
Imaging strategies for vascular rings
7
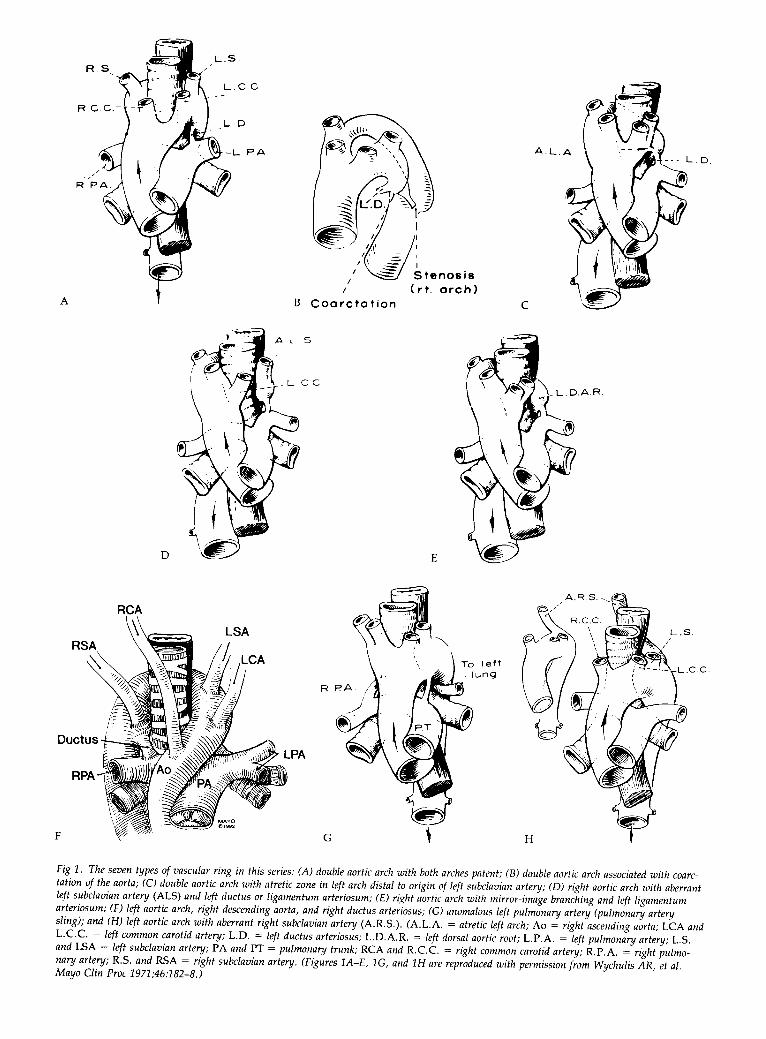
Imaging Strategies for Vascular Rings Jacques A. M. van Son, MD, PhD, Paul R. Julsrud, MD, Donald J. Hagler, MD, Eugene K. W. Sim, FRCS, Francisco J. Puga, MD, Hartzell V. Schaff, MD, and Gordon K. Danielson, MD Division of Thoracic and Cardiovascular Surgery, Department of Diagnostic Radiology, and Section of Pediatric Cardiology, Mayo Clinic, Rochester, Minnesota Thirty-nine patients have undergone operation for relief of tracheoesophageal compression resulting from vascu- lar rings and related entities at the Mayo Clinic. Nine- teen patients had a double aortic arch, 11 patients had a right aortic arch with an aberrant left subclavian artery, 5 patients had a left aortic arch with an aberrant right subclavian artery, 2 patients had a pulmonary artery sling, 1 patient had a right aortic arch with mirror-image branching and a left ligamentum arteriosum, and 1 patient had a left aortic arch, a right descending aorta, and a right ductus arteriosus. Diagnostic examinations included chest radiography, barium esophagography, angiography, and, more recently, transthoracic echocar- diography, computed tomography, and magnetic reso- nance imaging. A comparison among the various diag- ongenital vascular rings result from an abnormal C development of the branchial arch system in which its derivatives form a ring encircling the trachea and the esophagus. In this review, the term vascular ring includes not only complete vascular rings, such as double aortic arch, but also partial vascular rings, with or without ligaments or fibrous bands, causing tracheal or esopha- geal obstruction, such as left aortic arch with aberrant right subclavian artery and pulmonary artery sling. Vari- ous types of vascular rings have been described thor- oughly and classified embryologically by Stewart and associates [l]. Most of these anomalies produce symp- toms of varying degrees caused by esophageal or tracheal compression or both. Surgical treatment is frequently required, and early intervention is usually recommended [2-71. Although the use of barium esophagography and angiography in diagnosing vascular rings and related entities is well established, much less has been written about the possible role of echocardiography, computed tomography (CT), and magnetic resonance imaging (MRI) in this situation [2-61. This report reviews our experience with these diagnostic modalities in patients who were operated on for vascular rings at the Mayo Clinic. Patients and Methods The clinical records of 39 patients who underwent opera- tive treatment of vascular rings at the Mayo Clinic be- Accepted for publication May 3, 1993. Address reprint requests to Dr van Son, Division of Cardiothoracic Surgery, Children’s Hospital of Philadelphia, 34th and Civic Center Blvd, Philadelphia, PA 19104. 0 1994 by The Society of Thoracic Surgeons nostic techniques used in 12 patients during the last 12 years showed that angiography (n = 7), magnetic reso- nance imaging (n = 5), and computed tomography (n = 3) were the most reliable, as they always accurately delineated the anatomy. However, in the 6 patients who underwent transthoracic echocardiography, 1 of whom was an older child and 2 of whom were adults, the vascular abnormality was described correctly only once; in the other 5 patients, the results were false-negative or the technique failed to visualize the relevant vascular structures sufficiently. Currently, magnetic resonance imaging is our imaging technique of choice for the delineation of the vascular and tracheal anatomy in patients suspected of having a vascular ring. (Ann Thorac Surg 1994;57:60410) tween 1947 and 1993 were retrospectively reviewed to determine sex, age at operation, type of vascular anom- aly, diagnostic tests, surgical technique, and long-term results. Lesions were categorized as follows: double aortic arch with both arches patent and left ductus or ligamen- tum arteriosum (Figs lA, 1B); double aortic arch with atresia of the left arch distal to the orign of the left subclavian artery and left ligamentum arteriosum (Fig 1C); right aortic arch with aberrant left subclavian artery and left ductus or ligamentum arteriosum (Fig 1D); right aortic arch with mirror-image branching and left ligamen- tum arteriosum (Fig 1E); left aortic arch, right descending aorta, and right ductus arteriosus (Fig 1F); anomalous left pulmonary artery (pulmonary artery sling) (Fig 1G); and left aortic