
Potential Benefits of Glitazones for Cancer and Vascular Disease
15
Current Drug Therapy, 2008, 3, 111-125 111 1574-8855/08 $55.00+.00 ©2008 Bentham Science Publishers Ltd. Potential Benefits of Glitazones for Cancer and Vascular Disease José M. Pérez-Ortiz, Silvia Llorens, Juan Llopis, Pedro A. Tranque and Eduardo Nava * Department of Medical Sciences, University of Castilla-La Mancha School of Medicine and Regional Centre for Bio- medical Research (CRIB), Albacete, Spain Abstract: Glitazones were introduced into clinical use to offer type II diabetic patients an alternative to oral hypoglycae- mic agents. Unlike traditional agents based on -pancreatic overstimulation, glitazones raise peripheral insulin sensitivity allowing the patient to efficiently use his own insulin. Although glitazones are only approved for the treatment of diabetes, their beneficial effects extend to every symptom of the so-called metabolic syndrome: they protect against atherosclerosis, inhibit blood coagulation, decrease hypertension and improve vascular endothelial function. Moreover, glitazones coun- teract activation of macrophages and brain microglia, attenuate the expression of pro-inflammatory genes, and inhibit various signalling events involved in inflammation. In addition, glitazones are able to induce cell differentiation and apop- tosis in several cancer cells, suggesting possible use of these drugs for the treatment of gliomas and other tumors. The mo- lecular basis of such a vast array of glitazone actions is necessarily complex. Glitazone effects were originally attributed to activation of peroxisome proliferator activated receptor- (PPAR ). However, several properties of glitazones are unre- lated to PPAR . We review here the emerging actions of glitazones focusing on their antihypertensive and anti-tumoral ef- fects, PPAR -dependent and –independent, and also emphasizing the contribution of mitochondria and reactive oxygen and nitrogen species to these actions. INTRODUCTION Glitazones: Compounds with Clinical Applications Glitazones, also called thiazolidinediones, form a family of synthetic compounds that include troglitazone, ciglita- zone, pioglitazone and rosiglitazone. They were originally designed in an attempt to offer type II diabetic patients suf- fering insulin resistance an alternative to the existing oral hypoglycaemic agents. Until the early eighties no drugs able to increase insulin sensitivity were available with the excep- tion of sulfonylureas, which increase the number of insulin receptors [1]. However, such property of sulfonylureas was eclipsed by their main effect: a stimulation of insulin release from pancreatic cells that caused acute and chronic hypo- glycaemia, the most undesirable side effect of sulfonylureas and insulin itself. Sohda et al. [2] noticed that compounds possessing an acidic thiazolidine-2,4-dione were particularly effective as hypoglycaemic and hypolipidemic agents in genetically obese and diabetic yellow KK mice [3]. Ciglitazone (Fig. (1)) was a stand out in this study for its ability to decrease plasma insulin, glycaemia and plasma triglycerides, reducing also insulin secretion in response to oral glucose. Moreover, ciglitazone normalized the glycaemia response to insulin without causing acute or chronic hypoglycaemia. No adverse effects were observed in treated rats, demonstrating the po- tential medical usefulness of glitazones in insulin-resistant patients [4]. A few years later, the same pharmaceutical company, Takeda, introduced pioglitazone as a more potent compound [5]; whereas other laboratories produced troglita- zone (compound CS-045), [6] and rosiglitazone (compound *Address correspondence to this author at the Department of Medical Sci- ences, University of Castilla-La Mancha School of Medicine and Regional Centre for Biomedical Research (CRIB), 02006 Albacete, Spain; Tel: 34 967599200, Ext. 2938; Fax: 34 967 599327; E-mail: [email protected] Fig. (1). Chemical structure of ciglitazone, troglitazone, piogli- tazone and rosiglitazone. The first glitazone tried was ciglitazone: 5-[4-(1-methylcyclohexylmethoxy)-benzyl]-thiazolidine-2,4-dione as designated by Fujita et al. Troglitazone: 5-[4-(6-hydroxy-2,5,7,8- tetramethylchroman-2-yl-methoxy)benzyl]-2,4-thiazolidinedione as designated by Fujiwara et al. 1988. Pioglitazone: 5-[4-[2-(5-ethyl-2- pyridyl)ethoxy]benzyl]-2,4-thiazolidinedione, as designated by Ikeda et al. and rosiglitazone: 5-[(4-[2-methyl-2(pyridinylamino)ethoxy] phenyl)methyl]2,4-thiazolidinedione-(z)-2-butenedioate(1:1), as designated by Oakes et al. The acidic thiazolidine-2,4-dione group is the responsible for the biological activities of glitazones. CH 2 O CH 3 CH 2 S NH O O O CH 2 O CH 3 CH 3 H 3 C HO CH 3 CH 2 NH S H O O CIGLITAZONE TROGLITAZONE N H 3 C O S NH O O PIOGLITAZONE N N O S NH CH 3 O O ROSIGLITAZONE Not For Distribution
Transcript of Potential Benefits of Glitazones for Cancer and Vascular Disease
Current Drug Therapy, 2008, 3, 111-125 111
1574-8855/08 $55.00+.00 ©2008 Bentham Science Publishers Ltd.
Potential Benefits of Glitazones for Cancer and Vascular Disease
José M. Pérez-Ortiz, Silvia Llorens, Juan Llopis, Pedro A. Tranque and Eduardo Nava*
Department of Medical Sciences, University of Castilla-La Mancha School of Medicine and Regional Centre for Bio-
medical Research (CRIB), Albacete, Spain
Abstract: Glitazones were introduced into clinical use to offer type II diabetic patients an alternative to oral hypoglycae-mic agents. Unlike traditional agents based on -pancreatic overstimulation, glitazones raise peripheral insulin sensitivity allowing the patient to efficiently use his own insulin. Although glitazones are only approved for the treatment of diabetes, their beneficial effects extend to every symptom of the so-called metabolic syndrome: they protect against atherosclerosis, inhibit blood coagulation, decrease hypertension and improve vascular endothelial function. Moreover, glitazones coun-teract activation of macrophages and brain microglia, attenuate the expression of pro-inflammatory genes, and inhibit various signalling events involved in inflammation. In addition, glitazones are able to induce cell differentiation and apop-tosis in several cancer cells, suggesting possible use of these drugs for the treatment of gliomas and other tumors. The mo-lecular basis of such a vast array of glitazone actions is necessarily complex. Glitazone effects were originally attributed to activation of peroxisome proliferator activated receptor- (PPAR ). However, several properties of glitazones are unre-lated to PPAR . We review here the emerging actions of glitazones focusing on their antihypertensive and anti-tumoral ef-fects, PPAR -dependent and –independent, and also emphasizing the contribution of mitochondria and reactive oxygen and nitrogen species to these actions.
INTRODUCTION
Glitazones: Compounds with Clinical Applications
Glitazones, also called thiazolidinediones, form a family of synthetic compounds that include troglitazone, ciglita-zone, pioglitazone and rosiglitazone. They were originally designed in an attempt to offer type II diabetic patients suf-fering insulin resistance an alternative to the existing oral hypoglycaemic agents. Until the early eighties no drugs able to increase insulin sensitivity were available with the excep-tion of sulfonylureas, which increase the number of insulin receptors [1]. However, such property of sulfonylureas was eclipsed by their main effect: a stimulation of insulin release from pancreatic cells that caused acute and chronic hypo-glycaemia, the most undesirable side effect of sulfonylureas and insulin itself.
Sohda et al. [2] noticed that compounds possessing an acidic thiazolidine-2,4-dione were particularly effective as hypoglycaemic and hypolipidemic agents in genetically obese and diabetic yellow KK mice [3]. Ciglitazone (Fig. (1)) was a stand out in this study for its ability to decrease plasma insulin, glycaemia and plasma triglycerides, reducing also insulin secretion in response to oral glucose. Moreover, ciglitazone normalized the glycaemia response to insulin without causing acute or chronic hypoglycaemia. No adverse effects were observed in treated rats, demonstrating the po-tential medical usefulness of glitazones in insulin-resistant patients [4]. A few years later, the same pharmaceutical company, Takeda, introduced pioglitazone as a more potent compound [5]; whereas other laboratories produced troglita-zone (compound CS-045), [6] and rosiglitazone (compound
*Address correspondence to this author at the Department of Medical Sci-ences, University of Castilla-La Mancha School of Medicine and Regional Centre for Biomedical Research (CRIB), 02006 Albacete, Spain; Tel: 34 967 599200, Ext. 2938; Fax: 34 967 599327; E-mail: [email protected]
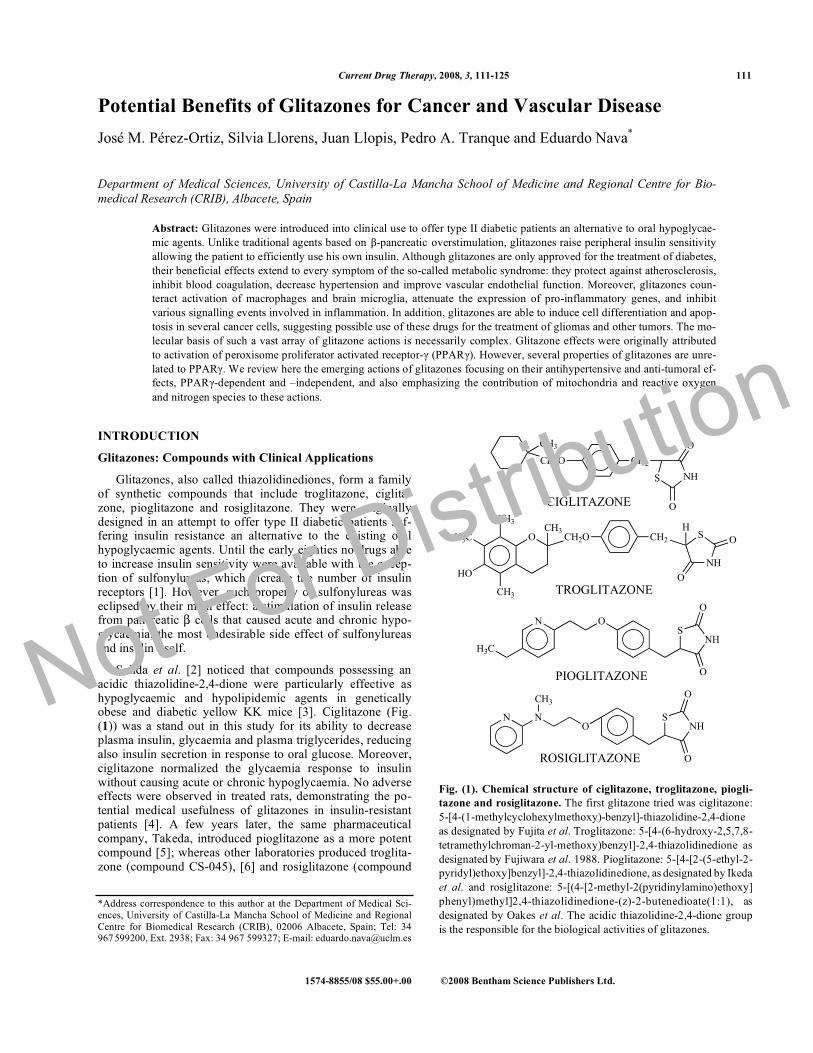
Fig. (1). Chemical structure of ciglitazone, troglitazone, piogli-
tazone and rosiglitazone. The first glitazone tried was ciglitazone: 5-[4-(1-methylcyclohexylmethoxy)-benzyl]-thiazolidine-2,4-dione as designated by Fujita et al. Troglitazone: 5-[4-(6-hydroxy-2,5,7,8-tetramethylchroman-2-yl-methoxy)benzyl]-2,4-thiazolidinedione as designated by Fujiwara et al. 1988. Pioglitazone: 5-[4-[2-(5-ethyl-2-pyridyl)ethoxy]benzyl]-2,4-thiazolidinedione, as designated by Ikeda et al. and rosiglitazone: 5-[(4-[2-methyl-2(pyridinylamino)ethoxy] phenyl)methyl]2,4-thiazolidinedione-(z)-2-butenedioate(1:1), as designated by Oakes et al. The acidic thiazolidine-2,4-dione group is the responsible for the biological activities of glitazones.
CH2O
CH3
CH2
S NH
O
O
O CH2OCH3
CH3
H3C
HO
CH3
CH2
NH
SH
O
O
CIGLITAZONE
TROGLITAZONE
N
H3C
OS
NH
O
OPIOGLITAZONE
N NO
SNH
CH3O
OROSIGLITAZONE
Not For Distribution
112 Current Drug Therapy, 2008, Vol. 3, No. 2 Pérez-Ortiz et al.
BRL49653) [7] (Fig. (1)). The first glitazone undergoing clinical trials, troglitazone [8], was launched to the market in 1997 [9]. However, reports showing hepatotoxicity [10,11] forced troglitazone withdrawal in less than a year [9]. Piogli-tazone and rosiglitazone, approved by the US Food and Drug Administration (FDA) in 1999, served as a quick replace-ment for troglitazone. These two glitazones are currently used in oral therapy as insulin sensitizers in type II diabetic patients under the commercial names Actos® (Takeda/Lilly) and Avandia® (Glaxo-SmithKline) respectively. Their bene-ficial effects on carbohydrate and lipid homeostasis derive from the synthesis of mediators of glucose and lipid trans-port and metabolism. Lipoprotein lipase, adipocyte fatty acid-binding protein aP2, fatty acid transport protein and acyl-CoA synthase [12] are only a few examples of the tar-gets through which glitazones ultimately reduce insulin resis-tance. Therefore, besides being well-tolerated drugs, the clinical use of pioglitazone and rosiglitazone is encouraged by their powerful metabolic effects in multiple cell types.
