
Postsurgical Hindfoot Deformity of a Patient With Rheumatoid ...
10
Postsurgical Hindfoot Deformity of a Patient With Rheumatoid Arthritis Treated With Custom-made Foot Orthoses and Shoe Modifications This case report describes the treatment of a 73-year-old woman with long-standing, severe rheumatoid arthritis, using custom-made foot orthoses and shoe modifications. The patient was referred for physical therapy 4 weeks after triple arthrodesis of her right foot. Her primary complaint was periodic unsteadiness during gait, which necessitated the use of a cane at all times. Other problems included a lower- extremity length discrepancy and right foot pain. Physical therapy included fabrication of bilateral semirigid foot orthoses, shoe modifi- cations, gait training, and instruction in strengthening exercises. After treatment, the patient reported feeling steady during walking without a cane, and she was able to resume community activities without right foot pain. Computerized movement analysis of gait revealed that the use of orthoses and modified footwear reduced weight bearing and movement-pattern abnormalities, as compared with barefoot walking. The findings in this case show that physical therapy including foot orthoses, shoe modifications, gait training, and strengthening exer- cises can be instrumental in the postsurgical rehabilitation of a patient with severe rheumatoid arthritis. [Shrader JA, Lohmann Siegel K. Postsurgical hindfoot deformity of a patient with rheumatoid arthritis treated with custom-made foot orthoses and shoe modifications. Phys Ther, 1997;77:296-305.1 Key Words: Foot orthoses, Rehabilitation, Rheumatoid arthritis, Shoe modifications, Triple arthrodesis. Joseph A Shrader Karen Lohmann Siegel i Physical Therapy. Volume 77 . Number 3 . March 1997 Downloaded from https://academic.oup.com/ptj/article/77/3/296/2633141 by guest on 04 February 2022
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Postsurgical Hindfoot Deformity of a Patient With Rheumatoid ...
Postsurgical Hindfoot Deformity of a Patient With Rheumatoid Arthritis Treated With Custom-made Foot Orthoses and Shoe Modifications
This case report describes the treatment of a 73-year-old woman with long-standing, severe rheumatoid arthritis, using custom-made foot orthoses and shoe modifications. The patient was referred for physical therapy 4 weeks after triple arthrodesis of her right foot. Her primary complaint was periodic unsteadiness during gait, which necessitated the use of a cane at all times. Other problems included a lower- extremity length discrepancy and right foot pain. Physical therapy included fabrication of bilateral semirigid foot orthoses, shoe modifi- cations, gait training, and instruction in strengthening exercises. After treatment, the patient reported feeling steady during walking without a cane, and she was able to resume community activities without right foot pain. Computerized movement analysis of gait revealed that the use of orthoses and modified footwear reduced weight bearing and movement-pattern abnormalities, as compared with barefoot walking. The findings in this case show that physical therapy including foot orthoses, shoe modifications, gait training, and strengthening exer- cises can be instrumental in the postsurgical rehabilitation of a patient with severe rheumatoid arthritis. [Shrader JA, Lohmann Siegel K. Postsurgical hindfoot deformity of a patient with rheumatoid arthritis treated with custom-made foot orthoses and shoe modifications. Phys Ther, 1997;77:296-305.1
Key Words: Foot orthoses, Rehabilitation, Rheumatoid arthritis, Shoe modifications, Triple arthrodesis.
Joseph A Shrader
Karen Lohmann Siegel i
Physical Therapy. Volume 7 7 . Number 3 . March 1997
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/3/296/2633141 by guest on 04 February 2022

When indicated,
foot orthoses and
F ifteen to 20 years ago, patients with long-stand-
appropriate well as cushioned
ing and unremitting rheumatoid arthritis (RA) fQOmear Can insoles and arch s u p were often expected to become dependent on a ports for patients with wheelchair for mobility. As a result, foot and q major role in the RA. Extradepth shoes
ankle care was not given high priority. Subsequent to and a multitude of successful total hip and knee reconstructive surgery in management of shoe modifications, patients with RA, health care professionals now need to direct more attention to disorders of the feet. Foot and ankle involvement has been reported in up to 90% of persons with RA.l A 1994 study of 99 outpatients with clinically proven RA revealed that 93 of those patients had foot or ankle involvement, and yet only 4 patients had received any treatment involving shoe inserts, foot orthoses, prescription footwear, or shoe modifications.2 Three of those 4 patients had received custom-molded shoes. These findings indicate that the three patients had advanced foot deformities and were unable to use standard or extradepth footwear. Because large joint replacements and pharmacological advances for patients with RA are allowing for ambulation for many more years, there is an increased need for early and ongoing foot care. One important area of this care is the use of foot orthoses. When indicated, we believe that the provision of foot orthoses and appropriate footwear can play a major role in the overall management of patients with RA.
Several authorss7 have advocated the use of pads of various shapes and sizes, strategically placed in shoes, as
-
people with including rocker bars, rocker or roller bot- toms, Thomas heels, rheumatoid adwitis. medial sole - medial stabilizers (which act like ex-
tended reinforced heel counters), and molded shoes, also are often recommended for patients with RA.S7 Dimonte and Light8 described the use of two kinds of foot orthoses for patients with arthritis: "functional" and "balance" types. Merrittg gave an extensive overview of the most common orthoses used for patients with arthri- tis and emphasized the need for controlled clinical studies of their efficacy. Locke et all0 conducted one of the few studies designed to demonstrate the value of an ankle-foot orthosis (AFO) in the treatment of patients with ankle and hindfoot pain and defonnity due to arthritis. Locke and colleagues used the extended C'ni- versity of California Biomechanics Laboratory orthosis. Although little has been written about the benefits of these devices, we have found that the use of foot orthoses, prescribed after a detailed biomechanical low- er-extremity evaluation, can help in the rehabilitation of patients with RA, either before or after surgery.
JA Shrader, PT, is Senior Staff Physical Therapist, Rehabilitation Medicine Department, Warren Grant Magnuson Clinical Center, National Institutes of Health, Bldg 10, Room 6 ~ 2 3 5 , 9000 Wisconsin Ave, Bethesda, MD 20892-1604 (USA) ([email protected]). Address all correspondence to Mr Shrader.
KLohmann Siegel, PT, is Senior Staff Physical TherapWResearch Coordinator, Biomechanics Laboratory, Rehabilitation Medicine Department, Warren Grant Magnuson Clinical Center, Kational Institutes of Health.
The opinions expressed in this article reflect the views of the authors and not necessarily those of the US Public Health Service or the National lnstitutes of Health.
Thrs ariicie was submitted Februaty 6, 1996, and war accepted November 22, 1996.