arch with aberrant right subclavian artery (Fig 1H). The distribution of the various lesions in our patients is shown in Table 1. Results There were 19 male and 20 female patients ranging from 1 month to 72 years old at the time of operation (mean age, 7.2 years; median age, 2.5 years) (see Table 1). A chest radiograph was obtained in all patients. Although the location of the ascending and descending aorta could frequently be determined and additional information about the thoracic structures was often helpful, the radio- graph was noncontributary to the diagnosis of the type of vascular ring in all instances. A barium esophagogram was obtained in all but 2 patients. It demonstrated an indentation suggesting extrinsic compression by a vascu- lar structure. The type of vascular ring was defined in 29 0003-4975/94/$7.00
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Imaging strategies for vascular rings

Imaging Strategies for Vascular Rings Jacques A. M. van Son, MD, PhD, Paul R. Julsrud, MD, Donald J. Hagler, MD, Eugene K. W. Sim, FRCS, Francisco J. Puga, MD, Hartzell V. Schaff, MD, and Gordon K. Danielson, MD Division of Thoracic and Cardiovascular Surgery, Department of Diagnostic Radiology, and Section of Pediatric Cardiology, Mayo Clinic, Rochester, Minnesota
Thirty-nine patients have undergone operation for relief of tracheoesophageal compression resulting from vascu- lar rings and related entities at the Mayo Clinic. Nine- teen patients had a double aortic arch, 11 patients had a right aortic arch with an aberrant left subclavian artery, 5 patients had a left aortic arch with an aberrant right subclavian artery, 2 patients had a pulmonary artery sling, 1 patient had a right aortic arch with mirror-image branching and a left ligamentum arteriosum, and 1 patient had a left aortic arch, a right descending aorta, and a right ductus arteriosus. Diagnostic examinations included chest radiography, barium esophagography, angiography, and, more recently, transthoracic echocar- diography, computed tomography, and magnetic reso- nance imaging. A comparison among the various diag-
ongenital vascular rings result from an abnormal C development of the branchial arch system in which its derivatives form a ring encircling the trachea and the esophagus. In this review, the term vascular ring includes not only complete vascular rings, such as double aortic arch, but also partial vascular rings, with or without ligaments or fibrous bands, causing tracheal or esopha- geal obstruction, such as left aortic arch with aberrant right subclavian artery and pulmonary artery sling. Vari- ous types of vascular rings have been described thor- oughly and classified embryologically by Stewart and associates [l]. Most of these anomalies produce symp- toms of varying degrees caused by esophageal or tracheal compression or both. Surgical treatment is frequently required, and early intervention is usually recommended [2-71. Although the use of barium esophagography and angiography in diagnosing vascular rings and related entities is well established, much less has been written about the possible role of echocardiography, computed tomography (CT), and magnetic resonance imaging (MRI) in this situation [2-61. This report reviews our experience with these diagnostic modalities in patients who were operated on for vascular rings at the Mayo Clinic.
Patients and Methods The clinical records of 39 patients who underwent opera- tive treatment of vascular rings at the Mayo Clinic be-
Accepted for publication May 3, 1993.
Address reprint requests to Dr van Son, Division of Cardiothoracic Surgery, Children’s Hospital of Philadelphia, 34th and Civic Center Blvd, Philadelphia, PA 19104.
0 1994 by The Society of Thoracic Surgeons
nostic techniques used in 12 patients during the last 12 years showed that angiography (n = 7), magnetic reso- nance imaging (n = 5), and computed tomography (n = 3) were the most reliable, as they always accurately delineated the anatomy. However, in the 6 patients who underwent transthoracic echocardiography, 1 of whom was an older child and 2 of whom were adults, the vascular abnormality was described correctly only once; in the other 5 patients, the results were false-negative or the technique failed to visualize the relevant vascular structures sufficiently. Currently, magnetic resonance imaging is our imaging technique of choice for the delineation of the vascular and tracheal anatomy in patients suspected of having a vascular ring.
