.39; P¼ 0.75). The preplanned subgroup analysis
revealed the greatest clinical benefit in (germline or somatic)BRCA-mutated patients (median: 11.2 vs 4.3 m; HzR, 0.19; 95% CI:0.11–0.32; Po0.0001) (Ledermann, ASCO 2013, abstract 5505).161
One of the major challenges of regimens combining olaparibwith conventional chemotherapeutics is myelotoxicity.162 However,the association of olaparib with metronomic cyclophosphamide orTMZ is rather well tolerated, allowing full-dose administration ofchemotherapy.163,164 In chemonaıve metastatic melanoma, thecombination therapy with TMZ seems of real interest. In a phase Itrial, one patient benefited from a complete response that hasbeen lasting for 45 years post therapy.164 A phase II trail yieldedencouraging results with a response rate of 17.4% and stabledisease in 36% of the patients 6 months post therapy.165
Several studies have associated olaparib with targeted therapies.Ongoing phase I studies are combining PARP inhibition with (i) thePI3K inhibitor BKM120 in recurrent TNBC and high-grade EOC(NCT01623349), (ii) the VEGFR inhibitor cediranib in ovarian andbreast cancer (NCT01116648), (iii) bevacizumab plus carboplatin andpaclitaxel in EOC (NCT00989651), (iv) the CDK inhibitor dinaciclibplus carboplatin in advanced solid tumors (NCT01434316) or (v) theanti-CD20 monoclonal antibody rituximab plus bendamustine inhematological malignancies (NCT01326702) (www.clinicaltrials.gov).The results of these studies are still elusive.
In synthesis, PARP inhibitors have been yielding promisingclinical results in several trials. When administered alone, PARPinhibitors are well tolerated and efficient provided that they areused against DNA repair deficient tumors. The subgroup ofpatients targeted by most ongoing clinical trials of PARP inhibitors
Table 2. Single agent trials involving the PARP inhibitor olaparib
Phase Patient population Trial design Results Grade 3/4 toxicity Reference
I BRCA1 or BRCA2 mutatedovarian cancer
Phase I (60 patients) witholaparibExpansion phase, 200mgbid in BRCA-mutatedadvanced ovarian cancer(50 patients)
MTD 400mg bidRadiological RR 28%CBR according to PFI in refractory,resistant and sensitive BRCA mutatedEOC: 23%, 45% and 69%, respectively
Lymphopenia 8%Anemia 8%GI symptoms 10%Fatigue 4%
95,155
II BRCA-mutated advancedrecurrent breast cancer
Olaparib 100 (27 patients)or 400mg (27 patients) bid
ORR, 21% vs 41% Fatigue 15%Nausea 15%Vomiting 11%Anemia 11%
156
II BRCA-mutated advancedovarian cancer
Olaparib 100 (24 patients)or 400 (33 patients) mg bid
ORR, 13% vs 33%CBR, 21% vs 52%PFS median, 1.9 (95% CI: 1.8–3.6)vs 5.8 (95% CI: 2.8–10.6)
Fatigue 3%Nausea 6%Anemia 3%
157
II Advanced recurrent high-grade ovarian or triple-negative breast cancer(TNBC). Stratificationaccording to BRCA1/2mutation
Olpaparib 400mg bidBRCA mutations in 17/64EOC patients and 10/26TNBC patients
OR 41% BRCA ovarian cancerOR 24% non-mutated ovarian cancerNo OR in breast cancerPFS in EOC with BRCA mutation(221 daily) or without (192 daily)PFS in breast cancer with BRCAmutation (109 daily) or without(54 daily)
Fatigue 11%Dyspnea 12%
158
II BRCA1- or BRCA2-mutatedovarian cancer recurrentwithin 12 months of priorplatinum therapy
Randomised 1:1:1 olaparib200 (32 patients) or 400mgbid (32 patients) or PLD50mg/m2 (33 patients)
PFS 6.5, 8.8 and 7.1 monthsHR 0.88, P¼ 0.66ORR 25, 31 and 18%GCIC 34, 56 and 33%
Anemia 13%Fatigue 9%Nausea 6%2 Toxic death(CV accident, MDSsyndrome)
159
II Platinum-sensitive relapsedhigh-grade EOC with twoor more platinum-basedprior regimens
Maintenance therapy witholaparib 400mg bid (136patients) versus placebo(129 patients). PFS as aprimary EP
PFS median, 8.4 months vs 4.8months; HR 0.35, 95% CI: 0.25–0.49,Po0.001OS interim analysis HR, 0.94; 95%CI: 0.63–1.39; P¼ 0.75
Anemia 5.1%,Fatigue 6.6%
161
Abbreviations: bid, twice a day; CBR, clinical benefit rate; CI, confidence interval; CV, cerebrovascular accident; EOC, epithelial ovarian cancer; EP, endpoint; GI,gastro-intestinal; HR, hazard ratio; MDS, myelodysplastic syndrome; OS, overall survival; OR, objective response rate; ORR, overall response rate; PARP,poly(ADP-ribose) polymerase; PD, pharmacodynamics; PFS, progression-free survival; PFI, platinum-free interval; RR, response rate; TNBC, triple-negative breastcancer.
Anticancer profile of PARP inhibitorsJ Michels et al
7
& 2013 Macmillan Publishers Limited Oncogene (2013) 1 – 14

carries BRCA mutations and platinum-sensitive tumors, becausethis subgroup showed the most promising results in early clinicaldevelopment.155 Although BRCA mutations render cells sensitiveto platinum and PARP inhibition,166 there is no absolutecorrelation between the BRCA mutational status, platinumsensitivity and clinical responses. Thus, a significant fraction ofpatients with BRCA non-mutated EOC demonstrated a prolongedPFS with olaparib.161 Moreover, a significant fraction of BRCA-mutated platinum-resistant EOC remained sensitive to PARPinhibitors.155 Clinical features considered as surrogatebiomarkers of HRD such as unfavorable pathobiologicalparameters (TNBC, high-grade serous EOC) and platinumresponsiveness in a BRCA-mutated context may not besufficiently specific in the prediction for the response to PARP I.
For instance, as reported by the Cancer Genome Atlas, only 50% ofhigh-grade EOCs are HRR deficient.167 Moreover, only 20% ofTNBC may be BRCA mutated.168 These findings underscore theneed for suitable biomarkers that diagnose DNA repair defectsand predict responses to PARP inhibitors.
CONCLUDING REMARKS: BIOMARKER DISCOVERYAs detailed in the clinical section of this review, PARP inhibitorsselectively target HR-deficient tumors, including tumors frompatients bearing hereditary BRCA1 and 2 mutations. Approxi-mately 15% of EOC bear mutations in BRCA1 or BRCA2.169,170
Moreover, an elevated proportion of sporadic EOC (up to 55%)—and in particular high-grade serous EOC—are HRR deficient for a
Table 3. Combination trials involving PARP inhibitors
PARPinhibitor
Othertherapeuticagents
Phase Patientpopulation
Trial design Results Grade 3/4 toxicity Reference
Olaparib Dacarbazine I Advancedcancer,Expansioncohort withchemonaıvemelanoma
Dacarbazine (600–800mg/m2)d1, plus olaparib (20–200mg)bid d1–d7, 21-day cycle (40patients)
OTDdacarbazine 600mg/m2 d1plus olpaparib100mg bid d1–d7,21-Day cycleTumor response: 2 PR, 8 SD, 30PD
Lymphopenia 15%Neutropenia 23%
203
Topotecan I Advanced solidtumors
Topotecan 0.5mg/m2/day, 3days or 1mg/m2/day, 3 days,plus olaparib 50, 100 or 200mgbid, d1¼d21 (19 patients)
MTD
Topotecan 1mg/m2/day 3 daysolaparib100mg bid
Neutropenia 204
CDDP andGemcitabine
I Advanced solidtumors
Olaparib 100mg bid d1-4 plusCDDP 60mg/m2 d3 plusGemcitabine 500mg/m2 d3,d10 (23 patients)
MTD, Olaparib 100mg/m2 d1plus CDDP 60mg/m2 d1 plusGemcitabine 500mg/m2 d1, d8Tumor response, 2 PR, 13 SD, 6PD
Neutropenia 61%Lymphopenia 61%Thrombo-cytopenia57%
162
Bevacizumab I Advanced solidtumors
Olaparib 100 (4 patients), 200(4 patients) or 400mg (4patients) bid plus bevacizumab10mg/m2 d1¼d15
No DLT None 205
Carboplatinand paclitaxel
II Platinum-sensitiverecurrent serousovarian cancer
6� 21 daily cycles P(175mg/m2 d1)þC(AUC4d1)þolaparib (200mg bidd1-10/21) (81 patients) thenolaparib (400mg bidcontinuous) (66 patients),or 6� 21 daily cyclesP(175mg/m2 d1)þC(AUC6 d1)(75 patients) then no further(55 patients)
PFS median, 12.2 months vs 9.6months; HR, 0.51, 95% CI: 0.34–0.77; P¼ 0.0012;ORR, 64% vs 58%OS, immature (14% totalevents)
65% vs 57% duringcombination phase29% vs 16% duringmaintenance
(Oza,ASCO2012,abstract5001)
Veliparib Topotecan I Advanced orrefractory solidtumors,lymphoma
Topotecan IV varyingschedules plus veliparib 10mgbid (24 patients)
MTDtopotecan 0.6mg/m2/day plusveliparib10mg bid d1-5,21-day cycletumor response: 8 SD
NeutropeniaThrombo-cytopenia
206
Cyclophosphamide
I Refractory solidtumors andlymphoidmalignancies
Metronomic dosing ofcyclophosphamide d1–d21plus veliparib d1–d7 or d1–d14or d1–d21 (35 patients)
MTD, cyclophosphamide50mg plus veliparib 60mgdailyTumor response: 8 PR, 6 SD
Lymphopenia 163
Rucaparib Temozolomide I Advanced solidtumors
Escalating doses of rucaparibplus temozolomide 100mg/m2
(18 patients) or 200mg/m2
d1–d5, 28-day cycle, for anexpansion cohort of metastaticmalignant melanoma (15patients)
PID 12mg/m2/daysMTD temozolomide 200mg/m2/days d1–d5, 28-day cycleTumor response: 1 CR, 2 PR, 6SD
Thrombo-cytopeniaNeutropenia
164
Temozolomide II Chemotherapynaıve metastaticmelanoma
Rucaparib 12mg/m2/day plustemozolomide 200mg/m2
d1–d5, 28-day cycle,(46 patients)
RR, 17.4%TTP median, 3.5 monthsOS median, 9.9 months
Myelo-suppressionrequiring a 25% dosereduction oftemozolomide
165
INO-1001 Temozolomide I Unresectablestage III/IVmelanoma
Escalating doses of INO-1001plus temozolomide 200mg/m2
d1–d5, 28-day cycle,(12 patients)
Tumor response: 1 PR, 4 SD,TTP median, 2.2 monthsOS median, 17 monthsHalf live of INO-1001 mean, 5 h
Thrombo-cytopeniaNeutropeniaAsthenia
207
Abbreviations: bid, twice a day; C, carboplatin; CB, clinical benefit; CDDP, cisplatin; CR, complete response; DLT, dose limiting toxicity; EOC, epithelial ovariancancer; MTD, maximal tolerated dose; NSCLC, non-small-cell lung cancer; ORR, overall response rate; OS, overall survival; OTD, optimal tolerated dose; P,paclitaxel; PARP, poly(ADP-ribose) polymerase; PD, progressive disease; PFS, progression-free survival; PID, PARP inhibitory dose; PI3K, PI3kinase; PLD, pegylatedliposomal doxorubicin; PR, partial response; SD, stable disease; TTP, time to progression.