Physical Therapy . Volume 7 7 . Number 3 . March 1997 Shrader and Lohmann Siegel . 297
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/3/296/2633141 by guest on 04 February 2022
Table 1. Medical/Surgical History
Age ( y ) Important Events
43 Diagnosed with rheumatoid arthritis; ~ainful hands and feet 45 Began use of gold, prednisone, Indocin@," and bndearil 49 Accepted at the National Institutes of Health for 1-month study of chloroquine 5 0 Left hip cup arthroplasty and synovectomy of right knee 5 1 Synovectomies of all meta~arpophalan~eal ioints and left thumb tendon repair 52 Silasticb joint implants of right rnetacarpophalangeal ioints 54 Hospitalization for septic right knee 60 Diagnosed with bronchitis 62 Hospitalization for acute tracheobronchitis; began use of methotrexate 63 left total hip replacement; left ankle fracture 65 Double Klansak orthosis prescribed by rhe~matolo~ist for right ankle pain 66 Right total knee replacement 68 Diagnosed with malignant carcinoma of breast; modified mastectomy 69 Continued malalignment of right hindfoot into varus position; discontinued use of brace due to pressureinduced ulceration of right
lateral rnalleolus 71 Right wrist fusion with tendon grah and transfer; tenolysis of right third flexor tendon
Referral made for rehabilitation at the National Institutes of Health Rehabilitation Medicine Department; triple arthrodesis of right hindfoot; fit with custom-made foot orthoses to accommodate postsurgical rigid hindfoot deformity
- -
Merck & Co Inc, West Point, PA 19486. Dow Coming Corp, PO Box 994. Midland, MI 48686.
The purpose of this report is to describe the improve- instructed to wear it for 3 months. In this case, the ment in ambulation in a patient with severe RA when surgeon felt that the leg-hindfoot orthosis would provide using accommodative foot orthoses and shoe modifica- sufficient immobilization of the surgical site and elimi- tion; after hindfoot surgery.
Methodology
nate the need for a heavy cast. This orthosis was designed to relieve subtalar joint pain by providing relative immo- bilization of the subtalar joint while allowing full ankle motion. The leg-hindfoot orthosis essentially looks like a
History short version of an AFO with anterior placement of the The patient was a 73-year-old woman with a 30-year medial and lateral trim lines (edges of the brace) but history of seropositive RA. She was nonambulatory due with a shortened footplate extending only to the mid- to a severe malalignment of her right hindfoot in a varus foot. The patient was referred for physical therapy position. Right-foot weight bearing occurred exclusively 1 month after surgery, with instructions to maintain through the fibular malleolus and the lateral head and partial weight bearing of the right lower extremity. The base i f the fifth metatarsal. The plantar surface of the primary reason for the referral for physical therapy was foot did not make contact with the floor. The patient to receive an evaluation for, and fabrication of, custom- could transfer independently to and from a wheelchair made foot orthoses to improve ambulation. The physical with the use of a standard cane. She reportedly had been therapist is a board-certified pedorthist with advanced using the cane for 6 years for community arnbulation training in the fabrication of foot orthoses, shoe modi- only because of right ankle pain. Her medical and fications, and other related devices for foot and ankle - surgical history was extensive, which is common for a rehabilitation. patient with long-standing severe RA (Tab. 1 ) .
Subjective Information The patient was initially seen in a multidisciplinary foot clinic of the Rehabilitation Medicine Department of the Warren Grant Magnuson Clinical Center at the National Institutes of Health (Bethesda, Md), with representation from physical therapy, orthopedics, rheumatology, physiatry, podiatry, and pedorthics. The team recom- mended that the patient should have surgery immedi- ately. The patient was treated by an orthopedic surgeon, who performed a triple arthrodesis procedure on the right hindfoot (fusion of three joints: talonavicular,
~ h d patient's primary complaint was a feeling of unsteadiness while walking, described as "losing my balance to the right side." Due to this problem, she did not feel comfortable walking without a cane. The patient denied any history of falls. Additional complaints, reported by the patient in order of importance to her, included pain in her right foot and ankle during walking (with partial weight bearing) rated as 3 on a scale of 0 to 10 (O=no pain, lO=excruciating pain). She also felt that her left hand and wrist were more painful than usual due
talocalcaneal, and calcaneocuboid).' Postoperatively, to increased reliance on cane use. She stated that all she was provided a leg-hindfoot orthosisl' and was these problems became worse when she tried to engage
298 . Shrader and Lohmann Siegel Physical Therapy. Volume 77 . Number 3 . March 1997
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/3/296/2633141 by guest on 04 February 2022
in social activities such as going shopping and attending bridge games, keeping hair appointments, and going to church. She had been accustomed to participating in each of these activities at least once per week and no longer could participate in such activities due to increas- ing pain in her right foot and ankle and left hand and wrist and to unsteadiness during gait.
Evaluafion A complete lower-extremity evaluation was performed in three l-hour sessions, per patient tolerance. The first two sessions were conducted 2 days apart; the third session was conducted 6 weeks later when stance and gait could be evaluated and the patient had full weight bearing.
The patient was evaluated while positioned sitting, supine, and prone. Range-of-motion testing (Tab. 2) revealed !.hat tibiotalar, subtalar, and midtarsal joint motions were severely limited bilaterally. Hip motion was full and pain-free bilaterally. The left knee was painful and had mild mediolateral instability. Manual muscle testing12 (Tab. 3) revealed that strength was Good at both hips, but there were limitations at the left knee and both feet and ankles. Reliability of the manual muscle test results was not established as part of this case.
Inspectior1 of both feet revealed tight shiny skin, with hair loss and dislocated metatarsophalangeal joints of toes 2 through 4. Both feet were cool to the touch, and there appeared to be widespread muscle atrophy of the anterior, posterior, and lateral compartments of both lower extremities below the knees. This clinical presen- tation is common in patients with long-standing RA, beginning with acute inflammation early in the course of the disease and progressing to chronic inflammation and scarring as the disease is "burning The left distal tibia was displaced laterally due to a previous ankle fracture (Tab. 1). The right hindfoot was fused in 25 degrees of varum (apparently the best result that could be obtained during surgery because of the severity of joint malalignment) .
