
Porcine buccal mucosa as in vitro model: Effect of biological and experimental variables
13
Porcine Buccal Mucosa as In Vitro Model: Effect of Biological and Experimental Variables UPENDRA KULKARNI, 1 RAVICHANDRAN MAHALINGAM, 1 INDIRAN PATHER, 2 XIAOLING LI, 1 BHASKARA JASTI 1 1 Department of Pharmaceutics and Medicinal Chemistry, Thomas J. Long School of Pharmacy and Health Sciences, University of the Pacific, Stockton, California 95211 2 California Northstate College of Pharmacy, 10811 International Drive, Rancho Cordova, California 95670 Received 4 February 2009; accepted 17 July 2009 Published online 8 September 2009 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/jps.21907 ABSTRACT: Porcine buccal mucosa has been used as an in vitro model to assess the potential of delivering a molecule via the transbuccal route. However, permeation studies across porcine buccal mucosa show high variability due to various experimental and biological factors. The variability associated with the use of different mucosal regions, tissue storage conditions and tissue processing methods on drug permeation was investigated in this study. The permeability of model diffusants was significantly higher in the region behind the lip when compared to the cheek region because the latter has a thicker epithelium. Porcine buccal mucosa retained its integrity in Kreb’s bicarbonate ringer solution at 48C for 24 h while many other storage conditions resulted in loss of epithelial integrity. Separation of the epithelium from underlying connective tissue either surgically or by heat treatment resulted in an epithelial thickness of approximately 150 mm. Separation of epithelium from the underlying connective tissue by heat treatment did not adversely affect its permeability and integrity characteristics. Investigation of these important biological and experimental variables provides gui- dance for conducting in vitro transbuccal permeation studies. ß 2009 Wiley-Liss, Inc. and the American Pharmacists Association J Pharm Sci 99:1265–1277, 2010 Keywords: buccal; mucosal delivery; membrane transport; permeability; physico- chemical properties INTRODUCTION The oral route is the most commonly employed route for administration of medications. Due to the limitations associated with this route, poten- tial use of other routes is being investigated for drug administration. Drug delivery via the buccal (cheek) mucosa possesses many advantages over other routes and is rapidly emerging as an alternate route for drug administration. 1–5 In buccal delivery, an adhesive patch or a tablet containing the drug could be placed in the buccal pouch allowing the absorption of the active drug across the buccal mucosa and into the blood circulation without degradation by the liver. The buccal mucosa appears to be better in terms of permeability, surface area, compliance, etc., when compared to the other mucosal and transdermal routes of delivery. Frequent exposure to food materials and rapid cell turnover make the buccal mucosa more resistant to tissue damage and irritation compared to other mucosal routes of administration. Hence, the buccal route of drug delivery is a logical alternative delivery route for drugs which undergo extensive degradation in the stomach and the liver. Ravichandran Mahalingam’s present address is Formurex, Inc., 2470 N. Wilcox Road, Stockton, CA 95215. Correspondence to: Bhaskara Jasti (Telephone: 209-946- 3162; Fax: 209-946-2410; E-mail: bjasti@pacific.edu) Journal of Pharmaceutical Sciences, Vol. 99, 1265–1277 (2010) ß 2009 Wiley-Liss, Inc. and the American Pharmacists Association JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010 1265
Transcript of Porcine buccal mucosa as in vitro model: Effect of biological and experimental variables
Porcine Buccal Mucosa as In Vitro Model:Effect of Biological and Experimental Variables
UPENDRA KULKARNI,1 RAVICHANDRAN MAHALINGAM,1 INDIRAN PATHER,2 XIAOLING LI,1 BHASKARA JASTI1
1Department of Pharmaceutics and Medicinal Chemistry, Thomas J. Long School of Pharmacy and Health Sciences,University of the Pacific, Stockton, California 95211
2California Northstate College of Pharmacy, 10811 International Drive, Rancho Cordova, California 95670
Received 4 February 2009; accepted 17 July 2009
Published online 8 September 2009 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/jps.21907
RavichandraInc., 2470 N. W
Corresponde3162; Fax: 209-
Journal of Pharm
� 2009 Wiley-Liss
ABSTRACT: Porcine buccal mucosa has been used as an in vitro model to assess thepotential of delivering a molecule via the transbuccal route. However, permeationstudies across porcine buccal mucosa show high variability due to various experimentaland biological factors. The variability associated with the use of different mucosalregions, tissue storage conditions and tissue processing methods on drug permeationwas investigated in this study. The permeability of model diffusants was significantlyhigher in the region behind the lip when compared to the cheek region because the latterhas a thicker epithelium. Porcine buccal mucosa retained its integrity in Kreb’sbicarbonate ringer solution at 48C for 24 h while many other storage conditions resultedin loss of epithelial integrity. Separation of the epithelium from underlying connectivetissue either surgically or by heat treatment resulted in an epithelial thickness ofapproximately 150mm. Separation of epithelium from the underlying connective tissueby heat treatment did not adversely affect its permeability and integrity characteristics.Investigation of these important biological and experimental variables provides gui-dance for conducting in vitro transbuccal permeation studies. � 2009 Wiley-Liss, Inc. and
the American Pharmacists Association J Pharm Sci 99:1265–1277, 2010
Keywords: buccal; mucosal delivery; m
embrane transport; permeability; physico-chemical propertiesINTRODUCTION
The oral route is the most commonly employedroute for administration of medications. Due tothe limitations associated with this route, poten-tial use of other routes is being investigated fordrug administration. Drug delivery via the buccal(cheek) mucosa possesses many advantages overother routes and is rapidly emerging as analternate route for drug administration.1–5 In
n Mahalingam’s present address is Formurex,ilcox Road, Stockton, CA 95215.nce to: Bhaskara Jasti (Telephone: 209-946-946-2410; E-mail: [email protected])
aceutical Sciences, Vol. 99, 1265–1277 (2010)
, Inc. and the American Pharmacists Association
JOURNAL OF P
buccal delivery, an adhesive patch or a tabletcontaining the drug could be placed in the buccalpouch allowing the absorption of the active drugacross the buccal mucosa and into the bloodcirculation without degradation by the liver. Thebuccal mucosa appears to be better in terms ofpermeability, surface area, compliance, etc., whencompared to the other mucosal and transdermalroutes of delivery. Frequent exposure to foodmaterials and rapid cell turnover make the buccalmucosa more resistant to tissue damage andirritation compared to other mucosal routes ofadministration. Hence, the buccal route of drugdelivery is a logical alternative delivery route fordrugs which undergo extensive degradation in thestomach and the liver.
HARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010 1265

1266 KULKARNI ET AL.
In vitro permeation studies using porcine buccalmucosa are being increasingly used to assess thepotential of a molecule to be administered by thebuccal route. Porcine buccal mucosa resembleshuman buccal mucosa in structure and perme-ability.6,7 It serves as an excellent model toexplore the feasibility of buccal delivery and tostudy the mechanism of drug transport across thebuccal mucosa. The permeation assembly can beeasily setup using different types of diffusionapparatus. The cost of conducting in vitro studiesis significantly lower than in vivo studies sinceonly a small piece of dissected buccal mucosa isused for each experiment. Sample analysis iseasier because the receiver side is a buffer solutionrather than a blood sample from in vivo studies.In vitro studies allow the control of experimentalconditions such as temperature, pH, and osmo-larity, which can be used to identify or isolate asingle factor that is responsible for variation.
Despite the above-mentioned advantages, thereare limitations and problems associated within vitro assessment. A significant variation hasbeen observed in the results of permeationexperiments across biological membranes. Inpermeation studies, reproducing observed per-meability characteristics of a diffusant is fairlydifficult. For example the permeability of 20,30-dideoxycytidine in porcine buccal mucosa hasbeen reported to be (1.75� 0.74)� 10�7 cm/s byXiang et al.8 and (4.09� 0.37)� 10�6 cm/s byShojaei et al.9 The variation in the permeabilityvalues is greater than 20 times under the differentconditions even within the same lab. It would notbe surprise to find the coefficient of variation (CV)is often between 20 and 50%, and one wouldoccasionally find CV values as high as 80% or morein the in vitro permeation studies. The variabilityin chemical, enzymatic, and instrumental ana-lyses of drugs is usually very low and can beavoided with the use of sensitive equipment andproper care. The relatively large CV observed inbuccal permeation experiment is mostly due to‘‘biological variation’’ or the lack of reproducibilityin living animals and the use of varying experi-mental conditions during such studies. It isimportant to determine the variables that areresponsible for such a high variation in per-meability experiments. Once these variables aredetermined, they can be controlled and thevariation can be minimized.
