The Rise, Fall and Potential Resilience Benefits of Jatropha in ...
Upload
khangminh22Category
view
2download
0
Evidence-Based and Potential Benefits ofMetformin in the Polycystic Ovary Syndrome:A Comprehensive Review
Stefano Palomba, Angela Falbo, Fulvio Zullo, and Francesco Orio, Jr.
Department of Obstetrics and Gynecology (S.P., A.F., F.Z.), University “Magna Graecia” of Catanzaro, 88100 Catanzaro,Italy; and Endocrinology (F.O.), University “Parthenope” of Naples, 80131 Naples, Italy
Metformin is an insulin sensitizer widely used for the treat-ment of patients affected by type 2 diabetes mellitus. Becausemany women with polycystic ovary syndrome (PCOS) are in-sulin resistant, metformin was introduced in clinical practiceto treat these patients also. Moreover, metformin’s effect hasother targets beside its insulin-sensitizing action. The presentreview was aimed at describing all evidence-based and po-
tential uses of metformin in PCOS patients. In particular, wewill analyze the uses of metformin not only for the treatmentof all PCOS-related disturbances such as menstrual disorders,anovulatory infertility, increased abortion, or complicatedpregnancy risk, hyperandrogenism, endometrial, metabolicand cardiovascular abnormalities, but also for the preventionof the syndrome. (Endocrine Reviews 30: 1–50, 2009)
I. IntroductionA. BackgroundB. Rationale and mechanism of actionC. PharmacokineticsD. Therapeutic regimensE. Adverse effectsF. Potential predictors
II. Menstrual DisordersIII. Anovulation
A. Metformin as first-step treatmentB. Metformin as second-step treatmentC. Metformin in patients who receive gonadotropins
IV. Adverse Pregnancy OutcomesA. MiscarriageB. Gestational diabetesC. Pregnancy-induced hypertension and preeclampsiaD. Poor infant outcomes
V. Endometrial AbnormalitiesA. Fertility implicationsB. Cancer implications
VI. HyperandrogenismVII. Malignancies
VIII. Quality of Life ImpairmentIX. ObesityX. Cardiovascular Risk
A. Cardiopulmonary impairmentB. Diabetes mellitusC. HypertensionD. DyslipidemiaE. Impaired fibrinolysisF. Chronic inflammationG. Endothelial impairmentH. Syndrome X
XI. Other Organ ImpairmentA. Liver impairmentB. Thyroid impairmentC. Cognitive functionD. Sleep disturbances
XII. High-Risk Patients for PCOS
XIII. Future PerspectivesXIV. Summary
I. Introduction
POLYCYSTIC OVARY SYNDROME (PCOS) is a hetero-geneous disorder. Although, essentially characterized
by hyperandrogenism, ovarian dysfunction, and polycysticovarian morphology, its definition remains somewhat fluidand controversial. Until now, two main criteria have beenproposed: the National Institute of Health (NIH)/NationalInstitute of Child Health and Human Development (NICHD)criteria proposed in April 1990 (1), and the European Society
First Published Online December 4, 2008Abbreviations: ADMA, Asymmetrical dimethylarginine; AGE, ad-
vanced glycation end-product; AMPK, 5�-AMP-activated protein ki-nase; AR, androgen receptor; AUC, area under the curve; BMI, bodymass index; CA, cyproterone acetate; CC, clomiphene citrate; CI, con-fidence interval; CRP, C-reactive protein; CVD, cardiovascular disease;DM, diabetes mellitus; E2, estradiol; EDS, excessive daytime sleepiness;EE2, ethinyl E2; ER�, estrogen receptor �; ET-1, endothelin-I; FAO, fattyacid oxidation; GFR, glomerular filtration rate; GLUT, glucose trans-porter; HDL, high-density lipoprotein; HOMA, homeostasis model ofassessment; HSC, hepatic stellate cell; IGFBP, IGF binding protein; IGT,impaired glucose tolerance; ISD, insulin-sensitizing drug; IVF, in vitrofertilization; LDL, low-density lipoprotein; LOD, laparoscopic ovariandiathermy; MIF, migration inhibitor factor; mTORC, mammalian targetof rapamycin; NAFLD, nonalcoholic fatty liver disease; NGT, normalglucose tolerance; NOS, nitric oxide synthase; OC, oral contraceptive;OCT, organic cation transporter; OHSS, ovarian hyperstimulationsyndrome; OR, odds ratio; OSA, obstructive sleep apnea; PAI, plas-minogen activator inhibitor; PCO, polycystic ovaries; PCOS, poly-cystic ovary syndrome; PE, preeclampsia; PI, pulsatility index; PIH,pregnancy-induced hypertension; QoL, quality of life; RCT, random-ized controlled trial; RI, resistance index; RR, relative risk; VO2max,maximal oxygen consumption; WHR, waist-hip ratio; WMD,weighted mean duration.Endocrine Reviews is published by The Endocrine Society (http://www.endo-society.org), the foremost professional society servingthe endocrine community.
0163-769X/09/$20.00/0 Endocrine Reviews 30(1):1–50Printed in U.S.A. Copyright © 2009 by The Endocrine Society
doi: 10.1210/er.2008-0030
1
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

for Human Reproduction and Embryology (ESHRE) and theAmerican Society for Reproductive Medicine (ASRM) pro-posed in May 2003 (2).
The 1990 NIH criteria (1) indicated the presence of hy-perandrogenism and/or hyperandrogenemia and chronicanovulation with exclusion of related ovulatory or otherandrogen excess disorders (e.g., thyroid dysfunction, hyper-prolactinemia, androgen-secreting neoplasms, or nonclassicadrenal hyperplasia) as PCOS features. The presence of poly-cystic ovaries (PCO), with morphology assessed by ultra-sound, was not included as a diagnostic criterion because itwas considered by some authors to be a finding with a lowspecificity (3). PCO can be present in women with normalovulation and sex hormone levels, whereas women with allthe endocrine PCOS features occasionally can have normalovarian morphology as assessed by ultrasound examination (3).
In 2003, an international conference in Rotterdam, TheNetherlands (2), proposed to revise the PCOS and PCO cri-teria. In particular, the ESHRE/ASRM conference proceed-ings expanded the definition of PCOS, establishing that itcould be diagnosed, even after the exclusion of related dis-orders, by at least two of the following features: 1) oligo- oranovulation; 2) clinical and/or biochemical signs of hyperan-drogenism; and 3) PCO. All women considered to be affectedby PCOS, according to the NIH criteria, would also be iden-tified through the Rotterdam criteria, which includedwomen with PCOS excluded by the NIH criteria: those withPCO affected by hyperandrogenism and ovulatory cycles orchronic anovulation and normal androgen levels. More re-cently, an expert panel of the Androgen Excess and PCOSSociety (AEPS) recommended that PCOS should be consid-ered an androgen excess disorder and that the NIH diag-nostic criteria should be used with some modifications, tak-ing into consideration the concerns expressed in theproceedings of the 2003 Rotterdam conference (4). In partic-ular, the AEPS Task Force concluded that PCOS was aboveall a disorder of androgen biosynthesis, utilization, and/ormetabolism in women. Thus, the AEPS criteria for PCOS arefulfilled by the combination of hyperandrogenism with atleast one of the following: ovarian dysfunction (includinginfrequent or irregular ovulation or anovulation) and PCO(4). In addition, the Task Force noted that support for thiscriterion is based on the risk for metabolic morbidity in thedisorder, not on whether hyperandrogenism per se is presentor not (4).
The phenotypes considered to represent the disorder mayvary according to the definition used, and several authors (5,6) questioned the points of agreement between the new phe-notypes according to the ESHRE/ASRM criteria and thefeatures classically related to the syndrome. Ovulatorywomen with PCO seem to be less insulin-resistant thananovulatory women with PCO (7–9). Barber et al. (10)showed that patients with PCO, chronic anovulation, andnormal androgen levels are not insulin-resistant. More-over, only women who fulfil the NIH criteria have beendemonstrated to be at high risk for metabolic sequelae ofPCOS, i.e., glucose intolerance (11) and metabolic syn-drome (12).
Notwithstanding the extreme variability of the diagnosticcriteria adopted, the main clinical features related to the
syndrome, albeit not pathognomonic, are menstrual disor-ders, anovulatory infertility, and signs of hyperandrogenism(2). Moreover, PCOS is characterized by a number of otherclinical traits and long-term sequelae.
The reduced fertility observed in PCOS patients cannot beattributed to anovulation alone. Other factors may be operantin PCOS to lower fertility in these women, including reducedoocyte and/or embryo quality, defects in endometrial de-velopment, and implantation abnormalities (13). In addition,pregnant women with PCOS seem to have a significantlyhigher risk for miscarriage, gestational diabetes mellitus(DM), pregnancy-induced hypertension (PIH), preeclampsia(PE), and poor infant outcome (13). Finally, even if no well-controlled prospective data have demonstrated a highermortality for cardiovascular disease (CVD) in PCOS patients,an increased prevalence of several surrogate end-points,mainly type 2 DM and metabolic syndrome, have been dem-onstrated in PCOS.
The pathogenesis of PCOS is still unclear, and a complexof genetic and environmental factors may be involved. Inparticular, family studies demonstrated that PCOS is signif-icantly more prevalent among family members than in thegeneral population (14, 15). Among first-degree female rel-atives of patients with PCOS, 35% of premenopausal mothersand 40% of sisters were affected by the disorder (16). Theserates are significantly higher than the 6–7% observed in thegeneral population (17). Other than PCOS itself, increasedandrogens, insulin secretion, and insulin resistance also ap-pear to be under significant genetic control, as established byfamily studies (15, 18–24). Several genes have been logicallychosen as candidates, but most of these studies were per-formed in small cohorts and confounded by several biases.Thus, no particular gene is universally recognized as impor-tantly contributing to PCOS risk, and several environmentalfactors probably modulate the clinical expression of geneticpredisposition. In particular, obesity, insulin resistance, pre-natal androgen excess during early gestation, birth weight,precocious pubarche, dietary intake, lifestyle, and stress mayact on the genetic substrate. Obesity is the most importantfactor contributing directly to insulin resistance and hyper-insulinemia. Low birth weight modifies the relationship be-tween insulin resistance and PCOS and seems to increase therisk of developing PCOS. Diet composition, eating disorders,and psychological stress seem to be related to the syndrome,even if no causality link has been clearly demonstrated. How-ever, insulin resistance with compensatory hyperinsulin-emia is probably a cornerstone of the pathogenesis of thePCOS, and this recognition has led to a much better under-standing of the syndrome and associated short- and long-term complications.
The molecular mechanisms of insulin resistance in PCOSdiffer from those in other common insulin-resistant states,such as obesity and type 2 DM (25). Despite the compensa-tory hyperinsulinemia that accompanies insulin resistance innondiabetic individuals, insulin-mediated glucose uptakeremains subnormal (26). Interestingly, insulin resistance oc-curring in PCOS patients is not evident in all tissues, but itseems to have a tissue peculiarity (26). Specifically, in skeletaland adipose tissue, insulin resistance led to a decreased glu-cose uptake and increased lipolysis, respectively, whereas,
2 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022
the ovary, adrenal, liver, and skin seem to remain insulinsensitive (26). Furthermore, recently a peripheral insulin re-sistance, which is related to ovarian (27) and uterine (28, 29)abnormalities detected in PCOS patients, has been demon-strated. Compensatory hyperinsulinemia exerts androgen-stimulating effects on the ovaries and adrenal glands and isresponsible for the main clinical manifestations of the syn-drome (see Section I.A).
Because insulin resistance with compensatory hyperinsu-linemia is widely considered the pivotal feature of PCOS,insulin-sensitizing drugs (ISDs) are introduced for the treat-ment of these patients.
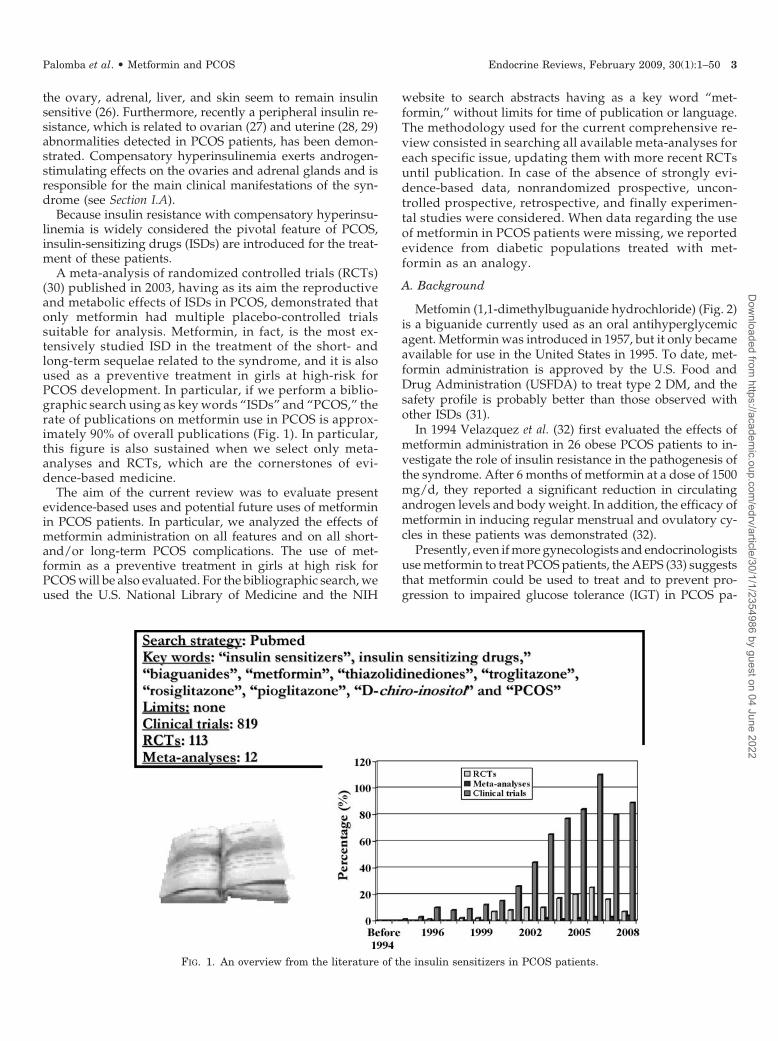
A meta-analysis of randomized controlled trials (RCTs)(30) published in 2003, having as its aim the reproductiveand metabolic effects of ISDs in PCOS, demonstrated thatonly metformin had multiple placebo-controlled trialssuitable for analysis. Metformin, in fact, is the most ex-tensively studied ISD in the treatment of the short- andlong-term sequelae related to the syndrome, and it is alsoused as a preventive treatment in girls at high-risk forPCOS development. In particular, if we perform a biblio-graphic search using as key words “ISDs” and “PCOS,” therate of publications on metformin use in PCOS is approx-imately 90% of overall publications (Fig. 1). In particular,this figure is also sustained when we select only meta-analyses and RCTs, which are the cornerstones of evi-dence-based medicine.
The aim of the current review was to evaluate presentevidence-based uses and potential future uses of metforminin PCOS patients. In particular, we analyzed the effects ofmetformin administration on all features and on all short-and/or long-term PCOS complications. The use of met-formin as a preventive treatment in girls at high risk forPCOS will be also evaluated. For the bibliographic search, weused the U.S. National Library of Medicine and the NIH
website to search abstracts having as a key word “met-formin,” without limits for time of publication or language.The methodology used for the current comprehensive re-view consisted in searching all available meta-analyses foreach specific issue, updating them with more recent RCTsuntil publication. In case of the absence of strongly evi-dence-based data, nonrandomized prospective, uncon-trolled prospective, retrospective, and finally experimen-tal studies were considered. When data regarding the useof metformin in PCOS patients were missing, we reportedevidence from diabetic populations treated with met-formin as an analogy.
A. Background
Metfomin (1,1-dimethylbuguanide hydrochloride) (Fig. 2)is a biguanide currently used as an oral antihyperglycemicagent. Metformin was introduced in 1957, but it only becameavailable for use in the United States in 1995. To date, met-formin administration is approved by the U.S. Food andDrug Administration (USFDA) to treat type 2 DM, and thesafety profile is probably better than those observed withother ISDs (31).
In 1994 Velazquez et al. (32) first evaluated the effects ofmetformin administration in 26 obese PCOS patients to in-vestigate the role of insulin resistance in the pathogenesis ofthe syndrome. After 6 months of metformin at a dose of 1500mg/d, they reported a significant reduction in circulatingandrogen levels and body weight. In addition, the efficacy ofmetformin in inducing regular menstrual and ovulatory cy-cles in these patients was demonstrated (32).
Presently, even if more gynecologists and endocrinologistsuse metformin to treat PCOS patients, the AEPS (33) suggeststhat metformin could be used to treat and to prevent pro-gression to impaired glucose tolerance (IGT) in PCOS pa-
FIG. 1. An overview from the literature of the insulin sensitizers in PCOS patients.
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 3
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

tients, and the American Association of Clinical Endocrinol-ogists’ guidelines (34) recommend metformin as an initialintervention in overweight and obese patients with PCOS; todate, neither in Europe nor in the United States has met-formin been approved for this type of treatment in PCOSpatients.
In March 2007, in Thessaloniki, Greece, a second interna-tional ESHRE/ASRM-sponsored PCOS Consensus Work-shop Group (35) was held to address the therapeutic chal-lenges raised in women with infertility and PCOS and toanswer important questions regarding the efficacy and safetyof various treatments available for these women, includingISDs. As in the Rotterdam meeting, a panel of internationalexperts was invited to discuss treatment in women affectedby PCOS to reach at a consensus regarding therapy. Thisworkshop group concluded that ISDs should not be used asfirst-choice agents in ovulation induction of women withPCOS, and their use should be restricted to those patientswith IGT. This is probably due to the fact that knowledgeregarding its effects and regimens of administration in PCOSpatients is still incomplete.
More recently, Nestler (36), in an interesting editorial, crit-icizes previous conclusions (35) maintaining the open debateon this issue.
B. Rationale and mechanism of action
The rationale for the use of an ISD, such as metformin, intreatment of patients with PCOS (as summarized in Figure 3)arises from the knowledge that insulin resistance with com-pensatory hyperinsulinemia has provided an insight into thepathogenesis of PCOS, although, not an essential criteria forthe diagnosis of PCOS.
Insulin resistance and secondary hyperinsulinemia affectapproximately 65 to 70% of PCOS women (37). PCOS pa-tients are more insulin resistant and hyperinsulinemic thanage- and body mass index (BMI)-matched non-PCOS con-trols, regardless of BMI (38). In addition, pancreatic �-celldysfunction with an increased basal secretion of insulin andan inadequate postprandial response has been described inPCOS patients, also after weight loss, despite an improve-ment in glucose tolerance (39).
The major defect of insulin action in PCOS patients isprobably a decrease in insulin sensitivity secondary to apostbinding abnormality in insulin receptor-mediated signaltransduction, with a less substantial, but significant, alter-ation in receptor binding (25). The decreased insulin sensi-tivity in patients affected by PCOS is potentially an intrinsicdefect in genetically predisposed subjects. In fact, indepen-dent of obesity, body fat distribution, sex hormone levels,and metabolic abnormalities, there may be genetic abnor-malities in the regulation of insulin receptor phosphoryla-tion, resulting in increased insulin-independent serine phos-phorylation and decreased insulin-dependent tyrosine
FIG. 2. Biochemical structure of 1,1-dimethylbuguanide hydro-chloride.
FIG. 3. Rationale for the use of metformin in PCOS patients.
4 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

phosphorylation (25). Although insulin resistance is presentindependently from BMI, obesity may further exacerbateinsulin resistance and exert a direct and synergistic or indi-rect deleterious impact on glucose metabolism with a pos-sible worsening of the clinical and biochemical features of thePCOS.
Insulin resistance and secondary hyperinsulinemia mightinfluence the spectrum of the disorders related to PCOS bymeans of various and still unclear mechanisms. Certainly, themost debated argument is the effect of insulin disorder onspecific characteristics of the syndrome, i.e., ovulatory dys-function and hyperandrogenism.
Central and peripheral mechanisms have been hypothe-sized to explain the role of insulin resistance on the patho-genesis of the PCOS.
At the central level, insulin was implicated in the regula-tion of LH secretion, but contrasting data rose from in vitroand in vivo studies (25). Particularly, rat pituitary cells pre-incubated with insulin showed an increased response of LHafter GnRH administration. On the other hand, insulin in-fusion in PCOS women did not cause significant alterationsin LH secretion or release after GnRH stimulation (25). Inaddition, the experimental reduction of hyperinsulinemiainduced a reduction in serum LH levels (25), even if it isunclear whether decreased serum LH is a direct result oflowered circulating insulin levels or secondary to the feed-back effect of increased ovarian estrogen production due toresumed folliculogenesis. Moreover, these data were not con-firmed by other studies (25). Recently, the influence of insulinon gonadotropin secretion in PCOS women and healthy con-trols was evaluated, and no alteration, due to insulin infu-sion, was observed in both groups over an interval of 12 h inepisodic gonadotropin secretion and LH response to mul-tidose GnRH stimulation by use of hyperinsulinemic-eugly-cemic clamp technique (25).
At the peripheral level, insulin resistance influences he-patic, muscle, and ovarian function.
At the hepatic level, hyperinsulinemia inhibits the syn-thesis of SHBG, increasing the free androgen amount andconsequently the peripheral androgen action; hyperinsulin-emia also inhibits the hepatic secretion of the IGF bindingprotein (IGFBP)-1, leading to increased bioactivity of IGF-Iand -II, two important regulators of ovarian follicular mat-uration and steroidogenesis (25). The IGF-I and -II systemicincrease augments ovarian androgen production from thecacells by acting on IGF-I receptors (25).
At the muscular level, insulin resistance is associatedwith reduced expression of genes involved in mitochon-drial oxidative metabolism (40). Moreover, experimentaldata indicated that insulin resistance induced transcrip-tional alterations in insulin signaling pathways, free fattyacid (FFA) metabolism, and calcium homeostasis in PCOSpatients (40).
At the ovarian level, compensatory hyperinsulinemiamight contribute to anovulation directly by interfering withfollicular development, causing premature follicular atresiaand antral follicular arrest (25), and indirectly by affectinggonadotropin effectiveness for abnormal intraovarian envi-ronment (25). On the other hand, increased insulin binds tothe IGF-I receptors, again enhancing the androgen theca cell
production in response to LH stimulation (25). Insulin stim-ulates the basal androgen secretion by cultured human thecacells from hyperandrogenic women, suggesting that thestimulatory effect of insulin on thecal steroidogenesis is aug-mented in PCOS (25). Insulin may also increase endogenousandrogen concentrations by increasing the cytochromeP450c17� activity, a key enzyme in the biosynthesis of ovar-ian and adrenal androgens having both 17�-hydroxylase and17,20-lyase activities. In ovarian theca cells, the P450c17�17�-hydroxylase activity converts progesterone to 17�-hy-droxyprogesterone, whereas its 17,20-lyase activity con-verts 17�-hydroxyprogesterone to androstenedione. An-drostenedione is then converted to testosterone by theenzyme 17�-reductase. Thus, the increase in P450c17� ac-tivity is accompanied by an increase in the serum testoster-one concentration. In this regard, in PCOS this abnormalitymay be responsible for exaggerating 17-hydroxyprogester-one response to stimulation by GnRH analog (41).
Intraovarian androgen levels may modulate follicularfunction by acting directly on the ovary. In particular, shortexposition to androgens suppresses granulosa cell apoptosisprolonging survival of small antral follicles, which in normal-cycling women either grow rapidly to become dominantfollicles or collapse in atresia (42, 43). On the other hand, aprolonged exposition to androgens, such as in PCOS, is re-sponsible for the collapse of these follicles into the ovarianstroma, leading to stromal hypertrophy and promoting theprocess of ovarian atresia and anovulation (44).
Even if this rationale initially induced several researchersto use metformin in PCOS patients, no clear evidence hasbeen provided yet regarding the effectiveness of metforminrelated to its insulin-sensitizing effects. On the other hand,other non-insulin-sensitizing mechanisms can be supposedor cannot be excluded.
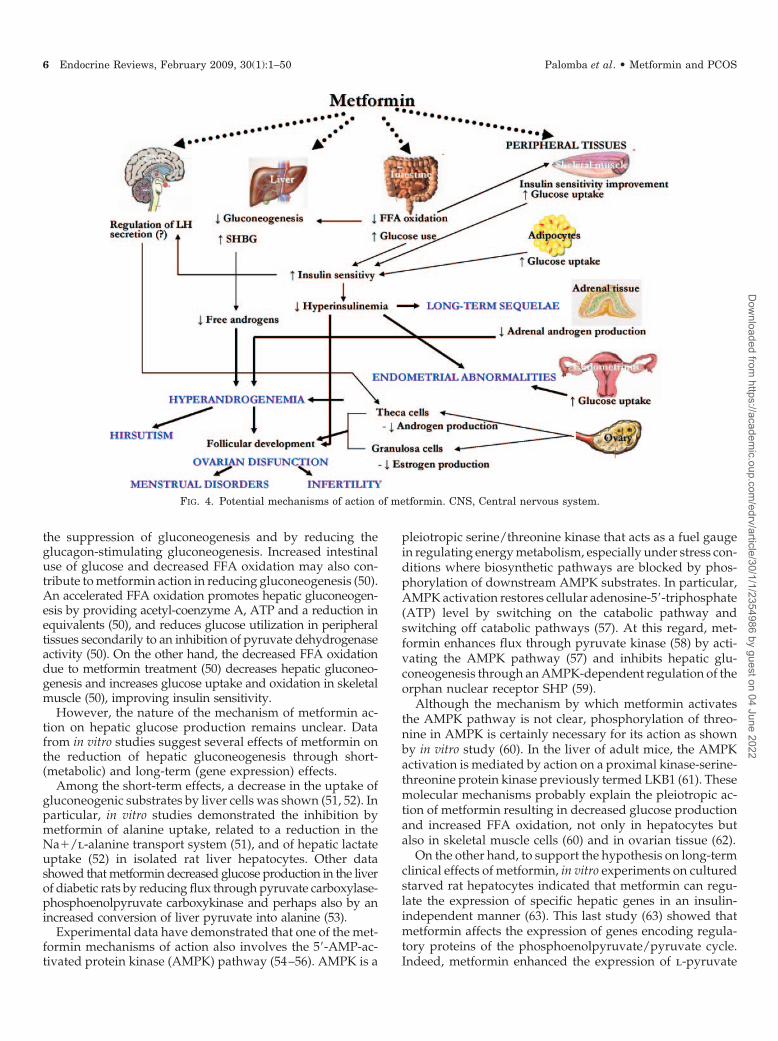
In Figure 4, all main potential mechanisms of action ofmetformin in PCOS patients are shown. Other mechanismsof metformin action on specific districts will be detailed inspecific paragraphs.
In an early meta-analysis on ISDs (30), metformin admin-istration in PCOS patients, when compared with placebo,resulted in a significant decrease in fasting glucose and in-sulin levels, as well as insulin levels in the area under thecurve (AUC) after oral glucose administration. Mechanisticstudies have shown that metformin improves insulin-medi-ated glucose disposal in women with PCOS (45). Further-more, to understand metformin’s main mechanisms of actionbetter, several data obtained in patients with type 2 DMcould be translated in PCOS patients.
Metformin has been shown to reduce basal hepatic glucoseproduction by 9 to 30% in patients with type 2 DM throughmultiple effects (46). The stimulating effect of this drug onnonoxidative glucose metabolism, including glycogenosynthe-sis, conversion to lactate, and incorporation to triglycerides, isresponsible for the insulin-stimulated glucose utilization esti-mated to be more than 50% in patients with type 2 DM (47) andfirst-degree relatives of patients with type 2 DM (48).
Experimental studies (49) evaluating glucose productionfrom collagenase-isolated hepatocytes of starved rats dem-onstrated that therapeutic concentrations of metformin po-tentiate the antigluconeogenic effect of insulin by enhancing
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 5
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022
the suppression of gluconeogenesis and by reducing theglucagon-stimulating gluconeogenesis. Increased intestinaluse of glucose and decreased FFA oxidation may also con-tribute to metformin action in reducing gluconeogenesis (50).An accelerated FFA oxidation promotes hepatic gluconeogen-esis by providing acetyl-coenzyme A, ATP and a reduction inequivalents (50), and reduces glucose utilization in peripheraltissues secondarily to an inhibition of pyruvate dehydrogenaseactivity (50). On the other hand, the decreased FFA oxidationdue to metformin treatment (50) decreases hepatic gluconeo-genesis and increases glucose uptake and oxidation in skeletalmuscle (50), improving insulin sensitivity.
However, the nature of the mechanism of metformin ac-tion on hepatic glucose production remains unclear. Datafrom in vitro studies suggest several effects of metformin onthe reduction of hepatic gluconeogenesis through short-(metabolic) and long-term (gene expression) effects.
Among the short-term effects, a decrease in the uptake ofgluconeogenic substrates by liver cells was shown (51, 52). Inparticular, in vitro studies demonstrated the inhibition bymetformin of alanine uptake, related to a reduction in theNa�/l-alanine transport system (51), and of hepatic lactateuptake (52) in isolated rat liver hepatocytes. Other datashowed that metformin decreased glucose production in the liverof diabetic rats by reducing flux through pyruvate carboxylase-phosphoenolpyruvate carboxykinase and perhaps also by anincreased conversion of liver pyruvate into alanine (53).
Experimental data have demonstrated that one of the met-formin mechanisms of action also involves the 5�-AMP-ac-tivated protein kinase (AMPK) pathway (54–56). AMPK is a
pleiotropic serine/threonine kinase that acts as a fuel gaugein regulating energy metabolism, especially under stress con-ditions where biosynthetic pathways are blocked by phos-phorylation of downstream AMPK substrates. In particular,AMPK activation restores cellular adenosine-5�-triphosphate(ATP) level by switching on the catabolic pathway andswitching off catabolic pathways (57). At this regard, met-formin enhances flux through pyruvate kinase (58) by acti-vating the AMPK pathway (57) and inhibits hepatic glu-coneogenesis through an AMPK-dependent regulation of theorphan nuclear receptor SHP (59).
Although the mechanism by which metformin activatesthe AMPK pathway is not clear, phosphorylation of threo-nine in AMPK is certainly necessary for its action as shownby in vitro study (60). In the liver of adult mice, the AMPKactivation is mediated by action on a proximal kinase-serine-threonine protein kinase previously termed LKB1 (61). Thesemolecular mechanisms probably explain the pleiotropic ac-tion of metformin resulting in decreased glucose productionand increased FFA oxidation, not only in hepatocytes butalso in skeletal muscle cells (60) and in ovarian tissue (62).
On the other hand, to support the hypothesis on long-termclinical effects of metformin, in vitro experiments on culturedstarved rat hepatocytes indicated that metformin can regu-late the expression of specific hepatic genes in an insulin-independent manner (63). This last study (63) showed thatmetformin affects the expression of genes encoding regula-tory proteins of the phosphoenolpyruvate/pyruvate cycle.Indeed, metformin enhanced the expression of l-pyruvate
FIG. 4. Potential mechanisms of action of metformin. CNS, Central nervous system.
6 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

kinase, whereas it decreased the phosphoenolpyruvate car-boxykinase gene expression (63).
Experimental studies on human muscle cell cultures (64)and rat adipocytes (65) demonstrated that metformin acts byincreasing glucose uptake through the glucose transport sys-tem. In fact, it facilitates the translocation of glucose trans-porters (GLUTs) from intracellular sites to the plasma mem-brane. In addition, metformin augmented the uptake of thenonmetabolizable sugar 3-O-methylglucose approximately,to the same extent, as the uptake of 2-deoxyglucose, sug-gesting a stimulation of hexose transport (64). The PCOS-related insulin-resistant state is associated both with de-creased ability of insulin to stimulate glucose disposal intotarget cells and with reduced glucose response to a givenamount of insulin. In fact, a reduction of the transporterGLUT-4 expression in the insulin target tissues has beendemonstrated (64). An experimental study (66) showed thata 6-month metformin course induces a significant improve-ment of the GLUT-4 mRNA expression in the adipose tissueof PCOS patients, demonstrating that metformin action im-proves the peripheral insulin signal transduction.
Besides its effects on glucose metabolism, metformin mayalso act on the insulin levels and, specifically, on insulinreceptor (46, 50, 67). In fact, significant reduction of bothinsulin and proinsulin levels in patients with type 2 DM hasbeen observed.
Controversial data are available regarding the effect ofmetformin on the extent of insulin binding (68–72). In fact,after addition of metformin to tissue, some authors found nometformin effect on the insulin receptor (69, 70), whereasothers reported that metformin elevated receptor tyrosinekinase activity (71, 72). In type 2 DM patients, metforminwas demonstrated to have no effect in erythrocyte insulinreceptor binding, but it increased both basal and insulin-stimulated insulin receptor tyrosine kinase activities ofsolubilized erythrocyte insulin receptors after 10 wk oftreatment (73).
However, the increase of insulin binding in various celltypes after metformin administration does not directly cor-relate with clinical and metabolic effects. In fact, Stith et al.(72) in an experimental model of Xenopus oocytes obtainedinteresting results regarding the intracellular mechanisms ofaction of metformin. Specifically, metformin must be inter-nalized to act, and it stimulates both insulin and IGF-I re-ceptors in oocytes (75) and mammalian tissue (74). Met-formin can also act independently from insulin to stimulatethe receptor tyrosine kinase and the �-isoform phospholipaseC activity and inositol 1, 4, 5-tris-phosphate production prob-ably through inositol 1,4, 5-tris-phosphate and Ca�� ele-vation (74). The addition of metformin was found to mimicinsulin action in cultured human skeletal muscle (76), humanerythrocytes (77), rat cardiomyocytes (78), rat adipocytes(79), and mouse soleus muscle (80).
Part of the efficacy of metformin in PCOS might be relatedto direct actions on steroidogenesis such as their insulin-sensitizing effects, although controversy exists as to whethermetformin has direct effects on steroidogenesis itself (81, 82).In fact, ovulation may be a result of a direct action of met-formin on the ovary that leads to normal steroid productionand likely steroid feedback effects that include a lowering of
LH and androgen levels. On the other hand, metformin couldact directly, improving abnormal steroidogenesis (systemicand/or local/ovarian) and, subsequently, the follicular func-tion. Several data suggest that metformin could act on hy-perandrogenism by interfering both with direct and specificmechanisms on peripheral androgen-secreting organs andwith free androgen fraction-regulating systems. In fact, areduced ovarian and adrenal secretion of androgens, a re-duced pituitary secretion of LH, and an increased liver SHBGproduction seem to be the mechanisms mediating metformineffect on hyperandrogenism (50).
A direct effect of metformin on androgen production bythecal cells could be hypothesized. In vitro experiments dem-onstrated that metformin significantly inhibits androstenedi-one and testosterone production from theca cells throughinhibition of the steroidogenic acute regulatory protein and17�-hydroxylase expressions (83). Nestler and Jakubowicz(84) demonstrated in obese PCOS patients that metforminadministration reduces the fasting and glucose-stimulatedinsulin levels and concomitantly decreases ovarian cyto-chrome P450c17� activity, inducing a reduction in the serumfree testosterone concentration. These results were also con-firmed in lean PCOS patients (85).
The reduction in insulin levels after metformin treatmentin PCOS patients is associated with an increase in IGFBP-1and a decrease in the IGF-I/IGFBP-1 ratio. IGF-I has auto-crine and paracrine mechanisms in stimulating estrogen pro-duction by granulosa cells (86) and acts synergistically withFSH and LH in controlling granulosa cell aromatase levels.Thus, by reducing plasma insulin levels and IGF-I availabil-ity to the ovaries, metformin may modify the hyperandro-genic intrafollicular milieu recognized in PCOS. Recent invitro studies have confirmed a significant effect of metforminon insulin and IGF-I pathway in granulosa cells (87). More-over, metformin may inhibit ovarian gluconeogenesisthrough a direct effect, thus reducing ovarian steroidogen-esis and, more specifically, androgen production (84). Inparticular, in bovine granulosa cells, metformin decreasessteroidogenesis and MAPK3/MAPK1 phosphorylationthrough AMPK activation (55). Experimental evidence (54)indicates that AMPK could also be implicated in reproduc-tive functions such as granulosa cell steroidogenesis andnuclear oocyte maturation in several species.
Keeping in mind that adrenal steroidogenic pathways areregulated much like those in the ovary, it is intuitive tohypothesize an effect of metformin on adrenal androgenproduction, too. In PCOS patients, 1 month of metforminadministration-regulated adrenal enzyme activities by re-ducing the ratio of 17�-hydroxyprogesterone to progester-one, which indicates 17�-hydroxylase activity, and the ratioof androstenedione to 17�-hydroxyprogesterone, which in-dicates 17,20-lyase activity (88).
On the other hand, the effect of metformin on hyperan-drogenism could also be due to a direct effect of metforminon LH secretion. In particular, metformin administrationmodulates LH secretion, decreasing LH pulse amplitude butnot pulse frequency (89). In this regard, it has been suggestedthat metformin acts at the hypothalamic level on AMPKpathway. Hypothalamic AMPK is a key regulator of foodintake in mammals, even if its role in reproduction at the
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 7
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

central level is unclear (54). In the rat model, metforminincreases in a dose-dependent and time-dependent way theAMPK activation by phosphorylation at Thr172 in GnRHneurones and, thus, the modulation of GnRH release (54).
Lastly, some metabolic hormones, such as adipokines(leptin, resistin, adiponectin) and ghrelin, which are in-volved in the control of the reproductive functions at thehypothalamus-pituitary-gonadal axis level (90) and of sev-eral processes of tumorogenesis (91), might act throughAMPK signaling (92). Thus, AMPK could be not only oneof the signaling pathways controlling the interactions be-tween energy balance and reproduction and/or tumoro-genesis, see also Section VII, but also a pivotal link ex-plaining the effects of metformin at the central level. Inother words, metformin could act on hypothalamicAMPK, exerting both a direct effect and an indirect effectvia paracrine/endocrine action of adipokines and ghrelin.
In conclusion, even if no study has currently demonstrateda cause-effect relationship for metformin effectiveness orexcluded its other mechanisms of action, the beneficial effectsof this drug on reproductive and nonreproductive parame-ters are seen only in association with a reduction in circu-lating insulin levels, consistent with the hypothesis that thisis the main mechanism by which metformin acts in patientsaffected by PCOS. Furthermore, it is possible that metforminmight also act by other parallel mechanisms not necessarilyimplicated with insulin resistance. In fact, several experi-mental data suggest an indirect effect of metformin by ovar-ian (and adrenal) steroidogenesis suppression and/or a di-rect cellular action by AMPK signaling.
C. Pharmacokinetics
The pharmacokinetic properties of metformin have beenevaluated in patients with type 2 DM and in healthy vol-unteers by using oral and iv preparations, although met-formin is always administered orally in clinical practice.Metformin pharmacokinetics has been described as a two-compartment open model with first-order absorption (93).It has an incomplete gastrointestinal absorption rangingfrom 20 to 30% (93). Absorption is complete within 6 hfrom administration and is slower than the elimination;thus it represents the phase that determines the drug’sdisposal rate (93). Metformin has been shown to have adose-dependent absorption in humans (93). Furthermore,the absorption is proportionally greater for a dose of 0.5 gthan for 1.5 g (93). In fact, transport occurs almost exclu-sively via the paracellular route (90%), and this transportis saturable (94).
The bioavailability of metformin is limited to 50–60% be-cause the amount available may result from presystemicclearance or binding to the intestinal wall (93). After absorp-tion of 1.5 g of metformin, a linear pharmacokinetics of met-formin was reported in both diabetic and nondiabetic sub-jects (93).
Once absorbed, metformin is rapidly accumulated in theesophagus, stomach, duodenum, salivary glands, and kid-neys. No binding with plasma proteins was reported; how-ever, a slight association with blood cells was hypothe-sized (93).
Metformin is not metabolized but is excreted by the kidneywith a mean 4- to 8-h half-life in healthy volunteers (93).Ranges of values for kidney and total clearance are reportedto be 20.1–36.9 and 26.5–42.4 liters/h, respectively (93), in-dicating active tubular secretion of the drug.
Metformin freely passes the placenta by a carrier thattransports cationic compounds bidirectionally, with ahigher transfer rate from the fetal to the maternal com-partment (95), resulting in the exposure of the fetus tometformin therapeutic concentrations (96). Furthermore,no effect on human placental glucose uptake or transporthas been demonstrated (97).
The concentrations of metformin in breast milk are gen-erally low. The mean infant exposure to metformin wasreported to be in the range 0.28–1.08% of the weight-nor-malized maternal dose, well below the level of concern forbreastfeeding (98).
The metformin pharmacokinetics can be influenced byseveral factors. In a rat model, metformin pharmacokineticschanges according to insulin resistance and/or presence/absence of streptozotocin-induced DM with significant vari-ation in hepatic and renal clearance (93). On the contrary, nodifference in metformin disposition seems to be present inpatients with type 2 DM or by using different oral prepara-tions (93). Coadministration of food was reported to decreaseslightly the rate of metformin absorption (93). Drug inter-actions have also been reported: coadministration of guargum was reported to interfere significantly with metforminabsorption, �-glucosidase inhibitor acarbose significantly re-duces the bioavailability of metformin (99), and histamineH2-receptor antagonist cimetidine has a competitive actionon renal tubular secretion (100). Excretion is prolonged inpatients with renal impairment and correlates with creati-nine clearance (93). Metformin is transported by at least twoorganic cation transporters (OCTs), OCT1 and OCT2 (101).These OCTs are saturable in the rat model (102), and geneticpolymorphism in these transporters was found to be asso-ciated with changes in pharmacokinetics and pharmacody-namics (103). In addition, genetic variants of the geneSLC22A2 encoding for the organic OCT2 protein result in areduced renal clearance and, thus, in increased metforminplasma concentrations (103).
D. Therapeutic regimens
Metfomin is available in two formulations: immediate andextended-release. Metformin at immediate-release is com-mercialized as 500-, 850-, and 1000-mg tablets, whereas thedrug at extended-release is available as 1000- and 2000-mgtablets.
Metformin is indicated in patients over the age of 10 yr,and the extended-release preparation is indicated in thoseover the age of 17 yr.
An extremely variable target dose of 1500 to 2550 mg/dwas proposed. A dose-finding study (104) showed that met-formin, at the upper limit of 2000 mg/d, had maximal benefitin lowering plasma glucose and glycated hemoglobin in di-abetic patients. However, to date, no dose-finding study isavailable for a PCOS population, probably due to the clinicalend-points used to test the effectiveness of metformin ad-
8 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

