
Clinical expression of rheumatoid arthritis in Chilean patients

Tofacitinib with Methotrexate in Third-Line Treatment of Patients with Active
Rheumatoid Arthritis: Patient-Reported Outcomes from a Phase 3 Trial
VIBEKE STRAND MD,1*
GERD R. BURMESTER MD,2*
CRISTIANO A.F. ZERBINI
MD,3 CHARLES A. MEBUS Ph.D.,
4 SAMUEL H. ZWILLICH MD,
4
DAVID GRUBEN Ph.D.,4 AND GENE V. WALLENSTEIN Ph.D.
4
*Both authors contributed equally to this work
1Biopharmaceutical Consultant, Portola Valley, CA, USA;
2Charité –
Universitätsmedizin Berlin, Berlin, Germany; 3Centro Paulista de Investigação Clinica,
São Paulo, Brazil; 4Pfizer Inc., Groton, CT, USA
Name and address for correspondence (and reprints):
Dr Gene Wallenstein
Pfizer Inc
445 Eastern Point Road
MS 8260-2515
Groton
CT 06340, USA
Tel: +1.860.441.5251
Fax: +1.860.686.7528
E-mail: [email protected]
Running head: Phase 3 study of tofacitinib plus methotrexate in TNF inhibitor-IR
population: patient-reported outcomes
Original Article Arthritis Care & ResearchDOI 10.1002/acr.22453
This article has been accepted for publication and undergone full peer review but has not beenthrough the copyediting, typesetting, pagination and proofreading process which may lead todifferences between this version and the Version of Record. Please cite this article as an‘Accepted Article’, doi: 10.1002/acr.22453© 2014 American College of RheumatologyReceived: Mar 21, 2014; Revised: Jul 29, 2014; Accepted: Aug 26, 2014
2
Previous presentations:
Burmester G-R, van der Heijde D, Strand V, Zerbini CAF, Connell CA, Mebus CA,
Zwillich SH, Bradley JD, Gruben D, Wallenstein G. Effects of tofacitinib on patient-reported
outcomes in patients with active rheumatoid arthritis receiving stable-dose methotrexate:
results of two Phase 3 studies. Poster presented at the ACR/ARHP Annual Scientific
Meeting, Washington, DC, USA, November 9–14, 2012; poster number 1283.
Funding:
This study was sponsored by Pfizer Inc.
Author disclosures of conflicts of interest:
V Strand, GR Burmester and CAF Zerbini have received research grants and fees from
Pfizer Inc. C Mebus, S Zwillich, D Gruben and G Wallenstein are employees and
stockholders of Pfizer Inc.
Word count: 2390
Page 2 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

3
ABSTRACT [247/250 WORDS]
Objective. Tofacitinib is an oral Janus kinase inhibitor for the treatment of rheumatoid
arthritis (RA). Patient-reported outcomes (PROs) in a 6-month, Phase 3, randomized
controlled trial (NCT00960440) are presented here.
Methods. Patients aged ≥18 years with active RA with an inadequate response to ≥1 tumor
necrosis factor inhibitor (TNFi) and on stable background methotrexate were randomized
2:2:1:1 to tofacitinib 5 mg or 10 mg twice daily (BID), or placebo advanced to 5 mg or 10 mg
BID at month 3. PROs measured at month 3 included: Patient Global Assessment of Disease
Activity (PtGA), pain, Health Assessment Questionnaire-Disability Index (HAQ-DI),
Medical Outcomes Study (MOS) Short-Form Health Survey Version 2 (acute; SF-36),
Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), and MOS Sleep
Scale.
Results. Patients received tofacitinib 5 mg (n = 133) or 10 mg (n = 134), or placebo advanced
to tofacitinib 5 mg (n = 66) or 10 mg (n = 66). HAQ-DI (reported previously), PtGA
(P<0.0001), and SF-36 physical and mental component (P<0.05) scores were improved for
both tofacitinib doses versus placebo. Furthermore, improvements ≥minimum clinically
important difference were more frequently reported by tofacitinib-treated patients versus
placebo: PtGA (P<0.05), pain (P<0.0001), HAQ-DI (P<0.05), SF-36 physical and mental
component scores (P<0.05), and FACIT-F (P<0.001 for 5 mg BID). No statistical differences
were observed in the MOS Sleep Scale.
Conclusion. Tofacitinib treatment resulted in significant, clinically meaningful improvements
in multiple PROs versus placebo over 3 months’ treatment in patients with active RA and
previous inadequate response to TNFi.
Page 3 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

4
SIGNIFICANCE & INNOVATIONS
• In this refractory, difficult-to-treat population with inadequate response to tumor
necrosis factor inhibitors (TNFi), tofacitinib in combination with methotrexate (MTX)
significantly improved patient-reported outcomes, including HRQoL, versus placebo
(on background MTX).
• These findings demonstrate, from the perspective of patients with inadequate response
to TNFi, clinically meaningful and relevant benefits of tofacitinib added to
background MTX. These patient-perceived benefits contribute importantly to overall
clinical efficacy.
Page 4 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