(Ann Thorac Surg 1994;57:60410)
tween 1947 and 1993 were retrospectively reviewed to determine sex, age at operation, type of vascular anom- aly, diagnostic tests, surgical technique, and long-term results. Lesions were categorized as follows: double aortic arch with both arches patent and left ductus or ligamen- tum arteriosum (Figs lA, 1B); double aortic arch with atresia of the left arch distal to the orign of the left subclavian artery and left ligamentum arteriosum (Fig 1C); right aortic arch with aberrant left subclavian artery and left ductus or ligamentum arteriosum (Fig 1D); right aortic arch with mirror-image branching and left ligamen- tum arteriosum (Fig 1E); left aortic arch, right descending aorta, and right ductus arteriosus (Fig 1F); anomalous left pulmonary artery (pulmonary artery sling) (Fig 1G); and left aortic arch with aberrant right subclavian artery (Fig 1H). The distribution of the various lesions in our patients is shown in Table 1.
Results There were 19 male and 20 female patients ranging from 1 month to 72 years old at the time of operation (mean age, 7.2 years; median age, 2.5 years) (see Table 1). A chest radiograph was obtained in all patients. Although the location of the ascending and descending aorta could frequently be determined and additional information about the thoracic structures was often helpful, the radio- graph was noncontributary to the diagnosis of the type of vascular ring in all instances. A barium esophagogram was obtained in all but 2 patients. It demonstrated an indentation suggesting extrinsic compression by a vascu- lar structure. The type of vascular ring was defined in 29
0003-4975/94/$7.00
n
3
3
3
Vd
a
V
606 VAN SON ET AL IMAGING OF VASCULAR RINGS
Ann Thorac Surg 1994;57&10
Table 1. Distribution of Vascular Anomalies
Anomaly No. of Mean
Patients Percent Age (y)
Double aortic arch Both arches patent and left
ductus or ligamentum arteriosum
Atresia of left arch distal to origin of left subclavian artery and left ligamentum arteriosum
Right aortic arch with aberrant left subclavian artery and left ductus or ligamentum arteriosum
Left aortic arch with aberrant right subclavian artery
Pulmonary artery sling Right aortic arch with mirror-
image branching and left ligamentum arteriosum
Left aortic arch with right descending aorta and right ductus arteriosus
Total
11 48.7
8
11 28.2
5 12.8
2 5.1 1 2.6
1 2.6
39
3.5
6.7
38.9
0.4 0.3
2.0
7.2
of the 37 patients who underwent barium esophagogra- phy. Angiography was performed in 30 patients and always demonstrated the anatomy of the vascular malfor- mation.
The results of the various diagnostic techniques used in 12 patients during the last 12 years (1982 through 1993) are summarized in Table 2. Transthoracic echocardiography was performed in 6 patients, in 4 prospectively (before angiography, MRI, or CT) and in 2 retrospectively (after CT or barium esophagography). In only 1 of the 6 patients did echocardiography correctly identify the vascular mal- formation (patient 3, Table 2); it also diagnosed a coexist- ing coarctation of the aorta that was not present. In 3
patients, the aortic arch was not adequately visualized by echocardiography and the examination was unable to provide a diagnostic opinion. In 2 patients, a false- negative diagnosis was made. In only 1 patient in our series (who underwent barium esophagography and echocardiography) (patient 12, Table 2), the type of vas- cular ring was not diagnosed preoperatively. The vascular ring in this patient was diagnosed as being a right aortic arch with an aberrant left subclavian artery; at operation, however, a double aortic arch with both arches patent and a left ductus arteriosus was identified.
In the same period, conventional or ultrafast CT was used in 3 patients and MRI in 5 patients. In all instances, CT and MRI precisely demonstrated the vascular anomaly (Figs 2, 3). In 3 of the most recent patients, MRI alone demonstrated the vascular anomaly, thereby obviating the need of either angiography or CT and avoiding the use of radiographic contrast material, ionizing radiation, or both. Volume reconstruction of the transverse MRI images can be done to render a three-dimensional image capable of providing enhanced demonstration of the anatomy (Fig 4).
The surgical approach is based on the underlying vas- cular anomaly. In 31 patients, access to the vascular ring was obtained through a left thoracotomy. A right thora- cotomy was used in 4 patients with a left aortic arch and an aberrant right subclavian artery (one of which was aneurysmal at its origin) and in the 1 patient with a left aortic arch, a right descending aorta, and a right ductus arteriosus. A median sternotomy was performed in 3 patients. One of them had a right aortic arch and an aberrant left subclavian artery as well as a ventricular septal defect; the median stemotomy facilitated repair of both lesions at the same operation. The second patient, a 72-year-old patient, had an aneurysm with a diameter of 6 cm at the origin of an aberrant right subclavian artery; using circulatory arrest, through an aortotomy, the os- tium of the aberrant vessel was closed with a Dacron
Table 2. Results of Diagnostic Techniques Used During Last 12 Years (1982-1993) in 12 Patients With Vascular Ring
Patient Age Date of Barium No. (y) Operation Diagnosis Esophagography Echocardiography Angiography MRI CT
1 2 3 4 5 6 7 8 9
10 11 12
8 mo 72 8 4 3 mo 30 9 32 1 19 34 7 mo
4/19/82 1/12/84
10/5/84 10/26/84 5/6/88 1/11/89 8/15/89 7/19/90 6/29/91 7/29/91 2/19/92 3/15/93
RAA, AbLSA, AbRSA RAA, AbLSA RAA, AbLSA DAA AbRSA DAA AbRSA RAA, AbLSA RAA, AbLSA RAA, AbLSA DAA
VSD + Not done + + + + + + + + Not done +, (1)
FV, prospective Not done (+), prospective Not done Not done -, retrospective Not done Not done -, retrospective Not done FV, prospective FV, prospective
+ + + + Not done Not done Not done
Not done + + Not done
+
Not done Not done + , retrospective Not done + , prospective Not done +, prospective Not done + , prospective + , prospective Not done Not done
Not done Not done Not done Not done Not done + , prospective Not done Not done Not done + , retrospective* +, retrospective* Not done
AbLSA = aberrant left subclavian artery; arch; FV = failed to visualize; arch; VSD = ventricular septal defect; - = false-negative; coarctation; * = ultrafast CT.