Use of different mucosal regions is a significantcontributor to the variability in permeabilitystudies. The different experimental conditions
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010
which may be likely to contribute to the variabilityin tissue permeability include different tissuestorage conditions and methods of tissue proces-sing before permeation studies.10–15 Some of thesevariables may also affect tissue integrity andhence the permeability of the drug. So far, theeffects of these variables have not been exploredsystematically in transbuccal permeation studies.It is essential to identify the contribution ofdifferent variables to the differences in thepermeability results and optimize the in vitropermeability conditions in order to obtain reliableand consistent permeability values. The objectiveof this research is to evaluate the influence ofthe mucosal region and the storage conditions onthe in vitro permeation of drugs across porcinebuccal mucosa as well as the methods of buccaltissue preparation—the surgical method and theheat separation method.
MATERIALS AND METHODS
Materials
Buspirone, bupivacaine, antipyrine, and caffeinewere obtained from Sigma-Aldrich (St. Louis, MO)and were used as model drugs since they havedifferent lipophilicities and physicochemical prop-erties.16 Tissue integrity was assessed by FD-20(fluorescein isothiocyanate (FITC)-labeled dextranof molecular weight 20,000 Da) which is an estab-lished integrity marker for the buccal mucosa.Acetonitrile and methanol were obtained fromVWR (West Chester, PA) and were of high perfor-mance liquid chromatography (HPLC) grade.
Tissue Preparation
Buccal mucosa was obtained from a local ranch(Long Ranch, Inc., Manteca, CA) after the pigswere freshly sacrificed. The mucosa was trans-ported to the laboratory in isotonic phosphatebuffer (pH 7.4) and used within 2 h of animalsacrifice. The majority of the underlying connec-tive tissue was removed with the help of a scalpelblade and then the remaining buccal mucosawas carefully trimmed with the help of surgicalscissors to a uniform thickness of about 500mm.The thickness of the tissues was measured with adigital micrometer and recorded. This helped tominimize variations between tissue specimens.
DOI 10.1002/jps

PORCINE BUCCAL MUCOSA AS IN VITRO MODEL 1267
Permeation Studies
The buccal mucosa was mounted on vertical Franzdiffusion cells in such a way that the epitheliumfaced the donor chamber and the connective tissueregion faced the receiver chamber. The exposedsurface area of the buccal mucosa for thepermeation studies was 0.76 cm2. A constanttemperature of 378C was maintained throughoutthe experiment in both the receiver and donorchambers to mimic the in vivo environment. Thiswas accomplished by mounting the diffusionassembly setup in a 378C walk-in incubator room.The tissues were allowed to equilibrate withbuffer for 15 min before commencement of thedrug permeability experiment. The permeabilityexperiments were carried out using phosphate-buffered saline (PBS) with pH 7.4 in the receiverchamber and known concentrations of drugsolutions at pH 6.8 in the donor chamber to mimicthe in vivo physiological pH conditions.17 Thereceiver chamber was filled with 5 mL of PBSwhile 1 mL of the drug solution was charged intothe donor chamber. Permeation studies werecarried out for up to 4 h and 1 mL samples werewithdrawn from the receiver chamber every30 min. In the case of bupivacaine, the sampleswere collected every hour for 8 h. At each samplingpoint, 1 mL of fresh buffer solution (pH 7.4) wasadded to the receiver chamber to compensate forthe volume of solution removed. All experimentswere conducted in triplicate. The steady state fluxof the model diffusants across the buccal mucosawas calculated from the slope of the linear portionof the cumulative amount permeated versus timeplots.
The apparent permeability, also known as thepermeability coefficient, was then calculated usingthe following equation:
P ¼ Jss
DC(1)
where Jss is the steady state flux and DC theconcentration gradient between the two surfacesof the membrane.
Table 1. Storage Conditions of Buccal Mucosa
Storage Condition
Phosphate-buffered saline, pH 7.4Kreb’s bicarbonate ringer, pH 7.4Dry, wrapped in aluminumCryoprotected in 20% glycerol solution
DOI 10.1002/jps JOU
Effect of Mucosal Region
Porcine buccal mucosa was carefully isolated fromthe rest of the connective tissue by scalpel/blade.The mucosa was then sliced from two differentsites of the buccal tissue, viz. the cheek region andthe region behind the lip. This mucosa was thentrimmed to a uniform thickness of 500mm usingsurgical scissors. The thickness was measuredusing a digital micrometer to achieve the requireduniform thickness among all mucosal samples.The tissues were processed within 2 h of animalslaughter and were then mounted between thetwo-halves of diffusion cells for permeationstudies.
Effect of Storage Conditions
The buccal mucosa specimens were trimmed to500mm thickness using surgical scissors andstored at the following conditions prior to thepermeation studies (Tab. 1).
A 20% glycerol in isotonic saline solution wasused as a cryoprotectant. The buccal tissues, afterbeing trimmed to a uniform thickness of 500mm,were immersed in the cryoprotectant solution for30 min to allow the solution to permeate thetissues. The tissues were then wrapped in alumi-num foil and placed in a desiccator to minimizemoisture contact. Alternatively, the tissues werefrozen in the cryoprotectant solution withoutdrying in a desiccator. Separate tissue sampleswere designated for storage at each of the con-ditions and times noted in Table 1. After storingfor the designated time, and prior to conductingthe diffusion experiments, the tissues werethawed to room temperature to minimize tissuedamage. The thawed tissues were then immersedin freshly prepared PBS (pH 7.4) to remove theresidual cryoprotective agent from the tissues.
The stored tissues were equilibrated withfreshly prepared PBS (pH 7.4) at room tempera-ture before mounting them on the Franz diffusioncells. Diffusion experiments with buspirone,
Temperature (8C) Storage Periods
4 6, 24, and 48 h4 6, 24, and 48 h
�20 6, 24, and 48 h�20 6, 24, and 48 h
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010

1268 KULKARNI ET AL.
antipyrine, and caffeine were conducted toobserve the effect of storage conditions on thepermeability rate. A change in the permeabilityof the stored tissues, when compared to freshtissues, would indicate a loss of integrity due tothe storage conditions.
Effect of Processing Method of Buccal Epithelium
Porcine buccal mucosa was carefully isolated fromthe rest of the connective tissue by scalpel/blade.Using surgical scissors, the mucosa was trimmedto a uniform thickness (�250mm) until theconnective tissue was completely removed. Forheat separation of the epithelium, the mucosaltissues were dipped for approximately 1 min insaline solution (0.9% NaCl) warmed to 608C. Thenthe connective tissue was peeled off from themucosa to obtain the heat-separated epithelium.The processing of the tissues was completedwithin 2 h of animal slaughter and then theepithelia were mounted on the Franz diffusioncells for permeation studies.
Tissue Integrity Studies
FITC-labeled dextran of molecular weight20,000 Da (FD-20) has been established as anintegrity marker for porcine buccal mucosa.10,18,19
To test whether the buccal tissues retain theirintegrity after various storage conditions anddifferent processing methods of the buccal epithe-lia, permeation studies were conducted using FD-20 at 100mg/mL concentration. A significantlyhigher permeation of the marker with respect topermeation in the control tissue would indicate aloss of integrity. Samples from the receiverchamber were collected every 30 min for 4 h.FD-20 samples were quantified using a Shimadzuspectrofluorimeter. An excitation wavelength of498 nm and emission wavelength of 518 nm wasused to quantify FD-20. All the permeationexperiments were conducted in triplicate.
Quantification of Model Diffusants
Known concentrations of model diffusants (anti-pyrine 50 mg/mL, buspirone 0.5 mg/mL, bupiva-caine 1 mg/mL, and caffeine 20 mg/mL) wereprepared using PBS at pH 6.8 and used as donorformulations. Steady state flux of model diffu-sants across buccal mucosa was calculated from
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010
the slope of the linear portion of the cumulativeamount permeated versus time plots. Concentra-tion of the model diffusants in the permeationsamples was quantified using methodologydescribed earlier.16 A HPLC system (consistingof Waters 590 HPLC pump, WISP 715 autosampler, Shimadzu SPD-M10AVP UV detector,and EZ chromatography software) was usedfor the analysis. A reverse phase C18—column(length 250 mm, thickness of capillary bore 5mm)was used to elute the diffusants. The HPLCconditions were developed and optimized foranalysis of individual diffusants.1 The assayrange for the four diffusants was established onthe basis of relationship between the peak areasand the diffusant concentrations. The assay rangebracketed the concentration of all permeationsamples. Excellent correlation was seen (R2¼ 0.99)between the peak area and drug concentrations inthe four diffusants.