Pleiotropic Actions of Glitazones
As mentioned, glitazones opened a new and unprece-dented perspective to treat insulin-resistant type II diabetic patients since, unlike traditional agents based on -pancreatic overstimulation, glitazones raise peripheral insulin sensitiv-ity allowing patients to efficiently use their own insulin. However, several lines of evidence indicate that the effects of glitazones highly exceed the control of glycaemia and lipidemia. Even more, some newly-identified actions of gli-tazones are attractive for their potential therapeutic implica-tions [13]. In particular, the fight against cardiovascular dis-ease and cancer has found in glitazones a promising ally.
A major hallmark in the pharmacological research of glitazones has been the finding that the transcription factor peroxisome proliferator-activated receptor (PPAR ) is an essential molecular target for the metabolic effects of glita-zones [14]. Evidence of the unambiguous role of PPAR in the mechanism of action of glitazones are, for example, that rare patients carrying heterozygous mutations in the ligand-binding domain of PPAR exhibit severe insulin resistance and the accompanying cardiovascular disease [15]. However, appealing alternative mechanisms unrelated to PPAR are also emerging, concerning glitazone actions on cardiovascu-lar disease and cancer. Therefore, in the present review we will go through the significance of glitazones for these two socially most-relevant diseases of Western countries, includ-ing a summary of the different mechanisms proposed to ex-plain glitazone effects in both pathologies.
GLITAZONES AND CARDIOVASCULAR DISEASE
Type II diabetes mellitus is typically associated with obe-sity, dyslipemia, hypertension, microalbuminuria, coagulo-paphy, atherosclerosis, and a number of other vascular dis-eases. This trend of symptom clustering was reported by Marañón as early as 1922 [16]. Six decades later, Reaven coined the name syndrome X for all these symptoms [17], more recently substituted by the term metabolic syndrome[18]. Interestingly, commercial glitazones are strictly pre-scribed as antidiabetic drugs. However, a large body of evi-dence indicates that glitazones improve all symptoms of the
metabolic syndrome along with insulin sensitivity [19]. The whole set of effects of glitazones on insulin resistance and the metabolic syndrome exceed the purposes of the present review, which specifically focuses on the metabolic actions of glitazones at the level of the vessel wall.
Effects of Glitazones on Vascular Smooth Muscle Cell
Contractility: Role of Glitazones in the Management of Hypertension
Glitazones ameliorate insulin resistance and all the ac-companying symptoms, including hypertension. Related to their antihypertensive properties, these drugs diminish vascu-lar contractility. After a first report on this issue quoted above [20], it was found that pioglitazone diminishes aortic contractility to potassium, norepinephrine, and vasopressin [21,22]. These properties have been ascribed to the inhibi-tory effects of pioglitazone [23] and troglitazone [24] on smooth muscle cell calcium channels. In addition to calcium channels, glitazones have been shown to modulate other smooth muscle cell channels (Fig. (2)). Thus, rosiglitazone inhibits ion currents through voltage-operated potassium channels and enhances potassium currents through calcium-activated potassium channels [25]. The latter current would be hyperpolarizing and, therefore, relaxant (Fig. (2)).
Modulation of Endothelial Secretory Function
Glitazones are also modulators of endothelial cell secre-tory functions related to both the control of inflammation and the modulation of blood vessel tone. As for the first case, glitazones have been shown to downregulate endothelial plasminogen activator inhibitor type 1 (PAI-1) [26], to en-hance endothelial adhesiveness by increasing intercellular adhesion molecule 1 (ICAM-1) expression [27] and to in-hibit leukocyte-endothelial interaction by diminishing vascu-lar adhesion molecule 1 (VCAM-1) expression [28]. As for the regulation of vascular tone, glitazones display effects on every player of the paracrine endothelial regulation of smooth muscle cells, namely: NO, prostaglandins, throm-boxane, endothelin-1, reactive oxygen species (ROS) and even ions associated to hyperpolarization (see previous sec-tion) [25].
Nitric Oxide
With few exceptions [29], it is quite unanimous that gli-tazones upregulate the NO pathway in vascular smooth mus-cle and endothelial cells (Fig. (2)). Most reports find in-creased NO release without changes in expression of NO synthases. Thus, troglitazone [30] and ciglitazone [31] en-hance NO release by increasing endothelial NO synthase (eNOS) activity without affecting expression of the enzyme in cultured endothelial cells. In the line, Ryan et al. 2004 [32] found that oral treatment of mice with rosiglitazone improves NO function without accompanying changes in eNOS or soluble guanylate cyclase (sGC) expression in aor-tic tissue. Interestingly, it has been reported that whereas the typical metabolic effects of pioglitazone are indeed NO-dependent, this glitazone does not affect NOS expression in rat skeletal muscle [33]. Finally, a few authors observe regu-lation of NOS levels by glitazones. Thus, it was found that pioglitazone increases eNOS expression [34] and troglita-zone upregulates NO synthesis [35] in cultured aortic smooth
Not For Distribution
Potential Benefits of Glitazones for Cancer and Vascular Disease Current Drug Therapy, 2008, Vol. 3, No. 2 113
muscle cells. Furthermore, the plasmatic concentrations of the endogenous inhibitor of NOS, asymmetric dimethy-larginine, were reduced by pharmacological intervention with rosiglitazone in volunteers [36].
Prostanoids: Prostaglandins and Thromboxane
Troglitazone increases prostacyclin production (Fig. (2))in isolated aortic rings from Wistar rats [37]. This could be applicable also for microcirculation because intervention with a cyclooxygenase inhibitor suppresses troglitazone-elicited rise in skin blood flow [37]. Our own data indicates that pioglitazone and rosiglitazone improve the endothelial control of vascular smooth muscle contraction, but only when the cyclooxygenase pathway is inhibited [38]. We con-cluded from this study that glitazones augment NO availabil-ity but, at the same time, promote endothelial generation of
vasoconstrictor prostanoids, most likely thromboxane A2 (Fig. (2)). Thus, a delicate balance existing between vasoac-tive substances determines the vascular response (vasodila-tory or constrictive) to glitazones [38].
Endothelin-1
Glitazones have been shown to inhibit endothelial bio-synthesis of endothelin-1 [39] as well as endothelin-1 release of both in vitro [40] and in vivo [41]. Therefore, the notion that glitazones are vasodilator substances is further rein-forced by the suppression of this strong endothelial vasocon-strictor (Fig. (2)).
Reactive Oxygen Species (ROS)
It is almost undisputed that, at least at the vascular level, glitazones relieve oxidative stress. Thus, troglitazone was
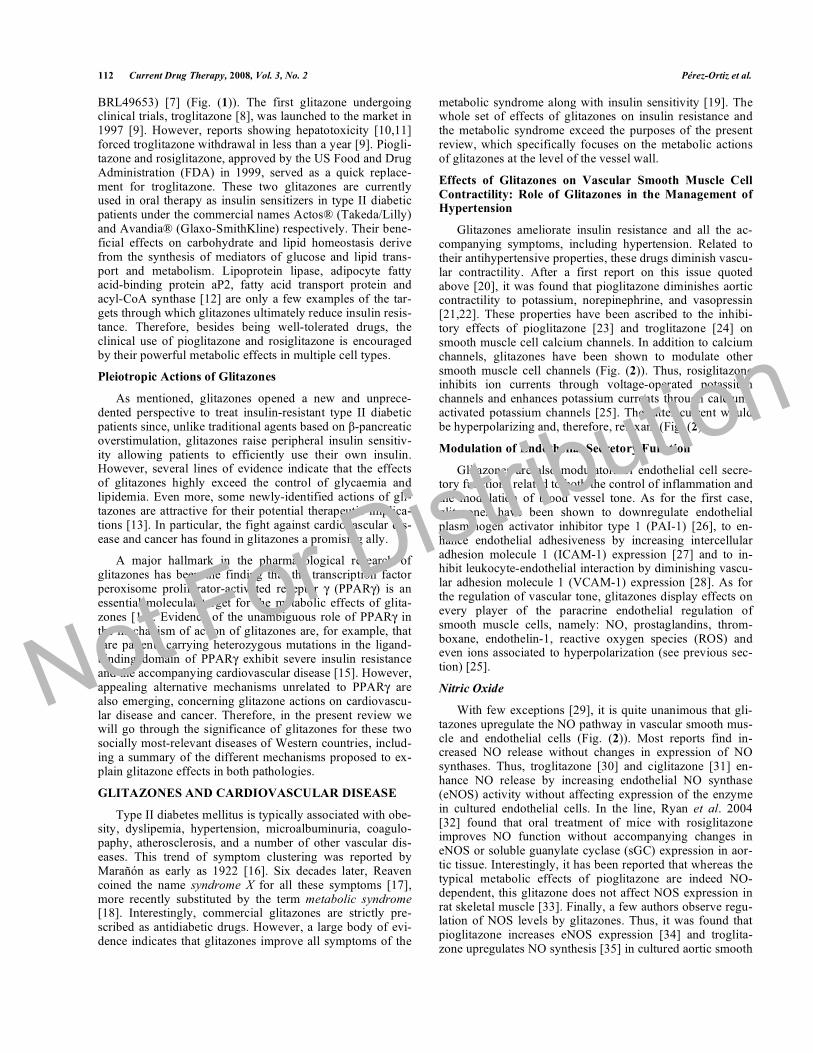
Fig. (2). The effects of glitazones on the endothelial cell and vascular smooth muscle cell.
In the endothelial cell, glitazones upregulate endothelial NO synthase (eNOS) to form nitric oxide (NO) which stimulates soluble guanylate cyclase (sGC) and dilates smooth muscle by enhancing cGMP synthesis. Glitazones also diminish superoxide anion (O2
.-) levels because they inhibit NADPH oxidase and activate superoxide dismutase enzyme (SOD). SOD accelerates the dismutation of O2
.- to form hydrogen perox-ide (H2O2) which in turn acts as an endothelium-derived hyperpolarizing factor (EDHF). EDHF opens potassium channels, leading to hyper-polarization and vasodilation. H2O2 also activates sGC causing vasorelaxation. Glitazones suppress endothelin-1 (ET-1) secretion (ECE: endothelin-converting enzyme). ETA and ETB are endothelin receptor subtypes which, in the smooth muscle lead to constriction whereas ETB, present in the endothelium, causes relaxation. The production of the prostanoid vasodilator, prostacyclin (PGI2) and vasoconstrictor prostanoids, thromboxane A2 (TXA2) and prostaglandin H2 (PGH2), from arachidonic acid (AA) via cyclooxigenase (COX) is enhanced by glitazones. Overall, in the endothelial cell, the balance is towards vasodilation. In the vascular smooth muscle cell, glitazones diminish Ca2+
currents through L-type Ca2+ channels and K+ currents through voltage-operated K+ channels (Kv) and increase K+ currents through calcium-dependent K+ channels (KCa). Again, the balance is towards vasodilation. Thus, glitazones are expected to be vasodilatory and antihyperten-sive. Stimulated by a glitazone: ; inhibited by a glitazone: . Final route stimulated (+) or inhibited (-).Not For Distribution
114 Current Drug Therapy, 2008, Vol. 3, No. 2 Pérez-Ortiz et al.
found to posses scavenging effects on ROS [42] and rosigli-tazone improves endothelium-dependent relaxation in type II diabetes mellitus through its antioxidant properties [43]. Comparable results have been obtained in hypercholes-terolemia [44] and obesity [34]. The findings by Calnek etal. (see NO section) indicating that ciglitazone increases NO release by promoting eNOS activity without an increase in eNOS expression were ascribed in a subsequent paper by the same authors to the ability of this glitazone to suppress NADPH oxidase and induce Cu/Zn-SOD (Fig. (2)) [45]. Finally, also supporting ROS-inhibition, a number of reports highlight the beneficial effects of glitazones on endothelial function [32,46-48], in different pathological conditions re-lated to insuline resistance.
Clinical Evidence of the Vascular Effects of Glitazones
It is needless to say that, after the initial clinical trials with troglitazone [8], a large number of studies have focused on the metabolic properties of these drugs. However, the success of glitazones over traditional antidiabetics is largely due to their benefits for the management of the accompany-ing cardiovascular problems of insulin resistance. For exam-ple, glitazones improve endothelial function studied by flow-mediated dilation, as well as plasma markers of endothelial function [49,50]. The same can be said about the blood pres-sure lowering abilities of glitazones (Table 1) [51]. Of par-ticular relevance are the micro- and macrovascular complica-tions of insulin resistance. Indeed, these precede the onset of diabetes mellitus [52], so that an early intervention in pa-tients with metabolic syndrome, but still no clear vascular complications, is essential [53]. While the traditional an-tidiabetics, like sulfonylureas, are not as useful in reducing macrovascular complications as they are with the microvas-cular ones [54], a recent trial demonstrates the promising effects of pioglitazone in reducing mortality in patients with a high risk of macrovascular events [55].
GLITAZONES AND CANCER
Effects on Human Cell Lines
Glitazones inhibit cell proliferation while inducing dif-ferentiation and apoptosis. These antiproliferative and cyto-toxic effects, initially observed in adipocytes [61], were later
confirmed in numerous cell types, generating a wide interest for these drugs in cancer research. Although we will focus in this section on the effects of glitazones on human cell lines, glitazones also act as antitumor agents on cancer cell types from other species.