AbRSA = aberrant right subclavian artery;
+ = true-positive;
CT = computed tomography; DAA = double aortic MRI = magnetic resonance imaging; RAA = right aortic
(+) = described vascular ring but was false-positive for (I) = described vascular ring but incorrect type;
Ann Thorac Surg 1994;5760&10
VAN SON ET AL 607 IMAGING OF VASCULAR RINGS
A B
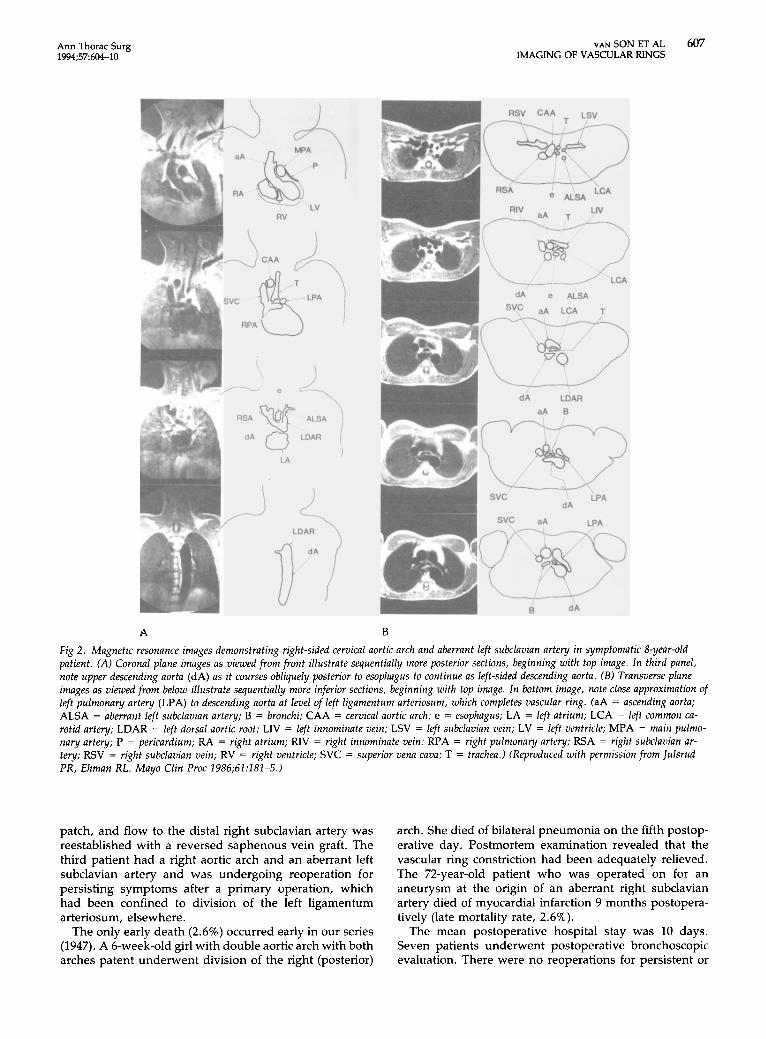
Fig 2 . Magnetic resonance images demonstrating right-sided cervical aortic arch and aberrant left subclavian artery in symptomatic 8-year-old patient. (A) Coronal plane images as viewed from front illustrate sequentially more posterior sections, beginning with top image. In third panel, note upper descending aorta (dA) as it courses obliquely posterior to esophagus to continue as left-sided descending aorta. ( B ) Transverse plane images as viewed from below illustrate sequentially more inferior sections, beginning with top image. In bottom image, note close approximation of left pulmonary artery (LPA) to descending aorta at level of left ligamentum arteriosum, which completes vascular ring. (aA = ascending aorta; ALSA = aberrant left subclavian artery; B = bronchi; CAA = cervical aortic arch; e = esophagus; LA = left atrium; LCA = left common ca- rotid artery; LDAR = left dorsal aortic root; LIV = left innominate vein; LSV = left subclavian vein; LV = left ventricle; MPA = main pulmo- nary artery; P = pericardium; RA = right atrium; RIV = right innominate vein; RPA = right pulmonary artery; RSA = right subclavian ar- tery; RSV = right subclavian vein; RV = right ventricle; SVC = superior vena cava; T = trachea.) (Reproduced with permission from Iulsrud PR, Ehman RL. Mayo Clin Proc 1986;61:181-5.)
patch, and flow to the distal right subclavian artery was reestablished with a reversed saphenous vein graft. The third patient had a right aortic arch and an aberrant left subclavian artery and was undergoing reoperation for persisting symptoms after a primary operation, which had been confined to division of the left ligamentum arteriosum, elsewhere.