Anticancer profile of PARP inhibitorsJ Michels et al
8
Oncogene (2013) 1 – 14 & 2013 Macmillan Publishers Limited

variety of reasons, including BRCA1 promoter methylation, MRE11mutation and EMSY amplification.167,171–173 Thus, reliablebiomarkers for the identification of patients with defects in theHR pathway would greatly facilitate the clinical development ofPARP inhibitor-based therapies (Figure 2).
Recently, 24 EOCs were classified as HRR-competent or HRR-deficient, based on the ability of primary tumor cells from asciticfluid cultures to form RAD51 foci, in vitro, upon short exposure toAG014699.174 In this study, the amount of RAD51 foci per nucleusinversely correlated with cytotoxicity of AG014699 in vitro.However, it remains unknown whether this functional marker ofHRR proficiency affects therapeutic outcome in vivo.174 In a cohortof 68 sporadic breast cancer patients, reduced in vivo formationof RAD51 foci (upon neoadjuvant anthracycline-based chemo-therapy) correlated with high histological grade and intenseproliferation rate (as determined by the Ki67 marker), yet waspredictive of pathologic complete responses.111 Remarkably,TNBCs, whose basal-like phenotype closely resembles that
caused by BRCA mutations, constituted the subgroup of breastcancers that most frequently exhibited a low RAD51 score.However, the use of RAD51 foci as a biomarker for HRRproficiency has two major intrinsic limits that would have to beovercome in future studies. First, RAD51 foci cannot be detected atbaseline and must be induced by DNA damage. Second, theexpression of RAD51 is restricted to the S and G2 phases ofproliferating cells, meaning that it cannot be detected in tumorcells that are dormant or arrested in the G1 phase.111 It remains tobe determined whether other types of DNA damage-elicited foci,such as Mre11 foci,29 might yield a more accurate biomarker topredict sensitivity to PARP inhibitors than RAD51 foci.
Several studies reported that PARP1 binding protein PARPBP(also known as PARI or CI2orf48), which is overexpressed inpancreatic human carcinoma cells,175 inhibited HRR and inducedan increase in PAR levels.176,177 This result suggests that PARPBPmight predict both HRD and sensitivity to PARP inhibition. PARP isalso hyperactivated in BRCA2 mutated—and thus HRR-deficient—cancer cell lines, as shown for instance for V-C8 hamster andCAPAN1 pancreatic cell lines, and this correlated with sensitivity toPARP inhibitors.96 Furthermore, the knockdown of HRR proteins(for example, RAD54, RAD52, BLM, WRN and XRCC3) in U2OSosteosarcoma cells induced HRD, PARP hyperactivation andincreased sensitivity to PARP inhibitors.96 Indeed, high levels ofPAR-modified proteins detectable by western blotting orimmunohistochemistry predicted the cytotoxic response to PARPinhibitors in vitro and in vivo, in CDDP-resistant human cancerscells of different histological origins.59 These finding suggest thatimmunohistochemical methods assessing the abundance of PARin cells (which correlates with PARP activity) may be useful topredict sensitivity to PARP inhibitors (Figure 3).
The genomic instability of HRR-deficient tumors might be usedas a predictive biomarker for the response to PARP inhibitors.
Figure 2. Predicitve biomarkers for PARP inhibitors. BRCA1/2 loss-of-function mutation impairs HRR and induces a PARP hyperactivationreflected by an increased abundance of poly(ADP)ribose polymers(PAR). HRD may occur without BRCA mutation in the context of‘BRCAness’. EMSY genes and ETS fusion genes that are reported indifferent tumors inhibit BRCA2. 53BP1 is a DDR factor that interactswith BRCA1 upstream of HRR and NHEJ. Concomitant 53BP1 andBRCA1 loss may reinitiate HRR and subsequent resistance to PARPinhibition. Genetic instability correlates with HRD according to aHRD score. PARPBP overexpression is reported in pancreatic cancers,inducing genetic instability and PARP hyperactivation. MRE11 fromthe MRN protein complex (MRE11, RAD50 and NBS1) acts at thestalled replication fork upstream of the HRR. RAD51 is one of themain effectors of HRR. Aurora A is an essential actor of mitosis andcell cycle regulation and is often overexpressed in tumors.Overexpression of Aurora A inhibits RAD51 recruitment. Apart fromHRR deficiencies, two main actors of the final steps of the BERpathway may be of interest. Downregulation of polymerase b andXRCC1 may induce increased PARylation. HER2 and PARP over-expression initiate an overexpression of the transcription factor NF-kB, actor of the immune response. Note that none of the depictedputative biomarkers is entirely specific for the response of tumorcells to PARP inhibitors. Aurora A, AURKA; BER, base excision repair;53BP1, p53-binding protein-1; BRCA, breast cancer gene; CDK1,cyclin-dependent kinase 1; DDR, DNA damage response; HER2,human epidermal growth factor receptor 2; HRD score, homologousrecombination deficiency score; HRR, homologous recombination;HR, homologous recombination repair; I PARP, inhibitors de PARP;MAPK, mitogen-activated protein kinase; MRE11, meiotic recombi-nation protein 11; NF-kB, nuclear factor-kappa B; PAR, poly-(ADP-ribose); PARPBP, poly-(ADP-ribose) polymerase-binding protein;PLK3, polo-like kinase-3; POLB, polymerase b; XRCC1, X-ray repaircross-complementing 1.
Figure 3. PARP hyperactivation. Preclinical data report that theabundance of PAR may reflect cellular DNA repair deficiencies orDDR (red box), thus constituting a universal predictive biomarkerfor the response to PARP inhibitors. PAR is detectable by differentmethods listed in the figure. BRCA, breast cancer gene; DDR, DNAdamage response; HRR, homologous recombination repair; MRE11,meiotic recombination protein 11; NADþ , nicotinamide dinucleo-tide; PAR, poly-(ADP-ribose); PI3K, phosphoinositide 3-kinase; POLB,polymerase b; XRCC1, X-ray repair cross-complementing 1.
Anticancer profile of PARP inhibitorsJ Michels et al
9
& 2013 Macmillan Publishers Limited Oncogene (2013) 1 – 14

A HRD score has been defined by assessing mutations of BRCA1and BRCA2, the methylation of their promoters, the level ofexpression of BRCA1 at the mRNA level, as well as LOH affectingthe loci coding for BRCA1 and BRCA2. This could be validated intwo independent human EOC cohorts.178–180 However, apart fromthe BRCA promoter methylation, these analyses cannot detectHRR deficiencies that fall into the category of ‘BRCAness’, andhence must be considered as intrinsically suboptimal.
In conclusion, there is ample awareness of the urgent need ofdefining reliable biomarkers that predict the clinical efficacy of PARPinhibitors. The definition and practical implementation of suchbiomarkers is still in its infancy. However, it is our hope that constantprogress in the comprehension of the complexities of DDRs willeventually lead to the development of simple and reproducibletests that facilitate the clinical application of PARP inhibitors.