A large body of evidence points to brain tumors as tar-gets of glitazones [62]. Ciglitazone, and less potently rosigli-tazone, inhibit human glioblastoma cell growth and induce cell death, involving in some cases apoptotic mechanisms [63-66]. Troglitazone was also shown proapoptotic in human glioma cells [67,68]. Several glitazones were also inhibitory for neuroblastoma cell lines [69]. As for cells from reproduc-tive organs, human breast carcinoma cells are also sensitive to glitazones. Glitazones reduce cell viability [70], prevent immortalization in vitro [71], and finally differentiate breast tumor cells into epithelial cells [72]. At the same time, cigli-tazone has been found to suppress the growth of multiple human cervical carcinomas [73]. There is also data available on several anaplastic thyroid cancer lines indicating that both rosiglitazone and ciglitazone induce cell cycle arrest [74], while troglitazone triggers apoptosis in human lung cancer cell lines [75]. Renal carcinoma cells exposed to pioglitazone or troglitazone undergo inhibition of proliferation and mas-sive apoptosis [76]. Human tumor cells from the gastrointes-tinal tract are also influenced by glitazones. Rosiglitazone sensitizes colon cancer cell lines to apoptotic stimuli [77], while suppressing in vitro growth of gastric cell lines [78]. Similarly, troglitazone significantly inhibits the growth of colon tumor cells [79]; and several glitazones slow down the proliferation rate of human adrenocortical cells [80,81]. Hu-man leukaemia cell lines undergo cell-cycle arrest upon pio-glitazone exposure [82], and human mantle lymphoma cell lines are sensitive to both pioglitazone and rosiglitazone, which respond undergoing apoptosis [83].
Distinctions Among Glitazones
Beyond the properties that are common to all family members, glitazones display characteristics that are specific of each compound [84-86]. One of the most striking episodes of glitazone individualism has been played by troglitazone, the first glitazone approved as an oral antidiabetic drug [9]. Although troglitazone shows beneficial metabolic properties common to other glitazones, it also has fatal cytotoxic ac-
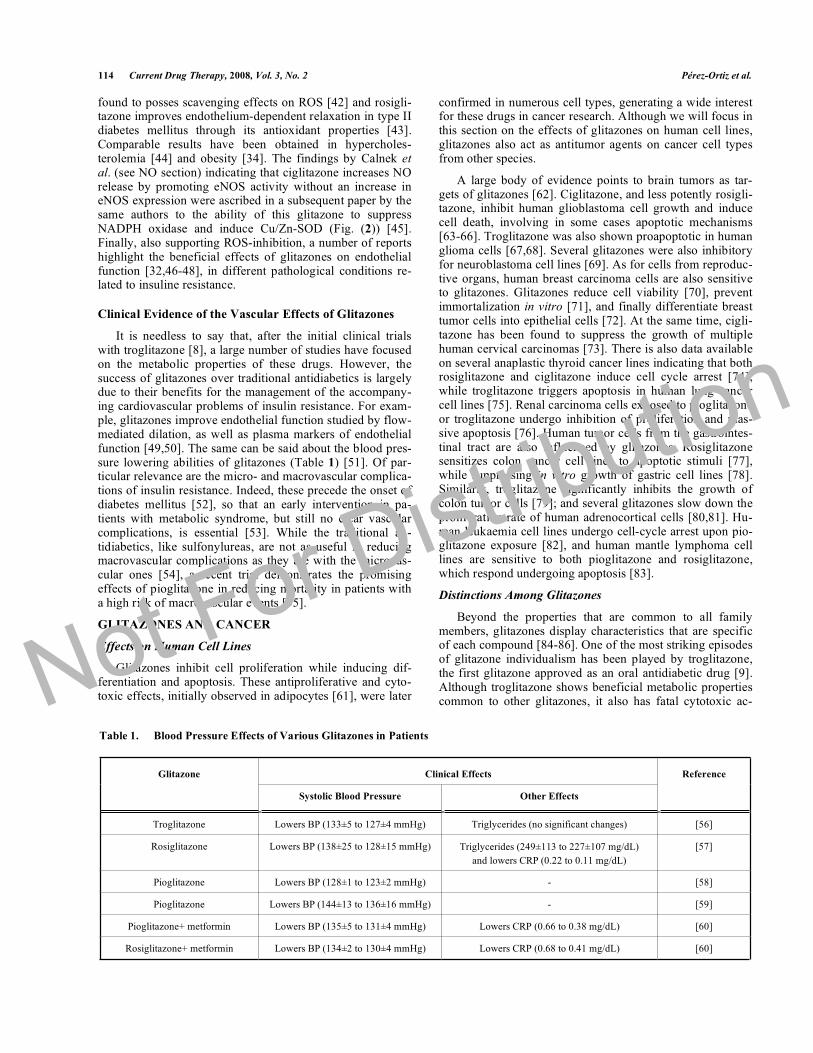
Table 1. Blood Pressure Effects of Various Glitazones in Patients
Clinical Effects Glitazone
Systolic Blood Pressure Other Effects
Reference
Troglitazone Lowers BP (133±5 to 127±4 mmHg) Triglycerides (no significant changes) [56]
Rosiglitazone Lowers BP (138±25 to 128±15 mmHg) Triglycerides (249±113 to 227±107 mg/dL)
and lowers CRP (0.22 to 0.11 mg/dL)
[57]
Pioglitazone Lowers BP (128±1 to 123±2 mmHg) - [58]
Pioglitazone Lowers BP (144±13 to 136±16 mmHg) - [59]
Pioglitazone+ metformin Lowers BP (135±5 to 131±4 mmHg) Lowers CRP (0.66 to 0.38 mg/dL) [60]
Rosiglitazone+ metformin Lowers BP (134±2 to 130±4 mmHg) Lowers CRP (0.68 to 0.41 mg/dL) [60]
Not For Distribution
Potential Benefits of Glitazones for Cancer and Vascular Disease Current Drug Therapy, 2008, Vol. 3, No. 2 115
tions that are not shared by pioglitazone or rosiglitazone [87]. There are numerous other examples to illustrate that individual glitazones may produce distinct effects. For ex-ample, upregulation of growth arrest and DNA damage-inducible gene 45 (GADD45) can be induced by troglita-zone, while pioglitazone and rosiglitazone are ineffective [88]. In our own work rosiglitazone showed cytotoxicity only in glioma cell lines, while ciglitazone affected the vi-ability of both glioma cells and primary astrocytes [65]. Meanwhile, ciglitazone and troglitazone treatment resulted in rapid death of Jurkat T cells, whereas rosiglitazone was inef-fective [89]. In conclusion, such diversity of actions raises the need to explore the antitumor effects of each glitazone individually.
Synergism Between Glitazones and Other Drugs
Glitazones promote apoptosis in MCF-7 breast cancer cells by a mechanism that involves a marked decrease in Bcl-2. Interestingly, this effect was highly enhanced by the combined stimulation with all-trans retinoic acid [90]. In another case of cooperation, rosiglitazone inhibits cell growth synergizing with the proteasome inhibitor borte-zomib, used to inactivate NF- B in human melanoma cell lines [91]. A different work showed that the histone deacety-lase inhibitor valproic acid enhances the antitumor action of pioglitazone on prostate cancer cells by a mechanism that implicates upregulation of the E-cadherin gene [92]. Surpris-ingly, pioglitazone actions are not always enhanced by the inhibition of histone deacetylase. In fact, histone deacetylase 3 is recruited by glitazone in cooperation with retinoblas-toma protein to induce cell arrest at the G1 phase [93]. Other synergisms observed using animal models are mentioned in the next section.
Animal Models
Data on the efficacy of glitazones collected from animal models for cancer therapy have not always been clarifying. The most recent and conclusive reports on the use of these models are listed in Table 2. The first study of this kind tested the effect of troglitazone on the growth of breast car-cinoma cells MCF-7 injected in nude mice and found that that this glitazone significantly reduces both tumor volume
and weight [90]. On the contrary, troglitazone acted as a tu-mor inducer in several mouse models of colon carcinogene-sis [94,95]. Finally, and enlarging the controversy, pioglita-zone showed a suppressive action on colonic polyps in mice models in which troglitazone promoted tumor growth [96].
With regard to gliomas, recent reports have shown en-couraging data. Orally administered pioglitazone drastically reduced tumor size in mice with C6 glioma cells intracere-brally implanted [97]. In the same line, pioglitazone showed clear antitumor properties on brain-injected GL261 glioma cells, although in this study pioglitazone was only effective when injected within the tumor bed, and not when adminis-tered orally [98]. Other authors have observed that troglita-zone potently inhibits glioma cell migration in a organotypic invasion model [99]. Animal models have also been useful to assess sensitivity of tumors of the reproductive tract to glita-zones. In this line, pioglitazone treatment inhibited the growth of OVCAR-3 ovarian cancer cells [100] and prostate cancer cells [92] subcutaneously xenotransplanted in nude mice models.
Interesting results have been obtained when cooperation among glitazones or synergism with other drugs have been tested in animal models. Thus, a recent study shows a potent synergism between rosiglitazone and carboplatin, a plati-num-based chemotherapeutic agent, to inhibit the growth of chemically-induced colonic tumors in mice. The same authors confirmed this synergism in vitro with other types of tumor cells, including lung adenocarcinoma, colon cancer and ovarian epithelial cell lines [101]. In another work, tro-glitazone and rosiglitazone were used to improve the antian-giogenic and antitumor effect of the thrombospondin-1 de-rivative ABT510 in mice with xenografted tumors. Both glitazones showed beneficial properties combined with ABT510, that promoted upregulation of the proapoptotic endothelial molecule CD36 [102]. Another appealing obser-vation is that pioglitazone induces glioma death in synergy with brain-implanted IL-2-secreting fibroblasts in a mouse model [98]. All these data obtained from combined-treat-ment strategies underline the potential value of glitazones as coadjuvant anticancer therapy, as an alternative to its use in monotherapy.
Table 2. Animal Models used to Test Antitumor Actions of Glitazones
Animal Species Model Glitazone Outcome Reference
Organotypic neuronal envi-
ronment
Glioma invasion Troglitazone Inhibits migration and brain inva-
sion
[98]
Immunodeficient mice Injected MCF-7 Troglitazone Inhibits tumor growth [89]
Rats Intrastriatal injection of C6
glioma cells
Pioglitazone Reduces tumor volume [96]
Min mice Intestinal polyp formation Pioglitazone Reduces intestinal polyps [95]
nu/nu mice Subcutaneous OVCAR-3
tumors
Pioglitazone Ciglitazone Supresses growth of tumors
Supresses growth of tumors
[99]
[102]
C57Bl/6 mice Intracerebral injection of
GL261 glioma cells
Pioglitazone Prolongs mice survival [187]
Not For Distribution

116 Current Drug Therapy, 2008, Vol. 3, No. 2 Pérez-Ortiz et al.
Clinical Trials
Despite the undeniable value of animal models, they pre-sent obvious limitations as predictors of the effect of glita-zones in humans. The efficacy of pre-clinical models may be undermined, among other factors, by the differences in the expression of mediators of glitazone actions, such as the transcription factor PPAR , between human and rodent. Therefore, it should be noted that negative findings using animal models could be misleading, and that positive results need further validation in humans.
In regard to the value of glitazones as antineoplastic drugs in humans, data are very limited. One of the most con-clusive pieces of evidence was recently obtained from a ret-rospective analysis of diabetic patients within a group of 87,678 individuals. Treatment with glitazones had no signifi-cant effect on colorectal and prostate cancers, but it reduced 33% lung cancer risk [103]. The PROACTIVE trial (PRO-spective pioglitAzone Clinical Trial In macroVascular Events, see also “Glitazones and cardiovascular disease”), another extensive study that included 5,238 diabetic patients, revealed a trend towards reduced breast cancer within the pioglitazone-treated group [55]. Less encouraging was the recently finished phase II clinical trial aimed to evaluate the therapeutic benefit of troglitazone in breast cancer (22 pa-tients). This trial found no response to treatment [104]. Tro-glitazone was also unable to modify disease progression in a phase II trial with 25 patients with colon cancer [105].
Although less data are available for rosiglitazone than for pioglitazone and troglitazone on cancer therapy, rosiglita-zone showed promising results in a thyroid cancer patient, as it improved radioiodine uptake and serum thyroglobulin lev-els [106]. This pilot study was further complemented by a phase II trial in which rosiglitazone treatment enhanced ra-dioiodine uptake in 4 out of 10 patients [107]. Meanwhile, 3 out of 4 patients with cutaneous T-cell lymphoma responded to therapy with rosiglitazone [108]; whereas rosiglitazone did not change the course of disease in a prostate cancer study with 106 men [109]. Short-term treatment with rosigli-tazone as a monotherapy was equally ineffective in 38 women with early-stage breast cancer [110].
As mentioned before, data gathered using cell lines and animal models indicate that the cytotoxic actions of glita-zones can be modulated by synergism with other cellular effectors. These observations have encouraged testing glita-zones in several clinical trials in combination with chemo-therapy or other antitumor agents. To date, results reported using this strategy are promising, at least for sarcoma treat-ment. Thus, pioglitazone combined with the selective cy-clooxygenase-2 inhibitor rofecoxib and with low-dose che-motherapy induced partial tumor remission in a patient with Kaposi´s sarcoma [111]. The effectiveness of this triple combination was later confirmed in larger studies with pa-tients presenting different types of sarcomas [112,113]. In addition, a phase II trial with patients showing metastatic melanoma and soft tissue sarcoma unresponsive to previous chemotherapy confirmed the significant action of pioglita-zone in association with angiostatic chemotherapy [114]. Contrarily to pioglitazone, rosiglitazone had no effect as antitumor drug in 12 patients with liposarcoma [115];
whereas troglitazone led to terminal adipocytic differentia-tion of tumor cells in 3 patients with liposarcoma [116]. All these reports on the use of glitazones as antitumor agents in humans, summarized in Table 3, has attracted a growing interest for these compounds, leading to new pilot tests and phase I/II clinical trials currently underway (www.Clinical Trials.gov).
MECHANISMS MEDIATING THE ANTITUMOR
AND VASCULAR ACTIONS OF GLITAZONES
Both antitumor and vascular effects of glitazones are currently under intense investigation because of their poten-tial therapeutic use, as outlined before. This section summa-rizes the latest molecular mechanisms proposed to explain these glitazone actions, distinguishing PPAR -dependent and -independent pathways.