5
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic, inflammatory disease characterized by progressive
joint destruction, and impairment in physical function and health-related quality of life
(HRQoL) (1–4). From a patient perspective, improvements in pain, physical function, fatigue,
and HRQoL are more important and meaningful than improvements in joint swelling,
tenderness, or inhibition of structural damage, when therapies for RA are evaluated (5).
Accordingly, the Outcomes Measures in Rheumatology (OMERACT) international
consensus effort, American College of Rheumatology (ACR), and European League Against
Rheumatism (EULAR) have recognized the importance of including a variety of
patient-reported outcomes (PROs) in randomized controlled trials (RCTs) (6–9). PROs
complement physician and laboratory measures in providing scientific evidence to support
decisions regarding clinical therapy (10).
Disease-modifying anti-rheumatic drugs (DMARDs), most prominently methotrexate
(MTX), represent the cornerstone of RA therapy. Patients with an inadequate response to
MTX frequently progress to receive biologic DMARDs, including tumor necrosis factor
inhibitors (TNFi). However, many patients do not respond well, lose their clinical response,
or experience adverse events with TNFi (11–14). Although patients with an inadequate
response to one TNFi may be switched to a second TNFi, patients may experience
progressive loss of efficacy with a subsequent TNFi (15). In addition, response to treatment,
physical function and other PROs decreases with more failed therapies and longer disease
duration (16). Patients with previously inadequate responses to TNFi, therefore, continue to
represent a challenging population to treat.
Tofacitinib is an oral Janus kinase inhibitor for the treatment of RA. Six Phase 3 RCTs have
demonstrated significant improvements in signs and symptoms of active RA compared with
Page 5 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

6
placebo (17–21) or MTX (22). PROs have been reported from all six Phase 3 trials; they have
demonstrated significant improvements with tofacitinib treatment versus placebo, with and
without background MTX across a range of patient populations (23–28).
In the Phase 3 ORAL Step trial (A3921032; clinicaltrials.gov identifier NCT00960440),
399 patients with active RA, with inadequate response to at least one TNFi and receiving
stable, background MTX were randomized to receive tofacitinib 5 mg, 10 mg, or placebo
twice daily (BID). Patients randomized to receive placebo advanced to tofacitinib 5 mg or
10 mg BID at month 3 (17). Co-primary endpoints – ACR20 response, mean change from
baseline in Health Assessment Questionnaire-Disability Index (HAQ-DI) and Disease
Activity Score-defined remission (DAS28-4, erythrocyte sedimentation rate [ESR] <2.6), all
measured at month 3 – were met for both doses of tofacitinib (17). Here, we report
improvements in additional PROs with tofacitinib (versus placebo) from this Phase 3 RCT.
Page 6 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

7
METHODS
Patients
Inclusion and exclusion criteria have been reported previously (17). Briefly, patients were
aged ≥18 years with moderate to severe active RA, defined as tender joint count ≥6 and
swollen joint count ≥6 (68/66-joint count) and either an ESR (Westergren method) >28 mm/h
or C-reactive protein >7 mg/L. Patients were required to have had previous inadequate
responses or intolerance to at least one approved TNFi. Patients had been receiving oral or
parenteral MTX with folate supplementation continuously for ≥4 months and had been
receiving stable doses, 7.5–25 mg weekly, for ≥6 weeks prior to the first dose of study
medication.
Study design and treatment
This 6-month, Phase 3 RCT was conducted at 82 centers in 13 countries worldwide. Patients
were randomized 2:2:1:1 to receive tofacitinib 5 mg or 10 mg BID, placebo advanced to
tofacitinib 5 mg BID, or placebo advanced to tofacitinib 10 mg BID. All patients receiving
placebo were blindly advanced to tofacitinib at month 3. Permitted concomitant medications,
wash-out schedules for prior DMARDS, and planned primary efficacy and safety analyses,
are described elsewhere (17).
Assessment of patient-reported outcomes
Patient Global Assessment of Disease Activity (PtGA) was recorded using a 100 mm visual
analog scale (VAS), higher scores indicating worse disease activity. Patient assessment of
arthritis pain was also recorded utilizing a 100 mm VAS. HAQ-DI, the co-primary endpoint
(17,29), assessed performance of activities of daily living, scored from 0 (able to perform
without difficulty) to 3 (unable to perform). HRQoL was evaluated using the Medical
Page 7 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

8
Outcomes Study (MOS) Short-Form (36-item) Health Survey (SF-36) Version 2 (acute) (30),
including eight domains scored from 0–100 and summarized into physical (PCS) and mental
(MCS) component scores. Visualizations of SF-36 data were generated from domain scores,
as previously described (31). The EuroQol 5-Dimensions (EQ-5D) Health State Profile was
also assessed. Fatigue was assessed by the Functional Assessment of Chronic Illness
Therapy-Fatigue (FACIT-F) scale (range 0–52), where higher scores represent less fatigue
(32). The MOS Sleep Scale (MOS-SS) assessed nine items of sleep disturbance to construct
an overall sleep problems score.
PtGA, pain, and HAQ-DI were assessed at baseline, week 2, months 1, 3, 4.5, and 6, or early
treatment discontinuation. SF-36, FACIT-F, and MOS-SS were assessed at baseline, week 2,
months 1, 3, and 6, or early treatment discontinuation. EQ-5D was assessed at baseline,
months 1, 3, and 6, or early treatment discontinuation.
Here, results in PROs are reported at month 3, before patients randomized to placebo
advanced to tofacitinib treatment. Data from the two placebo groups were pooled into a
single treatment group at month 3. At month 6, data were analyzed for each group in which
patients received placebo and then advanced to tofacitinib.
Statistical analysis
Determination of sample size is described elsewhere (17). With the exception of HAQ-DI,
which was a co-primary endpoint, PROs were pre-specified secondary endpoints.
Significance was declared at P ≤ 0.05, and there was no attempt to control for Type-1 error.
A longitudinal mixed-effect repeated-measures model was utilized to calculate mean changes
from baseline in the full analysis set (all patients who received ≥1 dose of study drug with
baseline and ≥1 post-baseline measures) without explicit imputation for missing values.
Page 8 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