ministration, which are various, and their intercorrelationsare unknown.
Therapeutic regimens of metformin administration are notwell standardized in clinical practice, and heterogeneous pro-tocols were used in the various studies available in literature.
To minimize the drug-related adverse effects (see SectionI.E), metformin is best taken on an empty stomach, startingwith a low dosage and gradually increasing over a period of4–6 wk. Nestler et al. (105, 106) suggested administeringimmediate-release metformin initially at a low dose at meals,beginning with 500 mg at dinner for 3–4 d, and then in-creasing by 500 mg every 3–4 d up to a maximal dosage of1000 mg twice daily.
Extended-release metformin is usually taken with theevening meal and the only suggestion to minimize potentialadverse affects is to divide the tablets into two administrations.
Previous data on patients with type 2 DM seemed to havedemonstrated that the extended-release preparation may beless efficacious in women with PCOS than the immediate-release metformin (107). Furthermore, this result was notconfirmed in a recent study (108) in which the extended-release preparation had similar efficacy at glycemic controlto the immediate-release form. In addition, in a multicenterRCT (109) on 150 Chinese patients with type 2 DM, no sig-nificant differences were found between the extended- andimmediate-release metformin formulation. In particular, theextended-release metformin administered at a daily dosageof 1500 mg was similarly effective as the immediate-releasemetformin at a 500-mg dosage three times daily (109). Asignificant difference between the two formulations was ob-served only for postprandial glycemia at 120 min, in favor ofthe immediate-release formulation (109).
Almost all published studies including PCOS patientsused metformin in immediate-release preparation; how-ever, in a recent RCT (110), PCOS patients were treatedwith the extended-release formulation (1 g twice daily). Inthat trial (110), there were significant decreases in BMI andtotal testosterone levels and significant increases in SHBGlevels with extended-release metformin, whereas no sig-nificant change in fasting markers of insulin resistance wasobserved.
A dose-response effect of immediate-release metformin inobese women with PCOS was suggested (111). In fact, fastingmarkers of insulin resistance did not change when 500 mg ofthis formulation was administered three times daily but im-proved when 850 mg of immediate-release metformin wasgiven three times daily.
Thus, different metformin preparations might have dif-ferent efficacy in PCOS.
In addition, most RCTs of ovulation induction in PCOSpatients used 1500–1700 mg/d, which could be a suboptimaldosage, rather than maximal doses of immediate-releasemetformin (30, 112).
The length of metformin treatment in PCOS patients is notstandardized. Although, several evidences (113) support theefficacy at the metabolic level of metformin treatment for alimited time in insulin-resistant PCOS women, it is still un-known whether metformin administration should be con-sidered as a symptomatic treatment or as a curative anddefinitive therapy. Thus, it is not clear for how long met-
formin should be administrated and which are the effects itmay have on insulin sensitivity at treatment suspension afterits short- or long-term administration.
A recent study (114) on infertile PCOS patients under-going in vitro fertilization (IVF) demonstrated that met-formin pretreatment did not affect androgen levels. Fur-thermore, within 36 h after metformin withdraw, anincrease in androstenedione and free-testosterone indexwas observed.
Our previous data (115) on a non-insulin-resistant PCOSpopulation showed that, after a long-term metformin treat-ment, drug suspension is related to a quick reversion of itsbeneficial effect on peripheral insulin sensitivity. In fact, aslightly, but significant, worsening of the insulin resistanceand hyperandrogenic state was observed in comparison withbaseline and with patients who received placebo, even if noPCOS patient developed IGT or DM at 12 months frommetformin suspension. In the same study (115), the quick lossof beneficial effects due to metformin on insulin resistanceand subsequently on hyperandrogenism after metforminsuspension seemed to be related to a worsening of menstrualcyclicity. In agreement with these findings, previous data(116) showed that the withdrawal of metformin treatmentseemed to be followed within 3 months by a significantreversal toward a pretreatment hyperandrogenic hyperin-sulinemic state in 10 nonobese adolescents with hirsutism,oligomenorrhea, dyslipidemia, and a history of precociouspubarche. However, because time could be considered aconfounding factor on the clinical evolution of PCOS, furtherdata on a wide sample, a long-time follow-up, having as itsprimary aim the evaluation of the effect of the time on ovar-ian function, and the clinical features in PCOS patients arenecessary to draw definitive conclusions.
Finally, because recent data seem to suggest that met-formin is more effective in insulin-resistant PCOS patientswith low BMI (see Section I.F), metformin dose should prob-ably be adjusted according to the patient’s BMI and insulinresistance (117). Unfortunately, no model is currently vali-dated to calculate the right dose according to these charac-teristics. From a clinical point of view and based on ourclinical experience, we suggest that it is appropriate anduseful to administer metformin in a slow and increasingmanner up to a maximal tolerated dosage (117).
E. Adverse effects
For several decades, metformin has been used worldwideto treat type 2 DM, and, during the last few years, severalstudies have been performed on women with PCOS usingmetformin. Thus, the safety profile of metformin is wellknown.
Potential side effects of metformin are listed in Table 1.In a recent meta-analysis (118), the rate of discontinuation
for adverse events in therapy-naive PCOS patients receivingmetformin, clomiphene citrate (CC), or both for anovulatoryinfertility was analyzed. Metformin and CC showed a similareffect on the discontinuation rate for adverse events [oddsratio (OR), 0.71; 95% confidence interval (CI), 0.22 to 2.25; P �0.765] with homogeneity data (118). In fact, the discontinu-ation rate for adverse events was similar between treatments
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 9
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

in studies of both Palomba et al. (119) (2.0% for each treatmentarm) and Legro et al. (110) (1.9 vs. 2.9% for CC and metformingroups, respectively), whereas no dropout for drug-relatedside effects was observed in the study by Zain et al. (120). Onthe other hand, when data obtained from studies comparingthe combination of metformin plus CC vs. CC alone (110, 119,120) were pooled, no significant effect of metformin on dis-continuation rate for adverse events (OR, 0.23; 95% CI, 0.04to 1.24; P � 0.096) was observed, even if a significant het-erogeneity was detected (118). No difference in the discon-tinuation rate for adverse events was recorded between treat-ments in studies by Legro et al. (110) (3.3 vs. 1.9%,respectively) and by Zain et al. (120) (no patients in bothgroups), whereas the study by Moll et al. (121) reported asignificantly higher adverse events rate in patients treatedwith combination therapy (16.2 vs. 5.3%, respectively). Fi-nally, no significant difference between metformin plus CCand metformin alone was observed in the discontinuationrate for adverse events (OR, 0.86; 95% CI, 0.23 to 3.04; P �0.993) (110). These data were homogeneous because nodifference in the discontinuation rate for adverse eventswas noted between treatments in both studies analyzed[3.3 vs. 1.9% for the Legro et al. study (110), and no case forthe Zain et al. study (120)].
1. Common side effects. Metformin is generally a well-tolerateddrug. A significantly increased incidence of nausea, vomit-ing, and gastrointestinal distress was reported in womenwith PCOS under metformin treatment (30, 110). In partic-ular, gastrointestinal symptoms are the most frequent drug-related adverse events occurring in about 30% of patientstaking metformin, limiting the compliance to treatment.
The rate of gastrointestinal side effects seems to be lowerwith the use of the extended-release formulation (122), butclear data are still unknown because the studies in which thiskind of formulation is used are very few. In the meta-analysisby Lord et al. (30), four trials (123–126) reporting details aboutside effects of metformin were analyzed. In all studies, met-
formin at immediate-release formulation was used, whereasthe treatment duration varied from 6 wk (125) to 12 wk ormore (123, 124, 126). Metformin caused a significantlyhigher incidence of nausea or vomiting (OR, 3.84; 95% CI,1.07 to 13.81; P � 0.05) and other gastrointestinal distur-bances (OR, 4.40; 95% CI, 1.82 to 10.66; P � 0.003). Successively,RCTs reported a rate of adverse events ranging from 7.9% (120)to 22.2% (119) in patients treated with immediate-release met-formin. On the other hand, a recent trial (110) showed a goodsafety profile of the extended-release formulation with an in-cidence of serious adverse events of 1.0%, whereas other ad-verse events ranged from 3.3% (anovulatory bleeding) to 66%(nausea).
In all cases of drug-related side effects, the dose should bereduced until symptoms disappear. Patients with intoleranceto metformin could benefit from the extended-release for-mulation, albeit given in divided doses.
2. Rare side effects. Serious adverse events are rare with met-formin administration.
Metfomin toxicity is manifested at a concentration of 100�g/ml or higher, but in vivo data showed plasma levels ofmetformin less than 5 �g/ml, even at maximum dosage.Moreover, cases of metformin overdose have also been re-ported in literature (127). Aggressive supportive care canresolve, without sequelae, potentially lethal metabolic alter-ation also in patients with serum metformin levels higherthan 100-fold in the therapeutic range (127).
Lactic acidosis is a rare complication of metformin admin-istration (5.1 cases per 100,000 patient-years) (128), even if,when it occurred, a mortality of 50% was detected. This riskincreases in patients with hepatic or renal impairment, car-diac or respiratory insufficiency, severe infection, or alco-holism, conditions that are, in themselves, associated withhypoxia and lactic acidosis (129, 130).
Almost all data on lactic acidosis in patients who receivedmetformin pertained to type 2 DM; nonetheless, even if nopublished reports on lactic acidosis with metformin therapyin women with PCOS are currently available, it can be as-sumed that this complication represented a very rare drug-related side effect in this specific population because thePCOS subjects are generally young and without other majormedical conditions.
A recent subanalysis of the Fremantle Diabetes Study, awide longitudinal observational study, confirmed that lacticacidosis incidence in type 2 DM patients is very low, but itincreases in older patients with a long duration of DM, thosewith the highest prevalence of cardiovascular and renal co-morbidities (131). Unfortunately, current risk determinantsfor metformin-associated lactic acidosis are largely disre-garded for patients with type 2 DM (132). Thus, appropriatecaution must always be taken in patient selection to avoidthis rare but potentially fatal side effect. A meta-analysis ofRCTs on metformin use in patients with type 2 DM confirmsthat this adverse event does not occur if precise precautionsare followed and if the drug is not administered to individ-uals with compromised renal or hepatic function (128). Fur-thermore, severe lactic acidosis can also be associated withhigh doses of metformin, i.e., higher than 3000 mg/d, in
TABLE 1. Metformin-related side effects
Rare side effectsSevere/serious
Lactic acidosisLiver failure
Slight/moderateChest painCoughMouth metallic tasteNail changesRashRunny noseSneezingSkin flushingAlopecia
Common side effectsAbdominal discomfortBloatingConstipationDiarrheaFlatulenceHeartburnIndigestionNauseaVomiting
10 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

patients with no known contraindications for metformin pre-scription (133).
Symptoms of metformin-associated lactic acidosis are un-specific, and physicians should be aware that metformin, ifprescribed in patients with renal impairment, can cause fatallactic acidosis due to drug accumulation (134). Symptomsand signs of lactic acidosis are abdominal pain and psy-chomotor agitation; the physical examination always revealssigns of poor perfusion. Laboratory evaluation shows hy-perkalemia, elevated creatinine and blood urea nitrogen, andmild leukocytosis, whereas arterial blood gases show severelactic acidemia. More rarely, renal impairment could be theonly alteration present in patients with metformin-in-duced lactic acidosis (134). The management of this severeadverse event consists of intensive care by use of vaso-pressor and ventilatory support and continuous veno-venous hemodiafiltration.
The available data regarding the deleterious effect of met-formin in patients with kidney disease are extremely limited,even if it is reasonable that metformin could be used at fulldosage in patients with a glomerular filtration rate (GFR) of60–90 ml/min (135). The doses should be reduced accordingto GFR with particular regard for patients with a GFR from30–60 mg/min, even if using the same caution as with anykidney-excreted drug (135). Lastly, metformin should not beadministered to women if serum creatinine is above 1.4mg/dl for women (135).
Because metformin may cause malabsorption of vitaminB12, patients on metformin should be monitored for signsand symptoms of vitamin B12 deficiency, including numb-ness, parasthesia, macroglossia, memory loss, and behav-ioral changes. Vitamin B12 deficiency can also lead to thedevelopment of pernicious anemia (106).
Metallic taste in the mouth is less frequently observed.Great attention should always be given to those subjectsundergoing treatment with different medications (136) orcontrast media use (137) due to the risk of acute kidneydysfunction and lactic acidosis. In this regard, acute renalfailure from contrast medium in patients taking metforminwas described (138).
A case of hepatitis after metformin administration wasdescribed as a likely rare idiosyncratic reaction with highserum transaminases and intrahepatic cholestasis (139). Inliterature, case reports describing very rare drug-related sideeffects, such as autoimmune neutropenia in a patient withlymphoma, are also available (140).
Osteoporosis could be another potential long-term ad-verse effect of ISD administration in patients with type 2 DM,a population notoriously known to have poor bone mineraldensity and/or quality. A subanalysis from the DiabetesOutcome Progression Trial (141) showed an increased frac-ture rate at 5 yr after rosiglitazone. Furthermore, metforminseemed to be safer than rosiglitazone, with a fracture rate ofabout half (7.3 vs. 15.1% for metformin and rosiglitazone,respectively). In fact, metformin seemed to have a directosteogenic effect on osteoblasts in culture, which could bemediated by activation/redistribution of phosphorylatedERK and induction of endothelial and inducible nitric oxidesynthase (NOS) (142). Contrarily, a case-control study (143)tested the effect of oral hypoglycemic treatments on bone
fractures in a population of diabetic patients demonstratingno significant association between fractures and metforminadministration.
Among very rare adverse events cited in literature, a caseof acute alopecia due to metformin treatment in a PCOSpatient was also reported (144).
3. Adverse effects on pregnancy evolution. Several authors stud-ied pregnancy outcomes in PCOS patients who receivedmetformin for ovulation induction (145). To date, metforminis still found in the B classification for USFDA pregnancycategory (31). This means that no teratogenic effect was dem-onstrated in animal models, and human safety studies arenot adequate. In fact, metformin has been tested in rat andrabbit models at doses up to 600 mg/kg�d, about 2- to 3-foldthe maximum recommended in humans according to bodysurface (31). On the other hand, a recent wide clinical trialconfirms that metformin alone or with supplemental insulinis as safe as insulin alone in patients with gestational DM(146).
To date, no teratogenic effects or adverse fetal outcomeswere reported from metformin when administered to preg-nant women with type 2 DM or gestational DM (147, 148),even if most treatments started after pregnancy had begun.
In 2006, a meta-analysis on metformin safety did not findany evidence for adverse pregnancy outcome in women un-dergoing treatment with metformin (149). More recently,another meta-analysis of eight studies focusing on preg-nancy outcome after metformin use in PCOS women con-firmed that there is no evidence of an increased risk for majormalformations (OR, 0.70; 95% CI, 0.11 to 4.39) (150). Not-withstanding these safety data, in clinical practice metforminis usually discontinued during pregnancy in women withPCOS who conceived while receiving the drug.
Currently, preliminary data on the use of metformin dur-ing pregnancy in patients with PCOS (151) seem to be reas-suring, suggesting also some beneficial effects on pregnancyloss reduction and pregnancy outcome improvement with-out affecting infant parameters (see Section IV). Also, a recentsemirandomized study (152) demonstrated the safety of themetformin administration during the first trimester of preg-nancy in regard to fetal growth and perinatal outcome inPCOS patients. In particular, no difference in major congen-ital malformations and in rate of babies admitted to theneonatal intensive care was observed between PCOS patientswho received metformin and those who did not (152).
F. Potential predictors
The beneficial effect of metformin might vary according tothe clinical characteristics of the patient to be treated. Thisconcern is even more important and complex in consider-ation of the different PCOS phenotypes (see Section I). Theknowledge of predictors for metformin response is crucialbecause their identification could lead clinicians to the bestindividualized treatment to improve metformin’s efficacy inoptimizing the safety profile (153).
1. Body weight. Some studies demonstrated that metforminappears to benefit PCOS subjects irrespective of their weightor degree of insulin resistance (154, 155). A study including
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 11
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

lean, overweight, and obese PCOS patients observed that allthree groups of patients demonstrated a significant decreasein fasting insulin and homeostasis model of assessment(HOMA) index after 6 months of metformin treatment, ir-respective of their pretreatment degree of insulin resistance(154). Additionally, the overweight and obese groups dem-onstrated a significant decrease in AUC for insulin (AUC-insulin) response to an oral glucose challenge. In normal-weight PCOS patients, metformin significantly improvedinsulin sensitivity and the AUC for glucose (AUCglucose) toAUCinsulin ratio in comparison with both the baseline as-sessment and against a placebo group (115). Even in studiesperformed to examine the effects of metformin in PCOSpatients with normal weight and with normal insulin sen-sitivity, significant decreases in fasting insulin, AUCinsulin,and HOMA were observed (156).
Several other data have demonstrated that metformin im-proves insulin sensitivity and is effective in decreasing ovar-ian androgen production and serum androgen levels withovarian function restoration regardless BMI (84, 85, 157).
On the contrary, a recent subanalysis (117) of a previouslypublished RCT (112) comparing metformin vs. CC was per-formed considering both ovulation and pregnancy as re-sponse markers to the treatment. These data showed signif-icant differences in BMI and insulin RIs between ovulatoryand anovulatory patients and between pregnant and non-pregnant patients treated with 1700 mg/d metformin. Inparticular, lower BMI was more likely associated with anovulatory response.
This finding is consistent with previous data found inliterature (124, 158–163). Specifically, Maciel et al. (158) firstdemonstrated in a randomized controlled fashion that a6-month course of 1500 mg/d metformin decreased serumandrogens and fasting insulin levels and improved men-strual cyclicity significantly better in nonobese than in obesePCOS patients. Subsequent studies agreed that metformininduces more pronounced endocrine effects and improvesovulation (159, 160, 162), particularly in nonobese PCOSpatients. Legro et al. (162) confirmed that metformin efficacyin terms of ovulation was significantly and directly asso-ciated with BMI. In particular, the adjusted ORs for ovu-lation rate comparing patients with BMI lower than 30Kg/m2 and those with BMI ranging between 30 and 34 kg/m2
vs. patients with BMI equal to or higher than 35 kg/m2 were2.36 (95% CI, 1.65 to 3.36) and 2.05 (95% CI, 1.46 to 2.88),respectively (162).
To date, it is plausible to consider patients with high BMIas subjects with a possible suboptimal response to met-formin. Metformin dosage might be crucial for a good re-sponse and for treatment success (111, 164). PCOS patientswho did not respond at a specific daily dose of metformincould probably respond clinically if higher doses were to beused. In this regard, it would be useful to administer met-formin in PCOS patients at the maximal tolerated dosageaccording to their BMI. Regarding this issue, two RCTs (111,164) tackling the problem of metformin dose were recentlypublished. The first study (111) showed that obese PCOSwomen, but not morbidly obese women, responded to met-formin reducing insulin sensitivity and body weight in adose- and BMI-related manner, even if there was no signif-
icant difference between either the dose or obesity subgroupsin the menstrual response to treatment. The latter study (164)confirmed that greater doses of metformin are more effectivein reducing BMI and waist circumference in an overweightand obese PCOS population. Furthermore, no data presentlyevaluated the optimal dosage of metformin according topatient BMI with ovulation and/or pregnancy as primaryoutcomes.
2. Insulin sensitivity. Insulin sensitivity indexes differed be-tween ovulatory and anovulatory patients treated with met-formin (117). This finding may be explained by hypothesiz-ing that insulin resistance is a common but not an imperativefeature in PCOS and might play, independently from BMI,a pathogenetic role only in a subset of women (25). Only theseinsulin-resistant subjects would substantially benefit fromimproved insulin sensitivity induced by metformin.
This suggestive hypothesis is supported by the results ofother studies (126, 160, 165), even if some authors (124, 154,159, 166) failed to demonstrate a predictive value of insulinRIs for ovulation under metformin. In these studies (124, 154,159, 166), patients were probably insulin resistant, but themethods used for assessing insulin sensitivity were not verythorough. In addition, a peripheral insulin resistance that didnot reflect in abnormal serum insulin sensitivity indexesshould be hypothesized in these PCOS patients. On the otherhand, it is possible to hypothesize that some insulin-resistantPCOS patients, notwithstanding the improvement of insulinsensitivity induced by metformin, have a poor clinical re-sponse because other mechanisms of ovarian dysfunction,independent from insulin resistance, could be involved.
3. Hyperandrogenism. Some authors (124, 126) observed thatresponders to metformin were less hyperandrogenic thannonresponders. In particular, in a randomized, double-blindcontrolled study, Fleming et al. (124) compared the baselinecharacteristics of the subgroups that responded to metforminwith those patients who did not respond with establishednormal ovarian function. Responders to metformin treat-ment showed significantly lower testosterone and higherSHBG levels. Another randomized, double-blind, placebo-controlled study (126) showed significant differences be-tween responders and nonresponders to metformin treat-ment. Logistic regression analysis demonstrated that lowerserum androstenedione was an independent predictor forclinical efficacy of metformin because responders had sig-nificantly lower serum androstenedione. A lower free an-drogen index (FAI) (OR, 1.59; 95% CI, 1.17 to 2.18 for FAI �10 vs. FAI � 10) was detected as a predictive factor forovulation under metformin in another study (162).
These data were not recently confirmed (117), probablybecause all PCOS patients were hyperandrogenic at studyentry.
Chang et al. (167) showed that the insulin levels and thedegree of �-cell function measured by HOMA index arehighest in oligoovulatory women with PCOS who are bothhirsute and hyperandrogenic, compared with PCOS patientswho are either hyperandrogenemic or hirsute only. In thisregard, a greater improvement in (biochemical) efficacy was
12 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

observed among PCOS women who were both hyperandro-genic and hyperinsulinemic (161).
4. Waist-hip ratio (WHR). Moll et al. (168), in a subanalysis ofa previous RCT (121), showed a significantly different chanceof ongoing pregnancy between PCOS patients receiving met-formin who were subgrouped according to age and WHR. Inparticular, metformin was demonstrated to have a positiveeffect in women older than 28 yr and with high WHR, anegative effect in women younger than 28 yr regardless oftheir WHR, and no effect in women older than 28 yr and withlow WHR (168).
5. Genetic factors. Genetic factors may also modulate the ef-fectiveness of metformin in inducing ovulation, resulting ina nonsufficient response on the part of some patients. Al-though the molecular reason for the variability in responseto metformin is not clear, the possibility for a pharmacog-enomic approach to the use of metformin may emerge in thenear future (101).
As previously discussed, genetic polymorphisms in OCT1 and OCT2 were found to be associated with changes inpharmacokinetic/pharmacodynamic responses to substratedrugs. In addition, data from the Pregnancy in PCOS (PP-COS) trial indicated that a polymorphism of a serine-threo-nine kinase gene expressed in the liver and site of metforminaction, STK11 (previously cited as LKB1), was associatedwith a significantly decreased chance of ovulation in PCOSpatients treated with metformin (162). In particular, the Callele of a single nucleotide polymorphism in the STK11 genewas associated with a significantly decreased chance of ovu-lation in PCOS women treated with metformin (162). In fact,the percentage of patients who ovulated increased with thenumber of G alleles present (48 vs. 67 vs. 79% for womenwithout alleles, with one allele, or with two alleles, respec-tively). In addition, the adjusted ORs for ovulation rate com-paring the C/C and G/G genotypes to the G/G genotypewere both 0.30 (95% CI, 0.14 to 0.66) (162).
Lastly, due to the lack of population-based studies in lit-erature, it is not known whether ethnic background maymodify the effectiveness of metformin. In a study conductedon Chinese women (123), no improvement was noted aftermetformin in the ovulation rate despite the significantreduction of BMI, serum testosterone, and fasting leptinconcentrations. Moreover, these data were not confirmed(169), demonstrating the efficacy of metformin in the im-provement of menstrual cyclicity, fertility, hirsutism, andPCO morphology.
II. Menstrual Disorders
Menstrual dysfunctions affect a high number of PCOSpatients, ranging between 80 and 100% depending on thediagnostic criteria; up to 40% of women with PCOS-relatedoligoovulation were referred with a history of eumenorrhea(170).
The main complaints about menstrual disorders fromPCOS patients are absence or infrequency of menstrualbleeding. Furthermore, other subclinical menstrual changesare frequent in PCOS patients, such as intermittent anovu-lation and related dysfunctional uterine bleeding (171–173).
Several pathogenetic mechanisms were proposed (174–176), although hyperinsulinemia could play a central role(see Section I. B) (25).
Based on these considerations, Velazquez et al. (32) firstreported resumption of menstrual cyclicity in 21 of 22 am-enorrheic PCOS women. Since then, several uncontrolledstudies (45, 177, 179) and RCTs (180, 181) evaluated theeffects of metformin on the restoration of regular menses.
Findings obtained from uncontrolled studies (45, 177–179)demonstrated that metformin was effective in restoring reg-ular menses in approximately 62% of PCOS women witholigoamenorrhea. In addition, a significant improvement inthe menses frequency under metformin was reported in twoRCTs (180, 181), although in one study (181) the number orpercentage of women reverting to regular menstrual cycleswas not reported, whereas, in the other (180), insufficientdata for this calculation were provided.
More recently, in a meta-analysis (30) on ISDs in PCOSpatients, only one trial was reported to improve the men-strual pattern showing a significant effect for metformin (OR,12.88; 95% CI, 1.85 to 89.61; P � 0.01). In particular, in arandomized, double-blind, placebo-controlled fashion, theeffects on menstrual abnormalities of a 6-month course ofmetformin in a group of 23 PCOS patients with normalglucose tolerance (NGT) were evaluated (126). After treat-ment, subjects treated with metformin showed a significantimprovement in menses frequency, whereas no change wasobserved in those receiving placebo. Five women in the met-formin group vs. none in the placebo group had a substantialimprovement in their menstrual pattern during treatment. Inaddition, in subjects experiencing regular menses after met-formin, the improvement was observed within 3 monthsfrom the beginning of treatment. In an open, long-termfollow-up of the same study (126), the frequency of mensesper month per patient continued to improve significantlyover time during the metformin administration period. Spe-cifically, after a follow-up of about 1 yr [11.0 � 1.3 months(mean � sd); median, 8 months; range, 4–26 months) in 13patients, a complete regularization of the menses was re-ported, whereas four other patients experienced a strikingamelioration of their menstrual cycle abnormalities.
The beneficial effect of metformin on menstrual cycle iscommonly attributed to its effectiveness on ovulatory func-tion. Furthermore, it is not infrequent to observe discordancebetween menstrual and ovulatory cycles. For example,Moghetti et al. (126) assessed ovulatory function measuringserum progesterone in the luteal phase of 39 cycles in 10PCOS women experiencing regular menses after treatmentwith metformin, which resulted in the confirmation of only32 of these assessments (79%). These observations may in-dicate that the effectiveness of metformin on menstrual cy-clicity is probably secondary not only to an indirect effect onthe ovary but also to a direct effect on the endometrium (seeSection V).
Finally, a meta-analysis (182) showed that metformin wassignificantly less effective in improving the menstrual pat-tern in comparison with oral contraceptives (OCs) (OR, 0.08;95% CI, 0.01 to 0.45; P � 0.004). Furthermore, metformin andOCs were compared in only two trials by the same group ofresearchers (183, 184). The first study (183) showed a resto-
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 13
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

ration of menstrual cyclicity in 75 and 100% of obese womenwith PCOS treated with metformin or OCs, respectively. Ina successive study (184), the same authors confirmed thesuperiority in improving menstrual pattern of OCs in com-parison with metformin in nonobese women with PCOS (50vs. 100%, respectively).
Unfortunately, no trial assessed whether this more favor-able OC effect leads to a reduction in the long-term risk ofendometrial cancer compared with metformin and/or animprovement of the quality of life (QoL). On the other hand,controversial data (185–187) are available on the metabolicand cardiovascular risks in OCs users. In fact, clinical datasuggested that OCs (188, 189) reduce insulin sensitivity inwomen with PCOS. These observations, combined with theknown actions of OCs to reduce insulin sensitivity and in-crease triglyceride levels in unselected patients, have re-sulted in the concern that these drugs could have adversemetabolic effects in women with PCOS (185).
Presently, no prospective long-term studies of OC use inwomen with PCOS are available. A small observationalstudy (189) did not find adverse metabolic outcomes inwomen with PCOS using OCs and followed for 6–18 yr.
In a recent meta-analysis, the metabolic effects of met-formin were compared with OCs (190). Metformin was moreeffective at lowering insulin and triglyceride levels than OCs,whereas there was insufficient evidence to assess clinicalend-points such as hirsutism, DM prevention, and weightloss. Unfortunately, the studies carried out in this meta-analysis (190) were obtained from small sample groups atshort term, and few estroprogestin combinations were tested[frequently ethinyl estradiol (EE2) plus cyproterone acetate(CA) association].
Two further studies (186, 191) comparing metabolic find-ings in PCOS patients receiving either metformin or OCshave been published. Metformin improved fasting parame-ters of insulin sensitivity, although EE2 plus CA did notworsen these end-points (187). OCs containing 35 �g EE2plus CA increased the AUCinsulin and arterial stiffness,compared with metformin and 20 �g EE2 plus levonorgestrelwith 100 mg daily spironolactone (191). On the other hand,serum uric acid levels, a cardiovascular risk factor andmarker, were significantly reduced in PCOS patients takingOCs (35 mg EE2 plus 2 mg CA) with a potential action onhyperandrogenic milieu, whereas no significant change wasobserved after 1700 mg metformin (192).
In conclusion, as well elucidated recently in a vignette byNestler (106), metformin should be considered the first-choice drug for treating oligomenorrhea in PCOS patients inwhom OCs are contraindicated.
III. Anovulation
Anovulation or oligoovulation is the cause of infertility inabout 25% of cases (193). In turn, PCOS is the most commoncause of anovulatory infertility (194). Thus, the treatment ofinfertile PCOS patients presently represents a social and eco-nomic burden.
Considering that insulin exerts several effects in regulatingnormal ovarian activity in all its compartments and insulin
resistance seems to play a pivotal role in the pathogenesis ofinfertility in obese and nonobese women affected by PCOS,metformin administration can be assumed to have a bene-ficial effect. Metformin could act directly on the ovary. More-over, very few experimental and clinical data are actuallyavailable. An interesting case report has shown the efficacyof metformin in an underweight young PCOS patient witholigomenorrhea and hirsutism (195). This case suggests thatmetformin could act exclusively at the ovarian level, prob-ably by insulin sensitization in a way completely unrelatedto weight loss or lifestyle modification (195). On the otherhand, experimental data seemed to suggest further mecha-nisms. In fact, as already discussed, in rat model, metforminhas been shown to inhibit GnRH release by activation of hy-pothalamic AMPK, a crucial regulator of food intake in mam-mals, in a dose-dependent and time-dependent fashion (54).
To clarify the exact role of metformin in the therapeuticstrategy of ovulation induction, it is pivotal to distinguishseveral conditions in which PCOS patients could take ad-vantage of ISDs.
The first issue regards the treatment of therapy-naivePCOS patients. CC was the first agent used in experimentsfor ovulation induction in oligomenorrheic women. It rep-resented for many years the first therapeutic option foranovulatory infertility treatment for its effectiveness, lowcost, limited dose-dependent side effects, and simplicity inadministration and management (196, 197). Therefore, theefficacy of metformin compared with placebo, or no treat-ment, should be demonstrated first. After this, metformincould be considered as a valid first-step option for ovulatoryinfertility in PCOS, once efficacy and safety have been provento be superior to CC. Moreover, metformin could have anadditive effect when combined with CC as the first-stepapproach to PCOS patients.
The second issue is whether PCOS patients who remainanovulatory after CC (CC resistance) or even those whoovulate but do not achieve a pregnancy (CC failure) couldbenefit by metformin, administrated as a single agent, incombination with CC, or as pretreatment. In fact, metforminmechanisms are still not completely clear, and whether itcould have beneficial effects on the ovary and endometrium,improving the response to CC, is yet to be understood.
Lastly, some PCOS patients treated with CC and met-formin alone or in combination and not affected by concom-itant infertility (tubal or male) factors do not achieve preg-nancy and can only turn to IVF as a possible solution; forthese patients, the administration of gonadotropins is thelast therapeutic step (198). Unfortunately, it is well docu-mented that the response of PCO to gonadotropin stimula-tion differs significantly from that of normal ovaries. Thisresponse was defined as “explosive” and is responsible forthe significantly higher risks of cancelled cycles and/or forovarian hyperstimulation syndrome (OHSS) (199). Clinical(200) and experimental (201) studies suggested that hyper-insulinemia and insulin resistance could be responsible forthis abnormal response. Thus, PCOS patients receiving go-nadotropins for controlled ovarian stimulation or IVF couldbenefit from the administration of ISDs.
For the above-mentioned reasons, we have separately an-alyzed the use of metformin as a first- and second-line drug
14 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

in anovulatory infertile patients with PCOS and in PCOSpatients scheduled for gonadotropin therapy.
A. Metformin as first-step treatment
Several systematic reviews and a meta-analyses (202–207)have evaluated the efficacy of metformin in the treatment ofanovulation due to PCOS. The unanimous conclusion ofthese reviews (202–207) was that metformin monotherapyrepresents a safe and valid therapeutic option for the im-provement of ovulation in PCOS patients.
Two meta-analyses (203, 204) demonstrated that met-formin is an effective drug, when compared with placebo orno treatment, in the restoration of normal menstrual cyclesand in inducing ovulatory cycles in oligoamenorrheic PCOSpatients [OR, 3.88; 95% CI, 2.25 to 6.69; P � 0.00001 (203), andOR, 1.50; 95% CI, 1.13 to 1.99; P � 0.004 (204)]. However, interms of pregnancies [OR, 2.76; 95% CI, 0.85 to 8.98; P � 0.09(203), and OR, 1.07; 95% CI, 0.20 to 5.74; P � 0.9 (204)] andlive births [OR, 1.00; 95% CI, 0.13 to 7.79; P � 1.00 (204)],no advantages resulted from metformin administration incomparison with placebo or no treatment. These data weresuccessively confirmed showing an OR for a clinical preg-nancy rate of 3.3 (95% CI, 0.92 to 11; P � 0.07), whereas nodata were provided regarding ovulation and live-birthrates (206).
A recent meta-analysis of 17 relevant placebo-controlledRCTs for a total sample of 1639 PCOS patients (207) wasaimed at updating the state of evidence on the efficacy ofmetformin, used alone or in combination with CC, on ovu-lation, early pregnancy, and live births in PCOS patients withunknown resistance to CC. Even if the P values were notreported for any meta-analytic comparison, the pooled sta-tistical estimate for ovulation showed an overall benefit forPCOS patients receiving metformin over placebo (OR, 2.94;95% CI, 1.43 to 6.02) with a number needed to treat usingmetformin of 4.0 (207). On the other hand, metformin didnot have any effect on pregnancy achievement (OR, 1.56;95% CI, 0.74 to 3.33) or live births (OR, 0.44; 95% CI, 0.03to 5.88) (208). For both end-points, no significant hetero-geneity was detected between studies. The reason met-formin was not effective in improving fertility could berelated to the short-term follow-ups and/or small popu-lation samples studied.
To define the role of metformin as first-line drug foranovulatory infertility in PCOS patients, CC, the traditionalgold standard ovulation inductor agent for PCOS-relatedanovulation, was also compared with metformin.
A meta-analysis (206) aimed at evaluating the efficacy ofmetformin, CC, or both drugs in therapy-naive PCOS pa-tients demonstrated no significant clinical benefit from met-formin administration over CC as first-line therapy for ovu-lation induction in PCOS patients (OR, 0.88; 95% CI, 0.19 to4.1; and OR, 0.96; 95% CI, 0.11 to 8.2, for clinical pregnancyand live-birth rates, respectively). However, the results ofthis last meta-analysis (206) were biased by two main factors(208): first, some studies not assessing the live-birth rate,which should have been the primary end-point, and othersin which a metformin pretreatment was administrated, wereincluded in the final analysis; and second, the conclusions
regarding the comparison of metformin vs. CC were drawnusing data analyzed with fixed model effects, although asignificant data heterogeneity was detected in both preg-nancy and live-birth rates.
More recently, a systematic review and meta-analysis ofthe head-to-head RCTs available in literature was conductedto better define the efficacy of CC and metformin, alone orin combination, as a first-step approach in treating anovu-latory infertility in PCOS patients (118). In this regard, a totalof four RCTs (110, 119–121) satisfied the exclusion and in-clusion criteria and were analyzed (118). Furthermore, onlyone study (110) was powered to demonstrate a difference inlive births, whereas the others were powered on pregnancy(119) and ovulation (120, 121) rates.
In the study by Palomba et al. (119), the cumulative ovu-lation rate was similar in women treated with CC or met-formin (62.0 vs. 84.0%, respectively), whereas the pregnancyrate was significantly higher (32.0 vs. 62.0%, respectively)in women treated with metformin compared with thosetreated with CC. There was no statistical difference in livebirths (18.0 vs. 5.2%, respectively) in women treated withCC vs. metformin, although a trend favoring the met-formin group was present. The subsequent study by Legroet al. (110) reported markedly different results. In thisclinical trial, CC was superior to metformin in increasingcumulative ovulation (75.1 vs. 55.3%, respectively), preg-nancy (29.7 vs. 12.0%, respectively), and live-birth (22.5 vs.7.2%, respectively) rates. Lastly, in the study by Zain et al.(120), the cumulative ovulation rate was significantlyhigher in CC than metformin (59.0 vs. 23.7%, respectively),whereas no differences between groups were reported inpregnancies (15.4 vs. 7.9%, respectively) and live births(15.4 vs. 7.9%, respectively).
Pooling the data obtained from the studies comparingmetformin to CC (110, 119, 120), metformin did not exertsignificant advantage over CC with respect to cumulativeovulation (OR, 1.55; 95% CI, 0.40 to 5.99; P � 0.527), preg-nancy (OR, 1.22; 95% CI, 0.23 to 6.55; P � 0.815) or live-birth(OR, 1.17; 95% CI, 0.16 to 8.61; P � 0.881) rates. However,the most interesting findings were the significant hetero-geneity detected for all reproductive end-points. Severalpotential explanations were given to justify the disagree-ment regarding the comparison between metformin andCC (209). However, the main concern is probably the greatheterogeneity in the protocol used and in the populationsstudied.
Regarding treatment schedules and formulations, in thestudy by Palomba et al. (119), both treatments were admin-istered at fixed dosages to simplify the double-blind design.Furthermore, a subsequent study (112) by the same authorsdemonstrated a higher safety and effectiveness of CC treat-ment at incremental doses in a similar population; thus,results could be biased in favor of metformin (119). On theother hand, in three RCTs (119–121) an immediate-releaseformulation of metformin was used, whereas the PPCOSTrial (110) used, for the first time in PCOS patients, theextended-release formulation of metformin.
The diagnosis of PCOS-related infertility was controver-sial between studies. Different criteria were adopted to assesseventual tubal and sperm patencies considered as potential
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 15
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