Glitazones and PPAR
It has been extensively shown that many glitazone ac-tions depend on the activation of PPAR . This transcription factor, together with the two other isoforms PPAR and PPAR , belongs to the nuclear hormone receptor superfa-mily. Its structure includes a transcriptional activation do-main, a ligand-binding domain and a DNA-binding motif [117]. The DNA-binding activity of PPAR is reinforced by heterodimerization with retinoid X receptor (RXR) [118]. Its more potent natural activating ligand is 15-desoxy- 12,14-prostaglandin J2 (15d-PGJ2), but polyunsaturated fatty acid derivatives are also effective. Meanwhile, glitazones are the best-characterized synthetic ligands of PPAR . They show a high specificity, with affinities (Kd) as low as 43 nM for rosiglitazone in humans, as shown in Table 4.
Ligand-dependent activation of PPAR induces nuclear translocation, resulting in the potential regulation of a large set of genes (at least 70 confirmed experimentally) [119]. PPAR is highly expressed in adipose tissue and was initially related to adipocyte differentiation as well as lipid and glu-cose homeostasis [120-123]. However, nowadays it is clear that PPAR is ubiquitous [124] and influences many proc-esses beyond cellular metabolism. The following parts of this review concentrate on the implications of PPAR in the anti-cancer and vascular effects of glitazones.
Vascular Actions of Glitazones: Dependency on PPAR
Endothelial cells [125] and vascular smooth muscle cells [126] express PPAR . Since Lehman et al. identified in 1995 PPAR as a molecular target of glitazones that mediates their metabolic effects [14], most vascular effects of glitazones have been ascribed to this pathway, especially those ob-served upon chronic treatments that do not impose time re-strictions for gene transcription and protein synthesis. How-ever, even before it was known that glitazones were PPARligands, Zhang et al. published in 1994 a prelude of what now we label as PPAR -independent effect, stating that “the hypotensive effect of pioglitazone is not invariably associ-ated with its capacity to improve insulin-induced utilization”[127]. A year later Buchanan et al. claimed that pioglitazone has direct vascular effects, providing the first evidence that glitazone stimulates calcium uptake in the vascular smooth muscle cell [21]. The natural agonist of PPAR 15d-PGJ2
Not For Distribution
Potential Benefits of Glitazones for Cancer and Vascular Disease Current Drug Therapy, 2008, Vol. 3, No. 2 117
elicited no clear actions on ion currents in the same cells [25]. Rapid vascular effects have also been found by others, including our own laboratory [22,38]. Finally, rosiglitazone lowers blood pressure in hypertensive transgenic mice by a PPAR -independent mechanism, as proven by the lack of effect of the PPAR antagonist bisphenol A diglycidyl ether (BADGE) [32]. This observation was later confirmed in clinical studies [50]. The notion that vascular contractility is not related to insulin or to PPAR collides with a few in-triguing reports. In one of them, troglitazone inhibits calcium influx and reduces contractility of smooth muscle cells, but only in the presence of insulin [128]. The authors conclude that a synergistic action of insulin with glitazones exists. Thus, a PPAR -dependent mechanism might be involved. Another intriguing report uses mice lacking PPAR expres-sion specifically in endothelial cells. In these animals in which hypertension develops after feeding with a high fat diet, rosiglitazone reduced insulinemia but was unable to lower blood pressure [129]. Again in contrast to the general view, the authors concluded that PPAR in endothelial cell mediates the antihypertensive effects of rosiglitazone.
Evidence available does not allow classification of every action of glitazones on vascular tissue as PPAR -dependent or –independent. However, it has been suggested that the actions of glitazones on smooth muscle growth are likely PPAR -independent considering the lack of correspondence between the antiproliferative potency of each glitazone and their affinities for PPAR [130]. Moreover, the natural PPAR ligand 15d-PGJ2 was unable to reproduce the anti-proliferative effects observed with glitazones [131].
The effects of glitazones on the endothelial NO pathway have been extensively characterized, and rely on both PPAR -dependent and -independent mechanisms. It has been reported that troglitazone increases NO production by a) an Akt-mediated eNOS-Ser1179 phosphorylation which is PPAR -dependent and b) a eNOS-Ser116 dephosphorylation which is PPAR -independent [30]. In this line, it has also been reported that ciglitazone stimulates NO release viaPPAR from endothelial cells without increasing the expres-sion of eNOS [31]. It is plausible that the lowering effects of glitazones on ROS production, also PPAR -dependent [43,44], protect from NO destruction.
Table 3. Clinical Trials to Study Antineoplastic Actions of Glitazones
Clinical Test Glitazone Outcome References
Liposarcoma (3 patients) Troglitazone Terminal adipocytic differentiation [116]
Refractory breast cancer (phase II) Troglitazone No significant response [104]
Liposarcoma (phase II) Rosiglitazone No significant response [115]
Advanced malignant vascular tumors (6 patients) Pioglitazone
+ rofecoxib
+ trofosfamide
2 patients complete remission
1 patient partial remission
3 patients no change
[112]
Endemic Kaposi sarcoma (1 patient) Pioglitazone
+ rofecoxib
+ trofosfamide
Partial and stable remission [111]
Refractory melanoma and soft tissue sarcoma
(phase II)
Pioglitazone
+ rofecoxib
+ trofosfamide
Prolonged progression-free survival [114]
Prostate carcinoma (106 patients) Rosiglitazone No effect in disease progression [109]
Advanced sarcoma (4 patients) Pioglitazone
+ rofecoxib
+ trofosfamide
Stabilization of disease (3 out of 4) [113]
Thyroid cancer (10 patients; phase II) Rosiglitazone Enhanced radioiodine uptake (4 out of 10) [107]
Thyroid cancer (1 patient) Rosiglitazone Improved radioiodine uptake and serum thy-
roglobulin levels
[106]
Cutaneous T-cell lymphoma (4 patients) Rosiglitazone
+ bexarotene
Decreased skin score (2 out of 4)
Pruritus alleviated (3 out of 4)
[108]
Early-stage breast cancer (38 women) Rosiglitazone
(short-term treatment)
No significant response [110]
Retrospective analysis of diabetic men (87,678
patients)
Glitazones Reduced risk of lung cancer
No significant response for colorectal and pros-
tate cancers
[103]
Not For Distribution
118 Current Drug Therapy, 2008, Vol. 3, No. 2 Pérez-Ortiz et al.
PPAR and Antitumor Actions
A genome search of putative PPAR -binding sequences within promoters reveals that the number of possible target genes implicated in cell cycle control and apoptosis is higher than genes related to metabolic control [119]. Moreover, there is compelling evidence indicating that PPAR activa-tion by glitazones leads to cell differentiation, while decreas-ing proliferation and apoptosis of different cells types [132]. Both human and rodent cancer cells have been shown sensi-tive to glitazones acting through PPAR –mediated mecha-nisms. This notion is further supported by the fact that tu-mors often display PPAR loss-of-function mutations, and that PPAR heterozygote knockout mice display an in-creased susceptibility to carcinogenesis [133]. Cancer cell types responsive to glitazones in which PPAR implication has been well proven include liposarcoma cells, breast ade-nocarcinoma, human hepatocellular cells, esophageal carci-noma cells, human colon carcinoma cells and colorectal can-cer among others [134].
Targeted Genes Related to Tumor Growth
Numerous genes involved in tumor growth are regulated by glitazones through PPAR -controlled pathways. A mi-croarray-based analysis of ovarian cancer cells was able to identify both upregulated and downregulated targets. Besides metabolic genes, most were associated with differentiation, tumor suppression or proliferation [135]. Supporting these findings, glitazones were also observed to activate propapop-totic genes Bax, caspase 3 and p53 in another human ovarian carcinoma [136], differentiation-related gene-1 (Drg-1) in colon cancer cells [137] and growth-inhibitory caveolin-1 and -2 in HT-29 colon carcinoma cells [138]. Meanwhile, glitazones promote the expression of anti-invasive genes such as gelatinase B (MMP-9) and MMP-1 in breast cancer cell lines [139], and E-cadherin in prostate cancer cells [92]. Complementing gene activation, there are also examples of gene inhibition by glitazones. Thus, these compounds reduce angiogenesis through repression of vascular endothelial growth factor (VEGF) [140], angiopoietin-1 [141], and chemokines CXCL1, CXCR4, CXCL5, CXCL8 [142,143]. The expression of the cell cycle regulator cyclin D1 is also inhibited [144].
PPAR Crosstalk with Other Signalling Pathways
Besides a direct regulation of gene expression, glitazone-stimulated PPAR may have antitumor actions by limiting or promoting other intracellular pathways. Thus, suppression of NF- B activity by PPAR stimulation may result in inhibi-
tion of the resistance to chemotherapy provided by NF- Bactivation [145-147]; whereas others have reported that rosiglitazone enhances binding of PPAR to the NF- B site in the promoter of p53, activating p53 transcription in breast carcinoma NCF7 cells [148].
Glitazones also oppose the tumor promoting activity of estrogen on breast cancer cells in part by reducing aromatase expression [149]. In addition, PPAR activation attenuates DNA binding of estrogen receptors [150]. Moreover, glita-zones inhibit the Wnt signalling pathway through PPAR .The consequence of this inhibition is a glycon synthasekinase -3 (GSK3 )-mediated degradation of -catenin that leads to blockage of cell proliferation and induction of apop-tosis in several tumor cell types [132]. On the other hand, rosiglitazone induces the suppressor gene phosphatase and tensin homolog deleted on chromosome TEN (PTEN). This action, together with the PTEN-induced decrease in Akt phosphorylation, limits cell growth and migration, and in-duces apoptosis in hepatocarcinoma cells [151,152], breast cancer and colorectal cancer [153,154]. In addition there is a crosstalk between PPAR and TGF signalling since glita-zones have been shown to inhibit the transcription of TGF 1[155], as well as the expression of TGF -regulated genes implicated in tumor invasiveness [156]. In addition, pioglita-zone has been observed to stimulate TGF release and the nuclear accumulation of SMAD2 in models in which TGFacts as a tumor suppressor [157].
Transrepression of Inflammatory Genes
Interestingly, patients with inflammatory bowel disease are under a significantly higher risk of developing colon can-cer, implicating that the antiinflammatory actions of glita-zones may be associated to their effectiveness against tumor progression. Stimulation of PPAR by glitazones inactivates the immune system at multiple levels [158,159]. In some cases, inhibition of proinflammatory genes involve interfer-ence with NF- B, AP-1 and STAT-1 pathways through tran-scriptional transrepression [160]. This mechanism implies physical interaction of PPAR with other transcription fac-tors impairing their binding to DNA [161]. Competition among PPAR and other transcription factors for a limited pool of common transcriptional coregulators could also ac-count for transrepression [162].
PPAR -Independent Actions of Glitazones
There is a growing body of evidence indicating that glita-zones may act by mechanisms independent of PPAR . Inter-estingly, these actions include antiproliferative and cytotoxic
Table 4. Glitazone Binding Affinity for PPAR
Glitazone Murine Receptor EC50 ( M) Human Receptor EC50
( M)
Rosiglitazone 0.076 0.043
Pioglitazone 0.55 0.58
Troglitazone 0.78 0.55
Ciglitazone 3 3
Not For Distribution

Potential Benefits of Glitazones for Cancer and Vascular Disease Current Drug Therapy, 2008, Vol. 3, No. 2 119
actions on cancer cells [65,163-166], stem cell proliferation [167] and macrophage differentiation [168]. Even some of the more classical actions of glitazones on energy metabo-lism, such as regulation of cholesterol biosynthesis, have been recognized as PPAR unrelated [169]. In addition, sup-pression of inflammatory mediators by glitazones may pre-sent a PPAR -independent pattern.
The idea that glitazones regulate signalling events unre-lated to PPAR are based in the following criteria: a) the antitumor efficacy of glitazones (troglitazone > ciglitazone > pioglitazone > rosiglitazone) usually differ from their affin-ity values for PPAR (measured as EC50) (Table 3), b) doses required for some of the antiproliferative and proapoptotic actions of glitazones highly exceed those needed to fully activate PPAR , c) lack of effect of non-glitazone PPARligands, d) glitazones show effects within minutes, whereas transcriptional regulation through PPAR requires several hours, e) effects happen in the absence of PPAR expression, and f) PPAR antagonists, expression of dominant negative forms of PPAR , or transcriptional and translational blockers do not abolish glitazone effects (reviewed by Grommes et al.[134] and Feinstein et al. [170]).
Moreover, the characterization of antitumor actions of glitazones by PPAR -independent mechanisms has benefited from the synthesis of a new class of glitazones, the 2 de-rivatives, which display a double bond adjoining the terminal thiazolidine-2,4-dione ring [171]. These compounds, al-though unable to activate PPAR , show antiproliferative actions more potent than those of troglitazone or ciglitazone [12].
Antitumor Effects Independent of PPAR
The current section reviews the most robust evidence sustaining PPAR independent pathways within the antican-cer effects of glitazones, giving special consideration to the mitochondria and the generation of reactive oxygen species among the alternative mechanisms proposed.
Implication of Mitochondria
Many proapoptotic actions of glitazones on cancer and other cells have been associated to mitochondrial dysfunc-tion [172-175]. To this respect, glitazone-induced death is preceded by mitochondrial membrane depolarization, cal-cium influx and caspase-3 activation in HepG2 hepatocarci-noma cells [176]. In addition, our own work in glioma cells described a rapid mitochondrial depolarization and a de-crease in mitochondrial pH associated to cell death induced by ciglitazone treatment [65,177] and similar depolarizing effects on mitochondria of glioma cells have been attributed to troglitazone by other authors [178]. Moreover, there is evidence indicating that depolarization induced by glitazones is more intense in glioma cells than in astrocytes, which is in line with the higher toxicity of glitazones on gliomas [178].