ABBREVIATIONSART, ADP-ribosyl transferases; ATM, ataxia-telangiectasia mutated;BER, base excision repair; bid, twice a day; CBR, clinical benefit rate;CDDP, cisplatin; CDK1, cyclin-dependent kinase 1; DDR, DNAdamage response; DiOC6(3), 3,30-dihexyloxacarbocyanine iodide;DLT, dose limiting toxicity; DNA-PK, DNA-dependent proteinkinase; DNA-PKcs, catalytic subunit of DNA-dependent proteinkinase; DR, direct repair; DSB, double-strand break; DSBR, double-strand break repair; EGBFr, epidermal growth factor receptor; EOC,epithelial ovarian cancer; GI, gastro-intestinal; HDAC, histonedeacetylase; HzR, hazard ratio; HR, homologous recombination;HRD, homologous recombination deficiency; HRR, homologousrecombinational repair; HSP90, heat-shock protein of 90 KDa; LOH,loss of heterozygosity; MAPK, mitogen-activated protein kinase;MGMT, O6-methylguanine DNA methyltransferase; MMR, mis-match repair; MTD, maximum tolerated dose; NAD, nicotinamideadenine dinucleotide; NER, nucleotide excision repair; NHEJ, non-homologous end joining; NSCLC, non-small-cell lung carcinoma;ORR, overall response rate; OS, overall survival; PAR, poly-(ADP-ribose); PARP, poly-(ADP-ribose) polymerase; PARPBP, PARP1-binding protein; PARP I, PARP inhibitor; PLD, pegylated liposomaldoxorubicin; PD, progressive disease; PFI, platinum-free interval;PFS, progression-free survival; PI, propidium iodide; PI3K, phos-phoinositide 3-kinase; PS, performance status; PSA, prostate-specific antigen; PTEN, phosphatase and tensin homolog; RECIST,response evaluation criteria in solid tumors; RNAi, RNA inter-ference; SNP, single-nucleotide polymorphism; SSB, single-strandbreak; SSBR, single-strand break repair; TMZ, temozolomide; TNBC,triple-negative breast cancer; XRCC1, X-ray repair cross-comple-menting 1
CONFLICT OF INTERESTThe authors declare no conflict of interest.
ACKNOWLEDGEMENTSThe authors would like to thank Lorenzo Galluzzi (Universite Paris Descartes, Paris,France) for assistance with manuscript preparation. The authors are supported by theLigue contre le Cancer (equipe labellisee), Agence National de la Recherche, AXAChair for Longevity Research, Association pour la Recherche sur le Cancer,Associazione Italiana per la Ricerca sul Cancro (AIRC), Canceropole Ile-de-France,Institut National du Cancer (INCa), Fondation Bettencourt-Schueller, Fondation deFrance, Fondation pour la Recherche Medicale, the European Commission (ArtForce),the European Research Council, the LabEx Immuno-Oncology, Action Lions ‘Vaincrele Cancer’, Luxembourg, the SIRIC Stratified Oncology Cell DNA Repair and TumorImmune Elimination (Socrate) and Cancer Research and Personalized Medicine(Carpem) and the Paris Alliance of Cancer Research Institutes.
REFERENCES1 Chambon P, Weill JD, Mandel P. Nicotinamide mononucleotide activation of new
DNA-dependent polyadenylic acid synthesizing nuclear enzyme. BiochemBiophys Res Commun 1963; 11: 39–43.
2 Rouleau M, Patel A, Hendzel MJ, Kaufmann SH, Poirier GG. PARP inhibition:PARP1 and beyond. Nat Rev Cancer 2010; 10: 293–301.
3 Krishnakumar R, Kraus WL. The PARP side of the nucleus: molecular actions,physiological outcomes, and clinical targets. Mol Cell 2010; 39: 8–24.
4 Herceg Z, Wang ZQ. Failure of poly(ADP-ribose) polymerase cleavage by cas-pases leads to induction of necrosis and enhanced apoptosis. Mol Cell Biol 1999;19: 5124–5133.
5 Galluzzi L, Vitale I, Abrams JM, Alnemri ES, Baehrecke EH, Blagosklonny MV et al.Molecular definitions of cell death subroutines: recommendations of theNomenclature Committee on Cell Death 2012. Cell Death Differ 2012; 19: 107–120.
6 Hassa PO, Haenni SS, Elser M, Hottiger MO. Nuclear ADP-ribosylation reactions inmammalian cells: where are we today and where are we going? Microbiol MolBiol Rev 2006; 70: 789–829.
7 Langelier MF, Planck JL, Roy S, Pascal JM. Structural basis for DNA damage-dependent poly(ADP-ribosyl)ation by human PARP-1. Science 2012; 336:728–732.
8 Jankevicius G, Hassler M, Golia B, Rybin V, Zacharias M, Timinszky G et al. A familyof macrodomain proteins reverses cellular mono-ADP-ribosylation. Nat StructMol Biol 2013; 20: 508–514.
9 Hottiger MO, Hassa PO, Luscher B, Schuler H, Koch-Nolte F. Toward a unifiednomenclature for mammalian ADP-ribosyltransferases. Trends Biochem Sci 2010;35: 208–219.
10 Durkacz BW, Omidiji O, Gray DA, Shall S. (ADP-ribose)n participates in DNAexcision repair. Nature 1980; 283: 593–596.
11 Dantzer F, Schreiber V, Niedergang C, Trucco C, Flatter E, De La Rubia G et al.Involvement of poly(ADP-ribose) polymerase in base excision repair. Biochimie1999; 81: 69–75.
12 Shall S, de Murcia G. Poly(ADP-ribose) polymerase-1: what have we learned fromthe deficient mouse model? Mutat Res 2000; 460: 1–15.
13 Wang ZQ, Stingl L, Morrison C, Jantsch M, Los M, Schulze-Osthoff K et al. PARP isimportant for genomic stability but dispensable in apoptosis. Genes Dev 1997;11: 2347–2358.
14 Tsutsumi M, Masutani M, Nozaki T, Kusuoka O, Tsujiuchi T, Nakagama H et al.Increased susceptibility of poly(ADP-ribose) polymerase-1 knockout mice tonitrosamine carcinogenicity. Carcinogenesis 2001; 22: 1–3.
15 Menissier de Murcia J, Ricoul M, Tartier L, Niedergang C, Huber A, Dantzer F et al.Functional interaction between PARP-1 and PARP-2 in chromosome stability andembryonic development in mouse. EMBO J 2003; 22: 2255–2263.
16 Farmer H, McCabe N, Lord CJ, Tutt AN, Johnson DA, Richardson TB et al.Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy.Nature 2005; 434: 917–921.
17 D’Amours D, Desnoyers S, D’Silva I, Poirier GG. Poly(ADP-ribosyl)ation reactionsin the regulation of nuclear functions. Biochem J 1999; 342(Pt 2): 249–268.
18 De Vos M, Schreiber V, Dantzer F. The diverse roles and clinical relevance ofPARPs in DNA damage repair: current state of the art. Biochem Pharmacol 2012;84: 137–146.
19 Luo X, Kraus WL. On PAR with PARP: cellular stress signaling through poly(ADP-ribose) and PARP-1. Genes Dev 2012; 26: 417–432.
20 Campalans A, Kortulewski T, Amouroux R, Menoni H, Vermeulen W, Radicella JP.Distinct spatiotemporal patterns and PARP dependence of XRCC1 recruitmentto single-strand break and base excision repair. Nucleic Acids Res 2013; 41:3115–3129.
21 Strom CE, Johansson F, Uhlen M, Szigyarto CA, Erixon K, Helleday T. Poly(ADP-ribose) polymerase (PARP) is not involved in base excision repair butPARP inhibition traps a single-strand intermediate. Nucleic Acids Res 2011; 39:3166–3175.
22 Noren Hooten N, Kompaniez K, Barnes J, Lohani A, Evans MK. Poly(ADP-ribose)polymerase 1 (PARP-1) binds to 8-oxoguanine-DNA glycosylase (OGG1). J BiolChem 2011; 286: 44679–44690.
23 Vodenicharov MD, Ghodgaonkar MM, Halappanavar SS, Shah RG, Shah GM.Mechanism of early biphasic activation of poly(ADP-ribose) polymerase-1 inresponse to ultraviolet B radiation. J Cell Sci 2005; 118(Pt 3): 589–599.
24 Pines A, Vrouwe MG, Marteijn JA, Typas D, Luijsterburg MS, Cansoy M et al.PARP1 promotes nucleotide excision repair through DDB2 stabilization andrecruitment of ALC1. J Cell Biol 2012; 199: 235–249.
25 Robu M, Shah RG, Petitclerc N, Brind’Amour J, Kandan-Kulangara F, Shah GM. Roleof poly(ADP-ribose) polymerase-1 in the removal of UV-induced DNA lesions bynucleotide excision repair. Proc Natil Acad Sci USA 2013; 110: 1658–1663.
26 King BS, Cooper KL, Liu KJ, Hudson LG. Poly(ADP-ribose) contributes to anassociation between poly(ADP-ribose) polymerase-1 and xeroderma pigmento-sum complementation group A in nucleotide excision repair. J Biol Chem 2012;287: 39824–39833.