subfertility factors. Fertility and subfertility tubal and malefactors formally excluded by appropriate testing in one study(119) were not evaluated in others (120, 121), whereas Legroet al. (110) excluded only patients with bilateral tubal abnor-malities and/or patients having a partner with a sperm con-centration less than 20 million per milliliter, regardless ofmotility or morphology. On the other hand, Moll et al. (121)used the 2003 ESHRE/ASRM criteria (2) to diagnose PCOS,even if the enrollment started before the validation and pub-lication of the criteria, suggesting that investigators per-formed a retrospective analysis on data prospectivelycollected.
The studied populations were very heterogeneous regard-ing the BMI distribution. In particular, Palomba et al. (119)excluded obese patients. It is well known that obesity ad-versely affects reproduction in PCOS patients (210) and met-formin may be more effective in nonobese than obese sub-jects (158); thus, the selection of a nonobese population mayhave contributed to the metformin efficacy in this study. Onthe other hand, no limitation for BMI was defined in the otherstudies (110, 120, 121) and the sd values of the BMI variedwidely, suggesting highly heterogeneous populations in-cluding a large proportion of obese and/or severely obesepatients. Furthermore, no information was given regardingeventual cotreatments frequently used by obese patients andpotentially influencing reproductive outcomes, such as ISDs,cholesterol-lowering drugs, dietary treatments, physical ex-ercise programs, or bariatric surgery (211–213).
In addition, although the RCTs were designed to evaluatethe best first-step treatment in inducing ovulation in anovu-latory PCOS patients, more than 50% of the population stud-ied by Legro et al. (110) was previously treated with ovulationinductors. This is critical because each specific treatmentmight influence response to the subsequent one as wellknown for CC, metformin, and OCs (214), and previoustreatment potentially results in the selection of “resistant”patients to the treatment or patients who ovulated undertreatment but did not conceive (treatment failure).
Whether the addition of metformin to CC could improvethe efficacy of CC alone was analyzed in a meta-analysis byMoll et al. (206). A significantly higher clinical pregnancy rate(OR, 1.9; 95% CI, 1.2 to 3.3) was observed in patients treatedwith metformin plus CC compared with those treated withCC alone, although a significant heterogeneity in treatmenteffect across the trials included in the meta-analysis wasreported (206). Seven RCTs comparing the combinationCC and metformin with CC in 985 infertile women withPCOS were included in the final analysis (206). Only threeof these RCTs reported data on live births. Furthermore,the meta-analysis of these last studies reported no signif-icant benefit on the live-birth rate of the combined therapy(OR, 1.0; 95% CI, 0.82 to 1.3; P � 0.74) and no significantheterogeneity in treatment effect (206).
By using a more strict criteria and updating of data foundin literature, three head-to-head RCTs (110, 120, 121) com-paring reproductive efficacy of metformin plus CC combi-nation vs. CC monotherapy in therapy-naive PCOS patientswere available. Metformin plus CC was no more effectivethan CC alone in inducing ovulation in the study by Moll etal. (121) (64.0 vs. 71.9%, respectively) and by Zain et al. (120)
(68.4 vs. 59.0%, respectively), whereas in the study by Legroet al. (110) the combination was significantly more effectivethan CC monotherapy (83.3 vs. 75.1%, respectively). Thepregnancy (39.6 vs. 45.6%, 38.3 vs. 29.7%, and 21.1 vs. 15.4%)and live-birth (18.9 vs. 26.3%, 26.8 vs. 22.5%, and 18.4 vs.15.4%) rates were similar between metformin plus CC com-bination and CC monotherapy in the studies by Moll et al. (121),Legro et al. (110), and Zain et al. (120), respectively. When thedata from these three studies (110, 120, 121) were combined ina meta-analysis (118), the metformin plus CC association wasshown to be no more effective than CC regarding rates ofovulation (OR, 0.84; 95% CI, 0.60 to 1.18; P � 0.360), pregnancy(OR, 0.85; 95% CI, 0.62 to 1.15; P � 0.326), or live births (OR, 0.99;95% CI, 0.70 to 1.40; P � 0.982). Of note, no significant heter-ogeneity was detected for all three parameters.
Presently, only two RCTs (118, 120) compared metforminplus CC with metformin alone. Both studies agreed in show-ing a clear advantage of combination therapy over met-formin alone in terms of ovulation rate (83.3 vs. 55.3% and68.4 vs. 23.7%, respectively). Conversely, Legro et al. (110)alone showed that the combination therapy was significantlymore effective than only metformin with regard to pregnan-cies (38.3 vs. 12.0%, respectively) and live births (26.8 vs. 7.2%,respectively), whereas no differences in pregnancies (21.1 vs.7.9%, respectively) and live births (18.4 vs. 7.9%, respectively)were observed in the study by Zain et al. (120). Pooling datafrom these last two studies (110, 120), metformin plus CC wasmore effective than metformin alone in inducing ovulation(OR, 0.23; 95% CI, 0.15 to 0.34; P � 0.0001), and no significantheterogeneity was detected (118). Similar results were ob-tained regarding pregnancy (OR, 0.23; 95% CI, 0.14 to 0.37;P � 0.0001) and live-birth (OR, 0.23; 95% CI, 0.13 to 0.40; P �0.0001) rates (118).
A main drawback in the design of the RCTs that assessedthe efficacy of combined CC plus metformin vs. CC (110, 120,121) or metformin (110, 120) alone was that metformin wasstarted either concurrently with (110, 120) or after only 1month (121) of CC initiation. Metformin has a slower onsetof action than CC; hence, the studies as such were uninten-tionally biased against demonstrating the value of the CCplus metformin combination.
Of note, multiple pregnancies occurred more frequentlyunder CC treatment (110), even if this result does not reacha statistical significance. In particular, 6.0% of patientstreated with CC and 3.1% receiving the combination therapyhad multiple births (110). On the other hand, only singletonbirths were observed under metformin alone (110, 120, 119).Assuming that the goal of infertility treatment is to achievea singleton gestation, it may be argued that CC is not quiteas successful as suggested by the data of the PPCOS trial(215). At the present time, only one case of multifetalpregnancy under metformin has been published (216).These data suggest that metformin may facilitate high-order pregnancies in predisposed patients who were pre-viously anovulatory.
Finally, a recent subanalysis (217) of the PPCOS trial (110)found that the distribution of the first ovulations occurringwith each CC dose was not different between patients undermetformin and those under metformin plus CC. Contrary toprevious studies (218, 219), this finding suggests that met-
16 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

formin does not benefit by the decrease in the CC doseneeded to induce ovulation in anovulatory PCOS women. Asstated by the same authors (217), the contrasting resultsfound in the PPCOS study population could be due to in-sufficient power, intrinsic differences in the subject popula-tions, use of extended-release formulation of metformin, andlack of a full effect of metformin due to an almost simulta-neous initiation of the two drugs. Certainly, the adherencewith metformin tables in the PPCOS trial was not the reasonfor the poor success rate observed in the metformin armbecause it was within acceptable limits and unrelated toovulation (220).
In conclusion, in anovulatory infertile therapy-naivePCOS patients, the combined approach of metformin plusCC is not better than CC or metformin monotherapy. On theother hand, the choice between CC and metformin as first-step treatment should be drawn considering also contingentcircumstances because of the lack of clear evidence.
B. Metformin as second-step treatment
Several studies were led to evaluate whether metformincan be effectively used as a second-step approach in thetreatment of anovulatory infertility in PCOS patients. In par-ticular, metformin was used as single agent (treatment), com-bined agent (cotreatment), and/or before other treatments(pretreatment).
1. Metformin as single agent. Only a few studies (123, 221, 222)addressed the potential role of metformin as a single agentin CC-resistant patients. In one RCT (123), 20 infertile CC-resistant patients with ultrasonographic evidence of PCOwere randomized to metformin or placebo. In this study, nobenefit of metformin over placebo was observed in ovula-tion, pregnancy, and live-birth rates. In particular, the risk forboth clinical pregnancies and live births in patients treatedwith metformin was calculated to be 0.50 (95% CI, 0.05 to 4.6;P � 0.54).
Palomba et al. (221) compared metformin as a single treat-ment with laparoscopic ovarian diathermy (LOD) in 120CC-resistant PCOS patients. No difference was present be-tween metformin and LOD in the ovulation rate (54.8 vs.53.2%, respectively), but significantly higher pregnancy (21.8vs. 13.4%, respectively) and live-birth (86.0 vs. 64.5%) rateswere observed. A successive meta-analysis (206) showed noevidence of difference in the clinical pregnancy rate (OR, 1.3;95% CI, 0.96 to 1.7; P � 0.09), whereas the live-birth rate wasstill higher after metformin (OR, 1.6; 95% CI, 1.1 to 2.5; P �0.02). However, metformin treatment was certainly not in-ferior to LOD and was about 20-fold less expensive than thesurgical ovulation induction (221).
2. Metformin combined with other treatments. The potentialeffects of metformin were assessed in PCOS patients receiv-ing other treatments. In particular, a great amount of dataregards the association of metformin plus CC, although sev-eral findings seem to show a role of metformin cotreatmentalso in patients that received aromatase inhibitors, otherkinds of ISDs, or surgical ovulation induction.
The efficacy of metformin cotreatment in CC-resistant pa-tients who received CC was evaluated in several studies
(203–207). Two meta-analyses (203, 204) agreed in demon-strating a significant benefit of metformin cotreatment incomparison with CC alone, even if a significant heteroge-neity was observed between studies included in both meta-analyses. In particular, in CC-resistant PCOS women, theaddition of metformin was demonstrated to be effective ininducing ovulation in the two meta-analyses by Lord et al.(203) (OR, 4.41; 95% CI, 2.37 to 8.22; P � 0.0001) and Kashyapet al. (204) (OR, 3.04; 95% CI, 1.77 to 5.24; P � 0.0005). In thesame manner, significant benefits of the combination therapyon pregnancy rate were demonstrated in both studies [OR,4.40; 95% CI, 1.96 to 9.85; P � 0.0003 (203); and OR, 3.65; 95%CI, 1.11 to 11.99; P � 0.03 (204)].
A successive meta-analysis (205), designed to assess met-formin coadministration as a second-step approach for CC-resistant PCOS patients, confirmed that metformin plus CCis significantly more effective than CC alone in terms ofovulations (OR, 6.82; 95% CI, 3.59 to 12.96; P � 0.00001), evenif a significant heterogeneity was demonstrated across stud-ies, and no data were provided regarding the effect on preg-nancy and live-birth rates.
Moll et al. (206) also compared metformin plus CC to CCalone and confirmed that metformin plus CC led to signif-icantly higher clinical pregnancy (OR, 5.6; 95% CI, 2.3 to 13;P � 0.0001) and live-birth rates (OR, 6.4; 95% CI, 1.2 to 34; P �0.03) without significant heterogeneity in treatment effectacross trials.
Recently, in the analysis of placebo-controlled RCTs only,Creanga et al. (207) showed a significant benefit of metforminover placebo in PCOS patients receiving CC in terms ofovulation (OR, 4.39; 95% CI, 1.94 to 9.96) and pregnancyachievement (OR, 2.67; 95% CI, 1.45 to 4.94) with a numberneeded to treat of 3.7 and 4.6, respectively. Furthermore, asignificant heterogeneity was detected between all studiesincluded in the analysis. Conversely, metformin did not haveany effect on live births (OR, 1.74; 95% CI, 0.79 to 3.86), andno significant heterogeneity data were present. Of note, insubanalyzing studies according to CC resistance, obesity,and duration of treatment, metformin was found to be morebeneficial than placebo among PCOS patients treated forshort periods and not CC resistant, whereas the benefits ofmetformin plus CC over CC were significantly higher inCC-resistant and obese PCOS patients (207).
The length of metformin administration is also a majorconcern. In fact, in meta-analytic studies (202–207), the ben-eficial effect of metformin could be diluted in time withlonger follow-up periods due to more time available forspontaneous ovulation in control group patients. On theother hand, short-course metformin (less than 4 wk) could bea suboptimal pretreatment period before beginning CC. Un-fortunately, there presently is no RCT assessing this aim, andthere is insufficient data to determine whether long-coursemetformin pretreatment, before initiation of CC for ovula-tory infertility treatment, is more effective than short-coursepretreatment (224).
The combination of metformin plus CC was demonstratedto be more effective than LOD in CC-resistant PCOS patientswith anovulatory infertility (225). In particular, metforminplus CC association was related to higher ovulation ratesthan LOD, even if no difference in the rates of pregnancies,
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 17
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

live births and miscarriages were detected between two pro-cedures (225).
The association of metformin plus letrozole, an aromataseinhibitor widely studied as an ovulation inductor for PCOSpatients, vs. metformin plus CC in CC-resistant PCOS pa-tients has been tested by Sohrabvand et al. (226) in a ran-domized controlled fashion. Serum estradiol (E2) levels andE2 levels per mature follicle were significantly higher in CCpatients without differences in mature follicles, ovulation,and pregnancy rates (226). However, endometrial thicknessand full-term pregnancies were significantly higher in pa-tients treated with metformin plus letrozole (226).
Metformin was also administrated in combination withrosiglitazone, an ISD afferent to the thiazolidinediones fam-ily, assuming that the combination of these two medicationscould have a greater effect on ovulation by modulating in-sulin sensitivity and insulin levels via different mechanisms.In a prospective study, 128 nonobese PCOS patients withnormal fasting and glucose-stimulated insulin levels wererandomized to receive metformin, rosiglitazone, or a met-formin plus rosiglitazone combination for 6 months (159). Nosignificant benefit of the rosiglitazone addition was detected,suggesting that the use of metformin plus rosiglitazone as-sociation is not presently supported by clinical evidence.Further studies are needed, given the selection biases of theenrolled population.
Finally, in one trial (222) 42 CC-resistant PCOS patientswere randomized to LOD followed by metformin or LODalone. Ovulation (86.1 vs. 44.6%) and pregnancy (47.6 vs.19.1%) rates were significantly higher in patients who re-ceived metformin. Furthermore, a successive meta-analysis(206) demonstrated no significant benefit in clinical preg-nancy rate (OR, 2.3; 95% CI, 0.82 to 6.2; P � 0.12) or live-birthrate (OR, 1.3; 95% CI, 0.39 to 4.0; P � 0.71) for the metforminadministration after LOD.
3. Metformin pretreatment. Several RCTs (113, 157, 219, 227–229) evaluated the efficacy of metformin pretreatment beforeCC in CC-resistant PCOS patients. Even if these studies werevery heterogeneous and were performed on small popula-tions, most of them (113, 157, 219, 227) seemed to suggest thatmetformin pretreatment improves the efficacy of CC inPCOS patients with CC resistance. In particular, one smallRCT (228) showed no beneficial effect on ovulation and preg-nancy rates after 3 months of metformin pretreatment, de-spite the improvement of insulin resistance and hyperan-drogenemia. On the contrary, other studies (113, 157, 219,227, 229) demonstrated that metformin pretreatment, alsowhen given in ultrashort protocols (227, 229), improvedCC response in terms of ovulation and pregnancy in CC-resistant PCOS patients. These findings support the ideathat decreasing insulin secretion while administering met-formin in PCOS patients facilitates the induction of ovu-lation by using CC (13).
C. Metformin in patients who receive gonadotropins
Metformin was also used in PCOS patients who receivedgonadotropins for inducing monoovulatory cycles or mul-tiple follicular development in IVF cycles. The effects of
metformin coadministration in patients who received go-nadotropins was the object of evaluation by two meta-anal-yses (206, 230).
1. Monoovulatory cycles. The first meta-analysis was pub-lished in 2006 by Costello et al. (230). Three RCTs evaluatingthe effect of metformin in patients who received gonadotro-pins for controlled ovarian stimulation were identified (230).Data obtained from the only available study showed thatmetformin does not improve ovulation rate during ovarianstimulation with gonadotropins (90 vs. 73.3%; OR, 3.27; 95%CI, 0.31 to 34.72; P � 0.33) (230). No significant metformineffect was observed regarding the improvement of preg-nancy rate during ovarian stimulation with gonadotropins(28 vs. 10%; OR, 3.46; 95% CI, 0.98 to 12.2; P � 0.05), whereasno RCT reporting live births as an outcome measure wasidentified. On the other hand, metformin was shown to besignificantly efficient in reducing the length of time forovarian stimulation while using gonadotropin [weightedmean duration (WMD) � �4.14 d; 95% CI, �6.36 to �1.93;P � 0.0002] and the total dose of FSH used (WMD ��425.05 IU; 95% CI, �507.08 to �343.03; P � 0.00001), evenif a significant heterogeneity was found between pooledstudies. Finally, no RCT reporting OHSS as an outcomemeasure was identified (230).
In updated literature, two RCTs (231, 232) evaluatingwhether metformin changes ovarian responsiveness in con-trolled ovarian stimulation cycles were recently published.The first RCT (231) on 70 nonobese insulin-resistant PCOSpatients who received a low-dose step-up gonadotropinstimulation protocol followed by timed intercourse or intra-uterine insemination demonstrated a significant effect ofmetformin in increasing the rate of monoovulatory cyclesand in reducing those of cancelled cycles. Furthermore, noeffect of metformin pretreatment and coadministration wasconfirmed in ovulation, cycle cancellation, pregnancy, abor-tion, live births, multiple pregnancies, or OHSS. The latterstudy (232) showed that metformin improved the endocrineprofile in insulin-resistant PCOS patients receiving gonad-otropins in a step-up protocol and confirmed that it facili-tated the monofollicular development during ovarian stim-ulation cycles. However, these findings also were includedin the Costello meta-analysis (230) as abstract.
Although the exact mechanisms by which metformin ex-erts its beneficial action remains unknown, the results ofprevious studies allow us to hypothesize that metformin actson the regulation of ovarian response to exogenous gonad-otropins improving insulin resistance. In fact, a reduction inserum testosterone and insulin levels in follicular fluid wasobserved after metformin treatment (233). Thus, the im-provement of the hyperinsulinemic and hyperandrogenicovarian environment might be crucial for a normal follicu-logenesis, homogeneous development, and responsivenessof follicles and atresia of the small cohort of follicles.
A more recent meta-analysis (206) on four RCTs demon-strated a pooled clinical pregnancy rate that was significantlyhigher when metformin was added to gonadotropins thanwith gonadotropins alone (OR, 1.7; 95% CI, 1.1 to 2.8; P �0.03). Furthermore, no significant difference in live-birth ratecould be proven (OR, 1.6; 95% CI, 1.0 to 2.9; P � 0.08). No
18 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

heterogeneity in treatment effect across trials was reportedfor either pregnancy or live-birth rate. In addition, metforminwas demonstrated to be effective in reducing multiple preg-nancies (OR, 0.26; 95% CI, 0.07 to 0.96), whereas no differencein OHSS (OR, 0.59; 95% CI, 0.17 to 2.1) was reported.
The lack of an effect of metformin on this end-point wasprobably due to the low incidence of OHSS during ovarianstimulation with low-dose step-up gonadotropin protocols(234). On the other hand, the employment of a step-up low-dose protocol tailoring the gonadotropin administrationseems to be a pivotal factor more and more in PCOS patientswho receive metformin because metformin coadministrationhas been shown to increase the incidence of multiple preg-nancies in patients who receive gonadotropins (235).
In conclusion, in patients who received gonadotropins astreatment for anovulation, metformin addition reduces theduration of gonadotropins administration and the doses ofgonadotropins required, and increases the rate of monoovu-lations, reducing the risk of cancelled cycles.
2. Multiple-ovulatory cycles for IVF procedures. Data obtainedfrom two meta-analyses (206, 230) seemed to suggest thatmetformin did not improve the efficacy of gonadotropinswhen it was prescribed in the context of adjuvant treatmentfor IVF cycles. In particular, Costello et al. (230) analyzed fourpublished RCTs and one trial published in abstract formatonly evaluating the effect of metformin addition to gonad-otropins in women undergoing IVF cycles. Metformin wasdemonstrated to have no significant effect on the number ofoocytes collected at IVF (WMD � 0.44; 95% CI, �0.98 to 1.86;P � 0.54), length of ovarian stimulation (WMD � �0.09 d;95% CI, �0.49 to 0.31; P � 0.66), pregnancy (34 vs. 29%; OR,1.29; 95% CI, 0.84 to 1.98; P � 0.25) and live-birth (36 vs. 22%;OR, 2.02; 95% CI, 0.98 to 4.14; P � 0.06) rates. No significantheterogeneity between studies for these last outcomes was re-ported. More recently, combining data from four RCTs, Moll et al.(206) confirmed previous results. Specifically, no significant dif-ferences in pregnancy (OR, 1.2; 95% CI, 0.85 to 1.6; P � 0.34) andlive-birth (OR, 1.5; 95% CI, 0.92 to 2.5; P � 0.10) rates in PCOSpatients undergoing IVF and treated with metformin were re-ported without significant heterogeneity between studies.
On the basis of these results, some authors concluded thatto date no adjuvant pretreatment in IVF cycles should besuggested in the clinical practice (236). Furthermore, in ahigh-risk population such as PCOS patients, metforminseemed to have improved the safety of gonadotropin admin-istration in IVF cycles. In fact, a significant decrease in the totaldose of gonadotropins used during IVF cycles (WMD ��290.42 IU; 95% CI, �450.34 to �130.51; P � 0.0004) and inOHSS risk (5.6 vs. 21.0%; OR, 0.21; 95% CI, 0.11 to 0.41; P �0.00001) was shown by Costello et al. (230), even if a significantheterogeneity across trials was reported. On the other hand,Moll et al. (206), pooling the data of the two RCTs who reportedmultiple pregnancy data, found no evidence of a significantbenefit of metformin on multiple pregnancy rate (OR, 0.93; 95%CI, 0.42 to 2.1), even if a significant reduced risk of OHSS infavor of metformin (OR, 0.33; 95% CI, 0.13 to 0.80) was detected.
In conclusion, metformin administration in infertile PCOSpatients scheduled for IVF cycles is useful to reduce theOHSS risk.
IV. Adverse Pregnancy Outcomes
Patients with PCOS have been shown to be at high risk ofpregnancy and neonatal complications. The specific effects of met-formin on miscarriage, gestational DM, PIH, PE, and poor infantoutcomes have been analyzed in the following paragraphs.
A. Miscarriage
An increased risk of miscarriage in PCOS patients afterspontaneous or assisted conception was reported up to amaximum of 30–50% (237), and the miscarriage rate seemsto be 3-fold higher in PCOS subjects than in healthy women(238). In addition, the syndrome was diagnosed in about40–80% of women with recurrent miscarriages (239, 240).
Unclear data explained the mechanisms underlying theincreased risk of miscarriage in the PCOS population. HighLH levels, hyperinsulinemia, hyperandrogenism, and hypo-fibrinolysis mediated by plasminogen activator inhibitor(PAI) activity could be involved alone or in combination.
Recent experimental findings (239, 240) showed that PCOSpatients have serum glycodelin and IGFBP-1 concentrationssignificantly lower during the first trimester of pregnancy,suggesting a deficient endometrial environment for implan-tation and pregnancy safekeeping. In addition, PCOS pa-tients who had miscarriages, when compared with patientswho did not, showed serum glycodelin and IGFBP-1 levelssignificantly lower during the third to eighth weeks andninth to 11th weeks of pregnancy, respectively (239). Gly-codelin is secreted by endometrial glands and acts by re-ducing the endometrial immune response against embryodevelopment (241). IGFBP-1 modulates adhesion processesat the feto/maternal interface (242) and hence may be im-portant in the periimplantation period. Besides being syn-thesized by the endometrium, IGFBP-1 is primarily synthe-sized in the liver, and insulin is known to inhibit hepaticIGFBP-1 production (170).
On the other hand, a microarray and PCR analysis ofoocyte cDNA revealed that normal and PCOS oocytes, whichare morphologically indistinguishable and of high quality,exhibit different gene expression profiles (243). Cluster anal-ysis suggested that androgens and other activators of nuclearreceptors may play a role in differential gene expression inthe PCOS oocyte (243). Several of these genes were associatedwith chromosome alignment and segregation during mito-sis/meiosis and/or early embryonic development, suggest-ing a potential role in the reduced developmental compe-tency of PCOS oocytes (243).
Considering the potential beneficial effects that metforminexerts at both systemic and local (endometrial, ovarian, em-bryonal) levels (see Section V.A), several authors (151, 244–248) suggested that metformin could play an important rolein abortion prevention.
In particular, metformin exerts systemic actions by reduc-ing body weight, insulin and PAI-1 levels (244, 248, 249),plasmatic endothelin-I (ET-1), androgen and LH concentra-tions (250, 251) and by increasing serum IGFBG-1 levels andglycodelin levels (240).
On the other hand, the success of implantation in humanreproduction is the result of endometrial and oocyte/embryo
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 19
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

factors. In this regard, metformin administration showedbeneficial effects on both factors involved. Particularly inPCOS patients, metformin improved the uterine artery bloodflow (28, 240) and several endometrial receptivity surrogatemarkers, as well as endometrial and subendometrial vascu-larization and endometrial pattern (28). Similarly, metforminnormalized the ovarian artery impedance and perifollicularand pericorpus luteum vascularization (28). Thus, metformincould induce a follicular development similar to that ob-served in healthy women, minimizing hypoxic damage andcytoplasmatic/chromosomal disorders related to poor vas-cularization (252), as observed in CC-stimulated ovulatorycycles (29), and improving the oocyte and embryo quality. Inthis regard, an interesting study showed that a 15-d met-formin pretreatment, at a dosage of 2000 mg/d, increased thehigh-quality embryos (37.8 vs. 24.3%), implantation (15.3 vs.6.2%), and pregnancy (38.2 vs. 16.7%) rates in CC-resistantPCOS patients who underwent in vitro matured oocyte treat-ment, confirming a potential beneficial role of metformin onoocyte/embryo factors, even if an effect of endometrial re-ceptivity cannot be excluded (254).
As already stated in Section I.B, experimental data dem-onstrated that metformin also acts by activating AMPK ingranulosa cells. In both bovine (55) and rat (56) granulosacells, metformin decreased steroidogenesis and MAPK3/MAPK1 phosphorylation through AMPK activation. Also inthe human granulosa cell line HGL5, cell viability and phos-phorylated protein kinase B/AKT and p44/42 MAPK ex-pression were significantly modulated by metformin prein-cubation (255).
Lastly, a very interesting experimental study (256) dem-onstrated that metformin also induced AMPK activationwithin the blastocyst, leading to improved insulin signalingand pregnancy outcomes. In fact, the preimplantation blas-tocyst stage embryo was demonstrated to be an insulin-sensitive tissue, responsive to insulin or IGF-I via the IGF-Ireceptor/translocation of GLUT-4 with an increased glucoseuptake (257). High insulin or IGF-I concentrations induced adown-regulation of IGF-I receptor (258) with consequentinsulin-stimulated glucose uptake reduction, intraembry-onic glucose levels dropping, and apoptosis triggering (257).Thus, the pregnancy outcome of these embryos transferredinto surrogate mice was poor (259). In the experimental de-sign, Eng et al. (256) exposed murine embryos to 200 nmIGF-I, by creating an experimental environment similar tothat observed in PCOS patients, and compared them to em-bryos cocultured with excess IGF-I plus metformin and em-bryos cultured in control media. Resulting blastocysts ex-posed to high IGF-I concentrations showed a decrease inAMPK activation and insulin-stimulated glucose uptake andan increase in the number of apoptotic nuclei (256). Con-trarily, blastocysts cocultured in metformin and excess IGF-Iwere similar to controls. In addition, the implantation rateand fetal size at d 14.5 were significantly lower among IGF-I-exposed embryos transferred into control mothers in com-parison with control embryos transferred into control mothers.However, these parameters were reversed by coincubationwith metformin and IGF-I before transfer (256).
Notwithstanding these hypothetical mechanisms bywhich metformin could reduce the abortion risk in PCOS
women, the findings from RCTs do not seem to support theuse of metformin in the preconceptional period concerningabortion risk reduction.
In particular, a recent meta-analysis (118) evaluating theeffects of CC vs. metformin or the combination of both drugsas first-line therapy in anovulatory PCOS patients seekingpregnancy, reported no significant difference in abortion riskwhen metformin was compared to CC (OR, 1.58; 95% CI, 0.77to 3.25; P � 0.219) and to CC plus metformin (OR, 0.47; 95%CI, 0.22 to 1.0; P � 0.069). No significant benefit of metforminaddition to CC over CC alone was also reported (OR, 0.74;95% CI, 0.43 to 1.26; P � 0.273).
More recently, a meta-analysis (260) of 17 RCTs, designedto clarify the role of preconceptional metformin administra-tion in PCOS patients, showed no significant overall effect ofmetformin administration on abortion rate on the entirePCOS population (OR, 0.89; 95% CI, 0.65 to 1.21; P � 0.452).When data were distinguished on the basis of treatment,again no significant effect of metformin on abortion rate wasobserved when compared either with CC (OR, 1.02; 95% CI,0.59 to 1.75; P � 0.941) or with no treatment or placebo intherapy-naive (OR, 0.76; 95% CI, 0.21 to 2.81; P � 0.683) andCC-resistant (OR, 1.43; 95% CI, 0.91 to 2.25; P � 0.125) PCOSpatients receiving CC. In addition, no significant effect ofmetformin on abortion risk was detected in patients treatedwith gonadotropins for monoovulation induction (OR, 0.84;95% CI, 0.24 to 2.95; P � 0.784) and for IVF cycles (OR, 0.96;95% CI, 0.40 to 2.34; P � 0.935).
On the other hand, encouraging data derived from retro-spective or prospective nonrandomized studies were ob-served. In fact, several authors experimented with the use ofmetformin during pregnancy showing a beneficial effect inreducing the incidence of pregnancy loss.
In a pilot study, Glueck et al. (244) firstly demonstrated thatPCOS women treated with metformin during pregnancy hada drastic reduction of spontaneous abortion when comparedwith historical outcome recorded in the same group ofwomen not receiving treatment in previous pregnancies (73vs. 10%). The same report (244) demonstrated that PAI ac-tivity was inversely associated with having live births, andit was speculated that the ability of metformin in reducingPAI activity was related to an improvement in the insulinresistance state and, thus, in abortion rate. This hypothesiswas subsequently confirmed (248). In particular, a subanaly-sis of a previous trial (221) showed a significant decrease inserum PAI-1 activity after metformin administration exclu-sively in women who had a favorable pregnancy outcome,whereas the serum PAI-1 activity was unchanged in womentreated with LOD and women receiving metformin whomiscarried (248).
A further retrospective study (246) showed a signifi-cantly lower rate of early pregnancy loss in PCOS womenwho received metformin during pregnancy in comparisonwith women who did not receive metformin (8.8 vs.41.9%). The reduction in the abortion rate was remarkableif considering the historical miscarriage rate in the samepopulation not treated with metformin in previous preg-nancies (8.8 vs. 70.6%). Also in this study (246), it wasproposed that the beneficial effect of metformin on an-
20 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

drogen levels and insulin sensitivity was a mechanism toexplain the reduced abortion rate.
Congruent with previous studies, Glueck et al. (261)showed in an observational report that metformin adminis-tration during pregnancy in PCOS patients was related to asignificant reduction in early pregnancy loss. The abortionrates in women taking metformin during pregnancy were5.4% in those who had never previously conceived, 24.0% inthose having a previous abortion, and 30.0% in those whohad previous live births without metformin. No difference inthe abortion rate was observed between patients who con-tinued metformin throughout pregnancy and those who in-terrupted treatment during the first trimester (261). This laststudy reached a power of 87%.
More recently, a prospective cohort study (262) was set upto determine the beneficial effects of metformin use duringpregnancy in patients previously diagnosed with PCOS. Anearly pregnancy loss was experienced in 11.6% of womenreceiving metformin throughout pregnancy and in 36.3% ofsubjects who discontinued metformin at the time of concep-tion or during pregnancy (OR, 0.23; 95% CI, 0.11 to 0.42; P �0.0001) (262).
A role for metformin could also be proposed in PCOSwomen with recurrent miscarriages, as suggested by a recentcase report (247) of an insulin-resistant PCOS woman whoreceived metformin successfully before and during preg-nancy. Recently, a placebo-controlled study on 29 PCOSwomen demonstrated that metformin administration, givenbefore and during pregnancy beyond the first trimester, re-duced significantly the abortion risk (15 vs. 55% for met-formin and placebo, respectively) in patients with an abnor-mal oral glucose tolerance test (263).
Finally, regarding abortion prevention, no definitive con-clusion on the efficacy of metformin administration duringpregnancy may be reached because well-powered double-blind RCTs having abortion rate as their aim are lacking.Currently, two protocols designed to evaluate the effects ofmetformin administration on pregnant women with PCOSare in a recruiting phase (264, 265); thus, before drawingdefinitive conclusions on the abortion risk in PCOS patientstreated with metformin, the results from these last RCTs (264,265) are needed.
B. Gestational diabetes
PCOS patients are likely to develop gestational DM in 20to 40% (266) of cases, whereas approximately 40% of womenwith gestational DM are likely to have underlying PCO mor-phology (267).
Meta-analytic data (268) demonstrated a significantlyhigher chance of gestational DM development in the PCOSpopulation (OR, 2.94; 95% CI, 1.70 to 5.08; P � 0.00001), evenif a significant heterogeneity between studies was detected.A subgroup analysis of five higher validity studies showedan OR of 3.66 (95% CI, 1.20 to 11.16; P � 0.02), but significantstatistical heterogeneity remained (268).
In this regard, metformin use during pregnancy has alsobeen advocated to reduce the risk of gestational DM inwomen with PCOS (269). The main mechanisms by whichmetformin could reduce the likelihood of developing gesta-
tional DM were: the reduction of preconceptional weight,insulin, insulin resistance, insulin secretion, and testosteronelevels, and the persistence of these effects during pregnancy(270). However, the effect of metformin on maternal andro-gen reduction in pregnant women was not confirmed in awell-designed RCT (271).
A randomized, placebo-controlled trial on a population of40 PCOS patients demonstrated that the rate of patients whofulfilled criteria for gestational DM at the eighth week ofpregnancy increased significantly at the end of pregnancy(from 20% to 40%), regardless of metformin administrationin this period (272).
In a combined prospective/retrospective, open-label, sin-gle center comparison (261), a significant reduction from 26to 4% in development of gestational DM in PCOS pregnantwomen under metformin, in comparison with previous preg-nancies not on metformin, was demonstrated. The rate ofgestational DM of the women who received metformin dur-ing pregnancy was similar to that observed in the generalpopulation (261). These encouraging results were confirmedin a subsequent series (245, 273) that demonstrated a sig-nificant reduction in risk for gestational DM in PCOSwomen taking metformin compared with those not takingmetformin.
In particular, in a prospective study Glueck et al. (245)showed that in PCOS subjects metformin use was associatedwith a 10-fold reduction in gestational DM. However, if thesefindings could be used to design a blinded RCT, 102 livebirths (51 randomized to metformin and 51 to placebo) strat-ified by age and BMI would be necessary to obtain a 95%chance for demonstrating that metformin significantly de-creases the development of gestational DM in women withPCOS (245). In a subsequent study (273), metformin plus dietregimen during pregnancy was demonstrated to be effectivefor primary and secondary prevention of gestational DM. Infact, gestational DM developed in 12% of metformin-treatedPCOS patients, in comparison with 30% of previous preg-nancies without metformin (273). In addition, in PCOS pa-tients affected by previous gestational DM, only 31% devel-oped DM in subsequent pregnancies on metformin (273).
One study found an increase in perinatal mortality indiabetic women receiving metformin compared with thosereceiving insulin or sulfonylureas (274). Moreover, thatstudy was biased by the presence of poorly controlled pre-gestational DM and other maternal comorbidities such as PE.
An overview (275) on the pharmacological management ofgestational DM concluded that data are inadequate to sup-port or refute the use of metformin in the treatment of ges-tational DM because metformin crosses the placenta andconsequently could be helpful or harmful to the developingfetus. Nonetheless, Moore et al. (276) showed no differencein glycemic control and neonatal outcomes in 63 women withgestational DM, not controlled for diet and exercise andrandomized to receive metformin or insulin. These findingshave been confirmed in the Metformin in Gestational Dia-betes (MiG) Trial (146). This is an open RCT on a widepopulation of women with gestational DM designed to eval-uate safety and efficacy of metformin compared with insulintherapy for gestational DM and having as its primary end-point a composite neonatal outcome (146). A total of 751
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 21
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

pregnant patients between 20 and 33 wk gestation wererandomized to metformin plus supplemental insulin when-ever they required suboptimal glycemic control or insulinalone. This trial confirms that metformin alone or with sup-plemental insulin is as safe as insulin alone in patients withgestational DM, demonstrating a higher satisfaction rate formetformin treatment (146).
C. Pregnancy-induced hypertension and preeclampsia
Women with PCOS have a greater risk of developing PIH(OR, 3.67; 95% CI, 1.98 to 6.81; P � 0.0001; and OR, 3.71; 95%CI, 1.72 to 17.49; P � 0.004, for total and high quality studies,respectively) and PE (OR, 3.47; 95% CI, 1.95 to 6.17; P �0.0001) than the general population (268).
The mechanisms underlying the increased risk for PIH andPE in PCOS patients remain unclear. However, our prelim-inary data showed that, similar to that observed in nonpreg-nant PCOS patients (28, 29), uterine artery resistance wassignificantly higher in PCOS women than in healthy controlsduring the first 12 wk of pregnancy. These findings could beinteresting, considering that pregnancy complications arealways characterized by a failure of normal trophoblasticinvasion and lack of uterine spiral artery remodeling leadingto a high-resistance uteroplacental circulation (277). In fact,a significant relationship between uterine artery Dopplerindexes and histological features of placentation in normaland preeclamptic pregnancies was observed (277), and anexperimental study (278) demonstrated an inverse relation-ship between vascular impedance of the uterine artery andpercentage of trophoblastic vessels.
Our preliminary data focused attention on the role ofmetformin in first phases of the implantation, showing thatmetformin administration during the first trimester of preg-nancy regularized the uterine artery RIs, and no differencebetween metformin-treated PCOS patients and healthy con-trols was observed. Thus, metformin in the first phases of thepregnancy might influence the trophoblastic invasion of thematernal decidua, myometrium, and blood vessels, allowinga successful placentation with consequent pregnancy out-come improvement. In agreement with our findings,Salvesen et al. (279) in a small RCT showed that metforminadministration in PCOS patients during pregnancy reduceduterine artery impedance between 12 and 19 wk gestation,and this was associated with reduced complication rate.
Unfortunately, few clinical data regarding the preventiveeffect of metformin in development of PIH and/or PE areavailable.
In preconceptional diabetic PCOS women treated withmetformin (270, 280), the incidence of PE was similar to thegeneral population and untreated PCOS patients. Further-more, women with pregestational type 2 DM treated withmetformin showed a higher prevalence of PE in comparisonwith women treated with insulin or sulfonylurea (281).
A RCT (279) assessing the potential benefit of metforminon maternal and fetal outcomes in 40 pregnant women withPCOS was recently published. Metformin administration re-duced, compared with placebo, pregnancy complicationssuch as preterm delivery before 32 wk, severe PE, or seriouspostpartum events (279).
In addition, data from a retrospective study (274) on di-abetic women suggested an increased rate of PE in womentreated with metformin compared with those treated withsulfonylureas or insulin during their pregnancies. How-ever, the groups in this study were not matched due to theretrospective nature of the study, and women who tookmetformin were more obese and had more poorly con-trolled DM, both of which are known as risk factors for PE.In addition, the excess perinatal mortality in the met-formin group in this study occurred in two subjects whohad poorly controlled DM and were noncompliant andtherefore cannot be attributed to metformin treatmentalone. In fact, these data were not subsequently confirmed(281), and metformin was shown not to be associated withPE in pregnant women with PCOS, appearing safe formother and fetus.
D. Poor infant outcomes
Unclear data are available regarding worse neonatal out-comes assumed in infants born to women with PCOS.
Pooling the data of all RCTs, a significantly lower neonatalbirth weight (WMD � �38.4 g; 95% CI, �62.2 to 14.6; P �0.002) was detected (268). However, when only higher va-lidity studies were analyzed, no significant difference wasfound (WMD � 26.5 g; 95% CI, �35.5 to 88.5; P � 0.40) (268).Similarly, no significant increase in the incidence of macro-somia (OR, 1.13; 95% CI, 0.73 to 1.75; and OR, 1.08; 95% CI,0.6 to 1.96, for total and high-quality studies, respectively)and neonates small for gestational age (OR, 1.16; 95% CI, 0.31to 5.12; and OR, 0.66; 95% CI, 0.05 to 7.91, for total andhigh-quality studies, respectively) was observed in PCOSpatients (274).
More recently, Bolton et al. (282) showed that metforminadministration throughout the first 12 wk of pregnancy isrelated to a lower incidence of neonates that are small or largefor gestational age, a lower risk of neonatal hypoglycemia,and fewer requests for iv glucose therapy.
No significant difference in incidence of neonatal malfor-mations was observed in PCOS patients (OR, 0.70; 95% CI,0.11 to 4.39) (268). However, a significantly higher rate ofadmission to a neonatal intensive care unit (OR, 2.31; 95% CI,1.25 to 4.26) and perinatal mortality (OR, 3.07; 95% CI, 1.03to 9.21) was observed among women with PCOS vs. controls(268). An increased perinatal mortality in women withtype 2 DM in treatment with metformin in comparisonwith those who received sulfonylurea or insulin was alsoreported (268).
The safety of metformin administration during pregnancywas evaluated by several authors, and all available studieswere in agreement that metformin use was not related to anyadverse fetal outcomes or congenital abnormalities.
These last data were confirmed by a meta-analysis (150)that showed no increased risk for major malformations whenmetformin is administered during the first trimester of preg-nancy (OR, 0.50; 95% CI, 0.15 to 1.60; P � 0.24).
Babies conceived during metformin administration hadgestational age, gestational length, head circumference, andbirth weight similar to those of normal gender-specific infantpopulations (280, 283). In addition, at routine 3- and 6-month
22 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