9
Treatment, week, and treatment-by-week interactions were included as fixed effects in the
model, with patients as a random effect. Estimates of least squares (LS) mean changes from
baseline and mean differences from placebo were derived from the model with 95%
confidence intervals (LS means from a model are means that are adjusted for other terms in
the model and, as such, provide more accurate estimates of changes from baseline for each
treatment group than do simple arithmetic means, and also are less sensitive to missing data).
SF-36 derived data were compared with values from healthy individuals in the US, which
were selected to match the specific age and gender distribution of this protocol population
(referred to as age- and gender-matched norms) (30).
RESULTS
Patients
Baseline demographics and disease characteristics were similar between treatment groups
(17). Three hundred and ninety-nine (399) patients were randomized to tofacitinib 5 mg
(n = 133), tofacitinib 10 mg (n = 134), placebo advanced to tofacitinib 5 mg (n = 66) or
tofacitinib 10 mg (n = 66) at month 3. The majority of patients in each group (81% – 91%)
were from North America and Europe and, as previously reported, over 80% were white (17).
Mean age ranged from 54.4 to 55.4 years, and mean duration of RA from 11.3 to 13.0 years.
The mean number of previous TNFi treatments was 1.4 to 1.5: 257 patients (64%) had
previously received one TNFi, 104 (26%) two, and 32 (8%) three or more. Forty-six patients
(12%) had also received biologic DMARDs other than TNFi (17).
Page 9 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

10
Patient-reported outcomes
At baseline, PROs were similar across treatment groups (Table 1). Significant improvements
versus placebo in HAQ-DI, pain score, and FACIT-F observed at month 3 with tofacitinib
5 mg and 10 mg BID were reported previously (17), and here we note that PtGA (Table1 and
Figure 1) and SF-36, PCS and MCS (Table 1 and Figure 2), significantly improved from
baseline in both tofacitinib groups versus placebo at month 3. In addition, all SF-36 domains
and EQ-5D scores improved significantly at month 3 with tofacitinib treatment versus
placebo (Table 1). There were no significant improvements (versus placebo) in MOS-SS
overall sleep problems score in any of the tofacitinib treatment groups (Table 1). Significant
improvements from baseline in PtGA, pain and SF-36 component scores were evident as
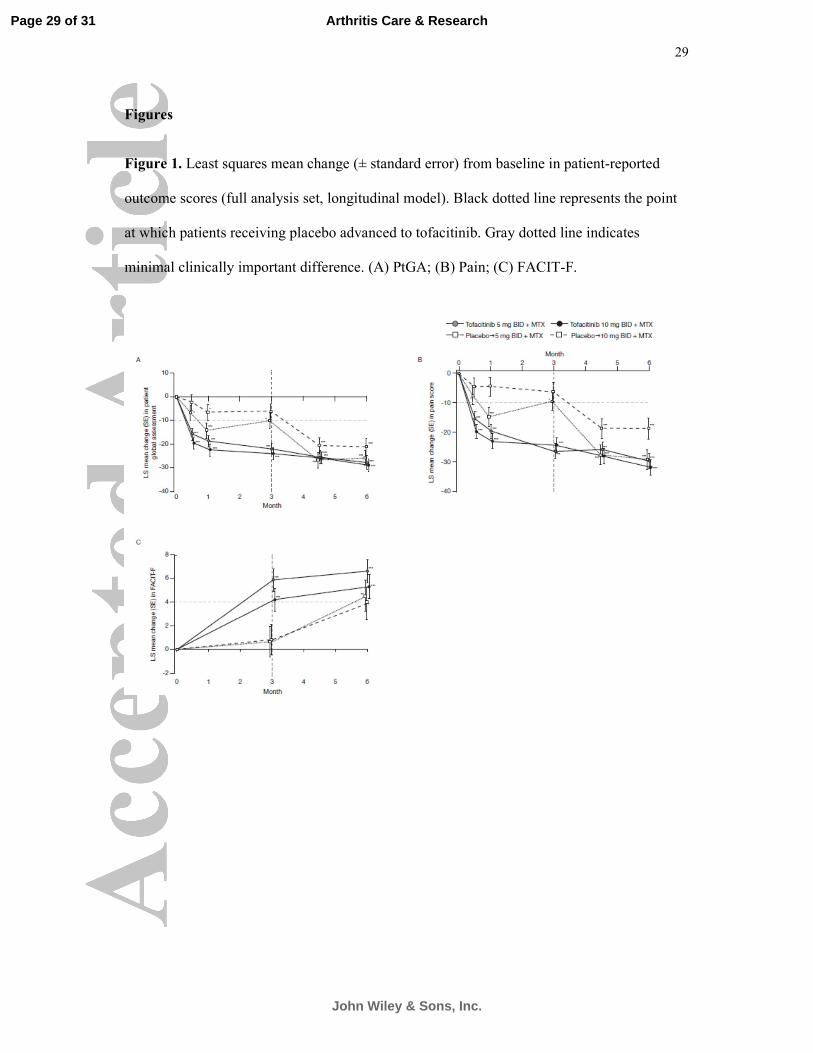
early as week 2 and continued to month 6 (Figures 1 and 2). Improvements from baseline in
FACIT-F, which was measured at month 3 and month 6, remained significant (versus
placebo) at month 6 (Figure 1). Improvements in PROs were similar in both tofacitinib
treatment groups, although frequently numerically higher with tofacitinib 10 mg BID (Table
1; Figures 1 and 2).
At month 3, LS mean changes from baseline exceeded minimal clinically important
differences (MCID) in PtGA (≥10 points (33)), pain (≥10 points (33)), HAQ-DI (≥0.22 points
(34)), SF-36 PCS and MCS (≥2.5 points (35)), and FACIT-F (≥4 points (36)) for both
tofacitinib doses. LS mean changes in SF-36 domain scores also exceeded MCID
(≥5.0 points (35)) in two domains (bodily pain [BP] and vitality [VT]) with tofacitinib 5 mg,
and five domains (physical functioning [PF], role physical [RP], social functioning [SF], BP,
and VT) with tofacitinib 10 mg. LS mean changes in PROs for patients receiving placebo did
not meet MCID (Table 1).
Page 10 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