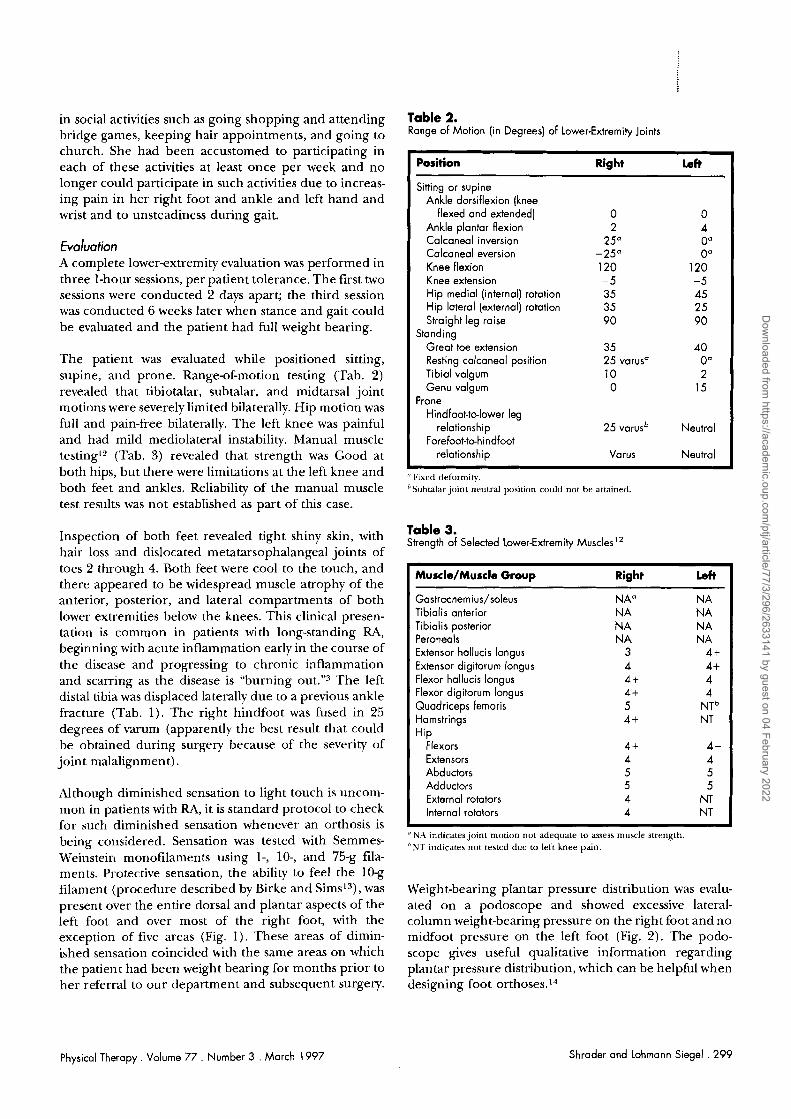
Although diminished sensation to light touch is uncom- mon in patients with RA, it is standard protocol to check for such diminished sensation whenever an orthosis is being considered. Sensation was tested with Semmes- Weiilsteir~ monofilaments using I-, lo-, and 75-g fila- ments. Protective sensation, the ability to feel the 10-g filament (procedure described by Birke and Sims13), was present over the entire dorsal and plantar aspects of the left foot and over most of the right foot, with the exception of five areas (Fig. 1) . These areas of dimin- ished sensation coincided with the same areas on which the patient had been weight bearing for months prior to her referral to our department and subsequent surgery.
Table 2. Range of Motion (in Degrees) of Lower-Extremity Joints
Position Right Left
Sitting or supine Ankle dorsiflexion (knee
flexed and extended] 0 0 Ankle plantar flexion 2 4 Calcaneal inversion 25" 0" Calcaneal eversion -25" 0" Knee flexion 120 120 Knee extension -5 - 5 Hip medial (internal) rotation 35 45 Hip lateral (external) rotation 35 2 5 Straight leg raise 90 90
Standing Great toe extension 35 40 Resting calcaneal position 25 varus" 0" Tibia1 valgum 10 2 Genu valgum 0 15
Prone Hindfoot-talower leg
relationship 25 varusb Neutral Forefoot-tehindfoot
relationship Varus Neutral
" Fixed deformity. "Subtalar joint neutral position could not be attained.
Table 3. Strength of Selected Lower-Extremity Muscles1'
Muscle/Muscle Group Right Left
Gastrocnemius/soleus N A" N A Tibialis anterior N A N A Tibialis posterior N A N A Peroneals N A N A Extensor hallucis longus 3 4+ Extensor digitorum longus 4 4 + Flexor hallucis longus 4 + 4 Flexor digitorum longus 4 + 4 Quadriceps femoris 5 N T ~ Hamstrings 4 + NT Hip
Flexors 4 + 4- Extensors 4 4 Abductors 5 5 Adductors 5 5 External rotators 4 NT Internal rotators 4 NT
a
"NA indicates joint motion not adequate to assess milscle strength. "NT indicates not tested due to left knee pain.
Weight-bearing plantar pressure distribution was evalu- ated on a podoscope and showed excessive lateral- column weight-bearing pressure on the right foot and no midfoot pressure on the left foot (Fig. 2). The podo- scope gives useful qualitative information regarding plantar pressure distribution, which can be helpful when designing foot orthoses.14
Physical Therapy. Volume 7 7 . Number 3 . March 1997 Shrader and Lohmann Siegel . 299
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/3/296/2633141 by guest on 04 February 2022
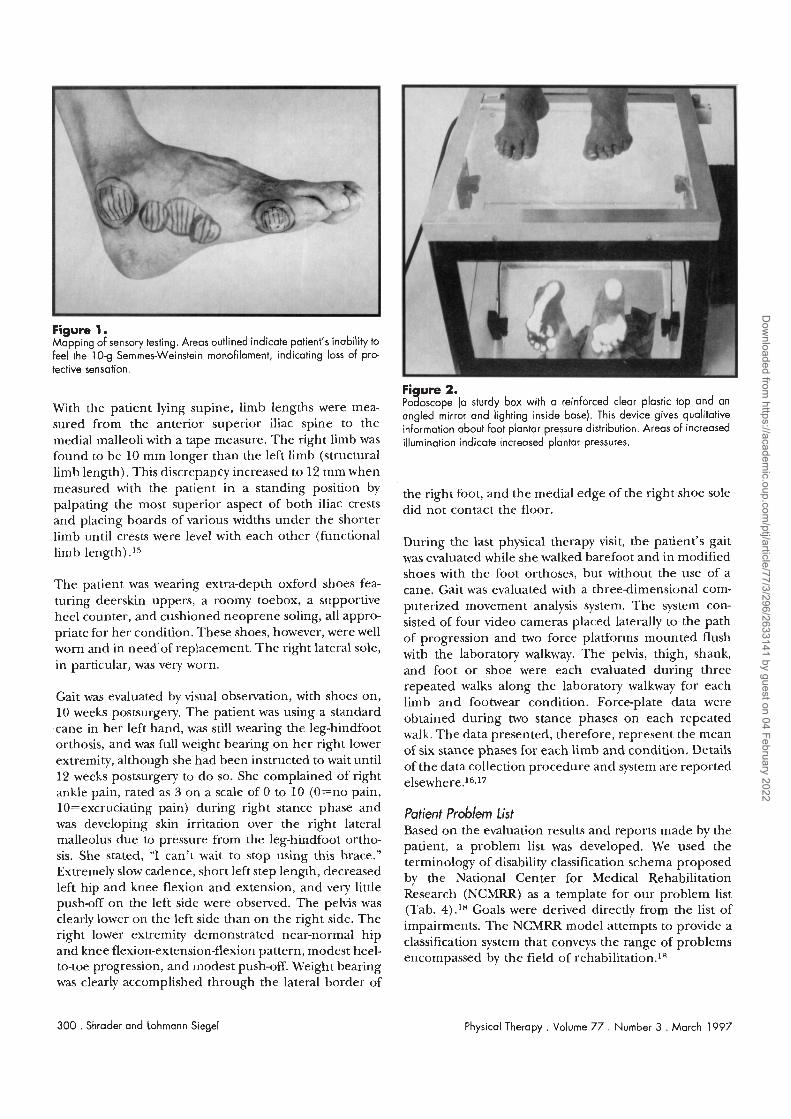
Figure 1. Mapping of sensory testing. Areas outlined indicate patient's inability to feel the 10-9 Semmes-Weinstein monofilament, indicating loss of pro- tective sensation.