A Shimadzu RF-5301 PC spectrofluorimeter(Columbia, MD) was used to quantify the FD-20marker for the tissue integrity studies. Anexcitation wavelength of 498 nm and emissionwavelength of 518 nm was used. A calibrationcurve was established using the FD-20 standardsolutions in the range of 0.02–2mg/mL. Theexperiments were conducted in triplicate.
Data Analysis
The transbuccal permeability data and lag timewere presented as mean or mean and standarderror of mean (SEM) for each variable studied anddiffusant (n¼ 3 replicates per experimental con-dition). For statistical analysis the software Excel20021 (Microsoft Co., Redmond, WA) was used.Statistical differences of permeability values fordifferent experimental and biological variableswere determined using the analysis of variance(one-way ANOVA). p< 0.05 was considered aslevel of significance.
Histological Examination
The histological changes in the buccal tissuesof differing mucosal thicknesses were evaluatedby sectioning carefully and fixing in vials con-taining 10% buffered formalin for 1 day at roomtemperature. Tissue samples were successivelydehydrated with increasing series of ethanolconcentrations—30%, 50%, 70% and absolutealcohol. This was followed by immersing in xylene
DOI 10.1002/jps

PORCINE BUCCAL MUCOSA AS IN VITRO MODEL 1269
and finally embedding in paraffin. Using amicrotome (Model 820, American Optical Co.,Buffalo, NY), thin slices (5mm) of the paraffincubes were prepared and then stained with HarrisHematoxylin and Eosin Y Stain. The stained sliceswere mounted on glass slides and were examinedunder a Nikon Eclipse E800 light microscope withplanfluor objective lenses (Nikon, Inc., Melville,NY). Two microscope slides per tissue samplewere prepared and examined. An Optronics DEI-750 three-chip CCD camera (Optronics Engineer-ing, Goleta, CA) was used to capture images.Images were processed by Image-Pro Plus soft-ware (Media Cybernetics, Silver Spring, MD).
RESULTS
Effect of Mucosal Region
All the model permeants showed significantlyhigher permeability in the region behind the lipsin comparison to the cheek region of the full thick-ness (500mm) buccal mucosa (Tab. 2) (ANOVA,p< 0.05). When the permeability experimentswere conducted with the epithelia only (allconnective tissue removed), the region behindthe lip again showed significantly higher perme-ability than the cheek region (Tab. 3) (ANOVA,p< 0.05).
When measured with a digital micrometer, thethickness of the epithelium in the region behindthe lip was about 170–200mm whereas thethickness of the epithelium in the cheek regionwas 250–280mm. The histological examination ofthe full thickness tissue specimens (epitheliumand connective tissue) showed that the thicknessof the epithelium is greater in the cheek regionwhen compared to that in the region behind the lip(see Fig. 1) which is annotated to show theepithelial and connective tissue regions. Both theimages were taken at the same magnification(125�).
Table 2. Permeability in the Full Thickness Mucosa–Beh
Mucosal Region Buspirone Bupivacai
Cheek (1.54� 0.04)� 10�5� (1.68� 0.04)�Behind-lip (1.74� 0.01)� 10�5� (1.97� 0.02)�
�p< 0.05, ANOVA (n¼ 3).
DOI 10.1002/jps JOU
Effect of Storage Conditions
The permeability of the model diffusants stored atdifferent conditions is given in Table 4. As shownin the table, the permeability of the buccalmucosae stored either in PBS at 48C for 6 h orin KBR at 48C for 24 h was similar to thepermeability of fresh buccal mucosa. The perme-ability of buccal mucosae stored in all otherconditions mentioned in the table was signifi-cantly higher than the permeability of fresh tissue(ANOVA, p< 0.05).
The permeability of all model permeantsincreased significantly (ANOVA, p< 0.05) whenthe tissues were stored at �208C for 6 h undereither of the following conditions: (a) wrapped inaluminum foil and frozen without medium; or (b)frozen in PBS buffer. The permeability and theintegrity of the buccal mucosa was also compro-mised when stored in Krebs bicarbonate ringer(KBR) for 48 h or in PBS for 24 h at pH 7.4 in arefrigerator at 48C. Cryoprotection with 20%glycerin in isotonic saline also compromisedthe integrity and permeability characteristics ofthe porcine buccal mucosa. Whether the tissueswere (a) pretreated with the cryoprotectant andwrapped in aluminum foil; or (b) immersed in thecryoprotectant solution and frozen, the tissueslost their barrier integrity resulting in increasedpermeability of the model drugs.
The cumulative amounts of FD-20 permeatedafter 4 h in buccal tissues stored at differentconditions are shown in Figure 2. Permeation ofmore than 0.1% of the integrity marker in thereceiver chamber over 4 h indicates a loss of tissueintegrity.9,20 As shown in Figure 2, the FD-20permeation was lower than 0.1% when the tissueswere stored in PBS for 6 h or in KBR for 24 h at48C. All other storage conditions led to an increasein FD-20 permeation (ANOVA, p< 0.05).
Light microscopic examination of buccalmucosa obtained after storage at various condi-tions is shown in Figure 3. The tissue specimenswith 6-h storage in PBS (Fig. 3b) and 24-h storage
ind-Lip Region and Cheek Region
ne Antipyrine Caffeine
10�5� (3.15� 0.5)� 10�6� (6.13� 0.75)� 10�6�
10�5� (5.75� 0.3)� 10�6� (8.15� 0.76)� 10�6�
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010
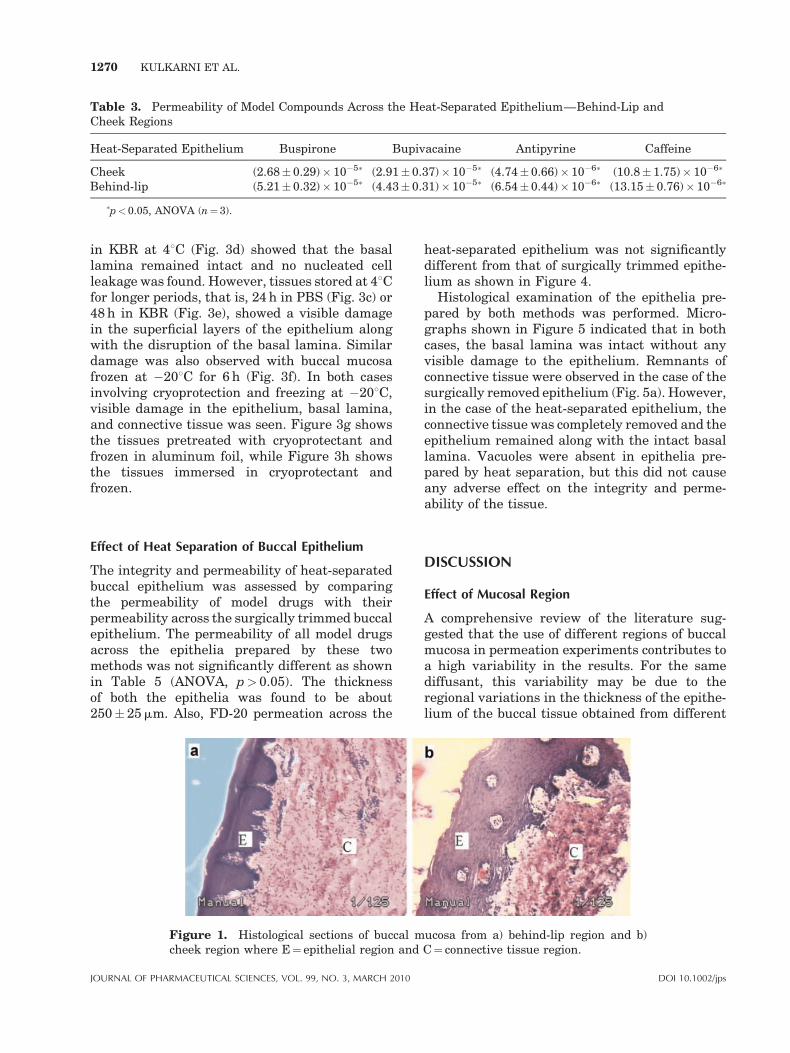
Table 3. Permeability of Model Compounds Across the Heat-Separated Epithelium—Behind-Lip andCheek Regions
Heat-Separated Epithelium Buspirone Bupivacaine Antipyrine Caffeine
Cheek (2.68� 0.29)� 10�5� (2.91� 0.37)� 10�5� (4.74� 0.66)� 10�6� (10.8� 1.75)� 10�6�
Behind-lip (5.21� 0.32)� 10�5� (4.43� 0.31)� 10�5� (6.54� 0.44)� 10�6� (13.15� 0.76)� 10�6�
�p<0.05, ANOVA (n¼3).