11
The proportion of patients reporting improvements ≥MCID in PROs at month 3 were
significantly higher in both tofacitinib groups versus placebo in PtGA, pain, HAQ-DI, SF-36
PCS and MCS, and in three (BP, VT, and general health [GH]) and five (PF, RP, BP, VT,
and SF) SF-36 domain scores with 5 mg and 10 mg respectively (Table 2). The proportion of
patients reporting improvements ≥MCID was also significantly higher for FACIT-F (Table 2)
in the tofacitinib 5 mg treatment group versus placebo.
When the proportion of patients reporting changes ≥MCID in PROs and the number needed
to treat (NNT) were compared between treatment groups, associations were observed
between particular PROs, although no formal statistical assessment was performed (Table 2).
The proportion of patients reporting improvements ≥MCID and NNTs was similar between
pain and SF-36 BP domain for both tofacitinib doses; between FACIT-F and SF-36 VT
domain in the tofacitinib 5 mg group; between HAQ-DI and SF-36 PF domain in the
tofacitinib 10 mg group; and between SF-36 RP and role emotional [RE] domains in the
tofacitinib 10 mg group, despite LS mean changes from baseline in SF-36 RE not being
statistically significant.
HRQoL: study and normative populations
SF-36 scores at baseline and month 3 are presented with SF-36 values from age-and gender-
matched norms to provide a benchmark comparison (Figure 3). SF-36 PCS and MCS at
baseline were approximately 2 and 1 standard deviations, respectively, below normative
scores of 50. At baseline, domain scores across all treatment groups were up to half of the
normative values (Figure 3 (30)). At month 3, VT domain scores in tofacitinib-treated
patients approached normative scores (Figure 3).
Page 11 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

12
DISCUSSION
In this Phase 3 RCT, treatment with tofacitinib 5 mg or 10 mg BID resulted in statistically
significant and clinically meaningful improvements versus placebo in HAQ-DI (month 3 data
reported previously (17)), PtGA, pain, physical function, HRQoL, and fatigue in patients with
RA and inadequate response to TNFi (TNFi-IR) receiving background MTX. These
improvements are of particular interest, as the central importance of these outcomes to
patients with active RA has been highlighted in previous RCTs (2,3,37).
Improvements in PROs were similar for both tofacitinib doses, but often numerically higher
with tofacitinib 10 mg BID. Significant improvements were observed after as little as two
weeks and maintained for the duration of tofacitinib treatment. Mean improvements from
baseline with tofacitinib were clinically meaningful, exceeding MCID and statistically
significant versus placebo, in PtGA, pain, HAQ-DI, SF-36 PCS and MCS, and in three and
five domains of SF-36 (with tofacitinib 5 mg and 10 mg BID, respectively). More patients in
both tofacitinib treatment groups reported clinically meaningful improvements in PROs than
did placebo-treated patients, with small NNTs. Together, these findings reflect a broad
beneficial effect of tofacitinib treatment on physical function, pain, fatigue, HRQoL,
including SF-36 domains of bodily pain and vitality, by not only reducing fatigue but
increasing patients’ energy levels. These improvements in PROs are consistent with the
primary efficacy data from the study, where ACR20/50/70 responses and DAS28-defined
remission and low disease activity rates were significantly improved in both tofacitinib
treatment groups versus placebo (17). No significant improvement in MOS-SS overall sleep
problems score was observed in any group, which remains unexplained. In other Phase 3
studies of tofacitinib, improvements from baseline in MOS-SS have been observed at
month 3 with tofacitinib 5 mg BID (26,27) and 10 mg BID (26–28) versus placebo.
Page 12 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

13
Changes in PROs with tofacitinib 5 mg and 10 mg BID appeared similar, although frequently
numerically higher with tofacitinib 10 mg BID, reflected in lower NNTs. Not surprisingly,
associations were observed between the number of patients reporting clinically meaningful
improvements in HAQ-DI and SF-36 PF domain, pain and SF-36 BP domain, and FACIT-F
and SF-36 VT domain, indicating that these PROs measure comparable aspects of HRQoL.
Baseline SF-36 domain scores were much lower than for age- and gender-matched norms,
indicating a substantial burden of disease in this population with incomplete response to
TNFi and long duration of disease (mean 11.3–13.0 years) . The broad range of
improvements in PROs observed in this treatment-refractory population, compared with those
in other Phase 3 tofacitinib RA trials, is encouraging.
Our findings are consistent with reported changes in PROs in other TNFi-IR populations
subsequently treated with established biologic agents. The proportion of patients reporting
improvements ≥MCID in FACIT-F and HAQ-DI after treatment with rituximab plus MTX
for 6 months were similar to those reported here (38). Again, similar proportions of patients
reported clinically meaningful changes in PtGA, pain, HAQ-DI, SF-36 PCS and MCS, and
FACIT-F, with 24 weeks’ tocilizumab + MTX (39). HAQ-DI responses ≥MCID (≥0.3 points)
were reported in 47% of TNFi-IR patients receiving abatacept + DMARD for 6 months (40).
In contrast to this study, improvements in sleep quality with abatacept were observed in
TNFi-IR patients (36).
This study focused on the first 3 months of this RCT to allow for comparison with the
placebo-treated population before advancement to tofacitinib. As RA is a chronic condition
requiring long-term treatment, ongoing extension studies are seeking to address whether
benefits observed in the short-term are maintained in the long term (41,42).
Page 13 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

14
In conclusion, tofacitinib therapy with background MTX improved HRQoL and reduced the
broad burden of active RA over 3 months’ treatment in TNFi-IR patients, compared with
placebo. These findings demonstrate both statistically and clinically meaningful benefits of
tofacitinib from the patient’s perspective, in addition to physician-reported outcomes.
ACKNOWLEDGMENTS
The authors would like to thank the patients who were involved in this study, and the
A3921032 investigators and study team. Medical writing support was provided by Kate
Silverthorne, PhD, and Claire Cridland at Complete Medical Communications and was
funded by Pfizer Inc.
Page 14 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