27 Bryant HE, Petermann E, Schultz N, Jemth AS, Loseva O, Issaeva N et al. PARP isactivated at stalled forks to mediate Mre11-dependent replication restart andrecombination. EMBO J 2009; 28: 2601–2615.
Anticancer profile of PARP inhibitorsJ Michels et al
10
Oncogene (2013) 1 – 14 & 2013 Macmillan Publishers Limited

28 Yang YG, Cortes U, Patnaik S, Jasin M, Wang ZQ. Ablation of PARP-1 does notinterfere with the repair of DNA double-strand breaks, but compromises thereactivation of stalled replication forks. Oncogene 2004; 23: 3872–3882.
29 Ying S, Hamdy FC, Helleday T. Mre11-dependent degradation of stalledDNA replication forks is prevented by BRCA2 and PARP1. Cancer Res 2012; 72:2814–2821.
30 Hochegger H, Dejsuphong D, Fukushima T, Morrison C, Sonoda E, Schreiber Vet al. Parp-1 protects homologous recombination from interference by Ku andLigase IV in vertebrate cells. EMBO J 2006; 25: 1305–1314.
31 Sugimura K, Takebayashi S, Taguchi H, Takeda S, Okumura K. PARP-1 ensuresregulation of replication fork progression by homologous recombination ondamaged DNA. J Cell Biol 2008; 183: 1203–1212.
32 Couto CA, Wang HY, Green JC, Kiely R, Siddaway R, Borer C et al. PARP regulatesnonhomologous end joining through retention of Ku at double-strand breaks.J Cell Biol 2011; 194: 367–375.
33 Wang M, Wu W, Wu W, Rosidi B, Zhang L, Wang H et al. PARP-1 and Ku competefor repair of DNA double strand breaks by distinct NHEJ pathways. Nucleic AcidsRes 2006; 34: 6170–6182.
34 Mansour WY, Rhein T, Dahm-Daphi J. The alternative end-joining pathway forrepair of DNA double-strand breaks requires PARP1 but is not dependent uponmicrohomologies. Nucleic Acids Res 2010; 38: 6065–6077.
35 Spagnolo L, Barbeau J, Curtin NJ, Morris EP, Pearl LH. Visualization of a DNA-PK/PARP1 complex. Nucleic Acids Res 2012; 40: 4168–4177.
36 Rulten SL, Fisher AE, Robert I, Zuma MC, Rouleau M, Ju L et al. PARP-3 and APLFfunction together to accelerate nonhomologous end-joining. Mol Cell 2011; 41:33–45.
37 Helleday T. The underlying mechanism for the PARP and BRCA syntheticlethality: clearing up the misunderstandings. Mol Oncol 2011; 5: 387–393.
38 Patel AG, Sarkaria JN, Kaufmann SH. Nonhomologous end joining drives poly(ADP-ribose) polymerase (PARP) inhibitor lethality in homologous recombi-nation-deficient cells. Proc Natl Acad Sci USA 2011; 108: 3406–3411.
39 Ha HC, Snyder SH. Poly(ADP-ribose) polymerase is a mediator of necrotic celldeath by ATP depletion. Proc Natl Acad Sci USA 1999; 96: 13978–13982.
40 Zong WX, Ditsworth D, Bauer DE, Wang ZQ, Thompson CB. Alkylating DNAdamage stimulates a regulated form of necrotic cell death. Genes Dev 2004; 18:1272–1282.
41 Ethier C, Tardif M, Arul L, Poirier GG. PARP-1 modulation of mTOR signaling inresponse to a DNA alkylating agent. PLoS One 2012; 7: e47978.
42 Jouan-Lanhouet S, Arshad MI, Piquet-Pellorce C, Martin-Chouly C,Le Moigne-Muller G, Van Herreweghe F et al. TRAIL induces necroptosisinvolving RIPK1/RIPK3-dependent PARP-1 activation. Cell Death Differ 2012; 19:2003–2014.
43 Sahaboglu A, Tanimoto N, Kaur J, Sancho-Pelluz J, Huber G, Fahl E et al. PARP1gene knock-out increases resistance to retinal degeneration without affectingretinal function. PLoS One 2010; 5: e15495.
44 Virag L, Robaszkiewicz A, Vargas JM, Javier Oliver F. Poly(ADP-ribose) signaling incell death. Mol Aspects Med S0098-2997: 00008-3.
45 Yu SW, Wang H, Poitras MF, Coombs C, Bowers WJ, Federoff HJ et al. Mediationof poly(ADP-ribose) polymerase-1-dependent cell death by apoptosis-inducingfactor. Science 2002; 297: 259–263.
46 Yu SW, Andrabi SA, Wang H, Kim NS, Poirier GG, Dawson TM et al. Apoptosis-inducing factor mediates poly(ADP-ribose) (PAR) polymer-induced cell death.Proc Natil Acad Sci USA 2006; 103: 18314–18319.
47 Wang Y, Kim NS, Haince JF, Kang HC, David KK, Andrabi SA et al.Poly(ADP-ribose) (PAR) binding to apoptosis-inducing factor is critical forPAR polymerase-1-dependent cell death (parthanatos). Science Signal 2011; 4:ra20.
48 Kashima L, Idogawa M, Mita H, Shitashige M, Yamada T, Ogi K et al. CHFR proteinregulates mitotic checkpoint by targeting PARP-1 protein for ubiquitination anddegradation. J Biol Chem 2012; 287: 12975–12984.
49 Munoz-Gamez JA, Rodriguez-Vargas JM, Quiles-Perez R, Aguilar-Quesada R,Martin-Oliva D, de Murcia G et al. PARP-1 is involved in autophagy induced byDNA damage. Autophagy 2009; 5: 61–74.
50 Yoon JH, Ahn SG, Lee BH, Jung SH, Oh SH. Role of autophagy in chemoresis-tance: regulation of the ATM-mediated DNA-damage signaling pathwaythrough activation of DNA-PKcs and PARP-1. Biochem Pharmacol 2012; 83:747–757.
51 Rodriguez-Vargas JM, Ruiz-Magana MJ, Ruiz-Ruiz C, Majuelos-Melguizo J,Peralta-Leal A, Rodriguez MI et al. ROS-induced DNA damage and PARP-1 arerequired for optimal induction of starvation-induced autophagy. Cell Res 2012;22: 1181–1198.
52 Huang Q, Shen HM. To die or to live: the dual role of poly(ADP-ribose) poly-merase-1 in autophagy and necrosis under oxidative stress and DNA damage.Autophagy 2009; 5: 273–276.
53 Huang Q, Wu YT, Tan HL, Ong CN, Shen HM. A novel function of poly(ADP-ribose) polymerase-1 in modulation of autophagy and necrosis under oxidativestress. Cell Death Differ 2009; 16: 264–277.
54 Zhou J, Ng S, Huang Q, Wu YT, Li Z, Yao SQ et al. AMPK mediates a pro-survivalautophagy downstream of PARP-1 activation in response to DNA alkylatingagents. FEBS Lett 2013; 587: 170–177.
55 Schultz N, Lopez E, Saleh-Gohari N, Helleday T. Poly(ADP-ribose) polymerase(PARP-1) has a controlling role in homologous recombination. Nucleic Acids Res2003; 31: 4959–4964.
56 d’Adda di Fagagna F, Hande MP, Tong WM, Lansdorp PM, Wang ZQ, Jackson SP.Functions of poly(ADP-ribose) polymerase in controlling telomere length andchromosomal stability. Nat Genet 1999; 23: 76–80.
57 Samper E, Goytisolo FA, Menissier-de Murcia J, Gonzalez-Suarez E, Cigudosa JC,de Murcia G et al. Normal telomere length and chromosomal end capping inpoly(ADP-ribose) polymerase-deficient mice and primary cells despite increasedchromosomal instability. J Cell Biol 2001; 154: 49–60.
58 Morrison C, Smith GC, Stingl L, Jackson SP, Wagner EF, Wang ZQ. Geneticinteraction between PARP and DNA-PK in V(D)J recombination and tumor-igenesis. Nat Genet 1997; 17: 479–482.
59 Michels J, Vitale I, Galluzzi L, Adam J, Olaussen KA, Kepp O et al. CisplatinResistance Associated with PARP Hyperactivation. Cancer Res 2013; 73:2271–2280.
60 Ba X, Garg NJ. Signaling mechanism of poly(ADP-ribose) polymerase-1 (PARP-1)in inflammatory diseases. Am J Pathol 2011; 178: 946–955.
61 Strosznajder RP, Czubowicz K, Jesko H, Strosznajder JB. Poly(ADP-ribose)metabolism in brain and its role in ischemia pathology. Mol Neurobiol 2010; 41:187–196.
62 Rosado MM, Bennici E, Novelli F, Pioli C. Beyond dna repair,the immunologicalrole of parp-1 and its siblings. Immunology 2013; 139: 428–437.
63 Szabo C. Roles of poly(ADP-ribose) polymerase activation in the pathogenesis ofdiabetes mellitus and its complications. Pharmacol Res 2005; 52: 60–71.
64 Pacher P, Szabo C. Role of poly(ADP-ribose) polymerase 1 (PARP-1) in cardio-vascular diseases: the therapeutic potential of PARP inhibitors. Cardiovas DrugRev 2007; 25: 235–260.