With the patient lying supine, limb lengths were mea- sured from the anterior superior iliac spine to the medial malleoli with a tape measure. The right limb was found to be 10 mm longer than the left limb (structural limb length). This discrepancy increased to 12 mm when measured with the patient in a standing position by palpating the most superior aspect of both iliac crests and placing boards of various widths under the shorter limb until crests were level with each other (functional limb length) .I5
The patient was wearing extra-depth oxford shoes fea- turing deerskin uppers, a roomy toebox, a supportive heel counter, and cushioned neoprene soling, all appro- priate for her condition. These shoes, however, were well worn and in need'of replacement. The right lateral sole, in particular, was very worn.
Gait was evaluated by visual observation, with shoes on, 10 weeks postsurgery. The patient was using a standard cane in her left hand, was still wearing the leg-hindfoot orthosis, and was full weight bearing on her right lower extremity, although she had been instructed to wait until 12 weeks postsurgery to do so. She complained of right ankle pain, rated as 3 on a scale of 0 to 10 (O=no pain, lO=excruciating pain) during right stance phase and was developing skin irritation over the right lateral malleolus due to pressure from the leg-hindfoot ortho- sis. She stated, "I can't wait to stop using this brace." Extremely slow cadence, short left step length, decreased left hip and knee flexion and extension, and very little push-off on the left side were observed. The pelvis was clearly lower on the left side than on the right side. The right lower extremity demonstrated near-normal hip and knee flexion-extension-flexion pattern, modest heel- to-toe progression, and modest push-off. Weight bearing
Fi ure 2. Po % oscope (a sturdy box with a reinforced clear plastic top and an angled mirror and lighting inside base). This device gives qualitative information about foot plantar pressure distribution. Areas of increased illumination indicate increased plantar pressures.
the right foot, and the medial edge of the right shoe sole did not contact the floor.
During the last physical therapy visit, the patient's gait was evaluated while she walked barefoot and in modified shoes with the foot orthoses, but without the use of a cane. Gait was evaluated with a three-dimensional com- puterized movement analysis system. The system con- sisted of four video cameras placed laterally to the path of progression and two force platforms mounted flush with the laboratory walkway. The pelvis, thigh, shank, and foot or shoe were each evaluated during three repeated walks along the laboratory walkway for each limb and footwear condition. Force-plate data were obtained during two stance phases on each repeated walk. The data presented, therefore, represent the mean of six stance phases for each limb and condition. Details of the data collection procedure and system are reported elsewhere.16."
Patient Problem fist Based on the evaluation results and reports made by the patient, a problem list was developed. We used the terminology of disability classification schema proposed by the National Center for Medical Rehabilitation Research (NCMRR) as a template for our problem list (Tab. 4) . I 8 Goals were derived directly from the list of impairments. The NCMRR model attempts to provide a classification system that conveys the range of problems encompassed by the field of rehabilitation.lR
was clearly accomplished through the lateral border of
300 . Shrader and Lohmann Siegel Physical Therapy . Volume 7 7 . Number 3 . March 1997
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/3/296/2633141 by guest on 04 February 2022
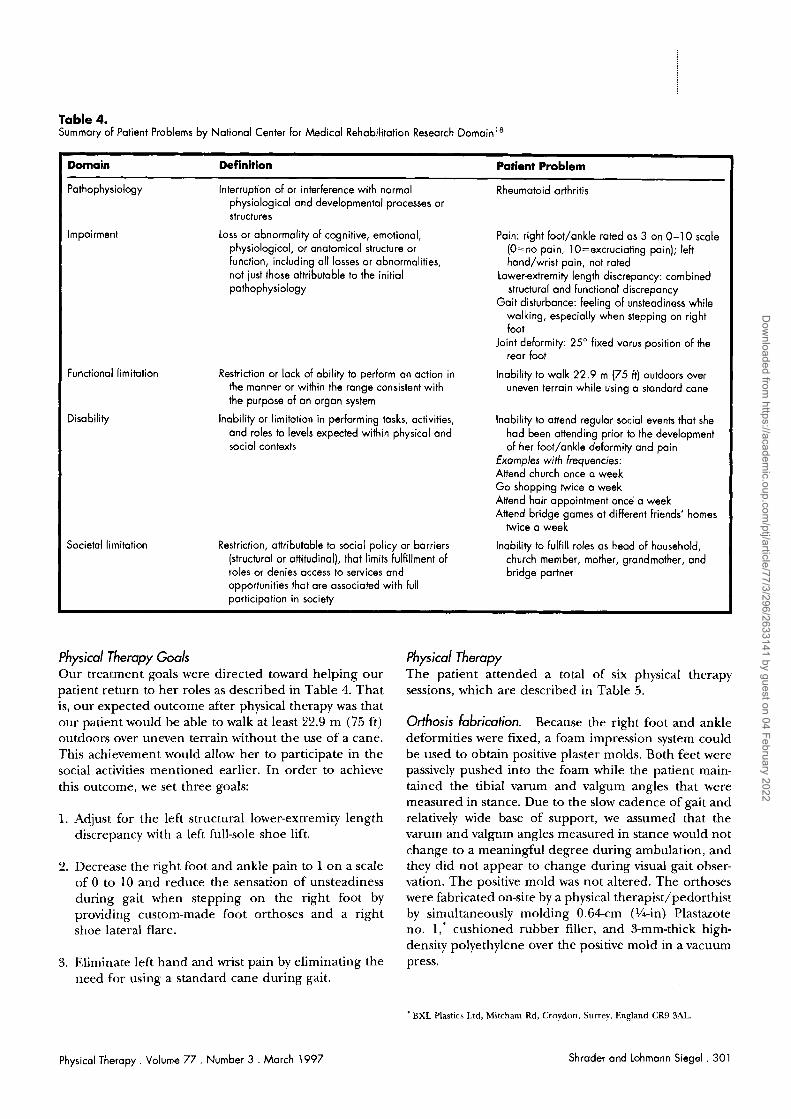
Table 4. Summary of Patient Problems by National Center for Medical Rehabilitation Research D o m ~ i n ' ~
Restriction or lack of ability to perform an action in the manner or within the range consistent with the purpose of an organ system
lnability or limitation in performing tasks, activities, and roles to levels expected within physical and social contexts