15
REFERENCES
1. Strand V, Singh JA. Newer biological agents in rheumatoid arthritis: impact on
health-related quality of life and productivity. Drugs 2010;70:121-45.
2. Strand V, Rentz AM, Cifaldi MA, Chen N, Roy S, Revicki D. Health-related quality
of life outcomes of adalimumab for patients with early rheumatoid arthritis: results
from a randomized multicenter study. J Rheumatol 2012;39:63-72.
3. Strand V, Smolen JS, van Vollenhoven RF, Mease P, Burmester GR, Hiepe F, et al.
Certolizumab pegol plus methotrexate provides broad relief from the burden of
rheumatoid arthritis: analysis of patient-reported outcomes from the RAPID 2 trial.
Ann Rheum Dis 2011;70:996-1002.
4. Hewlett S, Cockshott Z, Byron M, Kitchen K, Tipler S, Pope D, et al. Patients'
perceptions of fatigue in rheumatoid arthritis: overwhelming, uncontrollable, ignored.
Arthritis Rheum 2005;53:697-702.
5. Kirwan JR, Minnock P, Adebajo A, Bresnihan B, Choy E, de Wit M, et al. Patient
perspective: fatigue as a recommended patient centered outcome measure in
rheumatoid arthritis. J Rheumatol 2007;34:1174-7.
6. Felson DT, Anderson JJ, Boers M, Bombardier C, Chernoff M, Fried B, et al. The
American College of Rheumatology preliminary core set of disease activity measures
for rheumatoid arthritis clinical trials. The Committee on Outcome Measures in
Rheumatoid Arthritis Clinical Trials. Arthritis Rheum 1993;36:729-40.
Page 15 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

16
7. Gossec L, Dougados M, Rincheval N, Balanescu A, Boumpas DT, Canadelo S, et al.
Elaboration of the preliminary Rheumatoid Arthritis Impact of Disease (RAID) score:
a EULAR initiative. Ann Rheum Dis 2009;68:1680-5.
8. Kirwan JR, Hewlett SE, Heiberg T, Hughes RA, Carr M, Hehir M, et al. Incorporating
the patient perspective into outcome assessment in rheumatoid arthritis--progress at
OMERACT 7. J Rheumatol 2005;32:2250-6.
9. Kirwan JR, Tugwell PS. Overview of the patient perspective at OMERACT 10--
conceptualizing methods for developing patient-reported outcomes. J Rheumatol
2011;38:1699-701.
10. Pincus T. Are patient questionnaire scores as "scientific" as laboratory tests for
rheumatology clinical care? Bull NYU Hosp Jt Dis 2010;68:130-9.
11. Keystone EC, Kavanaugh AF, Sharp JT, Tannenbaum H, Hua Y, Teoh LS, et al.
Radiographic, clinical, and functional outcomes of treatment with adalimumab (a
human anti-tumor necrosis factor monoclonal antibody) in patients with active
rheumatoid arthritis receiving concomitant methotrexate therapy: a randomized,
placebo-controlled, 52-week trial. Arthritis Rheum 2004;50:1400-11.
12. Klareskog L, van der Heijde D, de Jager JP, Gough A, Kalden J, Malaise M, et al.
Therapeutic effect of the combination of etanercept and methotrexate compared with
each treatment alone in patients with rheumatoid arthritis: double-blind randomised
controlled trial. Lancet 2004;363:675-81.
13. Lipsky PE, van der Heijde DM, St Clair EW, Furst DE, Breedveld FC, Kalden JR, et
al. Infliximab and methotrexate in the treatment of rheumatoid arthritis. Anti-Tumor
Page 16 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research
17
Necrosis Factor Trial in Rheumatoid Arthritis with Concomitant Therapy Study
Group. N Engl J Med 2000;343:1594-602.
14. Hetland ML, Christensen IJ, Tarp U, Dreyer L, Hansen A, Hansen IT, et al. Direct
comparison of treatment responses, remission rates, and drug adherence in patients
with rheumatoid arthritis treated with adalimumab, etanercept, or infliximab: results
from eight years of surveillance of clinical practice in the nationwide Danish
DANBIO registry. Arthritis Rheum 2010;62:22-32.
15. Chatzidionysiou K, van Vollenhoven RF. When to initiate and discontinue biologic
treatments for rheumatoid arthritis? J Intern Med 2011;269:614-25.
16. Aletaha D, Strand V, Smolen JS, Ward MM. Treatment-related improvement in
physical function varies with duration of rheumatoid arthritis: a pooled analysis of
clinical trial results. Ann Rheum Dis 2008;67:238-43.
17. Burmester GR, Blanco R, Charles-Schoeman C, Wollenhaupt J, Zerbini C, Benda B,
et al. Tofacitinib (CP-690,550) in combination with methotrexate in patients with
active rheumatoid arthritis with an inadequate response to tumour necrosis factor
inhibitors: a randomised phase 3 trial. Lancet 2013;381:451-60.
18. Fleischmann R, Kremer J, Cush J, Schulze-Koops H, Connell CA, Bradley JD, et al.
Placebo-controlled trial of tofacitinib monotherapy in rheumatoid arthritis. N Engl J
Med 2012;367:495-507.
19. Kremer J, Li ZG, Hall S, Fleischmann R, Genovese M, Martin-Mola E, et al.
Tofacitinib in combination with nonbiologic disease-modifying antirheumatic drugs
Page 17 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