65 Moroni F, Cozzi A, Chiarugi A, Formentini L, Camaioni E, Pellegrini-Giampietro DEet al. Long-lasting neuroprotection and neurological improvement in strokemodels with new, potent and brain permeable inhibitors of poly(ADP-ribose)polymerase. Br J Pharmacol 2012; 165: 1487–1500.
66 Bai P, Canto C. The role of PARP-1 and PARP-2 enzymes in metabolic regulationand disease. Cell Metab 2012; 16: 290–295.
67 Strosznajder JB, Czapski GA, Adamczyk A, Strosznajder RP. Poly(ADP-ribose)polymerase-1 in amyloid beta toxicity and Alzheimer’s disease. Mol Neurobiol2012; 46: 78–84.
68 Abeti R, Abramov AY, Duchen MR. Beta-amyloid activates PARP causing astro-cytic metabolic failure and neuronal death. Brain 2011; 134(Pt 6): 1658–1672.
69 Russo AL, Kwon HC, Burgan WE, Carter D, Beam K, Weizheng X et al. In vitro andin vivo radiosensitization of glioblastoma cells by the poly (ADP-ribose) poly-merase inhibitor E7016. Clin Cancer Res 2009; 15: 607–612.
70 Dungey FA, Loser DA, Chalmers AJ. Replication-dependent radiosensitization ofhuman glioma cells by inhibition of poly(ADP-Ribose) polymerase: mechanismsand therapeutic potential. Int J Radiat Oncol Biol Phys 2008; 72: 1188–1197.
71 Senra JM, Telfer BA, Cherry KE, McCrudden CM, Hirst DG, O’Connor MJ et al.Inhibition of PARP-1 by olaparib (AZD2281) increases the radiosensitivity of alung tumor xenograft. Mol Cancer Ther 2011; 10: 1949–1958.
72 Taverna P, Catapano CV, Citti L, Bonfanti M, D’Incalci M. Influence ofO6-methylguanine on DNA damage and cytotoxicity of temozolomide in L1210mouse leukemia sensitive and resistant to chloroethylnitrosoureas. Anti-CancerDrugs 1992; 3: 401–405.
73 Sedgwick B. Repairing DNA-methylation damage. Nat Rev Mol Cell Biol 2004; 5:148–157.
74 Pan Q, Yang XJ, Wang HM, Dong XT, Wang W, Li Y et al. Chemoresistance totemozolomide in human glioma cell line U251 is associated with increasedactivity of O6-methylguanine-DNA methyltransferase and can be overcome bymetronomic temozolomide regimen. Cell Biochem Biophys 2012; 62: 185–191.
75 Taverna P, Liu L, Hanson AJ, Monks A, Gerson SL. Characterization of MLH1 andMSH2 DNA mismatch repair proteins in cell lines of the NCI anticancer drugscreen. Cancer Chemother Pharmacol 2000; 46: 507–516.
76 Tentori L, Turriziani M, Franco D, Serafino A, Levati L, Roy R et al. Treatment withtemozolomide and poly(ADP-ribose) polymerase inhibitors induces early apop-tosis and increases base excision repair gene transcripts in leukemic cellsresistant to triazene compounds. Leukemia 1999; 13: 901–909.
77 Daniel RA, Rozanska AL, Thomas HD, Mulligan EA, Drew Y, Castelbuono DJ et al.Inhibition of poly(ADP-ribose) polymerase-1 enhances temozolomide andtopotecan activity against childhood neuroblastoma. Clin Cancer Res 2009; 15:1241–1249.
Anticancer profile of PARP inhibitorsJ Michels et al
11
& 2013 Macmillan Publishers Limited Oncogene (2013) 1 – 14

78 Tentori L, Muzi A, Dorio AS, Scarsella M, Leonetti C, Shah GM et al. Pharmaco-logical inhibition of poly(ADP-ribose) polymerase (PARP) activity in PARP-1silenced tumour cells increases chemosensitivity to temozolomide and to aN3-adenine selective methylating agent. Curr Cancer Drug Targets 2010; 10:368–383.
79 Palma JP, Wang YC, Rodriguez LE, Montgomery D, Ellis PA, Bukofzer G et al.ABT-888 confers broad in vivo activity in combination with temozolomide indiverse tumors. Clin Cancer Res 2009; 15: 7277–7290.
80 Horton TM, Jenkins G, Pati D, Zhang L, Dolan ME, Ribes-Zamora A et al. Poly(ADP-ribose) polymerase inhibitor ABT-888 potentiates the cytotoxic activity oftemozolomide in leukemia cells: influence of mismatch repair status andO6-methylguanine-DNA methyltransferase activity. Mol Cancer Ther 2009; 8:2232–2242.
81 Huang SH, Xiong M, Chen XP, Xiao ZY, Zhao YF, Huang ZY. PJ34, an inhibitor ofPARP-1, suppresses cell growth and enhances the suppressive effects of cisplatinin liver cancer cells. Oncol Rep 2008; 20: 567–572.
82 Gambi N, Tramontano F, Quesada P. Poly(ADPR)polymerase inhibition andapoptosis induction in cDDP-treated human carcinoma cell lines. BiochemPharmacol 2008; 75: 2356–2363.
83 Cavallo F, Graziani G, Antinozzi C, Feldman DR, Houldsworth J, Bosl GJ et al.Reduced proficiency in homologous recombination underlies the high sensitivityof embryonal carcinoma testicular germ cell tumors to Cisplatin and poly (adp-ribose) polymerase inhibition. PLoS One 2012; 7: e51563.
84 Michels J, Vitale I, Senovilla L, Enot DP, Garcia P, Lissa D et al. Synergisticinteraction between cisplatin and PARP inhibitors in non-small cell lung cancer.Cell Cycle 2013; 12: 877–883.
85 Drew Y, Mulligan EA, Vong WT, Thomas HD, Kahn S, Kyle S et al. Therapeuticpotential of poly(ADP-ribose) polymerase inhibitor AG014699 in human cancerswith mutated or methylated BRCA1 or BRCA2. J Natl Cancer Inst 2011; 103: 334–346.
86 Wang JC. Cellular roles of DNA topoisomerases: a molecular perspective. Nat RevMol Cell Biol 2002; 3: 430–440.
87 Liu LF, Desai SD, Li TK, Mao Y, Sun M, Sim SP. Mechanism of action of camp-tothecin. Ann N Y Acad Sci 2000; 922: 1–10.
88 Park SY, Cheng YC. Poly(ADP-ribose) polymerase-1 could facilitate the religationof topoisomerase I-linked DNA inhibited by camptothecin. Cancer Res 2005; 65:3894–3902.
89 Thomas HD, Calabrese CR, Batey MA, Canan S, Hostomsky Z, Kyle S et al.Preclinical selection of a novel poly(ADP-ribose) polymerase inhibitor for clinicaltrial. Mol Cancer Ther 2007; 6: 945–956.
90 Delaney CA, Wang LZ, Kyle S, White AW, Calvert AH, Curtin NJ et al. Potentiationof temozolomide and topotecan growth inhibition and cytotoxicity by novelpoly(adenosine diphosphoribose) polymerase inhibitors in a panel of humantumor cell lines. Clin Cancer Res 2000; 6: 2860–2867.
91 Magan N, Isaacs RJ, Stowell KM. Treatment with the PARP-inhibitor PJ34 causesenhanced doxorubicin-mediated cell death in HeLa cells. Anti-cancer Drugs 2012;23: 627–637.
92 Munoz-Gamez JA, Quiles-Perez R, Ruiz-Extremera A, Martin-Alvarez AB,Sanjuan-Nunez L, Carazo A et al. Inhibition of poly (ADP-ribose) polymerase-1enhances doxorubicin activity against liver cancer cells. Cancer Lett 2011; 301:47–56.
93 Wesierska-Gadek J, Zulehner N, Ferk F, Skladanowski A, Komina O, Maurer M.PARP inhibition potentiates the cytotoxic activity of C-1305, a selective inhibitorof topoisomerase II, in human BRCA1-positive breast cancer cells. BiochemPharmacol 2012; 84: 1318–1331.
94 Kaelin Jr. WG. The concept of synthetic lethality in the context of anticancertherapy. Nat Rev Cancer 2005; 5: 689–698.
95 Fong PC, Boss DS, Yap TA, Tutt A, Wu P, Mergui-Roelvink M et al. Inhibition ofpoly(ADP-ribose) polymerase in tumors from BRCA mutation carriers. N Engl JMed 2009; 361: 123–134.
96 Gottipati P, Vischioni B, Schultz N, Solomons J, Bryant HE, Djureinovic T et al.Poly(ADP-ribose) polymerase is hyperactivated in homologous recombination-defective cells. Cancer Res 2010; 70: 5389–5398.
97 Zaremba T, Ketzer P, Cole M, Coulthard S, Plummer ER, Curtin NJ. Poly(ADP-ribose) polymerase-1 polymorphisms, expression and activity in selected humantumour cell lines. Br J Cancer 2009; 101: 256–262.
98 Seki A, Coppinger JA, Jang CY, Yates JR, Fang G. Bora and the kinase Aurora acooperatively activate the kinase Plk1 and control mitotic entry. Science 2008;320: 1655–1658.
99 Cazales M, Schmitt E, Montembault E, Dozier C, Prigent C, Ducommun B. CDC25Bphosphorylation by Aurora-A occurs at the G2/M transition and is inhibited byDNA damage. Cell Cycle 2005; 4: 1233–1238.