1270 KULKARNI ET AL.
in KBR at 48C (Fig. 3d) showed that the basallamina remained intact and no nucleated cellleakage was found. However, tissues stored at 48Cfor longer periods, that is, 24 h in PBS (Fig. 3c) or48 h in KBR (Fig. 3e), showed a visible damagein the superficial layers of the epithelium alongwith the disruption of the basal lamina. Similardamage was also observed with buccal mucosafrozen at �208C for 6 h (Fig. 3f). In both casesinvolving cryoprotection and freezing at �208C,visible damage in the epithelium, basal lamina,and connective tissue was seen. Figure 3g showsthe tissues pretreated with cryoprotectant andfrozen in aluminum foil, while Figure 3h showsthe tissues immersed in cryoprotectant andfrozen.
Effect of Heat Separation of Buccal Epithelium
The integrity and permeability of heat-separatedbuccal epithelium was assessed by comparingthe permeability of model drugs with theirpermeability across the surgically trimmed buccalepithelium. The permeability of all model drugsacross the epithelia prepared by these twomethods was not significantly different as shownin Table 5 (ANOVA, p> 0.05). The thicknessof both the epithelia was found to be about250� 25mm. Also, FD-20 permeation across the
Figure 1. Histological sections of buccal mcheek region where E¼ epithelial region and
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010
heat-separated epithelium was not significantlydifferent from that of surgically trimmed epithe-lium as shown in Figure 4.
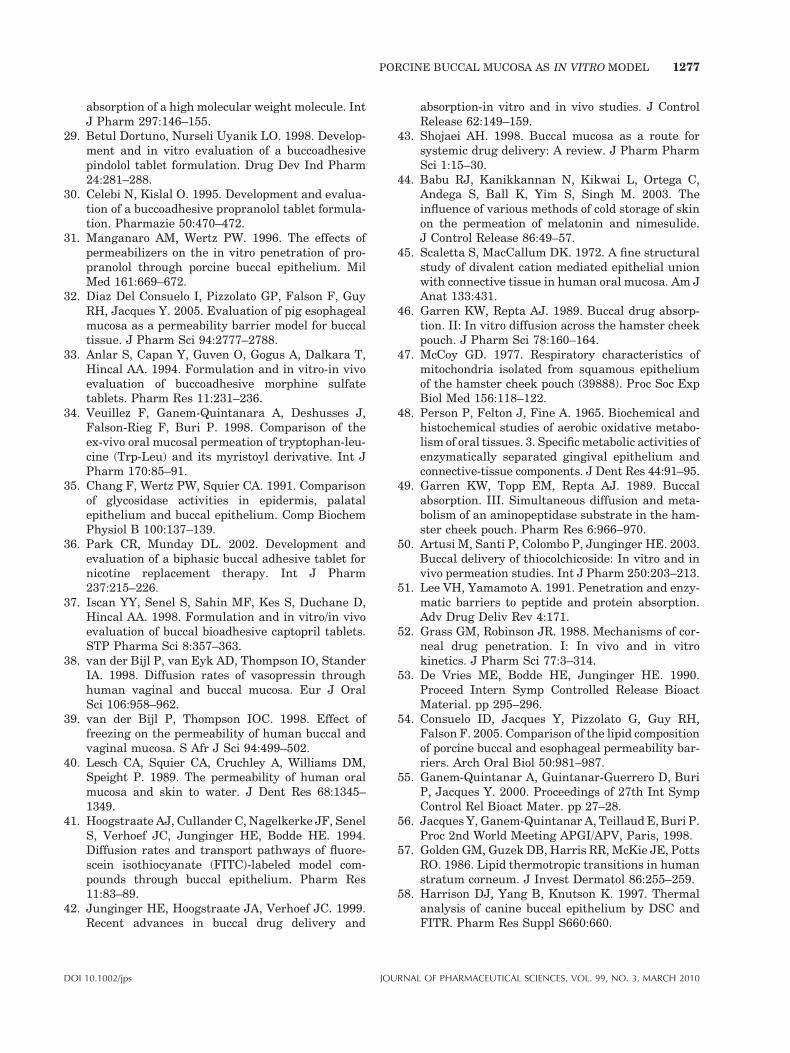
Histological examination of the epithelia pre-pared by both methods was performed. Micro-graphs shown in Figure 5 indicated that in bothcases, the basal lamina was intact without anyvisible damage to the epithelium. Remnants ofconnective tissue were observed in the case of thesurgically removed epithelium (Fig. 5a). However,in the case of the heat-separated epithelium, theconnective tissue was completely removed and theepithelium remained along with the intact basallamina. Vacuoles were absent in epithelia pre-pared by heat separation, but this did not causeany adverse effect on the integrity and perme-ability of the tissue.
DISCUSSION
Effect of Mucosal Region
A comprehensive review of the literature sug-gested that the use of different regions of buccalmucosa in permeation experiments contributes toa high variability in the results. For the samediffusant, this variability may be due to theregional variations in the thickness of the epithe-lium of the buccal tissue obtained from different
ucosa from a) behind-lip region and b)C¼ connective tissue region.
DOI 10.1002/jps
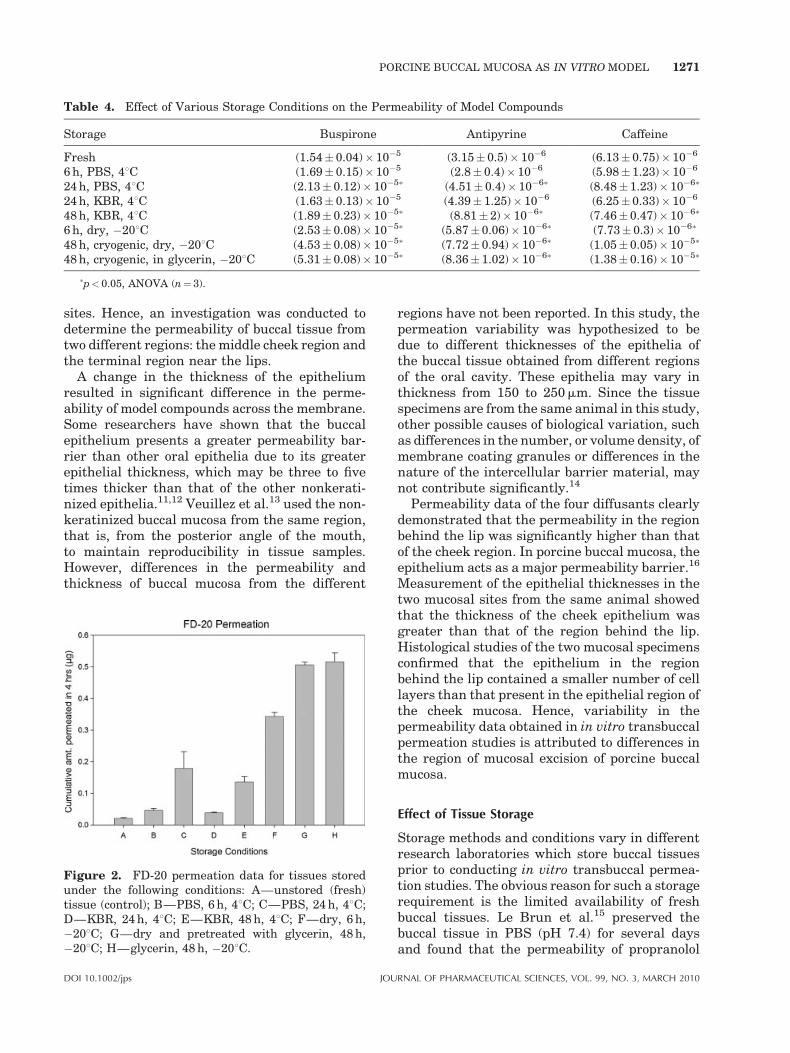
Table 4. Effect of Various Storage Conditions on the Permeability of Model Compounds
Storage Buspirone Antipyrine Caffeine
Fresh (1.54� 0.04)� 10�5 (3.15� 0.5)� 10�6 (6.13� 0.75)� 10�6
6 h, PBS, 48C (1.69� 0.15)� 10�5 (2.8� 0.4)� 10�6 (5.98� 1.23)� 10�6
24 h, PBS, 48C (2.13� 0.12)� 10�5� (4.51� 0.4)� 10�6� (8.48� 1.23)� 10�6�
24 h, KBR, 48C (1.63� 0.13)� 10�5 (4.39� 1.25)� 10�6 (6.25� 0.33)� 10�6
48 h, KBR, 48C (1.89� 0.23)� 10�5� (8.81� 2)� 10�6� (7.46� 0.47)� 10�6�
6 h, dry, �208C (2.53� 0.08)� 10�5� (5.87� 0.06)� 10�6� (7.73� 0.3)� 10�6�
48 h, cryogenic, dry, �208C (4.53� 0.08)� 10�5� (7.72� 0.94)� 10�6� (1.05� 0.05)� 10�5�
48 h, cryogenic, in glycerin, �208C (5.31� 0.08)� 10�5� (8.36� 1.02)� 10�6� (1.38� 0.16)� 10�5�
�p< 0.05, ANOVA (n¼ 3).