well-baby examinations, infants born to mothers with PCOStreated with metformin during pregnancy had normal motorand social development (280). These findings were con-firmed over the first 18 months of life.
The same authors extended their studies to investigategrowth and motor and social development in breast- andformula-fed infants born from metformin-treated PCOSwomen, demonstrating that metformin during lactation wassafe in the first 6 months of life (280).
In conclusion, to date no clear evidence is available re-garding a positive or negative effect of metformin adminis-tration on infant outcomes both during pregnancy andlactation.
V. Endometrial Abnormalities
Two main clinical concerns may be related to endometrialdysfunction in PCOS patients: first, endometrial receptivitymight be affected and, thus, the implantation impaired witha consequential increase in abortion risk; and second, the riskfor endometrial hyperplasia and cancer could be increased.In this regard, metformin administration may have, as de-tailed in Section IV.A, an impact on the endometrium, hy-pothetically both improving the potential for a successfulpregnancy implantation and reducing the long-term risks ofunopposed endometrial proliferation. Furthermore, beforeobtaining definitive and clinically valid conclusions, addi-tional research should be carried out.
A. Fertility implications
In human reproduction, endometrial receptivity is, in con-cert with oocyte/embryo factor, a pivotal factor for the im-plantation success (284). Several data seem to show thatPCOS patients have alterations of several surrogate end-points of endometrial receptivity. In particular, most PCOSpatients have endometrial vascularization, pattern, andthickness abnormalities (28, 29). An alteration of the expres-sion of various endometrial proteins has also been demon-strated (239, 240).
Anovulatory PCOS patients have an alteration in uter-ine vascularization (28, 29, 285, 286). In fact, at Dopplerultrasound, pulsatility index (PI) and RI values, two mea-sures of blood impedance inversely related to blood flow,were not only unchanged throughout the cycle (287) butwere also significantly higher in comparison with healthycontrols (28, 29).
Elevated impedance to blood flow in the uterine arteriesappears to be detrimental for endometrial receptivity (288–290). A high PI detected in the uterine arteries at the time ofimplantation predicts a poor chance of conception in spon-taneous and gonadotropin-stimulated transfer cycles, sug-gesting that uterine perfusion may be a pivotal factor for afavorable reproductive outcome (288–290). During IVF cy-cles, the implantation rate is decreased when uterine arteryPI is higher than 3.3–3.5 at the time of human chorionicgonadotropin administration (291). The reduction in uterineperfusion seems to be associated with a lower reproductiveprobability not only in patients affected by PCOS but also inpatients with unexplained recurrent abortion (292).
Interesting data (240) have demonstrated that metformintreatment enhanced uterine vascularity and blood flow inwomen with PCOS. More recently, it was confirmed thatmetformin has beneficial effects not only on uterine arteryblood flow (28, 240) but also on several surrogate markers ofendometrial receptivity. In particular, Palomba et al. (28)showed a significant decrease in subendometrial and endo-metrial vascularity in PCOS women, assessed as RI and/orPI and as number and/or areas of colored spots at comput-erized image analysis. In this regard, the evaluation of sub-endometrial vascularity seems to be a more accurate andsensible method for studying uterine receptivity (293).
Metformin increased the vascular penetration of the uterusin zones 3 (vessels penetrating the inner hypoechogenic areaof the uterine cavity) and 4 (vessels penetrating the layersurrounding the uterine cavity), zones corresponding to theendometrial layer (28).
Endometrial thickness was considered a marker for uter-ine receptivity and for pregnancy prediction with differentresults (294–296). Certainly, patients with a thick endome-trium have a higher pregnancy rate compared with thosehaving a thin endometrium, a minimum endometrial thick-ness being necessary for an effective endometrial receptivityand, thus, for pregnancy success (297). Furthermore, no effectof metformin monotherapy on endometrial thickness in com-parison with healthy women has been demonstrated (240,248). To the contrary, Kocak, et al. (223) demonstrated asignificant effect of metformin on endometrial thickness inPCOS women treated with CC.
Endometrial pattern is another critical factor influencingthe chance of pregnancy in spontaneous or drug-inducedcycles, and a triple-line pattern is associated with a signifi-cantly higher pregnancy rate (298). Fanchin et al. (299) dem-onstrated that endometrial echogenicity, studied using ob-jective methods as computer-assisted measurements, has asignificant relationship with implantation and pregnancyrates in IVF cycles, confirming that this parameter can beuseful to predict endometrial receptivity.
In this regard, PCOS women ovulating under metforminshowed a triple-line endometrial pattern in a percentage ofcases not different from those observed in healthy controls(28). Similarly, no difference in the high-grade pattern rate inthe midluteal phase was also observed between ovulatingPCOS patients under metformin and in healthy controls (28).
The mechanisms hypothesized for metformin action arevarious. Metformin can act directly and/or indirectly onendometrium.
A direct effect of metformin on endometrium via insulinaction can be hypothesized. In fact, insulin stimulates glucoseoxidation activity in the late luteal phase in human endo-metrium, suggesting its involvement in endometrial tissuemetabolic activities (300, 301). In addition, insulin receptorsare present at the endometrial level, reaching their maximalexpression in the secretory phase, further supporting thehypothesis that insulin directly influences endometrialgrowth by means of its mitogenic and metabolic effects (302).Finally, GLUT-1, a non-insulin-regulated transponder, is ex-pressed at endometrial levels in animals and humans (303,304), indicating the importance of glucose transport in theendometrium (304, 305). At this level, another insulin-de-
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 23
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

pendent transporter, GLUT-4, is also expressed and seems tobe regulated by body weight and insulin. Specifically, a re-cent experimental study showed that GLUT-4 expression isimpaired in PCOS patients, suggesting that in these subjectsinsulin resistance and hyperinsulinemia induce an inade-quate GLUT-4 expression, and thus a reduced glucose sup-ply. The consequences of this alteration could be responsiblefor the impaired endometrial receptivity, and metformincould be effective in endometrial functionality restorationthrough a direct effect.
The beneficial actions of metformin on the endometrium,and particularly on uterine vascularity, could be due to anindirect effect of the drug on serum androgen levels. In fact,it seems that insulin resistance did not play a key role inreducing uterine perfusion in a PCOS patient (307). On thecontrary, it is possible to suppose that metformin acts onuterine perfusion, reducing androgen levels and, thus, theirvasoconstrictive effect on vascular tissues (307).
In the endometrium of PCOS women, an altered modu-lation of the expression of the endometrial androgen recep-tors (ARs) is also present. Contrary to healthy women, anelevation in the endometrial expression of ARs during thelate luteal phase has been detected in PCOS women, and thiselevation seems to be strongly related to �3 integrin, a well-characterized biomarker of endometrial receptivity (308).The AR activation also seems to have a negative impact onthe expression of a homeobox gene, i.e., HOXA10, a geneimplicated in the endometrial plasticity during menstrualcycles and essential for endometrial receptivity (309).HOXA10, in fact, is significantly and inversely related totestosterone but is not regulated by insulin (310). Elevatedlevels of androgens, as observed in PCOS women, may havea detrimental effect on endometrial function via HOXA10modulation (310).
Jakubowicz et al. (240) showed that metformin increasedthe midluteal phase concentrations of serum glycodelin andIGF-I, two putative biomarkers of endometrial receptivity, 3-and 4-fold, respectively, and that this effect was related to thedecrease in androgen levels.
The beneficial effect of metformin on ET-1, a peptide syn-thesized in the vascular endothelial cells with vasoconstric-tive action, should be considered as another indirect mech-anism by which this drug acts on uterine vascularity. ET-1 isexpressed in human endometrium (311) and inversely re-lated to plasma E2 levels (312), suggesting that ET-1 and E2could operate in concert to modulate endometrial bloodflow. Clinical data demonstrated that in PCOS women thereare increased concentrations of serum ET-1 (313) and thatmetformin administration improves this alteration (251).
B. Cancer implications
An association between PCOS and endometrial carcinomawas first suggested in 1949 (314). Although another study(315) quoted a 37% prevalence of endometrial cancer, suc-cessive studies (316, 317) obtained controversial data prob-ably due to several confounding factors.
Coulam et al. (317) calculated a relative risk (RR) of 3.1 todevelop endometrial cancer after a diagnosis of chronicanovulation, whereas women with anovulatory infertility
were shown to have a RR of 4.2 for endometrial cancer. Inaddition, women with ovarian factor infertility are at risk fordeveloping endometrial hyperplasia, and when atypical en-dometrial type is present, it represents a potentially prema-lignant form. Finally, obesity, frequently present in PCOSpatients, seems to increase the risk of endometrial cancer 2.6-to 3-fold, suggesting that it is possibly a confounding factoror a pivotal cofactor in PCOS (318).
The main pathogenetic mechanism assumed to be respon-sible for increased risk for endometrial cancer in PCOS pa-tients was hyperestrogenic stimulation of endometrialgrowth, either unopposed by progesterone or opposed to aless extent than in normally cycling women. In fact, estrogensact by genetic and epigenetic mechanisms on cancer cells,and a close relationship between estrogens, growth factors,and oncogenes is important in the development of severalhuman cancers (319).
However, other mechanisms seem to be involved in thedevelopment of endometrial cancer in women with PCOS. Inparticular, LH hypersecretion could be associated with over-expression of LH/hCG receptors, and this condition could bea feature of endometrial hyperplasia and carcinoma in younganovulatory women, including PCOS subjects (320). In ad-dition, Li et al. (321) showed that the expression of the pro-gesterone receptor, of which dysregulation is involved in thepromotion of endometrial neoplasia in the stroma of hyper-plastic endometrium from PCOS women, is unevenly dis-tributed and significantly less than seen in the normal en-dometrium found in non-PCOS women.
In the normal menstrual cycle, during the late secretoryphase, active endometrial cell death occurs via apoptosis,and the Bcl-2/Bax system seems to play a role. Bcl-2 is anapoptotic inhibitor that promotes cell survival, whereas Baxinduces apoptosis. Endometrial apoptosis is regulated byestrogen and progesterone, which are known to modify theexpression of apoptotic proteins during the menstrual cycle.In women with PCOS, the endometrium displays increasedBcl-2 to Bax ratio in comparison with endometrium fromwomen without PCOS (322). The greater expression of Bcl-2activity in relation to Bax in endometrium of women affectedby PCOS resulted in prolonged cell survival (322).
Lastly, increased concentrations of plasma insulin in pa-tients with endometrial cancer (324) and insulin-binding siteshave been found in the endometrial stroma of premeno-pausal women and women with endometrial cancer (323).Thus, compensatory hyperinsulinemia could exert a delete-rious effect on endometrium acting on specific insulin-bind-ing sites exerting a mitogenic effect. In particular, an isoformof the insulin receptor, predominantly expressed in malig-nant tissues, may lead this mitogenic effect.
Several additional mechanisms have been proposed forthe mitogenic effect of insulin in endometrial cancer (325). Inaddition, insulin resistance may be associated with alter-ations of IGF and IGFBP expression or may inhibit the pro-tective effect of progesterone (326). Binding sites for IGF-Iand IGF-II have been confirmed in both normal and malig-nant endometrium. IGF-I binding is significantly higher inendometrial cancer compared with normal endometrium,and in the Ishikawa human endometrial cancer cell lineIGF-I was a more potent mitogen than insulin or IGF-II
24 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

(327). Interestingly, IGFBP-1 was undetectable or mini-mally expressed in endometrial cancers, and hyperinsu-linemia can decrease IGFBP-1 levels significantly; becauseinsulin up-regulates aromatase activity in endometrialglands and stroma, endogenous estrogen production isenhanced in women with high insulin levels as well asPCOS patients (325).
More recently, Pillay et al. (327) compared gene expressionin the endometrial proliferative phase with or without simplehyperplasia derived from women with PCOS matched forage, parity, and biochemical profile, showing differencesin gene expression related to hyperplasia. By microarrayanalysis, 24 genes were found to be up-regulated morethan 2-fold in the hyperplastic group, for which threegenes are known to have roles in endometrial carcinoma,namely human asialoglycoprotein receptor I, human-se-creted phosphoprotein I (osteopontin), and cytochromeP450 XVIIAI (327).
Based on these considerations, metformin could theoret-ically have a beneficial effect in reducing the risk for endo-metrial cancer in PCOS patients. In fact, its administrationmay have the power to reduce the risk of unopposed endo-metrial proliferation, hyperplasia, or carcinoma by improv-ing the regularity of ovulatory function and by reducing theeffect of hyperinsulinemia on the endometrium.
Increased insulin sensitivity may improve the metaboliceffect of insulin and decrease its mitogenic effect by tissue-specific mechanisms through the relative expression of theinsulin receptor isoforms (328).
Notwithstanding these theoretical mechanisms, prospec-tive studies providing clinical data are very few (329, 330).
Session et al. (329) first reported one case of atypical en-dometrial hyperplasia treated with metformin. In particular,the authors described a 37-yr-old patient treated with met-formin after failed progestogen treatment for endometrialhyperplasia. One month after initiating metformin therapy,the patient’s endometrial biopsy demonstrated an atypicalendometrial hyperplasia regression and the presence of pro-liferative endometrium (329).
A subsequent study (330) on a very small sample of sevenPCOS patients confirmed these data. Sequential endometrialbiopsies performed during metformin administrationshowed that endometrial histology normalized under treat-ment. In particular, patients with simple hyperplasia or ad-enocarcinoma at baseline showed no evidence of abnormalhistology after 6 months of insulin-sensitizing therapy. Un-fortunately, in this last study (330), the distinction betweenthe beneficial effects of the drug due to the ovarian functionimprovement/restoration and the direct effects of the drugon the endometrium itself remained unclear.
VI. Hyperandrogenism
Hirsutism is the main clinical feature of hyperandro-genism in PCOS patients, and it is present in approximately75% of these subjects (17). Moreover, there is no clear cor-relation between androgen levels and presence and grade ofhirsutism in PCOS women (167) because the clinical presen-tation is related to genetic susceptibility of the pilosebaceousunit to serum androgen levels (331).
Other signs of hirsutism, such as acne and androgenicalopecia, are less frequent, involving approximately 40% ofthe population (17). Finally, frank virilization with deepen-ing of the voice, clitoromegaly, severe androgenic alopecia,and/or masculine jaw is a very rare event.
Hyperandrogenemia may be affected by metformin. Pre-liminary in vitro data (83) indicated that metformin maydirectly decrease ovarian androgen production, and excel-lent experimental data (84, 85) demonstrated that metforminreduces the ovarian P450c17� activity with a consequentdecline in the serum free testosterone concentration.
Ample evidence supports the beneficial effect of metformin onhyperandrogenemia in PCOS patients.
The meta-analysis by Lord et al. (30) showed a significanteffect of metformin in comparison with placebo or no treat-ment regarding total testosterone (WMD � �0.34; 95% CI,�0.59 to �0.10; P � 0.005) and androstenedione (WMD ��1.21; 95% CI, �1.79 to �0.62; P � 0.00005), with and with-out significant heterogeneity, respectively. Decreases in freetestosterone levels could hypothetically be observed in PCOSpatients receiving metformin due to the up-regulation ofcirculating levels of SHBG caused by improved insulin sen-sitivity (30). Furthermore, clinical evidence is controversial.Meta-analytic data (30) reported a significant treatment effectof metformin (WMD � �4.40; 95% CI, �6.39 to �2.42; P �0.00001) on free testosterone with a significant heterogeneitycorrelated to two of the studies analyzed. Therefore, exclud-ing these studies, homogeneous data showing evidence oftreatment effect (WMD � �1.79; 95% CI, �4.14 to 0.56; P �0.14) were obtained (30). In addition, metformin was re-ported as not affecting SHBG levels (OR, 2.80; 95% CI, �1.11to 6.71; P � 0.2), but a significant heterogeneity was reported(30). Only one RCT (30) showed no evidence of effect fromboth metformin and CC on total testosterone (OR, 0.0; 95%CI, �0.59 to 0.59; P � 1.0) or SHBG (OR, 10.0; 95% CI, �10.17to 30.17; P � 0.3), but there was a significant treatment effecton free testosterone (WMD � �3.30; 95% CI, �5.07 to �1.53;P � 0.0003).
Whether metaformin is less effective than androgen-low-ering drugs, is a debated issue since an RCT found thatmetformin had similar androgen-lowering efficacy in bothobese and morbidly obese women affected by PCOS (111),whereas in another RCT nonobese women did not seem tobenefit from metformin (332). A result that was difficult tounderstand rose from the meta-analysis by Lord et al. (30)regarding the significant increase of adrenal androgen de-hydroepiandrosterone sulfate levels in metformin-treatedpatients (WMD � 0.66; 95% CI, 0.03 to 1.28; P � 0.04), but inthis study a significant heterogeneity was found. In thisregard, a recent double-blind, placebo-controlled, ran-domized study confirmed that the administration of 2000mg metformin for 14 wk increased serum dehydroepi-androsterone sulfate levels alone (333). Of note, the sus-pension of metformin induced a potential “rebound” ef-fect with an increase of serum androstenedione levels aswell as of free testosterone index (333).
A comparison of metformin (2250 mg/d), rosiglitazone (4mg/d), and the combination of both drugs to placebo dem-onstrated that the mean serum free testosterone levels innonobese non-insulin-resistant PCOS patients on therapy
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 25
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

were significantly lower than the levels found in subjects onplacebo without significant advantage for the combinationtreatment (159). The similar efficacy of metformin and otherthiazolinediones has also been confirmed in a further studycomparing 2250 mg/d metformin to 30 mg/d pioglitazonerandomly given for 6 months in 52 PCOS patients (334). Infact, both treatments demonstrated significant decreases infree testosterone, androstenedione, and LH levels with anapproximately 30% decrease in the hirsutism score (334). Onthe other hand, a significant decrease in androgens was ob-served only under 4 mg/d rosiglitazone, whereas no signif-icant change was detected in PCOS patients receiving 1700mg/d metformin (155). The length of treatment was 12 wk,and the population was composed of both lean and obesePCOS patients (155).
To date, there is an increasing interest for combinedtherapies. A prospective study (335) designed to evaluatethe effects of metformin plus flutamide on metabolic pa-rameters and insulin resistance in nonobese women withPCOS showed a similar reduction in free testosterone afteradministration of both 2250 mg/d metformin and 250mg/d flutamide. In addition, metformin plus OCs pro-vided benefits on hyperandrogenism and insulin resis-tance in nonobese PCOS women not desiring pregnancy,but the effects on central adiposity and dyslipidemia wereweaker (336). Recent studies showed that the combinationof metformin and low-dose flutamide was related to en-docrine and metabolic benefits in nonobese (337, 338) andobese (339) PCOS patients by acting on the upstream ab-normalities of PCOS without merely masking downstreamsymptoms such as OCs. Lastly, 6-month low-dose dexa-methasone administration further reduced androgen lev-els in PCOS patients treated with metformin and lifestyleinterventions (340).
Besides the metformin effect on biochemical hyperandro-genism, its efficacy on clinical manifestations of hyperan-drogenism is inconsistant. In this regard, the lack of signif-icant benefit from metformin administration in hirsute PCOSpatients could probably be explained with the need of longerfollow-ups.
In an open-label study of 39 women with PCOS, met-formin given at a dose of 500 mg three times daily signifi-cantly decreased the Ferriman-Gallwey score at the end ofthe 12-wk study period (341).
The meta-analysis by Lord et al. (30) analyzed two RCTsreporting hirsutism scores under metformin or metforminplus CC. Pooling data from these studies, a significanteffect of metformin on hirsutism without significant het-erogeneity (WMD � �5.12; 95% CI, �8.77 to �1.47; P �0.006) was observed. Another double-blind, placebo-con-trolled, crossover study confirmed the effect of metforminin improving hirsutism, assessed by using the Ferriman-Gallwey score, patient self-assessment, and hair growthvelocity (342).
Three RCTs compared the efficacy of metformin and OCs,consisting of 35 mg E2 and 2 mg CA (182, 183, 343). Inparticular, Harborne et al. (343) demonstrated a significantreduction in hirsutism with metformin, whereas two otherclinical trials (182, 183) showed a trend in the opposite di-rection. A greater decrease in the hirsutism score with 1500
mg/d metformin than the OCs was observed in 37 patientsafter 12 months of treatment (343). On the other hand, inanother study (182) a greater decrease in the hirsutism scorewith OCs was observed in 18 obese PCOS patients whoreceived either metformin (1000 mg/d for 3 months fol-lowed by 2000 mg/d for 3 additional months) or OCs (182).The same group of researchers published another analysis(183) confirming their results in nonobese PCOS subjectstreated with the same protocol. More recently, Luque-Ramírez et al. (186) demonstrated that OCs were moreeffective than 1700 mg/d of metformin in hyperandro-genism control and in restoration of menstrual cyclicity in34 PCOS patients receiving the treatment for 24 wk. Inaddition, OCs were not associated with any clinically rel-evant worsening in the classic metabolic and cardiovas-cular risk profile in their population (186). No significantdifference was seen in the development of type 2 DMbetween metformin and also OCs (OR, 0.17; 95% CI, 0.00to 8.54; P � 0.37) (190).
A meta-analysis (181) of three RCTs comparing the effectsof metformin and OCs on hirsutism demonstrated no dif-ference in efficacy between these two drugs (standardizedmean difference � �0.18; 95% CI, �0.67 to 0.32; P � 0.48).Furthermore, statistical heterogeneity, due to differences inthe selection criteria for PCOS participants, the assessmentmethod for hirsutism, and duration of treatment, waspresent.
The efficacy of metformin on hirsutism was also comparedwith antiandrogen therapy. A 6-month prospective, random-ized, placebo-controlled trial (344) on 76 obese PCOS womendemonstrated that PCOS patients who underwent a hypoca-loric diet 1 month before treatment had benefits significantlyhigher from flutamide (500 mg/d) than from metformin(1700 mg/d) and that a combination therapy with metforminplus flutamide did not add any further benefit in comparisonwith flutamide alone. The combination of flutamide plusmetformin could be efficient in normalizing the spectrum ofthe disorder in PCOS patients (338). However, addition ofOCs is advocated to avoid the potential embryotoxicity; thus,it cannot be considered a standard therapy for widespreadclinical practice (338).
Metformin seemed to be effective in improving achantho-sis nigricans in PCOS patients after 6 months of treatment,but no standardized measure to assess clinical manifestationwas used in the study (45). More recently, an open-label pilotstudy involving overweight or obese subjects with acantho-sis nigricans randomized to 12 wk of either metformin orrosiglitazone showed no effect on the severity of acanthosisnigricans and a modest improvement of skin texture in bothtreatment groups (345).
Similarly, 3 months of metformin administration had pooreffect on the acne score in young PCOS women (341). A singleRCT (343) comparing metformin vs. OCs regarding acnedemonstrated no significant difference in acne scores(WMD � 0.90; 95% CI, �0.40 to 2.20; P � 0.18) (181).
Briefly, metformin as well as OCs exert a relatively modestbeneficial effect on excess hair growth that is significantlyinferior to those observed with antiandrogen therapies. todate, other multi-drug regimens are under study. Currentguidelines derived from meta-analyses (346, 347) of RCTs on
26 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

medical treatments for hirsutism in women clearly statedthat there is strong evidence that metformin is not a choicetherapy for hirsutism and other strategies should be used(347). In fact, the random-effect meta-analyses of 16 RCTsshowed a small decrease in the Ferriman-Gallwey score inhirsute patients receiving ISDs when compared with placebo(WMD� �1.5; 95% CI, �2.8 to �0.2) (347). ISDs improvedhirsutism similarly to OCs (WMD� �0.5; 95% CI, �5.0 to3.9), but less than with spironolactone (WMD�1.3; 95% CI,0.03 to 2.6) and flutamide (WMD�5.0; 95% CI, 3.0 to 7.0)(347). Lastly, a recent Task Force behalf the Endocrine Societyin clinical practice guidelines suggested against the use ofISDs as therapy for hirsutism, whereas recommended OCs orantiandrogens (348).
VII. Malignancies
The association between PCOS and endometrial cancerhas been reported previously (see Section V.B). Anecdotalcases of low-grade endometrial stromal sarcoma and carci-nosarcoma in women with PCOS have been described in theliterature (349). Data regarding PCOS and epithelial ovarianand breast cancer derived from few studies, which seem toexclude any association between these conditions seems to beexcluded by few available data (349).
Some epidemiological and experimental evidence sug-gests that insulin and IGFs influence the risk and the prog-nosis of cancer with particular regard for the breast cancer(350). In the same manner, elevated androgen levels havebeen proposed as factors involved in the oncogenetic pro-cesses with several mechanisms (349).
It is intuitive that drugs that can reduce both insulin re-sistance and hyperandrogenism, i.e., metformin, could beproposed as treatments with potential roles in the preventionand treatment of some types of cancers.
A recent study (351) suggests that metformin may reducethe risk of cancer, but its mechanism of action remains un-clear. In vitro and in vivo experimental data have demon-strated that metformin led to a strong reduction of cyclin D1protein level in tumors, suggesting evidence for an ulteriormechanism in the explanation of metformin’s antitumoraleffect (351).
As detailed in Section I.B, in vitro and in vivo studies havedemonstrated that metformin induces LKB1, a serine-threonineprotein kinase that activates the AMPK by phosphorylation ofthe proximal site (60, 61), acting as tumor suppression.Recently, great attention has been given to the mammaliantarget of rapamycin (mTORC) pathway dysregulation inbreast cancer because several experimental and epidemi-ological data have shown that this pathway influencescancer development directly or through AMPK (352).
Based on these considerations, metformin could exert apleomorphic antiproliferative action on various malignan-cies. In fact, in diabetic patients treated with metformin, a lowincidence of cancer has been demonstrated targeting AMPKpathway activation as the main antiproliferative effect ofmetformin (352).
The deficiency of phosphatase and tensin homolog tumorsuppressor induces cell growth through an overactivation of
the mTORC1 kinase, which is activated in the majority ofhuman cancers. In mice deficient in phosphatase and tensinhomolog tumor suppressor, the tumor onset was delayedwith the use of metformin, which induces LKB1 and theconsequential activation of AMPK pathway that acts to in-hibit mTORC1 kinase (353).
Stimulation of AMPK by metformin resulted in a sig-nificant repression of cell proliferation and activeMAPK1/2 in both estrogen receptor � (ER�)-negative and-positive human breast cancer cell lines (354). Further-more, a different biological response to metformin wasdetected between ER�-negative and -positive human breastcancer cell lines. In fact, with metformin, only the first celllines demonstrated an AMPK-dependent increase of thevascular endothelial growth factor expression (352, 354).These findings obtained in vitro have also been tested inthe animal model (354). Athymic nude mice with ER�-negative breast cancer treated with metformin showedincreased vascular endothelial growth factor expression,microvascular density, and reduced necrosis, even if theserum IGF-I levels and the tumor cell proliferation rate invascularized regions were reduced (354). However, theoverall tumorogenic progression was improved comparedwith untreated controls (354). Unfortunately, the met-formin-induced neoangiogenesis could be a risk factor inbreast cancer development (355).
In conclusion and in consideration of the available data,great caution should be given to the potential beneficialeffects of metformin on tumorigenesis and to the translationof the in vitro findings to the in vivo model.
VIII. Quality of Life Impairment
Several data available in the literature (356) confirm thatPCOS negatively affects the patients’ health-related QoL, amultidimensional concept that includes physical, emotional,and social aspects.
In two studies, QoL in PCOS patients was found to beworse than in the healthy control group (357, 358). Thisfinding is understandable given several PCOS-related fea-tures. More interesting are the data comparing QoL in pa-tients with PCOS and/or other diseases. One study (359)designed to evaluate the Short-Form Healthy Survey (SF-36),a well-validated generic instrument to assess the QoL, in UKpeople affected by several diseases was recently published.In this survey, the PCOS patient’s QoL was similar to thoseof patients with asthma, epilepsy, DM, and back pain, andbetter than patients with arthritis and coronary heart disease.Furthermore, the items related to the psychological aspectswere significantly worse than in patients affected by otherdiseases (359).
As reported by a recent systematic review (356), obesityseems to exert the greatest negative influence on QoL inPCOS patients with a complex relationship with psychoso-cial well-being and sexual satisfaction. Infertility and men-strual disorders seemed to influence QoL assessed with bothgeneric and PCOS disease-specific questionnaires (356). Clin-ical signs of hyperandrogenism on both PCOS and non-PCOS patients had a negative impact on self-image and
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 27
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

esteem (356), and the treatment of these conditions improvedthe QoL and psychological well-being of the patients (360).In addition to somatic impairments, mood disturbances suchas depression, limitations in emotional well-being and lifesatisfaction, diagnosis of PCOS also has a negative impact onsexual self-worth and sexual satisfaction (361).
In this regard, treatments used in PCOS patients by ame-liorating the clinical aspects and preventing the long-termconsequences of the disease could improve their QoL. Pres-ently, few data (358, 362, 363) have evaluated the impact ofspecific treatment on QoL in PCOS patients.
Only one prospective observational study (358), not in-cluding placebo or control groups, evaluated the effect ofmetformin administration on QoL in a German PCOS pop-ulation by using four standardized questionnaires: theHealth-Related QoL (HRQL) and the SF-36 for generic mea-sure of QoL, the Symptoms Check List 90 (SCL-90-R) forpsychological disturbances, and the Visual Analog Scales(VAS) for sexual satisfaction. Metformin administration im-proved QoL, particularly for the psychological aspects ratherthan for physical ones, psychological disturbances, and sex-ual satisfaction. However, even if improved, these measure-ments remained worsened in PCOS patients compared withthe normal German female population used as control. Inaddition, the authors (358) computed a correlation to addresspossible associations between metformin-induced clinicaland/or biochemical improvements and psychological im-provement. An interesting correlation between the clinicaleffect of metformin and psychological improvement wasobserved.
Presently, comparative data on several treatment optionsin PCOS using a disease-specific questionnaire are lacking.In fact, even if the PCOS Questionnaire (PCOSQ), an instru-ment consisting of five domains formed by 26 questions onemotions, body hair, weight, infertility, and menstrual prob-lems, has been validated (364), no well-designed RCT eval-uating the impact of treatments on QoL is available.
IX. Obesity
Obesity is observed in up to 60% of patients with PCOS inthe United States (365), but it is less frequent in other pop-ulations (366).
More than a real presence of obesity or high BMI, thedistribution of fat is the main significant feature in PCOS(367). Visceral adiposity is known to be metabolically active,is more highly associated with hyperinsulinemia than scfat (368), and is more frequently noted in PCOS patients(369). In fact, regardless of ethnicity, most overweightwomen with PCOS have central obesity (android pattern)(369), and 70% of lean women with PCOS have an androiddistribution of fat (370).
Whether obesity is a promoting environmental factor or anintrinsic clinical sign of PCOS remains unclear. Certainly,obesity has a profound impact on the phenotypic expressionof PCOS, being associated with more severe hyperandro-genism, insulin resistance, and fertility disorders.
Obesity, particularly central obesity, is related to and re-sponsible for hyperinsulinemia that correlates with in-
creased cardiovascular risk (371). Moreover, obesity is inde-pendently associated with intermediate cardiovascular riskfactors, such as hypertension and type 2 DM. Lastly, obesityis also related to reduced fecundity (372). In fact, an increasedrate of menstrual disorders and anovulatory infertility (373)and a reduced clinical response to the infertility treatments(158, 374–377) was observed in obese women. Higher risk formiscarriage, gestational DM, hypertension, and unfavorableobstetrics outcomes was also reported in obese subjects (378).
Previous studies demonstrated that weight loss inducedby diet and/or physical activity causes endocrine, metabolic,and reproductive improvements in obese PCOS patientswishing to conceive (210, 211). In this regard, the UK guide-lines for the management of obese women with PCOS rec-ommend weight loss, preferably to a BMI of less than 30kg/m2, before starting drugs for ovarian stimulation (379).Unfortunately, lifestyle modification programs are oftennot followed by weight loss maintenance, probably be-cause of the low retention rate frequently related to life-style modifications (380). In fact, a high dropout rate fromthese programs often characterizes these interventions,even if performed for short periods (381). Although, bothdiet and exercise are effective in improving fertility inobese PCOS patients with anovulatory infertility, a struc-tured exercise program has a higher compliance than dietalone (382).
Data obtained from a type 2 DM population receivingmetformin seemed to clearly demonstrate that this drug,contrary to most antidiabetic agents, is not associated withweight gain (383). Thus, metformin can improve insulin sen-sitivity but does not reduce this effect with an increase inbody weight (383). In this regard, a recent clinical studydemonstrated that low-dose metformin pretreatment con-trasted the increase in BMI due to pioglitazone administra-tion, improved the glycemic control, and reduced the athero-genic index in type 2 DM patients (384). In addition,metformin, both as monotherapy (385) and combined withlifestyle intervention (386), has been demonstrated to reduceweight gain related to increased insulin resistance due toantipsychotic medication, and metformin alone was moreeffective in weight loss and insulin sensitivity improvementthan lifestyle intervention alone (386). Thus, indirect evi-dence seems to relieve concern about a potential increase ofbody weight in PCOS patients already at risk for obesity.
On the other hand, data regarding the potential beneficialeffects of metformin on obesity in PCOS patients arecontroversial.
The link between obesity and insulin resistance is strong(371), and the data showing a significant improvement ininsulin resistance seem to be a key factor in determining thatmetformin administration could be effective in reducingbody weight in several conditions in which insulin resistancecould have a role in weight gain, such as in PCOS (383).
Metformin could act to improve body weight in obesePCOS patients both directly on the central nervous systemand indirectly via adipokines modification. In fact, met-formin has been shown not only to stimulate catabolic pro-cesses in the peripheral organs but also to modulate appetitein the hypothalamus (387). Indeed, a recent experimentalstudy showed that acute and chronic administration of met-
28 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

formin increases anorectic gut hormone peptide YY fastingplasma levels in PCOS patients (388). Of note, this increasewas significantly related to waist circumference reduction(388). Thus, metformin probably acts not only in the reduc-tion of the total quantity of body fat, but also and especiallyin the visceral fat, which is the main endocrine organ pro-ducing metabolically active adipokines.
Not only insulin, ghrelin, neuropeptide Y, and leptin butalso several other adipokines interact in the regulation ofenergy homeostasis in healthy women. On the other hand, analteration of these metabolic signals was demonstrated inpatients with PCOS (389). In these patients, metformin ad-ministration had no effect on leptin levels, whereas it im-proved the blunted neuropeptide Y release induced by gh-relin injection (390). However, in patients with type 2 DM,metformin decreased plasma ghrelin levels after glucose load(391) and prolonged the postprandial fall in ghrelin concen-tration (392). Recently, Tan et al. (393) reported a high mRNAand protein expression of vaspin in omental adipose tissuein overweight PCOS women and a significant effect of6-month metformin administration on plasma vaspin levels.
Notwithstanding these intriguing experimental data on apotential effect of metformin on body weight, clinical dataregarding the effectiveness of metformin on the improve-ment of body weight in PCOS patients, with particular re-gard for the obese, are very controversial.
Initial data (32) of metformin treatment reported a loss inbody weight in women with PCOS. Successively, Tan et al.(154) analyzed data from three groups of PCOS patientsaccording to their BMI, i.e., normal weight, overweight, andobese. The authors (154) found that metformin use was sig-nificantly associated with decreased body weight and BMI inthe overweight and obese groups. On the other hand, the useof metformin was observed to decrease body weight, even innonobese PCOS women (335). Other investigators reporteda significant reduction in waist circumference, but no sig-nificant change was observed in weight in obese subjectstreated with metformin (147). In another study, researchersobserved that metformin reduced BMI in patients both withand without insulin resistance, but it had no influence on theWHR (394).
Lord et al. (30) showed no significant effect from met-formin on body weight (OR, �5.83; 95% CI, �18.43 to 6.78;P � 0.4) or BMI (OR, �0.27; 95% CI, �0.98 to 0.45; P � 0.5).In addition, no significant difference in waist circumference(OR, �4.00; 95% CI, �16.95 to 8.95; P � 0.5) or WHR (OR, 0.0;95% CI, �0.02 to 0.02; P � 0.7) was reported.
In a subsequent RCT (111) specifically designed to eval-uate the effects of metformin therapy on body weight, BMIdecreased significantly by approximately 4% in both obeseand morbidly obese women with PCOS after metformin ther-apy (500 or 850 mg three times daily) without lifestyle in-tervention. In the same study (111), obese PCOS patientsbenefited from greater weight loss at the highest dose (2550vs. 1500 mg/d) of metformin, whereas a similar degree ofweight loss at both doses of metformin was detected inmorbidly obese PCOS subjects.
Costello et al. (190), in a meta-analysis comparing the ef-fects of metformin vs. OCs on several end-points, demon-strated no difference in BMI or WHR between the two treat-
ments. Only one clinical trial comparing 6 months of OCs (35�g E2 combined with 250 �g norgestimate in a cyclic regimenof 21 d of active pills followed by a 7-d pill-free interval) alonevs. OCs combined with 1500 mg/d metformin reported nosignificant difference in body weight (336). Finally, meta-analysis (190) of two studies investigating OCs alone vs. OCscombined with metformin again revealed no difference inBMI between groups.
A recent RCT (110) demonstrated a significant BMI re-duction in PCOS patients receiving metformin alone or incombination with CC, although the treatment effect on BMIwas not an end-point of the trial.
The additive effects of metformin in PCOS patients underlifestyle modification programs were also investigated.
Pasquali et al. (181) compared the efficacy of a low-caloriediet combined with metformin or placebo in PCOS patientsand controls. Reduction of body weight, BMI, and visceral fatmass was greater in the metformin group than the placebogroup. A study (395) on overweight PCOS patients con-firmed that the combination of metformin plus lifestyle in-tervention was more effective in weight and androgen re-duction than placebo plus lifestyle intervention. Nodifference in ovulation rate was reported between groups,but ovulation rate was significantly higher in patients wholost weight (395). By contrast, a RCT (396) evaluating met-formin (850 mg twice daily) plus lifestyle modification inobese PCOS women did not find a significant improvementin body weight or menstrual frequency, even though thatstudy was not powered to examine weight loss as an end-point. Nevertheless, the metformin group lost twice as muchweight as the placebo group, and metformin therapy resultedin a significant reduction in waist circumference comparedwith lifestyle changes alone. In addition, a logistic regressionanalysis, used to analyze the independent predictors formenstrual restoration, showed that weight loss alone corre-lated with improvement in menses. These studies (395, 396)suggest that metformin therapy might facilitate modestweight loss and visceral fat reduction, particularly whencombined with a hypocaloric diet, but some of these effectscould be dose-related.
The effect of metformin on body weight was also inves-tigated in subjects at high risk for PCOS development (seeSection XII) or type 2 DM (397) and subjects with excessweight (398). In subjects at high risk for type 2 DM, met-formin reduced BMI (OR, �5.3; 95% CI, �6.7 to �3.5; P �0.00001) compared with placebo or no treatment (397). Sta-tistically significant reductions in BMI were seen in womenwith PCOS (OR, �5.3; 95% CI, �7.2 to �3.4) and withoutknown PCOS (OR, �5.4; 95% CI, �7.2 to �3.5), with obesity(OR, �5.1; 95% CI, �5.5 to �3.6) and without obesity (OR,�6.3; 95% CI, �9.4 to �3.3) (397). Lastly, as demonstrated ina recent 6-month clinical study (398) in a population of pa-tients with excess weight that chose their own management,2550 mg/d of metformin was significantly more effectivethan diet in reducing the incidence of overweight andobesity.
In conclusion, on the basis of the present data, metforminhad a marginal effect on weight loss as monotherapy. Thus,both clinicians and patients should be advised against the useof metformin as an antiobesity drug. On the other hand,
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 29
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