100 Yang G, Chang B, Yang F, Guo X, Cai KQ, Xiao XS et al. Aurora kinase A promotesovarian tumorigenesis through dysregulation of the cell cycle and suppressionof BRCA2. Clin Cancer Res 2010; 16: 3171–3181.
101 Sourisseau T, Maniotis D, McCarthy A, Tang C, Lord CJ, Ashworth A et al.Aurora-A expressing tumour cells are deficient for homology-directed DNAdouble strand-break repair and sensitive to PARP inhibition. EMBO Mol Med2010; 2: 130–142.
102 Salmena L, Carracedo A, Pandolfi PP. Tenets of PTEN tumor suppression. Cell2008; 133: 403–414.
103 Shen WH, Balajee AS, Wang J, Wu H, Eng C, Pandolfi PP et al. Essential role fornuclear PTEN in maintaining chromosomal integrity. Cell 2007; 128: 157–170.
104 Kumar A, Fernandez-Capetillo O, Carrera AC. Nuclear phosphoinositide 3-kinasebeta controls double-strand break DNA repair. Proc Natl Acad Sci USA 2010; 107:7491–7496.
105 Fraser M, Zhao H, Luoto KR, Lundin C, Coackley C, Chan N et al. PTEN deletion inprostate cancer cells does not associate with loss of RAD51 function: implica-tions for radiotherapy and chemotherapy. Clin Cancer Res 2012; 18: 1015–1027.
106 Mendes-Pereira AM, Martin SA, Brough R, McCarthy A, Taylor JR, Kim JS et al.Synthetic lethal targeting of PTEN mutant cells with PARP inhibitors. EMBO MolMed 2009; 1: 315–322.
107 McEllin B, Camacho CV, Mukherjee B, Hahm B, Tomimatsu N, Bachoo RM et al.PTEN loss compromises homologous recombination repair in astrocytes: impli-cations for glioblastoma therapy with temozolomide or poly(ADP-ribose) poly-merase inhibitors. Cancer Res 2010; 70: 5457–5464.
108 Dedes KJ, Wetterskog D, Mendes-Pereira AM, Natrajan R, Lambros MB, Geyer FCet al. PTEN deficiency in endometrioid endometrial adenocarcinomas predictssensitivity to PARP inhibitors. Sci Translation Med 2010; 2: 53ra75.
109 Fraser M, Harding SM, Zhao H, Coackley C, Durocher D, Bristow RG. MRE11promotes AKT phosphorylation in direct response to DNA double-strand breaks.Cell Cycle 2011; 10: 2218–2232.
110 Haince JF, McDonald D, Rodrigue A, Dery U, Masson JY, Hendzel MJ et al. PARP1-dependent kinetics of recruitment of MRE11 and NBS1 proteins to multiple DNAdamage sites. J Biol Chem 2008; 283: 1197–1208.
111 Graeser M, McCarthy A, Lord CJ, Savage K, Hills M, Salter J et al. A markerof homologous recombination predicts pathologic complete response toneoadjuvant chemotherapy in primary breast cancer. Clin Cancer Res 2010; 16:6159–6168.
112 Sultana R, Abdel-Fatah T, Abbotts R, Hawkes C, Albarakati N, Seedhouse C et al.Targeting XRCC1 Deficiency in Breast Cancer for Personalized Therapy. CancerRes 2013; 73: 1621–1634.
113 Sakata K, Someya M, Matsumoto Y, Tauchi H, Kai M, Toyota M et al. Gimeracil, aninhibitor of dihydropyrimidine dehydrogenase, inhibits the early step inhomologous recombination. Cancer Sci 2011; 102: 1712–1716.
114 Menisser-de Murcia J, Mark M, Wendling O, Wynshaw-Boris A, de Murcia G.Early embryonic lethality in PARP-1 Atm double-mutant mice suggests afunctional synergy in cell proliferation during development. Mol Cell Biol 2001;21: 1828–1832.
115 Lavin MF. Ataxia-telangiectasia: from a rare disorder to a paradigm for cellsignalling and cancer. Nat Rev Mol Cell Biol 2008; 9: 759–769.
116 Williamson CT, Muzik H, Turhan AG, Zamo A, O’Connor MJ, Bebb DG et al.ATM deficiency sensitizes mantle cell lymphoma cells to poly(ADP-ribose)polymerase-1 inhibitors. Mol Cancer Ther 2010; 9: 347–357.
117 Weston VJ, Oldreive CE, Skowronska A, Oscier DG, Pratt G, Dyer MJ et al. ThePARP inhibitor olaparib induces significant killing of ATM-deficient lymphoidtumor cells in vitro and in vivo. Blood 2010; 116: 4578–4587.
118 Schaffner C, Idler I, Stilgenbauer S, Dohner H, Lichter P. Mantle cell lymphoma ischaracterized by inactivation of the ATM gene. Proc Natl Acad Sci USA 2000; 97:2773–2778.
119 Veuger SJ, Curtin NJ, Richardson CJ, Smith GC, Durkacz BW. Radiosensitizationand DNA repair inhibition by the combined use of novel inhibitors of DNA-dependent protein kinase and poly(ADP-ribose) polymerase-1. Cancer Res 2003;63: 6008–6015.
120 Veuger SJ, Curtin NJ, Smith GC, Durkacz BW. Effects of novel inhibitors ofpoly(ADP-ribose) polymerase-1 and the DNA-dependent protein kinase onenzyme activities and DNA repair. Oncogene 2004; 23: 7322–7329.
121 Bryant HE, Helleday T. Inhibition of poly (ADP-ribose) polymerase activates ATMwhich is required for subsequent homologous recombination repair. NucleicAcids Res 2006; 34: 1685–1691.
122 Yuan ZM, Huang Y, Ishiko T, Nakada S, Utsugisawa T, Kharbanda S et al. Reg-ulation of Rad51 function by c-Abl in response to DNA damage. J Biol Chem1998; 273: 3799–3802.
123 Cousineau I, Belmaaza A. EMSY overexpression disrupts the BRCA2/RAD51pathway in the DNA-damage response: implications for chromosomal instabil-ity/recombination syndromes as checkpoint diseases. Mol Genet Genomics 2011;285: 325–340.
124 Verweij J, Casali PG, Zalcberg J, LeCesne A, Reichardt P, Blay JY et al. Progression-free survival in gastrointestinal stromal tumours with high-dose imatinib: ran-domised trial. Lancet 2004; 364: 1127–1134.
Anticancer profile of PARP inhibitorsJ Michels et al
12
Oncogene (2013) 1 – 14 & 2013 Macmillan Publishers Limited

125 O’Brien SG, Guilhot F, Larson RA, Gathmann I, Baccarani M, Cervantes F et al.Imatinib compared with interferon and low-dose cytarabine for newlydiagnosed chronic-phase chronic myeloid leukemia. N Engl J Med 2003; 348:994–1004.
126 Choudhury A, Zhao H, Jalali F, Al Rashid S, Ran J, Supiot S et al. Targetinghomologous recombination using imatinib results in enhanced tumor cellchemosensitivity and radiosensitivity. Mol Cancer Ther 2009; 8: 203–213.
127 Johnson N, Cai D, Kennedy RD, Pathania S, Arora M, Li YC et al. Cdk1 participatesin BRCA1-dependent S phase checkpoint control in response to DNA damage.Mol Cell 2009; 35: 327–339.
128 Johnson N, Li YC, Walton ZE, Cheng KA, Li D, Rodig SJ et al. Compromised CDK1activity sensitizes BRCA-proficient cancers to PARP inhibition. Nat Med 2011; 17:875–882.
129 Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, Brannigan BWet al. Activating mutations in the epidermal growth factor receptor underlyingresponsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med 2004; 350:2129–2139.
130 Karapetis CS, Khambata-Ford S, Jonker DJ, O’Callaghan CJ, Tu D, Tebbutt NCet al. K-ras mutations and benefit from cetuximab in advanced colorectal cancer.N Engl J Med 2008; 359: 1757–1765.
131 Li L, Wang H, Yang ES, Arteaga CL, Xia F. Erlotinib attenuates homologousrecombinational repair of chromosomal breaks in human breast cancer cells.Cancer Res 2008; 68: 9141–9146.
132 Nowsheen S, Bonner JA, Lobuglio AF, Trummell H, Whitley AC, Dobelbower MCet al. Cetuximab augments cytotoxicity with poly (adp-ribose) polymeraseinhibition in head and neck cancer. PLoS One 2011; 6: e24148.
133 Modi S, Stopeck A, Linden H, Solit D, Chandarlapaty S, Rosen N et al. HSP90inhibition is effective in breast cancer: a phase II trial of tanespimycin (17-AAG)plus trastuzumab in patients with HER2-positive metastatic breast cancer pro-gressing on trastuzumab. Clin Cancer Res 2011; 17: 5132–5139.
134 Hong DS, Banerji U, Tavana B, George GC, Aaron J, Kurzrock R. Targeting themolecular chaperone heat shock protein 90 (HSP90): lessons learned and futuredirections. Cancer Treat Rev 2013; 39: 375–387.