The only early death (2.6%) occurred early in our series (1947). A 6-week-old girl with double aortic arch with both arches patent underwent division of the right (posterior)
arch. She died of bilateral pneumonia on the fifth postop- erative day. Postmortem examination revealed that the vascular ring constriction had been adequately relieved. The 72-year-old patient who was operated on for an aneurysm at the origin of an aberrant right subclavian artery died of myocardial infarction 9 months postopera- tively (late mortality rate, 2.6%).
The mean postoperative hospital stay was 10 days. Seven patients underwent postoperative bronchoscopic evaluation. There were no reoperations for persistent or
608 VAN SON ET AL IMAGING OF VASCULAR RINGS
Ann Thorac Surg 1994;5760410
A
B
C
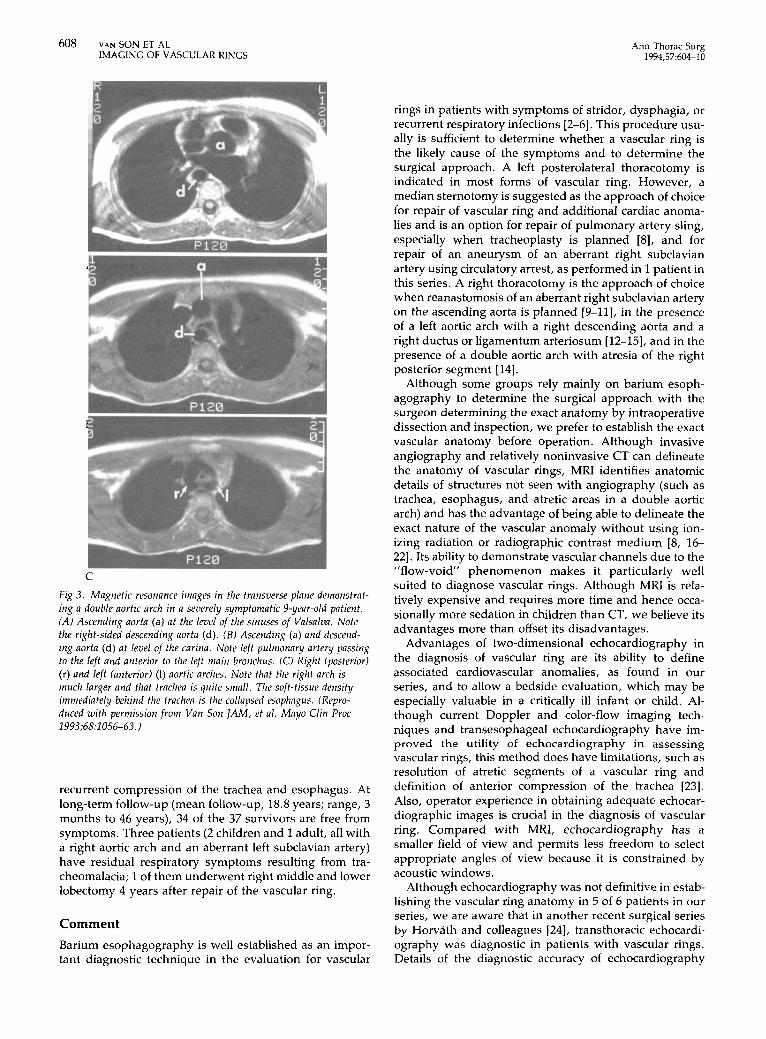
Fig 3 . Magnetic resonance images in the transverse plane demonstrat- ing a double aortic arch in a severely symptomatic 9-year-old patient. (A) Ascending aorta (a) at the level of the sinuses of Valsalva. Note the right-sided descending aorta (d). ( B ) Ascending (a) and descend- ing aorta (d) at level of the carina. Note left pulmonary artery passing to the left and anterior to the left main bronchus. (C) Right (posterior) (r) and left (anterior) (1) aortic arches. Note that the right arch is much larger and that trachea is quite small. The soft-tissue density immediately behind the trachea is the collapsed esophagus. (Repro- duced with permission from Van Son \AM, et a/ . Mayo Clin Proc 1993;68:1056-63.)
recurrent compression of the trachea and esophagus. At long-term follow-up (mean follow-up, 18.8 years; range, 3 months to 46 years), 34 of the 37 survivors are free from symptoms. Three patients (2 children and 1 adult, all with a right aortic arch and an aberrant left subclavian artery) have residual respiratory symptoms resulting from tra- cheomalacia; 1 of them underwent right middle and lower lobectomy 4 years after repair of the vascular ring.