Domain Definition Patient Problem
Pathophysiology Interruption of or interference with normal Rheumatoid arthritis physiological and developmental processes or structures
Impairmen1 Loss or abnormality of cognitive, emotional, Pain: right foot/ankle rated as 3 on 0-1 0 scale physiological, or anatomical structure or (O=no pain, lO=excruciating pain); left function, including all losses or abnormalities, hand/wrist pain, not rated not just those attributable to the initial Lowerextremity length discrepancy: combined pathophysiology structural and functional discrepancy
Gait disturbance: feeling of unsteadiness while walking, especially when stepping on right foot
Joint deformity: 25" fixed varus position of the rear foot
Functional limitation Inability to walk 22.9 m (75 ft) outdoors over uneven terrain while using a standard cane
Disability Inability to attend regular social events that she had been attending prior to the development of her foot/ankle deformity and pain
Exomples with frequencies: Attend church once a week Go shopping twice a week Attend hair appointment once a week Attend bridge games at different friends' homes
twice a week
Societal limitation Restriction, attributable to social policy or barriers Inability to fulfill roles as head of household, (structural or attitudinal), that limits fulfillment of church member, mother, grandmother, and roles or denies access to services and bridge partner opportunities that are associated with full participation in society
Physical Therapy Goals Our treal.ment goals were directed toward helping our patient return to her roles as described in Table 4. That is, our expected outcome after physical therapy was that our patient would be able to walk at least 22.9 m (75 ft) outdoors over uneven terrain without the use of a cane. This achievement would allow her to participate in the social activities mentioned earlier. In order to achieve this outcome, we set three goals:
1. Adjus~. for the left structural lower-extremity length discrepancy with a left full-sole shoe lift.
2. Decrease the right foot and ankle pain to 1 on a scale of 0 to 10 and reduce the sensation of unsteadiness during gait when stepping on the right foot by providing custom-made foot orthoses and a right shoe lateral flare.
3. Eliminate left hand and wrist pain by eliminating the need for using a standard cane during gait.
Physical Therapy. Volume 7 7 . Number 3 . March 1997
Physical Therapy The patient attended a total of six physical therapy sessions, which are described in Table 5.
Orthosis fabrication. Because the right foot and ankle deformities were fixed, a foam impression system could be used to obtain positive plaster molds. Both feet were passively pushed into the foam while the patient main- tained the tibia1 varum and valgum angles that were measured in stance. Due to the slow cadence of gait and relatively wide base of support, we assumed that the varum and valgum angles measured in stance would not change to a meaningful degree during ambulation, and they did not appear to change during visual gait obser- vation. The positive mold was not altered. The orthoses were fabricated on-site by a physical therapist/pedorthist by simultaneously molding 0.64cm (%-in) Plastazote no. 1,* cushioned rubber filler, and 3-mm-thick high- density polyethylene over the positive mold in a vacuum press.
* BXL Plastics Ltd, Mitcham Rd, Croydon, Surrey, England CR9 3AL.
Shrader and Lohmann Siegel . 301
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/3/296/2633141 by guest on 04 February 2022
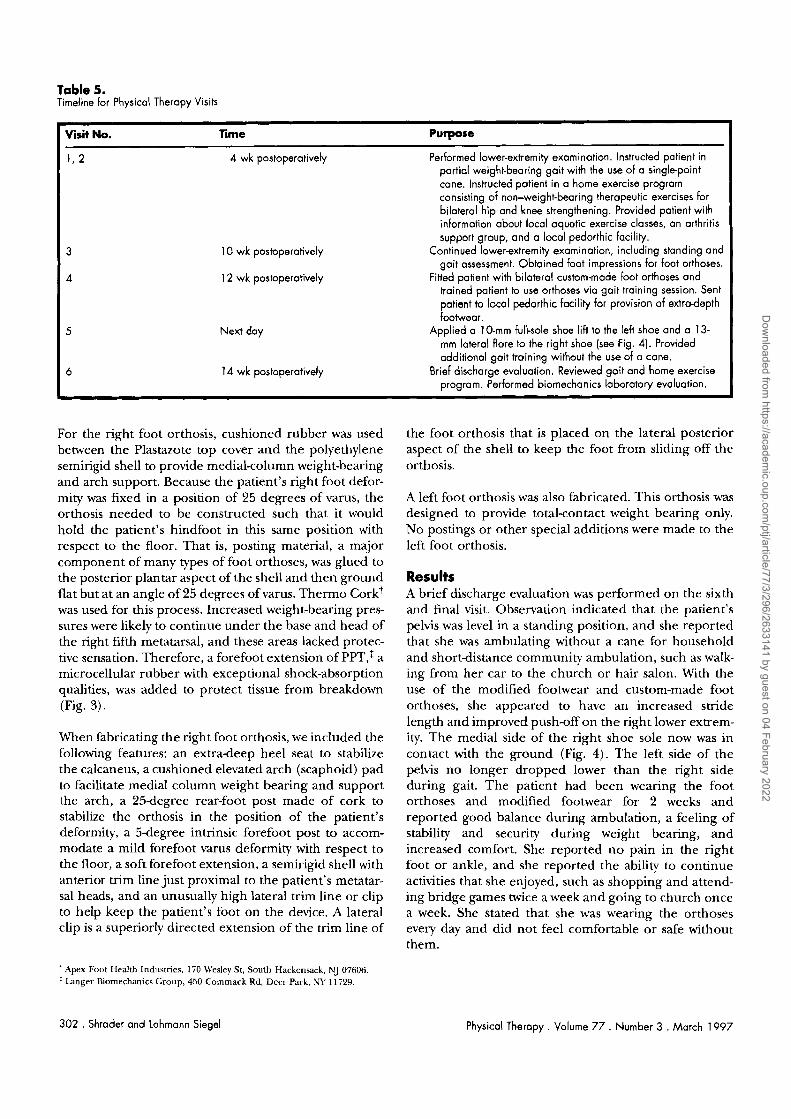
Table 5. Timeline for Physical Therapy Visits
Visit No. Time Purpose
1, 2 4 wk postoperatively Performed lower-extremity examination. Instructed patient in ~ar t ia l weight-bearing gait with the use of a singlepoint cane. Instructed patient in a home exercise program consisting of non-weight-bearing therapeutic exercises for bilateral hip and knee strengthening. Provided patient with information about local aquatic exercise classes, an arthritis support group, and a local pedorthic facility.