Along with mitochondrial depolarization, glitazones in-hibit oxygen consumption in glioma cells by blockage of the electron transport chain [177]. Although it has been sug-gested that pyruvate-driven state III respiration is inhibited, the mechanisms underlining these observations have not been completely elucidated [179]. A number of studies in
hepatocytes and muscle cells [173], as well as HL-60 cells [174] and glioma cells [177], suggest a site of inhibition lo-cated in a region that comprises complex I. Our own results suggest that glitazones may either a) bind to other mitochon-drial complexes, or b) block the flavin-proteins of complex I. When those flavins are reduced, their redox potential enables them to react with molecular oxygen, yielding superoxide.
The recently-described protein mitoNEET has also been proposed as a link between glitazones and mitochondria as it has a high affinity for pioglitazone [180]. MitoNEET is an integral protein of the outer mitochondrial membrane with a CDGSH domain oriented toward the cytoplasm [181]. Re-duction of cellular levels of mitoNEET by siRNA disrupts mitochondrial respiration [170]. The role of mitoNEET in the regulation of the mitochondrial respiratory function is also suggested by the fact that cardiac mitochondria obtained from mitoNEET-null mice exhibit a reduced oxidative ca-pacity [182].
Cytotoxicity Through Reactive Oxygen Species (ROS)
In fact, several reports support the contribution of oxida-tive stress to glitazone antitumor actions [65,87,89]. The mitochondrial respiratory chain is one of the major cellular sources of ROS in cells under stress. Our own studies illus-trate that superoxide released by glitazones in C6 glioma cells has a mitochondrial origin [177]. In the same line, other authors have proposed that proline oxidase, a mitochondrial redox enzyme implicated in ROS production, is upregulated by troglitazone in colon cancer cell lines [183].
On the other hand, the selective toxicity of glitazones on tumor cells may be related to their higher basal oxidative stress compared to normal cells, likely a consequence of a fast-paced metabolism and the presence of defective mito-chondria [184,185]. This notion may help to explain why pioglitazone induces a more potent superoxide boost in glioma cells than in primary astrocytes [98]. In addition, cancer cells have a lower threshold to survive under condi-tions of increased ROS, such as those induced by glitazones. Moreover, ROS produced by glitazones may act as signalling molecules that activate MAPK [186,187] or other intracellu-lar pathways involved in antiproliferative effects [188].
AMPK Activation: Another Consequence of Mitochondria
Disruption
AMP-activated protein kinase (AMPK) is activated in response to an increased AMP/ATP ratio [189]. Both rosigli-tazone and pioglitazone are activators of AMPK since they decrease ATP levels as a consequence of mitochondrial dis-ruption. In addition, there is evidence to suggest that glita-zones also trigger AMPK activation through stimulation of ROS [190] and reactive nitrogen species [191]. Independ-ently of the mechanism to activate AMPK, the result is a higher glycolytic rate [192,193]. To this respect, the long-known Warburg effect [194] proposes that the basal metabo-lism of tumor cells is often highly glycolytic due to poor mitochondrial respiration. Therefore, tumor cells would have a lower capacity to restore ATP levels by increasing glycoly-sis after a failure in mitochondrial function. Thus, it has been speculated that the selective death of tumor cells induced by glitazones relates to the inefficiency of AMPK to enhance
Not For Distribution
120 Current Drug Therapy, 2008, Vol. 3, No. 2 Pérez-Ortiz et al.
glycolysis in these cells after the inhibition of mitochondria respiration [194].
Other Pathways Regulated by Glitazones
Repression of cyclins by glitazones leads to cell cycle arrest. Both PPAR -dependent [144] and independent path-ways have been proposed for this glitazone effect [195-198]. Moreover, the reduction in cyclin D3 by glitazones sensitizes breast cancer cells to death induced by TNF -related apopto-sis-inducing ligand (TRAIL).
The antitumor properties of glitazones may also be asso-ciated to induction of growth response transcription factor (EGF-1) and nonsteroidal antiinflammatory drug-activated gene-1 (NAG-1) in human colon cancer cells [199], and to activation of tumorous sclerosis complex-2 (TSC2) in non-small cell lung carcinoma cells [200]. Meanwhile, mediators of tumor cell viability such as STAT3 [67] and Na+/H+ ex-changer (NHE) isoform 1 [201] are downregulated. Finally, some anticancer properties of glitazones may derive from an inhibitory effect on translation, given that the subunit of eukaryotic initiation factor 2 (eIF2) is inactivated by glita-zone-induced phosphorylation [167].
FUTURE DIRECTIONS
The list of mechanisms proposed as an alternative to PPAR activation has experienced a fast growth in the last few years. Such novel mechanisms have been found not only in association with antitumor and vascular actions, but with all the spectrum of glitazone actions including the more tra-ditional metabolic effects. Therefore, the growing relevance of PPAR -independent actions inspires the need to redefine glitazones, incorporating among glitazone properties the ability to interact with mitochondria and other targets cur-rently under investigation. Moreover, glitazones are now regarded as promising drugs for the treatment of cancer and the metabolic syndrome, as well as other inflammatory pa-thologies that include neurodegenerative diseases. Accord-ingly, we are witnessing a remarkable proliferation of pre-clinical and clinical trials intended to clarify the effective-ness of glitazones. In any case, future studies will be needed to select glitazone derivatives with higher potency and speci-ficity for each of the potential uses. As a concluding remark, it could be stated that the latest research advances have placed glitazones on the move from metabolic drugs to more pleiotropic agents.
ACKNOWLEDGEMENTS
This work was supported by: National I+D+i Plan from the Spanish Ministry of Science (SAF2005-02157), Conse-jería de Sanidad, Junta de Comunidades de Castilla-La Mancha. (06016-00, SAN06-010, 04007-00, GCS-2006-C/17) and FUCAMDI. J.M.P.O. was a fellow from Conse-jería de Sanidad, JCCM, Spain. We are grateful to Yolanda Mendizábal for her assistance with the management of the references and figures.
REFERENCES
[1] Feinglos MN, Lebovitz HE. Sulphonylureas increase the number of insulin receptors. Nature 1978; 276: 184-5.
[2] Sohda T, Mizuno K, Tawada H, Sugiyama Y, Fujita T, Kawamatsu Y. Studies on antidiabetic agents. I. Synthesis of 5-[4-(2-methyl-2-
phenylpropoxy)-benzyl]thiazolidine-2,4-dione (AL-321) and re-lated compounds. Chem Pharm Bull (Tokyo) 1982; 30: 3563-73.
[3] Sohda T, Mizuno K, Imamiya E, Sugiyama Y, Fujita T, Kawa-matsu Y. Studies on antidiabetic agents. II. Synthesis of 5-[4-(1-methylcyclohexylmethoxy)-benzyl]thiazolidine-2,4-dione (ADD-3878) and its derivatives. Chem Pharm Bull (Tokyo) 1982; 30: 3580-600.
[4] Fujita T, Sugiyama Y, Taketomi S, et al. Reduction of insulin resistance in obese and/or diabetic animals by 5-[4-(1-methylcyclohexylmethoxy)benzyl]-thiazolidine-2,4-dione (ADD-3878, U-63,287, ciglitazone), a new antidiabetic agent. Diabetes 1983; 32: 804-10.
[5] Ikeda H, Taketomi S, Sugiyama Y, et al. Effects of pioglitazone on glucose and lipid metabolism in normal and insulin resistant ani-mals. Arzneimittelforschung 1990; 40: 156-62.
[6] Fujiwara T, Yoshioka S, Yoshioka T, Ushiyama I, Horikoshi H. Characterization of new oral antidiabetic agent CS-045. Studies in KK and ob/ob mice and Zucker fatty rats. Diabetes 1988; 37: 1549-58.
[7] Oakes ND, Kennedy CJ, Jenkins AB, Laybutt DR, Chisholm DJ, Kraegen EW. A new antidiabetic agent, BRL 49653, reduces lipid availability and improves insulin action and glucoregulation in the rat. Diabetes 1994; 43: 1203-10.
[8] Kuzuya T, Iwamoto Y, Kosaka K, et al. A pilot clinical trial of a new oral hypoglycemic agent, CS-045, in patients with non-insulin dependent diabetes mellitus. Diabetes Res Clin Pract 1991; 11: 147-53.
[9] Parker JC. Troglitazone: the discovery and development of a novel therapy for the treatment of Type 2 diabetes mellitus. Adv Drug Deliv Rev 2002; 54: 1173-97.
[10] Graham DJ, Drinkard CR, Shatin D. Incidence of idiopathic acute liver failure and hospitalized liver injury in patients treated with troglitazone. Am J Gastroenterol 2003; 98: 175-9.
[11] Watkins PB, Whitcomb RW. Hepatic dysfunction associated with troglitazone. N Engl J Med 1998; 338: 916-7.
[12] Weng JR, Chen CY, Pinzone JJ, Ringel MD, Chen CS. Beyond peroxisome proliferator-activated receptor gamma signaling: the multi-facets of the antitumor effect of thiazolidinediones. Endocr Relat Cancer 2006; 13: 401-13.
[13] Yki-Jarvinen H. Thiazolidinediones. N Engl J Med 2004; 351: 1106-18.
[14] Lehmann JM, Moore LB, Smith-Oliver TA, Wilkison WO, Willson TM, Kliewer SA. An antidiabetic thiazolidinedione is a high affin-ity ligand for peroxisome proliferator-activated receptor gamma (PPAR gamma). J Biol Chem 1995; 270: 12953-6.
[15] Barroso I, Gurnell M, Crowley VE, et al. Dominant negative muta-tions in human PPARgamma associated with severe insulin resis-tance, diabetes mellitus and hypertension. Nature 1999; 402: 880-3.
[16] Marañón G. Über Hypertonie and Zuckerkrankheit. Zentralblatt für Innere Medizin 1922; 43: 169-76.
[17] Reaven GM. Banting lecture 1988. Role of insulin resistance in human disease. Diabetes 1988; 37: 1595-607.
[18] Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classi-fication of diabetes mellitus provisional report of a WHO consulta-tion. Diabet Med 1998; 15: 539-53.
[19] Martens FM, Visseren FL, Lemay J, de Koning EJ, Rabelink TJ. Metabolic and additional vascular effects of thiazolidinediones. Drugs 2002; 62: 1463-80.
[20] Dubey RK, Zhang HY, Reddy SR, Boegehold MA, Kotchen TA. Pioglitazone attenuates hypertension and inhibits growth of renal arteriolar smooth muscle in rats. Am J Physiol 1993; 265: R726-R732.
[21] Buchanan TA, Meehan WP, Jeng YY, et al. Blood pressure lower-ing by pioglitazone. Evidence for a direct vascular effect. J Clin In-vest 1995; 96: 354-60.
[22] Verma S, Bhanot S, Arikawa E, Yao L, McNeill JH. Direct vasodepressor effects of pioglitazone in spontaneously hyperten-sive rats. Pharmacology 1998; 56: 7-16.
[23] Zhang F, Sowers JR, Ram JL, Standley PR, Peuler JD. Effects of pioglitazone on calcium channels in vascular smooth muscle. Hy-pertension 1994; 24: 170-5.
[24] Song J, Walsh MF, Igwe R, et al. Troglitazone reduces contraction by inhibition of vascular smooth muscle cell Ca2+ currents and not endothelial nitric oxide production. Diabetes 1997; 46: 659-64.
Not For Distribution
Potential Benefits of Glitazones for Cancer and Vascular Disease Current Drug Therapy, 2008, Vol. 3, No. 2 121
[25] Eto K, Ohya Y, Nakamura Y, Abe I, Fujishima M. Comparative actions of insulin sensitizers on ion channels in vascular smooth muscle. Eur J Pharmacol 2001; 423: 1-7.
[26] Kato K, Satoh H, Endo Y, et al. Thiazolidinediones down-regulate plasminogen activator inhibitor type 1 expression in human vascu-lar endothelial cells: A possible role for PPARgamma in endothe-lial function. Biochem Biophys Res Commun 1999; 258: 431-5.
[27] Chen NG, Sarabia SF, Malloy PJ, Zhao XY, Feldman D, Reaven GM. PPARgamma agonists enhance human vascular endothelial adhesiveness by increasing ICAM-1 expression. Biochem Biophys Res Commun 1999; 263: 718-22.
[28] Jackson SM, Parhami F, Xi XP, et al. Peroxisome proliferator-activated receptor activators target human endothelial cells to in-hibit leukocyte-endothelial cell interaction. Arterioscler Thromb Vasc Biol 1999; 19: 2094-104.
[29] Ikeda U, Shimpo M, Murakami Y, Shimada K. Peroxisome prolif-erator-activated receptor-gamma ligands inhibit nitric oxide synthe-sis in vascular smooth muscle cells. Hypertension 2000; 35: 1232-6.
[30] Cho DH, Choi YJ, Jo SA, Jo I. Nitric oxide production and regula-tion of endothelial nitric-oxide synthase phosphorylation by pro-longed treatment with troglitazone: evidence for involvement of peroxisome proliferator-activated receptor (PPAR) gamma-dependent and PPARgamma-independent signaling pathways. J Biol Chem 2004; 279: 2499-506.
[31] Calnek DS, Mazzella L, Roser S, Roman J, Hart CM. Peroxisome proliferator-activated receptor gamma ligands increase release of nitric oxide from endothelial cells. Arterioscler Thromb Vasc Biol 2003; 23: 52-7.
[32] Ryan MJ, Didion SP, Mathur S, Faraci FM, Sigmund CD. PPAR(gamma) agonist rosiglitazone improves vascular function and lowers blood pressure in hypertensive transgenic mice. Hyper-tension 2004; 43: 661-6.
[33] Koshinaka K, Oshida Y, Han YQ, Ohsawa I, Sato Y. The effect of nitric oxide synthase inhibitor on improved insulin action by piogli-tazone in high-fructose-fed rats. Metabolism 2004; 53: 22-7.
[34] Dobrian AD, Schriver SD, Khraibi AA, Prewitt RL. Pioglitazone prevents hypertension and reduces oxidative stress in diet-induced obesity. Hypertension 2004; 43: 48-56.