PORCINE BUCCAL MUCOSA AS IN VITRO MODEL 1271
sites. Hence, an investigation was conducted todetermine the permeability of buccal tissue fromtwo different regions: the middle cheek region andthe terminal region near the lips.
A change in the thickness of the epitheliumresulted in significant difference in the perme-ability of model compounds across the membrane.Some researchers have shown that the buccalepithelium presents a greater permeability bar-rier than other oral epithelia due to its greaterepithelial thickness, which may be three to fivetimes thicker than that of the other nonkerati-nized epithelia.11,12 Veuillez et al.13 used the non-keratinized buccal mucosa from the same region,that is, from the posterior angle of the mouth,to maintain reproducibility in tissue samples.However, differences in the permeability andthickness of buccal mucosa from the different
Figure 2. FD-20 permeation data for tissues storedunder the following conditions: A—unstored (fresh)tissue (control); B—PBS, 6 h, 48C; C—PBS, 24 h, 48C;D—KBR, 24 h, 48C; E—KBR, 48 h, 48C; F—dry, 6 h,�208C; G—dry and pretreated with glycerin, 48 h,�208C; H—glycerin, 48 h, �208C.
DOI 10.1002/jps JOU
regions have not been reported. In this study, thepermeation variability was hypothesized to bedue to different thicknesses of the epithelia ofthe buccal tissue obtained from different regionsof the oral cavity. These epithelia may vary inthickness from 150 to 250mm. Since the tissuespecimens are from the same animal in this study,other possible causes of biological variation, suchas differences in the number, or volume density, ofmembrane coating granules or differences in thenature of the intercellular barrier material, maynot contribute significantly.14
Permeability data of the four diffusants clearlydemonstrated that the permeability in the regionbehind the lip was significantly higher than thatof the cheek region. In porcine buccal mucosa, theepithelium acts as a major permeability barrier.16
Measurement of the epithelial thicknesses in thetwo mucosal sites from the same animal showedthat the thickness of the cheek epithelium wasgreater than that of the region behind the lip.Histological studies of the two mucosal specimensconfirmed that the epithelium in the regionbehind the lip contained a smaller number of celllayers than that present in the epithelial region ofthe cheek mucosa. Hence, variability in thepermeability data obtained in in vitro transbuccalpermeation studies is attributed to differences inthe region of mucosal excision of porcine buccalmucosa.
Effect of Tissue Storage
Storage methods and conditions vary in differentresearch laboratories which store buccal tissuesprior to conducting in vitro transbuccal permea-tion studies. The obvious reason for such a storagerequirement is the limited availability of freshbuccal tissues. Le Brun et al.15 preserved thebuccal tissue in PBS (pH 7.4) for several daysand found that the permeability of propranolol
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010
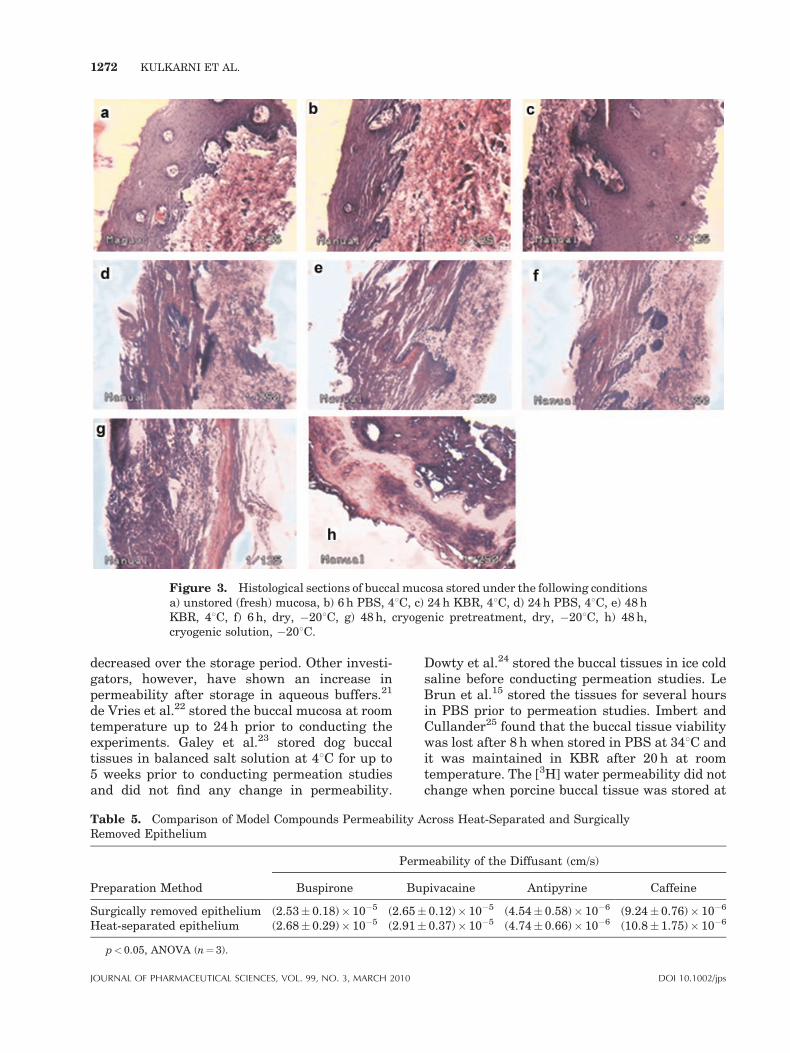
Figure 3. Histological sections of buccal mucosa stored under the following conditionsa) unstored (fresh) mucosa, b) 6 h PBS, 48C, c) 24 h KBR, 48C, d) 24 h PBS, 48C, e) 48 hKBR, 48C, f) 6 h, dry, �208C, g) 48 h, cryogenic pretreatment, dry, �208C, h) 48 h,cryogenic solution, �208C.
1272 KULKARNI ET AL.
decreased over the storage period. Other investi-gators, however, have shown an increase inpermeability after storage in aqueous buffers.21
de Vries et al.22 stored the buccal mucosa at roomtemperature up to 24 h prior to conducting theexperiments. Galey et al.23 stored dog buccaltissues in balanced salt solution at 48C for up to5 weeks prior to conducting permeation studiesand did not find any change in permeability.
Table 5. Comparison of Model Compounds Permeability ARemoved Epithelium
Preparation Method
Perm
Buspirone Bu
Surgically removed epithelium (2.53� 0.18)� 10�5 (2.65�Heat-separated epithelium (2.68� 0.29)� 10�5 (2.91�
p<0.05, ANOVA (n¼ 3).