Comment Barium esophagography is well established as an impor- tant diagnostic technique in the evaluation for vascular
rings in patients with symptoms of stridor, dysphagia, or recurrent respiratory infections [2-61. This procedure usu- ally is sufficient to determine whether a vascular ring is the likely cause of the symptoms and to determine the surgical approach. A left posterolateral thoracotomy is indicated in most forms of vascular ring. However, a median sternotomy is suggested as the approach of choice for repair of vascular ring and additional cardiac anoma- lies and is an option for repair of pulmonary artery sling, especially when tracheoplasty is planned [8], and for repair of an aneurysm of an aberrant right subclavian artery using circulatory arrest, as performed in 1 patient in this series. A right thoracotomy is the approach of choice when reanastomosis of an aberrant right subclavian artery on the ascending aorta is planned [9-111, in the presence of a left aortic arch with a right descending aorta and a right ductus or ligamentum arteriosum [12-151, and in the presence of a double aortic arch with atresia of the right posterior segment [14].
Although some groups rely mainly on barium esoph- agography to determine the surgical approach with the surgeon determining the exact anatomy by intraoperative dissection and inspection, we prefer to establish the exact vascular anatomy before operation. Although invasive angiography and relatively noninvasive CT can delineate the anatomy of vascular rings, MRI identifies anatomic details of structures not seen with angiography (such as trachea, esophagus, and atretic areas in a double aortic arch) and has the advantage of being able to delineate the exact nature of the vascular anomaly without using ion- izing radiation or radiographic contrast medium [8, 16- 221. Its ability to demonstrate vascular channels due to the "flow-void" phenomenon makes it particularly well suited to diagnose vascular rings. Although MRI is rela- tively expensive and requires more time and hence occa- sionally more sedation in children than CT, we believe its advantages more than offset its disadvantages.
Advantages of two-dimensional echocardiography in the diagnosis of vascular ring are its ability to define associated cardiovascular anomalies, as found in our series, and to allow a bedside evaluation, which may be especially valuable in a critically ill infant or child. Al- though current Doppler and color-flow imaging tech- niques and transesophageal echocardiography have im- proved the utility of echocardiography in assessing vascular rings, this method does have limitations, such as resolution of atretic segments of a vascular ring and definition of anterior compression of the trachea [23]. Also, operator experience in obtaining adequate echocar- diographic images is crucial in the diagnosis of vascular ring. Compared with MRI, echocardiography has a smaller field of view and permits less freedom to select appropriate angles of view because it is constrained by acoustic windows.
Although echocardiography was not definitive in estab- lishing the vascular ring anatomy in 5 of 6 patients in our series, we are aware that in another recent surgical series by Horvath and colleagues 1241, transthoracic echocardi- ography was diagnostic in patients with vascular rings. Details of the diagnostic accuracy of echocardiography