135 Noguchi M, Yu D, Hirayama R, Ninomiya Y, Sekine E, Kubota N et al. Inhibition ofhomologous recombination repair in irradiated tumor cells pretreated withHsp90 inhibitor 17-allylamino-17-demethoxygeldanamycin. Biochem Biophys ResCommun 2006; 351: 658–663.
136 Dungey FA, Caldecott KW, Chalmers AJ. Enhanced radiosensitization of humanglioma cells by combining inhibition of poly(ADP-ribose) polymerase withinhibition of heat shock protein 90. Mol Cancer Ther 2009; 8: 2243–2254.
137 Maeta Y, Shiota G, Okano J, Murawaki Y. Effect of promoter methylation of thep16 gene on phosphorylation of retinoblastoma gene product and growth ofhepatocellular carcinoma cells. Tumour Biol 2005; 26: 300–305.
138 Zhang JX, Li DQ, He AR, Motwani M, Vasiliou V, Eswaran J et al. Synergisticinhibition of hepatocellular carcinoma growth by cotargeting chromatinmodifying enzymes and poly (ADP-ribose) polymerases. Hepatology 2012; 55:1840–1851.
139 Brenner JC, Chinnaiyan AM. Translocations in epithelial cancers. Biochim BiophysActa 2009; 1796: 201–215.
140 Brenner JC, Ateeq B, Li Y, Yocum AK, Cao Q, Asangani IA et al. Mechanisticrationale for inhibition of poly(ADP-ribose) polymerase in ETS gene fusion-positive prostate cancer. Cancer cell 2011; 19: 664–678.
141 Ibrahim YH, Garcia-Garcia C, Serra V, He L, Torres-Lockhart K, Prat A et al.PI3K inhibition impairs BRCA1/2 expression and sensitizes BRCA-proficienttriple-negative breast cancer to PARP inhibition. Cancer Discov 2012; 2:1036–1047.
142 Baker KM, Wei G, Schaffner AE, Ostrowski MC. Ets-2 and components of mam-malian SWI/SNF form a repressor complex that negatively regulates the BRCA1promoter. J Biol Chem 2003; 278: 17876–17884.
143 Sharrocks AD. The ETS-domain transcription factor family. Nat Rev Mol Cell Biol2001; 2: 827–837.
144 Juvekar A, Burga LN, Hu H, Lunsford EP, Ibrahim YH, Balmana J et al. Combininga PI3K inhibitor with a PARP inhibitor provides an effective therapy for BRCA1-related breast cancer. Cancer Discover 2012; 2: 1048–1063.
145 Nowsheen S, Cooper T, Bonner JA, LoBuglio AF, Yang ES. HER2 overexpressionrenders human breast cancers sensitive to PARP inhibition independently ofany defect in homologous recombination DNA repair. Cancer Res 2012; 72:4796–4806.
146 Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, Bajamonde A et al. Use ofchemotherapy plus a monoclonal antibody against HER2 for metastatic breastcancer that overexpresses HER2. N Engl J Med 2001; 344: 783–792.
147 Merkhofer EC, Cogswell P, Baldwin AS. Her2 activates NF-kappaB and inducesinvasion through the canonical pathway involving IKKalpha. Oncogene 2010; 29:1238–1248.
148 Veuger SJ, Hunter JE, Durkacz BW. Ionizing radiation-induced NF-kappaB acti-vation requires PARP-1 function to confer radioresistance. Oncogene 2009; 28:832–842.
149 Montoni A, Robu M, Pouliot E, Shah GM. Resistance to PARP-Inhibitors in CancerTherapy. Front Pharmacol 2013; 4: 18.
150 Edwards SL, Brough R, Lord CJ, Natrajan R, Vatcheva R, Levine DA et al. Resis-tance to therapy caused by intragenic deletion in BRCA2. Nature 2008; 451:1111–1115.
151 Sakai W, Swisher EM, Karlan BY, Agarwal MK, Higgins J, Friedman C et al.Secondary mutations as a mechanism of cisplatin resistance in BRCA2-mutatedcancers. Nature 2008; 451: 1116–1120.
152 Bunting SF, Callen E, Wong N, Chen HT, Polato F, Gunn A et al. 53BP1 inhibitshomologous recombination in Brca1-deficient cells by blocking resection of DNAbreaks. Cell 2010; 141: 243–254.
153 Bouwman P, Aly A, Escandell JM, Pieterse M, Bartkova J, van der Gulden H et al.53BP1 loss rescues BRCA1 deficiency and is associated with triple-negative andBRCA-mutated breast cancers. Nat Struct Mol Biol 2010; 17: 688–695.
154 Patel AG, De Lorenzo SB, Flatten KS, Poirier GG, Kaufmann SH. Failure ofiniparib to inhibit poly(ADP-Ribose) polymerase in vitro. Clin Cancer Res 2012; 18:1655–1662.
155 Fong PC, Yap TA, Boss DS, Carden CP, Mergui-Roelvink M, Gourley C et al.Poly(ADP)-ribose polymerase inhibition: frequent durable responses in BRCAcarrier ovarian cancer correlating with platinum-free interval. J Clin Oncol 2010;28: 2512–2519.
156 Tutt A, Robson M, Garber JE, Domchek SM, Audeh MW, Weitzel JN et al. Oralpoly(ADP-ribose) polymerase inhibitor olaparib in patients with BRCA1 or BRCA2mutations and advanced breast cancer: a proof-of-concept trial. Lancet 2010;376: 235–244.
157 Audeh MW, Carmichael J, Penson RT, Friedlander M, Powell B, Bell-McGuinn KMet al. Oral poly(ADP-ribose) polymerase inhibitor olaparib in patients with BRCA1or BRCA2 mutations and recurrent ovarian cancer: a proof-of-concept trial.Lancet 2010; 376: 245–251.
158 Gelmon KA, Tischkowitz M, Mackay H, Swenerton K, Robidoux A, Tonkin K et al.Olaparib in patients with recurrent high-grade serous or poorly differentiatedovarian carcinoma or triple-negative breast cancer: a phase 2, multicentre, open-label, non-randomised study. Lancet Oncol 2011; 12: 852–861.
159 Kaye SB, Lubinski J, Matulonis U, Ang JE, Gourley C, Karlan BY et al. Phase II,open-label, randomized, multicenter study comparing the efficacy and safety ofolaparib, a poly (ADP-ribose) polymerase inhibitor, and pegylated liposomaldoxorubicin in patients with BRCA1 or BRCA2 mutations and recurrent ovariancancer. J Clin Oncol 2012; 30: 372–379.
160 Gordon AN, Fleagle JT, Guthrie D, Parkin DE, Gore ME, Lacave AJ. Recurrentepithelial ovarian carcinoma: a randomized phase III study of pegylated lipo-somal doxorubicin versus topotecan. J Clin Oncol 2001; 19: 3312–3322.
161 Ledermann J, Harter P, Gourley C, Friedlander M, Vergote I, Rustin G et al.Olaparib maintenance therapy in platinum-sensitive relapsed ovarian cancer.N Engl J Med 2012; 366: 1382–1392.
162 Rajan A, Carter CA, Kelly RJ, Gutierrez M, Kummar S, Szabo E et al. A phase Icombination study of olaparib with cisplatin and gemcitabine in adults withsolid tumors. Clin Cancer Res 2012; 18: 2344–2351.
163 Kummar S, Ji J, Morgan R, Lenz HJ, Puhalla SL, Belani CP et al. A phase I study ofveliparib in combination with metronomic cyclophosphamide in adults withrefractory solid tumors and lymphomas. Clin Cancer Res 2012; 18: 1726–1734.
164 Plummer R, Jones C, Middleton M, Wilson R, Evans J, Olsen A et al. Phase I studyof the poly(ADP-ribose) polymerase inhibitor, AG014699, in combination withtemozolomide in patients with advanced solid tumors. Clin Cancer Res 2008; 14:7917–7923.
165 Plummer R, Lorigan P, Steven N, Scott L, Middleton MR, Wilson RH et al. A phaseII study of the potent PARP inhibitor, Rucaparib (PF-01367338, AG014699), withtemozolomide in patients with metastatic melanoma demonstrating evidence ofchemopotentiation. Cancer Chemother Pharmacol 2013; 71: 1191–1199.
166 Adams SF, Marsh EB, Elmasri W, Halberstadt S, Vandecker S, Sammel MD et al. Ahigh response rate to liposomal doxorubicin is seen among women with BRCAmutations treated for recurrent epithelial ovarian cancer. Gynecol Oncol 2011;123: 486–491.
167 Cancer Genome Atlas Research Network. Integrated genomic analyses of ovariancarcinoma. Nature 2011; 474: 609–615.
168 Gonzalez-Angulo AM, Timms KM, Liu S, Chen H, Litton JK, Potter J et al. Incidenceand outcome of BRCA mutations in unselected patients with triple receptor-negative breast cancer. Clin Cancer Res 2011; 17: 1082–1089.
169 Moynahan ME, Chiu JW, Koller BH, Jasin M. Brca1 controls homology-directedDNA repair. Mol Cell 1999; 4: 511–518.
170 Moynahan ME, Cui TY, Jasin M. Homology-directed dna repair, mitomycin-cresistance, and chromosome stability is restored with correction of a Brca1mutation. Cancer Res 2001; 61: 4842–4850.