lifestyle modifications remain the cornerstone for weight lossin obese PCOS patients, although metformin cotreatmentmight improve the efficacy.
X. Cardiovascular Risk
Because of its association with insulin resistance, PCOScan lead to several metabolic complications. Although pro-spective controlled data on CVD morbidity and mortality inPCOS patients are lacking, various risk factors for CVD aredetected in the PCOS population. In particular, PCOS sub-jects have an increased incidence of obesity, hyperinsulin-emia, hypertension, dyslipidemia, elevated PAI-1 and ET-1,endothelial disarrangements, chronic inflammation, and im-paired fibrinolysis.
The pathogenetic mechanisms accounting for these abnor-malities are still controversial, but the most qualified datasuggested a relationship with both hyperandrogenism (399)and impaired peripheral insulin sensitivity (400). However,the main risk factors for CVD in PCOS patients are probablyIGT and type 2 DM.
In patients with type 2 DM, the UK Prospective DiabetesStudy (UKPDS) (401) showed that metformin may be car-dioprotective. In this large prospective trial on obese diabeticpatients, metformin significantly decreased all-cause mor-tality and stroke end-points. Recent epidemiological findingson 1181 patients with type 2 DM showed that, controlling forconfounders, i.e., glycemic control, metformin is as effectiveas insulin in terms of mortality and is probably more effectivethan insulin in terms of nonfatal myocardial infarction andstroke, suggesting a potential effect not mediated by insulinsensitivity (402). Also, other clinical data (396) have reportedthat metformin reduces cardiovascular end-points in subjectsat risk for type 2 DM by actions that cannot be attributedsolely to glucose-lowering effects. Based on these consider-ations, metformin might be used for long-term therapy de-signed to reduce the risk for CVD in normoglycemic patients,as frequently observed in PCOS.
Although the effects of ISDs on cardiovascular risk factorsare favorable, currently there are no RCT examining the useof these drugs in the prevention of DM or cardiovascularevents in women with PCOS. A recent experimental study(403) demonstrated that a very low dose of metformin ex-erted a cardioprotective effect in a nondiabetic murinemodel of myocardial ischemia-reperfusion injury, improv-ing AMPK activation, already activated by myocardialischemia as an endogenous protective signaling mecha-nism, and increasing endothelial NOS phosphorylation.Administrated after the start of reperfusion, metforminreduced infarct size in normoglycemic rats, reducing sub-sequent rigor contracture by inhibition of mitochondrialpermeability transition pore opening with a phosphoino-sitide-3 kinase inhibitor-mediated mechanism (404).
A. Cardiopulmonary impairment
PCOS patients have been shown to have a subclinicalcardiopulmonary impairment with a reduced cardiopulmo-nary functional capacity that could increase the risk for CVD,even at an early age (405).
The maximal oxygen consumption (VO2max), defined asthe maximal capacity of an individual to perform aerobicwork, is the product of cardiac output and arterial-venousoxygen difference at exhaustion, and it is probably the bestpredictor of functional capacity. This parameter is positivelycorrelated with insulin sensitivity and is considered a strongdeterminant of insulin sensitivity index in both men andwomen (406).
Several data demonstrated that an increased VO2max isassociated with a decreased cardiovascular mortality, even insubjects with CVD (407). In a recent study (405), there weresignificant differences in VO2max and in cardiovascular pa-rameters between young PCOS women and healthy age- andBMI-matched controls. On the other hand, a 3-month struc-tured exercise training program improved cardiopulmonaryfunctional capacity in overweight PCOS patients (408), prob-ably exerting a beneficial effect on mitochondrial biogenesisand insulin sensitivity.
It is unknown whether metformin could have a similar oradditive effect of exercise training in insulin-resistant sub-jects, as well as in PCOS women. Metformin has recentlybeen shown to inhibit complex I of the electron transportsystem, and thus it could exert some effect on aerobic ca-pacity (409). In a recent double-blind, placebo-controlledstudy, Braun et al. (409) demonstrated that 2000 mg/d met-formin exerts a significant effect on maximal exercise capac-ity in healthy patients without mitochondrial dysfunction.
B. Diabetes mellitus
Women with PCOS are at risk for developing IGT and type2 DM (272). In fact, in PCOS patients the prevalence of IGTand type 2 DM is 30–40% and 5–10%, respectively (272). Inaddition, the conversion from IGT to type 2 DM is increased(272). Women with PCOS and baseline NGT have a 16%conversion rate per year to type 2 DM (410), whereas by theage of 30 yr, 30–50% of obese women with PCOS develop IGTor overt type 2 DM. This is a 3- to 7-fold greater risk than anage-comparable population (272).
The mechanisms underlying the association betweenPCOS and glucose metabolism impairment are still unknown.
Fetal growth restraint and low birth weight and/or size forgestational age followed by catch-up of weight during in-fancy may lead to hyperinsulinemia and insulin resistance,obesity, PCOS, and type 2 DM in later life (411, 412). In uteroandrogen exposure has been also proposed to influence thephenotypic expression of PCOS. In fact, in nonhuman pri-mates, fetal exposure to high levels of androgen during earlyintrauterine development is associated with defects in insu-lin secretion and action in adult life (413), and prenatallyandrogenized female rhesus monkeys exhibit glucoregula-tory deficits similar to those seen in adult women with PCOS(414). Of note, the timing of the androgen exposure seems tohave different effects on glucose regulation: early androgenexposure has been associated with impaired pancreatic�-cell function, whereas exposure later in gestation ap-pears primarily to alter insulin sensitivity. However, thereis evidence that insulin resistance may play a major patho-physiological role in the development of glucose intoler-
30 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

ance in PCOS women like that which occurs in the healthypopulation (415).
The Diabetes Prevention Program (DPP) Research Grouprecently conducted a large placebo-controlled RCT spon-sored by the NIH (416) on 3234 subjects in the United Statesat high risk for developing type 2 DM (history of gestationalDM or presence of IGT and a first-degree relative with DM).Subjects were randomized to standard management, inten-sive lifestyle intervention, metformin, or troglitazone. Thisoriginal design changed because the treatment in the trogli-tazone arm was discontinued after 18 months due to theemerging risk of hepatic dysfunction (416). During the av-erage follow-up period of 2.8 yr, intensive lifestyle interven-tion reduced the incidence of newly developed DM by 58%,whereas subjects treated with metformin showed a RR forprogression to overt type 2 DM reduced by 31% in patients,and no difference based on gender was observed in any case(416). These results indicate that improvement in insulinsensitivity, through either intensive lifestyle modification ormetformin, reduces the risk of developing DM in high-riskindividuals (416).
At this point, three main concerns arise: 1) whether thebeneficial effects of metformin are maintained over the timeor disappeared at treatment suspension; 2) whether met-formin reduces only DM (as intermediate end-point) or alsothe cardiovascular events, which are the main cause of deathin DM patients; and 3) whether results from a heterogeneouspopulation at high risk for DM can be translated in the PCOSpopulation.
Data obtained from the same population studied in theDPP demonstrated that, after a short washout period, about25% of the beneficial effect of metformin on type 2 DMprevention did not persist when treatment was withdrawn(417). However, a significant reduction in the incidence ofDM was detected, supporting the hypothesis that metformindoes not mask the development of DM but provides a cur-ative effect in diabetic patients (417).
Different findings were obtained in a recent RCT on a smallbut well-selected population of normal-weight, non-insulin-resistant PCOS patients (115). In particular, metformin did notmaintain its benefits at a biochemical and clinical level after12-month treatment suspension (115). Conversely, a slight butsignificant worsening of the basal peripheral insulin sensitivitywas observed (115).
The UKPDS (401) reported a significantly reduced inci-dence of myocardial infarction in overweight patients withtype 2 DM treated with metformin. In addition, anotherstudy (418) demonstrated that metformin monotherapy ormetformin combined with sulfonylurea was associated withreduced all-cause and CVD mortality compared with sulfo-nylurea monotherapy among new users of these agents.
Unfortunately, data on CVD mortality in PCOS patientstreated with metformin are lacking at this time.
Although some evidences showed that metformin admin-istration in PCOS patients improves intermediate end-pointsfor DM, such as insulin sensitivity indexes, there are limiteddata on the long-term beneficial effects of metformin on therisk for type 2 DM in women with PCOS. One retrospectivestudy of PCOS women treated with metformin for an aver-age of 43 months found that metformin appeared to delay or
prevent the development of IGT and type 2 DM (419). Theseinvestigators found an 11-fold decrease in the annual con-version rate from NGT to IGT, with 55% of IGT patientsreverting to NGT.
Salpeter et al. (396) performed a meta-analysis of thepooled results of 31 clinical trials with 4570 participantsfollowed for 8267 patient-years to assess the effect of met-formin on metabolic risk in patients at high risk for DM.Fourteen trials included PCOS subjects, for a total of 620subjects. Metformin treatment significantly (P � 0.01) re-duced fasting glucose (OR, �4.5; 95% CI, �6.0 to �3.0),fasting insulin (OR, �14.4; 95% CI, �19.9 to �8.9), andHOMA index (OR, �23; 95% CI, �18.0 to �27.3), comparedwith placebo or no treatment. No statistically significantdifferences were found between subgroups, i.e., PCOS vs.non-PCOS and obese vs. nonobese. Metformin decreasednew-onset DM by 40% (95% CI, 0.5 to 0.8) and reduced theabsolute risk of DM by 6% (95% CI, 4 to 8); furthermore, nodata on subgroups were provided.
Finally, a recent position statement from the AEPS rec-ommended that women with PCOS, regardless of weight, bescreened for IGT or type 2 DM by an oral glucose tolerancetest at their initial presentation and every 2 yr thereafter (33).However, this statement noted that the use of metformin totreat or prevent the progression of IGT could be consideredbut should not be mandated at this point in time becausewell-designed RCTs demonstrating efficacy have yet to beconducted.
C. Hypertension
Controversial data are present in literature regarding theincidence of hypertension in PCOS women (420–422).
At a young age, PCOS patients generally do not manifestincreased blood pressure values (420), even if an increasedprevalence of labile daytime blood pressure, which is apredisposing factor to sustained hypertension later in life,has been reported (421). On the other hand, at menopause,women with PCOS have a risk of developing hypertensionthat is 2.5-fold higher than age-matched controls, andthis may be related in part to the obesity associated withPCOS (423).
Some authors (424) suggested that a mechanism respon-sible for hypertension in women with PCOS could be me-diated by ET-1. Diamanti-Kandarakis et al. (424) reportedthat serum ET-1 levels were higher in women with PCOSregardless BMI, and a positive correlation was found be-tween ET-1 and androgen levels. In this regard, Chen et al.(422) showed an independent relation between higher an-drogen levels and systolic and diastolic blood pressure innonobese PCOS women.
Notwithstanding these findings, the exact mechanisms bywhich androgens could influence the blood pressure inwomen with PCOS remain controversial.
Experimental data (425) support a role for the renin-an-giotensin system in mediating androgen-stimulated in-creases in blood pressure. In particular, in women withPCOS, plasma renin activity was found to be elevated com-pared with a nonoligomenorrheic group of age-matchedwomen (426). In fact, another possible mechanism inducing
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 31
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

hypertension in PCOS could be the increased serum aldo-sterone concentration (427). Aldosterone is a well-recognizedcardiovascular risk factor with an important role in thepathophysiology of hypertension, left ventricular hypertro-phy, and heart failure. In PCOS women, serum aldosteronelevels, even those within the normal range, were increasedin comparison with healthy women (427); increased aldo-sterone levels have been demonstrated to predispose to thedevelopment of hypertension.
Metformin administration could prevent structuralchanges that precede hypertension. In an animal model,Wang et al. (428) demonstrated that fructose-fed inducedadvanced glycation end-products (AGEs), well-knownatherogenetic molecules, significantly correlated with a re-duction in endothelial NOS and a structural remodeling ofthe vessel wall in the aorta and mesenteric artery in the rat,and that metformin administration reduces these structuralchanges.
In women with PCOS, 6 months of metformin adminis-tration reduced ET-1 levels and ameliorated insulin resis-tance and hyperandrogenism, without changes in bodyweight (424) (see Section X.G). A recent RCT (429) comparingthe effects of metformin vs. antiandrogenic OCs on PCOSpatients showed that metformin treatment decreased day-time ambulatory blood pressure monitoring, whereas OCsexerted the opposite effect.
In a wide multicenter trial (397), metformin reduced am-bulatory blood pressure in patients with type 2 DM and thewhite coat hypertension in an unselected population of over-weight and obese patients. Lastly, recent studies (430, 431)suggested that the combination of thiazolinediones and met-formin is associated with a slight but significant improve-ment in the long-term blood pressure control of patients withtype 2 DM.
D. Dyslipidemia
Dyslipidemia is the most common metabolic abnormalityin PCOS (415). Recent findings showed that women withPCOS have quantitative LDL alterations, with increased lev-els of atherogenic lipoprotein phenotype, associated with agreater cardiovascular risk (432).
In particular, serum total cholesterol, low-density lipopro-tein (LDL)-cholesterol, and triglycerides were significantlyhigher in women with PCOS compared with controls (432),and obese women with PCOS usually have higher levels oftriglycerides than normal-weight women with PCOS (432).Low concentrations of high-density lipoprotein (HDL)-cho-lesterol were also detected in this population (432).
Metformin action on lipoproteic metabolism can be director through a reduction of insulin concentration. Metforminimproved hepatic fatty acid metabolism from lipogenesistoward oxidation and ketone body production in rats withdiet-induced overweight and hypertriglyceridemia (433). Inparticular, the cumulative triglyceride output decreased bymore than 60% and the total ketone body output increasedby more than 100% from liver perfused with metformin (433).Moreover, AMPK plays a key role in the regulation ofcellular lipid metabolism increasing the rate of fatty acidoxidation (FAO) (59–60), and metformin could act as lipid-
lowering agent activating AMPK and, thus, increasingFAO (59 – 60). In fact, in a model liver cell line, metforminactivated AMPK, increasing immediately and for a pro-longed period the rate of constitutive exocytosis (triacyl-glycerol and apolipoprotein B) by about 2-fold (434). Thisaction is a mechanism independent from FAO increasebecause the FAO inhibition with R-etomoxir does not pro-duce a significant reduction of the lipid-lowering effects ofmetformin (434).
Although controversial data are available on the effectof metformin in reducing visceral fat, different beneficialeffects are reported on dyslipidemia in PCOS women (115,123, 124, 126, 203, 401, 432). Some evidence showed thatmetformin in PCOS women led to a decrease in plasmatotal and LDL cholesterol and in triglyceride levels (123,124, 126), as well as an increase serum HDL-cholesterolconcentrations (123, 124).
No significant effect of metformin on total cholesterol(WMD � �0.10; 95% CI, �0.41 to 0.21; P � 0.5), HDL-cholesterol (WMD � 0.04; 95% CI, �0.07 to 0.16; P � 0.4), andtriglycerides (WMD � �0.01; 95% CI, �0.29 to 0.27; P � 1)was detected by Lord et al. (30), whereas LDL-cholesterol wassignificantly reduced during treatment (WMD � �0.44; 95%CI, �0.79 to �0.08; P � 0.02).
Other investigators studying normal-weight PCOSwomen confirmed that 12 months of metformin administra-tion significantly improved LDL-cholesterol levels whencompared with baseline levels and the placebo group,whereas no effect on total cholesterol, HDL-cholesterol, andtriglycerides was found (115). In addition, at metformin sus-pension, LDL-cholesterol levels quickly worsened and re-turned to the baseline levels (115).
In a successive meta-analysis by Costello et al. (190), thelipid patterns of PCOS patients treated with metforminand OCs were compared, and no significant difference intotal cholesterol levels between treatments (WMD ��0.11; 95% CI, �0.53 to 0.30; P � 0.60) was observed.Contrarily, metformin resulted in a significantly lowertriglyceride level than OCs (WMD � �0.48; 95% CI, �0.86to �0.09; P � 0.01).
Lastly, Rizzo et al. (432) showed that metformin therapymay have a significant impact on atherogenic lipoproteinphenotype, which is considered a risk factor for PCOSwomen. The ISDs, and particularly metformin, have beenshown to improve this metabolic alteration, even if theycannot be considered as first-line therapy (432). In fact, asWild et al. (435) commented, the combination of metforminand thiazolinediones, although mechanistically attractive,has the potential to do harm. In addition, in the absence ofevidence from well-designed RCTs on PCOS subjects, weshould use the best evidence available from other popula-tions and the best clinical judgment to extrapolate (435).Thus, it is mandatory to use optimum tools to assess theburden of disease, and medication should be reserved onlyfor PCOS patients with remarkable lipid abnormalities in-cluding low HDL-cholesterol, high triglycerides, and thepresence of excess LDL-cholesterol (435).
Data obtained from a population at high risk for type 2 DM(396) and an unselected population of overweight and obesepatients (397) showed the beneficial effect of metformin on
32 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

lipoprotein pattern. In particular, metformin treatment wasshown to significantly increase HDL-cholesterol (OR, 5.0;95% CI, 1.6 to 8.3; P � 0.004) and to significantly reduceLDL-cholesterol (OR, �5.6; 95% CI, �8.3 to �3.0; P � 0.0001)and triglycerides (OR, �5.3; 95% CI, �10.5 to �0.03; P � 0.04)compared with placebo or no treatment, without signifi-cant differences between subgroups of PCOS/non-PCOSand obese/nonobese patients (396). Finally, in an uns-elected population of overweight and obese patients, met-formin reduced the incidence of dyslipidemia significantlymore than diet (397).
E. Impaired fibrinolysis
In PCOS patients, a significant increase in PAI-1, a 52-kDaglycoprotein whose main role is in the inhibition of plasminformation during plasminogen activation and fibrinolysis,has been demonstrated (248).
In several conditions, including not only PCOS (248) butalso type 2 DM and arterial/thrombotic diseases (436), PAI-1activity was related to insulin resistance and it increased,irrespective of obesity. Thus, it can be speculated that ele-vated PAI-1 activity increased cardiovascular morbidity seenin PCOS (437).
Recent data have, in fact, demonstrated that PAI-1 syn-thesis, expression in vitro, and action in vivo are up-regulatedby insulin (438). Adipose tissue is a major site of PAI-1mRNA expression, and visceral fat tissue expresses morePAI-1 than sc tissue (438).
Metformin inhibits PAI-1 production in human adiposecells in vitro (439). In fact, metformin decreases PAI-1production (and PAI-1 mRNA) under both basal and IL-1�-stimulated conditions. In particular, the metformin ef-fect on PAI-1 levels was dose dependent, and the PAI-1levels were inhibited by 47.8% at 1 mm metformin and by100% at 10 mm (439).
The role of metformin in reducing the PAI-1 levels hasbeen demonstrated in patients with type 2 DM (440).
Several authors (244, 247) also reported a significant re-duction in PAI-1 activity after metformin administration inPCOS patients, hypothesizing beneficial effects on preg-nancy outcomes. However, no clinical data are availableregarding the influence of metformin-related PAI-1 reduc-tion on cardiovascular risk in PCOS patients.
Finally, a significant reduction in circulating acylation-stimulating protein and in complement 3 was observed aftermetformin administration in 20 PCOS patients (441), sug-gesting further potential mechanisms by which metformincould act on impaired fibrinolysis in PCOS patients.
F. Chronic inflammation
An abnormal pattern of several markers of the chronic in-flammation has been demonstrated in women with PCOS (442,443).
Diamanti-Kandarakis et al. (442) evaluated the serum lev-els of cellular adhesion molecules, which reflect the degreeof low-grade chronic inflammation and have been associatedwith several insulin-resistant states. In particular, womenwith PCOS had levels of high sensitivity C-reactive protein
(CRP), soluble vascular cell adhesion molecule-1, and solubleendothelial leukocyte adhesion molecule-1 significantlyhigher in comparison to controls (442).
Metformin has been shown to exert a beneficial effect oninflammation markers with mediated and/or direct actions.It has been suggested that metformin acts on inflammatorymarkers by reducing insulin resistance (444). On the otherhand, a recent double-masked, double-dummy study dem-onstrated that metformin probably also exerts a direct actionon the inflammatory pattern because a similar improvementin insulin sensitivity in patients with type 2 DM with the useof metformin or the insulin secretagogue repaglinide wasobserved, even if the best benefits were observed undermetformin (445). In fact, metformin can exert a direct vas-cular antiinflammatory effect by dose-dependently inhibit-ing IL-1�-induced release of the proinflammatory cytokinesIL-6 and IL-8 in endothelial cells, human vascular smoothmuscle cells, and macrophages. Investigation of potentialsignaling pathways demonstrated that metformin dimin-ished IL-1�-induced activation and nuclear translocation ofnuclear factor-�B in smooth muscle cells. Furthermore, met-formin suppressed IL-1�-induced activation of the proin-flammatory phosphokinases Akt, p38, and Erk but did notaffect phosphoinositide-3 kinase activity (446).
In addition, it is well known that mitochondria have animportant role in intracellular energy generation, and recentdata have demonstrated their function in modulating cellularactivation and tissue injury associated with acute inflamma-tory processes with particular regard for neutrophil activa-tion. Metformin inhibits mitochondrial complex I, suggest-ing its effectiveness for the prevention or treatment of acuteinflammatory processes in which activated neutrophils havea crucial role (447).
Lastly, it was observed that plasma migration inhibitorfactor (MIF) concentrations and MIF mRNA expression inthe mononuclear cell are elevated in the obese, consistentwith a proinflammatory state in obesity (447). In this regard,metformin suppresses plasma MIF concentrations in theobese, suggestive of an antiinflammatory effect of this drug;thus, metformin may contribute to a potential antiathero-genic effect, which may have implications for the reducedcardiovascular mortality observed with metformin therapyin type 2 DM (448).
Clinical data confirmed the effects of metformin on chronicinflammatory markers observed in an experimental setting.
Metformin administration improved CRP and leukocytecount (442, 444) as well as serum high sensitivity CRP and solublevascular cell adhesion molecule levels in PCOS patients (442).
Some reports of Ibanez et al. (449, 450) clearly demon-strated that a high leukocyte count was present in girls withhyperinsulinemic hyperandrogenism, that metformin ther-apy decreased leukocyte count and neutrophil to lympho-cyte ratio, and also that a combination of metformin plus anoral or transdermal contraceptive could improve severalmarkers of low-grade chronic inflammation (450). In agree-ment with the Spanish data, Italian data (444) confirmed thebeneficial effect of metformin on the low-grade chronic in-flammation, specifically on leukocyte counts and CRP levels,in adult PCOS women. The decrease in serum CRP levelsduring metformin therapy is in agreement with the known
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 33
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

beneficial metabolic effects of this drug, and it suggests thatCRP or other inflammatory parameters could be used asmarkers for the efficiency of therapy in PCOS. The reduction incirculating levels of CRP with metformin therapy has also beendetected in obese women with PCOS (451). Moreover, whenmetforminisadministeredincombinationwithOCscontainingE2plus CA, the reduction seen in CRP was attenuated (451).
G. Endothelial impairment
Recent data support the hypothesis that PCOS is a con-dition associated with an increased vascular risk (452).
Our previous experience demonstrated that youngwomen of normal weight with PCOS , without dyslipidemiaand hypertension, when compared with age- and BMI-matched healthy subjects, had altered endothelial function,assessed by flow-mediated dilation of brachial arteries, andincreased intima-media thickness at carotid artery and serumET-1 values, suggesting early functional, structural, and bio-chemical preatherosclerotic vascular impairment (313).
Asymmetrical dimethylarginine (ADMA), a guanidino-substituted analog of l-arginine, is a potent endogenouscompetitive inhibitor of the endothelial NOS and has beenassociated with atherosclerosis, representing an independentmarker for cardiovascular morbidity and mortality (453).Recent data have demonstrated that ADMA is significantlyelevated in women with PCOS and that the degree of insulinresistance confers the greatest influence on ADMA level (453).
The effect of metformin on endothelium in PCOS patientshas been investigated. The rationale for supposing a bene-ficial effect of metformin on the PCOS-related dysfunctionconsists of its indirect effects on insulin sensitivity and hor-monal pattern and a direct action on cell proliferation.
Lund et al. (445) demonstrated, even if partially, a directaction of metformin on endothelium, whereas Romualdi et al.(454) showed a positive effect of metformin on the alteredvascular reactivity in normoinsulinemic normal-weightPCOS subjects, suggesting that the improvement might bemediated through hormonal changes, i.e., improved hy-perandrogenemia (454). On the other hand, in vitro studiesdemonstrated that metformin inhibited the proliferation ofHeLa or KB cells (455) and the drug may reduce atheroscle-rosis through its ability to inhibit tyrosine kinase prolifera-tion of smooth muscle cells (456).
A recent study (457) was designed to evaluate the effect ofmetformin on AGEs. This study involved 22 patients withPCOS who undertook metformin therapy for 6 months. At theend of the study, a significant reduction in AGE levels wasdetected. Several data (251, 458) evaluated the effects of met-formin on subclinical vascular disorders as surrogate end-points of atherosclerosis underlying CVD. A clinical study dem-onstrated that metformin improved coronary microvascularfunction and coronary flow reserve in 16 insulin-resistant PCOSpatients (458). Moreover, metaformin administration improvedendothelial structure and function in PCOS patients (251).
In particular, a 6-month metformin administration inyoung, normal-weight women with PCOS significantly re-duced the brachial artery diameter, flow-mediated dilation,diameter after reactive hyperemia, and intima-media thick-ness (251). The significant difference in insulin resistance
observed after only 6 months of metformin suggests an impor-tant role of insulin excess in the precocious development of ath-erosclerosis in PCOS patients. In fact, insulin could promoteatherogenesis by direct action on the arterial wall.
Finally, notwithstanding the generic notion of the ben-eficial effect of metformin on endothelium in PCOS pa-tients provided by these previous sparse data, future stud-ies are needed to establish the clinical relevance of thesefindings.
H. Syndrome X
The National Cholesterol Education Program Adult Treat-ment Panel (NCEPATP) defined the metabolic syndrome asthe presence of three of the five following factors: waistcircumference greater than 88 cm in females; fasting serumglucose 110 mg/dl or more; fasting serum triglycerides greaterthan 150 mg/dl; serum HDL-cholesterol less than 50 mg/dl;and blood pressure greater than 130/85 mm Hg (459). Thisclustering of abnormalities was also named dysmetabolic syn-drome or, in the female, syndrome X. The NCEPATP III guide-lines recognized syndrome X as a major cardiac risk factor anda specific ICD-9 code was assigned to the syndrome.
PCOS patients appear to have features of syndrome X. Syn-drome X has been reported to occur at an increased overallprevalence rate of 43–47% in women with PCOS (12) comparedwith the 24% prevalence rate in U.S. women (460). In addition,some authors suggested that in women with PCOS, an albuminto creatinine ratio greater than 7 mg/g is strongly associatedwith the metabolic syndrome, high blood pressure, and ele-vated alanine aminotransferase levels (461).
As detailed in the previous sections, metformin adminis-tration in patients with PCOS could theoretically result in animprovement of the single features of the metabolic syn-drome and a subsequent decreased risk for developing thesyndrome.
Obesity, type 2 DM, and metabolic syndrome are all dis-orders of energy balance, which the AMPK regulates at boththe cellular and whole body levels. As previously stated,AMPK switches cells from an anabolic state where nutrientsare taken up and stored to a catabolic state where they areoxidized. Based on these considerations, AMPK activationdue to metformin might be a potential mechanism for im-proving features of metabolic syndrome (462).
To date, no clinical data are available in literature re-garding the use of metformin in PCOS patients as a treat-ment for metabolic syndrome or as a preventive measurefor reducing the risk to develop metabolic syndrome.Thus, it is not currently possible to recommend metforminadministration in PCOS patients to prevent the risk andthe progression of metabolic syndrome. Thus, lifestylemodifications should always be considered the main ap-proach for these patients.
XI. Other Organ Impairment
A. Liver impairment
Nonalcoholic fatty liver disease (NAFLD) is a spectrum ofdiseases ranging from simple steatosis to steatohepatitis and
34 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

cirrhosis. NAFLD is closely associated with insulin resistanceand can be a hepatic manifestation of the metabolic syn-drome (463). Although insulin resistance and compensatoryhyperinsulinemia are frequently found in obese patientswith NAFLD, both are also noted in NAFLD patients withoutobesity and with NGT (463).
The incidence of NAFLD is significantly higher in PCOSpopulations, affecting up to 50% of patients, and these pa-tients have greater insulin resistance and are more likely tobe obese and have other features of the metabolic syndromethan PCOS patients without NAFLD (464–467).
Published data on the coexistence of PCOS and NAFLDare limited to only four retrospective studies (464–467), andit is unclear whether this clinical entity may be the result ofthe PCOS-related insulin resistance or whether NAFLD perse may contribute to insulin resistance frequently seen inpatients with PCOS.
Recent findings showed that reduced plasma high molec-ular weight adiponectin levels, as observed in PCOS patients,are closely associated with the severity of NAFLD (464–467).Normal high molecular weight adiponectin levels act to in-hibit hepatic stellate cells (HSCs), the key cells promotingliver fibrosis, by AMPK activation (468). Metformin might actindirectly increasing the adiponectin levels (469) but alsowith a direct effect of AMPK (468). In fact, metformin-me-diated activation of the AMPK seems to prevent hepaticfibrosis, inhibiting HSC proliferation via suppression of re-active oxygen species production and subsequent inhibitionof the AKT pathway (468). In addition, metformin-mediatedactivation of AMPK negatively modulates the platelet-de-rived growth factor-stimulated proliferation and migrationof human HSCs, reducing also the secretion of monocytechemoattractant protein-1 (470).
Clinical data on metformin administration demonstratedthat 500 mg of the drug given three times daily resulted ina significant improvement in serum alanine transaminaselevels in patients with NAFLD not responding to lifestyleinterventions (471). Metformin therapy was also associatedwith a reduction in surrogate liver fat markers in obesewomen with PCOS (472). A significant benefit of 12 monthsof metformin plus N-acetylcysteine was detected in 20patients with biopsy-proven NAFLD in terms of liver ste-atosis and fibrosis (473). Finally, ISDs can also lead toimprovement in histological abnormalities of nonalcoholicsteatohepatitis (474).
In conclusion, insulin resistance is a major feature ofNAFLD that, in some patients, can progress to steatohepa-titis. Treatments aimed at reducing insulin resistance havehad some success, but larger placebo-controlled studies areneeded to fully establish the efficacy of these interventions inreducing the deleterious effects of fat accumulation in theliver.
B. Thyroid impairment
Few data (475, 476) have shown a potential alteration of thethyroid function in PCOS patients.
Retrospective (475) and prospective (476) data suggestedthat metformin might modify thyroid hormone economy,causing suppression of TSH to subnormal levels. In partic-
ular, a recent study (476) on a very small sample of eightobese patients with DM and primary hypothyroidism underT4 replacement treatment demonstrated that 3-month met-formin (1700 mg daily) administration reduced significantlythe plasma TSH levels and increased those of free T4 (476).Furthermore, no data regarding metformin effects on thyroidimpairment in PCOS population are available in literature.
C. Cognitive function
Presently, no published studies specifically evaluated cog-nitive function in PCOS.
Hyperandrogenism and hyperestrogenism have been hy-pothesized to differentially influence cognitive functionacross cognitive domains in the PCOS population. A recentlarge internet-based study (477) compared neuropsycholog-ical functioning in right-handed women with and withoutPCOS, and it demonstrated that PCOS is not associated withmasculinized cognitive functioning and that the impairedperformance on tasks is subtle and unlikely to affect dailyfunctioning. A successive study by Schattmann et al. (478)showed that PCOS women had significantly worse perfor-mance on tests of verbal fluency, verbal memory, manualdexterity, and visuospatial working memory than thehealthy control women.
The same authors (479) showed that 3 months of treatmenteither with anti-androgen CA plus estrogen or with placebodid not have a significant impact on cognitive performancein women with PCOS, although reductions in free testoster-one may be beneficial for verbal fluency. However, no ex-perimental or clinical data on metformin administration onthis issue are actually available in the literature.
D. Sleep disturbances
PCOS is associated with poor sleep quality, excessive day-time sleepiness (EDS), and increased risk for obstructivesleep apnea (OSA) (480, 481).
To date, no data are available in literature on the potentialrole of metformin treatment in PCOS patients with sleepdisturbances. Moreover, its potential role is suggestible. Infact, insulin levels and measures of glucose tolerance inPCOS are strongly correlated with the risk and severity ofOSA. On the other hand, several data seem to indicate thatthe proinflammatory cytokines IL-6 and TNF-� were ele-vated, independently by obesity, in patients with disordersof EDS and that these cytokines could be the mediators ofdaytime sleepiness. Metformin could act on EDS (or OSA),reducing systemic inflammation (see Section X.F).
In obese patients, EDS and OSA may be manifestations ofsyndrome X, and an improvement of features of this syn-drome by metformin treatment might also result in an ame-lioration of the sleep disturbances.
XII. High-Risk Patients for PCOS
In the human species, prenatal growth restriction wasdemonstrated in a high percentage of cases to be followed bya postnatal catch-up of growth related to an exaggerated fatgain, particularly visceral fat (411). Girls with growth re-
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 35
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

striction and precocious pubarche are recognized to be at riskfor development of hyperinsulinemic androgen excess, lead-ing up to PCOS (411).
Some authors proposed to use metformin in post-preco-cious pubarche adolescents (116, 179) and in postmenarcheallow birth weight (482) as a treatment to prevent progressionto PCOS.
In particular, 6 months of metformin treatment in girlswith precocious pubarche was demonstrated to induce lessadipose body composition and proinflammatory state, toimprove lipid profile, and to attenuate adrenarche (116).
Early metformin therapy in precocious pubarche girls pre-vented the progression to PCOS (116, 179). Successive studies(482, 483) confirmed that prepubertal metformin therapy hasnormalizing effects on PCOS features in high-risk girls witha combined history of low birth weight and precociouspubarche, but its beneficial effects are reversed as soon asmetformin therapy is discontinued (483). However, in girlswith similar characteristics, long-term metformin treatmentreduced total and visceral fat and delayed menarche withoutattenuating linear growth (482, 483).
XIII. Future Perspectives
Notwithstanding so much clinical data on the uses of met-formin in diabetic and PCOS patients, the specific mecha-nisms of metformin action still must be completely eluci-dated, and only when these mechanisms are clarified shouldit be possible to understand all potential uses of this drug. Inparticular, recent data suggested a pleiotropic effect of thedrug across its action on AMPK, even if further investi-gations are necessary to elucidate the function of met-formin-related activation of the AMPK in reproductionand tumorogenesis.
From a clinical point of view, the crucial issue for the nextfew years will be to define predictive factors, including pos-sibly BMI and/or measures of insulin resistance, for a goodresponse to metformin to optimize the treatment(s) and de-fine the best protocol(s), especially in terms of timing, and themost effective dosages for different PCOS subpopulationsand for different end-points. In this regard, there is also thepotential for pharmacogenetic identification of women likelyto respond to metformin.
These problems could probably be solved by using well-designed RCTs focused on select phenotypes of the PCOSpopulation, instead of by conducting large-scale clinical tri-als on unselected patients, and successive wide clinical trialsshould be designed for evaluating the usefulness of met-formin not only as monotherapy or as a drug to be associatedwith other treatments but also as a therapeutic step in anintegrated strategy. In this regard, a wide multicenter ItalianRCT comparing different strategies for metformin use is inthe recruiting phase, and the data will not be available before2010 (484). Finally, a well-validated and clinically applicableprediction model should be constructed to select the patientswith the highest success chances, making the best patient-tailored therapeutic decision.
An interesting field of research will be the evaluation of theeffects of metformin on endometrium. The future studies
should establish whether metformin improves endometrialbiology and histology, reducing miscarriages and premalig-nancy endometrial diseases. Certainly, to obtain significantdata, a highly selected population must be studied.
Doubts existed until now regarding the use of metforminduring pregnancy. Available data seem to be reassuring withregard to metformin administration in diabetic patients. Fur-thermore, well-designed RCTs are advocated before met-formin would be safely prescribed in pregnant patients af-fected by PCOS as a preventive drug for reducing (potential)maternal and neonatal complications.
Even if metformin is not a cosmetic or anti-obesity drug,further research should clarify whether it has a role in themanagement of PCOS-related hirsutism and obesity and,specifically, its potential usefulness for optimizing thefirst-line treatments (e.g., antiandrogens and lifestyle mod-ifications, respectively).
More and more cellular, animal, and human data havedemonstrated the beneficial effects of metformin on severalmarkers of CVD. Unfortunately, no wide clinical trial hasdemonstrated any preventive effect of metformin in PCOSpatients. Thus, the long-term effect of metformin adminis-tration on morbidity and mortality in PCOS patients at highrisk for metabolic derangements should be also evaluated inthe future.
Finally, further studies on the clinical and metabolic effectsof metformin suspension are also needed before the use ofthis drug become common in clinical practice as treatment ofthe PCOS features and, specifically, as a preventive measurefor young girls at risk for developing PCOS.
XIV. Summary
In the clinical practice, metformin administration is lessuseful than OCs to regulate the menstrual cycle, but it shouldbe considered as initial intervention in (overweight or obese)PCOS patients in whom OCs are contraindicated or with aninitial metabolic derangement. In fact, clinical evidenceshows that this drug is an effective first treatment for re-storing ovulatory menstrual cycles in oligoamenorrheicPCOS patients, improving insulin sensitivity and, unlikeOCs, lipoprotein pattern. On the contrary, OCs might worseninsulin sensitivity, and prospective long-term trials areneeded to determine whether any of these changes translateinto differences in clinical outcomes between women treatedwith metformin and those treated with OCs.
In PCOS patients with anovulatory infertility who werenot previously treated, the administration of metformin plusCC is not better than monotherapy (metformin alone or CCalone); thus, the combined approach should be avoided as aninitial treatment of anovulatory infertility. To date, no spe-cific recommendation can be given regarding the use of CCor metformin because the best first-step option to induceovulation in infertile anovulatory PCOS patients remainsunclear and probably depends on the wishes of the patient.If time is of the essence, CC will work more quickly but couldresult in multiparity. If the woman is willing to wait for a fewmonths, metformin could be equally effective. Metformincould also be a valid option in those PCOS patients who
36 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