Ann Thorac Surg 1994;57604-10
A B
VAN SON ET AL 609 IMAGING OF VASCULAR RINGS
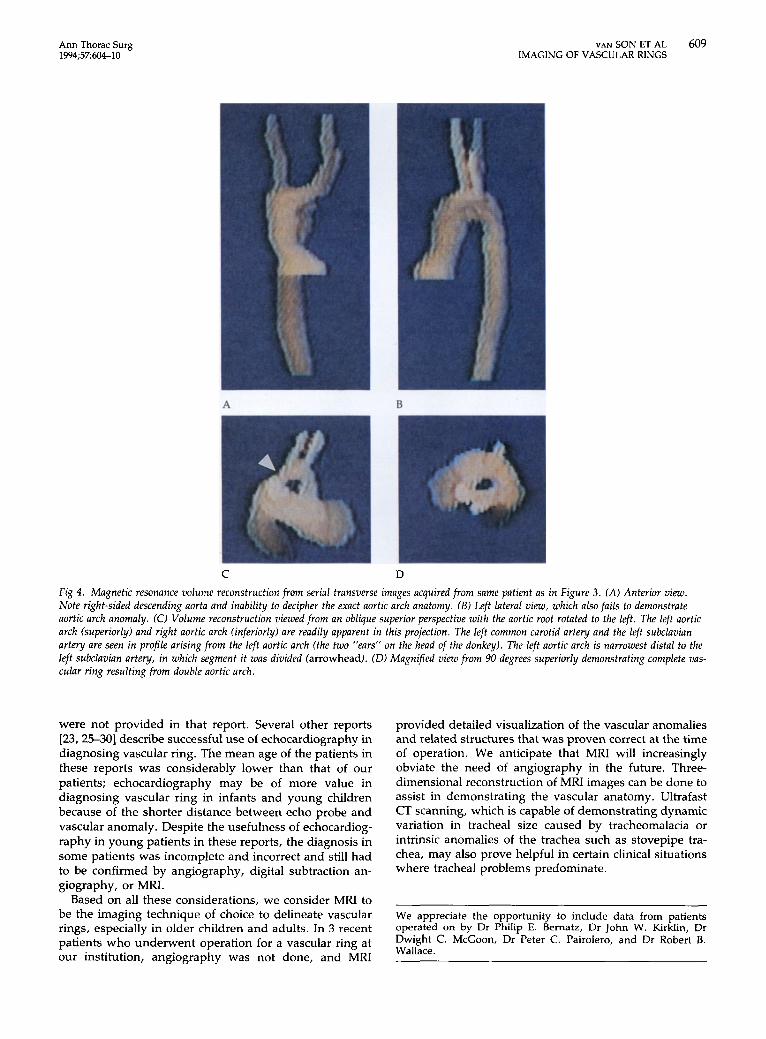
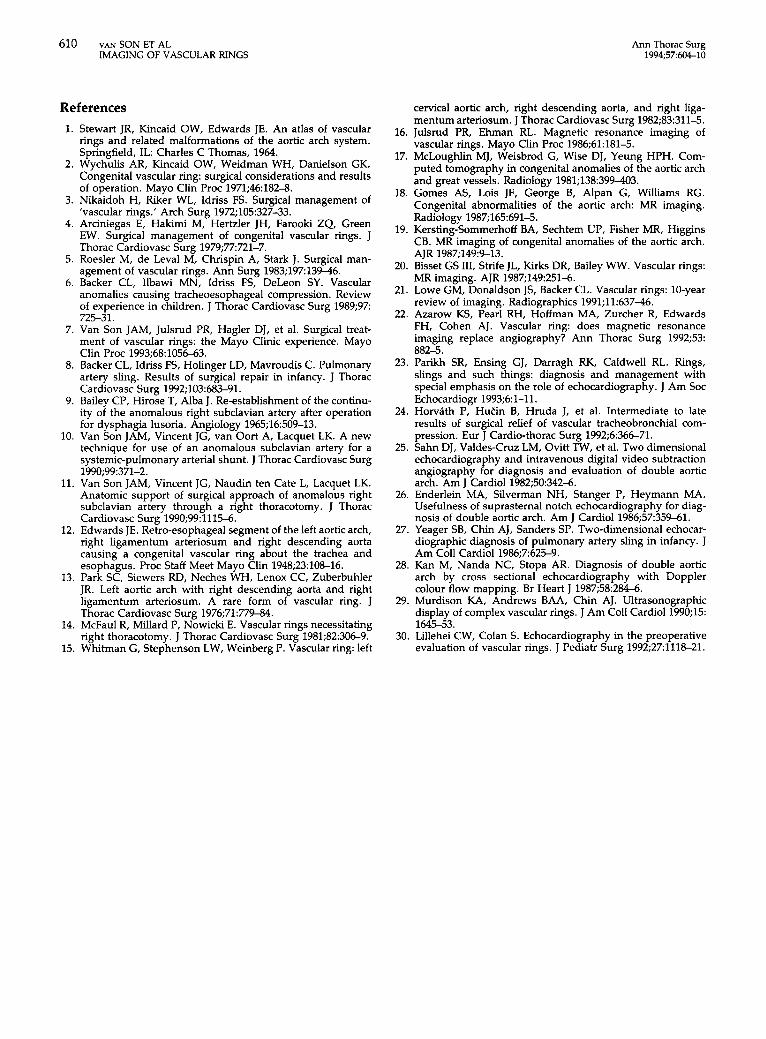
C D Fig 4. Magnetic resonance volume reconstruction from serial transverse images acquired from same patient as in Figure 3 . (A) Anterior view. Note right-sided descending aorta and inability to decipher the exact aortic arch anatomy. ( B ) Left lateral view, which also fails to demonstrate aortic arch anomaly. (0 Volume reconstruction viewed from an oblique superior perspective with the aortic root rotated to the left. The left aortic arch (superiorly) and right aortic arch (inferiorly) are readily apparent in this projection. The left common carotid artery and the left subclavian artery are seen in profile arising from the left aortic arch (the two "ears" on the head of the donkey). The left aortic arch is narrowest distal to the left subclavian artery, in which segment it was divided (arrowhead). (D) Magn$ed view from 90 degrees superiorly demonstrating complete vas- cular ring resulting from double aortic arch.
were not provided in that report. Several other reports (23, 25-30] describe successful use of echocardiography in diagnosing vascular ring. The mean age of the patients in these reports was considerably lower than that of our patients; echocardiography may be of more value in diagnosing vascular ring in infants and young children because of the shorter distance between echo probe and vascular anomaly. Despite the usefulness of echocardiog- raphy in young patients in these reports, the diagnosis in some patients was incomplete and incorrect and still had to be confirmed by angiography, digital subtraction an- giography, or MRI.
Based on all these considerations, we consider MRI to be the imaging technique of choice to delineate vascular rings, especially in older children and adults. In 3 recent patients who underwent operation for a vascular ring at our institution, angiography was not done, and MRI
provided detailed visualization of the vascular anomalies and related structures that was proven correct at the time of operation. We anticipate that MRI will increasingly obviate the need of angiography in the future. Three- dimensional reconstruction of MRI images can be done to assist in demonstrating the vascular anatomy. Ultrafast CT scanning, which is capable of demonstrating dynamic variation in tracheal size caused by tracheomalacia or intrinsic anomalies of the trachea such as stovepipe tra- chea, may also prove helpful in certain clinical situations where tracheal problems predominate.
We appreciate the opportunity to include data from patients operated on by Dr Philip E. Bernatz, Dr John W. Kirklin, Dr Dwight C. McGoon, Dr Peter C. Pairolero, and Dr Robert B. Wallace.
610 VAN SON ET AL IMAGING OF VASCULAR RINGS
Ann Thorac Surg 1994;5760&10
References 1. Stewart JR, Kincaid OW, Edwards JE. An atlas of vascular
rings and related malformations of the aortic arch system. Springfield, IL: Charles C Thomas, 1964.
2. Wychulis AR, Kincaid OW, Weidman WH, Danielson GK. Congenital vascular ring: surgical considerations and results of operation. Mayo Clin Proc 1971;46:182-8.