[35] Hattori Y, Hattori S, Kasai K. Troglitazone upregulates nitric oxide synthesis in vascular smooth muscle cells. Hypertension 1999; 33: 943-8.
[36] Stuhlinger MC, Abbasi F, Chu JW, et al. Relationship between insulin resistance and an endogenous nitric oxide synthase inhibi-tor. JAMA 2002; 287: 1420-6.
[37] Fujiwara T, Ohsawa T, Takahashi S, et al. Troglitazone, a new antidiabetic agent possessing radical scavenging ability, improved decreased skin blood flow in diabetic rats. Life Sci 1998; 63: 2039-47.
[38] Llorens S, Mendizabal Y, Nava E. Effects of pioglitazone and rosiglitazone on aortic vascular function in rat genetic hyperten-sion. Eur J Pharmacol 2007; 575: 105-12.
[39] Delerive P, Fruchart JC, Staels B. Peroxisome proliferator-activated receptors in inflammation control. J Endocrinol 2001; 169: 453-9.
[40] Satoh H, Tsukamoto K, Hashimoto Y, et al. Thiazolidinediones suppress endothelin-1 secretion from bovine vascular endothelial cells: a new possible role of PPARgamma on vascular endothelial function. Biochem Biophys Res Commun 1999; 254: 757-63.
[41] Iglarz M, Touyz RM, Amiri F, Lavoie MF, Diep QN, Schiffrin EL. Effect of peroxisome proliferator-activated receptor-alpha and -gamma activators on vascular remodeling in endothelin-dependent hypertension. Arterioscler Thromb Vasc Biol 2003; 23: 45-51.
[42] Inoue I, Katayama S, Takahashi K, et al. Troglitazone has a scav-enging effect on reactive oxygen species. Biochem Biophys Res Commun 1997; 235: 113-6.
[43] Bagi Z, Koller A, Kaley G. PPARgamma activation, by reducing oxidative stress, increases NO bioavailability in coronary arterioles of mice with Type 2 diabetes. Am J Physiol Heart Circ Physiol 2004; 286: H742-H748.
[44] Tao L, Liu HR, Gao E, et al. Antioxidative, antinitrative, and vas-culoprotective effects of a peroxisome proliferator-activated recep-tor-gamma agonist in hypercholesterolemia. Circulation 2003; 108: 2805-2811.
[45] Hwang J, Kleinhenz DJ, Lassegue B, Griendling KK, Dikalov S, Hart CM. Peroxisome proliferator-activated receptor-gamma ligands regulate endothelial membrane superoxide production. Am J Physiol Cell Physiol 2005; 288: C899-C905.
[46] Majithiya JB, Paramar AN, Balaraman R. Pioglitazone, a PPAR-gamma agonist, restores endothelial function in aorta of streptozo-tocin-induced diabetic rats. Cardiovasc Res 2005; 66: 150-61.
[47] Moroe H, Fujii H, Honda H, et al. Characterization of endothelium-dependent relaxation and modulation by treatment with pioglita-zone in the hypercholesterolemic rabbit renal artery. Eur J Pharma-col 2004; 497: 317-25.
[48] Walker AB, Chattington PD, Buckingham RE, Williams G. The thiazolidinedione rosiglitazone (BRL-49653) lowers blood pressure and protects against impairment of endothelial function in Zucker fatty rats. Diabetes 1999; 48: 1448-53.
[49] Fujishima S, Ohya Y, Nakamura Y, Onaka U, Abe I, Fujishima M. Troglitazone, an insulin sensitizer, increases forearm blood flow in humans. Am J Hypertens 1998; 11: 1134-7.
[50] Hetzel J, Balletshofer B, Rittig K, et al. Rapid effects of rosiglita-zone treatment on endothelial function and inflammatory biomark-ers. Arterioscler Thromb Vasc Biol 2005; 25: 1804-1809.
[51] Sarafidis PA, Nilsson PM. The metabolic syndrome: a glance at its history. J Hypertens 2006; 24: 621-626.
[52] Caballero AE, Arora S, Saouaf R, et al. Microvascular and mac-rovascular reactivity is reduced in subjects at risk for type 2 diabe-tes. Diabetes 1999; 48: 1856-1862.
[53] Tenenbaum A, Motro M, Schwammenthal E, Fisman EZ. Mac-rovascular complications of metabolic syndrome: an early interven-tion is imperative. Int J Cardiol 2004; 97: 167-172.
[54] Meriden T. Progress with thiazolidinediones in the management of type 2 diabetes mellitus. ClinTher 2004; 26: 177-90.
[55] Dormandy JA, Charbonnel B, Eckland DJ, et al. Secondary preven-tion of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In mac-roVascular Events): a randomised controlled trial. Lancet 2005; 366: 1279-89.
[56] Takase H, Hakamata M, Toriyama T, et al. Effect of troglitazone on endothelial function in type 2 diabetic patients. Arzneimittelfor-schung 2002; 52: 34-38.
[57] Wang TD, Chen WJ, Lin JW, Chen MF, Lee YT. Effects of rosigli-tazone on endothelial function, C-reactive protein, and components of the metabolic syndrome in nondiabetic patients with the meta-bolic syndrome. Am J Cardiol 2004; 93: 362-5.
[58] Negro R, Dazzi D, Hassan H, Pezzarossa A. Pioglitazone reduces blood pressure in non-dipping diabetic patients. Minerva Endocri-nol 2004; 29: 11-7.
[59] de RB, Luque M, Martell N, Fernandez C, Fernandez-Cruz A. Pioglitazone decreases ambulatory blood pressure in type 2 diabet-ics with difficult-to-control hypertension. J Clin Hypertens (Greenwich) 2007; 9: 530-7.
[60] Derosa G, Fogari E, Cicero AF, et al. Blood pressure control and inflammatory markers in type 2 diabetic patients treated with pio-glitazone or rosiglitazone and metformin. Hypertens Res 2007; 30: 387-394.
[61] Tontonoz P, Hu E, Spiegelman BM. Stimulation of adipogenesis in fibroblasts by PPAR gamma 2, a lipid-activated transcription fac-tor. Cell 1994; 79: 1147-56.
[62] Heneka MT, Landreth GE. PPARs in the brain. Biochim Biophys Acta 2007; 1771: 1031-45.
[63] Chattopadhyay N, Singh DP, Heese O, et al. Expression of perox-isome proliferator-activated receptors (PPARs) in human astrocytic cells: PPAR gamma agonists as inducers of apoptosis. J Neurosci Res 2000; 61: 67-74.
[64] Morosetti R, Servidei T, Mirabella M, et al. The PPARgamma ligands PGJ2 and rosiglitazone show a differential ability to inhibit proliferation and to induce apoptosis and differentiation of human glioblastoma cell lines. Int J Oncol 2004; 25: 493-502.
[65] Perez-Ortiz JM, Tranque P, Vaquero CF, et al. Glitazones differen-tially regulate primary astrocyte and glioma cell survival. Involve-ment of reactive oxygen species and peroxisome proliferator-activated receptor-gamma. J Biol Chem 2004; 279: 8976-85.
[66] Zander T, Kraus JA, Grommes C, et al. Induction of apoptosis in human and rat glioma by agonists of the nuclear receptor PPAR gamma. J Neurochem 2002; 81: 1052-60.
Not For Distribution
122 Current Drug Therapy, 2008, Vol. 3, No. 2 Pérez-Ortiz et al.
[67] Akasaki Y, Liu G, Matundan HH, et al. A peroxisome proliferator-activated receptor-gamma agonist, troglitazone, facilitates caspase-8 and -9 activities by increasing the enzymatic activity of protein-tyrosine phosphatase-1B on human glioma cells. J Biol Chem 2006; 281: 6165-74.
[68] Yao CJ, Lai GM, Chan CF, Cheng AL, Yang YY, Chuang SE. Dramatic synergistic anticancer effect of clinically achievable doses of lovastatin and troglitazone. Int J Cancer 2006; 118: 773-9.
[69] Valentiner U, Carlsson M, Erttmann R, Hildebrandt H, Schumacher U. Ligands for the peroxisome proliferator-activated receptor-gamma have inhibitory effects on growth of human neuroblastoma cells in vitro. Toxicology 2005; 213: 157-68.
[70] Mody M, Dharker N, Bloomston M, et al. Rosiglitazone sensitizes MDA-MB-231 breast cancer cells to anti-tumour effects of tumour necrosis factor-alpha, CH11 and CYC202. Endocr Relat Cancer 2007; 14: 305-15.
[71] Herbert BS, Pearce VP, Hynan LS, et al. A peroxisome prolifera-tor-activated receptor-gamma agonist and the p53 rescue drug CP-31398 inhibit the spontaneous immortalization of breast epithelial cells. Cancer Res 2003; 63: 1914-9.
[72] Mueller E, Sarraf P, Tontonoz P, et al. Terminal differentiation of human breast cancer through PPAR gamma. Mol Cell 1998; 1: 465-70.
[73] Jung TI, Baek WK, Suh SI, et al. Down-regulation of peroxisome proliferator-activated receptor gamma in human cervical carci-noma. Gynecol Oncol 2005; 97: 365-73.
[74] Aiello A, Pandini G, Frasca F, et al. Peroxisomal proliferator-activated receptor-gamma agonists induce partial reversion of epithelial-mesenchymal transition in anaplastic thyroid cancer cells. Endocrinology 2006; 147: 4463-75.
[75] Li M, Lee TW, Mok TS, Warner TD, Yim AP, Chen GG. Activa-tion of peroxisome proliferator-activated receptor-gamma by trogli-tazone (TGZ) inhibits human lung cell growth. J Cell Biochem 2005; 96: 760-74.
[76] Yang FG, Zhang ZW, Xin DQ, et al. Peroxisome proliferator-activated receptor gamma ligands induce cell cycle arrest and apop-tosis in human renal carcinoma cell lines. Acta Pharmacol Sin 2005; 26: 753-61.
[77] Zhang YQ, Tang XQ, Sun L, et al. Rosiglitazone enhances fluorouracil-induced apoptosis of HT-29 cells by activating perox-isome proliferator-activated receptor gamma. World J Gastroen-terol 2007; 13: 1534-40.
[78] Leung WK, Bai AH, Chan VY, et al. Effect of peroxisome prolif-erator activated receptor gamma ligands on growth and gene ex-pression profiles of gastric cancer cells. Gut 2004; 53: 331-8.
[79] Sarraf P, Mueller E, Jones D, et al. Differentiation and reversal of malignant changes in colon cancer through PPARgamma. Nat Med 1998; 4: 1046-52.
[80] Betz MJ, Shapiro I, Fassnacht M, Hahner S, Reincke M, Beuschlein F. Peroxisome proliferator-activated receptor-gamma agonists suppress adrenocortical tumor cell proliferation and induce differentiation. J Clin Endocrinol Metab 2005; 90: 3886-96.
[81] Ferruzzi P, Ceni E, Tarocchi M, et al. Thiazolidinediones inhibit growth and invasiveness of the human adrenocortical cancer cell line H295R. J Clin Endocrinol Metab 2005; 90: 1332-9.
[82] Saiki M, Hatta Y, Yamazaki T, et al. Pioglitazone inhibits the growth of human leukemia cell lines and primary leukemia cells while sparing normal hematopoietic stem cells. Int J Oncol 2006; 29: 437-43.
[83] Eucker J, Sterz J, Krebbel H, et al. Peroxisome proliferator-activated receptor-gamma ligands inhibit proliferation and induce apoptosis in mantle cell lymphoma. Anticancer Drugs 2006; 17: 763-9.
[84] Baek SJ, Wilson LC, Hsi LC, Eling TE. Troglitazone, a perox-isome proliferator-activated receptor gamma (PPAR gamma) ligand, selectively induces the early growth response-1 gene inde-pendently of PPAR gamma. A novel mechanism for its anti-tumorigenic activity. J Biol Chem 2003; 278: 5845-53.
[85] Kim KH, Cho YS, Park JM, Yoon SO, Kim KW, Chung AS. Pro-MMP-2 activation by the PPARgamma agonist, ciglitazone, in-duces cell invasion through the generation of ROS and the activa-tion of ERK. FEBS Lett 2007; 581: 3303-10.
[86] Narayanan PK, Hart T, Elcock F, et al. Troglitazone-induced intra-cellular oxidative stress in rat hepatoma cells: a flow cytometric as-sessment. Cytometry A 2003; 52: 28-35.
[87] Shishido S, Koga H, Harada M, et al. Hydrogen peroxide overpro-duction in megamitochondria of troglitazone-treated human hepa-tocytes. Hepatology 2003; 37: 136-47.
[88] Yin F, Bruemmer D, Blaschke F, Hsueh WA, Law RE, Herle AJ. Signaling pathways involved in induction of GADD45 gene ex-pression and apoptosis by troglitazone in human MCF-7 breast car-cinoma cells. Oncogene 2004; 23: 4614-23.
[89] Soller M, Drose S, Brandt U, Brune B, von Knethen A. Mechanism of thiazolidinedione-dependent cell death in Jurkat T cells. Mol Pharmacol 2007; 71: 1535-44.
[90] Elstner E, Muller C, Koshizuka K, et al. Ligands for peroxisome proliferator-activated receptor gamma and retinoic acid receptor in-hibit growth and induce apoptosis of human breast cancer cells in vitro and in BNX mice. Proc Natl Acad Sci USA 1998; 95: 8806-11.
[91] Freudlsperger C, Thies A, Pfuller U, Schumacher U. The protea-some inhibitor bortezomib augments anti-proliferative effects of mistletoe lectin-I and the PPAR-gamma agonist rosiglitazone in human melanoma cells. Anticancer Res 2007; 27: 207-13.
[92] Annicotte JS, Iankova I, Miard S, et al. Peroxisome proliferator-activated receptor gamma regulates E-cadherin expression and in-hibits growth and invasion of prostate cancer. Mol Cell Biol 2006; 26: 7561-74.
