
Ciliary dysfunction and ultrastructural abnormalities are features of severe asthma
Upload
independentCategory
view
4download
0
Pleomorphic Adenocarcìnoma of Ciliary Epithelium Simulating an Epibulbar Tumor
Merlyn Rodrigues, M . D . , Ahmed Hidayat, M . D . , and James Karesh, M . D .
A 72-year-old woman had epibulbar nodules and a blind eye following trauma in childhood. Histologie examination disclosed a pleomorphic adenocarcìnoma of ciliary epithelium with invasion of the epibulbar region, retina, retinal pigment epithelium, and optic nerve. The diagnosis was confirmed by histo-chemical stains and electron microscopy. The pigmented and nonpigmented neoplastic cells of the ciliary epithelium had a patchy basement membrane around the cell membrane and produced hyaluronic acid in the stroma.
ADENOCARCÌNOMA of the ciliary epithelium, a rare lesion, has been documented only by light microscopy.1,2 Using light and electron microscopy and immunocytochemistry, we studied an unusual epibulbar clinical appearance and rapid progression of this tumor, with intraocular involvement as well as invasion of the optic nerve.
Case Report
Over a two-month period this 72-year-old woman was noted to develop two rapidly enlarging, painless, fleshy, vascularized, epibulbar perilimbal masses involving the left eye (Fig. 1). During the previous ten years she had been closely followed up for chronic open-angle glaucoma of the right eye and sequelae of severe childhood trauma to the left eye. At the beginning of this period, visual acuity was L.E.: counting fingers eccentrically at 2 feet. There was opacification of the inferior cornea,
Accepted for publication July 28, 1988. From the Department of Ophthalmology, University
of Maryland at Baltimore, School of Medicine (Drs. Rodrigues and Karesh) and the Ophthalmic Pathology Branch, Armed Forces Institute of Pathology, Washington, DC (Dr. Hidayat).
Reprint requests to James Karesh, M.D., University of Maryland Hospital, 22 S. Green St., North Building, Rm. N6W45, Baltimore, MD 21201.
subluxation of the lens, rubeosis iridis, and a traction detachment of the inferior retina. Over the next several years, her visual acuity deteriorated to no light perception with the development of a large hyphema, a pupillary membrane, and extensive synechiae. Ultrasound examination five years before her most recent examination demonstrated a total retinal detachment and vitreous hemorrhage. Continued deterioration of the left eye resulted in complete corneal opacification and thickening as well as obliteration of the anterior chamber with a golden-yellow exudate-like material.
When the perilimbal nonpigmented epibulbar masses were first observed, they each measured 2 x 1 x 0.5 cm and appeared to originate from the conjunctiva. They were associated with large, dilated, feeding vessels and were firmly attached to the underlying sclera. While the two masses appeared to be separate, the intervening conjunctiva was moderately thickened and injected. Ultrasound examination demonstrated total disorganization of the intraocular contents. Results of biopsy of each tumor were initially considered to be consistent with an anaplastic conjunctival squamous cell carcinoma. Enucleation of the left globe was performed with extensive conjunctival resection and meticulous frozen section examination of the remaining conjunctiva. The anophthalmic defect was reconstructed with a dermis-fat graft. At the time of surgery, examination of the globe showed a small flesh-colored mass measuring 3 x 2 mm, firmly attached to the sclera adjacent to the optic nerve. Because of the patient's age and reluctance to undergo further surgery, several orbital surgeons were consulted; the consensus was to restrict long-term follow-up to frequent oph-thalmologic and radiologie examinations.
Gross examination—There were two irregular flesh-colored nodules in the epibulbar area, the larger measuring 10 x 9 mm. Behind the calcified lens there was a large white to black ciliary body mass that filled the vitreous cavity and posterior chamber with extension to the cho-roid, retina, and optic nerve (Fig. 2).
©AMERICAN JOURNAL OF OPHTHALMOLOGY 106:595-600, NOVEMBER, 1988 595

596 AMERICAN JOURNAL OF OPHTHALMOLOGY November, 1988
Fig. 1 (Rodrigues, Hidayat, and Karesh). Two epibulbar masses in the inferior perilimbal region.