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010
Dowty et al.24 stored the buccal tissues in ice coldsaline before conducting permeation studies. LeBrun et al.15 stored the tissues for several hoursin PBS prior to permeation studies. Imbert andCullander25 found that the buccal tissue viabilitywas lost after 8 h when stored in PBS at 348C andit was maintained in KBR after 20 h at roomtemperature. The [3H] water permeability did notchange when porcine buccal tissue was stored at
cross Heat-Separated and Surgically
eability of the Diffusant (cm/s)
pivacaine Antipyrine Caffeine
0.12)� 10�5 (4.54� 0.58)� 10�6 (9.24� 0.76)� 10�6
0.37)� 10�5 (4.74� 0.66)� 10�6 (10.8� 1.75)� 10�6
DOI 10.1002/jps
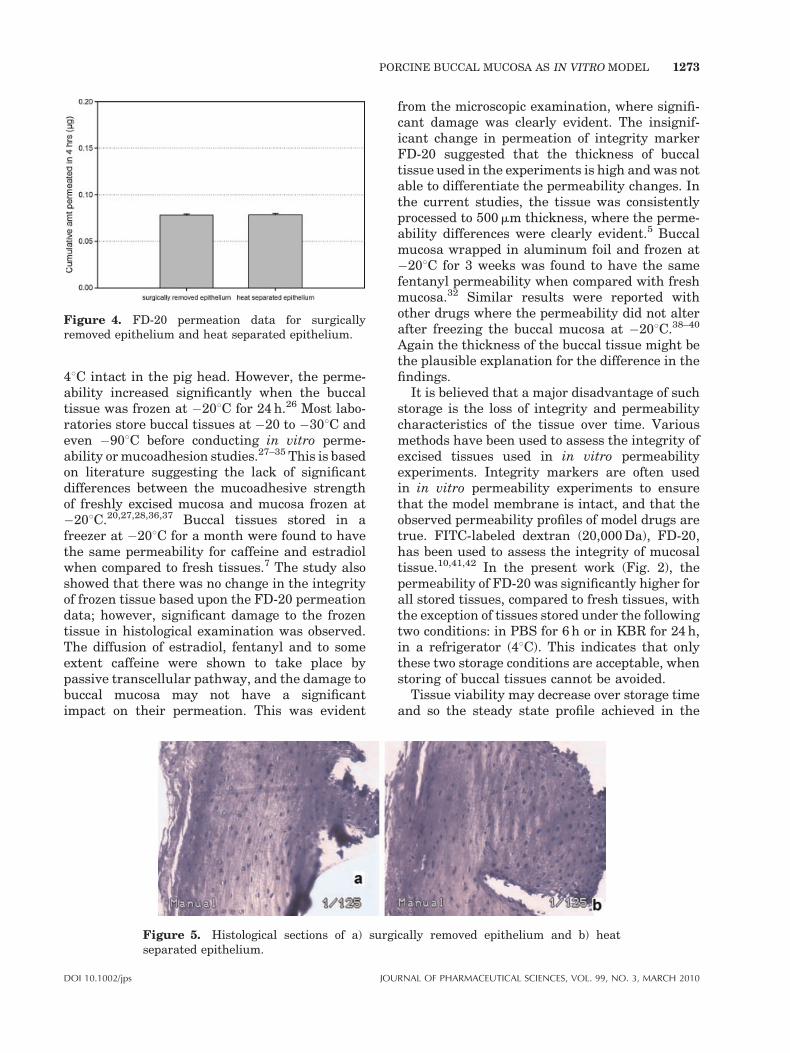
Figure 4. FD-20 permeation data for surgicallyremoved epithelium and heat separated epithelium.
PORCINE BUCCAL MUCOSA AS IN VITRO MODEL 1273
48C intact in the pig head. However, the perme-ability increased significantly when the buccaltissue was frozen at �208C for 24 h.26 Most labo-ratories store buccal tissues at �20 to �308C andeven �908C before conducting in vitro perme-ability or mucoadhesion studies.27–35 This is basedon literature suggesting the lack of significantdifferences between the mucoadhesive strengthof freshly excised mucosa and mucosa frozen at�208C.20,27,28,36,37 Buccal tissues stored in afreezer at �208C for a month were found to havethe same permeability for caffeine and estradiolwhen compared to fresh tissues.7 The study alsoshowed that there was no change in the integrityof frozen tissue based upon the FD-20 permeationdata; however, significant damage to the frozentissue in histological examination was observed.The diffusion of estradiol, fentanyl and to someextent caffeine were shown to take place bypassive transcellular pathway, and the damage tobuccal mucosa may not have a significantimpact on their permeation. This was evident
Figure 5. Histological sections of a) surgseparated epithelium.
DOI 10.1002/jps JOU
from the microscopic examination, where signifi-cant damage was clearly evident. The insignif-icant change in permeation of integrity markerFD-20 suggested that the thickness of buccaltissue used in the experiments is high and was notable to differentiate the permeability changes. Inthe current studies, the tissue was consistentlyprocessed to 500mm thickness, where the perme-ability differences were clearly evident.5 Buccalmucosa wrapped in aluminum foil and frozen at�208C for 3 weeks was found to have the samefentanyl permeability when compared with freshmucosa.32 Similar results were reported withother drugs where the permeability did not alterafter freezing the buccal mucosa at �208C.38–40
Again the thickness of the buccal tissue might bethe plausible explanation for the difference in thefindings.
It is believed that a major disadvantage of suchstorage is the loss of integrity and permeabilitycharacteristics of the tissue over time. Variousmethods have been used to assess the integrity ofexcised tissues used in in vitro permeabilityexperiments. Integrity markers are often usedin in vitro permeability experiments to ensurethat the model membrane is intact, and that theobserved permeability profiles of model drugs aretrue. FITC-labeled dextran (20,000 Da), FD-20,has been used to assess the integrity of mucosaltissue.10,41,42 In the present work (Fig. 2), thepermeability of FD-20 was significantly higher forall stored tissues, compared to fresh tissues, withthe exception of tissues stored under the followingtwo conditions: in PBS for 6 h or in KBR for 24 h,in a refrigerator (48C). This indicates that onlythese two storage conditions are acceptable, whenstoring of buccal tissues cannot be avoided.
Tissue viability may decrease over storage timeand so the steady state profile achieved in the
ically removed epithelium and b) heat
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010

1274 KULKARNI ET AL.
in vitro experiment using stored tissues maybe different from that observed in fresh, viabletissue. Various methods have been used to assessthe viability of excised tissues used in in vitropermeability experiments. Enzymatic methodssuch as the MTT assay have been used to evaluatetissue viability.18 However, Nicolazzo et al. foundinconsistency between results from the MTTassay and histological evaluation of frozen buccalmucosa. Although histological studies showedsignificant damage to the frozen mucosa, theMTT assay failed to show cell death because theactivity of the enzyme tetrazolium reductase wasnot affected by the freezing process.18 Thissuggests that the MTT assay cannot be used asan indicator of tissue viability and hence histolo-gical evaluation is very important in order toassess the viability of porcine buccal mucosa. Themost meaningful method to assess tissue viabilityis to conduct the actual permeability experi-ment.14,43 If the permeability of the stored tissueis similar to the permeability of fresh tissue whentested with a model drug, then the stored tissueis considered to be viable for the purpose ofconducting further permeability experiments.
The storage condition of tissues employed formucoadhesion purposes are different than storageconditions employed for permeation studies.In the case of mucoadhesion studies that areperformed with a tensile stress tester or a textureanalyzer, the storage of the tissues does notdamage the mucin layer that covers the epithe-lium. The integrity of the epithelial cells is notcrucial. However, in case of buccal permeationstudies integrity of the epithelium is most criticalfactor to obtain reliable results. Hence storagetimes and conditions used for mucoadhesionstudies may not be suitable for permeabilitystudies.
The influence of different storage conditionsused by different investigators in the buccal per-meation studies was investigated in the presentstudy. The duration for which buccal mucosaretains its integrity and permeability character-istics was determined. The studies were con-ducted with three model diffusants—buspirone,antipyrine, and caffeine. Bupivacaine shows ahigh lag time of 4 h and in order to achieve asteady state flux, its permeation needs to bedetermined over 8 h. Since the previous studiesin our laboratory indicated some loss of tissueintegrity beyond 8 h, the effect of storage condi-tions on bupivacaine’s permeability was notassessed. The results showed that the perme-
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010
ability characteristics of the buccal tissues weremaintained when they were stored for up to 6 h inPBS at 48C (Tab. 4). Similarly, the permeabilitycharacteristics of the tissue were maintained for alonger time (24 h) when the tissues were stored inKBR at 48C. A plausible reason for this is that theglucose in KBR nourishes the tissue. The influ-ence of cryoprotectant on retaining tissue integ-rity and viability was also studied. There is noreported literature on buccal tissue being storedwith a cryoprotective agent. Although the perme-ability of skin stored in a cryoprotective agent,viz. glycerol at �208C, did not change for up to60 days,44 the results of the present study indicatethat freezing with a cryoprotective agent (gly-cerol) damaged the integrity of the buccal tissuesin 48 h. Hence it would seem that the use of acryoprotective agent for buccal tissue storage in afreezer is not viable.
A histological evaluation was conducted toreveal any significant morphological changes inthe buccal tissues stored under different con-ditions. The microscopic examinations revealedsimilar trends as observed in the tissue perme-ability and integrity studies, with the tissuesrefrigerated in PBS and KBR for 6 and 24 h,respectively, showing less damage in cellularlayers as compared to tissues maintained underother storage conditions. This shows that KBRmaintained the buccal tissue integrity for a longerperiod than PBS.