18
in patients with active rheumatoid arthritis: a randomized trial. Ann Intern Med
2013;159:253-61.
20. van der Heijde D, Tanaka Y, Fleischmann R, Keystone E, Kremer J, Zerbini C, et al.
Tofacitinib (CP-690,550) in patients with rheumatoid arthritis receiving methotrexate:
twelve-month data from a twenty-four-month phase III randomized radiographic
study. Arthritis Rheum 2013;65:559-70.
21. van Vollenhoven RF, Fleischmann R, Cohen S, Lee EB, García Meijide JA, Wagner
S, et al. Tofacitinib or adalimumab versus placebo in rheumatoid arthritis. N Engl J
Med 2012;367:508-19.
22. Lee EB, Fleischmann R, Hall S, Wilkinson B, Bradley J, Gruben D, et al. Tofacitinib
versus Methotrexate in Rheumatoid Arthritis. N Engl J Med 2014;370:2377-86.
23. Strand V, van der Heijde D, Zerbini CAF, Connell C, Gruben D, Riese R, et al.
ORAL SCAN Effects Of The Oral JAK Inhibitor Tofacitinib In Combination With
Methotrexate On Patient Reported Outcomes In a 24-Month Phase 3 Trial Of Active
Rheumatoid Arthritis [abstract]. Arthritis and Rheumatism 2013;65 (Suppl 10):S996.
24. Strand V, Fleischmann R, Alten R, Koncz T, Zwillich SH, Bradley JD, et al. Oral
START: Effects Of The Oral JAK Inhibitor Tofacitinib Monotherapy Versus
Methotrexate On Patient Reported Outcomes In The Phase 3 Oral START Trial Of
Active Rheumatoid Arthritis [abstract]. Ann Rheum Dis 2013;72 (Suppl 3):252-3.
25. Burmester G, van der Heijde D, Strand V, Zerbini C, Connell C, Mebus C, et al.
Effects of tofacitinib on patient-reported outcomes in patients with active rheumatoid
Page 18 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

19
arthritis receiving stable dose methotrexate: results of two Phase 3 studies [abstract].
Arthritis and Rheumatism 2012;64 (suppl 10):549.
26. van Vollenhoven RF, Wallenstein G, Lee EB, Fleischmann R, Zwillich S, Gruben D,
et al. Effects of Tofacitinib (CP-690,550), an Oral Janus Kinase Inhibitor, or
Adalimumab on Patient Reported Outcomes in a Phase 3 study of active rheumatoid
arthritis [abstract]. Ann Rheum Dis 2012;71 S3:206.
27. Strand V, Kremer J, Li ZG, Hall S, Fleischmann R, Genovese M, et al. Tofacitinib
(CP-690,550) in combination with traditional disease-modifying anti-rheumatic drugs:
patient-reported outcomes from a Phase 3 study in patients with active rheumatoid
arthritis and an inadequate response to disease-modifying anti-rheumatic drugs.
Arthritis and Rheumatism 2011;63:S1032-S1033.
28. Strand V, Kanik K, Connell CA, Fleischmann R, Kremer J, Bradley J, et al. The
Effects of the Oral JAK Inhibitor CP-690,550 on Patient Reported Outcomes in a
Phase 3 Study of Active Rheumatoid Arthritis [abstract]. Ann Rheum Dis 2011;70
3:88-9.
29. Fries JF, Spitz PW, Young DY. The dimensions of health outcomes: the health
assessment questionnaire, disability and pain scales. J Rheumatol 1982;9:789-93.
30. Ware JE, Kosinski M, Dewey JE. How to score version two of the SF 36 Health
Survey. Lincoln, RI: Quality Metric, Incorporate; 2000.
31. Strand V, Crawford B, Singh J, Choy E, Smolen JS, Khanna D. Use of "spydergrams"
to present and interpret SF-36 health-related quality of life data across rheumatic
diseases. Ann Rheum Dis 2009;68:1800-4.
Page 19 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

20
32. Cella D, Lai JS, Chang CH, Peterman A, Slavin M. Fatigue in cancer patients
compared with fatigue in the general United States population. Cancer 2002;94:528-
38.
33. Strand V, Scott DL, Emery P, Kalden JR, Smolen JS, Cannon GW, et al. Physical
function and health related quality of life: analysis of 2-year data from randomized,
controlled studies of leflunomide, sulfasalazine, or methotrexate in patients with
active rheumatoid arthritis. J Rheumatol 2005;32:590-601.
34. Wells GA, Tugwell P, Kraag GR, Baker PR, Groh J, Redelmeier DA. Minimum
important difference between patients with rheumatoid arthritis: the patient's
perspective. J Rheumatol 1993;20:557-60.
35. Strand V, Bombardier C, Maetzel A. Use of minimum clinically important differences
[MCID] in evaluating patient responses to treatment of RA [abstract]. Arthritis
Rheum 2001;44 Suppl:S187.
36. Wells G, Li T, Maxwell L, Maclean R, Tugwell P. Responsiveness of patient reported
outcomes including fatigue, sleep quality, activity limitation, and quality of life
following treatment with abatacept for rheumatoid arthritis. Ann Rheum Dis
2008;67:260-5.
37. Strand V, Mease P, Burmester GR, Nikai E, Coteur G, van Vollenhoven R, et al.
Rapid and sustained improvements in health-related quality of life, fatigue, and other
patient-reported outcomes in rheumatoid arthritis patients treated with certolizumab
pegol plus methotrexate over 1 year: results from the RAPID 1 randomized controlled
trial. Arthritis Res Ther 2009;11:R170.
Page 20 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