[93] Fajas L, Egler V, Reiter R, Miard S, Lefebvre AM, Auwerx J. PPARgamma controls cell proliferation and apoptosis in an RB-dependent manner. Oncogene 2003; 22: 4186-93.
[94] Lefebvre AM, Chen I, Desreumaux P, et al. Activation of the per-oxisome proliferator-activated receptor gamma promotes the de-velopment of colon tumors in C57BL/6J-APCMin/+ mice. Nat Med 1998; 4: 1053-7.
[95] Yang K, Fan KH, Lamprecht SA, et al. Peroxisome proliferator-activated receptor gamma agonist troglitazone induces colon tu-mors in normal C57BL/6J mice and enhances colonic carcinogene-sis in Apc1638 N/+ Mlh1+/- double mutant mice. Int J Cancer 2005; 116: 495-9.
[96] Niho N, Takahashi M, Shoji Y, et al. Dose-dependent suppression of hyperlipidemia and intestinal polyp formation in Min mice by pioglitazone, a PPAR gamma ligand. Cancer Sci 2003; 94: 960-4.
[97] Grommes C, Landreth GE, Sastre M, et al. Inhibition of in VivoGlioma Growth and Invasion by Peroxisome Proliferator-Activated Receptor {gamma} Agonist Treatment. Mol Pharmacol 2006; 70: 1524-33.
[98] Spagnolo A, Glick RP, Lin H, Cohen EP, Feinstein DL, Lichtor T. Prolonged survival of mice with established intracerebral glioma receiving combined treatment with peroxisome proliferator-activated receptor-gamma thiazolidinedione agonists and interleu-kin-2-secreting syngeneic/allogeneic fibroblasts. J Neurosurg 2007; 106: 299-305.
[99] Coras R, Holsken A, Seufert S, et al. The peroxisome proliferator-activated receptor-gamma agonist troglitazone inhibits transform-ing growth factor-beta-mediated glioma cell migration and brain invasion. Mol Cancer Ther 2007; 6: 1745-54.
[100] Shigeto T, Yokoyama Y, Xin B, Mizunuma H. Peroxisome prolif-erator-activated receptor alpha and gamma ligands inhibit the growth of human ovarian cancer. Oncol Rep 2007; 18: 833-40.
[101] Girnun GD, Naseri E, Vafai SB, et al. Synergy between PPAR-gamma ligands and platinum-based drugs in cancer. Cancer Cell 2007; 11: 395-406.
[102] Huang H, Campbell SC, Bedford DF, et al. Peroxisome prolifera-tor-activated receptor gamma ligands improve the antitumor effi-cacy of thrombospondin peptide ABT510. Mol Cancer Res 2004; 2: 541-50.
[103] Govindarajan R, Ratnasinghe L, Simmons DL, et al. Thiazolidin-ediones and the risk of lung, prostate, and colon cancer in patients with diabetes. J Clin Oncol 2007; 25: 1476-81.
[104] Burstein HJ, Demetri GD, Mueller E, Sarraf P, Spiegelman BM, Winer EP. Use of the peroxisome proliferator-activated receptor (PPAR) gamma ligand troglitazone as treatment for refractory breast cancer: a phase II study. Breast Cancer Res Treat 2003; 79: 391-7.
[105] Kulke MH, Demetri GD, Sharpless NE, et al. A phase II study of troglitazone, an activator of the PPARgamma receptor, in patients with chemotherapy-resistant metastatic colorectal cancer. Cancer J 2002; 8: 395-9.
Not For Distribution
Potential Benefits of Glitazones for Cancer and Vascular Disease Current Drug Therapy, 2008, Vol. 3, No. 2 123
[106] Elias AN, Lizotte P. Enhanced radioiodine uptake in a patient with poorly differentiated papillary thyroid cancer after treatment with rosiglitazone. Clin Nucl Med 2006; 31: 517-9.
[107] Kebebew E, Peng M, Reiff E, et al. A phase II trial of rosiglitazone in patients with thyroglobulin-positive and radioiodine-negative differentiated thyroid cancer. Surgery 2006; 140: 960-6.
[108] Sepmeyer JA, Greer JP, Koyama T, Zic JA. Open-label pilot study of combination therapy with rosiglitazone and bexarotene in the treatment of cutaneous T-cell lymphoma. J Am Acad Dermatol 2007; 56: 584-587.
[109] Smith MR, Manola J, Kaufman DS, et al. Rosiglitazone versus placebo for men with prostate carcinoma and a rising serum pros-tate-specific antigen level after radical prostatectomy and/or radia-tion therapy. Cancer 2004; 101: 1569-74.
[110] Yee LD, Williams N, Wen P, et al. Pilot study of rosiglitazone therapy in women with breast cancer: effects of short-term therapy on tumor tissue and serum markers. Clin Cancer Res 2007; 13: 246-52.
[111] Coras B, Hafner C, Reichle A, et al. Antiangiogenic therapy with pioglitazone, rofecoxib, and trofosfamide in a patient with endemic kaposi sarcoma. Arch Dermatol 2004; 140: 1504-7.
[112] Kasper B, Ho AD, Egerer G. A new therapeutic approach in pa-tients with advanced sarcoma. Int J Clin Oncol 2005; 10: 438-40.
[113] Vogt T, Hafner C, Bross K, et al. Antiangiogenetic therapy with pioglitazone, rofecoxib, and metronomic trofosfamide in patients with advanced malignant vascular tumors. Cancer 2003; 98: 2251-6.
[114] Reichle A, Bross K, Vogt T, et al. Pioglitazone and rofecoxib com-bined with angiostatically scheduled trofosfamide in the treatment of far-advanced melanoma and soft tissue sarcoma. Cancer 2004; 101: 2247-56.
[115] Debrock G, Vanhentenrijk V, Sciot R, Debiec-Rychter M, Oyen R, Van Oosterom A. A phase II trial with rosiglitazone in liposarcoma patients. Br J Cancer 2003; 89: 1409-12.
[116] Demetri GD, Fletcher CD, Mueller E, et al. Induction of solid tumor differentiation by the peroxisome proliferator-activated re-ceptor-gamma ligand troglitazone in patients with liposarcoma. Proc Natl Acad Sci USA 1999; 96: 3951-6.
[117] Evans RM. The steroid and thyroid hormone receptor superfamily. Science 1988; 240: 889-95.
[118] Michalik L, Desvergne B, Wahli W. Peroxisome-proliferator-activated receptors and cancers: complex stories. Nat Rev Cancer 2004; 4: 61-70.
[119] Yu C, Markan K, Temple KA, Deplewski D, Brady MJ, Cohen RN. The nuclear receptor corepressors NCoR and SMRT decrease peroxisome proliferator-activated receptor gamma transcriptional activity and repress 3T3-L1 adipogenesis. J Biol Chem 2005; 280: 13600-605.
[120] Bajaj M, Suraamornkul S, Piper P, et al. Decreased plasma adi-ponectin concentrations are closely related to hepatic fat content and hepatic insulin resistance in pioglitazone-treated type 2 diabetic patients. J Clin Endocrinol Metab 2004; 89: 200-6.
[121] Miyazaki Y, Glass L, Triplitt C, et al. Effect of rosiglitazone on glucose and non-esterified fatty acid metabolism in Type II diabetic patients. Diabetologia 2001; 44: 2210-9.
[122] Nolan JJ, Ludvik B, Beerdsen P, Joyce M, Olefsky J. Improvement in glucose tolerance and insulin resistance in obese subjects treated with troglitazone. N Engl J Med 1994; 331: 1188-93.
[123] Suter SL, Nolan JJ, Wallace P, Gumbiner B, Olefsky JM. Meta-bolic effects of new oral hypoglycemic agent CS-045 in NIDDM subjects. Diabetes Care 1992; 15: 193-203.
[124] Fajas L, Auboeuf D, Raspe E, et al. The organization, promoter analysis, and expression of the human PPARgamma gene. J Biol Chem 1997; 272: 18779-89.
[125] Marx N, Bourcier T, Sukhova GK, Libby P, Plutzky J. PPAR-gamma activation in human endothelial cells increases plasmino-gen activator inhibitor type-1 expression: PPARgamma as a poten-tial mediator in vascular disease. Arterioscler Thromb Vasc Biol 1999; 19: 546-51.
[126] Iijima K, Yoshizumi M, Ako J, et al. Expression of peroxisome proliferator-activated receptor gamma (PPARgamma) in rat aortic smooth muscle cells. Biochem Biophys Res Commun 1998; 247: 353-6.
[127] Zhang HY, Reddy SR, Kotchen TA. Antihypertensive effect of pioglitazone is not invariably associated with increased insulin sen-sitivity. Hypertension 1994; 24: 106-10.
[128] Goud C, Pitt B, Webb RC, Richey JM. Synergistic actions of insu-lin and troglitazone on contractility in endothelium-denuded rat aortic rings. Am J Physiol 1998; 275: E882-E887.
[129] Nicol CJ, Adachi M, Akiyama TE, Gonzalez FJ. PPARgamma in endothelial cells influences high fat diet-induced hypertension. Am J Hypertens 2005; 18: 549-556.
[130] Hattori Y, Akimoto K, Kasai K. The effects of thiazolidinediones on vascular smooth muscle cell activation by angiotensin II. Bio-chem Biophys Res Commun 2000; 273: 1144-9.
[131] Aizawa Y, Kawabe J, Hasebe N, Takehara N, Kikuchi K. Pioglita-zone enhances cytokine-induced apoptosis in vascular smooth muscle cells and reduces intimal hyperplasia. Circulation 2001; 104: 455-60.
[132] Chou FS, Wang PS, Kulp S, Pinzone JJ. Effects of thiazolidinedi-ones on differentiation, proliferation, and apoptosis. Mol Cancer Res 2007; 5: 523-30.
[133] Rumi MA, Ishihara S, Kazumori H, Kadowaki Y, Kinoshita Y. Can PPAR gamma ligands be used in cancer therapy? Curr Med Chem Anticancer Agents 2004; 4: 465-77.
[134] Grommes C, Landreth GE, Heneka MT. Antineoplastic effects of peroxisome proliferator-activated receptor gamma agonists. Lancet Oncol 2004; 5: 419-29.
[135] Vignati S, Albertini V, Rinaldi A, et al. Cellular and molecular consequences of peroxisome proliferator-activated receptor-gamma activation in ovarian cancer cells. Neoplasia 2006; 8: 851-61.
[136] Yang YC, Tsao YP, Ho TC, Choung IP. Peroxisome proliferator-activated receptor-gamma agonists cause growth arrest and apopto-sis in human ovarian carcinoma cell lines. Int J Gynecol Cancer 2007; 17: 418-25.
[137] Yoshizumi T, Ohta T, Ninomiya I, et al. Thiazolidinedione, a per-oxisome proliferator-activated receptor-gamma ligand, inhibits growth and metastasis of HT-29 human colon cancer cells through differentiation-promoting effects. Int J Oncol 2004; 25: 631-9.
[138] Burgermeister E, Tencer L, Liscovitch M. Peroxisome proliferator-activated receptor-gamma upregulates caveolin-1 and caveolin-2 expression in human carcinoma cells. Oncogene 2003; 22: 3888-900.
[139] Liu H, Zang C, Fenner MH, Possinger K, Elstner E. PPARgamma ligands and ATRA inhibit the invasion of human breast cancer cells in vitro. Breast Cancer Res Treat 2003; 79: 63-74.
[140] Panigrahy D, Singer S, Shen LQ, et al. PPARgamma ligands in-hibit primary tumor growth and metastasis by inhibiting angiogene-sis. J Clin Invest 2002; 110: 923-932.
[141] Fu YG, Sung JJ, Wu KC, et al. Inhibition of gastric cancer cells associated angiogenesis by 15d-prostaglandin J2 through the down-regulation of angiopoietin-1. Cancer Lett 2006; 243: 246-54.
[142] Keshamouni VG, Arenberg DA, Reddy RC, Newstead MJ, Anthwal S, Standiford TJ. PPAR-gamma activation inhibits angio-genesis by blocking ELR+CXC chemokine production in non-small cell lung cancer. Neoplasia 2005; 7: 294-301.
[143] Richard CL, Blay J. Thiazolidinedione drugs down-regulate CXCR4 expression on human colorectal cancer cells in a perox-isome proliferator activated receptor gamma-dependent manner. Int J Oncol 2007; 30: 1215-22.
[144] Sharma C, Pradeep A, Pestell RG, Rana B. Peroxisome prolifera-tor-activated receptor gamma activation modulates cyclin D1 tran-scription via beta-catenin-independent and cAMP-response ele-ment-binding protein-dependent pathways in mouse hepatocytes. J Biol Chem 2004; 279: 16927-38.
[145] Chen F, Wang M, O'Connor JP, He M, Tripathi T, Harrison LE. Phosphorylation of PPARgamma via active ERK1/2 leads to its physical association with p65 and inhibition of NF-kappabeta. J Cell Biochem 2003; 90: 732-44.
[146] Montagut C, Tusquets I, Ferrer B, et al. Activation of nuclear fac-tor-kappa B is linked to resistance to neoadjuvant chemotherapy in breast cancer patients. Endocr Relat Cancer 2006; 13: 607-616.
[147] Pascual G, Fong AL, Ogawa S, et al. A SUMOylation-dependent pathway mediates transrepression of inflammatory response genes by PPAR-gamma. Nature 2005; 437: 759-63.
[148] Bonofiglio D, Aquila S, Catalano S, et al. Peroxisome proliferator-activated receptor-gamma activates p53 gene promoter binding to
Not For Distribution

124 Current Drug Therapy, 2008, Vol. 3, No. 2 Pérez-Ortiz et al.
the nuclear factor-kappaB sequence in human MCF7 breast cancer cells. Mol Endocrinol 2006; 20: 3083-92.
[149] Rubin GL, Zhao Y, Kalus AM, Simpson ER. Peroxisome prolifera-tor-activated receptor gamma ligands inhibit estrogen biosynthesis in human breast adipose tissue: possible implications for breast cancer therapy. Cancer Res 2000; 60: 1604-08.