The use of KBR in place of PBS for storage ofmucosal tissue seems more appropriate from thisdata and is in agreement with the results seen byImbert and Cullander.25 For reliable evaluationof in vitro permeability, use of fresh buccaltissues was found to be the best. If preservationis absolutely necessary, KBR seems to be theoptimal choice for storage. This is an importantfinding and provides guidance on storage of buccaltissues without compromising the integrity andpermeability characteristics. This finding alsosuggests that perhaps KBR might be a moreappropriate buffer medium for permeabilityexperiments than PBS.
Effect of Heat Separation of Buccal Epithelium
The connective tissue, like a stagnant layer,may significantly affect the permeability of thediffusant.7,19 Therefore, successful removal of theconnective tissue is essential to minimize thevariability between the tissue specimens and,hence, of the permeability measurements. Since
DOI 10.1002/jps

PORCINE BUCCAL MUCOSA AS IN VITRO MODEL 1275
the procedure of removing connective tissue withsurgical scissors is time consuming and requiresskill and patience, many researchers have devel-oped chemical,7,21,45 thermal,7 and enzymaticmethods (such as the use of collagenase46–49) forteasing away the buccal epithelium from theunderlying connective tissue. Mechanical sepa-ration with a dermatome7,50 or other surgicalinstrument18,26 was also tried. However, thedermatome may damage the tissue and renderit fragile.21 Mechanical separation with a derma-tome may also cut through the papillae,21 whilesurgical separation with scissors and forceps istechnically difficult and time-consuming. Also, thetissue needs to be frozen prior to dermatomiza-tion, resulting in changes to the integrity andpermeability characteristics of the buccal mucosa.
Some other methods utilize plastic adherenttapes or EDTA for stripping.15,21 In the case ofEDTA splitting, the tissues are incubated for up to50 min at 608C in 20 mM EDTA disodium salt inPBS (pH 7.4).15,21 The epithelium is then peeledoff from the connective tissue. These treatmentsmay substantially alter the permeability proper-ties of the buccal mucosa. Although Le Brun et al.have reported that there was no structuraldamage to the buccal mucosa, as seen by lightor electron microscopy, after EDTA treatment,15
other investigators have reported contrastingfindings. In fact, many chemical agents usedfor the removal of connective tissue from theepithelium (such as EDTA), have been shown toenhance drug absorption across the biologicalmembrane.51–53 An enzymatic treatment methodwas used to separate buccal epithelium from theconnective tissue in hamster pouch tissue.47 Itshould be noted that the rate limiting barrier inthe hamster pouch is a keratin layer. Althoughcollagenase did not affect the keratin layer, it ispossible that such an enzymatic treatment wouldaffect the viable portion of the epithelium.
Often buccal permeation studies have beenconducted using buccal epithelia after heattreating the tissues in saline solution at 608Cfor 1 min.32,54–56 The histological examinationshows that separation takes place at the basallayer without any compromise to the epithelialintegrity.32 Some laboratories also use the buccaltissues from pigs that have undergone postmortem heat treatment for 4 min in the slaughter-house.18,19 It has been shown that this treatmentdoes not affect epithelial morphology or perme-ability.18 Some researchers even treat the buccalmucosa at the higher temperature of 708C in
DOI 10.1002/jps JOU
saline solution.27,28,55 This helps with easyremoval of the connective tissue. In yet anothermethod, the epithelium was removed from theconnective tissue by holding an aluminum cylin-der, heated to 608C, close to the epithelialsurface.35 The use of higher temperatures mayraise concerns about the possibility of transitionsin lipid structure and organization, which areknown to occur in the skin’s stratum corneum.57
However, data from the literature using buccalmucosa from dogs suggest that irreversible effectsonly occur above 688C.58 Hence, 608C appears tobe a safe temperature at which to carry outseparation of the epithelium from the connectivetissue.
A comparison of the permeability, and theintegrity, of buccal mucosa prepared by heatseparation and surgical trimming conducted inthis study. The permeability of the model diffu-sants and the integrity marker FD-20 did notchange significantly in tissues processed using thetwo methods. Heat separation is easy and timeefficient when compared to surgical trimming.Additionally, complete and uniform removal ofconnective tissue was not achieved by surgicaltrimming as shown in the photomicrographs(Fig. 5).
From these studies, heat-separated epitheliumseems to have a potential to be used as an in vitromodel membrane to conduct transbuccal permea-tion studies.
CONCLUSION
The permeability of the model diffusants isaffected by the site of excision of the buccalmucosa used in permeation studies. The regionbehind the lip has lower epithelial thicknesswhich results in a higher permeability of modeldiffusants when compared to the middle-cheekregion. For assessing drug permeability in vitro,the appropriate storage time would be up to 24 h inKBR at 48C. Heat separation of buccal epitheliumdid not adversely affect the permeability andintegrity characteristics of the porcine buccalepithelium. While conducting in vitro permeabil-ity studies, use of fresh tissues and the sameregion of buccal mucosa are recommended.
ACKNOWLEDGMENTS
The authors wish to thank Long Ranch, Inc.(Manteca, CA) for providing fresh porcine buccal
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010
1276 KULKARNI ET AL.
tissues. The authors gratefully acknowledgeMarcia Fox in the Biology department at theUniversity of the Pacific for her help with tissuehistology and light microscopy studies.
REFERENCES
1. Kulkarni U, Mahalingam R, Pather SI, Li X, JastiB. 2009. Porcine buccal mucosa as an in vitro model:Relative contribution of epithelium and connectivetissue as permeability barriers. J Pharm Sci98:471–483.
2. Birudaraj R, Mahalingam R, Li X, Jasti BR. 2005.Advances in buccal drug delivery. Crit Rev TherDrug Carrier Syst 22:295–330.
3. Pather SI, Rathbone MJ, Senel S. 2008. Currentstatus and the future of buccal drug delivery sys-tems. Expert Opin Drug Deliv 5:531–542.
4. Smart JD. 2005. Buccal drug delivery. Expert OpinDrug Deliv 2:507–517.
5. Sudhakar Y, Kuotsu K, Bandyopadhyay AK. 2006.Buccal bioadhesive drug delivery-a promisingoption for orally less efficient drugs. J ControlRelease 114:15–40.
6. Wertz PW, Squier CA. 1991. Cellular and molecularbasis of barrier function in oral epithelium. Crit RevTher Drug Carrier Syst 8:237–269.
7. De Vries ME, Verhoef JC, Ponec M, Ine W, CraaneHM, Junginger HE. 1991. Localization of the per-meability barrier inside porcine buccal mucosa:A combined in vitro study of drug permeability,electrical resistance and tissue morphology. Int JPharm 76:25–35.
8. Xiang J, Fang X, Li X. 2002. Transbuccal delivery of2’,3’-dideoxycytidine: In vitro permeation study andhistological investigation. Int J Pharm 231:57–66.
9. Shojaei AH, Khan M, Lim G, Khosravan R. 1999.Transbuccal permeation of a nucleoside analog,dideoxycytidine: Effects of menthol as a permeationenhancer. Int J Pharm 192:139–146.
10. Hoogstraate AJ, Senel S, Cullander C, Verhoef J,Junginger HE, Bodde HE. 1996. Effects of bile saltson transport rates and routes of FITC-labelledcompounds across porcine buccal epithelium invitro. J Control Release 40:211–221.
11. Schroeder HE. 1981. Differentiation of human oralstratified epithelia, 7th edition. Basel: S. KargerAG.
12. Squier CA, Hall BK. 1985. The permeability of skinand oral mucosa to water and horseradish perox-idase as related to the thickness of the permeabilitybarrier. J Invest Dermatol 84:176–179.
13. Veuillez F, Rieg FF, Guy RH, Deshusses J, Buri P.2002. Permeation of a myristoylated dipeptideacross the buccal mucosa: Topological distributionand evaluation of tissue integrity. Int J Pharm231:1–9.
JOURNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010
14. Zhang H, Robinson JR. 1996. In vitro methods formeasuring permeability of the oral mucosa. In:Rathbone MJ, editor. Oral mucosal drug delivery,1st edition. New York: Marcel Dekker. pp 85–100.
15. Le Brun PP, Fox PL, De Vries ME, Bodde HE. 1989.In vitro penetration of some ß-adrenoreceptorblocking drugs through porcine buccal mucosa.Int J Pharm 49:141–145.
16. Kulkarni U, Mahalingam R, Pather SI, Li X, JastiB. 2008. Porcine buccal mucosa as an in vitro model:Relative contribution of epithelium and connectivetissue as permeability barriers. J Pharm Sci 98:471–483.
17. De Boer AG, De Leede LG, Breimer DD. 1984. Drugabsorption by sublingual and rectal routes. Br JAnaesth 56:69–82.
18. Nicolazzo JA, Reed BL, Finnin BC. 2003. The effectof various in vitro conditions on the permeabilitycharacteristics of the buccal mucosa. J Pharm Sci92:2399–2410.