Microscopic examination—The epibulbar portion of the neoplasm appeared as an extraocu-lar extension of a much larger intraocular mass, with continuity of both portions at the corneo-scleral limbus. The epibulbar portion of the tumor, although located in the substantia propria of conjunctiva, was not continuous with the overlying epithelium. In the epibulbar area, the tumor was composed of nonpigment-ed sheets of malignant cells, with hyperchro-matic pleomorphic nuclei, small nucleoli, and eosinophilic cytoplasm. In many areas, PAS-positive, thin linear basement membrane-like material partially surrounded the tumor cells. Many mitotic figures were noted (more than 20 per 10 high power fields) (Fig. 3).
The large intraocular portion of the tumor was located in the ciliary body, posterior chamber, and vitreous cavity, with invasion of the retina, pigment epithelium, choroid, sclera, episclera, and optic nerve. In contrast to the epibulbar area, the intraocular portion showed a variety of pigmented and nonpigmented cells. The pigmented areas were mostly necrot-ic except at the optic nerve where the pigmented cells appeared viable, arranged in a tubular pattern, with PAS-positive basement membrane-like material outside the base of the tumor cells (Fig. 4). Some nonpigmented intraocular tumor cells were similar to those in the epibulbar portion, whereas others had pale to clear cytoplasm containing neither glycogen nor mucinous material and most likely showing hydropic degeneration (Fig. 5). The stroma between the tumor cells contained Alcian blue-positive mucinous material that was sensitive to hyaluronidase digestion (Fig. 6). Immuno-histochemical studies showed no evidence of
Fig. 2 (Rodrigues, Hidayat, and Karesh). Gross photograph of the sectioned globe showing a large, white to dark brown tumor behind the lens (L) that has filled and replaced most of the intraocular contents. There is an anterior epibulbar nonpigmented extension of the neoplasm (asterisk) and a partly pigmented lesion invading the optic nerve (arrow).
cytokeratin using indirect peroxidase staining. The remainder of the ocular structures showed vascularization and scarring of the cornea, ne-crotic iris, calcified lens, and posterior intraocular ossification. The resected margin of the optic nerve was free of tumor cells.
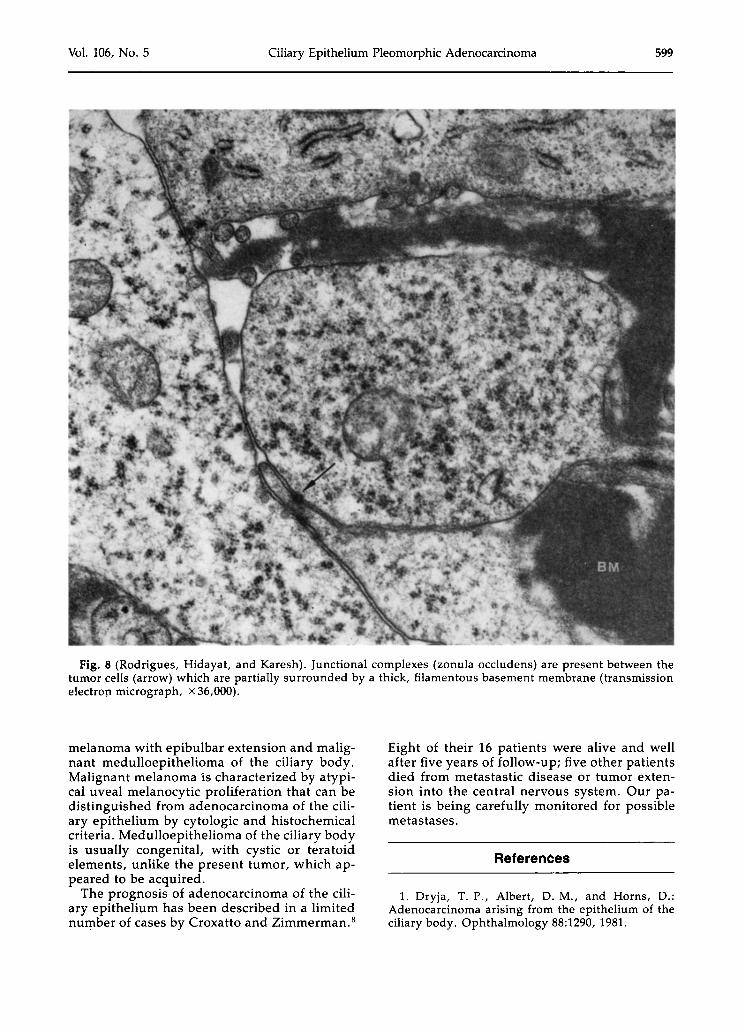
Electron microscopic studies of the formalin-fixed intraocular and epibulbar portions of the neoplasm disclosed necrotic and degenerating pigmented tumor cells. The nonpigmented tumor cells had few cytoplasmic organelles and were partially surrounded by a thick basement membrane that was either homogeneous, filamentous, or multilaminar (Figs. 7 and 8). Junc-tional complexes of the zonula occludens type were observed (Fig. 8).