3 10 wk postoperatively Continued lowerextremity examination, including standing and gait assessment. Obtained foot impressions for foot orthoses.
4 12 wk postoperatively Fitted patient with bilateral custom-made foot orthoses and trained patient to use orthoses via gait training session. Sent patient to local pedorthic facility for provision of extra-depth footwear.
5 Next day Applied a 10-mm full-sole shoe lift to the left shoe and a 13- mm lateral flare to the right shoe (see Fig. 4). Provided additional gait training without the use of o cane.
6 14 wk postoperatively Brief discharge evaluation. Reviewed gait and home exercise program. Performed biomechanics laboratory evaluation.
For the right foot orthosis, cushioned rubber was used between the Plastazote top cover and the polyethylene semirigid shell to provide medial-column weight-bearing and arch support. Because the patient's right foot defor- mity was fixed in a position of 25 degrees of varus, the orthosis needed to be constructed such that it would hold the patient's hindfoot in this same position with respect to the floor. That is, posting material, a major component of many types of foot orthoses, was glued to the posterior plantar aspect of the shell and then ground flat but at an angle of 25 degrees of varus. Thermo corkt was used for this process. Increased weight-bearing pres- sures were likely to continue under the base and head of the right fifth metatarsal, and these areas lacked protec- tive sensation. Therefore, a forefoot extension of PPT,: a microcellular rubber with exceptional shock-absorption qualities, was added to protect tissue from breakdown (Fig. 3).
When fabricating the right foot orthosis, we included the following features: an extra-deep heel seat to stabilize the calcaneus, a cushioned elevated arch (scaphoid) pad to facilitate medial column weight bearing and support the arch, a 25-degree rear-foot post made of cork to stabilize the orthosis in the position of the patient's deformity, a 5-degree intrinsic forefoot post to accom- modate a mild forefoot varus deformity with respect to the floor, a soft forefoot extension, a semirigid shell with anterior trim line just proximal to the patient's metatar- sal heads, and an unusually high lateral trim line or clip to help keep the patient's foot on the device. A lateral clip is a superiorly directed extension of the trim line of
the foot orthosis that is placed on the lateral posterior aspect of the shell to keep the foot from sliding off the orthosis.
A left foot orthosis was also fabricated. This orthosis was designed to provide total-contact weight bearing only. No postings or other special additions were made to the left foot orthosis.
Results A brief discharge evaluation was performed on the sixth and final visit. Observation indicated that the patient's pelvis was level in a standing position, and she reported that she was ambulating without a cane for household and shortdistance community ambulation, such as walk- ing from her car to the church or hair salon. With the use of the modified footwear and custom-made foot orthoses, she appeared to have an increased stride length and improved push-off on the right lower extrem- ity. The medial side of the right shoe sole now was in contact with the ground (Fig. 4). The left side of the pelvis no longer dropped lower than the right side during gait. The patient had been wearing the foot orthoses and modified footwear for 2 weeks and reported good balance during ambulation, a feeling of stability and security during weight bearing, and increased comfort. She reported no pain in the right foot or ankle, and she reported the ability to continue activities that she enjoyed, such as shopping and attend- ing bridge games twice a week and going to church once a week. She stated that she was wearing the orthoses every day and did not feel comfortable or safe without them.
Apex Foot Health Industries, 170 Wesley St, South Hackensack, NJ 07606. Langer Biomechanics Group, 450 Commack Rd, Deer Park, W 111529.
302 . Shrader and Lohmann Siegel Physical Therapy . Volume 7 7 . Number 3 . March 1997
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/3/296/2633141 by guest on 04 February 2022
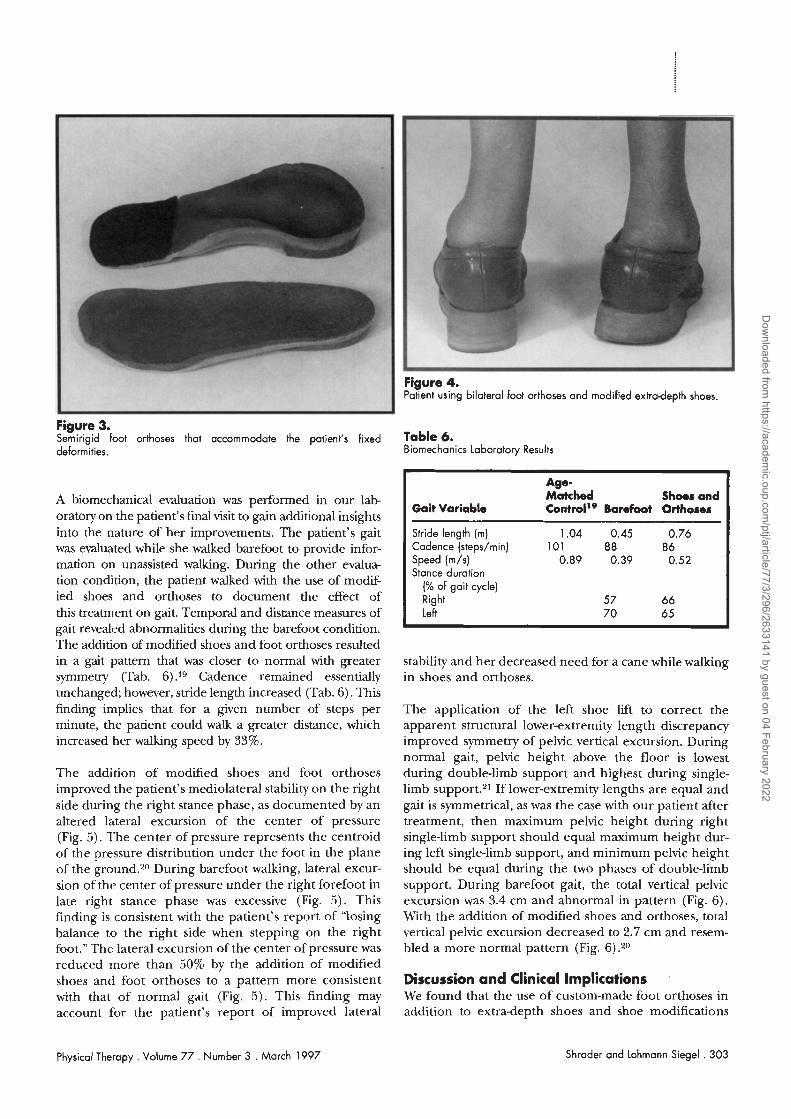
Figure 3. Semirigid foot orthoses that accommodate the patient's fixed deformities.