19. Nicolazzo JA, Reed BL, Finnin BC. 2004. Assess-ment of the effects of sodium dodecyl sulfate on thebuccal permeability of caffeine and estradiol.J Pharm Sci 93:431–440.
20. Rossi S, Sandri G, Ferrari F, Bonferoni MC, Car-amella C. 2003. Buccal delivery of acyclovir fromfilms based on chitosan and polyacrylic acid. PharmDev Technol 8:199–208.
21. Squier CA, Hall BK. 1985. In-vitro permeability ofporcine oral mucosa after epithelial separation,stripping and hydration. Arch Oral Biol 30:485–491.
22. de Vries ME, Bodde HE, Busscher HJ, JungingerHE. 1988. Hydrogels for buccal drug delivery: Prop-erties relevant for muco-adhesion. J Biomed MaterRes 22:1023–1032.
23. Galey WR, Lonsdale HK, Nacht S. 1976. The invitro permeability of skin and buccal mucosa toselected drugs and tritiated water. J Invest Derma-tol 67:713–717.
24. Dowty ME, Knuth KE, Irons BK, Robinson JR.1992. Transport of thyrotropin releasing hormonein rabbit buccal mucosa in vitro. Pharm Res 9:1113–1122.
25. Imbert D, Cullander C. 1999. Buccal mucosa invitro experiments. I. Confocal imaging of vitalstaining and MTT assays for the determination oftissue viability. J Control Release 58:39–50.
26. Lee J, Lee SK, Choi YW. 2002. The effect of storageconditions on the permeability of porcine buccalmucosa. Arch Pharm Res 25:546–549.
27. Sandri G, Rossi S, Ferrari F, Bonferoni MC, Muz-zarelli C, Caramella C. 2004. Assessment of chit-osan derivatives as buccal and vaginal penetrationenhancers. Eur J Pharm Sci 21:351–359.
28. Sandri G, Rossi S, Bonferoni MC, Ferrari F,Zambito Y, Di Colo G, Caramella C. 2005. Buccalpenetration enhancement properties of N-trimethylchitosan: Influence of quaternization degree on
DOI 10.1002/jps
PORCINE BUCCAL MUCOSA AS IN VITRO MODEL 1277
absorption of a high molecular weight molecule. IntJ Pharm 297:146–155.
29. Betul Dortuno, Nurseli Uyanik LO. 1998. Develop-ment and in vitro evaluation of a buccoadhesivepindolol tablet formulation. Drug Dev Ind Pharm24:281–288.
30. Celebi N, Kislal O. 1995. Development and evalua-tion of a buccoadhesive propranolol tablet formula-tion. Pharmazie 50:470–472.
31. Manganaro AM, Wertz PW. 1996. The effects ofpermeabilizers on the in vitro penetration of pro-pranolol through porcine buccal epithelium. MilMed 161:669–672.
32. Diaz Del Consuelo I, Pizzolato GP, Falson F, GuyRH, Jacques Y. 2005. Evaluation of pig esophagealmucosa as a permeability barrier model for buccaltissue. J Pharm Sci 94:2777–2788.
33. Anlar S, Capan Y, Guven O, Gogus A, Dalkara T,Hincal AA. 1994. Formulation and in vitro-in vivoevaluation of buccoadhesive morphine sulfatetablets. Pharm Res 11:231–236.
34. Veuillez F, Ganem-Quintanara A, Deshusses J,Falson-Rieg F, Buri P. 1998. Comparison of theex-vivo oral mucosal permeation of tryptophan-leu-cine (Trp-Leu) and its myristoyl derivative. Int JPharm 170:85–91.
35. Chang F, Wertz PW, Squier CA. 1991. Comparisonof glycosidase activities in epidermis, palatalepithelium and buccal epithelium. Comp BiochemPhysiol B 100:137–139.
36. Park CR, Munday DL. 2002. Development andevaluation of a biphasic buccal adhesive tablet fornicotine replacement therapy. Int J Pharm237:215–226.
37. Iscan YY, Senel S, Sahin MF, Kes S, Duchane D,Hincal AA. 1998. Formulation and in vitro/in vivoevaluation of buccal bioadhesive captopril tablets.STP Pharma Sci 8:357–363.
38. van der Bijl P, van Eyk AD, Thompson IO, StanderIA. 1998. Diffusion rates of vasopressin throughhuman vaginal and buccal mucosa. Eur J OralSci 106:958–962.
39. van der Bijl P, Thompson IOC. 1998. Effect offreezing on the permeability of human buccal andvaginal mucosa. S Afr J Sci 94:499–502.
40. Lesch CA, Squier CA, Cruchley A, Williams DM,Speight P. 1989. The permeability of human oralmucosa and skin to water. J Dent Res 68:1345–1349.
41. Hoogstraate AJ, Cullander C, Nagelkerke JF, SenelS, Verhoef JC, Junginger HE, Bodde HE. 1994.Diffusion rates and transport pathways of fluore-scein isothiocyanate (FITC)-labeled model com-pounds through buccal epithelium. Pharm Res11:83–89.
42. Junginger HE, Hoogstraate JA, Verhoef JC. 1999.Recent advances in buccal drug delivery and
DOI 10.1002/jps JOU
absorption-in vitro and in vivo studies. J ControlRelease 62:149–159.
43. Shojaei AH. 1998. Buccal mucosa as a route forsystemic drug delivery: A review. J Pharm PharmSci 1:15–30.
44. Babu RJ, Kanikkannan N, Kikwai L, Ortega C,Andega S, Ball K, Yim S, Singh M. 2003. Theinfluence of various methods of cold storage of skinon the permeation of melatonin and nimesulide.J Control Release 86:49–57.
45. Scaletta S, MacCallum DK. 1972. A fine structuralstudy of divalent cation mediated epithelial unionwith connective tissue in human oral mucosa. Am JAnat 133:431.
46. Garren KW, Repta AJ. 1989. Buccal drug absorp-tion. II: In vitro diffusion across the hamster cheekpouch. J Pharm Sci 78:160–164.
47. McCoy GD. 1977. Respiratory characteristics ofmitochondria isolated from squamous epitheliumof the hamster cheek pouch (39888). Proc Soc ExpBiol Med 156:118–122.
48. Person P, Felton J, Fine A. 1965. Biochemical andhistochemical studies of aerobic oxidative metabo-lism of oral tissues. 3. Specific metabolic activities ofenzymatically separated gingival epithelium andconnective-tissue components. J Dent Res 44:91–95.
49. Garren KW, Topp EM, Repta AJ. 1989. Buccalabsorption. III. Simultaneous diffusion and meta-bolism of an aminopeptidase substrate in the ham-ster cheek pouch. Pharm Res 6:966–970.
50. Artusi M, Santi P, Colombo P, Junginger HE. 2003.Buccal delivery of thiocolchicoside: In vitro and invivo permeation studies. Int J Pharm 250:203–213.
51. Lee VH, Yamamoto A. 1991. Penetration and enzy-matic barriers to peptide and protein absorption.Adv Drug Deliv Rev 4:171.
52. Grass GM, Robinson JR. 1988. Mechanisms of cor-neal drug penetration. I: In vivo and in vitrokinetics. J Pharm Sci 77:3–314.
53. De Vries ME, Bodde HE, Junginger HE. 1990.Proceed Intern Symp Controlled Release BioactMaterial. pp 295–296.
54. Consuelo ID, Jacques Y, Pizzolato G, Guy RH,Falson F. 2005. Comparison of the lipid compositionof porcine buccal and esophageal permeability bar-riers. Arch Oral Biol 50:981–987.
55. Ganem-Quintanar A, Guintanar-Guerrero D, BuriP, Jacques Y. 2000. Proceedings of 27th Int SympControl Rel Bioact Mater. pp 27–28.
56. Jacques Y, Ganem-Quintanar A, Teillaud E, Buri P.Proc 2nd World Meeting APGI/APV, Paris, 1998.
57. Golden GM, Guzek DB, Harris RR, McKie JE, PottsRO. 1986. Lipid thermotropic transitions in humanstratum corneum. J Invest Dermatol 86:255–259.
58. Harrison DJ, Yang B, Knutson K. 1997. Thermalanalysis of canine buccal epithelium by DSC andFITR. Pharm Res Suppl S660:660.
RNAL OF PHARMACEUTICAL SCIENCES, VOL. 99, NO. 3, MARCH 2010




