absolutely wish to avoid multiple gestations and/or in pa-tients who do not tolerate CC (i.e., secondary to moodchanges, visual disturbances, etc.). On the other hand, PCOSpatients who have failed to ovulate with CC (i.e., CC-resis-tant) may benefit from the addition of metformin. It is pos-sible to hypothesize that metformin therapy would augmentthe induction of ovulation in CC-resistant women because ofits favorable change in androgens, gonadotropins, and in-sulin through mechanisms distinct from those of CC. It isplausible to assume that women with CC resistance receivingmetformin have an increased response to CC secondary to animproved follicle steroidogenesis caused by the effect of met-formin administration.
Certainly, metformin monotherapy seems to be more effec-tive and cheaper than LOD for treating anovulatory infertileCC-resistant PCOS patients, and LOD should be reserved forinducing ovulation only in anovulatory PCOS patients withother suspected and/or diagnosed factors of subfertility (e.g.,endometriosis, uterine leiomyomas). Currently, data on the ef-ficacy of metformin pretreatment before CC in CC-resistantpatients are controversial and inconclusive. In patients whoreceived gonadotropins as treatment for anovulation, met-formin addition increases the rate of monoovulations, reducingthe risk of cancelled cycles, reduced the duration of gonado-tropins administrations and the doses of gonadotropins re-quired whereas in infertile PCOS patients scheduled for IVFcycles, metformin cotreatment reduces the OHSS risk and, thus,its use should be planned for patients at high-risk for OHSS.
Beneficial effects of metformin in reducing the rate ofmiscarriage in PCOS women have been widely suggested,but to date no advantage has been demonstrated when met-formin is administered before pregnancy. On the other hand,considering the lack of RCTs it is not possible to either sug-gest or advise against the use of metformin during pregnancyfor reducing the abortion risk. More relevant clinical data areneeded regarding the potential benefits of metformin ad-ministration during pregnancy on miscarriage prevention.
Observational and anecdotal findings suggest that met-formin may be beneficial in pregnancy by potentially reduc-ing the risk of gestational DM or other insulin resistance-associated pregnancy complications, e.g., PIH and PE.Furthermore, at present the routine use of metformin duringpregnancy in PCOS patients to prevent these morbidities isnot recommended. In fact, well-powered RCTs are neededbefore general use of metformin during pregnancy in PCOSpatients is advocated. Currently, there is no evidence sug-gesting a positive or negative effect of metformin adminis-tration on infant outcomes during both pregnancy and lac-tation. Furthermore, while waiting for definitive dataregarding the continuation of metformin during pregnancyfor women with documented insulin resistance to becomeavailable, the cessation of metformin after a positive preg-nancy test is still a reasonable course of action.
Preliminary clinical and experimental data showed thatmetformin could exert beneficial effects on endometrium,suggesting a potential and future role for the prevention andtreatment of endometrial degeneration due to PCOS-relatedchronic anovulation. Currently, it is not possible to drawdefinitive conclusions on these effects, and further researchon a large sample and with long-term follow-up is needed to
confirm these preliminary positive results. In addition, stud-ies on the potential beneficial effects of metformin in reduc-ing the long-term consequences of chronic anovulation aretotally lacking.
The clinical effectiveness of metformin on hirsutism seemsto be limited and inferior to that reported with OCs, whichis also low. In hirsute PCOS patients, metformin could becoadministered with antiandrogens, i.e., flutamide, and OCsto reduce the potentially increased metabolic and cardiovas-cular risks related to OC use.
Controversial data are available on the effects of met-formin on weight loss. Certainly, metformin should not beconsidered a treatment for weight loss, even in obese PCOSpatients. However, metformin administration in PCOS pa-tients who follow lifestyle modification programs seem re-lated to the best benefits in terms of weight loss and meta-bolic pattern improvement.
In addition, the role of metformin as a preventive measurefor PCOS development in girls at high risk for developingPCOS is strongly limited because the available data are stillscarce and long-term effects on these specific populations aretotally lacking.
Finally, metformin seems to be effective in amelioratingseveral intermediate markers of CVD in PCOS women dur-ing its administration. In particular, benefits may be seen inatherogenic profiles, including markers of subclinical inflam-mation, dyslipidemia, and insulin resistance. Enhanced en-dothelial function, coronary microvascular function, and cor-onary flow rate may also be seen. Notwithstanding theseimprovements in secondary CVD markers under metformintherapy in PCOS women, conclusive and prospective long-term studies have yet to be carried out, and the clinicalefficacy of metformin in the prevention of the developmentof type 2 DM or in reducing the cardiovascular accidents inPCOS women is to be still proven.
Acknowledgments
Received July 8, 2008. Accepted November 12, 2008.Address all correspondence and requests for reprints to: Stefano
Palomba, M.D., Department of Gynecology and Obstetrics, University“Magna Graecia” of Catanzaro, Via Pio X, 88100 Catanzaro, Italy. E-mail:[email protected]
Author Disclosure Statement: S.P., A.F., F.Z., and F.O. have nothingto declare.
References
1. Zawadzki JK, Dunaif A 1992 Diagnostic criteria for polycysticovary syndrome: towards a rational approach. In: Dunaif A, GivensJR, Haseltine FP, Merriam GR, eds. Polycystic ovary syndrome.Boston: Blackwell; 337–384
2. Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Work-shop Group 2004 Revised 2003 consensus on diagnostic criteria andlong-term health risks related to polycystic ovary syndrome. FertilSteril 81:19–25
3. Polson DW, Adams J, Wadsworth J, Franks S 1988 Polycysticovaries—a common finding in normal women. Lancet 1:870–872
4. Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E, Es-cobar- Morreale HF, Futterweit W, Janssen OE, Legro RS, Nor-man RJ, Taylor AE, Witchel SF; Androgen Excess Society 2006Position statement: criteria for defining polycystic ovary syndrome
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 37
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

as a predominantly hyperandrogenic syndrome: an Androgen Ex-cess Society guideline. J Clin Endocrinol Metab 91:4237–4245
5. Azziz R 2006 Controversy in clinical endocrinology: diagnosis ofpolycystic ovarian syndrome: the Rotterdam criteria are prema-ture. J Clin Endocrinol Metab 91:781–785
6. Franks S 2006 Controversy in clinical endocrinology: diagnosis ofpolycystic ovarian syndrome: in defense of the Rotterdam criteria.J Clin Endocrinol Metab 91:786–789
7. Robinson S, Kiddy D, Gelding SV, Willis D, Niththyananthan R,Bush A, Johnston DG, Franks S 1993 The relationship of insulininsensitivity to menstrual pattern in women with hyperandro-genism and polycystic ovaries. Clin Endocrinol (Oxf) 39:351–355
8. Adams JM, Taylor AE, Crowley Jr WF, Hall JE 2004 Polycysticovarian morphology with regular ovulatory cycles: insights intothe pathophysiology of polycystic ovarian syndrome. J Clin En-docrinol Metab 89:4343–4350
9. Chang PL, Lindheim SR, Lowre C, Ferin M, Gonzalez F, BerglundL, Carmina E, Sauer MV, Lobo RA 2000 Normal ovulatory womenwith polycystic ovaries have hyperandrogenic pituitary-ovarianresponses to gonadotropin-releasing hormone agonist testing.J Clin Endocrinol Metab 85:995–1000
10. Barber TM, Wass JA, McCarthy MI, Franks S 2007 Metaboliccharacteristics of women with polycystic ovaries and oligoam-enorrhoea but normal androgen levels: implications for the man-agement of polycystic ovary syndrome. Clin Endocrinol (Oxf)66:513–517
11. Sam S, Dunaif A 2003 Polycystic ovary syndrome: syndrome XX?Trends Endocrinol Metab 14:365–370
12. Apridonidze T, Essah PA, Iuorno MJ, Nestler JE 2005 Prevalenceand characteristics of the metabolic syndrome in women with poly-cystic ovary syndrome. J Clin Endocrinol Metab 90:1929–1935
13. Palomba S, Falbo A, Orio F, Zullo F 2008 Insulin sensitizing agentsand reproductive function in polycystic ovary syndrome patients.Curr Opin Obstet Gynecol 20:364–373
14. Legro RS, Strauss JF 2002 Molecular progress in infertility: poly-cystic ovary syndrome. Fertil Steril 78:569–576
15. Goodarzi MO 2008 Looking for polycystic ovary syndrome genes:rational and best strategy. Semin Reprod Med 26:5–13
16. Kahsar-Miller MD, Nixon C, Boots LR, Go RC, Azziz R 2001Prevalence of polycystic ovary syndrome (PCOS) in first-degreerelatives of patients with PCOS. Fertil Steril 75:53–58
17. Azziz R, Woods KS, Reyna R, Key TJ, Knochenhauer ES, YildizBO 2004 The prevalence and features of the polycystic ovary syn-drome in an unselected population. J Clin Endocrinol Metab 89:2745–2749
18. Legro RS, Kunselman AR, Demers L, Wang SC, Bentley-Lewis R,Dunaif A 2002 Elevated dehydroepiandrosterone sulfate levels asthe reproductive phenotype in the brothers of women with poly-cystic ovary syndrome. J Clin Endocrinol Metab 87:2134–2138
19. Nelson VL, Legro RS, Strauss JF, McAllister JM 1999 Augmentedandrogen production is a stable steroidogenic phenotype ofpropagated theca cells from polycystic ovaries. Mol Endocrinol13:946 –957
20. Legro RS, Bentley-Lewis R, Driscoll D, Wang SC, Dunaif A 2002Insulin resistance in the sisters of women with polycystic ovarysyndrome: association with hyperandrogenemia rather than men-strual irregularity. J Clin Endocrinol Metab 87:2128–2133
21. Sam S, Coviello AD, Sung YA, Legro RS, Dunaif A 2008 Metabolicphenotype in the brothers of women with polycystic ovary syn-drome. Diabetes Care 31:1237–1241
22. Kent SC, Gnatuk CL, Kunselman AR, Demers LM, Lee PA, LegroRS 2008 Hyperandrogenism and hyperinsulinism in children ofwomen with polycystic ovary syndrome: a controlled study. J ClinEndocrinol Metab 93:1662–1669
23. Recabarren SE, Smith R, Rios R, Maliqueo M, Echiburu B, Cod-ner E, Cassorla F, Rojas P, Sir-Petermann T 2008 Metabolic profilein sons of women with polycystic ovary syndrome. J Clin Endo-crinol Metab 93:1820–1826
24. Sam S, Sung YA, Legro RS, Dunaif A 2008 Evidence for pancreatic�-cell dysfunction in brothers of women with polycystic ovarysyndrome. Metabolism 57:84–89
25. Dunaif A 1997 Insulin resistance and the polycystic ovary syn-
drome: mechanism and implications for pathogenesis. Endocr Rev18:774–800
26. Legro RS, Castracane VD, Kauffman RP 2004 Detecting insulinresistance in polycystic ovary syndrome: purposes and pitfalls.Obstet Gynecol Surv 59:141–154
27. Palomba S, Orio Jr F, Falbo A, Russo T, Tolino A, Zullo F 2006Effects of metformin and clomiphene citrate on ovarian vascu-larity in patients with polycystic ovary syndrome. Fertil Steril86:1694 –1701
28. Palomba S, Russo T, Orio Jr F, Falbo A, Manguso F, Cascella T,Tolino A, Carmina E, Colao A, Zullo F 2006 Uterine effects ofmetformin administration in anovulatory women with polycysticovary syndrome. Hum Reprod 21:457–465
29. Palomba S, Russo T, Orio Jr F, Falbo A, Manguso F, SammartinoA, Tolino A, Colao A, Carmina E, Zullo F 2006 Uterine effects ofclomiphene citrate in women with polycystic ovary syndrome: aprospective controlled study. Hum Reprod 21:2823–2829
30. Lord JM, Flight IH, Norman RJ 2003 Insulin-sensitising drugs(metformin, troglitazone, rosiglitazone, pioglitazone, D-chiro-ino-sitol) for polycystic ovary syndrome. Cochrane Database Syst RevCD003053
31. Dunaif A 2008 Drug insight: insulin-sensitizing drugs in the treat-ment of polycystic ovary syndrome—a reappraisal. Nat Clin PractEndocrinol Metab 4:272–283
32. Velazquez EM, Mendoza S, Hamer T, Sosa F, Glueck CJ 1994Metformin therapy in polycystic ovary syndrome reduces hyper-insulinemia, insulin resistance, hyperandrogenemia, and systolicblood pressure, while facilitating normal menses and pregnancy.Metabolism 43:647–654
33. Salley KE, Wickham EP, Cheang KI, Essah PA, Karjane NW,Nestler JE 2007 Glucose intolerance in polycystic ovary syndrome:a position statement of the Androgen Excess Society. J Clin Endo-crinol Metab 92:4546–4556
34. Polycystic Ovary Syndrome Writing Committee 2005 AmericanAssociation of Clinical Endocrinologists position statements onmetabolic and cardiovascular consequences of polycystic ovarysyndrome. Endocr Pract 11:126–134
35. Thessaloniki ESHRE/ASRM-Sponsored PCOS Consensus WorkshopGroup 2008 Consensus on infertility treatment related to polycysticovary syndrome. Fertil Steril 89:505–522
36. Nestler JE 2008 Metformin in the treatment of infertility in poly-cystic ovarian syndrome: an alternative perspective. Fertil Steril90:14–16
37. DeUgarte CM, Bartolucci AA, Azziz R 2005 Prevalence of insulinresistance in the polycystic ovary syndrome using the homeostasismodel assessment. Fertil Steril 83:1454–1460
38. Dunaif A, Segal KR, Shelley DR, Green G, Dobrjansky A, LicholaiT 1992 Evidence for distinctive and intrinsic defects in insulin actionin polycystic ovary syndrome. Diabetes 41:1257–1266
39. Holte J, Bergh T, Berne C, Wide L, Lithell H 1995 Restored insulinsensitivity but persistently increased early insulin secretion afterweight loss in obese women with polycystic ovary syndrome. J ClinEndocrinol Metab 80:2586–2593
40. Skov V, Glintborg D, Knudsen S, Jensen T, Kruse TA, Tan Q,Brusgaard K, Beck-Nielsen H, Højlund K 2007 Reduced expres-sion of nuclear-encoded genes involved in mitochondrial oxidativemetabolism in skeletal muscle of insulin-resistant women withpolycystic ovary syndrome. Diabetes 56:2349–2355
41. Rosenfield RL, Barnes RB, Cara JF, Lucky AW 1990 Dysregulationof cytochrome P450c 17� as the cause of polycystic ovarian syn-drome. Fertil Steril 53:785–791
42. Weil SJ, Vendola K, Zhou J, Adesanya OO, Wang J, Okafor J,Bondy CA 1998 Androgen receptor gene expression in the primateovary: cellular localization, regulation, and functional correlations.J Clin Endocrinol Metab 83:2479–2485
43. Vendola KA, Zhou J, Adesanya OO, Weil SJ, Bondy CA 1998Androgens stimulate early stages of follicular growth in the pri-mate ovary. J Clin Invest 101:2622–2629
44. Hsueh AJ, Billig H, Tsafriri A 1994 Ovarian follicle atresia: ahormonally controlled apoptotic process. Endocr Rev 15:707–724
45. Diamanti-Kandarakis E, Kouli C, Tsianateli T, Bergiele A 1998Therapeutic effects of metformin on insulin resistance and hy-
38 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

perandrogenism in polycystic ovary syndrome. Eur J Endocrinol138:269–274
46. Stumvoll M, Nurjhan N, Perriello G, Dailey G, Gerich JE 1995Metabolic effects of metformin in non-insulin-dependent diabetesmellitus. N Engl J Med 333:550–554
47. Prager R, Schernthaner G, Graf H 1986 Effect of metformin onperipheral insulin sensitivity in non insulin dependent diabetesmellitus. Diabetes Metab 12:346–350
48. Widen EIM, Eriksson JG, Groop LC 1992 Metformin normalizesnonoxidative glucose metabolism in insulin-resistant normoglyce-mic first-degree relatives of patients with NIDDM. Diabetes 41:354–358
49. Wollen N, Bailey CJ 1988 Inhibition of hepatic gluconeogenesisby metformin: synergism with insulin. Biochem Pharmacol 37:4353– 4358
50. Bailey CJ, Turner RC 1996 Metformin. N Engl J Med 334:574–57951. Komori T, Hotta N, Kobayashi M, Sakakibara F, Koh N, Sakamoto
N 1993 Biguanides may produce hypoglycemic action in isolated rathepatocytes through their effects on L-alanine transport. Diabetes ResClin Pract 22:11–17
52. Radziuk J, Zhang Z, Wiernsperger N, Pye S 1997 Effects of met-formin on lactate uptake and gluconeogenesis in the perfused ratliver. Diabetes 46:1406–1413
53. Large V, Beylot M 1999 Modifications of citric acid cycle activityand gluconeogenesis in streptozotocin-induced diabetes and ef-fects of metformin. Diabetes 48:1251–1257
54. Coyral-Castel S, Tosca L, Ferreira G, Jeanpierre E, Rame C, LometD, Caraty A, Monget P, Chabrolle C, Dupont J 2008 The effect ofAMP-activated kinase activation on gonadotrophin-releasing hor-mone secretion in GT1-7 cells and its potential role in hypothalamicregulation of the oestrous cyclicity in rats. J Neuroendocrinol 20:335–346
55. Tosca L, Chabrolle C, Uzbekova S, Dupont J 2007 Effects of met-formin on bovine granulosa cells steroidogenesis: possible involve-ment of adenosine 5� monophosphate-activated protein kinase(AMPK). Biol Reprod 76:368–378
56. Tosca L, Solnais P, Ferre P, Foufelle F, Dupont J 2006 Metformin-induced stimulation of adenosine 5� monophosphate-activatedprotein kinase (PRKA) impairs progesterone secretion in rat gran-ulosa cells. Biol Reprod 75:342–351
57. Zhou G, Myers R, Li Y, Chen Y, Shen X, Fenyk-Melody J, Wu M,Ventre J, Doebber T, Fujii N, Musi N, Hirshman MF, GoodyearLJ, Moller DE 2001 Role of AMP-activated protein kinase in mech-anism of metformin action. J Clin Invest 108:1167–1174
58. Argaud D, Roth H, Wiernsperger N, Leverve X 1993 Metformindecreases gluconeogenesis by enhancing the pyruvate kinase fluxin isolated rat hepatocytes. Eur J Biochem 213:1341–1348
59. Youn D, Park K, Lee Y, Park Y, Kim D 2008 Metformin inhibitshepatic gluconeogenesis through AMP-activated protein kinase-dependent regulation of the orphan nuclear receptor SHP. Diabetes57:306–314
60. Zou MH, Kirkpatrick SS, Davis BJ, Nelson JS, Wiles WG, SchlattnerU, Neumann D, Brownlee M, Freeman MB, Goldman MH 2004Activation of the AMP activated protein kinase by the anti-diabeticdrug metformin in vivo. J Biol Chem 279:43940–43951
61. Shaw RJ, Lamia KA, Vasquez D, Koo SH, Bardeesy N, DepinhoRA, Montminy M, Cantley LC 2005 The kinase LKB1 mediatesglucose homeostasis in liver and therapeutic effects of metformin.Science 310:1642–1646
62. Elia E, Sander V, Luchetti CG, Solano ME, Di Girolamo G,Gonzalez C, Motta AB 2006 The mechanisms involved in the actionof metformin in regulating ovarian function in hyperandrogenizedmice. Mol Hum Reprod 12:475–481
63. Fulgencio JP, Kohl C, Girard J, Pegorier JP 2001 Effect of met-formin on fatty acid and glucose metabolism in freshly isolatedhepatocytes and on specific gene expression in cultured hepato-cytes. Biochem Pharmacol 62:439–446
64. Sarabia V, Lam L, Burdett E 1992 Glucose transport in humanskeletal muscle cells in culture. Stimulation by insulin and met-formin. J Clin Invest 90:1386–1395
65. Matthaei S, Hamann A, Klein HH 1992 Evidence that metforminincreases insulin-stimulated glucose transport by potentiating in-sulin-induced translocation of glucose transporters from an intra-
cellular pool to the cell surface in rat adipocytes. Horm Metab Res26:S34–S41
66. Jensterle M, Janez A, Mlinar B, Marc J, Prezelj J, Pfeifer M 2008Impact of metformin and rosiglitazone treatment on glucose trans-porter 4 mRNA expression in women with polycystic ovary syn-drome. Eur J Endocrinol 158:793–801
67. DeFronzo RA 1999 Pathogenesis of type 2 diabetes: implicationsfor metformin. Drugs 58:29–30
68. Nosadini R, Avogaro A, Trevisan R 1987 Effect of metformin oninsulin-stimulated glucose turnover and insulin binding to recep-tors in type II diabetes. Diabetes Care 10:62–67
69. Matthaei S, Hamann A, Klein HH, Benecke H, Kreymann G, FlierJS, Greten H 1991 Association of metformin’s effect to increaseinsulin-stimulated glucose transport with potentiation of insulin-induced translocation of glucose transporters from intracellularpool to plasma membrane in rat adipocytes. Diabetes 40:850–857
70. Jacobs DB, Hayes GR, Truglia JA, Lockwood DH 1986 Effects ofmetformin on insulin receptor tyrosine kinase activity in rat adi-pocytes. Diabetologia 29:798–801
71. Dominguez LJ, Davidoff AJ, Srinivas PR, Standley P, Walsh MF,Sowers JR 1996 Effects of metformin on tyrosine kinase activity,glucose transport, and intracellular calcium in rat vascular smoothmuscle. Endocrinology 137:113–121
72. Stith BJ, Goalstone ML, Espinoza R, Mossel C, Roberts D,Wiernsperger N 1996 The antidiabetic drug metformin elevatesreceptor tyrosine kinase activity and inositol 1,4,5-trisphosphatemass in Xenopus oocytes. Endocrinology 137:2990–2999
73. Santos RF, Nomizo R, Wajhenberg BL, Reaven GM, Azhar S 1995Changes in insulin receptor tyrosine kinase activity associated withmetformin treatment of type 2 diabetes. Diabete Metab 21:274–280
74. Klip A, Leiter LA 1990 Cellular mechanism of action of metformin.Diabetes Care 13:696–704
75. Khan NA, Wiernsperger N, Quemener V, Moulinoux JP 1994Internalization of metformin is necessary for its action on poten-tiating the insulin-induced Xenopus laevis oocyte maturation. J En-docrinol 142:245–250
76. Hundal HS, Ramlal T, Reyes R, Leiter LA, Klip A 1992 Cellularmechanism of metformin action involves glucose transporter trans-location from an intracellular pool to the plasma membrane in L6muscle cells. Endocrinology 131:1165–1173
77. Yoa RG, Rapin JR, Wiersnperger NF, Martinand A, Belleville I1993 Demonstration of defective glucose uptake and storage inerythrocytes from non-insulin dependent diabetic patients and ef-fects of metformin. Clin Exp Pharmacol Physiol 20:563–567
78. Fischer Y, Thomas J, Rosen P, Kammermeier H 1995 Action ofmetformin on glucose transport and glucose transporter GLUT1and GLUT4 in heart muscle cells from healthy and diabetic rats.Endocrinology 136:412–420
79. Kozka IJ, Holman GD 1993 Metformin blocks downregulation ofcell surface GLUT4 caused by chronic insulin treatment of ratadipocytes. Diabetes 42:1159–1165
80. Bailey CJ, Puah JA 1986 Effect of metformin on glucose metabolismin mouse soleus muscle. Diabete Metab 12:212–218
81. Arlt W, Auchus RJ, Miller WL 2001 Thiazolidinediones but notmetformin directly inhibit the steroidogenic enzymes P450c17 and3�-hydroxysteroid dehydrogenase. J Biol Chem 276:16767–16771
82. Mansfield R, Galea R, Brincat M, Hole D, Mason H 2003 Met-formin has direct effects on human ovarian steroidogenesis. FertilSteril 79:956–962
83. Attia GR, Rainey WE, Carr BR 2001 Metformin directly inhibitsandrogen production in human thecal cells. Fertil Steril 76:517–524
84. Nestler JE, Jakubowicz DJ 1996 Decreases in ovarian cytochromeP450c17� activity and serum free testosterone after reduction ofinsulin secretion in polycystic ovary syndrome. N Engl J Med335:617–623
85. Nestler JE, Jakubowicz DJ 1997 Lean women with polycystic ovarysyndrome respond to insulin reduction with decreases in ovarianP450c17� activity and serum androgens. J Clin Endocrinol Metab82:4075–4079
86. Erickson GF, Magoffin DA, Cragun JR, Chang RJ 1990 The effectsof insulin and insulin-like growth factors-I and -II on estradiolproduction by granulosa cells of polycystic ovaries. J Clin Endo-crinol Metab 70:894–902
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 39
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022
87. Sonnatag B, Gotte M, Wiilfing P, Schuring AN, Kiesel L, Greb RR2005 Metformin alters insulin signaling and viability of humangranulosa cells. Fertil Steril 84:1173–1179
88. la Marca A, Morgante G, Paglia T, Ciotta L, Cianci A, De Leo V1999 Effects of metformin on adrenal steroidogenesis in womenwith polycystic ovary syndrome. Fertil Steril 72:985–989
89. Genazzani AD, Strucchi C, Luisi M, Casarosa E, Lanzoni C,Baraldi E, Ricchieri F, Mehmeti H, Genazzani AR 2006 Metforminadministration modulates neurosteroids secretion in non-obeseamenorrhoic patients with polycystic ovary syndrome. GynecolEndocrinol 22:36–43
90. Budak E, Fernandez Sanchez M, Bellver J, Cervero A, Simon C,Pellicer A 2006 Interactions of the hormones leptin, ghrelin, adi-ponectin, resistin, and PYY3-36 with the reproductive system. FertilSteril 85:1563–1581
91. Barb D, Williams CJ, Neuwirth AK, Mantzoros CS 2007 Adi-ponectin in relation to malignancies: a review of existing basicresearch and clinical evidence. Am J Clin Nutr 86:s858–s866
92. Kadowaki T, Yamauchi T 2005 Adiponectin and adiponectin re-ceptors. Endocr Rev 26:439–451
93. Dunn CJ, Peters DH 1995 Metformin. A review of its pharmaco-logical properties and therapeutic use in non-insulin-dependentdiabetes mellitus. Drugs 49:721–749
94. Proctor WR, Bourdet DL, Thakker DR 2008 Mechanisms under-lying saturable intestinal absorption of metformin. Drug MetabDispos 36:1650–1658
95. Kovo M, Kogman N, Ovadia O, Nakash I, Golan A, Hoffman A2008 Carrier-mediated transport of metformin across the humanplacenta determined by using the ex vivo perfusion of the placentalcotyledon model. Prenat Diagn 28:544–548
96. Vanky E, Zahlsen K, Spigset O, Carlsen SM 2005 Placental pas-sage of metformin in women with polycystic ovary syndrome.Fertil Steril 83:1575–1578
97. Elliott BD, Langer O, Schuessling F 1997 Human placental glucoseuptake and transport are not altered by the oral antihyperglycemicagent metformin. Am J Obstet Gynecol 176:527–530
98. Glueck CJ, Wang P 2007 Metformin before and during pregnancyand lactation in polycystic ovary syndrome. Expert Opin Drug Saf6:191–198
99. Scheen AJ, de Magalhaes AC, Salvatore T, Lefebvre PJ 1994 Re-duction of the acute bioavailability of metformin by the �-gluco-sidase inhibitor acarbose in normal man. Eur J Clin Invest 24:50–54
100. Somogyi A, Stockley C, Keal J, Rolan P, Bochner F 1987 Reductionof metformin renal tubular secretion by cimetidine in man. Br J ClinPharmacol 23:545–551
101. Takane H, Shikata E, Otsubo K, Higuchi S, Ieiri I 2008 Polymor-phism in human organic cation transporters and metformin action.Pharmacogenomics 9:415–422
102. Umehara KI, Iwatsubo T, Noguchi K, Kamimura H 2008 Func-tional involvement of the organic cation transporter 2 (rOct2) in therenal uptake of organic cations in rats. J Int Med Res 36:123–136
103. Song I, Shin H, Shim E, Jung I, Kim W, Shon J, Shin J 2008 Geneticvariants of the organic cation transporter 2 influence the dispositionof metformin. Clin Pharmacol Ther 84:559–562
104. Garber AJ, Duncan TG, Goodman AM, Mills DJ, Rohlf JL 1997Efficacy of metformin in type II diabetes: results of a double-blind,placebo-controlled, dose-response trial. Am J Med 103:491–497
105. Nestler JE, Stovall D, Akhter N, Iuorno MJ, Jakubowicz DJ 2002Strategies for the use of insulin-sensitizing drugs to treat infertilityin women with polycystic ovary syndrome. Fertil Steril 77:209–215
106. Nestler JE 2008 Metformin for the treatment of the polycystic ovarysyndrome. N Engl J Med 358:47–54
107. Gusler G, Gorsline J, Levy G, Zhang SZ, Weston IE, Naret D,Berner B 2001 Pharmacokinetics of metformin gastric-retentivetablets in healthy volunteers. J Clin Pharmacol 41:655–661
108. Fujioka K, Pans M, Joyal S 2003 Glycemic control in patients withtype 2 diabetes mellitus switched from twice-daily immediate-release metformin to a once-daily extended-release formulation.Clin Ther 25:515–529
109. Gao H, Xiao W, Wang C, Zhang J, Yang Y, Yang J, Yang W, HongT 2008 The metabolic effects of once daily extended-release met-formin in patients with type 2 diabetes: a multicentre study. IntJ Clin Pract 62:695–700
110. Legro RS, Barnhart HX, Schlaff WD, Carr BR, Diamond MP,Carson SA, Steinkampf MP, Coutifaris C, McGovern PG, CataldoNA, Gosman GG Nestler JE, Giudice LC, Leppert PC, Myers ER;Cooperative Multicenter Reproductive Medicine Network 2007Clomiphene, metformin, or both for infertility in the polycysticovary syndrome. N Engl J Med 356:551–566
111. Harborne LR, Sattar N, Norman JE, Fleming R 2005 Metforminand weight loss in obese women with polycystic ovary syndrome:comparison of doses. J Clin Endocrinol Metab 90:4593–4598
112. Palomba S, Orio Jr F, Falbo A, Russo T, Tolino A, Zullo F 2007Clomiphene citrate versus metformin as first-line approach for thetreatment of anovulation in infertile patients with polycystic ovarysyndrome. J Clin Endocrinol Metab 92:3498–3503
113. George SS, George K, Irwin C, Job V, Selvakumar R, JeyaseelanV, Seshadri MS 2003 Sequential treatment of metformin and clo-miphene citrate in clomiphene-resistant women with polycysticovary syndrome: a randomized, controlled trial. Hum Reprod 18:299–304
114. Kjøtrød SB, von During V, Carlsen SM 2004 Metformin treatmentbefore IVF/ICSI in women with polycystic ovary syndrome; aprospective, randomized, double-blind study. Hum Reprod 19:1315–1322
115. Palomba S, Falbo A, Russo T, Manguso F, Tolino A, Zullo F, DeFeo P, Orio F Jr 2007 Insulin sensitivity after metformin suspensionin normal-weight women with polycystic ovary syndrome. J ClinEndocrinol Metab 92:3128–3135
116. Ibanez L, Valls C, Potau N, Marcos MV, de Zegher F 2000 Sen-sitization to insulin in adolescent girls to normalize hirsutism,hyperandrogenism, oligomenorrhea, dyslipidemia, and hyperin-sulinism after precocious pubarche. J Clin Endocrinol Metab 85:3526–3530
117. Palomba S, Falbo A, Orio F, Tolino A, Zullo F 26 April 2008Efficacy predictors for metformin and clomiphene citrate treatmentin anovulatory infertile patients with polycystic ovary syndrome.Fertil Steril 10.1016/j.fertnstert.2008.03.011
118. Palomba S, Pasquali R, Orio F, Nestler JE 7 August 2008 Clomi-phene citrate, metformin or both as first-step approach in treatinganovulatory infertility in patients with polycystic ovary syndrome(PCOS): a systematic review and meta-analysis. Clin Endocrinol(Oxf) 10.1111/j.1365–2265.2008.03369.x
119. Palomba S, Orio Jr F, Falbo A, Manguso F, Russo T, Cascella T,Tolino A, Carmina E, Colao A, Zullo F 2005 Prospective parallelrandomized, double-blind, double-dummy controlled clinical trialcomparing clomiphene citrate and metformin as the first-line treat-ment for ovulation induction in nonobese anovulatory women withpolycystic ovary syndrome. J Clin Endocrinol Metab 90:4068–4074
120. Zain MM, Jamaluddin R, Ibrahim A, Norman RJ 5 March 2008Comparison of clomiphene citrate, metformin, or the combinationof both for first-line ovulation induction, achievement of preg-nancy, and live birth in Asian women with polycystic ovarysyndrome: a randomized controlled trial. Fertil Steril 10.1016/j.fertnstert.2007.12.002
121. Moll E, Bossuyt PM, Korevaar JC, Lambalk CB, van der Veen F2006 Effect of clomifene citrate plus metformin and clomifene ci-trate plus placebo on induction of ovulation in women with newlydiagnosed polycystic ovary syndrome: randomised double blindclinical trial. BMJ 332:1485
122. Stepensky D, Friedman M, Srour W, Raz I, Hoffman A 2001Preclinical evaluation of pharmacokinetic-pharmacodynamic ra-tionale for oral CR metformin formulation. J Control Release 71:107–115
123. Ng EH, Wat NM, Ho PC 2001 Effects of metformin on ovulationrate, hormonal and metabolic profiles in women with clomiphene-resistant polycystic ovaries: a randomized, double-blinded place-bo-controlled trial. Hum Reprod 16:1625–1631
124. Fleming R, Hopkinson ZE, Wallace AM, Greer IA, Sattar N 2002Ovarian function and metabolic factors in women with oligomen-orrhea treated with metformin in a randomized double blind pla-cebo-controlled trial. J Clin Endocrinol Metab 87:569–574
125. Yarali H, Yildiz BO, Demirol A, Zeyneloglu HB, Yigit N, BukulmezO, Koray Z 2002 Co-administration of metformin during rFSH treat-ment in patients with clomiphene citrate-resistant polycystic ovariansyndrome: a prospective randomized trial. Hum Reprod 17:289–294
40 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022
126. Moghetti P, Castello R, Negri C, Tosi F, Perrone F, Caputo M,Zanolin E, Muggeo M 2000 Metformin effects on clinical features,endocrine and metabolic profiles, and insulin sensitivity in poly-cystic ovary syndrome: a randomized, double-blind, placebo-con-trolled 6-month trial, followed by open, long-term clinical evalu-ation. J Clin Endocrinol Metab 85:139–146
127. Dell’aglio DM, Perino LJ, Todino JD, Algren DA, Morgan BW 17March 2008 Metformin overdose with a resultant serum pH of 6.59:survival without sequalae. J Emerg Med 10.1016/j.jemermed.2007.09.034
128. Salpeter SR, Greyber E, Pasternak GA, Salpeter EE 2003 Risk offatal and nonfatal lactic acidosis with metformin use in type 2diabetes mellitus: systematic review and meta-analysis. Arch In-tern Med 163:2594–2602
129. Brown JB, Pedula K, Barzilay J, Herson MK, Latare P 1998 Lacticacidosis rates in type 2 diabetes. Diabetes Care 21:1659–1663
130. Jones GC, Macklin JP, Alexander WD 2003 Contraindications tothe use of metformin. BMJ 326:4–5
131. Kamber N, Davis WA, Bruce DG, Davis TM 2008 Metformin andlactic acidosis in an Australian community setting: the FremantleDiabetes Study. Med J Aust 188:446–449
132. Runge S, Alte D, Baumeister SE, Volzke H 2008 Prevalence of riskdeterminants for metformin-associated lactic acidosis and met-formin utilization in the study of health in Pomerania. Horm MetabRes 40:491–497
133. Silvestre J, Carvalho S, Mendes V, Coelho L, Tapadinhas C,Ferreira P, Povoa P, Ceia F 2007 Metformin-induced lactic acidosis:a case series. J Med Case Reports 1:126
134. Runge S, Mayerle J, Warnke C, Robinson D, Roser M, Felix SB,Friesecke S 2008 Metformin-associated lactic acidosis in patientswith renal impairment solely due to drug accumulation? DiabetesObes Metab 10:91–93
135. George JT, McKay GA 2008 Establishing pragmatic estimatedglomerular filtration rate thresholds to guide metformin prescrib-ing: careful assessment of risks and benefits is required. Diabet Med25:636–637
136. Audia P, Feinfeld DA, Dubrow A, Winchester JF 2008 Metformin-induced lactic acidosis and acute pancreatitis precipitated by di-uretic, celecoxib, and candesartan-associated acute kidney dys-function. Clin Toxicol (Phila) 46:164–166
137. Jain V, Sharma D, Prabhakar H, Dash HH 2008 Metformin-asso-ciated lactic acidosis following contrast media-induced nephrotox-icity. Eur J Anaesthesiol 25:166–167
138. Sayer JA 2006 Acute renal failure from contrast medium: bewarepatients taking metformin. BMJ 333:653
139. Babich MM, Pike I, Shiffman ML 1998 Metformin-induced acutehepatitis. Am J Med 104:490–492
140. Laporte F, Hamdi S, Oksman F, Huguet F 2008 Auto-immuneneutropenia associated with metformin in a patient with splenicmarginal zone lymphoma. Pharm World Sci 30:319–321
141. Kahn SE, Zinman B, Lachin JM, Haffner SM, Herman WH, HolmanRR, Kravitz BG, Yu D, Heise MA, Aftring RP, Viberti G; DiabetesOutcome Progression Trial (ADOPT) Study Group 2008 Rosigli-tazone-associated fractures in type 2 diabetes: an analysis from ADiabetes Outcome Progression Trial (ADOPT). Diabetes Care 31:845–851
142. Cortizo AM, Sedlinsky C, McCarthy AD, Blanco A, Schurman L2006 Osteogenic actions of the anti-diabetic drug metformin onosteoblasts in culture. Eur J Pharmacol 536:38–46
143. Monami M, Cresci B, Colombini A, Pala L, Balzi D, Gori F,Chiasserini V, Marchionni N, Rotella CM, Mannucci E 2008 Bonefractures and hypoglycemic treatment in type 2 diabetic patients:a case-control study. Diabetes Care 31:199–203
144. Jothilakshmi PK, Watson AJ, Jude E 2006 Acute alopecia due tometformin treatment for polycystic ovarian syndrome. J ObstetGynaecol 26:584–585
145. Checa MA, Requena A, Salvador C, Tur R, Callejo J, Espinos JJ,Fabregues F, Herrero J; Reproductive Endocrinology InterestGroup of the Spanish Society of Fertility 2005 Insulin-sensitizingagents: use in pregnancy and as therapy in polycystic ovary syn-drome. Hum Reprod Update 11:375–390
146. Rowan JA, Hague WM, Gao W, Battin MR, Moore MP; MiG Trial
Investigators 2008 Metformin versus insulin for the treatment ofgestational diabetes. N Engl J Med 358:2003–2015
147. Coetzee EJ, Jackson WPU 1979 Metformin in management of preg-nant insulin independent diabetes. Diabetologia 16:241–245
148. Coetzee EJ, Jackson WP 1985 The management of non-insulin-dependent diabetes during pregnancy. Diabetes Res Clin Pract 1:281–287
149. Koren G, Gilbert C, Valois M 2006 Metformin use during the firsttrimester of pregnancy. Is it safe? Can Fam Physician 52:171–172
150. Gilbert C, Valois M, Koren G 2006 Pregnancy outcome after first-trimester exposure to metformin: a meta-analysis. Fertil Steril 86:658–663
151. Thatcher SS, Jackson EM 2006 Pregnancy outcome in infertilepatients with polycystic ovary syndrome who were treated withmetformin. Fertil Steril 85:1002–1009
152. Bolton S, Cleary B, Walsh J, Dempsey E, Turner MJ 7 May 2008Continuation of metformin in the first trimester of women withpolycystic ovarian syndrome is not associated with increased peri-natal morbidity. Eur J Pediatr 10.1007/s00431-008-0737-7
153. Fauser BC, Diedrich K, Devroey P; on behalf of the Evian AnnualReproduction (EVAR) Workshop Group 2007 2008 Predictors ofovarian response: progress towards individualized treatment inovulation induction and ovarian stimulation. Hum Reprod Update14:1–14
154. Tan S, Hahn S, Benson S, Dietz T, Lahner H, Moeller LC, SchmidtM, Elsenbruch S, Kimmig R, Mann K, Janssen OE 2007 Metforminimproves polycystic ovary syndrome symptoms irrespective ofpre-treatment insulin resistance. Eur J Endocrinol 157:669–676
155. Yilmaz M, Biri A, Karakoc A, Toruner F, Bingol B, Cakir N, TirasB, Ayvaz G, Arslan M 2005 The effects of rosiglitazone and met-formin on insulin resistance and serum androgen levels in obeseand lean patients with polycystic ovary syndrome. J EndocrinolInvest 28:1003–1008
156. Marcondes JA, Yamashita SA, Maciel GA, Baracat EC, Halpern A2007 Metformin in normal-weight hirsute women with polycysticovary syndrome with normal insulin sensitivity. Gynecol Endo-crinol 23:273–278
157. Nestler JE, Jakubowicz DJ, Evans WS, Pasquali R 1998 Effects ofmetformin on spontaneous and clomiphene-induced ovulation inthe polycystic ovary syndrome. N Engl J Med 338:1876–1880
158. Maciel GA, Soares Junior JM, Alves da Motta EL, Abi Haidar M,de Lima GR, Baracat EC 2004 Nonobese women with polycysticovary syndrome respond better than obese women to treatmentwith metformin. Fertil Steril 81:355–360
159. Baillargeon JP, Jakubowicz DJ, Iuorno MJ, Jakubowicz S, NestlerJE 2004 Effects of metformin and rosiglitazone, alone and in com-bination, in nonobese women with polycystic ovary syndrome andnormal indices of insulin sensitivity. Fertil Steril 82:893–902
160. Onalan G, Goktolga U, Ceyhan T, Bagis T, Onalan R, Pabuccu R2005 Predictive value of glucose-insulin ratio in PCOS and profileof women who will benefit from metformin therapy: obese, lean,hyper or normoinsulinemic? Eur J Obstet Gynecol Reprod Biol123:204–211
161. Genazzani AD, Lanzoni C, Ricchieri F, Baraldi E, Casarosa E,Jasonni VM 2007 Metformin administration is more effective whennon-obese patients with polycystic ovary syndrome show bothhyperandrogenism and hyperinsulinemia. Gynecol Endocrinol 23:146–152
162. Legro RS, Barnhart HX, Schlaff WD, Carr BR, Diamond MP,Carson SA, Steinkampf MP, Coutifaris C, McGovern PG, CataldoNA, Gosman GG, Nestler JE, Giudice LC, Ewens KG, SpielmanRS, Leppert PC, Myers ER; Reproductive Medicine Network 2008Ovulatory response to treatment of polycystic ovary syndrome isassociated with a polymorphism in the STK11 gene. J Clin Endo-crinol Metab 93:792–800
163. Kumari AS, Haq A, Jayasundaram R, Abdel-Wareth LO, Al HaijaSA, Alvares M 2005 Metformin monotherapy in lean women withpolycystic ovary syndrome. Reprod Biomed Online 10:100–104
164. Bruno RV, de Avila MA, Neves FB, Nardi AE, Crespo CM,Sobrinho AT 2007 Comparison of two doses of metformin (2.5 and1.5 g/day) for the treatment of polycystic ovary syndrome and theireffect on body mass index and waist circumference. Fertil Steril88:510–512
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 41
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022
165. Eisenhardt S, Schwarzmann N, Henschel V, Germeyer A, vonWolff M, Hamann A, Strowitzki T 2006 Early effects of metforminin women with polycystic ovary syndrome: a prospective random-ized, double-blind, placebo-controlled trial. J Clin EndocrinolMetab 91:946–952
166. Liu KE, Tataryn IV, Sagle M 2006 Use of metformin for ovulationinduction in women who have polycystic ovary syndrome with orwithout evidence of insulin resistance. J Obstet Gynaecol Can 28:595–599
167. Chang WY, Knochenhauer ES, Bartolucci AA, Azziz R 2005 Phe-notypic spectrum of polycystic ovary syndrome: clinical and bio-chemical characterization of the three major clinical subgroups.Fertil Steril 83:1717–1723
168. Moll E, Korevaar JC, Bossuyt PM, van der Veen F 2008 Doesadding metformin to clomifene citrate lead to higher pregnancyrates in a subset of women with polycystic ovary syndrome? HumReprod 23:1830–1834
169. Misra S, Parida N, Das S, Parija BS, Padhi M, Baig MA 2004 Effectof metaformin in Asian Indian women with polycystic ovariansyndrome. Metab Syndr Relat Disord 2: 192–197
170. Goldzieher JW, Axelrod LR 1963 Clinical and biochemical featuresof polycystic ovarian disease. Fertil Steril 14: 631–653
171. Young RL, Goldzieher JW 1988 Clinical manifestations of polycysticovarian disease. Endocrinol Metab Clin North Am 17:621–633
172. Deaton R 1991 Hyperandrogenism and uterine bleeding. InfertilReprod Med Clin North Am 2:561–583
173. Azziz R, Waggoner WT, Ochoa T, Knochenhauer ES, Boots LR1998 Idiopathic hirsutism: an uncommon cause of hirsutism inAlabama. Fertil Steril 70:274–278
174. Barbieri RL, Makris A, Randall RW, Daniels G, Kistner RW, RyanKJ 1986 Insulin stimulates androgen accumulation in incubationsof ovarian stroma obtained from women with hyperandrogenism.J Clin Endocrinol Metab 62:904–910
175. Nestler JE, Powers LP, Matt DW, Steingold KA, Plymate SR,Rittmaster RS, Clore JN, Blackard WG 1991 A direct effect ofhyperinsulinemia on serum sex hormone binding globulin levels inobese women with the polycystic ovary syndrome. J Clin Endo-crinol Metab 72:83–89
176. Utiger R 1996 Insulin and the polycystic ovary syndrome. N EnglJ Med 335:657–658
177. Unluhizarci K, Kelestimur F, Bayram F, Sahin Y, Tutus A 1999 Theeffects of metformin on insulin resistance and ovarian steroido-genesis in women with polycystic ovary syndrome. Clin Endocri-nol (Oxf) 51:231–236
178. Glueck CJ, Wang P, Fontaine R, Tracy T, Sieve-Smith L 2001Metformin to restore normal menses in oligo-amenorrheic teenagegirls with polycystic ovary syndrome (PCOS). J Adolesc Health29:160–169
179. Ibanez L, Valls C, Ferrer A, Marcos MV, Rodriguez-Hierro F, deZegher F 2001 Sensitization to insulin induces ovulation in nono-bese adolescents with anovulatory hyperandrogenism. J Clin En-docrinol Metab 86:3595–3598
180. Crave JC, Fimbel S, Lejeune H, Cugnardey N, Dechaud H, PugeatM 1995 Effects of diet and metformin administration on sex hor-mone-binding globulin, androgens, and insulin in hirsute andobese women. J Clin Endocrinol Metab 80:2057–2062
181. Pasquali R, Gambineri A, Biscotti D, Vicennati V, Gagliardi L,Colitta D, Fiorini S, Cognigni GE, Filicori M, Morselli-Labate AM2000 Effect of long-term treatment with metformin added to hy-pocaloric diet on body composition, fat distribution and androgenand insulin levels in abdominally obese women with and withoutthe polycystic ovary syndrome. J Clin Endocrinol Metab 85:2767–2774
182. Costello MF, Shrestha B, Eden J, Johnson NP, Sjoblom P 2007Metformin versus oral contraceptive pill in polycystic ovary syn-drome: a Cochrane review. Hum Reprod 22:1200–1209
183. Morin-Papunen LC, Vauhkonen I, Koivunen RM, Ruokonen A,Martikainen HK, Tapanainen JS 2000 Endocrine and metaboliceffects of metformin versus ethinyl estradiol–cyproterone acetatein obese women with polycystic ovary syndrome: a randomizedstudy. J Clin Endocrinol Metab 85:3161–3168
184. Morin-Papunen L, Vauhkonen I, Koivunen R, Ruokonen A,Martikainen H, Tapanainen JS 2003 Metformin versus ethinyl
estradiol-cyproterone acetate in the treatment of nonobese womenwith polycystic ovary syndrome: a randomized study. J Clin En-docrinol Metab 88:148–156
185. Diamanti-Kandarakis E, Baillargeon JP, Iuorno MJ, JakubowiczDJ, Nestler JE 2003 A modern medical quandary: polycystic ovarysyndrome, insulin resistance, and oral contraceptive pills. J ClinEndocrinol Metab 88:1927–1932
186. Luque-Ramírez M, Alvarez-Blasco F, Botella-Carretero JI,Martínez-Bermejo E, Lasuncion MA, Escobar-Morreale HF 2007Comparison of ethinyl-estradiol plus cyproterone acetate versusmetformin effects on classic metabolic cardiovascular risk factorsin women with the polycystic ovary syndrome. J Clin EndocrinolMetab 92:2453–2461
187. Korytkowski MT, Mokan M, Horwitz MJ, Berga SL 1995 Meta-bolic effects of oral contraceptives in women with polycystic ovarysyndrome. J Clin Endocrinol Metab 80:3327–3334
188. Dahlgren E, Landin K, Krotkiewski M, Holm G, Janson PO 1998Effects of two antiandrogen treatments on hirsutism and insulinsensitivity in women with polycystic ovary syndrome. Hum Re-prod 13:2706–2711
189. Pasquali R, Gambineri A, Anconetani B, Vicennati V, Colitta D,Caramelli E, Casimirri F, Morselli-Labate AM 1999 The naturalhistory of the metabolic syndrome in young women with the poly-cystic ovary syndrome and the effect of long-term oestrogen-pro-gestagen treatment. Clin Endocrinol (Oxf) 50:517–527
190. Costello M, Shrestha B, Eden J, Sjoblom P, Johnson N 2007Insulin-sensitising drugs versus the combined oral contraceptivepill for hirsutism, acne and risk of diabetes, cardiovascular disease,and endometrial cancer in polycystic ovary syndrome. CochraneDatabase Syst Rev CD005552
191. Meyer C, McGrath BP, Teede HJ 2007 Effects of medical therapyon insulin resistance and the cardiovascular system in polycysticovary syndrome. Diabetes Care 30:471–478
192. Luque-Ramírez M, Alvarez-Blasco F, Uriol Rivera MG, Escobar-Morreale HF 2008 Serum uric acid concentration as non-classiccardiovascular risk factor in women with polycystic ovary syn-drome: effect of treatment with ethinyl-estradiol plus cyproteroneacetate versus metformin. Hum Reprod 23:1594–1601
193. World Health Organization 1992 Recent advances in medicallyassisted conception. WHO Tech Rep Ser 820:1-111. Geneva: WHO
194. McGovern PG, Legro RS, Myers ER, Barnhart HX, Carson SA,Diamond MP, Carr BR, Schlaff WD, Coutifaris C, SteinkampfMP, Nestler JE, Gosman G, Leppert PC, Giudice LC, NationalInstitutes for Child Health and Human Development-ReproductiveMedicine Network 2007 Utility of screening for other causes ofinfertility in women with “known” polycystic ovary syndrome.Fertil Steril 87:442–444
195. Al-Ozairi E, Quinton R, Advani A 2008 Therapeutic response tometformin in an underweight patient with polycystic ovarian syn-drome. Fertil Steril 90:1197.e1–e4
196. Hughes E, Collins J, Vandekerckhove P, Lilford R 2000 Clomi-phene citrate for ovulation induction in women with oligo-amen-orrhoea. Cochrane Database Syst Rev: CD000056
197. Palomba S, Oppedisano R, Tolino A, Orio F, Zullo F 2008 Met-formin use in infertile patients with polycystic ovary syndrome: anevidence-based overview. Reprod Biomed Online 16:327–335
198. Heijnen EM, Eijkemans MJ, Hughes EG, Laven JS, Macklon NS,Fauser BC 2006 A meta-analysis of outcomes of conventional IVFin women with polycystic ovary syndrome. Hum Reprod Update12:13–21
199. Fulghesu AM, Villa P, Pavone V, Guido M, Apa R, Caruso A,Lanzone A, Rossodivita A, Mancuso S 1997 The impact of insulinsecretion on the ovarian response to exogenous gonadotropins inpolycystic ovary syndrome. J Clin Endocrinol Metab 82:644–648
200. Dale PO, Tanbo T, Haug E, Abyholm T 1998 The impact of insulinresistance on the outcome of ovulation induction with low-dosefollicle stimulating hormone in women with polycystic ovary syn-drome. Hum Reprod 13:567–570
201. Rice S, Christoforidis N, Gadd C, Nikolaou D, Seyani L, DonaldsonA, Margara R, Hardy K, Franks S 2005 Impaired insulin-dependentglucose metabolism in granulosa-lutein cells from anovulatorywomen with polycystic ovaries. Hum Reprod 20:373–381
202. Costello MF, Eden JA 2003 A systematic review of the reproductive
42 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022
system effects of metformin in patients with polycystic ovary syn-drome. Fertil Steril 79:1–13
203. Lord JM, Flight IH, Norman RJ 2003 Metformin in polycystic ovarysyndrome: systematic review and meta-analysis. BMJ 327:951–953
204. Kashyap S, Wells GA, Rosenwaks Z 2004 Insulin-sensitizingagents as primary therapy for patients with polycystic ovariansyndrome. Hum Reprod 19:2474–2483
205. Siebert TI, Kruger TF, Steyn DW, Nosarka S 2006 Is the additionof metformin efficacious in the treatment of clomiphene citrate-resistant patients with polycystic ovary syndrome? A structuredliterature review. Fertil Steril 86:1432–1437
206. Moll E, van der Veen F, van Wely M 2007 The role of metforminin polycystic ovary syndrome: a systematic review. Hum ReprodUpdate 13:527–537
207. Creanga AA, Bradley HM, McCormick C, Witkop CT 2008 Use ofmetformin in polycystic ovary syndrome: a meta-analysis. ObstetGynecol 111:959–968
208. Palomba S, Falbo A 2008 Metformin in therapy naive patients withpolycystic ovary syndrome. Hum Reprod Update 14:193
209. Palomba S, Orio Jr F, Zullo F 2007 What is the best first-steptherapeutic approach in treating anovulatory infertility in patientswith polycystic ovary syndrome? Questions that are still unan-swered. Gynecol Endocrinol 23:245–247
210. Pasquali R, Gambineri A, Pagotto U 2006 The impact of obesityon reproduction in women with polycystic ovary syndrome. BJOG13:1148–1159
211. Norman RJ, Noakes M, Wu R, Davies MJ, Moran L, Wang JX2004 Improving reproductive performance in overweight/obesewomen with effective weight management. Hum Reprod Update10:267–280
212. Banaszewska B, Pawelczyk L, Spaczynski RZ, Dziura J, DulebaAJ 2007 Effects of simvastatin and oral contraceptive agent onpolycystic ovary syndrome: prospective, randomized, crossovertrial. J Clin Endocrinol Metab 92:456–461
213. Merhi ZO 2007 Weight loss by bariatric surgery and subsequentfertility. Fertil Steril 87:430–432
214. Branigan EF, Estes MA 2003 A randomized clinical trial of treat-ment of clomiphene citrate-resistant anovulation with the use oforal contraceptive pill suppression and repeat clomiphene citratetreatment. Am J Obstet Gynecol 188:1424–1428
215. Barbieri RL 2007 Editorial: clomiphene versus metformin for ovu-lation induction in polycystic ovary syndrome: the winner is. J ClinEndocrinol Metab 92:3399–3401
216. Clapauch R, Mattos TM 2008 Triplet pregnancy after metforminin a woman with polycystic ovary syndrome. Fertil Steril 89:1260.e1–e2
217. Cataldo NA, Barnhart HX, Legro RS, Myers ER, Schlaff WD, CarrBR, Diamond MP, Carson SA, Steinkampf MP, Coutifaris C,McGovern PG, Gosman G, Nestler JE, Giudice LC; for theReproductive Medicine Network 2008 Extended-release met-formin does not reduce the clomiphene citrate dose required toinduce ovulation in polycystic ovary syndrome. J Clin EndocrinolMetab 93:3124–3127
218. Vandermolen DT, Ratts VS, Evans WS, Stovall DW, Kauma SW,Nestler JE 2001 Metformin increases the ovulatory rate and preg-nancy rate from clomiphene citrate in patients with polycysticovary syndrome who are resistant to clomiphene citrate alone.Fertil Steril 75:310–315
219. Palomba S, Orio Jr F, Falbo A, Russo T, Caterina G, Manguso F,Tolino A, Colao A, Zullo F 2005 Metformin administration andlaparoscopic ovarian drilling improve ovarian response to clomi-phene citrate (CC) in oligo-anovulatory CC-resistant women withpolycystic ovary syndrome. Clin Endocrinol (Oxf) 63:631–635
220. McGovern PG, Carson SA, Barnhart HX, Myers ER, Legro RS,Diamond MP, Carr BR, Schlaff WD, Coutifaris C, Cataldo NA,Steinkampf MP, Nestler JE, Gosman G, Leppert PC, Giudice LC;for the NICHD-Reproductive Medicine Network 2008 Medica-tion adherence and treatment success in the National Institute ofChild Health and Human Development-Reproductive MedicineNetwork’s Pregnancy in Polycystic Ovary Syndrome Trial. FertilSteril 90:1283–1286
221. Palomba S, Orio Jr F, Nardo LG, Falbo A, Russo T, Corea D, DoldoP, Lombardi G, Tolino A, Colao A, Zullo F 2004 Metformin ad-
ministration versus laparoscopic ovarian diathermy in clomiphenecitrate-resistant women with polycystic ovary syndrome: a pro-spective parallel randomized double-blind placebo-controlled trial.J Clin Endocrinol Metab 89:4801–4809
222. Kocak I, Ustun C 2006 Effects of metformin on insulin resistance,androgen concentration, ovulation and pregnancy rates in womenwith polycystic ovary syndrome following laparoscopic ovariandrilling. J Obstet Gynaecol Res 32:292–298
223. Kocak M, Caliskan E, Simsir C, Haberal A 2002 Metformin ther-apy improves ovulatory rates, cervical scores, and pregnancy ratesin clomiphene citrate-resistant women with polycystic ovary syn-drome. Fertil Steril 77:101–106
224. Sinawat S, Buppasiri P, Lumbiganon P, Pattanittum P 2008 Longversus short course treatment with metformin and clomiphenecitrate for ovulation induction in women with PCOS. CochraneDatabase Syst Rev CD006226
225. Palomba S, Falbo A, Battista L, Russo T, Tolino A, Zullo F 2009Laparoscopic ovarian diathermy versus metformin plus clomi-phene citrate administration as second-line strategy for infertileanovulatory patients with polycystic ovary syndrome: a random-ized controlled trial. Fertil Steril, in press
226. Sohrabvand F, Ansari SH, Bagheri M 2006 Efficacy of combinedmetformin-letrozole in comparison with metformin-clomiphene ci-trate in clomiphene-resistant infertile women with polycystic ovar-ian disease. Hum Reprod 21:1432–1435
227. Khorram O, Helliwell JP, Katz S, Bonpane CM, Jaramillo L 2006Two weeks of metformin improves clomiphene citrate-inducedovulation and metabolic profiles in women with polycystic ovarysyndrome. Fertil Steril 85:1448–1451
228. Sturrock ND, Lannon B, Fay TN 2002 Metformin does not enhanceovulation induction in clomiphene resistant polycystic ovary syn-drome in clinical practice. Br J Clin Pharmacol 53:469–473
229. Hwu YM, Lin SY, Huang WY, Lin MH, Lee RK 2005 Ultra-shortmetformin pretreatment for clomiphene citrate-resistant polycysticovary syndrome. Int J Gynaecol Obstet 90:39–43
230. Costello MF, Chapman M, Conway U 2006 A systematic reviewand meta-analysis of randomized controlled trials on metforminco-administration during gonadotrophin ovulation induction orIVF in women with polycystic ovary syndrome. Hum Reprod 21:1387–1399
231. Palomba S, Falbo A, Orio Jr F, Manguso F, Russo T, Tolino A,Colao A, Dale B, Zullo F 2005 A randomized controlled trialevaluating metformin pre-treatment and co-administration in non-obese insulin-resistant women with polycystic ovary syndrometreated with controlled ovarian stimulation plus timed intercourseor intrauterine insemination. Hum Reprod 20:2879–2886
232. van Santbrink EJ, Hohmann FP, Eijkemans MJ, Laven JS, FauserBC 2005 Does metformin modify ovarian responsiveness duringexogenous FSH ovulation induction in normogonadotrophicanovulation? A placebo-controlled double-blind assessment. Eur JEndocrinol 152:611–617
233. Stadtmauer LA, Toma SK, Riehl RM, Talbert LM 2001 Metformintreatment of patients with polycystic ovary syndrome under-going in vitro fertilization improves outcomes and is associatedwith modulation of the insulin-like growth factors. Fertil Steril75:505–509
234. Gorry A, White DM, Franks S 2006 Infertility in polycystic ovarysyndrome: focus on low-dose gonadotropin treatment. Endocrine30:27–33
235. Shibahara H, Kikuchi K, Hirano Y, Suzuki T, Takamizawa S,Suzuki M 2007 Increase of multiple pregnancies caused by ovu-lation induction with gonadotropin in combination with metforminin infertile women with polycystic ovary syndrome. Fertil Steril87:1487–1490
236. Bromer JG, Cetinkaya MB, Arici A 2008 Pretreatments before theinduction of ovulation in assisted reproduction technologies: evi-dence-based medicine in 2007. Ann NY Acad Sci 1127:31–40
237. Balen AH, Tan SL, MacDougall J, Jacobs HS 1993 Miscarriagerates following in-vitro fertilization are increased in women withpolycystic ovaries and reduced by pituitary desensitization withbuserelin. Hum Reprod 8:959–964
238. Regan L, Braude PR, Trembath PL 1989 Influence of past repro-
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 43
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