-
A biomechanical evaluation was performed in our lab oratoly on the patient's final visit to gain additional insights into the nature of her improvements. The patient's gait was evaluated while she walked barefoot to provide infor- mation on unassisted walking. During the other evalua- tion condition, the patient walked with the use of modif- ied shoes and orthoses to document the effect of this treatment on gait. Temporal and distance measures of gait revealed abnormalities during the barefoot condition. The addition of modified shoes and foot orthoses resulted in a gait pattern that was closer to normal with greater symmetry (Tab. 6) .I9 Cadence remained essentially unchanged; however, stride length increased (Tab. 6). This finding implies that for a given number of steps per minute, the patient could walk a greater distance, which increased her walking speed by 33%.
Figure 4. Patlent using b~lateral foot orthoses and modified extradepth shoes.
The addition of modified shoes and foot orthoses improved the patient's mediolateral stability on the right side during the right stance phase, as documented by an altered lateral excursion of the center of pressure (Fig. 5). The center of pressure represents the centroid of the pressure distribution under the foot in the plane of the gr0und.2~ During barefoot walking, lateral excur- sion of the center of pressure under the right forefoot in late right stance phase was excessive (Fig. 5) . This finding is consistent with the patient's report of "losing balance to the right side when stepping on the right foot." The lateral excursion of the center of pressure was reduced more than 50% by the addition of modified shoes and foot orthoses to a pattern more consistent with that of normal gait (Fig. 5). This finding may account for the patient's report of improved lateral
Table 6. Biomechanics Laboratory Results
Age- Matched Shoes and
Gait Variable C o n t r ~ l ' ~ Barefoot Orthoses
Stride length (m) 1.04 0.45 0.76 Cadence (steps/min) 101 8 8 86 Speed (m/s) 0.89 0.39 0.52 Stance duration
(% of gait cycle) Right 5 7 6 6 Left 7 0 65
stability and her decreased need for a cane while walking in shoes and orthoses.
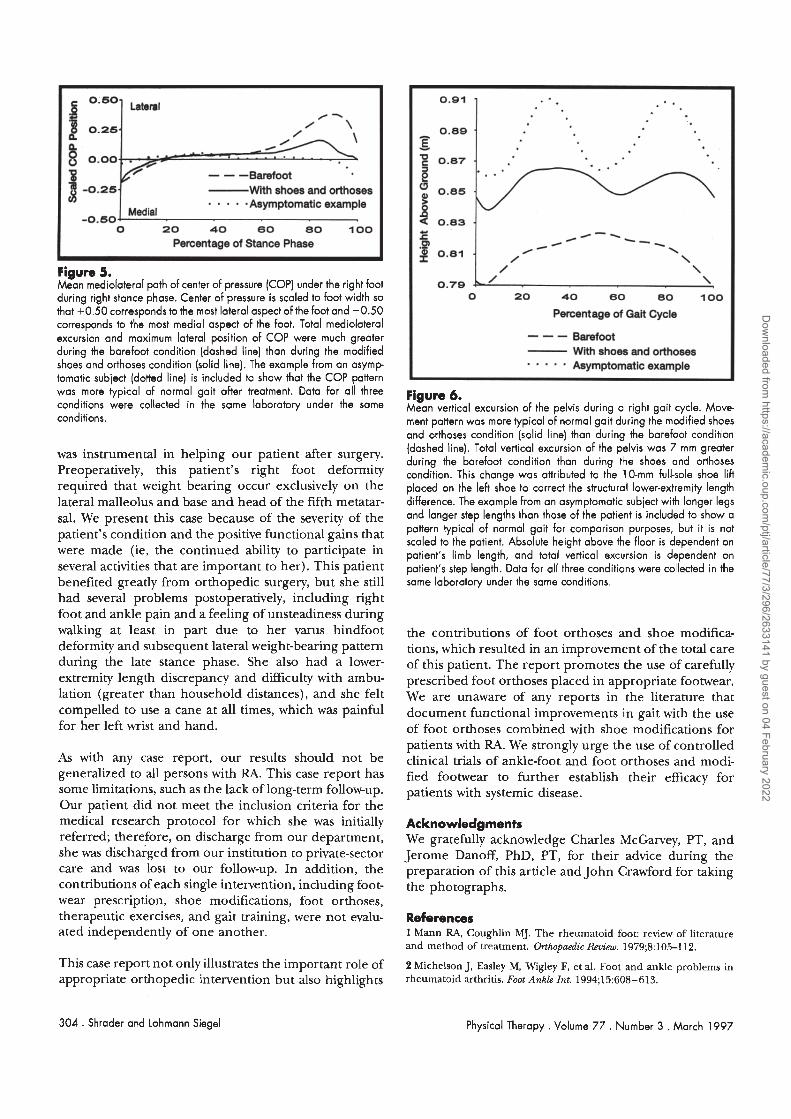
The application of the left shoe lift to correct the apparent structural lower-extremity length discrepancy improved symmetry of pelvic vertical excursion. During normal gait, pelvic height above the floor is lowest during double-limb support and highest during single- limb support.21 If lower-extremity lengths are equal and gait is symmetrical, as was the case with our patient after treatment, then maximum pelvic height during right single-limb support should equal maximum height dur- ing left single-limb support, and minimum pelvic height should be equal during the two phases of double-limb support. During barefoot gait, the total vertical pelvic excursion was 3.4 cm and abnormal in pattern (Fig. 6). With the addition of modified shoes and orthoses, total vertical pelvic excursion decreased to 2.7 cm and resem- bled a more normal pattern (Fig. 6) .zO
Discussion and Clinical Implications We found that the use of custom-made foot orthoses in addition to extra-depth shoes and shoe modifications
Physical Therapy . Volume 7 7 . Number 3 . March 1997 Shrader and Lohmann Siegel . 303
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/3/296/2633141 by guest on 04 February 2022
0.50- Lateral
/ - / \
#
- - -Barefoot With shoes and orthoses . . . . .Asymptomatic example
-0.50- Medial
0 20 40 60 80 100
Percentage of Stance Phase
Figure 5. Mean mediolateral path of center of pressure (COP] under the right foot during right stance phase. Center of pressure is scaled to foot width so that +0.50 corresponds to the most lateral aspect of the foot and -0.50 corresponds to the most medial aspect of the foot. Total mediolateral excursion and maximum lateral position of COP were much greater during the barefoot condition (dashed line) than during the modified shoes and orthoses condition (solid line). The example from an asymp tomatic subject (dotted line) is included to show that the COP pattern was more typical of normal gait after treatment. Data for all three conditions were collected in the same laboratory under the same conditions.
was instrumental in helping our patient after surgery. Preoperatively, this patient's right foot deformity required that weight bearing occur exclusively on the lateral malleolus and base and head of the fifth metatar- sal. We present this case because of the severity of the patient's condition and the positive functional gains that were made (ie, the continued ability to participate in several activities that are important to her). This patient benefited greatly from orthopedic surgery, but she still had several problems postoperatively, including right foot and ankle pain and a feeling of unsteadiness during walking at least in part due to her varus hindfoot deformity and subsequent lateral weight-bearing pattern during the late stance phase. She also had a lower- extremity length discrepancy and difficulty with ambu- lation (greater than household distances), and she felt compelled to use a cane at all times, which was painful for her left wrist and hand.