21
38. Keystone E, Burmester GR, Furie R, Loveless JE, Emery P, Kremer J, et al.
Improvement in patient-reported outcomes in a rituximab trial in patients with severe
rheumatoid arthritis refractory to anti-tumor necrosis factor therapy. Arthritis Rheum
2008;59:785-93.
39. Strand V, Burmester GR, Ogale S, Devenport J, John A, Emery P. Improvements in
health-related quality of life after treatment with tocilizumab in patients with
rheumatoid arthritis refractory to tumour necrosis factor inhibitors: results from the
24-week randomized controlled RADIATE study. Rheumatology (Oxford)
2012;51:1860-9.
40. Genovese MC, Becker JC, Schiff M, Luggen M, Sherrer Y, Kremer J, et al. Abatacept
for rheumatoid arthritis refractory to tumor necrosis factor alpha inhibition. N Engl J
Med 2005;353:1114-23.
41. Burmester G-R, Blanco R, Rubbert-Roth A, Hendrikx T, Kwok K, Bradley J, et al.
Short- and Long-term Efficacy of Tofacitinib, an Oral Janus Kinase Inhibitor, in the
Treatment of Patients with Rheumatoid Arthritis and an Inadequate Response to TNF
Inhibitors: Analyses of Pooled Phase 2, Phase 3, and Long-term Extension Studies.
Arthritis and Rheumatism 2012;64:4172 (L12).
42. Wollenhaupt J, Silverfield J, Lee EB, Curtis JR, Wood SP, Soma K, et al. Safety and
Efficacy of Tofacitinib, an Oral Janus Kinase Inhibitor, for the Treatment of
Rheumatoid Arthritis in Open-label, Longterm Extension Studies. J Rheumatol
2014;41:837-52.
Page 21 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

22
Table 1. Mean baseline values and LS mean changes from baseline at month 3 for
patient-reported outcomes
Baseline mean (SD) Month 3 LS mean change from baseline (SE)†
Placebo
+ MTX
Tofacitinib
5 mg BID
+ MTX
Tofacitinib
10 mg BID
+ MTX
Placebo
+ MTX
Tofacitinib
5 mg BID
+ MTX
Tofacitinib
10 mg BID +
MTX
n 131 127 128 117 114 120
PtGA (VAS) 61.87
(22.92)
64.69
(23.22)
58.79
(23.59)
–9.19
(2.42)
–23.39***
(2.43)
–25.05***
(2.48)
n 131 127 128 115 114 119
Pain (VAS) ‡ 60.74
(23.50)
65.73
(22.79)
60.10
(23.16)
–8.26
(2.41)
–27.16***
(2.43)
–24.95***
(2.48)
n 132 132 134 118 117 125
HAQ-DI‡ 1.63
(0.66)
1.60
(0.66)
1.50
(0.61)
–0.18
(0.04)
–0.43***
(0.04)
–0.46***
(0.04)
n 129 132 134 114 117 125
FACIT-F‡ 26.98
(11.52)
27.84
(11.12)
29.48
(11.39)
1.11
(1.04)
6.27***
(1.01)
4.57*
(1.03)
n 129 133 132 115 117 123
MOS-SS§ 46.08
(20.73)
43.10
(21.00)
41.57
(17.88)
–3.80
(1.45)
–6.80
(1.42)
–5.82
(1.46)
SF-36 component scores
n 132 133 134 116 118 125
PCS 29.98
(7.99)
30.72
(9.29)
32.13
(7.58)
2.03
(0.69)
5.65***
(0.68)
6.57***
(0.69)
MCS 41.34
(13.25)
42.82
(12.69)
43.24
(12.81)
0.37
(0.94)
3.52*
(0.92)
3.96*
(0.93)
SF-36 domain scores
n 132 133 134 117 118 125
Page 22 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

23
PF 28.32
(9.30)
30.54
(10.76)
31.61
(8.58)
1.55
(0.81)
4.61*
(0.79)
5.77***
(0.81)
RP 32.53
(9.66)
33.66
(10.21)
34.08
(9.67)
1.70
(0.85)
4.60*
(0.83)
6.24***
(0.85)
BP 31.95
(7.70)
31.09
(8.13)
32.55
(7.45)
2.49
(0.78)
8.05***
(0.77)
8.77***
(0.78)
GH 34.82
(8.67)
35.84
(9.50)
37.73
(9.18)
0.66
(0.64)
3.68**
(0.63)
3.52**
(0.64)
VT 38.41
(10.77)
39.71
(9.87)
40.11
(10.26)
2.20
(0.90)
6.40**
(0.89)
6.71***
(0.91)
SF 35.95
(12.39)
37.40
(13.10)
39.47
(12.11)
0.76
(0.93)
4.20*
(0.91)
5.27***
(0.92)
RE 35.52
(14.22)
37.58
(14.08)
36.75
(13.58)
–0.82
(1.12)a
3.00*
(1.10)
4.02**
(1.11)
MH 39.69
(12.66)
40.66
(11.63)
41.91
(11.99)
1.43
(0.89)
4.22*
(0.87)
4.47*
(0.88)
n 129 131 134 115 115 123
EQ-5D 0.38
(0.33)
0.38
(0.34)
0.47
(0.32)
0.03
(0.03)
0.15**
(0.03)
0.18***
(0.03)
*P < 0.05; **P < 0.001; ***P < 0.0001 versus placebo.
†Full analysis set, longitudinal model.
‡ LS mean change from baseline in HAQ-DI, pain score, and FACIT-F at month 3, and significance vs placebo
were reported previously (17) and are presented here for comparison
§Overall sleep problems score.
aN = 116.
BID = twice daily; BP = bodily pain; EQ-5D = EuroQol 5-Dimensions questionnaire; GH = general health;
LS = least squares; MCS = mental component score; MH = mental health; MOS-SS = Medical Outcomes Study-
Sleep Scale; MTX = methotrexate; PCS = physical component score; PF = physical functioning; PtGA = patient
global assessment of arthritis; RE = role emotional; RP = role physical; SD = standard deviation; SE = standard
Page 23 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

24
error; SF = social functioning; SF-36 = Medical Outcomes Study Short-Form (36-item) Health Survey Version
2 (acute); VAS = visual analog scale; VT = vitality.
Page 24 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