3. Nikaidoh H, Riker WL, Idriss FS. Surgical management of ‘vascular rings.’ Arch Surg 1972;105:327-33.
4. Arciniegas E, Hakimi M, Hertzler JH, Farooki ZQ, Green EW. Surgical management of congenital vascular rings. J Thorac Cardiovasc Surg 1979;77721-7.
5. Roesler M, de Leva1 M, Chrispin A, Stark J. Surgical man- agement of vascular rings. Ann Surg 1983;19713946.
6. Backer CL, Ilbawi MN, Idriss FS, DeLeon SY. Vascular anomalies causing tracheoesophageal compression. Review of experience in children. J Thorac Cardiovasc Surg 1989;97 725-31.
7. Van Son JAM, Julsrud PR, Hagler DJ, et al. Surgical treat- ment of vascular rings: the Mayo Clinic experience. Mayo Clin Proc 1993;68:1056-63.
8. Backer CL, Idriss FS, Holinger LD, Mavroudis C. Pulmonary artery sling. Results of surgical repair in infancy. J Thorac Cardiovasc Surg 1992;103:683-91.
9. Bailey CP, Hirose T, Alba J. Re-establishment of the continu- ity of the anomalous right subclavian artery after operation for dysphagia lusoria. Angiology 1965;16:509-13.
10. Van Son JAM, Vincent JG, van Oort A, Lacquet LK. A new technique for use of an anomalous subclavian artery for a systemic-pulmonary arterial shunt. J Thorac Cardiovasc Surg
11. Van Son JAM, Vincent JG, Naudin ten Cate L, Lacquet LK. Anatomic support of surgical approach of anomalous right subclavian artery through a right thoracotomy. J Thorac Cardiovasc Surg 1990;99:1115-6.
12. Edwards JE. Retro-esophageal segment of the left aortic arch, right ligamentum arteriosum and right descending aorta causing a congenital vascular ring about the trachea and esophagus. Proc Staff Meet Mayo Clin 1948;23:108-16.
13. Park SC, Siewers RD, Neches WH, Lenox CC, Zuberbuhler JR. Left aortic arch with right descending aorta and right ligamentum arteriosum. A rare form of vascular ring. J Thorac Cardiovasc Surg 1976;71:779-84.
14. McFaul R, Millard P, Nowicki E. Vascular rings necessitating right thoracotomy. J Thorac Cardiovasc Surg 1981;82:306-9.
15. Whitman G, Stephenson LW, Weinberg P. Vascular ring: left
1990;99:371-2.
cervical aortic arch, right descending aorta, and right liga- mentum arteriosum. J Thorac Cardiovasc Surg 1982;83:311-5.
16. Julsrud PR, Ehman RL. Magnetic resonance imaging of vascular rings. Mayo Clin Proc 1986;61:181-5.
17. McLoughlin MJ, Weisbrod G, Wise DJ, Yeung HPH. Com- puted tomography in congenital anomalies of the aortic arch and great vessels. Radiology 1981;138:399403.
18. Gomes AS, Lois JF, George B, Alpan G, Williams RG. Congenital abnormalities of the aortic arch: MR imaging. Radiology 1987;165:691-5.
19. Kersting-Sommerhoff BA, Sechtem UP, Fisher MR, Higgins CB. MR imaging of congenital anomalies of the aortic arch. AJR 1987;149:9-13.
20. Bisset GS 111, Strife JL, Kirks DR, Bailey WW. Vascular rings: MR imaging. AJR 1987;149:251-6.
21. Lowe GM, Donaldson JS, Backer CL. Vascular rings: 10-year review of imaging. Radiographics 1991;11:6374.
22. Azarow KS, Pearl RH, Hoffman MA, Zurcher R, Edwards FH, Cohen AJ. Vascular ring: does magnetic resonance imaging replace angiography? Ann Thorac Surg 1992;53:
23. Parikh SR, Ensing GJ, Darragh RK, Caldwell RL. Rings, slings and such things: diagnosis and management with special emphasis on the role of echocardiography. J Am Soc Echocardiogr 1993;6:1-11.
24. Horvith P, Hutin 8, Hruda J, et al. Intermediate to late results of surgical relief of vascular tracheobronchial com- pression. Eur J Cardio-thorac Surg 1992;6:36671.
25. Sahn DJ, Valdes-Cruz LM, Ovitt TW, et al. Two dimensional echocardiography and intravenous digital video subtraction angiography for diagnosis and evaluation of double aortic arch. Am J Cardiol 1982;50:342-6.
26. Enderlein MA, Silverman NH, Stanger P, Heymann MA. Usefulness of suprasternal notch echocardiography for diag- nosis of double aortic arch. Am J Cardiol 1986;57:359-61.
27. Yeager SB, Chin AJ, Sanders SP. Two-dimensional echocar- diographic diagnosis of pulmonary artery sling in infancy. J Am Coll Cardiol 1986;7625-9.
28. Kan M, Nanda NC, Stopa AR. Diagnosis of double aortic arch by cross sectional echocardiography with Doppler colour flow mapping. Br Heart J 1987;58:284-6.
29. Murdison KA, Andrews BAA, Chin AJ. Ultrasonographic display of complex vascular rings. J Am Coll Cardiol1990;15: 1645-53.
30. Lillehei CW, Colan S. Echocardiography in the preoperative evaluation of vascular rings. J Pediatr Surg 1992;271118-21.
882-5.




