ductive performance on risk of spontaneous abortion. BMJ 299:541–545
239. Jakubowicz DJ, Paulina AE, Seppa M, Jakubowicz S, BaillargeonJ-P, Koistinien R, Nestler JE 2004 Reduced serum glycodelin andinsulin-like growth factor-binding protein-1 in women with poly-cystic ovary syndrome during first trimester of pregnancy. J ClinEndocrinol Metab 89:833–839
240. Jakubowicz DJ, Seppala M, Jakubowicz S, Rodriguez-Armas O,Rivas-Santiago A, Koistinen H, Koistinen R, Nestler JE 2001Insulin reduction with metformin increases luteal phase serumglycodelin and insulin-like growth factor-binding protein 1 con-centrations and enhances uterine vascularity and blood flow in thepolycystic ovary syndrome. J Clin Endocrinol Metab 86:1126–1133
241. Bolton AE, Pockley AG, Clough KJ, Mowles EA, Stoker RJ,Westwood OM, Chapman MG 1987 Identification of placentalprotein 14 as an immunosuppressive factor in human reproduc-tion. Lancet 1:593–595
242. Giudice LC, Mark SP, Irwin JC 1998 Paracrine actions of insulin-like growth factors and IGF binding protein-1 in non-pregnanthuman endometrium and at the decidual-trophoblast interface.J Reprod Immunol 39:133–148
243. Wood JR, Dumesic DA, Abbott DH, Strauss 3rd JF 2007 Molecularabnormalities in oocytes from women with polycystic ovary syn-drome revealed by microarray analysis. J Clin Endocrinol Metab92:705–713
244. Glueck CJ, Phillips H, Cameron D, Sieve-Smith L, Wang P 2001Continuing metformin throughout pregnancy in women withpolycystic ovary syndrome appears to safely reduce first-trimesterspontaneous abortion: a pilot study. Fertil Steril 75:46–52
245. Glueck CJ, Wang P, Kobayashi S, Phillips H, Sieve-Smith L 2002Metformin therapy throughout pregnancy reduces the develop-ment of gestational diabetes in women with polycystic ovary syn-drome. Fertil Steril 77:520–525
246. Jakubowicz DJ, Iuorno MJ, Jakubowicz S, Roberts KA, Nestler JE2002 Effects of metformin on early pregnancy loss in the polycysticovary syndrome. J Clin Endocrinol Metab 87:524–529
247. Palomba S, Falbo A, Orio Jr F, Russo T, Tolino A, Zullo F 2006Metformin hydrochloride and recurrent miscarriage in a womanwith polycystic ovary syndrome. Fertil Steril 85:1511.e3–e5
248. Palomba S, Orio Jr F, Falbo A, Russo T, Tolino A, Zullo F 2005Plasminogen activator inhibitor 1 and miscarriage after metformintreatment and laparoscopic ovarian drilling in patients with poly-cystic ovary syndrome. Fertil Steril 84:761–765
249. Schachter M, Raziel A, Friedler S, Strassburger D, Bern O, Ron-ElR 2003 Insulin resistance in patients with polycystic ovary syn-drome is associated with elevated plasma homocysteine. HumReprod 18:721–727
250. Diamanti-Kandarakis E, Piperi C, Kalofoutis A, Creatsas G 2005Increased levels of serum advanced glycation end-products inwomen with polycystic ovary syndrome. Clin Endocrinol (Oxf)62:37–43
251. Orio Jr F, Palomba S, Cascella T, De Simone B, Manguso F,Savastano S, Russo T, Tolino A, Zullo F, Lombardi G, Azziz R,Colao A 2005 Improvement in endothelial structure and functionafter metformin treatment in young normal-weight women withpolycystic ovary syndrome: results of a 6-month study. J ClinEndocrinol Metab 90:6072–6076
252. Van Blerkom J 1998 Epigenetic influences on oocyte developmen-tal competence: perifollicular vascularity and intrafollicular oxy-gen. J Assist Reprod Genet 15:226–234
253. Van Blerkom J, Antczak M, Schrader R 1997 The developmentalpotential of the human oocyte is related to the dissolved oxygencontent of follicular fluid: association with vascular endothelialgrowth factor levels and perifollicular blood flow characteristics.Hum Reprod 12:1047–1055
254. Wei Z, Cao Y, Cong L, Zhou P, Zhang Z, Li J 2008 Effect ofmetformin pretreatment on pregnancy outcome of in vitro maturedoocytes retrieved from women with polycystic ovary syndrome.Fertil Steril 90:1149–1154
255. Sonntag B, Gotte M, Wulfing P, Schuring AN, Kiesel L, Greb RR2005 Metformin alters insulin signaling and viability of humangranulosa cells. Fertil Steril 84:1173–1179
256. Eng GS, Sheridan RA, Wyman A, Chi MM, Bibee KP, Jungheim
ES, Moley KH 2007 AMP kinase activation increases glucoseuptake, decreases apoptosis, and improves pregnancy outcomein embryos exposed to high IGF-I concentrations. Diabetes 56:2228 –2234
257. Chi MM, Schlein AL, Moley KH 2000 High insulin-like growthfactor 1 (IGF-1) and insulin concentrations trigger apoptosis in themouse blastocyst via down-regulation of the IGF-1 receptor. En-docrinology 141:4784–4792
258. Samoto T, Maruo T, Matsuo H, Katayama K, Barnea ER, MochizukiM 1993 Altered expression of insulin and insulin-like growth fac-tor-I receptors in follicular and stromal compartments of polycysticovaries. Endocr J 40:413–424
259. Pinto AB, Schlein AL, Moley KH 2002 Preimplantation exposureto high insulin-like growth factor I concentrations results in in-creased resorption rates in vivo. Hum Reprod 17:457–462
260. Palomba S, Falbo A, Orio F, Zullo F 2008 Preconceptional effect ofmetformin on abortion risk in polycystic ovary syndrome (PCOS):a systematic review and meta-analysis of randomized controlledtrials (RCTs). Fertil Steril, in press
261. Glueck CJ, Wang P, Goldenberg N, Sieve-Smith L 2002 Pregnancyoutcomes among women with polycystic ovary syndrome treatedwith metformin. Hum Reprod 17:2858–2864
262. Khattab S, Mohsen IA, Foutouh IA, Ramadan A, Moaz M, Al-Inany H 2006 Metformin reduces abortion in pregnant women withpolycystic ovary syndrome. Gynecol Endocrinol 22:680–684
263. Zolghadri J, Tavana Z, Kazerooni T, Soveid M, Taghieh M 2007Relationship between abnormal glucose tolerance test and historyof previous recurrent miscarriages, and beneficial effect of met-formin in these patients: a prospective clinical study. Fertil Steril90:727–730
264. Metformin in pregnant PCOS women. ClinicalTrials.gov Identifier:NCT00159536
265. Uterine artery blood flow in pregnant women with polycysticovary syndrome treated with metformin. ClinicalTrials.gov Iden-tifier: NCT00466622
266. Radon PA, McMahon MJ, Meyer WR 1999 Impaired glucose tol-erance in pregnant women with polycystic ovary syndrome. ObstetGynecol 94:194–197
267. Holte J, Gennarelli G, Wide L, Lithell H, Berne C 1998 Highprevalence of polycystic ovaries and associated clinical, endocrine,and metabolic features in women with previous gestational dia-betes mellitus. J Clin Endocrinol Metab 83:1143–1150
268. Boomsma CM, Eijkemans MJ, Hughes EG, Visser GH, Fauser BC,Macklon NS 2006 A meta-analysis of pregnancy outcomes inwomen with polycystic ovary syndrome. Hum Reprod Update12:673–683
269. Norman RJ, Wang JX, Hague W 2004 Should we continue or stopinsulin sensitizing drugs during pregnancy? Curr Opin ObstetGynecol 16:245–250
270. Glueck CJ, Goldenberg N, Wang P, Loftspring M, Sherman A2004 Metformin during pregnancy reduces insulin, insulin resis-tance, insulin secretion, weight, testosterone and development ofgestational diabetes: prospective longitudinal assessment ofwomen with polycystic ovary syndrome from preconceptionthroughout pregnancy. Hum Reprod 19:510–521
271. Vanky E, Salvesen KA, Heimstad R, Fougner KJ, Romundstad P,Carlsen SM 2004 Metformin reduces pregnancy complicationswithout affecting androgen levels in pregnant polycystic ovarysyndrome women: results of a randomized study. Hum Reprod19:1734–1740
272. Legro RS, Kunselman AR, Dodson WC, Dunaif A 1999 Prevalenceand predictors of risk for type 2 diabetes mellitus and impairedglucose tolerance in polycystic ovary syndrome: a prospective,controlled study in 254 affected women. J Clin Endocrinol Metab84:165–169
273. Glueck CJ, Pranikoff J, Aregawi D, Wang P 2008 Prevention ofgestational diabetes by metformin plus diet in patients with poly-cystic ovary syndrome. Fertil Steril 89:625–634
274. Hellmuth E, Damm P, Mølsted-Pedersen L 2000 Oral hypogly-caemic agents in 118 diabetic pregnancies. Diabet Med 17:507–511
275. Coustan DR 2007 Pharmacological management of gestational di-abetes: an overview. Diabetes Care 30:S206–S208
276. Moore LE, Briery CM, Clokey D, Martin RW, Williford NJ, Bofill
44 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