25
Table 2. Proportion of patients reporting improvements ≥MCID at month 3, and NNTs
(full analysis set, no imputation)
Tofacitinib
PRO MCID (threshold value)
Placebo
+ MTX
5 mg BID
+ MTX
10 mg BID
+ MTX
PtGA (VAS) Patients reporting change ≥MCID (–10), % 41.88 64.91** 59.17*
NNT 4.3 5.8
Pain (VAS) Patients reporting change ≥MCID (–10), % 39.13 69.30*** 65.55***
NNT 3.3 3.8
Physical function
(HAQ-DI)
Patients reporting change ≥MCID (0.22), % 46.61 60.68* 64.80*
NNT 7.1 5.5
Fatigue
(FACIT-F)
Patients reporting change ≥MCID (4), % 38.60 61.54** 48.00
NNT 4.4 10.6
Health-related quality of life (SF-36)
PCS Patients reporting change ≥MCID (2.5), % 49.14 67.80* 66.40*
NNT 5.4 5.8
MCS Patients reporting change ≥MCID (2.5), % 37.07 54.24* 49.60*
NNT 5.8 8.0
PF Patients reporting change ≥MCID (5), % 34.19 39.83 48.00*
NNT 17.7 7.2
RP Patients reporting change ≥MCID (5), % 30.77 38.98 47.20*
NNT 12.2 6.1
BP Patients reporting change ≥MCID (5), % 26.50 57.63*** 57.60***
NNT 3.2 3.2
GH Patients reporting change ≥MCID (5), % 22.22 35.59* 27.20
NNT 7.5 20.1
VT Patients reporting change ≥MCID (5), % 33.33 52.54* 54.40**
NNT 5.2 4.7
Page 25 of 341
John Wiley & Sons, Inc.
Arthritis Care & Research

26
SF Patients reporting change ≥MCID (5), % 42.74 51.69 56.00*
NNT 11.2 7.5
RE Patients reporting change ≥MCID (5), % 28.45 33.05 40.00
NNT 21.7 8.7
MH Patients reporting change ≥MCID (5), % 39.32 51.69 41.60
NNT 8.1 43.8
*P < 0.05, **P < 0.001, ***P < 0.0001 versus placebo.
BID = twice daily; BP = bodily pain; FACIT-F = Functional Assessment of Chronic Illness Therapy-Fatigue;
GH = general health; HAQ-DI = Health Assessment Questionnaire-Disability Index; MCS = mental component
score; MCID = minimal clinically important difference; MH = mental health; MTX = methotrexate;
NNT = number needed to treat; PCS = physical component score; PF = physical functioning;
PRO = patient-reported outcome; PtGA = patient global assessment of arthritis; RE = role emotional; RP = role
physical; SF = social functioning; SF-36 = Medical Outcomes Study Short-Form (36-item) Health Survey
Version 2 (acute); VAS = visual analog scale; VT = vitality.
Page 26 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

27
Figure legends
Figure 1. Least squares mean change (± standard error) from baseline in patient-reported
outcome scores (full analysis set, longitudinal model). Black dotted line represents the point
at which patients receiving placebo advanced to tofacitinib. Gray dotted line indicates
minimal clinically important difference. (A) PtGA; (B) Pain; (C) FACIT-F. BID = twice
daily; FACIT-F = Functional Assessment of Chronic Illness Therapy-Fatigue; LS = least
squares; MTX = methotrexate; PtGA = patient global assessment of arthritis; SE = standard
error.
Figure 2. Least squares mean change (± standard error) from baseline in SF-36 scores (full
analysis set, longitudinal model). Dotted line represents the point at which patients receiving
placebo advanced to tofacitinib. (A) SF-36 PCS; (B) SF-36 MCS. BID = twice daily;
LS = least squares; MCS = mental component score; MTX = methotrexate; PCS = physical
component score; SE = standard error; SF-36 = Medical Outcomes Study Short-Form
(36-item) Health Survey Version 2 (acute).
Figure 3. Visualization of mean overall SF-36 domain scores: (A) age- and gender-matched
norms versus weighted, combined baseline scores; (B) tofacitinib 5 mg BID, tofacitinib
10 mg BID and placebo at month 3; (C) tofacitinib 5 mg BID, tofacitinib 10 mg BID and
placebo at month 3 versus age- and gender-matched norms, and weighted, combined
baseline. Age- and gender-matched norms consist of SF-36 derived data from healthy
individuals in the US, which were selected to match the age and gender distribution of this
specific protocol population. Each spoke represents a domain, and the score for each group is
plotted along the spoke. BID, twice daily; BP = bodily pain; GH = general health;
MH = mental health; PF = physical functioning; RE = role emotional; RP = role physical;
SF = social functioning; SF-36 = Medical Outcomes Study Short-Form (36-item) Health
Page 27 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

28
Survey Version 2 (acute); US, United States; VT = vitality.
Page 28 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research
29
Figures
Figure 1. Least squares mean change (± standard error) from baseline in patient-reported
outcome scores (full analysis set, longitudinal model). Black dotted line represents the point
at which patients receiving placebo advanced to tofacitinib. Gray dotted line indicates
minimal clinically important difference. (A) PtGA; (B) Pain; (C) FACIT-F.
Page 29 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

30
Figure 2. Least squares mean change (± standard error) from baseline in SF-36 scores (full
analysis set, longitudinal model). Dotted line represents the point at which patients receiving
placebo advanced to tofacitinib. (A) SF-36 PCS; (B) SF-36 MCS.
Page 30 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research

31
Figure 3. Visualization of mean overall SF-36 domain scores: (A) age- and gender-matched
norms versus weighted, combined baseline scores; (B) tofacitinib 5 mg BID, tofacitinib
10 mg BID and placebo at month 3; (C) tofacitinib 5 mg BID, tofacitinib 10 mg BID and
placebo at month 3 versus age- and gender-matched norms, and weighted, combined
baseline.
Page 31 of 31
John Wiley & Sons, Inc.
Arthritis Care & Research
Copyright © 2022 FDOKUMEN




