[150] Kondoh K, Tsuji N, Asanuma K, Kobayashi D, Watanabe N. Inhi-bition of estrogen receptor beta-mediated human telomerase re-verse transcriptase gene transcription via the suppression of mito-gen-activated protein kinase signaling plays an important role in 15-deoxy-Delta(12,14)-prostaglandin J(2)-induced apoptosis in cancer cells. Exp Cell Res 2007; 313: 3486-96.
[151] Cao LQ, Chen XL, Wang Q, et al. Upregulation of PTEN involved in rosiglitazone-induced apoptosis in human hepatocellular carci-noma cells. Acta Pharmacol Sin 2007; 28: 879-87.
[152] Zhang W, Wu N, Li Z, Wang L, Jin J, Zha XL. PPARgamma acti-vator rosiglitazone inhibits cell migration via upregulation of PTEN in human hepatocarcinoma cell line BEL-7404. Cancer Biol Ther 2006; 5: 1008-14.
[153] Kim KY, Kim SS, Cheon HG. Differential anti-proliferative ac-tions of peroxisome proliferator-activated receptor-gamma agonists in MCF-7 breast cancer cells. Biochem Pharmacol 2006; 72: 530-40.
[154] Patel L, Pass I, Coxon P, Downes CP, Smith SA, Macphee CH. Tumor suppressor and anti-inflammatory actions of PPARgamma agonists are mediated via upregulation of PTEN. Curr Biol 2001; 11: 764-8.
[155] Weigert C, Brodbeck K, Bierhaus A, Haring HU, Schleicher ED. c-Fos-driven transcriptional activation of transforming growth factor beta-1: inhibition of high glucose-induced promoter activity by thi-azolidinediones. Biochem Biophys Res Commun 2003; 304: 301-7.
[156] Matsumoto E, Yoshida T, Kawarada Y, Sakakura T. Expression of fibronectin isoforms in human breast tissue: production of extra domain A+/extra domain B+ by cancer cells and extra domain A+ by stromal cells. Jpn J Cancer Res 1999; 90: 320-5.
[157] Redondo S, Ruiz E, Santos-Gallego CG, Padilla E, Tejerina T. Pioglitazone induces vascular smooth muscle cell apoptosis through a peroxisome proliferator-activated receptor-gamma, trans-forming growth factor-beta1, and a Smad2-dependent mechanism. Diabetes 2005; 54: 811-7.
[158] Jiang C, Ting AT, Seed B. PPAR-gamma agonists inhibit produc-tion of monocyte inflammatory cytokines. Nature 1998; 391: 82-6.
[159] Ricote M, Li AC, Willson TM, Kelly CJ, Glass CK. The perox-isome proliferator-activated receptor-gamma is a negative regulator of macrophage activation. Nature 1998; 391: 79-82.
[160] Blanquart C, Barbier O, Fruchart JC, Staels B, Glineur C. Perox-isome proliferator-activated receptors: regulation of transcriptional activities and roles in inflammation. J Steroid Biochem Mol Biol 2003; 85: 267-73.
[161] Zingarelli B, Sheehan M, Hake PW, O'Connor M, Denenberg A, Cook JA. Peroxisome proliferator activator receptor-gamma ligands, 15-deoxy-Delta(12,14)-prostaglandin J2 and ciglitazone, reduce systemic inflammation in polymicrobial sepsis by modula-tion of signal transduction pathways. J Immunol 2003; 171: 6827-37.
[162] Kamei Y, Xu L, Heinzel T, et al. A CBP integrator complex medi-ates transcriptional activation and AP-1 inhibition by nuclear recep-tors. Cell 1996; 85: 403-14.
[163] Chaffer CL, Thomas DM, Thompson EW, Williams ED. PPAR-gamma-independent induction of growth arrest and apoptosis in prostate and bladder carcinoma. BMC Cancer 2006; 6: 53.
[164] Emery MN, Leontiou C, Bonner SE, et al. PPAR-gamma expres-sion in pituitary tumours and the functional activity of the glita-zones: evidence that any anti-proliferative effect of the glitazones is independent of the PPAR-gamma receptor. Clin Endocrinol (Oxf) 2006; 65: 389-95.
[165] Phulwani NK, Feinstein DL, Gavrilyuk V, Akar C, Kielian T. 15-deoxy-Delta12,14-prostaglandin J2 (15d-PGJ2) and ciglitazone modulate Staphylococcus aureus-dependent astrocyte activation primarily through a PPAR-gamma-independent pathway. J Neuro-chem 2006; 99: 1389-402.
[166] Ray DM, Akbiyik F, Phipps RP. The peroxisome proliferator-activated receptor gamma (PPARgamma) ligands 15-deoxy-Delta12,14-prostaglandin J2 and ciglitazone induce human B lym-
phocyte and B cell lymphoma apoptosis by PPARgamma-independent mechanisms. J Immunol 2006; 177: 5068-76.
[167] Palakurthi SS, Aktas H, Grubissich LM, Mortensen RM, Halperin JA. Anticancer effects of thiazolidinediones are independent of peroxisome proliferator-activated receptor gamma and mediated by inhibition of translation initiation. Cancer Res 2001; 61: 6213-8.
[168] Chawla A, Barak Y, Nagy L, Liao D, Tontonoz P, Evans RM. PPAR-gamma dependent and independent effects on macrophage-gene expression in lipid metabolism and inflammation. Nat Med 2001; 7: 48-52.
[169] Wang M, Wise SC, Leff T, Su TZ. Troglitazone, an antidiabetic agent, inhibits cholesterol biosynthesis through a mechanism inde-pendent of peroxisome proliferator-activated receptor-gamma. Dia-betes 1999; 48: 254-60.
[170] Feinstein DL, Spagnolo A, Akar C, et al. Receptor-independent actions of PPAR thiazolidinedione agonists: is mitochondrial func-tion the key? Biochem Pharmacol 2005; 70: 177-88.
[171] Shiau CW, Yang CC, Kulp SK, et al. Thiazolidenediones mediate apoptosis in prostate cancer cells in part through inhibition of Bcl-xL/Bcl-2 functions independently of PPARgamma. Cancer Res 2005; 65: 1561-9.
[172] Brunmair B, Gras F, Neschen S, et al. Direct thiazolidinedione action on isolated rat skeletal muscle fuel handling is independent of peroxisome proliferator-activated receptor-gamma-mediated changes in gene expression. Diabetes 2001; 50: 2309-15.
[173] Brunmair B, Staniek K, Gras F, et al. Thiazolidinediones, like metformin, inhibit respiratory complex I: a common mechanism contributing to their antidiabetic actions? Diabetes 2004; 53: 1052-9.
[174] Scatena R, Bottoni P, Martorana GE, et al. Mitochondrial respira-tory chain dysfunction, a non-receptor-mediated effect of synthetic PPAR-ligands: biochemical and pharmacological implications. Biochem Biophys Res Commun 2004; 319: 967-73.
[175] Scatena R, Bottoni P, Martorana GE, et al. Mitochondria, ciglita-zone and liver: A neglected interaction in biochemical pharmacol-ogy. Eur J Pharmacol 2007; 567(1-2): 50-8.
[176] Bova MP, Tam D, McMahon G, Mattson MN. Troglitazone in-duces a rapid drop of mitochondrial membrane potential in liver HepG2 cells. Toxicol Lett 2005; 155: 41-50.
[177] Perez-Ortiz JM, Tranque P, Burgos M, Vaquero CF, Llopis J. Gli-tazones induce astroglioma cell death by releasing reactive oxygen species from mitochondria: modulation of cytotoxicity by nitric ox-ide. Mol Pharmacol 2007; 72(2): 407-17.
[178] Spagnolo A, Grant EN, Glick R, Lichtor T, Feinstein DL. Differen-tial effects of PPARgamma agonists on the metabolic properties of gliomas and astrocytes. Neurosci Lett 2007; 417: 72-7.
[179] Dello Russou C, Gavrilyuk V, Weinberg G, et al. Peroxisome proliferator-activated receptor gamma thiazolidinedione agonists increase glucose metabolism in astrocytes. J Biol Chem 2003; 278: 5828-36.
[180] Colca JR, McDonald WG, Waldon DJ, et al. Identification of a novel mitochondrial protein ("mitoNEET") cross-linked specifi-cally by a thiazolidinedione photoprobe. Am J Physiol Endocrinol Metab 2004; 286: E252-E260.
[181] Wiley SE, Paddock ML, Abresch EC, et al. The outer mitochon-drial membrane protein mitoNEET contains a novel redox-active 2Fe-2S cluster. J Biol Chem 2007; 282: 23745-9.
[182] Wiley SE, Murphy AN, Ross SA, van der GP, Dixon JE. Mi-toNEET is an iron-containing outer mitochondrial membrane pro-tein that regulates oxidative capacity. Proc Natl Acad Sci USA 2007; 104: 5318-23.
[183] Pandhare J, Cooper SK, Phang JM. Proline oxidase, a proapoptotic gene, is induced by troglitazone: evidence for both peroxisome pro-liferator-activated receptor gamma-dependent and -independent mechanisms. J Biol Chem 2006; 281: 2044-52.
[184] Carew JS, Huang P. Mitochondrial defects in cancer. Mol Cancer 2002; 1: 9.
[185] Hileman EO, Liu J, Albitar M, Keating MJ, Huang P. Intrinsic oxidative stress in cancer cells: a biochemical basis for therapeutic selectivity. Cancer Chemother Pharmacol 2004; 53: 209-19.
[186] Huang WC, Chio CC, Chi KH, Wu HM, Lin WW. Superoxide anion-dependent Raf/MEK/ERK activation by peroxisome prolif-erator activated receptor gamma agonists 15-deoxy-delta(12,14)-prostaglandin J(2), ciglitazone, and GW1929. Exp Cell Res 2002; 277: 192-200.
Not For Distribution
Potential Benefits of Glitazones for Cancer and Vascular Disease Current Drug Therapy, 2008, Vol. 3, No. 2 125
[187] Lennon AM, Ramauge M, Dessouroux A, Pierre M. MAP kinase cascades are activated in astrocytes and preadipocytes by 15-deoxy-Delta(12-14)-prostaglandin J(2) and the thiazolidinedione ciglitazone through peroxisome proliferator activator receptor gamma-independent mechanisms involving reactive oxygenated species. J Biol Chem 2002; 277: 29681-5.
[188] Kim JA, Park KS, Kim HI, et al. Troglitazone activates p21Cip/WAF1 through the ERK pathway in HCT15 human colo-rectal cancer cells. Cancer Lett 2002; 179: 185-95.
[189] Hayashi T, Hirshman MF, Fujii N, Habinowski SA, Witters LA, Goodyear LJ. Metabolic stress and altered glucose transport: acti-vation of AMP-activated protein kinase as a unifying coupling mechanism. Diabetes 2000; 49: 527-31.
[190] Nagata D, Takeda R, Sata M, et al. AMP-activated protein kinase inhibits angiotensin II-stimulated vascular smooth muscle cell pro-liferation. Circulation 2004; 110: 444-51.
[191] Zou MH, Kirkpatrick SS, Davis BJ, et al. Activation of the AMP-activated protein kinase by the anti-diabetic drug metformin in
vivo. Role of mitochondrial reactive nitrogen species. J Biol Chem 2004; 279: 43940-51.
[192] Bashan N, Burdett E, Guma A, et al. Mechanisms of adaptation of glucose transporters to changes in the oxidative chain of muscle and fat cells. Am J Physiol 1993; 264: C430-C440.
[193] Konrad D, Rudich A, Bilan PJ, et al. Troglitazone causes acute mitochondrial membrane depolarisation and an AMPK-mediated increase in glucose phosphorylation in muscle cells. Diabetologia 2005; 48: 954-66.
[194] Kim JW, Dang CV. Cancer's molecular sweet tooth and the War-burg effect. Cancer Res 2006; 66: 8927-30.
[195] Abe A, Kiriyama Y, Hirano M, et al. Troglitazone suppresses cell growth of KU812 cells independently of PPARgamma. Eur J Pharmacol 2002; 436: 7-13.
[196] Huang JW, Shiau CW, Yang YT, et al. Peroxisome proliferator-activated receptor gamma-independent ablation of cyclin D1 by thiazolidinediones and their derivatives in breast cancer cells. Mol Pharmacol 2005; 67: 1342-8.
[197] Laurora S, Pizzimenti S, Briatore F, et al. Peroxisome proliferator-activated receptor ligands affect growth-related gene expression in human leukemic cells. J Pharmacol Exp Ther 2003; 305: 932-42.
[198] Lu M, Kwan T, Yu C, et al. Peroxisome proliferator-activated receptor gamma agonists promote TRAIL-induced apoptosis by re-ducing survivin levels via cyclin D3 repression and cell cycle ar-rest. J Biol Chem 2005; 280: 6742-51.
[199] Baek SJ, Kim JS, Nixon JB, DiAugustine RP, Eling TE. Expres-sion of NAG-1, a transforming growth factor-beta superfamily member, by troglitazone requires the early growth response gene EGR-1. J Biol Chem 2004; 279: 6883-92.
[200] Han S, Zheng Y, Roman J. Rosiglitazone, an agonist of PPAR-gamma, inhibits non-small cell carcinoma cell proliferation in part through activation of tumor sclerosis complex-2. PPAR Res 2007; 2007: 29632.
[201] Turturro F, Friday E, Fowler R, Surie D, Welbourne T. Troglita-zone acts on cellular pH and DNA synthesis through a peroxisome proliferator-activated receptor gamma-independent mechanism in breast cancer-derived cell lines. Clin Cancer Res 2004; 10: 7022-30.
Received: November 26, 2007 Revised: January 04, 2008 Accepted: February 04, 2008
Not For Distribution




