As with any case report, our results should not be generalized to all persons with RA. This case report has some limitations, such as the lack of long-term follow-up. Our patient did not meet the inclusion criteria for the medical research protocol for which she was initially referred; therefore, on discharge from our department, she was dischaiged from our institution to private-sector care and was lost to our follow-up. In addition, the contributions of each single intervention, including foot- wear prescription, shoe modifications, foot orthoses, therapeutic exercises, and gait training, were not evalu- ated independently of one another.
Figure 6. Mean vertical excursion of the pelvis during o right gait cycle. Move ment pattern was more typical of normal gait during the modified shoes and orthoses condition (solid line) than during the barefoot condition (dashed line]. Total vertical excursion of the pelvis was 7 mm greater during the barefoot condition than during the shoes and orthoses condition. This change was attributed to the IO-mm full-sole shoe lift placed on the left shoe to correct the structural lower-extremity length difference. The example from an asymptomatic subject with longer legs and longer step lengths than those of the patient is included to show a pattern typical of normal gait for comparison purposes, but it is not scaled to the patient. Absolute height above the floor is dependent on patient's limb length, and total vertical excursion is dependent on patient's step length. Data for all three conditions were collected in the same laboratory under the same conditions.
0.91 -
0.89 - T - = 0.87 -
the contributions of foot orthoses and shoe modifica- tions, which resulted in an improvement of the total care of this patient. The report promotes the use of carefully prescribed foot orthoses placed in appropriate footwear. We are unaware of any reports in the literature that document functional improvements in gait with the use of foot orthoses combined with shoe modifications for patients with RA. We strongly urge the use of controlled clinical trials of ankle-foot and foot orthoses and modi- fied footwear to further establish their efficacy for patients with systemic disease.
. . . .
.
Acknowledgments We gratefully acknowledge Charles McGarvey, PT, and Jerome Danoff, PhD, PT, for their advice during the preparation of this article and John Crawford for taking the photographs.
References 1 Mann RA, Coughlin MJ. The rheumatoid foot: review of literature and method of treatment. Qlthopaedic Revim. 1979;8:105-112.
3 0.85 -
8 0.83 .
This case report not only illustrates the important role of 2 Michelson J, Easley M, Wigley F, et al. Foot and ankle problems in appropriate orthopedic intervention but also highlights rheumatoid arthritis. Foot Ankle Znt. 1994;15:608-613.
E P 2 0.81 -
304 . Shrader and Lohmann Siegel
A - \ / / / -- \
\ / \
/ \
Physical Therapy . Volume 77 . Number 3 . March 1997
0.79 + \ 0 20 40 60 80 100
Percentage of Gait Cycle
--- Barefoot With shoes and orthoses . . . . . Asymptomatic example
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/3/296/2633141 by guest on 04 February 2022

3 Gerber LH, Hunt GC. Evaluation and management of the rheuma- toid foot. Bull NYAcad Med. 1985;61:359-368.
4 Clayton ML, Smyth CJ. Surpyfor Rheumatoid Arthritis. New York, NY. Churchill Livingstone Inc; 1992:311-313, 329.
5 Ehrlich GE. Rehabilitation Management ofRheumahc Conditions. 2nd ed. Baltimore, Md: Williams & Wilkins; 1986:279-281.
6 McGuire T, Kumar VN. Rehabilitation management of the rheuma- toid foot. Orlhopaedtc Revim. 1987;16:671-676.
7 Glass MK, Karno ML, Sella EJ, Zeleznik R. An ofice-based orthotic system in treatments of the arthritic foot. Foot Ankle Int. 1982;3:37-40.
8 Dimonte P, Light H. Pathomechanics, gait deviations, and treatment of the rheumatoid foot: a clinical report. Phys Ther. 1982;62:1148- 1156.
9 Merritt JL. Advances in orthotics for the patient with rheumatoid arthritis. JRheumatol. 1987;14(suppl 15):62-67.
10 Locke M, PerryJ, Campbell J, Thomas L. Ankle and subtalar motion during gait in arthritic patients. Phys Ther. 1984;64:504-510.
11 Hunt GC, Fromherz WA, Gerber LH, et al. Hindfoot pain treated by a leg-hindfoot orthosis. Phys Ther. 1987;67:1384-1388.
12 Kendall FP, McCreary EK Muscles: Testing and Function. 3rd ed. Baltimore, Md: Williams & Wilkins; 1983.
13 Birke JA, Sims DS. Plantar sensory threshold in the ulcerative foot. L@ h. 1986;57:261-267.
Physical Therapy . Volume 77 . Number 3 . March 1997
14 Fromherz WA. Examination. In: Hunt GL, McPoil TG, eds. Physical Therapy of the Foot and Ankle. 2nd ed. New York, NY: Churchill Livingstone Inc; 1995: 11 1.
15 Schuitt D, lMcPoil TG, Mulesa P. Incidence of sacroiliac joint malalignment in leg-length discrepancies. J Am Podiatr Med Assoc. 1989;79:380-383.
16 Siegel KL, Stanhope SJ, Caldwell GE. Kinematic and kinetic adap tations in the lower limb during stance in gait of unilateral femoral neuropathy patients. Clin Biomech. 1993;8:147-155.
17 Siegel KL, Kepple TM, O'Connell PC, et al. A technique to evaluate foot function during the stance phase of gait. Foot Ankle Znt. 1995;16: 764-770.
18 Research Plan for the National Center for Medical Rehabilitation Research. Bethesda, Md: US Department of Health and Human Services, Public Health Senice, National Institutes of Health, National Institute of Child Health and Human Development; 1993:33. NIH Publication No. 93-3509.
19 Himann JE, Cunningham DA, Rechnitzer PA, Paterson DH. Age- related changes in speed of walking. Med Sci Spurts Exerc. 1988;20:161- 166.
20 Rogers MM, Cavanagh PR. Glossary of biomechanical terms, con- cepts, and units. Phys Ther. 1984;64:1886-1902.
21 Inman \T, Ralston HJ, Todd F. Human Walking. Baltimore, Md: Williams & Wilkins; 1981:38.
Shroder and Lohmann Siegel . 305
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/3/296/2633141 by guest on 04 February 2022




