JA, Morrison JC 2007 Metformin and insulin in the managementof gestational diabetes mellitus: preliminary results of a compar-ison. J Reprod Med 52:1011–1015
277. Brosens IA 1977 Morphological changes in the utero-placental bedin pregnancy hypertension. Clin Obstet Gynaecol 4:573–593
278. Prefumo F, Sebire NJ, Thilaganathan B 2004 Decreased endovas-cular trophoblast invasion in first trimester pregnancies with high-resistance uterine artery Doppler indices. Hum Reprod 19:206–209
279. Salvesen KA, Vanky E, Carlsen SM 2007 Metformin treatment inpregnant women with polycystic ovary syndrome—is reducedcomplication rate mediated by changes in the uteroplacental cir-culation? Ultrasound Obstet Gynecol 29:433–437
280. Glueck CJ, Salehi M, Sieve L, Wang P 2006 Growth, motor, andsocial development in breast- and formula-fed infants of met-formin-treated women with polycystic ovary syndrome. J Pediatr148:628–632
281. Glueck CJ, Bornovali S, Pranikoff J, Goldenberg N, Dharashivkar S,Wang P 2004 Metformin, pre-eclampsia, and pregnancy outcomes inwomen with polycystic ovary syndrome. Diabet Med 21:829–836
282. Bolton S, Cleary B, Walsh J, Dempsey E, Turner MJ 7 May 2008Continuation of metformin in the first trimester of women withpolycystic ovarian syndrome is not associated with increased peri-natal morbidity. Eur J Pediatr 10.1007/s00431-008-0737–7
283. Glueck CJ, Goldenberg N, Pranikoff J, Loftspring M, Sieve L,Wang P 2004 Height, weight, and motor-social development dur-ing the first 18 months of life in 126 infants born to 109 mothers withpolycystic ovary syndrome who conceived on and continued met-formin through pregnancy. Hum Reprod 19:1323–1330
284. Schwartz LB, Chiu AS, Courtney M, Krey L, Schmidt-Sarosi C1997 The embryo versus endometrium controversy revisited as itrelates to predicting pregnancy outcome in in-vitro fertilization-embryo transfer cycles. Hum Reprod 12:45–50
285. Battaglia C, Artini PG, D’Ambrogio G, Genazzani AD, GenazzaniAR 1995 The role of color Doppler imaging in the diagnosis of poly-cystic ovary syndrome. Am J Obstet Gynecol 172:108–113
286. Aleem FA, Predanic M 1996 Transvaginal color Doppler determi-nation of the ovarian and uterine blood flow characteristics inpolycystic ovary disease. Fertil Steril 65:510–516
287. Vrtacnik-Bokal E, Meden-Vrtovec H 1998 Utero-ovarian arterialblood flow and hormonal profile in patients with polycystic ovarysyndrome. Hum Reprod 13:815–821
288. Steer CV, Tan SL, Mason BA, Campbell S 1994 Midluteal-phasevaginal color Doppler assessment of uterine artery impedance in asubfertile population. Fertil Steril 61:53–58
289. Cacciatore B, Simberg N, Fusaro P, Tiitinen A 1996 TransvaginalDoppler study of uterine artery blood flow in in vitro fertilization-embryo transfer cycles. Fertil Steril 66:130–134
290. Tekay A, Martikainen H, Jouppila P 1996 Comparison of uterineblood flow characteristics between spontaneous and stimulatedcycles before embryo transfer. Hum Reprod 11:364–368
291. Dickey RP 1997 Doppler ultrasound investigation of uterine andovarian blood flow in infertility and early pregnancy. Hum ReprodUpdate 3:467–503
292. Habara T, Nakatsuka M, Konishi H, Asagiri K, Noguchi S, KudoT 2002 Elevated blood flow resistance in uterine arteries ofwomen with unexplained recurrent pregnancy loss. Hum Re-prod 17:190 –194
293. Ng EH, Chan CC, Tang OS, Yeung WS, Ho PC 2006 The role ofendometrial and subendometrial vascularity measured by three-dimensional power Doppler ultrasound in the prediction of preg-nancy during frozen-thawed embryo transfer cycles. Hum Reprod21:1612–1617
294. Basir GS, Lam TP, Chau MT, Ng EH, O WS, Ho PC 2001 ColourDoppler analysis of peri-implantation utero-ovarian haemody-namics in women with excessively high oestradiol concentrationsafter ovarian stimulation. Hum Reprod 16:2114–2117
295. Gonen Y, Casper RF 1990 Prediction of implantation by the sono-graphic appearance of the endometrium during controlled ovarianstimulation for in vitro fertilization (IVF). J In Vitro Fert EmbryoTransf 7:146–152
296. Dickey RP, Olar TT, Taylor SN, Curole DN, Matulich EM 1993Relationship of endometrial thickness and pattern to fecundity in
ovulation induction cycles: effect of clomiphene citrate alone andwith human menopausal gonadotropin. Fertil Steril 59:756–760
297. Yaman C, Ebner T, Sommergruber M, Polz W, Tews G 2000 Roleof three-dimensional ultrasonographic measurement of endome-trium volume as a predictor of pregnancy outcome in an IVF-ETprogram: a preliminary study. Fertil Steril 74:797–801
298. Hock DL, Bohrer MK, Ananth CV, Kemmann E 1997 Sonographicassessment of endometrial pattern and thickness in patients treatedwith clomiphene citrate, human menopausal gonadotropins, andintrauterine insemination. Fertil Steril 68:242–245
299. Fanchin R, Righini C, Ayoubi JM, Olivennes F, de Ziegler D,Frydman R 2000 New look at endometrial echogenicity: objectivecomputer-assisted measurements predict endometrial receptivityin in vitro fertilization-embryo transfer. Fertil Steril 74:274–281
300. Hackl H 1973 Metabolism of glucose in the human endometriumwith special reference to fertility and contraception. Acta ObstetGynecol Scand 52:135–140
301. Truchan B, Taylor P, Goren HJ, Lederis K, Hollenberg MD, OkabeT 1987 Basal, oxytocin- and insulin-stimulated glucose oxidation inhuman endometrium. Can J Physiol Pharmacol 65:323–327
302. Strowitzki T, Corleta Von Eye H, Kellerer M, Haring HU 1993Tyrosine kinase activity of insulin like growth factor I and insulinreceptors in human endometrium during the menstrual cycle: cy-clic variation of insulin receptor expression. Fertil Steril 59:315–322
303. Korgun ET, Denir R, Hammer A, Dohr G, Desoye G, Skofitch G,Hahn T 2001 Glucose transporter expression in rat embryo anduterus during decidualization, implantation, and early postim-plantation. Biol Reprod 65:1364–1370
304. Strowitzki T, Capp E, von Wolff M, Muller-Hocker J 2001 Ex-pression of glucose transporter 1 in human endometrial and de-cidual tissue. Gynecol Endocrinol 15:219–224
305. Jansson T, Wennergren M, Illsley NP 1993 Glucose transporterexpression and distribution in the human placenta throughoutgestation and in intrauterine growth retardation. J Clin EndocrinolMetab 77:1554–1562
306. Mioni R, Chiarelli S, Xamin N, Zuliani L, Granzotto M, MozzanegaB, Maffei P, Martini C, Blandamura S, Sicolo N, Vettor R 2004Evidence for the presence of glucose transporter 4 in the endometriumand its regulation in polycystic ovary syndrome patients. J Clin En-docrinol Metab 89:4089–4096
307. Ajossa S, Guerriero S, Paoletti AM, Orru M, Melis GB 2002 Theantiandrogenic effect of flutamide improves uterine perfusion inwomen with polycystic ovary syndrome. Fertil Steril 77:1136–1140
308. Apparao KB, Lovely LP, Gui Y, Lininger RA, Lessey BA 2002Elevated endometrial androgen receptor expression in womenwith polycystic ovarian syndrome. Biol Reprod 66:297–304
309. Taylor HS 2000 The role of HOXA genes in human implantation.Hum Reprod Update 6:75–79
310. Cermik D, Selam B, Taylor HS 2003 Regulation of HOXA-10expression by testosterone in vitro and in the endometrium ofpatients with polycystic ovary syndrome. J Clin Endocrinol Metab88:238–243
311. Economos K, MacDonald PC, Casey ML 1992 Endothelin-1 geneexpression and protein biosynthesis in human endometrium: po-tential modulator of endometrial blood flow. J Clin EndocrinolMetab 74:14–19
312. Cacciatore B, Simberg N, Tiitinen A, Ylikorkala O 1997 Evidenceof interplay between plasma endothelin-1 and 17 �-estradiol inregulation of uterine blood flow and endometrial growth in infer-tile women. Fertil Steril 67:883–888
313. Orio Jr F, Palomba S, Cascella T, De Simone B, Di Biase S, RussoT, Labella D, Zullo F, Lombardi G, Colao A 2004 Early impairmentof endothelial structure and function in young normal-weightwomen with polycystic ovary syndrome. J Clin Endocrinol Metab89:4588–4593
314. Speert H 1949 Carcinoma of the endometrium in young women.Surg Gynaecol Obstet 88:332–336
315. Dockerty MB, Jackson RL 1957 The Stein-Leventhal syndrome:analysis of 43 cases with special reference to association with en-dometrial carcinoma. Am J Obstet Gynecol 73:161–173
316. Navaratnarajah R, Pillay OC, Hardiman P 2008 Polycystic ovarysyndrome and endometrial cancer. Semin Reprod Med 26:62–71
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 45
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022
317. Coulam CB, Annegers JF, Kranz JS 1983 Chronic anovulationsyndrome and associated neoplasia. Obstet Gynecol 61:403–407
318. Calle EE, Thun MJ 2004 Obesity and cancer. Oncogene 23:6365–6378319. Lupulescu A 1993 Estrogen use and cancer risk: a review. Exp Clin
Endocrinol 101:204–214320. Konishi I, Koshiyama M, Mandai M, Kuroda H, Yamamoto S,
Nanbu K, Komatsu T, Matsushita K, Rao CV, Mori T 1997 In-creased expression of LH/hCG receptors in endometrial hyper-plasia and carcinoma in anovulatory women. Gynecol Oncol 65:273–280
321. Li L, Yang C, Qiaojie 1998 Pathological and immunohistochemicalstudy on estrogen and progesterone receptors in endometriumof polycystic ovarian syndrome. Zhonghua Fu Chan Ke Za Zhi33:89 –91
322. Maliqueo M, Clementi M, Gabler F, Johnson MC, Palomino A,Sir-Petermann T, Vega M 2003 Expression of steroid receptors andproteins related to apoptosis in endometria of women with poly-cystic ovary syndrome. Fertil Steril 80:812–819
323. Nagamani M, Stuart CA, Dunhardt PA, Doherty PA 1991 Specificbinding sites for insulin and insulin-like growth factor I in humanendometrial cancer. Am J Obstet Gynecol 165:1865–1871
324. Bershtein LM, Gamaiunova VB, Kvachevskaia IuO, Tsyrlina EV,Kovalenko IG 2000 The nature of hyperinsulinaemia (insulin re-sistance) in endometrial carcinoma: of plasma levels of insulin andc-peptide. Vopr Onkol 46:191–195
325. Pavelic J, Radakovic B, Pavelic K 2007 Insulin-like growth factor2 and its receptors (IGF 1R and IGF 2R/mannose 6-phosphate) inendometrial adenocarcinoma. Gynecol Oncol 105:727–735
326. Gunter MJ, Hoover DR, Yu H, Wassertheil-Smoller S, Manson JE,Li J, Harris TG, Rohan TE, Xue X, Ho GY, Einstein MH, KaplanRC, Burk RD, Wylie-Rosett J, Pollak MN, Anderson G, HowardBV, Strickler HD 2008 A prospective evaluation of insulin andinsulin-like growth factor-I as risk factors for endometrial cancer.Cancer Epidemiol Biomarkers Prev 17:921–929
327. Pillay OC, Leonard A, Catalano R, Sharkey A, Hardiman P 2005Endometrial gene expression in women with polycystic ovary syn-drome. Hum Reprod 20(Suppl 1):i96
328. Rutanen EM, Nyman T, Lehtovirta P, Ammala M, Pekonen F 1994Suppressed expression of insulin-like growth factor binding pro-tein-1 mRNA in the endometrium: a molecular mechanism asso-ciating endometrial cancer with its risk factors. Int J Cancer 59:307–312
329. Session DR, Kalli KR, Tummon IS, Damario MA, Dumesic DA2003 Treatment of atypical endometrial hyperplasia with an insu-lin-sensitizing agent. Gynecol Endocrinol 17:405–407
330. Legro RS, Zaino RJ, Demers LM, Kunselman AR, Gnatuk CL,Williams NI, Dodson WC 2007 The effects of metformin and ros-iglitazone, alone and in combination, on the ovary and endome-trium in polycystic ovary syndrome. Am J Obstet Gynecol 196:402.e1–e10
331. Rosenfield RL 1986 Pilosebaceous physiology in relation to hir-sutism and acne. Clin Endocrinol Metab 15:341–362
332. Trolle B, Flyvbjerg A, Kesmodel U, Lauszus FF 2007 Efficacy ofmetformin in obese and non-obese women with polycystic ovarysyndrome: a randomized, double-blinded, placebo-controlledcross-over trial. Hum Reprod 22:2967–2973
333. Kjøtrød SB, Sunde A, During VV, Carlsen SM 4 March 2008Possible metformin effect on adrenal androgens during pretreat-ment and IVF cycle in women with polycystic ovary syndrome.Fertil Steril 10.1016/j.fertnstert.2007.11.069
334. Ortega-Gonzalez C, Luna S, Hernandez L, Crespo G, Aguayo P,Arteaga-Troncoso G, Parra A 2005 Responses of serum androgenand insulin resistance to metformin and pioglitazone in obese,insulin-resistant women with polycystic ovary syndrome. J ClinEndocrinol Metab 90:1360–1365
335. Sahin I, Serter R, Karakurt F, Demirbas B, Culha C, Taskapan C,Kosar F, Aral Y 2004 Metformin versus flutamide in the treatmentof metabolic consequences of non-obese young women with poly-cystic ovary syndrome: a randomized prospective study. GynecolEndocrinol 19:115–124
336. Cibula D, Fanta M, Vrbikova J, Stanicka S, Dvorakova K, Hill M,Skrha J, Zivny J, Skrenkova J 2005 The effect of combinationtherapy with metformin and combined oral contraceptives (COC)
versus COC alone on insulin sensitivity, hyperandrogenaemia,SHBG and lipids in PCOS patients. Hum Reprod 20:180–184
337. Ibanez L, Valls C, Ferrer A, Ong K, Dunger DB, De Zegher F 2002Additive effects of insulin-sensitizing and anti-androgen treatmentin young, nonobese women with hyperinsulinism, hyperandro-genism, dyslipidemia, and anovulation. J Clin Endocrinol Metab87:2870–2874
338. Ibanez L, de Zegher F 2006 Low-dose flutamide-metformin ther-apy for hyperinsulinemic hyperandrogenism in non-obese adoles-cents and women. Hum Reprod Update 12:243–252
339. Gambineri A, Pelusi C, Genghini S, Morselli-Labate AM, CacciariM, Pagotto U, Pasquali R 2004 Effect of flutamide and metforminadministered alone or in combination in dieting obese women withpolycystic ovary syndrome. Clin Endocrinol (Oxf) 60:241–249
340. Vanky E, Salvesen KA, Carlsen SM 2004 Six-month treatmentwith low-dose dexamethasone further reduces androgen levels inPCOS women treated with diet and lifestyle advice, and met-formin. Hum Reprod 19:529–533
341. Kolodziejczyk B, Duleba AJ, Spaczynski RZ, Pawelczyk L 2000Metformin therapy decreases hyperandrogenism and hyperinsu-linemia in women with polycystic ovary syndrome. Fertil Steril73:1149–1154
342. Kelly CJ, Gordon D 2002 The effect of metformin on hirsutism inpolycystic ovary syndrome. Eur J Endocrinol 147:217–221
343. Harborne L, Fleming R, Lyall H, Sattar N, Norman J 2003 Met-formin or antiandrogen in the treatment of hirsutism in polycysticovary syndrome. J Clin Endocrinol Metab 88:4116–4123
344. Gambineri A, Patton L, Vaccina A, Cacciari M, Morselli-LabateAM, Cavazza C, Pagotto U, Pasquali R 2006 Treatment with flu-tamide, metformin, and their combination added to a hypocaloricdiet in overweight-obese women with polycystic ovary syndrome:a randomized, 12-month, placebo-controlled study. J Clin Endo-crinol Metab 91:3970–3980
345. Bellot-Rojas P, Posadas-Sanchez R, Caracas-Portilla N, Zamora-Gonzalez J, Cardoso-Saldana G, Jurado-Santacruz F, Posadas-Romero C 2006 Comparison of metformin versus rosiglitazone inpatients with Acanthosis nigricans: a pilot study. J Drugs Dermatol5:884–889
346. Koulouri O, Conway GS 2008 A systematic review of commonlyused medical treatments for hirsutism in women. Clin Endocrinol(Oxf) 68:800–805
347. Cosma M, Swiglo BA, Flynn DN, Kurtz DM, Labella ML, MullanRJ, Elamin MB, Erwin PJ, Montori VM 2008 Clinical review:insulin sensitizers for the treatment of hirsutism: a systematic re-view and metaanalyses of randomized controlled trials. J ClinEndocrinol Metab 93:1135–1142
348. Martin KA, Chang RJ, Ehrmann DA, Ibanez L, Lobo RA, RosenfieldRL, Shapiro J, Montori VM, Swiglo BA 2008 Evaluation and treat-ment of hirsutism in premenopausal women: an Endocrine SocietyClinical Practice Guideline. J Clin Endocrinol Metab 93:1105–1120
349. Gadducci A, Gargini A, Palla E, Fanucchi A, Genazzani AR 2005Polycystic ovary syndrome and gynecological cancers: is there alink? Gynecol Endocrinol 20:200–208
350. Guastamacchia E, Resta F, Triggiani V, Liso A, Licchelli B,Ghiyasaldin S, Sabba C, Tafaro E 2004 Evidence for a putativerelationship between type 2 diabetes and neoplasia with particularreference to breast cancer: role of hormones, growth factors andspecific receptors. Curr Drug Targets Immune Endocr MetabolDisord 4:59–66
351. Ben Sahra I, Laurent K, Loubat A, Giorgetti-Peraldi S, ColosettiP, Auberger P, Tanti JF, Le Marchand-Brustel Y, Bost F 2008 Theantidiabetic drug metformin exerts an antitumoral effect in vitroand in vivo through a decrease of cyclin D1 level. Oncogene 27:3576–3586
352. Hadad SM, Fleming S, Thompson AM 2008 Targeting AMPK: anew therapeutic opportunity in breast cancer. Crit Rev Oncol He-matol 67:1–7
353. Huang X, Wullschleger S, Shpiro N, McGuire VA, Sakamoto K,Woods YL, McBurnie W, Fleming S, Alessi DR 2008 Importantrole of the LKB1-AMPK pathway in suppressing tumourigenesis inPTEN-deficient mice. Biochem J 412:211–221
354. Phoenix KN, Vumbaca F, Claffey KP 7 February 2008 Therapeuticmetformin/AMPK activation promotes the angiogenic phenotype
46 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022
in the ER� negative MDA-MB-435 breast cancer model. BreastCancer Res Treat 10.1007/s10549-008-9916-5
355. Stambolic V, Woodgett JR, Fantus IG, Pritchard KI, Goodwin PJ26 April 2008 Utility of metformin in breast cancer treatment, isneoangiogenesis a risk factor? Breast Cancer Res Treat 10.1007/s10549-008-0015-4
356. Jones GL, Hall JM, Balen AH, Ledger WL 2008 Health-relatedquality of life measurement in women with polycystic ovary syn-drome: a systematic review. Hum Reprod Update 14:15–25
357. Ching HL, Burke V, Stuckey BG 2007 Quality of life and psycho-logical morbidity in women with polycystic ovary syndrome: bodymass index, age and the provision of patient information are sig-nificant modifiers. Clin Endocrinol (Oxf) 66:373–379
358. Hahn S, Benson S, Elsenbruch S, Pleger K, Tan S, Mann K,Schedlowski M, van Halteren WB, Kimmig R, Janssen OE 2006Metformin treatment of polycystic ovary syndrome improveshealth-related quality-of-life, emotional distress and sexuality.Hum Reprod 21:1925–1934
359. Coffey S, Bano G, Mason HD 2006 Health-related quality of lifein women with polycystic ovary syndrome: a comparison with thegeneral population using the polycystic ovary syndrome question-naire (PCOSQ) and the Short Form-36 (SF-36). Gynecol Endocrinol22:80–86
360. Lee AT, Zane LT 2007 Dermatologic manifestations of polycysticovary syndrome. Am J Clin Dermatol 8:201–219
361. Janssen OE, Hahn S, Tan S, Benson S, Elsenbruch S 2008 Moodand sexual function in polycystic ovary syndrome. Semin ReprodMed 26:45–52
362. van Wely M, Bayram N, van der Veen F, Bossuyt PM 2004 Aneconomic comparison of a laparoscopic electrocautery strategy andovulation induction with recombinant FSH in women with clomi-phene citrate-resistant polycystic ovary syndrome. Hum Reprod19:1741–1745
363. Clayton WJ, Lipton M, Elford J, Rustin M, Sherr L 2005 A ran-domized controlled trial of laser treatment among hirsute womenwith polycystic ovary syndrome. Br J Dermatol 152:986–992
364. Jones GL, Benes K, Clark TL, Denham R, Holder MG, Haynes TJ,Mulgrew NC, Shepherd KE, Wilkinson VH, Singh M, Balen A,Lashen H, Ledger WL 2004 The polycystic ovary syndrome health-related quality of life questionnaire (PCOSQ): a validation. HumReprod 19:371–377
365. Azziz R, Sanchez LA, Knochenhauer ES, Moran C, Lazenby J,Stephens KC, Taylor K, Boots LR 2004 Androgen excess in wom-en: experience with over 1000 consecutive patients. J Clin Endo-crinol Metab 89:453–462
366. Carmina E, Legro RS, Stamets K, Lowell J, Lobo RA 2003 Dif-ference in body weight between American and Italian women withpolycystic ovary syndrome: influence of the diet. Hum Reprod18:2289–2293
367. Lord J, Wilkin T 2002 Polycystic ovary syndrome and fat distri-bution: the central issue? Hum Fertil (Cambr) 5:67–71
368. Wajchenberg BL 2000 Subcutaneous and visceral adipose tissue:their relation to the metabolic syndrome. Endocr Rev 21:697–738
369. Strowitzki T, Halser B, Demant T 2002 Body fat distribution,insulin sensitivity, ovarian dysfunction and serum lipoproteinsin patients with polycystic ovary syndrome. Gynecol Endocrinol16:45–51
370. Kirchengast S, Huber J 2001 Body composition characteristics andbody fat distribution in lean women with polycystic ovary syn-drome. Hum Reprod 16:1255–1260
371. Despres JP, Couillard C, Gagnon J, Bergeron J, Leon AS, Rao DC,Skinner JS, Wilmore JH, Bouchard C 2000 Race, visceral adiposetissue, plasma lipids, and lipoprotein lipase activity in men andwomen: the Health, Risk Factors, Exercise Training, and Genet-ics (HERITAGE) family study. Arterioscler Thromb Vasc Biol20:1932–1938
372. Nelson SM, Fleming R 2007 Obesity and reproduction: impact andinterventions. Curr Opin Obstet Gynecol 19:384–389
373. Kiddy DS, Sharp PS, White DM, Scanlon MF, Mason HD, BrayCS, Polson DW, Reed MJ, Franks S 1990 Differences in clinical andendocrine features between obese and non-obese subjects withpolycystic ovary syndrome: an analysis of 263 consecutive cases.Clin Endocrinol (Oxf) 32:213–220
374. Imani B, Eijkemans MJC, te Velde ER, Habbema JDF, Fauser BC1999 Predictors of chances to conceive in ovulatory patients duringclomiphene citrate induction of ovulation in normogonadotropicoligoamenorrheic infertility. J Clin Endocrinol Metab 84:1617–1622
375. Mulders AG, Laven JS, Eijkemans MJ, Hughes EG, Fauser BC2003 Patient predictors for outcome of gonadotrophin ovulationinduction in women with normogonadotrophic anovulatory infer-tility: a meta-analysis. Hum Reprod Update 9:429–449
376. Amer SA, Li TC, Ledger WL 2004 Ovulation induction usinglaparoscopic ovarian drilling in women with polycystic ovariansyndrome: predictors of success. Hum Reprod 19:1719–1724
377. Gjønnaess H 1989 The course and outcome of pregnancy afterovarian electrocautery in women with polycystic ovarian syn-drome: the influence of body-weight. Br J Obstet Gynaecol 96:714 –719
378. Cedergren MI 2004 Maternal morbid obesity and the risk of ad-verse pregnancy outcome. Obstet Gynecol 103:219–224
379. National Institute for Clinical Excellence 2004 Fertility assessmentand treatment for people with fertility problems. A clinical guide-line. London: RCOG Press
380. Anderson JW, Konz EC, Frederich RC, Wood CL 2001 Long-termweight-loss maintenance: a meta-analysis of US studies. Am J ClinNutr 74:579–584
381. Stamets K, Taylor DS, Kunselman A, Demers LM, Pelkman CL,Legro RS 2004 A randomized trial of the effects of two types ofshort-term hypocaloric diets on weight loss in women with poly-cystic ovary syndrome. Fertil Steril 81:630–637
382. Palomba S, Giallauria F, Falbo A, Russo T, Oppedisano R, TolinoA, Colao A, Vigorito C, Zullo F, Orio F 2008 Structured exercisetraining programme versus hypocaloric hyperproteic diet in obesepolycystic ovary syndrome patients with anovulatory infertility: a24-week pilot study. Hum Reprod 23:642–650
383. Hermansen K, Mortensen LS 2007 Body weight changes associ-ated with antihyperglycaemic agents in type 2 diabetes mellitus.Drug Saf 30:1127–1142
384. Kawai T, Funae O, Shimada A, Tabata M, Hirata T, Atsumi Y, ItohH 2008 Effects of pretreatment with low-dose metformin on met-abolic parameters and weight gain by pioglitazone in Japanesepatients with type 2 diabetes. Intern Med 47:1181–1188
385. Wu RR, Zhao JP, Guo XF, He YQ, Fang MS, Guo WB, Chen JD,Li LH 2008 Metformin addition attenuates olanzapine-inducedweight gain in drug-naive first-episode schizophrenia patients:a double-blind, placebo-controlled study. Am J Psychiatry 165:352–358
386. Wu RR, Zhao JP, Jin H, Shao P, Fang MS, Guo XF, He YQ, LiuYJ, Chen JD, Li LH 2008 Lifestyle intervention and metformin fortreatment of antipsychotic-induced weight gain: a randomized con-trolled trial. JAMA 299:185–193
387. Christ-Crain M, Kola B, Lolli F, Fekete C, Seboek D, WittmannG, Feltrin D, Igreja SC, Ajodha S, Harvey-White J, Kunos G,Muller B, Pralong F, Aubert G, Arnaldi G, Giacchetti G, BoscaroM, Grossman AB, Korbonits M 2008 AMP-activated protein ki-nase mediates glucocorticoid-induced metabolic changes: a novelmechanism in Cushing’s syndrome. FASEB J 22:1672–1683
388. Tsilchorozidou T, Batterham RL, Conway GS 2008 Metforminincreases fasting plasma PYY in women with PCOS. Clin Endo-crinol (Oxf) 69:936–942
389. Gambineri A, Pelusi C, Vicennati V, Pagotto U, Pasquali R 2002Obesity and the polycystic ovary syndrome. Int J Obes Relat MetabDisord 26:883–896
390. Romualdi D, De Marinis L, Campagna G, Proto C, Lanzone A,Guido M 2008 Alteration of ghrelin-neuropeptide Y network inobese patients with polycystic ovary syndrome: role of hyperin-sulinism. Clin Endocrinol (Oxf) 69:562–567
391. Kusaka I, Nagasaka S, Horie H, Ishibashi S 2008 Metformin, butnot pioglitazone, decreases postchallenge plasma ghrelin levels intype 2 diabetic patients: a possible role in weight stability? DiabetesObes Metab 10:1039–1046
392. English PJ, Ashcroft A, Patterson M, Dovey TM, Halford JC,Harrison J, Eccleston D, Bloom SR, Ghatei MA, Wilding JP 2007Metformin prolongs the postprandial fall in plasma ghrelin con-centrations in type 2 diabetes. Diabetes Metab Res Rev 23:299–303
393. Tan BK, Heutling D, Chen J, Farhatullah S, Adya R, Keay SD,
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 47
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022
Kennedy CR, Lehnert H, Randeva HS 2008 Metformin decreasesthe adipokine vaspin in overweight women with polycystic ovarysyndrome concomitant with improvement in insulin sensitivityand a decrease in insulin resistance. Diabetes 57:1501–1507
394. Nawrocka J, Starczewski A 2007 Effects of metformin treatment inwomen with polycystic ovary syndrome depends on insulin re-sistance. Gynecol Endocrinol 23:231–237
395. Hoeger KM, Kochman L, Wixom N, Craig K, Miller RK, GuzickDS 2004 A randomized, 48-week, placebo-controlled trial of in-tensive lifestyle modification and/or metformin therapy in over-weight women with polycystic ovary syndrome: a pilot study.Fertil Steril 82:421–429
396. Tang T, Glanville J, Hayden CJ, White D, Barth JH, Balen AH 2006Combined lifestyle modification and metformin in obese patientswith polycystic ovary syndrome. A randomized, placebo-con-trolled, double-blind multicentre study. Hum Reprod 21:80–89
397. Salpeter SR, Buckley NS, Kahn JA, Salpeter EE 2008 Meta-anal-ysis: metformin treatment in persons at risk for diabetes mellitus.Am J Med 121:149–157.e2
398. Helvaci MR, Kaya H, Borazan A, Ozer C, Seyhanli M, Yalcin A2008 Metformin and parameters of physical health. Intern Med47:697–703
399. Wu FCW, Eckardstein A 2003 Androgens and coronary arterydisease. Endocr Rev 24:183–217
400. Muniyappa R, Montagnani M, Koh KK, Quon MJ 2007 Cardio-vascular actions of insulin. Endocr Rev 28:463–491
401. UK Prospective Diabetes Study (UKPDS) Group 1998 Effect ofintensive blood-glucose control with metformin on complicationsin overweight patients with type 2 diabetes (UKPDS 34). UK Pro-spective Diabetes Study (UKPDS) Group. Lancet 352:854–865
402. Mellbin LG, Malmberg K, Norhammar A, Wedel H, Ryden L;DIGAMI 2 Investigators 2008 The impact of glucose loweringtreatment on long-term prognosis in patients with type 2 diabetesand myocardial infarction: a report from the DIGAMI 2 trial. EurHeart J 29:166–176
403. Calvert JW, Gundewar S, Jha S, Greer JJ, Bestermann WH, TianR, Lefer DJ 2008 Acute metformin therapy confers cardioprotectionagainst myocardial infarction via AMPK-eNOS-mediated signal-ing. Diabetes 57:696–705
404. Bhamra GS, Hausenloy DJ, Davidson SM, Carr RD, Paiva M,Wynne AM, Mocanu MM, Yellon DM 2008 Metformin protectsthe ischemic heart by the Akt-mediated inhibition of mitochon-drial permeability transition pore opening. Basic Res Cardiol103:274 –284
405. Orio F, Giallauria F, Palomba S, Cascella T, Manguso F, Vuolo L,Russo T, Lombardi G, Colao A, Vigorito C 2006 Cardiopulmonaryimpairment in young women with polycystic ovary syndrome.J Clin Endocrinol Metab 91:2967–2971
406. Clausen JO, Borch-Johnsen K, Ibsen H, Bergman RN, HougaardP, Winther K, Pedersen O 1996 Insulin sensitivity index, acuteinsulin response, and glucose effectiveness in a population-basedsample of 380 young healthy Caucasians. Analysis of the impact ofgender, body fat, physical fitness, and life-style factors. J Clin Invest98:1195–1209
407. Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE2002 Exercise capacity and mortality among men referred for ex-ercise testing. N Engl J Med 346:793–801
408. Vigorito C, Giallauria F, Palomba S, Cascella T, Manguso F, LucciR, De Lorenzo A, Lombardi G, Colao A, Orio F 2007 Beneficialeffects of a three-month structured exercise training program oncardiopulmonary functional capacity in young women with poly-cystic ovary syndrome. J Clin Endocrinol Metab 92:1379–1384
409. Braun B, Eze P, Stephens BR, Hagobian TA, Sharoff CG, ChipkinSR, Goldstein B 2008 Impact of metformin on peak aerobic ca-pacity. Appl Physiol Nutr Metab 33:61–67
410. Legro RS, Gnatuk CL, Kunselman AR, Dunaif A 2005 Changes inglucose tolerance over time in women with polycystic ovary syn-drome: a controlled study. J Clin Endocrinol Metab 90:3236–3242
411. de Zegher F, Ibanez L 2006 Prenatal growth restraint followed bycatch-up of weight: a hyperinsulinemic pathway to polycysticovary syndrome. Fertil Steril 86:S4–S5
412. Hofman PL, Regan F, Jackson WE, Jefferies C, Knight DB, Robinson
EM, Cutfield WS 2004 Premature birth and later insulin resistance.N Engl J Med 351:2179–2186
413. Bruns CM, Baum ST, Colman RJ, Eisner JR, Kemnitz JW, WeindruchR, Abbott DH 2004 Insulin resistance and impaired insulin secretionin prenatally androgenized male rhesus monkeys. J Clin EndocrinolMetab 89:6218–6223
414. Eisner JR, Dumesic DA, Kemnitz JW, Abbott DH 2000 Timing ofprenatal androgen excess determines differential impairment ininsulin secretion and action in adult female rhesus monkeys. J ClinEndocrinol Metab 85:1206–1210
415. Hoffman LK, Ehrmann DA 2008 Cardiometabolic features of poly-cystic ovary syndrome. Nat Clin Pract Endocrinol Metab 4:215–222
416. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, LachinJM, Walker EA, Nathan DM; Diabetes Prevention ProgramResearch Group 2002 Reduction in the incidence of type 2 di-abetes with lifestyle intervention or metformin. N Engl J Med346:393– 403
417. Diabetes Prevention Program Research Group 2003 Effects ofwithdrawal from metformin on the development of diabetes in thediabetes prevention program. Diabetes Care 26:977–980
418. Johnson JA, Majumdar SR, Simpson SH, Toth EL 2002 Decreasedmortality associated with the use of metformin compared withsulfonylurea monotherapy in type 2 diabetes. Diabetes Care 25:2244–2248
419. Sharma ST, Wickham EP, Nestler JE 2007 Changes in glucosetolerance with metformin treatment in polycystic ovary syndrome:a retrospective analysis. Endocr Pract 13:373–379
420. Zimmermann S, Phillips RA, Dunaif A, Finegood DT, WilkenfeldC, Ardeljan M, Gorlin R, Krakoff LR 1992 Polycystic ovary syn-drome: lack of hypertension despite profound insulin resistance. J ClinEndocrinol Metab 75:508–513
421. Holte J, Pennarelli G, Berne C, Bergh T, Lithell H 1996 Elevatedambulatory day-time blood pressure in women with polycysticovary syndrome: a sign of a pre-hypertensive state? Hum Reprod11:23–28
422. Chen M-J, Yang W-S, Yang J-H, Chen C-L, Ho H-N, Yang Y-S2007 Relationship between androgen levels and blood pressurein young women with polycystic ovary syndrome. Hypertension49:1442–1447
423. Elting MW, Korsen TJM, Bezemer PD, Schoemaker J 2001 Prev-alence of diabetes mellitus, hypertension and cardiac complaints ina follow-up study of a Dutch PCOS population. Hum Reprod16:556–560
424. Diamanti-Kandarakis E, Spina G, Kouli C, Migdalis I 2001 In-crease in endothelin-1 levels in women with polycystic ovary syn-drome and the beneficial effect of metformin treatment. J ClinEndocrinol Metab 86:4666–4673
425. Reckelhoff JF 2001 Gender differences in the regulation of bloodpressure. Hypertension 37:1199–1208
426. Uncu G, Sozer M, Develioglu O, Cengiz C 2002 The role of plasmarenin activity in distinguishing patients with polycystic ovary syn-drome (PCOS) from oligomenorrheic patients without PCOS. Gy-necol Endocrinol 16:447–452
427. Cascella T, Palomba S, Tauchmanova L, Manguso F, Di Biase S,Labella D, Giallauria F, Vigorito C, Colao A, Lombardi G, OrioF 2006 Serum aldosterone concentration and cardiovascular risk inwomen with polycystic ovarian syndrome. J Clin Endocrinol Metab91:4395–4400
428. Wang X, Jia X, Chang T, Desai K, Wu L 2008 Attenuation ofhypertension development by scavenging methylglyoxal in fruc-tose-treated rats. J Hypertens 26:765–772
429. Luque-Ramírez M, Mendieta-Azcona C, Alvarez-Blasco F, Escobar-Morreale HF 18 June 2008 Effects of metformin versus ethinyl-estra-diol plus cyproterone acetate on ambulatory blood pressuremonitoring and carotid intima media thickness in women withthe polycystic ovary syndrome. Fertil Steril 10.1016/j.fertnstert.2008.03.082
430. Komajda M, Curtis P, Hanefeld M, Beck-Nielsen H, Pocock SJ,Zambanini A, Jones NP, Gomis R, Home PD; RECORD StudyGroup 2008 Effect of the addition of rosiglitazone to metformin orsulfonylureas versus metformin/sulfonylurea combination ther-apy on ambulatory blood pressure in people with type 2 diabetes:
48 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

a randomized controlled trial (the RECORD study). CardiovascDiabetol 7:10
431. Derosa G, Fogari E, Cicero AF, D’Angelo A, Ciccarelli L, PiccinniMN, Pricolo F, Salvadeo SA, Gravina A, Ferrari I, Fogari R 2007Blood pressure control and inflammatory markers in type-2 dia-betic patients treated with pioglitazone or rosiglitazone and met-formin. Hypertens Res 30:387–394
432. Rizzo M, Berneis K, Carmina E, Rini GB 2008 How should wemanage atherogenic dyslipidemia in women with polycystic ovarysyndrome? Am J Obstet Gynecol 198:28.e1–e5
433. Tessari P, Tiengo A 2008 Metformin treatment of rats with diet-induced overweight and hypertriglyceridemia decreases plasmatriglyceride concentrations, while decreasing triglyceride and in-creasing ketone body output by the isolated perfused liver. ActaDiabetol 45:143–145
434. Puljak L, Parameswara V, Dolovcak S, Waldrop SL, Emmett D,Esser V, Fitz JG, Kilic G 2008 Evidence for AMPK-dependentregulation of exocytosis of lipoproteins in a model liver cell line.Exp Cell Res 314:2100–2109
435. Wild RA 2008 Pioglitazone and metformin for increased smalllow-density lipoprotein in polycystic ovary syndrome: counter-point. Am J Obstet Gynecol 198:4–6
436. Juhan-Vague I, Alessi MC 1997 PAI-1, obesity, insulin resistanceand risk of cardiovascular events. Thromb Haemost 78:656–660
437. Orio Jr F, Palomba S, Cascella T, Tauchmanova L, Nardo LG, DiBiase S, Labella D, Russo T, Savastano S, Tolino A, Zullo F, ColaoA, Lombardi G 2004 Is plasminogen activator inhibitor-1 a car-diovascular risk factor in young women with polycystic ovarysyndrome? Reprod Biomed Online 9:505–510
438. Skurk T, Hauner H 2004 Obesity and impaired fibrinolysis: role ofadipose production of plasminogen activator inhibitor-1. Int J ObesRelat Metab Disord 28:1357–1364
439. He G, Pedersen SB, Bruun JM, Lihn AS, Richelsen B 2003 Met-formin, but not thiazolidinediones, inhibits plasminogen activatorinhibitor-1 production in human adipose tissue in vitro. HormMetab Res 35:18–23
440. Ersoy C, Kiyici S, Budak F, Oral B, Guclu M, Duran C, SelimogluH, Erturk E, Tuncel E, Imamoglu S 2008 The effect of metformintreatment on VEGF and PAI-1 levels in obese type 2 diabetic pa-tients. Diabetes Res Clin Pract 81:56–60
441. Oktenli C, Ozgurtas T, Dede M, Sanisoglu YS, Yenen MC,Yesilova Z, Kenar L, Kurt YG, Baser I, Smith J, Cianflone K2007 Metformin decreases circulating acylation-stimulating pro-tein levels in polycystic ovary syndrome. Gynecol Endocrinol23:710 –715
442. Diamanti-Kandarakis E, Paterakis T, Alexandraki K, Piperi C,Aessopos A, Katsikis I, Katsilambros N, Kreatsas G, Panidis D2006 Indices of low-grade chronic inflammation in polycystic ovarysyndrome and the beneficial effect of metformin. Hum Reprod21:1426–1431
443. Orio Jr F, Palomba S, Cascella T, Di Biase S, Manguso F, TauchmanovaL, Nardo LG, Labella D, Savastano S, Russo T, Zullo F, Colao A,Lombardi G 2005 The increase of leukocyte as a new marker of lowgrade chronic inflammation and early cardiovascular risk in the poly-cystic ovary syndrome. J Clin Endocrinol Metab 90:2–5
444. Orio F, Manguso F, Di Biase S, Falbo A, Giallauria F, Labella D,Tolino A, Lombardi G, Colao A, Palomba S 2007 Metformin ad-ministration improves leukocyte count in women with polycysticovary syndrome: a 6-month prospective study. Eur J Endocrinol157:69–73
445. Lund SS, Tarnow L, Stehouwer CD, Schalkwijk CG, Teerlink T,Gram J, Winther K, Frandsen M, Smidt UM, Pedersen O, ParvingHH, Vaag AA 2008 Impact of metformin versus repaglinide onnon-glycaemic cardiovascular risk markers related to inflammationand endothelial dysfunction in non-obese patients with type 2diabetes. Eur J Endocrinol 158:631–641
446. Isoda K, Young JL, Zirlik A, MacFarlane LA, Tsuboi N, GerdesN, Schonbeck U, Libby P 2006 Metformin inhibits proinflamma-tory responses and nuclear factor-�B in human vascular wall cells.Arterioscler Thromb Vasc Biol 26:611–617
447. Zmijewski JW, Lorne E, Zhao X, Tsuruta Y, Sha Y, Liu G, SiegalGP, Abraham E 2008 Mitochondrial respiratory complex I regu-
lates neutrophil activation and severity of lung injury. Am J RespirCrit Care Med 178:168–179
448. Dandona P, Aljada A, Ghanim H, Mohanty P, Tripathy C, HofmeyerD, Chaudhuri A 2004 Increased plasma concentration of macrophagemigration inhibitory factor (MIF) and MIF mRNA in mononuclearcells in the obese and the suppressive action of metformin. J ClinEndocrinol Metab 89:5043–5047
449. Ibanez L, Valls C, de Zegher F 2006 Discontinuous low-doseflutamide-metformin plus an oral or a transdermal contraceptive inpatients with hyperinsulinaemic hyperandrogenism: normalizingeffects on CRP, TNF-� and the neutrophil/lymphocyte ratio. HumReprod 21:451–456
450. Ibanez L, Jaramillo AM, Ferrer A, de Zegher F 2005 High neu-trophil count in girls and women with hyperinsulinaemic hyperan-drogenism: normalization with metformin and flutamide over-comes the aggravation by oral contraception. Hum Reprod 20:2457–2462
451. Morin-Papunen L, Rautio K, Ruokonen A, Hedberg P, Puukka M,Tapanainen JS 2003 Metformin reduces serum C-reactive proteinlevels in women with polycystic ovary syndrome. J Clin EndocrinolMetab 88:4649–4654
452. Battaglia C, Mancini F, Cianciosi A, Busacchi P, Facchinetti F,Marchesini GR, Marzocchi R, de Aloysio D 2008 Vascular risk inyoung women with polycystic ovary and polycystic ovary syn-drome. Obstet Gynecol 111:385–395
453. Heutling D, Schulz H, Nickel I, Kleinstein J, Kaltwasser P,Westphal S, Mittermayer F, Wolzt M, Krzyzanowska K,Randeva H, Schernthaner G, Lehnert H 2008 Asymmetricaldimethylarginine, inflammatory and metabolic parameters inwomen with polycystic ovary syndrome before and aftermetaformin treatment. J Clin Endocrinol Metab 93:82–90
454. Romualdi D, Costantini B, Selvaggi L, Giuliani M, Cristello F,Macrì F, Bompiani A, Lanzone A, Guido M 2008 Metformin im-proves endothelial function in normoinsulinemic PCOS patients: anew prospective. Hum Reprod 23:2127–2133
455. Rikimaru M, Nishikawa T, Shimizu Y, Ishida N 1965 Relationshipbetween tissue culture cytotoxicity and acute toxicity in mice ofbiguanide derivatives. J Antibiot 18:196–199
456. Koschinsky T, Bunting CE, Rutter R, Gries FA 1988 Influenceof metformin on vascular cell proliferation. Diabetes Metab 14:566 –570
457. Diamanti-Kandarakis E, Alexandraki K, Piperi C, Aessopos A,Paterakis T, Katsikis I, Panidis D 2007 Effect of metformin ad-ministration on plasma advanced glycation end product levels inwomen with polycystic ovary syndrome. Metabolism 56:129–134
458. Topcu S, Tok D, Caliskan M, Ozcimen EE, Gullu H, Uckuyu A,Erdogan D, Zeyneloglu H, Muderrisoglu H 2006 Metformin ther-apy improves coronary microvascular function in patients withpolycystic ovary syndrome and insulin resistance. Clin Endocrinol(Oxf) 65:75–80
459. Third Report of the National Cholesterol Education Program(NCEP) 2002 Expert Panel on Detection, Evaluation, and Treatmentof High Blood Cholesterol in Adults (Adult Treatment Panel III)final report. Circulation 106:3143–3421
460. Mokdad AH, Ford ES, Bowman BA, Dietz WH, Vinicor F, BalesVS, Marks JS 2003 Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 289:76–79
461. Patel AA, Bloomgarden ZT, Futterweit W 2008 Premicroalbumin-uria in women with polycystic ovary syndrome: a metabolic riskmarker. Endocr Pract 14:193–200
462. Hardie DG 2008 Role of AMP-activated protein kinase in the met-abolic syndrome and in heart disease. FEBS Lett 582:81–89
463. Angulo P 2002 Nonalcoholic fatty liver disease. N Engl J Med346:1221–1231
464. Schwimmer JB, Khorram O, Chiu V, Schwimmer WB 2005 Ab-normal aminotransferase activity in women with polycystic ovarysyndrome. Fert Steril 83:494–497
465. Setji TL, Holland ND, Sanders LL, Pereira KC, Diehl AM, BrownAJ 2006 Nonalcoholic steatohepatitis and nonalcoholic fatty liverdisease in young women with polycystic ovary syndrome. J ClinEndocrinol Metab 91:1741–1747
466. Cerda C, Perez-Ayuso RM, Riquelme A, Soza A, Villaseca P,Sir-Petermann T, Espinoza M, Pizarro M, Solis N, Miquel JF,
Palomba et al. • Metformin and PCOS Endocrine Reviews, February 2009, 30(1):1–50 49
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022

Arrese M 2007 Nonalcoholic fatty liver disease in women withpolycystic ovary syndrome. J Hepatol 47:412–417
467. Gambarin-Gelwan M, Kinkhabwala SV, Schiano TD, Bodian C,Yeh HC, Futterweit W 2007 Prevalence of nonalcoholic fatty liverdisease in women with polycystic ovary syndrome. Clin Gastro-enterol Hepatol 5:496–501
468. Adachi M, Brenner DA 2008 High molecular weight adiponectininhibits proliferation of hepatic stellate cells via activation of aden-osine monophosphate-activated protein kinase. Hepatology47:677–685
469. Elkind-Hirsch K, Marrioneaux O, Bhushan M, Vernor D, BhushanR 2008 Comparison of single and combined treatment withexenatide and metformin on menstrual cyclicity in overweightwomen with polycystic ovary syndrome. J Clin EndocrinolMetab 93:2670 –2678
470. Caligiuri A, Bertolani C, Guerra CT, Aleffi S, Galastri S, TrappoliereM, Vizzutti F, Gelmini S, Laffi G, Pinzani M, Marra F 2008 Aden-osine monophosphate-activated protein kinase modulates the acti-vated phenotype of hepatic stellate cells. Hepatology 47:668–676
471. Duseja A, Das A, Dhiman RK, Chawla YK, Thumburu KT,Bhadada S, Bhansali A 2007 Metformin is effective in achievingbiochemical response in patients with nonalcoholic fatty liver dis-ease (NAFLD) not responding to lifestyle interventions. Ann Hepa-tol 6:222–226
472. Preiss D, Sattar N, Harborne L, Norman J, Fleming R 2008 Theeffects of 8 months of metformin on circulating GGT and ALT levelsin obese women with polycystic ovarian syndrome. Int J Clin Pract62:1337–1343
473. de Oliveira CP, Stefano JT, de Siqueira ER, Silva LS, de CamposMazo DF, Lima VM, Furuya CK, Mello ES, Souza FG, Rabello F,Santos TE, Nogueira MA, Caldwell SH, Alves VA, Carrilho FJ2008 Combination of N-acetylcysteine and metformin improveshistological steatosis and fibrosis in patients with non-alcoholicsteatohepatitis. Hepatol Res 38:159–165
474. Idilman R, Mizrak D, Corapcioglu D, Bektas M, Doganay B,Sayki M, Coban S, Erden E, Soykan I, Emral R, Uysal AR, Ozden
A 2008 Clinical trial: insulin sensitizing agents may reduce conse-quences of insulin resistance in individuals with non-alcoholicsteatohepatitis. Aliment Pharmacol Ther 28:200–208
475. Vigersky RA, Filmore-Nassar A, Glass AR 2006 Thyrotropinsuppression by metformin. J Clin Endocrinol Metab 91:225–227
476. Isidro ML, Penín MA, Nemina R, Cordido F 2007 Metforminreduces thyrotropin levels in obese, diabetic women with pri-mary hypothyroidism on thyroxine replacement therapy. En-docrine 32:79 – 82
477. Barnard L, Balen AH, Ferriday D, Tiplady B, Dye L 2007 Cognitivefunctioning in polycystic ovary syndrome. Psychoneuroendocri-nology 32:906–914
478. Schattmann L, Sherwin BB 2007 Testosterone levels and cognitivefunctioning in women with polycystic ovary syndrome and inhealthy young women. Horm Behav 51:587–596
479. Schattmann L, Sherwin BB 2007 Effects of the pharmacologicmanipulation of testosterone on cognitive functioning in womenwith polycystic ovary syndrome: a randomized, placebo-controlledtreatment study. Horm Behav 51:579–586
480. Tasali E, Van Cauter E, Ehrmann DA 2006 Relationships betweensleep disordered breathing and glucose metabolism in polycysticovary syndrome. J Clin Endocrinol Metab 91:36–42
481. Vgontzas AN, Bixler EO, Chrousos GP 2005 Sleep apnea is amanifestation of the metabolic syndrome. Sleep Med Rev 9:211–224
482. Ibanez L, Ferrer A, Ong K, Amin R, Dunger D, de Zegher F 2004Insulin sensitization early after menarche prevents progressionfrom precocious pubarche to polycystic ovary syndrome. J Pediatr144:23–29
483. Ibanez L, Valls C, Marcos MV, Ong K, Dunger DB, De Zegher F2004 Insulin sensitization for girls with precocious pubarche andwith risk for polycystic ovary syndrome: effects of prepubertalinitiation and postpubertal discontinuation of metformin treat-ment. J Clin Endocrinol Metab 89:4331–4337
484. Strategies for ovulation induction in anovulatory infertile patientswith PCOS. ClinicalTrials.gov Identifier: NCT00461643
Endocrine Reviews is published by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving theendocrine community.
50 Endocrine Reviews, February 2009, 30(1):1–50 Palomba et al. • Metformin and PCOS
Dow
nloaded from https://academ
ic.oup.com/edrv/article/30/1/1/2354986 by guest on 04 June 2022
Copyright © 2022 FDOKUMEN