Vol. 106, No. 5 Ciliary Epithelium Pleomorphic Adenocarcinoma 597
Fig. 3 (Rodrigues, Hidayat, and Karesh). The epibulbar portion of the tumor discloses sheets of malignant cells with hyperchromatic pleomorphic nuclei and small nucleoli. In many areas, PAS-positive, thin linear, basement membrane-like material partially surrounds the tumor cells (periodic acid-Schiff, X250).
Discussion
One unusual aspect of this tumor was its initial clinical appearance as epibulbar nodules that simulated nonpigmented, poorly differentiated squamous carcinoma of the conjunctiva. However, clinically this tumor lacked the pear-
Fig. 5 (Rodrigues, Hidayat, and Karesh). Some intraocular tumor cells near the ciliary body have pale to clear cytoplasm. Other pigmented tumor cells contain melanin. The stroma is hyalinized and occasional linear PAS-positive, basement membrane-like material is present (periodic acid-Schiff, x 160).
Fig. 4 (Rodrigues, Hidayat, and Karesh). The pigmented portion of the tumor has invaded the optic nerve, showing a tubular pattern with PAS-positive, basement membrane-like material adjacent to the base of tumor cells (periodic acid-Schiff, x250).
ly white color that is typical of keratinized squamous carcinoma. Another unusual feature was the optic nerve invasion. The ciliary epithelial origin of the neoplasm was demonstrated by its arrangement in sheets, tubules, and cords surrounded by PAS-positive basement membrane-like material. The thick, patchy, sometimes multilaminar basement membrane was confirmed by electron microscopy. The pleomorphic nature of this tumor was demonstrated by atypical proliferation of different
Fig. 6 (Rodrigues, Hidayat, and Karesh). The stroma between the tumor cells contains blue staining mucinous material sensitive to hyaluronidase digestion (Alcian blue, x 125).

598 AMERICAN JOURNAL OF OPHTHALMOLOGY November, 1988
-4\ .,V'·
.if;t|êij*"
#lfv*v«#'", J!.»,
ρΑ:". ...JSP?
# ; * ♦ #
'Î />; ^
Fig. 7 (Rodrigues, Hidayat, and Karesh). Tumor cells are partially surrounded by a thick basement membrane (BM) that occasionally appears multilaminar (MLBM) (transmission electron micrograph, x 20,000).