Anticancer profile of PARP inhibitorsJ Michels et al
13
& 2013 Macmillan Publishers Limited Oncogene (2013) 1 – 14

171 Turner N, Tutt A, Ashworth A. Hallmarks of ’BRCAness’ in sporadic cancers.Nat Rev Cancer 2004; 4: 814–819.
172 Hughes-Davies L, Huntsman D, Ruas M, Fuks F, Bye J, Chin SF et al. EMSYlinks the BRCA2 pathway to sporadic breast and ovarian cancer. Cell 2003; 115:523–535.
173 Press JZ, De Luca A, Boyd N, Young S, Troussard A, Ridge Y et al. Ovariancarcinomas with genetic and epigenetic BRCA1 loss have distinct molecularabnormalities. BMC Cancer 2008; 8: 17.
174 Mukhopadhyay A, Elattar A, Cerbinskaite A, Wilkinson SJ, Drew Y, Kyle S et al.Development of a functional assay for homologous recombination status inprimary cultures of epithelial ovarian tumor and correlation with sensitivity topoly(ADP-ribose) polymerase inhibitors. Clin Cancer Res 2010; 16: 2344–2351.
175 Kashiwaya K, Hosokawa M, Eguchi H, Ohigashi H, Ishikawa O, Shinomura Y et al.Identification of C2orf18, termed ANT2BP (ANT2-binding protein), as one ofthe key molecules involved in pancreatic carcinogenesis. Cancer Sci 2009; 100:457–464.
176 Piao L, Nakagawa H, Ueda K, Chung S, Kashiwaya K, Eguchi H et al. C12orf48,termed PARP-1 binding protein, enhances poly(ADP-ribose) polymerase-1(PARP-1) activity and protects pancreatic cancer cells from DNA damage. GenesChromosome Cancer 2011; 50: 13–24.
177 O’Connor KW, Dejsuphong D, Park E, Nicolae CM, Kimmelman AC, D’Andrea ADet al. PARI Overexpression Promotes Genomic Instability and PancreaticTumorigenesis. Cancer Res 2013; 73: 2529–2539.
178 Abkevich V, Timms KM, Hennessy BT, Potter J, Carey MS, Meyer LA et al. Patternsof genomic loss of heterozygosity predict homologous recombination repairdefects in epithelial ovarian cancer. Br J Cancer 2012; 107: 1776–1782.
179 Stefansson OA, Jonasson JG, Johannsson OT, Olafsdottir K, Steinarsdottir M,Valgeirsdottir S et al. Genomic profiling of breast tumours in relation to BRCAabnormalities and phenotypes. Br Cancer Res 2009; 11: R47.
180 Birkbak NJ, Wang ZC, Kim JY, Eklund AC, Li Q, Tian R et al. Telomeric allelicimbalance indicates defective DNA repair and sensitivity to DNA-damagingagents. Cancer Dis 2012; 2: 366–375.
181 Gros L, Saparbaev MK, Laval J. Enzymology of the repair of free radicals-inducedDNA damage. Oncogene 2002; 21: 8905–8925.
182 Saparbaev M, Laval J. Excision of hypoxanthine from DNA containing dIMPresidues by the Escherichia coli, yeast, rat, and human alkylpurine DNA glyco-sylases. Proc Natl Acad Sc USA 1994; 91: 5873–5877.
183 Gros L, Ishchenko AA, Saparbaev M. Enzymology of repair of etheno-adducts.Mutat Res 2003; 531: 219–229.
184 Boiteux S, Radicella JP. The human OGG1 gene: structure, functions, and itsimplication in the process of carcinogenesis. Arch Biochem Biophys 2000; 377:1–8.
185 Ocampo MT, Chaung W, Marenstein DR, Chan MK, Altamirano A, Basu AK et al.Targeted deletion of mNth1 reveals a novel DNA repair enzyme activity. Mol CellBiol 2002; 22: 6111–6121.
186 Wilson 3rd DM, Barsky D. The major human abasic endonuclease: formation,consequences and repair of abasic lesions in DNA. Mutat Res 2001; 485:283–307.
187 Andressoo JO, Hoeijmakers JH, de Waard H. Nucleotide excision repair and itsconnection with cancer and ageing. Ad Exp Med Biol 2005; 570: 45–83.
188 Sugasawa K, Ng JM, Masutani C, Iwai S, van der Spek PJ, Eker AP et al. Xerodermapigmentosum group C protein complex is the initiator of global genomenucleotide excision repair. Mol Cell 1998; 2: 223–232.
189 Pegg AE. Mammalian O6-alkylguanine-DNA alkyltransferase: regulation andimportance in response to alkylating carcinogenic and therapeutic agents.Cancer Res 1990; 50: 6119–6129.
190 Gudmundsdottir K, Ashworth A. The roles of BRCA1 and BRCA2 and associatedproteins in the maintenance of genomic stability. Oncogene 2006; 25:5864–5874.
191 Jackson SP, Bartek J. The DNA-damage response in human biology and disease.Nature 2009; 461: 1071–1078.
192 Wooster R, Weber BL. Breast and ovarian cancer. N Engl J Med 2003; 348:2339–2347.
193 Cerbinskaite A, Mukhopadhyay A, Plummer ER, Curtin NJ, Edmondson RJ.Defective homologous recombination in human cancers. Cancer Treat Rev 2012;38: 89–100.
194 Jacinto FV, Esteller M. Mutator pathways unleashed by epigenetic silencing inhuman cancer. Mutagenesis 2007; 22: 247–253.
195 Bullrich F, Rasio D, Kitada S, Starostik P, Kipps T, Keating M et al. ATM mutationsin B-cell chronic lymphocytic leukemia. Cancer Res 1999; 59: 24–27.
196 Marsit CJ, Liu M, Nelson HH, Posner M, Suzuki M, Kelsey KT. Inactivation ofthe Fanconi anemia/BRCA pathway in lung and oral cancers: implications fortreatment and survival. Oncogene 2004; 23: 1000–1004.
197 Narayan G, Arias-Pulido H, Nandula SV, Basso K, Sugirtharaj DD, Vargas H et al.Promoter hypermethylation of FANCF: disruption of Fanconi Anemia-BRCApathway in cervical cancer. Cancer Res 2004; 64: 2994–2997.
198 Taniguchi T, Tischkowitz M, Ameziane N, Hodgson SV, Mathew CG, Joenje Het al. Disruption of the Fanconi anemia-BRCA pathway in cisplatin-sensitiveovarian tumors. Nat Med 2003; 9: 568–574.
199 Riffell JL, Lord CJ, Ashworth A. Tankyrase-targeted therapeutics: expandingopportunities in the PARP family. Nat Rev Drug Discov 2012; 11: 923–936.
200 Kraus WL, Lis JT. PARP goes transcription. Cell 2003; 113: 677–683.201 Carbone M, Rossi MN, Cavaldesi M, Notari A, Amati P, Maione R. Poly(ADP-
ribosyl)ation is implicated in the G0-G1 transition of resting cells. Oncogene2008; 27: 6083–6092.
202 Aurelius J, Thoren FB, Akhiani AA, Brune M, Palmqvist L, Hansson M et al.Monocytic AML cells inactivate antileukemic lymphocytes: role of NADPH oxi-dase/gp91(phox) expression and the PARP-1/PAR pathway of apoptosis. Blood2012; 119: 5832–5837.
203 Khan OA, Gore M, Lorigan P, Stone J, Greystoke A, Burke W et al. A phase I studyof the safety and tolerability of olaparib (AZD2281, KU0059436) and dacarbazinein patients with advanced solid tumours. Br J Cancer 2011; 104: 750–755.
204 Samol J, Ranson M, Scott E, Macpherson E, Carmichael J, Thomas A et al.Safety and tolerability of the poly(ADP-ribose) polymerase (PARP) inhibitor,olaparib (AZD2281) in combination with topotecan for the treatment of patientswith advanced solid tumors: a phase I study. Invest New Drugs 2012; 30:1493–1500.
205 Dean E, Middleton MR, Pwint T, Swaisland H, Carmichael J, Goodege-Kunwar Pet al. Phase I study to assess the safety and tolerability of olaparib in combi-nation with bevacizumab in patients with advanced solid tumours. Br J Cancer2012; 106: 468–474.
206 Kummar S, Chen A, Ji J, Zhang Y, Reid JM, Ames M et al. Phase I study of PARPinhibitor ABT-888 in combination with topotecan in adults with refractory solidtumors and lymphomas. Cancer Res 2011; 71: 5626–5634.
207 Bedikian AY, Papadopoulos NE, Kim KB, Hwu WJ, Homsi J, Glass MR et al. A phaseIB trial of intravenous INO-1001 plus oral temozolomide in subjects withunresectable stage-III or IV melanoma. Cancer Invest 2009; 27: 756–763.
Anticancer profile of PARP inhibitorsJ Michels et al
14
Oncogene (2013) 1 – 14 & 2013 Macmillan Publishers Limited
Copyright © 2022 FDOKUMEN









![Synthesis, [18F] radiolabeling, and evaluation of poly (ADP-ribose) polymerase-1 (PARP-1) inhibitors for in vivo imaging of PARP-1 using positron emission tomography](https://static.fdokumen.com/doc/165x107/6335c3a302a8c1a4ec01e906/synthesis-18f-radiolabeling-and-evaluation-of-poly-adp-ribose-polymerase-1.jpg)