cellular components that included nonpig-mented and pigmented cells, confirming its origin from pigmented and nonpigmented ciliary epithelium. The tumor involved the ciliary body as well as the retinal pigment epithelium, retina, optic nerve, and choroid. The extracellular matrix showed a hyaluronidase-sensitive, Alcian blue-positive mucopolysaccharide similar to that observed in benign tumors of ciliary epithelium.3,4 Secretion of hyaluronic acid by cysts and tumors of the ciliary epithelium has been described by Zimmerman and Fine.5,6
The tumor in the present study was composed of pleomorphic cells with abundant cytoplasm and hyperchromatic nuclei with prominent nucleoli. Our case differed from the one reported by Jakobiec and associates7 by its
greater pleomorphism with epibulbar as well as optic nerve invasion. Additionally, hyaluronic acid, one of the substances synthesized in the present tumor, was absent in the tumor described by Jakobiec and coworkers. Furthermore, unlike their case, we found no evidence of intracytoplasmic mucin. In the study by Croxatto and Zimmerman,8 more poorly differentiated tumors occurred in eyes with previous chronic inflammation or trauma, as in our patient. It is uncertain whether the neoplastic invasion of retinal pigment epithelium could have occurred either as direct extension from the ciliary epithelial tumor or as a neoplastic involvement of the retinal pigment epithelium with optic nerve invasion.
The differential diagnosis includes malignant
Vol. 106, No. 5 Ciliary Epithelium Pleomorphic Adenocarcinoma 599
Fig. 8 (Rodrigues, Hidayat, and Karesh). Junctional complexes (zonula occludens) are present between the tumor cells (arrow) which are partially surrounded by a thick, filamentous basement membrane (transmission electron micrograph, x 36,000).
melanoma with epibulbar extension and malignant medulloepithelioma of the ciliary body. Malignant melanoma is characterized by atypical uveal melanocytic proliferation that can be distinguished from adenocarcinoma of the ciliary epithelium by cytologie and histochemical criteria. Medulloepithelioma of the ciliary body is usually congenital, with cystic or teratoid elements, unlike the present tumor, which appeared to be acquired.
The prognosis of adenocarcinoma of the ciliary epithelium has been described in a limited number of cases by Croxatto and Zimmerman.8
Eight of their 16 patients were alive and well after five years of follow-up; five other patients died from metastastic disease or tumor extension into the central nervous system. Our patient is being carefully monitored for possible métastases.
References
1. Dryja, T. P., Albert, D. M., and Horns, D.: Adenocarcinoma arising from the epithelium of the ciliary body. Ophthalmology 88:1290, 1981.

600 AMERICAN JOURNAL OF OPHTHALMOLOGY November, 1988
2. Kuchynka, P.: Malignant epithelioma of the ciliary body. Ophthalmologica 178:190, 1979.
3. Shields, J. A., Augsberger, J. J., Wallar, P. H., and Shah, H. G.: Adenoma of the nonpigmented epithelium of the ciliary body. Ophthalmology 90:1528, 1983.
4. Patrinely, J. R., Font, R. L., Campbell, R. J., and Robertson, D. M.: Hamartomatous adenoma of the nonpigmented ciliary epithelium arising in iris-ciliary body colobomata. Ophthalmology 90:1540, 1983.
5. Zimmerman, L. E., and Fine, B. S.: Production of hyaluronic acid by cysts and tumors of the ciliary body. Arch. Ophthalmol. 72:365, 1964.
6. Zimmerman, L. E.: The remarkable polymorphism of tumors of the ciliary epithelium. Trans. Aust. Coll. Ophthalmol. 2:114, 1970.
7. Jakobiec, F. A., Zimmerman, L. E., Spencer, W. H., Slakter, J. S., and Krebs, W.: Metastatic colloid carcinoma versus primary carcinoma of the ciliary epithelium. Ophthalmology 94:1469, 1987.
8. Croxatto, J. O., and Zimmerman, L. E.: Malignant nonpigmented intraocular tumors of neuroecto-dermal origin in adults. A review of 21 cases. In Spencer, W. H. (ed.): Ophthalmic Pathology, ed. 3. Philadelphia, W. B. Saunders, 1985, vol. 2, pp. 1260-1262.
OPHTHALMIC MINIATURE It is at such moments I am called, in a voice so pure I have to close my eyes, and enter the breathing darkness just beyond my headlights. I have come back, I think, to something I had almost forgotten, a mouth that waits patiently, sighs, speaks and falls silent. No one else is alive. The blossoms are white, and I am almost there.
Robert Mezey, "White Blossoms'
Copyright © 2022 FDOKUMEN




















